Track 6 Cardiovascular system and obesity P152 - Nature
14
Track 6 Cardiovascular system and obesity P152 Urinary albumin excretion is independently associated with C-reactive protein levels in overweight and obese women N Pannacciulli 1 , FP Cantatore 2 , A Minenna 1 , M Bellacicco 1 , R Giorgino 1 , and G De Pergola 1 1 Department of Emergency and Organ Transplantation - Section of Internal Medicine, Endocrinology and Metabolic Diseases, University of Bari, Bari, Italy; 2 Department of Internal Medicine and Public Health - Section of Rheumatology, University of Bari, Bari, Italy INTRODUCTION: The aim of the present study was to evaluate the possible correlation between urinary albumin excretion (UAE), marker of endothelial dysfunction, and C-reactive protein (CRP), marker of chronic inflammation of the arterial wall, in overweight and obese premenopausal women. METHODS: CRP levels and UAE rate were measured in 103 overweight (BMI 25.0 – 29.9 Kg=m 2 ) and obese (BMI 30.0 Kg=m 2 ) premenopausal women, aged 18 – 45 years. Other measurements included central fat accumulation, as evaluated by waist circumference, insulin resistance, as calculated by home- ostasis model assessment (HOMA IR ), systolic and diastolic blood pressure, and fasting plasma levels of glucose, insulin, and lipids. RESULTS: UAE was positively correlated with BMI (P < 0.01), waist circumfer- ence (P < 0.00l), diastolic blood pressure (P < 0.01), triglyceride (P < 0.01), HOMA IR (P < 0.05), and CRP levels (P < 0.05), and negatively associated with HDL-cholesterol (P < 0.001). After multivariate analysis, diastolic blood pres- sure, HDL-cholesterol, and CRP levels maintained their significant correlation with UAE (P < 0.05, P < 0.01, and P < 0.01, respectively). Lastly, we observed a gradual increase in CRP plasma levels across the quartiles in which the whole population was divided according to UAE levels (F: 5.67, P 0.001 for linear trend). CONCLUSION: Our study shows a strong relationship between UAE rate and CRP concentrations, irrespective of age and other anthropometric and meta- bolic variables. On this basis, it can be argued that inflammation of the arterial wall, as indicated by higher CRP plasma levels, and endothelial dysfunction, as shown by higher UAE rate, might represent simultaneous phenomena in the development of atherosclerosis in overweight and obese premenopausal women. P153 C-reactive protein is independently associated with total body fat, central fat, and insulin resistance in adult women G De Pergola 1 , N Pannacciulli 1 , FP Cantatore 2 , A Minenna 1 , M Bellacicco 1 , and R Giorgino 1 1 Department of Emergency and Organ Transplantation - Section of Internal Medicine, Endocrinology and Metabolic Diseases, University of Bari, Bari, Italy; 2 Department of Internal Medicine and Public Health - Section of Rheumatology, University of Bari, Bari, Italy INTRODUCTION: The relationship between C-reactive protein (CRP) and atherotrombosis is well established. Moreover, the prevalence of elevated CRP levels has been shown to be higher in overweight and obese patients than in normal weight subjects. The aim of our study was to investigate whether CRP concentrations are influenced by body composition, insulin resistance and body fat distribution in apparently healthy women. METHODS: CRP plasma levels, body composition (fat mass, FM, and fat-free mass, FFM), as measured by bioimpedance analysis, central fat accumulation, as evaluated by waist circumference, and metabolic parameters, including fasting glucose, insulin levels and insulin resistance, as calculated by home- ostasis model assessment (HOMA IR ) have been determined in 201 apparently healthy normal weight, overweight, and obese women, aged 18 – 60 years. RESULTS: CRP was positively correlated with age (P < 0.001), BMI (P < 0.0001), waist circumference (P < 0.0001), fasting glucose (P < 0.0001), fasting insulin (P < 0.000l), HOMA IR (P < 0.000l), FFM (P < 0.0001), and FM (P < 0.0001). After multivariate analyses, age, HOMA IR , waist, and FM main- tained their independent association with CRP (P < 0.005, P < 0.00l, P < 0.05, and P < 0.05, respectively). Lastly, we observed a gradual increase in CRP plasma levels across the quartiles in which the whole population was divided according to HOMA IR levels (F: 4.83, P 0.003 for linear trend). CONCLUSION: Our study of apparently healthy adult women has shown a strong relationship of total body fat, central fat accumulation, and insulin resistance with CRP plasma levels, irrespective of age and other anthropo- metric and biochemical variables. Since CRP has been shown to be one of the most powerful predictors of risk of cardiovascular events, it can be hypothe- sized that atherogenic mild, chronic inflammation may be a further feature of the metabolic syndrome. P154 Association of early carotid atherosclerosis with hyperinsulinemia and low DHEA(S) in normotensive severe obese women S Savastano 1 , AM Belfiore 2 , R Valentino 3 , M Dorato 2 , N De Luca 4 , F Micanti 5 , C Mauriello 2 , C Falconi 2 , G Lupoli 1 , and G Lombardi 1 1 Department of Molecular and Clinical Endocrinology and Oncology, University Federico II Medical School Naples, Via S. Pansini n. 5 - 80131 Italy; 2 Department of Neurosciences, Unit of Physiology, University Federico II Medical School Naples, Via S. Pansini n. 5 - 80131 Italy; 3 C.E.O.S., CNR, Department of Cellular and Molecular Biology and Pathology, University Federico II Medical School Naples, Via S. Pansini n. 5 - 80131 Italy; 4 Department of Clinical Medicine and Cardiovascular Science, University Federico II Medical School Naples, Via S. Pansini n. 5 - 80131 Italy; 5 Unit of Psychotherapy, Department of Psychiatry, University Federico II Medical School Naples, Via S. Pansini n. 5 - 80131 Italy INTRODUCTION: Hypertension, hyperlipemia, smoking, and hyperinsulinae- mia are well known risk factors in the progression of atherosclerosis. Newer risk factors, such as hyperandrogenism or DHEAS and DHEA [DHEA(S)] levels have also been recently suggested, although the direct evidence that hyperinsuli- naemia or DHEA(S) per se are directly involved has been conflicting. We investigate the cross-sectional association of early carotid atherosclerosis, measured as intima-media thickness (IMT), with hyperinsulinaemia, and low circulating DHEA(S) levels in 17 normotensive severe obese premenopausal women and 10 normal-weight age-matched subjects. METHODS: Oral glucose tolerance test (OGTT), adrenal secretion, carotid diameter (CD), and left ventricular mass index (LVMi) were determined. RESULTS: Impaired glucose tolerance was present in 29% of the obese patients. DHEA(S) levels (P < 0.001) were lower and negatively correlated with simulated insulin (r70.7; P < 0.01), in spite of normal values of other androgens and increased plasma cortisol and urinary free cortisol were found in 53% of the obese patients, with normal dexamethasone suppression test. No differences were observed in systolic and diastolic blood pressure, heart rate, fasting triglycerides, or total cholesterol between the groups. CD, IMT, and LVMi were higher in obese women than in controls (P < 0.05); using simple regression analysis, we found that CD was also positively correlated with BMI (r 0.5; P < 0.05) and fasting insulin (r 0.6; P < 0.05); a weak positive correlation was present between IMT and LVMi (r 0.6; P < 0.05), while a strong negative correlation was present between IMT and DHEA(S) (r 0.9; P < 0.01). The multiple regression analysis, using insulin, BMI, and DHEA(S) as covariates, showed insulin (P < 0.01) and DHEA(S) (P < 0.001) to be the most powerful predictors for CD and IMT, respectively. CONCLUSION: In normotensive severe obese premenopausal women with- out hyperandrogenism, hyperinsulinaemia and low DHEA(S) as early carotid atherosclerosis can be detected in absence of other covariated risk factors for cardiovascular disease, suggesting their independent role in atherosclerosis progression. P155 Left ventricular hypertrophy regression: role of weight loss and insulin changes in obese normotensive subjects F Vetta 1,2 , S Ronzoni 1 , MR Lupattelli 1 , V Spallone 1 , MG Bendini 3 , A Meo 3 , P Fabbriconi 1 , B Novi 1 , A Pannone 1 , E Cicconetti 1 , C Ficoneri 1 , F Russo 2 , and MR Bollea 1 1 Department of Internal Medicine, "Tor Vergata" University, Rome, Italy; 2 Department of Internal Medicine, "SS. Gonfalone" Hospital, Monterotondo, Italy; 3 Institute of Cardiology U.C.S.C. Rome, Italy Obesity and hypertension are the most important determinants of left ventricular hypertrophy (LVH). Our previous reports have suggested the prime role of hyperinsulinism as determinant of LVH independently of blood pressure values in obese subjects. Therefore, on the ground of present knowledge, the aim of this study was to evaluate, in obese subjects, the influence of weight loss on left ventricular mass (LVM) in relation with changes in glycaemic and insulinemic metabo- lism, 24 h blood pressure values and centripetal adipose tissue distribution. We included in our study 24 obese subjects (BMI 34.3) mean age 38.9 years and 14 lean subjects (BMI 23.8) acted as controls age and sex matched. At enrollment and after a period of at least 6 months ensuing the weight loss (74.8 points of BMI), all subjects underwent a 24 h ABPM (Spacelabs 90202), a complete anthropoplicometric and bioimpedance analysis (Dietosystem) and biochemical determinations. Areas under glucose and insulin curves were assessed using Haffner’s formula by values obtained with OGTT, while insulin resistance was deter- mined indirectly (HOMA IR ). LVM was assessed with ATL Ultramark 8 system, International Journal of Obesity (2001) 25, Suppl 2, S74–S87 ß 2001 Nature Publishing Group All rights reserved 0307–0565/01 $15.00 www.nature.com/ijo
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of Track 6 Cardiovascular system and obesity P152 - Nature

Track 6 Cardiovascular system and obesityP152
Urinary albumin excretion is independently associated with C-reactiveprotein levels in overweight and obese women
N Pannacciulli1, FP Cantatore2, A Minenna1, M Bellacicco1, R Giorgino1, andG De Pergola1
1Department of Emergency and Organ Transplantation - Section of InternalMedicine, Endocrinology and Metabolic Diseases, University of Bari, Bari, Italy;2Department of Internal Medicine and Public Health - Section of Rheumatology,University of Bari, Bari, Italy
INTRODUCTION: The aim of the present study was to evaluate the possiblecorrelation between urinary albumin excretion (UAE), marker of endothelialdysfunction, and C-reactive protein (CRP), marker of chronic in¯ammation ofthe arterial wall, in overweight and obese premenopausal women.METHODS: CRP levels and UAE rate were measured in 103 overweight (BMI25.0 ± 29.9 Kg=m2) and obese (BMI �30.0 Kg=m2) premenopausal women,aged 18 ± 45 years. Other measurements included central fat accumulation, asevaluated by waist circumference, insulin resistance, as calculated by home-ostasis model assessment (HOMAIR), systolic and diastolic blood pressure, andfasting plasma levels of glucose, insulin, and lipids.RESULTS: UAE was positively correlated with BMI (P< 0.01), waist circumfer-ence (P< 0.00l), diastolic blood pressure (P<0.01), triglyceride (P< 0.01),HOMAIR (P< 0.05), and CRP levels (P< 0.05), and negatively associated withHDL-cholesterol (P<0.001). After multivariate analysis, diastolic blood pres-sure, HDL-cholesterol, and CRP levels maintained their signi®cant correlationwith UAE (P< 0.05, P< 0.01, and P< 0.01, respectively). Lastly, we observed agradual increase in CRP plasma levels across the quartiles in which the wholepopulation was divided according to UAE levels (F: 5.67, P�0.001 for lineartrend).CONCLUSION: Our study shows a strong relationship between UAE rate andCRP concentrations, irrespective of age and other anthropometric and meta-bolic variables. On this basis, it can be argued that in¯ammation of the arterialwall, as indicated by higher CRP plasma levels, and endothelial dysfunction, asshown by higher UAE rate, might represent simultaneous phenomena in thedevelopment of atherosclerosis in overweight and obese premenopausalwomen.
P153
C-reactive protein is independently associated with total body fat, centralfat, and insulin resistance in adult women
G De Pergola1, N Pannacciulli1, FP Cantatore2, A Minenna1, M Bellacicco1, andR Giorgino1
1Department of Emergency and Organ Transplantation - Section of InternalMedicine, Endocrinology and Metabolic Diseases, University of Bari, Bari, Italy;2Department of Internal Medicine and Public Health - Section of Rheumatology,University of Bari, Bari, Italy
INTRODUCTION: The relationship between C-reactive protein (CRP) andatherotrombosis is well established. Moreover, the prevalence of elevatedCRP levels has been shown to be higher in overweight and obese patients thanin normal weight subjects. The aim of our study was to investigate whetherCRP concentrations are in¯uenced by body composition, insulin resistanceand body fat distribution in apparently healthy women.METHODS: CRP plasma levels, body composition (fat mass, FM, and fat-freemass, FFM), as measured by bioimpedance analysis, central fat accumulation,as evaluated by waist circumference, and metabolic parameters, includingfasting glucose, insulin levels and insulin resistance, as calculated by home-ostasis model assessment (HOMAIR) have been determined in 201 apparentlyhealthy normal weight, overweight, and obese women, aged 18 ± 60 years.RESULTS: CRP was positively correlated with age (P<0.001), BMI(P<0.0001), waist circumference (P<0.0001), fasting glucose (P< 0.0001),fasting insulin (P< 0.000l), HOMAIR (P<0.000l), FFM (P< 0.0001), and FM(P<0.0001). After multivariate analyses, age, HOMAIR, waist, and FM main-tained their independent association with CRP (P<0.005, P<0.00l, P< 0.05,and P< 0.05, respectively). Lastly, we observed a gradual increase in CRPplasma levels across the quartiles in which the whole population was dividedaccording to HOMAIR levels (F: 4.83, P�0.003 for linear trend).CONCLUSION: Our study of apparently healthy adult women has shown astrong relationship of total body fat, central fat accumulation, and insulinresistance with CRP plasma levels, irrespective of age and other anthropo-metric and biochemical variables. Since CRP has been shown to be one of themost powerful predictors of risk of cardiovascular events, it can be hypothe-sized that atherogenic mild, chronic in¯ammation may be a further feature ofthe metabolic syndrome.
P154
Association of early carotid atherosclerosis with hyperinsulinemia and lowDHEA(S) in normotensive severe obese women
S Savastano1, AM Bel®ore2, R Valentino3, M Dorato2, N De Luca4, F Micanti5,C Mauriello2, C Falconi2, G Lupoli1, and G Lombardi11Department of Molecular and Clinical Endocrinology and Oncology, UniversityFederico II Medical School Naples, Via S. Pansini n. 5 - 80131 Italy;2Department of Neurosciences, Unit of Physiology, University Federico II MedicalSchool Naples, Via S. Pansini n. 5 - 80131 Italy; 3C.E.O.S., CNR, Departmentof Cellular and Molecular Biology and Pathology, University Federico II MedicalSchool Naples, Via S. Pansini n. 5 - 80131 Italy; 4Department of ClinicalMedicine and Cardiovascular Science, University Federico II Medical SchoolNaples, Via S. Pansini n. 5 - 80131 Italy; 5Unit of Psychotherapy, Departmentof Psychiatry, University Federico II Medical School Naples, Via S. Pansini n.5 - 80131 Italy
INTRODUCTION: Hypertension, hyperlipemia, smoking, and hyperinsulinae-mia are well known risk factors in the progression of atherosclerosis. Newer riskfactors, such as hyperandrogenism or DHEAS and DHEA [DHEA(S)] levels havealso been recently suggested, although the direct evidence that hyperinsuli-naemia or DHEA(S) per se are directly involved has been con¯icting. Weinvestigate the cross-sectional association of early carotid atherosclerosis,measured as intima-media thickness (IMT), with hyperinsulinaemia, and lowcirculating DHEA(S) levels in 17 normotensive severe obese premenopausalwomen and 10 normal-weight age-matched subjects.METHODS: Oral glucose tolerance test (OGTT), adrenal secretion, carotiddiameter (CD), and left ventricular mass index (LVMi) were determined.RESULTS: Impaired glucose tolerance was present in 29% of the obesepatients. DHEA(S) levels (P<0.001) were lower and negatively correlatedwith simulated insulin (r70.7; P<0.01), in spite of normal values of otherandrogens and increased plasma cortisol and urinary free cortisol were foundin 53% of the obese patients, with normal dexamethasone suppression test.No differences were observed in systolic and diastolic blood pressure, heartrate, fasting triglycerides, or total cholesterol between the groups. CD, IMT,and LVMi were higher in obese women than in controls (P< 0.05); usingsimple regression analysis, we found that CD was also positively correlatedwith BMI (r� 0.5; P<0.05) and fasting insulin (r� 0.6; P<0.05); a weakpositive correlation was present between IMT and LVMi (r� 0.6; P< 0.05),while a strong negative correlation was present between IMT and DHEA(S)(r� 0.9; P<0.01). The multiple regression analysis, using insulin, BMI, andDHEA(S) as covariates, showed insulin (P< 0.01) and DHEA(S) (P<0.001) tobe the most powerful predictors for CD and IMT, respectively.CONCLUSION: In normotensive severe obese premenopausal women with-out hyperandrogenism, hyperinsulinaemia and low DHEA(S) as early carotidatherosclerosis can be detected in absence of other covariated risk factors forcardiovascular disease, suggesting their independent role in atherosclerosisprogression.
P155
Left ventricular hypertrophy regression: role of weight loss and insulinchanges in obese normotensive subjects
F Vetta1,2, S Ronzoni1, MR Lupattelli1, V Spallone1, MG Bendini3, A Meo3,P Fabbriconi1, B Novi1, A Pannone1, E Cicconetti1, C Ficoneri1, F Russo2, andMR Bollea1
1Department of Internal Medicine, "Tor Vergata" University, Rome, Italy;2Department of Internal Medicine, "SS. Gonfalone" Hospital, Monterotondo,Italy; 3Institute of Cardiology U.C.S.C. Rome, Italy
Obesity and hypertension are the most important determinants of leftventricular hypertrophy (LVH). Our previous reports have suggested theprime role of hyperinsulinism as determinant of LVH independently of bloodpressure values in obese subjects.
Therefore, on the ground of present knowledge, the aim of this study wasto evaluate, in obese subjects, the in¯uence of weight loss on left ventricularmass (LVM) in relation with changes in glycaemic and insulinemic metabo-lism, 24 h blood pressure values and centripetal adipose tissue distribution. Weincluded in our study 24 obese subjects (BMI� 34.3) mean age 38.9 yearsand 14 lean subjects (BMI�23.8) acted as controls age and sex matched. Atenrollment and after a period of at least 6 months ensuing the weight loss(74.8 points of BMI), all subjects underwent a 24 h ABPM (Spacelabs 90202),a complete anthropoplicometric and bioimpedance analysis (Dietosystem)and biochemical determinations.
Areas under glucose and insulin curves were assessed using Haffner'sformula by values obtained with OGTT, while insulin resistance was deter-mined indirectly (HOMAIR). LVM was assessed with ATL Ultramark 8 system,
International Journal of Obesity (2001) 25, Suppl 2, S74±S87ß 2001 Nature Publishing Group All rights reserved 0307±0565/01 $15.00
www.nature.com/ijo

using Devereux and Reichek's formula according to Penn Convention criteria.Our data, beyond the expected differences between obese and controlsubjects with regard to LVMI (g� m72) and LVMC (g� m72.7) values,p<0.0001 with similar indices of RWT, have shown, in presence of nonsigni®cative differences in ABPM and AUGC levels, higher values in AUIC(p< 0.0001), HOMAIR (p< 0.0001), as well as in centripetal adipose tissuedistribution parameters (WHR) p<0.0001 in obese subjects.
Statistical analysis performed with linear regression method puts inevidence a strict correlation among LVMI, LVMC, RWT and hyperinsulinism,insulin-resistance, WHR and blood pressure variability (chie¯y systolic values)both before and after weight reduction, (p< 0.001) while the same dataanalyzed with multiple regression statistical method suggest the chie¯y role ofchanges in hyperinsulinism and insulin-resistance as determinants of LVMmodi®cations (p<0.001).
P156A speci®c lipolytic defect in visceral fat in polycystic ovary syndrome
M RydeÂn1, I Ek1, J Hoffstedt1, A ThoÈrne1, C Holm1, H Wahrenberg1, andP Arner1
1Lipidlaboratory, Centre for Metabolism and Endocrinology, Department ofMedicine, Karolinska Institute, Huddinge University Hospital, 141 86,Stockholm, Sweden
INTRODUCTION: Polycystic ovary syndrome (PCOS) is associated with insulinresistance, glucose intolerance, dyslipidemia and atherosclerosis, a similar riskpro®le as in visceral obesity. The etiology is unknown. In order to studypossible primary defects in omental adipose tissue from subjects with PCOS,we investigated visceral fat cells of 10 young non-obese PCOS women withnormal metabolic pro®le, except slightly decreased insulin sensitivity andnormal body fat distribution according to computerized tomography.METHODS: Lipolysis was measured in isolated fat cells by standard proce-dures. Protein was isolated from omental adipose tissue and separated by SDS-PAGE. Speci®c proteins were detected by Western blot. Speci®c lipolyticenzyme activity towards hormone sensitive lipase (HSL) was determined.RESULTS: In comparison to 13 control women, inhibition of lipolysis throughinsulin receptors and Gi receptors was normal but stimulation of lipolysisthrough all three beta-adrenergic receptor subtypes was two-fold increased inPCOS due to enhanced ability of cyclic AMP to activate lipolysis. Examinationof the lipolytic pathway demonstrated that PCOS cells display several differ-ences at the protein level compared to control cells. The short form of HSL,which is an enzymatically inactive splice variant, was highly expressed incontrol cells while PCOS cells showed a markedly reduced level. The expres-sion of the catalytic subunit of protein kinase A (PKA) was increased in PCOScells. Furthermore, detailed studies on the regulatory PKA subunits demon-strated that while Reg IIb was lowered, Regla levels were signi®cantly increasedin PCOS cells. This transition in regulatory subunits has been shown toenhance lipolytic activity in a transgenic animal models. All lipase activity invisceral fat cells could be attributed to hormone sensitive lipase.CONCLUSION: Young non-obese PCOS women with no apparent metabolicabnormality except slightly decreased insulin sensitivity have a markedincrease in the lipolytic function of visceral fat cells due to a superef®cientHSL-PKA complex. This in turn would increase fatty acid delivery to the liverand be an early and primary defect in the.
P157Greater increase in adipose tissue blood ¯ow after oral compared withintravenous glucose
BA Fielding1, F Karpe1, V Ilic1, SM Humphreys1, and KN Frayn1
1Oxford Lipid Metabolism Group, Oxford Centre for Diabetes, Endocrinologyand Metabolism, Radcliffe In®rmary, Oxford, OX2 6HE, UK
Adipose tissue blood ¯ow (ATBF) increases after meal intake and failure toregulate ATBF in the postprandial period may be a feature of insulin resistanceand obesity. The factors that regulate ATBF in the postprandial period are notwell understood, but insulin action is a potential mediator. The aim of thisstudy was to compare ATBF in subcutaneous abdominal adipose tissue afteroral glucose or intravenous glucose=insulin administration. The aim was toachieve similar peripheral glucose and insulin concentrations on the two visits.
15 healthy subjects (8 male) participated in the study after an overnightfast. Their mean age was 35.3 years (23 ± 52) and mean BMI was 23.8 kg=m2
(19 ± 30). On the ®rst visit, ATBF was measured by 133Xe washout, before andafter 75 g oral glucose. On the second, similar concentrations of insulin andglucose in plasma were achieved by dynamic i.v. infusions.
There was signi®cant heterogeneity in ATBF response between subjectson both days (P< 0.001). The mean peak ATBF was 7.9� 1.6 and 4.5�0.8 ml=min=l00 g tissue after oral and i.v. glucose respectively (P<0.05). Nineout of ®fteen subjects exhibited an increase in ATBF in response to oral glucose
that was greater than 50% and in the top tertile the increase was 212�49%.The respective value after i.v. glucose in the same ®ve subjects was 93�44%.There was a signi®cant correlation between peak ATBF in response to the twotreatments (Spearman's rs� 0.87, P<0.001). For both regimens, peak ATBFwas signi®cantly correlated with baseline ATBF (rs�0.60, P<0.05 andrs�0.72, P<0.05 for oral and i.v. glucose respectively). Peak ATBF wasnegatively correlated with BMI (rs�70.52, P<0.05 for both treatments).
The results show an ATBF response can be elicited either by oral or by i.v.glucose administration, but the effect is greater after oral ingestion. Thissuggests that factors in addition to an increasing postprandial insulin con-centration are associated with modulation of postprandial ATBF. Studies suchas this will increase the understanding of the regulation of ATBF in healthysubjects and the implications of dysregulation of ATBF in obesity.
P158Expression of endothelin-system genes and secretion of endothelin-1 byhuman adipocytes
S Engeli1, J Janke1, K Gorzelniak1, FC Luft1, AM Sharma1, Franz-Volhard-Klinik1, and Max-DelbruÈck1
1Center for Molecular Medicine, University Clinic ChariteÂ, Humboldt-UniversityBerlin, Germany
Recent studies have demonstrated that the potent vasoconstrictor peptideendothelin-1 inhibits adipogenesis and activity of lipoprotein lipase activity inrat and human adipocytes via endothelin receptor type A receptors. Further-more, endothelin-1 plasma levels have been reported to be higher in obeseindividuals. At present, no study has investigated the presence of endothelinsystem components in human adipose tissue.
We studied the expression pattern of endothelin system genes in humanadipose tissue, isolated adipocytes, and cultured preadipocytes by conven-tional RT-PCR (n�6 for each sample) and measured secretion of big-endothe-lin-1 into the culture medium of human primary cultured adipocytes byradioimmunoassay. We also measured the expression level of the endothe-lin-1 gene in lean and obese subjects by TaqMan-RT-PCR (n� 30).
Expression of the genes for endothelin-1, type A and type B endothelinreceptors, and the endothelin-1 regulating transcription factor GATA-2 weredetected in human adipose tissue as well as in isolated adipocytes andpreadipocytes. Radioimmunoassay studies revealed secretion of big-endothe-lin-1 by primary cultured human adipocytes into the culture medium.Endothelin-converting-enzyme, that liberates active endothelin-1 from itsprecursor big-endothelin-1, was not detected in adipose cells. Quantitativeexpression of the endothelin-1 gene was higher in obese normotensivesubjects compared to lean normotensive and obese hypertensive subjects.
Our data point to a potential contribution of adipocytes to increasedendothelin-1 plasma levels. Further studies must elucidate the regulation ofbig-endo-thelin-1 secretion by adipocytes and its possible contribution toadipose tissue physiology.
P159
Superoxide dismutase izoenzymes and glutathione peroxidase activity,and malondialdehyde concentration in obese women
K ZÇ wirska-Korczala1, J Jochem1, R Polaniak2, E Birkner2, B Rybus-Kalinowska1,and J JagodzinÂska1
1Department of Physiology; 2Department of Biochemistry, Silesian MedicalUniversity, ul. Jordana 19, 41-808 Zabrze, Poland
INTRODUCTION: Obesity is a metabolic disease associated with immunolo-gical complications. It is known that TNF a, pluripotent cytokine secreted inabundance by adipocytes in obesity, stimulates the antioxidant response ofmanganese-containing superoxide dismutase (MnSOD).METHODS: Lipid pro®le and plasma (pl) and erythrocytes (e) activities ofcopper=zinc superoxide dismutase (Cu=ZnSOD), MnSOD and glutathioneperoxidase (GSHpx), and concentration of malondialdehyde (MDA) wereexamined in 29 premenopausal obese and 14 lean women (age 34�7.2 vs27.3�3.2, BMI 38.2�4.5 vs 22.5� 1.2 kg=m2, respectively).RESULTS: Obese women demonstrated in comparison to the control groupincreased levels of total cholesterol (216.0�38.2 vs 166.3� 18.4 mg=dl;p<0.001), LDL-cholesterol (149� 28 vs 86� 10.1 mg=dl; p<0.00l) andtriglicerydes (162.8� 21.2 vs 85.5� 14.1 mg=dl; p<0.001), and decreasedlevel of HDL-cholesterol (46.3�9.1 vs 60.1�3.2; p< 0.05). In obese womenCu=ZnSOD(pl) and Cu=ZnSOD(e) activities were similar to those found in thecontrol group (8.4� 3.6 vs 9.8�1.7 NU=g protein and 25.1�1073� 3.8�1073 vs 24.8� 1073� 1.2� 1073 NU=g protein, respectively). Moreover, wefound in obese women enhanced activities of MnSOD(pl) (4.3�1.3 vs2.8� 1.7 NU=g protein; p< 0.00l) and PSHpx (40.3� 7.1 vs 5.5� 3.6 mmol=NADPH2=g protein=min; p< 0.00l), and concentrations of MDA(pl) (2.8� 0.3
Track 6 Cardiovascular system and obesity
S75
International Journal of Obesity

vs 2.2� 0.1 mmol=NADPH2=g protein=min; p< 0.05) and MDA(e) (2.5� 0.2vs 2.1� 0.3 mmol=NADPH2=g protein=min; p<0.05).CONCLUSION: Our data reveal the activation of plasma and erythrocytesenzymes involved in oxidative processes, mainly associated with lipid peroxi-dation, in premenopausal obese women with abnormal lipid pro®le.
P160Impact of the methylenetetrahydrofolate reductase (MTHFR) 677 C)Tmutation on folate requirements in obese adolescents during weightreduction
ML Frelut1,2, N Emery-Fillon3, JC Guillaud4, V Coppet2, JP ChristideÁs£,G Potier de Courcy£, and J Navarro1
1HoÃpital R. DebreÂ, 48 bd Serurier, 75019 Paris, France; 2CTP 95580 Margency,France; 3HoÃpital de Brabois Nancy, Dijon, France; 4CNRS Dijon, France
The 677 C)T MTHFR mutation increases the folates requirements in humans.Low folates in turn lead to increased plasma homocysteine (HCY) levels, anindependant cardiovascular risk factor. The aim of this study is to determinefolate requirements, based on HCY plasma concentrations, in obese adoles-cents during weight reduction.
97 obese adolescents (BMI� 36.1� 6.0 kg=m2) including 60 girls and 37boys, aged 14.1� 1.5 yrs were included. 73 completed an inpatient inter-disciplinary weight (Wt) reduction program during 6 to 12 months, 5 days perweek. Wt reduction program included a modertate caloric restriction (720%of national RDAs) at the expense of sucrose and saturated fat, within abalanced diet which provided 400 mg of folate per day. Regular submaximalphysical training was also included.
Folate intakes before Wt loss were assessed by mean of adapted foodfrequency questionnaire and food composition table. Folates in red blood cells(EF) were measured by a microbiological assay and plasma homocysteine(pHCY) by HPLC. MTHFR polymorphism was assessed by PCR.
BMI after Wt loss was 27.8�3.8 kg=m2 (p< 0.0001).Before Wt loss folates intakes were 270� 102 mg=d. Folate density in food
was positively correlated to EF (p<0.0006) and negatively to pHCY(p<0.003). 10% of the subjects are homozygote for the mutation (TT�), 47are heterozygote (CT) and 44% have the wild type (CC). During Wt loss EFincrease by 9% (p<0.04) and pHCY by 19% (p< 0.001). pHCY increase ishigher in CT (�27%, p< 0.001, n�35) than in CC (�15%, p<0.05,n�32). In TT, neither pHCY (9.06�2.46 mmol=l, n�6) nor EF (207�65 mg=l)vary. They remain higher than in CT and CC subjects.
Daily folates intakes above 400 mg=d seem to be required to prevent a risein pHCY in severely obese adolescents during Wt reduction. The increaserequired is proportional to the degree of the mutation (TT>CF>CC).
P161
Potential hypothalamic effects of leptin in cafeteria diet-inducedhypertension
C Plut1, C RibieÁre1, Y Giudicelli1, and JP Dausse1
1Service de Biochimie et de Biologie MoleÂculaire, Faculte de MeÂdecine de Paris-Ouest, France
Obesity is the most common cause of hypertension. Recent observationssuggest that leptin and its multiple interactions with neuropeptides in thehypothalamus may link excess weight gain with increased sympathetic activityand elevated blood pressure. In hypothalamus of cafeteria-fed rats, a model ofobesity-induced hypertension, we studied leptin receptor, neuropeptides andadrenergic system. After 10 weeks of diet, hyperleptinemia was associatedwith a decrease in leptin receptor mRNA (735 and 745% for the short andthe long isoform respectively). Leptin receptor belongs to cytokine receptor,we therefore ewamined inhibitors of cytokine signaling. Expressions of CIS andSOCS-3, known modulators of leptin signaling, were unchanged but SOCS-1was surprisingly increased. The leptin effect on SOCS-1 increase and its role inthe hypothalamic leptin signaling during obesity remain to be determined. Adecrease in proopiomelanocortin (POMC) gene expression was also observedwithout modi®cation in neuropeptide Y mRNA. The decrease in leptinreceptor could participate to the state of leptin resistance observed in obesityand contribute to decrease POMC. POMC down-regulation in cafeteria-fedrats could contribute to the onset of hypertension by a decrease in thehypotensive action of b-endorphin, a POMC product, or by conversion ofthis hypotensive response to a contrasting pressor response to b-endorphinpreviously observed in obese rats. On the other band, tyrosine hydroxylase(TH), the rate limiting enzyme in catecholamine synthesis, and a2B-adreno-ceptor were up-regulated. These modi®cations suggest an elevation in sym-pathetic activity and may participate to elavated blood pressure. If leptin hasbeen shown to increase TH mRNA levels in culture porcine adrenal medullary
chromaf®n cells, the leptin involment in the overexpression of TH mRNA in thehypothalamus of cafetria-fed rats remains to be determined.
P162
Blood pressure in relation to birth weight and weight history duringchildhood and adulthood in Danish men
L Schack-Nielsen1, C Holst1, and TIA Sùrensen1
1Danish Epidemiology Science Centre, Institute of Preventive Medicine,Kommunehospitalet, DK 1399 Copenhagen K, Denmark
INTRODUCTION: Obesity is associated with an increased risk of hypertension,but whether the duration of obesity has importance for blood pressure is notknown.METHODS: 245 obese men (body mass index (BMI)�31 kg=m2) and 236random controls were identi®ed retrospectively from draft board examinationmedical records. Weight and height during childhood (7 ± 13 years of age)were available from school health records in which birth weight, based onmothers recall when the child attended school, was also reported. Thesubjects were invited to participate in two follow up studies (median age 36years (interval 25; 53 years) and 47 (interval 37; 64 years), respectively),where height, weight and blood pressure were measured. By multiple regres-sion the importance of BMI and change in BMI in childhood and adolescencefor blood pressure as adults after taking current weight and age into accountwas estimated.RESULTS: Current BMI and age were positively associated with systolic anddiastolic blood pressure. While taking these effects into account, BMI duringchildhood, or change in BMI in childhood or adolescence, had no in¯uence onblood pressure. Birth weight was negatively related to systolic blood pressure(regression coef®cient 72.0 mmHg per kg; 95% con®dence interval 74.0;70.1 and 72.7 mmHg per kg; 95% con®dence interval 75.3; 0.0 at ®rst andsecond follow up, respectively), when adjusting for current BMI and age.Further adjustments for BMI measurements in childhood or adolescence didnot change these estimates.CONCLUSION: Obesity increases the risk of hypertension, but the duration ofobesity seems not to have an additional in¯uence on blood pressure. This hasimplications for the understanding of the relation between obesity and bloodpressure. However, birth weight was negatively related to blood pressure, onlyafter taking current BMI into account, indicating an adverse effect of a catch-up in weight. Since BMI measurements from the age of 7 years and change inBMI in childhood and adolescence had no in¯uence on blood pressure, thiscatch-up in weight has probably taken place before the age of seven.
P163
Obesity reduces muscle metabore¯ex control
IC Trombetta1, MM Ribeiro1, LT Batalha2, MUPB Rondon1, T Tinucci3,CLM Forjaz3, ACP Barretto1, A Halpern2, SMF Villares2, and CE NegraÄo1,3
1Heart Institute (InCor), University of SaÄo Paulo Medical School, SaÄo Paulo, Brazil;2Department of Endocrinology, University of SaÄo Paulo, SaÄo Paulo, Brazil; 3Schoolof Physical Education and Sports, University of SaÄo Paulo, SaÄo Paulo, Brazil
INTRODUCTION: There is no information about the muscle metabore¯excontrol in obese individuals.METHODS: In 40 normotensive obese women (OW) and 15 age-matchedlean women (LW), we measured muscle sympathetic nerve activity (MSNA)and forearm blood ¯ow (FBF) during static exercise at 10 and 30% of maximalvoluntary contraction (MVC).RESULTS: Baseline MSNA (38� 2 vs 31�1 bursts=min, P�0.001) and meanblood pressure (MBP, 100�2 vs 91� 3 mmHg, P�0.0036) were higherin OW compared with LW. FBF was lower (1.90� 0.07 vs 2.27� 0.15 mL=min=100 g, P�0.02), while forearm vascular resistance (FVR) was higher in OW(57� 3 vs 45�3 units, P� 0.03). During 10% MVC, MSNA increased similarlyin both groups, but during 30% MVC, MSNA increased was higher in LW. Theresponses of FBF and FVR during both 10 and 30% MVC were similar betweengroups. During post-handgrip circulatory arrest, MSNA remained signi®cantlyelevated compared with baseline in both groups, but this increase wassigni®cantly lower in OW compared with LW (3.8� 0.82 vs 9.4�1.03bursts=min, P�0.002). Further analysis showed the same results when wecompared a subset group 17 OW with similar MBP levels than LW.CONCLUSION: Muscle metabore¯ex control of MSNA is blunted in OW.MSNA responses are not augmented during selective activation of centralcommand=mechanoreceptors and metaboreceptor, despite increased MSNAlevels in OW. Muscle vasodilatory response during graded handgrip isometricexercise is preserved in OW.
Track 6 Cardiovascular system and obesity
S76
International Journal of Obesity

P164
Inhibitory effects of anti-diabetic compounds on interleukin-8 productionin human adipose tissue
JM Bruun1, SB Pedersen1, and B Richelsen1
1Department of endocrinology and metabolism C, Aarhus Amtssygehus, AarhusUniversity Hospital and Faculty of Health Sciences, Aarhus University, DK-8000Aarhus C, Denmark
INTRODUCTION: Obesity is known to be strongly associated with anincreased risk of developing Type 2 diabetes and cardiovascular disease.Reports have suggested that the chemokine, interleukin-8, may be involvedin the development of diabetic macroangiopathy as well as in the pathogen-esis of atherosclerosis, and is has been shown that interleukin-8 is producedand released form the human adipose tissue (Bruun et al, J. Clin. Endocrinol.Metab., In press). Two classes of drugs, the biguanides and the insulin-sensitizing thiazolidinediones seem to have additional bene®cial effects oncardiovascular risk-factors besides their effects on glucose homeostasis. In thisstudy we investigated the effects of the thiazolidinedione, Ciglitazone (aPPARg-agonist), the PPARa-agonist Eicosatetraynoic acid (ETYA) and thebiguanide, Metformin on interleukin-8 gene expression and production inhuman adipose tissue in vitro.METHODS: Adipose tissue obtained from the subcutaneous abdominal regionwere incubated up to 24 h together with increasing concentrations of thecompounds investigated stimulated with interleukin-1b (2 ng=mL). The con-centration of IL-8 in the media was measured by ELISA and the geneexpression was determined by real time RT-PCR. The mean stimulated con-centration of IL-8 was 42.9�3.1 nM.RESULTS: The PPARg, Ciglitazone 10 ± 100 mM inhibited interleukin-8 releaseand gene expression by 25 ± 50% (p<0.05). Metformin 0.1 ± 10 mM inhibi-ted interleukin-8 release and gene expression by 20 ± 80% (p< 0.05). How-ever, the PPARa-agonist, ETYA 1 ± 100 mM did not effect the production ofinterleukin-8 in the adipose tissue.CONCLUSION: We here demonstrate the ability of two anti-diabetic com-pounds to decrease the release of interleukin-8 from human adipose tissue invitro. These ®ndings could suggest that these anti-diabetic compounds mighthave additional bene®cial effects on the atherosclerotic process, besides theireffects on glucose homeostasis through the observed anti-in¯ammatorymechanism.
P165Associations of haemostatic variables with body mass index
LK Bowles1, PK MacCallum1, JA Cooper1, DJ Howarth1, J Af®eld1, TW Meade1,and GJ Miller1
1MRC Epidemiology and Medical Care Unit, Charterhouse Square, London,EC1M 6BQ, United Kingdom
INTRODUCTION: Obesity is a risk factor for venous and arterial thrombosisand this may be mediated partly through changes in the haemostatic system.We examined relationships between a range of haemostatic variables, mea-sured by standard methods, and BMI.METHODS: 150 adults (73 males, 77 females), age range 23 ± 80 years,identi®ed from a general practise list by strati®ed random sampling withingender and decade of age. Correlations with tertiles of BMI were sought afterage-adjustment.RESULTS: In women from the lowest to the highest tertile of BMI, ®brinogenrose from 2.66 to 3.24 g=l (p�0.0001), C1-inhibitor antigen rose from 96.2
to 112.2% (p�0.01), antithrombin III activity rose from 1.12 to 1.23 u=ml(p� 0.004) and median C-reactive protein rose from 3.8 to 4.2 mg=l(p� 0.0001). In men, these associations were not statistically signi®cant.There was no sex difference in the association of other variables with BMI,so results were combined.CONCLUSIONS: Increasing BMI is associated with elevation of coagulationfactors, inhibitors of ®brinolysis and inhibitors of coagulation. These changesmay partiy explain the increased tendency for thrombosis in obese subjects.Explanation for the sex differences requires further investigation.
P166
Left and right ventricular dysfunction in morbid obesity
LK Bowles1, TW Koh1, AD Timmis1, and PG Kopelman1
1St Bartholomew's and the Royal London School of Medicine, Whitechapel,London, E1 1BB, United Kingdom
INTRODUCTION: Circulatory volume expansion and increased cardiac outputaccompany increasing body weight. As a consequence, structural changesdevelop in the heart. Abnormalities of left ventricular (LV) function have beendescribed in obesity, but less is known about alterations in right ventricular(RV) function. The aim of this study was to assess cardiac adaptation to obesitywith particular reference to RV, in 22 young (age 45�11 yrs, 8 female)asymptomatic obese subjects without hypertension using transthoracic echo-cardiography (TTE). The results were compared to a control group of 21normal weight subjects of similar age (40�11 yrs) with structurally normalhearts.METHODS: 2-D guided M-mode echocardiographic measurements of thelongitudinal motion of the tricuspid and mitral annulus at the level of the LVand RV free walls, as well as trans-mitral and trans-tricuspid Doppler in end-expiration, were recorded by TTE. Pulmonary artery (PA) pressure wasestimated from tricuspid regurgitation. Body weight and BMI for the obesegroup was signi®cantly higher than the control group (150�32 kg vs73� 9 kg, 52� 10 kg=m2 vs 25� 3.0).RESULTS: Our LV observations con®rm previous ®ndings. Short axis measure-ments of the LV showed larger cavity size (LVEDD 5.2�0.6 vs 4.3�0.6 cm),increased wall thickness (1.3� 0.1 vs 1.0�0.1 cm) and greater LV mass (LVmass=height index 206�52 vs 96�19 g=m, p< 0.01 for all) in obese vscontrols. LV systolic excursion (SE) and shortening rate (SR) were no differentto controls, but lengthening rate (LR) was reduced (8.3�2.6 vs10� 2.5 cm=s), trans-mitral a wave was greater (0.7� 0.1 vs 0.5� 0.1 m=s)and e=a ratio was reduced (1.1�0.3 vs 1.4� 0.4) in obese vs controls.(p< 0.05 for all). We report for the ®rst time alterations in RV function. RVSE and SR were similar in the obese (2.4�0.3 vs 2.5�0.3 cm, 11.2�2.4 vs10� 2.5 cm=s p�ns). But LR was reduced in the obese vs controls (8.4� 2.4vs 10�2.5 cm=s, p<0.05). Trans-tricuspid a wave was greater (0.5�0.1 vs0.2� 0.1 m=s), e=a ratio was reduced (0.9� 0.2 vs 1.9�0.4), while RVisovolumic relaxation time increased, in obese vs control. (73� 22 vs40� 15 s, p<0.0l for all). PA pressure was similar in obese and controls(20�5 vs 18�6 mmHg).CONCLUSIONS: Extreme obesity is characterised by alterations in LV and RVdiastolic function. In addition, there are signi®cant alterations in LV mass andcavity size. These changes contribute to the increased risk of cardiovascularmorbidity and mortality in obese subjects.
P167Sibutramine improves clinical and metabolic parameters in obesepatients with polycystic ovary syndrome
T Sabuncu1, M Harma1, Y Nazligul1, and F Kilic1
1University of Harran, Faculty of Medicine, Research Hospital, 63200,Sanliurfa, Turkey
INTRODUCTION: It is known that polycystic ovary syndrome (PCOS) ischaracterized by hyperandrogenemia and may be associated with hyperinsu-linemia, insulin resistance and some other cardiovascular risk factors. Althoughtraditional oral contraceptive use can improve hyperandrogenemia, it isgenerally inadequate to correct other clinical and metabolic risk factors ofcardiovascular disease. Therefore, we aimed to evaluate the effectiveness ofsibutramine, an antiobesity drug, alone and combination with ethinyl estra-diol (35 mg)-cyproterone acetate (2 mg) (EE-CPA) on clinical and metabolicparameters of obese (BMI>30 kg=m2) patients with PCOS.METHODS: Group-1 patients (n� 14) were treated with EE-CPA alone, group-2 patients (n� 12) with sibutramine alone (l0 mg=d) and group-3 patients(n� 14) with EE-CPA plus sibutramine combination. All three groups ofpatients were advised to consume a diet of 1200 kcal=d. Body mass index(BMI), waist to hip ratio (WHR), systolic blood pressure (sBP), diastolic blood
Tertile of BMI (mean)
1 (21.7) 2 (25.1) 3 (29.3) p value
FVIIc1 109.9 (31.7) 124.2 (34.4) 139.8 (30.9) 0.0001
FVIIIc1 108.4 (25.6) 110.2 (31.2) 122.2 (30.2) 0.05
vWF 95.8 (27.3) 88.1 (26.7) 97.5 (25.7) 0.19
FXIIa1 1.69 (0.55) 1.98 (0.71) 2.33 (0.85) 0.0001
F1.21 1.32 (0.40) 1.41 (0.38) 1.51 (0.52) 0.12 (0.04)*
t-PA1 2.93 (1.23) 2.30 (1.14) 1.82 (1.22) 0.0002
PAI-1 9.5 (4.6) 10.7 (5.5) 13.6 (7.1) 0.003
Plasminogen 102.0 (13.1) 110.2 (11.3) 114.2 (11.4) <0.0001
a2-AP 88.4 (10.2) 95.3 (10.6) 99.0 (8.1) 0.0001
Protein C1 87.9 (12.0) 97.5 (17.6) 105.2 (17.4) <0.0001
APC1 2.99 (0.35) 2.81 (0.49) 2.61 (0.47) 0.002
Free PRS1 102.1 (33.3) 115.7 (27.4) 115.2 (28.1) 0.04
(All values are mean (sd) except, 1geometric mean (approx sd), *test for trend.)
Track 6 Cardiovascular system and obesity
S77
International Journal of Obesity

pressure (dBP), Ferriman-Gallwey hirsutism score (FG), serum levels of totaltestosterone (TT), free testosterone (FT), SHBG, DHEAS, total cholesterol (TC),HDL cholesterol (HDL-C), LDL cholesterol (LDL-C), triglyceride, glucose andinsulin during OGTT, insulin sensitivity index obtained from OGTT (ISI-composite), area under the curve for glucose (AUC-glucose) and insulin(AUC-insulin) were measured before and after 6 months of the treatment.RESULTS: BMI, FG, serum TT, FT and DHEAS levels signi®cantly decreased andSHBG signi®cantly increased at the end of the study in all groups. WHIR, dBPand serum triglyceride level signi®cantly reduced only in group-2. Bothgroup-2 and group-3 patients had signi®cantly reduction in the levels ofAUC-glucose, AUC-insulin and ISI-composite. Group-1 and group-3 patientsshowed signi®cantly increase in the serum level of HDL-C. Serum triglyceridelevel signi®cantly increased only in group-1 patients.CONCLUSION: This study has showed that treatment with the weight losingdrug sibutramine may improve hyperandrogenemia, and clinical and meta-bolic risk factors for cardiovascular disease in obese patients with PCOS.Sibutramine combination with EE-CPA may also enhance effectiveness in thetreatment of hirsutism, and further decrease cardiovascular risk by increasingserum HDL-C level.
P168The percentage of body fat and its relationship to age and blood pressurein men and women without cardiovascular medication
A Dzien1, C Dzien-Bischinger1, F Hoppichler 2, and M Lechleitner 3
1Medical Center Hentschelhof, Innsbruck, Austria; 2Hospital BarmherzigeBruÈder, Salzburg, Austria; 3Department of Internal Medicine, University ofInnsbruck, Austria
INTRODUCTION: Obesity is associated with a signi®cant increase in overallmorbidity and mortality, including an increased risk for hypertension. Adiposetissue is known to produce vasoactive substances, but clinical data on thelinkage between the percentage of body fat with blood pressure values is rare.METHODS: We have consecutively recruited 355 patients (234 women, 121men; mean age 56.7�17.5 years; mean BMI 25.5�4.4 kg=m2) withoutcardiovascular medication at a medical outdoor center. Beside laboratorycontrols, blood pressure measurements and calculation of the body massindex (BMI), the percentage of body fat was determined by a method ofbioimpedance applying the OMRON BF 302 body fat monitor. Patients wereassigned to a group with normal percentage of body fat (24% and less inwomen; 19% and less in men) and to a group with a more pronouncedpercentage of body fat (25% and more in women; 20% and more in men).RESULTS: The mean age of women in the group with a lower body fat content(14.5�4.5%) was 43.4� 17.7 years, and thus signi®cantly younger than inthe group with a more pronounced body fat content (30.6� 6.9%) witha mean age of 64.1�12.7 years (p<0.021). Blood pressure values weresigni®cantly lower in the leaner group (125.0�23.3 mm Hg and78.9� 12.6 mm Hg) than in the group with an increased body fat content(144.5� 16.6 mm Hg and 88.0� 14.1 mm Hg) (p< 0.050). The results in themale group were in accordance to the ®ndings obtained in women. Men witha lower percentage of body fat (15.2� 3.4%) were younger (52.7�17.4years) and revealed lower blood pressure values (130�19.2 mm Hg and79.7� 8.8 mm Hg) than men with a more pronounced percentage of bodyfat (25.7� 4.0%) with a mean age of 63.8� 12.7 years (146.4� 23.5 mm Hgand 90.7� 11.8 mm Hg). Systolic as well as diastolic blood pressure valuesshowed a strong positive correlation with the percentage of body fat in men(R�0.35; p< 0.033) and women (R�0.44; p< 0.015).CONCLUSIONS: Our results suggest that age and blood pressure values arerelated to the percentage of body fat content also in non-obese patientswithout cardiovascular medication.
P169
Body fat distribution and cardiovascular risk factors in pre- andpostmenopausal obese women with similar body mass index
N Ozbey1, M Taskale1, S Molvalilar1, E Sencer1, and Y Orhan1
1Department of Internal Medicine, Division of Endocrinology, Istanbul Facultyof Medicine, Capa, 34390, Istanbul, Turkey
An increase in the incidence of atherosclerotic cardiovascular disease isobserved in women after menopause. An increase in intraabdominal fat anda more atherogenic lipid pro®le might-in part-be operative for this observa-tion.The aim of this study is to determine the body fat distribution andcardiovascular risk factors in pre- and post menopausal obese womenmatched for weight, height and body mass index (BMI).
Study group consisted of 405 premenopausal obese (BMI>27 kg=m2,mean BMI 37.8�6.9 kg=m2) and 405 postmenopausal obese(BMI> 27 kg=m2), BMI-matched (mean BMI 37.7�6.8 kg=m2) women. Noneof the women were on hormone replacement therapy. After an overnight fast,
anthropometric parameters were determined and venous blood samples wereobtained for the measurements of glucose, uric acid, cholesterol, triglyceride,HDL-cholesterol, and insulin concentrations. Insulin resistance was evaluated by``homeostasis model assessment'' (HOMA) formula. Intraabdominal fat area(IAF) was calculated by a previously validated formula: IAF (cm2)� (waistcircumference�2.57)� (age� 0.92)� (suprailiac skinfold thickness� 0.69)7188.61. Waist circumference, waist to hip ratio and intraabdominal fat areawere signi®cantly higher in postmenopausai women compared with BMImatched-premenopausal women (p< 0.001 for all). Fasting glucose(109.6�33.6 vs 99.4� 19.1 mg=dL), uric acid (4.78�1.47 vs 4.34�1.12 mg=dL), cholesterol (232.2�43.2 vs 202.3� 37.0 mg=dL), triglyceride(172.6�79.9 vs 152.2� 74.9 mg=dL), systolic blood pressure (148.2�29.7vs 135.1�26.7 mm Hg) and diastolic blood pressure (91.79� 15.7 vs87.7� 15.0 mm Hg) were signi®cantly higher (p<0.001 for all) in postmeno-pausal women compared with premenopausals. No signi®cant differences wereobserved with respect to insulin levels and HOMA.
It is concluded that an increase in intraabdominal fat accumulation andmetabolic consequences of abdominal obesity disturb postmenopausalwomen even if total body weight and BMI do not change during menopause.
P170Angiotensiongen expression and angiotensin II secretion are stimulatedby insulin in human abdominal fat
CL McTernan1, AL Harte1, MC Eggo1, AH Barnett1, PG McTernan1, andS Kumar1
1University of Birmingham, Division of Medical Sciences, Clinical ResearchBlock, Edgbaston, Birmingham B15 2TH
Hypertension is a common disorder associated with obesity and Type IIdiabetes. The reninangiotensin system (RAS) is important for the regulationof blood pressure and previous studies have demonstrated the presence of thecomponents of an active tissue RAS in human adipose tissue. In this study weinvestigated the in¯uence of varying insulin doses on both the expression ofangiotensinogen and the secretion of angiotensin II in human subcutaneous(Sc) abdominal fat.
Isolated Sc adipocytes (n�10) were treated with varying doses of insulin(1 nM ± 1000 nM) for 48 hrs. Following treatment, the media from the adipo-cytes and the adipocytes were harvested. Western blotting was performed onthe protein extracted from the adipocytes to determine angiotensinogenexpression. ELISAs were performed on the collected media to determine thesecretion of angiotensin II from human adipocytes. Angiotensinogen mRNAlevels were also assessed.
Our results demonstrate that increasing doses of insulin (Ins) raisedangiotensinogen protein expression in a dose dependent manner (control1.0�0.0; (mean� SE), protein expression measured relative to control; 1 nMIns: 1.13�0.1; l0 nM Ins: 1.37�0.14:*; l00 nM Ins: 2.1� 0.3:**; 500 nM Ins:4.1�0.83:**; l000 nM Ins: 5.2� 8.7:**; *p< 0.05, **p<0.01). Insulin alsoraised angiotensin II secretion in a similar pattern to angiotensinogen proteinexpression (control: 155� (SEM) 6.4 pg=ml 1 nM Ins: 98�3.6 pg=ml;***;l0 nM Ins: 181�2.5 pg=ml:**; l00 nM Ins: 216� 8.7 pg=ml:***; 500 nM Ins:687.3�11.7 pg=ml***; 1000 nM Ins: 1964�18.2 pg=ml***:; ***p<0.001).
In conclusion, increasing insulin doses stimulate both angiotensinogenand angiotensin II production in adipocytes showing active regulation of therenin-angiotensin system in fat by insulin. This insulin regulated, adiposetissue-derived angiotensin may be important for obesity related hypertension.
P171
LDL phenotype B and triglyceride rich lipoproteins in overweight patientsrelated to platelet adhesion
J Hartwich1, I LeszczynÂska-Gol--bek1, M KwasÂniak1, A Gruca1, M Motyka1,L-- Partyka1, and A DembinÂska-KiecÂ1
1Department of Clinical Biochemistry, Collegium Medicum, JagiellonianUniversity, Krakow, Kopernika 15A str., Poland
INTRODUCTION: The genetically determined and environmentally in¯u-enced LDL pattern B (atherogenic lipid pro®le ALP) and triglyceride richlipoproteins have recently been recognised as an important risk factor ofCAD. The nongenetic factors shown to in¯uence LDL density include intra-abdominal fat accumulation, exercise and diet. Blood platelet adhesioncontributes to pathomechanism of atherosclerosis. The aim of the study wasto determine the in¯uence of lipoprotein composition on platelet adhesion inrelation to obesity.METHODS: Lipoproteins (VLDL, LDL, HDL) were isolated from fasting plasmaof overweight subjects (BMI> 25 kg=m2). VLDL after standard fat meal werealso used. The particle distribution pro®le (LDL, HDL), apoE phenotype, a
Track 6 Cardiovascular system and obesity
S78
International Journal of Obesity

tocopherol and b carotene contents, susceptibility to oxidation and reactivelysine amino groups (R-Lys) were estimated. Adhesion of human washedplatelets to native and oxidized lipoproteins immobilized in microtiter wellswas examined. The total number of adhered platelets was measured as theplatelet acid phosphatase activity.RESULTS: Platelet adhesion was activated by all the lipoproteins tested. VLDL,small dense LDL and oxidized lipoproteins were the most potent adhesionactivators. Platelet adhesion to VLDL was in¯uenced by apoE phenotype andR-Lys content. The standard fat meal augmented platelet adhesion to VLDL.Adhesion to LDL and HDL was related to antioxidant content, particle density,oxidative susceptibility and R-Lys level. High antioxidant content in LDL andHDL strongly limited platelet activation. Enrichment of LDL and oxLDL inoxidatively modi®ed lipids: 7-ketocholesterol and lyso-PC increased plateletadhesion. BMI correlated with platelet adhesion to VLDL (r� � 0.55,p.< 0.05) and to dense LDL (r� �0.48, p.<0.05).CONCLUSION: Particle distribution pro®le, apoE phenotype and antioxidantcontents strongly in¯uenced platelet adhesion to lipoproteins in overweightpatients. Fasting and postprandial VLDL, small, dense LDL, native antioxidant-poor and oxidized lipoproteins were the most potent adhesion activators.
P172
Cardiac autonomic neuropathy in obese children
K ToÈroÈk1, I Wittmann2, and D MolnaÂr1
1Department of Paediatrics, University of PeÂcs, Hungary; 2Second Department ofMedicine, University of PeÂcs, Hungary
INTRODUCTION: Obesity is associated with an increased incidence of hyper-tension, unexplained death, as well as an overall increase in mortality rate. Theautonomic nervous system is involved in the regulation of energy metabolismand cardiovascular system activity. Obese persons often have an alteration intheir autonomic nervous system, accounting for several clinical consequencesof obesity. Silent myocardial infarction and myocardial ischemia seem to beassociated with cardiac neuropathy in some cases. Long before the appear-ance of clinical signs of autonomic neuropathy, subclinical signs can bedetected. It has been suggested that subclinical signs of cardiovascularautonomic neuropathy appear in obese children and adolescents.METHODS: To evaluate the alterations in cardiac autonomic function, sub-clinical signs of autonomic neuropathy were investigated in 47 obese children(age: 13.4� 2.53 years, body weight: 81.64�16.3 kg, body fat: 32.9� 8.1 kg[mean� SD]) with different cardiovascular risk factors. Resting heart rate, heartrate variation to deep breathing, heart rate response to standing from a lyingposition, fall in systolic blood pressure on standing, and rise in diastolic bloodpressure during sustained handgrip were measured, by means of standardizedtests.RESULTS: Using reference ranges obtained in normal weight controls (Barkaiet al, Arch Dis Child 1995; 73: 515 ± 518), 19 obese children (40%) had 2 ormore abnormal autonomic test results (Table).CONCLUSION: Cardiovascular autonomic dysfunctions are detectable inobese children. According to the preliminary results further investigationsare needed to clarify subgroups being at risk of autonomic dysfunctions.
P173
Is the reduction of coronary heart disease risk by sibutraminedose-related?
KW Lauterbach1, and T Evers1
1Institute of Health Economics and Clinical Epidemiology, Gleueler Str.176 ± 178, D-50935 Cologne
INTRODUCTION: The additive nature and direct relationship between inde-pendent risk factors and the probability of CHD is well established. On thebasis of these risk factors equations have been developed which allow to
predict the probability of a CHD within a speci®ed time frame. As recentresults indicated that sibutramine signi®cantly reduces the probability of aCHD within 10 years we investigated whether this reduction is dose-related.METHODS: We applied the Whitehead and Whitehead meta-analysis techni-que and the Framingham risk equation on data from 5612 patients from 26studies. We compared patients receiving 10 mg or 15 mg sibutramine oncedaily with all placebo patients.RESULTS: Treatment difference in 10-year CHD-risk change1
1sibutramine minus placebo; Whitehead and Whitehead meta-analysis tech-nique; sibutramine categorical analysis vs all placebo.
CONCLUSION: The results indicate that sibutramine signi®cantly reduces therisk of CHD in a dose-dependent manner.
Table Abnormal autonomic test results in our patients
Abnormal autonomic test results
Obese children (n� 47)
n %
3 5 10.6
2 14 29.8
1 22 46.8
0 6 12.8
P174
An anthropometric index of obesity-linked risk factors based on thecombination of body weight and waist circumference values
F Bel®ore1, S Iannello1, and M Prestipino1
1Department of Internal Medicine, University of Catania Medical School,Ospedale Garibaldi, 95123 Catania, Italy
INTRODUCTION: We propose an anthropometric index of obesity-linked risk,resulting from the combination of the body weight and waist circumferencevalues, and compare this Index with the body mass index (BMI) and theWaist=Hip ratio (W=H). Our index is obtained with a formula similar to thatone previously described (Bel®ore et al Mol Gen Metab 1998; 63: 134 ± 141;Diabetes Care 23: 1595 ± 1596, 2000) to calculate an insulin sensitivity Index.METHODS: The commonly used indicators of obesity risk, the BMI and theW=H, are based on four anthropometric measures: body weight (WE), height(HE), waist circumference (WA) and the hip circumference (HI). We combinedthe WE and WA values into a single index, that we named WE7WA, throughthe following formula: WE7WA� 2=[(rWEp� rWAp)� 1], where rWEp andrWAp are the ``reciprocal'' values of WE and WA of the person studied. BothWE and WA are expressed by taking their ``mean normal value'' (MNV) as 1,i.e. by dividing the value recorded in the person studied by the MNV. The``reciprocal values'' (i.e., rWEp and rWAp) are calculated by dividing the MNVby the value measured in the person studied. In normal subjects WE7WA isalways close to 1, with maximal variations between 0 and 2. The MNV of WEand WA needs not be strictly de®ned or related to sex or groups. Rather, a``general mean normal value'' can be selected, leaving sex or group variationsto be re¯ected by small variations of the WE7WA obtained. We selected asmean normal values 70 (Kg) for WE and 80 (cm) for WA. We studied 95subjects (25 male and 70 female), age 18 ± 71 years, BMI 24.07 ± 52.76 andW=H 0.76 ± 1.13, and analyzed the correlations with several risk factors.RESULTS: In our study population, WE7WA ranged from 0.86 to 1.50, andwas signi®cantly correlated with an index of insulin sensitivity deduced fromthe OGTT data, triglycerides, uric acid and diastolic blood pressure(r�0.4070.45, p<0.001 in all instances). BMI and W=H (as well as thecombination of 3 or all the 4 anthropometric measures mentioned above)showed only � 3 of these correlations with weaker ``r'' and ``p'' values.CONCLUSION: WE7WA seems as a promising risk index in obese patients.
P175
Increased arterial pulse pressure in subjects with moderate obesity butnot in those with simple overweight
AJ Scheen1, I Geronooz1, Ph Ernest1, and M Marchand1
1Department of Medicine, CHU Sart Tilman LieÁge, Belgium
INTRODUCTION: The study aimed at comparing the changes in mean arterialpressure (PAM) and pulse pressure (PP) in obese, overweight and lean subjectssubmitted to an orthostatic test (``squatting'') and continuous cardiovascularmonitoring.
Track 6 Cardiovascular system and obesity
S79
International Journal of Obesity
METHODS: 30 obese subjects (BMI: 33.5�2.6 kg=m2 ± mean� SD ± ), 30overweight individuals (BMI: 26.7� 1.4 kg=m2) and 30 lean controls (BMI:22.2� 1.6 kg=m2) were submitted to an active orthostatic test (1 min stand-ing ± 1 min squatting ± 1 min standing). The three groups were matched forsex (11 women and 19 men) and age (around 42 years), and no subjects tookmedication interfering with cardiovascular regulation. Systolic, diastolic, meanand pulse arterial blood pressure were continuously monitored with a Fina-presR device (Ohmeda, USA).RESULTS: PAM (p�0.06) and heart rate (p�0.08) tended to be higher inobese vs lean subjects when averaged during the whole test. During squat-ting, PAM was higher in obese subjects (95.7� 13.6 vs 84.9�16.0 mm Hg,p� 0.007) while it was intermediate in overweight subjects(92.9�15.8 mm Hg, p� 0.06 vs lean; NS vs obese). Heart rate during squat-ting was higher in overweight (85� 14 beats=min; p� 0.005) and in obese(83� 13 beats=min; p�0.035) subjects than in lean controls(76� 9 beats=min). Average PP was similar in overweight and lean subjects(46.4�15.8 vs 45.7� 10.6 mm Hg, NS), whereas it was markedly increased inobese subjects (53.8� 12.2 mm Hg, p� 0.009 vs controls and p< 0.05 vsoverweight subjects). Such a difference was observed throughout the test andin each posture condition (standing or squatting).CONCLUSION: Increased heart rate, mean arterial pressure and pulse pressurelevels were observed in obese middle-aged subjects. Because high pulsepressure has been shown to be associated with a higher risk, such an increasemay contribute to the higher cardiovascular rnortality of obese patients.
P176
Low-fat, high-carbohydrate diets do not inevitably lead tohrypertriglyceridaemia
KS Culling1, KN Frayn1, F Karpe1, and HAW Neil21Oxford Lipid Metabolism Group, Oxford Centre for Diabetes, Endocrinologyand Metabolism, Radcliffe In®rmary, Oxford, OX2 6HE, UK; 2Division ofPublic Health and Primary Health Care, Institute of Health Sciences, Universityof Oxford, Old Road, Headington, Oxford, OX3 7LF, UK
INTRODUCTION: Low-fat diets are established as the best way to lose weightand maintain weight loss. Reducing dietary fat usually leads to an increase inthe carbohydrate (CHO). Recently, concern has been expressed that theselow-fat, high-CHO diets cause hypertriglyceridaemia (HTG), a known riskfactor for coronary heart disease. The objective of this study was to discoverif the type of carbohydrate consumed had any effect on the degree of HTGobserved.METHODS: Five normal-weight, normolipaemic subjects (3 female, 2 male)were recruited. Each followed 3 different 3-day, isoenergetic, weight main-tenance diets. Each diet was separated by at least one month. These consistedof one high-fat diet (50% fat, 35% CHO, 15% protein), a `high-sugar' diet(70% CHO, 40% as sucrose, 30% as complex-CHO, 15% fat, 15% protein),and a `high-starch' diet (70% CHO, 40% as complex-CHO, 30% as sucrose,15% fat, 15% protein). Each diet was followed by a study-day, where fastingand postprandial triacylglycerol (TG) concentrations were measured. Subjectsall received an identical mixed-meal.RESULTS: There was a signi®cant effect of diet on fasting TG (p< 0.0001 byrepeated measures ANOVA). Post-hoc tests with Bonferroni correction showedthat fasting TG was signi®cantly higher after the high-sugar diet comparedwith the high-fat (p< 0.005) and high-starch diet (p<0.008). There was nosigni®cant difference between fasting TG concentration on the high-starchcompared to the high-fat diet. The high-sugar diet signi®cantly increasedplasma TG compared with the high-starch diet (p< 0.03) and high-fat diet(p<0.05). However, there was no signi®cant difference between TG concen-trations on the high starch compared with the high-fat diet.CONCLUSION: A low-fat diet need not result in increased fasting andpostprandial TG concentrations if dietary fat is replaced with complex carbo-hydrate rather than sugar.
P177Improvement of cardio-vascular risk factors with a six months orlistattreatment in overweight and obese patients with comorbidities
B Guy-Grand1, H Gin1, P Drouin1, E Eschwege1, and P Valensi11Depts of Nutrition, Paris, Bordeaux, Nancy, INSERM U258 Villejuif, Bondy,France
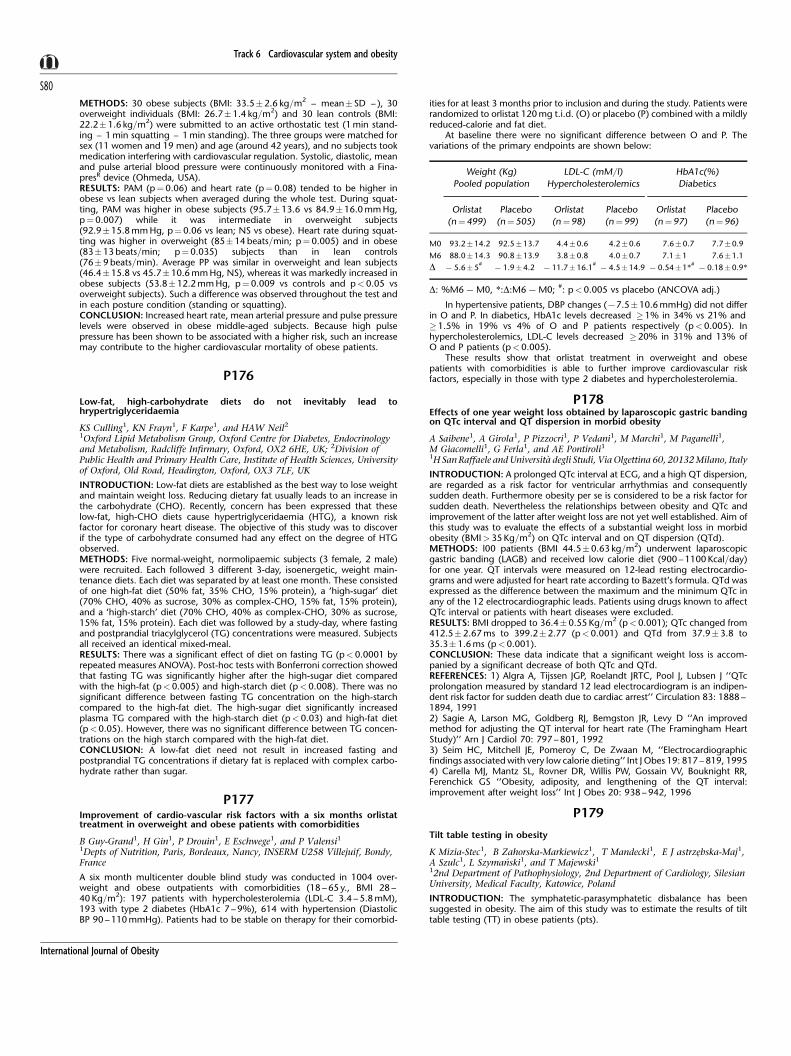
A six month multicenter double blind study was conducted in 1004 over-weight and obese outpatients with comorbidities (18 ± 65 y., BMI 28 ±40 Kg=m2): 197 patients with hypercholesterolemia (LDL-C 3.4 ± 5.8 mM),193 with type 2 diabetes (HbA1c 7 ± 9%), 614 with hypertension (DiastolicBP 90 ± 110 mmHg). Patients had to be stable on therapy for their comorbid-
ities for at least 3 months prior to inclusion and during the study. Patients wererandomized to orlistat 120 mg t.i.d. (O) or placebo (P) combined with a mildlyreduced-calorie and fat diet.
At baseline there were no signi®cant difference between O and P. Thevariations of the primary endpoints are shown below:
In hypertensive patients, DBP changes (77.5�10.6 mmHg) did not differin O and P. In diabetics, HbA1c levels decreased � 1% in 34% vs 21% and�1.5% in 19% vs 4% of O and P patients respectively (p<0.005). Inhypercholesterolemics, LDL-C levels decreased �20% in 31% and 13% ofO and P patients (p< 0.005).
These results show that orlistat treatment in overweight and obesepatients with comorbidities is able to further improve cardiovascular riskfactors, especially in those with type 2 diabetes and hypercholesterolemia.
P178Effects of one year weight loss obtained by laparoscopic gastric bandingon QTc interval and QT dispersion in morbid obesity
A Saibene1, A Girola1, P Pizzocri1, P Vedani1, M Marchi1, M Paganelli1,M Giacomelli1, G Ferla1, and AE Pontiroli11H San Raffaele and UniversitaÁ degli Studi, Via Olgettina 60, 20132 Milano, Italy
INTRODUCTION: A prolonged QTc interval at ECG, and a high QT dispersion,are regarded as a risk factor for ventricular arrhythmias and consequentlysudden death. Furthermore obesity per se is considered to be a risk factor forsudden death. Nevertheless the relationships between obesity and QTc andimprovement of the latter after weight loss are not yet well established. Aim ofthis study was to evaluate the effects of a substantial weight loss in morbidobesity (BMI> 35 Kg=m2) on QTc interval and on QT dispersion (QTd).METHODS: l00 patients (BMI 44.5�0.63 kg=m2) underwent laparoscopicgastric banding (LAGB) and received low calorie diet (900 ± 1100 Kcal=day)for one year. QT intervals were measured on 12-lead resting electrocardio-grams and were adjusted for heart rate according to Bazett's formula. QTd wasexpressed as the difference between the maximum and the minimum QTc inany of the 12 electrocardiographic leads. Patients using drugs known to affectQTc interval or patients with heart diseases were excluded.RESULTS: BMI dropped to 36.4� 0.55 Kg=m2 (p<0.001); QTc changed from412.5�2.67 ms to 399.2�2.77 (p<0.001) and QTd from 37.9�3.8 to35.3� 1.6 ms (p<0.001).CONCLUSION: These data indicate that a signi®cant weight loss is accom-panied by a signi®cant decrease of both QTc and QTd.REFERENCES: 1) Algra A, Tijssen JGP, Roelandt JRTC, Pool J, Lubsen J ``QTcprolongation measured by standard 12 lead electrocardiogram is an indipen-dent risk factor for sudden death due to cardiac arrest'' Circulation 83: 1888 ±1894, 19912) Sagie A, Larson MG, Goldberg RJ, Bemgston JR, Levy D ``An improvedmethod for adjusting the QT interval for heart rate (The Framingham HeartStudy)'' Arn J Cardiol 70: 797 ± 801, 19923) Seim HC, Mitchell JE, Pomeroy C, De Zwaan M, ``Electrocardiographic®ndings associated with very low calorie dieting'' Int J Obes 19: 817 ± 819, 19954) Carella MJ, Mantz SL, Rovner DR, Willis PW, Gossain VV, Bouknight RR,Ferenchick GS ``Obesity, adiposity, and lengthening of the QT interval:improvement after weight loss'' Int J Obes 20: 938 ± 942, 1996
P179
Tilt table testing in obesity
K Mizia-Stec1, B Zahorska-Markiewicz1, T Mandecki1, E J astrzeÎbska-Maj1,A Szulc1, L SzymanÂski1, and T Majewski112nd Department of Pathophysiology, 2nd Department of Cardiology, SilesianUniversity, Medical Faculty, Katowice, Poland
INTRODUCTION: The symphatetic-parasymphatetic disbalance has beensuggested in obesity. The aim of this study was to estimate the results of tilttable testing (TT) in obese patients (pts).
Weight (Kg)
Pooled population
LDL-C (mM=l)
Hypercholesterolemics
HbA1c(%)
Diabetics
Orlistat
(n� 499)
Placebo
(n�505)
Orlistat
(n�98)
Placebo
(n� 99)
Orlistat
(n� 97)
Placebo
(n�96)
M0 93.2�14.2 92.5�13.7 4.4�0.6 4.2�0.6 7.6�0.7 7.7�0.9
M6 88.0�14.3 90.8�13.9 3.8�0.8 4.0�0.7 7.1�1 7.6�1.1
D 75.6�5#
71.9�4.2 711.7�16.1#74.5�14.9 70.54�1*
#70.18�0.9*
D: %M67M0, *:D:M67M0; #: p<0.005 vs placebo (ANCOVA adj.)
Track 6 Cardiovascular system and obesity
S80
International Journal of Obesity

METHODS: We examined 59 pts with simplex obesity (F=M:50=9; BMI ±36.9�3.9 kg=m2) ± group A and 19 healthy persons as control group(F=M:16=3; BMI ± 24.7�4.3 kg=m2) ± group C. Additionally TT was per-formed in 11 pts from group A after 3-months of weight reducing treatment.The cardiovascular reactions to tilting were determined by the measurementsof HR, SBP and DBP. We assessed: baseline values, values after tilting,difference between maximal and minimal values during TT (A), and indexof change (%D�D=baseline value� 100%).RESULTS: Positive TT was observed in 10 obese pts (17%), and none of thecontrols. The comparison of HR, SBP and DBP between groups A and Crevealed higher DHR in group of obese pts (23.9� 13.7 vs 17.87� 8.9) only. Inpts with positive TT results signi®cant higher HR after tilting, DHR, and %DHRwere noted in comparison to pts with negative TT and to group C. Pts afterweight reducing treatment were characterised by: higher %DHR than groupA, and lower baseline HR, SBP, DBP in comparison both to group A and to theirresults before treatment.CONCLUSION: The positive results of TT are observed in 17% pts withsimplex obesity. Different HR reaction to tilting (increased HR ¯uctuation) ispresent in obese pts, especially in pts with positive TT. The 3-months weightreducing treatment decreases HR, SBP and DBP, but does not normalize thecardiovascular reaction to tilting. Our results can support the hypothesis ofautonomic disbalance in obesity.Supported by KBN grant C008=P05=2000
P1806 Mo high protein diet does not increase P-homocysteine in obese
N Haulrik1, S Toubro1, S Stender1, AR Skov1, and A Astrup1
1The Research Department of Human Nutrition, RVAU, Rolighedsvej 30,DK-1958 Frederiksberg, Denmark
Replacing carbohydrate with protein in ad lib fat-reduced diets increases fatloss without adverse effects on blood lipids and renal function1 ± 2
Plasma homocysteine (Hcy) is a risk factor for cardiovascular disease and isthought to be increased by a high protein intake. We studied the effect ofprotein intake in obese subjects in a 6 mo randomized intervention studycomparing two ad lib fat reduced diets (30% of total energy): Low-protein (LP,12 energy-%) or high-protein (HP, 22 energy-%). 65 overweight and obesesubjects were randomly assigned to LP (n� 25), HP (n� 25) or a controlgroup (C, n� 15). All food was provided by self selection in a shop at thedepartment. Compliance to the diet composition was evaluated by urinarynitrogen excretion.The protein intake was increased in the HP group mainlyby lean meat and low fat dairy products. Folate intake nearly doubled in the LPgroup and increased by 60% in the HP group (LP vs HP; P<0.05). It remainedunchanged in the C group (LP & HP vs C; P�0.0001). B12 intake decreased inthe LP and increased by 80% in the HP (P<0.0001), whereas B6 intakeincreased by 70 ± 90% in LP and HP groups with no change in the C group(P <0.0001). Plasma Hcy did not change in the LP or C groups, but there wasa non-signi®cant 20% decrease in the HP group. Fat loss was 4.3 kg in LP and7.6 kg in HP (P< 0.0001), with no change in the C group. In multiple linearregression analyses plasma Hcy after 3 mo intervention was determined bybaseline Hcy (r� �0.34, P�0.0001), folate intake (r�70.003, P� 0.0350),dietary protein content (r�70.17, P�0.0007), and by weight change(r�70.12, P� 0.0350). After 6 mo the same trends were seen (baselineHcy P� 0.0001; protein content P� 0.09). This study shows that increasingthe dietary protein from 12 to 22 energy-% does not increase plasmahomocysteine levels. By contrast, animal protein, independent of intake of Bvitamins and weight loss, may actually decrease plasma homocysteine con-centrations in obese subjects.1. Skov AR et al. Randomized trial on protein versus carbohydrate in ad libitumfat reduced diet for the treatment of obesity. It J Obes 1999;23:528 ± 536.2. Skov AR et al. Changes in renal function during weight loss induced byhigh vs low-protein low-fat diets in overweight subjects. It J Obes 1999;23:1170 ± 1177.
P181Orlistat reduces cardiovascular risk in overweight or obese patients withother risk factors
D Bellido1, JL Herrera-Pombo2, F Armero3, and M GenõÂs3
1Hospital Naval (El Ferrol); 2FundacioÂn JimeÂnez Diaz (Madrid) on behalf of theResearch group on Orlistat in diabetic and hypercholesterolemic patients (Spain);3Roche Farma Spain SA
INTRODUCTION: The present study was designed to evaluate the impact oftreatment for weight loss with 120 mg orlistat (Xenical1) t.i.d. versus placebo oncardiovascular risk in overweight or obese patients with other cardiovascular riskfactors (type 2 diabetic and non diabetic patients with hypercholesterolemia).
METHODS: Pooled data of two randomized, parallel groups, double blinded,multicenter clinical trials. 514 patients with BMI �27 kg=m2 were randomized(261 Orlistat, 253 placebo) after 4 weeks of placebo run-in and hypocaloricdiet (30% of calories from fat). Cardiovascular risk at 10 years was computedusing Framingham algorithm assuming all patients were smokers.RESULTS: Baseline cardiovascular risk was similar for Orlistat (ORL) andplacebo (PLA) (14.45% vs 13.36%). The change in predicted 10-year cardi-ovascular risk after 6 months treatment was threefold for Orlistat than forplacebo (71.43% vs 70.53%, p�0.063). Greater risk reduction wasobserved among hypercolesterolemic patients (73.02%) than diabeticpatients (71.46%). Signi®cant mean weight loss was achieved with Orlistatwhen pooling data from diabetic and non diabetic patients (77.1% vs73.46%, p<0.001). Diabetic mellitus group lost less weight than nondiabetic mellitus, consistent with previous reports than weight loss is moredif®cult for DM. Orlistat achieved a higher reduction of mean waist perimeter(76.36 vs 74.2 cm, p< 0.001) and BMI (72.66 vs 71.37, p< 0.001).31.5% and 38.3% of patients normalized total cholesterol and LDL choles-terol, respectively with ORL in comparison with 22.5% and 26.1% withplacebo (p�0.018 and p�0.003). Greater reduction of plasma glucosewas achieved with ORL than with placebo (1.59 vs 0.79, p< 0.001).CONCLUSION: Orlistat produces a signi®cant weight loss as well as a reduc-tion of cardiovascular risk through decreases of total and LDL cholesterol andan improvement of metabolic control of type 2 diabetes in overweight orobese patients with additional risk factors.
P182Sex hormone ± binding globulin levels and cardiovascular risk in morbidlyobese subjects before and after diet or biliopancreatic diversion
A Scarfone1, A Giancaterini1, AV Greco1, M Castagneto1, and G Mingrone1,1Institute of Internal Medicine, Catholic University, Rome, Italy
Several studies showed that in obese subjects low plasma SHBG levels wereassociated with high fasting insulin concentrations and with an altered lipid-lipoprotein pro®le, including reduced HDL cholesterol and an increasedatherogenic index. A cross-sectional study was conducted to verify thechanges of SHBG and lipid pro®le in 79 morbidly obese subjects, 27 menand 52 women (age: 30 ± 45yrs), randomly assigned to the diet protocol(20 kcal=kgFFM, 55% carbohydrates, 30% fat, and 15% proteins) or to BPDprocedure. We investigated the modi®cation of Coronary Heart Disease (CHD)risk in morbidly obese subjects after weight reduction treatment, either diet orbiliopancreatic diversion (BPD), and to evaluate whether SHBG changes mightplay any pathogenetic or diagnostic role.
Fatness parameters by dual-energy X-ray absorptiometry (Fat Mass andFat-Free Mass), SHBG and sex hormones plasma levels and lipid pro®le atbaseline and 1 year after the beginning of the study has been evaluated.
Pre-Post weight loss differences in SHBG plasma levels were signi®cantlyhigher in the BPD group compared to the dieting group (84.0� 25.2 nM=l vs143.4� 23.4, P<0.0001). Furthermore, surgical treated subjects largestchanges in insulin, total cholesterol, HDL-cholesterol and tryglicerides afterweight loss compared to the diet-group. (P<0.0001). The main result was thesigni®cant decrease of the atherogenic risk observed in BPD patients(6.58� 3.33 vs 2.90�0.58 after the treatment; P<0.0001), while no differ-ences were found in dieting patients.
A step-down regression analysis showed that FFM and SHBG were themost powerful independent variables for predicting HDL-cholesterol levels;while insulin did not in¯uence signi®cantly HDL-CH changes. The positiverelationship between low SHBG levels and increased CHD risk appears to bemediated, to a large extent, by concomitant variation in body fatnessmeasured directly. In this regard, SHBG level may be viewed as a re¯ectionof total adiposity rather than a predictor of an altered insulin=glucose home-ostasis.
P183Autonomic nervous system activity in obese subjects and during weightreduction
J Chaloupka1, P HluÂbik1, L OpltovaÂ1, H MalaÂ1, and S PelcaÂk1
1Purkyne Military Medical Academy, TrÏebesÏska 1575, 500 01 Hradec KraÂloveÂ,Czech Republic, [email protected]
Power spectral analysis of heart rate variability during modi®ed orthostatic testis the non-invasive method used for the evaluation of autonomic nervoussystem (NS) activity.
In the groups of 82 healthy volunteers (BMI 24.9�2.7 kg=m2) and 37healthy obese subjects (BMI 36.1�4.9 kg=m2) some of the vegetative NSparameters have been compared. In the group of 16 volunteers we measuredthe vegetative NS activity changes during the weight reduction regimen
Track 6 Cardiovascular system and obesity
S81
International Journal of Obesity

(10 day's hospitalisation, daily energy intake 3300 kJ, weight before101.5�18.1 kg, after 97.5�17.1 kg, p<0.0001). Acute reactions to theenergy restriction were evaluated in the groups of 10 volunteers during 3days of energy intake 3200, 6600 a 13 400 kJ.
Obese persons show a slight decrease of both sympathetic and parasym-pathetic NS activities. In the supine position, only few changes in thesympathetic=parasympathetic NS activity ratio were observed. In the standingposition, in the obese group, a decrease of sympathetic=parasympathetic NSactivity ratio was described. Signi®cant correlations between sympathetic NSactivity and lipid oxidation (r�0.329, p<0.01) as well as saccharide oxida-tion (r�70.258, p<0.05) were observed.
During the weight reduction, a slight increase of the parasympathetic NSactivity and a higher increase in the sympathetic NS activity were measured.Acute reaction to the low-energy diet was observed in a few days. Relativeincrease mainly in the sympathetic NS activity doesn't depend on the degreeof energy de®ciency only, but some subjective factors may play a signi®cantrole.
In the group of obese persons non-speci®c changes of the vegetative NSactivity were observed. They are modulated by some behavioural factors. Thetendency to the higher parasympathetic NS activity con®rms the MONA LISAtheory of the origin of obesity. The return of the indexes after overweightreduction is an important information.
P184Cardiac morphology and left ventricular function in children with simplexobesity
E Sadurska1, L Szewczyk1, and D Witkowski11Dept. of Paediatric Cardiology, Medical Academy, University Children'sHospital in Lublin, Poland; 2Dept. of Peadiatric Endocrinology and Neurology,Medical Academy, University Children's Hospital in Lublin, Poland
The purpose of this study was to assess left ventricular (LV) structure, systolicand diastolic function in obese children. The study group consist of 25 youngpatients (aged 12 ± 17) with body mass index (BMI) above 30 kg=m2. Theresults were compared with those in a control group of 15 healthy childrenwithout overweight.
Echocardiography was performed and echocardiographic measurementswere obtained in accordance with the recommendations of the AmericanSociety of Echocardiography with the exception of data for LV mass, whichwas derived using Penn convention methodology. LV diastolic ®lling wasassessed using pulsed-wave Doppler echocardiography, in accordance withthe methods of Nishimura at all.
It was established that LV mass, LV mass corrected for body surface and LVmass corrected for height were signi®cantly higher in obese children. Theprevalence of LV hypertrophy in children with obesity (using LV mass=heightindex) was almost 78%.
The tested parameters of the left ventricle systolic function: shorteningfraction (%SF), ejection fraction (%EF) were within normal values and therewere no signi®cant differences when compared to controls with normalweight. The date obtained from pulsed ± Doppler echocardiography indicatethat left ventricular ®lling pattern in obese children also was no signi®cantlydisturb. Peak early (MVE) left ventricular ®lling velocity, peak atrial (MVA)velocity, MVE=MVA velocities ratio were similiar in both groups.
P185MUFA enriched hypocaloric diet: effect on weight loss and onatherosclerosis
C Mary1, C Colette1, N Pares-Herbute1, TC Pham1, and L Monnier1
1Laboratoire de Nutrition et AtheÂrogeneÂse, IURC, 641 avenue du doyen Giraud,34093 Montpellier Cedex 5, France
In 23 obese patients, we compared the effects of 2 hypocaloric diets (730%of total energy expenditure) on weight loss rate, on smooth muscular cell(SMC) proliferation and on blood cardiovascular risk factors : TG, TC, HDLc,LDLc, ®brinogen, Lp(a), insulin resistance (HOMA).
In % of total energy intakes, the composition of the 2 diets (pro-teins=fats=CHO) was 20=25=55 (diet A, n�11) vs 20=40=40 (diet B,n�12). 65% of total energy intake was brought by CHO and MUFA inboth diets: 55�10 (diet A) and 40� 25 (diet B enriched in olive oil). Biologywas evaluated at days 0 and 60. Weight was measured at days 0, 30 and 60.
Neither at day 30 nor at day 60 was the weight loss dependent on thetype of the diet. At day 60, insulin resistance and plasma concentrations of TG,TC and LDLc were signi®cantly diminished independently of the type of thediet. HDLc, Lp(a) and ®brinogen remained unchanged. SMC proliferation wasenhanced with type A diet (�3.67%, p�0.025). Changes in SMC prolifera-tion (%) were negatively correlated to changes in HDLc (r�70.51,
p� 0.012) and to the compliance to the diet (r�70.48, p� 0.018). Instepwise multiple regression, changes in SMC proliferation could be explainedby changes in HDLc (step 1: 23%) and by compliance to the diet (step 2:16%).
In conclusion, during the early weight loss, diets enriched in olive oil couldhave a protective effect on SMC proliferation and therefore on atherosclerosis.
P186The effects of symptomatic and asymptomatic left ventricular systolicdysfunction on effort capacity and quality of life in 55 to 75 year oldsobese patients
D Rosu1, V Ivan1, and M Bordea1
1Academic Hospital Department of Cardiology Timisoara Romania
The effects of left ventricular systolic dysfunction (LVSD) in asymptomaticform, are less known as contributor to the disabling condition in chronic heartfailure.METHODS: We studied 69 obese patients aged 55 to 74 years, randomlyselected from hospitalized patients. Cardiovascular risk factors were observed.Each patient completed questionnaires regarding medical history, the symp-tom of breathlessnes, quality of life, current medication. Echocardiograms andmaximal exercise tests were performed. Left ventricular mass (LVM, Pennformula) and left ventricular ejection fraction (LVEF, Simpson's method) werecalculated. Data was compared with the same parameters in 30 nonobesepatients, with the same age and chronic heart failure.RESULTS: LVM in obese patients was 145� 25 g=m2, more then115� 15 g=m2 which was found in nonobese patients (p< 0.01). Themedian LVEF was 46.7% in 7 (10%) asymptomatic obese patients and50.9% in 5 (18%) nonobese patients (p< 0.05). The median LVEF of 35%,vs 42% was found in symptomatic patients, obeses and nonobeses. Themedian exercise time was lower in obese then nonobese patients (302.3 s vs380.0 s, p<0.001). Regarding asymptomatic patients, median exercise timewas also lower in obese then non obese patients (324.0 s v 456.0 s p<0.001)The multivariate analysis showed that for obese and nonobese patients, LVEFwas the signi®cant determinant of exercise time. In symptomatic and asymp-tomatic obese patients LVM was also the signi®cant determinant of exercisetime. The comparison of asymptomatic obese patients with asymptomaticnonobese patients showed lower LEVF, higher LVM and also lower quality oflife in obeses.CONCLUSION: The comparison between obese and nonobese patientsshowed a less number of asymptomatic patients with chronic heart failure,and lower quality of life between obeses. Apparently asymptomatic, obesepatients presented a signi®cant decrease of LVEF. The increase of LVM in obesepatients is an independent factor in the evolution of chronic heart failure. Inde®ning asymptomatic cardiac heart failure, we should include the quality oflife and the response to exercise tests, especially in obese pacients.
P187Gender-speci®ic associations of leptin and body composition in livercirrhosis
M Riedl1, B Tribl1, C MuÈller1, P Georg1, D David1, G Tappeiner1,W WaldhaÈusl1, and B Ludvik1
1Department of Internal Medicine III, Waehringer Guertel 18-20, 1090 Vienna
INTRODUCTION: Data on leptin levels and their association with bodycomposition in patients with liver cirrhosis are controversial, potentially dueto ignoring gender-speci®c differences.METHODS: We therefore measured leptin, body composition (BIA) andinsulin sensitivity (HOMA-Analysis) in 51 patients with liver cirrhosis (22females (LF) and 29 males (LM)) and in 55 healthy sex, age and BM1-matchedcontrol subjects (CF, CM).RESULTS: Compared o controls, patients with liver cirrhosis exhibiteddecreased insulin sensitivity (l.9�0.2 vs 4.4� 0.4, p<0.001) and increasedinsulin levels (50.4�4.2 vs 120.0�11.7 pmol=L, p<0.001). In both groups,leptin levels were increased in female vs male subjects (17.0�0.3 vs4.3�0.5 ng=mL, LF vs LM, p< 0.001, and I3.8� 3.3 vs 6.4� 0.9 ng=mL, CFvs CM, p<0.001). Leptin levels were higher (p< 0.05) in male, however notin female cirrhotic patients when compared to controls. FFM was slightlyreduced in LM (57.1�1.9 kg vs 57.8� 1.2 kg, LM vs CM, p< 0.05). Incontrast to CM, CF and to LM patients, plasma leptin concentrations didnot correlate with FM (r�0.4, p� 0.08), insulin levels (r�0.2, p� 0.44) orinsulin sensitivity (r� 0.1, p�0.65) in LF.CONCLUSION: In conclusion, only male, but not female cirrhotic patientsexhibit increased leptin levels when compared to controls. Circulating leptin isnot correlated to fat mass, insulin levels and insulin sensitivity in femalecirrhotic patients. These data point towards a gender-speci®c difference in
Track 6 Cardiovascular system and obesity
S82
International Journal of Obesity

the regulation of circulating leptin and the association of leptin with para-meters of body composition and glucose metabolism in cirrhotic patients.
P188
MUFA enriched hypocaloric diet: effect on weight loss and onatherosclerosis
C Mary1, C Colette1, N Pares-Herbute1, TC Pham1, and L Monnier 1
1Laboratoire de Nutrition et AtheÂrogeneÂse, IURC, 641 avenue du doyen Giraud,34093 Montpellier Cedex 5, France
During hypocaloric diets, weight loss but also the dietary composition cancontribute to the cardiovascular risk modi®cation. The aim of the study was tocompare the effects of 2 hypocaloric diets (730% of total energy expendi-ture) on weight loss rate, on smooth muscular cell (SMC) proliferation and onblood cardiovascular risk factors: TG, TC, LDLc, ®brinogeÁne, Lp(a). insulino-reÂsistance (HOMA).
23 obese patients were included. In % of total energy intakes, thecomposition of the 2 diets (proteins=fats=CHO) was 20=25=55 (diet A,n� 11) vs 20=40=40 (diet B, n�12). Monounsaturated fatty acids were10% of calories in diet A and 25% in diet B. 65% of total energy intake wasbrought by CHO and monounsaturated fats in both diets: 55�10 (diet A) and40�25 (diet B enriched in olive oil). Patients were asked to prepare theirmeals at home from pre-established menus, during 60 days. Biology wasevaluated at days 0 and 60. Weight was measured at days 0, 30 and 60.
Neither at day 30 (74.6 kg) nor at day 60 (77 kg) was the weight loss(adjusted on mean basal weight) dependent on the type of the diet. At day60, insulinoresistance and plasma concentrations of TG, TC and LDLc weresigni®cantly diminished independently of the type of the diet. HDLc, Lp(a) and®brinogen remained unchanged. SMC proliferation was enhanced with type Bdiet (� 3.6%, p� 0.025). Changes in SMC proliferation (%) were negativelycorrelated to changes in HDLc (r�70.51, p�0.012) and to the complianceto the diet (r�70.48, p�0.018). In stepwise multiple regression, changes inSMC proliferation (%) could be explained by changes in HDLc (step 1:23%)and by compliance to the diet (step 2 : 16%).
In conclusion, during the early weight loss, neither weight loss nor lipidmetabolism were dependent on dietary composition. However, during thisperiod, diets enriched in olive oil seem to have a protective effect on SMCproliferation and therefore on atherosclerosis.
P189
Effects of weight loss induced by gastric surgery on blood pressure levelsand metabolic parameters
AN Faria1, KMB Carvalho1, CH Arasaki1, JC Del Grande1, A Beani Jr1, andMT Zanella1
1Universidade Federal de SaÄo Paulo, SP-Brasil
INTRODUCTION: Gastric surgery has been indicated to treat obese patientswith body mass index above 40 kg=m2, mostly of them with associatedmorbidity, as hypertension, diabetes or dislipemia, which augment theircardiovascular risk.METHODS: In this study 15 severe obese patients (12F, 3M), aged 38� 10years old and BMI of 50� 6 kg=m2, were submitted to gastric surgery (band�by-pass) and evaluated for BMI, blood pressure (BP), fasting glucose (GLU),tryglicerides (TG) and cholesterol (CHOL) levels, before and after 6�3months. A 24 hour report of food ingestion was used to calculate the totalenergy consumed (TEC) after surgery.RESULTS: A reduction of 23.6� 6.0% (p< 0.01) in BMI correlated with periodafter surgery. The TEC ranged from 220 to 1400 kcal with a positive correla-tion with the time after surgery (r�0.79; p< 0.01), indicating an adaptativeprocess. Systolic and diastolic BP (SBP=DBP) fell from 136�12=78�8 to123� 17=71�12 mm Hg (p< 0.05),TG levels from 151� 85 to 106� 64(p<0.01) GLU levels from 101� 19 to 93� 7 mg=dl (p�0.06) withoutchanges in CHOL. No correlation was found between changes in BP andchanges in BMI.CONCLUSION: We concluded that the weight loss consequent to bariatricsurgery is effective in reducing blood pressure and, tryglicerides levels,tending also to diminish glucose levels in severe obese patients, contributingto a decrease of the cardiovascular risk of these patients. The increase in TEC,an expected adaptative behavior, probably responsible for the weight stabi-lization after an year of the procedure, otherwise may compromise the resultsof the surgery during long term follow-up and needs further evaluation.
P190
Reduction of smooth muscle cell contraction by perivascular adiposetissue
G Dubrovska1, M LoÈhn1, B Lauterbach1, FC Luft1, M Gollasch1, AM Sharma1,Franz-Volhard-Klinik1, and Max-DelbruÈck1
1Center for Molecular Medicine, University Clinic ChariteÂ, Humboldt-UniversityBerlin, Germany
In earlier studies, perivascular adipose tissue was shown to in¯uence theunderlying blood vessel contraction. We have pursued this intriguing notion.
We measured contraction of male Sprague-Dawley rat (200 ± 300 g) aorticrings in a Schuler organ bath system. Vessels were either stripped of surround-ing adipose tissue or were left intact and were incubated with severalsubstances in¯uencing vascular contraction.
Contractile responses to KCI were not different between stripped or intactvessels. However, a signi®cant reduction of smooth muscle cell contraction toserotonin and phenylephrine was measured in intact vessels. Dose-responsecurves for serotonin and phenylephrine in intact vessels showed a signi®cantlyrightward shift. The reduction of contraction response of intact vessels toserotonin and phenylephrine was abolished by preincubation of the vesselswith glybenclamide. Application of cromakalim to stripped vessels resulted ina reduction of the contractile response to serotonin and phenylephrine. Otherpotassium channel blockers did not modulate the reduced response of intactvessels to serotonin or phenylephrine. Additionally, vessels with perivascularadipose tissue were either denuded of endothelium or were left intact to ruleout an involvement of endothelium. No signi®cant differences were measuredin endothelium-denuded or endothelium-intact vessels with perivascularadipose tissue.
We conclude that perivascular adipose tissue exhibited a signi®cant effecton rat aortic smooth muscle cell contraction. This modulation did not dependon the endothelium. We suggest that perivascular adipose tissue affectssmooth muscle cell ATP-dependent potassium channels and thereby reducesserotonin or phenylephrine-evoked rat aortic smooth muscle cell contractions.
P191
Biochemical markers of patients with type 2 diabetes and orlistat inducedweight loss
CW le Roux1, J Alaghband-Zadeh1, J Suttard1, G Frost1, and JF Laycock1
1Departments of Metabolic Medicine, Dietetics and Neuroendocrinology,Imperial College School of Medicine, Charing Cross Hospital, London, UK
BACKGROUND: Obesity, insulin resistance, hypercholesterolaemia, Lp(a) andelevated homocysteine are all independent cardiovascular risk factors. Theinteraction between these factors, enhances the relative risk of cardiovasculardisease. Presently the reduction of weight through medical intervention hasnot yet been demonstrated to have cardiovascular mortality bene®ts. Thisstudy aimed to evaluate biochemical risk factors for cardiovascular disease inpatients with type 2 diabetes undergoing orlistat induced weight loss.METHODS: 7 patients (6 females, 1 male) with type 2 diabetes were followedas part of an on going Lifestyle clinic. A dietician followed patients monthlyand measured their body mass index (BMI) and hypoglycaemic agentrequirement. After 2.5 kg initial weight loss in 4 weeks, they were started onorlistat 120 mg tds. Fasting blood samples were obtained before any weightloss and 6 months after orlistat therapy. Plasma was analysed for insulin,glucose, fasting insulin resistance index (FIRI�glucose� insulin=25), totalcholesterol, triglycerides, high density lipoprotein (HDL), calculated lowdensity lipoprotein (LDL), Lp(a), HbAlc and homocysteine.RESULTS: The BMI of the patients decreased signi®cantly from40.2�3.23 kg=m2 (mean� SEM) to 37.8�3.23 kg=m2 (p< 0.001). Howeverthe majority of biochemical markers did not show any signi®cant change:FIRI (4.1� 1.2 to 5.6�1.3), total cholesterol (4.8�0.15 mmol=L to4.8� 0.18 mmol=L), triglycerides (1.4�0.19 mmol=L to 1.5�0.23 mmol=L),Lp(a) (284�87 mg=L to 258� 82 mg=L), homocysteine (8.6� 0.9 mmol=L to8.4� 0.5 mmol=L). The only signi®cant improvements were HbAlc(8.7�0.59% to 6.9� 0.29%, p� 0.01) and LDL=HDL ratio (2.88�0.3 to2.32�0.3, p�0.01) indicating a reduced cardiovascular risk.CONCLUSIONS: It was disappointing that the signi®cant weight reductiondid not translate into reductions in all of the individual biochemical markers ofcardiovascular risk. It could be postulated that a certain amount of weight lossneeds to be achieved over a longer follow up period, before reduction ofcardiovascular risk will be realised.
Track 6 Cardiovascular system and obesity
S83
International Journal of Obesity

P192
Effect of body fat and fat distribution on cardiovascular risk factors
F Magri1, B Pontiggia1, A Rebesco1, L Busconi1, D Camozzi1, S Precerutti1,and E Ferrari11Dept. of Int. Medicine and Med. Therapy, Chair of Geriatrics, University ofPavia, Italy
INTRODUCTION: It is well known that an excess of body fat is associated withalterations in metabolism homeostasis. In particular, changes in lipid metabo-lism are associated with central fat or visceral fat and there is a close correlationbetween fat distribution and cardiovascular risk.
The aim of this study was to evaluate the relationship between the supinesagittal abdominal diameter and others indicators of body fat distribution withcardiovascular (CVD) risk factors, such total cholesterol, HDL-cholesterol,triglycerides and blood pression, giving a particular attention to the genderdifferences.METHODS: One hundred and seventy eight obese women (BMI 34.4�0.41SE; age 41.2�1.12 ES) and 49 obese men (BMI 34.7�0.68 ES; age40.9� 2.02 ES) were studied. In each subjects we evaluated: degree ofoverweight (BMI), fat distribution (waist and hip circumference and abdom-inal sagittal diameter by a sliding-beam abdominal calliper), body composi-tion (bioelectric impedance measure), systolic and diastolic blood pressure,total and HDL cholesterol and tryglicerides.RESULTS: Both in women and in men, age was signi®cantly related to thedecrease of height and the increase of waist circumference or of the waist tohip ratio. In women BMI was signi®cantly correlated with systolic pressure,total and HDL cholesterol and tryglicerides. On the contrary, BMI wassigni®cantly related only with systolic pressure in men. In the group ofobese women, but not in the one of obese men, waist circumference andthe waist to hip ratio were signi®cantly related to systolic and diastolic bloodpressure and blood lipid parameters. A signi®cant association was also found,in women, between abdominal sagittal diameter, measured with sliding beamabdominal calliper, and blood arterial pressure, but this relation was notpointed in the group of men; in obese men the abdominal sagittal diameterwas signi®cantly related only to total cholesterol. In women there was acorrelation between fat mass (FM) and fat free mass (FFM) and systolic bloodpressure and cholesterol.CONCLUSION: Among the different measures of fat distribution, the sagittalabdominal diameter was very useful for the prediction of cardiovasculardisease risk factors both in obese women (signi®cant relationship with systolicand diastolic blood pressure) and in obese men (signi®cant relationship withtotal cholesterol).
P193
Obesity and risk of cardiovascular disease development
P HluÂbik1, S ByÂma1, J Chaloupka1, L OpltovaÂ1, and V BlaÂha1
1Purkyne Military Medical Academy, TrÏebesÏska 1575, 500 01 Hradec KraÂloveÂ,Czech Republic
The Czech Republic ranks among the countries with highest prevalence ofoverweight and obesity. It is important to recognize obesity as a seriousdisorder associated with several chronic deseases. The study provides exten-sive information on selected anthropometncal and biochemical parameters,especially on those, which are generally used as risk indices for the origin anddevelopment of cardiovascular disease (CVD): body mass index (BMI), bodyfat percentage (b.fat), waist circumference (waist), serum concentrations oftotal cholesterol (Tchol), HDL- and LDL-cholesterol (HDL-chol, LDL-chol),triacylglyceroles (TAG) and the atherogenic index (AI).
The nutritional status of a selected population ± 6267 male members ofthe Czech Army ± was assessed in 2000. The results of the study proved theconsiderable prevalence of the overweightness and obesity in the malepopulation group that was followed: according to the calculated BMI, 52%of volunteers were estimated to be overweight and 15% to be obese. As far aslipid parameters were concerned, increased serum levels were estimated in34% (TAG), 58% (Tchol) and 41% (LDL-chol) of volunteers. Decreased serumlevels of HDL-chol were found in 17% of volunteers. An AI higher than 3,5 a.u.was calculated for 73% of all subjects in study. The study concept made itpossible to reveal the relationships among the anthropometrical and bio-chemical parameters followed. The regression analysis results document astatistically signi®cant positive dependence among the BMI or waist valuesand the serum concentrations of Tchol, LDL-chol, TAG and AI. A signi®cantnegative correlation was found between the HDL-chol serum concentrationand the BMI or waist values.
The variance analysis results (the estimated lipid parameter values weredivided into groups according to the BMI and waist categories) document astatistically signi®cant increase of serum Tchol, LDL-chol, TAG and AI in boththe overweight and obese categories in comparison with the normal weight
category. An AI higher than 3,5 a.u. was found in 61% of males with normalweight, in 79% of overweight males and in 90% of obese males. A statisticallysigni®cant decrease in comparison with the normal weight category wasfound in the HDL-chol serum levels of both the overweight and obesitycategories. In the same way, an increase in Tchol and LDL-chol, TAG serumconcentrations and AI values in higher CVD category (according to the waistcircumference value: 94 ± 102 cm) and high risk CVD category (waist circum-ference value > 102 cm) was found in comparison with the low CVD riskcategory (waist circumference value < 94 cm).
P194
Estimation of visceral fat in obese patients with DEXA compare with CTscan
D Bellido1, J Carreira1, A Bouza1, B RodriÂguez1, V Blay2, A Becerra3,D De Luis4, G Piedrola5, and A HernaÂndez6
1Servicio de EndocrinologiÂa y NutricioÂn. H. Naval Ferrol; 2H. Militar Zaragoza;3H. Ramon y Cajal Madrid; 4H. Rio Hortega Valladolid; 5Virgen de las NievesGranada; 6Dr. Peset Valencia
INTRODUCTION: Computarized tomography (CT) scan is considered as goldstandard technique in estimation of visceral fat in obese patients, correlation ofthis technique with abdominal circumference, sagital diameter and cardio-vascular risk factors has been demonstrated. However estimation of visceral fatvolumen need a lot of CT scan slides, with low ef®cciency in clinical practice.PATIENTS AND METHODS: Fifty three patients (100% women) were studied,with a mean body mass index (BMI) 32,05 (5,28) Kg=m2, and a mean age 32(10) years. Total abdominal fat, intra-abdominal fat mass, and subcutaneousfat mass were determined in all patients (LUNARR DPX). Datas were comparedwith estimation of visceral fat from obese patients that previously has beenreported by our group (Int J Obes 2000; 24 (1): VF (cm2) � 764.5�(33.47� SD) 7 (7.15�A) 7 4.51�H) 7 (49� S): VF visceral fat, SD sagitaldiameter, A abdominal circumference, H height in cm, S sex: male�1,female� 2.
Linear correlation of Pearson were used in quantitative variables, withSTATISTICAR for WINDOWS.RESULTS AND CONCLUSIONS: A signi®cative correlation were obtainedamong between visceral fat estimated with our equation and intrabdominalfat mass determined by DEXA (r�0.73; p< 0.0001). Estimation of visceral fatin obese patients is an interesting area of investigation, although Ct scan is thegold standard technique, datas are correlated with DEXA results.
These results showed that aplication of DEXA in clinical practice is easy,and could be a good reference technique.
P195The bene®ts of very low calorie diet (VLCD) in the treatment extremelyobese persons
E Stokic1, and T Ivkovic-Lazar1
1Dept. of Endocrinology, Medical Faculty H.Veljkova 1-3, 21000 Novi Sad,Yugoslavia
Obesity is associated with a number of disorders such as glucose tolerancedisturbances, insulin resistance, hyperinsulinaemia, hypertension, dyslipidae-mia, impaired ®brinolysis, accelerated atherosclerosis which all lead to cardi-ovascular disease. VLCD therefore bene®ts the individual by reducing healthrisks and improving the quality of life.
In order to assess the in¯uence of VLCD on lipids, insulin, glucose,®brinogen and blood pressure, we have evaluated 36 extremely obese females(age 32,06 � =7 6.64 years), in whom, apart from standard measures (bodyweight, BMI, systolic and diastolic blood pressure), subcutaneous (SAT) andvisceral adipose tissue (VAT) had been measured by ultrasound. Patients weretreated with VLCD (1254 kJ) for 30 days. As for physical activities, during thisperiod only the light walking has been practiced. At the end of the study BMIsigni®cantly decreased (42.06� =77.64 to 37.58� =76.44 kg=m2, p< 0.05).VAT has been reduced signi®cantly (34.10� =73.25 to 24.78� =72.50 mm,p< 0.05), while SAT has been reduced but only on the edge of signi®cance(p�0.05). The signi®cant improvement of the lipid parameters was observed:total cholesterol (Ch) (5.68� =71.02 to 4.2� =70.84 mmol=l, p<0.001),triglycerides (2.25� =71.34 to 1.30� =70.59 mmol=l, p<0.001), LDL-Ch(3.37� =71.23 to 2.68� =70.86 mmol=l, p< 0.05). The study has shownthat the decrease of HDL-Ch happened on the bene®t of HDL3 subfraction.After weight reduction the level of ®brinogen and fasting insulin statisticallysigni®cantly decreased.
These results suggest that VLCD decreases signi®cantly body weight,mainly by reducing the VAT and improves the metabolic pro®le of extremelyobese persons. Also, this treatment is associated with reducing in ®brinogenlevel.
Track 6 Cardiovascular system and obesity
S84
International Journal of Obesity

P196The blood leptin concentrations are not corelated with trigliceride andglucose levels after functional tests in obese families from South Poland
M Malczewska-Malec1, I WybranÂska1, I LeszczynÂska-Golabek1, S Niedbal1,A Zdzienicka1, T Krzeszowska1, F Pietri-Rouxel2, and A DembinÂska-KiecÂ1
1Department of Clinical Biochemistry, Collegium Medicum, JagiellonianUniversity, KrakoÂw, Kopernika 15a, Poland; 2Institut Cochin de GenetiqueMoleculaire, Laboratoire d'ImmunoPharmacologie Moleculaire, CNRS UPR0415 and Universite de Paris VII 22, rue Mechain, 75014, Paris, France
INTRODUCTION: Leptin acts as a regulator of lipid reserves through changesin food intake, energy expenditure and fuel selection, and its direct effects oncellular lipid and carbohydrate metabolism is suggested.METHODS: The blood leptin, blood lipids (cholesterol, high-density lipopro-tein [HDL]- and low-density lipoprotein [HDL]-cholesterol, and triglycerides)were determined in 68 women and men from obese families from SouthPoland Glucose and insulin concentrations in the blood were measured beforeand 30, 60, 90 and 120 minutes after oral glucose (75 g) tolerance test(OGTT) according to WHO guidelines. The postprandial trigliceride levelswere determined after oral lipid tolerance test.RESULTS: The mean body mass index of study group was 33,2 kg=m2. Leptinlevel was strongly associated with percentage body fat (r�0.63; p< 0.001),fat mass (r�0.60; p<0.001), and body mass index (r�0.38; p� 0.04).However any correlation with basal metabolic rate (BMR) (r� 0.02;p�0.93) was observed. The occurrence of arterial hypertension in thegroup of highest values of BMI and leptin was 38% compared to referencegroup (BMI< 30 kg=m2; leptin < 10 ng=ml) 10%. There was no correlationbetween blood leptin level and parameters of lipid and carbohydratemetabolism.CONCLUSION: These ®ndings con®rm the associations between leptin andbody fat content and suggest the lack of direct relationship between serumleptin and triglicerides and glucose concentration in healthy humans.
P197
Blood pressure in relation to body fat distribution: gender differences
BZ Beleslin1, S Vujovic1, Z Penezic1, M Zarkovic1, B Trbojevic1, and M Drezgic1
1Institute of Endocrinology, Diabetes and Metabolic Diseases, 13 Dr Subotica,Belgrade, Yugoslavia
Several prospective studies have shown that the selective accumulation ofadipose tissue in the central or abdominal region is associated with anincreased risk for development of cardiovascular diseases. The aim of thisstudy was to asses gender differences in blood pressure (BP) in relation tobody fat distribution in extreme obese patients (pts).
The study population consisted of 56 extremely obese patients with nosigns of endocrine, cardiovascular and renal disease, divided according tobody fat distribution to lower-body (LB) obese men (7 pts; 39�4years, BMI52� 14 kg=m2), upper-body (UB) obese men (11 pts; 36�10 years, BMI47� 5 kg=m2), LB obese women (19 pts; 33�7 years; BMI 43� 5 kg=m2),and UB obese women (19 pts; 35�8 years; BMI 45� 6 kg=m2). Patientsunderwent 21 days of very low calorie diet. Results are presented in thefollowing Table including systolic (SBP) and diastolic (DBP) BP before and afterthe diet.
In conclusion, signi®cant reduction of BP (p<0.05) during very low caloriediet was observed in all groups except for DBP in LB obese women. Inaddition, BP was similar in both UB obese women and men, whereas bothSBP and DBP was signi®cantly (p<0.05) higher in LB obese men then women.
P198
Is leptin affect arterial hypertension in obesity Ð in¯uence of insulin anddifferent methods of obesity assessment
M L--uczak1, P BogdanÂski1, W Bryl1, and D Musialik1
1Department of Internal Diseases, University of Medical Sciences, PoznanÂ,Poland, [email protected]
INTRODUCTION: Hyperinsulinemia is regarded as one of most importantpathogenetic factors in obesity-related hypertension. Leptin, a peptide pro-duced in adipocite tissue, regulates food intake and energy expenditure. It isalso considered to participate in development of arterial hypertension mainly
through sympathetic activation and mitogenic action.METHODS: 45 untreated obese hypertensives (group 1) aged 40.7�7.5years, BMI 35.4� 4.9 kg=m2 were compared to 40 obese normotensives(group 2) aged 37.9� 6.9 years, BMI 36.3�5.8 kg=m2. 20 lean normoten-sives matched for age constituted the control group. We measured systolicand diastolic blood pressure (SBP, DBP), waist to hip ratio (WHR), fastingserum insulin and leptin (by RIA). Adipocite tissue content was assessed bybioelectrical impedance. Results were analysed by multivariate analysismethod.RESULTS:
In group 1 we found signi®cantly elevated WHR values, serum leptin andinsulin. In both groups leptin signi®cantly correlated positively with BMI, fatcontent, SBP, DBP and insulin. In group 1 after adjustment for BMI and insulin,leptin remained independent predictor of DBP, but this association disap-peared after adjustment for adipocite tissue content as a measure of fatness.CONCLUSIONS: we did not con®rm direct relationship between serum leptinand arterial hypertension. Insulin, degree of obesity and fat distributionremain most important factors in¯uencing obesity-related hypertension.
Table
Group 1 Group 2 Control
WHR 0.92�0.09 0.84�0.06* 0.77� 0.05*
Fat % 44.4�5.4 43.1� 5.1 22.3�3.2*
Fat kg 42.3�11.7 40.3� 10.7 16.8�6.1*
SBP mmHg 154.2�10.1 133.8� 5.3* 128.4�7.5*
DBP mmHg 101.9�6.7 85.6� 4.9* 78.9�6.4*
Leptin ng=ml 56.4�13.7 41.6� 10.9* 13.3�12.4*
Insulin mI=ml 29.4�11.9 22.5� 7.8* 11.2�6.3*
* p< 0.05 vs group 1
P199
Ad libitum intake of a low-fat diet fails to reduce blood pressure inoverweight adults
JM Moesenender1, and HJF Zunft11German Institute of Human Nutrition & University of Potsdam, D-14558Bergholz-Rehbruecke
INTRODUCTION: Aim of the study was to investigate whether the result ofthe DASH study can be con®rmed by (i) using a German hypertensivepopulation and (ii) replacing the well-controlled feeding design by allowingad libitum intake according to dietary advices.METHODS: 53 overweight subjects from Potsdam with borderline hyperten-sion and without medication were randomly assigned to either a combinationdiet low in fat and rich in dairy products, fruits and vegetables (I-group) or ahabitual diet as control (C-group). During 5 weeks the subjects were provided50% of their daily intake for free according to their dietary pattern. Single and24 h blood pressure measurements, dietary and physical activity records,blood and urine samples and anthropometnc measurements were collectedbefore, during and 5 weeks after the intervention period.RESULTS: No reduction of blood pressure could be observed in the I-group ofour trial. No change of body weight was observed during the whole studyperiod.CONCLUSION: Even convincing results of a controlled trial cannot be simplytransferred into dietary advices for the general public. For addressing food-based dietary guidelines to reduce the risk of hypertension it is necessary toconsider carefully (i) the genetic background, (ii) the dietary and (iii) lifestylesituation of the target population.
Table
UB obese women LB obese women
before after before after
SBP(mmHg) 141� 22 132� 13 134� 9 126�10
DBP(mmHg) 92� 17 89� 10 83� 8 83� 9
UB obese men LB obese men
before after before after
SBP(mmHg) 146� 26 131�8 154�15 143�15
DBP(mmHg) 93� 18 84�7 98�10 89� 9
Track 6 Cardiovascular system and obesity
S85
International Journal of Obesity

P200
Waist=hip circumference=height ratio and its relationship to athero-sclerotic risk factors in obese women
N Ozbey1, M Taskale1, S Molvalilar1, E Sencer1, and Y Orhan1
1Department of Internal Medicine, Division of Endocrinology, Istanbul Facultyof Medicine, Capa, 34390, Istanbul, Turkey
Anthropometric parameters can predict cardiovascular risk status in epide-miological studies. Waist girth and waist=hip ratio are known to be related tometabolic derangement induced by visceral obesity. Recently Asayama andHayashi used waist=hip circumference =height ratio (WHRH) standart devia-tion scores as an index of body fat distribution in children. The aim of thisstudy is to determine the validity of WHRH as a risk factor predictor in obesewomen.
Study group is composed of 1940 obese (BMI> 27 kg=m2, mean age37.1� 11.7 years) women. Fasting serum glucose level > 126 mg=dL, cho-lesterol and triglyceride levels > 200 mg=dL, HDL-cholesterol level <45 mg=dl, blood pressure> 140=90 mm Hg, serum uric acid level> 5.5 mg=dLand fasting serum insulin level>13 mU=mL are considered as risk factors.
WHRH were signi®cantly higher in women with risk factors than withoutrisk factors (p<0.001 for all). WHRH correlated positively with age (r�0.32,p> 0.001), BMI (r� 0.33, p<0.001), systolic and diastolic blood pressure(r�0.24, p<0.001 and r� 0.21, p<0.001 respectively), uric acid (r�0.13,p< 0.001), glucose (r�0.20, p<0.001), insulin (r�0.14, p<0.001), HOMA(r�0.17, p<0.001), cholesterol and triglyceride (r�0.20, p<0.001 andr� 0.26, p<0.001 respectively) and negatively with HDL-cholesterol(r�70.06, p� 0.01). According to receiver operating characteristics (ROC)analysis, a WHRH>0.70 indicated increased likelihood of presence of one ormore risk factors and a WHRH< 0.5 indicated low likelihood of presence of riskfactors.
It is concluded that WHRH can be used as an indicator for cardiovascularrisk status in obese women.
P201
The incidence of cardiovascular complications in the obese before and6 months after hypocaloric diet and physical exercise
C Tudor1, Jeberean Rorica1, Danciu Simina1, V Lungu1, Vizman Carmen1, andC Vizman1
1First Medical Clinic - University of Medicine and Pharmacy, B-dul TudorVladimirescu Nr.16, ap.2, 1900 Timisoara, Romania
Android obesity generates cardiovascular complications (increased bloodpressure, ischaemic cardiac disease, strokes and peripheral arteriopathy).Their incidence is directly related to the weight excess and to the metabolicdisorders evolution (glucose intolerance, diabetes mellitus, hyperlipoprotei-nemias and hyperuricemias). The metabolic disorders appear early during theobesity evolution representing major risk factors to the cardiovascular system.These require from practitioners to establish as soon as possible a hypocaloricdiet in order to bring back the metabolic parameters to normal values thusdiminishing the cardiovascular risk.
The authors analyze the incidence of cardiovascular complications in 350obese patients, 156 males with BMI� 35,3�5 kg=m2 and mean age 48� 12years, and 144 females with BMI� 37,4� 4 kg=m2 and mean age 44,6� 11years. The incidence of cardiovascular complications was 43% and after 6months it decreased signi®cantly. 210 (60%) obese patients were given1000 kcal=24 h for 6 months, together with dosed physical exercise, accordingto their cardiovascular and articular tolerance. 130 (40%) lost weight only bymeans of hypocaloric diet, being unable of physical efforts.
The weight loss was bigger in the group that exercised than in the othergroup, getting to a BMI� 30,4�3 and the incidence of cardiovascularcomplications was 12%, versus the group that couldn't afford the physicalexercises, which got to a BMI� 32,2�4 kg=m2 and incidence of cardiovas-cular complications of 28,2% (p<0.001).
In the time with the weight loss, the plasmatic lipids values and glucosetolerance improved signi®cantly. In conclusion the authors consider thehypocaloric diet and the dosed physical effort as the best therapeuticalmethod in the improvement of cardiovascular and osteoarticular perfor-mance. The returnal to normal values of metabolic parameters signi®cantlyreduces the cardiovascular risk.
P202
Association of fasting serum insulin, proinsulin and leptin levels withhypertension in obesity subjects
X Gao1, SF Jiang1, NQ Zhao1, and ZQ Lu1
1Department of endocrinology, Zhongshan, Hospitai, Shanghai MedicalUniversity, Shanghai 200032 P.R.China
PURPOSE: To investigate the association of fasting serum insulin, proinsulinand leptin levels with hypertension in obesity subjects.METHODS: 152 obesity or overweight subjects (BMI 29.5(28.2 ± 31.6) and28.8(27.9 ± 30.6), p� 0.072, aged 20 to 65 years were selected. The demo-graphic parameters and metabolic pro®le in 78 subjects were compared with74 normotesives. Fasting serum insulin proinsulin and leptin were mesured byRIA.RESULTS: Two groups had the same BMI, it was 29.5(28.2 ± 31.6) in hyper-sives and 28.8(27.9 ± 30.6) in normotesives, p� 0.072. Hypertensives (Bp133=90 mmHg) had signi®cantly higher W, WHR and fasting glucose andtriglyceride levels than normotesives (BP 118=77 mmHg). The groups did notdiffer in fasting serum insulin, leptin, and HOMA . In the hypertensive group,fasting serum proinsulin level was signi®cantly increased comparaed with it inthe normotesive group, it was 22.87 (8.99 ± 44.40) pmol=l and 14.90(8.27 ±25.45) pmol=l, respectively, p�0.0322. Proinsulin=insulin ratio was 18.0(9.0 ± 30.5) and 14.4 (7.2 ± 22.2) respectively in hypertensives and normote-sives, p� 0.0087. Age, waist-to-hip ratio, proinsuim level, hyperglycemia anddyslipidemia were associated with hypertension. But, after adjusted by BMI,those associations did not existence.CONCLUSIONS: Hypertensive and normotensive subjects with obesity hadthe same insulin sensitivity level. Hypertensive subjects had more visceral fatand higher glucose and triglyceride levels than normotensive ones. b celldysfunction were present in hypertensive patients, probably mediatedthrough dyslipidemia. Leptin seems not a major factor to cause hypertension.
P203
Obesity and cardiovascular risk in persons with newly diagnoseddiabetes mellitus (``EPIDIAB'' study in Romania ± 2000)
N HaÃncu1, G Roman1, A Cif 1, IA Veresiu1, A cerghizan1, and S Cernea1
1Clinical Center of Diabetes, Nutrition, Metabolic Diseases, 2 Clinicilor st.,3400 Cluj-Napoca, Romania
INTRODUCTION: Obesity alone or associated with other components of the``X metabolic syndrome'' is frequent met in diabetes. Its presence increasesboth global and cardiovascular risk, either by itself or by associated comor-bidity. Intensive care should be addressed to screen, evaluate and controlobesity and other risk factors in people with diabetes.OBJECTIVE: The study intended to evaluate the presence of obesity, othercardiovascular risk factors (CVRF) and the obesity-induced risk classes inpersons with newly diagnosed diabetes.METHOD: Data regarding the prevalence of CVRF: overweight, obesity, waistcircumference, dyslipidemia, blood pressure, lifestyle and familial history, havebeen recorded and assessed in 890 patients with newly diagnosed diabetesmellitus (DM) last year in Cluj-Napoca. This is a section of a larger study(EPIDIAB- epidemic of diabetes), including 12 counties, which aims toevaluate the prevalence of diabetes and its medical and socio-economicimpact. Patients have been selected in clinical risk classes according to BodyMass Index (BMI) adjustment with other risk factors (waist, hypertension,dyslipidemia) (D.H. Ryan, G. Bray, 1998).RESULTS: The prevalence of overweight=obesity in Type 1 DM patients is0.7%=0.3% and in Type 2 DM is 34.3%=51.2%. High waist circumference(>80 cm for females and >92 cm for males) has been found in 91.3% Type 2DM patients. A subgroup of 590 patients have been selected in clinical riskclasses, according to adjusted BMI, as follows:
5% at low risk (BMI�25 ± 29.9 kg=m2), 27.2% at moderate risk((BMI� 30 ± 35 kg=m2) and 67.47% at high risk (BMI>30 kg=m2).CONCLUSION: As we expected, the prevalence of overweight and obesity isvery high in newly diagnosed Type 2 DM patients mainly represented byabdominal fat distribution. When assessing the prevalence of the othercardiovascular risk factors among newly diagnosed Type 2 DM patients theglobal obesity-induced risk is extremely high. As a practical consequenceintensive weight management should be started from the moment of diabetesdiagnosis, in association with all CVRFs control.KEYWORDS: EPIDIAB, obesity, cardiovascular risk
Track 6 Cardiovascular system and obesity
S86
International Journal of Obesity

P204
Negative correlation between fat free mass and 24 hour heart rate
S Toubro1, H Hausner1, NF Johnsen1, and A Astrup1
1Royal Vet & Agri University, 1958- Frederiksberg, Denmark
INTRODUCTION: A positive correlation between resting heart rate andmortality has been observed. Weight gain increase resting heart rate andin¯uence the balance of the autonomic nervous system.METHODS: A sibling cohort of 7l (27 male and 43 femals) healthy mainly lean(BMI: 23.7�4.1 (range 16.9 ± 38.8 kg=m2) subjects aged 29.1� 4.5 years,had their body composition estimated by bioimpedance and 24-hour energyexpenditure (24-h EE) and heart rate (24-h HR) measured under standardisedlow physical activity conditions in open-circuit respiration chambers. Cate-cholamines and thyroid hormones assessed fasting after the stay. The day tonight decrease in heart rate were also tested for differences between lean andobese.RESULTS: The variation in heart rate correlated primarily with lean body mass(r�70.35, p< 0.01). The following prediction equations for 24-h HR wasfound by backward elimination:
24-h HR� 71.7 ± 1.13 x FFM� 0.15 x 24 hour EE(r� 0.57, p� 0.01). Nodifference in delta 24-h HR was found between obese and lean.CONCLUSION: On a low physical activity level lean body mass together with24-h EE are the best predictors of 24-h HR. There was no difference in day tonight drop in heart rate between lean and obese.
Track 6 Cardiovascular system and obesity
S87
International Journal of Obesity