tPA in the Central Nervous System: Relations Between tPA and Cell Surface LRPs
12
Send Orders of Reprints at [email protected] Recent Patents on Endocrine, Metabolic & Immune Drug Discovery 2013, 7, 000-000 1 1872-2148/13 $100.00+.00 © 2013 Bentham Science Publishers tPA in the Central Nervous System: Relations Between tPA and Cell Surface LRPs Saida Ortolano and Carlos Spuch* Department of Pathology and Neuropathology, University Hospital of Vigo, Vigo, Spain Received: October 25, 2012; Accepted: December 5, 2012; Revised: December 10, 2012 Abstract: A growing body of evidence has implicated the plasminogen activating system in various aspects of neuro- physiology and pathophysiology. In ischemic stroke, blood-brain barrier (BBB) regulations, typically involving matrix metalloproteinases (MMPs), inhibitors tissue inhibitors of metalloproteinases (TIMPs) and the low density lipoprotein re- ceptor-related protein/alpha 2-macroglobulin receptor (LRPs) as mediators became interesting since tissue plasminogen activator (tPA)-related BBB breakdown with risk of secondary hemorrhage was considered to involve these mediators too. The mechanism by which tPA implements its actions within the central nervous system (CNS) has been the topic of much controversy. Binding of plasminogen to surfaces is of crucial importance in regulating the function of this system. tPA can modulate permeability of the neurovascular unit in physiological conditions and pathological events exacerbating injury in ischemic stroke, vascular dementia, traumatic brain injury or neurotoxic events. The plasminogen activating en- zyme system is widely appreciated for its role in fibrinolysis and thrombolysis and in other areas related to remodelling of the extracellular matrix. However, this enzyme system also has a major impact in the central nervous system under patho- logical circumstances. The aim of this review is to revise the last patents and news to understand the mechanism by which t-PA modulates BBB permeability. Keywords: BBB, brain diseases, CNS, LRP, neurodegenerative diseases, plasmin, plasminogen, tPA. INTRODUCTION Biochemistry of tPA - tPA Receptors Thrombolysis relies on the activation of plasminogen into plasmin and a subsequent cascade of events leading to the degradation of fibrin clots [1]. The broad substrate protease plasmin is a key enzyme in a number of physiological and pathological processes, owing to its ability to degrade fibrin and extracellular matrix proteins, and to activate latent ma- trix metalloproteases and growth factors. Plasmin is formed when the Srg561-Val562 bond of plasminogen is hydrolyzed by one of the two plasmin activators, tPA or urokinase plas- minogen activator (uPA). Plasminogen is a single-chain gly- coprotein that is abundant in human plasma and extracellular fluids. It is converted to the active, proteolytic form plasmin by eukaryotic activators such as tPA and uPA as well as by prokaryotic activators such as staphylokinase and strepto- kinase. Plasminogen binds to specific cellular receptors with low affinity and high capacity. This cell binding has a number of important consequences. First, the rate of plasminogen acti- vation, that is, formation of active plasmin, is enhanced on the cell surface compared to the soluble phase. This results in efficient plasmin generation and, because active plasmin *Address correspondence to this author at the Department of Pathology and Neuropathology, University Hospital of Vigo (CHUVI), Hospital of Meixoeiro, Meixoeiro s/n, 36215, Vigo, Spain; Tel: +34 986814585; E-mails: [email protected]; [email protected] remains bound to the cell, leads to a pericellular proteolytic cascade and subsequent remodelling of the extracellular ma- trix or fibrin matrix surrounding the cell. Second, when bound to the cell, plasmin is inaccessible to physiological inhibitors such as its major inhibitor alpha-2-antiplasmin as well as alpha 2-macroglobulin, which rapidly inactivate soluble plasmin. Third, plasminogen binding to specific sur- face receptors allows the cell to regulate pericellular prote- olysis. By altering the expression and/or distribution of spe- cific receptors for plasminogen, the cell can spatially and temporally regulate the potentiation of plasmin activity on its surface Fig. (1). While plasmin activity is required for cell migration, tight regulation of pericellular proteolysis is absolutely re- quired for proper control of this process. Because the po- tency of plasmin and the breath of its substrates, excess amounts of plasmin activity would lead to loss of cell adhe- sion to the substratum, thus preventing migration. Regulation of plasmin generation can occur at a number of levels includ- ing: 1) Expression of receptors for plasminogen on the cell sur- face 2) Expression and activity of plasminogen activators. 3) Expression and distribution of plasminogen activator receptors on the cell surface. 4) Expression of plasminogen activator inhibitors (PAIs). In addition to their established fibrinolytic role in blood vessels, tPA and plasminogen/plasmin have also been impli-
Transcript of tPA in the Central Nervous System: Relations Between tPA and Cell Surface LRPs

Send Orders of Reprints at [email protected]
Recent Patents on Endocrine, Metabolic & Immune Drug Discovery 2013, 7, 000-000 1
1872-2148/13 $100.00+.00 © 2013 Bentham Science Publishers
tPA in the Central Nervous System: Relations Between tPA and Cell Surface LRPs
Saida Ortolano and Carlos Spuch*
Department of Pathology and Neuropathology, University Hospital of Vigo, Vigo, Spain
Received: October 25, 2012; Accepted: December 5, 2012; Revised: December 10, 2012
Abstract: A growing body of evidence has implicated the plasminogen activating system in various aspects of neuro-physiology and pathophysiology. In ischemic stroke, blood-brain barrier (BBB) regulations, typically involving matrix metalloproteinases (MMPs), inhibitors tissue inhibitors of metalloproteinases (TIMPs) and the low density lipoprotein re-ceptor-related protein/alpha 2-macroglobulin receptor (LRPs) as mediators became interesting since tissue plasminogen activator (tPA)-related BBB breakdown with risk of secondary hemorrhage was considered to involve these mediators too. The mechanism by which tPA implements its actions within the central nervous system (CNS) has been the topic of much controversy. Binding of plasminogen to surfaces is of crucial importance in regulating the function of this system. tPA can modulate permeability of the neurovascular unit in physiological conditions and pathological events exacerbating injury in ischemic stroke, vascular dementia, traumatic brain injury or neurotoxic events. The plasminogen activating en-zyme system is widely appreciated for its role in fibrinolysis and thrombolysis and in other areas related to remodelling of the extracellular matrix. However, this enzyme system also has a major impact in the central nervous system under patho-logical circumstances. The aim of this review is to revise the last patents and news to understand the mechanism by which t-PA modulates BBB permeability.
Keywords: BBB, brain diseases, CNS, LRP, neurodegenerative diseases, plasmin, plasminogen, tPA.
INTRODUCTION
Biochemistry of tPA - tPA Receptors
Thrombolysis relies on the activation of plasminogen into plasmin and a subsequent cascade of events leading to the degradation of fibrin clots [1]. The broad substrate protease plasmin is a key enzyme in a number of physiological and pathological processes, owing to its ability to degrade fibrin and extracellular matrix proteins, and to activate latent ma-trix metalloproteases and growth factors. Plasmin is formed when the Srg561-Val562 bond of plasminogen is hydrolyzed by one of the two plasmin activators, tPA or urokinase plas-minogen activator (uPA). Plasminogen is a single-chain gly-coprotein that is abundant in human plasma and extracellular fluids. It is converted to the active, proteolytic form plasmin by eukaryotic activators such as tPA and uPA as well as by prokaryotic activators such as staphylokinase and strepto-kinase. Plasminogen binds to specific cellular receptors with low affinity and high capacity. This cell binding has a number of important consequences. First, the rate of plasminogen acti-vation, that is, formation of active plasmin, is enhanced on the cell surface compared to the soluble phase. This results in efficient plasmin generation and, because active plasmin
*Address correspondence to this author at the Department of Pathology and Neuropathology, University Hospital of Vigo (CHUVI), Hospital of Meixoeiro, Meixoeiro s/n, 36215, Vigo, Spain; Tel: +34 986814585; E-mails: [email protected]; [email protected]
remains bound to the cell, leads to a pericellular proteolytic cascade and subsequent remodelling of the extracellular ma-trix or fibrin matrix surrounding the cell. Second, when bound to the cell, plasmin is inaccessible to physiological inhibitors such as its major inhibitor alpha-2-antiplasmin as well as alpha 2-macroglobulin, which rapidly inactivate soluble plasmin. Third, plasminogen binding to specific sur-face receptors allows the cell to regulate pericellular prote-olysis. By altering the expression and/or distribution of spe-cific receptors for plasminogen, the cell can spatially and temporally regulate the potentiation of plasmin activity on its surface Fig. (1). While plasmin activity is required for cell migration, tight regulation of pericellular proteolysis is absolutely re-quired for proper control of this process. Because the po-tency of plasmin and the breath of its substrates, excess amounts of plasmin activity would lead to loss of cell adhe-sion to the substratum, thus preventing migration. Regulation of plasmin generation can occur at a number of levels includ-ing: 1) Expression of receptors for plasminogen on the cell sur-
face 2) Expression and activity of plasminogen activators. 3) Expression and distribution of plasminogen activator
receptors on the cell surface. 4) Expression of plasminogen activator inhibitors (PAIs). In addition to their established fibrinolytic role in blood vessels, tPA and plasminogen/plasmin have also been impli-

2 Recent Patents on Endocrine, Metabolic & Immune Drug Discovery 2013, Vol. 7, No. 1 Ortolano and Spuch
cated in both normal and pathological situations in the cen-tral nervous system [2-8]. It is known that the plasminogen system plays a pivotal role in maintaining vascular patency and in cell migration. Interestingly, tPA participates in learn-ing and memory formation but can play a deleterious role under pathological conditions [2, 3]. It also exists in brain where tPA is the main plasminogen activator and is widely expressed in the hippocampus, hypothalamus, cerebellum, and amygdala [9]. Interestingly, fibrin has not been found in the brain, indicating that the plasminogen system has other functions than that of coagulation inhibitor. Indeed, substan-tial evidence now suggests that the brain tPA/plasminogen cascade is important for proper extracellular matrix degrada-tion during neuronal development and for events that require synaptic plasticity such as long-term potentiation [10], mem-ory [11] and motor learning [12]. Plasminogen is potentially the most likely substrate for tPA. Yet, the contribution to the generation of plasmin from plasminogen is not the sole func-tion of tPA. In fact, tPA plays a plasmin-independent role in microglial activation [13], mossy fiber outgrowth stimulation [14] and in the enhancement of NMDA receptor mediated signalling [15]. Thus, plasminogen activation by tPA has a protective role in certain neurological situations such as stroke, neurological diseases, Alzheimer’s disease and vas-
cular dementia. In fact, tPA is the only drug approved to treat ischemic stroke. Another pathological situation where the tPA-plasmin system has been suggested to play a role is in Alzheimer’s disease [16]. Recent evidence suggests that the plasminogen system may also play a key role in Alz-heimer’s disease pathogenesis. This is supported by the demonstration that plasmin can efficiently degrade the Ab peptide. In vitro experiments have shown that the main com-ponent of senile plaques, the Ab, can stimulate tPA activity and mRNA expression [17]. These reports showed that tPA modulates neuronal death in models of stroke, excitotoxicity, and oxidative stress and Ab appears central to Alzheimer's disease and is neurotoxic to neurons in vitro, resulting in plasmin generation and subsequent Ab degradation [14].
TPA-DEPENDENT SIGNALLING PATHWAYS IN THE CNS
Evidence has accumulated that point to the tPA, a serine protease associated with blood physiology, as an important regulator of the CNS functioning. Originally described as a circulating serine-protease, tPA is expressed within cerebral gray matter by neurons, astrocytes, and microglia [18, 19] and plays various roles primarily related to synaptic forma-tion and plasticity [20, 21]. Endothelial cells are the main
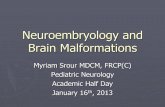
Fig. (1). The plasminogen activators uPA and tPA catalyse the proteolytic conversion of the zymogen plasminogen into the active protease plasmin, which can degrade fibrin and other extracellular matrix (ECM) proteins. uPA and tPA activity can be inhibited by either of two plasminogen activator inhibitors, PAI-1 and PAI-2, and plasmin activity can be inhibited by α2-antiplasmin.

Interaction between tPA and LRPs Recent Patents on Endocrine, Metabolic & Immune Drug Discovery 2013, Vol. 7, No. 1 3
source of tPA, but almost all cell types within and above the neurovascular unit (neurons, astrocytes, endothelial cells, microglia, oligodendrocytes and pericytes) express and re-spond to this factor [22]. tPA regulates physiological proc-esses in the brain, such as learning and memory, and plays a critical role in neuronal survival and neuroinflammation in pathological conditions. Interestingly, it was described that tPA is an important element of the cross talk between neu-rons and astrocytes. Recent paper showed that tPA released by neurons is constitutively endocytosed by astrocytes via the LRPs, and is then exocytosed in a regulated manner [23]. tPA would act as a double-edged sword when it enters the brain parenchyma [24]: on the one hand, it induces a deleterious effect in the gray matter as a result of the cleav-age of the N-methyl-D-aspartate (NMDA) receptor and in-creasing of Ca2+ entry [15, 25] and subsequent potentiation of excitotoxicity in neurons; on the other hand, it provides a beneficial effect protecting neurons from oxidative stress [26] as a result of the activation of EGFR, microglial activa-tion by binding to annexin II [27-29] or by binding to mem-brane receptors such as LRPs [30], inducing a subsequent protection against apoptosis. The extracellular protease cascade of tPA and plasmino-gen has been implicated in neuronal plasticity and degenera-tion. Most important that the synthesis of tPA by neurons in the brain is the tPA activator-catalyzed proteolysis that it is restricted to discrete areas, in particular within the hippo-campus and hypothalamus. This mechanism of the extracel-lular protease cascade of tPA and plasminogen has been im-plicated in neuronal plasticity and degeneration and the iden-tification of an extracellular proteolytic system active in the different regions of CNS may also help gain insights into the pathogeny of neurodegenerative disorders associated with extracellular protein deposition. Related to the implication of this molecule in the neu-ronal plasticity and cell migration, this year it was patented a novel invention relates to novel regulators of plasminogen activation and their use for regulating cell migration, plasmi-nolysis, angiogenesis, fibrinolysis. Although it was described its use for treating cancer and thrombo-embolic diseases such as heart stroke, could be a potential treatment for CNS diseases [31].
LOW DENSITY LIPOPROTEIN RECEPTOR-RELATED PROTEINS (LRPS)
The LRP family consists of more than 11 receptors that function in receptor-mediated endocytosis and cellular sig-nalling: LRP1, LRP-2, VLDLR, LRP5, LRP6, ApoE recep-tor 2 (ApoER2), also called LRP8, sorLA-1, LRP1B and the most recently identified the LRAD3 [32]. The two receptors of this family implicated in the tPA signalling are the LRP1 and LRP2. LRP1 is a massive pro-tein (600 kDa) that is proteolytically nicked during biosyn-thesis to give two stably associated polypeptides: an 85-kDa membrane-spanning C-terminal fragment and a 515-kDa extracellular N-terminal chain. LRP1 is expressed abun-dantly on neurons [33], where its fundamental role is the uptake of cholesterol and fatty acids required for synapse
formation [34]. LRP2, also called megalin, is one of the largest cell surface glycoproteins present in vertebrates, is a transmembrane protein with a non-glycosytaled molecular weigh of 517 kDa. This receptor is structurally very similar to LRP1. In addition, LRP1and LRP2 bind more than 30 ligands extracellularly, including ApoE, α2-macroglobulin, tPA, proteinase-inhibitors, blood coagulation factors, recep-tor-associated protein (RAP), Aβ, prion protein and aprotinin [32].
LRPS ARE EXPRESSED IN THE CNS.
LRP1 is highly expressed in neurons, mainly of the hip-pocampus, entorhinal cortex and cerebellum, astrocytes and microglia [35-37]. Importantly, LRP1 is further expressed in the CNS in different cell types within the neurovascular unit including vascular cells such as brain endothelial cells, vas-cular smooth muscle cells and pericytes, and it is also ex-pressed in the choroid plexus of the BBB [38]. In the healthy brain, the expression of LRP2 is classically identified in ependymal cells lining the ventricular wall, cap-illaries and choroid plexus [39]. Within the CNS, further ependyma of the choroid plexus [40]. LRP2 is widely ex-pressed on neurons and astrocytes [41, 42]. In astrocytes this receptor is required for albumin binding and internalization into astrocytes inducing synthesis of neurotrophic factors by the neighboring neurons. Other observations identified that LRP2 is present in retinal ganglion cells and in astrocytic processes of young and adult rats. Our group recently pub-lished the broad expression of this endocytic receptor in dif-ferent neuronal populations of the brain. In brain samples from healthy humans, monkeys, pigs, mice and rats we dem-onstrated LRP2 localization in different neuronal populations from cerebral cortex, hippocampus, striatum, thalamus, ol-factory bulb and cerebellum [43]. Interestingly, in brain tis-sues from patients diagnosed with Alzheimer’s disease (AD), LRP2 expression has been detected in neurons, even being up regulated in damaged neurons [41].
TPA IN PATHOLOGICAL PROCESSES OF THE CNS
It is well established that plasminogen system in many cells can be markedly modulated. While the tPA/plasmino-gen axis contributes to excitotoxic neuronal degeneration, tPA is also involved in other CNS pathologies. The role of tPA has been studied in AD, stroke, infarct formation, and seizure spreading. tPA expression is elevated during sei-zures, a state of synchronous, pathological hyperactivity in the CNS. Under pathological conditions, the deleterious con-sequences of tPA may be due to direct neurotoxicity or in-creased permeability of the BBB or a combination of both. The literature has amassed much data implicating tPA in cognitive function, memory, anxiety and in addictive behav-ior. Under pathological conditions, including ischemic stroke and traumatic brain injury, tPA has been shown to facilitate neurotoxic events via potentiation of glutamate receptor sig-nalling [6, 7] Fig. (2). tPA is highly expressed in the adult brain in regions in-volved in learning and memory (hippocampus), fear and anxiety (amygdale), motor learning (cerebellum), and auto-nomic and endocrine functions (hypothalamus) [44-50]. Cu-riously, tPA is involved in remodelling various non-neural

4 Recent Patents on Endocrine, Metabolic & Immune Drug Discovery 2013, Vol. 7, No. 1 Ortolano and Spuch
tissues and is associated with developing and regenerat-ing neurons. In the CNS both neurons and microglial cells express tPA. Different components of this system, such as, plasminogen, PAI-1, and neuroserpin are also present in the brain indicating that theses components are present in the CNS [50-52]. Thus, the literature has amassed much data implicating tPA and plasmin in cognitive function, memory and anxiety and in addictive behavior. Neuronal degeneration in the brain occurs in various pathological conditions, including AD, brain ischemia and epilepsy. When neuronal activity is stimulated in the adult rat and mouse hippocampus tPA, is transcriptionally induced [53, 54]. The activity of tPA in neural tissue is correlated with neurite outgrowth, regeneration and migration, suggest-ing that it might be involved in neuronal plasticity [55].
1. Neurotoxicity
Although thrombolysis with tPA is a stroke therapy ap-proved by the US Food and Drug Administration (FDA), its efficacy may be limited by neurotoxic side effects. Recently, proteolytic damage involving MMPs has been implicated, and non-fibrinolytic roles for t-PA have become prominent
in the CNS and mostly in relation to neurotoxicity and modulation of the BBB. The proteolytic damage involv-ing MMPs has been implicated in several papers. These pro-teins comprise a family of zinc endopeptidases that can mod-ify several components of the extracellular matrix. In par-ticular, MMP-2 and MMP-9 can degrade neurovascu-lar matrix integrity and promote neuronal death by disrupting cell-matrix interactions. In this context, tPA up-regulates MMP-9 mediated LRP, which avidly binds tPA and pos-sesses signalling properties. In experimental embolic stroke models, MMP inhibitors decreased cerebral hemorrhage and injury after treatment with tPA [56]. At the same time, the targeting of the tPA-LRP signalling pathway in brain may offer new approaches for decreasing neurotoxicity and im-proving stroke therapy. Thus, multiple clinical trials have been proven the efficacy of tPA in the treatment of acute focal cerebral ischemia [2], however the side effects due to breakdown of BBB, such as secondary hemorrhage obtained a poor outcome. The participation of the tPA/plasminogen axis has been defined in neuronal degeneration due to excitotoxicity. For example, an injection of kainate, an excitotoxic glutamate analog, into the CA1 region of the hippocampus of wild-type
Fig. (2). tPA promotes thrombolysis but increases neuronal death during stroke. Exogenous tPA is injected intravenously administered to ischemic stroke patients to dissolve the fibrin meshwork constituting the occluding clot (1). But this exogenous tPA can cross the BBB, and increase BBB leakage, thus pro-moting hemorrhage and oedema (2). tPA can also be released in the brain parenchyma by damaged neurons (3). In the synaptic cleft, both endogenous and exogenous tPA can interact with NMDA receptors, thus promoting excitotoxic neuronal death (4). tPA can also activate microglia, which in turn, release tPA, thus contributing to a vicious circle (5) and extracellular tPA can also be uptaken by astrocytes (6).

Interaction between tPA and LRPs Recent Patents on Endocrine, Metabolic & Immune Drug Discovery 2013, Vol. 7, No. 1 5
mice leads to neuronal damage, and this damage is reduced in either tPA-deficient or plasminogen-deficient mice [57]. Then, when it was co-injected in wild-type mice kainite and α2-antiplasmin, the neurodegeneration was prevented, sup-porting the role of plasmin in this neuronal injury paradigm. Using another model it was showed that tPA is produced primarily by microglia in the hippocampus and using toxins to induce neuronal cell loss, it was demonstrated that tPA-deficient mice are resistant to neuronal degeneration. These mice are also less susceptible to pharmacologically induced seizures than wild-type mice [58]. It well known that tPA induction and subsequent plasmin generation have been im-plicated in neuronal loss [57, 59]. This neuronal loss may be induced by extracellular matrix degradation because plasmin may degrade laminin directly or indirectly by activation of extracellular metalloproteases [60]. Indeed, matrix degrada-tion has been implicated in apoptosis in vitro [61]. However, the neurotoxic role of the plasmin system has been chal-lenged by reports that direct tPA infusion does not cause neuronal loss and, moreover, that tPA may be directly neu-roprotective in excitotoxicity models both in vitro and in vivo [62].
2. Alzheimer’s Disease
AD is the most common cause of dementia and cognitive decline in the elderly [63]. One of the characteristic patholo-gies of AD is the deposition of Aβ in the CNS parenchyma, leading to the activation of the inflammatory response. Ac-cumulation and deposition of Aβ is one of the main neuropa-thological hallmarks of AD and impaired Aβ degradation may be one mechanism of accumulation. In our plasminogen system, it was described that plasmin is the key protease of the plasminogen system and can cleave Aβ. Recently, the contribution of the tPA-plasmin system in the clearance of Ab has also been shown in vivo [64]. Plasmin is activated from plasminogen by tPA and uPA, Barker et al. found that the increases in tPA and uPA may also affect synaptic plas-ticity, excitotoxic neuronal death and apoptosis in these pa-tients [65]. The role of the plasmin system in neuronal death is under intense research. In the brain, tPA, uPA, and plas-minogen are synthesized in neurons, and tPA is synthesized by microglia as well. It has been known for some years that Aβ peptide stimu-lates the plasminogen system [66, 67] and also presented evidence that aggregated Aβ increases tPA levels, and that plasmin-mediated proteolytic activity is involved in amyloid plaque degradation. Interestingly, it was reported that aggre-gated, but not non- aggregated, Ab increases the level of the mRNAs encoding tPA and uPA. Unlike that work, Ledesma et al. demonstrated that reduced brain plasmin is one of the causes of amyloid plaque formation rather than its conse-quence. Consistent with this view, they found that plasmin and tPA increase APP cleavage and the activation of plasmin decreases the levels of Ab. Finally given the effects of plas-min activation on cleavage and Ab degradation, this work showed that plasmin levels are low in brains affected with AD [67, 68]. tPA/plasmin fibrinolytic activity is regulated by serine protease inhibitors, such as plasminogen activator inhibitor type one (PAI-1). Recently, it was reported that PAI-1 inac-
tivation can alleviate the symptoms of AD [69]. In mice, PAI-1 is up-regulated in the presence of Aβ, which agrees with the clinically observed elevation of PAI-1 levels in the cerebrospinal fluid of AD patients [70, 71] and decreased plasmin activity in the AD brain [69]. The tPA/plasmin system is down-regulated in AD, in accord with reductions in other naturally occurring Aβ-degrading proteases. The direct consequences of this general lack of protease activity might be the diminished clearance of Aβ peptide. The same results was described with LRPs receptors [72-74], where it was described the decrease of LRP-1 and LRP-2 levels in the BBB and neurons. However, it is possible that once amyloid plaques are formed, they trigger the upregulation of plasminogen as a compensatory mechanism. These studies propose that decreases in clear-ance of fibrin can also contribute to the progression of Aβ pathology. In any case, what appears clear is that the plasmi-nogen system is involved in APP processing, and this may create new possibilities for therapeutic approaches.
3. Seizures
Neuroserpin belongs to the serin proteases inhibitors (serpins) superfamily. It is a natural inhibitor of tPA, located almost exclusively in the CNS that has shown neuroprotec-tive effects in animal models of brain ischemic stroke [75]. The experimental evidence on the involvement of endoge-nous tPA in seizures is supported by human findings [76]. Thus, genetic point mutations in the neuroserpin gene are associated with aberrant deposition of neuroserpin in neu-rons, resulting in the formation of intracytoplasmatic bodies containing the mutant protein. These gene mutations in neu-roserpin are also characterized by generalized seizures, myo-clonus, and progressive dementia, that is, progressive myo-clonus epilepsy [77, 78]. Importantly, it was provided evi-dence that the mutated neuroserpin is inactive as a proteinase inhibitor, suggesting that the inactivity of this enzyme may result in uncontrolled activity of tPA and, thus, explain the epileptic seizures observed in the individuals carrying the mutation. It has also been found that both neuroserpin and tPA expression increase after brain ischemic stroke in rats. Immunohistochemical analysis has shown elevated neu-roserpin staining in neurons surrounding the ischaemic core as early as six hours after stroke, which reaches a peak value at 48 h and remains elevated for one week [79]. Addition-ally, transgenic mice overexpressing neuroserpin in the nervous system show a reduction in brain tPA activity, smaller lesion volume and attenuated microglial response after occlusion of the middle cerebral artery [80], whereas neuroserpin knockout mice have unchanged tPA activity [81]. Clinical evidence suggests that the inactivity of Ser52Arg neuroserpin in individuals carrying this mutation may exac-erbate the intrinsic ability of the intracellular inclusion to cause epilepsy. tPA and neuroserpin are therefore among the numerous endogenous factors that may contribute to the mechanisms of hyperexcitability in the CNS. Probably, an imbalance in their relative production or function may lead to exaggerated tPA activity in brain, thus resulting in harm-ful effects, including seizures and neuronal cell loss

6 Recent Patents on Endocrine, Metabolic & Immune Drug Discovery 2013, Vol. 7, No. 1 Ortolano and Spuch
4. Stroke
Stroke is a leading cause of adult death and disability with approximately 6 million deaths per year, with an alarm-ing projected incidence over the next decade due to the in-crease in the elderly population. Despite the significant ad-vances that have been made in understanding the cellular and molecular pathophysiology of cerebral ischemia, recombi-nant tPA remains the only approved acute treatment for ischemic stroke. Hundreds of compounds have been tested so far in clinical trials for ischaemic stroke, but aside from rtPA, none has proven effective. The use of recombinant tPA is limited by a short therapeutic window (4.5 hours post-onset) and by promotion of both intracerebral hemorrhage and neurotoxicity. Although, recent experimental evidences have raised controversy about the neurotoxic versus neuro-protective roles of tPA in acute brain injury. According to the complex behavior of tPA several molecular strategies for inhibiting the deleterious effects of tPA can be envisaged. Recently it was patented an interesting invention where the authors have found that proteins comprising of a kringle do-main or antibodies specifically binding to the amino-terminal domain of the NR1 subunit of the NMDA receptor (also called as anti-ATD-NR1 antibody) are active at two tPA relevant target sites: the BBB and the NMDA receptor and as a result exhibit vasoprotective and neuroprotective activity. This antibody and the kringle domain-containing proteinase working like a tPA inhibitor [82, 83]
PHYSIOLOGICAL ROLE OF TPA IN THE BLOOD BRAIN BARRIER
The CNS barriers consist of several hurdles in parallel formed by the cerebrovascular endothelial cells between blood and brain interstitial fluid (called as BBB), the choroid plexus epithelium between blood and ventricular cerebrospi-nal fluid CSF (called as B-CSFB), and the arachnoid epithe-lium between blood and subarachnoid cerebrospinal fluid [84]. The CNS barriers limit the entry of plasma compo-nents, red blood cells and leukocytes into the brain and the clearance of toxic products from the brain, exerting the greatest control over the immediate microenvironment of brain cells [40]. When any of these barriers is broken by ischemic injury, trauma, neurodegenerative processes in-flammation or vascular disorders; these generated neurotoxic products can get into the brain compromising synaptic and neuronal functions [84]. Three barrier layers regulate molecular exchange at the interfaces between the blood and the neural tissue or its fluid spaces: 1) the cerebrovascular endothelial cells, 2) the chor-oid plexus epithelium, 3) the arachnoid epithelium. Brain endothelial cells lining includes the lumen of brain capillar-ies, linked together by tight junctions that are composed of specific proteins, pinocytic vesicles, and specific transport mechanisms [85]. Surrounding the endothelial cells, we found the basement membrane, pericytes, and astroglial foot processes, creating a third continuous layer that separates these blood vessels from the brain tissue. The choroid plexus consists of highly differentiated epithelium and functions as a barrier at the interface between the blood-CSF. Choroid plexus is formed by a tight monolayer of epithelial cells sur-rounding a core of capillaries and loose connective tissue.
This epithelial layer is continuous with the ependymal cell layer that lines the ventricles, but unlike the ependyma, the choroid plexus has tight junctions in between the cells on the side facing the ventricle, known as the apical surface [8]. The last barrier is the arachnoid layer, this layer is character-ised by a distinct continuous basal lamina on its inner surface towards the innermost collagenous portion of the arachnoids. However the transport across the arachnoid membrane is not an important route for the entry of solutes into brain [86]. Except for the low passive permeability to many essential water-soluble nutrients and metabolites required by the nervous tissue, specific transport systems are expressed in the CNS barriers to ensure an adequate supply of nutrients [87]. To accomplish the task of nutrient transport, the brain endothelium and the choroid plexus epithelium are endowed with a diverse collection of molecular transport systems. One such class of transport system, known as a receptor-mediated transcytosis (RMT), employs the vesicular trafficking ma-chinery of the cell to transport substrates between blood and brain [88]. RMT utilizes the vesicular trafficking machinery of the endothelium or epithelium choroid plexus to transport nutrients such as iron, amyloid, apolipoproteins, and hor-mones via the transferrin receptor [89, 90], LRPs receptors [91], insulin or IGF-I receptor [92] into the parenchyma. RMT requires ligand binding to a specific receptor at the luminal side of the brain endothelial cells or apical epithe-lium choroid plexus, which initiates the process of endocyto-sis with the formation of intracellular transport vesicles that deliver the dissociated ligand to the parenchyma [93]. Some-times, further the binding lingand, also is needed the use of co-receptors. This is the case of plasminogen receptors or cubilin in the BBB, both receptors are needed to regulate the permeability properties of the BBB [94]. tPA is the only available treatment for acute stroke, in addition to its vascular fibrinolytic action, tPA exerts various effects within the brain, ranging from synaptic plasticity to control of cell fate. During stroke tPA is promoting throm-bolysis but increasing neuronal death. Exogenous tPA is injected intravenously administered to ischemic stroke pa-tients to dissolve the fibrin meshwork constituting the oc-cluding clot. But this exogenous tPA can cross the BBB, and can increase BBB leakage, thus promoting hemorrhage and oedema. tPA can also be released in the brain parenchyma by suffering neurons. In the synaptic cleft, both endogenous and exogenous tPA can interact with NMDA receptors, thus promoting excitotoxic neuronal death and can also activate microglia, which in turn, release tPA, thus contributing to a vicious circle [95]. During these events tPA have also detri-mental effects contributing to BBB disruption in ischemia-affected brain tissue. It is well described that tPA and espe-cially their simultaneous application differentially affects BBB permeability and alters plasma concentrations of MMPs and TIMPs. MMPs are a family of zinc-dependent endopeptidases involved in the pathogenesis of several cen-tral nervous system diseases including stroke [96, 97]. MMPs could challenge the integrity of the neurovascular unit by degrading matrix proteins. Moreover, a number of non-matrix proteins have been identified as possible MMP substrates [98]. It was suggested that some MMPs could have many functions in addition to extracellular matrix deg-

Interaction between tPA and LRPs Recent Patents on Endocrine, Metabolic & Immune Drug Discovery 2013, Vol. 7, No. 1 7
radation, and seems to be play a key role in BBB breakdown trough out mechanisms mediating of tPA toxicity. Interestingly, brain hemorrhage was significantly corre-lated with functional deficit and RAGE and Toll-Like-Receptors-4 (TLR4) expression, respectively. Treatment of stroke with tPA increased brain hemorrhage, BBB leakage and failed to improve functional outcome. tPA treatment also significantly increased the expression of RAGE, MMP-9 and TLR4 in the ischemic brain [99]. Much effort has been devoted to understanding the mechanism by which t-PA modulates BBB permeability. The tPA activity which increases permeability of the tissue in a subject results in oedema in the tissue is separate from tPA's thrombolytic activity. Delayed activation of tPA can lead to the disruption of the BBB, resulting in hemor-rhagic complications [100]. tPA delivered intravenously has been shown to cross brain endothelial cells via transcytosis without compromising BBB integrity [101] while others have shown that tPA can enter the parenchyma during patho-logical conditions where it further enhances BBB break-down. Hence, tPA-mediated modulation of BBB permeabil-ity may invoke more than one pathway involving plasmino-gen and other substrates. For example, it was reported the damaging effect of t-PA plasmin-dependent in the BBB breakdown [101, 102]. There are several patents that relate use of methods to reduce vascular permeability in tissues inhibiting the activity of tPA. The present invention more specifically relates to administering an amount of a tPA in-hibitor sufficient to reduce the vascular permeability increas-ing activity of tPA in a subject. Useful tPA inhibitors for the present method are neuroserpin, mutant neuroserpin, wild-type PAI-1, mutant PAI-1, an antibody that binds to tPA, an antibody that binds to the low-density lipoprotein (LDL) receptor or a low-density lipoprotein (LDL) receptor family antagonist [103, 104]. A recent therapy against the hemor-rhagic complications induced by tPA is the GM6001. Re-cently, it was described the use of GM6001 to prevent the hemorrhagic complications and improve the behavioral ab-normalities induced by tPA, partly via protection of tight junctions proteins [99]. This suggests that GM6001 may be a useful candidate for combination therapy against the hemor-rhagic complications induced by tPA. Another candidate patented in 2007 could be used for treating the stroke and could also be used for neuroprotection of cerebral injury and neurodegeneration is the tPA kringle-2 polypeptide. This polypeptide is offered after cerebral ischemia, can reduce the death rate of rats with the stroke, reduce the volume of the cerebral infarction, reduce the expression of endogenous tPA and adjust the BBB opening mode, makes the BBB permeability reduced after 24 hours of the cerebral ischemia, effectively prevents oedema, and reduces cerebral neuronal apoptosis [105] . Recently, the use of plasminogen activator was patented, also called desmoteplase, for the manufacture of a medica-ment for treating stroke in patients with cerebral artery oc-clusion [106]. Another potential use against inflammation of the CNS could be use a recent invention concerns a marker for low-grade inflammation-related diseases such as cardiovascular disease, ischemic heart disease and type 2 diabetes. This patent concerns the measurement of the
concentration of soluble urokinase plasminogen activator receptor (suPAR) in human biological fluids as a tool of diagnosing and/or prognosticating low-grade inflammation, such as sputum, cystic fluid, ascites, serum, plasma, urine [107, 108].
TPA-DEPENDENT SIGNALLING PATHWAYS: LRP-MEDIATED SIGNALLING
tPA regulates physiological processes in the brain, probably due to the different domains of the protein and in-teractions with other receptors, like LRP Fig. (3). The non fibrinolytic roles for tPA have become prominent in the CNS and mostly in relation to neurotoxicity and modulation of the BBB. While the literature is very consistent with regards to the effects of tPA on the BBB, the mechanism underlying this capacity of tPA remains controversial. It has been sug-gested that tPA is able to promote the leakage of the BBB, which is in agreement with the ability of tPA promote hem-orrhages. This effect of tPA on BBB leakage appears to be mediated by the LRP. Benchenane et al. showed that tPA crosses the intact BBB independently of its proteolytic activ-ity and this process is mediated through LRP family recep-tors [100]. Here, there are discrepancies because they dem-onstrated that tPA has no effect on the integrity of the BBB in physiological conditions either in vivo and in vitro, how-ever, Yepes et al. showed that tPA can lead to an opening of the BBB by a mechanism that involves LRP [109]. Some reports have suggested a plasmin-independent role for tPA via members of LRP family, while others have re-ported tPA-mediated plasmin generation as crucial for tPA activity on the BBB. Further, an interesting observation was that plasmin, although essential for tPA to promote an in-crease in permeability, was completely incapable of substi-tuting for tPA suggesting a requirement for an additional component. Indeed, our competition experiments using a catalytically inactive tPA gave credence to the idea that a cell-surface receptor for tPA was also required. The identity of this receptor was not revealed but was most likely a mem-ber of the LRP family since tPA mediated increase in perme-ability was inhibited by the panLRP blocking agent, RAP. A similar blocking effect was seen when tPA was added to our BBB model in the presence of the lysine analog. Together with the lack of effect of the truncated tPA variant, which retains its lysine-binding kringle 2 domain suggesting that tPA binding is lysine-independent, these observations point to a requirement for a second receptor, most likely a plasmi-nogen receptor. This group proposed a model where at least two cell surface receptors, one for tPA (an LRP) and another for plasminogen are required for this effect [30]. In contrast, to this date the role of LRP1 and tPA in the microglial cells has to be elucidated. Recent data indicated that after stroke the interaction between tPA and LRP1 in-duces microglial activation and the generation of an inflam-matory response with deleterious effects on the ischemic brain [110]. A growing body of evidence indicates that the interaction between tPA and LRP1 has a pro-inflammatory effect. Indeed, in vitro studies have demonstrated that bind-ing of tPA to LRP1 increases the synthesis of MMP-9 and NF-kb activation in the ischemic brain [111, 112]. Interest-ingly, this novel pathway for cerebral ischemia-induced mi-

8 Recent Patents on Endocrine, Metabolic & Immune Drug Discovery 2013, Vol. 7, No. 1 Ortolano and Spuch
croglial activation during cerebral ischemia is indicating that tPA has a direct effect on microglial cell activation and that this process, as previously reported by others, is independent of its proteolytic activity. Similar pathways was described in fibroblasts, tPA binds to LRP1, inducing a rapid and transient phosphorylation of its tyrosine residues that, in turn, transactivates the Erk1/2 pathway, initiating a cascade of cell survival, preventing the cleavage and activation of caspase-3, a major effectors cas-pase that degrades many physiologically important proteins and causes cells to die in an organized manner [113]. An additional role of tPA was affecting synaptic plastic-ity in hippocampus, tPA is highly expressed in the limbic system [114] where regulates neuronal viability and experi-ence induced plasticity mediated long-term potentiation (LTP). This additional role of tPA was identified as one of the immediate early genes induced by neuronal activity in-cluding LTP. Under normal physiological conditions, tPA is
widely expressed in the CNS, however tPA is highly ex-pressed in the limbic system [58] and the level of tPAI is finely regulated by its inhibitor and cell surface receptor LRP, and its synthesis is increased by activators of the cAMP-PKA pathway. More interestingly, late-phase-LTP but not early-phase-LTP is significantly decreased in mice lacking the gene encoding tPA [21, 115]. These findings indicate that tPA plays an important role in LTP in the hip-pocampus and probably the interaction between tPA and LRP participates in LTP. One possible candidate substrate of tPA is LRP itself, since recent studies have shown that the cytoplasmic domain of LRP can be released from the membrane through a proc-ess that involves proteolytic processing of the extracellular domain of LRP, and that the free intracellular domain can then regulate cell signalling pathways [116]. Clearly, block-ing either the proteolytic activity of tPA or its association with LRP could prevent this potential processing. Blocking
Fig. (3). tPA co-localize on the cell surface with plasminogen receptor, this co-localization provides the co-factor requires for effective plasmin generation. At the same time plasmin trigger signaling pathways (signaling 1). LRP1 is also able to trigger signaling pathways into the cell (signaling 3). However, when the activation of both receptors generates the interaction between LRP1 and plasminogen receptor triggers a different intracellular signaling (signaling 2).

Interaction between tPA and LRPs Recent Patents on Endocrine, Metabolic & Immune Drug Discovery 2013, Vol. 7, No. 1 9
either the proteolytic activity of tPA or its association with LRP would prevent this potential processing. Based on this mechanism, the role of astrocytes in the regulation of ex-tracellular tPA is very important and regulated by LRP. The astrocytes rapidly take up neuron-derived tPA through con-stitutive LRP-mediated, clathrin-dependent, and dynamin-dependent endocytosis. Astrocytes are also able to release tPA. Further, extracellular glutamate inhibits the release of tPA by astrocytes; and this inhibitory action of glutamate is mediated by kainate receptor-induced protein kinase C (PKC) signalling [23]. The interaction between this tPA and LRP in astrocytic end-feet processes results in cleavage of LRPs ectodomain. In the early stages of cerebral ischemia, the interaction between tPA and LRP in perivascular astro-cytes induces the activation of a cell signalling event medi-ated by pAkt that leads to increase in the permeability of the BBB [117]. It was shown that an antagonist of LRP, RAP, hinders tPA-induced late-phase-LTP and prevents rescue of synaptic potentiation by addition of tPA in tPA-deficient mice [118]. Additionally, the binding of tPA to LRP can lead to the up-regulation of MMP-9, a protease which can degrade the ex-tracellular matrix contributing to either synaptic plasticity or neuronal degeneration [112]. Interaction between LRP1 and tPA which was long considered only such as scavenging receptor for tPA and tPA/PAI-1 complexes. Furthermore, it recently became apparent that also binding of tPA to LRP triggers a cascade of intracellular signalling events. Target-ing the tPA-LRP signalling pathway in brain may offer new approaches for decreasing neurotoxicity and improving stroke therapy.
CURRENT & FUTURE DEVELOPMENTS
Cerebral injury induces dynamic changes in the BBB permeability, but the underlying mechanisms have remained largely unknown. More efforts are needed to better under-stand the molecular mechanism underlying the degradation and redistribution of various protein components of the BBB according to the type, severity and duration of cerebral ischemic insults. The tPA is the only FDA-treatment for acute stroke due to its thrombolytic properties, however the excitotoxic neuronal damage produced in animal models questions the validity of this approach as a convening ther-apy. During the last decade evidence has been emerging which suggests that MMPs play a central role in tPA-mediated neurotoxicity in thrombolytic therapy for acute stroke. Thus, pharmacological inhibition of MMPs, at an appropriate time, may hold promise as a safe and effective adjunct therapy for tPA in acute ischemic stroke. tPA neuro-toxicity is blocked either by co-treatment with neuroserpin or APC or by inhibiting LRP, PDGF-CC, or NMDA receptors during ischemic stroke. Targeting these pathways might of-fer new combinational therapies for decreasing tPA neuro-toxicity and improving stroke therapy. More efforts are needed to characterize either beneficial or detrimental effects of these pathways at different stages of stroke and to estab-lish the time window for tPA co-treatment of acute ischemic stroke.
CONFLICT OF INTEREST
None of the authors of this manuscript have any financial interest that has influenced the results or interpretation of this manuscript.
ACKNOWLEDGEMENTS
This work was supported by grants from Xunta de Galicia (INCITE2009, 09CSA051905PR), Ministerio de Ciencia e Innovación (PI11/00842) and “Isidro Parga Pon-dal” programme.
REFERENCES [1] Vassalli JD, Sappino AP, Belin D. The plasminogen activa-
tor/plasmin system. J Clin Invest 1991; 88(4): 1067-72. [2] Hacke W, Kaste M, Bluhrnki E, Bozman M, Davalos A, Guidetti
D, et al. Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. N Engl J Med 2008; 329(13): 1317-29.
[3] Strickland S. Tissue plasminogen activator in nervous system func-tion and dysfunction. Thromb Haemost 2001; 86: 138-43.
[4] Tsirka SE, Gualandris A, Amaral DG, Strickland S. Excitotoxin-induced neuronal degeneration and seizure are mediated by tissue plasminogen activator. Nature 1995; 377(6547): 340-4.
[5] Cesarman-Maus G, Hajjar KA. Molecular mechanisms of fibri-nolysis. Br J Haematol 2005; 129(3): 307-21.
[6] Sakharov DV, Barrertt-Bergshoeff M, Hekkenberg RT, Rijken DC. Fibrin-specificity of a plasminogen activator affects the efficiency of fibrinolysis and responsiveness to ultrasound: Comparison of nine plasminogen activators in vitro. Thromb Haemost 1999; 81(4): 233-40.
[7] Samson AL, Medcalf RL. Tissue-type plasminogen activator: A multifaceted modulator of neurotransmission and synaptic plastic-ity. Neuron 2006; 50(5): 673-8.
[8] Yepes M, Lawrence DA. New functions for an old enzyme: Non haemostatic roles for tissue-type plasminogen activator in the cen-tral nervous system. Exp Biol Med 2004; 229(11): 1097-104.
[9] Friedman GC, Seeds NW. Tissue plasminogen activator expression in the embryonic nervous system. Brain Res Dev Brain Res 1994; 81(1): 41-9.
[10] Madani R, Hulo S, Toni N, Madani H, Steimer T, Muller D, et al. Enhanced hippocampal long-term potentiation and learning by in-creased neuronal expression of tissue-type plasminogen activator in transgenic mice. EMBO J 1999; 18(1): 3007-12.
[11] Calabresi P, Napolitano M, Centonze D, Marfia GA, Gubellini P, Teule MA, et al. Tissue plasminogen activator controls multiple forms of synaptic plasticity and memory. Eur J Neurosci 2000; 12(3): 1002-12.
[12] Pawlak R, Nagai N, Urano T, Napiorkowska-Pawlak D, Ihara H, Takada Y, et al. Rapid, specific and active site-catalyzed effect of tissue-plasminogen activator on hippocampus-dependent learning in mice. Neuroscience 2002; 113(4): 995-1001.
[13] Rogove AD, Siao C, Keyt B, Strickland S, Tsirka SE. Activation of microglia reveals a nonproteolytic cytokine function for tissue plasminogen activator in the central nervous system. J Cell Sci 1999; 112(22): 4007-16.
[14] Wu YP, Siao CJ, Lu W, Sung TC, Frohman MA, Milev P, et al. The tissue plasminogen activator (tPA)/plasmin extracellular prote-olytic system regulates seizure-induced hippocampal mossy fiber outgrowth through a proteoglycan substrate. J Cell Biol 2000; 148(6): 1295-304.
[15] Nicole O, Docagne F, Ali C, Margaill I, Carmeliet P, MacKenzie ET, et al. The proteolytic activity of tissue-plasminogen activator enhances NMDA receptor-mediated signalling. Nat Med 2001; 7(1): 59-64.
[16] Selkoe DJ. Clearing the brain’s amyloid cobwebs. Neuron 2001; 32(2): 177-80.
[17] Sappino AP, Madani R, Huarte J, Belin D, Kiss JC, Wohlwend A, et al. Extracellular proteolysis in the adult murine brain. J Clin In-vest 1993; 92(2): 679-85.
[18] Rogove AD, Tsirka SE. Neurotoxic responses by microglia elicited by excitotoxic injury in the mouse hippocampus. Curr Biol 1998; 8:19-25.

10 Recent Patents on Endocrine, Metabolic & Immune Drug Discovery 2013, Vol. 7, No. 1 Ortolano and Spuch
[19] Docagne F, Nicole O, Marti HH, MacKenzie ET, Buisson A, Vivien D. Transforming growth factor-beta1 as a regulator of the serpins/t-PA axis in cerebral ischemia. FASEB J 1999; 13:1315-24.
[20] Frey U, Müller M, Kuhl D. A different form of long-lasting poten-tiation revealed in tissue plasminogen activator mutant mice. J Neurosci 1996; 16:2057-63.
[21] Baranes D, Lederfein D, Huang YY, Chen M, Bailey CH, Kandel ER. Tissue plasminogen activator contributes to the late phase of LTP and to synaptic growth in the hippocampal mossy fiber path-way. Neuron 1998; 21(4): 813-25.
[22] Vivien D, Ali C. Traumatic brain injury: Tissue-type plasminogen activator-harmful or beneficial? Nat Rev Neurol 2012; 11(8): 538-9.
[23] Cassé F, Bardou I, Danglot L, Briens A, Montagne A, Parcq J, et al. Glutamate controls tPA recycling by astrocytes, which in turn influences glutamatergic signals. J Neurosci 2012; 32(15):5186-99.
[24] Benchenane K, López-Atalaya JP, Fernández-Monreal M, Touzani O, Vivien D. Equivocal roles of tissue-type plasminogen activator in stroke-induced injury. Trends Neurosci 2004; 27:155-60.
[25] Chen ZL, Strickland S. Neuronal death in the hippocampus is pro-moted by plasmin-catalyzed degradation of laminin. Cell 1997; 91:917-25.
[26] Kim YH, Park JH, Hong SH, Koh JY. Nonproteolytic neuroprotec-tion by human recombinant tissue plasminogen activator. Science 1999; 284(5414):647-50.
[27] Lee HY, Hwang IY, Im H, Koh JY, Kim YH. Non-proteolytic neurotrophic effects of tissue plasminogen activator on cultured mouse cerebrocortical neurons. J Neurochem 2007; 101(5):1236-47.
[28] Liot G, Roussel BD, Lebeurrier N, Benchenane K, López-Atalaya JP, Vivien D, et al. Tissue-type plasminogen activator rescues neu-rones from serum deprivation-induced apoptosis through a mecha-nism independent of its proteolytic activity. J Neurochem 2006; 98(5):1458-64.
[29] Siao CJ, Tsirka SE. Tissue plasminogen activator mediates micro-glial activation via its finger domain through annexin II. J Neurosci 2002; 22(9): 3352-8.
[30] Benchenane K, Berezowski V, Fernández-Monreal M, Brillault J, Valable S, Dehouck MP, et al. Oxygen glucose deprivation switches the transport of tPA across the blood brain barrier from an LRP-dependent to an increase LEP-independent process. Stroke 2005; 36(5): 1065-70.
[31] Beliveau, R., Demuele, M., Bertrand, Y., Michaud-Levesque, J., Jodoin, J. Compound and method for regulating plasminogen acti-vation and cell migration. EP2497485 (2012).
[32] Spuch C, Ortolano S, Navarro C. LRP1 and LR2 receptors function in the membrane neuron. Trafficking mechanisms and proteolytic processing in Alzheimer’s disease. Front Physiol 2012; 3: 269.
[33] Kanekiyo T, Zhang J, Liu Q, Liu CC, Zhang L, Bu G. Heparan sulphate proteoglycan and the low density lipoprotein receptor re-lated protein-1 constitute major pathways for neuronal amyloid-beta uptake. J Neurosci 2011; 31: 1644-51.
[34] Fester L, Zhou L, Bütow A, Huber C, von Lossow R, Prange-Kiel J, et al. Cholesterol promoted synaptogenesis requires the conver-sion of cholesterol to estradiol in the hippocampus. Hippocampus 2009; 19; 692-705.
[35] Andersen OM, Willnow TE. Lipoprotein receptors in Alzheimer's disease. Trends Neurosci 2006; 29: 687-94.
[36] Rebeck GW, Harr SD, Strickland DK, Hyman BT. Multiple, di-verse senile plaque-associated proteins are ligands of an apolipo-protein E receptor, the alpha 2-macroglobulin receptor/low-density-lipoprotein receptor related protein. Ann Neurol 1995; 37: 211-7.
[37] Marzolo MP, von BR, Bu G, Inestrosa NC. Expression of alpha(2)-macroglobulin receptor/low density lipoprotein receptor-related protein (LRP) in rat microglial cells. J Neurosci Res 2000; 60: 401-11.
[38] Herz J, Bock HH. Lipoprotein receptors in the nervous system. Annu Rev Biochem 2002; 71: 405-34.
[39] Carro E, Spuch C, Trejo JL, Antequera D, Torres-Aleman I. Chor-oid plexus megalin is involved in neuroprotection by serum insulin-like growth factor I. J Neurosci 2005; 25: 10884-93.
[40] Spuch C, Navarro C. Expression and functions of LRP-2 in central nervous system: Progress in understanding its regulation and the potential use for treatment of neurodegenerative diseases. Immunol Endocr Metab Agents Med Chem 2010; 10(4): 249-54.
[41] LaFerla FM, Troncoso JC, Strickland DK, Kawas CH, Jay G. Neu-ronal cell death in Alzheimer’s disease correlates with ApoE up-take and intracellular Abeta stabilization. J Clin Invest 1997; 100: 310-20.
[42] Bento-Abreu A, Velasco A, Pólo-Hernandez E, Perez-Reyes PL, Tabernero A, Medina JM. Megalin is a receptor for albumin in as-trocytes and is required for the synthesis of the neurotrophic factor oleic acid. J Neurochem 2008; 106: 1149-59.
[43] Alvira-Botero X, Perez-Gonzalez R, Spuch C, Vargas T, Antequera D, Garzon M, et al. Megalin interacts with APP and the intracellu-lar adaptor protein Fe65 in neurons. Mol Cell Neurosci 2010; 45: 306-15.
[44] Seeds NW, Williams BL, Bickford PC. Tissue plasminogen activa-tor induction in Purkinje neurons after cerebellar motor learning. Science 1995; 270(5244): 1992-4.
[45] Seeds NW, Basham ME, Haffke SP. Neuronal migration is retarded in mice lacking the tissue plasminogen activator gene. Proc Nat Acad Sci USA 1999; 96(24): 14118-23.
[46] Salles FJ, Strickland S. Localization and regulation of the tissue plasminogen activator-plasmin system in the hippocampus. J Neu-rosci 2002; 22(6): 2125-34.
[47] Pawlak R, Margarinos AM, Melchor J, McEwen B, Strickland S. Tissue plasminogen activator in the amygdala is critical for stress-induced anxiety-like behavior. Nat Neurosci 2003; 6(2): 168-74.
[48] Seeds NW, Basham ME, Ferguson JE. Absence of tissue plasmino-gen activator gene or activity impairs mouse cerebellar motor learning. J Neurosci 2003; 23(19):7368-75.
[49] Rodrigues SM, Schafe GE, LeDoux JE. Molecular mechanisms underlying emotional learning and memory in the lateral amygdale. Neuron 2004; 44(1): 75-91.
[50] Teesalu T, Kulla A, Simisker A, Siren V, Lawrence DA, Asser T, et al. Tissue plasminogen activator and neuroserpin are widely ex-pressed in the human central nervous system. Thromb Haemost 2004; 92(2): 358-68.
[51] Masos T, Miskin R. mRNAs encoding urokinase type plasminogen activator and plasminogen activator inhibitor-1 are elevated in the mouse brain following kainate-mediated excitation. Brain Res Mol Brain Res 1997; 47(1-2): 157-69.
[52] Yepes M, Lawrence DA. New functions for an old enzyme: Non-hemostatic roles for tissue-type plasminogen activator in the central nervous system. Exp Biol Med 2004; 229(11): 1097-104.
[53] Seeds NW, Verrall S, Friedman G, Hayden S, Gadotti D, Haffke S, et al. Plasminogen activators and plasminogen ectivator inhibitors in neuronal development. Ann NY Acad Sci 1992; 4(667): 32-40.
[54] Lawson LJ, Perry VH, Dri P, Gordon S. Heterogeneity in the dis-tribution and morphology of microglia in the normal adult mouse brain. Neuroscience 1990; 39(1): 151-70.
[55] Bukhari N, Torres L, Robinson JK, Tsirka SE. Axonal regrowth after spinal cord injury via chondroitinase and the tissue plasmino-gen activator (tPA)/plasmin system. J Neurosci 2011; 31(42): 14931-43.
[56] Michalski D, Hobohm C, Weise C, Pelz J, Heindl M, Kamprad M, et al. Interrelations between blood-brain barrier permeability and matrix metalloproteinases are differently affected by tissue plasmi-nogen activator and hiperoxia in a rat model of embolic stroke. Med Gas Res 2012; 2(2): 1-5.
[57] Tsirka SE, Rogove AD, Bugge TH, Degen JL, Strickland S. An extracellular proteolytic cascade promotes neuronal degeneration in the mouse hippocampus. J Neurosci 1997; 17(2): 543-52.
[58] Indyk JA, Chen ZL, Tsirka SE, Strickland S. Laminin chain ex-pression suggests that laminin-10 is a major isoform in the mouse hippocampus and is degraded by the tissue plasminogen activator / plasmin protease cascade during excitotoxic injury. Neuroscience 2003; 116(2): 359-71.
[59] Chen ZL, Haegeli V, Yu H, Strickland S. Cortical deficiency of laminin gamma 1 impairs the AKT/GSK-3beta signaling pathway and leads to defects in neurite outgrowth and neuronal migration. Dev Biol 2009; 327(1): 158-66.
[60] Lijnen HR, Van Hoef B, Lupu F, Moons L, Carmeliet P, Collen D. Function of the plasminogen/plasmin and matrix metalloproteinase systems after vascular injury in mice with targeted inactivation of fibrinolytic systems genes. Arterioscler Thromb Vasc Biol 1998; 18(7): 1035-45.
[61] Basbaum CB, Werb Z. Focalized proteolysis: Spatial and temporal regulation of extracellular matrix degradation at the cell surface. Curr Opin Cell Biol 1996; 8(5): 731-8.
Interaction between tPA and LRPs Recent Patents on Endocrine, Metabolic & Immune Drug Discovery 2013, Vol. 7, No. 1 11
[62] Gravanis I, Tsirka SE. Tissue-type plasminogen activator as a therapeutic target in stroke. Expert Opin Ther Targets 2008; 12(2): 159-70.
[63] Spuch C, Navarro C. Liposomes for targeted delivery of active agents against neurodegenerative diseases (Alzheimer’s disease and Parkinson’ disease). J Drug Deliv 2011; 2011(469679): 1-12.
[64] Paul J, Strickland S, Melchor JP. Fibrin deposition accelerates neurovascular damage and neuroinflammation in mouse models of Alzheimer's disease. J Exp Med 2007; 204(8): 1999-2008.
[65] Barker R, Kehoe PG, Love S. Activators and inhibitors of the plasminogen system in Alzheimer's disease. J Cell Mol Med 2012; 16(4):865-76.
[66] Wnendt S, Wetzels I, Gunzler WA. Amyloid beta peptides stimu-late tissue-type plasminogen activator but not recombinant prourokinase. Thromb Res 1997; 85(3): 217-24.
[67] Ledesma MD, Da Silva JS, Crassaerts K, Delacourte A, De Strooper B, Dotti CG. Brain plasmin enhances APP alpha-cleavage and Abeta degradation and is reduced in Alzheimer's disease brains. EMBO Rep 2000; 1(6): 530-5.
[68] Melchor JP, Pawlak R, Strickland S. The tissue plasminogen acti-vator-plasminogen proteolytic cascade accelerates amyloid-beta (Abeta) degradation and inhibits Abeta-induced neurodegeneration. J Neurosci 2003; 23(26): 8867-71.
[69] Skrzypczak-Jankun E and Jankun J. The aflavin digallate inacti-vates plasminogen activator inhibitor: Could tea help in Alzheimer's disease and obesity? Int J Mol Med 2010; 26(1): 45-50.
[70] Sutton ET, Hellermann GR, Thomas T. β-Amyloid-induced endo-thelial necrosis and inhibition of nitric oxide production. Exp Cell Res 1997; 230(2): 368-76.
[71] Sutton R, Keohane ME, VanderBerg SR, Gonias SL. Plasminogen activator inhibitor-1 in the cerebrospinal fluid as an index of neuro-logical disease. Blood Coagul Fibrinolysis 1994; 5(2): 167-71.
[72] Zlokovic BV. Neurovascular pathways to neurodegeneration in Alzheimer’s disease and other disorders. Nat Rev Neurosci 2011; 12(12): 723-38.
[73] Alvira-Botero X, Pérez-Gonzalez R, Spuch C, Vargas T, Antequera D, Garzón M, et al. Megalin interacts with APP and the intracellu-lar adapter protein FE65 in neurons. Mol Cell Neurosci 2010; 45(3): 306-15.
[74] Hastings GA, Coleman TA, Haudenschild CC, Stefanson S, Smith EP, Barthlow R, et al. Neuroserpin, a brain-associated inhibitor of tissue plasminogen activator is localized primarily in neurons. Im-plications for the regulation of motor learning and neuronal sur-vival. J Biol Chem 1997; 272(52): 33062-7.
[75] Rodriguez-Gonzalez R, Millan M, Sobrino T, Miranda E, Brea D, Perez de la Ossa N, et al. The natural tissue plasminogen activator inhibitor neuroserpin and acute ischaemic stroke outcome. Thromb Haemost 2011; 105(3): 421-9.
[76] Takao M, Benson MB, Murrel JR, Yazaki M, Piccardo P, Unver-zagt FW, et al. Neuroserpin mutation S52R causes neuroserpin ac-cumulation in neurons and is associated with progressive myo-clonus epilepsy. J Neuropathol Exp Neurol 2000; 59(12): 1070-86.
[77] Spuch C, Ortolano S, Navarro C. Lafora progressive myoclonus epilepsy: Recent insights into cell degeneration. Rec Pat Endocr Metab Immune Drug Discov 2012; 6(2): 99-107.
[78] Yepes M, Sandkvist M, Wong MK, Coleman TA, Smith E, Cohan SL, et al. Neuroserpin reduces cerebral infarct volume and protects neurons from ischemia-induced apoptosis. Blood 2000; 96(2): 569-76.
[79] Cinelli P, Madani R, Tsuzuki N, Vallet P, Arras M, Zhao CN, et al. Neuroserpin, a neuroprotective factor in focal ischemic stroke. Mol Cell Neurosci 2001; 18(5): 443-57.
[80] Madani R, Kozlov S, Akhmedov A, Cinelli P, Kinter J, Lipp HP, et al. Impaired explorative behavior and neophobia in genetically modified mice lacking or overexpressing the extracellular serine protease inhibitor neuroserpin. Mol Cell Neurosci 2003; 23(3): 473-94.
[81] Vivien, D, Ali, C. Treatment of neurological or neurodegenerative disorders. EP2473185 (2012).
[82] Petersen, K., Vivien, D. Treatment of neurological or neurodegen-erative disorders. WO2011023249 (2011).
[83] Spuch C, Navarro C. Transport mechanisms at the blood-cerebrospinal-fluid barrier: Role of megalin (LRP2). Recent Pat Endocr Metab Immune Drug Discov 2010; 4(3): 190-205.
[84] Abbott NJ, Ronnback L, Hansson E. Astrocyte-endothelial interac-tions at the blood-brain barrier. Nat Rev Neurosci 2006; 7(1): 41-53.
[85] Zlokovic BV. Neurovascular mechanisms of Alzheimer’s neurode-generation. Trends Neurosci 2005; 28: 202-8.
[86] Kniesel U, Wolburg H. Tight junctions of the blood-brain bar-rier. Cell Mol Neurobiol 2000; 20(1): 57-76.
[87] Zlokovic BV. The blood-brain barrier in health and chronic neu-rodegenerative disorders. Neuron 2008; 57(2): 178-201.
[88] Carvey PM, Hendey B, Monahan AJ. The blood brain barrier in neurodegenerative disease: A rhetorical perspective. J Neurochem 2009; 111(2): 291-314.
[89] Morgan EH, Moos T. Mechanism and developmental changes in iron transport across the blood-brain barrier. Dev Neurosci 2002; 24(2-3): 106-13.
[90] Dietrich MO, Spuch C, Antequera D, Rodal I, de Yebenes JG, Molina JA, et al. Megalin mediates the transport of leptin across the blood-CSF barrier. Neurobiol Aging 2008; 29(56): 902-12.
[91] Bell RD, Zlokovic BV. Neurovascular mechanisms and blood-brain-barrier disorder in Alzheimer’s disease. Acta Neuropathol 2009; 118(1): 103-13.
[92] Carro E, Spuch C, Trejo JL, Antequera D, Torres-Aleman I. Chor-oid plexus megalin is involved in neuroprotection by serum insulin-like growth factor I. J Neurosci 2005; 25(47): 10884-93.
[93] Niego B, Freeman R, Puschmann TB, Turnley AM, Medcalf RL. t-PA-specific modulation of a human BBB involves plasmin medi-ated activation of the Rho-kinase pathway in astrocytes. Blood 2012; 119(20): 4752-60.
[94] Correa F, Gauberti M, Parcq J, Macrez R, Hommet Y, Objiang P, et al. Tissue plasminogen activator prevents white matter damage following stroke. J Exp Med 2011; 208(6): 1229-42.
[95] Gasche Y, Soccal PM, Kanemitsu M, Copin JC. Matrix metallopro-teinases and diseases of the central nervous system with a special emphasis on ischemic brain. Front Biosci 2006; 11: 1289-301.
[96] Rosenberg GA. Matrix metalloproteinases and their multiple roles in neurodegenerative diseases. Lancet Neurol 2009; 8(2): 205-16.
[97] McCawley LJ, Matrisian LM. Matrix metalloproteinases: They’re not just for matrix anymore. Curr Opinion Cell Biol 2001; 13(5): 534-40.
[98] Ning M, Chopp M, Yan T, Zacharek A, Zhang C, Roberts C, et al. Tissue plasminogen activator treatment of stroke in type-1 diabetes rats. Neuroscience 2012; 222: 326-32.
[99] Mishiro K, Ishiguro M, Suzuki Y, Tsuruma K, Shimazawa M, Hara H. A broad-spectrum matrix metalloproteinase inhibitor prevents hemorrhagic complications induced by tissue plasminogen activa-tor in mice. Neuroscience 2012; 205: 39-48.
[100] Benchenane K, Berezowski V, Ali C, Fernández-Monreal M, López-Atalaya JP, Brillault J, et al. Tissue-type plasminogen acti-vator crosses the intact blood-brain barrier by low-density lipopro-tein receptor-related protein-mediated transcytosis. Circulation 2005; 111(17): 2241-49.
[101] Yao Y, Tsirka SE. Truncation of monocyte chemoattractant protein 1 by plasmin promotes blood-brain barrier disruption. J Cell Sci 2011; 124(9): 1486-95.
[102] Lukic-Panin V, Deguchi, K, Yamashita T, Shang J, Zhang X, Tian F, et al. Free radical scavenger edaravone administration protects against tissue plasminogen activator induced oxidative stress and blood brain barrier damage. Curr Neurovasc Res 2010; 7(4): 319-29.
[103] Lawrence, D.A., Yapes, M.S., Strickland, D.M. Methods of reduc-ing vascular permeability in tissue by inhibition of tissue plasmino-gen activator (TPA) inhibitors useful therein. US20050019329 (2005) & US20087375076 (2008).
[104] Lawrence, D.A., Yapes, M.S., Strickland, D.M. Methods of reduc-ing vascular permeability in tissue by inhibition of tissue plasmino-gen activator (TPA) inhibitors useful therein. US20050019329 (2005).
[105] Jianning, L., Jing, Z., Haitao, Z. Treatment effect of tissue plasmi-nogen activator kringle-2 on stroke and preparation method for tis-sue plasminogen activator kringle-2. CN101886066 (2007).
[106] Sohngen, M., Ebel, A., Al-Rawi, Y. Use of plasminogen activator (desmoteplase) in the treatment of stroke. NZ584640 (2012).
[107] Eugen-Olsen, J., Haugaard, S., Andersen, O. Soluble urokinase plasminogen receptor (suPAR) as diagnostic marker for low-grade inflammation. EP2500730 (2012).

12 Recent Patents on Endocrine, Metabolic & Immune Drug Discovery 2013, Vol. 7, No. 1 Ortolano and Spuch
[108] Anderberg, J., Gray, J., McPherson, P., Nakamura, K. Methods and compositions for diagnosis and prognosis of renal injury and renal failure. US2012231472 (2012).
[109] Yepes M, Sandkvist M, Moore EG, Bugge TH, Strickland DK, Lawrence DA. Tissue type plasminogen activator induces opening of the blood-brain barrier via the LDL receptor-related protein. J Clin Invest 2003; 112(10): 1533-40.
[110] Zhang C, An J, Strickland DK, Yepes M. The low density lipopro-tein receptor related protein 1 mediates tissue-type plasminogen ac-tivator induced- microglial activation in the ischemic brain. Am J Pathol 2009; 174(2): 586-94.
[111] Hu K, Yang J, Tanaka S, Gonias SL, Mars WM, Liu Y. Tissue-type plasminogen activator acts as a cytokine that triggers intracellular signal transduction and induces matrix metalloproteinase-9 gene expression. J Biol Chem 2006; 281 (4): 2120-7.
[112] Wang X, Lee SR, Arai K, Lee SR, Tsuji K, Rebeck GW, et al. Lipoprotein receptor-mediated induction of matrix metallopro-teinase by tissue plasminogen activator. Nat Med 2003; 9(10): 1313-7.
[113] Hu K, Lin L, Tan X, Yang J, Bu G, Mars WM, et al. tPA protects renal interstitial fibroblasts and myofibroblasts from apoptosis. J Am Soc Nephr 2008; 19: 503-14.
[114] Skrzypiec AE, Buczko W, Pawlak R. Tissue plasminogen activator in the amygdale: A new role for an old protease. J Physiol Pharma-col 2008; 59(8): 135-46.
[115] Qian Z, Gilbert ME, Colicos MA, Kandel ER, Kuhl D. Tissue-plasminogen activator is induced as an immediate-early gene dur-ing seizure, kindling and long-term potentiation. Nature 1993; 361 (6411): 453-7.
[116] Spuch C, Ortolano S, Navarro C. LRP-1 and LRP-2 receptors func-tion in the membrane neuron. Trafficking mechanisms and prote-olytic processing in Alzheimer’s disease. Front Physiol 2012; 3:269.
[117] An J, Zhang C, Polavarapu R, Zhang X, Zhang X, Yepes M. Tis-sue-type plasminogen activator and the low-density lipoprotein re-ceptor-related protein induce Akt phosphorylation in the ischemic brain. Blood 2008; 112(7): 2787-94.
[118] Zhuo M, Holtzman DM, Li Y, Osaka H, DeMaro J, Jacquin M, et al. Role of tissue plasminogen activator receptor LRP in hippo-campal long-term potentiation. J Neurosci 2000; 20(2): 542-9.