TPA Spring 2002
40
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of TPA Spring 2002

American Professional Agency
Full
1c
pu Winter 2001 p9
IFC

Texas Psychologist 1SPRING 2002
Features
10 GUEST EDITOR: Focus on Bipolar DisorderJodi M. Gonzalez, PhD
13 Diagnosis and Treatment in the Broad Clinical Spectrum of Bipolar DisorderJodi M. Gonzalez, PhD
19 Medication Management Issues in Psychotherapy of Bipolar DisorderCheryl Gonzales, MD
24 Bipolar Disorder: Challenges for PregnancyBarbara Kertz, MS, LPC
Holly Zboyan, BA
28 An Interview with Charles Bowden on Research and Practice in Bipolar DisorderJodi M. Gonzalez, PhD
Departments
2 PRESIDENT’S MESSAGE: Sunrise...SunsetWalt Cubberly, PhD
4 LAW: Duty to Report Child Abuse, NeglectSam A. Houston
Merritt McReynolds Marinelli
6 Legislative Taskforce to Review Procedures for Forensic EvaluationsMary Alice Conroy, PhD, ABPP
8 New Members
9 Inside TPA
33 Psychopharmacology on the MoveDee Yates, PhD
34 Texas Psychology FoundationJoseph C Kobos, PhD, President
35 Classified Advertising
36 2001 PSY-PAC Contributors
Christopher Blazina, PhDEditor
The University of Houston
David White, CAEExecutive Director
Robert McPherson, PhDDirector of Professional Affairs
Lynda KeenBookkeeper
Sherry ReismanDirector of Conventions and Non-Dues
Revenue
Lila HolmesMembership Manager
TPA BOARD OF TRUSTEESPresident
Walt Cubberly, PhD
President-ElectDeanna F. Yates, PhD
President-Elect DesignateC. Alan Hopewell, PhD
Past-PresidentSam Buser, PhD
BOARD MEMBERSGary Brooks, PhDRon Cohorn, PhD
Patrick J. Ellis, PhDCharlotte Kimmel, PhDJoseph C. Kobos, PhD
Suzanne Mouton-Odum, PhDElizabeth L. Richeson, PhD
Ollie Seay, PhDJose Luis Torres, PhD
Jarvis A. Wright, Jr., PhD
EX-OFFICIO BOARD MEMBERSFederal Advocacy Coordinator
Paul Burney, PhD
Federal Advocacy CoordinatorRick McGraw, PhD
CAPP RepresentativeMelba J.T. Vasquez, PhD
Student Division DirectorJohn Hardie, MS
PUBLISHERRector Duncan & Associates
P.O. Box 14667Austin, Texas 78761
512-454-5262
Kim ScheberleManaging Editor
Pat HuberAdvertising Sales
Scott B. WilliamsArt Director
The Texas Psychological Association islocated at 1011 Meredith Drive, Suite 4,Austin, Texas 78748. Texas Psychologist(ISSN 0749-3185) is the official publicationof TPA and is published quarterly.
www.texaspsyc.org
SPRING 2002 VOLUME 53, ISSUE 1
These last three months do seem so
strange to me. Sometimes moods of
indescribable mental anguish,
sometimes moments when the veil of
time and the fatality of circumstances
seemed to be torn apart for an instant...
Vincent van Gogh
Letter Dated March 29, 1889
From the CoverVincent van Gogh Self-Portrait (1889)

2 Texas Psychologist SPRING 2002
My first LAS visit was to the RioGrande Valley Psychological
Association. I was surprised by the largeturnout. Over half of the psychologistsworking in the Valley attended and gave mea great deal of valuable input.I want to thank Dr. JosephMcCoy, the current president,and all the other psychologistswho attended. I shared withthem that if we could get thatpercentage of psychologists toshow up in our large metro-politan LASs, we would reallyfeel pleased.
If you would like to havethe same opportunity for inputand don’t have a TPA Board Member in yourLAS (or even if you do), call me (713-528-1510) or TPA (512-280-4099 or 888-872-3435) to arrange a visit.
For most psychologists, the major leg-islative issue before us is Sunset Review.Although Sunset Review doesn’t formallybegin until the 2005 legislative session, thecommittee is appointed following the con-clusion of the 2003 session (i.e. June 2003).This is closer than most psychologists real-ize. Much will be won or lost before thiscommittee is even appointed based on thequality of the prior relationships that havealready been built by TPA and our lobby-ists. The good news here is that we havehired the very best lobbyist to represent us.
Part of what makes Rusty Kelly andAssociates so valuable is that Rusty is high-ly regarded for his integrity and has manymore well developed, trusting friendshipswith state legislators than TPA could ever
build on its own. The legisla-tive process, fairly or unfairly,is based on these long-termfriendships, and we benefitfrom these friendships byassociation with Rusty. Theless good news is that hiring alobbying firm that enjoys avery good reputation costsmore money than hiring alobbyist that does not have somuch influence or enjoy such
a highly regarded reputation.TPA will be working diligently for the
next three years to insure passage of a licens-ing act that is favorable to psychology.Many psychologists believe that renewal ofour licensing act involves little more thanrenewing the previous one. This is not thecase. The state legislators assigned to ourSunset Review Committee are not assignedbecause they are friendly to psychology.They take apart our current licensing lawline by line and rebuild it line by line.Meanwhile, every non-psychology specialinterest group will try to influence this leg-islation in a way that favors its group andmay be very harmful for the profession ofpsychology. This will certainly include the
continuing attempt to lower the standard ofpractice for psychology to the master’sdegree level. For this reason we are asking
that each psychologist in Texas contribute$100 per year to our Sunrise Fund until weget our license renewed. If this is too muchto ask, we are requesting that you give atleast $25 a year to our Mid-AfternoonFund. (Please forgive our being so corny,but we can’t help ourselves.)
Another major effort of TPA involvespursuing prescription authority for appro-priately trained psychologists. President-Elect Dr. Dee Yates and President-ElectDesignate Dr. Alan Hopewell and othersare heading up this effort, which willinvolve a major push in 2003. Many psy-chologists who have completed the psy-chopharmacology training are already con-tributing $2,000 per year into a fund tosupport passage of this legislation. Updateswill be provided throughout the year as aninterim study is completed by the state leg-islature that addresses this issue. The statelegislators are trying to educate themselveson the merits of both sides of the issue.
Other projects already under considera-tion by your TPA Board include working
collaboratively with other professionalgroups on joint projects. I have invitedSusan Speight, Legislative Chair for theTexas Association of Marriage and FamilyTherapy, to dialogue with us at our firstBoard meeting. We have already had a pre-liminary discussion regarding issues of
mutual concern.Another group we are planning to work
more closely with is the Texas Association ofSchool Psychologists. We are hoping thatthe current President of TASP, Jan Opella,will also attend one of our Board meetingsto discuss ways we can work together. Theseefforts with TAMFT and TASP will help usbe better prepared for the issues likely tochallenge us in 2005.
The TPA Board is also trying to buildmore bridges within our profession. Schoolpsychology has been a recent focus. Wehave encouraged several school psycholo-gists to run for Board membership. If youbelong to a group that you believe is under-
Sunrise.. .Sunset
Walt Cubberly, PhD
Thank you for the opportunity to serve Texas psychologists and citizens as pres-
ident of TPA in 2002. I am excited to face the challenge of helping your Board of
Trustees create a comprehensive agenda for the legislative session that starts
in January of 2003. This year our TPA Board meetings will be largely devoted to
defining what our legislative goals will be, not only for 2003, but further out into
the future, as well. As your elected representatives, the Board Members want
input from you so that we best represent all of psychology. As part of putting
together your wishes, I will be traveling to various local area societies (LASs) to
collect ideas to put before the board.
FROM THE PRESIDENT
Wa l t Cubbe r l y, P hD
TPA P r e s i d en t
Texas Psychologist 3SPRING 2002
represented on your Board, let a currentBoard Member know and we will try tomentor your group in getting your grouprepresented. As a Board, we are committedto representing all of psychology.
Your Board is also trying to recruit morefaculty members to run for Board positions.If you are in academia, please considerbecoming more involved with TPA. Wewelcome you and consider your presencenecessary for our betterment.
As you probably know by now, TPAwent to Paris! The Paris workshop,Innovations in Marriage and FamilyTherapy, had over 70 people signed up. Tothe best of our knowledge, we are the firststate association to host a European work-shop. For many reasons, most of which aredue to our hard political work and not ourtravel plans, APA has grown to respect TPAas one of the two or three most outstandingstate associations in the country. My hat isoff to my colleagues who have put our stateassociation ahead of the curve in so manypositive ways. ✯
TPA has published NEW edition of the Texas Law andthe Practice of Psychology!
The new edition, Texas MentalHealth Law: A Sourcebook forMental Health Practitioners, is themost comprehensive book formental health practitioners everpublished. Get the latest informa-tion on supervising, ethics, sub-poenas, confidentiality, and more.If you have never purchased a ref-erence book on the laws that per-tain to your practice...the time todo so is NOW!
The book costs $35.00. Order your copy today! Please e-mail [email protected] or call 800-340-2034 to order your copy!
4 Texas Psychologist SPRING 2002
While there is no specific legal provi-sion to address this exact situation,
Chapter 261 of the Texas Family Code pro-vides in pertinent part:
(a) A person having cause to believethat a child’s physical or mental healthor welfare has been adversely affectedby abuse or neglect by any person shallimmediately make a report as providedby this subchapter. …
There is no language in the Code to sug-gest that a person is excused from this non-delegable affirmative duty just because thesuspected abuse or neglect took place in thepast, or may have taken place between minors.On the contrary, the triggering mechanism ofthe Code, is when the person becoming awareof the past abuse or neglect is made aware ofit, regardless of the age of the victim or perpe-trator at the time of disclosure.
Thus, the prudent course of action is toreport the information to the properauthorities, leaving it up to them to decidewhether to investigate or pursue the matterfurther. That way at least there is a recordmade regarding the incident, should futurereports regarding your client be made unbe-knownst to you. Simply put, just becauseyour client confessed to an incident thatoccurred while a minor, does not mean thathe or she is not capable of, or even worse, iscontinuing to abuse minors.
At the outset of a client relationship youare advised to put in writing and have yourclients acknowledge that you are requiredby law to report all suspected abuse andneglect, whether in the present or past. Youshould tell him or her you will follow the
law and your ethical obligation, and willmake such a report regardless of how youare made aware of it. This way it is out inthe open and there is no confusion aboutwhat you will do with such informationshould it be disclosed.
As a practical point you should make anote in a separate file stating why you report-ed despite the remoteness in time betweenthe alleged incident and the time when it wasdisclosed to you. If you choose not to report,document your reasoning, as well. This way,should the issue arise in the future, you havea written records of the incident. ✯
Sam A. Houston offers discounted legal con-sultation to TPA members. If you need to con-tact him regarding a legal matter, please do soat (713) 650-6600.
Duty to Report Child Abuse, Neglect
LAW
Sam A. Houston & Merritt McReynolds Marinelli
What are you required to do if an adult client discloses thatwhile a minor he or she sexually abused another minor?
A person having cause to
believe that a child’s physical
or mental health or
welfare has been adversely
affected by abuse or
neglect by any person shall
immediately make a report.

6 Texas Psychologist SPRING 2002
The taskforce held its first meeting onJan. 23 at the state capitol. Chaired
by Sen. Robert Duncan, R-Lubbock, withvice-chair Rep. Patricia Gray, D-Galveston, the 16-member group is tosubmit a final report to the next session ofthe state legislature.
Sen. Duncan noted that such a taskforceis rarely established, and the membersshould use the opportunity to make what-ever recommendations seem appropriate toimprove the quality of forensic evaluationsin the criminal justice system and theimpact of those evaluations on the continu-ity of care for those involved. Thus, thework of this taskforce could have far reach-ing implications for psychologists and psy-chiatrists who conduct forensic evaluationsor who otherwise work within the criminaljustice system.
Based upon the initial meeting, ques-tions addressed are likely to include the fol-lowing: 1) Who is a “disinterested expert?”2) What training, skills, credentials, orexperience should be required of profes-sionals who conduct mental health evalua-tions for the courts? 3) What specificallyshould a forensic report include? 4) Whereshould forensic work be conducted (e.g.,hospital, jail, community)? 5) Should theTexas insanity standard be reconsidered? 6)Is the competence for trial standard ade-quate as currently written? 7) Is the juvenilestatute regarding “unfitness to proceed/lackof responsibility” appropriate? 8) Should
Texas consider establishing mental healthcourts? 9) Under what circumstances isthere a compelling state interest to mandatecontinued treatment (including psy-chotropic medication)? 10) Can statutesregarding diversion and civil commitmentbe improved to facilitate continuity of care?11) Can statutory changes improve overallcommunication between law enforcementand the mental health community? 12) Can
electronic communication be used in evalu-ations and treatment?
The issues noted above are not all inclu-sive of what may be considered by the task-force. They do provide a starting point andhopefully will stimulate thinking amongpsychologists who practice in this arena.
Every indication is that recommendationsgenerated by this group will be taken veryseriously by the legislature. As your repre-sentative—and the only psychologistappointed to the taskforce—I would bevery interested in hearing about ideas, ques-tions and concerns that you may have.
Please feel free to contact me by e-mailat [email protected] or by phone (936)294-3806. ✯
Legislative Taskforce to Review Procedures for Forensic Evaluations
LEGISLATIVE NEWS
Mary Alice Conroy, PhD, ABPP (forensic)Sam Houston State University
During the 2001 legislative session, SB 553 established a taskforce to “review the methods and procedures used to evaluate a criminal defendant’s competency to stand trial anduse of the insanity defense.”
Do you conduct
forensic evaluations
or work in the criminal
justice system?
Texas Psychologist 7SPRING 2002
You can receive up to 15 hourscontinuing education creditthrough TPA Homestudy materials.
TPA's Homestudy offeringsinclude:
• Psychopharmacology I (4 hours) on CD-ROM
• Psychopharmacology II (4 hours) on CD-ROM
• Issues in Clinical Assessment(4 hours) on CD-ROM
• Testing Hispanic Populations(1 hour) printed article
• Overview of MulticulturalPsychotherapy (1 hour) printed article
• Ethical Principles That NeedConsideration When ProvidingServices Electronically (1 hour) printed article.
CD-ROM offerings cost $100for members and $140 for non-members.Printed article offerings cost$25 for members and $45 for non-members.
If you are in a CE jam andwould like more information onthese offerings, contact SherryReisman at 888-872-3435 or512-280-4099 [email protected].
In a CEJam?
A weekend conference devoted to finding, sustaining,
and sharing happiness.
The theme of our 2002 conference series is happiness—
happiness of mind, heart, body, and soul. Through
keynote talks, workshops, and full-day intensives, some
of the nation’s best-selling authors, teachers, and
spiritual leaders explore questions of the heart. Come
join us as we explore together the heart of happiness.
Austin, TexasRenaissance Austin Hotel
May 17-19, 2002Intensives May 17 & 20
OMEGAWorldwide Holistic Learning Centers
Omega Institute & The Crossings present
For 25 years Omega Institute has been aleader in organizing conferences that areequal parts education, relaxation, and cele-bration.
Omega is pleased to announce its partner-ship with The Crossings, a progressive learning centerand meeting place, opening in Austin inSeptember 2003. The Crossings is co-spon-soring this conference with Omega.
theheartofhappiness
Ram DassMarianne Williamson
Wayne DyerMitch Albom
Debbie FordOriah Mountain Dreamerdon Miguel RuizDavid Whyte
Faculty includes:
Information & Reservations
800.944.1001www.eomega.org
and others. . .
8 Texas Psychologist SPRING 2002
NEW MEMBERS
DoctoralArt Brownell, PhDGloria Chriss, PhDElizabeth Ann Cortez, PhDBarbara Hall, PhDWillam J. Holden, PhDJennifer Imming, PhDDavid B. Kelley, PhDGeorge Lazar, PhDWilliam Montgomery, PhDAnthony J. Rogers, PhDAnn I. Roose, PhDStephen Thorne, PhDCarol Walser, PhDDaniel Yancy, PhD
AssociateKaty Adams, MAJane Carr, MAMartha DuBose, MSDixie Valdez
StudentAmy Acosta, MEdVeronica AhueroLaura Alfonso, MSChrystina BacekKimberly BartonJohn BeachHelen Beckner, MSJoshua P. Bias, MSDonald Caudle, MA
John O. Charrier, MASusan Cromwell, PhDJames Deegear, MSKatherine DeGeorge, MEdNoel C. GonzalezMaryann HetrickCatherine G. KingKate Machemehl, MAMary MartinArlene Jean RiveroLisa SchreindorferMicheal Shafer, MSLee SheffermanKatherine TbabaDeborah Weber, MEdSharon Young, MA, MEd
The following individuals joined TPA between October 2, 2001 and
February 4, 2002. TPA welcomes all of our new members.
• Are you in the market for professional
liability insurance?
Call TPA’s preferred vendor, American Professional
Agency, (800) 421-6694.
• Psychological Tests and Confidential
Test Scoring Services
Download psychological tests for free. There is a
24-hour turnaround on our test scoring services.
Each test will be scored for $20. For more informa-
tion, please contact the Central Office or visit TPA's
“Practice Resources” link on our web page www.tex-
aspsyc.org.
• Discounted Legal Consultation Service:
Sam A. Houston (713) 650-6600.
• List serve subscription for timely updates.
• Director of Professional Affairs.
Psychologist on staff part-time to answer
member questions and requests for information
concerning professional affairs including, but not
limited to, ethics, insurance/managed care, and
practice management (512) 280-4099.
• Subscription to the Texas Psychologist.
Your quarterly journal is designed to provide you
with the most current information about professional
news and practice changes in the state.
• Continuing Education:
We offer both live and home study at substantially
discounted member rates.
• Fee Collection Service:
I.C. System (800) 325-6884.
TPA MEMBER BENEF I TSw w w. t e x a s p s y c . o r g
P A S S I N G S
Dr. Esme Williams passed away on Dec.
27, 2001 after a battle with cancer. Dr.
Williams was born in Guyana and made
Austin her home with her husband, Carlyle,
for the past four years. Dr. Williams
received a PhD from the Counseling
Psychology Training Program at the
University of Texas at Austin in December,
2001. Her major area of interest was how
women cope with the demands of working
in non-traditional careers, a passion she
developed from her own experiences work-
ing in the construction industry in the
Houston area prior to beginning her gradu-
ate studies at U.T. Dr. Williams presented
numerous papers on this topic at state and
local professional meetings, and defended
her dissertation, “Investigation of gender
stereotyping, stress, and coping strategies
for women and men in female- and male-
dominated occupations” in April, 2000. ✯

Texas Psychologist 9SPRING 2002
After 26 years at the same location,The Southwest Center for Psycho- logical Development has moved to newquarters in booming southwestLubbock. The new address of their free-standing building is: 5501 Spur 327,Lubbock, TX 79424.
Psychologists who are part of thisexpense-sharing association include:James E. Goggin, PhD, Cheryl L.Hall, PhD, Judy W. Halla, EdD,Charles W. Keller, PhD, and J. ScottRobertson, PhD. The SouthwestCenter, first established in 1969, hasbeen in business longer than any otherprivate practice psychology group inthis part of the state.
The National Organization forVictims Assistance called Houston psy-chologist Pauline Clansy and asked herto activate a team of 13 volunteers tosupport victims of the World TradeCenter disaster. Dr. Clansy immediate-ly gained the appropriate permissionsand alerted the All District Crisis Team,which includes 185 members.
During the week of Oct. 20, Dr.Clansy led an interdisciplinary team of13, which included six psychologists andone post-doctoral resident, to New Yorkand New Jersey to provide services forthe New York Children's AssistanceCenter staff and family members apply-ing for services at the Liberty State ParkFamily Assistance Center in New Jersey.It was a very gratifying experience for allinvolved. All were honored to be calledto serve at a trying time in our country'shistory.
A newly revised edition of JamesRandall Noblitt’s, PhD, and PamPerskin’s 1995 book has been published.
Cult and Ritual Abuse: Its History,Anthropology and Recent Discovery inContemporary America is available inboth hard and soft bound editions. Thefull citation is as follows.
Noblitt, J.R., & Perskin, P.S. (2000)Cult and Ritual Abuse: Its History,Anthropology and Recent Discovery inContemporary America. Westport, CT:Praeger Publisher.
John M. Velasquez, PhD, of theUniversity of the Incarnate Word (UIW;San Antonio) was awarded a two-yearHousing and Urban Development grantthrough the Office of UniversityPartnerships in the amount of $389,374to fund the expansion of PresaCommunity Center in San Antonio andthe extension of UIW service-learningprojects at Presa Community Center.
The HUD grant is an extension andoutgrowth of Dr. Velasquez's work withthe American Psychological Associa- tion's Psychology Partnerships Project(P3) and Campus Compact/ PewCharitable Trusts. The grant reflects Dr.Velasquez's role of psychologist as com-munity builder while addressing sys-temic influences on academic achieve-ment, economic development, andurban blight.
Dr. Lynn P. Rehm has been electedPresident of Division 6: Clinical andCommunity Psychology of theInternational Association of AppliedPsychology. The IAAP meets every fouryears as the International Congress ofApplied Psychology. In 2002 the meetingwill be held July 7-12 in Singapore. Dr.Rehm will become president-elect at thatmeeting and take over as president at theAthens meeting in 2006.
Dr. Rehm is also the currentPresident of the International Society ofClinical Psychology. This is a relativelynew organization that has been holdingannual meetings in conjunction withother international meetings. This sum-mer it will be meeting for one day inconjunction with the ICAP inSingapore.
Two long-time members of TPA,Rickie Moore, PhD, and HenryMarshall, PhD, have each releasedCDs that are aimed at helping manypeople reduce stress through excitingand innovating methods. Dr. Moorehas released an audio CD entitled“Yoga for Inner Peace,” which is medi-tative and easy to follow. The CDcomes with an illustrated instructionbooklet.
Dr. Marshall and the PlayshopFamily's latest CD, “Mantras 4 InnerPeace,” has been touted as inspiring,relaxing, and so beautiful it createschanges in the body/mind and spirit.Princess Christina of The Netherlands,interestingly enough, has been reportedto chant along with this CD.
Parachute Associates announces thatSue Cullen, owner of Sue Cullen andAssociates, has been selected as theauthorized Parachute Associate forAustin. Parachute Associates is thelife/work consulting firm authorized byRichard N. Bolles to offer "What ColorIs Your Parachute?" workshops for jobhunters and career changers in NorthAmerica. Sue Cullen and Associates pro-vides career development services, as wellas training and team building workshops, for a wide variety of individuals and organizations. ✯
INSIDE TPA
10 Texas Psychologist SPRING 2002
The contributors to this issueare investigators in an
unprecedented national study ofbipolar disorder, the largest clini-cal trial ever conducted for bipo-lar disorder. The SystematicTreatment Enhancement Programfor Bipolar Disorder (STEP-BD)began enrolling individuals in1999 and is both an efficacy andeffectiveness study. The principalsite of the study is HarvardUniversity, headed by Gary Sachs,MD, and Michael Thase, MD.The STEP-BD is funded by theNational Institute of MentalHealth and investigates bothpharmacological and psychosocialtreatments for an estimated 5,000patients.
The study will continue for upto eight years, possibly longer, inorder to follow these individuals long-term.Any person with a diagnosis of bipolar dis-order, cyclothymia or schizoaffective disor-der, bipolar type may be enrolled. Minimalexclusion criteria will provide researcherswith essential answers on the course andtreatment of bipolar disorder. Additionalinformation about STEP-BD, and contactinformation for interested clinicians orindividuals can be found on the web sitewww.stepbd.org.
This issue will provide an overview oftopics relevant to clinicians in the diagnosis
and treatment of bipolar disorder. Giventhe strong biological component of bipolardisorder, you will see contributions by psy-chiatrists, psychologists, and psychothera-pists. We take this approach because abiopsychosocial approach to treatment isparticularly relevant in bipolar disorder. Inthe first article I discuss current issues indiagnosis, and the state of the evidence ofpsychosocial treatments for bipolar disor-der. The seemingly increasing prevalencerate of bipolar disorder is explored, as wellas viewpoints about modern classifications
for bipolar disorder. I also sum-marize psychosocial treatment inbipolar disorder and promising
studies. From an integrative per-spective, I provide specific recom-mendations for determining a
psychotherapy treatmentapproach in bipolar disorder.
The second article by CherylGonzales, MD, provides clini-cians with an overview of themedication management issuesthat clinicians observe and maytreat in psychotherapy. First, psy-chological issues that emerge andmay impact adherence to medica-tions and successful psychothera-py are outlined. Dr. Gonzalesthen provides us with up-to-dateinformation on mood stabilizersand other medications used in thetreatment of bipolar disorder.
Common side effects and issues related topharmacological treatments are discussed,as increased awareness and intervention bythe psychotherapist can improve the effec-tiveness and adherence to treatment. Thisarticle will be a handy reference in workingwith the medical complexity of this disorderin psychotherapy.
The third article, by Barbara Kertz, MS,and Holly Zboyan, BA, takes a look at theissue of pregnancy for women who havebipolar disorder. Potential risks to themother, fetus and the newborn are out-
Guest Editor
Welcome to the spring issue of Texas Psychologist, focus on bipolar disorder. There has been an
increased public and professional interest in bipolar disorder, and mental health professionals are
treating individuals with bipolar disorder in increasing numbers. These patients seek answers from us
about the most beneficial treatments to this complex and chronic disorder.
Focus on Bipolar DisorderJodi M. Gonzalez, PhD
Focus on Bipolar Disorder

Texas Psychologist 11SPRING 2002
lined, whether the mother chooses toremain on medication or discontinue.Psychotherapy can be of primary impor-tance with women and their partners whenthe choice is to discontinue medication.Also, a promising new potential mood sta-bilizing agent of low risk to mother andfetus, omega 3 fatty acids, is described. Thisarticle provides information for clinicians toshare and discuss with women who are con-sidering pregnancy.
The last contribution to this issue is aninterview with Charles Bowden, MD, aninternationally recognized expert in bipolardisorder research and practice. Dr. Bowdendiscusses his viewpoints on the DSM IVdescriptions of bipolar disorder and changeswe might observe in the DSM in the future.He informs us about some of studies cur-rently underway in bipolar disorder. Finally,Dr. Bowden provides his opinions on pro-viding psychosocial treatment for bipolardisorder.
Our hope for this issue is to providethe reader with an up-to-date summary ofcurrent issues that researchers and clini-cians face in the diagnosis and treatmentof a complex disorder. Due to limitationsof time and space, important areas werenot covered. Areas that warrant furtherdiscussion include bipolar disorder inchildren and adolescents, bipolar disorderin the elderly, and psychological assess-ment for bipolar disorder. The field is wit-nessing numerous advances in these areasand in bipolar disorder in general, andthere will be much beneficial research infuture years that is relevant to the individ-uals that clinicians see in their psy-chotherapy practices.
An integrative approach to bipolar disor-der treatment guided this issue. In closingthis introduction, the words of a personwho suffers with bipolar disorder best sum-marize why in bipolar disorder thisapproach is of utmost importance.
At this point in my life, I cannot imagineleading a normal life without both takinglithium and being in psychotherapy. Lithiumprevents my seductive but disastrous highs,diminishes my depressions, clears out the wool
and webbing from my disordered thinking,slows me down, gentles me out, keeps me fromruining my career and relationships, keeps meout of a hospital, alive, and makes psychother-apy possible. But, ineffably, psychotherapyheals. It makes sense of the confusion, reins inthe terrifying thoughts and feelings, returnssome control and hope and possibility of learn-ing from it all. Pills cannot, do not, ease oneback into reality; they only bring one backheadlong, careening, and faster than can beendured at times. Psychotherapy is a sanctu-ary, it is a battleground, it is a place I havebeen psychotic, neurotic, elated, confused anddespairing beyond belief. But, always, it is
where I have believed – or have learned tobelieve – that I might someday be able to con-tend with all of this.
No pill can help me deal with the problemof not wanting to take pills; likewise, noamount of analysis alone call prevent mymanias and depressions. I need both. It is anodd thing owing life to pills, one’s own quirksand tenacities, and this unique, strange andultimately profound relationship called psy-chotherapy. ✯
Jodi M. Gonzalez, PhDUniversity of Texas Health Science CenterSan Antonio, Texas
To a person working toward recovery, every little bump, twist, turn or rough spot in the
journey can seem insurmountable. They look to you for support and guidance. That’s
where Hazelden can help. Hazelden Foundation offers professionals easy. access to a
world of adolescent & adult chemical dependency information, support, services and
training. Proven tools. that can help you better ease your clients down the road.
We can help you get your c l i ents over
t h o s e i n e v i ta b l e l i t t l e b u m ps o n t h e roa d t o re c o v e r y .
We can help you get your c l i ents over
t h o s e i n e v i ta b l e l i t t l e b u m ps o n t h e roa d t o re c o v e r y .
©2002 Hazelden Foundation
Texas Psychologist 13SPRING 2002
This article summarizes current knowledge in the diagnosis and treatment of bipolar disorder.Suggestions for new classification systems in bipolar disorder and viewpoints on broadening what isconsidered the bipolar spectrum are discussed. From these issues, we provide specific recommenda-tions in bipolar disorder diagnosis. The article then shifts focus to treatment, and the history of thepsychosocial treatment of bipolar disorder is reviewed. Psychotherapy studies are summarized, as wellas recommendations for approaches that may be particularly beneficial in bipolar disorder treatment.
Jodi M. Gonzalez, PhDUniversity of Texas Health Science Center
San Antonio, Texas
Bipolar disorder is a serious mental ill-ness characterized by a chronic course,
often requiring lifelong psychiatric and psy-chological intervention. In a national epi-demiological survey conducted in 1990 to1992, the prevalence rates for bipolar I dis-order were reported at 1.6% of the U.S.population (Kessler, 1994). In the lastdecade, the phenomenology considered toencompass bipolar disorder has evolved and
recent studies refer to the disorder morebroadly as the “bipolar spectrum” (Akiskalet al., 2000; Cassano et al., 1999). Withthis evolution, prevalence rates have recent-ly been proposed to be as high as 5%-8%(Akiskal et al.).
Consequently, psychologists are treat-ing more individuals who carry a bipolardiagnosis, and psychological treatmentsare being formalized and studied foreffectiveness. It is essential that psycholo-gists integrate and incorporate thisnascent literature on bipolar disorder intothe provision of effective psychologicaltreatments. This article will provide anoverview of current knowledge in thediagnosis and treatment of disorders inthe bipolar spectrum.
Diagnosing Bipolar DisorderDiscussions about nosology and diagno-
sis in psychiatry are commonplace. A cen-tral issue for classification systems is deter-mining what symptom, cluster of symp-toms, or characteristic of a disorder is itssine qua non, or essential element. In recentyears, the sine qua non of bipolar disorderhas been the existence of one manic orhypomanic episode, in the classic form as
DSM IV defines it. In the early 1900s,when Kraepelin developed the first widelyused nosological system in psychiatry, theessential element of manic-depression wasthe cyclical nature of the disorder. Kraepelinincluded unipolar depression in the manic-depressive spectrum, as depressive episodeswere cyclical. This was contrasted withDementia Praecox (Schizophrenia), whichhe viewed as having a chronic, non-cyclicalcourse (Kraepelin, 1913/1921).
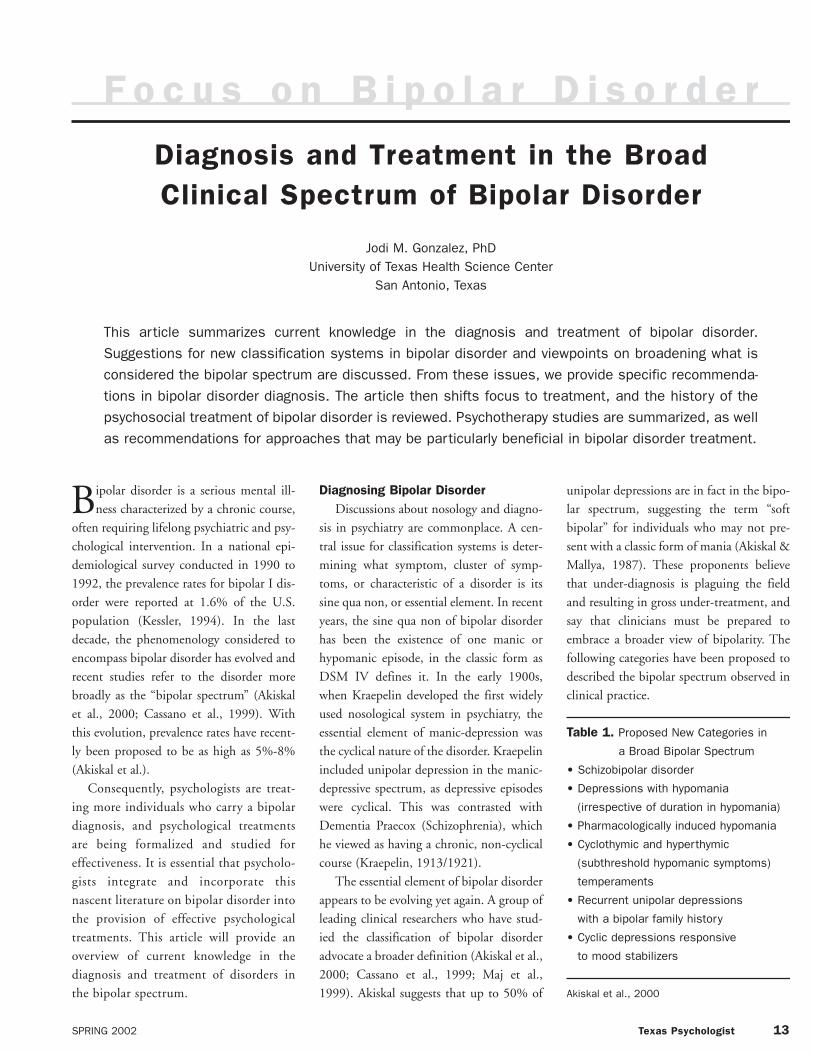
The essential element of bipolar disorderappears to be evolving yet again. A group ofleading clinical researchers who have stud-ied the classification of bipolar disorderadvocate a broader definition (Akiskal et al.,2000; Cassano et al., 1999; Maj et al.,1999). Akiskal suggests that up to 50% of
unipolar depressions are in fact in the bipo-lar spectrum, suggesting the term “softbipolar” for individuals who may not pre-sent with a classic form of mania (Akiskal &Mallya, 1987). These proponents believethat under-diagnosis is plaguing the fieldand resulting in gross under-treatment, andsay that clinicians must be prepared toembrace a broader view of bipolarity. Thefollowing categories have been proposed to
described the bipolar spectrum observed inclinical practice.
Table 1. Proposed New Categories in
a Broad Bipolar Spectrum
• Schizobipolar disorder
• Depressions with hypomania
(irrespective of duration in hypomania)
• Pharmacologically induced hypomania
• Cyclothymic and hyperthymic
(subthreshold hypomanic symptoms)
temperaments
• Recurrent unipolar depressions
with a bipolar family history
• Cyclic depressions responsive
to mood stabilizers
Akiskal et al., 2000
F o c u s o n B i p o l a r D i s o r d e r
Diagnosis and Treatment in the BroadClinical Spectrum of Bipolar Disorder

14 Texas Psychologist SPRING 2002
These categories describe the variety ofmood disturbance observed in clinical prac-tice today, and a suggested modern defini-tion of bipolar disorder. What is unclearfrom these categories is what will constitutethe essential element(s) of the disorder.
Not all experts agree that expanding thediagnosis of bipolar disorder is appropriate,and in the most troublesome case maymake the diagnostic entity meaninglessfrom both a clinical and research perspec-tive (Soares & Gershon, 2000; Baldessarini,2000). One example that Baldessarini(2000) cites is the emergent literature show-ing that lithium is not as effective in thecurrent treatment of bipolar disorder asreported in early studies of lithium. Inrecent literature describing the bipolarcourse, individuals are characterized asmore chronic and severe than previousstudies, suggesting a different population isbeing studied. The increased heterogeneitymay be especially relevant in genetic andpathophysiological research, which forsome purposes requires the most pure ofphenotypes to most efficiently elucidate thepathophysiology of bipolar disorder. Soaresand Gershon (2000) note, “the movetowards inclusion of increasing heteroge-neous groups of patients under this diag-nostic category threatens to jeopardize clin-ical research, and would be a disservice tothe field” (p. 1).
Another argument is the issue of moodvariation, which exists in many other disor-ders of putatively different etiologies. It isnoted, “Given the finite limits of how ourspecies can react psychopathologically, it ishardly surprising that affective instabilityand fluctuations of mood can be found inmany, if not most, other disorders”(Baldessarini, 2000, p. 5). Equally concern-ing is the significant risk of pathologizingnormal mood variation if we do not includerequirements of duration symptoms andsignificant impairment.
Recommendations for diagnosis. Itmay take a considerable length of time tofollow the course of an illness before aunipolar, bipolar, or other diagnosis can beapplied with confidence. One instrument
now being validated that has potentialfuture benefit is the SCI-MOODS, anadjunct to the Structured Clinical Interviewfor Diagnosis (SCID). The SCI-MOODSassesses the mood spectrum and relatedsymptoms in greater depth, allowing for amore accurate diagnosis (Cassano et al.,1999). Until the instrument or others areavailable, the following are recommenda-tions for improving diagnostic accuracy andclarity:• A thorough clinical history is required
with presentations of depression, as indi-viduals will rarely present for treatment ina manic state and may have little memoryor insight into past manic episodes.Obtaining past medical records and col-lateral information directly from lovedones can provide a more comprehensivehistory. Questions in attempting to elicit ahistory of mania when interviewingpatients are:
° How is your mood right before youbecome depressed (or directly after)?
° Are there times when others say youaren’t your usual self?
° Have there been times when you wereespecially productive?
• Asking for specific events such as financialdifficulties, relationship problems, druguse, etc. that someone may not haveattributed to their mood state.
• In treating someone diagnosed withunipolar depression who is not respond-ing to antidepressants, or responds atypi-cally to anti-depressant treatment, consid-er a re-evaluation of bipolar disorder. Itwill be especially important to considerthis in individuals with hyperthymic andcyclothymic temperaments.
• A significant family history of bipolar dis-order may be suggestive of a bipolar-typedepression (i.e., a depression that mayrespond better to a mood-stabilizer).
Mood stabilizers can reduce the severityof mood episodes significantly. That is,episodes while being treated may be “break-through” symptoms rather than full-blownepisodes. This is important to considerwhen diagnosing because the mood states
observed may not be of the same severity ofpast episodes prior to medication treat-ments. A diagnosis could be missed when a
hypomanic or irritable mood does not meetcriteria.
With the recent broadening of criteria,there currently are no agreed upon methodsfor classifying atypical mood disorders sure-ly being observed in psychologists’ prac-tices. Clinicians can include the above rec-ommendations for diagnosis so that theindividual receives the most beneficial phar-macological and psychological treatmentsavailable.
Psychosocial Treatment in Bipolar Disorder
Prior to the discovery of effective phar-macological interventions, psychoanalysispredominated in the outpatient treatmentof bipolar disorder. After the discovery oflithium, lithium clinics were opened toimprove management of the disease. Indescriptions of treatment provided in theseclinics, psychosocial treatment was animportant aspect of treatment, in the formof psychoeducation, formal therapy, andsupportive self-help therapy (e.g., Fieve,1975). From these promising psychothera-peutic beginnings, one might expect a pro-liferation of psychotherapy and then out-come studies for bipolar disorder. However,it is perplexing at times to see the lack of
emphasis in the psychotherapy research lit-erature on bipolar disorder. In a recentreview of psychotherapy outcome studies(Swartz & Frank, 2001), only 21 conduct-ed studies were identified as methodologi-cally sound for review.
There are various reasons for the insuffi-cient emphasis on psychological treatments.First, it is a general clinical belief that psy-chotherapy has little impact on mania, theessential element of bipolar disorder. Thisbelief is supported by research, especiallythose studies that have looked at moresevere manic episodes (Swartz & Frank,2001). This knowledge likely has led manypsychiatrists and psychologists to de-emphasize psychological interventions.Second, although the 1990s saw an explo-

Texas Psychologist 15SPRING 2002
sion of psychotherapy research, the 1990swere also labeled as the decade of the brain,and bipolar disorder is known a “brain dis-ease.” Thus, the productive explosion inbipolar research was seen in genetic, struc-tural, and psychopharmacological studies.A third contributor to the lack of psy-chotherapy research for bipolar disorder isfound in the amount of research fundingfor bipolar disorder, as compared to unipo-lar depression or anxiety. So, in more gener-al ways bipolar disorder has been neglected.Finally, and probably the most compellingargument, is that almost no clinician orresearcher would argue that medicationshould not be the first line of treatment anda primary focus of study in bipolar disorder.Even so, most pharmacological treatmentsdo not prevent recurrence and functionalimpairment in a substantial portion of indi-viduals with bipolar disorder (Goldberg &Harrow, 2001).
Fortunately, what psychotherapy litera-ture does exist suggests that psychologicaltreatments can have a significant impact ofthe clinical course and outcome for bipolardisorder (Swartz & Frank, 2001). TheAmerican Psychiatric Association, ExpertConsensus Guidelines, and the CanadianPsychological Association recommendadjunctive psychotherapy for treatment ofbipolar depression (APA, 1994; Frances etal., 1998; Kusumakar & Yatham, 1997).For example, the Consensus Guidelines rec-ommend mood stabilizers as a first line oftreatment in depression, followed by theaddition of either psychotherapy or antide-pressant medication (Frances et al., 1998).Guidelines also list psychodynamic, cogni-tive, interpersonal, behavioral, marital/fam-ily, and group therapy as potentially benefi-cial treatment modalities.
The 21 conducted studies reviewed bySwartz and Frank (2001) measured disease-specific outcomes, functional outcomes(e.g., quality of life, social or occupationalfunctioning), and in some cases cost-analy-ses (dollars lost or saved by individuals,organizations, or government). Positive out-comes documented were decreases in hospi-talization, decreased relapse rates, enhanced
medication adherence, and a clinicalimpression of overall improvement. For thedepressive phase of bipolar, psychotherapyshowed the most promise. Psychotherapiesdemonstrating significant improvement inbipolar depression were cognitive-behav-ioral therapy, family-focused therapy, andinterpersonal social rhythm therapy. Withthe exception of one important study(Perry, Tarrier, Morriss, McCarthy & Limb,1999), the authors found little evidencethat the emergence of mania (the moresevere type) can be prolonged or preventedwith psychotherapy. The Perry et al. (1999)study found that a psychoeducational/behavioral intervention produced a signifi-cantly longer time to relapse into mania.Finally, the review reported that psychoedu-cation, group, and psychodynamic thera-pies demonstrated beneficial outcomes,although it was not clear on what phase ofthe disorder.
Concerns and limitations in the reviewedpsychotherapy research are the ever-presentefficacy-effectiveness issue (i.e., will a clini-cal trial intervention be beneficial in real-world clinical practice?). That is, as bipolardisorder diagnoses are broadening, consen-sus guidelines for bipolar research studies areasking for a narrowing of eligible study par-ticipants. Specifically, the guideline is toexclude “less severe manic symptoms”(Angst et al., 2000). Thus, how likely arethese participants to be representative ofthose seen and treated in clinical practice?
Other studies on psychotherapy treat-ment take a more qualitative approach,describing key elements in the psychothera-py of individuals with bipolar disorder(Bauer & McBride, 1996). A review ofstudies on psychosocial treatments for bipo-lar disorder identified key elements that arelisted in Table 2.
The breadth of these key elementsshould not be too surprising, given that var-ious psychotherapy modalities seem to holdpromise in bipolar disorder. This breadthsupports the idea of an integrative model ofproviding psychotherapy, where factorssuch as disorder quality, stage of change,motivation level, support system and treat-
ment goals all inform the psychotherapyapproach (Norcross, 2001). This integra-tion may have various combinations—either phase-specific approaches or integra-tion throughout treatment. For phase-spe-cific, psychoeducation seems to be emerg-ing as an important first phase of treatment.We name a few examples although there areseveral. One group psychotherapy understudy, the Life Goals Program, has psychoe-ducation as the first phase and then behav-ioral and group methods in the later phaseof treatment (Bauer & McBride, 1996).The Family Focused Treatment approachutilizes psychoeducation in initial phasesand family and behavioral treatments inlater phases (Miklowitz & Goldstein,1997). Other approaches integrate tech-niques throughout treatment, such as a
group therapy approach that incorporatespsychoeducation, group theory and psycho-dynamic approaches throughout (Kanas,1999), or Interpersonal Social RhythmTherapy which utilizes interpersonal andbehavioral (circadian-rhythm) techniques(Frank et al., 1994).
Table 2. Key Elements in thePsychotherapy of BipolarDisorder Identified inDescriptive Reports
Predominantly psychoeducation
Education regarding illness and treatment
Illness management skills
Predominantly problem-solving/coping
Work Management
Family Management
Life goals outside of illness
Predominantly psychodynamic/interpersonal
Dealing with unstable interpersonal
relationships
Coping with loss
Vulnerability
Self-concept
M. Bauer & L. McBride (1996) Structured Group
Psychotherapy for Bipolar disorder: The Life Goals Program.

16 Texas Psychologist SPRING 2002
Bipolar-Specific ApproachesAlthough an integrative approach is
indicated when looking at the clinical andresearch literature, the literature alsoacknowledges specific techniques that maybe essential to incorporate in the treatmentof bipolar disorder. The followingapproaches can inform treatment and pro-vide important information and feedbackduring the course of treatment:
Psychoeducation. One significant dif-ference with bipolar disorder seems to bethe amount of education necessary toinform patients meaningfully about thischronic, episodic, and complex disorder.For example, there are at least potential fivetreatment foci, 1) mania, 2) depression, 3)relapse prevention, 4) sequelae of severeepisodes, and 5) substantial cognitive andphysical effects of medications.Additionally, assisting the individual inunderstanding and characterizing whichcriteria and course modifiers are or are notapplicable to them. Education also involves“working through” in an extreme degree,with repetition necessary in the context ofthe patient’s current experiences, both suc-cesses and travails.
At times patients will seek specialists,saying that their therapist has a lack ofunderstanding of bipolar disorder. Itbehooves clinicians who treat individualswith bipolar disorder to have a good basicknowledge about the disorder and commu-nicate this to patients. (See recommendedreadings).
Team Approach. Because of the severityof the illness and potential for suicide,mania, and psychosis, a team approach isoften necessary, involving both the psychia-trist and family. In some cases, the family isalready involved already in the patient’scaretaking. We recommend that if a familymember (or loved one) functions as a care-taker, regardless of the patient’s age, theyshould participate in treatment as needed.A value of this, unique to bipolar disorder,is that in many instances the family mem-ber will recognize and accurately report onimportant behavior, e.g., irritability, risk-taking involvements, and impulsivity that
the patient both does not perceive and doesnot display in the structured environmentof the office.
As well as educating the family and sum-moning their assistance during treatment,family involvement aids in conceptualiza-tion of the family system and the beneficialor harmful role to the person’s functioning.Having a family member attend a monthlysession, or for a specific period of time, willelucidate how bipolar disorder outcomesimpact the family and how the familyimpacts the disorder. Some opponentsmight suggest that family involvement pro-motes dependency, which indeed can occur.In the case of bipolar disorder, however,family involvement more serves to improveeffectiveness of relationships than to pro-mote or deal with dependency.
Charting. Bipolar experts advocate lifecharting, mood charting, and social rhythmcharting in bipolar disorder. Life chartingcan be indispensable in trying to under-stand the course of the disease, precipitatingfactors and treatment effects, for bothpatients and clinicians. Life charting is amacro documentation of the course of thedisorder, typically episode duration, fre-quency and severity, including time of year,medication regimen at the time of episodes,and relevant stressors that may have con-tributed to episodes. Mood charting docu-ments specific mood episodes or states indetail where weekly or even daily variationin mood are noted. Mood charting is bene-ficial in ascertaining if there are mood vari-ations related to time of day, menstrualcycle, dosing, medication changes, etc.Daily mood charting can also remind some-one to take medication, and promote activeparticipation in the treatment process.Mood charting can be taken to doctor visitsto serve as a reminder of previous weeks; fewof us can accurately recall past symptomswith clarity. Finally, there is emerging evi-dence that circadian rhythms may influencebipolarity and episode onset. For example,jet lag, loss of sleep, and irregular schedulesthat upset the regularity of circadianrhythms are suggested to increase the likeli-hood of episode onset. With individuals
whose daily routines, especially sleep pat-terns, are disrupted this would be importantto address. Other “rhythms” include inter-personal interactions, mealtimes, work andschool schedules, and travel.
Comorbity. Lifetime comorbidity ratesare high in bipolar disorder, with 71% forsubstance use and 93% for anxiety disorders(Kessler et al., 1997). In a recent study,25% of euthymic bipolar individuals werefound to meet criteria for personality disor-ders (Vieta et. al, 2001). Comorbid condi-tions are often additional if not primary fociof treatment. The iatrogenic effects of med-ications may also require therapeutic atten-tion, such as side effects of mood stabilizersand other psychiatric medication as well asthe possible changes in course of the diseasethat these medications may cause (e.g.,rapid cycling, mixed episodes).
Length of treatment. Length of treat-ment is an important consideration in bipo-lar disorder. As is true with the pharma-cotherapy for bipolar, we advocate a long-term approach to psychotherapy treatment.Estimates suggest that only about 15% to20% of patients have good overall function-ing or complete remission after an index
episode (Goldberg, Harrow & Grossman,1995). Thus, the expectation that short-term psychotherapy will significantly alterthe course of bipolar disorder seems over-optimistic. Often, however, clinicians andresearchers apply this short-term model inclinical trials and conclude that psychother-apy is not beneficial. We would argue thatthe dose-response issue should be resolvedbefore concluding a lack of efficacy. Forexample, suppose that someone is pre-scribed a daily dose of divalproex 1500 mgfor 6 months of treatment (short-term bypharmacotherapy standards), and thentitrated off.
Suppose the patient has a recurrence ofmania, and we conclude that divalproex hasno efficacy with bipolar disorder. It wouldbe spurious to conclude a lack of efficacy
for the medication yet that is what we oftenconclude with psychotherapy. Ellen Frank,a leading researcher in the psychotherapytreatment of bipolar disorder, noted that

Texas Psychologist 17SPRING 2002
because of the chronicity of the disease, ter-mination is often not indicated even afterlong-term treatment. Long-term treatmentshould not necessarily be translated thatweekly psychotherapy is indicated indefi-nitely, but may include monthly orbimonthly visits, for example. These visitsmaintain the connection with the providerin case emergencies or adherence issuesoccur, and is a similar model to treatment ofchronic disease in psychiatry and generalmedicine.
Summary and ConclusionsDiagnosis and treatment in bipolar dis-
order are primary concerns of clinicians andresearchers, as the course of the disorder canbe severe, chronic and very difficult to treat.New research suggests that what we view asbipolar and amenable to mood stabilizingtreatments would benefit from broadeningwhat we view as the bipolar spectrum.Broadening of the bipolar spectrum maylead to confusion and disagreements indiagnosis and classification, with some clin-icians following DSM IV criteria and otherstaking a broader, spectrum view. Untilmodern classification issues are resolved, wehave included recommendations forimproving diagnostic accuracy with boththe classic and broader views in mind.
Psychological treatments developed forbipolar disorder are increasing in the litera-ture. This literature suggests good evidencethat psychotherapy can have significantpositive clinical effects on the course andoutcome of the illness. In addition to thereview of therapy approaches, we have alsooutlined key elements and various tech-niques the clinician can emphasize duringtreatment.
Given the complexity of this disorderand heterogeneity of the population weadvocate an integrative, patient-specificapproach to treatment. A decision aboutwhat modality and interventions to use, inaddition to psychotherapist expertise andpreference, should be based on patientcharacteristics such as clinical presentationand phase, interpersonal issues, level offunctioning and comorbid problems. ✯
Recommended ReadingFor a review of studies of the relation-
ship of family functioning to bipolar disor-der and a family treatment based on thisresearch: Miklowitz, D.J. & Goldstein,M.J. (1999). Bipolar disorder: A family-focused treatment approach. New York, TheGuilford Press.
For a psychoeducational self-help guidefor families and individuals with bipolardisorder: Miklowitz, D.J. (2002). The bipo-lar disorder survival guide. New York:Guilford Press.
For a comprehensive review of bipolardisorder, with chapter contributions by lead-ing researchers: Goldberg, J. and Harrow,M. (eds.) (1999). Bipolar disorders: Clinicalcourse and outcome. Washington D.C.,American Psychiatric Press.
For a review of diagnostic issues in bipo-lar disorder: Akiskal, H., Bourgeois, M.L.,Angst, J., Post, R., Moller, H.J., Hirschfeld,R. (2000). Re-evaluating the prevalence ofand diagnostic composition within thebroad clinical spectrum of bipolar disorders.Journal of Affective Disorders, 59, S5-S30.
For a review of psychosocial treatmentsin bipolar disorder: Swartz, H.A., & Frank,E. (2001). Psychotherapy for bipolardepression: A phase specific treatment strat-egy? Bipolar Disorders, 3, 11-22.
REFERENCES
Akiskal, H., Bourgeois, M.L., Angst, J.,
Post, R., Moller, H.J., & Hirschfeld, R.
(2000). Re-evaluating the prevalence of
and diagnostic composition within the
broad clinical spectrum of bipolar disor-
ders. Journal of Affective Disorders, 59,
S5-S30.
Akiskal, H., & Mallya, G. (1987). Criteria
for the ‘soft’ bipolar spectrum:
Treatment implications. Psychopharm-
acological Bulletin, 23, 68-73.
Angst, J., Bowden, C.L., Calabrese, J.R.,
Chengappa, R., Goodwin, G., Lecrubier,
Y., Licht, R., Nolen, W.A., Sachs, G.,
Saint Raymond, A., Storosum, J.,
Suppes, P., & van Ree, J.M. (2001).
ECNP Consensus Meeting, March
2000, Nice guidelines for investigating
efficacy in bipolar disorder. European
Neuropsychopharmacology, 11, 79-88.
American Psychiatric Association (1994).
Practice guideline for the treatment of
patients with bipolar disorder. American
Journal of Psychiatry, 151(Suppl. 12),
1-36.
Baldessarini, R.J. (2000). A plea for the
integrity of the bipolar disorder concept.
Bipolar Disorders, 2, 3-7.
Bauer, M.S., & McBride, L. (1996).
Structured group psychotherapy for
bipolar disorder: The life goals program.
New York: Springer Publishing Company,
Inc.
Cassano, G.B., Dell’Osso, L., Frank, E.,
Miniati, M., Faglioni, A., Shear, K., Pini,
S., & Maser, J. (1999). The bipolar
spectrum: A clinical reality in search of
diagnostic criteria and assessment
methodology. Journal of Affective
Disorders, 54(3), 319-328.
Fieve, R. (1975). The lithium clinic. A new
model for the delivery of psychiatric ser-
vices. American Journal of Psychiatry,
132, 1018-1022.
Frances, A.J., Kahn, D.A., Carpenter, D.,
Docherty, J.P., & Donovan, S.L. (1998).
The expert consensus guidelines for
treating depression in bipolar disorder.
Journal of Clinical Psychiatry, 59
(Suppl. 4), 73-79.
Frank, E., Kupfer, D.J., Ehlers, C.L., Monk,
T.H., Cornes, C., Carter, S., & Frankel,
D. (1994). Interpersonal and social
rhythm therapy for bipolar disorder:
Integrating interpersonal and behavioral
approaches. The Behavior Therapist,
17, 143-149.
Goldberg, Harrow & Grossman (1995).
Course and outcome in bipolar affective
disorder: A longitudinal follow-up study.
American Journal of Psychiatry, 152,
379-384.
Kanas, N. (1999). Group therapy with
schizophrenic and bipolar patients:
Integrative approaches. In V. Schermer
& M. Pines (Eds.) Group psychotherapy
of the psychoses: Concepts, interven-
tions and contexts. London, Jessica
Kingsley Publishers.
18 Texas Psychologist SPRING 2002
Kessler, R. C., McGonagle, K.A., Zhao, S.,
Nelson, Ch.B., Hughes, M., Eshlemen,
S., Wittchen, H.U., Kendler, K.S.
(1994). Lifetime and 12-month preva-
lence of DSM III-R psychiatric disorders
in the United States: Results from the
National Comorbidity Survey. Archives
of General Psychiatry, 51(1), 8-19.
Kessler, R.C., Rubinow, D.R., Holmes, C.,
Abelson, J.M., & Zhao, S. (1997). The
epidemiology of DSM-III-R bipolar1 disor-
der in a general population survey.
Psychological Medicine, 27, 1079-1089.
Kraepelin, E. (1913/1921). Manic-depres-
sive insanity and paranoia. Edinburgh,
ES Livingstone.
Kusumakar, V., & Yatham, L.N. (eds.)
(1997). The treatment of bipolar disor-
der: Review of the literature, guide-
lines and options. The Canadian
Journal of Psychiatry, 42 (Suppl. 2),
67S-100S.
Maj, M., Pirozzi, R., Formicola, A.R., &
Tortorella, A. (1999). Reliability and valid-
ity of four alternative definitions of rapid-
cycling bipolar disorder. American Journal
of Psychiatry, 156(9), 1421-1424.
Norcross, J. (November, 2001). Empirically
Supported Psychotherapy Treatments.
Grand Rounds Presentation, Depart-
ment of Psychiatry, San Antonio, Texas.
Perry, A., Tarrier, N., Morriss, R.,
McCarthy, E., & Limb, K. (1999).
Randomised controlled trial efficacy of
teaching patients with bipolar disorder
to identify early symptoms of relapse
and obtain treatment. British Medical
Journal, 318, 149-153.
Soares, J.C., & Gershon, S. (1999). The
diagnostic boundaries of bipolar disor-
der. Bipolar Disorders, 1, 1-2.
Swartz, H.A., & Frank, E. (2001).
Psychotherapy for bipolar depression: A
phase specific treatment strategy?
Bipolar Disorders, 3, 11-22.
Vieta, E., Colom, F., Corbella, B., Martinez-
Aran, A., Reinares, M., Benabarre, A., &
Gasto, C. (2001). Clinical correlates of
psychiatric comorbidity in bipolar I
patients. Bipolar Disorders, 3, 253-258.
Help is hereOutside Medical Billing designed specifically for the Psychological and Licensed Therapy Industry.
• Many T.P.A. Member Testimonials on File• No more HCFA’s to make week after week• Free follow-up on any problem• Free office setup, free pickup and delivery• Working with over 600 Government and
Commercial Insurance Companies
Are you paper claims now? We cansolve a great deal of your problemswith medical billing. We havestate-of-the art software andstate-of-the-art knowledge.
Call or fax us today.
AMERICAN PROFESSIONAL ELECTRONIC SERVICES A.P.E.S.
Phone: 254-773-9000Fax: 254-773-9000
Let our muscles get you your money!
Texas Psychologist 19SPRING 2002
AbstractThe treatment of bipolar disorder is a complicated, multifaceted process. This article seeks to definethe common challenges faced by the non-physician professional treating the bipolar patient. It willdescribe the advantages and disadvantages of the traditional and newer medications physicians areprescribing for bipolar disorder, and address how these issues may ultimately affect the therapy of thebipolar patient. Upon the completion of this article, the clinician should have an increased under-standing of the common medications utilized in the treatment of bipolar disorder and related issuesthat ultimately affect adherence to treatment.
Medication Management Issues in Psychotherapy of Bipolar Disorder
Cheryl Gonzales, MDUniversity of Texas Health Science Center
San Antonio, Texas
Bipolar disorder is a common conditionaffecting between 1%-2% of the popu-
lation (Regier et al., 1988). Persons afflictedwith bipolar disorder are a heterogeneousgroup, and the condition affects personsequally irrespective of nationality, race, orgender. The commonality of bipolar disor-der lies in the severe mood disturbance,which, if left untreated, can lead to signifi-cant personal, familial, and occupationaldisruption. Fortunately, with good pharma-cological and psychological intervention,significant benefit and good outcomes canbe achieved.
It is well accepted by clinicians thatmedication should be the first line of treat-ment in bipolar disorder. The past 20 yearshave brought many changes to the field ofpsychiatry, including a host of new medica-tion options available with the potential totreat bipolar disorder. These are not neces-sarily new medications. Some, such as val-proic acid (Depakote) are established med-ications whose potential to treat bipolar dis-order was essentially untapped until theearly to mid 1990s. The trend in modern
psychiatry is to combine a variety of med-ications until the desired effect is achievedand the patient’s mood symptoms go intoremission. This approach has allowed manypatients to have fewer and less severe moodepisodes. However, the increased complexi-ty in medication regimens can lead to otherchallenges for psychiatrists. Medicationissues are also relevant for psychotherapists,who observe psychological and physicaleffects of pharmacology and then provideanswers to patients about the impact ofmedications. This article will provide a briefoverview of issues relevant for psychothera-pists treating individuals with bipolar disor-der, in order to provide essential feedbackboth to the patient and the collaboratingpsychiatrist.
Benefits of Psychotherapy for Bipolar Disorder
Given the complexity of the illness andtreatment, the person with bipolar disorderoften requires a multifaceted approach tohis or her care. Medications are of greatbenefit and can have dramatic improve-
ments on the severity and length of moodepisodes, but they are far from the idealtreatment we seek for our patients. The psy-chotherapy of the bipolar patient, while achallenge, can be a rewarding experience forboth patient and clinician alike, and aninvaluable contribution to their pursuit ofhealth.
One particularly challenging aspect oftreatment is the development of insightregarding the nature of the illness and theneed for ongoing treatment. As with any
chronic disease, particularly one that strikesat such a young age, the acceptance of bipo-lar disorder may be a struggle. While somepatients express relief that they have a diag-nosis and know what is wrong with them,others react with anger and denial. Helping
individuals deal with their anger and denialis profoundly important to the establish-ment of the long-term doctor/ patient rela-tionship needed to maximize recovery.
Another area where bipolar individualstypically need the help of an outside party isin recognition of certain target symptoms.Many patients with bipolar disorder will
F o c u s o n B i p o l a r D i s o r d e r

20 Texas Psychologist SPRING 2002
have a pattern of symptoms that herald animpending manic or depressive episode. Forexample, many patients experience subclin-ical changes in sleep, appetite, or energybefore they develop a clinical syndrome ofmania or depression. If recognized early andtreated aggressively, the potential exists tosideline the oncoming episode before itbegins; patients must be insightful andobservant of their mood and related symp-toms before this method can be successful.
A major mental illness is never con-tained solely in the person who suffers it.The effects on family and friends are signif-icant and sometimes profound. For this rea-son, psychotherapy with a bipolar individ-ual almost always involves some level offamily intervention, whether it be talking toa parent, spouse or child during a time ofcrisis, educating them after a new diagnosishas been made, or working with the familyduring a time of calm. Family members canbe invaluable to clinicians as observers, cue-ing into subtle signs the patient may notexhibit while in the therapist’s office, andalerting the patient to symptoms of whichhe or she may not yet be aware.
The development of a major mental dis-order during crucial developmental periodscan be devastating to the individual andinterfere with the healthy acquisition ofgoals. The most common age of onset inbipolar disorder occurs in late adolescenceand early adulthood, a time when mostpeople are finishing school, establishingrelationships, or starting careers. Also, theseverity of the mood disturbance can lead tosuicidal ideation (particularly in thedepressed and mixed manic states), disruptfamily relationships (leading to divorce oralienation from family), and cause the indi-vidual to engage in risky or dangerousbehaviors (with such consequences as lifethreatening sexually transmitted diseases,unplanned pregnancies, and accidentaldeath or serious injury). Persons sufferingfrom depressive disorders, including bipolardisorder, make up the vast majority of peo-ple who commit suicide each year.
Remission of the mood syndrome andmaintenance of remission is the goal of
pharmacotherapy as well as psychotherapy.Prevention of relapse determines the degreeto which the mood disorder is disruptive tothe patient’s life. While this may seemobvious to clinicians, it is not always so toour clients. The amount of insight intoone’s illness is quite variable among indi-viduals with bipolar disorder, and in com-bination with the iatrogenic effects of med-ications, may ultimately lead to adherencedifficulties.
Adherence to PharmacologicalTreatment
One of the greatest frustrations a clini-cian sees is the recurrence of disease due todiscontinuation of effective medications.Most often, the decision is made by ourpatients without our knowledge and againstour medical advice. What factors contributeto our patient’s ultimate decision to discon-tinue medications? A significant few thatdeserve further mention are discussed here.
As previously stated, many personsafflicted with bipolar disorder have signifi-cantly impaired insight into the nature andcourse of their disease. They may not acceptor understand the seriousness of their illnessor, having been stable for some time, mayno longer see the necessity of taking med-ication. Additionally, mild manic episodesoccurring during treatment may lead tomedication discontinuation, thus precipi-tating a full manic episode. Patients indepressive episodes may discontinue med-ications because they feel hopeless that amedication will benefit them, or will dis-continue medication hoping that they willbecome manic, thus ending a painfuldepressed phase.
Patient concerns are often medicationrelated. The medications used in the treat-ment of bipolar disorder may have signifi-cant, unpleasant side effects or associations.Lithium and Depakote, the two most wide-ly utilized mood stabilizers today, bothrequire periodic blood monitoring toensure that the patient’s blood level of med-ication is within a certain range. Low levelsof circulating medication leads to poormedication efficacy, while high levels lead
to a toxic syndrome. With long term use,both medications can begin to affect certainorgans (lithium the kidneys and thyroidgland, Depakote the liver and bloodplatelets). A third medication, Tegretol, alsorequires blood monitoring for levels and itseffects on bone marrow. Blood monitoringcan be a deterrent to take these medica-tions, due to time constraints, fear of nee-dles, or financial concerns.
Side effects to medications can also leadsome patients to discontinue them in frus-tration. Problematic side effects includesedation, acne, cognitive slowing, increasedappetite, hair loss, sexual dysfunction, and,most notably, weight gain. The followingsection will provide an overview of medica-tions and their most common or significantside effects.
A Brief Overview of MedicationsUtilized in Treatment
Medications used to treat bipolar disor-der come from a variety of medicationclasses. These include mood stabilizers,sedatives, antidepressants, and antipsy-chotics. Combinations of medications arefrequently needed to achieve the best out-come, which results in increasingly compli-cated regimens.
The established mood stabilizers consistof lithium, valproic acid, and to a lesserdegree Tegretol. Lithium is commonly
given in the salt form, lithium carbonate,and less frequently, lithium citrate. Lithiumis the first discovered mood stabilizer, andwas approved by the U.S. FDA in 1970 forthe treatment of acute mania. Between 70%and 80% of patients with bipolar disorderhave at least a partial response to lithiumtherapy when utilized in a manic state(Goodwin & Jamison, 1990). Lithium isalso used commonly with other mood sta-bilizers, benzodiazepines, and antipsychoticmedications. Daily dose is variable, butgenerally from 300mg daily to 1500mgdaily in adults. To be properly effective,lithium concentrations in the blood mustbe monitored routinely and kept within adefined therapeutic window. (0.5-1.4mEq/L). Lithium therapy has also been

Texas Psychologist 21SPRING 2002
shown to be a potentiating agent in thetreatment of refractory unipolar depression(de Montigny et al., 1983; Heninger et al.,1983; Price, 1989) and more research isshowing it to be an effective treatment forbipolar depression as well (Goodwin &Jamison, 1990). Lithium does haveunpleasant side effects including weightgain, acne, cognitive dulling, increased uri-nation and over time may affect the kidneysand thyroid gland.
Valproic acid (Depakote), has been inuse since 1978 in the United States as anantiepileptic, and has been utilized moreoften in the treatment of bipolar disordersince the late 1980s. Valproic acid is a firstline treatment for mania, is at least equallyefficacious as lithium, and has benefit inlithium non-responsive patients, particular-ly those who have elements of dysphoriawithin their manic syndromes (Bowden etal., 1994). As with lithium, daily dose isvariable in adults and depends on the serumlevel of the drug, but most patients achievetherapeutic blood levels between doses of500mg and 2000mg daily. Patients takingvalproic acid require blood monitoring tofollow serum drug concentrations, andmonitor any effect the medication is havingon the patient’s liver. Serum drug concen-trations should be between 50-100 micro-grams/mL for the average patient, but maybe titrated up into the low 100’s as thepatient’s clinical situation warrants. Patientson valproic acid may experience side effectssuch as weight gain, experience gastroin-testinal side effects such as nausea andincreased appetite, and neurological symp-toms such as tremor. Gastrointestinal sideeffects are lessened by using the enteric-coated form of the medication (Depakote).One fairly common and distressing sideeffect of Depakote is hair loss. Serious sideeffects to valproic acid are rare, but consistof liver toxicity, pancreatitis, and suppres-sion of blood platelets, which can potential-ly lead to fatal hemorrhage if not diagnosed.It is the clinician’s responsibility to monitora patient’s labs frequently (generally every4-6 weeks during the initial 6 months oftreatment). Intervals between lab work can
then be lengthened as the patient’s clinicalcondition remains stable.
Carbemazepine (Tegretol) is anotheranticonvulsant utilized in the treatment ofbipolar disorder. Tegretol, like lithium andDepakote, requires blood monitoring tocheck levels, with a serum level typicallybetween 4-12 micrograms/mL. Between33%-50% of Tegretol-treated patients expe-rience side effects such as double vision,blurred vision, fatigue, nausea, dizziness,and balance changes. Also limiting use areinteractions with other medications andbone marrow suppression, but it remains afairly common treatment in patients forwhom the standard medications are ineffec-tive.
Lithium and valproic acid both carryblack box warnings (the warning on a med-ication that alerts to a potentially life threat-ening side effect). Psychotherapists andclinicians with patients taking lithium whoobserve signs of neurotoxicity, such as sig-nificant cognitive impairment, lassitude,restlessness, and irritability will want toalert the treating physician. Unrecognized,neurotoxicity can progress to delirium,seizures, coma, and ultimately death.Although these are rare events, valproic acidis associated with hepatoxicity and pancre-atitis, with symptoms including abdominalpain, jaundice, and nausea. Patients takingeither of these medications require educa-tion about these syndromes, as early inter-vention is important in recovery from thesevery serious clinical events.
Several newer anticonvulsants are alsounder investigation for treatment of bipolardisorder. One of them, lamotrigine(Lamictal), appears to show good potentialfor treating the depressed phase of bipolardisorder. One drawback to using Lamictal isthe need for a slow titration due to the riskof developing a potentially life threateningskin rash, and patients need to be educatedabout the rash and contact their physicianimmediately should a rash appear. Becauseof the slow titration, it may take severalweeks to reach the dose that successfullytreats the individual patient.
Other potential medications currently
under investigation as mood stabilizersinclude topiramate (Topamax), tiagabine(Gabitril), and oxcarbazepine (Trileptal).Currently, these medications are predomi-nantly in use in the psychiatric communityas add-on medications to another mood sta-bilizer such as lithium or Depakote. Thesenewer medications are clinically in use, butwe await the study results to assess theirbenefit in the course and outcome of bipo-lar disorder.
AntipsychoticsAntipsychotics have long been used in
the treatment of acute mania and havedemonstrated significant benefits.Antipsychotics historically have had signifi-cant drawbacks with long-term use, includ-ing the risk of developing a serious and per-manent movement disorder (tardive dyski-nesia). The development of atypicalantipsychotics has resulted in improved tol-eration and a substantially reduced risk oflong-term side effects. In bipolar disorder,the primary use for antipsychotic medica-tions is in combination with a mood stabi-lizer, especially if psychotic symptoms occurwith mood episodes. There are currently
four FDA approved atypical antipsychoticsavailable for prescription: olanzapine,risperidone, quetiapine, and ziprasadone.
One particular antipsychotic, olanzapine(Zyprexa), has received FDA approval formonotherapy of an acute manic syndrome.Olanzapine is a demonstrated antimanicagent with few of the side effects of tradi-tional antipsychotics. However, it has sig-nificant side effects. It is associated withsedation, so it is most often taken at bed-time, and is also associated with significantweight gain. Patients who gain largeamounts of weight are also prone to devel-op illnesses related to obesity, such as dia-betes, high cholesterol, and joint problems.For these reasons, weight management canbecome an issue for patients treated withthis medication.
Risperidone (Risperdal) is another com-monly used atypical antipsychotic. Theretends to be less weight gain than with olan-zapine, but it is associated with more motor

22 Texas Psychologist SPRING 2002
side effects such as stiffness, especially at itshigher doses. Risperidone also has beenshown to elevate prolactin levels compara-bly to the older, typical antipsychotics(Umbricht & Kane, 1995), which can leadto such side effects as menstrual irregulari-ties, galactorrhea (abnormal lactation), andsexual dysfunction. Despite these potentialproblems, most patients tolerate risperidonevery well, and it is one of the more com-monly utilized atypical antipsychotics in thetreatment of bipolar disorder.
Quetiapine (Seroquel) and ziprasidone(Geodon) are the most recently arrivedatypical antipsychotics. Both are well toler-ated in general. Seroquel’s main side effect issedation, and is also associated with consti-pation and dry mouth. Geodon is notsedating, but has been shown to mildly slowdown the electrical system of the heart. Thisis seldom clinically significant (currentlythere is no FDA recommendation to evenmonitor EKGs in patients taking this med-ication), but care should be taken when pre-scribing Geodon to patients with heartproblems, and those who are taking certainother types of medications. Some patientson Geodon also experience dizziness. BothSeroquel and Geodon are new medications,but are becoming more widely utilized inthe treatment of bipolar disorder.
It is important to note that the atypicalantipsychotics, despite being much saferand better tolerated medications than theirearlier counterparts, still carry with them asmall but not insignificant risk of develop-ing tardive dyskinesia and other movementdisorders. All patients treated with themneed to be monitored for the emergence ofthese syndromes.
BenzodiazepinesBecause of the excitability and anxiety
inherent in the manic and mixed manicstates, sedating medications are commonlyutilized and medications in the benzodi-azepine family are frequently prescribed.The benzodiazepine family is a large one,and commonly prescribed medicationsinclude lorazepam (Ativan), oxazepam(Serax), diazepam (Valium), clonazepam
(Klonopin), and alprazolam (Xanax). Themain differences in these medications lies intheir half lives and length of time to onsetof action, with xanax, ativan, and serax hav-ing relatively shorter time to onset, and val-ium and klonopin having a longer time toaction. Sedation is the most common sideeffect of the benzodiazepines. Patients whotake benzodiazepines chronically canbecome physiologically dependent on themedication. Withdrawal symptoms includetremulousness, anxiety, irritability, sleep-lessness, and, in worst cases, seizures.Patients need to be monitored for their usepattern, and any drug seeking behaviorsnoted, such as seeking treatment and receiv-ing prescriptions from multiple physicians,and increased use of the medication.
AntidepressantsBipolar depression can be extremely dif-
ficult to treat, and antidepressants are com-monly prescribed in the treatment ofdepressive episodes. Antidepressants mustbe used with caution in the bipolar patient,as they hold certain risks. Antidepressantscan be destabilizing and cause cycle acceler-ation and manic switch ( Frye et al., 1996;Prien et al., 1984; Wehr & Goodwin 1987).For this reason, current clinical recommen-dations consist of short-term use of antide-pressants alongside a mood stabilizer, tominimize the occurrence of these seriousconsequences (Sachs et al., 2000).
Certain types of antidepressants, specifi-cally the selective serotonin reuptakeinhibitors (SSRIs) and Wellbutrin, havebecome the first line treatments for bipolardepression when an antidepressant isdeemed necessary. The SSRIs consist of thewell-known medications Prozac, Paxil,Zoloft, and now Celexa. The choice ofwhich antidepressant to use is generallydecided based on a careful evaluation of thepatient’s medical history, the pharmacoki-netics of the drug, and the psychiatrist’spreference and experience.
At present, no single antidepressant out-performs any others in the treatment ofbipolar depression, but Wellbutrin andSSRIs may have less risk of manic switch.
These medications are commonly used firstline treatments. The time course of a bipo-lar depressed state can last months to yearsif left to its own devices, and ending adepressive episode is often lifesaving. Forthis reason antidepressants are used,although there is not a large database sup-porting their clinical utility.
The newer atypical antidepressants(Remeron, Serzone, Effexor), as well as theolder medications such as the tricyclic anti-depressants and MAO inhibitors, are also inuse. Fewer patients are still on these oldermedications because the newer ones aremuch safer medically and well tolerated.
Medication Use and PregnancyPregnancy in the patient with bipolar
disorder creates issues not seen in the gener-al population. Ideally, the pregnancy shouldbe planned, as the medications used intreatment of bipolar disorder (particularly
the anticonvulsant mood stabilizers, lithi-um, and benzodiazepines) are associatedwith different types of birth defects. Mostpatients understandably express the inten-tion to discontinue their medication inorder to become pregnant. Women whobecome pregnant unintentionally will oftenabruptly stop their medications once theydiscover they are pregnant. This can lead toan acute manic or depressive syndrome.Slow discontinuation of medication pre-pregnancy, and close follow-up with aphysician and therapist can lessen the risk
of relapse and optimize the potential for ahealthy pregnancy and infant. More aboutpregnancy is discussed later in the article byB. Kertz and H. Zboyan, also in this issue.
Somatic TherapiesIt is lastly important to keep in mind
that, despite all our experience and training
as clinicians there are some cases of bipolardisorder that are so tenacious they will notrespond well to our intervention, or maynot respond at all. Despite all the advancesin pharmacology and psychotherapy thathave occurred over the years, there are stillmany chronically disabled or chronicallyhospitalized patients who suffer from this

Texas Psychologist 23SPRING 2002
disease, and remain cycling. In thesepatients it is a good idea to offer the optionof electroconvulsive therapy (ECT). ECTin patients with bipolar disorder is usefulfor the treatment of depression. It can alsobe used to treat mania, a lesser-known fact.While medication treatment is certainlyfirst line treatment for bipolar disorderexacerbations, ECT should not be over-looked. This treatment may have great ben-efit for patients with bipolar disorder, andfor refractory patients, this can be a lifeline.
Other investigational treatments forchronic mood disorders include transcranialmagnetic stimulation (TMS) and vagusnerve stimulation (VNS). In TMS, thepatient experiences repeated magnetic puls-es to the brain, and in VNS, the patient hasan implanted device that repeatedly stimu-lates the vagus nerve (cranial nerve 10).Both of these procedures are investigationaland not yet in clinical practice. TMS doesshow some promise as a treatment for bipo-lar disorder.
SummaryPsychiatrist/psychotherapist collabora-
tions are commonplace today, as profession-als and individuals are aware of the benefitof combining treatments such as medica-tion and structured psychotherapy in thelong-term treatment plan. Because the ther-apist generally sees the patient with greaterfrequency than the psychiatrist, and is oftenthe person the patient will go to with con-cerns or complaints about their symptomsand medications, they can be an importantlink to the psychiatrist. Clearly, educationabout medications is the responsibility ofthe physician prescribing the medication.Nevertheless, since the psychotherapist maybe the first person to observe an adverseeffect or a related concern, increased knowl-edge and education by the therapist canimprove the treatment and treatmentadherence. It is therefore important for thetherapist to have basic familiarity with themedications, in order to know when to referthe patient back to his psychiatrist forreevaluation. The therapist can also aid thepatient as he or she adjusts to a new med-
ication or treatment, and can alert the psy-chiatrist in the event of decompensation.This may allow for earlier medicationadjustment, and possibly prevent hospital-ization or another severe outcome.
The treatment of bipolar disorder canultimately be described as a rewarding chal-lenge. The future is promising for the devel-opment of new medications as well as newsomatic therapies. As we learn more aboutthe causes of bipolar disorder, the potentialfor development of new pharmacotherapiesand psychotherapies is bright, and the col-laboration of mental health professionalscan serve to greatly benefit our patients. ✯
ReferencesBowden C.L., Brugger, A.M., Swann, A.C.,
Calabrese, J.R., Janicak, P.G., Petty, F.,
Dilsaver, S.C., Davis, J.M., Rush, A.J., &
Small, J.G: (1994). Efficacy of dival-
proex vs lithium and placebo in the
treatment of mania. Journal of the
American Medical Association, 271,
918-924.
DeMontigny, C., Cournoyer, G., Morissette,
R., Langlois, R, & Caille, G: (1983).
Lithium carbonate addition in tricyclic
antidepressant resistant unipolar
depression: Correlations with the neu-
robiolgical actions of tricyclic antide-
pressant drugs and lithium ion on the
serotonin system. Archives of General
Psychiatry, 40, 1327-1334.
Frye, M.A., Altshuler, L.L., Szuba, M.P.,
Finch, N.N., & Mintz, J. (1996). The rela-
tionship between antimanic agent for
treatment of classic or dysphoric mania
and length of hospital stay. Journal of
Clinical Psychiatry, 57, 17-21.
Goodwin, F.K., & Jamison, K.R. (1990).
Manic Depressive Illness. New York,
Oxford University Press.
Heninger, G.R., Charney, D.S., &
Sternberg, D.E. (1983). Lithium carbon-
ate augmentation of antidepressant
treatment: An effective prescription for
treatment refractory depression.
Archives of General Psychiatry, 40,
1335-1342.
Price, L.A.(1989). Lithium augmentation in
tricyclic antidepressant resistant
depression. In Extein IL (Ed.), Treatment
of Tricyclic Antidepressant Resistant
Depression. (pp. 49-79). Washington
DC: American Psychiatric Press.
Prien, R.F., Kupfer, D.J., Mansky, P.A.,
Small, J.G., Tuason, V.B., Voss, C.B., &
Johnson, W.E. (1984). Drug therapy in
the prevention of recurrences in unipo-
lar and bipolar affective disorders:
Report of the NIMH collaborative study
group comparing lithium carbonate,
imipramine, and a lithium carbonate-
imipramine combination. Archives of
General Psychiatry, 41, 1096-1104.
Regier, D.A., Boyd, J.H., Burke, J.D. Jr.,
Rae, D.S., Myers, J.K., Kramer, M.,
Robins L.N., George, L.K. Karno, M., &
Locke, B.Z. (1988). One-month preva-
lence of mental disorders in the United
States, based on five epidemiologic
catchment area sites. Archives of
General Psychiatry, 45, 68-779.
Sachs, G.S., Printz, D.J., Kahn, D.A.,
Carpenter, D., Docherty, J.P. (2000).
The Expert Concensus Guideline
Series: Medication Treatment of Bipolar
Disorder 2000. Postgraduate Medicine,
Spec No:1-104. Review
Umbricht, D., & Kane, J.M. (1995).
Risperidone: Efficacy and safety.
Schizophrenia Bulletin, 21, 593-604.
Wehr, T.A., & Goodwin F.K. (1987). Can
antidepressants cause mania and wors-
en the course of affective illness?
American Journal of Psychiatry, 144,
1403-1411.
ARTICLEREPRINTSCall Pat Huber
at (512) 310-9795
for rates and
information.
24 Texas Psychologist SPRING 2002
This article offers practical information for clinicians and patients who are faced with the challenge oftreating women with bipolar disorder who are pregnant or planning pregnancy. A brief description ofbipolar disorder is followed by a review of the potential risks associated with standard treatments forbipolar disorder during pregnancy, as well as the potential risks associated with discontinuing standardtreatments. Recommendations and practical tips are provided to assist clinicians in this challengingdilemma.
For women with bipolar disorder, also known as manic-depressive illness, pregnancy presents aunique challenge. Standard treatment for bipolar disorder includes mood stabilizers, including lithiumand anticonvulsants such as valproate (Depakote), carbamazepine (Tegretol) and others, which areassociated with an increased risk of birth defects, particularly during the first trimester. Yet, womenwith bipolar disorder who choose to discontinue medications are at high risk of relapse. As such,patients and clinicians are faced with the challenge of balancing the risk of relapse with risk of poten-tial birth defects. Psychotherapy is an important adjunct in treating bipolar disorder, but, alone, is typ-ically not sufficient to prevent relapse.
Bipolar Disorder: Challenges for Pregnancy
Barbara Kertz, MS, LPCHolly Zboyan, BA
Baylor College of MedicineHouston, Texas
Bipolar Disorder: What is it?Bipolar disorder is a mood disorder char-
acterized by recurrent periods of depressionand elevated mood, often interspersed withintervals of mood stability. Cross-sectional-ly, the depressed phase of bipolar disorder isindistinguishable from unipolar majordepression. Periods of elevated mood areclassified as either mania or hypomania,depending on their severity and duration.Symptoms of mania include increased self-esteem, grandiose thinking, reduced needfor sleep, increased talkativeness, racingthoughts, distractibility, increased activity,psychomotor agitation, and high-riskbehavior. Mania usually has severe negativelife consequences. Hypomania is similar tomania, but generally has a shorter duration,
milder symptoms, and less severe life conse-quences.
Bipolar disorder is most commonly diag-nosed in young adulthood, which coincideswith the time that many women becomepregnant or plan pregnancy. Importantly,the disruptions in sleep cycles and/or dailyroutines that are common during pregnan-cy and the postpartum period may con-tribute to, or exacerbate, mood episodesassociated with bipolar disorder. Thus, it isimportant to evaluate the risk of changingor discontinuing treatment during this vul-nerable time. The challenge for practition-ers is to balance the risk of exposing thefetus to psychiatric drugs with the risk ofrelapse. This article will briefly review someof the potential risks associated with stan-
dard treatments for bipolar disorder, as wellas present some practical tips for cliniciansand patients who are faced with this chal-lenge. In some instances, continuing psy-chiatric medication may be the best choicefor both mother and baby.
Mood StabilizersLithium, valproate (Depakote), and car-
bamazepine (Tegretol) are effective moodstabilizers commonly used in the treatmentof bipolar disorder. Standard treatmentguidelines recommend that patients remainon a mood stabilizer in all phases of the ill-ness (depression, mania, hypomania, andperiods of mood stability) (AmericanPsychiatric Association, 1994; Sachs, Printz,Kahn, Carpenter & Docherty, 2000).
F o c u s o n B i p o l a r D i s o r d e r

Texas Psychologist 25SPRING 2002
During acute episodes, the use of additionalpsychiatric medications (antidepressants orantipsychotics) may be necessary.
Mood Stabilizers as TeratogensUnfortunately, first trimester exposure
to all of the established mood stabilizers(lithium, valproate and carbamazepine) isassociated with an increased risk of birthdefects. The primary concerns are cardiacabnormalities associated with exposure tolithium and neural tube defects associatedwith exposure to valproate and carba-mazepine.
The Register of Lithium Babies original-ly tracked infants exposed to lithium duringpregnancy (Schou, Goldfield & Weinstein,1973). An initial report based on the reg-istry estimated that infants exposed to lithi-um in the first trimester were 400 timesmore likely than unexposed infants to haveEbstein’s anomaly (Nora, Nora & Toews,1974). Since then, more data has been gath-ered and the risk of Ebstein’s anomaly hasbeen reevaluated. Two review articles byCohen address the risk of Epstein's anomalyin exposed infants. The risk is currentlythought to be about 10 to 20 times higherthan in the general population or about 1 in1,000 to 2,000 exposures (Cohen,Freidman, Jefferson, Johnson & Weiner,1994; Cohen & Rosenbaum, 1998).
Reports on the use of anticonvulsants(valproate, carbamazepine) during pregnan-cy come mostly from studies of womenwith epilepsy. Because birth defects aremore common in infants born to womenwith epilepsy than in the general popula-tion, it is possible that the risk of birthdefects will be lower in women withoutepilepsy who use these same medications asmood stabilizers for bipolar disorder.However, first trimester exposure to mostanticonvulsants is related to an increasedrisk for neural tube defects and orofacialmalformations such as cleft palate. Forcomprehensive reviews of the teratogenicrisks associated with mood stabilizers, seeCohen et al., 1998 and Altshuler, et al.,1996.
Additional concerns about the use of
mood stabilizers during pregnancy resultfrom the possibility of long term neurolog-ical and developmental problems. However,at least two studies have not reported anincreased long-term risk from use of amood stabilizer. In 1976, Schou reportedon a 5-year follow up study that compared60 children exposed to lithium during thesecond and third trimesters to 57 siblingswho were not exposed to lithium. Thisstudy found no significant developmentaldifferences between the two groups of chil-dren. Likewise, a study that compared theIQs of a group of children exposed to car-bamazepine with a group of unexposedchildren found no significant differencesbetween groups (Scolnik et al., 1994).
Risk of Recurrence FollowingDiscontinuation of Mood Stabilizers
Despite the potential for harm to thefetus, many factors must be weighed beforepsychiatric drugs are discontinued for anyreason, including pregnancy. An increasedrisk of relapse is the primary concern. It isimportant to keep in mind that, in general,the risk of relapse appears to be higher whenmood stabilizers are discontinued rapidly. Aslow taper of lithium over a two to four-week period lessens the risk of relapse(Faedda, Tondo, Baldessarini, Suppes &Tohen, 1993).
A study by Viquera and colleagues(2000) found that pregnancy did not offerprotection from relapse to women withbipolar disorder who discontinued treat-ment. Of 101 women, both pregnant andnon-pregnant, who discontinued lithiumtreatment, recurrences occurred in 52.4% ofthe pregnant women and 57.6% of the non-pregnant women in the 40 week period fol-lowing lithium discontinuation. Womenwho tapered their lithium gradually over 15to 30 days had a lower recurrence rate(37.14%). Of the pregnant women whoremained stable during the pregnancy, 70%relapsed during the postpartum period.
Use of Antidepressants Without a Mood Stabilizer
Because mood stabilizers are teratogenic,
it might seem reasonable to consider usingantidepressants by themselves to prevent ortreat depression during pregnancy, especial-ly since tricyclic antidepressants and selec-tive serotonin reuptake inhibitors (SSRIs)appear to be safe for prenatal use. However,the use of antidepressants without a moodstabilizer in patients with bipolar disordermay worsen the course of illness. In a recentnaturalistic study of patients with bipolardisorder who were treated with antidepres-sants, but not concurrent mood stabilizers,24% of patients “switched” from depressionto mania or hypomania (Henry, Sorbara,Lacoste, Gindre & Leboyer, 2001). In addi-tion to triggering mania/hypomania, anti-depressants can also trigger rapid cycling ormixed states in some patients. As a result, itis generally recommended that antidepres-sants be used in conjunction with moodstabilizers in patients with bipolar disorder.For acute episodes of depression or mania,electroconvulsive therapy (ECT) is general-ly considered safe for use during pregnancy.
Risks of Untreated Depression and Mania
Despite the high risk of relapse, many
women choose to discontinue their psychi-atric medications while they are attemptingto conceive and/or during pregnancy.However, untreated episodes of eitherdepression or mania also present serious risk
to the health of the mother and fetus. The risk of suicide in patients with bipo-
lar disorder is high. Goodwin and Jamison(1990) have estimated that up to 19% of
bipolar patients complete suicide. Althoughthere are no figures for suicide attemptsduring pregnancy in women with bipolardisorder, it is a serious concern, especiallyfollowing medication discontinuation.Suicide attempts expose the fetus to variousrisks depending on the method used.Completed suicide is, obviously, fatal to thefetus as well as to the mother.
Depression also carries serious risks forthe mother and fetus. Depression can exac-erbate the normal fatigue commonly expe-rienced in pregnancy and reduce the moth-er’s ability to care for herself. Reduced

26 Texas Psychologist SPRING 2002
appetite, especially when coupled withmorning sickness, can endanger the moth-er’s food intake and possibly the nutritionalstatus of the fetus. Reduced interest canaffect the mother’s adherence to her ownprenatal care, and disinterest and inabilityto attend to her own needs places both themother and the fetus at risk.
Newborns exposed to maternal depres-sion have exhibited both prolonged cryingand irritability, suggesting that maternaldepression affects the newborn’s ability toself–regulate (Weinberg & Tronick, 1998).Six-month old infants exposed to untreateddepression in utero have been found to bemore reactive to stress (Newport, Wilcox &Stowe, 2001).
Untreated manic episodes can also pre-sent risks for the mother and infant, as theyare frequently accompanied by high-riskbehavior. Lack of sleep, coupled withincreased physical activity and disregard forpersonal safety can create situations thatendanger the mother’s and the fetus’shealth.
Guidelines for DiscontinuingPsychiatric Medications
Although psychiatric drugs carry riskto the fetus, many factors must beweighed before treatment is discontinued.The woman’s psychiatric history, includ-ing the severity of her affective episodes,and her current clinical status are impor-tant elements (Packer, 1992). If thewoman has had prior pregnancies, the his-tory of her illness during the pregnanciesand the postpartum periods should also beconsidered. If a woman has a history ofsevere affective episodes when off medica-tion, it may not be reasonable to discon-tinue treatment, as the risk of relapse mayoutweigh the risk of birth defects. Inunplanned pregnancies, the fetus hasoften experienced the most damagingexposure by the time the pregnancy is rec-ognized. In cases such as these, the womanand her psychiatrist must work together todetermine a medication regime that willminimize risk to both the fetus and themother.
Omega-3 Fatty AcidsResearch continues to identify mood sta-
bilizers that are not teratogenic. Preliminaryresearch indicates that omega-3 fatty acids,naturally occurring compounds found infish, plant algae, and flaxseed, may havemood stabilizing properties (Stoll et al.,1999). Omega-3 fatty acids are non-toxicand safe during pregnancy and lactation(Hornstra, Al, van Houwelingen &Foreman-van Drongelen, 1995). As part ofthe STEP-BD research program (describedin the introduction to this issue), a study iscurrently underway to assess the use ofomega-3 fatty acids in women who havedecided voluntarily to discontinue medica-tion while planning pregnancy.
How Can Psychotherapy Help? Psychotherapy, combined with medical
management, is an important tool in treat-ing bipolar disorder. Psychotherapy canbenefit bipolar patients in many ways,including enhancing mood stability,improving functioning, and reducing thenumber of hospitalizations (Huxley, Parikh& Baldessarini, 2000). Resources for thera-pists working with bipolar patients includeMiklowitz and Goldstein’s book BipolarDisorder: A Family-Focused TreatmentApproach, Newman, Leahy, Beck & Reilly-Harrington’s book Bipolar Disorder: ACognitive Therapy Approach and Frank’swork with Interpersonal and SocialRhythm Therapy (Frank, Swartz & Kupfer,2000).
Because of the high risk of relapse duringpregnancy, psychotherapy should always beconsidered when a woman with bipolar dis-order is planning a pregnancy or is alreadypregnant. In our practice, psychotherapywith these women includes proactive plan-ning for pregnancy and the postpartumperiod. Whenever possible, the woman’spartner is included in sessions focusing onthe following issues:
Building a medical support team thatincludes the woman’s psychiatrist andobstetrician or midwife, building a socialsupport network, enhancing communica-tion skills, mood charting, managing sleep,
identifying and managing stressors, priori-tizing responsibilities, exploring physicaland emotional changes associated withpregnancy and the postpartum, and plan-ning for the postpartum period.
ConclusionThere are no perfect answers for the
woman with bipolar disorder who is plan-ning a pregnancy. All of the availableoptions carry risks. Remaining on psychi-atric medications during pregnancy carriesan increased risk of fetal malformations.Discontinuing psychiatric medicationsincreases the risk of relapse and the poten-tial negative effects of untreated moodepisodes on the mother and fetus. Whilethe risk of relapse can be reduced by aslow tapering of medication, it cannot beeliminated.
New treatments are under investiga-tion and may provide a safer alternative tomanaging bipolar disorder. For the pre-sent, a combination of close psychiatricsupervision and psychotherapy focused onissues surrounding pregnancy and post-partum in conjunction with a partner orother supportive person will serve to opti-mize outcomes for women planning preg-nancy.
ReferencesAltshuler, L., Cohen, L.S., Szuba, M.P.,
Burt, V.K., Gitlin, M. & Mintz, J. (1996).
Pharmacologic management of psychi-
atric illness during pregnancy:
Dilemmas and guidelines. American
Journal of Psychiatry, 153(5), 592-606.
American Psychiatric Association (1994).
Practice guideline for the treatment of
patients with bipolar disorder. American
Journal of Psychiatry, 151(12 Suppl), 1-
36.
Cohen, L.S., Freidman, J.M., Jefferson,
J.W., Johnson, E.M., & Weiner, M.L.
(1994). A reevaluation of risk of in utero
exposure to lithium. Journal of the
American Medical Association, 271(2),
46-150.
Cohen, L.S. & Rosenbaum, J.F. (1998).
Psychotropic drug use during pregnan-
Texas Psychologist 27SPRING 2002
cy: Weighing the risks. Journal of
Clinical Psychiatry, 59 (Suppl. 2), 18-
28.
Faedda, G.L., Tondo, L., Baldessarini, R.J.,
Suppes, T. & Tohen, M. (1993).
Outcome after rapid vs. gradual discon-
tinuation of lithium treatment in bipolar
disorders. Archives of General
Psychiatry, 50(6), 448-55.
Frank, E., Swartz, H.A., & Kupfer, D.J.
(2000). Interpersonal and social rhythm
therapy: Managing the chaos of bipolar
disorder. Biological Psychiatry, 48(6),
593-604.
Goodwin, F.K. & Jamison, K.R. (1990).
Manic-depressive illness. New York:
Oxford Press.
Henry, C., Sorbara, F., Lacoste, J., Gindre,
C. & Leboyer, M. (2001).
Antidepressant-induced mania in bipo-
lar patients: identification of risk fac-
tors. Journal of Clinical Psychiatry,
62(4), 249-255.
Hornstra, G., Al, M.D., van Houwelingen,
A.C., & Foreman-van Drongelen, M.M.
(1995). Essential fatty acids in preg-
nancy and early human development.
European Journal of Obstetrical and
Gynecological Reproductive Biology, 61,
57-62.
Huxley, N.A., Parikh, S.V., & Baldessarini,
R.J. (2000). Effectiveness of psychoso-
cial treatments in bipolar disorder:
state of the evidence. Harvard Review
of Psychiatry, 8(3), 126-40.
Miklowitz, D.J., & Goldstein, M.J. (1997):
Bipolar disorder: A family focused treat-
ment approach. New York: The Guilford
Press.
Newman, C., Leahy, R.L., Beck, A.T., &
Reilly-Harrington, N. (2001): Bipolar dis-
order: A cognitive therapy approach.
Washington DC: American Psychological
Association Press.
Newport, D.J., Wilcox, M.M., & Stowe, Z.N.
(2001). Antidepressants during preg-
nancy and lactation: defining exposure
and treatment issues. Seminal
Perinatology, 25(3), 177-90.
Nora, J.J., Nora, A.H., & Toews, W.H.
(1974). Letter: Lithium, Ebstein's
anomaly, and other congenital heart
defects. Lancet, 7; 2(7880), 594-595.
Packer, S. (1992). Family Planning for
women with bipolar disorder. Hospital
and Community Psychiatry, 43(5), 479-
482.
Sachs, G.S., Printz, D.J., Kahn, D.A.,
Carpenter, D., & Docherty, J.P. (2000).
The expert consensus guideline series:
Medication treatment of bipolar disor-
der. Postgraduate Medicine, Spec No:1-
104.
Schou, M., Goldfield, M.D., & Weinstein,
M.R. (1973). Lithium and pregnancy. I.
Report from the register of lithium
babies. British Medical Journal, 2, 135-
136.
Schou, M., (1976). What happened later to
the lithium babies? A follow-up study of
children born without malformations.
Acta Psychiatrica Scandinavica, 54(3),
193-7.
Scolnik, D., Nulman, I., Rovet, J.,
Gladstone, D., Czuchta, D., Gardner,
H.A., Gladstone, R., Ashby, P.,
Weksberg, R., & Einarson, T. (1994).
Neurodevelopment of children exposed
in utero to phenytoin and carba-
mazepine monotherapy. Journal of the
American Medical Association,
271(10), 767-770.
Stoll, A.L., Severus, W.E., Freeman, M.P.,
Rueter, S., Zboyan, H.A., Diamond ,E.,
Cress, K.K., & Marangell, L.B. (1999).
Omega 3 fatty acids in bipolar disorder:
a preliminary double-blind, placebo-con-
trolled trial. Archives of General
Psychiatry, 56(5), 407-412.
Viguera, A.C., Nonas, R., Cohen, L.S.,
Tondo, L., Murray, A.M., & Baldessarini,
R.J. (2000). Risk of recurrence of bipo-
lar disorder in pregnant and nonpreg-
nant women after discontinuing lithium
maintenance. American Journal of
Psychiatry, 157, 179-180.
Weinberg, M.K., & Tronick, E.Z. (1998).
The impact of maternal psychiatric ill-
ness on infant development.: Journal of
Clinical Psychiatry, 59 (Suppl. 2), 53-
61.

28 Texas Psychologist SPRING 2002
Charles Bowden, MD, is an internationally recognized expert on bipolar disorder and has authored over
200 articles, books, and book chapters. His research is principally on the symptomatic and biological
characterization of bipolar disorders and the efficacy and pharmacodynamics of mood stabilizing drugs.
Dr. Bowden is the Chairman of the Psychiatry Department at the University of Texas Health Science
Center in San Antonio. He is a member of the Scientific Advisory Board of the National Depressive and
Manic-Depressive Association and in 2001 received the association’s Gerald L. Klerman Senior
Investigator Award. He is named in Best Doctors in the U.S. in the area of mood disorders. Jodi
Gonzalez sat down with Dr. Bowden to discuss bipolar disorder research and practice.
An Interview with Charles Bowden onResearch and Practice in Bipolar Disorder
Jodi M. Gonzalez, PhD
JG: Why do you think bipolar disorder hasbeen receiving so much clinical and researchattention of late?
CB: It has always received some atten-tion. It has not had anywhere near thefinancial support in terms of the NationalInstitute of Mental Health funding; notuntil the early 90s was there much interestfrom pharmaceutical companies in terms ofdrug-related research. So, that’s what haschanged, I think. And, some of the reasonsfor that change have to do with the recog-nition that a substantial number of peoplewho might be diagnosed initially other thanbipolar disorder, fundamentally have bipo-lar disorders. So, the notion of how manypeople out there have some form of bipolardisorder has a different answer today than itwould have 25 years ago. That’s especiallytrue in select populations – children andadolescents where 25 even 10 years agoyou’d have a substantial number of childpsychiatrists say “I’ve never seen someonewith bipolar disorder.” You wouldn’t findthat point of view in the year 2002. Then,there have been more treatments added towhat was simply a solo treatment, standingalone, lithium, for 25 years and patients
who in many instances either didn’t benefitor didn’t tolerate the substantial side effectsof lithium, or both, now can benefit fromsome other alternatives. You put all thosetogether and you have a very different pro-fessional and public perception in the levelof interest in bipolar disorder.
JG: You are the site principal investigatorfor the national STEP-BD study. Can youprovide an update on that study?
CB: Well, the STEP study – let me firstexplain what is meant by STEP; theSystematic Treatment EnhancementProgram for Bipolar Disorder (STEP-BD).This is an NIMH sponsored, long-term,initially 5-year study possibly to continuelonger than that. STEP is a prospective fol-low-up of patients with bipolar disorder; allforms of bipolar disorder and people in allstages of the illness. STEP has an advantagein that it follows these people into thefuture. So you can start to ask the impor-tant questions. You can do this in partbecause you are pooling not only the SanAntonio center and another site in the stateof Texas at Baylor under the direction of Dr.Lauren Marangell, but also 15 other acade-
mic medical centers around the UnitedStates. So you have different people in dif-ferent urban settings studying such a largenumber of patients, instead of basing theanswer just on the impression of one inves-tigator with a handful of patients from hisor her experience, you have dozens of inves-tigators and you multiply your sample size.
JG: Is the STEP an efficacy or effectivenessstudy? (i.e., efficacy is evidence of benefit in aclinical trial; effectiveness is evidence of bene-fit in a real-world clinical setting)
CB: The STEP is a little bit of every-thing. I view the STEP as having more of animpact on effectiveness and not the generaldefinition of efficacy: does a drug work aswell as another treatment, does it work aswell or better than placebo, which would bethe usual, primary efficacy question.Rather, how does this treatment, and notjust the drugs—I emphasize the drugsbecause they are central but they certainlyare not used alone in the STEP—how doesthis treatment inform the world? Howmany people is it applicable to? Is it welltolerated by the patients? Are there seriousrisks, side effects or laboratory abnormali-
F o c u s o n B i p o l a r D i s o r d e r

Texas Psychologist 29SPRING 2002
ties that might not be side effects in thesense of someone complaining but still berisk factors that are added to the patient’shealth status over time if those laboratorytests are not followed up on. So, it’s muchmore along the lines of effectiveness.Having said that, the STEP has pathwaysfor smaller numbers of patients to test spe-cific treatments. Those specific treatmentsare for persons, for example, with depres-sion that have not responded to standardtreatments, what we call a refractory depres-sion. These patients, more like your stan-dard, pharmaceutical study at 50-60patients in each treatment group, would bein those kinds of studies. So, for a subset ofpatients, it’s an efficacy study as well as aneffectiveness study.
JG: You mentioned earlier that bipolar dis-order is recognized more often in cases whereit would previously not have been recognized.
CB: The recognition is at least that it’son the radar screen of physicians and behav-ioral health specialists in instances wherethey would have simply treated substanceabuse as an addictive disorder, alcoholism,whatever. Those persons are aware thatthere is a high comorbidity. They may notbe able to cite the references or the statistics,but even drug and alcohol counselors witha bachelor’s degree probably have someawareness that there is some linkage ofsome addictive disorders to bipolar disorderwith the stimulus seeking and impulsivitythat goes with a mood disorder.
JG: Bipolar disorder has previously beenunder-recognized in previous settings?
CB: Yes it has been under-recognizedbut that under-recognition has multiplefacets to it. It’s not that the person is notinclined to think bipolar or because they areunder-trained. Part of it is the way DSM IVis structured, where it takes criteria, forexample major depressive disorder, and saysthis is what major depression is in the con-text of bipolar disorder. The evidence is thatalthough there is a lot of overlap that thereare also some substantial differences in thedepression you see in bipolar and the
depression you see in unipolar. So, it’s easyto underestimate the true prevalence even ifone is aware of the pitfalls.
JG: What differences in depression does theDSM not account for?
CB: It tends to view depression as aconglomerate of physical, mood and cog-nition symptoms. A physical examplewould be complaining of body aches andpains. Mood would be feeling sad.Cognition would be preoccupation withparticular themes such as pessimism,impaired cognition or slowed thinking.Although all those are true, the physical orsomatic symptoms are relatively lackingand when present are mild in most bipolardepressive conditions, where they areprevalent in other depressions.
JG: What about the DSM IV classificationof mania?
CB: The DSM classification of maniaworks well, up to a point. A full-blownmanic episode is easy to recognize at leastin its classical form, and in fact has thehighest inter-rater reliability of any Axis Idisorder. So, there is reluctance to changeall the DSM IV criteria if it works so well.There are some problems with the criteria,and I am sympathetic to the problems thatthey pose even for experts. They tendedhistorically to require that a manic episodebe of such severity that it required hospital-ization to be called Bipolar Type I. Well, ata point where a psychiatrist chose hospital-ization strictly on the basis of clinicalgrounds that made sense. In the world thatwe live in now it does not, with heavilymanaged care restrictions such that impair-ing manic episodes do not result in hospi-talization. So, hospitalization probablyneeds to be removed from the diagnosticcriteria. And, only in the most recent DSMhas there been a classification of mixedmania; at least, a subclassification that aprofessional can make diagnostically.However, it is over-restrictive, requiringthat the person have the full spectrum ofmanic and depressive episodes. The rela-tionship at least in terms of response to
lithium is that it really doesn’t require nearthat much to put the person into a funda-mentally different category.
JG: Why would somebody need to be in amixed category? How would that informtreatment?
CB: Mixed manic episodes are associat-ed to poor response to lithium treatment. Itdoesn’t mean that no patients treated withlithium would respond, but one would bereluctant to treat a person with lithium ifyou view the person in a mixed group.
JG: Do you mean having mostly mixedepisodes or only having one mixed episodewould put them in the mixed group?
CB: You are asking more than we know.What the DSM would require is strictly a
cross-sectional look at things. So, the DSMis ahistoric. It doesn’t take into accountwhat health professionals know about thetreatment course and history, age of onsetor if so, DSM considers those in only thesoftest fashion. There is nothing that saysdo things differently because the personwas in a mixed episode two years ago. Theextent of systematic research on mixedmania isn’t that great. So, it’s an open ques-tion as to whether patients with mixedepisodes at one point will be highly likely,moderately likely or no more likely than anaverage patient to have another mixedepisode. You would think we would havegood information on that, but if you think
about it, that requires a long-term,prospective type study. If you tried to gleanthis information solely from the patient’sfamily and self-report your reliability of
information is increasingly poor. Evenwhen we try to get information frompatients on how they were six months ago,we’re on shaky ground. It’s not just in thisarea, but any clinician would have thatexperience with his or her patients.Fortunately, the STEP study will help toanswer these questions by looking at peoplewith a different set of criteria qualifyingthem as having some form of mixed state,comparing them to those who have the fullDSM criteria.

30 Texas Psychologist SPRING 2002
JG: There are a couple of new terms beingused in bipolar disorder to describe mania,such as ultra-rapid cycling and ultra-radiancycling. Can you talk about those a little bit?
CB: One of the problems is that as youunderstand more about a condition, theways you first defined it may seem inade-quate. Rapid cycling is not a diagnosis inthe DSM, it is what’s called a course modi-fier. So, you can call me Bipolar I, II, mixedor non-mixed and you could still add rapidcycling to the diagnostic label as a coursemodifier. And, it has its own specific set ofcriteria. It’s not that they are incorrect, butthey are inadequate for the degrees ofcycling. And there are some patients whodon’t cycle on a time frame that is measuredin weeks and months but on one that’s mea-sured in days - thus the term ultra-rapid - oreven within a day, hours or in someinstances, within matters of less than anhour; for those the modifier ultradian hasgenerally been used. I think they are helpfulterms, I think they deal with, at least tosome degree, different groups of personswith bipolar disorder. Having said that, nei-ther of these terms has worked its way intothe parlance of the DSM as we speak.
JG: So, you don’t have the durationrequirements, do you still like to have thesymptom requirements, the number of symp-toms in that 30 minutes or an hour?
CB: That’s a good question. The DSMgoes overboard on durational requirements.Actually, I think this is also true for manyother disorders than bipolar disorder.Certainly those patients who meet the dura-tion qualify for whatever the disorder, butthere are many patients who have all thesymptoms, the illness defining symptoms,but may have them in a time frame that issimply not what DSM spells out. I thinkthat some relaxation of those time framerequirements would be in the interest ofpracticing psychiatrists. I think that it’s like-ly we will see that incorporated into DSMto some degree. In rapid cycling, for exam-ple, there are a number of people that havebeen followed mostly naturalistically, butsystematically. The Italian psychiatrist for
whom I have substantial respect, MarioMaj, has a series of studies on this issue. Hehas shown that if we look at this in terms ofillness response to treatment, different bio-logical subtypes or abnormalities underly-ing rapid cycling, we would have better pre-dictive ability by relaxing or eliminatingthose durational requirements.
JG: The other requirement that can leadinto a more gray area is not having thegrandiosity of mania but being irritable.
CB: Yes, actually I think we know a greatdeal about that. That’s amenable simply todescriptive study, where you simply countthe portion of patients with symptoms in agiven period. And I think the irritabilityand hostility are more universal symptomsthan is grandiosity. It’s a little bit at oddswith the lay notion of mania of the personwanting to stay up all night, party all night,drink, have loose sexual relationships, planon making a million dollars on somegrandiose scheme. The degree of unadulter-ated pleasure in this illness is a lot lowerthan that notion, as you well know.
JG: In other words, you don’t see grandios-ity as a necessary component of mania?
CB: Well, I wouldn’t go so far as to sayit’s not necessary in the sense of necessary toexplain some of the behavior. Even whenthere is grandiosity it has a perverse or sec-ondary role. We can have a patient sent to usdepressed and describe how his depression isso bad that he has gone to all these top peo-ple and how none could help him and howhe is suffering in such a major way. So, whathe tells us in terms of content is of depres-sion but he tells us in a somewhat grandioseway. “My depression is worse than anyoneelse’s depression. My depression is beyondthe scope of the average mortal to inter-vene”. So, grandiosity can intrude in this ill-ness in a kind of back door fashion.
JG: Why is bipolar disorder so difficult totreat in children and adolescents?
CB: Foremost, we have fewer good stud-ies on which to base treatment. Also, fortreatment to be effective, both the child and
the parents must be involved, and many ofthe parents have bipolar symptomatology.Also, the treatment has to work around a
schedule of school and extracurricular activ-ities, and not have side effects that interferewith those activities.
JG: How important is it to differentiatebetween classifications of bipolar, such asbipolar I, bipolar II, and cyclothymia?
CB: Very important, at least to distin-guish bipolar I and II. The latter is frequentepisodes, including rapid cycling, and ismore prevalent in women. Antidepressantsare at present overused in bipolar IIpatients, with consequent mood destabiliza-tion. Lamictal has a potential large role forbipolar II’s, based on the evidence I see.
JG: In 1994 you conducted one of the effi-cacy trials for valproate that resulted in itsFDA approval. Since then other potentialmood stabilizers have entered the market.How are studies looking for these new agents?
CB: The study that I had the good for-tune to lead in a way defined a methodolo-gy that worked that allows you to comparea treatment with placebo plus usual care, orlithium. It led to results such that when psy-chiatrists started using valproate–dival-proex, they got essentially the same kind ofresults we reported in several articles. Oneof the main consequences was companiesthat had previously thought there was nopoint in involving themselves in bipolar dis-order research as far as drug developmentwas concerned came to understand thatthough lithium was, and remains to thisday, a very important, and for somepatients, effective treatment, that there wereclearly fewer than half of patients withbipolar disorder adequately treated by andtolerant of lithium. So here you have a com-bination of the recognition that those peo-ple being treated with lithium were oftenhaving poor outcomes and that there aremore people with bipolar disorder than hadbeen commonly understood. In addition,you had a methodology that allowed forstudy of treatments, at least on the manicside, so they went back to the drawing

Texas Psychologist 31SPRING 2002
boards and looked at what drugs they hadthat might have some sort of mood stabiliz-ing properties in them. There’s hardly amajor research pharmaceutical company inthe world now that does not have or is notendeavoring to develop a drug or a series ofdrugs that could have some role in improv-ing the lives of some of those patients.
JG: Any studies you are conducting nowinvolving these agents?
CB: We are nearly always involved inone or two studies. There have been twomajor directions for the mood stabilizersthat work on the manic side. One is to lookat every drug that was initially viewed as ananti-epilectic or seizure medication. That isthe class that valproate came from and it’sthe class that carbamazepine came from,but there are many others, just to mentiona couple of examples at present – topira-mate and levetiracetam. Both are marketedfor epilepsy but there are studies underwayto see what kind of benefit they bring most-ly for those in mania. The second is less anew story, but still an interesting one. Earlyon, it was understood that antipsychoticmedications helped in mania. In part it wasunderstood because a substantial percentageof manic episodes have psychotic features,but it also appeared to be the case that theantipsychotics helped some of the othermanic symptoms as well as the psychoticones. Now there is a group of drugs mostlyreferred to as atypical antipsychotics thathas better tolerated side effects, albeit sub-stantial side effects. There has been anequally great interest in the earlier antipsy-chotics, despite their side effects. It’s a morecomplex task to read this literature becausethe antipsychotic drugs have such broad,sedating, and motor slowing effects thatthey give you results that look like they arereally working, but some of that work isreally a function of sedative, non-specific,physical slowing kinds of activity.
I think that’s one reason that the antipsy-chotics have not been elevated to centerstage for treatment of bipolar disorder, andis unlikely to occur with the present groupof antipsychotics.
JG: The STEP also has psychosocial treat-ments being studied.
CB: Yes.
JG: How do you view the role of psychoso-cial treatment for bipolar disorder?
CB: Interestingly, to my way of think-ing, bipolar disorder more than any otherchronic, recurrent, severe mental disordermust have a psychosocial treatment com-ponent. For many patients that’s not goingto be standard, insight-oriented psy-chotherapy, but for some patients itincludes that. But at the very least thistreatment requires that patients activelyand only gradually over time develop anunderstanding about the role of environ-ment and psychosocial risk factors in theirillness. These include the importance ofsleep, the importance of avoiding certaindrugs of abuse, and certain drugs that to anon-bipolar patient might be innocuous.They need to understand the fact that thereis something about this illness—it’s still notadequately understood—but the illnessitself causes the person to start to think heor she is well. He thinks that he doesn’tneed the treatment, doesn’t need the med-ication, doesn’t need counseling, doesn’tneed to keep the next visit. So it’s notexactly the same as denial although it hasan element of that. The nature of this ill-ness causes people to make bad judgments,to lack insight, to behave impulsively. Thisoccurs to such an extent that it can placethem in danger of being put in jail, riskingtheir life, and avoiding the very treatmentsthat could provide at least temporaryrespite or more lasting benefits. So, the psy-chosocial aspect is critical for this illness. Itmay not be so critical for the person in thehospital for a week, but in the long-termmanagement of this illness where 90 per-cent of the care takes place, there has to bean active psychosocial component.
JG: I agree with that. At times psychiatriststreating bipolar disorder do not consider psy-chotherapy as an adjunctive treatment. Is thisbecause there is just not sufficient informationon psychosocial treatment available?
CB: Although there is some good psy-chosocial treatment research being done,the truth of the matter is that the researchlags behind some of the impressions that Ihave, based more on epidemiologic illnesscourse evidence than psychotherapy per se.I think there is some good work beingdone—David Miklowitz in Colorado is anexample of that—but there are othergroups, as well. But when one starts looking
at prospective, randomized kind of studies,the field of psychotherapy research is gener-ally weak in regard to that. Also, 90 percentof what has been developed in a really sys-tematic way on bipolar disorder hasoccurred in the past few years, so it’s notsurprising that there wouldn’t be a greatdeal psychotherapeutically or psychosocial-ly, as well.
JG: I have also heard individuals withbipolar disorder express that they want psy-chotherapists who specialize in or have a greatdeal of understanding of bipolar disorder.Why do you think that is?
CB: Well I think that’s true—of courseyou and I see perhaps a skewed sample.The patients that we see here tend to havehad the illness for some time. Most ofthem have some fundamentally basic goodunderstanding about the illness. Theyrealize that it’s complex. Often they haveseen psychiatrists for pharmacologicaltreatment, psychosocial treatment, othercounselors, and they have seen enough inboth camps of care that either misunder-stood some fundamental aspects of thisillness or may have actually been hurtfulin relationship to the current problem.Thus, they want to deal with professionalswho have current, in-depth knowledge ofthe complexities of this illness. There are amyriad number of reasons for this.Sometimes it’s influenced by their owngrandiosity, but sometimes it’s also influ-enced by their recognizing that they dohave these problems with impulsivity andjudgment and unless they are workingwith someone who has seen it all in termsof the spectrum of bipolar symptomatol-ogy, they are concerned that the well-

32 Texas Psychologist SPRING 2002
meaning professional might overlookthings that would cause that patient harmbecause they weren’t staying on top of hisor her problems.
JG: I think it’s difficult because whenpatients come in and they talk about theirmood lability, as psychotherapists we tend towant to focus on the psychological contribu-tors to that. It can be hard to differentiate ifthere is a psychological cause or if they wokeup that day and were feeling poorly because ofthe illness.
CB: I think many people who have psy-chotherapeutic practices, at least for thiscondition, are excessively inclined to lookfor some kind of psychological or conflictcause. It’s not that there is not often an ele-ment of one of those, but in bipolar disor-der what you see behaviorally is in manyways what you get. It’s better to deal withthat principally in terms of the conse-quences to present safety, present function,present well-being and not look into earlyor learned experiences. There are plenty ofexceptions. Many persons with bipolar dis-order have had more than their share ofearly life conflict for a somewhat uniquereason. Because of the high hereditarycomponent of at least the most commonform of bipolar disorder, many of thesepeople will have had one or both parentswith some form of bipolar disorder, some-times diagnosed, sometimes not diag-nosed. Such a parent would have displayedsome of the same unpredictability andimpulsivity toward the child that goes withthis illness.
JG: What are your views on how we canfocus on the relationship of stress to episodesduring treatment?
CB: First, we all have stress in our lives.Second, people with bipolar disorder havemore in the way of comorbid anxiety symp-toms and anxiety disorders. You name theanxiety disorder in terms of DSM labelingand it’s present with an increased prevalenceof cases over that of the general population.There are several reasons to pay attention tostress and stressful events. It’s a good way to
organize your major psychotherapeutic orpsychosocial effort for patients with bipolardisorder. It’s not the only way, but as far asthe entrée to what will be discussed over a30 or 45 minute appointment, it is proba-bly as good as any other.
JG: What about the collaborative role ofpsychologists/therapists and psychiatrists inworking with the disorder?
CB: Well, I don’t think there is any onesize fits all. In some ways, I think the issueis more of the time requirements and of theorganization of practices in the year 2002.On the issue of time requirements, manypsychiatrists simply lack the time to devotemajor portions of their efforts to counselingand psychotherapy. So, for those reasonsthey set up liaisons with psychologists.Psychologists, in turn recognizing thatmany of the clientele with whom they workneed medications, and have medically, bio-logically-based disorders to deal with, wantto work with psychiatrists. Also, more prac-tices are organized in a multidisciplinaryway rather than as solo practices as a psy-chiatrist, social worker, or psychologist.More practice is delivered in some form ofa multidisciplinary setting today than wasthe case 15 years ago. One reason for this isthat solo practices often place the profes-sional at somewhat of a disadvantage in thehealth care payor environment.
JG: If I am seeing someone weekly, andsee someone’s mood shift toward a differentepisode or phase, should I contact the psychi-atrist to change medications as soon as possi-ble? How important is that if the person doesnot see the psychiatrist for another month andthe symptoms are subclinical?
CB: It’s a good question. It is impor-tant. Having said that—and this isn’tsomething that is limited to psychiatristsand psychologists—you see it with physi-cians too, for example. Even if you haveyour offices next door to one another, it’snot as easy as the lay individual or thepatient might think for us to quickly con-vey to our colleague working with a patientwhat’s going on. I think if we found a wayto do that more patients would be the bet-
ter for it. There are more instances wherethere is less than optimal care—it’s not lim-ited to behavioral health—rather than toomuch.
Several themes can be extrapolatedfrom the discussion with Dr. Bowden. A
positive trend is that research in bipolardisorder are increasing, especially inquality and applicability to clinical set-tings. Additionally, Dr. Bowden men-tions investigations with a focus onincorporating modern classifications of
bipolar disorder into future DSM edi-tions, to better capture what is observedin clinical practice. Psychosocial treat-ment also seems to be gaining in promi-nence in comprehensive bipolar disordertreatments, and our patients are seekingour expert opinions and guidance toenhance their quality of life. ✯
AdvertisingOpportunities
Texas Psychologist
Conference Program
texaspsyc.org
Membership Directory
Take advantage of numerous
advertising opportunities to improve
your visibility with professionals
across the state of Texas.
Contact Pat Huber for more
information at 512-310.9795 or
e-mail [email protected]

Texas Psychologist 33SPRING 2002
Who will be first?As I sit down to write this article, New
Mexico’s RxP Bill has just passed out of itsHouse of Representatives. By the time thisjournal is delivered, New Mexico may verywell have prescription privileges for psy-chologists. How did New Mexico get to thispoint so quickly?
In their first try, during the 2001 NewMexico regular legislative session, the NewMexico Psychological Association got theirbill passed out of the House and out of twoSenate committees. MNA had the votes topass the bill in the Senate; however, on thelast day of the legislative session the leader inthe Senate kept the bill from being broughtup for a vote. After psychologists and psy-chiatrists debated the issue before the gover-nor, he requested the bill be brought upagain during the short 2002 session. Andnow New Mexico could be the first state topass an RxP bill. A few dedicated psycholo-gists already trained in psychopharmacology,with the backing of the AmericanPsychological Association and psychologistsall over the country, have gotten a prescrib-ing bill farther in a shorter time in NewMexico than any other state has.
At this time, 11 states have submittedRxP legislation at least once. Texas is one ofthose eleven. Texas began planning for pre-scriptive authority for psychologists as earlyas 1996. A time line was established thatwould put TPA in position to submit itsfirst bill in 2001. Task Forces were formed,debates were held and a new lobbyist washired. On schedule, TPA submitted its firstprescribing bill in the 2001 legislative ses-sion. With an abbreviated session becauseof redistricting, it was decided not to pushfor a vote in committee at that time. Ournext opportunity will be in 2003. With atleast one other state having passed RxP leg-islation that could be our year. The questionwas once, should psychologists prescribe?The question now is when? The momen-tum is here. The time is now!
Texas A&M PsychopharmacologyProgram
Over 100 psychologists in Texas havealready completed a psychopharmacologytraining program and many of those psychol-ogists are now completing a practicum underthe supervision of physicians. Recently, TexasA&M University, with the cooperation of theTexas Psychological Association, developed apsychopharmacology training program forpracticing psychologists. The program isoffered through Continuing Education in theCollege of Education. The program will betaught through Distance Learning at varioussites around the state. The program will beginwith sites in Dallas, San Antonio and CollegeStation. The first cohort is scheduled for April2002. It is not too late to enroll. Applicationsare available on line at www.coe.tamu.edu/~psypharm/ or by calling Kelli Phelan at 979-862-6529. ✯
Psychopharmacology on the MoveBy Dee Yates, PhD
For
TPA
Mem
bers
hip
Info
rmat
ion
visi
t w
ww
.tex
asps
yc.o
rg
@Does TPA have your
e-mail address?
If not, you could be missing out on
important announcements about
upcoming CE opportunities and
numerous other important updates.
If you have not been receiving
announcements from us via e-mail,
then we don’t have your current
address. To have your e-mail address
added, send your updated address to
E-mail Updates

34 Texas Psychologist SPRING 2002
TEXAS PSYCHOLOGY FOUNDATION
The mission of the Texas PsychologyFoundation is to support activities in
Texas that promote psychology and servicesfor the citizens of Texas. An example ofrecent Foundation activity was the TownHall on School Violence at the TPA AnnualConvention in October 2001. The TownHall brought together a diverse group ofprofessionals, including judges, school lead-ers, teenagers and parents from the commu-nity, to establish a framework to deal withviolence in the school setting.
The Foundation accepts gifts, memorialsto honor colleagues, family members andfriends, and bequests from estates. Gifts orbequests may include cash, securities, orinsurance proceeds. The Foundation isavailable to assist individuals in establishingmemorials or bequests from an estate. Allcontributions to the Foundation are taxdeductible.
• The Foundation accepts earmarked dona-tions to the following designated Funds:
• Schoenfeld-McCann-Schmidt-EhrismanFund for Ethics Education: Provides edu-cation in ethics in the field of psychologyin Texas.
• Rose Costello Education Fund: Providesawards for furthering education in psychology.
• Roy Scrivner Ga, Lesbian and BisexualIssues Award: Provides an annual awardfor the best student paper on Gay &Lesbian research issues.
• Bo and Sally Family Psychology ResearchAward: Provides awards for research pro-jects related to family psychology.
• TPA/TPF-Student Merit ResearchAwards: Given to one graduate student
and one undergraduate student to defraycosts of meritorious research projects.
• Alexander Award: Provides an award forthe best paper submitted by a graduatestudent in psychobiology, psychophysiol-ogy and related areas.
• Manuel Ramirez III Dissertation Awardfor Ethnic Minority Research: Providesawards for research projects related toEthnic Minority Psychology.
If you would like to make a donation,please make checks payable to TPF and mailto: 1011 Meredith Dr., Ste. 4, Austin, TX78748. Donations may also be charged toyour credit card by calling the central officeat 512-280-4099 or 888-872-3435. ✯
Joseph C Kobos, PhD, President
Have considered getting a doctorate?The Fielding Graduate Institute’s School of Psychology offers doctoral and certificate programs to midcareer adults in the areas of :• Clinical Psychology (Ph.D.) (APA approved)• Post-Doctoral Respecialization in Clinical Psychology (Certificate)• Contact www.fielding.edu for more information
Continuing Education Is As Close As Your Computer
Fielding Graduate Institute’s Webcast CE program. The most convenient way to renew your License.
TopicsADD/ADHD Anxiety Disorders Biological BasesBipoloar Disorders Child Therapy Couples TherapyDepression Divorce Medication Domestic ViolenceDSM-IV Eating Disorders Gerontology Legaland Ethical Multicultural NeuropsychologyParenting Psych. Testing PsychopharmSex Offenders Substance Abuse Supervision
What if you could renew your license on your own time, in you own home? Fielding’sWebcast CE program in the School of Psychology makes it possible. Courses are online andcan be completed in one sitting. Or, they can be done “your way”—to be completed in smallersegments—whichever is more convenient for you. For complete information, or to register,please call or visit our website:
www.fielding.edu/ce/online800-340-1099
ARTICLEREPRINTSCall Pat Huberat (512) 310-9795for rates and information.
Texas Psychologist 35SPRING 2002
Private Practice Psychologist Needed:
Psychologist needed to provide managed
care counseling and assessment in an
expanding private outpatient setting. Part
to full-time. Referrals, staff support, and
office space will be provided. Clients are
predominantly adults. Strong clinical
skills, extensive managed care eligibility
required. Apply to [email protected],
phone 713-774-2122, fax 713-774-3223.
Address: 8303 SW Frwy #303, Houston,
TX 77074.
EXPERIENCED PRESENTERS NEEDED!
Do you have an area of expertise?
Strong presentation skills? A desire to
increase your income but continue your
clinical practice? Meet new colleages and
expand your professional network?
Wisdom Springs, a company dedicated to
professional education, is seeking mental
health professionals to present to their
peers for CEUs throughout the state of
Texas. For more information, please call
Gail Chester, PhD at 1-866-329-4136 or
CLASSIFIEDS ADVERTISERS INDEX
Academic Review BC
Advanced Training IBC
AGS 18
American Professional Agency IFC
A.P.E.S. 18
CE Credit 4
Fielding Institute 34
Hazelden 12
Institute for Alternatives 35
Omega 7
Professional EDU 6
Professional Charges 27
Renfrew Center 3
Rockport 5
Senior Connections 11
36 Texas Psychologist SPRING 2002
$1,000Tim Branaman, PhDRon L. Cohorn, PhD
$500-$999Kevin G. Smith, PhD
$100-$249 *Laurence Abrams, PhD
Kyle Babick, PhDRay H. Brown, PhDSam J. Buser, PhD
Jim L..H. Cox, PhDRichard Fulbright, PhD
Ronald Alan Garber, PhDHumberto S. Gonzalez, PhD
Jerry R. Grammer, PhDCharles A. Haskovec, PhD
Sophia K. Havasy, PhDSheila Jenkins, PhDKevin T. Jones, PhDNancy A. Leslie, PhD
Marcia J. Lindsey, PsyDLeon Morris, EdD
J. Randall Price, PhDShannon E. Scott, PhD
Jana Swart, PhDThomas A. Van Hoose, PhD
David S. Wachtel, PhDJohn W. Worsham, Jr., PhD
Under $100Barbara Abrams, EdDElizabeth Barry, PhDConnie Benfield, PhDGlenn Bricken, PsyDBarry Bullard, PsyDCaren Cooper, PhD
Leslie Crossman, PhDC. Munro Cullum, PhDLinda M. Ingraham, PhD
Harry F. Klinefelter,III, PhDKaren Krause, PhDVictor E. Loos, PhD
Sam Marullo, Jr., PhDJoseph H. McCoy, PhD
Muriel Meicler, PhDShelley Probber, PsyD
Ollie J. Seay, PhDRobert M. Setty, PhD
Debbi S. Wagner-Johnson, BAB. R. Walker, PhD
Colleen A. Walter, PhDPatricia D. Weger, PhDMark J. Wernick, PhDConnie S. Wilson, PhD
Eirene Wong-Liang, PhD
*Individuals who contribute at least $100 may vote in PSY-PAC elections.
PSY-PAC
2001 PSY-PAC ContributorsJanuary 1 - February 4
Ron Cohorn, PhD, PSY-PAC President
The only organizations that represent psychologists in the Texas Legislature are the Texas Psychological Association and the PsychologyPolitical Action Committee (PSY-PAC). Legislative monitoring for bills that are detrimental to psychology and proactively introduce legis-lation to further the field are essential to the survival of our profession. These activities are not for just a few special interests, but for the pro-fession in general. As a group, psychologists have not understood the importance of contributing to the PSY-PAC fund, but the events of thenext few years will make consistent contributing absolutely necessary.
We will soon be facing sunset of our practice act and we must have funds to adequately protect our profession. Dealing with managedcare and promoting prescription privileges are also matters of priority. Unfortunately, only 10 percent of TPA. members contribute to thePAC and 2 percent contribute the majority of total funds. Please consider a contribution, consistent with your income, and help your pro-fession. We can do great things if everyone pulls together.
Please make a personal commitment to contribute regularly to PSY-PAC. Again, thank you for your support.