Toxicant-induced Loss of Tolerance-An Emerging Theory of ...
9
Toxicant-induced Loss of Tolerance-An Emerging Theory of Disease? Claudia S. Miller Department of Family Practice, The University of Texas Health Science Center, San Antonio, Texas This paper attempts to clarify the nature of chemical sensitivity by proposing a theory of disease that unites the disparate clinical observations associated with the condition. Sensitivity to chemicals appears to be the consequence of a two-step process: loss of tolerance in susceptible persons following exposure to various toxicants, and subsequent triggering of symptoms by extremely small quantities of previously tolerated chemicals, drugs, foods, and food and drug combinations including caffeine and alcohol. Although chemical sensitivity may be the consequence of this process, a term that may more clearly describe the observed process is toxicant-induced loss of tolerance. Features of this yet-to-be-proven mechanism or theory of disease that affect the design of human exposure studies include the stimulatory and withdrawallike nature (resembling addiction) of symptoms reported by patients and masking. Masking, which may blunt or eliminate responses to chemical challenges, appears to have several components: apposition, which is the overlapping of the effects of closely timed exposures, acclimatization or habituation, and addiction. A number of human challenge studies in this area have concluded that there is no physiological basis for chemical sensitivity. However, these studies have failed to address the role of masking. To ensure reliable and reproducible responses to challenges, future studies in which subjects are evaluated in an environmental medical unit, a hospital-based facility in which background chemical exposures are reduced to the lowest levels practicable, may be necessary. A set of postulates is offered to determine whether there is a causal relationship between low-level chemical exposures and symptoms using an environmental medical unit. Environ Health Perspect 1 05(Suppl 2):445-453 (1997) Key words: adaptation, chemical sensitivity, masking, multiple chemical sensitivity, sensitivity, sensitization, tolerance, addiction, habituation Introduction Clinical observations in North America (1-7) and Europe (8) point to an expand- ing group of patients who report sensitivities to extraordinarily low levels of environmen- tal chemicals. This phenomenon, termed chemical sensitivity or multiple chemical sensitivity, appears to develop de novo in some individuals following acute or chronic exposure to a wide variety of environmental agents including various pesticides, solvents, drugs, and air contaminants in so-called sick buildings. Some practitioners have attributed a broad spectrum of chronic medical condi- tions involving any and every organ system to chemical sensitivity (Figure 1) (4). Efforts to formulate a case definition for chemical sensitivity, to identify relevant biomarkers, and to explore a variety of mechanisms for the condition have esca- lated over the past decade. Several conflict- ing schools of thought have evolved with respect to underlying mechanisms, ranging from the purely psychological to the wholly physiological. In the midst of the tumult surrounding chemical sensitivity lies a pro- found but little-recognized scientific debate concerning the origins of disease. Some participants in this debate are challenging currently accepted notions concerning the causes for many chronic illnesses. This paper is based on a presentation .at the Conference on Experimental Approaches to Chemical Sensitivity held 20-22 September 1995 in Princeton, New Jersey. Manuscript received at EHP 6 March 1996; manuscript accepted 9 September 1996. Research for this paper was supported in part by an appointment to the Agency for Toxic Substances and Disease Registry (ATSDR) Clinical Fellowship Program in Environmental Medicine, administered by Oak Ridge Associated Universities through an interagency agreement between the U.S. Department of Energy and ATSDR. Address correspondence to Dr. C.S. Miller, Department of Family Practice, The University of Texas Health Science Center at San Antonio, 7703 Floyd Curl Drive, San Antonio, TX 78284-7794. Telephone: (210) 567- 4557. Fax: (210) 567-4579. E-mail: [email protected] Abbreviations used: EMU, environmental medical unit; TILT, toxicant-induced loss of tolerance. This paper attempts to clarify the nature of chemical sensitivity by describing a gen- eral mechanism that appears to underlie these cases; proposes a theory of disease based upon this general mechanism; and offers a set of testable postulates for corrobo- rating or refuting this theory. Science is not about opinion or belief; it is about "guess and test," that is, formulating hypotheses and then devising experiments to test them. Terminology Phenomenologically, chemical sensitivity appears to develop in two stages (3,4). First is the loss of tolerance (possibly but not necessarily due to sensitization) follow- ing acute or chronic exposure to various environmental agents such as pesticides, solvents, or contaminated air in a sick building. Second is the subsequent trigger- ing of symptoms by extremely small quan- tities of previously tolerated chemicals, drugs, foods, and food and drug combina- tions (Figure 2). Although sensitivity to chemicals may be one of the consequences of this two-stage process, the term chemical sensitivity does not appropriately describe the process involved. There are two principal reasons for this. First, although chemical sensitivity cer- tainly sounds like an inconvenient problem to have, the words fail to convey the poten- tially disabling nature of the condition and its postulated origins in a toxic exposure. Some researchers balk at using the word toxic in this manner. However, numerous investigators from different geographic regions have published strikingly similar descriptions of individuals who report dis- abling illnesses after exposure to recognized environmental contaminants, albeit at levels not generally regarded as toxic (1,9-12). Yet, for these individuals, the exposure appears to have been toxic. Paracelsus aptly opined that dose makes the poison. However, as our knowledge has grown, it has become evident that dose + host makes the poison (for example, pack- years of smoking plus a-l-antitrypsin defi- ciency). Similarly, in the case of chemical sensitivity, not everyone exposed in a sick building or to a chemical spill develops chronic illness. Thus, it may be concluded that individual susceptibility, whether physiological or psychological, must play a role in determining who gets sick. The term chemical sensitivity fails to convey this key observation that chemical exposures appear to initiate a process that results in chemical Environmental Health Perspectives - Vol 105, Supplement 2 * March 1997 445
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Toxicant-induced Loss of Tolerance-An Emerging Theory of ...
Toxicant-induced Loss of Tolerance-AnEmerging Theory of Disease?Claudia S. MillerDepartment of Family Practice, The University of TexasHealth Science Center, San Antonio, Texas
This paper attempts to clarify the nature of chemical sensitivity by proposing a theory of diseasethat unites the disparate clinical observations associated with the condition. Sensitivity tochemicals appears to be the consequence of a two-step process: loss of tolerance in susceptiblepersons following exposure to various toxicants, and subsequent triggering of symptoms byextremely small quantities of previously tolerated chemicals, drugs, foods, and food and drugcombinations including caffeine and alcohol. Although chemical sensitivity may be theconsequence of this process, a term that may more clearly describe the observed process istoxicant-induced loss of tolerance. Features of this yet-to-be-proven mechanism or theory ofdisease that affect the design of human exposure studies include the stimulatory andwithdrawallike nature (resembling addiction) of symptoms reported by patients and masking.Masking, which may blunt or eliminate responses to chemical challenges, appears to haveseveral components: apposition, which is the overlapping of the effects of closely timedexposures, acclimatization or habituation, and addiction. A number of human challenge studies inthis area have concluded that there is no physiological basis for chemical sensitivity. However,these studies have failed to address the role of masking. To ensure reliable and reproducibleresponses to challenges, future studies in which subjects are evaluated in an environmentalmedical unit, a hospital-based facility in which background chemical exposures are reduced to thelowest levels practicable, may be necessary. A set of postulates is offered to determine whetherthere is a causal relationship between low-level chemical exposures and symptoms using an
environmental medical unit. Environ Health Perspect 1 05(Suppl 2):445-453 (1997)
Key words: adaptation, chemical sensitivity, masking, multiple chemical sensitivity,sensitivity, sensitization, tolerance, addiction, habituation
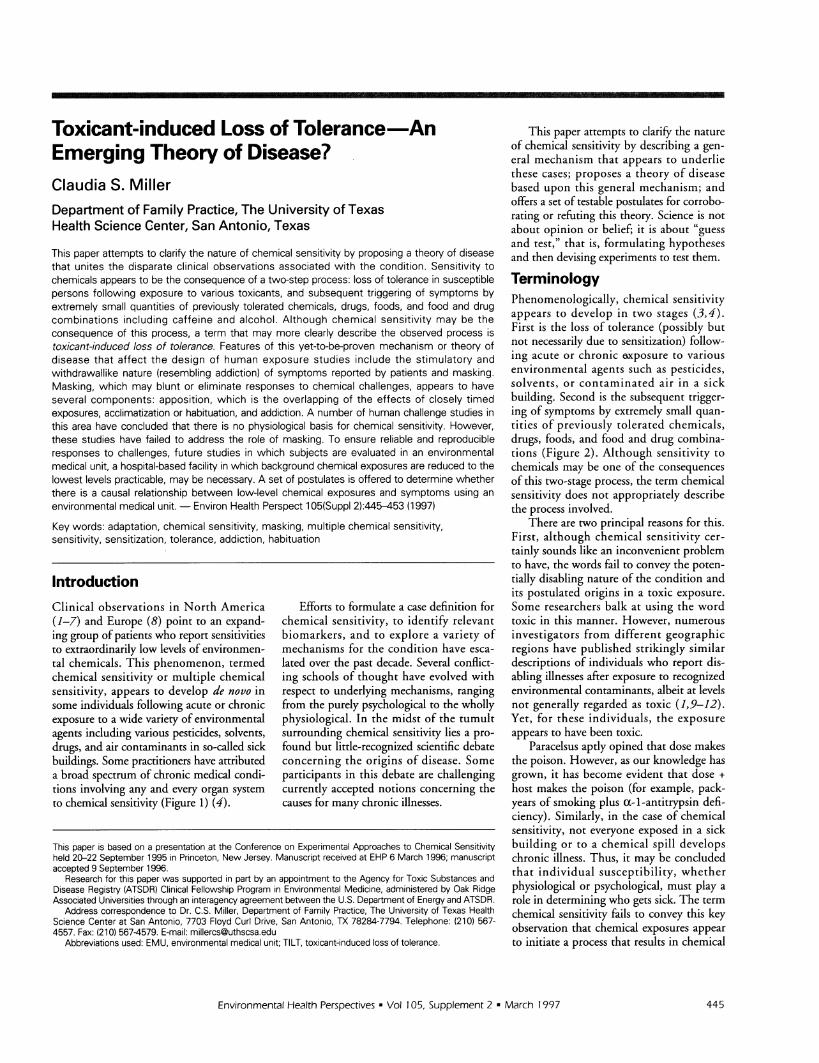
IntroductionClinical observations in North America(1-7) and Europe (8) point to an expand-ing group of patients who report sensitivitiesto extraordinarily low levels of environmen-tal chemicals. This phenomenon, termedchemical sensitivity or multiple chemicalsensitivity, appears to develop de novo insome individuals following acute or chronicexposure to a wide variety of environmentalagents including various pesticides, solvents,drugs, and air contaminants in so-called sickbuildings. Some practitioners have attributeda broad spectrum of chronic medical condi-tions involving any and every organ systemto chemical sensitivity (Figure 1) (4).
Efforts to formulate a case definition forchemical sensitivity, to identify relevantbiomarkers, and to explore a variety ofmechanisms for the condition have esca-lated over the past decade. Several conflict-ing schools of thought have evolved withrespect to underlying mechanisms, rangingfrom the purely psychological to the whollyphysiological. In the midst of the tumultsurrounding chemical sensitivity lies a pro-found but little-recognized scientific debateconcerning the origins of disease. Someparticipants in this debate are challengingcurrently accepted notions concerning thecauses for many chronic illnesses.
This paper is based on a presentation .at the Conference on Experimental Approaches to Chemical Sensitivityheld 20-22 September 1995 in Princeton, New Jersey. Manuscript received at EHP 6 March 1996; manuscriptaccepted 9 September 1996.
Research for this paper was supported in part by an appointment to the Agency for Toxic Substances andDisease Registry (ATSDR) Clinical Fellowship Program in Environmental Medicine, administered by Oak RidgeAssociated Universities through an interagency agreement between the U.S. Department of Energy and ATSDR.
Address correspondence to Dr. C.S. Miller, Department of Family Practice, The University of Texas HealthScience Center at San Antonio, 7703 Floyd Curl Drive, San Antonio, TX 78284-7794. Telephone: (210) 567-4557. Fax: (210) 567-4579. E-mail: [email protected]
Abbreviations used: EMU, environmental medical unit; TILT, toxicant-induced loss of tolerance.
This paper attempts to clarify the natureof chemical sensitivity by describing a gen-eral mechanism that appears to underliethese cases; proposes a theory of diseasebased upon this general mechanism; andoffers a set of testable postulates for corrobo-rating or refuting this theory. Science is notabout opinion or belief; it is about "guessand test," that is, formulating hypothesesand then devising experiments to test them.
TerminologyPhenomenologically, chemical sensitivityappears to develop in two stages (3,4).First is the loss of tolerance (possibly butnot necessarily due to sensitization) follow-ing acute or chronic exposure to variousenvironmental agents such as pesticides,solvents, or contaminated air in a sickbuilding. Second is the subsequent trigger-ing of symptoms by extremely small quan-tities of previously tolerated chemicals,drugs, foods, and food and drug combina-tions (Figure 2). Although sensitivity tochemicals may be one of the consequencesof this two-stage process, the term chemicalsensitivity does not appropriately describethe process involved.
There are two principal reasons for this.First, although chemical sensitivity cer-tainly sounds like an inconvenient problemto have, the words fail to convey the poten-tially disabling nature of the condition andits postulated origins in a toxic exposure.Some researchers balk at using the wordtoxic in this manner. However, numerousinvestigators from different geographicregions have published strikingly similardescriptions of individuals who report dis-abling illnesses after exposure to recognizedenvironmental contaminants, albeit at levelsnot generally regarded as toxic (1,9-12).Yet, for these individuals, the exposureappears to have been toxic.
Paracelsus aptly opined that dose makesthe poison. However, as our knowledge hasgrown, it has become evident that dose +host makes the poison (for example, pack-years of smoking plus a-l-antitrypsin defi-ciency). Similarly, in the case of chemicalsensitivity, not everyone exposed in a sickbuilding or to a chemical spill developschronic illness. Thus, it may be concludedthat individual susceptibility, whetherphysiological or psychological, must play arole in determining who gets sick. The termchemical sensitivity fails to convey this keyobservation that chemical exposures appearto initiate a process that results in chemical
Environmental Health Perspectives - Vol 105, Supplement 2 * March 1997 445
C.S. MILLER
Ear, nose, and throat* Sinusitis* Polyps* Tinnitus* Recurrent otitis
Miscellaneous* Chronic fatigue syndrome* Implant syndromes* Gulf War syndrome
Skin
Neuropsychological* Multiple chemical sensitivity* Attention deficit hyperactivitydisorder (ADHD)
* Depression/manic depression* Migraines and other headaches* Seizures
* Eczema* Hives* Other rashes, eruptions
Cardiovascular* Arrhythmias* Hypertension* Hypotension* Raynaud's phenomenon
Respiratory* Asthma* Reactive airways dysfunctionsyndrome (RADS)
*Toluene diisocyanate ITDI)hypersensitivity
Gastrointestinal* Irritable bowel*Reflux
Connective tissue/musculoskeletal* Fibromyalgia* Carpal tunnel syndrome* Temporomandibular joint (TMJ) dysfunction syndrome* Arthritis* Lupus
Figure 1. Some conditions that have been attributed to chemical sensitivity.
Symptoms -
©( Triggering Masking
Sensitive LowlvDerson epur
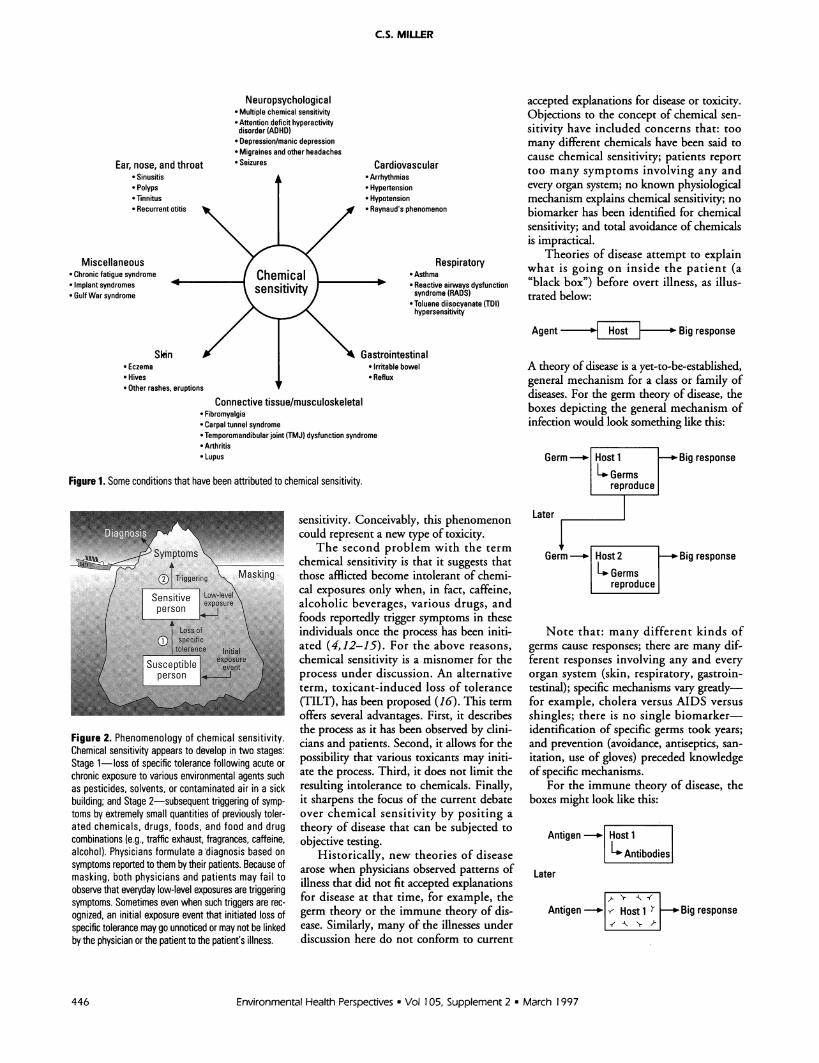
Figure 2. Phenomenology of chemical sensitivity.Chemical sensitivity appears to develop in two stages:Stage 1-loss of specific tolerance following acute orchronic exposure to various environmental agents suchas pesticides, solvents, or contaminated air in a sickbuilding; and Stage 2-subsequent triggering of symp-toms by extremely small quantities of previously toler-ated chemicals, drugs, foods, and food and drugcombinations (e.g., traffic exhaust, fragrances, caffeine,alcohol). Physicians formulate a diagnosis based onsymptoms reported to them by their patients. Because ofmasking, both physicians and patients may fail toobserve that everyday low-level exposures are triggeringsymptoms. Sometimes even when such triggers are rec-ognized, an initial exposure event that initiated loss ofspecific tolerance may go unnoticed or may not be linkedby the physician or the patient to the patient's illness.
sensitivity. Conceivably, this phenomenoncould represent a new type of toxicity.
The second problem with the termchemical sensitivity is that it suggests thatthose afflicted become intolerant of chemi-cal exposures only when, in fact, caffeine,alcoholic beverages, various drugs, andfoods reportedly trigger symptoms in theseindividuals once the process has been initi-ated (4,12-15). For the above reasons,chemical sensitivity is a misnomer for theprocess under discussion. An alternativeterm, toxicant-induced loss of tolerance(TILT), has been proposed (16). This termoffers several advantages. First, it describesthe process as it has been observed by clini-cians and patients. Second, it allows for thepossibility that various toxicants may initi-ate the process. Third, it does not limit theresulting intolerance to chemicals. Finally,it sharpens the focus of the current debateover chemical sensitivity by positing atheory of disease that can be subjected toobjective testing.
Historically, new theories of diseasearose when physicians observed patterns ofillness that did not fit accepted explanationsfor disease at that time, for example, thegerm theory or the immune theory of dis-ease. Similarly, many of the illnesses underdiscussion here do not conform to current
accepted explanations for disease or toxicity.Objections to the concept of chemical sen-sitivity have included concerns that: toomany different chemicals have been said tocause chemical sensitivity; patients reporttoo many symptoms involving any andevery organ system; no known physiologicalmechanism explains chemical sensitivity; nobiomarker has been identified for chemicalsensitivity; and total avoidance of chemicalsis impractical.
Theories of disease attempt to explainwhat is going on inside the patient (a"black box") before overt illness, as illus-trated below:
Agent Hs Big response
A theory of disease is a yet-to-be-established,general mechanism for a class or family ofdiseases. For the germ theory of disease, theboxes depicting the general mechanism ofinfection would look something like this:
Germ Host 1 _Big responseGermsreproduce
Later
Germ - Host 2 Big responseGermsreproduce
Note that: many different kinds ofgerms cause responses; there are many dif-ferent responses involving any and everyorgan system (skin, respiratory, gastroin-testinal); specific mechanisms vary gready-for example, cholera versus AIDS versusshingles; there is no single biomarker-identification of specific germs took years;and prevention (avoidance, antiseptics, san-itation, use of gloves) preceded knowledgeof specific mechanisms.
For the immune theory of disease, theboxes might look like this:
Antigen-| Host 1
Antibodies
Later
Antigen _ - Host 1 r Big response-t\ \, A)
Environmental Health Perspectives * Vol 105, Supplement 2 * March 1997446

TOXICANT-INDUCED LOSS OF TOLERANCE
Here, just as for the germ theory ofdisease: many different kinds of antigenscause responses; there are many differentresponses involving any and every organsystem (skin, respiratory, gastrointestinal);specific mechanisms vary greatly-forexample, poison ivy versus allergic rhinitisversus serum sickness; there is no singlebiomarker-identification of specific anti-bodies took years; and prevention (avoid-ance, allergy shots) preceded knowledge ofspecific mechanisms.
For toxicant-induced loss of tolerance,the boxes might look like this:
Chemical -_ Host 1Loss oftolerance
Later
chemicals - [ 3 _ Big response
For toxicant-induced loss of tolerance, asfor the germ and immune theories of dis-ease: many different kinds of chemicalsmay cause responses; there may be manydifferent responses involving any and everyorgan system; specific mechanisms mayvary greatly; it is conceivable that there isno single biomarker for response-identifi-cation of biomarkers may take years; andprevention (avoidance of initiators or trig-gers) may precede knowledge of specificmechanisms.
Although the concept loss of tolerancemay sound vague, in fact it is not. Whatthese individuals report is a loss of specifictolerance to particular chemicals, foods,and drugs. (16). Note that this theory doesnot exclude the possibility that toxicant-induced loss of tolerance could turn out tobe a special kind of toxicity or a variationon the immune theory of disease just asallergy and delayed-type hypersensitivityare special cases that fall under the generalclassification of immunologic disorders. Aconsequence of viewing TILT as a theoryof disease would be a shift in perspectivefrom chemical sensitivity as a syndrome tochemical sensitivity, now TILT, as a classof disorders parallel to infectious diseasesor immunologic diseases. Much effort hasbeen devoted to developing a case defini-tion for chemical sensitivity, with a singularlack of success. This lack of success wouldnot be surprising if in fact TILT repre-sented a new class or family of disorders.Certainly, it would not be feasible to
develop a single clinical case definitionthat would embrace all infectious or allimmunologic diseases.
Theories of disease that withstandscientific scrutiny arise infrequently. Thepast century has witnessed the inculcationof the germ and immune theories of dis-ease into medical practice. Equating toxi-cant-induced loss of tolerance to either oneof these theories, both of which have beenwidely corroborated, would be prematureand presumptuous. On the other hand,toxicant-induced loss of tolerance has cer-tain earmarks of an emerging theory of dis-ease, including the vituperative professionaldisputes that surround it (16).
Features of TILT Relevantfor Its TestingAs described by many investigators, thisphenomenon appears to involve a two-stage process. Because of ethical considera-tions, the first stage (initiation) is moredifficult to model in humans than the sec-ond stage (triggering). Ultimately, epi-demiologic studies and animal models mayelucidate the first stage. Fortunately, thesecond stage readily lends itself to testingvia direct human challenges, a potent formof scientific evidence. However, in thedesign of human challenge studies in thisarea, certain key clinical observations mustbe taken into account. First, the commonlyreported biphasic, stimulatory-and-with-drawallike pattern of the patients' symp-toms, particularly those symptoms involvingthe central nervous system, must be under-stood to perform meaningful test challengeson these patients. Second, a related phe-nomenon called masking (to be describedfurther) may hide responses to low-levelchemical challenges and therefore may needto be minimized before testing. Controllingmasking may be analogous to controllingbackground noise in studies on sound.
The following sections will discussthese clinical features, their incorporationin experimental designs, and how failure todo so might threaten research outcomes.
Stimulatory andWithdrawal SymptomsRandolph first described the time course ofthe responses of these individuals to chemi-cals and foods (17). He reported strikingparallels between their symptoms and thoseassociated with alcohol and drug addiction.Randolph viewed the food and caffeineaddictions his patients exhibited as thebottom rungs in a hierarchy of addiction,proceeding from foods and food and drug
combinations such as caffeine and alcoholon the lower rungs upward to nicotine andother naturally occurring and syntheticallyderived drugs (14).
Chemically sensitive patients resembledrug addicts in that members of bothgroups often report intense cravings anddebilitating withdrawal symptoms. How-ever, chemically sensitive patients' responsesare not primarily to drugs. These individu-als more commonly report addictions tocaffeine or certain foods. While drugaddicts manifest ad-dicted behaviors (Latinad "toward" + dicare "proclaim"), chemi-cally sensitive patients respond as thoughthey were ab-dicted (Latin ab "away from"+ dicare "proclaim") and assiduously avoidthe very substances addicted persons favorincluding alcohol, drugs and nicotine.
The stimulatory and withdrawal symp-toms reported by chemically sensitivepatients are frequently identical to thosereported by normal persons exposed tomuch greater amounts of the same sub-stances. For example, after drinking onecup of coffee, chemically sensitive patientsmay report feeling hyperactive, jittery, talk-ative, nervous, anxious, or experiencingpaniclike symptoms (stimulatory phase).Hours to days later, they may report with-drawal symptoms such as fatigue, yawning,confusion, indecisiveness, irritability,depression, loss of motivation, blurredvision, headaches, flulike symptoms, hot orcold spells, or heaviness in their arms andlegs (withdrawal phase). Similar symptomsoccur during caffeine withdrawal amongsome low-to-moderate caffeine users in thegeneral population (18). Large numbers ofchemically sensitive patients and manyGulf War veterans with unexplained ill-nesses report that one drink of an alcoholicbeverage causes inebriation and/or a severehangover (12,15,19). These augmentedresponses suggest that those afflicted havelost their previous natural or native tolerancefor such exposures.
Early in their illnesses, before elimi-nating caffeine from their diets, manychemically sensitive patients report havingconsumed chocolate, coffee, tea, or colaaddictively, often in very large quantities(15). Some carried large containers of cof-fee or tea around wherever they went.Many report later stopping use of all caf-feine and xanthines, generally on theadvice of a friend or physician, and subse-quently experiencing several days of intensewithdrawal symptoms. Frequently theyreport that it was only after eliminating allxanthines from their diets that they were
Environmental Health Perspectives * Vol 105, Supplement 2 * March 1997 447
C.S. MILLER
able to discern the effects of consuming asingle cup of coffee or a chocolate bar. Mostreport becoming aware of the unpleasanteffects of caffeine only after a trial of partialor complete caffeine avoidance. In thisregard, chemically sensitive patients resem-ble certain reformed smokers or alcoholicswho after quitting their addictants reportextreme sensitivity to minute amounts ofthe addicting agents. Terms like addiction,withdrawal, and detox pepper the vocabu-lary of chemically sensitive patients. Onepatient described the condition as being"like drug abuse without any of the fun."These parallels to addiction provide per-spective: they may help explain why themechanisms that underlie chemical sensi-tivity have been difficult to define and whybiological markers have proven elusive.
In summary, drug addiction and TILTshare a number of features in common.TILT also has features reminiscent of toxi-city and allergy (Table 1). However, it is itsresemblance to addiction that is perhapsmost striking and that has escaped the atten-tion ofmany physicians and researchers.
MaskingSuppose that TILT was a mechanismunderlying certain cases of chronic fatigue,migraine, asthma, or depression. It mightbe reasonable to wonder, then, why patientsexperiencing these symptoms do not alsoreport chemical intolerances. In fact, somebut not all patients do report them (21,22).Many chemically sensitive patients withthese same diagnoses report that it was notuntil they accidentally or intentionallyavoided a sufficient number of their prob-lem incitants that they noticed feeling bet-ter. Then, when they reencountered one ofthose incitants, robust symptoms occurred.As they repeated this iterative process ofavoidance and reexposure, they noticedthat particular symptoms occurred withparticular exposures. Most indicate thathad they not avoided many chemicals andfoods simultaneously, or unmasked them-selves, they might not have determinedwhat was making them sick.
Masking and unmasking are colorful layterms for which there is no scientific equiv-alent. Nevertheless, investigators' abilities tounderstand masking and unmasking andmanipulate these variables knowledgeablymay determine the success of studies in thisarea. When chemically sensitive patientsfollow a diet free of their problem foodsand live in a relatively chemical-free homein the hills of central Texas where thereare no major agricultural or industrial
Table 1. Features of toxicant-induced loss of tolerance compared with features of addiction, allergy, and toxicity.
Toxicant-inducedFeature loss of tolerancea Addictiona Allergya Toxicitya
Chemical/drug intolerance + + + +Ambient air incitants + + +Food intolerance + +Alcohol intolerance + +Caffeine intolerance + +Withdrawal symptoms + +Craving, binging + (foods) + (drugs)Sensitization + +Induction by chemicals + +b +Induction by biologicals +Multisystem symptoms + + + +Frequent CNS symptomatology + + +Well-defined mechanism(s) + +Genetic susceptibility + + + +Dose-response relationship +C +C +
"Categories are not pure and may overlap in a given host, e.g., haptenation of a chemical toxin may initiate animmunologic response; brain and liver toxicity may accompany alcohol addiction. bLow molecular weight chemi-cals may combine with tissue proteins producing haptens that evoke immune responses. cDose response doesoccur for allergens. With the first sensitizing exposure in a susceptible individual, there is a dose-response rela-tionship; with subsequent exposures, the sensitized person also responds in proportion to dose but at a muchlower dose level (20). The same kind of dose-response relationship may hold true for TILT but this has not beentested. Chemically sensitive individuals generally report increasingly severe symptoms the longer they remain inexposure situations, an observation that suggests a dose-response relationship.
operations or air contaminants, they saythey are in an unmasked state. Under thesecircumstances they claim that if a dieseltruck drove by they could identify specificsymptoms due to the diesel exhaust, forexample, irritability, headache, or nausea.
On the other hand, the patients reportthat when they travel to a large city likeHouston or New York City, stay in a hotelroom, and eat in restaurants, they becomemasked. In the presence of many concur-rent exposures (exhaust, fragrances, volatilesoffgassing from building interiors, variousfoods) in New York City many report feel-ing chronically ill, as if they had flu. If adiesel truck drove by under these circum-stances, most report they would not be ableto attribute any particular symptoms to theexhaust because of background noise fromoverlapping symptoms occurring as a con-sequence of overlapping or successive expo-sures. In theory, such background noise ormasking hides the effects of individualexposures-responses are blurred.
Masking appears to involve at least threeinterrelated components, any of which mayinterfere with the outcome of low-levelchemical challenges in these individuals:acclimatization, apposition, and addiction.In real life, these three components proba-bly operate concurrently, although herethey are considered individually.
There is some notation that can be usedto help depict these components. In theaddiction literature, responses to addictive
Increasingsymptomintensity
+ ++0-
Exposure
Time -
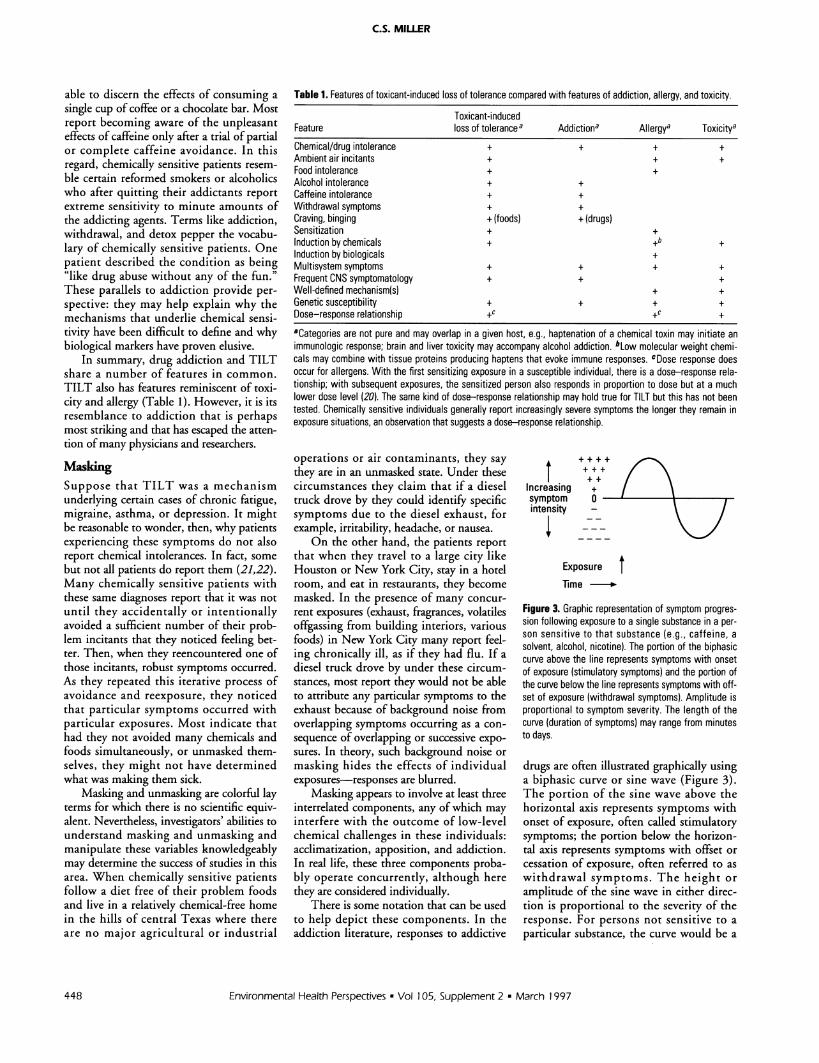
Figure 3. Graphic representation of symptom progres-sion following exposure to a single substance in a per-son sensitive to that substance (e.g., caffeine, asolvent, alcohol, nicotine). The portion of the biphasiccurve above the line represents symptoms with onsetof exposure (stimulatory symptoms) and the portion ofthe curve below the line represents symptoms with off-set of exposure (withdrawal symptoms). Amplitude isproportional to symptom severity. The length of thecurve (duration of symptoms) may range from minutesto days.
drugs are often illustrated graphically usinga biphasic curve or sine wave (Figure 3).The portion of the sine wave above thehorizontal axis represents symptoms withonset of exposure, often called stimulatorysymptoms; the portion below the horizon-tal axis represents symptoms with offset orcessation of exposure, often referred to aswithdrawal symptoms. The height oramplitude of the sine wave in either direc-tion is proportional to the severity of theresponse. For persons not sensitive to aparticular substance, the curve would be a
Environmental Health Perspectives * Vol 105, Supplement 2 * March 1997448
TOXICANT-INDUCED LOSS OF TOLERANCE
flat line with zero amplitude in eitherdirection. The length of the biphasic curverepresents the duration of symptoms fol-lowing an exposure, reportedly rangingfrom minutes up to several days dependingupon the exposure and the individual. Ofcourse, the particular nature of the symp-toms vary from one sensitive subject to thenext and from substance to substance.
Suppose researchers wished to test aputatively sensitive subject by exposing himto a low concentration of xylene. Xylene isa common indoor air contaminant and acomponent of Molhave's mixture (23) thathas been used in human inhalation chal-lenge studies. How would the researchersensure that their subject was unmasked (attrue baseline) before challenge? The follow-ing components of masking would need tobe considered and controlled:
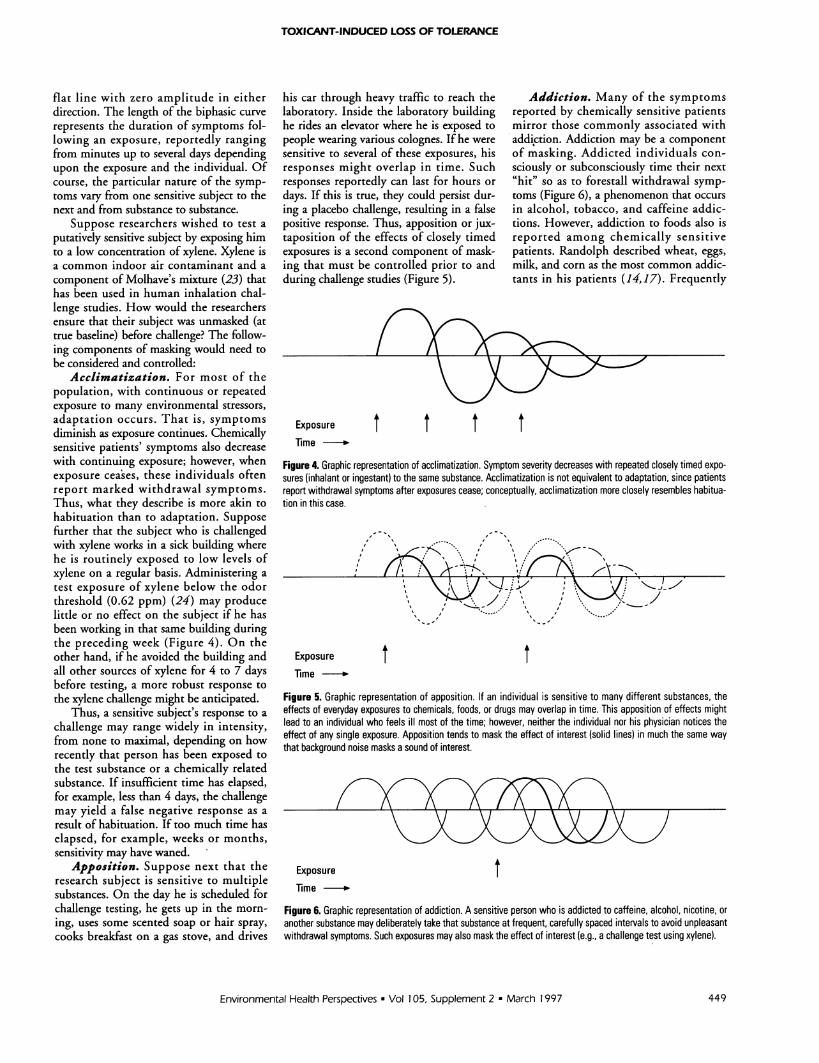
Acclimatization. For most of thepopulation, with continuous or repeatedexposure to many environmental stressors,adaptation occurs. That is, symptomsdiminish as exposure continues. Chemicallysensitive patients' symptoms also decreasewith continuing exposure; however, whenexposure ceases, these individuals oftenreport marked withdrawal symptoms.Thus, what they describe is more akin tohabituation than to adaptation. Supposefurther that the subject who is challengedwith xylene works in a sick building wherehe is routinely exposed to low levels ofxylene on a regular basis. Administering atest exposure of xylene below the odorthreshold (0.62 ppm) (24) may producelittle or no effect on the subject if he hasbeen working in that same building duringthe preceding week (Figure 4). On theother hand, if he avoided the building andall other sources of xylene for 4 to 7 daysbefore testing, a more robust response tothe xylene challenge might be anticipated.
Thus, a sensitive subject's response to achallenge may range widely in intensity,from none to maximal, depending on howrecently that person has been exposed tothe test substance or a chemically relatedsubstance. If insufficient time has elapsed,for example, less than 4 days, the challengemay yield a false negative response as aresult of habituation. If too much time haselapsed, for example, weeks or months,sensitivity may have waned.
Apposition. Suppose next that theresearch subject is sensitive to multiplesubstances. On the day he is scheduled forchallenge testing, he gets up in the morn-ing, uses some scented soap or hair spray,cooks breakfast on a gas stove, and drives
his car through heavy traffic to reach thelaboratory. Inside the laboratory buildinghe rides an elevator where he is exposed topeople wearing various colognes. If he weresensitive to several of these exposures, hisresponses might overlap in time. Suchresponses reportedly can last for hours ordays. If this is true, they could persist dur-ing a placebo challenge, resulting in a falsepositive response. Thus, apposition or jux-taposition of the effects of closely timedexposures is a second component of mask-ing that must be controlled prior to andduring challenge studies (Figure 5).
Addiction. Many of the symptomsreported by chemically sensitive patientsmirror those commonly associated withaddi,ction. Addiction may be a componentof masking. Addicted individuals con-sciously or subconsciously time their next"hit" so as to forestall withdrawal symp-toms (Figure 6), a phenomenon that occursin alcohol, tobacco, and caffeine addic-tions. However, addiction to foods also isreported among chemically sensitivepatients. Randolph described wheat, eggs,milk, and corn as the most common addic-tants in his patients (14,17). Frequently
Exposure t t t tTime -.
Figure 4. Graphic representation of acclimatization. Symptom severity decreases with repeated closely timed expo-sures (inhalant or ingestant) to the same substance. Acclimatization is not equivalent to adaptation, since patientsreport withdrawal symptoms after exposures cease; conceptually, acclimatization more closely resembles habitua-tion in this case.
ExposureTime -*
t tFigure 5. Graphic representation of apposition. If an individual is sensitive to many different substances, theeffects of everyday exposures to chemicals, foods, or drugs may overlap in time. This apposition of effects mightlead to an individual who feels ill most of the time; however, neither the individual nor his physician notices theeffect of any single exposure. Apposition tends to mask the effect of interest (solid lines) in much the same waythat background noise masks a sound of interest.
Exposure tTime -*
Figure 6. Graphic representation of addiction. A sensitive person who is addicted to caffeine, alcohol, nicotine, oranother substance may deliberately take that substance at frequent, carefully spaced intervals to avoid unpleasantwithdrawal symptoms. Such exposures may also mask the effect of interest (e.g., a challenge test using xylene).
Environmental Health Perspectives * Vol 105, Supplement 2 * March 1997 449
C.S. MILLER
these individuals report intense cravingsand consume astounding quantities offoods, for example, a pound of chocolate,several bags of popcorn, a dozen dough-nuts, or 30 cups of coffee in one day.Patients most often report this kind ofaddictive consumption in the early stages oftheir illness, before they practiced avoidingproblem exposures.
Foods may contain bioactive con-stituents such as tyramine, monosodiumglutamate, and opiates (13). Persons whoroutinely use tobacco, caffeine, alcohol, orfoods containing bioactive substances mayneed to avoid these substances before test-ing because the pharmacologic effects ofthese agents could override or mask theeffect of an experimental challenge. Failureto eliminate addictants before testing couldresult either in false positive challenges dueto lingering symptoms from an addictantused in the hours or days preceding aplacebo challenge or in false negativechallenges due to masking by an addictant.
Testing the TILT TheoryAfter the germ theory of disease was intro-duced in the late 1800s, many overly enthu-siastic investigators who were careless intheir bacteriological techniques announcedthey had discovered causative agents fortuberculosis, yellow fever, and other dis-eases. These pronouncements and subse-quent retractions became so frequent thatin 1884 the President of the New YorkAcademy of Medicine lamented that abacteriomania had swept over the medicalprofession (25). To prevent future suchpseudodiscoveries, Robert Koch, who iden-tified the organisms responsible for tuber-culosis, anthrax, and cholera, proposed aset of rules for etiological verification. Hispostulates required that: the microbe mustpresent in every case of the disease; it mustbe isolatable in pure culture; inoculating ahealthy animal with the culture mustreproduce the disease; and the microbemust be recoverable from the inoculatedanimal and be able to be grown again.
Just as bacteriomania engulfed the med-ical profession in the 1880s, chemomania ispoised to engulf it now. Chemical sensitiv-ity is in need of a set of postulates to ensurethat future causal determinations are scien-tifically based. Below is a set of postulatesthat, if met, would confirm (and if not met,refute) that a person's symptoms werecaused by a particular substance:
When a subject simultaneously avoids allchemical, food and drug incitants, remis-sion ofsymptoms occurs (unmasking).
EnterEMU
t t . 4 to 7 days - t- 4 to 7 days *t
Figure 7. Graphic representation depicting the testing of the toxicant-induced loss of tolerance postulates usingan environmental medical unit. In the left-hand portion of the figure, a chemically sensitive individual is experienc-ing symptoms in response to multiple exposures (chemicals, foods, drugs) before entering the environmental med-ical unit. Effects overlap in time. The effect of any particular exposure cannot be distinguished from the effects ofother exposures, and the person's symptoms may appear to wax and wane unpredictably over time. Postulate 1-When all chemical, food,and drug incitants are avoided concurrently, remission of symptoms occurs. Anecdotally,patients report going through withdrawal or detox for the first several days during which they experience symp-toms such as increased irritability, headaches, and depression. After 4 to 7 days, most report feeling well andtheoretically are at a clean baseline. Postulate 2-A specific constellation of symptoms occurs with reintroductionof an incitant. Postulate 3-Symptoms resolve when the incitant is again avoided. Postulate 4-Reexposure tothe same incitant within an appropriate window of time (estimated to be about 4-7 days) produces the samesymptoms. For research purposes, challenges should be conducted in a double-blind, placebo-controlled manner.
* A specific constellation of symptomsoccurs with reintroduction of aparticular incitant.
* Symptoms resolve when the incitant isagain avoided.
* With reexposure to the same incitant, thesame constellation of symptoms reoc-curs, provided that the challenge is con-ducted within an appropriate windowof time. Clinical observations suggestthat an ideal window is 4 to 7 days afterthe last exposure to the test incitant.To apply these postulates (illustrated in
Figure 7), the timing of exposures and thedegree of masking should be rigorously
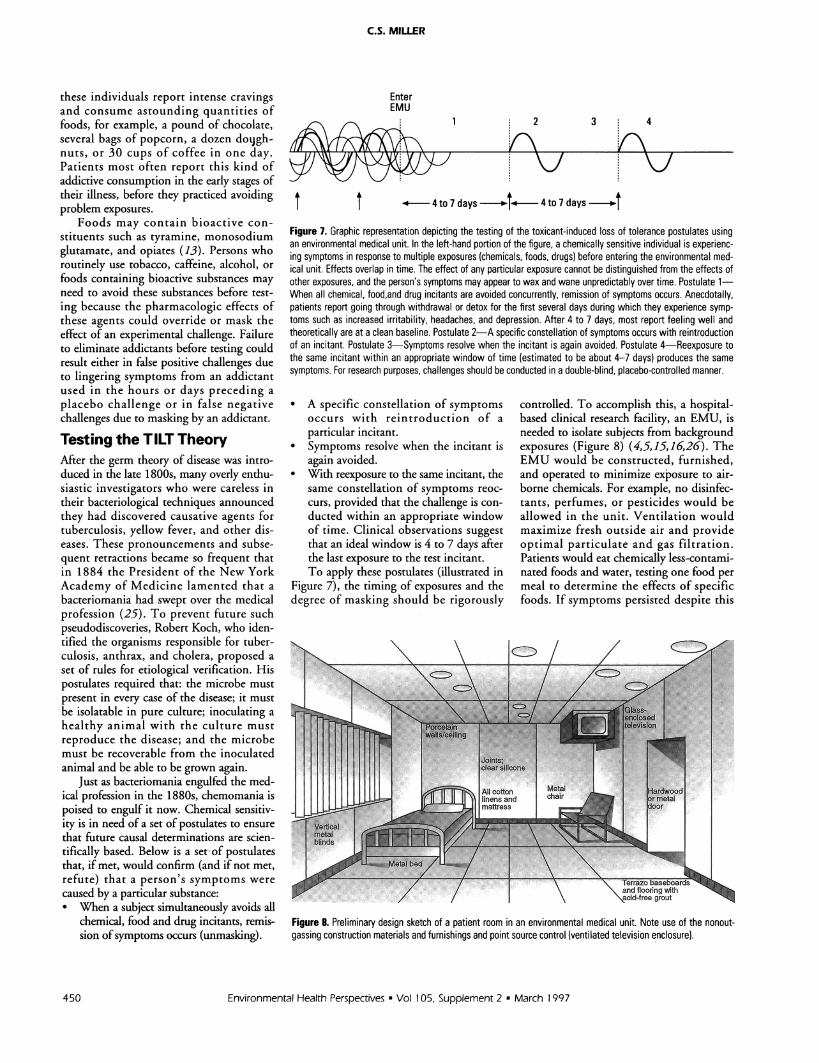
controlled. To accomplish this, a hospital-based clinical research facility, an EMU, isneeded to isolate subjects from backgroundexposures (Figure 8) (4,5,15,16,26). TheEMU would be constructed, furnished,and operated to minimize exposure to air-borne chemicals. For example, no disinfec-tants, perfumes, or pesticides would beallowed in the unit. Ventilation wouldmaximize fresh outside air and provideoptimal particulate and gas filtration.Patients would eat chemically less-contami-nated foods and water, testing one food permeal to determine the effects of specificfoods. If symptoms persisted despite this
Figure 8. Preliminary design sketch of a patient room in an environmental medical unit. Note use of the nonout-gassing construction materials and furnishings and point source control (ventilated television enclosure).
Environmental Health Perspectives * Vol 105, Supplement 2 * March 1997450

TOXICANT-INDUCED LOSS OF TOLERANCE
approach, fasting for a few days would beattempted before reintroducing single foods.
The rationale for housing subjects in anenvironmentally controlled facility for sev-eral days before challenges is 2-fold: to pre-vent extraneous exposure of patients toinhalants or ingestants so responses to themare not misinterpreted as positive responseswhen placebo challenges are administered(false positives), and to minimize maskingthat might blunt or eliminate responses toactive challenges (false negatives).
Although the terms exposure chamberand environmental medical unit appearsimilar, conceptually they differ in impor-tant ways with regard to patient safety andcontrol of interfering exposures.
By definition, an EMU is in a hospitalwhere patients can remain 24 hr a day in adean environment for up to several weeks.Like an intensive care unit or coronary careunit, the EMU would be a specialized, ded-icated hospital facility. The EMU must bein a hospital to accommodate very sickpatients; exposure chambers do not offercomparable levels of care. Because chemicalchallenges may precipitate bronchoconstric-tion, mental confusion, severe headaches,depression, and other disabling symptoms,these patients should not be tested in anexposure chamber on an outpatient basis.
Conventional exposure chambers donot reduce background chemical exposuresfor extended periods (up to several weeks)so the effects of a particular challenge in apatient can be assessed accurately. This isthe central limitation of exposure chambersand the reason they should not be used torule in or rule out chemical sensitivity. Ifsubjects are not kept in a clean environ-ment for several days before and duringchallenges, false positive responses mayoccur because of interfering exposures andfalse negative responses may occur becauseof masking. In contrast to an exposurechamber, an EMU would minimize inter-fering exposures before and during chal-lenges, thus maximizing the reliability andreproducibility of test responses.
Availability of an EMU would allowphysicians to refer a wide variety of cases inwhich environmental sensitivities were sus-pected to the unit for definitive evaluation.There physicians could observe first-handwhether a patient's symptoms improvedafter several days on a special diet in a cleanenvironment. If improvement occurred,single chemicals at concentrations encoun-tered in normal daily living as well as singlefoods could be reintroduced one at a timewhile the effects of each introduction were
observed. Thus, the EMU would be a toolto determine in the most direct and defini-tive manner possible whether chemical sen-sitivities exist. Studying patients withcomplicated conditions like chronic fatiguesyndrome or GulfWar syndrome in a con-ventional exposure chamber would notprovide the same information, since cham-bers allow only short-term residence, donot control the entire range of backgroundcontaminants, and provide inadequate sep-aration from background exposures priorto challenges.
An analogy may help illustrate theimportance of controlling exposures forextended periods before challenge. If onewished to determine whether a coffeedrinker's headaches were due to caffeine, itwould not be adequate simply to give theperson a cup of coffee and ask him how hefelt. It is obvious that the individual wouldhave to stop using caffeine for a periodbefore a meaningful test of caffeine sensi-tivity could be performed. In this instance,a false negative challenge likely would bethe result of failure to avoid coffee beforechallenge. Similarly, placing a putativelysensitive person in a conventional exposurechamber and exposing him to a low con-centration of a chemical might not pro-duce any noticeable effect. On the otherhand, if this same person remained in aclean environment such as an EMU for afew days before being tested and his condi-tion improved, one could then performmeaningful challenges.
Placing patients in an EMU wouldsimultaneously control all three componentsof masking: stopping all exposures severaldays before challenge testing and spacingtest exposures 4 to 7 days apart would pre-clude acclimatization or habituation; elimi-nating background chemical noise andallowing the effects of each challenge to sub-side before introducing the next one wouldcontrol apposition; and excluding drugs,alcohol, nicotine, and caffeine and spacingintroduction of individual foods 4 to 7 daysapart would interrupt any addiction.Individual sensitivity could then be evalu-ated in the EMU following the postulates inFigure 7 for etiological verification.
For research purposes, challenges mustbe performed in a double-blind, placebo-controlled manner. Patients with chronicfatigue syndrome, migraine headaches,seizures, depression, asthma, or unex-plained illnesses such as Persian Gulf illnesscould also be tested for sensitivities in anEMU using these postulates. Thus, theEMU could be used to determine whether
particular patients with these diagnoses hada masked form of this illness.
What evidence is there that unmaskingpatients in an EMU and conducting chal-lenges within a 4- to 7-day window of timeis either useful or necessary? Thousands ofcredible patients and dozens of physicianshave attempted this approach. They reportthat patients' symptoms resolve within afew days after they enter such a facility andthat robust symptoms occur when chal-lenges are conducted after several days ofavoidance. Other evidence corroboratesthese observations: Withdrawal symptomsof several days' to a week's duration areknown to occur in some persons followingcessation of exposure to nitroglycerine(dynamite workers' headaches) (27), caf-feine (18,28), nicotine, and alcohol. Notethat these substances are chemically unre-lated. In individuals chronically exposed toxylene (29) or ozone (30), reexposure afterseveral days' avoidance results in robustsymptoms. Foods may require one to sev-eral days to navigate the digestive tractbefore they are eliminated. Taken together,these observations suggest that individualswith sensitivities to multiple incitantsmight experience effects that linger as longas several days following initial avoidance.Thus, it may be argued that patientsshould be removed from their entire back-ground of food and chemical exposures for4 to 7 days before challenges, as Randolphfirst proposed (14,17).
While it is conceivable that synergistic oradditive chemical combinations may be nec-essary to reproduce certain symptoms, this isa limitation of any form of challenge testing.Wherever possible within the bounds ofsafety and feasibility, chemical combinationsbelieved to precipitate the most robust andmeasurable responses should be explored.However, 40 years of clinical observations,although anecdotal, suggest that single testsubstances may suffice for most sensitivesubjects. Confirmation or refutation ofthese claims seems a logical first step thatshould precede testing of complex mix-tures. Finally, because isolating patients ina hospital environment like the EMU mayhave unanticipated psychological conse-quences, early studies in this area shouldexamine the responses of control subjectsin the same environment.
ConclusionGood pathological and physiological theoriesprovide "a unified, clear, and entirely intelli-gible meaning for a whole series of anatomi-cal and clinical facts, and for the relevant
Environmental Health Perspectives * Vol 105, Supplement 2 * March 1997 451

C.S. MILLER
experiences and discoveries of reliableobservers..." (31). Theories and experi-ments that overlook salient observations ordo not control experimental conditions ade-quately may lead to erroneous conclusions.During the late 19th century, researcherscollected sputum from patients with tuber-culosis but were unsuccessful in culturingany organism. Some concluded that tuber-culosis was not an infectious disease. Theseearly investigators did not know that thetuberculin bacillus was fastidious and wouldgrow out only after many weeks on a spe-cialized culture medium. Correspondingly,scientists' abilities to observe and under-stand chemical sensitivity may depend onoptimizing experimental conditions, that is,appropriate timing of challenges and use ofan EMU for unmasking patients. To date,studies in this area have failed to unmaskpatients before challenge. When false posi-tive and false negative responses occurred,investigators concluded that chemical sensi-tivity was psychogenic in origin (32,33).
In summary, features of TILT overlapthose of allergy, addiction, and classicaltoxicity, yet TILT may be distinct fromeach of these. TILT appears to involve atwo-step process (resembling allergic sensi-tization) in which persons lose specific tol-erance (resembling addiction) for a widerange of common substances following achemical exposure event (resembling toxic-ity). Just as the germ theory describes aclass of diseases sharing the general mecha-nism of infection, the TILT theory of dis-ease posits a class of chemically induceddisorders characterized by loss of toleranceto chemicals, foods, drugs, and food anddrug combinations. In the same way thatfever is a symptom commonly associatedwith infectious diseases, chemical sensitiv-ity may be a symptom associated with theTILT family of diseases. Although clinicalcase definitions have been developed thatdescribe particular infectious diseases, noclinical case definition can be applied tothe entire class of infectious diseases. The
same may be true for TILT disorders. Thefact that this phenomenon does not fitalready accepted mechanisms for disease isoften offered as evidence that the condi-tion does not exist. However, the samecriticism would have applied to the germand immune theories of disease when theyfirst were proposed. What is plausibledepends on the biological knowledge ofthe time (34).
Looking to the future, carefully con-ducted epidemiological studies and animalmodels likely will play important roles incharacterizing the initiation stage of TILTduring which tolerance is lost. In themeantime, rigorous testing of the secondstage of TILT, that is, the triggering ofsymptoms by tiny doses of chemicals,foods, drugs, caffeine, or alcohol, is neededif progress in this area is to occur.Adopting a set of relevant testable hypothe-ses for etiological verification will ensurethe credibility of those endeavors.
REFERENCES
1. Cullen MR, ed. Workers with multiple chemical sensitivities.Occup Med:State Art Rev 2(4):655-806 (1987).
2. Bascom R. Chemical Hypersensitivity Syndrome Study:Options for Action, a Literature Review, and a NeedsAssessment. A Report to the State of Maryland Department ofEnvironment. Baltimore, Maryland 1989.
3. Ashford NA, Miller CS. Chemical Sensitivity. A Report to theNew Jersey State Department of Health. Trenton, NJ, 1989.
4. Ashford NA, Miller CS. Chemical Exposures: Low Levels andHigh Stakes. New York:Van Nostrand Reinhold, 1991.
5. National Research Council. Multiple Chemical Sensitivities:Addendum to Biologic Markers in Immunotoxicology.Washington:National Academy Press, 1992.
6. Association of Occupational and Environmental Clinics.Advancing the understanding of multiple chemical sensitivity.Toxicol Ind Health 8(4):1-257 (1992).
7. Thomson G. Report of the Ad Hoc Committee on Environ-mental Hypersensitivity Disorders. Ontario, Canada, 1985.
8. Ashford N, Heinzow B, Liitjen K, Marouli C, Molhave L,M6nch B, Papadopoulos S, Rest K, Rosdahl D, Siskos P,Velonakis E. Chemical Sensitivity in Selected EuropeanCountries: An Exploratory Study. Athens:Ergonomia, 1994.
9. Cone JE, Sult TA. Acquired intolerance to solvents followingpesticide/solvent exposure in a building: a new group of workersat risk for multiple chemical sensitivities? Toxicol Ind Health8(4):29-39 (1992).
10. Rosenthal N, Cameron CL. Exaggerated sensitivity to anorganophosphate pesticide (letter). Am J Psychiatry 148(2):270(1991).
11. Ziem GE. Multiple chemical sensitivity: treatment and fol-lowup with avoidance and control of chemical exposures.Advancing the understanding of multiple chemical sensitivity.Toxicol Ind Health 8(4):181-202 (1992).
12. Miller CS, Mitzel HC. Chemical sensitivity attributed to pesti-cide exposure versus remodeling. Arch Environ Health50(2):119-129 (1995).
13. Bell IR, Miller CS, Schwartz GE. An olfactory-limbic model ofmultiple chemical sensitivity syndrome: possible relationships
to kindling and affective spectrum disorders. Biol Psychiatry32:218-242 (1992).
14. Randolph TG, Moss RW. An Alternative Approach toAllergies. New York:Lippincott and Crowell, 1980.
15. Miller CS (1992). Possible models for multiple chemical sensi-tivity: conceptual issues and role of the limbic system.Advancing the understanding of multiple chemical sensitivity.Toxicol Ind Health 8(4):181-202 (1992).
16. Miller CS. Chemical sensitivity: symptom, syndrome or mech-anism for disease? Toxicology 11:69-86 (1996).
17. Randolph TG. Human Ecology and Susceptibility to theChemical Environment. Springfield, IL:Charles C Thomas, 1962.
18. Silverman K, Evans SM, Strain EC, Griffiths RR. Withdrawalsyndrome after the double-blind cessation of caffeine consump-tion. N Engl J Med 327(16):1109-1114 (1992).
19. Miller CS. Multiple chemical sensitivity and the Gulf War vet-erans. Paper presented at The Persian Gulf Experience andHealth, NIH Technology Assessment Workshop, Bethesda,Maryland, 27-29 April 1994.
20. Waddell WJ. The science of toxicology and its relevance toMCS. Reg Toxicol Pharmacol 18:13-22 (1993).
21. Fiedler N, Kipen HM, DeLuca J, Kelly-McNeil K, Natelson B.A controlled comparison of multiple chemical sensitivities andchronic fatigue syndrome. Psychosom Med 58:38-49 (1996).
22. Buchwald D, Garrity D. Comparison of patients with chronicfatigue syndrome, fibromyalgia, and multiple chemical sensitiv-ities. Arch Intern Med 154:2049-2053 (1994).
23. M0lhave L, Bach B, Pederson OF. Human reactions to lowconcentrations of volatile organic compounds. Environ Int12:167-175 (1986).
24. AIHA. Odor Thresholds for Chemicals with EstablishedOccupational Health Standards. Fairfax, VA:American IndustrialHygiene Association, 1989.
25. Warner M. Hunting the yellow fever germ: the principle andpractice of etiological proof in late nineteenth-century America.Bull Hist Med 59:361-382 (1985).
26. Miller CS. White paper: Chemical sensitivity: history and phe-nomenology. Toxicol Ind Health 10(4/5):2538-276 (1994).
452 Environmental Health Perspectives * Vol 105, Supplement 2 * March 1997

TOXICANT-INDUCED LOSS OF TOLERANCE
27. Daum S. Nitroglycerin and alkyl nitrates. In: Environmentaland Occupational Medicine (Rom W, ed). Boston:LittleBrown and Co, 1992;1013-1019.
28. Griffiths RR, Woodson PP. Caffeine physical dependence: areview of human and laboratory animal studies. Psychopharma-cology 94:437-451 (1988).
29. Riihimaki V, Savolainen K. Human exposure to m-xylene.Kinetics and acute effects on the central nervous system. AnnOccup Hygiene 23:411-432 (1980).
30. Hackney JD, Linn WS, Mohler JG, Pedersen EE, Breisacher P,Russo A. Experimental studies on human health effects of air
pollutants. Arch Environ Health 30:379-384 (1975).31. Carter KC. Ignaz Semmelweiss, Carl Mayrhofer, and the rise of
the germ theory. Med Hist 29:33-53 (1985).32. Leznoff A. Multiple chemical sensitivity: myth or reality? Prac
Allergy Immunol 8(2):48-52 (1993).33. Staudenmayer H, Selner JC, Buhr MP. Double-blind provoca-
tion chamber challenges in 20 patients presenting with "multi-ple chemical sensitivity." Reg Toxicol Pharmacol 18:44-53(1993).
34. Hill AB. The environment and disease: association or causa-tion? Proc Royal Soc Med 58:295-300 (1965).
Environmental Health Perspectives * Vol 105, Supplement 2 * March 1997 453