
Towards a medically approved technology for alginate-based microcapsules allowing long-term...
11
JOURNAL OF MATERIALS SCIENCE: MATERIALS IN MEDICINE 16 (2 0 0 5 ) 491 – 501 Towards a medically approved technology for alginate-based microcapsules allowing long-term immunoisolated transplantation H. ZIMMERMANN 1 , D. ZIMMERMANN 2 , R. REUSS 3 , P. J. FEILEN 4 , B. MANZ 5 , A. KATSEN 1 , M. WEBER 3 , F. R. IHMIG 1 , F. EHRHART 1 ,P. GEßNER 3 , M. BEHRINGER 3 , A. STEINBACH 3 , L. H. WEGNER 3 , V. L. SUKHORUKOV 3 , J. A. V ´ ASQUEZ 6 , S. SCHNEIDER 7 , M. M. WEBER 4 , F. VOLKE 5 , R. WOLF 8 , U. ZIMMERMANN 3, ∗ 1 Abteilung Kryobiophysik & Kryotechnologie, Fraunhofer-Institut f ¨ ur Biomedizinische Technik, 66386 St. Ingbert, Germany 2 Abteilung f ¨ ur Biophysikalische Chemie, Max-Planck-Institut f ¨ ur Biophysik, 60439 Frankfurt, Germany 3 Lehrstuhl f ¨ ur Biotechnologie, Biozentrum, Universit ¨ at W ¨ urzburg, 97074 W ¨ urzburg, Germany E-mail: [email protected] 4 Schwerpunkt Endokrinologie und Stoffwechselerkrankungen, Medizinische Klinik und Poliklinik, Universit ¨ atsklinik Mainz, 55131 Mainz, Germany 5 Arbeitsgruppe Magnetische Resonanz, Fraunhofer-Institut f ¨ ur Biomedizinische Technik, 66386 St. Ingbert, Germany 6 Depto. Biologia Marina, Facultad de Ciencias del Mar, Universidad Catolica del Norte, Coquimbo, Chile 7 Allgemeine Innere Medizin, Endokrinologie und Diabetologie, Berufsgenossenschaftliche Kliniken Bergmannsheil, Universit ¨ atsklinik Bochum, 44789 Bochum, Germany 8 Lehrstuhl f ¨ ur Zoologie I, Elektronenmikroskopie, Biozentrum, Universit ¨ at W ¨ urzburg, 97074 W ¨ urzburg, Germany The concept of encapsulated-cell therapy is very appealing, but in practice a great deal of technology and know-how is needed for the production of long-term functional transplants. Alginate is one of the most promising biomaterials for immunoisolation of allogeneic and xenogeneic cells and tissues (such as Langerhans islets). Although great advances in alginate-based cell encapsulation have been reported, several improvements need to be made before routine clinical applications can be considered. Among these is the production of purified alginates with consistently high transplantation-grade quality. This depends to a great extent on the purity of the input algal source as well as on the development of alginate extraction and purification processes that can be validated. A key engineering challenge in designing immunoisolating alginate-based microcapsules is that of maintaining unimpeded exchange of nutrients, oxygen and therapeutic factors (released by the encapsulated cells), while simultaneously avoiding swelling and subsequent rupture of the microcapsules. This requires the development of efficient, validated and well-documented technology for cross-linking alginates with divalent cations. Clinical applications also require validated technology for long-term cryopreservation of encapsulated cells to maintaining a product inventory in order to meet end-user demands. As shown here these demands could be met by the development of novel, validated technologies for production of transplantation-grade alginate and microcapsule engineering and storage. The advances in alginate-based therapy are demonstrated by transplantation of encapsulated rat and human islet grafts that functioned properly for about 1 year in diabetic mice. C 2005 Springer Science + Business Media, Inc. ∗ Author to whom all correspondence should be addressed. 0957–4530 C 2005 Springer Science + Business Media, Inc. 491
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Towards a medically approved technology for alginate-based microcapsules allowing long-term...

J O U R N A L O F M A T E R I A L S S C I E N C E : M A T E R I A L S I N M E D I C I N E 1 6 (2 0 0 5 ) 491 – 501
Towards a medically approved technology for
alginate-based microcapsules allowing long-term
immunoisolated transplantation
H. ZIMMERMANN1, D. ZIMMERMANN2, R. REUSS3, P. J. FEILEN4, B. MANZ5,A. KATSEN1, M. WEBER3, F. R. IHMIG1, F. EHRHART1, P. GE ß NER3,M. BEHRINGER3, A. STEINBACH3, L. H. WEGNER3, V. L. SUKHORUKOV3,J. A. V A SQUEZ6, S. SCHNEIDER7, M. M. WEBER4, F. VOLKE5, R. WOLF8 ,U. ZIMMERMANN3,∗1Abteilung Kryobiophysik & Kryotechnologie, Fraunhofer-Institut fur BiomedizinischeTechnik, 66386 St. Ingbert, Germany2Abteilung fur Biophysikalische Chemie, Max-Planck-Institut fur Biophysik,60439 Frankfurt, Germany3Lehrstuhl fur Biotechnologie, Biozentrum, Universitat Wurzburg,97074 Wurzburg, GermanyE-mail: [email protected] Endokrinologie und Stoffwechselerkrankungen, Medizinische Klinik undPoliklinik, Universitatsklinik Mainz, 55131 Mainz, Germany5Arbeitsgruppe Magnetische Resonanz, Fraunhofer-Institut fur Biomedizinische Technik,66386 St. Ingbert, Germany6Depto. Biologia Marina, Facultad de Ciencias del Mar, Universidad Catolica del Norte,Coquimbo, Chile7Allgemeine Innere Medizin, Endokrinologie und Diabetologie, BerufsgenossenschaftlicheKliniken Bergmannsheil, Universitatsklinik Bochum, 44789 Bochum, Germany8Lehrstuhl fur Zoologie I, Elektronenmikroskopie, Biozentrum, Universitat Wurzburg,97074 Wurzburg, Germany
The concept of encapsulated-cell therapy is very appealing, but in practice a great deal oftechnology and know-how is needed for the production of long-term functional transplants.Alginate is one of the most promising biomaterials for immunoisolation of allogeneic andxenogeneic cells and tissues (such as Langerhans islets). Although great advances inalginate-based cell encapsulation have been reported, several improvements need to bemade before routine clinical applications can be considered. Among these is the productionof purified alginates with consistently high transplantation-grade quality. This depends to agreat extent on the purity of the input algal source as well as on the development of alginateextraction and purification processes that can be validated. A key engineering challenge indesigning immunoisolating alginate-based microcapsules is that of maintainingunimpeded exchange of nutrients, oxygen and therapeutic factors (released by theencapsulated cells), while simultaneously avoiding swelling and subsequent rupture of themicrocapsules. This requires the development of efficient, validated and well-documentedtechnology for cross-linking alginates with divalent cations. Clinical applications alsorequire validated technology for long-term cryopreservation of encapsulated cells tomaintaining a product inventory in order to meet end-user demands. As shown here thesedemands could be met by the development of novel, validated technologies for productionof transplantation-grade alginate and microcapsule engineering and storage. The advancesin alginate-based therapy are demonstrated by transplantation of encapsulated rat andhuman islet grafts that functioned properly for about 1 year in diabetic mice.C© 2005 Springer Science + Business Media, Inc.
∗Author to whom all correspondence should be addressed.
0957–4530 C© 2005 Springer Science + Business Media, Inc. 491

1. IntroductionTreatment of hormone deficiency diseases, such as di-abetes mellitus or hypoparathyroidism, by the trans-plantation of immunoisolated living cells or tissue frag-ments that release the therapeutic factors is a very ap-pealing approach for overcoming the limitations of cur-rent therapies (see [1–4]). A matrix (e.g. cross-linkedalginate) protects cells against the immune responseof the host while simultaneously allowing unimpededtransfer of nutrients, oxygen, and therapeutic factors.This permits the imitation of moment-to-moment fineregulation of the missing therapeutic factors, avoidsa lifetime of immunosuppressive therapy and allowsthe use of non-human cells (thus overcoming the lim-ited supply of human donor cells). Small-scale clini-cal trials [3, 5] have given impressive evidence of thepotential of encapsulated cell therapy. Transplantationof Ba2+-alginate-encapsulated allogeneic parathyroidtissue pieces into the non-dominant forearm of pa-tients with hypoparathyroidism demonstrated normo-calcemia and normal levels of parathormone shortlyafter surgery. Without administration of any immuno-suppressives the grafts functioned for over three monthsbefore failure. During this time the patients were freeof symptoms of sequelae of hypoparathyroidism. Eval-uation of the clinical data and of the numerous re-sults obtained from animal studies using alginate andother matrices [1, 3] have shown that the biophysical,biochemical and immunological characteristics of theprotectant (such as biocompatibility, size, permeabil-ity, mechanical strength, elasticity, surface topography,swelling characteristics etc.) must be carefully tunedto prevent functional loss of the transplant and matrixbreakdown. However, the numerous matrix parameterscannot be adjusted independently [6]. Thus, seeminglyminor modifications of one property can have impor-tant implications for others. A further problem is thatthe demands placed on an immunoisolating matrix mayvary with the type of therapeutic application. A prereq-uisite for routine clinical application that has so far notbeen addressed is also the necessity of delivering well-characterized grafts “on demand” or the “pooling” ofgrafts, which implies the need for preservation.
Recent work in our laboratories demonstrated thatmicrocapsules of extremely high-viscosity alginate ex-tracted in a novel way from sterilized algae and uni-formly cross-linked with Ba2+ ions meet the variousdemands for a long-term immunoprotecting encapsu-lation matrix. The uniform gelling of alginate producesvery stable microcapsules and is achieved by the injec-tion of BaCl2 crystals into the cores of the microcap-sules before they come into contact with external Ba2+[7]. Application of the so-called “crystal gun” tech-nique allows reproducible cross-linking even for large-sized microcapsules (about 1 mm). Not only does thisincrease the efficiency of the process, it also minimizesthe risk of capsule damage during transplantation. The“crystal gun” method also allows the fine-tuning of mi-crocapsule parameters for factor delivery independentof the alginate composition and nature of the encapsu-lated cell/tissue. This leads to a robust and easy to vali-date protocol. Advanced technology is now also avail-
able for assessing of the quality of the alginate and theuniformity of the (surface and bulk) cross-linking.
These recent developments have paved the way forxenografts functional for about 1 year in rodents. Inthe light of these encouraging results together with im-provements in the storage of cells and tissues (cryop-reservation), clinical trials are obviously justified in thenear future. It is within the realms of possibility that thewhole process can be optimized under “Good Manu-facturing Practice” (GMP) conditions.
2. Alginate source and characteristicsAlginates are found in brown algae and in bacte-rial species [8]. They consist of unbranched binarycopolymers of 1-4 linked β-D-mannuronic acid (M)and α-L-guluronic acid (G), of widely varying compo-sition and sequential structure (MMM-blocks, GGG-blocks and MGM-blocks). The alkali-, ammonium- andmagnesium-alginates are soluble in water. Gelation ofalginates occurs when the carboxyl groups of the poly-mers are cross-linked with multi-valent cations (e.g.Ca2+, Ba2+, La3+, Fe3+) and poly-electrolytes. De-pending on the nature of the cross-linking cation, thelength of the polymeric chains, the M:G ratio and thepercentage of the block structures, hydrogels of varyingmechanical strength, elasticity and swelling character-istics can be produced (for more details, see [4]). Whencross-linked with Ba2+, high-M alginates result in elas-tic microcapsules, whereas microcapsules based onhigh-G alginate exhibit high mechanical strength. Mix-ing of high-M and high-G alginates is an elegant way fordesigning microcapsules of desired strength and forma-bility, particularly if such material is taken from algaeof the same genus. Suitable algal sources for such al-ginate mixtures are Lessonia nigrescens (Fig. 1A) andLessonia trabeculata (Fig. 1B). Both species grow fromcentral Peru to southern Chile. L. nigrescens grows inthe tidal zone and is exposed to strong surf. The stipesare very elastic and flexible because of high-M alginate(about 60%; [9]). In contrast, L. trabeculata occurs be-tween 0 and 30 m in subtidal habitats and is exposed toheavy currents [10]. The stipes of this species are verystiff due to an extremely high content of G (about 90%;[11]).
3. Alginate extraction andpurification technology
Crude commercial alginates are not recommended asstarting materials as they contain many inorganic andorganic impurities including non-natural constituentsthat would have to be removed. This is because dried al-gal material is washed ashore by the surf and the winds.This material is polluted with components of bacte-rial, fungal, animal and anthropogenic origin. Treat-ment of the raw algal material by formaldehyde causesfurther complications because of partially unknown in-teractions between alginate and impurities [3]. Com-mercial products can contain spores or components ofgram-positive bacteria commonly occurring in marineenvironments (e.g. Bacillus anthracis, Bacillus cereusand Bacillus thuringiensis; [12]). Contamination by
492

Figure 1 Source of alginates: stipes of Lessonia nigrescens (A) and Lessonia trabeculata (B). Note that the stipes in (A) are very flexible because ofhigh-M, while the stipes in (B) are mechanically very stiff due to high-G.
Figure 3 Stereo pair (i, ii) and anaglyphic 3-D image (iii) of microcapsules visualized by real-time 3-D dark field microscopy (A and C) and byCLSM (B; reconstructed from 64 optical sections). The microcapsules were made up of L. nigrescens alginate (0.8% w/v in A and 0.75% w/v in B andC) and cross-linked by external Ba2+ (A) and by the “crystal gun” method (B, C). Note that when fused by staring, the stereo pair (i and ii) shows adepth-reversed virtual view from the interior to the surface of the microcapsule (A, C). In (B) this virtual view is restricted to the 2nd quarter, otherwisethe abundant crystals adhering to the outer surface of the microcapsule calotte would disturb the view on the crystals within the microcapsule. Forviewing of the anaglyphic 3-D images (iii) red/green or red/blue glasses or filters must be used.
493
gram-positive debris has not received attention byworkers in the field, but is extremely important for theproduction of biocompatible alginates. Furthermore,due to the harvesting and extraction process the viscos-ity (closely linked to the molecular weight) of commer-cial alginates is also rather low (1–5 mPa s; 0.1% w/vsolution; [4]), enhancing the risk of graft failure sincethe cytotoxicity of polymers increases with decreasingmolecular mass [13].
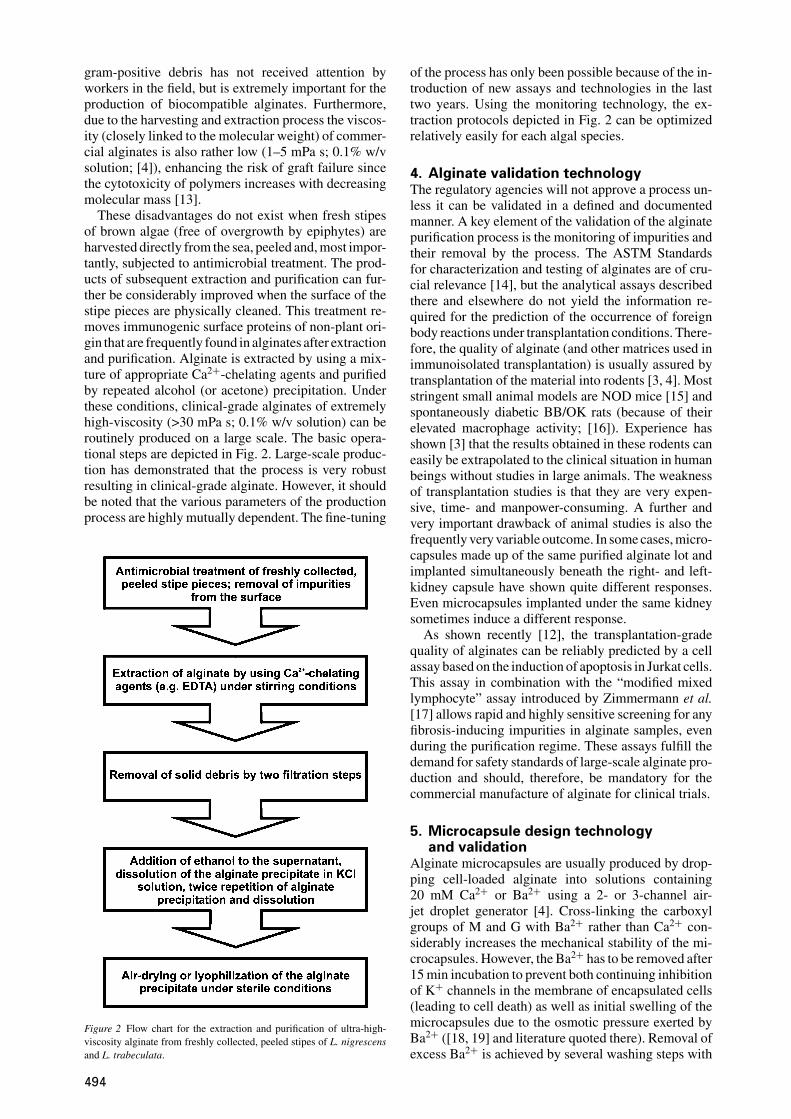
These disadvantages do not exist when fresh stipesof brown algae (free of overgrowth by epiphytes) areharvested directly from the sea, peeled and, most impor-tantly, subjected to antimicrobial treatment. The prod-ucts of subsequent extraction and purification can fur-ther be considerably improved when the surface of thestipe pieces are physically cleaned. This treatment re-moves immunogenic surface proteins of non-plant ori-gin that are frequently found in alginates after extractionand purification. Alginate is extracted by using a mix-ture of appropriate Ca2+-chelating agents and purifiedby repeated alcohol (or acetone) precipitation. Underthese conditions, clinical-grade alginates of extremelyhigh-viscosity (>30 mPa s; 0.1% w/v solution) can beroutinely produced on a large scale. The basic opera-tional steps are depicted in Fig. 2. Large-scale produc-tion has demonstrated that the process is very robustresulting in clinical-grade alginate. However, it shouldbe noted that the various parameters of the productionprocess are highly mutually dependent. The fine-tuning
Figure 2 Flow chart for the extraction and purification of ultra-high-viscosity alginate from freshly collected, peeled stipes of L. nigrescensand L. trabeculata.
of the process has only been possible because of the in-troduction of new assays and technologies in the lasttwo years. Using the monitoring technology, the ex-traction protocols depicted in Fig. 2 can be optimizedrelatively easily for each algal species.
4. Alginate validation technologyThe regulatory agencies will not approve a process un-less it can be validated in a defined and documentedmanner. A key element of the validation of the alginatepurification process is the monitoring of impurities andtheir removal by the process. The ASTM Standardsfor characterization and testing of alginates are of cru-cial relevance [14], but the analytical assays describedthere and elsewhere do not yield the information re-quired for the prediction of the occurrence of foreignbody reactions under transplantation conditions. There-fore, the quality of alginate (and other matrices used inimmunoisolated transplantation) is usually assured bytransplantation of the material into rodents [3, 4]. Moststringent small animal models are NOD mice [15] andspontaneously diabetic BB/OK rats (because of theirelevated macrophage activity; [16]). Experience hasshown [3] that the results obtained in these rodents caneasily be extrapolated to the clinical situation in humanbeings without studies in large animals. The weaknessof transplantation studies is that they are very expen-sive, time- and manpower-consuming. A further andvery important drawback of animal studies is also thefrequently very variable outcome. In some cases, micro-capsules made up of the same purified alginate lot andimplanted simultaneously beneath the right- and left-kidney capsule have shown quite different responses.Even microcapsules implanted under the same kidneysometimes induce a different response.
As shown recently [12], the transplantation-gradequality of alginates can be reliably predicted by a cellassay based on the induction of apoptosis in Jurkat cells.This assay in combination with the “modified mixedlymphocyte” assay introduced by Zimmermann et al.[17] allows rapid and highly sensitive screening for anyfibrosis-inducing impurities in alginate samples, evenduring the purification regime. These assays fulfill thedemand for safety standards of large-scale alginate pro-duction and should, therefore, be mandatory for thecommercial manufacture of alginate for clinical trials.
5. Microcapsule design technologyand validation
Alginate microcapsules are usually produced by drop-ping cell-loaded alginate into solutions containing20 mM Ca2+ or Ba2+ using a 2- or 3-channel air-jet droplet generator [4]. Cross-linking the carboxylgroups of M and G with Ba2+ rather than Ca2+ con-siderably increases the mechanical stability of the mi-crocapsules. However, the Ba2+ has to be removed after15 min incubation to prevent both continuing inhibitionof K+ channels in the membrane of encapsulated cells(leading to cell death) as well as initial swelling of themicrocapsules due to the osmotic pressure exerted byBa2+ ([18, 19] and literature quoted there). Removal ofexcess Ba2+ is achieved by several washing steps with
494

isotonic NaCl solution followed by a sulfate treatmentto precipitate any remaining free Ba2+ ions. Swellingof the microcapsules under transplantation conditionsand thus mechanical instability can be delayed furtherwhen proteins (e.g. up to 3% human serum albumin;HSA) are added to the alginate solution before mi-crocapsule formation [20, 21]. However, swelling andbreakage of microcapsules can still occur after long invitro incubations as well as after long-term transplan-tation times [22]. One major reason for microcapsuleswelling is the formation of concentration gradientsof alginate polymers and/or of proteins incorporatedfor stabilization resulting in microdomains of differentcomposition. Alginate polymer and protein concentra-tion gradients arise from demixing and shrinking pro-cesses during droplet formation and gelling by externalBa2+ (see e.g. [23, 24]). The extent of these problemsdepends on microcapsule dimensions, the M:G ratio,the viscosity (and thus the average molecular mass) aswell as on the molecular mass distribution of the algi-nate. The presence of non-gelling salts such as NaCl,the time of cross-linking and the spatial distribution ofthe cells play also an important role. Compared to com-mercial low-viscosity alginates these problems are lessfor ultra-high viscosity alginates extracted from freshlyharvested, peeled stipes. But the problem remains thata cross-linking time of 15 min (dictated by cell phys-iology) is too short for equilibration of external Ba2+between the core of the viscous alginate droplet and theexternal medium.
This has been demonstrated by the imaging of micro-capsules (made from alginate extracted from L. pallidaand cross-linked with Ba2+ for 15 min) with confo-cal laser scanning microscopy (CLSM) [7]. In orderto visualize the distribution of Ba2+, the excess ionswere not removed by washing before sulfate treatment.Solid BaSO4 particles appeared as white spots underthe CLSM reflection mode (see also further below). Asshown by H. Zimmermann et al. [7] many BaSO4 crys-tals were attached to the surface of the conventionallycross-linked alginate/protein microcapsule forming arather continuous peripheral layer. In contrast, therewere very few crystals within the interior of the micro-capsules indicating that diffusion of Ba2+ into the corewas apparently restricted.
This finding is confirmed by a novel real-time 3-Ddark field microscopy technique (Wolf, unpublished re-sults, see also [25, 26]) that provides a true 3-D imageat magnifications between 25:1 and 400:1 and can beused as an elegant tool for routine control of microcap-sule quality. Similar to conventional 3-D techniques insingle-lens light microscopy [25, 26] the microscopemust be equipped with three polarizing filters: an L-form double polarizing filter mounted at the backwardfocal plane of the objective lens and one polarizer inboth of the eyepieces. They serve as image switches andprovide the left eye with the microscopic image formedby the left half of the objective lens, and vice versa. Theunavoidable limitation of depth of focus is overcome bycontinuously focussing through the specimen. A typicalstereo pair and the corresponding anaglyphic 3-D im-age of a microcapsule cross-linked with external Ba2+
and visualized by real-time 3-D dark field microscopyis given in Fig. 3A. Focussing through the entire mi-crocapsule shows that only a very few, randomly dis-tributed BaSO4 crystals are found within the interior ofthe microcapsule.
As demonstrated recently by Manz et al. [24] ad-vanced 1H nuclear magnetic resonance (NMR) imag-ing also yields information about the quality of cross-linking within the interior of microcapsules. Ba2+-cross-linked microcapsules are placed in NMR tubescontaining a saline solution to which paramagneticCu2+ ions as contrast agent are added. Cu2+ diffusionand accumulation within the microcapsules is resolvedand quantified by taking spatially resolved maps of thespin-lattice relaxation time T1 and/or of the spin-spinrelaxation time T2. The T1 and T2 values of microcap-sules bathed for up to 20 h in Cu2+-containing mediumare significantly lower than the corresponding values ofthe surrounding due to accumulation of the paramag-netic Cu2+ ions within the microcapsules (see furtherbelow Fig. 5). Cu2+ has a similar affinity constant toalginate as Ba2+ [27]. After washing with Cu2+-free0.9% NaCl solution, the T1 and T2 relaxation times ofthe microcapsules (spatially resolved) are identical tothe corresponding values before the addition of Cu2+ tothe system. This implies that binding of Cu2+ to chargedor polar groups of the alginate (and the proteins) is veryunlikely.
Evaluation of the T1 and T2 values of the microcap-sules after washing has shown [24] that conventionalcross-linking with external Ba2+ at a physiological pHvalue is frequently not complete. It is subject to largevariations, even if the microcapsule production param-eters (such as monomer composition, size of the mi-crocapsules, time of exposure to Ba2+ etc.) are keptconstant ([24] and unpublished data). Cross-linking inthe peripheral layer of the microcapsules apparentlyrestricts diffusion of Ba2+ ions into the microcapsuleinterior, thus preventing complete cross-linking.
Predictable and reproducible results are expectedwhen external gelling is simultaneously accompaniedby internal gelling. A possible strategy for achievinguniform gelling is to add photo-releasable, caged Ba2+to the alginate solution before dropping [20]. The cagedions are not reactive, but free, reactive ions can be re-leased by UV-irradiation of the droplets in the BaCl2solution. The disadvantage of this approach is that thereleased organic cage compounds will not receive trans-plantation approval. Another possible way is to incor-porate tiny BaCO3 crystals into the alginate/cell sus-pension and to perform the gelling process in the BaCl2solution at lower pH, liberating Ba2+ ions [28]. Othermethods such as the incorporation of Ba2+-containingthermally unstable liposomes [29] or the addition ofantigelling cations [27] have also not resulted in long-term stable microcapsules. Best results have been ob-tained by the “crystal gun” method [7]. With this tech-nique, dried, sterilized, tiny BaCl2 crystals1are injected
1Nanosized crystals of BaSO4 which are very reactive because of theirlarge surface to volume ratio can also be used and may lead to anenhanced, and even more homogeneous gelling (unpublished results).
495
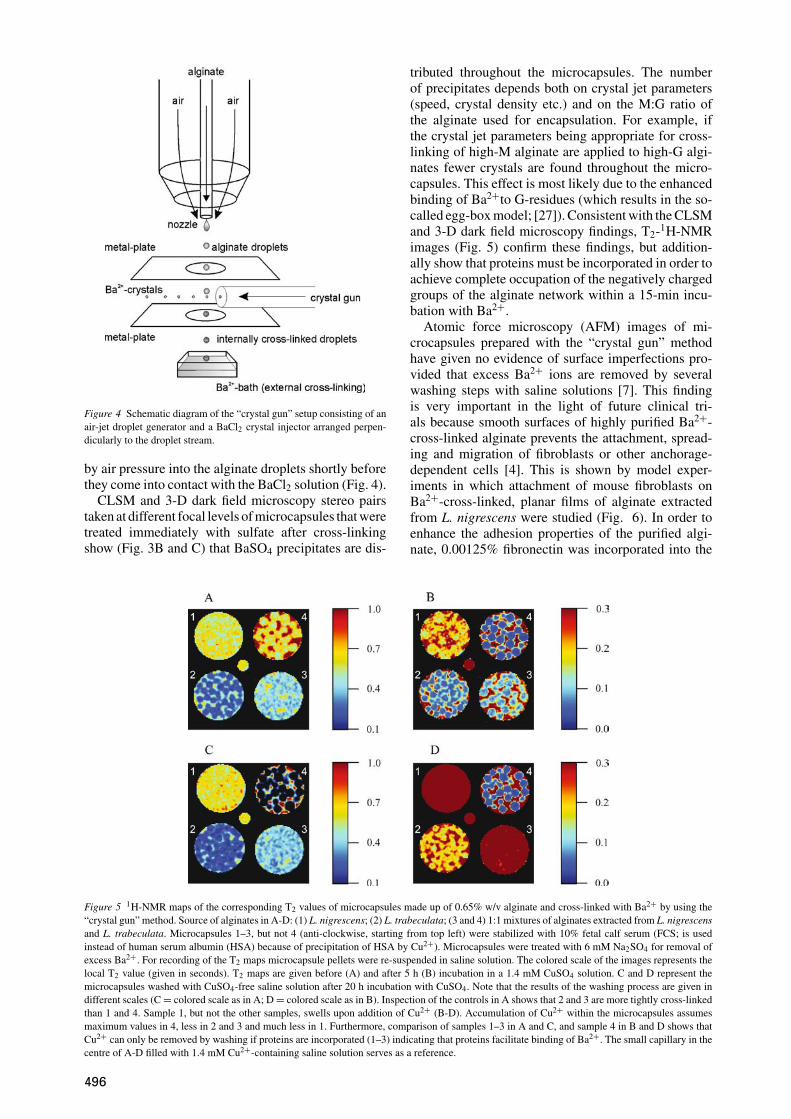
Figure 4 Schematic diagram of the “crystal gun” setup consisting of anair-jet droplet generator and a BaCl2 crystal injector arranged perpen-dicularly to the droplet stream.
by air pressure into the alginate droplets shortly beforethey come into contact with the BaCl2 solution (Fig. 4).
CLSM and 3-D dark field microscopy stereo pairstaken at different focal levels of microcapsules that weretreated immediately with sulfate after cross-linkingshow (Fig. 3B and C) that BaSO4 precipitates are dis-
Figure 5 1H-NMR maps of the corresponding T2 values of microcapsules made up of 0.65% w/v alginate and cross-linked with Ba2+ by using the“crystal gun” method. Source of alginates in A-D: (1) L. nigrescens; (2) L. trabeculata; (3 and 4) 1:1 mixtures of alginates extracted from L. nigrescensand L. trabeculata. Microcapsules 1–3, but not 4 (anti-clockwise, starting from top left) were stabilized with 10% fetal calf serum (FCS; is usedinstead of human serum albumin (HSA) because of precipitation of HSA by Cu2+). Microcapsules were treated with 6 mM Na2SO4 for removal ofexcess Ba2+. For recording of the T2 maps microcapsule pellets were re-suspended in saline solution. The colored scale of the images represents thelocal T2 value (given in seconds). T2 maps are given before (A) and after 5 h (B) incubation in a 1.4 mM CuSO4 solution. C and D represent themicrocapsules washed with CuSO4-free saline solution after 20 h incubation with CuSO4. Note that the results of the washing process are given indifferent scales (C = colored scale as in A; D = colored scale as in B). Inspection of the controls in A shows that 2 and 3 are more tightly cross-linkedthan 1 and 4. Sample 1, but not the other samples, swells upon addition of Cu2+ (B-D). Accumulation of Cu2+ within the microcapsules assumesmaximum values in 4, less in 2 and 3 and much less in 1. Furthermore, comparison of samples 1–3 in A and C, and sample 4 in B and D shows thatCu2+ can only be removed by washing if proteins are incorporated (1–3) indicating that proteins facilitate binding of Ba2+. The small capillary in thecentre of A-D filled with 1.4 mM Cu2+-containing saline solution serves as a reference.
tributed throughout the microcapsules. The numberof precipitates depends both on crystal jet parameters(speed, crystal density etc.) and on the M:G ratio ofthe alginate used for encapsulation. For example, ifthe crystal jet parameters being appropriate for cross-linking of high-M alginate are applied to high-G algi-nates fewer crystals are found throughout the micro-capsules. This effect is most likely due to the enhancedbinding of Ba2+to G-residues (which results in the so-called egg-box model; [27]). Consistent with the CLSMand 3-D dark field microscopy findings, T2-1H-NMRimages (Fig. 5) confirm these findings, but addition-ally show that proteins must be incorporated in order toachieve complete occupation of the negatively chargedgroups of the alginate network within a 15-min incu-bation with Ba2+.
Atomic force microscopy (AFM) images of mi-crocapsules prepared with the “crystal gun” methodhave given no evidence of surface imperfections pro-vided that excess Ba2+ ions are removed by severalwashing steps with saline solutions [7]. This findingis very important in the light of future clinical tri-als because smooth surfaces of highly purified Ba2+-cross-linked alginate prevents the attachment, spread-ing and migration of fibroblasts or other anchorage-dependent cells [4]. This is shown by model exper-iments in which attachment of mouse fibroblasts onBa2+-cross-linked, planar films of alginate extractedfrom L. nigrescens were studied (Fig. 6). In order toenhance the adhesion properties of the purified algi-nate, 0.00125% fibronectin was incorporated into the
496

Figure 6 Adhesion and spreading of mouse fibroblasts on a planar, mi-crostructured alginate film. The film was made by Ba2+-cross-linking ofhighly purified L. nigrescens alginate (0.7% w/v in 0.9% NaCl solutioncontaining 0.00125% fibronectin) on a glass substrate. Longitudinal im-perfections (slots) were mechanically introduced by lightly pressing ametal grid into the gelled alginate film. Then the film was air-dried andre-hydrated in culture medium before fibroblasts were added. Note thatfibroblast attachment, spreading and migration initially occurs preferen-tially along the imperfections even though the adhesivity of the alginatewas enhanced by the addition of fibronectin.
matrix before gelling with external Ba2+. When elon-gated crevices (or cracks) were mechanically intro-duced into the matrix, fibroblast attachment initiallyonly occurred at these surface imperfections before(very delayed) spreading and migration of the cellsover the entire surface of the planar film. Such pro-cesses are also expected under transplantation con-ditions. The alginate surface becomes more adhesivewhen anchorage-dependent cells attached to crevicesor cracks start to migrate, thereby releasing cellu-lar and membrane material. These materials togetherwith advanced glycation end products (AGEs) (arisingfrom non-enzymatic reactions of the polysaccharides;[30]) are immunogenic. “Topographical” biocompat-ibility is obviously equally important as “chemical”biocompatibility.
Microcapsules made up of alginates and alginatemixtures extracted from L. pallida, L. nigrescens andL. trabeculata incubated in 0.9% NaCl solution show adramatic increase in stability when cross-linked by the“crystal gun” method as proved by incubation in 0.9%NaCl solution. In contrast to conventional cross-linking(unpublished results), microcapsules of high-G alginateextracted from L. trabeculata as well as 1:1 mixturesof this alginate with high-M alginate extracted from L.nigrescens are still stable after 36 weeks of incubationdespite heavy stirring; the experiments are still contin-uing. There is also evidence that the amount of HSA (orFCS) added to the alginate for prevention of swellingcan be reduced if pure G-rich or 1:1 mixtures of G-rich and M-rich alginates are used because of the veryefficient cross-linking process. Complete omission ofprotein, however, is not advantageous because of in-complete cross-linking (see above and Fig. 5C and D)and deleterious effects on cellular function and integrityoccur without HSA.
The crystal bombardment does not affect the via-bility and function of encapsulated cells and islets [7,
21]. However, it is important to note, that concomitantwith the improvement of the cross-linking process, adecrease in permeability occurs that requires carefuladjustment of the alginate concentration. For example,long-term viability and insulin secretion of islets de-creased dramatically when 0.7% w/v instead of 0.65%w/v alginate extracted from L. pallida was used [21].
Unimpeded exchange of factors and nutrients be-tween the microcapsules and the environment is onlyexpected if pores exist in the alginate matrix. The exis-tence of such pores can be shown by water permeabil-ity studies through 1-mm thick 2-D Ba2+-cross-linkedalginate membranes. Transmembrane water flows canbe measured by the two-compartment setup in the in-set of Fig. 7. If an osmotic pressure gradient (e.g. bypolyethylene glycol, PEG 6000; reflection coefficientσ = 1; [31]) is generated across the alginate membraneseparating the two compartments, the osmotic perme-ability, Pf , of the matrix can be calculated from thewater flow Jv according to Pf = Jv RT/(πVw), withR = gas constant, T = absolute temperature in Kelvin,π = osmotic pressure of the osmolyte solution, Vw =molar volume of water [32]. Prerequisite is that the wa-ter efflux from the water-filled compartment, b, is equalto the water influx into the osmolyte-containing com-partment, a (see data in Fig. 7). At present data are onlyavailable for alginate membranes cross-linked by ex-ternal Ba2+. For these membranes Pf values of about2 × 10−2 cm/s were calculated from transmembranewater flow data. In contrast, the diffusive permeabil-ity of water, PD , of the 1-mm thick alginate matrix(PD = Dw/d ≈ 2.4 × 10−4 cm/s) is about 100 timessmaller (the diffusion coefficient of water, Dw, in cross-linked alginate can easily be determined by 1H-PGSE-NMR measurements; [33]). This finding provides clear-cut evidence [34] that water moves by viscous flow, i.e.through pores, rather than by diffusion. Assuming thatthe flow is laminar, the “equivalent pore radius”, r, [35]can be estimated from the Pf /PD ratio using the equa-tion Pf /PD = r2 RT/(8ηDwVw), with η = viscosityof water [36]. Calculations yield an equivalent pore ra-dius of about 4 nm (at room temperature). This is consis-tent with the finding that immunologically relevant pro-teins, which have an effective molecular radius of about7.5 nm [37], are excluded from the passage through thealginate pores whereas smaller molecules like insulin(1.5–4 nm; [37]) can freely pass the alginate barrier.
Measurements with alginate membranes cross-linked by the “crystal gun” method are planned. In-dependent of the outcome of these experiments it isclear from the above considerations that measurementof water (and also of solute) permeability through 2-D-alginate matrices yields valuable information for theassessment of microcapsule permeability while keep-ing the mechanical stability at an optimum value. Thisis because the data obtained on the 2-D matrices caneasily be extrapolated to the small-sized microcapsules.
6. Animal trialsThe improvements in purification of alginates and inencapsulation as well as the development of vari-ous validation protocols paves the way for long term
497

Figure 7 Osmotically-induced water flow across a 1-mm thick, planar alginate membrane of circular size (diameter 20 mm, 0.7% w/v L. nigrescensalginate, cross-linked with external Ba2+) at room temperature. The experimental setup (see inset) consisted of two glass chambers “a” (containing290 mM PEG 6000) and “b” (containing distilled water), each having a circular face with a 13-mm-diameter hole in it in which the alginate membrane(“d” in inset; integrated in a teflon support and stabilized by nylon nets) was clamped to form a fluid tight seal. Osmotically induced water flow occurredthrough the alginate membrane. Vigorous stirring in the bulk phases by small magnetic stirrers (c) minimized unstirred layer effects. Transmembranewater flow was determined by monitoring the movement of the menisci in the rectangular bent capillaries attached to the glass chambers (“e” in inset;→ water influx into compartment “a”, ← water efflux from compartment “b”). Note that the numerical slope of water influx and efflux are almostidentical, as expected when there is no water loss. Note further that diffusive water flow around the alginate membrane can be excluded because noPEG 6000 could be detected in the water-filled compartment “b” after the end of the experiment.
Figure 8 Long-term graft function of alginate-encapsulated rat (n = 5) as well as human (n = 2) islets transplanted into diabetic Balb/c mice (mean± SE); transplantation at t = 0.
transplantation studies. As shown in Fig. 8 encapsu-lated rat as well as human islets reversed chemically-induced diabetes in mice over extremely long times(experiments still continue) without the need for ad-ministration of immunosuppressives. These findingsare confirmed by intraperitoneal glucose tolerance tests(IPGTTs) and in vitro testing of explanted microcap-sules. The microcapsules showed normal regulation ofinsulin secretion upon glucose challenge. Furthermore,no significant fibrosis was observed on the surface of ex-planted, islet-containing microcapsules 10 or 36 weeksafter transplantation [38].
The peritoneum was selected as the site of xenografttransplantation. However, the preferred sites, at least
for the first clinical applications, are muscle pockets,e.g. in the non-dominant forearms and in the back be-cause oxygen concentration is high and in the case ofgraft failure, microcapsules can be retrieved easily. Afurther advantage is that location of the microcapsulesand their internal oxygen concentration can be moni-tored non-invasively by 19F-NMR-imaging [3, 4]. How-ever, the mechanical forces here are significant result-ing ultimately in fibrotic overgrowth and/or microcap-sule breakage as demonstrated by failure of parathyroidtransplants in the pilot clinical trial [5]. It is expectedthat encapsulated islets will have as long a lifetime inmuscle pockets as in the peritoneum provided that themicrocapsule design technology developed in recent
498

years is fully implemented. Especially useful may bethe “crystal gun” method and the very recent findingthat microcapsules made up of a 1:1 mixture of L. ni-grescens and L. trabeculata alginate are extremely sta-ble under in vitro conditions (see above) and do notprovoke any inflammatory or fibrotic response.
7. Cryopreservation technologyand validation
Considering the successful animal transplantation stud-ies and the large body of recent microcapsule de-sign technology, cryopreservation of encapsulatedislets (or other cells) is becoming a focus of re-search because just-in-time manufacturing of alginate-immunoprotected islets (or other cells and tissues) isdifficult to implement. Quality control, and the cre-ation of archives for validation of the manufacturingprocess of the alginates and the microcapsules alsorequire the long-term storage of the final transplants.Although progress in developing cryopreservation pro-cedures for cells is encouraging [39, 40], many chal-lenges remain because of the scale and complexity oftissues resulting in spatial, thermal, chemical, and os-motic (mechanical) gradients throughout the system
Figure 9 Freezing of Langerhans islets in micro-well-plates made from high-density polyethylene (HDPE). (A) Successive frames of a single wellat the time of ice growth made with infrared thermography. The temperature rise associated with transition from supercooled liquid (frames 2 to 4)to a 2-phase system (with release of latent heat) can be seen in the 5th frame and is complete in the 6th frame. Note that the temperature scale givenin (A) reached from +30 ◦C (red) to −30 ◦C (blue). Note that the time delay between the frames is different (1→2 640 ms, 2→3 160 ms, 3→4160 ms, 4→5 640 ms, 5→6 132 s). (B) Langerhans islet. Scanning electron microscopy (SEM) of a control preparation. The islets were placed onMilliporeTM filter inserts. Note the surface texture. Horizontal field width (HFW) = 92 µm. Bottom right: Cell viability assessed by double stainingwith fluorescein diacetate (green fluorescence for intact cells) and ethidium bromide (red fluorescence for nuclei of damaged cells). The cell viabilitytest (bottom right) showed about 87% viability. (C) SEM of Langerhans islet immediately after cryopreservation in HDPE–micro-well-plate with7% DMSO. Note the smooth, undamaged surface. HFW = 184 µm. A cell viability test (bottom right) showed about 64% viability. (D) SEM ofLangerhans islet immediately after cryopreservation in HDPE–micro-well-plate with 14% DMSO. Note the smooth surface with areas of damage.HFW = 184 µm. A cell viability test (bottom right) showed about 43% viability.
during the freezing or subsequent thawing processes.Membrane permeating (e.g. glycerol and dimethyl sul-foxide, DMSO) and nonpermeating (e.g. hydroxyethylstarch, trehalose, inositol) cryoprotectants are usuallyadded before freezing in order to increase the number ofviable cells recovered after thawing. DMSO is the mostcommonly used cryoprotectant. However, DMSO maybe cytotoxic, particularly if the time of exposure beforefreezing and after thawing is long, or if it is used in highconcentrations (usually up to 20%), precluding medi-cal approval. Reduction of the DMSO concentration orcomplete replacement of DMSO by equally powerful,but medically approved substances as well as technicalimprovements to the freezing and thawing process arethe current strategies for overcoming the problems ofcryopreservation of tissue.
The most promising technical improvements of thefreezing process are the significant reduction of totalsample volume, i.e. miniaturization of the cryosub-strates from typical 1 millilitre down to microlitres orbelow. The main advantages for the storage of encap-sulated and non-encapsulated tissue are the avoidanceof large temperature gradients and inhomogeneities[41]. The reduced temperature gradients in the smallercryosubstrates arise from the thermal conductivity of
499

water, that becomes, though small, increasingly impor-tant in determining heat flows with decreasing samplesize. Thus, either higher freezing rates or more homo-geneous freezing of the sample are possible. A furtheradvantage of small-sized cryosubstrates is the possibil-ity of fast and exact addition of cryoprotectant addi-tives by pipette robots. Fast addition results in an im-mediate and homogeneous distribution of the cryopro-tectants. Non-encapsulated islets cryopreserved in thisway were highly functional after thawing even thoughsignificantly lower final concentrations of DMSO thanusual were applied before freezing. For quality controlof transplants it is an extremely important advantagethat the surface temperature of the sample volume dur-ing the freezing and thawing process can directly beobserved by dynamic high-resolution thermo imaging(Fig. 9).
Parallel to these promising advances in technology,novel media for the cryopreservation of islets (andother mammalian cells) have been developed [42]. TheDMSO-free media are hypotonic (150 mOsm) and con-tain appropriate amounts of trehalose and/or inositol asmajor osmolytes. Mammalian cells (including islets)respond to hypotonic challenge by swelling until a max-imum volume is reached after 3–5 min (Fig. 10). In thepresence of trehalose, but not of inositol a regulatoryvolume decrease (RVD) is observed. According to theliterature [43] swelling activates Cl− channels. Effluxof Cl− leads to a depolarization of the membrane. Thisevokes activation of K+ channels. Thus, restoration ofthe original volume after about 15 min is accomplishedby release of intracellular KCl and water. While the K+channels are selective, the Cl− channels allow the pas-sage of other anions as well as of inositol (and other
Figure 10 Temporal changes in the relative volume, ν, of rat islets ofLangerhans in hypotonic 150 mOsm media containing inositol (open cir-cles) or trehalose (filled circles) as the major osmolyte. The islets wereoriginally (t < 0) exposed to an isotonic saline solution (300 mOsm).At zero time the islets were rapidly transferred into a hypotonic sugarsolution. After fast initial swelling (3–5 min), the islets either exhib-ited regulatory volume decrease (RVD, trehalose) or underwent slowsecondary swelling (inositol). The lack of RVD in the inositol mediumindicates that cell swelling rendered the membrane of islet cells highlypermeable to inositol (unlike the case for trehalose). Islet volumes, V ,were calculated from their microscopic cross-sectional areas by assum-ing spherical geometry. The relative islet volume is defined as ν = V/V0,where V and V0 are the cell volume and the initial (isotonic) volume,respectively. Each data point represents the mean ± SE of three inde-pendent measurements.
cryoprotectant monomeric sugar alcohols). In the pres-ence of inositol the volume of the swollen cells remainsconstant or even increases slightly (Fig. 10) indicatingthat KCl efflux is compensated by inositol uptake. Cry-opreservation of islets pre-loaded hypotonically withinositol and incubated in isotonic trehalose have yieldedhigh survival rates after thawing. A few dead cells (de-tected by propidium iodide staining under the cryomi-croscope) were seen occasionally in the periphery ofthe islets. Adoption of the technology described aboveto these media should lead to further improvements incryopreservation.
8. ConclusionsEven though significant advances have obviously beenmade in immunoisolated transplantation, many chal-lenges remain. Amongst these is, most importantly, thedevelopment of closed microfluidics platforms allow-ing automation of the microencapsulation process. In-corporating the entire process steps, from alginate/celldroplet formation, cross-linking by injection of Ba2+nanoparticles to microcapsule validation, in a chip-based platform (microlab) should meet the GMP stan-dards and demands for routine clinical applications ofencapsulated cells and tissues as well as for controlleddrug release. Together with this, the advanced cryotech-nology described here must be extended to alginate-encapsulated tissues (islets) in order to meet the de-mands of the granting agencies for long-term storageof transplants. The extremely high water content of al-ginate gels and the large component of bound water [44]pose enormous problems, but advances in micro- andnanotechnology offer a broad spectrum of solutions.Potential solutions can additionally be found amongdrought- and freezing-resistant and -tolerant plants asshown recently [45–47].
The remaining challenges are tremendous, but thesignificant advances described here were made by inter-disciplinary research activities. Therefore, we are con-fident that close interdisciplinary collaboration will findsolutions to the outstanding problems.
AcknowledgmentsThese studies were supported by grants from DeutscheForschungsgemeinschaft (Zi 99/15-1 to U.Z.), BMBF(16 SV 1329 and 0311 588 to U.Z.; 16 SV 1366/0and O3N8707 to H.Z.), Forum (AZ 437-2004 to S. S.),and research grants of Novo Nordisk Pharma GmbH,Germany, and the Stiftung Rheinland-Pfalz fur Innova-tion (386261/525 to M.M.W. and S.S.) as well as byFONDECYT (1000044 to J.A.V.).
References1. W. M. K U H T R E I B E R, R . P . L A N Z A and W. L . C H I C K ,
in “Cell Encapsulation Technology and Therapeutics” (Birkhauser,Boston, 1999).
2. R . P . L A N Z A, R . L A N G E R and J . V A C A N T I , in “Princi-ples of Tissue Engineering” (Academic Press, San Diego, 2000).
3. U . Z I M M E R M A N N, S . M I M I E T Z, H. Z I M M E R M A N N,M. H I L L G A R T N E R, H. S C H N E I D E R, J . L U D W I G, C .H A S S E, A. H A A S E, M. R O T H M U N D and G. R . F U H R ,BioTechniques 29(3) (2000) 564.
500

4. U . Z I M M E R M A N N, F . T H U R M E R, A. J O R K, M.W E B E R, S . M I M I E T Z, M. H I L L G A R T N E R, F .B R U N N E N M E I E R, H. Z I M M E R M A N N, I . W E S T P H A L,G. R . F U H R, U. N O T H, A. H A A S E, A. S T E I N E R T andC. H E N D R I C H , Ann. N.Y. Acad. Sci. 944(1) (2001) 199.
5. C . H A S S E, G. K L O C K, A. S C H L O S S E R, U.Z I M M E R M A N N and M. R O T H M U N D , Lancet 350(9087)(1997) 1296.
6. T . G . W A N G , in “Cell Encapsulation Technology and Thera-peutics,“ edited by W. M. Kuhtreiber, R. P. Lanza and W. L. Chick(Birkhauser, Boston, 1999) p. 29.
7. H . Z I M M E R M A N N, M. H I L L G A R T N E R, B . M A N Z, P .J . F E I L E N, F . B R U N N E N M E I E R, U. L E I N F E L D E R,M. W E B E R, H. C R A M E R, S . S C H N E I D E R, C .H E N D R I C H, F . V O L K E and U. Z I M M E R M A N N , Bio-materials 24(12) (2003) 2083.
8. B . H . A. R E H M , in “Biopolymers: Polysaccharides I: Polysac-charides from Prokaryotes,” edited by E. J. Vandamme, S. De Baetsand A. Steinbuchel (Wiley-VCH, Weinheim, 2002) Vol. 5, p. 179.
9. K . I . D R A G E T, O. S M I D S RøD and G. S K J A K-B R Æ K ,in “Biopolymers: Polysaccharides II: Polysaccharides from Eu-karyotes,” edited by S. De Baets, E. J. Vandamme and A.Steinbuchel (Wiley-VCH, Weinheim, 2002) Vol. 6, p. 215.
10. J . A . V A S Q U E Z , in “Coastal Plant Communities of Latin Amer-ica,” edited by U. Seeliger (Academic Press, San Diego, 1992)p. 77.
11. M. V E N E G A S, B . M A T S U H I R O and M. E . E D D I N G ,Botanica Marina 36 (1993) 47.
12. U . L E I N F E L D E R, F . B R U N N E N M E I E R, H. C R A M E R,J . S C H I L L E R, K. A R N O L D, J . A . V A S Q U E Z and U.Z I M M E R M A N N , Biomaterials 24(23) (2003) 4161.
13. B . M A T T I A S S O N , in “Immobilized Cells and Organelles,”edited by B. Mattiasson (CRC Press, Boca Raton, 1983) Vol. I,p. 3.
14. M. D O R N I S H, D. K A P L A N and Ø. SKAUGRUD, Ann. N.Y.Acad. Sci. 944(1) (2001) 388.
15. M. A. A T K I N S O N and E . H. L E I T E R , Nat. Med. 5(6) (1999)601.
16. J . W I J S M A N, P . A T K I S O N, R . M A Z A H E R I , B .G A R C I A, T . P A U L, J . V O S E, G. O‘S H E A and C.S T I L L E R , Transplantation 54(4) (1992) 588.
17. U . Z I M M E R M A N N, C. H A S S E, M. R O T H M U N D and W.K U H T R E I B E R , in “Cell Encapsulation Technology and Thera-peutics,” edited by W. M. Kuhtreiber, R. P. Lanza and W. L. Chick(Birkhauser, Boston, 1999) p. 40.
18. C . R Y S E R, J . W A N G, S . M I M I E T Z and U.Z I M M E R M A N N , J. Membr. Biol. 168(2) (1999) 183.
19. M. H E I D E C K E R, S . M I M I E T Z, L . H . W E G N E R and U.Z I M M E R M A N N , J. Membr. Biol. 192(2) (2003) 123.
20. M. H I L L G A R T N E R, H. Z I M M E R M A N N, S . M I M I E T Z,A. J O R K, F . T H U R M E R, H. S C H N E I D E R, U. N O T H,C . H A S S E, A. H A A S E, G. R . F U H R, M. R O T H M U N D
and U. Z I M M E R M A N N , Math.-Wiss. u. Werkstofftech. 30 (1999)783.
21. S . S C H N E I D E R, P . J . F E I L E N, H. C R A M E R,M. H I L L G A R T N E R, F . B R U N N E N M E I E R, H.Z I M M E R M A N N, M. M. W E B E R and U. Z I M M E R M A N N ,J. Microencapsul. 20(5) (2003) 627.
22. U . Z I M M E R M A N N, H. C R A M E R, A. J O R K, F .T H U R M E R, H. Z I M M E R M A N N, G. R . F U H R, C .H A S S E and M. R O T H M U N D , in “Biotechnology,” edited byH. J. Rehm and G. Reed (Wiley-VCH, Weinheim, 2001) Vol. 10,p. 547.
23. B . T H U, O. G A S E R O D, D. P A U L, A. M I K K E L S E N,G. S K J A K-B R Æ K, R. T O F F A N I N, F . V I T T U R and R.R I Z Z O , Biopolymers 53(1) (2000) 60.
24. B . M A N Z, M. H I L L G A R T N E R, H. Z I M M E R M A N N, D.Z I M M E R M A N N, F . V O L K E and U. Z I M M E R M A N N , Eur.Biophys. J. 33(1) (2004) 50.
25. R . W O L F , J. Microsc. (London) 153 (1989) 181.26. R . W O L F , in “Science, Technology and Education of Microscopy:
an Overview,” edited by A. Mendez-Vilas (Formatex, Madrid,2003) p. 720.
27. O . S M I D S R ø D and G. S K J A K-B R Æ K , Trends Biotechnol.8(3) (1990) 71.
28. C . D U L I E U, D. P O N C E L E T and R. J . N E U F E L D , in“Cell Encapsulation Technology and Therapeutics,” edited by W.M. Kuhtreiber, R. P. Lanza and W. L. Chick (Birkhauser, Boston,1999) p. 3.
29. P . B . M E S S E R S M I T H and S . S T A R K E , Chem. Mater. 10(1)(1998) 117.
30. M. E . W E S T W O O D and P . J . T H O R N A L L E Y , in “The Gly-cation Hypothesis of Atherosclerosis,” edited by C. Colaco (LandesBioscience, Georgetown, 1997) p. 57.
31. U . Z I M M E R M A N N and E. S T E U D L E , Adv. Bot. Res. 6 (1978)45.
32. J . D A I N T Y , Adv. Bot. Res. 1 (1963) 279.33. E . O . S T E J K A L and J . E . T A N N E R , J. Chem. Phys. 42 (1965)
288.34. M. M A U R O , Science 126 (1957) 252.35. A . K . S O L O M O N , J. Gen. Physiol. 51(5) (1968) 335.36. E . R O B B I N S and A. M A U R O , ibid. 43(3) (1960) 523.37. F . J . M A R T I N and C. G R O V E , Biomed. Microdiv. 3(2) (2001)
97.38. S . S C H N E I D E R, P . J . F E I L E N, F . B R U N N E N M E I E R,
U. Z I M M E R M A N N and M. M. W E B E R , Diabetes 53(2)(2004) A 615.
39. J . H . C R O W E and L. M. C R O W E , Nat. Biotechnol. 18(2)(2000) 145.
40. A . E R O G L U, M. J . R U S S O, R . B I E G A N S K I , A .F O W L E R, S . C H E L E Y, H. B A Y L E Y and M. T O N E R ,Nat. Biotechnol. 18(2) (2000) 163.
41. H . Z I M M E R M A N N, A. D. K A T S E N, F . R . I H M I G, C H.H. P . D U R S T, S T . G . S H I R L E Y and G. R . F U H R , IEEProc. Nanobiotechnol. 151(4) (2004) 134.
42. R . R E U S S , J . L U D W I G, R . S H I R A K A S H I , F .E H R H A R T, H. Z I M M E R M A N N, S . S C H N E I D E R, M.M. W E B E R, U. Z I M M E R M A N N, H. S C H N E I D E R andV. L . S U K H O R U K O V , J. Membr. Biol. 200(2) (2004) 67.
43. F . L A N G, G. L . B U S C H and H. V O L K L , Cell. Physiol.Biochem. 8(1/2) (1998) 1.
44. M. E S C H, V. L . S U K H O R U K O V, M. K U R S C H N E R andU. Z I M M E R M A N N , Biopolymers 50(3) (1999) 227.
45. H . S C H N E I D E R, N. W I S T U B A, H. J . W A G N E R, F .T H U R M E R and U. Z I M M E R M A N N , New Phytol. 148(2)(2000) 221.
46. H . S C H N E I D E R, B . M A N Z, M. W E S T H O F F , S .M I M I E T Z, M. S Z I M T E N I N G S, T . N E U B E R G E R, C .F A B E R, G. K R O H N E, A. H A A S E, F . V O L K E and U.Z I M M E R M A N N , New Phytol. 159(2) (2003) 487.
47. H . J . W A G N E R, H. S C H N E I D E R, S . M I M I E T Z, N.W I S T U B A, M. R O K I T T A, G. K R O H N E, A. H A A S E andU. Z I M M E R M A N N , New Phytol. 148(2) (2000) 239.
Received 15 Augustand accepted 15 October 2004
501




















