
Topotecan for relapsed small cell lung cancer: a systematic review and economic evaluation
8
General and Supportive Care Topotecan for relapsed small cell lung cancer: A systematic review and economic evaluation Debbie Hartwell * , Jeremy Jones a , Emma Loveman b , Petra Harris c , Andrew Clegg d , Alex Bird e Southampton Health Technology Assessments Centre (SHTAC), University of Southampton, First Floor Epsilon House, Enterprise Road, Southampton Science Park, Southampton SO16 7NS, UK article info Article history: Received 29 March 2010 Received in revised form 12 July 2010 Accepted 14 July 2010 Keywords: Small cell lung cancer Topotecan Treatment Systematic review Cost effectiveness summary Background: Topotecan is a relatively new drug for use as a second-line treatment in patients with relapsed small cell lung cancer (SCLC). We performed a systematic review and economic evaluation of topotecan, and consider it here in relation to the NICE end of life criteria. Methods: Seventeen bibliographic databases (including Cochrane library, Medline and Embase) were searched from 1990 to February 2009, and experts and manufacturers were consulted, to identify rele- vant randomised controlled trials (RCTs) which were selected according to prospectively defined criteria. An economic evaluation was undertaken to assess cost effectiveness compared with best supportive care (BSC) in the UK. Results: Five RCTs were included. The clinical evidence indicates a statistically significant benefit of oral topotecan plus BSC compared to BSC alone for overall survival. Intravenous topotecan was similar in effi- cacy to both oral topotecan and CAV (cyclophosphamide, doxorubicin and vincristine). In the survival model, oral topotecan plus BSC was associated with an average gain in life expectancy of approximately 4 months, resulting in a gain of 0.183 quality-adjusted life years (QALYs). At an incremental cost of approximately £6200 the incremental cost effectiveness ratio (ICER) is £33,851 per QALY gained. Conclusions: Compared with BSC alone, oral topotecan for patients with relapsed SCLC was associated with improved health outcomes but at increased cost. The ICER is at the upper extreme of the range con- ventionally regarded as cost effective from an NHS decision making perspective. However, this treatment may fall under supplementary guidance for life extending, end of life treatments. Crown Copyright Ó 2010 Published by Elsevier Ltd. All rights reserved. Introduction Small cell lung cancer (SCLC) is a devastating condition. Accounting for 10–20% of all lung cancers in the UK, 1 it has an aggressive course 2 growing rapidly and metastasising widely. 3 Without treatment the prognosis is poor, with a median survival of 2–4 months. 4 Survival can be prolonged with treatment 4 and of- ten the initial response to chemotherapy for SCLC is good. Unfortu- nately it is rarely long lasting. For some patients, where it is considered appropriate, a second-line treatment may be consid- ered. National Institute for Health and Clinical Excellence (NICE) guidelines for managing SCLC recommend that second-line chemotherapy should be offered if the disease has responded to first-line therapy. 5 Treatment can consist of a repeat of first-line therapy, if a good response was achieved, or an alternative. 6 For some, re-treatment with the first-line regimen may not be consid- ered appropriate due to resistance, contraindications, adverse events or patient refusal. 7 Options for these patients are limited. In the UK, combination therapy with cyclophosphamide, doxorubi- cin (adriamycin) and vincristine (CAV) has been the only second- line intervention used for those unable to undergo re-treatment with their first-line chemotherapy. Until recently there were no alternative treatments recommended for those ineligible for CAV. The emergence of both intravenous (IV) and oral forms of topotec- an (GlaxoSmithKline, UK) has provided other options for managing people with SCLC requiring second-line treatment. Prior to their widespread use, it is important to assess the relative benefits, risks and costs of the different interventions available to allow guidance to be provided to patients and the NHS. This study reports the results of a systematic review and eco- nomic evaluation to assess the clinical and cost effectiveness of topotecan within its licensed indications for treating people with relapsed SCLC. 8 It was commissioned to assist NICE in their 0305-7372/$ - see front matter Crown Copyright Ó 2010 Published by Elsevier Ltd. All rights reserved. doi:10.1016/j.ctrv.2010.07.005 * Corresponding author. Tel.: +44 23 8059 5632; fax: +44 23 8059 5662. E-mail addresses: [email protected] (D. Hartwell), [email protected] (J. Jones), [email protected] (E. Loveman), [email protected] (P. Harris), [email protected] (A. Clegg), [email protected] (A. Bird). a Tel.: +44 23 8059 7056; fax: +44 23 8059 5662. b Tel.: +44 23 8056 5628; fax: +44 23 8056 5662. c Tel.: +44 23 8059 5614; fax: +44 23 8059 5662. d Tel.: +44 23 8059 5597; fax: +44 23 8059 5662. e Tel.: +44 23 8059 5941; fax: +44 23 8059 5662. Cancer Treatment Reviews 37 (2011) 242–249 Contents lists available at ScienceDirect Cancer Treatment Reviews journal homepage: www.elsevierhealth.com/journals/ctrv
Transcript of Topotecan for relapsed small cell lung cancer: a systematic review and economic evaluation

Cancer Treatment Reviews 37 (2011) 242–249
Contents lists available at ScienceDirect
Cancer Treatment Reviews
journal homepage: www.elsevierheal th.com/ journals /c t rv
General and Supportive Care
Topotecan for relapsed small cell lung cancer: A systematic reviewand economic evaluation
Debbie Hartwell *, Jeremy Jones a, Emma Loveman b, Petra Harris c, Andrew Clegg d, Alex Bird e
Southampton Health Technology Assessments Centre (SHTAC), University of Southampton, First Floor Epsilon House, Enterprise Road,Southampton Science Park, Southampton SO16 7NS, UK
a r t i c l e i n f o
Article history:Received 29 March 2010Received in revised form 12 July 2010Accepted 14 July 2010
Keywords:Small cell lung cancerTopotecanTreatmentSystematic reviewCost effectiveness
0305-7372/$ - see front matter Crown Copyright � 2doi:10.1016/j.ctrv.2010.07.005
* Corresponding author. Tel.: +44 23 8059 5632; faE-mail addresses: [email protected] (D.
(J. Jones), [email protected] (E. Lov(P. Harris), [email protected] (A. Clegg), ab3o07@so
a Tel.: +44 23 8059 7056; fax: +44 23 8059 5662.b Tel.: +44 23 8056 5628; fax: +44 23 8056 5662.c Tel.: +44 23 8059 5614; fax: +44 23 8059 5662.d Tel.: +44 23 8059 5597; fax: +44 23 8059 5662.e Tel.: +44 23 8059 5941; fax: +44 23 8059 5662.
s u m m a r y
Background: Topotecan is a relatively new drug for use as a second-line treatment in patients withrelapsed small cell lung cancer (SCLC). We performed a systematic review and economic evaluation oftopotecan, and consider it here in relation to the NICE end of life criteria.Methods: Seventeen bibliographic databases (including Cochrane library, Medline and Embase) weresearched from 1990 to February 2009, and experts and manufacturers were consulted, to identify rele-vant randomised controlled trials (RCTs) which were selected according to prospectively defined criteria.An economic evaluation was undertaken to assess cost effectiveness compared with best supportive care(BSC) in the UK.Results: Five RCTs were included. The clinical evidence indicates a statistically significant benefit of oraltopotecan plus BSC compared to BSC alone for overall survival. Intravenous topotecan was similar in effi-cacy to both oral topotecan and CAV (cyclophosphamide, doxorubicin and vincristine). In the survivalmodel, oral topotecan plus BSC was associated with an average gain in life expectancy of approximately4 months, resulting in a gain of 0.183 quality-adjusted life years (QALYs). At an incremental cost ofapproximately £6200 the incremental cost effectiveness ratio (ICER) is £33,851 per QALY gained.Conclusions: Compared with BSC alone, oral topotecan for patients with relapsed SCLC was associatedwith improved health outcomes but at increased cost. The ICER is at the upper extreme of the range con-ventionally regarded as cost effective from an NHS decision making perspective. However, this treatmentmay fall under supplementary guidance for life extending, end of life treatments.
Crown Copyright � 2010 Published by Elsevier Ltd. All rights reserved.
Introduction
Small cell lung cancer (SCLC) is a devastating condition.Accounting for 10–20% of all lung cancers in the UK,1 it has anaggressive course2 growing rapidly and metastasising widely.3
Without treatment the prognosis is poor, with a median survivalof 2–4 months.4 Survival can be prolonged with treatment4 and of-ten the initial response to chemotherapy for SCLC is good. Unfortu-nately it is rarely long lasting. For some patients, where it isconsidered appropriate, a second-line treatment may be consid-ered. National Institute for Health and Clinical Excellence (NICE)guidelines for managing SCLC recommend that second-line
010 Published by Elsevier Ltd. All r
x: +44 23 8059 5662.Hartwell), [email protected]
eman), [email protected] (A. Bird).
chemotherapy should be offered if the disease has responded tofirst-line therapy.5 Treatment can consist of a repeat of first-linetherapy, if a good response was achieved, or an alternative.6 Forsome, re-treatment with the first-line regimen may not be consid-ered appropriate due to resistance, contraindications, adverseevents or patient refusal.7 Options for these patients are limited.In the UK, combination therapy with cyclophosphamide, doxorubi-cin (adriamycin) and vincristine (CAV) has been the only second-line intervention used for those unable to undergo re-treatmentwith their first-line chemotherapy. Until recently there were noalternative treatments recommended for those ineligible for CAV.The emergence of both intravenous (IV) and oral forms of topotec-an (GlaxoSmithKline, UK) has provided other options for managingpeople with SCLC requiring second-line treatment. Prior to theirwidespread use, it is important to assess the relative benefits, risksand costs of the different interventions available to allow guidanceto be provided to patients and the NHS.
This study reports the results of a systematic review and eco-nomic evaluation to assess the clinical and cost effectiveness oftopotecan within its licensed indications for treating people withrelapsed SCLC.8 It was commissioned to assist NICE in their
ights reserved.
D. Hartwell et al. / Cancer Treatment Reviews 37 (2011) 242–249 243
appraisal process and with the development of guidance to theNHS.9 As SCLC is considered a life-limiting disease, the appraisaladopted the supplementary advice issued by NICE in January2009 concerning such conditions.10 This provides the opportunity,when specific criteria apply, to raise the threshold for judging thecost effectiveness of an intervention. We discuss the possibleimplications appraising this technology.
Methods
A sensitive literature search was applied to seventeen electronicdatabases, including the Cochrane library, Medline and Embase,from 1990 to February 2009. Additional references were identifiedfrom bibliographies, key cancer resources and symposia, andthrough contact with experts and industry.
Randomised controlled trials (RCTs) and full economic evalua-tions of adults with relapsed SCLC, who responded to first-linetreatment and for whom re-treatment with first-line therapy wasnot considered appropriate, were included. Studies had to reportan evaluation of IV or oral topotecan. Outcomes included overallsurvival, time to disease progression (TTP), response rate (definedusing either the WHO criteria11 or the RECIST (Response EvaluationCriteria in Solid Tumours) guidelines12), response duration, adverseevents (symptoms and toxicity), health-related quality of life andmeasures of cost effectiveness or cost utility. Authors were con-tacted to check whether participants met the licensed indicationsfor topotecan.
Methodological quality was evaluated using standardcriteria13–15 and the risk of bias was assessed following the princi-pals of Cochrane Collaboration methodology.16 Inclusion criteriawere applied, data were extracted and study quality was assessedby one reviewer and checked by a second, with any differences inopinion resolved through discussion. Data were synthesisedthrough a narrative review with tabulation of results of all in-cluded studies. Quantitative meta-analysis was not possible owingto heterogeneity in the included studies. Further details on thesearch strategies and the systematic methods used to inform thereview are presented in the full research report.8
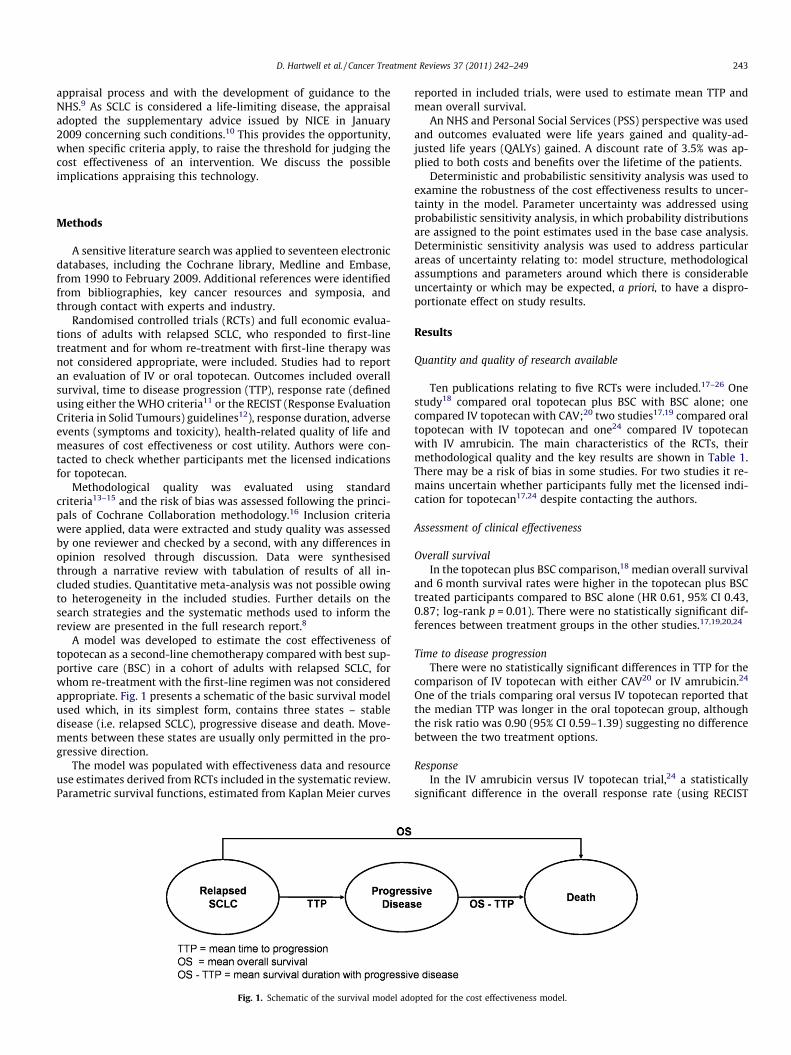
A model was developed to estimate the cost effectiveness oftopotecan as a second-line chemotherapy compared with best sup-portive care (BSC) in a cohort of adults with relapsed SCLC, forwhom re-treatment with the first-line regimen was not consideredappropriate. Fig. 1 presents a schematic of the basic survival modelused which, in its simplest form, contains three states – stabledisease (i.e. relapsed SCLC), progressive disease and death. Move-ments between these states are usually only permitted in the pro-gressive direction.
The model was populated with effectiveness data and resourceuse estimates derived from RCTs included in the systematic review.Parametric survival functions, estimated from Kaplan Meier curves
Fig. 1. Schematic of the survival model ado
reported in included trials, were used to estimate mean TTP andmean overall survival.
An NHS and Personal Social Services (PSS) perspective was usedand outcomes evaluated were life years gained and quality-ad-justed life years (QALYs) gained. A discount rate of 3.5% was ap-plied to both costs and benefits over the lifetime of the patients.
Deterministic and probabilistic sensitivity analysis was used toexamine the robustness of the cost effectiveness results to uncer-tainty in the model. Parameter uncertainty was addressed usingprobabilistic sensitivity analysis, in which probability distributionsare assigned to the point estimates used in the base case analysis.Deterministic sensitivity analysis was used to address particularareas of uncertainty relating to: model structure, methodologicalassumptions and parameters around which there is considerableuncertainty or which may be expected, a priori, to have a dispro-portionate effect on study results.
Results
Quantity and quality of research available
Ten publications relating to five RCTs were included.17–26 Onestudy18 compared oral topotecan plus BSC with BSC alone; onecompared IV topotecan with CAV;20 two studies17,19 compared oraltopotecan with IV topotecan and one24 compared IV topotecanwith IV amrubicin. The main characteristics of the RCTs, theirmethodological quality and the key results are shown in Table 1.There may be a risk of bias in some studies. For two studies it re-mains uncertain whether participants fully met the licensed indi-cation for topotecan17,24 despite contacting the authors.
Assessment of clinical effectiveness
Overall survivalIn the topotecan plus BSC comparison,18 median overall survival
and 6 month survival rates were higher in the topotecan plus BSCtreated participants compared to BSC alone (HR 0.61, 95% CI 0.43,0.87; log-rank p = 0.01). There were no statistically significant dif-ferences between treatment groups in the other studies.17,19,20,24
Time to disease progressionThere were no statistically significant differences in TTP for the
comparison of IV topotecan with either CAV20 or IV amrubicin.24
One of the trials comparing oral versus IV topotecan reported thatthe median TTP was longer in the oral topotecan group, althoughthe risk ratio was 0.90 (95% CI 0.59–1.39) suggesting no differencebetween the two treatment options.
ResponseIn the IV amrubicin versus IV topotecan trial,24 a statistically
significant difference in the overall response rate (using RECIST
pted for the cost effectiveness model.
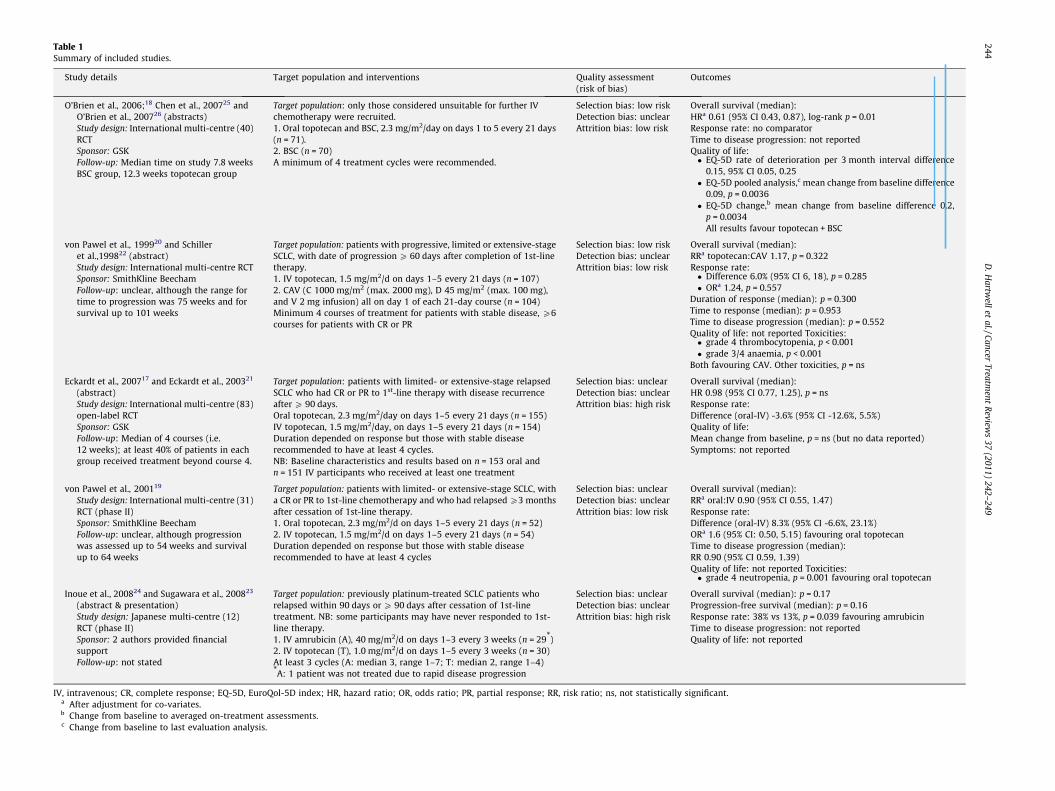
Table 1Summary of included studies.
Study details Target population and interventions Quality assessment(risk of bias)
Outcomes
O’Brien et al., 2006;18 Chen et al., 200725 andO’Brien et al., 200726 (abstracts)Study design: International multi-centre (40)RCTSponsor: GSKFollow-up: Median time on study 7.8 weeksBSC group, 12.3 weeks topotecan group
Target population: only those considered unsuitable for further IVchemotherapy were recruited.1. Oral topotecan and BSC, 2.3 mg/m2/day on days 1 to 5 every 21 days(n = 71).2. BSC (n = 70)A minimum of 4 treatment cycles were recommended.
Selection bias: low riskDetection bias: unclearAttrition bias: low risk
Overall survival (median):HRa 0.61 (95% CI 0.43, 0.87), log-rank p = 0.01Response rate: no comparatorTime to disease progression: not reportedQuality of life:� EQ-5D rate of deterioration per 3 month interval difference
0.15, 95% CI 0.05, 0.25� EQ-5D pooled analysis,c mean change from baseline difference
0.09, p = 0.0036� EQ-5D change,b mean change from baseline difference 0.2,
p = 0.0034All results favour topotecan + BSC
von Pawel et al., 199920 and Schilleret al.,199822 (abstract)Study design: International multi-centre RCTSponsor: SmithKline BeechamFollow-up: unclear, although the range fortime to progression was 75 weeks and forsurvival up to 101 weeks
Target population: patients with progressive, limited or extensive-stageSCLC, with date of progression P 60 days after completion of 1st-linetherapy.1. IV topotecan, 1.5 mg/m2/d on days 1–5 every 21 days (n = 107)2. CAV (C 1000 mg/m2 (max. 2000 mg), D 45 mg/m2 (max. 100 mg),and V 2 mg infusion) all on day 1 of each 21-day course (n = 104)Minimum 4 courses of treatment for patients with stable disease, P6courses for patients with CR or PR
Selection bias: low riskDetection bias: unclearAttrition bias: low risk
Overall survival (median):RRa topotecan:CAV 1.17, p = 0.322Response rate:� Difference 6.0% (95% CI 6, 18), p = 0.285� ORa 1.24, p = 0.557
Duration of response (median): p = 0.300Time to response (median): p = 0.953Time to disease progression (median): p = 0.552Quality of life: not reported Toxicities:� grade 4 thrombocytopenia, p < 0.001� grade 3/4 anaemia, p < 0.001
Both favouring CAV. Other toxicities, p = ns
Eckardt et al., 200717 and Eckardt et al., 200321
(abstract)Study design: International multi-centre (83)open-label RCTSponsor: GSKFollow-up: Median of 4 courses (i.e.12 weeks); at least 40% of patients in eachgroup received treatment beyond course 4.
Target population: patients with limited- or extensive-stage relapsedSCLC who had CR or PR to 1st-line therapy with disease recurrenceafter P 90 days.Oral topotecan, 2.3 mg/m2/day on days 1–5 every 21 days (n = 155)IV topotecan, 1.5 mg/m2/day, on days 1–5 every 21 days (n = 154)Duration depended on response but those with stable diseaserecommended to have at least 4 cycles.NB: Baseline characteristics and results based on n = 153 oral andn = 151 IV participants who received at least one treatment
Selection bias: unclearDetection bias: unclearAttrition bias: high risk
Overall survival (median):HR 0.98 (95% CI 0.77, 1.25), p = nsResponse rate:Difference (oral-IV) -3.6% (95% CI -12.6%, 5.5%)Quality of life:Mean change from baseline, p = ns (but no data reported)Symptoms: not reported
von Pawel et al., 200119
Study design: International multi-centre (31)RCT (phase II)Sponsor: SmithKline BeechamFollow-up: unclear, although progressionwas assessed up to 54 weeks and survivalup to 64 weeks
Target population: patients with limited- or extensive-stage SCLC, witha CR or PR to 1st-line chemotherapy and who had relapsed P3 monthsafter cessation of 1st-line therapy.1. Oral topotecan, 2.3 mg/m2/d on days 1–5 every 21 days (n = 52)2. IV topotecan, 1.5 mg/m2/d on days 1–5 every 21 days (n = 54)Duration depended on response but those with stable diseaserecommended to have at least 4 cycles
Selection bias: unclearDetection bias: unclearAttrition bias: low risk
Overall survival (median):RRa oral:IV 0.90 (95% CI 0.55, 1.47)Response rate:Difference (oral-IV) 8.3% (95% CI -6.6%, 23.1%)ORa 1.6 (95% CI: 0.50, 5.15) favouring oral topotecanTime to disease progression (median):RR 0.90 (95% CI 0.59, 1.39)Quality of life: not reported Toxicities:� grade 4 neutropenia, p = 0.001 favouring oral topotecan
Inoue et al., 200824 and Sugawara et al., 200823
(abstract & presentation)Study design: Japanese multi-centre (12)RCT (phase II)Sponsor: 2 authors provided financialsupportFollow-up: not stated
Target population: previously platinum-treated SCLC patients whorelapsed within 90 days or P 90 days after cessation of 1st-linetreatment. NB: some participants may have never responded to 1st-line therapy.1. IV amrubicin (A), 40 mg/m2/d on days 1–3 every 3 weeks (n = 29*)2. IV topotecan (T), 1.0 mg/m2/d on days 1–5 every 3 weeks (n = 30)At least 3 cycles (A: median 3, range 1–7; T: median 2, range 1–4)*A: 1 patient was not treated due to rapid disease progression
Selection bias: unclearDetection bias: unclearAttrition bias: high risk
Overall survival (median): p = 0.17Progression-free survival (median): p = 0.16Response rate: 38% vs 13%, p = 0.039 favouring amrubicinTime to disease progression: not reportedQuality of life: not reported
IV, intravenous; CR, complete response; EQ-5D, EuroQol-5D index; HR, hazard ratio; OR, odds ratio; PR, partial response; RR, risk ratio; ns, not statistically significant.a After adjustment for co-variates.b Change from baseline to averaged on-treatment assessments.c Change from baseline to last evaluation analysis.
244D
.Hartw
ellet
al./CancerTreatm
entR
eviews
37(2011)
242–249

Table 3Drug acquisition, chemotherapy administration and cost of patient monitoring whileon treatment for oral topotecan.
Item Resource useper course
Unit cost (£)
Oral topotecan 21.25 mga 30 per mg
Drug acquisition cost per course of oral topotecan 637.50Outpatient attendance to receive oral
chemotherapy1 184.97b
Pharmacy cost for dispensing oralchemotherapy
1 0.90c
FBC 1 2.90d
LFT 1 4.70d
d
D. Hartwell et al. / Cancer Treatment Reviews 37 (2011) 242–249 245
criteria) favouring amrubicin was reported (38% vs. 13%, p = 0.039).There were no statistically significant differences in response rate,response duration or time to response, where reported, in any ofthe other trials.
Adverse eventsGenerally, rates of adverse events were observed to be compa-
rable across treatments in the included studies but most were nottested for statistical significance. With respect to toxicities, topo-tecan-treated participants had a significantly higher incidence ofgrade 4 thrombocytopenia (p < 0.001) and grade 3/4 anaemia(p < 0.001) compared with CAV.20 Toxicities observed with oraland IV topotecan were broadly similar, with the exception of grade4 neutropenia which occurred significantly more frequently in theIV topotecan group (p = 0.001) in one trial.19 Rates of haematolog-ical toxicities in the topotecan versus amrubicin trial24 varied be-tween arms.
Quality of life (QoL)Only two trials17,18 measured QoL as an outcome. Differences in
the rate of deterioration of QoL (as measured by the EQ-5D) fa-voured those receiving topotecan in addition to BSC (difference0.15, 95% CI 0.05–0.25).18 Additional data on the EQ-5D index indi-cated a significantly smaller decline in health status for thosereceiving topotecan plus BSC.25 However, these results should beviewed with caution owing to a number of issues including theomission of any baseline data18 and the EQ-5D data being reportedin abstract form only and derived from a pooled estimate.25 In oneof the trials comparing oral versus IV topotecan,17 no statistical dif-ferences between groups were reported for QoL, although no actualdata was presented.
Assessment of cost effectiveness
No relevant economic evaluations were identified in the sys-tematic review, so a new economic model was developed. The costeffectiveness comparison reported in this paper concerns the addi-tion of oral topotecan to BSC in adults with relapsed SCLC forwhom re-treatment with the first-line regimen was not consideredappropriate and who were also unsuitable for further IV chemo-therapy (the population included by O’Brien and colleagues18).We did not include comparisons of oral topotecan with CAV or IVtopotecan due to the absence of a direct comparison of oral topo-tecan against CAV, uncertainties over the comparability of patientpopulations in included trials and limitations in the available datato support robust economic modelling.
Estimation of benefitsThe area under the survival curves was used to estimate mean
overall survival. Since some participants in each arm of the RCTby O’Brien and colleagues18 were still alive at the end of followup, the final portions of the survival curves were extrapolatedusing regression analysis (a log–logistic survival function provided
Table 2Health state utility values used in the cost effectiveness model.
Baselineutility
Percent reductionover 3 months(95% CI)
Percentreductionper day
Oral topotecan plus BSC 0.7 �5 (�11 to 2) �0.056BSC alone 0.7 �20 (�27 to �12) �0.244
BSC, best supportive care.Note: to estimate the percentage reduction per day, from the percent reduction over3 months, we calculated lnðUB�ð1�D3mÞÞ�lnðUBÞ
ð365:25=4Þ ,where UB = baseline utility, D3m = percent change in utility over 3 months and ln()indicates the natural logarithm.
the best fit to the observed Kaplan–Meier estimates). A similarmethod was used to estimate mean TTP, taking data supplied toNICE by the manufacturer for the topotecan-treated participantsonly. Further details can be found in the full research report.8
The estimated mean survival times were adjusted for quality oflife in the relapsed SCLC and progressive disease states of the costeffectiveness model (see Fig. 1), using appropriate health state util-ity valuations in order to calculate QALYs. Utilities used were basedon the EQ-5D utilities reported by O’Brien and colleagues.18 Base-line EQ-5D values, for participants in the RCT, were reported inan abstract.25 A baseline utility of 0.7 was assumed, as seen inTable 2.
Sources of cost and resource utilisationHealthcare costs included in the model were pre-medication,
drug acquisition costs, drug administration and patient monitor-ing, management of adverse events and palliative care costs.
Oral topotecan is administered at 2.3 mg/m2/day on five con-secutive days of each 21-day course of treatment.27 Allowing forthe fact that some participants in the RCT by O’Brien and col-leagues18 experienced dose reductions (reported as 8% of courses)or dose escalations (reported as 14% of courses), we estimated themean oral topotecan dosages to be between 2.29 and 2.38 mg/m2/day (corresponding to dosages of 4.13 to 4.28 mg per day oftreatment).
Chemotherapy administration and on-treatment monitoringcosts were based on patients attending hospital once (at the begin-ning of each course) for a consultation with their treating physicianand a series of biochemical, haematological and imaging tests. Atthe same time patients would collect the complete supply of oraltopotecan for each course of treatment along with a supply of anoral anti-emetic (domperidone, non-proprietary) and an anti-diar-rhoeal (loperimide) to use as required. Table 3 reports the assump-tions used in the cost effectiveness model to estimate the drugacquisition, chemotherapy administration and on-treatment mon-itoring costs per course for oral topotecan.
It was assumed that patients with relapsed SCLC received amean of four courses of oral topotecan based on quantities in theO’Brien and colleagues RCT.18 This corresponds to a total drugacquisition cost of £2550 and total chemotherapy administration
U&E 1 4.70Chest X-ray 1 28.64b
CT scan (every 2 courses) 0.5 94.68b
Total administration and monitoring cost per course of oraltopotecan
274.14
FBC, full blood count; LFT, liver function tests; U&E, urea and electrolytes (renalfunction tests).
a Assuming patient with body surface area of 1.8 m2, giving a daily dosage of4.25 mg. Oral topotecan is taken on five consecutive days of each 21-day course.
b Source for unit costs: NHS Reference Costs 2006/07, up-rated to 2007/08 pricesusing Hospital and Community Health Services (HCHS) Pay and Prices Index.28
c Prescription Prescribing Authority 2007/08 dispensing fee to communitypharmacists, from MS.29
d Finance Department, Southampton University Hospitals Trust.
246 D. Hartwell et al. / Cancer Treatment Reviews 37 (2011) 242–249
and on-treatment monitoring costs of £1097 per patient for oraltopotecan.
Cost of toxicities associated with oral topotecan treatment,were estimated based on the incidence (reported by O’Brien andcolleagues18) and estimates of the resources used to manage treat-ment related toxicity. Cost of managing these events were basedon validated estimates reported by Main and colleagues30 and,where necessary, updated for this model in consultation with clin-ical experts.
Patients were assumed to continue to attend out-patients forgeneral medical care and for monitoring of their condition, follow-ing the completion of their course of treatment with oral topotec-an. This continued monitoring is costed in the model until patientsdevelop progressive disease, assuming that patients attend out-pa-tients every four weeks, have a GP consultation every four weeksand undergo imaging (chest X-ray and a CT scan) once to confirmdisease progression.
Limited detail was reported on the supportive care provided topatients in the RCT by O’Brien and colleagues.18 While supportive
Table 4Base case analysis.
Treatment Costs (£) Lifeyears
Incrementalcost per lifeyear gained (£)
QALYs Incrementalcost per QALYgained (£)
BSC 4854 0.4735 0.2247Oral topotecan
and BSC11,048 0.7984 19,065 0.4077 33,851
BSC, best supportive care; QALY, quality-adjusted life year.
Table 5Treatment costs by phase of treatment.
Phase of treatment Oraltopotecan (£)
BSC (£)
Active treatment Drug 2550Drug administration 743On-treatment monitoring 353
Adverse event costs Haematological 1470Non-haematological 114
Non-progressive disease monitoring 1082Palliative care 4735 4854Total 11,048 4854
BSC, best supportive care.
0.00
0.25
0.50
0.75
1.00
20.00010.0000
Willingness to
Prob
abilit
y in
terv
netio
n is
cos
t effe
ctiv
e
Fig. 2. Cost effectiveness acceptability
care was a common component in both arms, it is likely that par-ticipants experienced palliative care at different times in the twoarms, given the survival advantage associated with topotecan. Anestimate of the cost of palliative care was included in the model,derived from a retrospective analysis of case notes for 109 SCLC pa-tients conducted in the UK,31 which includes in- and out-patientcosts, tests and procedures, surgery and radiotherapy (total cost£4977).
Estimates of cost effectivenessCosts and outcomes modelled for cohorts of patients receiving
oral topotecan plus BSC or BSC alone are presented in Table 4.The estimated gain in discounted life expectancy, associated withthe addition of oral topotecan to BSC, is 0.3249 years (16.9 weeks)and the estimated QALY gain is 0.1830. At the same time costs havemore than doubled (the incremental cost is £6194) yielding anincremental cost effectiveness ratio (ICER) for the addition of oraltopotecan to BSC of £33,851 per QALY gained.
Table 5 reports a breakdown of total cost, by phase of treatment,for each cohort. Palliative care is the only phase of treatment iden-tified for patients receiving BSC alone, and this represents 100% ofthe treatment cost for this cohort. While palliative care remains thesingle most costly phase for patients receiving treatment with oraltopotecan in addition to BSC, these have reduced to 43% of totalcosts for this cohort. Active treatment with oral topotecan repre-sents 33% of total costs for this cohort, the majority of which aredrug acquisition costs.
Sensitivity and probabilistic analysisThe cost effectiveness results were generally robust to variation
in the parameters included in the deterministic sensitivity analysis,with ICERs varying between approximately £30,000 and £37,000per QALY gained. Among the structural sensitivity analyses, the re-sults were most sensitive to assumptions over the functional formfor the survival functions. In terms of parameter inputs, the resultswere most sensitive to variation in the utility estimates applied inthe model, values of parameters in the survival functions (for over-all survival and TTP) and cost of outpatient attendance for theadministration of oral chemotherapy.
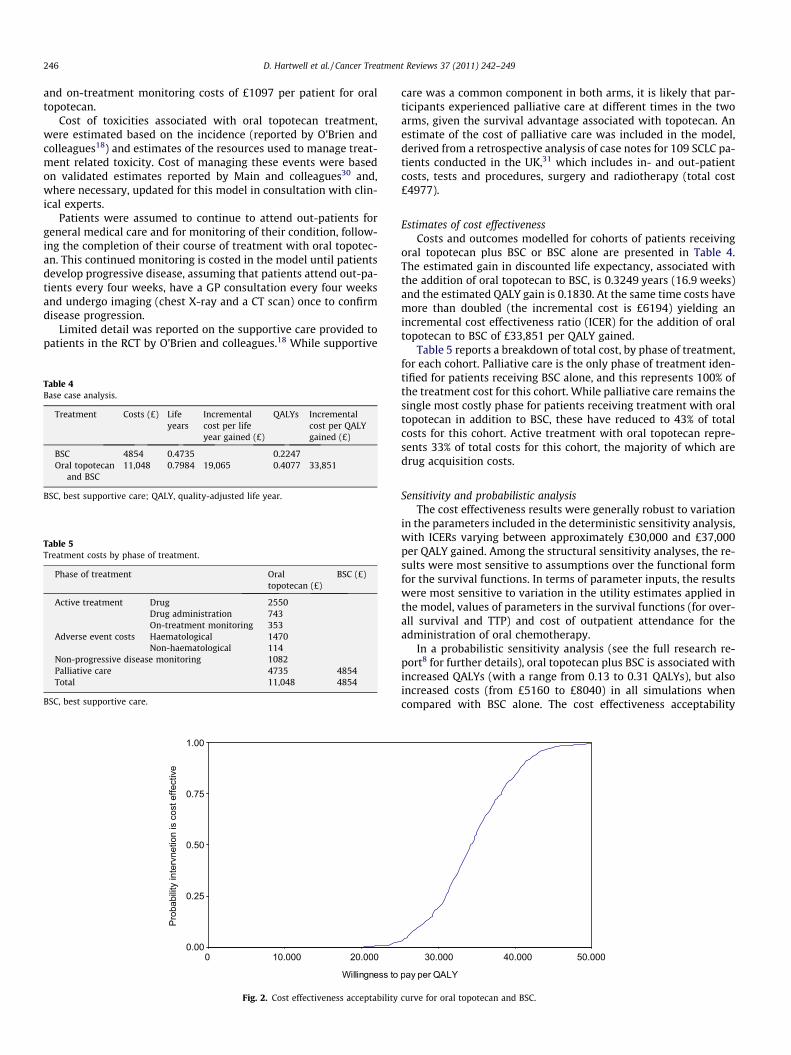
In a probabilistic sensitivity analysis (see the full research re-port8 for further details), oral topotecan plus BSC is associated withincreased QALYs (with a range from 0.13 to 0.31 QALYs), but alsoincreased costs (from £5160 to £8040) in all simulations whencompared with BSC alone. The cost effectiveness acceptability
50.00040.00030.000
pay per QALY
curve for oral topotecan and BSC.

D. Hartwell et al. / Cancer Treatment Reviews 37 (2011) 242–249 247
curve32 in Fig. 2 represents the proportion of simulations whereoral topotecan treatment is cost effective for a range of willingnessto pay thresholds, up to £50,000. In this analysis oral topotecanplus BSC had a probability of being cost effective of 0% at a willing-ness to pay threshold of £20,000 per QALY, 20% at a willingness topay threshold of £30,000 per QALY and 100% at a willingness to paythreshold of £50,000 per QALY.
Discussion
The clinical evidence presented in this systematic review of fiveRCTs, with varying degrees of risk of bias, indicates that oral topo-tecan is significantly better than BSC alone in terms of improvedsurvival, and is comparable to CAV, the current treatment stan-dard. Oral and IV topotecan were shown to be similar in efficacy.Topotecan appears to be less favourable than IV amrubicin in termsof response, but it should be noted that the dose of topotecan usedin this trial24 (1.0 mg/m2) was lower than the UK recommendeddose (1.5 mg/m2) and the population may be different. Rates of ad-verse events and toxicities were generally comparable across treat-ment groups, although most were not tested for statisticalsignificance. However, some haematological toxicities occurredsignificantly more frequently in the IV topotecan group comparedwith both CAV20 and oral topotecan.19 In the survival model usedin the economic evaluation, oral topotecan plus BSC was associatedwith an average gain in life expectancy of �4 months, resulting in again of 0.183 QALYs. At an incremental cost of approximately£6200, the ICER was £33,851 per QALY gained. The cost effective-ness results were sensitive to assumptions over the form of sur-vival functions adopted in the model, variation in values ofparameters in the survival functions and variation in the utilityestimates applied. In a probabilistic sensitivity analysis, we esti-mated a 0% probability of oral topotecan and BSC being cost effec-tive compared with BSC alone at a willingness to pay threshold of£20,000. At willingness to pay thresholds of £30,000 per QALY and£50,000 per QALY the probabilities of it being cost effective were20% and 100% respectively.
Oral topotecan is a comparatively expensive drug, with its ICERat the upper limit of the range generally deemed acceptable byNICE for issuing a positive recommendation, as noted in their cur-rent methods guide:
‘‘Above a most plausible ICER of £30,000 per QALY gained, theCommittee will need to identify an increasingly stronger casefor supporting the technology as an effective use of NHS resour-ces. . ..”(see paragraph 6.2.2532).
Despite this, NICE have recommended oral topotecan as an op-tion for people with relapsed SCLC for whom re-treatment with thefirst-line regimen is not considered appropriate and where CAV iscontraindicated.9 NICE’s guidance reflects the implementation of anew approach to the appraisal of health technologies that may ex-tend the life of people with a short life expectancy. Following theRichards review33 in 2008, which was prompted by the public de-bate over co-payments for drugs that meant people had to relin-quish their right to NHS treatment, NICE were advised to reviewthe cost effectiveness threshold used. NICE subsequently publishedsupplementary advice in January 2009, which was revised in July2009, identifying a set of criteria for the appraisal of so called‘end of life treatments’. These were that the treatment:
� is for patients with short life expectancy (normally less than24 months);� offers extension to life, normally of at least 3 months, compared
with standard treatment;� is licensed or indicated in small patient groups.
Originally another criterion had been included that stated thatthere should be no alternative treatment available with compara-ble benefits. The review in July 2009 by NICE of the applicationof these criteria resulted in an update of the supplementary ad-vice10,34 and this criterion was removed. However, it would appearlikely that this would still be an important factor for considerationand would probably be considered within the appraisal process.
The use of the supplementary advice on treatments for end oflife care in developing the guidance on oral topotecan for the treat-ment of relapsed SCLC provides an illustration of the process NICEhas adopted.9 It is evident that NICE consider the criteria in se-quence, so if a criterion were not met then there would be no fur-ther discussions concerning the other criteria.34 A life expectancyof normally less than 24 months is always considered first and ap-pears the most accessible criteria despite a lack of clarity over theprecision of its definition.34 The standard approach to establishingthis has been to use the median overall survival from the controlarms of the RCTs.34 For the appraisal of oral topotecan for relapsedSCLC, NICE noted that survival for those on best supportive carewas below the threshold of 24 months and was potentially aslow as 14 weeks.9 Having met the criteria on life expectancy, anassessment is made on whether the extension to life from thetreatment under consideration exceeds 3 months. Judgementmay be made through assessing the median overall survival andmean incremental life years gained provided by RCTs or the eco-nomic evaluations developed for the appraisal. Inevitably esti-mates may vary resulting in some uncertainty and differences ininterpretation and personal judgement. Oral topotecan was shownthrough sufficiently robust evidence to satisfy this criterion,extending survival compared to BSC by between 12 and 17 weeks.The final criterion, specifically licensed or indicated for a small pa-tient population, is thought to refer to the incidence of the popula-tion covered in the appraisal and the cumulative population acrossall indications for that treatment.34 In the case of topotecan thismay therefore include those with ovarian and cervical cancer. Withbetween 800 and 1600 people suffering from relapsed SCLC, NICEjudged that oral topotecan met this criterion. Although no longeridentified as a key criterion for appraising health technologies thatmay be considered end of life technologies, it is likely that someconsideration is given as to whether there is an alternative treat-ment with comparable benefit. Inevitably this criterion may besubject to different interpretations, whether it implies an impor-tant ‘step change’ in treatment (i.e. rewarding innovation) or anextension of the 3-month gain in length of life. While there are lim-ited treatment options for people with relapsed SCLC, it is unclearwhether oral topotecan offers a step-wise change from existingtreatments given it represents a new formulation of an existingtreatment. Having judged that oral topotecan represents a life-extending end of life treatment, NICE gave greater weight to thequality of life experienced by people with relapsed SCLC duringtheir extended survival period following treatment. As a conse-quence, NICE felt that the ICER for oral topotecan would lie belowthe threshold and would recommend its use as an option for peo-ple with relapsed SCLC for whom re-treatment with the first-lineregimen is not considered appropriate and where CAV iscontraindicated.9
It is evident from the review of the use of the supplementaryadvice on appraising treatments that may extend the life of peoplewith a short life expectancy and from the appraisal of oral topotec-an for relapsed SCLC, that the criteria used are open to differentialinterpretation. As consequence, it may be difficult to judge the pos-sible influence they may have in the long term. An analysis of pastNICE appraisals, which was undertaken before the change incriteria, suggested that the new arrangements may not improveavailability of the majority of treatments.35 However, this waspredominantly due to the interpretation of the criterion of no

248 D. Hartwell et al. / Cancer Treatment Reviews 37 (2011) 242–249
alternative treatment being available, so it is possible that this sit-uation will be different now that further guidance has been pub-lished. While there may still be different interpretations aroundthe criteria, NICEs’ report on the application of the advice statesthat so far, the end of life criteria has been applied consistently.34
Our evidence synthesis has a number of strengths. It is an inde-pendent assessment undertaken following the principles for con-ducting a systematic review and economic evaluation. Themethods were set out a priori explicitly and transparently andthe evidence was critically appraised. The clinical evidence to pop-ulate the economic model was extracted from reasonable qualityRCTs included in the systematic review. The effect of treatmentwas assessed using appropriate measures (survival and quality-ad-justed survival) to model cost and outcome differences over themodel time horizons. Additional relevant data on TTP were in-cluded to take account of expected differences in QoL followingdisease progression. However, in contrast, there is uncertainty overthe QoL data included in the model and adverse events may offsetQoL gains. To address this uncertainty we tested the impact ofassumptions regarding QoL in the model and attempted to identifywhich assumptions have greatest impact on the cost effectivenessresults.
Other issues to take into account when interpreting this reviewinclude the uncertainty over whether the participant groups inthese trials fully meet the licensed indication for topotecan, whatthe impact of dose escalations and reductions are, and how gener-alisable the participants are to the UK setting. A limitation of thecost effectiveness analysis is that it is based on only one publishedtrial. Further research is required into the QoL of patients with re-lapsed SCLC, to identify the impact of disease progression on QoL,the impact of response and the impact of treatment-related ad-verse events on QoL. Given that data collection on resource usein the RCT by O’Brien and colleagues18 was not comprehensive, fur-ther research on the impact of active treatment on resource use forpalliative care would improve cost effectiveness models fortopotecan.
Conclusion
The clinical evidence indicates that topotecan is better than BSCin terms of improved survival, is comparable to CAV and that oraland IV topotecan are similar in efficacy. In the cost effectivenessanalysis, oral topotecan for patients with relapsed SCLC was asso-ciated with improved health outcomes compared with BSC alone.However these improved outcomes were achieved at increasedcost. The ICER for oral topotecan compared with BSC is at the upperextreme of the range conventionally regarded as cost effectivefrom an NHS decision making perspective. However this treatmentmay fall under supplementary guidance for life extending, end oflife treatments.
Contributors
D. Hartwell developed the research protocol, drafted the back-ground section, assessed studies for inclusion, extracted data fromand quality assessed included studies, synthesised evidence,drafted the full research report, drafted the article, contributed tocritical revision of the article for intellectual content and final ap-proval of the article.
J. Jones developed the research protocol, assessed studies forinclusion, extracted data from and quality assessed included stud-ies, synthesised evidence, developed the economic evaluation,drafted the full research report, contributed to drafting the article,critical revision of the article for intellectual content and final ap-proval of the article.
E. Loveman developed the research protocol, drafted the back-ground section, assisted in the development of the search strategy,assessed studies for inclusion, extracted data from and quality as-sessed included studies, synthesised evidence, drafted and editedthe final full research report, contributed to drafting the article,critical revision of the article for intellectual content and final ap-proval of the article.
P. Harris drafted the background section, assessed studies forinclusion, extracted data from and quality assessed included stud-ies, synthesised evidence, drafted the full research report, draftedthe article, contributed to critical revision of the article for intellec-tual content and final approval of the article.
A. Clegg developed the research protocol, assessed studies forinclusion, extracted data from and quality assessed included stud-ies, synthesised evidence, drafted the full research report, contrib-uted to drafting the article, critical revision of the article forintellectual content and final approval of the article.
A. Bird assessed studies for inclusion, extracted data from andquality assessed included studies, synthesised evidence, developedthe economic evaluation, drafted the full research report, contrib-uted to drafting the article, critical revision of the article for intel-lectual content and final approval of the article.
Role of funding source
This report was funded by the NIHR Health Technology Assess-ment Programme (project number 08/36/01) and commissionedon behalf of the National Institute for Health and Clinical Excel-lence (NICE). It has been published in full in Health TechnologyAssessment 2010;14(9). See the HTA Programme website (www.hta.ac.uk) for further project information. The views and opinionsexpressed therein are those of the authors and do not necessarilyreflect those of the Department of Health.
Conflict of interest statement
None declared.
Acknowledgements
We would like to thank members of our advisory group panelwho provided expert advice and comments on the protocol and/ordraft of the full research report. We are also grateful to KarenWelch, Information Scientist, SHTAC, for generating and runningthe literature searches.
References
1. Rosti G, Bevilacqua G, Bidoli P, Portalone L, Santo A, Genestreti G. Small cell lungcancer. Ann Oncol 2006;17:ii5–ii10.
2. Hyde L, Yee J, Wilson R, Patno ME. Cell type and the natural history of lungcancer. JAMA 1965;193:52–4.
3. Rivera MP, Detterbeck FC, Loomis DP. Epidemiology and classification of lungcancer. In: Detterbeck FC, Rivera MP, Socinski MA, Rosenman JG, editors.Diagnosis and treatment of lung cancer. An evidence-based guide for the practicingclinician. Philadelphia: WB Saunders Company; 2001. p. 25–44.
4. Simon GR, Turrisi A. Management of small cell lung cancer. ACCP evidence-based clinical practice guidelines (2nd ed.). Chest 2007;132:324S–39S.
5. National Institute for Health and Clinical Excellence (NICE). The diagnosis andtreatment of lung cancer. London: NICE; 2005. Clinical Guideline No. 24.Available from:www.nice.org.uk/CG024NICEguideline accessed 03.11.08.
6. von Pawel J. The role of topotecan in treating small cell lung cancer: second-linetreatment. Lung cancer 2003;41:S3–8.
7. Cara S, Tannock IF. Re-treatment of patients with the same chemotherapy:implications for clinical mechanisms of drug resistance. Ann Oncol2001;12:23–7.
8. Loveman E, Jones J, Hartwell D, et al. The clinical and cost effectiveness oftopotecan for small cell lung cancer: a systematic review and economicevaluation. Health Technol Assess 2010;14(19).

D. Hartwell et al. / Cancer Treatment Reviews 37 (2011) 242–249 249
9. National Institute for Health and Clinical Excellence (NICE). Topotecan for thetreatment of relapsed small-cell lung cancer. London: 2009. Technology AppraisalNo. 184. Available from:www.nice.org.uk/TA184.
10. National Institute for Health and Clinical Excellence (NICE). Appraising life-extending, end of life treatments. London: 2009. Available from:<http://www.nice.org.uk/media/E4A/79/SupplementaryAdviceTACEoL.pdf> accessed21.08.09.
11. Miller AB, Hoogstraten B, Staquet M, Winkler A. Reporting results of cancertreatment. Cancer 1980;47:207–14.
12. Therasse P, Arbuck SG, Eisenhauer EA, et al. New guidelines to evaluate theresponse to treatment in solid tumors. J Natl Cancer Inst 2000;92:205–16.
13. NHS Centre for Reviews and Dissemination. Undertaking systematic reviews ofresearch on effectiveness: CRD’s guidance for those carrying out or commissioningreviews. York: York Publishing Services Ltd.; 2001. CRD Report No. 4 (2nd ed.).
14. Drummond MF, Sculpher MJ, O’Brien BJ, Stoddart GL, Torrance GW. Methods forthe economic evaluation of health care programmes. Oxford: Oxford UniversityPress; 2005.
15. Philips Z, Ginnelly L, Sculpher M, et al. Review of guidelines for good practice indecision-analytic modelling in health technology assessment. Health TechnolAssess 2004;8:1–158.
16. Cochrane Collaboration. Assessing risk of bias in included studies. In:Higgins J, Altman D, editors. Cochrane Handbook for Systematic Reviewsof Interventions 2007. Available from:<http://www.cochrane.org/resources/handbook/Handbook5_Bias_V10.pdf>.
17. Eckardt JR, von Pawel J, Pujol JL, et al. Phase III study of oral compared withintravenous topotecan as second-line therapy in small-cell lung cancer. J ClinOncol 2007;25:2086–92.
18. O’Brien ME, Ciuleanu TE, Tsekov H, et al. Phase III trial comparing supportivecare alone with supportive care with oral topotecan in patients with relapsedsmall-cell lung cancer. J Clin Oncol 2006;24:5441–7.
19. von Pawel J, Gatzemeier U, Pujol JL, et al. Phase II comparator study of oralversus intravenous topotecan in patients with chemosensitive small-cell lungcancer. J Clin Oncol 2001;19:1743–9.
20. von Pawel J, Schiller JH, Shepherd FA, et al. Topotecan versuscyclophosphamide, doxorubicin, and vincristine for the treatment ofrecurrent small-cell lung cancer. J Clin Oncol 1999;17:658–67.
21. Eckardt T, von Pawel J, Hainsworth JD, et al. Single agent oral topotecan (PO)versus intravenous topotecan (IV) in patients (pts) with chemosensitive smallcell lung cancer (SCLC). An international phase III study [abstract]. Proc Am SocClin Oncol 2003;22:619.
22. Schiller J, von Pawel J, Shepherd F, et al. Topotecan (t) versus (vs)cyclophosphamide (c), doxorubicin (a) and vincristine (v) for the treatment
(tx) of patients (pts) with recurrent small cell lung cancer (sclc): a phase IIIstudy [abstract]. Proc Am Soc Clin Oncol. 1998;17:1755.
23. Sugawara S, Inoue A, Yamazaki K, et al. Randomized, phase II trial comparingamrubicin with topotecan in patients (pts) with previously treated small celllung cancer (SCLC). J Clin Oncol 2008;26:8042.
24. Inoue A, Sugawara S, Yamazaki K, et al. Randomized Phase II trial comparingamrubicin with topotecan in patients with previously treated small-cell lungcancer: North Japan Lung Cancer Study Group Trial 0402. J Clin Oncol2008;26:5401–6.
25. Chen L, Antras L, Duh M, Pickard S, Cella D, Neary M, et al. Is treatment with oraltopotecan plus best supportive care associated with better health statuscompared to best supportive care alone in small cell lung cancer? [abstract]. JThoracic Oncol 2007;2:S391–2.
26. O’Brien ME, Duh MS, Chen L, Antras L, Neary M, Gralla RJ. An analysis of diseasecontrol: is major response associated with greater symptomatic benefits thanstable disease in small cell lung cancer (SCLC)? Results from the randomizedOral Topotecan (OT) vs. Best Supportive Care (BSC) trial [abstract]. J ThoracicOncol 2007;2:S827.
27. Hycamtin: summary of product characteristics. <http://www.emea.europa.eu/humandocs/PDFs/EPAR/Hycamtin/H-123-PI-en.pdf>; 2009 accessed 02.02.09.
28. Curtis L. Unit costs of health and social care. Canterbury: Personal Social ServicesResearch Unit, University of Kent; 2008.
29. GlaxoSmithKline UK. Multiple technology appraisal of topotecan for the treatmentof small cell lung cancer; 2008.
30. Main C, Bojke L, Griffin S, et al. Topotecan, pegylated liposomal doxorubicinhydrochloride and paclitaxel for second-line or subsequent treatment ofadvanced ovarian cancer: a systematic review and economic evaluation.Health Technol Assess 2006;10(9).
31. Oliver E, Killen J, Kiebert G, et al. Treatment pathways, resource use and costs inthe management of small cell lung cancer. Thorax 2001;56:785–90.
32. National Institute for Health and Clinical Excellence (NICE). Guide to themethods of technology appraisal. Available from:<http://www.nice.org.uk/media/B52/A7/TAMethodsGuideUpdatedJune2008.pdf> accessed 26.01.09.
33. Richards M. Improving access to medicines for NHS patients: a report for theSecretary of State for Health by Professor Mike Richards. Available from:www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_089927 accessed 14.08.09.
34. National Institute for Health and Clinical Excellence (NICE). Update report onthe application of the ‘end-of-life’ supplementary advice in health technologyappraisals. Available from:www.nice.org.uk/media/835/8E/item7endoflife-treatments.pdf accessed 14.08.09.
35. Raftery J. NICE and the challenges of cancer drugs. BMJ 2009;338:271–2.




















