Managing lung problems in scleroderma
20
It was only when I needed oxygen that I realised how scleroderma was affecting me. Susan morethanscleroderma.com Managing lung problems in scleroderma
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Managing lung problems in scleroderma

It was only when I needed oxygen that I realised
how scleroderma was affecting me.
Susan
morethanscleroderma.com
Managing lung problems in scleroderma
Lung problems in scleroderma
What lung problems might I get? ............ 3
Lung fibrosis (interstitial lung disease) ..4
Pulmonary arterial hypertension .............. 5
What medical tests might I have? .............7
Living with lung problems ...........................13
What could happen? .......................................15
Frequently asked questions (FAQs) ......17
ContentsScleroderma (also known as systemic sclerosis) is a condition that can affect the lungs.1–4 Most people don’t notice changes to their lungs at first. They just
think they’re unfit or tired. In some cases, this may be true. But you know your own body and what you’re capable of.
Try to be aware of any changes that could suggest a lung problem, such as getting out of breath easily, then tell your doctor as soon as possible. The earlier things are spotted, the sooner you can get expert help and support.
This booklet looks at a range of issues concerning lung problems in people with scleroderma, as well as answering some frequently asked questions. You can also visit morethanscleroderma.com to find out more.
3
What lung problems might I get?
Many people with scleroderma have some form of changes to their lungs. However, not everybody gets noticeable changes.2,3,5,6
There are two key ways in which scleroderma may affect your lungs:2,7
1. Lung fibrosis (also known as interstitial lung disease [or ILD]) occurs when your lungs become stiffer and thicker
2. Pulmonary arterial hypertension (or PAH) occurs when the pressure in the blood vessels in your lungs gets too high
It is possible to get one, or even both, of these conditions. Or you may get neither.
Shortness of breath or fatigue is common in scleroderma.7 This can be worrying, but it is not always serious and does not necessarily mean you have lung fibrosis or PAH.8 However, make sure you tell your doctor so they can check your lungs.
Phrases you might hear that describe problems with your lungs:
• Lung involvement
• Interstitial lung disease (or ILD)
• Pulmonary fibrosis
• Pulmonary disease
Type
s of
lung
pr
oble
ms
4
Lung fibrosis (interstitial lung disease)
How many people get it?
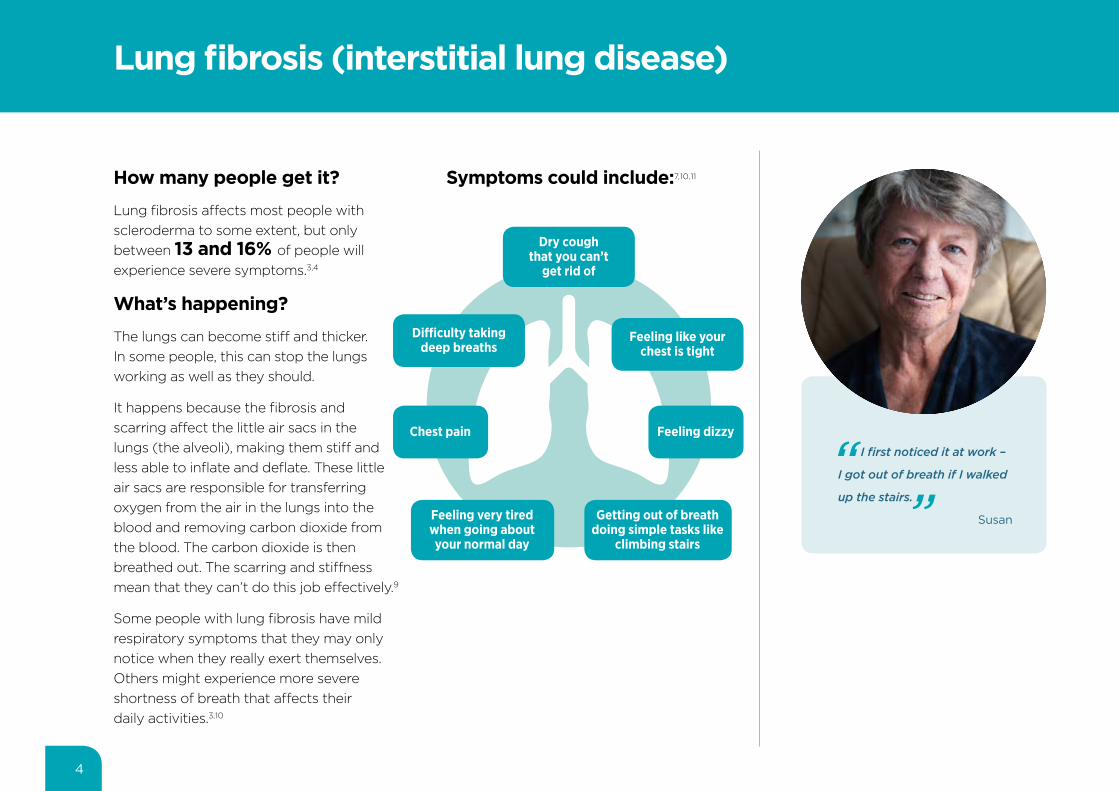
Lung fibrosis affects most people with scleroderma to some extent, but only between 13 and 16% of people will experience severe symptoms.3,4
What’s happening?
The lungs can become stiff and thicker. In some people, this can stop the lungs working as well as they should.
It happens because the fibrosis and scarring affect the little air sacs in the lungs (the alveoli), making them stiff and less able to inflate and deflate. These little air sacs are responsible for transferring oxygen from the air in the lungs into the blood and removing carbon dioxide from the blood. The carbon dioxide is then breathed out. The scarring and stiffness mean that they can’t do this job effectively.9
Some people with lung fibrosis have mild respiratory symptoms that they may only notice when they really exert themselves. Others might experience more severe shortness of breath that affects their daily activities.3,10
Feeling very tired when going about your normal day
Getting out of breath doing simple tasks like
climbing stairs
I first noticed it at work –
I got out of breath if I walked
up the stairs.
Susan
Feeling like your chest is tight
Feeling dizzy
Dry cough that you can’t
get rid of
Symptoms could include:7,10,11
Difficulty taking deep breaths
Chest pain
5
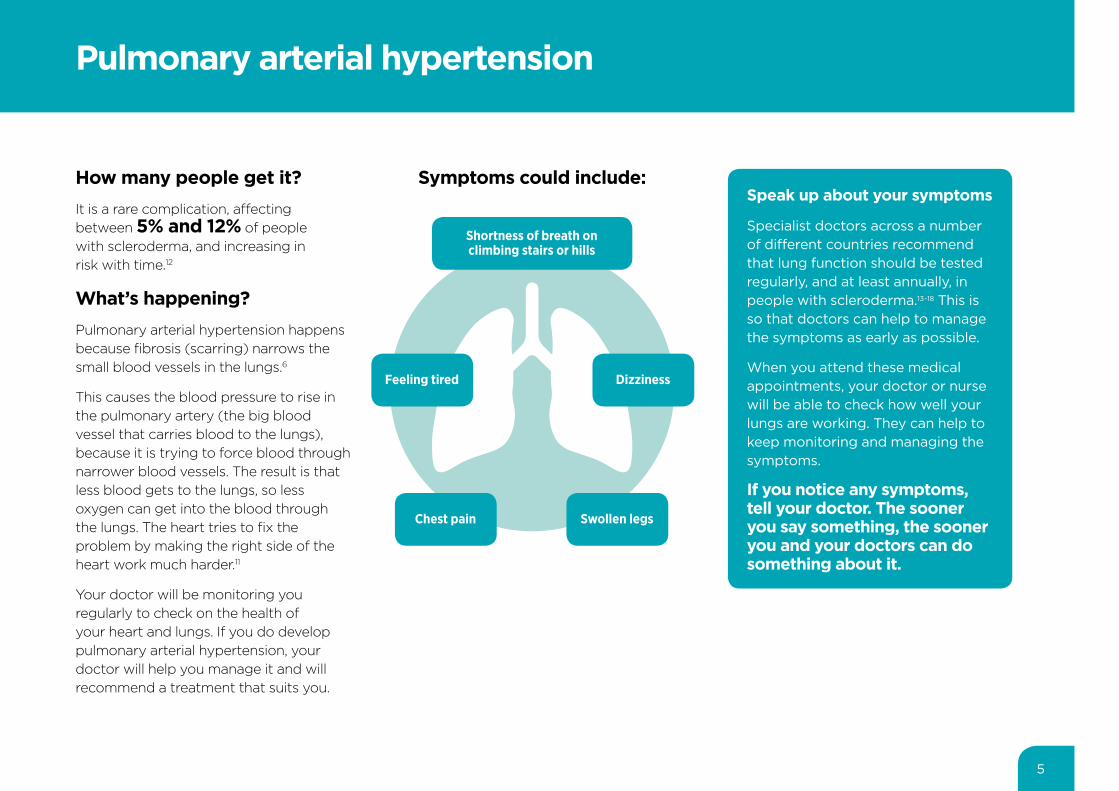
How many people get it?It is a rare complication, affecting between 5% and 12% of people with scleroderma, and increasing in risk with time.12
What’s happening? Pulmonary arterial hypertension happens because fibrosis (scarring) narrows the small blood vessels in the lungs.6
This causes the blood pressure to rise in the pulmonary artery (the big blood vessel that carries blood to the lungs), because it is trying to force blood through narrower blood vessels. The result is that less blood gets to the lungs, so less oxygen can get into the blood through the lungs. The heart tries to fix the problem by making the right side of the heart work much harder.11
Your doctor will be monitoring you regularly to check on the health of your heart and lungs. If you do develop pulmonary arterial hypertension, your doctor will help you manage it and will recommend a treatment that suits you.
Pulmonary arterial hypertension
Speak up about your symptoms
Specialist doctors across a number of different countries recommend that lung function should be tested regularly, and at least annually, in people with scleroderma.13–18 This is so that doctors can help to manage the symptoms as early as possible.
When you attend these medical appointments, your doctor or nurse will be able to check how well your lungs are working. They can help to keep monitoring and managing the symptoms.
If you notice any symptoms, tell your doctor. The sooner you say something, the sooner you and your doctors can do something about it.
Shortness of breath onclimbing stairs or hills
Chest pain Swollen legs
DizzinessFeeling tired
Symptoms could include:

7
What medical tests might I have?
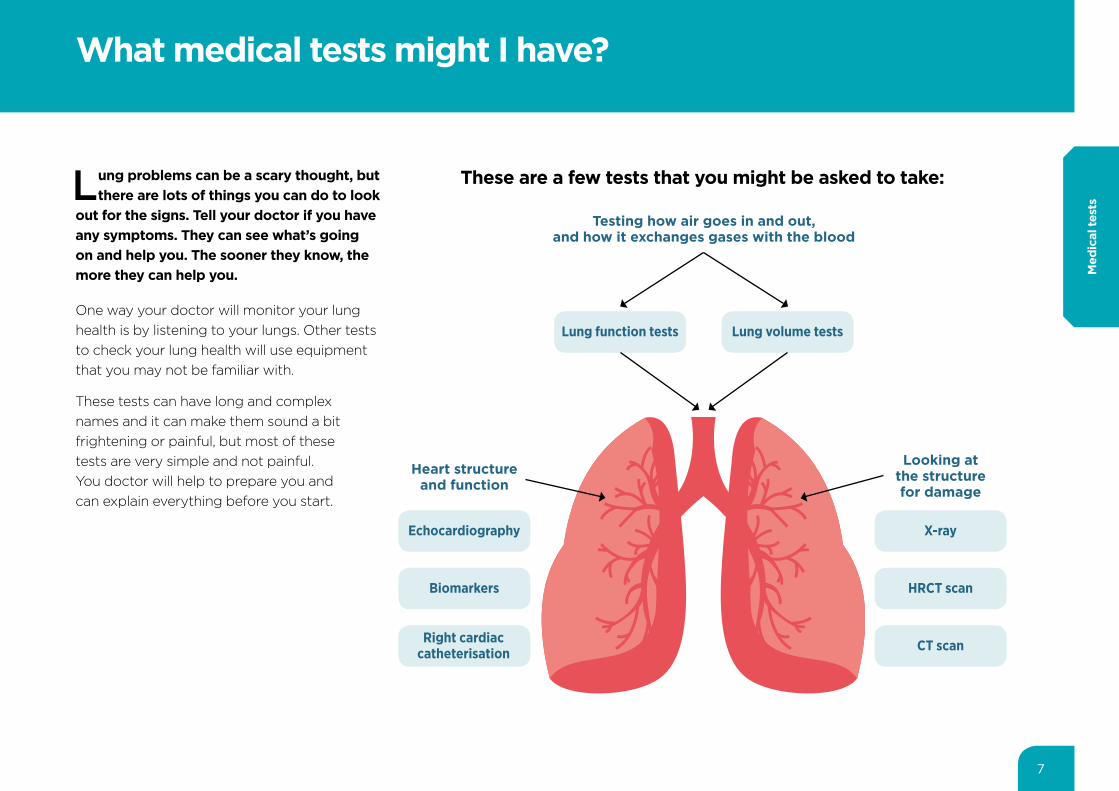
Lung problems can be a scary thought, but there are lots of things you can do to look
out for the signs. Tell your doctor if you have any symptoms. They can see what’s going on and help you. The sooner they know, the more they can help you.
One way your doctor will monitor your lung health is by listening to your lungs. Other tests to check your lung health will use equipment that you may not be familiar with.
These tests can have long and complex names and it can make them sound a bit frightening or painful, but most of these tests are very simple and not painful. You doctor will help to prepare you and can explain everything before you start.
X-rayEchocardiography
Lung function tests
HRCT scan
CT scan
Biomarkers
Right cardiac catheterisation
Lung volume tests
Testing how air goes in and out, and how it exchanges gases with the blood
Looking at the structure for damage
Heart structure and function
These are a few tests that you might be asked to take:
Med
ical
test
s
8
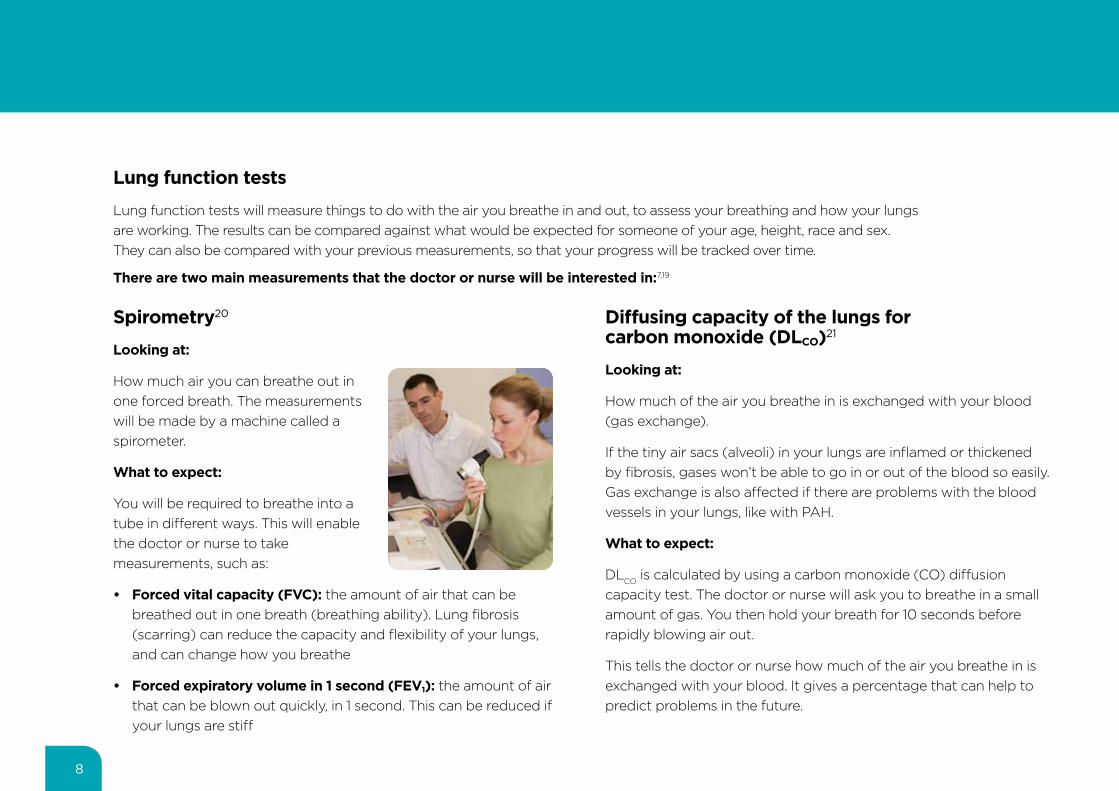
Spirometry20
Looking at:
How much air you can breathe out in one forced breath. The measurements will be made by a machine called a spirometer.
What to expect:
You will be required to breathe into a tube in different ways. This will enable the doctor or nurse to take measurements, such as:
• Forced vital capacity (FVC): the amount of air that can be breathed out in one breath (breathing ability). Lung fibrosis (scarring) can reduce the capacity and flexibility of your lungs, and can change how you breathe
• Forced expiratory volume in 1 second (FEV1): the amount of air that can be blown out quickly, in 1 second. This can be reduced if your lungs are stiff
Diffusing capacity of the lungs for carbon monoxide (DLCO)21
Looking at:
How much of the air you breathe in is exchanged with your blood (gas exchange).
If the tiny air sacs (alveoli) in your lungs are inflamed or thickened by fibrosis, gases won’t be able to go in or out of the blood so easily. Gas exchange is also affected if there are problems with the blood vessels in your lungs, like with PAH.
What to expect:
DLCO is calculated by using a carbon monoxide (CO) diffusion capacity test. The doctor or nurse will ask you to breathe in a small amount of gas. You then hold your breath for 10 seconds before rapidly blowing air out.
This tells the doctor or nurse how much of the air you breathe in is exchanged with your blood. It gives a percentage that can help to predict problems in the future.
Lung function tests
Lung function tests will measure things to do with the air you breathe in and out, to assess your breathing and how your lungs are working. The results can be compared against what would be expected for someone of your age, height, race and sex. They can also be compared with your previous measurements, so that your progress will be tracked over time.
There are two main measurements that the doctor or nurse will be interested in:7,19
9
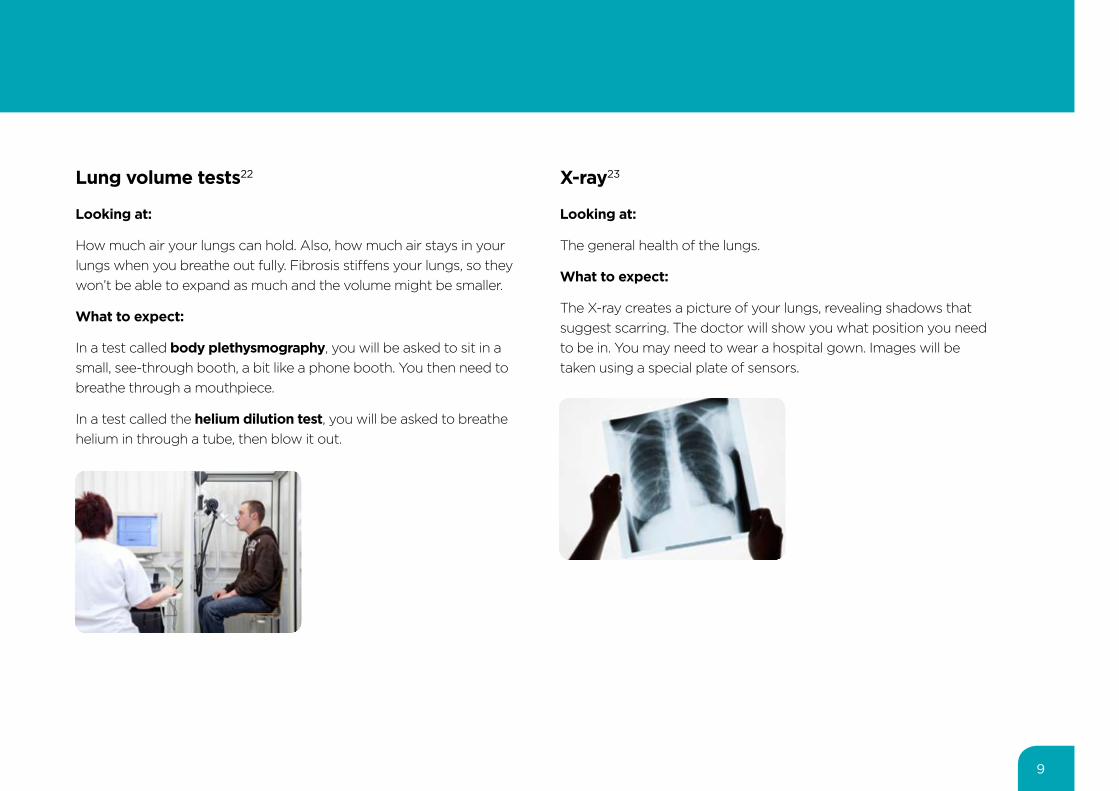
X-ray23
Looking at:
The general health of the lungs.
What to expect:
The X-ray creates a picture of your lungs, revealing shadows that suggest scarring. The doctor will show you what position you need to be in. You may need to wear a hospital gown. Images will be taken using a special plate of sensors.
Lung volume tests22
Looking at:
How much air your lungs can hold. Also, how much air stays in your lungs when you breathe out fully. Fibrosis stiffens your lungs, so they won’t be able to expand as much and the volume might be smaller.
What to expect:
In a test called body plethysmography, you will be asked to sit in a small, see-through booth, a bit like a phone booth. You then need to breathe through a mouthpiece.
In a test called the helium dilution test, you will be asked to breathe helium in through a tube, then blow it out.
10
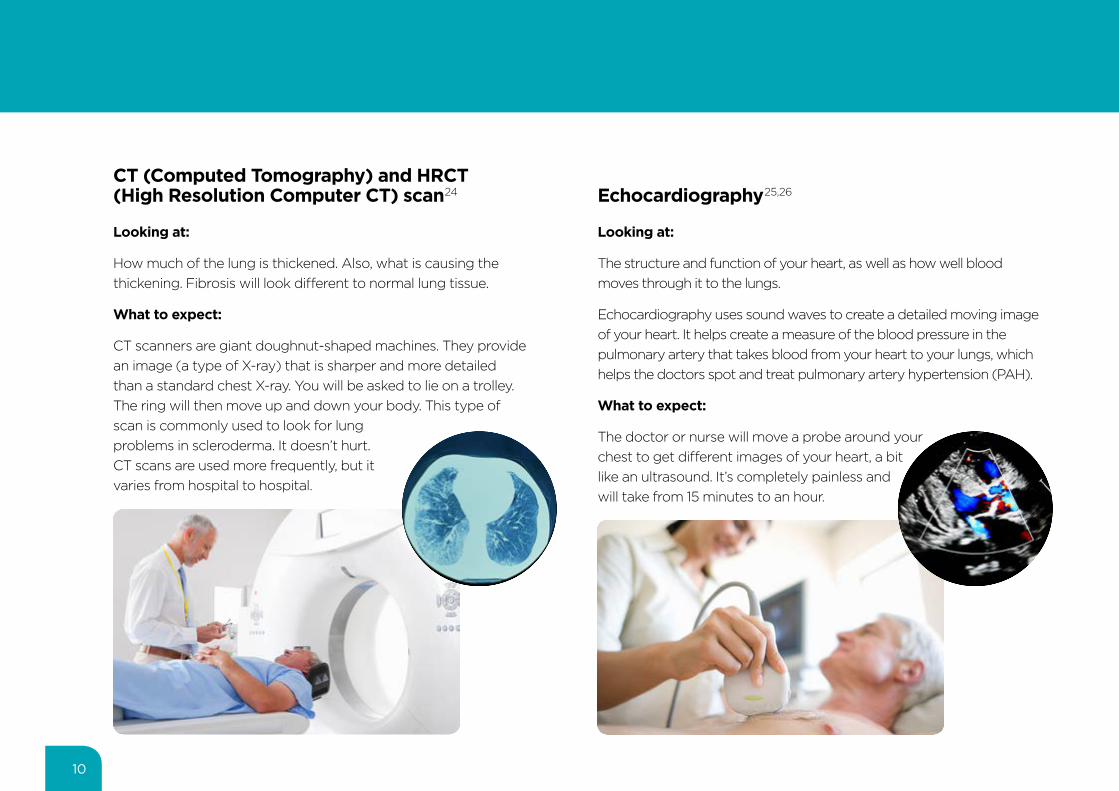
CT (Computed Tomography) and HRCT (High Resolution Computer CT) scan24
Looking at:
How much of the lung is thickened. Also, what is causing the thickening. Fibrosis will look different to normal lung tissue.
What to expect:
CT scanners are giant doughnut-shaped machines. They provide an image (a type of X-ray) that is sharper and more detailed than a standard chest X-ray. You will be asked to lie on a trolley. The ring will then move up and down your body. This type of scan is commonly used to look for lung problems in scleroderma. It doesn’t hurt. CT scans are used more frequently, but it varies from hospital to hospital.
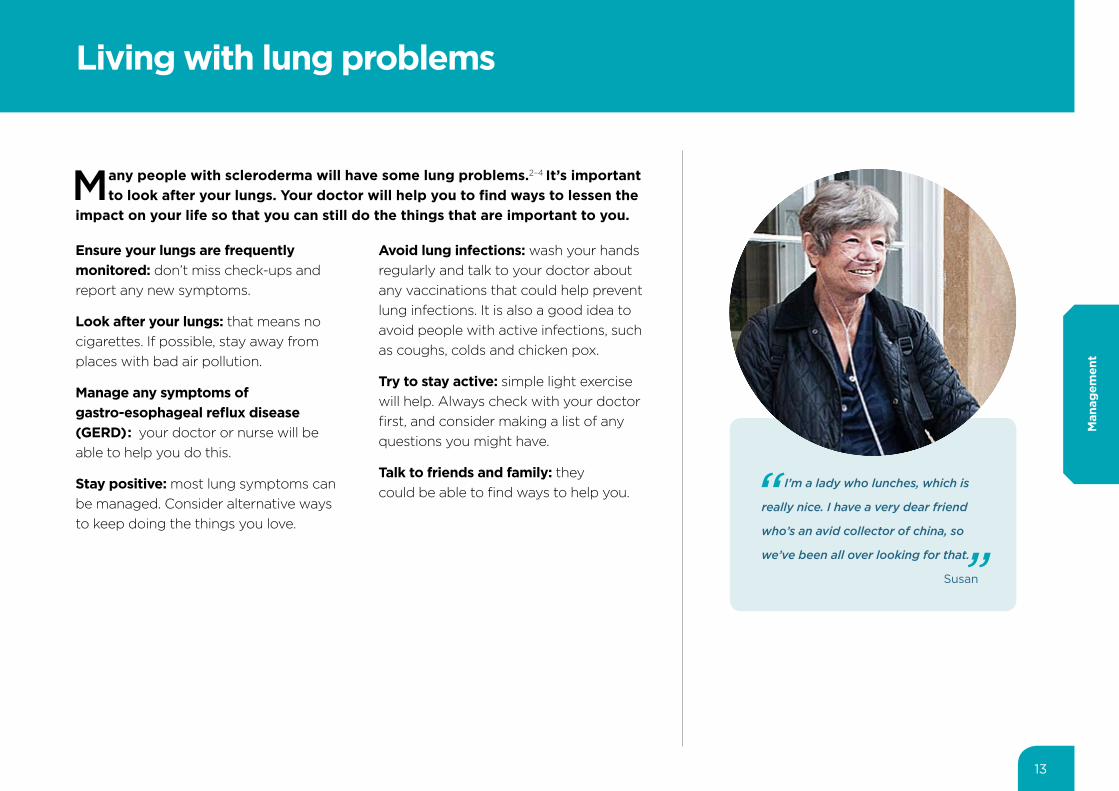
Echocardiography25,26
Looking at:
The structure and function of your heart, as well as how well blood moves through it to the lungs.
Echocardiography uses sound waves to create a detailed moving image of your heart. It helps create a measure of the blood pressure in the pulmonary artery that takes blood from your heart to your lungs, which helps the doctors spot and treat pulmonary artery hypertension (PAH).
What to expect:
The doctor or nurse will move a probe around your chest to get different images of your heart, a bit like an ultrasound. It’s completely painless and will take from 15 minutes to an hour.

Biomarkers26,27
Looking at:
Several substances called biomarkers in your blood. One example is a protein called N-terminal pro-brain natriuretic peptide (NT-proBNP). This is linked to heart function and helps to detect and predict pulmonary arterial hypertension (PAH).
What to expect:
A small needle will be used to collect a blood sample from you. Your doctor or nurse will let you know if you need to do anything to prepare.
Right heart catheterisation28
Looking at:
The blood pressure in the right side of your heart and in your pulmonary artery (the blood vessel that connects your heart with your lungs). It can help to diagnose PAH.
What to expect:
A thin, flexible tube will be passed into your pulmonary artery to take an accurate blood pressure measurement.
It is likely to be carried out in the hospital or a specialist heart centre.
11

13
Living with lung problems
Many people with scleroderma will have some lung problems.2–4 It’s important to look after your lungs. Your doctor will help you to find ways to lessen the
impact on your life so that you can still do the things that are important to you.
Ensure your lungs are frequently monitored: don’t miss check-ups and report any new symptoms.
Look after your lungs: that means no cigarettes. If possible, stay away from places with bad air pollution.
Manage any symptoms of gastro-esophageal reflux disease (GERD): your doctor or nurse will be able to help you do this.
Stay positive: most lung symptoms can be managed. Consider alternative ways to keep doing the things you love.
Avoid lung infections: wash your hands regularly and talk to your doctor about any vaccinations that could help prevent lung infections. It is also a good idea to avoid people with active infections, such as coughs, colds and chicken pox.
Try to stay active: simple light exercise will help. Always check with your doctor first, and consider making a list of any questions you might have.
Talk to friends and family: they could be able to find ways to help you.
I’m a lady who lunches, which is
really nice. I have a very dear friend
who’s an avid collector of china, so
we’ve been all over looking for that.
Susan
Man
agem
ent

15
What could happen?
As with everything to do with scleroderma, it is difficult to predict whose lungs will be affected or how badly. If you have any problems such as getting out
of breath easily, the best thing you can do is tell your doctor as soon as possible. The earlier things are spotted, the sooner you can get expert help and support.
Around 7 in 10 people with scleroderma report some shortness of breath, while 6 in 10 report difficulty climbing stairs or walking.10
Up to half of people who will be affected by lung problems develop symptoms within 3 years of having scleroderma.2,3,29–31
For most people with scleroderma and lung problems, their condition remains relatively stable, or declines slowly over many years.6 A small number of people will have symptoms that get worse quickly after they are diagnosed.
Over time, 1 in 10 people with severe scleroderma might develop serious lung symptoms that affect how they go about their life. In very severe cases, these symptoms can affect how long they live.3,4,32
I think to myself, ‘okay, I can
move, I can do things.’ I am far
more independent now than I
was, and happy.
Christina
Your
futu
re

17
Frequently asked questions
Can I exercise?
Light exercise can help your lungs continue to work well.33
It can be tempting to avoid exercise because you think it will make you breathless, or worsen your condition. But this will make you less fit and normal activities will become even harder. It’s a slippery slope.
Ask your doctor or nurse or a physiotherapist to help you make an exercise plan. Then you can stay active, confident in the knowledge that what you’re doing is safe and in keeping with what you’re capable of.
I’ve got a job or young family. How do I make it to my medical appointments?
It can be difficult to fit your medical appointments in around your other responsibilities. But it is important to find a way to get there. The tests and check-ups give the doctor an idea of what’s happening and how you’re doing.
It can help to talk with family, friends and colleagues about your scleroderma. They will be able to find ways to help you make it to your appointments. Don’t be afraid to ask. Most people will be glad to have found a way to help you.
Can medication make the lung problems go away? 2–4
There are some treatments for pulmonary arterial hypertension that can slow down the progression of lung problems. But as yet, no drugs can cure scleroderma or the lung fibrosis it causes. Scientists are working on it. For now, your doctors might suggest some medications that can make your symptoms easier to manage.
Do lung problems affect lifespan?
People are affected by scleroderma in different ways. It can be difficult to predict how it will progress. Don’t be afraid to ask your doctor or nurse this question. It’s an important thing to ask.
Around 1 in 10 people with severe scleroderma might develop fibrosis that reduces their lung capacity (measured by FVC) and affects how they go about their life. In very serious cases, these symptoms can affect how long they live. But this is only a small number of people.3,4,32
PAH can have an impact on how long somebody with scleroderma will live, but it depends on the type and nature of PAH.2,14 Your doctor will be able to give you some information that’s specific to your situation.
FAQ
s

References
1. Denton CP and Khanna D. Systemic sclerosis. 2017. The Lancet. In Press. Available at: http://thelancet.com/journals/lancet/article/PIIS0140-6736(17)30933-9/fulltext [Accessed November 2017].
2. Solomon J, et al. Scleroderma lung disease. Eur Respir Rev 2013;127:6–19.
3. Steen V, et al. Severe restrictive lung disease in systemic sclerosis. Arthritis Rheum 1994;66(6):1625–35.
4. Steen V and Medsger T. Severe organ involvement in systemic sclerosis with diffuse scleroderma. Arthritis Rheum 2000;43(11):2437–44.
5. Steen V, et al. Pulmonary involvement in systemic sclerosis (scleroderma). Arthritis Rheum 1985;28(7):759–67.
6. Iudici M, et al. Where are we going in the management of interstitial lung disease in patients with systemic sclerosis? Autoimmunity Reviews 2015;14(7):575–8.
7. University of Michigan Scleroderma Program. Lung Involvement. Available at: https://www.med.umich.edu/scleroderma/patients/lung.htm [Accessed May 2017].
8. Scleroderma of the lungs. Royal Brompton & Harefield NHS Foundation Trust. Available at: www.rbht.nhs.uk/patients/condition/scleroderma/lung-involvement-diagnosis/ [Accessed November 2017].
9. Scleroderma & Raynauds UK. Lung Fact Sheet. Updated March 2016. Available at: https://www.sruk.co.uk/media/filer_public/ac/74/ac749333-b083-4046-b688-366fd01ef19b/lungs_factsheet_v2_rgb.pdf [Accessed June 2017].
10. Willems L, et al. Frequency and impact of disease symptoms experienced by patients with systemic sclerosis in five European countries. Clin Exp Rheumatol 2014;32(S86):S88–93.
11. Mayo Clinic. Pulmonary hypertension. Updated March 2016. Available at: http://www.mayoclinic.org/diseases-conditions/pulmonary-hypertension/symptoms causes/dxc-20197481 [Accessed June 2017].
12. Denton C and Hachulla E. Risk factors associated with pulmonary arterial hypertension in patients with systemic sclerosis and implications for screening. Eur Respir Rev 2011;20(122):270–76.
13. Proudman S, et al. Pulmonary arterial hypertension in systemic sclerosis: the need for early detection and treatment. Int Med Journal 2007;37:485–94.
14. McLaughlin V, et al. Expert consensus document on pulmonary hypertension. J Am Coll Cardiol 2009;53(17):1573–1619.
15. Coghlan J, et al. Evidence-based detection of pulmonary arterial hypertension in systemic sclerosis: the DETECT study. Ann Rheum Dis 2014;73:1340–9.
16. Humbert M, et al. Screening for pulmonary arterial hypertension in patients with systemic sclerosis: clinical characteristics at diagnosis and long-term survival. Arthritis Rheum. 2011;63(11):3522–30.
17. Chatterjee S. The Cleveland Clinic Foundation. Published 2010. Available at: http://www.clevelandclinicmeded.com/medicalpubs/diseasemanagement/rheumatology/systemic-sclerosis/ [Accessed June 2017].
18. BMJ Best Practice. Systemic sclerosis (scleroderma): monitoring. Available at: http://bestpractice.bmj.com/best-practice/monograph/295/follow-up/recommendations.html [Accessed May 2017].
19. Cappelli S, et al. Interstitial lung disease in systemic sclerosis: where do we stand? Eur Respir Rev 2015;24:411–9.
20. NHS Choices. Spirometry. Available at www.nhs.uk/conditions/spirometry/[Accessed November 2017].
21. Plummer AL. The carbon monoxide diffusing capacity. Chest 2008;134:663–67.
22. National Heart, Blood and Lung Institute. Pulmonary function tests. Available at: www.nhlbi.nih.gov/health/health-topics/topics/lft [Accessed November 2017].
23. Radiological Society of North America Inc. X-ray (Radiography). Available at: https://www.radiologyinfo.org/en/submenu.cfm?pg=xray [Accessed August 2017].
24. Radiological Society of North America Inc. Computed Tomography. Available at: https://www.radiologyinfo.org/en/submenu.cfm?pg=ctScan [Accessed August 2017].
25. NHS Choices. Echocardiogram. Available at: http://www.nhs.uk/Conditions/echocardiogram/Pages/Introduction.aspx [Accessed July 2017].
26. Galiè N, et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: The Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT). Eur Heart J 2016;37(1):67–119.
27. Thakkar V, et al. N-terminal pro-brain natriuretic peptide in a novel screening algorithm for pulmonary arterial hypertension in systemic sclerosis: a case-control study. Arth Res & Ther 2012;14:R143.
28. NHS Choices. Diagnosing pulmonary hypertension. Updated March 2017. Available at: https://www.nhs.uk/Conditions/pulmonary-hypertension/Pages/diagnosis.aspx [Accessed July 2017].
29. Nihtyanova S, et al. Prediction of pulmonary complications and long-term survival in systemic sclerosis. Arthritis Rheum 2014;66(6):1625–35.
30. Jaeger V, et al. Incidences and risk factors of organ manifestations in the early course of systemic sclerosis: a longitudinal EUSTAR study. PLoS One 2016;11(10):e0163894.
31. McNearney T, et al. Pulmonary involvement in systemic sclerosis: Associations with genetic, serologic, sociodemographic, and behavioural factors. Arthritis Rheum 2007;57(2):318–26.
32. Steen V, et al. Changes in causes of death in systemic sclerosis. Ann Rheum Dis 2007;66:940–4.
33. de Oliveira NC, et al. Aerobic and resistance exercise in systemic sclerosis: State of the art. Musculoskeletal Care 2017;15(4):316–23
©Boehringer Ingelheim International GmbH (2017). This document and its contents are property of Boehringer Ingelheim (third party sources are indicated) and are, inter alia, protected by copyright law. Complete or partial passing on to third parties as well as copying, reproduction, publication or any other use by third parties is not permitted.
You can visit morethanscleroderma.com for more information.
PC-CDE-100326 Date of preparation: April 2018
Created in collaboration with: