
Lung Cancer Not Attributable to Smoking
14
Lung Cancer Not Attributable to Smoking OLAV AXELSON University Hospital S-58185 Linkoping, Sweden DEVRA LEE DAVIS. National Research Council Washington,D.C. 20418 FRANCESCOFORESTIERE Epidemiological Observatory Lazio Region, Italy MARVIN SCHNEIDERMAN National Research Council Washington,D.C. 20418 DIANE WAGENER National Center for Health Statistics Hyattsville, Maryland 20782 INTRODUCTION The great preponderance of lung cancer in industrial societies is attributable to cigarette smoking, although other causes are also involved. As the most common cancer for men in the industrial nations (excepting Japan) at least 85% of lung cancer in men is attributable to smoking as is about 75% in women.’” The overall impact on lung cancer mortality from factors other than smoking remains difficult to estimate, but is appreciable3 and will vary from time to time and between countries. Lung cancer mortality has peaked in the United Kingdom among men under age 7.5; and in the United States among men under age 55: where rates of smoking appear to be declining and proportionately more low-tar, high-filter cigarettes are now beingsmoked. In light of these welcome trends,factorsnot related to smoking that cause lung cancer merit closer attention. Recent research implicates a number of factors not related to direct smoking that #Address for correspondence: Devra Lee Davis, Ph.D., M.P.H., Scholar in Residence, National Academy of Sciences, 2101 Constitution Avenue, NW, Washington, DC 20418. 165
Transcript of Lung Cancer Not Attributable to Smoking

Lung Cancer Not Attributable to Smoking
OLAV AXELSON
University Hospital S-58185 Linkoping, Sweden
DEVRA LEE DAVIS. National Research Council
Washington, D.C. 20418
FRANCESCO FORESTIERE
Epidemiological Observatory Lazio Region, Italy
MARVIN SCHNEIDERMAN
National Research Council Washington, D.C. 20418
DIANE WAGENER
National Center for Health Statistics Hyattsville, Maryland 20782
INTRODUCTION
The great preponderance of lung cancer in industrial societies is attributable to cigarette smoking, although other causes are also involved. As the most common cancer for men in the industrial nations (excepting Japan) at least 85% of lung cancer in men is attributable to smoking as is about 75% in women.’”
The overall impact on lung cancer mortality from factors other than smoking remains difficult to estimate, but is appreciable3 and will vary from time to time and between countries. Lung cancer mortality has peaked in the United Kingdom among men under age 7.5; and in the United States among men under age 55: where rates of smoking appear to be declining and proportionately more low-tar, high-filter cigarettes are now beingsmoked. In light of these welcome trends,factorsnot related to smoking that cause lung cancer merit closer attention.
Recent research implicates a number of factors not related to direct smoking that
#Address for correspondence: Devra Lee Davis, Ph.D., M.P.H., Scholar in Residence, National Academy of Sciences, 2101 Constitution Avenue, NW, Washington, DC 20418.
165
166 ANNALS NEW YORK ACADEMY OF SCIENCES
increase the risk of contracting lung cancer; these include exposure to the decay products of radon gas indoors: non-occupational exposure to asbestos,’ passive ex- posure to cigarette smoke: pet birds: and possibly air pollution. Other factors are known to enhance the risk of lung cancer in smokers and non-smokers exposed to agents such as asbestos, ionizing radiation, nickel salts, wood dust, other industrial dusts, fibers, and fumes.1°
In light of discussions at this workshop indicating that lung cancer not attributable to smoking comprises a substantial proportion of all cancer, we have developed esti- mates of trends in non-smoking-attributable lung cancer, by using two different heuristic models: one based on survey data from the United States, Japan, and Italy, which takes into account smoking prevalence, passive smoking, and smoking cessa- tion; and one whichincorporates thesevariables alongwith two different estimates of the effect of duration on smoking.
LITERATURE REVIEW
Given past smokingpatterns, deaths attributable to smoking-induced lung cancer will continue to predominate into the next century, as this cancer has a latency of at least20yearsandasitsriskisafunctionofdurationandamount ofcigarettesmoking.2 In the United States, United Kingdom, and Italy, the proportion of smokers among men appears to have reached a peak in the 1960s and 1970s. More current smokers began smoking at younger ages. If the risk of lung cancer from smoking increases exponentially with duration of smoking or with time from “age started” smoking, therewould be littleneed to invoke other factors in explaining increasing time trends. Doll and Peto2 argue that the risk of lung cancer increases with the fourth or fifth power of duration of smoking. In contrast, Moolgavkar” suggests that the increase in risk is linear with duration of smoking, i.e., more directly related to total lifetime dose-possibly measured in units such as pack-years.
Brown and Kessler12 have developed a model for projecting lung cancer rates, employing data from middle-class volunteers enrolled in the American Cancer Society’s Continuing Population Survey13 from 1982 to 1986 and estimates of age- adjusted smoking prevalence, age-specific prevalence among new smoking cohorts, and tar content. Their model indicates that reductions in tar content of all brands of cigarettes coinciding with the introduction of low-tar and filtered brands in the late 1960sshould lead to lower lung cancerrisks of smoking. Their model incorporates the American Cancer Society conclusion that lung cancer rates have not increased in non- smokers. Based on the same American Cancer Society survey, Garfinkel and Si l~erberg’~ report that the increased risk of lung cancer among women can be explained by their post World War I1 increase in smoking. They conclude that the relative risk of lung cancer for smokers compared to non-smokers has increased to 22 for women enrolled in their study population.
In an analysis of a case control study of Swedish women, Carstensen and A x e l ~ o n ’ ~ report a slightly more than doubled increase inlung cancer mortality during a 30-year period that might possibly be all attributed tosmoking, although with some difficulty.
METHODS
Thispaperconsiderswhetherincreases in lung cancer amongwomen in theunited States, Japan, and Italy can be explained by smoking alone. Lack of detailed

AXELSON et aL: LUNG CANCER N o r ATTRIBUTABLE TO SMOKING 167
information on individuals represent.ative of their respective countries makes it necessary to apply a series of estimates, which employ models that rely on self- reporting surveys of smoking prevalence, passive smoking, and smoking cessation. Because cigarette smokers have higher mortality rates than non-smokers, estimates of the prevalence of cigarette smoking based on currently living persons may under- estimate the population prevalence of smoking in the past.12
ESTIMATE OF NONSMOKING LUNG CANCER IN JAPANESE WOMEN
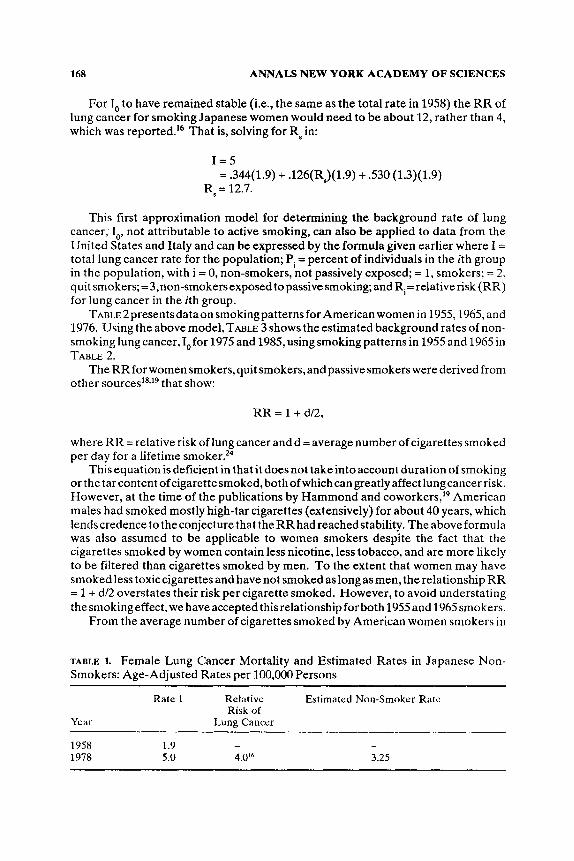
First consider a model of non-smoking-attributable lung cancer in Japanese women in 198 that includes a consideration of passive smoking. HirayamaI6 reported the relative risk of women active and passive smokers in Japan was 4.0 and 1.3, respectively. From these datawecanestimate the background rateof lungcancer (not attributable to smoking), I,, for Japanese women:
I = POIo + lJs(Rs)I,, + Pp(Rp)Io
or
I I =- O PiRi ’
where I = totalrate of lung cancer mortality (age-adjusted) in, say 1Y78(=5),P0= percent non-exposed women in 1958 (to allow for a 20-year latent period) = 34.4 (see below); Ps = percent women smokers, 1958 = ’12.6; R, = relative risk (RR) for women smok- ers = 4; Pp = percent women passive smokers in 1958 = 53.0 (see below); RP = relative risk for women passive smokers = 1.31; I, = background rate (in non-smoking, non- passively exposed women).
To estimate Pp, assume that 90% of (non-smoking) Japanese women married to male smokers are passively exposed.’4 In 1958,75.9% of Japanese men reported themselves as smokers.” Assume further that smoking prevalence for Japanese men is the same for married and unmarried men. For the percent of women non-smokers passively exposed, .759 x .9(1- .126) = .530. (As no data are reported from Japan on quit smokers, we assume that in 1958 there was a negligibleproportion of women quit smokers.) Smokingpatterns in 1958 should affect lung cancer rates in 1978. Thus, for 1978, lung cancer mortality, the equation given earlier can be solved for I,, yielding:
5 = .344(I,) + ,126 (4)I, + .530 (1.3)10
or
I, = 3.25.
As TABLE 1 shows, this estimated rate of lung cancer in non-smoking women in 1978of3.25ismore than60% greaterthanthetotallungcancerrateof 1.4 per 100,000, for Japanese women in 1958.
168 ANNALS NEW YORK ACADEMY OF SCIENCES
For I, to have remained stable (i.e., the same as the total rate in 1958) the R R of lung cancer for smoking Japanese women would need to be about 12, rather than 4, which was reported.16 That is, solving for Rs in:
I = 5 = .344(1.9) + .126(Rs)(1.9) + S30 (1.3)(1.9)
RS = 12.7.
This first approximation model for determining the background rate of lung cancer, I,, not attributable to active smoking, can also be applied to data from the United States and Italy and can be expressed by the formula given earlier where I = total lung cancer rate for the population; Pi = percent of individuals in the ith group in the population, with i = 0, non-smokers, not passively exposed; = 1, smokers; = 2, quit smokers;=3,non-smokersexposed to passive smoking; and R,=relativerisk (RR) for lung cancer in the ith group.
T ~ ~ ~ ~ 2 p r e s e n t s d a t a o n smokingpatternsfor Americanwomenin 1955,1965, and 1976. Using the above model, TABLE 3 shows the estimated background rates of non- smoking lung cancer, &for 1975 and 1985, using smoking patterns in 1955 and 1965 in TABLE 2.
The RR for women smokers, quit smokers, and passive smokers were derived from other source^^*^^^ that show:
RR = 1 + dl2,
where RR = relative risk of lung cancer and d = average number of cigarettes smoked per day for a lifetime ~moker .2~
This equation isdeficient in that it does not take into account duration of smoking or the tarcontent ofcigarettesmoked, bothofwhichcangreatlyaffectlungcancerrisk. However, at the time of the publications by Hammond and coworker^,'^ American males had smoked mostly high-tar cigarettes (extensively) for about 40 years, which lendscredence to the conjecture that the RR had reached stability. The above formula was also assumed to be applicable to women smokers despite the fact that the cigarettes smoked by women contain less nicotine, less tobacco, and are more likely to be filtered than cigarettes smoked by men. To the extent that women may have smoked less toxic cigarettes and have not smoked as long as men, the relationship RR = 1 + d/2 overstates their risk per cigarette smoked. However, to avoid understating thesmokingeffect, we haveaccepted thisrelationship for both 1955and 1965 smokers.
From the average number of cigarettes smoked by American women smokers in
TABLE 1. Female Lung Cancer Mortality and Estimated Rates in Japanese Non- Smokers: Age-Adjusted Rates per 100,000 Persons
Rate 1 Relative Estimated Non-Smoker Rate Risk of
Year Lung Cancer
1958 1.9 - -
1978 5.0 4.0’* 3.25

AXELSON et aL: LUNG CANCER NOT ATTRIBUTABLE TO SMOKING 169
TABLE 2 Percent of US. Women Smokers, Quit-Smokers, and Non-Smokers Age- Adjusted
Smokers' Former Passive Unexposedb Smoke:rs Smokers
1955 (18+)c 27.4 3.8 25.9 42.9 1965 (20+) 34.2 8.2 18.7 38.9 1976 (20+) 32.5 13.9 9.8 43.8
"Data for 1955 are from Haenszel et al.' Data for 1965 and 1976 are from the U.S. National Center for Health Statistics."
q h e s e values are estimated using a assortative mating model, assuming 90% of women who smoke are married to men who smoke. Thle remainder of the population is assumed to mate at random.
CData are for persons this age and older.
1965 in TABLE 2 we find: R, = 1.0 (non-smokers), Rl = 9.8 (smokers), R, = 3.9 (quit smokers, assuming the excess risk for quit smokers is one-third that of continuing smokers), and R, = 1.3 (passive smokers-from National Academy of Sciences/ National Research Council report on environmental tobacco smoke).8
Based on smoking patterns for women in 1955, we estimate: Po= .429, P, = .274, P, = .038,andP3=.259,andforsmokingpatternsin1965,P0=.389,P,= .342,P,= .082, and P3 = .187.
For 1955 smoking, 1975 lung cancar rates (American women)
= 4.79. 15.2 '0.1975 = .429+ .274(9.8)+ .038 (3.9) + 259(1.3)
For 1965 smoking, 1985 lung cancer rates (American women)
= 6.13. 26.4 I , , , = - .389+ .342(9.8)+ .082(3.9) + m(1.3)
TABLE 3 shows that the estimated rate of lung cancer in non-smoking women in 1985 is 45% higher than the estimated1 rate 10 years earlier. Moreover, the estimated 1985 backgroundrate of6.1 exceeds the total of alllung cancer recorded in 1955. That is, according to thismodel the lung cancer mortalityrate amongnon-smokingwomen has increased to such a large extent over the 30-year period from 1955 to 1985 that the 1985 1,rate is estimated to be greater than the total rate of lung cancer in 1955. This isastrikingincreasein light of the fact that themodelmay overstate the smokingeffect insofar as it does not take into account the lower tobacco contentmJ1 and the lower tar content1 of cigarettes smoked in the later time period. Hence, the 1985 non-smoking lungcancer rate would beunderestimated using thismodel. The possibility exists that the smoking contribution to the 1975 lung cancer mortality was overestimated, while the contribution to the 1985 rates was underestimated.
ITALIAN DATA ON ACTIVE AND FORMER SMOKERS
Italian data may be used for a similar modeling, although there are no good estimatesavailable for passivesmoking. The smoking habitsfor the Italian population

170 ANNALS NEW YORK ACADEMY OF SCIENCES
TABLE 3. FemaleLung CancerMortalityand Estimated RatesforNon-Smokersin the United States: Age-Adjusted Rates per 100,oOO Persons
Year Reported Rate# Estimated Non-Smoker Rate
1955 5.1 1965 7.4 1975 15.2 1985 26.4
- 4.8 6.1
“National Cancer Institute, 1988.
are available from two surveys conducted by DOXA (a private marketing research institute) during the years 1957 and 196522 and a random survey was also carried out by the Central Institute of Statistics (ISTAT)23in 1980 (TABLE 4). A decrease of the prevalence of smokers among men has recently occurred, while a rising prevalence in women is evident.24 Inconsistencies, between interview-based surveys and legal-sales data have been noted, however, and an underreporting of smoking prevalence and amount smoked in more recent periods has been suspected. It has nevertheless been concluded that the smoking habits among men have probably not changed markedly over the last three decades in Italy, whereas large increases have been observed among women. Furthermore, the average number of cigarettes smoked per day among smokers has increased both for males (13.3, 13.3, and 17.2 for the three surveys, respectively) and females (7.0, 5.8, and 10.9) in the period considered. Using the Hammond relationship to estimate relative risks and assuming that the excess risk for quit smokers is one-third that of current smokers, estimates of non-smoking lung cancer may be derived for the Italian data.
Sex-specific lung cancer death rates in the periods of the sample surveys are available from published statistics of the ISTAT.*’ The rates are consolidated on a three-year basis to reduce random fluctuation (Period 1: 1956-1958, Period 2: 1965- 1967, Period 3: 1980-1982) after direct standardization to the age distribution of the 1981 Italian population (TABLE 4). Given the amounts smoked, in the smokers group the relative risks are for males 7.7,7.7,9.6 and for female smokers are 4.5,3.9,6.5 for periods 1,2,3, respectively. In the quit smokers group the relative risks are for males 3.2,3.2,3.9 and for females 2.2,2.0,2.8 for periods 1,2,3, respectively.
Applying our model to Italian data on 1964-1966 smoking patterns to estimate 1980-1982 non-smoking lung cancer rates:
(MEN) I, = 76.6
= 14.2
.234+ .6a3 (7.7) + .163(3.2)
(WOMEN) I, = 10.8 .891+.w7(3.9)+.032(2.0)
= 8.6.
TAULB 4 shows that these estimates of non-smokinglungcancer for Italian women exceed the total lung cancer rate 1956-1958 and 1962-1964, and are nearly half the total rate for men at these times. These 1,values seem high, which would be expected

AXELSON et a/.: LUNG CANCER NOT ATTRIBUTABLE TO SMOKING 171
if the amount of cigarette smoking or the relative risks were underreported. To test our model further, we use theU.S. derived relativerisks, which are higher. Using the U.S. relative risks applied to Italian data, gives:
= 10.1 10.8 .891+ .07/(9.8) + .032(3.9)
(MEN) $= -
= 6.1. 10.8 .891+ .On( 9.8) + .032( 3.9)
(WOMEN) I,= -
These more conservative assumptitons produce an estimated background rate of non-smoking lung cancer I, for women of 6.1, in 198G1982, which is greater than the total rate for all women in 1956-1958 and a rate for men of 10.1, which is half of the total in 1956-1958. Thus, even under these assumptions, cigarette smoking only partially accounts for the large increase in recorded lung cancer mortality in Italian women.
MODEL INCORPORATING DURATION OF SMOKING
Yet another model can be proposed that incorporates average duration of smoking and related factors. This allows us to examine the possibility that an earlier age at which individuals started smoking accounts for much of the increase in lung cancer mortality over time-after prevalence, quitting, etc. are taken into account.
Assume that lung cancer mortality directly increases with duration to the fourth or fifth power.2 Thus, the finding of Gart and SchneidermanZ6 that the relative risk of lung cancer due to smoking equals 1 t. dl2 would need to be modified to read:
RR = 1 +d/2-, D"." where 1 +d,/2-, D"." Di Di
TABU 4. Prevalence of Cigarette Smtoking and Estimated Lung Cancer Mortality (Age-Adjusted) per 100,OOO Persons for Smokers and Non-Smokers in Italy
Year Men and Women Percent Lung Cancer Background Percent Ex-Smoker Mortality Rate
Current Smoker Rate Estimated
Men 1956-1 958 1965-1967 1980-1982
Women 1956-1 958 196% 967 1980-1982
65.0 12.5 23.0 Not computed 60.3 16.3 41.6 Not computed 54.3 9.9 76.6 10.8"
[10.1]
6.2 4.0 5.6 Not computed 7.7 3.2 7.6 Not computed
16.7 1.4 10.8 8.6" F.11
"Assuming relative risks for smokers, 1.0 for males and 4 for females, and for ex-smokers, 5
Brackets indicate estimated rate using US. assumptions of relative risk. for males and 2.5 for females

172 ANNALS NEW YORK ACADEMY OF SCIENCES
and d"=averagenumberofcigarettessmokedperdayinyearn,D,=durationofsmoking by an averagesmokerwhodiedoflungcancerinYear2,andD, =duration of smoking by an average smoker who died of lung cancer in Year 1.
Also assume that D, and D, are estimated by the median age of death from lung cancer minus age started smoking. For example, if average age started smoking is Year 1 = 20 and Year 2 = 15 and the median age at death is Year 1 = 66 and Year 2 = 65 (earlier because of heavier smoking and earlier starting smoking age) then d, = 15/ day and d, = 18Iday. Further assume that duration is estimated by taking the median age at deathof asmoker fromlungcancer minus the ageat which they started smoking.
The excess risk for quit smokers is 33% the excess risk for a continuing smoker. Smoking prevalence increased from Period 1 to Period 2. Lung cancer mortality rate is age-adjusted to the same base and assumes a 20-year lag. The lung cancer mortality rate is 15.1 for Period 1 and 26.4 for Period 2. These assumptions lead to the computation in TABLE 5 for the U.S., where the risk for quit smokers is the 33% the risk for current smokers.
Under the assumptions of RR,, the increase in percent of women who are current smokers20years earlierand their earlier ageof starting to smoke, account for the total increase in lung cancer mortality among white females in the U.S. from 1975 to 1985. If, however, one does not accept the assumption that mortality increases with the fourth to fifth power of the duration of smoking as in RR,, then the substantial in- crease in the proportion of ever smokers from 1955 to 1965 does not completely account for theincreaseinlung cancer mortalityratesfor U.S. white women from 1975 to 1985. Indeed, some data of Garfinkel and Stell~nan'~ imply that the increase in relative riskisnotproportional to theduration raised to some power greater than one. They report that the standard mortality ratio (SMR) for 1.5 or more packs per day smokersincreasedfrom18.9(duration21 to30years) to38.8 (duration41 to70years). This implies a duration effect of less than unity. Consider that the ratio of the SMRs is 2.05 (38.8:18.9) and the ratio of the average durations is 2.02 (55, the average duration of41 to70years, divided by25, theaveragedurationof21 to30years). Thus, the exponent characterizing the relationship of dose to risk of death with their data is .91,which is less than unity. Hence, the 4.5 factor may be much too high, based on the American Cancer Society data.
DISCUSSION
The models developed here for the calculation of background rates of lung cancer haveall thelimitsofmodelsapplied toanysubject. Forexample, they donot takeinto account the possibility of varying relative risks for smokers of different ages. It may also be argued that there are cohort effects, such that the longer duration of smoking in more recent cohorts produces an exponentially increased risk of lung cancer and that the relative risks employed are too low, especially for the recent years. They also do not take into account the low tobacco and lower tar content of cigarettes smoked after 1965.
However, considerable manipulation of recorded data is required to develop a set of assumptions in which smoking explains all of the change in lung cancer mortality in the countries examined here. For example, to reduce the estimated non-smoker ratesforItalianmenfrom10.8inPeriod3 toabout3.1 per100,OOOpersonsasinPeriod 1 it would be necessary to assume an average relative risk for smokers of about 40 and about 20 for ex-smokers in the years 1980 to 1982, and/or to lower the relative risks

TABL
E 5.
Uni
ted
Stat
es N
on-S
mok
ing Lung C
ance
r
Perio
d 1 (1955)’
Perio
d 2
(1%
5)b
Perio
d 2 (1965)’
Bas
elin
e M
odel
Usi
ng
Line
ar D
urat
ion
Fact
or
Dur
atio
n Fa
ctor
RR
? B
asel
ine M
odel
Usi
ng E
xpon
entia
l R
R
RR
, B
asel
ine
Mod
el Using O
nly
Dos
e
Cig
aret
tes p
er d
ay (d
) Sm
okin
g at
tribu
tabl
e fr
actio
n R
ate of lu
ng c
ance
r
Non
-sm
oker
s Ex
-sm
oker
s Sm
oker
s
Estim
ated
lung
can
cer r
ate
attri
buta
ble
to
Smok
ing
Non
-sm
okin
g
15
15.2
.a
Perc
ent
RR
,
49 (P
o)
1 (%
I 4
(P,)
3.5 (
R )
27
(P,)
8.5 (
R)
10.3
4.
9
18
26.4 .7
8
20.7
5.
7
18
26.4 83
21.9
4.5
‘No
“dur
atio
n” fa
ctor
: RR
. = 1
+ dt2
b
RR
= 1
+ dl2
ID-I
D.)
‘Exo
onen
tial d
urat
ion
fact
or
I 1
. 1
I’
65-15
d5
RR
,=l+
d/2
-
Dl =
1 + (
18/2
) -
=1+ 15
1-2
= 8
.5 fo
r sm
oker
s In
crea
sed
risk
for e
x-sm
oker
s = lL3
66-2
0 of sm
oker
risk
. i.e.
1 +
73
3 =
3.5.
=
10.8
65
- 19’
=1+1m _
__
66-20

174 ANNALS NEW YORK ACADEMY OF SCIENCES
(assumed to be lOand 5,respectively)for smokers and ex-smokers in theearly period. Relative risks as high as 40 and 20, respectively, have not yet been shown for any overall population of smokers and ex-smokers.
For women in Italy, relative risks of about 10 and 5 for smokers and ex-smokers, respectively, would be required by 1980 to 1982, to produce an estimate of a constant background rate over time. Similarly, some equally unlikely high rate ratios would have to be applied to the Japanese and US. data to obtain aconstant background rate over time. It seems reasonable to believe, therefore, that factors in addition to smoking play an important role for lung cancer in both smokers and non-smokers and that these have increased over time. This conclusion is certainly not new but rather in agreement with more specific studies, where synergistic effects between smoking and occupational factors have been directly indicated. The well-known-greater-than- additive effect of asbestos and smokingcombined is obviously also generally support- ive of theview that other factors have to be takeninto consideration for explaining the lung cancer trends in this century.
T A U L E ~ . Different Estimatesof Non-Smoking Lung Cancer Background Rate (White Women, United States)
1975 1985" 1985' 1985'
4.9 4.5 5.7 6.1
*Assuming mortality = ( d u ~ a t i o n ) ~ ~ . bAssurning mortality = (duration)'.O. 'No adjustment for duration. NOTE: The estimates for Period 2 (1985 deaths, 1965 smoking) probably overstate the
smoking-attributable fraction because no adjustment was made for the declining average tar content of the cigarettes smoked, the increasing number of cigarettes per pound of tobacco, and the partial replacement of sheet for leaf tobacco in cigarettes.
Available studies of predominantly middle and upper class persons who have been followedforlongperiodsof timein theunited States donot show any increase inlung cancer among nonsmoker^.^^ Persons such as those included in the American Cancer Society studies may exhibit reduced rates of lung cancer because they are subject to fewer carcinogenic exposures than are working-class persons. For instance, they are more likely to live in less polluted areas, consume diets rich in antioxidants, and have experienced less exposure to carcinogens in the workplace. In contrast to the finding of no increase in lung cancer among those studied, the exercises reported here on estimates of lung cancer for populations of Japanese, Americans, and Italians suggest that increases may have occurred in lung cancer not associated with active cigarette smoking. Moreover, other data from the United Kingdom and Sweden indicate that certain occupations entail high risks of lung cancer.
Exercises such as these are offered as heuristic devices for generating hypotheses for further testing. In that regard, several possibilities need to be considered as relevant explanations for the possible trends in lung cancer reported in this paper. First of all, models are only as good as the data on which they rest. It is possible that national surveys of reported smoking behavior are not reliable, especially in light of
AXELSON ef al.: LUNG CANCER NOT ATTRIBUTABLE TO SMOKING 175
the growing anti-smoking esprit de temps. Likewise, the quality of data on recorded mortality needs to be evaluated carefully. In the case of Japan, both of these factors may account for some part of the relatively low reported rates and smoking behaviors in women?'
In light of the important declines in cigarette smoking now underway in a number of countries, it is important for national studies to be undertaken on broadly repre- sentative samples of persons, throughout the economic spectrum, to assess better the effects of factors other than cigarette smoking on lung cancer. Finally, the possibility cannot bedismissed that smoker sin theseindustrialcountries todatehaveexperienced themajoreffect offactorsotherthancigarettesmokingon their lung cancer. As fewer persons smoke, the importance of nonsmoking factors may become evident and provide opportunities for further reductions of this important disease.
REFERENCES
1. U.S. Department of Health and Human Services. 1989. Reducing the Health Consequences of Smoking: 25 Years of Progress. A Report of the Surgeon General. U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control, Center for Chronic Disease Prevention and Health Promotion. Office on Smoking and Health. DHHS Publication No. (CDC) 89-8411.
DOLL, R. & R. PETO. 1978. Cigarette smoking and bronchial carcinoma: Dose and time relationships among regular smokers and lifelong non-smokers. J. Epidemiol. Commun. Hlth. 32: 303-313.
SCHNEIDERMAN, M. A., D. L. DAVIS & D. K. WAGENER. 1989. Lung cancer that is not attrib- utable to smoking. 269 2635-2636. [Correction in 1989 JAMA 262 904.)
Office of Censuses and Population Surveys. 1990. Review of the National Cancer Registra- tion Scheme. Report of the Working Group. London. Her Majesty's Stationery Office. London.
5. DEVESA, S. S., W. J. BLOT & J. F. FRAUMWI, JR. 1989. Declining lung cancer rates among young men and women in the United States: A cohort analysis. J. Natl. Cancer Inst. 81: 1568-1571.
6. National Research Council. 1988. Health Risks of Radon and Other Internally Deposited Alpha-Emitters: BEIR IV. National Academy Press. Washington, D.C.
7. National Research Council. 1984. Abestiform Fibers: Nonoccupational Health Risks. National Academy Press. Washington, D.C.
8. National Research Council. 1986. Environmental Tobacco Smoke: Measuring Exposures and Assessing Health Effects. National Academy Press. Washington, D.C.
9. HOLST,~. A., D. KROMHOUT& R. BRAND. 1988. For debate: Pet birds as an independent risk factor for lung cancer. Br. Med. J. 297: 1319-1321.
10. ROSENSTOCK, L. & M. R. CULLEN. 1986. Clinical Occupational Medicine. Saunders. Phila- delphia.
11. MOOLGAVKAR. S. H., A. DEWANJI & G. LUEBECK. 1989. Cigarette smoking and lung cancer: Reanalysis of the British doctors' data. J. Natl. Cancer Inst. 8k 415420.
12. BROWN, C. C. & L. G. KESSLER. 1989. Projections of lung cancer mortality in the United States: 1985-2025. J. Natl. Cancer Inst. 80: 43-51.
13. GARFINKEL, L. & S. D. STELLMAN. 1988. Smoking and lung cancer in women: Findings in a prospective study. Cancer Res. 4& 6951-6955.
14. GARFINKEL, L. & E. SILVERBERG. 1990. Lung cancer and smoking trends in the United States over the past 25 years. Ann. N.Y. Acad. Sci. This volume.
15. CARSTENSEN, J., 0. AXELSON & F. FORASTIERE. 1990. Changes in non-smoking related lung cancer-A theoretical exercise. Ann. N.Y. Acad. Sci. This volume.
16. HIRAYAMA, T. 1984. Cancer mortality in nonsmoking women with smoking husbands on a large-scale cohort study in Japan. Prev. Med. U: 680-690.
2.
3.
4.
176 ANNALS NEW YORK ACADEMY OF SCIENCES
17.
18.
19.
20.
21.
22. 23.
24.
2s.
26.
27.
28.
HIRAYAMA, T. 1981. Non-smoking wives of heavy smokers have a higher risk of lung cancer: A study from Japan. Br. Med. J. 282 183-185.
HAMMOND, E. C. 1966. Smoking in relation to death rates of one million men and women. Natl. Cancer Inst. Monogr. 19: 127-204.
HAMMOND, E. C., L. GARFINKEL, H. SEIDMAN & E. A. LEW. 1976. “Tar” and nicotine content of cigarette smoke in relation to death rates. Environ. Res. 12: 263-274.
U.S. Department of Agriculture, Tobacco Situation. 1989. Tobacco Products: Figure 2, Cigarettes Produced and Tobacco Used. December, 4.
U S . Department of Health and Human Services. 1981. The Health Consequences o€ Smoking: The Changing Cigarette, A Report of the Surgeon General. US. Department of Health and Human Services, Public Health Service, Office on Smoking and Health. DHHS Publication No. (PHS) 81-50156.
LA VECCHIA, C. 1986. Smoking in Italy, 1949-83. Prev. Med. 15c 274-281. LA VECCHIA, C. 1985. Patterns of cigarette smoking and trends in lung cancer mortality in
Italy. J. Epidemiol. Commun. Hlth. 3% 157-164. ISTAT. 1982. Indagine statistica sulk condizioni di salute della popolazione e sul ricorso ai
servize sanitari (Novembre 1980). Bollettino Mensile di Statistica 12 (Suppl.) ISTAT, ISS. 1988. Mortalita’ per causa e Unita’ Sanitaria Locale, 1980-1982. Istituto
Centrale di Statistica. Rome. GART, J. J. & M. A. SCHNEIDERMAN. 1979. “Low-risk’’ cigarettes: The debate continues
[letter]. Science 204 (4394): 690492. JABLON, S., D. THOMPSON, M. MCCONNEY & K. MAEUCHI. 1990. Accuracy of cause of death
certification in Hiroshima and Nagasaki, Japan. Ann. N.Y. Acad. Sci. Vol. 609. National Center for Health Statistics. 1986. Health, United States, 1986. DHHS Publ. No.
(PHS) 87-1232, Public Health Service. US. Government Printing Office. Washington, D.C.
DISCUSSION
OIAV ANDERSON (University Hospital, Linkoping, Sweden): As I am partially re- sponsible for these papers and models, I wish to make the comment that the question is, of course, if we have cohort effects involved here that are so strong that they can actually explain what is coming out from this simple model. Jan Carstensen tried t o adjust forthat and that seemstolead to theconclusion thattheriskof smokingexplains nearly all of the increase in lung cancer in Swedish women.
But the trend here in the Italian data is even stronger and unlikely to reflect smoking alone. It would be of interest, of course, to apply a similar adjustment and see if that would explain the differences. I really doubt that the increased risk of smokingcan completelyaccountfor theincreasesinlung cancer. But that is, of course, the question we have before us.
TAKESHI HIRAYAMA (Institute of Preventive Oncology, Tokyo): If it is a type of theoretical exercise, I think I should like to suggest a theoretical model of taking into consideration the possibility of passive smoking. You can make some model, like contagious disease, and see the effect of contact rates, something like that, in the family. If such is considered, I think it will also help.
AXFUON: We actually developed this relationship originally in the context of the passive smoking issue. We had plugged in that originally, but it contributed SO little. I really doubt that it plays a role here.
PHILLIP LANDRIGAN (Mount Sinai Medical Center, New York, N Y ) : Perhaps the
AXELSON et al.: LUNG CANCER NOT ATTRIBUTABLE TO SMOKING 177
approach needed is acombination of the theoretical and the practical. Model building is fine for a beginning. But what needs to be done next to follow-up on that is what we sometimes refer to as “shoe leather” epidemiology, where we actually wear out our shoes interviewing people. Of course, you have to move quickly because people with lung cancer don’t last too long-and do careful case control studies, as I know you’ve done, Dr. Forastiere, and track down the various factors: passive smoking, asbestos, silica, all the many different possible etiologies.
JOHN Fox (Office of Censuses and Population Surveys, London): I was struck that both for the males and the females the correlation between the background rate and the smoking-related rate of lung cancer is so high that I would have thought-I haven’t looked at the equations carefully-that you’ve actually got some circularity in the equations.
So that, in part, where you’ve got a massive rise in the smoking-related, you’re equally going to get a rise in the non-smoking related through the equations.
FRANCESCO FORESITERE (Epidemiology Observatory, Lazio Region, Italy): I have to add that in Italy for the smoking data used here, there is an average prevalence for smokers that is uniform in the country. It’s not correlated at all now with patterns of lung cancer mortality.
DIANE WAGENER (National Center for Health Statistics, Hyaitsville, Md): A number of matters can be raised. If smokers have a higher dose at an earlier age, passive smokers have the accumulated dose at a somewhat delayed age, and non- exposed have basically random risk factors that accumulate. The age of onset for lung cancer must have changed over the past 30 yearssince the conclusions have been that the proportion of lung cancers due to smoking changes. Is there any indication of changes in age-of-onset distributions? Of course, at the same time there has been a change in age-specific mortality rates so that the picture may be too complicated.
It seems that there are several factors that are potentially important for our models that werenot included in this analyses. Oneis age factor, such as age started smoking, age at exposure, age at death. Another is time lag. There absolutely must be some lag built into the models because the smoking patterns have changed remarkably over the past 40 years and because there is a generally agreed on latent period for this cancer. Another factor is competing causes of death, especially for certain socio-economic groups. Finally, all of the models assume the relative proportions of smokers and passive smokers do not change. The Brown models assume that smokers account for a certain attributable fraction of the lung cancer deaths. Based on that and current smokingpatterns, they project to the future. However, since fewer men are smoking, there must be fewer women passive smokers. Therefore, the relative proportion of women who are smokers and are passive smokers will be changing. However, the model projecting to the future does not allow for a change in the attributable fraction.
Insummary, it seems to me that there are many factors that we each, individually, have ignored for our own particular models. We do not have a good sense of the sensitivity of the models to these assumptions. M A R V I N S C H N E I D E R M A N ( N ~ ~ ~ ~ ~ ~ ~ R ~ ~ ~ ~ ~ ~ ~ Council, Washington, DC): Let me add
some comments on models of lung cancer and smoking. Consider whether rates for smokers should increase as follow-up time increases? Yes, as persons get older rates increase; No, if smoking effect is a multiplier on the background effect then, with aging, background will go up, and multiplying by a constant (the smoking effect) so will the rates for smokers. The relative risk should stay constant, i.e. be equal to the constant multiplier (+l). Doll-Pet0 argue that relative risk goes up with some high,

178 ANNALS NEW YORK ACADEMY OF SCIENCES
fourth or fifth, power of duration of exposure. In equations by Moolgavkar some minimum follow-up time is needed before the rates (and relative risks) stabilize. Perhaps as long as themedian latent period from time started smoking (e.g., if subject startedsmoking 10 years ago and medianlatent periodis 15 years) then subject should be followed for a minimum of 15 additional years. What mechanism would account for increasing relative risk with increasing follow-up duration? This must be mure than a simple relationship between response and cumulative dose.
As to dosemeasures,is there a better dose metameter thancigarette packs smoked per day? Consider cigaretteslday x days smoking x relative tarlcigarettes; packs per yearx a constant; lifetime relative tar intake. How about “wasted dose,” like among uranium miners? There appears to be no wasted dose. In results in quit smokers the rate begins to decline as soon as one quits. (Late-stagecarcinogenesis?) What do the ACS data tell us about tar content?
One further issue suggestsitself. Are blacksmore sensitive than whites to cigarette smoke? I don’t know. If blacks start from a higher base (for non-smokers), relative risks could still be the sarne,while absolute rates (background x a constant) would be higher. Is theconstant multiplier (for thesame smokingexposure) the same for whites and for blacks? If not, why not? In view of the fact that black women who smoke, smoke fewer cigaretteslday than white smokers, how does one account for the equivalence of their mortality rates?




















