Toll-like receptors 7 and 8 expression is associated with poor outcome and greater inflammatory...
6
Toll-like receptors 7 and 8 expression is associated with poor outcome and greater inflammatory response in acute ischemic stroke David Brea, Tomás Sobrino, Manuel Rodríguez-Yáñez, Pedro Ramos-Cabrer, Jesús Agulla, Raquel Rodríguez-González, Francisco Campos, Miguel Blanco, José Castillo ⁎ Clinical Neuroscience Research Laboratory, Department of Neurology, Hospital Clínico Universitario, University of Santiago de Compostela, Santiago de Compostela, Spain Received 4 September 2010; accepted with revision 1 February 2011 Available online 26 February 2011 KEYWORDS Ischemic stroke; Toll-like receptor; Outcome; TLR7; TLR8 Abstract Toll-like receptors are innate immunity receptors that activate inflammation and adaptive immunity. Our objectives were to analyze the association between TLR3, 7, 8 and 9 expressions and clinical outcome in patients with ischemic stroke and the expression of inflammatory molecules. One hundred-ten patients with ischemic stroke were included within 12 h of symptoms onset. Stroke severity was evaluated by the NIHSS, and functional outcome was assessed at 3 months by the modified Rankin Scale. Infarct volume at 4–7 days was measured on Computed Tomography imaging. TLR7 and TLR8 at different time points were independently associated with poor outcome. TLR8 was also correlated with infarct volumes. Furthermore, TLR7 and TLR8 on admission were correlated with levels of IL6 and IL1β at 24 h, 72 h and 7 days. In conclusion, TLR 7 and TLR8 expressions are associated with poor outcome and greater inflammatory response in acute ischemic stroke. © 2011 Elsevier Inc. All rights reserved. 1. Introduction Inflammation is a well known process that plays an important role in the outcome of ischemic stroke patients [1]. TLRs recognize specific structures, highly preserved in large groups of microorganisms, called Pathogen Associated Molecular Pattern. The receptors of the innate immune system that recognize such structures are called Pattern Recognition Receptors [2–4]. In recent years, several studies have shown that TLRs also recognize Damage Associated Molecular Patterns from endogenous molecules, which are Abbreviations: CT, Computed Tomography; mRS, modified Rankin Scale; ECG, Electrocardiogram; NIHSS, National Institute of Health Stroke Scale; Ct, Cycle threshold; CRP, C-Reactive Protein. ⁎ Corresponding author at: Servicio de Neurología, Hospital Clínico Universitario, 15706 Santiago de Compostela, Spain. Fax: +34 981951098. E-mail address: [email protected] (J. Castillo). 1521-6616/$ – see front matter © 2011 Elsevier Inc. All rights reserved. doi:10.1016/j.clim.2011.02.001 available at www.sciencedirect.com Clinical Immunology www.elsevier.com/locate/yclim Clinical Immunology (2011) 139, 193–198
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Toll-like receptors 7 and 8 expression is associated with poor outcome and greater inflammatory...
ava i l ab l e a t www.sc i enced i r ec t . com
C l i n i ca l Immuno logy
www.e l sev i e r . com/ loca te /yc l im
Clinical Immunology (2011) 139, 193–198
Toll-like receptors 7 and8expression is associatedwithpoor outcome and greater inflammatory response inacute ischemic strokeDavid Brea, Tomás Sobrino, Manuel Rodríguez-Yáñez, Pedro Ramos-Cabrer,Jesús Agulla, Raquel Rodríguez-González, Francisco Campos,Miguel Blanco, José Castillo⁎
Clinical Neuroscience Research Laboratory, Department of Neurology, Hospital Clínico Universitario,University of Santiago de Compostela, Santiago de Compostela, Spain
Received 4 September 2010; accepted with revision 1 February 2011Available online 26 February 2011
Abbreviations: CT, Computed TRankin Scale; ECG, ElectrocardiogramHealth Stroke Scale; Ct, Cycle thresho⁎ Corresponding author at: Servicio d
Universitario, 15706 Santiago de Co981951098.
E-mail address: [email protected]
1521-6616/$ – see front matter © 201doi:10.1016/j.clim.2011.02.001
KEYWORDSIschemic stroke;Toll-like receptor;Outcome;TLR7;TLR8
Abstract Toll-like receptors are innate immunity receptors that activate inflammation andadaptive immunity. Our objectives were to analyze the association between TLR3, 7, 8 and 9expressions and clinical outcome in patients with ischemic stroke and the expression ofinflammatory molecules. One hundred-ten patients with ischemic stroke were included within12 h of symptoms onset. Stroke severity was evaluated by the NIHSS, and functional outcome wasassessed at 3 months by the modified Rankin Scale. Infarct volume at 4–7 days was measured onComputed Tomography imaging. TLR7 and TLR8 at different time points were independently
associated with poor outcome. TLR8 was also correlated with infarct volumes. Furthermore,TLR7 and TLR8 on admission were correlated with levels of IL6 and IL1β at 24 h, 72 h and 7 days.In conclusion, TLR 7 and TLR8 expressions are associated with poor outcome and greaterinflammatory response in acute ischemic stroke.© 2011 Elsevier Inc. All rights reserved.omography; mRS, modified; NIHSS, National Institute ofld; CRP, C-Reactive Protein.e Neurología, Hospital Clínicompostela, Spain. Fax: +34
s (J. Castillo).
1 Elsevier Inc. All rights reserv
ed1. Introduction
Inflammation is a well known process that plays an importantrole in the outcome of ischemic stroke patients [1].
TLRs recognize specific structures, highly preserved inlarge groups of microorganisms, called Pathogen AssociatedMolecular Pattern. The receptors of the innate immunesystem that recognize such structures are called PatternRecognition Receptors [2–4]. In recent years, several studieshave shown that TLRs also recognize Damage AssociatedMolecular Patterns from endogenous molecules, which are
.

194 D. Brea et al.
released as a consequence of tissue damage. Thesemolecules, also known as endogenous ligands, are able toactivate TLRs in the same way that ligands coming frominfectious agents do [5,6].
The involvement of TLRs in the inflammatory response hasalso been established [7]. Consequently, the role of TLRs incerebral ischemia has also been studied. However, only TLRsexpressed on the cellular surface, such as TLR2 [8] and TLR4[9], have been associated to stroke outcome. Furthermore,studies performed with TLR4 knock-out mice have shownsmaller infarct sizes and improved scores in neurological testfor these animals as compared to wild type mice [10–12].Studies of TLR4 polymorphisms also showed associations withischemic stroke [13]. As with TLR4, the role of TLR2 inexperimental ischemia has also been evaluated [10,14].However, the role of intracellular TLRs, such as TLR3, TLR7,TLR8 and TLR9 in ischemic stroke remains unknown. Then, inthis study we analyze whether there is an associationbetween the expression of TLR3, TLR7, TLR8 and TLR9 onperipheral blood, and stroke outcome. Furthermore weanalyze the correlation between TLR3, TLR7, TLR8 and TLR9and the expression of inflammatory molecules.
2. Materials and methods
2.1. Study population and patients' characteristics
Between February 2009 and August 2009, 150 patients with afirst-ever stroke of less than 12 h duration and previouslyindependent for their daily living activities, were prospec-tively evaluated to be included in the study. The patients hadbeen admitted to the University Hospital of Santiago deCompostela. Patients with prior disability (mRSN1) (n=4),chronic inflammatory diseases (n=5), severe hepatic (n=2)or renal (n=3) diseases, hematological diseases (n=3),cancer (n=4), and infectious disease (n=5) or anti-inflam-matory treatment (n=6) in the 15 days prior to inclusionwere excluded. Furthermore, 5 patients did not accept theirparticipation in the study and 3 patients were lost duringfollow-up, so a total of 110 patients (male, 58.2%; mean age,74.6±9.8 years) were finally included in the study.
This protocol was approved by the corresponding ethicscommittee. Furthermore, informed consent was given bypatients or their relatives.
2.2. Clinical variables
All patients were admitted in the Acute Stroke Unit andtreated by the same stroke team according to the Guidelinesof the Cerebrovascular Diseases Study Group of the SpanishSociety of Neurology [15]. Medical history accounting forpotential vascular risk factors was recorded, and blood andcoagulation tests, 12-lead ECG, chest radiography, andcarotid ultrasonography were performed at admission.
Stroke subtype was classified according to the TOASTclassification [16]. To evaluate neurological deficits, theNIHSS was evaluated on admission, at 24 h, 72 h, 7 days and3 months. mRS was determined at 3 months on a routine visitof patients to the hospital. NIHSS and mRS were evaluated byinternationally certified neurologists.
2.3. Neuroimaging studies
CT scans were carried out on admission and between days 4and 7 of hospitalization. Early CT signs of infarction wereevaluated on admission, and infarct volume was assessed atthe second CT scan. Infarct volume was calculated on the CTimage by using the formula 0.5×a×b×c (where a is themaximal longitudinal diameter, b is the maximal transversediameter perpendicular to a, and c is the number of 10-mmslices containing infarct).
All CT scans were evaluated by neuroradiologists blindedto clinical and biochemical data.
2.4. Outcome variables
The primary endpoint was defined as good functionaloutcome (mRS≤2) at 3 months. Infarct volume was consid-ered as the secondary outcome variable.
2.5. TLR expression analysis
Expression of TLR3, 7, 8 and 9 was analyzed by real time-quantitative-RT-PCR on a Mx3005p system from Stratagene.For this analysis, RNA was extracted from 200 μL of EDTA-anticoagulated blood sample, with a semiautomatic robotMagnaPure Compact (Roche). RNA extracts were quantifiedwith a Nanodrop system (Thermo Scientific) and cDNA wassynthesized for each sample using the High Capacity RNA tocDNA kit (Applied Biosystems) according to the providedinstructions. The whole process was performed at T=37 Cduring 60 min, heating up to T=95 C during 5 min at the end,in a thermocycler T Professional (Biometra). Real time-quantitative-PCR was performed with commercially avail-able specific primers and probes for TLR3, TLR7, TLR8 andTLR9 (Applied biosystems). TLR amplifications were simul-taneously performed with a GAPDH amplification, which wasused as loading control. Amplification process was performedaccording to the following protocol; one cycle for 2 min atT=50 C, one cycle for 10 min at T=95 C and 60 cycles of 30 sat T=95 C and 1 min at T=60 C. Following RT–PCR, quanti-fication of gene expression was made by determining the Ct(for PCR cycle in what amplification it starts, these units areinverse to the TLR quantity), based on fluorescencedetection, within the geometric region of the semilog viewof the amplification plot. Relative quantization of targetgene expression was evaluated using the comparative Ctmethod as previously described by Ross et al. [17]. The ΔCtvalue was determined by subtracting the target Ct of eachsample from its respective GAPDH Ct value. Each value of ΔCtfor each sample was exported to a database in SPSS, to beanalyzed in combination with the clinical data. Finally, fold-changes in gene expression of the target gene wereestimated as: 2ΔCt poor outcome−ΔCt good outcome. For thiscalculation mean ΔCt for patients with good outcome andmean ΔCt for patients with poor outcome were used.
2.6. Laboratory tests
Blood samples, withdrawn from all patients on admission andat 24 h, 72 h and 7 days were collected in chemistry test
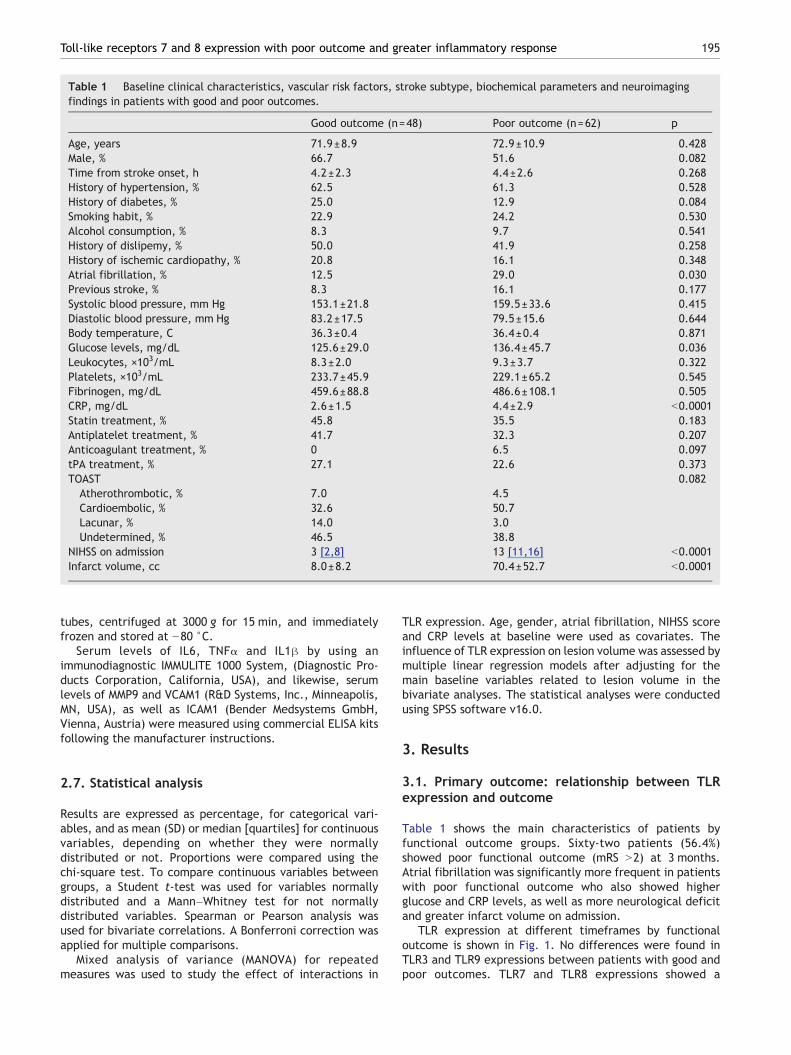
Table 1 Baseline clinical characteristics, vascular risk factors, stroke subtype, biochemical parameters and neuroimagingfindings in patients with good and poor outcomes.
Good outcome (n=48) Poor outcome (n=62) p
Age, years 71.9±8.9 72.9±10.9 0.428Male, % 66.7 51.6 0.082Time from stroke onset, h 4.2±2.3 4.4±2.6 0.268History of hypertension, % 62.5 61.3 0.528History of diabetes, % 25.0 12.9 0.084Smoking habit, % 22.9 24.2 0.530Alcohol consumption, % 8.3 9.7 0.541History of dislipemy, % 50.0 41.9 0.258History of ischemic cardiopathy, % 20.8 16.1 0.348Atrial fibrillation, % 12.5 29.0 0.030Previous stroke, % 8.3 16.1 0.177Systolic blood pressure, mm Hg 153.1±21.8 159.5±33.6 0.415Diastolic blood pressure, mm Hg 83.2±17.5 79.5±15.6 0.644Body temperature, C 36.3±0.4 36.4±0.4 0.871Glucose levels, mg/dL 125.6±29.0 136.4±45.7 0.036Leukocytes, ×103/mL 8.3±2.0 9.3±3.7 0.322Platelets, ×103/mL 233.7±45.9 229.1±65.2 0.545Fibrinogen, mg/dL 459.6±88.8 486.6±108.1 0.505CRP, mg/dL 2.6±1.5 4.4±2.9 b0.0001Statin treatment, % 45.8 35.5 0.183Antiplatelet treatment, % 41.7 32.3 0.207Anticoagulant treatment, % 0 6.5 0.097tPA treatment, % 27.1 22.6 0.373TOAST 0.082
Atherothrombotic, % 7.0 4.5Cardioembolic, % 32.6 50.7Lacunar, % 14.0 3.0Undetermined, % 46.5 38.8
NIHSS on admission 3 [2,8] 13 [11,16] b0.0001Infarct volume, cc 8.0±8.2 70.4±52.7 b0.0001
195Toll-like receptors 7 and 8 expression with poor outcome and greater inflammatory response
tubes, centrifuged at 3000 g for 15 min, and immediatelyfrozen and stored at −80 °C.
Serum levels of IL6, TNFα and IL1β by using animmunodiagnostic IMMULITE 1000 System, (Diagnostic Pro-ducts Corporation, California, USA), and likewise, serumlevels of MMP9 and VCAM1 (R&D Systems, Inc., Minneapolis,MN, USA), as well as ICAM1 (Bender Medsystems GmbH,Vienna, Austria) were measured using commercial ELISA kitsfollowing the manufacturer instructions.
2.7. Statistical analysis
Results are expressed as percentage, for categorical vari-ables, and as mean (SD) or median [quartiles] for continuousvariables, depending on whether they were normallydistributed or not. Proportions were compared using thechi-square test. To compare continuous variables betweengroups, a Student t-test was used for variables normallydistributed and a Mann–Whitney test for not normallydistributed variables. Spearman or Pearson analysis wasused for bivariate correlations. A Bonferroni correction wasapplied for multiple comparisons.
Mixed analysis of variance (MANOVA) for repeatedmeasures was used to study the effect of interactions in
TLR expression. Age, gender, atrial fibrillation, NIHSS scoreand CRP levels at baseline were used as covariates. Theinfluence of TLR expression on lesion volume was assessed bymultiple linear regression models after adjusting for themain baseline variables related to lesion volume in thebivariate analyses. The statistical analyses were conductedusing SPSS software v16.0.
3. Results
3.1. Primary outcome: relationship between TLRexpression and outcome
Table 1 shows the main characteristics of patients byfunctional outcome groups. Sixty-two patients (56.4%)showed poor functional outcome (mRS N2) at 3 months.Atrial fibrillation was significantly more frequent in patientswith poor functional outcome who also showed higherglucose and CRP levels, as well as more neurological deficitand greater infarct volume on admission.
TLR expression at different timeframes by functionaloutcome is shown in Fig. 1. No differences were found inTLR3 and TLR9 expressions between patients with good andpoor outcomes. TLR7 and TLR8 expressions showed a

Figure 1 Temporal profile of TLR expression by outcomegroup, in patients with acute ischemic stroke. Mean±SD TLR7(A) and TLR8 (B) expressions for patients with poor functionaloutcome showed a significant increase after admission up the7th day.
196 D. Brea et al.
significant increase after admission up to the 7th day forpatients with poor outcome. In the MANOVA analysis, therewas a significant interaction on TLR7 (F=15.54; pb0.0001)and TLR8 expression (F=9.46; pb0.0001), but no differencesby time point were found. Only TLR8 expression showed asignificant interaction with CRP levels (F=7.8; pb0.0001).
3.2. Secondary outcome: relationship between TLRexpression and infarct volume
Infarct volume was associated with history of diabetes(r=0.227, p=0.023), history of atrial fibrillation (r=0.208,p=0.038), CRP levels on admission (r=0.393, pb0.0001), andNIHSS on admission (r=0.560, pb0.0001).
On the other hand, no significant correlations or associa-tions were found between TLR3, TLR7 and TLR9 and infarctvolume (rb0.2). However, infarct volume was correlatedwith TLR8 expression at 24 h (r=−0.285, p=0.017), and 72 h(r=−0.394, pb0.0001). In the multivariate analysis, TLR8expression at 24 h (B,−3.6; 95%CI:−8.1 to 0.8) and 72 h (B,−5.8;95%CI: −9.9 to −1.8) was independently associated with infarct
volume after adjustment by history of diabetes and atrialfibrillation, CRP levels, and baseline stroke severity.
3.2.1. Relationship between the expressions of TLR3, 7, 8and 9 and levels of inflammatory markers
After a Bonferroni correction for multiple comparisons(n=12), TLR7 and TLR8 expressions at baseline were correlatedwith serum levels of IL1β (r=0.282, p=0.009 and r=0.324,p=0.002) and IL6 (r=0.231, p=0.036 and r=0.261, p=0.018).However no significant correlations were found between thoseTLRsandMMP9oradhesionmolecules, suchas ICAM-1orVCAM-1.No correlations were also found between TLR3 and TLR9expressions on admission and levels of any of the inflammatorymolecules analyzed on admission, at 24 h, 72 h and 7 days(Fig. 2).
4. Discussion
This is, to the best of our knowledge, the first prospectivestudy which has evaluated the relationship between intra-cellular TLR expression and brain injury in patients withacute ischemic stroke. Remarkably, greater expressions ofTLR7 and TLR8 were associated with poor functionaloutcome in ischemic stroke patients. TLR8 expression at24 h and 72 h was associated to infarct volume. Thus, TLR7and TLR8 can be considered good biomarkers of outcome forpatients with acute ischemic stroke. We also analyzed therole of TLR3 and TLR9, yet we did not find any association ofthese receptors with outcome or infarct volumes. Inaddition, TLR7 and TLR8 on admission were found to becorrelated with IL6 and IL1β but not with MMP9, ICAM1 orVCAM1. This indicates that TLR7 and TLR8 are involved in theactivation of the inflammatory response, though onlycytokines but not adhesion molecules are expressed as aconsequence of the activation of TLR7 and TLR8. Howeverthe exact mechanisms in which TLR7 and TLR8 are involved instroke pathophysiology remain to be clarified.
TLR7 and TLR8 are usually grouped with TLR3 and TLR9because they are predominantly locatedwithin endolysosomalcompartments. Their ligands are fundamentally single-strand-ed RNAs from RNA viruses [18], as well as small purine-basedanalog compounds (imidazoquinolines) [3]. TLR7 also detectsRNAs from bacteria in endolysosomes of dendritic cells [19].Since ligands of TLR7 and TLR8 are nucleic acids, these TLRsmay be activated by self nucleic acids, and to avoid thispossible interaction, they, together with TLR3 and TLR9, arelocated in intracellular compartments, detecting viral nucleicacids in late endosomes–lysosomes [20]. Because host nucleicacids are rarely accessible to these compartments, they do nottrigger the activation of TLRs. However, when necrotic/apoptotic cells are present in high amounts, a deficientclearance of cell debris can facilitate the availability of selfnucleic acids that activate TLRs [20]. Since accumulation ofapoptotic and necrotic cells is normal after stroke, self nucleicacids could actually activate TLR7 and 8, activating furtherexpression of these receptors and inflammation.
In this study we have quantified the expression of TLRs byanalyzing the expression of mRNA by quantitative RT–PCR inperipheral blood cells. The potential value of such analysison peripheral blood has been demonstrated in two studiesthat have stated the plausible values of TLR2 and TLR4 as
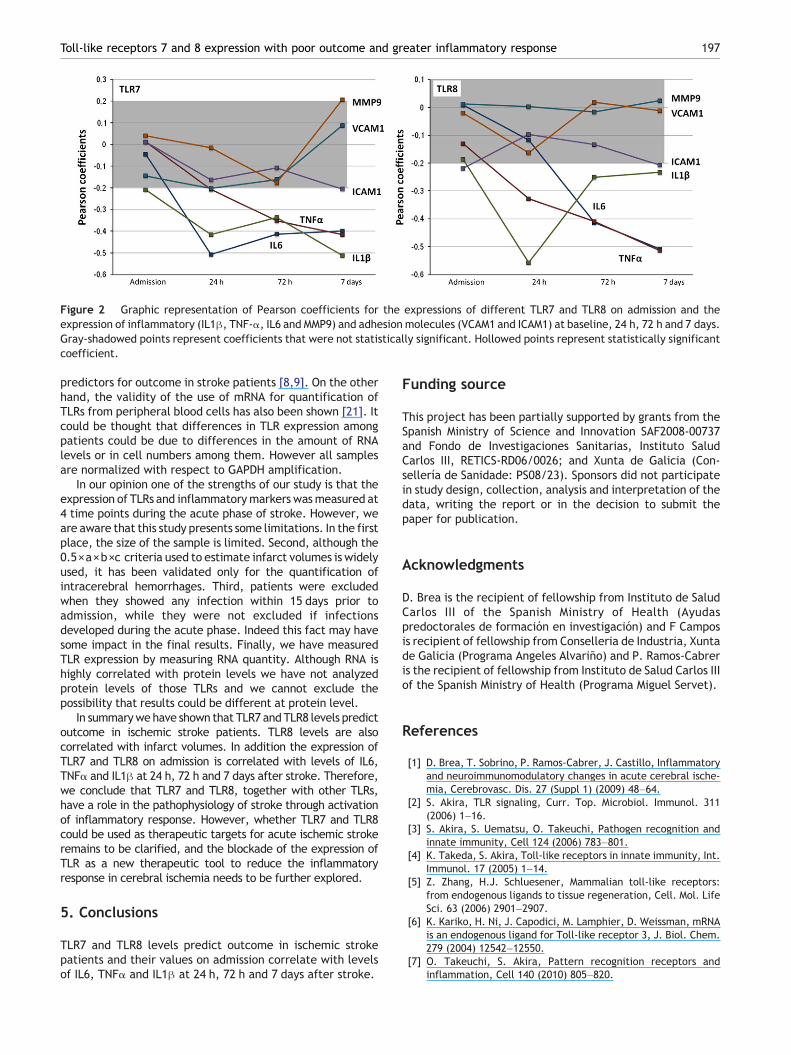
Figure 2 Graphic representation of Pearson coefficients for the expressions of different TLR7 and TLR8 on admission and theexpression of inflammatory (IL1β, TNF-α, IL6 and MMP9) and adhesion molecules (VCAM1 and ICAM1) at baseline, 24 h, 72 h and 7 days.Gray-shadowed points represent coefficients that were not statistically significant. Hollowed points represent statistically significantcoefficient.
197Toll-like receptors 7 and 8 expression with poor outcome and greater inflammatory response
predictors for outcome in stroke patients [8,9]. On the otherhand, the validity of the use of mRNA for quantification ofTLRs from peripheral blood cells has also been shown [21]. Itcould be thought that differences in TLR expression amongpatients could be due to differences in the amount of RNAlevels or in cell numbers among them. However all samplesare normalized with respect to GAPDH amplification.
In our opinion one of the strengths of our study is that theexpression of TLRs and inflammatorymarkers wasmeasured at4 time points during the acute phase of stroke. However, weare aware that this study presents some limitations. In the firstplace, the size of the sample is limited. Second, although the0.5×a×b×c criteria used to estimate infarct volumes is widelyused, it has been validated only for the quantification ofintracerebral hemorrhages. Third, patients were excludedwhen they showed any infection within 15 days prior toadmission, while they were not excluded if infectionsdeveloped during the acute phase. Indeed this fact may havesome impact in the final results. Finally, we have measuredTLR expression by measuring RNA quantity. Although RNA ishighly correlated with protein levels we have not analyzedprotein levels of those TLRs and we cannot exclude thepossibility that results could be different at protein level.
In summarywehave shown that TLR7 and TLR8 levels predictoutcome in ischemic stroke patients. TLR8 levels are alsocorrelated with infarct volumes. In addition the expression ofTLR7 and TLR8 on admission is correlated with levels of IL6,TNFα and IL1β at 24 h, 72 h and 7 days after stroke. Therefore,we conclude that TLR7 and TLR8, together with other TLRs,have a role in the pathophysiology of stroke through activationof inflammatory response. However, whether TLR7 and TLR8could be used as therapeutic targets for acute ischemic strokeremains to be clarified, and the blockade of the expression ofTLR as a new therapeutic tool to reduce the inflammatoryresponse in cerebral ischemia needs to be further explored.
5. Conclusions
TLR7 and TLR8 levels predict outcome in ischemic strokepatients and their values on admission correlate with levelsof IL6, TNFα and IL1β at 24 h, 72 h and 7 days after stroke.
Funding source
This project has been partially supported by grants from theSpanish Ministry of Science and Innovation SAF2008-00737and Fondo de Investigaciones Sanitarias, Instituto SaludCarlos III, RETICS-RD06/0026; and Xunta de Galicia (Con-sellería de Sanidade: PS08/23). Sponsors did not participatein study design, collection, analysis and interpretation of thedata, writing the report or in the decision to submit thepaper for publication.
Acknowledgments
D. Brea is the recipient of fellowship from Instituto de SaludCarlos III of the Spanish Ministry of Health (Ayudaspredoctorales de formación en investigación) and F Camposis recipient of fellowship from Conselleria de Industria, Xuntade Galicia (Programa Angeles Alvariño) and P. Ramos-Cabreris the recipient of fellowship from Instituto de Salud Carlos IIIof the Spanish Ministry of Health (Programa Miguel Servet).
References
[1] D. Brea, T. Sobrino, P. Ramos-Cabrer, J. Castillo, Inflammatoryand neuroimmunomodulatory changes in acute cerebral ische-mia, Cerebrovasc. Dis. 27 (Suppl 1) (2009) 48–64.
[2] S. Akira, TLR signaling, Curr. Top. Microbiol. Immunol. 311(2006) 1–16.
[3] S. Akira, S. Uematsu, O. Takeuchi, Pathogen recognition andinnate immunity, Cell 124 (2006) 783–801.
[4] K. Takeda, S. Akira, Toll-like receptors in innate immunity, Int.Immunol. 17 (2005) 1–14.
[5] Z. Zhang, H.J. Schluesener, Mammalian toll-like receptors:from endogenous ligands to tissue regeneration, Cell. Mol. LifeSci. 63 (2006) 2901–2907.
[6] K. Kariko, H. Ni, J. Capodici, M. Lamphier, D. Weissman, mRNAis an endogenous ligand for Toll-like receptor 3, J. Biol. Chem.279 (2004) 12542–12550.
[7] O. Takeuchi, S. Akira, Pattern recognition receptors andinflammation, Cell 140 (2010) 805–820.
198 D. Brea et al.
[8] X. Urra, A. Cervera, V. Obach, N. Climent, A.M. Planas, A.Chamorro, Monocytes Are Major Players in the Prognosis andRisk of Infection After Acute Stroke, Stroke (2009).
[9] Q.W. Yang, J.C. Li, F.L. Lu, A.Q. Wen, J. Xiang, L.L. Zhang, Z.Y.Huang, J.Z. Wang, Upregulated expression of toll-like receptor4 in monocytes correlates with severity of acute cerebralinfarction, J. Cereb. Blood Flow Metab. 28 (2008) 1588–1596.
[10] F. Hua, J. Ma, T. Ha, J.L. Kelley, R.L. Kao, J.B. Schweitzer, J.H.Kalbfleisch, D.L. Williams, C. Li, Differential roles of TLR2 andTLR4 in acute focal cerebral ischemia/reperfusion injury inmice, Brain Res. 1262 (2009) 100–108.
[11] J.R. Caso, J.M. Pradillo, O. Hurtado, J.C. Leza, M.A. Moro, I.Lizasoain, Toll-like receptor 4 is involved in subacute stress-induced neuroinflammation and in the worsening of experi-mental stroke, Stroke 39 (2008) 1314–1320.
[12] C.X. Cao, Q.W. Yang, F.L. Lv, J. Cui, H.B. Fu, J.Z. Wang,Reduced cerebral ischemia–reperfusion injury in Toll-likereceptor 4 deficient mice, Biochem. Biophys. Res. Commun.353 (2007) 509–514.
[13] Y.C. Lin, Y.M. Chang, J.M. Yu, J.H. Yen, J.G. Chang, C.J. Hu,Toll-like receptor 4 gene C119A but not Asp299Gly polymor-phism is associated with ischemic stroke among ethnic Chinesein Taiwan, Atherosclerosis 180 (2005) 305–309.
[14] S. Lehnardt, S. Lehmann, D. Kaul, K. Tschimmel, O. Hoffmann,S. Cho, C. Krueger, R. Nitsch, A. Meisel, J.R. Weber, Toll-likereceptor 2 mediates CNS injury in focal cerebral ischemia, J.Neuroimmunol. 190 (2007) 28–33.
[15] Comité ad hoc del Grupo de Estudio de EnfermedadesCerebrovasculares de la SEN, Guía para el diagnóstico ytratamiento del ictus, Prous Science, Barcelona, 2004.
[16] H.P. Adams Jr., B.H. Bendixen, L.J. Kappelle, J. Biller, B.B.Love, D.L. Gordon, E.E. Marsh III, Classification of subtype ofacute ischemic stroke. Definitions for use in a multicenterclinical trial. TOAST. Trial of Org 10172 in Acute StrokeTreatment, Stroke 24 (1993) 35–41.
[17] J.W. Ross, M.D. Ashworth, A.G. Hurst, J.R. Malayer, R.D.Geisert, Analysis and characterization of differential geneexpression during rapid trophoblastic elongation in the pigusing suppression subtractive hybridization, Reprod. Biol.Endocrinol. 1 (2003) 23.
[18] F. Heil, H. Hemmi, H. Hochrein, F. Ampenberger, C. Kirschning,S. Akira, G. Lipford, H. Wagner, S. Bauer, Species-specificrecognition of single-stranded RNA via toll-like receptor 7 and8, Science 303 (2004) 1526–1529.
[19] G. Mancuso, M. Gambuzza, A. Midiri, C. Biondo, S. Papasergi, S.Akira, G. Teti, C. Beninati, Bacterial recognition by TLR7 in thelysosomes of conventional dendritic cells, Nat. Immunol. 10(2009) 587–594.
[20] A. Iwasaki, R. Medzhitov, Toll-like receptor control of theadaptive immune responses, Nat. Immunol. 5 (2004) 987–995.
[21] N. Xu, H.P. Yao, Z. Sun, Z. Chen, Toll-like receptor 7 and 9expression in peripheral blood mononuclear cells from patientswith chronic hepatitis B and related hepatocellular carcinoma,Acta Pharmacol. Sin. 29 (2008) 239–244.