
Tolerability and dose-related effects of nebivolol in elderly patients with heart failure: Data from...
14
Tolerability and dose-related effects of nebivolol in elderly patients with heart failure: data from the SENIORS trial Daniela Dobre, MD, MPH 1 ; Dirk J. van Veldhuisen, MD, PhD 2 ; Marcus D. Flather, MD, PhD 3,4 ; Giacomo Mordenti, PhD 5 ; Marius Vintila, MD 6 ; Flora M. Haaijer-Ruskamp, PhD 7 ; Andrew J.S. Coats 8 , MD; Philip A. Poole-Wilson 4 , MD; on behalf of the SENIORS Investigators 1 Northern Centre for Healthcare Research, University Medical Centre Groningen, University of Groningen, e Netherlands 2 Department of Cardiology, University Medical Centre Groningen, University of Groningen, e Netherlands 3 Clinical Trials and Evaluation Unit, Royal Brompton and Harefield NHS Trust, London, UK 4 National Heart and Lung Institute, Imperial College of Science Technology and Medicine, London, UK 5 Clinical Research Department, Menarini Recerche SpA, Florence, Italy 6 Department of Internal Medicine & Cardiology, University Emergency Hospital “St Pantelimon”, Bucharest, Romania 7 Department of Clinical Pharmacology, University Medical Centre Groningen, University of Groningen, e Netherlands 8 Faculty of Medicine, University of Sidney, Sydney, Australia 8
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Tolerability and dose-related effects of nebivolol in elderly patients with heart failure: Data from...
Tolerability and dose-related eff ects of nebivolol in elderly patients with heart failure: data from the SENIORS trial
Daniela Dobre, MD, MPH1; Dirk J. van Veldhuisen, MD, PhD2;Marcus D. Flather, MD, PhD3,4; Giacomo Mordenti, PhD5; Marius Vintila, MD6; Flora M. Haaijer-Ruskamp, PhD7; Andrew J.S. Coats8, MD;Philip A. Poole-Wilson4, MD; on behalf of the SENIORS Investigators
1 Northern Centre for Healthcare Research, University Medical Centre Groningen, University of Groningen, Th e Netherlands2 Department of Cardiology, University Medical Centre Groningen, University of Groningen, Th e Netherlands3 Clinical Trials and Evaluation Unit, Royal Brompton and Harefi eld NHS Trust, London, UK4 National Heart and Lung Institute, Imperial College of Science Technology and Medicine, London, UK5 Clinical Research Department, Menarini Recerche SpA, Florence, Italy6 Department of Internal Medicine & Cardiology, University Emergency Hospital “St Pantelimon”, Bucharest, Romania7 Department of Clinical Pharmacology, University Medical Centre Groningen, University of Groningen, Th e Netherlands 8 Faculty of Medicine, University of Sidney, Sydney, Australia
8

Chapter 8
114
ABSTRACT
Aims To assess tolerability and dose-related eff ects of the β-blocker nebivolol in elderly patients with heart failure (HF). Methods and Results Th e SENIORS trial assessed the eff ects of nebivolol in elderly patients with HF. Th e present post-hoc analysis included patients who reached a maintenance dose or never tolerated any dose by the end of titration phase. Patients assigned to nebivolol (N=1031) were classifi ed into four groups, according to the last tolerated dose: 0 mg (n=74), low dose (1.25 or 2.5 mg, n=142), medium dose (5 mg, n=172), and target dose (10 mg, n=688). Patients tolerating low doses were remarkable similar to those tolerating high doses, although they had lower systolic and diastolic blood pressure, and were slightly older. Further, they had a higher prevalence of comorbidities. After adjustment, all cause mortality or cardiovascular (CV) hospitalisation was signifi cantly reduced in the target dose group compared to placebo (HR 0.75; 95% CI 0.63-0.90). Th e medium dose group had rather a similar benefi t compared to the target dose group, although not statistically signifi cant (HR 0.73; 95% CI 0.52-1.02), while the low dose group achieved no signifi cant benefi t (HR 0.88; 95% CI 0.64-1.20). Patients unable to tolerate any dose of nebivolol had a markedly increased risk of death or CV hospitalisation (HR 1.95; 95% CI 1.38-2.75).Conclusions Th e β-blocker nebivolol is well tolerated in elderly HF population. High doses (i.e medium to target) appear superior to low doses. Patients unable to tolerate any dose of nebivolol have the worst outcome.

Tolerability and dose-related eff ects of nebivolol in elderly patients with HF: data from the SENIORS trial
115
INTRODUCTION
Heart failure (HF) has emerged as a major public health problem among the elderly population. In Europe, 6-10% of people aged over 65 years have the disorder, and the average age of the patient in the community is 76 years.1-3 Th e syndrome of HF may arise in presence of either a depressed or a normal left ventricular ejection fraction (LVEF).4 In older patients, HF with preserved LVEF is common.5,6
In elderly patients with HF prescription of a β-blocker raises two major concerns, tolerability and effi cacy. Recent data suggest that β-blockers are well tolerated in the elderly7, yet target doses may be diffi cult to achieve in certain subgroups, such as patients with low blood pressure, and those with advanced disease.8-10 In turn, prescription of low doses may raise concerns over effi cacy since older patients may respond diff erently to medication.11
In patients with HF, one randomised trial has shown that β-blockade produce a dose-dependent improvement in survival.12 In contrast, subgroup analyses in major β-blocker trials have not shown a clear dose-response eff ect.13,14 Th e average age of the patients in these trials has been 63 years, and patients with a LVEF > 40% were excluded.
Th e SENIORS trial assessed the eff ects of the β-blocker nebivolol in elderly patients (age ≥ 70 years) with HF. About one third of the patients had a preserved LVEF.15 Nebivolol was initiated with a low dose, and, if tolerated, was carefully up-titrated to a target dose of 10 mg daily, or the highest tolerated dose. Overall, nebivolol reduced the combined end point of death or cardiovascular admission. Th is outcome represented an average-dose eff ect of nebivolol, as the trial was not designed as a dose-response study.
In this study, we aimed to assess tolerability and dose-related eff ects of nebivolol in eldely patients from the SENIORS trial.
METHODS
PatientsTh e present study is a post-hoc analysis of the SENIORS trial. Th e study design and results of SENIORS have been published previously.15 Briefl y, 2128 patients aged ≥ 70 years and with a history of HF were randomly assigned to nebivolol (1067 patients) or placebo (1061 patients). Th e initial dose of nebivolol was 1.25 mg once daily, and, if tolerated,
Chapter 8
116
it was increased to 2.5 and 5 mg, respectively, every 1-2 weeks, reaching a target of 10 mg once daily over a maximum of 16 weeks. Up-titration could be stopped or delayed depending on symptoms, side eff ects, or the judgment of the local investigator.
Th is study examine patients reaching a maintenance dose or not tolerating any dose by the end of titration phase. We analysed the data by classifying the patients assigned to nebivolol into four groups, according to the dose achieved at the end of the titration phase: 0 mg (patients who could not tolerate any dose), low dose (1.25 or 2.5 mg), medium dose (5 mg), and target dose (10 mg). A total of 67 patients (36 in the nebivolol group and 31 in the placebo group) were excluded from this analysis. Th ese were patients who discontinued the study before the end of titration phase despite initial tolerance of study drug. In the nebivolol group, discontinuation took place due to following reasons: patient request (16), death (11), lost to follow-up (4), adverse event, ie. stroke (1), hospitalisation (2), and worsening HF (2). In the placebo group, discontinuation took place as follows: patient request (17), death (9), lost to follow-up (1), adverse event, ie. myocardial infarction (1), patient not taking medication correctly (2), and mandatory indication to β-blocker (1). By excluding these patients, we identifi ed the group truly intolerant to any dose during up-titration. Th e population of the present study consisted therefore of 1031 patients in the nebivolol group and 1030 patients in the placebo group.
Clinical outcomesTh e primary outcome was the composite of death or cardiovascular (CV) hospitalisation. Secondary outcomes included the composite of CV mortality or CV hospitalisation, and the composite of all-cause mortality or all-cause hospitalisation. We analysed only composite outcomes because the number of events in medium and low-dose nebivolol groups was too small for appropriate analysis of individual outcomes.
Statistical analysisLogistic regression analysis was used to assess the relationship between each baseline characteristic and dose groups. Th e association between dose of nebivolol and clinical outcomes was assessed using multivariate Cox proportional hazard models. We controlled for baseline characteristics that had an independent association with the dose achieved up to p < 0.10. Adjustment was performed with the following variables: age, gender, heart rate, systolic blood pressure, diastolic blood pressure, creatinine, hypertension, myocardial infarction, prior CABG, prior PTCA, and prescription of aldosterone antagonists, antiarrhythmics, and calcium antagonists. In the Cox proportional analysis

Tolerability and dose-related eff ects of nebivolol in elderly patients with HF: data from the SENIORS trial
117
we compared each dose group with all placebo patients that reached the maintenance dose or never tolerated any titrated dose (N=1030). Results are expressed as hazard ratio (HR) with 95% confi dence interval (CI). Survival curves were estimated by the Kaplan-Meier method. Statistical analysis was performed by using SAS software (version 9.1, SAS Institute, NC, USA).
RESULTS
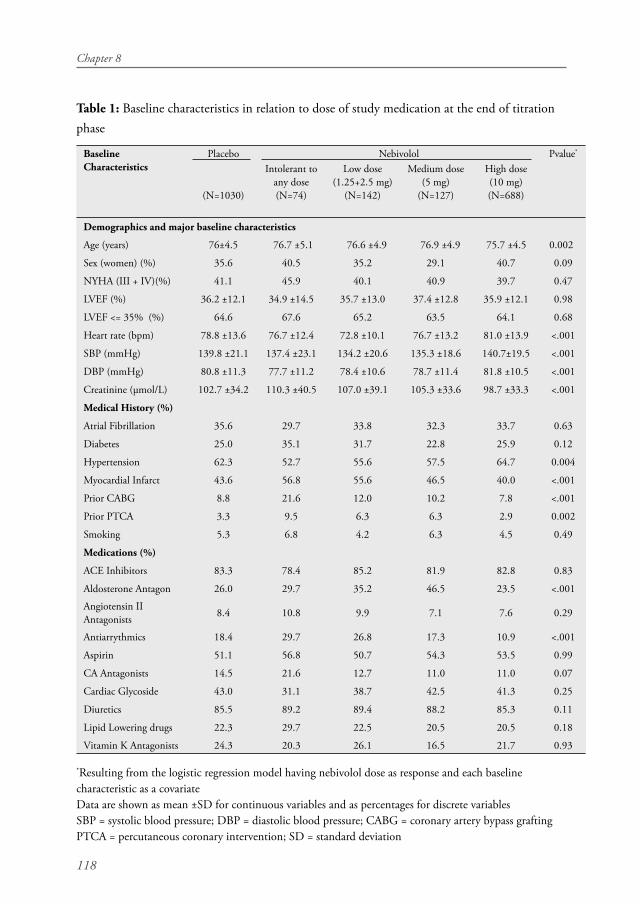
Baseline patient characteristicsPatient characteristics at baseline are shown in Table 1. In the nebivolol group (N=1031) a total of 668 (67%) patients reached the target dose, while 127 (12%), and 142 (14%) reached medium and target doses, respectively. A total of 74 (7%) patients were unable to tolerate any dose of nebivolol during up-titration. Patients who reached lower doses were remarkable similar with those who reached target doses, although they were signifi cantly older, and had a lower systolic and diastolic blood pressure. Also, they were more likely to have a lower heart rate, and higher creatinine levels. Patients tolerating low doses of nebivolol were also those who had a higher prevalence of myocardial infarction as the underlying cause of HF, whereas history of hypertension was more frequent among those tolerating target doses. No signifi cant diff erence was observed across the four groups with regard to well-defi ned measures of HF severity, such as NYHA class, and LVEF. Also, there was no signifi cant diff erence in associated comorbidities, such as atrial fi brillation or diabetes. However, there was a pattern of more severe disease among patients not tolerating any dose or low doses of medication. Th e use of antiarrythmics and calcium antagonists was higher among patients tolerating low doses, whereas a similar proportion received ACE Inhibitors or digitalis.
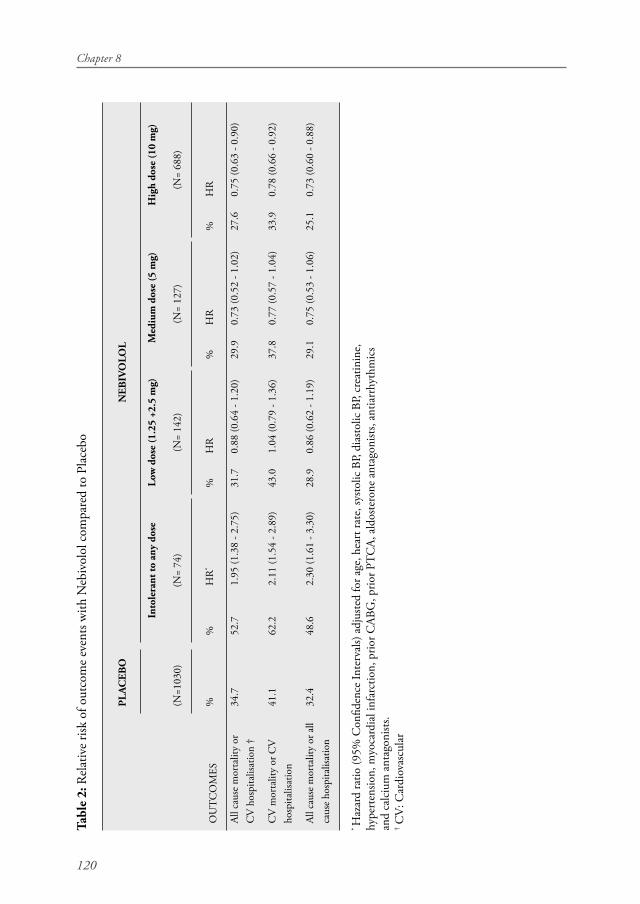
Clinical outcomesTh e proportion of patients who suff ered death or CV admission decreased with an increasing dose of nebivolol. Similarly, a higher proportion of patients on low doses experienced a secondary outcome.
Chapter 8
118
Table 1: Baseline characteristics in relation to dose of study medication at the end of titration phase
Baseline Characteristics
Placebo Nebivolol Pvalue*
(N=1030)
Intolerant to any dose(N=74)
Low dose(1.25+2.5 mg)
(N=142)
Medium dose(5 mg)
(N=127)
High dose(10 mg)(N=688)
Demographics and major baseline characteristics
Age (years) 76±4.5 76.7 ±5.1 76.6 ±4.9 76.9 ±4.9 75.7 ±4.5 0.002
Sex (women) (%) 35.6 40.5 35.2 29.1 40.7 0.09
NYHA (III + IV)(%) 41.1 45.9 40.1 40.9 39.7 0.47
LVEF (%) 36.2 ±12.1 34.9 ±14.5 35.7 ±13.0 37.4 ±12.8 35.9 ±12.1 0.98
LVEF <= 35% (%) 64.6 67.6 65.2 63.5 64.1 0.68
Heart rate (bpm) 78.8 ±13.6 76.7 ±12.4 72.8 ±10.1 76.7 ±13.2 81.0 ±13.9 <.001
SBP (mmHg) 139.8 ±21.1 137.4 ±23.1 134.2 ±20.6 135.3 ±18.6 140.7±19.5 <.001
DBP (mmHg) 80.8 ±11.3 77.7 ±11.2 78.4 ±10.6 78.7 ±11.4 81.8 ±10.5 <.001
Creatinine (μmol/L) 102.7 ±34.2 110.3 ±40.5 107.0 ±39.1 105.3 ±33.6 98.7 ±33.3 <.001
Medical History (%)
Atrial Fibrillation 35.6 29.7 33.8 32.3 33.7 0.63
Diabetes 25.0 35.1 31.7 22.8 25.9 0.12
Hypertension 62.3 52.7 55.6 57.5 64.7 0.004
Myocardial Infarct 43.6 56.8 55.6 46.5 40.0 <.001
Prior CABG 8.8 21.6 12.0 10.2 7.8 <.001
Prior PTCA 3.3 9.5 6.3 6.3 2.9 0.002
Smoking 5.3 6.8 4.2 6.3 4.5 0.49
Medications (%)
ACE Inhibitors 83.3 78.4 85.2 81.9 82.8 0.83
Aldosterone Antagon 26.0 29.7 35.2 46.5 23.5 <.001
Angiotensin II Antagonists 8.4 10.8 9.9 7.1 7.6 0.29
Antiarrythmics 18.4 29.7 26.8 17.3 10.9 <.001
Aspirin 51.1 56.8 50.7 54.3 53.5 0.99
CA Antagonists 14.5 21.6 12.7 11.0 11.0 0.07
Cardiac Glycoside 43.0 31.1 38.7 42.5 41.3 0.25
Diuretics 85.5 89.2 89.4 88.2 85.3 0.11
Lipid Lowering drugs 22.3 29.7 22.5 20.5 20.5 0.18
Vitamin K Antagonists 24.3 20.3 26.1 16.5 21.7 0.93
*Resulting from the logistic regression model having nebivolol dose as response and each baseline characteristic as a covariateData are shown as mean ±SD for continuous variables and as percentages for discrete variablesSBP = systolic blood pressure; DBP = diastolic blood pressure; CABG = coronary artery bypass graftingPTCA = percutaneous coronary intervention; SD = standard deviation

Tolerability and dose-related eff ects of nebivolol in elderly patients with HF: data from the SENIORS trial
119
In univariate survival analysis, nebivolol in high dose was associated with a signifi cant reduction of all cause mortality or CV hospitalisation compared to placebo (HR 0.74; 95% CI 0.62-0.88). Nebivolol in medium and low dose was associated with a non signifi cant eff ect (HR 0.81; 95% CI 0.58-1.13, and HR 0.94, 95% CI 0.69-1.29, respectively). Patients unable to tolerate any dose of nebivolol had a markedly risk of death or CV admission (HR 2.15, 95% CI 1.55-3.00).
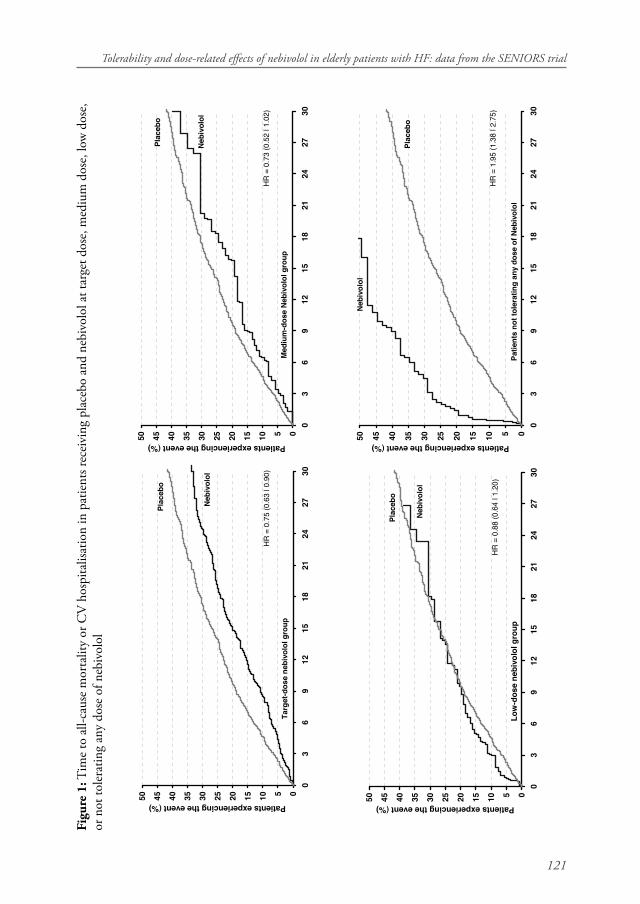
After adjustment, nebivolol in target dose remained associated with a signifi cant reduction of all cause mortality or CV hospitalisation (HR 0.75; 95% CI 0.63-0.90) (Table 2). Nebivolol in medium dose had a similar benefi t to the target dose (∼25% relative risk reduction), although of borderline statistical signifi cance (HR 0.73; 95% CI 0.52-1.02). In contrast, nebivolol in the low dose group achieved no signifi cant benefi t (HR 0.88; 95% CI 0.64-1.20). Patients unable to tolerate any dose of nebivolol remained with the worst outcome, with two-fold higher risk of death or CV hospitalisation (HR 1.95; 95% CI 1.38-2.75).
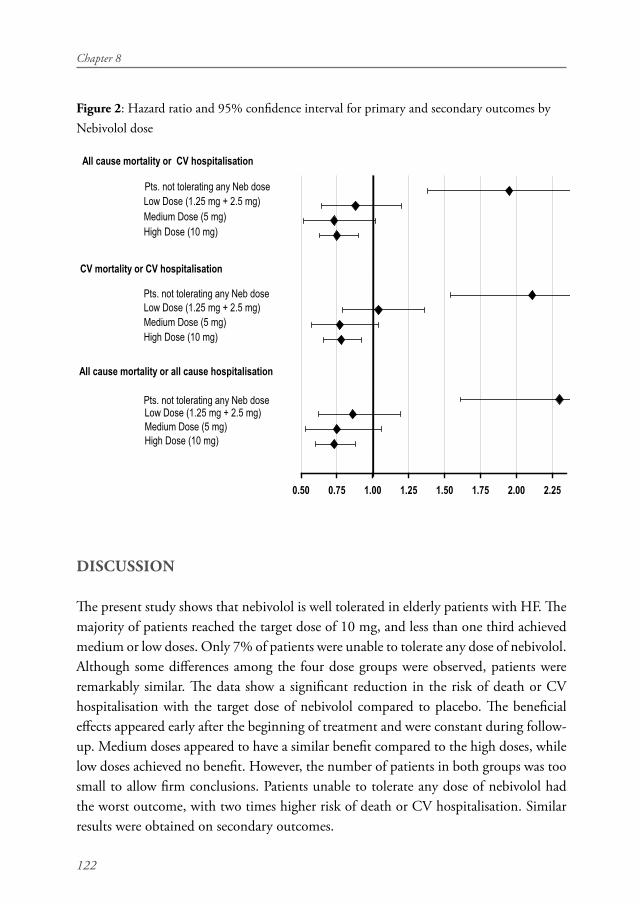
Figure 1 shows the Kaplan Meier survival curves in patients receiving nebivolol at diff erent doses or placebo. Th e benefi cial eff ects of target- and medium doses of nebivolol on primary outcome appeared early after the end of titration phase and were constant during follow-up. Patients intolerant to any dose of nebivolol had a clear higher risk of death or CV hospitalisation compared to the placebo. Similar results were obtained on secondary outcomes (Table 2 and Figure 2).
Chapter 8
120
Tabl
e 2:
Rel
ativ
e ris
k of
out
com
e ev
ents
with
Neb
ivol
ol c
ompa
red
to P
lace
bo
OU
TC
OM
ES
PLA
CEB
ON
EBIV
OLO
L
Into
lera
nt to
any
dos
eLo
w d
ose
(1.2
5 +2
.5 m
g)
Med
ium
dos
e (5
mg)
H
igh
dose
(10
mg)
(N=1
030)
(N=
74)
(N=
142)
(N=
127)
(N=
688)
%%
HR
*%
HR
%
HR
%H
R
All c
ause
mor
talit
y or
C
V h
ospi
talis
atio
n †
34.7
52.7
1.95
(1.3
8 - 2
.75)
31.7
0.88
(0.6
4 - 1
.20)
29.9
0.73
(0.5
2 - 1
.02)
27.6
0.75
(0.6
3 - 0
.90)
CV
mor
talit
y or
CV
ho
spita
lisat
ion
41.1
62.2
2.11
(1.5
4 - 2
.89)
43.0
1.04
(0.7
9 - 1
.36)
37.8
0.77
(0.5
7 - 1
.04)
33.9
0.78
(0.6
6 - 0
.92)
All c
ause
mor
talit
y or
all
caus
e ho
spita
lisat
ion
32.4
48.6
2.30
(1.6
1 - 3
.30)
28.9
0.86
(0.6
2 - 1
.19)
29.1
0.75
(0.5
3 - 1
.06)
25.1
0.73
(0.6
0 - 0
.88)
* H
azar
d ra
tio (9
5% C
onfi d
ence
Inte
rval
s) a
djus
ted
for a
ge, h
eart
rate
, sys
tolic
BP,
dias
tolic
BP,
crea
tinin
e,
hype
rten
sion,
myo
card
ial i
nfar
ctio
n, p
rior C
ABG
, prio
r PT
CA,
ald
oste
rone
ant
agon
ists,
antia
rrhy
thm
ics
and
calc
ium
ant
agon
ists.
† CV
: Car
diov
ascu
lar
Tolerability and dose-related eff ects of nebivolol in elderly patients with HF: data from the SENIORS trial
121
Figu
re 1
: Tim
e to
all-
caus
e m
orta
lity
or C
V h
ospi
talis
atio
n in
pat
ient
s rec
eivi
ng p
lace
bo a
nd n
ebiv
olol
at t
arge
t dos
e, m
ediu
m d
ose,
low
dos
e,
or n
ot to
lera
ting
any
dose
of n
ebiv
olol
05101520253035404550
03
69
1215
1821
2427
30
Patients experiencing the event (%)
HR
= 0
.75
(0.6
3 | 0
.90)
Tar
get
-do
se n
ebiv
olo
l gro
up
Neb
ivo
lol
Pla
ceb
o
05101520253035404550
03
69
1215
1821
2427
30
Patients experiencing the event (%)
HR
= 0
.73
(0.5
2 | 1
.02)
Med
ium
-do
se N
ebiv
olo
l gro
up
Neb
ivo
lol
Pla
ceb
o
05101520253035404550
03
69
1215
1821
2427
30
Lo
w-d
ose
neb
ivo
lol g
rou
p
Patients experiencing the event (%)
HR
= 0
.88
(0.6
4 | 1
.20)
Neb
ivo
lol
Pla
ceb
o
05101520253035404550
03
69
1215
1821
2427
30
Patients experiencing the event (%)
HR
= 1
.95
(1.3
8 | 2
.75)
Pla
ceb
o
Neb
ivo
lol
Pat
ien
ts n
ot
tole
rati
ng
an
y d
ose
of
Neb
ivo
lol
05101520253035404550
03
69
1215
1821
2427
30
Lo
w-d
ose
neb
ivo
lol g
rou
p
Patients experiencing the event (%)
HR
= 0
.88
(0.6
4 | 1
.20)
Neb
ivo
lol
Pla
ceb
o
Chapter 8
122
Figure 2: Hazard ratio and 95% confi dence interval for primary and secondary outcomes by Nebivolol dose
0.50 0.75 1.00 1.25 1.50 1.75 2.00 2.25
High Dose (10 mg)Medium Dose (5 mg)Low Dose (1.25 mg + 2.5 mg)
High Dose (10 mg)Medium Dose (5 mg)Low Dose (1.25 mg + 2.5 mg)
High Dose (10 mg)Medium Dose (5 mg)Low Dose (1.25 mg + 2.5 mg)
All cause mortality or CV hospitalisation
CV mortality or CV hospitalisation
All cause mortality or all cause hospitalisation
Pts. not tolerating any Neb dose
Pts. not tolerating any Neb dose
Pts. not tolerating any Neb dose
DISCUSSION
Th e present study shows that nebivolol is well tolerated in elderly patients with HF. Th e majority of patients reached the target dose of 10 mg, and less than one third achieved medium or low doses. Only 7% of patients were unable to tolerate any dose of nebivolol. Although some diff erences among the four dose groups were observed, patients were remarkably similar. Th e data show a signifi cant reduction in the risk of death or CV hospitalisation with the target dose of nebivolol compared to placebo. Th e benefi cial eff ects appeared early after the beginning of treatment and were constant during follow-up. Medium doses appeared to have a similar benefi t compared to the high doses, while low doses achieved no benefi t. However, the number of patients in both groups was too small to allow fi rm conclusions. Patients unable to tolerate any dose of nebivolol had the worst outcome, with two times higher risk of death or CV hospitalisation. Similar results were obtained on secondary outcomes.
Tolerability and dose-related eff ects of nebivolol in elderly patients with HF: data from the SENIORS trial
123
An important novel fi nding of the present study is that patients unable to tolerate any dose of nebivolol have the worst prognosis, on all clinical outcomes. Th e tolerability of nebivolol was dependent on the clinical status, as patients unable to tolerate any dose had lower systolic and distolic blood pressure, and lower heart rate. Further, they were slightly older, and had a higher prevalence of renal dysfunction and diabetes. However, it is of notice that patients unable to tolerate any dose did not diff er signifi cantly on well accepted markers of severity, such as LVEF. Th is is in consent with a previous study which shows that severity of HF, per se, does not appear to be a predictor of successful β-blocker titration in patients with idiopatic dilated cardiomyopathy. Instead, rather preserved blood pressure may be a predictor of normal titration.16 However, another study has found LVEF, along with low diastolic blood pressure, advanced age and chronic obstructive airway disease (COPD) as a predictor of tolerability in elderly patients with HF.7 While tolerability of nebivolol was clearly dependent on the clinical profi le, it is also possible that physicians were more likely to withhold the treatment if side eff ects occurred in patients with such profi le, i.e were older, and had lower blood pressure. Given the markedly increased risk on all outcomes in these patients, eff orts should be made to initiate β-blocker therapy.
Most RCTs with β-blockers in HF have not been designed as dose-response studies. To date, only the MOCHA trial, a small, 6-month study was designed to evaluate the dose-related eff ects of carvedilol in patients with mild to moderate HF. Th e study found a dose-related improvement in mortality and LVEF. In contrast to these fi ndings, posthoc subgroup analyses in both MERIT-HF and CIBIS II trials did not show a clear dose-response eff ect of metoprolol and bisoprolol on survival when compared to placebo.13,14 Subgroup analysis in the COMET trial has shown a higher benefi t of target versus subtarget doses of β-blockers, but subtarget doses included patients on both medium and low doses.17 However, posthoc fi ndings are generally limited by the fact that sicker patients are usually prescribed lower doses of β-blockers, when they may be the ones that need β-blockers the most.18
Data from observational studies are contradictory. A large observational study has found a similar benefi t on survival with prescription of high and low dose β-blocker therapy.19 In contrast, in the Euro Heart Failure Survey patients who were treated with high doses of β-blockers achieved a higher benefi t than patients treated with low doses.20 In a cohort of patients with advanced HF and preserved LVEF also a higher benefi t of high-dose therapy was observed.21 However, in observational studies high dose was defi ned as ≥ 50% of target dose achieved in RCTs, and therefore no clear distinction between the eff ect of target, medium and low dose therapy was made. Th e results of

Chapter 8
124
these studies rather suggest that patients who achieve at least medium doses do better than those on lower doses. In contrast to these studies, our trial data show the diff erential eff ects of various nebivolol doses. While target and medium doses appear to achieve a similar benefi t, lower doses seem the least benefi cial.
Th e titration of β-blockers in clinical trials is performed with a gradual increase in dosage guided by tolerance until the target dose is achieved. Compared to the randomised trial setting, in clinical practice a lower percentage of patients may receive target doses, and more patients may receive medium or low doses.21 Th e important fi nding of our study is that even medium doses of nebivolol may be eff ective in elderly HF population.
Th e proportion of patients who reached the target dose in SENIORS is higher than that reported in previous β-blocker trials.13,14 Nebivolol is a beta-1-selective blocker whose haemodynamic profi le is diff erent from that of classical β-blockers. Its mechanism of action combines beta-adrenergic blocking activity with vasodilating properties mediated by nitric oxide modulation on endothelial cells.22,23 Th is good tolerability of nebivolol may be related to its peculiar vasodilating properties.
Our study has a number of limitations. First, since it is a post-hoc analysis, it is not possible to ascertain whether a particular dose is optimal. Patients were not randomised to receive diff erent doses of nebivolol, and the dose prescribed was infl uenced by patients’ characteristics and physicians’ decisions. Second, medium and low dose groups included a small number of patients, and the analysis may have lacked the power to demonstrate a statistically signifi cant eff ect. Th ird, we assessed only composite outcomes as primary and secondary end-points, as the number of events in medium and low-dose nebivolol groups was too small for appropriate analysis of individual outcomes.
In conclusion, nebivolol is well tolerated in elderly heart failure patients. High doses (i.e medium to target) appear superior to low doses. Patients unable to tolerate any dose of nebivolol have the worst outcome.
REFERENCES
1. Cowie MR, Wood DA, Coats AJ, Th ompson SG, Suresh V, Poole-Wilson PA, Sutton GC. Survival of patients with a new diagnosis of heart failure: a population based study. Heart 2000;83:505-510.2. Kupari M, Lindroos M, Iivanainen AM, Heikkila J, Tilvis R. Congestive heart failure in old age: prevalence, mechanisms and 4-year prognosis in the Helsinki Ageing Study. J Intern Med 1997;241:387-394.
Tolerability and dose-related eff ects of nebivolol in elderly patients with HF: data from the SENIORS trial
125
3. Mosterd A, Hoes AW, de Bruyne MC, Deckers JW, Linker DT, Hofman A, Grobbee DE. Prevalence of heart failure and left ventricular dysfunction in the general population; Th e Rotterdam Study. Eur Heart J 1999;20:447-455.4. Gandhi SK, Powers JC, Nomeir AM, Fowle K, Kitzman DW, Rankin KM, Little WC. Th e pathogenesis of acute pulmonary edema associated with hypertension. N Engl J Med 2001;344:17-22.5. Masoudi FA, Havranek EP, Smith G, Fish RH, Steiner JF, Ordin DL, Krumholz HM. Gender, age, and heart failure with preserved left ventricular systolic function. J Am Coll Cardiol 2003;41:217-223.6. Pernenkil R, Vinson JM, Shah AS, Beckham V, Wittenberg C, Rich MW. Course and prognosis in patients > or = 70 years of age with congestive heart failure and normal versus abnormal left ventricular ejection fraction. Am J Cardiol 1997;79:216-219.7. Krum H, Hill J, Fruhwald F, Sharpe C, Abraham G, Zhu JR, Poy C, Kragten JA. Tolerability of beta-blockers in elderly patients with chronic heart failure: the COLA II study. Eur J Heart Fail 2006;8:302-307.8. Baxter AJ, Spensley A, Hildreth A, Karimova G, O’Connell JE, Gray CS. Beta blockers in older persons with heart failure: tolerability and impact on quality of life. Heart 2002;88:611-614.9. Tandon P, McAlister FA, Tsuyuki RT, Hervas-Malo M, Dupuit R, Ezekowitz J, Cujec B, Armstrong PW. Th e use of beta-blockers in a tertiary care heart failure clinic: dosing, tolerance, and outcomes. Arch Intern Med 2004;164:769-774.10. Macdonald PS, Keogh AM, Aboyoun CL, Lund M, Amor R, McCaff rey DJ. Tolerability and effi cacy of carvedilol in patients with New York Heart Association class IV heart failure. J Am Coll Cardiol 1999;33:924-931.11. Lamy PP. Physiological changes due to age. Pharmacodynamic changes of drug action and implications for therapy. Drugs Aging 1991;1:385-404.12. Bristow MR, Gilbert EM, Abraham WT, Adams KF, Fowler MB, Hershberger RE, Kubo SH, Narahara KA, Ingersoll H, Krueger S, Young S, Shusterman N. Carvedilol produces dose-related improvements in left ventricular function and survival in subjects with chronic heart failure. MOCHA Investigators. Circulation 1996;94:2807-2816.13. Simon T, Mary-Krause M, Funck-Brentano C, Lechat P, Jaillon P. Bisoprolol dose- response relationship in patients with congestive heart failure: a subgroup analysis in the cardiac insuffi ciency bisoprolol study(CIBIS II). Eur Heart J 2003;24:552-559.14. Wikstrand J, Hjalmarson A, Waagstein F, Fagerberg B, Goldstein S, Kjekshus J, Wedel H. Dose of Metoprolol CR/XL and clinical outcomes in patients with heart failure - Analysis of the experience in Metoprolol CR/XL Randomized Intervention Trial in Chronic Heart Failure (MERIT-HF). J Am Coll Cardiol 2002;40:491-498.
Chapter 8
126
15. Flather MD, Shibata MC, Coats AJ, Van Veldhuisen DJ, Parkhomenko A, Borbola J, Cohen-Solal A, Dumitrascu D, Ferrari R, Lechat P, Soler-Soler J, Tavazzi L, Spinarova L, Toman J, Bohm M, Anker SD, Th ompson SG, Poole-Wilson PA. Randomized trial to determine the eff ect of nebivolol on mortality and cardiovascular hospital admission in elderly patients with heart failure (SENIORS). Eur Heart J 2005;26:215-225.16. Anthonio RL, Van Veldhuisen DJ, Breekland A, Crijns HJ, van Gilst WH. Beta-blocker titration failure is independent of severity of heart failure. Am J Cardiol 2000;85:509-12, A11.17. Metra M, Torp-Pedersen C, Swedberg K, Cleland JG, Di Lenarda A, Komajda M, Remme WJ, Lutiger B, Scherhag A, Lukas MA, Charlesworth A, Poole-Wilson PA. Infl uence of heart rate, blood pressure, and beta-blocker dose on outcome and the diff erences in outcome between carvedilol and metoprolol tartrate in patients with chronic heart failure: results from the COMET trial. Eur Heart J 2005;26:2259-2268.18. Rouleau JL, Roecker EB, Tendera M, Mohacsi P, Krum H, Katus HA, Fowler MB, Coats AJ, Castaigne A, Scherhag A, Holcslaw TL, Packer M. Infl uence of pretreatment systolic blood pressure on the eff ect of carvedilol in patients with severe chronic heart failure: the Carvedilol Prospective Randomized Cumulative Survival (COPERNICUS) study. J Am Coll Cardiol 2004;43:1423-1429.19. Sin DD, McAlister FA. Th e eff ects of beta-blockers on morbidity and mortality in a population-based cohort of 11,942 elderly patients with heart failure. Am J Med 2002;113:650-656.20. Lenzen MJ, Boersma E, Reimer WJ, Balk AH, Komajda M, Swedberg K, Follath F, Jimenez-Navarro M, Simoons ML, Cleland JG. Under-utilization of evidence-based drug treatment in patients with heart failure is only partially explained by dissimilarity to patients enrolled in landmark trials: a report from the Euro Heart Survey on Heart Failure. Eur Heart J 2005;26:2706-2713.21. Dobre D, Van Veldhuisen DJ, DeJongste MJL, Lucas C, Sanderman R, Ranchor AV, Haaijer-Ruskamp FM. Prescription of beta blockers in patients with advanced heart failure and preserved left ventricular ejection fraction. Clinical implications and survival. Eur J Heart Fail 2006;10.1016/j.ejheart.2006.07.008.22. Ignarro LJ, Byrns RE, Trinh K, Sisodia M, Buga GM. Nebivolol: a selective beta(1)- adrenergic receptor antagonist that relaxes vascular smooth muscle by nitric oxide- and cyclic GMP-dependent mechanisms. Nitric Oxide 2002;7:75-82.23. Ignarro LJ. Experimental evidences of nitric oxide-dependent vasodilatory activity of nebivolol, a third-generation beta-blocker. Blood Press Suppl 2004;1:2-16.




















