
Cobalamin: a critical vitamin in the elderly
11
Review Cobalamin: a critical vitamin in the elderly Maike Wolters, Ph.D., * Alexander Stro ¨hle, Ph.D-student, and Andreas Hahn, Prof. Nutrition Physiology and Human Nutrition Unit, Department of Food Science, Centre of Applied Chemistry, University of Hanover, D-30453 Hannover, Germany Available online 11 June 2004 Abstract Vitamin B 12 deficiency is a common problem in elderly subjects. If a serum cobalamin level of about 150 pmol/L (200 pg/mL) is considered normal, 10– 15% of the elderly are deficient. Today, however, a threshold of 220– 258 pmol/L (300 –350 pg/mL) is recognized as desirable in the elderly, or else sensitive markers like the blood concentration of homocysteine or methylmalonic acid (MMA) are used. Then the prevalence of cobalamin deficiency rises to up to 43%. In the elderly, this high prevalence of poor cobalamin status is predominantly caused by atrophic gastritis type B. Atrophic gastritis results in declining gastric acid and pepsinogen secretion, and hence decreasing intestinal absorption of the cobalamin protein complexes from food. About 20 – 50% of the elderly are affected. Furthermore, the reduced acid secretion leads to an alkalinization of the small intestine, which may result in bacterial overgrowth and thus to a further decrease of the bioavailability of the vitamin. In addition, some drugs such as proton pump inhibitors or H2 receptor antagonists inhibit the intestinal absorption of vitamin B 12 . An already moderately reduced vitamin B 12 level is associated with vascular disease and neurocognitive disorders such as depression and impaired cognitive performance. Furthermore, a poor vitamin B 12 status is assumed to be involved in the development and progression of dementia (e.g., Alzheimer’s dementia). This is especially observable if the folic acid status is reduced as well. Due to the insecure supply, the cobalamin status of elderly persons (z60 years) should be regularly controlled and a general supplementation with vitamin B 12 (>50 Ag/day) should be considered. D 2004 The Institute For Cancer Prevention and Elsevier Inc. All rights reserved. Keywords: Vitamin B 12 ; Cobalamin; Homocysteine; Methylmalonic acid; Elderly; Atrophic gastritis; Vitamin – drug interactions; Atherosclerosis; Neurocognitive function Introduction There is a variety of reasons why elderly, especially geriatric subjects, are at high risk for nutrient deficiencies including age-associated physiological changes, chronic diseases, and a high prevalence of drug intake. Vitamin B 12 deficiency is one of the most important problems in the nutrition of the elderly [1,2] since the absorption of cobal- amin is often reduced in this group [3,4]. Current inves- tigations indicate that insufficient vitamin B 12 status may increase the risk for atherosclerotic [5–7] and neurodegen- erative diseases [2,8]. In the meanwhile, several nutrition boards recommend monitoring the vitamin B 12 status of elderly people and identifying risk persons at an early stage. The aim of this review is to describe the age-associated changes in cobalamin metabolism and to show pathophys- iological and therapeutic consequences. Metabolic function and sources of vitamin B 12 Vitamin B 12 contains a cobalt-centered corrin nucleus and shows a complex structure. The term vitamin B 12 includes all corrinoids qualitatively exhibiting the biolog- ical activity of cyanocobalamin. The coenzymatically ac- tive forms of vitamin B 12 are adenosylcobalamin and methylcobalamin, which are involved in two enzymatic reactions in human metabolism. One reaction requiring methylcobalamin is the remethylation of homocysteine to methionine catalyzed by the methionine synthetase [9]. In this reaction, 5-methyl tetrahydrofolic acid (5-methyl-FH 4 ) is involved as a methyl group donor (Fig. 1), whereas cobalamin is just intermediate acceptor of the methyl 0091-7435/$ - see front matter D 2004 The Institute For Cancer Prevention and Elsevier Inc. All rights reserved. doi:10.1016/j.ypmed.2004.04.047 * Corresponding author. Institute of Food Science, Department of Applied Chemistry, University of Hannover, Wunstorfer Str. 14, D-30453 Hannover, Germany. Fax: +49-511-762-5729. E-mail address: [email protected] (M. Wolters). www.elsevier.com/locate/ypmed Preventive Medicine 39 (2004) 1256 – 1266
-
Upload
uni-hannover -
Category
Documents
-
view
1 -
download
0
Transcript of Cobalamin: a critical vitamin in the elderly

www.elsevier.com/locate/ypmed
Preventive Medicine 39 (2004) 1256–1266
Review
Cobalamin: a critical vitamin in the elderly
Maike Wolters, Ph.D.,* Alexander Strohle, Ph.D-student, and Andreas Hahn, Prof.
Nutrition Physiology and Human Nutrition Unit, Department of Food Science, Centre of Applied Chemistry, University of Hanover,
D-30453 Hannover, Germany
Available online 11 June 2004
Abstract
Vitamin B12 deficiency is a common problem in elderly subjects. If a serum cobalamin level of about 150 pmol/L (200 pg/mL) is
considered normal, 10–15% of the elderly are deficient. Today, however, a threshold of 220–258 pmol/L (300–350 pg/mL) is
recognized as desirable in the elderly, or else sensitive markers like the blood concentration of homocysteine or methylmalonic acid
(MMA) are used. Then the prevalence of cobalamin deficiency rises to up to 43%. In the elderly, this high prevalence of poor
cobalamin status is predominantly caused by atrophic gastritis type B. Atrophic gastritis results in declining gastric acid and
pepsinogen secretion, and hence decreasing intestinal absorption of the cobalamin protein complexes from food. About 20–50% of the
elderly are affected. Furthermore, the reduced acid secretion leads to an alkalinization of the small intestine, which may result in
bacterial overgrowth and thus to a further decrease of the bioavailability of the vitamin. In addition, some drugs such as proton pump
inhibitors or H2 receptor antagonists inhibit the intestinal absorption of vitamin B12. An already moderately reduced vitamin B12 level
is associated with vascular disease and neurocognitive disorders such as depression and impaired cognitive performance. Furthermore,
a poor vitamin B12 status is assumed to be involved in the development and progression of dementia (e.g., Alzheimer’s dementia).
This is especially observable if the folic acid status is reduced as well. Due to the insecure supply, the cobalamin status of elderly
persons (z60 years) should be regularly controlled and a general supplementation with vitamin B12 (>50 Ag/day) should be
considered.
D 2004 The Institute For Cancer Prevention and Elsevier Inc. All rights reserved.
Keywords: Vitamin B12; Cobalamin; Homocysteine; Methylmalonic acid; Elderly; Atrophic gastritis; Vitamin–drug interactions; Atherosclerosis;
Neurocognitive function
Introduction
There is a variety of reasons why elderly, especially
geriatric subjects, are at high risk for nutrient deficiencies
including age-associated physiological changes, chronic
diseases, and a high prevalence of drug intake. Vitamin
B12 deficiency is one of the most important problems in the
nutrition of the elderly [1,2] since the absorption of cobal-
amin is often reduced in this group [3,4]. Current inves-
tigations indicate that insufficient vitamin B12 status may
increase the risk for atherosclerotic [5–7] and neurodegen-
erative diseases [2,8]. In the meanwhile, several nutrition
boards recommend monitoring the vitamin B12 status of
elderly people and identifying risk persons at an early stage.
0091-7435/$ - see front matter D 2004 The Institute For Cancer Prevention and
doi:10.1016/j.ypmed.2004.04.047
* Corresponding author. Institute of Food Science, Department of
Applied Chemistry, University of Hannover, Wunstorfer Str. 14, D-30453
Hannover, Germany. Fax: +49-511-762-5729.
E-mail address: [email protected] (M. Wolters).
The aim of this review is to describe the age-associated
changes in cobalamin metabolism and to show pathophys-
iological and therapeutic consequences.
Metabolic function and sources of vitamin B12
Vitamin B12 contains a cobalt-centered corrin nucleus
and shows a complex structure. The term vitamin B12
includes all corrinoids qualitatively exhibiting the biolog-
ical activity of cyanocobalamin. The coenzymatically ac-
tive forms of vitamin B12 are adenosylcobalamin and
methylcobalamin, which are involved in two enzymatic
reactions in human metabolism. One reaction requiring
methylcobalamin is the remethylation of homocysteine to
methionine catalyzed by the methionine synthetase [9]. In
this reaction, 5-methyl tetrahydrofolic acid (5-methyl-FH4)
is involved as a methyl group donor (Fig. 1), whereas
cobalamin is just intermediate acceptor of the methyl
Elsevier Inc. All rights reserved.

Fig. 1. Role of cobalamin in homocysteine metabolism (Ref. [30], modified). Abbreviations: SAH: S-adenosylhomocysteine; SAM: S-adenosylmethionine;
THF: tetrahydrofolate; 5-CH3-THF: 5-methyl tetrahydrofolic acid; TCC: tricarboxylic acid cycle.
M. Wolters et al. / Preventive Medicine 39 (2004) 1256–1266 1257
group. In cobalamin deficiency, methionine synthesis is
impaired and homocysteine can accumulate. Furthermore,
the methionine synthetase reaction provides tetrahydrofolic
acid (THF), which is the essential form for other folate-
dependent reactions [10]. Vitamin B12-deficient subjects
exhibit losses of this functional form of folate since 5-
methyl-FH4 is accumulated via the methyl-folate trap. This
explains why many symptoms of cobalamin deficiency are
similar to folate deficiency. Adenosylcobalamin, which is
located in the mitochondrion, is required as a coenzyme
for methylmalonyl-CoA mutase. Methylmalonyl-CoA mu-
tase catalyzes the conversion of methylmalonyl-CoA to
succinyl-CoA, a metabolite of the citric acid cycle. This is
an important biochemical reaction in the degradation of
odd-chain length fatty acids and requires first the carbox-
ylation of propionyl-CoA (supplied by the h-oxidation) tomethylmalonyl-CoA. Owing to loss of methylmalonyl-
CoA mutase activity, vitamin B12-deficient subjects show
accumulation of methylmalonic acid. Furthermore, the
degradation of the branched-chain amino acids valine
and isoleucine leads to methylmalonyl-CoA, which is then
rearranged to succinyl-CoA [11].
Cobalamins are exclusively synthesized by bacteria [12].
Rich sources of cobalamin are animal organ meats (espe-
cially liver and kidney), fish, mushrooms, eggs, and milk
products [13]. Food from plant sources does normally not
contain cobalamin, but very small amounts can be found in
fermented products or due to bacterial contamination. These
traces are not adequate to meet the vitamin B12 requirement.
Algae are often advertised as vitamin B12 sources. However,
algae contain only ineffective analogs of the vitamin, which
in addition are able to inhibit the metabolic functions of the
biologically active vitamin. Nor does yeast supply available
vitamin B12. Intestinal synthesis of the bacterial flora in

M. Wolters et al. / Preventive Medicine 39 (2004) 1256–12661258
humans is not sufficient; thus, dietary cobalamins are
required [14].
Diagnosis of vitamin B12 deficiency and status indicators
There are various methods for determining inadequate
vitamin B12 status. Deficiency of vitamin B12 leads to
impaired DNA synthesis and thus to delay or failure of
normal cell division, particularly in the erythropoiesis. A
reduction in mitotic rate results in macrocytosis (megalo-
blastic transformation) with an increased mean cellular
volume (MCV) of >100 fl. This MCV elevation with or
without anemia represents a relatively late sign of a pro-
gressed deficiency. It has to be considered that elevated
MCV is not a specific marker of vitamin B12 deficiency but
is also observed in folic acid deficiency. Vitamin B12 and
folate deficiencies are frequently found in hepatic diseases,
hemodialysis patients, and alcoholism; hence, elevated
MCV in those patients can also be a result of folic acid
or vitamin B12 deficiency [15,16]. The determination of the
cobalamin concentration in serum or plasma is more
specific but varies depending on the method and the
particular laboratory. In adults, a concentration of 150
pmol/L (200 pg/mL) is considered the lowest level for an
adequate supply. In a developing deficiency, serum con-
centrations are maintained by depleting stores of the vita-
min. Therefore, a concentration above the cutoff of 150
pmol/L does not inevitably reflect a sufficient vitamin B12
status as shown in some studies, indicating that the con-
centration is not a significant variable [17]. On the other
hand, if the cobalamin concentration is below this cutoff,
depleted stores can be assumed but are not necessarily
present [15,16]. Because of these results, a serum cobala-
min cutoff value of <220 pmol/L (<300 pg/mL) has been
proposed [18]. Based on studies with the more sensitive
indicators of cobalamin status, methylmalonic acid (MMA),
and homocysteine (see below), Lindenbaum et al. [19]
suggested a cutoff value of 258 pmol/L (350 pg/mL) in
elderly subjects. Subjects with low vitamin B12 concen-
trations exhibited significant elevations of MMA and
homocysteine concentrations. In the meanwhile, other
authors agree that the cutoff value of 150 pmol/L is too
low. For example, in a sample of elderly patients with
cobalamin concentrations below this value, 40% of the
subjects had increased serum MMA levels. In another
study, as many as 80% of the subjects aged 65 years with
cobalamin concentrations V148 pmol/L had increased
MMA and homocysteine values [18]. Thus, the limit
between sufficient and insufficient status is probably be-
tween serum cobalamin concentrations of 220–258 pmol/L
[18–20]. In the case of concentrations below 220 pmol/L,
further diagnostic measures are necessary. These early
markers of cobalamin deficiency could be elevated plasma
homocysteine, elevated serum MMA, and decreased serum
holotranscobalamin (holoTC) [21,22].
Elevated homocysteine is an important marker for vita-
min B12 and/or folate deficiency and it may also indicate a
low vitamin B6 status. In elderly people with normal folate
and vitamin B6 status, elevated homocysteine is generally a
consequence of cobalamin deficiency [23]. Homocysteine is
not a specific variable because it is not possible to differ-
entiate between a vitamin B12 and a folate deficiency.
Therefore, additional diagnostic measures such as the
MMA or the holoTC concentration are required (see below).
Homocysteine concentrations are also elevated in renal
insufficiency and hypovolemia [3]. Different levels of total
homocysteine in plasma have been suggested as normal:
<14 Amol/L [24], 5–13.6 Amol/L [25], and 4.9–11.7 Amol/
L [26]. Since results of many studies showed that the
prevalence and mortality of cardiovascular disease (CVD)
increased if a concentration of 10 Amol/L was exceeded
[27,28], this limit has been suggested as desirable [29].
Values of >12–30 Amol/L are classified as moderate hyper-
homocysteinemia [11].
A more specific and sensitive indicator of cobalamin
status is the serum methylmalonic acid (MMA) concentra-
tion. Elevated MMA is a direct metabolic consequence of
vitamin B12 deficiency, as shown in Fig. 1 [30]. Thus,
MMA is an important biochemical marker of cobalamin
status [3,25,31,32]. The reference range of serum MMA
concentrations in healthy adults is 73–271 nmol/L [33]. It
has to be considered that elevated MMA is also observed in
renal insufficiency and hypovolemia [3].
Beside MMA, which is an expensive measure, holo-
transcobalamin (holoTC) has been suggested to be an
early marker of cobalamin deficiency. holoTC contains
the biologically active vitamin B12 fraction bound to
transcobalamin II (TC II) because TC II promotes the
uptake of its vitamin B12 by all cells. Only 6–20% of total
serum cobalamin is present in the active form as holoTC
[21,34]. In recent studies, holoTC has been shown to be
the most sensitive marker of vitamin B12 deficiency
followed by MMA. However, in renal dysfunction, ho-
loTC increases and cannot be used as a marker of
cobalamin status [21].
Another indicator for vitamin B12 deficiency is the
increased amount of formiminoglutamic acid in the urine
following an orally administered dose of histidine. Since
formiminoglutamic acid excretion increases in folic acid
deficiency as well, this parameter lacks specificity for
cobalamin deficiency. In contrast, elevated propionate and
2-methylcitrate concentrations are specific markers of vita-
min B12 deficiency because both rise in cobalamin-deficient
subjects. However, both methods are not applied frequently
in routine laboratories [3,15].
Herbert (1994) suggested four stages of negative cobal-
amin balance in vitamin B12 deficiency: The first stage is
serum depletion indicated by low vitamin B12 on trans-
cobalamin II (i.e., low holoTC) [35]. The second stage is
cell depletion, which is also shown by decreased holoTC as
well as by low holohaptocorrin and low erythrocyte cobal-

Table 1
Causes of cobalamin deficiency [13,16,21]
Dietary deficiency
Strict vegetarian diet
Poor diet
Low intake
Malabsorption
M. Wolters et al. / Preventive Medicine 39 (2004) 1256–1266 1259
amin concentrations. The third stage is biochemical defi-
ciency with slowed DNA synthesis, elevated serum homo-
cysteine, and methylmalonic acid concentrations; and
finally, the fourth stage is anemia, the clinical deficiency.
Late clinical signs of vitamin B12 deficiency are megalo-
blastic anemia and neuropsychiatric disorders [21,35].
Pernicious anemia (type A chronic atrophic gastritis)Gastrectomy
Type B chronic atrophic gastritis (reduced release of cobalamin from its
bound form in food)
Zollinger–Ellison syndrome
Intestinal diseases, especially of the ileum (celiac disease, Crohn’s disease,
ileitis)
Resection of the ileum
Pancreatic insufficiency
Parasitism (broad tapeworm Diphyllobothrium latum)
Bacterial overgrowth
Antiepileptic agents (carbamazepine, phenytoin, primidone)
Proton pump inhibitors (omeprazole)
Histamine (H2) receptor antagonists (cimetidine, ranitidine)
Antidiabetic drug metformin
Antibiotics (chloramphenicol, neomycin)
Cholestyramine
Increased requirement
MTHFR mutation
Hyperthyroidism
Diabetes mellitus
Renal insufficiency
Smokers
Regular alcohol intake
Prevalence of cobalamin deficiency in the elderly
In elderly subjects, the prevalence of subnormal cobala-
min concentrations varies between 10% and 43% depending
on the diagnostic criteria [3,36–41]. If the previously
considered threshold of 150 pmol/L (200 pg/mL) for a
normal vitamin B12 status is used, only 10–15% of the
elderly subjects are classified as cobalamin deficient. Clas-
sical deficiency symptoms such as megaloblastic anemia
often fail to appear [42]. Today, however, a threshold of
220–258 pmol/L (300–350 pg/mL) is recognized as a
marker for a desirable status in the elderly [4,19,20] or
otherwise more sensitive markers such as the blood con-
centration of homocysteine or methylmalonic acid are used.
Then the prevalence of cobalamin deficiency rises to up to
43% [3,4]. As observed in several studies, cobalamin
deficiency appears in most cases together with insufficient
folate status [24,38,43–45]. For example, in 66% of the
participants of the Framingham study who exhibited low
serum folate and elevated homocysteine concentrations,
MMA was also increased [41].
We performed a study with healthy women aged 60–70
years (n = 176) who did not use supplements. Women with
serum cobalamin below 258 pmol/L exhibited significantly
higher methylmalonic acid concentrations than those with
higher serum cobalamin. In total, 9.6% of the women had
elevated MMA concentrations [36].
Aetiopathogenesis of cobalamin deficiency
There is a variety of reasons for inadequate cobalamin
status (Table 1) in the elderly. The main problems are
impaired absorption, and thus an increased need of vitamin
B12 whereas other reasons like dietary insufficiency are less
important.
Impaired absorption
In elderly subjects, decreased gastric secretion due to
type B chronic atrophic gastritis is the major cause of
vitamin B12 deficiency [3,46–48]. Studies suggest that
20–50% of elderly people are subject to chronic atrophic
gastritis, depending on the definition used [2]. As shown in
the Framingham Heart Study, the disease is highly prevalent
in very old people. Prevalence of chronic atrophic gastritis
in subjects aged 60–69 years was 24% and rose to 37% in
subjects aged 80 years and over [49]. Similar findings of an
age-dependent development have been found previously
[50–54] and have been confirmed by subsequent studies
[55,56]. The main characteristics of chronic atrophic gastri-
tis are reduced gastric secretion of HCl and pepsinogen, in
an advanced stage the secretion of intrinsic factor is also
diminished [2,3]. These changes have severe consequences
for the intestinal release of vitamin B12 from food. As
shown by Doscherholmen and Swaim [57] as well as
Bradford and Taylor [58], the bioavailability of dietary
cobalamin is low in atrophic gastritis. Normally, protein-
bound cobalamin is released by gastric acid and proteolytic
pepsin and is for the most part subsequently bound to
haptocorrins [59]. Cobalamin is liberated by pancreatic
proteases in the intestinal lumen and bound to IF, which
protects the vitamin from catabolism by intestinal bacteria.
This complex associates with cubilin, which initiates Ca2+-
dependent receptor-mediated endocytosis together with an-
other protein called megalin. Due to the low pH in the
endosomes, the release of cobalamin from its IF-B12 recep-
tor complex already starts here and continues in the emerg-
ing lysosomes. Afterwards, released cobalamin is bound to
transcobalamin II (TC-II) in secretory vesicles. (Fig. 2).
Subsequently, cobalamin transcytosis occurs with a 6- to 8-
h delay [60,61]. In inadequate gastric HCl and pepsinogen
secretion, the absorption process is impaired and cobalamin
absorption is limited [48]. Furthermore, reduced acid secre-
tion leads to an elevated pH in the small intestine, which
weakens the barrier protecting against microorganisms and
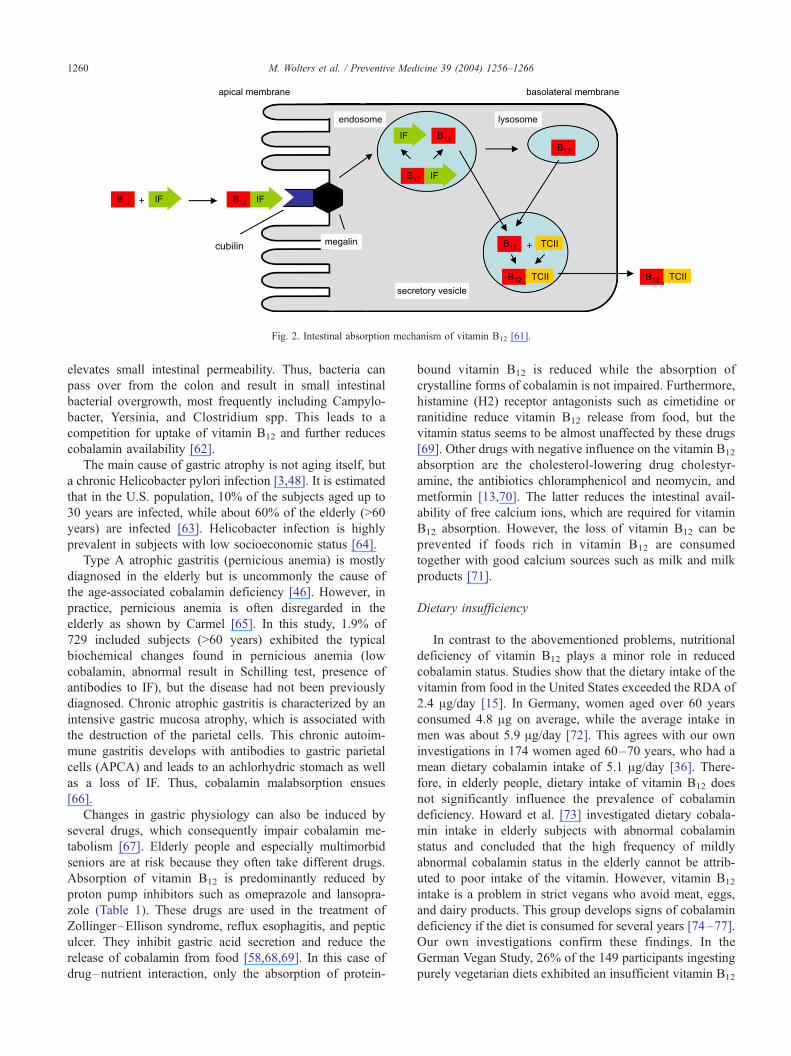
Fig. 2. Intestinal absorption mechanism of vitamin B12 [61].
M. Wolters et al. / Preventive Medicine 39 (2004) 1256–12661260
elevates small intestinal permeability. Thus, bacteria can
pass over from the colon and result in small intestinal
bacterial overgrowth, most frequently including Campylo-
bacter, Yersinia, and Clostridium spp. This leads to a
competition for uptake of vitamin B12 and further reduces
cobalamin availability [62].
The main cause of gastric atrophy is not aging itself, but
a chronic Helicobacter pylori infection [3,48]. It is estimated
that in the U.S. population, 10% of the subjects aged up to
30 years are infected, while about 60% of the elderly (>60
years) are infected [63]. Helicobacter infection is highly
prevalent in subjects with low socioeconomic status [64].
Type A atrophic gastritis (pernicious anemia) is mostly
diagnosed in the elderly but is uncommonly the cause of
the age-associated cobalamin deficiency [46]. However, in
practice, pernicious anemia is often disregarded in the
elderly as shown by Carmel [65]. In this study, 1.9% of
729 included subjects (>60 years) exhibited the typical
biochemical changes found in pernicious anemia (low
cobalamin, abnormal result in Schilling test, presence of
antibodies to IF), but the disease had not been previously
diagnosed. Chronic atrophic gastritis is characterized by an
intensive gastric mucosa atrophy, which is associated with
the destruction of the parietal cells. This chronic autoim-
mune gastritis develops with antibodies to gastric parietal
cells (APCA) and leads to an achlorhydric stomach as well
as a loss of IF. Thus, cobalamin malabsorption ensues
[66].
Changes in gastric physiology can also be induced by
several drugs, which consequently impair cobalamin me-
tabolism [67]. Elderly people and especially multimorbid
seniors are at risk because they often take different drugs.
Absorption of vitamin B12 is predominantly reduced by
proton pump inhibitors such as omeprazole and lansopra-
zole (Table 1). These drugs are used in the treatment of
Zollinger–Ellison syndrome, reflux esophagitis, and peptic
ulcer. They inhibit gastric acid secretion and reduce the
release of cobalamin from food [58,68,69]. In this case of
drug–nutrient interaction, only the absorption of protein-
bound vitamin B12 is reduced while the absorption of
crystalline forms of cobalamin is not impaired. Furthermore,
histamine (H2) receptor antagonists such as cimetidine or
ranitidine reduce vitamin B12 release from food, but the
vitamin status seems to be almost unaffected by these drugs
[69]. Other drugs with negative influence on the vitamin B12
absorption are the cholesterol-lowering drug cholestyr-
amine, the antibiotics chloramphenicol and neomycin, and
metformin [13,70]. The latter reduces the intestinal avail-
ability of free calcium ions, which are required for vitamin
B12 absorption. However, the loss of vitamin B12 can be
prevented if foods rich in vitamin B12 are consumed
together with good calcium sources such as milk and milk
products [71].
Dietary insufficiency
In contrast to the abovementioned problems, nutritional
deficiency of vitamin B12 plays a minor role in reduced
cobalamin status. Studies show that the dietary intake of the
vitamin from food in the United States exceeded the RDA of
2.4 Ag/day [15]. In Germany, women aged over 60 years
consumed 4.8 Ag on average, while the average intake in
men was about 5.9 Ag/day [72]. This agrees with our own
investigations in 174 women aged 60–70 years, who had a
mean dietary cobalamin intake of 5.1 Ag/day [36]. There-
fore, in elderly people, dietary intake of vitamin B12 does
not significantly influence the prevalence of cobalamin
deficiency. Howard et al. [73] investigated dietary cobala-
min intake in elderly subjects with abnormal cobalamin
status and concluded that the high frequency of mildly
abnormal cobalamin status in the elderly cannot be attrib-
uted to poor intake of the vitamin. However, vitamin B12
intake is a problem in strict vegans who avoid meat, eggs,
and dairy products. This group develops signs of cobalamin
deficiency if the diet is consumed for several years [74–77].
Our own investigations confirm these findings. In the
German Vegan Study, 26% of the 149 participants ingesting
purely vegetarian diets exhibited an insufficient vitamin B12

M. Wolters et al. / Preventive Medicine 39 (2004) 1256–1266 1261
status [78]. Because of long-term storage of vitamin B12 in
the liver, deficiency normally only develops after some
years of a vegan diet. However, in elderly subjects, defi-
ciency can develop sooner if absorption is impaired because
vitamin B12 is continually secreted in the bile and most of it
is reabsorbed in healthy individuals. Enterohepatic circula-
tion is important and vitamin B12 losses are much larger in
individuals who malabsorb B12 [13]. As shown in a recent
study, even lactovegetarians and lacto-ovo-vegetarians ex-
hibit metabolic features indicating vitamin B12 deficiency
[77].
Increased requirement of vitamin B12
Cobalamin deficiency in older adults is mostly due to
food cobalamin malabsorption. Since older people with low
cobalamin and elevated serum MMA mostly do not have
true pernicious anemia, they should be able to absorb free or
synthetic cobalamin. Screening of MMA, holoTC, and
homocysteine concentrations as well as cobalamin, folate,
and B6 concentrations in elderly adults indicated that
elevated concentrations of the metabolites are related to
subnormal vitamin status and decreased renal function.
Thus, elderly subjects may require higher circulating B
vitamin concentrations to maintain concentrations of
MMA and homocysteine within the normal range [79].
Moreover, individuals homozygous for methylenetetrahy-
drofolate reductase (MTHFR) polymorphism 677 may have
increased vitamin B12 and folate requirements [80]. Two
studies showed that high supplemental doses of cobalamin
are necessary to normalize serum MMA in older people
[20,81]. In 23 older cobalamin-deficient subjects, daily
intake of 25 or 100 Ag oral cobalamin for a 6-week period
was not sufficient to normalize serum MMA in all elderly
subjects whereas the concentrations were reduced by 1000
Ag daily. Since in screening studies doses of 30 Ag cobal-
amin daily decreased prevalence of increased MMA, a
longer treatment period might be necessary to normalize
serum MMA concentrations. Most elderly subjects with
cobalamin deficiency need larger doses than available in
usual cobalamin supplements [81]. This is confirmed by a
study with oral daily supplementation with 500 Ag cyano-
cobalamin, 800 Ag folic acid, and 3 mg vitamin B6 for 4
months, which was effective in normalizing plasma homo-
cysteine and serum MMA levels in 70- to 93-year-old
community-dwelling subjects [82].
Pathophysiological consequences of vitamin B12
deficiency and hyperhomocysteinemia in the elderly
Atherosclerotic vascular diseases
Even moderately elevated homocysteine concentrations
are associated with an increased risk for atherosclerotic [83]
and thrombotic events [11,84] and seem to be a risk factor
for congestive heart failure [85]. It is estimated that about
10% of atherosclerotic diseases is related to moderately
elevated homocysteine concentrations. A mild elevation of
plasma homocysteine can be found in about 5–7% of the
general population [86], whereas 20–50% of the subjects
with atherosclerotic diseases exhibit a mild homocysteine
elevation [87]. However, recent studies have shown contra-
dictory results. In some trials, highly significant associations
between cardiovascular diseases and homocysteine concen-
trations were found whereas in other studies no association
could be discovered [88]. A meta-analysis that evaluated the
results of 30 studies including 5,073 cases of ischemic heart
disease and 1,113 cases with stroke showed that elevated
homocysteine levels are a moderate independent predictor
for these diseases in healthy populations [88]. After data
correction for various confounders such as age, blood
pressure, smoking, and cholesterol concentration, it was
concluded that a 25% homocysteine reduction (about 3
Amol/L) was associated with 11% risk reduction for ische-
mic heart disease and with 19% risk reduction for stroke.
This result shows that decreasing the mean homocysteine
level in the population can significantly reduce important
health risks [88]. Another meta-analysis also yields strong
evidence that the association between homocysteine and
cardiovascular disease is causal. According to this study,
lowering homocysteine concentrations by 3 Amol/L would
reduce the risk of ischemic heart disease by 16%, deep vein
thrombosis by 25%, and stroke by 24% [89]. Furthermore,
treatment with homocysteine lowering B vitamins (folic
acid, vitamin B12, and vitamin B6) significantly decreases
the rate of restenosis and the need for revascularization of
the target lesion after coronary angioplasty [90].
Despite this empirical evidence, to date it is not definitely
known whether hyperhomocysteinemia is a cause of ath-
erosclerosis or only a result of the disease [5,83]. However,
in vitro studies and results of experimental animal studies
confirm the hypothesis that homocysteine plays a role in the
pathogenesis of atherosclerosis since it initiates various
atherogenetic mechanisms [4]. Fig. 3 gives some examples
for atherogenic effects of homocysteine [29].
Many clinical studies were able to show that supplemen-
tation with vitamin B12 and folic acid efficiently reduces
homocysteine concentrations [91]. In most individuals, folic
acid is the more effective substance because in the adult
population insufficient folic acid status is highly prevalent,
whereas vitamin B12 status is generally sufficient in young
adults. However, elderly people often exhibit vitamin B12
deficiency; thus, cobalamin supplementation may play a
major role in lowering homocysteine in this group.
Neuropsychiatric symptoms
Cognitive impairments are often associated with insuffi-
cient cobalamin status or elevated homocysteine or methyl-
malonic acid concentrations [4]. Plasma homocysteine
seems to be an important predictor for mental performance

Fig. 3. Examples for atherogenic effects of homocysteine [based on data of 29].
M. Wolters et al. / Preventive Medicine 39 (2004) 1256–12661262
[92]. In cognitively normal elderly community dwellers,
elevated plasma homocysteine and elevated serum levels of
methylcitric acid indicating insufficient cobalamin status
had an independent association with cognitive impairment
[93,94]. It is estimated that, independent of the intelligence,
homocysteine is responsible for 11% of the variance of
cognitive performance [95].
Furthermore, vitamin B12 can influence mood as shown
in an epidemiological study involving 700 persons aged >65
years. In the group with vitamin B12 deficiency, persons
with depression were twice the number than in the group
with normal cobalamin values [96]. An association had also
been found in a study with 3,884 seniors in the Netherlands.
The prevalence of depressive symptoms was associated with
vitamin B12 and homocysteine concentration in blood. This
association was especially pronounced in hospitalized
seniors. In this group, about 30% of all depressive patients
were classified as cobalamin deficient [97].
It is assumed that an insufficient vitamin B12 status may
also be involved in the pathogenesis and the progression of
dementia (e.g., Alzheimer’s dementia). In patients diag-
nosed with Alzheimer or vascular dementia, elevated homo-
cysteine concentrations were highly prevalent [98–103].
This observation is confirmed by the data of the Framing-
ham population, which shows that the risk of developing
Alzheimer’s dementia nearly doubles with plasma homo-
cysteine concentrations above 14 Amol/L [104]. In several
studies, an inverse correlation between plasma homocys-
teine concentrations and cognitive performance has been
assessed [105–108].
To date there is a lack of large interventional studies
showing a benefit of vitamin B12 supplementation in neuro-
cognitive impairment or dementia [109]. One effect of
supplemental vitamin B12, B6, and folate seems to be the
improvement of blood–brain barrier function [110]. Since
cobalamin metabolism is closely related to folic acid me-
tabolism and deficiency of both vitamins leads to elevated
homocysteine concentrations, the effects of both vitamins
can hardly be distinguished. Clinical studies evaluating the
effect of a combined therapy with folic acid and vitamin B12
have led to contradictory results. In some studies, an
improvement of cognitive performance was detected after
supplementation with both vitamins [111–113], whereas
other investigators found no positive results [114–116].
Results of a clinical study with high-dose cobalamin sup-
plementation indicated a prominent correlation between
duration of cognitive symptoms and response to therapy
[117]. It is assumed that for a successful therapy, an early
intervention plays a major role [118].
While the exact reasons for the correlations between
cobalamin deficiency and cognitive impairments are un-
known to date, there are some experimental findings that
may explain a relation between the metabolites S-adenosyl-
methionine (SAM) and homocysteine (Fig. 1). SAM is an
important methyl group donator in many neurophysiologi-
cally relevant reactions. Decreased SAM values in spinal
fluid have been observed in patients with Alzheimer’s
dementia and depression [119].
SAM-dependent reactions are the methylation of phos-
pholipids as well as the synthesis of various neurotrans-
mitters (e.g., acetylcholine). The demethylation of SAM
leads to S-adenosylhomocysteine (SAH), which is an
inhibitor of the SAM-dependent transmethylation reac-
tions [2,8,120]. Therefore, transmethylation reactions re-
quire a SAM concentration above the SAH concentration
[121]. In the case of insufficient vitamin B12 and folate
status, the vitamin-dependent remethylation of homocys-
teine to methionine is inhibited and as a consequence less

Fig. 4. Modified food pyramid for people >70 years [122].
M. Wolters et al. / Preventive Medicine 39 (2004) 1256–1266 1263
methionine is available for SAM synthesis. Thus, cerebral
SAM-dependent transmethylation reactions are inhibited
and homocysteine increases [121]. The resulting hypome-
thylation is seen as a responsible factor in various
neurological and psychiatric diseases such as dementia
and depression [2,8,121]. Furthermore, elevated homocys-
teine may contribute to the development and progression
of vascular dementia due to its involvement in athero-
sclerosis (see above).
Recommendations
Because of the problem of insufficient vitamin B12
status in the elderly, many institutions generally recom-
mend supplementation with cobalamin for elderly subjects.
For example, the food pyramid based on the Dietary
Guidelines for the Americans has been modified for people
aged 70 years and over (Fig. 4). In this pyramid for the
elderly, daily supplementation with vitamins B12, D, and
calcium is recommended, while folate fortified foods
should be used (flour has had to be fortified with folic
acid in the United States since 1998) [122]. The U.S. Food
and Nutrition Board recommends the use of supplements
and/or the intake of fortified food (e.g., grain products) for
elderly people as well because absorption of crystalline
vitamin B12 is not influenced by atrophic gastritis type B
[3]. However, studies have shown that the use of supple-
ments or enriched foods reduces the prevalence of cobal-
amin deficiency in the elderly, but there still remains the
risk of deficiency due mostly to low dosages
[19,20,123,124]. In a sample of elderly aged 65–100
years, 46% indicated regular consumption of cobalamin
supplements or enriched foods. Nevertheless, 13% was
classified as vitamin B12 deficient because of serum
cobalamin concentrations V221 pmol/L and MMA con-
centrations >271 nmol/L [20]. In the elderly, supplemen-
tation with up to 50 Ag/day vitamin B12 seems to be
insufficient to avoid poor cobalamin status [20]. Because
of the high prevalence of vitamin B12 deficiency and its
association with neurocognitive diseases, the daily use of
cobalamin supplements of >50 Ag/day can be recommen-
ded for elderly people aged 60 years and over. This
preventive measure assumes no side effects and would
be useful in respect to a risk–benefit analysis. Due to
insecure cobalamin supply, it is necessary to monitor the
vitamin B12 status regularly in elderly subjects (z60
years). Since serum vitamin B12 is no reliable marker of
subclinical cobalamin deficiency, measurement of more
sensitive markers like MMA and holoTC should be
considered.
In patients with diagnosed cobalamin deficiency, the
abovementioned preventive doses of cobalamin are insuffi-
cient. Therefore, it must be strictly distinguished between
preventive and therapeutic vitamin supplementation. For
therapy, oral doses of 1000–2000 Ag cyanocobalamin are
required, which can be used instead of parenteral therapy for
treatment in most cobalamin-deficient patients [125].
References
[1] Saltzman JR, Russell RM. The aging gut. Nutritional issues. Gastro-
enterol Clin North Am 1998;27:309–24.
[2] Selhub J, Bagley LC, Miller J, Rosenberg IH. B vitamins, homo-

M. Wolters et al. / Preventive Medicine 39 (2004) 1256–12661264
cysteine, and neurocognitive function in the elderly. Am J Clin Nutr
2000;71:614S–20S.
[3] Baik HW, Russell RM. Vitamin B12 deficiency in the elderly. Annu
Rev Nutr 1999;19:357–77.
[4] Wolters M, Strohle A, Hahn A. Altersassoziierte Veranderungen
im Vitamin-B12-und Folsaurestoffwechsel: Pravalenz, Atiopatho-
genese und pathophysiologische Konsequenzen. Z Gerontol Ger-
iatr 2004;37:109–35.
[5] Brattstrom L, Wilcken DE. Homocysteine and cardiovascular dis-
ease: cause or effect? Am J Clin Nutr 2000;72:315–23.
[6] Mangoni AA, Jackson SH. Homocysteine and cardiovascular dis-
ease: current evidence and future prospects. Am J Med 2002;112:
556–655.
[7] Nygard O, Vollset SE, Refsum H, Brattstrom L, Ueland PM. Total
homocysteine and cardiovascular disease. J Intern Med 1999;246:
425–54.
[8] Rosenberg IH. B vitamins, homocysteine, and neurocognitive func-
tion. Nutr Rev 2001;9:S69–73.
[9] Marsh EN. Coenzyme B12 (cobalamin)-dependent enzymes. Essays
Biochem 1999;34:139–54.
[10] Selhub J. Folate, vitamin B12 and vitamin B6 and one carbon me-
tabolism. J Nutr Health Aging 2002;6:39–42.
[11] Welch GN, Loscalzo J. Homocysteine and atherothrombosis. N Engl
J Med 1998;338:1042–50.
[12] Raux E, Schubert HL, Warren MJ. Biosynthesis of cobalamin (vi-
tamin B12): a bacterial conundrum. Cell Mol Life Sci 2000;57:
1880–93.
[13] Herbert V. Vitamin B12. In: Ziegler EE, Filer IF, editors. Present
knowledge in nutrition. Washington, DC: International Life Science
Institute Press; 1996. p. 191–205.
[14] Herbert V. Vitamin B12: plant sources, requirements, and assay. Am
J Clin Nutr 1988;852–8.
[15] Institute of Medicine, Food and Nutrition Board V. Dietary reference
intakes for thiamine, riboflavin, niacin, vitamin B6, folate, vitamin
B12, pantothenic acid, biotin, and choline. A report of the Standing
Committee on the Scientific Evaluation of Dietary Reference Intakes
and its Panel on Folate, Other B Vitamins, and Choline and Sub-
committee on Upper Reference Levels of Nutrients. Washington,
DC: National Academy Press; 1998. p. 9.1–9.33.
[16] Snow CF. Laboratory diagnosis of vitamin B12 and folate deficien-
cy: a guide for the primary care physician. Arch Intern Med
1999;159:1289–98.
[17] Carmel R. Current concepts in cobalamin deficiency. Annu Rev Med
2000;357–75.
[18] Yao Y, Yao SL, Yao SS, Yao G, Lou W. Prevalence of vitamin B12
deficiency among geriatric outpatients. J Fam Pract 1992;524–8.
[19] Lindenbaum J, Rosenberg IH, Wilson PW, Stabler SP, Allen RH.
Prevalence of cobalamin deficiency in the Framingham elderly pop-
ulation. Am J Clin Nutr 1994;60:2–11.
[20] Rajan S, Wallace JI, Beresford SAA, Brodkin KI, Allan RA, Stabler
SP. Screening for cobalamin deficiency in geriatric outpatients: prev-
alence and influence of synthetic cobalamin intake. J Am Geriatr Soc
2002;50:624–30.
[21] Herrmann W, Obeid R, Schorr H, Geisel J. Functional vitamin B12
deficiency and determination of holotranscobalamin in populations
at risk. Clin Chem Lab Med 2003;41:1478–88.
[22] Loikas S, Lopponen M, Suominen P, Moller J, Irjala K, Isoaho
R, et al. RIA for serum holo-transcobalamin: method evaluation
in the clinical laboratory and reference interval. Clin Chem
2003;49:455–62.
[23] Stabler SP, Lindenbaum J, Allen RH. The use of homocysteine and
other metabolites in the specific diagnosis of vitamin B12 deficiency.
J Nutr 1996;126(4 Suppl):1266S–72S.
[24] Selhub J, Jacques PF, Wilson PW, Rush D, Rosenberg IH. Vitamin
status and intake as primary determinants of homocysteinemia in an
elderly population. JAMA 1993;270:2693–8.
[25] Joosten E, Lesaffre E, Riezler R. Are different reference intervals for
methylmalonic acid and total homocysteine necessary in elderly
people? Eur J Haematol 1996;57:222–6.
[26] Ubbink JB, Becker PJ, VermaakWJ, Delport R. Results of B-vitamin
supplementation study used in a predictionmodel to define a reference
range for plasma homocysteine. Clin Chem 1995;41:1033–7.
[27] Gerhard GT, Duell PB. Homocysteine and atherosclerosis. Curr
Opin Lipidol 1999;10:417–28.
[28] OmennGS, Beresford SAA,MotulskyAG. Preventing coronary heart
disease. B vitamins and homocysteine. Circulation 1998;97:421–4.
[29] Stanger O, Herrmann W, Pietrzik K, Fowler B, Geisel J, Dierkes J, et
al. DACH-LIGA Homocystein e.V. DACH-LIGA homocystein
(German, Austrian and Swiss Homocysteine Society): consensus
paper on the rational clinical use of homocysteine, folic acid and
B-vitamins in cardiovascular and thrombotic diseases: guidelines
and recommendations. Clin Chem Lab Med 2003;41:1392–403.
[30] Herrmann W. The importance of hyperhomocysteinemia as a risk
factor for disease: an overview.ClinChemLabMed 2001;39:666–74.
[31] Green R, Kinsella LJ. Current concepts in the diagnosis of cobala-
min deficiency. Neurology 1995;45:1435–40.
[32] Naurath HJ, Joosten E, Riezler R, Stabler SP, Allen RH, Linden-
baum J. Effects of vitamin B12, folate, and vitamin B6 supplements
in elderly people with normal serum vitamin concentrations. Lancet
1995;346:85–9.
[33] Pennypacker LC, Allen RH, Kelly JP, Matthews LM, Grigsby J,
Kaye K, et al. High prevalence of cobalamin deficiency in elderly
outpatients. J Am Geriatr Soc 1992;40:197–204.
[34] Hvas AM, Nexo E. Holotranscobalamin as a predictor of vitamin
B12 status. Clin Chem Lab Med 2003;41:1489–92.
[35] Herbert V. Staging vitamin B-12 (cobalamin) status in vegetarians.
Am J Clin Nutr 1994;59:1213S–22S.
[36] Wolters M, Hermann S, Hahn A. B vitamins, homocysteine, and
methylmalonic acid in elderly German women. Am J Clin Nutr
2003;78:765–72.
[37] Bjorkegren K, Svardsudd K. Elevated serum levels of methylma-
lonic acid and homocysteine in elderly people. A population-based
intervention study. J Intern Med 1999;246:317–24.
[38] Bjorkegren K, Svardsudd K. Serum cobalamin, folate, methylma-
lonic acid and total homocysteine as vitamin B12 and folate tissue
deficiency markers amongst elderly Swedes—A population-based
study. J Intern Med 2001;249:423–32.
[39] Herrmann W, Schorr H, Bodis M, et al. Role of homocysteine,
cystathionine and methylmalonic acid measurement for diagnosis
of vitamin deficiency in high-aged subjects. Eur J Clin Invest
2000;30:1083–9.
[40] Klee GG. Cobalamin and folate evaluation: measurement of meth-
ylmalonic acid and homocysteine vs vitamin B12 and folate. Clin
Chem 2000;46:1277–83.
[41] Stabler SP, Lindenbaum J, Allen RH. Vitamin B-12 deficiency in the
elderly: current dilemmas. Am J Clin Nutr 1997;66:741–9.
[42] Stabler SP. Vitamin B12 deficiency in older people: improving diag-
nosis and preventing disability. J Am Geriatr Soc 1998;46:1317–9.
[43] Quinn K, Basu TK. Folate and vitamin B12 status of the elderly. Eur
J Clin Nutr 1996;50:340–2.
[44] Lindeman RD, Romero LJ, Koehler KM, Liang HC, LaRue A,
Baumgartner RN, et al. Serum vitamin B12, C and folate concen-
trations in the New Mexico elder health survey: correlations with
cognitive and affective functions. J Am Coll Nutr 2000;19:68–76.
[45] Charlton KE, Kruger M, Labadarios D, Wolmarans P, Aronson I.
Iron, folate and vitamin B12 status of an elderly South African
population. Eur J Clin Nutr 1997;51:424–30.
[46] Carmel R. Cobalamin, the stomach, and aging. Am J Clin Nutr
1997;66:750–9.
[47] Russell RM. The aging process as a modifier of metabolism. Am J
Clin Nutr 2000;72(2 Suppl):529S–32S.
[48] Russell RM. Factors in aging that effect the bioavailability of
nutrients. J Nutr 2001;131(4 Suppl):1359S–61S.
[49] Krasinski SD, Russell RM, Samloff IM, et al. Fundic atrophic gas-

M. Wolters et al. / Preventive Medicine 39 (2004) 1256–1266 1265
tritis in an elderly population. Effect on hemoglobin and several
serum nutritional indicators. J Am Geriatr Soc 1986;34:800–6.
[50] Cheli R, Simon L, Aste H, et al. Atrophic gastritis and intestinal
metaplasia in asymptomatic Hungarian and Italian populations. En-
doscopy 1980;12:105–8.
[51] Christiansen PM. The incidence of achlorhydria and hypochlorhy-
dria in healthy subjects and patients with gastrointestinal diseases.
Scand J Gastroenterol 1968;3:497–508.
[52] Ihamaki T, Varis K, Siurala M. Morphological, functional and im-
munological state of the gastric mucosa in gastric carcinoma fami-
lies. Comparison with a computer-matched family sample. Scand J
Gastroenterol 1979;14:801–12.
[53] Siurala M, Isokoski M, Varis K, Kekki M. Prevalence of gastritis in a
rural population. Bioptic study of subjects selected at random. Scand
J Gastroenterol 1968;3:211–23.
[54] Villako K, Tamm A, Savisaar E, Ruttas M. Prevalence of antral and
fundic gastritis in a randomly selected group of an Estonian rural
population. Scand J Gastroenterol 1976;11:817–22.
[55] Feldman M, Cryer B, McArthur KE, Huet BA, Lee E. Effects of
aging and gastritis on gastric acid and pepsin secretion in humans: a
prospective study. Gastroenterology 1996;110:1043–52.
[56] Hurwitz A, Brady DA, Schaal SE, Samloff IM, Dedon J,
Ruhl CE. Gastric acidity in older adults. JAMA 1997;278(4
Suppl):659–62.
[57] Doscherholmen A, Swaim WR. Impaired assimilation of egg Co 57
vitamin B12 in patients with hypochlorhydria and achlorhydria and
after gastric resection. Gastroenterology 1973;64:913–9.
[58] Bradford GS, Taylor CT. Omeprazole and vitamin B12 deficiency.
Ann Pharmacother 1999;33:641–3.
[59] Grasbeck R. Biochemistry and clinical chemistry of vitamin B12
transport and related diseases. Clin Biol 1984;17:99–107.
[60] Seetharam B. Receptor-mediated endocytosis of cobalamin (vitamin
B12). Annu Rev Nutr 1999;19:173–95.
[61] Seetharam B, Yammani RR. Cobalamin transport proteins and their
cell-surface receptors. Expert Rev Mol Med 2003;5:1–18.
[62] Saltzman JR, Russell RM. Nutritional consequences of intestinal
bacterial overgrowth. Compr Ther 1994;20:523–30.
[63] Peterson WL. Helicobacter pylori and peptic ulcer disease. N Engl J
Med 1991;324:1043–8.
[64] Logan RP, Walker MM. ABC of the upper gastrointestinal tract:
epidemiology and diagnosis of Helicobacter pylori infection. BMJ
2001;323:920–2.
[65] Carmel R. Prevalence of undiagnosed pernicious anemia in the el-
derly. Arch Intern Med 1996;156:1097–100.
[66] Toh BH, van Driel IR, Gleeson PA. Pernicious anemia. N Engl J
Med 1997;337:1441–8.
[67] Schumann K. Interactions between drugs and vitamins at advanced
age. Int J Vitam Nutr Res 1999;69:173–8.
[68] Kasper H. Vitamin absorption in the elderly. Int J Vitam Nutr Res
1999;69:169–72.
[69] Termanini B, Gibril F, Sutliff VE, Yu F, Venzon DJ, Jensen RT.
Effect of long-term gastric acid suppressive therapy on serum vi-
tamin B12 levels in patients with Zollinger–Ellison syndrome. Am
J Med 1998;104:422–30.
[70] Desouza C, Keebler M, McNamara DB, Fonseca V. Drugs affecting
homocysteine metabolism: impact on cardiovascular risk. Drugs
2002;62:605–16.
[71] Bauman WA, Shaw S, Jayatilleke E, Spungen AM, Herbert V. In-
creased intake of calcium reverses vitamin B12 malabsorption in-
duced by metformin. Diabetes Care 2000;23:1227–31.
[72] Stehle P. Ernahrung alterer Menschen. Deutsche Gesellschaft
fur Ernahrung e.V. Frankfurt am Main: Ernahrungsbericht,
2000. p. 147–78 [in German].
[73] Howard JM, Azen C, Jacobsen DW, Green R, Carmel R. Dietary
intake of cobalamin in elderly people who have abnormal serum
cobalamin, methylmalonic acid and homocysteine levels. Eur J Clin
Nutr 1998;52(4 Suppl):582–7.
[74] Haddad EH, Berk LS, Kettering JD, Hubbard RW, Peters WR.
Dietary intake and biochemical, hematologic, and immune status
of vegans compared with nonvegetarians. Am J Clin Nutr
1999;80(3 Suppl):586S–93S.
[75] Krajcovicova-Kudlackova M, Blazicek P, Kopcova J, Bederova A,
Babinska K. Homocysteine levels in vegetarians versus omnivores.
Ann Nutr Metab 2000;44:135–8.
[76] Herrmann W, Geisel J. Vegetarian lifestyle and monitoring of vita-
min B-12 status. Clin Chim Acta 2002;326:47–59.
[77] Herrmann W, Schorr H, Obeid R, Geisel J. Vitamin B-12 status,
particularly holotranscobalamin II and methylmalonic acid concen-
trations, and hyperhomocysteinemia in vegetarians. Am J Clin Nutr
2003;78:131–6.
[78] Waldmann A, Koschizke JW, Leitzmann C, Hahn A. Homocys-
teine and cobalamin status in German vegans. Public Health Nutr
2004;7:467–72.
[79] Obeid R, Schorr H, Eckert R, Herrmann W. Vitamin B12 status in
the elderly as judged by available biochemical markers. Clin Chem
2004;50:238–41.
[80] Herrmann W, Obeid R, Schorr H, Zarzour W, Geisel J. Homocys-
teine, methylenetetrahydrofolate reductase C677T polymorphism
and the B-vitamins: a facet of nature-nurture interplay. Clin Chem
Lab Med 2003;41(3 Suppl):547–53.
[81] Rajan S, Wallace JI, Brodkin KI, Beresford SA, Allen RH, Sta-
bler SP. Response of elevated methylmalonic acid to three dose
levels of oral cobalamin in older adults. J Am Geriatr Soc
2002;50(11):1789–95.
[82] Lewerin C, Nilsson-Ehle H, Matousek M, Lindstedt G, Steen B.
Reduction of plasma homocysteine and serum methylmalonate con-
centrations in apparently healthy elderly subjects after treatment with
folic acid, vitamin B12 and vitamin B6: a randomised trial. Eur J
Clin Nutr 2003;57(11):1426–36.
[83] Ueland PM, Refsum H, Beresford SA, Vollset SE. The controversy
over homocysteine and cardiovascular risk. Am J Clin Nutr
2000;324–32.
[84] Coppola A, Davi G, De Stefano V, Mancini FP, Cerbone AM, Di
Minno G. Homocysteine, coagulation, platelet function, and throm-
bosis. Semin Thromb Hemost 2000;243–54.
[85] Vasan RS, Beiser A, D’Agostino RB, Levy D, Selhub J, Jacques PF, et
al. Plasma homocysteine and risk for congestive heart failure in adults
without prior myocardial infarction. JAMA 2003;289:1251–7.
[86] McCully KS. Homocysteine and vascular disease. Nat Med
1996;2:386–9.
[87] Weiss N, Pietrzik K, Keller C. Atheroskleroserisikofaktor Hyperho-
mocyst(e)inamie: Ursachen und Konsequenzen. Dtsch Med
Wochenschr [in German] 1999;124:1107–13.
[88] N.N. Homocysteine and risk of ischemic heart disease and stroke: a
meta-analysis. JAMA 2002;288:2015–22.
[89] Wald DS, Law M, Morris JK. Homocysteine and cardiovas-
cular disease: evidence on causality from a meta-analysis. BMJ
2002;325:1202.
[90] Schnyder G, Roffi M, Pin R, Flammer Y, Lange H, Eberli FR, et al.
Decreased rate of coronary restenosis after lowering of plasma
homocysteine levels. N Engl J Med 2001;345:1593–600.
[91] N.N. Lowering blood homocysteine with folic acid based supple-
ments: meta-analysis of randomised trials Homocysteine Lowering
Trialists’ Collaboration. BMJ 1998;316:894–8.
[92] Riggs KM, Spiro III A, Tucker K, Rush D. Relations of vitamin B12,
vitamin B6, folate, and homocysteine to cognitive performance in the
Normative Aging Study. Am J Clin Nutr 1996;63:306–14.
[93] Ravaglia G, Forti P, Maioli F, Muscari A, Sacchetti L, Arnone G, et
al. Homocysteine and cognitive function in healthy elderly commu-
nity dwellers in Italy. Am J Clin Nutr 2003;77:668–73.
[94] Garcia AA, Haron Y, Evans LR, Smith MG, Freedman M, Ro-
man GC. Metabolic markers of cobalamin deficiency and cogni-
tive function in normal older adults. J Am Geriatr Soc 2004;
52:66–71.

M. Wolters et al. / Preventive Medicine 39 (2004) 1256–12661266
[95] Budge M, Johnston C, Hogervorst E, de Jager C, Milwain E,
Iversen SD, et al. Plasma total homocysteine and cognitive perfor-
mance in a volunteer elderly population. Ann NY Acad Sci
2000;903:407–10.
[96] Penninx BW, Guralnik JM, Ferrucci L, Fried LP, Allen RH, Stabler
SP. Vitamin B12 deficiency and depression in physically disabled
older women: epidemiologic evidence from the Women’s Health and
Aging Study. Am J Psychiatry 2000;157:715–21.
[97] Hutto BR. Folate and cobalamin in psychiatric illness. Compr Psy-
chiatry 1997;38:305–14.
[98] Clarke R, Smith AD, Jobst KA, Refsum H, Sutton L, Ueland PM.
Folate, vitamin B12, and serum total homocysteine levels in con-
firmed Alzheimer disease. Arch Neurol 1998;55:1449–55.
[99] Nilsson K, Gustafson L, Faldt R, Andersson A, Brattstrom L, Lindg-
ren A, et al. Hyperhomocysteinaemia—A common finding in a psy-
chogeriatric population. Eur J Clin Invest 1996;26:853–9.
[100] Nilsson K, Gustafson L, Hultberg B. The plasma homocysteine
concentration is better than that of serum methylmalonic acid as a
marker for sociopsychological performance in a psychogeriatric
population. Clin Chem 2000;46:691–6.
[101] Nilsson SE, Takkinen S, Tryding N, Evrin PE, Berg S, McClearn G,
et al. Association of biochemical values with morbidity in the elder-
ly: a population-based Swedish study of persons aged 82 or more
years. Scand J Clin Lab Invest 2003;63:457–66.
[102] Selley ML. Increased concentrations of homocysteine and asymmet-
ric dimethylarginine and decreased concentrations of nitric oxide in
the plasma of patients with Alzheimer’s disease. Neurobiol Aging
2003;24:903–7.
[103] Religa D, Styczynska M, Peplonska B, Gabryelewicz T, Pfeffer A,
Chodakowska M, et al. Homocysteine, apolipoproteine E and meth-
ylenetetrahydrofolate reductase in Alzheimer’s disease and mild cog-
nitive impairment. Dement Geriatr Cogn Disord 2003;16:64–70.
[104] Seshadri S, Beiser A, Selhub J, et al. Plasma homocysteine as a risk
factor for dementia and Alzheimer’s disease. N Engl J Med
2002;346:476–83.
[105] Teunissen CE, Blom AH, Van Boxtel MP, Bosma H, de Bruijn C,
Jolles J, et al. Homocysteine: a marker for cognitive performance? A
longitudinal follow-up study. J Nutr Health Aging 2003;7:153–9.
[106] Dufouil C, Alperovitch A, Ducros V, Tzourio C. Homocysteine,
white matter hyperintensities, and cognition in healthy elderly peo-
ple. Ann Neurol 2003;53:214–21.
[107] Miller JW, Green R, Ramos MI, Allen LH, Mungas DM, Jagust WJ,
et al. Homocysteine and cognitive function in the Sacramento Area
Latino Study on Aging. Am J Clin Nutr 2003;78:441–7.
[108] Polyak Z, Stern F, Berner YN, Sela BA, Gomori JM, Isayev M, et al.
Hyperhomocysteinemia and vitamin score: correlations with silent
brain ischemic lesions and brain atrophy. Dement Geriatr Cogn Dis-
ord 2003;16:39–45.
[109] Joosten E. Homocysteine, vascular dementia and Alzheimer’s dis-
ease. Clin Chem Lab Med 2001;39:717–20.
[110] Lehmann M, Regland B, Blennow K, Gottfries CG. Vitamin B12-
B6-folate treatment improves blood – brain barrier function in
patients with hyperhomocysteinaemia and mild cognitive impair-
ment. Dement Geriatr Cogn Disord 2003;16:145–50.
[111] van Asselt DZ, Pasman JW, van Lier HJ, et al. Cobalamin supple-
mentation improves cognitive and cerebral function in older, cobal-
amin-deficient persons. J Gerontol, Ser A 2001;56:M775–9.
[112] Martin DC, Francis J, Protetch J, Huff FJ. Time dependency of
cognitive recovery with cobalamin replacement: report of a pilot
study. J Am Geriatr Soc 1992;40:168–72.
[113] Nilsson K, Gustafson L, Hultberg B. Improvement of cognitive
functions after cobalamin/folate supplementation in elderly patients
with dementia and elevated plasma homocysteine. Int J Geriatr Psy-
chiatry 2001;16:609–14.
[114] Johnson MA, Hawthorne NA, Brackett WR, Fischer JG, Gunter EW,
Allen RH, et al. Hyperhomocysteinemia and vitamin B-12 deficien-
cy in elderly using Title IIIc nutrition services. Am J Clin Nutr
2003;77:211–20.
[115] Clarke R, Harrison G, Richards S. Vital Trial Collaborative Group:
effect of vitamins and aspirin on markers of platelet activation, ox-
idative stress and homocysteine in people at high risk of dementia.
J Intern Med 2003;254:67–75.
[116] Kwok T, Tang C, Woo J, Lai WK, Law LK, Pang CP. Randomized
trial of the effect of supplementation on the cognitive function of
older people with subnormal cobalamin levels. Int J Geriatr Psychi-
atry 1998;13:611–6.
[117] Abyad A. Prevalence of Vitamin B12 deficiency among demented
patients and cognitive recovery with cobalamin replacement. J Nutr
Health Aging 2002;6:254–60.
[118] Lokk J. Association of vitamin B12, folate, homocysteine and cog-
nition in the elderly. Scand J Nutr 2003;47:132–8.
[119] Bottiglieri T, Godfrey P, Flynn T, Carney MW, Toone BK, Reynolds
EH. Cerebrospinal fluid S-adenosylmethionine in depression and
dementia: effects of treatment with parenteral and oral S-adenosyl-
methionine. J Neurol Neurosurg Psychiatry 1990;53:1096–8.
[120] Bottiglieri T. Folate, vitamin B12, and neuropsychiatric disorders.
Nutr Rev 1996;54:382–90.
[121] Weir DG, Scott JM. Brain function in the elderly: role of vitamin B12
and folate. Br Med Bull 1999;55:669–82.
[122] Russell RM, Rasmussen H, Lichtenstein AH. Modified food guide
pyramid for people over seventy years of age. J Nutr 1999;129:
751–3.
[123] Koehler KM, Romero LJ, Stauber PM, Pareo-Tubbeh SL, Liang
HC, Baumgartner RN, et al. Vitamin supplementation and other
variables affecting serum homocysteine and methylmalonic acid
concentrations in elderly men and women. J Am Coll Nutr
1996;15:364–76.
[124] Seal EC, Metz J, Flicker L, Melny J. A randomized, double-blind,
placebo-controlled study of oral vitamin B12 supplementation in
older patients with subnormal or borderline serum vitamin B12 con-
centrations. J Am Geriatr Soc 2002;50:146–51.
[125] Lane LA, Rojas-Fernandez C. Treatment of vitamin b(12)-deficiency
anemia: oral versus parenteral therapy. Ann Pharmacother 2002;36:
1268–72.




















