
Incidence, Etiology, Histologic Findings, and Course of Thoracic Inflammatory Aortopathies
Upload
independentCategory
view
15download
0


I
INTERNATIONAL JOURNAL OFCONTEMPORARY SURGERY
www.ijocs.in
Volume 1 Number 02 July - December 2013
1. External Tube Drainage Versus no Drainage in Hepatic Hydatid Cysts with ...................................................................... 01
Cystobiliary Communications
Mubashir Ahmad Shah, Aakib Hamid Charag, Suhail Farooq Mir, Khursheed Alam Wani, Sameer Hassan Naqash,
Munir Ahmad Wani
2. Repair of Ruptured Neglected Quadriceps Tendon after Manipulation of Stiff Knee ....................................................... 05
Bikram Singla, SS Gill, Kapil Bansal
3. A Study of Role of Antibiotics in Cases of Acute Pancreatitis in Western Uttar Pradesh .................................................. 08
Dhawal Sharma, Atul Kumar Gupta, Shalabh Gupta, T S Bhagat, Rajiv Verma, Prateek Vardhan, Mamta Rai
4. Autoimmune Thyroid Dysfunction and Meniere's Disease .................................................................................................... 14
Rahil Muzaffar, Owais Mattoo, Anees Mir, Rauf Ahmad
5. Comparative Study of Surgical Site Infections in Elective Surgeries ..................................................................................... 18
Mamta Rai, T S Bhagat, Shalabh Gupta, Atul Kumar Gupta, Rajiv Verma, Dhawal Sharma, Pankaj Solanki
6. Delayed Presentation of Primarily Missed Fractures Reporting to a ..................................................................................... 23
Tertiary Care Centre: A Retrospective Study
Muzamil Ahmad Baba, Bashir Ahmed Mir, M A Halwai, Adil Bashir Shikari, Shakir Rasheed, Omar Khursheed, Qazi Manan
7. A Study to assess the effectiveness of Nesting on Posture and Movements ........................................................................ 27
among Preterm Babies in Selected Hospitals at Mysore
Neethu C Joseph, Ambika K, Sheela Williams
8. The Role of Caudal Epidural Steroid Injections in Management of Low Back Pain ........................................................... 31
Bikram Singla, Seema Jindal
9. Comparison of Analgesic effects between 'Interpleural Bupivacaine with Adrenaline ..................................................... 36
and Interpleural Bupivacaine with Adrenaline & Clonidine in Laparoscopic Cholecystectomy
Ovais Nazir, Mushtaq A Wani, B B Kapoor
10. Comparative Study of Infra-red Coagulation vs Haemorrhoidectomy in Patients of Haemorrhoids ............................ 42
Pankaj Solanki, Shalabh Gupta, T S Bhagat, Atul Kumar Gupta, Rajiv Verma, Dhawal Sharma, Mamta Rai
Contents
Content Final.pmd 10/10/2013, 9:23 AM1

II
11. Study of Incidence of Prolactin Level in Female Infertility in its
Correlation with the Hypothyroidism in Hapur ....................................................................................................................... 47
Poonam Mani, Pragya Maheshwari, Yogesh Kumar Rai
12. Comparison of Low Cost Net-mesh with Prolene Mesh in Management of Inguinal Hernia .......................................... 52
Prateek Vardhan, Shalabh Gupta, Rajiv Verma, T S Bhagat, Atul Kumar Gupta, Pankaj Solanki, Mamta Rai
13. A Study of Comparison of Cervical Epidural Anaesthesia with General ............................................................................. 56
Anaesthesia for Thyroid Surgery
Priyadarshini M Bentur, Ravi R
14. Morphometric Study of Sacral Hiatus with Significance in Interventional Clinical Procedure ....................................... 59
Ram Prakash Gupta, Nirupma Gupta, Anjulata Rai
15. Criteria for Defining Severe Septal Deviation ............................................................................................................................ 64
Owais Mattoo, Rahil Muzaffar, Raja Salman Khurshid, Shafqat Islam
16. Ruptured Rudimentary Horn Pregnancy at 20 Weeks of Gestation in a Primigravida: A Case Report .......................... 69
Girija B S, Sudha T R, Rajeshwari, Shridhar S K, Poornima
17. Dry Eye Syndrome. A Diagnostic Enigma .................................................................................................................................. 72
Kumar Prachi, Bhargava Rahul, Kumar Manjushri, Jyotsana Madaan
18. A Study of Rickets as an Avoidable Cause of Delayed Walking in Children in Rural Western Uttar Pradesh .............. 78
Bhawna Kohli, Rajesh Bhatia, Sumit Gupta
19. A Study of Urinary Tract Infections in Patients with Catheter in Tertiary ........................................................................... 83
Care Hospital in Western Uttar Pradesh
Sanjeev Dimri, Hemant Sharma, S K Datta, Deepak Gupta
20. To Study the Etiology and Various Treatment Modalities of Liver Abscess ......................................................................... 87
Shah Naveed, Hasina Quari, Asma Altaf , Maha Para, Tanveer Banday, V B Gupta
21. Anatomical Variation in Inferior Vena Cava- A Case Report and Review ............................................................................ 93
Shalini Chaudhary, Sarvesh
22. A Comparative Study of the Anti-inflammatory effect of Topical 1% Prednisolone and .................................................. 96
Topical 0.1% Dexamethasone Eye Drops after Cataract Surgery in Western Uttar Pradesh
Suman Bhartiya,Sunita Singh, Sudeep Sabbithi
23. Cytological Study of Cerebrospinal Fluid and Evaluation of its Role in the ...................................................................... 100
Diagnosis of Tubercular Meningitis
Uma Tayal, Aparna, Nishant, Emma Chaudhary
Content Final.pmd 10/10/2013, 9:23 AM2

III
24. A Study of Minimally Invasive Percutaneous Plate Osteosynthesis with Locking ........................................................... 104
Compression Plate for Distal Tibial Fractures
Rajesh Bhatia, Sumit Gupta, Firoz Khan
25. Study of Exfoliative Cytology of Ascetic Fluid & Evaluation of its Role in the Diagnosis of ......................................... 110
Abdominal Tuberculosis in Rural Population of National Capital Region
Uma Tayal, Nishant, Emma Chaudhary, Aparna
26. A Study of Incidence and Clinical Presentation of Deviated Nasal Septum in Western UP ........................................... 114
Vandana Singh, R K Singhal
27. Study and Evaluation of Cases of Total Condylar Knee Replacement ................................................................................ 119
Varun Vijay, Madan S Hardikar
28. Comparative Study of the Therapeutic efficacy of Cyproterone Acetate + Eflornithine .................................................. 124
(Topical) and Eflornithine (Topical) alone in the Treatment of Facial Hirsutism
Sachin Agarwal, Vinay Kumar, S K Sayal
29. Correlation between Fetal Heart Patterns in Labour and Cord Blood pH and its Perinatal Outcome ......................... 129
Seetha Panicker, T V Chitra, Meena Priyadharshini, A K Chithra
30. Clinico-social Profile and Surgical Management of Cases of Diabetic Foot: A Prospective Study ................................ 134
Md Shakeel, Arshiya Taranum
Content Final.pmd 10/10/2013, 9:23 AM3

International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 1
External Tube Drainage Versus no Drainage in HepaticHydatid Cysts with Cystobiliary Communications
Mubashir Ahmad shah1, Aakib Hamid Charag2, Suhail Farooq Mir2, Khursheed Alam Wani3,Sameer Hassan Naqash4, Munir Ahmad Wani5
1Associate Professor, 2Senior Resident, 3Professor and Head, 4Additional Professor, 5Asociate Professor, Department ofGeneral Surgery, Sher-I-Kashmir Institute of Medical Sciences, Srinagar, Jammu & Kashmir, India
ABSTRACT
Echinococcosis (hydatid disease) is a zoonosis caused by the larval stage of Echinococcus granulosus.About seventy-five per cent of all hydatid cysts are found in the liver. Surgical management of hepatichydatid cyst includes neutralization of the parasite, evacuation of cyst, removal of germinal liningand management of the residual cavity. Our study focussed on the management of the residualcavity in patients with cystobiliary communications. We divided the patients into two groups of 40patients each. In both the groups the cystobiliary communications were ligated using sutures. Afterclosing the cystobiliary communications, the residual cavity was left to drain externally using apolyvinyl chloride tube in group 1 whereas either capitonnage or omentoplasty was done in group 2.The results were studied in terms of the postoperative complications, mortality and hospital stay. Inthe patients managed by external tube drainage, average hospital stay was 6.95 ± 0.93 days while aspatients in group 2 had an average post operative stay of 4.54 ± 0.76 days (p value = 0.0001). Bile leakwas seen in 6 (15%) patients in group 1, while as only 1(2.5%) patient from group 2 developed anintra-abdominal bile collection. Wound infection and deep vein thrombosis was seen in one patienteach in group 1, whereas no such complication was seen in group 2. One (2.5%) patient from eachgroup had a recurrence of the disease during follow-up.
Keywords: Hydatid, External Drainage, Capitonnage, Omentoplasty
INTRODUCTION
Hydatid cyst infection is one of the oldest diseasesin animals and humans. It was first described in theTalmud as “bladders full of water.” Hippocratesdescribed it as “the liver is filled with water. Thecausative organism of hydatid disease is the post-larvalmetacestode stage of echinococcus granulosus. The lifecycle of E. granulosus requires two hosts. The adult
Corresponding author:Aakib Hamid CharagSenior ResidentDepartment of General Surgery, Sher-I-KashmirInstitute of Medical Sciences, Srinagar, IndiaRoom F-35, Unmarried Doctor's Hostel, SKIMS, Soura,Srinagar, Jammu & Kashmir, IndiaPostal code: 190011Phone: 09419776591Email: [email protected]
tapeworm lives in the intestine of the dog, which isthe most common definitive host for E. granulosus. (1)
Sheep and other animals such as goats and pigs arethe intermediate hosts which acquire the larval stageby ingesting the eggs. Humans are the accidentalintermediate hosts. Most commonly the parasite getslodged in the liver. Sometimes the eggs penetrate thecirculation and via blood stream may settle in anyorgan, including lung, spleen, brain, kidney and bone.Currently there are three treatment options for hydatiddisease of the liver: surgery, which remains the mostefficient treatment; percutaneous aspiration; andmedical treatment. Surgery is indicated in almost allthe cases except asymptomatic and small (< 5cm) CLtype cysts (2) and totally calcified cysts. After evacuationof the ectocyst, the management of the residual cavityhas been a subject of debate. External tube drainage,capsulorrhaphy, capitonnage, omentoplasty andinternal drainage are the commonly used methods todeal with the cavity.
DOI Number: 10.5958/j.2321-1024.1.2.018
1. Aakib --1-4.pmd 10/10/2013, 9:22 AM1

2 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
MATERIAL AND METHOD
The study was conducted in the department ofGeneral Surgery, Sher-i-Kashmir Institute of MedicalSciences, Srinagar, India from June 2010 to April 2012with a follow-up over a period of one year, upto April2013. It was a prospective study and total number ofpatients studied was 80. The patients were randomlyallocated to two groups using computer generatednumbers. Only those patients were selected who hada cystobiliary communication. The aim of the studywas to compare the results of external tube drainagewith no drainage (omentoplasty and capitonnage) formanagement of residual hepatic hydatid cyst cavitiesafter the suture ligation of cystobiliarycommunications. Forty patients were managed withexternal tube drainage and omentoplasty orcapitonnage was done in another forty.
The two groups were compared with respect to thefollowing parameters:
• Post operative complications
• Mortality
• Post operative hospital stay
The patients with infected, multiple, ruptured andrecurrent hydatid cysts were excluded from the study.Patients with ASA III or IV score were also excludedfrom the study. All the patients received albendazole(10mg/kg/day) for four days prior to surgery. For thediagnosis of hydatid disease, all the patients weresubjected to ELISA for hydatidosis, ultrasonographyand computed tomography scan of abdomen. Routineinvestigations like hemogram, liver and kidneyfunction tests and chest roentgenogram were done inevery patient.
A right subcostal incision was used in patientshaving cysts in right lobe of liver. Midline laparotomywas done in patients with left lobe cysts. Evacuationof the ectocyst was done while observing all thestandard precautions to prevent spillage. Sutureligation of the cystobiliary communications was doneusing vicryl. The residual cavity was finally managedby either of the two techniques (drainage or nodrainage). 28 Fr polyvinyl chloride tube was put inthe cavity for external drainage in 40 patients. In group2, omentoplasty was done in 31 patients andcapitonnage was done in 9 patients.
Every patient received two doses of Cephazolin,one at the time of induction and another dose was
given four hours later. Oral nutrition was allowed oncethe bowel sounds returned. All patients were givenoral albendazole (10mg/kg/day) for three monthsafter surgery, starting on first post operative day.Monitoring of liver function tests was done at the endof each month. All patients were subjected to regularultrasonography of abdomen during their follow-upto detect any recurrence.
Statistical analysis was done using Fischer’s exacttest and unpaired t-test.
RESULTS
Out of the 40 patients in group 1, thirty-one patientshad cyst in right lobe of liver while nine patients hadleft lobe cysts and thirty-six patients had a singlecystobiliary communication while four patients hadmultiple cystobiliary communications. In group 2,twenty eight patients had cyst in right lobe of liverwhile twelve patients had left lobe cysts and thirty-three patients had a single cystobiliary communicationwhile seven patients had multiple cystobiliarycommunications.
Biliary leak was seen in six patients in group 1.Biliary drainage began on 2nd day in 2 of the patientson the 3rd day in 4 patients. Of these six patients withpostoperative biliary fistulae, 5 benefitted fromendoscopic sphincterotomy. One patient had toundergo cystojejunostomy for persistent bile leak. Onepatient in group 2 developed an intra-abdominalcollection (bilioma), which was treated withendoscopic sphincterotomy followed by percutaneousdrainage under radiological guidance.
None of the patients in either group developedpleural effusion or any reactionary or secondarybleeding.
One patient in group 1 developed wound infection,which was managed conservatively with dailydressings and another patient developed deep veinthrombosis which was given medical treatment.
For patients in group 1, post operative hospital staywas 6.95 ± 0.93 days while as in group 2 it was only4.54 ± 0.76. The difference between the two wasstatistically significant.
None of our patients died during the period ofstudy. However, during the period of follow-up onepatient in each group had a recurrence. these twopatients are still on our follow-up.
1. Aakib --1-4.pmd 10/10/2013, 9:22 AM2

International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 3
Table 1: Intra operative findings
Intra operative Findings Group 1 Group 2(n=40) (n=40)
Right lobe cysts 31 (77.5) 28 (70)
Left lobe cysts 9 (22.5) 12 (30)
Single cystobiliary communication 36 (90) 33 (82.5)
Multiple cystobiliary communications 4 (10) 7 (17.5)
Table 2: Comparison with respect to variousparameters:
Parameters Group 1 Group 2 P value (n=40) (n=40)
Post operative bleeding 0 (0) 0 (0) -
Biliary leak 6 (15) 0 (0) 0.0255 (S)
Intra-abdominal fluid 0 (0) 1 (2.5) 1.000 (NS)collection (bilioma)
Pleural effusion 0 (0) 0 (0) -
Deep vein thrombosis 1 (2.5) 0 (0) 1.000 (NS)
Wound infection 1 (2.5) 0 (0) 1.000 (NS)
Post operative hospital 6.95 ± 0.93 4.54 ± 0.76 0.0001 (S)stay (days)
Mortality 0 (0) 0 (0) -
Recurrence 1(2.5) 1 (2.5) 1.000 (NS)
DISCUSSION
Echinococcosis is a near-cosmopolitan zoonosiscaused mostly by the larval stage of the parasite. Sixspecies of Echinococcus have been recognized, but themost important members of the genus areEchinococcus granulosus (which causes cysticechinococcosis) and Echinococcus multilocularis(which causes alveolar echinococcosis). (3) The greatestprevalence of E. granulosus in human and animal hostsis found in countries of the temperate zones. (4)
Surgery for hydatid cyst of liver can be eitherconservative or radical. Conservative surgery includesthe inactivation of protoscoleces, evacuation of the cystcontents, ligation of cystobiliary communications andmanagement of the residual cavity. The incidence oflocal recurrence after conservative surgery isapproximately 10%. (5) Radical surgery includescomplete removal of the cyst along with the pericyst,including exocysts when present and some adjacentliver parenchyma. This approach is the best treatmentfor all forms of hydatid cysts with least recurrence rates(1%). (6)
Methods for the management of residual cavityinclude open drainage of cyst cavity into the peritonealcavity or into an organ, or obliteration of cavity bycapsulorrhaphy, omentoplasty, myoplasty,capitonnage or introflexion, or external tubedrainage.(7)
External tube drainage is associated with themorbidity of hepatic abscesses, biliary fistulas and anincreased hospital stay. Therefore, procedures in whichexternal tube drainage is avoided should be thepreferred modality to deal with the residual hydatidcyst cavity. (8)
Mousavi SR and colleagues (9) studied drainageversus omentoplasty in 65 patients with hepatichydatid cysts. The residual cavity was treated withomentoplasty in 35 patients and drainage in 30patients. They concluded that overall complication ratewas more in patients treated with drainage procedure(16.6% vs 3.3%).
Arikan et al (10) in 2007 reported that tube drainageis a safe surgical modality in the treatment of hydatidcyst disease of liver if applied properly on appropriatepatients. However, their complication rate was 17.5%in patients who underwent any kind of surgery otherthan tube drainage whereas it was 28.1% with tubedrainage. Complications were more in patients treatedwith tube drainage, though the difference was notstatistically significant.
In our experience, the patients treated with externaltube drainage had an increased morbidity in the postoperative period. Bile leak was seen significant numberof patients treated with tube drainage. Bile leaks canoccur because of the improperly sutured cystobiliarycommunications or due to the opening up of the smallunapparent communications that are missed at thetime of surgery. Keeping a tube drain in place mayprovide a path of least resistance for bile to flow. Incases where omentoplasty or capitonnage is used todeal with the cavity, it may be argued that adhesionsmay form in the cavity with the omentum or with thewalls of the cyst itself, thereby helping in closure ofany potential source of bile leak. Bilioma can still be acomplication with non-drainage methods as was seenin one of our patients.
Patients with external tube drain are at a risk ofinfective complications as the drain paves a way forthe organisms to enter the body. Wound infection wasseen in one of our patients who had an external tubedrain, though complications like liver abscess was notseen in any patient.
Tube drains become a cause of restricted activityin patients who always feel discomfort in movingaround with the drain in place. Restriction of activityis a well known factor for causation of deep veinthrombosis as was seen in one of our patients.
1. Aakib --1-4.pmd 10/10/2013, 9:22 AM3

4 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
CONCLUSION
Therefore, we conclude, as have some otherauthors, that external tube drainage is not a preferredmethod to deal with the residual cavity in hepatichydatid cysts. Whenever possible tube drainageshould be avoided and other methods likeomentoplasty or capitonnage should be givenpreference.
Acknowledgements: None
Conflict of Interest: None
Source of Funding: None
Ethical Clearance: Not applicble
REFERENCES
1. Mandal S, Mandal MD. Humancystic echinococcosis: epidemiologic, zoonotic,clinical, diagnostic and therapeutic aspects. AsianPac J Trop Med. 2012 Apr;5(4):253-60.
2. Buttenschoen K, Carl i Buttenschoen D.Echinococcus granulosus infection: the challengeof surgical treatment. Langenbecks ArchSurg. 2003 Sep;388(4):218-30.
3. Grosso G, Gruttadauria S, Biondi A, MarventanoS, Mistretta A. Worldwide epidemiology of liverhydatidosis including the Mediterranean areaWorld J Gastroenterol 2012 April 7; 18(13):1425-1437.
4. Eckert J, Schantz PM, Gasser RB, Torgerson PR,Bessonov AS, Movsessian SO, et al. Geographic
distribution and prevalence. WHO/OIE Manualon Echinococcosis in Humans and Animals: aPublic Health Problem of Global Concern. Paris:Office International des Epizooties Paris, 2001:100-142
5. Yorganci K, Sayek I.Surgical treatment of hydatidcysts of the liver in the era of percutaneoustreatment. Am J Surg. 2002 Jul;184(1):63-9.
6. Alfieri S, Doglietto GB, Pacelli F, CostamagnaG, Carriero C, Mutignani M, et al. Radicalsurgery for liver hydatid disease: a study of 89consecutive patients. Hepatogastroenterology.1997 Mar-Apr;44(14):496-500.
7. Michael J Zinner, Seymour I. Schuxirtz, HaroldEllis. Liver abscess and hydatid disease;Maingot’s abdominal operations. Vol. II, 10thedition, Stamford, CT: Apleton and Lange: 1997;pp. 1513-1544.
8. Demirci S, Eraslan S, Anadol E, Bozatli L.Comparison of the results of different surgicaltechniques in the management of hydatid cystsof the liver. World J. Surg 1989; 13(1): 88-90.
9. Reza Mousavi S, Khoshnevis J, Kharazm.Surgical treatment of hydatid cyst of the liver:Drainage versus omentoplasty. Ann hepatol.2005; 4(4): 272-274
10. Arikan S, Kocakusak A, Yucel AF, Daduk Y.Evaluation of tube drainage method in thetreatment of hydatid cyst of liver.Hepatogastroenterology. 2007 Mar;54(74):470-4.
1. Aakib --1-4.pmd 10/10/2013, 9:22 AM4

International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 5
Repair of Ruptured Neglected Quadriceps Tendon afterManipulation of Stiff Knee
Bikram Singla1, SS Gill2, Kapil Bansal1
1Assitant Professor, Department of Orthopaedics, GGS Medical College & Hospital, Faridkot, 2Professor ofOrthopedics & Vice Chancellor, Baba Farid University of Health Sciences, Faridkot
ABSTRACT
We report the case of 28 year old male patient who suffered quadriceps rupture following manipulationof the stiff knee. We treated the patient with V-Y plasty procedure which is an uncommon procedurewith successful results. The final range of motion was 90 degrees with 10 degrees of extensor lag.
Keywords: Quadriceps, Stiff knee, V-Y Plasty
INTRODUCTION
Stiffness of the knee after trauma and/or surgeryfor femoral as well as tibial intraarticular fractures isone of the most common complications and is difficultto treat1. Stiffness in extension is more common whichcan be reduced by early vigorous physiotherapy1,2.Sometimes when the patient is not motivated enoughto undergo physiotherapy, the stiffness of knee isalmost certain. The surgeon may be tempted to tryother atypical options of treatment like manipulationunder anaesthesia. The results can be disastrous bothfor the patient as well as the surgeon if the extensormechanism ruptures. We encountered one such casein our clinical practice which we thought is worthwhilementioning.
CASE REPORT
The case pertains to a young male patient whosuffered multiple injuries in a road side accident. Heremained under ICU care on ventilator for head injury.The orthopaedic injuries consisted of fractures of neckand shaft of femur and ipsilateral femoral condylefracture. He was operated with proximal femoralnailing and percutaneous screw fixation respectively.The patient did not undergo physiotherapy after thedischarge from the hospital thereby developingstiffness of knee in extension. Six months later thescrews were removed from femoral condyle and kneewas manipulated under anaesthesia. Patient continuedwalking with an aid till he reported to us with thecomplaint of inability to lift the leg straight anddifficulty in walking without knee immobiliser.
On examination, the diagnosis of quadricepsrupture was made with healed fracture of femur and
interlocking nail in situ. Patella was relatively lessmobile sideways which suggested intraarticularadhesions. Also there was inability to actively extendthe knee. Radiographs revealed, patella alta in thelateral views.
Interlocking nail was removed from femur and MRIof the knee was done. MR images revealed the ruptureof quadriceps tendon from superior pole of patella.Patient was operated under spinal anesthesia in supineposition with tourniquet. A midline incision extendingfrom the middle third of the anterior aspect of the thighup to the tibial tuberosity was given3. After Submuscular dissesction rectus femoris was separatedfrom scarred vastus intermedius which was excisedextraperiosteally3 . Extensor expansions of the kneewere released on both sides and undersurface of thepatella4. There was more 4 cm. gap between proximalpole of patella and distal end of quadriceps tendon onfull extension of knee3.Codvilla V-Y plasty was doneto repair the ruptured extensor mechanism. It wasdecided to reinforce the repair at the tendon bonejunction with steel wire. The wire was passed throughthe patella and rectus tendon in an encirclagetechnique. Final range of motion achieved was 90degrees without undue stress at the repair site.Throughout the procedure, cautery was used toachieve haemostasis and negative suction drains wereused before closure. Loose stitches were applied toretinaculum. Posterior slab was applied with knee inflexion of about 45 degrees.
Post-operatively, limb was raised on Braun-Bohler’s splint and ice packs were applied for 72 hours.Epidural infusion with ropivacine was started duringthe wound closure and continued for 48 hours. Passiverange of motion exercises were allowed on second
DOI Number: 10.5958/j.2321-1024.1.2.019
2. Bikram singla-5-7.pmd 10/10/2013, 9:22 AM5

6 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
postoperative day within the range of 0-40 degrees andincreased as the pain settled3. Toe touch walking wasstarted with knee immobiliser and with the help ofwalker after the sutures were taken out3. Sero-sanguinous fluid continued to discharge fromproximal 1/3rd portion of the wound which settledwith debridement and antibiotics. Three months later,the range of motion at knee was about 60-70 degrees3.At the latest follow up, 12 months after the operation,the patient has demonstrated 90 degrees flexion and10 degrees of extension lag. Patient could easily domost of his activities without discomfort though thereis some limp while walking without any aid.
Fig. 1. MR image of ruptured quadriceps tendon
Fig. 2. Gap at the rupture site.
Fig. 3. Scarred adherent undersurface of rectus femoris
Fig. 4. Holes drilled in patella
Fig. 5. Gap closed by pulling sutures through patella
Fig. 6. Reinforcement with steel wire
2. Bikram singla-5-7.pmd 10/10/2013, 9:22 AM6

International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 7
Fig. 7. Final flexion 90 degrees
DISCUSSION
Most of the literature reviewed was on Thomson’squadricepsplasty for stiff knee in extension with onlyminimal amount of work on V-Y quadricepsplastyavailable1,2. Although, this is not a routine procedureand not a routine mode of injury, so the results can behighly unperdictable1. The procedure has morbidity
in the form of risk of scarring of rectus muscle, atrophyand extensor lag. Infection with subcutaneousplacement of sutures which is mentioned in theliterature is a potential problem1,2. We did notencounter wire breakage although some loosening isevident on follow up radiographs. Postoperative checkX-rays were did reveal patella baja which may be dueto contracture of patellar tendon. There are alwayschances of degenerative changes in patellofemoral jointdue to surgery and also in tibiofemoral joint. Wesuggest this as a salvage procedure when the stabilityof limb is the question. With good surgical techniqueand aggressive physiotherapy a practical range ofmotion can be achieved
CONCLUSION
Inspite of aggressive physiotherapy, results can bevariable depending upon the pre-operative stiffness,surgical expertise and motivation of the patient forphysiotherapy protocol. But this certainly a goodsalvage procedure in such cases.
REFERENCES
1. Kundu ZS, Sangwan SS, Guliani G, Siwach RC,Kamboj P, Singh R. Thompson’s quadricepsplastyfor stiff knee Indian Orthop 2007;41:390-394
2. Thompson TC. Quadricepsplasty to improveknee function. J Bone Joint Surg Am 1944;26:366-379
3. Campbell’s textbook of orthopaedic surgery
2. Bikram singla-5-7.pmd 10/10/2013, 9:22 AM7

8 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
A Study of Role of Antibiotics in Cases of AcutePancreatitis in Western Uttar Pradesh
Dhawal Sharma1, Atul Kumar Gupta2, Shalabh Gupta3, T S Bhagat4, Rajiv Verma5,Prateek Vardhan1, Mamta Rai1
1Post Graduate Student Third Year, 2Associate Professor, 3Professor, Head of Department, 4Professor, Unit Head,5Assistant Professor, Deptt. of General Surgery, Santosh Medical College & Hospital
ABSTRACT
Acute pancreatitis is a protean disease capable of wide clinical variation, ranging from mild discomfortto apocalyptic prostration. Infectious complications with incidence of 40-70% in severe acutepancreatitis are predominant cause of morbidity and mortality. The role of prophylactic antibiotictherapy in Acute Pancreatitis is still not clear. To assess the frequency of infection & role of antibiotictherapy in Acute Pancreatitis a study was conducted on 24 patients in Department of Surgery, SantoshMedical College & Hospital, Ghaziabad. All the patients underwent all specific investigations andmanaged with only supportive treatment unless infection was proven. In our study it was observedthat frequency of infection in acute pancreatitis is 4.16% and appropriate supportive therapy is themainstay of management of acute pancreatitis. Antibiotics are required in acute pancreatitis onlywhen there is a definite evidence of infection in terms of positive culture sensitivity or any interventionis done. Appropriate surgical intervention is the treatment of choice in those with infected pancreatitis.
Keywords: Acute Pancreatitis, Antibiotics, Infection
INTRODUCTION
Acute pancreatitis is a protean disease capable ofwide clinical variation, ranging from mild discomfortto apocalyptic prostration. Moreover the inflammatoryprocess may remain localized in the pancreas, spreadto regional tissues or even involve remote organsystems.
The incidence of acute pancreatitis is approximately5-70 cases per 10,000 per year. The causes of acutepancreatitis are protean with Biliary calculi and alcoholresponsible for 90% cases in U.S. Other causes includeDrugs, Infection, Postoperative, Trauma, Idiopathic.
Infectious complications are observed in 40-70% ofpatients with severe acute pancreatitis. Infectedpancreatic necrosis and pancreatic abscess are the mostdevastating of complications. Most deaths related toacute pancreatitis occur after first 7-10 days as a resultof infective complications particularly infectedpancreatic necrosis.
Sterile Pancreatic necrosis in the presence of severesystemic complications has a mortality rate of 20%while in the cases of infected necrosis it increases to50%. Infected necrosis is associated with high incidenceof organ failure irrespective of the extent of necrosis.
The diagnosis of infection in cases of acutepancreatitis causes difficulty, as the clinical profile ofinfected acute pancreatitis may well resemble that ofacute necrotizing pancreatitis. In these cases guidedaspiration is the only modality for definitive diagnosisof pancreatic infection. The establishment of this factis an important guide for further management in thesecases.
It is generally accepted that infected necrosis shouldbe managed surgically, whereas sterile pancreatitismay be managed conservatively also. However roleof antibiotics therapy in either of these cases needsfurther evaluation.
DOI Number: 10.5958/j.2321-1024.1.2.020
3. Dhawal Sharma--8-13.pmd 10/10/2013, 9:22 AM8

International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 9
Aims and Objectives
The aims and objectives of the present study were
1. To assess the frequency of infection in acutepancreatitis.
2. To study the role of antibiotic therapy in acutepancreatitis.
Materials and method
The study was conducted in Department ofSurgery, Santosh Medical College and Hospital. A totalnumber of 24 patients treated at Santosh Hospital,Ghaziabad for acute pancreatitis from June 2011 toDecember 2012.
PATIENT SELECTION
Inclusion Criteria
All fresh cases of Acute Pancreatitis within 48 hoursof attack were included in the study.
Exclusion Criteria
Patients who had been treated elsewhere andreceived antibiotics previously were excluded from thestudy.
All patients were admitted to the surgical serviceand a careful history and physical examination wereperformed.
• The following laboratory data were obtained oneach patient included in the study:
a) Hemoglobin, hematocrit, Total leukocyte counts,Differential Leukocyte counts.
b) Serum biochemistry including blood sugar,calcium, renal and liver function tests.
c) Serum amylase, serum lipase, serum LDH, serumCRP
d) Arterial blood gas analysis.
• Radiological studies: Chest X-ray, plain filmabdomen, USG abdomen to evaluate for gallbladder and pancreas in particular.
• Contrast Enhanced CT scan of abdomen was donein all patients within 48-72 hours of admission andmorphological severity of pancreatitis was gradedaccording to the Balthazar grade and CT severityindex(CTSI).
The clinical severity of illness was assessed usingRanson’s criteria.
All patients were treated with I.V. fluids,nasogastric suction, analgesics, antiemetics and othersupportive therapy as per condition and requirementof individual cases. None of the patients were givenantibiotics unless infection was proven.
Patients were carefully monitored for relief of pain,pulse rate, blood pressure, temperature and urineoutput. Laboratory investigations were repeated asand when required. Repeat USG scan or CT scan weredone in patients as per requirements.
Patients in whom infection was suspected basedon presence of fever, leukocytosis and deterioratingclinical condition, were subjected to furtherinvestigations:
a) Repeat USG abdomen or CECT abdomen.
b) Cultures of blood, urine, and pus.
c) USG or CT guided aspiration of fluid from acutefluid collection, pancreatic abscess or necrosis.
Observation and Results
This study included 24 patients. The patientsdiagnosed to have acute pancreatitis were studiedprospectively and following observations wererecorded.
Age distribution
The mean age was 40.66 years. Minimum age was16 years and maximum age was 68 years. Most of thecases were in the age group 31-40 years i.e. 50 % of thetotal number of cases in study.
Graph No. 1
Sex distribution
Out of total 24 cases in the study 9 were males andrest 15 were females
3. Dhawal Sharma--8-13.pmd 10/10/2013, 9:22 AM9

10 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
Presentation of cases
All the patients presented with complaints of painabdomen. Other common clinical presentations are asfollows
Table no. 1
Laboratory parameters
Laboratory parameters N % of N
S. amylase (>3 times normal) 20 83.33
S. lipase (n 0-60 U/L) 21 87.50
N= 24
Table no. 2
Average Ranson score
Average ranson score N % of total N
>2 7 29.16
<=2 17 70.83
N= Number of cases
Chart No. 1
Graph No. 2
Causes of Acute Pancreatitis
Four cases (16.66%) out of 24 had acute alcoholicpancreatitis and 17 cases (70.83%) had gallstoneinduced pancreatitis. In 3 cases cause of pancreatitiscould not be ascertained.
Chart No. 3
7(29.16%) cases were predicted to have severe acutepancreatitis based on ranson score and 17(70.83%) werepredicted to have mild acute pancreatitis. Out of 7 casesof severe pancreatitis 4 cases (57.14%) hadcomplications and 3(42.86%) of them had uneventfulrecovery and out of 17 predicted mild pancreatitis6(35.29%) cases had complications and 11(64%) casesof them recovered uneventfully.
Complications rates according to Ranson score
Graph no. 3Chart No. 2
3. Dhawal Sharma--8-13.pmd 10/10/2013, 9:22 AM10

International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 11
CT scan
Preliminary CT done on all 24 patients at the timeof admission demonstrated local complications in 9(37.5%) patients.
Table No. 3
Balthazar grade N % of total N
A 4 16.67
B 1 4.17
C 10 41.66
D 4 16.67
E 5 20.83
N = Number of case
Course in Hospital
5 patients (20.83%) had fever during stay in hospitaland 4 patients (16.67%) had leucocytosis . Howeveronly 3 (12.5%) had both fever and leucocytosis. Meanday of onset of fever was 7.4 days with earliest time ofoccurrence being 2 days and maximum 14 days afterthe attack of acute pancreatitis.
Table No. 4
Signs of Infection Present % o f Total N
Fever 5 20.83
Leucocytosis 4 16.67
Both 3 12.5
N = number of cases
Assessment of collection/ necrosis
Repeat scan was done on 11 patients (45.84%) forassessment of any collection or necrosis that waspresent either at time of admission or appeared in thecourse of disease during stay in the hospital .Out ofthese 8 (33.33%) patients showed collection on repeatscan.
Table No. 5
Follow up scan Present % of total N
Collection 8 33.33
No collection 3 12.5
N(Number of cases)= 24
Guided aspiration
Image guided aspiration was done in 4(16.67%)patients where infection was suspected. In 2 patientsultrasound guided and in 2 patients CT guidedaspiration was done.
Assessment of infection
In 4 cases suspected of harboring infection culturesobtained from blood and urine did not grow anypathological organisms in any patient. Culture of thefluid aspirated from the abdomen showed positiveresult in 1(4.16%) patient. In remaining 20 patientscultures were not required to be done.
Table No. 6
No growth Positive
Blood culture 4(16.67%) 0
Urine culture 4(16.67%) 0
Pus culture 3(12.5%) 1(4.16%)
In the patient with positive culture E.coli wasgrown from the pus aspirated from the abdomen underCT guidance.
Complication Rates
10 (41.67%) patients developed local complications,out of these 4 had pancreatic necrosis associated withacute fluid collection and 6(25%) only had acute fluidcollection/s. 3(12.5%) developed systemiccomplications.
Treatment Strategy
All patients were managed with only appropriatesupportive therapy initially and no antibiotics weregiven. 1 patient who had infected collection underwentsurgical drainage and received specific antibiotictherapy based on culture sensitivity result and 3patients with negative culture results of collectionaspiration were given broad spectrum antibiotics. Rest20 patients recovered from illness with supportivetherapy only without antibiotics.
Another patient underwent surgical drainage forpersistent pancreatic pseudocyst after 6 weeks.
DISCUSSION
In the present study a total of 24 patients with acutepancreatitis were prospectively studied. The mean agewas found to be 40.66 years(range 16-68 years).According to Carter, the mean age of presentation ofacute pancreatitis is usually the sixth decade of lifewith peak age incidence being slightly higher infemales(1).
From several large studies describing acutepancreatitis, the two most common causes are chronicalcohol abuse and gallstones. The combined incidence
3. Dhawal Sharma--8-13.pmd 10/10/2013, 9:22 AM11

12 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
varies from 80 to 90 percent(2).Combined frequency ofboth these cause in our study is 87.5% whichcorresponds with these studies.
The prognosis in acute pancreatitis depends mostimportantly on the presence of necrosis of pancreas.Infection if present further worsens the course of acutepancreatitis. In several series overall rate of infectionhas been found to be 1.2% - 9.5%(3). The rate of infectionin acute necrotizing pancreatitis is reported to be muchhigher (40-70%)(3). Pancreatic necrosis can be diagnosedaccurately with help of CT scan in most cases howeverdiagnosis of infection is rarely possible by CT.According to Freeny the characteristic air bubblephenomenon that is suggestive of infection in acutepancreatitis on CT scan is seen in only 20-50% of allpatients with infected necrosis(4). As the fever and otherconstitutional symptoms suggestive of infection mayoccur in sterile necrotizing pancreatitis also,differentiation of sterile necrosis from infected necrosisis not possible clinically. Image guided aspiration ofpus and /or collection is a safe and accurate methodfor identifying infection in cases of acutepancreatitis(5)(6) .
In this study all the patients were initially managedwith appropriate supportive therapy only. 4 patientssuspected to be having infection all sources of infectionwere excluded with proper clinical examination andsupported with blood and urine cultures. An imageguided fine needle aspiration along with culture andsensitivity of the aspirate was performed in these 4patients who had fever, leukocytosis and clinicaldeterioration features suggestive of infection, howeverinfection was found in only 1(4.16%) patient. In thisstudy though the frequency of infection corroborateswith the previous studies(3), it may not reflect the truepicture of the study population because of smallernumber of cases in the study. The actual rate ofinfection may be rather lower than observed in thisstudy.
Several guidelines have been proposed for routineuse of antibiotics in all the cases of severe acutepancreatitis, but still there is no common consensusabout the type of antibiotic to be used, timing andduration of its usage(7(8)(9(10)(11)(12). In our study patientswith culture proven infected collection underwentsurgical drainage along with culture guided specificantibiotic therapy.3 patients with negative culture onFNA were treated with broad spectrum antibioticsonly. These patients were treated with antibioticsbecause of risk of introducing infection during
aspiration. This observation challenges the usualpractice of using antibiotics in all cases of acutepancreatitis without any proven infection.
Though there is a theoretical possibility ofworsening of infection in patients with infectedpancreatic collection or necrosis due to delay ininitiating antibiotic therapy, this may not be absolutelytrue in practice as the appropriate management ofinfected pancreatitis depends more on appropriatesupportive treatment and surgical intervention ratherthan antibiotics.
The findings in this study are distinct from thepreponderance of prior literature regarding antibiotictherapy in acute pancreatitis and are important in theirsuggestion of use of specific antibiotic therapy ininfected acute pancreatitis based on CT scan evaluationand guided aspiration in acute pancreatitis.
CONCLUSIONS
1. Appropriate supportive therapy is the mainstayof management of acute pancreatitis in even thosewith severe necrotizing pancreatitis.
2. Prophylactic antibiotics are not required in acutepancreatitis & should be used only when there isevidence of infection or some intervention isperformed.
3. Image guided fine needle aspiration of pancreasremains a safe and good method of identificationand differentiation of infected acute pancreatitisfrom sterile pancreatitis.
4. Appropriate surgical intervention is the treatmentof choice in those with infected pancreatitis.
Acknowledgements: We greatly acknowledge thesupport of patients who participated in this study.There were no conflicts of interest amongst the authors.There was no source of funding.
Ethical clearance: The study was approved byethical committee of Santosh Medical College &Hospital, and the study was conducted after informedconsent from patient/guardian
REFERENCES
1. Carter DC, 2000. Diagnosis and prognosis inacute pancreatitis. In, Trede M, Cater DC Surgeryof pancreas,2nd ed. Churchill Livingstone ,p:221-235.
3. Dhawal Sharma--8-13.pmd 10/10/2013, 9:22 AM12

International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 13
2. Mayerle J, Simon P, Lerch MM. Medical treatmentof acute pancreatitis Gastroentrol Clin N Am2004;33:853-869.
3. Sphoenberg MH, Rau B, Beger HG. Newapproaches in surgical management of severeacute pancreatitis. Digestion 1999;60(suppi 1):22-26
4. Freeny PC.Incremental dynamic bolus computedtomography of acute pancreatitis. Int J Pancreatol1993;13:147-158
5. Reber HA, Widdision AL. Pathogenesis ofinfected pancreatic necrosis In: Bradly EL 3RD ;Acute Pancreatitis: Diagnosis and Therapy, NewYork, Raven 1994, p: 85-92
6. Widdison AL, Karanjia ND, Reer HA. Routes ofspread of bacteria to panceas in acute necrotizingpancreatitis. Pancreas 1990; A713
7. British socity of gastroenterology: UnitedKingdom guidelines for management of acutepancreatitis. Gut 1998;42(suppl):S1-S13.
8. Uhl W, Warshaw A, Imrie C et al. IAP guidelinesfor surgical management of acute pancreatitis.Pancreatology 2002;2:565-573.
9. Pederzoli P, Bassi C, Vesentini S, Campedelli A.A randomized multicenter trial clinical trial ofantibiotic prophylaxis of septic complications inacute necrotizing pancreatitis with Imipenum.Surg Gynaecol obstet 1993;176;480-3
10. Delcenserie R, Yzet T, Ducroix JP. Prophylacticantibiotics in treatment of severe acute alcoholicpancreatitis. Pancreas 1996;13:198-201
11. Sainio V, Kemppainern E, Puolakkaineu Pet al.Early antibiotic treatment in acute pancreatitis .Lancet 1995; 346:663-7
12. Sharma VK, Howden CK. Prophylactic antibioticadministration reduces sepsis and mortality inacute necrotizing pancreatitis: A meta analysis.pancreas 2001; 22(1):28-31.
3. Dhawal Sharma--8-13.pmd 10/10/2013, 9:22 AM13

14 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
Autoimmune Thyroid Dysfunction and Meniere'sDisease
Rahil Muzaffar1, Owais Mattoo2, Anees Mir3, Rauf Ahmad4
1Postgraduate Resident, ENT Head & Neck Surgery, 2Postgraduate Resident, ENT Head & Neck Surgery, 3SeniorResident, ENT Head & Neck Surgery, 4Professor, ENT Head & Neck Surgery, Govt. Medical College Srinagar, J&K
ABSTRACT
Title: Autoimmune thyroid dysfunction and Meniere's disease.
Study Design: Prospective Case-Control study.
Method: This study was conducted in the Department of Otorhinolaryngology, Head & Neck Surgery,S.M.H.S Hospital, an associated hospital of Government Medical College Srinagar, for a period of 22months w.e.f January 2011 to October 2012. In this study, we evaluated the association between thyroidautoimmunity and Meniere's disease. 35 Meniere's disease patients were enrolled in this study andtwo groups as controls: group A, 20 subjects suffering from acute unilateral peripheral vestibulopathyof non-Meniere origin; and group B, 30 healthy volunteers. All subjects were submitted to assessmentof cochlear-vestibular function and analysis of standard thyroid function test, anti-TSH receptorantibody (TR-Ab), anti-thyroperoxidase antibody (TPO-Ab) and anti-thyroglobulin antibody (Tg-Ab).
Results: The prevalence of autoimmune thyroiditis in Meniere's disease patients was higher (P <0·01)when compared to control groups.
Conclusion: Our data demonstrate a significant association between Meniere's disease and thyroidautoimmunity, which suggest that an autoimmune factor may be involved in the aetiopathogenesisof this disease.
Keywords: Meniere, Autoimmune, Thyroglobulin, Thyroid-peroxidase
INTRODUCTION
Meniere’s disease is an idiopathic disorder of theinner ear featuring fluctuating Sensorineural hearingloss, episodes of vertigo and tinnitus1-3. Meniere’sdisease is associated with endolymphatic hydrops withdistortion and distention of the membranousendolymph containing portions of the labyrinthinesystem. In spite of the well-known histopathologicallesion of Meniere’s disease its aetiopathogenesis
Corresponding author:Rahil MuzaffarC/o. Dr. Muzaffar AliR/o. Hilal Abad Colony,Sector 1, Qamarwari, Srinagar,J&K, India-190010Email-id: [email protected] .Mobile No.+919858321825
remains unclear. Although most patients have noidentifiable underlying otologic disease, multiplepotential causes of endolymphatic hydrops have beensuggested. The proposed etiologies include, blockageat the endolymphatic sac or duct, hypoplasia of thevestibular aqueduct, genetic predisposition, viral andvascular etiology4-11. An immunological basis ofMeniere’s disease has been claimed by variousauthors12-15. The possible association betweenautoimmune thyroid disease and Meniere’s diseasehas been postulated for more than 30 years, but it isstill controversial. Pulec and House16 first reported that3% of patients with Meniere’s disease had a positivehistory for hyperthyroidism, and Powers et al.17 founda much higher prevalence of association betweenMeniere’s disease and hypothyroidism (17%).However, at the beginning of the 1980s, a relationship
DOI Number: 10.5958/j.2321-1024.1.2.021
4. Rahil --14-17.pmd 10/10/2013, 9:22 AM14

International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 15
between altered thyroid function and Meniere’sdisease was actually excluded by Kinney18 and byMeyerhoff et al.19 while Evans et al.20 showedsubsequently that 17% of sera from Meniere’s diseasepatients contained positive anti-thyroid-microsomeantibody titres. Fattori B et al.21 in 2008 evaluated theassociation between thyroid autoimmunity andMeniere’s disease in a non-selected group of patientsand their data demonstrate a statistically significantassociation between Meniere’s disease and thyroidautoimmunity.
The aim of our study was to evaluate the prevalenceof thyroid autoimmunity in Meniere’s disease patientscompared with a group of healthy subjects and a groupof patients suffering from non-Meniere vestibulopathy.
MATERIAL AND METHOD
A prospective study was conducted in theDepartment of Otorhinolaryngology, Head & NeckSurgery, Shri Maharaja Hari Singh (SMHS) Hospital,an associated hospital of Government Medical CollegeSrinagar, for a period of 22 months w.e.f January 2011to October 2012.
Inclusion criteria
This study included female patients presentingwith symptom complex of Meniere’s disease and werediagnosed on the basis of diagnostic criteria’s proposedby the American Academy of Otolaryngology andHead and Neck Surgery (AAO-HNS).
Exclusion Criteria
Meniere’s syndrome patients, atypical Meniere’sdisease patients, patients with other known causes ofvertigo, patients with history of migraine, patients withCNS disorders were excluded from this study. Alsosubjects with any other known autoimmune disorderwere excluded from this study.
In this prospective study 35 patients presentingwith the symptom complex of Meniere’s disease wereenrolled. 25 patients were females (mean age 38.7±10.8years) and 10 patients were males (mean age 46.5±12.9years). Two groups of sex- and age-matched subjectsserved as controls; group A comprised 20 patients(mean age 43.1±3.2 years) suffering from acuteunilateral peripheral vestibulopathy and group Bincluded 30 healthy volunteers (mean age 39.7±6.2years).
All Meniere’s disease patients and group A patientswere submitted to clinical and instrumentalassessment of cochlear–vestibular function. The testsincluded pure tone audiometery, the head-shaking testand Fitzgerald–Hallpike caloric function test.
Blood samples were collected from all the studysubjects for the determination of serum thyroid-stimulating hormone (TSH), free triiodothyronine(FT3), free thyroxine (FT4), anti-TSH receptor antibody(TR-Ab), anti-thyroperoxidase antibody (TPO-Ab) andanti-thyroglobulin antibody (Tg-Ab) levels.
Serum FT3 levels (Normal range 2·1–4·6 pg/ml (3·2–7·1 pmol/l) and FT4 levels (Normal range 8·6–18·6 pg/ml (11·0–23·9 pmol/l) were measured by specificradioimmunoassay (RIA), TSH was determined withan ultrasensitive immunoradiometric assay (Normalrange 0·3–3·6 mU/l). Serum Tg-Ab (< 100IU/ml), TPO-Ab (<40IU/ml) & TR-Ab (<1IU/ml) levels weremeasured by specific RIA.
RESULTS
Thyroid function and autoimmunity tests of all thestudy subjects are shown in Table 1:
Table 1: Thyroid function & autoimmunity tests ofstudy subjects
Test Meniere’s Group A Group Bdisease (n=20) (n=30)
patients(n=35)
TSH 1.88(0.2-1.99) 1.1(0.1-3.3) 1.3(0.38-3.21)
T3 2.8±0.4 3.1±0.4 3.0±0.2
T4 10.8±4.9 8.9±1.9 10.3±1.8
TR-Ab 0.4±0.3 0.3±0.1 0.3±0.2
TPO-Ab 119±187.7 80.1±321.1 25.1±37.8
Tg-Ab 22.4±41.2 20.1±21.2 22.3±21.9
TSH-Thyroid stimulating hormone, T3-tri-iodothyronine, T4-thyroxine, TR-Ab-Thyroid receptorantibody, TPO-Ab-Thyro-peroxidase antibody, Tb-Ab-Thyroglobulin Antibody
In our study the prevalence of autoimmune thyroiddisease was higher in Meniere’s disease patients (p<0.01) as compared to control groups. However therewas statistically no significant difference (p> 0.05) inthe prevalence of autoimmune thyroid disease amongthe control groups (table 1).
4. Rahil --14-17.pmd 10/10/2013, 9:22 AM15

16 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
Table 2: Autoimmune profile of study groups:
Test Meniere’s Group A Group Bdisease (n=20) (n=30)
patients(n=35)
TR-Ab 1(2.85%) - -
TPO-Ab 12(34.2%) 3(15%) 5(16.6%)
Tg-Ab 5(14.2%) 1(5%) 2(6.6%)
Ab+ 18(51.4%) 4(20%) 7(23.3%)
Ab+ Antibody positive
Among the patients of Meniere’s disease, 18 (51.4%)patients were positive for thyroid antibodies, out ofwhich 12 (34.2%) were positive for TPO-Ab, 5 (14.2%)were positive for Tg-Ab and only 1(2.85%) patient ofMeniere’s disease was positive for TR-Ab (table 2).
In control group A 4 (20%) subjects were positivefor thyroid antibodies, out of which 3 (15%) werepositive for TPO-Ab, 1 (5%) were positive for Tg-Aband none of the subject in group A was positive forTR-Ab (table 2). In control group B 7 (23.3%) subjectswere positive for thyroid antibodies, out of which 5(16.6%) were positive for TPO-Ab, 2 (6.6%) werepositive for Tg-Ab and none of the subject in group Bwas positive for TR-Ab (table 2).
DISCUSSION
Meniere’s disease is an idiopathic disorder of theinner ear, in spite of the fact that environmental agentsand local factors have been postulated, the exactaetiopathogenesis of the disease remains unclear. Thereis most probably a multi-factorial pathogenesis behindthe disease and recent studies have reinforced thetheory of a possible involvement of the immunesystem. However, the role actually played byautoimmune reactions in the pathogenesis of Meniere’sdisease is still under debate.
Several authors have focused on the immuneresponse to antigens in the internal ear and on thepossibility of identifying the auto-antigens involvedin the genesis of hydrops. Wei and colleaguesdemonstrated antibodies against autologous ganglioncells in patients with Meniere’s disease. High levels ofanti-collagen II antibodies in the serum of thesepatients were detected by Yoo and co-workers.. On theother hand Fattori et al, analyzing the levels of auto-antibodies against basal membrane proteins as wellas collagen II, V and I, were not able to define any roleof these antibodies in the pathogenesis of Meniere’sdisease. More recently, the association between thepresence of anti-phospholipid antibodies and audio-
vestibular dysfunction has been reported22. Pendrin isa protein encoded by the Pendred syndrome (PDS)gene and expressed both in thyroid cells and theinternal ear, and could act as a shared auto-antigen.So far no data exist on the presence of serum auto-antibodies against pendrin (both in thyroid and eardiseases). However, a recent study suggests that PDSshould be considered a new susceptibility gene toautoimmune thyroid disorders23.
Brenner M et al. (2004) conducted a retrospectivecase-control study comparing the use of thyroidhormone supplements between patients withMeniere’s disease and controls. He reported thattreatment with L-T4 was significantly more frequentin patients with Meniere’s disease than in the normalcontrol population. Although the reason foradministering L-T4 therapy was not investigated, theauthors postulated chronic autoimmune thyroiditis tobe the main cause.
In our study the prevalence of autoimmune thyroiddisease was higher in Meniere’s disease patients (p<0.01) as compared to control groups. However therewas statistically no significant difference (p> 0.05) inthe prevalence of autoimmune thyroid disease amongthe control groups. Thus suggesting the possibleassociation between autoimmunity and Meniere’sdisease. However more studies need to be conductedin order to firmly establish the role of auto-immunityas the etiological factor of Meniere’s disease as differentauthors have come to different conclusions regardingthe role of auto-immunity in Meniere’s disease.
Conflict of Interest: There is no conflict of interest.
Source of Funding: Self funded.
Ethical Clearance: Sought from the ethical committee.
Acknowledgement: None
REFRENCES
1. N. J. P. Beasley and N. S. Jones.Meniere’s disease:evolution of a definition.The Journal ofLaryngology and Otology 1996; 110:1107-1113.
2. C. S. Hallpike. Postgraduate Medical Journal.1955 July; 31(357): 330–340.
3. P. H. Van De Heyning, F. L. Wuyts, J. Claes, et al.Definition, Classification and Reporting ofMeniere’s disease and its Symptoms. Deptt. ofOtorhinolaryngology, University of Hospital ofAntwerp, Belgium 1997, Vol. 117, Nos 526, Pages5-9.
4. Rahil --14-17.pmd 10/10/2013, 9:22 AM16

International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 17
4. Etsuo Yamamoto and Chikashi Mizukami.Development of the Vestibular Aqueduct inMeniere’s Disease. Acta Oto-laryngologica 1993;Vol. 113, Nos 504: Pages 46-50.
5. Jackler RK, Luxford WM, Brackmann DE et al.Endolymphatic sac surgery in congenitalmalformations of the inner ear.Deptt. ofOtolaryngology—Head and Neck Surgery,University of California, San Francisco.Laryngoscope. 1988 Jul; 98(7): 698-704.
6. Robert S. Kimura. Animal models of inner earvascular disturbances. American Journal ofOtolaryngology March 1986; Volume 7, Issue 2, 4Pages 130-139.
7. K.C. Horner Old theme and new reflections:Hearing impairment associated withendolymphatic hydrops. Hearing ResearchMarch 1991; Volume 52, Issue 1, Pages 147-156.
8. Wolfgang Arnold, Hans P. Niedermeyer. HerpesSimplex Virus Antibodies in the Perilymph ofPatients With Meniere Disease. Archives ofOtolaryngology Head and Neck Surgery. 1997;123(1): 53-56.
9. Klockars T, Kentala E. Inheritance of Meniere’sdisease in the Finnish population. ArchivesOtolaryngology Head Neck Surgery. 2007 Jan;133(1): 73-7.
10. Arweiler-Harbeck D, Horsthemke B, Jahnke K,et al Genetic aspects of familial Meniere’s disease.Otology and Neurotology. 2011 Jun; 32(4):695-700.
11. Frykholm, Carina; Larsen, Hans-Christian; Dahl,Niklas; et al. Familial Meniere’s Disease in FiveGenerations. Otology Neurotology. 2006 August;27(5): 681-6.
12. K. L. Evans, D. L. Baldwin, D. Bainbridge et al.Immune status in patients with Meniere’s disease.European archives of otorhinolaryngology 1998;Volume 245, Number 5: 287-292.
13. McCabe BF. Autoimmune sensorineural hearingloss. Annals of Otolaryngology Rhino-Laryngology. 1979;88:585–9
14. Hughes GB, Barna HP, Kinney SE, Calabrese LH,Hamid MA, Nalepa N. Autoimmuneendolymphatic hydrops: five yearreview. Otolaryngology Head & NeckSurgery. 1988;98:221–5.
15. Hughes GB, Barna BP, Kinney SE, Calabrese LH,Nalepa N. Clinical diagnosis of immune inner eardisease. Laryngoscope. 1988;98:251–3.
16. Pulec L, House WF. Meniere’s disease study:three-year progress report. Int J EquilibRes.1973;3:156–65.
17. Powers WH. Metabolic aspects of Meniere’sdisease. Laryngoscope. 1978;88:122–9.
18. Kinney SE. The metabolic evaluation in Meniere’sdisease. Otolaryngol Head NeckSurg.1980;88:594–8.
19. Meyerhoff WL, Paparella MM, GudbrandssonFK. Clinical evaluation of Menière’sdisease.Laryngoscope. 1981;91:1663–8.
20. Evans KL, Baldwin DL, Bainbridge D, MorrisonAW. Immune status in patients with Meniere’sdisease. Arch Otorhinolaryngol. 1988;245:287–92.
21. Fattori B, Nacci A, Dardano A, et al Possibleassociation between thyroid autoimmunity andMeniere’s disease. Clinical and ExperimentalImmunology. 2008 Apr; 152(1): 28-32.
22. Mouadeb DA, Ruckenstein HJ. Antiphospholipidinner ear syndrome. Laryngoscope. 2005;115:879–883.
23. Hadj Kacem H, Rebai A, Kaffel N, Masmoudi S,Abid M, Ayadi H. PDS is a new susceptibilitygene to autoimmune thyroid diseases: associationand linkage study. J Clin EndocrinolMetab. 2003;88:2274–80.
4. Rahil --14-17.pmd 10/10/2013, 9:22 AM17

18 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
Comparative Study of Surgical Site Infections in ElectiveSurgeries
Mamta Rai1, T S Bhagat2, Shalabh Gupta3, Atul Kumar Gupta4, Rajiv Verma5, Dhawal Sharma1,Pankaj Solanki1
1Postgraduate, Third year, 2Professor, Unit Head, 3Professor, Head of Department, 4Associate Professor, Unit Head,5Assistant Professor, Deptt of General Surgery, Santosh Medical College & Hospital
ABSTRACT
Surgical site infection [SSI] continues to be a major source of mortality and morbidity in developingcountries despite recent advances in aseptic technique. This study was conducted in Santosh MedicalCollege & Hospital Ghaziabad to determine the exact incidence of surgical site infection in electivesurgery and separately in each class of wound, the commonest bacterial pathogen, role of pre andpost operative antibiotic and the various predisposing factors influencing the development of SSI.The diagnosis of infection was made on clinical, bacteriological and epidemiological basis. In ourstudy the most common pathogen is Staphylococcus aureus and most sensitive antibiotic is Piperacillinplus Tazobactum. Older age group and females are more prone. Patient in whom diathermy wasused and drain was not used are less prone. Prevalence of SSI increased with increasing duration ofhospital stay and increased duration of surgery.
INTRODUCTION
Surgical site infection [SSI] is an infection thatoccurs at an infection site, or any part of the anatomythat was opened or manipulated during the procedurewithin 30 days of surgery if no implant in situ andwithin one year if implant is in situ [1].
Despite the advances made in asepsis, antimicrobialdrugs, sterilization and operative techniques, SSIcontinue to be a major problem in all branches ofsurgery in the hospitals [2]. It has been responsible forthe increasing cost, morbidity and mortality related tosurgical operations and continues to be a majorproblem in hospitals with modern facilities andstandard protocols of preoperative preparations andantibiotic prophylaxis.
In 1964 National Academy of Science classified thesurgical wounds according to the degree of microbialcontamination as clean, clean – contaminated,contaminated and dirty [3].
In the majority of SSI cases, the pathogen source isthe native flora of the patients skin, mucousmembrane, or hollow viscera[4]. Most typically aerobic
gram +ve cocci such as Staphylococcus aures andMRSA representing an increasing proportion of suchinfection in recent years[5][6]. Factors which influencethe occurrence of SSI can be classified as patient related,surgery related, anesthesia related.
MATERIAL AND METHOD
This study was conducted in department of GeneralSurgery at Santosh Medical College & HospitalGhaziabad from May 2009 to May 2011.The materialof this study consisted of 100 patients undergoingelective major surgeries.
All wounds were assessed 48 hours after primarydressing and then assessment done for ASEPSISwound scoring. If SSI occurred, next step was tocategorize it as Superficial SSI, Deep incision SSI andOrgan / space SSI. After classification of wound eachwound swab or pus swab was cultured on plates ofsheep-blood agar, Mac conkey’s agar and a tube ofglucose broth. These were then incubated at 370covernight. After obtaining pure culture of the pathogenits antibiotic sensitivity was determined by the Discdiffusion method as described by Kirby Bayer method.
DOI Number: 10.5958/j.2321-1024.1.2.022
5. mamta rai --18-22.pmd 10/10/2013, 9:22 AM18
International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 19
RESULTS
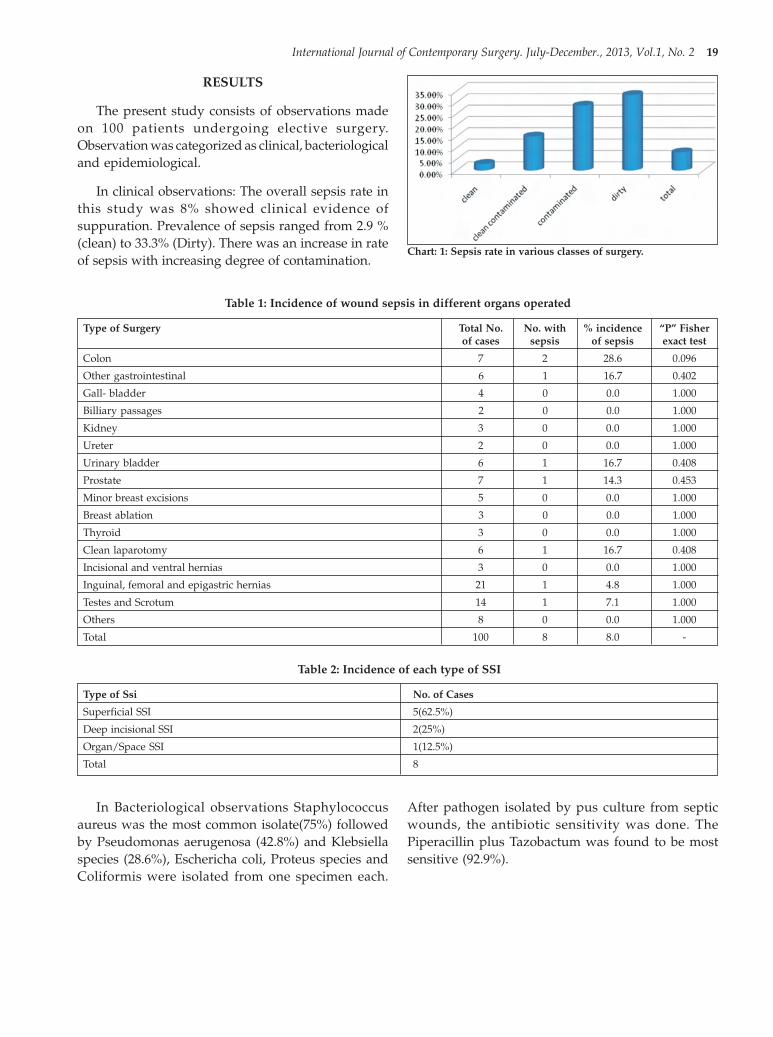
The present study consists of observations madeon 100 patients undergoing elective surgery.Observation was categorized as clinical, bacteriologicaland epidemiological.
In clinical observations: The overall sepsis rate inthis study was 8% showed clinical evidence ofsuppuration. Prevalence of sepsis ranged from 2.9 %(clean) to 33.3% (Dirty). There was an increase in rateof sepsis with increasing degree of contamination.
Chart: 1: Sepsis rate in various classes of surgery.
Table 1: Incidence of wound sepsis in different organs operated
Type of Surgery Total No. No. with % incidence “P” Fisherof cases sepsis of sepsis exact test
Colon 7 2 28.6 0.096
Other gastrointestinal 6 1 16.7 0.402
Gall- bladder 4 0 0.0 1.000
Billiary passages 2 0 0.0 1.000
Kidney 3 0 0.0 1.000
Ureter 2 0 0.0 1.000
Urinary bladder 6 1 16.7 0.408
Prostate 7 1 14.3 0.453
Minor breast excisions 5 0 0.0 1.000
Breast ablation 3 0 0.0 1.000
Thyroid 3 0 0.0 1.000
Clean laparotomy 6 1 16.7 0.408
Incisional and ventral hernias 3 0 0.0 1.000
Inguinal, femoral and epigastric hernias 21 1 4.8 1.000
Testes and Scrotum 14 1 7.1 1.000
Others 8 0 0.0 1.000
Total 100 8 8.0 -
Table 2: Incidence of each type of SSI
Type of Ssi No. of Cases
Superficial SSI 5(62.5%)
Deep incisional SSI 2(25%)
Organ/Space SSI 1(12.5%)
Total 8
In Bacteriological observations Staphylococcusaureus was the most common isolate(75%) followedby Pseudomonas aerugenosa (42.8%) and Klebsiellaspecies (28.6%), Eschericha coli, Proteus species andColiformis were isolated from one specimen each.
After pathogen isolated by pus culture from septicwounds, the antibiotic sensitivity was done. ThePiperacillin plus Tazobactum was found to be mostsensitive (92.9%).
5. mamta rai --18-22.pmd 10/10/2013, 9:22 AM19

20 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
Table: 3: Composite antibiotic sensitivities of various pathogens isolated by pus culture from septic wounds.
Antibiotics Staphy Pseudomonas Klebsiella Escherichia Proteus sp. Coliforms Sensitivitylococcus aureus aeruginosa species coli (n=1) %
(n=6) (n=3) (n=2) (n=1) (n=1) (out of 14)
Cefotaxime. 3 - - - - - 21.4
Amoxycillin. 1 - - - - - 7.1
Sulpha plus Trimeth. 1 - - - - - 7.1
Ciprofloxicin. 3 0 1 - - 1 35.7
Amikacin. 1 1 2 - - 1 35.7
Piperacillin plus Tazobactum 6 2 2 1 1 1 92.9
Ceftriaxone. 3 - - - - - 21.4
Ofloxacin. 3 1 - - 1 - 35.7
Linezolid 4 - - - - - 28.6
Poly. B - - - - 1 - 7.1
In epidemiological observations prevalence ofsepsis ranged from 4.2% to 28.6% in different agegroups. The prevalence was maximum in age groupof 61 years and above, minimum in 21 to 30 years ofage group. There is no significant association betweenage and incidence of sepsis (P= 0.444).
Table: 4: Frequency of Sepsis according to patient’sAge
Age in years. No. with Total No. PercentageSepsis of cases of SSI
13-20 1 15 6.7
21-30 1 24 4.2
31-40 1 17 5.9
41-50 1 16 6.3
51-60 2 21 9.5
61 and above 2 7 28.6
Total 8 100 8
Out of 100 pts 68 are males and 32 are females, inmales 5 pts (7.4%) developed sepsis and in females 3pts (9.4%) developed sepsis, therefore the prevalenceof sepsis was found to be more in females as comparedto males. But there is no statistically significantassociation (P=1).
Table 5: Frequency of sepsis according to Duration ofPreoperative stay:
Age in years. No. with Total No. PercentageSepsis of cases of SSI
0-2 4 63 6.3
3-6 1 10 10.0
7-14 2 19 10.5
15 and above 1 8 12.5
Total 8 100 8.0
Factors such as duration of hospital stay increasethe sepsis rate and order of the surgery. Prevalence ofsepsis in first order (out of 100 pts 40 were in first orderin which 3 had develop sepsis) 7.5% to third order (29pts taken in this category in which 3 had developsepsis) 10.3%. But there is no significant associationbetween them (P=0.880).
In patients in whom surgery was completed within30 minutes no sepsis developed but incidence increaseswith increase duration of surgery and no significantstatistic association found (P=0.631). Prevalence ofsepsis in which diathermy not used 7.5% (in 53 pts 4had develop sepsis) and 8.5% (in 47 pts 4 had developsepsis) in which diathermy used. There is no significantstatistical association was found. But incidence ofsepsis increased in which drain was used 11.4% (in 35pts 4 develop SSI) as compared to drain not used 6.1%(in 65 pts 4 develop SSI) and no significant associationstatistically (P=0.448) found. Prophylactic use ofantibiotic and sepsis also not made significantassociation (P=1).
Chart: 2: Incidence of Sepsis according to Patient’s Sex:
5. mamta rai --18-22.pmd 10/10/2013, 9:22 AM20

International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 21
DISCUSSION
In clinical consideration: overall sepsis rate inpresent study was 8%. Rates varying from 2.9% (clean)to 33.3% (dirty) for different classes of surgery. Thesefindings are in agreement with the findings quoted inthe literature wherein the rate of sepsis has beenreported to be varying from 1-2% in clean [7] to 40% indirty [7]. Maximum no of SSI in our study was foundin colon surgery (28.6%) which is fairly matching withthe Hnatko et al who found colon surgery (27.9%) wasassociated with maximum no sepsis.
In bacteriological consideration: Staphylococcusaureus (85.7%) most common pathogen isolated whichis agreed with the PHPLS [8] and HOWE and Mozden[9]. In antibiotic sensitivity of various pathogensPiperacillin plus Tazobactum combination is mostuseful antibiotic.
In epidemiological considerations: Present studyshowed an association between sepsis and advancingage supporting the similar findings of Barnes et al.Explanations for this finding include increasedprevalence of co-morbid conditions, an increasedseverity of acute illness, and a decreased host responseto bacterial invasion due to impaired immunity inolder patients[10][11].
Present study showed slightly higher rate of sepsisamong females but which is not significant statistically.All studies also not show significant variations withsex. PHLS, MINCHEW & CLUFF, NRC, Di Leo A etal[8][12][13][14]. There is no significant statistical associationbetween duration of pre- operative hospital stay andsepsis in our study. But other studies NRC study [15]
and Davidson et al found that greater length of preoperative hospitalization was associated with anincreased sepsis rate independent of other influencingfactor [16].
There is little association between the use ofdiathermy and wound sepsis which was not significantstatistically. Approximately in half of the operationsdiathermy was used and incidence of sepsis was nearlysame in both the groups. This is matching with thefindings of Wanabe et al 2008[17]. Sepsis rate was highin the cases where drain was used in the present studybut the difference was not significant statistically. It issupported by the findings of Alexander et al, ManzCW et al and Crowson WN et al[18][19][20].
Present study and the statement of the Bratzler DMet al who concluded that although prophylacticantibiotics have important role in reducing rate of SSIin clean-contaminated, contaminated and dirty classesbut there is no role in clean class of wounds exceptwhere we put implants in situ
CONCLUSIONS
This study comprised 100 electively operatedpatients admitted in the Dept. of General Surgery,Santosh
1. The overall incidence of sepsis was 8.0%.
2. The sepsis rate in clean class of surgery was 2.8%,in clean-contaminated class 15.0%, incontaminated class 28.5% and in dirty class was33.3%.
3. The incidence of sepsis was highest in colonsurgeries followed by other GI surgeries, urinarybladder surgeries and prostate sugeries.
4. Out of 8 cases of SSI 5 were of superficial type SSI,2were of deep incisional type and 1was of organ/space type.
5. The commonest bacterial pathogen isolated wasStaphylococcus aureus.
6. Most useful antibiotic in treating surgical woundsepsis apparently was pipracillin and Tazobactumcombination.
7. Age of the patient, duration of pre-operativehospital stay, duration of surgery, use of drains allstrongly influenced the rate of SSI.
8. There was little more incidence of SSI in females(which was not significant statistically) and caseswhere we used cautery.
Chart: 3: Incidence of Sepsis relative to use of Drains.
5. mamta rai --18-22.pmd 10/10/2013, 9:22 AM21

22 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
9. Use of prophylactic antibiotics in clean categoryof cases had no role in preventing SS
ACKNOWLEDGEMENTS
We greatly acknowledge the support of patientswho participated in this study. There were no conflictsof interest amongst the authors. There was no sourceof funding.
Ethical clearance
The study was approved by ethical committee ofSantosh Medical College & Hospital, and the studywas conducted after informed consent from patient/guardian
REFRENCES
1. Mangram AJ, Horan TC, Pearson ML, et al.Guideline for prevention of surgical site infection,1999. Hospital infection control practicesadvisory committee. Infect Control HospEpidemiol. Apr 1999; 20(4): 250-78; quiz 279-80.
2. Mahesh CB, Shivakumar S, Suresh BS,Chidanand SP, Vishwanath Y.A prospective studyof Surgical site infections in a teaching Hospital.Journal of clinical and diagnostic research 2010October;4: 3114-9.
3. Altemeier WA, Burk JF, Pruit BAJ, Sandusky WR.Definition and classification of surgical infections.In Manual on control of infection in surgicalpatients. 2nd Ed, Lippincott, Philadelphia,1984;2:28.
4. Altemeier WA, Culbertson WR, Hummel RP.Surgical considerations of endogenous infections-sources, types, and methods of control. Surg ClinNorth Am.1968;48: 227-240.
5. Schaberg DR. Resistant gram-positive organisms.Ann Emerg Med. 1994;24: 462-464.
6. Schaberg DR, Culver DH, Gaynes RP. Majortrends in the microbial etiology of nosocomialinfection. Am j Med.1991;91(3B):72S-75S.
7. Cruse PJE, Foord R. The epidemiological ofwound infection. A 10 year prospective study of62939 wounds. Surg. Clin. North Am. 1980;60(1):27-40.
8. Public Health Laboratory Service. Lancet. 1960;11: 659.
9. Nahmias AJ, Eickhoff TC. New Eng J Med. 1961;265: 74: 120-177.
10. Pessaux P, Msika s, Atalla D, Hay JM, Flamant Y.Risk factors for postoperative infectionscomplications in noncolorectal abdominalsurgery. a multivariate analysis based on aprospective multicentre study of 4718patients.Arch Surg 2003; 138: 314-24.
11. Raymond D, Pelletier S, Crabtree T, Schulman A,Pruett T, Sawyer R. Surgical infection and theaging population. Am Surg 2001;67:827-32.
12. Minchew BH, Cluff LE. J Chron Dis.1961; 13:354.13. National Research council-National Academy of
Sciences. Ann Surg1964;160(Suppl 2):1.14. Di Leo A, Piffer S, Ricci F, et al. Surgical site
infections in an Italian Surgical ward: aprospective study. Surg infect (Larchmt).2009;10(6):533-8.
15. National Research Council Associates Committeeon Control of Hospital Infection. Can Med Ass J.1960;82:403.
16. Davidson AI,Clark C, Smith G. Br. J.Surg.1970;57:847.
17. Wantanabe A, Kohnoe S, Shimabukuro R, et al.Risk factors associated with surgical site infectionin upper and lower gastrointestinal surgery. SurgToday. 2008;38: 404-412.
18. Tsujinaka S, Kawamura YJ, Konishi F, et al; Pelvicdrainage for anterior resection revisited: use ofdrains in anastomotic leaks. ANZ J Surg.2008 Jun;78(6): 461-5.
19. Guyot A, Layer G; MRSA – ‘bug-bear ’ of asurgical practice: reducing the incidence of MRSAsurgical site infections. Ann R Coll Surg Engl.2006Mar;88(2):222-3.
20. Gurusamy KS, Samraj K; Routine abdominaldrainage for uncomplicated opencholecystectomy. Cochrane Database SystRev.2007 Apr 18;(2):CD006003.
5. mamta rai --18-22.pmd 10/10/2013, 9:22 AM22

International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 23
Delayed Presentation of Primarily Missed FracturesReporting to a Tertiary Care Centre: A Retrospective Study
Muzamil Ahmad Baba1, Bashir Ahmed Mir2, M A Halwai2, Adil Bashir Shikari1, Shakir Rasheed3, OmarKhursheed3, Qazi Manan3
1Senior Resident, 2Associate Professor, Department of Orthopaedics, Govt. Medical College Srinagar, J&K3Postgraduate Resident, GMC Srinagar
ABSTRACT
Background: The purpose of the study was to evaluate the most frequently missed fractures byprimary care physicians and identify the most difficult areas of radiographic interpretation and suggestmeasures to avoid these in future.
Materials and Method: A retrospective study was carried on hospital based data of a period of threeyears from 2009 to 2012 of all patients with fractures which were initially missed by primary carephysicians and presented late to the hospital.
Results: A total of 50 fractures where confirmed to have been missed by primary care physiciansduring this period from the hospital records. Out of these 34 (68%) cases where seen in children lessthan 14 years of age (average 7.6 years) and 16 (32%) in adults. The most frequently missed fractureswhere around the elbow 14 (28%), wrist and hand 12 (24%), around hip 11 (22%), ankle 8 (16%) and5 (10%) in other regions including 2 in foot, 1 each in spine, shoulder and knee.
Conclusion: This study revealed that majority of missed injuries are seen around the elbow and thehip. If missed and not treated properly can lead to serious complications. So it is suggested that allprimary care physicians should undergo a specifically directed educational program in these areasto suspect and diagnose such injuries in time to avoid any complications related to such injuries.
Keywords: Missed Fractures, Complications, Delayed Presentation
INTRODUCTION
Majority of the patients in our state of a developingnation lack access to proper health care centres. Mostof the population belongs to the rural areas and anyhealth related issue including trauma are first seen bythe primary health care physicians in the peripheries.Any radiographs that are taken are interpreted by themand decisions made based on the initial interpretation.Misdiagnosing fractures in such situation is a verycommon occurrence and can have seriousconsequences because of delay in treatment and longterm disability.3 The consequences may range fromminor pain and inconvenience to the patients toadverse long term outcome and functional limitationsdue to fracture non-union, osteonecrosis, deformitiesand joint stiffness which may need more complexsurgeries.6,10 These cases are also a common reason formedical legal claims in developed nations like UnitedStates.1,10 The current study was done to identify the
potential sites of misdiagnosing fractures andsuggesting measures to decrease the incidence andprevent long term complications.
MATERIAL AND METHOD
After obtaining ethical board approval (IRB) aretrospective review was carried out on the records ofall patients over a three year period (2009 to 2012) atGovernment Hospital for Bone and Joint Surgery,Barzullah, Srinagar, Kashmir. The hospital is the onlymajor tertiary care centre in the valley dealing withorthopaedic trauma. The records of all the patientsadmitted with fractures which had been first seen byprimary care physicians at the primary care centres ofthe valley and had a delayed presentation to ourhospital from the hospital records where collected. Thedata concerning the residence, age, gender and thedistribution of fracture was recorded.
DOI Number: 10.5958/j.2321-1024.1.2.023
6. muzamil 26th--23-26.pmd 10/10/2013, 9:22 AM23

24 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
RESULTS
During the period of these three years the studyrevealed a total of 50 patients 22 males and 28 females,in the age group of 3 to 72 years. 34 (68%) cases werechildren in the age of less than 14 years (average 7.6years) and 16 (32%) were adults with an average ageof 56 years (Table 1).
Table 1. Age distribution
Age group Number of cases
0-10 years 18 (36%)
11 - 20 years 16 (32%)
21 - 30 years 1 (2%)
31 - 40 years 2 (4%)
41 – 50 years 0
51 – 60 years 2 (4%)
61- 70 years 9 (18%)
71 – 80 years 2 (4%)
The majority of patients belonged to south Kashmir (Table 2).
Table 2. Regional distribution
District Number of cases
Anantnag 10 (20%)
Bandipora 3 (6%)
Baramullah 2 (4%)
Budgam 1 (2%)
Ganderbal 1 (2%)
Kulgam 11 (22%)
Kupwara 10 (20%)
Pulwama 7 (14%)
Shopian 5 (10%)
Srinagar 0
Out of 50 cases the regional distribution of fractures includedelbow 14 (28%), wrist and hand 12 (24%), around hip 11 (22%),ankle 8 (16%) and 5 (10%) in other regions including 2 in foot, 1each in spine, shoulder and knee. The type of fracture is furtherdiscussed in table 3.
Table 3. Distribution of patients on anatomicallocation of fracture
Anatomical location No. of cases
Spine 1 (2%)
Shoulder 1 (2%)
Elbow 14 (28%)
Wrist and Hand 12 (24%)
Hip 11 (22%)
Knee 1 (2%)
Ankle 8 (16%)
Foot 2 (4%)
The most commonly missed fractures includefractures around the elbow such as lateral condyle inchildren, radial head and neck fractures, scaphoidfractures, undisplaced femoral neck fractures andmalleolar injuries around the ankle. There were 2 casesof lisfranc fracture dislocation and 1 case each of a tibialplateau fracture and a compression fracture of thelower dorsal spine (Table 3).
DISCUSSION
The diagnosis of an acute fracture is based uponan accurate history, a thorough clinical examinationand an appropriate imaging. The identification of highrisk patients (such as elderly and other patientssusceptible to fragility fractures) and mechanism ofinjury will lead to greater index of suspicion for certaininjuries.
The present study revealed that majority of thefractures missed on initial radiography where in theregion of elbow and the hip, followed by the ankleregion. Studies in the past have shown higherincidence of missed injuries around the ankle.4,5,10 Thereason behind our data could have been due to higherpaediatric population with injuries around the elbowand another group of elderly patients with osteoporoticfractures around the hip.
It is necessary to improve our health care at all levelsto improve our health care system. This would not onlyhelp to serve the patients better but would also reducethe cost. In a literature review the diagnostic errors inthe radiographic interpretation ranges from 8 – 11%.2,7,9
These errors can have significant clinical and legalconsequences.
Various measures have been suggested in the pastto avoid these errors in diagnosing fractures but mostof them are not applicable in our set up.6,7,9 The majorityof patients reporting to a tertiary care institute in ourvalley are first seen at the peripheral hospitals. Afocussed educational program in these hospitals hasto be carried out in order to avoid or at least decreasethe incidence of such missed injuries which is quitehigh in our set up. Various strategies includingeducational programs emphasizing on properassessment of patients, obtaining appropriate X-raysand assessing the adequacy of the views taken.Incomplete X-rays may miss obvious fractures if atleast two views are not obtained. Figure 1 and 2 depict
6. muzamil 26th--23-26.pmd 10/10/2013, 9:22 AM24

International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 25
a patient with an A/P view of the elbow which showssubtle changes and an obvious fracture on lateral viewwhich could have been easily missed (Fig.1, Fig.2).
Identifying a major long bone fracture from acrossthe room can be relatively straight forward; howevermore subtle injuries require a systematic approach toX-ray interpretation.
Finally it is important to keep in mind thelimitations of plain x-ray in identifying all fractures.In a patient with a fall and sustaining an injury aroundthe hip and clinical examination is suggestive of afracture a normal X-ray does not exclude the diagnosis.The primary care physicians need to identify suchpatients and refer them for further investigations andconfirmation of diagnosis as missing such injuries maylead to catastrophic results like osteonecrosis and non-union which may later on need complex surgeries.
We are aware of several limitations in our study.One is a part it is a retrospective study and all casesmay not have been included in the study, as many casesmay not have revealed the history also there was nocontrol group in our study which would have helpedin better statistical analysis. Nevertheless this is oneof the first of its kind of studies that was carried outwhich is a feat in itself and would lead to more studiesin the future.
CONCLUSION
This study although with its limitations showedmajority of missed injuries are seen around the elbowand the hip. If missed and not treated in time may leadto serious complications and medical legal issues. Soit is suggested that all primary care physicians shouldundergo a specifically directed educational programas suggested above in order to avoiding anycomplications related to such injuries.
Conflict of Interest: There is no conflict of interest
Source of funding: Self- funded
Ethical Clearance: Sought from the ethical committee
ACKNOWLEDGEMENTS
We thank Dr. Mubashir, Dr. Majid and Dr. Nailafor helping us in compiling the data. We also thankMr. Hameed for his technical assistance.
REFERENCES
1. Berlin L. Defending the “missed” radiographicdiagnosis. AJR Am J Roentgenol 2001;176:317-22.
2. Fleisher G, Ludwig S, McSorley M. Interpretationof pediatric x-ray films by emergency departmentpediatricians. Ann Emerg Med 1983;12:153-8.
3. Guly HR: Diagnostic errors in an accident and
Fig. 2. X-ray A/P and Lateral views of the same patient depictingan obvious fracture which could have been missed.
Fig. 1. X-ray A/P view of elbow which shows no gross abnormality.
6. muzamil 26th--23-26.pmd 10/10/2013, 9:22 AM25

26 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
emergency department.Emerg Med J 2001, 18:263-269.
4. Hallas P, Ellingsen T. Errors in fracture diagnosesin the emergency department characteristics ofpatients and diurnal variation. BMC Emerg Med2006;6:4.
5. James MR, Bracegirdle A, Yates DW. X-rayreporting in accident and emergencydepartments-an area for improvements inefficiency. Arch Emerg Med 1991;8:266-70.
6. Juhl M, Møller-Madsen B, Jensen J: Missedinjuries in an orthopaedicdepartment.Injury 1990, 21:110-112
7. Lufkin KC, Smith SW, Matticks CA, Brunette DD.Radiologists’review of radiographs interpretedconfidently by emergency physiciansinfrequently leads to changes in patientmanagement. Ann Emerg Med 1998;31:202-7.
8. Robinson PJ, Wilson D, Coral A, Murphy A,Verow P.Variation between experiencedobservers in the interpretation of accident andemergency radiographs. Br J Radiol1999;72(856):323-30.
9. Scott WW Jr, Bluemke DA, Mysko WK, WellerGE, Kelen GD, Reichle RL, et al. Interpretation ofemergency department radiographs byradiologists and emergency medicine physicians:teleradiology workstation versus radiographreadings. Radiology 1995;195:223-9.
10. Wei CJ, Tsai WC, Tiu CM, Wu HT, Chiou HJ,Chang CY.Systematic analysis of missedextremity fractures in emergency radiology. ActaRadiol 2006;47:710-7.
6. muzamil 26th--23-26.pmd 10/10/2013, 9:22 AM26

International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 27
A Study to assess the effectiveness of Nesting on Postureand Movements among Preterm Babies in Selected
Hospitals at Mysore
Neethu C Joseph1, Ambika K2, Sheela Williams3
1Nursing Student, Dept. of Pediatric Nursing, 2Assistant Professor, Dept.of Pediatric Nursing, 3Principal cumProfessor & HOD, JSS College of Nursing, Mysore
ABSTRACT
Background: Preterm babies are the most vulnerable group to get adjusted to the new environment.Following birth, the first few months acts as a transitory period during which the baby adjusts fromthe aquatic to the aerial environment. As a result, the way in which baby is positioned throughoutthis time is very important and his posture dictates the level of his wellbeing. Promoting goodpositioning and encouraging opportunities for flexion can prevent the problems like motor co-ordination, balance and posture difficulties. The correct positioning will help the baby to developgood posture and improve muscle control.
Method: In this study, a quasi-experimental control group pretest- posttest design was used and nonprobability convenience sampling technique was adopted to select 60 preterm babies, both inexperimental and control group. Pilot study was conducted, the tool and study design were found tobe feasible. Data were collected using structured observation checklist for posture and movement.An intervention, nesting was provided for the experimental group. The data were collected andanalyzed using descriptive and inferential statistics.
Results: The result of the study revealed that the significance of difference between the mean pretestand post test posture score which was statistically tested using paired 't' test and was found to behighly significant at 0.05 level of significance.(t(29) = 5.42 in post test 1, 46.14 in post test 2 and 56.82in post test 3 ; (p < 0.05) and the significance of difference between the mean post test posture scorebetween experimental and control group which was statistically tested using independent 't' testwas found to be highly significant at 0.05 level of significance t(58) = 7.41, 7.89 and 8.49; (p < 0.05 ).The significance of difference between the mean pretest and mean post test movement score whichwas statistically tested using paired 't' test was found to be highly significant at 0.05 level ofsignificance.(t(29) = 36.94 in post test 1, 15.59 in post test 2 and 22.80 in post test 3 ; p< 0.05 ) and thesignificance of difference between the mean post test movement score between experimental andcontrol group which was statistically tested using independent t test was found to be highly significantat 0.05 level of significance. (t(58) = 8.12, 5.26 and 4.88 ; p < 0.05 ). The result shows that the postureand movement score had no significant association with their selected personal variables.
Conclusion: Therefore, the study concluded that the nesting was an effective method to maintain thenormal posture and movement of preterm babies.
Keywords: Effectiveness, Nesting, Posture, Movement, Preterm babies
INTRODUCTION
Preterm babies are the most vulnerable group toget adjusts to the new environment. As a result, theway in which baby is positioned throughout this timeis very important, his posture dictates the level of his
well being1. Preterm babies are born before their littlemuscles are able to support them properly. Pretermbabies need some extra help from parents and medicalstaff to adopt good positioning that will help theirdevelopment2.
DOI Number: 10.5958/j.2321-1024.1.2.024
7. neetu c joseph--27-30.pmd 10/10/2013, 9:22 AM27

28 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
Danielle Salducci, a pediatric physiotherapist,started to design and make ‘nest’ which would enablepreterm to make movements similar to those made intheir mother’s womb. If the preterm lies flat on hisback on a very firm mattress, without the safe andsecure feeling he had in the womb, he could feel hewere falling into space. This posture could also be thestart of various physical aliments1. Developmentalbenefits may include achieving developmental milestones such as sitting, crawling, walking and movingtheir arms and legs normally2. Normal positionprevents frozen postures of arms and legs. Goodposture during growth and development keeps boneand joints in correct alignment and prevent abnormalwear and tear as well as keeping spine from becomingfixing in an abnormal position3.
HYPOTHESES
H1 : The mean post test posture score andmovement score of preterm babies in experimental
group will be significantly greater than the meanpretest posture score and movement score of pretermbabies in experimental group.
H2 : The mean post test posture score andmovement score of preterm babies in experimentalgroup will be significantly greater than the mean posttest posture score and movement score of pretermbabies in control group.
H3 : There will be significant association of postureand movements of preterm babies with their selectedpersonal variable viz age, gender, mode of deliveryand weight of preterm babies.
METHODOLOGY
Quasi experimental approach for an interventionstudy is the one in which subjects are not randomlyassigned to treatment condition, but the researcherexercises some control to enhance the study’s internalvalidity.
The schematic representation of research design
Group Day 1Morning Day 2Afternoon Day 3Night
Pretest Intervention Post test Pretest Intervention Post test Pretest Intervention Post test
Experimental SOCP Nx SOCP SOCP Nx SOCP SOCP Nx SOCP
Group
SOCM SOCM SOCM SOCM SOCM SOCM
Control group SOCP SOCP SOCP SOCP SOCP SOCP
SOCM SOCM SOCM SOCM SOCM SOCM
Fig (1) Schematic representation of research design
Keys
SOCP – Structured observation check list to assess posture
SCOM – Structured observation check list to assess movement
Nx - Nesting
The population comprises of pretermbabies inNICU and postnatal wards. Convenient sampling wasused to obtain the sample of 60 preterm babies inselected hospitals at Mysore. Data collection was basedon the structured observation check list to assess theeffectiveness of nesting on the posture and movementof preterm babies.It consist of 3 parts,
1. Porforma for selected personal variable (Consistof 4 items)
2. Observation checklist to assess posture of pretermbabies. (Consist of 4 items)
3. Observation checklist to assess movement ofpreterm babies (Consist of 12 items)
FINDINGS
The study samples composed of 60 preterm babies30 each in experimental and control group. Theselected personal variables were age, gender, mode ofdelivery and weight of the preterm babies. The datarelated to frequency and percentage distribution ofsample according to their selected personal variablesas shown in Table 1.
7. neetu c joseph--27-30.pmd 10/10/2013, 9:22 AM28
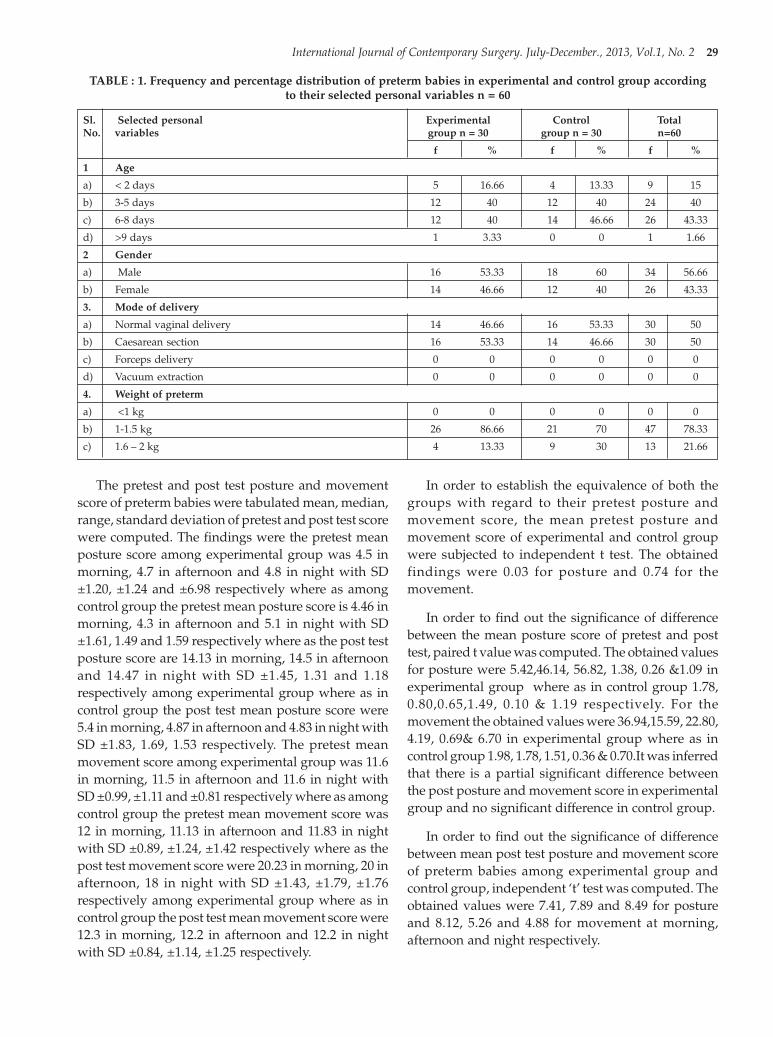
International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 29
TABLE : 1. Frequency and percentage distribution of preterm babies in experimental and control group accordingto their selected personal variables n = 60
Sl. Selected personal Experimental Control TotalNo. variables group n = 30 group n = 30 n=60
f % f % f %
1 Age
a) < 2 days 5 16.66 4 13.33 9 15
b) 3-5 days 12 40 12 40 24 40
c) 6-8 days 12 40 14 46.66 26 43.33
d) >9 days 1 3.33 0 0 1 1.66
2 Gender
a) Male 16 53.33 18 60 34 56.66
b) Female 14 46.66 12 40 26 43.33
3. Mode of delivery
a) Normal vaginal delivery 14 46.66 16 53.33 30 50
b) Caesarean section 16 53.33 14 46.66 30 50
c) Forceps delivery 0 0 0 0 0 0
d) Vacuum extraction 0 0 0 0 0 0
4. Weight of preterm
a) <1 kg 0 0 0 0 0 0
b) 1-1.5 kg 26 86.66 21 70 47 78.33
c) 1.6 – 2 kg 4 13.33 9 30 13 21.66
The pretest and post test posture and movementscore of preterm babies were tabulated mean, median,range, standard deviation of pretest and post test scorewere computed. The findings were the pretest meanposture score among experimental group was 4.5 inmorning, 4.7 in afternoon and 4.8 in night with SD±1.20, ±1.24 and ±6.98 respectively where as amongcontrol group the pretest mean posture score is 4.46 inmorning, 4.3 in afternoon and 5.1 in night with SD±1.61, 1.49 and 1.59 respectively where as the post testposture score are 14.13 in morning, 14.5 in afternoonand 14.47 in night with SD ±1.45, 1.31 and 1.18respectively among experimental group where as incontrol group the post test mean posture score were5.4 in morning, 4.87 in afternoon and 4.83 in night withSD ±1.83, 1.69, 1.53 respectively. The pretest meanmovement score among experimental group was 11.6in morning, 11.5 in afternoon and 11.6 in night withSD ±0.99, ±1.11 and ±0.81 respectively where as amongcontrol group the pretest mean movement score was12 in morning, 11.13 in afternoon and 11.83 in nightwith SD ±0.89, ±1.24, ±1.42 respectively where as thepost test movement score were 20.23 in morning, 20 inafternoon, 18 in night with SD ±1.43, ±1.79, ±1.76respectively among experimental group where as incontrol group the post test mean movement score were12.3 in morning, 12.2 in afternoon and 12.2 in nightwith SD ±0.84, ±1.14, ±1.25 respectively.
In order to establish the equivalence of both thegroups with regard to their pretest posture andmovement score, the mean pretest posture andmovement score of experimental and control groupwere subjected to independent t test. The obtainedfindings were 0.03 for posture and 0.74 for themovement.
In order to find out the significance of differencebetween the mean posture score of pretest and posttest, paired t value was computed. The obtained valuesfor posture were 5.42,46.14, 56.82, 1.38, 0.26 &1.09 inexperimental group where as in control group 1.78,0.80,0.65,1.49, 0.10 & 1.19 respectively. For themovement the obtained values were 36.94,15.59, 22.80,4.19, 0.69& 6.70 in experimental group where as incontrol group 1.98, 1.78, 1.51, 0.36 & 0.70.It was inferredthat there is a partial significant difference betweenthe post posture and movement score in experimentalgroup and no significant difference in control group.
In order to find out the significance of differencebetween mean post test posture and movement scoreof preterm babies among experimental group andcontrol group, independent ‘t’ test was computed. Theobtained values were 7.41, 7.89 and 8.49 for postureand 8.12, 5.26 and 4.88 for movement at morning,afternoon and night respectively.
7. neetu c joseph--27-30.pmd 10/10/2013, 9:22 AM29

30 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
Chi square value was computed to find out theassociation between the pretest posture score andmovement score of preterm babies and their selectedpersonal variables viz. Age, gender, mode of delivery,weight of baby. The obtained values for posture were0.76, 1.54, 0.33 and 0.003 was not found to be significantand for movement is not able to compute since allsample belongs to average group.
CONCLUSION
The analysis of the findings revealed that, there wasa significant improvement in the mean posture scoreand movement score of preterm babies in experimentalgroup when compared to control group. The nestingwas effective in improving the posture as the t(58) = 7.41in post test 1, t(58) = 7.89 in post test 2 and t(58) = 8.49 inpost test 3 was statistically significant at 0.05 level ofsignificance. As the same as the nesting was alsoeffective in improving the movement as the t(58)= 8.12in post test 1, 5.26 in post test 2 and 4.88 in post test 3was statistically significant at 0.05 level of significance.Chi-square test was computed to test the associationand the finding revealed that the posture of pretermbabies was not associated with their selected personalvariable viz age, gender, mode of delivery, weight ofbaby. The findings also revealed that chi squarecomputation is not applicable in case of movement ofthe preterm babies since all the sample belong to theaverage movement score.
Thus, it was concluded that, the nesting will helpto improve the posture and movement of pretermbabies. Nesting is simple, inexpensive interventionwhich is effective in improving the posture andmovement of preterm babies and the nurses canreadily use this intervention.
ACKNOWLEDGEMENT
We express our thanks to the parents of the subjectsfor giving their consent to be a part of this study andthe authorities who provided permission to conductthe study.
Conflict of Interest
Preterm babies are the most vulnerable group.Preterm babies is positioned throughout newbornperiod is very important and his posture dictates thelevel of his well being. The correct positioning will helpthe baby to develop good posture and improve musclecontrol. Hence a new technique is required to maintainthe posture and movement of preterm babies for it,nesting is introduced and it was effective too.
Ethical Clearance: Ethical clearance was obtained fromthe ethical committee of the college.
Funding Sources: Not obtained any funds from anysources.
REFERENCES
1. Oyen N Markestaad T Facilitation ofDevelopmental care for High Risk neonates: Aninterventional study Unpublished PhD( NursingScience) thesis [cited on 2011 oct 22 [availablefrom : http://upetd.up.ac.za/thesis]
2. Bradford, Preterm babies,2007, [ cited on2003September 08] [ available from : http: //preemiehelp.com
3. Slevin M, Farrington N, Duffy, Daly L, Mruphy JF. Altering the NICU and measuring infant’sresponses. Acta Paediatr 2000: 89(5): 577-81
4. Ferrari F et.al. Posture and movement in healthypreterm infants in supine position in and outsidethe nest. Archives of disease in childhood: Fetaland Neonatal. 2007, sep; 92 (5) : 48 – 52
5. Symington A, Pinelli J.Developmental Care forpromoting development and preventingmorbidity in preterm infants. 2003; 4: 119-30
6. Hunter J, Kenner C, McGrath JM. Developmentalcare of Newborn and Infant.A Guide for HealthProfessionals. 3rd ed. New Delhi. St. Louis ElevierPublishers (P) Ltd. 2004; 219 - 319
7. neetu c joseph--27-30.pmd 10/10/2013, 9:22 AM30

International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 31
The Role of Caudal Epidural Steroid Injections inManagement of Low Back Pain
Bikram Singla1, Seema Jindal2
1Assistant Professor, Department of Orthopaedics, 2Assistant Professor, Department of Anaesthesia, GGS MedicalCollege & Hospital, Faridkot
ABSTRACT
The role of caudal epidural steroid injection in management of low back pain is controversial. This isa prospective study done on 50 patients who reported to orthopaedic OPD over a period of 2 years.Patients were classified on the basis of MRI diagnosis. All the injections were given by same surgeonafter a trial of conservative treatment for at least six weeks. A combination of drugs containingmethylprednisolone, lignocaine 2% and normal saline was injected through sacral hiatus. Patientswere assessed at 24 hours, one week, three weeks and three months interval. No major complicationswere observed except for dural leak , headache and injection site pain. We believe that CEI is mainlyeffective in treating patients with acute low back pain refractory to conservative treatment, patientswith disc degeneration and discogenic grade I -II low back pain.The patients with chronic pain usuallydo not respond to CEI on long term follow up. Such patients must be referred to back school conditionprograms before taking up for surgery.
Keywords: CEI, HNP, PIVD, VAS
INTRODUCTION
Low back pain is remarkably a common disability.Patients with low back pain suffer from functional andpsychological disability adding to the intensity ofvisible impact of pain. Drugs help in the resolution ofpain to some extent but the disability of the patientpersists due to the psychological effect of chronicsymptoms. Waddell’s pain behaviour circlecomprehensively explains this point that painbehaviour is wrapped up into the theories of primaryand secondary pain and may include moaning,grimacing, limping, excessive talking, excessivesilence, refusing to work, seeking healthcare and takingmedications1.
Anatomically, there are five lumbar vertebrae andsacrum making the lumbar spine. The vertebral bodiesincrease in size from first to fifth indicative of loadbearing capacity1. The intervertebral dics have outerfibrous covering- the annulus fibrosus, central hyalinecartilage and the innermost nucleus pulposus, agelatinous material which is packed under pressure.With the changing biomechanics of the spine, as a partof degenerative process or congenital or trauma, thecartilage plate breaks and the nucleus pulposus packedunder pressure is pushed outwards rupturing the
posterior longitudinal ligament mostlyposterolaterally1 into spinal canal till the pressureinside it becomes neutral. The herniated nucleuspulposus (HNP) impinges the nerve root in theforamen or is extruded into the canal causing radicularsymptoms or neurogenic claudication adding to itcentral sensitisation magnifying the actual intensityof back pain.
Classification of low back pain
1. Spondylogenic back pain
2. Neurogenic pain
3. Viscerogenic back pain
4. Vascular back pain
MATERIAL AND METHOD
A total of 50 patients were included in the study.Patient with low back pain, radicular symptoms orboth and neurogenic claudication who reported toorthopaedic OPD were given conservative treatmentfor six weeks after routine x-rays. Patients wereassessed on follow up in OPD on VAS scale. If thepatient did not show improvement on VAS scale, MRI
DOI Number: 10.5958/j.2321-1024.1.2.025
8. bikram singla-31-35.pmd 10/10/2013, 9:22 AM31

32 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
of lumbosacral spine was done to find out the causeof low back pain and a diagnosis was arrived upon.
Exclusion criteria for the patients
1. Old osteoporotic fractures in the lumbar spine
2. Patients older > 65 years and younger < 25 years
3. Patients having co-morbid conditions like cardiacillness on drugs, antiplatlet drugs, epilepsy, onantipsychotic drugs, failed back syndrome
4. Patients having back pain due to osteopenia orosteoporosis
We assessed the patients on visual analogue scaleas this was the best measurement of subjective pain.
The VAS score was given from 0 – 10. The intensityof pain was divided as under:
1. None score 0-2 I
2. Uncomfortable score 2-4 II
3. Annoying score 4-6 III
4. Dreadful score 6-8 IV
5. Excruciating score 8-10 V
The patients who did not respond to conservativemeasures were taken up for CEI after informedconsent. The patients who did not meet exclusioncriteria were not a part of this study. After routineinvestigations and anaesthesia checkup, caudalepidural injection was given under MonitoredAnaesthesis care. All the injections were given by thesame surgeon.
The patients were lied in prone position onradiolucent table. The gluteal area was cleaned anddraped. The palpation was started from coccyxupwards and a step was felt 4cm.from the proximalend of natal crease. It was easy to feel in thin patientsthan those in obese. However with experience one can
easily feel the step. We did not give local infiltration atthe needle puncture site as we feel confident to putthe needle straight through sacral hiatus, also therewas C-Arm image intensifier to confirm the site ofneedle. 20G spinal needle was taken and inserted intosacral hiatus. As we insert the needle we get the feelingof give way which is when sacrococcygeal membraneis pierced. It is first aspirated to confirm that the needleis not in epidural blood vessel or inside the dura. 2cc.air is then injected through syringe to confirm theneedle in epidural space. We concluded that when aircould be freely injected, the needle was in epiduralspace. Position of the needle in sacral hiatus was alsoconfirmed under C-Arm. A 50cc syringe containing25cc normal saline, 5cc lignocaine 2% and 80mg.Depomedrol acetate was injected slowly underMonitored anaesthesia care. It was a stop and goprocedure. Sometimes it was difficult to inject the drugwhen the stenosis was severe. After the injectionpatient was put in supine postion and vitals monitoredfor five minutes. Patient was told to move toes andlegs actively to check the muscle power. The patientsin whom bloody tap was encounterd , the procedurewas abandoned and postponed for one week.
Patient was discharged on same day withinstructions to lie supine for next 6 hours to preventheadache, nausea and vomiting. He was called after24 hours to know about the pain and any adverseeffects if any. He was again started on conservativetreatment simultaneously. Subsequent follow ups inOPD were done one week, three weeks and threemonths intervals and assessed on VAS scale.
OBSERVATIONS AND RESULTS
Of the 50 patients who underwent CEI, 19 weremale and 31 were female with mean age of 47 years(range 25-65 years).
Table No. 1: Classification as per MR diagnosis
Diagnosis No. of patients % of patients complaint
Acute back pain (no cause on MRI) 10 20% Back pain
Spondylolisthesis 8 16% Claudication & low back pain
LCS 12 24% claudication
Disc deg. With/without root irritation 20 40% Back pain and Leg pain
We reached four major diagnoses on MR screeningof patients in whom we undertook CEI. Out of these,10 patients had acute back pain, 8 patients had various
grades of spondylolisthesis who complained ofclaudication symptoms and low back pain, 12 patientswho had lumbar canal stenosis (LCS) of various grades
8. bikram singla-31-35.pmd 10/10/2013, 9:22 AM32

International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 33
(we asked for sagittal diameters at disc levels)complained mainly of neurogenic claudicationsymptoms and 20 patients had disc degeneration with
or without root impingement complained of back painand leg pain (ref. Table no. 1).
Table no. 2: Improvement in VAS score on CEI
Diagnosis At first visit One week Three weeks Three months
Acute back pain (no cause) 6-8 (10) 0-2 (8) 2-4 (8) 2-4 (7)
Spondylolisthesis 2-4 (8) 0-2 (2) 2-4 (8) 2-4 (8)
LCS 2-4 (12) 2-4 (9) 0-2/2-4 (7) 2-4 (7)
Disc deg. With/without root irritation 4-6/2-4 (20) 0-2/0-2 (18) 0-2/2-4 (14) 2-4/4-6 (14)
Numerals out of bracket denote VAS score andfigures inside the bracket are number of patients.
Out of the 20% patients with acute low back painand 40% patients with discogenic pain, 70% had reliefwith caudal epidural injection.
Out of the 16% patients with spondylolisthesis only4% showed short term relief in VAS score. All of themhad same VAS score at three months, thus didnot showany improvement.
Out of the 24% patients with stenosis only 58%patients showed relief at three months.
Adverse effects
1. Immediate: Vertigo (52%)
2. Late onset: Injection site pain (70%), headache (8%)
DISCUSSION
Out of 50 patients studied, there was significantimprovement in patients with acute back pain andthose with grade I disc herniation as compared topatients with chronic back pain havingspondylolisthesis and lumbar canal stenosis. Thefemales and males were in ratio of 62:38 with meanage of 47 years. The controversy exists regardingapproach to lumbar epidural injections2 i.e.interlaminar or caudal epidural. Multiple guidelinesand systematic reviews have identified indications infavour of caudal epidural injections to treat radicularpain from herniated lumbar intervertebral discs2. Twoprospective evaluations 3,4 have shown positive resultsin patients without disc herniation or radiculitis, inchronic function-limiting LBP. These results are similarto the patients receiving caudal epidural injectionseither with or without steroids with disc herniationand radiculitis,5 but superior to patients suffering fromspinal stenosis and post-surgery syndrome.6,7
The underlying mechanism of action of epidurallyadministered steroid and local anaesthetic injectionsis still not well understood. It is believed that theachieved neural blockade alters or interruptsnociceptive input, reflex mechanism of the afferentfibers, self sustaining activity of the neurons, andpattern of central neuronal activities.8, 9 Furthercorticosteroids have been shown to reduceinflammation by inhibiting either the synthesis orrelease of a number of pro-inflammatory mediatorsand by causing a reversible local anaesthetic effect. 8, 10
In contrast, local anaesthetics have been described toprovide short to long-term symptomatic relief basedon various mechanisms. It has been described thatmultiple pathophysiologic mechanisms may beinvolved in chronic pain including noxious peripheralstimulation, excess nociceptive process resulting in thesensitization of the pain pathways at several neuronallevels11 and excess release of neurotransmitters causingcomplex central responses including hyperalgesia orwind-up,10 resulting in an increase in nociceptivesensitization of the nervous system12,13 and phenotypechanges which are also considered as part of neuronalplasticity.12 Consequently, it has been postulated thatlocal anaesthetics may provide analgesia bysuppression of nociceptive discharge, the block ofaxonal transport, 14 the block of reflex sympathetic arc,13 the block of sensitization,11 anti-inflammatory effect, and blockade of axonal transport of nerve fibres atlower concentrations compared with those that arenecessary for a block of a nerve conduction. 14 The longlasting effect of local anaesthetics in epidural injectionshas been demonstrated in a multitude of studies.15
Corticosteroids have therapeutic effects on radicularsymptoms caused by lumbar disc herniation due totheir anti-inflammatory function. Furthermore,corticosteroids reportedly ameliorate early vascularpermeability increases in spinal nerve roots and inhibitreductions in nerve conduction velocity induced byepidural application of nucleus pulposus. Finally
8. bikram singla-31-35.pmd 10/10/2013, 9:22 AM33

34 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
corticosteroids may exert anaesthetic like action onnociceptive C fiber condition independent of antiinflammatory properties16. However corticosteroidsare also known to possess direct neurotoxic effects onperipheral nerve tissue17, 18 unlike local anesthetics.
CONCLUSION
We conclude that acute back pain responds betterto CEI than chronic back pain. Patients with discdegeneration and the patients with low back pain ofdiscogenic origin (grade I-II) with or without nerveroot irritation showed improvement on VAS scale inback pain and leg pain on intermediate and long termfollow up but no long term improvement on VAS scalewas noted in patients with grade III-IV discs withspinal cord or nerve root irritation. There is noimprovement in neurogenic claudication symptomson CEI in chronic back pain. There is short termimprovement in neurogenic claudication in acute lowback pain of discogenic cause (grade III –IV) but noton intermediate and long term follow up. Patients withspondylolisthesis as a cause of chronic low back painimproved symptomatically in low back pain but noton neurogenic claudication on short term follow upbut not on intermediate and long term follow up.
We conclude that vast majority of patients withacute back pain respond to oral conservative treatmentin which there is no need for CEI. Around 70% patientswith acute refractory low back pain, patients with discdegeneration and discogenic grade I –II low back painrespond to CEI. The patients with chronic pain usuallydo not respond to CEI on long term follow up. Suchpatients must be referred to back school conditionprograms before taking up for surgery.
Prior Publication: Nil
Support: Nil
Conflicts of Interest: None
Permissions: Nil
REFERENCES
1. Wong David A.,Transfeldt Esnor. Macnab’sbackache. Fourth edition.
2. Gomal Journal of Medical Sciences July-December 2010, Vol. 8, No. 2 152
3. Manchikanti L, Singh V, Rivera JJ, PampatiV,Beyer CD, Damron KS, Barnhill RC.Effectiveness of caudal epidural injections indiscogram positive and negative chronic lowback pain. Pain Physician 2002; 5:18-29.
4. Manchikanti L, Singh V, Rivera JJ, PampatiV,Beyer CD, Damron KS, et al. Caudal epiduralinjections with sarapin steroid in chronic lowback pain. Pain Physician 2001; 4: 322-35.
5. Manchikanti L, Singh V, Cash KA, PampatiV,Damron KS, Boswell MV. Preliminary resultsof randomized, equivalence trial of fluoroscopiccaudal epidural injections in managing chroniclow back pain: part 2. Disc herniation andradiculitis. Pain physician 2008; 11: 801-15.
6. Manchikanti L, Singh V, Cash KA, PampatiV,Datta S. Preliminary results ofrandomized,equivalence trial of fluoroscopiccaudal epidural injections in managing chroniclow back pain: part 3. Post surgery syndrome.Pain physician 2008; 11: 817-31.
7. Manchikanti L, Cash KA, Mc Manus CD,PampatiV, Abdi S. Preliminary results ofrandomized,equivalence trial of fluoroscopiccaudal epidural injections in managing chroniclow backpain:part 4. Spinal stenosis. Painphysician 2008; 11: 833-48.
8. Manchikanti L. Role of neuraxial steroids ininterventional pain management. Pain Physician2002; 5: 182-99.
9. Manchikanti L. Pharmacology of neuralsteroids.In: Manchikanti L, Singh V. (eds).Interventional Techniques in chronic spinalpain, ASIPP publishing,Paducah, KY, 2007:p. 167-84.
10. Pasqualucci A, Varrasi G, Brashi A, PedutoVA,Brunelli A, Marinangeli F, et al. Epidural localanaesthetic plus corticosteroid for the treatmentof cervical brachial radicular pain: singleinjectionversus continuous infusion. Clin J Pain2007; 23: 551-7.
11. Melzack R, Coderre TJ, Katz J, VaccarinoAL.Central neuroplasticity and pathologicalpain.Ann N Y Acad Sci 2001; 933: 157-74.
12. Kawakami M, Weinstein JN, Chatani K, SprattKF, Meller ST, Gebhart GF. Experimental lumbarradiculopathy. Behavioral and histologicchanges in a model of radicular pain after spinalnerve root irritation with chromic gut ligaturesin the rat. Spine 1994; 19: 1795-1802.
8. bikram singla-31-35.pmd 10/10/2013, 9:22 AM34

International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 35
13. Decosterd I, Woolf CJ. Spared nerve injury: ananimal model of persistent peripheralneuropathic pain. Pain 2000; 87: 149-58.
14. Bisby MA. Inhibition of axonal transport innerves chronically treated with local anaesthetics.Exp Neurol 1975; 47: 481-9.
15. Tachihara H, Sekiguchi M, Kikuchi S, Konno S.Docorticosteroids produce additional benefit innerve root infiltration for lumbar discherniation.Spine 2008; 33: 743-7.
16. Johansson A, Hao J, Sjolund B. Localcorticosteroid application blocks transmission in
normalnociceptive c-fibres. Acta AnaesthesiolScand 1990; 34: 335-8.
17. Mackinnon SE, Hudson AR, Gentili F, KlineDG,Hunter D. Peripheral nerve injection injurywith steroid agents. Plast Reconstr surg 1982;69:482-9.
18. Shishido H, Kikuchi S, Heckman H, Myers RR.Dexamethasone decreases blood flow in normalnerves and dorsal root ganglia. Spine 2002;27:581-6.
8. bikram singla-31-35.pmd 10/10/2013, 9:22 AM35

36 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
Comparison of Analgesic effects between InterpleuralBupivacaine with Adrenaline and InterpleuralBupivacaine with Adrenaline & Clonidine in
Laparoscopic Cholecystectomy
Ovais Nazir1, Mushtaq A Wani1, B B Kapoor2
1Postgraduate Resident, 2Professor and Head, Department of Anesthesiology, Govt. Medical College,Jammu, J&K, India
ABSTRACT
Study Design: Prospective study.
Materials and method: This study was conducted in the Department of Anaesthesiology, Govt MedicalCollege, Jammu 2011-2012. In this study, 75 adult patients of age 18 -60 years of either sex belongingto ASA I & II, admitted in surgical ward for elective lapraoscopic cholcystectomy were taken for thisstudy. Patients were randomly divided into three groups.
• Group I - Patients who received normal saline 20ml at the end of surgery.
• Group II - Patients who received bupivacaine with adrenaline at the end of surgery.
• Group III- Patients who received bupivacaine with adrenaline and clonidine at the end of surgery.
Anaesthesia was standardized, consisting of glycopyrrolate 0.2 mg and ranitidine 50mg aspremedication i.v 30min before induction. Induction was done with thiopentone sodium 5mg/kgand atracurium 0.5mg/kg IV, followed by maintenance with isoflurane and nitrous oxide 60-70%with oxygen. Pain assessments were made using 'Visual Analogue Scale' first in recovery ward aftersurgery and then 15, and 30 minutes and 1, 2, 4, 6, 8, 10, 12, 14, 16 hours after injection till effect lasts.Systolic and diastolic blood pressures and heart rate were recorded before injection and at 15, and 30minutes, 1, 2, 4, 6, 8, 10, 12, 14 and 16 hours after injection.
Results: Onset of analgesia was 15min in group III where as it was 30min in group II and controlgroup do not show any analgesia. Quality of analgesia was much better in group III. Mean durationof analgesia was 14.5hrs in group III and it was 8.2hrs in group II.
Conclusions: To conclude, clonidine is a good adjuvant to 0.5% bupivacaine in interpleural block forpostoperative analgesia in cases of laparoscopic cholecystectomy.
Keywords: Analgesia, Bupivacaine, Clonidine, Adrenaline, VAS
INTRODUCTION
Uncontrolled postoperative pain may result insympathetic activation and increase myocardialoxygen consumption, which may lead to thedevelopment of myocardial ischemia and infarctionby decreasing myocardial oxygen supply throughcoronary vasoconstriction and attenuation of localmetabolic coronary vasodilation1. Poorly controlled
acute postoperative pain may be an importantpredictive factor in the development of chronic post-surgical pain (CPSP) 2. The relief of postoperative painis a subject, which is receiving increasing attention inthe past few years because effective pain control isessential for optimal care of surgical patients.Cholecystectomy is now commonly performed bylaparoscopic technique because it provides distinct
DOI Number: 10.5958/j.2321-1024.1.2.026
9. ovais--36-41.pmd 10/10/2013, 9:22 AM36

International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 37
advantages over open cholecystectomy3. The painproduced by laparoscopic cholecystectomy is mainlyvisceral. Recent reports have demonstrated that manypatients experience considerable pain afterlaparoscopic cholecystectomy, which is a relativelynew procedure, so there is no general agreement oneffective postoperative pain control. Visceral pain afterlaparoscopy usually occurs till 24Hr4. Differentmethods used with variable success include parenteralNSAID, infiltration of wounds with local anaesthetics,intermittent intramuscular narcotics, intraperitoneallocal anesthetics and interpleural block. Shoulder paindue to irritation of phrenic nerve usually occurs on2nd postoperative day5. Pain due to persistentpneumoperitoneum occurs till 3rd postoperative day6.
Reiestad et al (1984) published their results ofcontinuous intercostals nerve block for postoperativepain relief and presented their modification oftechnique, which is now termed as “interpleuralanalgesia”7. A preliminary report of the analgesicactivity of local anesthetics deposited into the pleuralcavity was published in 1986 by two Norwegiananesthesiologists, Reiestad and Stromskag. .Interpleural regional analgesia is a percutaneousintroduction of the local anaesthesia into the thoraciccage between parietal and visceral pleura.
Analgesia is thought to occur as a result of threemechanisms8 :
1. Diffusion of the local anaesthetic through theparietal pleura and the innermost intercostalsmuscles to reach the intercostal nerves whereblockade occurs.
2. Blockade of the intrathoracic sympathetic chain.
3. Direct action of the local anaesthetics on nerveendings within the pleural.
A unilateral analgesia is obtained by a rapid onset,but not sufficient enough for surgical procedure. Thearea covered by interpleural block includes the thoracicand upper part of abdomen. No hemodynamic adverseeffect occurs and ventilator function is ratherimproved9. First described in 1986, the technique hasrapidly captured the imagination of those responsiblefor the management of postoperative pain. Comparedwith multiple intercostal blocks, the technique has theadvantage of requiring only a single needle puncture,and compared with continuous intercostal blocks it hasthe advantage of the relative simplicity of thetechnique10 . Although exact dose & volume of local
anaesthetic is still controversial but 20ml of 0.5 %bupivacaine is the most convenient11 & adverse effects& hazards are uncommon and include mainlypnuemothorax and toxic effects of local anaestheticoverdose12. Fewer studies have been conducted tostudy the role of interplueral block for post operativepain relief for laparoscopic cholecystectomy.
MATERIALS AND METHOD
This study was conducted in the Department ofAnaesthesiology, Govt Medical College Jammu 2011-2012. After obtaining informed written consent andapproval from hospital ethics committee, this studywas conducted on 75 adult patients of age 18 -60 yearsof either sex belonging to ASA I & II, admitted insurgical ward for elective laparoscopic cholcystectomywere taken for this study. After pre-anaesthetic checkup and informed consent, patients were randomlydivided into three groups of 25 each.
• Group I – Patients who received normal saline20ml
• Group II - Patients who received bupivacaine withadrenaline
• Group III- Patients who received bupivacaine withadrenaline and clonidine
All the patients were explained details of visualanalogue scale and how to rate it on the scale of 0-10.All patients were made to fast overnight for 8 hoursprior to surgery and sedated with Alprazolam 0.25mgoral, bed time on night, before surgery. Anaesthesiawas standardized, consisting of glycopyrrolate 0.2 mgand ranitidine 50mg as premedication i.v 30min beforeinduction. Induction was done with thiopentonesodium 5mg/kg and atracurium 0.5mg/kg IV,followed by maintenance with isoflurane and nitrousoxide 60-70% with oxygen. At the end of surgicalprocedure, just before reversal patients of Group Ireceived 20ml of saline, group II receivedbupivacaine0.5% with adrenaline 5mcg/ml and GroupIII received 20ml bupivacaine0.5% with adrenaline5mcg/ml and 50mcg clonidine through interpleuralroute. Pain assessments were made first in recoveryward after surgery and then 15, and 30 minutes and 1,2, 4, 6, 8, 10, 12, 14, 16 hours after injection till effectlasts. Systolic and diastolic blood pressures and heartrate was recorded before injection and at 15, and 30minutes then 1, 2, 4, 6, 8, 10, 12, 14, 16 hours afterinjection upto 20hours.Duration of pain relief wasnoted till a VISUAL ANALOGUE SCORE of >7 is
9. ovais--36-41.pmd 10/10/2013, 9:22 AM37

38 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
reached (0:being no pain and 10:being unbearable pain)Patients at that time were given rescue analgesia inthe form of inj.diclofenac75 mg i/v in 100ml saline over15 minutes. Any side effects like
Hypotension (SBP<=90) was treated with i/vmephentermine 3 mg increments.
Bradycardia (HR<=55) was treated with i/vatropine 0.2 mg increments
Technique
Just before reversal 18 G Tuohy needle was used tomake puncture in the right 7th intercostal space inmidaxillary line perpendicular to skin with bevelturned cephalad just above the 8th rib with all theaseptic precautions. Needle was attached to loss ofresistance syringe having 2ml of sterile water and lossof resistance was identified in usual manner as inepidural. A first loss of resistance is felt as theintercostal membrane is pierced, and a second oneoccurs when the parietal pleura is traversed with the
characteristic click. Local anaesthetic was injected inpleural space.
Exclusion criteria:
• Allergy to local anaesthetic.
• History of respiratory disease
• Traumatic or spontaneous hemothorax orpneumothorax
• Bleeding disorder
• History of antiplatelet intake in one week previousto surgery.
• Chest deformity.
RESULTS
The results of this study are tabulated below.
The three groups did not differ preoperatively withrespect to age, weight, height, gender, andhemodynamic parameters (table1).
Table No. 1. Preoperative parameters:
Control Bupivacaine Bupivacaine p-valuewith with
adrenaline adrenaline+clonidine
Age(yrs) 47.73±8.22 46.72±8.32 50.15±8.88 0.52
Weight(kg) 55.35±4.33 59.8±5.03 56±5.33 0.54
M:F ratio 3:11 3:12 3:12 0.75
SBP(mmHg) 123±4.63 122.±4.63 124.±6.07 0.09
DBP(mmHg) 78±3.36 79±4.2 77.±7.16 0.41
PR per min 83±5.56 82±6.72 80±6.11 0.35
Mean pain score at 15min showed significantdifference between the three groups p=0.0 (p<0.05 issignificant) (table 2). All the patients in control grouprequired rescue analgesics by 30 min and hence weredeleted from study. Whereas all the patients of group
II required rescue analgesic by 10hrs and that of groupIII needed rescue analgesic by 14hrs(table 2). Qualityof analgesia was better in bupivacaine with clonidinegroup (table 2).
Table 2. Mean Pain Scores (Vas)
Control Bupivacaine with Bupivacaine withadrenaline adrenaline+clonidine
15min 6±1.4 3±2.15 1±1.230min 8±3.5 2±0.9 0±01hr 0±0 0±02hr 0±0 0±04hr 1±0.5 0±06hr 4±2.5 0±08hr 7±3.2 0±0
10hr 8±1.2 1±0.9
12hr 2±1.4
14hr 6±2.8
16hr 9±2.5
9. ovais--36-41.pmd 10/10/2013, 9:22 AM38

International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 39
Onset of analgesia was quicker in group III (15min)where as it was 30min in group II. Mean duration ofanalgesia (mean time for rescue analgesic) was about
14.54hrs in group III where as it was 8.26hrs in groupII (table 3).
Table No. 3. Duration and onset of analgesia
Group II Group III P Value
Onset of analgesia(min)* 30 15 <0.001
Duration of analgesia(hrs)** 8.26 ±1.49 14.54 ±0.98 <0.001
* Time of onset is time at which mean pain score reached VAS = 0, 1.
** Duration of analgesia is period starting when patients became pain free to the time when they further required the top up dose.
Table No. 4. Hemodynamic parameters
Time Control Bupivacaine Bupivacaine withwith adrenaline adrenaline+clonidine
HR SBP DBP HR SBP DBP HR SBP DBP
Preop 83±5.56 123±4.63 78±3.36 82±6.7 122±4.63 79±4.2 80±6.11 124±6.07 77±7.16
15 min 96±6.0 134±4.9 85±5.14 85±3.7 123±5.8 80±5.6 68±2.4 113±4.7 71±5.1
30 min 95±4.5 135±5.0 83±4.9 81±4.2 125±8.5 80±5.24 67±2.5 108±4.4 67±4.6
1 hr 80±3.5 120±6.0 80±5.7 66±2.8 108±3.9 68±5.2
2 hr 80±2.5 120±7.5 81±7.0 67±3.0 107±3.8 69±5.4
4 hr 81±5.4 120±7.2 79±3.5 67±2.9 110±4.3 71±5.4
6 hr 82±3.2 124±8.0 79±4.34 65±2.4 112±5.5 71±5.6
8 hr 85±3.6 129±9.0 82±5.0 66±2.5 113±5.8 73±5.5
10 hr 86±3.8 135±7.0 82±4.1 70±2.8 120±5.9 77±7.7
12 hr 75±4.5 127±6.5 78±8
14 hr 78±5.5 129±6.3 84±8.3
16 hr 84±4.5 131±7.9 85±7.4
DISCUSSION
This clinical research has shown the analgesic effectof both 20ml of 0.5% bupivacaine with adrenaline in1:2,00,000 concentration and 20ml of0.5% bupivacainewith adrenaline plus 50 mcg clonidine throughinterpleural route for postoperative analgesia in casesof laparoscopic cholecystectomy . In group III, themean time to rescue analgesic was significantlyprolonged (14.54 hours compared to 8.26 hours forgroup II).
Interpleural regional analgesia is the percutaneousintroduction of the local anaesthetic into thoracic cagebetween parietal and visceral pleural. Analgesia isthought to occur as a result of Local anaesthetic diffusesthrough the parietal pleura and the innermostintercostal muscles to reach the intercostal nerves.
Alpha-2 adrenergic agonists are known to havespinal and epidural antinociceptive effect via alpha-2receptor sub types. Several studies have beenpublished in the last decades describing the anestheticsparing effects and analgesic property of epiduralclonidine13. Clonidine, á-2 agonist agent, is causing
analgesia with a non-Opioid mechanism as analternative agent to Opioid. It was stated thatclonidine neither affects proprioception like localanesthetics nor causes respiratory depression, itching,nausea and vomiting like Opioids, but when given byepidural route with local anesthetics., it increaseanalgesia potency14. Additive effect of Clonidine tolocal anesthetics can be explained by variousmechanisms. á-2 agonists form their antinociceptiveeffects probably by affecting descending noradrenergictract in spinal cord that plays an important role in painmodulation by anon-opioidmechanism.15
In our study mean time of onset of analgesia was30min in group II, mean time for rescue analgesic orduration of analgesia was 8.26hrs.These findings in ourstudy after a single shot of bupivacaine with adrenalineare consistent with study of Stromskag et al (1988)16
which showed complete relief of pain by 15-30min,mean duration of analgesia with20ml 0.5%was 8hrs .
Bernard and Macarie, evaluating the effects ofadding 30-300 ìg clonidine to lignocaine for axillarybrachial plexus anesthesia, reported that the additionhastened the onset of the block and improved the
9. ovais--36-41.pmd 10/10/2013, 9:22 AM39

40 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
efficacy of surgical anesthesia17.. Susmita Chakrabortyet al. studied the effect of clonidine as adjuvant inbupivacaine-induced supraclavicular brachial plexusblock and concluded that addition of a small dose ofclonidine to 0.5% bupivacaine significantly prolongedthe duration of analgesia without producing anyclinically important adverse reactions other thansedation18. Our study also shows that addition ofclonidine to bupivacaine improved the onset time ofanalgesia (15min), mean duration of analgesia(14.54hr). Overall the duration and quality of analgesiawas better with group III. Though little work has beendone on interpleural bupivacaine with clonidine andanalgesia by interpleural route in cases of laparoscopiccholecystectomy, our results were consistent with otherstudies showing analgesic effect of clonidine withbupivacaine in epidural and peripheral nerve blockswithout increased incidence of side effects. Canver etal.19 reported excellent analgesia without side-effectswith the use of interpleural clonidine alone in twopatients in the first 48 h after open cholecystectomy.The first dose of 300mcg was effective within 30 minand was followed by subsequent ‘on demand’ 150mcgboluses.
To conclude, clonidine is a good adjuvant to 0.5%bupivacaine in interpleural block for postoperativeanalgesia in cases of laparoscopic cholecystectomywithout increased incidence of adverse affects.
Conflict of Interest: None.
Source of Funding: Self funded.
Ethical Clearance: Not Applicable.
Acknowledgement: None
REFERENCES
1. Liu S, Carpenter RL, Neal JM. Epiduralanaesthesia and analgesia. Their role inpostoperative outcome. Anesthesiology 1995; 82(6):1474-506.
2. Wu CL, Fleisher LA. Outcomes research inregional anesthesia and analgesia. Anesth Analg2000; 91 (5): 1232-42.
3. Nathaniel J. Soper, MD; Paul T. Stockmann, MD;Deanna L. Dunnegan, RN; Stanley W. Ashley,MD. Laparoscopic Cholecystectomy The New‘Gold Standard’. Arch Surg. 1992;127(8):917-923.
4. Cigarini, I., Joris, J., Jacquct, N., Lamy, M. Painand Pulmonary Dysfunction After
Cholecystectomy Under Laparoscopy andLaparotomy. Anesthesiology: September 1991 -Volume 75 - Issue 3 - pg A122
5. Psaqualucci A, Contrado R et al. Postoperativepain and management. Anaesthesia andIntensive Care 1999; 24: 1539-45.
6. F. F. Dobbs, V. Kumar, J.I. Alexander, M. G. R.Hull. Pain after laparoscopy related to postureand ring versus clip sterilization. BJOG: AnInternational Journal of Obstetrics &Gynaecology. Volume 94, Issue 3, pages 262–266, March 1987.
7. Reiestad F, Stromskag KE. Interpleural catheterin the management of postoperative pain. Apreliminary report. Reg Anaesth 1986; 11:89-91.
8. Yasin N. Khan MD, Shariq S. Raza MD, ElizabethA. Khan MD. Application of Spinal CordStimulation for the Treatment of AbdominalVisceral Pain Syndromes: Case Reports.Neuromodulation: Technology at the NeuralInterface. Volume 8, Issue 1, pages 14–27, January 2005.
9. Kastrissios H, Mogg GAG, Triggs EJ, Higbie JW.Interpleural bupivacaine infusion compared withintravenous pethidine infusion aftercholecystectomy. Anaesthesia and Intensive Care1991; 19: 539-545.
10. Stromaskag KE, Reiestad F, et al. IntrapleuralAdministration of 0.25%, 0.375%, and 0.5%Bupivacaine with Epinephrine afterCholecystectomy. A & A May 1988 vol. 67 no.5 430-434.
11. Benjema G.C. Analgesic and anaesthetic dosages.Anesth Analg. 1998 Oct; 210(5):710-15.
12. Orliajuet, carli et al. Toxic doses and adverseeffects of anesthetic drugs. Anesth Analg. 1994Oct; 5(3):210-13.
13. Eisenach JC, De Kock M, Klimscha W. Alpha (2)-adrenergic agonists for regional anesthesia. Aclinical review of clonidine (1984-1995) Anesthesiology. 1996; 85:655–74 14AnesthAnalg. 1995 Oct; 81(4):706-12.
14. Bernard JM, Kick O, Bonnet F. Comparison ofintravenous and epidural clonidine forpostoperative patient-controlled analgesia. A &A October 1995 vol. 81 no. 4 706-712
15. Shobhana Gupta, Dipak Raval, Mita Patel, NiravPatel, Nehal Shah. Addition of epiduralClonidine enhances postoperative analgesia: Adouble-blind study in total knee- replacementsurgeries. Anesth Essays Res 2010; 4: 70-4.
9. ovais--36-41.pmd 10/10/2013, 9:22 AM40

International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 41
16. Kjell Erik Strömskag, MD, Finn Reiestad, MD, Ewa L. O. Holmqvist, CRNA and StephanOgenstad, PhD. Intrapleural Administration of0.25%, 0.375%, and 0.5% Bupivacaine withEpinephrine after Cholecystectomy. A & A May1988 vol. 67 no. 5 430-434.
17. Bernard JM, Macarie P. Dose-range effects ofclonidine added to lidocaine for brachial plexusblock. Anesthesiology. 1997;87:277–84.
18. Susmita Chakraborty, Jayanta Chakrabarti, Mohan Chandra Mandal, Avijit Hazra,and Sabyasachi Das. Effect of clonidine asadjuvant in bupivacaine-induced supraclavicularbrachial plexus block: A randomized controlledtrial. Indian J Pharmacol. 2010 April; 42(2):
9. ovais--36-41.pmd 10/10/2013, 9:22 AM41

42 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
Comparative Study of Infra-red Coagulation vsHaemorrhoidectomy in Patients of Haemorrhoids
Pankaj Solanki1, Shalabh Gupta2, T S Bhagat3, Atul Kumar Gupta4, Rajiv Verma5,Dhawal Sharma1, Mamta Rai1
1Post Graduate, IIIrd year, 2Professor & Head of Department, 3Professor & Unit Head, 4Associate Professor & UnitHead, 5Assistant Professor, General Surgery, Santosh Medical College & Hospital
ABSTRACT
Hemorrhoid disease is the most common reason patients seek evaluation by a colon and rectal surgeon.The majority of hemorrhoids can be managed nonoperatively with medical management or as daycare procedures. Even though Milligan Morgan Hemorrhoidectomy(MMH) & Minimal InvasiveProcedure for Hemorrhoid (MIPH) is the gold standard for hemorrhoids, but newer techniques likeINFRA-RED Coagulation(IRC) for 1st, 2nd & 3rd degree hemorrhoids are showing promising resultsbecause of minimal complications, ease of procedure and a day care procedure most of the time.Besides that many patients are not ready for a definite surgical procedure and they can be benefittedby IRC.
Keywords: Hemorrhoids, Infra-red coagulation (IRC), Milligan-Morgan Hemorrhoidectomy (MMH), MinimalInvasive Procedure
INTRODUCTION
The word “hemorrhoids’ is derived from the greekword hemorrhoides meaning bleeding, which is mostprominent symptom in majority of cases. the term isalso used interchangeably with another term ‘piles’which is a derivation of the latin word pila meaning aball1. Haemorrhoids are classified according to theirplace in anal canal into internal & external in relationto dentate line. Mixed or combined hemorrhoids aredefined as the presence of both internal & externalhemorrhoids.
Open hemorrhoidectomy, also known as excision& ligation was originated by Frederick Salmon 2 in1830s. Milligan et al3 modified and popularized thetechnique which is now widely used known asMilligan Morgan hemorrhoidectomy.
Corresponding author:Pankaj SolankiPost Graduate, IIIrd yearB-6/73, Sector-4, Rohini-110085, DelhiMobile no. +91-8800234363,E-mail : [email protected]
Longo’s technique, commonly referred to as thestapled hemorrhoidectomy or stapledhemorrhoidopexy aka MIPH is another standardoperative technique but it is costly and has beenassociated with a number of serious complications,including anastomotic dehiscence necessitatingcolostomy, rectal perforation, severe pelvic infection,and acute rectal obstruction and therefore trainingbefore use is strongly recommended.
Among the newer technique for treatment ofhemorrhoids is Infra-Red Coagulation4, it utilizesinfrared radiation generated by tungsten halogen lampapplied to hemorrhoidal tissue through a solid quartzlight guide. In the infrared coagulator light is convertedto heat which coagulates tissue protein and evaporateswater from cells leading to inflammation, escharformation and eventual scarring which fixates thetissue and stops the bleeding5.
AIMS & OBJECTIVES
1) To study the comparative effects of IRC andMilligan-Morgan hemorrhoidectomy(MMH) for1st, 2nd, 3rd degree Hemorrhoids.
DOI Number: 10.5958/j.2321-1024.1.2.027
10. Pankaj Solanki--42-46.pmd 10/10/2013, 9:22 AM42

International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 43
2) To follow these patients post-IRC for 3 months.
3) To evaluate the efficacy of IRC andhemorrhoidectomy for the 1st, 2nd, & 3rd degreehemorrhoids respectively.
4) To assess IRC as a newer & simpler procedure fortreatment of hemorrhoids.
METHODOLOGY
The study was done on 120 patients attendingSurgery OPD at Santosh Medical College & HospitalGhaziabad. Patients were divided into two groups,with each group comprising 60 patients :
Group A : Patients underwent treatment by Infra-Red Coagulation.
Group B : Patients underwent treatment byMilligan-Morgan hemorrhoidectomy.
The patients included were of 18-95 years of age,symptomatic hemorrhoidal disease which would betreated by either surgical technique but not associatedwith fissure-in-ano, anal spasm or infectivepathologies, patient not fit for anesthesia, patients withgrade 4 hemorrhoids or with pre-existing medicalconditions i.e. IBDs, immune deficiency as AIDS ormalignancy.
All subjects were reassured and explained aboutthe study and thorough history & clinical examinationwere recorded along with routine investigations andsigmoidoscopy was done if required. All patientsunderwent surgical procedure with pre-op colonicpreparation (with enema) and prophylactic antibiotics-500mg of metronidazole and 1.5gm cefuroxime - onehour before the operation.
Group A patients who underwent IRC : IRCemploys a non-coherent, multi-spectrum light sourcewhose spectral maximum is 10000 A0 and works at1000 C. IRC penetrates the tissue to a predetermineddepth virtually at the speed of light & is instantlyconverted into heat. the coagulation time is brief (0.5-3 secs) & causes denaturation of proteins. The beam isfocused and coagulates only that tissue which is incontact with the applicator, which is gently pressedagainst the tissue.
With IRC left lateral position was preferred as itgives enough ease of maneuver with no specialpreference for the positions of hemorrhoids to begin
with; though the largest pile was dealt first & so on,done at all the three principle positions of hemorrhoidsi.e. 3, 7 & 11 o’clock position. The procedure wasperformed by applying the tip of infrared coagulatornear the apex of the hemorrhoid for a 1-1.5 sec pulseof energy. Approx. 3 to 4 applications per hemorrhoidwere performed and 1 to 3 hemorrhoids underwenttreatment per session6. All the pile bases werecoagulated one after the other. the mean treatmentduration was 3 minutes, having ranged between 2 to5 mins7. The application of the tip to hemorrhoidproduced a 3 to 4 mm diameter area of coagulationwith a depth of penetration approx 2.5 mm thatulcerated and scarred in 2 weeks providing fixation tothe hemorrhoid and cessation of bleeding. Patientswere sent home 1 hour post procedure, afterprescribing regular dose of laxative & xylocaine 5%ointment for local application.
Group B patients who underwent Milligan-Morgan haemorrhoidectomy : The patients in thisgroup were operated on in the lithotomy position. Theanal canal was gently dilated with two fingers andforceps was placed on the perianal skin just outsidethe the mucocutaneous junction at each primaryhemorrhoid. As the internal hemorrhoids were pulleddown, a second forceps was put onto the main bulk ofeach hemorrhoidal mass, producing the “triangle ofexposure”. The hemorrhoid was excised from theunderlying sphincter muscle. The dissection wascarried out proximally as far as the pedicles, where itwas stick tied with 3-0 chr catgut. The rest of the woundwas left open and a light dressing was applied to thewound. Other hemorrhoids were treated in a similarmanner. Operations usually lasted 28 mins (ranging15-50 mins). The sample was sent for histopathology.Patients were dismissed from the hospital averagely48-72 hours post procedure.
Each patient was then evaluated for
1. Post-op pain
2. Length of stay in the hospital
3. The time taken to return to normal activities
4. Post-op complications which include :
a) Post-op bleeding or haemorrhage
b) Retention of urine
c) Incontinence
10. Pankaj Solanki--42-46.pmd 10/10/2013, 9:22 AM43

44 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
d) Anal stenosis or narrowing of the anal canal
e) Recurrence of haemorrhoids if any
5. Effectiveness of symptom control like
a) Rectal bleeding
b) Prolapse
b) Discharge
d) Pain
e) Anal irritation
OBSERVATIONS & RESULTS
1) The avg mean age of patients in group A was 33.28+/- 7.62 yrs and 32.57 +/- 7.67 yrs for group B.
2) Total number of females in group A was 23% andthat in group B was 20%.
3) The mean duration of hospital stay in group A was0 days as patients were discharged on same day.However, the mean duration in group B was 2.33+/- 0.47 days.
4) Avg mean pain was calculated in both groupsusing VAS scale on days 0, 1, 5 & 14. The averagemean pain in the entire period was found to be2.11 +/- 0.20 in group A vs. 6.16 +/- in group B.This was extremely statistically significant(p<0.0001).
5) Avg. mean bledding was calculated in both groupson days 0, 1, 5 & 14. The avg mean bleeding in theentire period was found to be 0.766 +/-0.17 ingroup A vs. 1.86 +/-0.13 group B. This wasextremely statistically significant(p<0.0001).
6) Avg mean pruritis was calculated in both groupson days 0, 1, 5 & 14. The avg men pruritis in theentire period was found to be 0.3+/-0.12 in groupA vs 1.90+/-0.28 in group B. This was extremelystatistically significant (p<0.0001).
7) Avg mean excoriation was calculated in bothgroups on days 0, 1, 5 & 14. The avg meanexcoriation in the entire period was found to be0.948+/-0.19 in group A vs 2.096+/-0.19 in groupB. This was extremely statistically significant(p<0.0001).
8) 33% patients in both the groups had prolapsedthird degree hemorrhoids before the procedure. In
group B after open hemorrhoidectomy,theprolapsed portion of the pile mass regressed fromday 1 itself till a 98% regression by day 14 post-opperiod. In group A, the regression in prolapsed pilemass started from 7th day onwards till it reached98% regression on day 14 just as in the group B.
9) Post-op retention of urine was not seen in any casesin group A but was seen in 96% cases in group B.This was extremely statistically significant (0.0001).
DISCUSSION
In our study we found out that the average durationof stay in case of IRC was minimal i.e. only one hourwhereas in case of MMH, it was 2.33 days. For Bledayet al8 in their study it was 2.5 days of hospital stay forpatients underwent MMH. Ele and Okiemy9 studiedthe results of the MMH and the average time spent inhospital was five days (extremes 6 & 11 days). Accarpioet al10 assessed the advantage of nonsurgicaltechniques for haemorrhoids and found that IRC hadthe lowest duration of stay and complications.Templeton & colleagues11 and Marques et al12 alsopropounded that IRC due to its minimal duration ofhospital stay is an ideal procedure for outpatientprocedure for haemorrhoids.
In our study, using the VAS mean pain felt by thepatients in the IRCgroup was 2.11 as compared to 6.12.The pain was felt maximum on the day of theprocedure. In a study by Sielezneff et al13 it was foundthat most frequent complication in MMH was painexperienced by 71% of patients. Palimento et al14
compared the early results in 52 patients randomlyallocated to MMH. VAS score after 24 hours was 5(range b/w 3 to 7). Marquez et al12 in their studyobserved that the percentage of patients usninganalgesics was significantly lower in the IRC group at6 hours(19.2% cases) and 24 hours (13.5% cases) aftertreatment. In a study by Santiago et al15 63 of 358patients were treated with IRC. They found that onlyin the first day, mild anal pain was complained by 40/63 patients (63.4%), after which it subsided.
Our study showed that avg bleeding was 0.766during post-op period in group A vs 1.86 in group B.Palimento et al14 in 52 pateints undergoing MMHobserved that episodes of bleeding were 5/37(13.5%)patients. Bleday et al8 in their study found that delayedhaemorrhage was seen in 2.4% of patients. In 2007Candela et al16, among the pateints treated with MMHtechnique, 7.7% had post-op bleeding. Marquez et al12
10. Pankaj Solanki--42-46.pmd 10/10/2013, 9:22 AM44

International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 45
ascertained that there were significantly lowerincidence of bleeding immediately, 6 hours and 24hours after IRC (immediate-4.3%; 6 hours-3.6%;24hours-10.2%). According to Santiago et al15 of 63patients treated with IRC, mild bleeding was seen in1/63 (1.6%).
According to our study, mean pruritis over the postoperative period was 0.3 in the IRC group incomparison to 1.90 in the MMH group. Candela et al16
evaluated pruritis in 15.4%.
Urinary retention was found in none of the patientsin group A of our study while 96% of patients in groupB suffered urinary retention. In the study by Sielezneffet al13 1,134 patients were operated by MMH techniqueand urinary retention was seen in 16.4% cases.According to Bleday et al8 post MMH urinarycomplications was seen in 20.1% of patients.
In our study , mean excoriation was seen to be 0.948in IRC group whereas in group B was 2.096. Santiagoet al15 and Marquez et al12 separately in their studyfound that minimal or no excoriation was seen in anypatients undergoing IRC.
SUMMARY
Of 120 patients attending surgery OPD for 1st, 2nd
& 3rd degree hemorrhoids at Santosh Medical College& Hospital, Ghaziabad were incorporated into twogroups, divided equally of 60 patients each. On thebasis of the above a compariosn was done b/w groupsA and B, it was observed that :
• Mean Duration of hospital stay was lesser in groupA as compared to group B.
• Average post-op pain as calculated by VAS wassignificantly lower in group A than group B as wasthe average mean bleeding over a 14 day periodbetween the two groups.
• Also the average incidence of pruritis andexcoriation was much significantly lower in groupA as compared to group B.
• Post operative urinary retention was nil in groupA.
CONCLUSION
Even though MMH is the gold standard forhemorrhoids, newer techniques like INFRA-REDCoagulation for 1st, 2nd & 3rd degree hemorrhoids are
showing promising results because of minimalcomplications, ease of procedure and lesser in hospitalstay for the patient.The results in our study stronglyrecommend the use of hemorrhoidectomy only for fewpatients which include :
1. Failure of medical and non-operative therapy;
2. 4th degree, or mixed internal and externalhemorrhoids;
3. Symptomatic hemorrhoids in the presence of aconcomitant ano-rectal condition that requiressurgery.
And this is in accordance with recommendationsof AMERICAN GASTROENTEROLOGICALASSOCIATION17.
IRC is a effective non-operative therapy. Its quick,non-painful technique along with lack of complicationsmakes it an ideal OPD based treatment for 1st, 2nd & 3rd
degree hemorrhoids.
ACKNOWLEDGEMENT
We greatly acknowledge the support of patientswho participated in this study. There were no conflictsof interest amongst the authors. There was no sourceof funding.
Ethical Clearance
The study was approved by ethical committee ofSantosh Medical College & Hopitals, and the studywas conducted after informed consent from patient/guardian.
REFERENCES
1. Salvatore Vieni, Federica Latteri, Nello Grassi.Historical aspects of a frequent anal disease :haemorrhoids. CHIR ITAL.56 (5):745-8.
2. R C Benett et al. Late results ofhaemorrhoidectomy by ligature & excision.BRITISH MED JOURNAL 1963 july27;5351:216-219.
3. Milligan ET,Morgan CN,Jones LE. Surgicalanatomy of anal canal & operative treatment ofhaemorrhoids. Lancet 1937;2:119-1124.
4. A Neiger et al. Infrared-photo-coagulation forhaemorrhoids treatment. INT SURG.;74(3):142-32606612.
5. Nath G. The new principles of IRC in medicineand its physical fundamentals. Coloproctology,1983;379-81.
10. Pankaj Solanki--42-46.pmd 10/10/2013, 9:22 AM45

46 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
6. Walker AJ, Leicester RJ et al. A prospective studyof INFRA-RED coagulation, injection, and rubberband ligation in treatment of hemorrhoids. INTJOURNAL COLORECTAL DISEASE1990;5(2):113-116.
7. Jogen J, Bach S stubinger SH, Bock JU. Excisionof thrombosed external hemorrhoid under localanesthesia: a retrospective evaluation of 340patients DIS COLON RECTUM 2003’46:122.
8. Bleday R, Pena JP et al. Symptomatichemorrhoids: current incidence & complicationsof operative therapy. DISEASES COLONRECTUM 1992;35(5):477-481.
9. N Ele et al. Results from surgical treatment of thehemorrhoid disease according to Milligan &Morgan technique-about 56 cases. MALIMED.2007;22 (2):58-60.
10. Leicester RJ, Nicholls et al. Infrared coagulation:a new treatment for hemorrhoids. DISEASES OFCOLON RECTUM 1981;24(8)602-605.
11. Templeton JL, Spence RA, Kennedy TL, Parks TG,Mackenzie G, Hanna WA. Comparison ofinfrared coagulation & rubber band ligation forfirst & second degree hemorrhoids: a randomisedprospective clinical trial. BR MED J CLIN RESED 1983;286(6375):1387-1389.
12. C Marques et al. Early results of the treatment ofinternal hemorrhoid disease by infrared
coagulation & elastic banding: a prospectiverandomised cross-over trial. TECHCOLOPROCTOL.2006 Nov 27.
13. J Chir (Paris). Early postoperative morbidity afterhemorrhoidectomy using Milligan-Morgantechnique. A Retrospective studies of 1,134 cases.DIS COLON RECTUM. 1997 Nov;134(5-6):243-47 9772981.
14. Domenico Palimento et al. Stapled and openhemorrhoidectomy: randomised controlled trialof early results. WORLD J SURG.2003Feb;27(2):203-7.
15. E Linares Santiago et al. Effectiveness ofhemorrhoidal treatment by rubber band ligationand infrared photocoagulation. REV ESPENFERM DIG. 2001 Apr; 93(4):238-47 11488120.
16. G Candela et al. The gold standard in thetreatment of hemorrhoidal disease.Milligan-Morgan hemorrhoidectomy vs Longomucoprolapsectomy : comparing techniques.MINERVA CHIR. 2007 Jun; 62(3):151-159.
17. Clinical Practice Committee, AmericanGastroenterological Association(AGA). AGAmedical position statement: diagnosis andtreatment of hemorrhoids.GASTROENTEROLOGY 2004;126(5):1461-1462.
10. Pankaj Solanki--42-46.pmd 10/10/2013, 9:22 AM46

International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 47
Study of Incidence of Prolactin Level in Female Infertilityin its Correlation with the Hypothyroidism in Hapur
Poonam Mani1, Pragya Maheshwari2, Yogesh Kumar Rai3
1Assistant Professor, Department of Obstetrics & Gynecology, 2Senior Resident, 3Assistant Professor, Biochemistry,Saraswathi Institute of Medical Sciences, Hapur, Ghaziabad, U.P., India
ABSTRACT
Objectve: The aim of our study was to find out incidence of prolactin level in female infertility & itscorrelation with hypothyroidism .
Materials: The present study was conducted on 100 patients attending outpatient department ofobstetrics and Gynaecology SIMS, Hapur.
Result: Sixty patient had primary infertility and forty patient had secondary infertility. Anovulatorycycles were 52%.(40 % and 55% Primary & secondary infertility respectively). Galactorrhoea waspresent in 9% of the women. The incidence of Hyperprolactinemia i.e. serum prolactin level wasmore than 25% was 52% .The incidence of hypothyroidism 33.3%.
Conclution: There is high incidence of hyperprolactinemia in infertile women positive correlation of1:3 was found between hypothyroidism and hyperprolactinemia.
Keywords: Hyperprolactinemia ,Hypothyroidism & Infertility
INTRODUCTION
Infertility is defined as the inability to conceive afterone year of regular intercourse without contraception.According to standard protocol Infertility evaluationusually identifies different causes, including maleinfertility 30% female infertility 35% The combinationof both 20% and finally unexplained or idiopathicinfertility 15%..Prolactin is a polypeptide hormonesecreted by the anterior pituitary gland, whose mainrole is stimulation of lactation in the postpartumperiod. The increase in prolactin secretion can bephysiological (pregnancy and lactation) orpathological(hypothalamic and pituitary diseases,iatrogenic, etc). Hyper prolactinemia is usuallyassociated with menstrual and ovulatory disorders like
Corresponding author:Poonam ManiAssistant ProfessorDepartment of Obstetrics & gynaecology, SaraswathiInstitute of Medical Sciences, Hapur, Ghaziabad, U.P.Tel:991747766E-mail: [email protected]
amenorrhoea,.oligomenorrhoea, anovulation,ovulatory cycles with short or inadequate luteal phaseand galactorrhea3. Estimation of serum prolactin levelis recommended in women with unexplainedinfertility, any menstrual irregularity with or withouthirsutism, galactorrhea with or without amenorrhealuteal phase defects, anovulation, anovulatarybleeding and delayed puberty, Apart from these groupof some infertile women with regular menses also mayhave hyperprolactinemia with the determination ofserum prolactin levels. Some of the women withgalactorrhea and hyperprolactinemia might haveprimary hypothyroidism this disease is characterizedby low serum level of thyroxine (T4) and decreasednegative feedback on the hypothalamo pituitary axis.The resulting increased secretion of thyrotropinreleasing hormone (TRH) and prolactin.
Thyroid dysfunction is a condition known to reducethe likely hood of pregnancy and to adversely affectpregnancy outcome the aim of our study were to findthe incidence of hyperprolactinemia in femaleinfertility and its correction with hypothyroidism.
DOI Number: 10.5958/j.2321-1024.1.2.028
11. poonam mani --47-51.pmd 10/10/2013, 9:22 AM47

48 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
METHOD & MATERIAL
This was undertaken in department of obstetricsgynecology SIMS of Hapur. The study was conductedon 100 infertile women attending the out patientdepartment in a span of 2-3 years the exclusion criteriawere male factors infertility and amongst the femaletubal factors, any congenital anomaly of urogenitaltract. and any organic lesion.
A detailed history was taken examination carried
out and the infertility workup done which includedsemen analysis premenstrual endometrial sample,HSG, USG. Fasting Serum Prolactin levels, diagnosticlaparoscopy & when indicated Serum TSH levels incash of hyperprolactinemia. For prolactin estimationvenous sample in follicular phase was taken. Thenormal range taken was 2-25 ng/ml. serum whenprolactin level were >25 ng/ml, using auto analyzer.Women with serum prolactin levles >100 ng/ml wereadvised CT scan or MRI.
Table I. Menstrual irregularities and hyperprolactinemia (n=100)
Clinical condition n=100 Normal Prolactin level Increase Prolactin level(No. %) (n=49) (n=51)
Regular Menses 35 35% 17 35% 18 35%
Oligomenorrhea 57 57% 29 59% 28 55%
Amenorrhea 7 7% 3 6% 3 6%
Menorrhagia 1 1% 0 0 2 4 %
Total 100 100 49 100 51 100
RESULT
Out of the 100 patients, 60 (60%) had primaryinfertility and 40 (40%) secondary infertility. Most ofwomen were in the age group 24-30 years both thegroups the mean duration of infertility in the patientswith primary and 3.5 years and in those withsecondary infertility 3.3 years.
Galactorrhoea: was present in 10 (10%) five (5/
60, 8%) with Primary infertility five (5/40, 12.5%) withSecondary infertility. Galactorrhoea was either thechief complained or was detected on breastexamination.Normal menstrual cycles were present35% (35%, 35/100) infertility patients 23 (38.3%, 23/60) with Primary Infertility & 12 (30%, 12/40) withSecondary infertility the remaining 65 showed somemenstrual abnormalities as shown on (table-1)
Table 2. Endometrial sampling findings (n=100)
Non secretary Tuberculosis Secretary
No. % No. % No. %
Primary Infertility (n=60) 29 48% 4 6% 23 38%
Secondary Infertility (n=40) 23 55% 2 5% 19 47.5%
Total (n=100) 52 52% 6 6% 42 42%
Premenstrual endometrial abnormalities as shownin Table-2 Endometrial sampling done in all 100women and 52 (52%, 52/100) showed non secretaryendometrial suggestive of anovulatory &oligoovulatory cycle out of these (48% & 57% hadprimary infertility & secondary infertility respectively).Tuberculosis detected in 6(6% 6/100) out of these (4,(6%, 4/60) and 2 (5%, 2/40 with primary infertilityand secondary infertility respectively) The remaining
(42%, 42/100) showed secretary endometrial on HSG,all the patient had patent fallopian tubesUltrasonography (USG was done in all 100 patients &showed No abnormality in 86 women out to of this.52 (86%, 52/60) women with primary infertility and(85% 34/40) women with Secondary infertility. Table-3 shows the various pathologies found on Ultrasoundin two groups.
11. poonam mani --47-51.pmd 10/10/2013, 9:22 AM48

International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 49
Table 3: Abnormal finding on USG in two group.
Findings Primary Infertility(n=60) Secondary infer(n=40)
Uterine pathology
Endometrial hyperplasia 2 3.33% 0 0
fibroids 0 0 2 5%
Tubal pathology 0 0 0 0
Ovarian pathology
Polycystic ovaries 4 6.6% 2 5%
Adnexal cyst 2 3.3% 1 25%
chocolate cyst. 0 0 1 25%
Table 4. Diagnostic Laparoscopy findings (n=30)
Findings Primary SecondaryInfertility infertility
(n=16) (n=14)
No abnormality 4 1
Polycystic ovaries 4 2
Endometriosis 3 6
Fimbrial cyst 3 2
Bulky uterus 1 2
Flimsy adhesions 1 1
Diagnostic laparoscopy was done in 30 patient 16with primary infertility & 14 with Secondary infertilityas shown in. Table 4
Table 5 shows the serum prolactin levels theincidence of 51% (51/100) overall, 55% (33/60) and45% (18/40) in the Primary infertility & SecondaryInfertility groups respectively the an ovulation wasdetected in 40% (20/40) of the women with
normoprolactinemia and 62% (32/51) withhyperprolactinemia, 13 (thirteen women had prolactinlevel> 100 mg/ml, nine (15% 9/60) with primaryinfertility & four (10% 4/40) with secondary infertility.all the 13 were advised CT scan or MRI (one womenin each group had pituitary adenoma and both hadserum prolactin level) >200 mg/ml.
Table 5. Serum prolactin levels (n=100)
Serum prolactin Primary Percentage Secondary Percentage P valuelevel (ng/ml.) Infertility infertility
(n=60) (n=40
0-25 27 45% 22 55% 0.127
26-100 17 28% 6 15% 0.109
51-100 07 12% 8 20% 0.129
101-150 3 5% 2 5% 0.316
151-200 1 2% 1 2.5% 0.181
More than 200 5 8% 1 2.5% 0.128
Total 60 100% 40 100%
Table 6 shows the TSH level in 51hyperprolactinemia women the incidence ofhypothyroidism in hyperprolactinemia was 33.3% (17/out of 51) of this 13 (39%, 13/33) women had PrimaryInfertility and (22%, 4/18) had Secondary infertilitythe mean s. prolactin level in hyperprolactinemiawomen was 124.4. 64.32 mg/ml the mean serum TSH
level in women with hyperprolactinemia was 9.57 -+16.79 mIU and in hypothyroid women with hyperprolactinemia 27.88 + 32.57 mIU difference wasstatistically highly significant p (0.0004) The ratio ofproportions between hyperprolactinemia andhypothyroidism hyperprolactinemia patients one hadhypothyroidism. there was positive correlation.
11. poonam mani --47-51.pmd 10/10/2013, 9:22 AM49

50 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
The mean serum prolactin levels in women withgalactorrhea was 127.3 ng/ml. >out of the 51 womenwith hyperprolactinemia. 9 (17.6% 9/51) had
galactorrhea the most common cause ofhyperprolactinemia in our study idiopathic 18 (65% 33/51) followed by primary hypothyroidism 9((17.6 9/51).
Table 6. TSH Levels in Hyperprolactinemia (n=51)
Serum TSH level Primary Percentage Secondary Percentage(mIU/mL) Infertility infertility
(n=33) (n=18)
< 5 20 61% 14 78%
5-10 7 21% 1 5.5%
10-20 1 3% 1 5.5%
More than 20 15% 2 11%
Total 33 100% 18 100%
DISCUSSION
Hyperprolactinemia is a common problem ininfertility the understanding that hyperprolactinemianot onlycauses galactorrhea and amenorrhoea but alsogonodal dysfunction and infertility led. to the wideruse of prolactin estimation in our study there were 60%women with primary infertility 40% women withsecondary infertility, the menstrual irregularty foundin majority of infertile women in both group (60% withprimary infertility 70% in secondary infertility) suchfindings. have been reported by Mishra et al, 2002,Pappe K et al 2003, 2011 Ner et al 2001,
Reported hyperprolactinemia adversely affectsfertility potential by impairing GnRH pulsatility andthere by ovarian function.
Mishra R. et al 2002. Incidence of galactorrhea 25%has been reported in our study galactorrhea waspresent in 10%’ of in overall women incidence ofgalactorrhea in hyperprolactinemia women 18% andovulatary dysfunction has been report 51.4%.
Rangan. R. et al 1990. An incidence of hyperprolactinemia galactorrhic women 62.1% has beenreported and ovarian dysfunction had been report31.4% in our study 52% of all infertile women showedanovulatary cycle.
The incidence of hyperprolactinemia ingalactorrhoeic women was 90% out of ten, nine womenhad galactorrhea in our study.
In our study USG was done in all 100 women andpositive findings were seen in 14 only How’rediagnostic laparoscopy was done in 30 women andpositive findings were seen in 25 (83%) of them. Thedifference of proportions test shows a z value of 7.216
for diagnostic laparoscopic as compared to USG. ThisDiagnostic laparoscopy is a better tool for pelvicpathology in infertility in case of infertility.
The incidence of hyperprolactinemia in our studyis 51%.. Mishra et al have reported an incidence of 20%in infertility.Where as Mishra et al found to be 128.28 -+ 12.74 ng/ml.Mean prolactin level. In our study 80.6-+53.8. In our incidence of hypothyroidism inhyperprolactinemia women in 33.3% (17/51) so apositive correction 1:3 was found betweenhypothyroidism and hyperprolactinemia.Cramer DW.et al 2003. has been reported TSH and prolactin lavelwere positively correlated in femaleinfertility.Choudhary SD 1995. observe 16.6% inwomen with hypothyroidism in hyperprolactinemicwomen and singh et al hyperprolactinema in 5.7% withhypothyroidism women.
CONCLUSION
Serum prolactin level are mandatory in allovulatory dysfunction infertility, incidence ofhyperprolactinemia is very high in galactorrhoeicwomen hence serum prolactin levels are importantscreening procedures and high incidence & positivecorrelation with hypohthyrodsm in anovulatory /amenorrhoeic / oligomenorrhoeic women TSH levelshould be done in all hyperprolactinemic women.
ACKNOWLEDGEMENT:
We would like to thank the patients of SaraswathiInstitute of Medical Science Hapur. Who participatedin the study, we are also greatful to Dr. Rukma Idnaniprincipal of SIMS Hapur for her valuable suggestionsand guidance, without whose encouragement andassistance, this study was not possible.
11. poonam mani --47-51.pmd 10/10/2013, 9:22 AM50

International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 51
REFERENCES
1. Crammer DW, Sluss PM, Powers RD, MeshaneP, Ginsburgs ES, Hornstein MD, et al, SerumProlactin and TSH in an in vitro fertilizationpopulation: is there a link between fertilizationand thyroid function? J Assist Reprod Genet2003;20:210-5. (s)
2. Zollner U, Laning K, Steack T, Dietl J. Assessmentof endocrine status in patients undergoing in-vitro fertilization treatment. Is it necessary? ArchGynecol Obstet 2001;265:15-20. (s)
3. Mishra R, Baveja R, Gupta V et al. Prolactin levelin infertility with menstrual irregularities. JObstet Gynecol India 2002;52:40-3.
4. Shoupe D, Mishell DR. Hypoprolactinemia:Diagnosis and treatment. In: Mishell’s textbookof Infertility, COntraception and ReproductiveEndocrinlog. 4th edn. Massachusetts. BlackwellScience. 1997; 323-41.
5. Rajan R. Prolactin Metabolism in infertility. JObstet Gynecol India 1990;40:243-7.
6. Choudhary SD, Goswami A. Hyperprolactinemiaand reproductive disorders- a profile from northeast. J Assoc Physicians India 1995;43:617-8.
7. Singh L, Agarwal CG, Chowdhary SR Et al.Thyroid profile in infertile women. J ObstetGynecol India.
11. poonam mani --47-51.pmd 10/10/2013, 9:22 AM51

52 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
Comparison of Low Cost Net-mesh with Prolene Mesh inManagement of Inguinal Hernia
Prateek Vardhan1, Shalabh Gupta2, Rajiv Verma3, T S Bhagat4, Atul Kumar Gupta5,Pankaj Solanki1, Mamta Rai1
1Post Graduate Third Year, 2Professor, Head of Department, 3Assistant Professor, 4Professor, 5Associate Professor,Department of General Surgery, Santosh Medical College & Hospital
ABSTRACT
Hernia repair is one of the most commonly performed operations worldwide. The use of alloplasticmesh is now common place in hernia repair. However in developing countries cheaper alternativesto commercial mesh are available to the high associated cost. The cost of the mesh used normally foringuinal hernioplasty ranges from 1000-1500 rupees. The mesh used in the study costs Rs 40 only. Weaimed to investigate the use of mosquito net mesh in cases of inguinal hernioplasty in terms of costeffectiveness, handling, recurrence and complications.
Keywords: Inguinal Hernia, Alloplastic Mesh (Prolene Mesh), Mosquito Net Mesh, Cost Effective
INTRODUCTION
The word HERNIA means rupture or tear.Reference to the surgical treatment of an inguinalhernia dates back to the first century; however, theformal description of hernia repairs did not appearuntil the 15th century. Castration with woundcauterization or hernia sac debridement with healingallowed by secondary intention were the mostcommon operations. These early operations reflecteda complete lack of understanding of the anatomy ofthe groin. The latter part of 18th century heraldeddramatic changes as the anatomy of groin becomebetter understood. Edoardo Bassini is considered thefather of modern inguinal hernia surgery. Byincorporating the developing disciplines of antisepsisand anesthesia with a new operation that includedreconstruction of the inguinal floor along with high
Corresponding author:Prateek VardhanPost Graduate Third YearD-8/12, Teacher's Colony, Pratap ViharGhaziabad 201009, U.P.Mobile No. 8447266224E-mail id: [email protected]
ligation of the hernial sac, he was able to substantiallyreduce morbidity. Lotheissen, McVay, Halsted,Shouldice, and others described modifications ofBassini’s repair in an attempt to further reduce therecurrence rate and to avoid complications.
Although Bassini’s principle of the posterior wallreinforcement remains valid in surgical practice today,his operation has lost popularity and is used only inselected cases in which the use of prosthetic materialis either contraindicated. This change can be attributedto the widespread acceptance of the concept of theavoiding tension during hernioplasty, championed byLichtenstein. The history of inguinal hernia is notcomplete until mention about Stoppa’s repair. Theconcept of Stoppa’s repair has been the cornerstone ofthe evolution of laparoscopic technique of hernia.
Bard mesh is a unique knitted polypropylene meshindicated for use in inguinal hernias, femoral hernias,and incisional hernias. Bard mesh is permeable to thegrowth of granulation tissue and stimulates promptfibroplasia. Bard mesh has been widely used clinicallyover 30 years with excellent result. The only drawbackof using this mesh is, it is costly and hence it is beyondthe reach of poor population.
DOI Number: 10.5958/j.2321-1024.1.2.029
12. Prateek Vardhan-52--55.pmd 10/10/2013, 9:22 AM52

International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 53
Appropriate mesh materials should meet thefollowing criteria:
• Permanent
• Inert, Monofilament
• Non Oncogenic
• Resistant to infection
• Stimulates the growth of fibroblasts through itsholes
• Permits a strong layer of collagen deposition
• Fixed rapidly in place by the patient’s fibrin glue.
MATERIAL AND METHOD
A total 100 patients were included in the study over2 years from January 2011 to December 2012, 50patients were allocated to each arm of the study.
STUDY ARM: Net Mesh Hernioplasty
CONTROL ARM: Prolene Mesh Hernioplasty
I. Patient Selection
A. Inclusion Criteria:
All the patients of uncomplicated direct / indirect/ recurrent inguinal hernia over 18 years of age.
B. Exclusion Criteria
• Patients who are unfit for hernia repair undergeneral/ spinal anesthesia.
• Patients with bleeding diathesis and fungalinfection of inguinal area.
II. Equipments
• Net Mesh
• Prolene Mesh
Net mesh is a knitted monofilament of Polyethyleneand also is a co-polymer of polypropylene andPolyethylene. The melting point of the Net mesh is1400C, so it can be safely autoclaved.
PROCEDURE
All the patients underwent Lichenstein TensionFree Mesh hernioplasty in a random fashion using NetMesh/ Bard mesh in 50 patients in each group under
spinal/ general anesthesia with antibiotic cover. Thus100 patients were operated in 2 years.
OBSERVATION
Total 100 number of patients were included in thestudy. A randomized control trial was conducted byrandomly allocating patients to study and controlgroup of 50 each.
Table 1: Distribution of patients in two groups
Group Number of Patients
Study Group 50
Control Group 50
Total 100
In the study group the minimum age of patient is18 years and maximum is 70 years whereas in controlgroup the minimum age is 30 years and maximum is68 years.
Table 2: Distribution of Age for both study and controlgroups
Study Group Control Group(n=50) (n=50)
Minimum(years) 18 30
Maximum(years) 70 68
Range 52 38
Mean(years) 49.80 50.80
In the study group, 27 patients had hernia on rightside and 23 on left side. In the control group, 26 patientshad hernia on right side and 24 on the left side.
12. Prateek Vardhan-52--55.pmd 10/10/2013, 9:22 AM53

54 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
Post Operative Complications
There was only 1 wound infection and 2 seroma ineach study and control group. Wound infection wasmanaged conservatively without opening of stitch lineand seroma regressed spontaneously. There was 1hematoma in study group which was managed byopening the wound, evacuating the hematoma andclose it by secondary intention.
Complications Control Group Study Group
Wound Infection 1 1
Seroma 2 2
Hematoma 0 1
Rejection 0 0
Recurrence 0 0
Chart: Post Op. complications in both control and study group
Comparison of Cost of Net mesh and Prolene Mesh
Here, the graph which give us overview regardingthe comparison of cost of mosquito net mesh withprolene mesh which is rupees 40 as compared to thecost of prolene mesh is up to rupees 1500.
CONCLUSION
This study was being done as the cost of Net meshis very low. The cost of commercially available Prolenemesh which is widely used in inguinal hernioplastyranges from Rs. 1000-1500 whereas our Net mesh forthe same size costs just Rs.40. thus even the poor whoneeds hernioplasty can afford it.
Apart from the cost effectiveness if the results arethe same as with other meshes then we can use theNet mesh in all the patients and make a huge break-through in managing hernioplasty in managinghernioplasty at a very low cost.
ACKNOWLEDGEMENT
We greatly acknowledge the support of patientswho participated in this study. There were no conflictsof interest amongst the authors. There was no sourceof funding.
Ethical Clearance
The study was approved by ethical committee ofSantosh Medical College & Hospital, and the studywas conducted after informed consent from patient/guardian
REFERENCES
1. Article over use of mosquito net mesh by M GClark, C Oppong, R Simmermacher, K Park, MKurzer, L Vonotoo, A N Kingsnorth.
2. Halsted WS. Surgical papers by William papersby William Stewart Halsted: The operativetreatment of inguinal hernia, vol.1, baltimore,johns hopkins press, 1924 (special edition byclassics of surgery library.Birmingham, Albama,1984.)
3. Shouldice EE. The treatment of hernia. OntarioMed Rev 1953;20:670.
4. Lichtenstein IL, Shulman AG, Amid PK, et al: Thetension free hernioplasty. Am surg 1989,157:188-193.
5. Gilbert AI sutureless repair of inguinal hernia.Am surg 1992;163:331-335.
6. Robbins AW, Rutkow IM. The mesh-plughernioplasty.Surg clin North Am 1993;73:501-502.
7. Divilo LT. Inguinal Hernia and the Prolene(polypropylene) hernia system. Medical AffairsEthicon Inc 1997.
8. Albucasis. On surgery and instruments. Adefinitive edition of the Arabic text with Englishtranslation and commentary by M S Spink andGL Levels, London, The welcome institute of the
RESULTS
Excellent. The Net mesh was accepted by all thepatients and no recurrence has been reported till date.
Advantage of Net Mesh
a) Cost effective Rs.40/- only
b) Easily available
c) Ethylene Oxide sterilized
d) Easy to handle
e) Good tensile strength
f) Non degradable
No disadvantages there.
12. Prateek Vardhan-52--55.pmd 10/10/2013, 9:22 AM54

International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 55
History of Medicine and Oxford, The UniversityPress,1973.
9. Read RC. The development of inguinalherniorrhaphy. Surg Clin North Am 1984;64:185.
10. Bassini E. Nuovo Metodo per la cura radicaledell’ernia inguinale. Atti Congr Associ Med Ital1887;2;179.
11. Bassini E. Sulla Cura radicale dell’ernia inguinale.Arch Soc Ital Chir 1887;4:380.
12. Bassini E. Sopra 100 casi di cura radicale dell’erniainguinale. Arch Soc Ital Chir 1887;4:380.
13. Bassini E. Nuovo Metodo per la Cura Radiclaedell’ernia inguinale.Padua, Italy; Prosperini;1989.
14. Lotheissen G. Zur radikol operation derSchlenkelhernien. Zentralbi Chir 1898;23:548.
15. Lichtenstein IL, Shulman AG, Amid Pk, et al. Thetension free hernioplasty. Am J surg 1989; 157:188-193.
12. Prateek Vardhan-52--55.pmd 10/10/2013, 9:22 AM55

56 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
A Study of Comparison of Cervical Epidural Anaesthesiawith General Anaesthesia for Thyroid Surgery
Priyadarshini M Bentur1, Ravi R2
1Associate Professor, 2Professor, Department of Anaesthesia & Intensive Care J.J.M. Medical College, Davangere
ABSTRACT
Background: To compare cervical epidural anaesthesia (CEA) technique with general anaesthesia inthyroid surgeries.
Method: Fifteen patients were randomly selected to be operated under CEA for thyroid surgeriesand their results were compared with 15 other patients who underwent the same surgery underconventional GA technique.
Results: CEA was found to be comparable to GA in thyroid surgeries
Conclusion: We conclude that cervical epidural anaesthesia can be safely used for thyroid surgery.
Keywords: Cervical Epidural Anaesthesia, General Anaesthesia and Thyroid Surgery
INTRODUCTION
Thyroid surgeries have been performedconventionally/ traditionally under routine generalanaesthesia. Regional anaesthesia techniques haveprovided better patient and surgeon comfort and easedthe anaesthesiologist’s problems in certain patientpopulations for lower limb surgeries and (lower)abdominal surgeries. Whether the same advantagesof regional over general anaesthesia could be appliedto thyroid surgeries has been a subject of widespeculation. Several articles have been published inthe same regard1, 4, 12, 13. Huge goiters compressing /deviating the trachea can pose intubation challenges.Arrythmias can occur under the effect of generalanaesthetic gases and drugs especially in hypo/hyperthyroid patients. These are avoided. Additionaladvantages are lower cost, better surgical field,reduced stress response, prolonged postop analgesia,stable cardiovascular status, early patient ambulationand a conscious vocalizing patient.
MATERIALS AND METHOD
Ethical committee approval was obtained. 15patients were randomly selected to undergo thyroidsurgery under CEA during the period from Jan 2011to Jan 2013. Over the same period 15 comparablepatients were selected to undergo thyroid surgery
under GA. Patients with concomitant systemic illnesswere excluded from the study. Details are given inTable 1.
Selection Criteria
Patients were randomly allocated to the CEA andGA groups. The author is a proponent of CEA and heused this technique in all 15 cases. The other 15 caseswere done under the supervision of other colleaguesin the Dept of Anaesthesia under conventional generalanaesthesia technique.
CEA Technique
Patient was placed on a stool with neck flexed andhead resting on a table (figure 1). Skin was asepticallyprepared and landmark-vertebra prominens wasidentified. Skin over C7 –T1 interspace was infiltratedwith 2ml 2! Lignocaine. 18G Tuohy needle wasinserted parallel to the spine in C7 –T1 interspace andepidural space was located using Loss of resistancetechnique. After negative aspiration of CSF, 18G(BRAUN) catheter was inserted 3-4 cms into epiduralspace and fixed. Patient was placed supine and 10-15ml 1.5% lignocaine with Adrenaline was givenEpidural after test dose. After 15 mins, patient wasplaced in thyroid position .Monitoring of PR, BP, ECG,SaO2 and Respiratory rate were carried through outthe procedure.
DOI Number: 10.5958/j.2321-1024.1.2.030
13. Priyadarshini--56-58.pmd 10/10/2013, 9:22 AM56

International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 57
Table 1. (Patient Details)
CEA (n= 15) GA (n=15)
1. Mean age (yrs) 31 (20 -42) 37 (28 -46 )
2. Sex Ratio M : F 1:3 1:4
3. Thyroid status
• Euthyroid 8 8• Hyperthyroid 7 7
4. Tracheal compression/deviation
• Present 7 7• Absent 8 8
RESULTS
Among 15 patients, in CEA group, in 14 thetechnique was successfully accomplished. In onebecause of blood stained aspirate from Tuohy needle,the procedure was abandoned and the patientproceeded to undergo the surgery under conventionalGA. The rest of the 14 patients were comfortablymaintained in a state of conscious sedation during theprocedure (Figure 2). In 2 patients the surgery tooklonger than 90 min, 6ml 1.5% xylocaine was givenepidurally.
Out of the 15 patients selected for GA, in 2 patientswith huge goiter compressing the trachea, intubationwas difficult and achieved after multiple attempts witha bougie. Hypotension correctable with vasopressorswas seen in them following this episode. In these 2patients and 1 other hyperthyroid patient, arrhythmias(VPCs) appeared intraoperatively which was correctedwith I.V Lignocaine 1.5mg/kg and withdrawal ofinhalational anaesthetic.
Table 2: Comparison of results of CEA Vs GA
CEA GA(n = 15) (n =15 )
1. Technical success 14 15
2. Technical difficulty 1 2
3. Conversion to other technique 1 0
4. Intra-operative arrhythmia 0 3
5. Intra-operative hypotension 0 2
DISCUSSION
Anaesthesia for huge goitrous swelling of thethyroid with hypo/hyperthyroidism is fraught withhazards because of the delicate cardiovascular statusand airway difficulty. This is especially so wheninteraction with anesthetic gases and drugs occur.Multiple attempts at intubation can cause laryngealedema, a life threatening situation. In such situations,
where GA is a high risk proposition, regionaltechniques are safe.
CEA anaesthetises the brachial plexus, cervicalplexus and superior thoracic dermatomes. The incisionsite is anaesthetised by blockade of the nerves[Transverse cutaneous nerve (C3-C4) andSupraclavicular nerve (C3-C4)].
CEA can also be used for hand, upper limb,shoulder, upper thoracic wall surgeries likeMastectomy11, Carotid artery surgery2, Parathyroidsurgery3, neck dissection for head and neckcarcinomas4, treatment of complex regional painsyndrome of upper limbs 5, 11.
Adequate anaesthesia with a high degree of patientacceptance has been documented by theseAnaesthetists.
CEA is feared because of its potential complicationslike Phrenic nerve palsy, spinal cord trauma,cardiovascular dysfunction and pulmonarydysfunction.
Phrenic nerve (C3, C4, C5) mainly a motor nerve isnot blocked by the concentration that we used (1.5%Lignocaine). Steven6 et al found a measurable decreasein FEV and FVC by 10-15% after using 300mgLignocaine, but these were not clinically significant.Using USG Capdevilla7 found the diaphragmaticexcursion to decrease from 5.6 to 4.4 mm after CEA.None of our CEA patients experienced change inbreathing pattern, desaturation or postoperativepulmonary atelectasis.
CEA causes cardiac sympathetic denervation whichresults in depression of phasic and tonic dynamicmodulation of the cardiac cycle8.There is suppressionof reflex increase in heart rate and fall in MAP.Pancuronium9, Ketamine10 induced tachycardia aresuppressed. 10.9% developed hypotension and 2.9%bradycardia in articles .In our study none of ourpatients showed any cardiac destabilization. Incontrast, 2 patients who had difficult intubation in theGA group, proceeded to have hypotension followingthe intubation event. These 2 patients with one morepatient in the GA group later had VPCs intra-operatively.
Patients in the CEA group could vocalize, so earlydetection of recurrent laryngeal nerve palsy waspossible.
13. Priyadarshini--56-58.pmd 10/10/2013, 9:22 AM57

58 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
CONCLUSION
From review of literature and in our ownexperience we conclude that CEA is a safe and reliabletechnique. We anaesthetists being already familiar withthe lumbar epidural technique, it is easy for us tomaster the cervical epidural technique. With clearunderstanding of the anatomy of cervical spine, andtechnique related physiology, this method can be veryuseful in certain patient population. We recommendthis technique as a good alternative to GA for thyroidsurgery.
Conflict of Interest: None Declared.
Source of Funding: Nil
REFERENCES
1. Khanna R, Singh DK Cervical epiduralanaesthesia for thyroid surgery. Kathmandu UnivMed J 2009, July-Sep ; 7(27) : 242-5.
2. Bonnet F, Derosier JP, Pluskwa F, Abhay K,Gaillard A. Cervical epidural anaesthesia forcarotid artery surgery. Canadian JAnaesthesiology. 1990;37(3): 353-8.
3. Michalek P, David I ,Adamec M, Janousek L.Cervical epidural anaesthesia for combined neckand upper extremity procedure: a pilot study.Anaesth Analg .2004; 99(6): 1833 -6.
4. Wittich DJ Jr, Berny JJ, Davis RK. Cervicalepidural anaesthesia for head and neck surgery.Laryngoscope. 1984. 94(5):615 – 9.
5. Buchheit T, Crews JC. Lateral cervical epiduralcatheter placement for continuous unilateralupper extremity analgesia and sympathetic block.Regional Anaesthesia and Pain Medicine.2000;25(3): 313 – 7.
6. Stevens RA, Frey K ,Sheikh T, Kao TC, Milcat –Stevens M, Morales M. Time course of the effectsof cervical epidural anaesthesia on pulmonaryfunction. Regional Anaesthesia and PainMedicine. 1998;23(1): 20 – 4.
7. Capdevila X, Biboulet P, Rubenovitch J, Serre –Cousine O, Peray P, Deschodt J, et al. The effectsof cervical epidural anaesthesia with bupivacaineon pulmonary function in conscious patients.Anaesthesia and Analgesia. 1998; 86 (5):1033 – 8.
8. Tanaka M, Goyagi T, Kimura T, Nishikana T. Theeffects of cervical and lumbar epiduralanaesthesia on heart rate variability andspontaneous sequence baroreflex sensitivity.Anaesthesia and Analgesia. 2004;99(3):924-9.
9. Omete K, Iwasaki H, Namiki A. Cervicothoracicepidural anaesthesia blunts pancuroniuminduced increase in heart rate in humans. ActaAnaesthesiologica Scandinavica. 1993;37(4) :415 – 418.
10. Mayumi T, Dohi S, Takahashi T. Cardiovasculareffects of ketamine in humans with cervical orlumbar epidural blockade. Anaesthesiology.1985;62(1):39-43.
11. Jadon A, Agarwal P. Cervical epiduralanaesthesia for radical mastectomy and chronicregional pain syndrome of upper limb – a casereport. Indian J Anaesth.2009 December;53(6):696–699.
12. Ahsan SN, Faridi S. Cervical epidural anaesthesiafor sub total thyroidectomy in a patient withaortic incompetence. J Pak Med Assoc1998;48:281-3.
13. Kulkarni RS, Braverman LE, Patwardhan NA.Bilateral cervical plexus block for thyroidectomy& parathyroidectomy in healthy and high riskpatients. J Endocrinol Invest 1996;19:714-8.
13. Priyadarshini--56-58.pmd 10/10/2013, 9:22 AM58

International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 59
Morphometric Study of Sacral Hiatus with Significance inInterventional Clinical Procedure
Ram Prakash Gupta1, Nirupma Gupta2, Anjulata Rai2
1Assistant Professor, 2Associate Professor, Department of Anatomy, School of Medical Sciences & Research, ShardaUniversity, Greater Noida
ABSTRACT
Introduction: The sacral hiatus is an important portal for interventional clinical procedure.Identification of sacral hiatus is usually easy but sometime it becomes difficult particularly in obeseperson. Aim of present study was to identify additional anatomical landmarks to increase the successrate of trans-sacral hiatal procedure.
Methodology: The morphometric study was conducted on 31undamaged adult sacra. Themeasurements were done with the help of Vernier caliper and goniometer.
Results: The posterior superior iliac spines impose upon upper part of lateral sacral crest (superolateralcrest) . The distance between two superolateral crests was considered as the base and distance fromtwo superolateral crests to apex of sacral hiatus as two sides of the triangle. The base, right side andleft side of the triangle were 65. 81 mm ± 4.00mm,66.74 mm ± 6.18 mm and 66.84mm±6.07mrespectively. The mean depth (AP diameter) of sacral canal at the apex of sacral hiatus was 4.17 mm± 1.18 mm. An additional important landmark, the mean distance from the level of sacral cornua tothe level of S2 foramina was 59.23 mm±4.77mm.
Conclusion: The triangle formed by the two superolateral crests and apex of the sacral hiatus was anequilateral triangle in most of the sacra and this is very important parameter in localization of sacralapex in transacral hiatal procedures. The AP diameter of sacral canal at the apex was adequate forpassage of needle and endoscope in most of the specimens .
Keywords: Sacral Hiatus, Sacral Cornua ,Superolateral Crest ,Trans Sacral Hiatal Procedures
INTRODUCTION
The sacral hiatus is an important portal for variousclinical procedures like trans- sacral thecaloscopy,caudal epidural block for anesthesia and injection ofdrugs into epidural space for radiculopathy. Sacrumis a triangular bone formed by the fusion of five sacralvertebrae which is wedged between two hip bone1.It’sbase articulate with fifth lumber vertebra above andapex with coccyx below. The dorsal surface of sacrum
Corresponding author:R P GuptaAssistant ProfessorDepartment of Anatomy, School of Medical Sciences& Research, Sharda University, Greater NoidaEmail: [email protected] No. 9810321967
is rough, convex and marked by five prominentlongitudinal ridges.The central ridge, the mediansacral crest represents the fused rudimentary spinousprocesses of superior three or four sacral vertebrae.The intermediate sacral crests (right & left) representthe fused articular processes and the lateral sacral crests(right & left) formed by the fused transverse processes.The clinically important structure of dorsal surface ofsacrum is inverted U -shaped gap in the dorsal wall ofsacral canal, the sacral hiatus and sacral cornua2. Thesacral hiatus results from failure of fusion of laminaeof S5 and sometimes S4 in midline. The sacral cornuarepresent the inferior articular process of S5 vertebrawhich project downwards on each sides of sacralhiatus. Through the sacral hiatus filum terminale, fifthsacral and coccygeal nerves emerge.The sacral hiatusis covered by skin, subcutaneous fatty layer and
DOI Number: 10.5958/j.2321-1024.1.2.031
14. R P GUpta--59-63.pmd 10/10/2013, 9:22 AM59
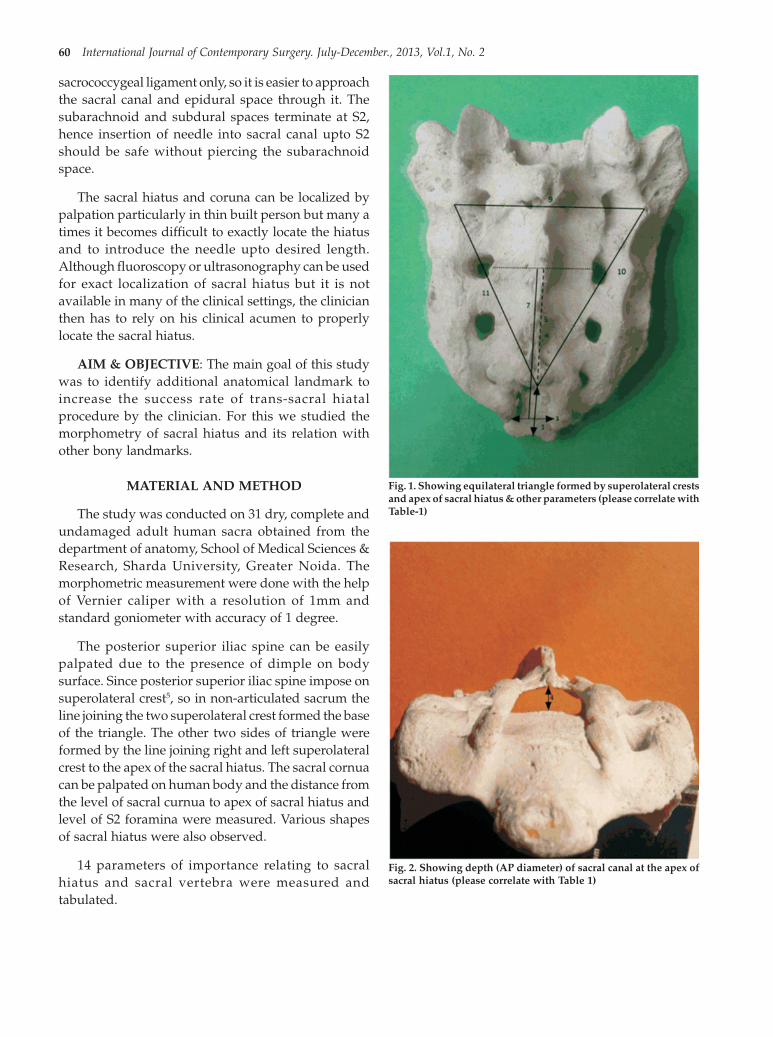
60 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
sacrococcygeal ligament only, so it is easier to approachthe sacral canal and epidural space through it. Thesubarachnoid and subdural spaces terminate at S2,hence insertion of needle into sacral canal upto S2should be safe without piercing the subarachnoidspace.
The sacral hiatus and coruna can be localized bypalpation particularly in thin built person but many atimes it becomes difficult to exactly locate the hiatusand to introduce the needle upto desired length.Although fluoroscopy or ultrasonography can be usedfor exact localization of sacral hiatus but it is notavailable in many of the clinical settings, the clinicianthen has to rely on his clinical acumen to properlylocate the sacral hiatus.
AIM & OBJECTIVE: The main goal of this studywas to identify additional anatomical landmark toincrease the success rate of trans-sacral hiatalprocedure by the clinician. For this we studied themorphometry of sacral hiatus and its relation withother bony landmarks.
MATERIAL AND METHOD
The study was conducted on 31 dry, complete andundamaged adult human sacra obtained from thedepartment of anatomy, School of Medical Sciences &Research, Sharda University, Greater Noida. Themorphometric measurement were done with the helpof Vernier caliper with a resolution of 1mm andstandard goniometer with accuracy of 1 degree.
The posterior superior iliac spine can be easilypalpated due to the presence of dimple on bodysurface. Since posterior superior iliac spine impose onsuperolateral crest5, so in non-articulated sacrum theline joining the two superolateral crest formed the baseof the triangle. The other two sides of triangle wereformed by the line joining right and left superolateralcrest to the apex of the sacral hiatus. The sacral cornuacan be palpated on human body and the distance fromthe level of sacral curnua to apex of sacral hiatus andlevel of S2 foramina were measured. Various shapesof sacral hiatus were also observed.
14 parameters of importance relating to sacralhiatus and sacral vertebra were measured andtabulated.
Fig. 1. Showing equilateral triangle formed by superolateral crestsand apex of sacral hiatus & other parameters (please correlate withTable-1)
Fig. 2. Showing depth (AP diameter) of sacral canal at the apex ofsacral hiatus (please correlate with Table 1)
14. R P GUpta--59-63.pmd 10/10/2013, 9:22 AM60

International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 61
Table 1: Results of the different morphometric measurements.
Sl. Measured parameters Mean Standard RangeNo. deviation
(SD)
1 Distance from apex of sacral hiatus to sacro-coccygeal junction (in mm) 31.74 3.53 28 – 41
2 Length of sacral hiatus from apex of sacral hiatus to the level of sacral cornua 20.71 3.63 15-28{base of sacral hiatus} ( in mm )
3 Width of sacral hiatus at the level of sacral cornua (in mm) 18.06 2.31 15 – 23
4 AP diameter of sacral hiatus at the level of apex (in mm) 4.77 1.18 3 – 7
5 Distance from the apex of sacral hiatus to the level of S2 foramina (in mm) 38.28 5.42 25 – 45
6 Distance from the sacrococcygeal junction to the level of S2 foramina, 1+5 (in mm) 69.90 5.41 63 – 80
7 Distance from the level of sacral cornua { base of sacral hiatus } 59.23 4.77 51 – 67to the level of S2 foramina, 2+5 ( in mm )
8 Distance between the upper margin of sacral canal to 70.45 9.24 47 – 91the apex of the sacral hiatus ( in mm)
9 Distance between two superolateral sacral crest ( in mm) 65.81 4.00 60 – 74
10 Distance between right superolateral sacral crest and apex 66.74 6.18 56 – 84of the sacral hiatus ( in mm)
11 Distance between left superolateral sacral crest and apex 66.84 6.07 56 – 84of the sacral hiatus ( in mm)
12 Angle between parameters 9 & 10 ( in degree) 60.32 1.68 56 – 63
13 Angle between parameters 9 & 11 (in degree) 60.26 1.63 56 – 63
14 Angle between parameters 10 & 11 ( in degree ) 59.42 3.22 54 – 68
Statistical analysis: The collected data wastabulated in New Microsoft office excel work sheet andanalyzed for mean, standard deviation and range.
OBSERVATION AND RESULTS
Most commonly observed shape of sacral hiatuswere Inverted U shaped3, 4(62%) with apex at S44,5,11,followed by inverted V shaped (30 %) and irregular (8%).The mean length from the sacrococcygeal junctionto the apex of sacral hiatus was 31.74 mm±3.53mm(range 28-41) and length from apex of sacralhiatus to the base of sacral hiatus ( level of sacralcornua) was 20.71mm± (range15- 28) [Table 1]. Themean distance from apex to level of S2 foramina andfrom base of sacral hiatus (level of sacral cornua) tothe level of S2 foramina were 38.28 mm±5.42mm(range 25-45) and 59.23 mm±4.77mm ( range 51-67 )respectively.[Table-1]. The mean distance between twosuperolateral crest (base of triangle ), distance betweenright superolateral crest and apex of sacral hiatus (rightside ) and distance between left superolateral crest andapex of sacral hiatus (left side) were 65.81 mm±4.00mm( range 60 – 84 ), 66.74 mm ±6.18mm(range 56 – 84)and 66.84 mm ±6.07mm( range56 – 84 )respectively.[Table-1]. So the three sides of triangle arealmost equal and forming equilateral triangle in mostof the sacrum except in three specimens where theywere isosceles triangle. Similarly the angle betweenbase and right side of triangle, angle between base and
left side and angle between right and left sides were60.32°±1.68 °( range 56 -63° ), 60.26°±1.63 ° (range 56-58° ) and 59.42°±3.22° (54 -68° ).
DISCUSSION
Approach to sacral epidural space through sacralhiatus for procedures like caudal epidural block, trans-sacral thecaloscopy and epidural injection of steroidsand other drugs for disc diseases, is a safe and reliableportal. Although fluoroscopy or ultrasound6 mayincrease the success rate of trans-sacral hiatalprocedure but these are not available in many clinicalsettings. Stitz et al8 have reported a success rate of 74%without the help of fluoroscopy. Similarly White andcolleagues13 have reported a failure rate of 25% inepidural steroid injection through sacral hiatal route.The reason for failure of trans-sacral procedure maybe attributed to difficulty in localizing the sacral hiatusand sacral cornua due to anatomical variations in theirsize and shape. Palpation of these bony landmarks isvery important as needle or canula is inserted throughthe skin at the level of sacral cornua and caudalepidural space is approached till a ‘pop’ is felt as thesacrococcygeal ligament is pierced6,11. Hence toovercome these difficulties other surface landmarksmay be used to correctly negotiate through the sacralhiatus, like apex of sacral hiatus and posterior superioriliac spine.The posterior superior iliac spine is easilyseen as a dimple on each side of sacral spine and it
14. R P GUpta--59-63.pmd 10/10/2013, 9:22 AM61

62 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
imposes upon the superolateral sacral crest. Senglu etal4 reported that two posterior superior iliac spine andapex of sacral hiatus constitute a equilateral triangle.Agrawal et al15 recorded this equilateral triangle in 45%cases. In the present study the mean distance betweenright and left superolateral crest (base of triangle) was65. 81mm±4.00mm, mean distance between rightsuperolateral crest and apex of sacral hiatus (right sideof triangle) was 66.74mm±6.18mm and mean distancefrom left superolateral crest to apex of the sacral crestwas 66. 84mm ±6.07mm. So the base, right side andleft side of the triangle are almost equal. In this study28 out of 31specimens formed equilateral triangleexcept 3 specimens where it was isosceles triangle.Thus localization of sacral hiatus on the basis ofequilateral triangle formed by apex of sacral hiatuswith right and left posterior superior iliac spine is animportant and useful anatomical landmark.
The midpoint of base of sacral hiatus between twosacral cornua is usually the point of entry of needle orendoscope as these are palpable. The distance frombase of sacral hiatus to the level of S2 foramina is themaximum length of the needle that can be introducedwithout entering into the subarachanoid space. Inpresent study emphasis is given on this distance sothe safe length of needle can be ascertained. In thisstudy the mean distance from base of sacral hiatus tothe level of S2 foramina was 59.23 mm ±4.77mm (range51 -67 mm),hence length of the needle that can safelyintroduced from the base of sacral hiatus should beless than 50mm. Needles of the length of 1.5 inches(38mm) and 1inch (25 mm) can be used without anydamage to dura and arachanoidmater if the sacralcoruna is palpable.
In this study the mean distance from apex of sacralhiatus to the level of S2 foramina was 38.28mm±5.42mm (range 25 - 45mm). In cases where apexof sacral hiatus is recognized on the basis of equilateraltriangle and entry point is immediately below the apex,needle with smaller length (25mm) will be safer.
Sekiguchi et5 al reported that the anteroposteriordiameter of sacral canal was less than 2mm in 1%specimen, resulting in difficulty in using 22 gauzeneedle for caudal epidural block. In this study theminimum AP diameter of sacral canal at apex of sacralhiatus was 3mm in 3 out of 31 specimens and meanAP diameter was 4.77mm±1.18mm ( range 3 -7 ).The22G needle has outer diameter of 0.7mm and 14 G(maximum) has diameter of 1.83 mm,so there is nodifficulty in passing a needle of 22G or more through
the sacral hiatus.The commonly used trans sacral hiatalendoscope has outer diameter of 3.8mm and difficultymay arise in introduction of endoscope through sacralhiatus in few cases. Mourgela S et7 al conducted MRIstudy of sacral canal for trans-sacral thecaloscopy.Preoperative assessment of sacral hiatus and sacralcanal by CT scan or MRI will be desired investigationbefore contemplating trans-sacral hiatal endoscopicsurgery.
The mean length of sacral canal from apex of sacralhiatus to upper margin of sacral canal was 70.45mm ±9.24mm (range 47 – 91mm). This is in importantparameter in trans-sacral hiatal endoscopy to knowhow far to push the endoscope to reach the upper limitof sacral canal.
CONCLUSION
The caudal epidural block and trans-sacral hiatalepidural injection of steroid and other drugs are verycommon procedure. Although fluoroscopy (C-armimage intensifier) and ultrasonography may add insuccess rate of these procedure, but such facilities arenot available in all setups. In this condition accuratelocalization of apex of sacral hiatus particularly inobese by equilateral triangle, determination of lengthof needle that has to be inserted inside and diameterof sacral hiatus are of paramount importance todevelop the clinical acumen.These procedure can becontemplated without the help of C-arm imageintensifier or ultrasonographic guidance. But in trans-sacral hiatal endoscopic procedure preoperativeassessment of sacral canal particularly AP diameter ofsacral canal at apex of sacral hiatus by CT scan or MRIare important and the procedure should be conductedunder C-arm image intensifier (fluoroscopy)vision.Further studies on human cadavers and clinical& interventional validation on patient are required tosupport the result of this study.
ACKNOWLEDGMENT
The authors are earnestly grateful to Prof (Dr.)Kamlesh Khatri, HOD of Anatomy,SMS & R for herkind guidance and support.We would like to thanktechnical and office staff of anatomy department fortheir cooperation.Our blessings are for Ishita forbeautiful photographs of sacrum.
Conflict of Interest: Nil
Source of Funding : Self
14. R P GUpta--59-63.pmd 10/10/2013, 9:22 AM62

International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 63
Ethical Clearance: Not Applicable
REFERENCES
1. Standring S, Newell RLM, Collins P, Healy JC(editors). In: Gray’s Anatomy, 40th Edition.Churchill Livingstone Elsevier, 2008; pp: 724 –728
2. Keith L. Moore, Arthur F. Dally, Anne M. R. Agur.Moore clinically oriented anatomy, 7th edition2012: 451-4532
3. Waldman SD. Caudal epidural nerve block:proneposition. In: Atlas of Interventional PainManagement, 2nd edn. Philadelphia: Saunders,2004; 380–925.
4. Senoglu N, Senoglu M, Oksuz H, Gumusalan Y,Yuksel KZ, Zencirci B, Ezberci M, Kizilkanat E.Landmarks of the sacral hiatus for caudalepidural block: an anatomical study.Br J Anaesth.2005; 95(5):692-695
5. Sekiguchi M, Yabuki S, Satoh K, Kikuchi S. Ananatomic study of the sacral hiatus: a basis forsuccessful caudal epidural block. Clin J Pain 2004;20: 51–41
6. Chen PC,Tang SFT, Hsu TC, et al. Ultrasoundguidance in caudal epidural needle placement.Anesthesiology 2004; 101: 181–4
7. MourgelaS,Sakellaropoulos A, AnagnostopoulouS, Warnke JP. The dimensions of the sacral spinal
canal in thecaloscopy: a morphometric MRIstudy. Neuroanatomy 2009;8 (1):1-3.
8. Stitz MY,Sommer HM. Accuracy of blind versusfloroscopically guided caudal epidural injection.Spine -199; 24: 1371 – 6.
9. Kumar V, Pandey SN, Bajpai RN, Jain PN, LongiaGS. Morphometrical study of sacralhiatus.J.Anat.Soc. India 1992; 41 (2):7-137.
10. Crighton IM, Barry BP. HobbsGJ.A study of theanatomy of the caudal space usingmagneticresonance imaging. Br J Anaesth.1997; 75
11. Tsui BC, Tarkkila P, Gupta S, Kearney R.Confirmation of caudal needle placement usingnerve stimulation. Anesthesiology1999; 91:374–378.
12. Spaccarelli KC. Lumbar and epiduralcorticosteroid injections. Mayo Clin Proc 1996;7:169–78.
13. White AH, Derby R, Wynne G. Epiduralinjections for the treatment of low back pain.Spine1980; 5: 78–866.
14. Aggarwal A, Aggarwal A, Harjeet, Sahni D.Morphometry of sacral hiatus and its clinicalrelevance incaudal epidural block.Surgical andRadiological Anatomy. 2009; 31(10):739-800.
14. R P GUpta--59-63.pmd 10/10/2013, 9:22 AM63

64 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
Criteria for Defining Severe Septal Deviation
Rahil Muzaffar1, Owais Mattoo1, Raja Salman Khurshid2, Shafqat Islam2
1Postgraduate Resident, ENT, 2Senior Resident, ENT, Govt. Medical College, Srinagar, JK, India
ABSTRACT
Objective: Criteria for defining 'severe septal deviation' and to describe the clinical profile of thesame.
Study: Retrospective study.
Materials and Method: Hundred patients who were diagnosed with Severe DNS and treated withExtracorporeal Septoplasty from September 2010 to August 2012 were retrospectively evaluated forthis study. A review of their clinical charts formed the basis of this study.
Results:
• In this study, majority of patients (97%) had nasal obstruction as their prime symptom followedby Post Nasal Discharge in 60 % cases, Headache in 40% cases and Anterior Nasal Discharge in30% cases. External Nasal deformity was reported by 22 patients. Snoring was seen in 20% ofpatients with same percentage complaining of altered sense of smell and throat discomfort.Epistaxis, sneezing and facial pain was seen in fifteen percent patients. Epiphora was complainedby only 8% of patients.
• In this study, nasal endoscopy/Anterior rhinoscopy was used to type the septal deformity. Thecommonest septal deviation was C-shaped cephalocaudal (48%), followed by S-shapedcephalocaudal (21%), C-shaped AP (16%), S-shaped AP (12%) and sharp septal deviation/angulation in 3 % cases.
• All but three patients had deviated nasal septum involving multiple Cottle's areas. These threepatients had sharp septal angulation involving Cottle's area 2 only.
• In this study, most common region involving DNS was area 1+2+3 (48%) followed by area 2+4+5(28%) and 1+2+3+4 (21%).
• Area 2 was invariably involved in 100% of cases.
• NOSE (Nasal Obstruction Symptom Evaluation) SCORES: n NOSE score was 67.60±5.26 (65.34to 72.86).
• NSS (Nasal Symptoms Score): Preoperatively mean NSS was -5.08±0.38 (-5.46 to -4.70).
Conclusions: A septal deviation is regarded as 'Severe' if patient satisfies all of the below mentionedcriteria
• Preoperatively mean NOSE score should be 65.34 or more.
• Preoperatively mean NSS should be -5.46 or more negative.
• The septal deviation must cause significant obstruction to Cottle's area 2 or nasal valve area.
• Patients of severe septal deviation report significantly higher rates of snoring (25% in our study)and PND (60% in our study) when compared with mild/moderate cases.
• All severe septal deviations display significant obstruction of Cottle's area 2/nasal valve areaand it is thus concluded that a severe septal deviation must cause significant obstruction of area2/ nasal valve.
Keywords: Severe, NOSE, NSS, PND, Snoring
DOI Number: 10.5958/j.2321-1024.1.2.032
15. owais--64-68.pmd 10/10/2013, 9:22 AM64

International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 65
INTRODUCTION
DNS may be developmental or it may be causedby impact trauma, such as by a blow to the face.Deviated septum is associated with genetic connectivetissue disorders such as Marfan syndrome,Homocystinuria1 and Ehlers-Danlos Syndrome. Therehave been studies describing the type of septaldeviations in patients based on anterior rhinoscopy/endoscopy findings. In one study, most common septaldeformity was septal tilt in 37 patients (40%). The nextcommon type of DNS was C- shaped anterioposteriorin 30 patients (32%) followed by localized septaldeviation/angulations/spurs in 13 patients (14%). S-shaped anterioposterior septal deviation was noticedin 8 patients (9.00%), C-shaped cephalocaudal in 4patients (4.30%) and S-shaped cephalocaudal in 1patient (0.9%) only2. No study so far has been done asto classify the type of septal deviation in ‘severe’ casesof septal deviation. Cottle (1961) suggested to dividethe internal nose into five areas: area 1, the externalostium or naris; area 2, the valve area; area 3, the areaunderneath the bony and cartilaginous vault, alsocalled the attic; area 4, the anterior part of the nasalcavity, including the heads of the turbinates, theinfundibulum or ostiomeatal complex; and area 5: thedorsal part of the nasal cavity, including the tails ofthe turbinates. Area 2 or nasal valve area is the mostsignificant area. This is the part of the nasal cavity withmajor air flow and a limited septal deviation here canresult in significant resistance to air flow enormoussymptoms3. Again, studies have been carried out totype the Cottle’s area involvement in septal deviationsbut there is a surprising lack of the same in cases ofsevere septal deviations. Defining criteria for severeseptal deviation is important because it has beenargued by many authors that severe septal deviationscannot be corrected by conventional septoplasty in asignificant proportion of patients and thatExtracorporeal Septoplasty should be the procedureof choice for such patients. Extracorporeal septoplastyhas been regarded as procedure of choice for correctingsevere septal deviations by many authors, the pioneerbeing Wolfgang Gubisch, 4, 5, 6. However, there is aremarkable absence of literature defining ‘criteria’ forsevere septal deviation. So far it is purely clinician’sjudgment which classifies a particular septal deviationas ‘severe’. The symptomatological profile of septaldeviations has been studied by many authors. In onestudy of J. Janardhan Rao symptomatology of patientswas as follows: nasal obstruction 74%, nasal discharge41%, headache 20%, sneezing 15% , throat discomfort8% , postnasal drip 8% , nasal bleeding 3% , snoring
3% and altered sense of smell in 4% cases7. LeandroCastro Velasco carried out a study to assess thesymptom improvement following septoplasty with orwithout turbinectomy. Most prevalent complaint in thepatients of deviated nasal septum among studysubjects was nasal obstruction (74%) followed byanterior nasal discharge (41%), headache (20%),sneezing (15%), post nasal drip (8%), epiphora (7%),hyposma (3%), bleeding (3%)and snoring (3%)8. Again,there is a remarkable absence of any similar study on‘severe’ septal deviations.
MATERIALS AND METHOD
This study was conducted in Department ofOtorhinolaryngology of S.M.H.S Hospital, anassociated hospital of Govt. Medical College, Sgr, JK,India. Review of the clinical charts of the patients whowere diagnosed as having ‘severe’ septal deviation andoperated using Extracorporeal Septoplasty (ECSP)technique was done. Hundred patients who werediagnosed with Severe DNS and treated with ECSPfrom September 2010 to August 2012 wereretrospectively evaluated for this study. The followingwere the inclusion/exclusion criteria used toundertake Extracorporeal Septoplasty.
Inclusion Criteria
1. All patients with markedly or severely deviatednasal septums.
2. Patients of age >12 years of either gender.However, younger patients with significantsymptoms were also operated.
Exclusion Criteria
1. Patients with mild to moderate septal deviationof all ages and either gender.
2. Patients with associated disorders like benignlesions, malignant lesions, cysts of nose or whereseptoplasty is done to gain surgical access only.
3. Patients with general medical contraindications tosurgery.
METHOD
The detailed and comprehensive study of eachpatient was made according to the proforma of studydesign. Detailed preoperative examination withanterior rhinoscopy and Nasal endoscopy aided in thediagnosis and thereby management of severe septal
15. owais--64-68.pmd 10/10/2013, 9:22 AM65

66 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
deviations. A complete history and clinicalexamination with relevant investigations aided inselecting the patient for Extracorporeal Septoplasty(ECSP). Nasal Obstruction Symptom Evaluation(NOSE) score and Nasal Symptoms Score (NSS) wascomputed preoperatively for each patient.
RESULTS
The following table shows the clinical profile ofpatients with severe septal deviation. (Table 1)
Table 1
Symptom Percentage
Nasal Obstruction 97%
Headache 40%
PND 60%
Ant. Nasal discharge 30%
END# 22%
Snoring 25%
Hyposmia /anosmia 20%
Throat discomfort 20%
Epistaxis 15%
Sneezing 15%
Facial pain 15%
Epiphora 8%
#END secondary to septal deviation only was considered.
In this study, majority of patients (97%) had nasalobstruction as their prime symptom followed by PostNasal Discharge in 60 % cases, Headache in 40% casesand Anterior Nasal Discharge in 30% cases. ExternalNasal deformity was reported by 22 patients. Snoringwas seen in 20% of patients with same percentagecomplaining of altered sense of smell and throatdiscomfort. Epistaxis, sneezing and facial pain wasseen in fifteen percent patients. Epiphora wascomplained by only 8% of patients.
The following table depicts the type of DNS inpatients of severe septal deviation (Table 2).
TABLE 2
Type of DNS Percentage
Simple tilt only 0%
C-shaped cephalocaudal 48%
S-shaped cephalocaudal 21%
C-shaped AP 16%
S-shaped AP 12%
Sharp septal deviation/angulation 3%
Total 100%
In this study, nasal endoscopy was used to typethe septal deformity. The commonest septal deviationwas C-shaped cephalocaudal (48%), followed by S-shaped cephalocaudal (21%), Cshaped AP (16%), S-shaped AP (12%) and sharp septal deviation/angulation in 3 % cases.
The following table depicts the Cottle’s areainvolvement in patients with severe DNS (Table 3).
TABLE 3
Type of DNS ECSPn = 50
Simple tilt only 0 (0%)
C-shaped cephalocaudal 27 (54%)
S-shaped cephalocaudal 10 (20%)
C-shaped AP 8 (16%)
S-shaped AP 4 (8%)
Sharp septal deviation /angulation 1 (2%)
Total 50 (100%)
#Sharp septal spur in relation to area 2
As is evident from the table, almost all the patientshad deviated nasal septum involving multiple Cottle’sareas. However, three patients had sharp septalangulation involving Cottle’s area 2 only. A limitedseptal deviation in this area causes significantresistance to air flow and hence significant symptoms.
The following table depicts the different Cottle’sarea involvement in multiple Cottle area involvement(Table 4).
TABLE 4
DNS in combined No. of casesn PercentageCottle’s area = 100
Cottle’s area 1+2+3 48 48%
Cottle’s area 2+4+5 28 28%
Cottle’s area 1+2+3+4 21 21%
Total 97 97%
In this study, most common region involving DNSwas area 1+2+3 (48%) followed by area 2+4+5 (28%)and 1+2+3+4 (21%). Area 2 was invariably involvedin all of the cases. In severe septal deviation, it istherefore, concluded that area 2 is invariably involvedin all.
NOSE SCORES
Preoperatively mean NOSE score was 67.60±5.26(65.34 to 72.86).
15. owais--64-68.pmd 10/10/2013, 9:22 AM66

International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 67
NSS SCORE
Preoperatively mean NSS was -5.08±0.38 (-5.46 to -4.70).
DISCUSSION AND CONCLUSION
Defining criteria for severe septal deviations isimportant since the literature presently lacks theobjective assessment of severe septal deviation andrelies mostly on the surgeon’s subjective valuation.Authors round the world are currently layingemphasis on ‘Extracorporeal Septoplasty’ (ECSP) andalmost all the authors favoring ECSP share a universalconsensus that ECSP should be the procedure of choicefor markedly or severely deviated nasal septums. Inour institution ECSP has been used to treat severeseptal deviations and a retrospective study of thesepatients formed the basis for defining criteria to treata particular septal deviation as ‘severe’. The criteriaused included both the symptomatological profile ofDNS as well as the objective clinical assessment/clinical examination by the clinician. Following are thecriteria and the clinical profile of severe DNS:
A septal deviation is regarded as ‘Severe’ if patientsatisfies all of the below mentioned criteria:
1. Preoperatively mean NOSE score should be 65.34or more.
2. Preoperatively mean NSS should be -5.46 or morenegative.
3. The septal deviation must cause significantobstruction to Cottle’s area 2 or nasal valve area.
The involvement of nasal valve or Cottle’s area 2was universally observed by us in all patients of severeseptal deviation. As is known, this is the area withmaximum air flow and a limited deviation in this arearesults in significant resistance to airflow dynamics andenormous symptoms. We had three patients with sharpseptal spurs obstructing area 2/ nasal valve onlywithout involvement of other areas. These patients hadsevere symptoms and a clinical profile similar to otherpatients, thus strengthening the fact that a septaldeviation causing significant obstruction of area 2 onlycan lead to severe symptoms. All hundred patientsdiagnosed as severe DNS in our series displayed a
significant obstruction of Cottle’s area 2 or nasal valvearea.
The clinical profile of severe septal deviations alsovaries when compared with the current literature.Patients of severe septal deviation report significantlyhigher rates of snoring (25% in our study) and PND(60% in our study) when compared with mild/moderate cases which is around 3% for snoring7,8 and8% for PND7,8. (This data was generated on comparingour results with the data available in current literature.)
ACKNOWLEDGEMENTS:
1. Prof. Rafiq Pampori, Professor & Head, Deptt. OfENT & HNS, Govt. Medical College, Srinagar, JK,India- [email protected]
2. Prof. Rauf Ahmad, Professor, Deptt. Of ENT &HNS, Govt. Medical College, Srinagar, JK, India
Conflict of Interest
As such, there is no conflict of interest, no secondarygains.
Source of Funding: Govt. Medical College, Srinagar,JK, India
Ethical Clearance: It was a retrospective study whichdid not need any ethical clearance.
REFERENCES
1. Finkbohner R, Johnston D, Crawford ES, CoselliJ, Milewicz DM (February 1995). “Marfansyndrome. Long-term survival and complicationsafter aortic aneurysm repair”. Circulation 91 (3):728–33.doi:10.1161/01.CIR.91.3.728. PMID7828300.
2. Bahman Guyuron, Cheryl d. Uzzo and HeatherScull. A practical classification of septonasaldeviation and an effective guide to septal surgery.Plast Reconstr Surg1999; 104:2202-2212.
3. Helmut Fischer, M.D; Wolgang Gubisch, M.D.nasal valves- Importance and SurgicalProcedures. Facial plastic surgery, volume 22,number 4, 2006.
4. Gubisch W. Extracorporeal Septoplasty for theMarkedly Deviated Septum. Arch Facial PlastSurg: 2005;7:218-226
15. owais--64-68.pmd 10/10/2013, 9:22 AM67

68 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
5. Gubisch W. The extracorporeal septoplasty: atechnique to correct difficult nasal deformities.Plast Reconstr Surg. 1995; 95:672-682.
6. Gubisch W. Constantinescu MA. Refinements inextracorporal septoplasty. Plas Reconstr Surg.1999; 104:1131-1142, AA.Gubisch W. Dasschwierige Septum. HNO. 1988; 36:286-289.
7. J.JanardhanRao , E.C. Vinay Kumar , K. Ram etal. Classification of nasal Septal Deviations-Relation to Sinonasal Pathology. Indian journal
of otolaryngology and head and neck surgery, vol57, no. 3, july-september, 2005
8. Leandro Castro Velasco, Lisandra MegumiArima, Romualdo Suzano LouzeiroTiago.Assessment of symptom improvementfollowing nasal septoplasty with or withoutturbinectomy. Braz J Otorhinolaryngol. 2011;77(5):577-83
15. owais--64-68.pmd 10/10/2013, 9:22 AM68

International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 69
Ruptured Rudimentary Horn Pregnancy at 20 Weeks ofGestation in a Primigravida: A Case Report
Girija B S1, Sudha T R2, Rajeshwari3, Shridhar S K4, Poornima4
1Associate Professor, Department of Obstetrics and Gynaecology, 2Professor and HOD, 3Resident, 4AssistantProfessors, Department of Obstetrics and Gynaecology, Hassan Institute of Medical Sciences, Hassan, Karnataka, India
ABSTRACT
Unicornuate uterus occurs due to a complete or partial non development of one mullerian duct1.Sometimes it is associated with a rudimentary horn, which may consist of functional cavity which isusually non - communicating or it may be small solid muscle with no functional endometrium.Pregnancy in rudimentary horn is rare and usually terminates in rupture during first or secondtrimester of pregnancy. Diagnosis is usually made at laparotomy. Ultrasound may help in pre-operativediagnosis. A case of 37 yr old primigravida with acute abdomen is reported here. Laparotomy revealedunicornuate uterus with rupture of rudimentary horn on left side. The incidence, diagnosis andmanagement of such cases are discussed.
Keywords: Rudimentary Horn Pregnancy, Ruptured Uterus, Uterine Anomaly
INTRODUCTION
Abnormalities of embryogenesis of Mullerian ductsystem resulting in congenital anomalies of femalegenital tract are relatively common. Unicornuateuterus is a congenital uterine anomaly resulting fromnon-developing Mullerian duct or agenesis ofMullerian system. Mullerian anomalies were classifiedin 1979 by Buttram and Gibbons and further revisedby the American Society of Reproductive Medicine in19882. Rupture uterus is an obstetric catastrophe. It ismore common in multigravida or with previousuterine scar, mostly in labour. Most rudimentary hornsare asymptomatic. Cyclic or chronic pelvic pain,endometriosis is often associated in these cases. Theuterine horn could represent a site of ectopicpregnancy, where natural course is rupture duringsecond trimester. Unicornuate uterus accounts for 5%of all Mullerian anomalies, occurring in generalpopulation approximately 1in 4020 women. In about84% of these cases a contra lateral rudimentary hornexists, almost always of a non communicating type.We report a case of unicornuate uterus with rupturedrudimentary horn.
CASE HISTORY
A 37 yr old primigravida came with history of 4months of amenorrhea on 19th April 2013. She hadconsumed medical termination pills for the same
without any prescription and got admitted to ourhospital with history of pain abdomen. She gaveconsent for termination of pregnancy as she waswidow and didn’t want her pregnancy to be continued.We started with tablet misoprostal 200µg sublingual,6th hourly. She did not respond and got dischargedagainst medical advice.
She again got admitted on 26th April 2013 withhistory of severe pain abdomen. On examination hergeneral condition was poor. She was pale, pulse 112bpm, Bp- 90/60 mm of Hg. Cardiovascular andRespiratory systems were normal. On per abdomenexamination, there was tenderness, guarding andrigidity. A tender 18weeks size gravid uterus was feltin hypo gastric region. On per vaginal examination,cervix was posterior, soft, cervix was 2 cm dilated andthere was no bleeding. Urgent ultrasound revealed abicornuate uterus with thickened endometrium inright horn and a single intrauterine foetus in left horn.A fibroid measuring 9.2x 9.7 cm in the anterior wall oflower segment. Patient was immediately shifted forlaparatomy with 2 pints of packed cells.
After taking aseptic precautions bladder wascatheterised, under spinal anaesthesia abdomen wasopened by suprapubic incision. Hemoperitoneum waspresent, around 1 litre of blood was drained.Unicornuate uterus with rudimentary horn on left sidewas found. There was rupture of rudimentary horn in
DOI Number: 10.5958/j.2321-1024.1.2.033
16. Girija BS--69-71.pmd 10/10/2013, 9:22 AM69

70 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
posterior aspect. Fig 1 shows rupture of rudimentaryhorn on left side. Amniotic sac along with foetus andplacenta was removed. The foetus weighed about500grams [Fig 2]. Resection of non-communicatingrudimentary left horn was done. Uterus was closed intwo layers. Right and left ovary conserved. There wasa cervical fibroid which was left undisturbed. Patientwithstood the procedure well. Two pints of packedcells were transfused. Her post operative period wasuneventful and stitches were removed on 8th day.Because renal abnormalities coexist in up to 40% casesof unicornuate uterus, patient was evaluated forassociated renal anomaly, which was not found.
be classified as those having an endometrial cavity andthose with no endometrial cavity, and 90% of the casesare those with endometrial cavity. A further divisioncan be between the communicating and non-communicating types. Identification of unicornuateuterus is almost always accidental, as it happened inour case, as it is asymptomatic until reproductive age.
Pregnancy in non- communicating rudimentaryhorn is uncommon, estimated to occur in 1 per 100000to 140000 pregnancies1. The pregnancy in a non-communicating horn is possible only throughtransperitoneal migration of the sperm or fertilisedovum. The timing of rupture varies from 5 to 35 weeksdepending on the horn musculature and its ability tohypertrophy and dilate with increasing gestational age.70 - 90 % of cases rupture before 20weeks of gestationand can be catastrophic2. As the uterine wall is thickerand more vascular, bleeding is more severe inrudimentary horn pregnancy rupture, which could belife threatening. Nowadays maternal mortality rate isestimated to be less than 0.5% 1.
Rupture is likely to occur in late first trimester orsecond trimester. Rarely pregnancy can go till latesecond trimester before rupturing. Chang et alreported rupture of rudimentary horn as late as 25weeks of gestation3. Mid trimester rupture generallyoccurs at fundus. Nwosu BO et al reported a case ofspontaneous rupture at 39 weeks4. In our case it wasunicornuate uterus with rupture of rudimentary hornon left side. Similar case was reported by SheelaJayaprakash et al5.Use of labour induction agents fortermination of pregnancy in a rudimentary horn isunsuccessful and can lead to rupture of the horn.Samuels and Awonuga reported rupture after use ofmisoprostol due to misdiagnosis6.
In our case when she presented first timeultrasound was not done, we got ultrasound donesecond time, when she presented with acute painabdomen. Ultrasound may be useful in diagnosingsuch anomalies before rupture. Achiron et al reported2 cases of pre-rupture ultrasound diagnosis in suchcases 7.
Treatment is removal of ruptured horn. Excisionusually carried out by laparatomy, but has beensuccessfully carried out laparoscopically inunruptured cases at 11 weeks of gestation8. Due to thepresence of scar in the upper part of uterus, pregnancyshould be avoided for at least 1 year.
Fig. 1. Ruptured rudimentary horn on left side.
Fig. 2. Foetus weighed about 500gms.
DISCUSSION
The incidence of uterine anomalies ranges between0.5% and 2%. Unicornuate uterus (TypeII) can further
16. Girija BS--69-71.pmd 10/10/2013, 9:22 AM70

International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 71
CONCLUSION
Pregnancy in rudimentary horn is rare. Antenataldiagnosis is challenging. Proper diagnosis and timelyintervention is needed. Therefore increased awarenessis needed to reduce the morbidity and mortality of thepatients.
ACKNOWLEDGMENT
We the authors would like to thank the patient andher family for having permitted us to publish her casehistory as an interesting case report.
Conflict of Interest: The authors have no conflicts ofinterest.
Source of Funding: This case did not involve anyexpenses, hence funding was not required.
Ethical Clearance: Patient and her family consent weretaken for publication, they agreed for the sameprovided her identity was not revealed andconfidentiality was maintained. Ethical committeegave the clearance.
REFERENCES
1. Elisabete Goncalves, Joao Pedro Prata, SandraFerreira, Rita Abreu, Jorge Mesquita, AgostinhoCarvalho and Paula Pinheiro. Case Rep ObstetGynecol. 2013;2013: 307828., April 27.doi:10.1155/2013/307828.[Pub med]
2. Deepa V Kanagal, Lokeshchandra C,Hanumanalu. Ruptured rudimentary horn
pregnancy at 25 weeks with previous vaginaldelivery: a case report, Case Rep Obstet Gynecol.2012; 2012: 985076.June 6.doi:10.1155/2012/985076. [ Pub med]
3. Chang JC, Lin YC.Rupture of rudimentary hornpregnancy. Acta Obstet Gynecol Scand1992;71:235 -238
4. Nwosu BO, Ugboaja JO. Obi Nwosu A.Spontaneous rupture of gravid horn of bicornuateuterus at term, a case report. Niger Med J [serialonline] 2010[ cited 2013 May 6]; 51: 184 – 5
5. Sheela Jayaprakash, Lakshmidevi Muralidhara,Sampathkumar G, Rajiv Kumar Sexsena. BMJcase reports 2011;doi:10.1136/ber.08.2011.4633
6. Samuels TA, Awonuga A. Second trimesterrudimentary horn pregnancy: rupture afterlabour induction with misoprostol. Obstetricsand Gynecology. 2005;106950:1160- 1162.[ Pubmed]
7. Achiron R, Tadmor O, Kamar R, Aboulafia Y,Diamant Y. Prerupture USG diagnosis ofinterstitial and rudimentary horn pregnancy in2nd trimester. A report of 2 cases J Reprod Med1992; 37: 89 – 92.
8. Kadan Y, Romano S.Rudimentary hornpregnancy diagnosed by ultrasound and treatedby laparoscopy-a case report and review of theliterature. J Minim Invasive Gynecol 2008 Sep-Oct; 15(5):527-30.doi:10.1016/j.jmig.2008.05.010.Epub 2008 Jul 10.
16. Girija BS--69-71.pmd 10/10/2013, 9:22 AM71

72 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
Dry Eye Syndrome. A Diagnostic Enigma
Kumar Prachi1, Bhargava Rahul2, Kumar Manjushri3, Jyotsana Madaan4
1Associate Professor, Department of Pathology, 2Associate Professor, Department of Ophthalmology, Santosh MedicalCollege and Hospital, Ghaziabad, 3Narayan Medical College and Hospital, Sasaram, 4Prof & Head, Department of
Pathology, Santosh Medical College and Hospital, Ghaziabad, U.P.
ABSTRACT
Purpose: To compare routine tear function tests and conjunctival impression cytology (CIC) in patientswith dry eye syndrome, and to determine the sensitivity, specificity and positive predictive values ofthese tests, considering CIC as the gold standard?
Material & method: A case control prospective study was done. The eyes of 276 patients with dryeyes, was compared with 216 eyes of controls. Patients were enrolled on basis of a questionnaire ofcommon symptoms of dry eye. Tear film break up time (TBUT), Schirmer's-1, Rose Bengal scores(RBS) were compared with impression cytology scores.
Results: The mean Schirmer's value in cases was 12.54 ± 4.73 and 16.32 ± 3.80 in controls (P=0.000).The mean tear film break up time in cases was 9.11 ± 2.90 and 14.21 ± 2.72 in controls (P=0.00). Themean goblet cell density in cases was 476 ± 238 and 1552 ± 598 in controls (P=0.000). 46.7% cases ofdry eye had abnormal CIC as compared to 32.8 % controls. The sensitivity of tear function tests indiagnosing dry eye was TBUT>Schirmer's>RBS and specificity was Schirmer's>TBUT>RBS indecreasing order, taking CIC as gold standard.
Conclusions: Dry eye diagnosis remains a diagnostic enigma. Routine tear function tests lacksensitivity and specificity. Therefore, they should be used in combination with tests like conjunctivalimpression cytology to improve diagnostic accuracy.
Keywords: Conjunctiva, Tears, Goblet cells
INTRODUCTION
Dryness of eyes has become a very commonproblem worldwide due to excess usage of computersand smartphones. In fact dry eye is one of the mostfrequent reasons that patient present to eye care clinics.Prevalence of dry eye varies from 7.8% to 93.2%. 1
Common patient complaints related to dry eyeinclude reduced vision, difficulty in reading, difficultyin driving at night and difficulty in doing computerwork. The disease is now prevalent in the youngerpopulation and, every individual has a degree ofsymptomatic dry eye. 2
International Dry Eye Workshop (DEWS) definesdry eye as a multifactorial disease of tears and ocularsurface. It is accompanied by increased osmolarity ofthe tear film and inflammation of ocular surface. 3
Although all Ophthalmologists are familiar withconventional tests like Schirmer’s and TBUT, most ofthese diagnostic tests for dry eye are poorlystandardized, making compare between studiestenuous at best. 4
A generally agreed upon ‘gold standard’ still doesnot exist due to lack of well-defined cut-off values,enabling a distinction to be made between healthy andaffected eyes. Additionally, some of these tests arepoorly associated with subjective symptoms, so therehas been a drift towards symptom based assessmentas a key diagnostic component. 5
The most commonly used Schirmer’s test is ameasure of tear production. However, it unrepeatable(due to reflex tearing) and overlooks evaporativeaspects of dry eye. It also lacks sensitivity andspecificity and may be difficult to perform in children.6
DOI Number: 10.5958/j.2321-1024.1.2.034
17. Rahul Bhargav--72-77.pmd 10/10/2013, 9:22 AM72

International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 73
TBUT assesses tear film stability. Manipulation oflid margins may affect the results. However, it seemsto be more reliable than Schirmer’s as it is somewhatrepeatable. 7
Staining with vital dyes like Rose Bengal measuresthe extent of damage to ocular surface, but may notdetect mild cases. Therefore they are often used incombination with other tests like TBUT, in dry eyestates.8
Conjunctival excision biopsy can be used forhistopathological diagnosis of dry eye. However, it isinvasive, and may not be accepted by patients. Inclinical practice, may not be possible to perform in allcenters.9
Conjunctival Impression Cytology (CIC) involvesremoving one to three cell layers of the surfaceepithelium, preserving the morphology. It is minimallyinvasive, relatively easy to perform, and yields reliableinformation about the area sampled with minimaldiscomfort to the patient. 10-12 However, it has not yetbecome the first line investigation in dry eye syndrome.
Currently, these tests are often used in combinationto diagnose and grade dry eye severity.
The purpose of the present study was to compareroutine tear function tests with CIC in patients withdry eye syndrome and normal individuals and todetermine the sensitivity and specificity of these testsin diagnosing dry eye syndrome.
MATERIAL & METHOD
A case control study was conducted in Laser EyeClinic, Noida from September, 2010-August, 2011.Patients were enrolled on the basis of a questionnairewith common symptoms of dry eye (n=276).Symptomatic score of 0-6 was mild, 6.1-12 moderate,and 12.1-18, severe dry eye (Table 1). 216 eyes of ageand sex matched controls without symptoms of dryeye were also selected from the same population.
Inclusion criteria were; age over16 years of age withsymptoms of dry eye (Table 1).
Exclusion criteria were: any pre-existing oculardisease other than DES; patients on oral tetracyclineor corticosteroids and; past history of herpetic eyedisease, liver disease, diabetes or laser in situkeratomileusis (LASIK). Other exclusion criteriaincluded pregnancy, or lactating mothers, cognitive orpsychiatric disorder, post-menopausal women, HIV
and Hepatitis B and C. Patients with inability toswallow soft gel capsules. Patients on aspirin or anti-coagulant therapy, allergy to fluorescein, patients witha malignancy or chronic infection of the lacrimal glandwere also excluded from the study.
A written consent was obtained from all patientswilling to take part in the case control study. The trialwas approved by the ethics committee. A singleexaminer performed all the tear function tests and wasmasked to the information obtained from dry eyequestionnaire.
TBUT was first performed as manipulation of theeyelids may affect the results. Two successive readingswere performed and averaged. The subject thenwaited for 30 minutes, and Schirmer ’s test withanesthesia was performed with eyes closed. Thesubject waited for another 30 minutes and the RoseBengal test was performed with the hanging dropmethod. A van Bijsterveld score of 4 or more wasconsidered positive for dry eye. 13
Conjunctival impression cytology was performedwith the eye anaesthetized with one drop of 4%Xylocaine. Then the lacrimal lake at inner canthus wasdried with a cotton tip applicator. A filter paper wasgrasped with blunt smooth edge forceps and appliedto the inferior bulbar conjunctiva. The filter paper wasgently pressed with a glass rod held in the other hand.The paper strip was removed in a peeling fashion after4-10 seconds and a specimen transferred to the lab forstaining and fixation.
The filter paper was placed on a glass slide withalbumin paste for specimen transfer. The slide waslabeled and numbered. It was stained with Periodicacid-Schiff (PAS) and counter stained withhaematoxylin and eosin. The mounted slide wasexamined under a microscope with 10x high powerfield (HPF). After localization, cells were thenexamined under 40x HPF for goblet cells and epithelialcells. At least 10 HPF were examined. Grading andscoring was recorded based on the criteria suggestedby Nelson et al. Grades 0 and 1 were normal andGrades 2 and 3 were abnormal. 14
Means of two groups was compared with t-test.Pearson Chi-Square test was used to compare crosstabulations between tear function tests. P value wascalculated at 1% and 5% level. P value <0.001 at 1%level and <0.005 at 5% level implied that thecomparison was statistically significant. Sensitivity,Specificity and Positive predictive values of tear
17. Rahul Bhargav--72-77.pmd 10/10/2013, 9:22 AM73

74 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
function tests were calculated using ConjunctivalImpression Cytology as gold standard.
RESULTS
The total number of valid cases (eyes) was 276 andcontrols 216. The mean age of cases was 24.03±10.12.The mean age of controls was 26.17 ±7.36 (P 0.000).
The mean Schirmer’s value in cases was 12.54 ±4.73 and 16.32 ± 3.80 in controls (P=0.000). The meantear film break up time in cases was 9.11 ± 2.90 and14.21 ± 2.72 in controls (P=0.00). The mean goblet celldensity in cases was 476 ± 238 and 1552 ± 598 in
controls (P=0.000). Likewise, the mean Rose Bengalscore in cases was 4.92 ± 3.16 and 1.02 ± 1.12 in controls(Table 1) (P 0.000).
The sensitivity, specificity and positive predictivevalue of Schirmer’s, TBUT and Rose Bengal stainingwas calculated taking CIC as the gold standard [Table3]. Sensitivity of Schirmer’s was 65.69 % and specificitywas 68.50 % with a PPV of 45.58%.
The sensitivity of TBUT was 80.43% and specificity64.96% with a PPV of 45.40%. The sensitivity of RBSwas 63.73%, specificity 64.17% and PPV of 41.67%respectively.
TABLE 1. Dry eye questionnaire and scoring system. ©
Symptom SCORE (Maximum 18)
Absent (0) Sometimes (1) Frequent (2) Always Present (3)
Itching or burning
Sandy or gritty sensation
Redness
Blurring of vision
Ocular fatigue
Excessive blinking
Dry Eye Scoring System (DESS©) Scores of 0-6 was mild, 6.1-12 moderate, and 12.1-18, severe dry eye. © Rahul Bhargava, Laser EyeClinic Noida.
TABLE 2. Mean Test Values
Group N Mean Std. t testDeviation
Age Case 276.00 24.03 10.12 Sig
Control 216.00 26.17 7.36 0.00
Schirmer’s Case 276.00 12.54 4.73 Sig
Control 216.00 16.32 3.80 0.00
TBUT Case 276.00 9.11 2.90 Sig
Control 216.00 14.21 2.72 0.00
RBS Case 276.00 4.92 3.16 Sig
Control 216.00 1.02 1.12 0.00
CIC Case 276.00 2.65 1.21 Sig
Control 216.00 1.69 0.88 0.00
GC Case 276.00 476.12 238.13 Sig
Control 216.00 1552.47 598.12 0.00
*Values in red indicate that the difference in two groups is statistically significant on application of t-test. Conjunctival ImpressionCytology (CIC), Goblet Cells (GC), Tear Film Break Up time (TBUT), Rose Bengal Score (RBS)
Table 3. Sensitivity, specificity and positive predictive value of tear function tests.
Test Sensitivity Specificity PositivePredictive
Value
Schirmer 65.69 % 68.50 % 45.58%.
TBUT 80.43% 64.96% 45.40%.
RBS 63.73%, 64.17% 41.67%
Conjunctival impression cytology was the gold standard test.
17. Rahul Bhargav--72-77.pmd 10/10/2013, 9:22 AM74

International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 75
Table 4. Tear film break up time (TBUT) and CIC cross tabulation.
Tear Film Break Up Time (Tbut) Tbut- Cic Cross Tab
Group
Case Control Normal Abnormal
N % N % N % N %
>10.1 s 52 24.10 131 93.6 147 68 36 25.7
5.1 to 10 s 80 37.0 9 6.4 44 20.37 45 32.14
<5 s 84 38.9 0 0 25 11.57 59 42.14
Total 216 100 140 100 216 100% 140 100
‡ Tear film break up time (TBUT) in cases and control (P 0.000).
DISCUSSION
The term ‘dye eye’ includes a wide spectrum ofalterations of ocular surface with different etiology andpathophysiology.
CIC is non-invasive, relatively easy to perform, andyields reliable information about the area sampled.Having said this, CIC is relatively a time consumingprocedure and may cause irritation and discomfort insome patients.
In the present study, tear functions tests we assessedvalidity of routine tear function tests in estimating dryeye disease in comparison to conjunctival impressioncytology.
In dry eye patients, 16.8% patients with Schirmer’sless than 10mm in 5 minutes had normal cytology and45.6 % had abnormal cytology (P 0.000) whereas only5.6 % controls with abnormal cytology had abnormalSchirmer’s.
GCD was significantly reduced in dry eye cases ascompared to controls. This result was similar to studydone by Murube and co-workers.15 Bandyopadhyayet al studied cytological changes in ocular surfacedisorders and found a statistically significant betweencases and control groups, similar to the present study.16
Although there has been some consensus on thecorrelation between assessment of ocular surface byCIC and conjunctival biopsy, Sood and co-workersdemonstrated a strong correlation betweenassessments made by tear function tests like Schirmer’sand CIC. 17 However, the results of our study weredifferent from their study. This was probably due to adifferent staging method used by the authors forgrading CIC (Tseng et al). 18
31.6% patients with dry eye and TBUT less than10 seconds had a normal cytology and 72.8% abnormal
cytology (P 0.000). On the contrary, in control group,28% had an abnormal cytology. TBUT is therefor abetter predictor of morphological and cytologicalchanges at the conjunctiva than Schirmer’s. A similarcorrelation was found in a study by Paschides and co-workers by using a simple linear regression analysisto compare the results. 19
24.1% patients with dry eye had a normal RBS scoreand 20.6 % had normal cytology. 65.3% had abnormalRBS score and 76.9% had abnormal cytology. Thisresult was different from results of study done byYayali et al. 20 These authors have establishedcorrelation between tear film profile and CIC forspecific causes of dry eye. The present study comparestear film profile and CIC in various etiologies of dryeye syndrome. A larger sample size in our study, couldexplain the difference in results.
Doughty MJ, 21 recently studied goblet cell densityof normal human subjects from impression cytologyspecimens. They found a wide variability in GCD insamples obtained from exposed (427± 376 cells/mm2)and non-exposed (973±789 cells/mm2) locations. Inanother study, the authors found that the use of a smallsampling area (high power field of view) is likely toresult in an unacceptably large uncertainty (variability)in the GCD estimates. 22
Slides were initially mounted on 10x high powerfield (HPF). At least 10 HPF were counted for gobletand epithelial cells to reduce the degree of variation.After localization, cells were then examined on 40xHPF magnification. However, in dry eye states, lessvariability is expected in samples obtained fromdifferent locations as compared to normal humansubjects.
The sensitivity and specificity of Schirmer ’sreported by Gupta et al was 81.3 % and 74.9 %,respectively. 23 This was comparable to the sensitivity
17. Rahul Bhargav--72-77.pmd 10/10/2013, 9:22 AM75

76 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
and specificity estimated in our study (80.43 and 64.96).Rahman et al reported that specificity of TBUT was75.57% and sensitivity of Rose Bengal was 92.85%. Thisresult was different from our study because their goldstandard was Schirmer’s test, as opposed to impressioncytology in our study. 24
CONCLUSION
Dry eye remains a diagnostic enigma. The accuracyof tear function tests in predicting morphological andcytological changes in the conjunctiva wasRBS>TBUT>Schirmer ’s. The sensitivity of tearfunction tests in diagnosing dry eye wasTBUT>Schirmer ’s>RBS and specificity wasSchirmer’s>TBUT>RBS in decreasing order, takingCIC as gold standard.
Acknowledgements: Dr. Puneet Gupta for statisticalanalysis.
Conflict of Interest: Nil
Financial Interest: Nil
REFERENCES
1. Schaumberg DA, Sullivan DA, Buring JE, DanaMR. Prevalence of dry eye syndrome among USwomen. Am J Ophthalmol 2003; 136:318-26.
2. Nelson JD, Helms H, Fiscella R, et al. A new lookat dry eye disease and its treatment. Adv Ther2000; 17(2):84-93.
3. Dry Eye Workshop. The definition andclassification of dry eye disease: report of thedefinition and classification subcommittee of theInternational Dry Eye Workshop. Ocul Surf. 2007;5: 75-92.
4. Foulks GN. Challenges and pitfalls in clinicaltrials of treatments for dry eye. Ocul Surf. 2003;1:20–30.
5. Nichols KK, Nichols JJ, Mitchel GL. The lack ofassociation between signs and symptoms inpatients with dry eye disease. Cornea 2004;23:762-70.
6. Nicholas KK, Mitchel GL, Zadnik K. Therepeatability of clinical measurements of dry eye.Cornea 2004; 23: 272-285.
7. Patel S, Murray D, McKenzie A, Shearer DS,McGrath BD. Effects of fluorescein on tear breakup time and tear thinning time. Am J OptomPhysiol Opt.1985; 62: 188-90.
8. Argüeso P, Tisdale A, Spurr-Michaud S,Sumiyoshi M, Gipson IK. Mucin characteristicsof human corneal-limbal epithelial cells thatexclude the rose Bengal anionic dye. InvestOphthalmol Vis Sci. 2006; 47:113–19.
9. Dart J. Impression cytology of the ocular surface-research tool or routine clinical investigation? BrJ Ophthalmol 1977; 81: 930.
10. Egbert PR, Lauber S, Maurice DM. A simpleconjunctival biopsy. Am J Ophthalmol 1977; 84:798-801.
11. Natadisastra G, Wittpenn JR, West KP Jr, Muhilal,Sommer A. Impression cytology for detectionof vitamin A deficiency. Arch Ophthalmol 1987;105:1224–8.
12. Puangsricharern V, Tseng SC. Cytologic evidenceof corneal diseases with limbal stem celldeficiency. Ophthalmology 1995; 102:1476–85.
13. van Bijsterveld OP. Diagnostic tests in the siccasyndrome. Arch Ophthalmol1969; 82 (1):10-4.
14. Nelson DJ. Impression cytology. Cornea 1988;7:71-81.
15. Murube J, Rivas L. Impression cytology onconjunctiva and cornea in dry eye patientsestablishes a correlation between squamousmetaplasia and dry eye clinical severity. Euro JOphthalmol.2003; 13:115-127.
16. Bandyopadhyay R, Nag D, Mondal SK,Gangopadhyay S, Bagchi K, Bhaduri G. Ocularsurface disorders in pterygium: Role ofconjunctival impression cytology. Ind J PatholMicrobiol.2010; 53:692-5.
17. Sood S, Shukla R, Nada M, Khurana AK, AroraB. Comparison of Tear film profile, ConjunctivalImpression Cytology, and Conjunctival biopsy inpatients with dry eye. Asian J Ophthalmol.2006;8: 24-27.
18. Tseng SCG. Staging of conjunctival squamousmetaplasia by impressioncytology. Ophthalmology1985; 92:728–33.
19. Paschides CA, Petroutsos G, Psilas K. Correlationof conjunctival impression cytology results withlacrimal function and age. Acta Ophthalmologica1991; 69: 422-25.
20. Yaylali V, Ozyurt C. Comparison of tear functiontests and impression cytology with the ocularfindings in acne rosacea. Euro J Ophthalmol. 2002;12:11-7.
17. Rahul Bhargav--72-77.pmd 10/10/2013, 9:22 AM76

International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 77
21. Doughty MJ. Goblet cells of the normal humanbulbar conjunctiva and their assessment byimpression cytology sampling. Ocular Surf.2012;10: 149-69.
22. Doughty MJ. Sampling area selection for theassessment of goblet cell density fromconjunctival impression cytology specimens. EyeContact Lens 2012; 38:122-9.
23. Gupta Y, Gupta M, Maheshwari R, Mittal T.Xerosis meter-an electro-physiological device forquick screening of dry eyes. Nepal J Ophthalmol2009; 1: 123-128.
24. Rahman A, Yahya K, Ahmed T, Sharif-Ul-HassanK. Validity of symptoms as a screening tool fordry eye. Pak J Ophthalmol 2007; 23:198-203.
17. Rahul Bhargav--72-77.pmd 10/10/2013, 9:22 AM77

78 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
A Study of Rickets as an Avoidable Cause of DelayedWalking in Children in Rural Western Uttar Pradesh
Bhawna Kohli1, Rajesh Bhatia2, Sumit Gupta3
1Assistant Professor, Department of Pediatrics, 2Associate Professor, 3Assistant Professor, Department of Orthopedics,Saraswathi Institute of Medical Sciences, Hapur, Uttar Pradesh, India
ABSTRACT
Aims and objective: To evaluate children with nutritional rickets presenting with complaints ofinability to walk and their responses to treatment. These children were investigated for rickets byappropriate history, clinical, radiological and biochemical examination.
Method: Children more than 1 year of age were inducted. Every child was properly examined anddiagnosed by clinical, radiological, biochemical findings and response to treatment. Every child wasevaluated keeping in mind all the other possible causes of delayed walking.
Results: 36(60%) children turned out to be affected by nutritional rickets out of 60 non-walkers duringthe study period. On follow-up at 3 weeks of treatment, all 36 patients (100%) showed radiologicaland biochemical response. 34(94%) patients started walking within 3 months of treatment. Radiologicalhealing averaged 5 months.
Conclusion: The study reveals that most of non-walkers with rickets start walking within 2 to 5months of appropriate treatment & it is preventable and easily curable if detected early, by simplemeasures, avoiding the crippling sequelae.
Keywords: Rickets, Children, Delayed Walking
INTRODUCTION
Rickets in infants due to either vitamin D deficiencyor inadequate intake has been reported with increasingfrequency around the world & especially in developingcountries.1, 2, 3 Vitamin D deficiency has been and is along standing public health issue. There are alsoconcerns for vitamin D deficiency in older children,adolescents & mothers of children with rickets.4Theincreased metabolic demands together with dark skinpigmentation, low vitamin-D intake, and lack ofsunlight exposure may predispose to nutritionalrickets. Actually biochemical rickets happen muchbefore clinical rickets.5, 6
Vitamin D deficient children may present eitherwith symptoms of hypocalcemia like convulsions,tetany and paraesthesias or with bony abnormalitieslike bowing of legs, knock knees, ricketic rosary of thecosto-chondral junction, swelling of ends of longbones, frontal bossing of the skull, pathological fracturein severe cases, as well as poor growth, delayeddentition, and slow motor development. 7, 8 One of themajor indicators of motor development in a child is
the age when the child starts to stand without supportand walk.9 Rickets as a cause of delayed motordevelopment has been proven before 10,11 but its role indelayed walking has never been studied in detail. Thecurrent study prospectively evaluated the response tovitamin D and calcium therapy in non-walkers due tonutritional rickets.
MATERIALS AND METHOD
The study was conducted between July 2010 andAugust 2012 in a medical college hospital located inrural western Uttar Pradesh. Most of the patientsvisiting the hospital belong to low to middle socio-economic group. The study evaluated children whowere brought to the setup with complaints of eitherdelayed walking or inability to stand despite being ofone year age. Only children who were past the ageconsidered to be the physiological age for walkingwere considered. The physiological age groups withinwhich a child usually starts to stand without supportand walk is around the first birthday of the child.9
Hence only children more than 1 year of age were
DOI Number: 10.5958/j.2321-1024.1.2.035
18. Rajesh Bhatia--78-82.pmd 10/10/2013, 9:22 AM78
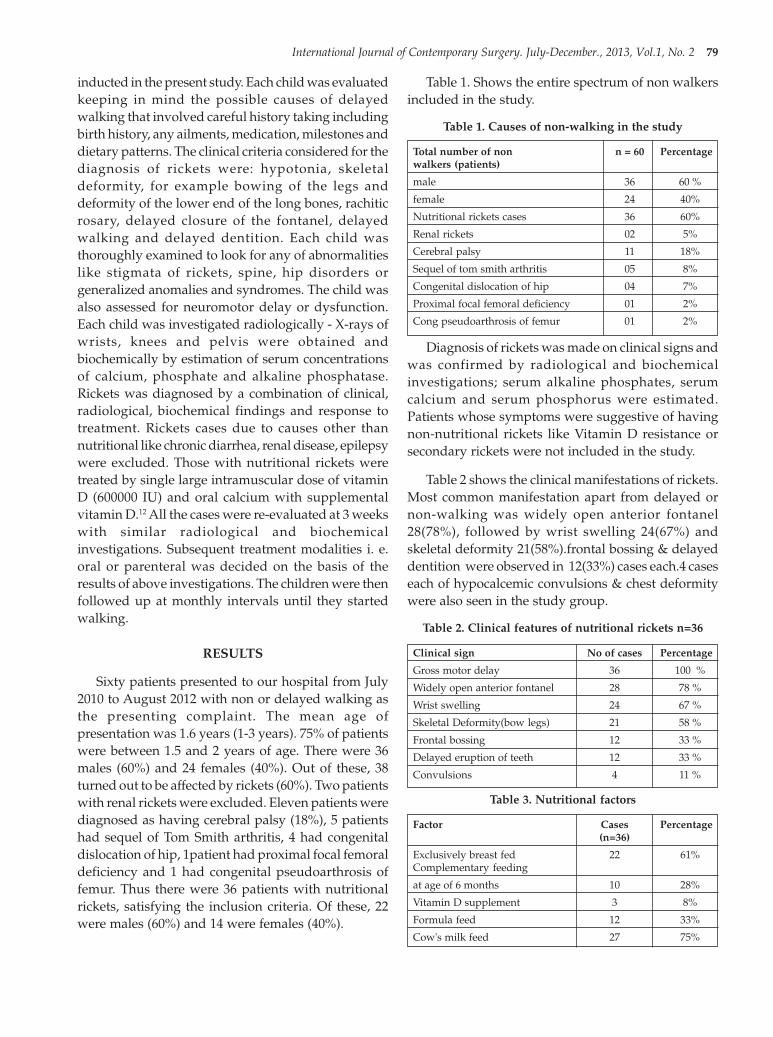
International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 79
inducted in the present study. Each child was evaluatedkeeping in mind the possible causes of delayedwalking that involved careful history taking includingbirth history, any ailments, medication, milestones anddietary patterns. The clinical criteria considered for thediagnosis of rickets were: hypotonia, skeletaldeformity, for example bowing of the legs anddeformity of the lower end of the long bones, rachiticrosary, delayed closure of the fontanel, delayedwalking and delayed dentition. Each child wasthoroughly examined to look for any of abnormalitieslike stigmata of rickets, spine, hip disorders orgeneralized anomalies and syndromes. The child wasalso assessed for neuromotor delay or dysfunction.Each child was investigated radiologically - X-rays ofwrists, knees and pelvis were obtained andbiochemically by estimation of serum concentrationsof calcium, phosphate and alkaline phosphatase.Rickets was diagnosed by a combination of clinical,radiological, biochemical findings and response totreatment. Rickets cases due to causes other thannutritional like chronic diarrhea, renal disease, epilepsywere excluded. Those with nutritional rickets weretreated by single large intramuscular dose of vitaminD (600000 IU) and oral calcium with supplementalvitamin D.12 All the cases were re-evaluated at 3 weekswith similar radiological and biochemicalinvestigations. Subsequent treatment modalities i. e.oral or parenteral was decided on the basis of theresults of above investigations. The children were thenfollowed up at monthly intervals until they startedwalking.
RESULTS
Sixty patients presented to our hospital from July2010 to August 2012 with non or delayed walking asthe presenting complaint. The mean age ofpresentation was 1.6 years (1-3 years). 75% of patientswere between 1.5 and 2 years of age. There were 36males (60%) and 24 females (40%). Out of these, 38turned out to be affected by rickets (60%). Two patientswith renal rickets were excluded. Eleven patients werediagnosed as having cerebral palsy (18%), 5 patientshad sequel of Tom Smith arthritis, 4 had congenitaldislocation of hip, 1patient had proximal focal femoraldeficiency and 1 had congenital pseudoarthrosis offemur. Thus there were 36 patients with nutritionalrickets, satisfying the inclusion criteria. Of these, 22were males (60%) and 14 were females (40%).
Table 1. Shows the entire spectrum of non walkersincluded in the study.
Table 1. Causes of non-walking in the study
Total number of non n = 60 Percentagewalkers (patients)
male 36 60 %
female 24 40%
Nutritional rickets cases 36 60%
Renal rickets 02 5%
Cerebral palsy 11 18%
Sequel of tom smith arthritis 05 8%
Congenital dislocation of hip 04 7%
Proximal focal femoral deficiency 01 2%
Cong pseudoarthrosis of femur 01 2%
Diagnosis of rickets was made on clinical signs andwas confirmed by radiological and biochemicalinvestigations; serum alkaline phosphates, serumcalcium and serum phosphorus were estimated.Patients whose symptoms were suggestive of havingnon-nutritional rickets like Vitamin D resistance orsecondary rickets were not included in the study.
Table 2 shows the clinical manifestations of rickets.Most common manifestation apart from delayed ornon-walking was widely open anterior fontanel28(78%), followed by wrist swelling 24(67%) andskeletal deformity 21(58%).frontal bossing & delayeddentition were observed in 12(33%) cases each.4 caseseach of hypocalcemic convulsions & chest deformitywere also seen in the study group.
Table 2. Clinical features of nutritional rickets n=36
Clinical sign No of cases Percentage
Gross motor delay 36 100 %
Widely open anterior fontanel 28 78 %
Wrist swelling 24 67 %
Skeletal Deformity(bow legs) 21 58 %
Frontal bossing 12 33 %
Delayed eruption of teeth 12 33 %
Convulsions 4 11 %
Table 3. Nutritional factors
Factor Cases Percentage(n=36)
Exclusively breast fed 22 61%Complementary feeding
at age of 6 months 10 28%
Vitamin D supplement 3 8%
Formula feed 12 33%
Cow's milk feed 27 75%
18. Rajesh Bhatia--78-82.pmd 10/10/2013, 9:22 AM79

80 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
All except two patients showed typical ricketicchanges on X-rays of wrist (95%) and 75 %( 27) showedchanges in knee X-rays. Changes in the upper end offemur were found in 12 patients (33%). 24 of these 36patients (66%) were found to have florid changes onX-rays. 2 patients had pathological fractures; one withfracture of bilateral neck femur and the other withfracture of the shaft of femur and ipsilateral ulnadetected on X-rays.
24 patients (67%) had low serum calcium withvalues ranging from 5.5-10.2 mg/dl (reference. 9.1-11.2mg/dl) and a mean value of 8.90 mg/dl; 60% had lowserum phosphate (2.5-5.0 mg/dl) with a mean of 3.2mg/dl and 100% had high serum alkaline phosphatasevalues ranging from 698-6050 IU/L (reference. <750IU/L). Average serum alkaline phosphatase value was2423.7 IU/L. On follow-up at 3 weeks of treatment, 4patients had started walking. All 36 patients (100%)showed radiological and biochemical response. Themean serum calcium levels
at 3 weeks were 9.4 mg/dl and mean phosphatelevels were 3.9 mg/dl. The average alkalinephosphatase levels at 3 weeks went down to 1235 IU/L. At 3 weeks, 80% (29 patients) had normal serumcalcium, 89% (32 patients) had normal phosphatelevels and 17% (6 patients) had normal alkalinephosphatase levels.32 children (89%) had biochemicalresolution by 2 months and all 36 (100%) at 6 months.78 % (28 patients) started walking within 2 months oftreatment and another 17% (6 patients) by 3 months.Two patients walked at 4.5 months. Hence all 36patients started walking by 4.5 months. Radiologicalresolution averaged 5 months (ranging from 3 to 8months).
Table 4. Laboratory Findings
Test Mean values Mean valuesin cases in at 3 weeks
the beginning
Serum calcium 8.9 9.4
Serum phosphorus 3.2 3.9
Serum alkaline phosphates 2423.70 1235
DISCUSSION
Vitamin D deficiency or nutritional rickets inchildren is almost eliminated in the developedcountries by prophylactic means. However, it stillremains major health problem in under developedcountries.13-15
Nutritional rickets is a multifactorial condition. Ithas been clear that some of the factors play moreimportant role for contribution of nutritional rickets.Maternal education, lack of exposure to sunlight dueto complete wrapping of the children and a poorweaning diet were more important than the otherfactors.
Most of the rickets patients were breast-fed.However, the value of breast milk as a source ofvitamin D is debated. Breast-fed infants are generallyprotected from vitamin D deficiency rickets during thefirst few months of life16, because vitamin D and itsmetabolites do cross the placenta. But this protectiondoesn’t last long as it is well recognized that breastmilk normally contains insufficient concentrations ofvitamin D.17, 18 Therefore if food fortification oradequate sunlight exposure17 is not given to the child,vitamin D deficiency is inevitable. In developingcountries as India, majority of children continue to takepredominantly breast feeds beyond 6 months of ageand complimentary feeds are inadequate, resulting innutritional deficiency.
Other similar studies were conducted depictingvarious presentations of rickets in infancy and earlychildhood with delayed walking as one of thepresentations.
70%(42) of a total of 60 patients were found to havegross motor delay in a study conducted in Pakistanby Rehana Majeed et al.19
Tahir, et al20 reported 20% of motor delay in a studyconducted in Pakistan.
Ten percent of a total of 56 patients in the age groupof 1-2 years had delayed walking in a study in Canadaby Ward et al.21
Ladhani et al22 found motor delay in only 2 (3%)of his 65 patients (considered age group 3 months to13 years with no further refinement of age groups).
15% of patients (total 60 in age group 3-36 monthswith 24 patients between 13 and 24 months) presentedwith delayed walking in a study in western SaudiArabia by Nadia23 and 5% as per Sedrani et al24 study.
We found an alarming 60% of non-walking cases(36 of 60) attributable to biochemical and radiologicalprofile and a definite response to vitamin D therapy.This signifies that in a country like India where the
18. Rajesh Bhatia--78-82.pmd 10/10/2013, 9:22 AM80

International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 81
disease is still rampant in the lower socio-economicstrata, which form a sizeable proportion of thepopulation, some serious measures needs to be taken.
Malnutrition has been reported in literature as acontributing factor for nutritional rickets & it issuggested that the rickets patients in general weremore malnourished. Maternal education may play animportant role. It is expected that an educated motherwill have better and improved child-rearing practices& will be more aware of the complementary feeding,its quality and for starting to wean.
CONCLUSION
According to our study rickets is a main cause ofdelayed walking in this area. Hence every child thatpresents as inability to stand or walk at more than oneyear age warrants a clinical examination to look forstigmata of rickets and appropriate radiological andbiochemical assessment as indicated.
Our study also reveals that majority of ricketic non-walkers start walking within 2 to 5 months ofappropriate treatment. The irony is that the disease istotally preventable and easily curable by simple means,if detected early.
Despite nutritional rickets still being quite prevalentin India it is not yet considered an important publichealth issue & no specific nutritional healthprogramme aims specifically at it. There is a strongneed for further population based studies to determinethe true impact of this disease on our society. Theseobservations can guide the nutrition interventionprogrammes for infant and toddlers for our country.It is suggested that a national campaign to promoteawareness of the risks of vitamin D deficiency,particularly among susceptible populations be doneto eliminate rickets as a cause of morbidity.
Conflict of Interest: Nil
Source of Funding: Self
Ethical Clearance: Taken
ACKNOWLEDGEMENT
The authors acknowledge the cooperation of thepatients & consent of their parents for participating inthe study. We would also like to thank the biochemistry& radiology departments of the institute.
There was no conflict of interest & no funding wasneeded.
Ethical Clearance
We would like to report that the study was carriedout in accordance with international and nationalethical guidelines and necessary approval fromInstitutional ethics committee was obtained andwritten informed consent was taken from the parentsof the participants or their legal guardian.
REFERENCES
1. Agarwal A, Gulati D et al. Rickets: A cause ofDelayed Walking in Toddlers. Indian J Pediatr2009; 76: 269 -272.
2. Pillow JJ, Forrest PJ, Rodda CP. Vitamin Ddeficiency in infants and young children born tomigrant parents. J Pediatr Child Health 1995; 31:180-184.
3. Robinson PD, Hogler W, Craig ME et al. The re-emerging burden of rickets: a decade ofexperience from Sydney. Arch Dis Child 2006; 91:564-568.
4. Nozza JM, Rodda CP. Vitamin D deficiency inmothers of infants with rickets. Med J Aust 2001;175: 253-255.
5. Working Group of the Australian and NewZealand Bone and Mineral Society, EndocrineSociety of Australia and Osteoporosis Australia.Vitamin D and adult bone health in Australia andNew Zealand: a position Statement. Med J Aust2005; 182: 281-285.
6. Hatun S, Ozkan B, Orbak Z et al. Vitamin Ddeficiency in early infancy. J Nutr 2005; 135:279-282.
7. Ladhani S, Srinivasan L, Buchanan C, Allgrove J.Presentation of vitamin-D deficiency. Arch DisChild 2004; 89: 781-784.
8. Mughal MZ, Salama H, Greenaway T, Laing I,Mawer EB. Florid rickets associated withprolonged breast-feeding without vitamin Dsupplementation. BMJ 1999; 318: 39-40.
9. Ghai OP, Paul VK, Gupta P. Growth anddevelopment. In Ghai OP, Gupta P, Paul VK, eds.Ghai Essential Pediatrics. Delhi; OP Ghai, 2004;1-48.
10. Fida NM. Assessment of nutritional rickets inwestern Saudi Arabia. Saudi Med J 2003; 24:337-340.
11. Blok BH, Grant CC, McNeil AR, Reid IR.Characteristics of children with florid vitamin D
18. Rajesh Bhatia--78-82.pmd 10/10/2013, 9:22 AM81

82 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
rickets in the Auckland region in 1998. N Z MedJ 2000; 113: 374-376.
12. Shah BR, Finberg L. Single day therapy fornutritional vitamin D deficiency rickets: apreferred method. J Pediatr 1994; 125: 487-490.
13. Bonnici F. Functional hypoparathyroidism ininfantile hypocalcaemia stage I vitamin Ddeficiency rickets. S Afr Med J.1978; 54: 611–12.
14. Jamal A, Khanani AR, Billo G, Asger A, Jafri Z.Rickets in a slum of Karachi. Pak J Med Sci. 1996;12(3) 247-50.
15. Iqbal SJ, Garrick DP, Howl A. Evidence ofcontinuing deprivational vitamin D deficiency inAsians in the UK. J Hum Nutr Diet.1994a; 7:47-52.
16. Hillman LS, Haddad JG. Human perinatalvitamin D metabolism- 1,25-hydroxyvitamin Din maternal and cord blood. J Paediatr 1974; 84:742-749.
17. Specker BL, Tsang RC, Hollis BW. Effect of raceand diet on human milk vitamin D and 25-Hydroxyvitamin D. Am J Dis Child 1985; 139:1134-1137.
18. Hollis BW, Roos BA, Draper HH, Lampert PW.Vitamin D and its metabolites in human andbovine milk. J Nutr 1981; 111: 1240-1248.
19. Rehana Majeed, Yasmeen Memon, MansoorKhowaja, Farrukh Majeed, Mohammad UsmanAli and Uzma Rajar. Contributing factors orrickets among children at Hyderabad. JLUMHS,MAY - AUGUST 2007
20. Tahir SS, Manzoor IR. Presentation andpredisposing factors of nutritional rickets inchildren of Hazara division. J Ayub Med CollAbbottabad 2005; 17(3).
21. Ward LM, Gaboury I, Ladhani M, Zlotkin S.Vitamin-D deficiency rickets among children inCanada. CMAJ 2007; 177: 161-166.
22. Ladhani S, Srinivasan L, Buchanan C, Allgrove J.Presentation of vitamin-D deficiency. Arch DisChild 2004; 89: 781-784.
23. Nadia MF. Assessment of nutritional rickets inwestern Saudi Arabia. Saudi Med J 2003; 24:337-340.
24. Sedrani SH, Abanmy A, Salman H, Al-Arabi K,Elidrissy A. Vitamin D status of Saudis: are Saudichildren at risk of developing vitamin Ddeficiency rickets? Saudi Med J 1992; 13: 430-433.
18. Rajesh Bhatia--78-82.pmd 10/10/2013, 9:22 AM82

International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 83
A Study of Urinary Tract Infections in Patients withCatheter in Tertiary Care Hospital in Western
Uttar Pradesh
Sanjeev Dimri1, Hemant Sharma2, S K Datta3, Deepak Gupta1
1Assistant Professor, Department of Microbiology, 2Assistant Professor, Department of Medicine, 3Professor and Head,Department of Microbiology, Saraswathi Institute of Medical Sciences, Hapur, U.P., India
ABSTRACT
Aim: The aim of this study was to determine microorganisms responsible for urinary tract infections(UTI) in patients with indwelling urinary catheter and their antibiotic susceptibility patterns tocommonly used antibiotics.
Subjects and Method: The study was carried out from April 2011 to January 2012 on 108 patientswith indwelling urinary catheters. The organisms were isolated by conventional culture methodsand identified by conventional biochemical methods. The antibiotic susceptibility pattern wasdetermined by Kirby-Bauer disc diffusion method on Muller-Hinton agar.
Results: In this study, 93 (86.1%) patients were found to be culture positive for microbial pathogensin their urine samples. Escherichia coli (50.5%) was the most frequently isolated bacteria followed byKlebsiella species (14%) and Pseudomonas aeruginosa (10.8%). The in-vitro susceptibility pattern offrequently isolated gram negative bacteria shows high resistance to commonly used antibiotics suchas ampicillin, amoxicillin+clavulanic acid and fluoroquinolones. Carbapenems and amikacin werefound to be the most effective antibiotics for frequently isolated gram negative bacteria.
Conclusion: Emphasis should be placed on good catheter management rather than using prophylacticantibiotic therapy to reduce the incidence of catheter associated urinary tract infection.
Keywords: Catheter, CAUTI, Pathogen, Kirby- Bauer, Resistance
INTRODUCTION
The urinary tract is the most common site ofnosocomial infection accounting for more than 40% ofthe total number reported by acute care hospitals andaffects approximately 600,000 patients per year1, 2, 3.Sixty six to 86% of these infections followinstrumentation of urinary tract, mainlycatheterization4. The risk of acquiring a urinary tractinfection (UTI) depends on method and duration ofcatheterization, the quality of catheter care and host
Corresponding author:Sanjeev DimriAssistant ProfessorDepartment of MicrobiologySaraswathi Institute of Medical Sciences, Hapur,Ghaziabad, U.P. IndiaTel: +91 9958322747E-mail: [email protected]
susceptibility. Host factors including advanced age,debilitation and post-partum state appear to increasethe risk of catheter associated urinary tract infection(CAUTI) 5, 6. Reported infection rates vary widely,ranging from 1 to 5 % after single brief catheterization7,over 20% of patients with indwelling cathetersmaintained on closed system8, 9 to virtually 100% forpatients with indwelling catheters draining into opensystem for more than 4 days10. Catheter associatedurinary tract infection is caused by a variety ofpathogens including Escherichia coli, Klebsiella,Pseudomonas aeruginosa, Enterobacter, Proteus,Enterococcus andCandida. Many of thesemicroorganisms are part of patients endogenous bowelflora but can also be acquired by cross contaminationfrom other patients, hospital personnel, by exposureto contaminated solution or non-sterile equipment9,11.Catheter associated urinary tract infection in healthypatient is often asymptomatic and is likely to resolve
DOI Number: 10.5958/j.2321-1024.1.2.036
19. Sanjeev Dimri Sims--83-86.pmd 10/10/2013, 9:22 AM83
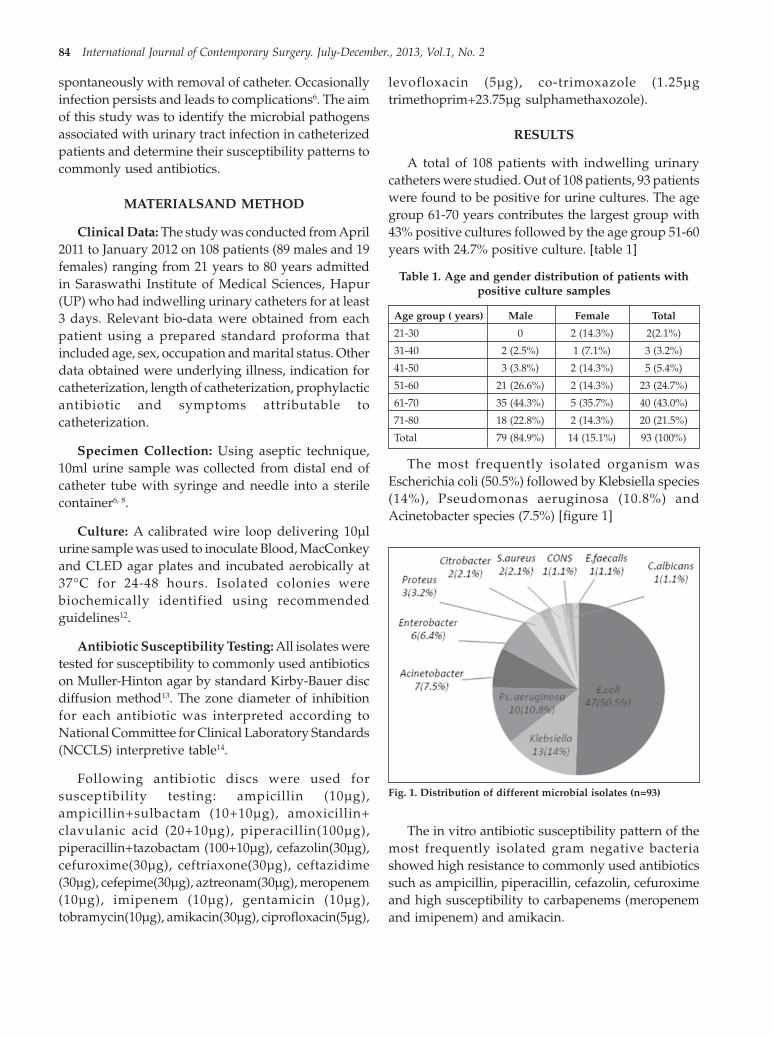
84 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
spontaneously with removal of catheter. Occasionallyinfection persists and leads to complications6. The aimof this study was to identify the microbial pathogensassociated with urinary tract infection in catheterizedpatients and determine their susceptibility patterns tocommonly used antibiotics.
MATERIALSAND METHOD
Clinical Data: The study was conducted from April2011 to January 2012 on 108 patients (89 males and 19females) ranging from 21 years to 80 years admittedin Saraswathi Institute of Medical Sciences, Hapur(UP) who had indwelling urinary catheters for at least3 days. Relevant bio-data were obtained from eachpatient using a prepared standard proforma thatincluded age, sex, occupation and marital status. Otherdata obtained were underlying illness, indication forcatheterization, length of catheterization, prophylacticantibiotic and symptoms attributable tocatheterization.
Specimen Collection: Using aseptic technique,10ml urine sample was collected from distal end ofcatheter tube with syringe and needle into a sterilecontainer6, 8.
Culture: A calibrated wire loop delivering 10µlurine sample was used to inoculate Blood, MacConkeyand CLED agar plates and incubated aerobically at37°C for 24-48 hours. Isolated colonies werebiochemically identified using recommendedguidelines12.
Antibiotic Susceptibility Testing: All isolates weretested for susceptibility to commonly used antibioticson Muller-Hinton agar by standard Kirby-Bauer discdiffusion method13. The zone diameter of inhibitionfor each antibiotic was interpreted according toNational Committee for Clinical Laboratory Standards(NCCLS) interpretive table14.
Following antibiotic discs were used forsusceptibility testing: ampicillin (10µg),ampicillin+sulbactam (10+10µg), amoxicillin+clavulanic acid (20+10µg), piperacillin(100µg),piperacillin+tazobactam (100+10µg), cefazolin(30µg),cefuroxime(30µg), ceftriaxone(30µg), ceftazidime(30µg), cefepime(30µg), aztreonam(30µg), meropenem(10µg), imipenem (10µg), gentamicin (10µg),tobramycin(10µg), amikacin(30µg), ciprofloxacin(5µg),
levofloxacin (5µg), co-trimoxazole (1.25µgtrimethoprim+23.75µg sulphamethaxozole).
RESULTS
A total of 108 patients with indwelling urinarycatheters were studied. Out of 108 patients, 93 patientswere found to be positive for urine cultures. The agegroup 61-70 years contributes the largest group with43% positive cultures followed by the age group 51-60years with 24.7% positive culture. [table 1]
Table 1. Age and gender distribution of patients withpositive culture samples
Age group ( years) Male Female Total
21-30 0 2 (14.3%) 2(2.1%)
31-40 2 (2.5%) 1 (7.1%) 3 (3.2%)
41-50 3 (3.8%) 2 (14.3%) 5 (5.4%)
51-60 21 (26.6%) 2 (14.3%) 23 (24.7%)
61-70 35 (44.3%) 5 (35.7%) 40 (43.0%)
71-80 18 (22.8%) 2 (14.3%) 20 (21.5%)
Total 79 (84.9%) 14 (15.1%) 93 (100%)
The most frequently isolated organism wasEscherichia coli (50.5%) followed by Klebsiella species(14%), Pseudomonas aeruginosa (10.8%) andAcinetobacter species (7.5%) [figure 1]
The in vitro antibiotic susceptibility pattern of themost frequently isolated gram negative bacteriashowed high resistance to commonly used antibioticssuch as ampicillin, piperacillin, cefazolin, cefuroximeand high susceptibility to carbapenems (meropenemand imipenem) and amikacin.
Fig. 1. Distribution of different microbial isolates (n=93)
19. Sanjeev Dimri Sims--83-86.pmd 10/10/2013, 9:22 AM84

International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 85
Table 2. Antibiotic susceptibility pattern of frequently isolated gram negative bacilli
Antibiotics E.coli Klebsiellaspp Enterobacterspp Acinetobacterspp P.aeruginosa(n=47) (n=13) (n=6) (n=7) (n=10)
Ampicillin 4.2% 0% 0% - -
Ampi/sul* 40.4% 38.6% 33.3% 28.5% -
Amoxi/clav** 36.2% 46.2% 16.6% - -
Piperacillin 6.4% 7.7% 16.6% 14.3% 10.0%
Piper/ tazo*** 46.8% 46.2% 33.3% 57.1% 70.0%
Cefazoline 19.1% 23.0% 0% - -
Cefuroxime 21.2% 30.0% 16.6% - -
Ceftriaxone 31.9% 38.6% 50.0% 28.6% -
Ceftazidime 38.3% 53.8% 66.6% 28.6% 30.0%
Cefepime 44.6% 61.5% 83.3% 42.8% 70.0%
Aztreonam 44.6% 46.2% 33.3% 28.6% 20.0%
Meropenem 87.2% 84.6% 100% 71.4% 70.0%
Imipenem 91.4% 92.3% 100% 85.7% 80.0%
Gentamicin 34.0% 38.6% 33.3% 42.8% 30.0%
Tobramycin 40.4% 53.8% 33.3% 42.8% 50.0%
Amikacin 80.8% 61.5% 66.6% 71.4% 60.0%
Ciprofloxacin 34.0% 30.7% 33.3% 28.5% 40.0%
Levofloxacin 36.2% 38.6% 33.3% 28.5% 50.0%
Co- trimoxazole 10.6% 30.7% 33.3% 28.5% -
*Ampicillin + sulbactam, **Amoxicillin+ clavulanic acid, ***Piperacillin+ tazobactam
DISCUSSION
An estimated 4 million patients are subjected yearlyto urinary catheterization and therefore are at risk forcatheter associated urinary tract infection and itsrelated sequelae15. One host factor that predisposes tocatheter associated urinary tract infection is advancedage5. In our study, the age group 61-70 years constitutesthe largest group (43.0%). Males (84.9%) werepredominantly affected in our study. The result of thisstudy showed that the rate of resistance to commonlyused antibiotics for gram negative bacteria was high.Escherichia coli (50.5%) was the most commonorganism causing catheter associated urinary tractinfection and showed least resistance to carbapenems.The most effective antibiotics against gram negativebacteria were carbapenems and amikacin. The mostfrequently used antibiotics used for the treatment ofcommunity based urinary tract infections such asampicillin, amoxicillin+clavulanic acid, cefuroxime,co-trimoxazole, gentamicin and tobramycin were theleast sensitive for frequently isolated gram negativebacteria in our study. The most important reason forresistance to antibiotics is the widespread use ofantibiotics such as beta-lactams and fluoroquinolones
in hospital16, 17. The microorganisms and theirresistance pattern vary from hospital to hospital andeven from clinic to clinic in the same hospital18.Although the systemic prophylactic antibiotics havebeen known to delay the onset of bacteriuria incatheterized patients, there is no justification for theirroutine use as this practice has been shown to beassociated with emergence of resistant pathogens3.
CONCLUSION
The antibiotic susceptibility pattern in our studyconfirms that most of the urinary isolates incatheterized patients are resistant to commonly usedantibiotics. The use of antibiotics should be kept undersupervision and be given in appropriate doses for anappropriate pair of time in order to preventdevelopment of resistance to antibiotics. The urinarycatheters should only be used when required andshould be inserted under aseptic conditions. Theyshould not be left in place for a long time andclosed drainage system should be used when possible.In addition, cultures and antibiotic susceptibilityresults should be taken into account when thetreatment is planned.
19. Sanjeev Dimri Sims--83-86.pmd 10/10/2013, 9:22 AM85

86 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
ACKNOWLEDGMENT
Authors are grateful to Ms. Shweta Rastogi, Ms.Gunjan Dutta and technical staff of the Department ofMicrobiology, Saraswathi institute of Medical Sciences,Hapur for technical assistance & valuable inputs.
Conflict of Interest: None
REFERENCES
1. Center for Disease Control. National NosocomialInfection Study Report. Atlanta: Centre forDisease Control, November 1979;2-14.
2. Meers PD. Infection control in developingcountries.J. Hosp. Infect. 11(Suppl A), 1988;406-410.
3. Warren JW. Catheter-associated urinary tractinfection.Infect. Dis. Clin. North Am, 1997;11:609- 622.
4. Martin CM, Bookrajian EN. Bacteriuriaprevention after indwelling catheterization.Arch.Intern. Med, 1962;110: 703-711.
5. Brumfitt W, Davies BL, Rosser E. The urethralcatheter as a cause of urinary tract infection inpregnancy and peuperium. Lancet.1961; 2:1059-1061.
6. Kunin CM. Detection, prevention andmanagement of urinary tract infections. 4thed.Lea and Febiger, Philadelphia, 1987;245-298.
7. Turck M, Goffe B, Petersdorf RG. The urethralcatheters and urinary tract infection.J. Urol, 1962;88: 834-837.
8. Kunin CM, McCormack RC. Preventionofcatheter-induced urinary tract infection by Sterileclosed drainage. N. Engl. J. Med, 1966; 274:1155-1162.
9. Garibaldi RA, Burke JP, Dickman ML, Smith CB.Factors predisposing to bacteriuria duringindwelling urethral catheterization. N. Engl. J.Med., 1974;291: 215-218.
10. Kass EH. Asymptomatic infection of the urinarytract.Trans. Assoc. Am. Physicians, 1956;69:56-63.
11. McLeod JW. The hospital urine bottle and bedpanas reservoir of infection by Pseudomonas. Lancet,1958;1: 394-395.
12. Barrow GI, Feltham RKA. Cowan and SteelManual for the Identification of MedicalBacteria.Third edition. Cambridge UniversityPress,London, 1993;23-26.
13. Bauer AW, Kirby WMM, Sherris JC, Turck M.Antibiotic susceptibility testing by a standardizedsingle disk method. Am. J. Clin. Pathol, 1966;.45:493-496.
14. Clinical and Laboratory StandardsInstitute.Performance standards for antimicrobialsusceptibility testing; Seventeenth informationalsupplement. CLSI document M100-S17.CLSI,2007; 27 (1):22-79.
15. TaiwoSS, Aderounmu AOA. Catheter AssociatedUrinary Tract Infection: Aetiologic Agents andAntimicrobial Susceptibility Pattern in LadokeAkintola University Teaching Hospital, Osogbo,Nigeria.African Journal of Biomedical Research,2006; 9:141–148.
16. Edmond MB, Wenzel RP .Organization forinfection control: Mandell GL Bennett JE, DolinR. Principles and Practice of Infectious Diseases.5thed Philadelphia: Churchill Livingstone,2000;2988-91.
17. Khurana CM, WojackBR .Prevalence ofciprofloxacin resistance in multi resistant gramnegative intensive care unit isolates. Infection,1994;22(Suppl 2):99-104.
18. Snydman DR .Clinical implications of multi-drugresistance in the intensive care unit.Scand J infectDis., 1991;78:54-63.
19. Sanjeev Dimri Sims--83-86.pmd 10/10/2013, 9:22 AM86

International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 87
To Study the Etiology and Various Treatment Modalitiesof Liver Abscess
Shah Naveed1, Hasina Quari2, Asma Altaf 3, Maha Para4, Tanveer Banday5, V B Gupta6
1Post Graduate Scholar Department of Surgery, ASCOMS & Hospitals, Sidhra, Jammu, Jammu & Kashmir, India,2Medical officer Department of Health Services, Jammu & Kashmir, India, 3Resident Department of Dental Surgery,
ITS College & Hospitals, Gaziabad U.P., 4Resident Department of Dental Surgery, GMC & Hospitals, Srinagar Jammu& Kashmir, India, 5Post Graduate Scholar Department of Medicine, 6Professor, Department of Surgery, ASCOMS &
Hospitals, Sidhra, Jammu, Jammu & Kashmir, India
ABSTRACT
Objective : "To study the etiology and various treatment modalities of liver abscess" a prospectivestudy over a period of one year from November 2011 to October 2012 in the department of Generalsurgery in Acharya Shri Chander College of Medical Sciences and Hospital Sidhra, Jammu.
(1) To study the etiology of liver abscess whether pyogenic or amoebic.
(2) How many were treated conservatively and how many needed intervention either aspiration orpig tail catheter drainage or open surgical drainage.
Mateial and Method: The patients of this study were admitted from the emergency wing, indoorand outdoor department of surgery and medicine over a period of one year from November 2011 toOctober 2012 in the department of General surgery in Acharya Shri Chander College of MedicalSciences and Hospital Sidhra, Jammu.
Patients of all age groups and either gender who presented with clinical suspicion of liver abscess oralready diagnosed were included in the study.
Results:
(1) Majority of the patients in our study had amoebic liver abscess (73.33%).
(2) E.coli and Klebsella were the most common organisms cultured from the pyogenic abscess.
(3) Majority of amoebic liver abscess patients were treated with drug therapy alone whereas allpyogenic liver abscesses required some form of drainage.
Keywords: Abscess, Liver, Amebic, Pyogenic, Tubercular
INTRODUCTION
Hippocrates is credited with the first descriptionof a hepatic abscess in the year 4000 BC. Hepaticabscesses are classified as those of bacterial origin andthose caused by Entamoeba-histolytica.
Modern times have seen a major shift in etiologyof pyogenic abscesses in the liver[1]. Liver abscessesnow rarely occur in young people secondary toappendicitis. They usually occur in older, moredebilitated patients, often in the setting of malignancy.
The incidence of pyogenic liver abscess is on the rise.At present the most common source of a pyogenic liverabscess is biliary tract obstruction [2]. The majority oflarge series published over the past 20 years citedbiliary disorders as the most common identifiablesource of the hepatic abscesses[2,3,4,5]. Although thereare no definitive studies, host factors that can weakenthe immune system are thought to predispose to liverabscess formation especially mycobacterial and fungal(e.g. cirrhosis, diabetes, or malignancy)[6].
DOI Number: 10.5958/j.2321-1024.1.2.037
20. Shah Naveed --87-92.pmd 10/10/2013, 9:22 AM87

88 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
In general, portal, traumatic, and cryptogenichepatic abscesses are solitary and large, while biliaryand arterial abscesses are multiple and small [4].
Diabetes has been cited in numerous studies fromacross the globe as a possible predisposing factor [7].
Amebiasis is a relatively common parasiticinfection caused by the protozoan E. histolytica withthe highest incidence in tropical and subtropicalclimates in Mexico, India, East and South Africa, andportions of Central and South America [8].
Cryptogenic abscesses, those of unknown etiology,occur in 10–45% of patients, depending on theaggressiveness of investigation used to define thesource [1].
Escherichia coli, Klebsiella species, enterococci, andPseudomonas species are the most common aerobicorganisms cultured in recent series [10,11], whereasBacteroides species, anaerobic streptococci, andFusobacterium species are the most commonanaerobes[12]. Klebsiella pneumonia is extremelyprevalent in liver abscesses in Asian countries as wellas in predominantly Asian population in the Westernworld for unclear reasons [13]. Mycobacteriumtuberculosis is a common infecting organism in theacquired immune deficiency syndrome [14].
Confirmation of pyogenic liver abscess involvesaspiration of the abscess as well as positive bloodcultures [13]. Amoebic serology is both a highly sensitiveand specific test in identifying patients with amebicinfection, thus aiding in differentiation betweenpyogenic and amebic hepatic abscess [15,16,17].
The practice of most authors is to reserve surgicalintervention for those patients failing less invasivemanagement, patients with complications of amebichepatic abscess, and those patients with large left sidedabscesses not amenable to catheter-based drainage thatare posing a risk of rupture into the pericardium [17].
MATERIAL AND METHOD
Study design : It is a hospital based prospectivestudy were the patients were admitted from theemergency wing, indoor and outdoor department ofsurgery and medicine over a period of one year fromNovember 2011 to October 2012 in the department ofGeneral surgery in Acharya Shri Chander College ofMedical Sciences and Hospital Sidhra, Jammu.
Inclusion Criteria
Patients of all age groups and either gender whopresented with clinical suspicion of liver abscess oralready diagnosed were included in the study.
Exclusion Criteria
All patients who refuse to give consent.
Total sample size was 30. The research wasapproved by ASCOMS ethical committee.
A detailed history of symptoms and detailedexamination was done. All necessary investigationswere done including amebic serology and USGabdomen. Culture and sensitivity of pus was done inthose patients in whom percutaneous aspiration orsurgical drainage of pus was done. Culture andsensitivity of blood in all patients.
Once the diagnosis of a single or multiple liverabscess was made, broad spectrum parenteralantibiotics were started. Routine haematological tests,liver function tests, amoebic serology to rule outamoebic abscess and blood culture (before onset ofantibiotic therapy were ever possible) were obtained.
A trail of antibiotics alone was given to patientswith multiple small abscesses, low risk of rupture andlack of toxaemia (i.e. is no hemodynamic instability,patient does not feel acutely ill). On getting the reportof amoebic serology, if it was negative we continuedwith parenteral antibiotics. After culture results andsensitivity profiles had been obtained, antibiotictherapy directed at the specific organism(s) wasadministered intravenously for at least two weeks andthen orally for up to six weeks. Lack of improvementafter a reasonable course (48 – 72hours) indicatedfailure of treatment. Worsening of fever, leucocytosis,and symptoms at any time also indicated failure oftreatment and would immediately qualify the patientfor a more aggressive treatment regimen in the formof percutaneous aspiration. As complete as possibledrainage of the abscess cavity was done on firstaspiration.
The aspirated pus was sent for culture andsensitivity. Response was measured by decrease infever and leucocytosis and symptomatic improvementand further aspiration will be done as and whenrequired.
Indications to proceed to percutaneous catheterdrainage was persistence of sepsis or worsening of
20. Shah Naveed --87-92.pmd 10/10/2013, 9:22 AM88

International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 89
clinical features, or failure to improve after a reasonabletime period or for whom aspiration fails or thickabscess contents.
Contraindications to percutaneous catheterdrainage included coagulopathy, the lack of a safe orappropriate access route (transpleural drainage) ,multiple macroscopic abscesses , ascites.
Operative drainage of pyogenic hepatic abscesswas indicated for the following patients, patients whorequire laparotomy for underlying problem, those inwhom percutaneous catheter drainage fails, patientswith contraindications to percutaneous drainage (inleft lobe of liver) , patients whose liver abscessesrupture into peritoneum and thoracic cavity.
If serology came out to be positive for amoeba thenmetronidazole remained the drug of choice as it ishighly effective, is inexpensive, and has the advantageof being effective for intestinal as well as extraintestinalamoebiasis. The dose regimen is 750mg three timesdaily for 10 days.
Percutaneous aspiration of amoebic abscesses isunnecessary unless bacterial suprainfection issuspected, a pyogenic liver abscess is suspected, theabscess is large (>5cm in diameter) and leftsided(segments 2 and 3) i.e concern of impendingrupture , persistance of symptoms beyond 48 to 72hrsor clinical deterioration with medical management.
Laparotomy is indicated for ruptured amoebicabscesses.
OBSERVATION
Table 1: Distribution of different Types of LiverAbscess (n=30)
Types of liver abscess No. of patients %age
Amebic liver abscess 22 73.33
Pyogenic liver abscess 7 23.33
Tubercular liver abscess 1 3.33
Table 2: Showing Organisms Cultured From Pus OfPyogenic Liver Abscess
Organism grown No. of patients n=7 Percentage
E.coli 4 66.66
Klebsiella 2 28.57
Table 3: Showing Results of Blood Culture of Patientsin our Study (n=30)
Culture Amebic Pyogenic Tubercularliver abscess liver abscess liver abscess
(n=22) (n=7) (n=1)No. %age No. %age No. %age
Positive culture 0(0) 3(42.85) 0(0%)
Table 4: Showing Organisms Cultured from Blood ofPyogenic Liver Abscess
Organism grown No. of patients n=7 Percentage
E.coli 2 66.66
Klebsiella 1 33.33
Table 5: Showing Various Modalities of ManagementUsed in Patients of our Study (N=30)
Treatment Amebic Pyogenic TubercularModality liver abscess liver abscess liver abscess
(n=22) (n=7) (n=1)No. %age No. %age No. %age
I.V. Drug 19(86.36) 0(0) 0(0)therapy only
Percutaneous 3(13.63) 5(71.42) 1(100)aspiration
Catheter drainage 0(0) 0(0) 0(0)
Open surgical 0(0) 2(28.57) 0(0)drainage
DISCUSSION
In our study, amoebiasis was the most predominantcause as 22(73.33%) of thirty cases belonged to thisgroup. Walsh JA: (1986) had found highest incidencesof amoebic liver abscess in Mexico, India, East andSouth Africa, and portions of Central and SouthAmerica. Incidence is increased in areas with higherpoverty levels, presumably a direct reflection of poorsanitation, public health, and hygiene [8]. In a studyconducted by Barnes PF, et al (1987) in Los AngelesCounty Hospital, 96 of 144 cases of liver abscesses wereamoebic [18].
19 cases (86.36%) of 22 amoebic liver abscesspatients were managed with antibiotics alone, with3(13.63%) patients requiring percutaneous drainagewhen they failed to respond to antibiotics for 72hours.These results match with those of McGarr PL, et al:(2003) a prospective study were 150 of 178 patientswere managed successfully with drug therapy alone,with those demonstrating clinical deterioration or noimprovement after 48 to 72 hours then receiving
20. Shah Naveed --87-92.pmd 10/10/2013, 9:22 AM89

90 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
percutaneous ultrasound-guided aspiration [19]. Thuswe conclude that conservative medical managementof uncomplicated amoebic liver abscesses is safe, withpatients who fail to respond medical therapy shouldbe considered for ultrasound guided percutaneousaspiration.
In bacterial culture Escherichia coli and kliebsellawere the most common organisms grown from thedrained abscess. This is in accordance to the studiesconducted by Rahimian J, et al (2004) andJohannsen EC, et al (2000) who also reportedEscherichia coli and Klebsiella to be the most commonorganism cultured [20,3].
In our study blood culture was positive in 3 patients(42.85%) of pyogenic liver abscess. This is inaccordance with the study conducted byChemaly, RF et al: (2003) who reported 50% of bloodcultures to be positive in pyogenic abscesses [13]. Thisdiscrepancy in blood culture with abscess culture isattributed to prior antibiotic use affecting organismrecovery from the blood. We advocate antibioticcoverage for common pathogens even in situationswhen these organisms are absent from blood culturedata, especially when abscess culture information isawaited.
In our study 5 of 7 patients (71.42%) of pyogenicliver abscesses required percutaneous aspiration outof which 4 were cured and 1 died of septicemia. A studyconducted by Giorgio A, et al: (1995) showed cure(normalization of clinical, laboratory, and imagingparameters) was achieved in 113 patients (98.3%) ofpyogenic liver abscess with percutaneous ultrasoundguided drainage of the abscess [21].
Surgery still plays a vital role in the comprehensivetreatment of hepatic abscesses. This is illustrated in aseries from Bertel CK, et al (1986) in which 61% ofpatients with hepatic abscesses required an additionalprocedure at time of operation to treat the causativecondition [22]. In our study 2 patients of pyogenic liverabscess who required surgical drainage hadunderlying hepatic hydatid cyst which had becomesecondarily infected. The diagnoses of hydatid cystwas hinted in the CT scan of the patient and confirmedintraoperatively and on histopathological report. Asthe contents of the abscess cavity appeared to be thickon the CT scan and as there was a strong possibility ofhydatid cyst getting infected we directly proceeded toopen surgical drainage in both these patients. Thesuper-infection probably occurs from sites next to the
hydatid cyst (e.g., biliary) or as a complication ofbacteremia of any cause. Chen YC, et al (2002) statedthat bacterial and fungal infections have beendescribed in hydatid cyst in case reports or in smallseries with a limited number of patients[23].
Essop AR, et al (1983) reported that the prevalenceof tubercular liver abscess was just 0.34% in patientswith hepatic tuberculosis [24]. In our study we had asingle patient (3.33%) of tubercular liver abscess whowas a female of 60years. She presented to us with fever,abdominal pain and significant weight loss. Onultrasound examination a single abscess was found inthe right lobe of the liver. 100 ml of pus was aspiratedunder ultrasound guidance and was sent formicrobiological investigations. Gram stain, stains foracid fast bacillus and fungus were negative. . In ourstudy diagnosis of tubercular liver abscess was madeonly by P.C.R detected in the abscess aspirated underultrasound guidance.
Four first line systemic anti-tubercular drugs(isoniazid, rifampicin, pyrazinamide and ethambutol)were started. Percutaneous aspiration of pus was donethree times. A routine bacteriological culture wassterile. Despite all these measures she died due toresistance to anti tubercular drug therapy.
A study conducted by Diaz ML et al: (1996) showedthat at least 57% of tuberculous hepatic granulomasgave positive PCR results compared to otherconventional diagnostic techniques for TB [25].
RESULTS
• Majority of the patients in our study had amoebicliver abscess (73.33%).
• E.coli and Klebsella were the most commonorganisms cultured from the pyogenic abscess.
• Pus culture was positive in 6 cases (85.71%) ofpyogenic abscess.
• E.coli was grown in 4 cases (66.66%) and Klebsiellawas grown in 2 cases (28.57%) of pus culturesfrom pyogenic abscess.
• Blood culture was positive in 3 cases (42.85%) ofpyogenic abscess while in amebic abscess it wasnegative in all cases.
• E.coli was grown in 2 cases (66.66%) of pyogenicabscess and klebsiella was grown in 1 case (33.33)of pyogenic abscess.
20. Shah Naveed --87-92.pmd 10/10/2013, 9:22 AM90

International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 91
• 19 cases (86.36%) of amoebic abscesses weretreated with i.v. drug therapy alone. 3 cases(13.63%) of amoebic abscesses requiredpercutaneous aspiration.
• 5 cases (71.42) of pyogenic abscesses requiredpercutaneous aspiration and 2 cases (28.57%) ofpyogenic abscesses required open surgicaldrainage as both these cases were secondary liverabscesses.
• Majority of amoebic liver abscess patients weretreated with drug therapy alone whereas allpyogenic liver abscesses required some form ofdrainage.
• Tuberculosis should be considered in thedifferential diagnosis of hepatic mass lesions,especially in the presence of immune-compromised states. Ruling out tuberculosis mayavoid delay in initiation of specific therapy. Agreater awareness of this rare clinical entity mayprevent needless surgical interventions and hencethe role of P.C.R. in the aspirated pus for thediagnosis of tuberculosis.
ACKNOWLEDGEMENT
I would like to pay my regards and express mysincere gratitude to all my teachers, viz, Dr.S.R.Anand,Dr.R.K.Chrungoo and others for their teaching,guidance and encouragement. I am highly grateful fortheir constant help and advice whenever sought for.
Conflict of Interest: ”The authors declare no conflictof interest whatsoever arising out of the publicationof this manuscript.”
Source of Funding: Self
Ethical Clearance: This study was approved by theEthical Review Committee of ASCOMS Hospital andMedical College Jammu.
REFERENCES
1. Branum GD, Tyson GS, Branum MA et al. Hepaticabscess: Changes in etiology, diagnosis andmanagement. Ann Surg 1990;212:655-662 .
2. Mohsen AH, Green ST, Read RC, et al: Liverabscess in adults: Ten years' experience in a UKcentre. Q J Med 2002; 95:797-802.
3. Johannsen EC, Sifri CD, Madoff LC: Pyogenicliver abscesses. Infect Dis Clin North Am 2000;14:547-563.
4. Chou FF, Sheen-Chen SM, Chen YS, et al: Singleand multiple pyogenic liver abscesses: Clinicalcourse, etiology, and results of treatment. WorldJ Surg 1997; 21:384-388.discussion 388-389.
5. Chu KM, Fan ST, Lai ECS et al. Pyogenic liverabscess: An audit of experience over the pastdecade. Arch Surg 1996;131:148-152 [PubMed:8611070].
6. Civardi G, Filice C, Caremani M et al. Hepaticabscesses in immunocompromised patients:Ultrasonically guided percutaneous drainage.GastrointestRadiol 1992;175:17-23.
7. Alvarez Perez JA, Gonzalez JJ, Baldonedo RF, etal: Clinical course, treatment, and multivariateanalysis of risk factors for pyogenic liver abscess.Am J Surg 2001; 181:177-186.
8. Walsh JA: Problems in recognition and diagnosisof amebiasis: Estimation of the global magnitudeof morbidity and mortality. Rev Infect Dis 1986;8:228-238.
9. Ochsner A. Pyogenic abscess of the liver. Am JSurg 1938;40:292.
10. Wong WM, Wong BC, Hui CK, et al: Pyogenicliver abscess: Retrospective analysis of 80 casesover a 10-year period. J GastroenterolHepatol2002; 17:1001-1007.
11. Seeto RK, Rocky DC. Pyogenic liver abscess:Changes in etiology, management, and outcome.Medicine1996;75:99-113.
12. Sabbaj J, Sutter VL, Finegold SM: Anaerobicpyogenic liver abscess. Ann Intern Med 1972;77:627-638.
13. Chemaly RF, Hall GS , Keys TF , et al.Microbiology of liver abscesses and the predictivevalue of abscess gram stain and associated bloodcultures. DiagnMicrobiol Infect Dis 2003; 46:245-248.
14. Bangaroo AK, Malhotra AS: Isolated hepatictuberculosis.J IndAssocPaediatrSurg 2005,10(2):105-107.
15. Conter RL, Pitt HA, Tompkins RK, et al:Differentiation of pyogenic from amebic hepaticabscesses. SurgGynecolObstet 1986; 162:114-120.
16. Lodhi S, Sarwari AR, Muzammil M, et al: Featuresdistinguishing amoebic from pyogenic liverabscess: A review of 577 adult cases. Trop MedInt Health 2004; 9:718-723.
17. Petri WA Jr, Singh U. Diagnosis and managementof amebiasis. Clin Infect Dis1999;29:1117-1125.
18. Barnes PF, De Cock KM, Reynolds TN, et al: Acomparison of amebic and pyogenic abscess ofthe liver. Medicine (Baltimore) 1987; 66:472-483.
20. Shah Naveed --87-92.pmd 10/10/2013, 9:22 AM91

92 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
19. McGarr PL, Madiba TE, Thomson SR, et al:Amoebic liver abscess: Results of a conservativemanagement policy. S Afr Med J 2003; 93:132-136.
20. Rahimian J, Wilson T, Oram V, et al: Pyogenic liverabscess: Recent trends in etiology and mortality.Clin Infect Dis 2004; 39:1654-1659.
21. Giorgio A, Tarantino L, Mariniello N et al.Pyogenic liver abscess: 13 years of experience inpercutaneous needle aspiration with U/Sguidance. Radiology 1995;195:122-124.
22. Bertel CK, van Heerden JA, Sheedy II PF:Treatment of pyogenic hepatic abscesses: Surgical
versus percutaneous drainage.Arch Surg 1986;121:554-558.
23. Chen YC, Yeh TS, Tseng J, et al.. Hepatic hydatidcysts with super-infection in a non-endemic areain Taiwan. Am J Trop Med Hyg. 2002;67:524-527.
24. Essop AR, Segal I, Posen J, et al:: Tuberculousabscess of the liver. S Afr Med J 1983, 63:825-826.
25. Diaz ML, Herrera T, Lopez-Vidal Y, etal:Polymerase chain reaction for the detection ofMycobacterium tuberculosis DNA in tissue andassessment of its utility in the diagnosis of hepaticgranulomas.J Lab Clin Med 1996, 127:359-363.
20. Shah Naveed --87-92.pmd 10/10/2013, 9:22 AM92

International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 93
Anatomical Variation in Inferior Vena Cava- A CaseReport and Review
Shalini Chaudhary1, Sarvesh2
1Assistant Professor, Department of Anatomy, 2Senior Resident, Department of Anaesthesia, B.P.S. Govt. MedicalCollege for women ,Khanpur kalan,Sonepat , Haryana
ABSTRACT
We highlight the case of a double Inferior Vena Cava (IVC) encountered in a routine dissection of a46 year old male cadaver. We outline gross anatomical details , summarize the embryologicaldevelopment of IVC and present the case as a reminder of this rare anatomical variation, as in suchcases ,pre-operative abdominal cross sectional imaging kis usually not available ;hence the operatingsurgeon needs to rely on vigilance and awareness of other potential anatomical variations that areassociated with the condition.
INTRODUCTION
The IVC is formed by the union of right and leftcommon iliac vein on the right anterior surface of fifthlumbar vertebra and conveys the venous blood tothe right atrium from all parts of the body below thediaphragm1.
The two common iliac veins failed to unite at thelevel of the aortic bifurcaktion. The two venae cavaeascend on both sides of the aorta. The left inferior venacava drains into the left renal vein. The left renal veincrosses anterior to the aorta to form the normal rightprerenal inferior vena cava. The prevalence of thisanomaly is 0.2%–3% 2 This arrangement of the left renalvein crossing anterior to thke inferior vena cava to formnormal right prerenal inferior vena cava is thecommonest arrangement in the duplication of inferiorvena cava 2
The embryogenesis of the inferior vena cava is acomplicated process involving development ,regression , anastomosis and replacement of threepairs of venous channels posterior cardinal ,subcardinal , and supracardinal .this complexity ofembryogenesis of the I.V.C. which accounts for thegreat diversity in its anomalies.
The majority of cases are clinically silent and arediagnosed incidentally by imaging (includingcomputed tomography [CT] and magnetic resonance[MR] imaging) done for other reasons. However, thesevenous anomalies may have significant clinicalimplications, especially during retroperitoneal surgeryor in the treatment of thromboembolic diseases.
CASE REPORT
A double inferior vena cava (I.V.C.) was observedduring routine dissection of the posterior abdominalwall in a middle aged cadaver. Both sided externaland internal iliac veins joined to form common iliacveins in a usual manner. These common iliac veinsjoined to form I.V.C. at the level of fifth lumbarvertebra. The right I.V.C. was normal in position withits normal course and tributaries. The abdominal partof right was 21 cm. in length and 1.4 cm. in dkikameter.The left I.V.C. began at the site of the formation of leftcommon iliac vein (fig. 1) . It was having 0.9 ckm.diakmeter and a length of 11 cm. Left I.V.C. receivedleft testicular vein aknd then opkened in to left renalvein. The left renal vein received its normal tributariesand then crossed kthe body of second lumbar vertebrato open in to right I.V.C. in front of the aorta.
DOI Number: 10.5958/j.2321-1024.1.2.038
21. Shalini --93-95.pmd 10/10/2013, 9:22 AM93

94 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
DISCUSSION
Embryogenesis of IVC is a complex processinvolving the development, regression, anastomosisand replacement of three pairs of embryonic veins(posterior cardinal, subcardinal and supracardinalveins). This process begins at the sixth week ofgestation and is completed by the tenth week. Theposterior cardinal veins appear first on the posterioraspect of the embryo. These veins regress, except forthe distal aspects which become the iliac bifurcation.The subcardinal veins then appear anterior and medialto the posterior cardinal veins. The right subcardinalvein remains to form the suprarenal IVC, while theleft subcardinal vein completely regresses.
Subsequently, the supracardinal veins appeardorsally to the subcardinal veins. The leftsupracardinal vein then regresses, and the rightsupracardinal vein forms the infrarenal IVC 2, 3. Theanomalies of IVC arise from the failure of normalembryogenesis. The most commonly-describedanomalies of IVC include circumaortic left renal vein(1.5%–8.7%), azygous or hemiazygous continuation ofIVC (0.6%), retroaortic left renal vein (2.1%), doubleIVC (0.2%–3%) and isolated left-sided IVC (0.2%–0.5%) 2.
Double IVC results from the failure of regressionin embryogenesis 2,4 The most common pathogenesisis the failure of regression of the left supracardinal vein.
The duplicated left IVC usually drains into the leftrenal vein, which then crosses anterior to the aorta andjoins the right IVC in a normal fashion.
It is speculated that the two inferior venae cavaeare derived from the right supracardinal andsubcardinal veins 3 . The majority of cases of doubleIVC are diagnosed incidentally by imaging for otherreasons, but these anomalies can have significantclinical implications. Radiologically, the presence ofdouble IVC can be mistaken as a pathological lesionsuch as lymphadenopathy, 5, 6. or left pyelouretericdilatation 7.
There are case reports describing patients whounderwent exploration for presumed metastatictesticular carcinoma based on the CT appearance ofthe anomaly 5, 8 . The presence of double IVC may alsocomplicate retroperitoneal surgery.9, 10 .
The double IVC can be inadvertently injured orligated during retroperitoneal surgery.Therefore, it isimportant to identify such anomalies preoperatively,There are several case reports of thromboembolicevents occurring in patients double IVC.11,12 . Thereappears to be an increased incidence of thrombosisformation in double IVC, but the exact cause isunknown.
In conclusion, double IVC is a rare congenitalanomaly. The majority of cases are diagnosedincidentally on imaging for other reasons. However,these venous anomalies should be recognised, as theycan have significant clinical implications, especiallyduring retroperitoneal surgery or in the treatment ofthromboembolic diseases
Acknowledgement: nil
Source of Funding: self
Conflict of Interest: nil
Ethical Clearance: from ethical committee of D.Y.Patilmedical college ,kolhapur
REFERENCES
1. Rosse C, Rosse PG. 1977. Hollinshead’s Text BookOf Anatomy . 5TH ED. Philadelphia: Lippincotts-Raven. P602.
2. Bass JE, Redwine MD, Kramer LA, Huynh PT,Harris JH. Spectrum of congenital anomalies ofthe inferior vena cava: cross sectional imagingfindings. Radiographics. 2000;20:639–652.
Fig.1. Duplicated left abdominal vena cava
21. Shalini --93-95.pmd 10/10/2013, 9:22 AM94

International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 95
3. Nagashima T, Lee J, Andoh K, et al. Right doubleinferior vena cava: report of 5 cases and literaturereview. J Comput Assist Tomogr 2006; 30:642-5.
4. Xue HG, Yang CY, Asakawa M, Tanuma K,Ozawa H. Duplication Of the inferior vena cavaassociated with othervariations. Anat Sci Int 2007; 82:121-5.
5. Klimberg I, Wajsman Z. Duplicated inferior venacava simulating retroperitoneallymphadenopathy in a patient with embryonalcell carcinoma of the testicle. J Urol 1986; 136:678-679.
6. Faer MJ, Lynch RD, Evans HO, Chin FK. Inferiorvena cava duplication: demonstration bycomputed tomography. Radiology 1979; 130:707-
7. Gay SB, Armistead JP, Weber ME, Williamson BR.Left infrarenal region: anatomic variants,pathologic conditions, and diagnostic pitfalls.Radiographics 1991; 11:549-70.
8. Cohen SI, Hochsztein P, Cambio J, Sussett J.Duplicated inferior vena cava misinterpreted by
computerized tomography as metastaticretroperitoneal testicular tumor. J Urol 1982;128:389-91. k
9. Radermecker MA, Van Damme H, Kerzmann A,Creemers E, Limet R. Association of abdominalaortic aneurysm, horseshoe kidneys, and left-sided inferior vena cava : report of two cases.JVasc Surg 2008; 47:645-8.
10. Shingleton WB, Hutton M, Resnick MI.Duplication of inferior vana cava: its importancein retroperitoneal surgery. Urology 1994; 43:113-115
11. Kouroukis C, Leclerc JR. Pulmonary embolismwith duplicated inferior vena cava . Chest 1996;109:1111-1113.
12. Sartori MT, Zampieri P, Andres AL, et al. Doubleinferior vena cava filter insertion in congenitalduplicated inferior vena cava : a case report andliterature review. Haematologica 2006; 91 (6Suppl):ECR30.
21. Shalini --93-95.pmd 10/10/2013, 9:22 AM95

96 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
A Comparative Study of the Anti-inflammatory effect ofTopical 1% Prednisolone and Topical 0.1% DexamethasoneEye Drops after Cataract Surgery in Western Uttar Pradesh
Suman Bhartiya1,Sunita Singh2, Sudeep Sabbithi3
1Assistant Professor, Department of Ophthalmology, 2Associate Professor, 3Demonstrator, Department ofPharmacology, Saraswathi Institute of Medical Sciences, Hapur, Ghaziabad, U.P., India
ABSTRACT
Purpose: The aim of this study is to compare the anti-inflammatory efficacy of topical 1% prednisoloneacetate and topical 0.1% dexamethasone sodium eye drops after uneventful small incision cataractsurgery with posterior chamber intraocular lens implantation in patients of Western Uttar Pradesh.
Method: This study was done at Saraswathi Institute of Medical Sciences (SIMS) Hapur. Data wascollected from Ophthalmic OPD from October 2012 to March2013.72 patients who underwentuneventful small incision cataract surgery with posterior chamber intraocular lens implantation weretaken for both study groups. The baseline parameters were same for both groups of patients. All thepatients were followed up post operatively on day 1, day 3, 1 week, 2 week, 4 week and 6 weeks andpost inflammatory response was graded according to severity. The anti-inflammatory efficacy of twostudy groups was compared by examination of operated eyes for anti-inflammatory response andvisual acuity.
Results: All results were correlated with final visual outcome, which showed that topical prednisoloneacetate is clinically and statistically more effective than dexamethasone sodium in early post operativeperiod to control the inflammation in uneventful small incision cataract surgery with posterior chamberintraocular lens implantation.
Conclusion: This study conclude that topical 1% Prednisolone acetate is more effective than topical0.1% Dexamethasone sodium eye drops in controlling postoperative inflammation and early visualrehabilitation after uneventful small incision cataract surgery with posterior chamber intraocularlens implantation.
Keywords: Prednisolone Acetate, Dexamethasone Sodium, Posterior Chamber Intraocular Lens Implantation,Visual Acuity
INTRODUCTION
The final visual outcome of cataract surgerypatients depends on various preoperative,peroperative and postoperative factors, out of whichpostoperative inflammation is the most importantfactor especially in early postoperative period. Thispostoperative inflammation occurs due to variousintraocular manipulations as irrigation of anteriorchamber, injection of viscoelastic agent, handling ofiris, intraocular lens implantation etc. as described byRoper Hall MJ et al1. All these intraocular manipulationleads to breakdown of blood aqueous barrier, leading
to release of various chemical mediators ofinflammation as prostaglandins, prostacyclins,leukotrienes, cytokines etc. and exudation of proteinsinto anterior chamber. The most important action ofsteroids is to inhibit the phospholipase A2 enzyme,which is the rate-limiting step for synthesis ofprostaglandins and other chemical mediators ofinflammation. They have many effects on theinflammatory and immune responses. Recent studiesstates that steroids act as immunosuppressive agent2,3.
In this study we compared the efficacy of topical1% Prednisolone acetate and topical 0.1%
DOI Number: 10.5958/j.2321-1024.1.2.039
22. Sunita Singh--96--99.pmd 10/10/2013, 9:22 AM96

International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 97
Dexamethasone sodium eye drops in controlling thepostoperative inflammation following uneventfulsmall incision cataract surgery with posterior chamberintraocular lens implantation4. This study wasconducted in a tertiary level hospital on 72 patientswho underwent uneventful small incision cataractsurgery with posterior chamber intraocular lensimplantation.
MATERIAL AND METHOD
72 patients who underwent uneventful smallincision cataract surgery with posterior chamberintraocular lens implantation from October 2012 toMarch 2013 were included for this study after obtaininginformed consent. Inclusion criteria for this study wereuncomplicated, small incision cataract surgery withposterior chamber intraocular lens implantation, noprevious ocular surgery, uncomplicated cataract,nontraumatic eye, nonallergic eye. Exclusion criteriawere patients suffering from bleeding disorders or onanticoagulant therapy, systemic diseases ashypertension, diabetes mellitus, bronchial asthma,ischemic heart disease, immunological disorders, andconnective tissue disorders. Preoperative workup ofall patients was done by testing visual acuity,measurement of intraocular pressure, syringing anddetailed slit lamp examination. Patients wererandomly taken and categorized into two groups,
Group A and Group B.1% Prednisolone acetate wasadministered to Group A (36 patients) and 0.1%Dexamethasone sodium was administered to GroupB (36 patients). Postoperative medication wasadministered 6 times a day for a week, 4 times a dayfor next week, 3times a day for next 2weeks and thentwice a week for rest of the period. Follow up was donefor 6 weeks as Day 1, Day3, Day 7, and at 2ndweek,4thweek and 6thweek. Grading of postoperativeinflammation was done according to followingobservations: lid oedema, circumcorneal congestion,corneal oedema, anterior chamber cells and flare5.Analgesia was subjectively estimated according tocomplaint of patient as pain and discomfort.
RESULTS
Pain, lid oedema and ciliary congestion were seenin most of the cases on early post operative day. Onday 7 follow up 15(41.67%) patients of Group A and17 (47.22%) patients of Group B had mild to moderatedegree of pain. At 2 weeks follow up 8 (22.22%)patients of Group A and 10 (27.78%) patients of GroupB and on 4thweek follow up 5(13.89%) patient of GroupA and 6 (16.67%) patients of Group B had pain butpain was very mild in severity. On final follow up i.e.6 weeks 3 (8.33%) patients of Group A and 4 (11.11%)patients of Group B had pain.
Table 1. Incidence of postoperative pain
Categories Post operative days
Day1 Day3 Day7 2Wks 4Wks 6Wks
Prednisolone1% 33(91.67%) 32(88.89%) 15(41.67%) 8(22.22%) 5(13.89%) 3(8.33%)
Dexamethasone0.1% 34(94.44%) 33(91.67%) 17(47.22%) 10(27.78%) 6(16.67%) 4(11.11%)
Almost all patients of Group A and Group B hadciliary congestion on early postoperative days, whichwas reduced to 6(16.67%) patient on day 7 in GroupA whereas it was exist in 13(36.11%) patients inGroup B on day 7. This congestion was further
reduced to 4(11.11%) patients and 1(2.78%) patientin Group A and 6(16.67%) patients and2(5.56%)patient in Group B on 2 week and 4 week follow up.No patient of both Groups had congestion on 6 week.
Table 2.Ciliary congestion
Categories Post operative days
Day1 Day3 Day7 2Wks 4Wks 6Wks
Prednisolone1% 35(97.22%) 33(91.67%) 6(16.67%) 4(11.11%) 1(2.78%) 0(0%)
Dexamethasone0.1% 36(100%) 36(100%) 13(36.11%) 6(16.67%) 2(5.56%) 0(0%)
Corneal oedema was seen in 18(50%) patients and28(77.78%) patients of Group A and Group Brespectively on early days which were reduced to5(13.89%) patients of Group A and 11(30.56%) patients
of Group B on day 7 follow up. Corneal oedema wasless in Group A. No oedema was seen in both Groupson 6-week follow up. On Slit Lamp Examination10(30.56%) patients of Group A and 14 (38.89%)
22. Sunita Singh--96--99.pmd 10/10/2013, 9:22 AM97

98 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
patients of Group B had anterior chamber reaction(flare and cells) during early postoperative period butthis number reduced to 2(5.56%) patients of Group Aand 5(3.89%) patients of Group B. This anteriorchamber reaction reduces on subsequent follow up andnone of the patient had this at the end of the study.
Visual acuity was tested on each visit. In Group Athe best visual acuity of 7(19.44%) patients was >18,20(55.56%) patients had between 6/60-6/18 and
9(25%) patients had visual acuity <6/60. In Group Bvisual acuity of 6(16.67%) patients was >18, 18 (50%)patients had visual acuity between 6/60-6/18 and 12(33.33%) patients had visual acuity <6/60 on firstpostoperative day. At the end of the follow up in GroupA the visual acuity of 29(80.56%) patients was>6/18and7 (19.44%) patients had between 6/60-6/18. InGroup B visual acuity of 22(61.11) patients was >18and 14 (38.89%) patients had between 6/60-6/18. Nopatient in both the Groups had visual acuity <6/60.
Table 3.Post operative visual acuity
Prednisolone 1%
Grade of visual acuity Day1 Day3 Day7 2Wks 4Wks 6Wks
>6/18 7(19.44%) 10(27.78%) 19(52.78%) 23(63.89%) 26(72.22%) 29(80.56%)
6/60-6/18 20(55.56%) 20(55.56%) 13(36.11%) 11(30.56%) 9(25%) 7(19.44%)
Total 27(75%) 30(83.33%) 32(88.89%) 34(94.44%) 35(97.22%) 36(100%)
<6/60 9(25%) 6(16.67%) 4(11.11%) 2(5.56%) 1(2.78%) 0(0%)
Table 4.Post operative visual acuity
Prednisolone 1%
Grade of visual acuity Day1 Day3 Day7 2Wks 4Wks 6Wks
>6/18 6(16.67%) 8(22.22%) 14(38.89%) 17(47.22%) 20(55.56%) 22(61.11%)
6/60-6/18 18(50%) 20(55.56%) 17(47.22%) 16 (44.44%)15(41.67%) 14(38.89%)
Total 24(66.67%) 28(77.78%) 31(86.11%) 33(91.67%) 35(97.22%) 36(100%)
<6/60 12(33.33%) 8(22.22%) 5(13.89%) 3(8.33%) 1(2.78%) 0(0%)
So this shows that topical 1% Prednisolone acetateis more effective clinically and statistically in earlypostoperative period than 0.1% Dexamethasonesodium to control inflammation in uneventful smallincision cataract surgery with posterior chamberintraocular lens implantation4.
DISCUSSION
Topical steroids are the most commonlyadministered steroids in the eye and following a singledrop, steroid is measurable in aqueous humor within15-30 minutes6,7,8. They are the main drugs that havebeen used so far for controlling postoperativeinflammation after intraocular surgery. Steroids act byinhibiting production of prostaglandins, leukotriensetc., which are critical in generating the inflammatoryresponse by different type of cells. Topical drugspenetrate the cornea across three barriers: cornealepithelium, which is lipophilic in nature, cornealstroma, which is hydrophilic in nature and cornealendothelium, which is again lipophilic in nature.Leopold IH et al9,10that lipophilic layer of the corneaprovide resistance to polar (water soluble) molecules,whereas stroma which is hydrophilic in nature has
resistance for lipid soluble molecules hence thesubstance which we used should be biphasic polarity.Leibowitz and Kupfermanet al11,studies withradiolabelled prednisolone and dexamethasone haveshown that acetate in the form of suspension canpenetrate through a normal, uninflammed cornea withan intact epithelium most easily and can attain themaximum concentration of 2336 microgram min/gmwithin 30 minutes of topical application in anteriorchamber12. Schoenwaldet al15 also showed inexperimental animals that prednisolone acetatesuspension reaches the higher corticosteroidconcentration in anterior chamber amongst the otherdrugs used. The bioavailability and effectiveness ofthe anti-inflammatory drugs were studied byLeibowitzet al12by using radiolabelledpolymorphonuclear leucocytes systemically beforethey invade the cornea. Studies of Leibowitz andKupferman et al12also showed that prednisoloneacetate was more effective agent in suppressinganterior chamber inflammation by using radiolabelledpolymorph nuclear leucocytes. Prednisolone acetateis the synthetic form with its prodrug as prednisone.It is 4 times more potent than cortisol and also hasmineral corticosteroid activity. The half life is 12 hours
22. Sunita Singh--96--99.pmd 10/10/2013, 9:22 AM98

International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 99
and is less toxic than Dexamethasone sodium with halflife of 36-72 hours. Leibowitz and Kupferman et al11,12studies in vivo showed that due to biphasic innature prednisolone attain its maximum concentrationof 2336 microgram min/gm within 30 minutes oftopical application in anterior chamber inuninflammed eye with an intact epithelium whichshowed that prednisolone acetate is more potent thanits sodium phosphate derivative, which attainconcentration of 968 microgram min/gm samecondition as it is available in solution form.Dexamethasone sodium 0.1% showed almost nopenetration through the cornea with intact epithelium.This study also showed that 1% Prednisolone acetateand 0.1% Dexamethasone sodium had similarconcentration in inflamed eyes or in eyes with erodedcornea. This showed that 1% Prednisolone acetate ismore potent than0.1% Dexamethasone sodium. Theseresults are similar to the study of Olejnik O et alandMcGhee CN et al13,14.
CONCLUSION
This study showed that topical 1% prednisoloneacetate is more effective than topical 0.1%dexamethasone sodium in controlling postoperativeinflammation and in early visual rehabilitation afteruneventful small incision cataract surgery withposterior chamber intraocular lens implantation inIndian patients. In spite of various adverse effects suchas increase in intraocular pressure, secondary infectionof topical steroids, prednisolone acetate 1% is moreeffective than 0.1% dexamethasone sodium for earlyvisual rehabilitation in uneventful cataract surgery.
Acknowledgement: I would like to thank the head ofdepartment, other colleagues & technical staff for theirkind support & cooperation.
Conflict of Interest: None.
Source of Funding: None.
Ethical Clearance: Obtained from the Ethical clearancecommittee.
REFERENCES
1. Roper Hall MJ: Stallard’s eye surgery. 7th edition:replica press Pvt. Ltd. Delhi. Butterworthinternational edition 1989; Pg. 286-329.
2. Black, P H. Central nervous system-immunesystem interactions: pyschoneuroendocrinologyof stress and its immune consequences.
Antimicrobial agents and chemotherapy 1994;38(1):1-6.
3. McMaster, P. Pancreatic transplantation. Britishmedical journal 1980;281(6253):1493.
4. Laurell, C-G Zettertrom, C. Effects ofdexamethasone, dicofenac, or placebo on theinflammatory response after cataract surgery. TheBritish Journal of Ophthalmology 2002;86(12):1380-1384.
5. Fong, Raymond Leitritz, Martin Siou-Mermet,RaphaeleErb, Tara. Loteprednoletabonate gel0.5% for postoperative pain and inflammationafter cataract surgery: results of a multicentertrail. Clinical Ophthalmology (Auckland, N.Z.)2012;6:1113-1124.
6. Watson D, Noble MJ, Dutton GN, Midgley JM,Healey TM. Penetration of topically applieddexamethasone alcohol into human aqueoushumor. Arch ophthalmol 1988 May;106(5):686-7.
7. McGhee CNJ, Noble, Watson DG, Dutton GN,Fern Al, Healey TM, et al. Penetration of topicallyapplied prednisolone sodium phosphate intohumans aqueous humour. Eye 1989; 3: 463-7.
8. Watson DG, McGhee CNJ, Midgley JM, DuttonGN, Noble MJ. Penetration of topically appliedbetamethasone sodium phosphate into humanaqueous humor. Eye1990; 4:603-6.
9. Lepold IH, kroman HS, Green H. Intraocularpenetration of prednisone and prednisone. TransAm AcadOphthalmolOtolaryngol 1955; 59:771-778.
10. Lepold IH, Sawyer JL, Green H. Intraocularpenetration of locally applied steroids. Archophthalmol 1955; 54; 916-21.
11. Leibowitz HM, Lass JH, Kupferman A:Quantitation of inflammation in the cornea. Archophthalmol 1974; 92: 427-30.
12. Leibowitz HM, Lass JH, Kupferman A: Anti-inflammatory effectiveness in the cornea oftopically administered prednisolone. InvestOphthalmol 1974; 13: 757-63.
13. Olejnik O, Weishecker CA. Ocular bioavailabilityof topical prednisolone preparations.ClinJrOphthalmol 1990;12(1): 2-11.
14. McGhee CN, Watsori DG, Midgley JM, Noble MJ,Dutton GN, Fern AI. Penetration of syntheticcorticosteroids into human aqueous humor. Eye1990; 4:526-30.
15. Schoenwald RD and Boltralik JJ. A bioavailabilityof comparison in rabbits of two steroidsformulated as high viscosity gels and referenceaqueous preparation. Invest ophthalmolvissci1979; 18:61-6.
22. Sunita Singh--96--99.pmd 10/10/2013, 9:22 AM99

100 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
Cytological Study of Cerebrospinal Fluid and Evaluationof its Role in the Diagnosis of Tubercular Meningitis
Uma Tayal1, Aparna2, Nishant3, Emma Chaudhary4
1Associate Prof. Pathology, 2Final Year MBBS Student, LLRM Meerut, 3Internee, PL Sharma Hospital Meerut,4Assistant Professor TB & Chest, Rama Medical College Hospital & Research Centre Ghaziabad,
ABSTRACT
Central nervous system involvement is the most common neurological complication in the course oftuberculosis. Lack of rapid and sensitive test delays the early diagnosis. Cytological study was carriedout in cerebrospinal fluid of patients which were clinically suspected patients of tubercular meningitis.Purpose of this study is to determine the cytomorphological patterns in cerebrospinal fluid whichwill help in making the diagnosis of tubercular meningitis by providing the additional supportiveevidence in clinically suspected cases. Technical aspect of this cytological study is rapid and simpletherefore it can be applied for early diagnosis of tubercular meningitis particularly in whichbacteriological methods did not demonstrate the presence of mycobacterium bacteria in cerebrospinalfluid.
Keywords: Cerebro Spinal Fluid, Tubercular Meningitis, Cytomorphologicalpatterns, MycobacteriumTuberculosis
INTRODUCTION
Tubercular meningitis still remains an importantcause of morbidity and mortality in India .Tuberculosiskills 5 lacks patients in India every year, out of which7-12%are with meningeal involvement [1] Due to lackof early and timely diagnosis and so delay in the startof effective treatment the fatality rate remains high.Even when it is not fatal the sequel are distressingand disabling4. Thus early and correct diagnosis isessential for a successful outcome in patients oftubercular meningitis. Any test which facilitates itscorrect and rapid diagnosis should be very valuable [3]
Available methods of diagnosis of tubercularmeningitis were evaluated [5] all of them were foundto have low sensitivity and specificity.
Diagnosis of tubercular meningitis cannot be madeor excluded solely on the basis of clinical findings.Variable natural history and accompanying clinicalfeatures of this disease hinder the diagnosis. Spinaltap is easy to perform and carries minimum risk. Ifmeningitis is suspected spinal tap must be performedand cerebrospinal fluid must be send for cytologicalexamination [2]
AIM
In view of lack of any sensitive, simple diagnosticmethod and considering the importance of earlydiagnosis, as the disease is curable in its earlier stages,present study was undertaken to overcome all theseshort comings and to ascertain whether there are anycellular constituents, peculiar to tubercular meningitiswhich are useful in making the diagnosis in cases oftubercular meningitis which were found persistentlynegative on bacteriological examination.
MATERIAL AND METHOD
Total 60 patients between the age group of 6 monthto 12 year attending Rama medical college Hospitaland Research CentreGhaziabadIndia during the periodof Dec 2010 -June 2012, were selected for study. Thesewere the clinically suspicious cases of tubercularmeningitis. Ten patients without any neurologicaldisorder, who had to be given spinal anesthesia, wereincluded as normally control.
Presence of first or more than one of the followingcriteria was adopted to label or suspect a case astubercular meningitis.
DOI Number: 10.5958/j.2321-1024.1.2.040
23. Uma tayal-100-103.pmd 10/10/2013, 9:22 AM100

International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 101
1. Bacteriological proof of mycobacteriumtuberculosis bacteria.
2. Clinical and radiological findings consistent withtuberculosis.
3. History of contact with T.B patients and a positivePPD.
In all the 60 patients, cerebrospinal fluid obtainedwas adequate and specific treatment not yetstarted. At least 5 smears were prepared in eachcase and were stained by-
• GIEMSA
• Papanicoloau
• Ziehl-Neelson staining for AFB
Hemorrhagicfluids were excluded from the study.In addition cerebrospinal fluid was subjected to grossexamination and culture by Lowen Stein Jensen Mediamethod.
OBSERVATIONS
GROSS--In all the control patients, the cerebrospinalfluid obtained was colorless, transparent and there wasno cobweb formation.
In the clinically suspected patients of tubercularmeningitis cerebrospinal fluid obtained was cloudyand there was presence of cob web formation in 76.5%of the cases.
In all the 10 control cases following features wereobtained
Table 1. Cytological Pattern In Normal [Control] C.s.f
Cytological findings Number of cases % of cases
Cellularity-scanty 100 100<5 cells/cumm
Increased Cellularity NIL 0
Mononuclear cells 100 100
Only Neutrophils NIL 0
Red Blood Cells NIL 0
Table2. Cytologicalpatternsof C.s.f. In TubercularMeningitis
Cytological findings Number of cases % of cases
Increased cellularity * 60 100
Predominantly or only 60 100mononuclear cells
Mixed cellularity 18 23.1
Red blood cells NIL 0
Only neutrophils NIL 0
*Total cell count 10-500 per cumm
Table 3. Z.N. Staining in tubercular Meningitis
Name of the fluid Positive Negative
Cerebrospinal Nil 60
Table 4. Culture for A.F.B
Name of the fluid Positive Negative
Cerebrospinal 01 59
Table 1 shows that normal cytological features ofcerebro spinal fluid are presence of only mononuclearcells and Total count is less than 5cells/cumm.
Table 2 shows that there isincreased cellularity andpresence of mononuclear cells inall the cases[100%] oftubercular meningitis. Presence of mononuclearcellwas the predominant findingamongst differentialcell counting.Only neutrophils and presence ofeosinophil were not seen even in a single case. In ourstudy Few neutrophils, [<30% of the total cell count]were found in 23.1% of the cases. The type of cellresponse can have a prognostic effect .A higherpercentage of neutrophils was associated to highersurvival rates.13.It has been suggested that neutrophilsmay have a protective role against MycobacteriumTuberclebacilli. In patients with symptoms of durationless than 2 weeks there may be predominance ofpolymorph nuclear leucocytes14Eosinophil were absentin all the cases. This finding goes in hand with Richard2003; which states that if eosinophil are found insignificant number(>10%) one can exclude thediagnosis of tuberculosis.14
Table 3 shows that Z-N staining was negative inall the cases.[100% negativity]
Table 4 shows that Culture for A.F.B. was positiveonly in 1 case.[1.7% positivity]
Tubercular bacilli are isolated very rarelyincerebrospinal fluid because Mycobacterium bacillioccur in small number (1x 102 to 1x 104/ml) as the Phis more acidic due to presence of inflammatory cells10.
DISCUSSION
There is a considerable urgency in establishing thecorrect diagnosis of tubercular meningitis becausespecific therapy is most effective when started earlyincourse of the disease.Demonstration of tubercularbacilli by Z-N staining, culture and genomicamplification are various means to confirm thetubercular meningitis, but visualization of A.F.B.isusually difficult in cerebrospinal fluid.[9,11] and in themost cases resultsobtained arenegative.
23. Uma tayal-100-103.pmd 10/10/2013, 9:22 AM101

102 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
Irreversiblebrain damage may result while waiting forculture reportto confirm the diagnosis. Newer methodssuch as those involving bacterial genomicamplification P.C.R. and other comparable methodslike CobasAmplicortest, Abbott LCX test,and B-Dprobe test[strand displacement amplification]test arenot available for wide spread use I n developingcountries because of their high cost.12 Result ofchemical test including ADA[adenosine di aminase]and ELISA test found to be seldomconclusive.[CBNAAT] cartridge based nucleic acidamplification test, Gene Xpert at certain centers is beingdone but is recommended at present, only forpulmonary cases.
There is a need to design an alternative diagnosticmethod so that an effective therapeutic modality canbe instituted quickly. To meet the above objective werecommend a simple cytological studyofCerebrospinalfluid in patients of tubercular meningitis. Thefundamental principal of this assay is that thecerebrospinal fluid in patients of tubercular meningitisduring active stages of the diseasecontainsmonocytoidcells [macrophages] andlymphocytes7 .We kept these cells in to the category ofmononuclear cells. Function of these cells is tophagocytize the tubercular bacilli.
SUMMARY AND CONCLUSION
Cytomorphological patterns in clinically suspectedcases of tubercular meningitis were studied to find outany cellular component peculiar to tuberculosis whichfacilitate in making the final diagnosis, especially incases persistently found negative for tubercle bacilli.Findings of present study can be summarized asfollows.
In tubercular patients good cellularity withpredominance of lymphocytes is the constant findings[>90%].Eosinophil were not found even in a singlecase. These findings were seen in all the bacteriologicalnegative cases. These are the diagnosticcytomorphological findings in patients of tubercularmeningitis .Same finding was obtained in abacteriological positive case, thus reconfirming thatabove cytological features are diagnostic for tubercularmeningitis.
Diagnosis of tubercular meningitis remains aproblem because of a typical clinical presentation,delay
in initiating the therapy thus causing high mortalityand frequent complications8. The disease is a result ofbacterial dissemination originating in another locationin the body6.
Aim of present study is to look for a simple rapidtest that can help in making the diagnosis of tubercularmeningitis. Results of the present study are veryencouraging and equivocal to other costlierinvestigations and thus confirm the usefulness ofcytological study for timely and early diagnosis oftubercular meningitis.Study exhibit fairly highaccuracy with sensitivity of 92.3% and specificity of84.6%.
In case where there is a dilemma in confirming thecause of meningitis cerebrospinal fluid cytology helpreaching out a conclusion and depending upon thefinding obtained patient may be diagnosed and treatedin time for a disease that is practically curable whichotherwise would have become fatal.
It can be concluded thatcytological examination ofcerebrospinal fluid is not only simple inexpensive andrapid,reports can be given on the same day but alsofairly specific method for making a diagnosis oftubercular meningitis .This test does not need speciallaboratory set up ,and the clinical procedure can bedone on an outpatient department also. For this reasonit should find a place as a routine investigation in casesof meningitis.
ACKNOWLEDGEMENT
Help and facilities provided by the institute andco-operation of the patient is deeply acknowledged.
1. Associate professor Pathology Rama medicalcollege hospital and research center Ghaziabad
2. Internee, Meerut district hospital
3. Final year medical student Meerut
4. Assistantprofessor chest & T.B. Rama medicalhospital and research center Ghaziabad
REFERENCES
1. Prasad R, Kumar A, Khanna BK. Mukerjip.k.,Agrawals.k. Kumar A. and Srivastav V.M.L...CSF- ADA for diagnosis of TBM. Ind J Tub.1991; 38:99-102
23. Uma tayal-100-103.pmd 10/10/2013, 9:22 AM102

International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 103
2. Mastroianni CM, Paoletti F, Lichtner M,D’Agostino C, Vullo V, Delia S. Cerebrospinalfluid cytokines in patients with tuberculousmeningitis. ClinImmunolImmunopathol.2006;84(2):171-176]
3. Thwaites G, Chau TT, Mai NT, Drobniewski F,McAdam K, Farrar J. Tuberculousmeningitis. JNeurosurgery Psychiatry. 2000; 68(3):289-299
4. Tandon P.N. Neurotuberculosis: Clinical aspects.In: Chopra J.S, Sawhney I.M.S., editors.Neurology in Tripica.Churchill Livingstone Ltd.;1999.pp. 358-389.
5. Bothamley GH. Serological diagnosis oftuberculosis.EurRespir J. 1995; 20(Suppl)(676s-688s)
6. Blake J, Berman P. The use of c.s.f. examinationin the diagnosis of tuberculosis.SAfr Med J. 1982;62(1):19-21.
7. M.G.Sumi, A.Mathai, S.reuben, C.Sarda andV.V.Radhakrishnan Methods for early diagnosisOf Tuberculous Meningitis. Clin.Microbiol.37:3925-3927.
8. Clark, W. C., J. C. Metcalf, Jr., M. S. Muhlbauer, F.C. Dohan, Jr., and J. H. Robertson. 1986.
Mycobacterium tuberculosis meningitis: a reportof twelve cases and a literature review.Neurosurgery 18:604-610.
9. Sutlas, P. N., A. Unal, H. Forta, S. Senol, and D.Kirbas. 2003. Tuberculous meningitis in adults:review of 61 cases. Infection 31:1387-389.
10. Jeren., T., and I. Beus. 1982. Characteristics ofcerebrospinal fluid in tuberculous meningitis.ActaCytol. 26:678-680.
11. Molavi A, LeFrock JL. Tuberculousmeningitis.MedClin North Am. 1994; 69(2):315-331.
12. Bharat KumarGupta, Anchitbharat,Bandyopadhyay c.s. fexamination of tuberculousmeningitis patientsJournal of clinical medicineresearch, Vol.2, No.5, Oct2010:220-224.
13. MachadoLR,Livramento JA,Bydlowski SP, BenditI ,Bravo LM, Polymerase chain reaction in thediagnosis of tuberculousmeningitis. ArqNeuropsiquiatr 1994;52:445-446.
14. Richard W Light, Yener S Eroyam(2003) ArchIntern Med. 132:854-9
23. Uma tayal-100-103.pmd 10/10/2013, 9:22 AM103

104 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
A Study of Minimally Invasive Percutaneous PlateOsteosynthesis with Locking Compression Plate for Distal
Tibial Fractures
Rajesh Bhatia1, Sumit Gupta2, Firoz Khan3
1Associate Professor, 2Assistant Professor, 3Senior Resident, Department of Orthopedics, Saraswathi Institute ofMedical Sciences, Hapur, U.P., India
ABSTRACT
Introduction: Distal tibial fractures present a serious challenge, often requiring operative treatmentbut are very difficult to deal with. Fixation with locking compression plate (LCP) by minimally invasivepercutaneous plate Osteosynthesis (MIPPO) technique has emerged as an alternative treatment optionbecause it respects biology of distal tibia and fracture hematoma and also provides biomechanicallysound fixation. The aim of this study was to find out the results of MIPPO with LCP for distal tibialfractures in our set up.
Method: Twenty nine patients were treated by minimally invasive technique (MIPPO with LCP) fordistal tibial fracture, only 24 patients were having proper follow-up. These 24 patients- (AOclassification: 14 type A, 5 type B & 5 type C) were prospectively followed up. Twenty two male andtwo female patients with a mean age of 35 years were included.
Results: In our study 17 (70.83%) patients had excellent results, 6(25%) patients had good results &1(4.17 %) patient was having poor result. One patient had delayed union & required bone grafting.Malleolar skin irritation and pain due to prominent hardware was observed in two patients. Onepatient had hardware failure due to non-compliance. Another patient had infection in fibular fixationsite that required hardware removal.
Conclusion: The MIPPO technique for distal tibia has shown good results with many additionaladvantages over the conventional methods. It appears to be a reliable & effective method ofstabilisation for these fractures. Rigid fixation allows the patient to be mobilized earlier & complicationslike displacement, contractures & stiffness can be avoided.
Keywords: Minimally Invasive Percutaneous Plate Osteosynthesis- MIPPO, Locking Compression Plate,Distal Tibial Fractures
INTRODUCTION
Distal tibial fracture comprises 1% of lower limbfracture & 5-10% of tibial fracture 1, 2, 3.These fracturesmay present with or without intra-articular extensionand are among the most difficult injuries to treat dueto soft-tissue damage from high-energy trauma.
High energy injuries such as road traffic accidentsor axial loading are associated with extensive softtissue injury, highly comminuted fractureconfiguration & displaced fracture pattern. 4 Disruptionof articular surface of the distal tibia occur in varyingdegrees with fragments of the articular surface being
driven proximally into the metaphysis of the tibia bythe impact.5
Fractures were classified according to AO/OTAclassification6
Type A: Extra articular fracture
Type B: Partial articular fracture
Type C: Complete articular fracture
Type B fractures are mostly associated withtraumatic torsion mechanism & type C fractures areassociated with high energy compression mechanism.7
DOI Number: 10.5958/j.2321-1024.1.2.041
24. Rajesh Bhatia--104-109.pmd 10/10/2013, 9:22 AM104

International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 105
Compound fractures were classified as per Gustilo-Anderson classification.8, 9Soft tissue injury wasclassified according to tscherne & Goetzen10, 11
classifications from grade 0 to 3.
Each of the fixation techniques has their own meritsand demerits. Nailing has been reported with higherrate of malunion because it is difficult to achieve twodistally locking screws.12,13,14 Wound infection, skinbreakdown and delayed union or non union requiringsecondary procedures like bone grafting are some ofthe complications associated with conventionalosteosynthesis with plates.15,16,17 Similarly, pin tractinfection, pin loosening, malunion and nonunionleading to osteomyelitis is potential complication ofexternal fixators and hence not preferred as definitivefixation method.18,19,20,21
This study presents minimally invasive plateosteosynthesis as a treatment method for these typesof fractures. Minimally invasive plate osteosynthesisinvolves
1) Respecting the soft tissue via small skin incisions,minimal surgical dissection, and gentle soft-tissueretraction; 2) indirect fracture reduction; and 3)minimal hardware application, e.g., screwsinsertion with stab incisions and avoidance ofexcess screw placement. This technique results inminimal periosteal disturbance, faster callusformation & offers the best possible option as itpermits adequate fixation in a biological manner.
MATERIAL & METHOD
29 patients were treated from Nov 2009 to Nov 2012by minimally invasive technique for distal tibialfractures; only 24 patients were having proper follow-up & were included in this study. Out of 24 patients,22 patients were male & 2 patients were female. Theage group of patients was from 17 year to 56 year &average age was 35 yrs. Mode of injury in most of thepatients was road traffic accident 17 (70.83%) and fallfrom height in 7(29.17%).Most of fractures were simple20(83.33%) & compounding of grade I was present in3 fractures and grade II in 1 patients – (3 from medialside and 1 from lateral side). We have not includedcompound grade III fractures in this study or whereskin loss is there.
Fractures were was classified according to AO/OTA classification
Type A- 14
Type B- 5
Type C- 5
6 patients were associated with head injury - 2 withsevere & 4 with mild head injury. Vertebral fractureswere associated in 2 patients & pelvic fractures wereassociated in 3 patients. 2 patients of distal tibia facturewere not associated with fibula facture.3 patients withcompound fracture were operated within 6 hours. Onepatient with compound fracture with severe headinjury was operated at 7th day. One patient of simplefracture, operated same day became drowsy at 2nd postoperative day. CT scan was done and extraduralhematoma was found which was managedconservatively.
Most of the patients which were not associated withany other injuries were discharged on the 1st dressing(2nd post of day). Maximum Stay in hospital was 12day for one head injury patient.
Surgical techniques
Patients who presented within six hours of injurywithout gross swelling of leg were operated on thesame day. Limbs with gross swelling were splinted andelevated till swelling subsided and wrinkles appearedover the ankle joint.
Fibula was fixed first to restore length of leg & tomaintain alignment, angulation & easy reduction oftibial fracture. Simple fibular fractures (transverse orslight oblique) were treated by close flexible nailingwhile comminuted fractures were treated by plating.
For fixation of tibia a 3-4 cm long incision startingjust distal to the medial maleoli was made, extendingit proximally overlying the subcutaneous surface ofthe tibia. Because periosteum of the tibia is veryprecious structure that supplies significant amount ofblood to bone, it should not be removed.22, 23 Anepiperiosteal plane over medial subcutaneous surfaceof tibia was developed 2-3 inches proximal fromfracture so that 3-4 screws can be used for fixation ofproximal segment by a 3.5 mm LCP low band medialdistal tibial plate.
Stab incision was given at proximal cortical screwhole seen in lateral view of leg by fluoroscopy. Platewas manipulated and when plate was in middle ofcortex, drilling with 2.8 mm drill bit was done andboth the cortex were pierced. Self tapping corticalscrews of 3.5 mm of appropriate length were placedand tightened. 3-5 locking screws of 4 mm were placedin distal segment where maximum purchase wassecured. Bone grafting was only done if gap persistedbetween fragments.
Post operative protocol
Post-operatively limb was kept in elevated position
24. Rajesh Bhatia--104-109.pmd 10/10/2013, 9:22 AM105

106 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
and active ankle and toe moments were started as perpain tolerance of the patient. Dressing and check x-ray was done 2nd post-operative day. Non weight-bearing was started from 2nd or 3rd day. Radiographs,including anteroposterior and lateral view were takenat 3 week, 6 week and 3 months post-operatively toassess healing and alignment. Partial weight-wearingwas started depending upon their clinical andradiographic evaluation generally from 6 weeks.24, 25, 26
RESULTS
24 patients were followed up for an average periodof 18 month from Nov-09 to Nov-12. 91.66 % were maleand 08.33% were female with an average age of 35 year.Mode of trauma was road traffic accident in 70.83 %and fall from height in 29.17 %. 83.33 % were simplefractures, 12.5 % compound grade 1 and 04.16 %compound grade II. Average period of partial weightbearing was 6 weeks and average period of union was18 weeks.
2 patients required bone-grafting at the time of
surgery. One patient developed infection in fibulawhere compounding was present and was cured afterhardware removal. Two patients developed superficialinfection at medial side that was cured by antibiotics.One patient required bone grafting at 14 week. Onepatient of compound grade II fracture had hardwarefracture because of being non compliant.
Final evaluation was done for distal tibial fracturesas per Teeny Wiss clinical assessment criteria whichare based on 100 points system.27
Table 1: Clinical results graded as excellent, good, fairor poor as per Teeny Wiss criteria
Rating Results
Excellent (>92 points)
Good (87-92 points)
Fair (65 - 86 points)
Poor (<65 points)
In our study 17 (70.83%) patients were havingexcellent, 6 (25 %) good and 1 (04.17 %) patient washaving poor result.
Table 2: Comparison of current study with previous clinical series
Study No of fractures Study Method Fixation Outcomes
Ronga M et al.28 19 Retrospective MIPO Union: 18 (22.3 wks, range 12-24)
Ahmad MA et al.29 18 Retrospective MIPO Union: 15 (21.2 wks)
Hasenbohehler E et al.30 32 (open fracture: 8) Retrospective MIPO Union: 29 ( 27.7 wks, range 24–60)
Hazarika S et al.31 20 (open fracture: 8) Retrospective MIPO Union: 18 ( 28.5 wks, range, 9–68)
Bahari S et al.32 42 (open fracture: 8) Prospective MIPO Union: 42 (22.4 wks)
Collinge C et al.33 38 (open fracture: 8) Prospective MIPO Union: 38 (21 wks, range 9–48)
Mushtaq A et al.34 21 (open fracture: 4) Prospective MIPO Union: 21( 5.5 months, range 3–13)
Gupta RK et al.35 80 (open fracture:19) Retrospective MIPO : 71, Open: 9 Union: 77 (19 wks, range 16-32)
Current study 24 Prospective MIPO Union: 20 (18 wks, range 14-28)
Clinical Photographs of a Patient
1 a: Pre-operative radiograph 1 b: Post-operative 2nd day radiograph
24. Rajesh Bhatia--104-109.pmd 10/10/2013, 9:22 AM106

International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 107
2 a: AP view after one year 2 b: LAT view after one year
3a, 3b: Foot in dorsiflexion and planter flexion after one year and showing minimal scar mark
DISCUSSION
The results of operative treatment are dependenton the severity of the initial injury and the quality andstability of the reduction. The mechanism of injury, thestatus of the soft tissue and the degree ofcommunication affect the long term clinical result. Themean interval for radiological union was 18 weeks inour study in accordance to previous study. However,the most important factor is to achieve stable fixationand to allow early range of motion withoutunnecessary osseous and soft tissuedevascularization.24 Minimally invasive techniques arebased on principles of limited exposure, indirectreduction methods and limited contact between boneand implant. As a result of these principles thistechnique, as seen in present study, we avoided majorsoft tissue complications and shortened the length ofthe patient’s stay in the hospital.24,25,26
The bone healing was excellent with this type offixation because the stresses were distributed over alonger segment of bone. This technique can be used infractures where locked nailing cannot be done likevertical slit and markedly comminuted fractures. Therewas rapid fractures consolidation due to preservedvascularity. There were fewer incidences of delayedunion and non-union. There was decreased need forbone grafting. There was less incidence of infectiondue to limited exposure. There were less chances ofrefracture. There was no chance of vascularcomplication by carefully inserting the plate submuscularly through limited incisions. There was noneed of any specialized instrumentation and themethod was less time consuming and cost effective inthe present study in a similar fashion as reported byprevious authors.36, 37 with the introduction of lockingcompression plates (LCP) minimally invasivetechniques have become widely used.
24. Rajesh Bhatia--104-109.pmd 10/10/2013, 9:22 AM107

108 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
CONCLUSION
Minimally invasive technique in distal tibial fourthfractures is relatively simple, safe and efficaciousmodality of treatment with following advantages:
• Biological reduction with least disruption of softtissue and fracture hematoma
• Reduced surgical time and tourniquet time
• Decrease risk of wound infection.
• Early mobilization and restoration of maximumankle moments
• Early union of fracture
ACKNOWLEDGEMENT
The authors acknowledge the cooperation of theanesthesia, physiotherapy & radiology departmentsof the institute.
Conflict of Interest: None
Ethical Clearance: Taken
Funding: Self
REFERENCES
1. Bedi A, Le TT, Karunakar MA. Surgical treatmentof nonarticular distal tibia fractures. J Am AcadOrthop Surg 2006 ; 14 : 406-416
2. Lee YS, Chen SH, Lin JC et al. Surgical treatmentof distal tibia fractures : a comparison of medialand lateral plating. Orthopedics 2009 ; 32 : 163
3. 3-Topliss CJ, Jackson M, Atkins RM. Anatomy ofpilon fractures of the distal tibia. J Bone Joint SurgBr 2005 ; 87 : 692-697.
4. Muller FJ, Nerlich M. Tibial pilon fractures. ActaChir Orthop Traumatol Cech 2010 ; 77 : 266-276.
5. Pollak AN, McCarthy ML, Bess RS, Agel J,Swiontkowski MF. Outcomes after treatment ofhighenergy tibial plafond fractures. J Bone JointSurg 2003 : 85-A : 1893-1900.
6. Weber BG. [Treatment of compression fracturesof the ankle from a biomechanical viewpoint.] (inGerman). Hefte Unfallkeilk 1965 ; 81 : 176-179
7. Zelle BA, Bhandari M, Espiritu M, Koval KJ,Zlowodzki M. Treatment of distal tibia fractureswithout articular involvement : a systematicreview of 1125 fractures. J Orthop Trauma 2006 ;20 : 76-79
8. Gustilo RB. Management of open fractures. Ananalysis of 673 cases. Minn Med 1971 ; 54 : 185-189.
9. Gustilo RB, Merkow RL, Templeman D. Themanagement of open fractures. J Bone Joint Surg1990 ; 72-A : 299-304
10. Tarkin IS, Clare MP, Marcantonio A, Pape HC.An update on the management of high-energypilon fractures. Injury 2008 ; 39 : 142-154
11. Tscherne H, Lobenhoffer P. Tibial plateaufractures. Management and expected results. ClinOrthop Relat Res 1993 ; 292 : 87-100
12. Ronga M, Longo UG, Maffulli N. Minimallyinvasive locked plating of distal tibia fracturesis safe and effective. Clin Orthop Relat Res 2010,468:975–82.
13. Mosheiff R, Safran O, Segal D, Liebergall M. Theunreamed tibial nail in the treatment of distalmetaphyseal fractures. Injury 1999,30:83–90.
14. Kneifel T, Buckley R. A comparison of one versustwo distal locking screws in tibial fractures treatedwith unreamed tibial nails: a prospectiverandomized clinical trial. Injury 1996, 27:271–273.
15. Redfern DJ, Syed SU, Davies SJM. Fractures ofthe distal tibia: minimally invasive plateosteosynthesis. Injury 2004, 35:615– 620.
16. Apivatthakakul T, Phornphutkul C, PatumasutraS. Idea and innovation: Simple minimallyinvasive plate osteosynthesis (MIPO)instruments. Injury Extra 2009,40:39–44.
17. Vallier HA, Le TT, Bedi A. Radiographic andclinical comparisons of distal tibia shaffractures(4 to 11 cm proximal to the plafond): platingversus intramedullary nailing. J Orthop Trauma2008, 22:307-11.
18. Yang SW, Tzeng HM, Chou YJ, Teng HP, Liu HH,Wong CY. Treatment of distal tibial metaphysealfractures: Plating versus shortenedintramedullary nailing. Injury 2006, 37:531–535.
19. Guo JJ, Tang N, Yang HL, Tang TS. A prospective,randomised trial comparing closedintramedullary nailing with percutaneous platingin the treatment of distal metaphyseal fracturesof the tibia. J Bone Joint Surg Br 2010, 92-B:984-8.
20. Hasenboehler E, Rikli D, Babst R. Lockingcompression plate with minimally invasive plateosteosynthesis in diaphyseal and distal tibialfracture: a retrospective study of 32 patients.Injury 2007, 38:365– 70.
21. Watson JT, Moed BR, Karges DE, Cramer KE.Pilon fractures. Treatment protocol based on
24. Rajesh Bhatia--104-109.pmd 10/10/2013, 9:22 AM108

International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 109
severity of soft tissue injury. Clin Orthop RelatRes 2000, 375:78–90.
22. Macnab I. The role of periosteal blood supply inhealing of fracture of tibia. ClinicalOrtho1974;105:27
23. Rhinelander WF. The normal microcirculation ofdiaphyseal cortex and its response to fracture.JBJS 1968; 50A:784-800
24. Helfet D, Paul Y S, David L, Joseph B Jr. Minimallyinvasive plate osteosynthesis of distal fracture oftibia.Injury 1998:28:S42- S48
25. Redfern DJ,Syed SU, DevisSJM. Fractures of thedistal tibia minimally invasive plateosteosynthesis.Injury 2004;35: 615-20
26. Nicola Mi, Andrew D , Andrew M, Francesco O.Percutaneous plating of distal tibial fractures.IntOrtho 2004;.28:159-62
27. Tenny SM, Wiss DA. Open reduction and internalfixation of tibial plafond fractures.ClinOrthop1993;292:108
28. Ronga M, Longo UG, Maffulli N. Minimallyinvasive locked plating of distal tibia fractures issafe and effective. Clin Orthop Relat Res 2010,468:975–82
29. Ahmad MA, Sivaraman A, Zia A, Rai A, PatelAD. Percutaneous locking plates for fractures ofthe distal tibia: Our experience and a review ofthe literature. J Trauma 2010, doi: 10.1097/TA.0b013e3181f140b3
30. Hasenboehler E, Rikli E, Babst R. LockingCompression Plate with Minimally Invasive PlateOsteosynthesis in diaphyseal and distal tibialfracture: A retrospective study of 32 patients.Injury 2007; 38; 365-70
31. Hazarika S, Chakravarthy J, Cooper J. Minimallyinvasive locking plate osteosynthesis for fracturesof the distal tibia-results in 20 patients. Injury2006, 37:877– 887.
32. Bahari S, Lenehan B, Khan H, Mcelwain JP.Minimally invasive percutaneous plate fixationof distal tibia fractures. Acta Orthop Belg 2007,73:635-640.
33. Collinge C, Protzman R. Outcomes of minimallyinvasive plate osteosynthesis for metaphysealdistal tibia fractures. J Orthop Trauma 2010,24:24–29.
34. Mushtaq A, Shahid R, Asif M, Maqsood M. Distaltibial fracture fixation with locking compressionplate (LCP) using the minimally invasivepercutaneous osteosynthesis (MIPO) technique.Eur J Trauma Emerg Surg 2009, 35:159–64.
35. Gupta RK, Rohilla RK, Sangwan K, Singh V, WaliaS. Locking plate fixation in distal metaphysealtibial fractures: series of 79 patients. Inter Orthop2010, 34:1285–1290.
36. Borrelli J Jr, Ellis E.Pilon fracture treatment andassessment.Ortho Clin North Am 2002; 33:231
37. Gerber C, Mast JW. Biological internal fixation offractures. J Ortho Trauma 1990;109:295-303
24. Rajesh Bhatia--104-109.pmd 10/10/2013, 9:22 AM109

110 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
Study of Exfoliative Cytology of Ascetic Fluid &Evaluation of its Role in the Diagnosis of AbdominalTuberculosis in Rural Population of National Capital
Region
Uma Tayal1, Nishant2, Emma Chaudhary3, Aparna4
1Associate Professor, Department of Pathology, RMCH & RC Ghaziabad, 2Internee, P.L.Sharma Hospital, Meerut,3Assistant Professor, Chest & TB department RMCH & RC Ghaziabad, 4Final yr MBBS Student LLRM Medical
College Meerut
ABSTRACT
Present study was carried out in 207 patients of ascites at Rama Medical College, Hospital and ResearchCenter [RMCHRH], Ghaziabad, India, during the period of July 2010 to June 2012.Amongs the patientsof ascites, majority of case were due to abdominal tuberculosis. Of the 207 patients, 180 [87%] werediagnosed as tubercular ascites on the basis of cytological examination of the centrifuge specimen ofascetic fluid received. The study correlated with clinical diagnosis. Sensitivity was 91.6%.
The present study advocated the efficiency of cytological examination of ascetic fluid in patients ofascites in low socio-economic population of rural and sub urban national capital region.
Keywords: Ascitic fluid, Abdominal Tuberculosis, Cytomorphological pattern, Ziehl-Nelson, Tuberculosis
INTRODUCTION
Tuberculosis can involve any part ofgastrointestinal tract and is the 6th most frequent siteof extra pulmonary involvement. About 0.4 millionpeople in India are co-infected with HIV andtuberculosis .Of the 3 million TB deaths reportedworldwide each year, the abdominal form accountsfor 1 to 3 %, according to the findings of a studyreported in the World Journal of Gastroenterology,2004.
Several recent developments, which haveinfluenced the incidence as well as clinical course oftuberculosis in general, warrant a fresh look atabdominal tuberculosis. The emergence of multidrugresistant bacilli [1] on the other hand, and the rapidspread of HIV-AIDS [2] have posed newer threats anda new dimension to the control of tuberculosis.
Despite being a treatable and curable disease, itcarries a mortality rate up to 12% in India. A highclinical index of suspicion and judicious use ofdiagnostic procedures certainly help in timely
diagnosis and treatment and thus will reduce the rateof mortality of this curable but potentially lethaldisease.
Hence there is a need for an early and reliablemethod for the diagnosis of abdominal tuberculosis.Conventional diagnosis of tuberculosis employsmicroscopic identification of AFB. However diagnosisby this method is difficult in pauci bacillary sampleslike ascetic fluid besides the long period needed forgrowth in culture. The objective of present researchwork is to evaluate the role of cytomorphologicalpatterns of ascetic fluid in the diagnosis of abdominaltuberculosis.
AIM
The above study was under taken in order to
1. To establish the role of exfoliative cytology ofascetic fluid as the best means in the diagnosis ofabdominal tuberculosis in rural and suburbanpopulation of national capital region, in casespersistently found negative on bacteriologicalexamination.
DOI Number: 10.5958/j.2321-1024.1.2.042
25. Uma tayal --110--113.pmd 10/10/2013, 9:22 AM110

International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 111
2. To determine the incidence of abdominaltuberculosis in patients presented with ascities inthe rural and sub urban population of nationalcapital region, India
3. To analyze the experience within our hospital.
MATERIAL AND METHOD
Study was conducted in the department ofpathology at Rama Medical College Hospital andResearch Center, Ghaziabad, U.P. Total 207 cases ofascitic fluid were studied. Patients were divided in totwo groups.
GROUP A--consists of ascites due to causes otherthan tuberculosis.
GROUP B--consists of ascites due to tuberculosis.These cases were clinically suspected patients oftuberculosis.
These are the cases where material obtained wasadequate for cytological study and specific treatmentnot yet started. Detail clinical history, routine bloodinvestigation and chest x-ray was undertaken in eachpatient,.
Smears were prepared from the Ascitic Fluidreceived. All the smears were stained with
• Giemsa
• PAP
• Z-N Staining
In addition gross appearance of ascitic fluid wasnoted and AFB Culture was also done by L.J. methodin all the cases.
OBSERVATION
TABLE 1. Year wise distribution of ascetic patients
Total No. Group A Group Bof Pts of Pts PtsAsites
1/07/10 – 30/06/11 95 16 79
1/07/11 – 30/06/12 112 11 101
Total 207 27 180
Study of Group A [Non Tubercular] patients
Ascitic fluid may be clear or turbid, color may bereddish and show various type of Cytomorphologicalpatterns like predominance of neutrophils, or mixedpopulation of inflammatory cells, presence of plenty
of mesothelial cells or malignant cell as per the etiology.The constant finding is presence of macrophages andmesothelial cells in large number along with fewlymphocytes and neutrophils. Mesothelial cells maybe seen in groups and sheets.
Study in detail of Group B [Tubercular] patients
Group B cases belong to different age group (18years to 65years,mean-39 years). including both malesand females.
Table 2. Gross Appearance
Appearance of Ascitic fluid Number of Cases % of Cases
Straw & Cloudy 174 96
Transparent 003 02
Cob Web formation 075 42
Reddish 003 02
Table 3. Cytomorphological Patterns
Cytological Pattern Number of Cases % of Cases
Good cellularity* 180 100
Predominantly Lymphocytes 158 88
Mixed inflammatory cells 072 40
Mesothelial cells occasional** 140 78
Histiocytes 013 08
*Good cellularity = 200-1000cells/mm3
** Occasional Measothelial = less than 5% of total cellularity
Table 4. Z-n Staining for A.f.b
Name of the Fluid Positive Negativecases (in %) Cases (in %)
Ascitic 05 (03%) 175 (97%)
Table 5. Culture For A.f.b.
Name of the Fluid Positive Negativecases (in %) Cases (in %)
Asitic 09 (05 %) 171 (95%)
Table 1. Show that tuberculosis is the most commoncause of ASCITES in rural and sub urban populationof national capital region of India.
Table 2. Shows that the fluid is mostly strawcoloured and cloudy. Next common finding is the cobweb formation.
Table 3. Shows that the most consistent finding isgood cellularity [100%], Next common finding is thepredominance of lymphocytes (96%) and absence oroccasional mesothelial cells (88%). Only in two casemesothelial cells were in groups and there number wasup to 08-10%.Neutrophils were always less than 50%of the differential count in all the cases.
25. Uma tayal --110--113.pmd 10/10/2013, 9:22 AM111

112 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
Table 4. Shows that only 3% of the cases were Z-Npositive.
Table 5. Shows that only 5% cases were found tobe positive for A.F.B. culture.
DISCUSSION
A patient presenting with ascites may be indicativeof non-specific inflammation, infection by tubercularbacilli, cirrhosis, cardiac or renal pathologies orneoplasms. Clinical examination alone usually presenta diagnostic challenge to the clinicians [3].An early andaccurate diagnosis is imperative to initiate earlyintervention & treatment. Most of the time treatmentis started on presumptive diagnosis due to absence ofany rapid and reliable method of diagnosis. Mantouxtest has little diagnostic value. Evidence of pulmonarytuberculosis on chest X ray is present only in about afifth of all cases of abdominal tuberculosis. Recentlydeveloped immunological investigations [ELISA] andsoluble antigen fluorescent antibody [SAFA] providemore information but their report of false positivity is12% and 8% with sensitivity of 80-84% and specificityof 88-95% for abdominal tuberculosis. However ELISAremains positive even after therapy and reproducibilityof ELISA is poor. This test is costlier and is not availableat all centers of rural and suburban areas. Hence thevalue of immunological tests remains undefined inmaking the diagnosis and more work is needed beforethey can be accepted as a useful diagnostic test [7]
Polymerase chain reaction [PCR] are far more specificup to 95% but there positivity is only 21.6% .These arenot at present commonly available and are costly hencebeyond the reach of low socio economic population.Use of chemical test like ADA [Adenosine deaminaseactivity] is under investigation [4] with few falsepositives [10].Peritoneal biopsy using a copes needle maybe useful [2,13] but their diagnostic yield is low. Howevercomplications including death may occur especiallywhen the peritoneal cavity is divided in to irregularcompartments by serous adhesions. Reproducibilityof other confirmatory tests like Z-N staining and A.F.B.culture is very poor also culture takes 6-8 weeksduration which is a definite draw back.
Paustian in 1964 stated that one or more of thefollowing three criteria must be fulfilled to diagnoseabdominal tuberculosis:
1. Histological evidence of tubercles with caseationnecrosis.
2. Animal inoculation or culture of suspected tissueresulting in growth of M.tuberculosis
3. Histological demonstration of acid fast bacilli in alesion
However several studies have shown that yield oforganisms on smear and culture is low. Staining foracid fast bacilli is positive in less than 3% of cases .Apositive culture is obtained in less than 20% of cases,and it takes 6-8 wk for the mycobacterial colonies toappear which a definite handicap [5] is. Result of ourstudy co related with this study.
SUMMARY AND CONCLUSION
Abdominal tuberculosis should be considered inall cases of ascites.It has a diverse and non-specificsymptomatology. Study conducted all over the worldhave highlighted that no single test is adequate for itsdiagnosis [8].
The cytomorphological features in 207 patients ofascites of which 180 were of abdominal tuberculosiswere studied with an aim to find out any cellularcomponent peculiar to abdominal tuberculosis whichcan facilitate the diagnosis in cases persistentlynegative for tubercle bacilli..Findings of the presentstudy can be summarized as follows—
1. In patients of abdominal tuberculosis presence ofgood cellularity, absence of mesothelial cells andpredominance of lymphocytes is a constantfinding. Eosinophils were not found even in asingle case. These are the definitivecytomorhological patterns of tuberculosis in caseswhich were consistently found negative fortubercular bacilli by conventional methods. Samefindings were obtained in patients who werepositive for tubercle bacilli thus reconfirming theabove cytological pattern as the diagnostic criteria.Smears showing large number of mesothelial cells[>5%] should be reported cautiously. Over allsensitivity obtained in this study is 91.6% which isreasonably good and comparable with othercostlier more sophisticated diagnostic modalities.
2. Abdominal tuberculosis is the commonest causeof ascities [ 86.9 % 180/207] at rural and sub urbanregion of national capital region..
3. Our experience with present study which wasundertaken in low income group of rural and
25. Uma tayal --110--113.pmd 10/10/2013, 9:22 AM112
International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 113
suburban population is that exfoliative cytologyof ascitic fluid is the best and reliable method todiagnose abdominal tuberculosis. The test beingmost economical, its diagnostic importance isreinforced. The procedure is easy to perform, canbe done in out patient department and results canbe obtained on the same day and thus providingearly diagnosis of tuberculosis. This test shouldbe advocated in all suspicious cases of abdominaltuberculosis.
ACKNOWLEDGEMENT
The help and facilities provided by the college andco operation of the patients is deeply acknowledged.
REFRENCES
1. Edlin, B.R., Tokars, J.I., Grieco, M.H., et al. Anoutbreak of multi-drug-resistant Jereh, J.A., Kelly,G.D., Dooley, S.W. Jr., et al. Tuberculosis mortalityin the United States; Final data, MMWR CDCSurveill Sum; 1990, 1991, 40 (SS-3), 23Tuberculosis among hospitalised patients withthe acquired immunodeficiency syndrome; N.Engl. J. Med 1992,326, 1514.
2. Manohar, A., Simjee,A.E., Hffejee, A.A., et al.Symptoms and investigative findings in 145patients with tuberculous peritonitis diagnosedby peritonioscopy and biopsy over a five yearperiod:;Gut 1990,31,1130.
3. Bhargava, D.K., Shriniwas, Chopra, P., etal.Peritoneal tuberculosis; Laparascopic patternsand its diagnostic accuracy; Am J Gastroenterol :1992,87,109.
4. Dwivedi, M., Misra, S.P., Misr,V. et al. Value ofadenosine deaminase estimation I the diagnosisof tuberculous ascitis; Am J Gastroenterol;1990:85,13.
5. Sharma M.P. Indian journal of Med.Research 2004120[4]:305-315
6. Bhansali SK. Abdominal tuberculosis.Experiences with 300 cases. Am J Gastroenterol1977;67:324-37.
7. Chawala T C, Sharma A Kiran U,BhargavaD.K.Tandon B.N. Serodiagnosis of intestinaltuberculosis by ELISA and SAFA using a salineextract antigen.Tubercle 1986:67:55-60
8. Jereh, J.A., Kelly, G.D., Dooley, S.W. Jr., et al.Tuberculosis mortality in the United States; Finaldata, MMWR CDC Surveill Sum; 1990, 1991, 40(SS-3), 23
9. Daniel, Thomas M., Tuberculosis; In Harrison’sPrinciples of Internal Medicine; 13th Edition, Vol.I, New Delhi, McGraw-Hill Inc., 1994, 710.
10. Marshall John, B. Tuberculosis of theGastrointestinal Tract and Peritoneum.TheAmerican Journal of Gastroenterology; 1993,88,989.
11. Bastani, B., Shariatzadeh, M.R., Dehdashti, F.:Tuberculous peritonitis; Report of 30 cases andreview of the literature; O J. Med; 1985, 56, 549.
12. Das, P., Shukla, H.S. : Clinical diagnosis ofabdominal tuberculosis : Br J. Surg., 1976, 63, 941.26. Borhanmanesh, F., Hekmat, K., Vaez/adch,K., et al. Tuberculous peritonitis; Prospectivestudy of 32 cases in Iran; Ann Intern Med; 1972,76, 567.
13. Singh, M.M., Bhargava, A.N., Jain, K.P.:Tuberculous peritonitis : An evaluation ofPathogenetic mechanisms, diagnostic proceduresand therapeutic measures; N Engl. J. Med, 1969,281, 1091.
14. Geake, TMS. Spitaels, J.M., Moshal, M.G., et al.Peritoneoscopy in the diagnosis of Tuberculousperitonitis. Gastrointest Endosc; 1981, 27, 66.
15. Phani Dhâr Abdominal tuberculosis; Indianjournal of tuberculosis 1998,45,9
25. Uma tayal --110--113.pmd 10/10/2013, 9:22 AM113

114 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
A Study of Incidence and Clinical Presentation ofDeviated Nasal Septum in Western UP
Vandana Singh1, R K Singhal2
1Associate Professor, Deptt of ENT, 2Assistant Professor, Deptt of Community Medicine, Saraswathi Institute ofMedical Sciences, Hapur, U.P.
ABSTRACT
Septal deformity is of two kinds, which may occur independently, or together: 1) anterior cartilagedeformity of the quadrilateral septal cartilage, caused by direct trauma or pressure at any age; and 2)combined septal deformity involving all the septal components, caused by compression across themaxilla from pressures occurring during pregnancy or parturition. This is part of a facial deformity.The incidence of septal deformity and symptoms attributed by it was investigated in 50 patients inthe out door of Saraswathi Institute of Medical Sciences.
It seems that the focus of attention in the recent studies have been shown towards finding out theincidence of deviated nasal septum in the general population.This possibility suggest that majorityof the authors believed that the septal deviation may be considered to be present in all but gainssignificance only when it is severe enough to cause disturbances in the physiology of nose.
Result: The present study showed the incidence of septal deviation to be maximum in the age groupof 21-30 yrs in which males were around 74% and females being 26%. In this students were foundmore affected that was around 30%. Trauma was found to be the aetiological factor of septal deviationand nasal blockage was the one of the major responses to this deviation.
Conclusion: Septal deviation is considered to be present in all but it gains significance only when itis severe enough to cause disturbance in the normal physiology of nose leading to clinical presentationof sinusitis.
Keywords: DNS, Septal Deflection
INTRODUCTION
The nasal septum is the armature of nose. Itmaintains the nose in the prominent position over theface. Besides the anatomical functions it also helps inphysiological functions of nose.
The construction of nose is such that inspite of itssmall size the surface area is greatly increased bypartition of nose into two by intervening nasal septumand each nasal cavity into three by three turbinates.The nose is divided into two cavities which do notfunction usually at the same time1,2. This is describedas a phenomenon, known as Naso-Pulmonary reflex.3
The nose is in direct communication with paranasalsinuses, the ear and the lower respiratory tract. If theseptum is deviated to one or both sides, the nasalphysiology will also be altered. If the air conditioning
becomes inefficient, the drainage, and aeration will alsobe embarrassed and due to the improper solution ofodiferous substance and disturbed eddie currents, theolfactory activity is also affected.
The septal deviations are extremely common, butare not usually severe enough to affect nasal functions.It is very surprising that many a times gross septaldefects are completely free from symptoms. In 25% ofpatients having deviated nasal septum is significantenough to produce symptoms. If left unattended forlong period then nasal physiology becomes impaired.This predisposes to episodes of more severe andprotracted rhinosinusitis and development of chronicdisease. The deviated nasal septum impinges uponlateral nasal wall causing obstruction and secondarynasal inflammation and then infection.
DOI Number: 10.5958/j.2321-1024.1.2.043
26. Vandana Singh--114-118.pmd 10/10/2013, 9:22 AM114

International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 115
Persistent growth of septum components aftercompletion of development of nasal and palatal bonesleads to lateral expansion and contortion, this processresults in varying degree of obstruction by formationof bulges, crest and ridges which may occur on eitherside of septum.
This explanation gives credence to the fact that thedeviations are less frequent in children than in adults.
Trauma is also a significant factor in etiology ofseptal deformity. The vomer and maxillary crest duringchildhood are not completely ossified. Trauma easilydisrupts this arrangement causing structures to growastride one another and leading to widening andcresting at the point of dislocation.
Other factors predisposing deviation of nasalseptum include irregularity of growth of maxilla,eruption of permanent incisor teeth, asymmetricdevelopment of maxillary sinuses, thumb sucking andtongue pressure habits,which cause shift in alveolarridge. Mouth breathing and congenital deformitiessuch as cleft lip and cleft palate are other noteworthyfactors.
The severity of symptoms owing to septalobstruction varies greatly among individuals and isoften related to the presence of processes such asinfection, allergy of vasomotor activity. Secondarypathological manifestations include snoring, sleepwake disturbances, loss of olfactory acuity, rhino lalia.Deviated nasal septum is also responsible for epistaxis.
Morgagni described septoturbinal pain syndromedue to compression of turbinate against the septumproduces pain over the medial canthus, supraorbitalregion and on temporozygomatic area.4
A structural disproportion in the nose createsvariety of symptoms whichis described as syndromeof nasal disharmony.5
It is rare for the nasal septum to be in midline 6,7.But it is also true that all the persons having deviatednasal septum do not suffer on account of this septaldeformity unless it is sufficiently severe to obstructthe respiration
MATERIAL AND METHOD
From April 2012 to October 2012, all patientspresented with nasal obstruction or chronic sinusitis
symptoms to ENT clinic were explained about the aimand design of the study .The study was conducted onpatients attending ENT outdoor of Saraswathi Instituteof Medical Sciences Hapur, who had symptomspertaining to deviated nasal septum .These patientswere selected from the total number of patientspresented in the OPD.
50 patients were selected for the study who hadsymtoms due to deflection.Detailed history was takenand extensive examination was done by anteriror andposterior rhinoscopy.Nose and throat were alsoexamined simultaneously.
Patients presented with chief complaint of nasalblockage,headache,recurrent cold,eutachian tubedysfunction,secretory otitis media,hearing impairment,tonsillitis,pahryngitis and other multiple responses.Besides the local examination air way patency testsand sinus examinations were done .Throatexaminations were carried out to see the post nasaldrip ,tonsils and pharynx.Ear was examined to findout the otological involvement.Eutachian tube patencytests were conducted and valsalva manouvere weregiven.Tuning fork tests with audiograms too weredone.
Table 1: Age wise incidence of Deviated Nasal Septum
S. No. Age Groups No. of cases Percentage
1 1-10 1 2%
2 11-20 14 28%
3 21-30 16 32%
4 31-40 12 24%
5 41-50 4 8%
6 50 and above 3 6%
Figures in Table -1 show the highest incidence (32%)of deviated nasal septum is in age group 21-30 years.The youngest patient recorded is 8 yrs while theoldest being 60 yrs.
Table 2: Sex wise incidence of Deviated Nasal Septum
S. No. Sex No. of cases Percentage
1 Male 37 74%
2 Female 13 26%
Total 50 100%
The study revealed the higher incidence of deviationin males (74%) than in females (26%) with the ratioof 3:1.
26. Vandana Singh--114-118.pmd 10/10/2013, 9:22 AM115

116 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
Table 3: Occupation wise incidence of Deviated Nasal Septum
S. No. Occupation No. of cases Percentage
1 Student 15 30.0%
2 Labourer 7 14.0%
3 Service 9 18.0%
4 House wives 10 20.0%
5 Businessman 4 8.0%
6 Carpenter 1 2.0%
7 Farmer 2 2.0%
8 Washer man 2 4.0%
9 Barber 1 2.0%
Total 50 100%
Study shows that majority of patients (30%) werestudents, the next common group was of the housewives 20%, service class 18%, labour 14%, businessman
8%, washer man 4% and barber, carpenter and farmer2% each.
Table 4: Showing Etiology of Deviation
S. No. Etiology No. of Types of Degree ofCases deviation & deviation &
No. of patients No. of patients
Ant. Post. Ant-Post. Mild Mode Severe
1. Birth trauma 1 1 - - - 1 -
2. Fall 2 2 - - - 2 -
3. Direct trauma 5 5 - - - 4 -
4. Tumour 1 - - 1 - - 1
5. Personal habits 7 4 2 1 2 4 1
Study shows that in majority of cases etiology couldnot be established but direct trauma was found to bethe most common cause of deflection in around 10%of patients and personal habits like nose picking inaround 14%.Birth trauma accounted for 2% of casesand fall from height in 4%.Tumaour was the cause in2% of cases . Anterior type of deviation of moderatedegree was found to be maximum in direct traumawhich was 100% followed by nose picking in 47%ofcases.
Table 5: Showing No. of cases and percentage inrelation to clinical presentation of DNS
S. No. Clinical Presentation No. of cases % age
1. Nasal blockage 49 98
2. Headache 21 42
3. Loss of smell 7 14
4. Epistaxis 7 14
5. Mouth breathing 14 28
6. Throat pain 15 30
7. Cough 16 32
8. Change in voice 5 10
9. Nasal discharge 8 16
Table 5: Showing No. of cases and percentage inrelation to clinical presentation of DNS
S. No. Clinical Presentation No. of cases % age
10. ET dysfunction 21 42
11. Pus discharge from ear 8 16
12. Diminished hearing 11 22
13. Tinnitus 1 2
14. Pain in teeth 6 12
15. Pain in cheek 19 38
16. External deformity 11 22
17. Overriding teeth 3 6
18. Sinusitis 34 68
19. Tonsilitis 7 14
20. Pharyngitis 8 16
21. Recurrent cold 38 76
22. Rhinolalia 4 8
Study shows that septal deviations causes multipleresponses in the patients.Nasal blockage was the mainsymptom almost found in all patients i.e is around98%.Recurrent cold was another main response todeflection which was found to be around 76% ofcases.Sinusitis was found to be in68% of cases.
26. Vandana Singh--114-118.pmd 10/10/2013, 9:22 AM116

International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 117
SUMMARY AND CONCLUSION
All the patients attending the outdoor ofdepartment of otorhinolaryngology, SaraswathiInstitute of Medical Sciences, Hapur during April 2012to October 2012 were studied.
A detailed history was obtained from every caseregarding the present complaints, past history,personal and family history.
The present study revealed that incidence ofdeviated nasal septum was found to be maximum inthe age group of 21-30 yrs. The incidence was founddecreasing towards the extremes of age. Males wereaffected more (74%) than females (26%).
Left sided deviation were more common 76% thanthe right sided deviation 26% in both the sexes.
Etiology could not be established but direct traumawas found to be the most common cause of deflectionin around 10% of patients and personal habits like
nose picking in around 14%.Birth trauma accountedfor 2% of cases and fall from height in 4%.Tumour wasthe cause in 2% of cases .
Majority of cases (30%) were students and least (2%each) were barbers, farmers and carpenters.
The most common symptom was nasal obstruction96%. On left side it was 48% and on right side it was28% and 20% of them complained of obstruction onboth sides. Other symptoms were headache 92%,sneezing in 68% of cases , 6% of cases had disorder ofsmell, 8% showed cosmetic deformities. Epistaxis wasnoticed in 14% of cases..
DISCUSSION
Obstructed nose is a non specific complaint anddiagnostic possibility includes every nasalabnormality. Among the local causes which canproduce obstruction in nose, nasal septal deformity isthe most important which either directly initiates thedisturbance in physiology of nose or can aggravatethe severity of other nasal symptom. The present studywas done on 50 selected cases of deviated nasalseptum. Only those patients were included in whomthe symptoms were attributable to the septal deformity.Attempts were made to find out the factor responsiblefor production of deviated nasal septum.
The present study reveals that there is a definiteincidence of deviated nasal septum which was also
earlier reported and straight septa could also be foundin many.8,9,10,11,12
The earlier worker reported a definite incidence ofdeviated nasal symptom, suggesting, thereby thatstraight septa could be in many.8,9,10,11,12
But still most of the authors claim that it is rare forthe nasal septum to be in midline.13,14
The deviation of nasal septum clinically manifestsin adult hood rather than childhood15,16,17,18.Thisobservation is the universal experience 6,7 and it is thatthe highest incidence is found in age group of 17-25yrs.19 In the present study the highest incidence foundin the age group of 21-30 yrs, the youngest patientrecorded is 8 yrs and the oldest is 60 yrs. This may bedue to the fact that trauma is more common in thisage group
The present study revealed that septal deformitiesare more common in males (74%) than in females(26%), ratio being 3:1 M:F. Although all the authorsreported higher incidence of septal deviation in males,but exact figure has been presented by few only. Atpresent it may be said that inspite of being universalexperience the question why the septal deviation aremore common in males is yet to be answeredsatisfactorily.
In present study left sided deviations were foundto be more common (76%) than right sided(20%).Similar results were also noted by others 11,12.
In present study both sexes showed higherincidence (76%) of septal deviation on left side(comprising 56% males and 20% females), whiledeviation on right side (20%) in which 18% were malesand 2% were females .This study coincides with thestudy of others too7,19.
a. Heredity- There is no role of heredity in causationof DNS.16
b. Occupation- In the present study the majority ofpatients were students 30%, others were housewives 20%, farmers 2%.Septal deviation is moreprevalent among civilised races and the reasongiven for this was enlargement in the facial angleand admixture of races. All these studies supportthe findings of the present study17,6,7
c. Trauma- Trauma to nose as a definite cause ofdeviated nasal septum deformity was observed in8% cases .15,18
26. Vandana Singh--114-118.pmd 10/10/2013, 9:22 AM117

118 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
d. Types of deviation- Majority of cases in the presentstudy showed ‘C’ type of deviation 96% and ‘S’shaped 4%. Spurs were found in 22% of cases andbony deviation was seen in 2% of cases 19,15,6,7.
Ethical approval
This study was a cross sectional study that wasapproved by ear-nose-throat (ENT) Head and principalSIMS,Hapur.Written informed consent was obtainedfrom the patient for publication of this research.
ACKNOWLEDGMENT
Heartfelt thanks to Dr.R.K.Singhal who helped mein compiling the data Dr.Ranjana Singh who helpedin editing the tables and my collegue Dr.Anuj Goel forall his help collecting and storing data of patients.
Source of Funding: This study was self funded andno grant from anywhere was taken.
Conflict of Interest: Nil
REFERENCES
1. Kayser 1895,Archieves of laryngol & Rhinolo1895,3:101-120. Ohki et al ,2005.Eccles.R.2000,Nasal airflow in health and disease.Actaotolaryngol 2000;120:580-595.
2. Stoksted .P.1952 ,1953,Obstruction in the nose andtheir influence on the pulmonary function.ActaOtolaryngol.suppl.1960 158 (suppl):110.
3. Sercer .A.1930, Research on homolateral reflex ofthe nasal cavity on Lung.Otolaryngol 1930; 14;82-90.
4. Stammberger.H, Wolf G. Headaches and Sinusdieases, the Endoscopic approach.Ann.Otolaryngol suppl 1988 ; 134:3-23.
5. Cottle M.H.1963 ,Mlandina (Mlamdina R .Therole of Maxilla morphology in development ofpathological septal deformities.Rhinology1987;25:199-205.
6. Negus .V. 1958, Comparative anatomy andphysiology of nose and paranasal sinuses, E & S,livingstone ,Ed. Edinberg & London.
7. St.Clair Thomson 1948 .Diseases of Nose andThroat, 6thedition E&S Livingstone ,London.
8. Speiss 1894 ,Diseaes of Nose and Throat ,byV.Negus & St.Clair Thomson.
9. Roe .J.O.1896 .Diseses of Nose and Throat byV.Negus & St.Clair Thomson.
10. Morell Mackerzie 1804,Diseases Of Nose andThroat.
11. Daoud Ali 1965 , Kennedy DW,ZinreichSJ,Rosenbaun AE : Functional Endoscopic SinusSurgery, Theory and Diagnostic Evaluation.Archives.Otolaryngol 1985 111: 576-582.
12. Sinha ,A, Maheshwari V.K, 1970 ClinicalObservations on Deviated Nasal Septum ILJO22:4
13. Lederer F.L.1952 ,Diseases of Ear Nose andThroat. 6thEd.
14. Scott Brown , 2008.Diseases Of Ear Nose Throat.7thEd. Butterworth ,London.
15. Ballenger H.C, & Ballenger J.J,1948 ,Diseases OfEar Nose Throat .Ed. Philadelphia .Lea & fegiber,pg 45-57.
16. Gray .L.(1980), DNS: Incidence and etiology .AnnOtolaryngol 87:320.
17. Delvan 1888.Diseases of Nose & Throat by Negus& St. Clair Thomson No.65 (183).
18. Jackson C.L.& Jackson C.1959 .Diseases Of NoseThroat and Ear.2nded. W.B.Saunders.
19. ConverseJ.M.(1964),Deformities of Nose.Ed.Reconstruction Plastic Surgery.Vol.2.SaundersPhiladelphia,London pg. 695.
26. Vandana Singh--114-118.pmd 10/10/2013, 9:22 AM118

International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 119
Study and Evaluation of Cases of Total Condylar KneeReplacement
Varun Vijay1, Madan S Hardikar2
1Resident in Department of Orthopedics, 2Senior Orthopedic Surgeon at Sushrut Medical Care and Research Society'sHardikar Hospital, Pune
ABSTRACT
Background: The incidence of chronic disabling conditions of the knee such as osteoarthritis,rheumatoid arthritis, inflammatory arthritis, osteonecrosis are on the rise. So patients prefer to getrid of these conditions permanently and this could be done only by means of Total Knee Replacement.Total knee arthroplasty is a generally effective procedure and is associated with substantial functionalimprovement [1].
Objectives:
1) To elaborate the role of Total Condylar Knee Replacement in osteoarthritic knees and rheumatoidarthritis.
2) To study the role of Total Knee Replacement in Indian patients keeping in mind their socioeconomicstatus & habits.
Method: In the present study 25 patients with 33 total condylar knee replacements were evaluated inSushrut Medical care & Research Society's Hardikar Hospital, Pune between July 2008 to June 2010using Nexgen LPS, high flex, fixed total condylar knee system.
Results: The patients were followed up for an average of 1 year (range 6 months to 2 years) after theprocedure.
According to Knee Society Score, 70% had excellent results, 24% good results and 6% fair results.
Conclusion: Osteo arthritic cases showed better results in all parameters of the score as compared torheumatoid patients. Relief of pain is predictable and often total. Rontgenographic study till lastfollow up did not show shift of prosthetic components, loosening, ectopic bone formation, though itmay be too short a follow up for such evidence.
Keywords: Knee Arthroplasty, Osteoarthritis Knee, Rheumatoid Arthritis
INTRODUCTION
The incidence of chronic disabling conditions of theknee such as osteoarthritis, rheumatoid arthritis,inflammatory arthritis, osteonecrosis is on the rise. Sopatients prefer to get rid of these conditionspermanently and this could be done only by means ofTotal Knee Replacement. Total knee arthroplasty is agenerally effective procedure and is associated withsubstantial functional improvement [1]. Therefore, theincidence of patients undergoing total kneereplacement is also on the rise.
In spite of number of treatment modalities, the endresult previously used to be painful and stiff jointwhich may disable the patient to the extent of beingbed ridden, thus significantly reducing his mobility atan age when he deserves to be active.
Till the discovery of total knee arthroplasty,arthrodesis was the final answer. Stiffness of the kneemay alleviate the pain but can significantly disable thepatient by limiting his activities, especially squattingand sitting cross-legged, as far as Indian patients areconcerned. Patients used to agree to arthrodesis, as a
DOI Number: 10.5958/j.2321-1024.1.2.044
27. Varun Vijay--119-123.pmd 10/10/2013, 9:22 AM119
120 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
means to get rid of pain, but soon realized theirlimitations after surgery and used to get frustrated.
The objectives of the study were:
1) To elaborate the role of Total Condylar KneeReplacement in osteoarthritic knees and rheumatoidarthritis.
2) To study the role of Total Knee Replacement inIndian patients keeping in mind their socioeconomicstatus & habits.
We all have been aware of the importance andbenefits of daily physical activity as it relates tocardiovascular and mental health. Disabling arthritisand other conditions of the knee can prevent patientsfrom all these day to day activities and lead to manycomplications. With the advent of total kneereplacement, all subjects with the above mentioneddisabilities are getting benefitted by this procedure.
MATERIALS AND METHOD
In the present study 25 patients with 33 totalcondylar knee replacements were evaluated in SushrutMedical care & Research Society’s Hardikar Hospital,Pune between July 2008 to June 2010.
The overriding indication was non-septicarthropathy causing severe incapacitating pain notresponding to NSAIDs, intraarticular steroid, weightreduction, topical anti inflammatory preparation &physical therapy .Pain was mainly due to deteriorationof joint surfaces demonstrable on X rays.
The inclusion criteria used: 1. Elderly patient notdoing heavy physical activities 2. Bi or tricompartmental diseases 3. Good functionalquadriceps muscle 4. No gross instability 5. Noevidence of infection in last 6 months 6. Varus orvalgus deformity<25 degrees 7. Fixed flexiondeformity<45 degrees.
The Prosthesis used: A total condylar knee system(Nexgen LPS, high flex, fixed) was used consisting of:femoral component tibial component patellarcomponent along with bone cement.
After proper pre-operative evaluation of thepatients and taking an informed written consent a totalknee replacement was performed and post operativeevaluation was done using Functional score and Kneesociety score.
RESULTS
A total of 33 condylar knee arthroplasties (17patients underwent unilateral knee replacementwhereas 8 patients underwent bilateral kneereplacement) were performed.
In the present study 21 patients were females and4 were males. The youngest patient was 49 years ofage while the eldest patient was 86 years old. The meanage of the patients undergoing knee replacement was63.36 years.
In the current study it was observed thatrheumatoid arthritis leading to knee replacement wasmore common in males when compared with females.Also, mean age of patients undergoing kneereplacement in rheumatoid arthritis group was 53years as compared to overall mean age of 63.36 years.
The anesthesia used during surgery in all 25patients (33 surgeries) was a combination of epiduralalong with spinal anesthesia.
The average pre operative range of motion was 69.5degrees and post operative range of motion was 104.4degrees
Tab.1: Pre-operative Knee Society Scores:
Knee society score No.
<60(Poor) 33
60-69(Fair) 0
70-79(Good) 0
>80(Excellent) 0
The average pre operative Knee Society Score was36.6 and post operative Knee Society Score was 82.15.
Average pre operative functional score was 33.9 andpost operative functional score was 65.75.
Tab 2: Pre-operative functional scores:
Pre-operative functional scores No.
0-20 12
21-40 6
41-60 15
61-80 0
81-100 0
There were no complications observed in our study.
The patients were followed up for an average of 1year (range 6 months to 2 years) after the procedure.
27. Varun Vijay--119-123.pmd 10/10/2013, 9:22 AM120

International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 121
Tab.3: Post-operative range of movement:
ROM NO.
0-25 0
26-50 0
51-75 0
76-100 15
101-125 18
According to Knee Society Score, we had 70%excellent results, 24% good results and 6% fair resultsat the latest follow up.
DISCUSSION
Various surgical modalities of treatment have beentried for treatment of arthropathy of the knee for thepast many years and obvious conclusion unanimouslydrawn is for tri compartmental affection of the diseasethe only answer is resection of the diseased jointsurface from all the three compartments. Taking intoaccount the dramatic relief of pain and restoration ofthe function after total knee arthroplasty, it is clearlythe optimum form of major reconstructive surgery forthe arthritic knee in the middle aged and elderlypatients unless contraindicated. At the same time onemust take into account the potential late disadvantagesof this procedure primarily the wear, infection,loosening, failure of HDPE etc. it is therefore veryimportant to evaluate each patient individually, hishabits, body weight, activity levels and socio-economicstatus before subjecting him to this procedure.
The goal of total knee arthroplasty is to providepain free, stable, mobile and functional joint.
For our study we chose osteo arthritis andrheumatoid arthritis with radiological evidence of bior tri compartmental affection as a primary indication.
It is now agreed that patients older than 60 yearsof age who are not heavily built, who do not participatein physical activities which places significant strain onthe knees and who have reasonable expectations canbe operated upon and their quality of life vastlychanged.
Obesity, young age, high medical risk, high activitylevels and pathological osteoporosis are relativecontraindications.
In addition to meticulous patient selection, properprosthetic design, sound surgical technique andequally meticulous post operative rehabilitation isinevitable for the success of total knee replacement.
Today a number of prosthetic designs are available tochoose from.
Total Condylar Knee Systen developed by Insalland Associates eliminates most of the undesired effectsof prosthetic components, limits complications, followsan easy technique with simple instrumentation andeasy reproducible technique [2,3,4].
The most important feature of this system is HDPEtibial component. It requires resection of both thecruciate ligaments and incorporates an inter-condylarridge and a concave plateau which gives excellentinherent stability to the system yet maintains itsmobility.
Insall and Associates reported after a long termstudy that Total Knee Replacement using this systemoffer results equivalent to Total Hip Replacement asregards with pain relief and improvement in function[5,6,7].
A total of 25 cases with 33 knees were selected fromOPD. A pre operative examination and assessmentproforma was made and used in all cases. Out of these,29 knees had osteo arthritis and 4 had rheumatoidarthritis. Thus osteo arthrhritic knee outnumbered therheumatoid arthritis knees by more than 7 times.
Second observation was that the average age ofpatients with rheumatoid arthritis was considerablyless (53 years) than those of osteo arthritis (64.8 years).
This is because rheumatoid arthritis is aninflammatory disease affecting the young anddestroying the joint much earlier than osteo arthritis,which is a degenerative condition of older age and isassociated with insidious progression of pain.
Ranawat, Padgett and Ohashi undertook the studyto evaluate the results of Total Knee Replacement inpatients younger than 55 years. Majority of 93 kneeswere from rheumatoid arthritis group ( RA 79, OA 17).The results indicated a cumulative survivorship rateof 96% at the end of 10 years. These are comparable toolder patients and better than Total Hip Replacementin younger patients [8].
Out of the 25 patients, all were females except 4,thus concluded that non infective arthropathy iscommon in females especially post menopausal.
In a study conducted by Lozango GMR, Ruiz FJ etal. for long term results (average 5 years, range 1-9years) of treatment of severe OA and RA with total
27. Varun Vijay--119-123.pmd 10/10/2013, 9:22 AM121

122 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
knee replacement. Out of the 193 posterior stabilizedcemented total knee replacements for OA and RAknees, the knee society score was 90.5% good orexcellent results for the OA group and 83.9% for theRA group. Thus they concluded that Insall-Burnsteinposterior stabilized total knee prosthesis is an excellentprimary replacement associated with long termsurvival in patients with severe degree of articulardistruction and functional incapacity [9].
In a similar study by Amenabar PP, Carrion M etal. regarding total knee replacement in patients withRA, a total of 25 posterior stabilized total kneeprosthesis in 19 patients were followed for an average
of 6 years. The mean Hospital For Special Surgery scoreincreased from 44 points(range 27-58) pre operativelyto 80 points(range 58-91) at final follow upexamination. Thus these authors concluded that totalknee replacement is a good choice in patients with RAin the medium term follow-up, with 80% good toexcellent results [10].
Ip D,Wu WC,Tsang WL studied early results ofNexGen Legacy posterior stabilized arthroplasty in 60knees(48 patients) at a mean follow up of 21 monthsshowed that the mean pre operative and post operativeKnee Society scores were 60 and 85. The mean postoperative knee flexion was 115 degrees [11].
Tab 4. Comparative overall results:
Series Knees Excellent Good Fair Poor Follow up
LozangoGMR 193 90% - - 10% Avg. 5 years
AmenabarPP 25 80% - 20% - Avg. 6 years
Ip D, WuWC 60 85% - 10% 5% 21 months
OurSeries 33 70% 24% 6% 0% Avg. 1 year
After reviewing the above published literatures, itis observed that results in patients with osteo arthritisare better and patients with RA do slightly poor in allcategories in the scoring system.
We did not have any poor results nor did we haveany post operative complications till the latest followup.
Patients with osteo arthritis did marginally betterthan patients with rheumatoid arthritis, but thoughthe patients with rheumatoid arthritis were moresatisfied due to marked improvement in their disabilityand function.
The good results that we observed can be attributedto careful patient selection, avoiding those withmultiple joint involvement, grossly deformed andunstable joints, precise surgical technique andmeticulous attention to post operative rehabilitation.
At the last follow up 29 knees had virtually no pain,4 knees had slight pain on climbing stairs, all the 4knees belonged to rheumatoid arthritis patients.
Thus we could provide a stable, pain free yetfunctional knee to each of our patients. The patientswere explained before surgery the modifications theywould have to do and the alterations in their life stylee.g. not to sit crossed legged, use western style toilets.All the patients preferred change in life style and werewell adapted to it and happy.
To conclude the total knee replacement using totalcondylar knee system appears to be a procedure ofchoice in older, non obese and low physically activepatients who are crippled with excruciating pain,deformity and instability due to osteo arthritis orrheumatoid arthritis. For a good result individualisticpatient selection, strict adherence to surgical technique,proper instrumentation and accurate alignment of theprosthesis are of at most importance.
Acknowledgements: None
Conflict of Interest: None
Source of Funding: None
Ethical Clearance: Yes
REFERENCES
1. Robert LK, Khaled JS, Timothy JW and Boris B2005: “The Functional Outcomes of Total KneeArthroplasty”, JBJS, 87A:1719-1724.
2. Insall JN, Ranawat CS, Scott WN and Walker PS.1976: “Total condylar knee replacement:preliminary report”, Clin Orthop, 120: 149-54.
3. Insall JN, Burstein AH and Lachiewicz PF 1982:“The posterior stabilized condylar prosthesis: Amodification of total condylar design: Two to fouryears clinical experience”, JBJS, 64A: 1317-1323.
4. Ranawat CS, Insall J 1989: “Duo condylar kneearthroplasty, Hospital for special surgery design”,Clin Orthop. 248: 27-33.
27. Varun Vijay--119-123.pmd 10/10/2013, 9:22 AM122

International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 123
5. Insall JN, Clarke HD. 2001: “Historicdevelopment classification and characteristics ofknee prostheses”, Insall JN, Scott WN (eds):Surgery of the knee, New York, Churchill-Livingstone, 1516 – 1553.
6. Insall JN, Dorr LD, Scott RD. 1989 b: “Rationaleof the knee society clinical rating system”, ClinOrthop, 248:13.
7. Insall JN, Ranawat CS, Aglietti P, Shine J. 1976: “A comparison of four models of total kneereplacement prosthesis”, JBJS, 58A: 754-765.
8. Ranawat CS, Padget DE, Ohashi Y 1989: “Totalknee arthroplasty for patients younger than 55years”, Clin Orthop 284: 27-33.
9. Lozango GMR, Ruiz FJ, Lopez AA, Gomez PL1997: “Long term results of treatment of severeosteo arthritis and rheumatoid arthritis with 193total knee replacements” ,Knee Surg SportsTraumatol Arthrosc, 5(2): 102--12.
10. Amenabar PP, Carrion M, Abablaza D, Paulos J2004: “Total knee arthroplasty in patients withrheumatoid arthritis”, Rev Med Chil, 132(3):337-345.
11. Ip D, Wu WC, Tsang WL 2003: “Early results ofposterior stabilized NexGen Legacy total kneearthroplasty”, J Orthop Surg (Hong Kong), 11(1):38-42.
27. Varun Vijay--119-123.pmd 10/10/2013, 9:22 AM123

124 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
Comparative Study of the Therapeutic efficacy ofCyproterone Acetate + Eflornithine (Topical) and Eflornithine
(Topical) alone in the Treatment of Facial Hirsutism
Sachin Agarwal1, Vinay Kumar2, S K Sayal3
1Assistant Professor, Department of Dermatology, SMC Ghaziabad, 2Assistant Professor, Department of Anatomy,SIMS, Hapur, 3Prof & HOD, Department of Dermatology, SMC Ghaziabad
ABSTRACT
Throughout the history of human civilization, excessive hair growth has been a concern to mankindthe object of superstition and mystery, as well as of cosmetic and medical interest. Hirsutism is acommon disorder affecting 5-10% of women; Although various modalities of treatment like cosmeticprocedures,laser are there but each of them has its own demerits.Since data concerning long termsafety and efficacy of the systemic drugs are also lacking, so studies have been conducted usingtopical agent Eflornithine Hydrochloride. The purpose of this study was to compare the efficacy andsafety of Cyproterone acetate + Eflornithine (topical) and Eflornithine (topical) alone in the treatmentof Facial Hirsutism. In this randomized comparative double-blind study, 45 patients with facialhirsutism consistent clinically were recruited. Patients were divided into two groups. In group- 1(23) patients were given eflornithine (13.9%) and cyproterone acetate and In group 2 (22) patientswere given topical eflornithine (13.9%)alone. The study showed that cyproterone acetate incombination with topical Eflornithine (13.9% is safe, well tolerated, and effective therapy for facialhirsutism.
Keywords: Facial Hirsutism, Topical Therapy,Eflornithine (Topical -13.9 %), Cyproterone Acetate
INTRODUCTION
Hirsutism refers to the occurrence of growth ofterminal hair in a male sexual pattern in women inandrogenic sensitive areas of the body. Hirsutism is acommon disorder affecting 5-10% of women; (1) and ismost often a result of ethnic background or heredity.In a small percentage of women, it may be caused byandrogen over production, increased sensitivity tocirculating androgens, or other metabolic or endocrinedisorders. The potential underlying causes ofHirsutism include ( 2,3,4,5)
(i) Familial/Ethnic & Idiopathic
(ii) Polycystic ovarian syndrome
(iii) Ovarian/Adrenal Tumors
(iv) Late onset adrenal hyperplasia
(v) Cushing’s syndrome
The currently available treatment methods forhirsutism include
(i) Cosmetic procedures- Bleaching, shaving,plucking, waxing, chemical depilatories andelectrosurgical epilation(6)
(ii) Light sources and Lasers(7.8)
(iii) Pharmacological treatment in the form of systemictreatment(9,10,11) includes drugs as:
(a) Androgen suppression drugs like oralcontraceptive pills glucocorticoids andgonadotropin releasing hormone agonist
(b) Antiandrogens like cyproterone acetate,spirinolactone, flutamide and finasteride.
(iv) Topical like the newly introduced moleculeeflornithine which is an ornithine decarboxylaseinhibitor in the hair follicles
DOI Number: 10.5958/j.2321-1024.1.2.045
28. Vinay Kumar--124-128.pmd 10/10/2013, 9:22 AM124

International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 125
Cyproterone acetate (CPA) (12) was first used to treathirsutism experimentally in 1965 and was brought tothe attention of dermatologists by Hammerstein andcolleagues in Germany. Since then it has become avery popular oral Antiandrogen. the primary actionof cyproterone acetate which makes it effective in thetreatment of hirsutism is competitive inhibition withdihydrotesterone for androgen receptor binding site.It also suppresses gonadotropin releasing hormone byits progestional activity, reduces androgen production,increases the metabolic clearance of testosterone andin addition long term therapy reduces 5 á reductaseactivity. In this way it decreases the androgen leveland in return reduces the hair growth
Since data concerning long term safety and efficacyof the systemic drugs are lacking, so studies have beenconducted using topical agent EflornithineHydrochloride. Eflornithine is a specific, reversibleinhibitor of the enzyme ornithine decarboxylase.Decarboxylation of ornithine by this enzyme is a keystep in the biosynthesis of polyamines which haveimportant roles in cell division and differentiation.Eflornithine is an ornithine analog that binds to theactive site of ornithine decarboxylase and forms acovalent bond with the enzyme, resulting in anirreversible inhibition. Animal data indicate thatinhibition of ornithine decarboxylase inhibits celldivision and synthetic function, which affect the rateof hair growth. Eflornithine cream has been shown toretard the rate of hair growth in non-clinical andclinical studies.(13)
It also appeared to be effective in hair unresponsiveto lasers like the white hair and vellus hairs.
AIM OF STUDY
The present study aims to compare the efficacy ofCyproterone acetate + Eflornithine (topical) andEflornithine (topical) alone in the treatment of FacialHirsutism and to give better option of treatment withleast side effects.
MATERIAL AND METHOD
A total of 45 patients, presenting with facialhirsutism at the Out Patient Department of theDepartment of Dermatology, S.T.D. & Leprosy,Rajendra Institute of Medical Sciences, Ranchi. Allpatients who were fulfilling the selection criteria weretreated and thoroughly followed up.
Before starting the above mentioned procedure,patients were carefully examined clinically, after goingthrough the history of the disease. Special referencewas made to the duration, extent, distribution of thedisease and the associated conditions. Procedure wasthoroughly explained to the patients and an informedconsent was taken from each of the patient. Apart fromroutine investigations some specific investigations like24-Hrs Urine Free Cortisol Test, Total and FreeTestosterone Level, DHEA Sulfate Level, LH and FSHRatio, Abdominal/Pelvic Ultrasound etc. were alsodone. Photographs were taken before the start of theprocedure and also after 32 weeks of starting thetherapy.
None of the patient had any systemic disease.Pregnant and breast feeding women were alsoexcluded. Any topical medication for treatment ofhirsutism was stopped for 2 weeks and systemictherapy for at least 4 weeks prior to the study.
The study was prospective randomized clinicalstudy. The study consisted of 45 female patients aged>= 18 years with presence of at least total 20 terminalhairs on upper lip and chin as determined by clinicalexamination.
Patients were divided into two groups (I and II)with Group I having 23 patients and Group II having22 patients.
• Group I patients given eflornithine (13.9%) andcyproterone acetate and
• Group II patients given eflornithine (13.9%) alone.
In Group I cyproterone acetate was given twicedaily (50 – 100 mg/day) depending upon the area ofinvolvement and severity for about 10 days in eachmenstrual cycle, starting from the fifth day of the cycle.Same schedule will be repeated in each cycle.Patientwas advised to apply a thin layer of eflornithine to theaffected areas of the face and adjacent involved areasunder the chin and rubbed thoroughly. The treatedareas should not be washed for at least 4 hours. Thecream should be applied twice daily at least 8 hoursapart. For better cosmetic results patient were advisedto apply the cream at least 5 minutes after shaving thearea.
Patients were reviewed after every 4 weeks and theresults were assessed according to Physician’s GlobalAssessment.
28. Vinay Kumar--124-128.pmd 10/10/2013, 9:22 AM125

126 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
Physician’s Global Assessment (PGA): (on fourgrade scale)
A Four-point Physician’s Global Assessment scalewas used for assessment. The response categories forthe treated areas of skin as per the scale are as follows:
(i) Grade 0: No improvement/ worse – no decrease/worsening in visibility of terminal hair withdarkening of skin by terminal hair not improved/worsened.
(ii) Grade 1: Improved – clinically apparent reductionin visibility of terminal hair and noticeablelightening in appearance of facial skin attributableto facial hair.
(iii) Grade 2: Marked improvement – considerablereduction in the visibility of terminal hair and onlyminimal darkening of skin by terminal hair.
(iv) Grade 3: Clear/ almost clear – no/almost no visibleterminal hair and no/ almost no darkening of skinby terminal hair.
Observations were recorded with respect to thefollowing parameters
(i) Comparative incidence of response observed infollow up
(ii) Complications.
(iii) Overall cosmetic results.
RESULTS
Results of the study are shown in table 1, 2 & 3
TABLE 1: Comparative Incidence of Response Observed in Follow Up
S. No. Responseobserved Group I
GRADES (According to PGA Scale)
0 1 2 3
No. % No. % No. % No. %
1. 4 WEEKS 23 100 0 0 0 0 0 0
2. 8 WEEKS 12 52.2 11 47.8 0 0 0 0
3. 12 WEEKS 10 43.5 13 56.5 0 0 0 0
4. 16 WEEKS 7 30.4 13 56.5 3 13.1 0 0
5. 20 WEEKS 6 26.1 10 43.5 7 30.4 0 0
6. 24 WEEKS 5 21.7 6 26.1 11 47.8 1 4.4
7. 28 WEEKS 4 17.4 5 21.7 12 52.2 2 8.7
8. 32 WEEKS 3 13.1 5 21.7 13 56.5 2 8.7
S. No. RESPONSEOBSERVED Group II
GRADES (According to PGA Scale)
0 1 2 3
No. % No. % No. % No. %
1. 4 WEEKS 22 100 0 0 0 0 0 0
2. 8 WEEKS 15 68.2 7 31.8 0 0 0 0
3. 12 WEEKS 13 59.1 9 40.9 0 0 0 0
4. 16 WEEKS 13 59.1 7 31.8 2 9.1 0 0
5. 20 WEEKS 12 54.5 8 36.4 2 9.1 0 0
6. 24 WEEKS 12 54.5 5 22.7 4 18.2 1 4.6
7. 28 WEEKS 11 50.0 6 27.3 4 18.2 1 4.6
8. 32 WEEKS 11 50.0 5 22.7 5 22.7 1 4.6
The response to the drugs at the end of 32 weeks isas shown in the tables above. There was no responseseen at the end of 4 weeks (i.e. all the patients were inGrade 0), in both, Group I & Group II. Initial responsewas seen during the 8th week in both the groups,
however maximum response in Group I was seen after16 weeks of treatment, i.e. in 20th week 10(43.5%)patients were in Grade 1 (i.e. some improvement),7(30.4%) patients in Grade 2 (i.e. markedimprovement) and at the end of 32nd week 13(56.5%)
28. Vinay Kumar--124-128.pmd 10/10/2013, 9:22 AM126

International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 127
patients were in Grade 2 and 2(8.7%) in Grade 3 (i.e.almost clear).
In Group II 2(9.1%) patients showed Grade 2improvement in 16th week, but at the end of 32 weeksnumber of patients increased up to 5(22.7%) in Grade2 and 1(4.6%) patient was in Grade 3.
As far as overall positive response (i.e. Grade I +Grade II + Grade III) is concerned 86.9% patients (i.e.20 out 23) showed positive response in Group I ascompared to only 50% patients (i.e. 11 out of 22) inGroup II
Table 2: Complications
S. No. Complications Groups
Group I Group II
No. % No. %
1. Acne 4 17.4 5 22.7
2. Pseudofolliculitis Barbae 2 8.7 2 9.0
3. Stinging Skin 1 4.4 0 0
4. Burning & Dry Skin 1 4.4 1 4.6
5. Pruritus 1 4.4 1 4.6
6. Erythema 0 0 0 0
7. Breast Enlargement 2 8.7 0 0
8. Weight Gain 3 13.1 0 0
9. Deep Vein Thrombosis 0 0 0 0
10. Liver Toxicity 0 0 0 0
11. Adrenal Suppression 0 0 0 0
Table 3: Overall Cosmetic Results at the end of 32Weeks
GroupsGrades Group I Group II
Grade 0 3(13.1%) 11(50.0%)
Grade I 5(21.7%) 5(22.7%)
Grade II 13(56.5%) 5(22.7%)
Grade III 2 (8.7%) 1 (4.6%)
Total 23 22
DISCUSSION
Out of 22 patients put in group II, to evaluate theeffect of eflornithine (topical – 13.9 %) only 50 %patients (i.e. 11 out of 22) showed positive response.To elaborate with grade 1 response was seen in 5 (22.7%), grade 2 was in 5 (22.7 %) and grade 3 responsewas seen only in 1 (4.6 %) patient and about half of thepatients were in grade 0 at the end of the study.
The response in our study is similar to other studiescarried out in past for evaluation of the effect ofeflornithine in the treatment of facial hirsutism, e.g.two multicenter, double blinded, vehicle controlled,randomized studies were carried out in U.S. and
Europe by Shapiro J and Lui M (2001), also found thesimilar results i.e. about 42 % patients were in grade 0(no improvement), 25 % patient were in grade 1(improvement), 27 % patients were in grade 2 (markedimprovement) and 6 % patient showed grade 3response, i.e. almost clear.
As far as cyproterone acetate is concerned it hasbeen an accepted treatment of hirsutism for almost twodecades with a reported good clinical response in sixtyto eighty percent of patients (Mowszowicz 1983;Kuttenn 1980; Hammerstein 1975; Hammerstein 1983).
However, various studies had been conducted toevaluate the effectiveness of cyproterone acetate forthe treatment of facial hirsutism, either given alone orin combination with other antiandrogenic drugs butvarious results have been obtained with no consistentfinding, e.g. Jones DV, Ibraham and Edwards in 1987found no difference in the reduction of overallhirsutism grades when cyproterone acetate given withor without ethinyl estradiol. In another study carriedout in South Africa where cyproterone acetatecombined with ethinyl estradiol, results in a subjectiveimprovement in hirsutism compared to placebo.
In this study cyproterone acetate was given incombination with eflornithine (topical) in group Ipatients and at the end of 32 weeks of treatment it wasfound to be very effective as compared to group IIpatients.
Out of 23 patients of facial hirsutism put in GroupI to evaluate the effect of cyproterone acetate andeflornithine ( topical) and eflornithine ( topical ) alone86.9% patients (i.e. 20 out 23) showed positive responseas compared to only 50% patients (i.e. 11 out of 22) inGroup II. Onset of improvement was seen after 8 weeksof therapy in both Group I & Group II. Best responsewas observed after 16 weeks of institution of therapyin both the Groups but response in Group I (13.1%) iscomparatively higher than in Group II (1%) becausethe effect of cyproterone start showing by the 16th weekof therapy. So far as cosmetic result is concerned 2(8.7%) patients in Group I revealed Grade 3improvement compared to 1 (4.6%) patient in GroupII. However, Grade 2 improvement was shown in 13(56.5%) patients in Group I compared to 5 (22.7%)patients in Group II.
Thus it is clear that the combination of cyproteroneacetate and eflornithine (topical) is more effective andsafe as compared to eflornithine (topical) alone in facialhirsutism.
28. Vinay Kumar--124-128.pmd 10/10/2013, 9:22 AM127

128 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
As far as complications are concerned these weresimilar to what have been reported in other studies ofeflornithine e.g. study carried out by Schrode K, HuberF, Staszak J, et al (2000) for the safety and efficacy ofeflornithine for facial hirsutism, observed Acne(21.3%), Pseudofolliculitis Barbae (16.3%), stinging andburning skin (14.2%), pruritus (3.8%), erythema (1.3%).We also observed similar complications in our studyin the form of acne, pseudofolliculitis barbae, burning& dry skin, stinging skin and pruritus in patients inboth the groups with similar frequency. All side effectswere primarily mild in intensity and generally resolvedwithout medical treatment.
As far as cyproterone is concerned, it is also foundto be safe in various studies when given for thetreatment for hirsutism e.g. one retrospective studycarried out by Van Wayjen RG et al (1995), of 188women taking cyproterone acetate 50 – 100 mg perday, described side effects in 23%. But many of theproblems were related to mood changes, weight gain,mild breast enlargement or menstrual disturbance.Within the group, 24 had been treated for 5 years ormore, 9 for 10 years or more and 2 for 15 years.Although, no serious side effects have been observed.
Similarly, no serious side effects of cyproteroneacetate like deep vein thrombosis, liver toxicity andadrenal suppression have been observed in my studyin Group I. However, some patients complained aboutbreast enlargement i.e. 2 (8.7%) and weight gain in 3(13.1%) patients.
CONCLUSION
Thus it can be concluded that eflornithine (topical– 13.9 %) when used in combination with cyproteroneacetate yields quicker and effective results as comparedto eflornithine (topical – 13.9 %) used alone.
Conflict of Interest: Nil
Sorce of Funding: Self
Ethical Clearance: Taken from the Institution(Enclosed)
ACKNOWLEDGMENT
Express my deep sense of gratitude, indebtness andsincere regards to my respected teacher and guide Dr.Shyam Sundar Chaudhary, M.B.B.S., M.D. & D.V.D,Professor and Head, Department of Dermatology,Venereology & Leprology, RIMS, Ranchi.
I express me humble and deep thankfulness to Dr.Arun Kumar Singh, Ex- Professor & Head, Departmentof Dermatology, Venereology & Leprology, RIMS,Ranchi.
REFERENCES
1. Hatch R, Rosenfield RL, Kim MH, Tredway D.Hirsutism: implications, etiology andmanagement. Am J Obstet Gynecol 1981;140:815-30.
2. Martin KA, Chang RJ, Ehrmann DA, et al.Evaluation and treatment of hirsutism inpremenopausal women: an Endocrine Societyclinical practice guideline. J Clin EndocrinolMetab. 2008;93(4):1105–1120.
3. Carmina E, Rosato F, Jannì A, Rizzo M, LongoRA. Extensive clinical experience: relativeprevalence of different androgen excess disordersin 950 women referred because of clinicalhyperandrogenism. J Clin Endocrinol Metab.2006;91(1):2–6.
4. Azziz R, Sanchez LA, Knochenhauer ES, et al.Androgen excess in women: experience with over1000 consecutive patients. J Clin EndocrinolMetab. 2004;89(2):453–462.
5. Fauci AS, et al., eds. 2008. Harrison’s Principlesof Internal Medicine. 17th ed. New York, NY:McGraw-Hill Medical; 2008
6. Wagner RF., Jr Physical methods for themanagement of hirsutism. Cutis. 1990;45:19–26.
7. Dierickx CC. Hair removal by lasers and intensepulsed light sources. Semin Cutan MedSurg. 2000;19:267–75.
8. Sanchez LA, Perez M, Azziz R. Laser hairreduction in the hirsute patient: A criticalassessment. Hum Reprod Update. 2002;8:169–81.
9. Burkman RT., Jr The role of oral contraceptivesin the treatment of hyperandrogenicdisorders. Am J Med. 1995;98:130–6.
10. Shaw JC. Spironolactone in dermatologicaltherapy. J Am Acad Dermatol. 1991;24:236–43.
11. Faloia E, Filipponi S, Mancini V, Di Marco S,Mantero F. Effect of finasteride in idiopathichirsutism. J Endocrinol Invest. 1998;21:694–8
12. van der Spuy ZM, le Roux PA. Cyproteroneacetate for hirsutism. Cochrane Database SystRev. 2003. CD001125
13. B, Noveck R, Behr D, Palmisano M. Percutaneousabsorption and pharmacokinetics of eflornithineHCl 13% cream in women with unwanted facialhair. J Clin Pharmacol. 2001;41:972–8.
28. Vinay Kumar--124-128.pmd 10/10/2013, 9:22 AM128

International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 129
Correlation between Fetal Heart Patterns in Labour and CordBlood pH and its Perinatal Outcome
Seetha Panicker1, T V Chitra2, Meena Priyadharshini3, A K Chithra4
1Professor & HOD of OBG, 2Professor and Unit II Chief of OBG, 3Assistant Professor of OBG, 4Junior Resident, P.S.GInstitute of Medical Sciences & Research, Peelamedu, Coimbatore, Tamilnadu
ABSTRACT
Objectives: To correlate the fetal heart patterns in labour with the cord blood PH and perinataloutcome.
Method: The study was carried out in the 104 women who required continuous electronic monitoringin labour. The CTG was assessed objectively using the Kerb's scoring system. Blood collection wasdone immediately after delivery from an isolated cord segment and PH was determined and correlatedwith the CTG scores and perinatal outcome.
Results: The study group was divided into three groups based on the CTG. There was significantcorrelation between low CTG score up to two hours before delivery and acidosis at birth (P = 0.01).
Conclusion: Application of a scoring system in interpretation of CTG increases the objectivity andreduces the intra & inter observer variation. Sensitivity of CTG with a poor score (zero to four) topredict acidosis was 55.81 % and the specificity was 77.04 %.
Keywords: CTG Scoring System, Cord Blood PH
INTRODUCTION
Electronic fetal monitoring (EFM) developed as anon-invasive tool to evaluate the fetal condition inlabour has been in clinical use from the 1960s. Fetalsurveillance in labour is performed mostly to identifyfetuses at risk of hypoxia. Electronic fetal heart ratemonitoring is the mainstay for assessing fetal healthduring labour, because the absence of FHRdecelerations is highly predictive of normal fetal bloodgas and pH at birth1,2,3,4. Fetal bradycardia on CTGeither persistent or progressive has been shown to bestrongly suggestive of fetal hypoxemia and an APGARscore of less than 7 at 5 mins, lower mean umbilicalartery pH and neonatal acidosis5,6,7,8,9. However thoughthe first results were promising it was found that EFMis associated with a high false positive rate. Thus itwould lead to unnecessary obstetric interventions likecaesarean section and instrumental deliveries for fetaldistress. Hence an attempt was made to correlate non-reassuring fetal heart patterns with the cord blood pHat birth and perinatal outcome.
MATERIALS AND METHOD
This study was carried out in the department ofObstetrics and Gynaecology at PSG Institute ofMedical Sciences & Research, Coimbatore. Onehundred and four women were included in the studyfrom Nov 2007 to Nov 2008.
The study group consisted of patients who requiredcontinuous electronic fetal heart monitoring in labour.The indications included risk factors like IUGR,oligohydramnios, pre-eclampsia, bad obstetric historyand hypothyroidism. Exclusion criteria weremalpresentation, fetal anomalies, multiple gestationand gestational age of less than 34 weeks.
All women were on continuous electronic fetalheart monitoring in the active phase of labour. Themonitor used in the study was Philips Avalon FM 30with an external transducer and a paper speed of onecm/min. Uterine contractions were recordedsimultaneously. CTG was assessed objectively usingKreb’s scoring system every two hrs to 30 minutes in
DOI Number: 10.5958/j.2321-1024.1.2.046
29. Seetha--129-133.pmd 10/10/2013, 9:22 AM129

130 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
active labour as indicated. Five parameters were usedin the Kreb’s scoring system (Table 1).
1. Baseline heart rate
2. Baseline variability
3. Amplitudes (Frequency)
4. Acceleration
5. Deceleration
Each parameter was scored zero to two giving tototal score of 10.
Table 1: Kreb’s Scoring system10
FHR Feature Score
0 1 2
Baseline FHR (bpm) < 100> 100-119 120 – 160180 161-180 -
VARIABLITYAmplitude (bpm) < 3 3-5 6 - 25
- >25 -Frequency (bpm) < 3 3-6 > 6
Accelerations 0 1-4 > 4(per 30 mins)
Decelerations Late Severe Moderate None EarlyVariable VariableAtypicalVariable
Three groups were made from the total score 0-3, 4-6 and 7- 10
Blood collection was performed immediately afterdelivery of baby and before delivery of placenta byapplying double clamps near the neonatal andplacental end enclosing 5cm of the umbilical cordbefore division.
The cord was cut between the two proximal andtwo distal clamps. Arterial blood was drawn from theisolated segment of cord with a two ml syringe thathad been flushed with Heparin containing 1000 units/ml. The needle was capped and the syringe transferredimmediately to the laboratory. The cord blood in adouble clamped cord is stable for upto an hour at roomtermperature11. Measurements of pH and base deificitwere performed using Cobasb-221 Omni- S analyser,Roche Company.
FINDINGS
The following results were noted
1. Parity: In the study group of 104 women 62 wereprimis and 42 were multigravidas.(Table 2)
2. Onset of labour: Spontaneous onset of labour in74 women and induced labour in 30 women.(Table 3)
3. Rupture of membranes: Artificial rupture ofmembranes was done in 79 women, eight hadspontaneous rupture of membranes and 17 hadpremature rupture of membranes. (Table 4)
4. Colour of liquor: Liquor was clear in 74 women,Grade I meconium in six, Grade II meconium in16 and Grade III meconium in eight women.(Table 5)
5. Mode of delivery: Thirty eight women had avaginal delivery with episiotomy. Twenty onewomen had an instrumental delivery, 13 withvacuum and eight with outlet forceps. Forty fivewomen were taken up for emergency LSCS withan incidence of 43.3 %.(Table 6) The commonestindication was fetal distress (30 women).
6. CTG score and correlation with cord blood PH:Based on the CTG score at the beginning of theactive phase of labour, 104 women were dividedwith three groups. Group I – initial CTG score ofseven to ten, Group II – initial CTG score of four tosix and Group III – initial CTG score of zero tothree.(Table 7)
Group I
Fifty eight women started active labour with a scoreof seven to ten. Of these 17 had a persistent score ofseven to ten up to delivery with a mean PH of 7.30.Twenty eight of the 58 women in group I who startedactive phase of labour with a CTG score of seven toten had a fall in score to four to six before delivery,they had a mean PH of 7.22. Thirteen of the 58 womenhad a progressive fall in score with time, they had ascore of four to six after one to two hrs and a score ofzero to three ½ hr prior to delivery. This group had amean PH of 7.21.
Group II
Thirty seven women had a CTG score of four to sixat the beginning of the active phase of labour. Fourteenof these had the same score till delivery. This grouphad a mean PH of 7.25. One of this group had a scoreof seven to ten after one hour of labour and deliveredwith the same score. This neonate had a cord bloodPH of 7.34. Twenty two of the 37 women had a scoreof zero to three half an hour prior to delivery. Thisgroup had a mean PH of 7.18.
Group III
Nine parturients had a CTG score of zero to threein the active phase on admission. Five of these had the
29. Seetha--129-133.pmd 10/10/2013, 9:22 AM130

International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 131
same score for three hours till delivery. They had meanPH of 7.07. Two of the nine delivered within one hourwith the same score. The mean PH of this group was7.14. Two of the nine in this group had this score foronly half an hour. Both delivered by LSCS. The meanPH of this group was 7.25.
Group I had 18 women
Group II had 28 + 14 = 42 women
Group III had 13 + 22 + 9 = 44 women.
Chi square analysis was used to correlate PH andCTG scores half an hour before delivery. P value = 0.01which is significant. Similarly there was a significantcorrelation between acidosis and CTG score one hourbefore delivery (P value 0.02) and two hours beforedelivery (P value 0.01) However there was nocorrelation between CTG scores taken 3 hours beforedelivery and acidosis.
The neonatal outcome was also analysed. (Table 8)Of the 104 deliveries 66 neonates had a good outcome.Eighteen belonging to Group I, 29 belonging to GroupII and 19 belonging to Group III. Thirty eight neonatesrequired NICU care. Seventeen were treated for mildrespiratory distress, 13 needed CPAP and eight neededventilatory support. There were no neonatal deaths.
Table 2: Parity-wise distribution
Parity Frequency (N) %
Primi gravidae 62 59.6 %
Multi gravidae 42 40.4 %
Total 104 100.0 %
Table 3: Onset of Labour
Onset of Labour Frequency (N) %
Spontaneous 74 71.2
Induced 30 28.8
Total 10 100.0
Table 4: Nature of Rupture of Membranes
Rupture of Membrane Frequency(N) %
Artificial Rupture 79 75.9of Membrane
Spontaneous Ruptureof Membrane 08 7.6
Premature Rupture 17 16.5of Membrane
Total 104 100.0
Table 5: Colour of Liquor
Colour of Liquor Frequency (N) %
Clear 74 71.1
Grade I Meconium 06 05.9Stained Liquor
Grade II Meconium 16 15.3Stained Liquor
Grade III Meconium 08 07.7Stained Liquor
Total 104 100.0
Table 6: Mode of Delivery
Mode of Delivery Frequency(N) %
Vaginal delivery 38 13with episiotomy
Vacuum 08 36.5
Forceps 12.5 07.7
LSCS 45 43.3
Total 104 100.0
Table 7 : Correlation between CTG score ½ hr beforedelivery and cord blood PH
CTG PH
7.15 > 7.15 Mean
Group I (8-10) 1 17 7.3
Group II (5-7) 8 34 7.2
Group III (0-4) 16 28 7.2
Table 8: Neonatal outcome based on CTG score
Outcome CTG Score Total
Group I Group II Group III (7-10) (4-6) (0-3)
Good 18 29 19 66
Mild respiratory 0 5 12 17distress
CPAP 0 5 8 13
Ventilator 0 3 5 8
Total 18 42 44 104
DISCUSSION
A pathological CTG detects acidaemia quite wellin that most cases of acidaemia are associated with anabnormal FHR12. Although CTG is a very useful toolfor fetal monitoring in labour it has been reported tobe associated with a high false positive rate13.
There is also a lot of inter & intra observe variation.Hence an objective analysis of the CTG is needed. Inthis study a scoring system was used to grade the CTGand the umbilical cord blood PH was determined tosee whether it correlated with the CTG. The perinataloutcome was also analysed.
29. Seetha--129-133.pmd 10/10/2013, 9:22 AM131

132 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
The study group consisted of women who requiredcontinuous CTG monitoring in labour with variousrisk factor like oligohydramnios, IUGR, PIH, BOH,gestational diabetes and hypothyroidism.
The parity, mode of onset of labour, rupture ofmembranes and colour of liquor in this group wereanalysed.
Analysis of the mode of delivery in this groupshowed 45 women were delivered by LSCS a rate of43.3 %. The commonest indication was fetal distressin 66.67%, the other indications being protracteddescent and dilatation, arrest of descent and dilatation.The parturients were divided into three groups basedon the CTG scores at the beginning of the active phaseof the labour.
Group I CTG score of seven to ten had 58 women.
Group II CTG score of four to six had 37 women.
Group III CTG score of zero to three had 9 women.
To evaluate the neonatal outcome, APGAR scorealone is a poor indicator of neonatal asphyxia and/oracidosis. The fetal acid-base status was the mostreliable index of fetal oxygenation14. Eighteen womenhad a CTG score of seven to ten from the beginning oflabour till delivery. They had a mean arterial PH of7.3.
Forty two women (28 from Group I and 14 fromGroup II) had a CTG score of four to six at delivery.They had a mean arterial PH of 7.22 and 7.25respectively.
Forty four women (13 from Group I, 22 from GroupII and nine in Group III) had a CTG score of zero tothree.
Five women had a CTG score of zero to three fromthree hours prior to delivery. They had a mean cordblood PH of 7.07.
Although fetal academia had been classicallydefined as an umbilical artery pH of < 7.20, significantor pathologic fetal academia had more recently benndefined as umbilical artery ph < 7.00 15,16. Changes inthe CTG score were observed. In women with a CTGscore of zero to three, if they were delivered withinhalf to one hour the risk of acidosis was 35.5 and 41.1
% respectively. If the delivery was prolonged to threehours or more the risk of acidosis was 60 %.
Correlation between CTG score at half an hour, onehour, two and three hours before delivery and the PHvalues were done. The CTG score at half an hour, onehour and two hours prior to delivery correlated wellwith cord blood PH at birth. Rapid deterioration ofthe CTG score requires immediate intervention toprevent acidosis17.
Joel D Larma et al found a sensitivity of 53.8 andspecificity of 61.7, positive predictive value of 50 %and negative predictive value of 88.6% with poor CTGscore for outcome as acidosis18.
In our study we found a sensitivity of 55.8 % andspecificity of 77.04 % for acidosis in the neonate whenthe CTG score was zero to three.
Positive predictive value ie. with a poor CTG scoreof zero to three the probability of acidosis for theneonate is 63.15%. Negative predictive value ie. witha good CTG of score of seven to ten the probability ofdelivering a non acidotic neonate is 71.21%.
CONCLUSION
Application of a scoring system in interpretationof CTG in labour increases the specificity and reducesthe inter & intra observer variability in interpretation.There was a significant correlation between low CTGscores and acidosis. Sensitivity of CTG with a poorscore of zero to three to predict acidosis was 55.81%and specificity was 77.04%. The longer the duration ofthe poor score the greater the chance for neonatalhypoxia and acidosis and rapid deterioration of CTGscores were found to require immediate interventionto prevent acidosis.
ACKNOWLEDGEMENT
We are thankful to Dr Anand CV, Professor ofBiochemistry, Dr. Sarah Paul, Professor of Paediatricsand Chief of Neonatology, Colleagues and Staff inlabour ward for being supportive for our study.
Conflict of Interest: None
Source of Funding: Hospital
Ethical Clearance: Obtained
29. Seetha--129-133.pmd 10/10/2013, 9:22 AM132

International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 133
REFERENCES
1. Liston R, et al., Fetal health surveillance in labour.J Obstet Gynaecol Can 24:250 – 276
2. Liston R, et al., Fetal health surveillance in labour.J Obstet Gynaecol Can 24: 342-355
3. Liston R, et al., Fetal health surveillance:antepatum and intrapartum consensus guideline.J Obstet Gynaecol Can 29: 53 – 56.
4. (1997) Electronic fetal heart rate monitoring:research guidelines for interpretation. NationalInstitute of Child Health and HumanDevelopment Research Planning Workshop. AmJ Obstet Gynecol 177 : 1385 – 1390. Doi 10.1016/s002-9378(97)70079-6
5. Krebs HB, et al., Intrapartum fetal heart ratemonitoring. V. Fetal heart rate patterns in thesecond stage of labor. Am J Obstet Gynecol 1981;140; 435-9
6. Cardoso CG, et al., A study on second stagecardiotocographic patterns and umbilical acid-base balance in cases with first stage normal fetalheart rates. J Maternal Fetal Invest 1995;5;144-7
7. Gilstrap LC, et al., Second stage fetal heart rateabnormalities and neonatal acidosis. ObstetGynaecol 1984;63; 209-13
8. Gilstrap LC, et al., Second stage fetal heart rateabnormalities and type of neonatal academia.Obstet Gynaecol 1987;70; 191-5.
9. Piquard F, et al., The validity of fetal heart ratemonitoring during the second stage of labor.Obstet Gynaecol 1988;72; 741-50.
10. Krebs H.B, et al., Intrapartum fetal heart ratemonitoring I. Classification and prognosis of fetal
heart rate patterns. Am J Obstet Gynaecol 1979;133: 762 – 780
11. Duerbeck NB, et al., A practical approach toumbilical artery pH and blood gasesdeterminations. Obstet Gynaecol. 1992; 79(6):959-962
12. FIGO News. Guidelines for the use of fetalmonitoring. Int J Gynaecol Obstet 1987; 25:159-167
13. Pattison.N, MC Cowanz. Cardiology for AntePartum Fetal assessment (Cochrane Review). IN:The Cochrane Library Issue 3, 2006. Oxford:Update software (Level I)
14. James LS. The acid-base status of human infantsin relation to birth asphyxia and onset ofrespiration. J Paediatr 1958;52;379-94
15. Goldaber KGD, et al., Pathologic fetal academia.Obstet Gynaecol 1991; 78; 1103-7 10.
16. American College of Obstetricians andGynecologists, Operative vaginal delivery, TheCollege, Washington, (1991) Technical BulletinNo. : 152)
17. Parer JT, King J, Flanders S, Fox M, Kilpatrick SJ.Fetal academia and Electronic FHR pattern : Isthere evidence of an association. J maternal, fetaland neonatal medicine 2006, 19:289-294
18. Larma JD, Silva AM, Holcroft CJ, Thompson RE,Donohue PK, Graham EM. Intra PartumElectronic FHR monitoring and the identificationof Metabolic acidosis and HIE. AMJ ObsetGynaecol 2007;197:301.el,301.e8.
29. Seetha--129-133.pmd 10/10/2013, 9:22 AM133

134 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
Clinico-social Profile and Surgical Management of Cases ofDiabetic Foot: A Prospective Study
Md Shakeel1, Arshiya Taranum2
1Asst Professor, Dept. of General Surgery, SSIMS & RC, Davanagere, Karnataka, 2Junior Resident, Dept ofCommunity Medicine, JJM Medical College Davanagere, Karnataka
ABSTRACT
Diabetes continues to be the most common chronic disease in the developed countries, with increasingtrend in India. Foot ulcers are among the leading causes of morbidity in diabetics3 and as suchdiabetic foot infection is a common cause for the hospital admissions of the diabetic patients in India.This could be attributed to several socio-cultural practices, low education and poor socio-economicconditions.
Objective: To study the clinico-social profile and surgical management of patients presenting withdiabetic foot.
Materials and Method: This is a descriptive cross-sectional study which was carried out on 150patients with diabetes mellitus with associated surgical complications who presented to SurgeryDepartment of SSIMS and Research Centre, Davanagere for a period of one year from February2012 to March 2013. Data was collected by detailed history followed by clinical examination diagnosticprocedures and surgical management.
Results: A total of 150 patients were selected for the study. There is a higher incidence in malepatients (70%) and majority of patients (42%) belonged to lower socioeconomic status
Average age of presentation was 56 years. Staph.aureus was the most common organism isolatedfrom diabetic foot infections and ulcer (60%) was the commonest presenting feature followed bycellulitis(15%).Severity of lesion correlated with severity and duration of diabetes. The averageduration of diabetes is 9.6 years. 24 % presented with osteomyletic changes on X-Rays of feet. Theaverage duration of hospital stay was 15 days.
Conclusion: Diabetic foot infections are the most common complication of diabetes mellitus resultingin disabilities, which get reported to surgeons and require multidisciplinary approach for itsmanagement. Prevention in the form of good diabetes control is the best modality. While muchemphasis should be given on patient education regarding diabetes control, foot care, early reportingof infections and continuing treatment even after leaving the hospital. A team approach with aggressiveand appropriate medical and surgical treatment according to grade of disease will go a long way inimproving the outcome and reducing the morbidity and mortality due to diabetes.
Keywords: Diabetes, Socio-Demographic, Clinical Profile, Foot Ulcers, Amputation
INTRODUCTION
Diabetes continues to be the most common chronicdisease in the developed countries, with more than100 million cases diagnosed worldwide.1 Based on acompilation of studies from different parts of theworld, the World Health Organisation (WHO) hasprojected that the maximum increase in diabetes
would occur in India.2 Considering the largepopulation and the high prevalence of diabetes, theburden of diabetes in India would become enormous.Foot ulcers are among the leading causes of morbidityin diabetics3 and as such diabetic foot infection is acommon cause for the hospital admissions of thediabetic patients in India.4 This could be attributed to
DOI Number: 10.5958/j.2321-1024.1.2.047
30. shakeel--134-140.pmd 10/10/2013, 9:22 AM134

International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 135
several socio-cultural practices such as barefootwalking; inadequate facilities for diabetic care, loweducation and poor socio-economic conditions.4
Diabetic foot amputations are the most frequent ofdiabetic complications in developing countries.
In recent years, the various factors resulting in thedevelopment of diabetic foot problems have beengaining attention because of the increasing disability,rising healthcare costs, and reduction in quality of lifeof patients that arise from diabetic foot problems.
Poor socioeconomic factors have been empiricallyaccepted as a risk factor for the development of diabeticfoot problems5. However, the role of socioeconomicfactors in Asian populations, like that of Indians, hasnot been well studied. Thus, this study was carriedout with the objective to look for the socio-demographic profile and clinical profile includingsurgical management of patients presenting withdiabetic foot problems.
MATERIALS AND METHOD
This is a descriptive cross-sectional study whichwas carried out in the Surgical Patients of SSIMS andResearch Centre, Davanagere for a period of one yearfrom February 2012 to March 2013. 150 patients havinglong standing diabetes mellitus with footcomplications presented to the surgical unit or theCasualty during the study period. Adult patients aged18 years and above, previously diagnosed or newlydiagnosed diabetic, presenting with lower extremityinfection. Data was collected by taking a detailedhistory including demographics, medical and surgicalhistory, duration of diabetes, and the type of treatmentthe patients received and any complication-relatedinformation followed by medical examination.Description of the wound or ulcer on the foot wasnoted and was assessed based on Wagner ’sclassification6 as follows:
Grade I: ulceration involving only the dermis
Grade II: ulceration involving tendons and/or jointcapsules
Grade III: extending to bone, usually causingosteomyelitis
Grade IV: localized gangrene
Grade V: gangrene involving a major part of thefoot.
Diagnostic procedures included the complete bloodexamination, complete urine examination, blood sugarprofile, renal parameters, radiograph of the affectedlimb, CXR,ECG. Pus from the ulcer was sent for cultureand sensitivity testing.
Plain Insulin was started and Broad spectrumantibiotics were prescribed accordingly.
Depending on the Grade of infection themanagement was planned which included bothsurgical and medical treatment methods. The patientswere followed up till their stay in the hospital.
RESULTS
Table 1: Demographic profile of study subjects
Patient Characteristics Number Percentage(n=150) (%)
Age (in years)
21-30 6 (4)
31-40 12 (8)
41-50 24 (16)
51-60 48 (32)
61-70 60 (40)
Gender
Male 105 (70)
Female 45 (30)
Residence
Urban 79 (53)
Rural 71 (47)
Family history of Diabetes
Positive 39 (26)
Negative 111 (74)
Table 2: Socioeconomic profile of study subjects
Socioeconomic Status Number Percentage(n=150) (%)
Lower 63 (42)
Middle 39 (26)
Upper Class 48 (32)
Occupation
Agriculture 45 (30)
Housewife 32 (21)
Coolie 24 (16)
Business 20 (13)
Office work 15 (10)
Teacher 15 (10)
30. shakeel--134-140.pmd 10/10/2013, 9:22 AM135

136 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
Table 3: Clinical and other diagnostic features of studysubjects
Clinical Characteristics Patients Percentage(n=150) (%)
Presenting features
Ulcer 90 (60)
Cellulitis 23 (15)
Abscess 19 (13)
Gangrene 18 (12)
Site of lesion
Sole 69 (46)
Dorsum 35 (23)
Leg 31 (21)
Leg and Foot 15 (10)
Organism
Staphylococcus aureus 60 (40)
Pseudomonas 29 (19)
Klebsiella 25 (17)
E.Coli 20 (13)
Streptococci 16 (11)
X-ray changes
Bone involvement 36 (24)
Non Bone involvement 114 (76)
Table 4: Surgeries secondary to diabetes relatedcomplications
Surgery Number Percentage(n=150) (%)
I & D 27 (18)
Debridement 90 (60)
Ray amputation 18 (12)
Below-knee amputation 12 (8)
Above-knee amputation 3 (2)
Split thickness Skin Grafting 30 (29)
RESULTS
The average age of presentation was 56 years. Themost common age group being 61-70 years. There is ahigher incidence in male patients with about threefourth (70%) of them presenting with the disease. Alsoin our study majority of patients (42%) belongs tolower socioeconomic status while only 26% in themiddle and 32% to the upper class.
A higher incidence (30%) was seen amongagriculturists, as this is the most common occupationof people here. 53% of diabetic patients were belongingto urban areas and 47% were belonging to rural areas.Contrary to the belief that diabetes is common amongthe sedentary workers but in our study it was foundto be common in moderate and even heavy workers.
The family history of diabetes is positive in 26% andnegative in 74% of patients.
The average duration of diabetes is 9.2 years. Thecommonest site of lesion was foot which included sole(46%), dorsum (23%) while leg (21%), combined legand foot lesions were seen in 10% of patients. The meanduration of wound was 25.4 days. Majority of footlesions developed without an apparent cause (54%),followed by infected nail bed (21%) or trauma(25%).Commonest type of lesion were ulcer (60%)followed by cellulitis (15%). Staph.aureus (40%) wasthe most common organism isolated from diabetic foot.On X-rays, bone involvement was seen in (24%) cases.
Minor operative procedures like incision anddrainage, slough excisions or debridement werecarried out in 78 % of patients. Ray amputation, Below-knee amputation and Above-knee amputation weredone in 12%, 8% and 2% respectively. Split thicknessSkin Grafting were done in 29% of patients.
DISCUSSION
Long standing diabetes mellitus leads tomultisystem complications. Foot ulcers develop in20-30% of such patients. The average duration ofdiabetes was 9.2years and in contrast to our studyGriffith and Jeffery7 study was 12 years, this may bedue to late detection of diabetes in our country.
In our study, diabetic foot infections were morecommon in males which form 70% of all patients.Study done by Munawar J8 and other studies 9alsoshowed male predominance. Diabetic foot infectionswere found to be common in 61-70 years which washigher than the studies by and Rooh-Ul-Muqim et al.10
Also in our study majority of patients (42%) belongedto lower socioeconomic status which is similar to thestudies by Gohel Jayesh.11 A higher incidence (30%)was seen among agriculturists, low average monthlyincome has been associated with worse diabeticoutcomes as it determines the ability to obtainmedication and services that improve health.12 Thedifference between urban and rural areas were meagreas such the prevalence of diabetes and diabetic footinfections were seen to be increasing in rural areaswhich is highlighted in study by Madan M.13
The family history of diabetes was positive inroughly one fourth of patients (26%) and nearly 96%had Type II diabetes while in study by Furqan
30. shakeel--134-140.pmd 10/10/2013, 9:22 AM136

International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 137
Siddiqui14, 89% patients had type II diabetes and familyhistory was positive in 79% patients.
The common presenting features were ulcer in 60%patients followed by cellulitis in 15% patients whereasin study by Gohel11, abscess (54%) was the commonestpresenting feature followed by gangrene (29%).Soleor foot was the commonest site for infection which isin agreement with other studies. The occurrence of thislesions are common in agriculturists who walkbarefoot and prone for infections.
Diabetic foot infection is usually polymicrobial innature consisting of gram positive and gram negativeaerobes as well as anaerobes. However the mostcommon microorganism isolated is staphylococcusaureus followed by streptococcus and pseudomonas.In this study staphylococcus aureus was isolated fromculture of pus in 40%, whereas staphylococcus aureuswas isolated in 54% of cases in a study done by ZafarA10. However when deeper tissues are invaded by theorganisms, anaerobes are more frequently found.
Bone involvement or osteomylitic changes on X-Ray was seen in one fourth of cases which is less thanthe findings by Khan A.H15 (40%) and by Gohel12(30%).
Depending upon the extent of foot infection, lesionsare graded into five groups as in Maggit-Wegnerclassification. Broad spectrum antibiotics such asclindamycin along with gentamicin or amoxicillin plusclavulenic acid are usually prescribed for at least 2-4weeks for grade I and II disease. Howeverciprofloxacin and metronidazole have also been founduseful. In our study 60% patients were treated withantibiotics and debridements Patients having gradeIII - grade V disease needed some form of amputationfor their management and comprises a bulk of patients.In our study 26% patients were in these grades likeother study16 whereas 20% needed amputations. In ourstudy 29% patients had skin grafting while in studyby Madan M13 54% patients were managed bydebridement,18 % by disarticulation, 10% by Incisionand Drainage, 8% managed by amputation andgrafting was done in 10%.
CONCLUSION
Diabetic foot infections are the most commoncomplication of diabetes mellitus which get reportedto surgeons and require multidisciplinary approachfor its management. Effective control of infection anddiabetes itself along with surgical procedures required
according to the grade of infection are the mostimportant steps in the management of such patients.
Males in the fifth and sixth decade belonging tolow socioeconomic status are more susceptible todiabetic foot infections because of increasedsusceptibility to trauma, smoking and unhygienicliving. Agriculturists were more affected because ofbarefoot walking and working in fields. As opposedto common belief that diabetes is common withsedentary lifestyle and in urban areas, we found ahigher prevalence in housewives who belong tomoderate work group and in agriculturists belongingto rural areas. This implies trend of diabetes is shifting.
Ulcers were the commonest presentation withstaphylococcus aureus being common organismisolated in our setup. Majority of foot infections weremanaged by controlling diabetes, antibiotics anddebridement. Amputation was done only for gangreneand uncontrolled spreading of infection, as a life savingmeasure.
A team approach must be adopted to managediabetic foot lesions in order to achieve good results.Much emphasis should be given on patient educationregarding diabetes control, foot care, early reportingof infections and continuing treatment even afterleaving the hospital. Knowledge about Rehabilitativemeasures, prosthesis and support must be given tothose patients who have undergone amputations.
ACKNOWLEDGEMENT
The authors are thankful to faculty members andinterns of surgery department, SSIMS and RC; for theirvaluable support during this study.
Conflict of Interest: Nil
Source of Funding: Self
Ethical Clearance: NA
REFERENCES1. Nathan DM, Meigs J, Singer DE: Lancet 350
(suppl): 4–9, 1997.2. Definition, diagnosis and classification of
diabetes mellitus and its complication. Reportof consultation. WHO, Geneva1999, Report 250.
3. Gibbons G, Habershaw G. Diabetic footinfections. Infect Dis Clin North Am 1995; 9:131-142.
30. shakeel--134-140.pmd 10/10/2013, 9:22 AM137

138 International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2
4. Vijay V, Snehalatha C, Ramachandran A.Socio-cultural practices that may affect thedevelopment of the diabetic foot. IDF Bulletin1997; 42:10–2
5. Peters EJD, Lavery LA, Armstrong DG. Diabeticlower extremity infection – influence of physicalpsychological and social factors. J DiabComplicat. 2005; 19:107–12.
6. Wagner FW. Algorithms of diabetic foot care. In;Levin MN, O’ Neal. The diabetic foot 2nd ed. StLouis: CV Mosby, 1983.
7. Griffiths GD. Diabetic foot disease. In CuschieriSA, Essential Surgical Practice 4th edition 2002Arnold. 785-94.
8. Munawar J, Asghar A, Amin M Osteomyelitis offoot in diabetic patients. J Surg Pak 2003; 8 (3);32-4.
9. Zafar A Management of diabetic foot- Two yearexperience. J Ayub Med Coll Abbottabad 2001;13 (1); 14-6.
10. Rooh-ul-muqim , Samson Griffin , MukhtarAhmed. Evaluation and Management of diabeticfoot according to Wagner classification: A studyof 100 cases. J Ayub Medical College2003; 15(3):39-42.
11. Gohel Jayesh B, Sharma Dinesh, Patel NaineshB, Raswan Uday S, Patil Salil. A study of sociodemographic and clinical Profile of cases ofdiabetic foot. Natl J Med Res. 2012; 2(3):279-81.
12. Bachmann MO, Eachus J, Hopper CD, DaveySmith G, Propper C, Pearson NJ, et al. Socio-economic inequalities in diabetes complications,control attitudes and health service use: acrosssectional study. Diabet Med 2003; 20: 921_9.
13. Madan M, Naveen T.K,Balachandra M. A studyof Surgical Management of Diabetic Limbcomplications among rural population.Indian JSurg;2012,74(2):131-135.
14. Furqan Siddiqui, Siriporn Janchai, DonaldMercante, William Dabdoub. Evaluation ofDiabetes-Related Complications.The Journal ofApplied Research In Clinical and ExperimentalTherapeutics.
15. Khan A.H, Bajwa G.R.Approach to ManagingDiabetic Foot Complications. A Study of 200Cases .Annals;2008, 14. ( 4) :129-32
16. Sanderson. PJ. Infection of the foot withpeptococcus Magnus. J Chin pathol 1990; 30;266-268.
30. shakeel--134-140.pmd 10/10/2013, 9:22 AM138

International Journal of Contemporary Surgery. July-December., 2013, Vol.1, No. 2 139
Call for Papers/Article Submission
International Journal of Contemporary Surgery is a double blind peer reviewed international journal
The following guidelines should be noted:
• The article must be submitted by e-mail only. Hard copy not needed. Send article as attachment in e-mail.
• The article should be accompanied by a declaration from all authors that it is an original work and has notbeen sent to any other journal for publication.
• As a policy matter, journal encourages articles regarding new concepts and new information.
• Article should have a Title
• Names of authors
• Your Affiliation (designations with college address)
• Abstract
• Key words
• Introduction or back ground
• Material and Methods
• Findings
• Conclusion
• Acknowledgements
• Interest of conflict
• References in Vancouver style.
• Please quote references in text by superscripting
• Word limit 2500-3000 words, MSWORD Format, single file
All articles should be sent to : [email protected]
Our Contact Info:
Prof. R K Sharma
Editor, International Journal of Contemporary Surgery
Institute of Medico-Legal Publications4th Floor, Statesman house buildingBarakhamba Road, Connaught Place
New Delhi-110001Tel No: +91 - 09971888542Fax No: +91 11 3044 6500
Email: [email protected]: www.ijocs.in
30. shakeel--134-140.pmd 10/10/2013, 9:22 AM139

INTERNATIONAL JOURNAL OF
CONTEMPORARY SURGERYInstitute of Medico-Legal Publications
4th Floor, Statesman house building, Barakhamba Road,Connaught Place, New Delhi-110001
Tel No: +91 - 09971888542Fax No: +91 11 3044 6500
Email: [email protected]: www.ijocs.in
CALL FOR SUBSCRIPTIONS FOR 2013
International Journal of Print Only Print+Online Online OnlyContemporary Surgery
INDIAN INR 7000 INR 9000 INR 5500
FOREIGN USD 550 USD 550 USD 250
Journal Title Pricing of Journals
NOTE FOR SUBSCRIBERS
• Advance payment required by cheque/demand draft in• the name of “Institute of Medico-Legal Publications” payable at Noida/New Delhi.• Cancellation not allowed except for duplicate payment.• Claim must be made within six months from issue date.• A free copy can be forwarded on request.
Our Contact Info:Prof. R K Sharma
Editor, International Journal of Contemporary SurgeryInstitute of Medico-Legal Publications
4th Floor, Statesman house buildingBarakhamba Road, Connaught Place
New Delhi-110001Tel No: +91 - 09971888542Fax No: +91 11 3044 6500
Email: [email protected]
Website: www.ijocs.in
ISSN 2320-9615 (Print Version) ISSN 2321-1024 (Online Version) Frequency Half yearly
International Journal of Contemporary Surgery is a double blind peer reviewed international journal whichhas commenced its publication from January 2013. The journal is half yearly in frequency. The journal coversall aspects of surgical practice. The journal has been assigned ISSN 2320-9615 (Print Version) andISSN 2321-1024 (Online Version). The journal is indexed in many international data bases
30. shakeel--134-140.pmd 10/10/2013, 9:22 AM140


Copyright © 2022 FDOKUMEN










![[Greeting modalities preferred by patients in pediatric ambulatory setting]](https://static.fdokumen.com/doc/165x107/6337af65d102fae1b6077daa/greeting-modalities-preferred-by-patients-in-pediatric-ambulatory-setting.jpg)









