Thumb Movements, Motions, and Moments
9
Thumb Movements, Motions, and Moments Anne Hollister, MD RilllcllO Los Amigos Medical Cellter, Dowlley, Califomia David J. Giurintano, MSME LCDR, u.s. PIIMic Health Service, Chief, Rehabilitatioll Research, Palll W. Bralld Biomechallics Laboraton/, Gillis W. LOllg Hallsell's Disease Center, Carville, LOllisa/w A n accurate model of thumb movements is essential for understanding thumb mechan- ics. The therapist treating a patient who has a thumb disorder will be more successful if he or she knows the effects of muscles and of applied loads on thumb function and posture. Evaluating the causes and planning treatment for deformities and functional loss in the thumb are easier when the mechanisms of motion of the thumb are understood. The form of a joint, its movements, and the forces acting about a joint are related. There has been a great deal of controversy regarding the motions of the thumb as a whole, the motions of its individual jOints, and the effects of muscles or tendon transfers on the thumb. Much of this confusion is due to the way thumb motions are defined. Anatomists have defined the three planes by which the locations of structures and joint movements may be described: the sagittal plane, which runs anteroposteriorly; the coronal plane, which runs side to side; and the transverse plane, which runs at right angles to the other two planes and is parallel to the ground when a person is standing (Fig. 1A). The classic diagram of a body shows the hands in supination, so that the palms face forward, and it is clear that the palm of the hand lies in the coronal plane. However, the arms are extended obliquely and thus do not lie parallel to the sagittal plane and are cut obliquely by the coronal plane. A compromise is to consider the length of the hand to be in the sagittal plane (Fig. 1B). The thumb still presents difficulty in matching movements and postures to classic planes. At rest, the thumb is usually thought of as lying halfway between pronation and supination. In this position, it is not aligned with any of the anatomic planes. This presents problems when precision is needed conforming the movements of the thumb with the anatomic planes. In the anatomic reference frame, the motions that hand surgeons call flexion and ex- tension become abduction and adduction. The other motions have similar descriptive problems. I Correspondence and reprint requests to Anne Hollister, MD, Ran- cho Los Amigos Medical Center ABIS, 8701 Imperial Highway, Downey, CA 90242. 106 JOURNAL OF HAND THERAPY ABSTRACT: An understanding of the movements of the thumb is essential for understanding thumb function and pathology and for planning therapeutic interventions. The thumb has three joints, which move about axes of rotation. The carpometacarpal and metacarpophalangeal joints have two offset axes of rotation and the interphalangeal joint has one. The thumb muscles act about these axes, and imbalances resulting from paralysis are explained by this model. The effects of tendon transfers and splints can be predicted by analyzing their effects at each joint and axis. J HAND THER 8:106-114, 1995. Another problem is the description of the move- ments of the joints themselves. Classically, joint mo- tion has been considered to occur about axes in the anatomic planes. Flexion and extension are move- ments that occur in the sagittal plane, abduction and adduction in the coronal plane, and internal and ex- ternal rotation in the transverse plane (Fig. 1C). For each joint, separate perpendicular axes for each set of motions-flexion-extension, internal rotation- external rotation, and abduction-adduction-have been proposed. These theories are based on the work of Fick,2 who analyzed the shapes of joint surfaces and felt that they were compatible with the bones moving about one or more fixed axes of rotation. The axis of rotation between two bones is defined as a line that does not move in relationship to either bone while they move around each other. Fick 2 never found any of these axes, but he felt that they were perpen- dicular to the bones and to each other. THE AXES OF ROTATION OF THE THUMB JOINTS The positions of these axes of rotation for the thumb joints have been found using a mechanical device. 3 .4 The carpometacarpal (eM C) and metacar- pophalangeal (MP) joints each have two fixed axes of rotation and the interphalangeal (IP) joint has one, as Fick 2 predicted. However, these axes are not per- pendicular to the bones or to each other. The ori- entation of the hinges relative to the bones and to each other, as shown in Figure 2, is of great impor- tance in understanding the mechanics of thumb mo- tion. When a body moves about fixed axes of rotation, the orientation of the axes determines the kind of motion that occurs. For a joint to exhibit pure flexion and extension, its axis of rotation must be perpen- dicular to the sagittal plane, similar to the hinge in Figure 3A. A point on the hinge will move in a circle about the hinge's axis and in a plane perpendicular to the hinge. This plane of motion is parallel to the sagittal plane because the hinge is perpendicular to the sagittal plane. A simple hinge has one degree of
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Thumb Movements, Motions, and Moments

Thumb Movements, Motions, and Moments
Anne Hollister, MD RilllcllO Los Amigos Medical Cellter, Dowlley, Califomia
David J. Giurintano, MSME LCDR, u.s. PIIMic Health Service, Chief, Rehabilitatioll Research, Palll W. Bralld Biomechallics Laboraton/, Gillis W. LOllg Hallsell's Disease Center, Carville, LOllisa/w
A n accurate model of thumb movements is essential for understanding thumb mechan
ics. The therapist treating a patient who has a thumb disorder will be more successful if he or she knows the effects of muscles and of applied loads on thumb function and posture. Evaluating the causes and planning treatment for deformities and functional loss in the thumb are easier when the mechanisms of motion of the thumb are understood.
The form of a joint, its movements, and the forces acting about a joint are related. There has been a great deal of controversy regarding the motions of the thumb as a whole, the motions of its individual jOints, and the effects of muscles or tendon transfers on the thumb.
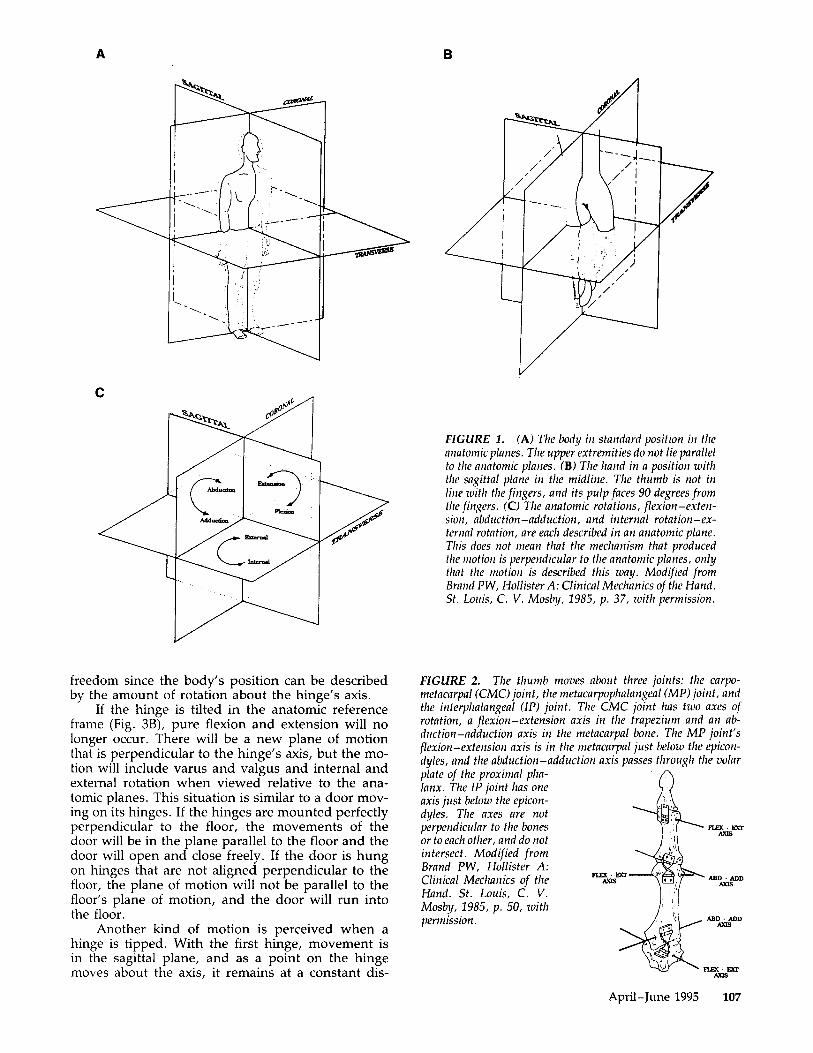
Much of this confusion is due to the way thumb motions are defined. Anatomists have defined the three planes by which the locations of structures and joint movements may be described: the sagittal plane, which runs anteroposteriorly; the coronal plane, which runs side to side; and the transverse plane, which runs at right angles to the other two planes and is parallel to the ground when a person is standing (Fig. 1A). The classic diagram of a body shows the hands in supination, so that the palms face forward, and it is clear that the palm of the hand lies in the coronal plane. However, the arms are extended obliquely and thus do not lie parallel to the sagittal plane and are cut obliquely by the coronal plane. A compromise is to consider the length of the hand to be in the sagittal plane (Fig. 1B). The thumb still presents difficulty in matching movements and postures to classic planes. At rest, the thumb is usually thought of as lying halfway between pronation and supination. In this position, it is not aligned with any of the anatomic planes. This presents problems when precision is needed conforming the movements of the thumb with the anatomic planes. In the anatomic reference frame, the motions that hand surgeons call flexion and extension become abduction and adduction. The other motions have similar descriptive problems. I
Correspondence and reprint requests to Anne Hollister, MD, Rancho Los Amigos Medical Center ABIS, 8701 Imperial Highway, Downey, CA 90242.
106 JOURNAL OF HAND THERAPY
ABSTRACT: An understanding of the movements of the thumb is essential for understanding thumb function and pathology and for planning therapeutic interventions. The thumb has three joints, which move about axes of rotation. The carpometacarpal and metacarpophalangeal joints have two offset axes of rotation and the interphalangeal joint has one. The thumb muscles act about these axes, and imbalances resulting from paralysis are explained by this model. The effects of tendon transfers and splints can be predicted by analyzing their effects at each joint and axis. J HAND THER 8:106-114, 1995.
Another problem is the description of the movements of the joints themselves. Classically, joint motion has been considered to occur about axes in the anatomic planes. Flexion and extension are movements that occur in the sagittal plane, abduction and adduction in the coronal plane, and internal and external rotation in the transverse plane (Fig. 1C). For each joint, separate perpendicular axes for each set of motions-flexion-extension, internal rotationexternal rotation, and abduction-adduction-have been proposed. These theories are based on the work of Fick,2 who analyzed the shapes of joint surfaces and felt that they were compatible with the bones moving about one or more fixed axes of rotation. The axis of rotation between two bones is defined as a line that does not move in relationship to either bone while they move around each other. Fick2 never found any of these axes, but he felt that they were perpendicular to the bones and to each other.
THE AXES OF ROTATION OF THE THUMB JOINTS
The positions of these axes of rotation for the thumb joints have been found using a mechanical device. 3.4 The carpometacarpal (eM C) and metacarpophalangeal (MP) joints each have two fixed axes of rotation and the interphalangeal (IP) joint has one, as Fick2 predicted. However, these axes are not perpendicular to the bones or to each other. The orientation of the hinges relative to the bones and to each other, as shown in Figure 2, is of great importance in understanding the mechanics of thumb motion.
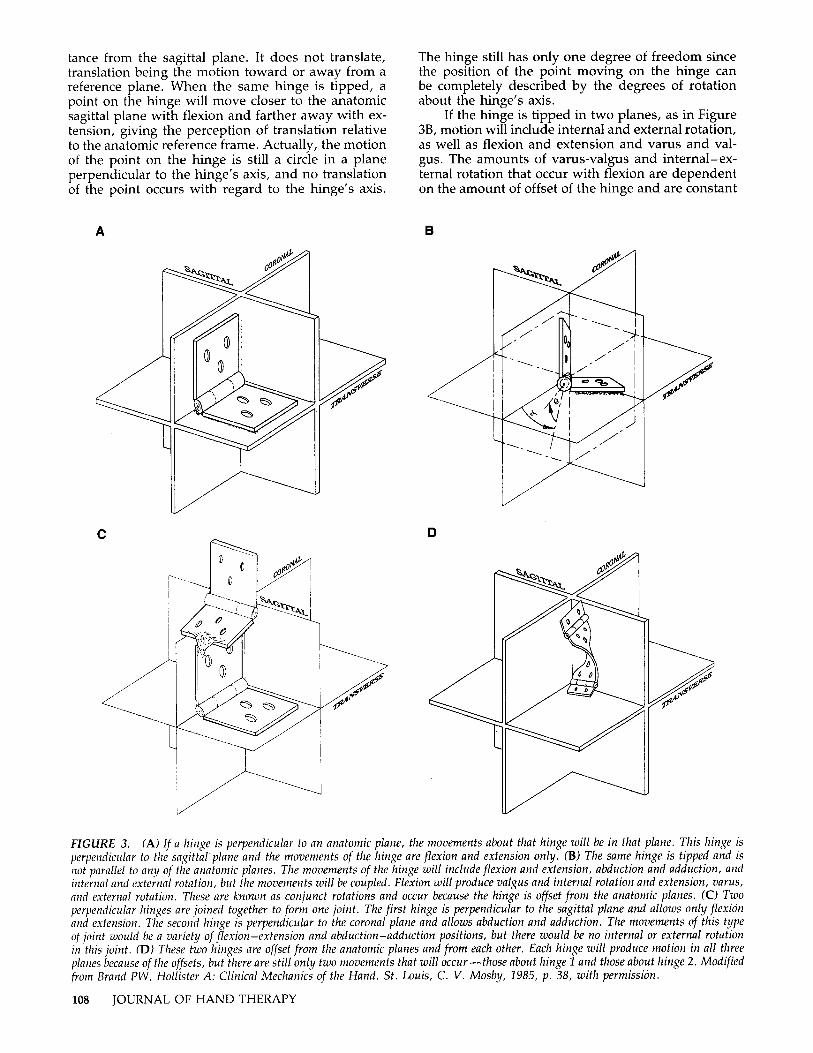
When a body moves about fixed axes of rotation, the orientation of the axes determines the kind of motion that occurs. For a joint to exhibit pure flexion and extension, its axis of rotation must be perpendicular to the sagittal plane, similar to the hinge in Figure 3A. A point on the hinge will move in a circle about the hinge's axis and in a plane perpendicular to the hinge. This plane of motion is parallel to the sagittal plane because the hinge is perpendicular to the sagittal plane. A simple hinge has one degree of
A
c
freedom since the body's position can be described by the amount of rotation about the hinge's axis.
If the hinge is tilted in the anatomic reference frame (Fig. 3B), pure flexion and extension will no longer occur. There will be a new plane of motion that is perpendicular to the hinge's axis, but the motion will include varus and valgus and internal and external rotation when viewed relative to the anatomic planes. This situation is similar to a door moving on its hinges. If the hinges are mounted perfectly perpendicular to the floor, the movements of the door will be in the plane parallel to the floor and the door will open and close freely. If the door is hung on hinges that are not aligned perpendicular to the floor, the plane of motion will not be parallel to the floor's plane of motion, and the door will run into the floor.
Another kind of motion is perceived when a hinge is tipped. With the first hinge, movement is in the sagittal plane, and as a point on the hinge moves about the axis, it remains at a constant dis-
B
FIGURE 1. (A) The body in standard position in the allatomic planes. The upper extremities do not lie parallel to the anatomic planes. (B) The hand in a position with the sagittal plane in the midline. The thumb is not in line with the fingers, and its pulp faces 90 degrees from the fingers. (C) The anatomic rotations, flexion-extensioll, abduction-adduction, and internal rotation-external rotation, are each described in an anatomic plane. This does not mean that the mechanism that produced the 1110tion is perpendicular to the anatomic planes, only that the motion is described this way. Modified from Brand PW, Hollister A: Clinical Mechanics of the Hand. St. LOllis, C. V. Mosby, 1985, p. 37, with permission.
FIGURE 2. The thumb moves about three joints: the carpometacarpal (CMC) joint, the metacarpophalangeal (MP) joint, and the interphalangeal (IP) joint. The CMC joint has two axes of rotation, a flexion-extension axis in the trapezium and an abduction-adduction axis in the metacarpal bone. The MP joint's flexion-extension axis is in the metacarpal just below the epicondyles, and the abduction-adduction axis passes through the volar plate of the proximal phalanx. The IP joint has one axis just below the epicondyles. The axes are not perpendicular to the bones or to each other, and do not intersect. Modified from Brand PW, Hollister A: Clinical Mechanics of the Hand. St. Louis, C. V. Mosby, 1985, p. 50, with permission.
FUX· DCI' AXIS
ADD· ADD AXIS
FUX· DCI' AXIS
April-June 1995 107
tance from the sagittal plane . It does not translate, translation being the motion toward or away from a reference plane. When the same hinge is tipped, a point on the hinge will move closer to the anatomic sagittal plane with flexion and farther away with extension, giving the perception of translation relative to the anatomic reference frame. Actually, the motion of the point on the hinge is still a circle in a plane perpendicular to the hinge's axis, and no translation of the point occurs with regard to the hinge's axis.
A
c
The hinge still has only one degree of freedom since the position of the point moving on the hinge can be completely described by the degrees of rotation about the hinge's axis.
If the hinge is tipped in two planes, as in Figure 38, motion will include internal and external rotation, as well as flexion and extension and varus and valgus. The amounts of varus-valgus and internal-external rotation that occur with flexion are dependent on the amount of offset of the hinge and are constant
B
o
FIGURE 3. (A) If a hinge is perpendicular to an anatomic plane, the movements about that hinge will be in that plane. This hinge is perpendiclliar to the sagitta/plane and the movements of the hinge are flexion and extension only. (B) The same hinge is tipped and is not parallel to any of the anatomic planes. The movements of the hinge will include flexion and extension, abduction and adduction, and internal and external rotation , but the movements will be coupled . Flexion will produce valgus and internal rotation and extension, varus, and external rotation. These are known as conjunct rotations and occur because the hinge is offset from the anatomic planes . (C) Two perpendicular hinges are joined together to form one joint . The first hinge is perpendicular to the sagittal plane and allows only flexion and extension. The second hinge is perpendicular to the coronal plane and allows abduction and adduction. The movements of this type of joint would be a variety of flexion-extension and abduction-adduction positions, but there would be no internal or external rotation ill this joint. (D) These two hinges are offset from the anatomic planes and from each other. Each hinge will produce motion in all three plal1es because of the offsets, but there are still only two movements that will occur-those about hinge 1 and those about hinge 2. Modified from Brand PW, Hollister A: Clinical Mechanics of the Hand. St. Louis, C. V. Mosby, 1985, p. 38, with permission.
108 JOURNAL OF HAND THERAPY

throughout the range of motion. These associated movements are called conjunct rotations and occur whenever an axis of rotation is offset from the anatomic planes.
There will also be perceived translation in all three anatomic planes as a point on the hinge will move closer to the sagittal, transverse, and coronal planes with flexion. A simple hinge tipped in two planes relative to the reference frame will give motion that includes rotations and translations in all three planes with regard to the reference frames. The motion of the point is still a circle in a plane relative to the hinge, and the hinge still has only one degree of freedom. This simple hinge is a key to understanding much of the controversy surrounding the motions of the thumb. The location of the thumb relative to the anatomic reference frames needs to be clearly defined, as do the locations of the joints' axes of rotation.
Two-axis joints can be thought of as two hinges that are welded together (Fig. 3C). The movements of a two-axis joint are combinations of motions about each axis. If the two hinges are perpendicular to the anatomic planes, as in Figure 3C, the motions about the first hinge will be flexion and extension. The second hinge will allow abduction and adduction. The position of the joint can be described in terms of the amount of flexion (motion about hinge 1) and the amount of abduction (hinge 2). These joints have two degrees of freedom. No internal or external rotation is allowed with this axis arrangement.
If the axes of rotation are offset from the anatomic planes, conjunct rotations will occur about each axis. Due to the way the first hinge in Figure 3D is offset from the anatomic planes, its motions are mainly flexion and extension with some varus and valgus, and internal and external rotation. The motions of the second hinge are mainly abduction and adduction, but flexion and extension and internal and external rotation also occur because the axis is not perpendicular to the anatomic planes. Only two kinds of movements occur in this joint-one about the first axis and the other about the second axis-but all three anatomic rotations are present. This is still a two degrees of freedom joint because it has only two axes of rotation. An interesting characteristic of this type of joint is that when two positions are known, the third position is known. In other words, when the position of flexion and the position of abduction are known, there is one and only one possible position of internal rotation. Or, when the position of rotation and the position of abduction are known, there is only one possible position of flexion.
The thumb joints have axes of rotation that are offset from the anatomic planes, and therefore have conjunct rotations. This is easily seen in the IP joint of the thumb. The proximal and distal phalanges lie in nearly a straight line when the IP joint is extended. As the IP joint is flexed, the tip pronates and adducts so that it can better interact with the index finger. There is a constant degree of varus and pronation with flexion. The tip of the thumb is actually tracing a shallow cone because the axis of rotation is not perpendicular to the proximal phalanx but runs be-
Tend .. A Tendon
B
FIGURE 4. The axes of rotation of the carpometacarpal (CMC) joint in the anatomic planes are similar to those of the hinges in Figure 3D. The tendons crossing the joint act on both axes. Tendon A is an adductor and a flexor of the carpometacarpal (CMC) joint; tendon B is an abductor and a flexor. It is not possible for either tendon to act on the flexion-extension axis without acting on the abduction-adduction axis. Each tendon has a moment arm for the flexion-extension axis and a separate moment arm for the abductioll-adduction axis. If the adductor moment for tendon A is exactly equal to the abductor moment for tendon B, the joint will 11/oue ill pure flexion. Modified from Brand PW, Hollister A: Clillical Mechanics of the Hand. St. Louis, C. V. Mosby, 1985, p. 42, with permission.
tween the tips of the flexion creases on the lateral sides of the thumb and is parallel to the volar and dorsal flexion creases. These lines are not perpendicular to the proximal phalanx, and the offset of the IP joint axis can be determined from these lines. The varus and internal rotation with flexion are the conjunct rotations that occur because the IP joint axis is offset from each of the anatomic planes.
The model of two offset hinges is actually a good model for the CMC joint of the thumb. Figure 4 shows the orientation of the thumb's CMC joint relative to the anatomic planes. Close examination of metacarpal bone movements (as opposed to the whole thumb, which includes MP joint and IP joint motions) reveals that extension is movement in a plane from the hypothenar eminence out of the palm. Flexion is in the same plane and is from the extended position toward the hypothenar eminence. Abduction and adduction occur about a cone whose apex is volar and ulnar to the joint. If a metacarpal is placed in 15 degrees of flexion and then in 5 degrees of abduction, there will be some pronation of the metacarpal as it moves from 15 degrees of flexion, neutral abduction to 15 degrees of flexion, and 5 degrees of abduction. But once in that position, the amount of pronation could not be changed without moving the thumb about either the flexion axis or the abduction axis (Fig. 2). The CMC joint has only two degrees of freedom and two axes of rotation, but the axes are not in the anatomic planes. 3 Again, the offset of the hinges allows for motion in three planes with only
April-June 1995 109
A B
Tendon
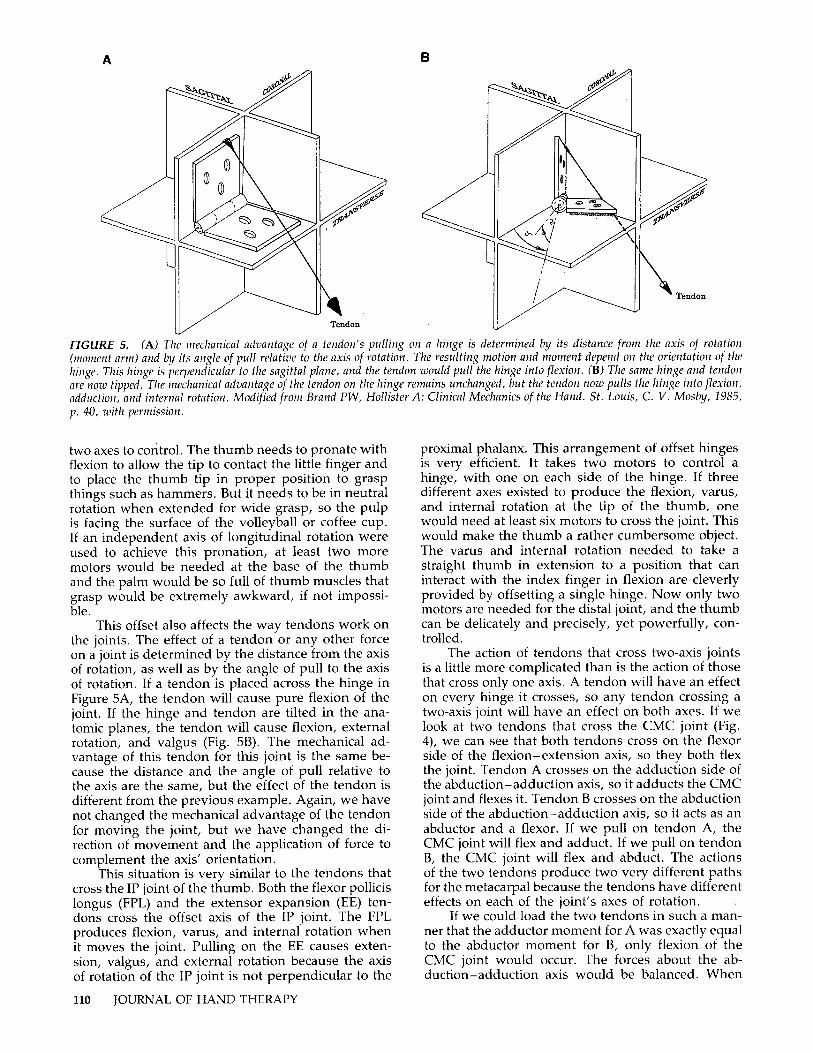
FIGURE 5. (A) The mechanical advantage of a tendon's pulling on a hinge is determined by its distance from the axis of rotation (moment ann) and by its angle of pull relative to the axis of rotation . The resulting motion and moment depend on the orientation of the hinge. This hinge is perpendicular to the sagittal plane, and the tendon would pull the hinge into flexion . (B) The same hinge and tendon are now tipped. The mechanical advantage of the tendon on the hinge remains unchanged, but the tendon now pulls the hinge into flexion , adduction, and internal rotation. Modified from Brand PW, Hollister A: Clinical Mechanics of the Hand. St . Louis, C. V. Mosby, 1985, p. 40, with permission.
two axes to control. The thumb needs to pronate with flexion to allow the tip to contact the little finger and to place the thumb tip in proper position to grasp things such as hammers. But it needs to be in neutral rotation when extended for wide grasp, so the pulp is facing the surface of the volleyball or coffee cup. If an independent axis of longitudinal rotation were used to achieve this pronation, at least two more motors would be needed at the base of the thumb and the palm would be so full of thumb muscles that grasp would be extremely awkward, if not impossible.
This offset also affects the way tendons work on the joints. The effect of a tendon or any other force on a joint is determined by the distance from the axis of rotation, as well as by the angle of pull to the axis of rotation . If a tendon is placed across the hinge in Figure SA, the tendon will cause pure flexion of the joint. If the hinge and tendon are tilted in the anatomic planes, the tendon will cause flexion, external rotation, and valgus (Fig. 5B). The mechanical advantage of this tendon for this joint is the same because the distance and the angle of pull relative to the axis are the same, but the effect of the tendon is different from the previous example. Again, we have not changed the mechanical advantage of the tendon for moving the joint, but we have changed the direction of movement and the application of force to complement the axis' orientation.
This situation is very similar to the tendons that cross the IP joint of the thumb. Both the flexor pollicis longus (FPL) and the extensor expansion (EE) tendons cross the offset axis of the IP joint. The FPL produces flexion, varus, and internal rotation when it moves the joint. Pulling on the EE causes extension, valgus, and external rotation because the axis of rotation of the IP joint is not perpendicular to the
110 JOURNAL OF HAND THERAPY
proximal phalanx. This arrangement of offset hinges is very efficient. It takes two motors to control a hinge, with one on each side of the hinge . If three different axes existed to produce the flexion, varus, and internal rotation at the tip of the thumb, one would need at least six motors to cross the joint. This would make the thumb a rather cumbersome object. The varus and internal rotation needed to take a straight thumb in extension to a position that can interact with the index finger in flexion are cleverly provided by offsetting a single hinge. Now only two motors are needed for the distal joint, and the thumb can be delicately and precisely, yet powerfully, controlled .
The action of tendons that cross two-axis joints is a little more complicated than is the action of those that cross only one axis . A tendon will have an effect on every hinge it crosses, so any tendon crossing a two-axis joint will have an effect on both axes. If we look at two tendons that cross the CMC joint (Fig. 4), we can see that both tendons cross on the flexor side of the flexion-extension axis, so they both flex the joint. Tendon A crosses on the adduction side of the abduction-adduction axis, so it adducts the CMC joint and flexes it. Tendon B crosses on the abduction side of the abduction-adduction axis, so it acts as an abductor and a flexor. If we pull on tendon A, the CMC joint will flex and adduct. If we pull on tendon B, the CMC joint will flex and abduct. The actions of the two tendons produce two very different paths for the metacarpal because the tendons have different effects on each of the joint's axes of rotation.
If we could load the two tendons in such a manner that the adductor moment for A was exactly equal to the abductor moment for B, only flexion of the CMC joint would occur. The forces about the abduction-adduction axis would be balanced. When
the thumb is used for pinch and grip, the abductors and the adductors are often fired together in perfect balance to stabilize the joint and give powerful CMC joint flexion for pinch.
The positions of the axes of rotation determine the position the finger or thumb can take. Understanding this concept helps one to predict the effect of surgery (e.g., a transferred tendon or an osteotomy) on the final range of positions available for the finger. A single-axis joint is pretty simple. The amount of conjunct rotation that will occur with motion can be determined by noting the offset of the axis from the anatomic planes as in Figure 3B.
THE MECHANICS OF THUMB MUSCLES
All of the muscles that cross the distal joints also cross the CMC joint. They tend to have bigger moment arms for the CMC joint than for the distal joints. The muscles that are abductors of the CMC joint are also abductors of the MP jointS (Fig. 6). Those that are adductors of the CMC joint are also adductors of the MP joint. This means that when the muscles that move the CMC joint into adduction are used, they also move the MP joint into adduction. In fact, it is
ElCIENSOR MECH..
FPL
DORSAL
ADD - ADD AXIS
VOlAR
IP JOINf 'IHUMB
RADIAL
FlEX - ElIT AXIS
DORSAL
ADD -ADD AXIS
VOlAR
MP JOINf 1HUMB
RADIAL
FlEX· ElIT AXIS
CMC JOINf 1HUMB
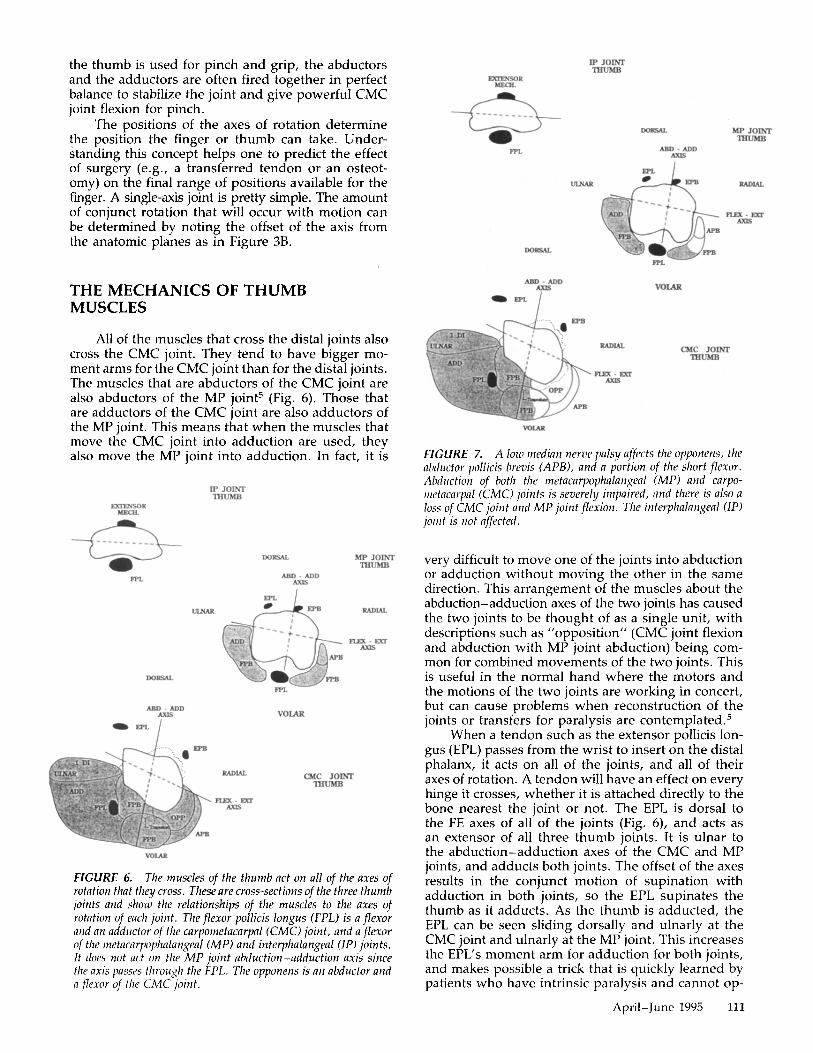
FIGURE 6. The muscles of the thumb act on all of the axes of rotation that they cross. These are cross-sections of the three thumb joints and show the relationships of the muscles to the axes of rotation of each joint. The flexor pollicis longus (FPL) is a flexor alld all adductor of the carpometacarpal (CMC) joint, and a flexor of the metacarpophalangeal (MP) and interphalangeal (IP) joints. It does not act on the MP joint abduction-adduction axis since the axis passes through the FPL. The opponens is an abductor and a flexor of the CMC joint.
EXDlNSOR MECIL
DORSAL
ADD - ADD
VOlAR
IP JOINf 'IHUMB
RADIAL
FlEX - ElIT AXIS
DORSAL
ADD - ADD AXIS
VOlAR
MP JOINf 1HUMB
RADIAL
FlEX· ElIT AXIS
CMC JOINf 1HUMB
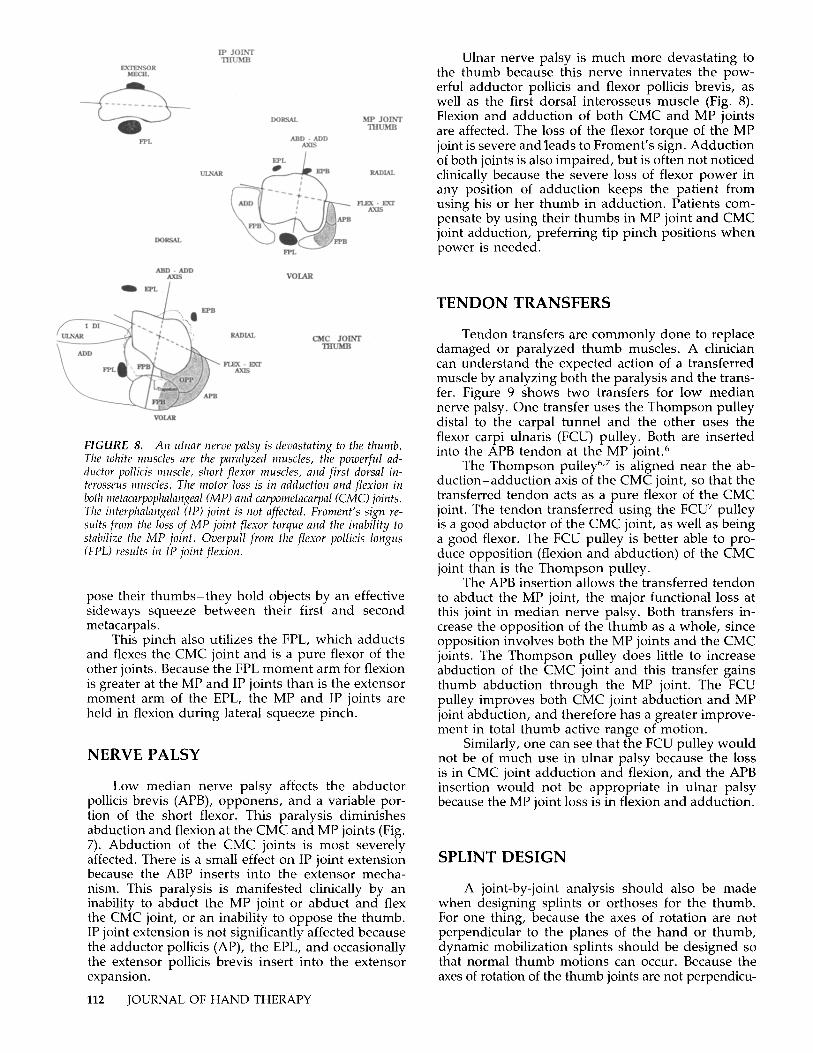
FIGURE 7. A low median nerve palsy affects the opponens, the abdl/ctor pol/icis brevis (APS), and a portion of the short flexor. Abdllction of both the metacarpophalangeal (MP) and carpometacarpal (CMC) joints is severely impaired, and there is also a loss of CMC joint and MP joint flexion. The interphalangeal (IP) joillt is Ilot affected.
very difficult to move one of the joints into abduction or adduction without moving the other in the same direction. This arrangement of the muscles about the abduction-adduction axes of the two joints has caused the two joints to be thought of as a single unit, with descriptions such as "opposition" (CMC joint flexion and abduction with MP joint abduction) being common for combined movements of the two joints. This is useful in the normal hand where the motors and the motions of the two joints are working in concert, but can cause problems when reconstruction of the joints or transfers for paralysis are contemplated. S
When a tendon such as the extensor pollicis longus (EPL) passes from the wrist to insert on the distal phalanx, it acts on all of the joints, and all of their axes of rotation. A tendon will have an effect on every hinge it crosses, whether it is attached directly to the bone nearest the joint or not. The EPL is dorsal to the FE axes of all of the joints (Fig. 6), and acts as an extensor of all three thumb joints. It is ulnar to the abduction-adduction axes of the CMC and MP joints, and adducts both joints. The offset of the axes results in the conjunct motion of supination with adduction in both joints, so the EPL supinates the thumb as it adducts. As the thumb is adducted, the EPL can be seen sliding dorsally and ulnarly at the CMC joint and ulnarly at the MP joint. This increases the EPL's moment arm for adduction for both joints, and makes possible a trick that is quickly learned by patients who have intrinsic paralysis and cannot op-
April-June 1995 111
ElCIENSOR MECH.
FPL
DORSAL
ABO· ADD AXJS
VOlAR
IP JOINT THUMB
RADIAL
FUX· EXT AXJS
DORSAL
ABD· ADD AXJS
VOIAR
MP JOINT 1HUMB
RADIAL
FUX· EXT AXJS
CMC 10INT 1HUMB
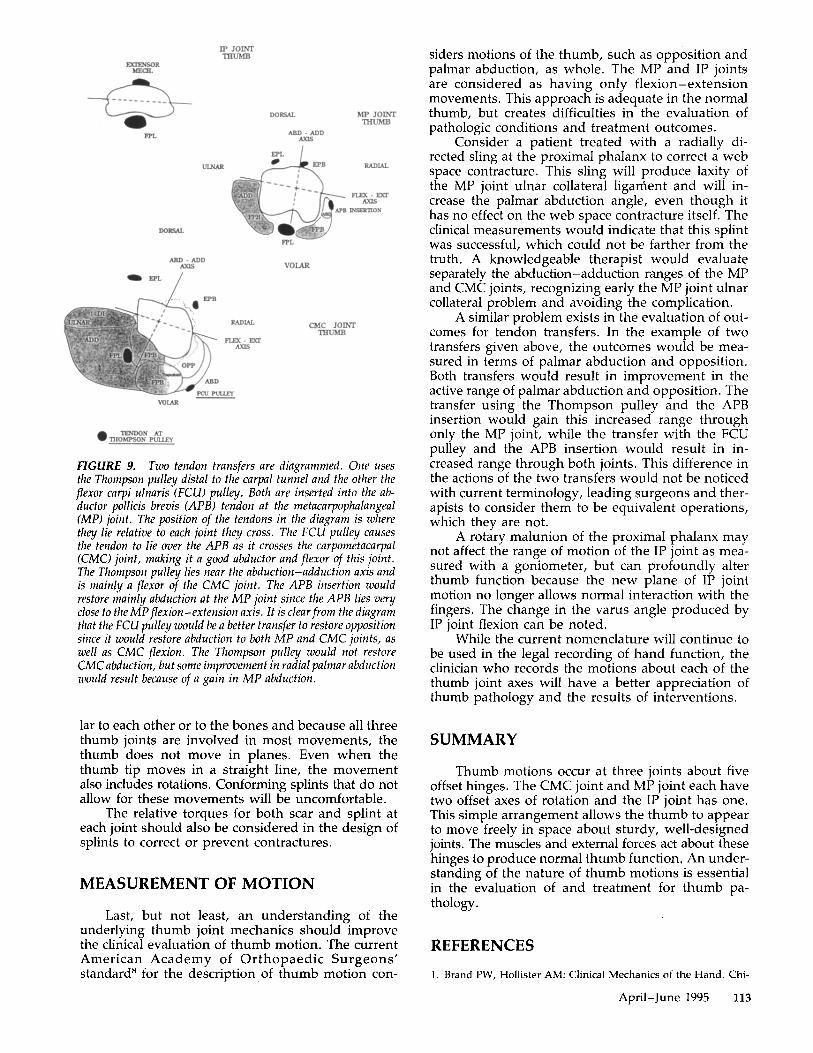
FIGURE 8. An ulnar nerve palsy is devastating to the thumb. The white muscles are the paralyzed muse/es, the powerful addllctor pol/icis muscle, short flexor muscles, and first dorsal interosseus muscles. The motor loss is in adduction and flexion in both metacarpophalangeal (MP) and carpometacarpal ((MC) joints. The interphalangeal (IP) joint is not affected. Froment's sign reSllltS from the loss of MP joint flexor torque and the inability to stabilize the MP joint. Overpul/ from the flexor pol/icis longus (FPL) results in IP joint flexion.
pose their thumbs-they hold objects by an effective sideways squeeze between their first and second metacarpals.
This pinch also utilizes the FPL, which adducts and flexes the CMC joint and is a pure flexor of the other joints. Because the FPL moment arm for flexion is greater at the MP and IP joints than is the extensor moment arm of the EPL, the MP and IP joints are held in flexion during lateral squeeze pinch.
NERVE PALSY
Low median nerve palsy affects the abductor pollicis brevis (APB), opponens, and a variable portion of the short flexor. This paralysis diminishes abduction and flexion at the CMC and MP joints (Fig. 7). Abduction of the CMC joints is most severely affected. There is a small effect on IP joint extension because the ABP inserts into the extensor mechanism. This paralysis is manifested clinically by an inability to abduct the MP joint or abduct and flex the CMC joint, or an inability to oppose the thumb. IP joint extension is not significantly affected because the adductor pollicis (AP), the EPL, and occasionally the extensor pollicis brevis insert into the extensor expansion.
112 JOURNAL OF HAND THERAPY
Ulnar nerve palsy is much more devastating to the thumb because this nerve innervates the powerful adductor pollicis and flexor pollicis brevis, as well as the first dorsal interosseus muscle (Fig. 8). Flexion and adduction of both CMC and MP joints are affected. The loss of the flexor torque of the MP joint is severe and 'leads to Froment's sign. Adduction of both joints is also impaired, but is often not noticed clinically because the severe loss of flexor power in any position of adduction keeps the patient from using his or her thumb in adduction. Patients compensate by using their thumbs in MP joint and CMC joint adduction, preferring tip pinch positions when power is needed.
TENDON TRANSFERS
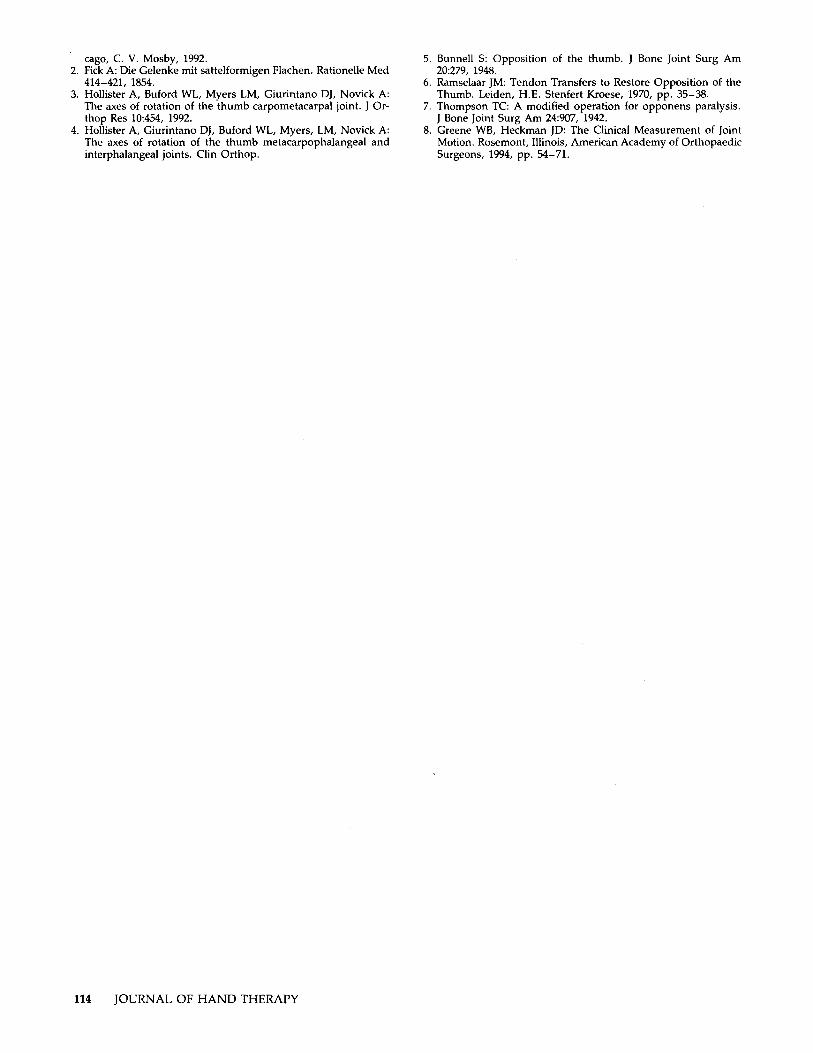
Tendon transfers are commonly done to replace damaged or paralyzed thumb muscles. A clinician can understand the expected action of a transferred muscle by analyzing both the paralysis and the transfer. Figure 9 shows two transfers for low median nerve palsy. One transfer uses the Thompson pulley distal to the carpal tunnel and the other uses the flexor carpi ulnaris (FCU) pulley. Both are inserted into the APB tendon at the MP joint.6
The Thompson pulley6,7 is aligned near the abduction-adduction axis of the CMC joint, so that the transferred tendon acts as a pure flexor of the CMC joint. The tendon transferred using the FCU7 pulley is a good abductor of the CMC joint, as well as being a good flexor, The FCU pulley is better able to produce opposition (flexion and abduction) of the CMC joint than is the Thompson pulley,
The APB insertion allows the transferred tendon to abduct the MP joint, the major functional loss at this joint in median nerve palsy, Both transfers increase the opposition of the thumb as a whole, since opposition involves both the MP joints and the CMC joints, The Thompson pulley does little to increase abduction of the CMC joint and this transfer gains thumb abduction through the MP joint. The FCU pulley improves both CMC joint abduction and MP joint abduction, and therefore has a greater improvement in total thumb active range of motion,
Similarly, one can see that the FCU pulley would not be of much use in ulnar palsy because the loss is in CMC joint adduction and flexion, and the APB insertion would not be appropriate in ulnar palsy because the MP joint loss is in flexion and adduction.
SPLINT DESIGN
A joint-by-joint analysis should also be made when designing splints or orthoses for the thumb, For one thing, because the axes of rotation are not perpendicular to the planes of the hand or thumb, dynamic mobilization splints should be designed so that normal thumb motions can occ.ur, Because the axes of rotation of the thumb joints are not perpendicu-
EXIENSOR MECH.
FPL
DORSAL
ABD· ADD AXIS
VOlAR
IP JOINI' THUMB
RADIAL
FlEX· EXT AXIS
DORSAL
ADD - ADD AXIS
VOLAR
MP JOINI' TIfUMB
RADIAL
FlEX· EXT AXIS
CMC JOINI' THUMB
FIGURE 9. Two tendon transfers are diagrammed. One uses the Thompson pulley distal to the carpal tunnel and the other the flexor carpi ulnaris (FCU) pulley. Both are inserted into the abductor pollicis brevis (APB) tendon at the metacarpophalangeal (MP) joint. The position of the tendons in the diagram is where they lie relative to each joint they cross. The FCU pulley causes the tendon to lie over the APB as it crosses the carpometacarpal (CMe) joint, making it a good abductor and flexor of this joint. The Thompson pulley lies near the abduction-adduction axis and is mainly a flexor of the CMC joint. The APB insertion would restore mainly abduction at the MP joint since the APB lies very close to the MP flexion-extension axis. It is clear from the diagram that the FCU pulley would be a better transfer to restore opposition sillce it would restore abduction to both MP and CMC joints, as well as CMC flexion. The Thompson pulley would not restore CMC abduction, but some improvement in radial palmar abduction would result because of a gain in MP abduction.
lar to each other or to the bones and because all three thumb joints are involved in most movements, the thumb does not move in planes. Even when the thumb tip moves in a straight line, the movement also includes rotations. Conforming splints that do not allow for these movements will be uncomfortable.
The relative torques for both scar and splint at each joint should also be considered in the design of splints to correct or prevent contractures.
MEASUREMENT OF MOTION
Last, but not least, an understanding of the underlying thumb joint mechanics should improve the clinical evaluation of thumb motion. The current American Academy of Orthopaedic Surgeons' standardS for the description of thumb motion con-
siders motions of the thumb, such as opposition and palmar abduction, as whole. The MP and IP joints are considered as having only flexion-extension movements. This approach is adequate in the normal thumb, but creates difficulties in the evaluation of pathologic conditions and treatment outcomes.
Consider a patient treated with a radially directed sling at the proximal phalanx to correct a web space contracture. This sling will produce laxity of the MP joint ulnar collateral ligament and will increase the palmar abduction angle, even though it has no effect on the web space contracture itself. The clinical measurements would indicate that this splint was successful, which could not be farther from the truth. A knowledgeable therapist would evaluate separately the abduction-adduction ranges of the MP and CMC joints, recognizing early the MP joint ulnar collateral problem and avoiding the complication.
A similar problem exists in the evaluation of outcomes for tendon transfers. In the example of two transfers given above, the outcomes would be measured in terms of palmar abduction and opposition. Both transfers would result in improvement in the active range of palmar abduction and opposition. The transfer using the Thompson pulley and the APB insertion would gain this increased range through only the MP joint, while the transfer with the FCU pulley and the APB insertion would result in increased range through both joints. This difference in the actions of the two transfers would not be noticed with current terminology, leading surgeons and therapists to consider them to be equivalent operations, which they are not.
A rotary malunion of the proximal phalanx may not affect the range of motion of the IP joint as measured with a goniometer, but can profoundly alter thumb function because the new plane of IP joint motion no longer allows normal interaction with the fingers. The change in the varus angle produced by IP joint flexion can be noted.
While the current nomenclature will continue to be used in the legal recording of hand function, the clinician who records the motions about each of the thumb joint axes will have a better appreciation of thumb pathology and the results of interventions.
SUMMARY
Thumb motions occur at three joints about five offset hinges. The CMC joint and MP joint each have two offset axes of rotation and the IP joint has one. This simple arrangement allows the thumb to appear to move freely in space about sturdy, well-designed joints. The muscles and external forces act about these hinges to produce normal thumb function. An understanding of the nature of thumb motions is essential in the evaluation of and treatment for thumb pathology.
REFERENCES
1. Brand PW, Hollister AM: Clinical Mechanics of the Hand. Chi-
April-June 1995 113
cago, C. V. Mosby, 1992. 2. Fick A: Die Gelenke mit sattelformigen Flachen. Rationelle Med
414-421, 1854. 3. Hollister A, Buford WL, Myers LM, Giurintano OJ, Novick A:
The axes of rotation of the thumb carpometacarpal joint. J Orthop Res 10:454, 1992.
4. Hollister A, Giurintano OJ, Buford WL, Myers, LM, Novick A: The axes of rotation of the thumb metacarpophalangeal and interphalangeal joints. Clin Orthop.
114 JOURNAL OF HAND THERAPY
5. Bunnell S: Opposition of the thumb. J Bone Joint Surg Am 20:279, 1948.
6. Ramselaar JM: Tendon Transfers to Restore Opposition of the Thumb. Leiden, H.E. Stenfert Kroese, 1970, pp. 35-38.
7. Thompson TC: A modified operation for opponens paralysis. J Bone Joint Surg Am 24:907, 1942.
8. Greene WB, Heckman JO: The Clinical Measurement of Joint Motion. Rosemont, Illinois, American Academy of Orthopaedic Surgeons, 1994, pp. 54-71.