
Thesis (whole)
100
14 Chapter 1 THE PROBLEM AND ITS BACKGROUND Introduction “When women are empowered to fulfill their potential, they invest in their families and work for lasting change as they cannot fully participate in society if they cannot expect to survive childbirth.” -Cooperative for Assistance and Relief Everywhere Organization (2008) Truly as it says above, the event of giving birth to a child is an experience that upholds a woman’s life experience. It gives an opportunity for nurses to help develop this important milestone because one’s actions may be empowered by one’s feelings and ability. It is also during this time wherein clients may find it critical to regain full physiological capacity especially after a caesarean section. In the nursing field, developing a plan
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Thesis (whole)
14
Chapter 1
THE PROBLEM AND ITS BACKGROUND
Introduction
“When women are empowered to fulfill their potential, they
invest in their families and work for lasting change as they
cannot fully participate in society if they cannot expect to
survive childbirth.”
-Cooperative for Assistance
and Relief Everywhere
Organization (2008)
Truly as it says above, the event of giving birth to a
child is an experience that upholds a woman’s life
experience. It gives an opportunity for nurses to help
develop this important milestone because one’s actions may
be empowered by one’s feelings and ability. It is also
during this time wherein clients may find it critical to
regain full physiological capacity especially after a
caesarean section. In the nursing field, developing a plan
15
is highly essential in the recovery process for these
clients in the process of providing holistic care. It is
also a vocation that defines the importance of dispensing
comfort, knowledge and most of all touching and nurturing
lives.
Caesarean section is described as the surgical removal
of the infant from the uterus through the incision made in
the abdominal wall and incision made in the uterus (Nettina,
2006). Because caesarean and section both refer to an
incision, some prefer the terms caesarean delivery or
caesarean birth to describe the procedure (Gabbe, et. al,
2007).
The origin of the term caesarean is obscureand three
principal explanations have been suggested. In the first
explanation, according to legend, Julius Caesar was born in
this manner, with the result that the procedure became known
as the Caesarean operation. Several circumstances weak this
explanation; First, the mother of Julius Caesar lived for
many years after his birth in 100 B.C and as late as the
16
17th century. The operation was almost invariably fatal.
Second the operation, whether performed on the living or
dead, is not mentioned by any medical writer before the
middle ages. Historical details of the origin of the family
name Caesar are found in the monograph. In the second
explanation, the name of the operation is derived from a
Roman law, supposedly created in the 8th century B.C by Numa
Pompilius, ordering that the procedure be upon women dying
in the last few weeks of pregnancy in the hope of saving the
child. The third explanation is that the word caesarean was
derived sometime in the middle age from the Latin word
Caedere which means “to cut” (Cunningham, 2005)
One in 10 live births was delivered through caesarean
section. Considering this, there may be other factors that
should be recognized (Kho, 2010). Rates of caesarean
section varies in different hospitalsin a national degree,
it can be as high as 50%. Caesarean rates are also twice
as high in urbanized areas than in the provinces. Another
factor is that not all women have access to hospital care.
Twenty percent of wealthier moms are said to give birth
17
through caesarean section, while only 1.7 percent of the
poorer moms do.
In a study conducted based on 133 countries, it was
calculated that approximately 18.5 million caesarean
sections (CS) are performed yearly worldwide. About 40% of
the countries have CS rates less than 10%, about 10% have CS
rates between 10 and 15%and approximately 50% have CS rates
greater than 15%, 56 countries with CS rates 10% account for
only 25% (4.5 millions) of the global CS but for 60% (77
millions) of the total number of births worldwide. On the
other hand, 73% (13.5 millions) of the total number of CS
are performed in the 65 countries with CS rates greater than
15% were 37.5% (48.4 millions) of the total number of births
occur (Gibbons et al., 2010).
Most women may not anticipate the need for a
complicated childbirth because they believe they are
healthy. This is a clear and helpful recommendation to
determine the necessity of a caesarean section (CS).
Undergoing this type of surgery, increases the risk for
18
complications in both the baby and the mother in comparison
with a vaginal birth.
There may be several reasons why the numbers of those
who undergo CS increases. First, better care has made the
operation safer. There have been improvements in the
way pain relief, antibiotics and blood transfusions are
administered. Babies also experience more monitoring and
increased medical intervention during low-risk labors.
Premature babies are given special care and have greater
chances for survival.
Activities of Daily Living (ADL) are the things or
tasks that most people perform every day. Necessity of
supervision, direction, personal assistance, or total care
for any dependent function can be recorded as parameters to
assess minute declines or increments of patients’ ADL. It
includes bathing, grooming, eating, dressing, toileting and
others. Knowing the individual’s ability to perform the
activities of daily living is important to determine the
specific care that will be rendered to the clients. It is
19
also serves as a guide in measuring the functional status of
the client. People that are unable to perform ADL tend to
be dependent to machines or gadgets or needs to be assisted
by other person or other family members. This can help
evaluate an individual’s ability to do basic tasks
especially in a hospital setting.
The researchers have chosen to proceed with this study
for several particular reasons, one of which is to gain
awareness and deeper understanding about the effects of
caesarean section on the performance of daily activities of
and individual. As there is an increasing necessity for
Cesarean Section (CS) due to the above-mentioned issues
faced by our society today, it is important for nurses to be
able to systematically assess the recovery of these clients
with the means of performing Activities of Daily Living
(ADL).
Theoretical / Conceptual Framework
The study was anchored on Virginia Henderson’s Need
Theory, which is a theory that focuses on the importance of
20
patient independence so that the patient will continue to
progress prior to discharge from the hospital (Henderson,
2007).
According to Henderson’s Need Theory, health is viewed
in terms of the individual’s ability to perform 14
components of nursing care unaided. Health is quality of
life basic to human functioning and requires independence
and interdependence. It is the quality of health rather
life itself that allows people to work most effectively and
to teach their highest potential level of satisfaction in
life. Individuals will achieve or maintain health if they
have necessary strength, will, or knowledge. Henderson
conceptualized the nurse’s role as assisting sick or well
individuals in a supplementary or complementary way. The
nurse needs to be a partner with the patient, a helper to
the patient and, when necessary, a substitute for the
patient. The nurse’s focus is to help individuals and
families to gain independence in meeting 14 fundamental
needs: Breathing normally, eating and drinking adequately,
eliminating body wastes, moving and maintaining desirable
21
position, sleeping and resting, selecting suitable clothes,
maintaining body temperature within normal range, keeping
the body clean and well-groomed, avoiding dangers in the
environment, communication with others, worshipping
according to one’s faith, working in such a way that one
feels a sense of accomplishment, playing or participating in
various forms of recreation, learning, discovering or
satisfying the curiosity that leads to normal development
and health and using available health facilities. She
described the role of the nurse as one of the following: (a)
substitutive, which is doing something for the patient; (b)
supplementary, which is helping the patient do something: or
(c) complementary, which is working with the patient to do
something. These all rely in the goal of helping the person
become as independent as possible. (Henderson, 2007)
In relation to the study, the performance of the daily
activities was theoretically being as unique as their
strength, will, or knowledge and variability. Each and
everyone have been exposed to experiences affirming the
difference of strength, will, or knowledge. This may also
22
influence how they work towards a goal of self independence.
Variability would have include age, family support systemand
parity. Existence of differences imposes significance to
knowing individual performances. Therefore, it is expected
that the performance of the clients involved in the study
regarding caesarean section vary depending on their
experiences and other factors that may affect their
respective viewpoints.
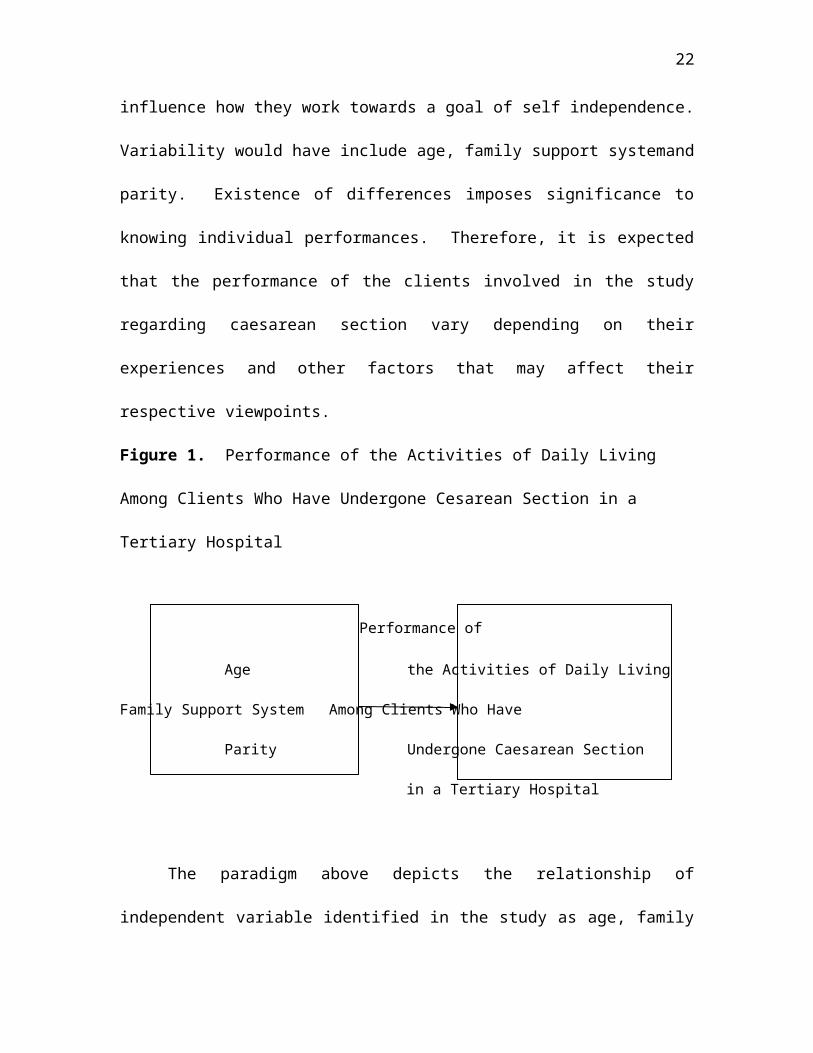
Figure 1. Performance of the Activities of Daily Living
Among Clients Who Have Undergone Cesarean Section in a
Tertiary Hospital
Performance of
Age the Activities of Daily Living
Family Support System Among Clients Who Have
Parity Undergone Caesarean Section
in a Tertiary Hospital
The paradigm above depicts the relationship of
independent variable identified in the study as age, family
23
support system and parity with the dependent variable which
is the performance of the activities of daily living of
patients who have undergone caesarean section.
Statement of the Problem
This study primarily aimed to determine the level of
performance of the activities of daily living among clients
who have undergone Caesarian Section in a tertiary hospital.
Specifically, it sought answers to the following
problems:
1. What is the profile of the respondents in terms of age,
family support systemand parity?
2. What is the level of performance of the activities of
daily living of the respondents?
3. Are there significant differences in the level of
performance of the activities of daily living when the
respondents are grouped according to age, family support
systemand parity?
24
Hypothesis of the study
It was hypothesized in this study that there are no
significant differences in the level of performance of the
activities of daily living when the respondents are grouped
according to age, family support systemand parity.
Scope and Delimitation of the Study
This study focused mainly on the performance of the
activities of daily living among clients who have undergone
Caesarian Section in a tertiary hospital.
This study involved 60 clients who have undergone
caesarean section two days post operatively and how many
births have already been undergone by the respondents. This
study was conducted in General Emilio Aguinaldo Memorial
Hospital in Trece Martires City, Cavite, a tertiary
hospital. The respondents were 18-37 years old and were
able to speak, read and write and understand English or
Filipino Language.
This study also included everyday routine, the things
the respondents normally perform for self-care such as
25
feeding, dressing/ undressing, grooming, ambulation, bed
mobility, bathing, use of toilet, continence and meal
preparation.
Significance of the Study
The researchers believed that the results of the study
may benefit the following:
Staff Nurses and Nursing Students. This may provide
both staff nurses and nursing students the awareness on
general abilities of clients who have undergone caesarean
section based on their performance of the activities of
daily living. Consequently, this study may encourage them
to start a careful assessment and provide essential
modifications when making a nursing care plan because they
know which type of daily activity is difficult to perform
individually.
College of Nursing and School of Midwifery.This study
may primarily provide the nursing educators an idea on how
to promote student nurse’s competencies when interacting
with clients who have undergone caesarean section. This may
help them have a better approach with these types of clients
26
because the area wherein they experience the most difficulty
is identified.
Clients who have undergone Caesarean Section.This may
help them have an improved understanding on their condition.
They may become more aware on their physical capabilities
and allow themselves to reach a new level of self
independence in order to be more active when performing
tasks on a daily basis.
Family of Caesarean Section Clients.They may benefit
from the study because this may increase their knowledge
about the effects of caesarean on the patient’s performance
of the activities of daily living. This may also enhance
their interaction with their relative as they develop a
sense of empathy and an understanding on their condition.
Future Researchers.Knowledge of the study would inform
the future researchers that clients who have undergone
caesarean section may have different responses as every
individual is unique. This study may serve as a road map
for the future researchers as this will provide additional
knowledge and information.
27
Definition of Terms
For the purpose of better understanding of the study,
the following terms used in this study are operationally
defined below:
Activities of Daily Living. It refers to the everyday
routine, the things the respondents normally perform for
self-care such as feeding, dressing/ undressing, grooming,
ambulation, bed mobility, bathing, use of toilet, continence
and meal preparation. ADL will be measured using a scale of
1-3 wherein; 1- Dependent, inability to perform the task
either by self of with support from others. This means a
complete dependence on a device or on someone else to
perform a task or has a low level of self-care 2- Needs
Assistance, ability to perform task only if with support
either by a person or a device or has a moderate level of
self-care, 3- Independent, ability to perform task by own
self or has a high level of self-care. The level of
performance of the activities of daily living of the
respondents are categorized into three, based on computed
28
mean scores mainly: (a) 1.00 to 1.67 – Performed
Dependently, (b) 1.68 to 2.34 – Performed with Assistanceand
(c) 2.35 to 3.00 – Performed Independently
Age. This pertains to the chronological age of the
respondents. The classifications are (a) 18-22 years old,
(b) 23-27 years old, (c) 28-32 years old, (d) 33-37 years
old. These are the indicators of the study.
Caesarean Section.This pertains to a type of operation
wherein the baby will be delivered through an incision made
in the abdominal wall.
Family Support System. It pertains to the support
given by the family to the clients who have undergone
caesarean section. It will be classified as: (a) with
family support, living with or being visited by family
members, friends, or relative, (b) without family support,
living without or not being visited by family members,
friends, or relatives.
Parity.This refers to the number of times the mother
has been pregnant but not less than 20 weeks of gestation.
It may be grouped into: (a) Primi-para refers to the mother
29
who is given birth for the first time and (b) Multi-para
refers to the mothers who has given birth two or more times.
Chapter 2
REVIEW OF RELATED LITERATURE
This chapter presents the review of both conceptual and
research literature, which were derived from education
books, journals, online sourcesand theses that provide the
researchers with necessary background knowledge to pursue
the study. The conceptual literature contains a brief
discussion of the following topics: Caesarean Section and
Activities of Daily Living.
Caesarean Section
Pliny the Elder theorized that Julius Caesar’s name
came from an ancestor who was born by caesarean section, but
the truth of this is debated. The Ancient Roman caesarean
section was first performed to remove a baby from the womb
of a mother died during childbirth. Caesar’s mother,
Aurelia, lived through childbirth and successfully gave
birth to her son, ruling out the possibility that the Roman
30
Dictator and General was born by caesarean section. The
Catalan saint, Raymond Nonnatus (1204-1240), received his
surname – from the Latin “non natus” (“not born”) – because
he was born by the caesarean section. His mother died while
giving birth to him. In 1316 the future Robert II of
Scotland was delivered by caesarean section – his mother,
Marjorie Bruce, died (Eubel, 2009)
Caesarean Section is defined as the birth of the fetus
trans abdominally after incising the gravid uterus (Daftray,
S.N. & Desai, S.V. 2005). Caesarean section is performed
when awaiting a vaginal birth would compromise the mother,
the fetus or both (McKinney, E. S. et al 2009). Dystocia,
or difficult labor, is the other common cause of c-sections.
The procedure is frequently used in cases where the mother
has had a previous caesarean section. The procedure is
frequently used cases where the mother has had a previous
caesarean section. The procedure is performed in the United
States on nearly one of every four babies delivered-more
than 900,000 babies each year (Heisler, 2009).
31
According to the American Congress of Obstetrician and
Gynecologist (ACOG) Practice Bulletin Number 49 (2003),
dystocia in labor (labor dystocia), a protraction disorder
or an arrest disorder, is a very commonly cited indication
for caesarean delivery, but it is not specific. These can
be primary or secondary disorders. Most dystocias are
caused by abnormalities of the power (uterine contractions),
the passage (maternal pelvis), or the passenger (the fetus).
The decision to proceed with a caesarean section for
the term frank breech singleton fetus has been challenged
based on the ACOG Committee Opinion No. 340 (2006).
Although most practitioners will always perform a caesarean
section in this situation, ACOG has left open the option to
consider a breech delivery under appropriate circumstances,
including practitioner experienced in the evaluation and
management of labor and skilled in the delivery of the
breech fetus.
Option of elective caesarean section on maternal
request (CDMR) has causes arise of debate. It is reasonable
to inform the pregnant woman requesting a caesarean section
32
of the associated risks and benefits for the current and any
subsequent pregnancies as the evidence shown. The
clinician’s role should be to provide the best possible
evidence-based counseling to the woman and to respect her
autonomy and decision-making capabilities when considering
route of delivery (Hankins, 2006).
A study conducted by Gagnon, Meierand Waghorn,
(2007) involved a representative sample of low-risk women
giving birth in an intrapartum unit at a university hospital
in Quebec, Canada, with approximately 3,700 births per year.
Data on all variables of interest were available for 467
women. These women were cared for the responsibility by 1-
17 nursesand it was range from 10 to 1045 minutes in which
the mean length of labor for which the same nurse was
responsible for a woman. The ratio for the caesarean
section due to the number of nurses was 1.17 (95%Cl 1.04,
1.32) after controlling for length of labor, maternal age,
maternal height, infant weight, gestational age, indication,
type of ruptureand epidural anesthesia. For 2 hours, 1 or
more nurses switch their shifts (i.e., number of times care
33
responsibilities changed hands), 1.04 (95% CL 0.42, 1.30).
In caring for a laboring woman who was at risk of caesarean
section, an association was observed between the numbers of
nurses in which it estimates that the other patterns of
nursing care responsibility on caesarean birth were not
sufficiently precise to draw conclusions.
Activities of Daily Living
ADL’s are defined as “the things we normally do such
as; feeding ourselves, bathing, dressing, grooming, work,
homemaking and leisure” (Wiley, 2012). Activities of Daily
Living can be classified into: basic ADL (e.g., eating,
dressingand toileting), instrumental ADL (e.g., cooking,
shoppingand laundry)and more complex functions requiring
greater intellectual effort (Sadock, B.J & Sadock, V.A.,
2005).
Activities of Daily Living (ADLs) is a term used by
health professionals to refer to activities being done
everyday either inside the house, outdoor, or can be both.
Health professionals refer to the ability in doing ADL to
measure the functional status of a person, especially with
34
people with disabilities and the elderly. Practitioners
conduct evaluations in order to determine how independent
patients are and what skills they would be able to
accomplish independently. It is also used to measure the
degree of independence an indvidual has gained after
performing the interventions prepared by the health
professionals. The goal of performing the evaluation of ADL
is to help the patient become independent using the
appropriate adaptations if needed. Many ADL indexes exist,
such as the Katz Index, Revised Kenny Self-Care
Evaluationand the Barthel Index. These indexes were used to
evaluate the patient’s self-care. Each individual is rated
according to how functional they are. Scoring is based on
how the patient performed with regard to the measure of
dependence or independence in which the patient performed
the tasks (Krapp, 2012).
Since the Katz index of Activities of Daily Living
(ADL) was developed in 1963, it has gained increased
acceptance as an accurate measure of physical functioning.
35
National databases, state long-term care programs, insurers
who offer private long-term care insurance policies, federal
legislationand a body of research literature routinely use
limitations in the ADL identified by Katz et al. (eating,
bathing dressing toileting, transferringand continence) as
appropriate proxies for an individual’s level of cognitive
transferringand continence, as appropriate proxies for an
individual’s level of impairment, depending on the wording
of the assessment instrument. For example, assessing
whether a person requires physical assistance to perform an
ADL primarily measures physical impairment. But assessing
whether a person needs prompting or cueing to initiate and
complete an ADL primarily measures cognitive impairment
(Rothwell, 2007).
An important aspect of the ADL program is the provision
of pain-free alternatives of daily living activities. For
example, if the patient finds it painful to walk for any
distance greater than 200 yards, the patient might be
advised to walk in a poll. The buoyancy of the water
decreases pressure on the joints, reducing the pain. If it
36
hurts the patient to lift things above the head, the patient
should be advised to get a step ladder to assist in reaching
high objects. If it hurts the patient to type, voice
recognition software could be utilized to make sure the
patients understands how to use proper body mechanics in
their daily activities to avoid additional injuries (Clover,
2007).
A functional limitation may include inability to remove
a coat from a hanger, inability to roll over in bed, or
difficulties with dressing, all of which are examples of
basic activities of daily living (ADL). Clients who are
independently incapable of performing ADL experience
problems in the areas of occupation, education, work,
leisure and social preparation. Overlap between physical
and occupational therapy most commonly occur when
facilitating movement or when promoting postural stability
during the performance of activities (Bertoti, 2004).
In a study done by Downs et. al (2009) entitled
“Impact of scoliosis surgery on activities of daily living
37
in females with Rett syndrome”, data from questionnaires
administered to caregivers biennially from 2000 to 2006 were
used to describe functional skill levels in subjects with
Rett syndromeand within-subject change in 16 subjects with
scoliosis surgery were compared with within-subject change
in 186 pairs of data from 86 subjects with conservatively
managed scoliosis. Post surgical assessment was conducted
after a mean of 17.8 months. Scoliosis is a common
orthopedic complication of Rett syndromeand surgery is
commonly used to reduce asymmetry in cases with severe
scoliosis. Surgery was associated with the improved
activities of daily living to those who were wheelchair-
bound. Mobility levels, social interaction, communication
skillsand the frequency of daytime napping remained similar
for the group as a whole.
Browning et. al (2207) explained in their study
entitled, “The Quantity of Early Upright Mobilization
Performed following Upper Abdominal Surgery is Low: An
Observational Study wherein they Quantified Early Upright
Mobilization in Patients following Upper Abdominal Surgery.”
38
Their findings indicate that there is a low duration of
uptime recorded with more than half of the sample dependent
on assistance to mobilize on day 3and a further 22% still
dependent on Day 5.
Another study which used activities of daily living as
a variable was by Meiners et. al (2002). Tetraplegic
patients were tested for hand strength before and after hand
surgery. They also answered questions on how they rated the
results of surgery. The study was conducted in the Werner
Wicker Clinic, Bad Wildungen, Germany, from 1991 to 1998.
The results of reconstruction surgery performed on 23
tetraplegic hands, as reflected in lifting the hand, lateral
gripand cylindrical grip were presented. In a follow-up
study with 22 patients, their management of activities of
daily living 34.1 months (9-51 months) after the surgery is
compared with the preoperative situation. Subjective
satisfaction levels were elicited for each of the 22
patients by means of a questionnaire. The gain in force
corresponded to 893 g (150-1500 g) for cyclindrical grip and
488 g (100-1200 g) for lateral grip, while they were able to
39
develop grade 4 force for lifting the hand. After the
operation, 28 aids/appliances that patients had formerly
used regularly were no longer necessary. There were 75
separate activities listed in the questionnaireand on
average the 22 patients were able to perform 8.7 (0-20) more
of these. Most patients, (19) said they would advise others
to have the operation and the rest,(18) said that they would
have the operation again.
In a study by La Pier et, al (2008) entitled “Analysis
of Activities of Daily Living Performance in Patients
Recovering from Coronary Artery Bypass Surgery”, they
completed the Functional Status Index, a self-report
instrument, at two weeks and two months post surgery. They
used the response frequency for each item of the Functional
Status Index and used chi-square for data analysis. The
purpose of this study was to investigate the impact of
coronary artery bypass grafting surgery (CABG) on the
ability to perform the activities of daily living. A
significant loss of function occurs immediately following
surgery. The number of patients who experienced limitations
40
or difficulty with opening containers, dressing and rising
from a chair increased two weeks after CABG surgery.
The activities of daily living in patients after
rotationplasty surgery with a long term follow up checkup
had a good outcome in the quality of life scores. But only
little is known about the actual level of activity and
distribution of activities in the daily life of this patient
group and whether the activity level remains reduced after
treatment due to a loss of confidence in physical capacity
and fitness. From the results of ADL monitoring, it became
apparent that the locomotion played a lesser role in
everyday life whereas sitting and standing were predominant.
(Winters et. al, 2007)
Synthesis
Most of the acquired literature regarding the chosen
study used experimental approaches and it shows that there
is an evidence of a perceived specific difficulty
demonstrated by each client with different medical
conditions in performing the activities of daily living.
41
The conceptual literature provided information regarding
caesarean section post operative patients, nursing care and
activities of daily living.
Based on the research literature presented, several
studies were conducted focusing on the activities of daily
living, which had a significant effect due to their
particular condition related to orthopedic and heart
surgeries.
Browning et. al (2007) explained in their study
entitled, “The Quantity of Early Upright Mobilization
Performed following Upper Abdominal Surgery is Low: An
Observational Study wherein they Quantified Early Upright
Mobilization in Patients following Upper Abdominal Surgery.”
Their findings indicate that there is a low duration of
uptime recorded with more than half of the sample dependent
on assistance to mobilize on day 3 and a further 22% still
dependent on Day 5. Similar to the study, most of the
respondents needed only a moderate level of care in
performing the activities of daily living.
42
Another study that shows improvement of ADL after
surgery is seen in a study done by Meiners et. al (2002),
entitled “Improvements in activities of daily living
following functional hand surgery for treatment of lesions
to the cervical spinal cord: Self-assessment by patients”.
From the title, the patients may be able to benefit as they
are allowed to assess themselves and therefore, understand
their condition better. This study is also experimental
just like the above mentioned. The study was conducted in
the Werner Wicker Clinic, Bad Wildungen, Germany, from 1991
to 1998. In a follow-up study in 22 patients, their
management of the activities of daily living 34.1 months (9-
51 months) after the surgery is compared with the
preoperative situation. Subjective satisfaction levels were
elicited for each of the 22 patients by means of a
questionnaire. Nineteen patients said they would advise
others to have the operation and eighteen of them said that
they would have the operation again. The age range used was
between 21-57 years old. There were 12 complications in
nine patients. Reconstructive surgery on the hands of
43
tetraplegic patients led to gains in both cylindrical grip
and lateral grip force and to increased manual dexterity.
Patient satisfaction with the procedure was high. This
coincides with our study, as we also allow patients to
assess themselves and as well as using subjective data as a
way of approaching the patients when asked to perform ADL.
Moreover, in the study done by Winters et. al,
entitled “The Activities of Daily Living in Patients after
Rotation plasty Surgery With a Long Term Follow up Checkup”,
there was a good outcome with the quality of life scores
yet, only little is known about the actual level of activity
and distribution of activities in the daily life of this
patient group and if the activity level remained reduced
after treatment due to a loss of confidence in physical
capacity and fitness. Although an experimental approach was
done, this research didn’t utilize questionnaires to assess
improvement when performing activities. The level of
activity was determined by the number of gait cycles
measured with the Step Watch Activity Monitor (SAM) (Cyma,
USA). This device is an ankle-worn accelerometer that
44
reliably assesses the number of gait cycles per day in one
minute intervals. It can be programmed to different gait
parameters and therefore provides a measurement precision of
about 99%. The SAM can store data of several weeks and
measures without providing feedback to the user thus
minimizing test bias. Similar with the study, the
researchers also took in consideration the gait of the
respondent in order to know if the clients are having
difficulty in performing the ADL.
In contrast to the above mentioned research, in this
study by La Pier, et. al (2008) entitled “Analysis of
Activities of Daily Living Performance in Patients
Recovering from Coronary Artery Bypass Surgery”, there was
no improvement when performing ADL. For data analysis, the
response frequency for each item of the Functional Status
Index and used chi-square was used. A significant loss of
function occurred immediately following surgery. Depressed
physical function immediately following surgery may be
related to surgeon-determined activity restrictions, fear of
activity and/or exacerbation of symptoms. In comparison with
45
the study, a few number of respondents expressed fear of
performing activity as they might aggravate negative effects
of surgery. This resulted in low level of activity for the
respondents.
Chapter 3
RESEARCH METHODOLOGY
This chapter presents the research design, population
and sampling, respondents/ participants of the study,
research instrument, validation of the instrument, data
46
gathering procedure and statistical tools utilized in the
treatment of data.
Research Design
The study utilized a quantitative, descriptive and non-
experimental method of research that aimed to observe,
describe and explain the effects of a certain phenomena.
The quantitative research design involved the investigation
of a phenomenon using numeric information, formal
measurement and quantification and was analyzed
statistically. The non-experimental type of quantitative
research explained the critical relationships between
relevant variables in the study and did not entail
introduction of treatment or changes to the variables (Polit
and Beck, 2008).
The researchers used the aforementioned research design
basically to aid in achieving their foremost intent of
describing the performance of the activities of daily living
among clients who have undergone caesarean section. These
variables were formally quantified without the introduction
of changes or alteration so as to make it more objective and
47
appropriate for accurate analysis and interpretation of
results.
Population and Sampling
The researchers utilized convenience and accidental
type of sampling. In convenience sampling, the most
conveniently available people as possible were used as the
participants who qualified for the eligibility criteria of
the study. On the other hand in accidental sampling, a
participant became part of the study because she happened to
be there (Polit and Beck, 2008).
Respondents of the Study
The study was conducted among clients who have
undergone caesarean section in the operating room complex of
General Emilio Aguinaldo Memorial Hospital in Trece Martires
City, Cavite, a tertiary hospital. There were 60 total
numbers of respondents who were two days postoperative, aged
48
18-37 years old and were able to speak, read, write and were
able to understand English or the Filipino language.
Research Instrument
In order to measure the performance of the activities
of daily living (ADL) among clients who have undergone
caesarean section, the researchers used the ADL (Activities
of Daily Living) Multidimensional Evaluation Checklist
(Mateo, 2009) based from Older American Resources and
Services (OARS) ADL Multidimensional Evaluation Checklist
(Bonito, 1998) as an instrument in the conduct of the study.
This tool was modified by excluding the following activities
such as household chores, handling money and personal
shopping. The researchers sent a letter or correspondence
to the originator of the instrument to ask permission to use
the aforementioned instrument. The items were translated in
Filipino.
The following instruments were used in this study:
49
1. Respondent’s Information Sheet – this was used to
gather the profile of the respondents in terms of age,
family support system and parity.
2. The Performance of the Activities of Daily Living –
measurement of the activities of daily living was based
on the ADL Multidimensional Evaluation Checklist
(Mateo, 2009). The ADL instrument contains a physical
ADL section and an instrument ADL section. Respondents
rated each item on a three-point scale based on the
ability to perform the activity independently. A score
of three (3) was given to items performed
independently, score of two (2) to those performed with
assistance, either through a person or device and a
score of one (1) to activities performed with great
dependence or not performed at all.
The activities included the following; (1) Eating,
(2) Drinking, (3) Preparing Meals, (4) Getting clothes
from the closet or bag, (5) Putting on clothes, (6)
Removing clothes, (7) Managing buttons, (8) Bathing
50
from head to toe, (9) Brushing teeth, (10) Moving from
bed to chair or vice versa, (11) Walking to and from
the toilet, (12) Urinating and (13) Defecating.
Validity and Reliability of Instrument
The research instrument was subjected to face and
content validation. The validators of the tool were the
faculty members of the College of Nursing and School of
Midwifery of De La Salle Health Sciences Institute, City of
Dasmariñas, Cavite.
The researchers requested the validators for their time
and consent regarding the validation of the tool. Letters
for the validators were made and were signed by the
researchers’ thesis adviser. The tool, together with the
letter, was given personally to the validators. The
research instrument was left to the validators for comments
and suggestions and was retrieved on the agreed date and
time.
51
It underwent the Cronbach’s alpha reliability testing
and showed 90.4% reliability indicating that the adapted
modified research tool was highly reliable.
Data Gathering Procedure
The following steps were undertaken for data gathering
and begun after pre-testing during the first week of August
until last week of August, 2012.
Social Preparation
Prior to the initiation of this study, permission to
utilize the tool for measuring the performance of the
activities of daily living was secured from the original
author of the tool from whom the instrument was adapted.
This was followed by seeking the approval of the College
Dean and thesis adviser to conduct the study in a Tertiary
Hospital. A letter of permission to conduct the study was
given to the Medical Services Director and Chief Nurse of
tertiary hospital. When permission was granted, the
researchers explained to the potential respondents the
objectives of the study before distributing the research
tool.
52
The whole process of this quantitative-descriptive
research was divided into two phases which were the
following: Phase I, coordination phase; Phase II Actual Data
Gathering
Phase 1: Coordination Phase
1. Formal letter was given to the Dean of College of
Nursing and School of Midwifery, the respective thesis
Adviser and the Medical Services Director and Chief
Nurse of the Tertiary Hospital.
2. The researchers went to a tertiary hospital to explain
to the potential respondents the research study and to
obtain an informed consent.
3. The researchers introduced themselves to the potential
respondents.
4. After the introduction, the researchers explained that
the purpose of why they were there was to conduct a
research study about the performance of the activities
of daily living of clients who have undergone caesarean
section.
53
5. The researcher explained that a participant should be
18-37 years of age who have undergone caesarean section
and at their two days postoperative. The respondents
must be able to speak, read, write and able to
understand English or Filipino language and were
willing to cooperate in the study. The researchers
explained that the process of gathering data needed for
the research study took about 10-15 minutes.
6. When the respondents consented to participate in the
study and when the specific criteria was met, the
researchers asked them to sign an informed consent form
which signified that the respondent agreed to be part
of the research study.
Phase II: Actual Data Gathering
1. The researchers asked the potential respondents to fill
out the Respondent’s Information Sheet for the
determination of the potential respondent’s profile.
2. Once the potential respondent was finished in filling
out the information sheet, the researchers assessed the
level of performance of activities of the daily living
54
of the potential respondents. The researchers used the
ADL Multidimensional Evaluation Checklist (Mateo, 2009)
to know the performance of the activities of daily
living of the potential respondents. In order to
assess the performance of the activities of daily
living of the potential respondents, the researchers
asked the patient if they could perform the items
included in the evaluation checklist. When the
respondent said that they could do it, then the
researchers asked the patient to do it. In cases where
in a respondent said that he/she was not able to
perform an item, the researchers did not force him/her
to do it. The researchers were the ones who filled out
the evaluation checklist as to how the patient
performed an item namely: (a) Independently, (b) Needs
Assistance and (c) Dependently.
Statistical Treatment of Data
55
The following statistical treatments were used to
answer the specific problems and to test the hypothesis of
the study.
Frequency distribution in percentage. This test was
used to organize the numeric data and this determined the
proportion of a part to a whole such as a given number of
respondents in relation to the sample population ( Polit, D.
et al, 2008). This was used to determine the profile of the
clients specifically age, family support system and parity.
Mean. This was the measurement of central tendency,
computed by summing all scores and diving by the number of
subjects (Polit and Beck, 2008). This statistical treatment
was used to determine the level of performance of the
activities of daily living when the respondents are grouped
according to age, family support systemand parity.
T-Test. This test employs the statistic (t), with n-
1degrees of freedom, to a test a given statistical
hypothesis about a population parameter. Usually used with
sample sizes (<30). It was used when the population
standard deviation was unknown (Roth, 2003). The t-test was
56
used to determine the significant differences on the
activities of daily living when the respondents are grouped
according to family support systemand parity.
F-Test. This was a test whether two samples are drawn
from different populations have the same standard
deviations, with specified confidence level. Sample may be
different sizes (Roth, 2003). In this study, the F-test was
used to determine any significant differences in the level
of performance of the activities of daily living when they
were grouped according to age.
57
Chapter 4
PRESENTATION, ANALYSIS and INTERPRETATION OF DATA
This chapter presents, analyzes and interprets the
findings on the specific problems and hypothesis of the
study. The data gathered regarding the profile of the
respondents are presented in graphs and are described,
analyzed and interpreted in narrative.
58
Problem 1. What is the profile of the respondents in terms
of age, family support system and parity?
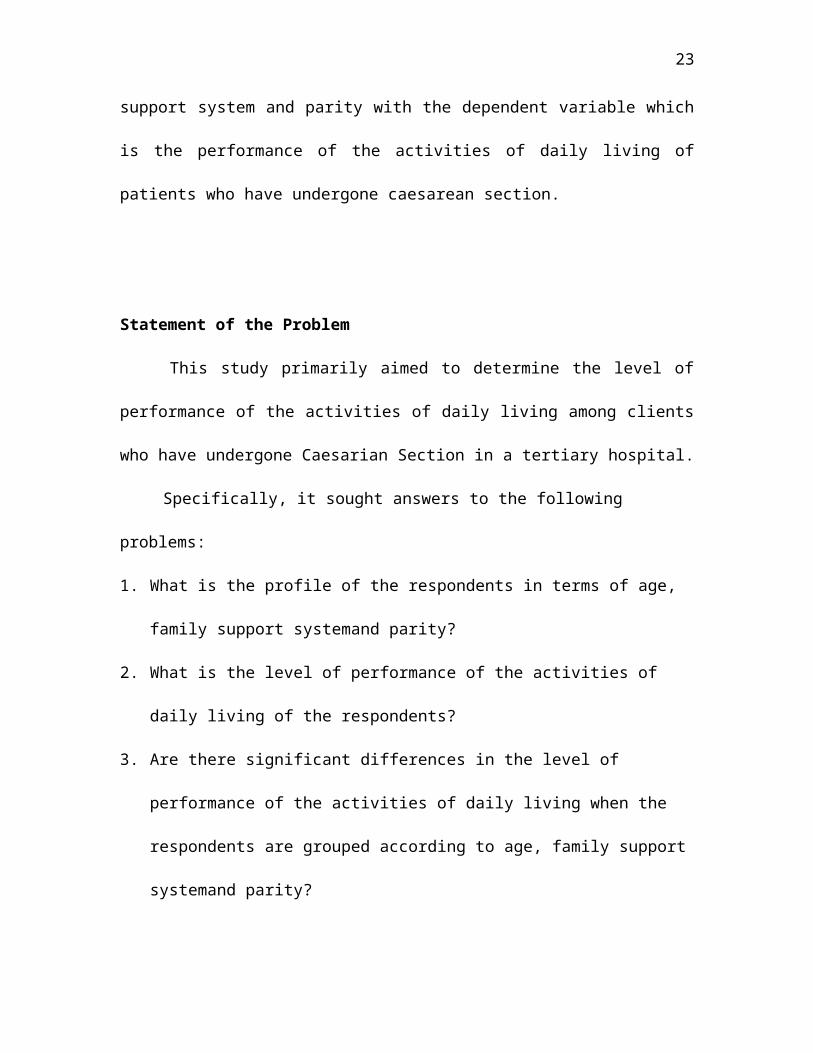
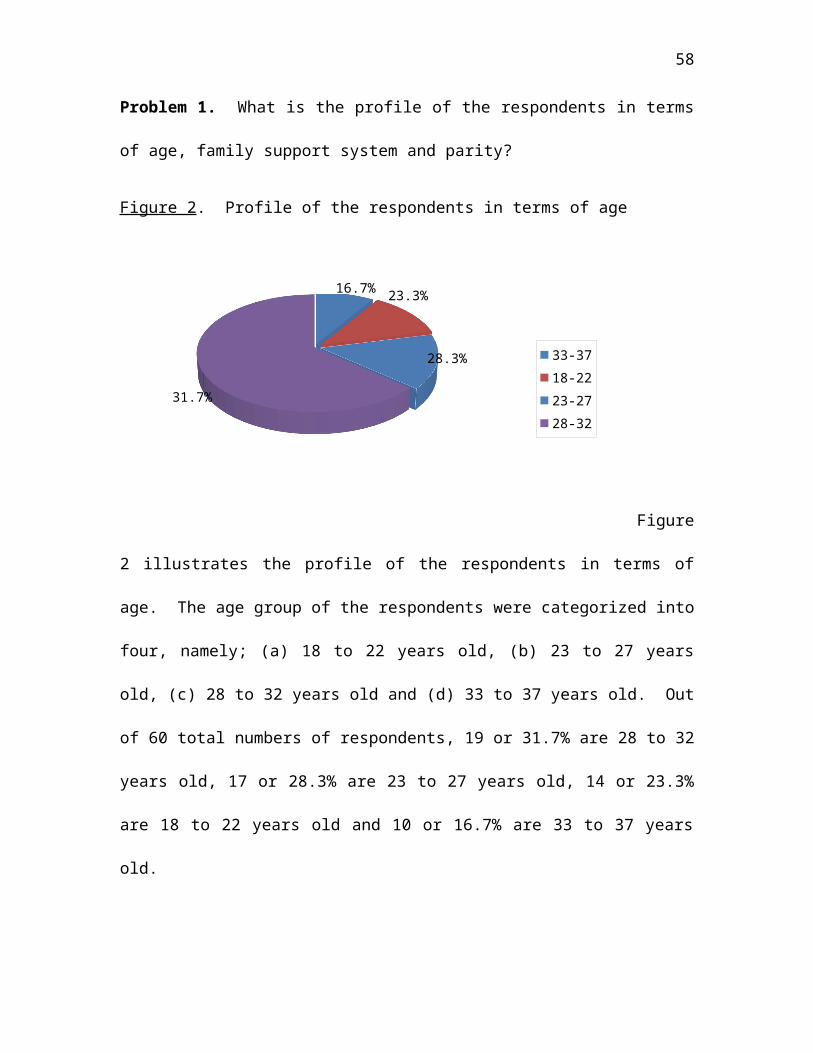
Figure 2. Profile of the respondents in terms of age
16.7% 23.3%
28.3%
31.7%
33-3718-2223-2728-32
Figure
2 illustrates the profile of the respondents in terms of
age. The age group of the respondents were categorized into
four, namely; (a) 18 to 22 years old, (b) 23 to 27 years
old, (c) 28 to 32 years old and (d) 33 to 37 years old. Out
of 60 total numbers of respondents, 19 or 31.7% are 28 to 32
years old, 17 or 28.3% are 23 to 27 years old, 14 or 23.3%
are 18 to 22 years old and 10 or 16.7% are 33 to 37 years
old.
59
This finding reveals that more of the clients who
have undergone caesarean section in a tertiary hospital are
28 to 32 years old.
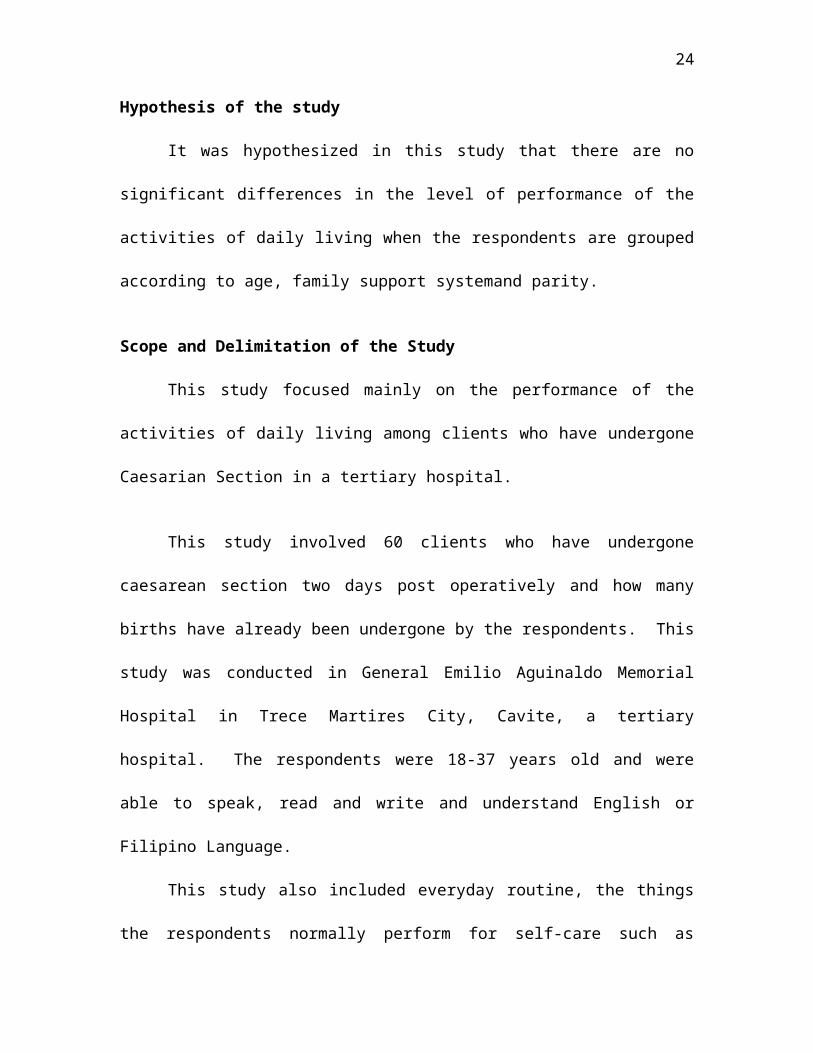
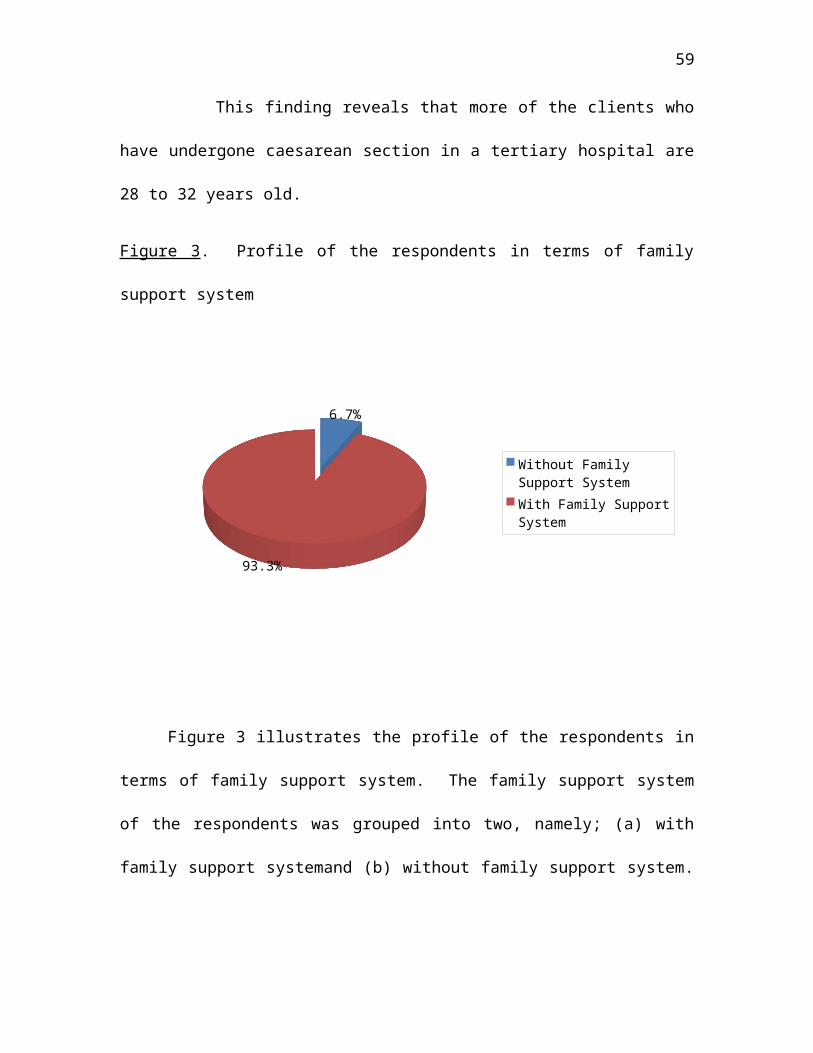
Figure 3. Profile of the respondents in terms of family
support system
6.7%
93.3%
Without Family Support SystemWith Family Support System
Figure 3 illustrates the profile of the respondents in
terms of family support system. The family support system
of the respondents was grouped into two, namely; (a) with
family support systemand (b) without family support system.
60
Out of 60 total numbers of respondents, 56 or 93.3% have
family support and 4 or 6.7% have no family support.
This finding shows that majority of clients who have
undergone caesarean section in a tertiary hospital have
family support system.
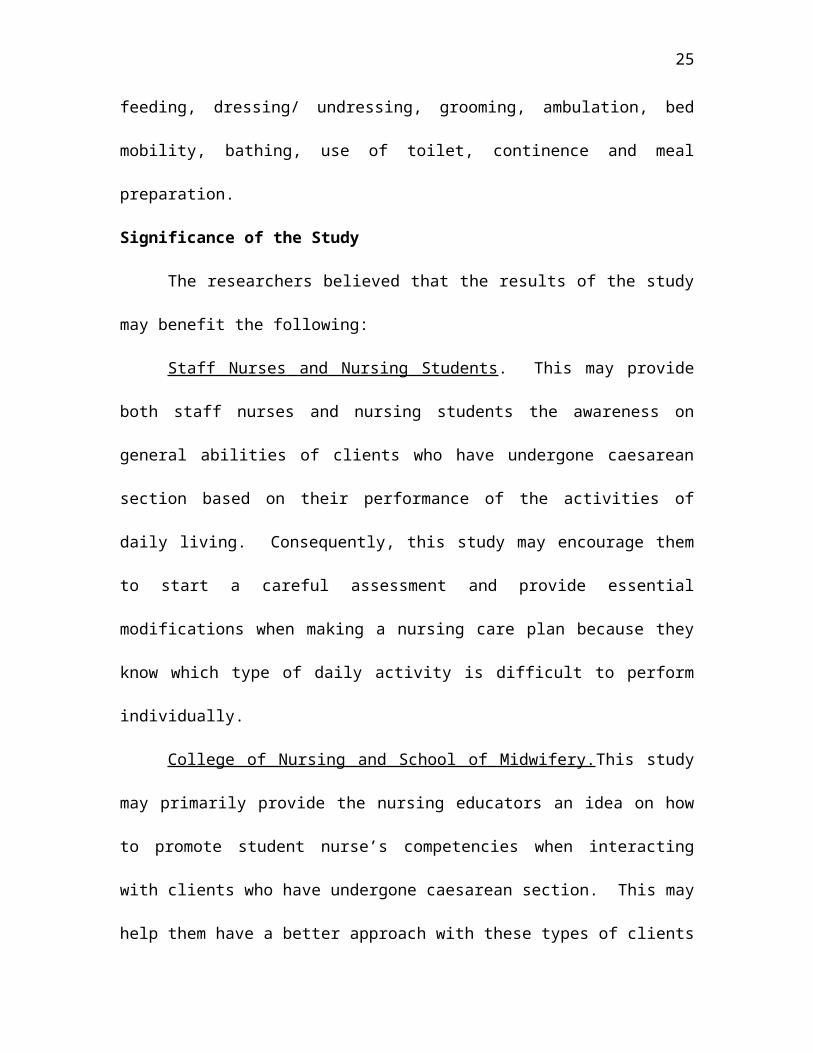
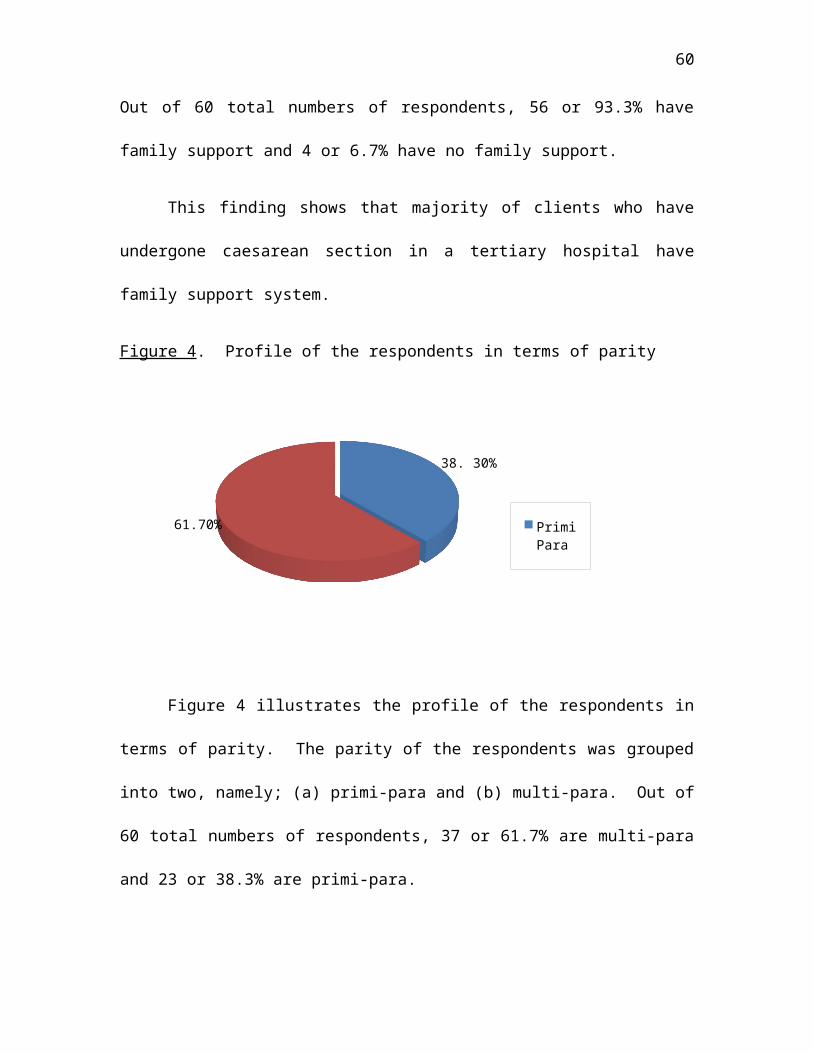
Figure 4. Profile of the respondents in terms of parity
38. 30%
61.70% Primi Para
Figure 4 illustrates the profile of the respondents in
terms of parity. The parity of the respondents was grouped
into two, namely; (a) primi-para and (b) multi-para. Out of
60 total numbers of respondents, 37 or 61.7% are multi-para
and 23 or 38.3% are primi-para.
61
This finding reveals that most of the clients who have
undergone caesarean section in a tertiary hospital are
multi-para.
Problem 2. What is the level of performance of the
activities of daily living of the respondents?
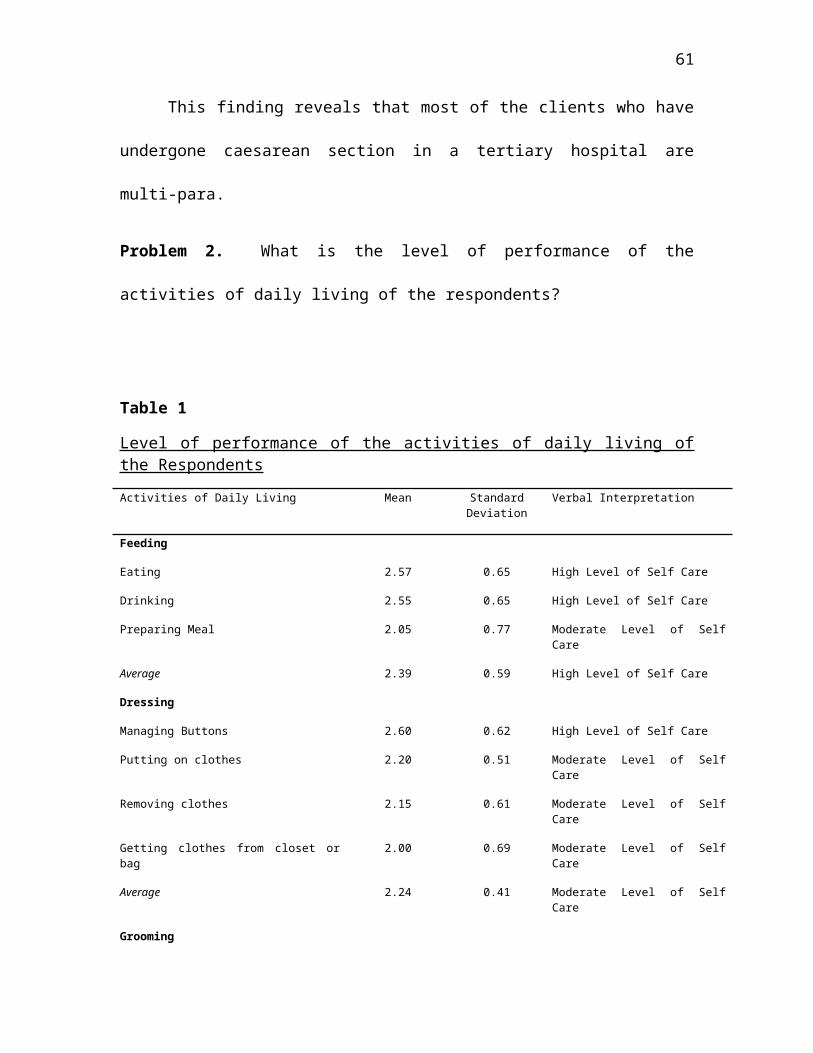
Table 1
Level of performance of the activities of daily living ofthe RespondentsActivities of Daily Living Mean Standard
DeviationVerbal Interpretation
Feeding
Eating 2.57 0.65 High Level of Self Care
Drinking 2.55 0.65 High Level of Self Care
Preparing Meal 2.05 0.77 Moderate Level of SelfCare
Average 2.39 0.59 High Level of Self Care
Dressing
Managing Buttons 2.60 0.62 High Level of Self Care
Putting on clothes 2.20 0.51 Moderate Level of SelfCare
Removing clothes 2.15 0.61 Moderate Level of SelfCare
Getting clothes from closet orbag
2.00 0.69 Moderate Level of SelfCare
Average 2.24 0.41 Moderate Level of SelfCare
Grooming
62
Combing Hair 2.67 0.64 High Level of Self Care
Brushing teeth 2.43 0.67 High Level of Self Care
Average 2.55 0.53 High Level of Self Care
Ambulation
Moving from bed to chair andvice versa
1.95 0.53 Moderate Level of SelfCare
Walking to and from the toilet 1.88 0.56 Moderate Level of SelfCare
Average 1.92 0.50 Moderate Level of SelfCare
Elimination
Defecating 1.87 0.65 Moderate Level of SelfCare
Urinating 1.58 0.67 Low Level of Self Care
Average 1.73 0.61 Moderate Level of SelfCare
Overall mean 2.17 2.15 Moderate Level of SelfCare
Interpretation: 2.35-3.00 High Level of Self Care/Performs Independently
1.68-2.34 Moderate Level of Self Care/Performs with Assistance
1.00-1.67 Low Level of Self Care/Performs Dependently
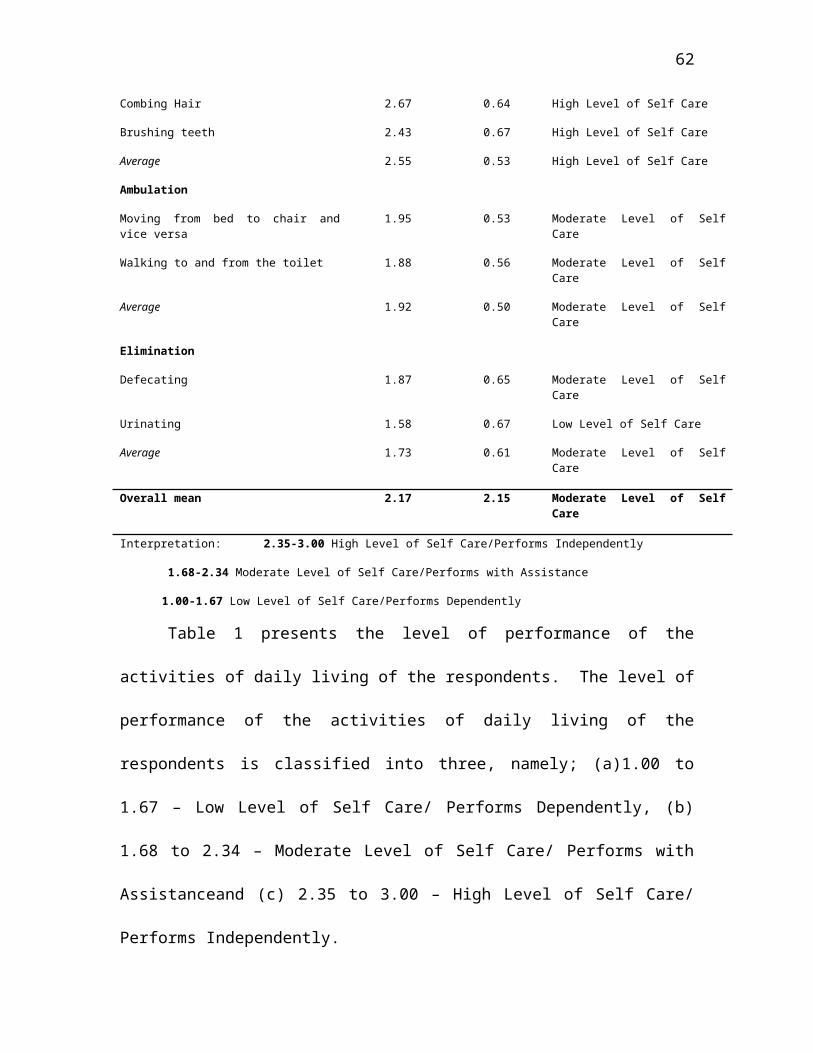
Table 1 presents the level of performance of the
activities of daily living of the respondents. The level of
performance of the activities of daily living of the
respondents is classified into three, namely; (a)1.00 to
1.67 – Low Level of Self Care/ Performs Dependently, (b)
1.68 to 2.34 – Moderate Level of Self Care/ Performs with
Assistanceand (c) 2.35 to 3.00 – High Level of Self Care/
Performs Independently.
63
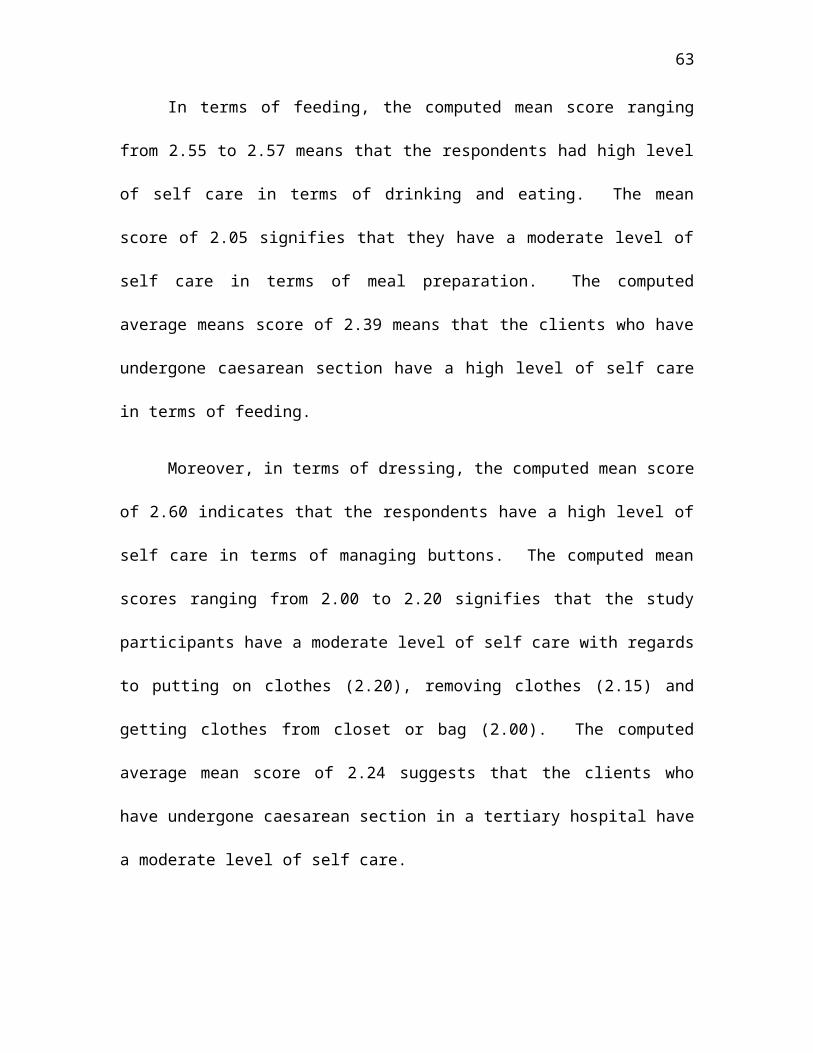
In terms of feeding, the computed mean score ranging
from 2.55 to 2.57 means that the respondents had high level
of self care in terms of drinking and eating. The mean
score of 2.05 signifies that they have a moderate level of
self care in terms of meal preparation. The computed
average means score of 2.39 means that the clients who have
undergone caesarean section have a high level of self care
in terms of feeding.
Moreover, in terms of dressing, the computed mean score
of 2.60 indicates that the respondents have a high level of
self care in terms of managing buttons. The computed mean
scores ranging from 2.00 to 2.20 signifies that the study
participants have a moderate level of self care with regards
to putting on clothes (2.20), removing clothes (2.15) and
getting clothes from closet or bag (2.00). The computed
average mean score of 2.24 suggests that the clients who
have undergone caesarean section in a tertiary hospital have
a moderate level of self care.
64
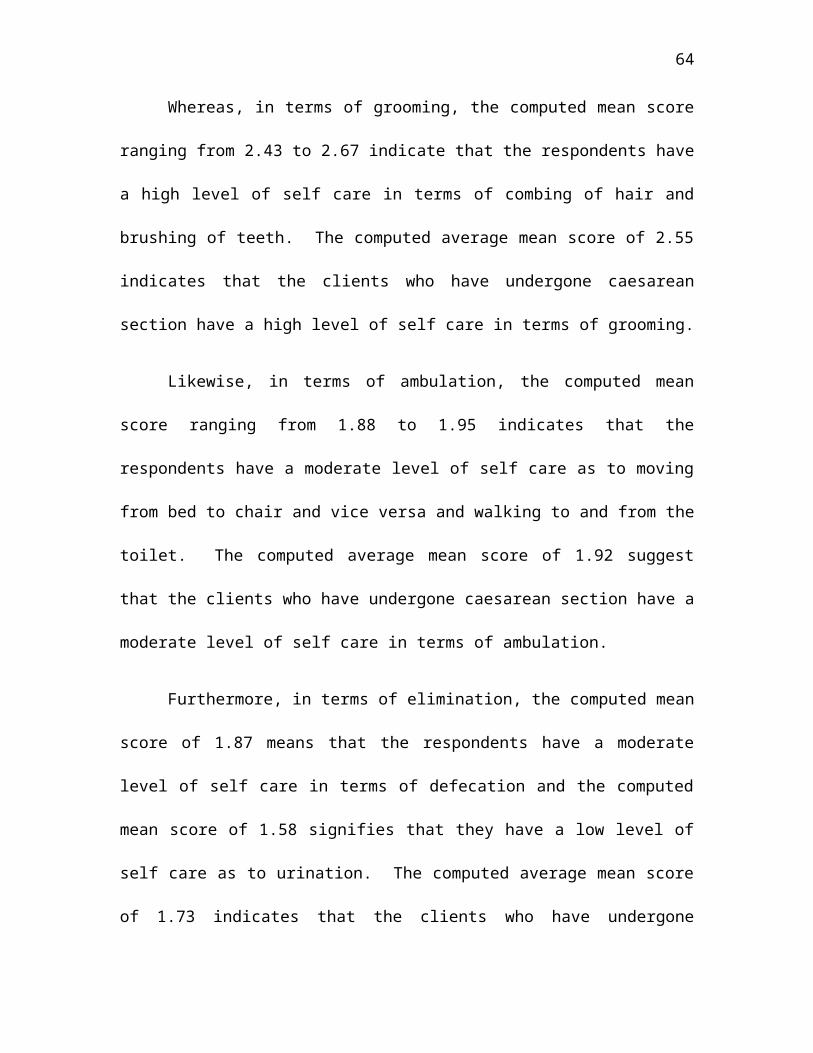
Whereas, in terms of grooming, the computed mean score
ranging from 2.43 to 2.67 indicate that the respondents have
a high level of self care in terms of combing of hair and
brushing of teeth. The computed average mean score of 2.55
indicates that the clients who have undergone caesarean
section have a high level of self care in terms of grooming.
Likewise, in terms of ambulation, the computed mean
score ranging from 1.88 to 1.95 indicates that the
respondents have a moderate level of self care as to moving
from bed to chair and vice versa and walking to and from the
toilet. The computed average mean score of 1.92 suggest
that the clients who have undergone caesarean section have a
moderate level of self care in terms of ambulation.
Furthermore, in terms of elimination, the computed mean
score of 1.87 means that the respondents have a moderate
level of self care in terms of defecation and the computed
mean score of 1.58 signifies that they have a low level of
self care as to urination. The computed average mean score
of 1.73 indicates that the clients who have undergone
65
caesarean section have a moderate level of self care in
terms of elimination.
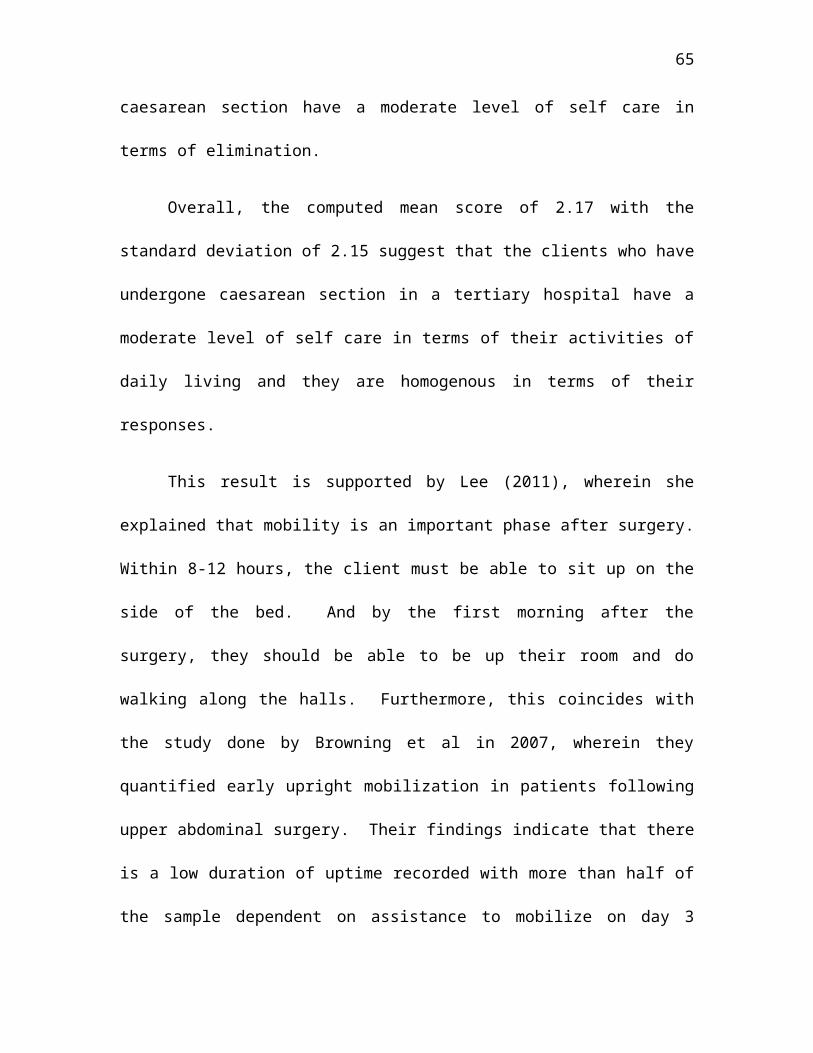
Overall, the computed mean score of 2.17 with the
standard deviation of 2.15 suggest that the clients who have
undergone caesarean section in a tertiary hospital have a
moderate level of self care in terms of their activities of
daily living and they are homogenous in terms of their
responses.
This result is supported by Lee (2011), wherein she
explained that mobility is an important phase after surgery.
Within 8-12 hours, the client must be able to sit up on the
side of the bed. And by the first morning after the
surgery, they should be able to be up their room and do
walking along the halls. Furthermore, this coincides with
the study done by Browning et al in 2007, wherein they
quantified early upright mobilization in patients following
upper abdominal surgery. Their findings indicate that there
is a low duration of uptime recorded with more than half of
the sample dependent on assistance to mobilize on day 3
66
while in a study by Mackay and Ellis (2002), 52% of the
respondents needed assistance to mobilize on day 5. Early
mobilization has no standard definition neither can it be
quantified but the activities included are: moving in bed,
sitting out of bed and standing, ambulating on the spot,
hallway ambulation and low intensity exercises (Dean 2006,
Kirkeby-Garstad et al 2005).
Problem 3. Are there significant differences in the
performance of daily living when respondents are grouped
according to age, family support system and parity?
Hypothesis: There are significant differences in the
performance of activities of daily living according to age
and parity and no significant difference in the performance
of activities of daily living when grouped according to
family support system.
67
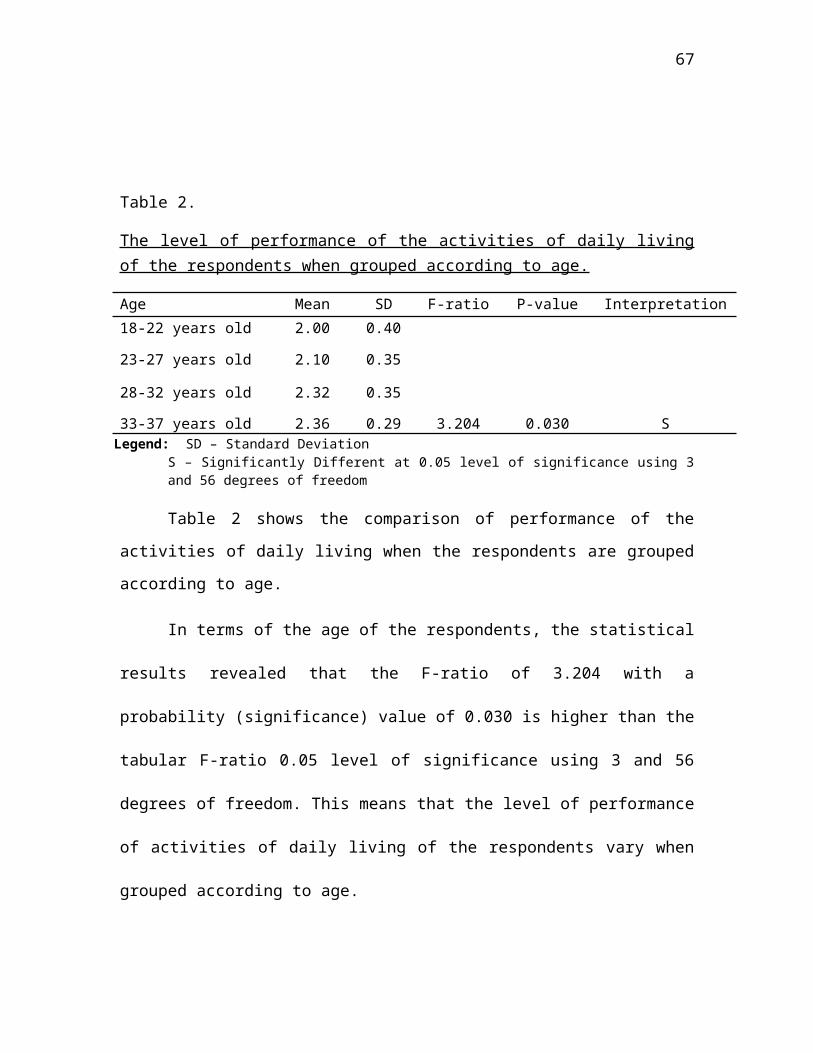
Table 2.
The level of performance of the activities of daily livingof the respondents when grouped according to age.
Age Mean SD F-ratio P-value Interpretation18-22 years old 2.00 0.40
23-27 years old 2.10 0.35
28-32 years old 2.32 0.35
33-37 years old 2.36 0.29 3.204 0.030 SLegend: SD – Standard Deviation
S – Significantly Different at 0.05 level of significance using 3and 56 degrees of freedom
Table 2 shows the comparison of performance of the
activities of daily living when the respondents are grouped
according to age.
In terms of the age of the respondents, the statistical
results revealed that the F-ratio of 3.204 with a
probability (significance) value of 0.030 is higher than the
tabular F-ratio 0.05 level of significance using 3 and 56
degrees of freedom. This means that the level of performance
of activities of daily living of the respondents vary when
grouped according to age.
68
The null hypothesis stating that there are no
significant differences in the level of performance of the
activities of daily living when the respondents are grouped
according to age is rejected and that the alternative
hypothesis which states that there are significant
differences in the level of performance of the activities of
daily living when the respondents are grouped according to
age, is accepted.
These findings confirm that the level of performance of
the activities of daily living of the respondents aged 18 to
37 years old vary. The clients who have undergone caesarean
section who were 33 to 37 years old are more likely to
exhibit better performance of the activities of daily living
in terms of feeding compared to the respondents in other age
groups.
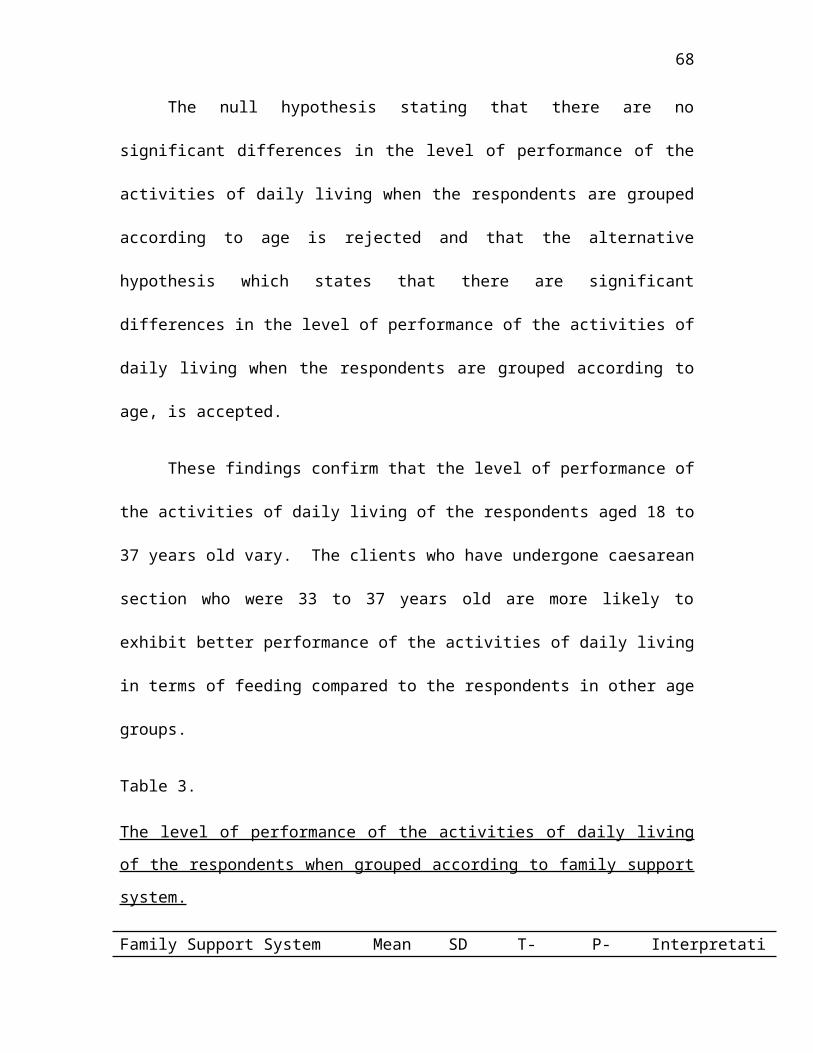
Table 3.
The level of performance of the activities of daily living
of the respondents when grouped according to family support
system.
Family Support System Mean SD T- P- Interpretati
69
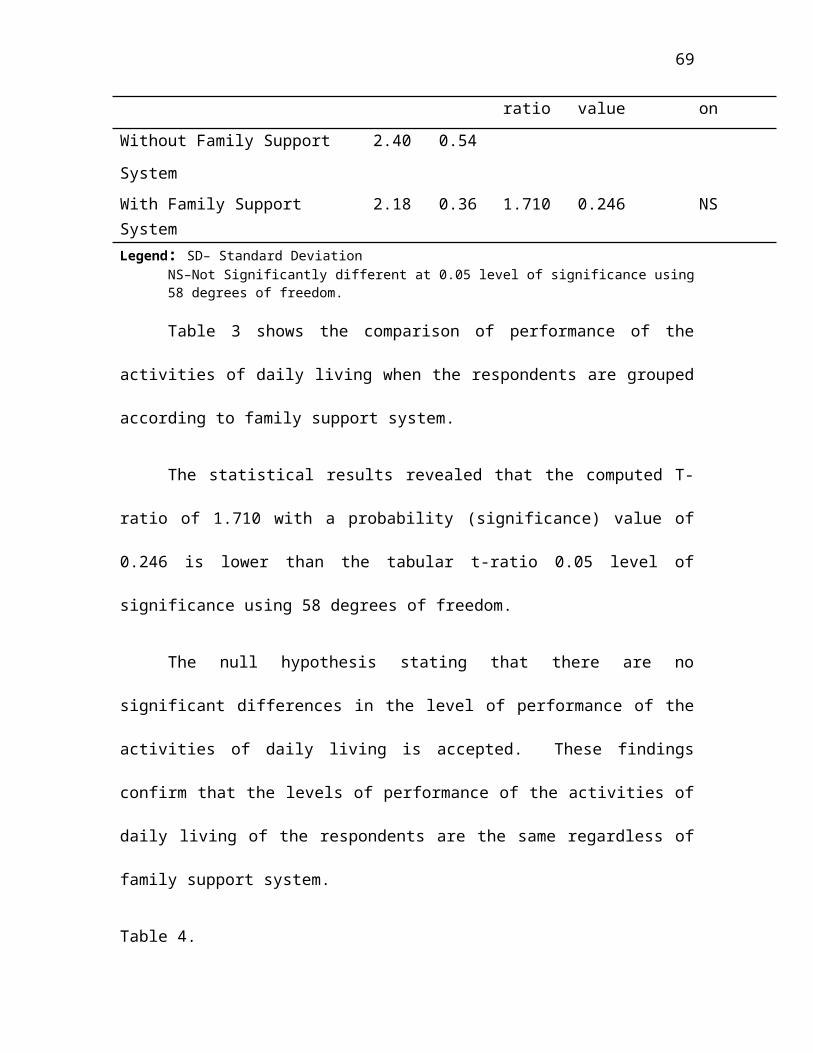
ratio value onWithout Family Support
System
2.40 0.54
With Family Support System
2.18 0.36 1.710 0.246 NS
Legend: SD– Standard DeviationNS–Not Significantly different at 0.05 level of significance using58 degrees of freedom.
Table 3 shows the comparison of performance of the
activities of daily living when the respondents are grouped
according to family support system.
The statistical results revealed that the computed T-
ratio of 1.710 with a probability (significance) value of
0.246 is lower than the tabular t-ratio 0.05 level of
significance using 58 degrees of freedom.
The null hypothesis stating that there are no
significant differences in the level of performance of the
activities of daily living is accepted. These findings
confirm that the levels of performance of the activities of
daily living of the respondents are the same regardless of
family support system.
Table 4.
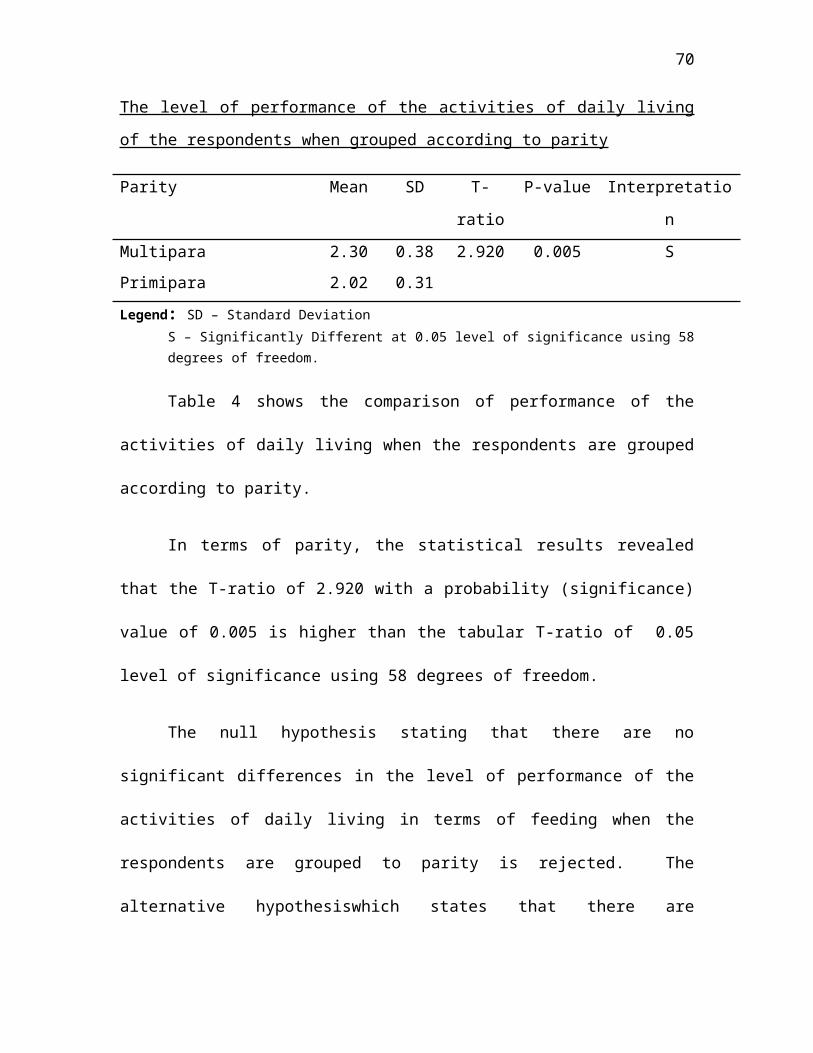
70
The level of performance of the activities of daily living
of the respondents when grouped according to parity
Parity Mean SD T-
ratio
P-value Interpretatio
nMultipara 2.30 0.38 2.920 0.005 SPrimipara 2.02 0.31Legend: SD – Standard Deviation
S – Significantly Different at 0.05 level of significance using 58degrees of freedom.
Table 4 shows the comparison of performance of the
activities of daily living when the respondents are grouped
according to parity.
In terms of parity, the statistical results revealed
that the T-ratio of 2.920 with a probability (significance)
value of 0.005 is higher than the tabular T-ratio of 0.05
level of significance using 58 degrees of freedom.
The null hypothesis stating that there are no
significant differences in the level of performance of the
activities of daily living in terms of feeding when the
respondents are grouped to parity is rejected. The
alternative hypothesiswhich states that there are
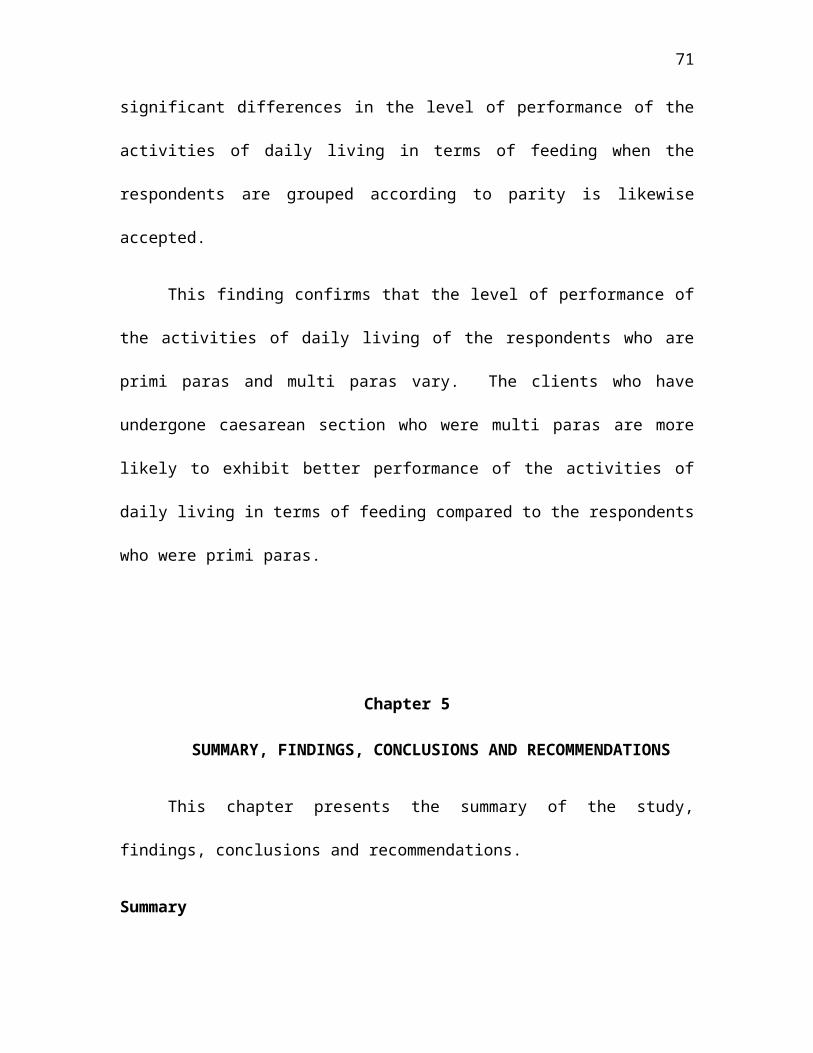
71
significant differences in the level of performance of the
activities of daily living in terms of feeding when the
respondents are grouped according to parity is likewise
accepted.
This finding confirms that the level of performance of
the activities of daily living of the respondents who are
primi paras and multi paras vary. The clients who have
undergone caesarean section who were multi paras are more
likely to exhibit better performance of the activities of
daily living in terms of feeding compared to the respondents
who were primi paras.
Chapter 5
SUMMARY, FINDINGS, CONCLUSIONS AND RECOMMENDATIONS
This chapter presents the summary of the study,
findings, conclusions and recommendations.
Summary
72
This study was undertaken to determine the level of
performance of the activities of daily living among clients
who have undergone caesarean section in a tertiary hospital.
Specifically, it sought answers to the following
problems:
1. What is the profile of the respondents in terms of age,
family support system and parity?
2. What is the level of performance of the activities of
daily living of the respondents?
3. Are there significant differences in the performance of
daily living when the respondents are grouped according
to age, family support system and parity?
Hypothesis of the Study
Specifically, this study tested the hypothesis that
there are no significant differences in the level of
performance of the activities of daily living when the
respondents are grouped according to age, family support
system and parity.
The study utilized a quantitative, descriptive and non-
experimental approach in order to observe, describe and
analyze the level of performance of the activities of daily
73
living of the respondents. The respondents of the study
were composed of 60 post-caesarean clients ages 18-37 year
old admitted in a tertiary hospital. The respondents were
selected using the criteria set by the researcher.
The following research instruments were used for the
data gathering. Respondent’s information sheet was used to
determine the profile of the clients who have undergone
caesarean section. The ADL Multidimensional Evaluation
Checklist in Mateo (2009) was used in identifying the level
of performance of the activities of daily living of clients,
two days after the caesarean section.
Prior to the actual gathering, permission was solicited
from the Medical Director and the Nursing Service Department
Administrator of the selected tertiary hospital. Upon
approval, the researcher proceeded with the data gathering.
In this study a standard script was utilized. The data
gathering started by evaluating the patients who were
admitted in the selected tertiary hospital after two days of
their post-operative caesarian section and ensuring they are
qualified for the study. The respondents were then asked to
74
sign the informed consent form and fill out the Respondent’s
Information Sheet. Using the ADL Multidimensional
Evaluation Checklist, the respondents were assessed.
The following statistical treatment utilized by the
researcher to be able to answer the problem stated and to
test the hypothesis of the study. This includes (a.)
Frequency distribution, (b.) meanand (c) t-test and (d) f-
test.
Frequency distribution was used to determine the
profile of the clients specifically age, family support
system and parity. The mean was used to measure the level
of performance of activities of clients who have undergone
caesarean section. The t-test and f-test was used to test
the significant difference in activities of daily living
when respondents are grouped according to age, family
support systemand parity.
Findings
The following findings were drawn from this study:
1. Out of 60 respondents in this study, their profileshowed that most of them are: (a) 28- 32years old
75
(31.7%), (b) with family support system, living with orbeing visited by family members, friends or relatives(93.3%), and (c) multi-para (61.7%).
2. The level of performance of the respondents who
have undergone caesarean section is moderate. This
evidenced by an overall mean score of 2.17 with a
standard deviation of 2.15 which signifies that the
respondents are able to perform activities of daily
living with assistance and they are homogenous in terms
of their respondents.
3. There is no significant differences in the level
of performance of activities of daily living when the
respondents are grouped are grouped according to family
support system as evidenced by a computed T-ratio of
1.710 that is lower than the tabular t-ratio at 0. 05
level of significance using 58 degrees of freedom.
There are significant differences however in the
level of performance of activities of daily living of
the respondents when grouped according to age and
parity. This is evidenced by an F-ratio of 3.204 and T-
76
ratio of 2.920 which are greater than the tabular as F-
ratio and T-ratio using 3 and 56 degrees of freedom and
58 degrees of freedom respectively.
Conclusions
Based on findings, generated by the study, thefollowing conclusions were drawn:
1. Most of the respondents are 28 to 32 years old, withfamily support system, and multi-para.
2. The clients who have undergone caesarean section in atertiary hospital were able to perform activities ofdaily living with assistance.
3. There are significant differences in the performance ofactivities of daily living according to age and parityand no significant difference in the performance ofactivities of daily living when grouped according tofamily support system.
Recommendations
Clients who have undergone Caesarean Section. Findingsof the study recommend the continuity of educating theclients regarding caesarean section to enhance theirperformance of activities of daily living. This would alsohelp them have an improved understanding of their condition;
77
they would become more aware of their physical capabilityand would be able to allow themselves to reach a new levelof self-independence in order to be more active inperforming their tasks on a daily basis.
Family of Clients who have undergone Caesarean Section.Families should be the primary providers of care to theclients as they would be more knowledgeable on their physicaland emotional needs. Therefore, family members arerecommended to collaborate with the nurses when providingcare and performing interventions as this would help theclients' recovery.
Future Researchers. The researchers encourage futureresearchers to contribute or to expand on this body ofknowledge. The researchers also recommend that the futureresearchers conduct further research and in-depthinvestigation regarding the study. Added factors such astheir past health history and lifestyle could be included toobtain a precise and unambiguous study. Other activities ofdaily living can be integrated as well. A replication ofthis study is recommended with longer time allocated in theprovision of intervention and with greater number ofrespondents.
78
REFERENCES
A. Books
Bertoti, D. (2004) Functional Neurorehabilitation Through The
Lifespan. Philadelphia. Davis Company
Clover, J. (2007) Core Concepts in Athletic Training and Fitness
Instruction (2nd. Ed.) New York. Thomson Delmar Learning
Cunningham, et. al, (2005). Williams Obstetrics (22nd ed.)
McGraw-Hills Companies, Inc.
Daftray, S.N. & Desai, S.V. (2005). Selected Topics in
Obstetrics and Gynecology- 1. B I Publications Pvt Ltd.
Gabbe, et. al, (2007). Obstetrics Normal and Problem
Pregnancies (5th ed.). Churchill Livingstone Publication.
Henderson, V. (2007). The Nature of Nursing in New York. New
YorkMacmillan Publishing
Krapp, K.. (2012) Activitiesof Daily Living Evaluation.
MichiganGale Group
79
McKinney, E. S. et al (2009) Maternal Child Nursing.
Missouri. Saunders Elsevier
Polit, D. & Beck C.T. (2008). Nursing Research: Generating
and Assessing Evidence for Nursing Practice (8th ed).
Philadelphia Lippincott Williams & Wilkins Publisher
Rothwell, P. et al (2007). Stroke Management (3rd ed).
USA: Blackwell Publishing
Sadock, B.J. & Sadock, V.A. (2005) Kaplan & Sadock's
Comprehensive Textbook of Psychiatry (8th ed.) Philadelphia.
Lippincott Williams & Wilkins
B. Periodicals and Other Materials
ACOG Committee Opinion No. 340.(2006) Mode of term
singleton breech deliveryObstet Gynecol; Vol. 108,
No.1
ACOG Practice Bulletin No. 49(2006) Dystocia and
augmentation of labor Obstet Gynecol; Vol. 108, No.1
ACOG Practice Bulletin Number 49, (2003): Dystocia and
augmentation of labor.. Obstet Gynecol.; Vol. 102 No.
6
80
Browning. et al (2007): The quantity of early upright
mobilisation performed following upper abdominal
surgery is low: an observational study Australian Journal
of Physiotherapy Vol. 53
Eubel C, (2009) St. Raymond Nonnatus. Hierarchia Catholica,
Vol. I
Hankins., et al (2006) .Cesarean section on request at 39
weeks: impact on shoulder dystocia, fetal trauma,
neonatal encephalopathyand intrauterine fetal
demise. Semin Perinatol.Vol. 30 No 5
Kirkeby-Garstad I, Sellevold OFM, Stenseth R, Skogvoll E
(2005) Mixed venous oxygen desaturation during early
mobilization after coronary artery bypass surgery.
Acta Anaesthesiologica Scandinavica Vol. 49: 827–834.
Mackay MR and Ellis E (2002) Physiotherapy outcomes and
staffing resources in open abdominal surgery
patients. Physiotherapy Theory and Practice Vol. 8: 75–
93.
C. Online Sources
81
Cooperative for Assistance and Relief Everywhere, Inc.
(CARE), (2007) Mothers Matter, Healthy Mothers, Healthy
Societies. Retrieved October 24, 2012 from.
http://www.care.org/getinvolved/advocacy/pdfs/agenda
2008/sp_mothersmatter.pdf
Downs et. al (2009) Impact of scoliosis surgery on activities of daily
living in females with Rett syndrome. Retrieved May 20,
2012. from.
http://www.ncbi.nlm.nih.gov/pubmed/19461379
Gagnon A.J, Meier K.M. & Waghorn K. (2007) Continuity of
nursing care and its link to caesarean birth rate. Retrieved
January 28, 2012 from
http://www.ncbi.nlm.nih.gov/pubmed/17324175
Gibbons., et al (2010) The Global Numbers and Costs of
Additionally Needed and Unnecessary Caesarean
Sections Performed per Year: Overuse as a Barrier to
Universal Coverage. Retrieved January 25, 2012,
from
http://www.who.int/healthsystems/topics/financing/he
althreport/30C-sectioncosts.pdf
82
Heisler, J. (2009) Do You Really Need Surgery. Retrieved
January 25, 2012, from
http://surgery.about.com/od/beforesurgery/a/NeedSurg
ery.htm
Kho, P. (2010) Labor complications. Retrieved from March
26, 2012 from
http://www.babycenter.com.ph/pregnancy/labourandbirt
h/labourcomplications/caesarean-rate/
La Pier et, al (2008) Analysis of Activities of Daily Living Performance
in Patients Recovering from Coronary Artery Bypass
SurgeryRetrieved May 20, 2012. from
http://informahealthcare.com/doi/abs/10.1080/0270318
0802206215
Meiners et. al (2002) Improvements in activities of daily living
following functional hand surgery for treatment of lesions to the
cervical spinal cord: Self-assessment by patient. Retrieved May
20, 2012. from
http://www.nature.com/sc/journal/v40/n11/full/310138
4a.html
83
Wiley. J. (2012) Definition of ADLs (activities of daily living)
Retrieved January 28,2012. from
http://www.medterms.com/script/main/art.asp?
articlekey=2152
Winters et. al,(2007) The Activities of Daily Living in Patients after
Rotationplasty Surgery With a Long Term Follow up Checkup
Retrieved May 20, 2012. From
http://www.isols2007.org/abstract.php?_IDA=431
D. Thesis
Mateo, J. (2009). Enhancement of performance of the
activities of daily living of Clients after
Cerebrovascular Accident Through Health Education
Intervention. Unpublished Master’s Thesis. De La
Salle Health Sciences Institute, Dasmariñas, Cavite.
84
APPENDICES
Appendix – A
Letter of Request for Actual Data Gathering
85
De La Salle Health Sciences InstituteCollege of Nursing and School of Midwifery
Dasmariñas City, Cavite
Naomi M. De Aro, RN, MAN, EdD
Dean, College of Nursing & School of Midwifery
De La Salle Health Sciences Institute
Dear Dr. De Aro:
Greetings in St. La Salle!
We, the third year nursing students of De la Salle
Health Sciences Institute, would like to inform you that we
are currently working on our thesis entitled “Performance of
the activities of daily living Among Clients who have
Undergone Caesarean Section in a Tertiary Hospital”.
In line with this, we would like to request from your
good office to allow us to distribute questionnaires to the
selected students of the college. Attached herewith are
parts of our research study consisting of the statement of
the problem, scope and delimitation, hypothesis and research
tool. The said data will be used in partial fulfillment of
the requirements in the nursing research. Attached here are
the statement of the problem and the tool to be used for our
thesis.
Hoping for your favorable response. More power and God
Bless!
86
Sincerely yours,Fatima Mae S. Baaclo Analen D.
Cagalpin
Emil John A. Medina Effienet Chioma
G. Onuh
Jeremiah Gael A. Stone
Noted by:
Rommel L. Salazar, RN, MAN, DrPH Naomi M. De Aro, RN, MAN, EdDThesis Adviser Dean, College of Nursing &
School of MidwiferyAppendix – B
Letter to the Medical Services DirectorDE LA SALLE HEALTH SCIENCES INSTITUTE
SCHOOL OF NURSING
George R. Repique Jr., MD, FPSRS, FPCSMedical DirectorGeneral Emilio Aguinaldo Memorial HospitalIndang Rd, Trece Martirez City, Cavite
Dear Sir,
Greetings in St. La Salle!
We are, Fatima Mae S. Baaclo, Analen D. Cagalpin,Emil John A. Medina, Effienet Chioma G. Onuh and JeremiahGael A. Stone, 4th year nursing students of the College ofNursing and School of Midwifery De La Salle – HealthSciences Institute School and currently conducting a studyentitled “Performance of the activities of daily livingAmong Clients who have Undergone Caesarean Section in aTertiary Hospital” in partial fulfillment of therequirements for the degree of Bachelor of Science inNursing.
87
In line with this, we would like to seek permissionfrom your good office to please allow us to have the pre-testing and data gathering of our research questionnairedone at your hospital.
We assure your good office that confidentiality anddata of findings will be upheld and with assurance thatclients who are post Caesarean Section will be handled withutmost care.
Your kind approval regarding our request will be agreat help in our present endeavor. Thank you very much.Respectfully Yours,
Fatima Mae S. Baaclo Analen D.
Cagalpin
Emil John A. Medina Effienet Chioma
G. Onuh
Jeremiah Gael A. Stone
Noted by:
Rommel L. Salazar, RN, MAN, DrPH Naomi M. De Aro, RN, MAN, EdDThesis Adviser Dean, College of Nursing &
School of MidwiferyAppendix – C
INFORMED CONSENT FORM
I, ___________________________, am being asked to
participate in a research entitled, “performance of the
88
activities of daily living among Clients who have Undergone
Caesarean Section in a Tertiary Hospital”. This research is
being conducted under the supervision of BSN students Ms.
Fatima Mae S. Baaclo, Ms. Analen D. Cagalpin, Mr. Emil
John A. Medina, Ms. Effienet Chioma G. Onuhand Ms.
Jeremiah Gael A. Stone.
The investigators hope to determine the performance of
the activities of daily living among clients who have
undergone caesarean section from this research.
While participating in this study, I will fill up the
Respondent’s Information Sheet. The researchers will assess
the level of performance of the activities of daily living
using the ADL Multidimensional Checklist by letting me
perform the said activity. The researchers are the ones to
fill up the evaluation checklist as to how the respondent
performed the item, Independently, Needs Assistance,
Dependently.
The nature of this study has been explained to me by
Ms. Baaclo, Ms. Cagalpin, Mr. Medina, Ms. Onuh and Ms.
Stone. I understand that the benefits of my participation
will be for my awareness on my physical capabilities and
allow myself to reach a new level of self independence in
order to be more active when performing tasks on a daily
basis.
The researchers will make every effort to safeguard the
confidentiality of the information that I will provide. Any
89
information obtained from this study that can be identified
with me will remain confidential and will not be given to
anyone without my permission.
If at anytime I would like additional information about
this project I can contact Ms. Onuh at 0915-835-55-56 or
(046) 416-4532.
I understand that I have the right to refuse to
participate in this study. I also understand that, if I do
agree to participate, I have the right to change my mind at
any time and stop participating in the above described
project. My signature also indicates that:
I have given opportunity to ask any and all questions
about the described project and that all of my
questions have been answered to my satisfaction.
I have been permitted to read this document and I have
been given a signed copy of it.
To the best of my knowledge and belief, I have no
physical or mental illness or weakness that would be
adversely affected by my participation in the described
project.
_____________________________ ________________
Signature of Participant Date
90
_____________________________ _________________
Signature of Witness Date
Appendix – D
PAHINTULOT NG KATUGON
Ako, si ______________________________________________,
ay hinilingang makilahok sa isang pananaliksik na
pinamagatang "Pagganap ng Mga Gawain sa Pang-araw-araw na
Pamumuhay sa Mga Kliyente Na Nakaranas ng Cesarean Section
sa Tersiyaryong Ospital." Ang pananaliksik na ito ay
isinasagawa sa pangangasiwa ng mga estudyante ng BSN na
sina: Bb. Fatima Mae S. Baaclo, Bb. Analen D. Cagalpin,
91
G. Emil John A. Medina, Bb. Effienet Chioma G. Onuh, at
Bb. Jeremiah Gael A. Stone.
Ninanais ng mga tagapagsiyasat na malaman mula sa
pananaliksik na ito ang pagganap ng mga gawain ng pang-araw-
araw na pamumuhay sa mga kliyente ng mga nakaranas na ng
Cesarian section.
Habang ako ay nakikilahok sa pag-aaral na ito,
sasagutan ko ang mga katanungan sa "Respondent Information
Sheet". Tatayahin ng mga mananaliksik ang antas ng aking
pagganap sa mga gawaing pang-araw-araw na pamumuhay sa
pamamagitan ng paggamit ng "ADL Multidimensional Checklist".
Ang mga mananaliksik ang siyang sasagot ng tseklist ng
pagsusuri kung paano gumanap ang katugon sa isang gawain:
ito ba ay kaya kong gawin ng mag-isa, kinakailangan ng
tulong, o umaasa nang husto sa tulong ng iba.
Ang uri ng pag-aaral na ito ay ipinaliwanag sa akin
nina Bb. Baaclo, Bb. Cagalpin, G. Medina, Bb. Onuh at
Bb. Stone. Naintindihan ko na ang mga benepisyo ng aking
paglahok sa pag-aaral na ito ay para sa aking kamalayan ng
aking pisikal na kakayahan at upang mapahintulutan ang aking
sarili na maabot ang bagong baitang ng pagiging
independente, upang maging lalong aktibo sa pagganap ng mga
pang-araw-araw na gawain.
Lubusang sisikapin ng mga mananaliksik na pangalagaan
ang pagiging kompidensyal ng mga impormasyong aking
92
ibabahagi. Ano mang impormasyong nakamit mula sa pag-aaral
na ito patungkol sa akin ay mananatiling kompidensyal at
hindi ibibigay kaninuman ng walang pahintulot mula sa akin.
At anumang oras na ninanais kong magkaroon ng
karagdagang impormasyon patungkol sa proyektong ito, maaari
kong kontakin si Bb. Onuh sa 0915-835-55-56 o(046) 416-
4532.
Naintindihan ko na may karapatan akong tanggihang
makilahok sa pag-aaral na ito. Naiintindihan ko rin na,
kung ako ay sumang-ayong makisali, may karapatan akong
magpalit ng aking desisyon anumang oras at ihinto ang
pakikilahok sa naturang proyekto. Ipahihiwatig ng aking
lagda na:
Binigyan ako ng pagkakataong magtanong ng kahit anumang
katanungan patungkol sa naturang proyekto at ang lahat
ng aking katanungan ay sasagutin ayon sa aking
kasiyahan.
Binigyan akong permiso na basahin ang dokumentong ito
at ako ay binigyan ng nilagdaang kopya.
Abot sa aking kaalaman at paniniwala, ako ay walang
pisikal o mental na sakit o kahinaan na makasasama sa
aking pakikilahok sa naturang proyekto.
93
__________________________________________Lagda ng Katugon
Petsa
__________________________
________________
Lagda ng Saksi
Petsa
Appendix - E
RESPONDENT’S INFORMATION SHEET
Name:___________________________ (optional)
Age: ( ) 18-22 years old
( ) 23-27 years old
( ) 28-32 years old
( ) 33-37 years old
Parity: number of times the mother has been pregnant but not
less than 20 weeks of gestation
( ) Primi para- has given birth for the first time
94
( ) Multi para - has given birth two or more times
Family Support System: (Please check if any of the following
support is available)
_____ With family support - living with or being
visited by family members, friends, or relative
_____ Without family support, living without or not
being visited by family members, friends, or relatives
Appendix - F
TALAAN NG IMPORMASYON NG RESPONDE
Pangalan : _______________________________
Edad: ( ) 18 – 22 taong gulang
( ) 23 – 27 taong gulang
( ) 28 – 32 taong gulang
95
( ) 33 – 37 taong gulang
Pagkakapareho : bilang ng pagkakataong nabuntis ang isang ina ngunit
hindi bababa sa dalawangpung linggong pagbubuntis
( ) Primipara – nakapagsilang sa unang pagkakataon
( ) Multi para – nakapagsilang ng dalawa o higit pang beses
Sistema ng Pagsuporta ng Pamilya : ( Lagyan ng tsek () kung ang mga
sumusunod na suporta ay matatagpuan )
____ sinusuportahan ng pamilya – kapisan ng pamilya o dinadalaw ng
miyembro ng pamilya
kaibigan, kamag-anak
____ walang suporta ng pamilya – hindi kapisan ng pamilya o hindi dinadalaw
ng pamilya, kaibigan,kamag-anak
Appendix - G
ADL Multidimensional Evaluation Checklist(Mateo, 2009)
96
Name (Pangalan): ______________________________
Direction: The following are the Activities of Daily Living(ADL). Place a check mark ( / ) on the box appropriate foreach ADL.Panuto : Ang mga sumusunod ay mga gawain sa pang-araw-araw na pamumuhay (ADL). Lagyan ng tsek ( ) ang kahon na angkop para sa bawat ADL.
1.) Dependent – inability to perform the task either by selfor with support from others. This means a completedependence on a device or on someone else toperform a task or has a low level of self care.
(Umaasa– Kawalan ng kakayahang makagawa ng gawain sa ganang sarili o maging sa tulong ng iba. Nangangahulugan ito ng ganap na pag-asa sa aparato o sa sinuman para gumawa ng gawain o may mababang antas ng pangangalaga sa sarili).
2.) Needs Assistance – ability to perform task only if withsupport either by a person or a device or has amoderate level of self-care.
(Nangangailangan ng Tulong – Kakayahang makagawa ng gawain basta may tulong ng ibang tao ng aparato o may katamtamang antasng pangangalaga sa sarili.)
3.) Independent – ability to perform task by own self or hasthe high level of self- care.
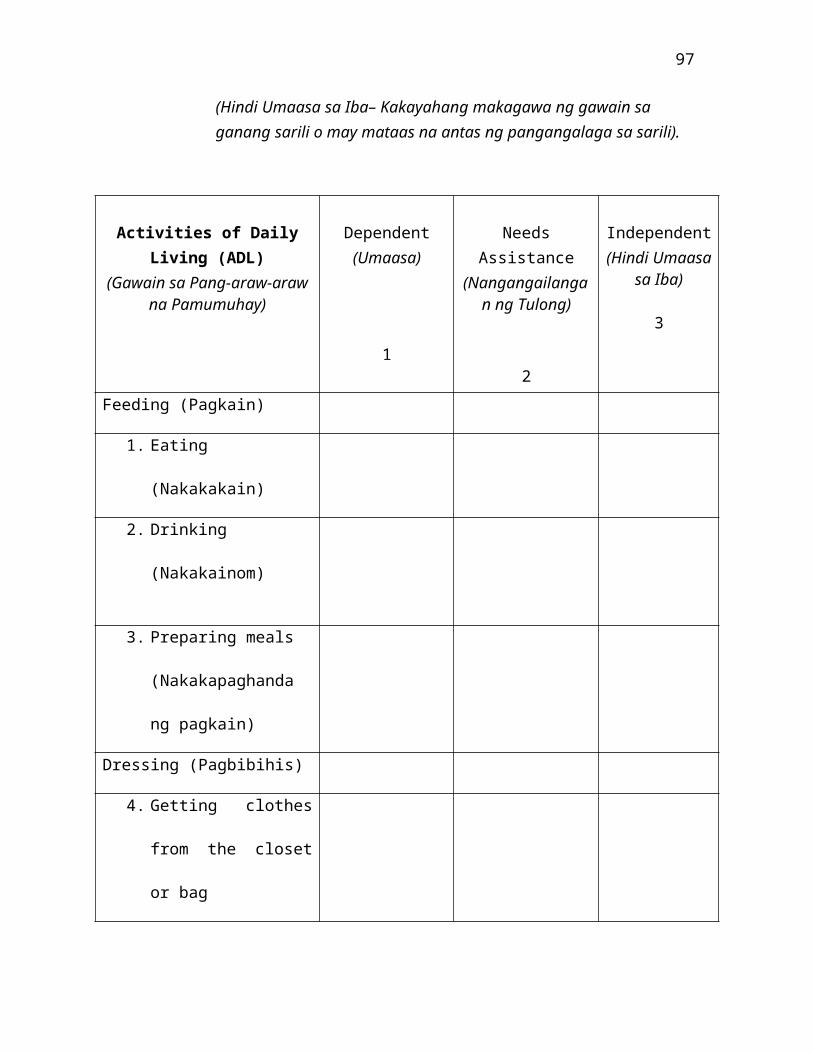
97
(Hindi Umaasa sa Iba– Kakayahang makagawa ng gawain sa ganang sarili o may mataas na antas ng pangangalaga sa sarili).
Activities of DailyLiving (ADL)
(Gawain sa Pang-araw-arawna Pamumuhay)
Dependent(Umaasa)
1
NeedsAssistance
(Nangangailangan ng Tulong)
2
Independent(Hindi Umaasa
sa Iba)
3
Feeding (Pagkain)
1. Eating
(Nakakakain)
2. Drinking
(Nakakainom)
3. Preparing meals
(Nakakapaghanda
ng pagkain)
Dressing (Pagbibihis)
4. Getting clothes
from the closet
or bag
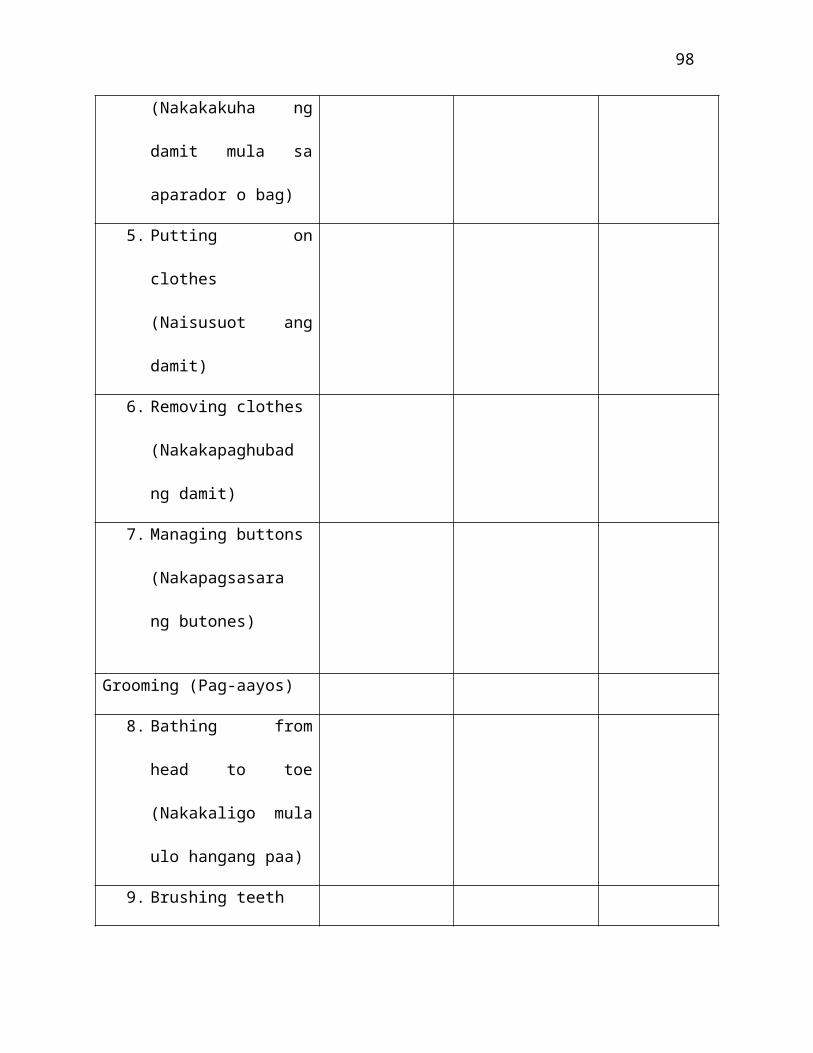
98
(Nakakakuha ng
damit mula sa
aparador o bag)
5. Putting on
clothes
(Naisusuot ang
damit)
6. Removing clothes
(Nakakapaghubad
ng damit)
7. Managing buttons
(Nakapagsasara
ng butones)
Grooming (Pag-aayos)
8. Bathing from
head to toe
(Nakakaligo mula
ulo hangang paa)
9. Brushing teeth
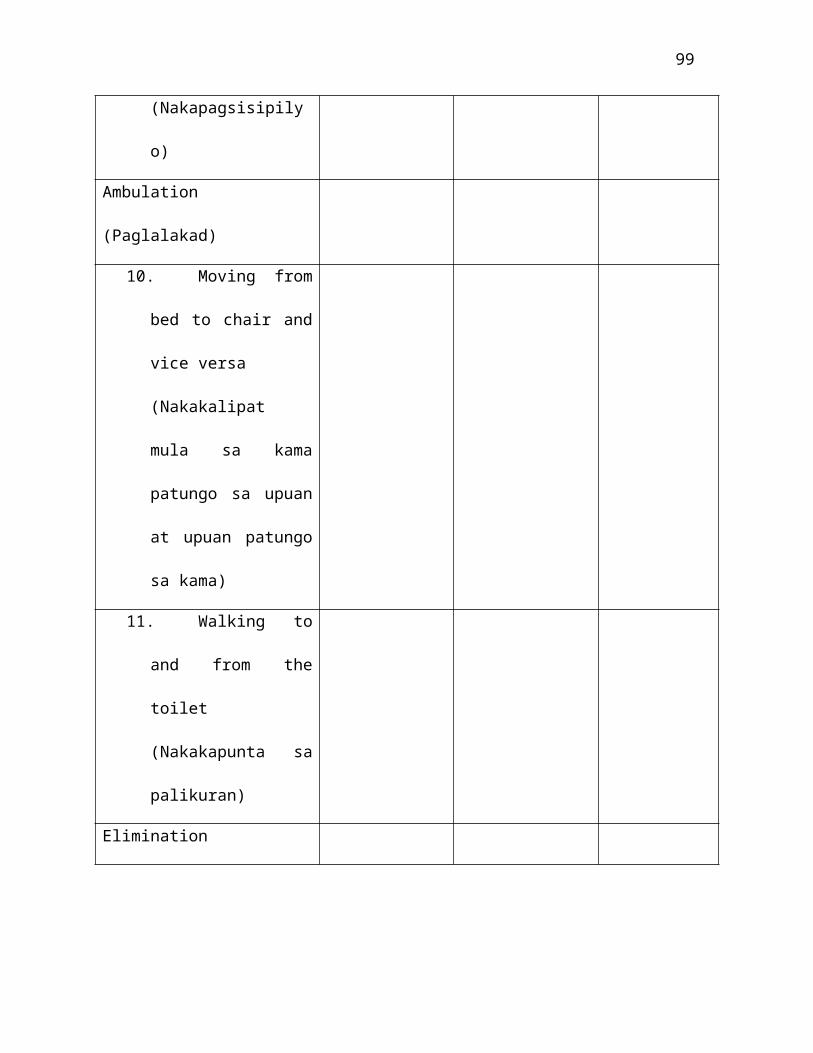
99
(Nakapagsisipily
o)
Ambulation
(Paglalakad)
10. Moving from
bed to chair and
vice versa
(Nakakalipat
mula sa kama
patungo sa upuan
at upuan patungo
sa kama)
11. Walking to
and from the
toilet
(Nakakapunta sa
palikuran)
Elimination
100
12. Urinating
(Pag-ihi)
13. Defacating
(Pagdumi)
Appendix – H
Letter of Permission to Use the Instrument
DE LA SALLE HEALTH SCIENCES INSTITUTESCHOOL OF NURSING
March 2012
To: Johnathan Mateo, RN, MAN
Dear Sir,
Greetings in peace!
The undersigned are currently enrolled in Research I as a requirement for the degree of Bachelor of Science in Nursingat De La Salle Health Sciences Institute. The thesis is entitled: “Performance of the activities of daily living Among Clients who have Undergone Caesarean Section in a Tertiary Hospital”.
In this regard, we respectfully ask permission from you thatwe will be allowed to adopt and use the ADL MultidimensionalAssessment Tool in your master’s thesis to be utilized in our study.
Hoping that this request will merit you favorable response.
101
Thank you very much and God bless you.
Respectfully Yours,
Sgd.Fatima Mae S. Baaclo Emil John A. MedinaAnalen D. Cagalpin Effienet Chioma G. Onuh
Jeremiah Gael A. Stone
Noted by:Rommel L. Salazar, RN, MAN, DrPHThesis Adviser
Approved:Naomi M. De Aro, RN, MAN, EdDDean, College of Nursing & School of Midwifery
APPENDIX I
CERTIFICATION FROM THE STATISTICIAN
CERTIFICATION
This is to certify that the undergraduate thesis
entitled, “Performance of the Activities of Daily Living
Among Clients who have Undergone Caesarean Section in a
Tertiary Hospital” prepared by Fatima Mae S. Baaclo, Analen
D. Cagalpin, Emil John A. Medina, Effienet Chioma G. Onuh
and F. Jeremiah Gael A. Stone, has been treated by the
undersigned.
102
_____________________________
Mr. Jerome Buhay
Statistician
APPENDIX J
DE LA SALLE HEALTH SCIENCES INSTITUTESCHOOL OF NURSING
CERTIFICATION OF TOOL VALIDATION
103
This is to certify that the main tool for the study of
Fatima Mae S. Baaclo, Analen D. Cagalpin, Emil John A.
Medina, Effienet Chioma G. Onuh, and Jeremiah Gael A. Stone
entitled, “Performance of Activities of Daily Living among
Clients who have Undergone Caesarean Section at Tertiary
Level Hospital” has been edited, critiqued and validated by
the undersigned.
Daisy H. Alberto, RN, MANFaculty, College of Nursing and School of Midwifery
Julieta M. Damian, RN, MSNFaculty, College of Nursing and School of Midwifery
Ma. Rodelyn T. Giron, RN, RM, MAEdFaculty, College of Nursing and School of Midwifery
The validated tool was checked and approved to be used bythe student researchers.
Rommel L. Salazar, RN, MAN, DrPHThesis Adviser
104
APPENDIX K
CERTIFICATION FROM THE FILIPINO EDITOR
CERTIFICATION
This is to certify that the undergraduate thesis
entitled, “Performance of the Activities of Daily Living
Among Clients who have Undergone Caesarean Section in a
Tertiary Hospital” prepared by Fatima Mae S. Baaclo, Analen
D. Cagalpin, Emil John A. Medina, Effienet Chioma G. Onuh
and F. Jeremiah Gael A. Stone, has been treated by the
undersigned.
105
_____________________________
Mrs. Emily Legaspi
Filipino Editor
APPENDIX L
CERTIFICATION FROM THE ENGLISH EDITOR
CERTIFICATION
This is to certify that the undergraduate thesis
entitled, “Performance of the Activities of Daily Living
Among Clients who have Undergone Caesarean Section in a
Tertiary Hospital” prepared by Fatima Mae S. Baaclo, Analen
D. Cagalpin, Emil John A. Medina, Effienet Chioma G. Onuh
and F. Jeremiah Gael A. Stone, has been treated by the
undersigned.
106
_____________________________
Ms. Dorothy Alforque
English EditorAPPENDIX M
CURRICULUM VITAE
107
PERSONAL DATA
Name: Fatima Mae S. Baaclo
Address: 16 Governor’s drive, Paliparan I, City of
Dasmariñas, cavite
Date of Birth: April 17, 1993
Civil Status: Single
Sex: Female
Religion: Roman catholic
Citizenship: Filipino
E-mail Address: [email protected]
Father’s name: Francis M. Baaclo
Occupation: Civil Engineer
Mother’s name: Merlinda S. Baaclo
Occupation: Housewife
EDUCATIONAL BACKGROUND
Tertiary De La Salle Health Sciences Institute
City of Dasmariñas, Cavite
2009 - 2013
108
Secondary Jabez Christian School
City of Dasmariñas, Cavite
2005 - 2007
Cavite Institute
Silang, Cavite
2007 - 2009
Elementary Jabez Christian School
City of Dasmariñas, Cavite
1999 - 2005
SEMINAR AND ACTIVITIES ATTENDED
109
SEMINARS/ TRAININGS
Study Habits and Stress
Management Seminar
Community Organizing
Participatory Research
(COPAR) Seminar
Integrated Management of
Childhood Illness Seminar
Research Seminar
Basic Life Support-
Cardiopulmonary
Resuscitation and Advanced
Cardiac Life Support
Training
VENUE
De La Salle Health Sciences
Institute
De La Salle Health Sciences
Institute
De La Salle Health Sciences
Institute
De La Salle Health Sciences
Institute
De La Salle Health Sciences
Institute
YEAR
2009
2010
2011
2011
2012
110
ORGANIZATION AND COMMITTEE
Lasallian Youth Lifeliner 2011-2012
Member
CURRICULUM VITAE
PERSONAL DATA
Name : Analen D. Cagalpin
Address : Brgy. Bignay 1 Pontor, Sariaya, Quezon
Email Address : [email protected]
Date of Birth : September 21, 1991
Age : 21 years old
111
Gender : Female
Civil Status : Single
Citizenship : Filipino
Religion : Roman Catholic
Father’s Name : Deceased
Mother’s Name : Leonora D. Cagalpin
Occupation : Housewife
EDUCATIONAL BACKGROUND
Tertiary Level : Bachelor of Science in Nursing
De La Salle Health Sciences Institute
Dasmariñas City, Cavite
2009 – 2013
Secondary Level : Lutucan National High School
Sariaya, Quezon
2004 – 2008
Primary Level : Bignay 1 Elementary School
112
Sariaya, Quezon
1998- 2004
SEMINARS AND ACTIVITIES ATTENDED
SEMINARS/ TRAININGS
Study Habits and Stress
Management Seminar
Integrated Management of
Childhood Illness
Seminar
Research Seminar
Job Search Tool Kit:
Winning Resume..
Winning Interview
Seminar
VENUE
De La Salle Health
Sciences Institute
De La Salle Health
Sciences Institute
De La Salle Health
Sciences Institute
De La Salle Health
Sciences
YEAR
2009
2010
2011
2012
113
Institute
ORGANIZATIONS AND COMMITTEE
CNSM LINGHAP 2011 Member




















