Therapeutic trial with glycine in myoclonus
11
Movement Disorders 8 1988 Movement Disorder Society Vol. 3. NO. 3, 1966. pp. 222-232 Therapeutic Trial with Glycine in Myoclonus Daniel Dung Truong and Stanley Fahn Department of Neurology, Columbia University College of Physicians and Surgeons, and Neurological Institute, Presbyterian Hospital, New York, New York, U.S.A. Summary: We investigated the therapeutic effects of glycine in seven patients with various forms of myoclonus. The initial phase was an open label trial. If benefit was seen in any patient, a double-blind substitution of placebo was carried out to determine if the benefit was due, in fact, to glycine. The dosage of glycine was initiated at 600 mg/day and was increased gradually until a maximum dosage of 6,000 mg/day was reached. This dosage was maintained for at least 6 weeks before lack of efficacy was declared. No improvement was seen in four patients. One patient reported improvement, but he discontinued the drug because of adverse effects encountered with the use of a concomitant medication and before he could be tested in a double-blind crossover phase. Two other patients also noticed improvement, but these improvements were not validated in the crossover phase. There were no adverse effects associated with glycine. Plasma glycine levels peaked at 30 min and returned to normal 1.5-h after 1 g of glycine p.0. Cerebrospinal fluid (CSF) glycine levels did not change during treatment, suggesting inadequate penetration into the central nervous system of glycine at the dosage used. Key Words: Myoclonus- Glycine-Glycine pharmacokinetics-Myoclonus rating scale. Myoclonus is defined as shock-like involuntary muscle jerks caused by mus- cular contractions or inhibitions arising from the central nervous system. These movements can be synchronous or asynchronous; unilateral or bilateral; gener- alized, segmental or focal; and rhythmic or arrhythmic (1). Myoclonus is associ- ated with many diseases of the central nervous system and is thought to be related to neuronal hyperexcitability (2). Serotonin (34, y-aminobutyric acid (GABA) (7-9), thyrotropin-releasing hormone (TRH) (10,l I), opioids (IZ), and recently, glycine (13,14) have been suspected of being involved in myoclonus. In urea- induced myoclonus, urea has been shown to displace glycine at its receptor sites in the brainstem (13). In the animal model of DDT-induced myoclonus, whole Address correspondence and reprint requests to Dr. D. D. Truong at Department of Neurology Wayne State University, Detroit, Michigan 48235. 222
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Therapeutic trial with glycine in myoclonus
Movement Disorders
8 1988 Movement Disorder Society Vol. 3. NO. 3, 1966. pp. 222-232
Therapeutic Trial with Glycine in Myoclonus
Daniel Dung Truong and Stanley Fahn
Department of Neurology, Columbia University College of Physicians and Surgeons, and Neurological Institute, Presbyterian Hospital, New York, New York, U.S.A.
Summary: We investigated the therapeutic effects of glycine in seven patients with various forms of myoclonus. The initial phase was an open label trial. If benefit was seen in any patient, a double-blind substitution of placebo was carried out to determine if the benefit was due, in fact, to glycine. The dosage of glycine was initiated at 600 mg/day and was increased gradually until a maximum dosage of 6,000 mg/day was reached. This dosage was maintained for at least 6 weeks before lack of efficacy was declared. No improvement was seen in four patients. One patient reported improvement, but he discontinued the drug because of adverse effects encountered with the use of a concomitant medication and before he could be tested in a double-blind crossover phase. Two other patients also noticed improvement, but these improvements were not validated in the crossover phase. There were no adverse effects associated with glycine. Plasma glycine levels peaked at 30 min and returned to normal 1.5-h after 1 g of glycine p.0. Cerebrospinal fluid (CSF) glycine levels did not change during treatment, suggesting inadequate penetration into the central nervous system of glycine at the dosage used. Key Words: Myoclonus- Glycine-Glycine pharmacokinetics-Myoclonus rating scale.
Myoclonus is defined as shock-like involuntary muscle jerks caused by mus- cular contractions or inhibitions arising from the central nervous system. These movements can be synchronous or asynchronous; unilateral or bilateral; gener- alized, segmental or focal; and rhythmic or arrhythmic (1). Myoclonus is associ- ated with many diseases of the central nervous system and is thought to be related to neuronal hyperexcitability (2). Serotonin ( 3 4 , y-aminobutyric acid (GABA) (7-9), thyrotropin-releasing hormone (TRH) (10,l I ) , opioids (IZ), and recently, glycine (13,14) have been suspected of being involved in myoclonus. In urea- induced myoclonus, urea has been shown to displace glycine at its receptor sites in the brainstem (13). In the animal model of DDT-induced myoclonus, whole
Address correspondence and reprint requests to Dr. D. D. Truong at Department of Neurology Wayne State University, Detroit, Michigan 48235.
222

GLYCINE IN MYOCLONUS 223
brain glycine levels have been reported to be decreased or unchanged (14,15). Even though regional determinations showed fluctuation of the glycine levels in the brainstem in the DDT model (14), they failed to prove the hypothesis that glycine is central to the induction of myoclonus. Nevertheless, drugs that increase brain glycine levels have been shown to have antimyoclonic (14) as well as an- tiepileptic properties (16-19). We report a crossover placebo-controlled study of glycine administered to myoclonic patients, as well as the pharmacokinetic profile of glycine.
MATERIALS AND METHODS
The computer data base of the Movement Disorder Group at the Columbia- Presbyterian Medical Center was utilized to search for patients with myoclonus. We selected patients with essential myoclonus, posthypoxic myoclonus, and seg- mental myoclonus to participate in this study. Essential myoclonus was diagnosed if myoclonus was not progressive, was the sole neurologic abnormality, and the etiology was unknown (20). Posthypoxic myoclonus was diagnosed when myoc- lonus was the permanent neurologic sequela of cerebral hypoxia (21). Segmental myoclonus was diagnosed by the presence of involuntary, rhythmical jerking movements limited to a segmental region of the body, such as the neck and shoulders or the soft palate and pharynx (22). The study protocol received ap- proval from the Food and Drug Administration and the Institutional Review Board. All enrolled patients gave informed, written consent prior to their entry into the study.
Seven patients were enrolled into the study (Table 1). There were two patients with posthypoxic myoclonus, two with essential myoclonus [including one with oscillatory myoclonus previously reported (23)1, one with idiopathic palatal my- oclonus, one with segmental rhythmical myoclonus associated with a porenceph-
TABLE 1. Patients’ characteristics
Age at Duration Patient Diagnoses onset of disease Etiology
A PHIM 23 17 Cardiac arrest due to penicillin allergy
B PHIM 48 10 Respiratory and cardiac arrest
C EM 1 30 No known etiology D EM 12 18 No known etiology E PM 31 8 Viral infection 1 week
prior to the onset of symptoms
in the 4th ventricle and rebleeding 2 years later
F OM 40 8 Atrioventricular malformation
G SRM 10 8 Porencephalic cyst
PHIM, posthypoxic intentional myoclonus; EM, essential myoclonus; PM, palatal myoclonus; OM, opsoclonus myoclonus; SRM, segmental rhythmical myoclonus.
Movement Disorders. Vol. 3, No. 3, 1988

224 D. D . TRUONG AND S. FAHN
alic cyst previously reported (24), and one with myoclonus secondary to a sub- arachnoid hemorrhage due to an arteriovenous malformation. The severity and quality of the myoclonus were rated according to a myoclonus rating scale (see Addendum) at the beginning of the study, at peak dosage of glycine, and after the crossover to placebo. A videotape recording of the myoclonus was also obtained at these time points. A lumbar puncture (LP) was performed prior to starting glycine and when glycine reached maximum dosage. The latter LP was performed 2 h after the maximum individual oral dose. Complete blood count, SMAC 20, urinalysis, and electrocardiogram (ECG) were obtained prior to the study and at specified intervals during the study. Previous medications that the patients were taking were kept unchanged during the entire study.
The initial dose of glycine was 200 mg t.i.d., and glycine was increased daily by 300 mg until a therapeutic effect was achieved or up to the maximum dose of 6 g/day in 3 divided doses. This maximum dose was kept constant for another 6 weeks to determine if a delay in onset of benefit could be observed. If no thera- peutic effects were achieved after 6 weeks of 6 g/day, glycine was considered to be a therapeutic failure, and the medication was discontinued. Prior to discontin- uation, the repeat lumbar puncture was performed to measure the CSF glycine level 2 h after the first 2-g dose taken in the morning after an overnight fast. If a therapeutic effect was observed in this open-label phase, the patient was switched to placebo medication at some point in the treatment without informing either the patient or the “blinded” observer. If symptoms recurred during the placebo phase, glycine was reintroduced, again without the patient or the “blinded observer” being aware of the change in medication.
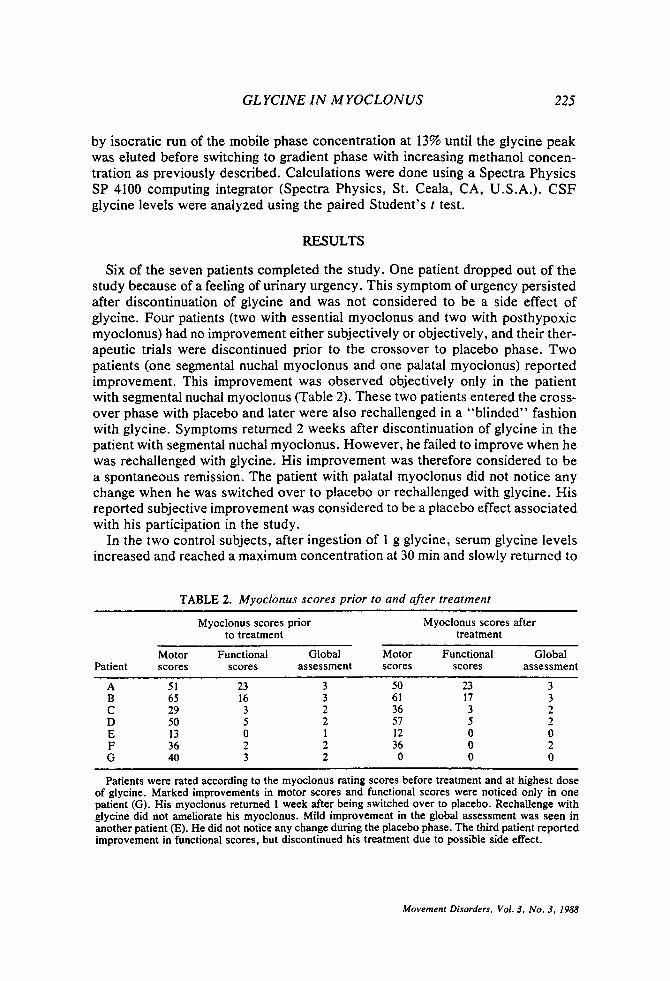
Glycine was obtained from Sigma Chemical Co. (St. Louis, MO, U.S.A.), tested ‘for purity, and encapsulated into lOO-mg, 200-mg, and 500-mg strength capsules. The peripheral pharmacodynamics of glycine were measured in two healthy individuals ingesting 1 g of glycine on an empty stomach; blood was drawn every 15 min from a heparin-locked indwelling venous catheter during the first hour and every 30 min afterwards up to 4 h. The serum was deproteinized with 5 vol of 0.6 M perchloric acid. The protein-free supernatant (and CSF) was frozen and later used to determine glycine concentrations. Glycine levels were measured using high-performance liquid chromatography (HPLC) with fluorometric detec- tion by the method previously described using a 3-p Ultrasphere column 4.5 mm x 7.5 cm (14,25). For determination of glycine in the CSF, the method was slightly modified to improve the sensitivity. In brief, 100 p1 of CSF was allowed to react with 20 p1 of o-phthaldialdehyde (OPA) for exactly 1 min. The pH of the solution was then lowered by diluting 90 p1 of the OPA-CSF solution with 30 p1 of 0.5 A4 sodium phosphate buffer, pH 4, to protect the HPLC column before injection. Due to the rapid decay of the fluorescent glycine-conjugated OPA compound (26), an automatic time-fixed Gilson 231 sample injector and Gilson Model 407 dilutor were used (Gilson, Middleton, WI, U.S.A.). Other equipment included a DuPont Instrument 850 gradient pump (Dupont, Wilmington, DE, U.S.A.) and a Kratos FS 950 fluorescence detector (Kratos, Ramsey, NJ, U.S.A.). Norvaline was used as internal standard. Good separation of glycine and threonine peaks was obtained
Movement Disorders. Vol. 3, N o . 3, 1988
GL YCINE IN M YOCLON US 225
by isocratic run of the mobile phase concentration at 13% until the glycine peak was eluted before switching to gradient phase with increasing methanol concen- tration as previously described. Calculations were done using a Spectra Physics SP 4100 computing integrator (Spectra Physics, St. Ceala, CA, U.S.A.). CSF glycine levels were analyzed using the paired Student’s t test.
RESULTS
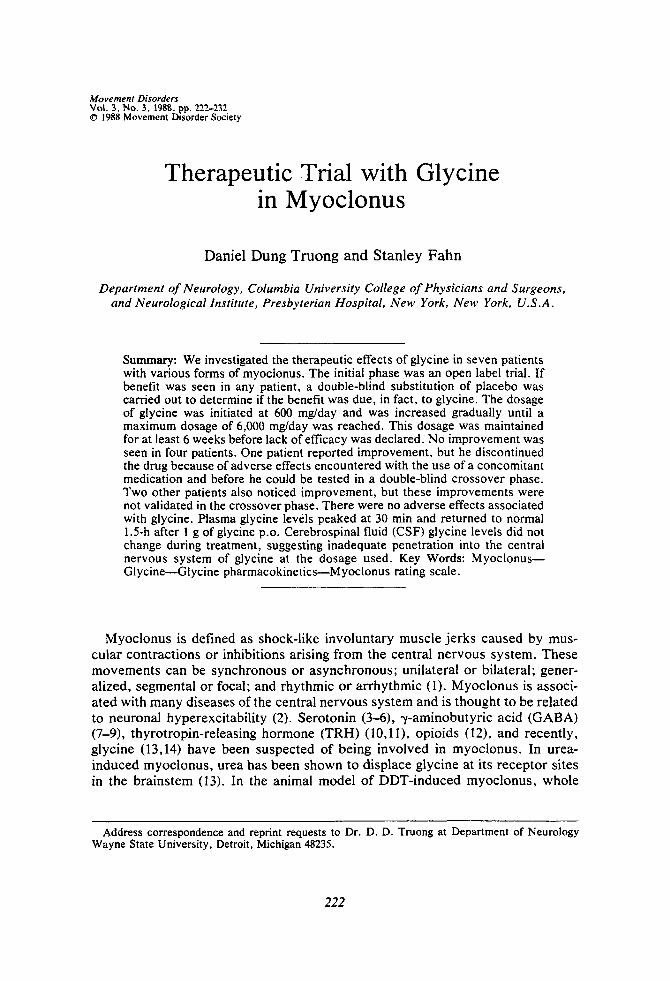
Six of the seven patients completed the study. One patient dropped out of the study because of a feeling of urinary urgency. This symptom of urgency persisted after discontinuation of glycine and was not considered to be a side effect of glycine. Four patients (two with essential myoclonus and two with posthypoxic myoclonus) had no improvement either subjectively or objectively, and their ther- apeutic trials were discontinued prior to the crossover to placebo phase. Two patients (one segmental nuchal myoclonus and one palatal myoclonus) reported improvement. This improvement was observed objectively only in the patient with segmental nuchal myoclonus (Table 2). These two patients entered the cross- over phase with placebo and later were also rechallenged in a “blinded” fashion with glycine. Symptoms returned 2 weeks after discontinuation of glycine in the patient with segmental nuchal myoclonus. However, he failed to improve when he was rechallenged with glycine. His improvement was therefore considered to be a spontaneous remission. The patient with palatal myoclonus did not notice any change when he was switched over to placebo or rechallenged with glycine. His reported subjective improvement was considered to be a placebo effect associated with his participation in the study.
In the two control subjects, after ingestion of 1 g glycine, serum glycine levels increased and reached a maximum concentration at 30 min and slowly returned to
TABLE 2. Myoclonus scores prior to and after treatment
Myoclonus scores prior Myoclonus scores after to treatment treatment
Motor Functional Global Motor Functional Global Patient scores scores assessment scores scores assessment
A 51 23 3 50 23 3 B 65 16 3 61 17 3 C 29 3 2 36 3 2 D 50 5 2 57 5 2 E 13 0 1 12 0 0 F 36 2 2 36 0 2 G 40 3 2 0 0 0
~ _ _ _ _ _ ~ ~ ~~ ~
Patients were rated according to the myoclonus rating scores before treatment and at highest dose of glycine. Marked improvements in motor scores and functional scores were noticed only in one patient (G). His myoclonus returned 1 week after being switched over to placebo. Rechallenge with glycine did not ameliorate his myoclonus. Mild improvement in the global assessment was seen in another patient (E). He did not notice any change during the placebo phase. The third patient reported improvement in functional scores, but discontinued his treatment due to possible side effect.
Movement Disorders. Vol. 3, No. 3, 1988
226 D. D. TRUONG AND S. FAHN
600r
500 in FIG. 1. The peripheral pharmacodynamics of glycine were measured in two healthy individ- uals (1 man and 1 woman) ingesting 1 g of gly- cine on an empty stomach; blood was drawn every IS min from a heparin-locked indwelling venous catheter during the first hour and every 30 min afterward up to 4 h. Serum glycine levels increased and reached a maximum concentra- tion at 30 min and slowly returned to normal at 1.5 h. (0, Male; ., female)
loo 153045 60 90 120 I50 180 210 240 Time lmin)
normal at 1.5 h (Fig. 1). CSF glycine levels were obtained in five patients. They did not change during glycine therapy when the glycine dose reached a maximum of 6 &/day (10.32 & 0.7 p,mol/L at baseline and 9.8 k 0.3 p,mol/L at peak dose).
DISCUSSION
Glycine showed no antimyoclonic property in the six patients who completed the study. There was no objective improvement that was obviously apparent or detected in the quantitative myoclonic scores except in one patient. Although he worsened after being on placebo for 2 weeks, he failed to improve again when glycine was reinstituted. Thus, we consider this lack of consistent benefit to be a reflection of spontaneous fluctuation of his segmental myoclonus. Subjective im- provement was reported by an additional patient, but he detected no difference during the double-blind phase between placebo and glycine administration.
Although deficiency of serotonin has been most often implicated in myoclonus, involvement of inhibitory amino acid neurotransmitters, such as glycine and GABA, have also been considered (7,8,14,15), and CSF GABA has been reported to be decreased in some patients with myoclonus (9). A therapeutic trial with progabide, a GABA precursor, was found to be ineffective (27). In our study, glycine similarly had no antimyoclonic effect. There are at least two distinct possibilities for the therapeutic failure. One possibility is that CNS glycine plays no role in the myoclonus seen in our patients. The other possibility is that glycine did not adequately enter the central nervous system (CNS) or failed to reach the proper target sites in the CNS. It has been thought that glycine is able to penetrate the blood-brain barrier when given in high doses (17,28), even though it has the lowest CSF:plasma concentration ratio of amino acids (29). However, CSF gly-
Movement Disorders, Vol. 3, No. 3, 1988
GLYCINE IN MYOCLONUS 22 7
cine levels in our patients 2 h after a large dose did not show any increase, suggesting that at the maximum dose used in our study, glycine did not penetrate the blood-brain barrier adequately. Perhaps the short half-life of glycine in the blood may not be adequate to raise brain glycine levels sufficiently or may have led us to miss a rise in CSF glycine, as we measured it 2 h after an ingested dose. Recently, milacemide, a glycine precursor, has been developed that has been shown to penetrate the blood-brain barrier easily before being converted into glycinamide and glycine (30). Milacemide has been shown to have an antiepileptic effect (31), and it also has an antimyoclonic property in one experimental model (14). It appears to be well tolerated (32). This drug may be more suitable for a therapeutic trial than glycine itself.
Acknowledgment: This study was supported by a grant from the Myoclonus Research Fund. We are grateful for the assistance from Tobjern Nygaard, M.D., and Mane-Helene Saint-Hilaire, M.D. and David Balch.
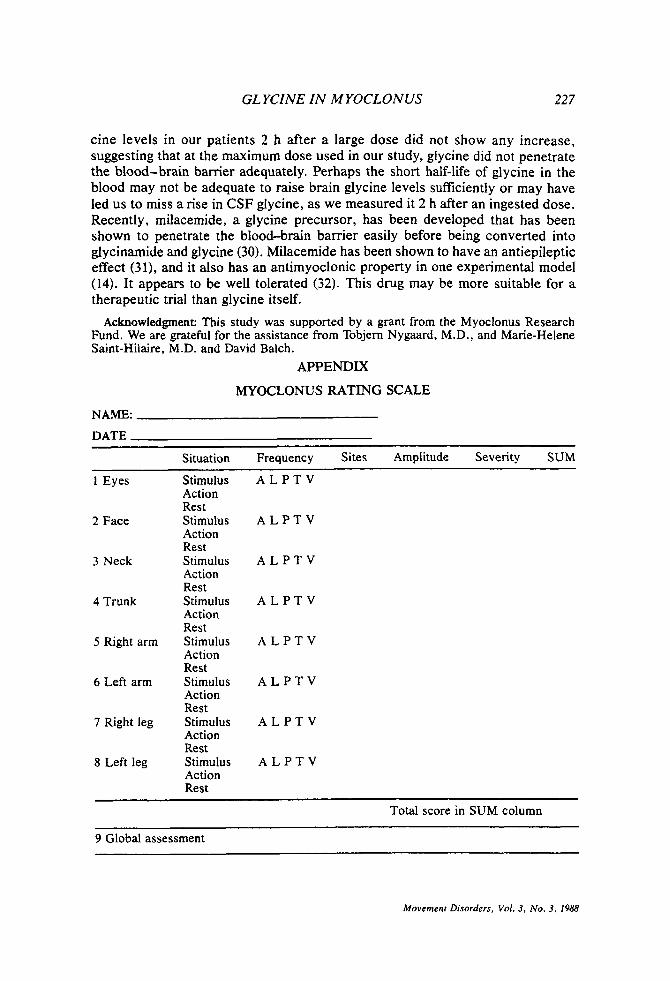
APPENDIX
MYOCLONUS RATING SCALE
NAME:
DATE
Situation Frequency Sites Amplitude Seventy SUM
1 Eyes Stimulus A L P T V Action Rest
2 Face Stimulus A L P T V Action Rest
3 Neck Stimulus A L P T V Action Rest
4 Trunk Stimulus A L P T V Action Rest
5 Right arm Stimulus A L P T V Action Rest
6 Left arm Stimulus A L P T V Action Rest
7 Right leg Stimulus A L P T V Action Rest
8 Left leg Stimulus A L P T V Action Rest
Total score in SUM column
9 Global assessment
Movement Disorders, Vol. 3, No. 3, 1988
228 D. D . TRUONG AND S . FAHN
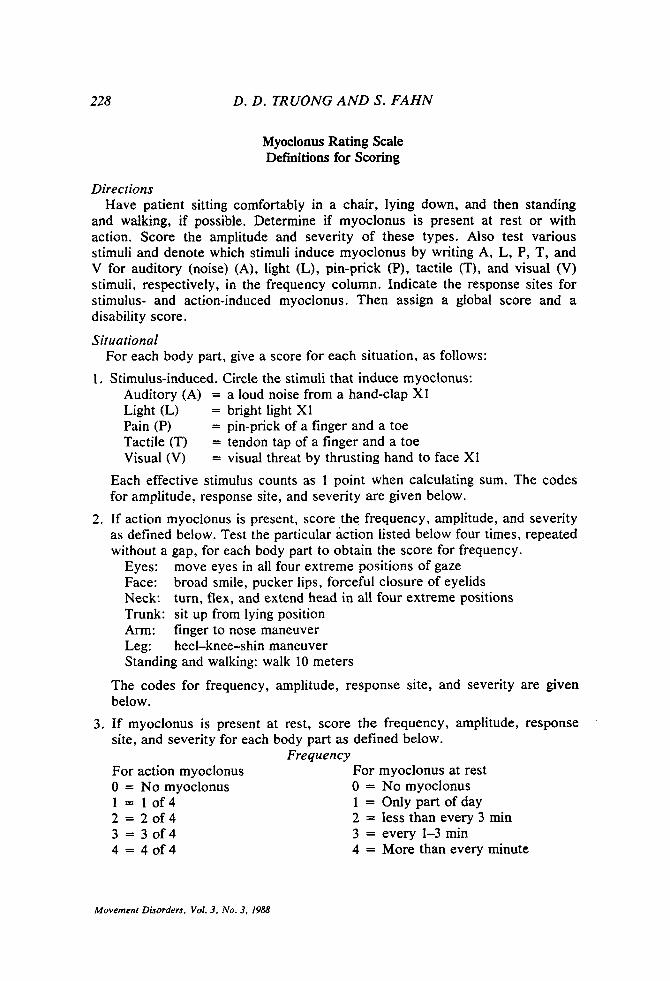
Myoclonus Rating Scale Definitions for Scoring
Directions Have patient sitting comfortably in a chair, lying down, and then standing
and walking, if possible. Determine if myoclonus is present at rest or with action. Score the amplitude and seventy of these types. Also test various stimuli and denote which stimuli induce myoclonus by writing A, L, P, T, and V for auditory (noise) (A), light (L), pin-prick (P), tactile (T), and visual (V) stimuli, respectively, in the frequency column. Indicate the response sites for stimulus- and action-induced myoclonus. Then assign a global score and a disability score.
Situational
1. Stimulus-induced. Circle the stimuli that induce myoclonus: For each body part, give a score for each situation, as follows:
Auditory (A) = a loud noise from a hand-clap XI Light (L) = bright light X1 Pain (P) = pin-prick of a finger and a toe Tactile (T) = tendon tap of a finger and a toe Visual (V) = visual threat by thrusting hand to face XI
Each effective stimulus counts as 1 point when calculating sum. The codes for amplitude, response site, and severity are given below.
2. If action myoclonus is present, score the frequency, amplitude, and seventy as defined below. Test the particular action listed below four times, repeated without a gap, for each body part to obtain the score for frequency.
Eyes: move eyes in all four extreme positions of gaze Face: broad smile, pucker lips, forceful closure of eyelids Neck: turn, flex, and extend head in all four extreme positions Trunk: sit up from lying position Arm: finger to nose maneuver Leg: heel-knee-shin maneuver Standing and walking: walk 10 meters
The codes for frequency, amplitude, response site, and severity are given below.
3. If myoclonus is present at rest, score the frequency, amplitude, response site, and seventy for each body part as defined below.
For action myoclonus 0 = No myoclonus 1 = 1 0 f 4 2 = 2 0 f 4 3 = 3 o f 4 4 = 4 0 f 4
Frequency For myoclonus at rest 0 = No myoclonus 1 = Only part of day 2 = less than every 3 min 3 = every 1-3 min 4 = More than every minute
Movement Disorders, Vol. 3# No. 3, 1988
GL YCINE IN MYOCLONUS 229
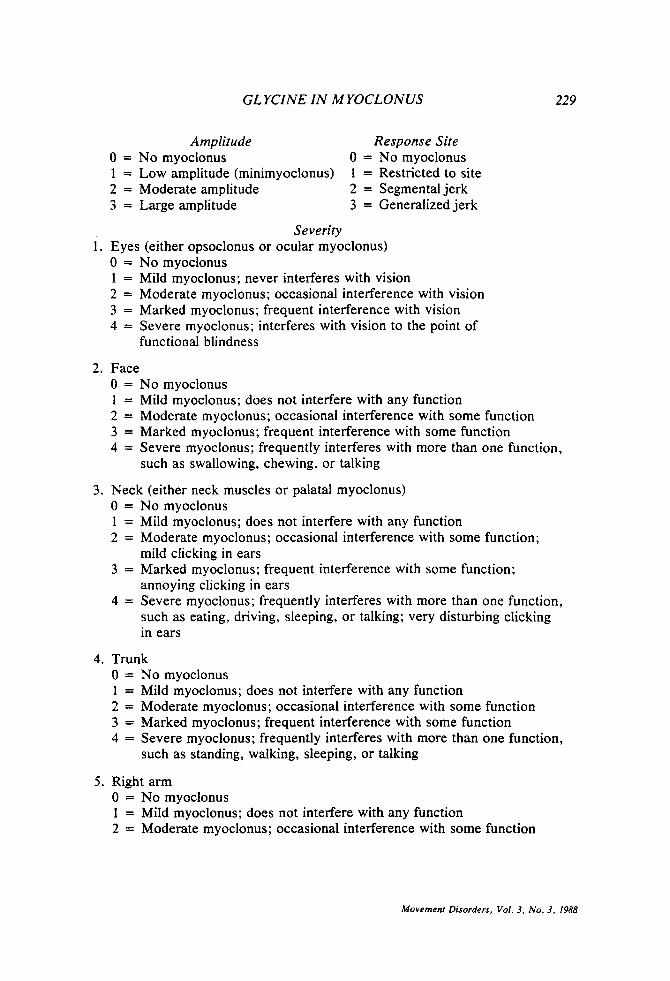
Amplitude Response Site 0 = No myoclonus 1 = Low amplitude (minimyoclonus) 2 = Moderate amplitude 3 = Large amplitude
0 = No myoclonus 1 = Restricted to site 2 = Segmental jerk 3 = Generalized jerk
Severity 1. Eyes (either opsoclonus or ocular myoclonus)
0 = N o myoclonus 1 = Mild myoclonus; never interferes with vision 2 = Moderate myoclonus; occasional interference with vision 3 = Marked myoclonus; frequent interference with vision 4 = Severe myoclonus; interferes with vision to the point of
functional blindness
2. Face 0 = N o myoclonus 1 = Mild myoclonus; does not interfere with any function 2 = Moderate myoclonus; occasional interference with some function 3 = Marked myoclonus; frequent interference with some function 4 = Severe myoclonus; frequently interferes with more than one function,
such as swallowing, chewing, or talking
3. Neck (either neck muscles or palatal myoclonus) 0 = N o myoclonus 1 = Mild myoclonus; does not interfere with any function 2 = Moderate myoclonus; occasional interference with some function;
3 = Marked myoclonus; frequent interference with some function;
4 = Severe myoclonus; frequently interferes with more than one function,
mild clicking in ears
annoying clicking in ears
such as eating, driving, sleeping, or talking; very disturbing clicking in ears
4. Trunk 0 = No myoclonus 1 = Mild myoclonus; does not interfere with any function 2 = Moderate myoclonus; occasional interference with some function 3 = Marked myoclonus; frequent interference with some function 4 = Severe myoclonus; frequently interferes with more than one function,
such as standing, walking, sleeping, or talking
5 . Right arm 0 = No myoclonus 1 = Mild myoclonus; does not interfere with any function 2 = Moderate myoclonus; occasional interference with some function
Movement Disorders, Vol. 3, No. 3, 1988
230 D . D. TRUUNG AND S. FAHN
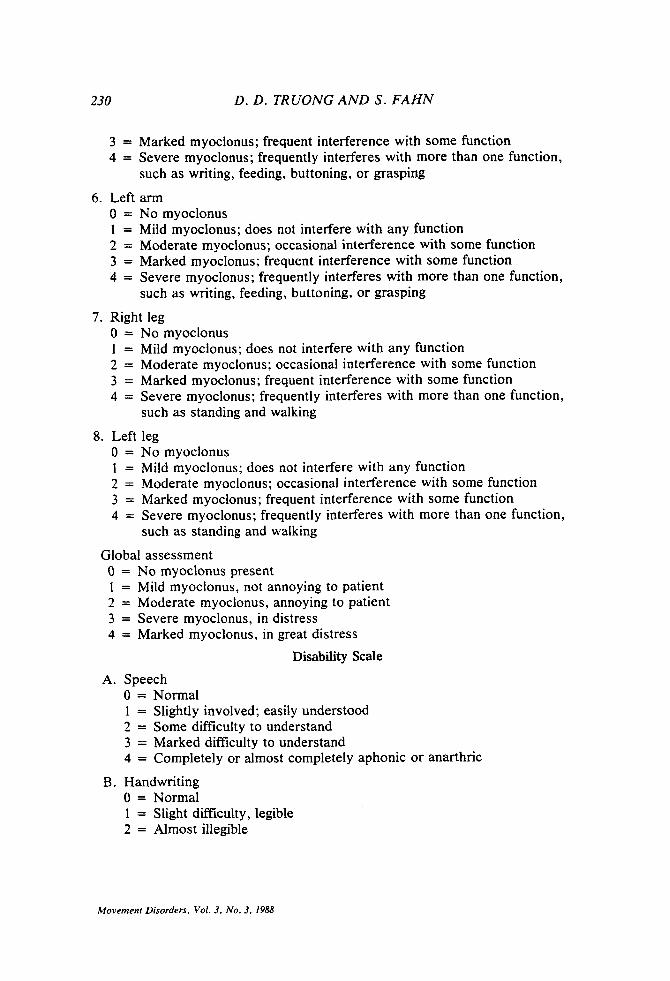
3 = Marked myoclonus; frequent interference with some function 4 = Severe myoclonus; frequently interferes with more than one function,
such as writing, feeding, buttoning, or grasping
6 . Left arm 0 = No myoclonus 1 = Mild myoclonus; does not interfere with any function 2 = Moderate myoclonus; occasional interference with some function 3 = Marked myoclonus; frequent interference with some function 4 = Severe myoclonus; frequently interferes with more than one function,
such as writing, feeding, buttoning, or grasping
7. Right leg 0 = No myoclonus 1 = Mild myoclonus; does not interfere with any function 2 = Moderate myoclonus; occasional interference with some function 3 = Marked myoclonus; frequent interference with some function 4 = Severe myoclonus; frequently interferes with more than one function,
such as standing and walking
8. Left leg 0 = N o myoclonus 1 = Mild myoclonus; does not interfere with any function 2 = Moderate myoclonus; occasional interference with some function 3 = Marked myoclonus; frequent interference with some function 4 = Severe myoclonus; frequently interferes with more than one function,
such as standing and walking
Global assessment 0 = No myoclonus present 1 = Mild myoclonus, not annoying to patient 2 = Moderate myoclonus, annoying to patient 3 = Severe myoclonus, in distress 4 = Marked myoclonus, in great distress
Disability Scale A. Speech
0 = Normal 1 = Slightly involved; easily understood 2 = Some difficulty to understand 3 = Marked difficulty to understand 4 = Completely or almost completely aphonic or anarthric
B. Handwriting 0 = Normal 1 = Slight difficulty, legible 2 = Almost illegible
Movement Disorders, Vol. 3. No. 3. 1988
GLYCINE IN MYOCLONUS 231
3 = Illegible 4 = Unable to grasp or maintain hold on pen
0 = Normal 1 = Uses “tricks,” independent 2 = Can feed, but not cut 3 = Finger food only 4 = Completely dependent
0 = Normal 1 = Occasional choking 2 = Choking frequently, difficulty swallowing 3 = Unable to swallow firm foods 4 = Marked difficulty swallowing soft foods and liquids
0 = Normal 1 = Clumsy, independent 2 = Needs help with some activities 3 = Needs help with most activities 4 = Needs help with all activities
0 = Normal 1 = Clumsy, independent 2 = Needs help with some 3 = Needs help with most 4 = Helpless
0 = Normal 1 = Slightly abnormal, hardly noticeable 2 = Moderately abnormal, obvious to naive observer 3 = Considerably abnormal 4 = Needs assistance to walk 5 = Wheelchair bound
C. Feeding
D. Eating
E. Hygiene
F. Dressing
G. Walking
REFERENCES 1 . Fahn S, Marsden D, Van Woert MH. Definition and classifcation of myoclonus. In: Myoclonus
Fahn S, Marsden CD, Van Woert MH eds. New York, Raven Press, 1986:l-5. (Advances in Neurology, Vol. 43).
2. Lance JW. Action myoclonus, Ramsay Hunt syndrome and the other cerebellar myoclonus syn- dromes. In: Myoclonus. Fahn J, Marsden CD, Van Woert MH, eds. New York Raven Press, 1986:33-55. (Advances in Neurology; V0143).
3. De Lean J , Richardson JC, Hornykiewicz 0. Beneficial effects of serotonin precursors in post- anoxic action myoclonus. Neurology 1976;26:863-8.
4. Growdon JH, Young RR, Shahani BT. L-5-Hydroxytryptophan in the treatment of syndromes in which myoclonus is prominent. Neurology 1976;26: 1135-40.
Movement Disorders, Vol. 3, No. 3, 1988

D. D . TRUONG AND S . FAHN
5. Lhermitte F, Marteau R, Degos CF. Analyse pharmacologique d'un nouveau cas de myoclonies d'intention et d'action postanoxique. Rev Neurol (Pans) 1972;126: 107-14.
6. Hwang EC, Van Woert MH. p,p'-DDT-induced neurotoxic syndrome: experimental myoclonus. Neurology 1978;lO: 1020-5.
7. Jenner P, Leigh PW, Marsden CD, Reavill C. Cortical involvement in forepaw myoclonus induced by intrastriatal administration of picrotoxin to rats. Br J Pharmacol 1981 ;72:503-4.
8. Patel S, Slater P. Analysis of the brain regions involved in myoclonus produced by intracerebral picrotoxin. Neuroscience 1987;20:687-93.
9. Enna SJ, Ferkany JW, Van Woert M, Butler IJ. Measurement of GABA in biological fluids: effect of GABA transaminase inhibitors. Advances in Neurology 1979;23:741-50.
10. Barbeau H, Bedard P. Similar motor effects of 5-HT and TRH in rats following chronic spinal transection and 5,7-dihydroxytryptamine injection. Neuropharmacology 1981 ;20:477-8 1.
11. Griffths EC, Widdowson PS, Slater P. Antagonism of TRH induced wet-dog shaking in rats by neurotensin and a neurotensin fragment. Neurosci Lett 1982;3 1: 171-4.
12. Snead OC. Bearden LJ. The epileptogenic spectrum of opiate agonist. Neuropharmacology l982;21: 1137-44.
13. Chung E, Yocca F, Van Woert MH. Urea-induced myoclonus: medullary glycine antagonism as mechanism of action. Lfe Sci 1985;36:1051-8.
14. Truong DD, de Yebenes JG, Pezzoli G, Jackson-Lewis V, Fahn S. Giycine involvement in DDT- induced myoclonus. Movement Dis 1987;3:77-87.
15. Kar PP, Matin MA. Possible role of cerebral amino acids in acute neurotoxic effects of DDT in mice. Eur J Pharmacol 1974;25:369.
16. Lapin IP. Antagonism of L-glycine to seizures induced by 2-kynurenine, quinolinic acid and strychnine in mice. Eur J Pharmacol 1981;71:495-8.
17. Toth E, Lajtha A, Sarhan S, Seiler N. Anticonvulsant effects of some inhibitory neurotransmitter amino acids. Neurochem Res 1983;8:291-302.
18. Seiler N, Sarhan S. Synergistic anticonvulsant effects of a GABA agonist and glycine. Gen Pharmacol 1984; l5:367-9.
19. Seiler N, Sarhan S , Krogsgaard-Larsen P, Hjeds H, Schousboe A. Amplification of glycine of the anticonvulsant effect of THPO, a GABA uptake inhibitor. Gen Pharmacol 1985;16:509-11.
20. Bressman S, Fahn S. Essential myoclonus. In: Myoclonus. Fahn S, Marsden CD, Van Woert MH, eds. New York: Raven Press, 1986:287-94. (Advances in Neurology; vol43).
21. Lance JW, Adams RD. The syndrome of intention or action myoclonus as a sequel to hypoxic encephalopathy. Brain 1963;86:111-36.
22. Lapresle J. Palatal myoclonus. In: Myoclonus. Fahn S , Marsden CD, Van Woert MH, eds. New York: Raven Press, 1986:265-73. (Advances in Neurology; vol 43).
23. Fahn S, Singh N. An oscillating form of essential myoclonus. Neurology 1981;31:80. 24. Fahn S, Singh N. Segmental tremor vs. rhythmic myoclonus: Successful treatment with serotonin
precursors. Neurology 1980;30:3834. 25. Jones BN, Gilligan JP. o-Phthaldialdehyde precolumn derivatization and reversed-phase high-
performance liquid chromatography of polypeptide hydrolysates and physiological fluids. J Chro- matog I983 ;266:47 1-83.
26. Jones BN, Paabo S, Stein S. Amino acid analysis and enzymatic sequences determination of peptides by an improved o-phthaldialdehyde precolumn labeling procedure. J Liq Chromatogr 1981 ;4:565-86.
27. Van Woert M, Rosenbaum D, Chung E. Biochemistry and therapeutics of posthypoxic myoclo- nus. In: Myoclonus. Fahn S , Marsden CD, Van Woert MH, eds. New York: Raven Press, 1986:171-81. (Advances in Neurology; vol43).
28. Toth E, Lajtha A. Elevation of cerebral levels of nonessential amino acids in vivo by adminis- tration of large doses. Neurochem Res 1981 ;6: 1309-17.
29. McGale EHF, Pye JF, Stonier C, Hutchinson EC, Aber GM. Studies of the inter-relationship between cerebrospinal fluid and plasma amino acid concentrations in normal individuals. J Neu- rochem 1977;29:291-7.
30. Christophe J, Kutzner R, Nguyen-Bui ND, Damien C, Chatelain P, Gillet L. Conversion of orally administered 2-n-pentylaminoacetamide into glycinamide and glycine in the rat brain. Life Sci 1983;33:53WI.
31. Van Drosser W, Barris DR, Cordi A, Roba J. Anticonvulsant activity of milacemide. Arch Znt Pharmacodyn 1983;226239-49.
32. Houtkooper MA, Oorschot CA, Rentmeester TW, Hoppener PJ, OnkeIinx C. Double blind study of milacemide in hospitalized therapy resistant patients with epilepsy. Epilepsia 1986;27:255-62.
Movement Disorders, Vol. 3, No. 3, 1988