
The skeletal manifestations of clubbing: A study in patients with cyanotic congenital heart disease...
11
The Skeletal Manifestations of Clubbing: A Study in Patients With Cyanotic Congenital Heart Disease and Hypertrophic Osteoarthropathy By Carlos J. Pineda, Jose Guerra, Jr, Michael H. Weisman, Donald Resnick, and Manuel Martinez-Lavin The skeletal manifestations of clubbing of the digits have been occasionally noted and only briefly dis- cussed in the literature. We investigated the radio- graphic features of digital clubbing in 37 patients with diverse diseases including cyanotic congenital heart disease, lung malignancy-associated hyper- trophic osteoarthropathy, and idiopathic cases. We identified two types of bone changes-osteolysis or bone dissolution, and bone formation or hypertro- phy. The changes were more evident in the feet than in the hands, and the degree of soft tissue change did not always reflect the underlying osseous abnor- C LINICAL and pathologic features of digital clubbing have been recognized for many years and are well documented.‘32 However, little attention has been directed to the underlying osseous abnormalities in the digits, particularly the terminal phalanges of the fingers and toes. Because of the obvious changes observed in a few patients, we undertook a controlled prospective study and retrospective analysis of the skeletal findings in the terminal tufts of patients with diseases or conditions regularly associated with clubbing. In order to accomplish this task, it is necessary to define terminology and clarify ambiguities. Clubbing is a descriptive term pertaining to the appearance of the fingers and/or toes and has been defined as the obliteration of the normal 160° angle between the nail and the nail bed (“the profile sign”).3 Clubbing should be distin- guished from the syndrome of hypertrophic osteoarthropathy (HOA), defined as chronic proliferative periostitis of the long bones, club- bing of the digits, and joint swelling.4 HOA is further divided into two basic forms, primary and secondary. The primary or idiopathic form is prone to develop in association with thickening of the skin, or pachydermia. In this situation the syndrome is termed pachydermoperiostosis and is diagnosed further by excluding all the recog- nized causes associated with HOA. The secon- dary forms of HOA are, by definition, associated with one of a variety of underlying conditions4 We have observed that two types of bone changes occur in the terminal tufts of these patients: (1) bone formation, or hypertrophy, and malities. The relationship of these changes (ie, osteolysis, hypertrophy) to each other appear to depend in part on the underlying disease as well as the time course or disease duration. Thus, clubbing and hypertrophic osteoarthropathy may not repre- sent distinct entities; our data suggest that they may be stages in an evolving, more generalized process of new bone formation or hypertrophy followed by osteolysis or atrophy affecting many parts of the skeleton. o 1985 by Grune & Stratton, Inc. (2) bone dissolution, or acre-osteolysis. The rela- tionship between these changes is complex, depending in part on the specific underlying disease and in part on disease duration or time course. In addition, the soft tissue changes in the digits, or clubbing, do not always reflect the underlying bone pathology. Our findings suggest that clubbing of the digits and hypertrophic osteoarthropathy of the long bones are not sepa- rate, distinct entities. An alternative view, sup- ported by these studies, is that these two clinical conditions are stages of an evolving, more gener- alized process producing hypertrophy and later resorption in the skeleton. PATIENTS AND METHODS Our study groups consisted of patients with the following: (1) cyanotic congenital heart disease (CCHD) with or with- out secondary HOA, (2) lung cancer associated with hyper- From the Department of Medicine, Division of Rheuma- tology, and Department of Radiology, University of Califor- nia Medical Center (UCSD); and Veterans Administration Medical Center, San Diego; and the Department of Rheuma- tology. Institute National de Cardiologia Ignacio Chavez. Mexico City. Carlos J. Pineda, MD: Department of Medicine, Division of Rheumatology, CJCSD: Jose Guerra, Jr, MD: Department of Radiology, CJCSD; Michael H. Weisman, MD: Depart- men1 of Medicine, Division of Rheumatology, UCSD; Don- ald Resnick, MD: Veterans Administration Medical Center; Manuel Martinez-Lavin, MD: Department of Rheumatolo- gy, Institute National de Cardiologia Ignacio Chavez. Address reprint requests to Michael H. Weisman. MD, UCSD Medical Center, H-81 1 G, 225 W Dickinson St, San Diego, CA 92103. o 1985 by Grune dl Stratton, Inc. 0049-0172/85/l 404-0005$5.00/O Seminars in Arthritis and Rheumatism, Vol 14, No 4 (May), 1985: pp 263-273 263
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of The skeletal manifestations of clubbing: A study in patients with cyanotic congenital heart disease...

The Skeletal Manifestations of Clubbing: A Study in Patients With Cyanotic Congenital Heart Disease
and Hypertrophic Osteoarthropathy
By Carlos J. Pineda, Jose Guerra, Jr, Michael H. Weisman, Donald Resnick, and Manuel Martinez-Lavin
The skeletal manifestations of clubbing of the digits have been occasionally noted and only briefly dis- cussed in the literature. We investigated the radio- graphic features of digital clubbing in 37 patients with diverse diseases including cyanotic congenital heart disease, lung malignancy-associated hyper- trophic osteoarthropathy, and idiopathic cases. We identified two types of bone changes-osteolysis or bone dissolution, and bone formation or hypertro- phy. The changes were more evident in the feet than in the hands, and the degree of soft tissue change did not always reflect the underlying osseous abnor-
C LINICAL and pathologic features of digital
clubbing have been recognized for many years and are well documented.‘32 However, little attention has been directed to the underlying osseous abnormalities in the digits, particularly the terminal phalanges of the fingers and toes. Because of the obvious changes observed in a few patients, we undertook a controlled prospective study and retrospective analysis of the skeletal findings in the terminal tufts of patients with
diseases or conditions regularly associated with
clubbing. In order to accomplish this task, it is necessary
to define terminology and clarify ambiguities. Clubbing is a descriptive term pertaining to the appearance of the fingers and/or toes and has been defined as the obliteration of the normal 160° angle between the nail and the nail bed (“the profile sign”).3 Clubbing should be distin-
guished from the syndrome of hypertrophic osteoarthropathy (HOA), defined as chronic proliferative periostitis of the long bones, club- bing of the digits, and joint swelling.4 HOA is
further divided into two basic forms, primary and secondary. The primary or idiopathic form is prone to develop in association with thickening of the skin, or pachydermia. In this situation the syndrome is termed pachydermoperiostosis and is diagnosed further by excluding all the recog- nized causes associated with HOA. The secon- dary forms of HOA are, by definition, associated with one of a variety of underlying conditions4
We have observed that two types of bone changes occur in the terminal tufts of these patients: (1) bone formation, or hypertrophy, and
malities. The relationship of these changes (ie, osteolysis, hypertrophy) to each other appear to depend in part on the underlying disease as well as the time course or disease duration. Thus, clubbing and hypertrophic osteoarthropathy may not repre- sent distinct entities; our data suggest that they may be stages in an evolving, more generalized process of new bone formation or hypertrophy followed by osteolysis or atrophy affecting many parts of the skeleton. o 1985 by Grune & Stratton, Inc.
(2) bone dissolution, or acre-osteolysis. The rela- tionship between these changes is complex, depending in part on the specific underlying disease and in part on disease duration or time course. In addition, the soft tissue changes in the digits, or clubbing, do not always reflect the underlying bone pathology. Our findings suggest that clubbing of the digits and hypertrophic
osteoarthropathy of the long bones are not sepa- rate, distinct entities. An alternative view, sup-
ported by these studies, is that these two clinical conditions are stages of an evolving, more gener- alized process producing hypertrophy and later resorption in the skeleton.
PATIENTS AND METHODS
Our study groups consisted of patients with the following:
(1) cyanotic congenital heart disease (CCHD) with or with-
out secondary HOA, (2) lung cancer associated with hyper-
From the Department of Medicine, Division of Rheuma-
tology, and Department of Radiology, University of Califor-
nia Medical Center (UCSD); and Veterans Administration
Medical Center, San Diego; and the Department of Rheuma- tology. Institute National de Cardiologia Ignacio Chavez.
Mexico City. Carlos J. Pineda, MD: Department of Medicine, Division
of Rheumatology, CJCSD: Jose Guerra, Jr, MD: Department
of Radiology, CJCSD; Michael H. Weisman, MD: Depart- men1 of Medicine, Division of Rheumatology, UCSD; Don-
ald Resnick, MD: Veterans Administration Medical Center; Manuel Martinez-Lavin, MD: Department of Rheumatolo-
gy, Institute National de Cardiologia Ignacio Chavez. Address reprint requests to Michael H. Weisman. MD,
UCSD Medical Center, H-81 1 G, 225 W Dickinson St, San Diego, CA 92103.
o 1985 by Grune dl Stratton, Inc. 0049-0172/85/l 404-0005$5.00/O
Seminars in Arthritis and Rheumatism, Vol 14, No 4 (May), 1985: pp 263-273 263

264 PINEDA F-1 AL
trophic pulmonary osteoarthropathy (HPOA). and (3) prl-
mary, idiopathic hypertrophic osteoarthropathy (HOA).
Skeletal surveys were obtained on 24 consecutive patients,
older than 7 years of age, admitted to the Institute National
de Cardiologia lgnacio Chavez (Mexico City) between I980
and 1982 for evaluation of CCHD. On clinical examination.
all patients demonstrated digital clubbing. Evidence of secon-
dary HOA was found in nine. Skeletal surveys from nine
cases of lung cancer associated with HPOA were selected
from the radiology department teaching files; in all of these
surveys, radiographs of the hands, feet, or both, were avail-
able, allowing retrospective analysis of the terminal tufts.
Four additional patients with clubbed digits, joint swelling.
and periostitis of the long bones were referred for evaluation
because of our interest in clubbing. Clinical scrutiny did not
show any associated organic disease in these patients. and
their disease was classified as primary or idiopathic HOA.
Eight controls with noncyanotic congenital heart disease and
no clubbing were selected and matched for age and sex to the
CCHD group.
The skeletal \urveya obtamcd on all patlent\ ~ncludrd
frontal radiographs of the long bones of the upper and Iwxcr
extremitica as well as the hands and feet. The latter wcrc
analyxd and xwred by two experienced skeletal radiologlxts
without prior knowjledge ofthe clinical diagnosis. Both radiul-
ogists agreed on spccilic criteria before Interpreting ihe
radiographs. Portions of the tilrnh were then scored indcpcn-
dcntly by both observers. and there was no significant Inter-
observer variation. One observer then scored all of the lilmh.
The radiographic criteria apecilically related to digital
abnormalities were as follows: grade 0 to grade 7 denoted
increasing order of severity. With regard to the soft tiswe
abnormalities in clubbing. grade 0 indicated normality. pradc
I (mild) reflected loss of the curvilinear lucency prehent at
the Junction between the nail and the skin. grade ? (moder-
ate) indicated the additional presence of ;I mild bulbouh
deformity of the distal aspect of the phalanx. and grade 3
(severe) denoted frank bulbous deformit) (Fig I ) Keith
respect to acre-osteolysis. grade 0 indicated normalit). (;rade
I (mild) indtcated minimal bone dtssolution ah manifested b\
Fig 1. Grades of soft tissue abnormalities in digital clubbing of the hand. (Al Grade 0: normal digit; note the curvilinear radiolucency at the junction of the nails and the skin. lBj Grade 1: the curvilinear radiolucency at the nail-skin junction is obliterated. The distal tuft is slightly rounded.

SKELETAL MANIFESTATIONS OF CLUBBING
the loss of the cortical dense line surrounding the distal half of
the terminal phalanx, grade 2 (moderate) indicated further
loss of bone of the distal phalanx with a tendency to trunca-
tion or tapering, and grade 3 (severe) indicated severe bone
loss with tapering or truncation (Fig 2). Occasionally, the
portion of bone just proximal to the tuft was destroyed, and
the tuft was preserved; this change merited a grade 3 rating.
Periostitis of the long bones was scored as present or absent.
RESULTS
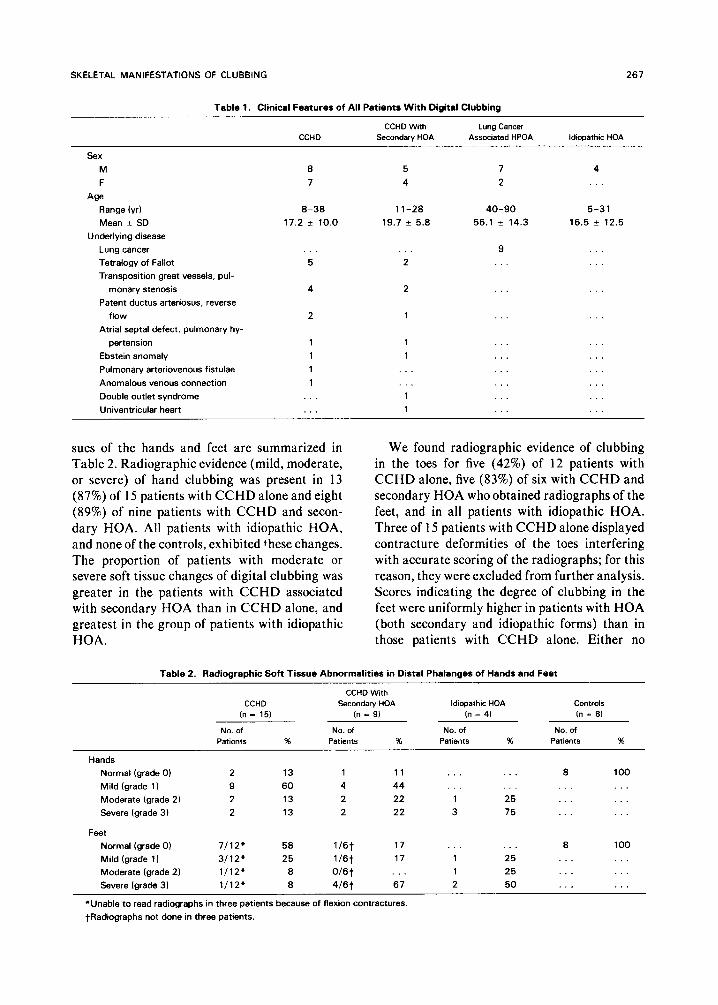
Table 1 includes the clinical features of all patients with digital clubbing. Fifteen patients had clubbing and CCHD alone, and nine had clubbing and CCHD associated with secondary HOA. Diverse types of heart disease were repre- sented in both subgroups of patients with CCHD; there appeared to be no major differences between these two groups in age, sex, or type of
265
heart disease. However, the severity of the heart disease as measured by right to left shunting and arterial oxygen desaturation was greater in the patients with both CCHD and secondary HOA than in those patients with CCHD alone.5
The nine patients with malignancy-associated HPOA were mostly men (seven of nine) ranging in age from 40 to 90 years (mean, 56 years). The four patients with idiopathic HOA were males ranging in age from 5 to 31 years. Two of these four patients were brothers. Of the eight controls with noncyanotic congenital heart disease and no clubbing, four were male and four were female, aged 11 to 34 years (mean, 21 .O + SD 8.5 years) similar to the CCHD patients. Five had patent ductus arteriosus, and three had atria1 septal defects.
Radiographic features related to the soft tis-
Fig 1. (Cont’d) (C) Grade 2: there is mild bulbous deformity of the distal phalanx. (DJ Grade 3: frank bulbous deformity indicating advanced clubbing is present.
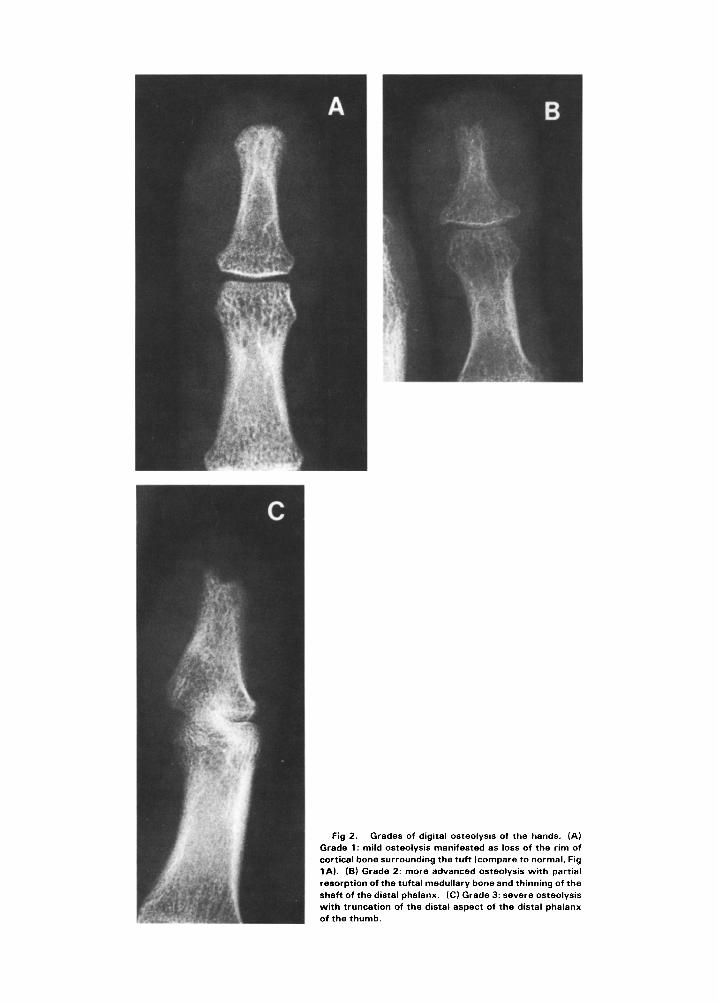
Fig 2. Grades of digital osteolysis of the hands. (A) Grade 1: mild osteolysis manifested as loss of the rim of cortical bone surrounding the tuft (compare to normal, Fig IA). (B) Grade 2: more advanced osteolysis with partial resorption of the tuftal medullary bone and thinning of the
shaft of the distal phalanx. (Cl Grade 3: savara osteolysis
with truncation of the distal aspect of the distal phalanx of the thumb.
SKELETAL MANIFESTATIONS OF CLUBBING 267
Table 1. Clinical Features of All Patients With Digital Clubbing
CCHD CCHD With Lung Cancer
Secondary HDA Associated HPDA Idiopathic HOA
sex M
F
Age
Range (vr) Mean k SD
Underlying disease
Lung cancer
Tetralogy of Fallot
Transposition great vessels, pul-
monary stenosis
Patent ductus arteriosus, reverse
flow
Atrial septal defect, pulmonary hy-
pertension
Ebstein anomaly
Pulmonary arteriovenous fistulae
Anomalous venous connection
Double outlet syndrome
Univentricular heart
a 7
8-38 1 l-28 40-90 5-31
17.2 + 10.0 19.7 f 5.8 56.1 + 14.3 16.5 f 12.5
5
4
2
5 7 4
4 2
9
2
2
1
1
1
1
1
sues of the hands and feet are summarized in We found radiographic evidence of clubbing Table 2. Radiographic evidence (mild, moderate, in the toes for five (42%) of 12 patients with or severe) of hand clubbing was present in 13 CCHD alone, five (83%) of six with CCHD and (87%) of 15 patients with CCHD alone and eight secondary HOA who obtained radiographs of the
(89%) of nine patients with CCHD and secon- feet, and in all patients with idiopathic HOA.
dary HOA. All patients with idiopathic HOA, Three of 15 patients with CCHD alone displayed
and none of the controls, exhibited these changes. contracture deformities of the toes interfering
The proportion of patients with moderate or with accurate scoring of the radiographs; for this severe soft tissue changes of digital clubbing was reason, they were excluded from further analysis. greater in the patients with CCHD associated Scores indicating the degree of clubbing in the with secondary HOA than in CCHD alone, and feet were uniformly higher in patients with HOA greatest in the group of patients with idiopathic (both secondary and idiopathic forms) than in
HOA. those patients with CCHD alone. Either no
Table 2. Radiographic Soft Tissue Abnormalities in Distal Phalanges of Hands and Feet
CCHD With CCHD Secondary HOA Idiopathic HOA Controls
In = 15) Ill = 91 In = 4) In = 8)
No. of No. of No. of No. of Patients % Patients % Patients % Patients %
Hands
Normal (grade 0)
Mild (grade 1)
Moderate (grade 2)
Severe (grade 3)
2 13 1 11 8 100
9 60 4 44
2 13 2 22 1 25
2 13 2 22 3 75
Feet Normal (grade 0) 7/12* 58 1/6t 17 8 100
Mild (grade 1) 3/12* 25 1/6t 17 1 25
Moderate (grade 2) l/12’ 8 0/6t . . . 1 25
Severe (grade 3) l/12” 8 4/6t 67 2 50 .
*Unable to read radiographs in three patients because of flexion contractures.
TRadiographs not done in three patients.
268 PINEDA tT AL
radiographic evidence of clubbing or a mild
degree of clubbing was found in the majority of
patients with CCHD alone. None of the controls
had radiographic evidence of clubbing in either
the hands or the feet.
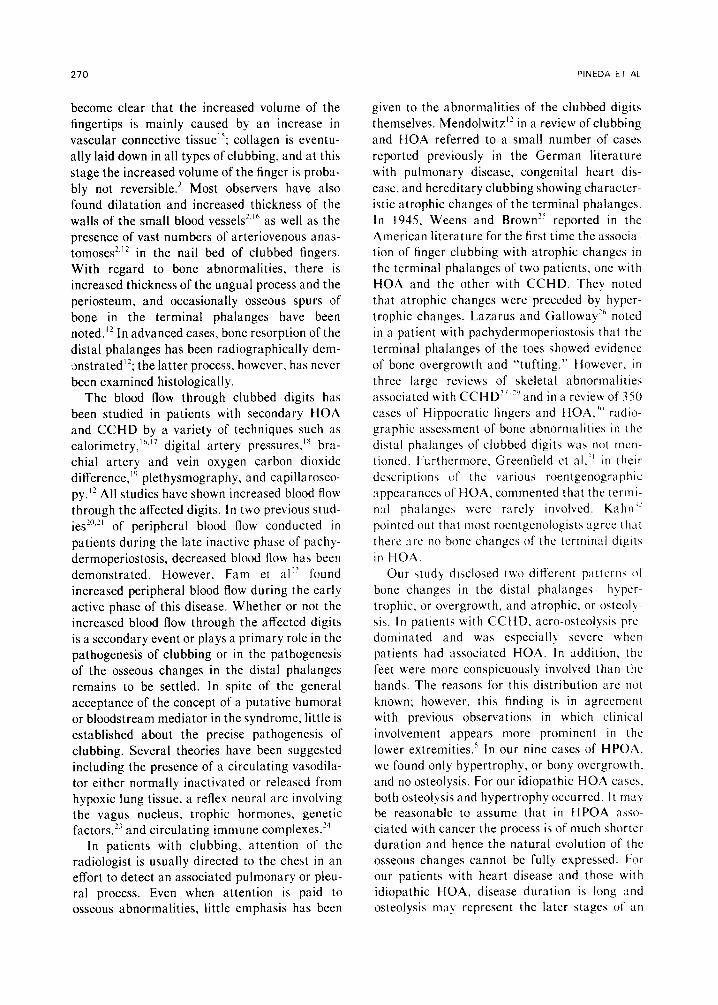
phalanx became pyramidal or “whtttled’ II~
appearance: and “truncation” (Fig 3). in which
the tuft was resorbed and the distal aspect of the
remaining bone was fattened.
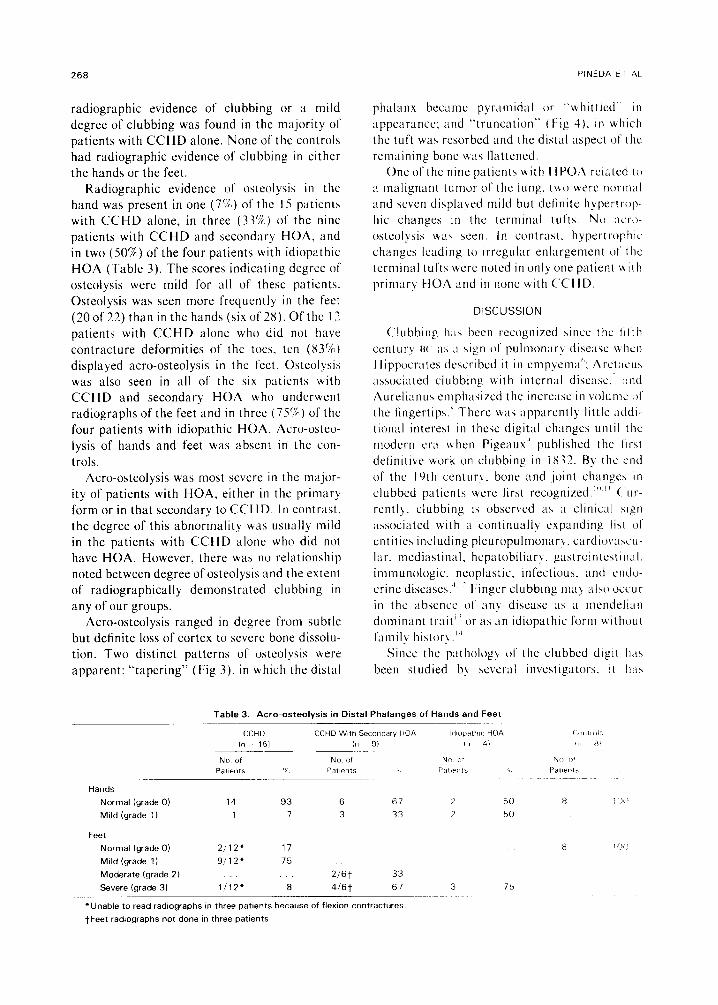
Radiographic evidence of osteolysis in the
hand was present in one (7X) of the I5 patients
with CCHD alone, in three (33%) of the nine
patients with CCHD and secondary HOA. and
in two (50%) of the four patients with idiopathic
HOA (Table 3). The scores indicating degree of
osteolysis were mild for all of these patients.
Osteolysis was seen more frequently in the feet
(20of22)thaninthehands(sixof28).Ofthc I3
patients with CCHD alone who did not have
contracture deformities of the toes, ten (83%)
displayed acre-osteolysis in the feet. Osteolysis
was also seen in all of the six patients with
CCHD and secondary HOA who underwent
radiographs of the feet and in three (75’1) of the
four patients with idiopathic HOA. Acro-osteo-
lysis of hands and feet was absent in the con-
trols.
One of the nine patients with tlPO:\ rclatcd to
a malignant tumor of the lung. tuo were normal
and seven displayed mild but detinitc hypertrop-
hit changes in the terminal tufts. No acre-
ostcolysix \+a> seen. In contrast, hypertrophic
changes leading II) Irregular enlargement of the
terminal tufts \+ere noted in only one patient with
primary HOA and in none uith C‘CHD
DISCUSSION
Acre-osteolysis was most severe in the major-
ity of patients with HOA, either in the primary
form or in that secondary to CCHD. In contrast,
the degree of this abnormality was usually mild
in the patients with CCHD alone who did not
have HOA. However, there was no relationship
noted between degree of osteolysis and the extent
of radiographically demonstrated clubbing in
any of our groups.
Acre-osteolysis ranged in degree from subtle
but definite loss of cortex to severe bone dissolu-
tion. Two distinct patterns of osteolysis were
apparent: “tapering” (Fig 3), in which the distal
C‘lubbing h:r\ been recognircd since the tit’th
centurv HU ;IX ;t \ipn of pulmonarv disease \+ hen
Hippocrates described it in empyema”: .:\rctacu\
associated clubbing with internal disease. ,~nd
:\urelianus cmphasircd the increase in volunrc 01‘
the fingertips.‘ There uas apparently little addl-
tional interest in these digital changes until the
modern era \chen Pigeaux” published the lir\t
definitive work on clubbing in IX32. By the cnci
of the 19th century. bone and joint changes in
clubbed patients wcrc first recognized.‘“” C ur-
rently. clubbing i\ observed ax ;I clinrcal ~1gt1
associated with a continually expanding list of
cntitics including pleuropulmonary. cardio\sascu-
lar. mediastinal. hepatobiliary. gastrointestinal.
immunologic. ncoplaatic, infectious. and cndv-
crinc diseases.’ ” Finger clubbing may also occur
in the absence of any disease ;LS ;I mcndelian
dominant trait’ ’ or as an idiopathic form Lvithout
family histot-) .“’
Since the pathology of the clubbed digrt 11;~s
been studied by several investigators. it ha\
Table 3. Acre-osteolysis in Distal Phalanges of Hands and Feet
CCHD CCHD With Secondary HOA In 151 /II 91
No of No of
Pat,k?lts ‘X Pat,ents
Hands
Normal (grade 0) 14 93 6 67
Mild (grade 1) 1 7 3 33
Feet
Normal (grade 0) 21121 17
Mild (grade 1) 9112’ 75
Moderate (grade 2) 2/6t 33
Severe (grade 31 1/12f 8 416t 67
*Unable to read radlographs in three patients because of flexlon contractures.
tFeet radngraphs not done in three panants

SKELETAL MANIFESTATIONS OF CLUBBING 269
Fig 3. Severe acre-osteolysis manifested as “tapering.” (A and B) In two different patients, note the tapering of multiple distal phalanges of the feet.
Fig 4. Severe acre-osteolysis as demonstrated by “truncation.” (A and B) Two different patients with truncation of multiple distal phalanges of the feet.
270 PINEDA ET AL
become clear that the increased volume of the fingertips is mainly caused by an increase in
vascular connective tissue”; collagen is eventu-
ally laid down in all types of clubbing, and at this stage the increased volume of the finger is proba-
bly not reversible.* Most observers have also
found dilatation and increased thickness of the walls of the small blood vessels*,” as well as the
presence of vast numbers of arteriovenous anas- tomoses*.’ * in the nail bed of clubbed fingers. With regard to bone abnormalities, there is
increased thickness of the ungual process and the periosteum, and occasionally osseous spurs of
bone in the terminal phalanges have been noted.” In advanced cases, bone resorption of the
distal phalanges has been radiographically dem- :,nstrated12; the latter process, however, has never
been examined histologically. The blood flow through clubbed digits has
been studied in patients with secondary HOA and CCHD by a variety of techniques such as calorimetry,“.” digital artery pressures,lx bra- chial artery and vein oxygen carbon dioxide
difference,” plethysmography, and capillarosco- py.‘? All studies have shown increased blood flow
through the affected digits. In two previous stud- ies’“,” of peripheral blood flow conducted in
patients during the late inactive phase of pachy-
dermoperiostosis, decreased blood flow has been demonstrated. However, Fam et al” found
increased peripheral blood flow during the early active phase of this disease. Whether or not the increased blood flow through the affected digits is a secondary event or plays a primary role in the pathogenesis of clubbing or in the pathogenesis
of the osseous changes in the distal phalanges remains to be settled. In spite of the general acceptance of the concept of a putative humoral or bloodstream mediator in the syndrome, little is established about the precise pathogenesis of
clubbing. Several theories have been suggested including the presence of a circulating vasodila- tor either normally inactivated or released from hypoxic lung tissue, a reflex neural arc involving the vagus nucleus, trophic hormones, genetic factors.2i and circulating immune complexes.‘J
In patients with clubbing, attention of the radiologist is usually directed to the chest in an effort to detect an associated pulmonary or pleu- ral process. Even when attention is paid to osseous abnormalities, little emphasis has been
given to the abnormalities of the clubbed digits themselves. Mendolwitz” in a review of clubbing
and HOA referred to a small number of case5
reported previously in the German literature with pulmonary disease, congenital heart dis-
ease, and hereditary clubbing showing character- istic atrophic changes of the terminal phalanges. In 1945, Weens and Brown” reported in the American literature for the first time the associa- tion of finger clubbing with atrophic changes in the terminal phalanges of two patients, one with HOA and the other with CCHD. They noted
that atrophic changes were preceded by hypcr- trophic changes. Lazarus and Galloway” noted
in a patient with pachydermoperiostosis that the terminal phalanges of the toes showed evidence
of bone overgrowth and “tufting.” However, in three large reviews of skeletal abnormalities
associated with CCHD” “and in a review of 350 cases of Hippocratic fingers and HOA.‘” radio- graphic assessment of bone abnormalities in the distal phalanges of clubbed digits was not mcn-
tioned. Furthermore, Greenfield et al.” in their descriptions of the various roentgenographic appearances of HOA, commented that the term- nal phalanges were rarely involved. Kahn”
pointed out that most roentgenologists ugrce that there arc no bone changes of the terminal digits
in HOA. Our study disclosed two diferent pattern\ ot
bone changes in the distal phalanges ~hyper-
trophic, or overgrowth, and atrophic, or osteolq- sis. In patients with CCHD. acre-osteolysis prc- dominated and was especial]!. severe when patients had associated HOA. In addition, the
feet were more conspicuously involved than the hands. The reasons for this distribution are not known; however. this finding is in agreement with previous observations in which clinical
involvement appears more prominent in the lower extremities.’ In our nine cases of HPOA. we found only hypertrophy, or bony overgrowth. and no osteolysis. For our idiopathic HOA caseh. both osteolysis and hypertrophy occurred. It ma! be reasonable to assume that in HPOA ;ISSO- ciated with cancer the process is of much shorter duration and hence the natural evolution of the osseous changes cannot be fully expressed. I-or our patients with heart disease and those with idiopathic HOA, disease duration is long and osteolysis may represent the later stages of an

SKELETAL MANIFESTATIONS OF CLUBBING 271
earlier hypertrophic process. In support of this hypothesis is an observation by Weens and Brown” of the combination of hypertrophic and
osteolytic changes in one patient with primary HOA, and osteolysis without hypertrophy changes in a second patient with longstanding
CCHD. Tufting,26 bowing,33 spurlike,” thumb tack,25
spatulation,34 burrlike, collar buttonlike,2s and atrophic25,35336 represent terms used to describe
the peculiar shape of the distal phalanges observed in cases of clubbing associated with CCHD, secondary HOA, and idiopathic HOA. We suggest that these presumed isolated mor-
phological changes are stages in the evolution of either acre-osteolysis or bony hypertrophy.
In spite of the fact that our 28 patients had
clinical evidence of clubbing (the profile sign) in both hands and feet, a radiographic approach did not demonstrate clubbing in the hands of three of the 28 patients and in the feet in eight of 25 patients. Clubbing in the feet was more difficult to assess radiographically; several factors may account for this difficulty including the presence of skeletal deformities, the normal flexed posi-
tion of the toes, and inadequate radiographic techniques. In our comparison of clinical and radiographic sensitivity in the diagnosis of club-
bing, the visual observation of obliteration of the angle between the nail and the rest of the finger, determined clinically, remained the essential
diagnostic sign. Scrutiny of previous observations in hereditary
or idiopathic forms of the syndrome may, as well, link clubbing to HOA. Idiopathic HOA or pachydermoperiostosis was first recognized as a distinct entity by Touraine et al” and was subdi-
vided into three different groups, the complete form consisting of pachydermia, periosteal new
bone formation, and digital clubbing, the incom- plete form without skin involvement of the scalp, and a form fruste with clubbing and thickening
of the skin but without periosteal changes. Recently, another varient, pachydermoperiosto- sis without pachydermia,33*38,39 has been reported; our four cases of idiopathic HOA have findings consistent with this variant form. In addition, acre-osteolysis has been described in ten patients with pachydermoperiostosis.22*25*3943 Such an association is also mentioned in textbooks by Kree144a,44b and Taybi.45 Hypertrophic changes of
the distal phalanges have also been noted in a case of pachydermoperiostosis.26 In our four cases of idiopathic HOA, bony abnormalities of
the distal phalanges were noted in three (osteoly- sis), and hypertrophic changes were noted in one,
suggesting that these abnormalities may repre- sent stages in the evolution of a more generalized
osseous process. Various explanations have been offered to
account for development of osteolytic changes in clubbed digits. Lippman,35 who observed this process in young patients with congenital heart disease, believed that swelling of the soft tissues
exerted a constant pressure on the terminal pha- langes resulting in atrophy. He arrived at this
conclusion because the atrophic changes were
most pronounced in those fingers and toes that
showed maximum clubbing. In our study we did not find any relationship between the degree of
clubbing and the presence or severity of osteo- lytic changes. Singer,46 who recorded a similar process in a patient with CCHD, suggested local circulatory disturbances as the cause of the changes in the terminal phalanges. On capillar- oscopic examination the investigator noted elon-
gation and dilatation of the small vessels of the
fingers and toes and he advanced the theory that dilated vessels could produce erosions of the
surface of the adjacent bone. No pathologic confirmation of this theory is available.
Hedayati et a142 and Rimoin2’ observing acro-
osteolysis in an advanced, inactive case of pachy- dermoperiostosis, believed that the bone resorp- tion came from a reduction in the peripheral blood flow. However, evidence of increased blood flow through the distal phalanges in an early active case of pachydermoperiostosis associated
with acre-osteolysis has recently been demon- strated.**
Older histologic observations4’ in the long tubular bones of the extremities have demon-
strated lacunar resorption and osteoporosis of both the newly formed subperiosteal bone and the underlying original bone in advanced cases of HOA. It is possible to unify these observations and hypothesize that, in the terminal phalanges, hypertrophic changes may be followed by the same resorptive process as in the long bones.25
In conclusion, our data gathered from a num- ber of patients with clubbing associated with diverse underlying diseases indicate that two
272 PINEDA ET AL
types of bone changes can be found in the distal
phalanges, hypertrophic and osteolytic. The rela- tionship between these changes may depend in part on the specific underlying disease as well as the duration. Acre-osteolysis is more pronounced when clubbing is associated with periosteal new bone formation in the long bones, except in malignancy-associated periostitis. Changes in the toes are more prevalent and more dramatic
than those in the hands. The degree of soft tissue changes in the distal phalanges does not reflect the underlying bone abnormality. The mecha-
nism for clubbing and HOA remains unknown
although a more generalized process of bone
hypertrophy followed by resorption IS suggested for the tufts as well as the long bones.
It is noteworthy that 25 centuries after the description of clubbing, one of the oldest clinical signs in medicine. there is debate over its mor- phological characteristics. Clubbing remains. as Samuel West remarked long ago. “one of those phenomena with which we are all so familiar that WC appear to know more about it than we rcall! do.“‘*
ACKNOWLEDGMENT
The ~nvcatigator\ gratefully acknoulcdge the ‘;ecrct;~r~;~I
skills of 1 isa Russell.
REFERENCES
I. Pyke DA, Camb MB: Finger clubblnp: Validity as a
physical sign. Lancet 2:352-354. 19.54
2. Bigler FC: The morphology of clubbing. Am .I Pathol
34:237 -248. 1958
3. Lovibond JL, Camb MD: Diagnosis of clubbed lingers.
Lancet I :363-364. 1938
4. Altman RD. Tenenbaun J: Hypertrophic osteoarthrop-
athy, in Kelly WN, Harris ED. Ruddy S, et al (eds):
Textbook of Rheumatology. Philadelphia, Saunders, 19x1.
~~1645-1657
5. Martinez-Lavin M. Bobadilla M, Casanova J. et al:
Hypertrophic osteoarthropathy in cyanotic congenital heart
disease: Its prevalence and relationship by bypass of the lung.
Arthritis Rheum 25:l 186-l 193, 1982
6. Hippocrates. The book of prognostics. in Adams F (ed.
transl): The Genuine Works of Hippocrates, vol I. London.
The Sydenham Society, 1849, p 249
7. Aretaeus: On the causes and symptoms of chronic
diseases. in Adams F (transl): Extant Works of Aretaeus. the
Cappadocian. Book I London, The Sydenham Society. 1856. p3ll
8. Aurelianus C: On chronic diseases. in Drabkin IE (ed.
transl): On Acute Diseases and On Chronic Diseases, vol 2.
Chicago, University of Chicago, 1950, p 697
9. Pigeaux DM: Recherches nouvells sur I’etiologie, la
symptomatologie et le mecanisme du development fusiforme
de I’extremite des doigts. Arch Gen de Med 29: 174. 1832
IO. Bamberger E: Uber knochenveranderugenn bei chron-
ischen lungen und herzkrankheiten. 2 Klin Med IX: 193-2 17.
1891
I I. Marie P: De I’osteoartrophic hypertrophiante pneu-
monique. Rev Med IO: l-36, 1890
12. Mendlowitz M: Clubbing and hypertrophic osteoar-
thropathy. Medicine (Baltimore) 21:269-306. 1942
13. Horsfall FL Jr: Congenital familial clubbing of the
fingers and toes. Can Med Assoc J 34: 145-I 49. I936
14. Buchman D, Hrowat EA: Idiopathic clubbing and
hypertrophic osteoarthropathy. Arch Intern Med 97:355
358, I955
15. Lovell R: Observations on the structure of clubbed
fingers. Clin Sci 9:299-321. 1950
16. Wilson GM: Local circulatory changes associated
I7 .lu\t-L’lew JO. C lubbed dIgit\. :\n cntgnl,, \rch
Intern Ued I Ii I71 17X. I ‘XVI
IX vendlow M: Some observation\ on clubbed lingcrr
(‘Iin SCI 3-387 401. 193X
IO Rashour 1,: < lubbing of the digits. Physiologic conhld-
oralion\;. J I.abC‘lin Mcd 5X:613 621. 1961
20. Rimotn Dl.. Pachyderrnopcrlostc\i\ (Idiopathic <tub-
bing and periostosis): Genetic and physiologic consideration
Z Engl J Med 272:923 931. 1961
2 I. Kerber RF. Vogl A Pach~dermoperlostuala. f’erlph-
era circulatrlr\ \tudiea. ,trch Intern Wed Ii2 245 24X.
I97 1
37 fFam \(;. (‘hln-Sang fi. Ramsa! ( .\ Pachydcrm~l
periostitts: Scintlgraphic. thermographic. plethyzmographlc.
and capillaro~copic obccr\ation\ ?\nn Rheum Dis 42-9X
102. 19x3
23 Shneeraon .fM. l>iglt;tl clubbing and hqper~rophlc
ostcoarthropath>: The underlying mechanism. Br J Di< (‘hcht
75:l I? 131. 19x1
‘4 Iwerbuch MS. Brooks PM. Role of Immune complcri
in hypertrophic wteoarthropathy and nonmctastatic polyar-
thritic Ann Rhcum Dis 40:470 472. 19X1
25. Wcens HS, Brown C‘E. .2trophy of terminal phalange\
In clubbing .Ind hlpertrophic osteoarthropathy. Rndtolop\
45:27 30. 1945
26 I warus .f Ii. (;allowa~ Jh. P;~cl~ydermopcrlu~ttr\l\
.Zn unusual cauw of tinger clubbing AJR 11X.70X II 1
1973
77 UICC (‘M Jr. Daveh Ml.. Wood (it]: C‘hangcb in bone
asroclated with qanotlc congenltal cardiac dwabc \ 11,
Heart .I 6X:75 3 I. I964
2X. Fellows KE .fr, Rosenthal !I: Extracardiac roentgcn(l-
graphic abnormalities in cyanotic congenital heart diaeace
AJR I14:317 379. 1972
29. Singh H, Parkash A. Saint M. et al: Bone changch II)
congenital cyanotic heart disease. Br Heart J 34:41? 417.
1972
30. C‘ourq C Hippocratic finger\ and hypertruphlc
osteoarthropathl: A study of 350 cases Br .f DIS (‘best
54:202 209, 1960

SKELETAL MANIFESTATIONS OF CLUBBING
3 1. Greenfield GB, Schorsch HA, Shkolnik A: The vari-
ous roentgen appearances of pulmonary hypertrophic
osteoarthropathy. AJR 101:927-931, 1967
32. Kahn D: Clubbing and hypertrophic osteoarthropa-
thy: Two unusual cases. Arch Intern Med 100:147-151,
1957
33. Bartolozzi G, Bernini G, Maggini M: Hypertrophic
osteoarthropathy without pachydermia: Idiopathic form. Am
J Dis Child 129:849-851, 1975
34. Hedstrand H, Berglund G, Werner 1: Ke-&odermia
palmaris et plantaris with clubbing and skeletal deformity of
the terminal phalanges of the hands and feet. Acta Derm
Venereol (Stockh) 52:278-280,1972
35. Lippman A: Uber einen interessanten rontgenbefund
bei trommelschlagelfingern. Fortschr Geb Rontgenstr Nuk-
learmed Erganzungsband 20:402404, 1913
36. Mankowsky BN, Heinismann Jl, Czerny LI: Osteopa-
thia dysplastica familiaris. Fortschr Geb Rontgenstr Nuk-
learmed Erganzungsband 30:542-549, 1934
37. Touraine A, Solente G, Gale L: Un syndrome osteo-
dermopatique: La pachyderma plicaturee avec pachyperios-
tose des extremites. Presse Med 43: 1820-I 824, 1935
38. Currarino G, Tierney RC, Giesel RG, et al: Familial
idiopathic osteoarthropathy. AJR 85:633-644, 1961
39. Schwartzman S, Spiera H: Idiopathic hypertrophic
osteoarthropathy without pachyderma and with acrolysis. Mt
Sinai J Med (NY) 49:335-337, 1982
40. Guyer PB, Brunton FJ, Wren MW: Pachydermo-
273
periostosis with acre-osteolysis: A report of five cases. J Bone
Joint Surg [Br] 60B:219-223, 1978
41. Herbert DA, Fessel WC: Idiopathic hypertrophic
osteoarthopathy (pachydermoperiostosis). West J Med
134:354-357,198l
42. Hedayati H, Barmada R, Skosey JL: Acrolysis in
pachydermoperiostosis: Primary or idiopathic hypertrophic
osteoarthropathy. Arch Intern Med 140:1087-1088, 1980
43. Sirinavin C, Buist NR, Mokkhaves P: Digital club-
bing, hyperhidrosis, acre-osteolysis and osteoporosis. A case _ resembling pachydermoperiostosis. Clin
1982
44a. Kreel L: Outline of Radiology.
Heinemann Medical, 1971, p 312
44b. Kreel L: Outline of Radiology.
Heinemann Medical, 1971, pp 363-364
Gdnet 22:83-89,
London, William
London, William
45. Taybi H: Touraine-Solente-Gale syndrome, in: Radi-
ology of Syndromes and Metabolic Disorders (ed 2). Chica-
go, Year Book Medical, 1983, pp 304-305
46. Singer S: Ueber destruktive veraunderungen an den
endphalangen bei trommelshlegelfingern. Wien Arch Finn
Med 16:51-60, 1928
47. Steckelmacher S: Ein bcitrag zur kenntnis der hyper-
plastisch-porotischen osteoperiostitis (osteoarthropathie
hypertrophiante pneumique). Dtsch Arch F Klin Med
127:242-260, 1918
48. West S: Two cases of clubbing of the fingers develop-
ing within a fortnight and four weeks respectively, with
remarks. Trans Clin Sot London 30:60, 1897




















