Computerized neuropsychological assessment: Issues and applications
Upload
manoa-hawaiiCategory
view
6download
0
Rachael Ann Polokoff, M.S. Pre-Doctoral Psychology Intern
Theresa Ratti, Ph.D., Supervising Psychologist
The Role of Computerized & Mobile
Technology in Therapy: Evidence Base,
Ethics, Limitations & Future Directions
Speaker Disclosure: The following speakers and/or
their spouse/partner have reported no relevant
financial relationship with a commercial interest:
•Rachael Polokoff, M.S.
•Theresa Ratti, Ph.D.
© 2013 Pine Grove
Opening Discussion Question:
How many of you already use
technology in your practice?

© 2013 Pine Grove
“Her” (2013)
© 2013 Pine Grove
Overview of Presentation
(1) Telepsychology: Definitions and Rationale
(2) Examples of New Technology Uses in Therapy
(3) Evidence Base
(5) Ethics of Telepsychology
(6) Limitations
(7) Future Directions
(8) Discussion Groups/Case Vignette

© 2013 Pine Grove
Key Definitions and Terms
• Important due to fact that literature often uses
terms interchangeably.
• Difficult to have a common language when
technology evolves so fast.
© 2013 Pine Grove
Telepsychology: Definitions
(APA, 2013)
• “Telepsychology”: the provision of psychological
services using telecommunication technologies.
• Often used synonymously with “teletherapy.”
• Include but are not limited to: telephone, mobile
devices, interactive videoconferencing, email, chat,
text and Internet (self-help websites, blogs, and
social media).
• May augment traditional in-person services or be
used as stand-alone services.
© 2013 Pine Grove
More Definitions: (APA, 2013)
• “Remote”: the provision of a service that is received at a different site than the therapist is located.
• “Jurisdictions”: governing bodies of states, nations, or provinces.
• “Confidentiality”: data or information is not disclosed to unauthorized persons.
• “Security measures”: terms that encompass all of administrative, physical and technical safeguards.
• “Information system”: interconnected set of information resources within a system.
© 2013 Pine Grove
Other Terms Used in the Literature
• “apps”: smartphone applications
• “CCBT”: computerized cognitive behavioral
therapy (Grist & Cavanagh, 2013)
• “mHealth”: mobile health (WHO, 2011)
• “SMS”: short message service or “text messaging” (Wagner, Hospital, Morris & Sawant, 2014)
• “TAP”: Technology-aided psychotherapy (Delucia,
Harold & Tang, 2013)
• “T2”: National Center for Telehealth & Technology
© 2013 Pine Grove
Telepsychology: Rationale
• With the use of new technology, psychologists can:
– Attract new patients/clients
– Provide services where previously unavailable
– Perform therapy
– Assist in suicide prevention
– Increase clients’ coping skills
– Increase therapeutic alliance and
communication (Overholser, 2013).
© 2013 Pine Grove
Rationale (continued)
• Teletherapy mobile apps and computer programs are
being developed and used at a fast rate.
• Often developed without significant effectiveness data.
• More than 200 unique mobile phone apps specifically
for behavioral health (Luxton et al, 2011).
• As consumer demand increases, it is essential that
therapists educate ourselves on new technology, and
continue to research efficacy and effectiveness.
• It will likely be increasingly used with or without our
professional input.
• Should we get “left behind” as a field?
© 2013 Pine Grove
Client/Patient Use of New
Technologies No meta-analyses exist yet that pin down
demographic of users but:
•3.8 million podcasts from thepsychfiles.com
downloaded worldwide (Luxton et al, 2011) .
•“PTSD Coach” app downloaded 135,000 times in 78
countries (Hoffman & Weingardt , 2014) .
•Over one billion subscribers to high speed mobile
connections (Gaggioli & Riva 2013) .
© 2013 Pine Grove
Practitioner Use of New Technologies
•Very few studies about the use of teletherapy in
practice today.
•9.8% of responding practitioners for a national
study use weekly email for clinical services (Jacobsen
& Kahout, 2010)
•Epocrates app is used by more than one million
health care providers in the U.S. (Luxton et al, 2011).
•Iris used by Forrest General Hospital and
Hattiesburg Clinic.

© 2013 Pine Grove
Example of New Technology : Computerized
Cognitive Behavioral Therapy (CCBT)
© 2013 Pine Grove
CCBT
• Any form of CBT that is delivered via an interactive computer interface, (offline computer program, or internet).
• Delivery of an effective evidenced based treatment may offer potential benefits:
-increased availability
-increased reach
-cost-effective treatment
-less stigma and no requirement to take off work
© 2013 Pine Grove
Coping with Craving Program (Kathleen Carroll and Yale University, 2013)
© 2013 Pine Grove
“Beating the Blues”
CCBT for Depression (Proudfoot, 2013).

© 2013 Pine Grove
Beating the Blues (Proudfoot, 2013)

© 2013 Pine Grove
Example of New Technology: Mobile
App Therapy
© 2013 Pine Grove
Different types of Apps:
• Self monitoring apps
• Relaxation apps
• Automated therapy apps
• Mood and memory apps
• CBT apps
• Symptom control apps
• Psychoeducation
• Suicide Prevention
• & More (see Luxton et al, 2011 for a comprehensive list )
© 2013 Pine Grove
Advantages of Mobile Mental Health Apps
• Treatment accessibility
• Real time behavior and mood
monitoring
• Increased participation engagement in
treatment
• Real time support and motivation
• Emotional & behavioral self-awareness
© 2013 Pine Grove
Disorders in Which Apps Have Been
Utilized
• Bulimia Nervosa • Depression • Stress • Anxiety • Smoking Cessation • Borderline Personality • Substance Abuse • PTSD • Sleep Disorders
(Luxton et al, 2011)
© 2013 Pine Grove
Some Apps available now • iQuit
• iBreathe
• eCBTMood
• DBT Diary Card and Skills
Coach
• promises
• Recovery Record
• PTSD Coach
• SleepCycle
• PE Coach

© 2013 Pine Grove
DBT Coach
© 2013 Pine Grove
PTSD Coach
• PTSD Coach is an app
designed to assist with
managing the symptoms
of PTSD in the moment
(Hoffman & Weingardt , 2014) .
• Developed by
Department of Veterans
Affairs’ National Center
for PTSD in collaboration
with T2.
© 2013 Pine Grove
MyCompass
• MyCompass is an application in which
participants can self monitor moods, mood
triggers, and behavioral symptoms in real
time.
• Developed by Australian government
grants to aid more people in free
healthcare.

© 2013 Pine Grove
MyCompass (Proudfoot, 2013)
© 2013 Pine Grove
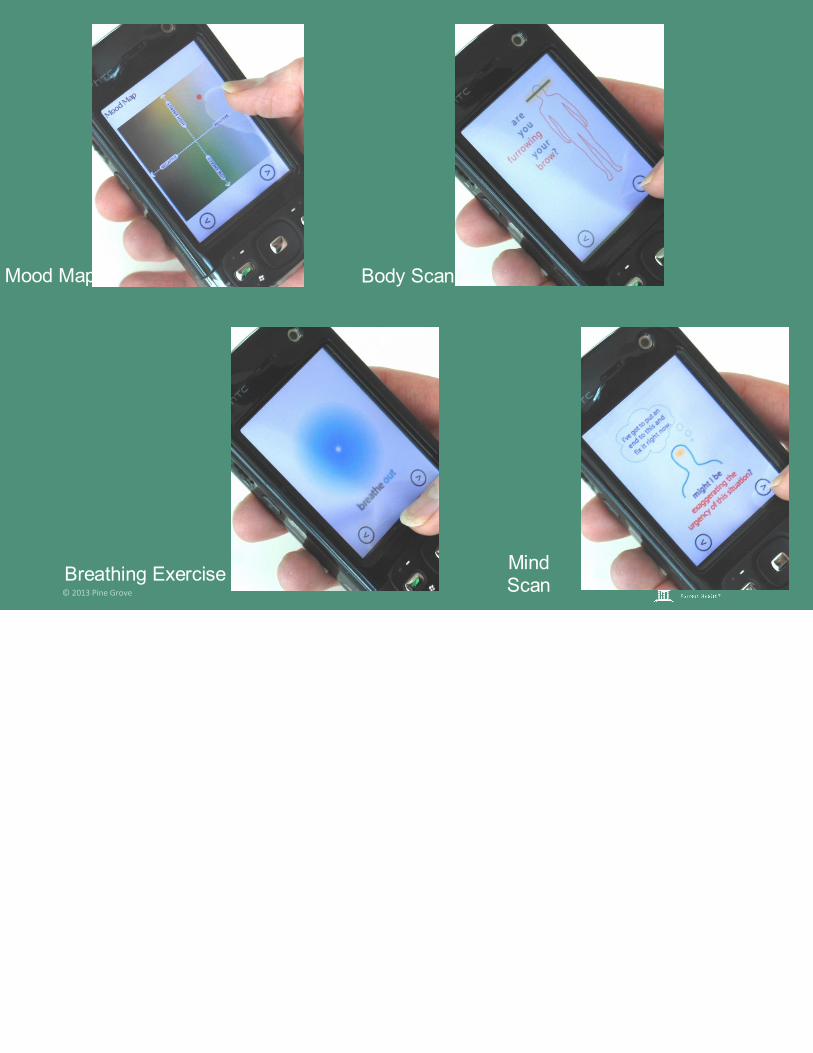
Mood Map
Breathing Exercise
Body Scan
Mind Scan

© 2013 Pine Grove
“Breath Awareness” App (Saagara,
2013)
© 2013 Pine Grove
Evidence Base for Telepsychology
As mentioned previously, there is very little
evidence base as these technologies are new.
•In a study of mental health patients,
hospitalization utilization decreased by an
average of 25% between 2006 and 2010
when telemental health services were
delivered with remote videoconferencing
(Maheu et al, 2012) .
© 2013 Pine Grove
Evidence Base (continued)
Meta-analysis on randomized control studies
comparing CCBT to other therapies and waiting
list controls for anxiety/depression.
•CCBT more effective than both waitlist and
active control conditions.
•Effective low-intensity intervention for anxiety
and depression.
© 2013 Pine Grove
Evidence Base: (continued)
• A preliminary analyses determined that overall
distress, self efficacy, and depression in the
participants after using MyCompass was
significantly lowered (Harrison et al., 2011).
• Participants given option of using “Mood Map”
app significantly lowered their sadness,
anxiety, and anger ratings in therapy (Morris et al.,
2010) .
© 2013 Pine Grove
Evidence Base (continued)
• At the end of study measuring effectiveness
of “DBT Coach,” participants had a major
decrease in urges to use substances and a
decrease in emotional distress (Rizvi et al., 2011) .
© 2013 Pine Grove
Ethical Issues in Telepsychology
(1) Possible breach in confidentiality in the
transmission of the information (Childress, 2000).
• Confidentiality could be in danger due to
availability of information (ex: patient’s family
members or friends maybe able to access an
application on a mobile device).
• Loss, theft or unauthorized access of client’s
equipment.
• The vendor of the equipment or programs could
access or distribute the information without the
client’s knowledge.
© 2013 Pine Grove
Ethical Issues (continued)
(2) The physical separation of the patient
and therapist (Childress, 2000).
• Could lead to miscommunications
which could alter the patient’s
treatment and lower the possibility for
success.
• Could also possibly increase risk of
Self-Injurious Behavior without
accurate assessment of risk.
© 2013 Pine Grove
Ethical Issues (continued)
(3) Concerns about therapist and patient competency (Childress, 2000).
•Therapist’s knowledge and skill in using new technologies may be limited
•The patient’s knowledge and skill may also be limited
-(Ex: Neither therapist nor patient knowing who has access to the data stored in a mobile app).
© 2013 Pine Grove
Ethical Issues (continued)
(4) Informed Consent (Childress, 2000).
• Is the patient aware of the risks and benefits
of using new technologies?
• Is the patient aware of the comparability to
in-person services?
© 2013 Pine Grove
What To Do?
• Guidelines in place from APA specific to
telepsychology (APA, 2013).
• However, will not apply in all situations with
all patients.
• Clinicians should use best “informed”
judgment in each situation.
© 2013 Pine Grove
Some Ethical Practices in Telepsychology
(1) Increase Competency:
• Increase one’s awareness about new technology (CEs, guideline review etc).
• Discuss with patients the issues surrounding confidentiality and the security conditions.
• Conduct an analysis of risks to practice with the patient.
-Ex: “Is the app you are using secure and confidential?” (APA, 2013)
© 2013 Pine Grove
Ethical Practices (continued)
(2) Utilize informed consent
• Informed consent should be in place when
using any mobile technology, whether
verbal or written.
• Policies, procedures, and safeguards
should be discussed with the patient
(Childress, 2000).
© 2013 Pine Grove
Ethical Practices (continued)
(3) Decrease Legal Risk
• Be aware of state regulations that address
delivery of services within and between
jurisdictions and consult licensing boards
when necessary (APA, 2013).
© 2013 Pine Grove
Jurisdiction Rules Infringement I
• Not all states have legislature surrounding
teletherapy.
• No federal guidelines either, so practicing
across state lines can be risky.
• There is not a high likelihood of litigation,
but it has happened….
© 2013 Pine Grove
Jurisdiction Rules Infringement II
• Ex: Dr. Rosemond, psychologist licensed in North Carolina.
• Ran an advice column in a paper that was syndicated in several states, including Kentucky.
• Received complaint letter from the board saying not to practice across state lines.
© 2013 Pine Grove
Limitations in Research
• There is a major lack of empirical evidence
on mobile applications within the mental
health field.
• Some research has been done, but most
studies include only posttest assessment
or a short-term follow-up (6 weeks).
• Most of the applications available today do
not have any research backing them.
© 2013 Pine Grove
Limitations for Therapeutic Use
• Under an ethical obligation at most clinical
sites to use “evidence-based treatment.”
• Yet: no significant evidence base…
• In Mississippi, no telehealth statues or
regulations although the practice of psychology
includes “internet or telehealth practices.”
• Coverage mandate= must be ‘real-time
consultation” (audio-only telephone, fax or
email excluded).
© 2013 Pine Grove
Future Directions in
Telepsychology
• More effectiveness research needed to
define what telepsychology techniques
work for whom.
• States should have specific
telehealth/telepsychology statutes to define
practice better.
• Journals specifically devoted to the study of
mobile technology would be highly useful in
dissemination of information J
© 2013 Pine Grove
Discussion:
• Would you use apps in your practice with
the possibility of a confidentiality breach?
• How could informed consent be used with
the applications?
• Do you think the lack of physical
interaction could lead to a decline in the
treatment?
• What is your personal reasoning for not
using applications?
© 2013 Pine Grove
Discussion: Case Vignette
• A 47- year old Caucasian female with a history of
depression and borderline personality disorder
presents in your office. She has tried Mindfulness
practice and finds it useful in session. She would
like you to recommend a DBT app on her phone to
help her in daily mindfulness practice. She has had
boundary issues with the internet in the past,
including chat rooms and cybersex. She also has
difficulty maintaining boundaries with privacy and
personal information. What do you do?
© 2013 Pine Grove
Acknowledgements
• Taylor Nocera, B.A., for her literature review
and slide design.
• Stephen Haynes, Ph.D. for his guidance on
programming phone applications.

© 2013 Pine Grove
References Childress, C. A. (2000). Ethical issues in providing online psychotherapeutic interventions.
Journal of Medical Internet Research, 2(1). Delucia, P., Harold, S. & Tang, Y. (2013). Innovations in Technology-Aided Psychotherapy
through Human Factors/Ergonomics: Toward a Collaborative Approach. Journal of Contemporary Psychotherapy, 2(1), 615-630.
Gaggioli, A., Riva, G. (2013). From mobile mental health to mobile wellbeing: Opportunities and challenges. Stud Health Technol Inform, 184, 141-7.
Grist, R. & Cavanagh, K. (2013).Computerized Cognitive Behavioral Therapy for Common Mental Health Disorders, What Works, for Whom Under What Circumstances? A systematic review and meta-analysis. Journal of Contemporary Psychotherapy, 43(4),
Harrison, V., Proudfoot, J., Wee, P. P., Parker, G., Pavlovic, D. H., & Manicavasagar, V. (2011). Mobile mental health: Review of the emerging field and proof of concept study. Journal of mental health, 20(6), 509-524.
Hoffman, J. & Weingardt, K. (2014). Is there an app for that? A consumer’s guide to tackling the invisible wounds of war using mobile apps and online technology. National Center for PTSD, webinar, March 2014. http://www.ptsd.va.gov
Kuhn, E., Greene, C., Hoffman, J., Nguyen, T., Wald, L & Schmidt, (2014). A preliminary evaluation of PTSD Coach, a smartphone app for posttraumatic stress symptoms. Military medicine, 179 (1), 12-18. doi:10.7205/MILMED-D-13-00271.

© 2013 Pine Grove
References
Luxton, D.,, McCann, R., Bush, N., Mishkind, M. &, Reger, G. (2011). mHealth for Mental Health: Integrating Smartphone Technology in Behavioral Healthcare. Professional Psychology: Research and Practice. 42(6), 505-512.
Morris, M. E., Kathawala, Q., Leen, T. K., Gorenstein, & E., Guilak (2010). Mobile therapy: case
study evaluations of a cell phone application for emotional self-awareness. Journal of
Medical Internet Research, 12(2), 205-212.
Overholser, J. Technology Assisted Psychotherapy (TAP): Adapting Computerized
Treatments into Traditional Psychotherapy for Depression (2013) J. Contemporary
Psychotherapy, 43(4) 235-252.
Rizvi, S., Dimmeff, L., Skutch, J., Carroll, D., & Linehan, M. (2011). A Pilot Study of the DBT
Coach: An Interactive Mobile Phone Application for Individuals With Borderline
Personality Disorder and Substance Use Disorder. Behavior Therapy, 42(4), 313-315.
World Health Organization, mHealth: New Horizons for Health Through Mobile
Technologies, Global Observatory for eHealth Series, 3, (2011), Retrieved from:
http://www.who.int/goe/publications/goe_mhealth_web.pdf, accessed October, 2013.
Copyright © 2022 FDOKUMEN