
The Relevance of Age of Onset to the Psychopathology of Social Phobia
18
BEHAVIOR THERAPY 34, 31-48, 2003 The Relevance of Age of Onset to the Psychopathology of Generalized Anxiety Disorder LAURA A. CAMPBELL TIMOTHY A. BROWN JESSICA R. GRISHAM Center for Anxiety and Related Disorders, Boston University The present study sought to clarify the relevance of age of onset to the psychopathol- ogy of generalized anxiety disorder (GAD) using a large clinical sample of 154 pa- tients with DSM-IV GAD. Most patients reported onset of GAD by early adulthood, although a smaller proportion of cases emerged in middle adulthood. Structural equation and regression models tested predictions that earlier onset GAD would be characterized by different levels of stress at disorder onset, disorder severity, lifetime comorbidity, and traits that predispose individuals to emotional disorders. Results showed that cases of GAD that emerged without any precipitating stressors were more likely to be of earlier onset. However, another sizable group of patients with earlier-onset GAD identified severely s~essful early environments that they linked to the emergence of GAD symptoms. In contrast, cases of GAD that began in adult- hood were most likely to emerge in the context of mild to moderate stress. Further analyses revealed that earlier-onset GAD was associated with higher levels of disor- der severity, comorbidity, and temperamental vulnerability to emotional disorders. These results are discussed in regard to their clinical and conceptual implications for anxiety disorders. Many patients with generalized anxiety disorder (GAD) report lifelong problems with excessive worry and tension (Brown, Barlow, & Liebowitz, 1994). The relatively early onset of GAD symptoms, along with their chro- nicity and pervasiveness, has led some authors to characterize GAD to be closer to personality disorders than Axis I conditions (Akiskal, 1985; Sander- son & Wetzler, 1991). Indeed, many patients claim that they "have always been a worrier" suggesting that worrying is a fundamental part of their iden- tity or personality. Although GAD often begins before adulthood, a signifi- cant proportion of patients also report later onset of symptoms. It has been noted that these later-onset cases of GAD tend to emerge in the context of Address correspondence to Laura A. Campbell, M.A., Center for Anxiety and Related Dis- orders, 648 Beacon Street, 6th Floor, Boston, MA 02215; e-mail: [email protected]. 31 005-7894/03/0031-004851.00/0 Copyright 2003 by Association for Advancement of Behavior Therapy All rights for reproductionin any form reserved.
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of The Relevance of Age of Onset to the Psychopathology of Social Phobia

BEHAVIOR THERAPY 34, 31-48, 2003
The Relevance of Age of Onset to the Psychopathology of Generalized Anxiety Disorder
LAURA A . CAMPBELL
TIMOTHY A . BROWN
JESSICA R . GRISHAM
Center for Anxiety and Related Disorders, Boston University
The present study sought to clarify the relevance of age of onset to the psychopathol- ogy of generalized anxiety disorder (GAD) using a large clinical sample of 154 pa- tients with DSM-IV GAD. Most patients reported onset of GAD by early adulthood, although a smaller proportion of cases emerged in middle adulthood. Structural equation and regression models tested predictions that earlier onset GAD would be characterized by different levels of stress at disorder onset, disorder severity, lifetime comorbidity, and traits that predispose individuals to emotional disorders. Results showed that cases of GAD that emerged without any precipitating stressors were more likely to be of earlier onset. However, another sizable group of patients with earlier-onset GAD identified severely s~essful early environments that they linked to the emergence of GAD symptoms. In contrast, cases of GAD that began in adult- hood were most likely to emerge in the context of mild to moderate stress. Further analyses revealed that earlier-onset GAD was associated with higher levels of disor- der severity, comorbidity, and temperamental vulnerability to emotional disorders. These results are discussed in regard to their clinical and conceptual implications for anxiety disorders.
Many patients with generalized anxiety disorder (GAD) report lifelong problems with excessive worry and tension (Brown, Barlow, & Liebowitz, 1994). The relatively early onset of GAD symptoms, along with their chro- nicity and pervasiveness, has led some authors to characterize GAD to be closer to personality disorders than Axis I conditions (Akiskal, 1985; Sander- son & Wetzler, 1991). Indeed, many patients claim that they "have always been a worrier" suggesting that worrying is a fundamental part of their iden- tity or personality. Although GAD often begins before adulthood, a signifi- cant proportion of patients also report later onset of symptoms. It has been noted that these later-onset cases of GAD tend to emerge in the context of
Address correspondence to Laura A. Campbell, M.A., Center for Anxiety and Related Dis- orders, 648 Beacon Street, 6th Floor, Boston, MA 02215; e-mail: [email protected].
31 005-7894/03/0031-004851.00/0 Copyright 2003 by Association for Advancement of Behavior Therapy
All rights for reproduction in any form reserved.

32 CAMPBELL ET AL.
life stressors (Blazer, Hughes, & George, 1987; Hoehn-Saric, Hazlett, & McLeod, 1993).
The pul~pose of the current study was to investigate the relevance of age of onset to the symptoms and impairment associated with GAD. At least two previous studies have directly examined the age-of-onset variable (Beck, Stanley, & Zebb, 1996; Hoehn-Saric et al., 1993). Hoehn-Saric et al. reviewed records of 103 patients with GAD who had been diagnosed according to DSM-III-R criteria. They classified individuals with GAD as "early onset" if subclinical symptoms had emerged during the first two decades of life. The "late onset" group was characterized by onset of anxious symptoms in the third decade of life or later.
Comparisons between these two groups revealed that the early-onset group was more likely to develop GAD independently of any precipitating stressors. The early-onset group also endorsed more disturbed environments in child- hood and more current marital distress. Patients in the early-onset group scored higher on measures of neuroticism, trait anxiety, depression, and obsessional features. However, they did not score higher on self-report mea- sures of current symptom severity, and their levels of autonomic arousal were not distinguishable from the late-onset group.
Beck et al. (1996) examined the age of onset of GAD symptoms as part of a broader investigation of GAD in older adults. Their sample, which con- sisted of older adults with DSM-III-R GAD, was divided into two groups. The early-onset group consisted of patients who reported excessive worry before age 15 (n = 16), whereas the late-onset group consisted of patients who reported problems with worry only after age 39 (n = 17). The early- onset group received higher clinician ratings of GAD severity, and obtained higher scores on measures of trait anxiety and depression. However, Beck et al. summarized their findings by stating, "examination of age of onset in the GAD sample suggested few differences between those who reported worry onset during childhood or adolescence vs. adulthood" (p. 232).
The present study attempted to extend our understanding of the role of age of onset in the psychopathology of GAD by addressing some of the limita- tions of previous studies. First, in both of the studies reviewed above, age of onset was treated as a categorical variable, with patients divided into early- onset and late-onset groups on the basis of arbitrary cutoff points. In order to retain more information about the variable of interest, age of onset was treated as a continuous variable for the analyses in this study. Secondly, pre- vious studies failed to directly examine the potentially confounding variable of duration of GAD. Duration of GAD is strongly associated with age of onset of GAD, and might better account for any differences observed between early- and late-onset groups.
In addition, the generalizability of the results from previous studies may be limited to patients who have relatively little comorbidity. Beck et al. (1996) excluded patients who had other principal or coprincipal Axis I disorders, which means that individuals with GAD who had more acutely interfering
AGE OF GAD O N S E T 33
problems (e.g., depression) were excluded from the study. Hoehn-Saric et al. (1993) studied an even more selective sample of individuals who had no additional Axis I disorders except for mild phobias. In the current study, any patient with a current diagnosis of GAD was included in the sample, even if he or she was presenting for treatment of another disorder. This may be a more representative clinical sample of individuals with GAD, because many people with lifelong worry seek treatment for comorbid disorders that cause more life interference.
The first specific aim of the current study was to examine the distribution of age of onset of GAD in a sample comprised of individuals who presented to an anxiety and mood disorders clinic for assessment and treatment. It was predicted that a substantial percentage of individuals with a clinical diagnosis of GAD would report onset of the disorder during childhood mid adoles- cence, and that fewer cases of GAD would emerge in middle to late adult- hood. Prior studies have reported an apparently bimodal distribution of age of onset of GAD (e.g., Blazer et al., 1987), so evidence for this type of distribu- tion was of particular interest.
Determining patterns of onset of GAD at different points in the lifespan was also a major focus of this study. Several authors have hypothesized that later-onset cases of GAD are more likely to emerge in the context of life stressors. In contrast, earlier-onset cases are thought to require fewer environ- mental catalysts to develop (Hoehn-Saric et al., 1993). We hypothesized that the onset of earlier-onset cases would coincide with fewer identifiable stressors, and that later-onset cases would be associated with increasingly higher levels of stress at onset.
Additional analyses tested hypotheses regarding the relationship of age of onset of GAD to disorder severity, comorbidity, and broader traits that predis- pose individuals to emotional disorders. It was hypothesized that earlier onset of GAD would reflect the presence of higher levels of traits that seem to pre- dispose individuals to emotional disorders. Specifically, it was predicted that earlier onset of GAD would be associated with higher scores on measures of negative affect, neuroticism, and behavioral inhibition. It was also hypothe- sized that earlier-onset GAD would be a more severe variant of the disorder, as reflected by higher clinician ratings of severity and higher levels of self- reported impairment. Finally, it was predicted that individuals with earlier- onset GAD would also be more susceptible to other emotional disorders, given that proneness to worry throughout various developmental periods would make these transitions more stressful (thereby increasing the likeli- hood that another disorder would become manifest). Age of onset of GAD was expected to account for unique variance in personality traits, disorder severity, and comorbidity even when contributions of duration of the dis- order were taken into account.
Although the study primarily aimed to resolve questions about the phe- nomenology of GAD, we also believed that the findings could have important clinical implications. Although cognitive-behavioral treatments have been
34 C A M P B E L L ET AL.
shown to be effective for reducing the worry and tension associated with GAD, treatment outcome has been less favorable for GAD than for the other anxiety disorders (Roemer & Orsillo, 2002). Identifying variables relevant to the presentation and course of GAD would be an important first step toward identifying groups of patients for whom interventions might need to be aug- mented or modified, thereby improving the overall efficacy of treatment for GAD. We predicted that the current study would shed light on whether age of onset of GAD might be an important vmiable to consider in assessing treat- ment outcome and developing new approaches to treating this disorder.
Method Participants
The sample for this study was selected from a larger group of patients (N = 1,127) who presented for assessment and treatment at an anxiety disor- ders specialty clinic. The larger sample has been described in detail in a study of the comorbidity of DSM-IV anxiety and mood disorders (Brown, Camp- bell, Lehman, Grisham, & Mancill, 2001). Individuals were selected for the current study if they received a current principal or additional diagnosis of GAD at the time of assessment (N = 154). The age range of the participants was 18 to 63, with a mean of 32.77 (SD -- 10.86). Females comprised 63% of the sample (37% male), and the sample was largely Caucasian (91%; 4% Asian, 2% African American, 2% Hispanic, and 1% Pacific Islander).
Measures
Anxiety Disorders Interview Schedule for DSM-IV: Lifetime Version (ADIS-IV-L; Di Nardo, Brown, & Barlow, 1994). The ADIS-IV-L is a semi- structured interview designed to facilitate reliable diagnosis of anxiety, mood, somatoform, and substance use disorders, and to screen for the presence of other clinical problems (e.g., psychosis). In addition, the ADIS-IV-L allows clinicians to rate the severity of symptoms and disorders on dimensional scales. These clinician severity ratings (CSRs) range from 0 (no interference/ distress) to 8 (extreme interference~distress). Disorders with CSRs of 4 or above are considered clinical diagnoses, whereas disorders with a CSR of less than 4 are judged to be subclinical. The disorder with the highest CSR is considered the principal diagnosis, and in the event that two disorders share the highest CSR, they are denoted "coprincipal" diagnoses. A recent study of reliability of DSM-IV anxiety and mood disorders suggests that clinicians achieve good to excellent reliability for the majority of these disorders when using the ADIS-IV-L (Brown, Di Nardo, Lehman, & Campbell, 2001). Results of Brown, Di Nardo, et al. (2001) demonstrated good agreement for GAD as a current principal or additional diagnosis (K = .65).
In the GAD diagnostic section of the ADIS-IV-L, clinicians rated the excessiveness and controllability of patients' worry about eight life matters using 0-to-8 scales. Clinicians also assigned ratings to each of the six associ-
AGE OF GAD ONSET 35
ated symptoms of GAD (e.g., irritability, muscle tension), as well as the over- all interference and distress associated with the disorder. Other ADIS-IV-L items that assisted the clinician in evaluating the presence and severity of GAD included, "On an average day over the past month, what percentage of the day did you feel worried?" Thus, the ADIS-IV-L provided four indica- tors of GAD severity that were used in subsequent analyses. The first indicator was the patient's estimate of the percentage of the day they felt worried. The second was an average of the clinician ratings pertaining to the patient's diffi- culty controlling worry in eight different domains (e.g., minor matters, work, health). An average of the clinician ratings of the six somatic symptoms of GAD was also calculated. Previous factor analyses support the use of these composite scores (Brown, Di Nardo, et al., 2001). Finally, clinician ratings for distress and interference associated with GAD were averaged and included as another indicator of severity. The four indicators of GAD severity from the ADIS-IV-L comprehensively cover the criteria for DSM-IV GAD (i.e., excessiveness of worry, controllability of worry, somatic symptoms, and interference/distress are all represented).
The thorough assessment of current and lifetime conditions with the ADIS- IV-L provided an estimate of comorbidity. For the purposes of this study, comorbidity was defined as the number of lifetime clinical diagnoses assigned in addition to GAD. The ADIS-IV-L also includes a diagnostic time line that requires clinicians to plot the dates of onset and remission of each clinical disorder and to identify stressors that were present at the time of onset. This diagnostic time line provided information about the age of onset of GAD and the duration of GAD. The stressors that were recorded by the clinician were rated by authors of this study on a 1-to-6 scale using the Axis IV scale contained in DSM-III-R (1 = none, 2 = mild, 3 = moderate, 4 = severe, 5 = extreme, 6 = catastrophic; American Psychiatric Association, 1987).
Behavioral Inhibition and Activation Scales (BIS/BAS; Carver & White, 1994). The BIS/BAS is a 20-item scale that asks individuals to rate the degree to which statements describe them. Patients provide ratings on a 4-point scale ranging from quite untrue of you to quite true of you. The questions address the broad traits of behavioral inhibition and behavioral activation. Psychometric studies have supported the construct validity of this measure (Carver & White, 1994; Jorm et al., 1999). Although the BAS items tend to load on three different facets of BA (drive, fun seeking, and reward dependence), the unidimensional- ity of the BIS scale has been consistent across studies (Carver & White; Jorm et al.). BIS scores have shown both traitlike temporal stability and significant associations with self-report and biological variables relevant to emotional dis- orders (Carver & White; Jorm et al.; Sutton & Davidson, 1997). For the pur- poses of this study, the BIS score was used as an indicator of the latent factor representing temperamental vulnerability to emotional disorders.
Eysenck Personality Inventory: Neuroticism Scale (EPI-N; Eysenck & Eysenck, I963). The Eysenck Personality Inventory is a measure that has been widely used over the last several decades as a measure of personality. Numerous
36 C A M P B E L L ET AL.
studies have supported the reliability and validity of the scales, and scores are stable over long periods of time (Eysenck & Eysenck, 1968). The EPI-N con- sists of 25 yes/no questions about a person's typical feelings and reactions. The total score reflects the individual's level of neuroticism, which was used as an indicator of temperamental vulnerability to emotional disorders in this study.
Positive and Negative Affect Scales (PANAS; Watson, Clark, & Tellegen, 1988). The PANAS contains 20 items that assess two dimensions of mood: positive affect and negative affect. Participants rated the degree to which moods characterized them in general on a scale from 1 (not at all~very slightly) to 5 (extremely). The PANAS has been shown to have sound psychometric properties (Watson et al., 1988). Scores from the general version of the PANAS have been shown to have a significant, moderate level of temporal stability (Watson & Walker, 1996) and have defined a higher-order factor that underlies expression of the more specific emotional disorders (Brown, Chorpita, & Bar- low, 1998). The Negative Affect (NA) scale of the PANAS was used as an indi- cator of temperamental vulnerability to emotional disorders in this study.
Procedure
Patients who contacted the clinic with interest in assessment and treatment were first screened by telephone to establish that their primary complaint was an anxiety or mood problem. Individuals were excluded from the study if they had current hallucinations or delusions, current or recent (within the past 6 months) alcohol or substance abuse or dependence, current suicidal or homicidal risk meriting crisis intervention, or multiple hospitalizations in the past 5 years for severe mental illness (psychosis). Individuals were also required to be between the ages of 18 and 65.
Patients who met the inclusion criteria were scheduled for a formal assess- ment with a clinician trained in the administration of the ADIS-IV-L. A ran- dom subset of the participants in the current study (n = 55) were asked to complete two independent ADIS-IV-L interviews as part of a study of the reliability of DSM-IV anxiety and mood disorders (Brown, Di Nardo, et al., 2001). In the current study, these dual interviews were utilized to obtain information about the reliability of the major variables of interest. All partici- pants also completed a battery of self-report questionnaires that measured anxiety, mood, and personality features. Data from both the ADIS-IV-L and the self-report questionnaires were utilized in the current study.
Data Analysis
The variables of interest in this study were age of onset of GAD, life stressors at onset of GAD, GAD severity, temperamental vulnerability to emotional dis- orders, and number of lifetime comorbid disorders. The potentially confounding influence of duration of GAD also was evaluated. Because there were no cases of remission of GAD in this sample (i.e., all cases had been present continu- ally from the time of original onset), the contribution of duration of the disorder was addressed by including patient age as a covariate in the relevant analyses.
AGE OF GAD ONSET 37
Measurement error of the variables was estimated and adjusted for using two methods in a structural equation modeling framework. First, when pos- sible, multiple indicators of the same variable were used. With this method, indicators of GAD severity were clinician ratings of patients' difficulty con- trolling worry, patients' estimated percentage of the day worried, clinician rat- ings of somatic symptoms of GAD, and clinician ratings of interference and distress associated with GAD. Indicators of temperamental vulnerability to emotional disorders were NA scores on the PANAS, BIS scores on the BIS/ BAS, and EPI-N scores. Second, for variables where only one indicator was available, reliability coefficients were computed using the subsample of 55 patients who received two independent ADIS-IV-L interviews. The reliability of patients' retrospective reports of the age of onset of GAD and reports of additional clinical problems (i.e., comorbidity) were evaluated. These reliability data were used to impose constraints on the error matrices of the age of onset and comorbidity variables in the sU'uctural equation models (cf. Bollen, 1989).
Structural regression models were tested to determine the unique contribu- tions of age of GAD onset to prediction of GAD severity, comorbidity, and temperamental vulnerability to emotional disorders. Prior to testing these structural models, confirmatory factor analysis was performed to evaluate the validity of the measurement model (e.g., to ensure that indicators of tempera- ment and GAD severity loaded on distinct factors).
Separate analyses addressed the question of the relationship between age of GAD onset and stress present at the time of onset. As noted above, stress level at GAD onset was rated on an ordinal scale from 1 to 6 (no stress to cat- astrophic stress). For the subsample of cases used for test-retest reliability analyses (n = 55), these stress ratings were independently assigned by two of the authors (LC and JG) and examined for interrater reliability. The remain- ing cases (n = 99) were rated by one of the authors (LC).
Results Interrater Reliability
The reliability of patients' reports of age of GAD onset was estimated by a Pearson's correlation coefficient using the 55 cases that received two inde- pendent ADIS-IV-L interviews. Reliability for self-reports of age of GAD onset was in the good range (r = .73). Reliability of lifetime comorbidity was also analyzed. The Pearson's correlation between the number of lifetime diagnoses assigned in the first and second interviews was .72, indicating good reliability. Finally, good interrater reliability was obtained for the ratings of life stress at the time of GAD onset (r = .84).
Distribution of Age of GAD Onset
Reported age of GAD onset ranged from 4 to 48. Some patients with very early onsets (n = 5) could not identify a precise age of onset beyond stating that their GAD symptoms had been problematic "since early childhood" or
38 C A M P B E L L ET AL.
"as long as I can remember." Under these circumstances, age of onset was coded as age 5, in the middle of the first decade of life.
The mean age of onset for the sample was 18.82 (SD = 10.79). Twenty- five percent of the sample reported the onset of GAD at age 10 or younger, 50% at age 18 or younger, and 75% at age 26 or younger. Visual exalmnation of the distribution suggested two peaks: the first in early childhood (between 5 and 8 years), and the second in the late teenage years (between 16 and 19 years). However, the first peak may have been partly an artifact of the data coding strategy that we adopted to include childhood onset cases where a precise age of onset was not specified. Moreover, tests for normality using PRELIS 2.14 (J6reskog & S6rbom, 1993) indicated that the skew and kurto- sis of age of GAD onset were within the limits of those that characterize nor- mal distributions (skew = .636, kurtosis = - .383) . Therefore, conclusive evidence for a bimodal distribution was not obtained.
Relationship of Age of Onset to Life Stress at Onset of GAD
Inspection of the ADIS-IV-L interviews of the 154 participants revealed that 150 had enough information about life circumstances at the time of GAD onset to make a stress rating. The remaining four cases (2.6%) were omitted from subsequent analyses because of interviewer error in obtaining stressor information or patient's inability to provide this information. The raters did not assign a stress rating of 6 to any case; they assigned a stress rating of 5 to only four cases. Due to the low frequency of extreme and catastrophic stress at onset of GAD, cases with a rating of 4 or above were grouped together for subsequent statistical analyses.
A preliminary correlational analysis demonstrated that there was no linear relationship between age of GAD onset and stress present at onset (r = .01, ns). Inspection of the data revealed that earlier-onset cases tended to report either no stress or severe stress at GAD onset, whereas later-onset cases appeared to arise during times of mild to moderate stress. These observations, along with the absence of a linear effect, prompted us to consider other pos- sible relationships between these variables. In particular, it seemed that the relationship between age of GAD onset and stress might be quadratic. A non- linear hierarchical regression with age of GAD onset as the dependent vari- able was conducted to explore this possibility. Because the linear and qua- dratic terms of' the raw stress ratings were highly correlated (r = .98), these data were mean centered. Centering the values was successful in eliminating multicollinearity between the linear and quadratic terms (r = .31).
The linear and quadratic terms of the stress ratings were entered in the first and second steps of the regression, respectively. Whereas the first step of the analysis (linear effect) was once again nonsignificant (R = .01), the quadratic term accounted for significant unique variance in age of GAD onset, as indi- cated by the hierarchical F test, F(2, 147) = 32.22, p < .001, R = .42, p < .001. The change in R 2 from Step 1 to Step 2 of the regression was .18, indi- cating an effect size of 18% of the quadratic term. Finally, the nature of the
AGE OF GAD ONSET 39
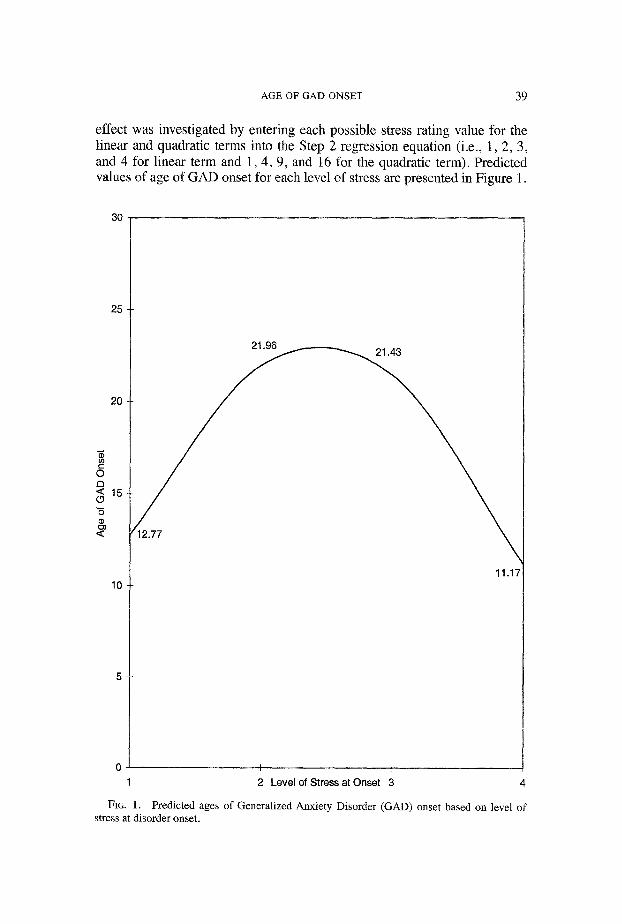
effect was investigated by entering each possible stress rating value for the linear and quadratic terms into the Step 2 regression equation (i.e., 1, 2, 3, and 4 for linear term and 1, 4, 9, and 16 for the quadratic term). Predicted values of age of GAD onset for each level of stress are presented in Figure 1.
30
25
20
0 El < 15
"5
<
10
21.96
1/~2.77
FIG. 1.
17
I I - -
2 Level of Stress at Onset 3 4
Predicted ages of Generalized Anxiety Disorder (GAD) onset based on level of stress at disorder onset.
40 CAMPBELL ET AL.
As depicted in Figure 1, the quadratic effect indicates that earlier onset cases of GAD are more likely to emerge either in the context of no identifi- able stress or in the context of severely distressing environments. Of the 30 individuals with no identifiable stress at GAD onset, 25 (or 83%) had the onset of GAD occur during childhood or adolescence (i.e., prior to age 18). On the other hand, many individuals who reported earlier-onset GAD did in fact experience considerable stressors. Many of these cases received stress ratings of 4 (severe) or above due to the presence of childhood abuse or neglect, death of a parent, or other exceedingly stressful circumstances in their homes. All four cases that had received a stress rating of 5 (extreme) were childhood-onset cases. Many individuals who reported clinical GAD from childhood or adolescence also described circumstances that were rated as moderately stressful, such as contending with the unpredictability of alco- holic parents.
Individuals who reported later onset of GAD were much less likely to report that no identifiable stressors were present at the time of disorder onset. Cases of GAD that began in adulthood were most often associated with life events that were rated as mildly stressful, such as job strain or starting college. Some patients linked the later onset of their GAD to more severely stressful events, such as birth of their first child. However, the major- ity (84%) of later-onset cases were associated with mild or moderate levels of stress at onset.
Relationship of Age of Onset to GAD Severity, Comorbidity, and Temperamental Vulnerability to Emotional Disorders
Confirmatory factor analysis was conducted to determine whether a five- factor model, in which onset, age, severity, comorbidity, and vulnerability were distinct factors, provided an adequate fit for the data. The sample variance- covariance matrix of the indicators was analyzed using a linear structural relations program and maximum-likelihood estimation (LISREL 8.14; J6reskog & Srrbom, 1993). The five factors were permitted to be intercorrelated. Cor- related error was specified between certain indicators of GAD severity. Because interference/distress ratings are influenced by clinicians' ratings of worry and somatic symptoms, error covariances were specified between interference/distress and controllability of worry, and between interference/ distress and somatic symptom ratings (cf. Brown, Chorpita, & Barlow, 1998). For latent variables defined by single indicators (age of onset and comorbid- ity), error variances were derived from the reliability estimates and sample variances of the indicators. The resulting values were used to impose con- straints on the error matrices of the measurement model and subsequent structural models (Bollen, 1989).
Goodness of fit was evaluated using the following indices: chi-square (X2), standardized root mean square residual (SRMR), goodness of fit index (GFI), root mean square error of approximation (RMSEA), p value for test of close fit (RMSEA < .05; Cfit), and the comparative fit index (CFI). These indices
AGE OF GAD ONSET 41
were used because they provide information about various aspects of model fit including absolute fit, fit adjusting for model parsimony, and fit relative to a null model. Used together, these indices provide a more conservative and reliable evaluation of the specified models (Jaccard & Wan, 1996).
Prior to analysis of measurement and structural models, the data were eval- uated for possible departures from normality. Skewness and kurtosis of each variable distribution was examined using PRELIS 2.14 (J6reskog & S6rbom, 1993). The results of these analyses suggested that none of the indicators' distributions departed substantially from a normal distribution.
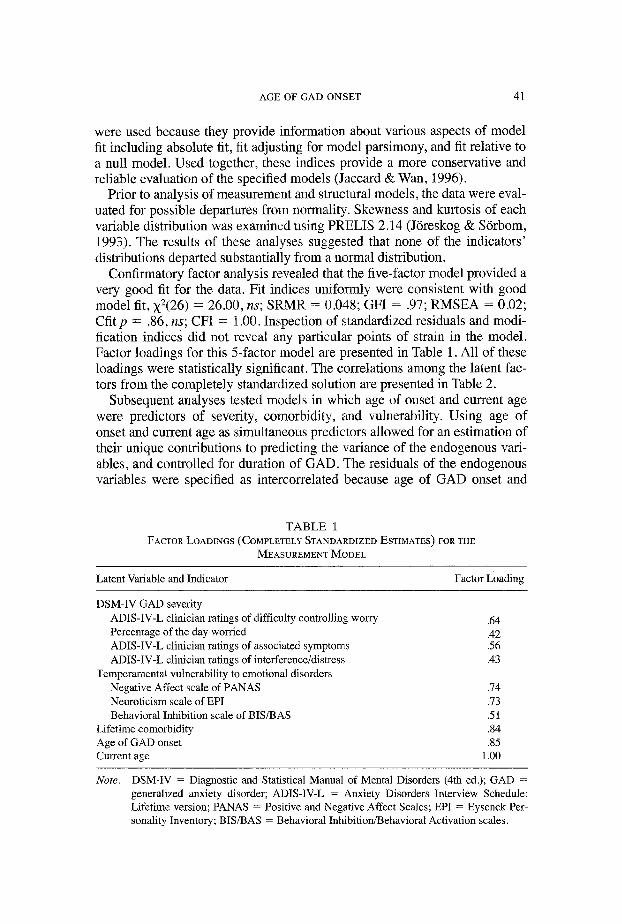
Confirmatory factor analysis revealed that the five-factor model provided a very good fit for the data. Fit indices uniformly were consistent with good model fit, X2(26) = 26.00, ns; SRMR = 0.048; GFI = .97; RMSEA = 0.02; Cfit p = .86, ns; CFI = 1.00. Inspection of standardized residuals and modi- fication indices did not reveal any particular points of strain in the model. Factor loadings for this 5-factor model are presented in Table 1. All of these loadings were statistically significant. The correlations among the latent fac- tors from the completely standardized solution are presented in Table 2.
Subsequent analyses tested models in which age of onset and current age were predictors of severity, comorbidity, and vulnerability. Using age of onset and current age as simultaneous predictors allowed for an estimation of their unique contributions to predicting the variance of the endogenous vari- ables, and controlled for duration of GAD. The residuals of the endogenous variables were specified as intercorrelated because age of GAD onset and
T A B L E 1 FACTOR LOADINGS (COMPLETELY STANDARDIZED ESTIMATES) FOR THE
MEASUREMENT MODEL
Latent Variable and Indicator Factor Loading
DSM-IV GAD severity ADIS-IV-L clinician ratings of difficulty controlling worry Percentage of the day worried ADIS-IV-L clinician ratings of associated symptoms ADIS-IV-L clinician ratings of interference/distress
Temperamental vulnerability to emotional disorders Negative Affect scale of PANAS Neuroticism scale of EPI Behavioral Inhibition scale of BIS/BAS
Lifetime comorbidity Age of GAD onset Current age
.64
.42
.56
.43
.74
.73
.51
.84
.85 1.00
Note. DSM-IV = Diagnostic and Statistical Manual of Mental Disorders (4th ed.); GAD = generalized anxiety disorder; ADIS-IV-L = Anxiety Disorders Interview Schedule: Lifetime version; PANAS = Positive and Negative Affect Scales; EPI = Eysenck Per- sonality Inventory; BIS/BAS = Behavioral Inhibition/Behavioral Activation scales.
4 2 C A M P B E L L ET AL.
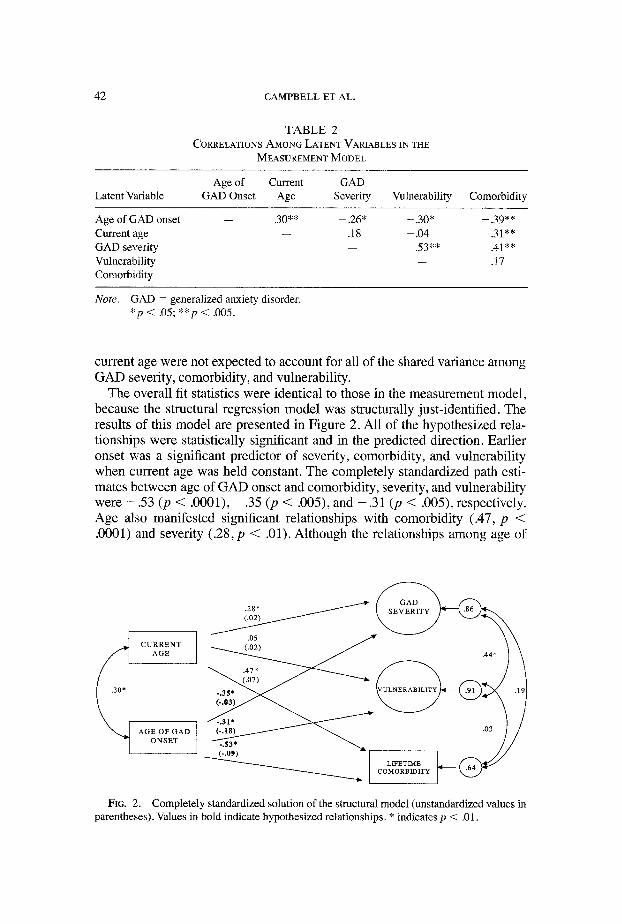
T A B L E 2
CORRELATIONS AMONG LATENT VARIABLES IN THE
MEASUREMENT MODEL
Age of Current G A D
Latent Variable GAD Onset Age Severity Vulnerability Comorbidity
Age of GAD onset - - .30** - .26* - .30* - .39**
Current age - - .18 - .04 .31 **
G A D s e v e r i t y - - .53** .41 **
Vulnerability -- .17 Comorbidity
Note. G A D = generalized anxiety ~sorder. * p < . 0 5 ; * * p < .005.
current age were not expected to account for all of the shared variance among GAD severity, comorbidity, and vulnerability.
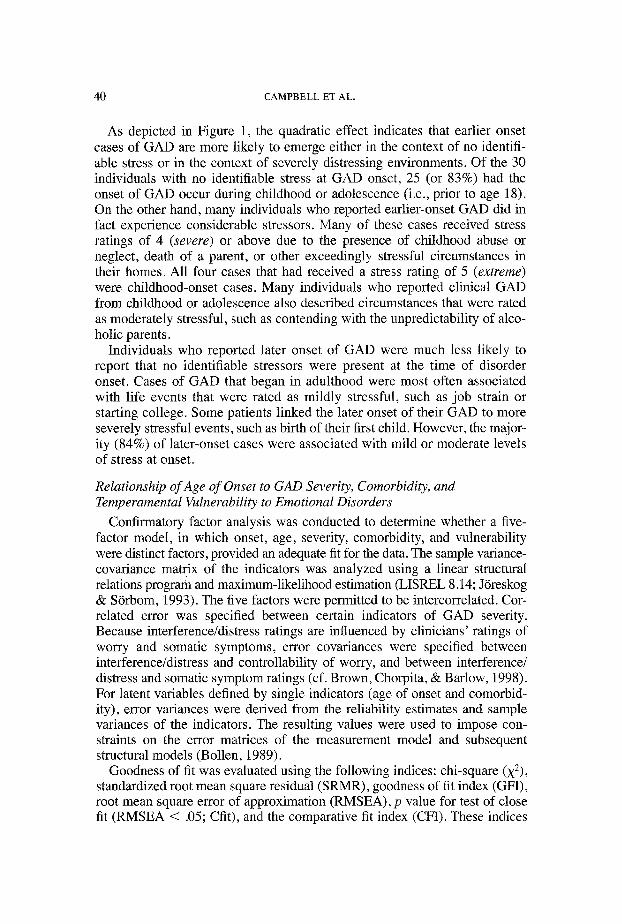
The overall fit statistics were identical to those in the measurement model, because the structural regression model was structurally just-identified. The results of this model are presented in Figure 2. All of the hypothesized rela- tionships were statistically significant and in the predicted direction. Earlier onset was a significant predictor of severity, comorbidity, and vulnerability when current age was held constant. The completely standardized path esti- mates between age of GAD onset and comorbidity, severity, and vulnerability were - . 5 3 (p < .0001), - . 3 5 (p < .005), and - .31 (p < .005), respectively. Age also manifested significant relationships with comorbidity (.47, p < .0001) and severity (.28, p < .01). Although the relationships among age of
CURRENT AGE
AGE OF GAD ONSET
44 /\
03/ / i.".:; - - . - . / /
FIG. 2. Completely standardized solution of the structural model (unstandardized values in parentheses). Values in bold indicate hypothesized relationships. * indicates p < .01.
AGE OF GAD ONSET 43
GAD onset and current age and these endogenous variables were statistically significant, the amount of unexplained variance in GAD severity, comorbid- ity, and vulnerability was large (completely standardized disturbances were .86, .64, and .91, respectively).
Discussion This study sought to clarify the relevance of age of onset to predicting the
symptoms and impairment associated with GAD. Many participants in this study reported clinically significant problems with worry and tension from very early ages. For the 50% of the sample who developed GAD during childhood or adolescence, the life circumstances at onset varied considerably. There was a substantial portion of individuals who could not identify any stressors present at the time of disorder onset. Indeed, cases that arose in the absence of life stress were much more likely to occur in childhood or adoles- cence than in adulthood. On the other hand, many other individuals who reported GAD at an early age indicated that severely stressful environments contributed to the development of their disorder. Reports of childhood abuse, mental illness or substance abuse in parents, and other traumatic circum- stances were common.
The clustering of earlier-onset cases at the two extremes of the stress scale and the preponderance of later-onset cases triggered by intermediate levels of stress were best described as a quadratic relationship between age of GAD onset and degree of stress present at onset. Individuals who developed GAD while under no stress or while under severe stress had similarly younger ages of onset (12 years old, on average). In contrast, individuals who developed GAD in response to mild or moderate levels of life stress were apt to have older ages of GAD onset (21 years old, on average). These results seem to partly clarify Hoehn-Saric et al.'s (1993) finding that individuals with early- onset GAD reported more severely disturbed childhood environments, yet also were more likely to report that their problems with worry began indepen- dently of any precipitating life stressors.
The results of the current study lend further support to the idea that most adult-onset cases of GAD occur in response to some identifiable stressor (typically a mild to moderate one). The findings also support two distinct-- but not incompatible--theories about the early development of GAD. The first is that some individuals seem to be anxious by temperament, and may develop clinically significant problems with worry without the catalyst of life stress. Other individuals unfortunately experience unpredictable, uncontrolla- ble negative events from a very early age, and in response to this severe stress may develop a threat-oriented perspective on the world. Their environments rather than their native temperaments seem to foster problems with worry and tension.
The results pertaining to stress present at disorder onset lend preliminary support to a multifaceted model of the development of anxiety disorders
44 C A M P B E L L ET AL.
recently articulated by Barlow (2002). Barlow identifies three major contrib- utors to the development of pathological anxiety: genetic/biological predis- positions, early experiences that foster anxious temperaments, and more spe- cific sets of learning experiences that focus anxiety on certain aspects of life. Earlier-onset cases of GAD seemed to develop as a result of one or both of the first two types of vulnerabilities: either a native propensity for anxious apprehension reflected by high levels of worry even in the absence of life stress, or a psychological vulnerability to experience worry that develops as a result of negative formative experiences (typically occurring within the fam- ily). Later-onset cases of GAD, on the other hand, seem to develop more in response to acute stressors that focus anxiety on different aspects of life, such as work or relationships. Although other types of vulnerability may have been present for these individuals, they were not of sufficient "strength" for the GAD to manifest itself until a precipitating stressor occurred. Of course, it is likely that the different forms of vulnerability combine in different ways to produce any individual case of clinical GAD. However, it is interesting that the patterns of onset observed for earlier- and later-onset GAD in this sample are easily interpreted within Barlow's model.
The second portion of this study evaluated the relationship between age of GAD onset and disorder severity, comorbidity, and personality features that predispose individuals to anxiety and mood disorders. Age of GAD onset was significantly related to each of these variables. The associations were signifi- cant even with the influence of duration of GAD controlled for by using cur- rent age as a covariate. The substantial association between earlier-onset GAD and higher levels of comorbidity suggests that the presence of GAD symptoms throughout different developmental phases increases the likeli- hood of developing additional clinical problems. The stress associated with typical life events and transitions may be exacerbated by the presence of excessive worry and tension, leading to additional anxiety or mood disorders.
In the current sample, GAD was not always the first lifetime disorder to develop, and therefore the above interpretation of the relationship between age of GAD onset and comorbidity will not apply in all cases. However, in a recent study of comorbidity of anxiety and mood disorders that included the participants of this study, Brown, Campbell, et al. (2001) reported that GAD was temporally primary to other psychological disorders in the majority of cases. GAD frequently preceded mood disorders, substance use disorders, and all other anxiety disorders except social phobia (Brown, Campbell, et al., 2001). For many individuals in the current study, it seems that the presence of GAD throughout the lifespan increased their susceptibility to the negative effects of stress and to the manifestation of other clinical problems. In terms of clinical significance, the tested model predicts that for every decade later that a person develops GAD, he or she will have one fewer additional lifetime psychological disorder.
The relationship of age of GAD onset to traits of vulnerability to emotional disorders provides additional evidence that a significant proportion of earlier-
AGE OF GAD ONSET 45
onset GAD cases may be characterized by a strong temperamental compo- nent. Earlier-onset GAD may reflect an anxious temperament that has been shaped by genetic or early environmental factors, whereas acute life stressors have a more prominent role in development of adulthood-onset GAD. The fact that the severity of GAD symptoms was somewhat higher in earlier-onset cases also may relate to the idea that these individuals are more anxious by temperament. Individuals with temperamental GAD seem naturally inclined to approach most situations with an anxious attitude, and this style likely becomes completely ingrained over time. These individuals probably have had few life experiences in which they learned that worry was unproductive or unnecessary. On the other hand, individuals who develop GAD later in life may already have learned that certain aspects of their lives are not causes for extreme worry. Their worry may be more circumscribed and they may seem to have more respite from worry and tension, leading clinicians to rate their symptoms as lower in severity.
Several limitations of this study are noteworthy. The most significant is the reliance on retrospective report for patients' reports of both their age of GAD onset mad the life circumstances that were present when they developed the disorder. The fact that many individuals with earlier-onset GAD reported no identifiable stressors at the time of disorder onset may have been attributable to poorer memory for events that occurred in childhood and adolescence. Perhaps individuals with adult-onset GAD were better able to recall events that were occurring at the time they noticed problems with worry and tension. Although many individuals with childhood-onset GAD did identify specific stressors that were present during the period of onset, it is certainly possible that milder stressors had since faded from memory. This may have contrib- uted to the quadratic effect obtained in the present results, where individuals with earlier onset GAD were most likely to either report no stress or severe stress at onset.
A second potential limitation of the study involved the measurement of the latent factors of temperamental vulnerability to emotional disorders and GAD severity. The exclusive reliance on self-report questionnaires to define the vulnerability factor and the prominence of clinician ratings in the severity factor may have led these factors to be discriminated (at least in part) on the basis of method variance. Ideally, these factors would have been modeled with a combination of self-report and clinician-rated measures to maximize their validity.
Additionally, the measurement of temperamental traits was not ideal in that it relied on self-report by adults at the time of diagnostic assessment. Much purer estimates of temperament would be attained if participants could have completed assessment earlier in life and before they were symptomatic. Scores on measures of temperament were likely influenced to some degree by individuals' mood states and/or heightened symptomatology at the time of assessment. In addition, the cross-sectional measurement of variables in the current study precludes claims about directionality of any of the effects; we can
46 C A M P B E L L ET AL.
only observe that the variables were significantly correlated and relate in a meaningful way to study hypotheses and current theories of emotional disorders.
Finally, it should be noted that the findings of the current study are not gen- eralizable to all patients with GAD. Our sample was quite homogeneous in terms of race, and results might have differed for a more racially diverse group of patients. In addition, some studies of GAD have suggested that the disorder may be particularly prevalent in older adulthood (Beck et al., 1996; Blazer, George, & Hughes, 1991). Because the oldest participant in our study was 63, we were unable to comment on the possibility of a second peak of GAD onset occurring in older adulthood. This may explain our failure to find evidence for a clear bimodal distribution in age of GAD onset (cf. Blazer et al.). Exclusion of participants with current alcohol and substance use disorders may also limit the applicability of our findings, although inclusion of individu- als with past substance use difficulties remedies this limitation to some degree.
This study offers evidence that earlier-onset cases of GAD distinguish themselves in terms of temperamental factors, circumstances at onset, symp- tom severity, and impairment. Prospective studies of children with GAD would provide the most conclusive information about the relative influence of genetic factors and stressful early environments on the development and course of the disorder. Prospective studies would also shed light on the influ- ence of GAD symptoms on the development of other clinical problems, such as depression and other anxiety disorders.
Future studies should also examine whether earlier-onset or "temperamen- tal" GAD is more resistant to short-term cognitive-behavioral interventions focused on reducing worry and tension. Extant treatments for GAD might benefit from incorporation of approaches that recognize that, for many patients with GAD, their patterns of worry and tension are long-standing and grounded in relatively stable temperamental traits. For patients who seem to fit the description of a more characterological form of GAD, approaches that stress acceptance of internal states such as worrisome thoughts or anxiety symptoms could prove helpful (Roemer & Orsillo, 2002). In addition, tech- niques that increase insight into the counterproductive nature of worry and other anxious responses might be a useful addition to standard treatments for these patients. Finally, cognitive approaches might need to be more schema- focused (i.e., addressing core beliefs and attitudes that are reflective of per- sonality) than focused on patients' day-to-day worries in earlier onset cases of GAD, if significant progress is to be made.
Perhaps the most significant clinical implication of this study is the impor- tance of effectively treating GAD early in its course. Successful early inter- vention would not only alleviate the impairment and distress caused by gen- eralized anxiety, but might also preempt the emergence of later-onset comorbid disorders. Reducing the incidence of these comorbid disorders would have substantial public health benefits in addition to the immeasurable benefits to individual patients of not having to struggle with additional psy- chological disorders.
AGE OF GAD ONSET 47
References
Akiskal, H. S. (1985). Anxiety: Definition, relationship to depression, and proposal for an inte- grative model. In A. H. Tnma & J. D. Maser (Eds 3, Anxiety and the anxiety disorders (pp. 787-797). Hillsdale, NJ: Lawrence Erlbaum.
American Psychiatric Association. (1987). Diagnostic and statistical manual of mental disor- ders (3rd ed., rev.). Washington, DC: Author.
American Psychiatric Association. (1994). Diagnostic and statistical manual of mental disor- ders (4th ed.). Washington, DC: Author.
Barlow, D. H. (2002). Anxiety and its disorders: The nature and treatment of anxiety and panic (2nd ed.). New York: The Guilford Press.
Beck, J. G., Stanley, M. A., & Zebb, B. J. (1996). Characteristics of generalized anxiety disor- der in older adults: A descriptive study. Behaviour Research and Therapy, 34,225-234.
Blazer, D., George, L. K., & Hughes, D. (1991). The epidemiology of anxiety disorders: An age comparison. In C. Salzman & B. D. Lebowitz (Eds.), Anxiety in the elderly: Treatment and research (pp. 1%30). Berlin: Springer.
Blazer, D., Hughes, D., & George, L. K. (1987). Stressful life events and the onset of general- ized anxiety syndrome. American Journal of Psychiatry, 144, 1178-1183.
Bollen, K. A. (1989). Structural equations with latent variables. New York: Wiley. Brown, T. A., Barlow, D. H., & Liebowitz, M. R. (1994). The empirical basis of generalized
anxiety disorder. American Journal of Psychiatry, 151, 1272-1280. Brown, T. A., Campbell, L. A., Lehman, C. L., Grisham, J. R., & Mancill, R. B. (2001). Current
and lifetime comorbidity of the DSM-IV anxiety and mood disorders in a large clinical sample. Journal of Abnormal Psychology, 110,585-599.
Brown, T. A., Chorpita, B., & Barlow, D. H. (1998). Structural relationships among dimensions of the DSM-IV anxiety and mood disorders and dimensions of negative affect, positive affect, and autonomic arousal. Journal of Abnormal Psychology, 107, 179-192.
Brown, T. A., Di Nardo, P. A., Lehman, C. L., & Campbell, L. A. (2001). Reliability of DSM-IV anxiety and mood disorders: Implications for the classification of emotional disorders. Journal of Abnormal Psychology, 110, 49-58.
Carver, C. S., & White, T. L. (1994). Behavioral inhibition, behavioral activation, and affective responses to impending reward and punishment: The BIS/BAS scales. Journal of Personal- ity and Social Psychology, 67, 319-333.
Di Nardo, R A., Brown, T. A., & Barlow, D. H. (1994). Anxiety Disorders Interview Schedule for DSM-IV: Lifetime version (ADIS-IV-L). San Antonio, TX: Psychological Corporation.
Eysenck, H. J., & Eysenck, S. B. G. (1963). The Eysenck Personality Inventory. San Diego, CA: Educational and Industrial Testing Service.
Eysenck, H. J., & Eysenck, S. B. G. (1968). Manual for the Eysenck Personality Inventory. San Diego, CA: Educational and Industrial Testing Service.
Hoehn-Saric, R., Hazlett, R. L., & McLeod, D. R. (1993). Generalized anxiety disorder with early and late onset of anxiety symptoms. Comprehensive Psychiatry, 34,291-298.
Jaccard, J., & Wan, C. K. (1996). LISREL approaches to interaction effects in multiple regres- sion. Thousand Oaks, CA: Sage.
J6reskog, K., & S6rbom, D. (1993). LISREL 8.14 and PRELIS 2.14 [Computer software]. Chi- cago: Scientific Software International.
Jorm, A. F., Christensen, H., Henderson, A. S., Jacomb, P. A., Korten, A. E., & Rodgers, B. (1999). Using the BIS/BAS scales to measure behavioural inhibition and behavioural acti- vation: Factor structure, validity, and norms in a large community sample. Personality and Individual Differences, 26, 49-58.
Roemer, L., & Orsillo, S. M. (2002). Expanding our conceptualization of and treatment for gener- alized anxiety disorder: Integrating mindfulness/acceptance-based approaches with existing cognitive-behavioral models. Clinical Psychology: Science and Practice, 9, 54-68.
48 CAMPBELL ET AL.
Sanderson, W. C., & Wetzler, S. (1991). Chronic anxiety and generalized anxiety disorder: Issues in comorbidity. In R. M. Rapee & D. H. Barlow (Eds.), Chronic anxiety: General- ized anxiety and mixed anxiety-depression (pp. 119-135). New York: The Guilford Press.
Sutton, S. K., & Davidson, R. J. (1997). Prefrontal brain asymmetry: A biological substrate of the behavioral approach and inhibition systems. Psychological Science, 8,204-210.
Watson, D., Clark, L. A., & Tellegen, A. (1988). Development and validation of brief measures of positive and negative affect: The PANAS scales. Journal of Personality and Social Psy- chology, 54, 1063-1070.
Watson, D., & Walker, L. M. (1996). The long-term stability and predictive validity of trait measures of affect. Journal of Personality and Social PsychoIogy, 70, 567-577.
RECEIVED: January 30, 2002 ACCEVTED: July t0, 2002




















