U.S. National Security Culture: From Queer Psychopathology to Queer Citizenship
Upload
independentCategory
view
0download
0
Prq. NeumPsychophannd. &Bid. Psychtat. 1998, Vol. 22, pp. 331-340
CopyrIght 0 1998 Elsetier Science Inc.
PrInted in the USA. AU rights reserved
027%5846/98 $19.00 + .OO
ELSEVIER PII 8027th5846(98)00008-6
EFFECTS OF PIMOZIDE ON THE PSYCHOPATHOLOGY OF DELUSIONAL DISORDER
HERNAN SILVA4, SONIA JEREZ4, ALEJANDRA RAMIREZ’, PATRICIA RENTERIA”, NELLY ARAVENA,‘, DIEGO SALAZARZand RODRIGO LABARCA’
’ Departamento de Psiquiatrla y Salud Mental, Campus Norte, and ’ Escuela de Salud Publica, Universidad de Chile;3 Centro
Neuropsiquiatrico de Santiago, Chile.
(Final form. November 1997)
Abstract
Silva Hernan, Sonia Jerez, Alejandra Ramirez, Patricia Renteria, Nelly Aravena, Diego Salazar and Rodrigo Labarca: Effects of pimozide on the psychopathology of delusional disorder. Prog. Neuro-Psychopharmacol & Biol Psychiat. 1998, 22. pp. 331-340. o 1998 Elsevier Science Inc.
1.
2.
3.
4.
The effects of pimozide on the psychopathology of delusional disorder were studied. After six weeks, pimozide (2-l 2 mg/day) administration had no effect on the Brief Psychiatric Rating Scale, or in the psychological, social and occupational functioning, as measured by the Global Assessment of Functioning Scale. When the different dimensions of the delusional experience were looked upon, no modifications were observed in any of them after six weeks of pimozide treatment.
These data failed to support the therapeutic role of pimozide in the treatment of delusional disorder and may suggest, when compared to other disorders with prominent delusions such as schizophrenia, a different neurobiology for the illness.
Kevwords: delusional disorder, delusional experience, dimensions, pimozide.
ws: Brief Psychiatric Rating Scale (BPRS), Global Assessment of Functioning Scale (GAF), high performance liquid chromatography (HPLC), Structured Clinical Interview for DSM-III-R (SCID).
331
332 H. Sflva et cd.
Introduction
The presence of persistent nonbizarre delusions characterize delusional
disorders. Patients with this disorder have delusions as primary
symptoms. In most cases, behavior is not obviously odd or bizarre, and
impairment in daily functioning is rare (American Psychiatric
Association, 1987). Besides delusions, the rest of psychic life remains
normal in most of the patients suffering a delusional disorder, whereas in
other psychotic disorders such as schizophrenia or depressive disorders
this is not the case (Kendler and Tsuang, 1981).
The literature on the pharmacologic treatment of delusional disorders
suggests that these disorders do not respond well to standard neuroleptic
medications. These observations are consistent with the distinctness of
delusional disorders from schizophrenia and affective disorders
(Manschreck, 1995). However, a few open neuroleptic trials suggest that,
at least for a subgroup, patients with delusional disorder do respond to
some extent to neuroleptics (Bilikiewict et al., 1957; Blanc et al.,l970; Ey
and Bohard, 1970; Riding and Munro, 1975; Munro, 1978). The combination
of antidepressants with neuroleptics (Cheng and Fogel, 1963) or lithium
(Forssman and Walinder, 1969; Morrison, 1972) has in anecdotal reports
been claimed to be useful. Moreover, electroconvulsive therapy may not be
a good choice for delusional disorders patients (Huston and Lecher, 1948).
Since none of these are controlled studies, the question still remains as
to whether neuroleptics are effective in the treatment of delusional
disorder (Kendler, 1980).

Pimozide on the psychopathology of delusional disorder 333
Non controlled studies and case reports have suggested that pimotide
may be a good choice in the treatment of some delusional disorders
subtypes such as the somatic (Riding and Munro, 1975; Munro, 1978),
jealous (Pollock, 1982; Byrne and Yatham, 1989) and erotomanic (Munro et
al., 1985) types.
In the present paper the authors report the effects of pimozide on the
psychopathology of patients with delusional disorder.
Methods
Patients
Seven patients (1 male, six female; age range, 29 to 60) (Table 1)
meeting DSM-III-R (American Psychiatric Association, 1987) and ICD-10
(World Health Organization, 1992) criteria for the diagnosis of delusional
disorder and free of physical illness were studied at the day hospital at
Clinica Psiquiatrica Universitaria, Universidad de Chile. Diagnosis was
made by the Structured Clinical Interview for DSM-III-R (SCID) (Spitzer et
al., 1987). The study was approved by the Institutional Review Board.
Drua Administration
After giving informed consent to participate in a double-blind study,
patients were put on placebo for a minimum of two weeks (range:2-4
weeks) after which pimozide was substituted and administered in ranging
doses between 2 and 12 mg/day for six weeks. Patients were started at 2
or 4 mg/day during the first week, and from then on the dose was
increased according to tolerance so by the last of the second week

334 H. Sflva et al
patients received a dose of pimozide of 4.57k1.9 (meanfS.D.). Whenever
necessary, trihexiphenidile was added to avoid extrapiramidal symptoms.
Table 1
Clinical and Demographic Characteristics
----a-_----_-__- -----_-_11 -_-_----- Patients Age Sex Delusional Theme Duration of
(years) (DSM-III-R) Illness (years) ---__-__---_--__l-l_____I____________________
1 60 F Persecutor-y 11 2 35 F Persecutory 11 3 36 F Persecutory 9 4 29 F Persecutory 9 5 32 M Persecutor-y 11 6 48 F Somatic/Persecutory 12 7 56 F Somatic/persecutory 6
Assessment Instruments
Clinical
Behavioral ratings with the Brief Psychiatric Rating Scale
(BPRS)(Overall and Gorman, 1961), the Global Assessment of Functioning
Scale (GAF) (American Psychiatric Association, 1987) and the scale to
measure five dimensions of delusional experience (Kendler et al., 1983)
were obtained weekly by two psychiatrist, none of whom were aware of
the medication status of the patient.
j_aboratory
Plasma pimozide levels were determined once a week by HPLC according

Pimozide on the psychopathology of delusional disorder
to Miyao et al (1983).
335
Data Analvsis
Clinical changes comparing the last week on placebo and the sixth week
on pimozide were analyzed with a paired t test.
Results
In the group of patients, insignificant changes in the behavior were
observed after six weeks of pimozide treatment (Table 2). Thus, BPRS
scores during the last week of placebo were 38.36k6.22 (meanfS.D.) and
34.36*5.86(meanfS.D.) during the sixth week of pimozide; this change did
not reach statistical significance. Moreover, changes in patients
psychological, social and occupational functioning as assessed by the GAF
scale was also marginal (57.36i8.24 (meanfS.D.) during the last week on
placebo vs 60.57k6.72 (meanfS.D.) during the last week of pimozide
treatment). According to the these results, when the effects of pimozide
on the different dimensions of delusional experience were analyzed, no
changes were observed on conviction, extension, bizarreness and
disorganization; a meaningless, non-significant decrease on pressure was
the only change.
The compliance for pimozide was good enough as weekly plasma pimozide
leveis were determined in each patient. In fact, after the second week of
treatment patients received dose of pimozide of 4.57&l .9 (mean+S.D.),
achieving plasma levels of 2.41f0.82 ng/ml (meanfS.D.) and during the
sixth week while patients were receiving a dose of pimozide of 6.57k3.41
336 H. Silva et al.
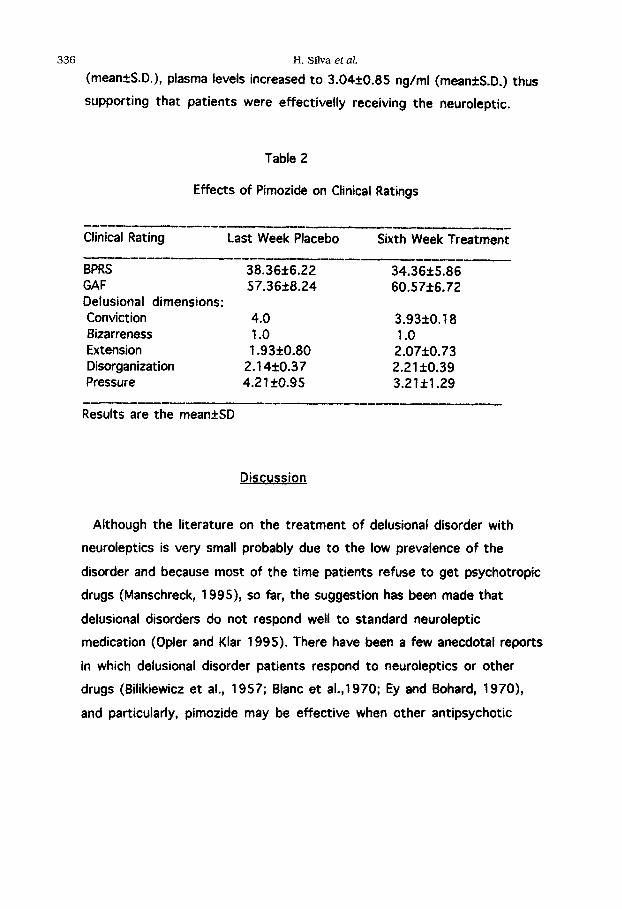
(meaneS.D.), plasma levels increased to 3.04+0.85 ng/ml (meanfS.D.) thus
supporting that patients were effectivelly receiving the neuroleptic.
Table 2
Effects of Pimozide on Clinical Ratings
_L_-__--_______I_---__l___l_l -_-_-_---
Clinical Rating Last Week Placebo Sixth Week Treatment
BPRS 38.36k6.22 34.36k5.86 GAF 57.3628.24 60.57f6.72 Delusional dimensions: Conviction 4.0 3.93&O. 18 Bizarreness 1 .o 1 .o Extension 1.93kO.80 2.07f0.73 Disorganization 2.14f0.37 2.21 *to.39 Pressure 4.21 zto.95 3.21fl.29
Results are the mean&SD
Discussion
Although the literature on the treatment of delusional disorder with
neuroleptics is very small probably due to the low prevalence of the
disorder and because most of the time patients refuse to get psychotropic
drugs (Manschreck, 1995), so far, the suggestion has been made that
delusional disorders do not respond well to standard neuroleptic
medication (Opler and Klar 1995). There have been a few anecdotal reports
in which delusional disorder patients respond to neuroleptics or other
drugs (Bilikiewicz et al., 1957; Blanc et al.,1 970; Ey and Bohard, 1970),
and particularly, pimozide may be effective when other antipsychotic

Pimozide on the psychopathology of delusional disorder
failed (Riding and Munro, 1975; Munro, 1978; Pollock, 1982; Byrne and
Yathan, 1989; Munro et al., 1985).
337
Clinical Response to Pimozide in Delusional Disorder
The results of the present report failed to support the therapeutic role
of pimozide in the treatment of delusional disorder. In fact, despite the
good patient compliance, no changes were observed in the scores of BPRS,
GAF or the different dimensions of delusional experience after six week
of pimozide treatment. It could be argued that six weeks is not a long
enough period to expect changes. This is not the case with schizophrenia
in which time-dependent changes in psychopathology can be seen after
four weeks of neuroleptic treatment (Pickar et al., 1984), even when low
dosis of standard neuroleptics are used (Labarca et al., 1993).
Dimensions of Delusional Experience and Response to Pimozide
A very important goal of the following protocol was to see whether or
not pimozide would modify the different dimensions of delusional
experience. Clearly the answer was no. The question then become as to
whether delusions reported by delusional patients are neurobiologically
different from the ones reported by schizophrenic patients that do respond
to current neuroleptic treatment (Pickar et al., 1984) and, in this regard,
at least in part, may be dopamine mediated. If newer neuroleptics such as
clozapine, risperidone, olanzapine or others fail to work on delusional
disorders, it would suggest that the neurobiology of delusional disorder
may be different from other psychotic disorders such as schizophrenia.

338 H. Sflva et aL
Conclusions
After six weeks of treatment with pimozide, seven patients with
delusional disorder showed no changes on BPRS, GAF or the different
dimensions of delusional experience. These results suggest that the
neurobiology of delusional disorder may be different from other disorders
such as schizophrenia in which delusion may be also prominent.
Acknowledoements
Supported by a grant from Fondo National de Desarrollo Cientifico y
Tecnologico (FONDECM No 193 1037).
References
AMERICAN PSYCHIATRIC ASSOCIATION (1987). Diagnostic and Statistical Manual of Mental Disorders, Third Edition, Revised, Washington DC.
BILIKIEWICZ T., SULESTROWSKI W. and WDOWIAK L-(1957) Les resultats du traitment de la paranoia et de la paraphrenie par le largactil. Annee Medico-Psycho1 115:52-69.
BLANC M., BORENSTEIN P., BRION S. and BONNER H.( 1970) Etude comparative de I’activite de deux neuroleptiques. Encephale =:97-l 61.
BYRNE A., and YATHAM L.N.( 1989) Pimozide in pathological jealousy. Br J Psychiatry m:249-25 1.
CHENG S.F., and FOGEL,E.J.( 1963) Trifluoperazine combined with amitriptyline in paranoid psychosis. Am J Psychiatry 119:780-781.
EY H. and BOHARD F.( 1970) Resultats d’une therapeutique medicamenteuse dans les delires chroniques. Evolution Psychiatrique s25 l-295.

Pimozide on the psychopathology of delusional disorder
FORSSMAN H. and WALINDER J.( 1969) Lithium treatment on atypical indication. Acta Psychiatr Stand 207(suppl):34-40.
339
HUSTON P.E. and LOCHER L.M.( 1948). involutional psychosis: Course when untreated and when treated with electric shock. Arch Neurol Psychiatry
%:385-394.
KENDLER K.S.( 1980). The nosologic validity of paranoia (Simple delusional disorder). A review. Arch Gen Psychiatry =:699-706.
KENDLER K.S. and TSUANG M.T.( 1981) Nosology of paranoid schizophrenia and other paranoid psychoses. Schizophr Bull 2:594-610.
KENDLER K.S., GLAZER W.M. and MORGENSTERN H.( 1983) Dimensions of delusional experience. Am J Psychiatry M:466-469.
LABARCA R., SILVA H., JEREZ S., RUIZ A., FORRAY M.I., GISLYNG K., ANDRES M.E., BUSTOS G,. CASTILLO Y. and HONO J.(1993) Differential effects of haloperidol on negative symptoms in drug-naive schizophrenic patients: effects on plasma homovanillic acid. Schizophr Res. 9: 29-34.
MANSCHRECK T.C. (1995) Delusional disorder and shared psychotic disorder. In: Comprehensive Textbook of Psychiatry, Sixth edition, H. Kaplan and B. Sadock (Eds), pp ‘I 031-1049, Williams & Wilkins, Baltimore.
MIYAO Y., SUZUKI A., NODA K. and NAGUCHI H.( 1983) A sensitive assay method for pimozide in human plasma by high-performance liquid chromatography with fluorescence detection. J. Chrom. =:443-449.
MORRISON S.D.( 1972). Nonmanic responders to lithium. South Med J =:822.
MUNRO A.( 1978) Monosymptomatic hypochondriacal psychosis manifesting as delusions of parasitosis. A description of four cases succesfully treated with pimozide. Arch Dermatol m:940-943.
MUNRO A., O’BRIEN J.W., and ROLL D.( 1985) Two cases of “pure” or “primary” erotomania succesfully treated with pimozide. Can J Psychiat
x:619-622.
340 H. Sflva et al
OPLER L.A. and KLAHR D. (1995) Pharmacological treatment of delusions. The Psychiatric Clinics of North America =:379-39 1.
OVERALL J.E. and GORHAM D.E.(1961) The Brief Psychiatric Rating Scale. Psycho1 Rep =:799-8 12.
PICKAR D., LABARCA R., LINNOILA M., ROY A., HOMMER D., EVERETT D. and PAUL S.( 1984) Neuroleptic-induced decrease in plasma homovanillic acid and antipsychotic activity in schizophrenic patients. Science
a:954-957.
POLLOCK B.G.( 1982) Succesfull treatment of pathologicai jealousy with pimozide. Can J Psychiat 27:86-87.
RIDING J. and MUNRO A.( 1975) Pimozide in the treatment of monosymptomatic hypochondriacal psychosis. Acta Psychiatr Stand
x:23-30.
SPITZER R.L., WILLIAMS J.B.W. and GIBBON M.(1987) Structured Clinical Interview for DSM-III-R. New York State Psychiatric Institute. Biometrics Research, New York.
WORLD HEALTH ORGANIZATION (1992). The ICD-10 Classification of Mental and Behavioural Disorders: Clinical descriptions and diagnostic
guidelines, Geneve.
Inquiries and reprint requests should be addressed to:
Dr. Hernan Silva 1. Clinica Psiquiatrica, Universidad de Chile. Av. La Paz 1003. Santiago de Chile.
Copyright © 2022 FDOKUMEN