
Mapping resting-state functional connectivity using perfusion MRI
Upload
uni-rostockCategory
view
4download
0
To be submitted to:
Psychiatry Research: Neuroimaging
The relation of regional cerebral perfusion and atrophy in mild cognitive
impairment (MCI) and early Alzheimer’s dementia
Christian Luckhaus*a, Mathias Cohnenb, Michael Oliver Flüßc, Michaela Jännera,
Brigitte Grass-Kapanked, Stefan J. Teipele, Harald Hampelf,g, Tillmann Suppriana,
Hans-Jörg Wittsackf
a. Department of Psychiatry and Psychotherapy, Heinrich-Heine-University,
Duesseldorf, Germany
b. Department of Radiology, Städtische Kliniken Neuss, Lukaskrankenhaus
GmbH, Neuss, Germany
c. Institute of Radiology and Nuclear Medicine, Mönchengladbach, Germany
d. Department of Geriatric Psychiatry, Alexian Hospital, Krefeld, Germany
e. Department of Psychiatry and Psychotherapy, University of Rostock, Germany
f. Department of Psychiatry, Ludwig-Maximilian University, Munich, Germany
g. Discipline of Psychiatry, School of Medicine & Trinity College Institute of
Neuroscience (TCIN), Laboratory of Neuroimaging and Biomarker Research,
Trinity College Dublin, The Adelaide and Meath Hospital incorporating the
National Children’s Hospital (AMiNCH), Dublin, Ireland
h. Department of Diagnostic Radiology, Heinrich-Heine-University, Duesseldorf,
Germany

- 2 -
* Address for Correspondance:
Christian Luckhaus, M.D. Department of Psychiatry and Psychotherapy Heinrich-Heine-University Bergische Landstrasse 2 40629 Düsseldorf Tel.: xx49-211-9222741 Fax: xx49-211-9222745 Email: [email protected]

- 3 -
Abstract
The spatial and temporal relationship between regional cerebral blood flow (rCBF)
and brain volume changes in incipient and early Alzheimer’s dementia (AD) are not
yet fully understood.
In the present study a cohort of 30 subjects with mild cognitive impairment (MCI) and
15 patients with mild AD were examined by structural perfusion weighted magnetic
resonance imaging (MRI). Hippocampus and amygdala volumes were measured
using manual volumetry. Using a region of interest (ROI) based co-localisation
methodof structural and perfusion weighted MRIs rCBF values of various brain
regions were calculated. From a total of 36 subjects DNA samples were available for
ApoE4 genotyping.
The main findings are: (1) Reduced rCBF of the posterior cingulum and reduced
volumes of both amygdala and the right hippocampus in mild AD vs. MCI. (2) No
correlation hippocampus and amygdale perfusion and volumes in MCI or AD. (3)
Negative correlations of left hippocampal volume with bilateral frontobasal perfusion
and with perfusion of left thalamus in MCI. (4) Positive correlations in mild AD of right
hippocampal volume with perfusion of both thalami and of right amygdalon volume
with perfusion of bilateral mesotemporal regions. (5) Association of reduced
hippocampal but not amygdala volume with presence of one or two apoE ε4 alleles in
MCI and mild AD; no apoE ε4 allele association with rCBF.
The present data support the concept of functional compensatory brain activation in
MCI and the diachisis hypothesis in early AD. rCBF and brain volume changes are at
least partly dissociated in the early pathogenesis of AD and heterogeneously
associated with the ApoE risk allele for AD.
Kommentar [T1]: Singular ist amygdalon, Plural amygdala

- 4 -
Keywords:
cerebral perfusion, cerebral blood flow, brain volume, atrophy, ApoE, mild cognitive
impairment, MCI, Alzheimer’s disease, dementia

- 5 -
1. Introduction
Mild cognitive impairment (MCI) is a condition that is often transitional to Alzheimer’s
disease (AD) (Petersen et al., 1999, 2001). It likely resembles pre-dementia stages of
AD in the majority of cases and is, therefore, an approximate model to study early
disease mechanisms. The ApoE 4 genotype is a genetic at risk marker for sporadic
AD, its prevalence is increased in MCI patients that later develop AD (Modrego PJ.
(2006): Predictors of conversion to dementia of probable Alzheimer type in patients
with mild cognitive impairment. Curr. Alzheimer Res. 3(2):161-70).
. Recent reports have demonstrated reductions of regional cerebral blood flow (rCBF)
in MCI employing arterial spin labelling (Johnson et al., 2005) or perfusion weighted
magnetic resonance imaging (MRI) (Luckhaus et al., 2008). Hypopersfusion
compared to cognitively normal controls was most pronounced in the mesiotemporal
regions in MCI (-23 %) with no further decline in mild AD and in the amygdala in MCI
(-20%) and mild AD (-28%) (Luckhaus et al., 2008).
A large range of morphometric MRI studies have shown regional brain volume loss in
MCI compared to healthy controls, particularly of mediotemporal structures, using
both region of interest (ROI) methods (Devanand et al., 2007; Horinek et al., 2007;
Colliot et al., 2008) and automated voxel-based analysis (Duarte et al., 2006; Teipel
et al., 2007).
The question of the temporal sequence, spatial relationship and causality of brain
perfusion and volume changes in MCI and AD is still unsolved.
In the presenmt study, we report a correlation analysis of rCBF and brain volume
data of hippocampi and amygdala that have been obtained in the same set i of
Kommentar [T2]: Mit dem aktuellen Ansatz können Sie keine kausalen Aussagen ma-chen. Dazu müssten Sie z.B. Pfadmodelle verwenden. Wenn da Interesse besteht, können wir eine solche Analyse mal bespre-chen.

- 6 -
patients with MCI or mild AD. Furthermore, we analyse the association of ApoE
genotypes with regional brain perfusion and volume, respectively.

- 7 -
2. Materials and Methods
2.1. Subjects
The original study cohort comprised a total of 68 cognitively normal, MCI or mild AD
subjects recruited from the memory clinic of our institute or from a community-based
senior citizen organisation. The MR-based rCBF data from these subjects have
recently been described (Luckhaus et al., 2008).
From a reduced cohort of 30 subjects with MCI and 15 subjects with mild AD brain
volume data were calculated. DNA samples for ApoE genotyping were available in
the majority of these cases.
All subjects had received a thorough diagnostic assessment prior to study inclusion
which comprised of a detailed psychiatric, medical and neurological history, a
physical examination, an extensive laboratory blood screen and a CT- or MR-
structural brain image. The comprehensive psychometric testing applied consisted of
the Test for the Early Detection of Dementia with Differentiation from Depression (Ihl
& Grass-Kapanke, 2000), the neuropsychological test battery of the Consortium to
Establish a Registry for Alzheimer´s Disease (CERAD-NP, Thalmann et al., 1998)
including the Mini-Mental-Status-Examination (MMSE, Folstein et al. 1975), the
Clock-Drawing-Test (CDT, Shulman et al., 2000), the Wechsler Memory Scale
Revised, Subtest Logical Memory (WMS-R-LM, Härting et al., 2000), the Trail Making
Test (TMT-A and –B, Reitan, 1979), the Brief Cognitive Rating Scale and the Global
Detoriation Scale (BCRS and GDS, both: Reisberg et al., German translation by Ihl &
Frölich 1991) and the Clinical Dementia Rating Scale (CDR, Morris, 1997). A
caregiver interview consisted of the Informant Questionnaire on Cognitive Decline in
Kommentar [T3]: Warum wurde gerade diese Subgruppe ausgewählt?

- 8 -
the Elderly (IQCODE, Jorm, 1994) , the Bayer Activities of Daily Living (B-
ADL,Hindmarch et al. 1998) and the Frontal Behavioral Interview (Kertesz, 2000).
A consensus-based diagnosis for each subject had been made by a senior
psychiatrist, a psychologist and a radiologist based upon the results of the above
examinations. MCI was defined according to the diagnostic criteria of Petersen et al.,
(1999). These define MCI as a decline in memory function, isolated or associated
with a decline in intellectual abilities, such as abstract thinking, judgement and
problem solving. These symptoms may interfere with complex Activities of Daily
Living (ADL), e.g. handling finances, whereas basic ADL skills are preserved.
AD-diagnosis was based on the NINCDS-ADRDA-criteria (McKhann et al., 1984) for
probable AD. Only mildly demented AD subjects (GDS 3-4) had been included.
Prior to study enrolment, informed consent had been obtained from all subjects or, in
case of impaired capacity to consent, from their legally authorised guardians. The
study had been approved by the local ethics review board.
2.2. Image acquisition
All MRI investigations were performed using a 1.5-T hole-body MR scanner
(Magnetom Vision Plus, Siemens Medical Solutions, Erlangen, Gemany). The
imaging protocol comprised a high-resolution 3D gradient echo sequence (3D-MPR),
a fluid attenuated inversion recovery sequence (FLAIR), a T2-weighted gradient echo
sequence (T2W), a dynamic T2*-weighted echo planar imaging sequence for the
imaging of perfusion (PWI) and a T1-weighted spin echo sequence after the
administration of gadolinium-containing contrast agent (gadopentetate dimeglumine
[Magnevist], Schering Berlin, Germany). The MR measurement sequences had the
following characteristics:

- 9 -
3D-MPR: gradient echo, TR = 11.6 ms, TE = 4.9 ms, flip angle = 12°, slab thickness
= 180 mm, 180 partitions, field of view (FOV) = 256 mm, matrix = 256 x 256, scan
time = 11min 30 sec.
FLAIR: turbo inversion recovery, TR = 9000ms, TE = 105ms, TI = 2500ms, flip angle
= 180°, 21 slices, thickness = 5mm, distance factor = 0.3, FOV = 250mm, matrix =
224 x 256, scan time = 4min 57sec.
T2W: gradient echo, TR = 840ms, TE = 26ms, flip angle = 25°, 21 slices at 5mm
thickness, distance factor = 0.3, FOV = 250mm, matrix = 224 x 256, scan time =
3min 10sec.
PWI: single shot echo planar imaging, TE = 54ms, flip angle = 90°, FOV = 240mm,
12 slices, distance factor = 0.3, matrix = 128 x 128, 50 measurements at an interscan
interval of 1600ms, scan time 1min 20sec.
T1W: spin echo, TR = 560ms, TE = 17ms, flig angle = 70°, 19 slices, distance factor
= 0.1, matrix = 192 x 256, FOV = 230mm, scan time = 3min 38sec.
During the dynamic perfusion imaging sequence 10 seconds after starting the
measurement a 15ml bolus of gadolinium-containing contrast agent [Magnevist] was
injected in an antecubital vein at a rate of 5 ml/sec and was immediately followed by
15 ml of sodium chloride injected at the same rate.
2.3. Perfusion image analysis
The employed method was described recently (Luckhaus et al., 2008).
For the sake of completeness the procedure of PWI analysis is described in brief in
the following. The dynamic EPI data were transferred to an external workstation and
processed using the software stroketool (http://www.digitalimagesolutions.de,
Frechen, Germany). Maps of the regional cerebral blood flow (rCBF), the regional

- 10 -
cerebral blood volume (rCBV) and the mean transit time (MTT) were calculated using
the singular value decomposition (SVD) technique (Ostergaard et al., 1996). For the
quantification of rCBF normal white matter served as an internal standard
(Ostergaard et al. 1996, Leenders et al. 1990, Luckhaus et al. 2008).
For the regional analysis of the cerebral perfusion rCBF images were coregistered to
the high resolution 3D gradient echo images using rigid body transformation on a
patient by patient basis. The cerebral blood flow then was determined in manually
placed regions of interest (ROI’s). The ROI’s were drawn in the 3D anatomical
images guided by anatomical landmarks. Then the ROI’s were copied to the rCBF
maps.
The following cerebral regions were analyzed: frontobasal (FROB) including parts of
the superior and medial frontal gyrus, temporoparietal (TPAR, superior temporal and
angulate gyrus), mesotemporal (MTMP, hippocampus), anterior/posterior cingular
cortex (ACING, PCING, cingulate gyrus), amygdalae (AMYG), thalami (THAL) and
cerebellar cortex (CEREBELL). ->Figure???
(Further details in Luckhaus et al. 2008).
2.4. Volumetric image analysis
Volumetric analyses were performed with the interactive software package Display,
developed at McConnell Brain Imaging Centre at the Montreal Neurologic Institute.
Four raters blinded to subjects identity, clinical diagnosis and left/right orientation of
scans conducted the volumetry. The number of scans per rater was balanced for
diagnosis. The anatomical boundaries used for segmentation of hippocampus and
amygdala have been described in detail in a previous study (Pruessner JC, Li LM,
Serles W, Pruessner M, Collins DL, Kabani N, Lupien S, Evans AC. (2000):

- 11 -
Volumetry of hippocampus and amygdala with high-resolution MRI and three-
dimensional analysis software: minimizing the discrepancies between laboratories.
Cerebral Cortex 10(4):433-442).
Inter-rater reliability was established through four raters independently measuring the
same set of 10 MRI scans The relative error for each pairwise comparison between
the four raters was below 5% for all volumetric measures obtained by the four raters.
The intra-class correlation coefficients across the four raters were 0.92 for right and
0.93 for left hippocampus, and 0.69 for right and 0.80 for left amygdala.
2.5. Apolipoprotein E genotyping
Blood samples for DNA acquisition were available from a total of 36 MCI and AD
subjects. For DNA analysis, leukocyte DNA was isolated with the Qiagen blood
isolation kit (Qiagen, Hilden, Germany). The apoE ε4 genotyped was studied as
previously described (Hixson and Vernier, 1990)
2.6. Statistical analysis The two groups MCI and AD were compared by t-tests in case of continuous data
and χ²-test in case of categorical data. Correlation analysis were carried out using the
Pearson product-moment correlation coefficient, whereas correlations were
computed separately for MCI and AD. Differences between patients without apoE ε4
allels and patients with 1 or 2 apoE ε4 allels referring to brain volume were again
investigated by t-tests.
A value of p <= 0.05 was defined to be significant.

- 12 -
3. Results
Table 1 gives basic demographic and psychometric data of the two groups under
study. MMSE and GDS psychometric scores were significantly different between the
MCI and AD group, while group differences in age and gender distribution were non-
significant.
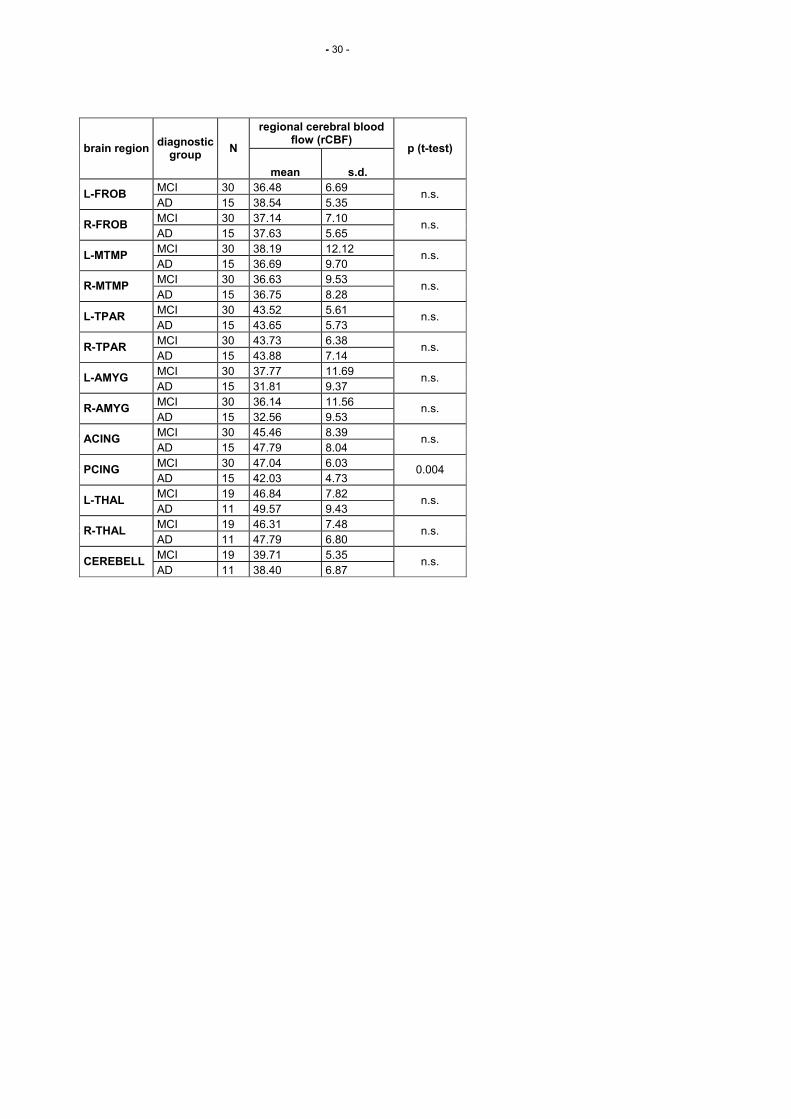
Table 2 summarizes rCBF values of MCI and AD patients. A lower rCBF (-11 %) was
detected in the posterior cingulum of AD vs. MCI subjects. The perfusion of all other
cerebral regions under study was not different between both groups.
Table 3 gives regional brain volume data of MCI and AD patients. Significant volume
reductions in AD vs. MCI were found for both amygdala (left: -15 %; right: -21 %)
and the right hippocampus (-14 %), while the left hippocamal volume (-11 %)
reduction was not significant.
Tables 4 and 5 show correlations between regional perfusion and volumes for the
MCI and AD group, respectively.
In MCI left hippocampal volume was negatively correlated with frontobasal perfusion
of both hemispheres and with perfusion of the left thalamus (Fig. 1). All other
examined regions showed no significant correlations between perfusion and volume.
In mild AD right hippocampal volume was positively correlated with perfusion of left
and right thalami. Also right amygdala volume was positively correlated with left and
right mesotemporal perfusion. (Fig. 2)
Kommentar [T4]: Beii 13*4 Einzelvergleichen/Gruppe macht man sich schon etwas Sorgen wegen des Alphafehlers. Sollte zumindest diskutiert werden

- 13 -
Tables 6 depicts the association of the apoE ε4 allele with regional brain volume in
the merged group of MCI and AD. Decreased volumes of the right hippocampus and,
as a trend, of the left hippocampus, but not of amygdala were associated with the
presence of the apoE ε 4 allele. In contrast rCBF of all analysed regions including the
mesiotemporal and amygdala regions were not assciated with apoE ε4 genotype
(data not shown).
4. Discussion
The major findings of our study are:
1. Significant brain volume reductions were observed in mild AD vs. MCI for both
amygdala and the right hippocampus.
2. No rCBF changes were apparent in mild AD vs. MCI in the above brain
regions or in all other analysed regions except for reduced rCBF in the
posterior cingulum.
3. There was no correlation between rCBF and volumes in hippocampi or
amygdala, neither in MCI nor in mild AD.
4. In MCI we found negative correlations of left hippocampal volume with
frontobasal perfusion of both hemispheres and with perfusion of left thalamus.
5. In AD we found positive correlations of the right hippocampal volume with
perfusion of both thalami and of right amygdala volume with perfusion of left
and right mesotemporal regions.
6. Presence of one or more apoE ε4 alleles was associated with reduced
hippocampal but not amygdala volumes in MCI and mild AD, while there was
no association with rCBF.

- 14 -
The observed hippocampal volume reductions in mild AD vs. MCI are in close
accordance with Colliot et al. (2008), who reported reductions of 15 %. They also
described a substantial hippocampal volume loss in MCI vs. controls, as did
Devanand et al. (2007), suggesting that hippocampal atrophy begins in preclinical
AD and continues throughout the clinical onset of dementia. Amygdala volume
reductions have previously been described in very mild AD patients vs. controls
(Basso et al., 2006), and further reductions have been reported in mild to
moderate AD (Horínek et al., 2006). Volume losses of both structures have been
associated with compromised memory performance in AD (Basso et al., 2006).
Significant rCBF reductions in MCI vs. controls have been described for the
hippocampi, amygdalae and anterior cingulum (Johnson et al., 1998; Fakhri et al.,
2003; Luckhaus et al., 2008). Regarding the transition from MCI to AD, further
rCBF reductions seem to be largely limited to the posterior cingulum (Ishiwata et
al., 2006; Luckhaus et al., 2008). This suggests that hypoperfusional changes in
hippocampi and amygdalae occur in incipient AD and reach a plateau at the MCI
stage, while cerebral volume loss of the same regions continues further into
clinical AD stages. Regional CBF and volume changes, thus, appear to be
dissociated in early AD in respect to time course and localisation. Accordingly, we
saw no correlations of hippocampal and amygdala volumes with the respective
mesiotemporal and amygdala rCBF in MCI or mild AD.
On the other hand, in MCI we found negative correlations of left hippocampal
volume with frontobasal perfusion of both hemispheres and with perfusion of the
left thalamus (Fig. 1). Prefrontal cortex function is particularly involved in strategic
aspects of memory retrieval, such as establishing a retrieval mode and goals,
initiating and guiding search, and monitoring and verifying the memories that have
Kommentar [T5]: Wahrschein-lich meinen Sie das umgekehrt: zunächst MCI dann AD

- 15 -
been retrieved, while the thalamus subserves as a relay station (Moscovitch et al.,
2005). Frontal brain regions are typically spared from atrophy in MCI (Pennanen
et al., 2006). Increased prefrontal activation, as depicted by increased blood flow
or BOLD response, may, thus, constitute a functional compensatory mechanism
of hippocampal dysfunction in incipient AD. In accordance, analysis of regional
low-frequency fluctuations of fMRI signal intensity showed increased left
hippocampal connectivity with the right prefrontal cortex in early AD (Wang et al.,
2006). Gould et al. (2005) described a corresponding trend towards increased
BOLD responses in frontal brain areas during an associate learning task in mild
AD.
In contrast to the findings in MCI, we saw positive correlations in mild AD of
hippocampal and amygdala volume loss with reduced rCBF in functionally
connected brain areas, i.e. both thalami and mediotemporal regions, respectively
(Fig. 2). These results match the diachisis hypothesis of morphological and
functional brain changes in early Alzheimer’s disease, which postulates distant
hypofunctional effects caused by neuronal damage in the hippocampus via a
disconnection process (Villain et al., 2008). A recent voxel-based comparison of
structural MRI- and 18FDG-PET-data in early AD showed opposite atrophy –
hypometabolism ratios of the hippocampus (atrophy > hypometabolism) as
compared to other functionally connected brain areas (hypometabolism > atrophy)
(Chételat et al., 2008). Regarding white matter loss in relation to glucose
metabolism, deterioration of the cingular bundle, a major fibre tract linking the
hippocampi with functionally related structures, was highly correlated with
hypometabolism of the thalami (Villain et al., 2008).

- 16 -
The observed dissociation of regional cerebral atrophy and perfusion in incipient
and early AD suggests that underlying pathogenetic mechanisms may also
diverge. We, therefore, analysed the association of both variables with the ApoE
ε4 allele. ApoE ε4 is the most consistently confirmed genetic risk factor of AD and
has been implicated in biochemical disease mechanisms (Saunders et al., 2000).
In the merged group of MCI and mild AD subjects we distinguished ApoE ε4
carriers with one or two alleles from non-carriers. We found significantly reduced
hippocampal, but not amygdala volume in carriers. Wang et al. (2006) also
described the association of the ApoE ε4 allele with smaller hippocampal volume
in MCI and mild AD. Van de Pol et al. (2007) found a higher hippocampal atrophy
rate in MCI subjects carrying a ApoE ε4 allele. Regarding amygdala atrophy, two
studies suggest that an association with the ApoE ε4 genotype in MCI and early
AD becomes apparent in ApoE ε4 homocygotes only (Lehtovirta et al., 1995;
Pennanen et al., 2006). Hashimoto et al. (2001) described a negative correlation
of the number of ApoE ε4 alleles with both hippocampal and amygdala volume in
probable AD. Possibly, a higher ApoE ε4 gene dose effect underlies the
association with amygdala atrophy, as is also suggested by the data of Pennanen
et al., 2006. Alteratively, amygdala volume association with the ApoE genotype
may be detectable in ApoE ε4 homocygotes only, because of limitations in
imaging technology and sample sizes.
The observed lack of ApoE genotype association with rCBF is in association with
findings by Sakamoto et al. (2003). They used SPECT longitudinally in
conjunction with MRI in very mild AD and found that declines of rCBF did not
differ in ApoE ε4 carriers vs. non-carriers, when partial volume effects were
corrected. An earlier report by Lehtovirta et al. (1998) on a positive association of

- 17 -
the ApoE ε4 allele with temporoparietal hypoperfusion in AD using SPECT
images uncorrected for partial volume effects is probably spurious due to the
above methodological concern.
Regarding the collective evidence, one can conclude that in MCI and early AD an
ApoE ε4 genetic effect is stronger on hippocampal than amygdala atrophy and
that functional rCBF changes are not driven by ApoE ε4. This divergent genetic
effect on regional brain atrophy and perfusion strengthens the argument that
these variables, although functionally interacting, are dissociated regarding their
causation and pattern of occurence in the complex AD process.
Prospective longitudinal studies assessing combined structural and functional
imaging data together with genotypes in incipient AD are thought to be promising
for further research on this topic.

- 18 -
Acknowledgement
This study was carried out in association with the German Competence Network for
Dementias (Kompetenznetz Demenzen), which is supported by the Federal Ministry
for Education and Research (Bundesministerium für Bildung und Forschung, grant
no. 01GI0420).

- 19 -
References
Basso, M., Yang, J., Warren, L., MacAvoy, M.G., Varma, P., Bronen, R.A., van Dyck,
C.H., 2006. Volumetry of amygdala and hippocampus and memory performance in
Alzheimer’s disease. Psychiatry Research: Neuroimaging 146, 251-261.
Chételat, G., Desgranges, B., Landeau, B., Mézenge, F., Poline, J.B., de la Sayette,
V., Viader, F., Eustache, F., Baron, J.-C., 2008. Direct voxel-based comparison
between grey matter hypometabolism and atrophy in Alzheimer’s disease. Brain
131, 60-71.
Colliot, O., Chételat, G., Chupin, M., Desgranges, B., Magnin, B., Benali, H., Dubois,
B., Garnero, L., Eustache, F., Lehéricy, S., 2008. Discrimination between
Alzheimer disease, mild cognitive impairment, and normal aging by using
automated segmentation of the hippocampus. Neuroradiology, Epub May 5, 2008.
Desgranges, B., Baron, J.C., de la Sayette, V., Petit-Taboué, M.C., Benali, K.,
Landeau, B., Lechevalier, B., Eustache, F. (1998). The neural substrates of
memory systems impairment in Alzheimer's disease. A PET study of resting brain
glucose utilization. Brain 121, 611-31.
Devanand, D.P., Pradhaban, G., Liu, X., Khandji, A., De Santi, S., Segal, S.,
Rusinek, H., Pelton, G.H., Honig, L.S., Mayeux, R., Stern, Y., Tabert, M.H., de
Leon, M.J., 2007. Hippocampal and entorhinal atrophy in mild cognitive
impairment. Prediction of Alzheimer disease. Neurology 68, 828-836.
Duarte, A., Hayaska, S., Du, A., Schuff, N., Jahng, G.-H., Kramer, J., Miller, B., Wei-
ner, M., 2006. Volumetric correlates of memory and executive function in normal

- 20 -
elderly, mild cognitive impairment and Alzheimer’s disease. Neuroscience Letters
406, 60-65.
Fakhri, G.E., Kijewski, M.F., Johnson, K.A., Syrkin, G., Killiany, R.J., Becker, J.A.,
Zimmermann, R.E., Albert, M.S., 2003. MRI-guided SPECT perfusion measures
and volumetric MRI in prodromal Alzheimer disease. Arch. Neurol. 60, 1066-1072.
Folstein, M.F., Folstein, S.E., McHugh, P.R., 1975. Mini-mental-state. Psychiatric
Research 12, 189-198.
Gould, R.L., Brown, R.G., Owen, A.M., Bullmore, E.T., Williams, S.C.R., Howard,
R.J., 2005. Functional neuroanatomy of successful paired associate learning in
Alzheimer’s disease. Am. J. Psychiatry 162, 2049-2060.
Härting C, Markowitsch HJ, Neufeld H et al. (Eds.), 2000. WMS-R Wechsler Ge-
dächtnistest – revidierte Fassung. Deutsche Adaption der Wechsler Memory Sca-
le. Verlag Hans Huber, Bern, Göttingen.
Hashimoto, M., Yasuda, M., Tanimukai, S., Matsui, M., Girono, N., Kazui, H., Mori,
E., 2001. Apolipoprotein E ipsilon 4 and the pattern of regional brain atrophy in
Alzheimer’s disease. Neurology 57, 1461-1466.
Hindmarch, I., Lehfeld, H. Jongh, P., Erzigkeit, H., 1998. The Bayer Activities of
Daily Living Scale (B-ADL). Dementia and Geriatric Cognitive Disorders, 9 (Suppl.
2), 20-26.
Hixson, J.E., Vernier, D.T., 1990. Restriction isotyping of human apolipoprotein E by
gene amplification and cleavage with HhaI. Journal of Lipid Research 31, 545-548.
Horínek, D., Varjassyova, A., Hort, J., 2007. Magnetic resonance analysis of
amygdalar volume in Alzheimer’s disease. Current Opinion in Psychiatry 20, 273-
277.

- 21 -
Ihl, R., Frölich, L., 1991. Die Reisberg-Skalen. Beltz Verlag, Weinheim.
Ihl, R., Grass-Kapanke, B., 2000. Manual – Test zur Früherkennung von Demenzen
mit Depressionsabgrenzung. Libri Books on Demand, Hamburg.
Ishiwata, A., Sakayori, O., Minoshima, S., Mizumura, S., Kitamura, S., Katayama, Y.,
2006. Preclinical evidence of Alzheimer changes in progressive mild cognitive
impairment: a qualitative and quantitative SPECT study. Acta Neurol. Scand. 114,
91-96
Johnson, K.A., Jones, K., Holman, B.L., Becker, J.A., Spiers, P.A., Satlin, A., Albert,
M.S., 1998. Preclinical prediction of Alzheimer’s disease using SPECT. Neurology
50, 1563-1571.
Johnson, N.A., Jahng, G.-H., Weiner, M.W., Miller, B.L., Chui, H.C., Jagust, W.J.,
Gorno-Tempini, M.L., Schuff, N., 2005. Pattern of cerebral hypoperfusion in
Alzheimer disease and mild cognitive impairment measured with arterial spin-
labeling MR imaging: Initial experience. Radiology 234, 851-859.
Jorm, A., 1994. A short form of the Informant Questionnaire on Cognitive Decline in
the Elderly (IQCODE): development and cross-validation. Psychological Medicine
24, 145-153.
Kertesz, A., Nadkarni, N., Davidson, W., Thomas, A.W., 2000. The Frontal
Behavioral Inventory in the differential diagnosis of frontotemporal dementia. J. Int.
Neuropsychol. Soc. 6, 460-468.
Lehtovirta, M., Kuikka, J., Helisalmi, S., Hartikainen, P., Mannermaa, A., Ryynänen,
M., Riekkinen, P. Sr., Soininen, H., 1998. Longitudinal SPECT study in
Alzheimer’s disease: relation to apolipoprotein E polymorphism. Journal of
Neurology, Neurosurgery and Psychiatry 64, 742-746.

- 22 -
Lehtovirta, M., Laako, M.P., Soininen, H., Helisalmi, S., Mannermaa, A., Helkala, E.-
L., Partanen, K., Ryynänen, M., Vainio, P., Hartikainen, P., Riekinen, P.J., 1995.
Volumes of hippocampus, amygdale and frontal lobe in Alzheimer patients with
different apolipoprotein E genotypes. Neuroscience 67, 65-72.
Luckhaus, C., Flüß, M.O., Wittsack, H.-J., Grass-Kapanke, B., Jänner, M., Khalili-
Amiri, R., Friedrich, W., Supprian, T., Gaebel, W., Mödder, U., Cohnen, M., 2008.
Detection of changed regional cerebral blood flow in mild cognitive impairment and
early Alzheimer’s dementia by perfusion-weighted magnetic resonance imaging.
Neuroimage 40, 495-503.
McKhann, G., Drachman, D., Folstein, M., Katzman, R., Price, D., Stadlan, E.M.,
1984. Clinical diagnosis of Alzheimer’s disease: report of the NINCDS-ADRDA
work group under the auspices of Department of Health and Human Services Task
Force on Alzheimer’s disease. Neurology 34, 939-944.
Morris, J.C. , 1997. The Clinical Dementia Rating (CDR): Current version and scoring
rules. Neurology, 43, 2412-2414.
Moscovitch, M., Rosenbaum, R.S., Gilboa, A., Addis, D.R., Westmacott, R., Grady,
C., McAndrews, M.P., Levine, B., Black, S., Winocur, G., Nadel, L., 2005.
Functional neuroanatomy of remote episodic, semantic and spatial memory: a
unified account based on multiple trace theory. Journal of Anatomy 207, 35-66.
Pennanen, C., Testa, C., Boccardi, M., Laasko, M.P., Hallikainen, M., Helkala, E.-L.,
Hänninen, T., Kivipelto, M., Könönen, M., Nissinen, A., Tervo, S., Vanhanen, M.,
Vanninen, R., Frisoni, G.B., Soininen, H., 2006. The effect of apolipoprotein
polymorphism on brain in mild cognitive impairment: a voxel-based morphometric
study. Dementia and Geriatric Cognitive Disorders 22, 60-66.

- 23 -
Petersen, R.C., Doody, R., Kurz, A., Mohs, R.C., Morris, J.C., Rabins, P.V., Ritchie,
K., Rossor, M., Thal, L., Winblad, B, 2001. Current concepts in mild cognitive
impairment. Archives of Neurology 58, 1985-92.
Petersen, R.C., Smith, G.E., Waring, S.C., Ivnik, R.J., Tangalos, E.G., Kokmen, E.,
1999. Mild cognitive impairment. Clinical characterization and outcome. Archives
of Neurology 56, 303-308.
Reitan, R. M., 1979. Trail Making Test (TMT). Hogrefe Verlag, Bern, Göttingen.
Sakamoto, S., Matsuda, H., Asada, T., Ohnishi, T., Nakano, S., Kanetaka, H., Taka-
saki, M., 2003. Apolipoprotein E genotype and early Alzheimer’s disease: A
longitudinal SPECT study. Journal of Neuroimaging 13, 113-123.
Saunders, A.M., Trowers, M.K., Shimkets, R.A., Blakemore, S., Crowther, D.J.,
Mansfield, T.A., Wallace, D.M., Strittmatter, W.J., Roses, A.D., 2000. The role of
apolipoprotein E in Alzheimer's disease: pharmacogenomic target selection.
Biochimica Biophysica Acta 1502, 85-94.
Shulman, K.I., 2000. Clock-drawing: is it the ideal cognitive screening test? Int. J.
Geriatr. Psychiatry 15, 548-561.
Teipel, S.J., Born, C., Ewers, M., Bokde, A.L.W., Reiser, M.F., Möller, H.-J., Hampel,
H., 2007. Multivariate deformation-based analysis of brain atrophy to predict
Alzheimer’s disease in mild cognitive impairment. Neuroimage 38, 13-24.
Thalmann, B., Monsch, A.U., Bernasconi, F., Berres, M., Schneitter, M., Ermini-
Fuenfschilling, D., Spiegel, R., Staehelin, H.B., 1998. Die CERAD Neuropsycholo-
gische Testbatterie - Ein gemeinsames minimales Instrumentarium zur Demenz-
abklärung. Memory Clinic, Geriatrische Universitätsklinik Basel.

- 24 -
van de Pol, L.A., Korf, E.S., van der Flier, W.M., Brashear, H.R., Fox, N.C., Barkhof,
F., Scheltens, P., 2007. Magnetic resonance imaging predictors of cognition in
mild cognitive impairment. Archives of Neurology 64,1023-1028.
Villain, N., Desgranges, B., Viader, F., de la Sayette, V., Mézenge, F., Landeau, B.,
Baron, J.-C., Eustache, F., Chételat, G., 2008. Relationships between
hippocampal atrophy, white matter disruption, and gray matter hypometabolism in
Alzheimer’s disease. The Journal of Neuroscience 28, 6174-6181.
Wang, L., Zang, Y., He, Y., Liang, M., Zhang, X., Tian, L., Wu, T., Jiang, T., Li, K.,
2006. Changes in hippocampal connectivity in the early stages of Alzheimer’s
disease: Evidence from resting state fMRI. Neuroimage 31, 496-504.

- 25 -
Figure Legends
Table 1: Psychometric and demographic data of study groups (MCI, mild cognitive
impairment; AD, Alzheimer’s dementia).
Table 2: Regional cerebral blood flow (rCBF) in millilitres per 100 g brain matter per
minute in various brain regions of subjects with mild cognitive impairment (MCI) vs.
Alzheimer’s dementia (AD). (L, left hemisphere; R, right hemisphere; FROB,
frontobasal; MTMP, mesotemporal; TPAR, temporoparietal; AMYG, amygdale;
ACING, anterior cingulum; PCING, posterior cingulum; THAL, thalamus; CEREBELL,
cerebellum)
Table 3: Regional brain volumes in ??Herr Teipel, bitte Maßeinheit ergänzen?? of
hippocampi (HIPPOCAMP) and amygdalae (AMYG) of subjects with mild cognitive
impairment (MCI) vs. Alzheimer’s dementia (AD). (L, left hemisphere; R, right
hemisphere)
Table 4: Pearson’s correlation analysis of regional cerebral blood flow (rCBF) of
various brain regions and hippocampal (HIPPOCAMP) and amygdalar (AMYG)
volumes in subjects with mild cognitive impairment (MCI). Yellow markings denote
significant correlations. (L, left hemisphere; R, right hemisphere; FROB, frontobasal;
MTMP, mesotemporal; TPAR, temporoparietal; AMYG, amygdale; ACING, anterior
cingulum; PCING, posterior cingulum; THAL, thalamus; CEREBELL, cerebellum)

- 26 -
Table 5: Pearson’s correlation analysis of regional cerebral blood flow (rCBF) of
various brain regions and hippocampal (HIPPOCAMP) and amygdalar (AMYG)
volumes in subjects with Alzheimer’s dementia (AD). Yellow markings denote
significant correlations. (L, left hemisphere; R, right hemisphere; FROB, frontobasal;
MTMP, mesotemporal; TPAR, temporoparietal; AMYG, amygdale; ACING, anterior
cingulum; PCING, posterior cingulum; THAL, thalamus; CEREBELL, cerebellum)
Table 6: Regional brain volumes of MCI and AD subjects in relation to the absence
or presence of apoE ε4 alleles. (L, left hemisphere; R, right hemisphere;
HIPPOCAMP, hippocampus; AMYG, amygdale).
Figure 1: Schematic picture of correlative changes of regional brain volumes and
perfusion in mild cognitive impairment (MCI). (L, left hemisphere; R, right
hemisphere; FROB, frontobasal; HIPPOCAMP, hippocampus; AMYG, amygdale;
THAL, thalamus)
Figure 2: Schematic picture of correlative changes of regional brain volumes and
perfusion in mild Alzheimer’s dementia (AD). (L, left hemisphere; R, right
hemisphere; FROB, frontobasal; HIPPOCAMP, hippocampus; MTMP, mesotemporal;
AMYG, amygdale; THAL, thalamus)
Kommentar [T6]: Unklar, insbesodnere werden auch Farben nicht erklärt, eher weg-lassen.

- 27 -
L-FROB
R-FROB Perfusion ↑
L-
CAMP
R-IPPO
CAMP HIPPO- H -
Volumen ↓
L-AMYG
R-AMYG
L-THAL
R-THAL
Perfusion ↑

- 28 -
Volumen ↓
Perfusion ↓
Perfusion ↓
Volumen ↓
THAL
right
THAL
left
AMYG
right
AMYG
left
L-MTMP
R-HIP-
POCA
L-HIP-
POCA
L-MTMP
R-FROB
L-FROB

- 29 -
group N mean s.d. p (t-test)
MMSE MCI 30 27.5 1.8
AD 15 23.3 2.0 0.0001
GDS MCI 30 2.2 0.4
AD 15 3.5 0.5 0.0001
age MCI 30 63.9 9.5
AD 15 68.7 7.6 0.091
% male p (χ²-test)
gender MCI 30 56.7
AD 15 26.7 0.057
- 30 -
regional cerebral blood flow (rCBF)
brain region diagnostic
group N
mean s.d.
p (t-test)
MCI 30 36.48 6.69 L-FROB
AD 15 38.54 5.35 n.s.
MCI 30 37.14 7.10 R-FROB
AD 15 37.63 5.65 n.s.
MCI 30 38.19 12.12 L-MTMP
AD 15 36.69 9.70 n.s.
MCI 30 36.63 9.53 R-MTMP
AD 15 36.75 8.28 n.s.
MCI 30 43.52 5.61 L-TPAR
AD 15 43.65 5.73 n.s.
MCI 30 43.73 6.38 R-TPAR
AD 15 43.88 7.14 n.s.
MCI 30 37.77 11.69 L-AMYG
AD 15 31.81 9.37 n.s.
MCI 30 36.14 11.56 R-AMYG
AD 15 32.56 9.53 n.s.
MCI 30 45.46 8.39 ACING
AD 15 47.79 8.04 n.s.
MCI 30 47.04 6.03 PCING
AD 15 42.03 4.73 0.004
MCI 19 46.84 7.82 L-THAL
AD 11 49.57 9.43 n.s.
MCI 19 46.31 7.48 R-THAL
AD 11 47.79 6.80 n.s.
MCI 19 39.71 5.35 CEREBELL
AD 11 38.40 6.87 n.s.

- 31 -
brain volume brain region
diagnosticgroup
N mean s.d.
p (t-test)
MCI 30 1975.5 378.0 L-HIPPOCAMP
AD 15 1759.8 438.2
0.094
MCI 30 1999.5 385.7 R-HIPPOCAMP
AD 15 1716.5 526.3
0.046
MCI 30 556.3 127.1 L-AMYG
AD 15 473.0 107.2
0.035
MCI 30 579.8 163.2 R-AMYG
AD 15 458.9 91.6
0.011

- 32 -
regional cerebral blood flow (rCBF)
regional brain volume
L-HIPPOCAMP R-HIPPOCAMP L-AMYG R-AMYG Pearson correlation -0.407 -0.292 -0.223 -0.359 significance (2-sided) 0.026 0.118 0.236 0.051
L-FROB N 30 30 30 30
Pearson correlation -0.484 -0.334 -0.179 -0.308 significance (2-sided) 0.007 0.072 0.345 0.098
R-FROB N 30 30 30 30
Pearson correlation -0.123 0.058 0.025 -0.258 significance (2-sided) 0.517 0.762 0.896 0.169
L-MTMP N 30 30 30 30
Pearson correlation -0.052 0.031 0.090 -0.316 significance (2-sided) 0.787 0.872 0.635 0.089
R-MTMP N 30 30 30 30
Pearson correlation -0.177 -0.118 -0.239 -0.109 significance (2-sided) 0.349 0.535 0.202 0.566
L-TPAR N 30 30 30 30
Pearson correlation -0.163 -0.236 -0.095 -0.200 significance (2-sided) 0.390 0.208 0.618 0.288
R-TPAR N 30 30 30 30
Pearson correlation -0.155 0.008 0.103 0.034 significance (2-sided) 0.415 0.967 0.588 0.858
L-AMYG N 30 30 30 30
Pearson correlation -0.004 0.063 0.089 0.096 significance (2-sided) 0.981 0.742 0.640 0.613
R-AMYG N 30 30 30 30
Pearson correlation -0.068 -0.022 -0.268 -0.347 significance (2-sided) 0.721 0.909 0.152 0.060
ACING N 30 30 30 30
Pearson correlation -0.146 0.062 0.050 -0.024 significance (2-sided) 0.442 0.744 0.794 0.901
PCING N 30 30 30 30
Pearson correlation -0.460 -0.219 -0.152 0.161 significance (2-sided) 0.047 0.368 0.533 0.510
L-THAL N 19 19 19 19
Pearson correlation -0.329 -0.201 -0.116 0.095 significance (2-sided) 0.169 0.409 0.636 0.700
R-THAL N 19 19 19 19
Pearson correlation 0.284 0.426 0.213 0.255 significance (2-sided) 0.239 0.069 0.381 0.292
CEREBELL N 19 19 19 19

- 33 -
regional cerebral blood flow (rCBF)
regional brain volume
L-HIPPOCAMP R-HIPPOCAMP L-AMYG R-AMYG L-FROB Pearson correlation -0.190 0.022 -0.144 -0.114
significance (2-sided) 0.498 0.938 0.610 0.686 N 15 15 15 15
R-FROB Pearson correlation -0.389 -0.229 -0.261 0.081 significance (2-sided) 0.151 0.412 0.348 0.775 N 15 15 15 15
L-MTMP Pearson correlation -0.072 0.116 0.373 0.571 significance (2-sided) 0.799 0.681 0.171 0.026 N 15 15 15 15
R-MTMP Pearson correlation -0.216 0.038 0.140 0.609 significance (2-sided) 0.440 0.893 0.620 0.016 N 15 15 15 15
L-TPAR Pearson correlation 0.126 0.342 0.186 0.460 significance (2-sided) 0.654 0.212 0.507 0.085 N 15 15 15 15
R-TPAR Pearson correlation 0.018 0.202 0.081 0.496 significance (2-sided) 0.950 0.471 0.774 0.060 N 15 15 15 15
L-AMYG Pearson correlation -0.141 -0.201 0.166 0.081 significance (2-sided) 0.617 0.472 0.555 0.774 N 15 15 15 15
R-AMYG Pearson correlation 0.001 -0.162 -0.015 -0.199 significance (2-sided) 0.998 0.563 0.959 0.477 N 15 15 15 15
ACING Pearson correlation 0.149 0.311 0.177 0.098 significance (2-sided) 0.597 0.259 0.528 0.729 N 15 15 15 15
PCING Pearson correlation -0.295 -0.001 0.048 0.465 significance (2-sided) 0.285 0.997 0.865 0.081 N 15 15 15 15
L-THAL Pearson correlation 0.258 0.694 0.057 -0.126 significance (2-sided) 0.444 0.018 0.869 0.711 N 11 11 11 11
R-THAL Pearson correlation 0.251 0.654 0.111 -0.109 significance (2-sided) 0.456 0.029 0.746 0.749 N 11 11 11 11
CEREBELL Pearson correlation -0.168 0.092 0.306 0.551 significance (2-sided) 0.621 0.788 0.361 0.079 N 11 11 11 11

- 34 -
brain volume
??Einheit, Herr Teipel???
brain region
apoE ε4 alleles
N
mean
s.d.
p (t-test)
none 18 2083,7 407,5 L-HIPPOCAMP
1 or 2 18 1809,6 427,9
0,057
none 18 2149,3 362,5 R-HIPPOCAMP
1 or 2 18 1788,7 507,7
0,019
none 18 544,9 138,8 L-AMYG
1 or 2 18 501,7 116,1
0,319
none 18 568,9 184,3 R-AMYG
1 or 2 18 508,6 133,1
0,268
Copyright © 2022 FDOKUMEN








![[Posterior cortical atrophy]](https://static.fdokumen.com/doc/165x107/6331b9d14e01430403005392/posterior-cortical-atrophy.jpg)











