Working memory, attention, and executive function in Alzheimer’s disease and frontotemporal dementia
Upload
johnshopkinsCategory
view
0download
0
Selectivity of Executive Function Deficits in Mild Cognitive Impairment
Jason Brandt, Eleni Aretouli, Eleanor Neijstrom,Jaclyn Samek, Kevin Manning,
and Marilyn S. AlbertThe Johns Hopkins University School of Medicine
Karen Bandeen-RocheThe Johns Hopkins Bloomberg School of Public Health
Impairment in executive cognition (EC) is now recognized as relatively common among older personswith mild cognitive impairment (MCI) and may be predictive of the development of dementia. However,both MCI and executive functioning are broad and heterogeneous constructs. The present study soughtto determine whether impairments in specific domains of EC are associated with specific subtypes ofMCI. MCI patients (n � 124) were divided into 4 subgroups (amnestic vs. nonamnestic, and single- vs.multiple-domain) on the basis of their performance of widely used neuropsychological screening tests.These patients and 68 normal older persons were administered 18 clinical and experimental tests ofexecutive function. Principal components analysis suggested 2 highly reliable EC components, planning/problem solving and working memory, and a less reliable 3rd component, judgment. Planning/problemsolving and working memory, but not judgment, were impaired among the MCI patients. This was trueeven among those with “pure amnestic” MCI, the least impaired group overall. Multiple-domain MCIpatients had more severe impairments in planning/problem solving and working memory than single-domain patients, leading to the supposition that they, not pure amnestic MCIs, are at highest risk ofimminent dementia.
Keywords: executive function, mild cognitive impairment, dementia, principal components analysis
Supplemental materials: http://dx.doi.org/10.1037/a0015851.supp
The status of mild cognitive impairment (MCI) as an importantclinical entity remains debated. Expert opinion ranges from itbeing early Alzheimer’s disease (AD) in virtually all cases (Morriset al., 2001) to it being a diagnostic nonentity (Gauthier & Tou-chon, 2005; Milwain, 2000; Whitehouse, 2007). Most opinions fallsomewhere between these two extremes, and view MCI as aheterogeneous cognitive state that sometimes heralds the onset ofprogressive dementia (Chertkow et al., 2007). Much recent re-search has focused on determining the characteristics of patientswith MCI that predict the progression to AD or another dementia.
It is now widely recognized that several subtypes of MCI can beidentified, and the prognoses for them may differ (Lopez, Jagust,DeKoskey, et al., 2003; Winblad et al., 2004). The most studiedvariety is pure amnestic MCI, an isolated and otherwise unex-
plained memory impairment in an older person (Ganguli, Dodge,Shen, & DeKoskey, 2004; Petersen, 2004b). Although estimatesvary, patients with this condition appear to “convert to” (i.e.,develop) AD at a rate of 6%�15% per year (Daly et al., 2000; J. D.Fisk, Merry, & Rockwood, 2003; Grundman, Petersen, & Morris,1996). Patients with isolated impairments in other cognitive do-mains (e.g., language, spatial cognition) have also been identified,as have patients with mild impairments in multiple cognitivedomains who remain functionally intact and do not meet criteriafor dementia. The prognoses for the various subtypes of MCIremain unknown (Chertkow et al., 2007).
The present study investigated the status of executive function-ing in four subtypes of MCI. We conceptualize executive functionsas Miyake et al. (2000) does: “general purpose control mechanismsthat modulate the operation of various cognitive subprocesses andthereby regulate the dynamics of human cognition” (p. 50). Al-though the identification and operation of these control processeshave been the subject of much experimentation and discussion, ageneral model of executive cognition (EC) has yet to be validatedor universally accepted (Burgess, 1997; Miyake et al., 2000). Thepresent study is seen as a step toward that goal in that it attemptedto identify, empirically, the latent structure underlying a largenumber of executive function tests.
There are many reasons to believe that decline in some aspectsof EC is a strong risk factor for the imminent development ofdementia. First, Baddeley and colleagues demonstrated 20 yearsago that selective impairment of the central executive componentof working memory is a prominent feature of Alzheimer’s-typedementia (Baddeley, Bressi, Della Sala, Logie, & Spinnler 1991;Baddeley, Logie, Bressi, Della Sala, & Spinnler, 1986). Second,onset of executive dysfunction typically follows onset of episodic
Jason Brandt and Marilyn S. Albert, Department of Psychiatry andBehavioral Sciences, and Department of Neurology, The Johns HopkinsUniversity School of Medicine; Eleni Aretouli, Eleanor Neijstrom,Jaclyn Samek, and Kevin Manning, Department of Psychiatry andBehavioral Sciences, The Johns Hopkins University School of Medicine;Karen Bandeen-Roche, Department of Biostatistics, The Johns HopkinsBloomberg School of Public Health.
We thank Laura Wulff, Chiadi Onyike, and the staff and participants ofthe Johns Hopkins Alzheimer’s Disease Research Center. Arnold Bakkerand Egberdina J. van der Hulst assisted in data collection. This study wassupported by Grant AG-005146 from the National Institute on Aging.
Correspondence concerning this article should be addressed to JasonBrandt, Department of Psychiatry and Behavioral Sciences, The JohnsHopkins Hospital, 600 North Wolfe Street, Meyer 218, Baltimore, MD21287-7218. E-mail: [email protected]
Neuropsychology © 2009 American Psychological Association2009, Vol. 23, No. 5, 607–618 0894-4105/09/$12.00 DOI: 10.1037/a0015851
607

memory impairment in AD and precedes impairment of languageor spatial cognition (Binetti et al., 1996; Bondi et al., 2002;Lafleche & Albert, 1995). Third, many of the cognitive tests thatare most helpful for predicting which nondemented older personswill subsequently develop dementia have substantial executivecontrol requirements (Albert, Blacker, Moss, Tanzi, & McArdle,2007; Albert, Moss, Tanzi, & Jones, 2001; Bondi et al., 1994; Eliaset al., 2000; Jacobs et al., 1995; Rapp & Reischies, 2005). Finally,even among patients with pure amnestic MCI, impairments inexecutive function can be found (Crowell, Luis, Vanderploeg,Schinka, & Mullan, 2002; Griffith et al., 2003; Kramer et al., 2006;Royall et al., 2004). These observations have led to the hypothesisthat only when executive functioning becomes impaired should anMCI patient be considered to have prodromal AD (Albert et al.,2001; Royall, Palmer, Chiodo, & Polk, 2002).
Not only is the development of executive impairment poten-tially predictive of the development of dementia, it also appearsto be uniquely associated with functional impairment in elders.One study reported that just two executive function tasks (Wis-consin Card Sorting Test [WCST] and Trail Making Test—Part B[TMT-B]) accounted for more than 50% of the variance in func-tional abilities of normal elders (Bell-McGinty, Podell, Franzen,Baird, & Williams, 2002). Among community-dwelling elders,executive function tests have predictive value above and beyonddemographic and health variables, overall cognitive integrity (e.g.,Mini-Mental State Exam [MMSE] score), and other specific cog-nitive functions (language, spatial skills, and memory) for bothself-reported and empirically measured everyday functioning(Cahn-Weiner, Malloy, Boyle, Marran, & Salloway, 2000;Grigsby, Kaye, Baxter, Shetterly, & Hamman, 1998; Lewis &Miller, 2007; Royall, Cabello, & Polk, 1998; Royall, Chiodo, &Polk, 2004). Thus, subtle changes in EC can have a major impacton the lives of older persons.
Questions remain as to (a) whether impairments in specificexecutive domains are associated with specific subtypes of MCI,and (b) whether these impairments have particular prognosticvalue. The present study addressed the first of these questions bystudying normal elders, patients with amnestic MCI (both single-and multiple-domain), and patients with nonamnestic MCI (bothsingle- and multiple-domain) with an extensive set of clinical testsand experimental tasks of executive control. We selected 18 testsrepresenting six conceptually distinct domains of EC: (a) sponta-neous flexibility and generativity, (b) inhibition of prepotent re-sponses, (c) planning and sequencing, (d) concept/rule learningand set shifting, (e) decision making and judgment, and (f) work-ing memory and resource sharing. The cognitive test data werereduced using principal components analysis, and the profile ofeach of the four MCI subgroups on the derived components wascompared to each other and to normal elders.
Method
Participants
Persons with MCI (n � 124) and cognitively normal olderadults (n � 68) participated in this study. Most participants (81%)were recruited from the Johns Hopkins Alzheimer’s Disease Re-search Center and other research studies. They responded to direct-mail and posted announcements, newspaper ads, and solicitations
of research volunteers at community lectures. A small number ofsubjects (19%) were referred from university clinics and physi-cians in the community from whom they sought evaluation ofmemory or other cognitive complaints. A health conditions check-list was used to gather information about major physical andpsychological disorders. Volunteers were excluded from studyparticipation if they had any history of psychosis, central nervoussystem disorder, or active systemic illness (e.g., cancer). Personswith histories of depression were not excluded given that depres-sion is both very common in MCI and may be an importantpredictor of incident dementia (Jorm, 2001; Lyketsos et al., 2002;Mondrego & Ferrandez, 2004; Visser, 2000) or a very earlymanifestation (Chen, Ganguli, Mulsant, & DeKosky, 1999).
Every participant was required to have a family member or closefriend available to be interviewed for a clinical dementia rating(CDR; Hughes, Berg, Danziger, Coben, & Martin, 1982). Onlythose with overall CDR scores of 0 or 0.5 were eligible. Inaddition, every participant was required to score in the normalrange (i.e., at or above the 20th percentile for age and education)on the MMSE (Bravo & Hebert, 1997).
Each participant was administered the following screening teststo determine group assignment: Logical Memory subtest (Story A)of Wechsler Memory Scale—Revised (WMS–R; Wechsler, 1987),a 30-item version of the Boston Naming Test (Brandt et al., 1989;Goodglass & Kaplan, 1983), word list generation (for the lettersFAS and the semantic categories animals and vegetables; Rascov-sky, Salmon, Hansen, Thal, & Galasko, 2007; Salmon, Heindel, &Lange, 1999), and clock drawing to request (Rouleau, Salmon,Butters, Kennedy, & Mcquire, 1992). These specific tests werechosen for their brevity and their widespread use in the neuropsy-chological evaluation of geriatric cognitive disorders (Attix &Welsh-Bohmer, 2006). Tests of EC were not included in thisscreening/subtyping battery because they constitute the outcomevariables of interest. In addition, the Activities of Daily Living—Prevention Instrument (ADL–PI) developed by the Alzheimer’sDisease Cooperative Study (Galasko et al., 2006) was completedby each participant’s “study partner” to supplement the CDR’sassessment of functional capacity in everyday life.
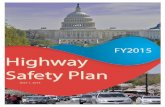
MCI groups. Participants were diagnosed with MCI accordingto the Petersen (2004) criteria. Specifically, each participant or hisor her study partner reported excessive decline in one or morecognitive domain and obtained an overall CDR score of 0.5,indicating questionable dementia. In addition, participants wererequired to perform at or below 1.5 standard deviations below themean for age and education (i.e., 6.7th percentile), according topublished norms, on one or more of the screening tests. Applyingthe criteria described in Figure 1 allowed the MCI sample to bedivided into four groups: amnestic single domain (AS; n � 36),amnestic multiple domain (AM; n � 45), nonamnestic singledomain (NAS; n � 26), and nonamnestic multiple domain (NAM;n � 17).
Normal control group. All participants in the normal control(NC) group were free of significant cognitive complaints. Theabsence of cognitive decline was confirmed by interview with thestudy partner; all normal control subjects obtained an overall CDRscore of 0. In addition, they all scored at or above 1.5 standarddeviations below the mean for age and education on all fourscreening tests.
608 BRANDT ET AL.
Procedure
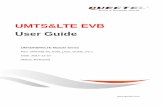
Three clinical tests or experimental tasks were selected to eval-uate each of the six EC domains proposed. Although our selectionof tasks was based on previous literature, the very large number ofexecutive tests and tasks available (Burgess, Alderman, Evans,Emslie, & Wilson, 1998; Lezak, Howieson, & Loring, 2004;Miyake et al., 2000) makes the ones selected somewhat arbitrary.It is also appreciated that our description of tasks as representativeof particular domains is rationally based, rather than empiricallybased. However, this categorization was only preliminary, servingto guide test selection. An empirical categorization of tasks wasachieved in the present study, using principal components analysis.
The tasks chosen to represent each domain are shown in Table 1.More detailed descriptions of the tasks, and the metrics derivedfrom them, may be found in the online Appendix.
The Johns Hopkins University Institutional Review Board fullyreviewed and approved the study protocol. All participants andtheir study partners gave written informed consent to participate.
Statistical Analysis
The baseline demographic and clinical characteristics of the fivegroups (four MCI and one normal control) were compared withone-way analyses of variance (ANOVAs), with planned compar-isons between (a) NC versus all MCI, (b) NC versus AS, (c) AS �AM versus NAS � NAM, and (d) AS � NAS versus AM �NAM. Given the large number of comparisons, alpha for both theomnibus ANOVAs and the planned comparisons was set to .01;this was viewed as a compromise between risking Type I and TypeII statistical errors. One-way ANOVAs were also performed oneach of the 18 executive function measures.
To derive composite scores summarizing executive test perfor-mance, we performed an exploratory principal components anal-ysis of the 18 EC variables. The number of components retainedwas determined by examination of the scree function and by factoranalysis fitted by the maximum likelihood method and using theAkaike information criterion (AIC; Akaike, 1974). Because the
distributions of many of the EC variables were highly skewed, wefirst transformed the 18 variables to probit scores using the per-centile method in which the ith sorted value is assigned thepercentile z score of (i/(n � 1)) � 100, for each i � 1, . . . , n(Rosner & Glynn, 2007). These analyses were restricted to datafrom the MCI participants only because large differences betweenthe MCI and normal groups were found in descriptive analyses.The normal control group performed near test ceiling on severalmeasures, producing clearly bimodal distributions for many of thetests. We restricted the principal components analysis to MCIparticipants because our primary aim was to discover covarianceamong tests in MCI rather than to identify scores that distinguishMCIs from controls. The derived components were subjected toorthogonal rotation using the varimax method and were standard-ized to have variance of 1 to maximize their interpretability. Inlight of our sample size and composition, we relied primarily onprincipal components analysis rather than factor analysis to min-imize reliance on model assumptions.
Component scores were computed for each participant using theprincipal components coefficients derived from analysis of the MCIparticipants. Cronbach’s alpha was used to estimate the reliabilitiesof the derived component scores. The mean component scores ofthe five groups were compared using analysis of covariance, withthe same four planned comparisons described earlier. Given thetotal of five tests per component score (the omnibus comparisonplus four planned comparisons), alpha was set to .01 (.05 dividedby 5 � .01). In light of the descriptive nature of our study, this wasseen as a reasonable compromise between risking Type I and TypeII statistical errors.
Results
Table 2 shows demographic and clinical characteristics for thefive groups of participants. The groups were well matched foreducation, but they differed in age, with the NCs being slightlyyounger than the MCI groups, contrast � 3.55, t(187) � 3.11, p �.002. For reasons that are not clear, the sex distribution of thegroups differed, �2(4) � 17.43, p � .002; men predominated
Amnestic
Nonamnestic
Single
Domain
Only
WMS-R Logical Memory
(delayed recall of Story A)
Boston Naming Test
or
Word List Generation (sum of letter and category trials)
or
Clock Drawing Test
Multiple Domains
WMS-R Logical Memory
(delayed recall of Story A)
and
any one or more tests
At least two of:
Boston Naming Test
Word List Generation
(sum of letter and category trials)
Clock Drawing Test
Figure 1. Operational criteria for four groups of participants with mild cognitive impairment. Subjects in eachgroup performed at or below 1.5 SD below age and education norms on the test(s) indicated.
609SELECTIVITY OF EXECUTIVE FUNCTION DEFICITS
Tab
le1
Mea
n(a
ndSt
anda
rdD
evia
tion
)P
erfo
rman
ceof
Fiv
eSu
bjec
tG
roup
son
18E
xecu
tive
Fun
ctio
nT
ests
Prop
osed
dom
ain
Tes
tN
orm
alco
ntro
l(C
DR
�0.
0)
Am
nest
icM
CI
(CD
R�
0.5)
Non
amne
stic
MC
I(C
DR
�0.
5)
�2
pSi
ngle
dom
ain
Mul
tiple
dom
ain
Sing
ledo
mai
nM
ultip
ledo
mai
n
Spon
tane
ous
flexi
bilit
yan
dge
nera
tivity
Alte
rnat
eU
ses
Tes
t(r
awsc
ore)
15.1
2(5
.65)
11.8
6(5
.34)
7.49
(5.8
3)11
.27
(4.9
0)7.
82(5
.60)
.244
�.0
01R
ando
mnu
mbe
rge
nera
tion
(wri
tten
tria
lR
NG
�or
altr
ial
RN
G)
0.60
(0.0
9)0.
65(0
.24)
0.68
(0.2
1)0.
73(0
.31)
0.71
(0.2
5).0
52.0
41
Tin
ker
Toy
Tes
t(r
awsc
ore)
9.19
(1.8
0)8.
69(1
.98)
7.31
(2.4
7)8.
65(1
.79)
7.25
(1.8
8).1
39�
.001
Inhi
bitio
nof
prep
oten
tre
spon
ses
D-K
EFS
and
Stro
opte
st(i
nhib
ition
tria
lsc
aled
scor
e)10
.70
(2.2
3)10
.26
(2.8
8)9.
73(3
.94)
9.38
(3.4
4)10
.18
(3.0
1).0
24.3
49
Hay
ling
Tes
t(t
otal
scal
edsc
ore)
5.22
(1.4
5)4.
67(1
.55)
3.89
(1.6
4)4.
50(1
.68)
3.71
(1.6
9).1
20�
.001
Com
plet
ions
&C
orre
ctio
nsT
est
(tot
alco
rrec
t)11
.06
(1.2
6)9.
75(1
.95)
9.18
(2.3
4)9.
65(1
.81)
9.18
(2.0
4).1
64�
.001
Plan
ning
and
sequ
enci
ngPo
rteu
sM
aze
Tes
t(t
est
age)
15.6
0(1
.74)
15.0
7(1
.62)
12.9
2(3
.50)
13.8
3(2
.32)
11.0
0(3
.86)
.254
�.0
01D
-KE
FST
ower
Tes
t(t
otal
achi
evem
ent
scal
edsc
ore)
11.8
1(2
.59)
10.1
7(2
.43)
9.00
(3.0
4)9.
77(2
.37)
8.53
(3.2
6).1
75�
.001
Tic
-tac
-toe
(tot
alsc
ore)
�4.
57(2
.44)
�4.
69(1
.85)
�4.
76(2
.59)
�5.
08(1
.65)
�5.
47(1
.70)
.014
.603
Con
cept
/rul
ele
arni
ngan
dse
tsh
iftin
gD
-KE
FSSo
rtin
gT
est
(con
firm
edso
rts
scal
edsc
ore)
13.1
6(1
.85)
11.9
4(2
.51)
10.6
7(2
.73)
10.7
7(2
.41)
10.1
2(2
.64)
.201
�.0
01
Bri
xton
Tes
t(s
cale
dsc
ore)
5.26
(2.1
2)4.
64(2
.22)
3.80
(2.0
6)4.
73(2
.01)
2.76
(1.7
9).1
24�
.001
Ver
bal
Con
cept
Atta
inm
ent
Tes
t(r
awsc
ore)
19.5
0(2
.47)
17.3
3(3
.14)
14.7
8(4
.03)
16.9
6(3
.28)
15.4
1(3
.20)
.263
�.0
01
Dec
isio
nm
akin
gan
dju
dgm
ent
Stan
ford
–Bin
etA
bsur
ditie
sT
est
(raw
scor
e)29
.47
(2.8
9)29
.31
(2.0
5)25
.93
(4.4
1)27
.08
(2.9
4)23
.88
(3.8
7).2
58�
.001
Iow
aG
ambl
ing
Tes
t(a
dvan
tage
ous
sele
ctio
nson
Blo
ck5
min
usB
lock
1)
3.95
(6.4
5)4.
36(6
.85)
2.60
(5.5
2)1.
77(6
.53)
2.47
(6.3
8).0
22.4
03
Exp
erim
enta
lJu
dgm
ent
Tes
t(m
ean
perc
enta
gede
viat
ion)
7.75
(4.7
9)10
.25
(6.7
5)10
.61
(5.5
8)6.
68(3
.04)
7.50
(4.4
3).0
81.0
04
Wor
king
mem
ory
and
reso
urce
shar
ing
Tra
ilM
akin
gT
est
(tim
eon
Part
Bm
inus
time
onPa
rtA
)39
.15
(20.
57)
67.3
6(1
4.31
)78
.64
(63.
71)
74.7
2(4
3.21
)94
.53
(50.
02)
.173
�.0
01
Bri
efT
est
ofA
ttent
ion
(tot
alco
rrec
t)15
.31
(3.2
8)14
.31
(3.2
9)12
.53
(4.2
3)14
.12
(3.5
8)10
.71
(3.4
6).1
43�
.001
Tes
tof
Eve
ryda
yA
ttent
ion
Tel
epho
neSe
arch
Whi
leC
ount
ing
(dua
lta
skde
crem
ent
scor
e)
1.35
(1.8
1)1.
48(1
.83)
4.16
(5.3
6)1.
58(2
.34)
4.44
2(5
.48)
.130
�.0
01
Not
e.M
CI
�m
ildco
gniti
veim
pair
men
t;C
DR
�cl
inic
alde
men
tiara
ting;
RN
G�
rand
omnu
mbe
rge
nera
tion;
D-K
EFS
�D
elis
–Kap
lan
Exe
cutiv
eFu
nctio
nSy
stem
.
610 BRANDT ET AL.
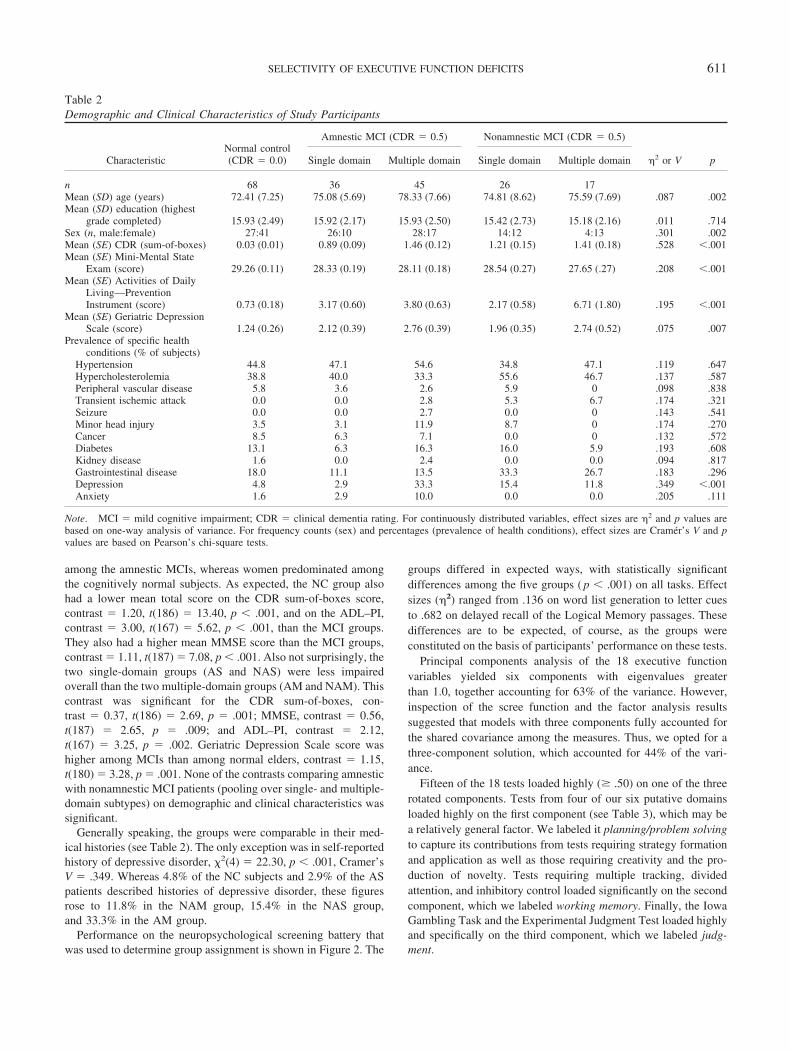
among the amnestic MCIs, whereas women predominated amongthe cognitively normal subjects. As expected, the NC group alsohad a lower mean total score on the CDR sum-of-boxes score,contrast � 1.20, t(186) � 13.40, p � .001, and on the ADL–PI,contrast � 3.00, t(167) � 5.62, p � .001, than the MCI groups.They also had a higher mean MMSE score than the MCI groups,contrast � 1.11, t(187) � 7.08, p � .001. Also not surprisingly, thetwo single-domain groups (AS and NAS) were less impairedoverall than the two multiple-domain groups (AM and NAM). Thiscontrast was significant for the CDR sum-of-boxes, con-trast � 0.37, t(186) � 2.69, p � .001; MMSE, contrast � 0.56,t(187) � 2.65, p � .009; and ADL–PI, contrast � 2.12,t(167) � 3.25, p � .002. Geriatric Depression Scale score washigher among MCIs than among normal elders, contrast � 1.15,t(180) � 3.28, p � .001. None of the contrasts comparing amnesticwith nonamnestic MCI patients (pooling over single- and multiple-domain subtypes) on demographic and clinical characteristics wassignificant.
Generally speaking, the groups were comparable in their med-ical histories (see Table 2). The only exception was in self-reportedhistory of depressive disorder, �2(4) � 22.30, p � .001, Cramer’sV � .349. Whereas 4.8% of the NC subjects and 2.9% of the ASpatients described histories of depressive disorder, these figuresrose to 11.8% in the NAM group, 15.4% in the NAS group,and 33.3% in the AM group.
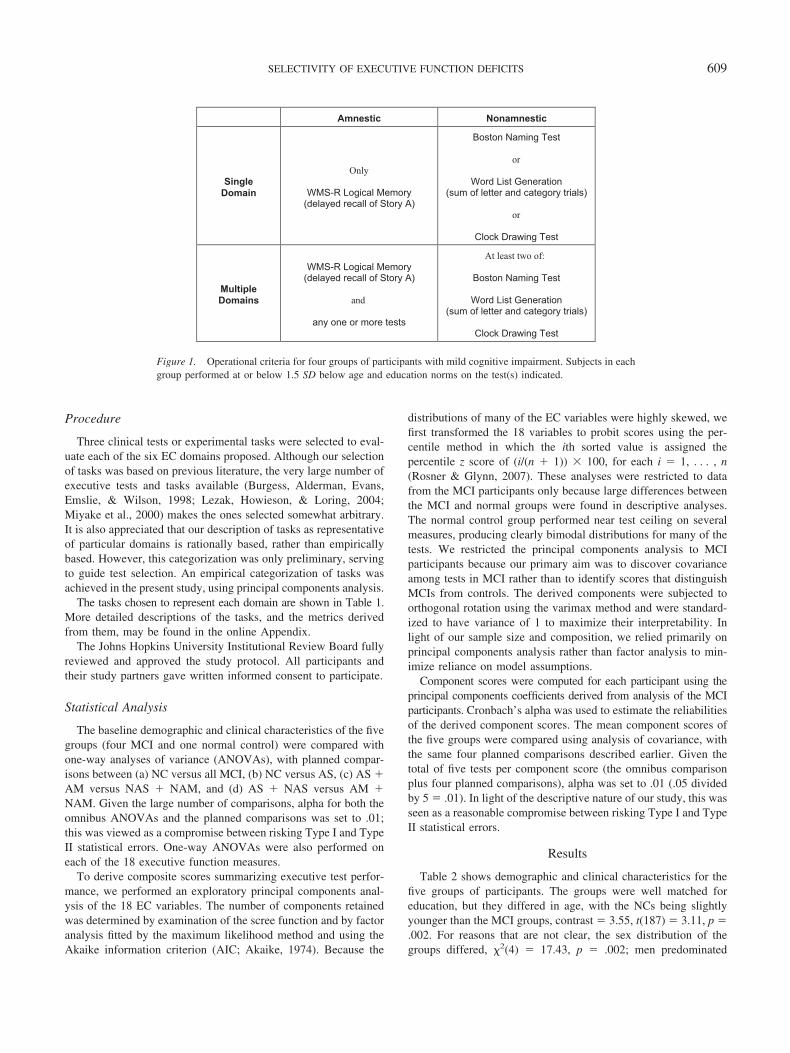
Performance on the neuropsychological screening battery thatwas used to determine group assignment is shown in Figure 2. The
groups differed in expected ways, with statistically significantdifferences among the five groups ( p � .001) on all tasks. Effectsizes (�2) ranged from .136 on word list generation to letter cuesto .682 on delayed recall of the Logical Memory passages. Thesedifferences are to be expected, of course, as the groups wereconstituted on the basis of participants’ performance on these tests.
Principal components analysis of the 18 executive functionvariables yielded six components with eigenvalues greaterthan 1.0, together accounting for 63% of the variance. However,inspection of the scree function and the factor analysis resultssuggested that models with three components fully accounted forthe shared covariance among the measures. Thus, we opted for athree-component solution, which accounted for 44% of the vari-ance.
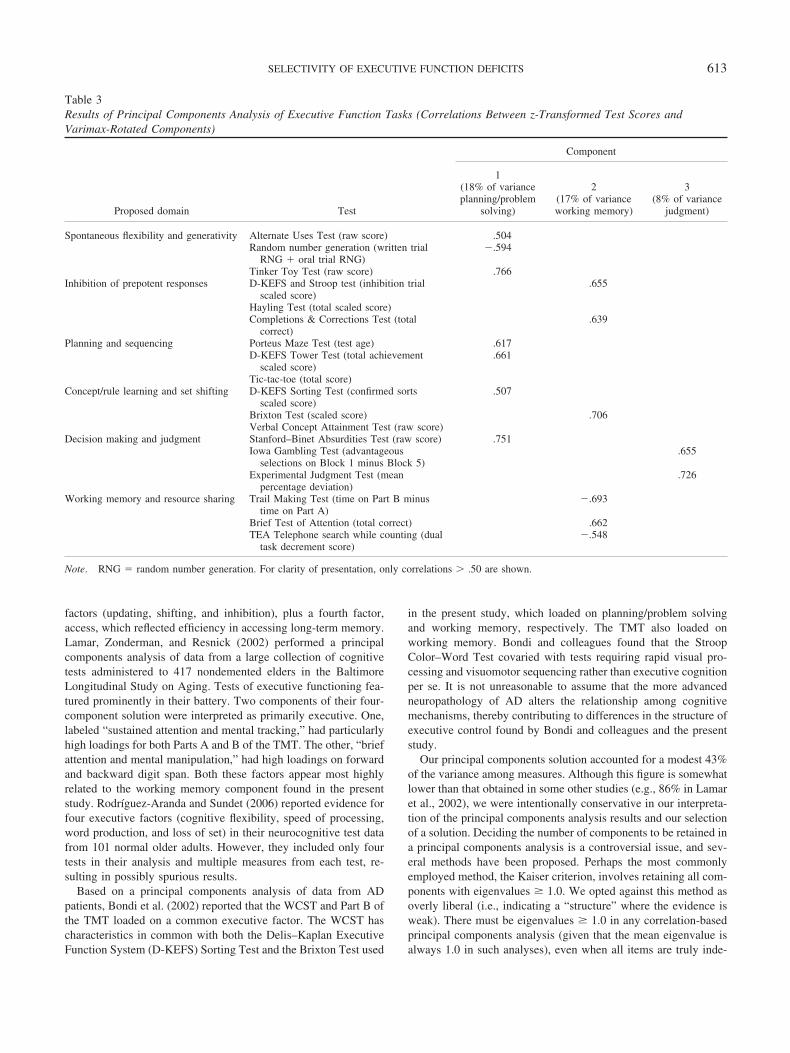
Fifteen of the 18 tests loaded highly (� .50) on one of the threerotated components. Tests from four of our six putative domainsloaded highly on the first component (see Table 3), which may bea relatively general factor. We labeled it planning/problem solvingto capture its contributions from tests requiring strategy formationand application as well as those requiring creativity and the pro-duction of novelty. Tests requiring multiple tracking, dividedattention, and inhibitory control loaded significantly on the secondcomponent, which we labeled working memory. Finally, the IowaGambling Task and the Experimental Judgment Test loaded highlyand specifically on the third component, which we labeled judg-ment.
Table 2Demographic and Clinical Characteristics of Study Participants
CharacteristicNormal control(CDR � 0.0)
Amnestic MCI (CDR � 0.5) Nonamnestic MCI (CDR � 0.5)
�2 or V pSingle domain Multiple domain Single domain Multiple domain
n 68 36 45 26 17Mean (SD) age (years) 72.41 (7.25) 75.08 (5.69) 78.33 (7.66) 74.81 (8.62) 75.59 (7.69) .087 .002Mean (SD) education (highest
grade completed) 15.93 (2.49) 15.92 (2.17) 15.93 (2.50) 15.42 (2.73) 15.18 (2.16) .011 .714Sex (n, male:female) 27:41 26:10 28:17 14:12 4:13 .301 .002Mean (SE) CDR (sum-of-boxes) 0.03 (0.01) 0.89 (0.09) 1.46 (0.12) 1.21 (0.15) 1.41 (0.18) .528 �.001Mean (SE) Mini-Mental State
Exam (score) 29.26 (0.11) 28.33 (0.19) 28.11 (0.18) 28.54 (0.27) 27.65 (.27) .208 �.001Mean (SE) Activities of Daily
Living—PreventionInstrument (score) 0.73 (0.18) 3.17 (0.60) 3.80 (0.63) 2.17 (0.58) 6.71 (1.80) .195 �.001
Mean (SE) Geriatric DepressionScale (score) 1.24 (0.26) 2.12 (0.39) 2.76 (0.39) 1.96 (0.35) 2.74 (0.52) .075 .007
Prevalence of specific healthconditions (% of subjects)
Hypertension 44.8 47.1 54.6 34.8 47.1 .119 .647Hypercholesterolemia 38.8 40.0 33.3 55.6 46.7 .137 .587Peripheral vascular disease 5.8 3.6 2.6 5.9 0 .098 .838Transient ischemic attack 0.0 0.0 2.8 5.3 6.7 .174 .321Seizure 0.0 0.0 2.7 0.0 0 .143 .541Minor head injury 3.5 3.1 11.9 8.7 0 .174 .270Cancer 8.5 6.3 7.1 0.0 0 .132 .572Diabetes 13.1 6.3 16.3 16.0 5.9 .193 .608Kidney disease 1.6 0.0 2.4 0.0 0.0 .094 .817Gastrointestinal disease 18.0 11.1 13.5 33.3 26.7 .183 .296Depression 4.8 2.9 33.3 15.4 11.8 .349 �.001Anxiety 1.6 2.9 10.0 0.0 0.0 .205 .111
Note. MCI � mild cognitive impairment; CDR � clinical dementia rating. For continuously distributed variables, effect sizes are �2 and p values arebased on one-way analysis of variance. For frequency counts (sex) and percentages (prevalence of health conditions), effect sizes are Cramer’s V and pvalues are based on Pearson’s chi-square tests.
611SELECTIVITY OF EXECUTIVE FUNCTION DEFICITS

Within the MCI group, Cronbach’s alpha coefficients were .73,.72, and .34 for Components 1, 2, and 3, respectively. For theentire sample, the reliabilities were .76, .76, and .22. Thus, theplanning/problem solving and working memory components hadreasonably high internal consistency reliability. Although the re-liability of the judgment component was low, we choose to reportit because of its clear interpretability. However, we recognize thatability to detect meaningful associations with the judgment factoris limited by the measure’s low reliability.
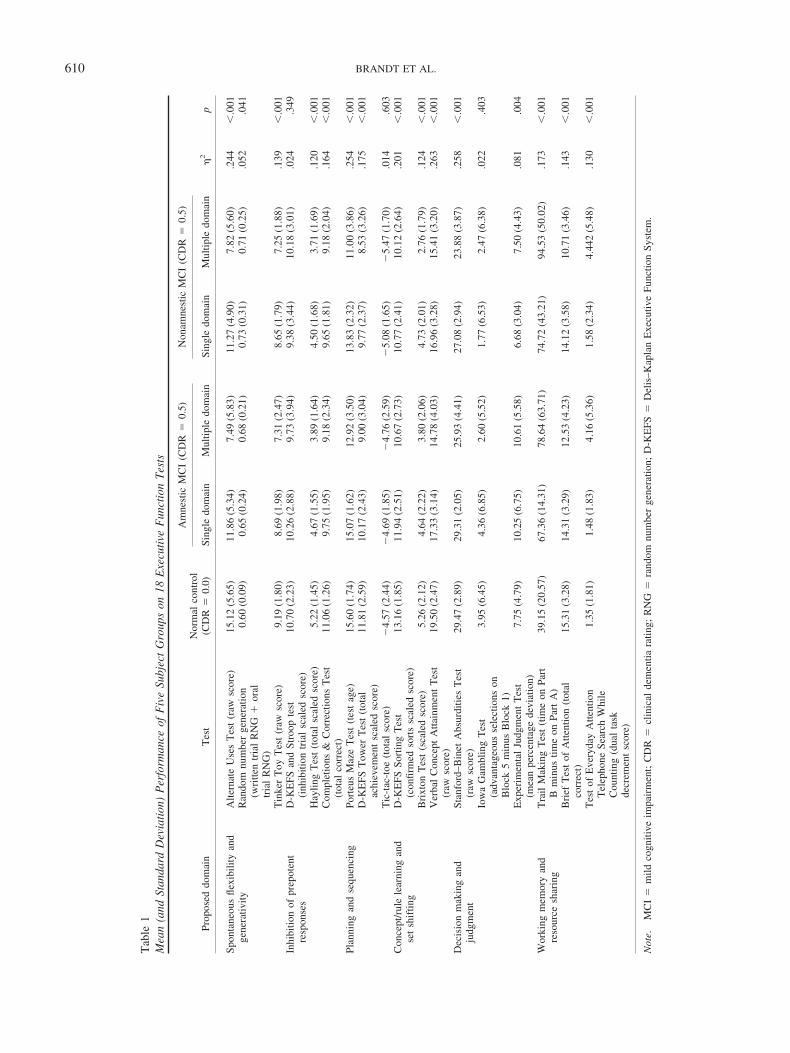
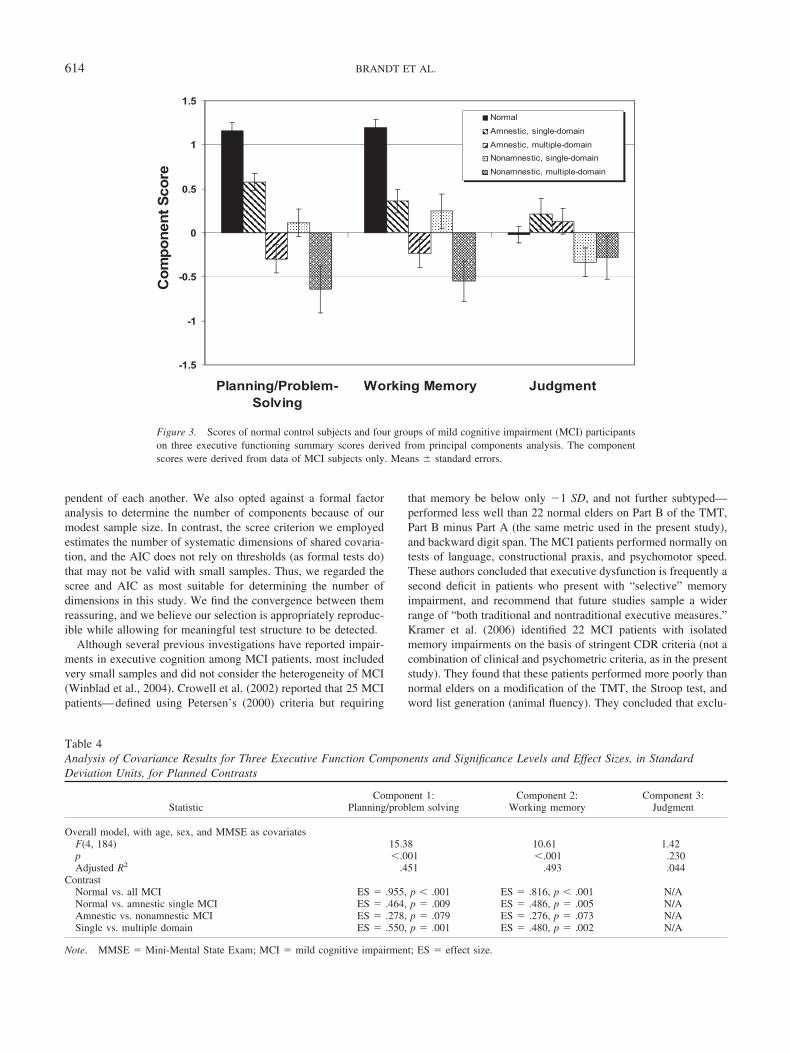
The mean score on each of the executive function componentsfor each group of participants is shown in Figure 3. A regressionmodel, with age, sex, and MMSE scores as covariates, was com-puted on each of the three components. For Component 1, therewas a significant effect of group, F(4, 184) � 15.38, p � .0001,adjusted R2 � .451. The results of the four planned contrastsappear in Table 4. The MCI patients, as a whole, performed lesswell than the NC subjects. Even the AS group, the least impairedMCI subgroup overall, was severely impaired in planning/problemsolving compared with normal participants. The difference be-tween amnestic and nonamnestic MCI patients in this EC domainwas not statistically significant, but the multiple-domain patientsperformed less well than single-domain patients.
For Component 2, working memory, the five groups differedsignificantly, F(4, 184) � 10.61, p � .0001, with the normalparticipants again outperforming the MCI patients as a group. Asin Component 1, the AS group differed from the normal group, andsingle-domain patients outperformed multiple-domain patients,but the amnestics did not outperform the nonamnestics.
For Component 3, judgment, the five groups did not differsignificantly, F(4, 184) � 1.42, p � .230. Therefore, no plannedcomparisons were undertaken.
Discussion
There are four major findings of this study. First, using a broadarray of clinical tests and experimental tasks, we found moderatesupport for the existence of two highly reliable domains of exec-utive functioning—planning/problem solving and working mem-ory—among elderly persons with MCI, and a less reliable thirddomain, judgment. Second, we found planning/problem solvingand working memory, but not judgment, to be selectively impairedin MCI compared with cognitively normal elders. Third, evenpatients with “pure” amnestic MCI, the least impaired subgroupoverall, displayed major impairments in these two executive do-mains. Finally, multiple-domain MCI patients (i.e., those withdeficits in at least two domains [of episodic memory, language,and spatial cognition]) had more significant planning/problem-solving and working memory deficits than single-domain patients.
Much of the previous research on the latent structure of exec-utive cognition, including the elegant work of Miyake and col-leagues on inhibitory control (Friedman & Miyake, 2004), useddata from young normal subjects performing experimental para-digms. Few previous studies have used latent structure methods todetermine the components of executive functions in older persons.J. E. Fisk and Sharp (2004) studied normal subjects rangingfrom 20 to 81 years of age and found evidence for Miyake’s three
0
5
10
15
20
25
30
35
40
45
50
Mini-Mental State WMS-R LogicalMemory, (story Adelayed recall)
Boston NamingTest, 30 item
Clock DrawingTest
Word ListGeneration:categories
Word ListGeneration:
letters
Scor
eNormalAmnestic, single-domainAmnestic, multiple-domainNon-amnestic, single-domainNon-amnestic, multiple-domain
Figure 2. Performance of five subject groups on neuropsychological screening battery. Age- and education-adjusted means � standard errors. Note that although the data are drawn on one set of axes, the possible rangeof scores for the tests differs.
612 BRANDT ET AL.
factors (updating, shifting, and inhibition), plus a fourth factor,access, which reflected efficiency in accessing long-term memory.Lamar, Zonderman, and Resnick (2002) performed a principalcomponents analysis of data from a large collection of cognitivetests administered to 417 nondemented elders in the BaltimoreLongitudinal Study on Aging. Tests of executive functioning fea-tured prominently in their battery. Two components of their four-component solution were interpreted as primarily executive. One,labeled “sustained attention and mental tracking,” had particularlyhigh loadings for both Parts A and B of the TMT. The other, “briefattention and mental manipulation,” had high loadings on forwardand backward digit span. Both these factors appear most highlyrelated to the working memory component found in the presentstudy. Rodrıguez-Aranda and Sundet (2006) reported evidence forfour executive factors (cognitive flexibility, speed of processing,word production, and loss of set) in their neurocognitive test datafrom 101 normal older adults. However, they included only fourtests in their analysis and multiple measures from each test, re-sulting in possibly spurious results.
Based on a principal components analysis of data from ADpatients, Bondi et al. (2002) reported that the WCST and Part B ofthe TMT loaded on a common executive factor. The WCST hascharacteristics in common with both the Delis–Kaplan ExecutiveFunction System (D-KEFS) Sorting Test and the Brixton Test used
in the present study, which loaded on planning/problem solvingand working memory, respectively. The TMT also loaded onworking memory. Bondi and colleagues found that the StroopColor–Word Test covaried with tests requiring rapid visual pro-cessing and visuomotor sequencing rather than executive cognitionper se. It is not unreasonable to assume that the more advancedneuropathology of AD alters the relationship among cognitivemechanisms, thereby contributing to differences in the structure ofexecutive control found by Bondi and colleagues and the presentstudy.
Our principal components solution accounted for a modest 43%of the variance among measures. Although this figure is somewhatlower than that obtained in some other studies (e.g., 86% in Lamaret al., 2002), we were intentionally conservative in our interpreta-tion of the principal components analysis results and our selectionof a solution. Deciding the number of components to be retained ina principal components analysis is a controversial issue, and sev-eral methods have been proposed. Perhaps the most commonlyemployed method, the Kaiser criterion, involves retaining all com-ponents with eigenvalues � 1.0. We opted against this method asoverly liberal (i.e., indicating a “structure” where the evidence isweak). There must be eigenvalues � 1.0 in any correlation-basedprincipal components analysis (given that the mean eigenvalue isalways 1.0 in such analyses), even when all items are truly inde-
Table 3Results of Principal Components Analysis of Executive Function Tasks (Correlations Between z-Transformed Test Scores andVarimax-Rotated Components)
Proposed domain Test
Component
1(18% of varianceplanning/problem
solving)
2(17% of varianceworking memory)
3(8% of variance
judgment)
Spontaneous flexibility and generativity Alternate Uses Test (raw score) .504Random number generation (written trial
RNG � oral trial RNG)�.594
Tinker Toy Test (raw score) .766Inhibition of prepotent responses D-KEFS and Stroop test (inhibition trial
scaled score).655
Hayling Test (total scaled score)Completions & Corrections Test (total
correct).639
Planning and sequencing Porteus Maze Test (test age) .617D-KEFS Tower Test (total achievement
scaled score).661
Tic-tac-toe (total score)Concept/rule learning and set shifting D-KEFS Sorting Test (confirmed sorts
scaled score).507
Brixton Test (scaled score) .706Verbal Concept Attainment Test (raw score)
Decision making and judgment Stanford–Binet Absurdities Test (raw score) .751Iowa Gambling Test (advantageous
selections on Block 1 minus Block 5).655
Experimental Judgment Test (meanpercentage deviation)
.726
Working memory and resource sharing Trail Making Test (time on Part B minustime on Part A)
�.693
Brief Test of Attention (total correct) .662TEA Telephone search while counting (dual
task decrement score)�.548
Note. RNG � random number generation. For clarity of presentation, only correlations .50 are shown.
613SELECTIVITY OF EXECUTIVE FUNCTION DEFICITS
pendent of each another. We also opted against a formal factoranalysis to determine the number of components because of ourmodest sample size. In contrast, the scree criterion we employedestimates the number of systematic dimensions of shared covaria-tion, and the AIC does not rely on thresholds (as formal tests do)that may not be valid with small samples. Thus, we regarded thescree and AIC as most suitable for determining the number ofdimensions in this study. We find the convergence between themreassuring, and we believe our selection is appropriately reproduc-ible while allowing for meaningful test structure to be detected.
Although several previous investigations have reported impair-ments in executive cognition among MCI patients, most includedvery small samples and did not consider the heterogeneity of MCI(Winblad et al., 2004). Crowell et al. (2002) reported that 25 MCIpatients—defined using Petersen’s (2000) criteria but requiring
that memory be below only �1 SD, and not further subtyped—performed less well than 22 normal elders on Part B of the TMT,Part B minus Part A (the same metric used in the present study),and backward digit span. The MCI patients performed normally ontests of language, constructional praxis, and psychomotor speed.These authors concluded that executive dysfunction is frequently asecond deficit in patients who present with “selective” memoryimpairment, and recommend that future studies sample a widerrange of “both traditional and nontraditional executive measures.”Kramer et al. (2006) identified 22 MCI patients with isolatedmemory impairments on the basis of stringent CDR criteria (not acombination of clinical and psychometric criteria, as in the presentstudy). They found that these patients performed more poorly thannormal elders on a modification of the TMT, the Stroop test, andword list generation (animal fluency). They concluded that exclu-
-1.5
-1
-0.5
0
0.5
1
1.5
Planning/Problem-Solving
Working Memory Judgment
Com
pone
nt S
core
Normal
Amnestic, single-domain
Amnestic, multiple-domainNonamnestic, single-domain
Nonamnestic, multiple-domain
Figure 3. Scores of normal control subjects and four groups of mild cognitive impairment (MCI) participantson three executive functioning summary scores derived from principal components analysis. The componentscores were derived from data of MCI subjects only. Means � standard errors.
Table 4Analysis of Covariance Results for Three Executive Function Components and Significance Levels and Effect Sizes, in StandardDeviation Units, for Planned Contrasts
StatisticComponent 1:
Planning/problem solvingComponent 2:
Working memoryComponent 3:
Judgment
Overall model, with age, sex, and MMSE as covariatesF(4, 184) 15.38 10.61 1.42p �.001 �.001 .230Adjusted R2 .451 .493 .044
ContrastNormal vs. all MCI ES � .955, p � .001 ES � .816, p � .001 N/ANormal vs. amnestic single MCI ES � .464, p � .009 ES � .486, p � .005 N/AAmnestic vs. nonamnestic MCI ES � .278, p � .079 ES � .276, p � .073 N/ASingle vs. multiple domain ES � .550, p � .001 ES � .480, p � .002 N/A
Note. MMSE � Mini-Mental State Exam; MCI � mild cognitive impairment; ES � effect size.
614 BRANDT ET AL.

sively amnestic MCI patients are probably extremely rare, and thatconcomitant executive dysfunction is common. They recom-mended comprehensive cognitive assessments for all MCI pa-tients, even when patients and families report only memory de-cline. Albert et al. (2007) found that scores on an executivefunctioning factor were lower at baseline in MCI patients whosubsequently converted to dementia than in normal subjects or inMCI patients who declined but did not convert. Rate of change inexecutive cognition over longitudinal assessments was greatestamong those MCI patients who subsequently converted.
A major finding of the present study is that the impairment ofexecutive cognition in MCI is not global; only certain empiricallydefined domains are affected. This is consistent with previousobservations that some specific executive tests are performednormally and others are impaired in MCI. For example, Traykov etal. (2007) found their 20 MCI patients to be impaired on the Strooptest and a modified WCST, but normal on the TMT, the Bells Test(a visual search task), and the Wechsler Adult Intelligence ScaleDigit Symbol subtest. The authors conclude that response inhibi-tion, switching, and cognitive flexibility are selectively impaired,whereas sustained and divided attention are intact. Zhang, Han,Verhaeghen, and Nilsson (2007) reported that the TMT, PorteusMaze Test, and verbal fluency tests—which they described asmeasures of planning—were impaired among 32 MCI patients,whereas no-go accuracy, Stroop task performance, and negativepriming—described as measures of inhibition—were not. In thepresent study, the Porteus Maze Test contributed to a planning/problem-solving factor, and the TMT and Stroop loaded togetheron a working memory factor, both of which were impaired amongMCI patients. Differences in assignment of tasks to domains (doneempirically in our study and conceptually in the Traykov andZhang studies) may be a primary reason for the apparent discrep-ancies.
No previous study of EC in either normal or cognitively im-paired elders has identified a specific factor related to judgment.Judgment, especially as it involves risk taking and decision mak-ing, appears to rely on neural circuitry (orbitofrontal cortex and itsstriatal, thalamic, and limbic connections) that is distinguishablefrom that supporting planning/problem solving and working mem-ory (primarily dorsolateral prefrontal cortex; Rogers et al., 1998,1999). Our finding that judgment is selectively spared in MCI maysuggest that orbitofrontal cortex is largely unaffected in thesepatients, although the low reliability of our judgment componentscore dictates extreme caution in its interpretation.
Few previous studies of executive cognition in MCI have con-sidered differences among MCI subtypes. In the present study, allfour MCI subtypes, even the group with “pure” memory impair-ment, displayed deficits in planning/problem solving and workingmemory, and multiple-domain patients were more severely im-paired than single-domain patients. In contrast, neither the 10amnestic nor the 28 “multiple cognitive deficits” MCI patients inthe Cardiovascular Health Study were found to have impairmentson a composite executive function measure (Lopez et al., 2006).The specifics of the sample characteristics and cognitive testsemployed are likely responsible for the differences among studies.
The present study found differences in the lifetime prevalence ofmajor depression among our groups, with the highest rate (33.3%)in the amnestic multiple-domain group. Other investigators havealso found an association of depression with MCI (Jorm, 2000;
Lopez et al., 2003), although differences in prevalence by MCIsubtype have not, to our knowledge, been previously reported.There is a large and complex literature on neuropsychologicaldeficits associated with late-life depression (Steffens et al., 2006),and several studies suggest that executive function deficits pre-dominate (Butters et al., 2004; Lockwood, Alexopoulos, Kakuma,& Van Gorp, 2000). However, we do not believe that the executivefunctioning deficits of our patients can be accounted for entirely bytheir histories of affective disorder given that our MCI group withthe most severe executive impairment (NAM) had an only mod-estly elevated lifetime prevalence of depression (11.8%). Addi-tional studies are clearly needed to resolve this issue.
Needless to say, the findings of the present study are not definitiveand require replication. First, our MCI sample was recruited largelyfrom other research studies and from memory disorder clinicsrather than from population screening. Although this undoubtedlyresults in some selection bias, we suspect that our sample is quitecomparable to most MCI samples described in the clinical litera-ture. Second, the specific criteria we used for diagnosing MCI andclassifying patients into subtypes may be questioned. Although ourscreening battery was composed of frequently used, standardizedneuropsychological tests, it was admittedly very brief, and “single-domain” deficits were identified by failure of single tests. Inaddition, we relied on the report of knowledgeable informants forthe assessment of functional capacity rather than direct assessmentof participants (as in Cahn-Weiner, Boyle, & Malloy, 2002; Cahn-Weiner et al., 2000). However, we contend that our requirement ofa cognitive test failure (score � 7th percentile) in the setting of anormal MMSE score and the report of borderline functioning by aknowledgeable informant (i.e., CDR � 0.5) conforms to the cur-rent standard for the diagnosis of MCI (Winblad et al., 2004). Andalthough our MCI groups differed from each other and from theNC group on both the CDR sum-of-boxes score and ADL–PIscore, with a particularly high ADL–PI score in the NAM group,their functional deficits were not of sufficient magnitude to inter-fere significantly with daily life or to merit the diagnosis ofdementia.
Among the other limitations of this study was that we did notallow MCI to be defined by a selective impairment in executivecontrol. This was done to avoid conflating the independent and thedependent variables. However, it does complicate the meaning of“single-domain” (memory, language, or spatial cognition) MCI, asdefined in this study. Another limitation of the study is its modestsample size for multivariate statistical approaches. Given the largenumber of executive function measures we employed (18), basinga principal components analysis on data from 124 subjects mayresult in a somewhat unstable structure. Because of this, we chosea relatively conservative approach to analysis.
A major implication of this study is that whether patients haveimpairment in memory or some other cognitive domain (languageor spatial cognition) is less important in predicting their executivefunctioning (and, hence, their vulnerability to everyday functionalimpairment) than whether they are impaired in only one or morethan one domain. It is our prediction that patients with multiple-domain MCI are at higher risk for the development of dementia, orto develop it sooner, than patients with pure amnestic MCI. This issupported by the findings of several recent studies (Alexopoulos,Grimmer, Perneczky, Domes, & Kurz, 2006; Rasquin, Lodder,Visser, Lousberg, & Verhey, 2005; Tabert et al., 2006), but not all
615SELECTIVITY OF EXECUTIVE FUNCTION DEFICITS

(Fischer et al., 2007; Yaffe, Petersen, Lindquist, Kramer, & Miller,2006). Continued follow-up of the participants in this study willallow us to test this prediction.
References
Akaike, H. (1974). A new look at the statistical model identification. IEEETransactions on Automatic Control, 6, 716–723.
Albert, M., Blacker, D., Moss, M. B., Tanzi, R., & McArdle, J. J. (2007).Longitudinal change in cognitive performance among individuals withmild cognitive impairment. Neuropsychology, 21, 158–169.
Albert, M. S., Moss, M. B., Tanzi, R., & Jones, K. (2001). Preclinicalprediction of AD using neuropsychological tests. Journal of the Inter-national Neuropsychological Society, 7, 631–639.
Alexopoulos, P., Grimmer, T., Perneczky, R., Domes, G., & Kurz, A.(2006). Progression to dementia in clinical subtypes of mild cognitiveimpairment. Dementia and Geriatric Cognitive Disorders, 22, 27–34.
Attix, D. K., & Welsh-Bohmer, K. A. (Eds.). (2006). Geriatric neuropsy-chology: Assessment and intervention. New York: Guilford Press.
Axelrod, B. N., & Millis, S. R. (1994). Preliminary standardization of theCognitive Estimation Test. Assessment, 1, 269–274.
Baddeley, A. D., Bressi, S., Della Sala, S., Logie, R., & Spinnler, H.(1991). The decline of working memory in Alzheimer’s disease. Brain,114, 2521–2542.
Baddeley, A., Logie, R., Bressi, S., Della Sala, S., & Spinnler, H. (1986).Dementia and working memory. Quarterly Journal of ExperimentalPsychology: Human Experimental Psychology, 38(A), 603–618.
Bechara, A., Damasio, H., Tranel, D., & Anderson, S. W. (1998). Disso-ciation of working memory from decision making within the humanprefrontal cortex. Journal of Neuroscience, 181, 428–437.
Bell-McGinty, S., Podell, K., Franzen, M., Baird, A. D., & Williams, M. J.(2002). Standard measures of executive function in predicting instru-mental activities of daily living in older adults. International Journal ofGeriatric Psychiatry, 17, 828–834.
Binetti, G., Magni, E., Padovani, A., Cappa, S. F., Bianchetti, A., &Trabucchi, M. (1996). Executive dysfunction in early Alzheimer’s dis-ease. Journal of Neurology, Neurosurgery & Psychiatry, 60, 91–93.
Bondi, M. W., Monsch, A. U., Galasko, D., Butters, N., Salmon, D. P., &Delis, D. C. (1994). Preclinical cognitive markers of dementia of theAlzheimer type. Neuropsychology, 8, 374–384.
Bondi, M. W., Serody, A. B., Chan, A. S., Eberson-Shumate, S. C., Delis,D. C., Hansen, L. A., & Salmon, D. P. (2002). Cognitive and neuro-pathologic correlates of Stroop Color-Word Test performance in Alz-heimer’s disease. Neuropsychology, 16, 335–343.
Bornstein, R. A. (1982). A factor analytic study of the Verbal ConceptAttainment Test. Journal of Clinical Neuropsychology, 4, 43–50.
Bornstein, R. A., & Leason, M. (1985). Effects of localized lesions on theVerbal Attainment Test. Journal of Clinical and Experimental Neuro-psychology, 7, 421–429.
Brandt, J. (2008). Tic-tac-toe as a simple test of planning and problem-solving for use in dementia research. Manuscript in preparation.
Brandt, J., Mellits, E. D., Rovner, B., & Gordon, B. (1989). Relation of ageat onset and duration of illness to cognitive functioning in Alzheimer’sdisease. Neuropsychiatry, Neuropsychology and Behavioral Neurol-ogy, 2, 93–101.
Bravo, G., & Hebert, R. (1997). Age- and education-specific referencevalues for the Mini-Mental and modified Mini-Mental State Examina-tions derived from a non-demented elderly population. InternationalJournal of Geriatric Psychiatry, 12, 1008–1018.
Brugger, P., Monsch, A. U., Salmon, D. P., & Butters, N. (1996). Randomnumber generation in dementia of the Alzheimer type: A test of frontalexecutive functions. Neuropsychologia, 34, 97–103.
Burgess, P. W. (1997). Theory and methodology in executive functionresearch. In P. Rabbitt (Ed.), Methodology of frontal and executivefunction (pp. 81–116). East Sussex, England: Psychology Press.
Burgess, P. W., Alderman, N., Evans, J., Emslie, H., & Wilson, B. A.(1998). The ecological validity of tests of executive function. Journal ofthe International Neuropsychological Society, 4, 547–558.
Burgess, P. W., & Shallice, T. (1997). The Hayling and Brixton Testsmanual. Bury St. Edmunds, England: Thames Valley Test Company.
Butters, M. A., Whyte, E. M., Nebes, R. D., Begley, A. E., Dew, M. A.,Mulsant, B. H., et al. (2004). The nature and determinants of neuropsy-chological functioning in late-life depression. Archives of General Psy-chiatry, 61, 587–596.
Cahn-Weiner, D. A., Boyle, P. A., & Malloy, P. F. (2002). Tests ofexecutive function predict instrumental activities of daily living incommunity-dwelling older individuals. Applied Neuropsychology, 9,187–191.
Cahn-Weiner, D., Malloy, P. F., Boyle, P. A., Marran, M., & Salloway, S.(2000). Prediction of functional status from neuropsychological tests incommunity-dwelling elderly individuals. The Clinical Neuropsycholo-gist, 14, 187–195.
Chen, P., Ganguli, M., Mulsant, B. H., & DeKosky, S. T. (1999). Thetemporal relationship between depressive symptoms and dementia. Ar-chives of General Psychiatry, 56, 261–266.
Chertkow, H., Nasreddine, Z., Joanette, Y., Drolet, V., Kirk, J., Massoud,F., et al. (2007). Mild cognitive impairment and cognitive impairment,no dementia: Part A, concept and diagnosis. Alzheimer’s & Dementia, 3,266–282.
Crowell, T. A., Luis, C. A., Vanderploeg, R. D., Schinka, J. A., & Mullan,M. (2002). Memory patterns and executive functioning in mild cognitiveimpairment and Alzheimer’s disease. Aging, Neuropsychology, andCognition, 9, 288–297.
Crowley, K., & Siegler, R. S. (1993). Flexible strategy use in youngchildren’s tic-tac-toe. Cognitive Science, 17, 531–561.
Daly, E., Zaitchick, D., Copeland, M., Schmahmann, J., Gunther, J., &Albert, M. (2000). Predicting “conversion” to AD using standardizedclinical information. Archives of Neurology, 57, 675–680.
Delis, D. C., Kaplan, E., & Kramer, J. H. (2001). Delis–Kaplan ExecutiveFunction System examiner’s manual. San Antonio: Psychological Cor-poration.
Elias, M. F., Beiser, A., Wolfe, P. A., Au, R., White, R. F., & D’Agostino,R. B. (2000). The preclinical phase of Alzheimer disease. Archives ofNeurology, 57, 808–813.
Evans, F. J. (1978). Monitoring attention deployment by random numbergeneration: An index to measure subjective randomness. Bulletin of thePsychonomic Society, 12, 35–38.
Fischer, P., Jungwirth, S., Zehetmayer, S., Weissgram, S., Hoenigschnabl,S., Gelpi, E., et al. (2007). Conversion from subtypes of mild cognitiveimpairment to Alzheimer dementia. Neurology, 68, 288–291.
Fisk, J. D., Merry, H. R., & Rockwood, K. (2003). Variations in casedefinition affect prevalence but not outcomes of mild cognitive impair-ment. Neurology, 61, 1179–1184.
Fisk, J. E., & Sharp, C. A. (2004). Age-related impairment in executivefunctioning: Updating, inhibition, shifting, and access. Journal of Clin-ical and Experimental Neuropsychology, 26, 874–890.
Friedman, N. P., & Miyake, A. (2004). The relations among inhibition andinterference control functions: A latent variable analysis. Journal ofExperimental Psychology: General, 133, 101–135.
Galasko, D., Bennett, D. A., Sano, M., Marson, D., Kaye, J., & Edland,S. D. (2006). ADCS Prevention Instrument Project: Assessment ofinstrumental activities of daily living for community-dwelling elderlyindividuals in dementia prevention clinical trials. Alzheimer’s Diseaseand Associated Disorders, 20, S152–169.
Ganguli, M., Dodge, H. H., Shen, C., & DeKosky, S. T. (2004). Mildcognitive impairment, amnestic type: An epidemiologic study. Neurol-ogy, 63, 115–121.
616 BRANDT ET AL.
Gauthier, S., & Touchon, J. (2005). Mild cognitive impairment is not aclinical entity and should not be treated. Archives of Neurology, 62,1164–1166.
Gillespie, D. C., Evans, R. I., Gardener, E. A., & Bowen, A. (2002).Performance of older adults on tests of cognitive estimation. Journal ofClinical and Experimental Neuropsychology, 24, 286–293.
Goodglass, H., & Kaplan, E. (1983). Boston Diagnostic Aphasia Exami-nation. Philadelphia: Lea & Febiger.
Griffith, H. R., Belue, K., Sicola, A., Krzywanski, S., Zamrini, E., Harrell,L., & Marson, D. C. (2003). Impaired financial abilities in mild cognitiveimpairment. Neurology, 60, 449–457.
Grigsby, J., Kaye, K., Baxter, J., Shetterly, S. M., & Hamman, R. F. (1998).Executive cognitive abilities and functional status among community-dwelling older persons in the San Luis Valley Health and Aging Study.Journal of the American Geriatrics Society, 46, 590–596.
Grundman, M., Petersen, R. C., & Morris, J. C. (1996). ADCS CooperativeStudy: Rate of dementia of the Alzheimer’s type (DAT) in subjects withmild cognitive impairment. Neurology, 46, A403.
Guilford, J. P., Christensen, P. R., Merryfield, P. R., & Wilson, R. C.(1978). Alternate uses, Form B, Form C; manual of instructions andinterpretations. Orange, CA: Sheridan Psychological Services.
Hughes, C. P., Berg, L., Danziger, W. L., Coben, L. A., & Martin, R. L.(1982). A new clinical scale for the staging of dementia. British Journalof Psychiatry, 140, 566–572.
Jacobs, D. M., Sano, M., Dooneief, G., Marder, K., Bell, K. L., & Stern, Y.(1995). Neuropsychological detection and characterization of preclinicalAlzheimer’s disease. Neurology, 45, 957–962.
Jahanshshi, M., Dirnberger, G., Fuller, R., & Frith, C. D. (2000). The roleof the dorsolateral prefrontal cortex in random number generation: Astudy with positron emission tomography. NeuroImage, 12, 713–725.
Jorm, A. F. (2000). Is depression a risk factor for dementia or cognitivedecline? Gerontology, 46, 219–227.
Jorm, A. F. (2001). History of depression as a risk factor for dementia: Anupdated review. Australian and New Zealand Journal of Psychiatry, 35,776–781.
Koss, E., Paterson, M. B., Mack, J. L., Smyth, K. A., & Whitehouse, P. J.(1998). Reliability and validity of the Tinker Toy Test in evaluatingindividuals with Alzheimer’s disease. The Clinical Neuropsycholo-gist, 12, 325–329.
Kramer, J. H., Nelson, A., Johnson, J. K., Yaffe, K., Glenn, S., Rosen,H. J., & Miller, B. L. (2006). Multiple cognitive deficits in amnestic mildcognitive impairment. Dementia and Geriatric Cognitive Disorders, 22,306–311.
Lafleche, G., & Albert, M. S. (1995). Executive function deficits in mildAlzheimer’s disease. Neuropsychology, 9, 313–330.
Lamar, M. L., Zonderman, A. B., & Resnick, S. (2002). Contribution ofspecific cognitive processes to executive functioning in an aging popu-lation. Neuropsychology, 16, 156–165.
Lewis, M. S., & Miller, L. S. (2007). Executive control functioning andfunctional ability in older adults. The Clinical Neuropsychologist, 21,274–285.
Lezak, M. D. (1982). The problem of assessing executive functions.International Journal of Psychology, 17, 281–297.
Lezak, M. D., Howieson, D. B., & Loring, D. W. (2004). Neuropsycho-logical assessment (4th ed.). New York: Oxford University Press.
Lockwood, K. A., Alexopoulos, G. S., Kakuma, T., & Van Gorp, W. G.(2000). Subtypes of cognitive impairment in depressed older adults.American Journal of Geriatric Psychiatry, 8, 201–208.
Lopez, O. L., Becker, J. T., Jagust, W. J., Fitzpatrick, A., Carlson, M.C.,DeKosky, S. T., et al. (2006). Neuropsychological characteristics of mildcognitive impairment subgroups. Journal of Neurology, Neurosurgery &Psychiatry, 77, 159–165.
Lopez, O. L., Jagust, W. J., DeKosky, S. T., Becker, J. T., Fitzpatrick, A.,Dulberg, C., et al. (2003). Prevalence and classification of mild cognitive
impairment in the Cardiovascular Health Cognition Study, Part 1. Ar-chives of Neurology, 60, 1385–1389.
Lopez, O. L., Jagust, W. J., Dulberg, C., Becker, J. T., DeKosky, S. T.,Fitzpatrick, A., et al. (2003). Risk factors for mild cognitive impairmentin the Cardiovascular Health Cognition Study, Part 2. Archives ofNeurology, 60, 1394–1399.
Lyketsos, C. G., Lopez, O., Jones, B., Fitzpatrick, A. L., Breitner, J., &DeKosky, S. (2002). Prevalence of neuropsychiatric symptoms in de-mentia and mild cognitive impairment: Results from the CardiovascularHealth Study. Journal of the American Medical Association, 288, 1475–1483.
Manning, K. J., & Brandt, J. (2006, February). “Completions and correc-tions” as a test of executive control. Presented at the 34th AnnualMeeting of the International Neuropsychological Society, Boston.
Milwain, E. (2000). Mild cognitive impairment: Further caution [Letter].The Lancet, 355, 1018.
Miyake, A., Friedman, N. P., Emerson, M. J., Witzki, A. H., Howerter, A.,& Wager, T. D. (2000). The unity and diversity of executive functionsand their contributions to complex “frontal lobe” tasks: A latent variableanalysis. Cognitive Psychology, 41, 49–100.
Mondrego, P. J., & Ferrandez, J. (2004). Depression in patients with mildcognitive impairment increases risk of developing dementia of Alzhei-mer type. Archives of Neurology, 61, 1290–1293.
Morris, J. C., Storandt, M., Miller, J. P., McKeel, D. W., Price, J. L., Rubin,E. H., & Berg, L. (2001). Mild cognitive impairment represents early-stage Alzheimer disease. Archives of Neurology, 58, 397–405.
Petersen, R. C. (2000). Mild cognitive impairment: Transition betweenaging and Alzheimer’s disease. Neurologica, 15, 93–101.
Petersen, R. C. (2004a). Challenges of epidemiological studies of mildcognitive impairment. Alzheimer’s Disease and Associated Disor-ders, 18, 1–2.
Petersen, R. C. (2004b). Mild cognitive impairment as a diagnostic entity.Journal of Internal Medicine, 256, 183–194.
Porteus, S. D. (1965). Porteus Maze Test: Fifty years’ application. NewYork: Psychological Corporation.
Rapp, M. A., & Reischies, F. M. (2005). Attention and executive controlpredict Alzheimer disease in late life: Results from the Berlin AgingStudy (BASE). American Journal of Geriatric Psychiatry, 13, 134–141.
Rascovsky, K., Salmon, D. P., Hansen, L. A., Thal, L. J., & Galasko, D.(2007). Disparate letter and semantic category fluency deficits in autop-sy-confirmed frontotemporal dementia and Alzheimer’s disease. Neuro-psychology, 21, 20–30.
Rasquin, S. M. C., Lodder, J., Visser, P. J., Lousberg, R., & Verhey, F. R. J.(2005). Predictive accuracy of MCI subtypes for Alzheimer’s diseaseand vascular dementia in subjects with mild cognitive impairment: A2-year follow-up study. Dementia and Geriatric Cognitive Disor-ders, 19, 113–119.
Reitan, R. M. (1958). The validity of the Trail-Making Test as an indicatorof organic brain damage. Perceptual and Motor Skills, 8, 271–276.
Robertson, I. H., Ward, T., Ridgeway, V., & Nimmo-Smith, I. (1994). TheTest of Everyday Attention (TEA) manual. Bury St. Edmunds, England:Thames Valley Test Company.
Rodrıguez-Aranda, C., & Sundet, K. (2006). The frontal hypothesis ofcognitive aging: Factor structure and age effects on four frontal testsamong healthy individuals. Journal of Genetic Psychology, 167, 269–287.
Rogers, R. D., Owen, A. M., Middleton, H. C., Williams, E. J., Pickard,J. D., Sahakian, B. J., & Robbins, T. W. (1999). Choosing betweensmall, likely rewards and large, unlikely rewards activates inferior andorbital prefrontal cortex. Journal of Neuroscience, 20, 9029–9038.
Rogers, R. D., Sahakian, B. J., Hodges, J. R., Polkey, C. E., Kennard, C.,& Robbins, T. W. (1998). Dissociating executive mechanisms of taskcontrol following frontal lobe damage and Parkinson’s disease. Brain,121, 815–842.
617SELECTIVITY OF EXECUTIVE FUNCTION DEFICITS

Rosner, B., & Glynn, R. J. (2007). Interval estimation for rank correlationcoefficients based on the probit transformation with extension to mea-surement error correction of correlated ranked data. Statistics in Medi-cine, 26, 633–646.
Rouleau, I., Salmon, D. P., Butters, N., Kennedy, C., & Mcquire, K.(1992). Quantitative and qualitative analyses of clock drawings in Alz-heimer’s and Huntington’s disease. Brain and Cognition, 18, 70–87.
Royall, D. R., Cabello, M., & Polk, M. J. (1998). Executive dyscontrol: Animportant factor affecting the level of care received by older retirees.Journal of the American Geriatric Society, 46, 1519–1524.
Royall, D. R., Chiodo, L. K., & Polk, M. J. (2004). Misclassification islikely in the assessment of mild cognitive impairment. Neuroepidemi-ology, 23, 185–191.
Royall, D. R., Lauterbach, E. C., Cummings, J. L., Reeve, A., Rummans,T. A., Kaufer, D. I., et al. (2002). Executive control function: A reviewof its promise and challenges for clinical research. Journal of Neuro-psychiatry and Clinical Neurosciences, 14, 377–405.
Royall, D. R., Palmer, R., Chiodo, L. K., & Polk, M. J. (2004). Decliningexecutive control in normal aging predicts change in functional status:The Freedom House Study. Journal of the American Geriatrics Soci-ety, 52, 346–352.
Salmon, D. P., Heindel, W. C., & Lange, K. L. (1999). Differential declinein word generation from phonemic and semantic categories during thecourse of Alzheimer’s disease: Implications for the integrity of semanticmemory. Journal of the International Neuropsychological Society, 5,692–703.
Schretlen, D., Brandt, J., & Bobholz, J. H. (1996). Development andpsychometric properties of the Brief Test of Attention. The ClinicalNeuropsychologist, 10, 80–89.
Steffens, D. C., Otey, E., Georgeopoulos, G. S., Butters, M. A., Cuthbert,B., Ganguli, M., et al. (2006). Perspectives on depression, mild cognitiveimpairment, and cognitive decline. Archives of General Psychiatry, 63,130–138.
Tabert, M. H., Manly, J. J., Liu, X., Pelton, G. H., Rosenblum, S., Jacobs,M., et al. (2006). Neuropsychological prediction of conversion to Alz-heimer disease in patients with mild cognitive impairment. Archives ofGeneral Psychiatry, 63, 916–924.
Thorndike, R. L., Hagen, E. P., & Sattler, J. M. (1986). The Stanford–BinetIntelligence Scale: Guide for administration and scoring (4th ed.).Chicago: Riverside.
Towse, J. N., & Neil, D. (1998). Analyzing human random generationbehavior: A review of methods used and a computer program fordescribing performance. Behavior Research.
Traykov, L., Raoux, N., Latour, F., Gallo, L., Hanon, O., Baudic, S., et al.(2007). Executive functions deficit in mild cognitive impairment. Cog-nitive and Behavioral Neurology, 20, 219–224.
Visser, P., & Verhey, F. (2000). Distinction between preclinical Alzhei-mer’s disease and depression. Journal of the American Geriatrics Soci-ety, 48, 479–484.
Wechsler, D. (1987). The Wechsler Memory Scale—Revised manual. NewYork: The Psychological Corporation.
Whitehouse, P. J. (1007). Mild cognitive impairment—A confused con-cept? Nature Clinical Practice Neurology, 3, 62–63.
Winblad, B., Palmer, K., Kivipelto, M., Jelic, V., Fratiglioni, L., Wahlund,L.-O., et al. (2004). Mild cognitive impairment—Beyond controversies,towards a consensus. Journal of Internal Medicine, 256, 240–246.
Yaffe, K., Petersen, R. C., Lindquist, K., Kramer, J., & Miller, B. (2006).Subtype of mild cognitive impairment and progression to dementia anddeath. Dementia and Geriatric Cognitive Disorders, 22, 312–319.
Zhang, Y., Han, B., Verhaeghen, P., & Nilsson, L.-G. (2007). Executivefunctioning in older adults with mild cognitive impairment: MCI haseffects on planning, but not on inhibition. Aging, Neuropsychology, andCognition, 14, 557–570.
Received June 6, 2008Revision received February 23, 2009
Accepted March 9, 2009 �
618 BRANDT ET AL.
Copyright © 2022 FDOKUMEN