Investigation of cool and hot executive function in ODD/CD independently of ADHD
19
REVIEW “Cool” Inferior Frontostriatal Dysfunction in Attention-Deficit/Hyperactivity Disorder Versus “Hot” Ventromedial Orbitofrontal-Limbic Dysfunction in Conduct Disorder: A Review Katya Rubia Attention-deficit/hyperactivity disorder (ADHD) and conduct disorder overlap behaviorally, clinically, and cognitively. An important ques- tion of potential future clinical relevance is whether these two overlapping disorders are mediated by similar or distinct underlying brain substrates. This article reviews the modern neuroimaging literature on brain structure, function, and connectivity in both disorders, shaping out commonalities and differences. Findings show that ADHD is characterized predominantly by abnormalities in inferior frontal, striatal, parietotemporal, and cerebellar regions and networks that mediate “cool”-cognitive, i.e., inhibitory, attention and timing functions associ- ated with the disorder. Conduct disorder, by contrast, has consistently been associated with abnormalities of the “hot” paralimbic system that regulates motivation and affect, comprising lateral orbital and ventromedial prefrontal cortices, superior temporal lobes, and underly- ing limbic structures, most prominently the amygdala. Direct comparisons in functional imaging show that these associations of cool inferior fronto-striato-cerebellar dysfunction in ADHD and of hot orbitofrontal-paralimbic dysfunction in conduct disorder are disorder-specific. There is, hence, evidence for dissociated underlying pathophysiologies for these two disorders that may have implications for future anatomy-based differential diagnosis and prevention and intervention. Key Words: ADHD, attention-deficit/hyperactive disorder, CD, con- duct disorder, executive functions, fMRI, frontal lobe, functional magnetic resonance imaging, motivation, MRI A ttention-deficit/hyperactivity disorder (ADHD) is character- ized by symptoms of age-inappropriate inattention, impul- siveness, and hyperactivity (DSM-IV) (1). It disrupts academic and social development and is associated with significant psychiat- ric comorbidities (2) and mental health problems in adult life (3,4). Conduct disorder (CD) is defined by the violation of the rights of others and societal rules and the persistent display of antisocial behaviors such as deception, theft, vandalism, and violence within a 6- to 12-month period before age 18 (DSM-IV) (1). Conduct disor- der is considered a risk factor for various psychiatric conditions beginning in adolescence or adulthood, including antisocial per- sonality disorder and mood disorders (5–13). Oppositional defiant disorder (ODD) is characterized by recurrent patterns of negativis- tic, defiant, disobedient, and hostile behavior toward authority fig- ures. Oppositional defiant disorder is often comorbid with CD and has been considered a less severe subtype, although there is em- piric evidence to distinguish the two disorders. In the DSM-IV, a diagnosis of CD is given if an individual meets criteria for both CD and ODD. The lower age of onset of CD before age 10 has been associated with a worse outcome, such as a greater risk for adult antisocial behavior and for emotional and behavioral dysregulation (14). A more pervasive subtype of CD is seen in those with callous- unemotional (CU) traits, defined as low fearfulness and a lack of empathy, guilt, and emotion (15), present in approximately 25% of cases of child-onset conduct disorder (16,17). This subtype is asso- ciated with poorer outcomes compared with non-CU CD groups, including substance use disorders, criminality, violent offending, and increased risk of psychopathy, as well as higher genetic risk factors (15,16,18 –20). Neuropsychological Findings Attention-deficit/hyperactivity disorder is associated most con- sistently with neuropsychological deficits in tasks of motor re- sponse and cognitive inhibition (such as tasks of interference inhi- bition or cognitive switching), sustained attention, and timing functions (21–23). Children with CD have also shown deficits in tasks of motor and cognitive inhibition (24 –27). Furthermore, like ADHD patients, they are also impaired in tasks of cognitive switch- ing and reversal (28 –31), as well as of sustained attention (32–37). However, studies have included comorbidity with ADHD, and the evidence for impairment in CD without comorbid ADHD compared with control subjects is less consistent; in fact, several studies found no independent deficits from ADHD for these tasks (37– 43). An exception, however, is in functions of motivation control, where children with CD seem as impaired or more impaired than children with ADHD. Thus, children with CD or psychopathy are consistently impaired in reversal tasks, where previously valid and learned rewarded stimulus-response contingencies change and are no longer rewarded or even punished (28,44). This seems to be due to a reduced sensitivity to punishment in children with CD com- pared with control subjects or children with ADHD. In fact, response perseveration (i.e., hyposensitivity to increasing punishment) using the Newman Card Playing Task paradigm (45) or other task variants has been found to be independently related to CD but not “nonco- morbid” ADHD (39,46,47). In gambling tasks that measure reward- related long-term advantageous decision making versus impulsive short-term decisions, both pathologies have been shown to be impaired, although none of these studies excluded comorbidity with the other disorder (48 –50). Regression analyses, however, showed that the antisocial behavior traits were responsible for the impulsive reward-related choice pattern in this task, whereas ADHD traits accounted for the “cool” executive function deficits in tasks of motor inhibition and attention (50). From the Department of Child Psychiatry/Medical Research Council Center for Social, Genetic and Developmental Psychiatry, Institute of Psychiatry, London, United Kingdom. Address correspondence to Katya Rubia, Ph.D., Institute of Psychiatry, King’s College, Department of Child Psychiatry, 16 De Crespigny Park, London SE5 8AF, United Kingdom; E-mail: [email protected]. Received Apr 20, 2010; revised Sep 16, 2010; accepted Sep 18, 2010. BIOL PSYCHIATRY 2011;69:e69 – e87 0006-3223/$36.00 doi:10.1016/j.biopsych.2010.09.023 © 2011 Society of Biological Psychiatry
Transcript of Investigation of cool and hot executive function in ODD/CD independently of ADHD

REVIEW
“Cool” Inferior Frontostriatal Dysfunction inAttention-Deficit/Hyperactivity Disorder Versus“Hot” Ventromedial Orbitofrontal-LimbicDysfunction in Conduct Disorder: A ReviewKatya Rubia
Attention-deficit/hyperactivity disorder (ADHD) and conduct disorder overlap behaviorally, clinically, and cognitively. An important ques-tion of potential future clinical relevance is whether these two overlapping disorders are mediated by similar or distinct underlying brainsubstrates. This article reviews the modern neuroimaging literature on brain structure, function, and connectivity in both disorders, shapingout commonalities and differences. Findings show that ADHD is characterized predominantly by abnormalities in inferior frontal, striatal,parietotemporal, and cerebellar regions and networks that mediate “cool”-cognitive, i.e., inhibitory, attention and timing functions associ-ated with the disorder. Conduct disorder, by contrast, has consistently been associated with abnormalities of the “hot” paralimbic systemthat regulates motivation and affect, comprising lateral orbital and ventromedial prefrontal cortices, superior temporal lobes, and underly-ing limbic structures, most prominently the amygdala. Direct comparisons in functional imaging show that these associations of cool inferiorfronto-striato-cerebellar dysfunction in ADHD and of hot orbitofrontal-paralimbic dysfunction in conduct disorder are disorder-specific.There is, hence, evidence for dissociated underlying pathophysiologies for these two disorders that may have implications for future
anatomy-based differential diagnosis and prevention and intervention.iaf
N
ssbftAiHewn
wcclntppthmrsiwsit
Key Words: ADHD, attention-deficit/hyperactive disorder, CD, con-duct disorder, executive functions, fMRI, frontal lobe, functionalmagnetic resonance imaging, motivation, MRI
A ttention-deficit/hyperactivity disorder (ADHD) is character-ized by symptoms of age-inappropriate inattention, impul-siveness, and hyperactivity (DSM-IV) (1). It disrupts academic
and social development and is associated with significant psychiat-ric comorbidities (2) and mental health problems in adult life (3,4).
Conduct disorder (CD) is defined by the violation of the rights ofothers and societal rules and the persistent display of antisocialbehaviors such as deception, theft, vandalism, and violence withina 6- to 12-month period before age 18 (DSM-IV) (1). Conduct disor-der is considered a risk factor for various psychiatric conditionsbeginning in adolescence or adulthood, including antisocial per-sonality disorder and mood disorders (5–13). Oppositional defiantdisorder (ODD) is characterized by recurrent patterns of negativis-tic, defiant, disobedient, and hostile behavior toward authority fig-ures. Oppositional defiant disorder is often comorbid with CD andhas been considered a less severe subtype, although there is em-piric evidence to distinguish the two disorders. In the DSM-IV, adiagnosis of CD is given if an individual meets criteria for both CDand ODD. The lower age of onset of CD before age 10 has beenassociated with a worse outcome, such as a greater risk for adultantisocial behavior and for emotional and behavioral dysregulation(14). A more pervasive subtype of CD is seen in those with callous-unemotional (CU) traits, defined as low fearfulness and a lack ofempathy, guilt, and emotion (15), present in approximately 25% ofcases of child-onset conduct disorder (16,17). This subtype is asso-ciated with poorer outcomes compared with non-CU CD groups,
From the Department of Child Psychiatry/Medical Research Council Centerfor Social, Genetic and Developmental Psychiatry, Institute of Psychiatry,London, United Kingdom.
Address correspondence to Katya Rubia, Ph.D., Institute of Psychiatry, King’sCollege, Department of Child Psychiatry, 16 De Crespigny Park, LondonSE5 8AF, United Kingdom; E-mail: [email protected].
mReceived Apr 20, 2010; revised Sep 16, 2010; accepted Sep 18, 2010.
0006-3223/$36.00doi:10.1016/j.biopsych.2010.09.023
ncluding substance use disorders, criminality, violent offending,nd increased risk of psychopathy, as well as higher genetic riskactors (15,16,18 –20).
europsychological Findings
Attention-deficit/hyperactivity disorder is associated most con-istently with neuropsychological deficits in tasks of motor re-ponse and cognitive inhibition (such as tasks of interference inhi-ition or cognitive switching), sustained attention, and timing
unctions (21–23). Children with CD have also shown deficits inasks of motor and cognitive inhibition (24 –27). Furthermore, likeDHD patients, they are also impaired in tasks of cognitive switch-
ng and reversal (28 –31), as well as of sustained attention (32–37).owever, studies have included comorbidity with ADHD, and thevidence for impairment in CD without comorbid ADHD comparedith control subjects is less consistent; in fact, several studies foundo independent deficits from ADHD for these tasks (37– 43).
An exception, however, is in functions of motivation control,here children with CD seem as impaired or more impaired than
hildren with ADHD. Thus, children with CD or psychopathy areonsistently impaired in reversal tasks, where previously valid and
earned rewarded stimulus-response contingencies change and areo longer rewarded or even punished (28,44). This seems to be due
o a reduced sensitivity to punishment in children with CD com-ared with control subjects or children with ADHD. In fact, responseerseveration (i.e., hyposensitivity to increasing punishment) using
he Newman Card Playing Task paradigm (45) or other task variantsas been found to be independently related to CD but not “nonco-orbid” ADHD (39,46,47). In gambling tasks that measure reward-
elated long-term advantageous decision making versus impulsivehort-term decisions, both pathologies have been shown to bempaired, although none of these studies excluded comorbidity
ith the other disorder (48 –50). Regression analyses, however,howed that the antisocial behavior traits were responsible for thempulsive reward-related choice pattern in this task, whereas ADHDraits accounted for the “cool” executive function deficits in tasks of
otor inhibition and attention (50).
BIOL PSYCHIATRY 2011;69:e69–e87© 2011 Society of Biological Psychiatry

drtdv
S
S
sitTr(rtdyeisfvbmistmtcsdflcc3b
F
iccra1hppnushfttn
e70 BIOL PSYCHIATRY 2011;69:e69–e87 K. Rubia
Cool and Hot Executive Functions and TheirUnderlying Neurobiology
Recent developmental theorists have proposed the distinction be-tween cool cognitive executive functions such as attention, workingmemory, planning, and inhibition that are known to be mediated bylateral inferior and dorsolateral frontostriatal and frontoparietal net-works (51–54) and “hot” executive functions that involve incentivesand motivation (55) and are mediated by the paralimbic orbitomedialand ventromedial frontolimbic structures (51,56–60).
Emotion regulation and motivation are mediated by lateral or-bitofrontal and ventromedial frontal regions, including the anteriorcingulate, amygdala, insula, hippocampus and hypothalamus, theventral striatum, and other connected areas (61,62). The amygdalais important for the processing of negative affect and threat andtogether with ventral striatum mediates stimulus-reward associa-tions and motivation functions (63– 66). Orbitofrontal and temporallobes have been associated with impulsivity and aggression in le-sion, animal, and imaging studies (67– 69). Together with ventro-medial frontal cortex, including anterior cingulate, they mediatetop-down affect regulation in their interconnection to underlyinglimbic areas (61,62,65,66). These networks of affect regulation andmotivation have been shown to be implicated in hot executivefunctions (70).
Cool higher level cognitive processes are mediated by fronto-striato-temporo-parietal and frontocerebellar circuitries in childrenand adults (51–54). Higher order temporal and parietal sensorycortices mediate bottom-up attention based on stimulus salience,with the temporoparietal junction being crucial for visual-spatialand executive attention functions (71–73). The prefrontal cortex(PFC) provides goal-directed top-down attention and cognitivecontrol through several functions: inhibitory control of irrelevantacts and attention to irrelevant stimuli; sustaining, dividing, andselecting attention; working memory; and cognitive flexibility, aswell as timing functions such as temporal foresight (74 –76). Frontal,temporal, and parietal cortical areas are reciprocally intercon-nected with each other and project to basal ganglia and thalamus,as well as cerebellum in fronto-parieto-striatal and corticocerebel-lar circuitries that, in concert, mediate these attention and cognitivecontrol functions (65,66,72,73).
It thus seems that the neuropsychological evidence shows def-icits in children with ADHD in cool executive function tasks medi-ated by fronto-striato-cerebellar and frontoparietal neural net-works, while children with CD appear to be more prominentlyimpaired in tasks of affect and motivation control, such as gam-bling, or stimulus-response contingency reversal tasks that are me-diated by ventromedial and orbitofrontal limbic neural networks.The association between motivation control deficits and antisocialbehaviors is in line with behavioral studies showing that contin-gency association learning involving reward and punishment isstrongly implicated in the development and maintenance of anti-social behaviors (77).
Comorbidity Between ADHD and CDConduct disorder and ODD overlap clinically, behaviorally, and
cognitively with ADHD. The odds ratio for comorbidity with ADHDin children with CD is over 40, while this increases to 79 in childrenwith ODD (78,79). Comorbid patients are often considered severecases of ADHD (28) and the notion of a separate neurobiologicalbasis for CD has been debated (80). Comorbid cases have a moresevere clinical outcome than the individual diagnoses (81,82).
An important question yet to be addressed is whether these two
similar and often clinically and neuropsychologically overlapping dwww.sobp.org/journal
isorders differ in their underlying etiopathophysiology. The sepa-ation of associated neural networks for each disorder would po-entially be very helpful for the development of a more objectiveifferential diagnosis and of disorder-specific prevention and inter-entions.
tructural and Functional Neuroimaging of ADHD
tructural StudiesNeuroimaging studies in children with ADHD have shown con-
istent abnormalities relative to control subjects in late-developingnferior frontostriatal and frontocerebellar circuitries that mediatehese cognitive control functions that are impaired in the disorder.hus, structural magnetic resonance imaging (MRI) studies foundeduced volume and cortical thickness in inferior prefrontal cortexIFC) but also other frontal brain regions, as well as parietotemporalegions, the basal ganglia, the splenium of the corpus callosum, andhe cerebellum (83– 86). Two recent meta-analyses of structuralata in childhood ADHD have been published. The first meta-anal-sis was conducted on region of interest studies showing the great-st significant reductions relative to control subjects in posterior
nferior vermis of the cerebellum, the splenium of the corpus callo-um, total and right cerebral volumes, right caudate, and variousrontal regions (87). The other meta-analysis was of whole-brainoxel-based morphometry imaging studies, avoiding the a prioriias of region selection, and identified a significant regional grayatter reduction in ADHD children compared with control subjects
n right putamen and globus pallidus (88). Diffusion tensor imagingtudies have furthermore provided evidence for abnormalities athe neural network level, showing abnormalities in multiple white
atter tracts in cingulate and frontostriatal, as well as frontoparie-al, frontocerebellar, and parieto-occipital white matter tracts, inhildren, as well as adults, with ADHD compared with comparisonubjects (89 –92). Longitudinal imaging studies have provided evi-ence that the structural abnormalities in these late-developing
ronto-striato-cerebellar and frontoparietal systems are due to aate structural maturation of these regions (86,93). Thus, the peak ofortical thickness maturation has been shown to be delayed inhildren with ADHD compared with healthy peers by an average ofyears, with some regions, including frontal and temporal areas,
eing delayed in their cortical maturation by up to 4 to 5 years (93).
unctional Imaging StudiesIn line with the frontostriatal hypothesis of ADHD, functional
maging studies have shown reduced activation compared withontrol subjects, in particular in the IFC, anterior cingulate, andaudate, but also in temporoparietal regions, during tasks of motoresponse inhibition (69,94 –100), interference inhibition (101–103),nd of sustained, selective, and flexible attention (100,102,104 –11) (for meta-analysis, see [112]). Furthermore, ADHD childrenave also shown reduced activation in dorsal and ventrolateralrefrontal, cingulate, and cerebellar brain regions during tem-oral processes, including tasks of motor timing, time discrimi-ation, and temporal foresight (94,113–115), as well as temporalnpredictability (116). The cerebellum has furthermore beenhown to be dysfunctional in children with ADHD relative toealthy control subjects during tasks of attention and timing
unctions (108,109,114,116). A few recent studies have alsoested for neurofunctional deficits in children with ADHD relativeo healthy control subjects during tasks of motivation, finding ab-ormalities in ventral striatum, orbitofrontal, and cingulate cortices
uring reward-related processes (108,109,114,117).
pA
S
S
bdsc(ffsMmaccctlrdtwdtafAaC(glaApdtbapmuhtctmsasatcs(w
K. Rubia BIOL PSYCHIATRY 2011;69:e69–e87 e71
More recent functional imaging studies have tested for deficitsin interregional functional connectivity. During the resting state,children with ADHD have been shown to have reduced functionalconnectivity relative to healthy control subjects in frontostriatal,frontoparietal, temporoparietal, and frontocerebellar networks(118 –120), although increased interregional connectivity betweenanterior cingulate, striatum, and temporocerebellar regions hasalso been reported (118,121–123). In the context of cognitive tasks,I am only aware of two published papers in childhood ADHD. Onefound a reduced degree of functional connectivity relative tohealthy control subjects between IFC and the basal ganglia, parietallobes, and cerebellum, as well as between cerebellum and parietaland striatal brain regions during sustained attention (108); theother study found reduced connectivity between frontoparietaland frontocerebellar regions during interference inhibition andtime estimation, respectively (124). These findings suggest that thedysfunctions observed in ADHD patients not only affect isolatedbrain regions but also the functional interregional interconnectivitybetween affected regions, thus demonstrating deficits in fronto-striato-cerebellar and frontoparietal neural networks.
Relatively fewer studies have been conducted in adult ADHDand findings have been more inconsistent. This is likely due to thefact that confounding factors are more pronounced in adult com-pared with childhood ADHD imaging studies, such as the inclusionof small sample sizes, the elevated rate of comorbid conditions inadult ADHD, long-term medication history, and the need for retro-spective diagnosis (125). Structural imaging studies in adult ADHDobserved abnormalities in the volumes of left orbitofrontal cortex(126); in overall cortical gray matter, right anterior cingulate, andleft superior/dorsolateral prefrontal cortex (127); and cortical thick-ness in bilateral dorsolateral and orbitofrontal cortices, anterior andposterior cingulate, and in the temporo-occipitoparietal junction(128), as well as reduced structural connectivity between theseregions (91). Functional underactivation has been observed in adultADHD relative to healthy control subjects in orbital and dorsolateralprefrontal cortices and striatal, anterior cingulate, cerebellar, andparietotemporal brain regions, with, however, also some evidencefor compensatory increased activation in some of these regions insome studies (for review, see [125]). Functional task-related connec-tivity studies show deficits in interregional connectivity relative tohealthy control subjects during motor response inhibition betweenright and left IFC cortices and between the right inferior frontal lobeand other areas, including basal ganglia, anterior and posteriorcingulate, and parietotemporal and cerebellar areas (129), whichwas also observed by another study in adult ADHD patients duringworking memory (130). However, in the study of Wolf et al. (130),compensatory-increased connectivity was also observed betweenleft dorsal anterior cingulate, superior frontal lobe, and cerebellum.Rest-associated functional connectivity studies have found abnor-mal functional connectivity between anterior and posterior cingu-late (91,131,132).
ConclusionsIn summary, childhood ADHD is characterized by structural and
functional deficits compared with healthy children in predomi-nantly inferior but also medial and dorsolateral prefrontal cortices,anterior cingulate, the basal ganglia, cerebellum, and temporopa-rietal brain regions and their functional and structural interconnec-tivity, causing poor top-down control over inhibitory, attention,and timing functions. An important caveat, however, is that themajority of imaging studies in children with ADHD have not ex-
cluded comorbidity with ODD or CD. The extent to which antisocial croblems may have confounded the neuroimaging literature ofDHD can therefore not be assessed.
tructural and Functional Neuroimaging of CD
tructural Imaging StudiesUnfortunately, the imaging literature in CD is very confounded
y ADHD comorbidity. Very few imaging studies have tested chil-ren with CD independently of ADHD. A small, underpoweredtructural study compared 7 comorbid children with ADHD � CD, 5hildren with noncomorbid ADHD, and 19 healthy control subjects133). While the children with noncomorbid ADHD did not differrom those with comorbid ADHD and CD, both groups differedrom control subjects in the volume of the left and total posterioruperior and inferior lobes of the cerebellar vermis (133) (Table 1).ore recent structural studies found reduced volume and grayatter concentration/thickness of temporal lobes and other limbic
nd paralimbic regions in childhood-onset CD relative to healthyontrol subjects (134,135). In the study of Kruesi et al. (134), allhildren had lower IQ and a history of ADHD, with 6 out of 10hildren having current ADHD and 4 having substance abuse. Pa-ients relative to control subjects showed reduced total temporalobe and reduced right temporal gray matter volumes, and findingsemained after controlling for IQ and substance abuse. Attention-eficit/hyperactivity disorder, however, was not controlled for in
he study. In the study of Huebner et al. (135), most CD patientsere comorbid with ADHD (17 of 23 patients) but had no affectiveisorder. They showed reduced total gray matter volumes relative
o control subjects, in particular in bilateral temporal lobes, leftmygdala and hippocampus, and orbitofrontal and ventromedialrontal regions, but increased gray matter in bilateral cerebellum.lthough the majority of CD children also had ADHD, regressionnalyses within patients revealed significant associations betweenD symptoms and gray matter reductions in temporal, limbic
amygdala, hippocampus), cerebellar, medial, and mesial frontalray matter, while hyperactivity/impulsiveness symptoms corre-
ated inversely with gray matter reductions in left inferior frontalnd parietal cortices and bilateral temporo-occipital regions (135).study by Sterzer et al. (136) scanned 10 patients with CD; 7 of the
atients also met criteria for ADHD and scored high for anxiety andepression. Reduced gray matter volumes were observed relative
o healthy control subjects in bilateral insula and left amygdala,oth of which correlated with aggressive and inattentive but notnxiety/depression symptoms. A study by DeBrito et al. (137) com-ared 23 community adolescent boys with no psychiatric abnor-alities or mood or anxiety problems but high levels of callous-
nemotional (CD-CU), as well as CD and ADHD problems, with theirealthy twins. Covarying for both inattentive-hyperactivity symp-
oms and IQ, they found that gray matter concentration was in-reased compared with control boys in posterior medial orbitofron-al cortex, dorsal and rostral anterior cingulate, as well as in gray
atter concentration and volumes in superior parietotemporal anduperior frontal regions, cerebellum, insula, posterior cingulate,nd hippocampus. The most interesting finding of their study was aignificant deviation in CD-CU children from the norm-typical neg-tive correlation between age and cortical thickness in orbitofron-al and left dorsal anterior cingulate. The fact that patients, unlikeontrol subjects, showed no negative age correlation in this mea-ure could potentially indicate a delay of normal brain maturation137), similar to that observed in ADHD (93). Longitudinal studies
ill be needed, however, to corroborate this observation based on
ross-sectional data.www.sobp.org/journal
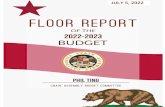
Table 1. Summary of Main Findings of Structural and Functional Magnetic Resonance Imaging Studies that Directly Compared Children with ADHD and with CD
StudyImagingMethod Task WB/ROI Subjects F/M
AgeRange
Med/MedHistory Results
Bussing et al.2002 (133)
sMRI — WB 5 ADHD only7 CD/ADHD10 control subjects
F and M 8 –12 Yes CD/ADHD and ADHD alone versus control subjects: reduced mean volumesin total and L posterior superior and inferior cerebellar vermis. Nodifferences between the pure and the comorbid groups. No groupdifferences in cerebral hemispheres or caudate.
Rubia et al.2008 (96)
fMRI Stop taska) Successful
stopb) Failed stop
WB 20 ADHD13 CD20 control subjects
M 9 –17 No 3-group interaction effects:a) Successful stop: ADHD versus CD and versus control subjects: reduced
activation in L DLPFC/IFCb) Failed stop: CD versus ADHD and versus control subjects: reduced
activation in L and R IPL and R STLBoth patient groups versus control subjects: reduced activation in L and R
PCC/precuneus.Rubia et al.
2009 (109)fMRI Rewarded CPT WB 18 ADHD
14 CD16 control subjects
M 9 –17 No 3-group interaction effects:CPT: ADHD versus CD and control subjects: reduced L and R IFC and
enhanced L and R Cb/hippocampus/PCC activation.L and R IFC activation was correlated with omission errors that were
enhanced at trend level in ADHD.CD versus ADHD and control subjects: reduced activation in R insula,
hippocampus, PMC, ACC.Reward effect: CD versus ADHD and control subjects: reduced activation
in R ventromedial OFC.ADHD versus CD and control subjects: reduced activation in precuneus
and PCC.Rubia et al.
2009 (102)fMRI Simon and oddball
tasksROI 8 ADHD
8 control subjectsM 10 –17 No 3-group interaction effects:
Oddball: ADHD versus CD and control subjects: reduced activation in LDLPFC/IFC.
ADHD and CD versus control subjects: reduced activation in R DLPFC butno differences between patient groups.
Simon: ADHD and CD versus control subjects: reduced activation in R STLand MTL and R precuneus but no differences between patient groups.
Rubia et al.2010 (107)
fMRI Switch task WB 14 ADHD14 CD20 control subjects
M 9 –17 No 3-group interaction effects:ADHD versus CD and control subjects: reduced activation in L and R IFC/
DLPFC.2-group comparisons:CD versus control subjects: reduced activation in L and R IPL and R STL/
precuneus but no differences between patient groups.Marsh et al.
2008 (148)fMRI Neutral, fearful,
and angryfaces
ROI 12 ADHD/CD/ODD � CU12 ADHD12 control subjects
M 10 –17 Yes Group by expression effect:ADHD/CD/ODD � CU versus ADHD pure and control subjects: reduced R
amygdala activation for fearful faces (trend). Also reduced functionalconnectivity between R amygdala and R OFC.
Connectivity abnormalities correlated with CU severity. No groupdifferences for angry or neutral faces.
e72B
IOL
PSY
CH
IATRY
2011;69:e69–e87
K.Rubia
ww
w.so
bp
.org
/jou
rnal

ablmobc
F
svjC(cjwbtlisrt(aawestacmaata
8ctpttlFvts
tpppcvttble
1.
Co
nti
nu
ed
dy
Imag
ing
Met
ho
dTa
skW
B/R
OI
Sub
ject
sF/
MA
ge
Ran
ge
Med
/Med
His
tory
Resu
lts
ger
etal
.00
8(1
95)
fMRI
Reve
rsal
lear
nin
gta
skW
B12
AD
HD
/CD
/OD
D�
CU
14A
DH
D14
con
tro
lsu
bje
cts
M10
–17
Yes
Dia
gn
osi
sb
yre
spo
nse
typ
ein
tera
ctio
n:
AD
HD
/CD
/OD
D�
CU
vers
us
con
tro
lsu
bje
cts
and
vers
us
AD
HD
:en
han
ced
acti
vati
on
inL
and
Rvm
PFC
du
rin
gp
un
ish
edre
vers
aler
rors
.C
orr
elat
ion
bet
wee
nvm
PFC
acti
vati
on
and
anti
soci
alan
dC
Utr
aits
.A
DH
D/C
D/O
DD
�C
Uve
rsu
sco
ntr
ols
ub
ject
s:en
han
ced
cau
dat
eac
tiva
tio
nd
uri
ng
pu
nis
hed
reve
rsal
erro
rs.N
od
iffer
ence
toA
DH
Dal
on
e.D
iag
no
sis
effe
ct:b
oth
AD
HD
/CD
/OD
D�
CU
and
AD
HD
alo
ne
vers
us
con
tro
lsu
bje
cts
hav
een
han
ced
acti
vati
on
inL
pre
cun
eus
and
RSF
C.
All
fMRI
task
sw
ere
even
t-re
late
dd
esig
ns.
AC
C,a
nte
rio
rci
ng
ula
teco
rtex
;AD
HD
,att
enti
on
defi
cit
hyp
erac
tivi
tyd
iso
rder
;Cb
,cer
ebel
lum
;CD
,co
nd
uct
dis
ord
er;C
PT,c
on
tin
uo
us
per
form
ance
task
;CU
,cal
lou
s-u
nem
oti
on
alsy
mp
tom
s;D
LPFC
,so
late
ralp
refr
on
talc
ort
ex;F
,fem
ale;
fMRI
,fu
nct
ion
alM
RI;I
FC,i
nfe
rio
rfr
on
talc
ort
ex;I
PL,i
nfe
rio
rp
arie
tall
ob
e;L,
left
;M,m
ale;
Med
,med
icat
ion
;MFC
,med
ialf
ron
talc
ort
ex;M
RI,m
agn
etic
reso
nan
ceg
ing
;MTL
,med
ialt
emp
ora
llo
be;
OD
D,o
pp
osi
tio
nal
defi
ant
dis
ord
er;O
FC,o
rbit
ofr
on
talc
ort
ex;P
CC
,po
ster
ior
cin
gu
late
cort
ex;P
MC
,pre
mo
tor
cort
ex;R
,rig
ht;
ROI,
reg
ion
ofi
nte
rest
anal
ysis
;SFC
,er
iorf
ron
talc
ort
ex;s
MRI
,str
uct
ura
lMRI
;STL
,su
per
iort
emp
ora
llo
be;
Sto
p,s
top
sig
nal
task
;vm
PFC
,ven
tro
med
ialp
refr
on
talc
ort
ex;W
B,w
ho
leb
rain
anal
ysis
.
K. Rubia BIOL PSYCHIATRY 2011;69:e69–e87 e73
In conclusion, the structural evidence, therefore, points towardbnormalities in CD of the paralimbic system, comprising the or-itofrontal cortex (OFC), anterior cingulate, superior temporal
obes, and underlying limbic structures that are known to mediateotivation and affect (29,138). So far, however, there are no studies
f structural connectivity in CD that have tested for potential distur-ance of white matter tracts belonging to the paralimbic system toonfirm a neural network disturbance.
unctional Imaging StudiesFunctional imaging studies in children with CD have been con-
istent with the structural evidence, finding abnormalities in theentromedial orbitofrontal temporolimbic system in CD. The ma-
ority of functional magnetic resonance imaging (fMRI) studies inD have used emotion processing tasks. A study by Sterzer et al.
139) found more pronounced deactivation in right dorsal anterioringulate gyrus in children with CD relative to healthy control sub-ects during the viewing of pictures with negative valence, which
as interpreted by the authors as reduced inhibition of emotionalehavior. Although 62% of patients also met criteria for ADHD and
he group scored high on depression-anxiety, the anterior cingu-ate deactivation correlated negatively with the aggressive behav-or scores and remained when controlling for attention, depres-ion/anxiety scores, and IQ (139). This is in line with the notion ofeduced emotion processing as the basis of aggression, given thathe amygdala is a key region for the processing of negative affect140). A subsequent correlation analysis on the same dataset found
correlation between abnormal functioning of anterior cingulatend sensation seeking (141). A later study on a group of 22 childrenith CD with no affective disorder, 16 of which had ADHD, found
nhanced left amygdala activation compared with healthy controlubjects to the same negative affect stimulation, suggesting emo-ional hyperresponsivity. The effect remained when controlling forffective/depressive symptoms and was not observed in a patientontrol group with ADHD only (142). Although the findings re-ained when covaried for affective symptoms, the group was char-
cterized by high symptoms of emotion and anxiety, which could,t least partly, explain the enhanced amygdala activation that isypically enhanced in anxiety in relation to negative emotions suchs fear (143).
A recent fMRI study in children with early-onset childhood CD,8% of which also met criteria for ADHD, found abnormal activationompared with control subjects in relation to empathy and sympa-hy. Children with CD had reduced activation in the somatosensoryain matrix, typically activated in healthy children in response to
he observation of pictures showing humans undergoing acciden-al body harm, but enhanced activation in anterior midcingulate,eft amygdala, right caudate, and bilateral temporal pole (144).urthermore, the extent of prefrontal and amygdala activation toiewing pain in others was significantly positively correlated toheir number of aggressive acts and their ratings of daring andadism score on behavioral questionnaires.
The comparison of pictures showing intentional versus acciden-al body harm also showed enhanced activation in the antisocialatients compared with healthy control subjects in somatosensoryain regions of left anterior insula, supplementary motor area, andrecentral gyrus but decreased activation in lateral IFC, posterioringulate, and the temporoparietal junction. Furthermore, the acti-ation in the temporoparietal junction and insula correlated withhe subjective ratings of the pain experienced by the individuals inhe pictures (144). Connectivity analyses showed that pain inflictedy others versus accidental pain led to enhanced connectivity be-
tween ventromedial prefrontal cortex and amygdala in control sub-Tab
Stu
Fin 2
do
rim
asu
p
www.sobp.org/journal

pwav
dagAwa
scwmsmc
Co
twl(wioddiiatctttgdh(dfdt(ttacw1(b(csb
e74 BIOL PSYCHIATRY 2011;69:e69–e87 K. Rubia
jects but not in CD patients (144). The findings suggest that highlyaggressive antisocial youth are hypersensitive in their brain re-sponse to seeing victims in pain and show diminished regulation ofemotion-processing networks, as shown by reduced PFC/amygdalaconnectivity relative to control subjects. The fact that these activa-tion and connectivity patterns correlated with sadism and antiso-cial behavioral ratings suggests either that the hypersensitivity re-flects greater enjoyment of the other’s pain or enhanced reactivityand reduced control over networks that process negative emotions(144). The correlation findings also suggest that the brain abnor-malities are associated with the antisocial core ratings, which isimportant, given the high comorbidity. Aggression may thus berelated to poor regulation over hypersensitive negative affect pro-cessing brain regions, resulting in harmful patterns of interpersonalbehavior (144 –146).
Another more recent fMRI study found reduced activation com-pared with healthy control subjects in the amygdala in patientswith CD and callous-unemotional traits who had elevated ADHDscores but no elevated affective symptoms (147). The findings re-mained after covarying for ADHD symptoms.
In conclusion, parallel to structural studies, functional imagingstudies show evidence that children with CD and CD-CU suffer froma dysregulation of ventromedial prefrontal amygdala regions andnetworks that mediate affect regulation (29,138).
Overall ConclusionIn conclusion, imaging studies of children with CD show struc-
tural and functional abnormalities compared with healthy controlsubjects in ventromedial and orbital prefrontal, superior temporal,and limbic brain regions that are known to regulate motivation andaffect and abnormal functional connectivity within these frontolim-bic networks. A caveat is that all studies have included a largeproportion of patients that were comorbid with ADHD, with themajority of studies including over 50% comorbidity. The observedabnormalities in brain abnormalities, however, were shown to cor-relate with antisocial symptoms or to survive covariation for ADHDin several structural (135–137) and functional imaging studies(139,144,148). Some studies, however, did not control for ADHD(136) or found that the main findings correlated with both CD andADHD symptoms (136) or only presented the correlation with CD,but not ADHD, symptoms (144). Anxiety and depression are othercommon comorbidities with CD. The majority of studies, however,have either excluded comorbidity with affective disorders and/orcovaried for anxiety and depression (139,142,147,148). However,while this suggests that anxiety and depression cannot alone ac-count for the deficits, this does not exclude the possibility that theymay have contributed to some extent. Lastly, all imaging studiesfocused on children with CD, and ODD was not assessed separatelyin any study. Future studies will need to investigate the neuroimag-ing correlates of ODD and whether they differ from those associ-ated with CD.
Structural and Functional Neuroimaging ComparisonsBetween ADHD and CD
Given the substantial clinical overlap between ADHD and CDsymptoms, with between 50% and 90% comorbidity (19,149), thepossibility of an objective differentiation through imaging technol-ogy is attractive. Modern functional neuroimaging could be animportant aid in the differentiation of clinically and behaviorallysimilar disorders, if it can identify differences in the objectivelymeasurable underlying pathophysiological mechanisms, the bio-markers that underlie overlapping behavior features of these two
disorders. Disentangling the disorder-specific underlying patho- rwww.sobp.org/journal
hysiology of behaviorally and cognitively overlapping disordersill be crucial to develop more objective differential diagnostics
nd more informed and disorder-specific targeted methods on pre-ention and early intervention.
Very few studies, however, have directly compared these twoisorders in neuroimaging. As mentioned, only one structural im-ging study compared whole brain volume abnormalities in smallroups of comorbid children with CD and ADHD and noncomorbidDHD, finding no significant differences between the disorders,hereas both groups showed reduced volumes in the posterior
nd inferior cerebellar vermis (133) (Table 1).Few fMRI studies have compared the neurofunctional sub-
trates between the two disorders. Furthermore, few of them haveontrolled for differences in IQ or tested medication-naive patientsith ADHD or CD that were clinically not comorbid. Long-termedication with stimulants appears to have effects on both brain
tructure (150,151) and brain function development (152), andedication naivety is, hence, crucial when comparing between
hild psychiatric disorders.
omparison Between Noncomorbid Groups of ADHD and CDn Tasks of Executive Functions and Reward
A series of fMRI studies from our group compared well-differen-iated, medication-naive IQ-matched groups of children with CD,ho had no clinical diagnosis of ADHD and scored significantly
ower on ADHD symptoms on a questionnaire of symptom severitythe Strength and Difficulties Questionnaire [153]), with children
ith ADHD, who had no clinical diagnosis of CD and scored signif-cantly lower on the questionnaire for CD symptoms. Affective dis-rders and anxiety were excluded and both patient groups did notiffer from control subjects in their affective symptom scores. Theisorders were compared in their neurofunctional activation dur-
ng five disorder-relevant executive function tasks, shown to bempaired in both disorders: motor response inhibition, sustainedttention, cognitive switching, interference inhibition, and atten-ional oddball. One of the tasks, the sustained attention task, in-luded an additional motivational aspect, where sustained atten-ion was compared in both rewarded and nonrewarded conditionso assess the effects of motivation on attention networks. Despitehe fact that performance measures did not differ between patientroups, in four of the five tasks we observed disorder-specific re-uced activation in patients with ADHD compared with bothealthy control subjects and CD patients in the IFC (96,102,107,109)
Table 1). The location of disorder-specific abnormality was moreorsolateral for the stop and oddball tasks and more ventrolateral
or the sustained attention and switching tasks. Furthermore, theysfunction was bilateral for the sustained attention and switching
asks (107,109) but left hemispheric for the stop and oddball tasks96,102) (Figure 1A, Table 1). During the sustained attention condi-ion, we also observed a disorder-dissociated effect in a large pos-erior activation cluster comprising the cerebellum, hippocampus,nd inferior temporal lobe, which was enhanced in activation inhildren with ADHD but reduced in children with CD comparedith each other and healthy control subjects (109) (Figure 1A, Table
). The cerebellum is an essential part of frontocerebellar networks72), and in particular, the later-developing anterior cerebellum haseen shown to be crucially implicated in attention functions
154,155). We hypothesized that the disorder-specific enhancederebellar/temporal activation in children with ADHD was compen-atory for the reduced IFC activation during the task, corroboratedy the finding of a negative correlation between these two brain
egions in ADHD children but not the other two groups.

abpns(rri
a(bpcwaa ore d
K. Rubia BIOL PSYCHIATRY 2011;69:e69–e87 e75
The disorder-specific reduced IFC activation in ADHD patientsacross four different tasks is a consistent finding that may suggestthat IFC dysfunction is a disorder-specific neurofunctional bio-marker for ADHD, at least when compared with CD. This is in linewith the fact that we also found disorder-specific reduction in IFCactivation in children with ADHD during two tasks, motor responseinhibition and switching, when compared with healthy childrenand children with obsessive-compulsive disorder (156). Obsessive-compulsive disorder patients, in turn, had shared abnormalities
Figure 1. (A) Disorder-specific underactivation in inferior prefrontal cortconduct disorder (CD) and healthy children. Disorder-specific underactivat
ge-matched healthy control children (n � 20) and children with conduct dcontinuous performance task), attention allocation (oddball task), and cogut decreased in CD children relative to control subjects and each other. Inrefrontal activation that was reduced in ADHD compared with healthy contompared with ADHD and healthy children in areas of the paralimbic systemith healthy children and children with ADHD in areas of the paralimbic sy
ttention task); the ventromedial orbitofrontal cortex (during rewarded comnterior cingulate, insula and hippocampus (sustained attention task). For m
with ADHD patients in other prefrontal regions, including the OFC m
nd dorsolateral prefrontal cortex (106,156) (Figure 2). The IFC haseen associated with a range of cognitive control processes. It has arominent role in motor response inhibition, more prominently butot exclusively in the right hemisphere, as demonstrated by fMRItudies of children and adults during motor inhibition tasks22,52,53,157), as well as lesion (158) and transcranial magneticesonance imaging studies (159). The IFC, however, is also a keyegion for other related functions that may share elements of inhib-tory control, such as interference inhibition, which has more com-
attention-deficit/hyperactivity disorder (ADHD) children compared withinferior prefrontal cortex in children with ADHD (n � 20) compared with
er (n � 14) during tasks of motor inhibition (stop task), sustained attentionswitching. The cerebellum activation was increased in activation in ADHDpatients, the cerebellum activation correlated negatively with the inferior
bjects and CD children. (B) Disorder-specific underactivation in CD childrenorder-specific underactivation in children with conduct disorder comparedincluding the temporal lobe (inhibition failures in the stop task; sustained
d with nonrewarded attention trials); and in underlying limbic structures ofetails, see Rubia et al. (96,102,107,109).
ex inion inisordnitiveADHDrol su. Dis
stem,pare
only been found to be mediated by left hemispheric inferior
www.sobp.org/journal

t(
agfawwewrsrdps
lhcstmT
wtncn(tvgc
cand h).
e76 BIOL PSYCHIATRY 2011;69:e69–e87 K. Rubia
frontal cortex (51,53,160 –162). It is also involved in cognitiveswitching, in a typically bilateral location, presumably mediatingthe inhibition of previously valid but no longer relevant stimulus-response associations (right IFC) and the re-engagement of novelstimulus-response associations (left IFC) (51,53,163). It has alsobeen suggested that the IFC junction may have a more generic rolefor the update of information in tasks of cognitive control, whichcould explain its ubiquitous activation across cognitive controltasks (160). Furthermore, the bilateral IFC is also consistently acti-vated in children and adults during tasks of selective and sustainedattention (108,164) and attention allocation in oddball tasks(54,110). The finding that IFC may be a disorder-specific neurofunc-tional biomarker of ADHD, when compared with CD, is in line withneuropsychological findings. Attention-deficit/hyperactivity disor-der children have consistent impairment in tasks that are mediatedby IFC (21,23,113) and this is more prominent than in children withCD (24). Furthermore, children with CD or ODD are often not im-paired in these tasks when ADHD is controlled for (38 – 43). It is alsoparallel to regression analyses that show that ADHD, but not CD,traits account for poor performance in these IFC mediated coolexecutive function tasks (50).
For the reward contrast, however, it was the CD children whoshowed deficits in the recruitment of task-relevant prefrontal brainregions (109). Children with CD, relative to control subjects andchildren with ADHD, showed reduced activation in ventromedialOFC, which is known to be crucial for executive reward processingand the mediation of motivation (51,165,166) (Figure 1B, Table 1).The orbitofrontal cortex is thought to be important for holdinginformation in representational memory, as well as incentive moti-vation (58), and thus mediates stimulus-reinforcement learning(58,167). The ventromedial part, in particular, is associated withreward as opposed to punishment-driven processes (168 –170).The disorder-specific abnormality in ventromedial PFC for CD is inline with evidence for abnormal activation in ventromedial PFC andOFC in patients with impulsive aggression and psychopathy duringemotional tasks. For example, reduced orbitofrontal activation was
Figure 2. Disorder-specific underactivation in attention-deficit/hyperactivihildren in inferior prefrontal cortex. Disorder-specific underactivation in ch
cortex compared with children with obsessive-compulsive disorder (n � 10)and cognitive switching (switch task). For more details, see Rubia et al. (156
observed in patients with impulsive aggression in relation to nega- d
www.sobp.org/journal
ive emotional stimuli (171), as well as in patients with psychopathy172,173).
Furthermore, the lateral and ventromedial orbitofrontal cortexlso plays a crucial role in the modulation of paralimbic brain re-ions that mediate aggression (138,174). As mentioned, the orbito-
rontal cortex, together with temporal areas including amygdaland hippocampus, was reduced in gray matter in adolescent boysith CD (135). It has been hypothesized that abnormalities in re-ard computations mediated by orbitofrontal cortex leading to
nhanced frustration could trigger reactive aggression, whichould explain the link between aggression, abnormalities with the
eward system, and orbitofrontal abnormalities (174). The disorderpecificity of the dysfunction of the ventromedial frontal cortex inelation to reward compared with ADHD is also in line with evi-ence of reduced autonomic response in patients with CD com-ared with ADHD and healthy control subjects during emotionaltimuli (175).
It thus seems that there is a disorder-specific and process-re-ated dissociation in prefrontal lobe deficits, where ADHD childrenave consistent problems with the recruitment of IFC systems in theontext of cool executive inhibitory and attention control acrosseveral cognitive domains, while CD children have problems withhe recruitment of hot ventromedial OFC systems that mediate
otivation in the context of reward processing (109) (Figure 1B,able 1).
Attention-deficit/hyperactivity disorder children, during the re-ard contrast, showed disorder-specific reduced activation relative
o control and CD children in the posterior cingulate and precu-eus, brain regions known to mediate visual-spatial attention pro-essing of saliency (176,177). The posterior cingulate and precu-eus are reciprocally connected with the anterior cingulate cortex
ACC) (178), which monitors action outcomes to support learninghe value of actions (179), and the parietal cortex, which directsisual attention (180) and has hence been associated with the inte-ration of incentives with attention modulation (181). The posterioringulate and precuneus are typically reduced in activation in chil-
order children compared with obsessive-compulsive disorder and healthywith attention-deficit/hyperactivity disorder (n � 18) in inferior prefrontal
ealthy children (n � 20) during tasks of motor response inhibition (stop task)
ty disildren
ren with ADHD during salient stimuli such as errors (95,96) and

stgt
tnoddldCrvbhk
pdmh(tridpftAacG(aecdtdctbTwbmww
Bacderjtap
K. Rubia BIOL PSYCHIATRY 2011;69:e69–e87 e77
oddball or incongruent targets (102,108,110). Reduced activation ina region of saliency processing is consistent with the catecholaminedeficiency hypothesis of ADHD, given that catecholamine defi-ciency diminishes and catecholamine agonists enhance the sa-lience of stimuli (182). In fact, methylphenidate, the treatment ofchoice and an indirect catecholamine agonist, has been shown toupregulate the activation of posterior cingulate in children withADHD, leading to better attention performance (108). Abnormalcingulate activation in ADHD children may thus be the neurobio-logical substrate of catecholamine deficiency-related abnormal sa-lience processing.
Apart from the abnormal ventromedial OFC activation, conductdisorder patients demonstrated disorder-specific reductions of ac-tivation compared with control subjects in several other regions ofthe paralimbic system during all tasks. During the sustained atten-tion task, where ADHD children showed disorder-specific inferiorfrontal underactivation relative to control and CD children, thatfurthermore correlated with the main performance indicator (i.e.,omission errors), children with CD showed reduced activation rela-tive to ADHD and control children in areas of the limbic system thathave been shown to contribute to sustained attention throughtheir mediation of motivation, such as hippocampus, the insula,superior temporal lobe, and the dorsal ACC. Furthermore, they alsoshowed reduced activation relative to control and ADHD children ina cluster comprising the cerebellum, the hippocampus, and theinferior temporal lobes (109) (Figure 1B, Table 1). These regions ofthe paralimbic system lie at the interface between emotion andcognition. The dorsal anterior cingulate is connected to frontal-parietal attentional networks but is also crucial for motivation andarousal (183,184). Hippocampus and insula form part of the limbicsystem and visuomotor pathways and are an interface betweenmotivation and spatial attention (185). Thus, a more anterior part ofthe insula has been shown to contribute to sustained attention(164), while the hippocampus plays a role in selective visual atten-tion to targets (186). As mentioned, the cerebellar hemispheresform part of frontocerebellar attention systems (72,154,155,187).The superior and inferior temporal lobes are closely connected tothe limbic system and contribute to cognitive functions such asperceptual selective attention (188). Together, it thus appears thatCD children show disorder-specific underactivation in subcorticaland paralimbic brain regions that lie at the interface between mo-tivation and attention and contribute to attention functions, pre-sumably through their mediating role between motivation andcognition. The key performance measure of omission errors did notdiffer between patient groups but were lower than those of controlsubjects, which reached significance for ADHD. This suggests thatthe underrecruitment of cool IFC networks, as well as the reducedrecruitment of motivational paralimbic brain regions, can lead tosimilar performance underachievement.
In addition, CD children showed disorder-specific underactiva-tion of the superior temporal lobes during failures in the stop taskcompared with both ADHD children and healthy control subjects(96) (Figure 1B, Table 1). The reduced activation of superior tempo-ral regions after mistakes may reflect reduced recruitment of per-formance monitoring systems, in line with evidence that CD chil-dren care less about their mistakes and respond less to negativefeedback than healthy children (39,47). Disorder-specific reducedactivation in this brain region was also observed in children with CDcompared with control subjects, but not ADHD patients, duringcognitive switching (107) and sustained attention (109) (Figure 1B,Table 1).
Dysfunction of the temporal lobes during attention and perfor-
mance monitoring in patients with CD is in line with evidence for structural abnormalities in this brain region (134,135,137). Fur-hermore, temporal lobe lesions have been associated with ag-ression and antisocial behavior (189,190), as well as with empa-
hy (191).In conclusion, the findings of disorder-specific deficits in these
wo clinically overlapping disorders suggest distinct underlyingeurofunctional abnormalities, both of which may be related toverlapping behavioral features. Attention-deficit/hyperactivityisorder appears to be associated with disorder-specific cool top-own inferior prefrontal and bottom-up cerebellar-posterior cingu-
ate cognitive control/attention networks, presumably causing re-uced top-down executive inhibitory and attention control.onduct disorder, by contrast, appears to be associated with neu-
ofunctional deficits in areas of the paralimbic system, in top-downentromedial OFC and underlying bottom-up limbic and paralim-ic structures (anterior cingulate, superior temporal lobes insula,ippocampus) that together mediate motivation and affect and arenown to feed into attention systems (164,183,184,186).
The findings of disorder-specific abnormalities in areas of thearalimbic system in CD are in line with neuropsychological evi-ence that shows specific impairment in these children in tasks ofotivation control compared with children with ADHD. They show
yposensitivity to punishment in reward-related paradigms39,45– 47,192). Furthermore, symptom-regression analyses showhat CD/ODD symptoms account for the deficits in hot reward-elated gambling tasks, while ADHD symptoms accounts for deficitsn cool executive function tasks (50). This neuropsychological evi-ence, combined with our imaging findings of disorder-specificaralimbic dysfunction, suggests that impairment in cool executive
unctions in CD may be related to an underlying pathophysiology ofhe motivational limbic system—that is different from that ofDHD—that disturbs the normal interaction between motivationnd cognition, leading to reduced motivational upregulation of theool executive system, necessary for normal optimal performance.iven that motivation and reward upregulate cognitive processes
185,193,194), both a dysfunction of the hot motivation system, asppears to be the case in CD, as well as a dysfunction of the coolxecutive system directly, as observed in ADHD, would lead toognitive impairment. The difference is that the neurobiologicaleficit in ADHD is directly affecting the cool cognitive control sys-
ems, while the deficit in CD affects these systems indirectly, via aysregulation of the neuronal interplay between motivation andognition. The dissociative imaging findings hence show that func-ional imaging is more sensitive than performance to differentiateetween behaviorally and cognitively overlapping patient groups.his is illustrated, in particular, for the sustained attention task,here both disorders shared the same number of omission errorsut the underlying disorder-specific dysfunctions were in perfor-ance correlated cool IFC frontocerebellar activation in patientsith ADHD and in hot paralimbic motivation regions in CD thatere not directly related to task performance.
We also observed shared abnormalities in the two disorders.oth disorders showed reduced posterior cingulate and precuneusctivation during inhibition failures and during incongruent stimuliompared with control subjects, presumably reflecting shared re-uced activation to salience, given that both errors and incongru-nt trials are salient stimuli (96,102). Another brain region that waseduced in activation in both disorders compared with control sub-ects was the right medial frontal lobe during visual-spatial atten-ion to oddball stimuli (102) (Table 1). It thus appears that a sharedbnormality in both disorders is the recruitment of dorsolateralrefrontal and posterior parietal brain regions that mediate visual-
patial attention to salient events.www.sobp.org/journal

mttartpaopsaCmpws
vtiopcwcewi
swvattra
G
aCbIa(drdAbtiwthasws
e78 BIOL PSYCHIATRY 2011;69:e69–e87 K. Rubia
Comparisons Between Children with CD-CU and ComorbidADHD with Noncomorbid Children with ADHD
Two fMRI studies from within the same research group com-pared children with callous-unemotional traits and either CD orODD with children with noncomorbid ADHD as well as controlsubjects (148,195). The groups were not well separated in clinicalsymptomatology because the group with CD/ODD-CU also hadADHD symptoms (7 out of 12). Hence, the comparison was betweenchildren with ADHD and no comorbidities and children with ADHDand/or CD or ODD and CU symptoms and healthy control subjects.Mood and anxiety disorders were excluded. Furthermore, the ma-jority of children with ADHD in either group were medicated withpsychostimulants. In the study of Marsh et al. (148), reduced rightamygdala activation was found to fearful compared with neutralfaces in the group with CD/ODD-CU and ADHD relative to controlsubjects and relative to noncomorbid ADHD, while the lattergroups did not differ from each other (148). No group effects wereobserved for angry or neutral faces. Furthermore, both control sub-jects and ADHD patients without CD/ODD-CU had a higher degreeof functional connectivity between right amygdala and right ven-tromedial prefrontal activation during fear compared with the CD/ODD-CU and ADHD group, which furthermore correlated with theseverity of the psychopathy symptom scores (Table 1). Theamygdala plays an important role in fear processing and socializa-tion (140), and its abnormal response may be the neural substratefor reduced distress cue processing and socialization problems inpsychopathy (29,138,196). The underconnectivity findings are in-teresting with respect to evidence showing that the closely inter-connected ventromedial prefrontal cortex and amygdala (197) arecrucial to affect control (198). Together, they mediate appropriatebehavioral decision making based on positive and negative feed-back (51,199) and moral decision making (200 –202). These twostructures are also known to regulate reactive aggression (174,203).
The second study by Finger et al. (195), on the same sample,compared 14 children with CD/ODD-CU, allowing for ADHD symp-toms, with 14 children with noncomorbid ADHD with low scores onantisocial traits and 14 healthy control subjects in a reversal task.While healthy and ADHD children showed reduced activation inbilateral ventromedial prefrontal cortex and caudate during pun-ished reversal errors compared with rewarded correct responses,this effect was not observed in children with CD-CU who showedenhanced activation in this region during punished reversal errorsrelative to the other two groups. The disorder-specific abnormali-ties in ventromedial prefrontal activation in the CD-CU and ADHDgroup were furthermore correlated with total scores on antisocialand callous-unemotional traits (Table 1). Although some of thepatients were medicated, the findings remained when these wereexcluded from the analysis (195). Both the ADHD only group andthe group with psychopathy and CD/ODD/ADHD showed en-hanced activation in left precuneus and right superior frontal gyrusrelative to control subjects (Table 1). The enhanced activation in thegroup of ADHD without comorbid CD-CU compared with controlsubjects in precuneus and medial frontal lobe is unusual and not inline with the underactivation findings of the majority of fMRI stud-ies of ADHD during tasks of cognitive flexibility (100,107) or errorprocessing (95,96,156). The negative findings may potentially berelated to the fact that the children in this group had a higher IQcompared with the other two groups. While at first the findings ofenhanced ventromedial frontal activation may seem in the oppo-site direction to our finding of reduced ventromedial OFC activationin children with CD during rewarded attention trials (109), theyare, in fact, consistent with each other. The children with psychop-
athy in the study of Finger et al. (195) also showed reduced ventro- bwww.sobp.org/journal
edial PFC activation during rewarded correct trials, even thoughhis did not reach significance, but showed enhanced activation inhis region during punished error trials relative to control subjectsnd ADHD patients. It thus may be that reward and punishmentesult in patients with CD in dissociated abnormal response pat-erns in ventromedial and orbitofrontal brain regions, showing hy-osensitive activation in the context of reward and hypersensitivectivation during punishment, suggesting a contingency-sensitiverbitofrontal dysregulation. Alternatively, it is also possible thatsychopathy and CD have qualitatively different underlying neuralubstrates, as demonstrated with evidence with respect tomygdala hyperactivation in CD (139,144) and hypoactivation inD-CU (148). The disorder-specific abnormality findings in ventro-edial prefrontal and amygdala activation in the children with
sychopathy compared with control and ADHD children are in lineith evidence for dysfunction and dysmorphology of these two
tructures in adults with psychopathy (29,138,145,204 –206).Another interesting dissociation was found for the caudate acti-
ation, which was exclusively enhanced in patients with psychopa-hy compared with control subjects and ADHD patients for pun-shed reversal errors compared with correct rewarded trials, thepposite pattern as in control subjects. However, the caudate hy-eractivation did not differ from ADHD patients (195) (Table 1). Theaudate is a key region of typically reduced activation in childrenith ADHD during tasks of cognitive control (94,97,113,207), in-
luding tasks of cognitive flexibility (100,156,208). The finding ofnhanced caudate activation in antisocial pathologies comparedith ADHD may potentially be related to different dopamine levels
n these disorders.In summary, the disorder-specific functional imaging findings
uggest that CD and CD-CU compared with ADHD are associatedith disorder-specific abnormalities of the paralimbic system of
entromedial and OFC, the limbic part of the anterior cingulate, themygdala, hippocampus, and the superior temporal lobes, knowno regulate affect and motivation. The disorder-specific dysfunc-ions in children with ADHD, by contrast, appear to be in brainegions that mediate a more cognitive form of top-down inhibitorynd attention control, most prominently in IFC-striatal circuitries.
enetic Associations
The findings of disorder-specific cool IFC dysfunction in ADHDnd disorder-specific hot ventromedial-paralimbic dysfunction inD is further interesting with respect to the genotypes that haveeen associated most prominently with each of the two disorders.
n ADHD, dopamine dysregulation is thought to play a crucial rolend the dopamine genotypes of DAT1 and dopamine receptor D4DRD4) 7-repeat allele are most commonly associated with theisorder (209). The DRD4-7-7 genotype has been associated with
educed volume and cortical thickness of the right IFC in normalevelopment, which was, furthermore, particularly pronounced inDHD children with the genotype (210). The DAT1 genotypes haveeen associated with abnormal caudate volume, as well as activa-
ion in patients with ADHD (211,212). Antisocial behaviors, includ-ng psychopathy and CD, have more commonly been associated
ith serotonin genotypes. Thus, the short allele of the serotoninransporter has been associated with impulsive and antisocial be-avior features in alcohol abuse (213,214) and violent crime (215) indults. In children, the short variant has been associated with anti-ocial and aggressive behavioral features in adoptees (216) andith childhood aggression (217). Furthermore, the short allele
howed an interaction with childhood adversity on later-life violent
ehavior (218). In healthy adults, the short allele of the serotonin
CttscowntlsmittscCctnwtitswp4A
K. Rubia BIOL PSYCHIATRY 2011;69:e69–e87 e79
transporter has consistently been associated with the brain struc-tures that have been associated with CD. It has been related to adysmorphology and dysregulation of the ventromedial prefrontalcortex, including anterior cingulate and medial frontal cortex, andthe amygdala, as well as the functional connectivity between bothstructures (219 –221) (for review, see [222]). Abnormal connectivitybetween amygdala hyperactivity and orbitofrontal hyporesponsiv-ity in relation to negative emotions has been suggested to underlieimpulsive aggression (171). Genetic predisposition, hence, mayplay a role in the development of the disorder-specific dysregula-tion of IFC-striatal and ventromedial-limbic neural networks inADHD and antisocial-aggressive behaviors, respectively.
Conclusion and Future Directions
This review shows that ADHD is most prominently associatedwith the dysmorphology, dysfunction, and the underconnectivityof cool fronto-striato-cerebellar and frontoparietal neural networksthat regulate cognition and attention. Furthermore, these regions,most prominently the IFC, are disorder-specific underfunctioningwhen compared with CD. Antisocial and aggressive behaviors inthe form of CD and CD-CU, by contrast, are associated with struc-tural and functional deficits in areas of the paralimbic system, in-cluding the orbitofrontal cortex, superior temporal lobes, and un-derlying limbic structures, as well as ventromedial frontolimbicunderconnectivity. Furthermore, compared with ADHD, this para-limbic system dysfunction and underconnectivity are disorder-spe-cific (Figure 3).
Comorbidity Between DisordersThere are several potential caveats, however, that need to be
taken into account. All structural studies have tested children with
Figure 3. Schematic representation of the magnetic resonance imagingchildren with attention-deficit/hyperactivity disorder and those with condufrom head-to-head functional and structural imaging comparisons betweencontrol studies may suggest overlapping abnormalities in several of these re
figure is focusing on evidence for disorder-specific association findings between rconduct disorder. ADHD, attention-deficit/hyperactivity disorder; CD, conduct diD with over 50% comorbidity with ADHD. Consequently, struc-ural abnormality findings apply mostly to the comorbid presenta-ion of CD and ADHD. This is also the case for all functional imagingtudies, except for those conducted in my laboratory, where weompared noncomorbid patient groups. Although in the majorityf studies, brain structure and function abnormalities correlatedith antisocial behaviors or survived covariance with ADHD, it can-ot be excluded that the comorbid ADHD features may have con-
ributed to the abnormalities. The fact that the studies from ouraboratory, however, were conducted in noncomorbid groups andhowed disorder-specific functional brain abnormalities in nonco-
orbid CD relative to noncomorbid ADHD in paralimbic regions,ncluding superior temporal lobes, orbitofrontal cortex, insula, an-erior cingulate, and hippocampus, reinforces the association be-ween these paralimbic functional deficits, also observed in thetudies of comorbid cases and antisocial behaviors. However, non-omorbid patient groups may be less representative of the typicalD or ADHD population. According to epidemiological studies,hildren with noncomorbid CD or noncomorbid ADHD are rela-ively rare (19,78,149). An epidemiological prevalence study inorth England schools showed that while hyperactivity prevalenceithout CD can be relatively high (30%), CD without ADHD is rela-
ively uncommon (1.5%) (223). Epidemiological data from the Brit-sh Child Mental Health Survey, however, using diagnostic criteriahat elicit a relatively conservative ADHD prevalence of 1.5%,howed that only 23% of children with CD had ADHD comorbidity,hile 50% of ADHD children had CD comorbidity (224). In US sam-les, this ratio appears to be higher, however, with odds ratios of1.3 for concurrent comorbidity of ADHD given CD and of 79 forDHD given ODD (78). The comorbid presentation is likely to suffer
nce for disorder-specific structural and functional brain abnormalities insorder. The figure is based on evidence for disorder-specific abnormalitiesomorbid and comorbid disorders. While evidence from individual disorder-(such as anterior cingulate, dorsolateral prefrontal, or temporal lobes), the
evidect dinoncgions
egional abnormalities and either attention-deficit/hyperactivity disorder orsorder; PFC, prefrontal cortex.
www.sobp.org/journal

ts
paehmtrcoshtifCtipcasspcbf
PF
wbalteautrgctwpmpoapttob
llfm
e80 BIOL PSYCHIATRY 2011;69:e69–e87 K. Rubia
from a dysregulation of both cool fronto-striato-parieto-cerebellaras well as hot ventromedial fronto-temporo-limbic neural net-works. Future studies will need to compare 100% comorbid caseswith noncomorbid CD and noncomorbid ADHD patients to eluci-date to what extent the comorbid presentation shares the etio-pathophysiology of the noncomorbid disorders or whether it is amore complex disorder, characterized by a qualitatively differentunderlying pathology.
Furthermore, although most studies in ADHD and CD have ex-cluded affective comorbidity and controlled for anxiety and depres-sive symptoms, it cannot be completely excluded that underlyingproblems of anxiety and depression may have contributed to theobserved brain abnormalities. Future studies are needed to assessthe contribution of affective symptomatology on brain abnormali-ties in these disorders, by comparing children with noncomorbiddepression and anxiety with children with noncomorbid ADHD andCD, as well as comorbid presentations of these disorders.
Bias in Structural and Functional Imaging StudiesThere has been a bias in structural studies, where regions of
interest in ADHD have more commonly targeted frontal and striatalbrain regions, while areas of the paralimbic motivation circuitrieshave more commonly been selected as regions of interest in struc-tural studies in CD. More recent structural imaging studies of ADHDthat have selected limbic areas as regions of interest have, in fact,found limbic structural abnormalities in ADHD children. A study byPlessen et al. (225) found enhanced volumes in the head of thehippocampus in 51 children with the combined type of ADHDcompared with 63 healthy control subjects. This structural abnor-mality, however, was associated with fewer ADHD symptoms andhence interpreted as a compensatory plastic hypertrophic re-sponse, possibly for reduced prefrontal parts of frontal-hippocam-pal circuitries. Surface morphology analyses also showed reducedsize bilaterally of the basolateral complex of the amygdala in ADHDchildren relative to control subjects, which correlated with prefron-tal cortex size, suggesting reduced frontal-amygdala connectivity.The amygdala surface morphology was negatively associated withinattention but positively associated with hyperactivity symptoms,suggesting distinct associations between amygdala neurobiologyand different ADHD symptoms (225). Although there were poten-tial confounds such as history or current symptoms of depression/anxiety, ODD, or medication history and status, these were notassociated with the findings. Abnormalities in medial frontal re-gions and their connections to amygdala and hippocampus couldbe associated with abnormal performance in some of the hot exec-utive functions associated with ADHD, most typically reward-re-lated decision making in the form of delay aversion or hypersensi-tivity to immediate rewards, as well as attention and mnemonicprocesses. Another recent structural study found smaller volume ofthe pulvinar of the thalamus in 46 children with ADHD comparedwith healthy control subjects. A dissociation of thalamic volumeswith ADHD symptoms was observed, with hyperactivity being as-sociated with smaller left ventrolateral and pulvinar regions andinattention with larger right pulvinar and medial dorsal thalamicregions (226). The pulvinar is part of fronto-parieto-cortico-tha-lamic networks important for attentional saliency processing(227,228). However, this region is also connected to the limbicsystem, including the amygdala (229,230), and hence part of anemotional regulation network (228). Moreover, recent positronemission tomography studies that carefully selected noncomorbidadults with ADHD observed abnormal dopamine transporter levelsrelative to healthy adults in areas of the limbic system including
nucleus accumbens and midbrain, amygdala, and hippocampus mwww.sobp.org/journal
hat furthermore correlated with inattention but not hyperactivityymptoms (231,232).
In fMRI studies of both disorders, there has also been a bias inaradigm selection, where cool cognitive paradigms have beenpplied in the majority of fMRI studies of ADHD to test the hypoth-sis of frontostriatal deficits, while hot motivational paradigmsave been more commonly chosen for fMRI research of CD. In fact,ore recent fMRI studies that have tested for deficits in motiva-
ional networks in ADHD using paradigms of emotion processing oreward-related functions have, indeed, found underfunctioning inhildren and adults with ADHD in limbic brain regions, includingrbital and ventromedial prefrontal cortex, amygdala, and ventraltriatum (114,117,233–235). Comorbidity with antisocial behaviors,owever, was not excluded and could potentially have confounded
he results. This, however, also applies to the majority of fMRI stud-es that observed frontostriatal dysfunctions during cool executiveunction in ADHD patients and did not exclude comorbid cases withD. In support of an association with ADHD, however, is the fact
hat several of these studies found a correlation between activationn limbic regions, such as ventral striatum and amygdala, with hy-eractive/impulsive but not inattentive symptoms (117,233,235). Inonclusion, given the bias in the neuroimaging literature of ADHDnd CD in the selection of regions of interest in structural imagingtudies and paradigm selection for fMRI studies, future imagingtudies should combine structural and functional analyses in largeatient numbers to conduct head-to-head comparisons betweenhildren with noncomorbid CD, noncomorbid ADHD, and comor-id cases using whole-brain structural imaging analyses and using
MRI tasks that tap into both hot and cool executive functions.
otential Overlap Between Disorders in Brain Structure andunction Abnormalities
Ventromedial-limbic circuitries and mesolimbic dopamine re-ard pathways may potentially be a shared abnormality betweenoth ADHD and CD. The nucleus accumbens is located betweennd reciprocally connected to both cool frontocortical as well as hot
imbic areas and is thought to be a key mediator between motiva-ion and attention functions (64). It is ideally placed to integratemotional salience and contextual constraints, processed inmygdala and hippocampus, respectively, and goal-directed exec-tive plans from the PFC. The mesolimbic dopamine system main-
ains the balance between limbic and cortical drive within thisegion (64). This region is closely interconnected with anterior cin-ulate, ventromedial frontal cortex, and amygdala, which, in con-ert, mediate reward-related decision making (67,236,237). Fur-hermore, abnormalities in these circuitries have been associatedith impulsiveness and behavioral disinhibition (67,238), overlap-ing features between ADHD and CD (28). While orbital and ventro-edial frontal cortices, anterior cingulate, amygdala, and hip-
ocampus have been shown to be associated with CD, no structuralr functional MRI study, however, has as yet tested for structuralbnormalities of nucleus accumbens in children with CD or forotential activation abnormalities in reward-related paradigms
hat specifically activate this region. It is likely that the ventral stria-um, in its role as interface between motivation and attention, is notnly impaired in ADHD but also in children with CD, and this shoulde tested in future studies.
Another area of potential overlap could be the anterior cingu-ate. This paralimbic area lies at the interface between the frontalobes and the limbic system and has been associated with severalunctions, depending on exact location, including performance
onitoring, error detection, arousal, motivation, and outcome
onitoring to modulate executive attention (157,179,183,184,239).
Tamspt
datcbPnc
wabbtCtas
suwmdhat
NS
sdWndbdt
tsapdql(ocnjsdt
tCa
a
K. Rubia BIOL PSYCHIATRY 2011;69:e69–e87 e81
Both rostral and dorsal anterior cingulate have consistently beenfound to be abnormal in structural and functional imaging studiesof CD (see above). This brain region has also been found to beabnormal in brain structure and function in ADHD children(94,102,110,156,240) and adults (125,127,241,242). Direct compari-sons between ADHD and CD, however, point toward more severeabnormalities in this region in CD. Functional MRI comparisonshave found dorsal ACC underactivation to be specifically associatedwith noncomorbid CD when contrasted with noncomorbid ADHD(109) and dysfunction in this area remained when ADHD was con-trolled for (139) or correlated specifically with antisocial and CUsymptoms (144). Structural studies found ACC to be specificallyassociated with CD but not ADHD symptoms in regression analyses(135) and to be associated with CD when ADHD was covaried (137).
he ACC abnormality may thus be more strongly associated withntisocial behavioral features than ADHD symptoms and abnor-ality findings in ACC in ADHD patients—more commonly ob-
erved in adult than childhood ADHD (for review, see 125])—mayotentially be associated with underlying, and mostly uncon-
rolled, antisocial features.Lastly, we found that in children with ADHD and emotional
ysregulation, both the DRD4 7-repeat allele as well as the shortllele of the serotonin transporter have been associated with emo-ion dysregulation, suggesting that this behavioral feature, which isommon in ADHD children and associated with CD and/or ODDehavior, may be mediated by the abnormality of both top-downFC control systems, the cool executive lateral PFC-striatal controletwork as well as the hot ventromedial PFC-limbic pathway thatontrols affect and motivation (243).
In conclusion, there is evidence that some brain regions thatintermediate between hot motivation and cool attention functionsmay be affected in both disorders, but this needs to be furthertested in head-to-head comparisons between noncomorbid andcomorbid patient groups.
Heterogeneity Within ADHD and CDBoth ADHD and CD are heterogeneous disorders. More effort
needs to be undertaken to disentangle the neurobiological sub-strates within subgroups of these disorders. For example, childrenwith inattention only are likely to suffer from different neurobiolog-ical abnormalities than children with the combined type ADHD.Children with inattention are less likely to have oppositional defiantdisorder than those with the combined subtype (244), while impul-siveness is a key feature shared between the impulsive-hyperactivesubtype of ADHD and CD, in particular the impulsive-aggressivesubtype of CD. It has been argued that the inattentive symptoms ofADHD may be associated with deficits in frontostriatal mediatedcool EF, whereas hyperactivity/impulsivity symptoms may reflecthot executive function deficits, mediated by paralimbic brain re-gions (245). This would suggest that the different subtypes of ADHDmay be mediated by different brain abnormalities, with the impul-sive-hyperactive subtype resembling more CD than the inattentivesubtype. This is, however, only in part supported by evidence. In linewith this theory, limbic brain abnormalities in orbitofrontal,amygdala, and ventral striatum correlated with impulsive-hyperac-tive but not inattentive symptoms (117,233,235). Symptoms of in-attention, however, and not impulsive-hyperactive symptoms havebeen shown to correlate with limbic abnormalities in children withADHD and CD in structural MRI and positron emission tomographystudies (136,231). By contrast, hyperactivity/impulsiveness symp-toms and not inattention symptoms correlated inversely with graymatter reductions in cool fronto-temporo-parietal brain regions
(135). Furthermore, there is some evidence to suggest that childrenith inattention and sluggish cognitive tempo have more anxietynd depression and fewer externalizing problems (246). This would,y contrast, point toward abnormalities in orbitofrontal-limbicrain regions that are typically associated with depression (72) and
hat overlap substantially with the observed brain abnormalities inD. Clearly, large-scale imaging studies that compare children with
he inattentive, impulsive-hyperactive, and the combined subtypesre needed to clarify potential differences in the underlying neuralubstrates of each of the subtypes.
Along the same lines, future imaging studies should investigateubtypes of CD because there are likely to be differences in thenderlying neurobiological substrates of CD children with andithout callous-unemotional traits or with either reactive or instru-ental aggression. Lastly, there are likely to be neurophysiological
ifferences between children with CD and ODD. To my knowledge,owever, no imaging studies have as yet investigated the neuroim-ging substrates of ODD, independent from CD, or compared be-ween different subtypes of CD.
eed for Longitudinal and Combined Structure-Functiontudies
All published studies comparing ADHD and CD have been cross-ectional. Longitudinal imaging studies will be needed to assessifferences in the developmental trajectories of the disorders.hile in ADHD there is evidence for a maturational delay (93,247),
othing is known on the longitudinal trajectories of CD. Childhoodisorders are more likely to differ in the temporal dynamics of theirrain abnormalities, i.e., in the onset of their deviance from normalevelopment and/or in their developmental trajectories, rather
han at any chosen cross-sectional time point.Furthermore, no studies have combined structural and func-
ional information. Future, large-scale multimodal imaging studieshould compare ADHD and CD in brain structure, brain function,nd structural and functional connectivity. Modern multivariateattern recognition analysis classification systems applied to MRIata, which differentiate cases and control subjects on the basis ofuantitative, spatially distributed neural networks rather than iso-
ated brain regions with the ability to make individual classifications248 –250), could potentially be of clinical use by providing a morebjective, neuroimaging-based differential diagnosis. A successfullassification of these two patient groups based on their underlyingeurobiological abnormalities would not only provide a more ob-
ective differential diagnosis but also deliver a target for disorder-pecific preventions and interventions aimed at normalizing disor-er-specific abnormal brain and neurotransmitter systems and
heir abnormal development.
The research reported in this article has been funded by Grants fromhe Wellcome Trust (053272/Z/98/Z/JRS/JP/JAT), the Medical Researchouncil (G9900839), and the PPP Healthcare Foundation (1206/1140)nd (1206/1568), United Kingdom.
KR has received funding from Eli Lilly for another research projectnd speakers honoraria from Eli Lilly and Medice.
1. American Psychiatric Association(1994): Diagnostic and StatisticalManual of Mental Disorders, 4th ed. Washington, DC: American Psychi-atric Association.
2. Spencer T, Biederman J, Mick E (2007): Attention-deficit/hyperactivitydisorder: Diagnosis, lifespan, comorbidities, and neurobiology. AmbulPediatr 7:73– 81.
3. Faraone SV, Wilens TE, Petty C, Antshel K, Spencer T, Biederman J(2007): Substance use among ADHD adults: Implications of late onset
and subthreshold diagnoses. Am J Addict 16(suppl 1):24 –32; quiz33–34.www.sobp.org/journal

e82 BIOL PSYCHIATRY 2011;69:e69–e87 K. Rubia
4. Taylor E, Chadwick O, Heptinstall E, Danckaerts M (1996): Hyperactivityand conduct problems as risk factors for adolescent development.J Am Acad Child Adolesc Psychiatry 35:1213–1226.
5. Beyers JM, Loeber R (2003): Untangling developmental relations be-tween depressed mood and delinquency in male adolescents. J Ab-norm Child Psychol 31:247–266.
6. Creemers HE, Van Lier PAC, Vollebergh WAM, Ormel J, Verhulst FC,Huizink AC (2009): Predicting onset of cannabis use in early adoles-cence: The interrelation between high-intensity pleasure and disrup-tive behavior. The TRAILS Study. J Stud Alcohol Drugs 70:850 – 858.
7. Green JG, McLaughlin KA, Berglund PA, Gruber MJ, Sampson NA,Zaslavsky AM, Kessler RC (2010): Childhood adversities and adult psy-chiatric disorders in the national comorbidity survey replication I: As-sociations with first onset of DSM-IV disorders. Arch Gen Psychiatry67:113–123.
8. Kessler RC, Wang PS (2008): The descriptive epidemiologv of com-monly occurring mental disorders in the United States. Annu Rev PublicHealth 29:115–129.
9. Loeber R, Farrington DP, Stouthamer-Loeber M, Moffitt TE, Caspi A,Lynam D (2001): Male mental health problems, psychopathy, and per-sonality traits: Key findings from the first 14 years of the PittsburghYouth Study. Clin Child Fam Psychol Rev 4:273–297.
10. McBurnett K, Raine A, Stouthamer-Loeber M, Loeber R, Kumar AM,Kumar M, Lahey BB (2005): Mood and hormone responses to psycho-logical challenge in adolescent males with conduct problems. BiolPsychiatry 57:1109 –1116.
11. McLaughlin KA, Green JG, Gruber MJ, Sampson NA, Zaslavsky AM,Kessler RC (2010): Childhood adversities and adult psychiatric disor-ders in the national comorbidity survey replication II: Associations withpersistence of DSM-IV disorders. Arch Gen Psychiatry 67:124 –132.
12. Riehman KS, Stephens RL, Schurig ML (2009): Substance use patternsand mental health diagnosis among youth in mental health treatment:A latent class analysis. J Psychoactive Drugs 41:363–368.
13. Zoccolillo M, Meyers J, Assiter S (1997): Conduct disorder, substancedependence, and adolescent motherhood. Am J Orthopsychiatry 67:152–157.
14. Dandreaux DM, Frick PJ (2009): Developmental pathways to conductproblems: A further test of the childhood and adolescent-onset dis-tinction. J Abnorm Child Psychol 37:375–385.
15. Frick PJ, Stickle TR, Dandreaux DM, Farrell JM, Kimonis ER (2005): Cal-lous-unemotional traits in predicting the severity and stability of con-duct problems and delinquency. J Abnorm Child Psychol 33:471– 487.
16. Frick PJ (2009): Extending the construct of psychopathy to youth:Implications for understanding, diagnosing, and treating antisocialchildren and adolescents. Can J Psychiatry 54:803– 812.
17. Lynam DR, Gudonis L (2005): The development of psychopathy. AnnuRev Clin Psychol 1:381– 407.
18. Fanti KA, Frick PJ, Georgiou S (2009): Linking callous-unemotionaltraits to instrumental and non-instrumental forms of aggression. J Psy-chopathol Behav Assess 31:285–298.
19. Frick PJ, Viding E (2009): Antisocial behavior from a developmentalpsychopathology perspective. Dev Psychopathol 21:1111–1131.
20. Moffitt TE, Arseneault L, Jaffee SR, Kim-Cohen J, Koenen KC, Odgers CL,et al. (2008): Research review: DSM-V conduct disorder: Research needsfor an evidence base. J Child Psychol Psychiatry 49:3–33.
21. Rubia K, Smith A, Brammer M, Taylor E (2007): Performance of childrenwith attention deficit hyperactivity disorder (ADHD) on a test batteryfor impulsiveness. Child Neuropsychol 30:659 – 695.
22. Rubia K, Russell T, Overmeyer S, Brammer MJ, Bullmore ET, Sharma T, etal. (2001): Mapping motor inhibition: Conjunctive brain activationsacross different versions of go/no-go and stop tasks. Neuroimage 13:250 –261.
23. Willcutt EG, Doyle AE, Nigg JT, Faraone SV, Pennington BF (2005):Validity of the executive function theory of attention-deficit/hyperac-tivity disorder: A meta-analytic review. Biol Psychiatry 57:1336 –1346.
24. Oosterlaan J, Logan GD, Sergeant JA (1998): Response inhibition inAD/HD, CD, comorbid AD/HD�CD, anxious, and control children: Ameta-analysis of studies with the stop task. J Child Psychol Psychiatry39:411– 425.
25. Herba CM, Tranah T, Rubia K, Yule W (2006): Conduct problems in
adolescence: Three domains of inhibition and effect of gender. DevNeuropsychol 30:659 – 695.www.sobp.org/journal
26. Geurts HM, Vertie S, Oosterlaan J, Roeyers H, Sergeant JA (2004): Howspecific are executive functioning deficits in attention deficit hyperac-tivity disorder and autism? J Child Psychol Psychiatry 45:836 – 854.
27. Pliszka SR, Borcherding SH, Spratley K, Leon S, Irick S (1997): Measuringinhibitory control in children. J Dev Behav Pediatr 18:254 –259.
28. Banaschewski T, Hollis C, Oosterlaan J, Roeyers H, Rubia K, Willcutt E,Taylor E (2005): Towards an understanding of unique and shared path-ways in the psychopathophysiology of ADHD. Dev Sci 8:132–140.
29. Blair RJR, Peschardt KS, Budhani S, Mitchell DGV, Pine DS (2006): Thedevelopment of psychopathy. J Child Psychol Psychiatry 47:262–275.
30. Lueger RJ, Gill KJ (1990): Frontal-lobe cognitive dysfunction in conductdisorder adolescents. J Clin Psychol 46:696 –706.
31. Toupin J, Dery M, Pauze R, Mercier H, Fortin L (2000): Cognitive andfamilial contributions to conduct disorder in children. J Child PsycholPsychiatry 41:333–344.
32. Dougherty DM, Bjork JM, Harper RA, Marsh DM, Moeller FG, MathiasCW, Swann AC (2003): Behavioral impulsivity paradigms: A compari-son in hospitalized adolescents with disruptive behavior disorders.J Child Psychol Psychiatry 44:1145–1157.
33. Dougherty DM, Bjork JM, Marsh DM, Moeller FG (2000): A comparisonbetween adults with conduct disorder and normal controls on a con-tinuous performance test: Differences in impulsive response charac-teristics. Psychol Rec 50:203–219.
34. Shapiro SK, Garfinkel BD (1986): The occurrence of behavior disordersin children: The interdependence of attention-deficit disorder andconduct disorder. J Am Acad Child Psychiatry 25:809 – 819.
35. Schachar R, Logan G, Wachsmuth R, Chajczyk D (1988): Attaining andmaintaining preparation—a comparison of attention in hyperactive,normal, and disturbed control children. J Abnorm Child Psychol 16:361–378.
36. Halperin JM, Obrien JD, Newcorn JH, Healey JM, Pascualvaca DM, WolfLE, et al. (1990): Validation of hyperactive, aggressive, and mixed hy-peractive/aggressive childhood disorders: A research note. J Child Psy-chol Psychiatry 31:455– 459.
37. Matier K, Halperin JM, Sharma V, Newcorn JH, Sathaye N (1992): Meth-ylphenidate response in aggressive and nonaggressive ADHD chil-dren: Distinctions on laboratory measures of symptoms. J Am AcadChild Adolesc Psychiatry 31:219 –225.
38. Klorman R, Hazel-Fernandez LA, Shaywitz SE, Fletcher JM, MarchioneKE, Holahan JM, et al. (1999): Executive functioning deficits in atten-tion-deficit hyperactivity disorder are independent of oppositionaldefiant or reading disorder. J Am Acad Child Adolesc Psychiatry 38:1148 –1155.
39. van Goozen SHM, Cohen-Kettenis PT, Snoek H, Matthys W, Swaab-Barneveld H, van Engeland H (2004): Executive functioning in children:A comparison of hospitalised ODD and ODD/ADHD children and nor-mal controls. J Child Psychol Psychiatry 45:284 –292.
40. Avila C, Cuenca I, Felix V, Parcet MA, Miranda A (2004): Measuringimpulsivity in school-aged boys and examining its relationship withADHD and ODD ratings. J Abnorm Child Psychol 32:295–304.
41. Schachar R, Mota VL, Logan GD, Tannock R, Klim P (2000): Confirmationof an inhibitory control deficit in attention-deficit/hyperactivity disor-der. J Abnorm Child Psychol 28:227–235.
42. Scheres A, Oosterlaan J, Sergeant JA (2001): Response inhibition inchildren with DSM-IV subtypes of AD/HD and related disruptive disor-ders: The role of reward. Child Neuropsychol 7:172–189.
43. Scheres A, Oosterlaan J, Sergeant JA (2001): Response execution andinhibition in children with AD/HD and other disruptive disorders: Therole of behavioural activation. J Child Psychol Psychiatry 42:347–357.
44. Budhani S, Blair RJR (2005): Response reversal and children with psy-chopathic tendencies: Success is a function of salience of contingencychange. J Child Psychol Psychiatry 46:972–981.
45. Newman JP, Schmitt WA, Voss WD (1997): The impact of motivationallyneutral cues on psychopathic individuals: Assessing the generality ofthe response modulation hypothesis. J Abnorm Psychol 106:563–575.
46. Lynam DR (1998): Early identification of the fledgling psychopath:Locating the psychopathic child in the current nomenclature. J Ab-norm Psychol 107:566 –575.
47. Matthys W, van Goozen SHM, Snoek H, van Engeland H (2004): Re-sponse perseveration and sensitivity to reward and punishment in
boys with oppositional defiant disorder. Eur Child Adolesc Psychiatry13:362–364.
K. Rubia BIOL PSYCHIATRY 2011;69:e69–e87 e83
48. Garon N, Moore C, Waschbusch DA (2006): Decision making in childrenwith ADHD only, ADHD-anxious/depressed, and control children us-ing a child version of the Iowa Gambling Task. J Atten Disord 9:607– 619.
49. Toplak ME, Jain U, Tannock R (2005): Executive and motivational pro-cesses in adolescents with attention-deficit-hyperactivity disorder(ADHD). Behav Brain Funct 1:8.
50. Hobson C, Scott S, Rubia K (in press): Cool and hot executive functiondeficits related to ODD/CD symptoms independently of ADHD in ado-lescents with early onset conduct problems. J Child Psychol Psychiatry.
51. Christakou A, Halari R, Smith AB, Ifkovits E, Brammer M, Rubia K (2009):Sex-dependent age modulation of frontostriatal and temporo-parietalactivation during cognitive control. Neuroimage 48:223–236.
52. Rubia K, Smith AB, Taylor E, Brammer M (2007): Linear age-correlatedfunctional development of right inferior fronto-striato-cerebellar net-works during response inhibition and anterior cingulate during error-related processes. Hum Brain Mapp 28:1163–1177.
53. Rubia K, Smith AB, Woolley J, Nosarti C, Heyman I, Taylor E, Brammer M(2006): Progressive increase of frontostriatal brain activation fromchildhood to adulthood during event-related tasks of cognitive con-trol. Hum Brain Mapp 27:973–993.
54. Rubia K, Hyde Z, Giampietro V, Smith A (2010): Effects of age and sex ondevelopmental neural networks of visual-spatial attention allocation.Neuroimage 51:817– 827.
55. Kerr A, Zelazo PD (2004): Development of “hot” executive function: Thechildren’s gambling task. Brain Cogn 55:148 –157.
56. Fellows LK, Farah MJ (2005): Dissociable elements of human foresight:A role for the ventromedial frontal lobes in framing the future, but notin discounting future rewards. Neuropsychologia 43:1214 –1221.
57. Northoff G, Grimm S, Boeker H, Schmidt C, Bermpohl F, Heinzel A, et al.(2006): Affective judgment and beneficial decision making: Ventrome-dial prefrontal activity correlates with performance in the Iowa Gam-bling Task. Hum Brain Mapp 27:572–587.
58. Schoenbaum G, Roesch MR, Stalnaker TA (2006): Orbitofrontal cortex,decision-making and drug addiction. Trends Neurosci 29:116 –124.
59. Remijnse PL, Nielen MMA, Uylings HBM, Veltman DJ (2005): Neuralcorrelates of a reversal learning task with an affectively neutral base-line: An event-related fMRI study. Neuroimage 26:609 – 618.
60. Hampton AN, Adolphs R, Tyszka MJ, O’Doherty JP (2007): Contribu-tions of the amygdala to reward expectancy and choice signals inhuman prefrontal cortex. Neuron 55:545–555.
61. Davidson RJ, Jackson DC, Kalin NH (2000): Emotion, plasticity, context,and regulation: Perspectives from affective neuroscience. Psychol Bull126:890 –909.
62. Davidson RJ, Putnam KM, Larson CL (2000): Dysfunction in the neuralcircuitry of emotion regulation--a possible prelude to violence. Science289:591–594.
63. Dolan RJ (2007): The human amygdala and orbital prefrontal cortex inbehavioural regulation. Philos Trans R Soc Lond B Biol Sci 362:787–799.
64. Goto Y, Grace AA (2008): Limbic and cortical information processing inthe nucleus accumbens. Trends Neurosci 31:552–558.
65. Haber S (2008): Parallel and integrative processing through the basalganglia reward circuit: Lessons from addiction. Biol Psychiatry 64:173–174.
66. Haber SN, Kim KS, Mailly P, Calzavara R (2006): Reward-related corticalinputs define a large striatal region in primates that interface withassociative cortical connections, providing a substrate for incentive-based learning. J Neurosci 26:8368 – 8376.
67. Bechara A, Tranel D, Damasio H (2000): Characterization of the deci-sion-making deficit of patients with ventromedial prefrontal cortexlesions. Brain 123:2189 –2202.
68. Bechara A, Van der Linden M (2005): Decision-making and impulsecontrol after frontal lobe injuries. Curr Opin Neurol 18:734 –739.
69. Durston S, Tottenham NT, Thomas KM, Davidson MC, Eigsti IM, YangYH, et al. (2003): Differential patterns of striatal activation in youngchildren with and without ADHD. Biol Psychiatry 53:871– 878.
70. Zelazo PD, Müller U (2002): Executive Function in Typical and AtypicalDevelopment. Oxford, UK: Blackwell.
71. Rushworth MF, Johansen-Berg H, Gobel SM, Devlin JT (2003): The leftparietal and premotor cortices: Motor attention and selection. Neuro-image 20(suppl 1):S89 –S100.
72. Arnsten A, Rubia K (in press): Neurobiological circuits regulating atten-
tion, movement and emotion and their disruptions in pediatic neuro-psychiatric disorders. Journal of ADHD and Related Disorders.73. Arnsten AFT (2009): Emerging neurobiology of attention deficit hyper-activity disorder: The key role of the prefrontal association cortex.J Pediatr 154:I–S43.
74. Fuster JM (2001): The prefrontal cortex—an update: Time is of theessence. Neuron 30:319 –333.
75. Fuster JM (1999): Synopsis of function and dysfunction of the frontallobe. Acta Psychiatr Scand Suppl 395:51–57.
76. Fuster JM (1997): The Prefrontal Cortex, 4th edition. London: AcademicPress, 392.
77. Patterson GR, Chamberlain P, Reid JB (1982): A comparative-evaluationof a parent-training program. Behav Ther 13:638 – 650.
78. Costello EJ, Mustillo S, Erkanli A, Keeler G, Angold A (2003): Prevalenceand development of psychiatric disorders in childhood and adoles-cence. Arch Gen Psychiatry 60:837– 844.
79. Spencer T, Biederman J, Wilens T (1999): Attention-deficit/hyperactiv-ity disorder and comorbidity. Pediatr Clin North Am 46:915–927, vii.
80. Taylor E, Sandberg S, Thorley G, Giles S (1991): The Epidemiology ofChildhood Hyperactivity. Oxford, England: Oxford University Press.
81. Biederman J, Newcorn J, Sprich S (1991): Comorbidity of attentiondeficit hyperactivity disorder with conduct, depressive, anxiety, andother disorders. Am J Psychiatry 148:564 –577.
82. Johansson P, Kerr M, Andershed H (2005): Linking adult psychopathywith childhood hyperactivity-impulsivity-attention problems and con-duct problems through retrospective self-reports. J Pers Disord 19:94 –101.
83. Krain AL, Castellanos FX (2006): Brain development and ADHD. ClinPsychol Rev 26:433– 444.
84. Mackie S, Shaw P, Lenroot R, Pierson R, Greenstein DK, Nugent TF, et al.(2007): Cerebellar development and clinical outcome in attention def-icit hyperactivity disorder. Am J Psychiatry 164:647– 655.
85. Shaw P, Lerch J, Greenstein D, Sharp W, Clasen L, Evans A, et al. (2006):Longitudinal mapping of cortical thickness and clinical outcome inchildren and adolescents with attention-deficit/hyperactivity disor-der. Arch Gen Psychiatry 63:540 –549.
86. Castellanos FX, Lee PP, Sharp W, Jeffries NO, Greenstein DK, Clasen LS,et al. (2002): Developmental trajectories of brain volume abnormalitiesin children and adolescents with attention-deficit/hyperactivity disor-der. JAMA 288:1740 –1748.
87. Valera EM, Faraone SV, Murray KE, Seidman LJ (2007): Meta-analysis ofstructural imaging findings in attention-deficit/hyperactivity disorder.Biol Psychiatry 61:1361–1369.
88. Ellison-Wright I, Ellison-Wright Z, Bullmore E (2008): Structural brainchange in attention deficit hyperactivity disorder identified by meta-analysis. BMC Psychiatry 8:51.
89. Ashtari M, Kumra S, Bhaskar SL, Clarke T, Thaden E, Cervellione KL, et al.(2005): Attention-deficit/hyperactivity disorder: A preliminary diffu-sion tensor imaging study. Biol Psychiatry 57:448 – 455.
90. Davenport ND, Karatekin C, White T, Lim KO (2010): Differential frac-tional anisotropy abnormalities in adolescents with ADHD or schizo-phrenia. Psychiatry Res 181:193–198.
91. Konrad A, Dielentheis TF, El Masri D, Bayerl M, Fehr C, Gesierich T, et al.(2010): Disturbed structural connectivity is related to inattention andimpulsivity in adult attention deficit hyperactivity disorder. Eur J Neu-rosci 31:912–919.
92. Pavuluri MN, Yang S, Kamineni K, Passarotti AM, Srinivasan G, HarralEM, et al. (2009): Diffusion tensor imaging study of white matter fibertracts in pediatric bipolar disorder and attention-deficit/hyperactivitydisorder. Biol Psychiatry 65:586 –593.
93. Shaw P, Eckstrand K, Sharp W, Blumenthal J, Lerch JP, Greenstein D, etal. (2007): Attention-deficit/hyperactivity disorder is characterized by adelay in cortical maturation. Proc Natl Acad Sci U S A 104:19649 –19654.
94. Rubia K, Overmeyer S, Taylor E, Brammer M, Williams SC, Simmons A,Bullmore ET (1999): Hypofrontality in attention deficit hyperactivitydisorder during higher-order motor control: A study with functionalMRI. Am J Psychiatry 156:891– 896.
95. Rubia K, Smith AB, Brammer MJ, Toone B, Taylor E (2005): Abnormalbrain activation during inhibition and error detection in medication-naive adolescents with ADHD. Am J Psychiatry 162:1067–1075.
96. Rubia K, Halari R, Smith AB, Mohammed M, Scott S, Giampietro V, et al.(2008): Dissociated functional brain abnormalities of inhibition in boys
with pure conduct disorder and in boys with pure attention deficithyperactivity disorder. Am J Psychiatry 165:889 – 897.www.sobp.org/journal

1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
e84 BIOL PSYCHIATRY 2011;69:e69–e87 K. Rubia
97. Booth JR, Burman DD, Meyer JR, Lei Z, Trommer BL, Davenport ND, etal. (2005): Larger deficits in brain networks for response inhibition thanfor visual selective attention in attention deficit hyperactivity disorder(ADHD). J Child Psychol Psychiatry 46:94 –111.
98. Durston S, Mulder M, Casey BJ, Ziermans T, van Engeland H (2006):Activation in ventral prefrontal cortex is sensitive to genetic vulnera-bility for attention-deficit hyperactivity disorder. Biol Psychiatry 60:1062–1070.
99. Pliszka SR, Glahn DC, Semrud-Clikeman M, Franklin C, Perez R, Xiong JJ(2006): Neuroimaging of inhibitory control areas in children with at-tention deficit hyperactivity disorder who were treatment naive or inlong-term treatment. Am J Psychiatry 163:1052–1060.
00. Smith AB, Taylor E, Brammer M, Toone B, Rubia K (2006): Task-specifichypoactivation in prefrontal and temporoparietal brain regions duringmotor inhibition and task switching in medication-naive children andadolescents with attention deficit hyperactivity disorder. Am J Psychi-atry 163:1044 –1051.
01. Konrad K, Neufang S, Hanisch C, Fink GR, Herpertz-Dahlmann B (2006):Dysfunctional attentional networks in children with attention deficit/hyperactivity disorder: Evidence from an event-related functionalmagnetic resonance imaging study. Biol Psychiatry 59:643– 651.
02. Rubia K, Halari R, Smith AB, Mohammad M, Scott S, Brammer MJ (2009):Shared and disorder-specific prefrontal abnormalities in boys withpure attention-deficit/hyperactivity disorder compared to boys withpure CD during interference inhibition and attention allocation. J ChildPsychol Psychiatry 50:669 – 678.
03. Vaidya CJ, Bunge SA, Dudukovic NM, Zalecki CA (2005): Altered neuralsubstrates of cognitive control in childhood ADHD: Evidence fromfunctional magnetic resonance imaging. Am J Psychiatry 162:1605–1613.
04. Stevens MC, Pearlson GD, Kiehl KA (2007): An FMRI auditory oddballstudy of combined-subtype attention deficit hyperactivity disorder.Am J Psychiatry 164:1737–1749.
05. Tamm L, Menon V, Reiss AL (2006): Parietal attentional system aberra-tions during target detection in adolescents with attention deficithyperactivity disorder: event-related fMRI evidence. Am J Psychiatry163:1033–1043.
06. Rubia K, Cubillo A, Woolley J, Brammer MJ, Smith AB (2010): Disorder-specific dysfunctions in patients with attention-deficit/hyperactivitydisorder compared to patients with obsessive-compulsive disorderduring interference inhibition and attention allocation [published on-line ahead of print June 28]. Hum Brain Mapp.
07. Rubia K, Halari R, Cubillo A, Mohammad A, Scott S, Brammer M (2010):Disorder-specific inferior frontal dysfunction in boys with pure atten-tion-deficit/hyperactivity disorder compared to boys with pure CDduring cognitive flexibility [published online ahead of print March 4].Hum Brain Mapp.
08. Rubia K, Halari R, Cubillo A, Mohammad M, Taylor E (2009): Methyl-phenidate normalises activation and functional connectivity deficits inattention and motivation networks in medication-naïve children withADHD during a rewarded continuous performance task. Neurophar-macology 57:640 – 652.
09. Rubia K, Smith A, Halari R, Matukura F, Mohammad M, Taylor E, et al.(2009): Disorder-specific dissociation of orbitofrontal dysfunction inboys with pure conduct disorder during reward and ventrolateral pre-frontal dysfunction in boys with pure attention-deficit/hyperactivitydisorder during sustained attention. Am J Psychiatry 166:83–94.
10. Rubia K, Smith AB, Brammer MJ, Taylor E (2007): Temporal lobe dys-function in medication-naive boys with attention-deficit/hyperactivitydisorder during attention allocation and its relation to response vari-ability. Biol Psychiatry 62:999 –1006.
11. Tamm L, Menon V, Reiss AL (2006): Parietal attentional system aberra-tions during target detection in adolescents with attention deficithyperactivity disorder: event-related fMRI evidence. Am J Psychiatry163:1033–1043.
12. Dickstein SG, Bannon K, Castellanos FX, Milham MP (2006): The neuralcorrelates of attention deficit hyperactivity disorder: An ALE meta-analysis. J Child Psychol Psychiatry 47:1051–1062.
13. Rubia K, Taylor E, Smith AB, Oksanen H, Overmeyer S, Newman S(2001): Neuropsychological analyses of impulsiveness in childhoodhyperactivity. Br J Psychiatry 179:138 –143.
14. Rubia K, Halari R, Christakou A, Taylor E (2009): Impulsiveness as atiming disturbance: Neurocognitive abnormalities in attention-
www.sobp.org/journal
deficit hyperactivity disorder during temporal processes andnormalization with methylphenidate. Philos Trans R Soc Lond B BiolSci 364:1919 –1931.
15. Smith AB, Taylor E, Brammer M, Halari R, Rubia K (2008): Reducedactivation in right lateral prefrontal cortex and anterior cingulate gyrusin medication-naive adolescents with attention deficit hyperactivitydisorder during time discrimination. J Child Psychol Psychiatry 49:977–985.
16. Durston S, Davidson MC, Mulder MJ, Spicer JA, Galvan A, Tottenham N,et al. (2007): Neural and behavioral correlates of expectancy violationsin attention-deficit hyperactivity disorder. J Child Psychol Psychiatry48:881– 889.
17. Scheres A, Milham MP, Knutson B, Castellanos FX (2007): Ventral stria-tal hyporesponsiveness during reward anticipation in attention-defi-cit/hyperactivity disorder. Biol Psychiatry 61:720 –724.
18. Zang YF, He Y, Zhu CZ, Cao QJ, Sui MQ, Liang M, et al. (2007): Alteredbaseline brain activity in children with ADHD revealed by resting-statefunctional MRI. Brain Dev 29:83–91.
19. Cao QJ, Zang YF, Sun L, Sui MQ, Long XY, Zou QH, Wang Y (2006):Abnormal neural activity in children with attention deficit hyperactiv-ity disorder: A resting-state functional magnetic resonance imagingstudy. Neuroreport 17:1033–1036.
20. Cao XH, Cao QJ, Long XY, Sun L, Sui MQ, Zhu CZ, et al. (2009): Abnormalresting-state functional connectivity patterns of the putamen in med-ication-naive children with attention deficit hyperactivity disorder.Brain Res 1303:195–206.
21. Tian LX, Jiang TZ, Wang YF, Zang YF, He Y, Liang M, et al. (2006): Alteredresting-state functional connectivity patterns of anterior cingulatecortex in adolescents with attention deficit hyperactivity disorder.Neurosci Lett 400:39 – 43.
22. Zhu CZ, Zang YF, Liang M, Tian LX, He Y, Li XB, et al. (2005): Discrimina-tive analysis of brain function at resting-state for attention-deficit/hyperactivity disorder. Med Image Comput Comput Assist Interv 8:468 –475.
23. Wang L, Zhu CZ, He Y, Zang YF, Cao QJ, Zhang H, et al. (2009): Alteredsmall-world brain functional networks in children with attention-defi-cit/hyperactivity disorder. Hum Brain Mapp 30:638 – 649.
24. Vloet TD, Gilsbach S, Neufang S, Fink GR, Herpertz-Dahlmann B, KonradK (2010): Neural mechanisms of interference control and time discrim-ination in attention-deficit/hyperactivity disorder. J Am Acad ChildAdolesc Psychiatry 49:356 –367.
25. Cubillo A, Rubia K (2010): Structural and functional brain imaging inadult attention deficit hyperactivity disorder (ADHD): A review. ExpertRev Neurother 10:603– 620.
26. Hesslinger B, Tebartz van Elst L, Thiel T, Haegele K, Hennig J, Ebert D(2002): Frontoorbital volume reductions in adult patients with atten-tion deficit hyperactivity disorder. Neurosci Lett 328:319 –321.
27. Seidman LJ, Valera EM, Makris N, Monuteaux MC, Boriel DL, Kelkar K, etal. (2006): Dorsolateral prefrontal and anterior cingulate cortex volu-metric abnormalities in adults with attention-deficit/hyperactivity dis-order identified by magnetic resonance imaging. Biol Psychiatry 60:1071–1080.
28. Makris N, Biederman J, Valera EM, Bush G, Kaiser J, Kennedy DN, et al.(2007): Cortical thinning of the attention and executive function net-works in adults with attention-deficit/hyperactivity disorder. CerebCortex 17:1364 –1375.
29. Cubillo A, Halari R, Ecker C, Giampietro V, Taylor E, Rubia K (2010):Reduced activation and inter-regional functional connectivity offronto-striatal networks in adults with childhood attention deficit hy-peractivity disorder (ADHD) and persisting symptoms during tasks ofmotor inhibition and cognitive switching. J Psychiatr Res 44:629 – 639.
30. Wolf RC, Plichta MM, Sambataro F, Fallgatter AJ, Jacob C, Lesch KP, et al.(2009): Regional brain activation changes and abnormal functionalconnectivity of the ventrolateral prefrontal cortex during workingmemory processing in adults with attention-deficit/hyperactivity dis-order. Hum Brain Mapp 30:2252–2266.
31. Castellanos FX, Margulies DS, Kelly C, Uddin LQ, Ghaffari M, Kirsch A, etal. (2008): Cingulate-precuneus interactions: A new locus of dysfunc-tion in adult attention-deficit/hyperactivity disorder. Biol Psychiatry63:332–337.
32. Uddin LQ, Kelly AMC, Biswal BB, Margulies DS, Shehzad Z, Shaw D, et al.
(2008): Network homogeneity reveals decreased integrity of default-mode network in ADHD. J Neurosci Methods 169:249 –254.
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
K. Rubia BIOL PSYCHIATRY 2011;69:e69–e87 e85
133. Bussing R, Grudnik J, Mason D, Wasiak M, Leonard C (2002): ADHD andconduct disorder: An MRI study in a community sample. World J BiolPsychiatry 3:216 –220.
34. Kruesi MJ, Casanova MF, Mannheim G, Johnson-Bilder A (2004): Re-duced temporal lobe volume in early onset conduct disorder. Psychia-try Res 132:1–11.
35. Huebner T, Vloet TD, Marx I, Konrad K, Fink GR, Herpertz SC, Herpertz-Dahlmann B (2008): Morphometric brain abnormalities in boys withconduct disorder. J Am Acad Child Adolesc Psychiatry 47:540 –547.
36. Sterzer P, Stadler C, Poustka F, Kleinschmidt A (2007): A structuralneural deficit in adolescents with conduct disorder and its associationwith lack of empathy. Neuroimage 37:335–342.
137. De Brito SA, Mechelli A, Wilke M, Laurens KR, Jones AP, Barker GJ, et al.(2009): Size matters: Increased grey matter in boys with conduct prob-lems and callous unemotional traits. Brain 132:843– 852.
138. Kiehl KA (2006): A cognitive neuroscience perspective on psychopa-thy: Evidence for paralimbic system dysfunction. Psychiatry Res 142:107–128.
139. Sterzer P, Stadler C, Krebs A, Kleinschmidt A, Poustka F (2005): Abnor-mal neural responses to emotional visual stimuli in adolescents withconduct disorder. Biol Psychiatry 57:7–15.
140. Phelps EA, LeDoux JE (2005): Contributions of the amygdala to emo-tion processing: From animal models to human behaviour. Neuron48:175–187.
141. Stadler C, Sterzer P, Schmeck K, Krebs A, Kleinschmidt A, Poustka F(2007): Reduced anterior cingulate activation in aggressive childrenand adolescents during affective stimulation: Association with tem-perament traits. J Psychiatr Res 41:410 – 417.
142. Herpertz SC, Huebner T, Marx I, Vloet TD, Fink GR, Stoecker T, et al.(2008): Emotional processing in male adolescents with childhood-onset conduct disorder J Child Psychol Psychiatry 49:781–791.
43. Etkin A, Wagner TD (2007): Functional neuroimaging of anxiety: ameta-analysis of emotional processing in PTSD, social anxiety disorder,and specific phobia. Am J Psychiatry 164:1476 –1488.
44. Decety J, Michalska KJ, Akitsuki Y, Lahey BB (2009): Atypical empathicresponses in adolescents with aggressive conduct disorder: A func-tional MRI investigation. Biol Psychol 80:203–211.
45. Raine A, Lencz T, Bihrle S, LaCasse L, Colletti P (2000): Reduced prefron-tal gray matter volume and reduced autonomic activity in antisocialpersonality disorder. Arch Gen Psychiatry 57:119 –127.
46. Lewis DM (2002): Responding to a violent incident: Physical restraint oranger management as therapeutic interventions. J Psychiatr MentHealth Nurs 9:57– 63.
47. Jones AP, Laurens KR, Herba CM, Barker GJ, Viding E (2009): Amygdalahypoactivity to fearful faces in boys with conduct problems and cal-lous-unemotional traits. Am J Psychiatry 166:95–101.
48. Marsh AA, Finger EC, Mitchell DG, Reid ME, Sims C, Kosson DS, et al.(2008): Reduced amygdala response to fearful expressions in childrenand adolescents with callous-unemotional traits and disruptive be-haviour disorders. Am J Psychiatry 165:712–720.
49. Klein RG, Abikoff H, Klass E (1998): Attention deficit and bad behavior.Harv Ment Health Lett 14:7.
50. Shaw P, Sharp WS, Morrison M, Eckstrand K, Greenstein DK, Clasen LS,et al. (2009): Psychostimulant treatment and the developing cortex inattention deficit hyperactivity disorder. Am J Psychiatry 166:58 – 63.
51. Bledsoe J, Semrud-Clikeman M, Pliszka SR (2009): A magnetic reso-nance imaging study of the cerebellar vermis in chronically treatedand treatment-naive children with attention-deficit/hyperactivity dis-order combined type. Biol Psychiatry 65:620 – 624.
52. Konrad K, Neufang S, Fink GR, Herpertz-Dahlmann B (2007): Long-termeffects of methylphenidate on neural networks associated with exec-utive attention in children with ADHD: Results from a longitudinalfunctional MRI study. J Am Acad Child Adolesc Psychiatry 46:1633–1641.
53. Goodman DW (2007): The consequences of attention-deficit/hyperac-tivity disorder in adults. J Psychiatr Pract 13:318 –327.
54. Allen G, McColl R, Barnard H, Ringe WK, Fleckenstein J, Cullum CM(2005): Magnetic resonance imaging of cerebellar-prefrontal and cer-ebellar-parietal functional connectivity. Neuroimage 28:39 – 48.
55. Bonnet MC, Dilharreguy B, Allard M, Deloire MSA, Petry KG, Brochet B(2009): Differential cerebellar and cortical involvement according to
various attentional load: role of educational level. Hum Brain Mapp30:1133–1143.1
56. Rubia K, Cubillo A, Smith AB, Woolley J, Heyman I, Brammer MJ (2010):Disorder-specific dysfunction in right inferior prefrontal cortex duringtwo inhibition tasks in boys with attention-deficit hyperactivity disor-der compared to boys with obsessive-compulsive disorder. Hum BrainMapp 31:287–299.
57. Rubia K, Smith AB, Brammer MJ, Taylor E (2003): Right inferior prefron-tal cortex mediates response inhibition while mesial prefrontal cortexis responsible for error detection. Neuroimage 20:351–358.
58. Aron AR, Fletcher PC, Bullmore ET, Sahakian BJ, Robbins TW (2003):Stop-signal inhibition disrupted by damage to right inferior frontalgyrus in humans. Nat Neurosci 6:1329.
59. Chambers CD, Bellgrove MA, Stokes MG, Henderson TR, Garavan H,Robertson IH, et al. (2006): Executive “brake failure” following deacti-vation of human frontal lobe. J Cogn Neurosci 18:444 – 455.
60. Derrfuss J, Brass M, Neumann J, von Cramon DY (2005): Involvement ofthe inferior frontal junction in cognitive control: Meta-analyses ofswitching and Stroop studies. Hum Brain Mapp 25:22–34.
61. Liu X, Banich MT, Jacobson BL, Tanabe JL (2004): Common and distinctneural substrates of attentional control in an integrated Simon andspatial Stroop task as assessed by event-related fMRI. Neuroimage22:1097–1106.
62. Fan J, Flombaum JI, McCandliss BD, Thomas KM, Posner MI (2003):Cognitive and brain consequences of conflict. Neuroimage 18:42–57.
63. Smith AB, Taylor E, Brammer M, Rubia K (2004): Neural correlates ofswitching set as measured in fast, event-related functional magneticresonance imaging. Hum Brain Mapp 21:247–256.
64. Voisin J, Bidet-Caulet A, Bertrand O, Fonlupt P (2006): Listening insilence activates auditory areas: A functional magnetic resonance im-aging study. J Neurosci 26:273–278.
65. Elliott R, Deakin B (2005): Role of the orbitofrontal cortex in reinforce-ment processing and inhibitory control: Evidence from functionalmagnetic resonance imaging studies in healthy human subjects. IntReview Neurobiol 65:89 –116.
66. Kringelbach ML, Rolls ET (2004): The functional neuroanatomy of thehuman orbitofrontal cortex: Evidence from neuroimaging and neuro-psychology. Prog Neurobiol 72:341–372.
67. Baxter MG, Murray EA (2002): The amygdala and reward. Nat Rev Neu-rosci 3:563–573.
68. Knutson B, Fong GW, Bennett SM, Adams CM, Homme D (2003): Aregion of mesial prefrontal cortex tracks monetarily rewarding out-comes: Characterization with rapid event-related fMRI. Neuroimage18:263–272.
69. O’Doherty JP (2004): Reward representations and reward-relatedlearning in the human brain: Insights from neuroimaging. Curr OpinNeurobiol 14:769 –776.
70. Windmann S, Kirsch P, Mier D, Stark R, Walter B, Gunturkun O, Vaitl D(2006): On framing effects in decision making: Linking lateral versusmedial orbitofrontal cortex activation to choice outcome processing. JCogn Neurosci 18:1198 –1211.
71. Coccaro EF, McCloskey MS, Fitzgerald DA, Phan KL (2007): Amygdalaand orbitofrontal reactivity to social threat in individuals with impul-sive aggression. Biol Psychiatry 62:168 –178.
72. Veit R, Flor H, Erb M, Hermann C, Lotze M, Grodd W, Birbaumer N (2002):Brain circuits involved in emotional learning in antisocial behavior andsocial phobia in humans. Neurosci Lett 328:233–236.
73. Birbaumer N, Viet R, Lotze M, Erb M, Hermann C, Grodd W, Flor H (2005):Deficient fear conditioning in psychopathy: A functional magneticresonance imaging study. Arch Gen Psychiatry 62:799 – 805.
74. Blair RJR (2004): The roles of orbital frontal cortex in the modulation ofantisocial behavior. Brain Cogn 55:198 –208.
75. Herpertz SC, Mueller B, Qunaibi M, Lichterfeld C, Konrad K, Herpertz-Dahlmann B (2005): Response to emotional stimuli in boys with con-duct disorder. Am J Psychiatry 162:1100 –1107.
76. Mesulam MM, Nobre AC, Kim YH, Parrish TB, Gitelman DR (2001):Heterogeneity of cingulate contributions to spatial attention. Neuro-image 13:1065–1072.
77. Small DM, Gitelman DR, Gregory MD, Nobre AC, Parrish TB, MesulamMM (2003): The posterior cingulate and medial prefrontal cortex me-diate the anticipatory allocation of spatial attention. Neuroimage 18:633– 641.
78. Kobayashi Y, Amaral DG (2003): Macaque monkey retrosplenial cortex.II. Cortical afferents. J Comp Neurol 466:48 –79.
www.sobp.org/journal

1
1
1
1
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
e86 BIOL PSYCHIATRY 2011;69:e69–e87 K. Rubia
179. Kennerley SW, Walton ME, Behrens TEJ, Buckley MJ, Rushworth MFS(2006): Optimal decision making and the anterior cingulate cortex. NatNeurosci 9:940 –947.
180. Kastner S, Ungerleider LG (2000): Mechanisms of visual attention in thehuman cortex. Annu Review Neurosci 23:315–341.
181. Hayden BY, Heilbronner SR, Nair AC, Platt ML (2008): Cognitive influ-ences on risk-seeking by rhesus macaques. Judgm Decis Mak 3:389 –395.
82. Volkow ND, Wang GJ, Ma YM, Fowler JS, Wong C, Jayne M, et al. (2006):Effects of expectation on the brain metabolic responses to methyl-phenidate and to its placebo in non-drug abusing subjects. Neuroim-age 32:1782–1792.
183. Critchley HD (2005): Neural mechanisms of autonomic, affective, andcognitive integration. J Comp Neurol 493:154 –166.
184. Ridderinkhof KR, Ullsperger M, Crone EA, Nieuwenhuiss S (2004): Therole of the medial frontal cortex in cognitive control. Science 306:443–447.
185. Mohanty A, Gitelman DR, Small DM, Mesulam MM (2008): The spatialattention network interacts with limbic and monoaminergic systemsto modulate motivation-induced attention shifts. Cereb Cortex 18:2604 –2613.
186. Wu ZH, Guo AK (1999): Selective visual attention in a neurocomputa-tional model of phase oscillators. Biol Cybern 80:205–214.
187. Schmahmann JD (1991): An emerging concept. The cerebellar contri-bution to higher function. Arch Neurol 48:1178 –1187.
188. Corbetta M, Shulman GL (2002): Control of goal-directed and stimulus-driven attention in the brain. Nat Rev Neurosci 3:201–215.
189. Herzberg JL, Fenwick PB (1988): The aetiology of aggression in tempo-ral-lobe epilepsy. Br J Psychiatry 153:50 –55.
190. van Elst LT, Woermann FG, Lemieux L, Thompson PJ, Trimble MR(2000): Affective aggression in patients with temporal lobe epilepsy: Aquantitative MRI study of the amygdala. Brain 123:234 –243.
191. Perry RJ, Rosen HR, Kramer JH, Beer JS, Levenson RL, Miller BL (2001):Hemispheric dominance for emotions, empathy and social behaviour:Evidence from right and left handers with frontotemporal dementia.Neurocase 7:145–160.
192. Matthys W, van Goozen SHM, de Vries H, Cohen-Kettenis PT, van Enge-land H (1998): The dominance of behavioural activation over behav-ioural inhibition in conduct disordered boys with or without attentiondeficit hyperactivity disorder. J Child Psychol Psychiatry 39:643– 651.
93. Krawczyk DC, Gazzaley A, D’Esposito M (2007): Reward modulation ofprefrontal and visual association cortex during an incentive workingmemory task. Brain Res 1141:168 –177.
94. Pochon JB, Levy R, Fossati P, Lehericy S, Poline JB, Pillon B, et al. (2002):The neural system that bridges reward and cognition in humans: AnfMRI study. Proc Natl Acad Sci U S A 99:5669 –5674.
95. Finger EC, Marsh AA, Mitchell DG, Reid ME, Sims C, Budhani S, et al.(2008): Abnormal ventromedial prefrontal cortex function in childrenwith psychopathic traits during reversal learning. Arch Gen Psychiatry65:586 –594.
196. Murphy FC, Nimmo-Smith I, Lawrence AD (2003): Functional neuro-anatomy of emotions: A meta-analysis. Cogn Affect Behav Neurosci3:207–233.
197. Amaral DG, Price JL, Pitkanen A, Carmichael ST (1992): Anatomicalorganisation of the primate amygdaloid complex. In: Aggleton JP,editor. The Amygdala: Neurobiological Aspects of Emotion, Memory, andMental Dysfunction. New York: Wiley-Liss, Inc., 1– 66.
198. Best M, Williams JM, Coccaro EF (2002): Evidence for a dysfunctionalprefrontal circuit in patients with an impulsive aggressive disorder.Proc Natl Acad Sci U S A 99:8448 – 8453.
199. De Martino B, Kumaran D, Seymour B, Dolan RJ (2006): Frames, biases,and rational decision-making in the human brain. Science 313:684 –687.
200. Moll J, de Oliveira-Souza R, Eslinger PJ (2003): Morals and the humanbrain: A working model. Neuroreport 14:299 –305.
201. Blair RJR (2007): Aggression, psychopathy and free will from a cogni-tive neuroscience perspective. Behav Sci Law 25:321–331.
202. Blair RJR (2007): The amygdala and ventromedial prefrontal cortex inmorality and psychopathy. Trends Cogn Sci 11:387–392.
203. Whittle S, Yap MBH, Yucel M, Fornito A, Simmons JG, Barrett A, et al.(2008): Prefrontal and amygdala volumes are related to adolescents’
affective behaviors during parent-adolescent interactions. Proc NatlAcad Sci U S A 105:3652–3657.www.sobp.org/journal
04. Deeley Q, Daly E, Surguladze S, Tunstall N, Mezey G, Beer D, et al. (2006):Facial emotion processing in criminal psychopathy. Preliminary func-tional magnetic resonance imaging study. Br J Psychiatry 189:533–539.
05. Kiehl KA, Smith AM, Hare RD, Mendrek A, Forster BB, Brink J, Liddle PF(2001): Limbic abnormalities in affective processing by criminal psy-chopaths as revealed by functional magnetic resonance imaging. BiolPsychiatry 50:677– 684.
06. Rilling JK, Glenn AL, Jairam MR, Pagnoni G, Goldsmith DR, ElfenbeinHA, Lilienfeld SO (2007): Neural correlates of social cooperation andnon-cooperation as a function of psychopathy. Biol Psychiatry 61:1260.
07. Shafritz KM, Marchione KE, Gore JC, Shaywitz SE, Shaywitz BA (2004): Theeffects of methylphenidate on neural systems of attention in attentiondeficit hyperactivity disorder. Am J Psychiatry 161:1990–1997.
08. Silk T, Vance A, Rinehart N, Egan G, O’Boyle M, Bradshaw JL, Cunning-ton R (2005): Fronto-parietal activation in attention-deficit hyperactiv-ity disorder, combined type: Functional magnetic resonance imagingstudy. Br J Psychiatry 187:282–283.
09. Asherson P, Brookes K, Franke B, Chen W, Gill M, Ebstein RP, et al. (2007):Confirmation that a specific haplotype of the dopamine transportergene is associated with combined-type ADHD. Am J Psychiatry 164:674 – 677.
10. Shaw P, Gornick M, Lerch J, Addington A, Seal J, Greenstein D, et al.(2007): Polymorphisms of the dopamine D-4 receptor, clinical out-come, and cortical structure in attention-deficit/hyperactivity disor-der. Arch Gen Psychiatry 64:921–931.
11. Durston S, Fossella JA, Casey BJ, Hulshoff Pol HE, Galvan A, Schnack HG,et al. (2005): Differential effects of DRD4 and DAT1 genotype on fronto-striatal gray matter volumes in a sample of subjects with attentiondeficit hyperactivity disorder, their unaffected siblings, and controls.Mol Psychiatry 10:678 – 685.
12. Durston S, Fossella JA, Mulder MJ, Casey BJ, Ziermans TB, Vessaz MN,Van Engeland H (2008): Dopamine transporter genotype conveys fa-milial risk of attention-deficit/hyperactivity disorder through striatalactivation. J Am Acad Child Adolesc Psychiatry 47:61– 67.
13. Hallikainen T, Saito T, Lachman HM, Volavka J, Pohjalainen T, RyynanenOP, et al. (1999): Association between low activity serotonin trans-porter promoter genotype and early onset alcoholism with habitualimpulsive violent behavior. Mol Psychiatry 4:385–388.
14. Matsushita S, Yoshino A, Murayama M, Kimura M, Muramatsu T, Higu-chi S (2001): Association study of serotonin transporter gene regula-tory region polymorphism and alcoholism. Am J Med Genet 105:446 –450.
15. Liao DL, Hong CJ, Shih HL, Tsai SJ (2004): Possible association betweenserotonin transporter promoter region polymorphism and extremelyviolent crime in Chinese males. Neuropsychobiology 50:284 –287.
16. Cadoret RJ, Langbehn D, Caspers K, Troughton EP, Yucuis R, SandhuHK, Philibert R (2003): Associations of the serotonin transporter pro-moter polymorphism with aggressivity, attention deficit, and conductdisorder in an adoptee population. Compr Psychiatry 44:88 –101.
17. Beitchman JH, Baldassarra L, Mik H, De Luca V, King N, Bender D, et al.(2006): Serotonin transporter polymorphisms and persistent, perva-sive childhood aggression. Am J Psychiatry 163:1103–1105.
18. Reif A, Rosler M, Freitag CM, Schneider M, Eujen A, Kissling C, et al.(2007): Nature and nurture predispose to violent behavior: Serotoner-gic genes and adverse childhood environment. Neuropsychopharma-cology 32:2375–2383.
19. Pezawas L (2009): Serotonin transporter gene polymorphism and sus-ceptibility to depression. Eur Neuropsychopharmacol 19:S216 –S217.
20. Pezawas L, Meyer-Lindenberg A, Drabant EM, Verchinski BA, MunozKE, Kolachana BS, et al. (2005): 5-HTTLPR polymorphism impacts hu-man cingulate-amygdala interactions: A genetic susceptibility mech-anism for depression. Nat Neurosci 8:828 – 834.
21. Scherk H, Gruber O, Menzel P, Schneider-Axmann T, Kemmer C, UsherJ, et al. (2009): 5-HTTLPR genotype influences amygdala volume. EurArch Psychiatry Clin Neurosci 259:212–217.
22. Munafo MR, Brown SM, Hariri AR (2008): Serotonin transporter (5-HTTLPR) genotype and amygdala activation: A meta-analysis. Biol Psy-chiatry 63:852– 857.
23. McArdle P, Obrien G, Kolvin I (1995): Hyperactivity: Prevalence and
relationship with conduct disorder. J Child Psychol Psychiatry 36:279 –303.
2
2
2
2
2
2
2
2
2
2
2
2
K. Rubia BIOL PSYCHIATRY 2011;69:e69–e87 e87
224. Maughan B, Rowe R, Messer J, Goodman R, Meltzer H (2004): Conductdisorder and oppositional defiant disorder in a national sample: Devel-opmental epidemiology. J Child Psychol Psychiatry 45:609 – 621.
225. Plessen KJ, Bansal R, Zhu HT, Whiteman R, Amat J, Quackenbush GA, etal. (2006): Hippocampus and amygdala morphology in attention-def-icit/hyperactivity disorder. Arch Gen Psychiatry 63:795– 807.
226. Ivanov I, Bansal R, Hao XJ, Zhu HT, Kellendonk C, Miller L, et al. (2010):Morphological abnormalities of the thalamus in youths with attentiondeficit hyperactivity disorder. Am J Psychiatry 167:397– 408.
227. McAlonan K, Cavanaugh J, Wurtz RH (2006): Attentional modulation ofthalamic reticular neurons. J Neurosci 26:4444 – 4450.
228. Haber SN, Calzavara R (2009): The cortico-basal ganglia integrativenetwork: The role of the thalamus. Brain Res Bull 78:69 –74.
229. Jones EG (1998): A new view of specific and nonspecific thalamocorti-cal connections. Adv Neurol 77:49 –73.
230. Morel A, Magnin M, Jeanmonod D (1997): Multiarchitectonic and ste-reotactic atlas of the human thalamus. J Comp Neurol 387:588 – 630.
231. Volkow ND, Wang GJ, Kollins SH, Wigal TL, Newcorn JH, Telang F, et al.(2009): Evaluating dopamine reward pathway in ADHD: Clinical impli-cations. JAMA 302:1084 –1091.
232. Volkow ND, Wang GJ, Newcorn J, Telang F, Solanto MV, Fowler JS, et al.(2007): Depressed dopamine activity in caudate and preliminary evi-dence of limbic involvement in adults with attention-deficit/hyperac-tivity disorder. Arch Gen Psychiatry 64:932–940.
233. Plichta MM, Vasic N, Wolf RC, Lesch KP, Brummer D, Jacob C, et al.(2009): Neural hyporesponsiveness and hyperresponsiveness duringimmediate and delayed reward processing in adult attention-deficit/hyperactivity disorder. Biol Psychiatry 65:7–14.
234. Brotman MA, Rich BA, Guyer AE, Lunsford JR, Horsey SE, Reising MM, etal. (2010): Amygdala activation during emotion processing of neutralfaces in children with severe mood dysregulation versus ADHD orbipolar disorder. Am J Psychiatry 167:61– 69.
235. Strohle A, Stoy M, Wrase J, Schwarzer S, Schlagenhauf F, Huss M, et al.(2008): Reward anticipation and outcomes in adult males with atten-tion-deficit/hyperactivity disorder. Neuroimage 39:966 –972.
236. Christakou A, Brammer M, Giampietro V, Rubia K (2009): Right ventro-medial and dorsolateral prefrontal cortices mediate adaptive deci-sions under ambiguity by integrating choice utility and outcome eval-uation. J Neurosci 29:11020 –11028.
237. Lawrence NS, Jollant F, O’Daly O, Zelaya F, Phillips ML (2009): Distinctroles of prefrontal cortical subregions in the Iowa Gambling Task.Cereb Cortex 19:1134 –1143.
238. Bechara A, Damasio H, Tranel D, Anderson SW (1998): Dissociation ofworking memory from decision making within the human prefrontal
cortex. J Neurosci 18:428 – 437.39. Ullsperger M, von Cramon DY (2004): Decision making, performance andoutcome monitoring in frontal cortical areas. Nat Neurosci 7:1173–1174.
40. Tamm L, Menon V, Ringel J, Reiss AL (2004): Event-related FMRI evi-dence of frontotemporal involvement in aberrant response inhibitionand task switching in attention-deficit/hyperactivity disorder. J AmAcad Child Adolesc Psychiatry 43:1430 –1440.
41. Bush G, Frazier JA, Rauch SL, Seidman LJ, Whalen PJ, Jenike MA, et al.(1999): Anterior cingulate cortex dysfunction in attention-deficit/hy-peractivity disorder revealed by fMRI and the counting Stroop. BiolPsychiatry 45:1542–1552.
42. Bush G, Spencer TJ, Holmes J, Shin LM, Valera EM, Seidman LJ, et al.(2008): Functional magnetic resonance imaging of methylphenidateand placebo in attention-deficit/hyperactivity disorder during themulti-source interference task. Arch Gen Psychiatry 65:102–114.
43. Chen W, Tobias Banaschewski T, Barbara Franke B, Taylor A, EdmundJS, Sonuga-Barke E, et al. (in press): Emotional lability, SLC6A4/5-HTTand DRD4 genotypes in attention deficit hyperactivity disorder(ADHD): Genetic substrates for emotional dysregulation or distinctiveADHD subtypes? Am J Psychiatry.
44. Willcutt EG, Pennington BF, Chhabildas NA, Friedman MC, Alexander J(1999): Psychiatric comorbidity associated with DSM-IV ADHD in anonreferred sample of twins. J Am Acad Child Adolesc Psychiatry 38:1355–1362.
45. Castellanos FX, Sonuga-Barke EJS, Milham MP, Tannock R (2006): Char-acterizing cognition in ADHD: Beyond executive dysfunction. TrendsCogn Sci 10:117–123.
46. Carlson CL, Mann M (2002): Sluggish cognitive tempo predicts a differ-ent pattern of impairment in the attention deficit hyperactivity disor-der, predominantly inattentive type. J Clin Child Adolesc Psychol 31:123–129.
47. Rubia K (2007): Neuro-anatomic evidence for the maturational delayhypothesis of ADHD. Proc Natl Acad Sci U S A 104:19663–19664.
48. Ecker C, Rocha-Rego V, Johnston P, Mourao-Miranda J, Marquand A,Daly EM, et al. (2010): Investigating the predictive value of whole-brainstructural MR scans in autism: A pattern classification approach. Neu-roimage 49:44 –56.
49. Fu CH, Mourao-Miranda J, Costafreda SG, Khanna A, Marquand AF,Williams SC, Brammer MJ (2008): Pattern classification of sad facialprocessing: Toward the development of neurobiological markers indepression. Biol Psychiatry 63:656 – 662.
50. Davatzikos C, Shen D, Gur RC, Wu X, Liu D, Fan Y (2005): Wholebrainmorphometric study of schizophrenia revealing a spatially complex
set of focal abnormalities. Arch Gen Psychiatry 62:1218 –1227.www.sobp.org/journal