
Asymmetrical temporal lobe atrophy with massive neuronal inclusions in multiple system atrophy
9
Journal of the Neurological Sciences 179 (2000) 50–58 www.elsevier.com / locate / jns Asymmetrical temporal lobe atrophy with massive neuronal inclusions in multiple system atrophy a,b, b b c * Katsuhiko Shibuya , Hideki Nagatomo , Kiyoshi Iwabuchi , Masayuki Inoue , c c Saburo Yagishita , Yoji Itoh a Department of Neurology and Psychiatry, Numazu Central Hospital, Nakasecho 24-1, Numazu, Shizuoka, 410-8575 Japan b Department of Neurology and Psychiatry, Kanagawa Rehabilitation Center, Nanasawa 516 Atugi, Kanagawa 243-0121, Japan c Department of Pathology, Kanagawa Rehabilitation Center, Nanasawa 516 Atugi, Kanagawa 243-0121, Japan Received 11 December 1998; received in revised form 6 June 2000; accepted 3 July 2000 Abstract This report concerns a rare association of asymmetrical temporal lobe atrophy with multiple system atrophy (MSA). A 53-year-old Japanese woman developed cerebellar ataxia and parkinsonism and was diagnosed as olivopontocerebellar atrophy (OPCA). This patient showed forgetfulness and subsequent disorientation even in the early stage of the disease. She fell into a decorticate state at the age of 64, and died a year later. The autopsy showed MSA with asymmetrical atrophy of temporal lobes, intraneuronal globular inclusions mostly confined to the hippocampus, amygdaloid nucleus, and most abundant in the granule cells in the dentate fascia. These inclusions were intensely argyrophilic and expressed marked immunoreactivity to ubiquitin, but not to neurofilament (NF), tau and paired helical filaments (PHF). Ultrastructurally, they were composed of scattered short filamentous structures of 15 to 30 nm in diameter, ribosome-like granules, mitochondria and lipofuscin. The lack of immunoreactivity against tau, NF and PHF suggests that the inclusions are distinct from Pick bodies. To our knowledge, MSA in association with asymmetrical temporal lobe atrophy with the present neuronal inclusions has not been reported. This case is distinct from MSA combined with atypical Pick’s disease in the distribution and immunohistochemical properties of neuronal inclusions, and may present a new variant of MSA since the neuronal inclusions are similar, in many respects, to those of neuronal inclusions reported in MSA. Globular inclusions are also discussed in variants of Pick’s disease, amyotrophic lateral sclerosis and Alzheimer’s disease. 2000 Published by Elsevier Science B.V. Keywords: Multiple system atrophy; Globular argyrophilic neuronal bodies; Pick body; Immunohistochemistry; Ultrastructure 1. Introduction of a patient with MSA who displays asymmetrical tempo- ral lobe atrophy with neuronal intracytoplasmic inclusions Multiple system atrophy (MSA) includes olivopon- having some features of Pick bodies. tocerebellar atrophy (OPCA), striatonigral degeneration (SND) and Shy–Drager syndrome [1]. The clinicopathological unity of these syndromes is supported 2. Case report by the presence of characteristic argyrophilic cytoplasmic inclusions in the oligodendroglia and neurons [2–9]. A 53-year-old woman, the proprietress of ‘ryokan’ Rarely, this disease may be associated with Alzheimer’s (Japanese inn) developed an unsteady gait, dysarthria, and disease [10], progressive supranuclear palsy [11], or impairment of memory. The dysmnesia gradually became atypical Pick’s disease [12]. This study documents the case worse. She often forgot the telephone number of booking visitors and was unable to continue her work as propriet- ress. At age 55 years, she was diagnosed as having OPCA *Corresponding author. Tel.: 181-559-314-100; fax: 181-559-319- 221. by one of the authors (K.I.). The patient developed 0022-510X / 00 / $ – see front matter 2000 Published by Elsevier Science B.V. PII: S0022-510X(00)00364-6
-
Upload
independent -
Category
Documents
-
view
8 -
download
0
Transcript of Asymmetrical temporal lobe atrophy with massive neuronal inclusions in multiple system atrophy

Journal of the Neurological Sciences 179 (2000) 50–58www.elsevier.com/ locate / jns
Asymmetrical temporal lobe atrophy with massive neuronal inclusionsin multiple system atrophy
a,b , b b c*Katsuhiko Shibuya , Hideki Nagatomo , Kiyoshi Iwabuchi , Masayuki Inoue ,c cSaburo Yagishita , Yoji Itoh
aDepartment of Neurology and Psychiatry, Numazu Central Hospital, Nakasecho 24-1, Numazu, Shizuoka, 410-8575 JapanbDepartment of Neurology and Psychiatry, Kanagawa Rehabilitation Center, Nanasawa 516 Atugi, Kanagawa 243-0121, Japan
cDepartment of Pathology, Kanagawa Rehabilitation Center, Nanasawa 516 Atugi, Kanagawa 243-0121, Japan
Received 11 December 1998; received in revised form 6 June 2000; accepted 3 July 2000
Abstract
This report concerns a rare association of asymmetrical temporal lobe atrophy with multiple system atrophy (MSA). A 53-year-oldJapanese woman developed cerebellar ataxia and parkinsonism and was diagnosed as olivopontocerebellar atrophy (OPCA). This patientshowed forgetfulness and subsequent disorientation even in the early stage of the disease. She fell into a decorticate state at the age of 64,and died a year later. The autopsy showed MSA with asymmetrical atrophy of temporal lobes, intraneuronal globular inclusions mostlyconfined to the hippocampus, amygdaloid nucleus, and most abundant in the granule cells in the dentate fascia. These inclusions wereintensely argyrophilic and expressed marked immunoreactivity to ubiquitin, but not to neurofilament (NF), tau and paired helical filaments(PHF). Ultrastructurally, they were composed of scattered short filamentous structures of 15 to 30 nm in diameter, ribosome-like granules,mitochondria and lipofuscin. The lack of immunoreactivity against tau, NF and PHF suggests that the inclusions are distinct from Pickbodies. To our knowledge, MSA in association with asymmetrical temporal lobe atrophy with the present neuronal inclusions has not beenreported. This case is distinct from MSA combined with atypical Pick’s disease in the distribution and immunohistochemical properties ofneuronal inclusions, and may present a new variant of MSA since the neuronal inclusions are similar, in many respects, to those ofneuronal inclusions reported in MSA. Globular inclusions are also discussed in variants of Pick’s disease, amyotrophic lateral sclerosisand Alzheimer’s disease. 2000 Published by Elsevier Science B.V.
Keywords: Multiple system atrophy; Globular argyrophilic neuronal bodies; Pick body; Immunohistochemistry; Ultrastructure
1. Introduction of a patient with MSA who displays asymmetrical tempo-ral lobe atrophy with neuronal intracytoplasmic inclusions
Multiple system atrophy (MSA) includes olivopon- having some features of Pick bodies.tocerebellar atrophy (OPCA), striatonigral degeneration(SND) and Shy–Drager syndrome [1]. Theclinicopathological unity of these syndromes is supported 2. Case reportby the presence of characteristic argyrophilic cytoplasmicinclusions in the oligodendroglia and neurons [2–9]. A 53-year-old woman, the proprietress of ‘ryokan’Rarely, this disease may be associated with Alzheimer’s (Japanese inn) developed an unsteady gait, dysarthria, anddisease [10], progressive supranuclear palsy [11], or impairment of memory. The dysmnesia gradually becameatypical Pick’s disease [12]. This study documents the case worse. She often forgot the telephone number of booking
visitors and was unable to continue her work as propriet-ress. At age 55 years, she was diagnosed as having OPCA*Corresponding author. Tel.: 181-559-314-100; fax: 181-559-319-
221. by one of the authors (K.I.). The patient developed
0022-510X/00/$ – see front matter 2000 Published by Elsevier Science B.V.PII : S0022-510X( 00 )00364-6
K. Shibuya et al. / Journal of the Neurological Sciences 179 (2000) 50 –58 51
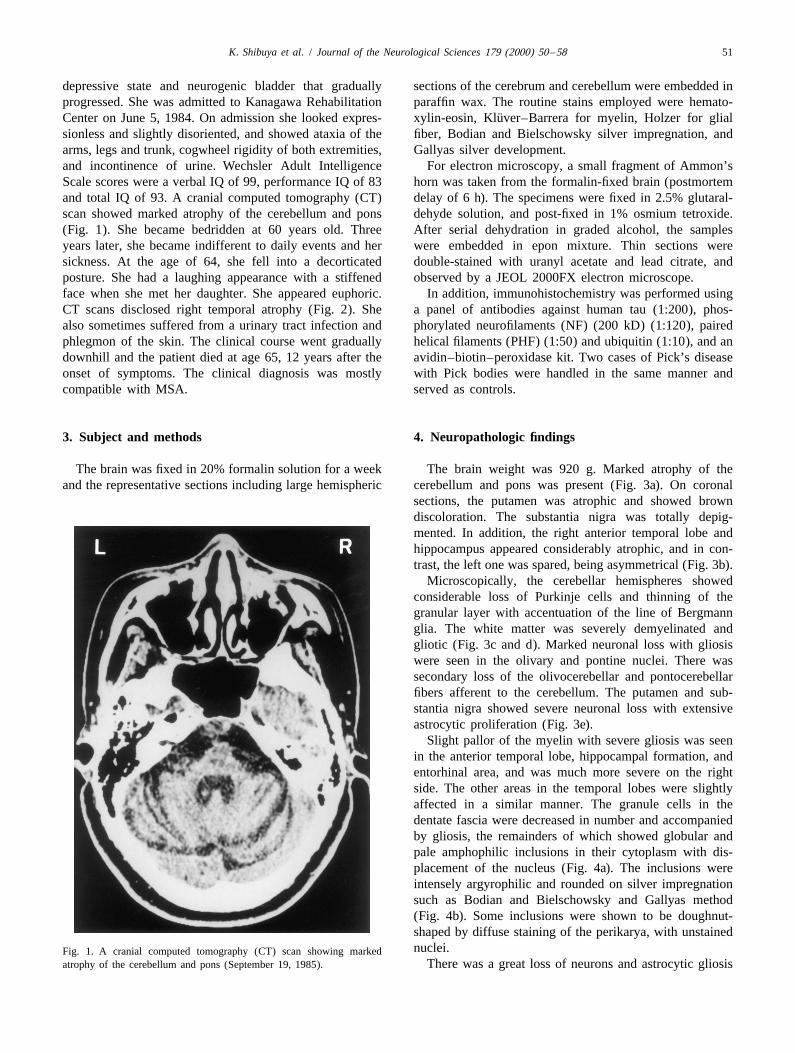
depressive state and neurogenic bladder that gradually sections of the cerebrum and cerebellum were embedded inprogressed. She was admitted to Kanagawa Rehabilitation paraffin wax. The routine stains employed were hemato-
¨Center on June 5, 1984. On admission she looked expres- xylin-eosin, Kluver–Barrera for myelin, Holzer for glialsionless and slightly disoriented, and showed ataxia of the fiber, Bodian and Bielschowsky silver impregnation, andarms, legs and trunk, cogwheel rigidity of both extremities, Gallyas silver development.and incontinence of urine. Wechsler Adult Intelligence For electron microscopy, a small fragment of Ammon’sScale scores were a verbal IQ of 99, performance IQ of 83 horn was taken from the formalin-fixed brain (postmortemand total IQ of 93. A cranial computed tomography (CT) delay of 6 h). The specimens were fixed in 2.5% glutaral-scan showed marked atrophy of the cerebellum and pons dehyde solution, and post-fixed in 1% osmium tetroxide.(Fig. 1). She became bedridden at 60 years old. Three After serial dehydration in graded alcohol, the samplesyears later, she became indifferent to daily events and her were embedded in epon mixture. Thin sections weresickness. At the age of 64, she fell into a decorticated double-stained with uranyl acetate and lead citrate, andposture. She had a laughing appearance with a stiffened observed by a JEOL 2000FX electron microscope.face when she met her daughter. She appeared euphoric. In addition, immunohistochemistry was performed usingCT scans disclosed right temporal atrophy (Fig. 2). She a panel of antibodies against human tau (1:200), phos-also sometimes suffered from a urinary tract infection and phorylated neurofilaments (NF) (200 kD) (1:120), pairedphlegmon of the skin. The clinical course went gradually helical filaments (PHF) (1:50) and ubiquitin (1:10), and andownhill and the patient died at age 65, 12 years after the avidin–biotin–peroxidase kit. Two cases of Pick’s diseaseonset of symptoms. The clinical diagnosis was mostly with Pick bodies were handled in the same manner andcompatible with MSA. served as controls.
3. Subject and methods 4. Neuropathologic findings
The brain was fixed in 20% formalin solution for a week The brain weight was 920 g. Marked atrophy of theand the representative sections including large hemispheric cerebellum and pons was present (Fig. 3a). On coronal
sections, the putamen was atrophic and showed browndiscoloration. The substantia nigra was totally depig-mented. In addition, the right anterior temporal lobe andhippocampus appeared considerably atrophic, and in con-trast, the left one was spared, being asymmetrical (Fig. 3b).
Microscopically, the cerebellar hemispheres showedconsiderable loss of Purkinje cells and thinning of thegranular layer with accentuation of the line of Bergmannglia. The white matter was severely demyelinated andgliotic (Fig. 3c and d). Marked neuronal loss with gliosiswere seen in the olivary and pontine nuclei. There wassecondary loss of the olivocerebellar and pontocerebellarfibers afferent to the cerebellum. The putamen and sub-stantia nigra showed severe neuronal loss with extensiveastrocytic proliferation (Fig. 3e).
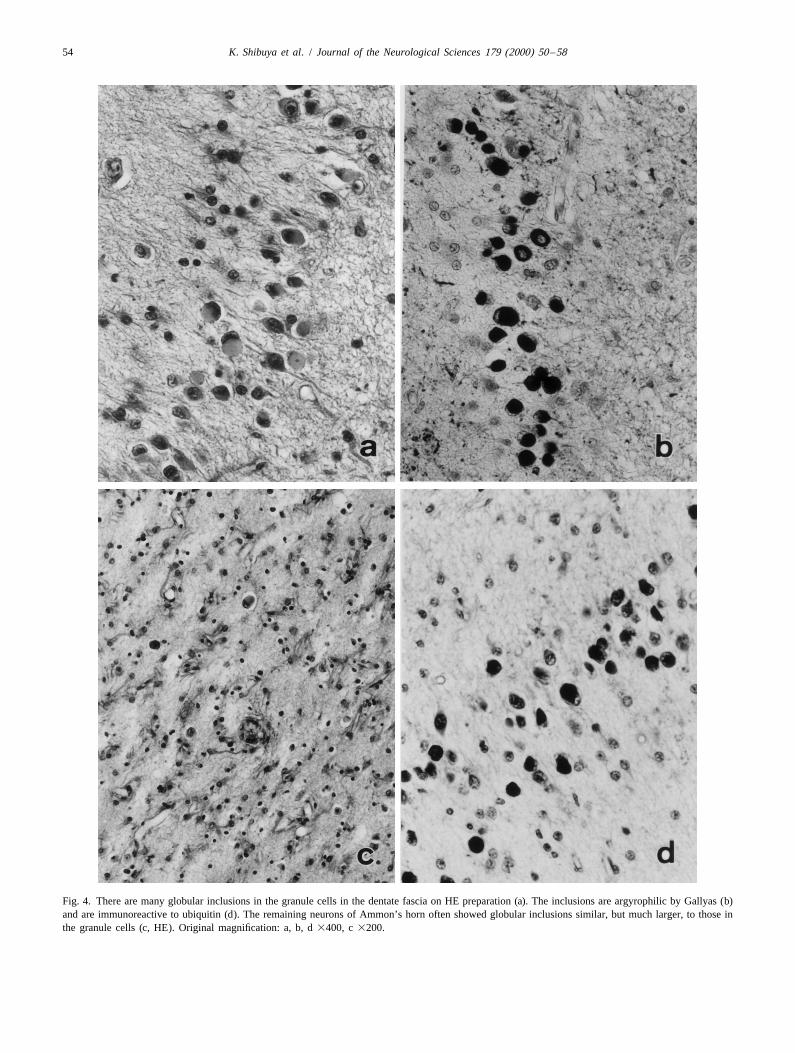
Slight pallor of the myelin with severe gliosis was seenin the anterior temporal lobe, hippocampal formation, andentorhinal area, and was much more severe on the rightside. The other areas in the temporal lobes were slightlyaffected in a similar manner. The granule cells in thedentate fascia were decreased in number and accompaniedby gliosis, the remainders of which showed globular andpale amphophilic inclusions in their cytoplasm with dis-placement of the nucleus (Fig. 4a). The inclusions wereintensely argyrophilic and rounded on silver impregnationsuch as Bodian and Bielschowsky and Gallyas method(Fig. 4b). Some inclusions were shown to be doughnut-shaped by diffuse staining of the perikarya, with unstainednuclei.Fig. 1. A cranial computed tomography (CT) scan showing marked
atrophy of the cerebellum and pons (September 19, 1985). There was a great loss of neurons and astrocytic gliosis

52 K. Shibuya et al. / Journal of the Neurological Sciences 179 (2000) 50 –58
Fig. 2. CT scans disclosing right temporal atrophy (a) and mild cerebral atrophy (b) (August 6, 1993).
in the pyramidal cell layer of Ammon’s horn and dria were displaced to the periphery of the cytoplasm (Fig.prosubiculum. The subiculum and presubiculum were 6a). They consisted of scattered fibrillary structures, somespared. The remaining neurons often showed globular mitochondria and abundant osmiophilic granules. Theargyrophilic inclusions similar, but much larger, to those in fibrillary structures were randomly distributed and in-the granule cells (Fig. 4c). Many similar inclusions were frequently arranged in bundles. The fibrils were 15 to 30also seen in the amygdala, entorhinal and insular cortices, nm in diameter to which many osmiophilic structures wereand a few in the middle and superior temporal and parietal attached along the entire length (Fig. 6b).cortices. The distribution of the neuronal loss is illustrated These neuronal inclusions were similar in ultrastructurein Fig. 5. The inclusions were also seen in the left cerebral to oligodendroglial argyrophilic inclusions, but they werehemisphere but were much fewer than in the right. easily differentiated by their shape and location, morePrimitive plaques were scattered in the cerebral cortex.
Table 1Neither Lewy bodies, Pick cells (swollen neurons) norProperties of inclusions of this case
typical Alzheimer’s neurofibrillary tangles were presentStainingsanywhere.Hematoxylin-eosin EosinophilicImmunohistochemically, the inclusions were immuno-
¨Kluver–Barrera Slightly bluereactive to ubiquitin (Fig. 4d), but not to tau, NF or PHF Bodian Argyrophilic(Table 1). In contrast, Pick bodies in two Pick’s disease Bielschowsky Argyrophilic
Gallyas–Braal Argyrophilicexpressed intense immunoreactions to tau and PHF. Thehistochemical properties of the inclusions are listed in
ImmunohistochemistryTable 2.Tau Negative
Ultrastructurally, the inclusions were recognized as PHF Negativeglobular structures that were fairly well demarcated from Neurofilament 200 kD Negative
Ubiquitin Positivethe other cytoplasmic structures, but had no limitingb-Amyroid Negativemembranes.Synaptophisin NegativeLipofuscin, granular endoplasmic reticula and mitochon-

K. Shibuya et al. / Journal of the Neurological Sciences 179 (2000) 50 –58 53
Fig. 3. The brain showing marked atrophy of the cerebellum and pons (a). Coronal section of the right hemisphere. The anterior temporal lobe and¨ ¨hippocampus appeared atrophic (b, Kluver–Barrera). The cerebellar white matter is severely demyelinated and gliotic (c, Holzer; d, Kluver–Barrera). The
substantia nigra showing severe neuronal loss with extensive astrocytic proliferation (e, HE, original magnification 3200).
easily in the granule cells of the dentate fascia. Oligoden- gliosis in the olivopontocerebellar system involving thedroglial inclusions were widely distributed throughout the cerebellar cortex, and in the striatonigral system. Incentral nervous system as previously described [2–5]. addition, oligodendroglial argyrophilic inclusions [2–
4,8,9,13] were widely distributed throughout the brain. So,this case was easily diagnosed as MSA [1,14].
5. Discussion Interestingly, the patient developed dysmnesia and sub-sequent disorientation even in the early stage of the
In the present case, there was severe neuronal loss and disease. The cerebrum showed asymmetrical atrophy of the
54 K. Shibuya et al. / Journal of the Neurological Sciences 179 (2000) 50 –58
Fig. 4. There are many globular inclusions in the granule cells in the dentate fascia on HE preparation (a). The inclusions are argyrophilic by Gallyas (b)and are immunoreactive to ubiquitin (d). The remaining neurons of Ammon’s horn often showed globular inclusions similar, but much larger, to those inthe granule cells (c, HE). Original magnification: a, b, d 3400, c 3200.

K. Shibuya et al. / Journal of the Neurological Sciences 179 (2000) 50 –58 55
Fig. 5. Schema showing the distribution of the inclusions in the cerebral cortex (right hemisphere). Black, numerous; dark gray, many; light gray, a few.
anterior temporal lobe including Ammon’s horn, being and entorhinal cortex where many neurons disappearedmore severe on the right side. Numerous argyrophilic with reparative gliosis. The other cortical areas such asinclusions were seen in the neuronal cytoplasm, and were insular and inferior temporal cortices were also, but to amainly confined to the hippocampus, amygdaloid nucleus, lesser extent, involved.

56 K. Shibuya et al. / Journal of the Neurological Sciences 179 (2000) 50 –58
Fig. 6. (a) Ultrastructurally, a neuronal inclusion shows globular filamentous structures, fairly well-demarcated from the other cytoplasmic organellae andno limiting membranes. Lipofuscin, granular endoplasmic reticula and mitochondria are displaced toward the periphery of the cytoplasm (granule cell ofdentate fascia, 32000). (b) Higher magnification of Fig. 6a. The fibrillary structures are randomly distributed and infrequently arranged in bundles,measuring 15 to 30 nm.
The inclusions were intensely argyrophilic on Bodian, with classical [15,16] and atypical Pick bodies [12], andBielschowsky and Gallyas stains, and immunoreactive Pick-body-like inclusions in some other diseases [17–19].only to ubiquitin, not to tau, phosphorylated NF or PHF. Pick bodies were immunoreactive to tau and PHF. SomeThe histochemical and topographical properties of the Pick bodies, but not all, were immunoreactive to ubiquitinpresent inclusions are summarized in Table 2, compared [16]. Love et al. [20] reported that most of the Pick bodies
Table 2aNeuronal cytoplasmic inclusions, immunohistochemistry, ultrastructure and distribution
Case Lobar Immunohistochemistry Ultrastructure Distribution
atrophy Bodian Biel Gal PHF Tau NF Ub Diameter Granules DG HP EC Am Insula Cortex BG BS
Typical Pick [16] 1 1 11 11 11 21 21 15 nm 2 11 11 1 11 1 1 1 1
Generalized variant [15] 1 21 21 15 nm 1 2 2 2 2 2 2 1 1
MSA1Pick [12] F 11 Alz50(2) 2 21 1 11 nm 1 1 1 2 1 1 P 1 1
Alzheimer [18] 1 ANT(1) 1 15–18 nm 1 1
ALS1Pick [19] F,T 1 12–16 nm 1 1 1 F 1
ALS1Pick [17] 1 9–15 nm 1 F 1
Pick variant [25] F,T 1 1 2 2 1 2 12 nm 1 1 1 1 1 1 2 2
Our case T 1 1 1 2 2 2 1 15–30 nm 1 1 1 1 1 1 F,P,T 1 1
Our two Pick cases F,T 1 1 1 1 1 2 21 15 nm 2 1 1 1 1 1 F,T 1 1
a Biel, Bielschowsky; Gal, Gallyas; NF, neurofilament 200 kD; Ub, ubiquitin; DG, dentate granular cell layer; HP, hippocampal pyramidal cell layer; EC,entorhinal cortex; Am, amygdala; BG, basal ganglia; BS, brain stem nucleus; F, frontal cortex; P, parietal cortex; T, temporal cortex.

K. Shibuya et al. / Journal of the Neurological Sciences 179 (2000) 50 –58 57
[2] Papp MI, Kahn JE, Lantos PL. Glial cytoplasmic inclusions in thewere positive to ubiquitin. Thus, the present neuronalCNS of patients with multiple system atrophy (striatonigral degene-inclusions were superficially similar to but apparentlyration, olivopontocerebellar atrophy and Shy–Drager syndrome). Jdistinct from Pick bodies.Neurol Sci 1989;94:79–100.
Neuronal cytoplasmic inclusions (NCIs) in MSA were [3] Nakazato Y, Yamazaki H, Hirato J, Ishida Y, Yamaguchi H.positive for ubiquitin and occasionally positive for neuro- Oligodendroglial microtubular tangles in olivopontocerebellar atro-
phy. J Neuropathol Exp Neurol 1990;49:521–30.filament, while negative for tau and PHF [21]. Therefore,[4] Arai N, Nishimura M, Oda M, Morimatsu Y, Oue R. Immuno-the present inclusions are very similar, in their stainability,
histochemical study of glial cytoplasmic inclusion in multipleto the neuronal inclusions reported in MSA [21], but theirsystem atrophy. Brain Nerve 1991;43:857–62, (in Japanese).distribution is quite different since the latter are mainly
[5] Abe H, Yagishita S, Amano N, Iwabuchi K, Hasegawa H, Kowa Kconfined to the pontine neurons in their cases. The et al. Argyrophilic glial intracytoplasmic inclusions in multipleinclusions in a case of MSA reported by Horoupian and system atrophy: immunocytochemical and ultrastructural study. Acta
Neuropathol 1992;84:273–7.Dickson [12] were also different in distribution form.[6] Kobayashi K, Miyazu K, Katsukawa K, Fukutani Y, Mukai M,Ultrastructurally, the present inclusions were composed
Nakakura I et al. Cytoskeletal protein abnormalities in patients withof scattered short fibrillary structures of 15 to 30 nm inolivopontocerebellar atrophy — an immunocytochemical anddiameter to which many osmiophilic granules were at-Gallyas silver impregnation study. J Neuropathol Appl Neurobiol
tached along the entire length of the fibrils. In contrast, the 1992;18:237–49.inclusions of classical Pick disease [15,16] consisted of [7] Mochizuku A, Mizusawa H, Ohkoshi N, Yoshizawa K, Komatsuzaki
Y, Inoue K et al. Argentophilic intracytoplasmic inclusions instraight filaments [22,23], paired twisted profiles [16] ormultiple system atrophy. J Neurol 1992;239:311–6.periodically constricted filaments or NF with a geometrical
[8] Papp MI, Lantos PL. The distribution of oligodendroglial inclusionspattern [22,24]. Thus, the inclusions of the present case arein multiple system atrophy and its relevance to clinical symp-
distinct from that of classical Pick disease. Munoz-Garcia tomatology. Brain 1994;117:235–43.et al. [15] described generalized variants of Pick’s disease [9] Nakazato Y, Suzuki S. Oligodendroglial microtubular tangles inin which the bodies consisted of straight fibrils coated with multiple system atrophy. Neuropathology 1996;16:145–50.
[10] Kosaka K, Iizuka R, Mizutani Y, Kondo T, Nagatsu T. Striatonigralgranular material. The bodies were composed primarily ofdegeneration combined with Alzheimer’s disease. Acta Neuropatholskeins of neurofilaments studded with granular substances1981;54:253–6.[25].
[11] Renkawek K, Horstink MWIM. Striatonigral degeneration withPick-body-like inclusions in motor neuron disease con- neurofibrillary tangles. Acta Neuropathol 1993;86:405–10.sisted of fibrils decorated by granular and fuzzy materials [12] Horoupian DS, Dickson DW. Striatonigral degeneration, olivopon-along their entire length [17,19]. Neuronal cytoplasmic tocerebellar atrophy and ‘atypical’ Pick disease. Acta Neuropathol
1991;81:287–95.inclusions (NCIs) in MSA also consisted of fibrils with[13] Abe H. Multiple system degeneration. Clinical and pathologicalgranular materials [21,26]. The inclusions of generalized
observation of 15 cases of multiple system atrophy (Oppenheimer).variants of Pick’s disease, motor neuron disease withYokohama Med Bull 1992;43:17–35.
dementia and NCIs in MSA resemble each other in the ´ ´ ´ ´[14] Dejerine J, Thomas A. L’atrophie olivo-ponto-cerebelleuse. Nouvcomponents of fibrillary structures with granular sub- Incongr Salpet 1990;13:330–70.stances, and are also similar in some respects to the [15] Munoz-Garcia D, Ludwin SK. Classical and generalized variants of
Pick’s disease. A clinicopathological, ultrastructural, and immuno-inclusions of the present case. The inclusions in MSA withcytochemical comparative study. Ann Neurol 1984;16:467–80.atypical Pick disease reported by Horoupian and Dickson
[16] Murayama S, Mori H, Ihara Y, Tomonaga M. Immunocytochemical[12] were formed from the skeins of straight intermediateand ultrastructural studies of Pick’s disease. Ann Neurol
filaments with a smooth surface. They are different from 1990;27:394–405.the inclusions of the present case. This case had some [17] Oda M, Akagawa N, Tabuchi Y, Tanabe H. A sporadic juvenile case
of the amyotrophic lateral sclerosis with neuronal intracytoplasmicfeatures of generalized variant of Pick’s disease, but theinclusions. Acta Neuropathol 1978;44:211–6.present inclusions in this case were found mostly in the
[18] Dickson DW, Yen S-H, Horoupian DS. Pick body-like inclusions inhippocampus. The inclusions in generalized variant ofthe dentate fascia of the hippocampus in Alzheimer’s disease. Acta
Pick’s disease [15] are absent or rare in this region. Neuropathol 1986;71:38–45.Interestingly, the present neuronal inclusions were virtu- [19] Hamada K, Fukazawa T, Yanagihara T, Yoshida K, Hamada T,
Yoshimura N et al. Dementia with ALS features and diffuse Pickally identical, in ultrastructure as well as in their immuno-body-like inclusions (atypical Pick’s disease). Clin Neuropatholhistochemical stainability, to oligodendroglial inclusions in1995;14:1–6.MSA [2,5,27]. Thus, pathological changes might develop
[20] Love S, Saitoh T, Quijada S, Cole GM, Terry RD. Alz-50, ubiquitinin neurons and oligodendroglial cells in the same mecha- and tau immunoreactivity of neurofibrillary tangles, Pick bodies andnism. So this case may be a new variant of MSA and not a Lewy bodies. J Neuropathol Exp Neurol 1988;47:393–405.
[21] Arima K, Murayama S, Mukoyama M, Inose T. Immunocytochemi-mere co-existence of Pick’s disease or its variant.cal and ultrastructural studies of neuronal and oligodendroglialcytoplasmic inclusions in multiple system atrophy. 1. Neuronalcytoplasmic inclusion. Acta Neuropathol 1992;83:453–60.
References [22] Mikol J, Brion S et al. A new case of Pick’s disease. ActaNeuropathol 1980;49:57–61.
[1] Graham JG, Oppenheimer DR. Orthostatic hypotension and nicotine [23] Shibayama H, Kitoh J, Marui Y, Kobayashi H, Iwase S, Kayukawasensitivity in a case of multiple system atrophy. J Neurol Neurosurg Y et al. An unusual case of Pick’s disease. Acta NeuropatholPsychiatry 1969;32:28–34. 1983;59:79–87.

58 K. Shibuya et al. / Journal of the Neurological Sciences 179 (2000) 50 –58
[24] Oyanagi S, Tanaka M, Omori T, Matsushita M, Ishii T. Regular neurons of pontine nuclei in patients with olivopontocerebellarrearrangements of tubular structures in Pick bodies in an autopsy atrophy: immunohistochemical and ultrastructural study. Actacase of Pick’s disease. Adv Neurol Sci (Tokyo) 1979;23:441–51, (in Neuropathol 1990;79:584–94.Japanese). [27] Papp MI, Komoley S. Filamentous glial cytoplasmic inclusions in
[25] Yokoo H, Oyama T, Hirato J, Sasaki A, Nakazato Y. A case of the CNS of patients with various combinations of striatonigralPick’s disease with unusual neuronal inclusions. Acta Neuropathol (SND), olivopontocerebellar atrophy (OPCA) and Shy–Drager1994;88:267–72. syndrome (SDS). Clin Neuropathol 1988;7:195.
[26] Kato S, Nakamura H. Cytoplasmic argyrophilic inclusions in




















