Structural and functional neuroimaging in mild-to-moderate head injury

www.elsevier.com/locate/ynbdi
Neurobiology of Disease 17 (2004) 29–43
The pathobiology of moderate diffuse traumatic brain injury as
identified using a new experimental model of injury in rats
Ibolja Cernak,a,* Robert Vink,a,b David N. Zapple,c Maria I. Cruz,a Farid Ahmed,a
Taeun Chang,a,d Stanley T. Fricke,a and Alan I. Fadena
aDepartment of Neuroscience, Georgetown University, Washington, DC 20057-1464, USAbDepartment of Pathology, University of Adelaide, Adelaide, SA, AustraliacAdvanced Research Computing, Office of Information Services, Georgetown University, Washington, DC 20057-1464, USAdDepartment of Pediatric Neurology, Children’s Hospital, Washington, DC, USA
Received 5 April 2004; revised 11 May 2004; accepted 28 May 2004
Available online 25 July 2004
Experimental models of traumatic brain injury have been developed to
replicate selected aspects of human head injury, such as contusion,
concussion, and/or diffuse axonal injury. Although diffuse axonal
injury is a major feature of clinical head injury, relatively few
experimental models of diffuse traumatic brain injury (TBI) have been
developed, particularly in smaller animals such as rodents. Here, we
describe the pathophysiological consequences of moderate diffuse TBI
in rats generated by a newly developed, highly controlled, and
reproducible model. This model of TBI caused brain edema beginning
20 min after injury and peaking at 24 h post-trauma, as shown by wet
weight/dry weight ratios and diffusion-weighted magnetic resonance
imaging. Increased permeability of the blood–brain barrier was
present up to 4 h post-injury as evaluated using Evans blue dye.
Phosphorus magnetic resonance spectroscopy showed significant
declines in brain-free magnesium concentration and reduced cytosolic
phosphorylation potential at 4 h post-injury. Diffuse axonal damage
was demonstrated using manganese-enhanced magnetic resonance
imaging, and intracerebral injection of a fluorescent vital dye (Fluoro-
Ruby) at 24-h and 7-day post-injury. Morphological evidence of
apoptosis and caspase-3 activation were also found in the cerebral
hemisphere and brainstem at 24 h after trauma. These results show
that this model is capable of reproducing major biochemical and
neurological changes of diffuse clinical TBI.
D 2004 Elsevier Inc. All rights reserved.
Keywords: Diffuse traumatic brain injury; Rat; Model; Manganese-
enhanced magnetic resonance
Introduction
Traumatic brain injury (TBI) is the most common cause of high
morbidity rates in individuals under 44 years of age and often leads
to severe disability (Bruns and Hauser, 2003; Harris et al., 2003). It
0969-9961/$ - see front matter D 2004 Elsevier Inc. All rights reserved.
doi:10.1016/j.nbd.2004.05.011
* Corresponding author. Department of Neuroscience, Georgetown
University, 3970 Reservoir Road NW, Research Building, Room EP04,
Washington, DC 20057-1464. Fax: +1-202-687-0617.
E-mail address: [email protected] (I. Cernak).
Available online on ScienceDirect (www.sciencedirect.com.)
is now well established that neuronal cell death after TBI is caused
by both primary and secondary injury mechanisms and is the major
factor underlying post-traumatic neurological deficits (Faden,
2002; Vink and Nimmo, 2002). Primary injury is defined as
mechanical disruption occurring at the time of trauma and includes
laceration, contusion, shearing, and axonal stretching, among
others. Secondary injury mechanisms include complex biochemi-
cal and physiological processes, which are initiated by the primary
traumatic event, but manifest over a period of hours to days. It has
been acknowledged that such secondary injury may substantially
contribute to chronic neurological disability (DeKosky et al., 1998;
Faden, 1993). Diffuse axonal injury (DAI), which is characterized
by morphologic changes to axons throughout the brain and
brainstem, has contributions from both primary and secondary
mechanisms and is recognized as one of the main consequences of
non-missile TBI leading to the diffuse degeneration of cerebral
white matter (Adams et al., 1989). An important methodological
limitation in neurotrauma research has been the ability to consis-
tently reproduce the pathological mechanisms of clinical injury in
experimental animals, particularly the diffuse component of axonal
injury (Lighthall and Anderson, 1994).
A variety of closed head impact models have been designed to
imitate the biomechanics and pathobiology of human concussive
and diffuse brain injury (Bakay et al., 1977; Beckman and Bean,
1970; Chen et al., 1996; Hall, 1995; Marmarou et al., 1994;
Nilsson et al., 1977; Shapira et al., 1988). This type of trauma is
especially difficult to mimic in small animals using common
experimental models such as fluid-percussion, cortical impact or
focal brain contusion, which cause more focal damage, and are
often accompanied by subdural-, subarachnoid-, and/or intracere-
bral hemorrhages, as well as convulsions. Nonetheless, the
development of such a model is critical for the characterization
of the pathobiology of injury and the subsequent development of
interventional therapies. The first objective of this study was
therefore to develop a highly controlled rat model of diffuse
traumatic brain injury, and to establish the parameters necessary
to cause a reproducible moderate severity of injury, the most
frequent injury group encountered in clinical practice. Having
established these parameters, we characterize the pathobiology of

I. Cernak et al. / Neurobiology of Disease 17 (2004) 29–4330
moderate diffuse traumatic brain injury, describing major mor-
phological, physiological, and biochemical changes comparable
to those observed after moderate clinical TBI.
Materials and methods
All protocols involving the use of animals were in compliance
with the Guide for the Care and Use of Laboratory Animals
published by NIH (DHEW publication NIH 85-23-2985) and
were approved by the Georgetown University Animal Use
Committee.
The injury device
The device consists of an air-driven high-velocity impactor that
is targeted to contact a steel disc cemented onto the rodent skull.
The impactor is of the same diameter as the steel disc, which in the
case of the adult rats used in the present study, is 10 mm. The
animal’s head is supported by a molded, gel-filled base (Hand-
stands, Taiwan), which also acts to decelerate the head after impact.
The middle diameter of the gel is 1.7 cm and its compressibility is
approximately 64 kPa/mm. To ensure precise and even contact
with the steel disc on the animal’s skull, the 14-cm length impactor
can be manually lowered onto the steel disc such that the two
surfaces meet. A laser beam guide is used to confirm that the two
surfaces are parallel and in contact with each other. Having
established this point of contact, the impactor is retracted to a 4-
cm fixed distance above the steel disc. Impact is then initiated
wherein the velocity of the impactor is constant (3.25 m/s),
however, the distance the impactor travels after contacting the
steel disc is under user control. This distance thus determines the
injury severity. Force of impact is controlled and recorded on a
personal computer connected to the device through a PowerLab
(Stoelting, Wood Dakem IL, USA). In this study, the total impact
energy at the end of the impactor was 512.717 N, meaning that
6.528 N/mm2 of impact energy was delivered to the disc.
Induction of injury
Male Sprague–Dawley rats (380F 30 g; n = 360) had access to
food and water ad libitum. Animals were initially anesthetized with
4% isoflurane and 1–1.5% for maintenance; the anesthetic was
evaporated in a gas mixture containing 30% oxygen/70% nitrous
oxide and applied through a nose-mask. The animals were allowed
to breathe spontaneously without tracheal intubation. A midline
incision exposed the dorsal surface of the skull upon which a 10 �3 mm diameter steel disc was cemented centrally between lambda
and bregma using a polyacrylamide adhesive. Rectal temperature
was maintained at 37jC using a thermostatically controlled heating
blanket. After targeting the point of contact between the device
impactor and the steel disc, the impactor was retracted and an
impact displacement was manually entered. Injury was then
induced by activating the air-driven piston.
Groups
The animals were divided into eight groups.
Group I (n = 100): the rats were injured with increasing impact
displacement to determine mortality rates.
Group II (n = 14): included 7 animals with moderate DTBI and
7 sham control rats, used for blood pressure and blood gas
analyses after injury.
Group III (n = 60): 35 animals with moderate DTBI and 25
sham control rats, used for edema study.
Group IV (n = 60): 35 moderately injured and 25 sham control
rats, used for blood–brain barrier study.
Group V (n = 30): 15 moderately injured and 15 sham control
rats, used in studies of neurological outcome and magnetic
resonance spectroscopy (MRS).
Group VI (n = 48): 30 animals with moderate DTBI and 18
sham controls used for morphological (histology and immuno-
cytochemistry) studies.
Group VII (n = 40): 25 moderately injured and 15 sham control
rats, used for fluorescent vital staining.
Group VIII (n = 8): 5 animals with moderate DTBI and 3 sham
control rats, used for functional, manganese T1-weighted
magnetic resonance imaging (MRI).
Acute neurological evaluation and mortality
In Group I, the anesthetized animals were subjected to various
levels of injury, depending on the impact displacement: 16, 17, 18,
19, or 20 mm (n = 20/displacement). Immediately following injury,
anesthesia was discontinued and the animals were maintained on
room air alone. No resuscitation was performed after trauma. Acute
neurological recovery was assessed in all rats by recording indi-
cators of sensorimotor function: recovery of hind paw-flexion
following the gradual application of pressure and the latency to
recovery of the righting reflex. The mortality rate was assessed at
24 h post-trauma.
Arterial pressure and blood gases
Seven animals in Group II were anesthetized and a catheter
(PE-50) was placed into the tail artery. After surgical preparation as
previously described, the animals were subjected to moderate
traumatic brain injury (18 mm vertical head displacement). A
further seven animals served as sham (uninjured) controls. Blood
pressure was monitored with an ITT Cannon transducer (Interna-
tional Biomedical, Austin, TX, USA) and a Narcotrace 40 physio-
graph (Narco Biosystems, Houston, TX, USA) before and at 1 min,
30 min, 1 h, 1.5 h, and 2 h after injury. Arterial blood gases were
measured with a NOVA 8 Blood Gas Analyzer (Nova Biomedical,
Waltham, MA, USA) before injury and at 30 min, 1 h, 1.5 h, and 2
h after injury. Values of blood pressure, as well as pH, pO2, SO2,
pCO2, and HCO3�, were compared both with pre-injury findings
and values measured in control animals.
Edema development assessed by diffusion-weighted magnetic
resonance imaging (MRI) and wet/dry method
The 60 animals in Group III were anesthetized and 35 were
subjected to moderate TBI. At 20 min, 40 min, 2 h, 4 h, and 24
h post-trauma, a subgroup of animals (n = 7/time point) were
reanesthetized with isoflurane and assessed for edema formation by
diffusion-weighted image (DWI) as previously described (Albensi
et al., 2000; Hanstock et al., 1994). A further five uninjured
animals were used as sham controls at every time points. Briefly,
animals were placed in the heated plexiglas holder and a respira-

I. Cernak et al. / Neurobiology of Disease 17 (2004) 29–43 31
tory motion detector positioned over the thorax to facilitate
respiratory gating. The plexiglas holder was then positioned in
the center of the 7 T magnet bore (Bruker 7 T/21 cm Biospec-
Avance system; Bruker, Karlsruhe, Germany) where a 72-mm
proton tuned birdcage coil had been positioned. Field homogeneity
across the brain was then optimized, and sagittal and coronal scout
images obtained to orient the transverse slices throughout the brain
region of interest. Diffusion weighted (DWI) images were then
acquired with a spin echo pulse sequence that had diffusion
gradients added before and after the refocusing pulse. Gradient
strength was varied in six steps using sensitization values ranging
from 10 to 1000 s/mm2. A 256 � 256 matrix was used with a 4-cm
field of view, TR 0.5 s, TE 52.7 ms, slice thickness of 2 mm and 4
echoes. The DWI images were converted to diffusion maps by
applying the Stejskal-Tanner equation in association with a Mar-
quart algorithm using the commercially available Paravision soft-
ware (Bruker, Billerica, MA, USA) so as to highlight changes in
MR signal associated with changes in molecular diffusion. Appar-
ent diffusion coefficients (ADCs) were calculated for four regions:
left cortex, right cortex, left hippocampus and right hippocampus,
and expressed as 10�5 mm2/s F SD. ADC values of left and right
cortices, as well as left and right hippocampi were pooled for
statistical analysis due to a lack of any difference between them,
respectively. As there were no differences between sham control
animals at any time point, they were pooled into one group (C) for
statistical analysis (n = 25).
After completion of DWI, the animals were anesthetized with
sodium pentobarbital (100 mg/kg, i.p.) and decapitated. The brains
were removed rapidly and parietal cortex and hippocampal samples
were collected. The samples were then dried for 72 h at 100jC and
reweighed. Water content was calculated and expressed as a per-
centage of a brain tissue (Elliott and Jasper, 1949).
Blood–brain barrier permeability
A time course for blood–brain barrier (BBB) permeability in
cortex and hippocampus was investigated in animals (n = 60)
assigned to Group IV. The integrity of the BBB was assessed using
Evans blue (EB) extravasation according to Uyama et al. (1988).
Evans blue dye (4 ml/kg of 2% solution, i.e., 0.08 g/kg, in
phosphate-buffered saline) was injected intravenously 30 min
before decapitation at 20 min, 40 min, 2 h, 4 h, and 24 h after
injury (n = 7/time point) or sham surgical procedure (n = 5/time
point). At assigned time points, the animals were anesthetized
using sodium pentobarbital (65 mg/kg i.p.) and intracardially
perfused with saline. The meninges and outer vessels were re-
moved, and samples of cortex and hippocampi were then isolated
and weighed. Brain samples were homogenized in 60% trichloro-
acetic acid solution and centrifuged. The absorbance of the
extracted dye in supernatant at 620 nm was determined with a
Perkin-Elmer spectrometer, and the tissue content of EB quantified
from a linear standard curve obtained using known amounts of the
dye, and expressed as Ag/g of tissue. Because there were no
differences between sham controls, they were pooled for statistical
analysis (n = 25).
Magnetic resonance spectroscopy
Magnetic resonance spectroscopy (MRS) was performed on a
Bruker 7.0 T system operating Paravision 2.0 software. Phosphorus
magnetic resonance spectra were obtained before and at 4 h after
injury as previously described (Heath and Vink, 1996; Vink et al.,
1996) in a subgroup (n = 7 injured and n = 7 sham controls) of
randomly chosen animals assigned to Group V. Briefly, the animal
was placed in a plexiglas holder in which a heating pad warmed to
37jC was fixed to maintain the animal’s temperature. A 5 � 9 mm
surface coil was then placed centrally over the skull and skin and
temporal muscle retracted well clear of the coil to ensure that there
was no contribution from these tissues to the brain spectrum. The
plexiglas holder containing the animal was then positioned in the
center of the magnet bore and the B1 field optimized to less than
0.25 ppm at the half height of the proton water signal. Phosphorus
spectra were subsequently obtained in a 20-min block using a 90jpulse width set at a 2-mm cortical depth, a 800-ms delay time, and
a 6000-Hz spectral width containing 2048 data points. Previous
studies have shown that the sensitive volume of this type coil
extends to approximately one-diameter depth (5 mm) directly
under the coil (Vink et al., 1997). The accumulated free induction
decays were analyzed after convolution difference (20/500 Hz
exponential filter) and peak frequencies determined using the
computer peak-picking program.
Intracellular pH was determined from the chemical shift of the
inorganic phosphate peak (yPi) relative to phosphocreatine (PCr)
using the equation:
pH ¼ 6:77þ logyPi � 3:29
5:68� yPi
� �ð1Þ
Similarly, free magnesium concentration was determined from
the chemical shift difference between the a and h peaks of ATP
(Gupta et al., 1978) using the equation:
½Mg2þ� ¼ Kd
10:82� ya�b
ya�b � 8:35
� �ð2Þ
where ya–b is the chemical shift difference between the a and bpeaks of ATP. The Kd for MgATP was initially assumed to be 50
AM at pH 7.2 and 0.15 M ionic strength and was corrected for pH
by multiplying by a correction factor calculated as (Bock et al.,
1987):
f ¼ ð1þ 106:5�pHÞð1þ 106:5�7:2Þ ð3Þ
Cytosolic phosphorylation potential (PP), which is commonly used
as an indicator of cell bioenergetic status, was determined accord-
ing to the equation
PP ¼ ½AATP�½AADP�½APi�
ð4Þ
where A represents all the ionic forms of the free species. The
concentration of ADP was calculated from the creatine kinase
equilibrium equation after correcting the equilibrium constant for
pH and free magnesium concentration as previously described in
detail elsewhere (Vink et al., 1994). Concentrations of the other
metabolites were determined from the integrated peak areas of the
respective MRS peaks, assuming that pre-injury the normal values
for PCr and ATP were 4.72 and 2.59 Amol/g, respectively, and that
the total creatine pool remained constant at 10.83 Amol/g (Siesjo,
1981; Veech et al., 1979). Brain water content was assumed to be
80%, with the intracellular compartment accounting for 78% of the
total water (Siesjo, 1981).

ogy of Disease 17 (2004) 29–43
Neurological outcome
Motor and cognitive functions were assessed in animals
assigned in Group V (n = 15 injured and n = 15 sham controls).
Motor scoring was performed on days 1, 2, 3, and 7 after
moderate TBI using three separate tests (Faden et al., 2003b),
each of which is scored via an ordinal scale ranging from zero
(no function) to five (normal function). Tests included the ability
to maintain position on an inclined plane in two vertical and two
horizontal positions, forelimb flexion, and forced lateral pulsion.
Forelimb flexion measures the reflex extension of the forelimb to
break a fall when suspended by the tail. Lateral pulsion measures
the degree of resistance to a lateral push. Each of seven
individual scores (vertical angle with the animal positioned head
up, vertical angle with the animal positioned head down, right
and left horizontal angle, forelimb flexion, right and left lateral
pulsion) was added to yield a composite neurological score
ranging from 0 to 35.
Cognitive outcome (spatial learning) was determined using the
hidden platform version of the Morris water maze (MWM) as
previously described (Faden et al., 2003b). Briefly, rats are trained
to locate a hidden, submerged platform using constant extra-maze
visual information. The apparatus consists of a large, white circular
pool (165 cm diameter, 500 mm high, water temperature 24 F1jC) with a 110 mm2 plexiglas platform painted white and
submerged 20 mm below the surface of the water. The surface of
the water is rendered opaque with the addition of dilute, white,
nontoxic paint (Crayola). During training, the platform remained in
a constant location hidden in one quadrant 14 cm from the
sidewall. The rat was gently placed in the water facing the wall
at one of four randomly chosen locations separated by 90j. Thelatency to find the hidden platform within a 90-s criterion time was
recorded by a blinded observer. Trials were conducted on days
14,15, 16, and 17 post-injury.
Histology and immunocytochemistry
At assigned time points (24 h, 48 h, 72 h, 7, 15 and 21 days
post-trauma, Group VI: n = 5/time point), the animals were
anesthetized using sodium pentobarbital (65 mg/kg i.p.) and
prepared for histopathological and morphological analysis. Briefly,
the rats were perfused transcardially with isotonic saline, followed
by 4% formaldehyde. After perfusion, the brains were immersed in
30% of sucrose at 4jC for 24 h. The brains were then removed,
blocked and embedded in paraffin for tissue sectioning. Coronal
10-Am sections were then cut with a cryostat and mounted on glass
slides. Sections were either stained with hematoxlin and eosin
(H&E), used for the immunocytochemical visualization of amyloid
precursor protein (APP; monoclonal primary antibody 22C11
obtained as a gift from Prof. Colin Masters, University of Mel-
bourne, Australia), cleaved caspase-3 [cleaved caspase-3(Asp175)
(5A1) monoclonal antibody; Cell Signaling Technology, Beverly,
MA, USA), or to assess in situ internucleosomal DNA fragmen-
tation, used for TUNEL staining. TUNEL was performed using a
commercially available FD NeuroApopTM kit (FD NeuroTechno-
logies, Ellicott City, MD, USA). All sections were examined by
light microscopy (Zeiss Axioplan; Carl Zeiss Inc., Thoronwood,
NY, USA).
Functional integrity of neuronal cell body and visualization of
axons were analyzed using a vital fluorescent dye and anterograde
tracer Fluoro-Ruby (Molecular Probes Inc., Eugene, OR, USA).
I. Cernak et al. / Neurobiol32
Briefly, the animals (Group VII, n = 40) were initially anesthetized
with 4% isoflurane and anesthesia subsequently maintained on
1.5% isoflurane. The animal’s head was then immobilized stereo-
taxically, and small holes were drilled in the skull with a dental
drill at the sites corresponding to the right and left cingulum.
Fluoro-Ruby (3 Al of 15% solution in PBS, pH 7.4) was injected
into each cingulum using a Hamilton syringe with tip diameter of
50 Am. To avoid diffusion of the dye from the cingulum, the
syringe was left in place for 5 min after the injection before slowly
withdrawing it from the brain. Three days following the injection
of the dye, the animals were subjected to TBI as previously
described. At assigned time points (24 h, 72 h, 7, 15, and 21 days
post-trauma, n = 5/time points), the rats were anesthetized, trans-
cardially perfused, and their brains removed as previously de-
scribed. After 24 h incubation in 30% sucrose at 4jC, the brains
were snap-frozen using 2-methyl-butane pre-cooled in dry ice for 2
h. Coronal 30-Am sections were then cut with a cryostat, with
every fifth section mounted on a glass slide and examined under a
fluorescent microscope using a rhodamine filter (Zeiss Axioplan;
Carl Zeiss Inc.). An additional 15 (n = 3/time point) sham control
animals were used for comparison.
Manganese-dependent contrast magnetic resonance imaging
(MRI)
It has been demonstrated that MnCl2 shows potential as an MRI
contrast agent that may reflect neuronal pathway activation (Lin
and Koretsky, 1997). MnCl2 (120 mM solution, 88 mg/kg) was
administered intravenously, with a flow rate of 2.25 ml/h using a
syringe pump (Harvard Bioscience Inc., Holliston, MA, USA), to
eight rats assigned to Group VIII (n = 5 injured and n = 3 uninjured
sham controls) 48 h before injury or sham procedure. This regime
of MnCl2 administration has been shown to be safe for the animal,
without any toxic effects (Lin and Koretsky, 1997). Moderate 18-
mm injury was then induced as previously detailed. Twenty-four
hours following injury, the animals were prepared for MRI analysis
(see detailed description above). Following optimization of the
field homogeneity across the brain, and obtaining sagittal and
coronal scout images to orient the transverse slices throughout the
brain region of interest, T1-weighted images were acquired (128 �128 matrix, TR 0.5 s, TE 6.4 ms, field of view 3.40 cm, slice
thickness 30 mm, slice separation 30 mm). Regions of hyper-
intensity showed localization of activated neural fibers.
Statistical analysis
All continuous data are shown as mean F SD and were
analyzed by repeated measures analysis of variance followed by
individual Student–Neuman–Keuls tests. Wet weight/dry weight
ratios were compared using Student’s t test. Neurological motor
outcome was analyzed using nonparametric repeated measures
Kruskal–Wallis ANOVA followed by individual Mann–Whitney
U tests.
Results
Acute neurological evaluation and mortality
The 16-mm vertical displacement of the head did not result in
any mortality, whereas the 17-mm head depression produced a

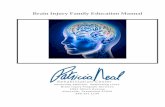
Fig. 1. Systemic, mean arterial and diastolic blood pressures expressed in
mm Hg following moderate traumatic brain injury, induced by 18-mm head
depression in rats. Significant transient increase (5 s post-injury) followed
by a significant reduction in all blood pressures occurred at 1 min following
injury. *P < 0.05 compared to pre-injury levels.
I. Cernak et al. / Neurobiology of Disease 17 (2004) 29–43 33
mortality rate of 12%. Moderate severity of head injury (26%
mortality) was caused by 18-mm head depression. Severe TBI was
produced by 19 mm (56% mortality) and 20 mm (90% mortality)
of head depression. Death occurred within 5 min of injury and
resulted from cardiorespiratory depression. The moderate injury
level (18 mm) was subsequently used in all further experiments.
There was no mortality later than 24 h post-trauma.
Following cessation of anesthesia, sham-injured control rats
recovered the pedal withdrawal reflex after a mean 1.56 F 0.18
min and righting reflex after 2.67 F 0.30 min. The 16-mm vertical
displacement did not significantly change these parameters com-
pared to controls (pedal withdrawal reflex: 1.63 F 0.32 min;
righting reflex: 2.90 F 0.31 min). However, animals subjected to
a 17-, 18-, or 19-mm injury levels recovered the pedal withdrawal
reflex more slowly: pedal withdrawal reflex 3.07 F 0.65 min,
6.92 F 0.83 min, or 12.12 F 1.17 min, respectively (for all
groups P < 0.0001 vs. sham-injured group). Similarly, recovery of
the righting reflex took significantly longer (P < 0.0001 vs. sham-
control) in these injury groups: 5.79 F 1.13 min for 17 mm,
11.52 F 1.84 min for 18 mm, and 20.46 F 3.27 min for 19 mm
injury levels.
Arterial pressure and blood gases
Arterial blood pressure increased immediately after induction
of moderate injury, and then declined, reaching a minimum at 1
min post-trauma (Fig. 1). This was followed by a gradual
normalization such that there was no significant difference at
30 min post-injury compared to control values. These changes are
similar to what has been previously described after weight-drop
injury (Marmarou et al., 1994). There were no significant changes
in arterial blood pH, pCO2 or HCO3� at any time point compared
to control animals as well as to pre-trauma levels (Table 1). Since
the animals inhaled a mixture of 30% oxygen and 70% nitrous
oxide, the baseline of pO2 was significantly higher (approximate-
ly 140 mm Hg) than it would be if they would inhale air. Hence,
although pO2 levels were significantly decreased compared to the
baseline, even the lowest values were over 100 mm Hg suggest-
ing that the animals were never hypoxic after injury. Indeed, SO2
remained normal during the 2-h observation period following
injury (Table 1).
Edema development and blood–brain barrier integrity: vasogenic
vs. cytotoxic edema
The percentage water content in cortex of sham control animals
was 78.45 F 0.24%, whereas in hippocampus, it was 77.94 F0.18%; this is consistent with values reported in rats by others
(Bareyre et al., 1997; Kita and Marmarou, 1994). At 20 min after
injury, the water content in cortex of injured animals was 79.20 F0.17% (P < 0.05) and in hippocampus 79.77 F 0.26% (P < 0.001)
indicating acute edema development after moderate diffuse trau-
matic brain injury (Fig. 2A). Increased cortical water content was
also seen at 4 h (79.40F 0.10%, P < 0.05) and 24 h (80.25F 0.22)
post-trauma. In hippocampus, the water content was also increased
at 4 h (80.52 F 0.22, P < 0.001) and 24 h (82.38 F 0.64, P <
0.001) after injury.
The changes in edema measured by wet/dry weight method
were confirmed using diffusion-weighted MRI. Additionally, this
method is accepted as a sensitive tool for distinguishing between
vasogenic and cytotoxic edema following traumatic brain injury
(Li and Fisher, 1996). Increased apparent diffusion coefficient
(ADC) in the brain indicates vasogenic edema whereas reduced
ADC suggests cytotoxic edema (Li and Fisher, 1996). Significant
changes in ADC were found in both cortex and hippocampus at
20 min, 4 h, and 24 h following injury, compared to control
values (Fig. 2B). ADC maps derived from the DWI are shown in
Fig. 2C. ADC was significantly increased in cortex and hippo-
campus of injured animals at 20 min and 4 h following injury,
which reflects vasogenic edema. This is manifested as areas of
hyperintensity on the ADC maps. At 24 h post-trauma, decreased
ADC suggested development of cytotoxic edema. Indeed, the
ADC map showed regions of hypointensity diffusely scattered
throughout the brain, reflecting a decrease in the molecular
motion of water, consistent with accumulation of water within
the intracellular space. Such a biphasic development of edema
has been previously reported in other diffuse models of brain
trauma (Barzo et al., 1997).
Increase in ADC was associated with a significant increase in
the permeability of the blood–brain barrier (BBB) at 20 min and 4
h after injury as assessed by penetration of Evans blue dye (Fig. 3).
Since increased BBB permeability associated with edema at early
time points following TBI has been seen to correspond to vaso-
genic edema (Tanno et al., 1992), these results support our DWI
findings suggesting a vasogenic origin of acute edema. Moreover,

Table 1
Blood gas changes in spontaneously breathing animals after moderate diffuse traumatic brain injury
Post-trauma
Variable Group Pre-trauma 30 min 1 h 1.5 h 2 h
pH Control 7.44 F 0.04 7.45 F 0.03 7.47 F 0.04 7.45 F 0.04 7.46 F 0.05
Injured 7.45 F 0.03 7.43 F 0.07 7.45 F 0.05 7.47 F 0.02 7.44 F 0.06
pO2 Control 141.6 F 7.5 147.5 F 9.1 142.4 F 8.8 139.3 F 9.7 132.7 F 7.5
Injured 139.3 F 7.7 115.1 F 17.3* 107.8 F 16.8* 104.2 F 16.1* 102.7 F 14.3*
SO2 Control 98.9 F 0.4 99.3 F 0.6 98.3 F 0.5 98.9 F 0.6 98.2 F 0.7
Injured 98.7 F 0.4 98.1 F 0.4 97.9 F 0.5 97.9 F 0.7 97.3 F 1.3
pCO2 Control 30.2 F 4.4 30.4 F 5.6 32.3 F 6.7 34.9 F 6.6 33.2 F 2.7
Injured 33.0 F 7.6 36.7 F 5.2 37.2 F 5.5 36.5 F 3.5 39.7 F 8.7
HCO3� Control 24.0 F 2.2 25.3 F 1.8 25.6 F 1.7 24.0 F 2.6 26.0 F 2.1
Injured 25.9 F 2.7 26.5 F 1.8 27.1 F 2.3 27.4 F 0.7 26.9 F 2.7
Statistical significance of difference: *P < 0.05, **P < 0.01, ***P < 0.001 compared to pre-trauma level.
I. Cernak et al. / Neurobiology of Disease 17 (2004) 29–4334
significantly reduced ADC and the lack of a significant increase in
Evans blue dye concentration in brain structures at 24 h post-
trauma confirm cytotoxic edema formation at this time point.
Magnetic resonance spectroscopy
The phosphorus magnetic resonance spectroscopy (MRS) at
4 h after trauma demonstrated that there were no significant
Fig. 2. (A) Changes in water content measured in cortex in hippocampus by wet
Apparent diffusion coefficients (ADC) obtained in cortex and hippocampus follo
***P < 0.001 compared to sham control values. (C) Apparent diffusion coeffici
obtained in sham control animals and in animals with moderate traumatic brain in
animals at 4 h postinjury indicates vasogenic edema, while scattered regions of
cytotoxic edema.
changes in ATP concentration at this time point compared to
sham controls (results not shown). Similarly, there was no
significant difference in pH at 4 h post-trauma (7.15 F 0.04)
compared to sham values (7.13 F 0.04). This lack of significant
change in ATP concentration and pH after trauma is consistent
with previous studies of moderate diffuse brain injury (Heath and
Vink, 1995; Smith et al., 1998). There was, however, a significant
decline (P < 0.05) in intracellular brain-free magnesium concen-
weight/dry weight method following moderate traumatic brain injury. (B)
wing moderate traumatic brain injury in rats; *P < 0.005, **P < 0.01, and
ent maps derived from the diffusion weighted magnetic resonance images
jury at 4 and 24 h postinjury. Areas of subcortical hyperintensity in injured
hypointensity (white arrows) at 24 h postinjury suggests development of

Fig. 3. Changes in blood–brain barrier (BBB) permeability to Evans
blue dye in cortex and hippocampus of rats subjected to moderate
traumatic brain injury. *P < 0.05 and **P < 0.01 compared to sham
controls (C).
I. Cernak et al. / Neurobiology of Disease 17 (2004) 29–43 35
tration, with the free concentration of the ion falling to 0.31 F0.02 mM by 4 h post-trauma compared to the sham control value
of 0.50 F 0.06 mM (Fig. 4A). The change in free magnesium
Fig. 4. (A) Brain-free magnesium concentration at 4 h after moderate
traumatic brain injury in rats. (B) Brain cytosolic phosphorylation potential
at 4 h following diffuse traumatic brain injury in rats. *P < 0.05 compared
to preinjury levels.
concentration paralleled a significant reduction in phosphorylation
potential 4 h following injury (21 F 2 in injured vs. 40 F 4
mM�1 (Fig. 4B). Previous studies have shown that this decline is
typical in traumatic brain injury and occurs irrespective of the
model or the species used (for review, see (Vink and Cernak,
2000). The preservation of ATP and the lack of acidosis at 4 h
after injury also indicate an absence of ischemic indicators,
consistent with the vasogenic origin of the observed edema at
this time point following moderate traumatic brain injury.
Motor and cognitive outcomes
Motor and cognitive outcomes are summarized in Fig. 5. All
animals demonstrated a significant decline (P < 0.05) in motor
function after moderate (18 mm) trauma (Fig. 5A). Rats subjected
to an 18-mm head trauma exhibited similar reduction in com-
Fig. 5. (A) Changes in composite neuroscore 1, 2, 3, and 7 days after
moderate traumatic brain injury in rats; (B) Water maze cognitive score
after moderate traumatic brain injury in rats measured at 14, 15, 16, and
17 days postinjury. *P < 0.05 and ***P < 0.001 compared to sham control
animals.

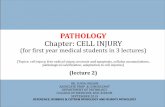
Fig. 6. The brain of a moderately brain-injured rat 24 h following injury.
(A) Superior surface; (B) inferior surface; (C) coronal section. No focal
lesions or contusions were observed. Subarachnoid hemorrhage and
intraventricular hemorrhage (black arrows) were frequent findings.
I. Cernak et al. / Neurobiology of Disease 17 (2004) 29–4336
posite neuroscore at 1, 2, and 3 days post-injury (30.67 F 0.8,
30.33 F 0.5, and 29.67 F 0.4, respectively, vs. 35 F 0 before
injury), and showed a trend toward neurological improvement at
7 days after injury (31.33 F 0.3). Although the deficits are
moderate, they are consistent with those previously described in
other rodent models of diffuse trauma as determined by the
composite motor tests used in the present study (Heath and Vink,
1995). We found that the forelimb flexion and forced lateral
pulsion tests lacked sensitivity to show motor deficits after
diffuse traumatic brain injury. This can be explained by the fact
that these methods are based upon the ‘‘lateralization effect’’
induced by unilateral brain injury, which develops as the undam-
aged hemisphere attempts to compensate for the damaged or
disconnected region. On the other hand, the impact energy in our
model is delivered centrally to the skull, and distributed homo-
genously over the brain surface. However, the method of inclined
plate examining fine motor coordination and balance proved to be
sensitive to indicate motor deficits following diffuse TBI induced
by our model, and the reduction in composite neuroscore reflects
changes measured by these tests.
The Morris Water Maze was performed over 4 consecutive days
starting at 14 days after sham surgery or TBI (Fig. 5B). The mean
latency to locate the platform immersed below the surface of the
water was significantly increased in injured animals at 15 (P <
0.001), 16 (P < 0.05) and 17 (P < 0.001) days postinjury, compared
to sham control animals.
Pathological changes: histology and immunocytochemistry
Gross pathological observation of the brains following moder-
ate (18 mm) brain injury show an absence of focal lesions or
contusion. Subarachnoid hemorrhage was usually observed in the
basal cisterns, cisterna magna, and over the cerebral hemispheres
(Fig. 6).
Histological examination of hematoxylin and eosin (H&E)-
stained tissue sections demonstrated profound dark cell change
and reduced neuronal density in the CA3 pyramidal layer of the
hippocampus (Fig. 7). There were also shrunken neurons
associated with perineuronal vacuolation in supraventricular
cortical areas and the dentate gyrus after injury, together with
pericapilllary edema in supraventricular regions of the cerebral
cortex, brainstem, and thalamus; in these areas, several con-
gested capillaries also were seen (results not shown). A pro-
found increase in APP immunoreactivity in neuronal cell bodies
was also present at 24 h, particularly in the brainstem (Fig. 8).
This increase in APP has been noted in other models of diffuse
traumatic brain injury and is thought to represent an acute
phase post-traumatic stress response (Van den Heuvel et al.,
1999).
Induction of moderate (18 mm) TBI resulted in internucleo-
somal DNA fragmentation as assessed by the positive Terminal
Deoxynucleotidyl Transferase Biotin-dUTP Nick End Labeling
(TUNEL) histochemistry. TUNEL-stained cells were clearly ap-
parent throughout the brain at 1, 2, and 3 days post-trauma.
These TUNEL-positive cells were found mainly in cortex, thala-
mus, and brainstem. The largest number of TUNEL-positive cells
was seen 24 h following injury (Fig. 9B), whereas no TUNEL-
positive cells were detected after 7 days post-trauma. Sham
control (non-injured) tissue did not demonstrate any TUNEL-
positive cells at any time point. The TUNEL findings were
confirmed by the Fluoro-Ruby technique, which showed cells
with condensed nuclei and marginated chromatin in cortex and
thalamus (Fig. 9D).
To elucidate whether caspase-3-mediated apoptosis was asso-
ciated with the TBI-induced cell death, the distribution of a
cleaved (active) caspase-3 in the brain if injured animals was
measured by qualitative immunocytochemistry (Fig. 10). The
antibody used [cleaved caspase-3(Asp175) (5A1) monoclonal
antibody; Cell Signaling Technology] does not detect the pro-
caspase-3 form; it identifies endogenous levels of the large
fragment (17/19 kDa) of activated caspase-3 resulting from
cleavage adjacent to Asp175. As such, this antibody can be used
as a cellular marker of caspase activation. The cleaved form of
caspase-3 was expressed in cortex, hippocampus (not shown),
and widely distributed throughout the entire region of brainstem
by 24 h after injury (Fig. 10).
Analysis of morphological characteristics and distribution of
Fluoro-Ruby labeled cells showed microglia and cell debris in
supraventricular cortical areas (Figs. 11C and D) and in brain-
stem (not shown) at 24 h after injury. At 7 day post-trauma, a
significant reduction of neurons and further increase in micro-
glia were observed (Figs. 11G and H). Similarly, Fluoro-Ruby-

Fig. 7. Representative photomicrograph of the hippocampal CA3 region 24 h after the 18-mm injury (C and D) compared to a sham injured animal (A and B);
H&E staining. Magnifications A and C �3, B and D �20. Reduced neuronal density and cell loss as well as profound dark cell changes are shown.
I. Cernak et al. / Neurobiology of Disease 17 (2004) 29–43 37
labeled axons in the caudate putamen showed mild axonal
pathology 24 h after injury (Fig. 12B), whereas retraction balls,
broken fibers, and disrupted axons were observed at 7-day post-
injury (Fig. 12D).
Manganese-dependent contrast magnetic resonance imaging
(MRI)
Manganese-enhanced T1-weighted MRI was used to demon-
strate and compare the regional difference of manganese accumu-
lation in injured vs. non-injured animals. Our results demonstrated
hyperintense areas corresponding to dentate gyrus and interpedun-
Fig. 8. Representative photomicrograph of amyloid precursor protein (APP) accu
injury 24 h after the insult (C and D), compared to a sham-injured animal (A and
and D �20. The APP protein accumulation in axons and neuronal cell body is s
cular nuclei (Fig. 13) at 24 h post-injury, whereas absence of
positive contrast enhancement was shown in the brains of naive
(not shown) and sham-injured animals (Fig. 13).
Discussion
Methodological aspects
Several models of traumatic brain injury have been developed
to reproduce diffuse axonal injury (DAI), which is one of the
primary aspects of human head trauma (Chen et al., 1996;
mulation in the brain of an animal with moderate (18 mm) traumatic brain
B). APP 22C11 monoclonal antibody used. Magnifications A and C � 3, B
hown as darkly staining immunoreactivity.

Fig. 9. (A and B) TUNEL immunocytochemistry in rat brain cortex at 24 h
after moderate traumatic brain injury. Darkly stained TUNEL-positive
nuclei (arrows) are clearly observed distributed throughout the cortex (B).
Such dark staining nuclei are absent in sham control (A). Scale bar = 100
Am. (C and D) Representative photomicrographs of Fluoro-Ruby-labeled
cells in thalamus. Cells with condense nuclei and marginated chromatin
(arrows) are clearly observed at 24 h postinjury (D) compared to a sham
control (C) Scale bar = 50 Am.
I. Cernak et al. / Neurobiology of Disease 17 (2004) 29–4338
Gennarelli, 1994; Lighthall and Anderson, 1994; Povlishock et al.,
1994; Shapira et al., 1988). While many earlier brain injury models
used higher species such as primate, sheep, and cat, recent models
Fig. 10. Immunocytochemical staining of paraffin-embedded rat brain shows dar
injury using cleaved Caspase-3 (Asp175) (5A1) Rabbit Monoclonal Antibody, whi
caspase-3. Scale bar = 100 Am.
have often focused on rodents (Povlishock et al., 1994). The non-
impact acceleration injury models in nonhuman primates and
miniature swine appear to closely reproduce the complex pathobi-
ology of human traumatic brain injury (Smith et al., 1997).
Although these techniques offer valuable information on morpho-
logical, cellular and molecular responses to diffuse brain injury,
their use is difficult for most laboratories due to the cost and size of
the animal, as well as the sophisticated technical requirements
(Povlishock et al., 1994). Moreover, the models of acceleration
head injury using large experimental animals lack established
functional outcome tests, which are critical to the preclinical
assessment of neuroprotective strategies. Since rodent models are
inexpensive, easy to use, and generally involve highly inbred
strains of one sex, they have been found to be useful tools to
reduce intersubject and outcome variability (Faden, 2001).
One of the most frequently used rodent models of impact
acceleration head injury is Marmarou’s weight drop model (Foda
and Marmarou, 1994; Marmarou et al., 1994). The trauma device
utilized in this model consists of a column of brass weights falling
freely by gravity from a designated height through a Plexiglas tube
onto a stainless steel disc fixed to the skull. This model has been
shown to produce graded brain injury in rodents depending upon
the mass and the height from which the brass weight is released
(De Mulder et al., 2000; Marmarou et al., 1994; Piper et al., 1996).
The popularity of the weight drop model is based on the fact that it
is inexpensive, easy to perform, and capable of producing graded
diffuse axonal injury. However, the biomechanics of the impact
produced by this model are not strictly controlled. For example,
there is a possibility of a ‘‘second hit’’ induced by the weight after
rebounding from the skull of the animal resting on the flexible
sponge. Furthermore, although the weight is enclosed within a
Plexiglas tube, some lateral movement occurs during its fall, which
has the potential to cause lateralization of the impact, uneven
kly stained apoptotic cells (white arrows) in the brainstem 24 h following
ch detects endogenous levels of the large fragment (17/19 kDa) of activated

Fig. 11. Representative photomicrographs of Fluoro-Ruby-labeled cells in cortex. A, B, E and F show cortex in a sham control animal, while C, D, G, and H show
cortex in an injured animal. A, C, E, and G are with a lower magnification (the scale bar represents 50 Am), whereas B, D, and H demonstrate a region (white box)
with a higher magnification (the scale bar represents 200 Am). At 24 h postinjury (C), there are few microglia (white arrows) and cell debris (yellow arrows); at 7-
day postinjury (F) decrease in neuronal cell number, increased number of microglia (white arrows), and presence of debris (yellow arrows) are observed.
Fig. 12. Representative photomicrographs of Fluoro-Ruby labeled axons in
the caudate putamen. A and C show caudate putamen in a sham control
animal, while B and D represent caudate putamen in a moderately injured
rat. At 24-h postinjury (B), there is no noticeable change compared to a
sham control (A); at 7 days (D) postinjury, retraction balls (black arrow)
and broken fibers (white arrow) are visible. Scale bar = 50 Am.
I. Cernak et al. / Neurobiology of Disease 17 (2004) 29–43 39
distribution of the impact energy and increased variability of
outcome measures. As with Marmarou’s model, we also use a
stainless-steel disk to protect the skull, as well as to disperse the
impact energy over the surface of the brain. However, our device
enables control of the velocity as well as of the dwell time during
which the impactor is in contact with the disk, that is, with the
animals’ head. It is well known that these biomechanical factors
are the most important determinants of the injury severity (Gold-
smith, 2001); thus, their inconsistency inevitably increases the
variability of the injury outcome. Moreover, using a laser-beam
guide incorporated in our device permits precise centralization of
the hit, preventing uneven delivery of impact energy to the skull.
Our model also demonstrates a direct relationship between the
injury outcomes/mortality and the vertical displacement of the head
(i.e., intensity of the impact energy inflicting the injury), thus
fulfilling one of the most important criteria for a reliable experi-
mental model of TBI.
In the present studies, recovery latencies for pedal withdrawal
and righting reflexes measured immediately after injury were
dependent upon vertical displacement of the head, that is, levels
of injury. In clinical practice, severity of brain injury is routinely
graded by the Glasgow Coma Scale, which is based upon eye
opening, as well as verbal and motor responses (Teasdale and
Jennett, 1976). Although translation of neurological parameters
observed in experimental animals into outcome parameters of
patients has proven to be difficult (Teasdale et al., 1999), our
results demonstrate a causal relationship between acute neurolo-
gical/motor dysfunction and injury severity.
Physiological and functional responses to diffuse traumatic brain
injury
The systemic response to traumatic head injury can significant-
ly modify complex cellular and molecular changes in the brain
induced by impact. Indeed, the hypertensive response to fluid

Fig. 13. Manganese-dependent contrast T1-weighted MRI in sham control and moderately injured rats at 24 h postinjury. Hyperintense areas correspond to
dentate gyrus (white arrow) and interpeduncular nuclei (black arrows).
I. Cernak et al. / Neurobiology of Disease 17 (2004) 29–4340
percussion injury, in which blood pressure exceeds 180 mm Hg for
several minutes (Yuan et al., 1991), has been shown to cause loss
of autoregulation and a marked elevation of cerebral blood flow
(Lewelt et al., 1980). Such pathological alterations due to hyper-
tension could significantly compromise investigation of trauma-
induced changes in blood–brain barrier integrity and cerebral
autoregulation. In contrast, TBI induced using our model caused
only a small and transient elevation of blood pressure (5–10 s)
followed by mild hypotension at 1 min post-trauma, with the blood
pressure returning to normal, pre-injury levels by 30 min post-
trauma. Similar dynamics of blood pressure were shown after
impact injury inflicted by Marmarou’s model (Marmarou et al.,
1994). Hypotension was also shown in patients with isolated brain
injury (Mahoney et al., 2003).
Because many of the critical energetic processes occurring in
the cell are essentially phosphate transfer reactions, phosphorus
MRS is one of the most widely used techniques used in the study
of brain metabolism. It has been established that trauma, which
results in mild to severe levels of motor dysfunction does not cause
loss of ATP or sustained lactic acidosis, but rather induces more
subtle changes in bioenergetics reflected as reduction in calculated
cytosolic phosphorylation potential and decrease in free magne-
sium concentration (Vink et al., 1988, 1994). In our study, MRS
analysis of the brain confirmed the absence of indicators of
cerebral ischemia/hypoxia, and demonstrated significant decrease
in cytosolic phosphorylation potential parallel with a reduction in
free Mg2+, suggesting increased energy demand in response to
attempts to maintain ionic gradients after injury (Vink and Cernak,
2003). Our findings are comparable with changes found after
impact-acceleration brain injury induced by Marmarou’s model
(Heath and Vink, 1995). The similarity in metabolic events
associated with production of neurologic deficits in our and
Marmarou’s model, as well as in other classical experimental
models of traumatic brain injury (Vink et al., 1988) suggests that
these bioenergetic changes may be common to major experimental
models of brain trauma. Indeed, MRS showed similar alterations in
the brain of head-injured patients (Garnett et al., 2001).
Currently, two major forms of brain edema are recognized
(Klatzo, 1987b): (1) vasogenic, which involves a breakdown of
the blood–brain barrier (BBB) leading to accumulation of edema
fluid in the extracellular spaces, and (2) cytotoxic, where swelling
of cellular elements of brain parenchyma occurs without BBB
breakdown. While the wet and dry weight method measures total
tissue water content (Elliott and Jasper, 1949) without giving
information on the type of edema, diffusion-weighted imaging
(DWI), and calculation of apparent diffusion coefficient (ADC)
offer the opportunity of a real-time detection and differentiation of
the edema formation (Hanstock et al., 1994). In our study, wet and
dry weight results show significant increase in water content at 20
min, 4 h and 24 h after injury (Fig. 2A). Increased ADC (Fig. 2B)
together with BBB breakdown (Fig. 3) at 20 min and 4 h post-
trauma suggest an early and rapid opening of the BBB and
development of vasogenic brain edema at these time points. Early
vasogenic edema was also shown after impact acceleration injury
induced by Marmarou’s weight-drop model (Barzo et al., 1997),
controlled cortical impact injury (Baskaya et al., 1997), closed
head injury (Assaf et al., 1999), and following major cerebral
artery occlusion (Klatzo, 1987a). Although total tissue water
content, measured by wet and dry method, is significantly in-
creased at 24 h post-trauma, absence of increased BBB permeabil-
ity at the same time point implies that the brain edema is not of
vasogenic origin. Indeed, significantly decreased ADC at 24 h after

I. Cernak et al. / Neurobiology of Disease 17 (2004) 29–43 41
injury suggests cytotoxic edema (Hanstock et al., 1994). Complex
secondary injury factors initiated at the time of traumatic brain
injury (TBI) and manifesting for minutes or even days after the
traumatic insult have been shown to induce cytotoxic edema in
various models of TBI (Assaf et al., 1999; Ito et al., 1996;
Loubinoux et al., 1997). These findings suggest that our traumatic
brain injury model induces early vasogenic edema followed by
more delayed cytotoxic edema. The fact that alterations in water
content and ADC values showed similar trends in both cortex and
hippocampus suggests that the trauma in this model results in
diffuse injury rather than a more focal brain damage. Brain edema
has been shown as one of the main consequences of TBI in
patients. Rozsa et al. (1989) analyzed 107 patients with head
injury and indicated that diffuse swelling was present in 91% of
patients. These findings are consistent with the results published by
Marmarou et al. (2000), showing brain edema development in 87%
(66 of 76) of head-injured patients. The temporal profile of edema
development following our experimental TBI is comparable with
the temporal profile of the brain swelling in injured patients
(Bullock et al., 1991; Marmarou et al., 2000).
Our model, similar to various rodent models of TBI including
fluid percussion (Faden et al., 2003b; Hamm et al., 1993),
controlled cortical impact (Faden et al., 2003a; Scheff et al.,
1997), and impact-acceleration brain injury (Chen et al., 1996;
Schmidt et al., 2000; Zohar et al., 2003), induces cognitive deficits
using the Morris water maze test. The model also induces moderate
motor deficits measured by composite neuroscore, which are
comparable to motor impairments observed in certain rodent TBI
models (Chen et al., 1996; Heath and Vink, 1995; Raghupathi et al.,
1998).
Pathological changes induced by diffuse traumatic brain injury
Adams et al. (1989) identified diffuse axonal injury as major
pathological feature of human fatal non-missile head injury, and
classified it into three grades. Grade 1 is associated with histolo-
gical evidence of axonal injury in the white matter of the cerebral
hemispheres, the corpus callosum, and the brain stem, and less
commonly, the cerebellum. In Grade 2, there is also a focal lesion
in the corpus callosum. Grade 3 is characterized by an additional
focal lesion in the dorsolateral parts of the rostral brain stem.
Amongst experimental models of TBI, Marmarou’s model (Foda
and Marmarou, 1994) successfully replicated Grade 1 DAI ob-
served in cerebral hemisphere and brain stem following mild
injury, without focal lesion in the corpus callosum or in the brain
stem. Furthermore, Marmarou’s severe injury model has been
shown to reproduce Grade 3 DAI, which was in cerebellum and
in the brain stem. However, there was a lack of evidence for similar
changes in the corpus callosum (Foda and Marmarou, 1994). The
authors hypothesized that focal lesions in the corpus callosum
could be caused only by a head acceleration oriented in coronal
plane and not in the sagittal plane (Foda and Marmarou, 1994).
Indeed, Gennarelli et al. (1982), using the acceleration-rotational
head injury model in primates, has demonstrated that coronal head
acceleration is a major cause of prolonged traumatic coma and
underlying DAI, whereas acceleration in sagittal plane caused less
neurological deficits and less DAI. In our study, we demonstrated
diffuse axonal injury in the cerebral hemispheres and in the brain
stem, and observed reduced numbers of intact fibers in the corpus
callosum without signs of focal lesions. Furthermore, we found
progressive reduction of neuronal cells with a parallel increase in
microglia. Neuronal cell death due to impact showed features of
both necrosis and apoptosis, similar to previously developed
models of closed head injury (Stahel et al., 2000). Additionally,
the involvement of caspase-3 activation in injury-induced cell
death was demonstrated, which is consistent with our previous
findings using Marmarou’s model of diffuse traumatic brain injury
(Cernak et al., 2002), as well as with fluid percussion induced
injury (Knoblach et al., 2002; Yakovlev et al., 1997).
Recently, Lin and Koretsky (1997) demonstrated that focal
injections of manganese (Mn2+) within the mouse central nervous
system combined with in vivo high-resolution magnetic resonance
imaging (MRI) demarcate neuronal tracts originating from the site
of injection. Others, using alternative (intraarterial) route of injec-
tion coupled with artificial opening of the blood–brain barrier,
confirmed the usefulness of Mn2+ contrasted magnetic resonance
imaging in rats (Aoki et al., 2003; Morita et al., 2002). Manganese,
similarly to Ca2+ in various biological systems (Shibuya and
Douglas, 1993), is known to enter glial cells and/or neurons via
voltage-gated Ca2+ channels following the triggering of an action
potential (Narita et al., 1990). Indeed, this new visualization
method is described as a useful tool to detect manganese accumu-
lation caused by permanent ischemia in rat brain, whereas manga-
nese hyperintensity reflected the increased Ca2+ influx (Aoki et al.,
2003). Here, we demonstrate for the first time the utilization of this
method in experimental TBI, and show its usefulness in differen-
tiation of neuronal structures activated by trauma. Since traumatic
brain injury induces blood–brain barrier breakdown, which is well
documented by literature data as well as our own results, in this
study, there was no need for artificial opening the blood–brain
barrier by administration of a hyperosmolar agent, necessary for
the entry of MnCl2 into brain parenchyma. Although future
experimental work is necessary to fully define the potential and
limitations of this methodology in TBI, these findings indicate that
Mn2+ contrasted MRI may be a useful technique for investigating
the trauma-induced functional changes in the brain.
In conclusion, we have developed a new model for diffuse
traumatic brain injury, which induces biochemical and neurological
changes consistent with the diffuse axonal injury produced in other
models and comparable to alterations found after clinical TBI. This
model offers a high level of control of mechanical force inflicting
the injury, thereby reducing the intersubject and outcome variabil-
ity. Moreover, by reproducing both features of necrosis and
apoptosis, this model is suitable for studying complex mechanisms
of post-traumatic cell death and testing novel therapeutic
approaches targeting diffuse axonal damage.
Acknowledgments
We acknowledge Jill MacLeod, Lilia Ileva and Thomas Krupica
Jr. for their outstanding technical assistance, along with Drs. Jung
Hee Lee and Alan P. Koretsky (Laboratory of Functional and
Molecular Imaging, NINDS, NIH) for their valuable directions
concerning manganese-enhanced MRI.
References
Adams, J.H., Doyle, D., Ford, I., Gennarelli, T.A., Graham, D.I., McLellan,
D.R., 1989. Diffuse axonal injury in head injury: definition, diagnosis
and grading. Histopathology 15, 49–59.

I. Cernak et al. / Neurobiology of Disease 17 (2004) 29–4342
Albensi, B.C., Knoblach, S.M., Chew, B.G., O’Reilly, M.P., Faden, A.I.,
Pekar, J.J., 2000. Diffusion and high resolution MRI of traumatic brain
injury in rats: time course and correlation with histology. Exp. Neurol.
162, 61–72.
Aoki, I., Ebisu, T., Tanaka, C., Katsuta, K., Fujikawa, A., Umeda, M.,
Fukunaga, M., Takegami, T., Shapiro, E.M., Naruse, S., 2003. Detec-
tion of the anoxic depolarization of focal ischemia using manganese-
enhanced MRI. Magn. Reson. Med. 50, 7–12.
Assaf, Y., Holokovsky, A., Berman, E., Shapira, Y., Shohami, E., Cohen,
Y., 1999. Diffusion and perfusion magnetic resonance imaging follow-
ing closed head injury in rats. J. Neurotrauma 16, 1165–1176.
Bakay, L., Lee, J.C., Lee, G.C., Peng, J.R., 1977. Experimental cerebral
concussion. Part 1: an electron microscopic study. J. Neurosurg. 47,
525–531.
Bareyre, F., Wahl, F., McIntosh, T.K., Stutzmann, J.M., 1997. Time course
of cerebral edema after traumatic brain injury in rats: effects of riluzole
and mannitol. J. Neurotrauma 14, 839–849.
Barzo, P., Marmarou, A., Fatouros, P., Hayasaki, K., Corwin, F., 1997.
Contribution of vasogenic and cellular edema to traumatic brain
swelling measured by diffusion-weighted imaging. J. Neurosurg. 87,
900–907.
Baskaya, M.K., Rao, A.M., Dogan, A., Donaldson, D., Dempsey, R.J.,
1997. The biphasic opening of the blood–brain barrier in the cortex
and hippocampus after traumatic brain injury in rats. Neurosci. Lett.
226, 33–36.
Beckman, D.L., Bean, J.W., 1970. Pulmonary pressure–volume changes
attending head injury. J. Appl. Physiol. 29, 631–636.
Bock, J.L., Wenz, B., Gupta, R.K., 1987. Studies on the mechanism of
decreased NMR-measured free magnesium in stored erythrocytes. Bio-
chim. Biophys. Acta 928, 8–12.
Bruns Jr., J., Hauser, W.A., 2003. The epidemiology of traumatic brain
injury: a review. Epilepsia 44 (Suppl. 10), 2–10.
Bullock, R., Maxwell, W.L., Graham, D.I., Teasdale, G.M., Adams, J.H.,
1991. Glial swelling following human cerebral contusion: an ultrastruc-
tural study. J. Neurol., Neurosurg. Psychiatry 54, 427–434.
Cernak, I., Chapman, S.M., Hamlin, G.P., Vink, R., 2002. Temporal char-
acterisation of pro- and anti-apoptotic mechanisms following diffuse
traumatic brain injury in rats. J. Clin. Neurosci. 9, 565–572.
Chen, Y., Constantini, S., Trembovler, V., Weinstock, M., Shohami, E.,
1996. An experimental model of closed head injury in mice: patho-
physiology, histopathology, and cognitive deficits. J. Neurotrauma 13,
557–568.
DeKosky, S.T., Kochanek, P.M., Clark, R.S., Ciallella, J.R., Dixon, C.E.,
1998. Secondary injury after head trauma: subacute and long-term
mechanisms. Semin. Clin. Neuropsychiatry 3, 176–185.
De Mulder, G., Van Rossem, K., Van Reempts, J., Borgers, M., Verlooy, J.,
2000. Validation of a closed head injury model for use in long-term
studies. Acta Neurochir., Suppl. 76, 409–413.
Elliott, K.A., Jasper, H., 1949. Measurement of experimentally induced
brain swelling and shrinkage. Am. J. Physiol. 157, 122–129.
Faden, A.I., 1993. Experimental neurobiology of central nervous system
trauma. Crit. Rev. Neurobiol. 7, 175–186.
Faden, A.I., 2001. Neuroprotection and traumatic brain injury: the search
continues. Arch. Neurol. 58, 1553–1555.
Faden, A.I., 2002. Neuroprotection and traumatic brain injury: theoretical
option or realistic proposition. Curr. Opin. Neurol. 15, 707–712.
Faden, A.I., Fox, G.B., Di, X., Knoblach, S.M., Cernak, I., Mullins, P.,
Nikolaeva, M., Kozikowski, A.P., 2003a. Neuroprotective and noo-
tropic actions of a novel cyclized dipeptide after controlled cortical
impact injury in mice. J. Cereb. Blood Flow Metab. 23, 355–363.
Faden, A.I., Knoblach, S.M., Cernak, I., Fan, L., Vink, R., Araldi, G.L.,
Fricke, S.T., Roth, B.L., Kozikowski, A.P., 2003b. Novel diketopiper-
azine enhances motor and cognitive recovery after traumatic brain in-
jury in rats and shows neuroprotection in vitro and in vivo. J. Cereb.
Blood Flow Metab. 23, 342–354.
Foda, M.A., Marmarou, A., 1994. A new model of diffuse brain injury in
rats: Part II. Morphological characterization. J. Neurosurg. 80, 301–313.
Garnett, M.R., Corkill, R.G., Blamire, A.M., Rajagopalan, B., Manners,
D.N., Young, J.D., Styles, P., Cadoux-Hudson, T.A., 2001. Altered
cellular metabolism following traumatic brain injury: a magnetic reso-
nance spectroscopy study. J. Neurotrauma 18, 231–240.
Gennarelli, T.A., 1994. Animate models of human head injury. J. Neuro-
trauma 11, 357–368.
Gennarelli, T.A., Thibault, L.E., Adams, J.H., Graham, D.I., Thompson,
C.J., Marcincin, R.P., 1982. Diffuse axonal injury and traumatic coma
in the primate. Ann. Neurol. 12, 564–574.
Goldsmith, W., 2001. The state of head injury biomechanics: past, present,
and future: Part 1. Crit. Rev. Biomed. Eng. 29, 441–600.
Gupta, R.K., Benovic, J.L., Rose, Z.B., 1978. The determination of the free
magnesium level in the human red blood cell by 31P NMR. J. Biol.
Chem. 253, 6172–6176.
Hall, E.D., 1995. The mouse head injury model: utility in the discovery
of acute cerebroprotective agents. In: Ohnishi, S.T. (Ed.), Central
Nervous System Trauma Research Techniques. CRC Press, Boca
Raton, pp. 213–233.
Hamm, R.J., Lyeth, B.G., Jenkins, L.W., O’Dell, D.M., Pike, B.R., 1993.
Selective cognitive impairment following traumatic brain injury in rats.
Behav. Brain Res. 59, 169–173.
Hanstock, C.C., Faden, A.I., Bendall, M.R., Vink, R., 1994. Diffusion-
weighted imaging differentiates ischemic tissue from traumatized tissue.
Stroke 25, 843–848.
Harris, C., DiRusso, S., Sullivan, T., Benzil, D.L., 2003. Mortality risk after
head injury increases at 30 years. J. Am. Coll. Surg. 197, 711–716.
Heath, D.L., Vink, R., 1995. Impact acceleration-induced severe diffuse
axonal injury in rats: characterization of phosphate metabolism and
neurologic outcome. J. Neurotrauma 12, 1027–1034.
Heath, D.L., Vink, R., 1996. Traumatic brain axonal injury produces sus-
tained decline in intracellular free magnesium concentration. Brain Res.
738, 150–153.
Ito, J., Marmarou, A., Barzo, P., Fatouros, P., Corwin, F., 1996. Character-
ization of edema by diffusion-weighted imaging in experimental trau-
matic brain injury. J. Neurosurg. 84, 97–103.
Kita, H., Marmarou, A., 1994. The cause of acute brain swelling after the
closed head injury in rats. Acta Neurochir. (Suppl. 60), 452–455.
Klatzo, I., 1987a. Blood–brain barrier and ischaemic brain oedema.
Z. Kardiol. 76 (Suppl. 4), 67–69.
Klatzo, I., 1987b. Pathophysiological aspects of brain edema. Acta Neuro-
pathol. (Berl.) 72, 236–239.
Knoblach, S.M., Nikolaeva, M., Huang, X., Fan, L., Krajewski, S., Reed,
J.C., Faden, A.I., 2002. Multiple caspases are activated after traumatic
brain injury: evidence for involvement in functional outcome. J. Neuro-
trauma 19, 1155–1170.
Lewelt, W., Jenkins, L.W., Miller, J.D., 1980. Autoregulation of cerebral
blood flow after experimental fluid percussion injury of the brain.
J. Neurosurg. 53, 500–511.
Li, F.H., Fisher, M., 1996. Diffusion-weighted and perfusion magnetic
resonance imaging and ischemic stroke. Drugs Today 32, 615–627.
Lighthall, J.W., Anderson, T.E., 1994. In vivo models of experimental brain
and spinal cord trauma. In: Salzman, S.K., Faden, A.I. (Eds.), The
Neurobiology of Central Nervous System Trauma. Oxford Univ. Press,
New York, pp. 3–12.
Lin, Y.J., Koretsky, A.P., 1997. Manganese ion enhances T1-weighted MRI
during brain activation: an approach to direct imaging of brain function.
Magn. Reson. Med. 38, 378–388.
Loubinoux, I., Volk, A., Borredon, J., Guirimand, S., Tiffon, B., Seylaz, J.,
Meric, P., 1997. Spreading of vasogenic edema and cytotoxic edema
assessed by quantitative diffusion and T2 magnetic resonance imaging.
Stroke 28, 419–426 (discussion 426–417).
Mahoney, E.J., Biffl, W.L., Harrington, D.T., Cioffi, W.G., 2003. Isolated
brain injury as a cause of hypotension in the blunt trauma patient.
J. Trauma 55, 1065–1069.
Marmarou, A., Foda, M.A., van den Brink, W., Campbell, J., Kita, H.,
Demetriadou, K., 1994. A new model of diffuse brain injury in rats:
Part I. Pathophysiology and biomechanics. J. Neurosurg. 80, 291–300.

I. Cernak et al. / Neurobiology of Disease 17 (2004) 29–43 43
Marmarou, A., Fatouros, P.P., Barzo, P., Portella, G., Yoshihara, M., Tsuji,
O., Yamamoto, T., Laine, F., Signoretti, S., Ward, J.D., Bullock, M.R.,
Young, H.F., 2000. Contribution of edema and cerebral blood volume to
traumatic brain swelling in head-injured patients. J. Neurosurg. 93,
183–193.
Morita, H., Ogino, T., Seo, Y., Fujiki, N., Tanaka, K., Takamata, A., Naka-
mura, S., Murakami, M., 2002. Detection of hypothalamic activation by
manganese ion contrasted T(1)-weighted magnetic resonance imaging
in rats. Neurosci. Lett. 326, 101–104.
Narita, K., Kawasaki, F., Kita, H., 1990. Mn and Mg influxes through Ca
channels of motor nerve terminals are prevented by verapamil in frogs.
Brain Res. 510, 289–295.
Nilsson, B., Ponten, U., Voigt, G., 1977. Experimental head injury in the
rat. Part 1: mechanics, pathophysiology, and morphology in an impact
acceleration trauma model. J. Neurosurg. 47, 241–251.
Piper, I.R., Thomson, D., Miller, J.D., 1996. Monitoring weight drop ve-
locity and foam stiffness as an aid to quality control of a rodent model
of impact acceleration neurotrauma. J. Neurosci. Methods 69, 171–174.
Povlishock, J.T., Hayes, R.L., Michel, M.E., McIntosh, T.K., 1994. Work-
shop on animal models of traumatic brain injury. J. Neurotrauma 11,
723–732.
Raghupathi, R., Fernandez, S.C., Murai, H., Trusko, S.P., Scott, R.W.,
Nishioka, W.K., McIntosh, T.K., 1998. BCL-2 overexpression attenu-
ates cortical cell loss after traumatic brain injury in transgenic mice.
J. Cereb. Blood Flow Metab. 18, 1259–1269.
Rozsa, L., Grote, E.H., Egan, P., 1989. Traumatic brain swelling studied
by computerized tomography and densitometry. Neurosurg. Rev. 12,
133–140.
Scheff, S.W., Baldwin, S.A., Brown, R.W., Kraemer, P.J., 1997. Morris
water maze deficits in rats following traumatic brain injury: lateral
controlled cortical impact. J. Neurotrauma 14, 615–627.
Schmidt, R.H., Scholten, K.J., Maughan, P.H., 2000. Cognitive impairment
and synaptosomal choline uptake in rats following impact acceleration
injury. J. Neurotrauma 17, 1129–1139.
Shapira, Y., Shohami, E., Sidi, A., Soffer, D., Freeman, S., Cotev, S., 1988.
Experimental closed head injury in rats: mechanical, pathophysiologic,
and neurologic properties. Crit. Care Med. 16, 258–265.
Shibuya, I., Douglas, W.W., 1993. Indications from Mn-quenching of Fura-
2 fluorescence in melanotrophs that dopamine and baclofen close Ca
channels that are spontaneously open but not those opened by high
[K+]O; and that Cd preferentially blocks the latter. Cell Calcium 14,
33–44.
Siesjo, B.K., 1981. Cell damage in the brain: a speculative synthesis.
J. Cereb. Blood Flow Metab. 1, 155–185.
Smith, D.H., Chen, X.H., Xu, B.N., McIntosh, T.K., Gennarelli, T.A.,
Meaney, D.F., 1997. Characterization of diffuse axonal pathology and
selective hippocampal damage following inertial brain trauma in the
pig. J. Neuropathol. Exp. Neurol. 56, 822–834.
Smith, D.H., Cecil, K.M., Meaney, D.F., Chen, X.H., McIntosh, T.K.,
Gennarelli, T.A., Lenkinski, R.E., 1998. Magnetic resonance spec-
troscopy of diffuse brain trauma in the pig. J. Neurotrauma 15,
665–674.
Stahel, P.F., Shohami, E., Younis, F.M., Kariya, K., Otto, V.I., Lenzlinger,
P.M., Grosjean, M.B., Eugster, H.P., Trentz, O., Kossmann, T., Mor-
ganti-Kossmann, M.C., 2000. Experimental closed head injury: anal-
ysis of neurological outcome, blood – brain barrier dysfunction,
intracranial neutrophil infiltration, and neuronal cell death in mice
deficient in genes for pro-inflammatory cytokines. J. Cereb. Blood
Flow Metab. 20, 369–380.
Tanno, H., Nockels, R.P., Pitts, L.H., Noble, L.J., 1992. Breakdown of the
blood–brain barrier after fluid percussive brain injury in the rat: Part 1.
Distribution and time course of protein extravasation. J. Neurotrauma 9,
21–32.
Teasdale, G., Jennett, B., 1976. Assessment and prognosis of coma after
head injury. Acta Neurochir. (Wien.) 34, 45–55.
Teasdale, G.M., Maas, A., Iannotti, F., Ohman, J., Unterberg, A., 1999.
Challenges in translating the efficacy of neuroprotective agents in ex-
perimental models into knowledge of clinical benefits in head injured
patients. Acta Neurochir., Suppl. (Wien.) 73, 111–116.
Uyama, O., Okamura, N., Yanase, M., Narita, M., Kawabata, K., Sugita,
M., 1988. Quantitative evaluation of vascular permeability in the gerbil
brain after transient ischemia using Evans blue fluorescence. J. Cereb.
Blood Flow Metab. 8, 282–284.
Van den Heuvel, C., Blumbergs, P.C., Finnie, J.W., Manavis, J., Jones,
N.R., Reilly, P.L., Pereira, R.A., 1999. Upregulation of amyloid pre-
cursor protein messenger RNA in response to traumatic brain injury:
an ovine head impact model. Exp. Neurol. 159, 441–450.
Veech, R.L., Lawson, J.W., Cornell, N.W., Krebs, H.A., 1979. Cytosolic
phosphorylation potential. J. Biol. Chem. 254, 6538–6547.
Vink, R., Cernak, I., 2000. Regulation of intracellular free magnesium in
central nervous system injury. Front. Biosci. 5, D656–D665.
Vink, R., Cernak, I., 2003. Brain injury, investigating metabolic aspects
using magnetic resonance I. In: Adelman, G., Smith, B. (Eds.), Ency-
clopedia of Neuroscience. Elsevier, Amsterdam. CD-ROM.
Vink, R., Nimmo, A.J., 2002. Novel therapies in development for the
treatment of traumatic brain injury. Expert Opin. Investig. Drugs 11,
1375–1386.
Vink, R., Faden, A.I., McIntosh, T.K., 1988. Changes in cellular bioener-
getic state following graded traumatic brain injury in rats: determination
by phosphorus 31 magnetic resonance spectroscopy. J. Neurotrauma 5,
315–330.
Vink, R., Golding, E.M., Headrick, J.P., 1994. Bioenergetic analysis of
oxidative metabolism following traumatic brain injury in rats. J. Neuro-
trauma 11, 265–274.
Vink, R., Heath, D.L., McIntosh, T.K., 1996. Acute and prolonged alter-
ations in brain free magnesium following fluid percussion-induced
brain trauma in rats. J. Neurochem. 66, 2477–2483.
Vink, R., Golding, E.M., Williams, J.P., McIntosh, T.K., 1997. Blood glu-
cose concentration does not affect outcome in brain trauma: a 31P MRS
study. J Cereb. Blood Flow Metab. 17, 50–53.
Yakovlev, A.G., Knoblach, S.M., Fan, L., Fox, G.B., Goodnight, R., Faden,
A.I., 1997. Activation of CPP32-like caspases contributes to neuronal
apoptosis and neurological dysfunction after traumatic brain injury.
J. Neurosci. 17, 7415–7424.
Yuan, X.Q., Wade, C.E., Clifford, C.B., 1991. Immediate hypertensive
response to fluid percussion brain injury may be related to intracerebral
hemorrhage and hypothalamic damage. J. Neurotrauma 8, 219–228.
Zohar, O., Schreiber, S., Getslev, V., Schwartz, J.P., Mullins, P.G., Pick,
C.G., 2003. Closed-head minimal traumatic brain injury produces long-
term cognitive deficits in mice. Neuroscience 118, 949–955.
Copyright © 2022 FDOKUMEN