Augmented Exercise in the Treatment of Deconditioning From Major Burn Injury

Rehabilitation Aftera Burn Injury
Michael Serghiou, MBA, OTRa,*, April Cowan, OTR, CHTb,Christopher Whitehead, PTbKEYWORDS� Burn � Rehabilitation � Splinting � Positioning � Casting� Therapeutic exercise � Scar management� Physical therapy � Occupational therapy
.com
Physical and occupational therapists becomeinvolved with burn patients as soon as they areadmitted to the burn unit and provide therapeuticinterventions along the rehabilitation continuum ofcare as indicated. The distribution and depth ofthe burn injury may be used to predict the potentialfor joint contractures and diminished function andguide the rehabilitative process. The most imme-diate goals of therapy are to preserve range ofmotion (ROM) and function. The long-term goalsof therapy are to maximize independence in activi-ties of daily living and train the burn survivor to be asfunctional as possible despite any loss of extremity.This article provides a comprehensive overview ofhow burn therapists approach rehabilitation alongthe continuum of care.
POSTBURN POSITIONING OF THE ENTIRE BODY
As soon as the patient is admitted to the burn unit,rehabilitation therapists design a positioningprogram tailored to the patient’s specific needs.Positioning is crucial early in rehabilitation becauseit aids in (1) decreasing the incidence of edema, (2)preventing future contractures and deformities, (3)preventing neurologic trauma, (4) preserving func-tion, and (5) promoting wound healing.
Head and Neck
A burn injury involving the head warrants elevationof the patient’s head above the level of the heart.Elevation of the head causes gravitational forcesto aid in edema reduction. This position can be
a Rehabilitation and Outpatient Services, Shriners HosGalveston, TX 77550, USAb Rehabilitation Services Department, Shriners HospiGalveston, TX 77550, USA* Corresponding author.E-mail address: [email protected] (M. Serghiou).
Clin Plastic Surg 36 (2009) 675–686doi:10.1016/j.cps.2009.05.0080094-1298/09/$ – see front matter ª 2009 Elsevier Inc. All
easily achieved by elevating the head of the bedor, in cases of large-body-surface-area injuryinvolving the lower extremities, by positioning theentire bed on an incline of approximately 30�. Ther-apists may use wooden blocks beneath the head ofthe bed to achieve the total-bed inclined position.Modern hospital beds come equipped witha mechanism that allows for achieving the total-bed inclined position (reverse Trendelenburg posi-tion). Depending on the size of the patient, thera-pists can use foam cutouts and wooden wedgesto prevent the patient from sliding downward inthe bed and altering the anticontracture positioning(Fig. 1).1 When the patient’s ears are burned, ther-apists can fabricate ear cups (ear protectors) tohelp prevent further injury to the ear cartilage andsubsequent chondritis. Ear cups can also serveas anchors for securing patient lines and tubesinstead of using ties wrapped around the headand risking damage to the ear cartilage.2–5
The neck should be positioned in neutral toslight extension (0–15�) by using positioningdevices placed behind the neck or along the scap-ular line. Therapists may use foam mattresses aspart of the positioning regimen, cutting them toallow the neck of the patient to extend.1 Patientswho are severely burned and are intubated mayhave the tendency to rotate and laterally flex theneck toward the ventilator side. This deformity,known as burn torticollis, can be prevented byfrequently altering the ventilator from one side ofthe patient’s bed to the other, placing the ventilatordirectly behind the patient’s head, or fabricating
pitals for Children—Galveston, 815 Market Street,
tals for Children—Galveston, 815 Market Street,
rights reserved. plas
tics
urge
ry.th
ecli
nics
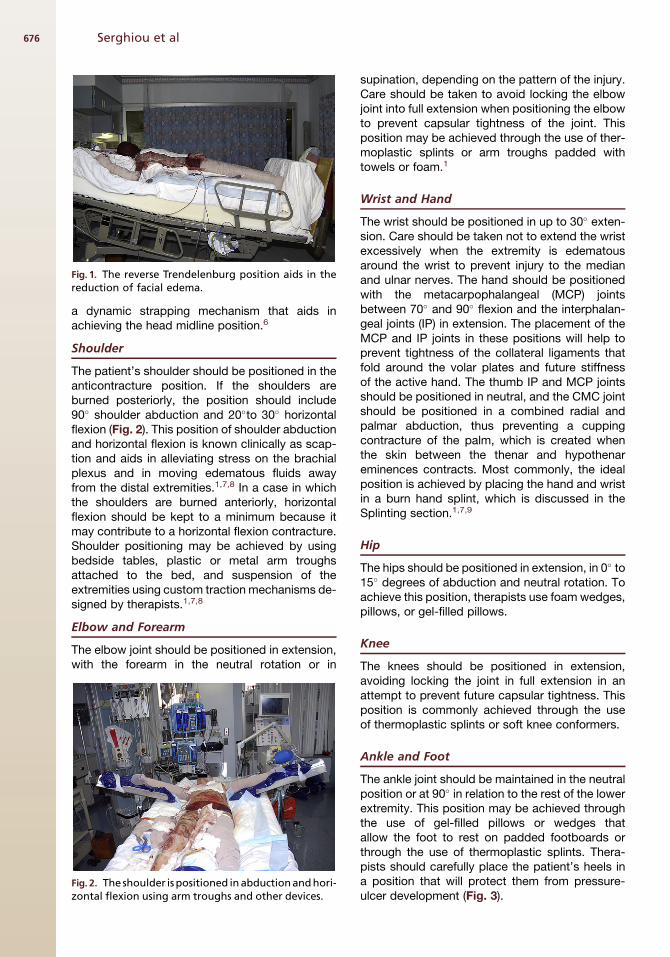
Fig. 1. The reverse Trendelenburg position aids in thereduction of facial edema.
Serghiou et al676
a dynamic strapping mechanism that aids inachieving the head midline position.6
Shoulder
The patient’s shoulder should be positioned in theanticontracture position. If the shoulders areburned posteriorly, the position should include90� shoulder abduction and 20�to 30� horizontalflexion (Fig. 2). This position of shoulder abductionand horizontal flexion is known clinically as scap-tion and aids in alleviating stress on the brachialplexus and in moving edematous fluids awayfrom the distal extremities.1,7,8 In a case in whichthe shoulders are burned anteriorly, horizontalflexion should be kept to a minimum because itmay contribute to a horizontal flexion contracture.Shoulder positioning may be achieved by usingbedside tables, plastic or metal arm troughsattached to the bed, and suspension of theextremities using custom traction mechanisms de-signed by therapists.1,7,8
Elbow and Forearm
The elbow joint should be positioned in extension,with the forearm in the neutral rotation or in
Fig. 2. The shoulder is positioned in abductionand hori-zontal flexion using arm troughs and other devices.
supination, depending on the pattern of the injury.Care should be taken to avoid locking the elbowjoint into full extension when positioning the elbowto prevent capsular tightness of the joint. Thisposition may be achieved through the use of ther-moplastic splints or arm troughs padded withtowels or foam.1
Wrist and Hand
The wrist should be positioned in up to 30� exten-sion. Care should be taken not to extend the wristexcessively when the extremity is edematousaround the wrist to prevent injury to the medianand ulnar nerves. The hand should be positionedwith the metacarpophalangeal (MCP) jointsbetween 70� and 90� flexion and the interphalan-geal joints (IP) in extension. The placement of theMCP and IP joints in these positions will help toprevent tightness of the collateral ligaments thatfold around the volar plates and future stiffnessof the active hand. The thumb IP and MCP jointsshould be positioned in neutral, and the CMC jointshould be positioned in a combined radial andpalmar abduction, thus preventing a cuppingcontracture of the palm, which is created whenthe skin between the thenar and hypothenareminences contracts. Most commonly, the idealposition is achieved by placing the hand and wristin a burn hand splint, which is discussed in theSplinting section.1,7,9
Hip
The hips should be positioned in extension, in 0� to15� degrees of abduction and neutral rotation. Toachieve this position, therapists use foam wedges,pillows, or gel-filled pillows.
Knee
The knees should be positioned in extension,avoiding locking the joint in full extension in anattempt to prevent future capsular tightness. Thisposition is commonly achieved through the useof thermoplastic splints or soft knee conformers.
Ankle and Foot
The ankle joint should be maintained in the neutralposition or at 90� in relation to the rest of the lowerextremity. This position may be achieved throughthe use of gel-filled pillows or wedges thatallow the foot to rest on padded footboards orthrough the use of thermoplastic splints. Thera-pists should carefully place the patient’s heels ina position that will protect them from pressure-ulcer development (Fig. 3).

Fig. 3. The ankle joint is maintained in the neutralposition with the focus on protecting the heel frompressure irritation in the supine and prone positions.
Fig. 4. This photo shows a combination of splints usedto manage neck and upper extremity contractures.
Rehabilitation After a Burn Injury 677
SPLINTING
In general, patients who have experienced severeburn injuries are at risk for the development oflimited ROM and decreased joint mobility.10
Management of scar contractures is a majoraspect of the work of burn therapists, and splintinghas become an essential tool in their clinical reper-toire.11 A splint program for contracture manage-ment should include multiple splint designs(Fig. 4).12 A well-designed splint program, usingactive and passive mobilization, is essential toprevent and convert joint contractures anddeformity.12,13
The development of deformities after burn injurycan be avoided by the prompt institution of splint-ing techniques to prevent contracture andcompensate for functional deficits.14 Splints areused most commonly to counteract the initialand ongoing contraction of wounded tissue tothe time of scar maturation. Additionally, splintsare used for protection of exposed anatomicstructures, prevention or correction of deformitiescaused by nerve injuries, and postoperative immo-bilization of grafted or reconstructed areas.7 Someclinicians consider splinting to be an extension of
a patient-positioning program. It has been estab-lished that patients who are unable to complywith rehabilitation programs need to receivesplints.15
Richard and colleagues16 found that burn thera-pists apply splints at the time of hospital admis-sion, when a decrease in ROM is apparent, atthe time of skin grafting, and immediately afterreconstructive surgery. The areas of burn that aremost often splinted at the time of patient admis-sion to the burn unit are the hand–wrist complex,axilla, elbow, and ankle. The current trend is towait until a decreased ROM has been demon-strated before splinting. Additionally, Richard andcolleagues16 noted an overall tendency to applysplints more often after reconstructive surgerythan after initial placement of a skin graft.However, hand burns and full-thickness injuriesshould and do continue to receive prioritytreatment.
The burned hand requires immediate splinting tocombat edema, protect exposed structures, andbalance soft tissue lengths.14 Splinting of thehand should place healing tissues at maximumlength, protect grafts and reconstructed sites,and stretch soft tissue adhesions (Fig. 5). Hand-positioning protocols vary from one burn centerto another, but most therapists agree thata severely burned hand should be positionedopposite the anticipated deformity.10
Pulliam14 provides a thorough discussion of thepatient factors to be considered before institutinga splinting program. Additionally, Richard andWard10 describe the strategies for clinical
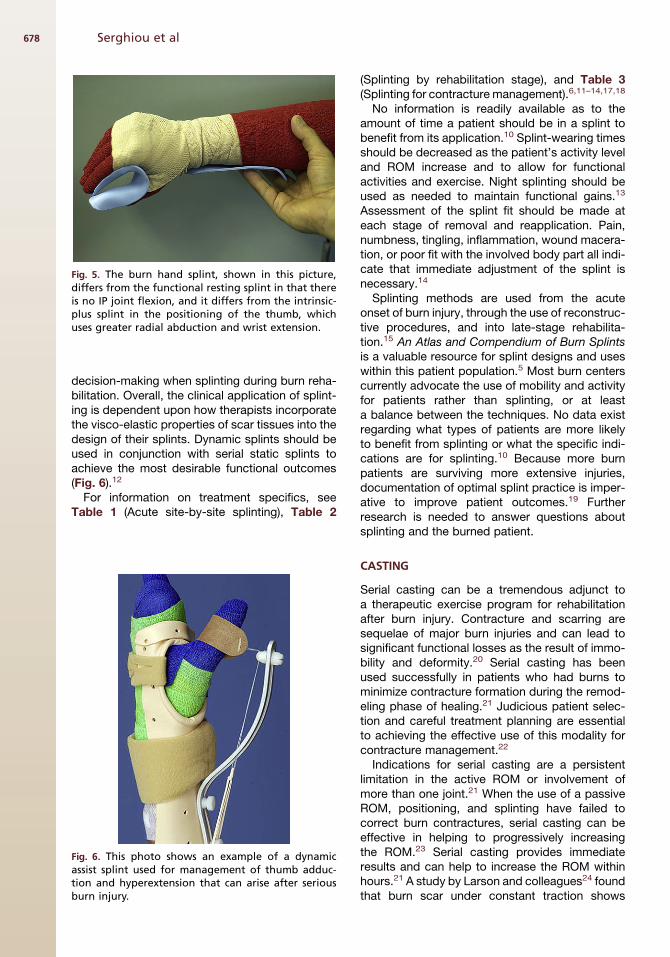
Fig. 5. The burn hand splint, shown in this picture,differs from the functional resting splint in that thereis no IP joint flexion, and it differs from the intrinsic-plus splint in the positioning of the thumb, whichuses greater radial abduction and wrist extension.
Serghiou et al678
decision-making when splinting during burn reha-bilitation. Overall, the clinical application of splint-ing is dependent upon how therapists incorporatethe visco-elastic properties of scar tissues into thedesign of their splints. Dynamic splints should beused in conjunction with serial static splints toachieve the most desirable functional outcomes(Fig. 6).12
For information on treatment specifics, seeTable 1 (Acute site-by-site splinting), Table 2
Fig. 6. This photo shows an example of a dynamicassist splint used for management of thumb adduc-tion and hyperextension that can arise after seriousburn injury.
(Splinting by rehabilitation stage), and Table 3(Splinting for contracture management).6,11–14,17,18
No information is readily available as to theamount of time a patient should be in a splint tobenefit from its application.10 Splint-wearing timesshould be decreased as the patient’s activity leveland ROM increase and to allow for functionalactivities and exercise. Night splinting should beused as needed to maintain functional gains.13
Assessment of the splint fit should be made ateach stage of removal and reapplication. Pain,numbness, tingling, inflammation, wound macera-tion, or poor fit with the involved body part all indi-cate that immediate adjustment of the splint isnecessary.14
Splinting methods are used from the acuteonset of burn injury, through the use of reconstruc-tive procedures, and into late-stage rehabilita-tion.15 An Atlas and Compendium of Burn Splintsis a valuable resource for splint designs and useswithin this patient population.5 Most burn centerscurrently advocate the use of mobility and activityfor patients rather than splinting, or at leasta balance between the techniques. No data existregarding what types of patients are more likelyto benefit from splinting or what the specific indi-cations are for splinting.10 Because more burnpatients are surviving more extensive injuries,documentation of optimal splint practice is imper-ative to improve patient outcomes.19 Furtherresearch is needed to answer questions aboutsplinting and the burned patient.
CASTING
Serial casting can be a tremendous adjunct toa therapeutic exercise program for rehabilitationafter burn injury. Contracture and scarring aresequelae of major burn injuries and can lead tosignificant functional losses as the result of immo-bility and deformity.20 Serial casting has beenused successfully in patients who had burns tominimize contracture formation during the remod-eling phase of healing.21 Judicious patient selec-tion and careful treatment planning are essentialto achieving the effective use of this modality forcontracture management.22
Indications for serial casting are a persistentlimitation in the active ROM or involvement ofmore than one joint.21 When the use of a passiveROM, positioning, and splinting have failed tocorrect burn contractures, serial casting can beeffective in helping to progressively increasingthe ROM.23 Serial casting provides immediateresults and can help to increase the ROM withinhours.21 A study by Larson and colleagues24 foundthat burn scar under constant traction shows

Table1Acute site-by-site splinting
Body Part Splint
Neck Anterior/posterior/lateral conformers; soft collars
Shoulder Abduction wedges; airplane splints
Elbow Anterior/posterior conformers
Hand Dorsal burns 5 volar resting hand splintPalmar burns 5 dorsal hand extension splintCircumferential burns with grafting 5 volar positioning splint or banjo splint
Trunk T-shirt splint
Hip Abduction wedge; anterior hip spica splint
Knee Posterior knee conformer, knee immobilizer, or three-point extension splint
Ankle and foot Ankle-foot orthoses, dorsiflexion assist splint, footplate or total contactsandal
Data from Pullium GF. Splinting and pasitioning. In: Fisher SV, editor. Comprehensive rehabilitation of burns. Philadelphia:Lippincott Williams & Wilkins; 1984. p. 64–95.
Rehabilitation After a Burn Injury 679
changes in collagen alignment along the forces ofstress.
Serial casting techniques have been describedby Cusick25 and Ridgway and colleagues.26 Safecasting considerations include the use of lukewarmdip water for plaster of paris, cool dip water forfiberglass materials, and padding to avoid sharpedges or pressure points.27 At the time of eachcast change, the following are recommended: theuse of wound care techniques, scar massage usinga skin lubricant, ROM exercises, and taking gonio-metric measurements to assess treatment efficacy(Fig. 7).23 Serial casts are sometimes wedgedbetween cast changes to decrease the effort andexpense of recasting. The best results when usingserial casting are achieved by alternating castchanges with cast wedging on a daily basis. Forpatients who have open wounds, casts changesshould be performed at more frequent intervals.22
Serial casting should be terminated when either
Table 2Splinting by rehabilitation stage
Stage Splint Purposes
Acute Used for positioning and alleviatioedema; serially adjusted tocounteract scar contracture
Intermediate Essential for positioning and stretchlengthening of contracted tissue
Long-term Used to provide stretch, promote tgliding, decrease stiffness, andstrengthen weakened structures
Data from Refs.12,13,17
normal ROM is restored or no further gains areachieved.21
PROSTHETICS
Burn injuries can require amputation because ofthe depth of the injury, severe infection, or lossof function.28 The use of prosthetics greatly aidesin the restoration of function to patients whohave sustained amputations.
Prosthetic fitting and training can begin on theburn unit before complete wound closure isachieved and provides a difficult challenge forthe patient and the rehabilitation therapist.Common problems that occur in burn patientswho have sustained an amputation includecompromised skin integrity, skin fragility, jointcontracture, formation of bone spurs, edema,and phantom pain.29 Many patients also havesevere limitations in the functioning of intact
Splint Types
n of Static splints
ing/s
Static splints, static progressive splints,or dynamic splints
issue Static progressive and dynamic splints
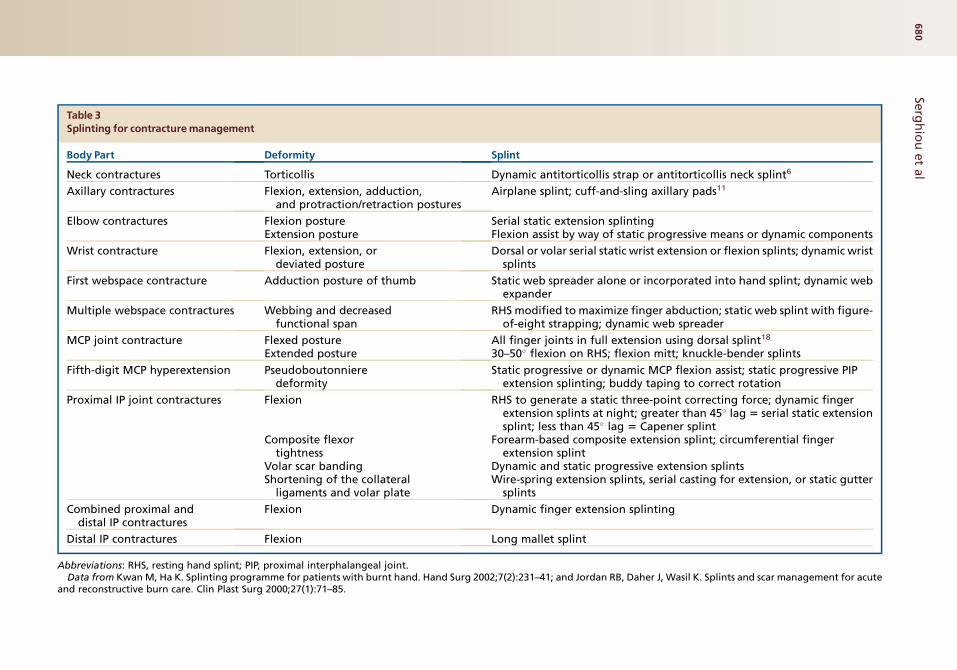
Table 3Splinting for contracturemanagement
Body Part Deformity Splint
Neck contractures Torticollis Dynamic antitorticollis strap or antitorticollis neck splint6
Axillary contractures Flexion, extension, adduction,and protraction/retraction postures
Airplane splint; cuff-and-sling axillary pads11
Elbow contractures Flexion posture Serial static extension splintingExtension posture Flexion assist by way of static progressive means or dynamic components
Wrist contracture Flexion, extension, ordeviated posture
Dorsal or volar serial static wrist extension or flexion splints; dynamic wristsplints
First webspace contracture Adduction posture of thumb Static web spreader alone or incorporated into hand splint; dynamic webexpander
Multiple webspace contractures Webbing and decreasedfunctional span
RHS modified to maximize finger abduction; static web splint with figure-of-eight strapping; dynamic web spreader
MCP joint contracture Flexed posture All finger joints in full extension using dorsal splint18
Extended posture 30–50� flexion on RHS; flexion mitt; knuckle-bender splints
Fifth-digit MCP hyperextension Pseudoboutonnieredeformity
Static progressive or dynamic MCP flexion assist; static progressive PIPextension splinting; buddy taping to correct rotation
Proximal IP joint contractures Flexion RHS to generate a static three-point correcting force; dynamic fingerextension splints at night; greater than 45� lag 5 serial static extensionsplint; less than 45� lag 5 Capener splint
Composite flexortightness
Forearm-based composite extension splint; circumferential fingerextension splint
Volar scar banding Dynamic and static progressive extension splintsShortening of the collateral
ligaments and volar plateWire-spring extension splints, serial casting for extension, or static gutter
splints
Combined proximal anddistal IP contractures
Flexion Dynamic finger extension splinting
Distal IP contractures Flexion Long mallet splint
Abbreviations: RHS, resting hand splint; PIP, proximal interphalangeal joint.Data from Kwan M, Ha K. Splinting programme for patients with burnt hand. Hand Surg 2002;7(2):231–41; and Jordan RB, Daher J, Wasil K. Splints and scar management for acute
and reconstructive burn care. Clin Plast Surg 2000;27(1):71–85.
Serg
hio
uet
al
680
Fig. 7. This photo shows an example of documentingROM status during the serial casting process for treat-ment of elbow contracture.
Rehabilitation After a Burn Injury 681
extremities that affect their ability to use a pros-thesis.1 After a prosthetic has been applied,common problems include skin breakdown,formation of blisters or sebaceous cysts,neuromas, stump pain, muscle weakness, andjoint contractures.29
THERAPEUTIC EXERCISE
The use of therapeutic exercise in conjunction witha comprehensive rehabilitation plan helps toprevent the formation of deforming contracturesand maintain strength in the involved and unin-volved extremities.30 It is through the use of thera-peutic exercise programs that rehabilitationtherapists seek to restore functional movement ina burn patient.
Acute Rehabilitation Phase
The acute rehabilitation phase is defined as thetime from admission until about the time thata patient’s wounds are 50% closed or the use ofskin grafting to achieve wound closure hasbegun.19
The use of active ROM exercises is vital to coun-teract the effects of prolonged bed rest andmuscle atrophy, maintain joint ROM, and preventcontractures. The use of active assistive ROMexercises is an appropriate intervention whena patient cannot actively move through the fullROM. In conditions in which patients cannotparticipate actively, passive exercise is used tomaintain ROM, assess joint motion, and elongatetissue.31
Resistive exercises are used to maintain orincrease strength, ROM, proprioception, andcoordination.32 Rehabilitation therapists shouldbegin with simple exercises such as manual
resistance and isometric strengthening, progress-ing to more difficult exercises as the patient’sstatus improves.
Another important aspect of a patient’s recoveryis the ability to ambulate. Severe weakness,impaired motor control, decreased cognitivestatus, pain, and risk for graft shearing are allfactors that can make ambulation a difficulttask.33 The primary goals of ambulation includemaintaining lower extremity ROM, reducing therisk for thrombophlebitis, preventing the formationof decubiti, providing mild cardiovascular condi-tioning, and maintaining or increasing strengthand endurance.34
Intermediate Rehabilitation Phase
The intermediate phase is from about 50% ofwound closure to the time of complete woundclosure.19 The prevention of functional impair-ments becomes the focus of therapeutic exerciseas patients begin to achieve wound coverage,and the therapy program focus shifts to sustainedstretching of the affected areas, with increasedfrequency and intensity of active ROM andstrengthening exercises. Sustained stretching isconsidered to be one of the most effectivemethods to combat the strong destructive forcesthat lead to contracture formation.35
Strengthening exercises change from manualresistance to the use of weights and resistivetubing. Areas to be concentrated on shouldinclude those where weakness is found duringstrength assessments and the muscles opposingscar tissue contractures.31
Long-Term Rehabilitation Phase
The long-term phase occupies the timeframe fromwound closure or patient discharge from the acutehospital setting until such time that a patient hasreceived maximal benefit from rehabilitationservices.19 As patients near their discharge fromthe acute hospital setting, they will be givenmore responsibility for their exercise program.
Supplemental exercise programs complimentbasic rehabilitation services by addressing theoverall conditioning of the patients and letting therehabilitation therapists focus on exercises andstretching that promote the restoration of move-ment and function. If deficits in ROM are present,the rehabilitation therapist should make it a priorityto treat the limitation in motion rather than workingto increase the patient’s strength because normal,healthy muscle is unable to generate the forcerequired to elongate burn scar tissue.31

Serghiou et al682
SCARMANAGEMENT
As a burn wound heals, it forms scar tissue at thesite of the injury that is characterized by an abun-dance of collagen fibers. These collagen fibershave properties of connective tissue and continueto be produced at the injury site, serving as themechanism by which the wound heals andbecomes stronger.1 Initially, the newly developedscar seems to be red, raised, and rigid, and iscommonly known as an immature scar. Clinicalstudies indicate that an immature burn scarresponds best to pressure therapy that is incorpo-rated in the overall therapy regimen to depress thescar in an attempt to prevent scar hypertrophy. Ithas been reported that delayed wound closure,wound infection, patient age, the location anddepth of the burn injury, the patient’s geneticmakeup, and repeated harvesting of donor sitesare factors that may contribute to the developmentof scar hypertrophy.1 Clinical observationsuggests that scar hypertrophy may be evidentat approximately 12 weeks after a burn woundhas closed.1 The overall goals of burn rehabilita-tion when it comes to scar management are todepress the scar’s height, which is attempted byexerting pressure on the scar, and to maintainscar pliability, which in turn contributes to main-taining the patient’s mobility and ROM. Burn reha-bilitation professionals have developed the use ofvarious technologies to study and assess thescar maturation process. Such technologiesinclude ultrasonography, tonometry, laser Dopplerflowmetry and colorimetry, which all provideobjective ways of rating the burn scar.1 The Van-couver Scar Scale Assessment is used to ratethe burn scar based on its pigmentation, vascu-larity, pliability, and height. It is widely used, simpleto administer, and an inexpensive way assessingthe burn scar; however, this technique seems toprovide a subjective assessment of the burnscar.1,36–38 The treatment of hypertrophic scarsis very problematic and poses significant chal-lenges for burn rehabilitation professionalsbecause the mechanism of how scars are formedand how they progress toward maturation remainselusive. Currently, burn scars are treated by meansof pressure therapy, application of physical agentmodalities, massage, and exercise.
Fig. 8. Custom-made pressure garments provide from24 to 28 mm Hg of pressure and should be worn untilscars are matured.
Pressure Therapy
Clinically, scar hypertrophy is managed throughthe use of pressure garments and inserts. Studieshave shown that when an active (red, raised, andrigid) scar is compressed, it becomes devascular-ized. Decreased blood flow to the scar leads to
decreased production of collagen fibers, causinga balance in the synthesis and breakdown (lysis)of collagen. Such a balance, when established,produces a flatter, softer, and less vascularizedscar.1 Even though the use of pressure garmentshas been observed to decrease scar hypertrophy,no scientific evidence exists to support the use ofpressure garments as the standard of care in scarmanagement.1,39 When used, pressure garmentsmust be worn on a 24-hour basis in conjunctionwith insert materials (used in areas in which opti-mized pressure cannot be achieved by usinggarments alone). The use of pressure garmentsmay be initiated as soon as all burn wounds haveclosed sufficiently to tolerate wear, and their useshould be continued until the burn scar hasmatured. A mature scar appears devascularized,depressed, and pliable.
The scar maturation process appears to bedependant on the individual patient’s geneticpredisposition to scar formation and various otherfactors described previously in this article.1 Initially,the pressure applied is low (15–17 mm Hg, or insome cases as low as 10 mm Hg) and is deliveredusing pressure garments. Low-pressure garmentsinclude tubular elastic bandages, elastic self-adherent wraps and prefabricated garments thatare commercially available and fit the entirebody.1 As the burn scar progresses in the matura-tion process and is able to withstand higher pres-sures without breaking down, custom-madepressure garments providing 24 to 28 mm Hg ofpressure may be fabricated for the patient (Fig. 8).Custom pressure garments, if properly managed,last approximately 12 weeks before they beginlosing their elasticity, which results in a decreasein the amount of pressure they can apply to thehypertrophic scar.1 Various insert materials may

Fig. 10. Silicone elastomer is used to fabricate facialorthotics to depress scar hypertrophy.
Rehabilitation After a Burn Injury 683
be used beneath pressure garments on areaswhere optimal pressure cannot be achieved, suchas concave areas of the body (Fig. 9). Insert mate-rials include foam, silicone elastomers, silicone gel,gel polymers, and various semirigid elastic mate-rials formed from elastomer putties.1,40,41 High-temperature thermoplastic materials and liquid sili-cone elastomers may be used to fabricate facialorthotics that provide pressure to areas of scarringand may be worn in conjunction with pressuregarments (Fig. 10).1
Massage
Despite the controversy as to whether massage isbeneficial in burn rehabilitation, therapistsfrequently incorporate massage in their attemptsto soften and elongate tissue and to allow extrem-ities to be more mobile.42 Various massage tech-niques are used to treat the burn scar. Thechoice of massage technique is generally dictatedby the strength of the scar tissue and its ability towithstand frictional forces acting on it. Initially,the massage used is gentle and primarily nonfric-tional and then progresses to a more deep fric-tional (pinch-and-roll) method.1,8 Therapistscommonly apply heat before massaging and
Fig. 9. Various materials are used as inserts beneathpressure garments in areas where good pressureprovided by garments cannot be achieved.
stretching the scar tissue. Patients and caregiversare instructed on massage as part of a home exer-cise program.
Modalities in Scar Management
Although they are underused, therapeutic modali-ties should be employed in a rehabilitation thera-pist’s treatment plan for scar management. Theapplication of therapeutic heat may permit easierelongation of scar tissue by way of an increasedextensibility of connective tissue.43 The use ofhot packs, ultrasonography, and paraffin have allbeen found to provide tissue extensibility to scartissue.44–46 Although caution needs to be takenin cases of increased or decreased levels of sensi-tivity, the use of therapeutic heat in burn patientscan provide an effective method of increasingburn scar extensibility.
FUNCTION
The improved survival rates of individuals whohave large burn injuries have made the restorationof function and the role of rehabilitation increas-ingly important.47 A greater focus exists on thephysical consequences of surviving a massiveburn and the social and psychological factorsinvolved in recovery.48 Functional independenceis the ultimate long-term goal in burn rehabilita-tion.49 Short-term goals focus on modification ofactivities of daily living, return to work or school,acceptance of one’s altered appearance, and rein-tegration into society.50
The following factors may preclude the burnedindividual from becoming fully independent inactivities of daily living: limited ROM, poordexterity, loss of mobility, intolerance for standingand walking, and pain and decreased strength orendurance.51 Salisbury52 described 12 postburndeformities of the upper extremities that may limitfunctioning. Sheridan and colleagues53 noteddifferences in functional outcomes that were

Serghiou et al684
associated with the overall severity of thermalinjury. Full-thickness hand burns involving thetendons have the greatest potential to limit func-tioning after a thermal injury.50 Clinical studieshave shown that burn injury results in decondition-ing and persistent fatigue that can significantlyimpact functional aptitudes.54
Following significant thermal insult, quality of lifebecomes one of the most important aspects ofrecovery.55,56 Current research indicates that thestrongest independent predictors of physicalquality of life are total full-thickness injury andhand functioning.49,57 Being young at the time ofa burn injury and the patient’s level of socialsupport were the strongest predictors of improvedmental quality of life after massive burn injury.57
Becoming reinvolved in preburn roles and produc-tive activities are very important to a person’sperception that life has positive qualities afterrecovering from burn injury.58
The resumption of work roles may requiregradual reintegration into the workplace, modifica-tion of work duties, and close coordination with theemployer.59 ‘‘Work hardening’’ and other voca-tional programs appear to be useful in rehabilita-tion from burn injury.60 Furthermore, patients’subjective assessments of functional ability,appearance, pain, and generic health status havebeen found to correlate with work status afterburn injury.61 Those patients who are working afterserious burn injury reported better health-relatedquality of life and better physical health and hadbetter psychological health.48
The first study to report on quality of life aftermassive burn injuries in the adult population wascompleted by Anzarut and associates.57 Theirdata supported the hypothesis that adult survivorsof massive burn injury have a quality of life compa-rable to the national norms. Baker andcolleagues62 studied young burn survivors andfound that as a group they rated their overallquality of life significantly lower than the normativereference group. On the positive side, Baker andcolleagues’ results suggest that most childrenwho experience moderate to severe burns will beable to address their own self-care and mobilityneeds as young adults.
The outlook for those who experience a severeburn injury is generally positive. Thus, the authorsare able to reassure patients and their familiesthat they can achieve functional independenceand a reasonable quality of life in the long term.63
Attempts should be made to evaluate specificinterventions and their impact on outcome afterburn injury.64 Clinical efforts and research shouldfocus on improving patient hand function,enhancing social support, and identifying other
predictors of quality of life after massive burninjury.57 Long-term follow-up of patients whosuffer severe burns is critical,65 and continuedcollaboration between specialized burn centers isneeded to advance the effectiveness of burnrehabilitation.
DISCHARGE
In preparation for discharge from acute hospitali-zation, the patient and caregivers meet with theburn therapist to discuss the patient’s currentfunctional abilities and to prepare a home treat-ment program that includes exercise, splinting,positioning, and scar management. A hospital-based outpatient rehabilitation program may berequired after discharge from the hospital fora period of time based on the patient’s needs. Insome cases, therapists may conduct home andwork-site assessments in preparation for thepatient to return to work and the home environ-ment. This is done to address the need for adap-tive equipment that may be necessary tomaximize the patient’s independence. A schoolreentry program may be organized in preparationfor a child who sustained serious burn injuries toreturn to school. This program may be organizedby members of the burn team and should include,among others, child life specialists, occupationaland physical therapists, psychologists, andnurses. Community reintegration is a crucialcomponent of burn rehabilitation and contributessignificantly to the total and successful completionof the rehabilitative process. After discharge fromthe hospital setting, outpatient clinic appointmentsfor the patient and caregivers should be scheduledat regular intervals as indicated. The patient andburn therapist should remain in touch for as longas necessary to successfully complete the rehabil-itative process. Home exercise programs shouldbe adjusted as needed for the patient to achieveoptimal functional outcomes.1
REFERENCES
1. Serghiou MA, Ott S, Farmer S, et al. Comprehensive
rehabilitation of the burn patient. In: Herndon D,
editor. Total burn care. Philadelphia: Saunders
Elsevier; 2007. p. 620–51.
2. Harries CA, Pegg SP. Foam ear protectors for burnt
ears. J Burn Care Rehabil 1989;10:183–4.
3. Gallagher J, Leman C, Alley R, et al. A pressure
prevention device for burned ears. J Burn Care
Rehabil 1992;13:673–7.
4. Manigandan C, Dhanaraj P. An innovative, cost-
effective, pressure-relieving device for burned
ears. Burns 2004;30:269–71.

Rehabilitation After a Burn Injury 685
5. Richard R, Chapman T, Dougherty M, et al, editors.
An atlas and compendium of burn splints. San
Antonio, TX: Reg Richard Inc; 2005.
6. Serghiou M, McLaughlin A, Herndon D. Alternative
splinting methods for the prevention and correction
of burn scar torticollis. J Burn Care Rehabil 2003;
24:336–40.
7. Daugherty MB, Carr-Collins JA. Splinting techniques
for the burn patient. In: Richard RL, Staley MJ,
editors. Burn care and rehabilitation: principles and
practice. Philadelphia: FA Davis Co.; 1994. p. 243–4.
8. Serghiou MA, Farmer SA. A practical approach to
acute burn rehabilitation. In: Barret-Nerı́n JP,
Herndon DN, editors. Principles and practice of burn
surgery. New York: Marcel Dekker; 2005. p. 317–63.
9. Serghiou M, McLaughlin A. Rehabilitation of the
burned hand. In: McCauley R, editor. Functional
and aesthetic reconstruction of burned patients.
Boca Raton (FL): Taylor and Francis; 2005.
p. 489–519.
10. Richard R, Ward S. Splinting strategies and contro-
versies. J Burn Care Rehabil 2005;26(5):392–6.
11. Obaidullah, Ullah H, Aslam M. Figure-of-8 sling for
prevention of recurrent axillary contracture after
release and skin grafting. Burns 2005;31:283–9.
12. Kwan M, Ha K. Splinting programme for patients
with burnt hand. Hand Surg 2002;7(2):231–41.
13. Jordan RB, Daher J, Wasil K. Splints and scar
management for acute and reconstructive burn
care. Clin Plast Surg 2000;27(1):71–85.
14. Pullium GF. Splinting and positioning. In: Fisher SV,
editor. Comprehensive rehabilitation of burns. Phila-
delphia: Lippincott Williams & Wilkins; 1984. p. 64–95.
15. Richard R, Staley M, Miller S, et al. To splint or not to
splint—past philosophy and present practice: part I.
J Burn Care Rehabil 1996;17(5):444–53.
16. Richard R, Staley M, Miller S, et al. To splint or not to
splint: past philosophy and current practice—part II.
J Burn Care Rehabil 1997;18(1):64–71.
17. Richard RL, Hedman TL, Quick CD, et al. A clarion
to recommit and reaffirm burn rehabilitation. J Burn
Care Res 2008;29:425–32.
18. Schwanholt C, Daugherty MB, Gaboury T, et al.
Splinting the pediatric palmar burn. J Burn Care
Rehabil 1992;13(4):460–4.
19. Richard R, Staley M, Miller S, et al. To splint or not to
splint—past philosophy and present practice: part
III. J Burn Care Rehabil 1997;18(3):251–5.
20. Abston S. Scar reaction after thermal injury and
prevention of scars and contracture. In: Boswick J,
editor. The art and science of burn care. Gaithers-
burg (MD): Aspen Publishers Inc; 1987. p. 359–71.
21. Bennett GB, Helm P, Purdue GF, et al. Serial casting:
a method for treating burn contractures. J Burn Care
Rehabil 1989;10(6):543–5.
22. Leahy P. Precasting work sheet—an assessment
tool: a clinical report. Phys Ther 1988;68(1):72–4.
23. Johnson J, Silverberg R. Serial casting of the lower
extremity to correct contractures during the acute
phase of burn care. Phys Ther 1995;75(4):262–6.
24. Larson DL, Abston S, Evans EB, et al. Techniques
for decreasing scar formation and contractures in
the burned patient. J Trauma 1971;11:807–23.
25. Cusick BD. Serial casts: their use in the manage-
ment of the spasticity-induced foot deformity. Tuc-
son (AZ): Therapy Skill Builders; 1990.
26. Ridgway CL, Daugherty MB, Warden GD. Serial
casting as a technique to correct burn scar contrac-
tures: a case report. J Burn Care Rehabil 1991;
12(1):67–72.
27. Hutchinson MJ, Hutchinson MR. Factors contrib-
uting to the temperature beneath plaster or fiber-
glass cast material. J Orthop Surg 2008;3:10.
Available at: http://www.josr-online.com/content/3/1/
10. Accessed September 3, 2008.
28. Saffle JR, Schnelby WA. Burn wound care. In:
Richard RL, Staley MJ, editors. Burn care and reha-
bilitation principles and practice. Philadelphia: F.A.
Davis; 1994. p. 119–76.
29. Ward RS, Hayes-Lundy C, Schnebly WA, et al. Pros-
thetic use in patients with burns and associated limb
amputations. J Burn Care Rehabil 1990;11:361–4.
30. Braddom RL, Boe L, Floers L, et al. The physical
treatment and rehabilitation of burn patients. In:
Hummel RP, editor. Clinical burn therapy. Boston:
John Wright-PSG; 1982. p. 279–99.
31. Humphry CN, Richard RL, Staley MJ. Soft tissue
management and exercise. In: Richard RL,
Staley MJ, editors. Burn care and rehabilitation: prin-
ciples and practice. Philadelphia: F.A. Davis; 1994.
p. 324–59.
32. Wright PC. Fundamentals of acute burn care and
physical therapy management. Phys Ther 1984;64:
1217–31.
33. Trees D, Ketelsen CA, Hobbs JA. Use of a modified
tilt table for preambulation strength training as an
adjunct to burn rehabilitation: a case series. J Burn
Care Rehabil 2003;24:97–103.
34. Nothdurft D, Smith PS, LeMaster JE. Exercise and
treatment modalities. In: Fisher SV, Helm PA, editors.
Comprehensive rehabilitation of burns. Baltimore
(MD): Williams & Wilkins; 1984. p. 97–127.
35. Blassingame WM, Bennett GB, Helm PA, et al.
Range of motion of the shoulder performed while
patient is anesthetized. J Burn Care Rehabil 1989;
10:539–42.
36. Sullivan T, Smith J, Kermode J, et al. Rating the burn
scar. J Burn Care Rehabil 1990;11:256–60.
37. Baryza MJ, Baryza GA. The Vancouver Scar Scale:
an administration tool and its inter-rater reliability.
J Burn Care Rehabil 1995;16:535–8.
38. Forbes-Duchart L, Marsall S, Strock A, et al. Deter-
mination of inter-rater reliability in pediatric burn
scar assessment using a modified version of the

Serghiou et al686
Vancouver Scar Scale. J Burn Care Res 2007;28:
460–7.
39. Linares HA, Larson DL, Willis-Galstaum BA. Histor-
ical notes on the use of pressure in treatment of
hypertrophic scars or keloids. Burns 1993;19:17–21.
40. Van den Kerchove E, Boechx W, Kochreyt A. Sili-
cone patches as a supplement for pressure therapy
to control hypertrophic scarring. J Burn Care Reha-
bil 1992;12(4):361–9.
41. Quinn KJ, Evans JH, Courtney JM, et al. Non-pres-
sure treatment of hypertrophic scars. Burns 1985;
12:102–8.
42. Patino O, Novick C, Merlo A, et al. Massage in hyper-
trophic scars. J Burn Care Rehabil 1999;20:268–81.
43. Ward RS. The use of physical agents in burn care.
In: Richard RL, Staley MJ, editors. Burn care and
rehabilitation principles and practice. Philadelphia:
F.A. Davis; 1994. p. 419–46.
44. Ward RS, Hayes-Lundy C, Reddy R, et al. Evaluation
of topical therapeutic ultrasound to improve response
to physical therapy and lessen scar contracture after
burn injury. J Burn Care Rehabil 1994;15:74–9.
45. Head M, Helm P. Paraffin and sustained stretching in
treatment of burn contractures. Burns 1977;4:136–9.
46. Kowalske K, Holavanahalli R, Hynan I, et al. A
randomized-controlled study of the effectiveness of
paraffin and sustained stretch in treatment of burn
contractures. J Burn Care Rehabil 2003;24:S67.
47. Spires MC, Bowden ML, Ahrns KS, et al. Impact of
an inpatient rehabilitation facility on functional
outcome and length of stay of burn survivors. J
Burn Care Rehabil 2005;26(6):532–8.
48. Dyster-Aas J, Kildal M, Willebrand M. Return to work
and health-related quality of life after burn injury. J
Rehabil Med 2007;39:49–55.
49. Holavanahalli RK, Helm PA, Gorman AR, et al.
Outcomes after deep full-thickness hand burns.
Arch Phys Med Rehabil 2007;88(Suppl 2):S30–5.
50. Klein MB, Lezotte D, Fauerbach J, et al. The National
Institute on Disability and Rehabilitation Research
burn model system database: a tool for the multi-
center study of outcome of burn injury. J Burn
Care Res 2007;28(1):84–96.
51. St-Pierre DM, Choiniere M, Forget R, et al. Muscle
strength in individuals with healed burns. Arch
Phys Med Rehabil 1998;79:155–61.
52. Salisbury R. Reconstruction of the burned hand. Clin
Plast Surg 2000;27(1):65–9.
53. Sheridan R, Hurley J, Smith M, et al. The acutely
burned hand: management and outcome based
on a ten-year experience with 1047 acute hand
burns. J Trauma 1995;38(3):406–11.
54. Helm P, Herndon DN, DeLateur B. Restoration of
function. J Burn Care Res 2007;28(4):611–4.
55. Baker CP, Rosenberg M, Mossberg K, et al. Relation-
ships between the Quality of Life Questionnaire
(QLQ) and the SF-36 among young adults burned as
children. Burns 2008;34:1163–8.
56. Cochran A, Edelman LS, Saffle JR, et al. Self-re-
ported quality of life after electrical and thermal
injury. J Burn Care Rehabil 2004;25(1):61–6.
57. Anzarut A, Chen M, Shankowsky H, et al. Quality-of-
life and outcome predictors following massive burn
injury. Plast Reconstr Surg 2005;116(3):791–7.
58. Cromes GF, Holavanahalli R, Kowalske K, et al.
Predictors of quality of life as measured by the
Burn Specific Health Scale in persons with major
burn injury. J Burn Care Rehabil 2002;23(3):229–34.
59. Esselman PC, Askay S, Carrougher G, et al. Barriers
to return to work after burn injuries. Arch Phys Med
Rehabil 2007;88(Suppl 2):S50–6.
60. Saffle JR, Tuohig GM, Sullivan JJ, et al. Return to
work as a measure of outcome in adults hospitalized
for acute burn treatment. J Burn Care Rehabil 1996;
17(4):353–61.
61. Moi AL, Wentzel-Larsen T, Salemark L, et al. Long-
term risk factors for impaired burn-specific health
and unemployment in patients with thermal injury.
Burns 2007;33:37–45.
62. Baker CP, Russell WJ, Meyer W III, et al. Physical
and psychological rehabilitation outcomes for young
adults burned as children. Arch Phys Med Rehabil
2007;88(12 Suppl 2):S57–64.
63. Druery M, Brown TLH, Muller M. Long term func-
tional outcomes and quality of life following severe
burn injury. Burns 2005;31:692–5.
64. Kildal M, Willebrand M, Andersson G, et al. Coping
strategies, injury characteristics and long-term
outcomes after burn injury. Injury 2005;36:511–8.
65. Noble J, Gomez M, Fish JS. Quality of life and return
to work following electrical injuries. Burns 2006;32:
159–64.
Copyright © 2022 FDOKUMEN