Control of the sugar/ethanol conversion rate during moderate ...
Upload
independentCategory
view
1download
0
JOURNAL OF NEUROTRAUMAVolume 22, Number 3, 2005© Mary Ann Liebert, Inc.Pp. 333–344
Frontal and Temporal Morphometric Findings on MRI inChildren after Moderate to Severe Traumatic Brain Injury
ELISABETH A. WILDE,1 JILL V. HUNTER,4 MARY R. NEWSOME,1RANDALL S. SCHEIBEL,1 ERIN D. BIGLER,5,6,7,8 JAMIE L. JOHNSON,5
MICHAEL A. FEARING,5 HOWARD B. CLEAVINGER,5 XIAOQI LI,1PAUL R. SWANK,9 CLAUDIA PEDROZA,9 GARLAND STALLINGS ROBERSON,1
JOCELYNE BACHEVALIER,10 and HARVEY S. LEVIN1,2,3
ABSTRACT
In vivo MRI volumetric analysis enables investigators to evaluate the extent of tissue loss followingtraumatic brain injury (TBI). However, volumetric studies of pediatric TBI are sparse, and therehave been no volumetric studies to date in children examining specific subregions of the prefrontaland temporal lobes. In this study, MRI volumetry was used to evaluate brain volume differences inthe whole brain, and prefrontal, temporal, and posterior regions of children following moderate tosevere TBI as compared to uninjured children of similar age and demographic characteristics. TheTBI group had significantly reduced whole brain, and prefrontal and temporal regional tissue vol-umes as well as increased cerebrospinal fluid (CSF). Confidence interval testing further revealedgroup differences on gray matter (GM) and white matter (WM) in the superior medial and ven-tromedial prefrontal regions, WM in the lateral frontal region, and GM, WM, and CSF in the tem-poral region. Whole brain volume and total brain GM were reduced, and total ventricular volume,total CSF volume, and ventricle-to-brain ratio (VBR) were increased in the TBI group. Additionalanalyses comparing volumetric data from typically developing children and subgroups of TBI pa-tients with and without regional focal lesions suggested that GM loss in the frontal areas was pri-marily attributable to focal injury, while WM loss in the frontal and temporal lobes was related toboth diffuse and focal injury. Finally, volumetric measures of preserved frontotemporal tissue wererelated to functional recovery as measured by the Glasgow Outcome Scale (adapted for children)with greater tissue preservation predicting better recovery.
Key words: children; frontal lobes; morphometry; MRI; temporal lobes; traumatic brain injury
333
Departments of 1Physical Medicine and Rehabilitation, 2Neurosurgery, and 3Psychiatry, Baylor College of Medicine, Hous-ton, Texas.
4Department of Diagnostic Imaging, Texas Children’s Hospital, Houston, Texas.Departments of 5Psychology and 6Neuroscience, Brigham Young University, Provo, Utah.Departments of 7Radiology and 8Psychiatry, University of Utah, Salt Lake City, Utah.Departments of 9Pediatrics and 10Neurobiology & Anatomy, University of Texas Health Science Center, Houston, Texas.

INTRODUCTION
TRAUMATIC BRAIN INJURY (TBI) is the most commoncause of death and disability among children in the
United States, with an annual incidence of about 70/100,000hospitalizations (Langlois et al., 2003). Despite similar-ities in the mechanisms of primary and secondary injuryassociated with TBI in adults and children (Graham etal., 2002), patient outcome studies (Levin et al., 1992;Adelson and Kochanek, 1998; Kochanek et al., 2000) andanimal models (Bittigau et al., 1999) suggest that the im-mature brain is especially vulnerable to insult. Suscepti-bility to excitotoxicity and hypoxic-ischemic insult arepurportedly greater in developing than in mature neurons(Kochanek et al., 2000), relatively unmyelinated axonsin the young brain are especially vulnerable to traumaticaxonal injury (TAI) (Adelson and Kochanek, 1998;Kochanek et al., 2000), and apoptotic neurodegenerationfollowing trauma is inversely related to age at injury us-ing a rodent weight-drop model (Bittigau et al., 1999).Following injury, it has been proposed that the immaturebrain is also more susceptible to cerebral blood flow dys-regulation (Muizelaar et al., 1989a,b; Grundl et al., 1994;Biagas et al., 1996) and generalized swelling (Bruce etal., 1981; Graham et al., 1989; Aldrich et al., 1992; Gor-rie et al., 2001).
The frontal and temporal lobes are among the areasmost vulnerable to injury in TBI. Neuropathologic (Gra-ham et al., 1989; Graham et al., 2002) and magnetic res-onance imaging (MRI) studies (Levin et al., 1997) havereported an anterocaudal gradient of focal brain lesionsin children sustaining TBI, a finding attributed to prox-imity of the orbitofrontal and anterior temporal regionsto bony protuberances (Graham et al., 2002). Further-more, the frequent impairment of executive function(Levin et al., 1993; Dennis et al., 1996; Anderson et al.,2002), learning and memory (di Stefano et al., 2000), andbehavioral disturbance (Brown et al., 1981; Max et al.,1998) following moderate to severe TBI in children isconsistent with frontotemporal dysfunction.
Volumetric analysis and segmentation of MRI—tech-niques that quantify gray matter (GM), white matter(WM), and cerebrospinal fluid (CSF) of brain regions andwhole brain—enable investigators to evaluate the extentof tissue loss following TBI. However, volumetric MRIstudies of pediatric TBI are sparse (Berryhill et al., 1995;Bigler, 1999; Levin et al., 2000; Verger et al., 2001), re-vealing enlarged ventricles, generalized atrophy (Bigler,1999; Verger et al., 2001), reduced prefrontal cortical vol-ume (Berryhill et al., 1995), and reduced growth of thecorpus callosum over a 36–month period following se-vere, but not mild TBI (Levin et al., 2000). However,there have been no volumetric studies to date in children
examining specific subregions of the prefrontal and tem-poral lobes. Consequently, we (1) compared frontotem-poral and whole brain volumes of children who had sus-tained a moderate to severe TBI at least 1 year earlierwith findings in an age- and gender-matched comparisongroup of uninjured children; (2) examined whether tissueloss following moderate to severe TBI in children wasdisproportionately higher in frontotemporal cortex ascompared to the parieto-occipital cortex; (3) explored therelative contributions of diffuse and focal injury to fron-totemporal volume loss; and (4) evaluated the relationbetween volumetric changes in the frontotemporal areaand functional outcome of pediatric TBI with parallelanalysis of posterior volume.
MATERIALS AND METHODS
Subjects
Sixteen children who had sustained moderate to severeTBI were selected from cohorts in Houston and Dallaswho had been recruited for an ongoing, IRB-approvedproject concerning outcome of pediatric TBI. Inclusioncriteria were TBI arising from closed head trauma witha postresuscitation score of 3–12 on the Glasgow ComaScale (GCS) of Teasdale and Jennett (1974) recorded inthe emergency center, availability for this study at 1 yearor longer postinjury, and consent to undergo MRI. Ad-ditional selection criteria included an Abbreviated InjuryScale (AIS) (Committee on Injury, 1998) score of lessthan 4 for areas of the body other than the head, and nohistory of post-resuscitation hypoxia or hypotension ex-ceeding 30 min in duration. Subject characteristics, in-cluding age, handedness (Oldfield, 1971), and maternaleducation, are summarized in Table 1.
Sixteen typically developing children were recruitedfor the comparison group from the local communitythrough advertising on bulletin boards and selected tomatch the TBI patients on age (within 6 months), gen-der, handedness, and maternal education. All children in-cluded in the study were English-speaking and had nopre-existing head injury, neurologic disorder associatedwith cerebral dysfunction and/or cognitive deficit (e.g.,cerebral palsy, mental retardation, epilepsy), diagnosedlearning disability, psychiatric disorder, or child abuse.
MRI Acquisition
All subjects underwent MRI without sedation onPhilips 1.5-T Intera scanners (Philips, Best, Netherlands)at Texas Children’s Hospital–Houston (TCH) or at theRogers MRI Center, University of Texas SouthwesternMedical Center, Dallas. T1-weighted (T1-w; 15 msec TR,
WILDE ET AL.
334

4.6 msec TE, 1.0-mm slices) and T2-weighted (T2-w;3500 msec TR, 114 msec TE, 1.5-mm slices) three-di-mensional sagittal acquisition series were used for volu-metric analysis of the frontal and temporal areas. A 256-mm field of view (FOV) was used for these series witha reconstructed voxel size of 1 � 1 � 1 mm for the T1-w images and a reconstructed voxel size of 1 � 1 � 1.5mm for the T2-w series. A dual-echo acquisition protondensity/T2-w (2200 msec TR, 20/120 msec TE, 5.0-mmslices) axial sequence was used for whole brain quan-tification. A 240-mm FOV was used with a reconstructedvoxel size of 0.47 � 0.47 � 5.0 mm. Imaging parame-ters included flow compensation and an inferior satura-tion pulse. For lesion analysis, a coronal T2-w fluid at-tenuated inversion recovery (FLAIR) sequence was used(1100 msec TR, 140 msec TE, 5.0-mm slices). For thissequence, a 220-mm FOV was used with a reconstructedvoxel size of 0.86 � 0.86 � 5.0 mm.
Volumetric Analysis
Each data set was imported into ANALYZE 5.0/6.0(Biomedical Imaging Resource, Mayo Foundation,Rochester, MN), converted into a three-dimensional vol-ume, and re-sliced to create 1-mm isovoxels. T1-w andT2-w image sets were co-registered after realignment tothe anterior to posterior commissure (AC-PC) line andthe interhemispheric fissure. Next, interactive manualsegmentation of GM, WM, and CSF was performed us-ing the ANALYZE multispectral tool. To minimize ef-fects of nonuniformity in pixel intensity (i.e., gradient ar-tifact) and to obtain optimal classification within eachregion of interest (ROI), separate segmentation was per-formed for each of three protocols: (1) whole brain, (2)frontal lobe, and (3) temporal lobe. Manual tracings were
performed using ANALYZE trace and editing tools. Fi-nally, volumes (cm3) of GM, WM, and CSF for wholebrain and for each ROI were calculated by summing pix-els designated as GM, WM, or CSF across the slices.
Anatomical Protocols
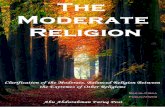
Frontal protocol. Regions of the frontal protocol in-cluded (a) lateral, comprising dorsolateral and ventrolat-eral prefrontal cortex (Brodmann areas (BA) 8, 9, 10, 11,44, 45, 46, 47); (b) superior medial (BA 8, 9, 24, 32); (c)inferior medial (BA 10, 24, 32); (d) orbitofrontal (BA 11,12, 47); and, (e) frontal pole (BA 10). Although (c) and(d) were traced separately, these regions were combinedto obtain the ventromedial region (Fig. 1A). All areas,including the frontal poles, were combined to obtain ameasure of the total prefrontal areas. Bolded numbers in-dicate those Brodmann areas that form a substantial por-tion of the region. Figure 1B depicts a three-dimensionalreconstruction of a typically developing subject’s brainand our tracing of frontal subregions.
A limited number of clearly definable landmarks werechosen to enhance reliability in marking the frontal ar-eas. Although all final tracings were done in the coronalplane, sagittal and axial planes were also utilized to iden-tify anatomic landmarks and to place visual markers to ensure consistent tracings. Briefly, the superior or-bitofrontal (OF) boundary was identified by first view-ing the image in the axial plane to determine the most in-ferior slice in which GM surrounding the olfactory sulciwas continuous through the length of the sulci, therebydefining the gyri recti. On this slice, a line was drawnaround the OF region to create a marker that persistedwhen the images were transposed into the coronal plane.Next, the boundary between superior and inferior medial
MORPHOMETRIC FINDINGS IN PEDIATRIC TBI
335
TABLE 1. DEMOGRAPHIC CHARACTERISTICS OF TBI AND TYPICALLY DEVELOPING GROUPS
TBI group Typically developing children(n � 16) (n � 16)
Age at testing (years) M � 12.9; SD � 2.5; range 9.0–16.8 M � 12.8; SD � 2.4; range 9.0–16.4Age at injury (years) M � 9.75; SD � 3.0; range 3.7–13.8 N/ATime post-injury (years) M � 3.1; SD � 2.4; range 1.0–10.1 N/AGender distribution 8 males, 8 females 8 males, 8 femalesEthnicity distribution 6 Caucasian, 10 African American 6 Caucasian, 6 African-American,
3 Hispanic, 1 AsianMaternal education (years) M � 13.2; SD � 1.8; range 10–17 M � 13.2; SD � 1.6; range 12–16Handedness 14 right-handed, 2 left-handed 14 right-handed, 2 left-handedMechanism of injury 7 auto-pedestrian, 1 auto-bicycle, N/A
(accident type) 5 MVA, 1 motorcycle, 2 RVGlasgow coma score M � 5.7; SD � 2.8; range 3–11 N/A
MVA, motor vehicle accident; RV, recreation vehicle accident; M, mean; SD, standard deviation; N/A, not applicable.

areas was marked by placing a horizontal line originat-ing from the anterior-most aspect of the genu of the cor-pus callosum extending forward on the midsagittal im-age, also forming a marker observed when the ROIs weretraced in the coronal plane. Images were then transferredto the coronal plane. Tracing commenced at the posteriorborder for this protocol, at the slice just anterior to thegenu of the corpus callosum, and proceeded anteriorlyuntil there was no discernible parenchyma. The lateralareas were defined by tracing through the superior frontalsulcus (in the coronal plane) down to the boundary be-tween GM and WM below the sulcus and dropping a ver-tical line to the superior OF boundary. The frontal polewas defined as all tissue anterior to gyrus rectus and me-dial orbital gyri (when no tissue was visible beneath theboundary between the OF areas and the IM areas), withno further attempt to specify subregions, aside from rightor left hemisphere.
We performed initial analyses to determine whetherthere was any appreciable difference when every slicewas measured versus every third slice with a correctionfactor applied to account for the skipped slices. To dothis, we used an intraclass correlation coefficient (ICC)that considered both relative and absolute differences inorder to ensure that differences in the means betweenmethods were also small. Specifically, we used the for-mula ��
2/(��2 � ��
2 � ��2), where ��
2 represents thevariance component for subjects, ��
2 represents the vari-ance component for subject by slice, and ��
2 representsthe variance component for slice (Cronbach et al., 1972;Brennan, 1983). The ICC values for six subjects (threepatients and three typically developing children) in whomevery slice was measured and compared to volumes es-timated from every third slice ranged from 0.92 to 0.99for all subregions. Therefore, we utilized measures ofevery third slice for this study.
Temporal lobe protocol. Whole temporal lobe volumeencompassed portions of BA 20, 21, 22, 25, 27, 28, 34,36, 37, 38, 41, and 42. Tracing for this protocol was donein the coronal plane, and as in the frontal protocol, allthree planes were used to cross check markings. We fol-lowed previously published protocols for the temporallobes, utilizing a protocol that could practicably incor-porate most of the parahippocampal gyrus (Bigler et al.,2002, 2003).
Whole brain protocol. Whole brain volumes were ob-tained using proton density/T2-w image sets. T1-w vol-umes were also referenced to ensure accuracy in distin-guishing brain tissue from other tissue (e.g., dura, skull).Well-established protocols were utilized for measure-ment of all whole brain variables, including GM, WM,
total ventricular CSF, and total brain CSF (Blatter et al.,1997; Bigler et al., 2003), using an image editing toolwithin the ANALYZE software package. We examinedmeasures of total brain WM, total brain GM, and totalbrain CSF, which included both subarachnoid and ven-tricular CSF. Total intracranial volume (TICV) was thesum of total brain (GM and WM) and total CSF volume.The ventricle-to-brain ratio (VBR), which was calculatedby dividing the total ventricular volume by total brainvolume and multiplying by 100, provided an overall mea-sure of atrophy.
Interoperator Reliability
Experienced raters (E.W., M.N., R.S., J.J., M.F.), in-cluding three research neuropsychologists and the chiefresearch technician in a laboratory of volumetric brainimaging, performed segmentation and tracing under thesupervision of both a neuroradiologist (J.H.) and an ex-pert in volumetric imaging (E.B.). Although the raterswere not given information about the group identity ofthe children, the presence of focal brain lesions was in-dicative of the TBI patients. Intra- and interrater relia-bilities were computed on each measure utilized in thefrontal, temporal, and whole brain protocols. In deter-mining reliability, at least six cases (18.75% of the sam-ple) were re-traced by either the same rater (for intraraterreliabilty) or two raters (for interrater reliability). TheICCs of both intra- and interrater reliability exceeded 0.90for all measures used in this study. In calculating thesevalues, we considered only relative error as any absoluteerror would be equal across groups. Specifically, we uti-lized the formula ��
2/(��2 � ��
2), where ��2 represents
the variance component for the subject, and ��2 repre-
sents residual variance.
Posterior Brain Regions
To obtain an estimate of the volume of occipital andparietal cortex, we edited the whole brain volumes to ex-clude the brain stem and cerebellum. From this volumeof total cortex, we then subtracted the frontal and tem-poral areas so that remaining tissue provided an estimateof parietal and occipital lobe volumes. We calculated botha total posterior cortex volume as well as posterior GMand WM volumes.
Lesion Volumes
Areas of signal abnormality were identified and tracedby a board-certified neuroradiologist (J.H.) using FLAIRimages, which facilitate lesion conspicuity and measure-ment (Pierallini et al., 2000). Areas were reported in cm2,summed, and converted to volume measures (area mul-tiplied by slice thickness). Pathologic type and anatomic
WILDE ET AL.
336

locations corresponding to regions that were defined forthe volumetric analysis were recorded.
Assessment of Outcome
The Glasgow Outcome Scale (GOS) of Jennett andBond (1975) was used to assess functional outcome. TheGOS is a five-point categorical scale that includes (1)good recovery, (2) moderate disability, (3) severe dis-ability, (4) persistent vegetative state, and (5) death. Wemodified the criteria for grading the GOS by emphasiz-ing participation in the typical activities of a child (Ap-pendix). The GOS was graded after a mean post-injuryinterval of 830.75 days (SD � 688.53 days; range,151–2845 days) by an experienced examiner based onfindings obtained in an interview with the primary care-giver, available cognitive test data in relation to estimatedpre-injury functioning, and neurologic sequelae such asa motor deficit. Examiners grading the GOS had noknowledge of the brain volumetric findings.
Design and Statistical Analysis
A multivariate analysis approach was used to examinegroup differences in whole brain and regional brain vol-umes. Critical assumptions of multivariate analysis wereexamined using chi-square plots for the ordered distancesto check for multivariate normality and Bartlett’s test toensure equal variance and covariance structure; no es-
sential violations were noted. Multivariate analyses of co-variance (MANCOVA) were used to test the overall ef-fect of group on subregions in each area (i.e., whole brain,prefrontal areas except frontal pole, temporal lobes, pos-terior cortex). Bonferroni simultaneous confidence inter-vals (SCI; 95%) were then used to further examine thecontribution of each variable to the group difference inanalyses where overall group differences for the regionwere significant. Finally, an analysis of covariance (ANCOVA) was used to examine the differences in VBR.In view of age-related change in brain volume (Giedd etal., 1999; Gogtay et al., 2004), age was included as a co-variate in each group.
To evaluate the effect of concomitant lesions on volumeloss measured from MRI, we subdivided the TBI groupinto two subgroups based on focal lesion volume in thefrontal and temporal regions of interest (ROIs): (1) TBI-lesion, children with a total lesion volume of greater than1 cc in the ROI, and (2) TBI–no lesion, children with to-tal lesion volume of less than 1 cc in the ROI. For thefrontal lobes, the TBI–no lesion volume group includedthree children with very small and generally isolated imag-ing abnormalities (no single lesion volume of �0.5 cc) inthe frontal lobes. Since these children had substantiallysmaller lesion volumes than other children in the TBI-le-sion group and to mitigate the possibility that abnormali-ties of this size may represent false positives due to arti-fact, we set the cutoff for inclusion in the TBI-lesion group
MORPHOMETRIC FINDINGS IN PEDIATRIC TBI
337
A B
FIG. 1. Measurement of frontal regions. (A) Coronal slice illustrating eight of the 10 regions included in the frontal protocol:right and left lateral areas (RL and LL, respectively) represented in yellow, superior medial areas (RSM, LSM) represented ingreen, and inferior medial areas (RIM, LIM) and orbitofrontal areas (ROF, LOF), represented in red. The right and left frontalpole areas are not included at this level. (B) Colored/shaded areas of the three-dimensional reconstruction of a subject’s brain de-pict the pre-frontal regions included in volumetric quantification. The frontal pole area has been removed to more clearly viewthe inferior medial and orbitofrontal areas. The square highlights the acquisition plane and level for the coronal slice in A.

to be lesion volume of �1 cc. For the temporal areas, onechild had a single abnormality in the temporal lobes mea-suring 0.189 cc. Again, since this child’s lesion volumewas a clear outlier in relation to other children in the TBI-lesion group, we utilized the same cut-off and includedthat child in the TBI–no lesion group. With TBI-lesion pa-tients differing in the relative involvement of frontal ver-sus temporal areas, two separate univariate ANCOVAs andplanned pair-wise comparisons were utilized with age asa covariate to examine differences between the compari-son group and the two TBI subgroups in (1) percentage ofpreserved frontal WM and GM and (2) percentage of pre-served temporal WM and GM. For this analysis, we con-verted raw volumes to percentages of tissue in the frontaland temporal regions using tissue volume for the regiondivided by the intracranial volume for the region, and mul-tiplied by 100 [e.g., frontotemporal tissue volume/(fron-totemporal tissue volume � frontotemporal CSF) * 100].Using percentages of preserved tissue allowed us to con-trol for differences in head size on volumetric measureswithout decreasing statistical power by using TICV as anadditional covariate.
Finally, we utilized a multinomial logistic regressionmodel (assuming proportional odds) to examine whetherthe GOS score could be predicted by percentage of pre-served tissue in the (1) frontotemporal and (2) posteriorcortex. We again used percentages of preserved tissue inthe frontotemporal and posterior regions for this analy-sis rather than raw volumes for the reason describedabove. Percentage of preserved tissue in the posterior re-gion of the brain was calculated as 100 * [(posterior cor-tex)/(posterior cortex � posterior cortex CSF)].
RESULTS
Demographic Characteristics
The TBI group and the typically developing children didnot significantly differ in gender, age, maternal education,or socioeconomic status, as measured by the SocioeconomicComposite Index (Yeates et al., 1995). However, the groupsdiffered in race/ethnicity (Fisher’s exact p � 0.02). Table 1shows that the groups differed in the number of Asian, His-panic, and African-American children.
MRI Volumetric Findings for Whole Brain,Frontal Lobes, and Temporal Lobes
Mean whole brain and brain region volumes are pre-sented in Table 2 as are the confidence intervals for thedifferences between the comparison group and the TBIpatients. MANCOVA revealed a significant main effect(F(4,26) � 12.87, p � 0.0001) for group, and the 95%
confidence intervals indicated statistically significantgroup differences on total brain volume and whole brainGM, which were decreased in the TBI group, as well astotal CSF, total ventricular volume, and subarachnoidCSF, which were increased in the TBI group (Table 2).Head size tended to differ between the groups (t(30) �1.914, p � 0.065). The ventricle-to-brain ratio (VBR), ameasure of generalized atrophy which inherently controlsfor head size, was also significantly different between thegroups (F(1,29) � 16.86, p � 0.0003), with larger VBRsin the TBI patients (Table 2).
Prefrontal regional volumes (frontal tissue anterior tothe genu of the corpus callosum) were also significantlydifferent in the TBI patients as compared to the uninjuredcomparison group (F(7,23) � 3.65, p � 0.009). Superiormedial GM and WM, lateral frontal WM, and ventro-medial GM and WM were all significantly smaller in theTBI group using 95% confidence interval testing (Table2). In addition, the amount of CSF in the prefrontal ar-eas differed significantly between the groups (Table 2),with TBI patients having increased subarachnoid CSF.MANCOVA also revealed an overall significant dif-ference between the TBI and comparison groups on temporal lobe volumes (F(3,27) � 11.16, p � 0.0001).Again, 95% confidence intervals revealed significant dif-ferences for temporal lobe GM, WM, and CSF, with at-rophic changes evident in the TBI group (Table 2). Fi-nally, MANCOVA did not yield a significant groupdifference for posterior cortex, though there was a ten-dency toward decreased volumes in the TBI group(F(2,28) � 2.83, p � 0.076).
Lesion Volume on MRI
Areas of abnormal signal on MRI were detected in allof the TBI patients, with total lesion size for each childranging from 2.50 to 249.22 cc3 (mean � 67.11 cc3 �89.44). Consistent with lesion findings from MRI stud-ies in adult (Pierallini et al., 2000) and child TBI patients(Levin et al., 1997), the majority of the lesions were inthe frontal (52.8%) and temporal areas (19.5%), and thesealso represent regions with the largest lesion volumes(Table 3). Eighty-nine percent of patients with focalfrontal pathology on MRI exhibited more than one le-sion. The distribution of frontal lesions by tissue com-partment was WM (25% of lesions), GM-WM junction(25%), and GM (50%). The pathology of most lesionswas hemosiderin deposit (56.3%) and gliosis (29.9%).
Analysis of TBI Patient Subgroups with andwithout Lesions
Comparison of subgroups of patients with (n � 6) andwithout (n � 10) total frontal lesion volume of �1 cc and
WILDE ET AL.
338

the uninjured comparison group indicated significantoverall group differences on ANCOVA testing for per-centage of preserved total frontal WM (F(2,28) � 8.07,p � 0.002) and GM (F(2,28) � 6.43, p � 0.005). Pair-
wise comparisons disclosed significant or near-signifi-cant differences on all between-group comparisons forfrontal WM, with the TBI-lesion group having the small-est mean WM volume, followed by the TBI-no lesion
MORPHOMETRIC FINDINGS IN PEDIATRIC TBI
339
TABLE 2. WHOLE BRAIN AND REGIONAL BRAIN VOLUMES
Typically 95%TBI developing p-value Confidence
LS mean (SD), LS mean (SD), (group intervalBrain variable volumes (in cm3) n � 16 n � 16 effect) (UB, LB)
Ventricle-to-brain ratio (VBR) 2.05 (0.96) 1.02 (0.32) �0.001 N/ATotal ventricular 22.60 (11.49) 12.51 (4.28) 0.003 �16.04, �4.14Total whole brain 1082.63 (97.57) 1217.05 (108.27) 0.001 63.61, 205.01Total whole brain gray matter 796.55 (77.26) 884.27 (77.20) 0.003 34.86, 140.82Total whole brain white matter 286.07 (66.36) 332.78 (70.60) 0.054 �0.53, 93.47Total whole brain CSF 122.01 (46.09) 72.00 (33.25) 0.002 �77.50, �22.37Total frontal CSF 26.88 (12.50) 15.03 (7.83) 0.008 �19.34, �4.32Lateral frontal gray matter 41.54 (8.24) 46.10 (7.66) 0.112 �1.18, 10.28Lateral frontal white matter 18.39 (5.85) 23.12 (6.45) 0.037 0.31, 9.18Ventromedial frontal gray matter 20.27 (5.64) 25.58 (4.13) 0.006 1.75, 8.88Ventromedial frontal white matter 7.12 (3.20) 10.67 (3.09) 0.004 1.30, 5.83Superior medial frontal gray matter 26.97 (5.49) 31.74 (5.53) 0.023 0.80, 8.73Superior medial frontal white matter 11.13 (3.77) 14.08 (3.93) 0.040 0.18, 5.72Temporal gray matter 90.88 (11.93) 107.11 (11.27) 0.002 8.87, 23.56Temporal white matter 23.20 (4.51) 32.01 (4.49) �0.001 5.95, 11.64Temporal CSF 12.52 (6.93) 7.34 (1.82) 0.003 �8.38, �1.97Posterior cortex gray matter 504.15 (57.09) 536.46 (57.96) 0.105 N/APosterior cortex white matter 164.43 (52.26) 192.72 (51.02) 0.132 N/ATotal intracranial volume 1204.63 (122.70) 1289.06 (126.82) 0.065 N/A
N/A, CI interval testing not performed since result is from univariate analysis (VBR), post-hoc analysis (TICV) or non-significantMANCOVA (Posterior Cortex GM and WM); UB, upper bound; LB, lower bound.
TABLE 3. NEUROANATOMIC SITE AND LESION VOLUME IN TBI GROUP
Patients with lesionin area, n (%) Mean (SD) Range
Whole brain 16 (100) 67.11 (89.44) 2.50–251.71Right hemisphere 15 (93.8) 17.40 (24.65) 0–73.66Left hemisphere 14 (87.5) 29.47 (53.54) 0–203.12
Total temporal lobes 9 (56.3) 9.32 (25.07) 0–99.36Total frontal lobes 9 (56.3) 28.80 (63.57) 0–219.60
Lateral frontal 6 (37.5) 4.96 (16.66) 0–67.00Superior medial 8 (50) 8.89 (21.34) 0–79.79Ventromedial 5 (31.3) 8.05 (18.73) 0–67.91
Posterior areas 8 (50) 7.81 (15.26) 0–53.82Corpus callosum 4 (25) 0.98 (1.86) 0–5.69Parietal lobes 4 (25) 1.88 (5.23) 0–18.35Occipital lobes 3 (18.8) 1.14 (4.14) 0–16.67Cerebellum 4 (25) 3.21 (8.18) 0–28.84Brain stem 0 (0) N/A N/A
Lesion volume for area (cc)

group (comparison group vs. TBI-lesion, p � 0.001;Comparison group versus TBI–no lesion, p � 0.042; TBIlesion vs. TBI–no lesion, p � 0.062). However, pair-wisecomparisons of frontal GM revealed significant groupdifferences between the comparison and TBI-lesiongroups (p � 0.001) and between TBI-lesion and TBI–nolesion groups (p � 0.033), but not between the compar-ison group and TBI–no lesion groups (p � 0.186). Sim-ilar to the pattern observed in frontal WM, the TBI-le-sion group demonstrated the smallest percentage ofpreserved frontal GM, followed by the TBI–no lesionGroup (Fig. 2A,B).
Similarly, comparison of subgroups of children with(n � 8) and without (n � 8) temporal lesions indicated asignificant group difference on ANOVA testing for tem-poral WM (F(2,28) � 10.08, p � 0.0005), with the TBI-lesion group demonstrating the smallest percentage ofpreserved tissue, followed by the TBI-no lesion group.Pair-wise testing indicated significant differences in tem-poral lobe WM between the uninjured and TBI-lesiongroups (p � 0.004) as well as between the comparisongroup and the TBI–no lesion patients (p � 0.0004). Therewas no significant overall group difference in volume oftemporal GM despite a tendency for reduced percentageof preserved tissue in the TBI-lesion patients relative tothe comparison group (Fig. 2A,B).
Outcome of TBI in Relation to Brain Regional Volumes
Multinomial logistic regression indicated that percent-age of frontotemporal tissue predicted the GOS score(�2 � 6.69, df � 2, p � 0.035), with greater frontotempo-ral tissue percentage associated with better recovery (Fig.3A). However, the percentage of preserved posterior braintissue did not contribute significantly as a predictor of GOSscore (�2 � 0.706, df � 2, p � 0.703; Fig. 3B).
DISCUSSION
Whole Brain and Frontotemporal Volume Lossfollowing TBI
Our findings show a reduction in whole brain, ventro-medial frontal, superior medial frontal, lateral frontal, andtemporal lobe volumes at 1–10 years following moder-ate to severe TBI in children. VBR, a measure of gen-eralized cerebral atrophy, and CSF volume were consis-tently increased in the TBI patients, indicating degener-ative changes (Anderson et al., 1995; Bigler, 2001; Gra-ham et al., 2002). Despite variation in age, lesion size,and total intracranial volume, the group differences re-flect a generalized brain volume loss in TBI patients.
Our findings of reduced WM and GM are consistentwith volumetric studies of both adult TBI and experi-mental models of TBI. Diffuse white matter degenera-tion (Gale et al., 1995) and decreased temporal lobe WM(Bigler et al., 2002) have been identified in volumetricstudies of adults sustaining moderate and severe TBI. Al-though volumetric analysis of MRI in children followingTBI has shown enlarged ventricles, generalized atrophy(Bigler, 1999; Verger et al., 2001), reduced prefrontalcortical volume (Berryhill et al., 1995), and diminishedgrowth of the corpus callosum (Levin et al., 2000), thesestudies have not differentiated the contributions of focallesions from diffuse injury to volume loss, and theylacked a matched group of uninjured children.
In the experimental literature, the fluid percussion (FP)model of TBI in rodents has produced loss of ipsilateralGM at 2 months postinjury, involving the cerebral cor-tex, thalamus, dentate gyrus, and hippocampus with en-largement of the ipsilateral lateral ventricle (Bramlett etal., 1997). Serial findings up to 1 year following FP in-jury have documented progressive loss of GM volume,including cerebral cortex and hippocampus (Smith et al.,1997). Although histopathological findings following FPbrain injury have emphasized GM, ipsilateral WM loss
WILDE ET AL.
340
FIG. 2. Comparison of GM and WM differences between typically developing children and those with and without focallesions in the area of interest. Bar graphs demonstrating the meandifference in percentage of preserved GM (A) or WM (B) be-tween typically developing children and TBI patients with andwithout lesions in the area of interest (frontal or temporal areas).
A
B

specific to the external capsule and cerebral pedunclewere found at 1 year postinjury (Bramlett and Dietrich,2002), and widespread WM damage throughout the ipsi-lateral hemisphere has also been demonstrated as earlyas 14–35 days post-injury in rodents (Carbonell andGrady, 1999).
Specificity of Frontotemporal Volume Loss
In addition to global degenerative changes, we alsofound a selective vulnerability for frontotemporal tissueloss in these children as MRI demonstrated a higher fre-quency and larger volume of frontotemporal lesions rel-ative to more posterior sites. Finally, the percentage ofpreserved frontotemporal tissue predicted the GOS score,whereas percentage of preserved posterior cortex was un-related to outcome. With frontal lesions frequently pre-sent in our sample, it may be that regional difference inpredicting the GOS may simply reflect more frequent fo-cal injury in the frontal lobes. Although our sample sizeprecluded a more detailed analysis of lesion size and lo-cation in relation to brain volume change in other areassuch as the posterior regions of the brain, this issue mer-its further study given recent evidence for region-specific
cortical thinning in the FP brain injury model (Bramlettand Dietrich, 2002).
Focal Lesion versus Diffuse Injury
While limitations of this initial study (e.g., small sam-ple size, heterogeneity of post-injury interval, and age atinjury) preclude definitive conclusions regarding the rel-ative impact of focal versus diffuse injury on subsequentbrain region volume, our MRI data revealed a degree ofdissociation between the effects of focal lesions on thevolume of GM as compared with WM. Lesion presencein the frontal and/or temporal lobes appeared to account,at least in part, for GM loss in the frontotemporal regionsbecause a significant difference in GM volume was notfound between the TBI–no lesion and typically develop-ing children in either frontal or temporal lobes. Addi-tionally, the significant difference between the TBI-le-sion and TBI–no lesion groups on frontal GM supportsthis conclusion. This is consistent with findings from ex-perimental rodent models of pediatric TBI, where mini-mal GM glial swelling underlying the site of impact wasobserved on histopathologic study (Adelson et al., 2001).Therefore, although GM may be damaged during injury,the effects appear to remain relatively focal as opposedto the more far-reaching impact of WM injury.
The findings reported by Adelson et al. (2001) for im-mature animals indicate axonal degeneration and diffuseinjury to WM. Similarly, in our study, the presence offocal concomitant lesions could not fully account for re-gional volume changes in frontal or temporal WM, whichwe found to be reduced in both the TBI-lesion andTBI–no lesion groups relative to findings in typically de-veloping children. A recent study (Tong et al., 2004) using high-resolution, susceptibility-weighted imaging(SWI) within 2 weeks after TBI in children showed thatthe number and volume of small hemorrhagic lesionswere strongly related to the initial GCS score and to out-come at 6–12 months postinjury. Tong et al. (2004) in-terpreted these lesions as markers of traumatic axonal in-jury (TAI). Although 56% of the lesions we identified atleast 1 year postinjury were interpreted as hemosiderindeposits, longitudinal investigation using SWI is neces-sary to determine whether these lesions are similar tothose observed acutely by Tong et al. (2004). Progres-sive axonal pathology (Povlishock, 1992) and myelin de-generation (Bramlett and Dietrich, 2002) are candidatemechanisms to explain the WM changes in the presentstudy, especially in view of the severe impairment of con-sciousness in most of our patients following motor vehi-cle and pedestrian–motor vehicle injury (Adams et al.,1982). Such severe impairment of consciousness isknown to be associated with diffuse axonal injury(Adams et al., 1982; Gennarelli et al., 1982; Meythaler
MORPHOMETRIC FINDINGS IN PEDIATRIC TBI
341
A
B
FIG. 3. Atrophic volumetric change and GOS score. Box-plots indicating the percentage of preserved frontotemporal (A)and posterior (B) tissue in comparison group children (n � 16)and TBI patients with Good Recovery (n � 6), Moderate Dis-ability (n � 8), and Severe Disability (n � 2) ratings on theGOS. Horizontal bars within the boxes represent means.

et al., 2001). In comparison with the effects of TBI inadults, the children in our study sustained TAI during aperiod of developmental axonal connectivity (Gogtay etal., 2004). Longitudinal investigation using alternativeimaging sequences such as diffusion tensor imaging mayfurther elucidate the impact of TBI in children on the de-velopmental course of myelination.
Level of Recovery following Injury
Volumetric measures of frontotemporal tissue predictedlevel of outcome, as measured by the GOS, with betterrecovery associated with greater volume. This is consis-tent with previous evidence indicating a relationship be-tween frontal lesion volume and functional recovery us-ing the Disability Rating Scale score at 1 year post-injuryin adults (Pierallini et al., 2000). Interestingly, in our studythere was no significant relationship between outcome asmeasured by the GOS and percentage of preserved tissuein the posterior cortex. This finding could be due to thehigher frequency of lesions in the frontotemporal regionof our patients. Another possibility is that disproportion-ate damage to the frontotemporal areas may result in spe-cific cognitive and behavioral difficulties that render chil-dren less able than adults to adapt following brain injury.These also represent important areas for further study.
Limitations of the Study and Future Directions
Limitations of this study include the cross-sectional de-sign, small sample size, and heterogeneity in gender, ageat injury, and post-injury interval. We also acknowledgethat mild TBI was not included in the study design, andwe caution against extrapolating our findings to intentionalinjury or injury caused by falls. Apart from these limita-tions, we posit that morphometric study of MRI in pedi-atric TBI could also be applied to clinical trials to evalu-ate the effects of interventions and to understand the effectsof TBI on brain maturation. Brain morphometric study ofchildren after TBI could also provide a bridge to experi-mental pediatric brain models (Prins and Hovda, 2003) andenhance understanding of brain–behavior relationships inchildren with TBI, given previous findings of a relation-ship between volumetric measures of frontal tissue andcognitive function (Reiss et al., 1996; Sowell et al., 2001;Castellanos et al., 2002). Despite the aforementioned lim-itations, this is the first study to demonstrate quantitativebrain regional volumetric changes in pediatric TBI rela-tive to age-matched, typically developing children.
ACKNOWLEDGMENTS
This study was supported in part by NIH grants NS-21889 and U19 HD035476 and a grant from the Ira Ful-
ton Foundation. We gratefully acknowledge the contri-butions of Stacey Martin and JoAnn Petrie in manuscriptassistance and the technical expertise of Tracy J. Abild-skov, David Chu, Ph.D., and Stephen R. McCauley,Ph.D.
APPENDIX A: GLASGOW OUTCOMESCALE, WITH SPECIFIC CRITERIA FOR RATING THE FUNCTIONING
OF CHILDREN
1. Good recoverya. If child has returned to school and is performing at
the preinjury level in the same curriculum (e.g., reg-ular classes), and
b. Child is exhibiting psychosocial adjustment similarto pre-injury level, taking age-related expectationsinto account, e.g., leisure activities/hobbies main-tained; family/social relations maintained, and
c. Child is exhibiting no disability due to focal neu-rological deficit.
2. Moderate disabilitya. If child has been assigned to special education/ re-
source classes (or now needs curriculum modifica-tions in regular classes) which were not neededprior to injury, or
b. Child has developed a new behavioral disturbancewhich was not present before the injury but can bemanaged through outpatient treatment, or
c. Child has partial disability due to neurologicaldeficits which limits activities.
3. Severely disableda. If child is unable to participate in full-time studies
due to a neurobehavioral disturbance, orb. Child requires psychiatric hospitalization or pro-
longed neurobehavioral rehabilitation dictated bybehavior or physical problems which were not pres-ent before the injury, or
c. Child requires chronic institutionalization or con-finement to home (homebound instruction) due todevastating neurological deficit, receives intensivehome care, and is dependent for daily support.
4. Vegetative Statea. Child exhibits an absence of cortical function, e.g.,
does not speak, does not have meaningful contactwith other persons, is unresponsive. Child may openeyes, or have sleep/wake cycles.
5. Deatha. If child died as a direct result of brain trauma, orb. Child regained consciousness, and then died there-
after from secondary complications or other causes.
WILDE ET AL.
342

REFERENCES
ADAMS, J.H., GRAHAM, D.I., MURRAY, L.S., and SCOTT,G. (1982). Diffuse axonal injury due to nonmissile head injuryin humans: an analysis of 45 cases. Ann. Neurol. 12, 557–563.
ADELSON, P.D., and KOCHANEK, P.M. (1998). Head injuryin children. J. Child Neurol. 13, 2–15.
ADELSON, P.D., JENKINS, L.W., HAMILTON, R.L., RO-BICHAUD, P., TRAN, M.P., and KOCHANEK, P.M.(2001). Histopathologic response of the immature rat to dif-fuse traumatic brain injury. J. Neurotrauma 18, 967–976.
ALDRICH, E.F., EISENBERG, H.M., SAYDJARI, C., et al.(1992). Diffuse brain swelling in severely head-injured chil-dren. A report from the NIH Traumatic Coma Data Bank. J.Neurosurg. 76, 450–454.
ANDERSON, C.V., BIGLER, E.D., and BLATTER, D.D.(1995). Frontal lobe lesions, diffuse damage, and neuropsy-chological functioning in traumatic brain-injured patients. JClin Exp Neuropsychol. 17, 900–908.
ANDERSON, V., LEVIN, H.S., and JACOBS, R. (2002). Ex-ecutive functions following frontal lobe injury: a develop-mental perspective, in: Principles of Frontal Lobe Function.D.T. Stuss and R.T. Knight (eds), Oxford University Press:New York, pps. 504–527.
BERRYHILL, P., LILLY, M., LEVIN, H.S., et al. (1995).Frontal lobe changes after severe diffuse closed head injuryin children: A volumetric study of magnetic resonance imag-ing. Neurosurgery 37, 392–399.
BIAGAS, K.V., GRUNDL, P.D., KOCHANEK, P.M., SCHID-ING, J.K., and NEMOTO, E.M. (1996). Posttraumatic hyper-emia in immature, mature, and aged rats: autoradiographic de-termination of cerebral blood flow. J. Neurotrauma 13, 189–200.
BIGLER, E.D. (1999). Neuroimaging in pediatric traumatic headinjury: diagnostic considerations and relationships to neu-robehavioral outcome. J. Head Trauma Rehabil. 14, 406–423.
BIGLER, E.D. (2001). Quantitative magnetic resonance imagingin traumatic brain injury. J. Head Traum Rehabil. 16, 117–134.
BIGLER, E.D., ANDERSON, C.V., and BLATTER, D.D.(2002). Temporal lobe morphology in normal aging and trau-matic brain injury. AJNR Am. J. Neuroradiol. 23, 255–266.
BIGLER, E.D., TATE, D.F., NEELEY, E.S., et al. (2003).Temporal lobe, autism and macrocephaly. AJNR Am. J. Neu-roradiol. 24, 2066–2076.
BITTIGAU, P., SIFRINGER, M., POHL, D., et al. (1999).Apoptotic neurodegeneration following trauma is markedlyenhanced in the immature brain. Ann. Neurol. 45, 724–735.
BLATTER, D.D., BIGLER, E.D., GALE, S.D., et al. (1997).MR-based brain and cerebrospinal fluid measurement aftertraumatic brain injury: correlation with neuropsychologicaloutcome. AJNR Am. J. Neuroradiol. 18, 1–10.
BRAMLETT, H.M., and DIETRICH, W.D. (2002). Quanti-tative structural changes in white and gray matter 1 year fol-
lowing traumatic brain injury in rats. Acta Neuropathol.(Berl).103, 607–614.
BRAMLETT, H.M., DIETRICH, W.D., GREEN, E.J., andBUSTO, R. (1997). Chronic histopathological consequencesof fluid-percussion brain injury in rats: effects of post-trau-matic hypothermia. Acta Neuropathol. (Berl). 93, 190–199.
BRENNAN, R.L. (1983). Elements of Generalizability Theory.ACT Publications: Iowa City, IA.
BROWN, G., CHADWICK, O., SHAFFER, D., RUTTER, M.,and TRAUB, M. (1981). A prospective study of children withhead injuries: III. Psychiatric sequelae. Psychol. Med. 11, 63–78.
BRUCE, D.A., ALAVI, A., BILANIUK, L., DOLINSKAS, C.,OBRIST, W., and UZZELL, B. (1981). Diffuse cerebralswelling following head injuries in children: the syndromeof “malignant brain edema.” J. Neurosurg. 54, 170–178.
CARBONELL, W.S., and GRADY, M.S. (1999). Regional andtemporal characterization of neuronal, glial, and axonal re-sponse after traumatic brain injury in the mouse. Acta Neu-ropathol. (Berl). 98, 396–406.
CASTELLANOS, F.X., LEE, P.P., SHARP, W., et al. (2002).Developmental trajectories of brain volume abnormalities inchildren and adolescents with attention-deficit/hyperactivitydisorder. JAMA 288, 1740–1748.
COMMITTEE ON INJURY. (1998). Abbreviated Injury Scale.Association for the Advancement of Automotive Medicine:Barrington, IL.
CRONBACH, L.J., GLESER, G.C., NANDA, H., and RA-JARATNAM, N. (1972). The Dependability of BehavioralMeasurement: Theory of Generalizability for Scores andProfiles. John Wiley & Sons, Inc.: New York.
DENNIS, M., BARNES, M.A., DONNELLY, R.E., WILKIN-SON, M., and HUMPHREYS, R.P. (1996). Appraising andmanaging knowledge: metacognitive skills after childhoodhead injury. Dev. Neuropsychol. 12, 77–103.
DI STEFANO, G., BACHEVALIER, J., LEVIN, H.S., SONG,J.X., SCHEIBEL, R.S., and FLETCHER, J.M. (2000). Vol-ume of focal brain lesions and hippocampal formation in re-lation to memory function after closed head injury in chil-dren. J. Neurol. Neurosurg. Psychiatry 69, 210–216.
GALE, S.D., JOHNSON, S.C., BIGLER, E.D., and BLATTER,D.D. (1995). Nonspecific white matter degeneration fol-lowing traumatic brain injury. J. Int. Neuropsychol. Soc. 1,17–28.
GENNARELLI, T.A., THIBAULT, L.E., ADAMS, H., GRA-HAM, D.I., THOMPSON, C.J., and MARCINCIN, R.P.(1982). Diffuse axonal injury and traumatic coma in the pri-mate. Ann. Neurol. 12, 564–574.
GIEDD, J.N., BLUMENTHAL, J., JEFFRIES, N.O., et al.(1999). Brain development during childhood and adoles-cence: a longitudinal MRI study. Nat. Neurosci. 2, 861–863.
GOGTAY, N., GIEDD, J.N., LUSK, L., et al. (2004). Dynamicmapping of human cortical development during childhood
MORPHOMETRIC FINDINGS IN PEDIATRIC TBI
343

through early adulthood. Proc. Natl. Acad. Sci. U.S.A. 101,8174–8179.
GORRIE, C., DUFLOU, J., BROWN, J., GIBSON, T., andWAITE, P.M. (2001). Extent and distribution of vascular braininjury in pediatric road fatalities. J. Neurotrauma 18, 849–860.
GRAHAM, D.I., FORD, I., ADAMS, J.H., et al. (1989). Fatalhead injury in children. J. Clin. Pathol. 42, 18–22.
GRAHAM, D.I., GENNARELLI, T.A., and MCINTOSH, T.K.(2002). Trauma, in: Greenfield’s Neuropathology, Vol. 2. D.I.Graham and P.L. Lantos (eds), Oxford University Press: NewYork, pps. 823–898.
GRUNDL, P.D., BIAGAS, K.V., KOCHANEK, P.M., SCHID-ING, J.K., BARMADA, M.A., and NEMOTO, E.M. (1994).Early cerebrovascular response to head injury in immatureand mature rats. J. Neurotrauma 11, 135–148.
JENNETT, B., and BOND, M. (1975). Assessment of outcomeafter severe brain damage. Lancet 1, 480–484.
KOCHANEK, P.M., CLARK, R.S.B., RUPPEL, R.A., et al.(2000). Biochemical, cellular, and molecular mechanisms inthe evolution of secondary damage after severe traumaticbrain injury in infants and children: Lessons learned from thebedside. Pediatr. Crit. Care Med. 1, 4–19.
LANGLOIS, J.A., KEGLER, S.R., BUTLER, J.A., et al.(2003). Traumatic brain injury-related hospital discharges.MMWR Surv. Summ. 52, 1–18.
LEVIN, H.S., ALDRICH, E.F., SAYDJARI, C., et al. (1992).Severe head injury in children: experience of the TraumaticComa Data Bank. Neurosurgery 31, 435–443.
LEVIN, H.S., BENAVIDEZ, D.A., VERGER-MAESTRE, K.,et al. (2000). Reduction of corpus callosum growth after severe traumatic brain injury in children. Neurology 54,647–653.
LEVIN, H.S., CULHANE, K.A., MENDELSOHN, D., et al.(1993). Cognition in relation to magnetic resonance imagingin head injured children and adolescents. Arch. Neurol. 50,897–905.
LEVIN, H.S., MENDELSOHN, D., LILLY, M.A., et al. (1997).Magnetic resonance imaging in relation to functional out-come of pediatric closed head injury: a test of the Ommaya-Gennarelli model. Neurosurgery 40, 432–440.
MAX, J.E., KOELE, S.L., SMITH, W.L., JR., et al. (1998). Psy-chiatric disorders in children and adolescents after severetraumatic brain injury: a controlled study. J. Am. Acad. ChildAdolesc. Psychiatry 37, 832–840.
MEYTHALER, J.M., PEDUZZI, J.D., ELEFTHERIOU, E.,and NOVACK, T.A. (2001). Current concepts: diffuse ax-onal injury–associated traumatic brain injury. Arch. Phys.Med. Rehabil. 82, 1461–1471.
MUIZELAAR, J.P., MARMAROU, A., DESALLES, A.A., etal. (1989a). Cerebral blood flow and metabolism in severely
head-injured children. Part 1: Relationship with GCS score,outcome, ICP, and PVI. J. Neurosurg. 71, 63–71.
MUIZELAAR, J.P., WARD, J.D., MARMAROU, A.,NEWLON, P.G., and WACHI, A. (1989b). Cerebral bloodflow and metabolism in severely head-injured children. Part2: Autoregulation. J. Neurosurg. 71, 72–76.
OLDFIELD, R.C. (1971). The assessment and analysis of handedness: the Edinburgh inventory. Neuropsychologia 9,97–113.
PIERALLINI, A., PANTANO, P., FANTOZZI, L.M., et al.(2000). Correlation between MRI findings and long-term out-come in patients with severe brain trauma. Neuroradiology42, 860–867.
POVLISHOCK, J.T. (1992). Traumatically induced axonal in-jury: pathogenesis and pathobiological implications. BrainPathol. 2, 1–12.
PRINS, M.L., and HOVDA, D.A. (2003). Developing experi-mental models to address traumatic brain injury in children.J. Neurotrauma 20, 123–137.
REISS, A.L., ABRAMS, M.T., SINGER, H.S., ROSS, J.L., andDENCKLA, M.B. (1996). Brain development, gender, andIQ in children. A volumetric impact study. Brain 119,1763–1774.
SMITH, D.H., CHEN, X.H., PIERCE, J.E., et al. (1997). Pro-gressive atrophy and neuron death for one year followingbrain trauma in the rat. J. Neurotrauma 14, 715–727.
SOWELL, E.R., DELIS, D., STILES, J., and JERNIGAN, T.L.(2001). Improved memory functioning and frontal lobe mat-uration between childhood and adolescence: a structural MRIstudy. J. Int. Neuropsychol. Soc. 7, 312–322.
TEASDALE, G., and JENNETT, B. (1974). Assessment of comaand impaired consciousness. A practical scale. Lancet 2, 81–84.
TONG, K.A., ASHWAL, S., HOLSHOUSER, B.A., et al.(2004). Diffuse axonal injury in children: clinical correlationwith hemorrhagic lesions. Ann. Neurol. 56, 36–50.
VERGER, K., JUNQUE, C., LEVIN, H.S., et al. (2001). Cor-relation of atrophy measures on MRI with neuropsycholog-ical sequelae in children and adolescents with traumatic braininjury. Brain Inj. 15, 211–221.
YEATES, K.O., BLUMENSTEIN, E., PATTERSON, C.M., andDELIS, D.C. (1995). Verbal learning and memory followingpediatric closed-head injury. J. Int. Neuropsychol. Soc. 1, 78–87.
Address reprint requests to:Harvey S. Levin, Ph.D.
Cognitive Neuroscience Laboratory6560 Fannin St., Ste. 1144, Box 67
Houston, TX 77030
E-mail: [email protected]
WILDE ET AL.
344
Copyright © 2022 FDOKUMEN