Moderate hyperhomocysteinaemia and immune activation in Parkinson's disease
8
Moderate hyperhomocysteinaemia and immune activation in patients with rheumatoid arthritis Katharina Schroecksnadel a , Barbara Frick a , Sabine Kaser b , Barbara Wirleitner a , Maximilian Ledochowski b , Erich Mur b , Manfred Herold b , Dietmar Fuchs a,c, * a Institute of Medical Chemistry and Biochemistry, University of Innsbruck, Fritz Pregl Strasse 3, A-6020 Innsbruck, Austria b Department of Internal Medicine, Leopold Franzens University of Innsbruck, Innsbruck, Austria c Ludwig-Boltzmann Institute of AIDS Research, Innsbruck, Austria Received in revised form 22 August 2003; accepted 5 September 2003 Abstract Background: Moderate hyperhomocysteinaemia related to folate deficiency has been described in patients with cardiovascular risk and also in patients with autoimmune diseases including rheumatoid arthritis (RA). Methods: In 33 patients with RA, serum concentrations of homocysteine and cysteine, of B-vitamins folate and vitamin B 12 , and of immune activation markers neopterin and soluble 75-kDa TNF-receptor (sTNF-R75) were measured. Results: A significant proportion of patients presented with elevated homocysteine and cysteine concentrations in comparison to reference ranges of healthy control persons. Moderate hyperhomocysteinaemia coincided with decreased serum folate and with higher concentrations of sTNF-R75 and neopterin, but it was rather independent from methotrexate (MTX) therapy. Conclusions: The coincidence of higher homocysteine and lower folate concentrations with increased concentrations of immune activation markers in patients with RA suggests that immune activation could be involved in the development of hyperhomocysteinaemia. D 2003 Elsevier B.V. All rights reserved. Keywords: Rheumatoid arthritis; Homocysteine; Immune activation; Neopterin; Oxidative stress; Vitamin deficiency 1. Introduction Moderate hyperhomocysteinaemia has been estab- lished as an independent risk factor for atherosclerosis and other vascular diseases [1]. Moderate hyperho- mocysteinaemia is also common in autoimmune dis- eases, e.g., rheumatoid arthritis (RA) [2,3], Behcet’s disease [4], and Raynaud’s phenomenon [5]. Hyper- homocysteinaemia in patients with RA is often asso- ciated with folate and vitamin B 12 deficiency [2]. Methotrexate (MTX), a cytostatic drug frequently used for the treatment of RA, could increase homo- cysteine by interfering with folate metabolism and thereby blocking methionine synthesis from homo- cysteine [6,7]. Folate supplementation in patients with RA being treated with MTX is able to decrease homocysteine concentrations [8,9]. 0009-8981/$ - see front matter D 2003 Elsevier B.V. All rights reserved. doi:10.1016/j.cccn.2003.09.003 * Corresponding author. Institute of Medical Chemistry and Biochemistry, University of Innsbruck, Fritz Pregl Strasse 3, A- 6020 Innsbruck, Austria. Tel.: +43-512-507-3519; fax: +43-512- 507-2865. E-mail address: [email protected] (D. Fuchs). www.elsevier.com/locate/clinchim Clinica Chimica Acta 338 (2003) 157 – 164
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Moderate hyperhomocysteinaemia and immune activation in Parkinson's disease

www.elsevier.com/locate/clinchim
Clinica Chimica Acta 338 (2003) 157–164
Moderate hyperhomocysteinaemia and immune activation in
patients with rheumatoid arthritis
Katharina Schroecksnadela, Barbara Fricka, Sabine Kaserb, Barbara Wirleitnera,Maximilian Ledochowskib, Erich Murb, Manfred Heroldb, Dietmar Fuchsa,c,*
a Institute of Medical Chemistry and Biochemistry, University of Innsbruck, Fritz Pregl Strasse 3, A-6020 Innsbruck, AustriabDepartment of Internal Medicine, Leopold Franzens University of Innsbruck, Innsbruck, Austria
cLudwig-Boltzmann Institute of AIDS Research, Innsbruck, Austria
Received in revised form 22 August 2003; accepted 5 September 2003
Abstract
Background: Moderate hyperhomocysteinaemia related to folate deficiency has been described in patients with
cardiovascular risk and also in patients with autoimmune diseases including rheumatoid arthritis (RA). Methods: In 33
patients with RA, serum concentrations of homocysteine and cysteine, of B-vitamins folate and vitamin B12, and of immune
activation markers neopterin and soluble 75-kDa TNF-receptor (sTNF-R75) were measured. Results: A significant proportion of
patients presented with elevated homocysteine and cysteine concentrations in comparison to reference ranges of healthy control
persons. Moderate hyperhomocysteinaemia coincided with decreased serum folate and with higher concentrations of sTNF-R75
and neopterin, but it was rather independent from methotrexate (MTX) therapy. Conclusions: The coincidence of higher
homocysteine and lower folate concentrations with increased concentrations of immune activation markers in patients with RA
suggests that immune activation could be involved in the development of hyperhomocysteinaemia.
D 2003 Elsevier B.V. All rights reserved.
Keywords: Rheumatoid arthritis; Homocysteine; Immune activation; Neopterin; Oxidative stress; Vitamin deficiency
1. Introduction
Moderate hyperhomocysteinaemia has been estab-
lished as an independent risk factor for atherosclerosis
and other vascular diseases [1]. Moderate hyperho-
mocysteinaemia is also common in autoimmune dis-
0009-8981/$ - see front matter D 2003 Elsevier B.V. All rights reserved.
doi:10.1016/j.cccn.2003.09.003
* Corresponding author. Institute of Medical Chemistry and
Biochemistry, University of Innsbruck, Fritz Pregl Strasse 3, A-
6020 Innsbruck, Austria. Tel.: +43-512-507-3519; fax: +43-512-
507-2865.
E-mail address: [email protected] (D. Fuchs).
eases, e.g., rheumatoid arthritis (RA) [2,3], Behcet’s
disease [4], and Raynaud’s phenomenon [5]. Hyper-
homocysteinaemia in patients with RA is often asso-
ciated with folate and vitamin B12 deficiency [2].
Methotrexate (MTX), a cytostatic drug frequently
used for the treatment of RA, could increase homo-
cysteine by interfering with folate metabolism and
thereby blocking methionine synthesis from homo-
cysteine [6,7]. Folate supplementation in patients with
RA being treated with MTX is able to decrease
homocysteine concentrations [8,9].

K. Schroecksnadel et al. / Clinica Chimica Acta 338 (2003) 157–164158
A relationship between increased homocysteine
concentrations, antiphospholipid antibodies and
thrombotic events was demonstrated in patients with
RA [10]. Although the pathogenesis of RA is still
unclear, the activation of T-lymphocytes and macro-
phages and the production of cytokines seem to play a
crucial role in the initiation and perpetuation of the
disease [11]. Recently, it has been demonstrated that
serum soluble markers of immune activation like
soluble cytokine receptors, e.g., sTNF-R [12–14]
and sIL-2R [14–18], or neopterin [19,20], are raised
in patients with RA, correlating well with disease
activity. On the other hand, homocysteine was found
to accumulate in supernatants of stimulated peripheral
blood mononuclear cells [21] indicating that immune
activation can be responsible for the development of
hyperhomocysteinaemia.
In this study, serum concentrations of homocys-
teine and cysteine were measured in patients with RA
and were compared to B vitamin status and to con-
centrations of immune activation markers sTNF-R75
and neopterin.
2. Materials and methods
Thirty-one women and two men (mean age: 56.9
yearsF 9.2, range: 37–77 years) with RA were
recruited from the University Hospital of Innsbruck.
Diagnosis was based on the Steinbrocker criteria.
According to these criteria, 15 patients suffered from
RA stage 2, the other 18 patients were classified as
stage 3. All 33 patients with RA were under therapy
Table 1
Treatment of 33 patients with rheumatoid arthritis
NSAIDs (Diclofenac: 25–100 mg/day;
Meloxicam/Lomoxicam: 4–15 mg/day;
Rheumotrop: 60–90 mg/day;
Ibuprofen: 300–600 mg/day)
Steroids (Methyl-prednisolone: 1–8 mg/day)
Immunosuppressants (Methotrexate: 2.5–15 mg/week;
Cyclosporin A: 50–100 mg/day; Leflunomide: 20 mg/day;
Azathioprin: 100 mg; Sulfasalazine: 1000–1500 mg/day)
Opioids: (Tramadol 50–200 mg/day)
NSAIDs = non-steroidal anti-inflammatory drugs.
(see details in Table 1). Of 21 patients treated with
MTX, 10 were supplemented with 6 or 7.5 mg/week
folate, all other patients did not receive vitamin
supplementation within their treatment regimen.
Patients were asked to keep a record of their diet
(normal diet, no adaptation of their normal eating
habits), and according to these records, vitamin intake
was calculated. Patients gave informed consent to
participate in this study, which was approved by the
local ethics committee.
Pregnant women and women in the puerperium,
patients with malignant diseases or clinical relevant
gastrointestinal, renal, hepatic, cardiorespiratoric, hae-
matological, neurological, or psychiatric diseases as
well as patients with metabolic disorders or chronic
infections were excluded from the study.
Blood samples from patients were obtained within
the scope of routine blood examinations and centri-
fuged immediately, sera were stored at � 20 jC for
later analysis. Total homocysteine and cysteine were
measured by reversed phase high-performance liquid
chromatography (HPLC). Sixty microliters of speci-
mens was used, and after reduction with tris-(2-
carboxylethyl)-phosphine (TCEP) and derivatization
with ammonium-7-fluorobenzo-2-oxa-1,3-diazole-4-
sulfonate (SBD-F), separation was performed using
a 55-mm cartridge, RP18 LiChroCART 55-4 and RP18precolumns (Merck, Darmstadt, Germany). Homocys-
teine and cysteine concentrations were monitored by
fluorescence detection at 385 nm excitation wave-
length and 515 nm emission wavelength [22].
For the determination of concentrations of folate
and vitamin B12 double-labelled radioimmunoassay
No therapy Therapy on
demand
Regular
therapy
13 12 8
6 23 4
6 0 27
27 5 1

K. Schroecksnadel et al. / Clinica Chimica Acta 338 (2003) 157–164 159
(Chiron Diagnostic, Walpole, MA, USA) was used.
Concentrations of neopterin (BRAHMS Diagnostica,
Berlin, Germany) and sTNF-R75 (R&D Systems,
Minneapolis, MN) were measured by ELISA.
For statistical comparisons between subgroups of
patients, non-parametric Mann–Whitney U test was
employed. Spearman rank correlation analysis was
applied to assess correlations. p-Values < 0.05 were
considered to indicate statistical significance.
3. Results
A significant percentage of patients with RA pre-
sented with elevated homocysteine and cysteine con-
centrations (Table 2) in comparison to reference
ranges of healthy control persons [23,24]. In 14 of
33 patients, homocysteine concentrations above 15
AM (upper limit of normal) were observed. Concen-
trations of vitamin B12 and folate were within the
normal range in most of the patients (Table 2). Also,
neopterin concentrations were elevated in a significant
percentage of patients (Table 2).
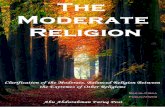
In the 14 patients with homocysteine concentrations
above 15 AM, the concentrations of immune activation
markers sTNF-R75 and neopterin were higher than in
the other 19 patients with normal homocysteine con-
centrations (Fig. 1). Cysteine concentrations were also
higher, whereas folate concentrations were lower in the
patients with hyperhomocysteinaemia. Vitamin B12
concentrations showed only a tendency towards lower
concentrations in patients with elevated homocysteine
concentrations compared to the other 19 patients
( p < 0.06; Fig. 1).
Table 2
Median and range of serum concentrations of homocysteine, cysteine, folate
reference ranges of these parameters and the percentage of patients with c
Medians Range
Homocysteine (AM) 13.9 4.7–31.3
Cysteine (AM) 416 268–701
Folate (nM) 16.8 1.8–49.5
Vitamin B12 (pM) 244 129–979
sTNF-R75 (ng/ml) 2.73 1.6–4.7
Neopterin (nM) 8.08 3.5–27.7
*p< 0.01.
**p< 0.001.
There existed correlations between concentrations
of homocysteine and folate and between homocys-
teine and sTNF-R75 (Fig. 2). Concentrations of
vitamin B12 and folate were associated as well
(rs = 0.462; p < 0.01). Cysteine correlated with homo-
cysteine (rs = 0.713; p < 0.001) and sTNF-R75
(rs = 0.487; p < 0.01); sTNF-R75 concentrations also
correlated with neopterin concentrations (rs = 0.607;
p< 0.001).
Patients treated with non-steroidal anti-inflamma-
tory drugs (NSAIDs) had higher ( p < 0.01) and those
treated with MTX had lower ( p < 0.05) vitamin B12
concentrations. Furthermore sTNF-R75 concentra-
tions were lower in patients treated with MTX
( p < 0.05). There was no such difference of neopterin
concentrations between groups with different treat-
ment regimens. Dosage of MTX did not correlate with
any of the parameters investigated.
The median calculated dietary intake of vitamin
B12 was 5.0 mg/day (range: 1.77–25.5) and 202 Ag/day for folate, respectively (range: 69.2–933.0),
which was much lower than the recommended daily
intake of 300 Ag/day. Only three patients had a folate
intake higher than this recommendation. Patients
with a higher folic acid intake also had a higher
vitamin B12 intake (rs = 0.448, p < 0.05). Dietary
intake of vitamins C and E was also below recom-
mendations. No association was found between cal-
culated dietary intake and blood concentrations of B
vitamins.
Ten of 21 MTX-treated patients were supplemented
with folate, and two other patients had an calculated
dietary intake of folate much higher than the recom-
mended daily intake of 300 Ag. In patients treated with
, vitamin B12, sTNF-R75, and neopterin in 33 patients with RAwith
oncentrations above or below the reference range
Reference limits
(95th percentile)
Outside reference limit
15.0 [23] 42% increased*
347 [24] 85% increased**
4.0 [25] 12% decreased
150 [25] 21% decreased
4.8 [26] 0% increased
8.7 [27] 36% increased*

Fig. 1. Boxplots of serum concentrations of folate and vitamin B12 (upper) and of immune activation markers sTNF-R75 and neopterin (lower)
in 33 patients with RA (divided into two groups—patients with homocysteine (HCy) concentrations V 15 AM and >15 AM).
K. Schroecksnadel et al. / Clinica Chimica Acta 338 (2003) 157–164160
MTX and supplemented with folate, serum folate
concentrations were higher ( p < 0.02) and homocys-
teine concentrations tended to be lower ( p < 0.06) in
comparison with unsupplemented patients. In supple-
mented patients, serum folate concentrations weakly
correlated with the amount of folate supplemented
(rs = 0.371, p < 0.05). Inverse relationships between
homocysteine and serum folate concentrations were
of similar strength in MTX-treated patients with
(rs =� 0.612, p < 0.06) and without (rs =� 0.700,
p < 0.02) folate supplementation. Concentrations of
sTNF-R 75 and homocysteine correlated in MTX-
treated patients without folate supplementation
(rs = 0.718; p < 0.02) but not in supplemented patients
(rs = 0.45; p>0.1). The correlation between neopterin
and sTNF-R75 was somewhat stronger in MTX-trea-

Fig. 2. Correlations of homocysteine with immune activation marker sTNF-R75 (rs = 0.508; p< 0.01) and serum folate (rs =� 0.519; p< 0.01) in
33 patients with RA.
K. Schroecksnadel et al. / Clinica Chimica Acta 338 (2003) 157–164 161
ted patients with folate supplementation (rs = 0.821,
p < 0.01) compared to those without (rs = 0.685,
p < 0.03).
4. Discussion
This study confirms that patients with RA may
present with increased serum homocysteine and cys-
teine concentrations in comparison with healthy con-
trol persons. Homocysteine concentrations in patients
with RA were demonstrated to depend on vitamin
availability [2,3]. In our patients, a significant inverse
correlation existed between homocysteine and folate
concentrations, although concentrations of B vitamins
were well above the lower limit of normal in most
patients. Twelve of 33 patients even presented with
serum folate concentrations above 20 nM, the upper
limit of normal in humans. In the 14 patients with
hyperhomocysteinaemia, significantly lower concen-
trations of serum folate were found in comparison
with the other 19 patients with low homocysteine
concentrations. Also, vitamin B12 tended to lower
concentrations in patients with higher homocysteine.
Interestingly, differences in marker concentrations
were rather small between patients with and without
MTX therapy and between MTX-treated patients with
and without folate administration. In MTX-treated
patients supplemented with folate, homocysteine con-
centrations were only slightly lower, folate concen-
trations slightly higher than in unsupplemented
patients. These results, however must be regarded
with care, because numbers in the subgroups of
MTX-treated patients with/without folate were low.
No significant relationship was found between
calculated folic acid intake and concentrations detect-
able in the circulation. Interestingly, Houcher et al.
[28] reported earlier that an association found between
calculated folic acid intake and circulating concen-
trations in healthy controls could not be detected in
patients with cardiovascular disease. Discrepancy be-
tween dietary intake of vitamins and circulating con-
centrations may relate to an increased consumption of
vitamins in inflammatory conditions.
Elevated concentrations of homocysteine and cys-
teine occurred concomitantly with increased concen-
trations of immune activation marker sTNF-R75 and
neopterin, indicating a link between immune activa-
tion and moderate hyperhomocysteinaemia. Concen-
trations of immune activation markers were higher in
patients with lower vitamin concentrations. This
association as well as the high percentage of hyper-
homocysteinaemia (42%) in patients with RA per se
suggests a relationship between the autoimmune

K. Schroecksnadel et al. / Clinica Chimica Acta 338 (2003) 157–164162
process and homocysteine metabolism. This link
between higher homocysteine concentrations and
immune activation was observed also in other auto-
immune disorders [4,5]. Cysteine concentrations,
which correlated well with homocysteine concentra-
tions, also showed a strong association with concen-
trations of sTNF-R75, but there was no evident
association with vitamin availability. The positive
correlation between homocysteine and cysteine may
indicate that transsulfuration pathway of homocys-
teine is intact.
The concentrations of homocysteine and immune
activation markers did not differ between patients with
RA stage 2 or stage 3. However, most patients were
under treatment while blood specimens were taken,
which will have influenced disease activity. In agree-
ment, concentrations of immune activation markers
usually much better correlate with the activity than
with stage of RA [16–20].
Interestingly, we did not find a difference in
homocysteine and folate concentrations in patients
with or without MTX treatment, which contrasts
earlier findings of others [6,8]. Concentrations of
vitamin B12 were lower in patients with MTX therapy
and also concentrations of sTNF-R75 were markedly
lower in those patients indicating an influence of
MTX on immune activation on the one hand, and
possibly also on homocysteine metabolism on the
other hand. Under regular treatment with NSAIDs,
concentrations of vitamin B12 were higher than in
untreated patients ( p < 0.01), anti-inflammatory treat-
ment therefore seems to influence vitamin B12 avail-
ability in a positive manner.
In parallel to the raised homocysteine concentra-
tions, elevated blood concentrations of immune acti-
vation markers sTNF-R75 and neopterin are found,
and also the strong correlation between homocys-
teine and sTNF-R75 indicates a link between homo-
cysteine metabolism and immune system activation.
A relationship between immune activation and
hyperhomocysteinaemia was already demonstrated
in patients with peripheral vascular disease [29],
atherosclerosis [30,31], and also in patients with
neurodegenerative disorders like dementia and Par-
kinson’s disease [32,33]. Interestingly, oxidative
stress appears to be deeply involved in the patho-
genesis of all the diseases listed. Enhanced immune
activation associated with production of reactive
oxygen species (ROS) and developing oxidative
stress may enhance consumption of antioxidant vita-
mins [34]. In this way, also blood concentrations of
oxidation-sensitive tetrahydrofolate could be dimin-
ished by oxidative stress developing during immune
activation, leading to raised homocysteine and cys-
teine concentrations [35,36]. Since B vitamin cofac-
tors, necessary for the conversion of homocysteine,
are oxidation sensitive, the observation accords well
with the assumption that an enhanced consumption
of these vitamins is likely during conditions going
along with prolonged immune activation and oxida-
tive stress. Similarly, in patients with Alzheimer’s
disease McCaddon et al. [37] recently suggested an
enhanced consumption of vitamin B12 as a conse-
quence of oxidative stress impairing the metabolism
of homocysteine.
We conclude that immune activation, involved in
the pathogenesis of RA, could be the reason for the
increased requirement of B vitamins and the develop-
ment of hyperhomocysteinaemia in patients. Further
studies will be necessary to support the possible role
of oxidative stress to increase the demand for B
vitamins including folate in RA patients.
Acknowledgements
This work was supported by the Austrian Funds
‘‘Zur Forderung der wissenschaftlichen Forschung’’,
project 14942, and by the Austrian Federal Ministry
of Social Affairs and Generations.
References
[1] Boushey CJ, Beresford SA, Omenn GS, Motulsky AG. A
quantitative assessment of plasma homocysteine as a risk fac-
tor for vascular disease. Probable benefits of increasing folic
acid intakes. JAMA 1995;274:1049–57.
[2] Pettersson T, Friman C, Abrahamsson L, Nilsson B, Norberg
B. Serum homocysteine and methylmalonic acid in patients
with rheumatoid arthritis and cobalaminopenia. J Rheumatol
1998;25:859–63.
[3] Roubenoff R, Dellaripa P, Nadeau MR, et al. Abnormal ho-
mocysteine metabolism in rheumatoid arthritis. Arthritis
Rheum 1997;40:718–22.
[4] Aksu K, Turgan N, Oksel F, et al. Hyperhomocysteinaemia in
Behcet’s disease. Rheumatology 2001;40:687–90.
[5] Marasini B, Casari S, Bestetti A, et al. Homocysteine concen-

K. Schroecksnadel et al. / Clinica Chimica Acta 338 (2003) 157–164 163
tration in primary and systemic sclerosis associated Raynaud’s
phenomenon. J Rheumatol 2000;27:2621–3.
[6] Slot O. Changes in plasma homocysteine in arthritis patients
starting treatment with low-dose methotrexate subsequently
supplemented with folic acid. Scand J Rheumatol 2001;30:
305–7.
[7] Allegra CJ, Fine RL, Drake JC, Chabner BA. The effect of
methothrexate on intracellular folate pools in human MCF-7
breast cancer cells. Evidence for direct inhibition of purine
synthesis. J Biol Chem 1986;261:6478–85.
[8] Erb N, Kitas GD. Homocysteine modulation as a reason for
continuous folic acid supplementation in methotrexate-trea-
ted rheumatoid arthritis patients. Rheumatology 2001;40:
715–6.
[9] Morgan SL, Baggott JE, Lee JY, Alarcon GS. Folic acid sup-
plementation prevents deficient blood folate levels and hyper-
homocysteinemia during long-term, low dose methotrexate
therapy for rheumatoid arthritis: implications for cardiovascu-
lar disease prevention. J Rheumatol 1998;25:441–6.
[10] Seriolo B, Fasciolo D, Sulli A, Cutolo M. Homocysteine and
antiphospholipid antibodies in rheumatoid arthritis patients:
relationships with thrombotic events. Clin Exp Rheumatol
2001;19:561–4.
[11] Wilder RL. Rheumatoid arthritis: epidemiology, pathology
and pathogenesis. In: Schumacher HR, editor. Primer on
Rheumatic Diseases. Atlanta: Arthritis Foundation; 1993.
p. 86–9.
[12] Cope AP, Aderka D, et al. Increased levels of soluble tumor
necrosis factor receptors in the sera and synovial fluid of
patients with rheumatic disease. Arthritis Rheum 1992;35:
1160–9.
[13] Barrera P, Boerbooms AM, Janssen EM, et al. Circulating
soluble tumor necrosis factor receptors, interleukin-2 recep-
tors, tumor necrosis factor-a and interleukin-6 levels in rheu-
matoid arthritis. Arthritis Rheum 1993;36:1070–9.
[14] Steiner G, Studnicka-Benke A, Witzmann G, Hofler E, Smo-
len J. Soluble receptors for tumor necrosis factor and interleu-
kin-2 in serum and synovial fluid of patients with rheumatoid
arthritis, reactive arthritis and osteoarthritis. J Rheumatol
1995;22:406–12.
[15] Keystone EC, Snow KM, Bombardier C, Chang CH, Nelson
DL, Rubin LA. Elevated soluble IL-2 receptor levels in the
sera and synovial fluids of patients with rheumatoid arthritis.
Arthritis Rheum 1988;31:1358–64.
[16] Symons JA, Wood NC, Di Giovine FS, Duff GW. Soluble IL-
2 receptor in rheumatoid arthritis: correlation with disease
activity, IL-1 and IL-2 inhibition. J Immunol 1988;141:
2612–8.
[17] Rubin LA, Snow KM, Kurman CC, Nelson DL, Keystone EC.
Serial levels of soluble interleukin 2 receptor in the peripheral
blood of patients with rheumatoid arthritis: correlations with
disease activity. J Rheumatol 1990;17:597–602.
[18] Tebib JG, Letroublon MC, Bienvenu J, Bouvier M. sIL-2R
levels in rheumatoid arthritis: poor correlation with clinical
activity is due to part to disease duration. Br J Rheumatol
1995;34:1037–40.
[19] Reibnegger G, Egg D, Fuchs D, et al. Urinary neopterin re-
flects clinical activity in patients with rheumatoid arthritis.
Arthritis Rheum 1986;29:1063–70.
[20] Maerker-Alzer G, Diemer O, Strumper R, Rohe M. Neopterin
production in inflamed knee joints: high levels in synovial
fluids. Rheumatol Int 1986;6:151–4.
[21] Schroecksnadel K, Frick B, Wirleitner B, Schennach H, Fuchs
D. Homocysteine accumulates in supernatants of stimulated
human peripheral blood mononuclear cells. Clin Exp Immunol
2003;134:53–6 .
[22] Frick B, Schrocksnadel K, Neurauter G, Wirleitner B, Artner
Dworzak E, Fuchs D. Rapid measurement of total plasma
homocysteine by HPLC. Clin Chim Acta 2003;331:19–23.
[23] Selhub J, Jacques PF, Rosenberg IH, et al. Serum total homo-
cysteine concentrations in the third National Health and Nu-
trition Examination Survey (1991–1994): population refer-
ence ranges and contribution of vitamin status to high serum
concentrations. Ann Intern Med 1999;131:331–9.
[24] van den Brandhof WE, Haks K, Schouten EG, Verhoef P. The
relation between plasma cysteine, plasma homocysteine and
coronary atherosclerosis. Atherosclerosis 2001;157:403–9.
[25] Burtis CA, Ashwood ER. In: Tietz ER, editor. Textbook of
Clinical Chemistry. 2nd ed. Philadelphia: WB Saunders
Publishers; 1994. p. 2057.
[26] Zangerle R, Gallati H, Sarcletti M, et al. Increased serum
concentrations of soluble tumor necrosis factor receptors in
HIV-infected individuals are associated with immune activa-
tion. J Acquir Immune Defic Syndr 1994;7:79–85.
[27] Fuchs D, Weiss G, Reibnegger G, Wachter H. The role of
neopterin as a monitor of cellular immune activation in trans-
plantation, inflammatory, infectious and malignant diseases.
Crit Rev Clin Lab Sci 1992;29:307–41.
[28] Houcher B, Candito M, Gibelin P, et al. Assessment of folate
status: measurement of homocysteine versus vitamin B12 and
folate. Pteridines 2003;14:27–34.
[29] Mansoor MA, Bergmark C, Svardal AM, Lonning PE, Ueland
PM. Redox status and protein binding of plasma homocys-
teine and other aminothiols in patients with early-onset periph-
eral vascular disease. Arterioscler Thromb Vasc Biol 1995;
15:232–40.
[30] Gottsater A, Forsblad J, Mattiasson I, Lindgarde F. Decreasing
plasma endothelin-1 and unchanged plasma neopterin during
folate supplementation in hyperhomocysteinemia. Int Angiol
2002;21:158–64.
[31] Erren M, Reinecke H, Junker R, et al. Systemic inflammatory
parameters in patients with atherosclerosis of the coronary and
peripheral arteries. Arterioscler Thromb Vasc Biol 1999;19:
2355–63.
[32] Leblhuber F, Walli J, Arthner-Dworzak E, et al. Hyperho-
mocysteinemia in dementia. J Neural Transm 2000;107:
1469–74.
[33] Widner B, Leblhuber F, Frick B, Laich A, Artner-Dworzak E,
Fuchs D. Moderate hyperhomocysteinemia and immune acti-
vation in Parkinson’s disease. J Neural Transm 2002;109:
181–9.
[34] Halliwell B, Clement MV, Long LH. Hydrogen peroxide in
the human body. FEBS Lett 2000;486:10–3.
[35] Fuchs D, Jaeger M, Widner B, Wirleitner B, Artner-Dworzak,

K. Schroecksnadel et al. / Clinica Chimica Acta 338 (2003) 157–164164
E, Leblhuber F. Is hyperhomocysteinemia due to the oxidative
depletion of folate rather than to insufficient dietary intake?
Clin Chem Lab Med 2001;39:691–4.
[36] Mezzano D, Pais EO, Aranda E, et al. Inflammation, not
hyperhomocysteinemia, is related to oxidative stress and he-
mostatic and endothelial dysfunction in uremia. Kidney Int
2001;60:1844–50.
[37] McCaddon A, Regland B, Hudson P, Davies G. Functional
vitamin B12 deficiency and Alzheimer disease. Neurology
2002;58:1395–9.