The Learning Curve of Laparoendoscopic Single-Site (LESS) Cholecystectomy: Definable, Short, and...
6
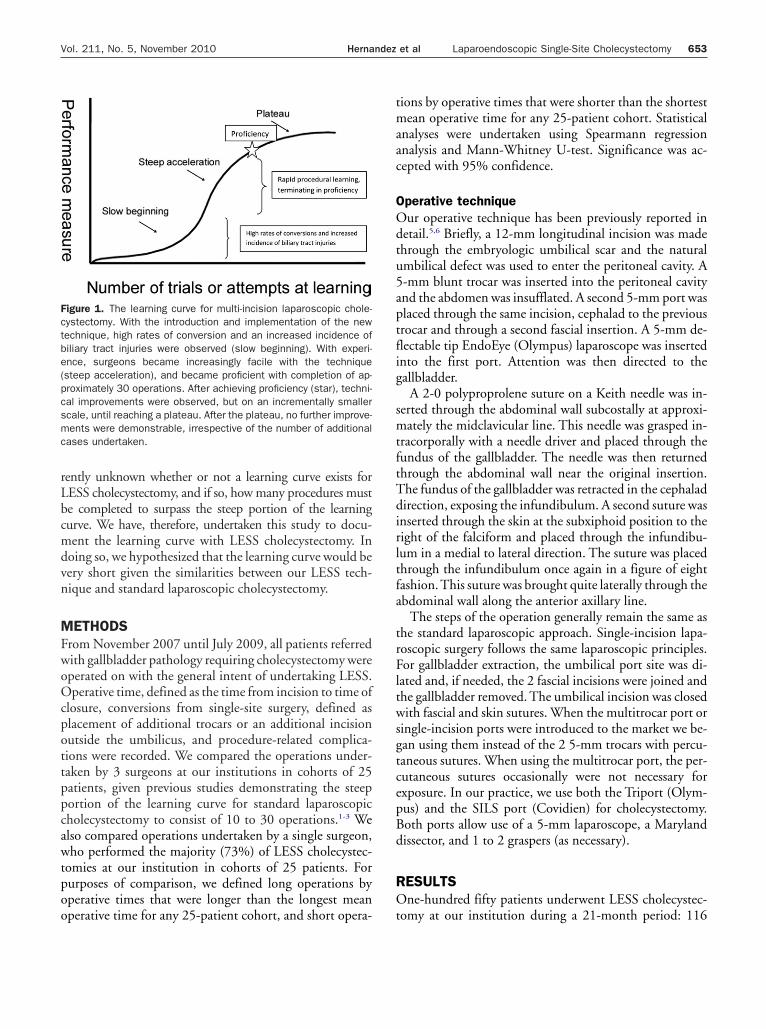
The Learning Curve of Laparoendoscopic Single-Site (LESS) Cholecystectomy: Definable, Short, and Safe Jonathan Hernandez, MD, Sharona Ross, MD, Connor Morton, BS, Kellie McFarlin, MD, Sujat Dahal, MD, Farhaad Golkar, MD, Michael Albrink, MD, FACS, Alexander Rosemurgy, MD, FACS BACKGROUND: The applications of laparoendoscopic single-site (LESS) surgery, including cholecystectomy, are occurring quickly, although little is generally known about issues associated with the learning curve of this new technique including operative time, conversion rates, and safety. STUDY DESIGN: We prospectively followed all patients undergoing LESS cholecystectomy, and compared oper- ations undertaken at our institutions in cohorts of 25 patients with respect to operative times, conversion rates, and complications. RESULTS: One-hundred fifty patients of mean age 46 years underwent LESS cholecystectomy. No signif- icant differences in operative times were demonstrable between any of the 25-patient cohorts operated on at our institution. A significant reduction in operative times (p 0.001) after completion of 75 LESS procedures was, however, identified with the experience of a single surgeon. No significant reduction in the number of procedures requiring an additional trocar(s) or conversion to open operations was observed after completion of 25 LESS cholecystectomies. Complication rates were low, and not significantly different between any 25-patient cohorts. CONCLUSIONS: For surgeons proficient with multi-incision laparoscopic cholecystectomy, the learning curve for LESS cholecystectomy begins near proficiency. Operative complications and conversions were infrequent and unchanged across successive 25-patient cohorts, and were similar to those reported for multi-incision laparoscopic cholecystectomy after the learning curve. ( J Am Coll Surg 2010;211:652–657. © 2010 by the American College of Surgeons) In the last several years surgery has witnessed an unprece- dented expansion of minimally invasive procedures, both in application (ie, colectomy, splenectomy, pancreatec- tomy, etc) and in technique (ie, use of fewer trocars, single site surgery, and natural orifice translumenal endoscopic surgery [NOTES]). Although admittedly on a smaller scale, this expansion mirrors that seen in the late 1980s as laparoscopic cholecystectomy quickly became the standard of care for symptomatic gallstone disease. Enthusiasm for the adoption of laparoscopic cholecystectomy over the open procedure was, however, somewhat tempered, and understandably so, by an increase in operative times and procedure-related complications associated with the learn- ing curve of the new technique. 1-3 As we move forward to provide patients with single-site surgical procedures, we realize that documentation of safety and any associated learning curve will be especially important. The learning curve of any procedure is the number of times that particular procedure must be done in order to complete the procedure repeatedly with high accuracy and precision. 4 With the transition to multi-incision laparo- scopic cholecystectomy in the late 1980s, the initial slope of the learning curve, or slow beginning, was associated with high rates of conversion to open procedures and in- creased rates of biliary tract injuries. As experience was gained, a transition to the steep portion of the learning curve was seen, which correlated with rapid learning and ended with the surgeon attaining proficiency.This rise then changed slowly; the improvement in outcomes became more modest until the curve flattened (plateau), without any further detectable change irrespective of additional procedures performed (Fig. 1). Experience with laparoendoscopic single-site (LESS) surgery, particularly as applied to cholecystectomy, is grow- ing rapidly. We have previously reported our experience 5,6 and have begun to disseminate our technique by frequently teaching courses for practicing surgeons. However, it is cur- Disclosure Information: Drs Ross, Albrink and Rosemurgy have received honoraria from Covidien Corporation for teaching LESS surgery using Covidien instruments, and from Olympus Corporation for teaching LESS surgery using Olympus instruments. All other authors have nothing to disclose. Received February 4, 2010; Revised July 13, 2010; Accepted July 15, 2010. From the Department of Surgery, University of South Florida College of Medicine, Tampa General Hospital, Tampa, FL. Correspondence address: Alexander S Rosemurgy, MD, University of South Florida, c/o Tampa General Hospital, PO Box 1289, Room F-145, Tampa, FL 33601. email: [email protected] 652 © 2010 by the American College of Surgeons ISSN 1072-7515/10/$36.00 Published by Elsevier Inc. doi:10.1016/j.jamcollsurg.2010.07.008
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of The Learning Curve of Laparoendoscopic Single-Site (LESS) Cholecystectomy: Definable, Short, and...

T(JS
Iditssslotoup
DhCsd
RFMCFF
©P
he Learning Curve of Laparoendoscopic Single-SiteLESS) Cholecystectomy: Definable, Short, and Safe
onathan Hernandez, MD, Sharona Ross, MD, Connor Morton, BS, Kellie McFarlin, MD,ujat Dahal, MD, Farhaad Golkar, MD, Michael Albrink, MD, FACS, Alexander Rosemurgy, MD, FACS
BACKGROUND: The applications of laparoendoscopic single-site (LESS) surgery, including cholecystectomy, areoccurring quickly, although little is generally known about issues associated with the learningcurve of this new technique including operative time, conversion rates, and safety.
STUDY DESIGN: We prospectively followed all patients undergoing LESS cholecystectomy, and compared oper-ations undertaken at our institutions in cohorts of 25 patients with respect to operative times,conversion rates, and complications.
RESULTS: One-hundred fifty patients of mean age 46 years underwent LESS cholecystectomy. No signif-icant differences in operative times were demonstrable between any of the 25-patient cohortsoperated on at our institution. A significant reduction in operative times (p � 0.001) aftercompletion of 75 LESS procedures was, however, identified with the experience of a singlesurgeon. No significant reduction in the number of procedures requiring an additional trocar(s)or conversion to open operations was observed after completion of 25 LESS cholecystectomies.Complication rates were low, and not significantly different between any 25-patient cohorts.
CONCLUSIONS: For surgeons proficient with multi-incision laparoscopic cholecystectomy, the learning curvefor LESS cholecystectomy begins near proficiency. Operative complications and conversionswere infrequent and unchanged across successive 25-patient cohorts, and were similar to thosereported for multi-incision laparoscopic cholecystectomy after the learning curve. (J Am Coll
Surg 2010;211:652–657. © 2010 by the American College of Surgeons)iprl
tcpsowcgcecmap
sia
n the last several years surgery has witnessed an unprece-ented expansion of minimally invasive procedures, both
n application (ie, colectomy, splenectomy, pancreatec-omy, etc) and in technique (ie, use of fewer trocars, singleite surgery, and natural orifice translumenal endoscopicurgery [NOTES]). Although admittedly on a smallercale, this expansion mirrors that seen in the late 1980s asaparoscopic cholecystectomy quickly became the standardf care for symptomatic gallstone disease. Enthusiasm forhe adoption of laparoscopic cholecystectomy over thepen procedure was, however, somewhat tempered, andnderstandably so, by an increase in operative times androcedure-related complications associated with the learn-
isclosure Information: Drs Ross, Albrink and Rosemurgy have receivedonoraria from Covidien Corporation for teaching LESS surgery usingovidien instruments, and from Olympus Corporation for teaching LESS
urgery using Olympus instruments. All other authors have nothing toisclose.
eceived February 4, 2010; Revised July 13, 2010; Accepted July 15, 2010.rom the Department of Surgery, University of South Florida College ofedicine, Tampa General Hospital, Tampa, FL.orrespondence address: Alexander S Rosemurgy, MD, University of Southlorida, c/o Tampa General Hospital, PO Box 1289, Room F-145, Tampa,
tL 33601. email: [email protected]
6522010 by the American College of Surgeons
ublished by Elsevier Inc.
ng curve of the new technique.1-3 As we move forward torovide patients with single-site surgical procedures, weealize that documentation of safety and any associatedearning curve will be especially important.
The learning curve of any procedure is the number ofimes that particular procedure must be done in order toomplete the procedure repeatedly with high accuracy andrecision.4 With the transition to multi-incision laparo-copic cholecystectomy in the late 1980s, the initial slopef the learning curve, or slow beginning, was associatedith high rates of conversion to open procedures and in-
reased rates of biliary tract injuries. As experience wasained, a transition to the steep portion of the learningurve was seen, which correlated with rapid learning andnded with the surgeon attaining proficiency.This rise thenhanged slowly; the improvement in outcomes becameore modest until the curve flattened (plateau), without
ny further detectable change irrespective of additionalrocedures performed (Fig. 1).Experience with laparoendoscopic single-site (LESS)
urgery, particularly as applied to cholecystectomy, is grow-ng rapidly. We have previously reported our experience5,6
nd have begun to disseminate our technique by frequently
eaching courses for practicing surgeons. However, it is cur-ISSN 1072-7515/10/$36.00doi:10.1016/j.jamcollsurg.2010.07.008
rLbcmdvn
MFwoOcpottppcawtpoo
tmaac
OOdtu5aptfig
smtftTdirltfa
trFltwsgtcepBd
RO
Fctbe(pcsmc
653Vol. 211, No. 5, November 2010 Hernandez et al Laparoendoscopic Single-Site Cholecystectomy
ently unknown whether or not a learning curve exists forESS cholecystectomy, and if so, how many procedures muste completed to surpass the steep portion of the learningurve. We have, therefore, undertaken this study to docu-ent the learning curve with LESS cholecystectomy. In
oing so, we hypothesized that the learning curve would beery short given the similarities between our LESS tech-ique and standard laparoscopic cholecystectomy.
ETHODSrom November 2007 until July 2009, all patients referredith gallbladder pathology requiring cholecystectomy wereperated on with the general intent of undertaking LESS.perative time, defined as the time from incision to time of
losure, conversions from single-site surgery, defined aslacement of additional trocars or an additional incisionutside the umbilicus, and procedure-related complica-ions were recorded. We compared the operations under-aken by 3 surgeons at our institutions in cohorts of 25atients, given previous studies demonstrating the steeportion of the learning curve for standard laparoscopicholecystectomy to consist of 10 to 30 operations.1-3 Welso compared operations undertaken by a single surgeon,ho performed the majority (73%) of LESS cholecystec-
omies at our institution in cohorts of 25 patients. Forurposes of comparison, we defined long operations byperative times that were longer than the longest mean
igure 1. The learning curve for multi-incision laparoscopic chole-ystectomy. With the introduction and implementation of the newechnique, high rates of conversion and an increased incidence ofiliary tract injuries were observed (slow beginning). With experi-nce, surgeons became increasingly facile with the techniquesteep acceleration), and became proficient with completion of ap-roximately 30 operations. After achieving proficiency (star), techni-al improvements were observed, but on an incrementally smallercale, until reaching a plateau. After the plateau, no further improve-ents were demonstrable, irrespective of the number of additional
ases undertaken.
perative time for any 25-patient cohort, and short opera- t
ions by operative times that were shorter than the shortestean operative time for any 25-patient cohort. Statistical
nalyses were undertaken using Spearmann regressionnalysis and Mann-Whitney U-test. Significance was ac-epted with 95% confidence.
perative techniqueur operative technique has been previously reported in
etail.5,6 Briefly, a 12-mm longitudinal incision was madehrough the embryologic umbilical scar and the naturalmbilical defect was used to enter the peritoneal cavity. A-mm blunt trocar was inserted into the peritoneal cavitynd the abdomen was insufflated. A second 5-mm port waslaced through the same incision, cephalad to the previousrocar and through a second fascial insertion. A 5-mm de-lectable tip EndoEye (Olympus) laparoscope was insertednto the first port. Attention was then directed to theallbladder.
A 2-0 polyproprolene suture on a Keith needle was in-erted through the abdominal wall subcostally at approxi-ately the midclavicular line. This needle was grasped in-
racorporally with a needle driver and placed through theundus of the gallbladder. The needle was then returnedhrough the abdominal wall near the original insertion.he fundus of the gallbladder was retracted in the cephaladirection, exposing the infundibulum. A second suture was
nserted through the skin at the subxiphoid position to theight of the falciform and placed through the infundibu-um in a medial to lateral direction. The suture was placedhrough the infundibulum once again in a figure of eightashion.This suture was brought quite laterally through thebdominal wall along the anterior axillary line.
The steps of the operation generally remain the same ashe standard laparoscopic approach. Single-incision lapa-oscopic surgery follows the same laparoscopic principles.or gallbladder extraction, the umbilical port site was di-
ated and, if needed, the 2 fascial incisions were joined andhe gallbladder removed. The umbilical incision was closedith fascial and skin sutures. When the multitrocar port or
ingle-incision ports were introduced to the market we be-an using them instead of the 2 5-mm trocars with percu-aneous sutures. When using the multitrocar port, the per-utaneous sutures occasionally were not necessary forxposure. In our practice, we use both the Triport (Olym-us) and the SILS port (Covidien) for cholecystectomy.oth ports allow use of a 5-mm laparoscope, a Marylandissector, and 1 to 2 graspers (as necessary).
ESULTSne-hundred fifty patients underwent LESS cholecystec-
omy at our institution during a 21-month period: 116
wpyuTdtap3ih
3w(ttW2ttWgUpf
3aucoppet
at
3csSp2ppspc
DAwgtctgtwcapm
wwsatg
TP(
1
1
*† r any
654 Hernandez et al Laparoendoscopic Single-Site Cholecystectomy J Am Coll Surg
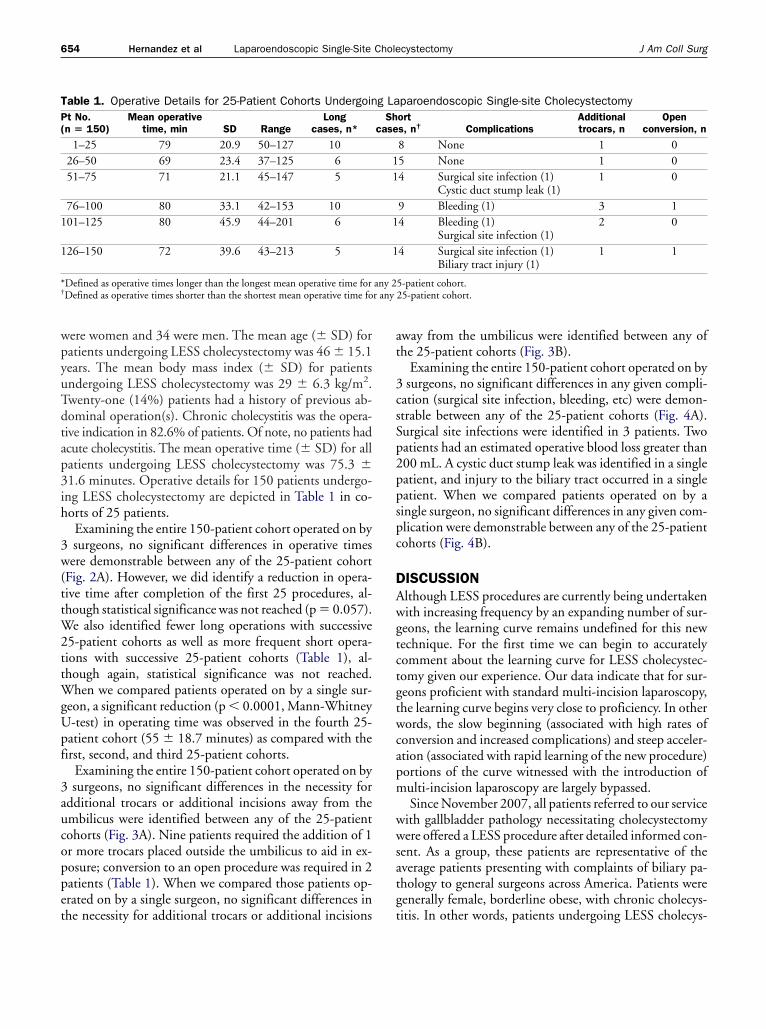
ere women and 34 were men. The mean age (� SD) foratients undergoing LESS cholecystectomy was 46 � 15.1ears. The mean body mass index (� SD) for patientsndergoing LESS cholecystectomy was 29 � 6.3 kg/m2.wenty-one (14%) patients had a history of previous ab-ominal operation(s). Chronic cholecystitis was the opera-ive indication in 82.6% of patients. Of note, no patients hadcute cholecystitis. The mean operative time (� SD) for allatients undergoing LESS cholecystectomy was 75.3 �1.6 minutes. Operative details for 150 patients undergo-ng LESS cholecystectomy are depicted in Table 1 in co-orts of 25 patients.Examining the entire 150-patient cohort operated on bysurgeons, no significant differences in operative timesere demonstrable between any of the 25-patient cohort
Fig. 2A). However, we did identify a reduction in opera-ive time after completion of the first 25 procedures, al-hough statistical significance was not reached (p � 0.057).
e also identified fewer long operations with successive5-patient cohorts as well as more frequent short opera-ions with successive 25-patient cohorts (Table 1), al-hough again, statistical significance was not reached.
hen we compared patients operated on by a single sur-eon, a significant reduction (p � 0.0001, Mann-Whitney-test) in operating time was observed in the fourth 25-atient cohort (55 � 18.7 minutes) as compared with theirst, second, and third 25-patient cohorts.
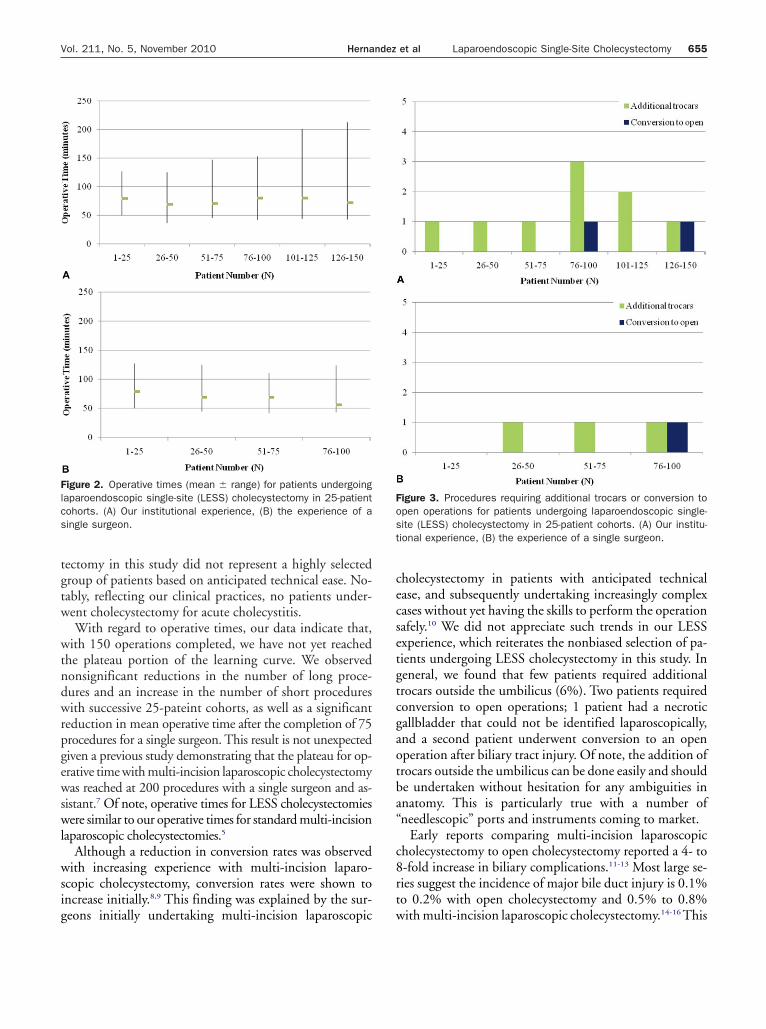
Examining the entire 150-patient cohort operated on bysurgeons, no significant differences in the necessity for
dditional trocars or additional incisions away from thembilicus were identified between any of the 25-patientohorts (Fig. 3A). Nine patients required the addition of 1r more trocars placed outside the umbilicus to aid in ex-osure; conversion to an open procedure was required in 2atients (Table 1). When we compared those patients op-rated on by a single surgeon, no significant differences in
able 1. Operative Details for 25-Patient Cohorts Undergoint No.n � 150)
Mean operativetime, min SD Range
Longcases, n*
1–25 79 20.9 50–127 1026–50 69 23.4 37–125 651–75 71 21.1 45–147 5
76–100 80 33.1 42–153 1001–125 80 45.9 44–201 6
26–150 72 39.6 43–213 5
Defined as operative times longer than the longest mean operative time forDefined as operative times shorter than the shortest mean operative time fo
he necessity for additional trocars or additional incisions t
way from the umbilicus were identified between any ofhe 25-patient cohorts (Fig. 3B).
Examining the entire 150-patient cohort operated on bysurgeons, no significant differences in any given compli-
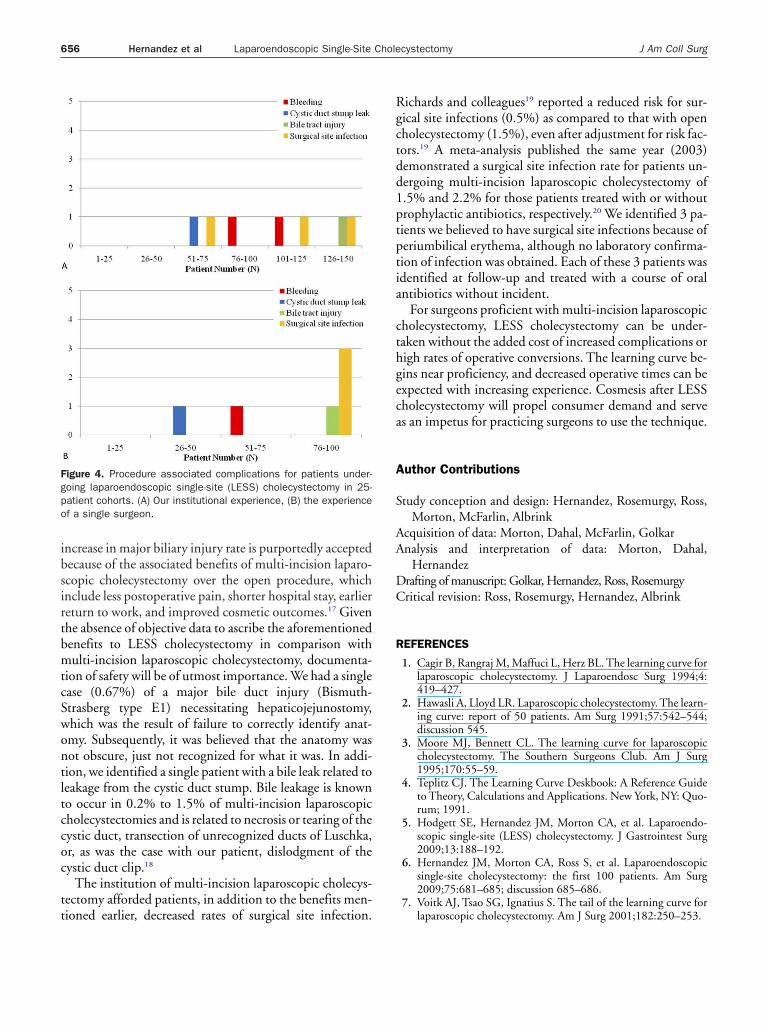
ation (surgical site infection, bleeding, etc) were demon-trable between any of the 25-patient cohorts (Fig. 4A).urgical site infections were identified in 3 patients. Twoatients had an estimated operative blood loss greater than00 mL. A cystic duct stump leak was identified in a singleatient, and injury to the biliary tract occurred in a singleatient. When we compared patients operated on by aingle surgeon, no significant differences in any given com-lication were demonstrable between any of the 25-patientohorts (Fig. 4B).
ISCUSSIONlthough LESS procedures are currently being undertakenith increasing frequency by an expanding number of sur-eons, the learning curve remains undefined for this newechnique. For the first time we can begin to accuratelyomment about the learning curve for LESS cholecystec-omy given our experience. Our data indicate that for sur-eons proficient with standard multi-incision laparoscopy,he learning curve begins very close to proficiency. In otherords, the slow beginning (associated with high rates of
onversion and increased complications) and steep acceler-tion (associated with rapid learning of the new procedure)ortions of the curve witnessed with the introduction ofulti-incision laparoscopy are largely bypassed.Since November 2007, all patients referred to our service
ith gallbladder pathology necessitating cholecystectomyere offered a LESS procedure after detailed informed con-
ent. As a group, these patients are representative of theverage patients presenting with complaints of biliary pa-hology to general surgeons across America. Patients wereenerally female, borderline obese, with chronic cholecys-
paroendoscopic Single-site Cholecystectomyorts, n† Complications
Additionaltrocars, n
Openconversion, n
8 None 1 05 None 1 04 Surgical site infection (1)
Cystic duct stump leak (1)1 0
9 Bleeding (1) 3 14 Bleeding (1)
Surgical site infection (1)2 0
4 Surgical site infection (1)Biliary tract injury (1)
1 1
5-patient cohort.25-patient cohort.
g LaSh
case
11
1
1
any 2
itis. In other words, patients undergoing LESS cholecys-
tgtw
wtndwrpgewswl
wsig
cecsetgtcgaotba“
c8rt
Flcs
Fost
655Vol. 211, No. 5, November 2010 Hernandez et al Laparoendoscopic Single-Site Cholecystectomy
ectomy in this study did not represent a highly selectedroup of patients based on anticipated technical ease. No-ably, reflecting our clinical practices, no patients under-ent cholecystectomy for acute cholecystitis.With regard to operative times, our data indicate that,
ith 150 operations completed, we have not yet reachedhe plateau portion of the learning curve. We observedonsignificant reductions in the number of long proce-ures and an increase in the number of short proceduresith successive 25-pateint cohorts, as well as a significant
eduction in mean operative time after the completion of 75rocedures for a single surgeon. This result is not unexpectediven a previous study demonstrating that the plateau for op-rative time with multi-incision laparoscopic cholecystectomyas reached at 200 procedures with a single surgeon and as-
istant.7 Of note, operative times for LESS cholecystectomiesere similar to our operative times for standard multi-incision
aparoscopic cholecystectomies.5
Although a reduction in conversion rates was observedith increasing experience with multi-incision laparo-
copic cholecystectomy, conversion rates were shown toncrease initially.8,9 This finding was explained by the sur-
igure 2. Operative times (mean � range) for patients undergoingaparoendoscopic single-site (LESS) cholecystectomy in 25-patientohorts. (A) Our institutional experience, (B) the experience of aingle surgeon.
eons initially undertaking multi-incision laparoscopic w
holecystectomy in patients with anticipated technicalase, and subsequently undertaking increasingly complexases without yet having the skills to perform the operationafely.10 We did not appreciate such trends in our LESSxperience, which reiterates the nonbiased selection of pa-ients undergoing LESS cholecystectomy in this study. Ineneral, we found that few patients required additionalrocars outside the umbilicus (6%). Two patients requiredonversion to open operations; 1 patient had a necroticallbladder that could not be identified laparoscopically,nd a second patient underwent conversion to an openperation after biliary tract injury. Of note, the addition ofrocars outside the umbilicus can be done easily and shoulde undertaken without hesitation for any ambiguities innatomy. This is particularly true with a number ofneedlescopic” ports and instruments coming to market.
Early reports comparing multi-incision laparoscopicholecystectomy to open cholecystectomy reported a 4- to-fold increase in biliary complications.11-13 Most large se-ies suggest the incidence of major bile duct injury is 0.1%o 0.2% with open cholecystectomy and 0.5% to 0.8%
igure 3. Procedures requiring additional trocars or conversion topen operations for patients undergoing laparoendoscopic single-ite (LESS) cholecystectomy in 25-patient cohorts. (A) Our institu-ional experience, (B) the experience of a single surgeon.
ith multi-incision laparoscopic cholecystectomy.14-16 This
ibsirtbmtcSwontltccoc
tt
Rgctdd1ptptia
cthgeca
A
S
AA
DC
R
Fgpo
656 Hernandez et al Laparoendoscopic Single-Site Cholecystectomy J Am Coll Surg
ncrease in major biliary injury rate is purportedly acceptedecause of the associated benefits of multi-incision laparo-copic cholecystectomy over the open procedure, whichnclude less postoperative pain, shorter hospital stay, earliereturn to work, and improved cosmetic outcomes.17 Givenhe absence of objective data to ascribe the aforementionedenefits to LESS cholecystectomy in comparison withulti-incision laparoscopic cholecystectomy, documenta-
ion of safety will be of utmost importance. We had a singlease (0.67%) of a major bile duct injury (Bismuth-trasberg type E1) necessitating hepaticojejunostomy,hich was the result of failure to correctly identify anat-my. Subsequently, it was believed that the anatomy wasot obscure, just not recognized for what it was. In addi-ion, we identified a single patient with a bile leak related toeakage from the cystic duct stump. Bile leakage is knowno occur in 0.2% to 1.5% of multi-incision laparoscopicholecystectomies and is related to necrosis or tearing of theystic duct, transection of unrecognized ducts of Luschka,r, as was the case with our patient, dislodgment of theystic duct clip.18
The institution of multi-incision laparoscopic cholecys-ectomy afforded patients, in addition to the benefits men-
igure 4. Procedure associated complications for patients under-oing laparoendoscopic single-site (LESS) cholecystectomy in 25-atient cohorts. (A) Our institutional experience, (B) the experiencef a single surgeon.
ioned earlier, decreased rates of surgical site infection.
ichards and colleagues19 reported a reduced risk for sur-ical site infections (0.5%) as compared to that with openholecystectomy (1.5%), even after adjustment for risk fac-ors.19 A meta-analysis published the same year (2003)emonstrated a surgical site infection rate for patients un-ergoing multi-incision laparoscopic cholecystectomy of.5% and 2.2% for those patients treated with or withoutrophylactic antibiotics, respectively.20 We identified 3 pa-ients we believed to have surgical site infections because oferiumbilical erythema, although no laboratory confirma-ion of infection was obtained. Each of these 3 patients wasdentified at follow-up and treated with a course of oralntibiotics without incident.
For surgeons proficient with multi-incision laparoscopicholecystectomy, LESS cholecystectomy can be under-aken without the added cost of increased complications origh rates of operative conversions. The learning curve be-ins near proficiency, and decreased operative times can bexpected with increasing experience. Cosmesis after LESSholecystectomy will propel consumer demand and serves an impetus for practicing surgeons to use the technique.
uthor Contributions
tudy conception and design: Hernandez, Rosemurgy, Ross,Morton, McFarlin, Albrink
cquisition of data: Morton, Dahal, McFarlin, Golkarnalysis and interpretation of data: Morton, Dahal,
Hernandezrafting of manuscript: Golkar, Hernandez, Ross, Rosemurgyritical revision: Ross, Rosemurgy, Hernandez, Albrink
EFERENCES
1. Cagir B, Rangraj M, Maffuci L, Herz BL. The learning curve forlaparoscopic cholecystectomy. J Laparoendosc Surg 1994;4:419–427.
2. Hawasli A, Lloyd LR. Laparoscopic cholecystectomy. The learn-ing curve: report of 50 patients. Am Surg 1991;57:542–544;discussion 545.
3. Moore MJ, Bennett CL. The learning curve for laparoscopiccholecystectomy. The Southern Surgeons Club. Am J Surg1995;170:55–59.
4. Teplitz CJ. The Learning Curve Deskbook: A Reference Guideto Theory, Calculations and Applications. New York, NY: Quo-rum; 1991.
5. Hodgett SE, Hernandez JM, Morton CA, et al. Laparoendo-scopic single-site (LESS) cholecystectomy. J Gastrointest Surg2009;13:188–192.
6. Hernandez JM, Morton CA, Ross S, et al. Laparoendoscopicsingle-site cholecystectomy: the first 100 patients. Am Surg2009;75:681–685; discussion 685–686.
7. Voitk AJ, Tsao SG, Ignatius S. The tail of the learning curve for
laparoscopic cholecystectomy. Am J Surg 2001;182:250–253.
1
1
1
1
1
1
1
1
1
1
2
657Vol. 211, No. 5, November 2010 Hernandez et al Laparoendoscopic Single-Site Cholecystectomy
8. Shea JA, Berlin JA, Bachwich DR, et al. Indications for andoutcomes of cholecystectomy: a comparison of the pre and post-laparoscopic eras. Ann Surg 1998;227:343–350.
9. Nair RG, Dunn DC, Fowler S, McCloy RF. Progress with cho-lecystectomy: improving results in England and Wales. Br J Surg1997;84:1396–1398.
0. Shea JA, Healey MJ, Berlin JA, et al. Mortality and complica-tions associated with laparoscopic cholecystectomy. A meta-analysis. Ann Surg 1996;224:609–620.
1. Woods MS, Shellito JL, Santoscoy GS, et al. Cystic duct leaks inlaparoscopic cholecystectomy. Am J Surg 1994;168:560–563;discussion 563–565.
2. Woods MS, Traverso LW, Kozarek RA, et al. Characteristicsof biliary tract complications during laparoscopic cholecys-tectomy: a multi-institutional study. Am J Surg 1994;167:27–33; discussion 34.
3. Doctor N, Dooley JS, Dick R, et al. Multidisciplinary approachto biliary complications of laparoscopic cholecystectomy. Br JSurg 1998;85:627–-632.
4. Richardson MC, Bell G, Fullarton GM. Incidence and nature
of bile duct injuries following laparoscopic cholecystectomy:an audit of 5913 cases. West of Scotland LaparoscopicCholecystectomy Audit Group. Br J Surg 1996;83:1356–1360.
5. Gouma DJ, Go PM. Bile duct injury during laparoscopic andconventional cholecystectomy. J Am Coll Surg 1994;178:229–233.
6. Chapman WC, Abecassis M, Jarnagin W, et al. Bile duct injuries12 years after the introduction of laparoscopic cholecystectomy.J Gastrointest Surg 2003;7:412–416.
7. McMahon AJ, Russell IT, Baxter JN, et al. Laparoscopic versusminilaparotomy cholecystectomy: a randomised trial. Lancet1994;343:135–138.
8. Mulvihill SJ. Surgical management of gallstone disease and post-operative complications. Semin Gastrointest Dis 2003;14:237–244.
9. Richards C, Edwards J, Culver D, et al. Does using a laparo-scopic approach to cholecystectomy decrease the risk of surgicalsite infection? Ann Surg 2003;237:358–362.
0. Al-Ghnaniem R, Benjamin IS, Patel AG. Meta-analysis suggestsantibiotic prophylaxis is not warranted in low-risk patients un-dergoing laparoscopic cholecystectomy. Br J Surg 2003;90:365–
366.



















