
Evaluation of fracture resistance of ceramics: Edge fracture tests
d e n t a l m a t e r i a l s 2 9 ( 2 0 1 3 ) 1280–1286
Available online at www.sciencedirect.com
ScienceDirect
jo ur nal ho me pag e: www.int l .e lsev ierhea l th .com/ journa ls /dema
The influence of substance loss and ferrule heighton the fracture resistance of endodontically treatedpremolars. An in vitro study
Abdulaziz Samrana,b,c,∗, Shadi El Bahraa,d, Matthias Kerna
a Department of Prosthodontics, Propaedeutics and Dental Materials, School of Dentistry, Christian-AlbrechtsUniversity at Kiel, Kiel, Germanyb Department of Fixed Prosthodontics, School of Dentistry, Ibb University, Ibb, Yemenc Al-Farabi Dental College, Riyadh, Saudi Arabiad Department of Removable Prosthodontics, School of Dentistry, Damascus University, Damascus, Syria
a r t i c l e i n f o
Article history:
Received 3 February 2013
Received in revised form
14 August 2013
Accepted 7 October 2013
Keywords:
Residual coronal wall
Ferrule height
Glass fiber post
Resin cement
a b s t r a c t
Objective. This study evaluated the effect of different ferrule heights and varying degrees of
substance loss on the fracture resistance of endodontically treated premolars.
Methods. Eighty extracted and endodontically treated lower premolars were used and divided
into 5 test groups (n = 16) depending on the ferrule height: A (0.0 mm), B (0.5 mm), C (1.0 mm),
D (1.5 mm) and E (2.0 mm) respectively. Teeth in subgroups were either with 1 or 2 residual
coronal dentin walls which were 3 mm in height and 1 mm in thickness. Teeth were restored
with glass fiber posts and cast crowns. All specimens were then subjected to dynamic load-
ing in a masticatory simulator for 1,200,000 loading cycles with a nominal load of 5 kg at
1.2 Hz combined with thermal cycling (5–55 ◦C, dwell time 30 s). Then specimens were quasi-
statically loaded at 30◦ in a universal testing machine until fractured. Data were analyzed
with 2-way ANOVA, followed by multiple comparisons using Tukey HSD test ( ̨ = .05).
Results. Mean (SD) failure loads for groups ranged from 679.5 ± 164.9 N to 1084.5 ± 269.9 N.
Two-way ANOVA revealed that both the ferrule height and the number of residual coronal
walls had a significant influence on the fracture resistance (P < .001 and P = .006, respectively).
Significant increases were produced in the final fracture resistance, when the ferrule height
was increased, which was reduced to approximately 37% when teeth with 2 mm ferrule
height were compared with teeth without a ferrule.
Significance. Under the conditions of this in vitro study, increasing the number of resid-
ual coronal walls and ferrule height had a significant effect on the fracture resistance of
ed pr
emy
in an increase of the likelihood of fracture of the treated
endodontically treat
© 2013 Acad
1. Introduction
Endodontically treated teeth (ETT) have been problematicbecause of coronal destruction from dental caries, fractures,
∗ Corresponding author at: Department of Prosthodontics, PropaedeutUniversity at Kiel, Arnold-Heller Strasse 16, 24105 Kiel, Germany. Tel.: +
E-mail addresses: [email protected], [email protected]/$ – see front matter © 2013 Academy of Dental Materials. Puhttp://dx.doi.org/10.1016/j.dental.2013.10.003
emolars restored with prefabricated posts.
of Dental Materials. Published by Elsevier Ltd. All rights reserved.
previous restoration, and endodontic therapy. This results
ics and Dental Materials School of Dentistry, Christian-Albrechts49 431 5972877; fax: +49 431 597 2860.
(A. Samran).
tooth during function [1]. The prognosis of ETT is influencedby different parameters such as amount of hard tissue loss[2], presence of a minimum of 1.5–2.0 mm ferrule height
blished by Elsevier Ltd. All rights reserved.

9 ( 2
priltlus
rpadeupblor
rttNeasrivfati
rwihar
2
2
EwsHa
ctfsCr
d e n t a l m a t e r i a l s 2
reparation [3], material and design of post and core mate-ial used [4]. The susceptibility to fracture of a restored tooths increased with the loss of coronal dentin. Therefore, toothongevity will depend on the amount of remaining tooth struc-ure and the efficiency of the restorative procedures to replaceost structural integrity [5]. A treatment using posts should besed only for retention of a core within the remaining toothtructure but not for aiming to strengthen the tooth [6].
Several post system techniques are available for theestoration of ETT and can be divided into custom-made castost and core systems and prefabricated post systems. Therere many concerns when using custom-made metallic postsue to their inhomogeneous stress distribution, biological sideffects due to microleakage and corrosion, and the dark colornder all-ceramic restorations [7]. The popularity of the fiberosts is due to their favorable physical properties [8] and theirond strength is equivalent to adhesively or conventionally
uted gold posts [9]. They were reported to reduce the riskf tooth fracture and display higher survival rates than teethestored with rigid zirconia posts [10].
An important element for tooth preparation is the incorpo-ation of a ferrule design. Sorensen and Engelman describedhe ferrule as the coronal dentinal extension of the tooth struc-ure occlusal to the shoulder preparation [11]. Libman andicholls suggested that to achieve the full benefits of ferruleffect, it should be a minimum of 1.5 mm in height with par-llel dentin walls, totally encircling the tooth and ending onound tooth structure [12]. Many studies investigating the fer-ule effect have used cast posts and cores [13–15], but theres little information as to whether the ferrule is of additionalalue in providing reinforcement in teeth restored with pre-abricated glass-fiber posts and composite cores [16]. Mangoldnd Kern [17] described the influence of posts on fracture resis-ance of ETT with varying substance loss but they did notndicate the effect of the different ferrule height in their study.
Therefore, the aim of this study was to evaluate the fractureesistance of endodontically treated premolars (ETPs) restoredith glass-fiber posts when different ferrule heights and vary-
ng degrees of substance loss were incorporated. The nullypothesis of the study was that neither ferrule height nor themount of residual coronal dentin would affect the fractureesistance of crowned premolars.
. Materials and methods
.1. Test groups
ighty recently extracted caries-free lower premolars, whichere removed for orthodontics or periodontal reasons, were
elected and then stored in 0.1% thymol solution (Caelo,ilden, Germany). The teeth were cleaned with a hand scalernd stored then at room temperature during the study.
Endodontic access cavities were prepared using a waterooled air turbine handpiece. During root canal preparationhe working length was set at 1 mm short of the apical
oramen. The teeth were endodontically prepared using thetep-back technique to an ISO size 50 (K-files; Dentsply De Trey,onstance, Germany), irrigated with 3% sodium hypochlo-ite solution (Hedinger, Stuttgart, Germany) and dried with0 1 3 ) 1280–1286 1281
paper points (Coltene/Whaledent Inc., Langenau, Germany).Each canal was obturated using the lateral condensationmethod with gutta-percha points (Coltene/Whaledent Inc.)and sealed with an eugenol-free epoxyamine resin sealer(AH Plus; Dentsply De Trey). After 24-h water storage at37 ◦C, gutta-percha was removed using no. 2,3,4 Gates-Gliddenburs (Maillefer, Ballaigues, Switzerland). The teeth roots wereembedded into brass tubes, using an auto-polymerizing resin(Technovit 4000; Heraeus Kulzer, Wehrheim, Germany) up to2 mm apical to the cemento-enamel junction (CEJ) and ori-ented their long axes perpendicular to horizontal using acustom-made surveyor. The ETPs received 0.8 mm shoulderfinish lines which were mesial and distal 1 mm more coronalthan the facial and lingual surfaces and which were cervicalto the (CEJ). Burs were replaced after 8 preparations, in orderto ensure high cutting efficacy. For teeth preparations, dia-mond rotary cutting instruments (Brasseler, Lemgo, Germany)under copious air-water cooling were used (with a 2◦ taper toachieve a 4◦ convergence angle) in a high-speed handpiecemounted on a custom-made parallelometer to standardizethe preparation for all specimens. The teeth were assignedrandomly to 5 groups of 16 teeth each according to the fer-rule height. The properties of the specimens included in eachgroup were as follows: group A: specimens without circumfer-ential ferrule; group B: circumferential ferrule 0.5 mm abovethe finish line; group C: circumferential ferrule 1 mm abovethe finish line; group D: circumferential ferrule 1.5 mm abovethe finish line; group E: circumferential ferrule 2 mm above thefinish line. Teeth in subgroups had either 1 residual facial wall(A1, B1, C1, D1 and E1) or 2 residual facial and lingual walls(A2, B2, C2, D2 and E2). The walls were 3 mm high and 1 mmthick.
Post spaces were accomplished with a tapered drill (ER-postkit; Brasseler) of ISO size 90 to achieve an intraradicular postlength of 7.5 mm for all teeth. The coronal opening of the postspace was enlarged in a facio-lingual direction to a 3 mm inwidth and 2 mm in depth to resist rotation and to standardizethe coronal openings and the thickness of residual coronalwalls. The walls of the post preparation were roughened usinga diamond-coated hand instrument 3 times (ER Post Systems;Brasseler) [18].
The glass-fiber posts (Komet ER DentinPost; ISO size 90,Brasseler) were airborne-particle abraded for 5 s at a distanceof 30-mm with 50 �m alumina particles (Heraeus Kulzer) at0.25 MPa and ultrasonically cleaned in 96% isopropanol (Ger-man Federal Monopoly Administration for Spirits, Hamburg,Germany) for 3 min. The post spaces were then irrigated witha 3% sodium hypochlorite solution and dried with paperpoints, followed by irrigating with 70% ethanol (German Fed-eral Monopoly Administration for Spirits) and drying withpaper points.
The posts were luted with adhesive composite-resincement using a microbrush (Panavia 21 TC; Kuraray Medical,Osaka, Japan) after conditioning the dentin with the system’sautopolymerizing primer (ED-Primer; Kuraray) for 60 s. Theresin cements were mixed and applied according to the man-ufacturer’s instructions. Excess luting resin was used to coat
the coronal portion of the post. An auto-polymerizing com-posite resin (Clearfil Core; Kuraray Medical, Osaka, Japan) wasapplied as the core material according to the manufacturer’s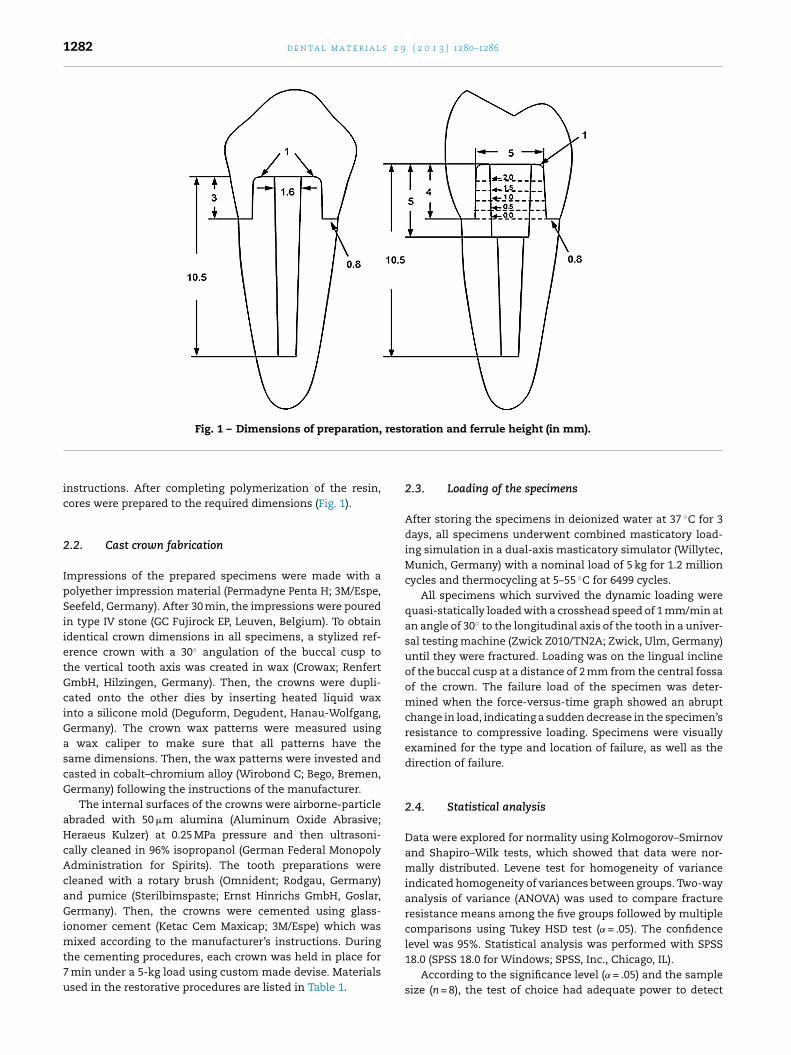
1282 d e n t a l m a t e r i a l s 2 9 ( 2 0 1 3 ) 1280–1286
Fig. 1 – Dimensions of preparation, restoration and ferrule height (in mm).
instructions. After completing polymerization of the resin,cores were prepared to the required dimensions (Fig. 1).
2.2. Cast crown fabrication
Impressions of the prepared specimens were made with apolyether impression material (Permadyne Penta H; 3M/Espe,Seefeld, Germany). After 30 min, the impressions were pouredin type IV stone (GC Fujirock EP, Leuven, Belgium). To obtainidentical crown dimensions in all specimens, a stylized ref-erence crown with a 30◦ angulation of the buccal cusp tothe vertical tooth axis was created in wax (Crowax; RenfertGmbH, Hilzingen, Germany). Then, the crowns were dupli-cated onto the other dies by inserting heated liquid waxinto a silicone mold (Deguform, Degudent, Hanau-Wolfgang,Germany). The crown wax patterns were measured usinga wax caliper to make sure that all patterns have thesame dimensions. Then, the wax patterns were invested andcasted in cobalt–chromium alloy (Wirobond C; Bego, Bremen,Germany) following the instructions of the manufacturer.
The internal surfaces of the crowns were airborne-particleabraded with 50 �m alumina (Aluminum Oxide Abrasive;Heraeus Kulzer) at 0.25 MPa pressure and then ultrasoni-cally cleaned in 96% isopropanol (German Federal MonopolyAdministration for Spirits). The tooth preparations werecleaned with a rotary brush (Omnident; Rodgau, Germany)and pumice (Sterilbimspaste; Ernst Hinrichs GmbH, Goslar,Germany). Then, the crowns were cemented using glass-ionomer cement (Ketac Cem Maxicap; 3M/Espe) which was
mixed according to the manufacturer’s instructions. Duringthe cementing procedures, each crown was held in place for7 min under a 5-kg load using custom made devise. Materialsused in the restorative procedures are listed in Table 1.2.3. Loading of the specimens
After storing the specimens in deionized water at 37 ◦C for 3days, all specimens underwent combined masticatory load-ing simulation in a dual-axis masticatory simulator (Willytec,Munich, Germany) with a nominal load of 5 kg for 1.2 millioncycles and thermocycling at 5–55 ◦C for 6499 cycles.
All specimens which survived the dynamic loading werequasi-statically loaded with a crosshead speed of 1 mm/min atan angle of 30◦ to the longitudinal axis of the tooth in a univer-sal testing machine (Zwick Z010/TN2A; Zwick, Ulm, Germany)until they were fractured. Loading was on the lingual inclineof the buccal cusp at a distance of 2 mm from the central fossaof the crown. The failure load of the specimen was deter-mined when the force-versus-time graph showed an abruptchange in load, indicating a sudden decrease in the specimen’sresistance to compressive loading. Specimens were visuallyexamined for the type and location of failure, as well as thedirection of failure.
2.4. Statistical analysis
Data were explored for normality using Kolmogorov–Smirnovand Shapiro–Wilk tests, which showed that data were nor-mally distributed. Levene test for homogeneity of varianceindicated homogeneity of variances between groups. Two-wayanalysis of variance (ANOVA) was used to compare fractureresistance means among the five groups followed by multiplecomparisons using Tukey HSD test ( ̨ = .05). The confidence
level was 95%. Statistical analysis was performed with SPSS18.0 (SPSS 18.0 for Windows; SPSS, Inc., Chicago, IL).According to the significance level ( ̨ = .05) and the samplesize (n = 8), the test of choice had adequate power to detect

d e n t a l m a t e r i a l s 2 9 ( 2 0 1 3 ) 1280–1286 1283
Table 1 – Materials used for restorative procedures.
Material Company Batch number
ER Dentin Post Brasseler, Lemgo, Germany 676303Clearfil Core Kuraray, Osaka, Japan 041523Permadyne Penta H 3M/Espe, Seefeld, Germany Heavy 434544Light 422524Panavia 21 Kuraray, Osaka, Japan 041344Ketac Cem Maxicap 3M/Espe, Seefeld, Germany 347837Cobalt-chromium alloy Wirobond C, Bego, Bremen, Germany 3533
Table 2 – Fracture loads in N [means (SD)].
Group 1 residual coronal wall 2 residual coronal walls
A A1: 679.5 (164.9) A2: 754.9 (193.4)B B1: 742.6 (166.6) B2: 824.0 (157.7)C C1: 824.7 (194.3) C2: 933.9 (145.5)D D1: 854.0 (232.1) D2: 1052.3 (187.0)
.4)
2 mm
srsc
3
NTttircw(sr
dTsamapaftbtc
4
ThTdm
E E1: 932.2 (206
A, no ferrule; B, 0.5 mm ferrule; C, 1 mm ferrule; D, 1.5 mm ferrule; E,
tatistical differences which could be used to provide clinicalecommendations (F = .11). Failure modes were recorded andtatistically analyzed with Chi-square (X2) testing for signifi-ant correlation between design and failure modes.
. Results
one of the specimens failed during masticatory simulation.he mean values of the fracture strength and standard devia-
ions are displayed in Table 2. They ranged from 679.5 ± 164.9 No 1084.5 ± 269.9 N. The fracture resistance of each groupncreased when the ferrule height increased and a secondesidual coronal wall existed. Two-way ANOVA (Table 3) indi-ated that both the ferrule height and the number of residualalls had a significant influence on the fracture resistance
P ≤ .001 and P = .006, respectively). There was no statisticallyignificant interaction between the factors ferrule height andesidual coronal walls (P = .889).
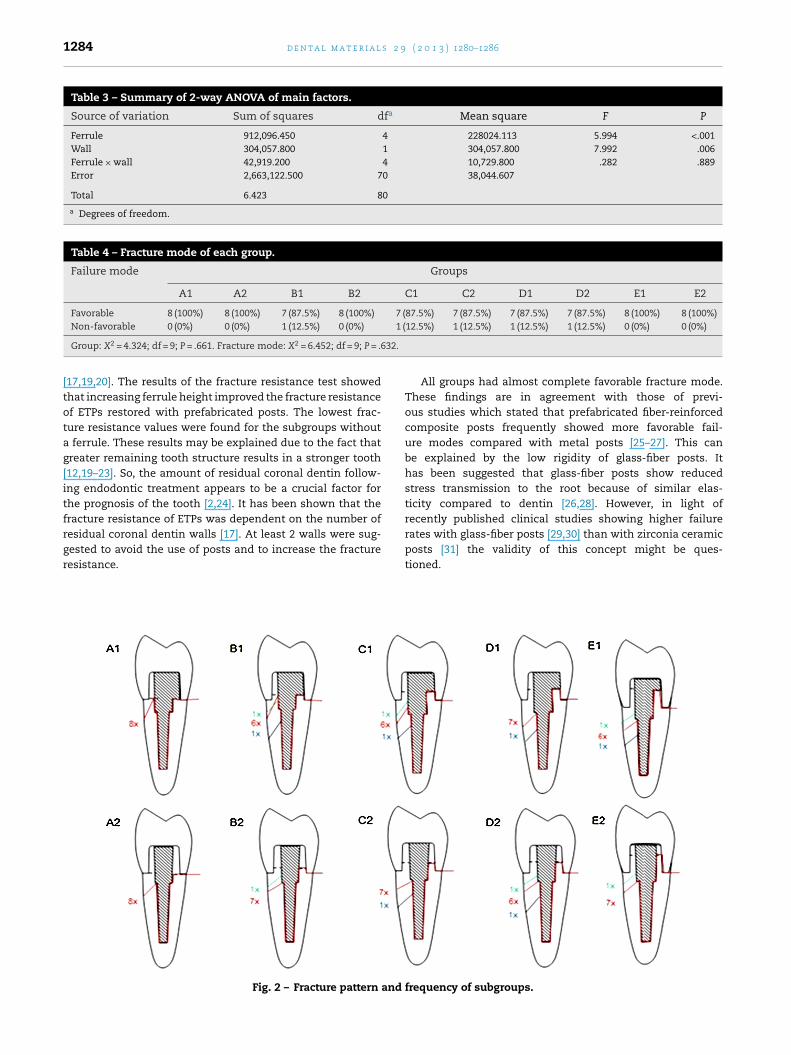
Chi-square (X2) test revealed that there were no significantifferences in fracture modes among the 10 groups (Table 4).he mode of failure was determined by visual inspection of allpecimens. The type of fracture behavior and the frequencyre illustrated in Fig. 2. There were 2 typical root fractureodes: cervical third fracture (favorable mode), middle and
pical third (catastrophic mode). All groups had almost com-lete favorable fracture mode. The fracture behavior in A1, B1,nd C1 subgroups with 1 residual coronal wall differed slightlyrom that in subgroups with 2 residual coronal walls, wherehe fracture line crossed into the dental substance whichegan further facially. Nearly all the teeth had a facial frac-ure by 2–4 mm below the crown margin and lingual along therown margin.
. Discussion
he present study investigated the influence of five ferrule
eights on the fracture resistance of crowned lower premolars.eeth in subgroups were either with 1 or 2 residual coronalentin walls. Eight specimens per group were exposed to ther-al cycling and mechanical loading and loaded until theyE2: 1084.5 (269.9)
ferrule height; 1, 1 residual wall; 2, 2 residual walls.
fractured. Eight specimens per subgroup were chosen because8 specimens can be loaded at a time in the masticatory simu-lator. Teeth are generally prepared; however, with their finishlines following the coronal extension of the gingival tissuelevel interproximally. To mimic this clinical condition, thefinish lines in this study were mesial and distal 1 mm morecoronal than the facial and lingual surfaces and which werecervical to the CEJ.
A custom-made parallelometer was used to standardizethe preparation for all specimens and the required dimensionswere obtained prior to core fabrication by reducing the toothstructure in a stepwise manner using a digital sliding caliperto control dimensions. After core fabrication only a low speedhandpiece with a fine grain diamond was used to finish thepreparation and only a minimal additional amount of dentinwas removed by that procedure. It must be admitted that thisresulted in a slight overestimation of the remaining coronaltooth structure. However, as this was done in the same man-ner in each group it is assumed that this did not affect theresults considerably.
The first hypothesis that the ferrule height would notaffect the fracture resistance of crowned premolars had tobe rejected. The ferrule height had a significant influenceon the final fracture resistance (P ≤ .001), which was reducedby approximately 37% when teeth with 2 mm ferrule heightwere compared with teeth without ferrule. In addition, theamount of residual coronal dentin had a significant influenceon the final fracture resistance of the restored teeth (P = .006).Therefore, the second hypothesis that the amount of resid-ual coronal dentin would not affect the fracture resistance ofcrowned premolars was also rejected.
Unfortunately, the authors identified no other studies thatevaluated the effect of the ferrule height and the numberof residual walls on the fracture strength of the crownedpremolars. None of the specimens failed during masticatorysimulation. For that reason, the fracture resistance of the agedspecimens to quasi-static loading could be determined in all
groups.The fracture resistance of the restored premolars rangedfrom 679.5 ± 164.9 N (group A1) to 1084.5 ± 269.9 N (groupE2) and can be compared well to previous in vitro studies
1284 d e n t a l m a t e r i a l s 2 9 ( 2 0 1 3 ) 1280–1286
Table 3 – Summary of 2-way ANOVA of main factors.
Source of variation Sum of squares dfa Mean square F P
Ferrule 912,096.450 4 228024.113 5.994 <.001Wall 304,057.800 1 304,057.800 7.992 .006Ferrule × wall 42,919.200 4 10,729.800 .282 .889Error 2,663,122.500 70 38,044.607
Total 6.423 80
a Degrees of freedom.
Table 4 – Fracture mode of each group.
Failure mode Groups
A1 A2 B1 B2 C1 C2 D1 D2 E1 E2
Favorable 8 (100%) 8 (100%) 7 (87.5%) 8 (100%) 7 (87.5%) 7 (87.5%) 7 (87.5%) 7 (87.5%) 8 (100%) 8 (100%)1 (
632.
Non-favorable 0 (0%) 0 (0%) 1 (12.5%) 0 (0%)
Group: X2 = 4.324; df = 9; P = .661. Fracture mode: X2 = 6.452; df = 9; P = .
[17,19,20]. The results of the fracture resistance test showedthat increasing ferrule height improved the fracture resistanceof ETPs restored with prefabricated posts. The lowest frac-ture resistance values were found for the subgroups withouta ferrule. These results may be explained due to the fact thatgreater remaining tooth structure results in a stronger tooth[12,19–23]. So, the amount of residual coronal dentin follow-ing endodontic treatment appears to be a crucial factor forthe prognosis of the tooth [2,24]. It has been shown that thefracture resistance of ETPs was dependent on the number of
residual coronal dentin walls [17]. At least 2 walls were sug-gested to avoid the use of posts and to increase the fractureresistance.Fig. 2 – Fracture pattern and
12.5%) 1 (12.5%) 1 (12.5%) 1 (12.5%) 0 (0%) 0 (0%)
All groups had almost complete favorable fracture mode.These findings are in agreement with those of previ-ous studies which stated that prefabricated fiber-reinforcedcomposite posts frequently showed more favorable fail-ure modes compared with metal posts [25–27]. This canbe explained by the low rigidity of glass-fiber posts. Ithas been suggested that glass-fiber posts show reducedstress transmission to the root because of similar elas-ticity compared to dentin [26,28]. However, in light ofrecently published clinical studies showing higher failure
rates with glass-fiber posts [29,30] than with zirconia ceramicposts [31] the validity of this concept might be ques-tioned.frequency of subgroups.
9 ( 2
suritntabfet
5
Rso
A
Tctpoc
r
d e n t a l m a t e r i a l s 2
In light of the results of this study, preservation of toothtructure is an important factor and maximizing the resid-al amount of coronal tooth structure will increase the toothesistance against fracture load. As in many in vitro studies,t is difficult to extrapolate the results of this study directlyo a clinical situation. The limitations of this study include:atural variations among natural teeth that lack a periodon-
al ligament and the preparation of the ferrule was placed at constant height around the periphery of the teeth. In vivo,y contrast, ferrule height usually varies around the circum-erence of the tooth. Therefore, further research is needed tovaluate the effects of non-uniform ferrule heights and theype of posts on the fracture resistance of ETTs.
. Conclusions
esidual walls should be preserved and the ferrule heighthould be kept maximal to increase the fracture resistancef ETPs.
cknowledgments
he authors thank Dr. Sandra Freitag-Wolf, Institute of Medi-al Informatics and Statistics, University of Kiel, for help withhe statistics. The authors acknowledge Brasseler-Komet forroviding the glass-fiber posts and corresponding drills freef charge and also Kuraray for providing the resin cement andomposite core materials free of charge.
e f e r e n c e s
[1] Carter JM, Sorensen SE, Johnson RR, Teitelbaum RL, LevineMS. Punch shear testing of extracted vital andendodontically treated teeth. J Biomech 1983;16:841–8.
[2] Bitter K, Noetzel J, Stamm O, Vaudt J, Meyer-Lueckel H,Neumann K, et al. Randomized clinical trial comparing theeffects of post placement on failure rate of postendodonticrestorations: preliminary results of a mean period of 32months. J Endod 2009;35:1477–82.
[3] Stankiewicz NR, Wilson PR. The ferrule effect: a literaturereview. Int Endod J 2002;35:575–81.
[4] Sidoli GE, King PA, Setchell DJ. An in vitro evaluation of acarbon fiber-based post and core system. J Prosthet Dent1997;78:5–9.
[5] Fernandes AS, Dessai GS. Factors affecting the fractureresistance of post-core reconstructed teeth: a review. Int JProsthodont 2001;14:355–63.
[6] Trope M, Maltz DO, Tronstad L. Resistance to fracture ofrestored endodontically treated teeth. Endod DentTraumatol 1985;1:108–11.
[7] Mannocci F, Ferrari M, Watson TF. Microleakage ofendodontically treated teeth restored with fiber posts andcomposite cores after cyclic loading: a confocal microscopicstudy. J Prosthet Dent 2001;85:284–91.
[8] Freedman GA. Esthetic post-and-core treatment. Dent ClinNorth Am 2001;45:103–16.
[9] Kremeier K, Fasen L, Klaiber B, Hofmann N. Influence ofendodontic post type (glass fiber, quartz fiber or gold) and
luting material on push-out bond strength to dentin in vitro.Dent Mater 2008;24:660–6.[10] Mannocci F, Ferrari M, Watson TF. Intermittent loading ofteeth restored using quartz fiber, carbon-quartz fiber, and
0 1 3 ) 1280–1286 1285
zirconium dioxide ceramic root canal posts. J Adhes Dent1999;1:153–8.
[11] Sorensen JA, Engelman MJ. Ferrule design and fractureresistance of endodontically treated teeth. J Prosthet Dent1990;63:529–36.
[12] Libman WJ, Nicholls JI. Load fatigue of teeth restored withcast posts and cores and complete crowns. Int J Prosthodont1995;8:155–61.
[13] Gegauff AG. Effect of crown lengthening and ferruleplacement on static load failure of cemented cast post-coresand crowns. J Prosthet Dent 2000;84:169–79.
[14] Sendhilnathan D, Nayar S. The effect of post-core andferrule on the fracture resistance of endodontically treatedmaxillary central incisors. Indian J Dent Res 2008;19:17–21.
[15] Tan PL, Aquilino SA, Gratton DG, Stanford CM, Tan SC,Johnson WT, et al. In vitro fracture resistance ofendodontically treated central incisors with varying ferruleheights and configurations. J Prosthet Dent 2005;93:331–6.
[16] Juloski J, Radovic I, Goracci C, Vulicevic ZR, Ferrari M. Ferruleeffect: a literature review. J Endod 2012;38:11–9.
[17] Mangold JT, Kern M. Influence of glass-fiber posts on thefracture resistance and failure pattern of endodonticallytreated premolars with varying substance loss: an in vitrostudy. J Prosthet Dent 2011;105:387–93.
[18] Balbosh A, Ludwig K, Kern M. Comparison of titanium dowelretention using four different luting agents. J Prosthet Dent2005;94:227–33.
[19] Akkayan B. An in vitro study evaluating the effect of ferrulelength on fracture resistance of endodontically treated teethrestored with fiber-reinforced and zirconia dowel systems. JProsthet Dent 2004;92:155–62.
[20] Pereira JR, de Ornelas F, Conti PC, do Valle AL. Effect of acrown ferrule on the fracture resistance of endodonticallytreated teeth restored with prefabricated posts. J ProsthetDent 2006;95:50–4.
[21] Zhi-Yue L, Yu-Xing Z. Effects of post-core design and ferruleon fracture resistance of endodontically treated maxillarycentral incisors. J Prosthet Dent 2003;89:368–73.
[22] Naumann M, Preuss A, Rosentritt M. Effect of incompletecrown ferrules on load capacity of endodontically treatedmaxillary incisors restored with fiber posts, compositebuild-ups, and all-ceramic crowns: an in vitro evaluationafter chewing simulation. Acta Odontol Scand 2006;64:31–6.
[23] Aykent F, Kalkan M, Yucel MT, Ozyesil AG. Effect of dentinbonding and ferrule preparation on the fracture strength ofcrowned teeth restored with dowels and amalgam cores. JProsthet Dent 2006;95:297–301.
[24] Peroz I, Blankenstein F, Lange KP, Naumann M. Restoringendodontically treated teeth with posts and cores—a review.Quintessence Int 2005;36:737–46.
[25] Cormier CJ, Burns DR, Moon P. In vitro comparison of thefracture resistance and failure mode of fiber, ceramic, andconventional post systems at various stages of restoration. JProsthodont 2001;10:26–36.
[26] Fokkinga WA, Kreulen CM, Vallittu PK, Creugers NH. Astructured analysis of in vitro failure loads and failuremodes of fiber, metal, and ceramic post-and-core systems.Int J Prosthodont 2004;17:476–82.
[27] Sherfudhin H, Hobeich J, Carvalho CA, Aboushelib MN, SadigW, Salameh Z. Effect of different ferrule designs on thefracture resistance and failure pattern of endodonticallytreated teeth restored with fiber posts and all-ceramiccrowns. J Appl Oral Sci 2011;19:28–33.
[28] Lassila LV, Tanner J, Le Bell AM, Narva K, Vallittu PK. Flexuralproperties of fiber reinforced root canal posts. Dent Mater2004;20:29–36.
s 2 9
[31] Bateli M, Kern M, Wolkewitz M, Strub JR, Att W. Aretrospective evaluation of teeth restored with zirconiaceramic posts: 10-year results. Clin Oral Invest 2013
1286 d e n t a l m a t e r i a l
[29] Schmitter M, Hamadi K, Rammelsberg P. Survival of two postsystems—five-year results of a randomized clinical trial.Quintessence Int 2011;42:843–50.
[30] Naumann M, Koelpin M, Beuer F, Meyer-Lueckel H. 10-yearsurvival evaluation for glass-fiber-supported postendodonticrestoration: a prospective observational clinical study. JEndodont 2012;38:432–5.
( 2 0 1 3 ) 1280–1286
http://dx.doi.org/10.1007/s00784-013-1065-5
Copyright © 2022 FDOKUMEN




















