
academic performance of substance abusing secondary ...
119
1 ACADEMIC PERFORMANCE OF SUBSTANCE ABUSING SECONDARY SCHOOL STUDENTS IN ABAKALIKI. A DISSERTATION SUBMITTED TO THE NATIONAL POSTGRADUATE MEDICAL COLLEGE IN PART FULFILMENT OF THE REQUIREMENTS FOR THE AWARD OF FELLOWSHIP OF THE COLLEGE IN THE FACULTY OF PEDIATRICS. BY DR ANYANWU, ONYINYE UCHENNA MBBS (SEPTEMBER 2001) EXAMINATION DATE: MAY 2015
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of academic performance of substance abusing secondary ...
1
ACADEMIC PERFORMANCE OF SUBSTANCE
ABUSING SECONDARY SCHOOL STUDENTS IN
ABAKALIKI.
A DISSERTATION SUBMITTED TO THE NATIONAL POSTGRADUATE
MEDICAL COLLEGE IN PART FULFILMENT OF THE
REQUIREMENTS FOR THE AWARD OF FELLOWSHIP OF THE
COLLEGE IN THE FACULTY OF PEDIATRICS.
BY DR ANYANWU, ONYINYE UCHENNA
MBBS (SEPTEMBER 2001)
EXAMINATION DATE: MAY 2015
2
DECLARATION
I hereby declare that this work, titled “ACADEMIC PERFORMANCE OF
SUBSTANCE ABUSING SECONDARY SCHOOL STUDENTS IN ABAKALIKI.”,
is original unless otherwise acknowledged. This work has neither been presented to
any College for the award of Fellowship, nor submitted elsewhere for publication.
..............................................................................
ANYANWU, ONYINYE UCHENNA
DATE ………………………………………….
3
ATTESTATION
The study reported in this dissertation was carried out by the candidate Anyanwu
Onyinye Uchenna under our supervision. We also supervised the writing of the
dissertation.
PROF. N.C OJINNAKA.
CONSULTANT PAEDIATRICIAN
UNIVERSITY OF NIGERIA TEACHING HOSPITAL, ENUGU
SIGNATURE___________________________________
DATE ________________________________________
DR R.C. IBEKWE
CONSULTANT PAEDIATRICIAN
UNIVERSITY OF NIGERIA TEACHING HOSPITAL, ENUGU
SIGNATURE___________________________________
DATE ________________________________________

4
TABLE OF CONTENTS
PAGE
Title i
Declaration ii
Attestation iii
Table of contents iv
List of abbreviations vi
Definitions viii
List of Tables x
List of appendices xii
Dedication xiii
Acknowledgement xiv
Summary xv
Introduction and Justification 1
Literature review 5
Aims and objectives 28
Participants and methods 29
Results 40
Discussion 57

5
Conclusion 64
Recommendation 65
Limitations 66
Lines of future study 67
References 68
Appendices 81
6
LIST OF ABBREVIATIONS
ADI-Adolescent Drinking Index
ASADA-Assessing the Seriousness of Adolescent Drug Abuse.
ASI-Addiction Severity Index
AUDADIS-Alcohol Use Disorders and Associated Disabilities Interview Schedule
CAGE- Cutting down, Annoyance by criticism, Guilty feeling, and Eye-openers.
CBCL-Child Behavior Checklist.
CIDI-Composite International Diagnostic Interview
Conner's CBRS-Conner's Comprehensive Behaviour Rating Scales.
CRAFFT- Car (have you ever been driven in the car of someone high on drugs?) Relax (do
you use drugs to relax?) Alone (do you use drugs while alone?) Friends/family (has your
friends or family members felt you had a drug problem?) Forget (do you forget/regret the
things you did while using drugs? ) Trouble (have you ever gotten into trouble for using
drugs?)
IQ-Intelligence Quotient.
LGA-Local Government Area.
NECO-National Examinations Council.
PESQ-Personal Experience Screening Questionnaire
PIAT-Peabody Individual Achievement Test.
PRISM-Psychiatric Research Interview for Substance and Mental Disorders

7
PSC-Pediatrics Symptom Checklist.
SAT-M Score-Scholastic Aptitude Test Mathematics score.
SCID-Structured Clinical Interview for DSM-IV
SCPS-School Children Problem Scale.
SDQ-Strength and Difficulty Questionnaire.
SPSS-Statistical Package for Social Sciences.
SSADDA-Semi-Structured Assessment for Drug Dependence and Alcoholism.
SSCE-Senior Secondary Certificate Examination.
TRF-Teacher Report Form.
UBE-Universal Basic Education.
WAEC-West African Examinations Council
WASC-West African School Certificate.
WHO-World Health Organization..
WRAT-Wide Range Achievement Test.
YSR-Youth Self Report.
8
DEFINITIONS
SUBSTANCE: A substance is any psychoactive or mood altering agent that is consumed for
pleasurable or other reasons rather than therapeutic purposes and also possesses habit forming
potential.
LICIT AND ILLICIT SUBSTANCES: Licit substances are substances which are not
prohibited by law example alcohol, coffee, kola nut and cigarette. While illicit substances are
substances whose use and possession are prohibited by law such substances are cannabis,
cocaine, and heroine.
SUBSTANCE USE: This implies that a person is in control of his/her use of a substance, or
is using it in a manner that is not harmful to health and is experiencing no social or
occupational impairment from its use. However for illicit substances they are liable for
possession and use of the substance prohibited by law.
SUBSTANCE ABUSE: The use of substances when they are not physiologically or
pharmacologically necessary; when they are used against legal prohibition like any use of
illicit drugs, or when there is a culturally inappropriate as well as excessive use of socially
acceptable substances like alcohol and tobacco especially if the abuser is unable to stop the
use of the substance. There is continuous abuse within 30days before the survey.
CURRENT SUBSTANCE USE: Substance abuse in the past 12months with continuous use
within 30days before the survey.
LIFETIME SUBSTANCE USE: Use of substance at least once in life.
PAST USE OF SUBSTANCE: Substance use but not within the last 12 months before the
survey.
9
DEPENDENCE: This occurs when a person is unable to lead a normal life without ingesting
the substance he is depended on. Psychological dependence implies that there is craving or an
overpowering drive or desire for the use of the substance to avoid discomfort that may arise
from not using the substance.
ADDICTION: It is a specific cluster of symptoms experienced by the addict when the
substance is abruptly or completely withdrawn, e.g. delirium tremens occurring in alcoholics
who suddenly withdraws from taking alcohol.
ACADEMIC PERFORMANCE: It is the extent to which a student has achieved his or her
educational goal. It is usually measured by performances in school examinations and
continuous assessment.
ADOLESCENT: Adolescence is defined by World Health Organisation (WHO) as the age
between 10-19 years, and is characterized by increased adventurous tendencies and peer
influences. Hence an adolescent is one aged 10 to 19 years.

10
LIST OF TABLES
Page
Table I: Number of Respondents and Number of Substances Abused 40
Table II: Socio-demographic characteristics of subjects and controls 41
Table III: Prevalence of Substance Abuse 42
Table IV: Prevalence of individual and combination substances of abuse. 43
Table V: Prevalence of Substance abuse within Age groups 44
Table VI: Prevalence of Substance abuse according to Gender 45
Table VII: Association between substance abuse and age at first use 46
Table VIII: Family structure of total respondents and its association with abuse of various
substances 48
Table IX: Overall academic score of subjects and control 49
Table X: Mean scores of subjects and controls in selected key class subjects and their overall
score 50
Table XI: Association between school absence and overall academic score of subjects and
controls 51
Table XII: Association between psychosocial dysfunction and overall academic score of
substance abusers and controls 52

11
Table XIII: Academic performance of subjects using different substances of abuse. 53
Table XIV: Association between the number of substances abused and overall academic score
of subjects 55
Table XV: Multiple regression analysis of factors associated with academic performance of
substance abusers and controls 56
12
LIST OF APPENDICES
Page
APPENDIX I: Letter of ethical approval from research and ethics committee Federal
Teaching Hospital Abakaliki (FETHA). 81
APPENDIX II: Letter of introduction from Ministry of Education Ebonyi. 83
APPENDIX III: Consent letter (students). 84
APPENDIX IV: Consent letter (parents/guardian). 86
APPENDIX V: Consent letter (principal) 88
APPENDIX VI: WHO student’s drug use questionnaire. 89
APPENDIX VII: Social classification by OLUSANYA et al 108 99
APPENDIX VIII: Assessing the seriousness of adolescent drug abuse (ASADA) scoring
method. 100
APPENDIX IX: Paediatrics Symptoms Checklist (PSC) – Youth report version 101
APPENDIX X: School data/ report 103
13
DEDICATION
To my ever loving and supportive husband CHUKWUEMEKA,
With whom I have these 6 lovely daughters,
Thank you for enduring till the very end of this program.
You Inspire Me.
I LOVE YOU.
14
ACKNOWLEDGEMENTS.
I express my heartfelt appreciation to my supervisors, Prof N C Ojinnaka, and Dr
R.C Ibekwe for painstakingly guiding me through my research work and manuscript writing.
Your constructive criticisms and patient guidance helped me perfect this work.
I thank all my teachers for guiding me through the various stages of residency
training. I will continue to make you proud. I also appreciate Mrs G C Ngwu of the Ministry
of Education Ebonyi State and the authorities of the various schools used for this study
whose approval made this work possible.
I appreciate Dr L U Ogbonnaya (Professor of Community Medicine), and his wife,
Dr C.E Ogbonnaya both of whom made my residency training dream come true. To my
father Eze (Dr) E.O Nwigwe, and mother Prof H.C Nwigwe (Ugoeze), I'm eternally grateful
for your support all through my stay here in Abakaliki. My siblings Obiyo, Chinenye, and
Munachiso, your individual encouragement have helped me all the way.
I appreciate my lovely daughters Hadassah, Shalom, Tehilah, Nagge, and my twins
Orna and Rinnah who had to endure the burden of being without their mother so many times
because mummy had to work and study. Your prayers kept me strong at my lowest moments.
Above all I thank God Almighty for being my source of strength all through the
training.

15
SUMMARY
Academic performance of students may be influenced by substance abuse. Substance
abuse could result in increased school absence while increasing predisposition to behavioral
disorders which may result in poor concentration thereby hindering the abuser from
benefiting from schooling. Poor academic performance undermines efforts made by parents
and teachers to impart knowledge on students in a bid to improve their future income
capabilities.
Six hundred and twenty senior secondary 2 and 3 students selected in a multi-staged
manner were screened for substance abuse using the WHO students’ drug use questionnaire.
Academic performance, school absence, psychosocial impairment of substance abusing
students was compared with those of their classmates matched for age, sex and socio-
economic class.
Prevalence rate of substance abuse obtained was 32.9% and alcohol was the most
commonly abused substance. There was a general poor academic performance of students
although the academic performance of substance abusing students(67.3%) was significantly
(p<0.001) poorer than that of control(35.8%). Substance abusers also had lower scores in the
four subjects studied (biology, English, Igbo and mathematics) when their scores were
compared with non-substance abusing students. There was also higher mean number of days
absent from school (14.68+4.79 for subjects; 9.50+3.84 days for controls; p<0.001) as well as
a higher prevalence of psychosocial dysfunction amongst substance abusers (43.7% of
subjects against 13.9% of controls). Age at initiation of substance (p=0.006) as well as use of
multiple substances (p=0.003), were the most important determinants of academic
performance of substance abusers. However, school absenteeism (p<0.001) was the
16
underlying determinant of academic performance of all students whether substance abusing
or non-substance abusing.
It is concluded that substance abuse is high among secondary school students in
Abakaliki and that the academic performance of substance abusers is poorer than that of
those who do not abuse substances. It is therefore recommended that substance abuse and
school absenteeism should be considered in students with poor academic performance in
senior secondary schools in Abakaliki.
17
INTRODUCTION
Substance abuse is a complex behavior seen amongst young people all over the
world.1 Reports from epidemiological studies in Nigeria,2-4 Ghana,5 South Africa,6,7 Kenya,8
and the United States 9 have shown alarming figures of substance abuse among young people.
Abuse of substance is now recognized as a significant public health problem worldwide.10
Adolescence which is defined by World Health Organization (WHO)11 as the age
between 10-19 years, is characterized by increased adventurous tendencies and peer
influences.12 During this period, children establish their individuality and become
independent. They tend to form gangs, and are often seen 'hanging' around with peers
experimenting with new things including the use of substance.13 Young people often start by
taking ‘gateway’ substances like cigarette and alcohol from which they gradually progress to
other substances to degrees that control their behavior.14
Previous authors13,15,16 have identified some reasons for the use of substances by
adolescents. These include curiosity, suppression of anxiety or mustering courage to speak to
the opposite sex, a way of fitting into the desired gang or social clubs, and as a means to
feeling ‘high’ at all times. Other reported reasons include availability of substances, parental
influence, as children from homes where parents take substances are often more likely to do
the same. Kola nut and coffee are often consumed to keep awake during examinations.15,16
Adolescents’ who abuse substances are exposed to risks and consequences that can
manifest physically, psychosocially and behaviorally.17 For instance, the abuse of
psychoactive substances is known to increase the incidence of psychosocial disorders in the
adolescent.17,18 In addition, drunkenness, risky sexual behavior and other delinquent behavior
18
like stealing and running away from home have also been reported amongst substance
abusers.19,20
Several authors21-23especially in the developed countries have noted poor school
performance in adolescents who abuse substances. Such students have been reported to have
declining school grades, dropping out of school and impaired concentration, memory and
thinking.21-23 It has also been found that college students who used marijuana regularly had
impaired skills related to memory, attention and learning 24 hours after using the substance.24
Furthermore deficits in mathematical skills, verbal expression, as well as selective
impairments in memory-retrieval processes were observed in those who used marijuana
seven or more times weekly.24 Lukoye et al25 reported poor academic performance amongst
4.4% of first year university students in Kenya who abuse cigarette. Similarly, Cox et al26 in
a survey of academic performance and substance use among public high school students
noted low academic performance in those that drunk heavily, smoked frequently and used
marijuana. The authors26 adjudged participants who had mostly grade-C and below as having
low academic performance.
Academic performance of an adolescent affects the individual as well as the society at
large. Poor academic performance may frustrate a student and lead to dropout on the short-
term while affecting the individual’s future occupational prospects.27 Poor performance
academically of a large group of adolescents, affects the society by increasing unemployment
and reducing the development of human capital, while undermining the mission of investing
in schooling.27
Abakaliki, the capital of Ebonyi state in South Eastern Nigeria is an emerging city.
People migrate from the rural to the urban center. A prevalence of 27.1% was observed as the
rate of adolescent substance abuse in an earlier study in Abakaliki.30 There has been empirical
19
observation of increasing crime rate such as rape and armed robbery, majority of the culprits
were young adolescents who should be in secondary schools. Studies have shown that such
crimes and behaviors may be associated with substance abuse.19,20,28 The government of
Ebonyi state has tried to encourage literacy in the populace by introducing the Universal
Basic Education (UBE) scheme and improving the states of boarding facilities in secondary
schools so that students can have conducive environments for studying to improve their
performance academically. However, students have performed poorly at recent exit external
examinations, West Africa School Certificate (WASC) exams and the National Examination
Council’s (NECO) exams. Less than 30% of students who took these exams achieved the five
credits with English language and mathematics inclusive required for entrance into higher
institutions in Nigeria.29 Many reasons have been postulated as being responsible for this
worrying academic trend, one of which is the high prevalence of substance abuse reported
among adolescents in Abakaliki.30 This association is anecdotal, there has been no study to
test this hypothesis. This study aims at establishing the pattern of substance abuse amongst
secondary school students in Abakaliki and the academic performance of such substance
abusing students. It also hopes to determine if there is any association between substance
abuse and the academic achievement of these students.
JUSTIFICATION
The school is a place where young people gather to learn. In schools students not only
receive the instructions given during each subject, they also learn to interact with each other.
Peer pressure and the need to belong to a certain group of friends arise in schools especially
in the period of adolescence. Most substance abusers were introduced to it by friends at
school.30-32 This makes the school a good site for the study of substance abuse.
Substance abuse is an increasing problem amongst youths in Nigeria and the world at
large. Data from school surveys in Nigeria have shown a rising prevalence and a decreasing
20
age at onset of substance use.33-36 Other studies have shown not just a rise in consumption,
but also increasing female involvement and a trend towards multiple substance use among
Nigerian adolescents.33,34 Substance abuse has negative effects on the user’s physical, mental,
behavioral and emotional health which may affect performances in school.
Academic performance of students may be influenced by substance abuse since
substance use could result in poor concentration, memory loss and absences from studies.
Poor academic performance undermines the efforts parents and teachers put into imparting
knowledge on students while frustrating the student and may lead to school dropout. Also,
failing to achieve good grades in school could be a pointer to delinquent behavior in
adolescents who abuse substances. Although there is a high prevalence of substance abuse
among secondary school students in Abakaliki, 30 there has been no report on the academic
performance of such students. The absence of any study describing the academic performance
of such students in Abakaliki and the factors influencing their academic performance justifies
the study.
This study aims not only at adding to existing data on the prevalence and factors
associated with substance abuse among secondary school students, but also to describe the
academic performance of such substance abusing adolescents with the aim of forming the
basis for policies for their educational program.
21
LITERATURE REVIEW
Definitions of Substance Abuse
A substance is any chemical agent other than food which affects a living organism.37
These agents interact with the body system to modify its physiological and biological
processes.38 Odejide39 and Obianwu40 both defined substances as agents that act mainly on
the brain and affect psychological function resulting in effects such as sedation, stimulation
and change in mood or behavior. Substances also possess the potential for habit
formation.39,40
Substance abuse as defined by the World Health Organization Expert committee on
Drug Dependence is the persistent or sporadic excessive substance use inconsistent with or
unrelated to acceptable medical practice.41 By this definition, intentional use of large
quantities and the intentional use of therapeutic doses for purposes other than that for which
the drug is indicated are inclusive. The terms, misuse and non-medical use were used
synonymously with abuse in this definition.41 This definition however, includes all
pharmaceutical agents and not just psychoactive substances. Abiodun42 defined substance
abuse as taking a substance which harms or threatens to harm the physical or mental health of
an individual or the society at large. The author42 opined that the effect of substance use was
not just on the individual but involved the society. Odejide39 on the other hand, defined
substance abuse as the use of agents, when they are not medically indicated, when they are
used against legal prohibition or when there is an excessive use of socially acceptable
substances such as tobacco and alcohol. These socially acceptable substances were termed
licit while the legally prohibited substances were termed illicit substances.43 In addition,
Obot44 defined substance use as consumption, in any form, of a substance to alter mood or
behavior, and that when a substance is used beyond culturally accepted limits it becomes
22
abuse. This supposes that substance use and abuse are stages of a process with abuse being a
severe form of substance use. Furthermore, Burns45 defined substance abuse as a pathological
pattern of use of a substance, characterized by the inability to control its use resulting in
impairment in social and occupational functioning with the duration of abuse being at least
one month. Ebie and Ebie38 brought in the aspect of society, by defining substance abuse as
the use of a substance viewed by the society concerned as posing a problem. The authors38
suppose that a person is termed as abusing a substance only if it poses a problem to the
society.
History of Adolescent Substance Abuse in Nigeria
Cannabis, in the form of marijuana or Indian hemp leaves, was the first illicit drug of
abuse in Nigeria.46 It was introduced into Nigeria by sailors and retiring soldiers returning
from the Middle East and North Africa during and after the Second World War.47 The abuse
of cannabis was first noticed in 1960, and in 1966, the Indian hemp Decree was promulgated
to control the wide spread use of the substance.47 By the 1970’s and early 80’s the abuse of
alcohol and other prescribed drugs by young people came to the forefront.46 In the early
1980’s cocaine and heroin were introduced to the scene as the country became a trans-
shipment route for drugs meant for Europe and America.48 Since then, urbanization, with the
adoption of the western life-style, in addition to increased availability and affordability of
substances have contributed to the shifts in the pattern and types of substances abused in
Nigeria.16,31
Scope and Prevalence of Adolescence Substance Abuse
Alcohol

23
Alcohol is a substance of dependence which is produced by fermentation, a process
which turns sugar into ethanol.39 Alcoholic beverages abound in Nigeria, from the traditional
drinks such as palm wine (the sap of either the oil or raffia palm tree), burukutu (produced by
fermentation of millet) and ogogoro (a gin-like distillate of palm wine) to the western types
such as beer, rum and gin introduced to Nigeria by Europeans.39,49 Since the advent of the
Europeans, beer has become the most popular type of alcoholic beverage in Nigeria and has
resulted to an increase in the number of breweries in Nigeria.36 Furthermore, the availability
of alcoholic beverages has made its consumption common especially amongst adolescents in
secondary schools. It was consumed more by males than females, however authors38 have
observed that the difference in prevalence rates of alcohol consumption between males and
females is narrowing.
Epidemiological studies33,34 have shown alcohol as the most commonly abused
substance. This is because it is readily available and can be easily accessed by adolescents. In
Enugu South Eastern Nigeria, Igwe et al50 working amongst secondary school students in
SS2 and SS3 showed that 31.6% of respondents currently used alcohol, majority of whom
were males (67.3%). In contrary, 12% of senior secondary students were reported to abuse
alcohol in Ilorin, Middle belt Nigeria.51 On the other hand, Odejide and Olatawura32 in
Western Nigeria reported an abuse rate of 9% in a rural community, while Anochie et al52
reported that 36.4% of secondary school students in Port Harcourt, had tried alcohol at least
once. The authors52 also reported that, 12% of their participants were currently using it on a
regular basis. The varied prevalence rate may be attributed to the differing case definitions
used by the different authors as well as cultural behaviors in different localities. While Igwe
et al50 and Anochie et al52 studied current alcohol use and obtained higher figures, Abiodun et
al51 and Odejide and Olatawura32 studied those whose current use of alcohol was to such a
degree as can be adjudged abuse, and hence obtained lower prevalence rates. Cultural
24
practices may also contribute as some tribes in Rivers state introduce alcohol to their
newborn and young children. It is also worthy of note that the study by Odejide and
Olatawura32 was conducted in a rural community where limitations of access exists to alcohol
use. The low rate of 9%, reported may be due to strong cultural inhibitions which may have
resulted in actual low prevalence rates, and or to under-reporting. All except the study by
Anochie et al52 showed male preponderance in alcohol abuse. This observation may be due to
the fact that Port Harcourt is a highly industrialized city which supposes that there may be an
increased availability of alcohol to both males and females alike. Alcohol acts primarily as a
central nervous system depressant resulting in euphoria, talkativeness, impaired short-term
memory and reduced inhibition.53
Cannabis
Cannabis is a mind altering substance made from a plant called cannabis sativa which
thrives in both temperate, and tropical climates including Nigeria.53 It has many street names
in Nigeria such as weewee, ganja, grass, daga, bang, hashish, charas, stone, kaya, pot, weed,
igbo, morocco and Indian hemp amongst others.54
Several authors50,55,56 have reported variable prevalence rates of cannabis abuse
amongst secondary school students in Nigeria. Igwe et al50 reported cannabis abuse rate of
4.1% in senior secondary school students in Enugu South Eastern Nigeria and noted that
cannabis was used exclusively by males. In Port Harcourt, Southern Nigeria, Anochie and
Nkanginieme2 reported that amongst secondary school students, 3.6% of males,and 2.2% of
female participants were current abusers of cannabis. Similarly, Oshodi and Aina55 in Lagos,
Western Nigeria, reported cannabis abuse rate of 4.4% amongst secondary school students.
The authors55 report however, was of those who had ever used cannabis in their lifetime and
did not bring into cognizance those who were currently using the substance suggesting that
25
the actual prevalence of cannabis abuse in their population may have been lower than they
reported. Males also had a higher lifetime use of this substance in the study.55 Furthermore,
Shehu and Idris56 working in Zaria, Northern Nigeria reported cannabis abuse rate of 9.4%
among secondary school students with 90% of them being males. The reported low
prevalence rates of cannabis abuse may represent its true prevalence or may be attributable to
denial since cannabis use is prohibited by law. This supports the postulation of Fatoye and
Morakinyo34 who observed that there remained a low reported prevalence rate of cannabis
use among secondary school students in Nigeria in spite of the high cannabis-related
psychiatric disorders observed amongst students in Nigerian psychiatric clinics. This they
attributed to denial because of the legal consequences associated with cannabis use.
Cannabis contains tetrahydrocannabinol which exerts its effect on the central nervous
system (CNS) to produce euphoria, loss of inhibition, hallucinations, reduced concentration,
feeling of relaxation and sleepiness.31,39
Tobacco
Tobacco is derived from a plant named nicotiana tabacum which was cultivated for
its medicinal and mystical uses in the 14th century.34 Recently the use of tobacco has changed
from its use for mystical reasons to consumption in the form of cigarette, cigar, pipe tobacco,
chewing tobacco and the traditional snuff.30 Cigarette smoking has become the most favored
form of tobacco use in Nigeria while snuffing remains popular in the rural areas amongst
older persons.30
Advertisements and promotion of sporting, cultural and social activities by cigarette
manufacturing companies have increased the rate of cigarette smoking.36 Nigerian studies2-
4,16,50,52 have revealed a high prevalence rate of cigarette smoking among secondary school
boys and girls. Igwe et al50 reported that 14.3% of senior secondary school students in Enugu,
26
South Eastern Nigeria currently used cigarette. In their study50 all respondents who used
cigarettes were males. This report is remarkably higher than that documented by Anochie et
al52 in Port Harcourt metropolis where a prevalence rate of 2.7% was reported and higher also
than the 6.4% prevalence reported by Odey et al57 in Calabar South East Nigeria. These later
studies52,57 not only reported current cigarette use rather, their report was on the participants
who currently used cigarette excessively and had tried but were unable to stop cigarette use
which defines abuse. Salawu et al58 on the other hand studied adolescents aged between 12
and 17 years in communities in Yola, Adamawa state Northern Nigeria and reported a
prevalence of 33.6%. Their study58 was carried out on adolescents randomly selected from
the market area. It is worthy of note that their participants were out of school, reasons for
being out of school, and at the market area instead were unknown to the researchers. This
therefore, may have accounted for the remarkably high prevalence rate for cigarette use.
Cigarette smoking has been associated with so many illnesses like lung cancer, stroke,
heart disease and chronic lung diseases like emphysema. Those who chew tobacco have been
reported to have an increased risk of oropharyngeal carcinoma in adulthood.53
Coffee
Coffee is a substance that is derived from a shrub coffee canephora which grows in
different parts of the world including Southern Nigeria.30 Its active ingredient, caffeine is a
central nervous system stimulant which causes increased alertness and decreased sleepiness
by increasing the release of cathecolamines.59,60 This effect on arousal has made coffee abuse
very common amongst adolescents in schools especially during preparation for examinations.
Despite its beneficial effect on arousal and decreasing sleep, caffeine use has been associated
with poor learning.61 Mednick et al61 conducted a study to compare the use of caffeine,
having some daytime sleep (“nap”) and a placebo on verbal, motor and perceptual memory.
27
The authors61 observed that moderate dosage of caffeine impairs motor skill and may not be
an adequate substitute for memory enhancements or daytime sleep. This effect is due to
caffeine induced increase in hippocampal acetylcholine which may have negative effects on
cognition, perceptive memory and learning. Wentz and Magavi60 on the other hand,
demonstrated that caffeine depressed hippocampal neurogenesis by observing this effect
when administering high doses of caffeine into mice.
Igwe et al50 reported a current use prevalence of 20.7% among secondary school
students in Enugu Nigeria. More males abused coffee and more students in SS3 abused
coffee. The authors50 attributed the high prevalence to the fact that these students were
preparing for exams and used kola and coffee as stimulant to stay awake at night. Contrary to
the previous report, Abdulkarim et al62 in Ilorin, Southwest Nigeria, reported a combined
prevalence of 26.2% for coffee and kola nut abuse amongst students aged 10-19 years in
secondary schools. The authors62 found no gender disparity in the prevalence rates in this
study and students enrolled for the study were in both junior and senior secondary schools
and were probably not involved in active preparation for exams.
Kola nut
Kola nut is derived from the plant cola nitida which is found in West Africa. It is
shared traditionally in several Nigerian cultures as a sign of hospitality.39 Kola nut is also
used by the poor to ward-off pangs of hunger and by students to keep awake when preparing
for exams.39 Its active ingredient is caffeine.
The prevalence of Kola nut abuse by secondary school students in Nigeria was
reported as 13.3% amongst students aged 10-18 years in Enugu, Nigeria by Okwaraji.4 On the
other hand, Okonkwo et al47 had reported a prevalence rate of 16% for coffee and kola nut
abuse put together. While Okwaraji13 used a self-constructed questionnaire for his study on
28
substance abuse, Okonkwo et al47 had used the modified WHO questionnaire for students
drug use. Moreover, Okwaraji's study may be a better representation of Enugu since he
studied a total of five schools while Okonkwo’s participants were selected from a single
school. As with other substances, both studies showed a male preponderance in the use of
kola nut. Abdulkarim et al62 also reported a higher combined rate for coffee and kola of 26%
in Ilorin. The difference between the reported prevalence in Enugu and Ilorin may be
attributed to the availability of the substance and cultural variations in the two locales.
Though the Igbos of Southeast Nigeria use kola nut for traditional purposes, kolanut is
planted and produced in Western Nigeria, it is thus more affordable and accessible to
adolescents in Western Nigeria. The effect of kola nut use is similar to that of coffee since
they have similar active agent.
Cocaine
Cocaine is an alkaloid derived from the coca plant.53 It is usually supplied as the
hydrochloride salt which can be snorted or dissolved in water and injected intravenously.53 It
is primarily a stimulant giving the user a ‘high’ feeling after its use.
Three decades ago cocaine abuse was not heard of in Nigeria until the explosion of
drug trafficking in the 1980’s.46 However surveys still report minimal prevalence rates
probably due to denial since it is illegal. Fatoye35 in his study of five hundred and sixty two
senior secondary school students in Ilorin reported a cocaine abuse rate of 0.2% with a male
preponderance in its abuse. On the other hand, Abdulkarim et al62 reported a remarkably
higher prevalence rate of 3.6% amongst adolescent students in a recent study in the same
area. Although a similar finding of male preponderance in cocaine abuse was observed, the
huge difference in prevalence of both studies may reflect changing societal trend with
increasing availability and affordability of this substance. In Port Harcourt Southern Nigeria,
29
Anochie and Nkanginieme52 reported a prevalence rate of 2.2% and 0.7% amongst male and
female senior secondary 3(SS3) students. It is plausible that the reported low prevalence rates
of cocaine abuse may be “apparent” rather than “real” because of under-reporting due to
denial since cocaine is an illicit drug in Nigeria.
Stages and Seriousness of Substance Abuse in Adolescents
Substance use in adolescents has been studied and found to occur in an increasing
manner.63 Adolescents, usually start with licit substances like alcohol and cigarette and
progress to cannabis use which in turn leads to the use of other illicit substances.63 Cormerci
and Schwebel64 defined various stages of adolescent use of alcohol and other substances
which are;
Experimentation is the use of socially acceptable substances minimally, for instance
use at social outings;
Recreational is the progression to illicit substances like cannabis;
Problematic is regular substance use leading to personality changes associated with
difficulties at home and at school;
Compulsive is the final stage, where the individual is truly addicted with need to avoid
abstinence effects.
Factors Influencing Substance Abuse
Initiation into substance use and progression to abuse is influenced by the complex
interaction of the pharmacologic effects of the drug, its availability, the personality of the
user and the environment in which the substance is used.44 Studies have identified such
factors as economic hardship, unemployment, failed relationships and poor academic
attainment as contributing factors. 36,51,52 Substance use amongst adolescents have been
30
linked to their exploratory behavior which is part of their development.53 Other contributing
factors identified by previous authors were peer influence,4,15,51 advertisements that
encourage the use of these substances15,36 urbanization and migration.36 Family structure and
parental influence is also contributory.36 Previous authors have reported a higher prevalence
rate of substance abuse amongst students from divorced homes, those who had lost their
parents or those who had strained relationships with their parents.4,15,31 The finding may be
attributed to lack of parental supervision and discipline. Parental use of substances has also
been identified as a risk factor for substance use by adolescents36 as the availability of the
substances and observation of their parents may result in trial of substances and ultimately
abuse in adolescents.
Although both gender are reported to be involved with substance abuse, it is said to be
more common among the male gender because of their more adventurous nature.2,4,16
Additionally, adolescents who engage in substance abuse have been found to have
commenced the use of substances in their early teens due to increased peer pressure in early
adolescence.4,36,47-49
Consequences of Substance Abuse
Substance abuse has consequences on the individual. The adolescent who abuses
substances is at risk of physical, psychological and social consequences. He or she
experiences acute physical problems like central nervous system stimulation resulting in
restlessness, seizures, cerebral hemorrhage, insomnia, fainting attacks from hypoglycemia
and irritant cough from cocaine and cannabis use.31,39 Psychological problems such as
hallucinations, poor perception, illusions and delusions have been linked with cannabis
use.31,39 Alcohol abuse has also been associated with other psychological problems such as
deterioration of personality, blackout, morbid jealousy, and hallucinations.65,66 Social
31
consequences of substance abuse include delinquency, risky sexual behavior, drunkenness
and poor school performance.31,39
Academic Performance and Substance Abuse.
Academic performance is the extent to which a student achieves his or her educational
goal.67 It is usually measured by performances in school examinations and continuous
assessment.67 Students substance use have been shown to be a risk factor for academic
problems such as lower school grades, absenteeism and high dropout rates.68 Alcohol for
instance interferes with a student’s ability to think making learning and concentration more
difficult. The more alcohol a student uses the lower his grade point average and the more
likely he is to drop out of school.68
Cox et al26 in a survey of academic performance and substance use among public
high school students in USA, noted low academic performance in those that abused alcohol,
cigarette, or marijuana. They defined poor academic performance as having a grade C or
below. The authors26 studied academic performance in mathematics and Spanish language
and assessment was made using school records. Similarly, Ingles et al69 using the same
measure for assessment of academic performance in grade 8-10 students, reported poor
academic performance in adolescents who abused alcohol or smoked daily probably because
their interest is not positioned on school achievement or because consumption of substances
interferes with their study tasks. Lukoye et al25 in Eldoret, Western Kenya, reported poor
academic performance evidenced by a low grade point average in 4.4% of first year
university students in Kenya who abuse cigarette. However, self-rating of academic
performance was used by the respondents with the tendency of under assessment with this
method. Substances has been shown to have varying effects on the central nervous system
which can decrease cognition generally.16,21-24,39,53,60 Those who abuse substances have been
32
shown to manifest other delinquent behavioral attitudes such as truancy which has been
shown to affect academic performance.20-22,70
In a study carried out by Fatoye,35 amongst Nigerian senior secondary school students
in Ilesha, Osun state, poor academic performance was reported in participants who used
coffee and tobacco. Academic performance was assessed using the respondents self-rating of
his/her performance. This method of assessing academic performance may be unreliable and
non-reproducible as it relies largely on own perception of academic performance. A similar
finding of poor academic performance was made of secondary school students who abused
marijuana when compared to controls in Zaria Northern Nigeria by Shehu and Idris.56 The
authors56 assessed academic performance using class positions of subjects and controls which
is relative to the academic performances of the other students in the class and so not reliable
such that a subject with 70% average may be the first position in one class but may take the
last position in a more competitive class.
Varying mechanisms by which substance abuse may result in poor academic
performance have been postulated by different authors.21-24 One mechanism being that
substance use itself may have a direct effect on cognitive development which results in
academic under achievement and disruption of academic progress.21-24 Studies22-24 have
shown that heavy substance use can lead to problems in working memory and attention due
to changes in adolescent brain activity. This results in poor academic performance and
engagement in school, ultimately increasing the risk for school problems and dropout.
Alternatively, substance use during adolescence leads to association with antisocial
peer groups which diminish school engagement while increasing other behavioral and social
problems resulting in school absences and decreased motivation to attend school.71 Langas et
al72 in Norway, reported that 46% of first admission substance use patients in the
33
neuropsychiatric ward had at least one personality disorder. Those who had personality
disorders were younger at initiation of substance use, used more illicit substances, and less
often attended school.72 Although the study was done in an adult population, subjects had
become abusers of substances in their adolescence. Similarly, Igwe and Ojinnaka73 in
Nigeria, reported a higher prevalence of psychosocial disorders amongst substance abusing
adolescents when compared to controls, however his study employed the definition of current
use of substances. Other authors have also collaborated increased delinquent behavioral
attitudes which can affect academic performance in substance abusers.20-22
Factors Influencing Academic Performance in Substance Abusers
Students’ academic performance is a product of several socioeconomic, psychological
and environmental factors.67 A student's natural ability, his/her motivation, and the quality of
primary education obtained may go a long way in determining how he/she performs in
subsequent levels of education.70
Various factors may contribute to the academic performance of substance abusers
irrespective of their natural abilities and motivation.71 The detrimental effect of substance use
has been supported by reports that maturation of the brain is not complete until after
adolescence.71 Therefore, increased use of various substances can cause injury to the
immature brain thereby resulting in reduced intelligence and poor school performance.71
Gender.
Athough previous authors have reported higher prevalence rates of substance abuse in
males more than occurs in females2,4,16,50 which may be due to the more adventurous nature
of boys, the association between gender and academic performance is yet to be explored.
34
Socioeconomic class.
Socioeconomic class has been found to be an important factor in substance abuse.30
Authors have reported a higher prevalence of substance abuse among the lower and middle
socioeconomic classes.30,50,74 This finding was attributed to permissive attitude of parents to
the use of these substances. It may also be due to poor supervision by the parents of these
adolescent substance abusers. However, Anochie et al2 reported that there was no significant
correlation between substance abuse and social class. It is noteworthy that in a highly
commercial city of Nigeria, Port Harcourt, substances are readily available to adolescents of
all socioeconomic classes so that there is no difference in prevalence rates of abuse of
substances in the different socioeconomic classes.
Academic performance however, has been reported to be poor in the lower social
class and students from the lower social class were more likely to drop out of school.75 Some
authors75-77 believe that low social class negatively affects academic performance because it
prevents access to vital resources and creates additional stress at home. The economic
hardship caused by low social class leads to conflicts in the home which results in a poor
quality of home life for these children. On the contrary, children from higher social class
generally have a more favorable learning environment with access to extra learning facilities
which aids their performances in school, their parents are more likely to be more educated
hence there is a better supervision of their school work.75-77
Psychosocial impairment.
Substance abuse has been linked with various deviant behaviors which could affect
academic performance negatively.71 Alcohol abuse is associated with depression, anxiety and
personality deterioration.65 Students who abuse substances are more likely to be involved in
other social vices such as stealing and truancy which has been linked to psychosocial
35
impairment.19,20,28 Psychosocial impairment in substance abusers make them lose
concentration during lessons and assessments making their overall academic performance
poor.71 Gruber et al78 found an increased prevalence of inattention in heavy substance
abusers. Their study of 129 American students found that, heavy marijuana users (those who
used the substance at least 27 of the preceding 30 days), lacked critical skills related to
attention, memory, and learning was significantly impaired, even after they had not used the
drug for at least 24 hours. The heavy marijuana users in the study had more trouble sustaining
and /or shifting their attention, as well as in registering, organizing, and using information
than did the study participants who had used marijuana no more than 3 of the previous 30
days.78 Heavy smokers of cannabis were more fidgety and had more records of truancy much
more than those who were not smokers of canabis.78 Langas et al72 also reported that 46% of
their subjects who used substances had personality disorders which was more associated to
the age at the initiation of substance use.
School absenteeism
School absenteeism has been associated with poor academic performance because
students who are absent at lessons miss out on the daily class lessons.79 Substance abusers
often indulge in risky behaviors including truancy in school.70 Truants ‘hang out’ with peers
rather than sit in class for lessons. In doing so, they lose interest in schooling which could
finally result in school drop-out. Okike,30 found school absenteeism as one of the
consequences of cigarette, alcohol and cannabis abuse in Abakaliki South eastern Nigeria.
The author30 inferred that the centrally acting substances may produce ''hang over'' effects on
the abusers, thereby making school attendance difficult. Okike30 also postulated that since the
abuse of substances leads to impaired concentration, the abusers may decide to stay away
from school to avoid the embarrassment their poor concentration in school might cause them.
Although increased school absences has been reported in substance abusers, there has been
36
no report of the relationship between school absences and academic performance in substance
abusers.
Severity of substance abuse
Severity of substance use may also affect the academic performance of substance
abusers. Cormerci and Schwebel64 defined various stages of adolescent use of alcohol and
other substances. At initial stages of experimental and recreational use there may be little
symptomatology of substance use disorders. Later on, in the problematic and compulsive
stages, the adolescent experiences difficulties at school and at home. These difficulties may
affect their performance in class work.64
Instruments for Assessing Substance use and abuse
The objectivity of detecting recent substance use by urine testing in adolescents is
undisputed, however this does not provide information about the adolescent's history of
substance use problems. More over some substances require quick assessment in order to
detect it in the urine, like alcohol whose evidence of use in urine disappears after eight
hours.80 It therefore supposes that self-report, especially when confidentiality is ensured and
no legal contingency is attached, in describing pattern and factors affecting substance use and
abuse is reliable.65 Studies carried out with self-report are cheap, easily accepted and the
refusal rate has been found to be minimal.81 Various instruments of self-report have been used
to study substance abuse. The cutting down, annoyance by criticism, guilty feeling and eye-
opener’s (CAGE) questionnaire82 is one of such instruments which has been used for
screening of alcoholism and has been validated for use in American Indian population by
Saremi et al.83 It consists of a set of four questions for which scores are given for a yes (score
1) or a no ( score 0) answer. A total score of two or above is significant in diagnosing alcohol
abuse. This questionnaire is strictly for alcoholism, however some authors have modified it to

37
study the abuse of other substances. Other instruments used are; the car, relax, alone, friends,
forget, trouble (CRAFFT) questionnaire, Adolescent drinking index (ADI) and the Personal
experience screening questionnaire (PESQ).80 These instruments are culture specific and have
not been validated for use in Nigeria. Self-constructed questionnaires have also been used in
the study of substance abuse,84 which has resulted in a wide variation in prevalence rates of
substance abuse reported.
It is based on this that the WHO81 constructed a questionnaire for students’ drug use
which can be used in epidemiological studies of substance abuse. The WHO student’s drug
use questionnaire consists of two sections. The first describes the socio-demography of the
respondent such as age and sex. Parental education has been added as a modification by
Nigerian authors to aid in establishing the socioeconomic class of respondents.30,73 The 2nd
section describes the use of various substances in the past 30 days (current users), before the
past 1year (past use) and ever in their lifetime (lifetime use). Other questions try to evaluate
who introduced the respondent to substance use, age at first use of a substance and attempts
made at stopping substance use. A ''yes'' to the question ''have you ever tried to stop the use of
this substance and found that you were unable to'' signifies an addiction to the substance
hence its abuse. Current use of illicit substances which is included in the WHO questionnaire
was also considered as abuse as defined by Odejide et al.39 Several modifications can be
made to the questionnaire to suit the cultural differences in different countries such as
introducing local names of the substances like "ogogoro" which was used for alcohol in the
study by Okike.30 The author30 also introduced a fictitious substance "flexinal" which `was
used to check over-reporting of abuse of substances. The advantage of the WHO
questionnaire is that it can be completed within 30 minutes. The questionnaire also brings
standards and makes the study reproducible. Hence studies within and outside a country can
be compared making planning for educational and treatment program for drug users easier.
38
On the other hand its disadvantage is that a lot of expertise is required in the analysis of data
collected by it because it has 30 or more items in the questionnaire. However, this can be
circumvented by using statistical packages like the statistical package for social sciences
(SPSS) and a well-trained biostatistician. This questionnaire has been further revalidated for
use in Nigeria85 and has since been used by several authors on substance abuse in
Nigeria.30,33,34,73
Assessment of Severity of Substance Abuse.
The Addiction Severity Index (ASI) is a structured interview designed to provide
important information or screen for problems in individuals who abuse substances.86 It
contains questions which try to explain certain problem areas. Such areas are interpersonal
difficulties with family, friends, and co-workers; medical conditions such as hepatitis B,
HIV/AIDS, sexually transmitted diseases, alcoholic liver disease, acute myocardial
infarction, pneumonia, metabolic and endocrine complications; and legal problems. It uses
questions in the different subscales, interpersonal difficulties, medical problems, and legal
problems of people who abuse substances. The questionnaire requires about 60 minutes to
administer and describes the seriousness of the individual’s substance abuse problem by
determining the degree of complications of substance abuse such as the presence of
interpersonal and legal problems. The coexistence of medical problems with substance use
also worsens the individual’s clinical state. The ASI has been used extensively for planning
of treatment and evaluation of the outcome of treatments for substance use disorders, but
because it also deals with other problem areas aforementioned it is cumbersome to
administer. It also requires that the researcher personally interviews each individual using the
questions.
39
Other instruments used in assessing seriousness of substance abuse disorder are,
Composite International Diagnostic Interview (CIDI), Structured Clinical Interview for
DSM-IV (SCID), Alcohol Use Disorders and Associated Disabilities Interview Schedule
(AUDADIS), Psychiatric Research Interview for Substance and Mental Disorders (PRISM),
and Semi-Structured Assessment for Drug Dependence and Alcoholism (SSADDA).68 These
instruments have been tested and found valid and reliable in assessing seriousness of
substance abuse however they all require between 60 and 90 minutes to administer and
require lots of training to use. They are also culture specific and have not been used in
Nigerian studies.
Assessing the seriousness of adolescent drug abuse (ASADA) score53 is an
instrument for assessing the seriousness of substance use. ASADA questionnaire (see
Appendix 9) uses an aggregate of variables to assess the seriousness of students’ substance
abuse. Variables include type of drug used, setting of drug use, effect of drug use and use of
drug during driving. School performance, history of accident after drug use, time of week and
day of drug use and family history of drug use were also variables. Scoring is done by
assigning 0, 1 or 2 points for each selected variable and aggregate scores of 0-3, 4-8 and 9-18
are designated as less worrisome, serious, and very serious respectively. It is very easy to
administer and requires five to 10 minutes to complete hence can be used to assess
seriousness of substance abuse on a vast number of people at the same time. It has also been
used amongst Nigerian students.48 The ASADA questionnaire has its draw back being that the
self-report nature may introduce some bias since the truthfulness of reports may be
questionable. However, as with all other anonymous reports, it is believed that the reporter
will be truthful after he/she has understood the study and the need for a truthful response.
40
Instruments for Assessing Academic Performance
Academic achievement measures are standardized tests used to assess academic skills
of children.87 It is used to assess weather a condition or disease affects a child’s learning in
school.87 These measures include standard educational tests, like the Wide Range
Achievement Test (WRAT), the Peabody individual achievement test (PIAT), the
Woodcock–Johnson tests of achievement and the Schonnel attainment test, all of which are
curriculum based tests assessing the child’s performance in areas such as spelling, reading,
written language and mathematics.88 A student is problematic with these academic
achievement measures if he/she performs ≥1.5 standard deviation below age expectation on
either broad reading or broad mathematics measures.88 The advantage of these achievement
measures is that they are standardized tests, hence are reproducible. However, they are mostly
culture specific and are cumbersome to administer and assess. Moreover, none of these
academic achievement tools has been validated for use in Nigeria.
Academic attainment measures are direct measures of school performance that are
partially independent of formal testing situations.87 The school examination report is an
example of academic attainment measure.89 It involves the use of the sectional aggregate
score and scores in core, specific subjects like mathematics, English language, sciences and
social studies. This academic attainment measure was used by Ogunfowora et al89 in their
comparative studies of academic performance in children with sickle cell anemia. Ibekwe et
al90 also used the same methodology in assessing the academic performance of school
children with epilepsy. Using this attainment measure, a score <50% represents poor
academic performance. This measure has its disadvantage as being the lack of
standardization. Although the same subjects are being assessed, participants may have other
cofounders that may affect their scores in the individual subject such as having different
teachers. However since controls are selected from the same environment as the cases, it is
41
believed that both cases and controls are exposed to similar circumstances. In addition, this
measure of assessing academic performance is less cumbersome and has been used severally
by Nigerian authors.89-91
Other measures of assessing academic attainment include the school grade level
placement which has been found to correlate with IQ.88 However, the “social promotion” of
students, where a student is promoted despite the fact that he does not merit promotion, could
affect the accuracy of grade placement as an outcome measure.87
Assessment of Behavioral Problems.
Substance abuse has been associated with psychological and behavioral problems.
Some authors31,39,65,92-94 have described association between substance abuse and emotional
disturbances, anxiety, restlessness and chronic patterns of aggression, hostility defiance and
disruption all of which may affect academic performance.
A number of valid and reliable screening tools are available for assessing behavioral
problems in children and adolescents. These include the Strength and difficulty questionnaire
(SDQ),95 the School children problem scale (SCPS),96 the Rutter children’s behavior
questionnaire,97 the Conner’s comprehensive behavior rating scales (Conner’s CBRS),98 the
Paediatrics Symptoms Checklist(PSC)99 and the Child Behavior Checklist (CBCL).100
SDQ95 is a 25-item questionnaire that describes attributes of a child, including the
positive or negative attributes. It is divided between fives scales which describe emotional
symptoms, conduct problems, hyperactivity/inattention, peer relationship problems and social
behavior. Two versions exist, the informant-rated version for parents or teachers of younger
children four to 10 years and another self-report version suitable for 11-17 year olds to fill
themselves. This rating scale has the advantage of being useful in both young and older
42
children and describes five domains of behavioral disorders, however it is cumbersome to
administer because it requires that a follow-up administration of questionnaire be done,
moreover it is culture specific and has not been validated for use in Nigerian children.
The Child Behavior Checklist (CBCL)101 has the youth self-report (YSR) and the
teacher report form (TRF). Although it is used by authors outside Nigeria, its use in Nigeria
has not been possible due to the fact that it has not been validated for use.
The Rutter scale97 is used to assess behavioral disorders in children and has been
validated for use in Nigerian children.101 This scale has also been used by other authors102
who assessed behavioral disorders in school children in Nigeria. This tool however, can only
be used for children aged four to 12 years.
Conner's CBRS rating scale98 is an instrument designed to provide a complete
overview of child and adolescent behaviors, emotions and academic problems. It is suitable
for ages six to 18 years (for the parent and teachers forms) and eight to 18 years (for the self-
report forms). It has the advantage of excellent reliability, validity and measures academic
difficulties in mathematics, language and total academic difficulties as well as aggressive
behaviors, separation fears, hyperactivity/impulsivity, social problems, perfectionist and
compulsive behaviors. However, it is a comprehensive tool which describes many disorders
and so cumbersome to administer. It is also culture specific and has not been validated for use
amongst Nigerian children and adolescents.
The PSC99 is a psychosocial screen designed to facilitate the recognition of cognitive,
emotional, and behavioral problems. Items in the questionnaire include questions based on
major diagnostic categories listed in the American Psychiatric Association Diagnostic and
Statistical Manual of Mental Disorders III (DSM-111).103 Two versions exist, the
parent‐completed version-PSC and the youth self-report‐PSC. The YSR‐PSC can be

43
administered to adolescents aged 11 and above. The PSC consists of 35 items that are rated as
“Never,” “Sometimes,” or “Often” present and scored 0, 1, and 2, respectively. The total
score is calculated by adding together the score for each of the 35 items. A cutoff score of 28
or higher indicates psychological impairment for children six years to adolescence. For
children aged two to five years, the scores on the items 6, 7, 14 and 15 are ignored and the
total score based on the remaining 31 items are used. The PSC cutoff score for the two to five
age group is 24 or higher. The PSC has been validated for use in general paediatric office
screening and its case classification has been correlated with the Child Behavior Checklist
(CBCL) of Achenbach and Edelbrock .104 Jellinek et al100 also reported its reliability and
consistency. The PSC had a specificity and sensitivity of 68% and 95% respectively with
clinician’s ratings.100 It has also been used to assess Nigerian adolescents73
AIMS AND OBJECTIVES

44
Aim
To describe the academic performance of substance abusing secondary school students in
Abakaliki.
Specific Objectives.
To determine the prevalence and pattern of substance abuse amongst secondary
school students in Abakaliki.
To identify the factors predisposing to substance abuse among the students.
To determine the academic performance of substance abusing secondary school
students and their non-substance abusing classmates.
To identify factors associated with academic performance of students abusing
substances.
MATERIALS AND METHODS

45
Study Area
Abakaliki is the capital city of Ebonyi state in the South eastern part of Nigeria. The
metropolis comprises parts of 2 Local Government Areas (LGAs) namely Abakaliki and
Ebonyi. The inhabitants are mainly Igbo-speaking though other ethnic groups are found. The
metropolis has a total population of 141,438 inhabitants according to the 2006 census
records.105 It’s inhabitants are of different educational attainment and religion. Majority of
them are farmers. There are a total of 13 approved secondary schools both public and
privately owned with about 5,748 students in SS2-3 in 2012/2013 session.106
Study Population
Students who were in SS2 and SS3 aged 10-19 years in the 13 secondary schools in
the metropolis constituted the study population for screening for substance abuse. This is
because they are the ones who are more likely to have abused substances for some time and
would have completed at least one session of senior secondary school. Subjects were those
that abuse substance while the control group consists of non-substance abusing classmates of
the subjects.
Study Design
It was a cross-sectional study.
Ethical Approval
Institutional ethical approval was obtained from the medical and ethics committee of
the Federal Teaching Hospital Abakaliki (see Appendix 1). Approval was also obtained from
the secondary education board of the state ministry of education, Ebonyi state (see Appendix
II). Similarly, informed written consent was also obtained from the Principals, selected
students and their parents/guardian before commencement of the study.
46
Inclusion Criteria
Students in SS2 and SS3 aged 10-19 years in the selected schools who were abusing
various substances.
Exclusion Criteria
Students less than 10 or more than 19 years of age.
Those who were unwilling to participate in the study were excluded.
Students with chronic diseases like sickle cell anemia, diabetes mellitus, epilepsy that
may affect a person’s academic performance as reported by previous studies.89-91
Sample Size
The desired sample size was determined in two stages. First, the sample size
appropriate for an infinite population (i.e. greater than 10,000) was calculated using the
formula107
n = z2pq/d2
where n = the desired sample size when the population is more than 10,000
z = the standard normal deviate, usually set at 1.96 (which corresponds to 95%
confidence interval)
p = the proportion in the target population estimated to have a particular characteristic
(prevalence of substance abuse amongst secondary school students in a previous study done
in Abakaliki Nigeria =27.1%).30
q = 1.0-p

47
d = degree of accuracy desired, which is usually set at 0.05
Substituting the values in the formula gives
n = (1.96)2(0.271)(0.729)
(0.05)2
=303.57708
However the target population is 5,748 which is the total number of students in SS2-3 in
Abakaliki. This population size is less than 10, 000, therefore the minimum sample size was
calculated using a correction formula 107
nf = n
1+ (n)
(N)
Where nf = minimum sample size for population less than 10,000
n = the desired sample size when the population is more than 10,000
Here n = 303.57708
N= the estimate of the population size which is 5748
Therefore,
nf = 303.57708
1+ (303.57708)
(5748)
= 303.57708
48
1.0528144
= 288.34815 ≈288.
Two hundred and eighty eight was the calculated minimum proportion of students
that was included in the survey for substance abuse. WHO recommendation for substance
abuse study is that 10% of the sample frame be recruited which for this population is 574.
Since the minimum calculated sample size is less than the WHO recommendation, therefore
574 was used for this study in line with WHO recommendation. A 20% attrition rate
allowance was made which resulted in an additional 115 persons. Therefore 689 students
were recruited for screening. 68
Training of research assistants
The researcher recruited two research assistants for the study who were registrars in
Paediatrics department. The assistants were trained to administer the study tools in an exam
like manner. They also helped to supervise the participants while they completed their
questionnaires unitarily.
Level of participation
Apart from assistance in administering the questionnaires, the rest of the data
collection was done by the researcher personally.
Pilot Study.
A pilot study was carried out with 50 student from Hope High international
Secondary school (not included in the sampling procedure) to assess the appropriateness of
study tools, perfect the intended methodology and provide a training opportunity for research
assistants before the commencement of the study. Out of the 50 consenting students selected

49
for the pilot study, 40 questionnaires were fully filled giving 20% attrition. Adjustments in
language were then made on the questionnaire before administering same at the subsequent
study.
Sampling Procedure
Selection of schools.
There were 13 approved secondary schools in Abakaliki. Schools were stratified by
gender into male, female, and coeducational schools. Two schools were girls only, two were
boys only, while nine were coeducational. Excluding the school where a pilot study was
carried out reduced the number of mixed schools to eight. Furthermore, the authorities of two
schools declined consent leaving the researcher with six schools to select from. All schools
had their names written on sheets of paper for blinding and subsequently grouped into strata.
The mixed schools were grouped into three strata with two schools in each stratum which
when combined with the boys only and girls only gave a total of five. One school was
subsequently selected from each stratum by ballot method. One male, one female and three
mixed, schools were therefore selected. The schools selected and the respective number of
students in SS2 and SS3 are shown in Appendix VI.
Selection of respondents.
Respondents were selected from each school pro rata, according to their school
population, and the number of class arms. The population of the SS2 and 3 students of the
selected schools were obtained. A ratio of the percentage of the population in each school to
the total population of SS2 and SS3 students was established, and this ratio was used to select
the required number from each school such that the more populous schools had a higher
number recruited for study. Viz;
50
Population at each school X calculated sample size (689)
Total population of students in selected schools (2210)
Subsequently, the respondents were selected from the various classes using the systematic
interval width (I) which was calculated using the fomular,108
I = N
n
Where N is the number of students in the whole arms of a class and
n is the number to be selected from the class. For instance in Nnodo boys secondary school
which had a total of 402 from which 125 were selected, the sample width was 3.3 therefore
every 3rd student was selected from the last one selected from the class according to their
appearance on the class register. The first person was selected randomly and subsequently the
interval width was applied to avoid bias. At the coeducational schools, students were
stratified further into male and female, equal proportions were then selected from both male
and female strata using systematic sampling as previously described. The schools selected
and the respective number of participants selected in each school is represented in Appendix
VI.
Coding of participants
All selected participants were given a code which was known only to the researcher.
The code was written on their Questionnaire. With the code all participants could be
recognized from the class register by the researcher alone.
Selection of subjects and control
Having administered the drug use questionnaire, respondents who abused any
substance were included in the study if they satisfy the inclusion criteria. A respondent was
51
selected as a substance abuser if he/she had an uncontrollable (excessive) use of licit
substances like alcohol, coffee, cigarette and kola nut. This was estimated by the number of
respondents who responded affirmatively to the question ‘have you tried to stop or reduce
your use of substances in the past 12 months and found that you were unable to do so?’.
Secondly any use of an illicit substance like cannabis or cocaine was regarded as abuse as
defined by Odejide.39 However, subjects had to be current users of illicit substances, which is
use within the past 30 days preceding the study, to be selected as a substance abusers.
Controls were selected from the class registers if they were matched with subjects for age,
sex, and socioeconomic class and were in the same arm and class with the subjects in the
academic session that was reviewed. Controls were selected from those who filled the drug
use questionnaire and were found to be non-substance-abusing.
SCHOOLS SELECTED, TOTAL AND SELECTED POPULATION OF SS 2 AND
3 STUDENTS.
School Total Number in SS2 and SS3(Selected)
1. Nnodo boys secondary school…………………………….………..402(125)
2. Urban Model Secondary School, Abakaliki (public, co-educational).623(194)
3. Girls Secondary School, Abakaliki ………………………………….321(100)
4. Holy Ghost College, Abakaliki (private, co-educational)…...............320(100)
5. Presco Secondary School(public, co-educational)…………..............544(170)
Total population in SS2 and SS3 in selected school…………………….2210(689)
Survey Instruments and Parameters to be evaluated.
The study instruments used for the study were:

52
(1) The WHO students drug use questionnaire81 (see Appendix VI) for assessing the prevalence
and factors associated with substance abuse. The first part of the questionnaire, described
basic socio-demographic information like age, sex, religion, year of study at school, parental
education and occupation from which socioeconomic class was determined as proposed by
Olusanya108(see Appendix VII). Section B described the substances abused. Substances that
were studied were alcohol, cigarette, kola nut, coffee, cannabis and cocaine and the popular
local names like ‘igbo’, ‘wee-wee’, ''grass'' were added in the questionnaire for easy
identification by respondents.30 This section also described when and how the respondent was
initiated into substance use.
A participant was selected as a substance abuser if he/she had an uncontrollable
(excessive) use of licit substances like alcohol, coffee, cigarette and kola nut. This was
estimated by the number of respondents who responded affirmatively to the question ‘have
you tried to stop or reduce your use of substances in the past 12 months and found that you
were unable to do so?’. Secondly any use of an illicit substance like cannabis or cocaine was
regarded as abuse as defined by Odejide.39 However, subjects had to be current users of illicit
substances, which is use within the past 30 days preceding the study, to be selected as a
substance abusers. Respondents who did not meet these criteria were considered users not
abusers.
(2) Assessing the seriousness of adolescent drug abuse (ASADA) score53 (see Appendix VIII)
for assessing the severity of substance use. Severe substance use was taken as a total score of
4 and above.
(3) The class attendance register was used to assess school absences in the preceding school
session. High absence was taken as >12 school days absence from the school in a year as
recommended by Weitzman et a,79 while low absence is 1 – 12 school days absence.
53
(4) The Paediatric Symptom Checklist (PSC)- Youth Report Version99 (see Appendix IX) for
assessing psychosocial impairment in substance abusers. A total score of 28 and above was
taken as an indication of significant psychosocial impairment.24
(5) The proforma on school academic report (see Appendix X) adopted from Ogunfowora’s
study109 was used for assessing academic performance of these children. It used information
obtained from the class examination result register. A modification of this tool was made by
substituting Biology for integrated science and Igbo for social studies. This is because this
study was carried out amongst senior secondary students who do not offer social studies and
science as subjects but offer biology and Igbo language since one of biology, chemistry, and
physics and one Nigerian language must be subjects of choice according to WAEC
registration criteria.110
The overall score in percentage in the three terminal examinations of the school
session preceding the study was documented and the average taken. This was used as an
index of general academic performance. The performance was scored as high if ≥75%
whereas 50-74% and <50% were scored as average and low, respectively.87-89 Scores of
<50% were considered as poor academic performance. Scores in 4 subjects, English,
Mathematics, Biology, and Igbo were also compared likewise in accordance with
Ogunfowora’s criteria.
Procedure
The researcher recruited two assistants. Pre-tests of the drug use questionnaire,
ASADA score questionnaire and the PSC- Youth Report Version were done with 50 students
in a co-educational secondary school that was not included in the selected schools. This
helped to identify and modify any ambiguity in the instrument. A familiarization visit was
then paid to each selected school during which the researcher obtained consent from the
54
schools’ authority and obtain a convenient date for the study. The researcher was also
introduced to the parents by school authorities during their parents’ teachers’ association
termly meeting. Parental consent was obtained thereafter and those who were absent had
other subsequent visits scheduled to obtain consent.
On the selected day of study, the researcher was introduced to all students by the
principal or a representative. Selected participants were gathered in a school hall, not in their
classrooms, to fill the questionnaire independently. Explanation on the nature of the
questionnaire, and the need for truthful responses was done. The students were assured of
anonymity and confidentiality to reduce their anxiety regarding victimization and to detect
their real pattern of substance use. Their teachers were not allowed into the hall during the
filling of the questionnaire. The session lasted 60 minutes during which the participants filled
the drug use questionnaire, the ASADA score questionnaire and the PSC questionnaire.
Adequate guidance was given to the respondents by the researcher and/or her assistants
during the questionnaire administration without influencing their responses.
Data collected at this visit was analyzed with the help of a biostatistician to determine
prevalence and pattern of substance abuse. Substance abusing students were then identified
based on the code they were given on the day they filled the substance use questionnaire.
Control subjects were selected subsequently from their class registers systematically.
School absence and academic performances were evaluated for both subjects and
controls. Psychosocial impairment for both subjects and control were assessed by
determining those who had PSC scores of 28 and above. Also, seriousness of drug abuse was
assessed by determining the subjects with ASADA score of 4 and above.
55
Data from these was used to compare the academic performance of substance abusers
and non-abusers and to assess the influence of school absence, severity of substance abuse
and psychosocial impairment on academic performance in subjects and controls.
Data Analysis
Data obtained was analyzed using SPSS Version 20 (IBM SPSS Statistics for
Windows, Version 20.0. Armonk, NY: IBM Corp 2011). Descriptive statistics was used to
find the prevalence of substance abuse. The student’s t-test was used to compare means of
overall scores and scores in key subjects of substance abusers and controls while frequencies
in 2 X 2 tables were compared using the Pearson’s chi-square test or fishers’ exact test as
appropriate. Multiple linear regressions were used to find the associations between
independent variables and the dependent variable, academic performance. All calculations
were based on a significant level of p<0.05.
RESULTS
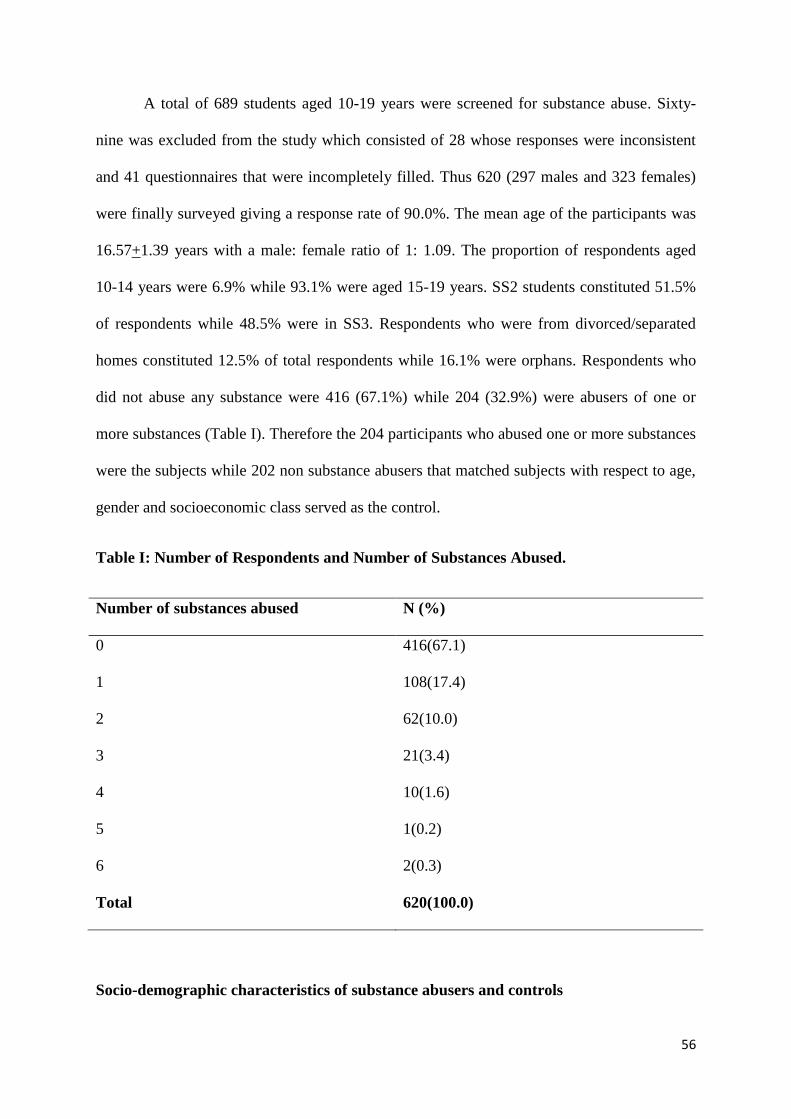
56
A total of 689 students aged 10-19 years were screened for substance abuse. Sixty-
nine was excluded from the study which consisted of 28 whose responses were inconsistent
and 41 questionnaires that were incompletely filled. Thus 620 (297 males and 323 females)
were finally surveyed giving a response rate of 90.0%. The mean age of the participants was
16.57+1.39 years with a male: female ratio of 1: 1.09. The proportion of respondents aged
10-14 years were 6.9% while 93.1% were aged 15-19 years. SS2 students constituted 51.5%
of respondents while 48.5% were in SS3. Respondents who were from divorced/separated
homes constituted 12.5% of total respondents while 16.1% were orphans. Respondents who
did not abuse any substance were 416 (67.1%) while 204 (32.9%) were abusers of one or
more substances (Table I). Therefore the 204 participants who abused one or more substances
were the subjects while 202 non substance abusers that matched subjects with respect to age,
gender and socioeconomic class served as the control.
Table I: Number of Respondents and Number of Substances Abused.
Number of substances abused N (%)
0 416(67.1)
1 108(17.4)
2 62(10.0)
3 21(3.4)
4 10(1.6)
5 1(0.2)
6 2(0.3)
Total 620(100.0)
Socio-demographic characteristics of substance abusers and controls

57
Table II shows the socio-demographic characteristics of subjects and control. The
mean age for subjects was 17.09+1.33 years while that of controls was 17.02+1.34years
(t=21.402, p=0.623). Subjects were made up of 120 (58.8%) males and 84 (41.2%) females
giving a male: female ratio of 1.4:1. Males were 120(59.4%) while females were 82 (40.6%)
in the control group (χ2=0.634, p=0.541). Socioeconomic stratification showed that 151
(74.5%), 32 (15.5%) and 21 (10.2%) of subjects belonged to the lower, middle and the upper
strata (χ2=1.139, p=0.566). There were no significant differences in age, gender and
socioeconomic class between subjects and controls.
Table II: Socio-demographic characteristics of subjects and controls.
Socio-demographic
variable
Subjects n(%) Control n(%) P
Age range (years)
10-14 9(4.5) 9(4.5) 0.623
15-19 195(95.5) 193(95.5)
Gender
Male 120(58.8) 120(59.4) 0.541
Female 84(41.2) 82(40.6)
Socioeconomic class
Lower 151(74.5) 147(72.7) 0.566
Middle 32(15.5) 40(20.0)
Upper 21(10.0) 15(7.3)
Prevalence of Substance Abuse.
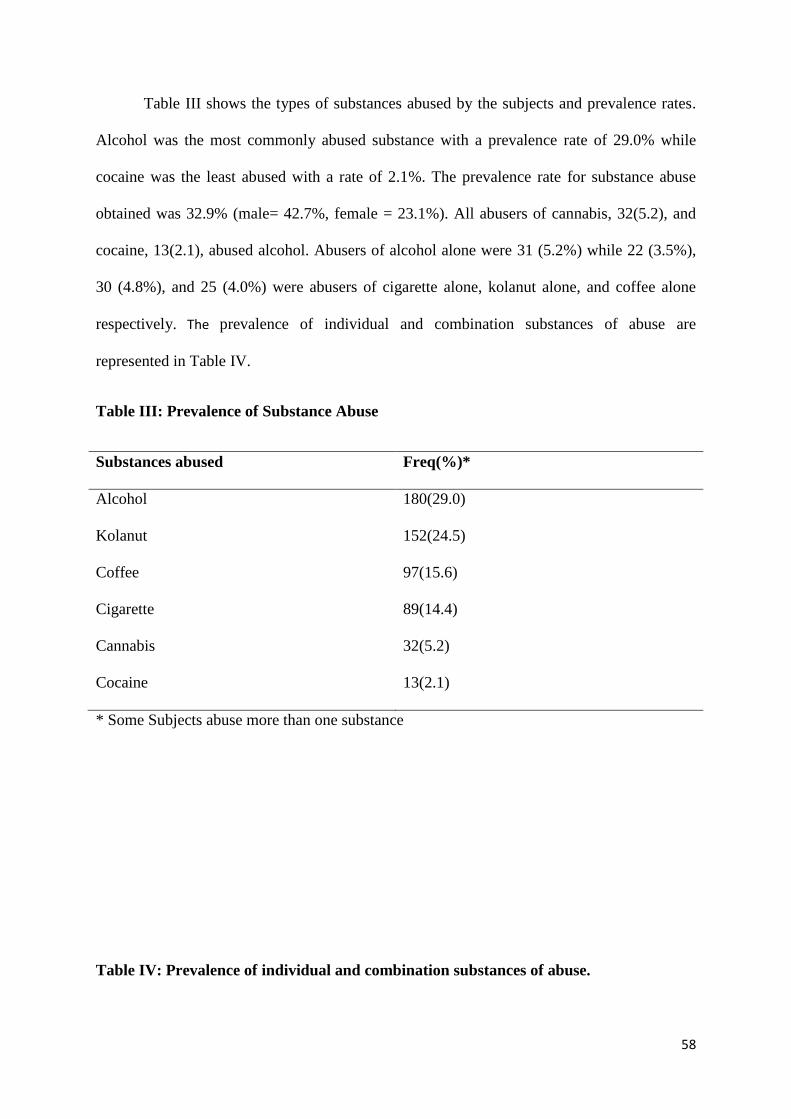
58
Table III shows the types of substances abused by the subjects and prevalence rates.
Alcohol was the most commonly abused substance with a prevalence rate of 29.0% while
cocaine was the least abused with a rate of 2.1%. The prevalence rate for substance abuse
obtained was 32.9% (male= 42.7%, female = 23.1%). All abusers of cannabis, 32(5.2), and
cocaine, 13(2.1), abused alcohol. Abusers of alcohol alone were 31 (5.2%) while 22 (3.5%),
30 (4.8%), and 25 (4.0%) were abusers of cigarette alone, kolanut alone, and coffee alone
respectively. The prevalence of individual and combination substances of abuse are
represented in Table IV.
Table III: Prevalence of Substance Abuse
Substances abused Freq(%)*
Alcohol 180(29.0)
Kolanut 152(24.5)
Coffee 97(15.6)
Cigarette 89(14.4)
Cannabis 32(5.2)
Cocaine 13(2.1)
* Some Subjects abuse more than one substance
Table IV: Prevalence of individual and combination substances of abuse.

59
Substances abused Frequency(%)
Alcohol alone 31(5.2)
Kolanut alone 30(4.8)
Coffee alone 25(4.0)
Cigarrete alone 22(3.5)
Cannabis alone 0(0.0)
Cocaine alone 0(0.0)
Kolanut + Coffee 24(11.8)
Alcohol + Cigarette 21(10.3)
Alcohol + Cannabis 11(5.4)
Alcohol + Cocaine 6(2.9)
Cigarette + Coffee + Kolanut 10(4.9)
Alcohol + Coffee + Kolanut 8(3.9)
Alcohol + Cigarette + Kolanut 3(1.5)
Alcohol + Cigarrete + Cannabis + Kolanut 4(2.0)
Alcohol + Cigarette + Cocaine + Canabis 4(2.0)
Alcohol + Cigarette + Cocaine + Canabis + Kolanut 1(0.5)
Alcohol + Cigarette + Cocaine + Canabis + Kolanut + Coffee 2(1.0)
Factors Influencing Prevalence of Substance Abuse.
Age.

60
Table V shows the prevalence of substance abuse by age group. It demonstrates that
90.8%, 44.6% and 76.9% of 15-19 years old subjects abused alcohol, cigarette and kolanut
respectively. These were statistically significant. There were no significant differences in the
ages of those who abused cannabis, cocaine, and coffee.
Table V: Prevalence of Substance abuse within Age groups.
Age group(years)
Substances
abused
10-14
N=9
15-19
N=195
Fishers exact P
Alcohol n(%) 3(33.3) 177(90.8) 18.201 0.001*
Cannabis n(%) 1(11.1) 31(15.9) 0.961 0.348
Cigarette n(%) 2(22.2) 87(44.6) 10.346 0.002*
Cocaine n(%) 0(0.0) 13(6.7) 1.230 0.623
Coffee n(%) 3(33.3) 94(48.2) 1.670 0.134
Kolanut n(%) 2(22.2) 150(76.9) 2.342 0.243*
N= total number of subjects in that age group
n= number of subjects who abused the various substances within the age group
*=significant
Note some were abusers of more than one substance.
Gender.
The association between abuse of the various substances studied and gender is shown
in Table VI below. More males (99.2%, 46.7%, and 7.5%) were abusers of alcohol, cigarette
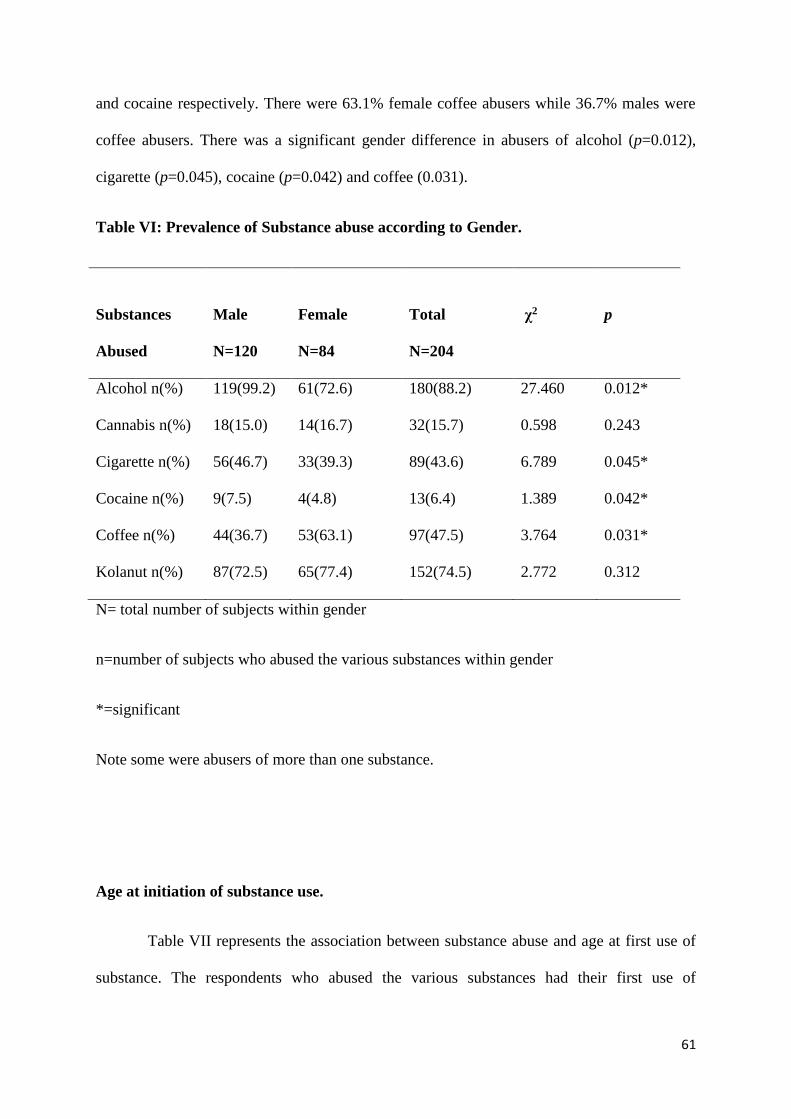
61
and cocaine respectively. There were 63.1% female coffee abusers while 36.7% males were
coffee abusers. There was a significant gender difference in abusers of alcohol (p=0.012),
cigarette (p=0.045), cocaine (p=0.042) and coffee (0.031).
Table VI: Prevalence of Substance abuse according to Gender.
Substances
Abused
Male
N=120
Female
N=84
Total
N=204
χ2 p
Alcohol n(%) 119(99.2) 61(72.6) 180(88.2) 27.460 0.012*
Cannabis n(%) 18(15.0) 14(16.7) 32(15.7) 0.598 0.243
Cigarette n(%) 56(46.7) 33(39.3) 89(43.6) 6.789 0.045*
Cocaine n(%) 9(7.5) 4(4.8) 13(6.4) 1.389 0.042*
Coffee n(%) 44(36.7) 53(63.1) 97(47.5) 3.764 0.031*
Kolanut n(%) 87(72.5) 65(77.4) 152(74.5) 2.772 0.312
N= total number of subjects within gender
n=number of subjects who abused the various substances within gender
*=significant
Note some were abusers of more than one substance.
Age at initiation of substance use.
Table VII represents the association between substance abuse and age at first use of
substance. The respondents who abused the various substances had their first use of
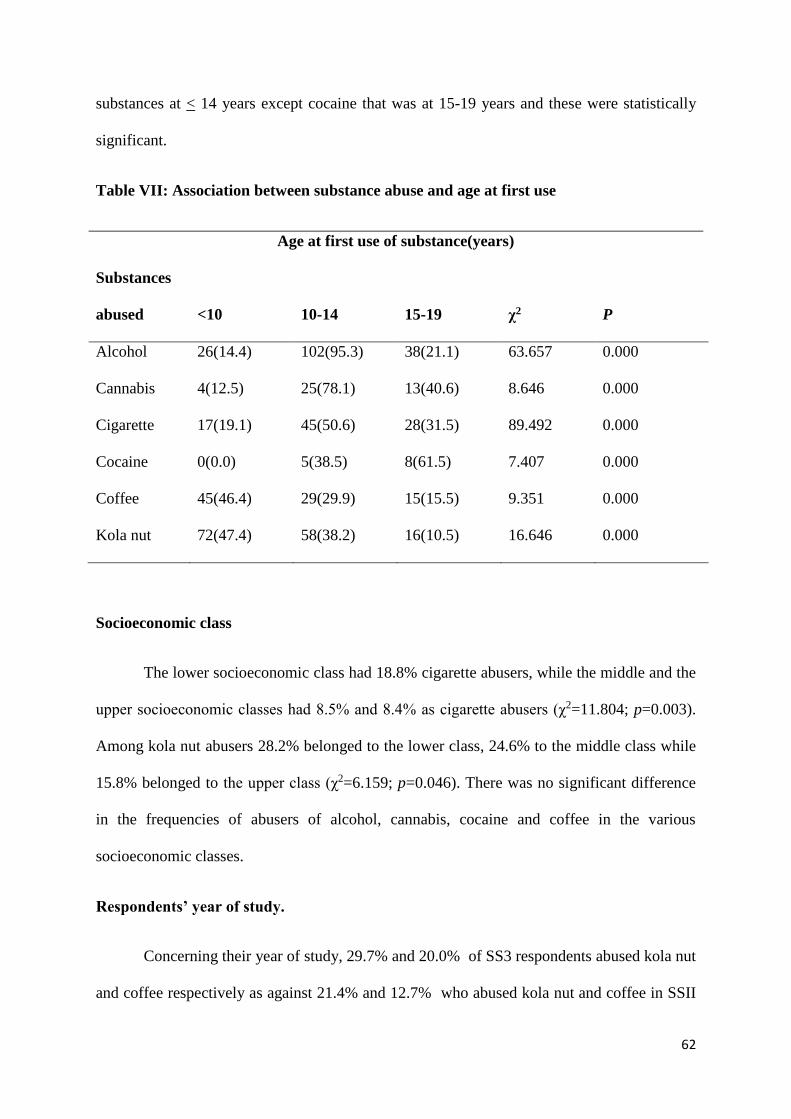
62
substances at < 14 years except cocaine that was at 15-19 years and these were statistically
significant.
Table VII: Association between substance abuse and age at first use
Age at first use of substance(years)
Substances
abused
<10
10-14
15-19
χ2
P
Alcohol 26(14.4) 102(95.3) 38(21.1) 63.657 0.000
Cannabis 4(12.5) 25(78.1) 13(40.6) 8.646 0.000
Cigarette 17(19.1) 45(50.6) 28(31.5) 89.492 0.000
Cocaine 0(0.0) 5(38.5) 8(61.5) 7.407 0.000
Coffee 45(46.4) 29(29.9) 15(15.5) 9.351 0.000
Kola nut 72(47.4) 58(38.2) 16(10.5) 16.646 0.000
Socioeconomic class
The lower socioeconomic class had 18.8% cigarette abusers, while the middle and the
upper socioeconomic classes had 8.5% and 8.4% as cigarette abusers (χ2=11.804; p=0.003).
Among kola nut abusers 28.2% belonged to the lower class, 24.6% to the middle class while
15.8% belonged to the upper class (χ2=6.159; p=0.046). There was no significant difference
in the frequencies of abusers of alcohol, cannabis, cocaine and coffee in the various
socioeconomic classes.
Respondents’ year of study.
Concerning their year of study, 29.7% and 20.0% of SS3 respondents abused kola nut
and coffee respectively as against 21.4% and 12.7% who abused kola nut and coffee in SSII
63
(χ2=5.332; p=0.021; for kolanut and χ2=5.918; p=0.015; for coffee). Cigarette, alcohol,
cannabis, and cocaine showed no significant difference in the frequency of abusers in the two
years of study (p=0.532, 0.246, 0.346, and 0.498 respectively).
Family structure
Cannabis and cigarette abusers were more amongst those who were orphaned
(p=0.042 and 0.027 respectively). Cigarette, alcohol, cannabis and kola nut showed a
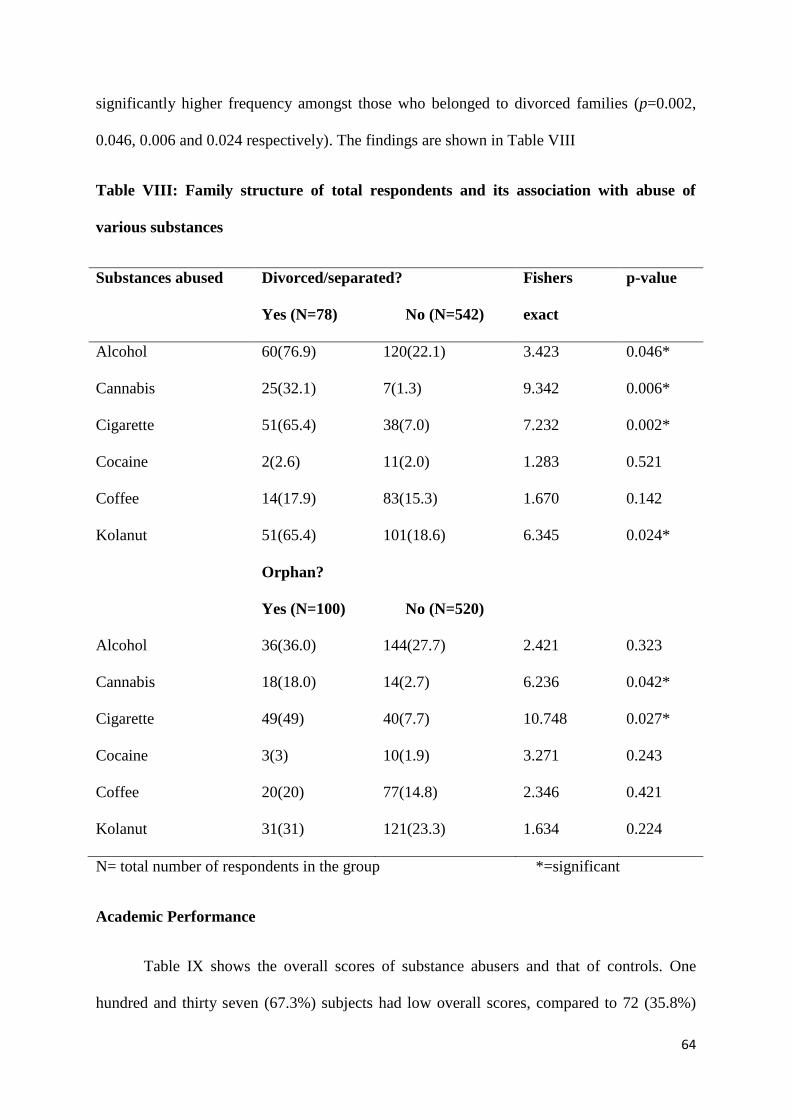
64
significantly higher frequency amongst those who belonged to divorced families (p=0.002,
0.046, 0.006 and 0.024 respectively). The findings are shown in Table VIII
Table VIII: Family structure of total respondents and its association with abuse of
various substances
Substances abused Divorced/separated?
Yes (N=78) No (N=542)
Fishers
exact
p-value
Alcohol 60(76.9) 120(22.1) 3.423 0.046*
Cannabis 25(32.1) 7(1.3) 9.342 0.006*
Cigarette 51(65.4) 38(7.0) 7.232 0.002*
Cocaine 2(2.6) 11(2.0) 1.283 0.521
Coffee 14(17.9) 83(15.3) 1.670 0.142
Kolanut 51(65.4) 101(18.6) 6.345 0.024*
Orphan?
Yes (N=100) No (N=520)
Alcohol 36(36.0) 144(27.7) 2.421 0.323
Cannabis 18(18.0) 14(2.7) 6.236 0.042*
Cigarette 49(49) 40(7.7) 10.748 0.027*
Cocaine 3(3) 10(1.9) 3.271 0.243
Coffee 20(20) 77(14.8) 2.346 0.421
Kolanut 31(31) 121(23.3) 1.634 0.224
N= total number of respondents in the group *=significant
Academic Performance
Table IX shows the overall scores of substance abusers and that of controls. One
hundred and thirty seven (67.3%) subjects had low overall scores, compared to 72 (35.8%)
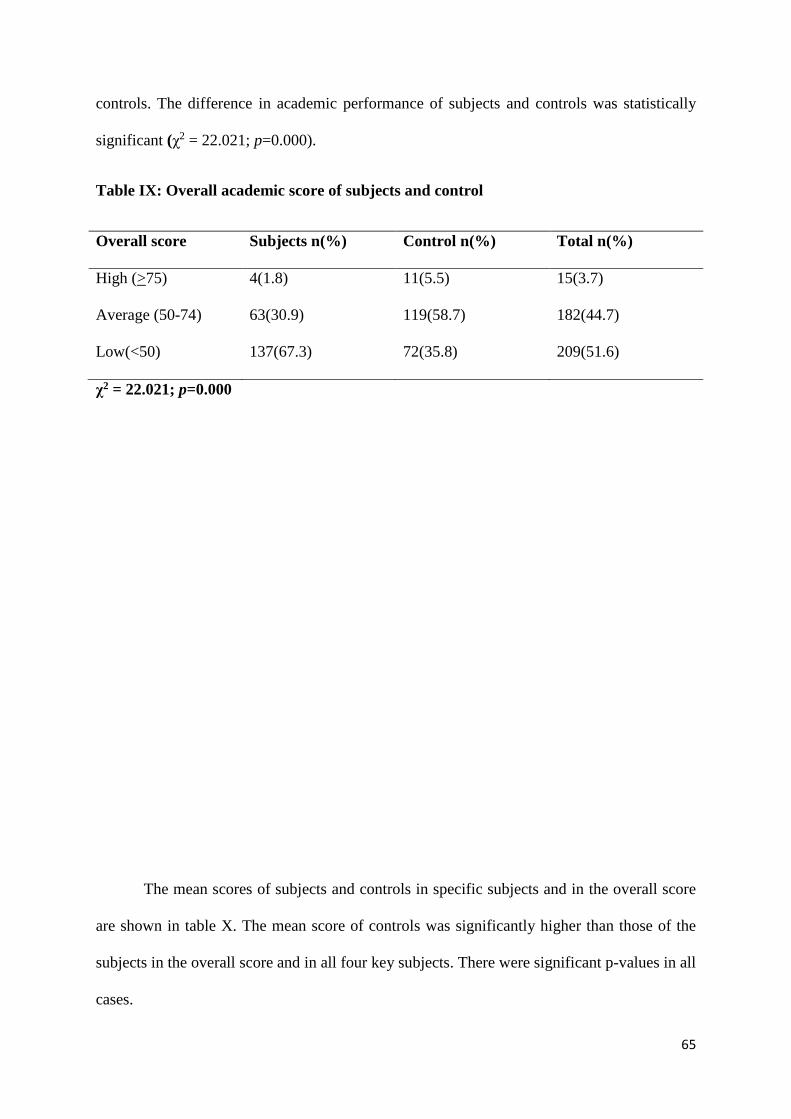
65
controls. The difference in academic performance of subjects and controls was statistically
significant (χ2 = 22.021; p=0.000).
Table IX: Overall academic score of subjects and control
Overall score Subjects n(%) Control n(%) Total n(%)
High (>75) 4(1.8) 11(5.5) 15(3.7)
Average (50-74) 63(30.9) 119(58.7) 182(44.7)
Low(<50) 137(67.3) 72(35.8) 209(51.6)
χ2 = 22.021; p=0.000
The mean scores of subjects and controls in specific subjects and in the overall score
are shown in table X. The mean score of controls was significantly higher than those of the
subjects in the overall score and in all four key subjects. There were significant p-values in all
cases.
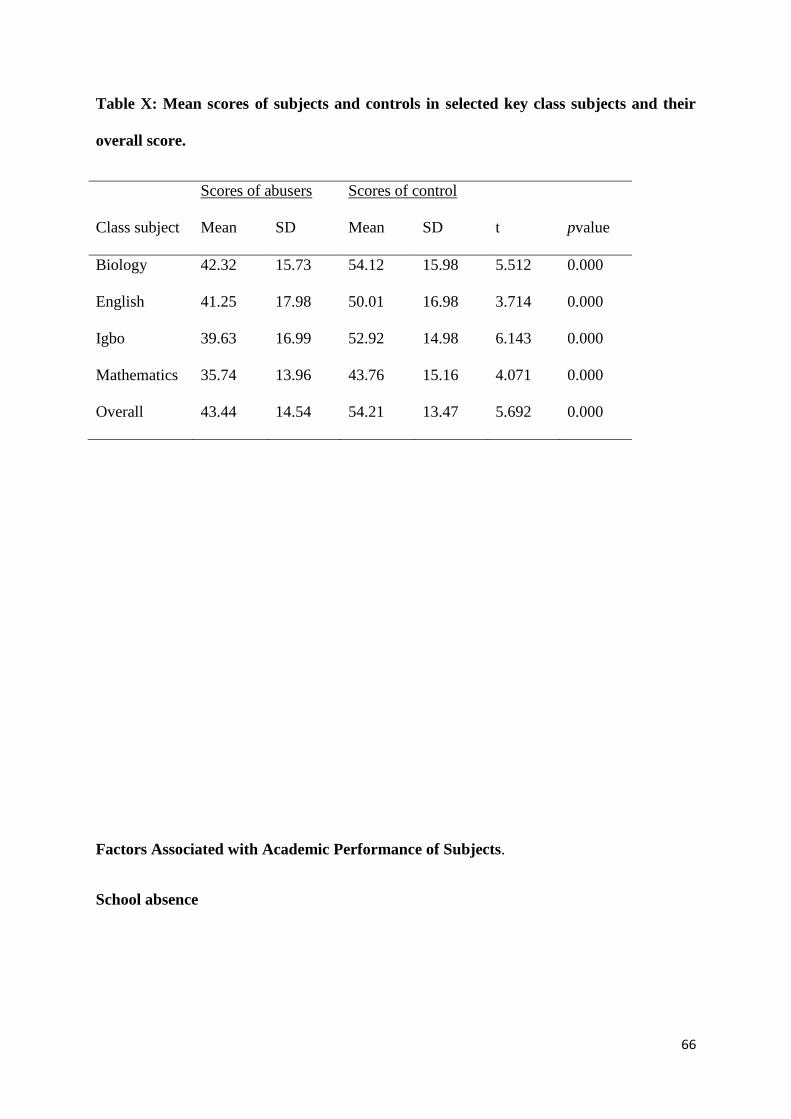
66
Table X: Mean scores of subjects and controls in selected key class subjects and their
overall score.
Scores of abusers Scores of control
Class subject Mean SD Mean SD t pvalue
Biology 42.32 15.73 54.12 15.98 5.512 0.000
English 41.25 17.98 50.01 16.98 3.714 0.000
Igbo 39.63 16.99 52.92 14.98 6.143 0.000
Mathematics 35.74 13.96 43.76 15.16 4.071 0.000
Overall 43.44 14.54 54.21 13.47 5.692 0.000
Factors Associated with Academic Performance of Subjects.
School absence
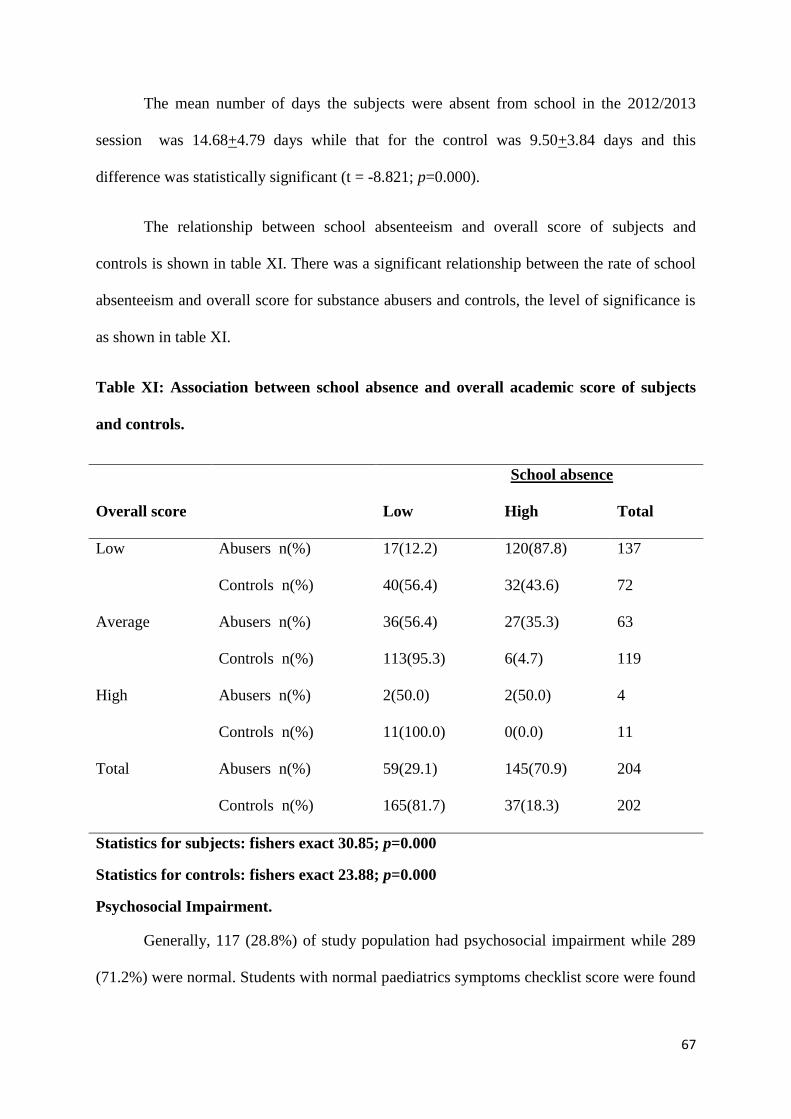
67
The mean number of days the subjects were absent from school in the 2012/2013
session was 14.68+4.79 days while that for the control was 9.50+3.84 days and this
difference was statistically significant (t = -8.821; p=0.000).
The relationship between school absenteeism and overall score of subjects and
controls is shown in table XI. There was a significant relationship between the rate of school
absenteeism and overall score for substance abusers and controls, the level of significance is
as shown in table XI.
Table XI: Association between school absence and overall academic score of subjects
and controls.
School absence
Overall score Low High Total
Low Abusers n(%) 17(12.2) 120(87.8) 137
Controls n(%) 40(56.4) 32(43.6) 72
Average Abusers n(%) 36(56.4) 27(35.3) 63
Controls n(%) 113(95.3) 6(4.7) 119
High Abusers n(%) 2(50.0) 2(50.0) 4
Controls n(%) 11(100.0) 0(0.0) 11
Total Abusers n(%) 59(29.1) 145(70.9) 204
Controls n(%) 165(81.7) 37(18.3) 202
Statistics for subjects: fishers exact 30.85; p=0.000
Statistics for controls: fishers exact 23.88; p=0.000
Psychosocial Impairment.
Generally, 117 (28.8%) of study population had psychosocial impairment while 289
(71.2%) were normal. Students with normal paediatrics symptoms checklist score were found

68
to perform significantly better academically ( χ2=8.75 ; p=0.024). The mean PSC score for
substance abusers was 21.96+10.77 while that for controls was 16.07+8.69. The difference
was statistically significant (t=-6.74; p=0.000). Eighty-nine subjects (43.7%) and 28 controls
(13.9%) had abnormal PSC scores. The association between PSC score and the overall
academic score of substance abusers, as shown in table XII, was statistically significant.
Table XII: Association between psychosocial dysfunction and overall academic score of
substance abusers and controls
PSC Score
Overall score Normal Abnormal Total
Low Abusers n(%) 70(51.4) 67(48.6) 137
Controls n(%) 61(84.7) 11(15.4) 72
Average Abusers n(%) 45(71.0) 18(29.0) 63
Controls n(%) 104(87.3) 15(12.7) 119
High Abusers n(%) 0(0.0) 4(100.0) 4
Controls n(%) 9(83.3) 2(16.7) 11
Total Abusers n(%) 115(56.3) 89(43.7) 204
Controls n(%) 174(86.1) 28(13.9) 202
Statistics for subjects: Fishers exact 5.54;p = 0.046
Statistics for controls: Fishers exact 0.55;p = 0.821
Type of substance abused
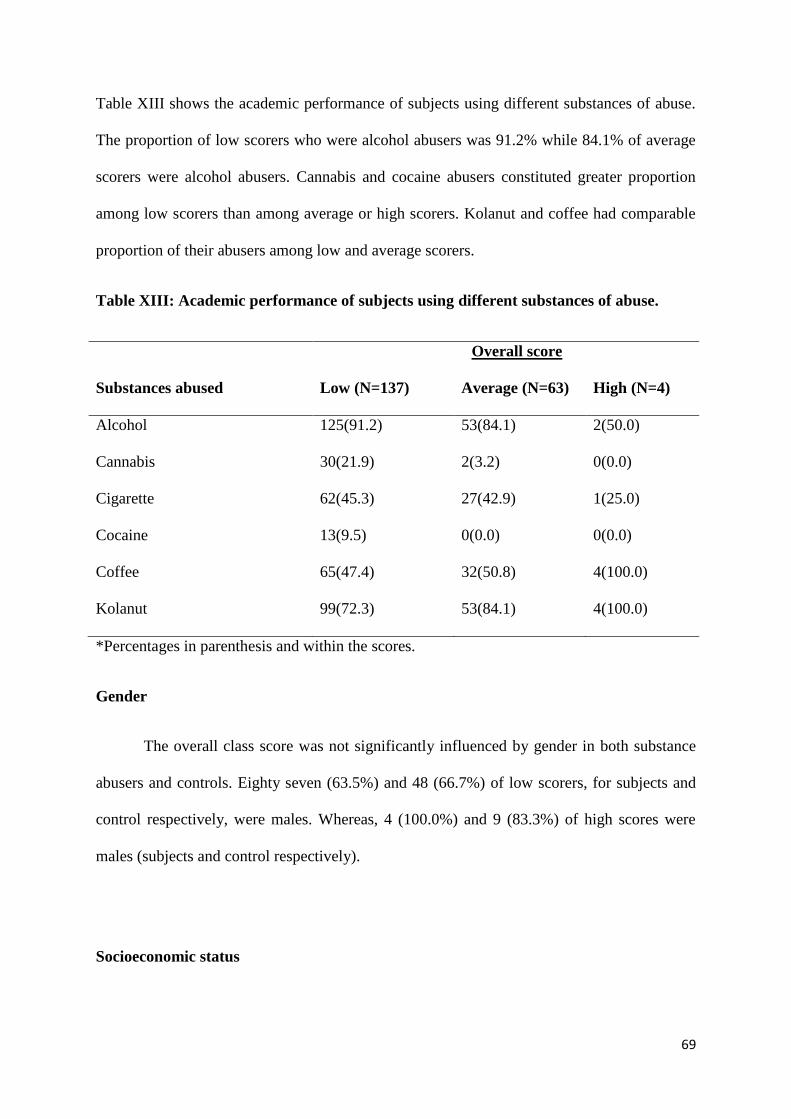
69
Table XIII shows the academic performance of subjects using different substances of abuse.
The proportion of low scorers who were alcohol abusers was 91.2% while 84.1% of average
scorers were alcohol abusers. Cannabis and cocaine abusers constituted greater proportion
among low scorers than among average or high scorers. Kolanut and coffee had comparable
proportion of their abusers among low and average scorers.
Table XIII: Academic performance of subjects using different substances of abuse.
Overall score
Substances abused Low (N=137) Average (N=63) High (N=4)
Alcohol 125(91.2) 53(84.1) 2(50.0)
Cannabis 30(21.9) 2(3.2) 0(0.0)
Cigarette 62(45.3) 27(42.9) 1(25.0)
Cocaine 13(9.5) 0(0.0) 0(0.0)
Coffee 65(47.4) 32(50.8) 4(100.0)
Kolanut 99(72.3) 53(84.1) 4(100.0)
*Percentages in parenthesis and within the scores.
Gender
The overall class score was not significantly influenced by gender in both substance
abusers and controls. Eighty seven (63.5%) and 48 (66.7%) of low scorers, for subjects and
control respectively, were males. Whereas, 4 (100.0%) and 9 (83.3%) of high scores were
males (subjects and control respectively).
Socioeconomic status

70
There was no significant association between the overall scores of both subjects and
controls and their socioeconomic status. The proportion of low scorers among the lower
socioeconomic class for subjects and control were 83.8% and 84.6% respectively, those of
the middle socioeconomic class were 9.5% (subjects) and 12.8% (control) while the
proportion of low scorers among the upper socioeconomic class were 6.8% (subjects) and
2.6% (control).
Severity of substance use using ASADA score and academic performance.
Fifty nine (29.1%) of subjects had ASADA scores >4. Fourty one (69.5%) of subjects
with severe substance abuse had low scores while 97(66.8%) of subjects who had ASADA
score less than 3 had low academic scores. There was no significant association between the
severity of substance use, measured by the ASADA score, and the overall score in 2012/2013
session ( χ2=4.081; p=0.092).
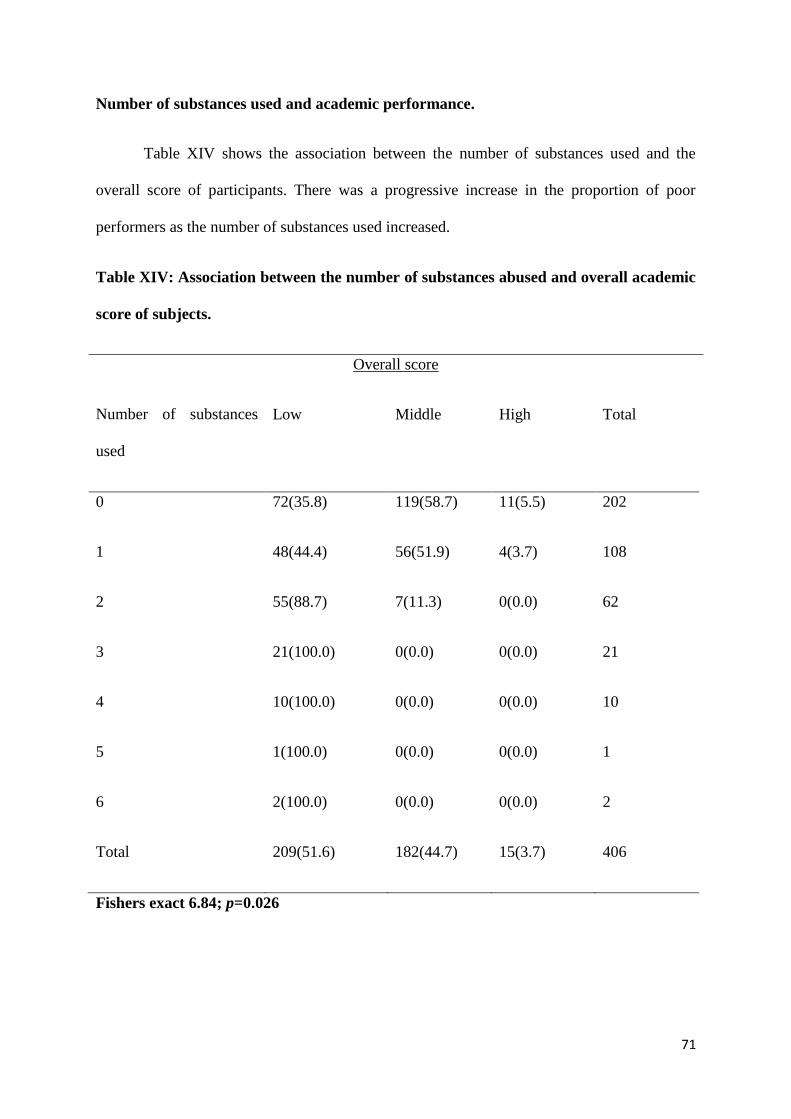
71
Number of substances used and academic performance.
Table XIV shows the association between the number of substances used and the
overall score of participants. There was a progressive increase in the proportion of poor
performers as the number of substances used increased.
Table XIV: Association between the number of substances abused and overall academic
score of subjects.
Overall score
Number of substances
used
Low Middle High Total
0 72(35.8) 119(58.7) 11(5.5) 202
1 48(44.4) 56(51.9) 4(3.7) 108
2 55(88.7) 7(11.3) 0(0.0) 62
3 21(100.0) 0(0.0) 0(0.0) 21
4 10(100.0) 0(0.0) 0(0.0) 10
5 1(100.0) 0(0.0) 0(0.0) 1
6 2(100.0) 0(0.0) 0(0.0) 2
Total 209(51.6) 182(44.7) 15(3.7) 406
Fishers exact 6.84; p=0.026
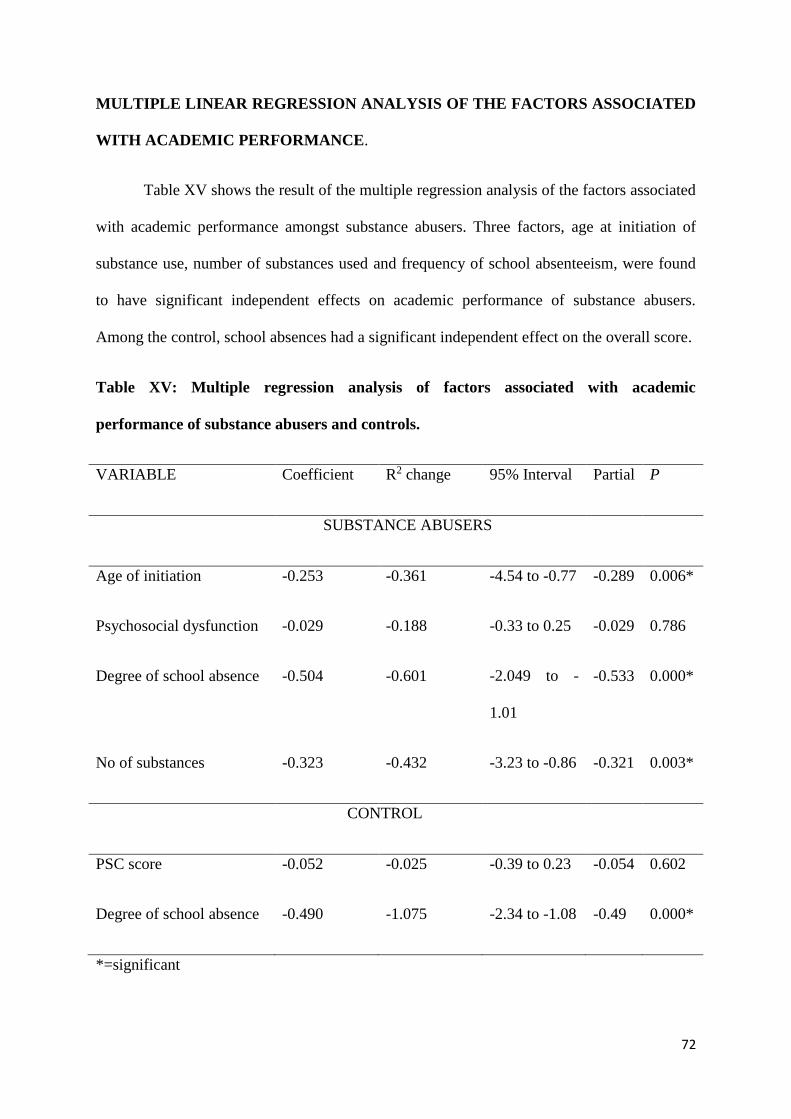
72
MULTIPLE LINEAR REGRESSION ANALYSIS OF THE FACTORS ASSOCIATED
WITH ACADEMIC PERFORMANCE.
Table XV shows the result of the multiple regression analysis of the factors associated
with academic performance amongst substance abusers. Three factors, age at initiation of
substance use, number of substances used and frequency of school absenteeism, were found
to have significant independent effects on academic performance of substance abusers.
Among the control, school absences had a significant independent effect on the overall score.
Table XV: Multiple regression analysis of factors associated with academic
performance of substance abusers and controls.
VARIABLE Coefficient R2 change 95% Interval Partial P
SUBSTANCE ABUSERS
Age of initiation -0.253 -0.361 -4.54 to -0.77 -0.289 0.006*
Psychosocial dysfunction -0.029 -0.188 -0.33 to 0.25 -0.029 0.786
Degree of school absence -0.504 -0.601 -2.049 to -
1.01
-0.533 0.000*
No of substances -0.323 -0.432 -3.23 to -0.86 -0.321 0.003*
CONTROL
PSC score -0.052 -0.025 -0.39 to 0.23 -0.054 0.602
Degree of school absence -0.490 -1.075 -2.34 to -1.08 -0.49 0.000*
*=significant
73
DISCUSSION
The prevalence rate of substance abuse obtained from this study is 32.9%. A previous
study30 done five years ago in this environment obtained a prevalence of 27.1%. In keeping
with previous studies in south eastern Nigeria,30,33,47,50 alcohol was the most commonly
abused substance. This finding, may be attributable to the availability of various brands of
alcoholic beverages in the study area. However, reports from western32,51 and northern56
Nigeria showed that cigarette was the most commonly abused substance. The difference in
finding may be due to cultural differences between the South Eastern, Northern and Western
Nigeria.
It is pertinent to note that 47% of subjects, abused more than one substance.
Substance abuse disorders therefore may be causing significant morbidity amongst our
adolescent population. As a result, more efforts need to be exerted to bring the use and abuse
of substances to the barest minimum. Substance abuse is more common among male
adolescents. This is consistent with observed trend in Nigeria2,4,15,16,30,48,50 and globally.7,13,14
The reason may be attributable to the more adventurous nature of males especially during
adolescence.30
Cigarette and kola nut abuse were more amongst adolescents of lower socioeconomic
class. The abuse of other substances did not show any significant association with
socioeconomic class. This observation contrasts with the findings of Abiodun et al31 in Ilorin,
and Odejide et al49 in Ibadan, Western Nigeria. They reported that adolescents from upper
socioeconomic class abused substances more than those from other socioeconomic classes.
Abiodun et al31 as well as Odejide et al49 attributed this to increased availability of these
substances to this class of adolescents based on costs. The reason for the preponderance of
cigarettes and kola nut abuse among the adolescents of lower socioeconomic class in
74
Abakaliki may be economic. Kola nuts and cigarettes are cheap and readily available. The
practice of giving kolanut as a sign of acceptance of a visitor among the Igbos could also
account for a high preponderance of kalanut abuse in Abakaliki. Another possible
contributing factor could be parenting style. Adolescents with permissive parents; and those
whose parents abuse substance are more likely to abuse substances.36 Parents of the lower
socioeconomic classes have been reported to have less supervision of their adolescent
students. This may make them vulnerable to negative peer influences at school.36
Age of the respondent was found to be significantly associated with the abuse of
cigarettes and alcohol. Most of the abusers were older and in the late adolescence. Ngesu et
al8 in Kenya and Adelakan and Ndom16 in Nigeria made similar observations. Older students
have stayed longer in school, and therefore have been exposed to stronger and sustained peer
influences. Adolescents found to be substance abusers were observed to have had their first
use of these substances in early adolescence. This is because the use of substance has strong
appeal for those beginning their independence as they search for identity.4,41,48 Early
adolescence is characterized by innate curiosity and thirst for new experiences. They are
therefore susceptible to experimentation with drugs at this age.36 Furthermore, because
adolescents at this stage lack the knowledge of consequences of actions and self-will, they
may progress from experimentation with substances to addiction in later years.36,49
Adolescents who were orphaned were more likely to abuse cannabis and cigarettes
while the abuse of cigarettes, alcohol, cannabis and kola nuts were more in adolescents from
divorced homes. Similar findings of high prevalence of substance use and or abuse among
students from dysfunctional homes have been reported severally in the literature. 30,43,52 This
may be due to lack of discipline, poor supervision and poor personality development which is
often associated with single parenting.4,15,31
75
The mean overall academic score of substance abusing adolescents, was significantly
lower than that of the control. The poor academic achievement of these students may be due
to the direct effect of these substances on cognition or the associated increased school
absence. School absence was more common among substance abusing students. In this
report, high school absence is associated with poor school performance. This finding supports
the assertion of Cox et al26 that heavy drinking of alcohol, frequent smoking of cigarette and
cannabis use resulted in low academic performance as measured by school reports of
performances in mathematics and Spanish language. Ingles et al69 corroborated this, having
observed poor academic performance in adolescents who abused alcohol or smoked daily.
Ingles et al69 attributed poor academic performance to lack of interest on school
achievements or interference with study tasks induced by the use of substances. In addition,
the “hang-over” effect of alcohol use for instance may result in poor concentration and sleep
during lessons and examinations.
It is worthy to note that despite the poorer performance of subjects when compared to
that of control, students in both groups performed generally poor academically. This finding
is consequent upon the observation of the high prevalence of low overall score of 67.3% and
35.8% in substance abusers and controls respectively. High scorers were 1.8% and 5.5% in
subjects and controls respectively. There are obviously other factors contributing to this poor
academic performance in the general population of students in Abakaliki. The reason for this
was not explored in this study.
However, academic failure amongst controls in this study (35.8%) is remarkably
higher than previous studies by Ibekwe et al90 and Ogunfowora et al89 who reported
prevalence rates of 16% and 7.7% respectively in their controls. Ogunfowora‘s participants
were mainly from the upper socioeconomic class and Ibekwe’s study had equal
representation of all socioeconomic classes. In present study, more of the participants were

76
from the lower socioeconomic class. Previous report have highlighted the relationship
between socioeconomic class and academic performance.75 This may partly explain the
higher prevalence of academic underachievement in controls demonstrated in the my study.
Another contributing factor may be the high proportion(70.9% for subjects and 18.3% for
controls) of adolescent with high school absence rate in in my study population. School
absenteeism is known to affect academic performance especially in substance abusing
students.75-77
Substance abusing students performed worse than controls in all the key subjects
studied. Cox et al26 who studied public high school students observed lower scores in
mathematics and Spanish language amongst heavy substance users. However my study shows
poor performance in mathematics amongst both substance abusers and controls. The reason
for this is not clear. Lynsky21 had suggested that the reason for poor academic performance in
substance abusers is that substance use itself may have a direct effect on cognitive
development which in turn results in academic underachievement and disruption of progress.
Similarly, Engberg and Moral,22 King et al,23 and Pope and Yurelun-Todd24 reported that
heavy substance use can result in problems in working memory and attention due to changes
in brain activity induced by the use of substances which may culminate into school problems
and eventual dropout. The same studies,21-24 emphasized that the degree of substance use, as
well as the use of multiple substances rather than the type of substances used was associated
with poor academic performance.
School absenteeism was more amongst substance abusers than control. Similar
findings were made by Godley70 who reported more risky behaviours such as truancy among
substance abusers. This finding was corroborated by Okike30 who performed a similar study
on substance abuse in adolescents in Abakaliki five years ago. He observed that school
absenteeism was a consequence of the various substances he studied. It has been posited that
77
these substances produce “hang over” effects on the abuser thereby making school attendance
difficult. Other reason given is that these students prefer to “hang out” with peers rather than
participate in school activities. School attendance is a critical factor in school success of
students. Students who absent themselves from school lose out on the preparatory classes and
tend to perform worse than their peers.79 This is confirmed by the finding of academic
underachievement among children with high school absence rate in the present study.
Substance abusers in this study had higher rate of psychosocial dysfunction, 43.7%
compared to 13.9% among controls. The fact that psychosocial dysfunctions are common
among substance abusers has been previously reported.65,66,73 However, the prevalence of
psychosocial dysfunction,43.7%, obtained in this study is higher than 24.1% reported in a
previous study using similar rating scale in 2010.73 The observed difference may be due to
the varying definitions used for subjects. While this study recruited all substance abusers as
subjects, the previous study73 recruited only current users of substances. Langas et al72
reported that 46% of their substance users had personality disorders which were more or less
a function of the age at which substance abusers initiated substance use. Substance abusing
students with psychosocial impairment performed significantly worse than those without
psychosocial impairment. This corroborates the finding of Gruber et al78 that there is
increased prevalence of inattention in heavy substance abusers. Gruber et al78 reported that
the impaired critical skills are related to attention, memory and learning problems amongst
heavy users of cannabis. Poor performance may also be due to loss of concentration during
lessons and class assessments from psychosocial dysfunctions as postulated by Gruber et al.78
Although this study has shown a significant association between gender and the abuse
of some substances with more males as substance abusers, there was however no significant
association between the overall scores of substance abusers and control with respect to
gender. The reason for this is unclear. Although it suggests that there may be other factors

78
affecting academic performance such as the individual’s natural ability, conscientious study
and school attendance. Similarly socioeconomic class was noted not to be significantly
associated with academic performance a trend that has been noted by other authors.89-91 The
performance of all the students was generally poor in spite of their social class. This shows
that participants, both abusers and control, may be exposed to similar factors which could
account for their general poor performance.
The type of substance abused rather than the severity of substance used was noted to
be associated with the academic performance of these students. Students that abuse cigarettes,
alcohol, and cannabis and cocaine performed poorly in school. Abusers of kolanut and coffee
had similar proportion of subjects within the low and average score group. This may be due
to the central acting nature of alcohol, cigarrete , cannabis, and cocaine and their tendency to
cause addiction. It could also be due to inattention, and impairment in memory and thought
caused by these substances as reported by Gruber et al.78 Unlike these substances, kola nut
and coffee has been shown to have less central toxicities .30,73
The number of substances used has been shown to be significantly associated to
academic performance in this study. There was a significant increase in proportion of
participants with a low overall score as the number of substances used increased. This may be
due to the additive pharmacologic toxicities of these substances. Igwe and Ojinnaka73 had
earlier noted multiple substance use as a risk factor for psychiatric morbidity in students that
abuse substances. The resultant psychosocial impairment of multiple substance use may
result in poor concentration and poor thought which could adversely affect school
performance.
Multiple linear regressions showed that school absences, age at initiation of substance
use and number of substances used had significant independent effects on academic
79
performance of substance abusers. This finding agrees with the known relationship between
school absenteeism and academic performance79 as well as the effect of multiple substance
use on mental health of substance abuser which in turn can affect their school
performance.73,78 However the finding of significant independent effect of school
absenteeism on academic performance among control shows that the poor academic
performance of substance abusers may largely be due to school absenteeism rather than
substances related factors. Furthermore, the age of initiation of substance use and the use of
multiple substances rather than the type of substance abused are what preclude good
academic performance in substance abusers.
80
CONCLUSION
The following conclusions can be drawn from the results of this study:
1. Substance abuse is high among secondary school students in Abakaliki and alcohol is
the most commonly abused substance
2. The academic performance of substance abusers is worse than that of students who do
not abuse substances.
3. High school absence, age at initiation of substance use and abuse of multiple
substances are the most important determinants of academic performance of substance
abusers in secondary schools in Abakaliki.
4. School absenteeism is the underlying determinant of academic performance of all
secondary school students whether substance abusing or non-substance abusing in
Abakaliki.
81
RECOMMENDATIONS
Based on the findings of this study, the following recommendations are made:
1. Awareness campaign on the finding of significant prevalence of substance abuse and
its consequences should be made to the general public and inculcated in the
curriculum of secondary school students.
2. School absenteeism should be considered in poor performing students in schools.
82
LIMITATIONS
The direct effect of substance abuse on cognition of the individual could not be ascertained
especially using a cross-sectional means. However a longitudinal study carried out to observe
the substance abuser over a period of time would require enormous resources and participants
may be lost to follow up after they leave the secondary school.
LINES OF FUTURE STUDY

83
Substance abusers in this study had a higher rate of psychosocial impairment than was
previously reported. A study, to determine the factors responsible for this in Abakaliki should
be conducted
REFERENCES
84
1. Abdulkarim AA. Opinion of adolescents on how best to tackle the problem of drug
abuse among students. Nig J Pediatr 2004; 31:144-45.
2. Anochie IC, Nkanginieme KEO. Social correlates of drug use among secondary school
students in Port Harcourt, Southern Nigeria. Sahel Med J 2000; 3: 87-92.
3. Ayuba NL, Audu DM. Illicit drug abuse among children and adolescents in Jos Nigeria.
Highland Med Res J 2003; 1:18-22.
4. Okwaraji FE. Substance abuse among secondary school adolescents in Enugu. J Coll
Med 2006; 1: 130-55.
5. Lamptey JJ. Socio-demographic characteristics of substance abusers admitted to a
private specialist clinic. Ghana Med J 2005; 39: 2-07.
6. Bronwyn M, Charles DHP. Access to substance abuse treatment services for black
South Africans: Findings from audits of specialist treatment. SA Psychiat Rev 2005; 8:
15-19.
7. Betencourt OA, Herrera MM. Alcohol and drug problems and sexual and physical
abuse at three urban high schools in Mthatha. SA Fam Pract 2006; 48:17-17c.
8. Ngesu LM, Ndiku J, Masese A. Drug dependence and abuse in Kenyan secondary
schools: strategies for intervention. Edu Res Rev 2008; 3: 304-08.
9. Wu L, Woody GE, Yang C, Pan J, Blazer DG. Racial/ethical variations in substance-
related disorders amongst adolescents in the United States. Arch Gen Psychiatry 2011;
68: 1176-85.
10. Belfer ML. International child and adolescent mental health review. WHO, Department
of Mental Health and Substance Dependence, Geneva 2003;17-22.
85
11. World Health Organization (WHO). World Bank Special Programme of Research,
Development and Research Training in Human Reproduction (HRP), author Guidelines
for research on reproductive health involving adolescents. From the Programme's
document Preparing a Project Proposal, Guidelines and Forms. 3rd ed. 2003.
www.who.int/reproductivehealth/hrp/guidelines_adolescent.en.html,. Retrieved august
3rd, 2012.
12. United Nations Population Fund. State of the world population. Making 1 billion count:
investing in adolescent's health and rights. 2003.
http://www.unfpa.org/swp/2003/english/ch1/index.htm#1 Retrieved august 3rd, 2012.
13. Greydanus DE, Patel DR. Substance abuse in adolescents: A complex conundrum for
the clinician. Pediatr Clin North Am 2003; 50: 1179-23.
14. McArdle P. Substance use by children and young people. Arch Dis Child 2004; 89:
701-04.
15. Okolie KC, Obinwanne SC. Substance use among students of tertiary institutions in
Anambra State, Nigeria. Medzik J 2002; 4: 25-30.
16. Adelekan ML, Ndom RJE. Trends in prevalence and pattern of substance use among
secondary school pupils in Ilorin, Nigeria. Werst Afr J Med 1997; 16: 157-64.
17. Goodman E, Huang B. Socioeconomic status, depressive symptoms and adolescent
substance use. Arch Paediatr Adolesc Med 2002; 156: 448-53.
18. Shrier LA, Harry SK, Kurland M, Knight JR. Substance use problems and associated
psychiatric symptoms among adolescents in primary care. Pediatrics 2003; 3: 699-05.
86
19. Brook DW, Brook JS, Pahl TIM. The Longitudinal Relationship between drug use and
risky behaviors among Colombian adolescents. Arch Pediatr Adolesc Med 2002; 156:
1101–07.
20. Kebede D, Alem A, Mitike G, Enquselassie F, Berhane F, Abebe Y, Ayele R, Lemma
W, Assefa T, Gebremichael T. Khat and alcohol use and risky sex behavior among in-
school and out-of-school youth in Ethiopia. BMC Public Health. 2005; 5: 109.
21. Lynsky MT. Substance use and educational attainment. Addiction. 2006; 101: 1684–85.
22. Engberg J, Morral AR. Reducing substance use improves adolescents’ school
attendance. Addiction. 2006; 101:1741–51.
23. King KM, Meehan BT, Trim RS, Chassin L. Marker or mediator? The effects of
adolescent substance use on young adult educational attainment. Addiction. 2006; 101:
1730–40.
24. Pope HG, Yurelun-Todd D. The residual cognitive effects of heavy marijuana use in
college students. J Am Med Assoc 1996; 275: 521-27.
25. Lukoye A,Mungla PA, Ndung MN, Kinoti KC, Ogot EM. Prevalence of substance use
among college students in Eldoret, Western Kenya. BMC Psychiatry 2011; 11: 34-38.
26. Cox RG, Zhang L, Johnson WB, Bender DR. Academic performance and substance
use: Findings from a state survey of public high school students. J Sch Health ASHA
2007; 77: 109-15.
27. Needham BL, Crosnoe R, Muller Chandra. Academic failure in secondary school: The
inter-related role of health problems and educational context. Soc Probl 2004; 51: 569-
86.
87
28. Sigqueirra LM, Brook JS. Tobacco use as a predictor of illicit drug use and related
problems in Columbian youths. J Adolesc Health 2003; 32: 50-57.
29. Oyedeji B. Federal centralism and Nigerian university governance. Cont J Arts Human
2012; 4: 20-36.
30. Okike CO. Prevalence of substance abuse among secondary school adolescents in
Abakaliki, Ebonyi state, South Eastern Nigeria. Dissertation: West African College of
Physicians. 2009.
31. Abiodun OA, Adelakan ML, Ogenremi OO, Oni GA, Obayan AO. Psychosocial
correlates of alcohol, tobacco and cannabis use amongst secondary school students in
Ilorin Nigeria. West Afr J Med 1994; 3: 213-17.
32. Odejide AO, Olatawura MO. Alcohol use in a Nigerian rural community. Afr J
Psychiat 1977; 12: 69-74.
33. Egbuonu I, Ezechukwu CC, Chukwuka JO, Unakwe R. Substance abuse among female
secondary school students in Anambra State, South Eastern Nigeria. Nig J Clin Pract
2004; 7: 53-55.
34. Fatoye FO, Morakinyo O. Substance use among secondary school students in rural and
urban communities in South Western Nigeria. East Afri Med J 2002; 79: 299-305.
35. Fatoye FO. Psychosocial correlates of substance use amongst secondary school students
in South Western Nigeria. East Afri Med J 2003; 80: 154-58.
36. Obot IS. The epidermiology of tobacco and alcohol abuse in Nigeria. In Obot IS ed.
Epidermiology and Control of Substance Abuse in Nigeria. Centre for Research and
information on Substance Abuse (CRISA), Jos 1993; 67-87.
88
37. Ahmed AM. Pharmacological principles in drug dependence. In: Ebie JC, Tongue EJ,
editors. Handbook of African Training Courses on Drug Dependence. 1st ed.
International Council on Alcohol and Addiction (ICAA) Publication, Switzerland,
1988: 64-68.
38. Ebie JC, Ebie EJ. Drug abuse: Overview of the current situation in Nigeria. In: Ebie JC,
Tongue EJ. editors. Handbook of the African Training Courses on Drug Dependence.
1st ed. International Council on Alcohol and Addiction (ICAA) Publication,
Switzerland, 1988: 19-25.
39. Odejide AO. A nation at risk: Alcohol and substance abuse among Nigerian youth.
Inaugural Lecture Delivered at the University of Ibadan 1989: 1-39.
40. Obianwu HO. Drug classification. In: Ebie JC, Tongue EJ. editors. Handbook of
African Training Courses on Drug Dependence, 1st ed. International Council on
Alcohol and Addiction (ICAA) Publication, Switzerland, 1988:5-7
41. Report of WHO Committee on Drug Dependence. WHO Technical Report Series
Geneva 2003; 915: 6. Retrieved august 3rd, 2012.
42. Abiodun OA. Drug abuse and its clinical implications with special reference to Nigeria.
Centr Afr J Med 1991; 37: 24-30.
43. Galea S, Pandi A, Vlahor D. The social epidemiology of substance use. Epidemiol Rev
2004; 26: 36-52.
44. Obot IS. Alcohol and Drug -related disorders. In: Peltzer K, Ebigbo PO, editors.
Clinical Psychology in Africa. 1st ed. Chuks printing Co Enugu 1989; 329-44.

89
45. Burns EM. The nature of dependence. In: Ebie JC, Tongue EJ. editors. Handbook of
African Training Courses on Drug Dependence, 1st ed. International Council on
Alcohol and Addiction (ICAA) Publication, Switzerland, 1988; 43-52.
46. Obot IS. Pattern of Drug Use and Abuse in Nigeria. CEWG 1992; 432-438.
47. Okonkwo KOB, Ezeani PO, Ihezue UH, Nwagbo DFE. Psychoactive substance abuse
amongst an urban secondary school population in Enugu, Nigeria: Prevalence and
pattern of use. J Coll Med 1999; 4: 24-6.
48. Akhabue VO. Pattern of drug abuse among adolescents in secondary schools in Benin
City. Dissertation: National Postgraduate Medical College of Nigeria. 2000.
49. Odejide AO, Ohaeri JU, Adelakan ML, Ikuesan BA. Alcohol treatment system in
Nigeria. Alcohol Alcoholism 1989; 24: 347-53.
50. Igwe WC, Ojinnaka N, Ejiofor SO, Emechebe GO, Ibe BC. Socio-Demographic
correlates of psychoactive substance abuse amongst secondary school students in
Enugu Nigeria. Euro J Soc Sci 2009; 12: 277-83.
51. Abiodun OA, Adelekan ML, Ogunremi OO, Oni GA, Obayan AO. Pattern of substance
use amongst secondary school students in Ilorin, Northern Nigeria. West Afr J Med
1994; 13: 91-94.
52. Anochie IE, Nkanginieme KEO, Alikor EAD. Drug abuse among secondary school
students in Port-Harcourt Metropolis. Nig J Med 1999; 8: 17-23.
53. Jenkin RR, Adger H. Substance abuse. In: Kliegman RM, Behrman RE, Jenson HB,
Stanton BF. editors. Nelson Textbook of Paediatrics. 18th ed. WB Saunders 2007: 653-
61.
90
54. Omadjohwoefe OS. Drug prohibition and the problem of conformity in Nigeria. J
Psychology 2010; 1: 91-97.
55. Oshodi OY, Aina OF, Onajole AT. Substance use among secondary school students in
an urban setting in Nigeria: Prevalence and associated factors. Afr J Psychiatry 2010;
13: 52-57.
56. Shehu AU, Idris SH. Marijuana smoking among secondary school students in Zaria,
Nigeria: Factors responsible and effects on Academic Performance. Al Afri Med 2008;
7: 175-79.
57. Odey FA, Okokon IB, Ogbeche JO, Jombo GT, Ekanem EE. Prevalence of cigarette
smoking among adolescents in Calabar city, South-eastern Nigeria. J Med Sci 2012; 3:
237-42.
58. Salawu FK, Danburam A, Desalu OO, Olokoba AB, Agbo J, Midala JK. Cigarette
smoking habits among adolescents in Northeast Nigeria. Afri J Resp Med 2009; 2: 8-11.
59. Barry RJ, Rushby JA, Wallace ML, Clarke AR, Johnstone SJ, Zlojutro I. Caffeine
effect on resting-state arousal. Clin Neurophysiol 2005; 116: 2693-00.
60. Wentz CT, Magavi SSP. Caffeine alters proliferation of neuronal precursors in the
adults hippocampus. Neuropharmacology 2009; 56: 994–00.
61. Mednick SC, Cai DJ, Kanady J, Drummond SPA. Comparing the benefits of caffeine,
naps and placebo on verbal, motor and perceptual memory. Behav Brain Res 2008; 193:
79–86.
62. Abdulkarim AA, Mokuolu OA, Adeniyi A. Drug use among adolescents in Ilorin,
Nigeria. Trop Doct 2005; 35: 225-28.

91
63. Kandel DB. Does marijuana cause the use of other drugs? JAMA 2003; 289: 482-83.
64. Comerci GD, Schwebel R. Substance abuse: An overview. Adolsc Med State Art Rev
2000; 11: 87-89.
65. Rehm J, Mathers C, Popova S, Thavorncharoensap M, Teerawattananon Y, Patra J.
Global burden of disease and injury and economic cost attributable to alcohol use and
alcohol use disorders. Lancet. 2009; 373: 2223–33.
66. Rehm J, Taylor B, Room R. Global burden of disease from alcohol, illicit drugs and
tobacco. Drug Alcohol Rev 2006; 25: 503–13.
67. en.wikipedia.org/wiki/Academic_achievement (assessed 14th may 2012).
68. Dewey JD. “Reviewing the relationship between school factors and substance use for
elementary, middle and high school students.” J Prim Prevent 1999;19: 177-25.
69. Ingles CJ, Torregrosa MS, Rodriguez-Marin J, Garcia del Castillo JA, Gazquez JJ,
Garcia-Fernandez JM, Delgado B. Alcohol and tobacco use and cognitive-motivational
variables in school settings: effects on academic performance in Spanish adolescents.
Adicciones 2013; 25: 63-70.
70. Godley SH. Substance use, academic performance and the village school. Addiction.
2006; 101: 1685–87.
71. Meltem D, Serap T. Gender differences in academic performance in a large public
university in Turkey. Higher Education 2007; 53: 255-77. Springer L Science +
Business Media B.V DOI10.1007/s 10734-005-2464-6. (assessed 22nd march 2013)
72. Langas A, Malt UF, Opjordsmoen S. In-depth study of personality disorders in first
admission patients with substance use disorders. BMC Psychiatry 2012; 12:180.
92
73. Igwe WC, Ojinnaka NC. Mental health of adolescents who abuse psychoactive
substances in Enugu Nigeria – A cross-sectional study. Italian J Paediatr 2010; 36: 36-
53.
74. Breyer J, Winter K. Adolescent brain development: Implication for drug use
prevention. Center for substance abuse research. Department of psychiatry; University
of Minnesota and Mentor USA.1-8.
www.mentorfoundation.org/pdfs/prevention_perspectives/19.pdf. (assessed 21st march
2013.)
75. Odejide AO, Ohaeri JU, Adelekan ML, Ikuesan BA. Drinking behavior and social
change among youth in Nigeria: A study of two cities. Drug Alc Depend 1987; 20: 227-
33.
76. Eamon MK. Social-demographic, school, neighbourhood, and parenting influences on
academic achievements of latino young adolescents. J Youth Adol 2005; 34: 163-75.
77. Hochschild JL. Social class in public schools. J Soc Issues 2003; 59: 821-40.
78. Gruber AJ, Pope HG, Hudson HI, Yurgelun-Todd D. Attributes of long-term heavy
cannabis users: A case control study. Psychol Med 2003; 33:1415-22.
79. Weitzman M, Klerman LV, Lamb G, Menary J, Alpert JJ. School absence: a problem
for the Paediatrician. Pediatrics 1982; 69: 739-46.
80. Winter KC, Kaminer Y. Screening and assessing adolescent substance use disorders in
clinical populations. J Am Acad Child Adolesc Psych 2008; 47: 740-44.
81. Smart RG, Hughes HS, Johnson LD. A methodology for students’ drug use surveys.
Who Offset Publications, WHO Geneva, 1980: 35-52.
93
82. en.wikipedia.org/wiki/CAGE_questionnaire
83. Saremi A, Hanson RL, Wiliams DE, Roumain J, Robon RW, Long JC, Goldman D,
Knowler WC. Validity of the CAGE questionnaire in an American Indian population. J
Stud Alcohol 2001; 62: 294-00.
84. Ojo OO, Lawani AO, Adedigba MA, Nwhafor SO. Influences on smoking behaviour of
adolescents and young adults in a Nigerian university. Afri J Drug Alchohol Stud 2009;
7: 2-05.
85. Adelakan ML, Odejide AO. The reliability and validity of the WHO students drug use
questionnaire among Nigerian students. Drug Alc Depend 1989; 24: 245-49
86. Saffier K, Colombo C, Brown D, Mundt MP, Fleming MF. Addiction severity index in
a chronic pain sample receiving opiod therapy. J Subst Abuse Treat 2007; 33: 303-11.
87. Schatz J. Brief report: academic attainment in children with sickle cell disease. J
Paediatr Psychol 2004; 29: 627-33.
88. Karadel S, Kulkarni M. Poor school performance. Indian J Peditr 2005; 72: 961-67.
89. Ogunfowora OB, Olanrewaju DM, Akenzua GI. A comparative study of academic
achievement of children with sickle cell anemia. J Natl Med Assoc .2005; 97: 405-08.
90. Ibekwe RC, Ojinnaka NC, Iloeje SO. Academic performance of school children with
epilepsy. West Afr J Med 2008; 27: 74-77.
91. Akpan MU, Ojinnaka NC, Ekanem EE. Academic performance of school children with
behavioural disorders in Uyo, Nigeria. Afr Health Sci 2010; 10: 154 – 8.
94
92. Perkonigg A, Goodwin RD, Fiedler A, Behrendt S, Beesdo K, Lieb R, et al. The natural
course of cannabis use, abuse and dependence during the first decades of life.
Addiction. 2008;103: 439–49.
93. Lovallo WR, Farag NH, Vincent AS, Thomas TL, Wilson MF. Cortisol responses to
mental stress, exercise and meals following caffeine intake in men and women.
Pharmacol Biochem Behav 2006; 83: 441–47.
94. Nardi AE, Lopes FL, Valenca AM, Freire RC, Veras AB, de-Melo-Neto L, Nascimento
I, King AL, Mezzasalma MA, Soares-Filho GL, Zin WA. Caffeine challenge test in
panic disorder and depression with panic attacks. Compr Psychiatry 2007; 48: 257–63.
95. Goodman R. The strengths and difficulties questionnaire: A research note. J child
Psychology Psychiatry 1997; 38: 581-86.
96. Salem S, Mehmood Z. Development of a scale for assessing emotional and behavioral
problems of school children. Pakist J social clinical Psychol 2011; 9: 73-78.
97. Rutter MA. Children’s behavior questionnaire for completion by teachers, preliminary
findings. J Child Psychology Psychiatry 1967; 8: 1-11.
98. Conner CK. Conners Comprehensive Behaviour Rating Scales (CBRS) Manual.
2008.3rd edition.
99. Achenbach T, Rescorla L. Manual for the ASEBA (Achenbach System of
Empirically Based Assessment) school-age forms & profiles. Burlington, VT:
University of Vermont, Research Center for Children, Youth, and Families. 2001.
100. Jellinek MS, Murphy MJ. Brief psychosocial screening in outpatient paediatric
practice. J Paediat 1986; 109: 374-78.

95
101. Iloeje SO, Meme J. Rutter’s behavior Scale (B2) for children (Teacher’s scale):
Validation and standardization for use in Nigerian children. J Trop Pediatr 1992; 38:
235-39.
102. Akpan MU, Ojinnaka NC, Ekanem E. Behavioural problems among school children in
Nigeria. SAJP 2010; 16: 50-55.
103. American Psychiatric Association. Diagnostic and statistical manual of mental
disorders, 3rd ed. Washington DC 1980.
104. Achenbach TM, Edelbrock CS. Manual for the Child Behaviour Checklist and Revised
Child Behaviour Profile. Burlington VT Queencity Printers 1983.
105. National Population Commission. Provisional census figures. Official gazette. 2007;
24: B-185.
106. Ebonyi State ministry of education, Statistics and Planning Unit. 2012 school
enrolment: 12-24.
107. Araoye MO. Research methodology with statistics for health and social sciences. Ilorin:
Nathadex Publishers. 2003; 115-29.
108. Olusanya O, Okpere EE, Ezimokhai M. The importance of social class in voluntary
fertility control in a developing country. West Afr J Med. 1985; 4: 252-55.
109. Ogunfowora OB. A comparative study of school absence and academic performance of
children with sickle cell anemia and healthy controls. West African Postgraduate
Medical College Dissertation 1994.
110. The West African Examinations Council. Regulations for the West African Senior
School Certificate Examination (WASSCE). Pg 13.

96
registration.waecdirect.org/pdf/Syllabus/INTRODUCTION.pdf assessed 1st
September 2012.
APPENDIX Ia. LETTER OF ETHICAL APPROVAL FROM RESEARCH AND
ETHICS COMMITEE FEDERAL TEACHING HOSPITAL ABAKALIKI (FETHA)
97
APPENDIX Ib. LETTER OF EXTENSION OF DATE OF ETHICAL APPROVAL
98
99
APPENDIX II. LETTER OF INTRODUCTION FROM MINISTRY OF EDUCATION
EBONYI.
100
APPENDIX III: CONSENT LETTER (STUDENTS).
Subjects Identification Number…………………………………
TITTLE OF STUDY: ACADEMIC PERFORMANCE OFSUBSTANCE ABUSING
SCONDARY SCHOOL STUDENTS IN ABAKALIKI.
Dear respondent,
This study is aimed at describing the academic performance of substance abusing
students. You will be asked to fill 3 questionnaires which will take a total of 60 minutes to
do. Thereafter your class attendance and averages in the terms of last academic sessions will
be obtained.
I seek your co-operation to participate in this study and promise that your
confidentiality will be maintained. You will not be victimized for not participating, you are
not exposed to any risks and you have the right to withdraw from the study at any time you
deem it necessary. In addition, your name will not be mentioned in any publication emanating
from this study. You may contact the chairman, Research and Ethics Committee Federal
Teaching Hospital Abakaliki if there is any need to do so.
Thank you.
Dr Onyinye Anyanwu
Principal Investigator.

101
I …………………………………………………….having read this consent letter am willing
to participate in the study on my own freewill without inducement or coercion.
I hereby affirm my willingness to participate in this study.
…………………………… ………………………………..
Name of participant Name of researcher
…………………………. ………………………………
Signature/date of participant Signature/date of researcher

102
APPENDIX IV: CONSENT LETTER (PARENTS/GUARDIAN).
Subjects Identification Number…………………………………
TITTLE OF STUDY: ACADEMIC PERFORMANCE OF SUBSTANCE ABUSING
SCONDARY SCHOOL STUDENTS IN ABAKALIKI.
Dear Sir/Madam,
This study is aimed at assessing the pattern of substance abuse and its influence on
academic performance. Your child will be asked to fill 3 questionnaires which will take a
total of 60 minutes to do. Thereafter his/her class attendance and averages in the terms of the
last academic session will be obtained.
I seek your consent to allow him/her participate in this study and promise that
confidentiality will be maintained. He/she will not be victimized for not participating, is not
exposed to any risks by participating and you have the right to withdraw him/her from the
study at any time you deem it necessary. In addition, his/her name will not be mentioned in
any publication emanating from this study. You may contact, the chairman, Research and
Ethics Committee Federal Teaching Hospital Abakaliki if there is any need to do so.
Thank you.
Dr Onyinye Anyanwu
Principal Investigator.
103
I …………………………………………………………………….having read this consent
letter am willing to allow my child/ward …………………………………………………….
participate in the study on my own freewill without inducement or coercion.
I hereby affirm my willingness to allow my child/ward participate in this study.
…………………………… ………………………………..
Name of parent/guardian Name of researcher
…………………………. ………………………………
Signature/date of parent/guardian Signature/date of researcher
104
APPENDIX V: CONSENT LETTER (PRINCIPAL)
Department of Pediatrics
Federal Teaching Hospital Abakaliki
Sir,
I wish to inform you of my intent to carry out a research on the title “Academic
performance of substance abusing secondary school students in Abakaliki metropolis”. It will
entail filling three questionnaires and assessment of students’ class performance and
attendance. Selected students will be from SS2 and 3. This research will pose no negative
effect to your administration nor your students. I therefore solicit your consent and support to
carry out this exercise in your school. Attached herewith is a letter of introduction from the
Ebonyi State Secondary Education Board.
Thank you.
Dr Anyanwu Onyinye
Principal Researcher.
[email protected](08033230292)
Consent Given:
Name of Principal…………………………………………………………………
Signature ……………………………………………………………………………
Date …………………………………………………………………………………..
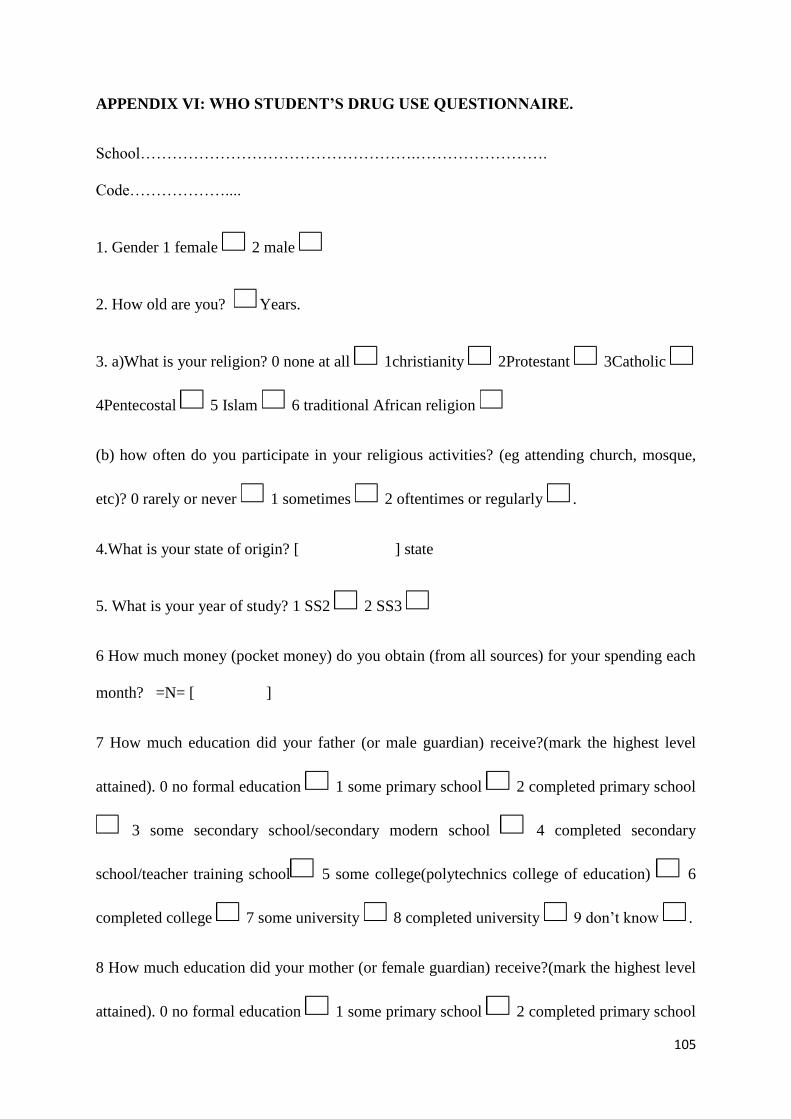
105
APPENDIX VI: WHO STUDENT’S DRUG USE QUESTIONNAIRE.
School…………………………………………….…………………….
Code………………....
1. Gender 1 female 2 male
2. How old are you? Years.
3. a)What is your religion? 0 none at all 1christianity 2Protestant 3Catholic
4Pentecostal 5 Islam 6 traditional African religion
(b) how often do you participate in your religious activities? (eg attending church, mosque,
etc)? 0 rarely or never 1 sometimes 2 oftentimes or regularly .
4.What is your state of origin? [ ] state
5. What is your year of study? 1 SS2 2 SS3
6 How much money (pocket money) do you obtain (from all sources) for your spending each
month? =N= [ ]
7 How much education did your father (or male guardian) receive?(mark the highest level
attained). 0 no formal education 1 some primary school 2 completed primary school
3 some secondary school/secondary modern school 4 completed secondary
school/teacher training school 5 some college(polytechnics college of education) 6
completed college 7 some university 8 completed university 9 don’t know .
8 How much education did your mother (or female guardian) receive?(mark the highest level
attained). 0 no formal education 1 some primary school 2 completed primary school
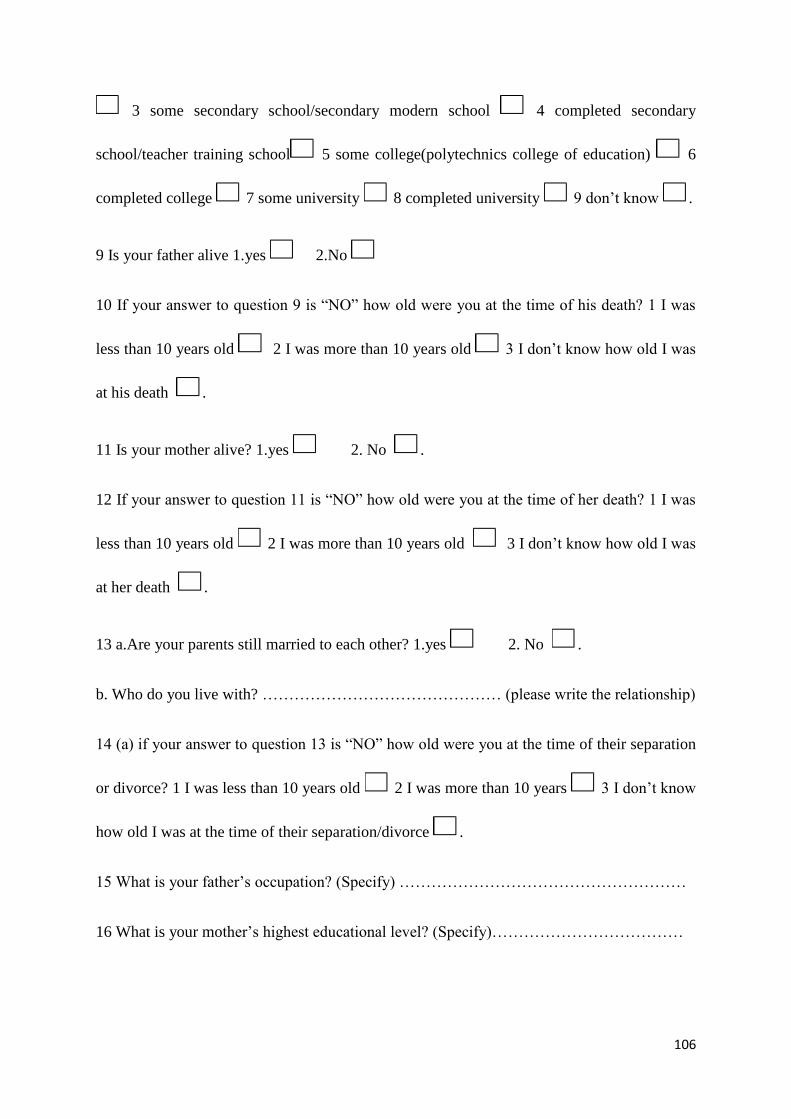
106
3 some secondary school/secondary modern school 4 completed secondary
school/teacher training school 5 some college(polytechnics college of education) 6
completed college 7 some university 8 completed university 9 don’t know .
9 Is your father alive 1.yes 2.No
10 If your answer to question 9 is “NO” how old were you at the time of his death? 1 I was
less than 10 years old 2 I was more than 10 years old 3 I don’t know how old I was
at his death .
11 Is your mother alive? 1.yes 2. No .
12 If your answer to question 11 is “NO” how old were you at the time of her death? 1 I was
less than 10 years old 2 I was more than 10 years old 3 I don’t know how old I was
at her death .
13 a.Are your parents still married to each other? 1.yes 2. No .
b. Who do you live with? ……………………………………… (please write the relationship)
14 (a) if your answer to question 13 is “NO” how old were you at the time of their separation
or divorce? 1 I was less than 10 years old 2 I was more than 10 years 3 I don’t know
how old I was at the time of their separation/divorce .
15 What is your father’s occupation? (Specify) ………………………………………………
16 What is your mother’s highest educational level? (Specify)………………………………
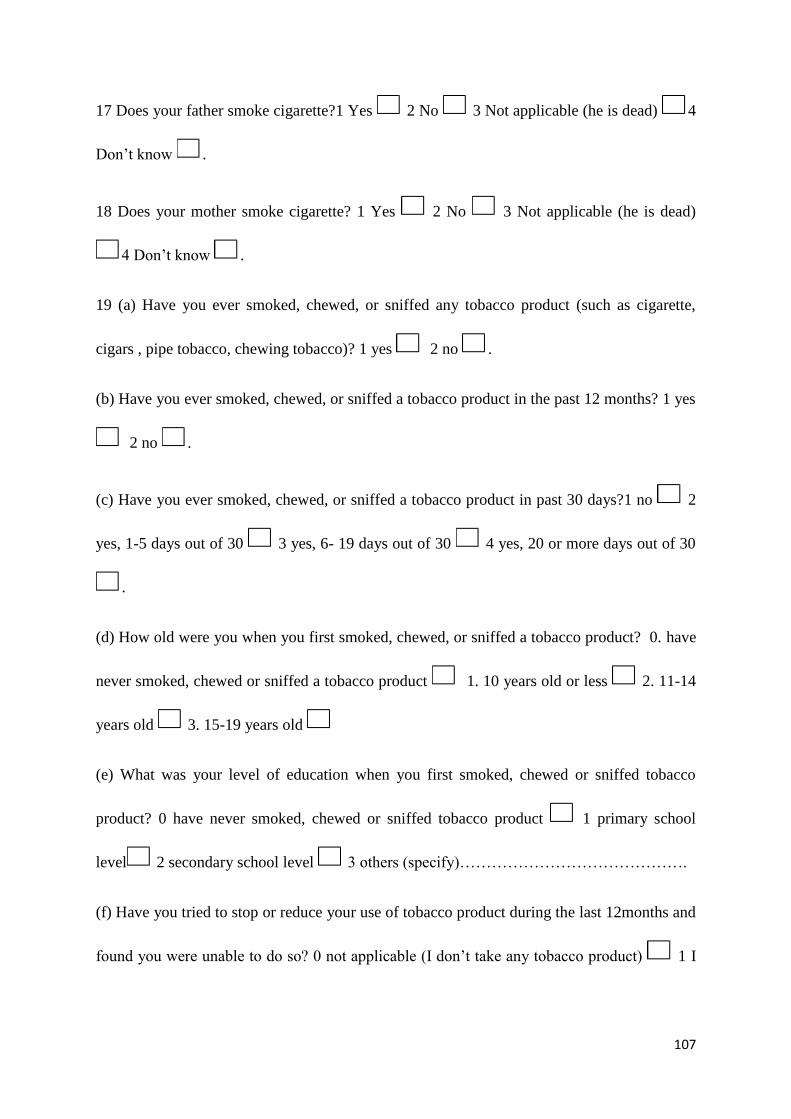
107
17 Does your father smoke cigarette?1 Yes 2 No 3 Not applicable (he is dead) 4
Don’t know .
18 Does your mother smoke cigarette? 1 Yes 2 No 3 Not applicable (he is dead)
4 Don’t know .
19 (a) Have you ever smoked, chewed, or sniffed any tobacco product (such as cigarette,
cigars , pipe tobacco, chewing tobacco)? 1 yes 2 no .
(b) Have you ever smoked, chewed, or sniffed a tobacco product in the past 12 months? 1 yes
2 no .
(c) Have you ever smoked, chewed, or sniffed a tobacco product in past 30 days?1 no 2
yes, 1-5 days out of 30 3 yes, 6- 19 days out of 30 4 yes, 20 or more days out of 30
.
(d) How old were you when you first smoked, chewed, or sniffed a tobacco product? 0. have
never smoked, chewed or sniffed a tobacco product 1. 10 years old or less 2. 11-14
years old 3. 15-19 years old
(e) What was your level of education when you first smoked, chewed or sniffed tobacco
product? 0 have never smoked, chewed or sniffed tobacco product 1 primary school
level 2 secondary school level 3 others (specify)…………………………………….
(f) Have you tried to stop or reduce your use of tobacco product during the last 12months and
found you were unable to do so? 0 not applicable (I don’t take any tobacco product) 1 I
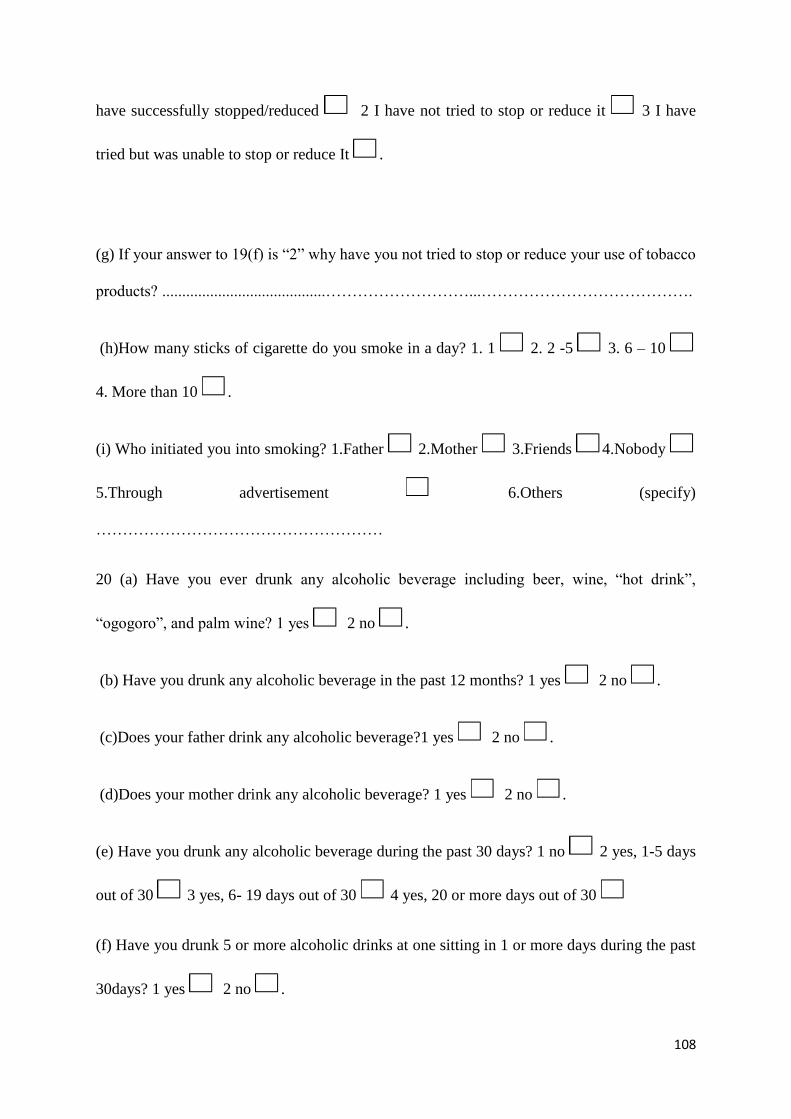
108
have successfully stopped/reduced 2 I have not tried to stop or reduce it 3 I have
tried but was unable to stop or reduce It .
(g) If your answer to 19(f) is “2” why have you not tried to stop or reduce your use of tobacco
products? .........................................………………………...………………………………….
(h)How many sticks of cigarette do you smoke in a day? 1. 1 2. 2 -5 3. 6 – 10
4. More than 10 .
(i) Who initiated you into smoking? 1.Father 2.Mother 3.Friends 4.Nobody
5.Through advertisement 6.Others (specify)
………………………………………………
20 (a) Have you ever drunk any alcoholic beverage including beer, wine, “hot drink”,
“ogogoro”, and palm wine? 1 yes 2 no .
(b) Have you drunk any alcoholic beverage in the past 12 months? 1 yes 2 no .
(c)Does your father drink any alcoholic beverage?1 yes 2 no .
(d)Does your mother drink any alcoholic beverage? 1 yes 2 no .
(e) Have you drunk any alcoholic beverage during the past 30 days? 1 no 2 yes, 1-5 days
out of 30 3 yes, 6- 19 days out of 30 4 yes, 20 or more days out of 30
(f) Have you drunk 5 or more alcoholic drinks at one sitting in 1 or more days during the past
30days? 1 yes 2 no .
109
(g) How old were you when you first had a drink of an alcoholic beverage more than just a
sip? 0. have never drunk alcoholic beverage 1.10 years old or less 2.11-14 years old
3.15-19 years old .
(h) What was your level of education when you first had a drink of an alcoholic beverage
more than just a sip? 0 have never drunk alcoholic beverages 1.primary school level
2 secondary school level 3.others (specify) ……………………………………………….
(i) Have you tried to stop or reduce your use of alcoholic beverage during the last 12months
and found you were unable to do so? 0 not applicable (I don’t take any alcoholic beverage)
1 I have successfully stopped/reduced 2 I have not tried to stop or reduce it 3 I
have tried but was unable to stop or reduce it.
(j) if your answer to 20(i) is “2” why have you not tried to stop or reduce your use of
alcohol?..............................................................................................………………………….
(k)How much alcohol do you take at a sitting?1. Half beer bottle 2. 1 bottle 3. 2 – 4
bottles 4. More than 5 bottles .
(l) Who initiated you into drinking alcohol? 1. Father 2.Mother 3.Friends
4.Nobody 5.Through advertisement 6.Others
(specify)……………………………….
21 (a) Have you ever taken any cannabis (Indian hemp, marijuana, hashish, ganga, igbo etc)?
1 yes 2 no .
(b) Does your father take cannabis? 1 yes 2 no .
110
(c) Does your mother take cannabis? 1 yes 2 no .
(d) Have you taken any cannabis during the past 12 months? 1 yes 2 no .
(e) Have you taken any cannabis during the past 30 days? 1 no 2.yes, 1-5 days out of 30
3 yes, 6- 19 days out of 30 4 yes, 20 or more days out of 30 .
(f) How old were you when you first took cannabis? 0. have never taken cannabis 1. 10
years old or less 2. 11-14 years old 3. 15-19 years old .
(g) What was your level of education when you first took cannabis? 0 have never taken
cannabis 1 primary school level 2 secondary school level 3 others (specify)
……………………………………………………….
(h) Have you tried to stop or reduce your use of cannabis during the last 12months and found
you were unable to do so? 0 not applicable (I don’t take cannabis) 1 I have successfully
stopped/reduced 2 I have not tried to stop or reduce It 3 I have tried but was unable
to stop or reduce it .
(i) if your answer to 21(h) is “2” why have you not tried to stop or reduce your use of
cannabis?..........................................……………………………………………………………
(j) Who initiated you into taking cannabis? 1.Father 2.Mother 3.Friends 4.
Nobody 5.Through advertisement 6.Others (specify) ……………………………….
22 (a) Have you ever taken any cocaine? 1 yes 2 no .
(b)Does your father take cocaine? 1 yes 2 no .
111
(c)Does your mother take cocaine? 1 yes 2 no .
(d) Have you taken cocaine during the past 12 months? 1 yes 2 no .
(e) Have you taken any cocaine during the past 30 days?1 no 2 yes, 1-5 days out of 30
3 yes, 6- 19 days out of 30 4 yes, 20 or more days out of 30 .
(f) How old were you when you first took cocaine? 0. have never taken cocaine 1. 10
years old or less 2. 11-14 years old 3. 15-19 years old .
(g) What was your level of education when you first took cocaine? 0 have never taken
cocaine 1 primary school level 2 secondary school level 3 others (specify)
………………………………………………………
(h) Have you tried to stop or reduce your use of cocaine during the last 12months and found
you were unable to do so? 0 not applicable (I don’t take cocaine) 1 I have successfully
stopped/reduced 2 I have not tried to stop or reduce it 3 I have tried but was unable
to stop or reduce it .
(i) if your answer to 22(h) is “2” why have you not tried to stop or reduce your use of
cocaine?................................................…………………………………………………………
(j)if you have ever taken any cocaine, write the route through which you took it(eg sniffing,
injections):....................................................................…………………………………………
(k) Who initiated you into taking cocaine? 1.Father 2.Mother 3.Friends
4.Nobody 5. Through advertisement 6.Others (specify)
…………………….……….
112
23 (a) Have you ever taken kola nut before? 1 yes 2 no .
(b) Does your father take kola nut? 1 yes 2 no .
(c) Does your mother take kola nut? 1 yes 2 no .
(d) Have you taken kola nut in the past 12 months? 1 yes 2 no .
(e)Have you taken any kola nut in the past 30 days? 1.no 2.Yes 1-5 days out of 30
3. Yes 6-19 days out of 30 4.yes, 20 or more days out of 30
(f)How old were you when you first took kola nut? 1 I have never taken kola nut before
2. 10 years old or less 3. 11-14 years old 4. 15-19 years old
(g) What was your level of education when you first took kola nut? 0.have never taken kola
nut before 1. Primary school level 2. Secondary school level 3 others (specify)
…………………………………………………………
(h) Have you tried to stop or reduce your use of kola nut during the last 12 months and found
that you were unable to do so? 0. Not applicable (I don’t take kola nut) 1. I have
successfully stopped/reduced it 2. I have not tried to stop or reduce it 3. I have tried
but was unable to stop or reduce it .
(i) if your answer to 23(h) is “2” why have you not tried stopping or reducing your use of
kola nut …………………………………..……………………………………………………
(k) Who initiated you into taking kola nut? 1. Father 2. Mother 3. Friends
4.Nobody 5.Through advertisements 6.Others (specify) ……………………………
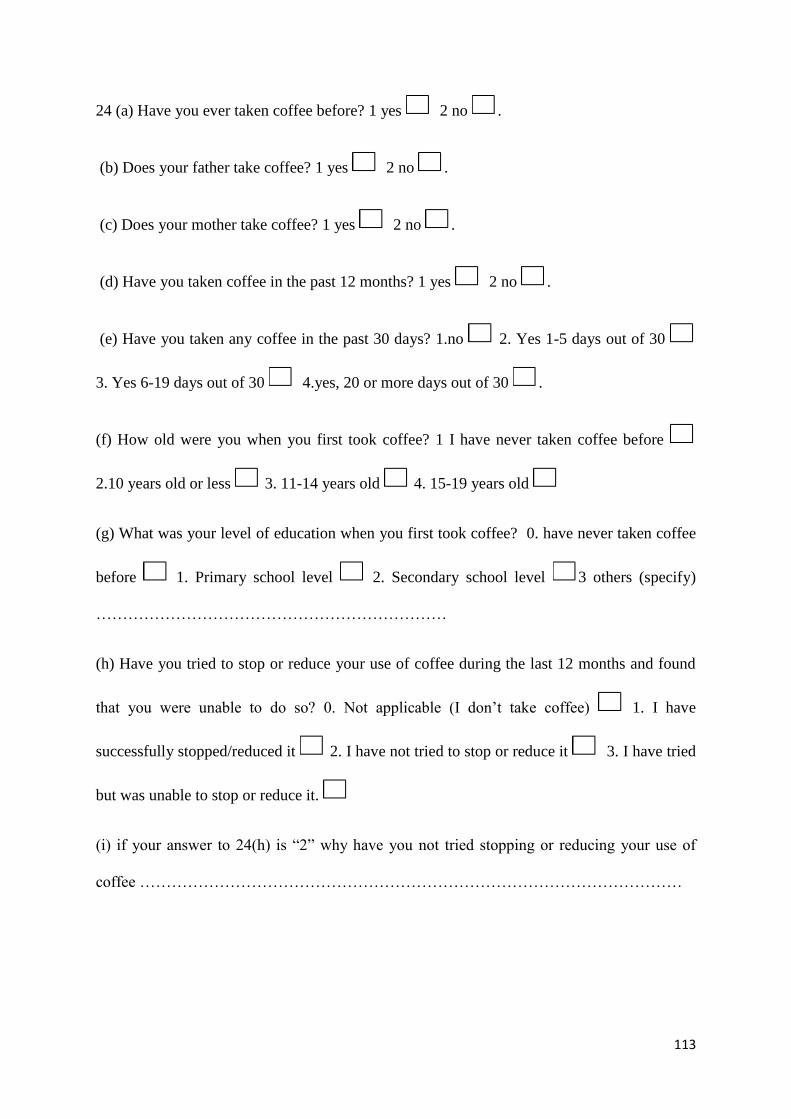
113
24 (a) Have you ever taken coffee before? 1 yes 2 no .
(b) Does your father take coffee? 1 yes 2 no .
(c) Does your mother take coffee? 1 yes 2 no .
(d) Have you taken coffee in the past 12 months? 1 yes 2 no .
(e) Have you taken any coffee in the past 30 days? 1.no 2. Yes 1-5 days out of 30
3. Yes 6-19 days out of 30 4.yes, 20 or more days out of 30 .
(f) How old were you when you first took coffee? 1 I have never taken coffee before
2.10 years old or less 3. 11-14 years old 4. 15-19 years old
(g) What was your level of education when you first took coffee? 0. have never taken coffee
before 1. Primary school level 2. Secondary school level 3 others (specify)
…………………………………………………………
(h) Have you tried to stop or reduce your use of coffee during the last 12 months and found
that you were unable to do so? 0. Not applicable (I don’t take coffee) 1. I have
successfully stopped/reduced it 2. I have not tried to stop or reduce it 3. I have tried
but was unable to stop or reduce it.
(i) if your answer to 24(h) is “2” why have you not tried stopping or reducing your use of
coffee …………………………………………………………………………………………

114
(j) Who initiated you into taking coffee? 1. Father 2. Mother 3.Friends
4.Nobody 5.Through advertisements 6. Others (specify)
….…………………………
25 Are there any other drug not mentioned that you have taken in the past year to make you
feel good or intoxicated? 1 yes 2 no .
(b) If yes write the name/s of the drug here ………………………………………………….
26 Do you know of any other drug that some of your classmates are taking to make them feel
good or intoxicated? 1 yes 2 no .
(b) If yes what are the drugs called? ………………………………………………………..
27 If you had used any cannabis, would you have mentioned it in this questionnaire? 1. No
2. Not sure 3. Yes
28 Do you know all these drugs are dangerous to health? 1 yes 2 no .
Thank you for responding
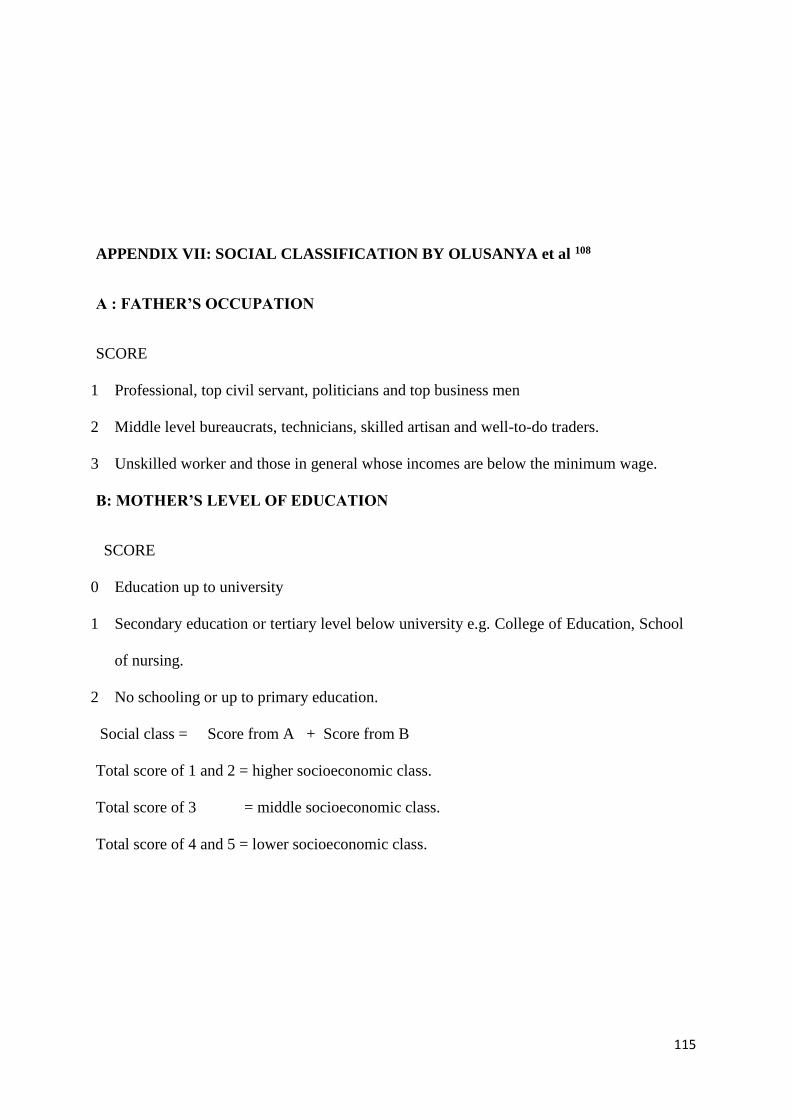
115
APPENDIX VII: SOCIAL CLASSIFICATION BY OLUSANYA et al 108
A : FATHER’S OCCUPATION
SCORE
1 Professional, top civil servant, politicians and top business men
2 Middle level bureaucrats, technicians, skilled artisan and well-to-do traders.
3 Unskilled worker and those in general whose incomes are below the minimum wage.
B: MOTHER’S LEVEL OF EDUCATION
SCORE
0 Education up to university
1 Secondary education or tertiary level below university e.g. College of Education, School
of nursing.
2 No schooling or up to primary education.
Social class = Score from A + Score from B
Total score of 1 and 2 = higher socioeconomic class.
Total score of 3 = middle socioeconomic class.
Total score of 4 and 5 = lower socioeconomic class.

116
APPENDIX VIII: ASSESSING THE SERIOUSNESS OF ADOLESCENT DRUG
ABUSE (ASADA) SCORING METHOD.
School…………………………………………….…………………….
Code………………....
VARIABLES SCORE
0 +1 +2
1 Type of drug used None Beer, wine,
local gin,
cigarette,
coffee, kola
nut.
Marijuana, Indian hemp,
cocaine, crack, heroine,
amphetamine,
hallucinogens.
2 Setting of drug abuse Group Alone
3 Affect before drug use Happy Always poor Sad
4 Time of drug use After school Before school
5 Time of week drug is
used
Weekend Week days
6 Use before driving No Yes
7 History of accidents None Yes
8 School performance Good/impr
oving
Always poor Recently poor
9 Positive history of family
drug abuse
No Yes
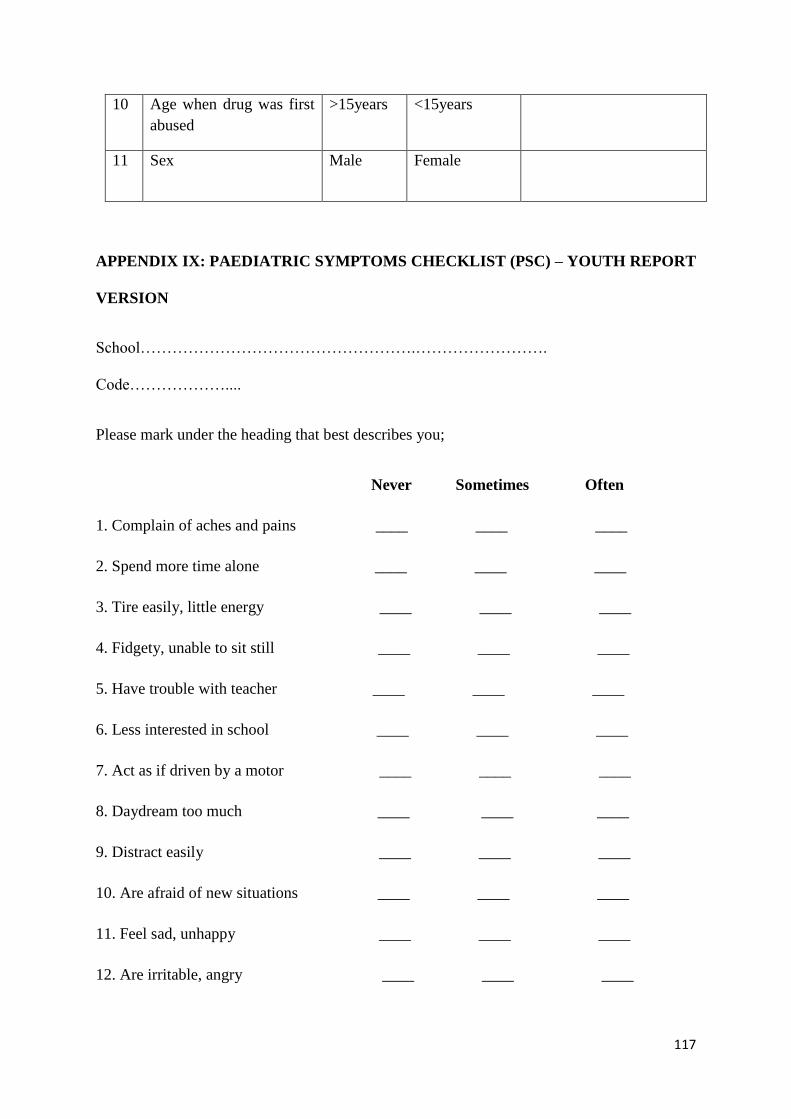
117
10 Age when drug was first
abused
>15years <15years
11 Sex Male Female
APPENDIX IX: PAEDIATRIC SYMPTOMS CHECKLIST (PSC) – YOUTH REPORT
VERSION
School…………………………………………….…………………….
Code………………....
Please mark under the heading that best describes you;
Never Sometimes Often
1. Complain of aches and pains ____ ____ ____
2. Spend more time alone ____ ____ ____
3. Tire easily, little energy ____ ____ ____
4. Fidgety, unable to sit still ____ ____ ____
5. Have trouble with teacher ____ ____ ____
6. Less interested in school ____ ____ ____
7. Act as if driven by a motor ____ ____ ____
8. Daydream too much ____ ____ ____
9. Distract easily ____ ____ ____
10. Are afraid of new situations ____ ____ ____
11. Feel sad, unhappy ____ ____ ____
12. Are irritable, angry ____ ____ ____
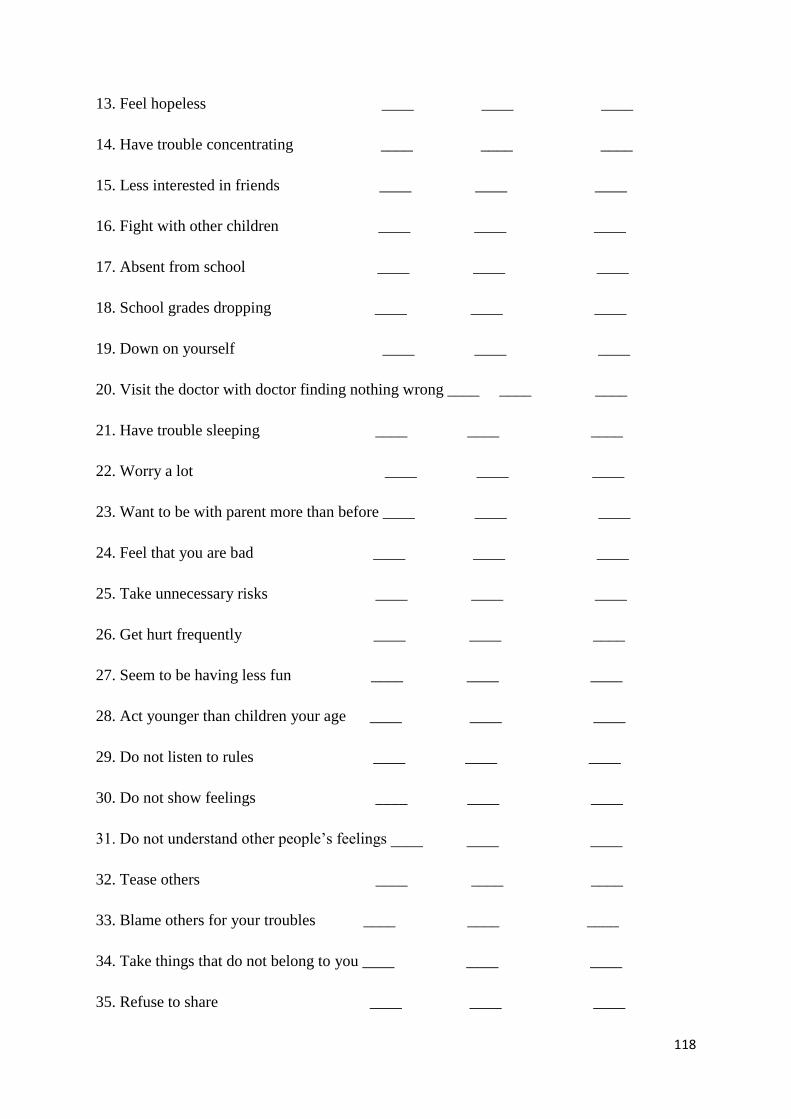
118
13. Feel hopeless ____ ____ ____
14. Have trouble concentrating ____ ____ ____
15. Less interested in friends ____ ____ ____
16. Fight with other children ____ ____ ____
17. Absent from school ____ ____ ____
18. School grades dropping ____ ____ ____
19. Down on yourself ____ ____ ____
20. Visit the doctor with doctor finding nothing wrong ____ ____ ____
21. Have trouble sleeping ____ ____ ____
22. Worry a lot ____ ____ ____
23. Want to be with parent more than before ____ ____ ____
24. Feel that you are bad ____ ____ ____
25. Take unnecessary risks ____ ____ ____
26. Get hurt frequently ____ ____ ____
27. Seem to be having less fun ____ ____ ____
28. Act younger than children your age ____ ____ ____
29. Do not listen to rules ____ ____ ____
30. Do not show feelings ____ ____ ____
31. Do not understand other people’s feelings ____ ____ ____
32. Tease others ____ ____ ____
33. Blame others for your troubles ____ ____ ____
34. Take things that do not belong to you ____ ____ ____
35. Refuse to share ____ ____ ____
119
Total Score -------------------------------------------------
APPENDIX X: SCHOOL DATA/ REPORT
Name of Child…………………………………………….. Code…………………
Class in 2012/2013 Academic Session……………………………………….
Academic Performance 1st Term 2nd Term 3rd Term
I Class Position .......... ……….. ………..
II Overall Score ………. ……….. ………..
III % Score Mathematics ………. ……….. ………..
IV % Score English ………. ……….. ………..
V % Score Igbo ………. ……….. ………..
VI % Score biology ………. ……….. ………..
Total number of days absent from school……… ………. .………
Total for the year……………………………………………………………………
Total No. of students in the Class ……………………………………………………




















