
Adolescent Substance Use and Aggression: A Review
23
http://cjb.sagepub.com/ Behavior Criminal Justice and http://cjb.sagepub.com/content/39/6/748 The online version of this article can be found at: DOI: 10.1177/0093854812437022 2012 39: 748 originally published online 20 March 2012 Criminal Justice and Behavior Neal Doran, Susan E. Luczak, Nicole Bekman, Igor Koutsenok and Sandra A. Brown Adolescent Substance Use and Aggression: A Review Published by: http://www.sagepublications.com On behalf of: International Association for Correctional and Forensic Psychology can be found at: Criminal Justice and Behavior Additional services and information for http://cjb.sagepub.com/cgi/alerts Email Alerts: http://cjb.sagepub.com/subscriptions Subscriptions: http://www.sagepub.com/journalsReprints.nav Reprints: http://www.sagepub.com/journalsPermissions.nav Permissions: What is This? - Mar 20, 2012 OnlineFirst Version of Record - May 10, 2012 Version of Record >> by guest on October 11, 2013 cjb.sagepub.com Downloaded from by guest on October 11, 2013 cjb.sagepub.com Downloaded from by guest on October 11, 2013 cjb.sagepub.com Downloaded from by guest on October 11, 2013 cjb.sagepub.com Downloaded from by guest on October 11, 2013 cjb.sagepub.com Downloaded from by guest on October 11, 2013 cjb.sagepub.com Downloaded from by guest on October 11, 2013 cjb.sagepub.com Downloaded from by guest on October 11, 2013 cjb.sagepub.com Downloaded from by guest on October 11, 2013 cjb.sagepub.com Downloaded from by guest on October 11, 2013 cjb.sagepub.com Downloaded from by guest on October 11, 2013 cjb.sagepub.com Downloaded from by guest on October 11, 2013 cjb.sagepub.com Downloaded from by guest on October 11, 2013 cjb.sagepub.com Downloaded from by guest on October 11, 2013 cjb.sagepub.com Downloaded from by guest on October 11, 2013 cjb.sagepub.com Downloaded from by guest on October 11, 2013 cjb.sagepub.com Downloaded from by guest on October 11, 2013 cjb.sagepub.com Downloaded from by guest on October 11, 2013 cjb.sagepub.com Downloaded from by guest on October 11, 2013 cjb.sagepub.com Downloaded from by guest on October 11, 2013 cjb.sagepub.com Downloaded from by guest on October 11, 2013 cjb.sagepub.com Downloaded from by guest on October 11, 2013 cjb.sagepub.com Downloaded from by guest on October 11, 2013 cjb.sagepub.com Downloaded from
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Adolescent Substance Use and Aggression: A Review

http://cjb.sagepub.com/Behavior
Criminal Justice and
http://cjb.sagepub.com/content/39/6/748The online version of this article can be found at:
DOI: 10.1177/0093854812437022
2012 39: 748 originally published online 20 March 2012Criminal Justice and BehaviorNeal Doran, Susan E. Luczak, Nicole Bekman, Igor Koutsenok and Sandra A. Brown
Adolescent Substance Use and Aggression: A Review
Published by:
http://www.sagepublications.com
On behalf of:
International Association for Correctional and Forensic Psychology
can be found at:Criminal Justice and BehaviorAdditional services and information for
http://cjb.sagepub.com/cgi/alertsEmail Alerts:
http://cjb.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
What is This?
- Mar 20, 2012OnlineFirst Version of Record
- May 10, 2012Version of Record >>
by guest on October 11, 2013cjb.sagepub.comDownloaded from by guest on October 11, 2013cjb.sagepub.comDownloaded from by guest on October 11, 2013cjb.sagepub.comDownloaded from by guest on October 11, 2013cjb.sagepub.comDownloaded from by guest on October 11, 2013cjb.sagepub.comDownloaded from by guest on October 11, 2013cjb.sagepub.comDownloaded from by guest on October 11, 2013cjb.sagepub.comDownloaded from by guest on October 11, 2013cjb.sagepub.comDownloaded from by guest on October 11, 2013cjb.sagepub.comDownloaded from by guest on October 11, 2013cjb.sagepub.comDownloaded from by guest on October 11, 2013cjb.sagepub.comDownloaded from by guest on October 11, 2013cjb.sagepub.comDownloaded from by guest on October 11, 2013cjb.sagepub.comDownloaded from by guest on October 11, 2013cjb.sagepub.comDownloaded from by guest on October 11, 2013cjb.sagepub.comDownloaded from by guest on October 11, 2013cjb.sagepub.comDownloaded from by guest on October 11, 2013cjb.sagepub.comDownloaded from by guest on October 11, 2013cjb.sagepub.comDownloaded from by guest on October 11, 2013cjb.sagepub.comDownloaded from by guest on October 11, 2013cjb.sagepub.comDownloaded from by guest on October 11, 2013cjb.sagepub.comDownloaded from by guest on October 11, 2013cjb.sagepub.comDownloaded from by guest on October 11, 2013cjb.sagepub.comDownloaded from

748
CRIMINAL JUSTICE AND BEHAVIOR, Vol. 39, No. 6, June 2012, 748-769DOI: 10.1177/0093854812437022© 2012 International Association for Correctional and Forensic Psychology
AUTHORS’ NOTE: This article is part of a special issue titled “Treatment Considerations for Aggressive Adolescents in Secure Settings,” edited by Calvin M. Langton of the University of Toronto, Canada. All cor-respondence should be addressed to Neal Doran, 151B, VMRF room 317, 3350 La Jolla Village Drive, San Diego, CA 92161; e-mail: [email protected].
ADOLESCENT SUBSTANCE USE AND AGGRESSION
A Review
NEAL DORANUniversity of California, San Diego
SUSAN E. LUCZAKUniversity of California, San DiegoUniversity of Southern California
NICOLE BEKMAN IGOR KOUTSENOK University of California, San Diego
SANDRA A. BROWN University of California, San DiegoVA San Diego Healthcare System
Substance use disorders (SUDs) in youth are strongly associated with aggression, delinquency, and involvement with the juvenile justice and mental health systems. This article reviews the relationship between aggression and SUDs and discusses evidence-based approaches to assessment and intervention, with a focus on youth in secure settings. While evidence indicates etiological overlap, SUDs also confer risk for aggression and delinquent behavior. SUDs and aggression are each influenced by executive functions that develop as youth transition toward adult roles. Additionally, the effects of substance use on the adolescent brain impair neurocognitive function and increase the risk for aggression and further substance use. In terms of assessment, it is important to identify function and form of aggression in order to understand motives and associations with substance use and to select appropriate interventions. Evidence-based screening and assessment of aggression, substance involvement, and related domains is also critical. In terms of treatment, youth with SUDs tend to be underserved, particularly when they are also involved with the juvenile justice system. Multiple modes of evidence-based treatment for substance use are available. Approaches that address risk factors common to SUDs and aggression across multiple domains (e.g., family therapies) have been found to be most effective but may be difficult to adapt for use in secure settings. Individual therapy approaches also have empirical support and may generally be more practical in secure settings.
Keywords: aggression; delinquency; substance use; adolescence
Youth substance use disorders (SUDs) are strongly associated with involvement in the juvenile justice and mental health systems (Chassin, 2008; Grisso & Underwood,
2004). School and community samples have yielded SUD prevalence estimates of 6% to 10% (Kandel, Johnson, & Bird, 1999; Rohde, Lewinsohn, & Seely, 1996), compared with 62% to 81% (Aarons, Brown, Hough, Garland, & Wood, 2001; Milin, Halikas, Meller, & Morse,

Doran et al. / ADOLESCENT SUBSTANCE USE AND AGGRESSION 749
1991) and 33% to 41% (Aarons et al., 2001; Deas-Nesmith, Campbell, & Brady, 1998; Piazza, 1996) in the juvenile justice and mental health systems, respectively. Consequently, it is important that clinicians working with youth be sensitive to the possibility of SUDs even for youth whose involvement in these systems is not explicitly SUD-related.
Substance use is associated with recidivism (Young, Dembo, & Henderson, 2007), likely reflecting etiological overlap and shared risk factors (Mason & Windle, 2002). Substance use also contributes to behaviors that result in juvenile justice involvement. For example, early use is a strong predictor of violent behavior (J. D. Hawkins et al., 2000). SUD inter-ventions also reduce behavioral risks for juvenile justice involvement (Fisher & Harrison, 2000). This is particularly important in light of evidence that most juvenile-justice-involved youth in need of SUD treatment do not receive it (Nissen, 2007), indicating that improving treatment access within the system may reduce recidivism.
Substance-involved youth are also likely to become involved in the mental health sys-tem, and the majority meet criteria for another Axis I disorder (Deas, 2006). There are multiple pathways through which co-occurrence may develop. Some disorders, including mood and conduct disorders, are associated with increased SUD risk (Armstrong & Costello, 2002). Alternatively, SUDs, especially with early onset, may increase the risk of other psychiatric conditions (Armstrong & Costello, 2002; Lamps, Sood, & Sood, 2008). Additionally, there is evidence of neurobiological and genetic overlap between SUDs and other disorders (McQuown, Belluzzi, & Leslie, 2007).
The goals of this article are to provide an overview of the relationship between aggres-sion and substance use in youth and to discuss the implications of this relationship for clinical work in secure settings. Below, we broadly describe aggression and substance use in the context of adolescent social and neurocognitive development, and we discuss assess-ment of aggression and substance use. These issues are then tied into discussion of evi-dence-based approaches to treatment of substance abuse and aggression or related problems such as delinquency and involvement with the juvenile justice system.
DEVELOPMENTAL CONSIDERATIONS
It is well-established that substance use has negative consequences for the brain (Oscar-Berman & Marinkovic, 2003) but only recently has the impact on the adolescent brain been explored (Squeglia, Jacobus, & Tapert, 2009). Although the adolescent brain may be more resistant to the neurotoxic effects of substance use, drug exposure may interrupt brain development (D. B. Clark, Thatcher, & Tapert, 2008; Crews, He, & Hodge, 2007), poten-tially leading to cognitive, social, and psychological deficits (Squeglia et al., 2009). Normal adolescent brain development includes changes in efficiency and specialization, via synap-tic refinement and myelination (Yakovlev & Lecours, 1967), and changes in prefrontal and limbic systems thought to contribute to normative adolescent impulsivity, risk-taking, and substance use (Casey, Jones, & Hare, 2008; Chambers & Potenza, 2003; Spear, 2000). Adolescent substance use has been linked to subsequent changes in brain volume, white matter integrity, and function and to neurocognitive deficits, including spatial, learning, memory, and inhibitory dysfunction (De Bellis et al., 2000; De Bellis et al., 2005; Medina, Schweinsburg, Cohen-Zion, Nagel, & Tapert, 2006; Squeglia et al., 2009). These deficits may result from substance-related reductions in the volume of important brain structures (e.g., hippocampus) (Squeglia et al., 2009) and may increase the risk for aggression in addi-tion to the risk for further substance use. For example, inhibitory (Blair, 2001; Kirisci,

750 CRIMINAL JUSTICE AND BEHAVIOR
Tarter, Vanyukov, Reynolds, & Habeych, 2004) and executive (Morgan & Lilienfeld, 2000) dysfunction are associated with both SUDs and aggression.
Social factors also play a role in linking aggression and SUDs in adolescence. Following the onset of puberty, there are normative increases in risk-taking (Reyna & Farley, 2006) and social affiliation drives that enhance substance use and delinquency. These changes are particularly problematic for youth who associate with deviant peers; such youth are themselves more likely to engage in substance use, aggression, and other problem behav-iors (Allen, Porter, & McFarland, 2006; Sullivan, 2006). Evidence indicates that teens are far more likely to take risks in the presence of peers (Gardner & Steinberg, 2005) or in strong affective states, suggesting that risk taking may partially reflect youth affiliative needs. Additionally, environmental stress from social role transitions fuels emotional dis-tress, further increasing risk for impulsive decision making (Cyders & Smith, 2007) and thus for substance use and aggressive behavior.
Overall, normative brain maturation and social processes during adolescence are associated with increased impulsivity, which in turn increases the risk for both aggression and substance use. These risks are compounded by substance use during adolescence, which appears to be associated with changes in brain structure and consequent changes in neurocognitive abilities that further increase risks for substance use and for aggressive, antisocial behavior.
ASSESSMENT OF AGGRESSION AND SUBSTANCE USE
Childhood aggression predicts early onset and frequency of substance use in adolescence (Pulkkinen & Pitkanen, 1994), consistent with a common cause or deviance proneness model (Martel et al., 2009). This model appears to operate through both direct and indirect pathways, although underlying mechanisms are not yet clear (Zucker, 2008). Aggression has been classified in terms of both function and form. Function can be classified as either proactive (i.e., calculated and goal-oriented, motivated by external reward) or reactive (i.e., defensive, impulsive responding to threat or frustration) (Dodge & Coie, 1987). Proactive aggression is associated with delinquency and violence in youth, but reactive aggression has been a less consistent predictor (Card & Little, 2006; Fite, Stoppelbein, & Greening, 2009; Raine et al., 2006). Proactive and reactive aggression have been prospectively linked to SUDs via separate pathways (Fite, Colder, Lochman, & Wells, 2008). Proactive aggres-sion predicts substance use directly and via association with delinquent peers, whereas reactive aggression is indirectly associated with peer delinquency and rejection by peers (Fite & Colder, 2007).
Aggression form can be categorized as either direct or relational (Card, Stucky, Sawalani, & Little, 2008). Direct aggression is defined as behavior directed at individuals with the intent to harm (Coie & Dodge, 1998), while relational aggression refers to acts intended to manipulate or damage relationships (Crick & Grotpeter, 1995). Early direct (Swaim, Deffenbacher, & Wayman, 2004) and relational (Herrenkohl, Catalano, Hemphill, & Toumbourou, 2009; Skara et al., 2008) aggression are associated with subsequent sub-stance use. However, substance involvement may be more strongly related to direct aggres-sion in boys and to relational aggression in girls (Skara et al., 2008). Additionally, youth with high levels of both direct and relational aggression appear to have the worst substance use outcomes (Herrenkohl et al., 2009).
These studies highlight the importance of examining relationships of substance involve-ment with different functions and forms of aggression separately. Assessing these aspects of
Doran et al. / ADOLESCENT SUBSTANCE USE AND AGGRESSION 751
aggression is crucial for understanding aggressive behaviors and underlying motives, their associations with substance use, and potential targets of intervention. It is also important that assessment of aggression and substance use be empirically based. The use of standardized, evidence-based tools allows for comparisons across settings and aids our understanding of the scope of problems such as aggression and substance involvement (Wasserman et al., 2003). At the individual level, evidence-based assessment may reduce bias that can influ-ence treatment and placement recommendations (Niarhos & Routh, 1992).
A number of factors have been identified as common risks for both aggression and SUDs in youth. Individual common risk factors include impulsivity and risk-taking ten-dencies (Cooper, Wood, Orcutt, & Albino, 2003; Farrington, 1989) and early manifesta-tions of violence or delinquency, and low academic achievement (Herrenkohl et al., 2000). Importantly, there is evidence that individual risk factors may lead to different types of delinquent or aggressive behavior, depending on sex. Researchers have suggested that early childhood impulsivity is typically the first step on the developmental pathway toward delinquency, substance use, and criminality (Beauchaine, Klein, Crowell, Derbridge, & Gatzke-Kopp, 2009). Impulsivity is about 80% heritable and increases risk for multiple externalizing disorders (Crowell, Beauchaine, & Lenzenwger, 2008; Kendler, Prescott, Myers, & Neale, 2003; Krueger & Markon, 2006; Price, Simonoff, Walderman, Asherson, & Plomin, 2001; Sherman, Iacono, & McGue, 1997); it appears to result from dysfunction in serotonergic and dopaminergic brain systems (Beauchaine et al., 2009). A number of genes that influence serotonergic and dopaminergic neurotransmission are associated with vulnerability to impulsive, aggressive behavior, but in at least some cases (e.g., MAO-A, COMT, 5HTT) the behavioral expression of this vulnerability appears to differ by sex, with males more prone to outward aggression and females to emotional instability and self-injury (Beauchaine et al., 2009; Courtet et al., 2001; Perez et al., 2007).
Family risk factors include poor family management and parental monitoring (J. D. Hawkins et al., 1998), patterns and values that model or normalize violence (Brewer, Hawkins, Catalano, & Neckerman, 1995), and parental SUDs (Brook & Brook, 1992). Children from minority ethnic groups, urban areas, and families with fewer resources are more likely to be exposed to such risks and may also be more vulnerable to developing aggressive behaviors and substance use following exposure (T. L. Brown, Miller, & Clayton, 2004; Burchinal, Roberts, Hooper, & Zeisel, 2000; Wallace & Muroff, 2002; Wilson, Hurtt, Shaw, Dishion, & Gardner, 2009). Notably, however, data indicate that childhood aggression decreases when in competent families that respond adaptively to early aggression (Andreas & Watson, 2009).
Socially, association with antisocial peers strongly predicts both aggression and sub-stance involvement (J. D. Hawkins et al., 1998; Lipsey & Derzon, 1998). These common risk factors influence both substance use and aggression, which in turn exert reciprocal influence on each other (H. R. White, Loeber, Stouthamer-Loeber, & Farrington, 1999). Consequently, clinicians engaged in assessment and treatment of youth aggression and SUDs should focus on common risk factors; interventions that focus on aggression alone or SUDs alone are likely to be less successful (Brewer et al., 1995). In terms of moderators of peer influence, studies have suggested that delinquent behavior among girls is more closely related to peer deviance, whereas in boys this effect is mitigated by their perception of adult monitoring of behavior (O’Donnell, Richards, Pearce, & Romero, in press). Additionally, there is evidence that, relative to rural youth, urban children may be more

752 CRIMINAL JUSTICE AND BEHAVIOR
TABLE 1: Measures Assessing Form and Function of Aggression
Measure Psychometric PropertiesPopulations
Normed Administration
Aggression functionTeacher Rating
Scale (Dodge & Coie, 1987)
Good internal consistency (Dodge & Coie, 1987) and criterion validity (Poulin & Boivin, 2000). Factor analyses consistent with two-factor model (Day, Bream, & Pal, 1992; Poulin & Boivin, 2000), but high correlations between scales in normative samples suggest it may not sufficiently differentiate the two factors.
Normative and aggressive children and adolescents
Six-item observer-rated scale
Reactive-Proactive Aggression Questionnaire (Raine et al., 2006)
Good internal consistency and criterion and construct validity; high correlations between reactive and proactive subscales (Fossati et al., 2009; Raine et al., 2006).
Normative and antisocial adolescents
23-item self-report scale
Aggression function and formSelf-Report Scale
(Little, Jones et al., 2003)
Good internal consistency and criterion validity. Direct and relational aggression correlated but distinct; low correlation between proactive and reactive aggression. Invariant across sex, race/ethnicity, and age (Little, Brauner, Jones, Nock, & Hawley, 2003; Little, Jones et al., 2003).
Normative adolescents
36-item self-report scale
heavily influenced by aggressive models and deviant peers in terms of behavior outside the home (Hope & Bierman, 1998; Lanza, Rhoades, Nix, & Greenberg, 2010).
Aggression screening. Several measures of aggression form are available (see Table 1), including observer rating scales (K. Brown, Atkins, Osborne, & Milnamow, 1996; Dodge & Coie, 1987) and the self report Reactive-Proactive Aggression Questionnaire (Raine et al., 2006). Two methodological issues are common to these measures. First, they typically find substantial overlap (e.g., r = .5-.7) between proactive and reactive aggression (Little, Jones, Henrich, & Hawley, 2003). Second, while designed to assess function, item wordings from these scales typically include form. Little, Jones et al. (2003) recently developed an instru-ment designed to distinguish function from form. With this measure, when form is controlled for, the relationship between proactive and reactive aggression is minimal (Little, Jones et al., 2003). In terms of clinical utility, in light of their brevity and good criterion validity, the measures designed to address function would appear to be useful measures for screening for potential aggression problems. However, accurate assessment of both function and form are important in identifying targets for intervention. For exam-ple, appropriate interventions for reactive relational aggression and proactive relational aggression may differ. Consequently, the more comprehensive instrument developed by Little et al. may be more useful to clinicians working with youth with identified aggression problems. However, when considering appropriate treatment targets for youth with prob-lems in multiple domains, the comprehensive assessments described below for substance use and related domains are likely to provide the most complete information regarding risk factors for both aggression and substance involvement.
SUD screening. While youth in secure settings are at increased risk for substance use, the purpose of screening and assessment is to identify those needing treatment (Chassin, 2008; National Institute on Drug Abuse, 2006). Current best practices include screening followed

Doran et al. / ADOLESCENT SUBSTANCE USE AND AGGRESSION 753
by thorough assessment (Chassin, 2008). Screening is most effective at system entry, when all youth are screened, and when standardized instruments are used (Winters & Yifrah, 2008). While most institutions conduct screening, many only screen youth already identified as having substance-related problems, and up to half do not use standardized measures (Snyder & Sickmund, 2006). Informal questions about quantity and frequency of use are not sufficient for screening, and standardized measures are recommended (Winters & Yifrah, 2008). A number of brief, multisubstance screeners are available. For example, the CRAFFT (Knight et al., 1999) assesses dangerous use, consequences of use, using for positive or negative reinforcement, using alone, blackouts, and a desire to cut down, with good sensitivity and specificity for SUDs. Other brief screeners include the Drug Abuse Screening Test (DAST; Gavin, Ross, & Skinner, 1989; Skinner, 1982) and the Alcohol, Smoking and Substance Involvement Screening Test (ASSIST; World Health Organization, 2002).
A limitation of self-report screeners is their reliance on honest responding. One study suggests that up to half of respondents with a positive bioassay for cocaine use denied recent use (McClelland, Teplin, & Abram, 2004). For this reason, current guidelines endorse the inclusion of objective measures (e.g., urinalysis) in screening protocols (NIDA, 2006). Some tools have been developed to indirectly screen for SUDs by assessing related risk factors, including the Problem-Oriented Screening Instrument for Teenagers (Rahdert, 1991a) and the Substance Abuse Subtle Screening Inventory (F. G. Miller, 1997). However, these meas-ures are less useful, given their length and evidence that indirect SUD assessments tend to be less accurate (Feldstein & Miller, 2007). Effective screening may be best accomplished by combining a brief, face valid screener with objective assessment of recent use.
Comprehensive assessment tools. Positive screens should trigger a comprehensive assessment to identify needs and plan interventions. There are a number of tools with good psychometric properties for thoroughly assessing substance involvement and related domains (e.g., psychiatric history and symptoms, family functioning, school and legal sta-tus; see Table 2). The Teen version of the Addiction Severity Index, or T-ASI-2 (Kaminer, Bukstein, & Tarter, 1991) is a semistructured interview that assesses 18 substance-related domains, including substance use, service utilization, and social, family, and school function-ing (Skinner, 1982), yielding scores on each domain to assist clinicians in identifying treat-ment targets.
The Global Appraisal of Individual Needs (GAIN; Dennis, 1999) is a semistructured interview that assesses recent and lifetime substance use; psychiatric, school, and legal status; risk behavior; living environment; physical health; and other domains. The GAIN can be used to generate diagnoses (Dennis, White, Titus, & Unsicker, 2008) and has been extensively studied, with norms available for a variety of populations (Dennis et al., 2008). Administration requires relatively extensive training and takes up to 2 hours, although shorter forms are available.
A final comprehensive assessment tool is the self-report Personal Experience Inventory, or PEI (Winters, Stinchfield, & Henly, 1989). The PEI core module assesses drug use severity, psychosocial risk, and response distortion; supplemental modules are available for eating disorders, suicide risk, abuse history, and family drug use history. Scoring software provides nonclinical and substance-involved norms. While other comprehensive tools with similarly appropriate psychometric properties are available, the T-ASI, GAIN, and PEI were selected based on ease of administration and accessibility. In addition to providing

754 CRIMINAL JUSTICE AND BEHAVIOR
TABLE 2: Substance Use Screening and Assessment Measures
Measure Test Type and PsychometricsFee/Training Required? Admin, Scoring
Screening ToolsCRAFFT Interview or self-report, six items. Good reliability, validity
(Knight et al., 1999), sensitivity and specificity with scores ≥2 (Cummins, Chan, Blume, Larimer, & Marlatt, 2003; Knight, Sherritt, Shrier, Harris, & Chang, 2002).
N/N 2 min
DAST Interview or self-report, 10 or 28 items. Adequate reliability and validity (Gavin et al., 1989; Skinner, 1982).
N/N 1-5 min
ASSIST Interview, eight items. Good validity, sensitivity, and specificity for multiple substances (Newcombe, Humeniuk, & Ali, 2005).
N/N 5 min
POSIT Interview or self-report, 139 items. Can discriminate between treatment samples and general population, but 10 domain subscales are overly sensitive (Rahdert, 1991b). Acceptable reliability for most subscales (Knight, Goodman, Pulerwitz, & DuRant, 2001).
N/N 20-30 min
SASSI Self-report, 93 items. Good reliability and construct validity; excellent sensitivity and specificity for detecting SUDs (Lasowski, Miller, Boye, & Miller, 1998).
N/N 15 min
Assessment ToolsT-ASI Interview assessing 18 SUD-related domains. Domain sub-
scales have excellent internal consistency and strong validity (Skinner, 1982).
N/Y 20-45 min, 10 min
GAIN Interview that uses 99 scales and subscales to assess SUD-related domains, including lifetime and recent severity. Extensively normed with excellent psychometric properties (Gavin et al., 1989; WHO, 2002).
Y/Y 90-120 min, 15 min
PEI Self-report measure assessing drug use severity, psychosocial risk, and response distortion; supplemental modules available. Good psychometric properties (Newcombe et al., 2005).
Y/N 45-60 min, 10 min
baseline information on client needs, these measures are useful for periodically assessing response to treatment.
TREATMENT
Treatment for adolescent SUDs and comorbid problems such as aggression has often been poorly integrated (Lamps et al., 2008). Barriers to successful treatment include poor coordination between delivery systems (E. H. Hawkins, 2009), a relative lack of research into developmentally appropriate interventions (Lysaught & Wodarski, 1996), and a lack of funding specific to SUDs and comorbid disorders (E. H. Hawkins, 2009). Additionally, aggression is associated with poor treatment outcomes (Crowley, Mikulich, MacDonald, Young, & Zerbe, 1998). Consequently, there is increasing interest in interventions that address youth needs across multiple areas, including problem-solving and communication skills, family, mental health, and SUDs (Libby & Riggs, 2005).
When treating youth in secure settings, five general strategies are recommended (Greenwood, 2008). First, intervention should focus on malleable problem behaviors (e.g., problem-solving skills, peer associations, family dysfunction). Second, interventions should be evidence-based and tailored to individual needs. Third, institutional treatment

Doran et al. / ADOLESCENT SUBSTANCE USE AND AGGRESSION 755
programs should focus on youth at highest risk for relapse and recidivism, who have both the most room for improvement and for whom failure will tend to have more severe con-sequences (Latessa, Listwan, & Hubbard, 2005). Fourth, consistent implementation of evidence-based interventions is critical to positive outcomes. Finally, interventions are most effective when provided by mental health professionals (Greenwood, 2008).
The use of evidence-based approaches is a key component of treating youth with aggression and SUDs in secure settings. In criminal justice settings in particular, imple-mentation of such interventions can be more difficult because of the systemic focus on public safety and control of offenders, and because providers may not be fully aware of the effectiveness literature. Additionally, SUD programs are often discretionary and therefore are eliminated when budget cuts occur (Chandler, Peters, Field, & Juliano-Bult, 2004). However, all treatments are not equally effective (W. L. White, 2005). Those with demonstrated effectiveness for SUDs are more likely to reduce recidivism and relapse (Chandler et al., 2004; Farabee, Shen, Hser, Grella, & Anglin, 2001) and the incidence of violence during incarceration (Lovell, Allen, Johnson, & Jemelka, 2001). Selected studies of evidence-based interventions for youth substance abuse are shown in Table 3.
Family approaches. Family therapy aims to create more adaptive patterns of family inter-action, reducing problem behaviors thought to be a result of family dysfunction (Waldron, 1997). Multiple family therapies have been developed for the treatment of youth SUDs, aggression, and delinquency. Those with the most empirical support include Multisystemic Therapy (MST; Henggeler et al., 1991), Functional Family Therapy (FFT; Alexander & Parsons, 1973; Gordon, Graves, & Arbuthnot, 1995), Brief Strategic Family Therapy (BSFT; Szapocznik, Kurtines, Santisteban, & Rio, 1990), and Multidimensional Family Therapy (MDFT; Liddle, 2010). Evidence indicates that family therapy is more effective than indi-vidual therapy for youth SUDs and other problem behaviors (Diamond & Josephson, 2005; Slesnick & Prestopnik, 2005).
MST is an intensive, in-home intervention designed as an alternative to secure placement for youth with severe social, emotional, or behavioral problems. Therapists are available to families at all times, and they work with caregivers to adjust the ecological context of problem behaviors (Schoenwald, Ward, Henggeler, Pickrel, & Patel, 1996). A strong evidence base shows that MST is effective for both SUDs and delinquent, aggressive behavior (Henggeler, Melton, & Smith, 1992; Schaeffer & Borduin, 2005). It produces better family, SUD, and criminal justice outcomes than usual services or individual therapy (Henggeler, Clingempeel, Brondino, & Pickrel, 2002; Henggeler, Melton, Brondino, Scherer, & Hanley, 1997; Letourneau et al., 2009) and is more effective and cost-effective than hospitalization or incarceration (Henggeler et al., 1992; Sheidow et al., 2004).
FFT combines the family systems and social learning approaches (Gordon et al., 1995), focusing on increasing engagement and motivation for change before using behavioral techniques to develop healthier interaction patterns (Flicker, Turner, Waldron, Brody, & Ozechowski, 2008). FFT increases family engagement in treatment (Friedman, 1989) and is effective for adolescent SUDs (Lewis, Piercy, Sprenkle, & Trepper, 1990; Stanton & Shadish, 1997) and for delinquency among adolescents with SUDs (Chamberlain & Reid, 1998). FFT is also superior to usual services in preventing criminal activity in adolescents and young adults (Barton, Alexander, Waldron, Turner, & Warburton, 1985; Gordon et al., 1995; Hansson, 1998). Like MST, FFT has been shown to be more cost-effective than secure placement (Aos & Barnoski, 1998; Sexton & Alexander, 2000).

756 CRIMINAL JUSTICE AND BEHAVIOR
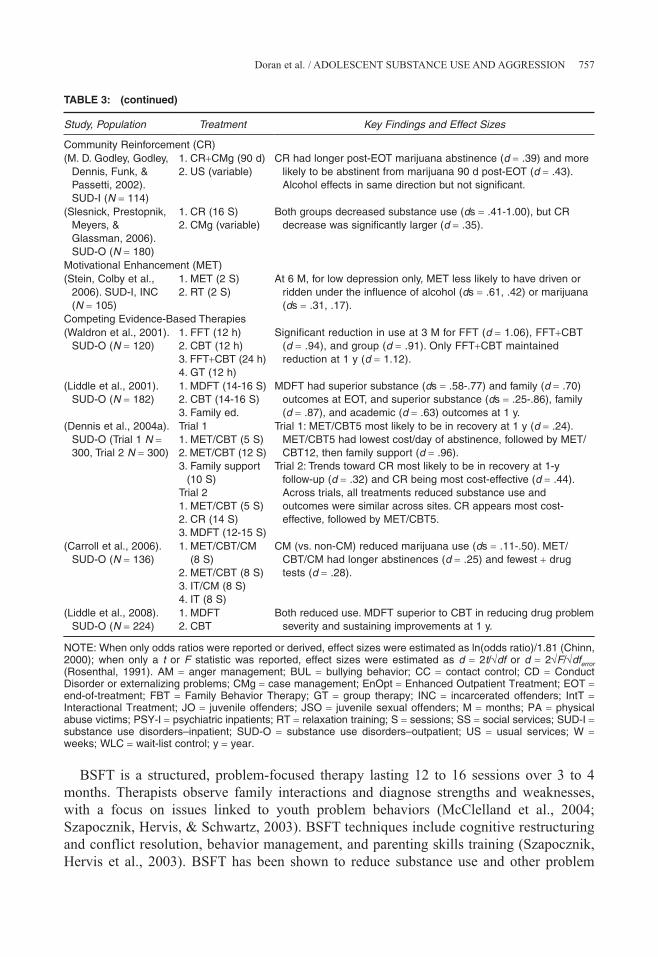
TABLE 3: Selected Studies of Evidence-Based Treatments for Youth Aggression and Substance Involvement
Study, Population Treatment Key Findings and Effect Sizes
Multisystemic Therapy (MST)(Henggeler et al.,
1992). JO (N = 84)1. MST (33 h)2. US
MST had less recidivism (d = .45-.62) and aggression (d = .34) and greater family cohesion (d = .56) at 59 W.
(Timmons-Mitchell, Bender, Kishna, & Mitchell, 2006). JO (N = 93)
1. MST (145 d)2. US
MST had lower recidivism (d = .57) and higher functioning across substance use and other domains (ds = 1.46-1.53).
(Borduin, Schaeffer, & Heiblum, 2009). JSO (N = 48)
1. MST (31 W)2. GT (30 W)
MST had better psychiatric (d = 1.31-1.47), conduct (d = 1.85), family (d = 1.67-1.81), social (d = .46-1.53), academic (d = 1.40) outcomes at EOT, and recidivism outcomes (ds = .41-.87) at 9 years.
(Letourneau et al., 2009). JSO (N = 127)
1. MST (7 M)2. US (15 M)
MST had less deviant interest (d = .28-.36) and behavior (d = .36-.56), delinquency (d = .51), and substance use (d = .66).
Functional Family Therapy (FFT)(Friedman, 1989).
SUD-O (N = 166)1. FFT (6 M)2. Parenting (6 M)
Both groups reduced use; FFT had greater parent participation in treatment (d = .18).
(Gordon et al., 1995). JO (N = 54)
1. FFT (16 S)2. Probation
FFT had lower recidivism over 3 y post-treatment (d = .86).
(Sexton & Turner, 2010). JO (N = 917)
1. FFT (12 S)2. Probation
High FFT fidelity associated with decreased and low fidelity with increased recidivism versus controls (d = .27-.28).
Brief Strategic Family Therapy (BSFT)(Szapocznik et al.,
1983). SUD-O (N = 37)
1. BSFT (12 S)2. BSFT-I (12 S)
Improved substance use (d = 1.26), conduct (d = 1.39), and family (ds = .62-1.46) outcomes for both groups.
(Santisteban et al., 2003). CD (N = 126)
1. BSFT (11 S)2. GT (9 S)
BSFT superior in change in behavior problems (d = .63-.67), drug use (d = .63), and family functioning (d = .70).
(Nickel et al., 2006). BUL (N = 40)
1. BSFT (12 S)2. CC (12 S)
BSFT associated with significant reductions in anger, substance use, disinhibition, and bullying at EOT and 1 y.
Multidimensional Family Therapy (MDFT)(Hogue, Dauber,
Samuolis, & Liddle, 2006). SUD-O (N = 63)
1. MDFT (14 S) Increased use of family techniques reduced psychiatric symptoms (ds = .48-.76) at 6 mos. when youth focus also high (d = .76) and increased family cohesion at 1 y (d = .68).
Cognitive-Behavioral Therapy (CBT)(Feindler, Ecton,
Kingsley, & Dubey, 1986). PSY-I (N = 21)
1. CBT AM (8 W)2. WLC
CBT had EOT improvements in patient self-control (d = 1.36) and frequency of rule violations (d = .71).
(Kaminer & Burleson, 1999; Kaminer et al., 1998). SUD-O (N = 32)
1. CBT (12 W)2. IntT (12 W)
CBT had greater reduction in use at 3 M (d = 1.40); no differences for those with data (n = 15) at 15 M.
(Latimer et al., 2003). SUD-O (N = 43)
1. IFCBT (16 W)2. Psychoed.
(16 W)
IFCBT had superior use (ds = .47-.84), problem-solving skills (ds = .08-.60), and family (ds = .08-.75) outcomes.
(Cann, Falshaw, Nugent, & Friendship, 2003). INC (N = 3068)
1. CBT2. US
CBT completers had less recidivism at 1 y (d = .10). In completers, CBT better for those at medium-low risk for recidivism (d = .62) versus those at higher risk (ds = .07)
Contingency Management (CM)(Larzelere et al.,
2001). PSY-I (N = 43)
1. CM + social skills (Med 165 d)
At EOT and 6 M reductions in internalizing (d = 1.48) and externalizing (d = 1.58) symptoms, delinquency (d = 1.53), and aggression (d = 1.49).
(continued)
Doran et al. / ADOLESCENT SUBSTANCE USE AND AGGRESSION 757
Study, Population Treatment Key Findings and Effect Sizes
Community Reinforcement (CR)(M. D. Godley, Godley,
Dennis, Funk, & Passetti, 2002). SUD-I (N = 114)
1. CR+CMg (90 d)2. US (variable)
CR had longer post-EOT marijuana abstinence (d = .39) and more likely to be abstinent from marijuana 90 d post-EOT (d = .43). Alcohol effects in same direction but not significant.
(Slesnick, Prestopnik, Meyers, & Glassman, 2006). SUD-O (N = 180)
1. CR (16 S)2. CMg (variable)
Both groups decreased substance use (ds = .41-1.00), but CR decrease was significantly larger (d = .35).
Motivational Enhancement (MET)(Stein, Colby et al.,
2006). SUD-I, INC (N = 105)
1. MET (2 S)2. RT (2 S)
At 6 M, for low depression only, MET less likely to have driven or ridden under the influence of alcohol (ds = .61, .42) or marijuana (ds = .31, .17).
Competing Evidence-Based Therapies(Waldron et al., 2001).
SUD-O (N = 120)1. FFT (12 h)2. CBT (12 h)3. FFT+CBT (24 h)4. GT (12 h)
Significant reduction in use at 3 M for FFT (d = 1.06), FFT+CBT (d = .94), and group (d = .91). Only FFT+CBT maintained reduction at 1 y (d = 1.12).
(Liddle et al., 2001). SUD-O (N = 182)
1. MDFT (14-16 S)2. CBT (14-16 S)3. Family ed.
MDFT had superior substance (ds = .58-.77) and family (d = .70) outcomes at EOT, and superior substance (ds = .25-.86), family (d = .87), and academic (d = .63) outcomes at 1 y.
(Dennis et al., 2004a). SUD-O (Trial 1 N = 300, Trial 2 N = 300)
Trial 11. MET/CBT (5 S)2. MET/CBT (12 S)3. Family support
(10 S)Trial 21. MET/CBT (5 S)2. CR (14 S)3. MDFT (12-15 S)
Trial 1: MET/CBT5 most likely to be in recovery at 1 y (d = .24). MET/CBT5 had lowest cost/day of abstinence, followed by MET/CBT12, then family support (d = .96).
Trial 2: Trends toward CR most likely to be in recovery at 1-y follow-up (d = .32) and CR being most cost-effective (d = .44). Across trials, all treatments reduced substance use and outcomes were similar across sites. CR appears most cost-effective, followed by MET/CBT5.
(Carroll et al., 2006). SUD-O (N = 136)
1. MET/CBT/CM (8 S)
2. MET/CBT (8 S)3. IT/CM (8 S)4. IT (8 S)
CM (vs. non-CM) reduced marijuana use (ds = .11-.50). MET/ CBT/CM had longer abstinences (d = .25) and fewest + drug tests (d = .28).
(Liddle et al., 2008). SUD-O (N = 224)
1. MDFT2. CBT
Both reduced use. MDFT superior to CBT in reducing drug problem severity and sustaining improvements at 1 y.
NOTE: When only odds ratios were reported or derived, effect sizes were estimated as ln(odds ratio)/1.81 (Chinn, 2000); when only a t or F statistic was reported, effect sizes were estimated as d = 2t/√df or d = 2√F/√dferror (Rosenthal, 1991). AM = anger management; BUL = bullying behavior; CC = contact control; CD = Conduct Disorder or externalizing problems; CMg = case management; EnOpt = Enhanced Outpatient Treatment; EOT = end-of-treatment; FBT = Family Behavior Therapy; GT = group therapy; INC = incarcerated offenders; IntT = Interactional Treatment; JO = juvenile offenders; JSO = juvenile sexual offenders; M = months; PA = physical abuse victims; PSY-I = psychiatric inpatients; RT = relaxation training; S = sessions; SS = social services; SUD-I = substance use disorders–inpatient; SUD-O = substance use disorders–outpatient; US = usual services; W = weeks; WLC = wait-list control; y = year.
TABLE 3: (continued)
BSFT is a structured, problem-focused therapy lasting 12 to 16 sessions over 3 to 4 months. Therapists observe family interactions and diagnose strengths and weaknesses, with a focus on issues linked to youth problem behaviors (McClelland et al., 2004; Szapocznik, Hervis, & Schwartz, 2003). BSFT techniques include cognitive restructuring and conflict resolution, behavior management, and parenting skills training (Szapocznik, Hervis et al., 2003). BSFT has been shown to reduce substance use and other problem

758 CRIMINAL JUSTICE AND BEHAVIOR
behaviors and to improve family functioning (Santisteban et al., 2003; Szapocznik, Amaro et al., 2003; Szapocznik, Kurtines, Foote, Perez-Vidal, & Hervis, 1983).
MDFT is a manualized, short-term approach that focuses on risk and protective behav-iors for adolescent and family functioning (Liddle, 2010). Therapists conduct interven-tions with youth and caregivers individually and jointly; in joint sessions, family members try new ways of problem solving with active therapist guidance (Liddle, 1999). MDFT has strong empirical support as an effective treatment for adolescent SUDs, outperforming group, residential, and cognitive behavioral comparisons (Liddle & Dakof, 2002; Liddle et al., 2001; Liddle, Dakof, Turner, Henderson, & Greenbaum, 2008; Liddle, Rowe, Dakof, Henderson, & Greenbaum, 2009; Liddle, Rowe, Dakof, Ungaro, & Henderson, 2004). MDFT has recently been adapted for institutional settings as MDFT-Detention to Community (MDFT-DTC; Liddle, Dakof, Henderson, & Rowe, in press), which includes treatment pre- and postrelease. MDFT-DTC has been shown to be more effective than juvenile detention (Liddle et al., in press) and day treatment (Liddle et al., 2006) in terms of treatment participation, patient satisfaction, substance use, and delinquency.
Family therapies are typically designed to be delivered in the home and/or community (Henggeler, 2011; Sexton & Alexander, 2005). Evidence of equal or superior outcomes and superior cost-effectiveness indicate that they should be considered as alternatives to insti-tutional placement and individual therapy when possible. Unlike individual interventions, family therapies are explicitly designed to address risk factors at multiple levels that con-tribute to substance abuse, which may explain why they have demonstrated better out-comes. Some components of these interventions (e.g., therapist availability, frequent family sessions) may be difficult to fully adapt to secure settings. However, other components (e.g., engaging family in treatment, working to reduce family dysfunction) may be useful approaches for clinicians in such settings. Additionally, some family-based interventions (e.g., MDFT) have been effective when specifically adapted for secure settings.
Cognitive-behavioral therapy (CBT). CBT for SUDs (Wright, Beck, Newman, & Liese, 1993) is based on the idea that problem behaviors result from maladaptive cognitions (Winters, 1999). Youth who use drugs may have distorted expectancies about the positive effects of drugs and may not consider the negative consequences. Failure to develop problem-solving, social, and self-control skills or adaptive strategies for coping with peer pressure and negative emotions are also thought to contribute to substance use, aggression, and delinquency (Kaminer, Burleson, Blitz, Sussman, & Rounsaville, 1998). CBT aims to correct maladaptive beliefs by examining their rational basis and substituting beliefs that are consistent with adaptive behavior (Winters, 1999). Meta-analytic studies and reviews have shown CBT to effective for SUDs (Dennis et al., 2004a; Dennis et al., 2004b) and delinquency (Lipsey, Landenberger, & Wilson, 2007) in male and female adolescents. The inclusion of anger management and problem-solving components appears to be particularly important in terms of minimizing aggression (Lipsey et al., 2007).
CBT may be the best studied approach with adolescents in secure settings (Bray, 2000). Evidence indicates that the brief (4-10 session) CBT interventions that focus on interper-sonal, behavioral, and anger management skills reduce recidivism and substance use among institutionalized and noninstitutionalized youth offenders (Goldstein, Glick, & Gibbs, 1998; Lipsey, Wilson, & Cothern, 2000). CBT is also well-suited for use with youth

Doran et al. / ADOLESCENT SUBSTANCE USE AND AGGRESSION 759
in secure settings, due to its brevity, structure, and focus on symptom-reduction rather than insight. Additionally, while it is directive, CBT is also collaborative, which may increase its attractiveness and accessibility to adolescents in residential institutions who may experi-ence little control over their lives and environments (Desai et al., 2006).
While CBT addresses certain specific individual risk factors for aggression and SUDs that family therapies do not, it is limited in that it fails to address common risk factors in family and other systems. Consequently, some researchers have combined CBT with fam-ily therapy to address youth SUDs. Integrated Family and Cognitive-Behavioral Therapy (IFCBT) is an intensive program that includes one family and two peer group sessions each week (Latimer, Winters, D’Zurilla, & Nichols, 2003). Initial research suggests that IFCBT may be effective in reducing substance abuse as well as aggression and delinquency (Latimer et al., 2003). Another study (Waldron, Slesnick, Brody, Turner, & Peterson, 2001) compared marijuana outcomes in adolescents randomly assigned to either CBT, FFT, CBT+FFT, or a drug education group. Significant reductions in marijuana use were observed across groups, but the FFT, CBT+FFT, and drug education groups used marijuana less frequently than the CBT group. These studies suggest that individual and family therapy approaches can be usefully combined to treat adolescents with substance abuse and other delinquency problems.
Motivational enhancement therapy (MET). MET is a brief therapy based on motivational interviewing (W. R. Miller & Rollnick, 1991). MET interventions focus on increasing motivation to change by addressing ambivalence. Therapists empathize with clients and collaboratively assist clients in developing discrepancy between their current behaviors and their goals (Feldstein & Ginsburg, 2006). MET has been shown to be an effective treatment for SUDs (Dunn, Deroo, & Rivara, 2001). For example, brief emergency department inter-ventions with adolescents admitted for alcohol-related injuries have been associated with reduced drinking, alcohol-related problems, and risky behavior (Barnett, Monti, & Wood, 2001; Monti et al., 1999). It has also been shown to improve engagement in substance abuse treatment in incarcerated adolescents (Stein, Monti et al., 2006). Although further research is needed, from a theoretical perspective MET is likely to be useful in secure set-tings, either as a stand-alone treatment or as an adjunct to other approaches (Feldstein & Ginsburg, 2006). It is brief and has demonstrated effectiveness with clients with high levels of anger or hostility (Waldron et al., 2001). Additionally, the collaborative nature of MET may be particularly useful in working with incarcerated adolescents who are resistant to authority (Marlatt & Witkiewitz, 2002).
Contingency management (CM) and community reinforcement (CR). CM interventions are based on operant conditioning principles, in which behavior is a function of its conse-quences (Higgins, 1997; Higgins & Silverman, 2008). CM requires that nonabstinence be readily detectible (Higgins, Budney, & Bickel, 1994). Rewards are given for verified absti-nence and other targeted behaviors (e.g., nonaggression), but withheld for nonabstinence (Higgins, Alessi, & Dantona, 2002). Abstinent clients may receive vouchers with monetary values that increase with longer abstinence (Higgins et al., 1991) or may draw slips of paper from a bowl which may contain either written reinforcement or a voucher (Petry & Martin, 2002). CM is well-established as an effective treatment for adult SUDs (Higgins &
760 CRIMINAL JUSTICE AND BEHAVIOR
Silverman, 2008; Prendergast, Podus, Finney, Greenwell, & Roll, 2006), and several recent studies have assessed its use for youth SUDs and conduct problems. For example, adoles-cent outpatient interventions combining CM with CBT and/or motivational enhance-ment have been reported to reduce marijuana use and externalizing behaviors (Carroll et al., 2006; Kamon, Budney, & Stanger, 2005) and cigarette smoking (Krishnan-Sarin et al., 2006).
Like CM, CR interventions aim to rearrange environmental contingencies so that refraining from problem behavior is more rewarding than engaging in it (S. H. Godley et al., 2001). CR focuses on the interaction between youth and others in their environment, teaching them how to build a positive support system and additional reinforcers, how to replace maladaptive behaviors with newly developed prosocial alternatives, and how to utilize community resources (S. H. Godley et al., 2001). Initial studies suggest that CR for adolescents is an effective community SUD treatment (Dennis et al., 2004a).
Although additional research is needed, studies suggest that MET, CM, and CRA may be effective approaches for adolescent SUDs. Like CBT, they are individual approaches that do not systematically address common risk factors outside the individual and are not preferred over family approaches when either is feasible. However, individual approaches have the advantage of being better-suited to secure environments such as juvenile deten-tion and residential treatment facilities. For example, youth who maintain abstinence or refrain from aggressive behavior can be rewarded with additional visits or other privileges. Similarly, training adolescents to develop and use strategies for more rewarding social interactions in a controlled environment may be a step toward generalizing such behaviors to a less controlled environment following discharge.
Pharmacotherapy. Most SUD treatment studies in the literature involve psychosocial interventions, due to concerns about the efficacy and safety of psychotropic medications in youth and to legal restrictions on use in youth. However, an increasing number of youth are being treated with pharmacotherapy for SUDs (D. Clark, Wood, Cornelius, Bukstein, & Martin, 2003), and a few studies have examined the efficacy of specific agents. Some evi-dence supports the use of naltrexone for adolescent alcohol dependence (Deas, May, Randall, Johnson, & Anton, 2005), and nicotine replacement therapy and bupropion for adolescent tobacco dependence (Upadhyaya, Deas, & Brady, 2005). Some studies also sug-gest that opiate replacement may be useful for older adolescents with highly treatment-refractory SUDs (Ebner, Schreiber, & Zierer, 2004; Woody et al., 2008). Overall, more systematic, controlled research is needed to determine the utility of pharmacotherapy for youth SUDs, and considerable caution is warranted in the use of pharmacologic agents approved for adults in younger populations (Toumbourou et al., 2007).
Interestingly, pharmacotherapy for comorbid disorders may also reduce substance use (Waxmonsky & Wilens, 2005). These findings are important in light of research suggest-ing that more than half of youth with SUDs have comorbid disorders (Armstrong & Costello, 2002) and that those with comorbid disorders tend to have more severe refractory SUDs (Rowe, Liddle, Greenbaum, & Henderson, 2004). The combination of SUDs with internalizing or externalizing psychopathology has been associated with worse outcomes in terms of aggression and physical and mental health (Clingempeel, Britt, & Henggeler, 2008). Consequently, these findings suggest that effective pharmacologic or psychosocial treatments for psychiatric disorders may be an effective way to reduce later substance use and aggression in adolescents.

Doran et al. / ADOLESCENT SUBSTANCE USE AND AGGRESSION 761
SUMMARY
Substance involvement is a critical factor in the assessment and treatment of youth aggression and delinquency. Evidence suggests that shared underlying mechanisms con-tribute to both behaviors and that each reciprocally influences the other. In light of the strong relationship between the two, it is important that SUD status be considered during assessment and treatment of youth aggression and delinquency. Across settings, it is recom-mended that clinicians use brief, evidence-based tools to screen for aggression- and sub-stance-related problems. Objective measures (e.g., urinalysis) should also be used to screen for substance use. Positive screening results should be followed by comprehensive, evi-dence-based assessment to more thoroughly identify problem behaviors and intervention targets (Chassin, 2008; Grisso & Underwood, 2004).
Despite high levels of need, adolescents with aggression and comorbid substance use tend to be underserved. Studies demonstrating reduced aggression and criminality associ-ated with SUD treatment (Bernberg & Thorlindsson, 1999; Rossow & Wichstrom, 1999) suggest a need for increased integration and emphasis in this area. Several interventions have been developed that are effective in reducing aggressive, delinquent behaviors and substance use. Treatment is most likely to be effective when it addresses dysfunction and risk factors across multiple domains (e.g., individual, family, school, peer systems).
Family-based therapies focus on reducing dysfunction in family and other systems that is thought to influence problem behaviors. The literature demonstrates that family therapies are superior to other modalities (Diamond & Josephson, 2005) and should be considered first-line treatments for youth SUDs and aggression. However, these interventions were designed for use in the community, and with the exception of MDFT have not been adapted for use in secure or residential settings. Some elements of these approaches may be practical for use in secure settings. Additionally, further research is needed to adapt family-based interventions to these settings. While less effective than family therapy, other treatment approaches have dem-onstrated effectiveness with institutionalized youth, including CBT, CM, CRA, and MET. Because these interventions can be conducted one-on-one, they are practical for use in secure settings. These approaches may also have more appeal for adolescents, as they allow a measure of control over the environment. This may be particularly attractive for incarcerated adoles-cents, who may be more resistant to authority and whose environment is subject to stringent controls.
REFERENCES
Aarons, G. A., Brown, S. A., Hough, R. L., Garland, A. F., & Wood, P. A. (2001). Prevalence of adolescent substance use disorders across five sectors of care. Journal of the Academy of Child Adolescent Psychiatry, 40, 419-426.
Alexander, J., & Parsons, B. (1973). Short-term behavioral intervention with delinquent families: Impact on family process and recidivism. Journal of Abnormal Psychology, 81, 219-225.
Allen, J. P., Porter, M. R., & McFarland, F. (2006). Leaders and followers in adolescent close friendships: Susceptibility to peer influence as a predictor of risky behavior, friendship instability, and depression. Development and Psychopathology, 18, 155-172.
Andreas, J. B., & Watson, M. W. (2009). Moderating effects of family environment on the association between children’s aggressive beliefs and their aggression trajectories from childhood to adolescence. Development and Psychopathology, 21, 189-205.
Aos, S., & Barnoski, R. (1998). Watching the bottom line: Cost-effective interventions for reducing crime in Washington. Olympia, WA: Institute for Public Policy.

762 CRIMINAL JUSTICE AND BEHAVIOR
Armstrong, T. D., & Costello, E. J. (2002). Community studies on adolescent substance use, abuse, or dependence and psy-chiatric comorbidity. Journal of Consulting and Clinical Psychology, 70, 1224-1239.
Barnett, N. P., Monti, P., & Wood, M. D. (2001). Motivational interviewing for alcohol-involved adolescents in the emergency room. In E. F. Wagner & H. Waldron (Eds.), Innovations in adolescent substance abuse interventions (pp. 143-168). Oxford, UK: Elsevier Science, Ltd.
Barton, C., Alexander, J. F., Waldron, H., Turner, C. W., & Warburton, J. (1985). Generalizing treatment effects of Functional Family Therapy: Three replications. American Journal of Family Therapy, 13, 16-26.
Beauchaine, T. P., Klein, D. N., Crowell, S. E., Derbridge, C., & Gatzke-Kopp, L. (2009). Multifinality in the development of personality disorders: A biology × sex × environment interaction model of antisocial and borderline traits. Development and Psychopathology, 21, 735-770.
Bernberg, J. G., & Thorlindsson, T. (1999). Adolescent violence, social control, and the subculture of delinquency. Youth and Society, 30, 445-461.
Blair, R. J. R. (2001). Neurocognitive models of aggression, the antisocial personality disorders, and psychopathy. Journal of Neurology, Neurosurgery & Psychiatry, 71, 727-731.
Borduin, C. M., Schaeffer, C. M., & Heiblum, N. (2009). A randomized clinical trial of multisystemic therapy with juvenile sexual offenders: Effects on youth social ecology and criminal activity. Journal of Consulting and Clinical Psychology, 77, 26-37.
Bray, C. (2000). Cognitive behavioral curricula in correctional settings: A review of the literature. Minneapolis, MN: University of Minnesota Press.
Brewer, D., Hawkins, J. D., Catalano, R. F., & Neckerman, H. J. (1995). Preventing serious, violent, and chronic juvenile offending: A review of evaluations of selected strategies in childhood, adolescence, and the community. In J. C. Howell, B. Krisberg, J. D. Hawkins, & J. J. Wilson (Eds.), Sourcebook on serious, violent, and chronic juvenile offenders (pp. 61-141). Thousand Oaks, CA: Sage.
Brook, D. W., & Brook, J. S. (1992). Family processes associated with alcohol and drug abuse. In E. Kaufman & P. Kaufman (Eds.), Family therapy of drug and alcohol abuse (pp. 15-33). Needham Heights, MA: Allyn & Bacon.
Brown, K., Atkins, M. S., Osborne, M. L., & Milnamow, M. (1996). A revised teacher rating scale for reactive and proactive aggression. Journal of Abnormal Child Psychology, 24, 473-480.
Brown, T. L., Miller, J. D., & Clayton, R. R. (2004). The generalizability of substance use predictors across racial groups. Journal of Early Adolescence, 24, 274-302.
Burchinal, M. R., Roberts, J. E., Hooper, S., & Zeisel, S. A. (2000). Cumulative risk and early cognitive development: A comparison of statistical risk models. Development and Psychopathology, 36, 793-807.
Cann, J., Falshaw, L., Nugent, F., & Friendship, C. (2003). Understanding what works: Accredited cognitive skills pro-grammes for adult men and young offenders. London: Home Office Communication Development Unit.
Card, N. A., & Little, T. D. (2006). Proactive and reactive aggression in childhood and adolescence: A meta-analysis of dif-ferential relations with psychosocial adjustment. International Journal of Behavioral Development, 30, 466-480.
Card, N. A., Stucky, B. D., Sawalani, G. M., & Little, T. D. (2008). Direct and indirect aggression during childhood and adolescence: A meta-analytic review of gender differences, intercorrelations, and relations to maladjustment. Child Development, 79, 1185-1229.
Carroll, K. M., Easton, C., Nich, C., Hunkele, K. A., Neavins, T. M., Sinha, R., et al. (2006). The use of contingency manage-ment and motivational/skills-building therapy to treat young adults with marijuana dependence. Journal of Consulting and Clinical Psychology, 74, 955-966.
Casey, B. J., Jones, R. M., & Hare, T. A. (2008). The adolescent brain. Annals of the New York Academy of Sciences, 1124, 111-126.Chamberlain, P., & Reid, J. B. (1998). Comparison of two community alternatives to incarceration for chronic juvenile
offenders. Journal of Clinical and Consulting Psychology, 66, 624-633.Chambers, R. A., & Potenza, M. N. (2003). Neurodevelopment, impulsivity, and adolescent gambling. Journal of Gambling
Studies, 19, 53-84.Chandler, R. K., Peters, R. H., Field, G., & Juliano-Bult, D. (2004). Challenges in implementing evidence-based treatment
practices for co-occurring disorders in the criminal justice system. Behavioral Sciences & the Law, 22, 431-448.Chassin, L. (2008). Juvenile justice and substance use. The Future of Children, 18, 165-183.Chinn, S. (2000). A simple method for converting an odds ratio to effect size for use in meta-analysis. Statistics in Medicine,
19, 3127-3131.Clark, D., Wood, D., Cornelius, J., Bukstein, O. G., & Martin, C. (2003). Clinical practices in the pharmacological treatment of
comorbid psychopathology in adolescents with alcohol use disorders. Journal of Substance Abuse Treatment, 25, 293-295.Clark, D. B., Thatcher, D. L., & Tapert, S. F. (2008). Alcohol, psychological dysregulation, and adolescent brain development.
Alcoholism: Clinical and Experimental Research, 32, 375-385.Clingempeel, W. G., Britt, S. C., & Henggeler, S. W. (2008). Beyond treatment effects: Comorbid psychopathologies and
long-term outcomes among substance-abusing delinquents. American Journal of Orthopsychiatry, 78, 29-36.Coie, J. D., & Dodge, K. A. (1998). Aggression and antisocial behavior. In W. Damon & N. Eisenberg (Eds.), Handbook of
child psychology, 5th Ed.: Vol 3. Social, emotional, and personality development (Vol. 3, pp. 779-862). Hoboken, NJ: John Wiley and Sons.

Doran et al. / ADOLESCENT SUBSTANCE USE AND AGGRESSION 763
Cooper, M. L., Wood, P. K., Orcutt, H. K., & Albino, A. (2003). Personality and the predisposition to engage in risky or problem behaviors during adolescence. Journal of Personality and Social Psychology, 84, 390-410.
Courtet, P., Baud, P., Abbar, M., Boulenger, J. P., Castelnau, D., Mouthon, D., et al. (2001). Association between violent suicidal behavior and the low activity allele of the serotonin transporter gene. Molecular Psychiatry, 6, 338-341.
Crews, F., He, J., & Hodge, C. (2007). Adolescent cortical development: A critical period of vulnerability for addiction. Pharmacology, Biochemistry and Behavior, 86, 189-199.
Crick, N. R., & Grotpeter, J. K. (1995). Relational aggression, gender, and social-psychological adjustment. Child Development, 66, 710-722.
Crowell, S. E., Beauchaine, T. P., & Lenzenwger, M. F. (2008). The development of borderline personality disorder and self-injurious behavior. In T. P. Beauchaine & S. P. Hinshaw (Eds.), Child and adolescent psychopathology (pp. 510-539). Hoboken, NJ: Wiley.
Crowley, T. J., Mikulich, S. K., MacDonald, M., Young, S. E., & Zerbe, G. O. (1998). Substance-dependent, conduct-disordered adolescent males: Severity of diagnosis predicts 2-year outcome. Drug and Alcohol Dependence, 49, 225-237.
Cummins, L. H., Chan, K. K., Blume, A. W., Larimer, M., & Marlatt, G. A. (2003). Validity of the CRAFFT in American-Indian and Alaska-native adolescents: Screening for drug and alcohol risk. Journal of Studies on Alcohol, 64, 727-732.
Cyders, M. A., & Smith, G. T. (2007). Mood-based rash action and its components: Positive and negative urgency. Personality and Individual Differences, 43, 839-850.
Day, D. M., Bream, L. A., & Pal, A. (1992). Proactive and reactive aggression: An analysis of subtypes based on teacher perceptions. Journal of Clinical Child Psychology, 21, 210-217.
Deas, D. (2006). Adolescent substance abuse and psychiatric comorbidities. Journal of Clinical Psychiatry, 67, 18-23.Deas, D., May, K., Randall, C., Johnson, N., & Anton, R. (2005). Naltrexone treatment of adolescent alcoholics: An open-
label pilot study. Journal of Child and Adolescent Psychopharmacology, 15, 723-728.Deas-Nesmith, D., Campbell, S., & Brady, K. T. (1998). Substance use disorders in an adolescent inpatient psychiatric popu-
lation. Journal of the National Medical Association, 90, 233-238.De Bellis, M. D., Clark, D. B., Beers, S. R., Soloff, P., Boring, A. M., Hall, J., et al. (2000). Hippocampal volume in adoles-
cent-onset alcohol use disorders. American Journal of Psychiatry, 157, 737-744.De Bellis, M. D., Narasimhan, A., Thatcher, D. L., Keshavan, M. S., Soloff, P., & Clark, D. B. (2005). Prefrontal cortex,
thalamus, and cerbellar volumes in adolescents and young adults with adolescent-onset alcohol use disorders and comor-bid mental disorders. Alcoholism: Clinical and Experimental Research, 29, 1590-1600.
Dennis, M. (1999). Global Appraisal of Individual Needs (GAIN): Administration guide for the GAIN and related measures. Bloomington, IL: Chestnut Health Systems.
Dennis, M., Godley, S. H., Diamond, G., Tims, F., Babor, T., Donaldson, J., et al. (2004a). The Cannabis Youth Treatment (CYT) study: Main findings from two randomized trials. Journal of Substance Abuse Treatment, 27, 197-213.
Dennis, M., Godley, S. H., Diamond, G., Tims, T. M., Babor, T., Donaldson, J., et al. (2004b). The Cannabis Youth Treatment (CYT) study: Main findings from two randomized trials. Journal of Substance Abuse Treatment, 27, 197-213.
Dennis, M., White, M., Titus, J. C., & Unsicker, J. (2008). GAIN: Global Appraisal of Individual Needs: Administration guide for the GAIN and related measures (Version 5). Normal, IL: Chestnut Health Systems.
Desai, R. A., Goulet, J. L., Robbins, J., Chapman, J. F., Migdole, S. J., & Hoge, M. A. (2006). Mental health care in juvenile detention facilities: A review. Journal of the American Academy of Psychiatry & Law, 34, 204-214.
Diamond, G., & Josephson, A. (2005). Family-based treatment research: A 10-year update. Journal of the American Academy of Child & Adolescent Psychiatry, 44, 872-887.
Dodge, K. A., & Coie, J. D. (1987). Social-information-processing factors in reactive and proactive aggression in children’s peer groups. Journal of Personality and Social Psychology, 53, 1146-1158.
Dunn, C., Deroo, L., & Rivara, F. P. (2001). The use of brief interventions adapted from motivational interviewing across behavioral domains: A systematic review. Addiction, 96, 1725-1742.
Ebner, R., Schreiber, W., & Zierer, C. (2004). Buprenorphine or methadone for detoxification of young opioid addicts? Psychiatrische Praxis, 31(Suppl. 1), S108-S110.
Farabee, D., Shen, H., Hser, Y., Grella, C. E., & Anglin, M. D. (2001). The effects of drug treatment on criminal behavior among adolescents in DATOS-A. Journal of Adolescent Research, 16, 679-696.
Farrington, D. P. (1989). Early predictors of adolescent aggression and adult violence. Violence and Victims, 4, 79-100.Feindler, E. L., Ecton, R. B., Kingsley, D., & Dubey, D. R. (1986). Group anger-control training for institutionalized psychi-
atric male adolescents. Behavior Therapy, 17, 109-123.Feldstein, S. W., & Ginsburg, J. I. D. (2006). Motivational interviewing with dually diagnosed adolescents in juvenile justice
settings. Brief Treatment and Crisis Intervention, 6, 218-233.Feldstein, S. W., & Miller, W. R. (2007). Does subtle screening work? A review of the SASSI. Addiction, 102, 41-50.Fisher, G. L., & Harrison, T. C. (2000). Substance abuse: Information for school counselors, social workers, therapists, and
counselors. Needham Heights, MA: Allyn & Bacon.Fite, P. J., & Colder, C. R. (2007). Proactive and reactive aggression and peer delinquency: Implications for prevention and
intervention. The Journal of Early Adolescence, 27, 223-240.

764 CRIMINAL JUSTICE AND BEHAVIOR
Fite, P. J., Colder, C. R., Lochman, J. E., & Wells, K. C. (2008). The relation between childhood proactive and reactive aggression and substance use initiation. Journal of Abnormal Child Psychology, 36, 261-271.
Fite, P. J., Stoppelbein, L., & Greening, L. (2009). Proactive and reactive aggression in a child psychiatric inpatient popula-tion. Journal of Clinical Child and Adolescent Psychology, 38, 199-205.
Flicker, S. M., Turner, C. W., Waldron, H. B., Brody, J. L., & Ozechowski, T. J. (2008). Ethnic background, therapeutic alli-ance, and treatment retention in functional family therapy with adolescents who abuse substances. Journal of Family Psychology, 22, 167-170.
Fossati, A., Raine, A., Borroni, S., Bizzozero, A., Volpi, E., Santalucia, I., et al. (2009). A cross-cultural study of the psycho-metric properties of the Reactive‚ Proactive Aggression Questionnaire among Italian nonclinical adolescents. Psychological Assessment, 21, 131-135.
Friedman, A. S. (1989). Family therapy vs. parent groups: Effects on adolescent drug abusers. American Journal of Family Therapy, 17, 335-347.
Gardner, M., & Steinberg, L. (2005). Peer influence on risk taking, risk preference, and risky decision making in adolescence and adulthood: An experimental study. Developmental Psychology, 41, 625-635.
Gavin, D. R., Ross, H. E., & Skinner, H. A. (1989). Diagnostic validity of the drug abuse screening test in the assessment of DSM-III drug disorders. British Journal of Addiction, 84, 301-307.
Godley, M. D., Godley, S. H., Dennis, M., Funk, R., & Passetti, L. (2002). Preliminary outcomes from the assertive continu-ing care experiment for adolescents discharged from residential treatment. Journal of Substance Abuse Treatment, 23, 21-32.
Godley, S. H., Meyers, R. J., Smith, J. E., Karvinen, T., Titus, J. C., Godley, M. D., et al. (2001). The Adolescent Community Reinforcement Approach for Adolescent Cannabis Users, Cannabis Youth Treatment (CYT) Series, Volume 4 (DHHS Pub. No. 01-3489). Rockville, MD: Center for Substance Abuse Treatment, Substance Abuse and Mental Health Services Administration.
Goldstein, A., Glick, B., & Gibbs, J. (1998). Aggression replacement training: A comprehensive intervention for aggressive youth. Champaign, IL: Research Press.
Gordon, D. A., Graves, K., & Arbuthnot, J. (1995). The effect of functional family therapy for delinquents on adult criminal behavior. Criminal Justice and Behavior, 22, 60-73.
Greenwood, P. (2008). Prevention and intervention programs for juvenile offenders. The Future of Children, 18, 185-211.Grisso, T., & Underwood, L. A. (2004). Screening and assessing mental health and substance use disorders among youth in
the juvenile justice system. Washington, DC: U.S. Department of Justice.Hansson, K. (1998). Program replication in Sweden. In J. F. Alexander, C. Pugh, & B. Parsons (Eds.), Book three: Blueprints
for violence prevention (pp. 87-109). Golden, CO: Venture Publishing.Hawkins, E. H. (2009). A tale of two systems: Co-occurring mental health and substance abuse disorders treatment for ado-
lescents. Annual Review of Psychology, 60, 197-227.Hawkins, J. D., Herrenkohl, T. I., Farrington, D. P., Brewer, D., Catalano, R. F., & Harachi, T. W. (1998). A review of predic-
tors of youth violence. In R. Loeber & D. P. Farrington (Eds.), Serious and violent juvenile offenders: Risk factors and successful interventions (pp. 106-146). Thousand Oaks, CA: Sage.
Hawkins, J. D., Herrenkohl, T. I., Farrington, D. P., Brewer, D., Catalano, R. F., Harachi, T. F., et al. (2000). Predictors of youth violence. In Wilson, J. J. (Ed.), Juvenile justice bulletin: Predictors of youth violence (pp. 1-12). Washington, DC: U.S. Department of Justice.
Henggeler, S. W. (2011). Efficacy studies to large-scale transport: The development and validation of multisystemic therapy programs. Annual Review of Clinical Psychology, 7, 351-381.
Henggeler, S. W., Borduin, C. M., Melton, G. B., Mann, B. J., Smith, L., & Hall, J. A. (1991). Effects of multisystemic therapy on drug use and abuse in serious offenders: A progress report from two outcome studies. Family Dynamics of Addiction Quarterly, 1, 40-51.
Henggeler, S. W., Clingempeel, W. G., Brondino, M. J., & Pickrel, S. G. (2002). Four-year follow-up of multisystemic therapy with substance-abusing and substance-dependent juvenile offenders. Journal of the American Academy of Child and Adolescent Psychiatry, 41, 868-874.
Henggeler, S. W., Melton, G. B., Brondino, M. J., Scherer, D. G., & Hanley, J. H. (1997). Multisystemic therapy with violent and chronic juvenile offenders and their families: The role of treatment fidelity in successful dissemination. Journal of Consulting and Clinical Psychology, 65, 821-833.
Henggeler, S. W., Melton, G. B., & Smith, L. A. (1992). Family preservation using multisystemic therapy: An effective alternative to incracerating serious juvenile offenders. Journal of Consulting and Clinical Psychology, 60, 953-961.
Herrenkohl, T. I., Catalano, R. F., Hemphill, S. A., & Toumbourou, J. W. (2009). Longitudinal examination of physical and relational aggression as precursors to later problem behaviors in adolescents. Violence and Victims, 24, 3-19.
Herrenkohl, T. I., Maguin, E., Hill, K. G., Hawkins, J. D., Abbott, R. D., & Catalano, R. F. (2000). Developmental risk factors for youth violence. Journal of Adolescent Health, 26, 176-186.
Higgins, S. T. (1997). Applying learning and conditioning theory to the treatment of alcohol and cocaine abuse. In B. A. Johnson & J. D. Roache (Eds.), Drug addiction and its treatment: Nexus of neuroscience and behavior (pp. 367-385). Philadelphia: Lippincott, Williams & Wilkins.

Doran et al. / ADOLESCENT SUBSTANCE USE AND AGGRESSION 765
Higgins, S. T., Alessi, S. M., & Dantona, R. L. (2002). Voucher-based incentives: A substance abuse treatment innovation. Addictive Behaviors, 27, 887-910.
Higgins, S. T., Budney, A. J., & Bickel, W. K. (1994). Applying behavioral concepts and principles to the treatment of cocaine dependence. Drug and Alcohol Dependence, 34, 87-97.
Higgins, S. T., Delaney, D. D., Budney, A. J., Bickel, W. K., Hughes, J. R., Foerg, F., et al. (1991). A behavioral approach to achieving initial cocaine abstinence. American Journal of Psychiatry, 148, 1218-1224.
Higgins, S. T., & Silverman, K. (2008). Contingency management in substance abuse treatment. In S. T. Higgins, K. Silverman, & S. H. Heil (Eds.), Contingency management in substance abuse treatment (pp. 1-18). New York: Guilford Press.
Hogue, A., Dauber, S., Samuolis, J., & Liddle, H. (2006). Treatment techniques and outcomes in Multidimensional Family Therapy for Adolescent Behavior Problems. Journal of Family Psychology, 20, 535-543.
Hope, T. L., & Bierman, K. L. (1998). Patterns of home and school behavior problems in rural and urban settings. Journal of School Psychology, 36, 45-58.
Kaminer, Y., Bukstein, O. G., & Tarter, R. E. (1991). The Teen-Addiction Severity Index: Rationale and reliability. International Journal of Addictions, 26, 219-226.
Kaminer, Y., & Burleson, J. (1999). Psychotherapies for adolescent substance abusers: 15-month follow-up of a pilot study. American Journal on Addictions, 8, 114-119.
Kaminer, Y., Burleson, J., Blitz, C., Sussman, J., & Rounsaville, B. (1998). Psychotherapies for adolescent substance abusers: A pilot study. Journal of Nervous and Mental Disease, 186, 684-690.
Kamon, J., Budney, A. J., & Stanger, C. (2005). A contingency management intervention for adolescent marijuana abuse and conduct problems. Journal of the American Academy of Child & Adolescent Psychiatry, 44, 513-521.
Kandel, D. B., Johnson, J. G., & Bird, H. R. (1999). Psychiatric comorbidity among adolescents with substance use disorders: Findings from the MECA study. Journal of the Academy of Child & Adolescent Psychiatry, 38, 693-699.
Kendler, K. S., Prescott, C. A., Myers, J., & Neale, M. C. (2003). The structure of genetic and environmental risk factors for common psychiatric and substance use disorders in men and women. Archives of General Psychiatry, 60, 929-937.
Kirisci, L., Tarter, R. E., Vanyukov, M., Reynolds, M., & Habeych, M. (2004). Relation between cognitive distortions and neurobehavior disinhibition on the development of substance use during adolescence and substance use disorder by young adulthood: A prospective study. Drug and Alcohol Dependence, 76, 125-133.
Knight, J. R., Goodman, E., Pulerwitz, T., & DuRant, R. H. (2001). Reliability of the problem oriented screening instrument for teeneragers (POSIT) in adolescent medical practice. Journal of Adolescent Health, 29, 125-130.
Knight, J. R., Sherritt, L., Shrier, L. A., Harris, S. K., & Chang, G. (2002). Validity of the CRAFFT substance abuse screen-ing test among adolescent clinic patients. Archives of Pediatric Adolescent Medicine, 156, 607-614.
Knight, J. R., Shrier, L. A., Bravender, T. D., Farrell, M., Vander Bilt, J., & Shaffer, H. J. (1999). A new brief screen for adolescent substance abuse. Archives of Pediatric Adolescent Medicine, 153, 591-596.
Krishnan-Sarin, S., Duhig, A. M., McKee, S. A., McMahon, T. J., Liss, T., McFetridge, A., et al. (2006). Contingency man-agement for smoking cessation in adolescent smokers. Experimental and Clinical Psychopharmacology, 14, 306-310.
Krueger, R. F., & Markon, K. E. (2006). Reinterpreting comorbidity: A model-based approach to understanding and classify-ing psychopathology. Annual Review of Clinical Psychology, 2, 111-133.
Lamps, C. A., Sood, A. B., & Sood, R. (2008). Youth with substance abuse and comorbid mental health disorders. Current Psychiatry Reports, 10, 265-271.
Lanza, S. T., Rhoades, B. L., Nix, R. L., & Greenberg, M. T. (2010). Modeling the interplay of multilevel risk factors for future academic and behavior problems: A person-centered approach. Development and Psychopathology, 22, 313-335.
Larzelere, R. E., Dinges, K., Schmidt, M. D., Spellman, D. F., Criste, T. R., & Connell, P. (2001). Outcomes of residential treatment: A study of the adolescent clients of Girls and Boys Town. Child and Youth Care Forum, 30, 175-185.
Lasowski, L. E., Miller, F. G., Boye, M. W., & Miller, G. A. (1998). Efficacy of the Substance Abuse Subtle Screening Inventory 3 (SASSI-3) in identifying substance dependence disorders in clinical settings. Journal of Personality Assessment, 71, 114-128.
Latessa, E. J., Listwan, S. J., & Hubbard, D. J. (2005). Correctional interventions: Changing offender behavior. Boston: Roxbury Publishing.
Latimer, W. W., Winters, K. C., D’Zurilla, T., & Nichols, M. (2003). Integrated family and cognitive-behavioral therapy for adolescent substance abusers: A Stage I efficacy study. Drug and Alcohol Dependence, 71, 303-317.
Letourneau, E. J., Henggeler, S. W., Borduin, C. M., Schewe, P. A., McCart, M. R., Chapman, J. E., et al. (2009). Multisystemic therapy for juvenile sexual offenders: 1-year results from a randomized effectiveness trial. Journal of Family Psychology, 23, 89-102.
Lewis, R. A., Piercy, F. P., Sprenkle, D. H., & Trepper, T. S. (1990). Family-based interventions for helping drug-abusing adolescents. Journal of Adolescent Research, 5, 82-95.
Libby, A. M., & Riggs, P. D. (2005). Integrated substance use and mental health treatment for adolescents: Aligning organi-zational and financial incentives. Journal of Child and Adolescent Psychopharmacology, 15, 826-834.

766 CRIMINAL JUSTICE AND BEHAVIOR
Liddle, H. A. (1999). Theory development in a family-based therapy for adolescent drug abuse. Journal of Clinical Child Psychology, 28, 521-532.
Liddle, H. A. (2010). Multidimensional Family Therapy: A science-based treatment system. The Australian and New Zealand Journal of Family Therapy, 31, 133-148.
Liddle, H. A., & Dakof, G. A. (2002). A randomized controlled trial of intensive outpatient, family-based therapy versus residential drug treatment for comorbid adolescent drug abusers. Drug and Alcohol Dependence, 66, S2-S202.
Liddle, H. A., Dakof, G. A., Henderson, C., & Rowe, C. L. (in press). Implementation outcomes of Multidimensional Family Therapy-Detention to Community: A reintegreation program for drug-using juvenile detainees. International Journal of Offender Therapy and Comparative Criminology.
Liddle, H. A., Dakof, G. A., Parker, K., Diamond, G. S., Barrett, K., & Tejeda, M. (2001). Multidimensional family therapy for adolescent drug abuse: Results of a randomized clinical trial. American Journal of Drug and Alcohol Abuse, 27, 651-688.
Liddle, H. A., Dakof, G. A., Turner, R. M., Henderson, C., & Greenbaum, P. E. (2008). Treating adolescent drug abuse: A randomized trial comparing Multidimensional Family Therapy and Cognitive Behavior Therapy. Addiction, 103, 1660-1670.
Liddle, H. A., Rowe, C. L., Dakof, G. A., Henderson, C., & Greenbaum, P. E. (2009). Multidimensional Family Therapy for early adolescent substance abusers: Twelve month outcomes of a randomized controlled trial. Journal of Consulting and Clinical Psychology, 77, 12-25.
Liddle, H. A., Rowe, C. L., Dakof, G. A., Ungaro, R. A., & Henderson, C. (2004). Early intervention for adolescent substance abuse: Pretreatment to posttreatment outcomes of a randomized controlled trial comparing multidimensional family therapy and peer group treatment. Journal of Psychoactive Drugs, 36, 2-37.
Liddle, H. A., Rowe, C. L., Gonzalez, A., Henderson, C., Dakof, G. A., & Greenbaum, P. E. (2006). Changing provider practices, program environment, and improving outcomes by transporting Multidimensional Family Therapy to an ado-lescent drug treatment setting. The American Journal on Addictions, 15, 102-112.
Lipsey, M. W., & Derzon, J. H. (1998). Predictors of violent and serious delinquency in adolescence and early adulthood: A synthesis of longitudinal research. In R. Loeber & D. P. Farrington (Eds.), Serious and violent juvenile offenders: Risk factors and successful interventions (pp. 86-105). Thousand Oaks, CA: Sage.
Lipsey, M. W., Landenberger, N. A., & Wilson, S. J. (2007). Effects of cognitive-behavioral programs for criminal offenders (Campbell Collaboration Systematic Review). Retrieved November 2, 2009 from http://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.124.6626&rep=rep1&type=pdf
Lipsey, M. W., Wilson, D. B., & Cothern, L. (2000). Effective intervention for serious juvenile offenders. Washington, DC: Office of Juvenile Justice and Delinquency Prevention.
Little, T. D., Brauner, J., Jones, S. M., Nock, M. K., & Hawley, P. H. (2003). Rethinking aggression: A typological examina-tion of the functions of aggression. Merrill-Palmer Quarterly (Special Issue: Aggression and Adaptive Functioning: The Bright Side to Bad Behavior), 49, 343-369.
Little, T. D., Jones, S. M., Henrich, C. C., & Hawley, P. H. (2003). Disentangling the “whys” from the “whats” of aggressive behaviour. International Journal of Behavioral Development, 27, 122-133.
Lovell, D., Allen, D., Johnson, C., & Jemelka, R. (2001). Evaluating the effectiveness of residential treatment for prisoners with mental illness. Criminal Justice and Behavior, 28, 83-104.
Lysaught, E., & Wodarski, J. S. (1996). A dual-focused intervention for depression and addiction. Journal of Child and Adolescent Substance Abuse, 5, 55-71.
Marlatt, G. A., & Witkiewitz, K. (2002). Harm reduction approaches to alcohol use: Health promotion, prevention, and treat-ment. Addictive Behaviors, 27, 867-886.
Martel, M. M., Pierce, L., Nigg, J. T., Jester, J. M., Adams, K. M., Puttler, L. I., et al. (2009). Temperament pathways to childhood disruptive behavior and adolescent substance abuse: Testing a cascade model. Journal of Abnormal Child Psychology, 37, 363-371.
Mason, W. A., & Windle, M. (2002). Reciprocal relations between adolescent sbustance use and deliquence: A longitudinal latent variable analysis. Journal of Abnormal Psychology, 111, 63-76.
McClelland, G., Teplin, L., & Abram, K. (2004). Detection and prevalence of substance use among juvenile detainees. OJJDP Juvenile Justice Bulletin. Retrieved March 12, 2011 from http://www.usdoj.gov
McQuown, S. C., Belluzzi, J. D., & Leslie, F. M. (2007). Low dose nicotine treatment during early adolescence increases subsequent cocaine reward. Neurotoxicology and Teratology, 29, 66-73.
Medina, K. L., Schweinsburg, A. D., Cohen-Zion, M., Nagel, B. J., & Tapert, S. F. (2006). Effects of alcohol and combined marijuana and alcohol use during adolescence on hippocampal volume and asymmetry. Neurotoxicology and Teratology, 29, 141-152.
Milin, R., Halikas, J. A., Meller, J. E., & Morse, C. (1991). Psychopathology among substance abusing juvenile offenders. Journal of the Academy of Child & Adolescent Psychiatry, 30, 569-574.
Miller, F. G. (1997). SASSI: Application and assessment for substance-related problems. Substance Use and Misuse, 2, 163-166.Miller, W. R., & Rollnick, S. (1991). Motivational interviewing: Preparing people to change addictive behavior. New York:
Guilford Press.
Doran et al. / ADOLESCENT SUBSTANCE USE AND AGGRESSION 767
Monti, P., Colby, S. M., Barnett, N. P., Spirito, A., Rohsenow, D. J., Myers, M. G., et al. (1999). Brief intervention for harm reduction with alcohol-positive older adolescents in a hospital emergency department. Journal of Consulting and Clinical Psychology, 67, 989-994.
Morgan, A. B., & Lilienfeld, S. O. (2000). A meta-analytic review of the relation between antisocial behavior and neuropsy-chological measures of executive function. Clinical Psychology Review, 20, 113-136.
National Institute on Drug Abuse. (2006). Principles of drug abuse treatment for criminal justice populations: A research-based guide (NIH Publication No. 06-5316). Washington, DC: National Institutes of Health.
Newcombe, D. A. L., Humeniuk, R. E., & Ali, R. (2005). Validation of the World Health Organization Alcohol, Smoking and Substance Involvement Screening Test (ASSIST): Report of results from the Australian site. Drug and Alcohol Review, 24, 217-226.
Niarhos, F., & Routh, D. K. (1992). The role of clinical assessment in the juvenile court: Predictors of juvenile dispositions and recidivism. Journal of Child Clinical Psychology, 21, 151-159.
Nickel, M., Luley, J., Krawczyk, J., Nickel, C., Widermann, C., Lahmann, C., et al. (2006). Bully girls—Changes after Brief Strategic Family Therapy: A randomized, prospective, controlled trial with one-year follow-up. Psychotherapy and Psychosomatics, 75, 47-55.
Nissen, L. B. (2007). The reclaiming futures initiative: Improving substance abuse interventions for justice-involved youth, a reclaiming futures national program report. Portland, OR: Portland State University.
O’Donnell, P., Richards, M., Pearce, S., & Romero, E. (in press). Gender differences in monitoring and deviant peers as predictors of delinquent behavior among low-income urban African American youth. Journal of Early Adolescence.
Oscar-Berman, M., & Marinkovic, K. (2003). Alcoholism and the brain: An overview. Alcohol Health & Research World, 27, 125-133.
Perez, M., Burns, A. B., Brown, J. S., Sachs-Ericsson, N., Plant, A., & Joiner, T. E. (2007). Associations of serotonin trans-porter genotypes to components of the tripartite model of depression and anxiety. Personality and Individual Differences, 43, 107-118.
Petry, N. M., & Martin, B. (2002). Low-cost contingency management for treating cocaine- and opioid-abusing methadone patients. Journal of Consulting and Clinical Psychology, 70, 398-405.
Piazza, N. J. (1996). Dual diagnosis and adolescent psychiatric inpatients. Journal of Substance Use and Misuse, 31, 215-223.Poulin, F., & Boivin, M. (2000). Reactive and proactive aggression: Evidence of a two-factor model. Psychological
Assessment, 12, 115-122.Prendergast, M., Podus, D., Finney, J., Greenwell, L., & Roll, J. (2006). Contingency management for treatment of substance
use disorders: A meta-analysis. Addiction, 101, 1546-1560.Price, T. S., Simonoff, E., Walderman, I., Asherson, P., & Plomin, R. (2001). Hyperactivity in pre-school children is highly
heritable. Journal of the American Academy of Child & Adolescent Psychiatry, 40, 1342-1364.Pulkkinen, L., & Pitkanen, T. (1994). A prospective study of the precursors to problem drinking in young adulthood. Journal
of Studies on Alcohol, 55, 578-587.Rahdert, E. (1991a). The Adolescent Assessment and Referral Manual (DHHS Publication No. ADM-91-1735). Rockville,
MD: National Institute on Drug Abuse.Rahdert, E. (1991b). The adolescent assessment/referral system manual. Rockville, MD: .Raine, A., Dodge, K., Loeber, R., Gatzke-Kopp, L., Lynam, D., Reynolds, C., et al. (2006). The reactive-proactive aggression
questionnaire: Differential correlates of reactive and proactive aggression in adolescent boys. Aggressive Behavior, 32, 159-171.
Reyna, V. F., & Farley, F. (2006). Risk and rationality in adolescent decision making: Implications for theory, practice, and public policy. Psychological Science in the Public Interest, 7, 1-44.
Rohde, P., Lewinsohn, P. M., & Seely, J. R. (1996). Psychiatric comorbidity with problematic alcohol use in high school students. Journal of the Academy of Child & Adolescent Psychiatry, 35, 101-109.
Rosenthal, R. (1991). Meta-analytic procedures for social research. Thousand Oaks, CA: Sage.Rossow, L., & Wichstrom, L. (1999). Young, wet and wild? Associations between alcohol intoxication and violent behavior
in adolescence. Addiction, 94, 1017-1031.Rowe, C. L., Liddle, H. A., Greenbaum, P. E., & Henderson, C. E. (2004). Impact of psychiatric comorbidity on treatment of
adolescent drug abusers. Journal of Substance Abuse Treatment, 26, 129-140.Santisteban, D. A., Coatsworth, J. D., Perez-Vidal, A., Kurtines, W., Schwartz, S. J., LaPerriere, A., et al. (2003). Efficacy of
brief strategic family therapy in modifying Hispanic adolescent behavior problems and substance use. Journal of Family Psychology, 17, 121-133.
Schoenwald, S. K., Ward, D. M., Henggeler, S. W., Pickrel, S. G., & Patel, H. (1996). Multisystemic therapy treatment of substance abusing or dependent adolescent offenders: Costs of reducing incarceration, inpatient, and residential place-ment. Journal of Child and Family Studies, 5, 431-444.
Sexton, T. L., & Alexander, J. F. (2000). Family-based empirically supported intervention programs. The Counseling Psychologist, 30, 238-261.
Sexton, T. L., & Alexander, J. F. (2005). Functional family therapy for externalizing disorders in adolescents. In J. L. Lebow (Ed.), Handbook of clinical family therapy (pp. 164-194). Hoboken, NJ: John Wiley and Sons.

768 CRIMINAL JUSTICE AND BEHAVIOR
Sexton, T. L., & Turner, C. W. (2010). The effectiveness of Functional Family Therapy for youth with behavioral problems in a community practice setting. Journal of Family Psychology, 24, 339-348.
Sheidow, A. J., Bradford, W. D., Henggeler, S. W., Rowland, M. D., Halliday-Boykins, C., Schoenwald, S. K., et al. (2004). Treatment costs for youths receiving multisystemic therapy or hospitalization after a psychiatric crisis. Psychiatric Services, 55, 548-554.
Sherman, D. K., Iacono, W. G., & McGue, M. K. (1997). Attention-deficit hyperactivity disorder dimensions: A twin study of inattention and impulsivity-hyperactivity. Journal of the American Academy of Child & Adolescent Psychiatry, 36, 745-753.
Skara, S., Pokhrel, P., Weiner, M. D., Sun, P., Dent, C. W., & Sussman, S. (2008). Physical and relational aggression as pre-dictors of drug use: Gender differences among high school students. Addictive Behaviors, 33, 1507-1515.
Skinner, H. A. (1982). The Drug Abuse Screening Test. Addictive Behaviors, 7, 363-371.Slesnick, N., & Prestopnik, J. L. (2005). Ecologically based family therapy outcome with substance abusing runaway ado-
lescents. Journal of Adolescence, 28, 277-298.Slesnick, N., Prestopnik, J. L., Meyers, R. J., & Glassman, M. (2006). Treatment outcome for street-living, homeless youth.
Addictive Behaviors, 32, 1237-1251.Snyder, H., & Sickmund, M. (2006). Juvenile offenders and victims: 2006 national report. Washington, DC: U.S. Department
of Justice, Office of Justice Programs, Office of Juvenile Justice and Delinquency Prevention.Spear, L. P. (2000). The adolescent brain and age-related behavioral manifestations. Neuroscience and Biobehavioral
Reviews, 24, 417-463.Squeglia, L. M., Jacobus, J., & Tapert, S. F. (2009). The influence of substance use on adolescent brain development. Clinical
EEG and Neuroscience, 40, 31-38.Stanton, M. D., & Shadish, W. R. (1997). Outcome, attrition, and family/couples treatment for drug abuse: A review of the
controlled, comparative studies. Psychological Bulletin, 122, 170-191.Stein, L. A. R., Colby, S. M., Barnett, N. P., Monti, P., Golembeske, C., & Lebeau-Craven, R. (2006). Effects of motivational
interviewing for incarcerated adolescents on driving under the influence after release. American Journal on Addictions, 15(Suppl. 1), 50-57.
Stein, L. A. R., Monti, P., Colby, S. M., Barnett, N. P., Golembeske, C., Lebeau-Craven, R., et al. (2006). Enhancing substance abuse treatment engagement in incarcerated adolescents. Psychological Services, 3, 25-34.
Sullivan, C. J. (2006). Early adolescent delinquency: Assessing the role of childhood problems, family environment, and peer pressure. Youth Violence and Juvenile Justice, 4, 291-313.
Swaim, R. C., Deffenbacher, J. L., & Wayman, J. C. (2004). Concurrent and prospective effects of multi-dimensional aggres-sion and anger on adolescent alcohol use. Aggressive Behavior, 30, 356-372.
Szapocznik, J., Amaro, H., Gonzalez, G., Schwartz, S. J., Castro, F. G., & Bernal, G. (2003). Drug abuse treatment for Hispanics. In H. Amaro & D. E. Cortes (Eds.), National strategic plan on Hispanic drug abuse research: From the mol-ecule to the community (pp. 91-117). Boston: National Hispanic Science Network on Drug Abuse, Northeastern University Institute on Urban Health Research.
Szapocznik, J., Hervis, U., & Schwartz, S. (2003). Breif strategic family therapy for adolescent drug abuse (NIH Publication No. 03-4751). Bethesda, MD: National Institute on Drug Abuse.
Szapocznik, J., Kurtines, W., Foote, F. H., Perez-Vidal, A., & Hervis, O. (1983). Conjoint versus one-person family therapy: Some evidence for the effectiveness of conducting family therapy through one person. Journal of Consulting and Clinical Psychology, 51, 889-899.
Szapocznik, J., Kurtines, W., Santisteban, D. A., & Rio, A. T. (1990). Interplay of advances between theory, research, and application in treatment interventions aimed at behavior problem children and adolescents. Journal of Consulting and Clinical Psychology, 58, 696-703.
Timmons-Mitchell, J., Bender, M. B., Kishna, M. A., & Mitchell, C. C. (2006). An independent effectiveness trial of Multisystemic Therapy with juvenile justice youth. Journal of Clinical Child and Adolescent Psychology, 35, 227-236.
Toumbourou, J. W., Stockwell, T., Neighbors, C., Marlatt, G. A., Sturge, J., & Rehm, J. (2007). Interventions to reduce harm associated with adolescent substance use. Lancet, 369, 1391-1401.
Upadhyaya, H., Deas, D., & Brady, K. (2005). A practical clinical approach to the treatment of nicotine dependence in ado-lescents. Journal of the Academy of Child & Adolescent Psychiatry, 44, 942-946.
Waldron, H. B. (1997). Adolescent substance abuse and family therapy outcome: A review of randomized trials. In T. H. Ollendick & R. J. Prinz (Eds.), Advances in clinical child psychology (Vol. 19, pp. 199-234). New York: Plenum.
Waldron, H. B., Slesnick, N., Brody, J. L., Turner, C. W., & Peterson, T. R. (2001). Treatment outcomes for adolescent sub-stance abuse at 4- and 7-month assessments. Journal of Consulting and Clinical Psychology, 69, 802-813.
Wallace, J. M. J., & Muroff, J. R. (2002). Preventing substance abuse among African American children and youth: Race differences in risk factor exposure and vulnerability. Journal of Primary Prevention, 22, 235-261.
Wasserman, G. A., Jensen, P. S., Ko, S. J., Cocozza, J., Trupin, E., Angold, A., et al. (2003). Mental health assessments in juvenile justice: Report on the consensus conference. Journal of the American Academy of Child & Adolescent Psychiatry, 42, 752-761.

Doran et al. / ADOLESCENT SUBSTANCE USE AND AGGRESSION 769
Waxmonsky, J. G., & Wilens, T. E. (2005). Pharmacotherapy of adolescent substance use disorders: A review of the literature. Journal of Child and Adolescent Psychopharmacology, 15, 810-825.
White, H. R., Loeber, R., Stouthamer-Loeber, M., & Farrington, D. P. (1999). Developmental associations between substance use and violence. Development and Psychopathology, 11, 785-803.
White, W. L. (2005). Treatment works: Is it time for a new slogan? Addiction Professional, 3, 22-28.Wilson, M. N., Hurtt, C. L., Shaw, D. S., Dishion, T. J., & Gardner, F. (2009). Analysis and influence of demographic and
risk factors on difficult child behaviors. Prevention Science, 10, 353-365.Winters, K. C. (1999). Treating adolescents with substance use disorders: An overview of practice issues and treatment out-
come. Substance Abuse, 20, 203-225.Winters, K. C., Stinchfield, R., & Henly, G. (1989). Personal Experience Inventory and manual. Los Angeles: Western
Psychological Services.Winters, K. C., & Yifrah, K. (2008). Screening and assessing adolescent substance use disorders in clinical populations.
Journal of the American Academy of Child & Adolescent Psychiatry, 47, 740-744.Woody, G. E., Poole, S. A., Subramaniam, G., Dugosh, K., Bogenschutz, M., Abbott, P., et al. (2008). Extended vs. short-term
buprenorphine-naloxone for treatment of opioid-addicted youth: A randomized trial. Journal of the American Medical Association, 300, 2003-2011.
World Health Organization. (2002). The Alcohol, Smoking and Substance Involvement Screening Test (ASSIST): Development, reliability and feasibility. Addiction, 97, 1183-1194.
Wright, F. D., Beck, A. T., Newman, C. F., & Liese, B. S. (1993). Cognitive therapy of substance abuse: Theoretical rationale. National Institute on Drug Abuse Research Monograph Series, Behavioral Treatments for Drug Abuse and Dependence, 137, 123-146.
Yakovlev, P. I., & Lecours, A. R. (1967). The myelogenetic cycles of regional maturation of the brain. In A. Minkowski (Ed.), Regional development of the brain in early life (pp. 3-70). Boston: Blackwell Scientific.
Young, D., Dembo, R., & Henderson, C. (2007). A national survey of substance abuse treatment for juvenile offenders. Journal of Substance Abuse Treatment, 32, 255-266.
Zucker, R. A. (2008). Anticipating problem alcohol use developmentally from childhood into middle adulthood: What have we learned? Addiction, 103(Suppl. 1), 100-108.
Neal Doran is an assistant professor of psychiatry at the University of California, San Diego, and a research scientist at the Veterans Medical Research Foundation in San Diego. His research focuses on mechanisms that promote the initiation and maintenance of addictive behaviors, particularly alcohol and tobacco use.
Susan E. Luczak is an associate research professor of psychology at the University of Southern California and assistant professor of psychiatry at the University of California, San Diego. Her work has centered on assessment of etiological factors that contribute to the development of alcohol problems and on methodological issues in alcohol research. Her current NIAAA-funded research examines ethnic differences in predictors of alcohol use and real-time assessment of alcohol-metabolizing gene effects on naturalistic drinking patterns.
Nicole Bekman is an assistant project scientist in the University of California, San Diego Department of Psychology. Her research focuses on cognitive and affective predictors of alcohol use in adolescents.
Igor Koutsenok is an assistant professor of psychiatry and director of the Center for Criminality and Addiction Research, Training, and Application at the University of California, San Diego. His work focuses on the development and provision of training to providers of substance abuse treatment in correctional settings, the judicial system, and law enforcement.
Sandra A. Brown is a professor of psychology and psychiatry at the University of California, San Diego. Her research centers on models of the course of alcohol and other substance abuse, psychiatric comorbidity, and neurocognitive and psychosocial factors that influence transitions out of substance abuse disorders. Her current work is focused on key factors in the etiology, progression, and resolution of substance abuse; the long-term impact of multiple substance abuse; and gen-erational differences in substance abuse and treatment outcomes.




















