
Internalizing and externalizing problems in adolescent aggression perpetrators, victims, and...
23
55 Brian J. Sherman, M.A., is a doctoral candidate in clinical psychology at the Department of Counseling and Clinical Psychology, Teachers College, Columbia University. He has conducted research in developmental psychopathology from a risk and resilience framework among at-risk populations in the United States and Brazil. Cristiane S. Duarte, Ph.D., M.P.H., is an assistant professor of clinical psychology in psychiatry at the Division of Child and Adolescent Psychiatry, Columbia University, New York State Psychiatric Institute, New York. She has contributed to influential innovative large-scale studies of youth mental health in Brazil, the United States, Puerto Rico, and other countries. Helen Verdeli, Ph.D., is an assistant professor at the Department of Counseling and Clinical Psychology, Teachers College, Columbia University, and an adjunct assistant professor of psychology at the College of Physicians and Surgeons, Columbia University, New York State Psychiatric Institute, New York. Her research focuses on treatment and prevention of mood disorders. Dr. Verdeli is involved in adapting and testing psychotherapy for depressed people in developing countries, and she has collaborated with academic and humanitarian groups in the United States and International Journal of Mental Health, vol. 40, no. 3, Fall 2011, pp. 55–76. © 2011 M.E. Sharpe, Inc. All rights reserved. ISSN 0020–7411/2011 $9.50 + 0.00. DOI 10.2753/IMH0020-7411400304 BRIAN J. SHERMAN, CRISTIANE S. DUARTE, AND HELEN VERDELI Internalizing and Externalizing Problems in Adolescents from Bahia, Brazil Sociodemographic Correlates and Family Environment in Boys and Girls ABSTRACT: This study examines the associations between sociodemographic and family environment factors, and adolescent internalizing and externalizing problems in a socioeconomically disadvantaged community in the northeast- ern state of Bahia, Brazil. Three-hundred and forty-four adolescents, age 11 to 18 (mean age = 13.6 years) responded to a school-based survey that assessed sociodemographic indicators of risk (e.g., race, parental marital status, parental education, parental employment), intrinsic religiosity, family
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Internalizing and externalizing problems in adolescent aggression perpetrators, victims, and...
55
Brian J. Sherman, M.A., is a doctoral candidate in clinical psychology at the Department of Counseling and Clinical Psychology, Teachers College, Columbia University. He has conducted research in developmental psychopathology from a risk and resilience framework among at-risk populations in the United States and Brazil. Cristiane S. Duarte, Ph.D., M.P.H., is an assistant professor of clinical psychology in psychiatry at the Division of Child and Adolescent Psychiatry, Columbia University, New York State Psychiatric Institute, New York. She has contributed to influential innovative large-scale studies of youth mental health in Brazil, the United States, Puerto Rico, and other countries. Helen Verdeli, Ph.D., is an assistant professor at the Department of Counseling and Clinical Psychology, Teachers College, Columbia University, and an adjunct assistant professor of psychology at the College of Physicians and Surgeons, Columbia University, New York State Psychiatric Institute, New York. Her research focuses on treatment and prevention of mood disorders. Dr. Verdeli is involved in adapting and testing psychotherapy for depressed people in developing countries, and she has collaborated with academic and humanitarian groups in the United States and
International Journal of Mental Health, vol. 40, no. 3, Fall 2011, pp. 55–76.© 2011 M.E. Sharpe, Inc. All rights reserved.ISSN 0020–7411/2011 $9.50 + 0.00.DOI 10.2753/IMH0020-7411400304
Brian J. Sherman, CriStiane S. Duarte, anD helen VerDeli
Internalizing and Externalizing Problems in Adolescents from Bahia, BrazilSociodemographic Correlates and Family Environment in Boys and Girls
ABSTRACT: This study examines the associations between sociodemographic and family environment factors, and adolescent internalizing and externalizing problems in a socioeconomically disadvantaged community in the northeast-ern state of Bahia, Brazil. Three-hundred and forty-four adolescents, age 11 to 18 (mean age = 13.6 years) responded to a school-based survey that assessed sociodemographic indicators of risk (e.g., race, parental marital status, parental education, parental employment), intrinsic religiosity, family

56 INTERNATIONAL JOURNAL OF MENTAL HEALTH
conflict, and family cohesion. Results indicate that high family cohesion and low family conflict are associated with lower risk for probable internalizing and externalizing disorders among girls but not boys. This gender difference is particularly important as it suggests that mechanisms of risk and protection vary for boys and girls. These findings shed light on risk factors in adolescence in the context of vast socioeconomic disparity found in Brazil.
Adolescent and child development is best understood from an ecological perspective in which individual and contextual characteristics interact to produce myriad pathways of normal and abnormal development [1–3]. Early exposure to risk at the individual, family, and community level is as-sociated with maladjustment across psychological, behavioral, and cognitive domains [3–5] and predicts high rates of recurrent mental health problems in adulthood [6, 7]. Likewise, protective factors such as a close relationship with a supportive adult [8] and a positive family environment [9, 10] serve to reduce the impact of developmental risk. Understanding risk and protective mechanisms of psychopathology during adolescence is of utmost importance to informing prevention and intervention strategies geared toward reducing lifetime prevalence rates of mental illness and minimizing long-term effects of high-risk environments. While extensive research has been conducted in the United States, less is known about adolescent mental health and its key correlates in developing nations.
This study was conducted in the rapidly developing nation of Brazil. In the last decades, Brazil has witnessed considerable urbanization and, in recent years, fast economic growth. Regrettably, this process is occurring within a context of extreme social inequity, including vast economic disparity that translates into poor living conditions for a substantial proportion of the population. Although Brazil boasts the world’s eighth largest economy [11], it remains the tenth most economically disparate country [12]. Socioeconomic
abroad, playing a major role in the cultural modification of interpersonal psychotherapy for randomized controlled trials with depressed adults in Southern Uganda, depressed adolescents in IDP camps in Northern Uganda, and distressed patients in primary care in Goa, India.
The authors thank research assistant and agent of the Justice of Childhood and Youth, Lidiane Conceição da Silva, from Salvador, Bahia, Brazil, for her dedicated assistance and support in developing, coordinating, and conducting this study.
There are no conflicts of interest regarding this study or its publication. Brian Sherman was supported by the Tinker Foundation through the Institute of Latin American Studies (ILAS) at Columbia University. ILAS has also supported Dr. Du-arte. Helen Verdeli is supported by National Institute of Mental Health K23 Award (MH071530).

FALL 2011 57
inequities provide the context in which sociodemographic risk factors exert their influence, contributing to the development of common mental health problems including anxiety and affective disorders, conduct disorders, an-tisocial behavior, and substance use disorders [5, 13, 14]. Indeed, the vast inequalities found in Brazil contribute to the social and economic burden of psychiatric morbidity highlighted by the “inverse care law” [15, 16], which posits “lower-income populations, with an excess of morbidity, do not receive minimal care for mental health, while the more privileged population could be receiving excessive assistance” [16, p. 165].
Socioeconomic Indicators of Risk and Adolescent Mental Health
Prevalence rates of adolescent mental health problems in Brazil have been examined. For example, Paula, Duarte, and Bordin [17] examined 479 chil-dren and adolescents between the ages of 6 and 17 years in the low-income municipality of Embu in southeastern Brazil. They found that 24.6 percent of these 6- to 17-year-olds reported clinical levels of current psychiatric symptoms. Other studies have reported rates of mental health problems in Brazilian samples ranging from 13 percent to 23 percent [18–21]. These num-bers suggest that almost one in four Brazilian children and adolescents suffer from a mental disorder. It is now time to move beyond the determination of prevalence rates and to address potential mechanisms of risk and protection associated with adolescent mental health problems in Brazil.
Psychological research in Brazil increased between 1995 and 2005 [22], shedding light on the deleterious effects of poverty and socioeconomic dis-advantage on mental health. For example, Almeida-Filho et al. [13] examined social inequality defined across racial, gender, and social class lines among adults in northeastern Brazil. They found an inverse relation between educa-tion and depressive symptoms, and a higher prevalence of depression in racial minority groups and divorced or widowed persons. In a study of high-risk adolescents from a low socioeconomic status community in southeastern Brazil, community, economic, and familial risk were associated with higher substance use and negative emotionality (e.g., low self-esteem) [23].
Other indicators of socioeconomic disadvantage such as public school attendance, low parental education, high unemployment, and single-parent families are associated with poor mental health outcomes in children and adolescents in Brazil [14, 24–26]. In a study of the relation between common mental disorders and indicators of social inequality in 515 adolescents, strong predictors of adolescent mental disorder included less formal schooling (<5 years) and parental unemployment [27]. Similarly, in a cross-sectional study
58 INTERNATIONAL JOURNAL OF MENTAL HEALTH
of 960 adolescents from an urban area, Pinheiro et al. [28] found that single-family households and low parental education were associated with increased rates of common mental disorders.
Family Environment and Adolescent Mental Health
The family environment plays an integral role in adolescent development. Specifically, family conflict and family cohesion have been linked with inter-nalizing and externalizing problems across cultures. A multi-informant study (parent, child, teacher-report) examining predictors of internalizing problems in 415 Moroccan immigrant adolescents in the Netherlands, found strong as-sociations between parent–child, and parent–parent conflict and adolescent internalizing problems [29]. In a separate longitudinal study of 354 adoles-cents transitioning to adulthood, early adult major depression was linked to low family cohesion and adolescent internalizing problems [7]. These effects are pronounced in disadvantaged youth. For example, Gorman-Smith, Tolan, Henry, and Florsheim [30] showed that skilled parenting and high family cohesion moderated the risk of socioeconomic disadvantage on externalizing behaviors, and other research has corroborated the findings that high family cohesion protects at-risk youth against maladjustment [9, 31] and that family conflict confers risk for internalizing and externalizing disorders [32]. These findings highlight the protective effect of a positive family environment de-fined by low levels of conflict and high levels of cohesiveness, particularly among disadvantaged youth.
Religiosity and Adolescent Mental Health
Research on religiosity and mental health suggests that religiosity buffers against psychiatric illness, especially in the context of socioeconomic dispar-ity. In a review by Moreira-Almeida, Neto, and Koenig [33], religiosity and spirituality were positively correlated with psychological well-being and were associated with decreased rates of depression, substance use, and suicidal ideation. In a study comparing 178 African-American young adults (M age = 20) exposed to community violence with 163 of their white counterparts, private religiosity was associated with reduced rates of externalizing prob-lems [34]. Similarly, private religiosity and religious identification among African-American teenagers exposed to high levels of community violence was associated with fewer conduct problems [35]. Research suggests that the buffering effects of religiosity on adolescent maladjustment operate through increased social capital resources and the promotion of prosocial behavior [36].
FALL 2011 59
Gender and Adolescent Mental Health
Gender differences in adolescent mental health are also notable. Girls are consistently found to have elevated rates of internalizing disorders, while boys tend to show higher rates of externalizing problems [37, 38]. In addition, specific types of risk may differ in how they predict adolescent mental health problems according to the adolescent’s gender. A comprehensive study by Raffaelli et al. [23] examined community, economic, and familial risk in an impoverished community sample of 918 Brazilian youth age 14–19. Results showed that type of risk factor interacted with gender such that girls reported higher rates of familial risk (e.g., physical/sexual abuse) and economic risk (e.g., unemployed parent), while boys reported greater community risk (e.g., peer violence). For boys, community risk was associated most strongly with substance use, whereas, for girls, familial and economic risk was associated most strongly with negative emotionality and low self-esteem. These gender differences in risk exposure and type of mental health problem support the importance of considering gender when assessing risk exposure and adoles-cent psychopathology.
Regional Disparities in Brazil
Mental health problems experienced by Brazilian youth occur within a cultur-ally complex environment of socioeconomic disadvantage and inequity. In the northeastern state of Bahia where this study was conducted, social inequity is particularly prominent and socioeconomic indicators of risk have predomi-nated historically. Bahia, as the center of the African slave trade during the colonial period, is comprised of the largest population of slave descendants in the country, and currently it is estimated that roughly 80 percent of Bahia’s population is nonwhite [39]. Within this historical context, economic and educational opportunities have not paralleled those of more affluent states in the southeast. In the municipality from which our sample is drawn, the 2000 census reported that 23 percent of persons age 10 or older had three years or less of formal schooling, and 11 percent were illiterate. The average monthly income was US$716 (converted based on historical exchange rates). Comparatively, in the city of Sao Paulo, Brazil, only 5 percent were illiterate and the average monthly income was US$2,175 [40].
The historical oppression and poverty endemic to the region allow for the examination of the insidious effects of socioeconomic disadvantage. Examin-ing the effects of socioeconomic disadvantage in the context of vast disparity found in Brazil adds a highly relevant dimension to our understanding of the nature of psychological disorders in this unique sample of adolescent youth.

60 INTERNATIONAL JOURNAL OF MENTAL HEALTH
It is not only the oft-studied sociodemographic risk factors but also living within sharp contrast to those benefitting from national economic prosperity that may contribute to demoralization, resentment, and overall poor psycho-logical health.
While most research is being conducted in the more affluent regions of southeastern Brazil, there is a dearth of research in the socioeconomically disadvantaged regions in the northeast. Goodman et al. [21] conducted one of the few large-scale studies in northeastern Brazil assessing prevalence rates of common mental disorders among adolescents from a small island near Salvador, Bahia. Compared to findings from southeastern Brazil, participants reported higher symptom levels but lower rates of psychiatric disorders. Good-man et al. concluded that the regional variability and discrepancy between symptom levels and rates of disorder indicates a need for further research on adolescent mental health nationwide, particularly in the socioeconomically and ethnically diverse regions in the northeast. The current study starts to fill this gap, offering a unique look into the relation between socioeconomic dis-advantage and mental health among a historically impoverished population.
The Current Study
This study seeks to better understand risk and protective factors associated with adolescent mental health problems in the context of social and economic disparity in a resource-poor setting in Bahia, Brazil. Specifically, we examine the following hypotheses: (a) girls have higher rates of internalizing problems whereas boys have higher rates of externalizing problems; (b) low parental education, having unmarried or unemployed parents, and nonwhite racial status are associated with higher risk for internalizing and externalizing problems; and (c) intrinsic religiosity, high family cohesion, and low family conflict are associated with lower rates of internalizing and externalizing problems.
Method
Participants
The sample is drawn from a public school in a municipality outside of Salvador, Bahia. Participants include 344 adolescents between the ages of 11 and 18 years (M = 13.6 years, SD = 1.8 years). Participants were recruited through school visits by the principal investigator and a native Brazilian research as-sistant over a two-day period. An introduction to the study was provided in each classroom, and all students were given the opportunity to participate. Of the 704 students enrolled in the school, we received parental consent and

FALL 2011 61
child assent from 346. Two respondents were excluded from analyses due to missing data. The majority of the sample (87 percent) is nonwhite, which is slightly higher than the percentage of nonwhites in the state of Bahia (78.8 percent) [39]. Sixty-one percent are girls. Highest parental education attained is generally low, and more than one-half of the participants have unmarried parents (e.g., divorced, separated, widowed).
Measures
Adolescent Internalizing and Externalizing Problems
We use the Brazilian version of the Youth Self-Report (YSR) [41, 42] to assess internalizing (anxiety, depression) and externalizing (rule-breaking, oppositional) problems. The YSR is the adolescent self-report component of the Achenbach System of Empirically Based Assessment, a standardized screening system for assessing internalizing and externalizing mental health problems. The YSR yields three symptom level categories based on norma-tive data from U.S. samples: clinical (T-score >63; above 90th percentile), borderline (T-score 60–63), and nonclinical (T-score <60). For the purposes of the present analysis, we collapsed borderline and clinical categories to define presence of internalizing or externalizing mental health problems. YSR symptom structures have shown consistency across cultures [43], and the YSR has demonstrated psychometrically sound properties for use in Brazil [17, 44, 45]. In our study sample, the YSR demonstrates good internal consistency for both internalizing (0.84) and externalizing scales (0.87).
Impact: Functional Impairment and Distress Related to Problems
To assess the impact of internalizing and externalizing symptoms reported on the YSR, we use the Impact Supplement of the Strength and Difficulties Questionnaire (SDQ) [46]. This scale assesses the impact of current symptoms, defined by the combination of subjective distress and impairment in social functioning. Children are asked to rate how much their reported difficulties “upset or distress [them],” and how much they “interfere with everyday life in the following areas: home life, friendships, classroom learning, leisure activities.” For each item, the child selects from the following options, not at all, only a little, quite a lot, and a great deal. Their responses are scored to indicate clinically significant impact, or caseness [46]. We consider the impact of symptoms clinically significant for children who report quite a lot or a great deal of distress in at least one area. The SDQ–Impact scale dem-onstrates good internal consistency in our sample (0.73).
62 INTERNATIONAL JOURNAL OF MENTAL HEALTH
Probable cases
To determine rates of probable internalizing and externalizing disorders, we create a composite index by combining YSR symptom levels and SDQ–Impact ratings. We define probable cases as children who (a) score in the borderline or clinical range on the YSR and (b) report clinically significant impact on the SDQ–Impact Supplement. We apply these criteria for internalizing and externalizing cases separately. Inclusion of the SDQ–Impact Supplement is essential, because although the YSR is used extensively worldwide, it is a symptom checklist rather than a diagnostic measure. Operationalizing disor-ders based only on symptoms alone does not accurately assess an individual’s level of distress and functional impairment related to experienced symptoms [47]. Psychiatric disorder, as defined by both the Diagnostic and Statistical Manual of Mental Disorders [48] and the International classification of Dis-eases [49] require either significant distress or impairment in everyday role expectations. The SDQ–Impact Supplement has shown powerful predictive utility, exceeding that of symptom checklists alone [46, 47].
Sociodemographic Risk Factors
We developed a brief demographic questionnaire for the purposes of this study. Participants were asked to report their age, gender, and race, as well as their parents’ marital status (married, divorced, separated, never married, widowed), highest level of education for mother and father (illiterate, fourth grade or less, eighth grade or less, high school graduate, college or graduate degree), and employment status for mother and father (yes or no response). Responses were then dichotomized. For example, parental education was recoded into eighth grade or less and high school or more, and parental marital status was recoded into married and nonmarried. Risk factors included in the models are nonwhite race, having unmarried parents, having parents with eighth grade education or less, and families with one or more unemployed parents.
Family Environment
To assess levels of family conflict and family cohesion, we use the Family Environment Scale [50]. The Family Environment Scale consists of ten sub-scales including cohesion, expressiveness, conflict, independence, assertive-ness, intellectual interests, leisure, religion, organization, and control. In a validation study of the Brazilian version, Vianna, Silva, and Souza-Formigoni [51] found good internal consistency for the subscales family conflict and family cohesion. As part of the current study, we also find acceptable internal

FALL 2011 63
consistency coefficients for both family conflict (0.65) and family cohesion (0.67). Data analyses use standardized scores for family conflict and cohesion because the sample distribution was skewed.
Intrinsic Religiosity
The Duke Religion Index [52] is a five-item scale that assesses public, pri-vate, and total religiosity. Intrinsic (i.e., private) religiosity was defined by items such as “how much do you lead your life by your religious beliefs and values?” We use the intrinsic religiosity subscale to ascertain the extent to which participants attempt to integrate religious beliefs into their daily lives; this scale had an acceptable level of internal consistency (0.62).
Procedures
Data collection was conducted in accordance with the Teachers College, Columbia University Institutional Review Board and with approval from the Justice of Childhood and Youth of the State of Bahia, as well as school ad-ministrators. Informed parental consent and child assent were obtained. Data collection took place over a two-day period and participation was voluntary. Confidentiality was assured by the use of random identification numbers. Student names and assent forms were detached from response sheets prior to survey completion. Teachers were not present during the survey to encourage open and honest responding.
The research team consisted of the principal investigator (Sherman), two native Brazilian agents of the Justice of Childhood and Youth, and one native licensed child psychologist. The team worked in pairs, and the survey was read aloud by a native Brazilian Portuguese speaker to assure proper pronunciation and timely completion. The second member served as a “floater,” answering any questions the students had regarding survey items or procedure. Students who did not want to participate completed other academic activities in a separate classroom. Completion of the survey took approximately forty-five minutes.
Data Analysis
Initially, we compare, between boys and girls, the frequency of adolescent internalizing and externalizing problems with and without the SDQ–Impact scale. We then conduct a series of logistic regression analyses to assess the associations between sociodemographic and family environment factors with probable cases of internalizing and externalizing disorders. First, we examine unadjusted logistic regression models for each of the factors of interest, with
64 INTERNATIONAL JOURNAL OF MENTAL HEALTH
internalizing and externalizing probable cases as the dependent variable. Next, we examine adjusted models including all factors simultaneously to adjust for combined effects. We conduct all regression models separately for girls and boys, given anticipated gender differences.
Results
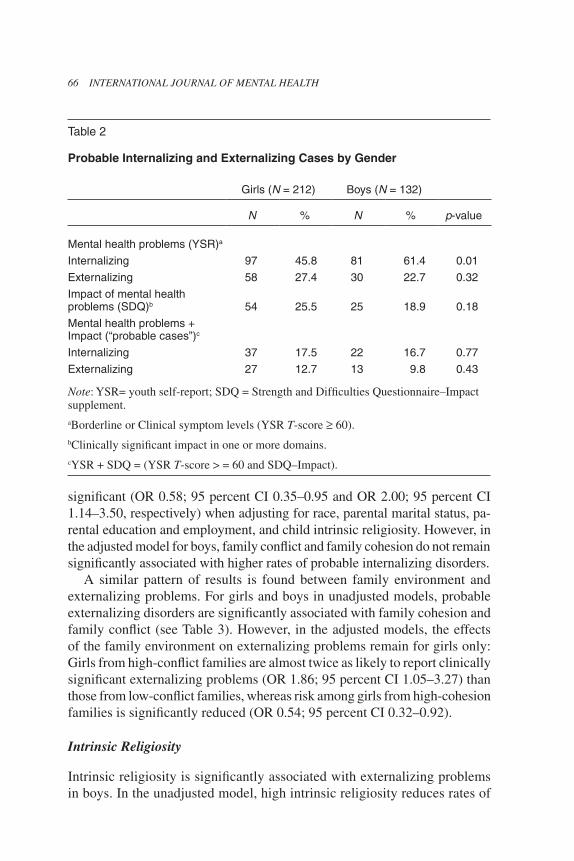
Table 1 provides demographic, family, and religiosity characteristics of the sample. Boys and girls did not differ significantly on any factors, although the overall breakdown was notable in regards to race (87 percent nonwhite) and education (roughly 50 percent of parents had an eighth grade education or less). Frequencies for levels of YSR internalizing and externalizing symptoms are found in Table 2. Results indicate a significant difference in presence of internalizing problems between girls and boys (p = 0.01), however, when impact is considered, no significant gender differences exist in rates of prob-able internalizing or externalizing problems.
Sociodemographic Risk Factors
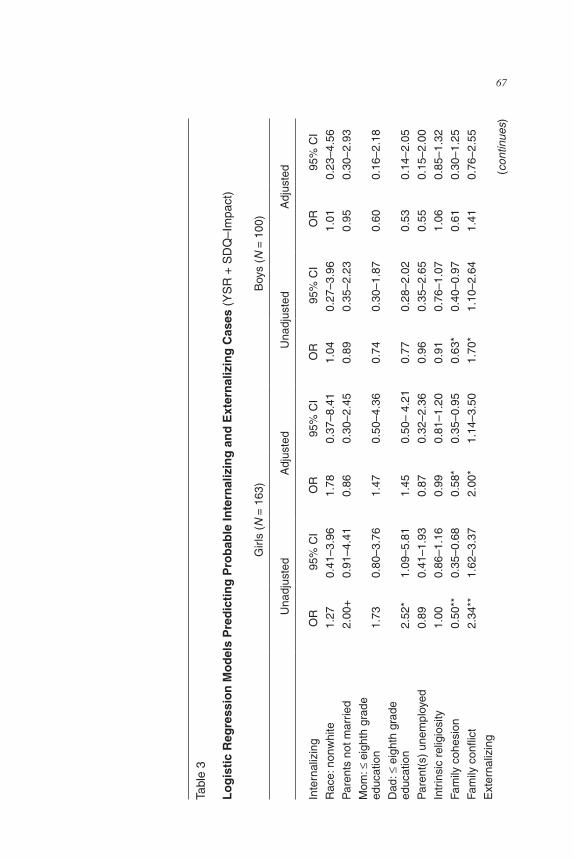
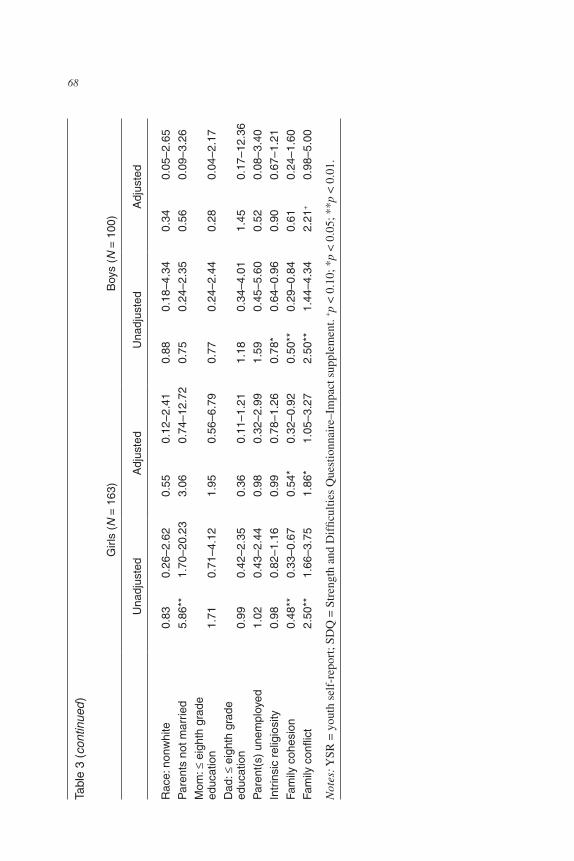
Unadjusted models indicate significant associations between demographic factors and internalizing and externalizing problems for girls only (see Table 3). Girls reporting paternal education of eighth grade or less are 2.5 times more likely to report clinically significant internalizing symptoms (OR 2.52; 95 percent CI 1.09–5.81), while girls with unmarried parents are almost six times as likely to report clinically significant externalizing problems (OR 5.86; 95 percent CI 1.70–20.23). In the adjusted model including all demographic, family, and religiosity factors these associations are no longer significant.
Family Environment
Family conflict and family cohesion show robust associations with probable internalizing and externalizing disorders (see Table 3). In the girls’ unadjusted models, high family cohesion is significantly associated with lower risk for internalizing problems (OR 0.50; 95 percent CI 0.35–0.68), whereas high fam-ily conflict is significantly associated with higher risk (OR 2.34; 95 percent CI 1.64–3.42). Similarly, boys from high-conflict families are almost two times more likely than boys from low-conflict families to report significant internalizing problems (OR 1.70; 95 percent CI 1.10–2.64), whereas boys from high-cohesion families are at lower risk for internalizing problems (OR 0.63; 95 percent CI 0.40–0.97). Gender differences emerge in the adjusted models. Among girls, the effects of family cohesion and family conflict remain
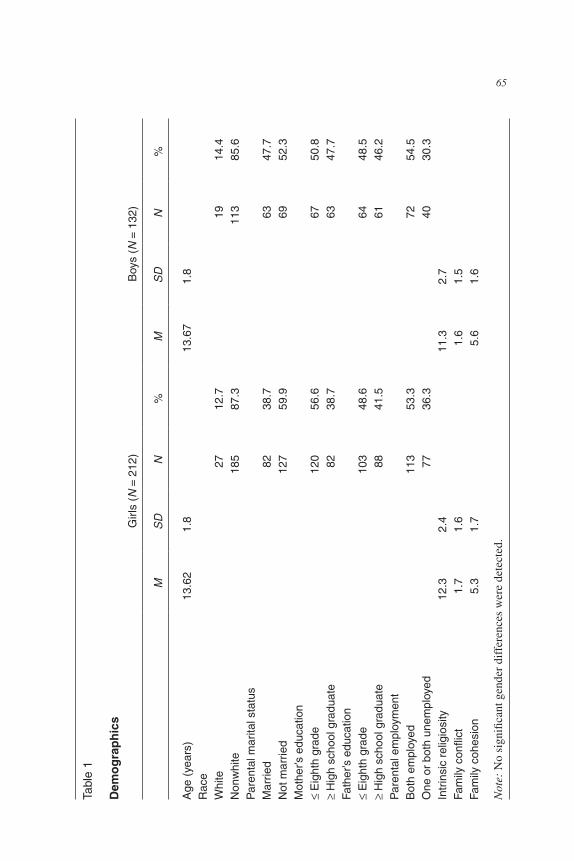
FALL 2011 65Ta
ble
1
Dem
og
rap
hic
s
Girl
s (N
= 2
12)
Boy
s (N
= 1
32)
MS
DN
%M
SD
N%
Age
(ye
ars)
13.6
2 1.
813
.67
1.8
Rac
eW
hite
27
12.7
19
14.4
Non
whi
te
185
87.3
11
385
.6P
aren
tal m
arita
l sta
tus
Mar
ried
82
38.7
63
47.7
Not
mar
ried
12
759
.9
6952
.3M
othe
r’s e
duca
tion
≤ E
ight
h gr
ade
12
056
.6
6750
.8≥
Hig
h sc
hool
gra
duat
e
8238
.7
6347
.7Fa
ther
’s e
duca
tion
≤ E
ight
h gr
ade
10
348
.6
6448
.5≥
Hig
h sc
hool
gra
duat
e88
41.5
61
46.2
Par
enta
l em
ploy
men
tB
oth
empl
oyed
11
353
.372
54.5
One
or
both
une
mpl
oyed
77
36.3
4030
.3In
trin
sic
relig
iosi
ty
12.3
2.
411
.3
2.7
Fam
ily c
onfli
ct1.
7 1.
61.
6 1.
5Fa
mily
coh
esio
n5.
3 1.
75.
6 1.
6
Not
e: N
o si
gnifi
cant
gen
der
diff
eren
ces
wer
e de
tect
ed.
66 INTERNATIONAL JOURNAL OF MENTAL HEALTH
significant (OR 0.58; 95 percent CI 0.35–0.95 and OR 2.00; 95 percent CI 1.14–3.50, respectively) when adjusting for race, parental marital status, pa-rental education and employment, and child intrinsic religiosity. However, in the adjusted model for boys, family conflict and family cohesion do not remain significantly associated with higher rates of probable internalizing disorders.
A similar pattern of results is found between family environment and externalizing problems. For girls and boys in unadjusted models, probable externalizing disorders are significantly associated with family cohesion and family conflict (see Table 3). However, in the adjusted models, the effects of the family environment on externalizing problems remain for girls only: Girls from high-conflict families are almost twice as likely to report clinically significant externalizing problems (OR 1.86; 95 percent CI 1.05–3.27) than those from low-conflict families, whereas risk among girls from high-cohesion families is significantly reduced (OR 0.54; 95 percent CI 0.32–0.92).
Intrinsic Religiosity
Intrinsic religiosity is significantly associated with externalizing problems in boys. In the unadjusted model, high intrinsic religiosity reduces rates of
Table 2
Probable Internalizing and Externalizing Cases by Gender
Girls (N = 212) Boys (N = 132)
N % N % p-value
Mental health problems (YSR)a
Internalizing 97 45.8 81 61.4 0.01
Externalizing 58 27.4 30 22.7 0.32
Impact of mental health problems (SDQ)b 54 25.5 25 18.9 0.18
Mental health problems + Impact (“probable cases”)c
Internalizing 37 17.5 22 16.7 0.77
Externalizing 27 12.7 13 9.8 0.43
Note: YSR= youth self-report; SDQ = Strength and Difficulties Questionnaire–Impact supplement.aBorderline or Clinical symptom levels (YSR T-score ≥ 60).bClinically significant impact in one or more domains.cYSR + SDQ = (YSR T-score > = 60 and SDQ–Impact).
FALL 2011 67
Tabl
e 3
Lo
gis
tic
Reg
ress
ion
Mo
del
s P
red
icti
ng
Pro
bab
le In
tern
aliz
ing
an
d E
xter
nal
izin
g C
ases
(Y
SR
+ S
DQ
–Im
pact
)
Girl
s (N
= 1
63)
Boy
s (N
= 1
00)
Una
djus
ted
Adj
uste
dU
nadj
uste
dA
djus
ted
Inte
rnal
izin
gO
R95
% C
IO
R95
% C
IO
R95
% C
IO
R95
% C
I
Rac
e: n
onw
hite
1.27
0.41
–3.9
61.
780.
37–8
.41
1.04
0.27
–3.9
61.
010.
23–4
.56
Par
ents
not
mar
ried
2.00
+0.
91–4
.41
0.86
0.30
–2.4
50.
890.
35–2
.23
0.95
0.30
–2.9
3
Mom
: ≤ e
ight
h gr
ade
ed
ucat
ion
1.73
0.80
–3.7
61.
470.
50–4
.36
0.74
0.30
–1.8
70.
600.
16–2
.18
Dad
: ≤ e
ight
h gr
ade
ed
ucat
ion
2.52
*1.
09–5
.81
1.45
0.50
– 4.
210.
770.
28–2
.02
0.53
0.14
–2.0
5
Par
ent(
s) u
nem
ploy
ed0.
890.
41–1
.93
0.87
0.32
–2.3
60.
960.
35–2
.65
0.55
0.15
–2.0
0
Intr
insi
c re
ligio
sity
1.00
0.86
–1.1
6 0.
990.
81–1
.20
0.91
0.76
–1.0
71.
060.
85–1
.32
Fam
ily c
ohes
ion
0.50
**0.
35–0
.68
0.58
*0.
35–0
.95
0.63
*0.
40–0
.97
0.61
0.30
–1.2
5
Fam
ily c
onfli
ct2.
34**
1.62
–3.3
72.
00*
1.14
–3.5
01.
70*
1.10
–2.6
41.
410.
76–2
.55
Ext
erna
lizin
g(c
ontin
ues)
68 INTERNATIONAL JOURNAL OF MENTAL HEALTH
Rac
e: n
onw
hite
0.83
0.26
–2.6
20.
550.
12–2
.41
0.88
0.18
–4.3
40.
340.
05–2
.65
Par
ents
not
mar
ried
5.86
**1.
70–2
0.23
3.06
0.74
–12.
720.
750.
24–2
.35
0.56
0.09
–3.2
6
Mom
: ≤ e
ight
h gr
ade
ed
ucat
ion
1.71
0.71
–4.1
21.
950.
56–6
.79
0.77
0.24
–2.4
40.
280.
04–2
.17
Dad
: ≤ e
ight
h gr
ade
ed
ucat
ion
0.99
0.42
–2.3
50.
360.
11–1
.21
1.18
0.34
–4.0
11.
450.
17–1
2.36
Par
ent(
s) u
nem
ploy
ed1.
020.
43–2
.44
0.98
0.32
–2.9
9 1.
590.
45–5
.60
0.52
0.08
–3.4
0
Intr
insi
c re
ligio
sity
0.98
0.82
–1.1
60.
990.
78–1
.26
0.78
*0.
64–0
.96
0.90
0.67
–1.2
1
Fam
ily c
ohes
ion
0.48
**0.
33–0
.67
0.54
*0.
32–0
.92
0.50
**0.
29–0
.84
0.61
0.24
–1.6
0
Fam
ily c
onfli
ct2.
50**
1.66
–3.7
51.
86*
1.05
–3.2
72.
50**
1.44
–4.3
42.
21+
0.98
–5.0
0
Not
es: Y
SR =
you
th s
elf-
repo
rt; S
DQ
= S
tren
gth
and
Dif
ficul
ties
Que
stio
nnai
re–I
mpa
ct s
uppl
emen
t. +p
< 0
.10;
*p
< 0
.05;
**p
< 0
.01.
Tabl
e 3
(con
tinue
d)
Girl
s (N
= 1
63)
Boy
s (N
= 1
00)
Una
djus
ted
Adj
uste
dU
nadj
uste
dA
djus
ted

FALL 2011 69
probable externalizing disorders (OR 0.78; 95 percent CI 0.64–0.96). However, this association is not significant when adjusting for combined effects of other factors. Intrinsic religiosity is not associated with probable internalizing or externalizing disorders among girls.
Discussion
To better understand risk and protective factors operating during adolescence in a context of socioeconomic disparity, and to begin applying developmental psychopathology theory cross-culturally, this study explores the associations between internalizing and externalizing problems and sociodemographic and family correlates in a sample of public school adolescents in a low-income region in northeastern Brazil. Rates of probable internalizing and externalizing disorders among girls are associated with family conflict and family cohesion when adjusting for demographic and religious factors. Also, girls’ internalizing problems are independently associated with low paternal education, whereas girls’ externalizing problems are independently associated with having non-married parents. For boys, demographic factors are not related to internalizing or externalizing problems, and family environment factors are not associated with mental health problems when adjusting for other factors.
Sociodemographic Risk Factors
The absence of a relation between the sociodemographic risk factors included in this study and mental health problems is notable given the evidence in the literature showing the relation between these factors and adolescent malad-justment. While paternal education and parental marital status are associated with internalizing and externalizing problems in girls, we find no significant associations between sociodemographic factors and boys’ mental health problems. In addition, the effects among girls are not retained in adjusted models. There may be various explanations for these findings. It is possible that within the studied community sociodemographic risk factors are not important determinants of mental health problems or that we did not have information on relevant aspects of socioeconomic factors, such as house-hold income. However, it is also important to consider that the study had a low response rate of roughly 50 percent. Low response rates are associated with high absenteeism and, importantly, increased rates of adolescent risky behavior [53]. High absenteeism is not uncommon in low-income Brazilian communities [54]. Therefore, it is plausible that youth from low sociode-mographic groups and with mental health problems were less likely to be part of the sample.

70 INTERNATIONAL JOURNAL OF MENTAL HEALTH
Family Environment
The study reveals important gender-specific associations between family environment and rates of probable internalizing and externalizing disorders. The protective effect of a family environment characterized by low levels of conflict and high levels of cohesion is associated with internalizing and externalizing problems among girls but not boys. Low-conflict families are associated with lower risk of internalizing and externalizing problems in girls, even when adjusting for sociodemographic factors and religiosity. Similarly, among girls, the protective effect of high family cohesion on both internalizing and externalizing problems is significant in the adjusted models. These findings, consistent with the literature showing the deleterious effects of family conflict and protective effects of family cohesion [9, 30, 31, 55], also offer fresh evidence for important gender-specific patterns that are less well-documented. One possible explanation for this gender effect may be related to the interaction between type of risk and gender. Raffaelli et al. [23] found that female adolescents reported greater familial and economic risk, which was related to low self-esteem and negative emotionality. In contrast, boys reported more community risk than familial or economic, which was related to elevated rates of substance use. Given that we focus primarily on familial and economic factors, our findings are consistent with Raffaelli et al.’s results. It stands to reason that because adolescent boys are less susceptible to familial and economic risk factors, they will likewise be less responsive to the protective mechanisms of a positive family environ-ment, as our results illustrate.
Intrinsic Religiosity
High intrinsic religiosity appears to buffer against externalizing problems in adolescent boys. Research has shown that religiosity may be linked with psychological well-being [33] and may reduce externalizing problems includ-ing alcohol and drug abuse [56, 57], sexual promiscuity, and teen pregnancy [58]. Moreover, in high-risk samples, private religiosity is associated with lower rates of externalizing problems in male children [59] and adolescents [35]. The mechanisms by which religiosity protects against externalizing problems are not well understood, but evidence suggests a pathway through morality and social capital [36]. However, the nonsignificance of our finding when adjusting for family environment and other demographic factors may reflect recent evidence demonstrating that the correlation between religios-ity and alcohol use (age at first drink) is entirely accounted for by family environment [60].
FALL 2011 71
Overall Rates of Probable Disorders
Despite the impact of gender in response to risk and protective factors ex-amined in this study, we find no significant differences in overall rates of probable internalizing and externalizing disorders (YSR + Impact). The non-significant differences in probable cases does not support most of the literature on adolescent mental health, which generally finds girls with higher rates of internalizing disorders and boys with higher rates of externalizing disorders (see [38] for review). Moreover, when symptom severity is considered alone (YSR only), boys report more internalizing symptoms than girls. Thus, the standard conclusion that girls show higher rates of internalizing disorders and boys externalizing disorders should not be assumed across all adolescent populations. Our rare finding importantly highlights the need for continued exploration of gender differences in adolescent psychiatric disorders across socioeconomically and geographically disparate contexts.
Limitations
Certain limitations should be considered when interpreting the results of the study. First, due to the cross-sectional design, no inferences regarding causality can be made. Ideally, a longitudinal research design would be used to assess mechanisms of developmental psychopathology, but, given the limited financial resources and short timeline for this study, that was not feasible. However, the sample size is substantial and significant associa-tions are demonstrated. Cross-sectional research is characterized by high ecological validity, which is important when examining adolescence from an ecological perspective.
Second, the cross-cultural nature of the research raises questions regarding the validity of the measures. Measures developed with U.S. and other Western samples cannot be assumed to translate to Brazilian language and culture. While the YSR subscales demonstrated good internal constancy (0.82–0.87), the Duke Religion Index and Family Environment Scale reveal lower internal consistency (0.62–0.67), which may raise concerns about the quality of the translations, validity of these constructs, and, likewise, the interpretation of the results. Low alpha levels may introduce greater error variance into the models, thus restricting the power or even masking important associations. One consideration is that the Family Environment Scale uses a dichotomous true/false response scale, which inherently reduces the amount of variability. Although alpha levels ranging from 0.60 to 0.70 are considered acceptable, particularly in nonclinical research samples [61], we urge the reader to interpret the results with some caution.

72 INTERNATIONAL JOURNAL OF MENTAL HEALTH
Finally, the study would have benefited from using multiple informants. Self-report surveys have several drawbacks, including underreporting of symptoms and testing fatigue. Participants may have feared evaluation from teachers or parents for reporting illegal substance use or conduct problems, or they may not have been comfortable reporting emotional distress due to stigma. In addition, the response rate was somewhat low for a school-based survey, which may result in underestimates of adolescent risky behavior [53]. Ideally, school-based research should employ a tri-informant design in which teachers and parent measures are also used; however, this format is rarely possible. Additionally, more precise and detailed information about socioeconomic status and family context could have been obtained if family members were also assessed.
Despite these limitations, the results of the study are important, providing a more nuanced understanding of adolescent development in the context of socioeconomic disadvantage. Further research is warranted to confirm our findings on the gender-specific associations between family environment and adolescent mental health problems. Future research would benefit from a longitudinal design using multiple informants.
Conclusion
This study explores the relation between sociodemographic and family cor-relates of internalizing and externalizing disorders in a school sample of Brazilian adolescents. The setting of northeastern Brazil, outside of Salva-dor, Bahia, reflects a unique at-risk population within a broader context of national economic disparity. Our findings provide corroborating evidence for the protective effects of a positive family environment characterized by low family conflict and high family cohesion. Most important, we find that adolescent girls are more strongly affected by family factors than their male counterparts. Research suggests that adolescence is a time of increasing peer-influence, with adolescents spending less time at home and more time, usually unsupervised, with peers [62]. Our findings suggest this scenario may not be as relevant for adolescent girls, specifically in areas of economic inequality and national disparity. To tease apart these complicated gender differences, future research on adolescent mental health should consider gender-specific responses to different types of risk.
Finally, further research examining the broader context of national dispar-ity in conjunction with the range of sociodemographic risk factors obtained from multiple informants is warranted. While this study offers insight into the risk and protective mechanisms of adolescent developmental psychopa-thology, more research is needed across cultures and socioeconomic strata
FALL 2011 73
to gain a clearer picture of the myriad pathways of development worldwide. Only with greater clarity of knowledge and insight can we inform prevention and intervention strategies geared toward reducing mechanisms of risk and promoting mechanisms of protection.
References
1. Bronfenbrenner, U. (1979) The Ecology of human development: Experiments by nature and design. Cambridge, MA: Harvard University Press.
2. Bronfenbrenner, U. (Ed.). (2004) Making human beings human: Bioecological perspectives on human development. Thousand Oaks, CA: Sage.
3. Masten, A.S., & Garmezy, N. (1985) Risk, vulnerability, and protective factors in developmental psychopathology. In B.B. Lahey & A.E. Kazdin (Eds.), Advances in clinical child Psychology (Vol. 8, pp. 1–52). New York: Plenum.
4. Cowan, P.A.; Cowan, C.P.; & Schulz, M.S. (1996) Thinking about risk and resilience in families. In E.M. Hetherington & E.A. Blechman (Eds.), Stress, coping, and resiliency in children and families (pp. 1–38). Mahwah, NJ: Erlbaum.
5. Luthar, S. (Ed.). (2003) Resilience and vulnerability: Adaptation in the context of childhood adversities. Cambridge: Cambridge University Press.
6. Green, J.G.; McLaughlin, K.A.; Berglund, P.A.; Gruber, M.J.; Sampson, N.A.; Zaslavsky, A.M.; et al. (2010) Childhood adversities and adult psychiatric disorders in the national comorbidity survey replication I: Associations with first onset of DSM-IV disorders. Archives of General Psychiatry, 67(2), 113–123.
7. Reinherz, H.Z.; Paradis, A.D.; Giaconia, R.M.; Stashwick, C.K.; & Fitzmaurice, G. (2003) Childhood and adolescent predictors of major depression in the transition to adulthood. American Journal of Psychiatry, 160(12), 2141–2147.
8. Hetherington, E.M., & Elmore, A.M. (2003) Risk and resilience in children coping with their parents’ divorce and remarriage. In S. Luthar (Ed.), Resilience and vulnerability: Adaptation in the context of childhood adversities (pp. 182–212). Cambridge: Cambridge University Press.
9. Masten, A.S., & Shaffer, A. (2006) How families matter in child development. In A. Clarke-Stewart & J. Dunne (Eds.), Families count: Effects on child and adolescent development (pp. 5–25). Cambridge, MA: Cambridge University Press.
10. Yates, T.M.; Egeland, B.; & Sroufe, L.A. (2003) Rethinking resilience: A developmental process perspective. In S. Luthar (Ed.), Resilience and vulnerability: Adaptation in the context of childhood adversities (pp. 243–266). Cambridge: Cam-bridge University Press.
11. World Bank. (2010). World development indicators database. Washington, DC. Available at http://siteresources.worldbank.org/DATASTATISTICS/Resources/GDP .pdf, accessed September 27, 2010.
12. Central Intelligence Agency. World factbook: Gini index, 2007/2008. Wash-ington, DC. Available at www.cia.gov/library/publications/the-world-factbook/rankorder/2172rank.html, accessed June 1, 2011.
13. Almeida-Filho, N.; Lessa, I.; Magalhães, L.; Araujo, M.J.; Aquino, E.; James, S.A.; et al. (2004) Social inequality and depressive disorders in Bahia, Brazil: In-teractions of gender, ethnicity, and social class. Social Science & Medicine, 59(7), 1339–1353.
14. Curto, B.M.; Paula, C.S.; Nascimento, R.; Murray, J.; & Bordin, I.A. (in press)

74 INTERNATIONAL JOURNAL OF MENTAL HEALTH
Environmental factors associated with adolescent antisocial behavior in a poor urban community in Brazil. Social Psychiatry and Psychiatric Epidemiology.
15. Lima, M.S.; Hotopf, M.; Mari, J.J.; Beria, J.U.; Bastos, A.B.; & Mann, A. (1999) Psychiatric disorder and the use of benzodiazepines: An example of the inverse care law from Brazil. Social Psychiatry and Psychiatric Epidemiology, 34(6), 316–322.
16. Mari, J.J.; Bressan, R.A.; Almeida-Filho, N.; Gerolin, J.; Sharan, P.; & Saxena, S. (2006) Mental health research in Brazil: Policies, infrastructure, financing and hu-man resources. Revista de Saúde Pública, 40(1), 161–169.
17. Paula, C.S., Duarte, C.S., & Bordin, I.A.S. (2007) Prevalence of mental health problems in children and adolescents from the outskirts of Sao Paulo City: Treatment needs and service capacity evaluation. Revista Brasileira de Psiquiatria, 29(1), 11–17.
18. Anselmi, L.; Piccinini, C.A.; Barros, F.C.; & Lopes, R.S. (2004) Psychosocial determinants of behavior problems in Brazilian preschool children. Journal of child Psychology and Psychiatry, 45(4), 779–788.
19. Cury, C.R., & Golfeto, J.H. (2003) Strengths and Difficulties Questionnaire (SDQ): A study of school children in Ribeirão Preto. Revista Brasileira de Psiquia-tria, 25(3), 139–145.
20. Fleitlich-Bylik, B., & Goodman, R. (2003) Prevalence of child and adolescent psychiatric disorders in southeast Brazil. Journal of the American Academy of child & Adolescent Psychiatry, 43(6), 727–734.
21. Goodman, R.; Santos, D.N.; Nunes, A.P.R.; Miranda, D.P.; Fleitlich-Bilyk, B.; & Almeida-Filho, N. (2005) The Ilha de Maré study: A survey of child mental health problems in a predominantly African-Brazilian rural community. Social Psychiatry and Psychiatric Epidemiology, 40(1), 11–17.
22. Razzouk, D.; Zorzetto, R.; Dubugras, M.T.; Gerolin, J.; & Mari, J.D. (2007) Leading countries in mental health research in Latin America and the Caribbean. Revista Brasileira de Psiquiatria, 29(2), 118–122.
23. Raffaelli, M.; Koller, S.H.; Cerqueria-Santos, E.; & Morais, N.A. (2007) De-velopmental risks and psychosocial adjustment among low-income Brazilian youth. Development and Psychopathology, 19(2), 565–584.
24. Cuchiaro, G., & Dalgalarrondo, P. (2007) Mental health and quality of life in pre- and early adolescents: A school-based study in two contrasting urban areas. Revista Brasileira de Psiquiatria, 29(3), 213–221.
25. Ferriolli, S.H.T.; Marturano, E.M.; & Puntel, L.P. (2007) Family context and child mental health problems in the Family Health Program. Revista de Saúde Pública, 41(2), 251–259.
26. Ponde, M.P., & Freire, A.C.C. (2007) Prevalence of attention deficit hyper-activity disorder in schoolchildren in the city of Salvador, Bahia, Brazil. Arq de Neuropsiquiatr, 65(2A), 240–244.
27. Marin-Leon L.; Oliveira H.B.; Barros M.B.; Dalgalarrondo P.; & Botega N.J. (2007) Social inequality and common mental disorders. Revista Brasileira de Psiquiatria, 29(3), 250–253.
28. Pinheiro, K.A.; Horta, B.L.; Pinheiro, R.T.; Horta, L.L.; Terres, N.G.; & Silva, R.A. (2007) Common mental disorders in adolescents: A population based cross-sectional study. Revista Brasileira de Psiquiatria, 29(3), 241–245.
29. Stevens, G.W.J.M.; Vollebergh, W.A.M.; Pels, T.V.M.; & Crijnen, A.A.M. (2005) Predicting internalizing problems in Moroccan immigrant adolescents in the Netherlands. Social Psychiatry and Psychiatric Epidemiology, 40(12), 1003–1011.
FALL 2011 75
30. Gorman-Smith, D.; Tolan, P.H.; Henry, D.B.; & Florsheim, P. (2000) Patterns of family functioning and adolescent outcomes among urban African American and Mexican American families. Journal of Family Psychology, 14(3), 436–457.
31. Richmond, M.K., & Stocker, C.M. (2006) Associations between family cohe-sion and adolescent siblings’ externalizing behavior. Journal of Family Psychology, 20(4), 663–669.
32. Mamorstein, N.R., & Iacono, W.G. (2004) Major depression and conduct dis-order in youth: Associations with parental psychopathology and parent-child conflict. Journal of child Psychology and Psychiatry, 45(2), 377–386.
33. Moreira-Almeida, A.; Neto, F.L.; & Koenig, H.G. (2006) Religiousness and mental health: A review. Revista Brasileira de Psiquiatria, 28(3), 242–250.
34. Fowler, P.J.; Ahmed, S.R.; Tompsett, C.J.; Jozefowicz-Simbeni, D.M.H.; & Toro, P.A. (2008) Community violence and externalizing problems: Moderating ef-fects of race and religiosity in emerging adulthood. Journal of community Psychology, 36(7), 835–850.
35. Pearce, M.J.; Jones, S.M.; Schwab-Stone, M.E.; Ruchkin, V. (2003) The protective effects of religiousness and parent involvement on the development of conduct problems among youth exposed to violence. child Development, 74(6), 1682–1697.
36. King, P.E., & Furrow, J.L. (2004) Religion as a resource for positive youth development: Religion, social capital, and moral outcomes. Developmental Psychol-ogy, 40(5), 703–713.
37. Rutter, M.; Caspi, A.; & Moffitt, T.E. (2003) Using sex differences in psy-chopathology to study causal mechanisms: Unifying issues and research strategies. Journal of child Psychology and Psychiatry, 44(8), 1092–1115.
38. Zahn-Waxler, C.; Shirtcliff, E.A.; & Marceau, K. (2008) Disorders of child-hood and adolescence: Gender and psychopathology. Annual Review of clinical Psychology, 4, 275–303.
39. Pesquisa Nacional por Amostra de Domicílios. (2005) Maior população negra do país [Largest Black population in the country]. Available at www.seade.gov.br/produtos/idr/download/populacao.pdf, accessed June 1, 2011.
40. Instituto Brasileiro de Geografia e Estatística. (2000) Resultados da amostra do censo Demográfico 2000 [Sample results of the 2000 population census]. Avail-able at www.ibge.gov.br/home/estatistica/populacao/censo2000/default_tendencias .shtm, accessed June 1, 2011.
41. Achenbach, T.M. (1991) Integrative guide for the 1991 cBcL/4-18, YSR, and TRF profiles. Burlington: University of Vermont, Department of Psychiatry.
42. Achenbach, T.M., & Rescorla, L.A. (2001) Manual for the ASEBA school-age forms and profiles. Burlington University of Vermont, Research Center for Children, Youth, and Families.
43. Crijnen, A.A.M., Achenbach, T., & Verhulst, F.C. (1997) Comparisons of problems reported by parents of children in 12 cultures: Total problems, external-izing, and internalizing. Journal of the American Academy of child and Adolescent Psychiatry, 36(9), 1269–1277.
44. Bordin, I., Mari, J., Caeiro, M. (1995) Validacão da versão brasileira do Child Behavior Checklist (CBCL) (Inventário de comportamentos da infância e adolescên-cia): Dados preliminares. [Validation of the Brazilian version of the Child Behavior Checklist (CBCL) (Behavior inventory for children and adolescents): Preliminary data]. Revista ABP/APAL, 17(2), 55–66.
76 INTERNATIONAL JOURNAL OF MENTAL HEALTH
45. Rocha, M.M.; Araujo, L.G.S.; & Silvares, E.F.M. (2008) A comparative study between two Brazilian translations of the “Youth Self-Report” (YSR). Psicologia: Teoria e Practica, 10(1), 14–24.
46. Goodman, R. (1999) The extended version of the Strength and Difficulties Questionnaire as a guide to child psychiatric caseness and consequent burden. Journal of child Psychology and Psychiatry, 40(5), 791–799.
47. Goodman, R.; Renfrew, D.; & Mullick, M. (2000) Predicting type of psychiatric disorder from Strength and Difficulties Questionnaire (SDQ) scores in child mental health clinics in London and Dhaka. European child and Adolescent Psychiatry, 9(2), 129–134.
48. American Psychiatric Association. (2000) Diagnostic and statistical manual of mental disorders (4th ed., text rev.). Washington, DC.
49. World Health Organization. (1992) International Statistical classification of disease and related health problems (10th rev.). Geneva.
50. Moos, R., & Moos, B. (1994) Family environment scale manual: Development, applications, research (3d ed.). Palo Alto, CA: Consulting Psychologist Press.
51. Vianna, V.P.T.; da Silva, E.A.; & Souza-Formigoni, M.L.O. (2007) Portuguese version of the Family Environment Scale: Application and validation. Revista de Saúde Pública, 41(3), 419–426.
52. Koenig, H.G.; Meador, K.; & Parkerson, G. (1997) Religion index for psychi-atric research: A 5-item measure for use in health outcomes studies. American Journal of Psychiatry, 154(6), 885–886.
53. Weitzman, B.C.; Guttmacher, S.; Weinberg, S.; & Kapadia, F. (2003) Low response rate schools in surveys of adolescent risk taking behaviors: Possible biases, possible solutions. Journal of Epidemiology and community Health, 57(1), 63–67.
54. Carnoy, M.; Gove, A.K.; Loeb, S.; Marshall, J.H.; & Socias, M. (2008) How schools and students respond to school improvement programs: The case of Brazil’s PDE. Economics of Education Review, 27(1), 22–38.
55. Andreas, J.B., & Watson, M.W. (2009) Moderating effects of family environ-ment on the association between children’s aggressive beliefs and their aggression trajectories from childhood to adolescence. Development and Psychopathology, 21(1), 189–205.
56. Wallace, J.M., & Forman, T.A. (1998) Religion’s role in promoting health and reducing risk among American youth. Health Education and Behavior, 25(6), 721–741.
57. Wills, T.A.; Yaeger, A.M.; & Sandy, J.M. (2003) Buffering effect of religiosity for adolescent substance use. Psychology of Addictive Behaviors, 17(1), 24–31.
58. Hardy, S.A., & Raffaelli, M. (2003) Adolescent religiosity and sexuality: An investigation of reciprocal influences. Journal of Adolescence, 26(6), 731–739.
59. Kim, J. (2008) The protective effects of religiosity on maladjustment among maltreated and nonmaltreated children. child Abuse and Neglect, 32(7), 711–720.
60. Harden, K.P. (2010) Does religious involvement protect against early drinking? A behavior genetic approach. Journal of child Psychology and Psychiatry, 51(7), 763–771.
61. Nunnally, J.C. (1967) Psychometric theory. New York: McGraw-Hill. 62. Windle, M.; Spear, L.P.; Fuligni, A.J.; Angold, A.; Brown, J.D.; Pine, D.; et al.
(2008) Transitions into underage and problem drinking: Developmental processes and mechanisms between 10 and 15 years of age. Pediatrics, 121(4), 273–289.
Copyright of International Journal of Mental Health is the property of M.E. Sharpe Inc. and its content may not
be copied or emailed to multiple sites or posted to a listserv without the copyright holder's express written
permission. However, users may print, download, or email articles for individual use.




















