
Assessing the Generalization of Psychopathy in a Clinical Sample of Domestic Violence Perpetrators
16
Law Hum Behav (2006) 30:571–586 DOI 10.1007/s10979-006-9052-x ORIGINAL ARTICLE Assessing the Generalization of Psychopathy in a Clinical Sample of Domestic Violence Perpetrators Matthew T. Huss · Jennifer Langhinrichsen-Rohling Published online: 9 May 2006 C American Psychology-Law Society/Division 41 of the American Psychological Association 2006 Abstract This study proposed that domestic violence perpetrators in a clinical sample could be categorized into distinct subgroups and that a particular subgroup of batterers would exhibit suf- ficient psychopathic characteristics to be clinically meaningful. Participants were interviewed in order to gather a relevant social, familial, educational, criminal, and substance abuse his- tory. They were then administered several psychological measures including the Psychopathy Checklist: Screening Version (PCL:SV). Results lent support to the empirical batterer typol- ogy identified by Holtzworth-Munroe, A., Meehan, J. C., Herron, K., Rehman, U., & Stuart, G. L. (2000). However, despite the presence of a more antisocial subgroup, psychopathy did not consistently differentiate among batterers across the measured dependent variables. Keywords Psychopathy . Domestic violence . Batterers . Batterer typologies There has been an increasing focus on the heterogeneity of domestic violence perpetrators (Dixon & Browne, 2003). Although a number of different batterer typologies have been presented, in 1994, Holtzworth-Munroe and Stuart advanced the most widely accepted ty- pology in the literature. They proposed that domestically violent batterers formed three dis- tinct subtypes: family only, borderline/dysphoric and generally violent/antisocial. Holtzworth- Munroe and Stuart theorized that these three groups of batterers would be differentiated along dimensions of psychopathology, whether they committed generalized vs. partner-specific violence, and the severity and frequency of the partner violence they perpetrated. The family Funding from a National Institute of Mental Health Research Grant R03 MH058929-01, a Harry Frank Guggenheim Foundation Dissertation Fellowship, and a Creighton University Summer Research Fellowship supported portions of this research. M. T. Huss () Department of Psychology, Creighton University, Room 307 Hixon-Lied Science Building, Omaha, NE 68178, USA e-mail: [email protected] J. Langhinrichsen-Rohling University of South Alabama, USA Springer
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Assessing the Generalization of Psychopathy in a Clinical Sample of Domestic Violence Perpetrators

Law Hum Behav (2006) 30:571–586DOI 10.1007/s10979-006-9052-x
ORIGINAL ARTICLE
Assessing the Generalization of Psychopathy in a ClinicalSample of Domestic Violence Perpetrators
Matthew T. Huss · Jennifer Langhinrichsen-Rohling
Published online: 9 May 2006C© American Psychology-Law Society/Division 41 of the American Psychological Association 2006
Abstract This study proposed that domestic violence perpetrators in a clinical sample could becategorized into distinct subgroups and that a particular subgroup of batterers would exhibit suf-ficient psychopathic characteristics to be clinically meaningful. Participants were interviewedin order to gather a relevant social, familial, educational, criminal, and substance abuse his-tory. They were then administered several psychological measures including the PsychopathyChecklist: Screening Version (PCL:SV). Results lent support to the empirical batterer typol-ogy identified by Holtzworth-Munroe, A., Meehan, J. C., Herron, K., Rehman, U., & Stuart,G. L. (2000). However, despite the presence of a more antisocial subgroup, psychopathy did notconsistently differentiate among batterers across the measured dependent variables.
Keywords Psychopathy . Domestic violence . Batterers . Batterer typologies
There has been an increasing focus on the heterogeneity of domestic violence perpetrators(Dixon & Browne, 2003). Although a number of different batterer typologies have beenpresented, in 1994, Holtzworth-Munroe and Stuart advanced the most widely accepted ty-pology in the literature. They proposed that domestically violent batterers formed three dis-tinct subtypes: family only, borderline/dysphoric and generally violent/antisocial. Holtzworth-Munroe and Stuart theorized that these three groups of batterers would be differentiatedalong dimensions of psychopathology, whether they committed generalized vs. partner-specificviolence, and the severity and frequency of the partner violence they perpetrated. The family
Funding from a National Institute of Mental Health Research Grant R03 MH058929-01, a Harry Frank GuggenheimFoundation Dissertation Fellowship, and a Creighton University Summer Research Fellowship supported portionsof this research.
M. T. Huss (�)Department of Psychology, Creighton University, Room 307 Hixon-Lied Science Building,Omaha, NE 68178, USAe-mail: [email protected]
J. Langhinrichsen-RohlingUniversity of South Alabama, USA
Springer
572 Law Hum Behav (2006) 30:571–586
only batterers are largely free of psychopathology, commit the least severe partner violence andare unlikely to generalize their violence. Borderline/dysphoric batterers are characterized bydepression and anger, are likely to perpetrate more domestic violence than the family-only andare expected to commit some generalized violence. The generally violent/antisocial batterersare characterized by general antisocial features and greater substance abuse, the most severepartner violence, and the commission of violence both against the partner and against others.Holtzworth-Munroe and Stuart also delineated a different etiology for the violence perpetratedby each subtype of batterer and suggested that batterer treatment would be more efficacious ifit were subtype-specific. Perhaps as a result, the Holtzworth-Munroe and Stuart typology hasbecome the theoretical standard for batterer typologies (see Holtzworth-Munroe & Meehan,2004). Recently, this typology has even been expanded and applied to general criminal offenders(Stalans, Yarnold, Seng, Olson, & Repp, 2004).
Of particular relevance to the current study is the generally violent/antisocial subtype ofbatterer described by Holtzworth-Munroe and Stuart (1994). Generally violent/antisocial (GVA)batterers are expected to engage in more antisocial behavior, express more generalized violence,and perpetrate more severe violence as compared to the family only or the dysphoric border-line batterer. We have argued that there is a subgroup of especially violent criminal offenders(i.e., psychopaths) who exhibit characteristics similar to those ascribed to the generally vio-lent/antisocial subgroup of batterers by Holtzworth-Munroe and Stuart (1994) and others (seeHuss & Langhinrichsen-Rohling, 2000). For example, both GVA batterers and psychopaths arethought to constitute about 25% of their respective populations (i.e., domestic violence perpe-trators and prison inmates). Both groups also are expected to exhibit heightened familial andgeneralized violence, perpetrate more severe violence, engage in elevated rates of substanceabuse, show evidence of similar specific cognitive deficits such as a narrowed attentional focus,express controlled physiological reactivity, and are thought to exhibit a poor response to treat-ment compared to their peers (see Huss and Langhinrichsen-Rohling, 2000). After comparing theexpectations derived from disparate literatures across multiple constructs, we proposed that thegenerally/violent antisocial subgroup of batterers should exhibit sufficient levels of psychopathyto warrant the attention of clinical and legal professionals (Huss, Covell, & Langhinrichsen-Rohling, 2006; Huss & Langhinrichsen-Rohling, 2000; Spidel et al., in press). This notion hasnot been tested empirically, however. Thus, the purpose of the current study was to examineempirically the degree to which the Holtzworth-Munroe and Stuart three-subgroup batterer ty-pology would replicate in an outpatient clinical sample of batterers and whether psychopathiccharacteristics, as measured by a standard and well-accepted measure of psychopathy, exist in aclinical sample of batterers who presented for domestic violence treatment.
In 2000, Holtzworth-Munroe, Meehan, Herron, Rehman, and Stuart reported on their ownempirical testing of their theoretical model in a community sample of 102 men. They concludedthat there was empirical support for the existence of their three proposed batterer sub-groups;GVA (16% of the sample, more extensive criminal behavior and greater substance abuse);family only; and dysphoric/borderline. Surprisingly, however, their empirical data suggested thepresence of a fourth subgroup of batterers. They labeled this unexpected fourth group low-levelantisocial (LLA). Thirty-three percent of their total sample was placed into this group. The low-level antisocial batterers usually fell between the family only and the generally violent/antisocialgroups across the different descriptive dimensions. Most recently, a follow-up study completedby this same group demonstrated reasonable long-term (i.e., 1.5 to 3 years post initial assessment)consistency of the four groups (Holtzworth-Munroe et al., 2003). These data also showed thatbatterers who were classified as generally violent/antisocial or GVA, were the most likely tocontinue being violent which supported the clinical utility of this designation.
Springer
Law Hum Behav (2006) 30:571–586 573
Other researchers have also considered the validity of the original Holtzworth-Munroeand Stuart (1994) theoretically derived typology. These efforts have employed a variety ofmeasurement devices (e.g., Hamberger, Lohr, Bonge, & Tolin, 1996; Langhinrichsen-Rohling,Huss, & Ramsey, 2000; Lawson et al., 2003; Waltz, Babcock, Jacobson, & Gottman, 2000)and have typically found support for the three group solution theorized by Holtzworth-Munroe& Stuart (1994). However, there have been some inconsistent findings as well (i.e., Tweed &Dutton, 1998).
Evidence from these initial attempts at validating the Holtzworth-Munroe and Stuart (1994)typology reveals some variability in the number of subgroups of batterers (2–4) which emerge,minor differences in the characteristics of the delineated groups, and some variety in the measureswhich have been submitted to the statistical grouping procedures. However, there appears to bealmost universal convergence about the presence of one subgroup of batterers: a generally violent,antisocial group. However, the relative degree to which this group also exhibits features similarto psychopathic offenders has not been fully considered in previous samples of domesticallyviolent perpetrators. Initial attempts to determine the utility of assessing for psychopathy amongdomestic violence perpetrators and whether one group of batterers exhibited elevated clinicallymeaningful levels of psychopathy have some obvious limitations. For example, several of thestudies assessing domestic violence perpetrators have relied on a self-report measure (i.e., theSelf-Report Psychopathy Scale-II) to assess psychopathy in their samples of male batterers(e.g., Holtzworth-Munroe et al., 2000; Taft, Murphy, Musser, & Remington, 2004). Yet, the useof a self-report measure to assess psychopathy has been routinely criticized because a centralfeature of psychopaths is their ability to con and manipulate (see Rogers, Vitacco, & Jackson,2002).
There also is a relevant body of work that has examined the presence of psychopathy in malecriminal offenders who have a concurrent history of domestic violence. In contrast to studies inthe domestic violence literature, these studies have utilized the most widely accepted measure ofpsychopathy, the Psychopathy Checklist-Revised (PCL-R; Grann & Wedin, 2002; Hilton, Harris,& Rice, 2001; Kropp & Hart, 2000). However, these studies focused on criminal offenders with ahistory of domestic violence and not solely batterers. Moreover, it is more appropriate to use thePsychopathy Checklist: Screening Version (PCL:SV), rather than the Psychopathy Checklist-Revised in a clinical sample of batterers who are not otherwise in the criminal justice system(Hart, Cox, & Hare, 1995).
Therefore, based on previous literature, in the current study, we propose that three subgroupsof batterers will be identified via cluster analytic procedures. One of these subgroups is expectedto be analogous to the Generalized Violence/Antisocial batterer subgroup that has been found innumerous subtyping studies. It is expected that, consistent with the original Holtzworth-Munroe& Stuart (1994) theory and more recent empirical studies, this subgroup of batterers will compriseapproximately 25% of the total sample of batterers. It is also hypothesized that this subgroup:(1) will exhibit more frequent and more severe violence partner violence and general violence,(2) will be more likely to use and abuse alcohol and drugs, and (3) will report less depressionand more anger than the other batterer subgroups as Holtzworth-Munroe and Stuart (1994)originally theorized. Furthermore, we propose that there is a subgroup of maritally violent menwho exhibit sufficient psychopathic characteristics over and above simple antisocial behaviorto be clinically relevant. We expect that the majority of these men will have been originallyclassified as Generally Violent/Antisocial. Furthermore, we expect that batterers with highlevels of psychopathy will differ from batterers with low levels of psychopathy in the frequency,generalizability, and severity of their violence; regardless of the degree to which they exhibitantisocial behavior. This finding, if obtained, would support the clinical utility of assessing forpsychopathy within domestically violent perpetrators who are being treated in the community.
Springer

574 Law Hum Behav (2006) 30:571–586
Method
Participants
One hundred and thirty-one men who were either court-referred (59%) or self-referred (41%)for treatment as a result of partner assault participated in this study. This distinction representsa conservative delineation of court-referral because while 41% percent of the current samplewas not court referred, some of these men were referred to treatment by their attorneys anddid have pending legal issues because of domestic violence incidents that had not yet beenadjudicated. Participants were individuals seeking outpatient treatment for the perpetration ofdomestic violence against an intimate partner at a large public hospital that generally providedlow-cost services to the community. This agency provided a psycho-educational Duluth basedintervention that incorporated elements of cognitive-behavioral therapy. Participants were onaverage 35.53 years of age (SD = 9.76), had 12.0 years of education (SD = 1.97), and reportedan average income of $29,716 (SD = 18,192). Almost 85% of the participants were Caucasian,8.4% were African-American, 2.3% Hispanic/Latino, 3.1% Native American, and 1.5% were ofother races (not Asian-American). Forty-one percent (41.2%) of the participants were marriedand 91.6% were employed at the time of the intake evaluation. These demographics are similarto the general population in this Midwestern community.
Procedure
Upon referral, participants were interviewed in order to gather a relevant social, familial, educa-tional, criminal, and substance abuse history. This interview was a semi-structured interview asidentified in the manual for the Psychopathy Checklist-Revised: Screening Version (PCL:SV).The PCL:SV was used because it has been normed on less pathological populations, it has areduced administration and scoring time over the PCL-R, and it has high reliability and validity(see Hart et al., 1995). Collateral information for each man was obtained through several sourcesincluding but not limited to parole/probation reports, correctional records, mental health records,hospital records, and Child Protective Services reports. Upon completion of the intake interview,participants scheduled a 2-hour testing session to complete a series of psychological measures.
Measures
Psychopathy Checklist: Screening Version (Hart et al., 1995)
The PCL:SV consists of a semi-structured interview that lasts approximately 30–45 min. It isaccompanied by a collateral check of records, which takes about the same amount of time tocomplete. The PCL:SV contains 12 items that are scored on a 0–2 point scale but cover largelythe same content as the PCL-R. Several of the items dropped from the PCL-R (pathological lyingand shallow affect) overlap with some of the retained items (manipulative and lacks empathy).The PCL:SV also excludes items that are more difficult to assess (promiscuous sexual behaviorand parasitic lifestyle). In general, the PCL:SV has similar psychometric properties to the fullversion. The average internal consistency of the PCL:SV is .84 with a mean interrater reliabilityof .92. The mean weighted correlation between total scores on the PCL:SV and the PCL-R is .80.Interrater reliability in the current study was .82 for the PCL-SV. The interrater reliability wasidentified by selecting a random sample of 26 (20%) coded PCL:SVs, scored by the graduateresearch assistants, and comparing them with the first author’s coding of these same individuals.The two-factor structure of the PCL-R has also been found for the PCL:SV (Hart et al., 1995).
Springer
Law Hum Behav (2006) 30:571–586 575
The traditional two-factor structure is normally composed of an interpersonal/affective factor(Factor 1) that many argue represents the core of psychopathy and the more behavioral antiso-cial/deviant factor that is more similar to general antisocial behavior (Factor 2; Harpur, Hare, &Hakstian, 1989).
The Millon Clinical Multiaxial Inventory (MCMI-III; Millon, Davis, & Millon, 1997)
The MCMI-III is composed of 175 true-false items that form 24 clinical scales intended tomeasure both Axis I and Axis II disorders from DSM-IV (American Psychiatric Association,2000). The MCMI-III also contains validity scales (Validity Index, Disclosure Index, DesirabilityIndex, and Debasement Index). The first eleven scales are normal personality scales (Schizoid,Avoidant, Depressive, Dependent, Histrionic, Narcissistic, Antisocial, Aggressive, Compulsive,Passive-Aggressive, and Self-Defeating). The three other personality scales assess severe per-sonality disorders (i.e., Schizotypal, Borderline, and Paranoid). The ten clinical scales offerinformation on the presenting clinical problem and are highly dependent on current stressful sit-uations (Millon et al., 1997). These scales are divided into three indices of severe syndromes (i.e.,Thought Disorder, Major Depression, and Delusional Disorder) and the remaining seven includeAnxiety, Somatoform, Bipolar: Manic, Dysthymia, Alcohol Dependence, Drug Dependence,and Post-Traumatic Stress Disorder.
Alpha coefficients in past studies have ranged from .66 to .90 across the clinical scales of theMCMI-III, suggesting high internal consistency. Test-retest correlations have ranged from .82to .96 with a median stability of .91 across scales. In addition, high correlations with other testscores and clinical ratings have demonstrated the overall validity of the MCMI-III in previousresearch (Millon et al., 1997).
Conflict Tactics Scale-2 (CTS2; Straus, Hamby, Boney-McCoy, & Sugarman, 1996)
The CTS2 is a self-report measure that assesses the extent to which romantic partners engage inpsychological and physical violence and their use of noncoercive means to solve their conflicts.The CTS2 also includes an injury-related scale that assesses the extent of the injuries in a violentaltercation. Furthermore, the CTS2 differentiates between minor and severe psychological,physical, and injury acts. The internal consistency and reliability indices of the CTS2 haveranged from .79 to .95 in previous research (Straus et al., 1996).
Differences in the level of violence in the batterer’s relationships were examined with modifiedforms of the CTS2. The first version asked participants to respond regarding their most recentromantic partner, Conflict Tactics Scale for Partners (CTS-P). The second version asked theparticipants to make similar responses regarding their extended family, friends, acquaintances,and family members, Conflict Tactics Scale for Others (CTS-O). Responses on both the CTS-P and CTS-O were scored on a 5-point scale from 1 (very rare) to 5 (very frequent) on thefive subscales of the CTS-P (physical assault, psychological aggression, negotiation, injury, andsexual coercion) and the four subscales of the CTS-O (physical assault, psychological aggression,negotiation, injury). The sexual coercion subscale was dropped from the CTS-O because of arelative absence of reported instances of sexual violence against someone other than a romanticpartner. Items on each of these subscales were totaled to produce continuous scores for each ofthe subscales. Alpha levels for the subscales of the CTS-O and CTS-P ranged from .81 to .92 inthe current sample.
Springer

576 Law Hum Behav (2006) 30:571–586
Substance Abuse Subtle Screening Inventory-3 (SASSI-3; Miller & Lazowski, 1999)
The SASSI-3 is a self-report questionnaire that assesses the respondents likelihood of both al-cohol and substance dependence. It is composed of 10 total subscales. Two of these subscalesare identified as face-valid scales for alcohol (FVA) and drugs (FVD) and assess how frequentlyparticipants experienced particular situations related to substance use. There are also six subtlescales that consist of items that are less easily recognized as pertaining to substance use (ObviousAttributes (OAT), Subtle Attributes (SAT), Defensiveness (DEF), Supplemental Addiction Mea-sures (SAM), Family vs. Controls (FAM), and Correctional (COR)). There is also a subscale thatmeasures substance misuse symptoms (SYM) and a subscale that identifies random answering(RAM). Overall, the SASSI has been found to have a true positive rate of .94 and a true negativerate of .93 (Miller & Lazowski, 1999). Furthermore, the subscales of the SASSI have been foundto demonstrate acceptable internal consistency while having the ability to differentiate amongdivergent populations.
Multidimensional Anger Inventory (MAI; Siegel, 1986)
The MAI is a 38-item self-report instrument rated on a scale from 1 (completely undescriptive ofyou) to 5 (completely descriptive of you) assessing different aspects of anger: (1) Anger Arousal,(2) Range of Anger Eliciting Situations, (3) Hostile Outlook), (4) Anger-in, (5) Anger-out, (6)Guilt, (7) Brood, and (8) Anger-Discuss. Specifically, a scale like Anger-Discuss focuses onverbal discussion of issues to avoid or elicit anger. Siegel (1986) reports appropriate test-retestreliability (r = .75) and internal consistency for the subscales of the MAI (α = .51 to .83) andthe entire MAI (α = .89 and .84 for two separate samples). Its high associations with other angerand hostility measures have established the construct validity of the MAI. The alpha level forthe entire scale in the current sample was .95.
Beck Depression Inventory-II (BDI-II; Beck, Steer, & Brown, 1996)
The BDI-II is a 21-item measure in which the respondent must choose one of four possibleresponses for each item that suggest an increase in the severity of depressive symptoms. As aresult, scores range from 0 to 63. Meta-analytic studies of the BDI have found it to demonstrategood psychometric properties with high reliability and validity (Beck, Steer, & Garbin, 1988;Nietzel, Russell, Hemmings, & Gretter, 19871987). Studies using the BDI-II also have foundacceptable construct and convergent validity and a coefficient alpha of .91 for the BDI-II (Beck,Steer, Ball, & Ranieri, 1996; Steer, Ball, Ranieri, & Beck, 1997). The alpha level for the entirescale in the current sample was .94.
Data preparation
Though the PCL:SV manual recommends that individuals who score 18 and above on thePCL:SV should be assessed on the PCL-R and potentially confirmed as psychopaths (Hart et al.,1995), additional information suggested that given the less antisocial nature of this outpatientpopulation, it was unlikely that many participants would meet this stringent criteria. As expected,only one domestic violence perpetrator scored above 18 in the current sample. Instead, it wasrecommended that scores above 7 were meaningful for domestic violence perpetrators (R. Hare,personal communication April 10, 1999), although norms have not been published on thisspecific population (F. Dunford, personal communication April 13, 1998), Dunford has used
Springer
Law Hum Behav (2006) 30:571–586 577
the PCL:SV in a sample of batterers in the military (see Dunford, 2000 for a description of theoverall project and results) and recommended the use of 7 as a cut-off score based on his data.The dichotomization of PCL:SV scores using 7 as a cut-off resulted in 97 low psychopathybatterers and 34 high psychopathy batterers. This procedure appears to be in keeping with thePCL-R literature that uses cutoff scores (i.e., 25 or as low as 15; Seto & Barbaree, 1999) belowthat recommended in the PCL-R manual (i.e., 30) because of the utility of the lower thresholds.Overall, the sample yielded an average of 5.53 for a total score on the PCL:SV (SD = 3.84), 1.80(SD = 2.06) on Factor 1, and 3.74 (SD = 2.74) on Factor 2 of the PCL:SV.
There has been agreement about the general constructs to include in replicating theHoltzworth-Munroe and Stuart (1994) typology, but less agreement about the specific mea-sures that should be used to assess those constructs. Almost all studies have used scales fromthe MCMI, although some studies also have used the MMPI, but even among studies utilizingthe MCMI, there is not consistent agreement about which scales of the MCMI to use. As aresult, we utilized the empirical literature, current theory, clinical utility, and preliminary exam-ination of data from the current sample to establish the variables to include when creating thebatterer cluster groups. Holtzworth-Munroe et al. (2000) identify three dimensions, personality,partner violence, and generalized violence that are central to their theory. As a result we firstselected the physical violence scale of the CTS-P to assess violence within the relationshipand the physical violence subscale of the CTS-O to assess generalized violence in the pastyear. Because of significant skew in both scales, as would be expected (see Holtzworth-Munroeet al., 2000); we performed log transformations on all violence scales of the CTS-P and CTS-O.For easier comparison to previous studies, the uncorrected means are largely presented in thetext and tables. In selecting the personality/pathology measures to include we used scales fromthe MCMI-III. In keeping with our previous focus on the clinical utility of batterer typologies(Langhinrichsen-Rohling et al., 2000), we decided to utilize single scales from the MCMI-III tofacilitate use in practice settings. The Antisocial scale was first selected as the best true measureof antisocial behavior on the MCMI-III. Because of the criticism of the MCMI for item-overlap,we then examined the bivariate correlations between the additional scales under considerationfor inclusion (Borderline, Depressive, and Dependent). Results showed that the Antisocial andBorderline scales were highly correlated (r = .72) because these two scales share all but threeitems in common. In addition, we found significant correlations between Borderline scale andthe Dependent scale (r = .78) but not as strong a relationship between the Antisocial scale andthe Dependent scale (r = .48). As a result, we excluded the Borderline scale and selected theDependent and Depressive scales of the MCMI-III to include in the cluster analysis along withthe previously identified variables. Finally, all scores were standardized prior to entry in thecluster analysis as z-scores.
Results
Cluster analytic techniques
We chose Ward’s Method for delineating the batterer subgroups. Ward’s Method has beenwidely used in psychology (e.g., Langhinrichsen-Rohling et al., 2000), it has previously beenused to examine the batterer typologies (Holtzworth-Munroe et al., 2000), and it performs betterthan most other clustering methods (Blashfield & Aldenderfer, 1988). Ward’s Method attemptsto minimize within-Cluster variability and thereby produce clusters with very little variabilityamong the members. In general, hierarchical cluster analysis uses an algorithm in which a caseis assigned to a cluster for which the distance between the case and the center of the cluster (i.e.,
Springer

578 Law Hum Behav (2006) 30:571–586
centroid) is the least. Squared Euclidean distance is the distance measurement for the algorithm.This is a commonly used index of distance measurement, but it depends on the scale and units ofmeasurement for the variables to be included in the cluster analysis (Milligan & Cooper, 1987).When performing cluster analysis, there are also no clear rules for determining the appropriatenumber of clusters (Milligan & Cooper, 1987). Two criteria were employed to determine themost reasonable number of clusters in this study. First, the dendogram for the overall solutionwas examined. Second, the numbers of participants in each cluster were considered. Inspectionof the dendogram suggested that the three- and four-cluster solutions were most likely. Thefour-cluster solution appeared to be the most appropriate solution based on a review of thedendograms, cluster size, and current theory. In addition, it appeared that cluster homogeneitysignificantly decreased and explanatory power was lost with a three-cluster solution.1
Despite being one of the largest samples of batterers in the typology literature, the currentsample was insufficient to split for cross-validation. As a result, we followed similar proceduresto Holtzworth-Munroe et al. (2000) by using the cluster centers produced in the initial clusterin a K-means cluster analysis, to confirm the original cluster membership, setting it for 2, 3, 4,and 5 clusters. The 4 cluster solution best fit the data and resulted in 122 of the 131 batterersbeing placed in the same cluster for both analyses. In order to help maintain statistical power,we elected to keep the 9 batterers who were not classified in identical cluster groups in theseanalyses. For these 9 batterers, two independent raters examined their obtained cluster ratingson the individual variables, similar to the procedures of Langhinrichsen-Rohling et al. (2000).In all nine cases, the two raters independently placed each of the nine batterers into the samesubgroups. These groups also were in keeping with these batterers designation according to theoriginal Wards Method cluster solution.
Examination of cluster groups
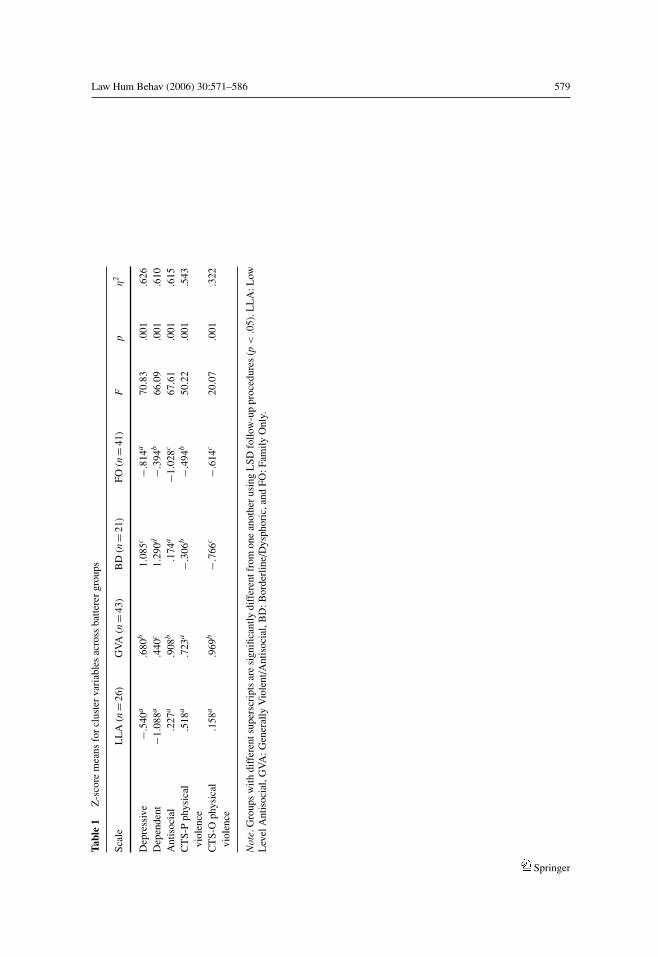
Statistical analyses revealed that the four obtained subgroups can be clearly distinguished fromone another on the basis of MCMI-III scores and batterer’s self-reports of their perpetration ofphysical violence within and outside the family. See Table 1 for an examination of cluster z-scoremeans and differences across the cluster variables, as statistically indicated by the multivariateanalysis of variance (MANOVA) results, F(3, 131) = 43.50, p = .001, η2 = .627. In order tobest interpret these groups, both the BR (base rate) scores of the MCMI-III (non standardizedmean scores are referred to in the text below for easier interpretation) and the z-score meansfor the MCMI-III (see Table 1 for Z-score means for all cluster variables) were examinedalong with scores on the CTS-P and CTS-O (see Table 1)2. Group four did not exhibit clinicalelevations on any of the MCMI-III scales3 and generally exhibited the lowest mean scores onthe MCMI-III. Though none of elevations rose to the level of a clinical disorder, group threeexhibited trait clinical elevations on the Depressive (M = 83) and Dependent (M = 80) scales ofthe MCMI-III and the group means were significant greater than the other three groups. Grouptwo exhibited trait clinical elevations only on the Antisocial scale (M = 76) and produced thehighest overall mean on the Antisocial scale of the MCMI-III. Similar to group four, group
1 In the three cluster solution, the LLA batterers were placed as a group in their entirety into the FO batterercluster. Given the clear distinctions between the LLA batterers and the FO batterers in the resulting analyses, itseems appropriate that they should be in different clusters.2 All independent measures (CTS-P, CTS-O, SASSI scales, BDI, and MAI) were correlated at less than r = .4with most correlations being well below r = .20.3 Authors of the MCMI-III recommend that BR scores of 75 indicate the presence of a particular trait while scoresof 85 indicate the presence of a particular disorder (Millon, Davis, & Millon, 1997).
Springer
Law Hum Behav (2006) 30:571–586 579Ta
ble
1Z
-sco
rem
eans
for
clus
ter
vari
able
sac
ross
batte
rer
grou
ps
Scal
eL
LA
(n=
26)
GV
A(n
=43
)B
D(n
=21
)FO
(n=
41)
Fp
η2
Dep
ress
ive
−.54
0a.6
80b
1.08
5c−.
814a
70.8
3.0
01.6
26D
epen
dent
−1.0
88a
.440
c1.
290d
−.39
4b66
.09
.001
.610
Ant
isoc
ial
.227
a.9
08b
.174
a−1
.028
c67
.61
.001
.615
CT
S-P
phys
ical
viol
ence
.518
a.7
23a
−.30
6b−.
494b
50.2
2.0
01.5
43
CT
S-O
phys
ical
viol
ence
.158
a.9
69b
−.76
6c−.
614c
20.0
7.0
01.3
22
Not
e.G
roup
sw
ithdi
ffer
ents
uper
scri
pts
are
sign
ifica
ntly
diff
eren
tfro
mon
ean
othe
rus
ing
LSD
follo
w-u
ppr
oced
ures
(p<
.05)
.LL
A:L
owL
evel
Ant
isoc
ial,
GV
A:G
ener
ally
Vio
lent
/Ant
isoc
ial,
BD
:Bor
derl
ine/
Dys
phor
ic,a
ndFO
:Fam
ilyO
nly.
Springer
580 Law Hum Behav (2006) 30:571–586
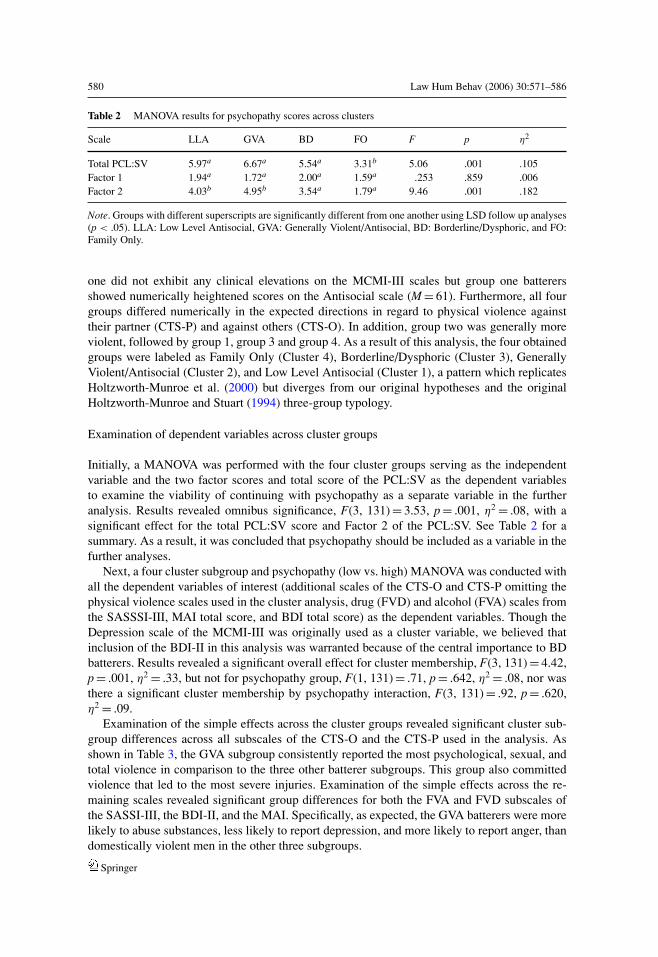
Table 2 MANOVA results for psychopathy scores across clusters
Scale LLA GVA BD FO F p η2
Total PCL:SV 5.97a 6.67a 5.54a 3.31b 5.06 .001 .105Factor 1 1.94a 1.72a 2.00a 1.59a .253 .859 .006Factor 2 4.03b 4.95b 3.54a 1.79a 9.46 .001 .182
Note. Groups with different superscripts are significantly different from one another using LSD follow up analyses(p < .05). LLA: Low Level Antisocial, GVA: Generally Violent/Antisocial, BD: Borderline/Dysphoric, and FO:Family Only.
one did not exhibit any clinical elevations on the MCMI-III scales but group one batterersshowed numerically heightened scores on the Antisocial scale (M = 61). Furthermore, all fourgroups differed numerically in the expected directions in regard to physical violence againsttheir partner (CTS-P) and against others (CTS-O). In addition, group two was generally moreviolent, followed by group 1, group 3 and group 4. As a result of this analysis, the four obtainedgroups were labeled as Family Only (Cluster 4), Borderline/Dysphoric (Cluster 3), GenerallyViolent/Antisocial (Cluster 2), and Low Level Antisocial (Cluster 1), a pattern which replicatesHoltzworth-Munroe et al. (2000) but diverges from our original hypotheses and the originalHoltzworth-Munroe and Stuart (1994) three-group typology.
Examination of dependent variables across cluster groups
Initially, a MANOVA was performed with the four cluster groups serving as the independentvariable and the two factor scores and total score of the PCL:SV as the dependent variablesto examine the viability of continuing with psychopathy as a separate variable in the furtheranalysis. Results revealed omnibus significance, F(3, 131) = 3.53, p = .001, η2 = .08, with asignificant effect for the total PCL:SV score and Factor 2 of the PCL:SV. See Table 2 for asummary. As a result, it was concluded that psychopathy should be included as a variable in thefurther analyses.
Next, a four cluster subgroup and psychopathy (low vs. high) MANOVA was conducted withall the dependent variables of interest (additional scales of the CTS-O and CTS-P omitting thephysical violence scales used in the cluster analysis, drug (FVD) and alcohol (FVA) scales fromthe SASSSI-III, MAI total score, and BDI total score) as the dependent variables. Though theDepression scale of the MCMI-III was originally used as a cluster variable, we believed thatinclusion of the BDI-II in this analysis was warranted because of the central importance to BDbatterers. Results revealed a significant overall effect for cluster membership, F(3, 131) = 4.42,p = .001, η2 = .33, but not for psychopathy group, F(1, 131) = .71, p = .642, η2 = .08, nor wasthere a significant cluster membership by psychopathy interaction, F(3, 131) = .92, p = .620,η2 = .09.
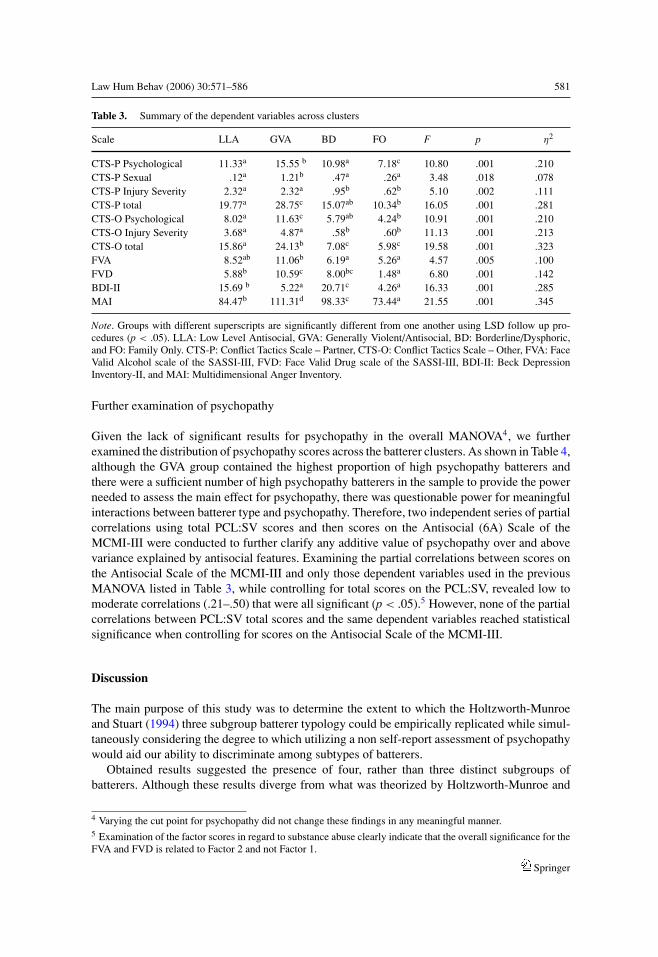
Examination of the simple effects across the cluster groups revealed significant cluster sub-group differences across all subscales of the CTS-O and the CTS-P used in the analysis. Asshown in Table 3, the GVA subgroup consistently reported the most psychological, sexual, andtotal violence in comparison to the three other batterer subgroups. This group also committedviolence that led to the most severe injuries. Examination of the simple effects across the re-maining scales revealed significant group differences for both the FVA and FVD subscales ofthe SASSI-III, the BDI-II, and the MAI. Specifically, as expected, the GVA batterers were morelikely to abuse substances, less likely to report depression, and more likely to report anger, thandomestically violent men in the other three subgroups.
Springer
Law Hum Behav (2006) 30:571–586 581
Table 3. Summary of the dependent variables across clusters
Scale LLA GVA BD FO F p η2
CTS-P Psychological 11.33a 15.55 b 10.98a 7.18c 10.80 .001 .210CTS-P Sexual .12a 1.21b .47a .26a 3.48 .018 .078CTS-P Injury Severity 2.32a 2.32a .95b .62b 5.10 .002 .111CTS-P total 19.77a 28.75c 15.07ab 10.34b 16.05 .001 .281CTS-O Psychological 8.02a 11.63c 5.79ab 4.24b 10.91 .001 .210CTS-O Injury Severity 3.68a 4.87a .58b .60b 11.13 .001 .213CTS-O total 15.86a 24.13b 7.08c 5.98c 19.58 .001 .323FVA 8.52ab 11.06b 6.19a 5.26a 4.57 .005 .100FVD 5.88b 10.59c 8.00bc 1.48a 6.80 .001 .142BDI-II 15.69 b 5.22a 20.71c 4.26a 16.33 .001 .285MAI 84.47b 111.31d 98.33c 73.44a 21.55 .001 .345
Note. Groups with different superscripts are significantly different from one another using LSD follow up pro-cedures (p < .05). LLA: Low Level Antisocial, GVA: Generally Violent/Antisocial, BD: Borderline/Dysphoric,and FO: Family Only. CTS-P: Conflict Tactics Scale – Partner, CTS-O: Conflict Tactics Scale – Other, FVA: FaceValid Alcohol scale of the SASSI-III, FVD: Face Valid Drug scale of the SASSI-III, BDI-II: Beck DepressionInventory-II, and MAI: Multidimensional Anger Inventory.
Further examination of psychopathy
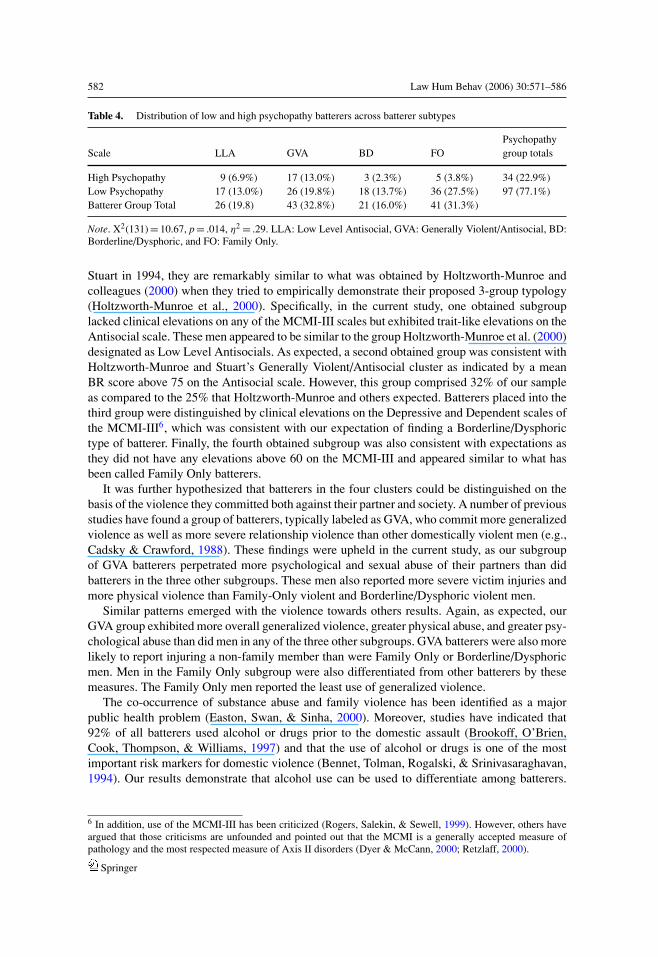
Given the lack of significant results for psychopathy in the overall MANOVA4, we furtherexamined the distribution of psychopathy scores across the batterer clusters. As shown in Table 4,although the GVA group contained the highest proportion of high psychopathy batterers andthere were a sufficient number of high psychopathy batterers in the sample to provide the powerneeded to assess the main effect for psychopathy, there was questionable power for meaningfulinteractions between batterer type and psychopathy. Therefore, two independent series of partialcorrelations using total PCL:SV scores and then scores on the Antisocial (6A) Scale of theMCMI-III were conducted to further clarify any additive value of psychopathy over and abovevariance explained by antisocial features. Examining the partial correlations between scores onthe Antisocial Scale of the MCMI-III and only those dependent variables used in the previousMANOVA listed in Table 3, while controlling for total scores on the PCL:SV, revealed low tomoderate correlations (.21–.50) that were all significant (p < .05).5 However, none of the partialcorrelations between PCL:SV total scores and the same dependent variables reached statisticalsignificance when controlling for scores on the Antisocial Scale of the MCMI-III.
Discussion
The main purpose of this study was to determine the extent to which the Holtzworth-Munroeand Stuart (1994) three subgroup batterer typology could be empirically replicated while simul-taneously considering the degree to which utilizing a non self-report assessment of psychopathywould aid our ability to discriminate among subtypes of batterers.
Obtained results suggested the presence of four, rather than three distinct subgroups ofbatterers. Although these results diverge from what was theorized by Holtzworth-Munroe and
4 Varying the cut point for psychopathy did not change these findings in any meaningful manner.5 Examination of the factor scores in regard to substance abuse clearly indicate that the overall significance for theFVA and FVD is related to Factor 2 and not Factor 1.
Springer
582 Law Hum Behav (2006) 30:571–586
Table 4. Distribution of low and high psychopathy batterers across batterer subtypes
PsychopathyScale LLA GVA BD FO group totals
High Psychopathy 9 (6.9%) 17 (13.0%) 3 (2.3%) 5 (3.8%) 34 (22.9%)Low Psychopathy 17 (13.0%) 26 (19.8%) 18 (13.7%) 36 (27.5%) 97 (77.1%)Batterer Group Total 26 (19.8) 43 (32.8%) 21 (16.0%) 41 (31.3%)
Note. X2(131) = 10.67, p = .014, η2 = .29. LLA: Low Level Antisocial, GVA: Generally Violent/Antisocial, BD:Borderline/Dysphoric, and FO: Family Only.
Stuart in 1994, they are remarkably similar to what was obtained by Holtzworth-Munroe andcolleagues (2000) when they tried to empirically demonstrate their proposed 3-group typology(Holtzworth-Munroe et al., 2000). Specifically, in the current study, one obtained subgrouplacked clinical elevations on any of the MCMI-III scales but exhibited trait-like elevations on theAntisocial scale. These men appeared to be similar to the group Holtzworth-Munroe et al. (2000)designated as Low Level Antisocials. As expected, a second obtained group was consistent withHoltzworth-Munroe and Stuart’s Generally Violent/Antisocial cluster as indicated by a meanBR score above 75 on the Antisocial scale. However, this group comprised 32% of our sampleas compared to the 25% that Holtzworth-Munroe and others expected. Batterers placed into thethird group were distinguished by clinical elevations on the Depressive and Dependent scales ofthe MCMI-III6, which was consistent with our expectation of finding a Borderline/Dysphorictype of batterer. Finally, the fourth obtained subgroup was also consistent with expectations asthey did not have any elevations above 60 on the MCMI-III and appeared similar to what hasbeen called Family Only batterers.
It was further hypothesized that batterers in the four clusters could be distinguished on thebasis of the violence they committed both against their partner and society. A number of previousstudies have found a group of batterers, typically labeled as GVA, who commit more generalizedviolence as well as more severe relationship violence than other domestically violent men (e.g.,Cadsky & Crawford, 1988). These findings were upheld in the current study, as our subgroupof GVA batterers perpetrated more psychological and sexual abuse of their partners than didbatterers in the three other subgroups. These men also reported more severe victim injuries andmore physical violence than Family-Only violent and Borderline/Dysphoric violent men.
Similar patterns emerged with the violence towards others results. Again, as expected, ourGVA group exhibited more overall generalized violence, greater physical abuse, and greater psy-chological abuse than did men in any of the three other subgroups. GVA batterers were also morelikely to report injuring a non-family member than were Family Only or Borderline/Dysphoricmen. Men in the Family Only subgroup were also differentiated from other batterers by thesemeasures. The Family Only men reported the least use of generalized violence.
The co-occurrence of substance abuse and family violence has been identified as a majorpublic health problem (Easton, Swan, & Sinha, 2000). Moreover, studies have indicated that92% of all batterers used alcohol or drugs prior to the domestic assault (Brookoff, O’Brien,Cook, Thompson, & Williams, 1997) and that the use of alcohol or drugs is one of the mostimportant risk markers for domestic violence (Bennet, Tolman, Rogalski, & Srinivasaraghavan,1994). Our results demonstrate that alcohol use can be used to differentiate among batterers.
6 In addition, use of the MCMI-III has been criticized (Rogers, Salekin, & Sewell, 1999). However, others haveargued that those criticisms are unfounded and pointed out that the MCMI is a generally accepted measure ofpathology and the most respected measure of Axis II disorders (Dyer & McCann, 2000; Retzlaff, 2000).
Springer
Law Hum Behav (2006) 30:571–586 583
Specifically, the GVA batterers consistently reported more severe alcohol and drug abuse acrossthe SASSI-3 scales with the FO batterers exhibiting the lowest levels of abuse. The LLA batterersand BD batterers generally fell between the GVA and FO batterers numerically with no statisticaldifferences between one another. These findings suggest that concomitant alcohol treatment maybe more beneficial for some subtypes of batterers. Future research will be needed to explore thisissue.
The four subgroups of batterers also differed in regard to their depressive symptoms,as indicated by their BDI-II scores. Not surprisingly, the borderline/dysphoric batterersscored the highest on the depression measures, followed by the GVA batterers. The FOand LLA batterers were statistically equivalent to one another and reported fewer depressivesymptoms.
The expected patterns also were obtained with regards to the self-reported expression ofanger. GVA batterers reported the most anger, followed by statistically significant differencesamong the BD, LLA, and FO batterers. It is worth noting that although LLA batterers reportedgreater levels of partner and generalized violence than did BD batterers, BD batterers reported,as expected, greater emotional dysregulation in the form of anger than did LLA batterers. Thispattern of findings is consistent with Holtzworth-Munroe and Stuart’s conjecture that there maybe different etiological processes underlying the violence of particular subgroups of batterers.
Overall, our results provide support the four batterer subgroup first empirically identifiedby Holtzworth-Munroe et al. in 2000. Furthermore, although Holtzworth-Munroe & Meehan(2004) expressed concern about the relative lack of empirical differentiation between GVAand BD batterers, our results support the notion that these two groups of batterers are dis-tinct from one another. However, it should also be mentioned that the available measureswere arguably the least consistent in support of a BD batterer group relative to our initialexpectations.
However, contrary to expectation, the results examining the utility of including a state-of-theart assessment of psychopathy failed to garner empirical support.7 Though the four clustersdiffered according to their scores on the PCL:SV and the number of high psychopathy battererspresent in each batterer subtype was found to differ as expected, there were no significantdifferences among the four groups on the interpersonal/affective factor (Factor 1) of the PCL:SV.This non-finding is important because many have argued that it is this factor, rather than Factor2 of the PCL, which separates psychopathy from antisocial behavior. Although there werestatistical differences among the four groups on Factor 2 and on total PCL:SV scores, thesefindings were almost exclusively driven by the reduced scores of the FO batterers on Factor2 compared to similar and significantly higher scores on Factor 2 by all three other batterersubgroups. Moreover, there were no significant differences between low and high psychopathybatterers across any of the relevant dependent variables. The potential limitation of reducedpower in regard to psychopathy as a categorical variable in the present sample should again beidentified. Results may be due in part to small cell sizes for low psychopathy batterers across thebatterer clusters. However, examination of psychopathy as a continuous variable revealed similarresults. The partial correlations between the dependent measures using PCL:SV total scores andtotal scores on the Antisocial Scale of the MCMI-III further clarify these results. Although itappears that psychopathy does differentiate the batterer subtypes in this sample, this may belargely a function of the antisocial component of psychopathy and not the Factor 1 characteristics.As a result, it is difficult at this time to recommend that clinicians spend additional time and
7 Using scores on the PCL:SV as a continuous variable in a series of regressions resulted in nearly identicalfindings. Clusters did not differ regarding their level of psychopathy.
Springer
584 Law Hum Behav (2006) 30:571–586
expense administrating the PCL:SV in a clinical outpatient sample of batterers. However, thesenon-findings may be due in part to the heterogeneity of psychopathy. Scholars are increasinglysuggesting that there are meaningful subtypes of psychopaths themselves (Skeem, Poythress,Edens, Lilienfeld, & Cale, 2003). As a result, it might be that individuals in a domestic violencesample will exhibit few of the primary features of psychopathy. Future research should explorethis possibility as an alternative explanation.
The obtained results also suggest possible differences in the predictive mechanisms associatedwith domestic violence and generalized violence within a clinical sample of batterers. These mayprovide fertile ground for future research. Psychopathy has been one of the most powerful, if notthe single most powerful predictor of continued violence across a variety of different samplesincluding general criminal offenders, sex offenders, substance abusers, psychiatric patients, menand women, adolescents, and in various countries throughout the world. Furthermore, there wasa great deal of overlap between the GVA batterers and many dimensions of psychopathy. Thus,while the present study may be one of the first to demonstrate a limitation of using psychopathyto explain violent behavior, it is also possible that the utility of measuring psychopathy is in itsability to predict response to treatment or recidivism. Longitudinal research will be needed toconsider this possibility.
In general, caution should be exercised when interpreting these findings as these results maybe somewhat sample-specific. The county that all the batterer-participants resided in during thestudy was mandated to refer all batterers to one specialized court, which was handling all thedomestic violence cases for that jurisdiction. It was observed that the presiding judge during theduration of this study consistently sentenced batterers with more extensive criminal histories tojail or prison rather than to outpatient treatment. As a result, it is likely that the current samplerepresents a less antisocial group of batterers than would normally be expected (i.e., restriction ofrange). Furthermore, there were some challenges using the PCL:SV with an outpatient sample ofbatterers. Many of the batterers did not have any contact with typical collateral sources (mentalhealth agencies, criminal justice involvement, probation/parole, Child Protective Services etc.)so although our efforts at obtaining collateral information were extensive, often times little mean-ingful collateral information could be obtained to score the PCL:SV. Instead, we had to rely uponcurrent testing results and batterer self-reports. As a result, psychopathy scores may have beensuppressed or at least influenced in some manner by the relative lack of collateral information.This is important because Factor 1 of the PCL:SV may be more sensitive to collateral informationdeficits than is Factor 2. It could also be argued because of the low split value between the high andthe low psychopathy batterers that there simply is not much going on at this level of the construct.Furthermore, the current study can also be criticized, as can many of the studies in the psychopa-thy literature, for relying on one measure of psychopathy and exhibiting a potential mono methodbias in using a version of the PCL. Nonetheless, taken as a whole, these results provide supportfor the existence of specific batterer subtypes within a clinical sample of domestically violentmen. The present results are the first to replicate Holtzworth-Munroe et al.’s (2000) four grouptypology. Moreover, they expand upon Holtzworth-Munroe et al. (2000) by examining a clinicalsample of batterers seeking treatment, rather than a recruited community sample. Though otherempirical examinations of typologies (Langhinrichsen-Rohling et al., 2000; Waltz et al., 2000)have identified three groups of batterers, this subtype solution may be too simplistic given theseempirical findings in conjunction with those obtained by Holtzworth-Munroe et al. (2000). TheLLA batterers were clearly differentiated on the relevant dependent measures from the FO batter-ers. However, it remains to be seen whether these statistical differences are clinically discernableand convey clinically relevant information about response to treatment or likelihood of futureabusiveness.
Springer

Law Hum Behav (2006) 30:571–586 585
Acknowledgments The authors would like to acknowledge the invaluable assistance of the administration andstaff of the BryanLGH Medical Center West, particularly Jodi Henning and Dave Miers. We also would liketo thank Stephanie Bruhn, Christmas Covell, Russell Palarea, and Mitch Sartin for their assistance in the datacollection and Travis Huss for his assistance with data entry.
References
American Psychiatric Association (2000). Diagnostic and Statistical Manual-IV Text Revised (DSM-IV TR).Washington, DC: Author.
Blashfield, R. K., & Aldenderfer, M. S. (1988). The methods and problems of cluster analysis. In J. R. Nesselroade& R. B. Cattell (Eds.), Handbook of multivariate experimental psychology (2nd Ed.) (pp. 447–473). NewYork: Plenum Press.
Beck, A. T., Steer, R. A., & Brown, G. K. (1996). Beck Depression Inventory-II Manual (2nd ed.). San Antonio,TX: Psychological Corporation.
Beck, A. T., Steer, R. A., Ball, R., & Ranieri, W. F. (1996). Comparison of Beck Depression Inventories-IA and-II in psychiatric outpatients. Journal of Personality Assessment, 67, 588–597.
Beck, A. T., Steer, R. A., & Garbin, M. G. (1988). Psychometric properties of the Beck Depression Inventory:Twenty-five years of evaluation. Clinical Psychology Review, 8, 77–100.
Bennett, L. W., Tolman, R. M., Rogalski, C. J., & Srinivasaraghavan, J. (1994). Domestic abuse by male alcoholand drug addicts. Violence and Victims, 9, 59–368.
Brookoff, D., O’Brien, K., Cook, C. S., Thompson, T. D., & Williams, C. (1997). Characteristics of participantsin domestic violence. Journal of the American Medical Association, 277, 1369–1373.
Cadsky, O., & Crawford, M. (1988). Establishing batterer typologies in a clinical sample of men who assault theirfemale partners. Canadian Journal of Community Mental Health, 7, 119–127.
Dixon, L., & Browne, K. (2003). The heterogeneity of spouse abuse: A Review. Aggression and Violent Behavior,8, 107–130.
Dunford, F. W. (2000). The San Diego Navy Experiment. An assessment of interventions for men who assaulttheir wives. Journal of Consulting and Clinical Psychology, 68, 468–476.
Dyer, F. J., & McCann, J. T. (2000). The Millon clinical inventories: Research critical of their forensic applicationand Daubert criteria. Law and Human Behavior, 24, 487–498.
Easton, C., Swan, S., & Sinha, R. (2000). Motivation to change substance use among offenders of domesticviolence. Journal of Substance Abuse Treatment, 19, 1–5.
Grann, M., & Wedin, I. (2002). Risk factors for recidivism among spousal assault and spousal homicide offenders.Psychology, Crime, & Law, 8, 5–23.
Hamberger, L. K., Lohr, J. M., Bonge, D., & Tolin, D. F. (1996). A large sample empirical typology of male spouseabusers and its relationship to dimensions of abuse. Violence and Victims, 11, 277–301.
Harpur, T. J., Hare, R. D., & Hakstian, A. R. (1989). Two-factor conceptualization of psychopathy: Constructvalidity and assessment implications. Psychological Assessment, 1, 6–17.
Hart, S. F., Cox, D. E., & Hare, R. D. (1995). The Hare Psychopathy Checklist: Screening Version, Toronto:Multi-Health Systems.
Hilton, N. Z., Harris, G. T., & Rice, M. E. (2001). Predicting violence by serious wife assaulters. Journal ofInterpersonal Violence, 16, 408–423.
Holtzworth-Munroe, A., & Meehan, J. C. (2004). Typologies of men who are martially violent: Scientific andclinical implications. Journal of Interpersonal Violence, 19, 1369–1389.
Holtzworth-Munroe, A., & Stuart, G. L. (1994). Typologies of male batterers: Three subtypes and the differencesamong them. Psychological Bulletin, 116, 476–497.
Holtzworth-Munroe, A., Meehan, J. C., Herron, K., Rehman, U., & Stuart, G. L. (2000). Testing theHoltzworth-Munroe and Stuart Typology. Journal of Clinical and Consulting Psychology, 68, 1000–1019.
Holtzworth-Munroe, A., Meehan, J. C., Herron, K., Rehman, U., & Stuart, G. L. (2003). Do subtypes of maritallyviolent men continue to differ over time? Journal of Consulting and Clinical Psychology, 71, 728–740.
Huss, M. T., Covell, C. N., & Langhinrichsen-Rohling, J. (2006). Clinical implications for the assessment andtreatment of antisocial and psychopathic domestic violence perpetrators. Journal of Aggression, Maltreatment,and Trauma, 13, 61–87.
Huss, M. T., & Langhinrichsen-Rohling, J. (2000). The identification of the psychopathic batterer: Clinical, legal,and policy implications. Aggression and Violent Behavior, 5, 403–422.
Kropp, P. R., & Hart, S. D. (2000). The Spousal Assault Risk Assessment (SARA) Guide: Reliability and validityin adult male offenders. Law and Human Behavior, 24, 101–118.
Springer

586 Law Hum Behav (2006) 30:571–586
Langhinrichsen-Rohling, J., Huss, M. T., & Ramsey, S. (2000). The clinical utility of batterer typologies. Journalof Family Violence, 15, 37–53.
Lawson, D. M., Weber, D., Beckner, H. M., Robinson, L., Marsh, N., & Cool, A. (2003). Men who use violence:Intimate violence versus non-intimate violence. Violence and Victims, 18, 259–277.
Miller, F. G., & Lazowski, L. E. (1999). The Adult Substance Abuse Subtle Screening Inventory Manual (2nd ed.).Springville, IN: The SASSI Institute:.
Milligan, G. W., & Cooper, M. C. (1987). Methodology review: Clustering methods. Applied PsychologicalMeasurement, 11, 329–354.
Millon, T., Davis, R., & Millon, C. (1997). MCMI-III Manual (2nd ed.). Minneapolis, MN: National ComputerSystems.
Nietzel, M. T., Russell, R. L., & Hemmings, K. A. (1987). Clinical significance of psychotherapy for unipolardepression: A meta-analytic approach to social comparison. Journal of Consulting and Clinical Psychology,55, 156–161.
Retzlaff, P. D. (2000). Comment on the validity of the MCMI-III. Law and Human Behavior, 24, 499–500.Rogers, R., Salekin, R. T., & Sewell, K. W. (1999). Validation of the Millon Clinical Multiaxial Inventory for Axis
II disorders: Does it meet the Daubert standard? Law and Human Behavior, 23, 425–444.Rogers, R., Vitacco, M. J., & Jackson, R. L. (2002). Faking psychopathy? An examination of response styles with
antisocial youth. Journal of Personality Assessment, 78, 31–46.Seto, M. C., & Barbaree, H. E. (1999). Psychopathy, treatment behavior, and sex offender recidivism. Journal of
Interpersonal Violence, 24, 1235–1248.Siegel, J. M. (1986). The Multidimensional Anger Inventory. Journal of Personality and Social Psychology, 51,
191–200.Skeem, J. L., Poythress, N., Edens, J. F., Lilienfeld, & Cale (2003). Psychopathic personality or personalities?
Exploring potential variants of psychopathy and their implications for risk assessment. Aggression & ViolentBehavior, 8, 513–546.
Spidel, A., Vincent, G., Huss, M. T., Winters, J., Thomas, L., & Dutton, D. G. (in press). Psychopathy: Subtypingperpetrators of domestic violence. In H. F. Herve & J. C. Yuille (Eds.). Psychopathy: Theory, research, andimplications for society.
Stalans, L. J., Yarnold, P. R., Seng, M., Olson, D. E., & Repp, M. (2004). Identifying three types of violent offendersand predicting violent recidivism while on probation: A classification tree analysis. Law and Human Behavior,28, 253–272.
Steer, R. A., Ball, R., Ranieri, W. F., & Beck, A. T. (1997). Further evidence for the construct validity of the BeckDepression Inventory-II with psychiatric outpatients. Psychological Reports, 80, 443–446.
Straus, M. A., Hamby, S. L., Boney-McCoy, S., & Sugarman, D. B. (1996). The revised Conflict Tactics Scales(CTS2): Development and preliminary psychometric data. Journal of Family Issues, 17, 283–316.
Taft, C. T., Murphy, C. M., Musser, P. H., & Remington, M. A. (2004). Personality, interpersonal, and motivationalpredictors of the working alliance in group cognitive behavioral therapy for partner violent men. Journal ofClinical and Consulting Psychology, 72, 349–354. 349–354.
Tweed, R. G., & Dutton, D. G. (1998). A comparison of impulsive and instrumental subgroups of batterers.Violence and Victims, 13, 217–230.
Waltz, J., Babcock, J. C., Jacobsen, N. S., & Gottman, J. M. (2000). Testing a typology of batterers. Journal ofConsulting and Clinical Psychology, 68, 658–669.
Springer




















