Meshoil language description - Adelaide Research & Scholarship
Upload
khangminh22Category
view
0download
0
THE EMERGENCY CARE
OF
ROAD CRASI"I VICTIMS
P. D. Clark, M.8.,, B.S. (Adelaide, 1967)
A Thesls presented for the degree of Doctor of Medlcineln the Universlty of Adelalde, based on a sfudy conducted
in the Departmenf of Social and Preventive Mediclne,Monash Universlty, Melbourne, Vicforla, and supporled by
the National Health and Medical Research Counci I of Austral ia.
SubmíTted May, 1972
CONTENTS
tt
Page
vl
lx
x
1
33
1216l62328
63646467676969737475767980
Summary
Dec larat ion
Acknow I edgements
Chapter I INTRODUCTION
Chapter 2
Chapter 5
HISTORICAL OUTLINE AND REVIEI,ll OF THE LITERATUREThe Development of Emergency ServlcesCrash lnjury Studies in AustraliaSludies of Emergency Servlces
Ambu I ance ServicesHospital Casualty DepartmentsEmergency Care System Studles
THE STUDY BACKGROUND
Stafement of the ProblemThe Emergency Care Sysfem ln Melbourne
Obj ecf i vesE I ements
The General PublicTowi ng ServicesPol iceThe Fire BrigadeThe Ambulance Servíce
Descriptlve Model
THE STUDY OEJECTIVES
THE STUDY METHOD
The Study Design: Phase OneEmergencies in MelbourneThe Sample AreaThe Sampl ing ScheduleSelection of lhe CrashesOperatlon of the Research Team
The Study Design: Phase TwoThe Samp I i ng Schedu leSelectîon of Sludy PatientsData Col lection Methods
Data Recording and ProcessingDefínitions
393941
4243434343444452
61Chapler 4
Chapter 5
ilt
85Chapter 6
Chapler 7
THE CRASHES, THE PATIENTS AI.ID THEIR INJURIESPhase One:
The CrashesThe PatientsPatterns of lnjurySeat BeltsAlcohol
Phase Two:The PatlentsPatlerns of I nJurySeal BelfsAlcoholThe CrashesVal idity of the SampleThe Quesfionnaire Sample
OPERATION OF THE EMERGENCY CARE SYSTEM IN I,4ELBOURNEThe Communications Subsystem:
Crash Detection and NotífícatlonAmbulance DispatchCommunications during Ambulance ServiceCommunications between Hospitals and lhe
Ambulance ServlceCommunications withi n Hospifa I
The Transport Subsystem:Response of fhe Emergency ServicesProtection al the Crash SceneAmbulance TransporfLift¡ng and Moving fhe lnjuredTime Delays during Ambulance Service
Trave I T imeTlme at SconeTransport TlmeAmbu lance Response TimeTrealmenf and Transport TimeAmbulance Service Time
The Treatment Subsystem:Care beforo Hospital
First Aid at the SceneAmbu lance Care
Care in CasualtyTr i ageIreatment ProceduresIreatmenl De I ays
Reception TlmeNursing Assessmenf DelayWaifing Time to See a Medical
0ff i cerX-Ray Service TlmeObservation and Treatment TimeTolal Casualty Treafment Time
B989919292939B
101
83858687B8
101103105
110113
n5118120121123124124125126127128
129129130134134135139140140
141143145146
Chapter 7 (Contd. )
The Documentatlon Subsystem:Crash Data CollectionAmbu lance RecordsCasua I ty Documental i on
Chapler I EVALUATION OF THE EMERGENCY CARE SYSTEMOutcomes of CareThe Slrucfure of CareThe Care Process
Time Delays in the Emergency Care System:The Significance of Tíme DelaysThe Observed Time DelaysWaifíng Times in Hospltal Casualty
DepartmentsThe Effects of Alternative Patterns of
Ambulance Servíce on Time Delays
The Qual îty of Emergency Medical Care:Standa rdsThe Method of EvaluationThe Quality of Care for the Phase One
Paf i entsThe Qual ify of Care for the Phase Two
Patients - comprising:Ihe Histony and PhysieaT EnønínøtionIhe Tneahnent Penformed:
Int ensío e Re sus eitationfntnauenous IhetapyFnaettpe MannganentWounå Manngement
Ihe SuaLitA of CasuaLty CaneReLíabiLíta of the AssessmentePatients' Attítttdee to CareSwrmaz,y
An Analysis of Patterns of Casualfy Servlcefor Road Crash Victlms
ïhe Technique of Simulated Sampl ingSimulaÌion of fhe Observed Sysïem
A lms of the S imu laf ionThe S imu lat ion Mode I
D i scuss ionConclusions
CONCLUS IONS AND RECOÍ\4MENDAT IONSCommunicationsTransportDocumentaf ionTreatmentSumma ry
iv
148t48152
155155158162163163164
166
168
171172
174
17A179
185187192195202205206212
212213215219219225225
228229231233235238
Chapter 9
Appendix 1 TABLES
Appendix 2 AMBULANCE EQUIPMENT LtST
Appendix 3 EMERGENCY CARE SysTEJvt sTUDy coDEs
Appendix 4 QUESTIONNAIRE
Bibl iography
Appendix 5 TREATMENT DELAYS BY TIME 0F I,rIEEK
v
239
251
25t
268
270
286
V¡
SUMMARY
The lhesis describes the findings of a study conducted by a
research team, consisting of Dr. G. A. Ryan and lhe author, from fheDepartmenl of Social and Preventive Medicine, Monash Universíty,l4elbourne. The aim of the study u¡as to descrlbe and evaluate theopenation of the emergency care system in Melbourno.
The study was conducted ín two distinct phases. ln fhe firsfphase the research feam attended the scene of 100 road crashes ln a
selected metropol itan area. Delai ls of fhe crashes, the operatíon ofthe omergency services, and the care provided for the 310 persons
involved in fhe crashes, wore observed and recorded by the fwo
researchers. Pallenls who required hospital trealment were fol lowed
to the hospital and observed untll their dlscharge from fhe casualtydepartment. ln the second phase, the author observed the care pro-vided Íor 328 crash victims during fheir frealment in lhe casualfydepartment of a major Melbourne feaching hospífal. This phaso of thestudy was designed to investigate in greater detai I the performance
of emergency care within the casualty department.
ln the thesis a systems approach is used to describe theemergency services and the care provided at the crash scene, duringambulance care, and in the hospital casualty department. Care beforehospital is compared with that provlded in the casualfy department,
using the time delays ln the varlous freatment phases and the qualityof the treafment performed as varíables for evaluafing performance inthe omergency care system.
Deficiencies dotocted in the system included poor communication
betwoen ambulance and casualty staff members, the lack of an effectlvedocumentation subsysfem for recording posf-crash dafa, and defects lnthe provisions for patient safety and comfort during transport.
vi¡
Ïhe major time delays during treatment occurred within fhehospltal casualty department. lt was observed that the median elapsedtime for ambulances to reach the crash scene affer the service was
notif ied was 12 minutes with a median delay oÍ 25 minutes from receiptof thc notification cal I untî I patients reached hospital. Afterarriving in hospital the median waiting time to see a doctor was 17
minutes, just eight minutes less than-lhe total elapsed tlme duringlhe ambulance cal l. 0n the average, study patients spenf approximatelythree hours in receiving casualfy treatment.
Deficiencies were found in the qual ity of the lreatmenfprovided in the casualfy deparfmenT. Major discrepancies were observed
belween the care provided and fhat expected on the basis of fhenormative standards for the managemenf of road traffic casualtiesdefined by the Royal Ausfralasian Col lege of Surgeons. Less than
21, oÍ patients received care commensurable wlih these standards.Ïhirfeen per cenf of patients were assessed by the observers as receivlngunsatisfactory casualty treatment. ln contrasf, the differences befween
the standards for ambulance care and the care acfually performed were
less marked, wifh approximately 6% of patienfs receîving care thaf was
assessed as unsatisfactory.
Many of the emergency care sysfem problems are problems oforganization and managemenf. As such, they lend themselves to operationsresearch analysís and, in the f inal section of the thesis, a simulationmodel is used to demonstrate the applicability of these lechniques tothe problems under study. Data collected during the study are used as
inpufs for the model and the cffects of two changes in casualty depart-menf operafions are examined.
The study, which is lhe first of its kind fo be conducted inAustral ia, contributes to knowledge by descríbing and documentíng the
vl¡l
operat¡on of the emergency care system and demonstrating the confrlb-utions of fhe separafe omergency services to the overalr systemperformance. The major conclusion drawn is that important deflclenciesin the emergency care system occur durlng care wilhin hospital casualtydepartments. lt is recommended that planners of emergency servlcesshould consider care within the casualty department when plannlng changes
in fhe exlsting system.
ix
DECLARAT ION
This thesis is my own composition and fho work thereln
has nof been presented for the award of any other Degree in this
or any other University.
P. D. CLARK
X
ACKNOWLEDGEMENTS
The firsf phase.of Ìhis study was planned and direcled byDr. G. A. Ryan who, as leader of fhe research team, assis-led wifh thecollection and analysis of the data. H¡s advice, guldance andsupervlsion were invaluable throughout bofh phases of the sÌudy.
Professor B. S. Hetzel and o1'her members of the Departmentof Social and Preventive Medicine. Monash University, gave help andadvice on many occasions. Dr. Tony McMichael wrote many of thecomputer programs and Dr, Graeme 0l iver advised on statistical andprogramming problems. Mr. Steven Lazarus, of the Department ofEconomics, Monash University, derived lhe model used in the simulafionsludy and assisted with the calculations and analysis of the results.
The study could not have been performed without the co-operatlonof the Hospitals and Charilies Commission of Vicforia and the boards ofmanagement and employees of the Victorian CÌvi I Ambulance Service,Alf red llospital, Prince Henryrs Hospilal and the Box Hi ll and DistrictHospital. ln particular, I am indebted to Mr. Gordon Ortmann, thechief executive officer of the Vicforian Civi I Ambulance Service, forhis help on meny occasions and to the many staff members of the casualtydeparlments of the hospitals who lolerated a redundant docfor wilhoutreal ly understanding what he was doing.
Mrs. Dorothy Chappel l, Dr. Gabor Kovacs and Mr. Shane Fennessyassisted on many occasions wilh preparation of lhe research matorial.Sandra, ffiy wife, assisted with preparalion of the manuscript and sufferedlhe rigorous sampl ing schedules used in lhe study.
The study was supported by fhe National Healfh and MedicalResearch Council of Ausfralia, with the aulhor wcrking as a postgraduatescholar of -lhe Council.
Finally, I wish lo acknowledge the assistance of Dr. David Dqntand Dr. Tony Ryan, who read and criticised -lhe manuscripl.
xl
,The
adequnte eare(1)
(2)
(3)
(4)
abiT.ity of any ønbuLanee sertsiee to giue pronpt and.to and transportation of the iraju.t,ed depends on:-Effieient eo¡nrntnícatíon beü¡een eontrol anå. ønbuLances.
Suffieient ønbuLanees positioned ín eueh a,lnaA that onLyshort distanees mtst be eoüeyed from eaLL to píek up.Adequate nwtbens of traíned staff to deal uíth theaecídent uictíms.Effíeient first aíd en route. I
(4. Howard Toyne, President,Victorlan Civi I Ambulance Service, 1970)
tThe Casunlty Departrnent nendere a seyuiee to the eomnunítyoultase funetion may be diuided into a series of separate actiuities:-
(1) Ebornpt reeeption, doeumentation and, transfer of patientsfrom the qnbu\anees and uaLking entnanees to theirappnopríat e destinøtíon.
( 2) Pnoyp-t eæønination, app"opz.íate speeíaL inuestigationsand díagnosis of the eondit.ion oi eondítions.
(3) Pronpt and adequate treatment uheyaobsen)atíon if neeessqrA and speedyrequåned destination.
appnopriate,díspateh to the
Ihe department shouLd be regæded as a uard of the hospí,taL. l
( I nsfructions for Casua lty Resl denfs,Alf red Hospital, Melbourne, 1969)
O,t¡
Chapfer 1
I NTRODUCT ION
A steady lncrease in the number of víolent and accidentaldeafhs in recent years, combined with an ahrareness of fheir causes and
cosfs, has led many people to express concern about the adequacy ofemergency services and their faci I lties. An important factor con-tributing to this sítuation has been the prevalence and severlty oflosses due to motor vehlcle crashes.
ln 1969, 31502 people dled on Ausfralian roads as a resulf ofnotor vehicle crashes and a further 87,864 were injured. ln theMelbourne statlstical divlsion, one area of which was studied in thisresearch project, 548 persons wore killed and 16,196 injured in 11,739casualty accldenfs in the same perlod. (Commonwealth Bureau of Census
and Statislics, 1970.)
The load which fhis epidemic of traumatic injury places upon
The emorgency care syslem is one of many factors whlch have caused
concern over the operation of the sysfem in general, and ambulance
servlces and hospital casualfy departments in particular. Cases ofrunnecessary? death at the roadside, delay in ambulance service, and
deficiencies ln lroatment have received comment in fhe public press and,occasionally, f rom medical personnel. ln Australia, the problems ofhospítal casualfy departments have remained comparatively free from
crilical investigation. The population tends lo accept the long waitlngtimes and discomfort, which accompany casualty and outpatient care lnhospltals, as an inevitable part of receiving what is often lhought tobo the best medícal care.
ln 1959 fhere were 15,266 casualty admisslons to fhe AlfredHospltal in Melbourne, of which 1,458 were traf f ic crash victlms.(Hocking, 1962.) By 1969 +hls figure had risen to 46,997 adnisslons
")
2
tv¡th f,788 crash víctlms (Alfred Hospltal, 197ü. An important aspectof this growth in fhe overall numbers of caeualty attendances has been
the use of the department by non-emergency patienfs seeklng prlmarymedical care. This addif ional load has major lmplicallons for- theemergency services. The consumers of emergency medical cane, fhepafients, are confronted wlth increased waiting and treatment timeswhich, apart from the inconvenience they generate, may affect theirconditíon and treatment. Administraflve and sfaffing problems arecreated by the overloading of avallable f acil¡+les, and the abi lity ofthe avaí lable staff to handle the work load decreases proportfonately.
Several authors have suggested thaf deficiencies in emergency
services may exist, but there have been relatively few atfempts toidentify and evaluate those deflcîencies. Vlews have been expressed on
the desirability of improvements in patienf care from the scene of fhecrash to and through the casualty department. Standards for ambulance
vehîcles, their equlpment and operaf lon, ancj the operation, f aci litíesand staffing of casualty departments have been examined by commitfeesin the uniled Kingdom and the u.s.A. ln Australia, the managemenl ofroad traffic casualties was fhe subJect of a seminar held by the Royal
Australasian college of surgeons in 1969. ln 1971, the Expert Group on
Road Safety of the commonwealth Department of shipping and Transportincluded a review of emergency services in a detailed investlgatlon ofthe state of road safety in Australia. There has been li+fle workdocumenting what actually happens at the scene of the crash and durlngsubsequent emergency care, to define the exisfing system and ldentifythose areas of it which may warrant closer investigation and subsequent
npdification.
This lhesis relates the findíngs of a study which was designedto descrlbe the operation of the emergency care system in an area ofMelbourne and lo evaluate the quality of care provided for a group ofroad crash victims,
3
Chapter 2
HISTORICAL OUTLINE AND REVIEI{ OF THE LITERATURE
THE DEVELOPI4EN.T OF EMERGENCY Í\4EDIC,qL SERVICES
Among 'the earl iest recorded descrlpf ions of organized medical
services are those relating fo Roman milîlary medicine. ln Roman times
a syslem of emergency cðre evolved with medici providing firsl ald forwounded in the field. (Nutton, 1969.) Severoly injured victims wero
evacuated to ualetu&inaria, the hospilals which were establ ished in
stralegic positions as the armies advanced. Expeditionary armies
returned lo Rome carrying their sick and wounded and if became a mark
of palriolism among lady patricians to establ ish temporary hospitalsln fhelr houses, in which casualties were nursed and treated.
With the decline of lhe Roman Empire and the spread ofChristianity, thescr houses opened their doors to lhe sick and suffering,and tho system of Christian hospiTals evolved. Ihe hospitals were
staffed by i-he various monastic and other Orders which sprang up during
the mediaeval period. (Poynter & Keele, 1961.) Among these Orders was
a group of Benedictlne monks who served în hospìlals ín Jerusalem. This
Order treated many of the Crusaders and, after the capture of Jerusalem
in 1099, acquired the monastery of St. John fhe Baptîst in Jerusalem.
St. John was adopted as lhe Patron Saint of the Order, which was recog-
nized by the Pope in 1113. Subsequently throughoul the succession ofholy wars between Chris'fians and Moslems, the activities of tho hosplt-allers of the Order were closely associaled with charilable and nursing
functions. An English tongue of the Order developed in London, buf fhe
dissolulion of the monasleries which fol lowed the quarrel between Henry
Vlll and the Pope saw the end of the activities of the Order in England
in 1540. (Ronwick & hlilliams, 1969.)
Religious wars in the sixteenth an<j seventeenlh centuriesprovided surgeons of the time with ample experience in wound treafmenT.
Notable advances in techniques of surgical repair and the alleviaffon of
t\
ì
ê
ra
a
,ù
t)
Z1\v,,
l .f!
I
..-¡.! J
I II
-
-t4t'rl
Larrey's 'Flyi ng Ambul ance ' (tlgZ)
4
suffering fol lowed the work of such surgeons as Ambrose Paré. Neverfhe-
less, developments in lhe organizalion of emergency servlces were few and
were restricted to lhe bafllefiolds. (Singer & Underwood, 1962.)
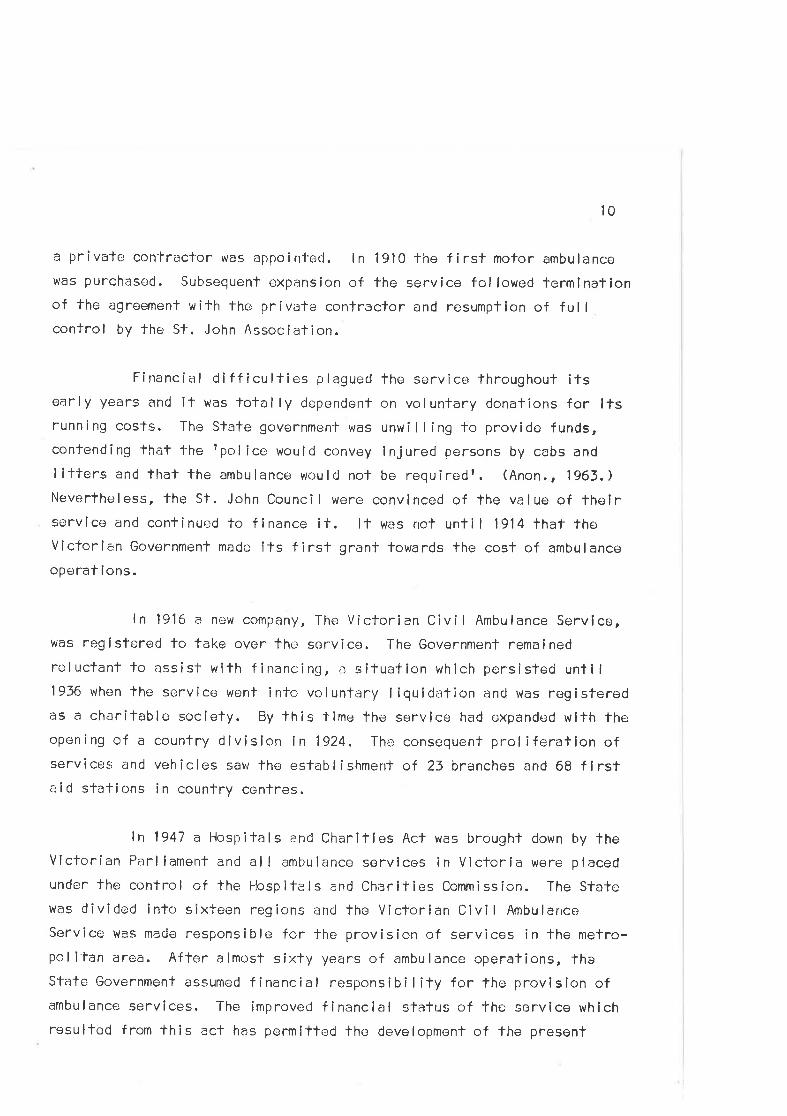
One of the greafesf mi I itary surgeons was Dominique Jean
Larrey who, after his appointment as a surgeon major ln lhe Army of the
Rhine in 1792, introduced the use of I ighf-weight, horse-drawn ambul-
ances to evacuale the wounded from -lhe battlefield. The Baron Percy, a
contemporary of Larrey in Napoleonts army, lrained a corps of lifterbearers who gathered patients from the front lines and transported them
to surgical aid posts. (McKenny, 1967,)
Other armies were slow to recognize the developments in
emergency service¡s initiated by the French. ln the United States, forexample, there was no effecf ive system for handling casualties at the¡
outbreak of the Civil frlar in 1861 . ln late 1862, Major Jonathan
Letterman, a medical officer in the Army of the Potomac, devised a plan
for an organized ambulance corps which was so practical that it has
formed the b¿¡sis for subsequent ar,'ny f ield medical services lhroughout
the world. Leltermanrs complete syslem was first employed at Fredericks-
burg on December 13, 1862. Approximately ten lhousand wounded were re-moved from the battlefield and shellered within twelve hours. (Key,
1968. ) Ambulances were used duríng thís war, initial ly two and four
wheeled horse-drawn types and, later, the I ight-weight Rosencrans ambul-
ance, capable of carrying either len seated patients or two sitling and
two rec I i n i ng pat i ents. (McKenny, 1967 . )
Significant advances in care of lhe wounded fol lowed the work
of iJenri Dunant, v,/ho, appalled by the suf fering he wifnessed at the
Batlle of Sclferino in 1859, was responsible for the foundation of the
Red Cross and the organizalion of lhe Geneva Convention of 1864. Ïhe
St. John Organization had been revived in England in 1831 but it was not
until the 1870ts that the first aid work of lhe Order recommenced. ln
5
Europe, Friedrlch von Esmarch foundod the Samarltan Movement, and
Jarom i r Fre i herr von lrlundy the V iennese Vo I untary Rescue Soc iety.( Fi scher-Homberger, 1 971 . )
The development of these services was the result of several
faclors. The pressures of war and its effects, 1'he humanitarian approach
of particular individuals and the social and spirifual climate of the
lime all conÌribuled to the cJevelopmenl of civilian hospltal and
emergency care services.
Systems of care evolved according to the patlerns of health
and hospÌtal service in the separate countries. ln Europe, first aid
and rescue Services were regarded as an additional duty for lhe Fire
Brigade and as early as 1877 fire fighting organieations included firstaid as parl of lheir service in Germany and Switzerland. ln Germany in
the lBBOts insurance organizatlons establ ished a network of remergency
stationsr for the treatment of insured and non-insured citizens' This
development led, preclictably, to clashes, based on pol itical, economlc
and ethical grounds, with The medlcal profession which, fortunately,wero soon resolved. The present system of Accident Hospital s ln Austria
was founded by Bôhler in conjunction with the compulsory accident insur-ance company in 1925. (Böhler, 1965.)
The first accldent service in Britain was organized by Robert
Jones during lhe bui lding of fhe Manchester Ship Canal. The service
consisled of a chain of f irst aid stations with fhree base hospitals
strategically placed along thc waterway. The importanl feature of thisunif ied organization was that it became possible to treat the ln.jured
v¡ithout undue delay. (Platt, .l969. ) Ambulance services in Britaindeveloped under the auspices of the St. John and St. Andrewfs Ambulance
Associations, staffecJ mainly by voluntary workers, who provided treat-ment for lhe sick and injured before fransporting them to the major
hospitals which had developed.
6
Throughoul the twenlíelh century significant developments in
lhe management of trauma have conlinued to follow medical experience in
war. The Flrst World War saw advances in wound care associated with thedevelopment of plastic surgery and the acceptance of the principles ofsplInling fraclures at the scene. Little atfention hacl been paid to themanagemenl of shock t¡efore the war but the value of blood transf uslon
was established al that lime. (Cave, 1968. ) ln Vlorld War ll lhe valueof resuscilaTion ín the r.ìanagement of shock was recognized and methods
of trealing major injuries were refined. Further improvemenfs in
surgical techniques resulted from experience in Korea and Vietnam.
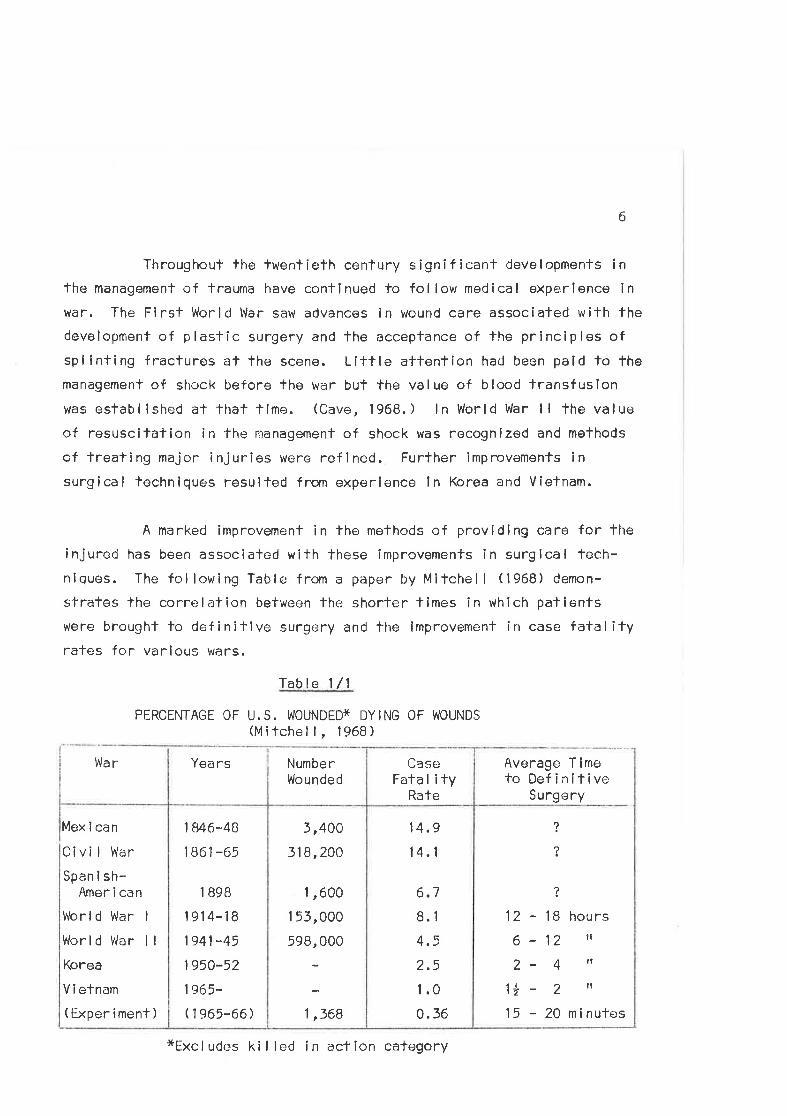
A marked improvemenl in tho methods of providing care for theinjured has been assoclated with these improvemenfs in surgical tech-nlques. The following Table from a paper by Mitchell (1968) demon-
strates the correlation befween the shorter tlmes in which patientswere brought to definitive surgery and the improvement in case fatalityrates for various wars.
Table l/1
PERCENTAGE OF U.S. WOUNDËDX DYING OF WOUNDS(Mitchell, ,l968)
War Yea rs Average Timoto Definítive
Surgery
,l
?
12 - 18 hours
6-12 tl
2- 4 'l{ I â lltT - ¿
15 - 20 minules
?
6.7
8.1
4.5
2.5
1.0
0. 36
14,9
14. I
3,400
318,200
1 ,600
1 53,000
598,000
1,568
1 846*48
1861 -65
1 B9B
19r4-i81941 -45
1950-52
1e65-
( 1 965-66 )
Mex i can
Ci vi I War
Span i sh-Amer i can
Worl d War I
World VJar I I
Korea
V i efnam
( Exper i ment )
CaseFata I i ty
Rate
Numbe rlllounded
*Excludes kil led in action cafegory
7
lmprovemenls în surgical expertise undoubtedly accounled formuch of the improvemenf ín fatal ity rates demonstrated. Nevertheless,
it is generally acknovrledged lhat the ef f iciency of the militaryemergency care syslem în bringing rapicl, ski I led treatment to the
palient has made a substantial contribution to the observed improvement
rales. (Howard , 1956; Eiseman , 1967; I'leel , 1968; Haacker , 1969,)
The mi I itary emergency care system is characterized by llsconstant preparedness for the treatment of the injured. An extenslve
communications system is supported by transport faci I ltíes, notably
helicopfens, which ensure that injured victims receive prornpt lreatment
on fhe batf lef leld f rom ski I led personnel . Subsequontly, victims are
rapidly evacualed to triage centres and base hospitals where medícal
and surgical teams are ready to províde definitive treaTment.
ln contrasl lo the improvements in the mi I ltary emêrgoncy
care system, civi I ian systems have been extnemely slow to develop.
Surgical lessons learnt during war have been adopted rapidly by the
med ical profession, but, unti I recenl years, there have been f a:w
attempts to adopt the supporting techniques which have proved effectivein war zones. Thís sifuafion is anomalous in thaf, sínce the advent and
universal acceptance of the motor car as a transport vehicle, lhe major
source of trauma in this century has moved from the military battlefieldto 1'he civi I ian road.
The firsl motor car accident death is believed to have occurred
in 1895 but it was nol until the 1920ts that the significance of the
motor car as a cause of lrauma was recognized in the medical literature.(Ryan, 1965,) Further references to motor vehicle frauma arppeared
sporadically during the 1930ts and 1940ts but only during lho last
twenty years has a scientific approach been adopted in sludying crashes
and thei r epidemiology.
B
Th,: importance of lhe motor car as a cause of death and injuryneeds no subsfantiation, but the comparison betwêen civi I ian and mi I lt-ary lrauma is demonstrated by Austral ian Army statislics relafing toarmy personncl killed or wounded in Vietnam and Australía. ln the periodfrom May 1, 1966, to May 28, 1911, the Ausfralian Army suffered 2,439Battle Casualties - 369 men ki lled and 2,070 injured. ln the same
period; 324 soldiers were killed and 2,7Q8 injured in non-battle accid-enls, many of which involved motor vohicles. (Derpt. of Army, 1971.)
ln the same period, 17,483 civilians were ki lled on Australlan roads.(Commonwealth Bureau of Census and Slatislics, 1971.)
ln summary, the developmenf of services and techniques for thetreatment of the injured throughout history has fol lowed the fortunes ofwar. ln this cenlury, the road has replaced fhe bafllefield as themajor source of traumatic injury. ln spile of this fransposition,civillan emergency services have evolved slowly in comparison with Ìhemi I itary system, a situation which reflects many influences, among themost important of which is the general apalhy of the corrnunity towards
lhe problems of road safefy.
THE DEVELOFI4ENT OF EI4ERGENCY MEDICAL SERVICES IN VICTORIA
(a) Casua lty Departments
The first hospital in Victoría was the Melbourne Hospital,founded in 1848 as a voluntary hospilal to cater for the needs of thesick and injured of the cify. The hospifal was financed by a government
grant from ils inception and relied upon grants and donations from ilspatrons and supporters for additÍonal supporf. By 1865 the hospitalwôs ln an unsanitary stale and was unable to cope with fhe numbers ofpatients who required admission. Hence, following the shooting ofPrince Alfred in Sydney in 1868, the Prince Alfred Memorial Fund, which
hacj been set up as a loken of thanksgivlng thaf the Prince had not been
killed, was used fo build the f irs't two pavilion style units of the
. ,...ii-¡ .4.7
h,*¡' l
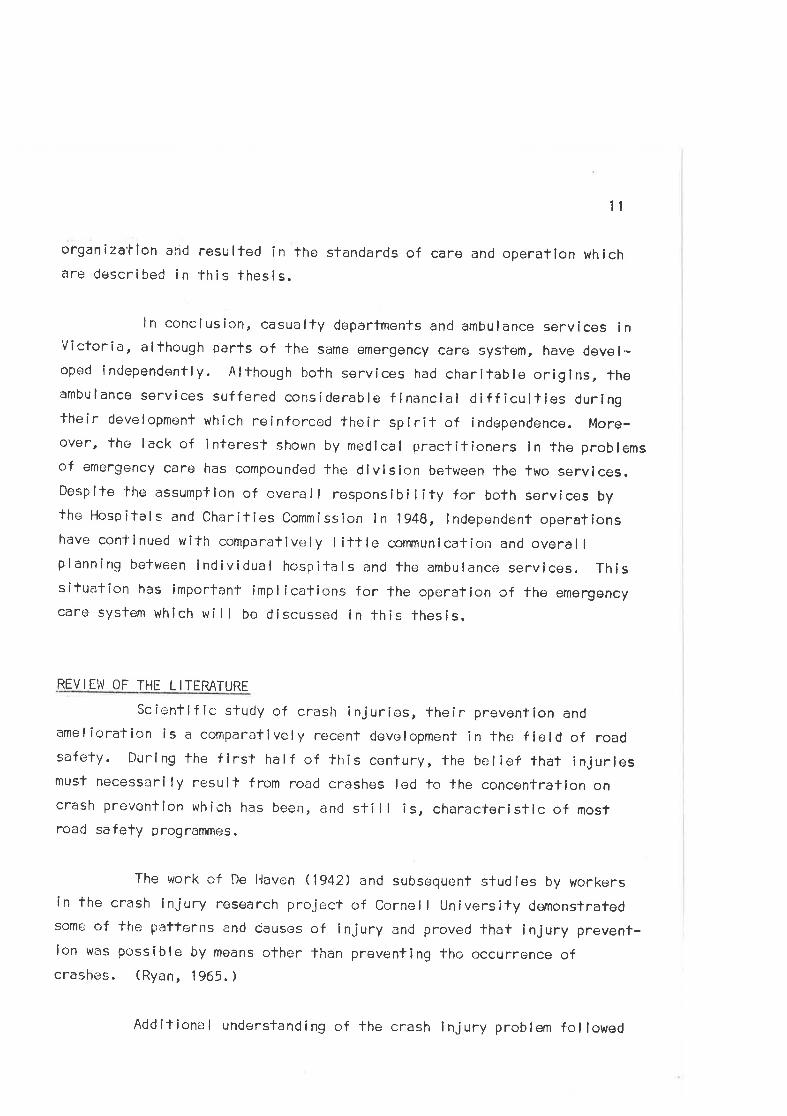
The first horse-drown ombulonce, outside the Eostern Hill Fire Stotion'
t
S\'
9
Alfred Hcspital. The hospi'fal accepted its f irst outpatients in March
1871. (Milchel l, ,l970.)
A number of hospitals ancl charilable inslitutions were erectedin Victoria during lhe l860ts and 1B7Ots, a situation which has been
ascribed to the humanitarian spiri-l- abroad in the community in thoseyears. These large public hospilals l"raVê ôlways constituted ono of theStaters main responsibilities to the sick and seriously lnjured and theprovision of emergency medical care has been centred on them. Successive
Eovernmenfs con'f inued fo combine with charltable institutions to f lnancethe hospilals, fhus avoiding the more fînancial ly unpalatable alter-native of direct responsibi I ity for hospital services. (Mitchel l, 1972,)Whi ls'l the founding and financlng of lhese institutions fostered thenotion of fhe sick poor, fhe hospitals have always catered for allsectlons of the community, and, lo this day, these hospitals provicletroafment for the majority of road crash vicfims and many other emergencypat i ents.
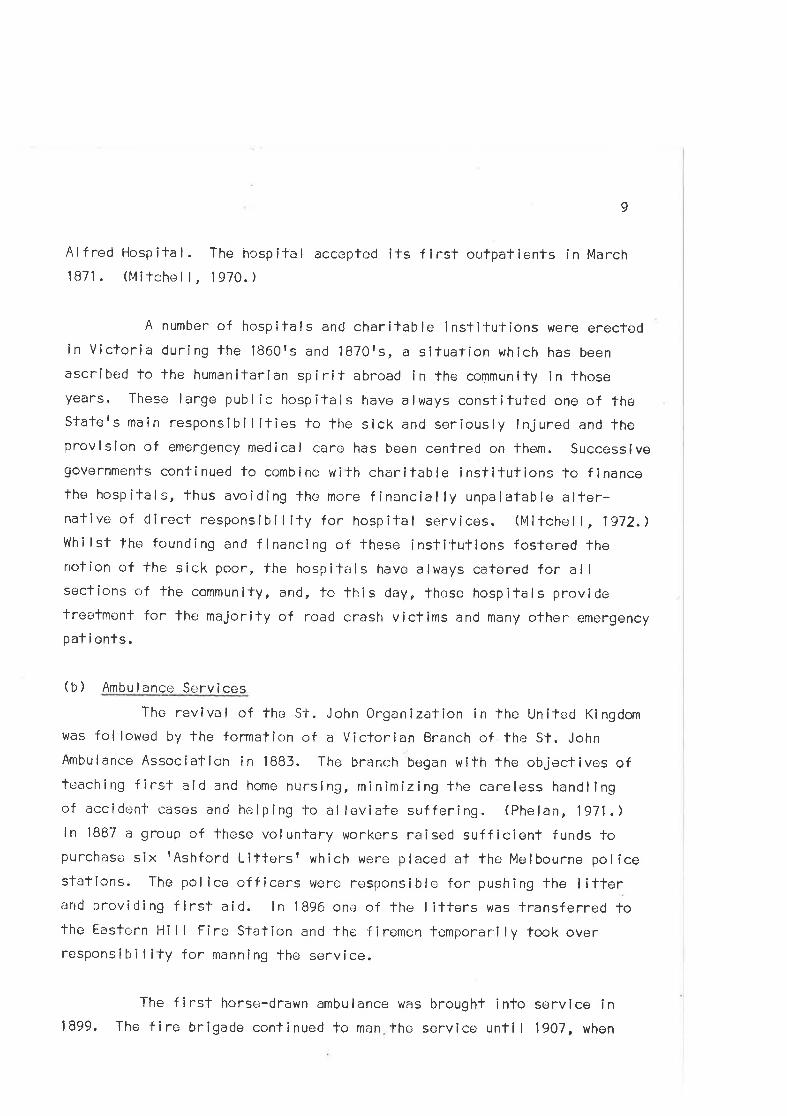
(b) Ambulance Services
The revival of the St. John Organization in the United Kingdom
was followed by the formalîon of a Victorian Branch of the st. John
Ambulance Association in 1883. The branch began with the objectives ofteaching f irst aid and home nursíng, minimizing fhe careless handlingof accidenl casos and helping lo al leviate suffering. (phelan, 1971.)ln 1BB7 a group of lhese volunfary workers raised sufficient funds topurchase six tAshford Littersr which were placed at the Melbourne policesfations. The pol ice officers were responsible for pushing the I itterand providing first aid. ln 1896 one of the litters was lransferred tothe Easfern Hill Firc stalion and the firemen temporarily took overresponsibi I ¡ty for manning lhe service.
The first horsc+-drawn ambulance was brought into service ini899. The fire brîgade continuod fo man the service unfil 1907, when
:&..::
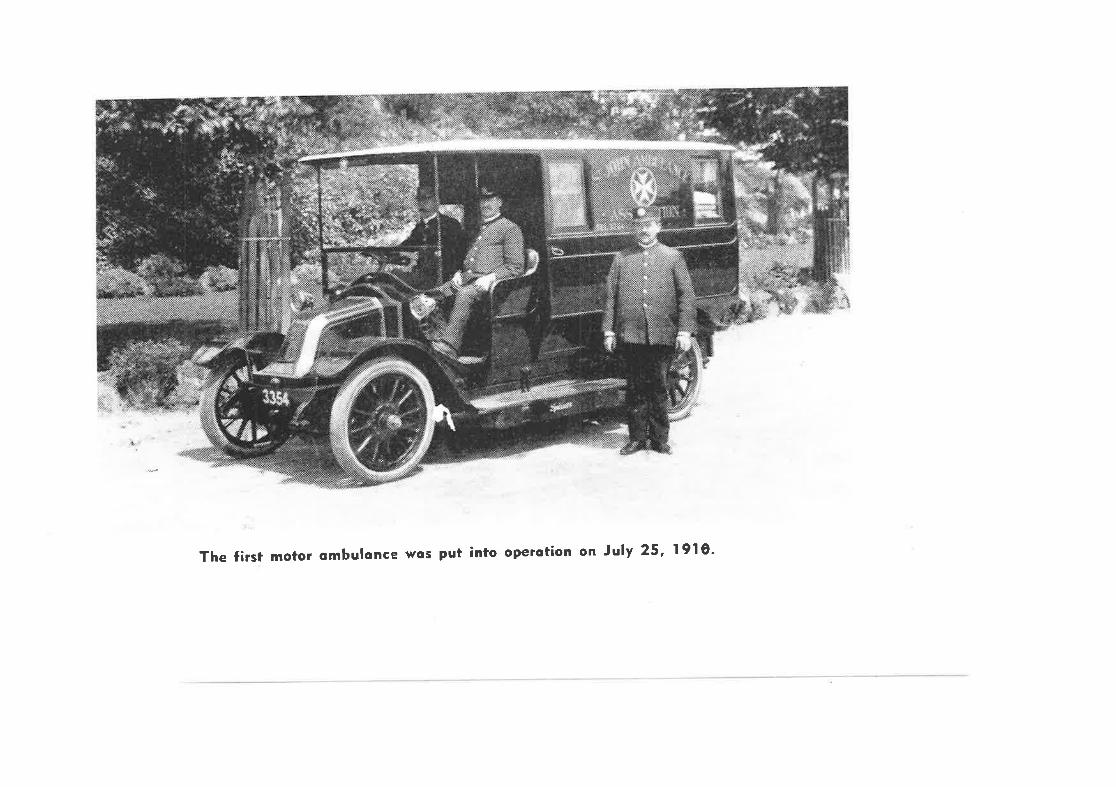
The first motor ombulonce wos put into operotion on July 25, I9l0'
l0
a privale contractor was appoinl'ed. ln 19lO'ihe f irst mofor ambulance
was purchased. Subsequenl expansion of fhe service fol lowed terminatíonof the agreement with the private conlractor and resumption of fullcontrol by the St. John Association.
Financial difficulties plagued lhe servico throughout itsearly years and lt was totally dependenf on voluntary donations for ltsrunning cosls. The state governmenl was unwi I I ing fo provide funds,conlending fhat the ?police would convey injured persons by cabs and
lifters and that the ambulance would not bo requiredr. (Anon., 1963.)Nevertheless, the St. John Council were convinced of the value of theirservice and continued to flnance ¡t. lt was not until 1914 that theVíctorien Government made its first grant towards the cosl of ambulance
ope rat i ons .
ln 1916 a new company, The Victorian Civi I Ambulance Service,was registered to fake over thc service. The Government remained
reluctanf to assist wi+h f inancing, a situaf ion which persistecj untl I
1936 when the servîce went into voluntary liquid¿¡tion and was rogisteredas a charitable society. By lhis lime the service had expanded wlth theopening of a country cllvision in 1924, The consequent proliferaf ion ofservices and vehicles saw the esfablishmenl of 23 branches and 68 firstaid stalions ín country centres.
ln 1947 a Hospitals and Charities Act was broughl down by theVictorian Parl iament and al I ambulance services in Victoria were placed
under the contro I of the l-losp ita I s and Char it ies Comm i ss ion. The Statewas divided into sixteen regions and the Victorian Civi l Ambulance
Service was made responsible for the provision of services in the melro-pol itan area. After a lmost sixty years of ambu lance operaf ions, theState Government assumed financial responsib¡ I ity for the provision ofambulance services. The improved financial slatus of the service whichresulted from this act has permitted the development of fhe present
11
organizatlon and resulted in the standards of care and operation whichare described in this thesis.
ln conclusion, casualty departments and ambulance services inVictoria, although parls of fhe same emergency care system, have devel-opecl incJependently. A lthough both services hacj charitab le orig lns, theambulance services suffered considerable f inancial d¡ff iculties duringtheir development which reînforcod the¡ir spi rit of independence. More-over, the lack of interest shown by medical praclitioners ln the problemsof emergency care has compoundecj the divislon belween fhe two services.Despite the assumption of overal I responsibi I ity for both services bythe Hospilals and Charities Commissîon ln 1948, lndependent operationshave continued with comparatively little communication and overallplanning between individual hospitals and the ambulance services. Thissitueltion has imporlant implications for lhe operation of the emergencycaro system which wi I I be discussed in this thesls.
REVIEW OF THE LITE RATURE
scientiflc study of crash injuries, their prevention andamelioration ls a comparatively recent development in the field of roadsafety. Durlng the f lrst half of this century, the t¡elief that injuriesmusl necessarily result from road crashes led to the concontratlon oncrash prevention which has been, and still is, characlerisflc of moslroad safety programmes.
The work of De Haven (1942) and subsequent studîes by workersín the crash injury research project of Cornel I University demonstratedsome of the patterns and causes of injury and proved that injury prevent-ion was possible by means other Ìhan preventing lho occurrence ofcrashes. (Ryan, 1 965. )
Additional understanding of the crash injury problem fol lowed
12
the applícalion of epidemiological prlnciples to the study of crashes by
Gordon (1949), McFarIand and Mocrc (962) and Haddon (1963). Man, as
the host, was relaled to lhe energy exchanged in the crash as the agent,with the crash environment completing the epidemiologlcal triarJ.
Haddon (1968, 1970) described an extenslon of this epidemiolog-ical approach in which emphasis was placed on aetirclogical factors intrauma. The primary objeclive of the road safety system was seen to be
reductlon of the losses, in terms of personal injury and propertydamage, caused by crashes. Crash events were cafegorized ln fhreephases'- pre-crash, crash and pos'f-crash - and identified as eitherhuman, vehicle, or environmental in origîn. By comparing these phases
and factors, a matrix was developed which is of considerable value forcafegorizing the various road safety phenomena.
The use of an epidemiological approach for investigating crash
injury requires that the'tyoes and causes of injury should first be
defíned. Many studies havo been undertaken in differenf countries todelermine the patterns of road crash injury. The following secf ion
reviews the major studies performeci in Austral ia.
CRASH INJURY STUDIES IN AUSTRALIA
One of the eerliesl studies of crash injury in Australia was
reported by Hodge (1962)" He reviewed a series of 174 aufopsies per-formed ¡:n victims of road crashcs which occurred in and around theAdelaide metropol ilan area over a lwo year period. The analysis included
descripfions c'¡f the types anci time distribufion of lhe crashes, the age
and sex distribution of lhe victims, and the types of injury sustained.Elevatod blood alcohol levels were detected in 38ß of drivers.
A second study based on aufopsy findings was reported from
Brisbane by Tonge et al, (1964). The resulls of 2,214 post mortem
13
examlnatîons performed between 1935 and 1963 were reviewed and theinjury patterns of the victims analysed. This series was much largerthan that observed by Hodge. lt included 90$ of all deaths from 1958-
1963. The study prrcv i decj descr i pt ions of the patterns of crash i nj ury
and demonstrated changes ín the patterns of injury over fhe periodstud i ed.
A sludy by Jamlesorr and Tail (1966) used hospital admission
records to detecl 1,000 consecutive victims of crashes in Brisbane.Patients who were; treated in hsopital were examined and their injuriesrecorded. A ful I autopsy was performed on the 1BB viclims who died.Detai ls of the crashes were col lected, whenever posslble, by inter-viewing patients and pol ice officers and by lnspectlng the crashed
vehicles. Approximalely one quarter of the patienls Q62) had sufferedminor lnjuries,416 had major injuries of one body region and 322 had
major injuries To more than one body area. The study extended the know-
ledge of injury patterns, lhe management of injuries and provided
limited information on fhe causes of injury for a population of victimswho received hospital treatment.
A different melhod for studying crashes was introduced by
Robertson and his co-workers in Adelaide in 1963-64. An ton-therspotf
study used the ambulance service to delect crashes in which persons
had been injured. A research team consisting of a doctor and an
engineer atlended the scene of 408 mefropol itan road crashes, rcpresent-ing a 12.3 per cent sample of all crashes attended by ambulances duríng
thcl sample period. The patterns of injury of 1,029 car occupants,82 pedestrians, 44 pedal cycl isfs and 74 motor cycl ists were documented.
Crash mechanisms were studied and injuries were relaled lo lhe parts ofthevehicle which had caused lhem. Although lhe study concentrated on crash
injury, lhc numbers of palienls J'aken to hospital, their trea-lment and
duration of stay were among the post-crash events recorded. A defect
14
in the study method was the sampling bias caused by the omission ofcnashes occurring during lhe late night hours on Fridays and Saturdays.
A second ron-the-spo'tt study was performed in Brisbane. Agaln
the ambulance service was used as a means of detecting crashes and a
team consisting of a doctor, social worker and an engineer atlended thecrash scene within 15 minutr:s of the collision. Findings of the previous
studies on the patterns and mechanisms of injury were confirmed. Parfic-ular attenlion t,las paid to elucidaTing the effects of the ejectlon ofvictims from vehicles and it was suggested that, when most of the energy
of collisîon had been expended in fhe collision, ojectlon was a relative-ly unimportant cause of injury. Sociological and psychological facforslrlere examined by fhe social worker in the team. Drivers were classifledas reckless, negl lgent or involved by chance. The characteristics ofeach group in lerms of their social, occupational and financial back-grounds were described. lt was fcund that 25 per cent of driversinvolved in single vehlcle crashes to which an ambulance was called were
known to police because of a previous criminal rocord. The experience ofthe Adelaide sfudy was available fo lhe workers and thus statisticaldesign of the sampling melhod r:nsured thaf lhe sample of crashes repres-ented fhe patfern of crashes in all areas of Brisbane at all hours ofthe week. (Jamieson et a I . , 1911 .)
A s'ludy of rural crashes was performed by Adams (1967) using
a questionnaire sent lo 56 general praclilioners in country areas. The
doctors \¡/ere requested to complete the questíonnairos for road crashes
occurring in the country ôreas surrounding thoír practice. Data was
analysed fron 320 of a fotal of 359 queslionnaires returned to therecorder. Single vehicle and rol l-over crashes were found to be common
and the aulhor concluded lhat high impact speeds wilh correspondinglyhigh degrees of injury were responsible for the high dealh rales ob-served. 0f particular importance for the emergency care system vÌas thefinding that a large number of deaths occurred during extra-hospítal
15
care. Delay in the provision of adequate medical care was suggesfed as
a causalive faclor. The sample was probably biased towards severecrashes. Nevertheless, the 'lypes and patterns of injury differed from
lhose observed in tha previous studies of urban crashes.
The imporlance of time de|ays In the survivaI of crash victimswas discussed by Robertson and Tonge (1968), who studied survival timesby comparing data from aufopsy studies in A<Jelaide and Brisbane. ltwas found that 50Í of fatally injured victims were dead within one hour,B0É in a day, goiÅ in a week, and tess than 4Í líved beyond a month. The
authors strongly recommended the adoption of a thirty day cuf off periodfor the defínitlon of road crash Ceaths for statistical purposes. The
influence on survival of such factors as agê, sex and type of involve-ment were compared for the victims. ll was found that the main facforsinfluencíng survival for severely injured pedestrians from the lwocities were.; the nafure, degree and dístribution of their injuríes.
More recenf injury studies in Austral ia include a review offhe crashes involving heavy vehlcles ln New South frlales by Henderson(1970) and a study of the mcchanisms of pedestrian injury by vaughan(1971), The Royal Aus'tralasian C<¡ll¡'.;ge of Surgeons is conducting a
pattern of injur^y survey in Victoria, results of which are, as ye-|-,
unpublished.
As a resull of 1'hese studies, patterns of crash injury inAustralia have been delineate¡d, particularly for urban crashos. Furtherinvesllgalion of rural crashes would be desirable to expand knowledge
of the palterns and mechanisms of crash injury in the counfry areas.Moreover,although research has defined many of the problems in the crashand pre-crash phascs of the epiderniological matrix, there have been few
invesfigations of post-crash avents. Emergency services, which help loamel iorale the effecls of crashes and crash injury, are importanfelemenfs of fhe post-crash phase. The dearlh of studies of these
16
services in Austral ia reflecls a simi lar lack in overseas countries.Sludies which have contribul'ecJ lo knowledge in this ¿:rea will be dis-cussed ín the fol lowing secfion.
STUDIES OF EMERGENCY SERVICËS
Most studies of emergency serrvices have concentrated on
either ambulance services or hospital casualfy departments withoufrelating each to the ofher as importanl elements of the emergency caresystem. Neverlheless, as a resull of lhe increasing attention whichhas been paid to emergency services in the last five years, many papershave been publ ished which describe exisling services and suggest methods
of improving them. The studios fal I into three broad categories accord-ing to the area of emergency care which forms theír main focus. These
categories are:(a) Studies of Ambulance Services(b) Studies of Hospital Casualty Deparfmenls(c) Emergency Care System studiesThe fol lowi ng review wi I I considor the publ i shed I iterafure
in these three categories.
(a) Ambulance Servicos
Several papers l-rave described existing ambuf¿lnce servÍces inlocal areas by using data gathered from questionnoire surveys. Hampton(1960) reported one of ther earliest such surveys in the United Slates.A questionnaire designed to gather information on patterns of ambulance
service was mailed to 1,560 cilîes. Replies f rom 865 cilies describedthe number and types of ambulance vehicles used, the sfaffing patternsof the sf:r-vice, training standards, legal con-lrols of service, and theagencios responsi ble for ambu lance service. Oiher i nvestigators used
quest ionna í i-e and i nterv iew methocjs lo descr i be ambu I ance serv i ces i n
several local areas in tne United States (Lehman & Hollingsworth, 1960;
cadmus, 1965; t4aine De¡rartment of Hearlth and welfare, 1966; owens, 1965,
17
1966; Cooper, 1968. ) The studles provided invenlories of ambulance
faci I ities which were used for eval uating existing services and re-commending changes lo improve them.
Olher aufhors have analysed servict: records or introduced
special recording forms as methods of gathelring operational data tocomplement avai lable invcntory data and permit assessments of perform-
ance to be made. Caldwell (1961) usod such forms to gather data on
the elapsed times during the phases of the ambulance call, the injuriessustaîned by victims, and the trealment performed for fhose injuries,for an Ont¡¡rio ambulance service. He concluded that substantialdeficiencies existed in all aspects of the servic;e and recommended thata major reorganization of ambulance services should be undertaken.
Vlallc-r (1966) examinecJ trip records for 923 ambulance runs performed by
a service in rural Cal ifornia, supplemonting the ambulance Cefa wifhadditional material gathered from hospilal records. Thc populafion
using the service was delineated and census tracts were used to delermine
utilization rates. A gross annual utillzation rate of 29.6 trips per
1,0C0 members of 'the resîdeinl oopulation was noted. Heavy uti lizationby elclerly persons was found and types of illnesses for which ambul-
ances were used were determined. Traffic crashes accounted for 33.1
per cenl of the tnips and 23.6 per cent of the fafalities attended.
In the Uniled Kingciom, Boughey (I968) reviewed dala coI lected
by ambulance of f icers in Portsmouth. A card lvas completed for each of1,612 paf ients of whom 597 ß71,) were crash victims. Thc adequacy ofthe lrealmcnt performed was ¿rssessed and rç:laled to lhe availabilityof equipment and olher faci I ities. Allhough the criteria and methods
of assessment of lhe adequacy c.rf treatment were not def i ned i n thepaper, the author concluded thaf morlal ity and morbidity from accldentsrcould be appreciably reduced by better training, equipment and improved
communicatíons befween the ambulance service and hospîtalsr.
1B
Ambulance services in European countries vary în several
respecfs frorn those described in the Llnited States. A description ofseveral services is contained în a World Health Organization report ofresuscilation and casualty sorvices iri Europe. (W.l-1.0., 1968. ) Kimball(1967) also describes features of several Ëuropean services in reporlingobservations made during a study tour of Europe. Emergency ambulances,
especial ly equipped for resuscitation and infensive care a-l- the scene,
are widely used. (Gregorieva, 1967; Böhler, 1970; Bourrel, 1971; Storey
& Rothr 1971.) ln most countries thcse arnbulances are manned by skilledmedical or para-medical personnel. Their use in Germany has been des-
cribed in many papers, although Few data are avai lable f rom which theírI ife saving potential and cosl-effectiveness may be evaluated.
Frledhoff (1959) discussed the use of such an ambulance in Cologne,
detailing the types of treatment used and lhe particular value of the
un i -l' f or 579 emergency cases. An extens i vo rev iew of emergency serv i ces
i n Germ¿:ny (Gog ler, 1969) inc I uded data f rom He ide I berg, where a doctor
travels ïo the scene of incídents, meeting lhe ambulance on arrival.For J'he period under review, 1,666 patlenls f rom 1,300 incidents had
been lreated (an averagc. of 300 irrciden-ls per year); 517 paf ients ß1%)
were dangerously il l, of whom l83 ß5/") were rsavedr. (Brechmann, 1969.)
The {'avourable descriptions of the use of these vehicles have
led to the adoption of similar services in other countries, parlicularlyas mobilo cnronary care unils. (l'lagel, 1968; Nagel ef a. , 1970; Audette,
1970; Safar, 1971.) Robinson (1970) descríbed the use of such a vehicle
i n Perth, Western Austra I ia.
The demand for emergency ambulances hars grown markedly in
recent years, largely as a result of a widespread feelíng that existingambulance services are inadequate. Nevertheless, there have been few
sfudies evaluating their cosl-effectiveness. ln parficular, the advant-
ages of taking medical care to the scene over those of rapidly carryingpatients Tc; a hospital wilh ef f icient cmergency faci lities have not been
19
demonstraled. l.levertheless, favourable reports of their use, coupled
with fheir undoubted usefulness when injured víctims arc trapped and incertain medical emergencies, suggcsl that they represent a val uable
adjunct fo existing ambulance services.
Alternative suggestions for prcviding medical care at thecrash scene have included the use of Accident Flying Squads. Experiences
wíth the operaf ion of such a squad were <Jescribed by Collins (1966) forthe area surrounding the Derbyshire Royol lnfirmary. ln differenlschemes in Bath (Snc¡ok,1969 (1) & (2);1971) and in Yorkshire (Easton,
1969; 19701, general practilioners join ambulance, police and f ireservices in providing care ¿t the scene. Again lhere is little publisheddata by which the erffectiveness of the schemes may be assessed, but lheservices do marshal I community rcsources and develop publ ic interest inemergency care, as well as enabling docfors to aftend emergencies when
lhey are required.
A sîmi lar community project operates in fhe Tea Gardens areaol' New South Wrrles. (Pacy , 1967.) Bush (1971) dlscussed the merifs ofthese schernes and announced plans for a similar service to be started inthe Me I bo u rne met ropo I i -t an a rea .
The costs ancl difficullies involved in providing and staffingemergency ambulances, coup led with a general awareness of the deficienc-ic;s in cornmunication which exist between ambulances and hospitalcasualty departments, has led several aufhors to investigate thefeasibilily of direct radio links between the ambulance and the hospital.Hal I and Garden ( l9€.¡7) reported the use of such a I ink, which was found't<¡ be cffective in warning the hospi-lal of the ambulancess arrival.Moreover, it provided support for ambulence officers at lhe scene, who
could communicate with the doclor in hospital. Telemetry of physio-logical data is another communications development which has been invest-igated (Nagel ef al., 1910; Safar,19-11) and which may be used in future
20
emergency servi ces.
There have been few publ ished reports of ambulance services inAuslral ia. Gartrel I (1965) revíewed the developments in ambulance trans-port nursing in South Auslralia in describing traíning meì'hods and dis-cussing recent innovations in ambulance treal-ment. He also listed theslandard equi pmenf carri ed on Sc¡ulh Austra I i an ambu l ances. Descri ptionsof ambulance operations in Vicforia were provided by several speakers atthe seminar of lhe Royal Australasian College of Surgeons in 1969.(Roya I Austra I as ian Co I lege of Surgec-:ns, 1970.)
Robr:rtson (1971) stucjied the rural ambulance load in South
Aus-iral ia in 1968 and 1970. Sixly-three ambulance services were sur-veyed using a postai questionnaire direcled to fhe acjministrators ofeach service. Dat¡: w¿:re gathererJ on the numbers and types of emergenciesaltr:ncled, the total mileage travelled and ther number of victims involvedfor the various catr:gories of service. The study documenled ambulance
work loads and operat i ng cha r¿rc-ler î s'f lcs, and represe nts f he on I y rev i ew
of ifs type yel pubI ished for AustraI ian ambuIance services. The
Australîan N4edical Association has commissioned an Ausfralia-wide surveyof ambulance and casually services but the survey is still in progress
and its resulfs to dale are no'l' published. Data f rom this survey will,no doubl, provide an inventory of Australian services upon which fufurep I ann i ng of ambu I ance servi cos may be based.
Many authors concl ude thci r descriptions of exi sli ng ambul ance
services by recommcnding changes -lo improve the quality of service. The
need for standards as operatir¡nal and evalualory quides for ambulance
services has been recognized in many countries. ln the Uniled l(ingdom,
a working party was established in 'the early l960rs to invesf igateambulance services. The resulting report recommended standards forambulanc': operafions, eguipment and trainirrg in that country. (Mi I lar,1966, ) Sfandards for al I aspecfs of ambulance operations in lhe tJnited
21
States were recommended by the American College of Surgeons (1961), theAmerican Society of Anaesthesiologists ( 1968) and the U.S. Dr:parlment ofTransportation ( 1 968) .
ln Austral ia, stancjards vary from service fo service and fromSla-le tc¡ Stale. The re are nc naf iona I standards for an¡bu länce operations.ln Victoria tha Hospilals and Charifies Commission supervíses servicesand publ ishos a handbook r,¡hich prescnibes standards. (Hospifals and
Charities Commission, 1970. )
Ïhe establishment of standards for organizatic'rn and stafftraining provides a means of ímproving and evalua'fing the eff iciencyand effectiveness of ambulance services. Moreover, êQUipment standardsênsure lhal adequate facîl¡fies are available for use by the traineds-laff. Several papers have reported the findings of committees invest-igating vohicle dcsign and equîpment slandards. (Millar, 1966; 0glo,1969; Mackay, 1969; Berry, 1971,) Uniformlty of vehicle an<J equipmentdesign Îs desirable sitrce stretchers and other items of equipmenf need
to be interchangeable belwer¡n vehicles and bctween services. ln spiteof these recommendetions, I ittle progress has been made fowar<Js theach i evemenl of such un i form i ty betwc;en serv i ces.
Further emphasis has bcen plced on'lhe good design of oquip-ment and vehicles because of the effects thaf road transport may have
on the comfort and clinical condition of th¿; palient. This aspect ofambulance care has received I ittle objective study. Although soveralauthors have; e>xpressed concern thaf road transporl'may have an adverseeffecl on a patien'tts condition, no studles have been performed toconfirm these suspicions. Harbison (1969) asserted lhat road transportcoulrJ dol'rimontally affect patients on long country lrips and supportedhis assertion with examples from his personal observations of ruralgeneral practice in Austral ia. ln advocating fhe use of air ambulancos
as a desir¿lble alternative to road transport, he discussed the operations
22
of the Viciorian Air Ambulance Service.
The question of the spss¿ing ambulance, i1-s hazards and
advanlages, is closely related to lhis problem of road transport and
its effects on the patient. Af'l-er studying 2,500 ambulance emergency
calls in Michigan, Curry and Ly-t'tle (19i7 ) ccncluded that speed was
unnecessary in 98.2 per cent of the cases. ln The remaining 'l .B percent íl was concluded thatrexpeditious han<lling was necessary, but a
speeding ambulance could have increased the severity of injuryr.
ln one of lhe most comprehensive studies of fhe effects ofambulence fransporf on patients, west e;t al. (1964) examined over 5,000emergency lrips in Cal ifornia. The primary objecfive was to determinelhe need for, and effects of, speed during ambulance transport. The
allending ambulance and medical slaff were asked to record fheir opiníonson the urgency of the cases ancl the consequenf need for speedy transport.It was c<¡ncluded that speed during transport to hospital may have been
of benef it in B,q' of the côses reviewecl buf was not essential in any ofl¡e cases. l4oreover, the medical observors considercd that speed was
nol !-f-%sry.j¡9. in -any of the cases studied. Nor was there any evi<jencethat the ambulance ride had dclrîme¡nfally affecfcci the patientrs coh-dilion. The mean time saved by exceedirrg the speed limît was 2 minutc:s.I n conc I us ion , i-t' was cons i dered thal tlre i ncreased hazards of spe;ed i ng
were such lha't its use was contra-inclicated in view of the marg inalt i rne-sav i ng i: dvanf ages .
Ro¡;d transport has sr¡vera I obvious I imitalîons and theefficiency of the helicopten as an ambulance verhicle in war zones has
led many people lo advocale its use as an alternative to road ambulances.
Ïhe use of ambulance hel ícopters has been extensively investigated inthe lJnited States (Bordner, 1968- Karthauser et al., 1969; Arizona Slafeuniversîfy, 1970; Turner & EllÍngson, 1g7o; Barflett, I97l) and lhey areused in several European countries. An evaluation of fheir usefulness
23
and opereling costs in an Australian settlng was performed by Berry(1968). Hel icopters have significant operating advantages c¡ver ambul-ances in certain sifuations, notably when road access ls difflculf forany reasoÍ1. However, the costs of operatlons are high and represenfmajrrr restricfions on the use of these vehícles. These cosls can be
modif ied by using the helicop-ters for police, f ire and rescue as wellas ambulance work. Such multi-service usage, howu-ver, restricfs fheavai labi I ity of the aircraft for ambulance purposes.
(b) Hosp i ta I Casua I tv Deoartmenl's
Many aulhors of pðpers describing hospital emergency depart-menls express dissatisfaction with the quality of care provided în thedepartmen'l-s and suggest the need for changes in methods of departmental
organ izat ion. However, mos't reports f ocus on specif ic hosp íta I s orgroups of hospitals and the ir f indings.,are thus.of limíted general
applicåbîlity.
United Kinqdom Studies
The British Orthopaedic Association (1959) described defic-iencies in Accident Services, attributing them to fai lures in organiz-ation, staffing, accommodation and surgical fraining. The Associationcalled for a major nalional reorganization of accident services for theinjured, to remedy the sifuafion. This call was followed by the reportof a commitlee of lhe Nuff ield Provincial Hospitals Trust, who surveyedtwenly casualty departments ar-rd lheir facili-ties in fourtcen areas ofthe United Kingdom. They concluded lhal (a) publ ic dissafisfaction withcasualty services was jusfified; (b) hospital leadership and execufiveaclion were needed to improve service;s; (c) hosp ita ls shou ld be class-if ied and listed according Io their faci lities for accidenf anc,i emergency
care; (d) general practifioner services affect casually department uti l-ization; and (e) there r¡/as a need for detailed surveys of services by
mu lt i -d i sci p I i nary teams compri si ng stati sti ci ans, sociolog i sts and
doctors. (Fry, 1960. )
24
ln Jarruary, 1965, a committee of the lrish tledical Associationinvesfigated hospitals and ambulance services in Dubl in, by requestingpatients who presented fo eleven of the ciÌyts major casualty depart-ments-fo complele survey queslionnaires. The findings of the surveyincluded informalion on the source of pafienl referrals and the patternand nature of casualty workloads. Changes in the organizatîon and sfaff-îng of the departments were recommended as a result of lhe committeersf i ndi ngs. (Corcoran , 1967 ,)
ln London, Fairley and Hewett (1969) surveyed workloads on 126
casualty departments in the Greater London area. ln noting deficíenciesin the organization of serviccs, they commented on the facl that approx-imately 50 per cent of the depantments freated less fhan 5 palients pernight. Non-emergency cases represented o largc proportion of thecasua I ty vrork load.
Jenkins eT al. (1969) review<¡d the medical records of a seriesof 100 emergency pafients who required admission to the resuscitationroom of the Edinburgh Royal lnfîrmary. This group represented 0.45 percent of al I patients admitJ'ed to the casualfy department. Trafficcrashes and drug overdose wene the commonest causes of admission. Two-
fhirds of the injured patlents had susTained multiple injuries. The
sludy doscríbod injury types, lreatmenl mothods and fime delays duringtreafmenl for the observed patienls.
Although these and simi lar studies had described 'the sifualionin casually deparfmenls, several authors nofed that the organization ofaccident services in the U.K. had remained basica I ly unaltered duringthe decade to 1970. (Anon., 1g7O; Sc<¡tt, 1970; London, 1970,)
Studies of Emerqencv Deoarfmenls in the Un ited StalesThe problems of erncrgency departments in the United States
have; been exacerbated by lhe marked increases in usage of fhe depart-ments in recent years. A postal survey of 300 hospital emergency
25
deparTments lhroughout the coun'try revealed a 120 per cent increase inemergency depanfment visíts deom 1944 to 1951. (Skudder & McCarrol l,1961 . ) From 1954 to 1964, vísíts lo emerrgency de;partments increased aT
a rate of 6 per cent annually (American Medical Association, 1966) and
the increase has confinued steadi ly since that time. (webb, 1969.) The
implications of theso changing usage patterns were díscussed by Kennedy(1963) and Skudder and Wade (196Ð.
0ther sTudies have investigatetl workloads on departmenls inaffempting fo def ine the problcrms and suggest solutions lo them. Freyel al. (1970) used the casuírlty department log book to determine work-.
loads on the universîty of Michigan Medical centre during 1960-67,Staffing and edminisfrative arrangements were considered in the I ight oftheir findings, and fhe authors concluded that improvements in recordlngsystems, sÌaff ratios, communications between hospltals and rescueunils, teaching, and quality conÌrol of care were indicatod. A similarmelhod was used by Jacobs et al. (1971) to study hospitals in theRochester, New York aroa. They suggested fhal an integrated primarycare system t,ias needed on a coñìmunity-wide basís fo overcome The problemsof hospital emergency departments.
Patient interviews were useci as a means of determining usage
patterns by White and 0rConnor (1970) and Torrens and Yedvab (1970).
EioJ'h sfudies invesllgaled the types of patients using emergency depart-menls and theír reasons for seeking merdîcal care from the departmentsin preference t<¡ other sources of care. ln the secon,l study it was
noted that 12 per cent of palienis receîved more than half their carefrom emergency departments, with approximately 7 per cent using itexclusively.
Several authors heve considered alternatívo methods ofcasualty department organization as a means of improving the serviceprovided. worman et al. (1962) were highly critical of an accident
26
service in þ1ílwaukes which was separaled from the local general hospital.
The service was considered fo be expensíve, inefficienl, a poor trainingarea for surgical staff, and a freatment service that was detrimental to
the care of lhe trauma patient.
Weinerman el al, (1963; 1965; 1966), after studying the work-'
loads in lhe emergency departmenl of lhe Yale - New Haven hospital,
introduced a system of rtriaget for new patients pre;senting to fhe
emergency department. An area of the department was sef asíde for the
assessment of new patienls and a senior medical officer was appolnted
to.screen patìenïs and refer them lo the appropriate treatment service.
The service proved effective in rectucing waitlng times and the congestion
in the emergency treatment areas. Experiences with this scheme were
reviewed by Beloff (1969). The scheme is effectíve in helplng lo solve
some of the problems of emergency departments, but is not a panacea. The
authors concluded lhat the solution to emergency cleparÌment problems
lies in an inlegratr:d system of emergency care for the whole community.
Austral lan Studies
Although several speakers at the seminar conducted by the
Royal Austr¿:lasian Col loge of Surcleons in 1969 expressed concern about
lhe care provided in casualty departme,.n'is, fhere have been few sfudies
i nvestigatl ng the subject i n Ausfra I ia. Hocki ng (1962) descr i bed the
incidence of various condilions in patienls presenting to fhe casualty
department of the Alfred Hospital in i\4elbourne in 1969. Brand (1971 )
in a series of papcrs discusse<l workloads, waiting times and the eff lc-iency of staffing of several Victorian hospitals, using data gathered
during a spccial survey of lhe departmonls. Grounds (1969) discussed
the needs of accident and emergency services in a general revir¡w of lhe
Australian situalion for the Australian Mr':dical Assoclation Study Group
on l'1ed ica I P lann ing.
27
Standards for Emerqencv Deoartments
ln recognition of these probable deficiencies in emergency
care in hospilals many professional associations have prescribed sfand-ards for al I aspecfs of casualty department operations. (American
l{ospital Associatlon, 1960; 1962; Amorican Medical Assocíation , 1966;American College of Surgeons, 1963; 1964. ) Staf f ing policíes arereviewed in several papers and recommr¡ndatíons made as to lhe numbers
of s'taff members required lo provide adequate care in the dopartments.(Kennedy, 1963; Am<;rican Hospital Association, 1962; 1g66; Gibson,1970.)
Although fhe managemenl of road crash viclims is an area ofparticu!ar concern to those sludying casualty departments, mosl papers
on this subject have been rcstricted to descriptions of fhe clinicalmanagemenT of inj urles. The im¡rorfance of p lanned managemenf in thetreatment of the severely injured is emphasized by Mustard (1961).
Several ¡rapers have discussed tho surgical principles involved lntreating r:rash injurics. (Currie, 1966; Curry et al., 1967; Howell,1967; Pizzi, 1968; Jones & Shires, 1969; Lewin,1969; Royal AustralasianCol I ege of Surgeons. I 970. )
The Quqf ity of Care in Emerqency Departmenfs
It will be apparenl from the studies discussed so far, fhatmany researchers have described r;xisting servlces and discussed stand-ards for care in casualty deparlments. Few, however, have aftempted toeva luate the qual lfy of the rnedical care provided by matchíng the careperformcd with the establ is;hed standards. Nevertheless, the recentupsurge of interest in med ìca I care reser-rrch genera I ly has led to stud lesbeing underfaken to investígafe methods of evaluating the qual ity ofemergency care.
t'or example, Helfer (1967) examined the performance of internsin a paediatric emergency room using a charf review technique. A panel
of paediatricians defined sfandards for the trealmenf cf cerfaln diseases
28
in the emergcncy roorn. These standards were fhen used to evaluate thec:rre performed by interns as recorded in the medical assessmenf chartfor each paf ient. The interns were raled for prof iciency, ef'f lciencr¡
and competence. After an inilial assessment period, the interns were
made aware that fhe chart review was being performed. Subsequently'the records, and, prcJsumably, the quality of care, were observed foimprove. Chart review was then introduced lo the department as an
on-going process clesigned lo maintain'lhe improvement.
Brook of al , (1970) ev¡¡luatc+d the quality of care provided
for patients in an emorgency room in Ballimore by reviewing the medical
records of 141 patients who presented wi'lh gastro-intestinal disease.
Qual ity was assessed by examining Ìhe relaÌionship between the adequacy
of lhe diagnostic and therapeulic processes employed by the doctor and
the outcome of the disr:ase episodc. The methodology of the study in-volved both charf roviews and oatienl inlerviews. The qual ily of the
medical care was assessed as both inadequafe and ineff icien1- by every
criterion used.
A prel iminary report of a survey beíng conducted ín lheemergoncy departmenf of the Albany l.4edical Cenlre included reviews oflhe care provided for 4,029 trauma vicfims, 514 of whom were from road
crashes. (Carfer, 1971. ) 'Ihe¡ sludy involved colla'tion of data obtained
f rom ambu I ance reports, eme rgency dt> ¡,.artment records, hosp ita I records
and fol low-up patient interviews. A 1.7 per cenf diagnostic error rafewas reported for the roed crash vici-ims; none of lhese mis-diagnoses
werc fatal. The survey was felt -lo be extromely valuable for staf f ln
providing continuing evaluation and feedback of the results of theirwork.
(c) Emerqencv tlare Syslem Studies
ln recent yeôrs, lhe real ization thal the objectíve of high
qual ify emergency care requircs co-ordination between the separate
29
emergency services ôs well as eff iciency of operation wifhin each
service has led reseorchers to use a systems approach for sludyíngemBrgency care problems. ln the case of road crashes, the services pro-viding emergency care may be considerecl as elemen-ls of a system which
intoracl in pursuil of rhe common objcctive of reducing the losses, interms of injury and properfy danrage, resulting from the crashes.
The systems approach involves defining objectives and ident-ifying the critical factors ope;rating in a given situation, so thatalternative methods of achieving ttie stafed objectives may be evaluatedand related to the operation ol the total system under study. Severalsteps are involvecJ in such an approach. Firstly, the objectives ofthe system must be consídered ancl sfated in sufficiently operationalterms lo allow the development of mcasures of performance of the system.
Secondly, alternative methods of saïisfying lhe objectives must be
defined, and, thirdly, these alternatives must bc; evaluaterd to cletermine
the contribution crach could make lo the sfated objective. Finally, lhecosl of each alternatîve should be measured" (Boodman, 1967.)
t¡/ade (1964) was cne of the f irst aufhors to <Jiscuss the need
for an examination of emergency services whích would include servicesoperating at the crash scene as well as the hospital casualty depart-ment. ln 1965, Drye and Hyde clescribecl a system for providing emergency
care in Louisvi I le, Kcntucky. They discussed freatmenf at the crashscene and in hospilal and sta'teC that injured patíeni's receivedrcompef-ent first aid af fhe scene within 5 to 15 rninutes of the crash and were
in hospÍfal within 3C minuTc,.sr. Few data were presented to supportlhese claims.
The passage of the National t"lighway Safety Act by the 89th
Congress of ihe United States in 1966 provided lhc stimulus for wide-spread invesligaTion of emergency services. Several sludies of emergency
caro syslems were commenced under the auspices of.the National Highway
30
Safely Bureau of tho U.S. Deparfment of Transportation.
Particular emphasis was placed on the design of methods forthe analysis and evaluation of services. (Owen (1966, 1967) describeddetailed check lists which coulcJ be used by local authorities to clocument
êmergency s+rvíce workloads. Ir4ancgolC and Silver (1967 ) discussed theconcept of an Êmergency care system which íncluded - as system elemenfs -f irst aid, communícation, transporf and medical facilities. principalproblems in existing systerns were deemed to be the delays in the varioustrealment phases and inadequacies in the quality of the freatment pro-vided. The authors saw the solution to these problems in better educ-ation, comprehenslve planning, accreditation and control of services,and research into the various elemenls of .the syslem.
The commiftee on acufe medicine of the American Society ofAnaesthes iolog ísts -(
I 968) recommended community-wi <Je organ ization ofemergency care. The goal of hígh qualÍty emergency care was seen torequire ma.lor improvements in services af the scene, during ambulance
carÉ), ancJ in the hosp ita I emergency deparfmenf . Starrdards for the organ-ization, sfaffíng and equipment of ambulance servicr¡s and casualtydepartments were stated. l4edical staffing of ambulance was considereddesirable and recommenda'tions wcre made for the catogorlzation ofemergency deparfments accorrli ng to thei r size, faci I ilies and staffavailabîlity.
King and Sox (961) reported one of the f irst studios fo use a
systems approach in gathering data on emergency service operations.Report forms wcìre completod by ambulance drivers, casualty receivingnurses and admitting medical offlcers who treated emergency patlents inthe San Francisco emergency senvice area. The characteristlcs of theemergency services systom and the workloads on the varíous faci I itieswûre recorded by analysing the data containr¡d in 3,431 reports on
ambulance palients and 7,894 reports on non-ambulance patients from the
31
part¡cipating hospitals. Defails c''n the management of palients, lhetypes of care; providr:d and i-l-s effect on the patienfs were recorded,
along with The total times spenf irr receiving casualty care. Although
The findings were specific fo the local situation, lhe authors suggested
that the data may bo useful in subscquent simulalion studies, or for thederivation of ô genere I predicf ive mathema-licel model. The study didnot involve defined populalion and thus iis general appl icabi I ity was
I imited. ln a later paper King dcscribed the approaches lhal are
necessary in formulating plans for systems studies of emergency care.(King, 19ti8.) ln this paper he emphasized lhe difficulties inherent in
measuring fhe quality of emergëncy care and suggested the need for more
sensitive, prcferably time based, criteria for assessing care.
Several studies commissioned bry the National Highway Safety
Bureau tJevised morJels for the analysis of emergency care systems and
designed data systems for L¡se as recording and evalua-lion instrumentsby emc:rgency services. (Borclner, 1968; Dunlap, 1968; SfanforcJ Research
lnstifute, 1968. ) The studies predominantly focusscd on the provisionof servict s outside the hospital. A program for the analysls and sub-
sc':quent improvement of omergency services throughoul'the United Staleswas developed from the findings of such sludieE. (U,S. Deparlment ofTransporfation, 1969. ) The achievcment of emergency cere system object-Îves, as defined, would requirc individual slates to undertake compre-
hensive planning and development programs. Guidel ines for such programs
were suggested.
Th¿ Yalo lrauma survey (Keggi et al. 1970) was designed foexploro the re:lationships belween lhe communications, lreatmenf and
transport componenls of lhe emcrqency care system by using a cenlraltrauma registry. Adinitting nurses used specia I data forms to col lectinformalion from injurod palienls admitted to the Yale - Now Haven
Hospitolfs emergency cJepartmenf. Tho dala related to =l I phases of thepalientst emergency care and documenled demands on several areas of the
32
syslem as well ôs providing such assessments of performance as tlmedelays and treatment procedures used.
ln Austral ia, a: survey conducted by Hughes (1970) investigatedthe availabilify of acciclenJ and emergcncy servîces in the Melbourne
metnopol ilan arca. Questionnaires were used to determino the workloads
and response cðpacitles of N4elbourners casua lty departmcnts and ambulance
services. The findings were related to the clemographic characferisticsof the Melbourne metropol itan ereð. The author concluded lhat the number
of casualfy services in Mr:Ibourne was adequate, but that their distrib-ution in the metropol itan area was unsatisfactory.
Two comprehensive studies in the Uniled States used a systems
approach to evaluate problems of -l'he emergency care syslem in Baltimoreand Chícago. Webb (1969) investigated the patterns of staffing and
uti I izalion of emergency departments in Baltimore and compared the usage
patterns wilh those of 7-25 privately practising physicians. The studywas designed to investígate lhe faclors influencing lhe increasing use
of emergency clepartments by palients seeking primary care. Components ofthe emergency medical care sys-tem which wcre investigaterd included ambul-artce services, poison conf rol centres, prival'e physicians and emergency
deparlments. The steady increase in emergency department usage by non-urgent patients was found to have a weak negafive correlation wiihgeneral practitioner avai labi I ity. Greal variabi I ity in types ofphysician staffing of t;merqency rooms was found, although mosf depart-ments wr-'re staf f ed by i nterns and res i cJcnts. Pat ients wa i-led longer i n
hospitals staffed by housemen, who look longer fo treat patients and
ordered more diagnostic'tesfs. T¡me delays during ambulance care were
deferminecl from records, and the ambulance service tlme was found to be
22.8 ninutes. The mean f ime spent in waif ing for freatment in hospitalwas 42.5 minutes, with a mean tolal system'fine of 121 minufes.
A detai led analysîs of emergcncy servîces in the Chicago area
33
was performed by Gibson et al. (1970) '¡¿ho used a variety of techniques
to collect data about patienl's using J'he various emergency services.Ambulance services and hospital rèmergency de;partments were studied, and
a systems approach was used'to describe the transporl freatmenl, commun-
ications and documentation subsysfems. ln documenÌing changes in
pal-lerns of emergency servíce usage, the study bof h descr i bed a ncj eva I -!_dg!_ lhe opera-l i on of the emergency serv i ces . Ambu la nce serv i ces were
found to be def lclent in terms of their numbers and availability foruse, and standards of service varied widely between the differentservíces. lìecommendations for improving communications lncluded the
inlroduction of an emergency telephone numbcr and cenlral dispatching
faci I ifies. The survoy of' hospital emergency departmenfs in lhe Chicago
area suggesfed lhat the hospitals compared favourably with those in
other meÌropol itan areas and compl ied substantial ly with the relevanfstandards. Fînal ly, the survey investígafed the characferistics ofpatients trealed at hospilaI emergency dr:partments and reviewed the
cos'ts of lhis -l-reatment.
Thes,l 'l-wo studies are among the; most comprehensive reports ofemergency care syslems yet pubi ished. ln addiTion fc describing the
operation of the system in lwo major melropolifan areas, the authors
evalualed fhe performance of tlie system by consideríng the ínteractionsand perfoflflânctl of the various conrponent services.
Melhods of evaluating the performance of emergency care are
poorly defined and relafively unsophisticafed and have thus presented a
major stumbl ing-block to morc wîdespread eva luations of lhe qual ity ofcare. Andrews (1969) saw a necd for a genêral evaluatory model ofemergency care syslems which would take into ¿:ccount the occurrence of
emergency and emergency-l íke incidents, the outcome of those incidents,the operational characferistics of tho system, and fhe total cost ofoperating lhe system. He stated tha-t lhe u ltimale crìf eria for assossing
emergency care should be -
34
(a)
(b)
(c)
MedicaI oufcomes.
Reduction of sufferi ng.
l'ota I cosf .
Cosf is the only one of these lhree criferia which may be
âssrrssed objectively with presen-l rnefhodology, although even this isdiff¡cult because of lhe large number of hiddon cosfs involved. Never-
theless, cost htls, until recently, rarely been usecj as a measurc ofmedical care. Medical oulcomes are extremely difficult to predlct and
measure, and consequently death has been the outcome moasure mosf
common I y used.
lrr tl"re absence of adequate oulcome measurês, operalional cri-feria and nof ultimate criteria must be used to evaluate qualfty.Andrews suggested fhat time delays during freatment would be an appro-priate surrogatr: for fhe reducTion of suffering and thaf operationalcriteria fr:r the quality r:f omergency care were needed lo permit meanlng-
f ul evaluations of the systemrs performance. Simi larly, Nahum (1971),
in advocaling the use of a syslems approach for studying emorgency care,sfaled that functional analyses of lhe sysfem were Fequired. He con-
sidered that such analyses slrould include descriptions of the system
components and evalualion of their operating characterlsllcs, notably-iime delays and the qualily of the care provided.
Severa I stud les have desc¡-ibed tofa I t ime de lays i n e ílherambulance service or casualty core, bul only three - the systems sfudiesby King (967), Webb (1969) and Gibson et al. (1970) - have systematic-ally sturJiod the time delays experienced by patienfs in the variousphases of emergency care by recording delays in ambulance care and
de I ays i n recei vi ng freatment i n hosp ita I .
An important local study by membors of the Austral lan
lnsllfute of Hospital Adminisfrators examincd the waiTing and treatment
35
t îmes exper îenced by ¡ral ients i n scvera I hosp ita I c¿i sua I 'f y depa rfments
in Victoria. A recording fornr was complete<j for patients as theypassed through lhe; several stagcs of lheir casually treatment and
delays werr.: noted. Visits of 4,125 pa'fir>n1's'to eleven hospifals were
documented. Subscquent analysis of the recorded data showed thatpatients w¿riled considerable limes in the various treafmenf phases.
(Brand el al., 1971, (1), (2), (3).) ln a subse;quent paper standards
for waifing times were suggested (Brand,1971, (4).) and the offects ofa mc,thod of ensuring that thr: standarrls were recognízed by attending
staff were discussed. lt was founcj that improvements in waiting limesoccurred as a result of enforcirrg an adrninis;trative instruction thatall patienls should be secn r¡ri-fhin 45 minutes of arriving in casualty.
The use of time cjr:lays as a substitute for reduction ofsuffenirrg presupposes lhat the provision of care în tho shortestpossible time is likely to be a sig.¡nif icant faclor in reducing
morbidity and mortalîty. I'ievertheless, lhe relalionship befween treaf-menf delays and thc development of morbidil'y is difficult to define inmosl silualions and is a ma.jor reason for lhe facl lhat precise standards
for delays have never been suggesfed beyond the usual and somewhat
ncbulous eshorlest possible? delay. More precise definitíon of reason-
able time inÌervals ís of some importance for planncrs of emergency
care sys-lerns, however, sinco many of the major recommended changes loexisting services are based on the assumption thal adequate treatmentis _¡ç.!._ being provided ín reasonable tîme. For examplc, one importanl
advantagr: quolod Lry thosc: who ¿¡dvocate Ìhe replacement of road ambul-
ances by hc-.licopters is lhs recJuction of lhe time delays which accompany
road transport. Unless lime delays in'j-he existinçl system, and the i rsiqnif icance, are known , such measures as the introductíon of hel icoptersmay nol have the effects desired and expecled of lhem.
Several authors have investigaled lhe importance of time
delays in emergency carr: by reviewing the f indings of autopsies on road
36
crash victims. Roberfson and Tonge (1968) and Ruffel-Smith (1970) exam-
ined'lhe duration of survival of victims af-ler crashes. lt was estimated
that approxÍmately two-thirds of'all the dealhs in lhe second study
occurred within the first 25 minutes after The crash and that, if the
ambulance response tlme could have been halved, only 1.5 per cent ofthoso persons rvho diecJ within lhe firsl twelve hours mighl have been
saved.
Frey ef al. (1969) estimated thal 2B (18fr) of 159 persons who
died afier fatal crashes in Michigan could have survlved had oarlier oralternative Ireatment been avai lable. lf was noted, however, thatresuscilation of these patients would have required the ski I ls ofpersons well versed in intravenous fluid therapy and airway control.Furthermore, this lreatment wculd have been required at the crash scene
and within minutes of the cr¿:sh for 15 of the victims, during transportlo hospifal for 11, and in hospilal 'for 2 paf íents.
Furfhcr evidence in supporf of the importance of delays in
receiving emergency treatmenf is provided by the di fferenccs in fafal ityrates cbserved belween rural and urban crashes. Wal ler (1964) attributedthese differences fo problems in crash detection, delays in providing
care, poor communications between personnel at the scene and back-up
medical staff, and the inexperience anci lesser availability of staff in
rural areas. Victims were ob,si:rved to die sooner, morê commonly at Ìhc
scene, and of less severe injuries in rural than in urban crashes.
Adams (1961) made similar observations in his study of rural cr¿islles in
Ausfra I ia.
Mi I ler and Page ( 1968), however, €XP lorc¡d f he ef f ects of
delays ín receiving emergency medical care on the probabi I ity of
survival, given thal patienls had rsurvived Ìhe initial col lisionr.Time delays during ambulance care for 275 crash viclims in Louisiana
wero calculated from data in police f iles and the patientrs injuries
37
vlere classified by sevcrity. LiTl'le difference existed befween the
fatal ancl non-fatal groups arrcJ if was not possible to relate the delay
before. treatmt-.nt to lhe ultimate outcome f'or the paTicnls studied.
Van Wagoner (196i ) investigaled the meCical records of 606
male soldiers who died from traumalic injury in the United Stafes. He
found thatlspeed in reerching medic;:l altention did not seem to be a
primary facfor in survival of the injuredl and noled lhaf one-sixth of
lhe patienls had received inadcquate trealment in hospifal which had
contributetl to lheir death. This lack of proper care was a.tf ributed to
a combinaf ion of faulty díagnosis and inaclequate therapy by'the attend-
ing surgeons. The author wenl on to suggest that, rwhile proper trans-portatÌon, physical facilitîos, blood, X-ra'ys and laboralory tests havr>
all been pointcd ouT as important facÌors in the proper care of the
injured, perhaps the weake.:st I ink is the doctor hirnself | .
Lougheed (1965) report':rd the quality of the e:mergency care
received by a group of rr:ad crash vicfims in er paper which discussed fhe
arrangemen-ls for treating crash injury ín Tennessee. Although the
criteria of adequacy of carc and fhe methocls of assessment were not
defined in the paper, it was slatcd thal only 5 per cent of 616 patients
had received adequale f irst aid befor-e admission to hospita l.
Such evidence reinfcrces the need for studies evaluating the
qual ily of care. Assessments of qual ify have proved exlremely difficultin all areas of medical care becausi: of the limitations of available
mt:thocJology. Nevertl¡eless, s-tudîes have been underfaken to investigate
:issessin(rnt methods. These represenl a large f ield of modical care
rcsearch i n the ir own right., ancJ are comprehens lve ly rev iewed by
Donabedian (1966; 1969) ancj Peterson (1963;1966).
One of fhe reasons that deta relating lo the porformance of
care and its effects on the patienÌ havc rarely been obfained, is that
38
i+ is exlremely diff icull to Ce-t'ermine retrospectively wl'relher or not
proper care h¿rs been given by ambulance officers and rnedical personnel.
It is one-thirrg fo examîne fhe potential lreafment thaT personnel
should be able to deliver; it is another lo de'i'ermine how lhey actuallyperform.
DirecT observatic¡n of physician perfcrm¿lnce has boen used fo
overcorne lh is prob lern in othcr tneclica I care areas, notab ly in the
sludies of gr.jneral practice conducted by PeTerson ef al. (1956), Clute(1963) and .Jungfer and Last (1965). Whi lst such studies have the
obvious aCvantages of diroct observation in any scientific investigat-ion, fhey are ¡:lso accompanied by problems of sampling, observer bias,
cost and re¡rroducibi I ity. Direct observation, as a sludy method, has
not been used in any of fhe reported studies of emergency care.
ln recent vears, wÎclespread use has been made of operations
rc:search lechniques in tl're stucJy of queue Ìng and resource allocationproblems and as aids'to admÍnistrative decision making in industry. 'Ihe
application of fhese techniques lo road safeÌy and emergency care pro-
blems is, however, a comparalively recent development. (Little, 1966l'
Leinirìgor, 1968. ) Bonner (1966) used waif ing time data in a simulation
sludy of hosp ita I outpal ienf and emergr,\ncy services. Savas (1969 ) used
a compuler s imu I at ion fr: ana I yse the poss ib le.: improvements f hat wou ld
result from proposed changcs in lhe nunrber and locatîon of ambulances in
New York City. The cosf-.effcr:'tivoness of several alTernatives ivas eval-
ualed and the advantages of a <lispersed ambulance system wifh central
dispalching faci I it¡es was demons'trated. Kel ler (1971 ) reported the
results of a simulation sf u<1y which investigated service and detection
syslems on freeways. lt w¿rs found that-l-he combinafion of discretecommunication terminals along lhe freeway, monitored at a central clis-
patching system, with station¿:l pol ice and mechanical service unlts
werc the most cost-effectîve operotions. The usefulness of fhese tech-
niques as administrative aids suggests that They will be of consideratrle
benefit in planning future modificalions c¡f emergency care systems.
39
Chapter 3
THE STUDY BACKGROUND
STAÏEMENT OF 'IHE PROBLE¡4
The review of the publ ished I iterature shows that stuclles ofroad crash epidemiology in Austral la have concentratecJ on fhe causesand patterns of crash injury. consequenfly I ittle information has
been available from which the performance of post-crash events can be
assessed. ln particular, I iÌtle has been known abouf the care pro-vided by emergency services a-t lhe scene of the crash, durlng ambul-ance treatment, and in fhe hospltal casualty department. Nevertheless,a general awareness lhat lmprovements ln emergency services may be
desirable has meant thaf planners and administrators are under pressurefrom many seclions of the community to infroduce changes in existingservices. For example, tlre use of helicopters and emergency careambulances has been suggestecl as a means whereby the consequences ofroad crashes and other medical emergencies may be reduced. The lack ofdata on existing operations makes the raflonal planning of services and
evaluation of such a lfernative patferns of operation extremely dif f icult,
As the review of the literature has shown, Ausfralla is notalone in thls need for emergency care sTudies, although fhe increaslngatlention being paid to €mergency care problems is reflected in thegrowing number of studies being reported f rom overseas cenlres. f,4ore-
over, further studíes of emergency care systems are sfi I I required.These needs were well summarised by Frey who, in discussing the dlrect-ions further research in fhe united sfates shourd take, sfated:
'There muet be a systems analyaís of the openation of theemegeneA medieal senùíce" from the seene of the aeeident untíL lospí,taLdiselwnge. Eaeh eLement inuoLued ín patí,ent eare (transpont" eonnmtnie-atíon" training the neeeue worken, in-hospital treabnent of the patienta,nd vøspitaL staffing) mtst be eæønined, in oyder to d.etect a?ea,B ohiehneed improuement. t (Frey, 1971,)
40
The systems approach for studying emergency care was brieflydiscussed in lhe preceding chapter. The use of such an approach re-quires that elements of lhe system should be examinecJ in the contextof thc+ overall system, that syslem objecf ives should be def îned, and
that alternafive means of achieving those objectives should be eval-uated in the lighl of their possible effects on the overall system.ln this study a systems approach is used whereby the separate servicesinvolved in providing emergency care are regardeci as elements of an
emergency care system.
ln fhe pas-|, most studies of emergency care have concentratedon the operalion of emergency services oulside the hospital withoutrelating fhe care provided by'these services to events whlch occurwlthin'the hosoital. The importance of each soparate phase i n fhemanagement of an injured pa'tient ls diff lcult lo def ine, since medlcalcare is a conlinuous process which commences soon after a pafíontreceives his injury and continues through his deflnitive freatment.Nevertheless, for practical reasons, cut-off poinls for each of fhevarious phases of care must be used. Traditional ly emergency care has
been considered as ending with the arrival of the patient at the hospitalemergency department. ln contradistinction, th¡s study wi l l argue thatstudies of the emergency care system should include consideration of thecare provided wilhin lhe hospital casualty rlepartment.
There are several reasons why such an epproach should be used.
Firsf, al-lhough the patientrs arrival at the casualfy departmenf usual lyrepresenfs lhe beginning of his medical treatment, lhe care providedfor patients with severe ínjuries is usually limited lo resuscitatlonand stabilization of their condition before they are admitfed fordefinltive freatment. As such l't is probably most appropriately des-cribed as emerqency medical care. secondly, projecfed changes in theoperation of one ôrea of the system musf be viewed in the overall system
context. For example, time delays în bringing medical care to the
41
pat¡enl (or the potierrt to medical care) are often quoted as reasons formodîficalions to lho transport and treatment subsystems. Time saved in
transport, whi lsl it may bc¡ of cri tícal value, musl be viewed against
The background of time spenl stabilizing lhe condition of the patlenlaf the crash scenê and, more parficularly, againsl the time delays in-volved in receiving medical carc after arrival in casualty deparlments.
It is worth noting In fhis regard that the Task Force on
Emergency Medical Services of the National Hlghway Safety Bureau in the
Uníted Stales recordcd lhe fol lowing observatlon at lhe Highway Safety
Program Priorities Seminar in July, 1969,
'ALtlnugh in the work of N,H,S,B. ue ¡'haLtedrt mo?e or Less atthe TrcspitaL door, the emengeneA ?oom and the medical eare requined
uhen the oietin reaehee that faeiLity, makes this phase of the aystem a
uitaT element of the totaL Ernerge-ney MedícaL Servíees System, and one
in uhích eonsídepabLe upgnadíng is requined. rf ilnt' faeility ispoonLy staffed or badly deficðent - as ís often the ease - then írnpnou-
íng othen eLements of the system outside the emez'gency ?oom uiLL ob-
uiousLy not produee paA offs.'
THE EMERGENCY CARE SYSTENî IN MELBOURNE
Extensive use wÌ I I be made throughout +his thesis of an
analytical model which describes the emergency care sysiem in terms of
four functional subsystems - communications, transport, treatment and
documentation. The mode i t'ras de ve loped by the Frank I I n I nsf iluteResearch Laborafories (Bordner, 1968) to describe lhe services providing
care before pafients reached hospital. ln lhis study the model is
adapted and expanded to includo care within the hospifal casualty
department.
ln lhe fol lowlng two sectlons fhe objeclives of the emergency
care system are stated and the services which comprise the elements of
42
the sysfem for road crashes in MelLrourne are dÌscussed. These servicesinclude the general publ ic, pol ice, fire, fowing and ambulance services,and lhe casually departments of the major metropol ltan hospitals. ln
the th ird sect ion, the mocle I is described. ln a laler sect lon(Chapter 7) the model will be used to discuss the performance of emerg-
ency care within the system as it was observed in Melt¡ourne.
(a) Emerqencv Care Svstem 0biectivesThe primary objective of the emergency care system, as ¡t
operates for road crash victims, is to reduce the losses due tc injury,death and property damage incurred as a result of road crashes. ln
functlonal lerms, this objective impl ies fhat a comprehensive emergency
care system should ber capable of:1. Providing prompt idenliflcation and response lo crashes
under a range of emergency conditions.2. Suslaining and prolonging I ife through proper first ald
and resuscitation measures, both at lhe scene, duringtransport and in the hospital casualty department.
3. Providing fhe co-ordination, lransport and communicalions
necessary to bring fhe injured person and definitivemedical care 1'ogether in the shortest praclicable tlme,wilhoui simultaneously crcating additional hazards.
(U.S. Dept. of Transporfation, 1969.)
The achlevement of these objectives would ensure that crash
vicf lms received prompt and adequate ernergency care. The followlnganalysis aims to determine to what exten'l such cbjectives are mef by
the existing system, and to provide a data base from which performance
standarcJs can be developed, system defects determined and appropriatemod i f icalions p lanned.
43
(b) Elements of the Emerqency Care Svstem
The fol lowing groups and services are normal ly involved lnprovlding care for road crash victims in Melbourne:
( I ) Memtrers of the Genera I Pub I lc(2) Towing Scrvices(5) Pol ice(4) The Fire Brigade(5) Ambu lance Services(6) Publ ic Hospilal Casual ty Deparfments
(1 ) The General Publ icMembers of fhe public are usually the first to arrive af fhe
scene of a road crash. They frequently provide first aid for the
injured, undertake traffic control and, most importanfly, notify the
formal emergency servicos thaf fhe incidenl has occurred. Hence fhey
play an important role ln the early post-crash phase.
(2) -low i nq Serv lces
Towing services are usually the f lrst c¡f the formal emergency
services to reach the scene of road crashes in f,lelbourner ê situationwhich results parfly from the competitive nature of the towing business
and partly from lhe fact that cach service works within a relativelysmall geographical area. Theîr primary role is to remove vehicles and
debris from the crash scene. They rarely provide first ald for the
i nj ured.
(l) Pol lce
Police play an importanl role: in lhe post-crash phase. Thelrresponsîbi I ities include protection of the crash scene, maintenance oftraff ic f low, and crash investigation. They collect informaf ion forofficial recording purposes, assist communicafion between the separate
emergency services, notify the next of kin of the injured and conduct
44
fol low-up investlgations to assess and apportion blame. This is an
extremely complex and time-consuming role.
First aid skills may be required by police in a wide range ofemergency siluations. Police in Victoria receive f irst aid instruclionduring their basic training on joining the force. Any further first aid
trainíng is undertaken on a voluntary basis.
(4) The_ Life Briqade
The f ire brigade a-ltends road crashes in response to speclal
requests from ambulance or police officers at the scene. As the omerg-
ency service equipped with the heavy duty povrer tools occasionally ro-quired for extrícating Trapped viclîms, fhe brigade is summoned when
such equipment is needod. They also altend crashes when the risk ofpost-crash firo is high, nc¡tably when fuel line rupture results in
pefrol spi I lage.
ln Victoria, firemen do nol receive first aid instruclion as
a roufine part of their trainlng. Some firemen attend firsf aid courses
of the St. John Ambulance Association on a voluntary basis.
( 5 ) Ambu lance Serv ice i n t''le I bourne
The ambulance service is fhe major provider of emergency care
at the scene of road crashes in Melbourne. Ambulance treatmenl and
transport facilities in the metro¡rolitan area are provided by the
Victorian Civil Ambulanco Servlce (V.C.A.S. ) which operates oul of 10
ambulance stafions in the city and surrounding suburbs. The service isgovernmenl subs i d i zed and depends on vo I untary subscr i pt i ons, donaf ions
and the collection of fees for service for the remainder of its income.
Fourteen other ambulance services operate in outer urban and rural areas
of thc Sfate of Victorla, each wilh a defined area of operaTion and
simi lar arrangementsfor financing, equipmenl and personnel training.Overall control of ambulance services in lhe Stale of Victoria is
45
maintained by the Viclorian Hospitals and Charities Commission.
ln addition to treatment and transport for emergency cases,
the Victorlan Civi I Ambulance Service provides routine transport forsick patients befween hospilals and belween home and hospltal. Whi lsta tClinic Carr service provides facil¡t¡es for the rouline fransport ofnon-stretcher patlents, the majorily of ambulance runs are made forpatienf transfer cases, with emergency cal ls forming approximately l0Íof al I calls aftendod by the ambulance service. 0f the emergency callsapproximately 501 are i'o the scene of road crashes. (V.C.4.S., 1970.)
This pattern of operafion has evolved as an apparently efficlentand economicaI melhod of servicÌng fhe demands on lhe st:rvlce, althoughthe efficiency and economy of the operation has never been fhoroughlyinvestigated. ln particular it is worth noting that there is no system
of emergency ambulances staffed with ski I led medical or paramedical
personnel providing care in emergencies. The use of such ambulances has
been suggested in view of the claims made for their effectiveness inEuropean counÌnies and in the U.S.A. and a unif is currently being testedin an experimenTal project conducted jointly by the V.C.A.S. and theRoyal Melbourne Hospital. Evaluation of fhe effectiveness of such
units in the light of the present crpera'tion of the emergency care system
wi I I be referred to later in this study.
Ambulance Staffln 1969/70 the V.C.A.S. employed a slaff of 285 persons of
whon 2?.5 were directly associated with ambulance operaf ions. A def inifecareer structure exisls for ambulance officers within the service. Pro-mofion through fhe ranks of Ambulance Officer Grades I - lll, two grades
of Slatlon Officer, two gracles of Divisíonal Officer, fo executive staffpositions is dependent on experîence, seniority, attendance at resident-ial fraining schools and successful complefion of correspondence coursesconducted by the Victorian Hospítals and Charifîes Commission Ambulance
46
Training School. 0f the lB7 Ambulance Officers employed by the serviceat the end of the 1969/70 fiscal year, 4of were of Ambulance officerGrade lll rank, 50% Grade ll and lOÍ Grade l. (V.C.4.S., 1970.) Con-
difíons of service for these men are governed by a determination under
the V íctor ian Lat¡our and I ndustry Act.
Staff Recruilment
Standards for the recruitment of officers to the service areunder conÌinual review. At the time of lhis sfudy the only prerequisitefor joining the service was the possession of a current driverrs licence.Applicants who possess a f irst ¿:id certif icate from the St. John Assoc-iation or some similar volunfary society are preferred. A recruit was
required to present a medical ccrtif icato to af f irm his suil'ability forambulance work, bul recenl modîfìcations to service pol icy have meant
that recruits are now examined by lhe servicers own Medical Officerbefore lhey are employe,.d. The general level of education of recruits islow and less than 5% nold the Victorian lntermediafe Certîficafe or ílsequivalenf. This fact presents some diff iculty urith the dosign oftrainíne courses. (tierry & Toyne, 1970,) Nevertheless, recruitingsultable off icers is not a problem for thesorvice and, a't present,approximately 7 app I icants are i ntervicwed for each man emp loyed.(Ortmann , 1971.)
Staff TrainingTraining procedures irr the service also undergo conlinuing
review. Soveral changes in training methods took place during the sfudyperiod ancj the fol lowîng descriplîon of tra ín ing courses represcntsthose applying at the end of 1971.
0n joining thc service, V.C.A.S. recruifs atfernd a fhroe¡ week
course which includes instruction in basic anatomy, physiology, firslaid, the fundamenfals of ambulance transport nursing.and demonstrations
of the r:se of ambulance equipment.
47
Visits are arranged during this period to fhe casualty departmenl of a
major city toaching hospital, the city mortuary and lhe recovery and
intensive-: care warC of a teaciiîng hospifal. After completing this basic
lraining lhe; officcr is roslerod for normal ambulance duty. For the
f irst four weel.ls of such dufy, a recruit is p laced under the supervision
of an Aml¡ulance Of f icer Gradr,: lll. After this period of supervised
scrvice ttre officer joins tl¡c normal roster, but e servicc regulation
stipulafes that no ambulance should be manned by fwo Ambulance Officersof Gr¿:de I standard. Anothcr administralive instruction requires thatthe senior officer manning an ambulance should be responsible forpa1-ient care.
Tho Victorian Hospit¡¡ls and Charifies Commission conducts a
training school for Ambulance Cfficers which is attended by offìcorsf rom all 16 of 1'he Victoriar¡ Ambulance services. All ambulance off icers
musf apply for such lrainîng wilhin twclve months of joining a service
and promotion through the separal-c grades of Ambulance 0ff icer, Sfafion
Off icer, Divisional 0ff icer and Superintenden-t is conditional on success
in lhese courses as well as expcrience and seniority in the service.
The subjecf material of the courses covers all aspects of ambulance
service and lectures and practical materÎal are presented by oxperts
in the separate fields.
Affer compleTing lhe necerssary courses, an Arnbulance Officer
Grade ll should be competont to lre¿¡l the unconscious patient, maintain
ef feclive airway confrol, ventili-:'te the patienl using mouth to moulh
lechniques or a Lrag and mask, and be able fo diagnose the need for and
perform ex'ternal cardiac mossage. As well as these life-saving procod-
ures he should be conrpetent in minor firsT aicl pror:edLtFersr and be able
to control haemorrhage, apply spl ints, anil perform aPpropriate exlric-ation and I ¡ft¡ng manoeuvres.
St¿rndards for ambulance officer training in Victoria are
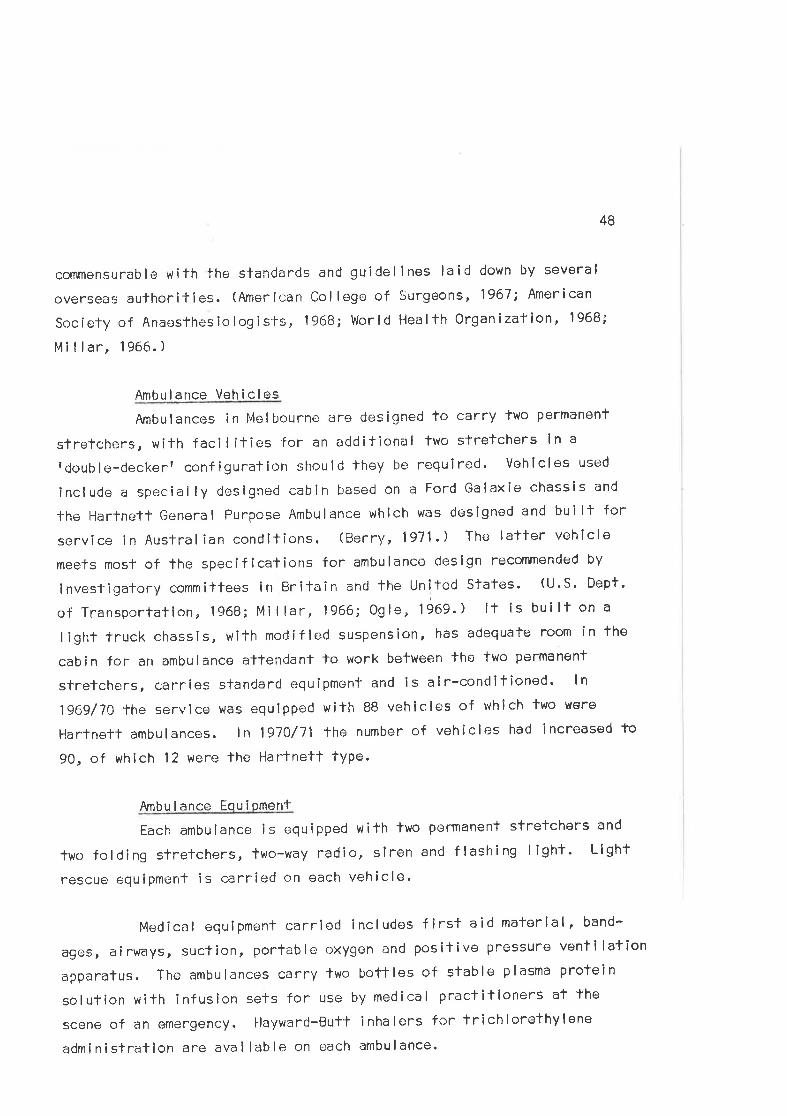
48
commensurable with the slandards and guidel lnes laid down by several
overseôs aufhorities. (American Col loge of Surgeons, 1967; American
SocÍety of Anaesthesiologlsts, 1968; World Health Organization, 1968;
l,lillar, 1966. )
Amt¡ulance Vehicles
Ambulances in Melbourno are designed to carry fwo permanent
stretchers, with faci l it¡es for an additional two slretchers in a
fdouble-deckert configuralion should lhey ber reguired' Vohicles used
lnclude a specially designed cabin based on a Ford Galaxie chassis and
Ìhe Hartnetl General Purpose Ambulance which was designed and builf for
service in Austral ian conditions. (Berry , 1971,) The latter vehlcle
meefs mosf of lhe specifications for ambulance deslgn recornmended by
invesf igatory committees in Britain and the United Stales' (U'S' Dept'
of Transportation, 1968; Millar, 1966; Ogle, 1969.) lf is built on a
light truck chassis, with modífied suspension, has adequate room in the
cabin for an ambulance attendant to work between lhe two permanent
stretchers, carries stanclard oquipmenf and is air-conditîoned' ln
1969/70 lhe servlce was equlpped with 88 vehicles of which two were
Hartnett ambulances. ln l97O/71 the number of vehicles had increased fo
90, of which 12 were lhe Harfnett fype.
fur¡bu I ance Eou i omenf
Each ambulance is equipped with lwo permanent stretchers and
two folding sfretchers, two-¡,ay radio, siren ancl flashing I ight' Llght
rescue equ ipment i s carri<;d on each veh ic le.
Medical equipment carried includes first aid matorial, band-
ages, airways, suction, portable oxygen and pos¡tive pressure venti lation
apparatus. The ambulances carry two bottles of stable plasma prolein
solulíon with infusion sets for use by medical praclitioners at the
scene of an emergency. Hayward-Bul't inha lers for trichlorethylene
administration are available on each ambulance'
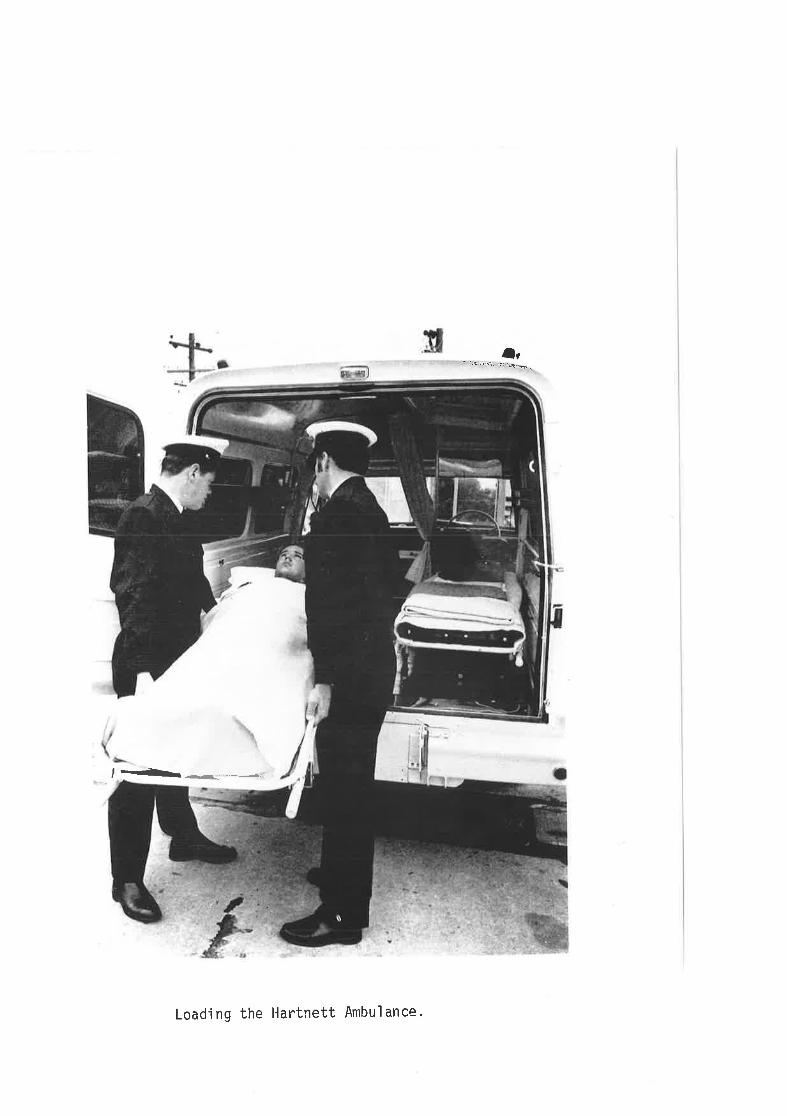
lr- ,È irrri: -1i '-\,Þ ,
,- .-
Load'ing the Hartnett Ambul ance.
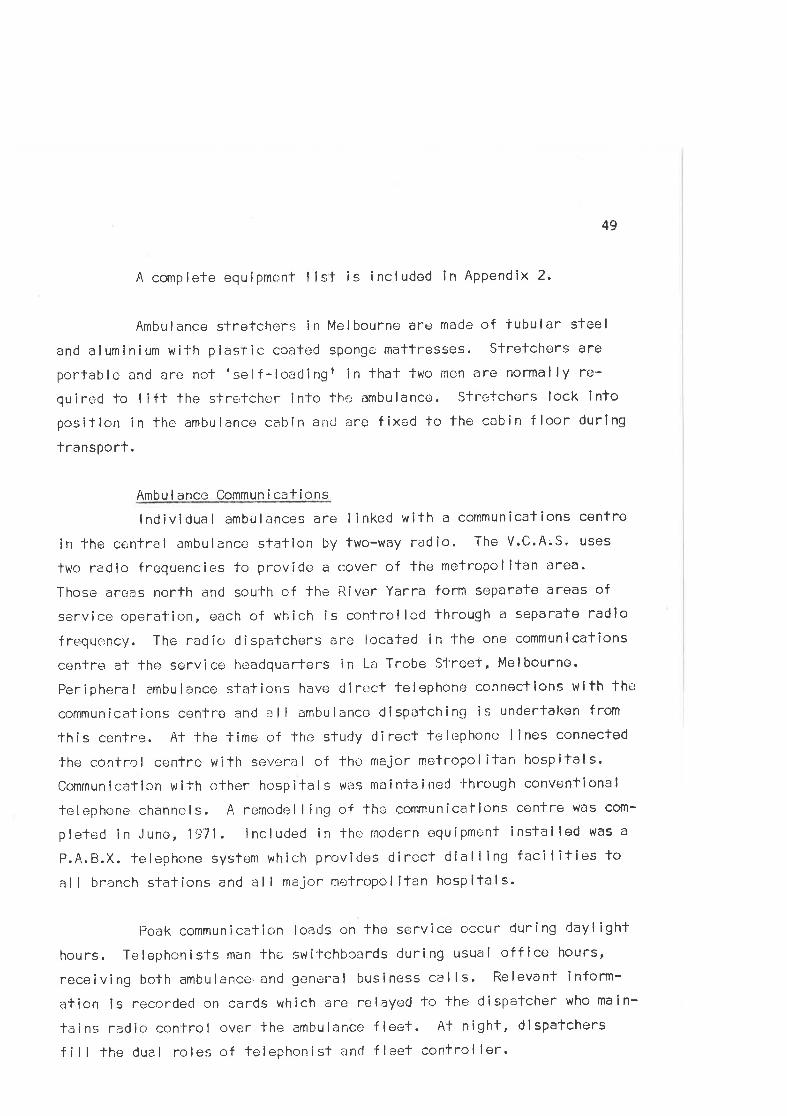
49
A complete equipmcnt I lst is included in Appendix 2-
Ambulance stretchers in Melbourne are made of iubular steel
and aluminium wilh plastic coated sponge mattresses. Slretchors are
porlable and arc notrself-loedingt in that two men are normally re-
quired to lift the s'lrotchcr into fhe ambulance. Stretchers lock into
posilion in the ambulance cabin and are fixed to lhe cabin floor during
transporf.
Ambul ance Commun í cationslndividual ambulances are I inked wiTh a communications centre
in the central ambulancc station by two-way radio. The V.C.A.S. uses
lwo radic frequencies to provide a cover of the metropolitan area.
Those arcjas north and south of fhe Fìiver Yarra form separate areas of
service operation" each of which is controlled lhrough a separate radio
frerquoncy. The radio dispatchers are locafed in the one communications
cenlre al lhe.service headquarters in La Trobe Street, Melbourne.
Peripheral ambulance stations have direct telephone conneclions wifh The
communications centre and a I I ambulance dispafching¡ is undertal<on f rorn
fhis centre. Al the time of the study direct lelephone lines connected
the control centre with several of fhe major metropol itan hospitals.
Communication with other hospitals was môintained thrc¡ugh conventional
telephone channels. A remodellirrg of the communicalions centre wðs com-
pleted in June,1971. lncluded in lhe modern equipment installed was a
P.A.B.X. telephone system which provides direct dialling facil¡ties Ioal I branch stations and al I major rnetropol itan hospitals.
Peak communication loads on the service occur during dayl ight
hours. Telephonists man lhe switchboards during usual office hours,
receiving both ambulance,and general business calls. Relevanl inform-
ation ¡s ¡s66rdecl on cards which are relayed to the dispatcher who main-
lainE radio control over the ambulance fleet. At night, dlspatchers
fi I I the duel roles of felephonisl ancl fleet control ler.
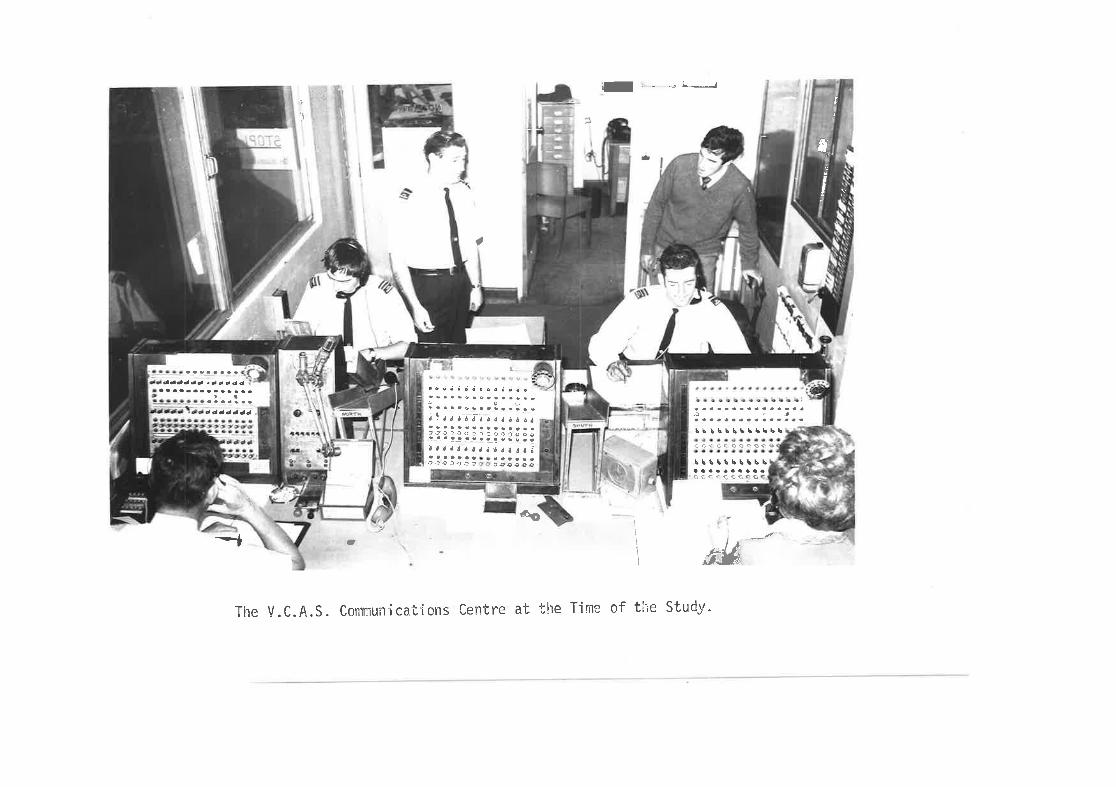
T*
I, _ _4L- t
a
t
)
\r
I
I
.oiJ
r'iìl ..,
bi lb\L5b5l.bbù,:t:ùcooÔÔse
Lltlrbb\\baaaaaaaaaaaçtrccc G
\êO
-t\ t,z
dÅlJ
The V.C.A.S. Commuilícalfons Centre at the Tirne of the Study.
¿aôððé )a¿ccddd d d ó ó ó o ô ¡ ó e o ó
.)a8a.aco oaa9a€
I
¡,
¡,
50
Dispatchers are senlor ambulance personnel, usual ly of SJation
Offlcer rank and above, who have had considerable training and experience
in ambulanc<; work on the road as well as special training in the radlo
and olher procedures associated with fleel control. The control room lsmanned lhroughout the day by af least tr,¿o dispatchers and a supervisory
divlsional off icer who is responslb,le for overall control of the f leet.
( 6 ) l-losp i ta I Casua lty Dep¿rrtmenls
Victims of road crashes in Melbourne usual ly receive emergency
medical care in the casualTy department of major public hospitals. Two
of these hospltals in lhe area of Melbourne under sfudy are teaching
hospitals and the lhird, on fhe periphery of the study area, is a rnajor
district hospítal. Each is equippeld fo handle medlcal emergencies of
al I types. The distribution of major hospitals in the Melbourne mefro-
politan area was invesligated by Hughes (970) and found to be unsatis-
factory. That study was conducted at the same time as this and his con-
clusions and recommendalions are thus germane to the present discussíon.
Those interested in fhin problem are roferred to Hughesf thesis.
Med i ca I Staff i nq Patterns
At the time of fhe s'l'udy each of fhe casualty departments was
manned throughoul the day by junior resident medical offlcers (flrstyear gradua'tes in medicine). Their immediate supervision \,úas provided
by senior resident medîcal officers. These are usual ly doctors in theirsecond post-graduate year. Administrative responsibi I ity for the depart-
menl lies with fhe medical superinlendent, or his deputy, and casualty
surgeons were ¿ìppointed, on a half-time basis, to oversee casualfy
services. Ofher medical supporf was provided by members of the in-paticnt meclical staff .
Nurs I nq StaffNursing care in fhe deparlments is provided by both lralned
and trainee nursing staff. At the timc¡ of the study frained staff were
51
read¡ ly avai lable for casually dulies during the morning, afternoon and
evening shifts, bul'slaff ratios fell off markedly during the night
shift. One sisfer and three or four trainee nurses were normal ly
rostered for night duty in the Alfred Hospitalfs deparfment. A senior
nursing sisler was responsiblo for supervising casualty nursing services
and was present in lhe departmenl during normal workíng hours. During
the night hours, the cenfral nursing administration assumed administrat-ive responsibi I ity for nursing services in casualty.
Anci I larv Staff and Services
Casualty clerks normally inferview patienls on admission and
perform the necessary recording and documontafion procedures. The
medical reccrds library is located clc¡s¡; to lhe casuälty clepartment in
lhe hospifals studied, particularly fhe Alf red Hospital, whero the
casual'ly department is relatively modern and wel I equipped, having beon
opened in 1966.
ln keeping wi-fh its modern design and facilities, the Alf red
Hospilal has an X-ray machine anC 90 seconcj film processor in the casual-
fy department. Radiographers ere rostered for dut'y in the deparlment
throughout the day. The X-ray deparlrnent is conveniently located ln
lhe Box l.lill HospiTal, t¡ut in Prince Henryrs is several f loors removeC
from the casualty department in the same wing of the building. ln the
lalter hospital, at the time of the sÌudy, a radiographer was rostered
on call during the night hours, but was nol required to bo present in
the deparfment - or even within the hospiial confines.
Other casua lly staff members i ncl ude medical orderl ies,
nurslng aides and domeslic sfaff.
52
(c) A Model for ribino the Emeroencv Care Svstem
The Emerqencv Care Cycle
It is useful to consider the events which occur during emerg-
ency care in lerms of flow pattorns in the system. After a road crash,
several emergency services are involved in the various care phases.
The flow of events is, to some oxtent, sequential and each stage is
described as an cperational stage of the Emergency Care Cycle.
CRASH
An incídcnt occurs with patient injury and property damage.
DETECT I ON
Members of the publ ic, who are usual ly the firsl helping
personnel on the scene, detect fhe crash and may Perform
important emergency procedures (e.9. first ald, protectlon
of the scene, extrication of victims).
NOTIFICATION
The emergency services are alertod and thelr resources
mobi I ized.
D I SPATCH
Emergency si¡rv ice veh ic les â Fê srîñ't to lhe scene.
5. TRAVEL TO THE SCËNE
The emergency services travel to the scene with al I reason-
able haste. The relalive localions of the ambulance and the
incident and lhe accessib¡ I ify of the site are important
factors in delermining time delays ln ambulance response.
TR I AGE
The injured are assessed to determine priori'l-ies forfreatment.
2
3
4
6
7
B
53
TREATMENT
First aîd is performed, the paf ientrs condilion is slabil-ized and preparations mado for transport.
TRANSPORT
The injured are laken to hospital for definilive medical
care.
9. TREATMENT IN 'I-RANSIT
Sk¡ l led treatment may be required to maintain the patienttscond it ion.
.IO. TRANSFER TO CASUALTY CARE
The events associated with del ivery of the patient tomedical care inclucle fhe transfer of the patient from the
ambulance to the casualty department and the fransmission,
from th<l ambulance officers to lhe casualty staff, of al I
relevant informalion rela'f ing fo the patientrs condition
and lreatment before admission.
1 1. AMBULANCE RETURN TO READINESS
The ambulance personnel prepare fhe vehicle for another
cal I and notify the dispalcher of their readiness for such
a call.
12. CASUALTY RECEPT ION
Personal detai ls are recorded, the patienfis medical record
is generated, and lhe pallent is admitled to the casualty
assessment area.
13. TRIAGE
Examination and assessment of patient injury is undertaken
by the nursing and medical staff.
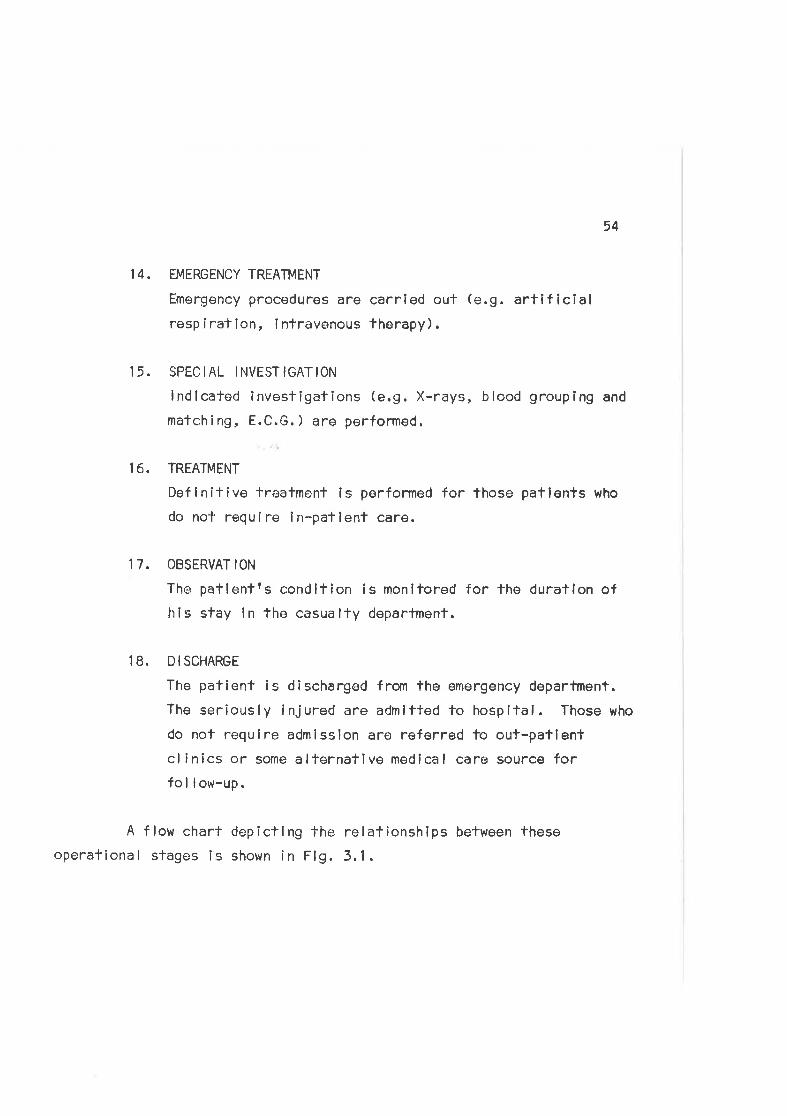
54
14. EMERGENCY TREATMENT
Emergency procedures are carrled out (e.9. artlficialresp íralion, intravenous therapy).
15. SPECIAL INVESTIGATION
lndlcated investigafions (e.9. X-rays, blood grouping and
matching, E.C.G.) are performed.
I6. TREATMENT
Deflnltive treatment is performed for those patients who
do not require ln-pallent care.
17. OBSERVAT ION
The patienfrs condífion is monitored for the duraflon ofhis stay in the casualty department.
18. DISCHARGE
The patient is dischargod from the emergency department.
The seriously injured are admltted to hospital. Those who
do not requlre admission are referred fo out-patlentcl inics or some alternative medical care source forfo I I ow-up.
A flow chart depictlng The relalionships befween theseoperational stages ls shown in Flg. 3.1.
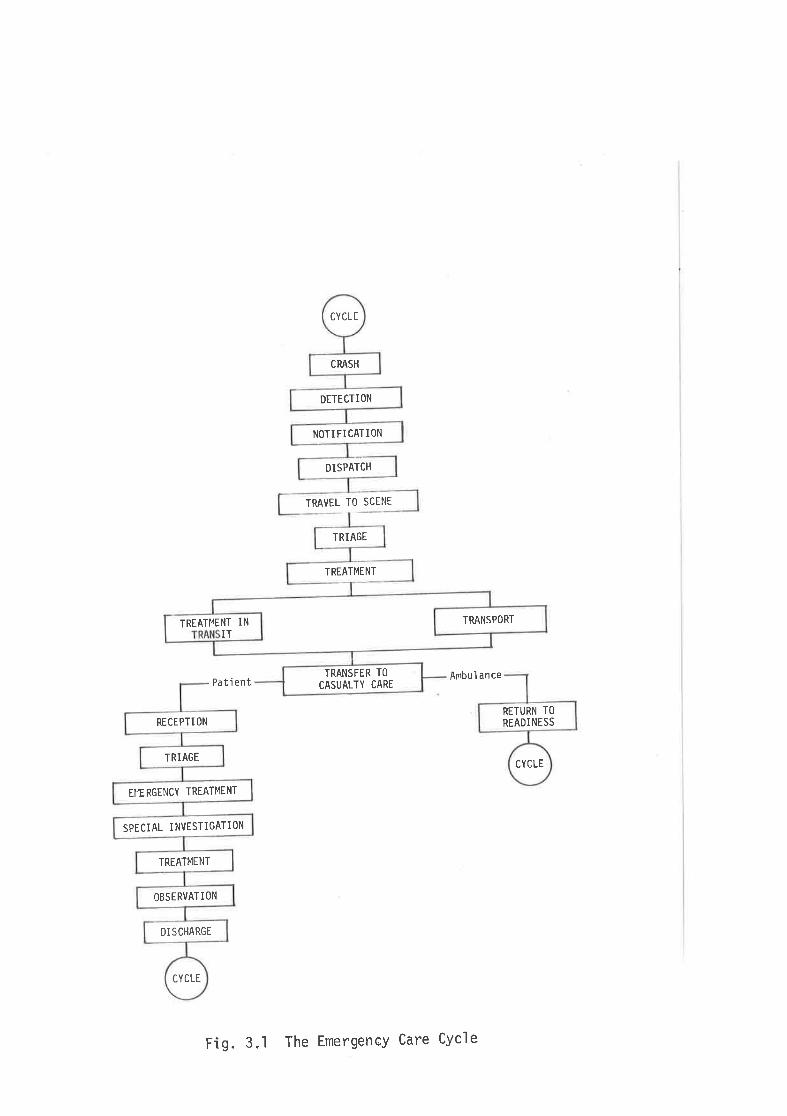
CYCLE
DI SCHARGE
OBSERVATION
TREATMENT
SPECIAL INVESTIGATION
EI4ERGENCY TREATMENT
TRIAGE
RECEPTI ON
DISPATCH
NOTI FI CATION
DETECTION
CRASH
CYCLE
CYCLE
RETURN TO
READINESS
TRANSFER TO
CASUALTY CARE
TREATI'IENT INIT
TRANSPORT
TREATMENT
TRIAGE
TRAVEL TO SCENE
Ambul ancePa ti ent
Fig.3.1 The Emerge'ncy Care CYcle
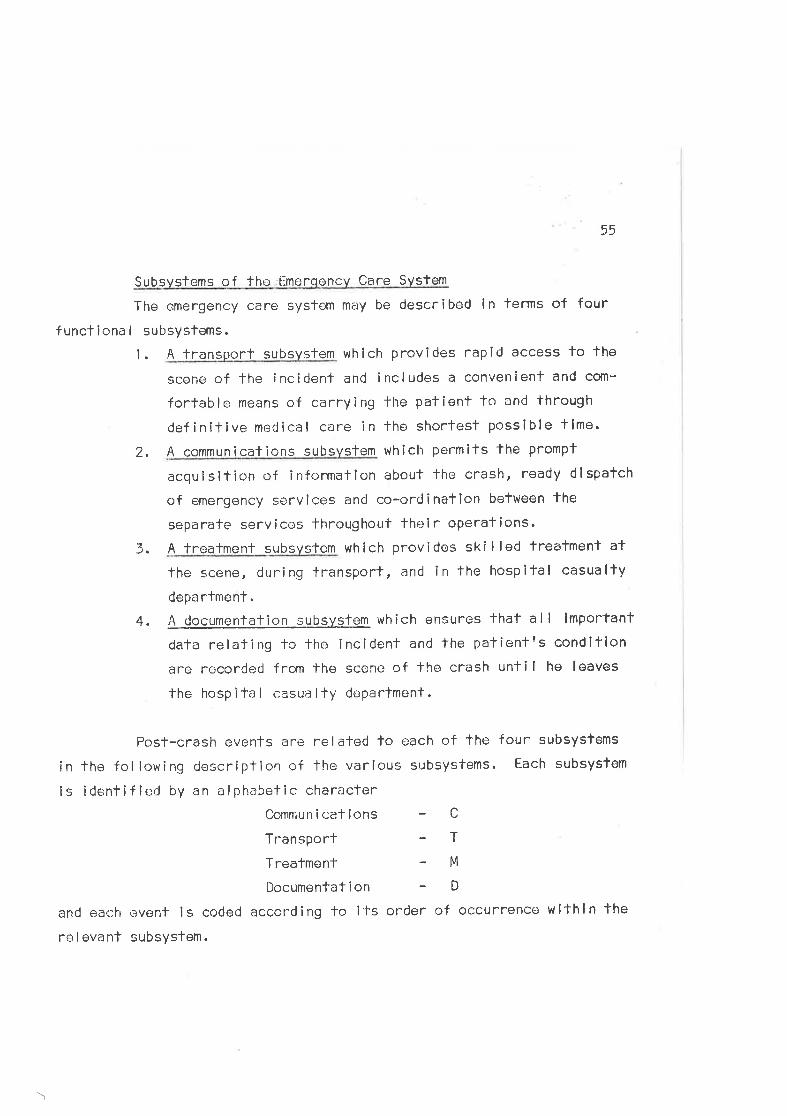
55
Subsvstems of the :Emerooncv Care System
The emergency care system may be described in terms of four
functlona I subsystems.
1. A transport subsvslem which provides rapid access to the
scene of the incident and includes a convenient and com-
forlable means of carrying the patient to and through
definitive medical care in the shortest possible tlme.
2 . A communicafions subsystem which permits lhe prompl
acquisition of information about the crash, ready dlspatch
of emergency services and co-ordination between the
separafe servicos lhroughout their operations.
3. A treatment subsvstem which provides ski I led treatmenl at
the scene, during tra¡sport, and in the hospifal casualty
depa rtment .
4. A rlocumgntation subsvg!_em which ensures fhat all lmportant
dala relating to the incident and the palienl?s condition
are recorded from the scene of the crash until he leaves
the hosp Ì ta I casua I ty departmenl.
Posf-crash events are relafed lo cach of the four subsystems
in tho fol lowing description of lhe various subsystems. Each subsyslem
is idenfífied by an alphabetic character
Commun i cat lons - C
Transporl - T
TreafmenT - M
Documentation - D
and each evenl is coded according to ifs order of occurrence lvlthin the
relovant subsyslem.
\
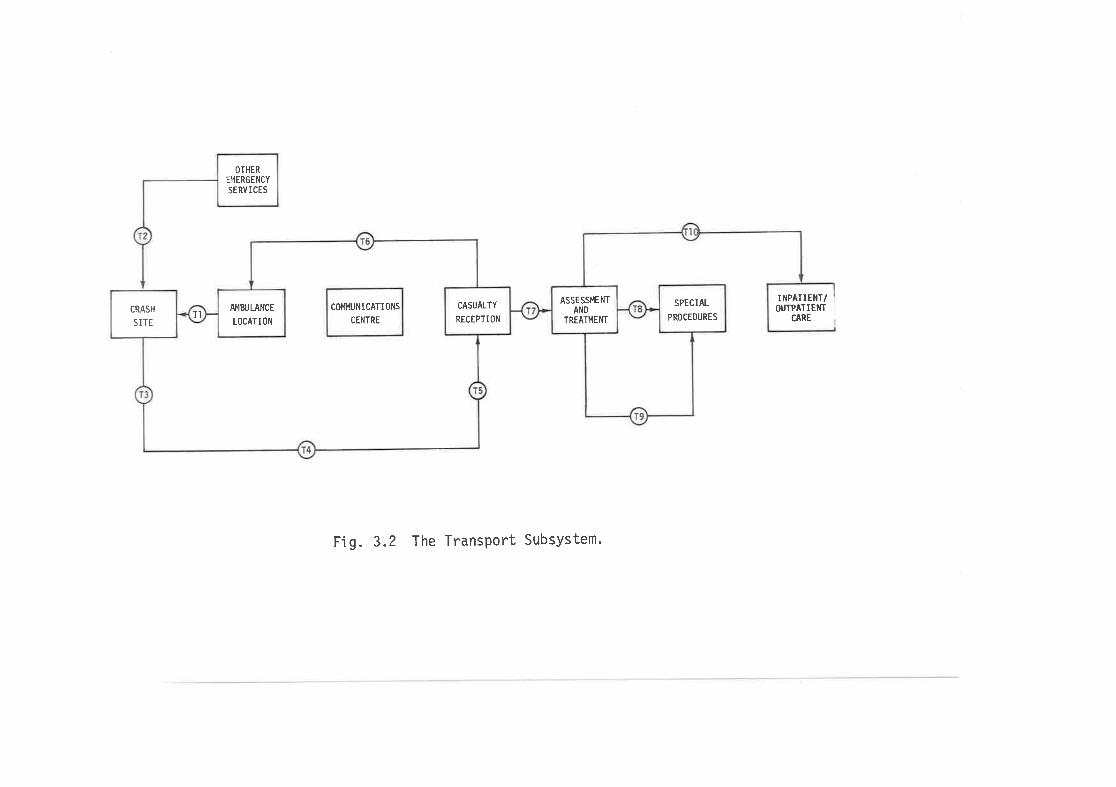
CRASH
S ITETI
OTHER
E14ERGENCY
SERVI CES
A,I4zuLANCE
LOCATION
COI4I'IUNICAÏIONS
CENTRE
CASUALTY
RECEPTION
ASSESS¡.IENT
AND
TREATT'.IENÏ
SPECIAL
PROCEDURES
IÎ{PATIEIIT/OUTPATIEI{T
CARE
Fig. 3.2 The TransPort SubsYstem.
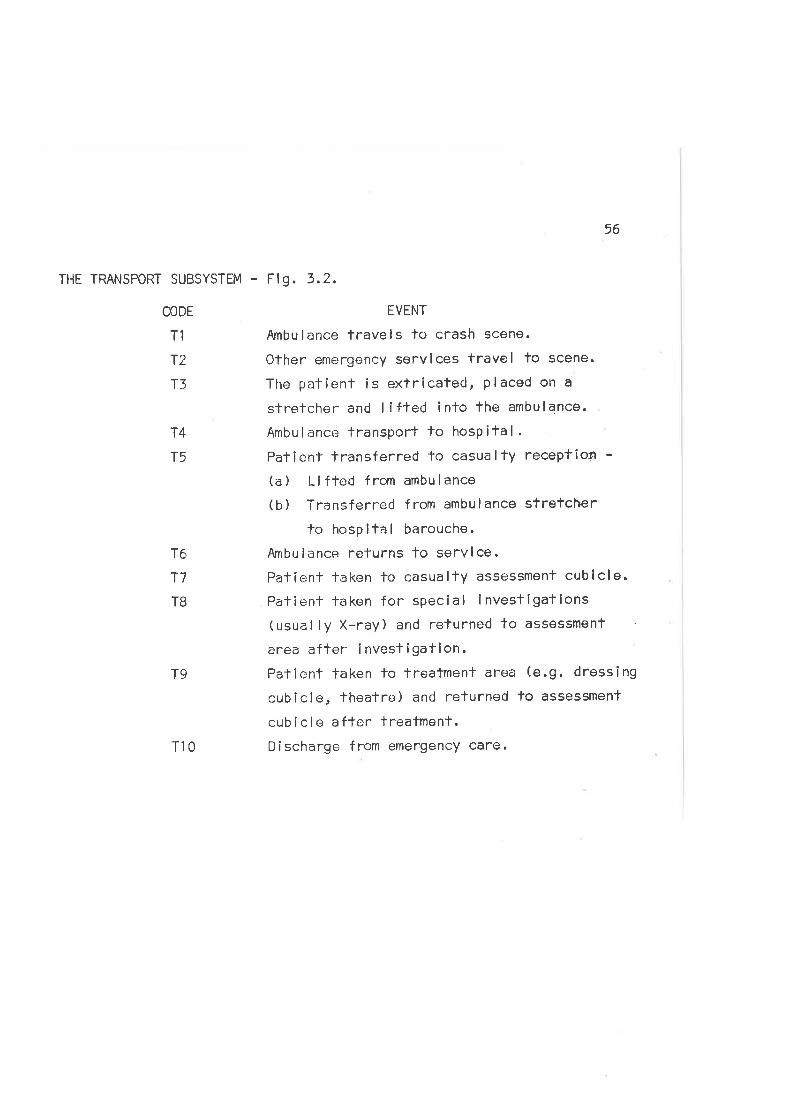
THE TRANSPORT SUBSYSTEM -
CODE
T1
r2
r3
14
T5
T6
T7
TB
T10
56
Fig.3.2,
EVENT
Ambulance travels lo crash scene.
Other emergency servlces travel to scene.
The patient is extricated, placed on a
stretcher and I lfled into fhe ambulance.
Ambulance transport to hosPital.Patienf lransferred to casualty receptiott -(a ) Li fted from ambu I ance
(b) Transferred from ambulance strefcher
to hospital barouche.
Ambulance refurns to servlce.Patíent taken to casualfy assessment cublcle.
Palienl taken for special invesligatlons(usual ly X-ray) and returned to assessment
area after ínvesllgation.Patient taken lo treatmenl area (e.9. dresslng
cubicle, thealre) and returned lo assessment
cubi cle afler treatment.
Discharge from emergency care.
T9
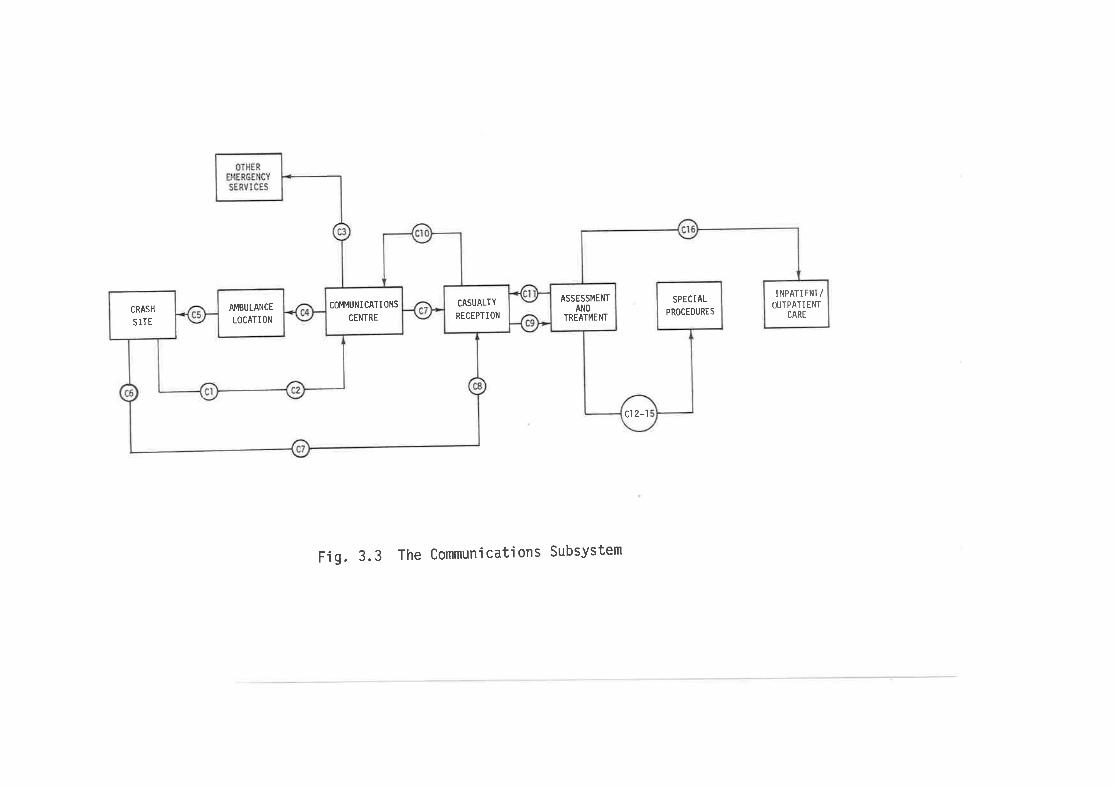
CRASH
SITE
OTHEREMERGENCY
SERVICES
AMBULANCE
LOCATION
coÈll'IuNI CATt 0NS
CENTRE
CASUALTY
RECEPTIONAND
TREATMEl{T
ASSESSMENT
cl 2-l
SPECI AL
PROCEDURES
INPATIENT/OT'TPATIENT
CARE
Fig. 3.3 The Communications Subsystem
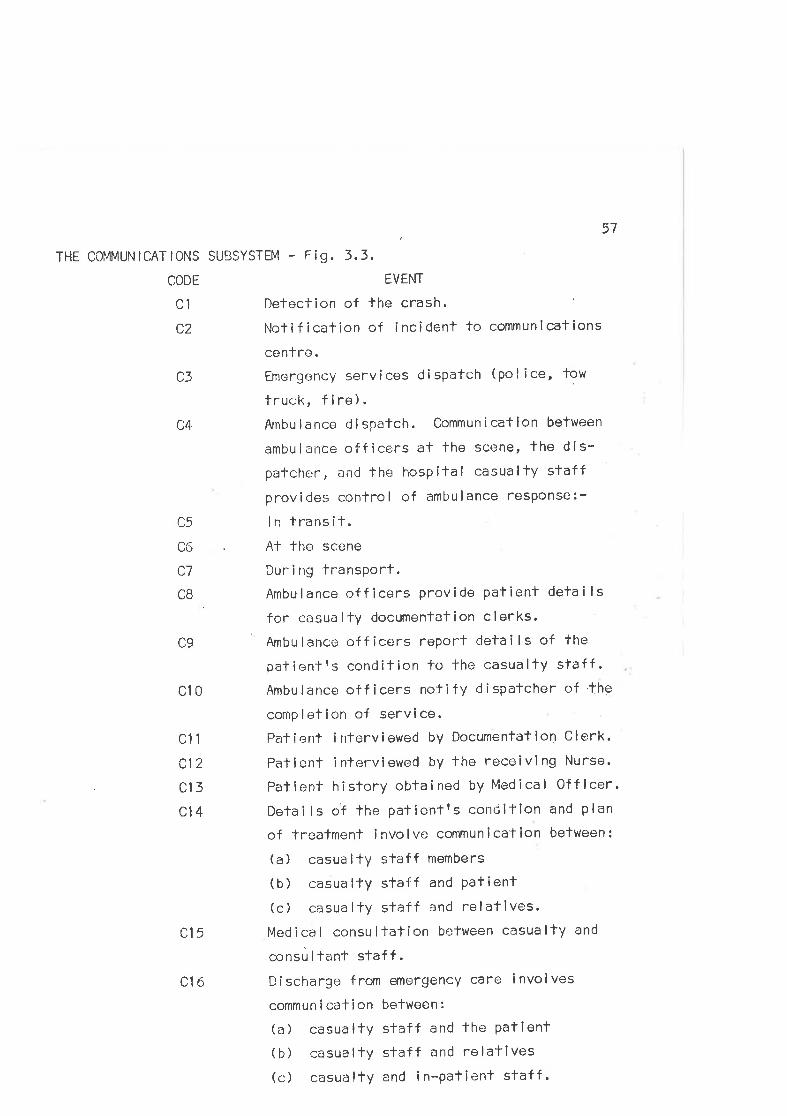
,57THE COi4MUN ICAT lONg SUBSYSTEM - F ig , 3.3
CODE EVENT
Cl Deloclion of lhe crash
CZ Notification of inciclent to communications
cenlre.C3 Emergency services dispatch (pol ice, tow
truck, f i re).C4 Arnbulance dispatch. CommunicatÌon between
ambulance officers at the scene, lhe dis-patcher, and the hospitaI casualty staffprovides control of ambulance response:-
C5 ln transil.C6 Al the scene
C7 Duri ng fransPort.CB Ambulance officers provide patient detai ls
for casua I ty documenlat i on c I erks.
C9 Ambu I ance off ícers report deta i I s of the
palientts condition fo-the casualty sfaff .
Cl O Ambu lance of f icers no't if y d ispatcher of 'the
complelion of service.
Cl1 Patient interviowed by Documentation Clerk'
Clz Patienl intr¿rviewed by the receivlng Nurse'
Cl3Patieni.hÎstoryobfainedbyMedicalOfficer.Cl4 DefaiIs of the pafienff s contlitlon and plan
of treatment i rlvo I ve commun ical ion belween :
(a) casualtY staff members
(b) casualtY staff and Patienl(c) casua ltY staff and relatives.
Cl 5 Med i ca I consLl I lat i on bertween casua lÌy and
consùltanf staff.C16 Discharge from emergency care involves
commun i caf ion between :
(a) casualtY slaff and the Patient(b) casualtY staff and relatives(c) casuölty and in-patient staff.
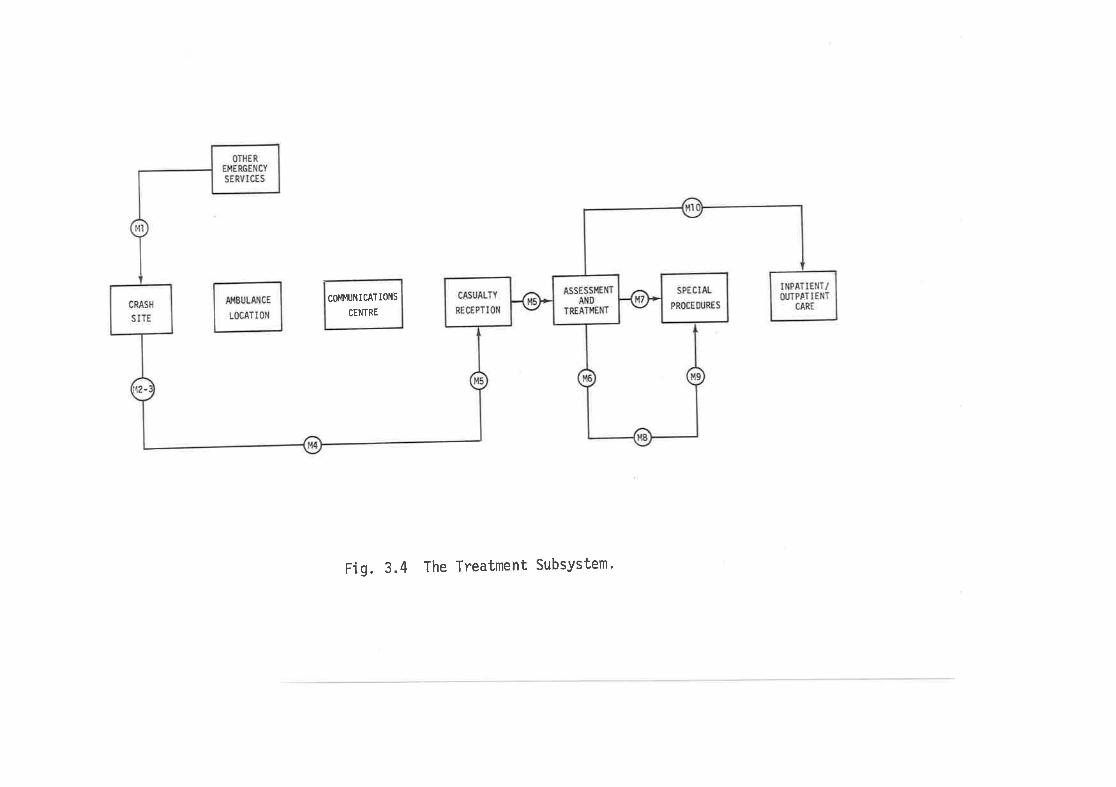
CRASH
SITE
OTHER
EMERGENCY
SERVICES
CASUALTY
RECEPTION
ASSESSI,IE¡lTAND
TREATI,IENT
SPECIAI
PROCEfN'RES
INPATIENT/ü,TP¡TIENT
CAREAI'IBULANCE
LOCATION
COIO4UNICATIONS
CENTRE
Fig. 3.4 The Treatment SubsYstem'
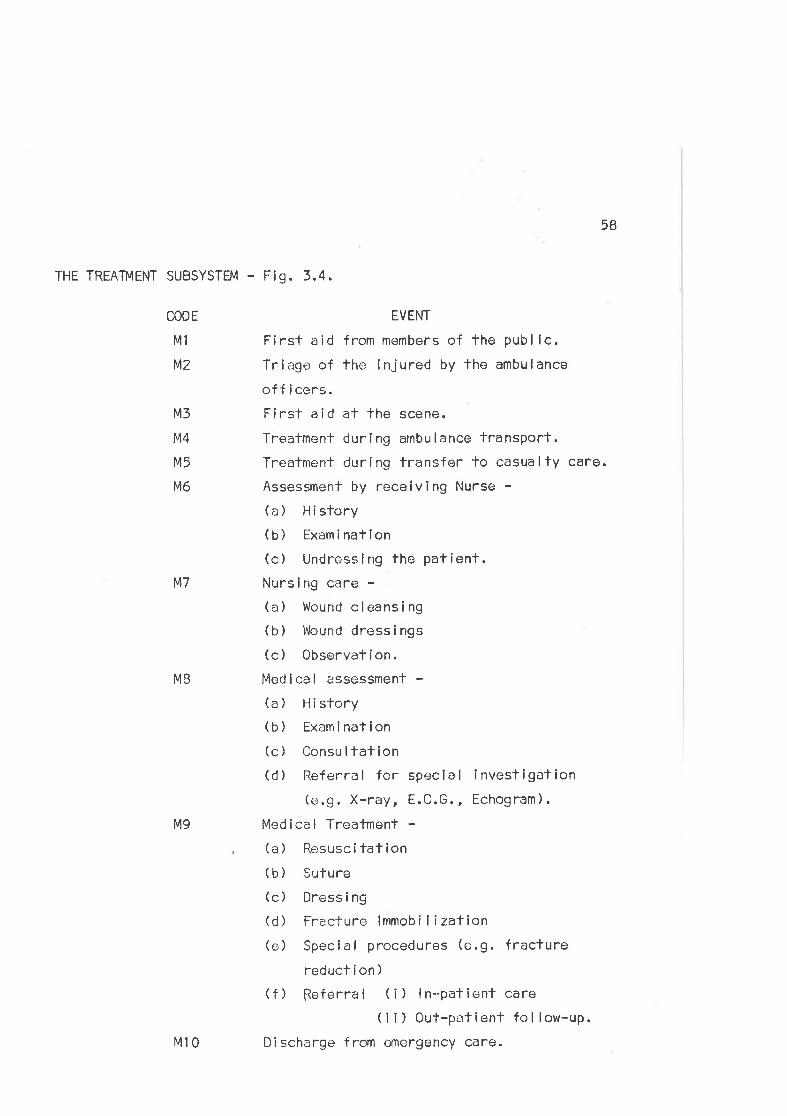
58
THE TREA1ï4ENT SUBSYSTEM - Fig. 3,4.
CODE
M1
tú2
M3
M4
M5
lvl6
M7
MB
M9
EVENT
First aid from members of the publ ic.Tríage of the injured by lhe ambulance
officers.Firs't aid at lhe scene.
Treatmenl duri ng ambu lance transport.Treatment during transfer to casualty care.
Assessment by receiving Nurse -(a) History(b) Exami nation(c) Undressing tho patient.Nursing care -(a) Wound cleansing(b) Wound dressings(c) 0bservation.Med i ca I assessmenf -(a) History(b) Examination(c) Consu ltation(d) Referral for special investigation
(e.9. X-ray, E.C.G., Echogram).
Medical Treatment -(a) Resuscitation( b ) Sufure(c) Dressi ng
(d) Fracture immobi lizalion(e) Special procedures (e.9. fracture
reducl í on )
(f) fleferral (¡) ln-palient care( i i ) Out-patient fol low-up.
Dischargo from cmergency care.M10
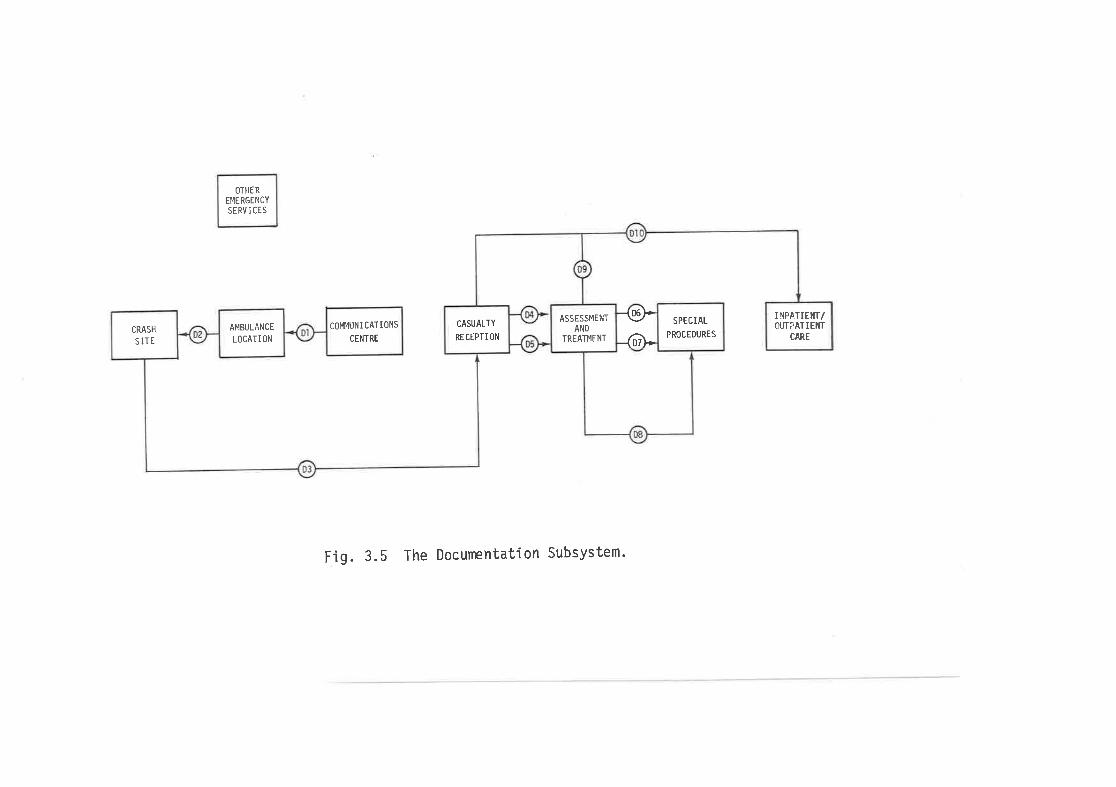
OTHER
EI.IERGENCY
SE RV I CES
CRASH
SITE
AMBULANCE
LOCATION
COII4UN ICAT IONS
CENTRE
CASUALTY
RECTPTION
ASSESSÌVIENT
AND
TREATMENT
{sÞ{)}'
SPECIAL
PROCEDURES
I ¡tPAlIEr{t/OI'T?ATIEIfI
CARE
Fig. 3.5 The DocurrpntatÍon Subsystem'
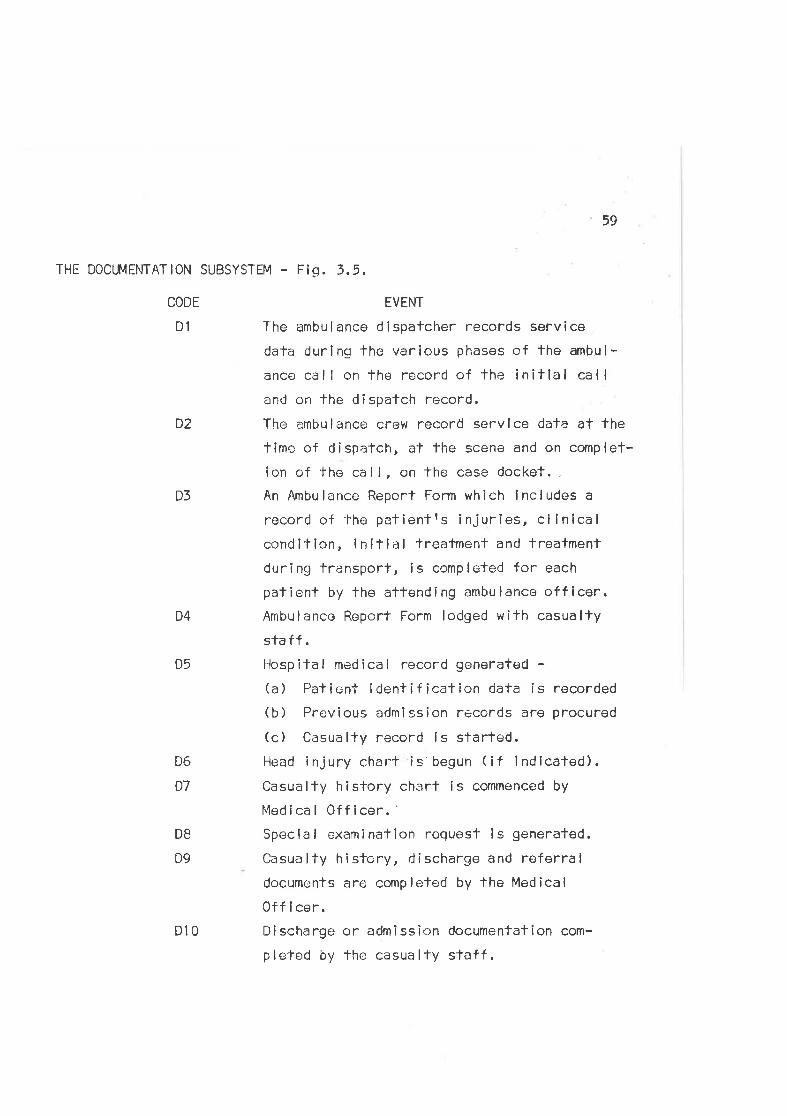
59
THE DOCUMENTATION SUBSYSTËM - Fig. 3.5.
CODE
DI
D6
D7
EVENT
Tlre ambu I ance d lspalcher records serv ice
dafa during the various phases of the ambul-
ance côll on the record of the initlal callan<J on the d i spatch record.
The ambulance crew record servlce data at thetimc of dispatch, a't the scene and on complet-
ion of the cal l, on the case docket. -
An Ambulance Report Form which lncludes a
record of the petientrs injuries, cl lnicalcondition, initial treafment and treatment
during transport, is comploted for each
pafient by the aftending ambulance officer.Ambulance Report Form lodged with casuallysta ff .
Hospital medical record generated -(a) Palient Ídentificafion data is recorded(b) Previous arJmlssion records are procured
(c) Casually record ls started.Hoad injury chart is'begun (if lndicaled).Casualty history charl is commenced by
Medical 0fficer.'Speclal oxamination request ls generated.
Casua lty hÌstory, discharge and referraldocuments are completed by the Medical
Off i cer.Discharge or admission documentation com-
ple'ted by lhe casualty sfaff .
D2
D3
D4
D5
DB
D9
010
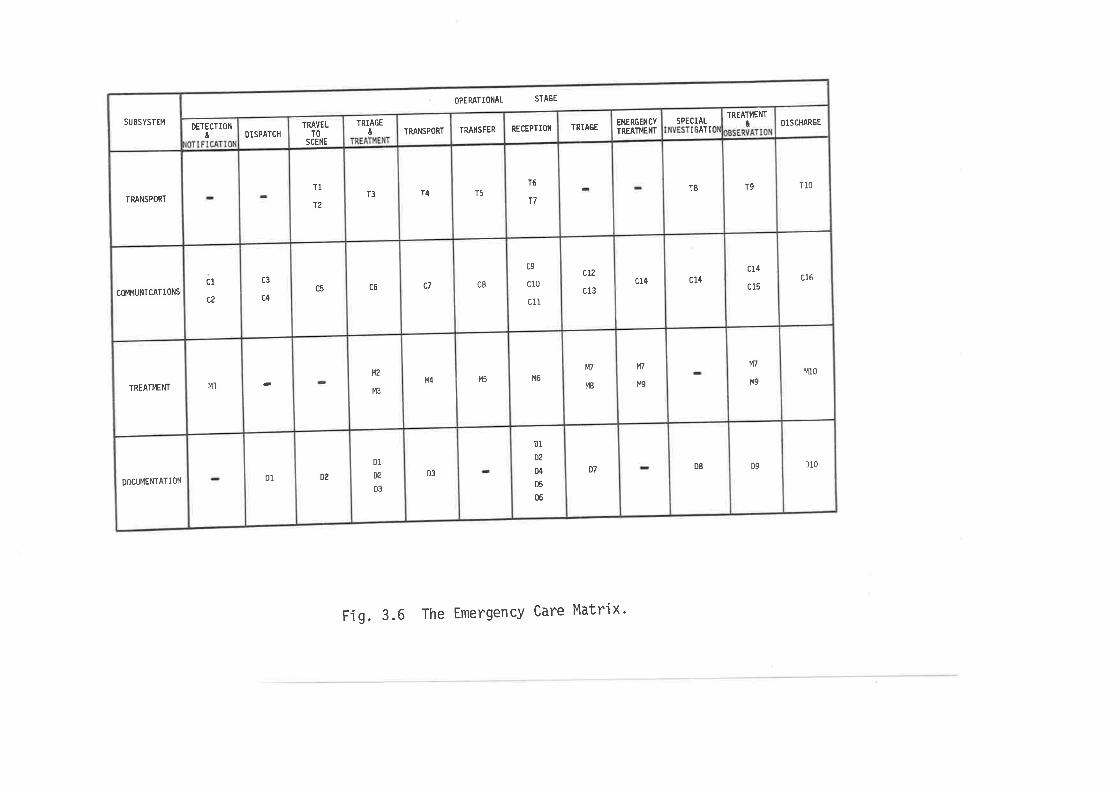
SUBSYSTEM
TRANSPORT
COII4UNI CATI ONS
TREATI4ENT
DOCUMENTATION
tDETECTION
cl
c2
M]
DISPATCH
c3
c4
D1
TRAVELTO
SCENE
TI
12
c5
D2
ûTRIAGE
T3
c6
M2
M3
D1
æ
D3
TRANSPORT
T4
c7
t44
D3
TRANSFER
T5
c8
M5
RECEPTION
T6
T7
ao
cl0
c11
M6
DI
D2
D4
D5
ü
TRIAGE
ctz
c13
t17
r'18
D7
EI.IERGENCY
TREATI'IENT
c14
t{/
M9
SPECIALIGATI
T8
c14
D8
&TREATI,IEI{T
T9
cI4
c15
M7
M9
D9
DISCHARGE
OPERATIOI{AL STAGE
T10
c16
M10
Dl0
Fig. 3.6 The Emergency Care Matrix'
60
A matrix relating the four subsystems and lheir events tothe operatíonal stages of the emergency care cycle is shown in Fig. 3.6.Entries in indlvidual cells of the matrix rarpresent fhe subsystem eventswhich occur during each stage of'lhe cycle. The matrlx thus depictsthe interactions between the elements of fhe emergency care sysfem.
For example, during transport to -lhe hospiTal, communications (C7)
between fhe ambulance ancl the clispalcher and subsequenfly belwoon thedlspatcher and'lhe hospital provide advance warnlng of the lmminent
arrival of a seríously injured pa'lient. Al 1'he same time necessaryresuscitalion and Trealment (M4) is performed by the ambulance officerfo onsure the stabilization of the patienf rs condition. S¡gnif icantevents relatlng to lhe patientes injuries, condition, and managemeht
arê recorded by the ambulance officer on lhe ambulance report form (D5).
ln addition lo shot^ring the relationships betwu.en the operaf-ional stages and subsystem events in diagrammatic form, the mafrixdemonstrates the interfaces between the separate subsystems. A selectionof these interfaces are described ín Flg. 3.7.
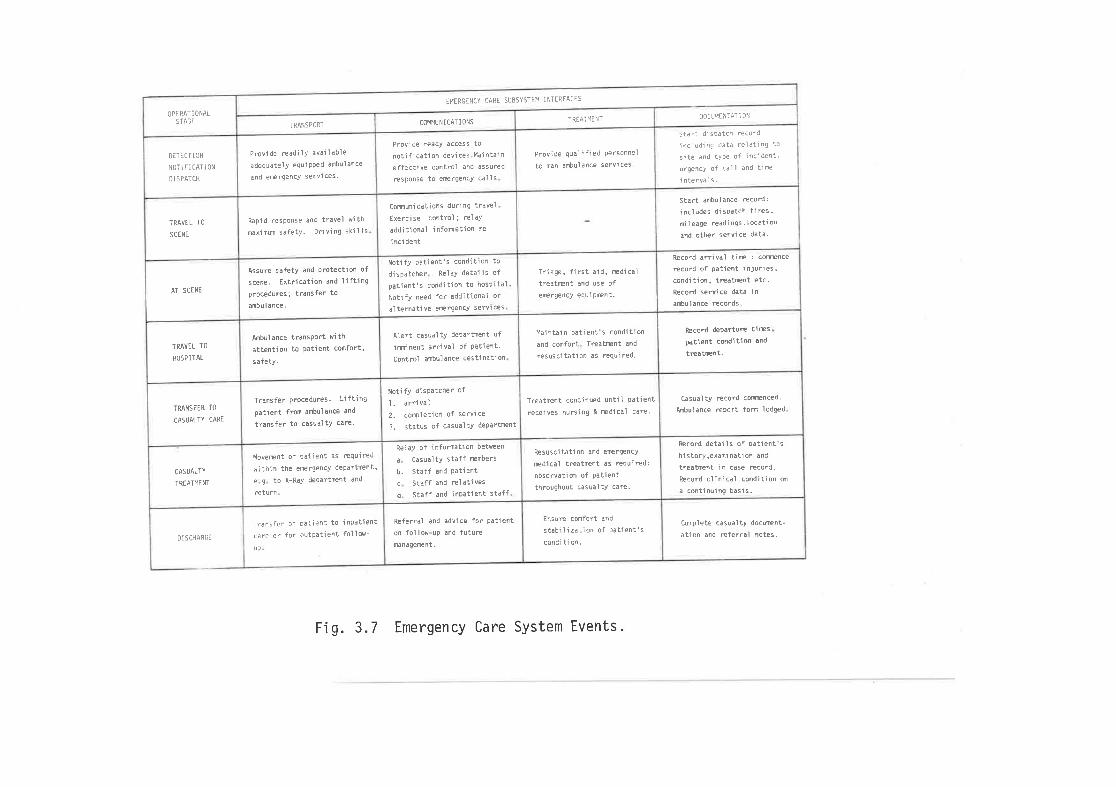
DETECTION
NOII FlCATION
OISPATCH
OPIRATIONALSfAGI
TRAVEL TO
SCENE
AT SCENE
TRÁVEL TO
HOSPITAL
TR,ANSFIR fO
CASIJALfY CARE
CASUALTY
TREAT14EIfI
DISCHARCE
TRANSPORT
Provide readiìY available
adequ¿tely equi PPed ambulance
and erergency servlces.
Rapjd response and travel with
maximum safety. Driving skills
Assure safetY and Protection of
scene. txtrication and liftingproceduæs; transfer toambul ance.
Anbulance transPort with
âttention to P¿tient confort's afetY.
Trônsfer Prccedures. Liftingpatient frcn anbulance and
transfer to casualtY care.
Moverent of gatient as required
\rithin the erergencY departrent'
e g to X-R¿Y depÀrtrent and
return.
Tr¿¡sfer of Datient to inpatient
c¿re or for outpatient foì low-
U¡
COI4I,IIJNICAT¡ONS
comunications during travel
Exercise controì; relaY
additìonal infomation re
incident
Provìde ready access to
noti fi cati on devi ces.l'lai nt¿in
effective control and assured
resPonse to erergency cal I s
Notify patient's condition to
dispatcher RelaY details of
patient' s condi tion to hosPi tal
Notify need for additional or
al ternôti ve emergencY servl ces ,
Alert cðsualtY departnent of
iminent arrival of Patient.control ômbulance destinetion
Notify dispatcher of
completion of service
status of casualtY depôrtment
arri valt.,:r.
Rela-v of infornation between
a CasualtY staff rembers
b. Staff and Patientc Staff and relativesd. Staff and inpðtient staff
Referrðl ðnd advice for oatienton follow-uÞ and futurenanôgeænt.
fREAT14ENT
Provide qual jfied Personnel
to man anbulance servjces.
Trjage, first aid, redic¿l
treatrent and use ofemrgency equi prent.
liajntâin patíent's condition
and comfort Treatrent and
resuscitation as required.
Treatrent continued until Patient
receives nursing & mdical care.
Resuscitation and erergencY
redical treatrent as requíredi
observation of Datient
throughout casualty cðre.
Ensure comfort ànd
staÈilizà!ion of patient's
condi ti on.
TI'IERCENCY CARE SUBSYSTEI¡ INTERFACES
l0cu,4il{fAfi 0N
Stàrt ambulance record:
includes diso¿tch tires'mi leðge readi ngs.l ocàtion
and other service dàta.
Stðri disoatch record
includinç data reì¿ting to
site ¿nd t-vDe of incident'
urgency of.all and tìæintervals.
Record arrival tiÉ : colmnce
record of pôtient iniuríes,condition, treatrent etc.Record service dàt¿ in
ànbulance records.
RÊcord depðrture ti@spatient condition and
tÉatrent.
Casu¿l ty æcord comnced.Ambulance reoort fom lodæd
Record detaiìs of o¿tient'shi story,exômi nôti on ànd
treatænt in case record.
Record cì i ni cal condi ti on on
a continuing basìs.
Complete cèsuèì ty docurent-
àtion ànd Éferraì notes-
Fig. 3.7 Emergency Care System Events.
61
Chapfer 4
THE STUDY OBJECTIVES
An lmporïant stlmulus to the planning and dosign of lhisstudy was the dearth of information avai lable fo administrators and
planners of emergency services. Al the time the study was commenced,
lhe only operationaI dala normaI ly reported by fhe ambulance service
were fhe number of ambulance trips performed annually and the pro-
porlion of emergency and non-emergency trips within lhat group. No
details were available on the types of emergencies atlended and llttleinformation was ava í lab le on such importanf operaf ional characteristlcsas the elapsed times in the various phases of the ambulance call. Much
basic service information was not avai lable to administration. ( ltshould be said, however, lhaf recording procedures have since been
upgraded and many of these data are now recorded. ) Simi larly, hospitalrecords did nol provide detaîled breal<downs of the lypes of cases
treateo in casualty, although the inforrna'tion cculd be determined by
special studies of existing medical records. Many detai ls of patient care
in casualty were, and sti I I are, unavai lable from existing records.
Hence, in early 1969, tltis study was undertaken wilh lhe aim
of gathering data relal-ing to the i:mergency care of road crash victimsin the Melbr:urne metropolitan arÉ)a. This thesis records fhe study
findings and provides an analysis of the available data, with the
fo I low ing ob.iect ives.
The first and major objective ls to describe the emergency
care system as il operales for road crash viclims in an area of Melbourne.
The services involved and fheir inleractions were discussed in the pre-
ceding chapter and the performance and contributiorr of each to the over-all system operations will be reviewed in detail in a later sectlon.
The second objeclive is to describe the patterns of injurysustalncrd by víclims of a sample of metropolifan crashes and to discuss
62
the care provided for those patienfs from the scene of the crash untilthe completion of thelr emergency treatment.
A third aim is to evaluate tho qualily of the firsf aid and
emergency medical care provlded for fhe crash victims, by relating the
care performed to the standards of care expec'fed of ambulance and
casualty servlces in Melbourne.
The fourth objoctive is lo determine the time delays exper-
lenced by patlenfs during the various phases of emergency care and to
relate fhese <Je lays in the sc;parate treatment phases 'io the totalsystem times. To complemont this descriplion, a slmulatlon model willbe used to study fhe possiblo effecls of certain organizational changes
on time delays during patienf flow through lhe hospital casualty
depa rtment.
The f inal objective of fhe sfucly is to ideni-ify def iciencies
in presenl operations, to recommend methods of overcoming these defic-iencies, and to examlne the probable effecfs of these changes on the
emergency care system.
63
Chapter 5
THE STUDY I"IETHOD
ln plannlng this study, it was declcled to observe the care
provided for a sample of road crash vicfims al the scene of the crash
and dur i ng ambu I ance and casua I ty trr:atrnent. D i rect observat ion by
physicîan observers v¡as choserr as the method of sludy because of the
need, as d¡scussed in Chapter 2 of this thesis, for evaluatíons of fhe
quality of emergency care using operational criferia. Measurernenfs of
time delays during the various phases of care are nol available from
existing ambulance ancJ hospital records and Thus specÎal study was
necessary to oblain this imporlant data. Furthermore, the dirr-'ct
observation method permits evaluation of the appropriateness and
qualify of lhe care provided for the injured. Although several of the
disa<Jvantages of this me'thod of s1'udy wcre inevifably involved - small
sample popula'l ions, possible observer bias, questions as to the¡ valldity,rel iabi I ify and reproducibi I ity of the observations - lhe advantages,
notably the accurafe recc.rrding of 'lime data and the use of operational
criferia for the assessrnenl' of quality, were felt to far outwelgh any
dísadvanlages of the methocl. Moreover, by wor^king in close contact with
the various emcrgency services, it was possible for the observers togain aclditional insight and exporience of 1'he problems facing each ofthe services in providing emerqency care.
Dala were qalherecl on two sample potulafions during two
dislincl study phases.
Phase one. lhe on-scenc sfudy, involved the attendance of a
research team, consisfing of Dr. G. A. Ryan and lhe author, at fhe
scenc of a sample of 100 road crashes in an area of Melbourne. These
crashes were attended between August 4,. i969 and February 7, 1970.
Phase fwo of lhe study involved a more intensive examination
of the medical care provided for crash victims within lhe casualfy
64
deparlmenl of tho Alfred Hospilal. The study was performed by the
author, as sole observer, between itay 25, 1970 and December 12, 1970.
The sampl ing methods varied between the separate phases and
thus each study phase is considered separalely in the following cliscuss-
lon of thr: study methocj and sampl ing procedures.
THE STUDY DESIGN: PHASE ONE
(l) Emerqencies in M¿+lbourne
ln order fo determine the pattern of ambulance emergency
cal ls, and 'thus the patfern of occurrence of injury-producing crashes
in Melbourne, the records of tho Vîctorian Civi I Ambulance Servlce(V.C.A.S. ) for the months January fo Apri I 1968 were analysed. Unfort-unately, the V.C.A.S. records for lhis period dld not differentiateroad crash calls from other Êmergency calls made on the ambulance
service. Thus drug overdosôge, drowning, d<¡mestic accidents, and
rnedical conditions such as myocardial inf'arction which require urgent
ambulance attendance, were inclucled with the road crashes in a general
omergency category for ambulancc recording purposes. Each emergency
call could be identif ied from the records. lnformation on the time ofnolif ication of each call, the localion of the incidenl, and lhe hospital
to which the persons involved were subsequently taken was recorded.
During the period under revicrw there were 3,701 such emergency
calls in fhe area def ined by the Sands and MacDougall Postc<¡de l4ap ofMelbourne and Suburbs. These accidenfs werè plotted on tlre rnap and each
vvas given co-ordinates locating it lo a map area of { square mile. ln
addition tho time of occurrence of each emergency by hour of day and
day of week was recorded, along with the hospital to which the injured
victims were laken. Thîs coded informafion was punched on B0 column
cards, verified and anaIysed, usirrg lhe CDC 3200 Computer at the Monash
University Computi ng Centre.
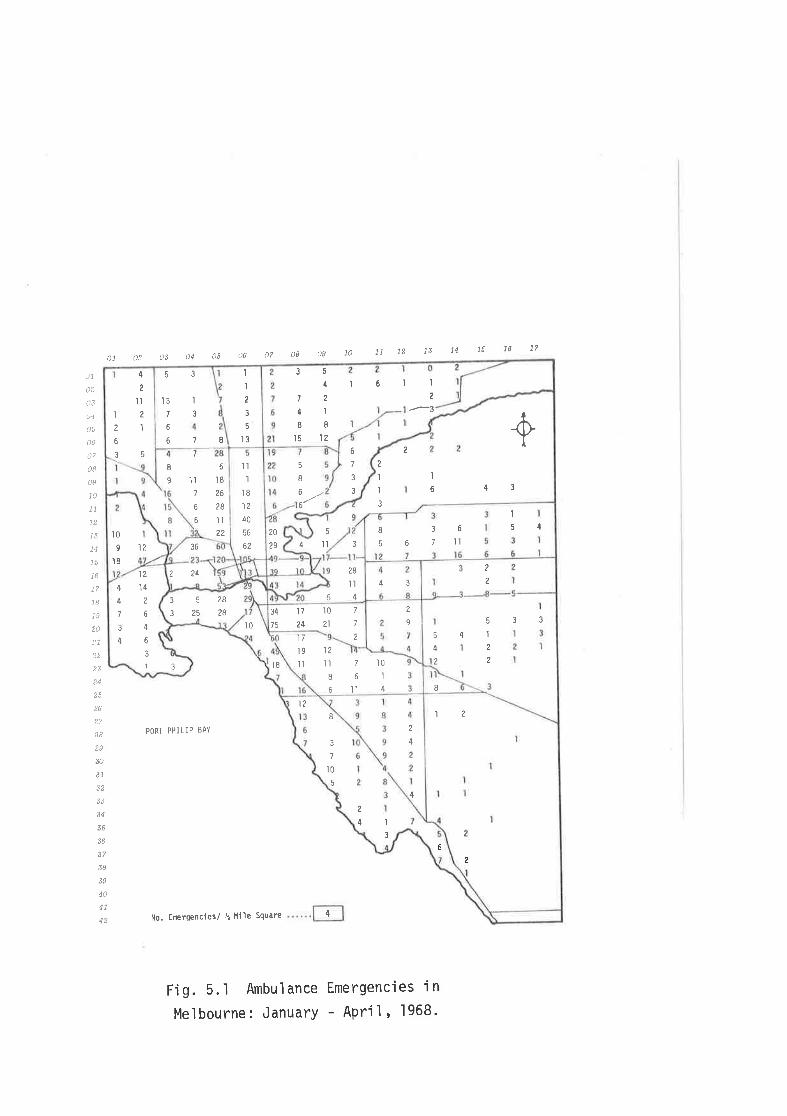
01 ()2 A3 04 ¿r5 dd 07 0B 0g 10 11 12 1s 14 16 18 1?
ù1
o2
03
o5
Ò7
o8
o9
10
11
13
14
16
17
18
19
20
24
27
28
29
30
34
38
40
41
42
PORT PHILIP BAY
No. EíErgencles/ ! Mlìe Square
Fig. 5.1 Ambulance Emergencies 'in
Melbourne: January - APrÍl ' 1968.
I
3
2
4
12
6
8
5
3
7
t0
4
4
2
2
12
B
't7
l91l
t2
lìI6
7 ì061l1 4
7
7
2
34
75
't0
21
l724 I
2
't8
l0
352832528
12't4
?
6
4
6
3
1
4
4
7
3
4
3
43
4
2
'I
2
?
2
4
533
36
224
6
1t
'ì
5o 3 4
5bl1?
10
9
l8
I9
7
'Iì6
'ì8
26
?8
Il?2
7
6
6
'tl
ll812
40
56
ô¿
2
I
ì
3
,l
6
5
3
2+
5
4 ll
43
28
ll4
I
2
3 5
6
4
2
1l
2
I 6
6
I
37
'ì3
78
53 I
I
2
3
5
t3
20
29
6
7
3
3
5
I6
6
I
2
.-3
r6l35
4
724l88]s 12
4
65
The data were used lo examíne lhe distribution of V.C.A.S.
emergency calls in time and space, and determine fhe pattern of accidentoccurrence as a pre-requisite to the derivation of a suifable sampling
plan. The computer map of these 3,701 accidonts is shown in Fig. 5.1.The map demonstrates lhe concenlralîon of emergency calls ín the cenfralcity aroa, with a gradient of decreasing frequency extending from fheinner urban areas to thc; outer suburbs. Concentrations of emergency
calls were noted along the lines of major highways, presumably reflecf-ing lhe signif icant contributic¡n of road frauma lo the tofal number ofemergency cal ls. Simi lar maps were produced to relate the site ofoccurrence of each ernergency to the hospital to which the patients were
transported, and a geographical twatorshedt arêa was demonstrated foreach hospilal. This, no cJoubt, reflectod tho result of lhe ambulance
service policy which required that each patient should be taken lo thenearest publ ic hospital for emerqency care.
The distrlbution of these emergencies by hour of day of week
is shown in Table 5/1 (see p.66). The concenTration of emergencles
during the daytime hours and particularly during peak road crash periods
in the evening hours on week nights, and the late night and early morn-
ing hours on Friday, Saturday arrd Sunday confirm the lmportanf contrlb-ution of road crashes to this group in addltÌon to reflecting thepaftern of road crash occurrence which has been demonstrated by ofherstudies in Austral ia. (Robertson et al., 1966; Jamieson et al., 1971.,
A sampling plan for uso during the on-scene study was derived
f rom this analysis of V.C.A.S. emergency calls. The following sectionsdescribo the choice of the study area, Ìhe sampling schedule, and the
method of operatíon of the research team"
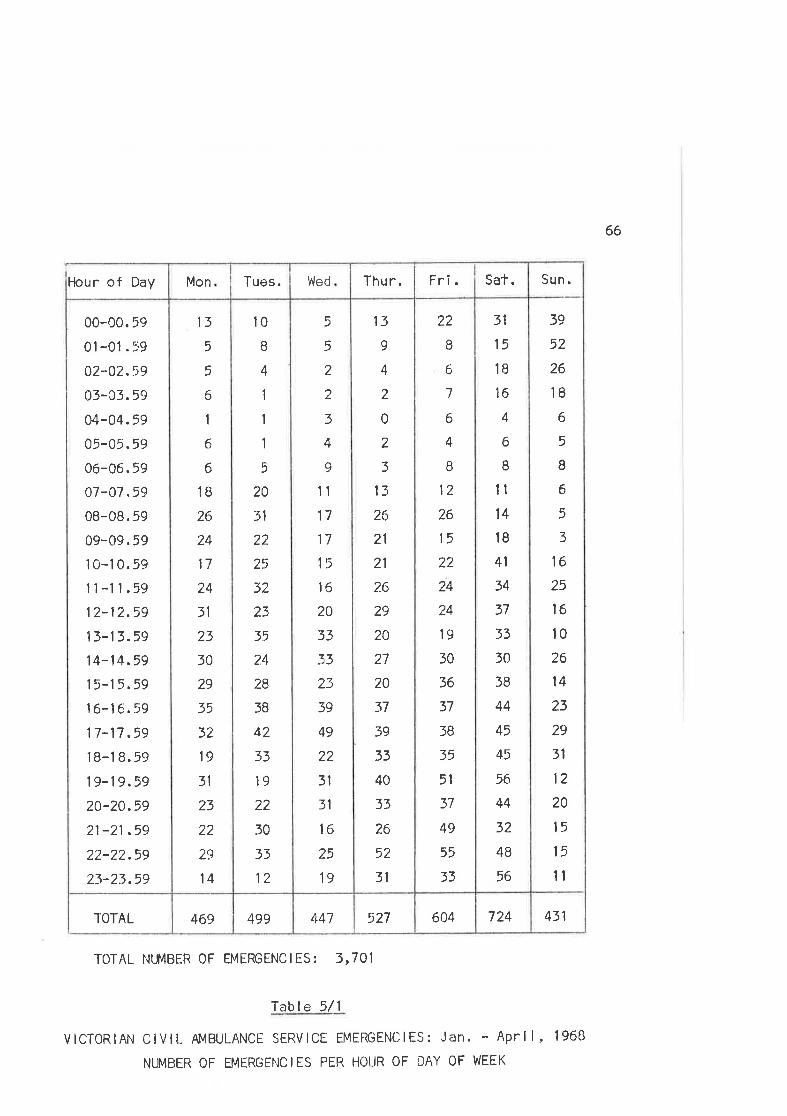
66
431724604527447499469TOTAL
39
52
26
18
6
5
I6
5
3
16
25
l6l026
14
23
29
31
12
20
l5
15
tl
31
15
1B
16
4
6
Illl4
l8
41
34
37
33
30
38
44
45
45
56
44
32
48
56
22
B
6
7
6
4
I12
26
15
22
24
24
l9
30
36
37
3B
35
51
37
49
55
33
13
9
4
2
0
2
3
13
26
21
21
?.6
29
20
27
20
37
39
33
40
33
26
52
31
5
5
2
2
3
4
-Q
11
17
17
15
16
20
33
33
23
39
49
22
3l
31
16
25
19
10
I4
1
1
1
5
20
31
22
25
32
23
35
24
28
3B
42
33
19
22
30
33
12
13
5
5
6
1
6
6
1B
26
24
17
24
31
23
50
29
35
32
19
31
23
22
29
14
00..00.59
01-01.59
02-02.59
03-03.59
04-04.59
05-05. 59
06-06,59
07-07.59
08-08. 59
09-09. 59
1 0-1 0.59
11-11.59
12-12.59
13-13.59
1 4-1 4 .59
1 5-1 5.59
16-16.59
17-17.59
1B-1 8.59
19-19.59
20-20.59
21-21 .59
22-22.59
23-23.59
Sun.Sat.Fri.Thur.WedTues.MonHour of Day
TOTAL NTMBER 0F EMERGENC I ES z 3,7O1
fable 5/1
vlcTORlAN CIVIL AMBULANCE SERVICE EMETENC|ES: Jan. - April, 1968
NUMBER OF EMERGENC IES PER HOI.IR OF DAY OF WEEK
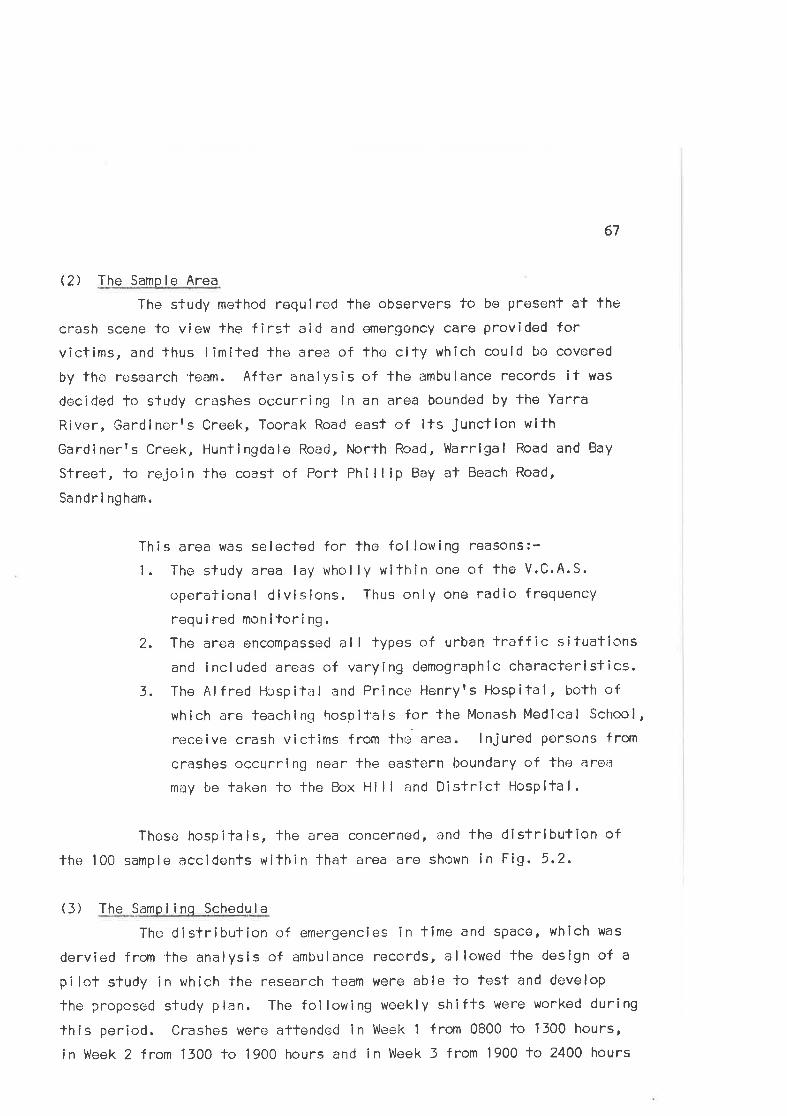
67
Q) The Sample Area
The study method requ i red the observers to be present at fhe
crash scene to view fhe firsf aid and emergency care provided forvîctims, and thus limited lhe area of the city whlch could L¡e covered
by the research team. After analysis of the ambulance records it was
decided lo study crashes occurring ln an area bounded by the Yarra
River, Gardinerrs Creek, Toorak Road easf of its junctlon wlth
Gardinerfs Creek, Huntingdale Road, North Road, V,larrlgal Road and Bay
Sfreet, to rejoln tho coast of Port Ph¡llip Bay at Beach Road,
Sandri ngham.
This area was selected for the fol lowing reasons:-
1. The study area lay wholly within one of the V.C.A.S.
operational divlsions. Thus only one radio frequency
required monltoring.2. The area encompassed al I types of urban traffic situations
and included areas of varying demographic characteristics.3. The Alfred Hospifal and Princo Henryts Hospilal, both of
which are teaching hospitals for the Monash Medical School,
receive crash victims from the-area. lnjured persons from
crashes occurring near lhe eastern boundary of tho area
may be taken lo lhe Box Hi I I and Distrlct Hospital.
These hospitals, the area concerned, and the dlslribution of
the 100 sample accidents within that area are shown in Fig. 5.2.
(3) The Sampl inq Schedule
The distribution of emergencies in time and space, which was
dervied from fhe analysis of ambulance records, allowed fhe design of a
pilot s'tudy in which the research team were able to test and develop
lhe proposed study plan. The fol lowing woekly shifts were worked during
this period. Crashes were attended in Week 1 from 0800 lo 1300 hours,
in Week 2 Íron 1300 to 1900 hours and in Week 3 from 1900 to 2400 hours
Og TO LL t2 L3 14 L5 L8 L7
0t t2 t3 j'4 )s c6 07 08
OL
t2.
t4
tea7
o8
o9
LO
LL
L3
L5
Lb
L7
L8
20
2L
24
26
27
28
29
30
3L
34
35
38
39
40
4l
PORf PHILIP
BAY
IIo. OF CRASHES/å I:ILE SQUARE
STUDY AREA
A - ALFRED HOSPITAL
P. PRINCE HENRY'5 HOSPITAL
B - 8O)( HILL HOSPITAL
.l-ã-l
Fi g. 5.2 The D'i stri buti on of the
Study Crashes in the SamPle Area'
II¡III
2
2
2
IIII
-J
4
6l
@
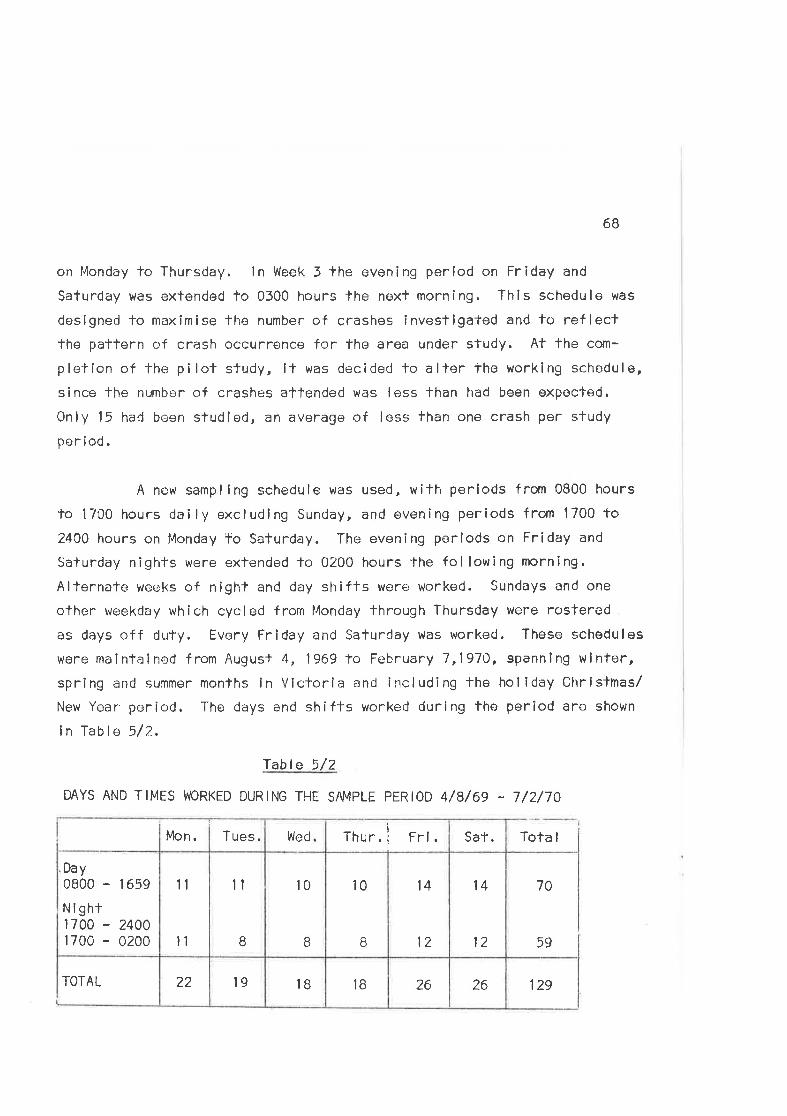
6B
on lvlonday to Thursday. ln Week 3lhe evening perlod on Friday and
Saturday was extended to 0300 hours lhe nexl morning. This schedule was
designed to maximise the number of crashes investlgated and t<¡ ref lectthe pattern of crash occurrence for the area under study. At the com-
pletlon of the pilot study, lt was decided lo aller the working schedule,
since lhe number of crashes attended was less than had been expocted.
Only 15 had been studied, an average of less than one crash per study
per iod .
A new sampling schedule was used, with periods from 0800 hours
lo 17û0 hours daily excluding Sunday, and evening periods from 1700 to2400 hours on l.londay To Saturday. The evening periods on Friday and
Saturday nights were extended to 0200 hours 'the following morning.
Alternate wecks of night and day shifts were: worked. Sundays and one
other weekday which cycled from l4onday through Thursday vvere rostered
as days off duty. Every Friday and Saturday was worked. These schedules
were rnaintained from Augusl 4, 1969 to February 7,1970, spannÎng wintor,spring and summer months in Victoria and including the holiday Chrisltnas/
New Year period. The days and shif-l-s worked during the period are shown
in Table 5/7-.
Table 5/2
DAYS AND TIMES WORKED DURING THE SAMPLE PERIOD 4/8/69 - 7/2/70
Tota I
70
59
12926261BIB1922TOTAL
l4
12
14
12
10
B
10
I
il
B
11
ll
'Day0800 - I 659
Night1700 - 24001700 - 0200
Sat.Thur. Frí.WedTues.Mon.
69
(4) Seleclion of the Crashes
An essential feature of the sample plan was that the team
should attend the first crash which occurred duríng the sample periodwithin lhe area under study. Thus, since fhe nature of the crash was
nol known before arrival at the scene, the sample of crashes obtainedshould be represenlative of lhe range of types and severity of crashesoccu rr i ng .
lf the in'¡estigation of a crash was completed before the end
of a study period, the team awailed fhe occurrence of lhe next crashwithin lhat period. ln practlce, due to the long delays involved infol lowing the viclims during their stay ln hospifal, it was not possîbleto investigate more than fwo crashes in any single study period. lnpractice, fhe number of crashes studied in each working period averaged0.8 over the entire study period.
(5) Operation of the Research Team
The method chosen for the sfudy required that the team shoutdlravel lo the scene of a sample of injury-producing crashes in a seloctedarea of Melbourne. For the purpose of the study an injury-producingcrash was defíned as any road crash to v¡hich an ambulance was calledwithin the study area during the time fhe team was on duty. whilst fheco-operation of the ambulance service was essential for the me"thod
chosen, it was considered importanf'lhaf the team should not be depend-ent on that service for transport to the crashes. llence, to make indep-endent travel possíble, the Department of Social and Preventive Medicinepurchased a car equipped wilh a two-way raclio tuned to the ambulancefrequency. The car was equipped with warning devices (a flashlng I ightand reflecting lriangles for protection at fhe scene), a f irst aid kit,photographic equipment, sphygmomanometer and cJata recording forms.
During the times on duty, as dofermíned by the sampling plan,f he team rnon itored lhe arnbu I a nce rad i o conÌ i nuous I y. To ensure lhat
70
the response time to calls was as small as possible, the team wailed inor near the car, which was kept slraiteglcally placed within the study
area whilst nol actually invesligating a crash. ln this way the prob-
abilify of the team reaching the site of a crash before the ambulance
was increased. lt was arranged with the ambulance service that the
controller should dlspalch lhe rcsearch vehlcle at the same time as
he sent the ambulance to a crash. The feam arrived at fhe scene bofore
the ambulance on 25{. of occasíons, at lhe same lime in 14fi of callsand after lhe ambulance in thc remairrlng 6l#. lrrespective of the
separaì'e arrival patterns of the team and ambulance, if was a require-
ment for sludy of a case lhat the team should Lre able to vlew f lrstaid anc] palient care at tho scene. Thus even in those cases where the
team arrived aflor The ambulance, the llme differencos were minimal
ancl did not preclude inclusion of the case in the sludy.
There were occasions whe¡n the team arrived at fhe scene too
late to observe firsl ald and emergency caro and lhese cases were
excluded from the sample. No detailed record was kept of the frequency
with which lhese cases occurred, their type or the severity of fhe
injuries of those involved. lt is eslimated that less than 5 per cent
of crashes were discarded for such reasons and that those discarded
were predominantly minor crashes involving minor injury. This exclusion
policy wes nof considerc¡d to be a major source of bias in fhe sample.
At lhe sconc of the crash one member of the team was respons-
ible for gathering data on the mechanisms of injury and the crash con-
f iguration as well as obtaining informa'tion from bystanders, Police and
other emergoncy service personnel. The second obsorver v/as thus free
to concentrate on lhe first aid an<l emergency care provided for the mosl
seriously injured victims. Neither observer was directly involved in
the provision of medícal care at the scene and observer interference
with the work carried out by emergency services personnel was kept to a
min imum. ln add it ion lo observing the emergency care of injured vlctlms,
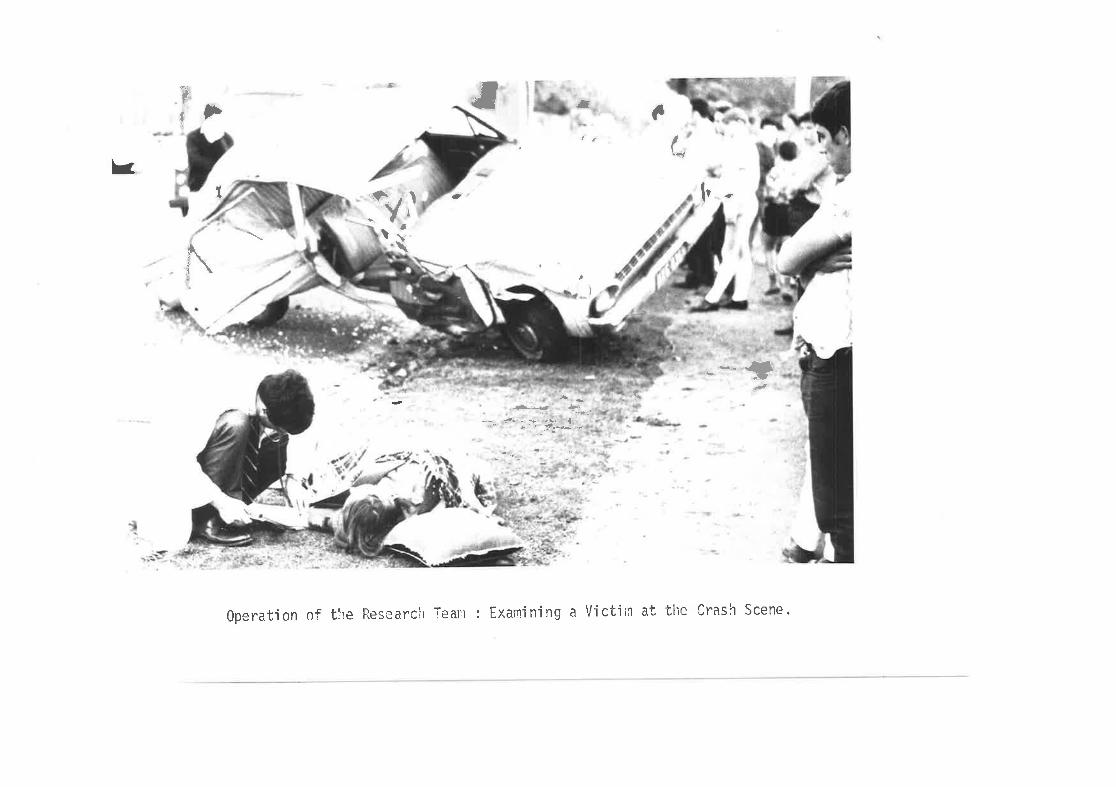
à tfI Þ a a
(,k
3 'ì¡
1
a
\ì
ta I l-
\ ,).
__.{¡¿
ç,,.r;-4 J-.
.. --t.l
.,,\'.- d" .-- '.;-$..* þ-.:
gperat.ion 0f tire Research Tearn : Examining a Victjln at the Cra.sh Scene.
71
measures of pulse, blood pressure, pupl I lary reactions and state ofconsciousness were obfained for each victim at the scene, usually afterthe ambulance officors had completed their initlal assessment of fhe
v i ct ims.
ln practice it was possible for such observations to be made
wilhout ínferfering with the work of fhe ambulance and first aldpersonnel. The ambulance offîcois were aware of the survey as belng a
study of crash injury, lts causes and its effects on fhe patient, and
were aware that if was not the observerrs intention to partlclpate inproviding medlcal care at the scene. 0n two occasions the obsorvers
were obllged to assist when no other help was available. Vlhllst thereis always the posslb¡l¡ty that the presence of the observer ls lik.ely lolnfluence the practlces under observafion, ln fhe busy sltuallons thatare usual at the scene of crashes, observer influence on the system
was felt to be smal l.
All persons involved in the crash were inlervlewed at the
scene. The observed populafion thus included fhose wlth no or mlnor
inJury, as well as fhose whose injuries were sufficienfly severe fowarrant their being laken lo hospttal by ambulance. After first ald atthe scene had been comploted and the victlms placed ln the ambulance
for transport to hospital, fhe team followed the ambulance fo the
casua I ty deparl'ment.
It was not possible for a member of the research team toaccompany tl're patienl to hospital ln the ambulance. The board of the
V.C.A.S. preferred lo have the obsc¡rvers travel lndependently of the
ambulance at al I limos. Hence the procoss of ambulance care during
transport and the effect of the ambulance ride on the patient could not
be assessed.
After arrlving at fhe hospilal, the team observed tho
72
procedures associated with the patientfs transfer fo the casualty
department and continued to observe the patient throughout his medical
care in the department.
A detai led physical examinalion was performed by one of fheobservers after the pationt had been admltted lo tha casualty depart-ment, to complement the roadside dlagnosls and complete the injurydescrlpllon for each patienf.
Significanl events were recorded in each phase of treatmentas they occurred. The patienlfs conditlon was monitored with quarter-hourly estimalions of pulse rate, blood pressure, pupillary reactlonsand state of consciousness.
All evc¿nfs rrJere recorded on work sheets, using a time base
for al I lmportanf treafment events. Time intervals befween the varloustreatment phases h,ere recordod during bolh ambulance and casualty care.It was fhus possible to build up a picture of llme delays ln the variousstages of the emergency care cycle, and to relafe them fo the overallsystem. Simultaneously, judgements on the appropriateness of the care
and the performance of the professionals providing it were made by theobservers.
Each palient was observed until his medical care in the cas-
ualty department was completed. The research team was then free toatlend anofher crash should it occur durlng the remalnder of lhe dutyperlod. Those victlms of crashes which occurred towards the end of theduty periods were obsorved unli I their dlscharge, whether this event
fell vrilhín lhe samplo period or not. Thus, if a crash was attended af0145 hours on a Saturday morning, lhe patients concorned were observed
durlng the course of their emergency care although lhis lnvariablyextended well beyond lhe end of lhe sampling period at 0200 hours.
73
THE ST DESIGN: PHASE TV'IO
(1) I ntroduct i on
Analysis of lhe data col lected during the on-scene study of
crash operations indicated lhal lhe care provided for patients within
hospital casualty deparfments warranted more intenslve investigalion'
The major anphasis of the first study was directed at lhe
investigation of emergency care outside the hospifal and the operafion
of emergency Services at the scene of the crash. Slnce an lmporfant
objective of lhe study was to obtain an overview of the emergency care
syslem, il was logical lhat the focus of thls second phase of fhe study
should be fhe care provided within lhe hospltal emergency department'
A further stimulus for this more intenslve study was the teamrs impress-
ion, backed by a preliminary analysis of the data collected during lhe
on-scene study, that dsficiencies in care within hospital casualty
departmenls had important implications for lhe oporalion of the emerg"
ency care system as a whole, and pa¡ticular relevance for lhe plannlng
of any changes in fhe systom which may be undertaken. Hence if was
decided thaf lhe author should undertake a more detalled analysis of
lhe care of a sample of road crash victims during their treatment in the
casualty deparlment of the Alfred Hospifal '
The Alfred Hospital was chosen as the site for this more
intensive sfudy for several reasons. First, lt is the maJor toaching
hospilal for the trealmenf of road crash vlcfims in the area chosen for
the earl ier, on-scene study. secondly, the analysis of v.c.A.s. emerg-
encìes which was conclucted during Phase one of lhe study showed fhat
more emergency patients werej'aken to the Alfred Hospital than to any
other hospital in the clly. Furfhermore, the Alfred is renowned for the
busyness of lts casualty deparfment, and for the large numbers of roacJ
accident victims who are treated in lhat department (and, subsequently'
as in-palients in the hospital). Thirdly, the casualTy department of
the hospital is relatively new, having been buí lt ancl equipped as part
74
of an extenslve rebuilding of the hospital which is still in progress.
The department thus has the advantages over fhe other deparfmenfs
studîed in Phase One of being well equipped, of modern design and
compact. A patient admitted to the Alf red Hospital fol lowing a road
crash receives all phases of his emergency medical care within fhe
casualty department before being admitfed to lhe wards for elective
treatment. ,Moreover, the ambulance bay, clerical documentation section,
admitting office and X-ray department are built around a cenlral cas-
ualty lreatment area, and it was thus possible lo maintain close sur-
vei I lance of more than one patienï concurrently.
Q) The Samp I i nq Schedu le
Experience in Phase One of the sfudy combined with a review
of the casualty admission records of the Alfred Hospital resulted in the
use of a sampllng plan similar to fhaf used in the on-scene sfudy.
Sundays were included as sampllng days in thls study to permil analysls
of casually operations throughout the week. Sampl ing limes used during
each day of the week were similar fo thoso worked during the on-scene
study, with the addítÎon of fhe Sunday periods as shown'
DAY SHI FT
MONDAY-SATURDAY:0800hoursto1700hoursSUNDAY: 1000 hours to lB00 hours
N IGHT SH I FT
MONDAY-THURSDAY:1700hoursto2400hoursFRIOAY/SAT. - SAT,/SUN.: 1700 hours to 0200 hours
SUNDAY: 1800 hours to 24OO hours
As in lhe on-scene study, evêry Friday and salurday were
worked. Two days were rostered off duty each vJeek, rotafing from Sunday
through Thursday. Allernate weeks of day and night shifts were worked
throughoul the studY Perlod.
The samplÍng period extended f rom l4ay 25, 1970 unlll Augusf 12
and from September 1B unlll December 12,1970. The numbers of days and
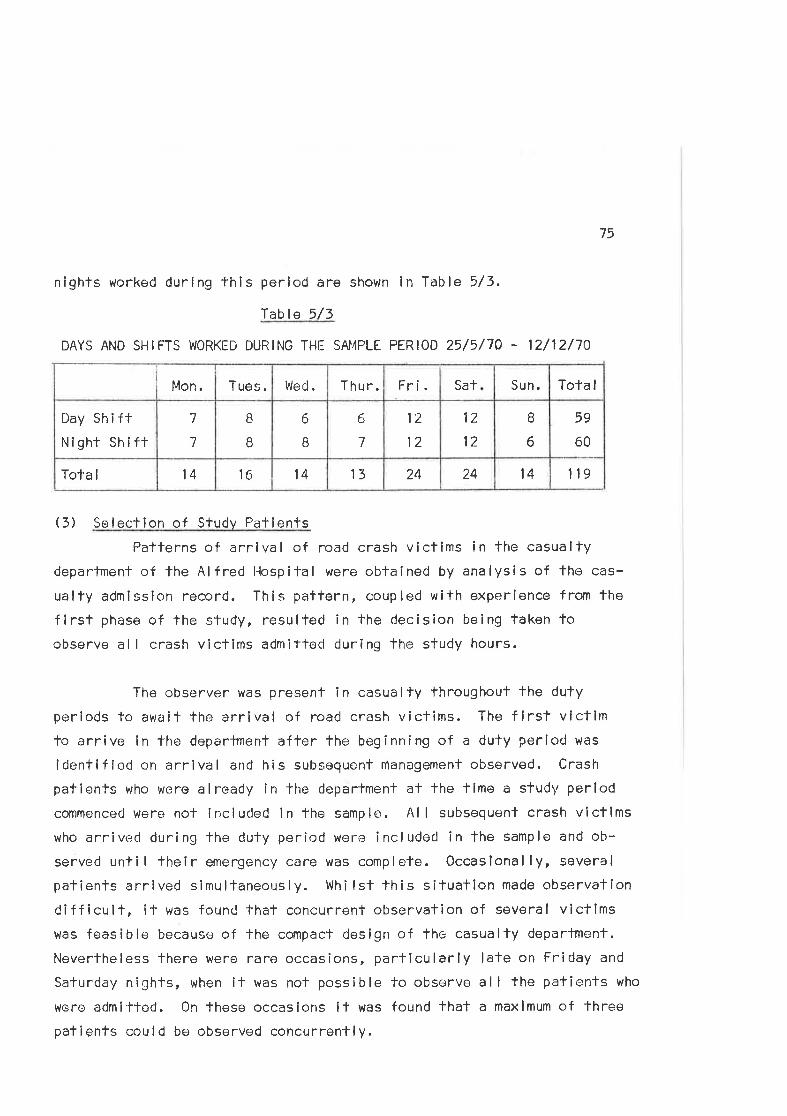
75
nights worked during this period are shown in Table 5/3.
lable 5/3
DAYS AND SHIFTS WORKED DURING THE SAI4PLE PERIOD 25/5/70 - 12/12/70
11914242413l41614Tota I
59
60
B
6
12
12
1'2
12
6
7
6
B
B
I7
7
Day Sh i ftNight Sh ¡ fl
Tota ISun.Fri. SatThu r.Wed.Tues.Mon.
(3) Selecfion of Study PatientsPatferns of arrlval of road crash victims in the casualty
department of the Alf red llospital were obtained by analysis of tho cas-
ualty admission record. This pattern, coupled with experíence from the
first phase of the study, resulted in the decision being taken foobserve al I crash vlctims admitted during the study hours.
The observer vlas present in casually throughout the duty
periods to await the arrival of road crash vicfims. The first victimto arrive in the department after the beginning of a dufy period was
identlfied on arrival and his subsequent nlanagemenl observed. Crash
pafients who were already in lhe department at the tíme a study perlod
commenced were nol included in the sample. Al I subsequent crash victimswho arrived during the duty period were included in the sample and ob-
served unti I their emergency care was complele. Occasional ly, several
patienls arrlved simultaneously. Whilsl this situation made observatlon
difficult, it was found that concurrent observalion of several victlmswas feasible because of the compacf design of the casualty deparfment.
Nevertheless there were rare occasions, parlicularly late on Friday and
Saturday nights, when it was not possible to observe all the pafients who
were admitted. 0n these occasions il was found lhat a maxÌmum of three
pafienfs could be observed concurrently.
76
Three hundred and twenty-elght victlms were admitted to the
casualty department during the study perlod; an average of 2.8 patlentsper duty period worked.
(4) Dala Col lecf ion Methods
This phase of the study was considereC complementary to the
first phase and dlrect observatlon of the care provided for a sample ofpatients was selected as the method for col lectlng data. The author
acfed as the sole observer, recordlng the patientst lniuries, cllnicalcondltion and managemenf throughouf their casualty care. Slnce the
observer had no other clinical responsibllities if was possible for hlm
to be present whilsf the patient was being admitted lo the department by
lhe nursing staff, examined and treated by fhe docfor on duty, and trans-ported between the various areas of the departmenl by the medlcal order-
lles. Patients were also observed whilst receiving X-ray and other
díagnostic and treatment procedures.
A plan of management has evolved for all patients admltted fothe casualty department for dlagnosls and frealrnenl. Since crash
victims form a sub-set of this larger group, ll was posslble for the
observer fo document the various slgnificanl evenfs whlch occurred
during the patientrs care ln a structured manner withouf interferingwith fhe medical or nursing staff who were actually looking after him.
This sysfem of management is described in detail ln a later chapter.
Mosf patients who are admltfed to casualfy departments exper-
ience waitlng times of variable lengfhs between the various stages of
lheir care. During these tfmes it was possíble for fhe observer to
obtain a history and perform clinical examlnatlons on the study vlcflms.
The history obfained from the patlent was supplemented by interviews
with tho ambulance officers who had brought the patlent fo hospital.
Consequently informatîon about the type of crash, its sife, the condlt-
lon of lhe patienl and treatmenf provided bofh at the scene and duning
77
transport was galhered. Whenever possible, conlact was made wíth
relatives or other persons who may have accompanied the pafient to
hospitol, and the políce, who f requently înterview victims in hospital.
As a resull.of these enquirios it was possible lo obtain a
piclure of both the crash and the emergency care provided outsíde the
hospilal, to supplement lhe observations made wi-lhln the hospital.
As in Phase one of lhis study, the problems associated wlth
direcl observation of care were presenl in thís Phase. ln this regard
the observer was fortunate in that tho second study followed closely on
the first. Casualty staff, who were acquainted with the study from our
previous contacts, regarrJed the observer as another membor of staff and
thus accepled his presence.
lndividual patíerrls were observed in a manner similar to fhat
describcd for thc casualty care section of the first phase. A continuing
rocord was kepl-, at approximately 15 minute inlervals, of each patienfis
pulse, bloorj pressure, slate of consciousness, and pupi I lary reactions.
Olher relevant infonnation relating to the patientrs injuries, condifion
and treafment was notecj.
Procedures and signifîcanl events were recorded on a Time base
and informatlon relating to specific aspects of departmental operation
was col lected and codcd in pre-designated categories. The waiting and
service tlmr:s withín the department, the numbers of sfaff in attendance'
the numbers cf patients receiving and awaiting treatment, work loads on
the respective services, and the equipment and facililies used in troat-ment were recorded.
Particular emphasis was placed in lhís second phase on record-
ing the time spenl in the various lreatment stages by each patient and
on assessing the quality of the care provided for each patient.
78
The observer assessed the qual ity of emergency care by compar-
ing the care actually performed by the casualty staff with that expected
of provlders of emergency care as defined by fhe Alfred Hospitalrs pro-
cedure manual I lnstructions for Casualty Residentsr, and the standards
for the management of road traffic casualtîes defined by the Royal
Australasian Col lege of Surgeons (1970), The performance of each treat-ment procedure was assessed according to predetermined criteria(Appendix 5) based on the melhods used by Peferson (1956) and Clute(1963).
As an oufcome measure of the qual ity of care, 313 of the 328
patients who were observed during this phase of the study wore invitedfo complete a postal questionnaire designed to assess their attitudesto fhe care they had received in casualty (Appendix 4).
Fifteen of the patients were not included in thls sample,
either because they had died as a result of their inJuries or because
their postal addresses could not be determined from study or hospital
records.
Three hundred and thirleen questionnalres were posfed at the
end of January 1971, two months after the lasf sampling day and approx-
imately eight months from the beginning of the sample perÎod. One
hundred and thirty replies were received fo thls firsÌ malling. At fhe
end of March a second mailing wes performed in whlch fhe non-respondents
were invited to complete an identlcal questionnaire. A further 53
replies were received, making a tofal of 183 respondents - a 5B/' overall
response rate.
Each patientrs questlonnalre was identified try lhe five digitpatient identlflcafion number and thus repondents could be identified.Date from fho questionnaire were added to the data file for each paflent
and il was thus possible to compare questionnaire dafa wifh other data
gathered during the direct observatlon study.
79
DATA RECORDING AND PROCESSING
Record i nq Forms
Data were rocorded on pre-codod forms i n each phase of thestudy. Scparate data forms were used for crash and pa'l'ient data duringthe first phase. Tho crash data form recorded data relatlng to each
crash and thrs performance of the emergency services at the scene. A
patient record form was completed for each person involved ln fhecrash and included data describing the patient, his injuries and thecare provided for lhose injuries from the scene of fhe crash until fhetime of the patientrs discharge from fhe hospital casually department.
ln the second phase, a palient data form was compleled foreach new road crash vicfim admitted to the casualty department. The
form was similar to thal used in the first phase of the study wíthmodifícations to allow fho recording in greater detail of fhe qualityof the care provided for the patient.
Data Process i nq
Data from fhe first phase uiere coded and recorded sfraighton to computer disc files. The recorded data were veriflod by compar-
ison with the original dala. The disc f lles were¡ transferred to magnef ictape and these tape files were uscd for subsequent data procêssing and
analysis. A card deck was punched by the compuler from the tape file,to provide a hard copy for minor sorting and security purposes.
Data from Phase Two were coded and punched on to B0 col umn
cards. The cards were verified and punchÌng errors corrected aften com-
parison of the output with the oríginal data. Tho coded data were
transferred to magnetic tape fi les for data processing.
All sortlng and analysls of the data was undertaken usîng thefaci I ities of the Monash Universíty Computing Centre, predominantly theRemofe Terminal Monitor sysfem I inked with the Centrers CDC i200
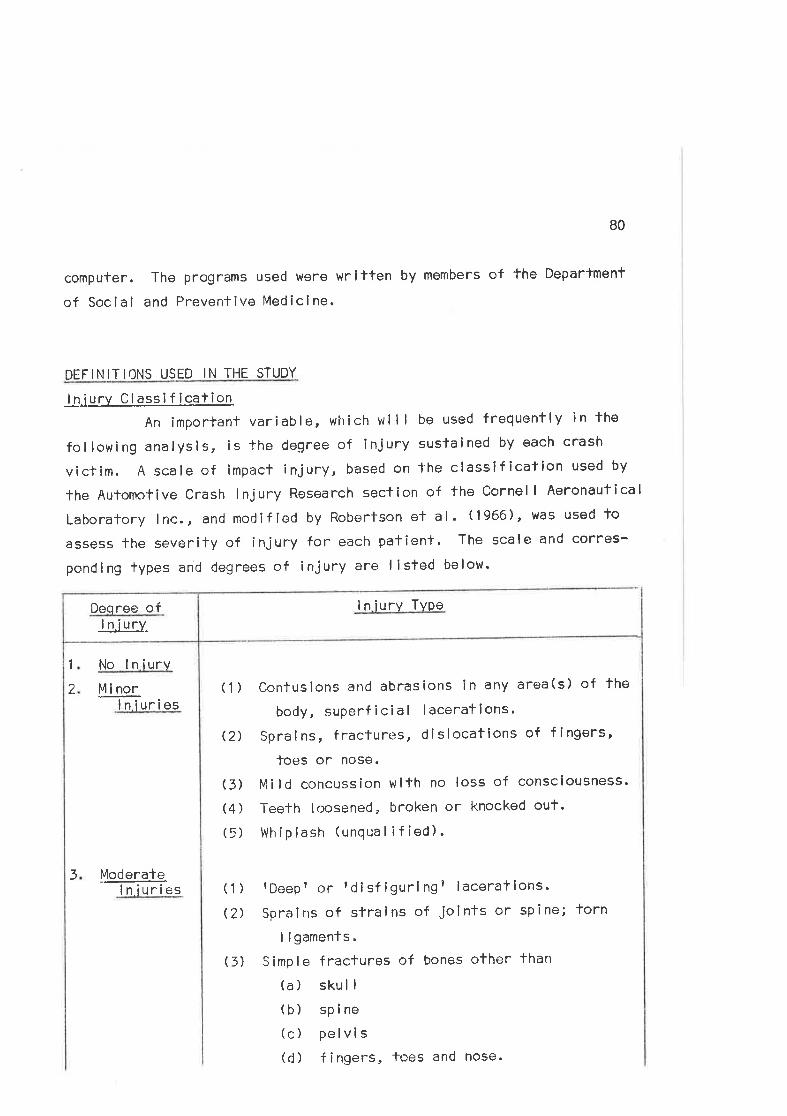
80
computer. The programs used were writfen by members of the Departmenf
of Social and Preventive Mediclne.
DEFINI TIONS USED IN THE STUDY
I n.i u ry C l._a_ss i f icat ion
An important variable, which wll I be used frequently in the
following analysis, is the degree of injury sustained by each crash
victim. A scale of impact ínjury, based on the classlf ication used by
The Automofive Crash lnjury Rosearch section of fhe Cornel I Aeronautical
Laboratory lnc., and modified by Robertson ef al. (1966), was used to
assess the severity of injury for each patient. The scale and corres-
ponding lypes and degrees of injury are I isted below'
I n iury Type
1
2
No I n iurv
Uj norlniuries
Ug!_era+e.ln iuries
(1)
Q)
(3)
(4)
(5)
Contusions and abrasions in any area(s) of the
body, superf icial lacerations.
Spralns, fractures, dislocations of fingers,
loes or nose.
Mild concussion wifh no loss of consciousness'
Teeth loosened, broken or knocked out.
Whiplash (unqual if ied).
3(1)
(2)
rDoepr or tdisf igurl ngt laceratlons.
Sprains of sfralns of joints or spine;
I i gaments.
Simple fraclures of bones other than
(a) skull(b) spine(c) pelvis(d) fingers, toes and nose.
I n.iuj^yDeqree of
(3)
torn
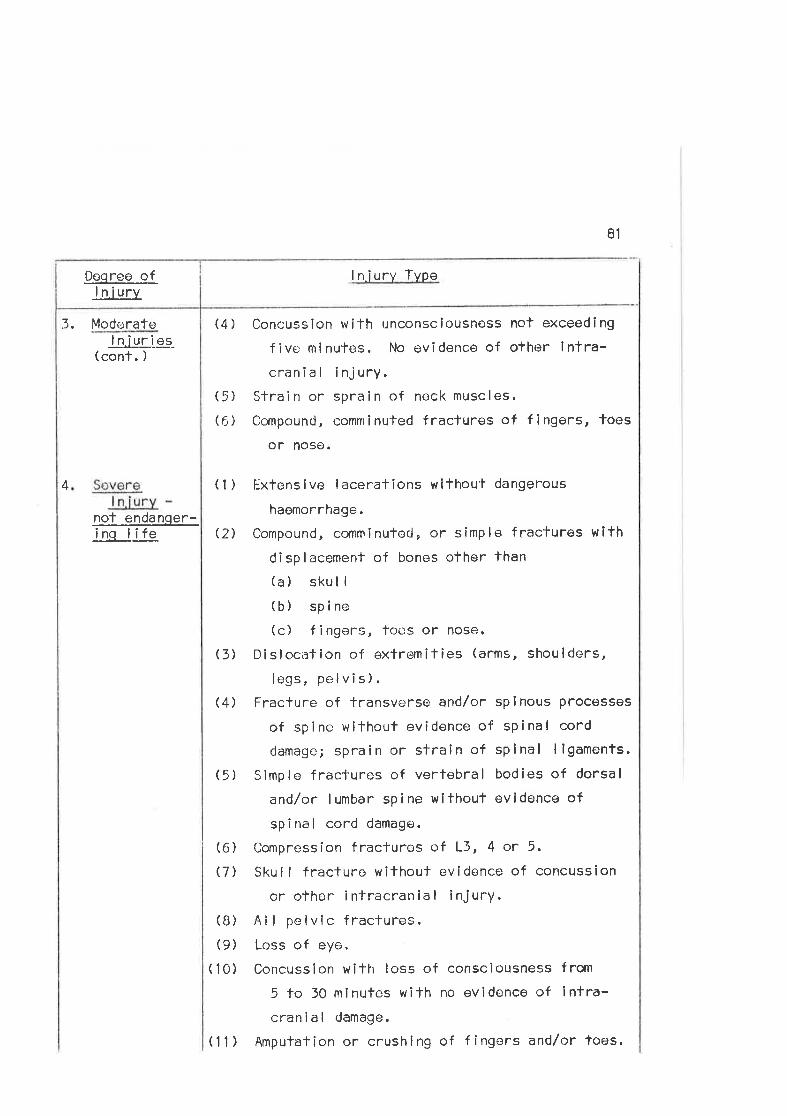
Deoree ollniury
3. Moderate
81
I n.iury ïype
Concussion wifh unconsciousness not exceeding
f i ve m i nutes . No ev i dence of other i ntra-cranial injury.
Stra i n or spra i n of neck musc I es.
Compound, comminuled fractures of fingêrs, toes
or nose.
Extensive laceratlons wlthout dangerous
haemorrhage.
Compound, comminutecJ, or simple fractures with
displacement of bones other than(a) skul I
(b) spine(c) fingers, toes or nose.
Disloci:tion of extremif ies (arms, shoulders,
legs, pelvis).Fracture of transverse and/or spinous processes
of spine without evidence of spinal cord
damage; sprain or strain of splnal I igaments.
Simple fractures of verfebral bodies of dorsal
and/or lumbar spine without evidence of
spinal cord damage.
Compression fraclures of L3, 4 or 5.
Skul I fracture without evidence of concussion
or other intracranial injurY.
Al I pelvlc fractures.Loss of eyo.
Concussion with loss of consciousness from
5 to 50 mlnutes wifh no evidence of lntra-cranial damage.
Amputation or crushing of fingers and/or toes.
lnjur.ig-(cont. )
(4)
(1)
Q)
(5)
(6)
4
nof endanqer-inq life
(3)
(4)
(5)
(6)
(7)
(B)
(9)
(10)
(11)
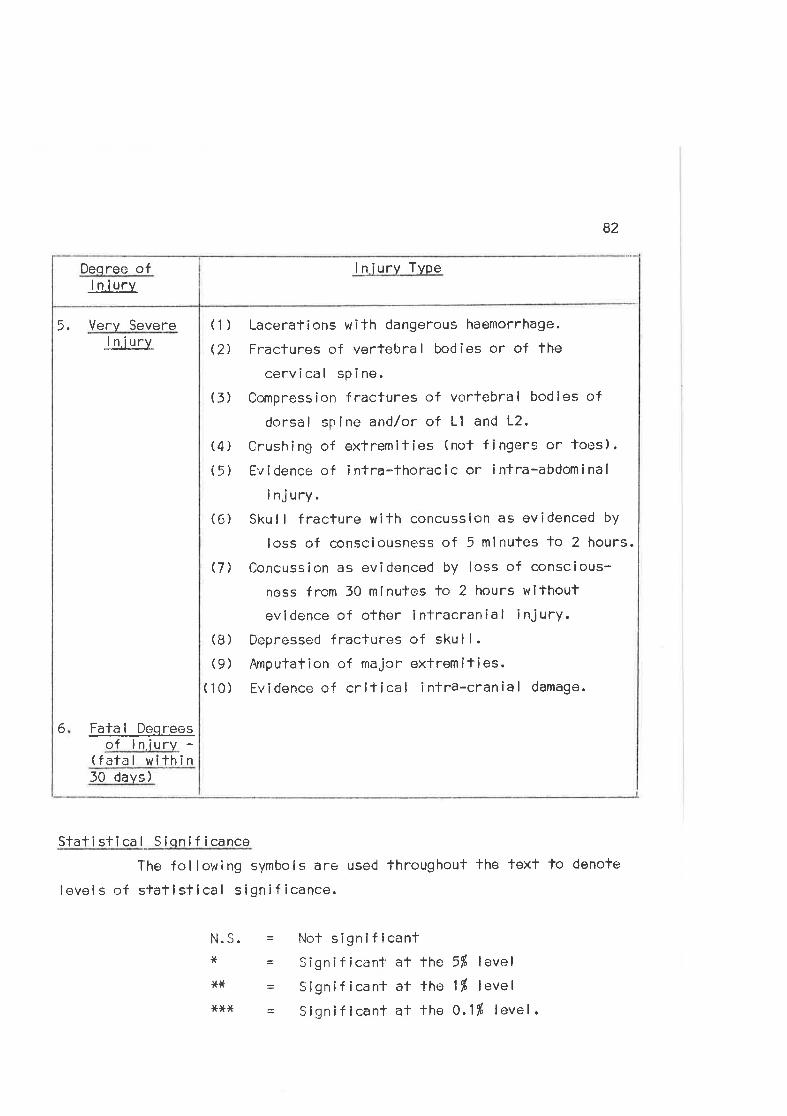
I n iury TypeDeqree ofI n.iurv
5, Very SevereJn.iury
(1)
(2)
82
Lacerations with dangerous haemorrhage.
Fractures of vertebral bodies or of the
cervical spine.
Compression fractures of vertebral bodies of
dorsal spine andlor of Ll and 12,
Crushing of exfremilíes (not fingers or toes).
Evidence of intra-thoraclc or intra-abdominal
i nj ury.Skul I fracture with concussion as ovidenced by
loss of consciousness of 5 mlnutes fo 2 hours.
Concussion as evidenced by loss of conscious-
ness from 30 minutos to 2 hours without
evldence of other intracranial injury.Depressed fractures of skul l.Amputation of majcr extremities.Evidence of critical intra-cranial damage.
= Nol significanl= gignificant at the 5É lovel
- Signíficant at the 1Í level
= $ignif icant at the 0.1tÚ level.
(3)
(6)
(4)
(5)
(7)
(B)
(9)
( 10)
6 Fafa I Deqreesof lniurv -
(fafal wlthin30 days)
Slati sti ca I S iqni f icance
The fol lowing symbols are used fhroughout the fext to denofe
level s of statistical significance.
N.S.******
83
Chapter 6
TI]E CRASHES, THE PAT I ENTS AND TIjE I R INJ UR I ES
PHASE ONE
l. The Sample Crashes
Between Augus't 4, 1969 and February 7, 1970, 100 crashes
involvîng 310 persons an<J 174 vehicles were sfudîed. Ambulance records
showed that, during the same period, 2,501 emergencies occurred withinthe study area, of which 803 occurred during fhe lime the research feam
was on duty. These records did not differentiate the lype of emorgency
attended but an estimate of the proportion of road crashes among these
emergencies was obtained from a special study conducted by the ambulance
authorities <Juring one month in 1969. (V.C.A. S. , 1970, ) lf was found
in that sludy 1'hat road crashes formed approximately a0% of all emerg-
ency cal ls on Mondays, 50f" of the cal ls on Tuesdays, Wednesdays,
Thursdays, Fridays and Surrdays and 607l of emergency cal ls on Saturdays.
Thus, by adjusting the above figures, it was estimated that 1,264 crashes
occurred in the tolal population of 2,501 emergencies and thal 410
crashes occurred during the lime in which the study team was on duty.
The proportion of crashes studied was thus approximately 25% of allthose which occurred during the study poriod.
Table 6/1 (Appendix 1) shows the distribution of those emerg-
encies and estimated crashes by tíme of day and day of week. fable 6/2(Appendix 1 ) shows the dislribution of emergencies and eslimated crashes
during the sarnpl ing perîods. Table 6/3 (see p.B4) depicts fhe distrib-tribution of lhe sample crashes by four hourly periods for each day ofthe week worked. More crashes were observecl on Fridays and Saturdays as
a rcsult of the fact fhat more of fhese days were worked lo reflect thepaftern of crash occurrence whích peaks on these days. Tablo 6/4(Appendix 1) shows the time disÌribution of the study cases as a pro-
portion of the eslimated crashes occurring during the sfudy period. ltcan be seen that thcrc is variation from day fo day and hour to hour
with an overall 24fi sanple. The large variation betwet:n time periods is
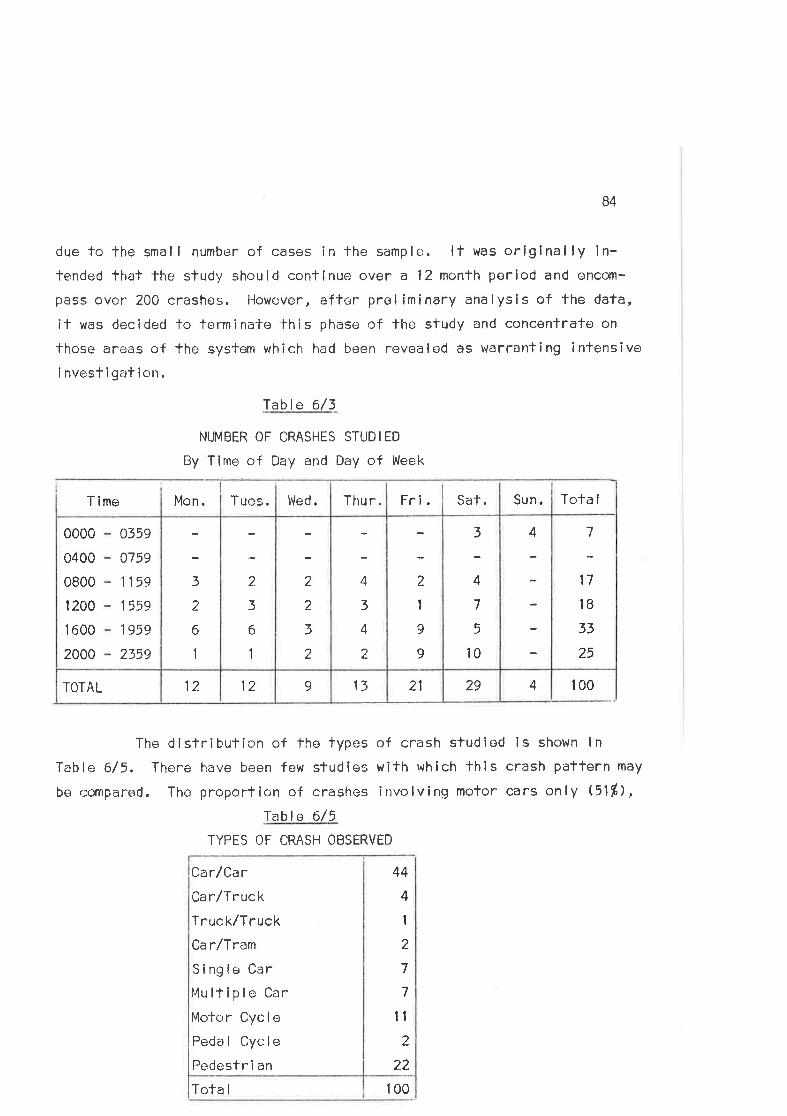
84
due to the small number of cases in the sample. lt was orlginally ln-tended that the study should conflnue over a 12 month period and encom-
pass ovor 200 crashes. llowever, aftor preliminary analysis of the data,
it was decided lo terminate this phase of lhe study and concenfrate on
those areils of the system which had been revealed as warranting intensive
i nvest igat ion.
Iable 6/3
NUMBER OF CRASHES STUDIED
By Time of Day and Day of Week
429211391212TOTAL
7
17
18
33
25
43
4
7
5
10
2
1
9
9
4
3
4
2
2
2
3
2
2
3
6
1
3
2
6
0000
0400
0800
1 200
1 600
2000
0359
0759
1 15e
1 559
1959
2359
Tola ISat. Sun.Fri.Thu r.Wed.Tues.T ime Mon.
100
The distribution of lhe types of crash studied is shown ln
Table 6/5, There have been few sludies with which thls crash pattern may
be compared. The proportion of crashes involving motor cars only $1ß),Ïable 6/5
TYPES OF CRASH OBSERVED
100Tota I
44
1
4
1
2
7
7
I
2
22
Ca r/Ca rCarlTruckTruck/Truck
Ca r/Tram
Single Car
l4ultiple Car
Motor Cycle
Pedal Cycle
Pedestr i an
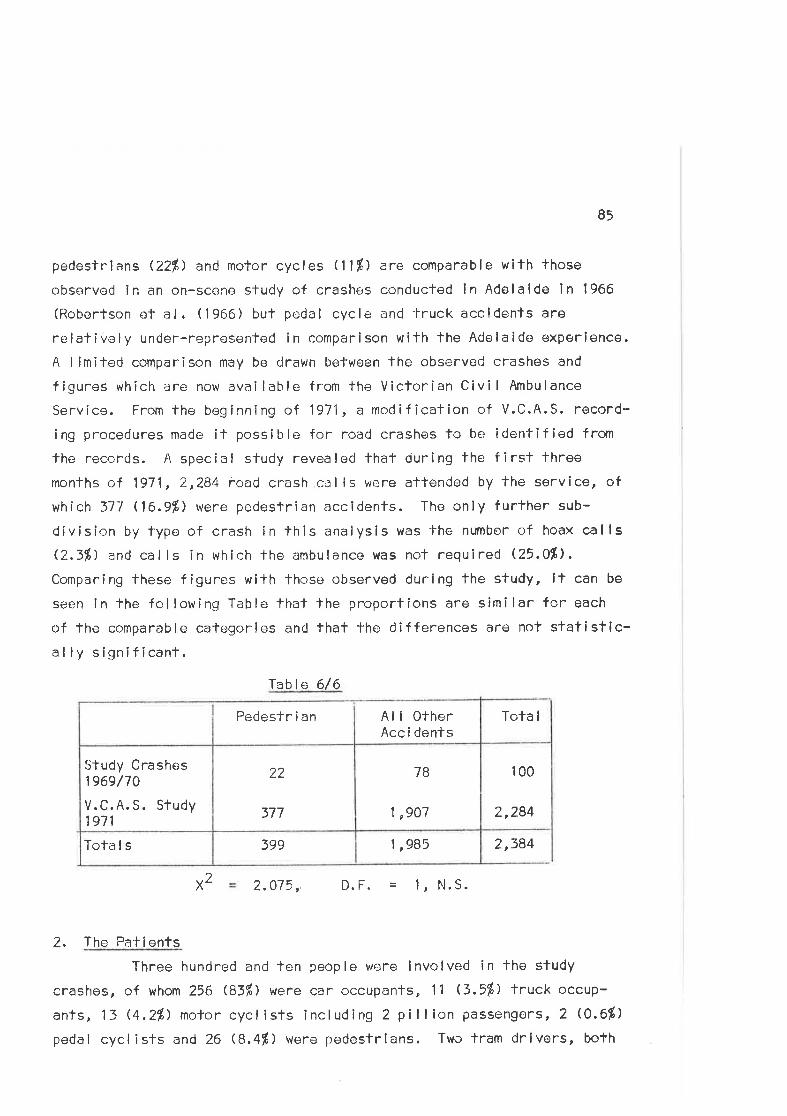
85
pedeslrians (22ß) and motor cycles U1%) are comparable wifh those
obsorved in an on-scene study of crashes conducted in Adelaíde in 1966
(Robertson ef al. (1966) but pedal cycle and 'lruck accldents are
relaliVely under-represented in comparison wifh the Adelaide experience.
A limiled comparison may be drawn be'l'ween lhe observed crashes and
f igures which are now available from the Viclorian Civi I Ambulance
Service. From the beginning of 1971 , a moc!if ication of V.C.A.S. record-
ing procedures made it possit¡le for road crashes to be idenfified frorn
the records. A special sludy revêaled thaf during the first three
months of 1971,2,284 road crash cells were attended by the service, of
which 577 (16.9%) were pcdestrian accldents. The only further sub-
division by type of crash in this analysis was the number of hoax callsQ..3fi) and calls in which the ¿rmbulance was nol required Q5.0Ð,Comparing these figures with those observed during the study, it can be
seen in lhe fcllowing Table that the proportions are similar for each
of the comparable categories and that lhe differences arê not statistlc-ally sif¡nif icanf .
Table 6/6
1 ,985399To1'a I s
100
2,284
7B
1 ,907
22
377
Study Crashes1969/70
V.C.A. S. Study1971
Tota IAl I OtherAcc i dents
Pedeslr i an
2,384
X 2.075, D.F. 1, N.S.
2. The PatientsThree hundred and len people were involved in fhe study
crashes, of whom 256 ß3í') were car occupantso 11 ß.51) truck occup-
ants, 13 ø.2%) no'ror cyclists including 2 pillion passengers, 2 (0,6fi)
pedal cyclists and 26 ß,4f ) were pedestrlans. Two tram drivers, bofh
2
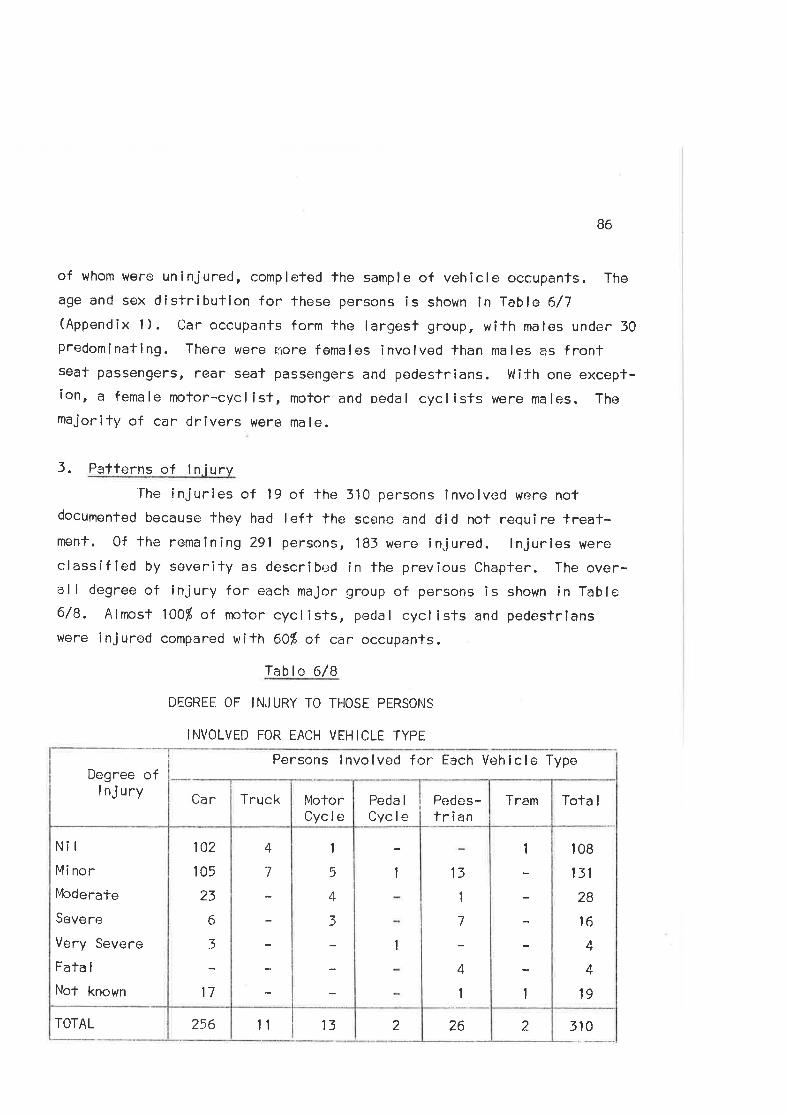
B6
of whom were uninjured, complefed the sample of vehicle occupanfs. The
age and sex distríbulion for these persons is shown ln Table 6/7(Appendlx 1). Car occupants form Ìhe largest group, with males under 30
predomlnating. There were more females involved than males as frontseat passengers, rear seat passengers and pedestrians. With one except-ion, a female nr¡tor-cyclisf , motor and pedal cyclîsts were males. The
majority of car drivers were male.
3 . Pafferns of I n.iury'The
i nj ur i es of 1 9 of the 310 persons i nvo lved were notdocumented because they had left the scene and did not require treat-ment. 0f fhe remaîning 291 persons, 183 were injured. lnjurles were
classified by severify as descrîbed in the previous Chapfer. The over-all degree of injury for each maJor group of persons is shown ln Table6/8. Alnpst 100Í of motor cycl isls, pedal cycl ists and pedestrianswere injured compared with 601 of car occupants.
Table 6/8
DEGREE 0F INJ URY T0 THOSE PERSOI'|S
INVOLVED FOR EACH VEHICLE TYPE
Persons lnvolved fr:r Each Vehiclo Type
2262256
Tota I
108
131
28
16
1
4
19
1
t
13
I
7
4
I
1
1
1
5
4
3
4
7
102
105
23
6
3
17
N¡I
Minor
l4cderafe
Severe
Very Severe
Fata I
Not known
TramPeda I
CyclePedes-trian
MotorCycle
Truck
Degree ofI nj ury Car
TOTAL 11 13 310
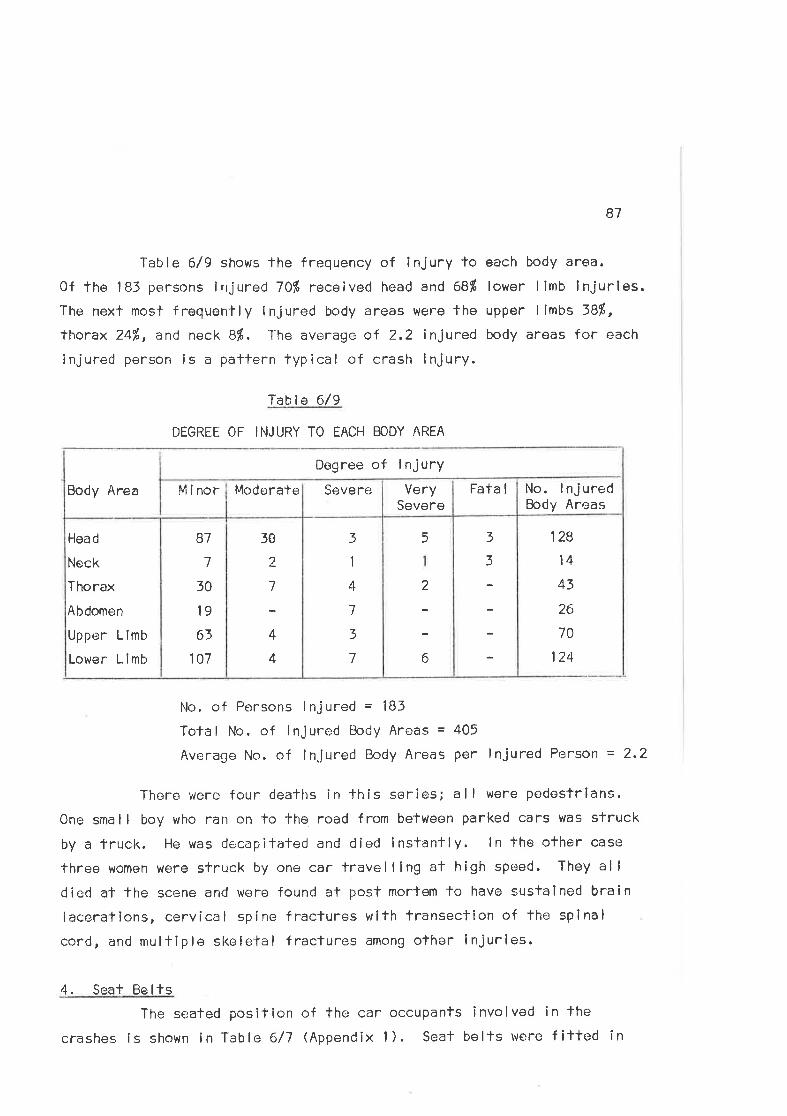
Table 6/9 shows lhe frequency of injury toOf fhe 183 persons injured 7Ol' received head and 6Bf
The next most frequently ínjured body areas were fhe
thorax 24%, and neck Bf . 'Ihe average of 2.2 injuredinjured person is a paltern typical of crash injury.
B7
each body area.
lower I imb i nj ur ies.
upper I lmbs 38Í,body areas for each
Table 6/9
DEGREE OF INJURY TO EACH BODY AREA
Body Area M inor
No. of Porsons lnjured = l8jTotal No. of lnjured Body Areas = 405
Average No. of ln.jured Body Areas Per lnjured Person = 2.2
Thero were four deaths in fhis serles; al I were pedesfrians,
One sma I I boy who ran on to the road from between parked cars was sfruck
by a fruck. He was decapitated and clied instantly. ln the ofher case
three women were struck by one car lravelllng at high speed. They alldied at the scone and were found at post morlem to have sustained brain
lacerations, cervical spine fraclures with fransection of lhe spinal
cord, and mulfiple skeletal fractures among other lnjurles.
4. Seaf Be I tsThe seated poslTion of the car occupants involved in the
crashes is shown in Table 6/7 (Appendix 1). Seat belts were fitted in
128
14
43
2(,
70
124
3
3
5
2
6
3
1
4
I
3
7
30
2
7
4
4
87
7
30
19
63
107
Head
Neck
Thorax
Abdomen
Upper L imb
Lower Limb
No. I nJ urectBody Areas
Fata IVerySevere
Modorate Severe
Degree of lnjury
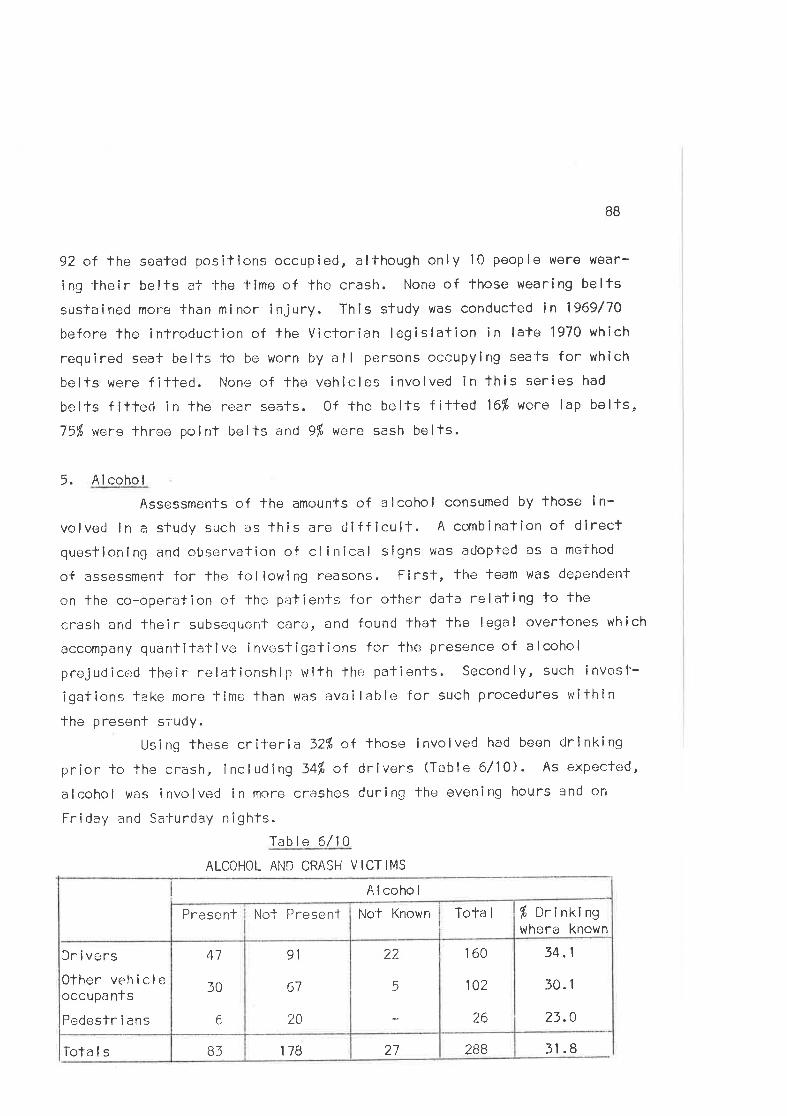
BB
92 oÍ the sealed positlons occupied, although only 10 people were wear-
ing'lheir belts at the time of the crash. None of those wearing belfs
sustained moro than minor injury. This study was conducted in 1969/70
before lhe inlroduction of the Victorian legislation in late 1970 which
requîred seat belts J'o be worn by all persons occupying sea'ts for whlch
belts were fitted. None of the vehicles involved in lhis seríes had
belts f ilted in the rear seats. Of the belts f itled 16$ were lap belts,75% were three; point bel'ts and 9dp wcre sash belts.
5. Alcohol
Assessments of the amounts of a I coho I consumed by those i n-
volved in a sludy such as lhis are diff icult. A combination of direclquestioning and observation of clinical signs was adopted as a meihod
of assessment folthe folloviing reasons. First, the team was dependernt
on the co-operation of thc patients for other dala relating to fhe
crash and their subsequenÌ care, and found that the legal overtones which
accompany quanlifalive investigations for the presence of alcohol
prejudiced lheir rc--lalionship with lhe patients. Secondly, such invtrst-
igations take more time than was available for such procedures within
the present siudy.Usi ng these criteria 32% of those i nvol ved had been dri nki ng
prior to lhe crash, including S4dp of drivers (Table 6/10). As expected,
alcohol was involved in more crashes during The evening hours and on
Fr i day and Sa-lurclay n i ghfs.
Table 6/10
ALCOHOL AND CRASH VICTIMS
Alcohol
28B27178B3Tota I s
34.1
30. 1
23.0
160
102
26
22
5
91
67
20
41
30
6
Dr i vers
Other vehicleoccupa nts
Pedestr i ans
þ Drt nKr ngwhere known
Tota INol KnownNo-l PresentPresernt
31 .8
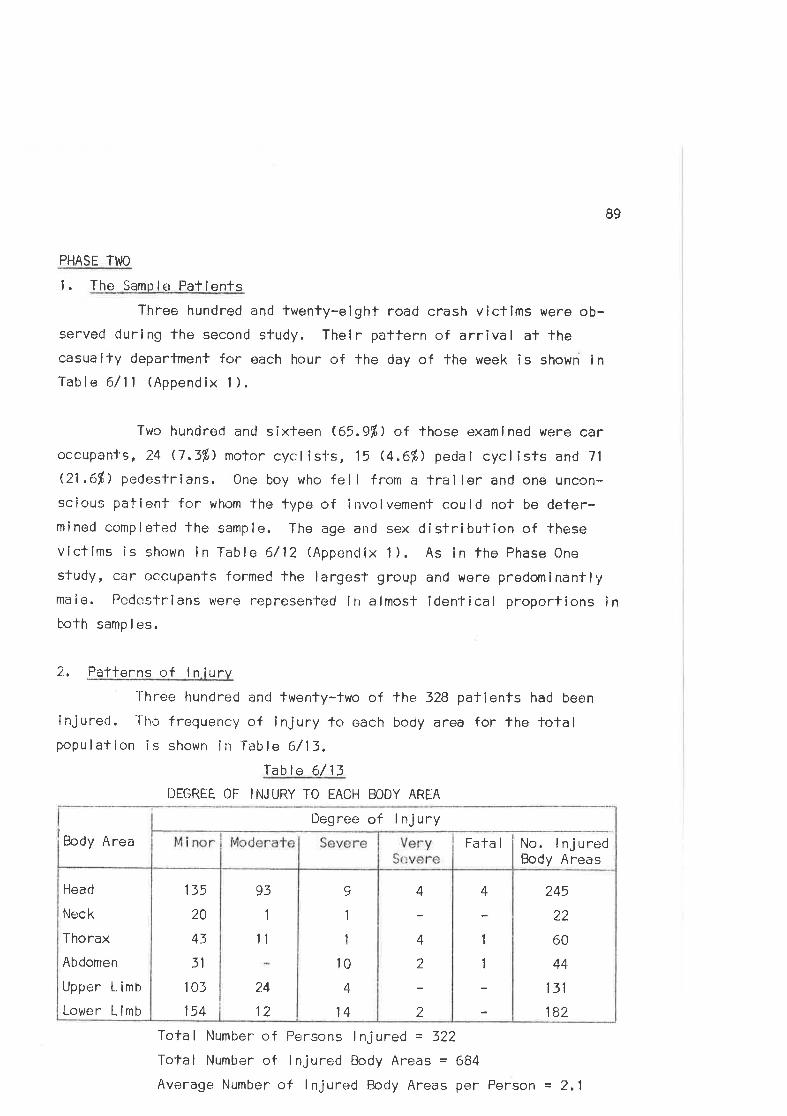
89
PHASË ThIO
l. The Sample PatientsThree hundred and twenty-eighf road crash victims were ob-
served during the second study. Their pattern of arrival af thecasualty department for each hour of the day of the week is shown inTable 6/11 (Appendix 1).
Two hundred and sixteen (65.91,) of those examlned were caroccupanl's, 24 (7.31,) motor cyclisi's, 15 G.6%) pedal cyclists and 71
Q1 .6%) pedes-f'rians. One boy who fell f rom a trailer and one uncon-scious patien-t'for whom the fype of involvement could not be deter-m i ned comp I eted the samp I e. The age and sex cI í stri but ion of -lhese
victims is shown in Table 6/12 (Appendix 1). As in fhe Phase One
study, car occupants formed the largest group and were predominanflymale. Pedestrians were nepresented in almost idenfical proportions inboth samp I es.
2., Paflerns of ln iurvl-hree hundred and twenty-two of the 328 pationts had been
injurecl. The frequency of injury to each body area for the totalpopu I at ion i s shown î n Tab le 6/13,
Table 6/11I]EGRËE OF INJURY TO EACH BODY AREA
Body Area
Tota I Number of Persons I nj ured = 327-
Tofal Number of lnjured Body Areas = 684
Average Number of I njured Body Areas per Person = 2.1
245
22
60
44
131
182
4
1
1
4
4
2
?_
9
1
1
10
4
14
93
1
t1
24
12
135
20
43
3l
103
154
HearJ
Neck
ïhoraxAbdomen
Upper L imb
Lower Limb
Degree of lnjuryFatal i No. lnjured
I ao¿y Areas
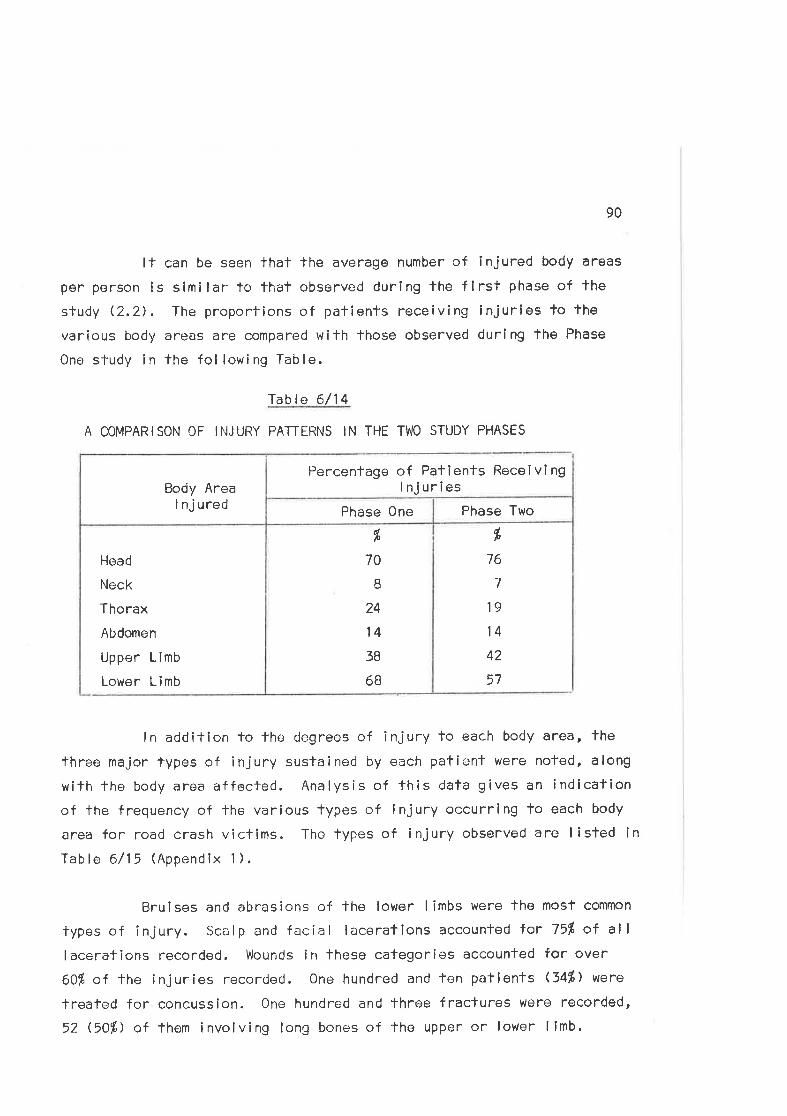
90
It can be seen thaf the average number of injured body areas
per person is similar to thal observed during lhe first phase of the
study (2.2). The proporfions of pafients receiving injuries to the
various body areas are compared with lhose observed during the Phase
Ono s-ludy i n the fo I low i ng Tab I e.
Tab le 6/l 4
A COMPARISON OF INJURY PATTERNS IN THE TWO STUDY PHASES
dþ
76
7
19
14
42
57
dþ
70
B
24
l438
6B
Hoad
Neck
Thorax
Al¡domen
Upper Limb
Lower Limb
Phase TwoPhase One
Body AreaI nj ured
Percentage of Patients ReceivingI njuries
ln addition lo Ìhe degrees of injury to each body area, the
lhree major types of injury suslained by each patient were noted, along
with the body area affected. Analysis of fhis data gives an indlcafionof the frequency of the various types of lnjury occurring to each body
area for road crash viclims. The types of injury observed are lisled lnTable 6/15 (Appendlx 1).
Bruises and abrasíons of the lower limbs were the mosf common
types of injury. Scalp and facíal laceratlons accounted for 75l of al I
lacerations recorded. Wounds in these categories accounled for over
60Í of the injuries recorded. One hundred and Ten patients (34%) were
treafed for concussion. One hundred and throe fractures werê recorded,
52 $O%) of them involving long bones of the upper or lovrer limb.
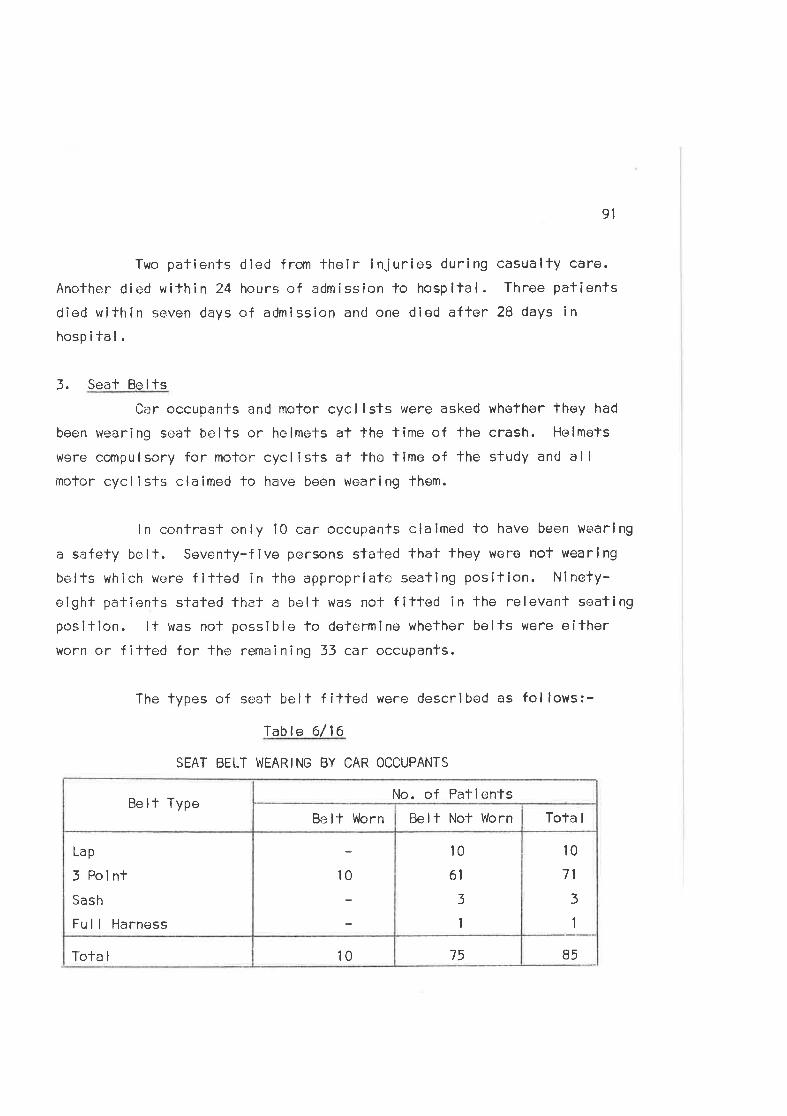
9l
Two patienfs died from lheir injuries during casualty care.
Another died within 24 hours of admission to hospital. Three patientsdiod within seven days of admission and one died affer 28 days in
hospital.
3. Seat BeltsCa:r occupants and motor cyc I i sls were asked whether they had
been wearing seat belts or helmets at the time of the crash. Helmets
were compulsory for motor cycliEts at fhe time of the study anrJ allmotor cycl ists claimed to have been wearing them.
ln contrasf only 10 car occupants clalmed lo have been wearing
a safety bell. Seventy-five persons sfated that lhey were not wearlng
belts which were fitted in lhe appropriate seatlng position. N¡nefy-
eight patienfs staled that a bell was not filted in the relevant seatingposition. lt was not possible to delermlne whether belfs were eitherv/orn or f ilted for the remaining 33 car occupants.
The types of seat belt f ittecl were described as follows:--lable 6/ l6
SEAT BELT WEARING BY CAR OCCUPANTS
7510Tola I
l071
3
1
't0
61
3
1
10
Lap
3 Poi ntSash
Fu I I Harness
Tota IBelt Nol WornBelt WornBelt Type
No. of Patients
85
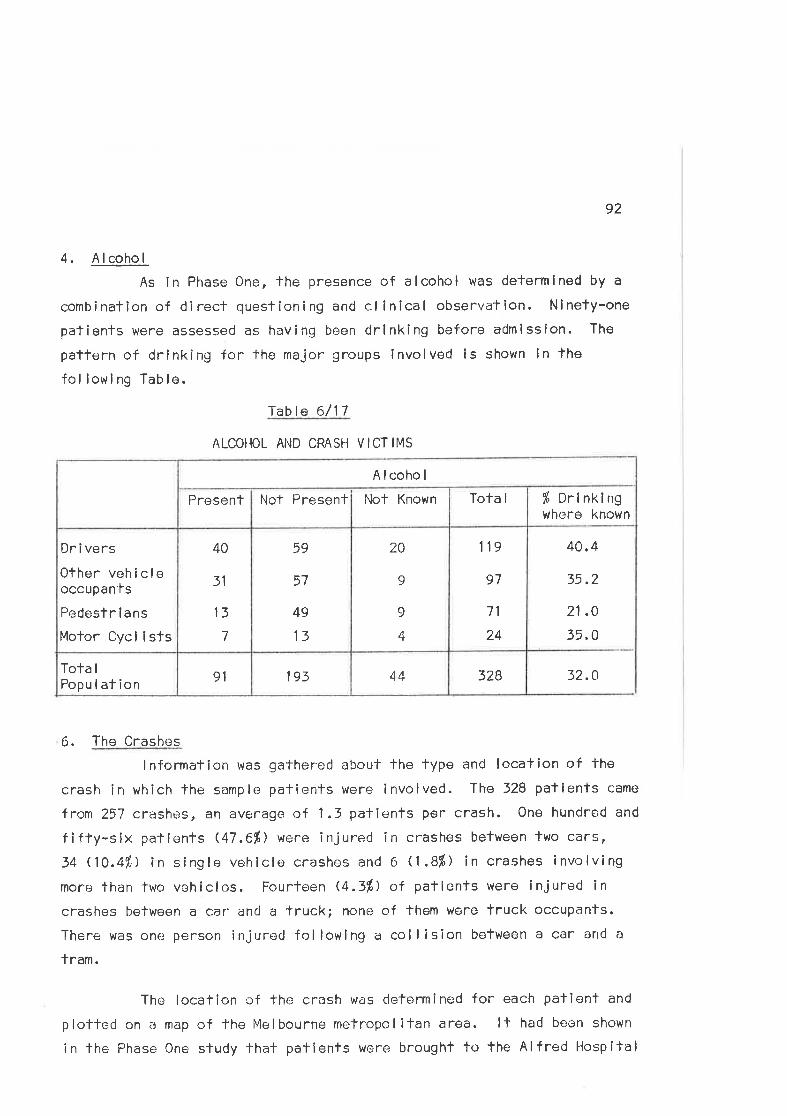
92
4, Alcohol
As ln Phase One, the presence of alcohol was determlned by a
combination of direct questloning and clinical observetion. Ninety-one
patîents were assessed as having been drinking before admission. The
pattern of drinking for the major groups involved is shown ln lhe
fol lowi ng Tab le.
'fable 6/17
ALCOHOL AhID CRASI.I VICTIMS
6. The Crashes
lnformation was gathered about the fype and location of the
crash in which lhe sample patients were involved. The 328 patients came
fron 257 crashes, an average of 1.3 patienls per crash. One hundrod and
fifty-six patients (47.6%) were injured in crashes between two cars,
34 (10.41,) in single vohicle crashes and 6 (,8Ð in crashes involving
moro than two vehicles. Fourtoen Q.3%) of patienls were injured incrashes belween a car and a truck; none of them Were lruck occupants.
There was one person injurod following a collision between a car and a
lram.
The locaTion cf the crash was delermined for each palient and
plotted on a map of the l,4elbourne melropolitan area. ll had beon shown
in lhe Phase One study that patients were brought to the Alfred Hospital
40,4
35.2
21 ,0
35.0
32.03284419391Tota I
Popu I at ion
lr9
97
71
24
20
9
9
4
59
57
49
13
40
31
13
7
Dr i vers
Other vehicleoccupan'ls
Pedestr i ans
Molor Cycl isfs
% Drinkingwhere known
Tota INot KnownNot PresentPresent
Alcohol
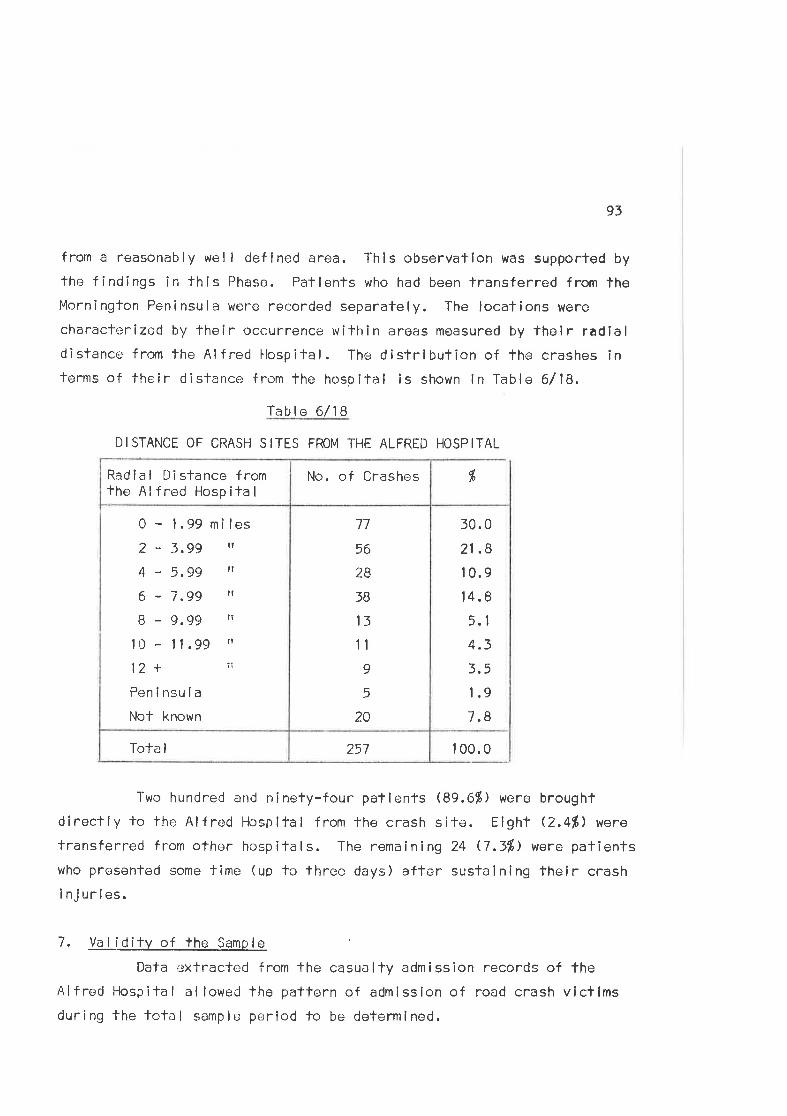
93
from a reasonably wel I defined area. This observation was supporfed by
the findings in this Phase. Patlents who had been lransferred from theMornington Feninsula were recorded separately. The locations were
characterized by fheir occurrence within areas measured by their radlaldistance f rom the Alf red llospital. The distribuf ion of the crashes interms of their distance from the hospifal is shown in Table 6/18.
TaLrle 6/18
DISTANCE OF CRASH SITES FROM THE ALFRÊD HOSPITAL
1 00.0257ToTa I
30.0
21 .B
1 0.9
14.8
5.1
4.3
3,5
1.9
7.8
77
56
2B
5B
13
11
9
5
20
0 - 1.99 mî les
2-3.gg il
4-5,99 l'
6 - 7.gg rt
8 - g.gg rr
10 - 11.99 ,,
12 + ïi
Peninsula
Not known
No. of CrashesRadial Dislance fromfhe Al fred Hosp ita I
dþ
Two hundred and ninefy-four patienfs (89.6%) were broughtdireclly to the Alfred Hospilal from the crash site. Eight Q.4ft) were
transferred from other hospilals. The remaining 24 0.3%) were patienlswho presented some time (up to three days) after sustaining their crash
injurles.
7 . Va t 'l O itv o+ +ne Samp le
Data oxtracted from the casualty admisslon records of theAlfred llospilal allowed the pattern of admission of road crash victimsduring the tolal sample period to be determined.
94
A casualty admlssion regisler is maintained in the hospitalwhich records the name¡ âge, sex, time of admission, admission diagnosísand approximate duration of stay ín the casuâlty department for each
patient seen in fhal deparTment. Road crash victims receive specialnotation in this record and can fhus be readily identif ied fro¡n ¡1.
This admission register is kept for the convenience of casualty sfaffand inaccuracies occasional ly occur in the detai ls relating fo each
patient (due largely fo lhe facl that the information is recorded by
different members of staff at different times during the patientrs stayin the department). I'levertheless, if was possible lo positively identifylhe records of 324 of the 328 persons observed, and fo compare characf-eristics of the study populaTion wifh those road crash vicfims who were
admitted buf not seen durîng the duty periods. The numbor of road crash
victims admitted during the total sample period was also identifiedfrom lhe record.
Durlng the total sample period of 170 days, 26,236 pat ientswere frealed in the casualty departmenÌ of the Alfred Hospifal, of whom
1,382 $.3%) were vlctims of road crashes. The distrlbution of fhe times
of arrival of these crash patients at the casualty department is shown in
Table 6/19 (Appendix 1).
The toTa I numbe.¡r of crash pat ient arr iva I s at the casua ltydepartment during the limes the observer was on duty were also deter-mined from the admission record. Three hundred and ninety-four patientswere admi-lfed during these duly periods. The observed population thus
represented an 83ß sample of all patients admitted cf uring the duty
periods and a 241" sanple of the road crash patients treated in the cas-
ualty department during lhe total study per¡od. ln Íable 6/20(Appendix 1) the dîsfribulion of the observed patients is compared wifhthal of -lhe tc'tal population admitted during dufy periods.
The number of palients seen during each throe hourly period of
95
the week is expressed as a proportion of the total number of crash
vicf ims admitted to the department in Table 6/21 (Appendix I ). lt can
be seen tha't the proporfion of patients seen varies from time period to
time period fhroughout the week, with an overal I 24fi sanple.
ln 'the fol lowlng discussion, data obtained from fhe casualty
admission records are used lo compare the observed population with those
admitted bul not seen during the duty periods and wi'fh fhe crash popul-
atlon admifted during the folal sample perlod. Age, sex, to+al time
spent in casualty and discharge patterns are usecl for comparing the
three pop u I arl ions .
Table 6/22 (Appendix l) shows the age and sex distrÎbutlon of
the three populations. Comparing the sex distributions, the difference
between those observerl and those admitted duríng duty periods bu'|" not
otrserved is not slatislically signif icant. Similarly, comParison of
fhose observed wilh those not observed bul admitfed during the totalsanrple period reveals lhaf fhe differences between lhe fwo populations
are not slatistical ly sigttificant.
Comparison of the three populations by age in 10 year groups
shows that the observed dlfferences are, once again, not statistical lysignificant, (Observed versus not observed during duty periods
x2 = 6.177; D.F. = 7; N.s.; observed versus not observed during the
tolal sample Period X2 = 12,042; D.F. = 7; lrl.S. )
Since lhe presence of the observer is a potenfial source of
interference in lhe system under study, it is imporfant lhaf an assess*
ment of thls influencc should be obtained. This is of part¡cular import-
ance in this study, where elapsed times in the various -treatrnent phases
are amorìg the major variables under examination.
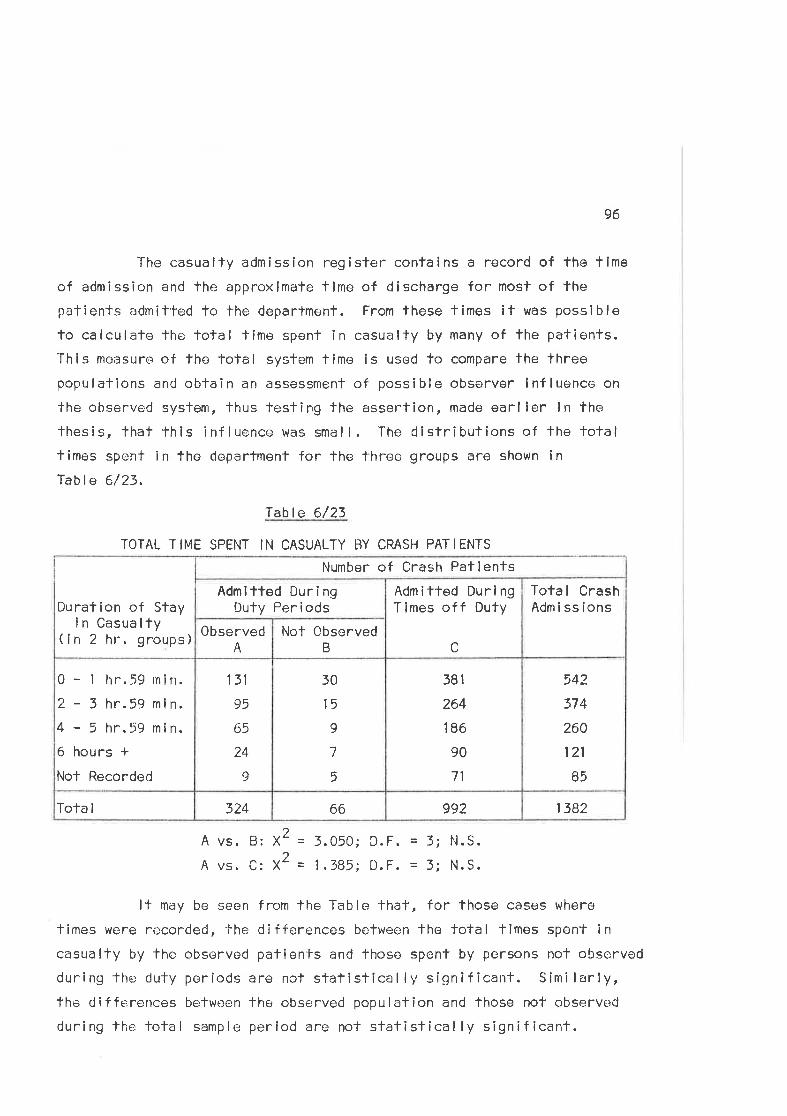
96
The casualty admission register contaíns a record of the time
of admission and the approximate time of discharge for most of thepatients admit'ted to the department. From these times if was possible
to calculate the fotal tlme spent in casualty by many of the pafients.Thís measure of the tolal system time is used fo compare the threepopulations and obtain an assessment of possible observer lnfluence on
the observed syslem, thus testing the assertion, made earlier ln the
fhesis, that lhis influence was smal l. The distributions of the totalfimes spent in the department for the three groups are shown ln
Table 6/23.
Table 6/23
TOTAL TIME SPENT IN CASUALTY BY CRASH PATIENTS
A vs.
A vs.
2B: X
C: X
= 3.050;
= 1.385;2D. F.
D. F. - z.N. S.
N. S.
lf may be seen from the Table that, for those cases where
times were recorded, the differences between the total times spent incasualty by the observed palients and lhose spenl by persons not observed
during lhe duty periods are not statistically sígnlf icant. Similarly,the differences between the observed population and those not observed
during lhe fotal sample period are not statistically signif icant.
138299266324Tota I
542
374
260
121
85
381
264
186
90
71
50
15
9
7
5
131
95
65
24
I
0 - t hr.59 rnin.
2-3hr.59min.4-5hr.59min.6 hours *Nol Recorded
Tota I CrashAdmisslons
Adm i tted Dur i ngTimes of f Duty
cNot 0bserved
B
0bservedA
Duration of Stayin Casualty
(in 2 hr. groups)
Admltted Duri ngDuty Periods
Number of Crash Patlenls
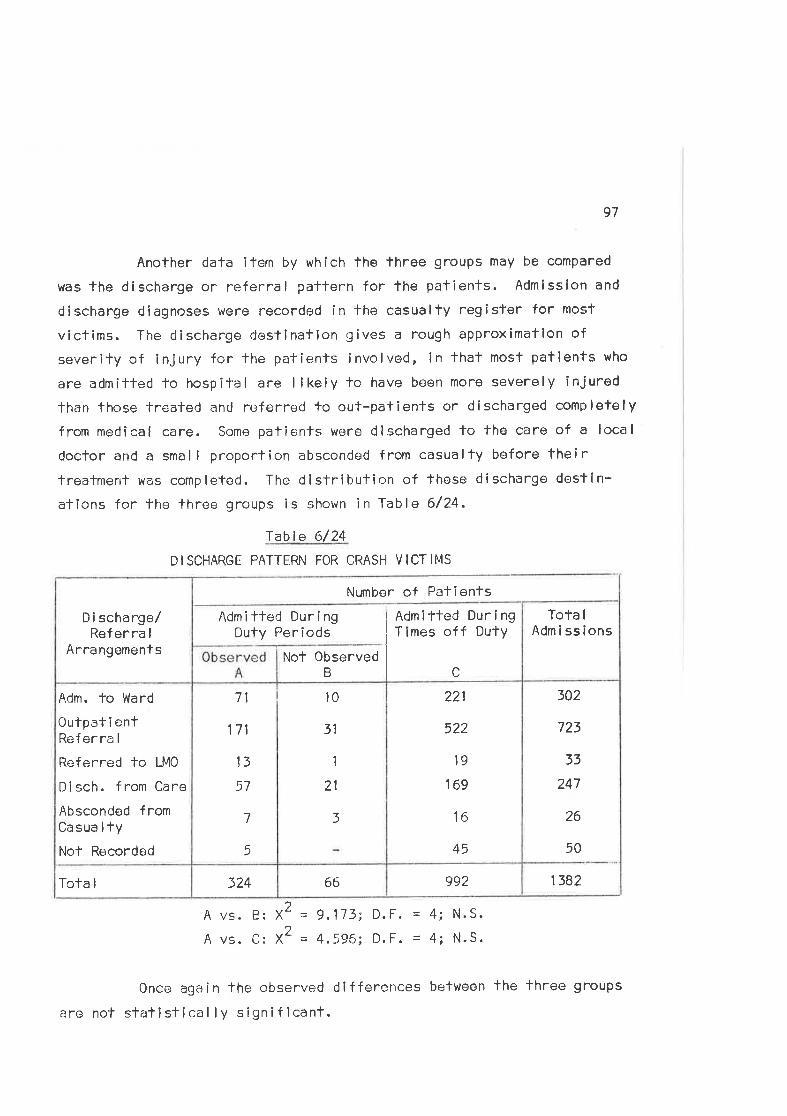
97
Another data itern by whích the lhree groups may be compared
was the discharge or referral patfern for lhe patients. Admission and
discharge diagnoses were recorded in the casualty register for most
victims. The discharge destinaflon qives a rough apProximation of
severity of injury for lhe patienfs involved, in that most patlents who
are admitted lo hospital are likely to have been more severely injured
than those treated and referred to out-pafients or discharged completely
from medical care. Somo patients were discharged to the care of a local
doclor and a smal I proportion absconded from casualty before theirtreatmenl was comp leted. The d I stri but ir:,n of these d i scharge dest I n-
ations for the lhree groups is shown in Table 6/24.
rable 6/24
DISCHARGE PATTERN FOR CRASH VICTIMS
138299266324Tota I
302
723
33
247
26
50
221
522
19
169
16
45
71
171
13
57
7
rì
10
31
1
21
5
Adm. to Ward
0ulpat i entReferra I
Referred to LMO
Disch. from Care
Absconded fromCasua I fyNof Recorded
Tota I
AdmissionsAdmitled Duri ng
Duty PeriodsI Admitted During
Times of f Duty
Not ObservedB c
D i schargo/Referra I
Arrangoments
Numbor of Patienfs
2 = 9,173; D.F. = 4; N.S.
= 4,596; D.F. = 4; N.S.
A vs. B; X
A vs. C: X2
Oncu again the cbserved differences beTween lhe fhree groups
are not slalislical ly signiflcant.
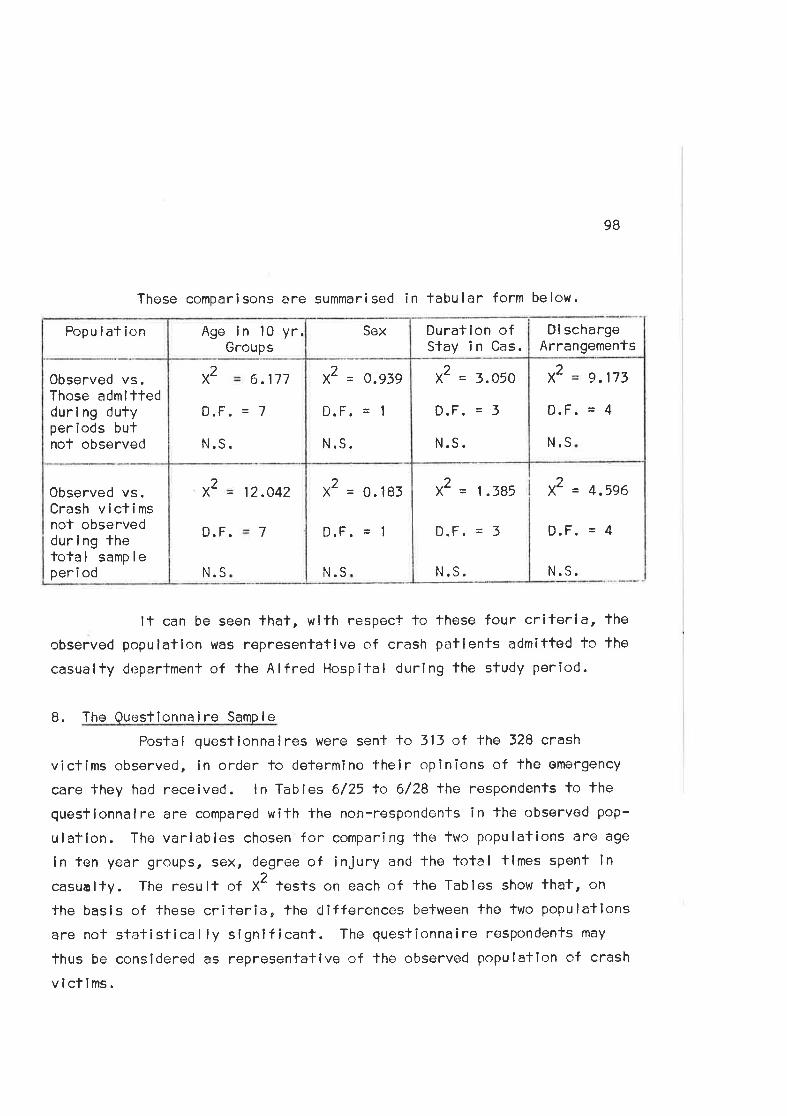
These comparisons are summarised in tabular form below.
98
Di schargeArrangemenfs
x2 = 4,596
D,F. = 4
N.S.
It can be seen that, with respect to these four criterla, the
observed populallon lvas rêpresentatlve of crash patients admitfed to the
casualfy deparfment of the Alfred Hospifal during the study period.
8. The Questîonna i ro Samp I e
Postal questlonnalres were sent to 313 of fhe 328 crash
vicfims observed, ln order to determine their opinions of the emergency
care fhey had receivod. ln Tables 6/25 to 6/28 lhe respondents to the
quesÌionnaire are compared wifh fhe non-respondents in the observed pop-
ulation. The variables chosen for comparing the lwo populations are age
in ten year groups, sex, degree of injury and the lotal tlmes spenf ln
casualty. The result of X2 lests on each of fhe Tables show that, on
the basls of these criferia, the clifferences between The two populallons
are not statistical ly significant. The questionnaire respondenfs may
thus be considered as representative of the observed population of crash
vlcflms.
x2 = 1.385
D.F. = 3
N. S.
X2 = 0. 183
D.F. = I
N.S
x2 12.042
D. F. 7
N.S
Observed vs.Crash victimsnot observeddurl ng thefotal sampleper i od
x2 9.173
D. F. 4
N.S
X2 = 3.050
D.F. = 3
N.S.
X2 = O.939
D.F. = 1
N.S.
x2 6.177
D. F.
N.S.
7
0bserved vs.Those admittedduri ng dufyperiods butnof observed
Durat ion ofStay i n Cas.
SexAge in 10 yr.Groups
Popu lat ion
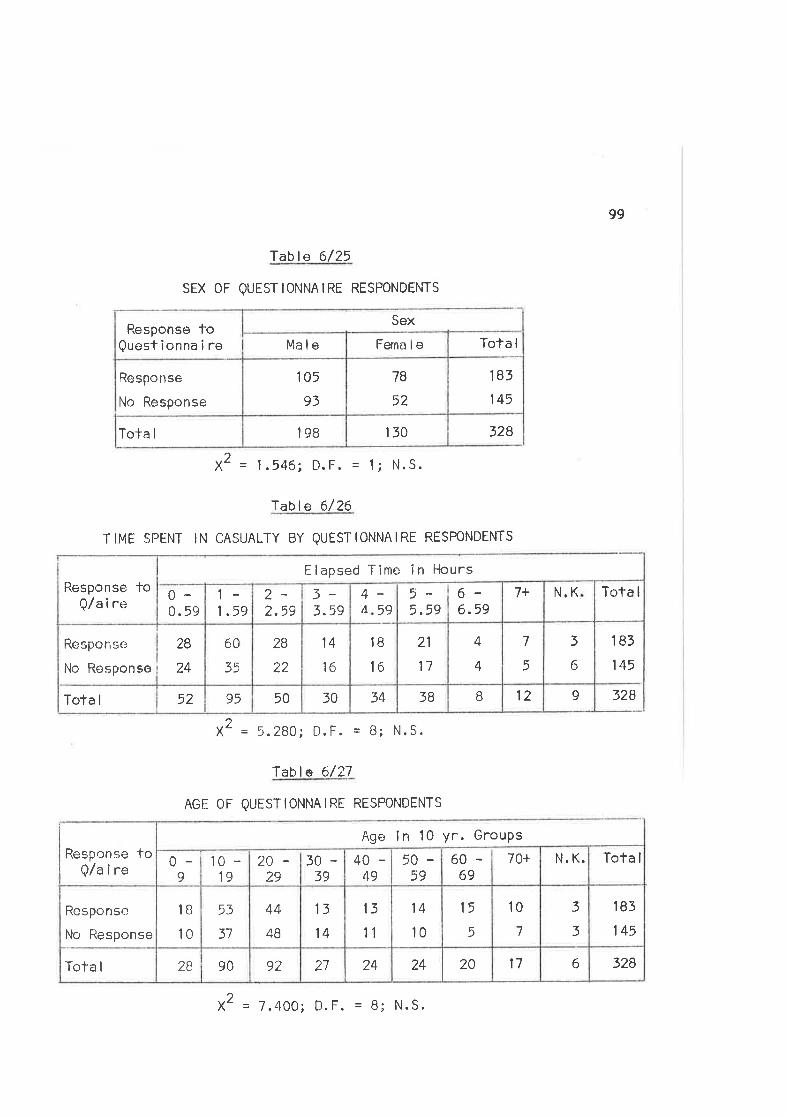
Table 6/25
sEX 0F QUESTIoNNAIRE RESPoNDENTS
2X = 1.546; D.F. = 1i N.S.
lable 6/26
TIME SPËNT IN CASUALTY BY QUESTIONNAIRE RESPONDENTS
2X = 5.280; D.F. = B; N.S.
lablø 6/27
AGE OF QUESTIONNAIRE RESPONDENTS
X
99
183
145
328
328150198Tota I
183
145
78
52
105
93
Response
No Response
Response toQuest ionna i re
Sex
Ma le Ferna le Tota I
91283B3430509552Tota I
3
6
7
5
4
4
21
17
IB
16
14
16
28
2?_
60
35
Response
No Response
28
24
Tota IN.K7+6-6.59
5-5.59
44 59
3-3.59
2-2.59
1-I .59
0-0. 59
Response toQ/aire
Elapsed Time in Hours
32861720242427929028Tofa I
183
145
3
3
10
7
15
5
14
10
13
11
13
14
44
48
53
37
1B
l0Responso
No Response
Tota IN. K.70+60-69
50-59
40-49
20-29
3039
10 -19
0-<)
Response toQ/a i re
Age in 10 yr. GrouPs
2 = 7.400; D.F. = B; N.S.
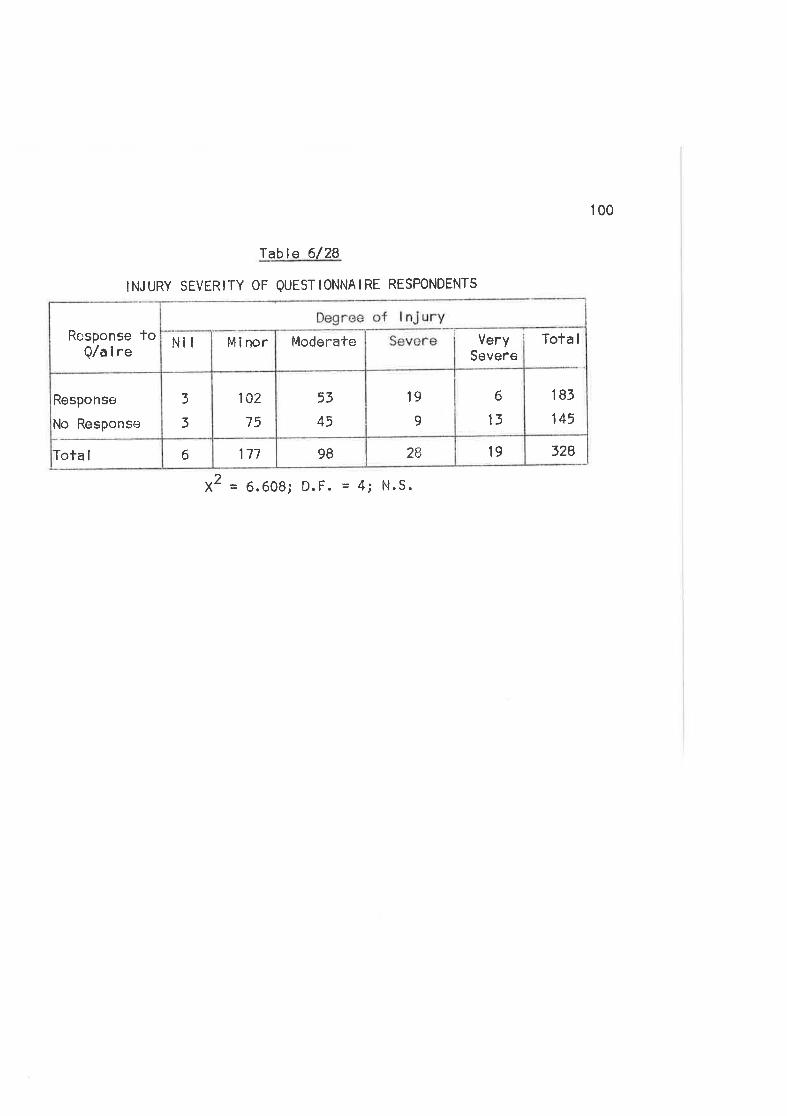
100
Table 6/28
INJURY SEVERITY OF QUESTIONNAIRE RESPONDENTS
2X = 6.608; D.F. = 4; N.S.
3281928981776Tota I
183
145
6
13
19
I53
45
102
75
3
3
Response
No Response
Tota IVerySevere
ModerateMinorNilRcsponse toQ/a i re
lot \.,ìi )j
1ii'i,r(:. "OPERATION OF THE ET4ERGENCY CARE SYSTEM
I N MELBOURNE
The fol lowing discussion of fhe study findings uses the
emergency care system modc-;l (see Chapler 3) lo descríbe the emergency
servîces provided for road crash victims in lerms of the fourfuncfional systems:
(a) Commun i cat ions(b) T'ransporf(c) Treatment(C ) Documentat lon.
TIIE COMNIUN ICAT IONS SUBSYSTEM
(a ) Crash De tecf ion and l,'lot i f icat ion
The firsf helping porsonnel to arrive on the scene of a crash
are usually members of the -c¡eneral public. From observation of fhe
study crashes it seems lhat most crashes in metropolitan aroas are
detected and notified to the ernergency services oromptly.
ll was dîfficull lo determine -lhe length of the notificationdolays for the sludy crashes but bystanders at lhe crash scene were
questioned in an attempt to determine which emergency service was
summorred and by whom. These enquiries were supplemented by examination
of the ambu lance ca I I record kept in lhe ambu lance commun ications cen-tre,
which records the origin of lhe nofification cal I when thls is known.
The origin of the call was delermined for forty of Ìhe
crashes. Thirfy-elght Í were nofified to the ambulance servlce from
the universal omergency number i000t , 16'/" were relayed by the policecommunÎcafions centre and 16Í by taxi radio control lers. The remaining
30Í were nolif ied by direct felephone calls to the ambulance sorvice
from persons al lhe crash scene.
Chapler 7at
l02
The emergency telephone number t000u ls avai lable fhroughout
Ausfral ia for al I major trunk exchanges of the Postmaster Generalrs
Department. Emergency cal ls may be made through this exchange and are
directed to the appropriate emergency service. ln 12 months fo June 50,
1971,397,757 calls were made on the number ln Vlctoria, of which
120,039 were connected fo the fol lovring servlces:
Pol lce
FireAmbu I ance
83,627
10,322
?6,090(Austral ian Post Office, 1971,)
A critical factor which affects the response of the emergency
servlco is the quality of the information fransmitted in the notifyingcal l. lnformafion on the number of persons injured, the nalure oftheir injuries and the slte of the crash allows the dlspatcher loassess 1'he needs and send several ambulances lf necessary. Volce
communication between fhe person notifying the cal I and lhe dispatcher
is the only satisfactory method of ensuring fhat this lnformatlon isavailable. ln practico most notif icaf ions are recelved by telephone
and the dispalcher is fhus al¡le fo exfract the relevant informationf rom fhe caller. ln addif ion lo holping the dlspatcher assign prlorlt-ies, the abilily fo discuss the incident with fhe caller assists him
to assess the seriousness of the incident. lf also helps to reduce
the number of hoax cal ls on the service.
Several authors have commented on the importance of thisinifial call and have suggested methods of improving lhe quality ofthe information transmitted ln ¡f. (Archer,1970; Pacy, l97l;Berry, 1972.,
102A
Communi cations Belween Emerqencv Servlces
Each emergency servÎce has an independenf communicatlons
network with central dispatching faci I ities. Two-way radio and
telephone equipment is used to mainlain confact belween services and
between the vehicles in each servíce. Since towing services are
privately run and competitlve, fhere is no system of central dlspatch
or rational ized operation of low trucks. The olher services - pol lce,
ambulance and fire - have control centres which are linked by telephone
during normal operations. StanCby connections are available formajor emergencies.
ln metropol itan areas, road crashes usual ly result ln several
notlf icatlon calls to the relevant emergency services. A call of any
one of the.services may be relayed to the other services, bul fhis does
not necessarily occur unless members of the Service at the scene
specifical ly request the attendance of another service. For example,
ambulance officers at fhe crash scene will ask for police to be nollfiedif lhey are required and vice versa. The conlrol ler lhen notlflesthe other service, uslng lhe direct telephone line which connects the
lwo services. A sirnî lar procedure is used lo summon flre appl iances.,
Communi cations Equ i pment
The Victorian Civi I Ambulance Service has recently remodel led
its communicafions cenfre, lnstal led modern telephone sysfems and modif-
ied operating procedures within lhe centre. The Victoria Police
communications centre is reported to be severely taxed by current
pol ico operafions and recommendations have been made that the centre
and lts oquipment shoul d be moderni zed. (St. Johnston, 1971.)
Electronic systems which provide data processing and recording
facilîf ies in addition to co-ordinaling emergency service operations
103
have been descrlbed for several overseas contres. (Storey, 1971;
Phel an , 191 1; W.H.0. , 1 968. ) Liftl e consi deration has apparentl y been
given to the instal lation of such equipment in Melbourne. Ambulance
communications are adequate for present operations but more sophisticated
communications and data systems could be expected to contribute signif*icantly to improving the efflciency of the servíce.
It may be opportune, if pol ice co¡nmunications are to be
upgraded by the i nsta I lat ion of ccmputer i zed data syslems, for the
ambulônce Service lo investlgate concurrenf use of the faci I ilies.These systems may be used in solvíng such ambulance servlce problems as
planning ambulance locations and routine fransport schedules, as wel I
as thelr obvious usefulness for accounfing and data processing purposes.
(b) Ambulance Disoatch
Aflor receiving the notification cal l, the ambulance control ler
dlspatches an ambulance to the crash. This usual ly involves sênding the
nearest available vehicle. Allernatively a standby vehicle is sent
from the nearest base station. During daylight hours, when mosf of the
ambulances are involved in lhe routine transport of sick patlents, fhe
control ler may re-route an ambulance from a non-emergency cal l. Durlng
off-peak hcurs and at night, proporlionately more ambulances are on
sland-by in base stations. Dispatching ls usual ly performed by radio,
allhough ambulances in base stations may be cal led out by lelephone.
ln dispatching the ambulance, the control ler transmits inform-
atlon relating to lhe site and nature of the incldent as well as service
data which is required for recording and accounting purposes. ln emerg-
ency calls to road crashes this information includes:
Se¡rvice Data:- DailY Job Number
Time of Day
Crash Data:- Sife of the lncídent
Type of Crash (if known)
Urgency of the Ca I I .
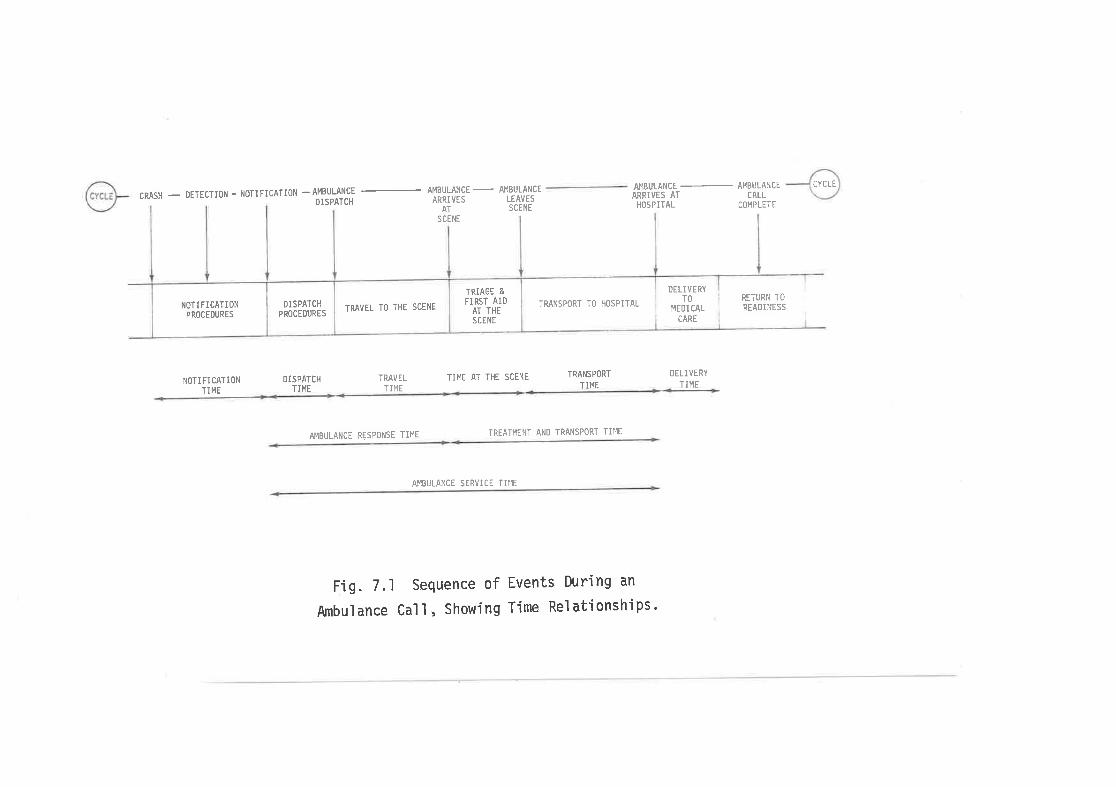
CRASH - DETECTION - NOTIFICATION -AMBULANCE
DISPATCH
AMBULANCE
- A¡|BULANCE
ARRIVES LEAVES
AT SCENE
SCENE
TII1E AT THE SCENE
AÎ'.IBULANCE SERVICT ÏIIIE
AI1BULANCE AMBULANCE
ARRIVES AT CALLHOSPITAL COHPLETE
RETURN TO
READINESS
NOTI FICATIONTIME
DISPATCHTIME
TRAVET
TII4E
TRANS PORT
TII4E
DELIVERY
TII'IE
AMBULANCE RESPONSE TII''IE TREATI4ENT AND TRANSPORT TIME
Fig. 7.1 Sequence of Events During an
Arnbul ance Cal I , Showi ng Time Rel ati onshi ps '
CYCLE
NOTIFICATIONPROCEDT'RES
DISPATCHPROCEruRES
TRAVEL fO THE SCENE
TRIAGE E
FIRSl AIDAT THESCENE
TRANSPORT TO HOSPITAL
DELIVERYTO
MEDI CAL
CARE
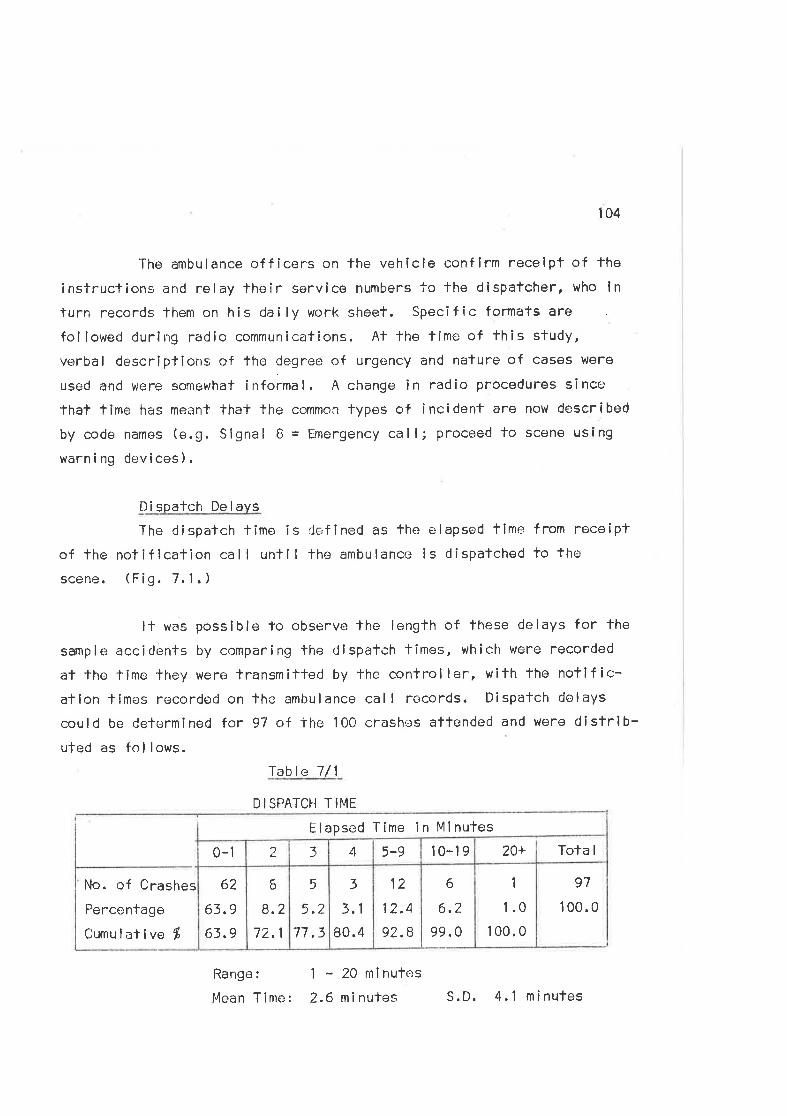
104
The ambulance officers on the vehicle conflrm recelpt of fhe
instrucïions and relay their service numbers fc the dispatcher, who in
turn records them on his dai ly work sheet. Specifîc formats are
followed durirrg radio communícations. At the time of this study,
verbal descriplions of the degree of urgency and nature of cases were
used and were sonewhat informal. A change in raclio procedures since
that time has meant that the common lypes of incident are now described
by code names (e.g. Signal B = Emergency call; proceed to scene usíng
warn i ng dev I ces ) .
Di soatch De I avs
The dispatch fime is defined as fhe elapsed time from roceiptof fhe notiflcation call untll lhe ambulance is dispatched to thc'
scene. (Fig. 7.1,)
ll was possible to observe lhe length of these delays for the
sample acciclents by comparing lhe dispatch fimes, which were recorded
al the time lhey were transmitted by the controller, with the notif ic-atlon times recorded on the ambulance cal I records. D¡spatch delays
could be determined for 97 of fhe 100 crashes aftended and were dislrlb-uted as fol lows.
Table 7/1
DISPATCH TIME
Range:
Mean Time:
1 - 20 minutes
2.6 ninutes
62
Ã?o
63.9
3
3.1
80.4
5
5.2
77,3
6
8.2
72.1
6
6.2
99.0
12
12.4
92.8
1
.l.0
100.0
97
I 00.0
)0-1 43 10-195-9 20+ Tota I
Elapsed Time in Mlnutes
No. of Crashes
Percentage
Cumu I at ive $
S.D. 4.1 minufes
t05
It may be seen lhat dispatch times are usually short, with a
median delay of one minute. Nevertheless, on 7% of occasions the delay
vras greater lhan '10 minutes. During peak hours the availabilify ofambulances for emergency calls irr a given area is a complex queuelng
and schedul ing problem. Ihe ambulance dispatcher must balanco the
desirabi I lty of sending a given ambulance against the estimated work
loads facing the service and the availability of other ambulances in
the area. Such ollrer variables as knowledge of the site of the incident,d¡ff¡culties of access, roacJ condilions and traffic densities at the
time of dispafch complicafe the fask. He is frequently faced with the
decision as to whether to r¿rail for a nearby ambulance to complete a
case or dispatch anofher ambulance from a more remote site. The
decision involves balancing a dispatch tirne of indeterminafe (but
presumably short) length against a relatively long travel lime from the
remote site. The solulion of lhese dispalching problems could be
assistcd by elocfronic syslems whích record vehicle locaïíons and
incorporate visual displays. Such systoms have been described foroverseas centres where lhey are used as mefhods of keeping the dis-p¡rtchor informed on the whereabouts and status of hís fleet and provid-
ing solutions to the probabilify decisions involved in lhe various
di spatch i ng a lternaf ives.
(c) Communications duri nq Ambulance Service
Rad io con'f act is ma inla i ned belween the cen-lra I d ispalcherand lhe ambulance cr€rw throughout each ambulance ca I I . Relevant
information may thus be passed between conlrol ler and crew, ensuring
overal I control of ambulance operalions. During travel to the scene,
details of the localion of the crash, redirection of the ambulance or
even cancellation of the call may be reasons for additional radio
c'ontacts. The crew notífy tlre controller of their arrival at lhe
scene and assess the crash, after which they may request additionalaid íf such ls requíred. þJhen the injured have been treated and placed
in the ambulance the driver reports lheir condition, the type and
106
severify of their injuries, and notifies his intention of faking fhepatients to a partlcular hospital.
Current service pol icy requires that crash víctims should be
fakcn to the nearest publ ic hospital casualty department. Occasional lypatients are taken elsewhere for medical care. For example, a doctor
al the scens may wish To manage a palîc-.nt privafely and will direclthat he be takon to a particular hospilal. Occasionally the ambulance
control lcr may suggest thal' palienl's should be taken to an a lternativehospiTal Ìf their clinical conclítion permits the diversion and he knows
that the nearest hospifal is overloaded. Normal ly, however, the choice
of hosp ita I is leff To 'the atnbu lance of f icers at the scene, and they
usually elecT lo take the patient to fhe nearest hospital. This policyis based on the legitimate essumption that fhe ambulance officer in
atfendance is the person besi'equipped to assess the patientrs conditionand need for urgent care. Although this prc+mise is sound, the pol icy
has ímportant impl ications for the operation of the emergency care
system in thaf it affects lhe distribution of paTients between hospitals,which, in lurn, affects palient waiting times and care within fhose
hospitals. This situafion wi I I be discussed laler in this chapter.
During transport to hospifal the crew may provide the con-
lroller with progress reports on the condifion of the injured and
request that lhe hospital be nolified of their impending arrival. There
is, at present, no facility for dîrect cornmunication belwoen the ambul-
ance of f îcers at the scene and cloctors in lhe receiving hospltal.Particular advantages of these I inks which have been described include:
(1) Early warning of lhe patientes condition and impending
arrival allows lhe-- casualfy staff to prepare fhe
necessany faci I itiesQ) The I i nk prov i dos back-up med ica I adv ice f or ambu I ance
officers al the scene.
ß) V ita I phys io log i ca I pa rameters may be transm itted f or
107
interpretation by the hospital staff.(4 ) Hosp i-f'a I based f I y i ng squads may be summoned to lhe
scene. (Hall & Garden, 1967; Nagel el al., 1968.)
ln the existing system in Melbourne, the ambulance service and
the separate metropol iTan hospilals are connecled by direct telephone
lines. lnformation f low, before lhe ambulancers arrival at hospital,is normal ly restricted to telephone communications beïween the ambulance
conïrol lers and members of the hospital staff. The member of the
hospifal staff who receives The incoming cal I under this arrangement
varies f rom hospital to hospi'lal. ln the Alfred Hospital calls on the
direct line are usually taken by a hospifal medical orderly who then
relays fhe informalion lo the casually sistcr. ln cases where patienls
wifh I ife-threatening injuries are being transporled, the confrol lerusually altempls to nof ify the admílting medical off icer, thus alelrtingthe medical staff directly. The present communication system has
several defocTs. Firsl, lhe introduction of the ambulance conlrol lerand a casualty medical orderly into the line of communication between
ambulance offlcers af thc scene and receivíng medical and nursing slaffis undesirablo in lhat the advanlages of direct communicalion are
mitigated or lost. Secondly, it was occasional ly observed that the
ambulance servicets notíficatiorìs w€re ignored because of a rwait and
seer altitude on the part of fhe casually s1-aff . Thirdly, although the
existing system has lhe capacily for providing advanced warning ofpalient arrivals, 'these warnirìgs are not always heeded. As one example
of this, the admiïting officer of one of the study hospilals was advised
by the ambulance conlroller thal a severely înjured crash vicf im would
arrive in casualty wiThin five minutes. The admilting off icer was not
in fhe deparTment at the time he received the telephone call. He did
nol nolify the casualty staff and they were thus not prepared to receive
the pat i enf, who requ i red i ntens i ve resusc i fat i on.
The advantages of direcl ambulance lo hospital radio I inks as
l0B
outl lned previously are consîderable, but several observaf ions made
during the study suggest lhat these advantages may nol be readilyachieved by their introduction into the exisling system. Flrsf,casualty medical sfaf f are usua I ly busy and thus may no'f be readi ly
available for radio consultation. Secondly, fhey are usually iuniormembers of the mec1ical staff who are roslered for relafively briefterms of casu¿¡lty duty and are thus unlikely lo be experienced in radio-
diagnosis and consultation. Thirdly, in busy departments, fhe responslb-
ilily for manning and moni'toring radio equipment is likely to be dele-
gatc:d fo a junior staff memberr or even, as is the case wilh the present
telephone connecf ions, a medical orderly. Finally, in a large cify wilhseveral hospitals receiving casualties, the duplication of facllitíesnecessary to provide links to all of the required hospilals may be a
relatively inefficient way of providing fhe service. An alternativemethod of achieving the objectives will be suggested in a later section.
0n reaching the hospil'al the ambulance crev'' notify theirarrival lo the dispalcher. After removing the patienl from tho vehicle
and transferring him to the casLlôlTy stretcher one member of the ambulance
crew usually accompanies the palient into -lhe casualty receiving area,
while the sec;ond ambulance off icer provides details of the paf ienl fortho'casu¡:lty documentation clerks. Ambulance off icers continue fo main-
tain patien't care unlil responsibilify for this care is fransferred tolhe casualty nursing and medical staff. Al lhe time of transferring the
patient, the ambulance officer normally provides a brief history of the
patientrs injurics and clinical condí-lion during lransport fo a member
of tho casualty staff. lf an ambulance report form has been completed
for thr.; palient, il is lodged with the slaff member at fhis tlme.
A further breakdown in communicalions can occur af fhis point.Arnbulance off icers are usually the only para-medical personnel to have
observed lhe patienl durlng the early post-crash phase. They thus have
information relating lo thc+ patientts injuries and clinical condltion
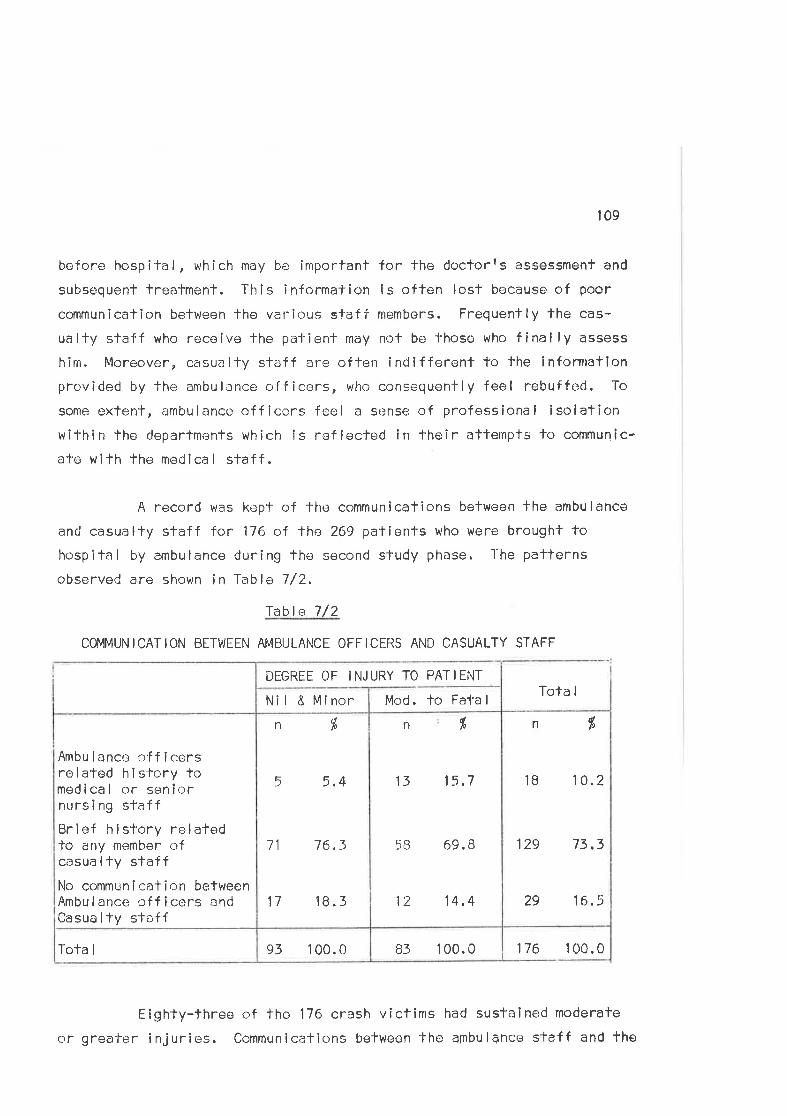
109
bcfore hospilal, which may be important for the doctorrs assessmenf and
subsequent treatmenl. This ìnformalion is often lost because of poor
communication belween the various staff members. Frequently the cas-
ualty slaff who receive the patient may not be fhose who finally assess
him. lr'loreover, casua lty staf f are of ten indif ferent to the infornlatlonprovided by the ambul¡nce off icers, wlio consequently feel rebuffcd. To
some extent, arnbulance off icers feel ô sense of professional isolationwilhin lho departments which is reflecled in fheir attempts lo communic-
ate with the medlcal sfaff.
A record was kepf of the communications befween lhe ambulance
and casualty sfaff for 176 of the 269 patienfs who were brought tohospital by ambulance during the second study phase. l-he patferns
observed are shown in Tablo 7/2,
Table 7/2
COMMUNICATION BETWEEN AI'4BULANCE OFFICERS AND CASUALTY STAFF
176 100.083 100.093 100.0Tota I
n dþ
18 10.2
129 73,3
29 16.9
n %
13 15.7
5B 69.8
12 14.4
n tr
5 5.4
11 76.3
17 18. 3
Ambu lance o'f f icersrelated history tomed i ca I or sen iornursing sfaffBrief hisl'ory relatedlo any member ofcasua I ty sfaffNo communlcalion betweenAmbulance officers andCasualty staff
Mod. lo FatalNil & Minor
DEGREE OF INJURY TO PATIENTTota I
Eighty-three of lhe '176 crash victims had sustalned moderate
or greater injuries. Communicalions between fhe alnbulance staff and the
110
medical and nursing staff who managed I'he patient occurred for onlV 16Í,
of these patients. The situatíon wherein ambu lance of f icers describe a
brief hislory fo a member of the casualty slaff on arriving in thedeparfment îs oftcn unsalisfacl'cry in that, often, the member of staffis not presenf when the patient is assessed by the medical officer. An
awareness by i:mbulanco aufhorities of the d¡ff iculfies associaled vrith
this communications problem led to the development of the Ambulanco
Report Form as a tangible record ol a patientrs ambulance tneatmenf.
The use of ihis dc)cumen't will l¡e discussecl in a later secfion. Paflernsof crash injury are, to scrme extcrnt." pre<Jiclable, and much useful dia-gnostic materlal c¿rn be gained by knowing whether lhe pafienf was, forexample, a pedes-trian or a vchiclL- occupant. ln many cases, lheireating medîcal officers did not have such basic informaticn nt lher
fime c¡f examination and, on occasions, were not even aware that thei nj u rod person had been i nvr-¡ | ved i n ¡: road crash .
After the patienl'has been fransferred lo casualty care, theambulance officers relurn to their vehicle, prepare it for a subsequent
trip and notify the dispatcher of th<¡ir refurn to readiness by radio,or by direct telephone call from fhe hospítal. This final radio contacfcould be used as a means of providirrg the ambulance controller with an
estimale of the loads on lhe crersualty dc-:partmenl so that distribution ofemergency calls between casualty deparfmenfs could be facililated. ln
pracfice this feedback raroly occurs.
(d) Communications between Hosoit¿:ls and belween the Ambulance Service
and Hosp i ta I s
Several areas of communication between hospitals and between
the ambulance service and hospitals warrant commenl in view of observ-
alions made during lhe sfudy. The dis-i'ribution of palients between the
separate hospital emergency departments in Melbourne is a problem whîch
affects severôl areas of pa-l'ien-l care. As menfioned previously, thedecisic¡n as lo which a hospíta I a patient should be taken after a crash
111
is normally lefl to the ambulance off icer at fhe scene. ln 'the absence
of any cenfral confrol of emergency deparl-ments or accident servicebeds, this policy dlrectly af fects fhe number of patients waif ing forcare in the separate departmenÌs. During peak periods, one department
may be overloadod whilst a second department as liltle as one or two
miles away is relatively f rcr-i of w¡¡iting pa-l'ienfs. E¡ght major publichospitals in the Melbourne metropol îtan area receive road crash victimsand 1-here is a need for an effectîve system for recording casualtydepartmenl loads and emergency bed occupanc)', lo ensure fhe distributionof pal i ents between these hosp i ta I s.
ln an atlempt to r¡vercome this problem in patient distrit¡ufiona fbed bureauf co-ordinated by fhe ambulance service has been in oper-ation in Melbourne for several years. Several fimes each day theambulance conlrol ler contacts lhe admifting offlcen at every Melbourne
public hospilal to de'termine the bed stafe of his hospital. This inform-ation is galhered in an attempt lo ensure the distribufion of ambulance
cases befween lhe major hospi lals. Each hospital is autonomous wifhrespect lo ils admitting policies and it has become the practice c.¡f
admifling offîcers to under-report the number of empty beds in theirrespective hospi-fals. This practice has lod to the breakdown of the
bure¿:u with consequenl effects on the distribufion of palients between
hospitals. Furlher inefficiencies result from the fai lure of this system,
since patienls who are admitted to the casualfy deparlments of hospitalswhich genuinely have no beds must be placed ín other hospitals. Thisplacement requires consultation between the separa"le hospital admittingoff icers. As a rcsull, valuable medical off icer lime is wasted and
furlher ambulance services are involverl în Ìransfcrring patients between
ho.sp ita I s.
Much of the responsibi I ity for this breakdown in communicalions
between fhe ambulence conÌrol centre and lhe hospilal casuälty depart-ment can be allributed lo poor inferpr of essiona I cornmunication. The
112
relatively junior medical staff who act as hospital admilting off icersin Melbourne hospilals have I itlle appreciation of the importance ofthe bed bureau for patienl care. Equal ly, ambulance control lers have
Iittle comprehensíon of the dÌf f iculties facing admitting of f icers inmanaglng the few unoccupied be<Js wilhin fheir hospitals. These cornmunic-
ations diff iculties are likely -lo persist for as long as casualtydeparlments are manned by rclal'ively junior medical staff and ambulance
off icers are trained outside the hospital environment. With existingorganizational arrangemenls there are few opportunities for hospital and
ambulance staff to develop mutual uirderstanding and respect for each
olherts lasks within lhe emergency care system.
These breakdowns i n commun i cat ions have sevena I imp I i cat ions
for lhe ernergency care of road crash v ict ims. An uneven d i slr i but íon
of patients belween casualty departments occurs commonly, particularlyduring such peak periods as'the laTe night hours on Friday and Safurday
nights. As a resull, crash,¡ictims experience long delays in receívingcare and fhe pressures of Ìhe heavy work loads on the attending medical
staff make mistakes ln diagrrosis and trealment more likely. These
problems could be alleviated if the work loads were distribulecJ more
evenly between the avai lable departments.
The introducfion of a sysfem whereby ambulance officers, inconjunction with the hospita I ca!ìualty staf f , provided some feedback tothe ambulance confroller on casualty patient loads would help to resolvethis problem.
A more efficìent means cf ensuring distribution may be a
system of accident or emerqcncy units within hospilals with centralcontrol over admissions to their cmergency beds. Such systems have
boen descr i bed for cerfa i n European countr ies. (1,4u I , 1 956; Storey
& Rofh, 1971,) There has been considerable debate between members ofthe medical profession about the desirabi I ity of accident or trauma
113
un¡ls to undertakæ the man¿rgemcnt of lrauma patíents. Whilsl thisproblem is related to the overall problem of management of crash victims,it may be regarded as a separate issue from that relating fo lhe avail-ability, dislribuf ion, and control of admissions to, emergency beds in
hospitals. Central control of such beds could help to reduce lime
delays in casualfy departmenTs and increase the overal I efficiency of
emergency care sysÌem operalions.
A first step in the developmenf of such a system would be the
appointment of a medical officer to the ambulance control centre. This
officer could assume respons¡bilify for the bed bureau and would be well
placed to discuss admission pric¡rlties with the separate hospital
admitling officers. As a frained medical officer he should be able tc>
overcome many of the difficulties in communicalion which beset the
existing sys-t'em. ln addition such a person would be well placed loprovide medical advice for ambulance officers at lhe crash scene and
during transport to hospîtal. ln this capacity he could advise the
conlroller and fhe ambulance crew on the risks lnvolved in by-passing
the nearest hospital department in f¿:vour of a second less-crowded
department. ln the event of telemetry of physiological data becoming
a feasible adjuncf lo ambulance care, such a medical officer would be
well placed to monitor lhe equlpment and advise the crew accordingly.
Considerable savings in manpower, equipment and time should result from
such centra I i zed faci I íti es.
(e ) Commun i cal ions w ilh i n l-losp ita I
Pat i enf-Sf,af f Commun i cat ions
Many pafients who have been ínvolved in road crashes regard
themselves as emergency casos warnanting urgent attention and had
difficulty reconci I ing the long waiting flmes experienced in casualty
deparTments wilh the apparent urgency of their condition. TwenÌy per
cent of patients who were asked lheir opinion of casually waitlng times
before discharge from the department statod that wailing times were too
r14
long. ln response fo a postal ques'l'ionnaire asklng opinions about
several aspects of casualty care,35/ o1 respondents regarded the wáit-ing times in casualty as longer than they had expected.
Patients can be holped lo understand fheir condition, thetroatment whích is being performed and lhe reasons for delays in treal-ment by adequale communication urith lhose members of lhe casualty staffwho are carinE for them. Because casualty departmenls are busy lhere lsa Tendency for staff to regard païients as pathological entitíes to be
processed. Allhough the emphasis in casualty is on prompl díagnosis,-treatment and referral, lhe explanaf ion of a paf ienlf s situation need
not be time consuming and does rnuch to allevia'te anxiely. Twenty-fourper cent of the observed pal'ients were unaware of the reason for theirbeing kept in casualty and displayed anxiety about their condition and
fulure management as a resul'l'. Only 3lí of palíents were kepf informed
of their condition, the reasons for freatmenf delays, and fhe trealmenfbe i ng performed, throuqhoul lhei r stay in the casually deparfment.
Those patienls who do not reqr:ire admission for f urther lreat-ment of i njuries are discharged for oul-palienf fol low-up. Speci ficwritten instructions are issued t<: patients who have undergone such
special procedures as lhe application of a plaster casl or who have been
observed for heacl injuries. ln addition a medical officer, casualtysisfer or senior member of the nursing sfaff explains fhe necessary
steps the palient should take lc, ensure fol low-up cane. Nevertheless,
many patients were confused about lhe arrangements for fheir futuremanagement at the time of discharge. Thirteen (28%) of the 47 patientswho were questioned about errangements for fol low-up care w<;re uncertainas to what arrangernenfs had been made for them and what was required ofthem in fr.rlf illing their future care requirements. This lack of under-
standing no doubt contributes to the fall off in attendance at out-patient accident cl inics.
115
Communicalions between Casuallv Staff and a Patientrs RelativesAn administralive ins-t'rucÌion requires casualty residenf
medical officers in the Alfred Hospital fo give \,vailing rç:lativos a briefsummary of the palientrs condition either directly, or through a member
of the senior nursing staff, affcr his examination is compleled. The
insl'rucf icn requíres that particular attention should be paid to estim-ating the tirnc the patient will be in the department. Moreover, a
summary of the palienlrs contlilion and management instrucf ions should
be given to fhe relalives aT lhe fime of the patientrs discharge. ln
pracf i ce cornmun icat ion betwtl r¡n ll-¡c casua lty staf f and re I at i ves i s
usually lefl to senior nursirrg slz:f f . The lack of an established
rcutine for this procedure meanÌ fhat relatives were often unaware ofthe patientts clinical progross. Hospital siaff conlacted the waitingrelatives of 106 ß6%) of fhe 160 patients for vihom it was possible toobserve this evenl in casual'ty care at least once. Nevertheless,
relatives were rarely kept informed of a patienlfs progress on an
ongoing basîs. Several pafients made particular comment fo this effectin thei r questionna i re respor'rses.
Reassurance of bo1-h pationts and relatives is an imporlant
aspect of tho medical care process which reflects on the quality ofthe care provlded and which markedly influences fhe attitude of the
patients to bolh lhe care and the insfilution providing lhe care. The
sc¡cial dimensions of medical care warrant attentíon from treafmenf
personnel, even though lhey may appear to be of peripheral imporfance
in busy casualty departments.
THE TRANSPORT SUBSYSTEJVI
(a) Response cf the Emerqency Services
Road transport is used by each of lhe services in responding
to emergency cal ls in Melbourne. Ambulance and pol ice vehicles aro
equipped with warníng devices for use during travel to and from the
116
scene. Tow trucks have flashing amber lighfs for use at fhe scene but
are not classed as emergency vehlcles within the meaning of the Road
Traffic Act. Legal ly they do not have emergency priority whi le trav-elling to lhe scene. All the services usually travel to the scene at
speed. The usual pattern of arrival of emergency services for the
crashes sfudied was towing service, ambulance and then pol íce.
(1 ) Towinq Services
The f i rst emergency serv i ces at the scene of a crash i n
Melbourne are uSuAl ly the toiv trucks. Towing companies operate in
limited but overlapping areas and may offer financial reward to a callerwho notifies them of a crash in which they oblain Ìhe tow. The towing
business in Melbourne is fiercely compelitive since the financialrewards for resuscltafing cars are considerable. Several differentsenvices are usually presenl at the scene of each crash. The firsltowing service on the scene has a good chance of obtaining lhe tow and
drivers thus use all measures in lheir atlempls to achieve this end.
Al I of fhese factors assist the early notification and arrival of the
towing services. l4oreover, the possibilify of f lnancial reward may
induce members of the public to call the towing company before the
ambulance or police when first notífying the crash.
Q) Pol ice
ln police operations in Vic1-oria' mossages concerning emerg-
encies are given precedence over all ofher radio messages and dispatch
of police to lhe scene is prompt. (Braybrook, 1970.) This applies inparticular to road crashes where the profection of life and property at
the scene requires pol ice control in co-operation with other emergency
services. (Pol ice attend the scene of lhe majority of injury-producing
road crashes ín Melbourne.) Police had arrived at the scene of 59 of
the 1OO crashes studied by the time the ambulance had left the scene.
117
(3) The Ambu I ance Servi ce
ln responding to en emergency cal I ambulancês use lheírwarning devices and travel at speeds which will ensure their rapidarrival at the scene. Service rules and training programs emphasize
that safel'y is more important than speed in ambulance work. (Hospitals
and Charif ies Commission, 1970,) Road traff ic regulations allowpriority for emerqency vehicles using lheir warning devices, but do notpermît dangerous driving in the course of exercising fhat priority.
The research team was able lo observe the driving pracflcesof ombulance officers during several of the sludy cases and for many
non-sfudy emergencies. 0n most occasions ambulances are driven wilhinthe limits of speed and safety specif íed by Ìhe services. Violationsof this code are difficult to determine, although some measure of itseffectiveness could be gainod from the rate of ambulance crashes duringcmergency cal ls, were these fo be avai lable. There are, however, no
figures available on the numbers and lypos of crashes in which V.C.A.S.
ambulances are involved. A sfudy of crashes for another Vicforianservíce revealed that lhe risk is 4å times greater for ambulances duringemergency calls lhan during transport calls, with a ra'i-e of one crash
for every 629 energency cal ls. (Watson, 1970.) Since the majority ofthese crashos occurred al intersections, speed is probably a less
critical facfor ln ambulance crashes than lhe failure of other motorisfsto delect and heed viarning devices.
Ambulance off icers unclorgo training on recruitment which
acquaints them with the praclical requirements for ambulance drlving toensure patient comfort. There is no specific înstruction in the drivingand handl ing of vehicles at speed. Such instruction should be unnecess-
ary, but for pract i ca I purposes may b,e des i rab I e.
llB
(b) Proteclion of the Crash Scene
Prolection from secondary collislons is an important area ofpost-crash control which warranfs comment in view of observations made
at the scene of sfudy crashes. lrlo dala are available f rom police
records on the incidence of second collisions in Victoria but Braybrook
(197ü, in commenting on this aspoct cf emergency care operations,
stated that'bflen furlher crashos occur resuiting in ser¡ous or fafalinjurics lo essentlal service workers or bysïundersl'
ln one of the study crashes a car collided with one of two
cars involved in an inlersec-fion smash. A tow lruck operalor, who was
examining lhe front chassis of the stationary vehicle, was dragged along
the road beneath tho car for sorne ten yards. He suffered abrasions fohis arms, legs and trunk, without further serious injury. No acfive
measures had been laken by cmergency service personnel to prolect the
scène of lhis crash.
Protectíon of the crash scene may be dlvided lnto two sections:(1 ) Site Prolectícn(2) Personal Protection.
(l ) Sile ProtectionEach of lhe emergency services should be involved in this
lmportanl area of post-crash safety. ln most cases second col I isions
are due fo lhe lnadequate use of warning devices. At mosf crashes,
byslanders or police redirect traffic and thus maintaÎn some degree ofprotecïion. The only other protective measure routinely faken by the
services is lhal emergency vehicles are parked close to the crashed
vehicles. These vehicles are equipped with flashing I ights (red fcrambulances, blue for police and amber for all other emergency sorvfcos)
which offer some warning for oncoming motorisls. Nevertheless, they
are invariably parked close to llre scene, and this limits their usef ul-ness as warning devices.
119
Emergency services in lulelbourne do not use such proven
de,¡ices, as Twitches hatstor ref lecting triangles as a warning for on-
coming motorists. Experience ín the Unifed Kingdom has shown lhat these
devices need to be placecl up to 900 yarcis from the scene (presumably for
motorway crashes). (Anderson, 1969,) Road and other fransport workers
in Victoria use these protective devices and they should be used
routinely by the emergency servîces.
(2) Personal Protection
Ambulance and pol ice officers ln Melbourne wear dark uniforms
during norma I duty and no addltional c¡r alternative clolhing is worn at
lhe scene of crashes. These colours are difficult to distinguish,parlicularly r:f night, and the resultlng lack of visibility adds to the
risk of injury from socondary col I isions. Pol îcemen on point duty at
busy intersections are similarly at risk, although white armlels are
occasionally t,ilorn by lhese off icers. Tow fruck drivers do not use
sfandard for¡ns of dress allhough many wear overalls, some of which are
white or I ighÌ coloured.
Fluorescent orange has been shown fo be an effective colour
for use ln safety clolhíng (lvlichon, 1969) and jackets of this material
are used by Counlry Roads Board workers in Victoria. The use of fhese
dustco¿its or jackets would contribufe to the safety of emergency service
personnel at the Scene. Moreover, the clothing could be expected to
contribule lo the effectiveness of the task of Those involved in trafflccontrol by ensuring that lhey are visible to the oncoming motorist.
The rlsks incurrr¡d by fai lure to use protecting devices are
considerable and demonstrably useful saf'ety measures should be inlro-ducecl and used roulinely by emergency servíce personnel.
120
(c) Ambu I ance Transporf
Patienls are carriecl in the rear cabin of V.C.A.S. ambulances
on stretchers fixed on either side of a central corridor. An ambulance
officer ri<ies in fhe cabir¡ rr,ilh lhe patient and maintains patient care
during lransporl. Patienls wifh minor injuries may be seated on fhese
strelchers or in the Passengerrs seal next to fhe driver. V.C.A.S.
anlbulances are equipoed to load an addìJ'ional two stretcher patienfs in
fhe rear cabin in emengencies. This confíguration Ìs rarely used and
was no-f required for any of the study crashes, ln practice lhe con-
trollers usually dispal-ch ¿: strcond ambularrce when rnore than fwc stretcher
patients need transport from any ono inciden'|.
One hunclrecl and t'lenfy-one injured victims f rom the 100 study
crashes were transporled to hospÎtal by ambulance. EÌghty-six of fhese
persons were stretcher palients carried lying in the rear cabin. The
remainîng fhirty-five patienls were sealed in either lhe rear cabin or
in the front passenger seat of the vehicle. Ambulances frequently
carrîc;d several victims from the same crash. Two victims were trans-
ported fron 21 of the stu<iy crashes and lhree or morÈ patients from 9
of thE: crashes. The ambulanc€) was not roquired for transporT in 16
cases. Tw i ce pat i ents were la kc-.n lo hosp îla I i n pr i ,¿ate ca rs bef ore
the ambulance arriveci. Orr bolh occasions lhe hospital was nearby, the
patíentst injuries were minor ancJ they were laken to hospifal by
bysta n de rs .
Seat Belts în Ambulances
At lhc time of thc s'lucly arnbulances were not f ítted wilh
devices to restrain patients in 'the event of a collision. All ambulance
stretchr:rs ar(? now f illed wilh yir,-bbing harness to restrain stretcher
paticrnts. Seat bells are fittod in lhe fronf seats of vehicles bul
fhere arü no restraining mechanisms for those; palienls who sit in the
rear cabin during transport. A signifîcant proportion of the 35 patienls
who were carried as silling pa-fîenfs, were seated in the rear cabin and
121
were thus unprolected in the event of a crash.
Road TransoorT and its Effocts on the Patient
As was menlíoned in the revisw of the I iterafure, several
authors have commented on the possible effects of road transport on fhe
injured palient and have related experiences of lhe discomfort felt by
patients during ambulance 'lrips. Since it was nof possiblo for the
observer lo ride in the ambulance wífh the patients, observations ofpatientsr condition wcre linriled to lhose which were obtained lmmediafely
before the ambulance leff the scene and on arrival af the hospital.These íncluded measuroments of pulso rate and blood pressure and observ-
ations of pupillary reacf ions, colour, state of consciousness, as
îndicalîons of the patienlts cl inical condition. lf was not posslble todemonstrate any changes i n pa'fi ent cond it ion wh i ch cou I d be attr I buted
to the ambulance ride. ln particular, there wero no marked changes in
pulsc or blood pressure associaled wìlh ambulance transport for those
patients with moderafe or greatcr injuries. Nor was it possible todemonstrate marked changes in the clinical condi-lion of these patienls
affer ambulance transport.
After arriving in the casualty department, study patients
were asked
whether the ambulancer ride had made them feel sick;whether The ambulance ride had increascd the pain from
their injurit=;s.
(i)(¡i)
lnvariably the patients responded to these dlrect questions lnlhe negalive. Several pationts did comment, however, on the pain assoc-
ialed with lîf+îng nìanoeuvres during fhe various phases of their caro.
(d) Liftinq and Movinq lhe lniuredtion of C h Vic-t'ims f V
Forty-four of lhe 310 persons involved in the study crashes
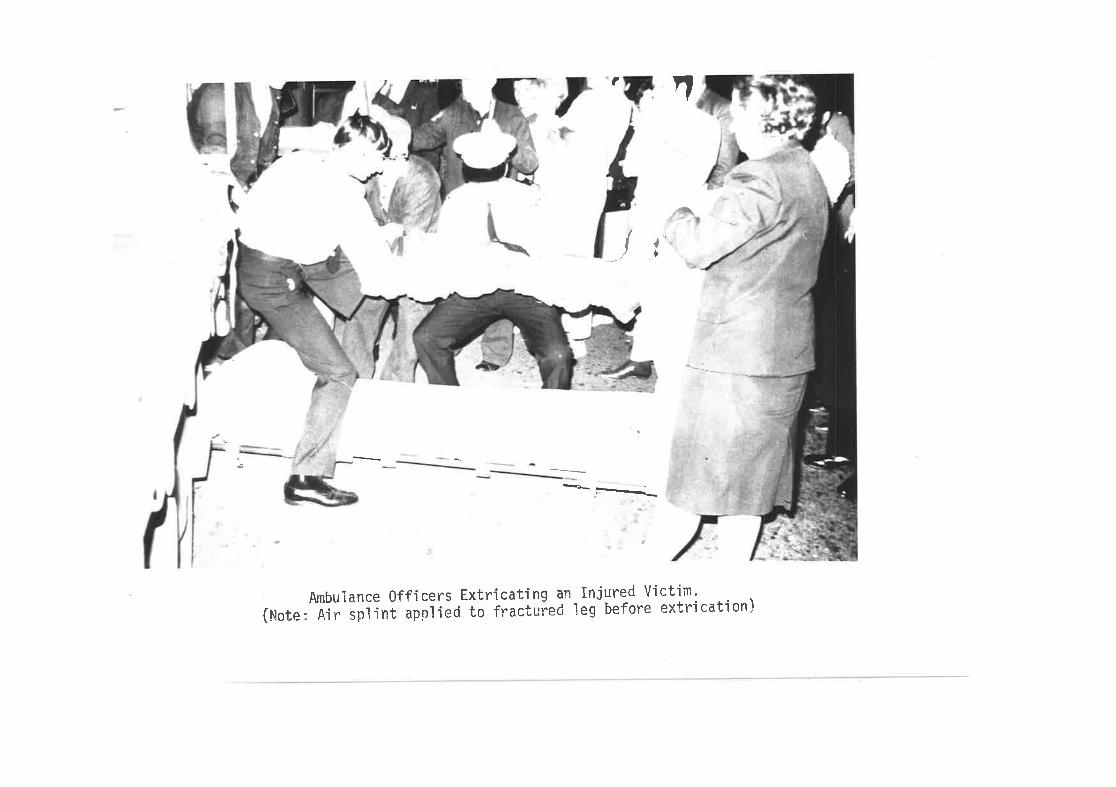
(uorlecUlxa oroJaq 6ai pe;nllerJ ol pol¡dde 1u'rlds r'!'V:0+0hl)'rutlo!A pã.rnçu1 up 6u!1PrlJxxl sroslJJg aouPInquy
-Ê---
a
tI
laÐ )
122
were sti I I inside their vehicles when the ambulance officers arrivedat lhe scL'ane. Twelve of fheso patients were either unconscious or had
suffered limb fracfures ancJ had to be lifted from the vehicle. One
patienf was trappelC in an overturned car and a power saw was used toassisÌ wíth extricating him. Overal l, the methods uscd to extricalevictims were considerod satisfactory. Eight of these viclims had
sustained limb fracturcs, of whom'lhree were rèmoved from the vehiclebefore theír f ractures were splinted, when splints could and should
havo been applie:d before moving them.
Liftin<l and Movinq Patients durinq Emerqencv Care
Ambulanc,r of f icers ¿:re trained Ìn methods of lifting and
extrica'ling injured patîents and are thus more ski I led lhan most
bystanders (including most mcdical practitionors) in lhese procedures.
They were observed to perforrr these manoeuvres satisfactori ly for the
study patîents. Lifting movements arc often painful for the injuredpatients and may cause fur-lher in.jury in certain situalions. lt thusfollows that pafienfs should be lifted and moved as liltle as possible.ldeally, once a patient is placcd on a stretcher it should not be
necessary to move him f rom J'l-rat s-lrelcher until he is 1'ransferred to a
hospital bed.
ln practicel, paticnls are moved from the strelcher several
f imes during emergency care. 0n ¿:rriving a1' the casualty deparfment
patients are usual ly transferred from the ambulance stretcher to a
hospital barouche. This transfer is made because changeover ambul-ance strelchcrs are n,;-f ava i lab le in the casua lty departmenf s,
Frequently lhe patient îs liftod manually from lhe stretcher on to thebarouche allhough canv¿)s s-lretchcrs ârc occasionally used for -lhis pro-ceCure. The procedure is of-len painful for lhe patient and represenlsan avoidable source of discomfort"
Nlos-l patients are lransferred f rom fhc barouche af le¿:st once
123
more dur¡ng emergency care. Those patients -r.rho require X-ray are
lifted from tho barouche lo lhe X-ray table and back. Most barouches
are equipped wilh a canvas which may be convertecl into a stretcher by
mêans of two poles with melal spreaders to tension fhe cÐnvas. Occasion-
al ly staf f members were obsc:rved tc I ift patients without using the
metal spreaders. Thls resultcrd ín unnecessary pain and discomfort forthe patient.
Changeover stretchers, which al low the patient to remain on
the one stretcher throughout emergency care, are used in other AustrallanStates and eliminalo lhe need for multlple patient lifts. A recent
invenfion which promises to solve somc of lhe problems associated wilh
change;over stretchers is the Jordan I ¡ f ting f rame. ([3erry ' 1972., The
davice is light, compact, clreap, simple to operafe and may be used atthe crash scene or in hospifals. lt overcomes many of the dísadvanfages
of changeover slretchors slnce it is easily stored, is radio-lucent and
fits on exisfing stretchers and barouches. lts particular advantage
for emergency care lies ín fho fact that the patienf, once placed on ¡lat lhe crash scene, remains on -l-he frame until lifted into the hospítal
bed.
(e) Time Delavs durinq Ambulance Service
The sequenc(r and time¡ relationships of evenfs occurring
durlng the various phases of an ambulance call are shown in Fig. 7,1.
ln lhe first phase of the study, fime delays during these phases were
measured for the majority of the sludy cases. ln some cases it was
nelth--r possible nor appropriate to record elapsed times during allphases of the ambulance cal l. For example, ambulance transport was not
requlred for patients from 16 of the 100 study crashes and thus lreatment
and transirort times were noI recorded for those paf ients. 0n anolher
c)ccäsion a patient was taken to a privafe doctorrs surgery and sub-
sequently to a private hospital for care. Since this represented an
a-lypical situation, da-l-a from this crash were also precluded from
the analysis"
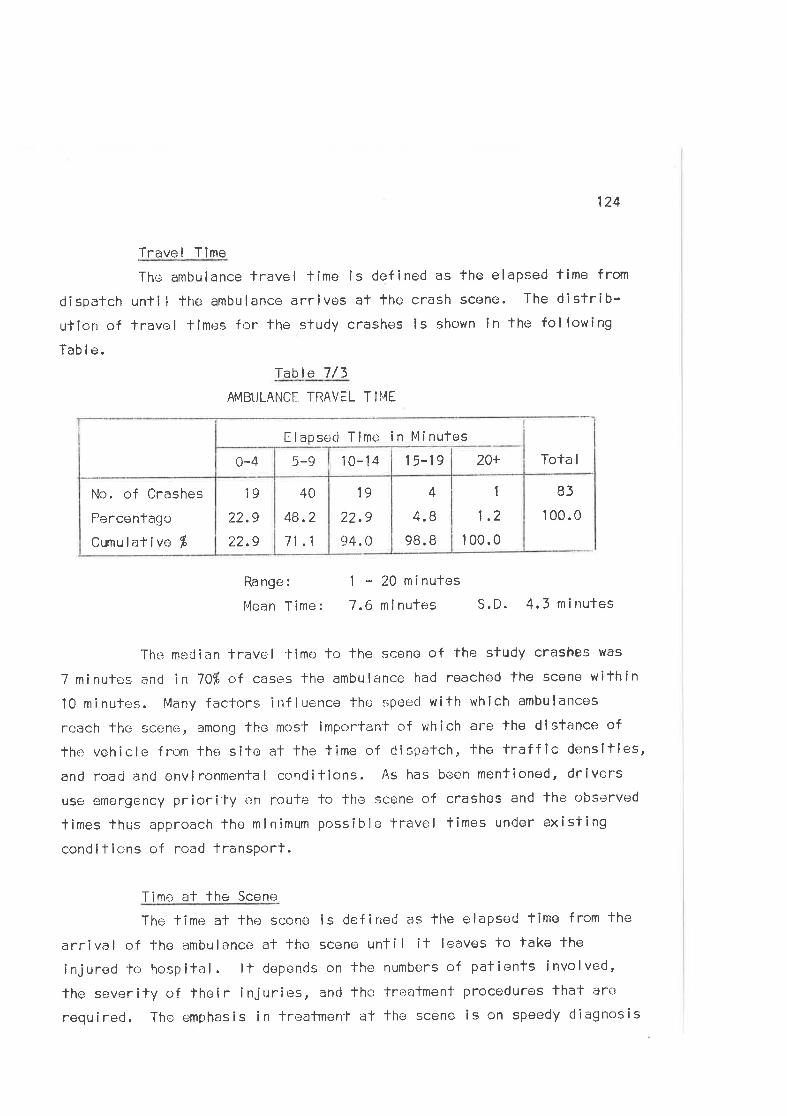
124
Trave I T lme
The ambulance lravel lime is defined as the elapsed time from
dispatch unti I the ambulance arrive¡s al fhe crash scene. The distrib-ution of travel limes for the study crashes is shown in the following
Tab I e.
Table 7/3
AMBI.JLANCE TRAVEL T II'"{E
1
1.2
I 00.0
4
4.8
98. B
19
22.9
94. 0
40
48.2
71 .1
19
22.9
22.9
No. of Crashes
Percentaç¡c
Cumulative f
Tota I20+1 5-1910-145-90-4
Elapsecl Time in Minufes
83
1 00.0
Ra nge :
Mean Time:
1 - 20 minutes
7 .6 ninutes S. D. 4.3 ni nutes
The meCian fravel time to the scene of the sludy crashes was
7 minulcs and in 7O% of cases the ambulance had reached lhe scone within
10 minutes. lvlany factors inf luence thc speecl with which ambulances
reach the scene, among the most important of whích are the distance of
the vehicle frt:lm the site at the time of dispatch, the traffic densltles,
and roacj and envlronmental conditions. As has been mentioned, drivers
use emergency priority cn route lo the scene of crashes and lhe observed
limes thus approach the minimum possible travel times under existing
condifions of road transPort.
Time at the Scene
The time at lhe scene ls defined as lhe elapseC time from the
arrival of the ambulance at the scene until it leaves to take fhe
injured to hospital. lt depen<1s on the numbers of patienls involved,
lhc severily of lheir injuries, anri the trealmeni-procedures that are
required. The emphasis in freafmenl at the scene is on speedy cliagnosis
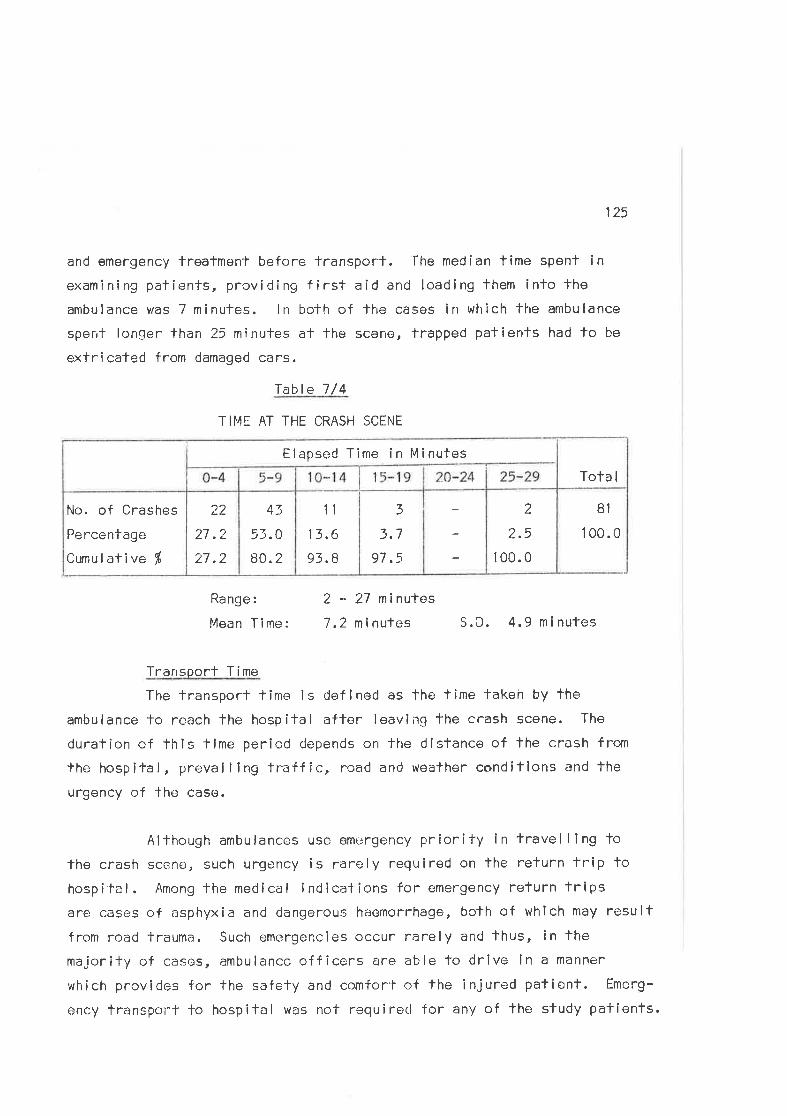
125
and emergency treatment before lransporf. 'Ihe median time spent inexamining patients, provídirrg f irst aid and loading them into the
ambulance was 7 minutes. ln both of lhe cases in which the ambulance
spent longer than 25 minutes al fhe scene, trapped patients had to be
extricaled from damaged cars.
fable 7/4
TIME AT THE CRASH SCENE
81
1 00.0
2
?_.5
1 00.0
z)3.7
97.5
1t
13,6
93,8
43
53.O
80.2
22
27.2
27,2
No. of Crashes
Percentage
Cumul ative %
Tota I
Elapsed Time in Minutes
Range:
Mean Time:
2 - 27 minutes
7 ,2 n inutes S. D. 4.9 ni nutes
Transport Time
The transport time is cJefined as the lime takeír by the
ambulance to reach the hospital after leaving fhe crash scene. The
duration of this lime period depends on the distance of lhe crash from
the hospilal, prevai I ing traffic, road and wealhen condíllons and the
urgency of the case.
Al though ambu lances use emergency Pr ior i fy i n trave I I I ng to
the crash scene, such urgency is rarely required on lhe refurn trip lohospital. Among fhe medical indicalions for emergency return tripsare cases of asphyxia and dangerous haemorrhage, bolh of which may resultfrom road trauma. Such emergencies occur rarely and thus, in the
majority of cases, ambulance officers are able to drive ln a manner
which provides for the safety and comforf of the injured patient. Emerg-
ency transport to hospital was nof required for any of the study patients.
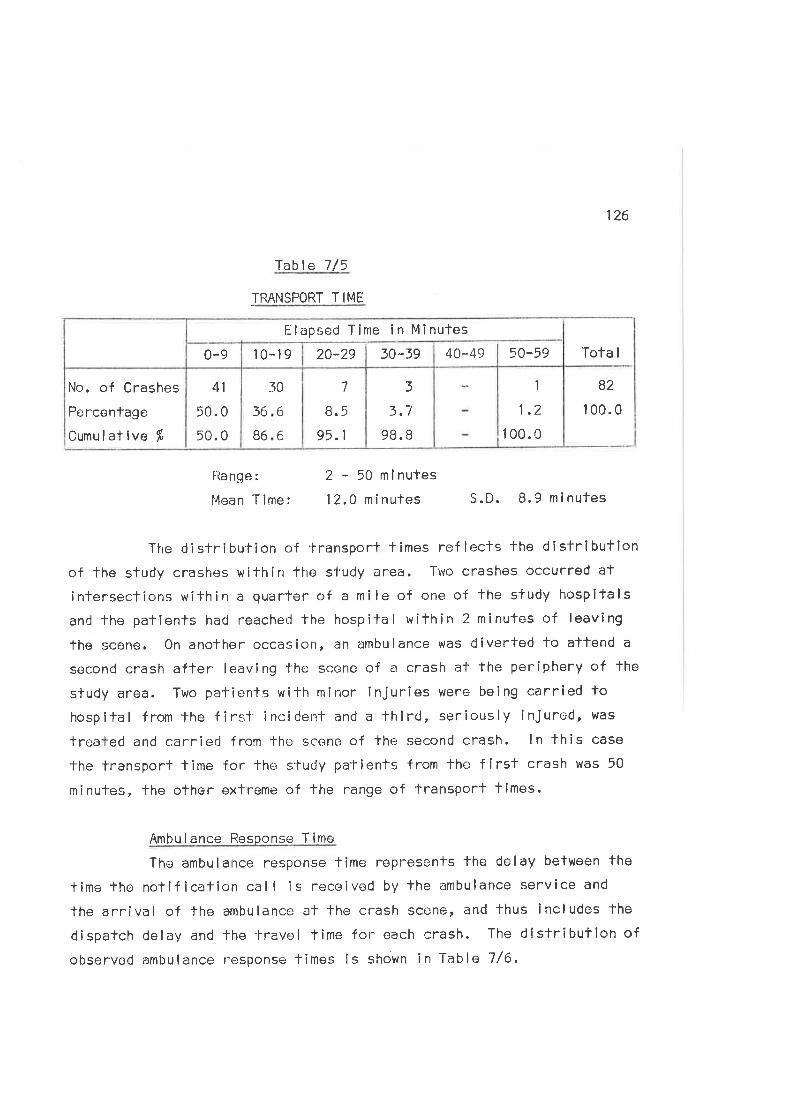
126
Iable 7/5
TRANSPORT T IME
Tota I
82
I 00.0
1
1,2
1 00.0
3
3.7
98. I
7
8.5
95.1
30
36
B6
6
6
41
50. 0
50.0
No. of Crashes
Percentage
Cumulative fl
40-49 50-5930*3920-29l0-190-9
Elapsed Tíme in Minufes
llange:
Mean 'f ime:
2 - 50 mlnutes
12.0 n inutes S.D. 8.9 minutes
The distribution of transport times reflecls the dfstributionof the study crashes within the study area. Two crashes occurred at
intersections within a quarter of a mile of otre of lhe sfudy hospifals
and lhe patients had reachecl the hospital within 2 minutes of leaving
the scene. On another occasion, an ambulance was diverted to atlend a
qecond crash after leaving'l-he scene of a crash at the poriphery of the
study area. Two pafients with minor Injuries were being carried tohospital from the firsf inciderrT and a third, seriously ¡niured, was
trealed and carried from the scene of the second crash. ln this case
the transport lime for lhe study patients from the first crash was 50
minutes, The other extreme of fhe range of transport times.
Ambulance Resoonse Time
The ambulance response tíme represents the delay between the
time the notif ication call is received by the ambulance service anC
the arrival of fhe ambulance at the crash scene, and thus includes the
dispatch delay and the lravol time for- each crash. The distribufion ofobservod ambulance r-esponse times Îs shown in Table 7/6.
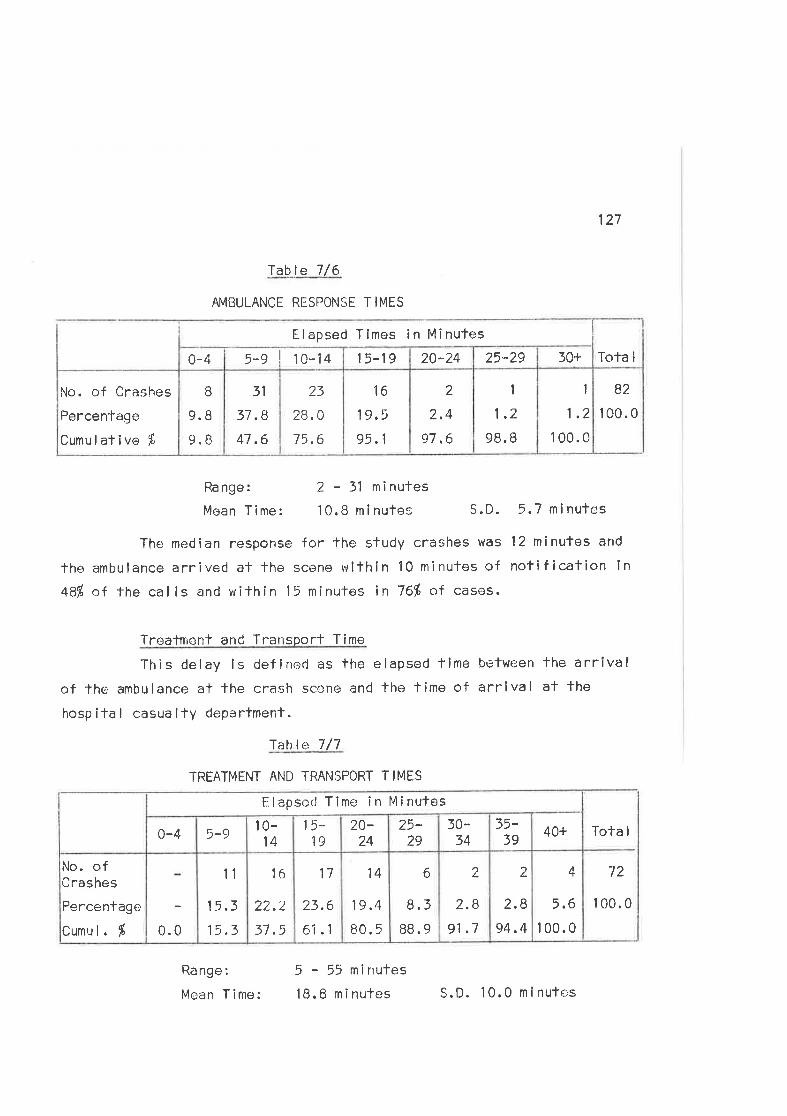
127
-lable 7/6
AMBULANCE RESPONSE TIMES
Rangez 2-31 minutes
MeanTime: l0.Bminules S.D. 5.Tminufes
The median response for the study crashes was 12 mínutes and
lhe ambulance arrived at lhe scene wilhin 10 minufes of notif ication inqA% of the calls and wilhin 15 minutes in 76% of casos.
Treatment and Transporf Time
This delay is definecl as the elapsed time befween fhe arrivalof the ambulance al the crash sccne and the time of arrlval af the
hosp ita I casua l-ly depa rtment.
f able 7 /7
TRËATMENT AND TRANSPORT TIMES
B2
100.0
1
1.2
1 00.0
1
1.2
98. B
2
2.4
97.6
16
19.5
95.1
23
28.0
75,6
31
37.8
47.6
B
9.8
9.8
No. of Crashes
Percenfage
Cumul ative f
Tota I30+25"2920..2415-195-s I ro-t+0-4
Elapsed Tlmos in Minufes
Tota I
72
1 00.0
4
5,6
100.0
2
2.8
94,4
2
2.8
91 .7
6
8.3
BB.9
14
19.4
80.5
17
23.6
6i .1
16
22.2
37.5
11
15.3
15.30.0
No, ofCrashes
Percentago
Cumul. É
40+35-39
t0-34
25-29
20-24
15-19
10-14
5-90-4
Elapsed Time in Mînules
Ra nge :
Mean Time:
5 - 55 mirrutes
lB.B minutes S.D. 10.0 minutes
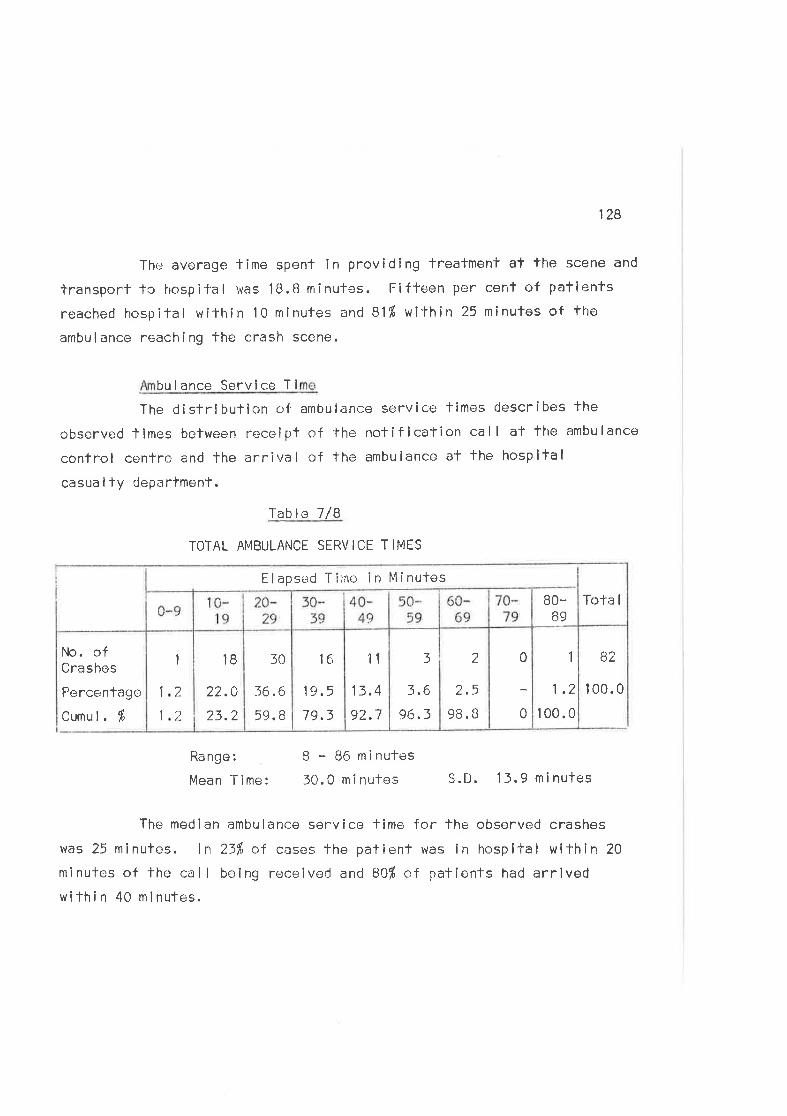
128
The average time spent in providing Treatment af the scene and
Ìransport to hospil'al was 1B.B minutes. Fifteen per cent of patients
reached hospital wi'l'hin 10 minutes ancl 81'Á within 7-5 tninutes of tiroambulance reaching the crash scene.
bulance Service Ti
The distribulion of ambulance service tlmes describes the
observed limes between receipt of the notification call al the ambulance
conlro I cenlre and the arr i va I of the ambu lance a't the hosp ita I
casualty departmenf.
Iablct 7/B
TOTAL AMBULANCE SERVICE T IES
B2
I 00.0
1
1.2
100.0
0
0
3
3,6
96.3
2
2.5
98. B
11
13.4
92.7
1e'
19.5
79.3
l0
36.6'
59. B
18
22.0
23.2
1
1 2
21
Tota I
Elapse.d Tilne in MinutosB0-
B9
No. ofCrashes
Percentage
Cumul. Í
Ra nge :
Mean Time:
B - 86 minutes
30.0 m i nutes S.D. 13.9 minutes
The median ambulance service lime follhe observed crashes
was 25 minules. ln 23fr of cases the patient was in hospl-lal wilhin 20
minutes of lhe call being receiveC and BOf of patients had arrivedwilhin 40 minutes.
1?9
THE TREATI'4ENÏ SUBSYSTEM
Treafment subsystem elemenls include lhe various measures used
in providlng care from the scene of lhe crash until the time of dlscharge
from emergency caro. They may be broadly divlded inlo two groups:(a) care before casualty, and (b) care within fhe casualty department.
Care Before Hospifal(a) Firsl Aid at lhe Scene
First aid had been performed by members of the public forpersons lnvolved in 23 of the study crashes. V¡cfims from 12 crashes
had been taken to nearby houses or buildings where they were made com-
fortable whi lst awaiting the ambulance. There were three instancos oftowels or other makeshift dressings being used to staunch blood flow
from lacerations. Only once u/as ð first aid kit used by a bystander.
A motorist stopped after witnessing the crash and used materlals from
a kit he carried in his car fo bandage a head laceration. There were
no casos in which first aid provided by members of the public lvas detri-mental to the patient?s conCition.
Tow truck drivers occasional ly assisted fhe injured before
the ambulance service arríved and helped with the exlricalion of Trapped
persons. Some truck operators are genuinely interesfed ln first aid and
carry first aid equipment in lheir trucks. (Murcott, 1971. ) Neverthe-
less, lheir job is to obtain lhe towing rlghts and this takes precedence
over fîrst aid. Some ambulance drfvers acf as tow truck drivers durlng
off-duty periods and openly admit that fhey rarely perform first ald
because They have to compete with other services for ïhe towing rights.(Kovacs, 1971.)
Police were not involved in the provision of f f rst aid at lhescene of any of tho study crashes. They altend to the imporlant tasks
of site prolection and traff ic control and this llmits their avail-abllity as flrst aid personnel.
t50
None c¡f the vehicles lnvolved in the study crashes caught
fire, allhough the flre brigade altended two crashes to hose spiltpetrol from fhe road and maínlain general surveillance in case firebroke ouf. 0n one occasion the brigaders salvage van was called foassist with the exTricatíon of a lrapped victim.
Doctors were present at the scene of 3 of fhe 100 crashes
studied. One of the patients treeted by a doctor at the scene was
subsequently managed privately by that practifíoner. These observations
support previous stafements that doctors in urban areas rarely attend
the scene.¡f road crashes and even more rarely confinue to manage the
patients after providing emergency care. (Bush, 1971; Royal Austral-asian Col lege of Surgeons, 1970. )
(b) Ambulance Care
Ambulance c¡fficers are frained to provide f lrst aid, withparlicular emphasis on speedy díagnosis and correct emergency lreatment.0n arrivîng af the scene they assess the condition of the injured,delermino treatment priorities and porform necessary first ald before
loading patients into the ¿rmbulance for transport to hospital.
Trlaqo at the Sceno
Three hundred and ten persons were involved in the
crashes, of whom 183 wore injured. One hundred and forty-seven (80Í)
of the injurecl were treated by ambulance officers. Those injured but
not treated had sustained minor injurles and ln most cases did not
requlre treatment. Overal I the ambulance offlcers were thorough in
their altempts to locate and assess the irrjured and friage of those
lnvolved was completed within a short limo of arrival at the crash site.Five victims, who had lacerations requlring suture. or t'lere concussed,
refused ambulance troatment and transporf, despite repeated attempts
by fhe ambulance men lo have them attend hospital.
131
Ambulance cfficers encourage al I palients with a hlsïory,signs, or symptoms suggeslive of concussion to accompany them tohospilal. Many patienls wilh minor injuries (e,9. bruises or abrasions)
who, on questioning, have an incomple-l-e recollection of the crash and
evonls leading up to il, are broughf to hospital wiÌh suspected con-
cussion. These patients with minor injuries contribute signiflcantlyto the loads on casualty departments, particularly in the late night,peak poriods. Nevertheless, fhe cautîon of the ambulance offlcers isjusfified and reflects the current service (and medical ) pol ïcy which
requires lhaT al I palients with possible head injuries should be
assessed by qual ifíed medical personnel before thely are discharged from
emergency care.
Treatment Procedures
Particular importancc^ is placed on the management of the
unconscious patlent with emphasis on the maintenance of the patientrs
airway, breathing and circulation. None of the sample patien'ts required
inlensive resuscilation at the scene, buT the necessary faci I íties,which included suction, oxygen and intravonous infusion equipment, were
available on ambulances if required. The suction equipment was used to
clear blood from the naso-pharynx of ono of the study patlents.
Five of the palients werc unconscious at the crash scene.
Four were managed in the coma position ('three-quartor prone) which is
sfandard practice within the service. The fiflh was a young man' one
of four victims involved in a single vehicle crash in which a car
col I ided with a pole.
cAsE 51 041 An 1B year-old unconscious male was
extricated from the rear seal of a car. Three other viclims in the
crash had been assessed by thc ambulance officers and loaded into the
ambulance be;fore his extrication was completed. A second ambulance was
thus summoned to take him J-o hospital. The f irsl ambulance left the
132
scene before the second had arrived, leaving the unconscious man lyingon his back at the roadside ín lhe care of bystanders. ïhe second
ambulance arrived approximately five minutes later.
This was one of the few cases of unsatisfactory ambulance
care that were observed. The anrbulance officers should have nursed thepafien-f in the coma position and waited for the second ambulance before
leaving lhe crash scene. Triage and treatmenf of several injuredvictims is ciiff icult at tho crash scene and mistakes in priorities are
bound to occur. Nevertheless, it is important that few such mistakes
wore made by ambulance offlcers al lhe sfudy crashes.
Dress i ngs were app I ied 'to 35 vict ims w íth I acerat ions
and abrasions. They were usual ly used to achieve haemostasis. Dressings
are not always applied to op.:n wounds, but there were few occasions on
whlch dressings were not applled when indicated. ln general, the dress-ings used and the technique of applying them were satisfactory.
Seventeen persons required I imb spl ints for fracturss.Air splints are stanclard equipment in thls service and were used forsuspectcrJ fractures in al I cases. Deficlencies in the uso of these
spl ints were noted on three occasions, when ambulance officers removed
victims f rom vehicles before applying splints. 0n another occaslon a
short leg splint was used for a tibial f racture when a long leg splintwas indicated. The re-use of air spl ints, whlch is sfandard practice,makes it important lhat splints should be checked for leaks before they
are repackaged. Sevoral splints were partially def lated by the time
the patienl reached hospital. ln general, the judgement used by
ambulance officers in applying splints for suspected fractures was
sat i sfactory.
Forty-one patients with I imb fraclures were included infhe series of 328 patienfs examined affer admission to casualty in fhe
133
second phase of lhe study. ln 7 cases, splints had nof been appliedby ambulance offîcers when indicated; 1'wice for upper limb fractures,once for a fraclured tibia and fibula and on four occasions for fracturesof the femoral shaft. Each ambulance carries a modifled Thomas Spl intwhlch is narticularly suifable for immobilizing f ractures of fhe femoral
slraft, bul which is rarely used for vicfims of urban cnashes.
ln cases of suspected spinal fraclure, of which fherewere two in Phase One, no special immobilizafion measures were used.
Spinal boards are not carried on Victorian ambulances. Sand bags forsupporting suspected cervical fractures have been introduced as standard
equlpmenf since the lime of lhe study. Ambulance officers are acutelyaware of the dangers of manipulatlng spinal injuries and showed care inmanaging cases in whlch fractures were suspected.
Trichlorethylene is used as an an¿:esthetic for ambulance
purposes and Hayward-Butt inhalers are carried on al I ambulances. An
inhaler was used only once in ihis sample of patients. lts use isparticularly lncJicated when patients are being extricated f rom vehiclesor undergoing procedures which can be expected to be painful, nofablyI ¡ft¡ng movements and lhe appl icatíon of spl ints. Despite iÌs avai l-ability the inhalêr was not used during such procedures. 0n the one
occasion in which lhe inhaler was used, it was offered to the patientafter she had been ex1'ricated and her fraclure spl inted. The operationof the device was inadequately explained and it was thus ineffective.
The fol lowing Table summarizes lhe freatment procedures
carried ouî by ambul¿¡nce officers for the victims of the study crashes.
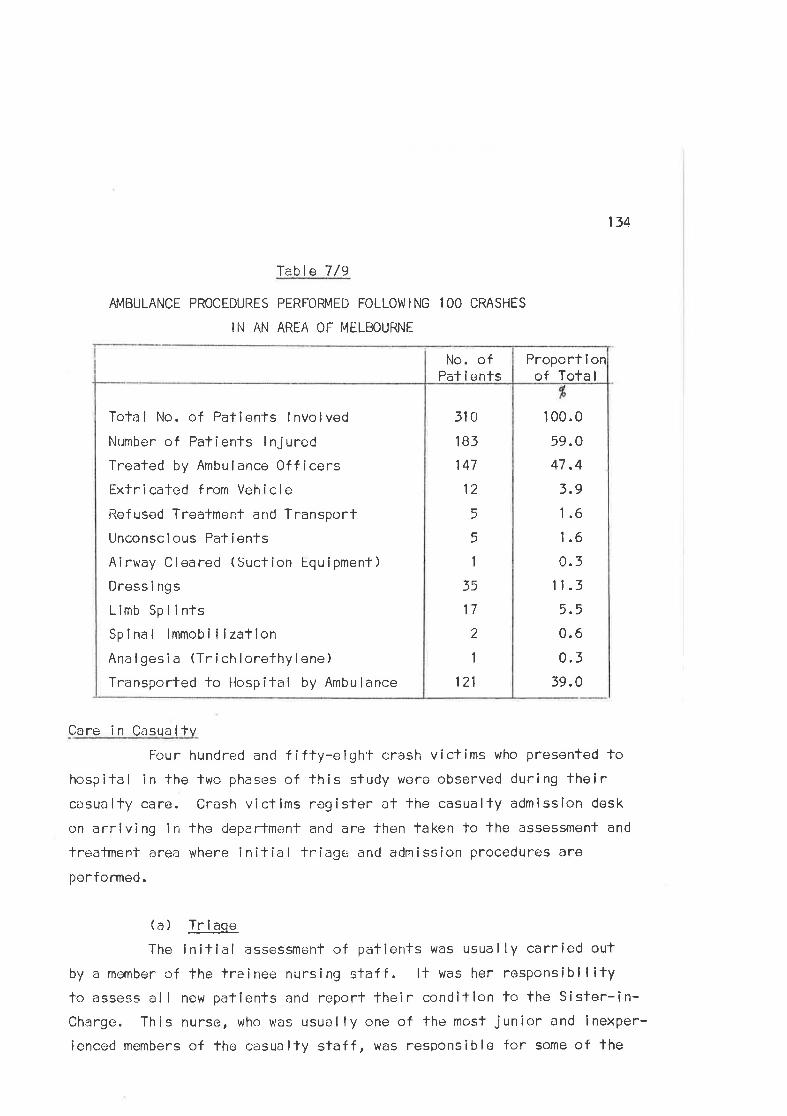
134
Table 7/9
APIBULANCE PROCEDURES PERFOFMED FOLLOI4IING l OO CRASHES
lll AN AREA 0F Í"|ËLBOURNE
510
lBl147
12
5
5
1
35
17
2
1
121
Total No. of Patients lnvolved
Number of Patients lnjuredTreated by Ambulance 0fficersExfricated from Vehicle
Refused Treafment and Transport
Unconscious Patíents
Airway Cleared (Suction Equipment)
Dress i ngs
Limb SplintsSpinal lmmobilization
Anal gesi a (Tr ich lorethyl ene)
Transported fo Hospital by Ambulance
Proport I onof Total
No. ofPat ie+nts
100.0
59.0
47,4
3.9
1.6
1.6
0.3
11.3
5.5
0.6
0.339.0
Care in Casualtv
Fou r hundrecl and f i f ty-e igh't crash v i ct íms who presented tohospital in the two phases of this study u¡ero observed during thelrcasualty care. Crash victims regisler at the casualty admission desk
on arriving in tho departmenÍ and are lhen faken to the assessmënf and
treatment area where initial tr iage and admission procedures are
performed.
(a) Trl.aqe
The initlal assessment of palients was usual ly carr¡ed out
by a momber of the trainee nursing staff. lt was her responsibllitylo assess all new patients and reporl fheir conditlon to the Sister-in-Charge. This nurse, who was usuôlly one of the most junior and lnexper-
ienced members of the casualty staff, was responsible for some of the
135
most important decisions affecting priorities in patient care, since
she was frequently the only member of the casualty staff to see the
patient immediately after admission.
This triage mechanism was unsatisfaclory. Many of the
observed patients wifh severe injuries did not receive apPropriate
priority in the patient queue because they had been inadequately
assossed. Road crash victims were not automatical ly rogarded as
emergency cases requiring urgent care in casualty. Hence they j'oined
the normal patient queue, unless lhe assessmenf by 'fhe triage nurse
or some other staff member suggested lhaf they should be seen more
urgently. The distributîon of waiting tîmes to see the medical officer,described in the next section, supports llre conclusion that the methoo
of Ìriage presently employed is unsuitable and ineffectlve.
Four hunclred and forty-eight of the patients who presenfed
lo thc casually doparfment tliere examined by a medical officer and
subsequenlly received invesligation and treatment of their injuries.Ten patients absconded from the departments before they were seen by a
doctor. The .types and sevority of -ihe injuries susfalned by these
patients was described in Chapter 6. ln lhe fol lowing section fhe
lreatmcnt procedures penformed for them wi I I be described.
(b) Treatment Procedures
There were 110 patients treated for concussion in the second
study phase. They were observed for a pcriod of at least four hours
bofore being allowed to leave lhe casualty department. Thoy received
assessment by a resiclenf medical officer and regular half-hourlyobsorvation by the nursing staff before being discharged from emergency
medical care. These oatienfs are observed in the acute receiving
cubicles in the treatmenl and assessment area.
Unconscious patîeni's were usually admitted to lhe emergency
136
cubicles in 'lhe departmenf and received prompt assessment from members
of the medîcal and nursing staf f . Ten Q.2% ) of fhe patients were
unconscious on admission to lhe casua lty department. l4ost unconscious
palients were nursed supine, which increased the risk of inhalatlon ofsecretions. Several of these patienJ-s had facial fnjuries, with
bleeding from and into the naso-pharynx, or had been drinking heforo
the crash occurred. Active measuros, which incl uded oro-pharyngeal
airways and suction, were used lo clear the alrway of flve pafienfs.
Two patients with multiple severe injuries required intensiveresuscitation, incl uding endotrachea I íntubation, artlf icial respirationand exlernal cardiac massage. Both died in lhe casualfy department.
Twenty pallents G.4%) had inTravenous infusions commenced
in the casualty dopartment. Al I were severely injured and cl inical lyshocked al the time fhe drips were sel up. Seventy of lhe study
patienls had received severe or greater injuries. Doctors in casually
were conservative in lheir use of intravenous lherapy and usually waited
until patients had developed clinical slgns and symptoms of shock before
commencing infusions, Those patients who had intravenous infusions had
blood senl for grouping and matching. 0nly one patienl received a blood
transf usion in the casualty departrnenl. Stable plasma protein solution
was used in those cases where ungent plasma expansion was required.
Thirty-six of the 58 patienfs who had sustained I ímb fractureshad their fracturos imrnobi I ized by spl inTs in casualfy, As was staTed
in an earlier secticn, ambulance officers apply air splints af lhe scene
in lhe majority of cases where fractures are suspectod. ln the hospitals
under study, it is ncrmal practice for lhese splints to be removed soon
after the pafient is admitted. The splint is either replaced by a
wooden splint or, as hap¡;ened in 3B/' of cases where fractures were
present, nol reapplîed at all.
137
Eight patienls were suspected of having spinal injuries at thetime of admission. Three of these were subsequently confirmed as having
fractures of lhe cervical spine, A fourth victim who was admîtted lohospilal for lreatment of multiple pelvic and limb fractures was found
to have an undisplaced fraclure of his seconcl cervícal verfebrae two
days after his admlssion tc¡ lrospital, when he complained of a sore neck.
A furlher two patients had frac'tures of luml¡ar transverse processes.
The adequacy of the communications between ambulance officersand casualty staff is of paramount importance in the management of spinalinjury. 0n onc occasion, poor communicatîon befween fhe ambulance
off icers and members of the casualty s-l'aff at the fime of admission
meant that the oatient was undressed without due care by nurses who were
unaware of the suspecled cervical fnacture. 0n a second occasion nurses
undressed a patient whc had.iust been examined by a doc'tor who suspected
a spînal fracture. ln both cases manipulalion of the pafienlfs head and
neck was involved in removing lhe clotlies. Fortunately, fractures were
not present in either case.
M i nor wounds, bru i ses, abras i ons and I acerat ions ¿:re the
commonest injuries suffered in road crashcs. Abrasions were usual lycleaned and painled wilh mercurochrome by members of lhe nursing s'taff.It4ost laceralions were clcaned a¡rd dressc-:d by nurses before sutures were
insertecl. One hundred and twenty*seven patients received sutures in lhedepartment. Although casualty theatres and procedure rooms were avai l-able for the perfonnance of'these procedures, many of them were performed
i n f he acule rece i v i ng and treatm.-.,nf are¿J.
Two hundred and sixfy-nine patients had casually X-rays
performed, buf few other special diagnostic services were required forthe study patients. One echogram was performed on a pa-fient with a
head injury and suspected întra-cranial lesion.
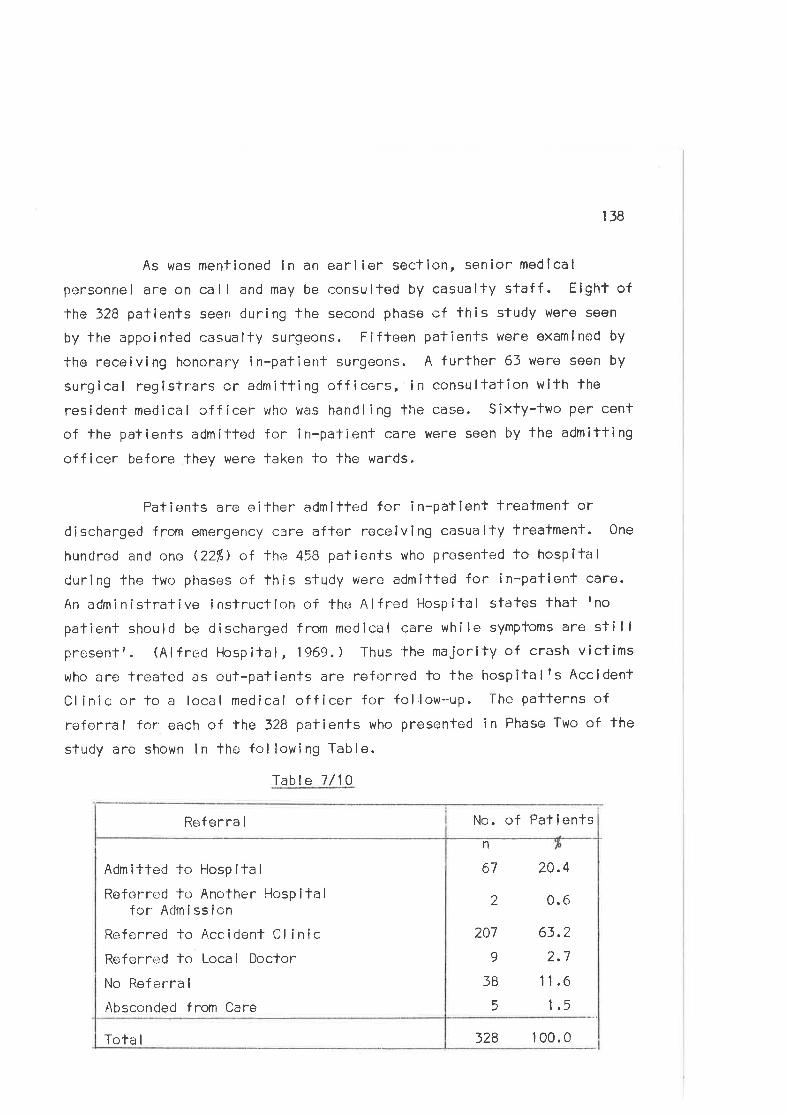
138
As was mentîoned in an earlier section, senior medlcal
personrìel are on call and may be consulted by casualty sfaff . E¡ght of
fhe 328 patienls seen during the second phase of this study were seen
by the appointed casualfy surgeons. Fifteen patients were examined by
the receiving honorary in-patienf surgeons. A further 63 werr¡ seen by
surgical registrars cr admitling officers, in consultation with the
res i dent med ica I of f icer i,rho was hancl I i ng lhe case. S ixty-two per cent
of the palienls admilted for in-patienl care were seen by the admitting
officer before they were laken to lhe wards.
Patients are eilher admilted for in-patient treafment or
discharged from emergerìcy care after receiving casualty treatment. One
hundred and one Q2Ð of the 458 patients who presented to hospilal
during the two phases of this study wero admitted for in-pationt care.
An edminisfrative inslrucfion of the Alfred Hospilal stafes That Ino
patient shoulcJ be dischargecl frorn medical care while symptoms are stillpresentr. (Alfred Hospital, 1969. ) Thus the majority of crash victims
who are trealed as oul-pafients are referred lo the hospitalfs Accldent
Clinic or lo a local medical officer for fol.low*up. The paTterns of
referral for each of the 328 patients who presented in Phase Ïwo of fhe
study are shown in the following Table.
Table 7/10
No. of Pafientsn
67
2
207
9
]B
5
20.4
0.6
63.?
2.7
11.6
1.5
Tota I
Admitted to Hospital
Referred to Another Hospitalfor Admission
Referred to Accidenl Cl inicReferr+:d lo Local Doclor
No Referra I
Absconded from Care
Referra I
328 100.0
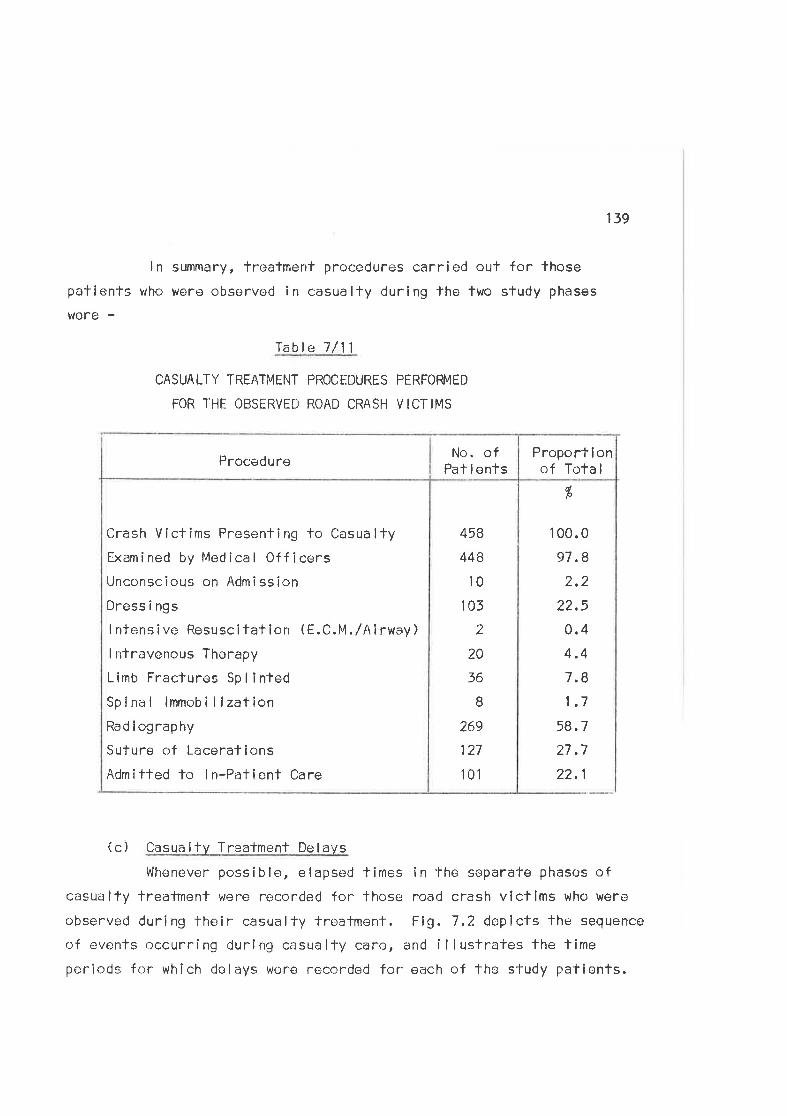
ln summary, treatment procedures carried out for those
patients who were observod in casualty during the two study phases
were -
lable 7/11
CASUALTY TREATMENT PROCI.DURES PERFOFMED
FOR THE OBSERVED ROAD CRASI.I VICTIMS
139
458
448
10
103
2
20
36
B
269
127
101
Crash Viclims Presenling lo Casualty
Examined by Modical OfficersUnconscious on Admi ssion
Dress i ngs
I ntensive Resuscitaf ion (E.C.M./Airway)
I ntravenous Therapy
Limb Fraclures Sp I i nted
Sp ina I lmmob i I lzat ion
Radiography
Suture of Lacerations
Admitfed lo ln-Patient Care
Proporf I onof Tota I
No. ofPat i entsProcedure
I 00.0
97.8
2.2
22,5
0.44,4
7.8
1.7
58.7
27.7
22.1
%
(c) Casualty Treatment Delays
V'lhenever poss ib le, e lapsed times in the separate phases ofcasualty lreatment were recorded for fhose road crash victims who were
observerl during their casualfy troafment. Flg. 7.2 dep icts fhe sequence
of events occurring during casualty care, and i I lustrates fhe time
periods for which delays wene recorded for each of the study patients.
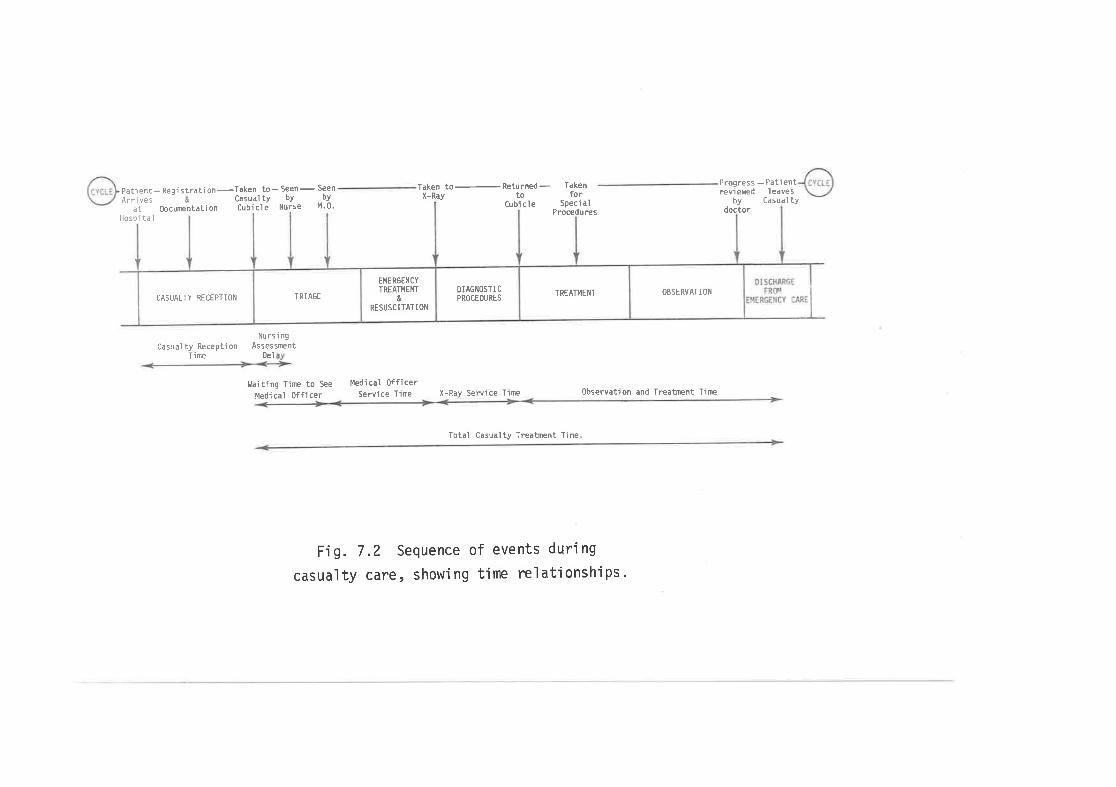
Patient- Regi stratj on-Casual ty bY by
M.0.tbcurentati on Cubi cl e Nurse
Nursingcasualty Reception Assessment
Ti me Del
l,laiting Tine to See
Medical 0fficer
Taken to-Seen-Seen Taken to- Returned -to
Takenfor
speci aìProcedures
Progressreviered - Pati ent
I eave sby Casual ty
doctor
X-RayArri vesat
Hospi taìCubi cle
X-Ray Service Time
-l-otal Casualty Treatnent Time
0bservatìon and Treatnent TireMed'ical officer
Service Time
F'ig. 7.2 Sequence of events during
casualty care, show'ing time relationsh'ips.
CASUALTY RECEPTION TRIAGE
EMERGENCYTREAI},IENT
&
RESUSCITATION
DIAGNOSTI C
PROCEOURESTREATMENT OBSERVAT IOIi
140
Recept ion TÌme
The recepfion time represenls lhe delays experienced by
pafients durirrg transfer to the casualty trealment and assessment area.
This corresponds to the ambulance delivery time (Flg. 7.1.) for those
crash victims brought to hospital by ambulance. ll încludes delays
incurred in transfer from ambulance stretcher to hospifal barouche and
in documentation and registrafion en route fo the assessment and treat-rnent area. Non-emergency patients usual ly complete this lransfer in
less than five minutes. These procedures may be waived for emergency
patients and they are usually lransferred in one or two mlnutes.
Walking patienfs regíster at the casualfy admissions
desk before being faken fo the treafment area. Queues form at thispolnt anC delays depend on the number of patÌents waÎting to reglsÌer,the tlme of day, and the severlty of their injuries. Pallenfs wifh
disabling injuries are usual ly taken straight to the assessment area
where registration and documentation procedures are completed by lho
casualty clerks.
Two hundrecJ and slxty-seven (81Ð of the 328 patienTs
in the second phase of fhe study were broughf to hospltal by ambulance
and avoided the reglstratlon and documentation queue. Many of lhe
remaining 19/ of patients also passed by fhÌs queue because of thelrovert lnjuries.
Nurs i nq Assessment De I ay
It was stated earl ier in
inltlal ly assessed by a receivîng nurse
patientls conditlon and then reports fonursing assessment delay represents thepatientrs arrlval in the assessment and
î s soen by fhe assess i ng nurse.
this chapter that patients are
who gathers deta i I s of the
lhe sister in charge. The
elapsed time befween the
treatment area and the time he
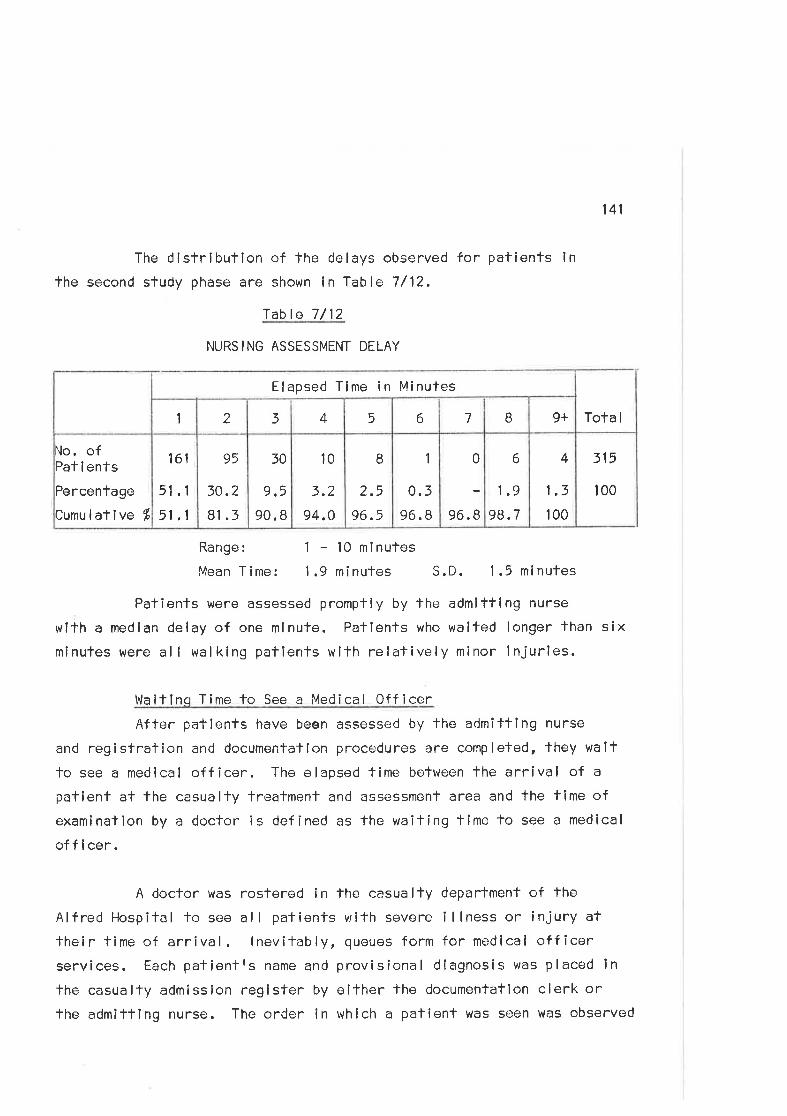
141
The distribufion of the delays observed for patients lnfhe second study phase are shown in Table 7/12.
Table 7/12
NURSING ASSESSMENT DELAY
315
100
Range: 1-l0minutesMean Time: 1.9 minutes S.D. 1.5 minutes
Patienfs were assessed prompfly by the admitting nurse
wlth a median delay of one mlnute. Patients who waifed longer than sixminufes were all walking patients with relatively minor injuries.
Waltinq Time to See a Medical OfficerAfter patients have been assessed by the admitting nurse
and registration and documentalíon procedures are completed, they wait
to see a medlcal officer. The elapsed time befween the arrival of a
patient at the casualty trealment and assessment area and the time ofexamination by a doctor is defined as the waiting time to see a medical
of f i cer.
A doctor was rostered ín the casualty department of fhe
Alfred Hospifal to see all pafienfs wifh severe illness or injury attheir time of arrival. lnevitably, queues form for medical officerservices. Each patientfs name and provisional diagnosis was placed in
the casualty admission register by oither lhe documentation clerk orthe admittlng nurse. The order in whlch a patient was seen was observed
4
1.3
100
6
1.9
98.7
0
96.8
1
0.396.8
I2.5
96.5
l0
3.2
94.O
30
9,5
90. I
95
30.2
Bt .3
161
51 .1
51 .1
No. ofPat i ents
Percentage
Cumulatlve Í
Tota I9+B765432I
Elapsed Time in Minutes
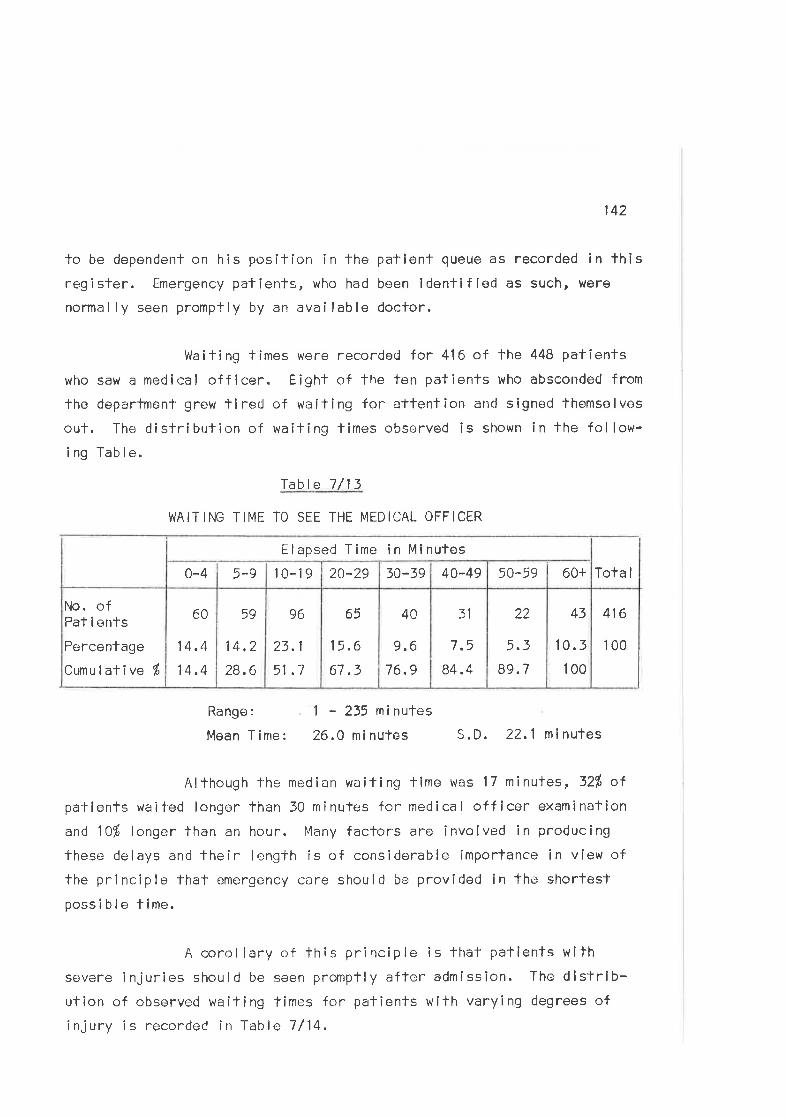
142
lo be dependenl on his posiTîon in the patienl queue as recorded in lhisregister. Êmergency palienls, who had boen identifled as such, were
normal ly seen promptly by an avai lable docfor.
Waiting times were recorded for 416 of the 448 patients
who saw a medical offîcer. E¡ght of the ten patients who absconded from
the departmen't grerl tlred of waiting for a'ltention ancJ signed lhemselves
out. The distribution of waiting times observed is shown in the follow-ing Table.
Tabla 7/13
I¡JAITING TIME TO SEE THE MEDICAL OFFICER
416
100
43
10.5
100
22
5.3
89. 7
31
7.5
84.4
4A
9.6
76.9
65
1 5.6
67.3
96
23.1
51 .1
59
14,?
28.6
60
14.4
14 .4
No. ofPat i enÌs
Percentage
Cumulative É
ïota I60+50-5940-4930-3920-29t0-195-90-4
Elapsed Tíme in Mlnutes
Range:
Mean Time:
1 - 235 minutes
26.0 mi nutes S.D. 22.1 ninutes
Although the median waiting lime was 17 minutes, 32% ofpatienfs waited longor than 30 minules for medical officer examination
and 10f longcr than an hour. l{any factors are involved in producing
these delays and their length is of considerable importance in view ofthe principle thal emergency care shoulrJ be provided in the shortestpossible time.
A corollary of this principle is that paf ients wilhsevere injuries should be seen promptly afler admission. The dlstrib-ution of observed wailing times for patients with varying degrees of
injury is recorded in Table 7/14,
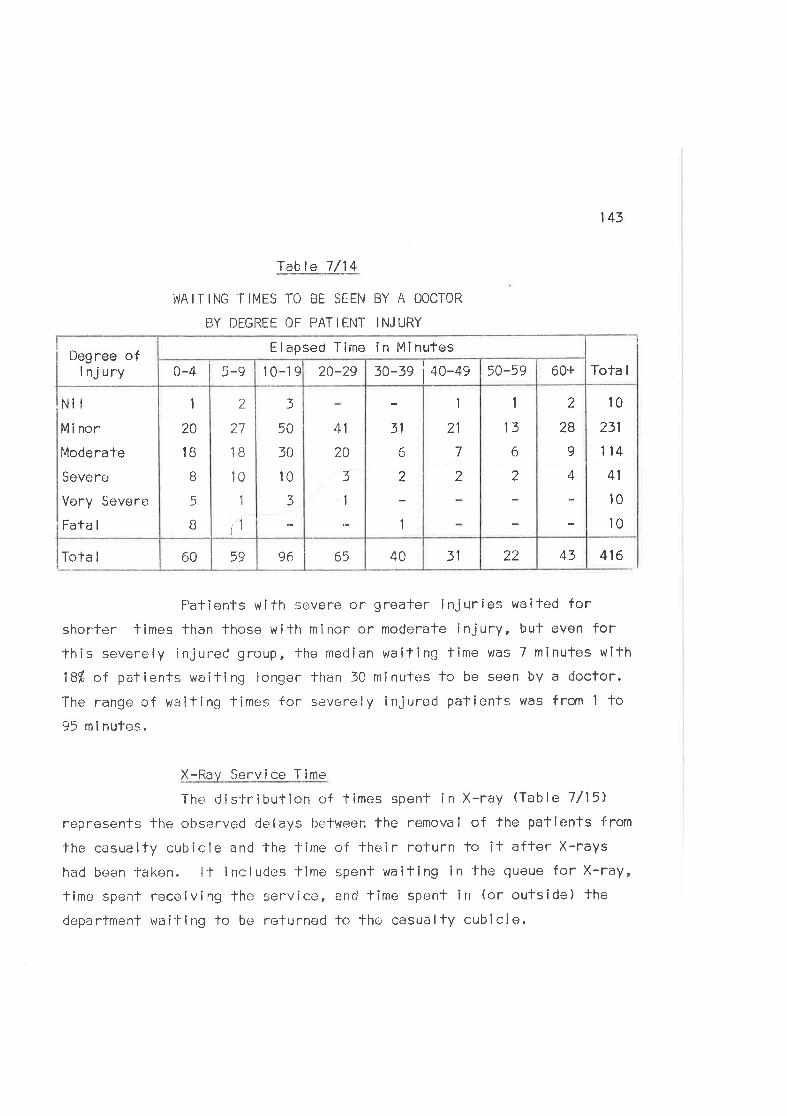
143
Table 7 /14
WAITING TIMES TO i3E SEEN BY A DOCTOR
BY DEGREË OF PATIENT INJURY
Nit
Minor
Moderate
Severe
Very Severe
Fata I
416
Patients wilh severe or greater injuríes waited forshortcr limes than those with minor or moderate injury, but even forthis severoly injurerl group, fhe rnedian waiting time was 7 minutes with
18% of palients waiting longer than 30 minutes to be seen by a doctor.
The range cf waiting¡ times for severely injured pafiente was from 1 to95 m i nules.
X-Ray Service Time
The dis-lribution of times spent in X-ray (Table 7/15)
represents the observed delays between fhe removal of the patients from
the casualfy cubicle and the fime of their return to it affer X-rays
had been-faken. lt include-s tlme spent wailing in fhe queue for X-ray,
time spent receiving lhe service, an<i time spent in (or outside) the
department wai'llng to be returned to the casualty cubicle.
4322314065965960Tota I
10
231
114
41
10
10
2
28
9
4
1
13
6
2
1
21
7
2
31
A
2
1
41
20
3
1
3
50
30
10
3
,)1-
27
1B
10
1
t1
1
20
1 B
B
5
B
Tota I60+50-593o-3s j +o-+s20-2910-190-4 5-9Degree of
I nj ury
Elapsed Tirne ín Minutes
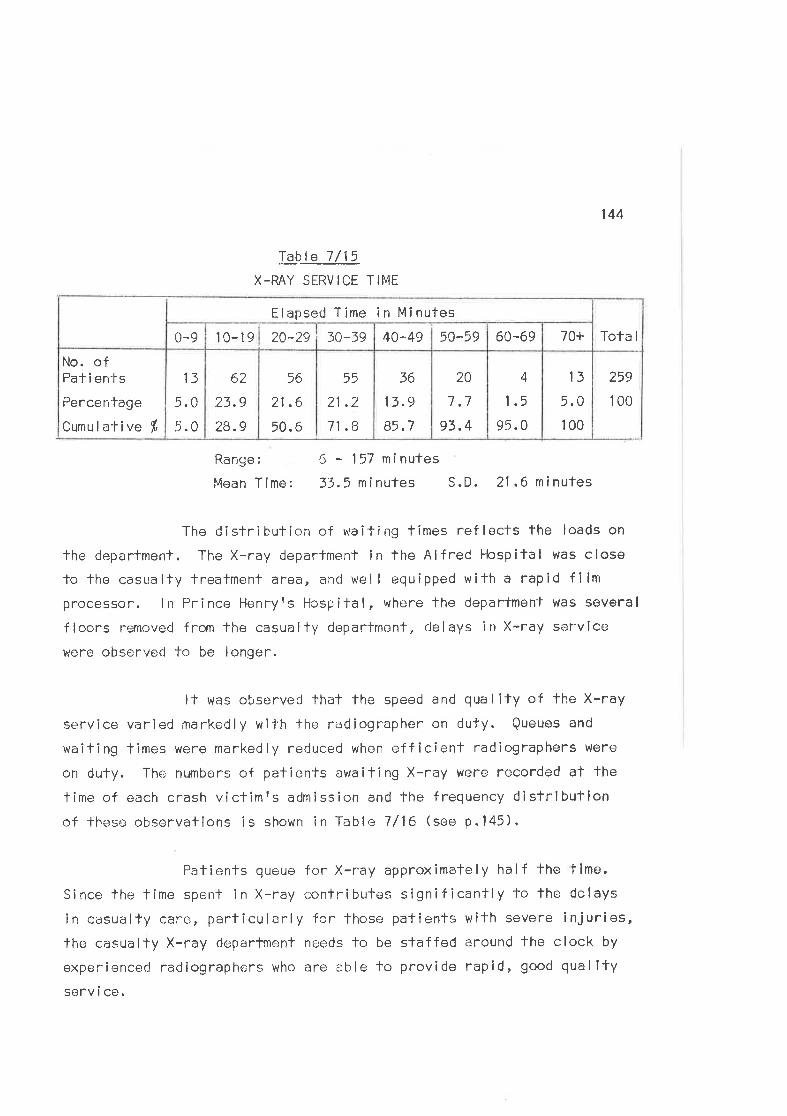
þ_b..te 7/15
X-RAY SERVICE TIME
144
259
100
Range:
Mean Time:
6 - 157 minutes
33.5ninutes S.D. 21 .6minutes
The distribution of waifing times ref lects the loads on
the deparlment. The X-ray department in the Alfred Hospital was close
to the casualty treatment area, and wel I equipped with a rapid fllmprocessor. I n Pr i nce llenryrs Hosp î fa I , where the department was severa I
floors removed from the casually deparfmenf, cJelays in X-ray service
were observed to be longer.
It was observed thal the speed and qua I iÌy of the X-ray
service varied markedly wil'h the racjiographer on duïy. Queues and
waiting times were markecJly reduced when efficient radiographers were
on duty. The numbers of patients awaiting X-ray were recorded at the
time of each crash victîmrs admission and the frequency distríbutionof lhese observalions is shown in Table 1/16 (see p.1a5).
Patients queue for X-ray approximately half the time.
Since lhe time spenl in X-ray conlributes significantly To the delays
in cosualty care, particularly for lhose patients with severe injuries,the casualty X-ray departmr:nt ne¡eds to be slaffecl around the clock by
experienced radiographers who are able to provide rapid, good qual itysorv i ce.
13
5.0
100
4
1.5
95.0
20
7.7
93.4
36
13.9
85.7
55
21 .2
71.8
56
21 .6
50.6
62
23.9
28.9
13
5.0
5.0
No. ofPat i en'ts
Percentage
Cumulative f
Tota I70+60-6950-594A^4930-3920-2910-190-9
Elapsed Time in Minutes
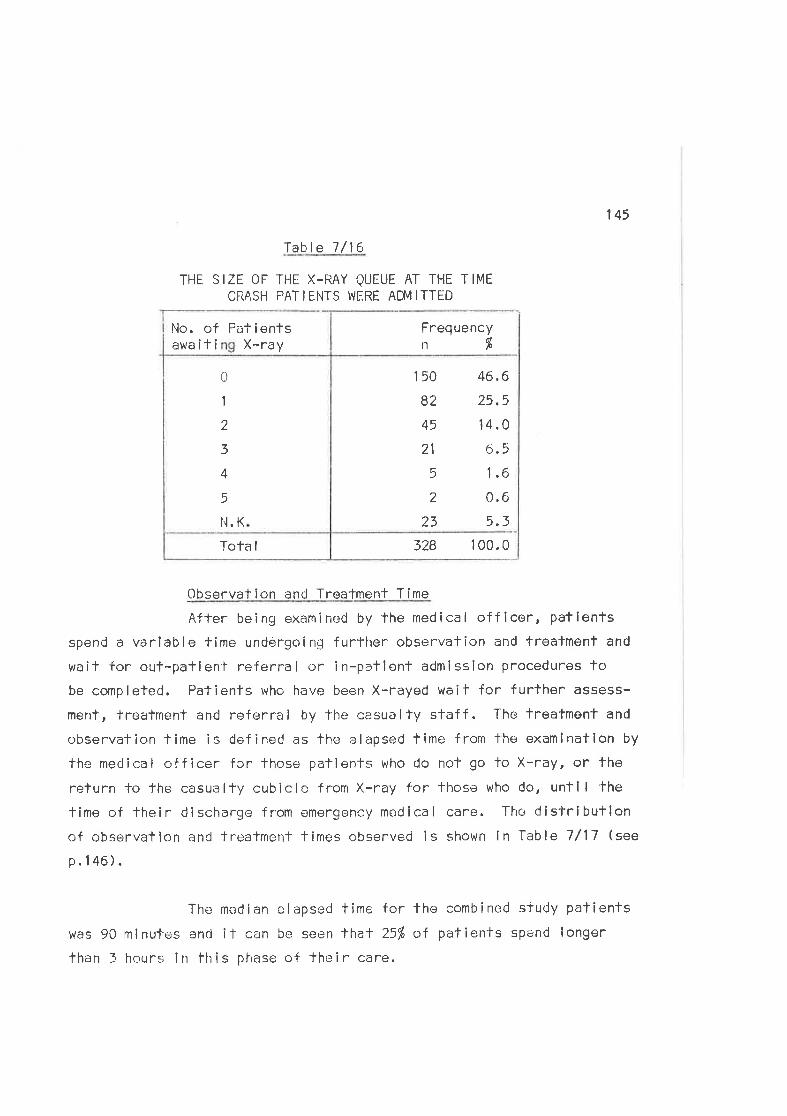
145
lable 7/16
THE SIZE OF THE X-RAY QUEUE AT THE TIMECRASH PAT I ENTS I.i FRE ADÍ\4 ITTËD
150
82
45
21
5
2
23
46.6
25,5
14.0
6.5
1.6
0.6
5.3
328 100.0Tota I
0
1
2
3
4
5
N.K
Frequencyn%
No. of Patientsawaiti X-ray
_Observation and Treatment Time
Afler being examined by lhe medical officor, patienlsspend a variable time undergoinE further observation and trealmenl and
wail for out-patlen'l referra I or in-patlent admission procedures tobe cornpleled. Patients lvho have been X-rayed wait for f urther assess-
ment, treatment and referral by The casualty staff. The treafment and
observation time is defined as the elapsed time from fho examination by
the medical officer for lhose pallents who do not go to X-ray, or the
return to J'he casualfy cubicle from X-ray for those who do, until the
time of their discharge from emergency medÍcal care. The dislribufionof observation and treatment times observeci is shown in Table 7/17 (see
p.146).
The median elapsed time for the combined sludy patients
was 90 minutes and il can be seen that 25% of patients spend longer
than 3 hours ín th is pl'rase of the i r care.
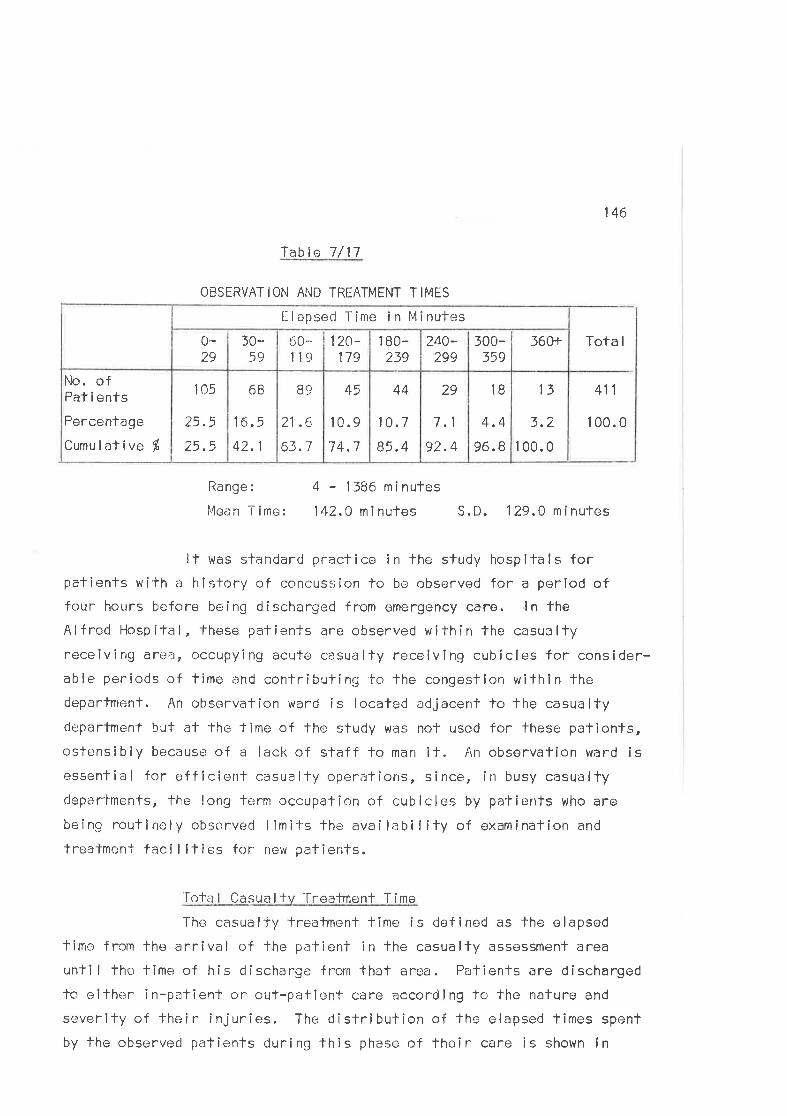
Table 7/17
OBSERVATION AND TREATMENT TIMËS
146
Tota I
411
1 00.0
Range:
l4ean Time:
4 - 1386 minutes
142.0 minutes S. D. 129,0 m i nufes
It was standard practice in the stucjy hospifals forpafients with a history of concussion to be observed for a period offour hours before being discharged from omergency caro. ln the
Alfred Hospital, lhese patients aro observed withín the casualtyreceivîng are-.¡, occupy¡ng acute casualty recoiving cubícles for consider-able periods of time and contributing to the congesfion withln thedepartmenl. An observalion ward is located adjacenl to the casualtydepartment but at the -lime of lhe study was nol used for these patients,ostcnsibly becauser of a lack of staff to man il. ftn observation ward isessenfial for eff icíent cesualty opere.itions, since, in busy casualtydepartmenfs, the long teirm occupatíon of cubicles by patienls who are
bein.o routinely observe..d limits the availabilify of examinaf ion and
trealmenf faci I ities for new patients.
'[ota I Casua I lv Trealmont T ime
The casually treatment time is defined as the elapsed
lime frcm the arrival of the patient in fhe casually assessment area
until lhe time of his discharge frorn thaf area. Patients are discharged
lo eifher in-patîent or ouf-patient care according to the nature and
severify of their injuries. The distribution of the elapsed fimes spent
by the observed patients during lhis phase of lheir care is shown in
13
3.2
1 00.0
1B
4.4
96.8
29
7,1
92.4
44
10.7
85.4
45
10.9
7 4.7
B9
21 .6
63.7
6B
1ô.5
42.1
105
25.5açE
No. ofPaf i ents
Percentage
Cumu I alive $
560+300-359
240-299
1 80-239
120-179
õ,0*119
30..59
0-29
F-lapseci Time in Minutes
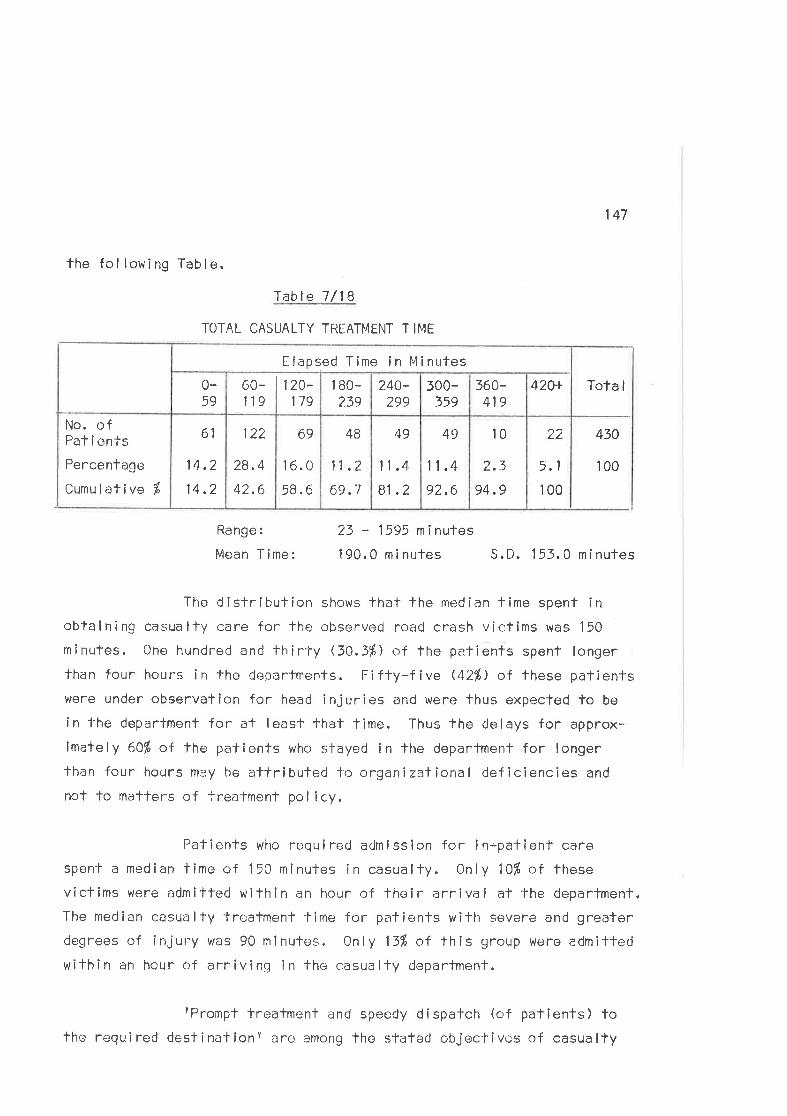
the fol lowing Table.
22
5.1
100
147
Tota I
430
100
lable 7/18
TOTAL CASUALTY TREATI4ENT T IME
Range:
Mean T ime:
23 - 1595 minutes
190.0 minutes S,D. 1 53.0 mi nutes
The distribulion shows that the median fime spent inobtaining casua lfy care for the observed rc-:ad crash victims was 150
minutes. Cne hundred and thirly ß0,3%) of the patients spent longerthan four hours in the deparfments. Fifly-five (42Ð of these paTients
were under observation for head injuries and were fhus expecfed to be
in lhe department for at least lhat lime. Thus the delays for approx-imately 60f" of lhe palients who stayed in lhe department for longerlhan four hours mey be allribuled to organizational deficiencies and
not to matters of treatment pol icy.
Pafients who required admission for in-pafienf care
spen-l- a median time of 150 minutes in casualty. 0nly 10ft of these
victims were admitted within an hour of thoir arrival at the department,
The median casualty treatment time for pafients with severe and greaterdegrees of injury was 90 minutes. 0nly 13% of this group were admitfedwiïhi n an hour of arrivi ng I n the casua lty department.
fPrompt treatment and speedy dîspatch (of patienfs) tothe required destinatione are among the sfated objectives of casualty
10
17
94.9
49
11 .4
92.6
49
11 .4
81 .2
4B
11,2
69.1
69
1 6.0
58.6
122
28.4
42.6
61
14.2
14.2
No. ofPat i ents
Percentage
Cumul ative f,
420+360-419
500-359
2.40-299
1 BO-239
120-179
60-119
0-59
Elapsed Time in 14inutes
148
trealment. (Alfred Hospital, 1969.) TreaÌment times as long as those
observed suggest that the present organization of services is not
ach ievi ng the des i red object i ves.
THE DOCUI.4ENTAT ION SUBSYSTEM
The documentation subsys-lem i nc I udes the var ious methods of
recording data describing the crash, the response of the emergency
sorvices,-fhe patienlst injuries and their management.
(a) Crash Data CoI IectionAccidenl invesligation and the collection of crash data for
statistical purposes is undertaken by the V!cforia Police. The VictoriaPolice Accident Report Form con'tains four, closely typewritten, foolscap
pages of question relating to matlers of fact and opinion based on the
pol icemanrs observafions of the incident. Much of the form ls pre-coded
and thus suitable for completion al the scene. The policemanf s role atlhe scene is complex and ir¡volves such important functions as slleprotection and supervision of the olher emergency services. Consequently
lhe form was rarcly filled oul at the scenü and the officers presumably
relied on lheir memory to complete the clata record af a lafer date. ln
many cases pollce were observed to make long-hand notes of their find-îngs, presumably fo assisl with subsequenl completion of lhe reoorlforms. The rel iabi I ity of data recorded under such conditions is opon
to question and, although it is nol appropriate lo comment on the con-
tenÌs or requiremenfs of the polico accidenl record, it may be thal a
review of both recordìng melhods and the content of the record could
procluce more itccurate data for bolh stat ist ica I record i ng and genera I
pol ice purposes.
(b) Ambulanco Records
Ambulance service dala are recorded for each ambulance cal I on
three separale forms. A fourth form records data rolating to the
149
injuries and condition of fhe patient and îs deslgned to be handed tothe casualty staff at fhe time of 'the patientts admission for inclusioni n fhe med i ca I record.
Ambulance Call Record
0n receiving the notif ication call, the lelephonist or ambul-
ance dispatcher comple'tes a case card on which lhe details of the callare listed. lncluded among these details are
1. The time of lhe call;2, The slte of the incident;3, The nature of the incident;4. The name of the cal ler;5. The origin of the call (e.9. police, taxi
company etc. ).This record ls then passed on fo the ambulance dispalcher who
notes the relevant informatíon on lhe díspatch recond.
Di spatch Record
Each dispatcher maintains a dai ly work sheet which provides
a record of the location and distribution of lhe ambulances under hlsconf rol. On receiving the cal I record he notes the tlme of the day,
the timc of dispatch and the site and nafure of the incidenf on the
work sheet. When an ambulance is dispafched he records the ambulance
and crew I denli f i calion numbers.
At lhe time of the sfudy fhe service did not record fimes ofarrival and departure from fhe scene and arrival at hospital. As a
rosult of changes in adminislrative pol icy these significant servicoflmes are now recorded. The dispatcher also records fhe hospital towhich the injured are taken.
Service Docket
The ambulance crew complete a case docket on each ambulance
150
call. Data recorded on lhls docket lnclude1. The name and acldress of the palient;2. The d¿ri ly job number;-5. Di spatch and job cornp I et ion f imes;
4. The site and na.ture of the incident;5. The nurnbcr of patients and their injuries;6. 14ileage dala (from odorneter readings);7. lnformation requîred for bill¡ng and accounting
DUrposes.
This dockel is completed during the approprlate phases of theambulance call: dispatch data at the lime of dispatch, crash data atthe scene, and patient defai ls, accounJ'ing and bi I I ing informafionduring transport to hospital or orì completion of the call.
Ambulance Officerfs Report on a Casualtv
The fourth p iece of ambu l¡rnce service documentation ls thecasualty report form, designed to provide a record of the patientfsinjuries and cl inical condition as observed during ambulance care. A
form should be compleled for each emergency paflent. This form is theonly tangible and permanent record of lhc patientrs condition at the
scene and during transport. As such, il should provide a valuablesource of infr¡rmation for subsequent emergency care in casua lty. The
form, which is divided into six seclions, is used by all Victorianambulance services. ln addition to brie f personal details on thepatienlts name, âgo, sex, it contains thc following observations ofpatient conditîon at fhe scene and durÌng transporf.
Patient Data: Stata of consciousness;
Pupillary reactions;Pu I se;
Resp i rafory rate;Suspecterd injuríes;Other abnormal ities noticed.
151
Trealmenl Performed: Oxygen adminislration;Tri lene admi n istration;Other lreatmenf.
'fhe report form was rarely used for patients carried by theVictorian Civi I Ambulance Servlce. Ten of the ?67 patients brought tohospital by ambulance in the Eecond phase werê accompanied by completed
report forms. Soven of these patients were carriecl by the Peninsula
Anrbulance Servíce which used the fcrms routinely as part of the ambul-
ênce service rocord. Thus approximately lfi of cresh victims carrledby the V.C.A.S. had ambulance report'Éonns completed.
Since the reporf form was fhe only record of the patientf s
condition and treatment before hospllal, the arnbulance of f icersr fai lurefo complete it was reprehensible. Novertheless, it was, to some extenl,understandable. The form is designed to be included in the patient?shospilal record buf, in practice, none of them were subsoquently
included in the hislory. They wone usual ly left lying around thecasualty deparlment or consîgne<J to the waste paper baskel. Ambulance
officers were aware Ìhat casualty medical staff rarely read the reportform and had thus developed thc attitude that completion of fhe form
was a waste of time.
This represents a furfher example of poor communicalion
befween the ambulance and casualty sfaffs which may affecf subsequenf
palienl' care. Although ambulance men usual ly attempt to relate detal lsof a patientts injuries and management to a member of the casualtystaff, the only satisfactory way of ensuring that the relevant inform-ation gets to the medical officer who ultimately assesses the patientis to provide a written history. Equally, fhere is an obligaTion on
the casualty staff to take note of fhe hisfory whlch is provide<1.
152
(c) Casua I ty Documentat ion(1 ) Documentalion Procedures
Casually Documenfation clerks were among the first members oflhç casualty staff to inferview pationts, recording the personal data
necessary to eifhor procure an exísfing medical history or generate a
new hisTory. ln pracfice this procedure was a pre-requislte for exam-
inatíon by a medical officer in all cases except those where seriouslyi njured patients requi red i nfens i ve resuscí tation and care. On comp I et-ion of casualty documentation, paf lents were listed in the casualtyadmission bcok and theircby joinod the queue for examÍnallon.
Documentation delays in casualty were not recorded in thisstudy, buf two of the observed patlents did not receive medical carebecause they had not been docurnenled on admission to the clepartment.ln both cases, affer a delay of an hour, thc¡ observer reporTed theomission to thrs c.:sualty clerks who promptly completed the documontationand the patienfs jcined the queue for medical attention.
P.'tients who require':d admlssion to hospifal wero frequentlydelayed in casualty because of lhc documenfation procedures requiredbefore they were admitted. The admilting medical officor on duly was
required to sign thc medical record and allot lhe palient fo a ward.Often, during evening and nighf hours whan admit'ting officers were
absent from the department, long delays occurred because the document-
ation procedures couId noï be compIeterj. The delays caused by thedocumen-i-ation procedures pûr se were rìegligible in comparison with thedelays cat¡sed by the norì-availability of the admi'l-ting medical off icers.There are good medical reasons why aCmitting officers should be presenfin the deparlment thrcughout their rostc.:rod duty periods, since they arethe personnel who should be available for immediate consultation by thejunior resident staff. Equal ly, fhey should be presonT at al I times To
ensure the rapid admission or discharge of those patients who have com-
p leted thei r casua I ly treatment.
153
Q) The Medical HistorvCasua lly h istory and exam ination sheets tvere comp leted f or
each pat ie¡lt seen i n the clepa r1-ment. Record i ng proc;eclures i n the sludyhospitals followed the traditional patTern whereby medical informationwas noted in long-hand in fhe medical history. structured recordingformafs offer several advantages over the traditional methods ofrecorciing medical cjata. (Weed, 1970; Race, 1972.) Recording forms
have been de.signed especially for trauma victims (Bordner, 1968;
Stanford Research lnstitute, 1968) and evaluafed as an effecfive means
of recording and s.toring clinical and statistical data. (Cashman, 1970).
The existing system has several obvious deficiencies. Firsf,it I eads to lhe record i ng of i ncomp le'l-e ancj, f requent I y, i rre levanfdata. secondly, observations made during'this study suggest that lhemosf severely injurr:d paf ients are often those for whom lhe least datais recorded in the medical hislory. Data recorcling is rightful ly low
in the order of priorities in the l'lurry of aclivity that surrounds fheadmission of these palienls. Nevertheless, data on the early management
of fhe seriously injured may be of consiclerable importance for subsequent
care and relevant signs, symptoms and treatmenf detai ls should be
included in the patîentts history.
The casually medicai records of each of ihe palients admittedduring fhe second phaser of fhis sludy rvere reviewed after the patienfhad been discharged from tho casualty departmenf. Twelve (4/ù of therecords reviewed contalned complete documentation of the patientrshís'lory, examinalion, and subsequent casualty troatment. Two hundred
and forfy-nine ß2%) of the records contaíned a record of the majorf ind ings and treatment performed . ln 44 (4%) of the cases importantinformation on the patienlrs condition ancJ lrealment was omitted from
the casualty record. 'Table 7/19 describes the observed relationshipbetween the qualily of the medical necord and the degnee of injurysustaíned by patlents.
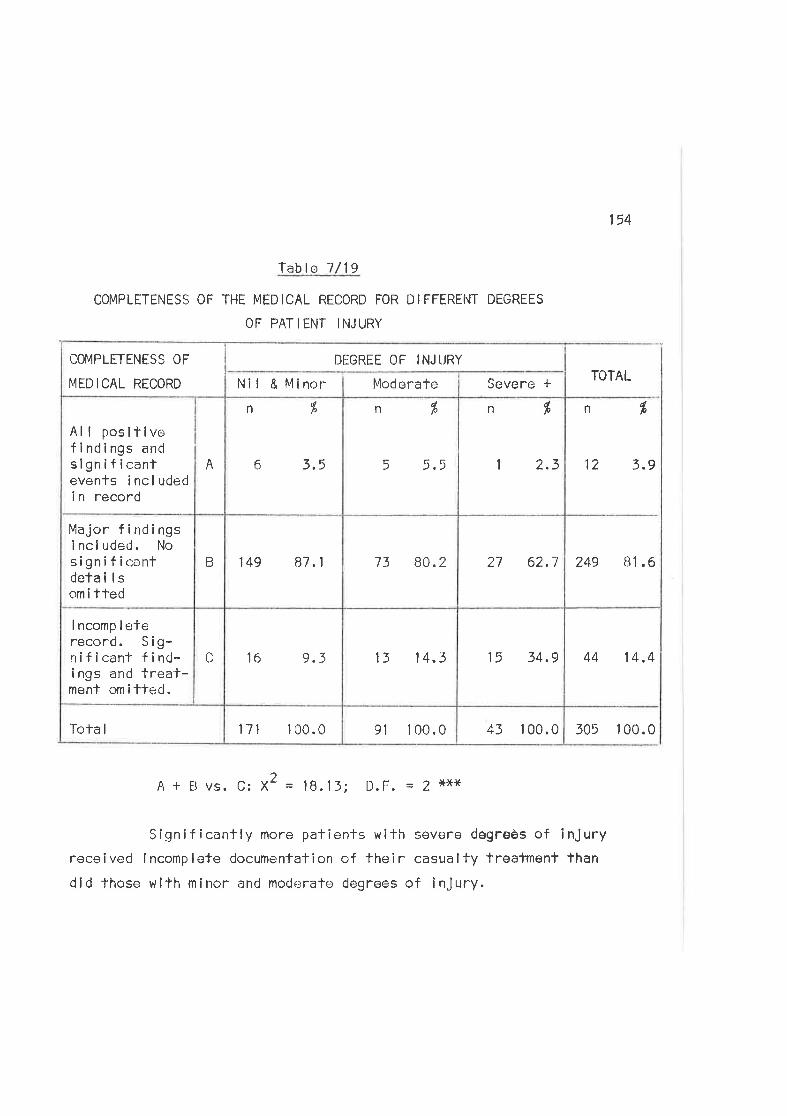
lable 7/19
COMPLETENESS OF THE MEDICAL RECORD FOR DIFFERËNT DEGRËES
OF PATIENT INJURY
154
TOTAL
ndlo
12 3.9
249 81.6
44 14 .4
305 100.0
2A + I vs. C: X = 18.15; D.F. = I tr*x
Significanfly more paf¡ents with severe dêgreès of injuryreceived Incomplote documentafion of their casualfy treatmont than
did fhose wilh minor and modc¡rate degrees of injury.
43 100.091 1 00.0171 1 00.0'Iola I
15 34,913 14.316 9.3C
I ncomp I eferecord. S i g-rrif icant f ind-i ngs and treat-ment omitte<J.
27 62.773 80.2149 87.1B
Major findingsi nc I uded. l.losigníficantdetai lsom i tted
I 2.3
n í
5 5.5
n %
6
n dle
3,5A
Al I posilívofindings andsignifícanfevents í ncl udedi n record
Severe *ModerateNll & Minor
DIGREE OF INJ I.JRYCOI,4PLETENESS OF
T4EDICAL RECORD
155
Chapter I
F THE EM ENCY CARE S
The use of a systems approach for examining emergency servlces
requires that the operations of the existing system should be evaluated
and alternative methods of achlevlng the objecflves of the system con-
sidered in the light of their likely effects on lt. Moreover, fhe
approach implies that the system should be examined as a whole, using
specific criterla to evaluate its various elements.
The problem in evaluating emergency care, as in many olher
areas of medical care, lles malnly in f indlng valid and reliablecrlteria. Few slandards have been defined and thus reference polnts
wilh whlch perfofinance ln the system may be compared are few. Many ofthe criteria that do exist are subjective and assessments based on them
are usually slmilarly subjective.
lnvestlgators of medlcal care have used three main approaches
in studying qual ity. These have been described as
(a) Studies of Care Outcornes;
(b) Studles of the Structure of Care;
(c) Studles of the Process of Care. (Donabedian, 1969.)
(a) OUTCOMES 0F CARE
Assessments of the outcomes of care involve evaluation of the
end results of the care process. Quality ls determined by the extent fo
which fhe results accord wlth curren'l- social and professional expect-
ations. Crlteria used frequently in outcome assessments include case
fatality or disability rates, measures of recovery such as length ofabsenteeism, and patienf attitudes to and satisfaction wlth the care pro-
vided. Outcomes are diffícult to measure and usual ly fai I to provlde
insight into the specific strengths or wraaknesses of the system. They
represent broad measures of perf'ormance and are dependent on the
156
assumption that good results are consequenl on good care. ln Ìheory,
outcome measures provide lhe best measure of quality because they assess
lhe ultimate effectiveness of the process under review. Nevertheless,
the diff iculties wilh def inition limil lheir usefulness and aPplicabil-ity as qual ity measures.
This appl los particularly to fhe assessment of the outcome of
emerqencv care, since emergency care forms the inifial part of a continu-
ous medical care process which lncl udes definifive treatment and rehabi l-llation. The outcomes of care are înfluenced by treatment in all fhe
separate phases and it is extremely difficult to distinguish the parflc-ular significance of any one of these phases for the ultimate result.Thus, for example, the recovery of the severely fnjured patÎent may be
influenced by the rapiclity with which he receives emergency care and the
competence of those who provide it. Bul it is also affected by lhe
compelence of the doclors who provide deflnitlve care, the nurslng care
and many other factors.
Two outcome measures were used in thls study and both were
based on pafientst assessments of the care they had received. As an
outcome measure of recovery frcm crash injury, patlents who responded
lo questionnai re sunvey were asked to make an assessment of the length
of the time between the occurrence of fhe crash and their return fofheir normal activities. The distribution of lhe responses is shown in
Table 8/1. (See p.157.)
The median time for crash vlctims to resumo normal activítleswas approximalely a fortnight with 20% of patienfs laking three months
or more.
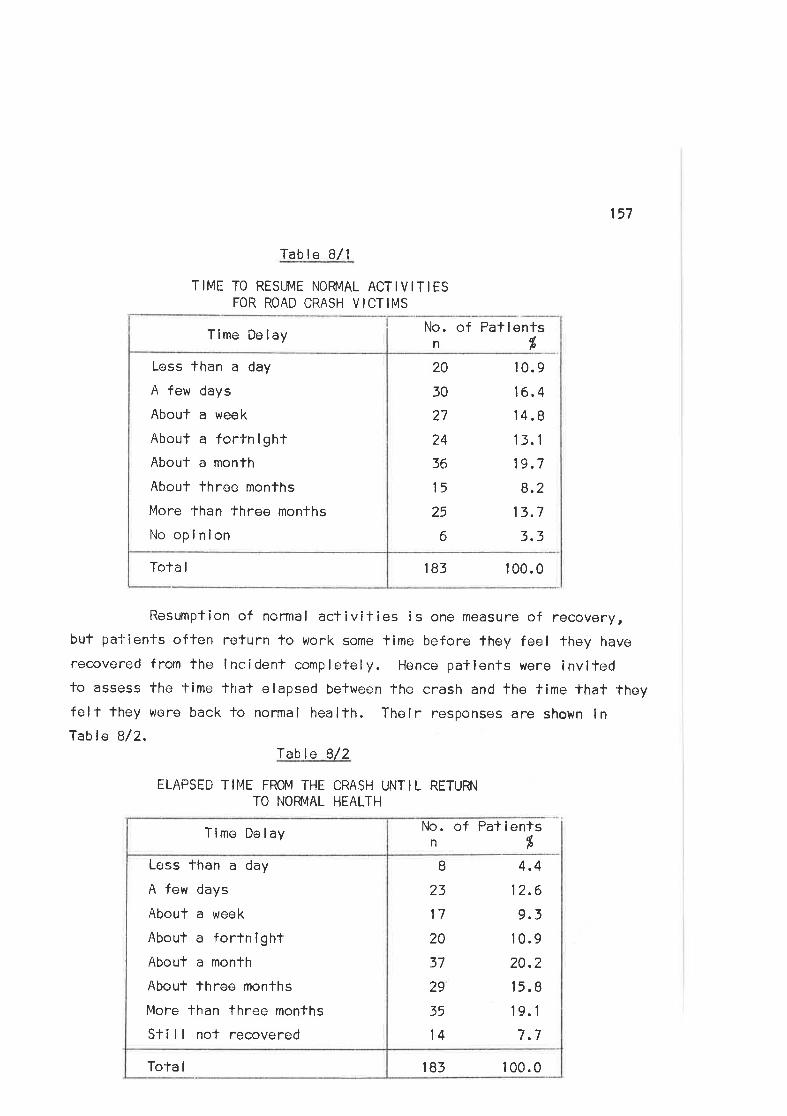
157
Tab le B/1
T IME TO REStJfl4E NOFMAL ACT I V IT IESFOR ROAD CRASH VICTIMS
No. of Patlentsnfi
183 1 00,0Tola I
Less than a day
A few days
About a week
About a forfníghtAbout a monfh
About Ihree months
More than three months
No opi nion
Tlme Delay
20
30
27
24
36
15
25
6
I23
17
20
37
29
35
14
10.9
16.4,l4.
B
13. 1
19,7
8.2
13.7
3.3
4.4
12.6
9.310.9
20.2
15.8
19.1
7.7
Resumption of normal activities is one measure of recovery,but pa'i'ienfs often return to work some time before they feel they have
recovered from the lncident completely. Hence patients were invitedfo assess the lime that elapsed belween the crash and the fime that theyfelr they were back to normal health. Their responses are shown lnTable Bl2.
Table B/2
ELAPSED TII"1E FROM THE CRASH UNTIL RETURN
TO NOFMAL HEALTH
183 1 00.0ïota I
Less lhan a day
A few days
About a week
About a fortnightAbouf a month
About three months
More than three months
S+¡ll not recovered
Time Delay No. of Patientsn%
158
The median tîme before patients felf back to normal health was
approximately a month. That morbidity from crash injury ls considerable
is demonstrated by the fact lhaf The distribution is skewed fowards fhe
longer llme intervals" No dat¿: are avai lable with which theso assess-
ments can be compared, and thus the ef'fect of the care provided on thislreatment oulcome cannot be evaluated.
Evaluatlons using outcome measures are cornpl icated by such
variables as lhe characlerlstics of the populafion, the types of injurysuffered, the d¡fficulty in defining the exact measure used, and lhe
lack of comparable criteria as reference points. These facfors al I need
to be considered in making assessmenls and it is oflen d¡fflculf torelate tho outcome fo a specific causo. Thus assessments using less
ultimate criteria must be useC. Such criteria are used in studies of
the slrucfure and process of care.
(b) THË STRUCTURE OF CARE
Assessmenls of the structure of care involve evaluatÎon of the
facilifies used for providing care and examination of such areas as the
administration and organizalion of fhe services, equipment and faci I itiesused, staff qualif ications and availabillty, and the f inancing of the
serv i ces.
Qual ily assessments based on these crileria have the advant-
ages of deal ing wifh objective data. The underlying premises in the
evaluation are that -1. Betler qual ity care is more I ikely to be provided when
, qualif ied staf f , good physical facllities and sound
organizafional sfructures are avai lable.
?-. EnouEh is known to idenfify whaf is good with respect
to these items.
3. A relationship exists between these sfructural elements
159
and The qual ity of care.
Given good structural qual ifies, good care wi I I result.
ln chapter 3 it was shown that the sfrucfure of ambulance
services in Melbourne in lerms of organization, equipmenf, personnol
and staff fraining compared favourably with similar services elsewhero
in Auslralia and wilh the published standards for services in several
overseas countries. The lack of a system of emergency ambulances
staffed uri-t'h rnedical or para-medical personnel, such as ls employed in
several European countries, was noted, although the particular value of
these services in lhe Austral ian setting, partícularly for road crash
victims, has yet to be defined.
Slmí larly, the sfructure of hospital casualty departmenls was
oull ined. Ëxisling departments in Melbourne aro equipped to cater for
all lypes of emergencies although facîlif ies, in ferms of equipmenf and
manpower, are strained by the demancJs placed on lhe system by patients
seeking primary medical care.
ln evaluating struclural aspects of the emergency caro syslem,
'the medical staff ing of hospifal casualty departments warrants particular
comment. Most hospital casualty deparfments ln Melbourne are staffed by
doctors in their firsl year after graduation. These doctors are resPon-
sible for thr: initial aesessment and managoment of injured patients.
Since it is generally acknowledged that the early freatment of injuriesmay be of importance for the outcome of care, it is paradoxical that
emergency care is provided by the most ínexperienced medical personnel.
The casualty departmenl of oach of fhe sfudy hospltals was
manned throughout tho 24 hour's of the day by junior resident medical
officers. ln the casualty departmenl of lhe Alfred Hospital, four of
these doctors were orì duty each weekday morníñ9, With either 2, 3 or 4
docïors at other times and on vleekends between the hc'urs of 0830 hours
4
160
and 2300 hours. One residenl medical officer was on dufy at night tocover the emergency cases presenling between 2300 hours and 0830 hours
the following morning. An additional doctor vras rostered unti I midnight
on Friday and 0300 hours on Sunday morning to help cope with the addition-al workloads which occurred on lhose nights, due largely to the admission
of road crash victims.
Duties are allocaled to each of lhe residents according to hìs
working shift. _The duties required of lhe resident working lhe so-calledrfirst cnf shift included the lmmediate assessment and management ofemergency cases as they arrived in the department. The doctor working
this shift was on duty from 0830 hours until 2300 hours - a 14.5 hour
shift. ln a busy casualty departmenl this involved consfant work under
pressure. The medical officers accepted the long hours which they
worked as a necessary, if undesirable part of lheir training and exper-
ience. Few other professionals work for such long periods under such
constant stress. lt is doubtful whether fhese work patterns are conducive
to maximum efficiency and there can be little doubt that the fatíguewhich most doctors experience affects both their judgement and perform-
ance. The minimum weekly working períod for a casualty resldent medical
officer al the lime of the sfudy was 62.5 hours.
ln these hospitals, immediate supervision of residenl medical
of f icers was provided by 'lhe hospital admitting of f icers, who were
usual ly doctors in their second year afler graduation. Three of these
doctors were rosfered for duTy ín the casualty department of the AlfredHospital during the day. Al night one of them was responslble forhospifal admissions and overseeing the casualty department.
Responsib¡ l ity for the overal l supervision of the deparfment
lay with the medical superintendent or his deputy. ln addition most
hospîfals employed qualified surgeons on a part or full-tlme basis toconduct casually cl înics, supervise in-service trai ning and deparfmental
161
oPeralions, and provide consultanÌ services for the casualty staff. lnlhe Alf red lìospital two cersualty surgeons were employed on a half -'limebasis to provide these supenvisory arrd consultant services. One of them
was rostered for duty in the deparfment each day and on Friday and
salurday evenings. Further t.'ack-up medical support was provided by lhein-patiçnl staff. þledical and surgical registrars were frequently con-su I ted by lhe casuô I ty staff.
lf is thus apparenf that a large number of medical practition-ers witlr varying levels of lraining and experience were pofentiallyavai lable to assist casualty staff. ln praclice these back-up staffwere offen not avaílable for immediate ccnsultation. This situationusual ly arose cluring late nighl' hours when consulting and supervisingstaff were nof presenf in the department and junior sfaff were fhusso le ly respons ib le for the prov ís ion of emergency care. i'vlany road
crash vicl ims we-.re adm itted during these hours, particu larly on Frídayand Safurday nights, and experienced Treatment delays and deficienciesas a nesu I t of the staff i ng def i ci enci es.
Ther.: is a need for f ul l-time supe rvision of casualty depart-ments by trained and experienced medical practitioners. The special istfor this position shculd Lrc cxperiencecJ in resuscitation ancl the manage-
menf of f rauma ancj, above all, be înteresled in fhe organization and
adminîslration of lhe department. Experienccd personnel should be
avai lable in the casualty deparlment on ô round-the-clock basis provid-ing assistance and advice for resident medical officers. Several
hospitals in Melbourne have advertised for ful l -Ìime casualty super-visors in an attompt to remedy some of the deficiencies in casual'lystaffing and orqanization. ln general, it has proved Cifficult to finddoctors 'to f i I I these positions. The compromise arrangement wtrich isadopte<l in many hospítals, of employing two half-f ime pe; rsons, usuallyjunior surgeons, to perform this funcfion is unsatisfacfory. Such
personnel are rarely interesfed in the organizational and supervisory
162
functions which are of prime imporlance for mainlaining and promotlng
thc-, ef f i ci ency of casua I ty operat ions.
The recommendaf ions on caslralty staf f ing prepared by theNew Soulh Wales State Commîttee of the Royal Australasian Col lege of
Surgeons and publ ished by lhe Col lege (Royal Australasian Col lege ofSurgeons, 1970) stafe thal rjunior residents should nof be unsupervised
in a Casualty Departmentr. ln practice, în the hospilals studied, lheywere unsupervised during mosl of fhe night hours on all days of the woek.
Di,l'icienci,¡s in the structural aspects of care are inevitablein any systemn especially when normative Etandards are used as a basls
for evalualion. The particular significance of the structural deficien-cies for fhe operation of fhe system cannot be evaluatcd unless theprocیs_ of ca re i s cons i dered.
(c) THÊ CARE PFOCESS
Assessmenls of the process of care consider the performance ofdoctors and olher professionals in managing pafienls wifhln the system.
The criteria used are the currently accepted standards of praclice as
formulated by leaders of the professions. Qual íty is determined by the
degree to which observed performance matches 'these accepted standards.
lmplicît in the assessments is the assumptîon that particular aspects ofcare are known to be specifically relatod to successful heallh outcomes.
Sludies o'f process have usually involved detailed assessment of theperformance of professionals by direct observation or by record revlew.
The judgements c.rf qualily are based on such faclors as the complefeness
of lhe cl inical history and examinafion, the technical competence dis-played in lhe performance of therapy., the choice of diagnosfic aids and
fhe compleleness of the medical record.
ln considering the process of emergency care additlonal facfors
163
must be laken inlo consideration. The use of the term emengeney lodescribe lhe care syslem has two importanÌ implications for lts function.First, lhe system should have the capabílily to handle serious illness orinjury. Secondly, the def inif ion implies fhat timo or, more partlcularly,time delays are imporTant variables to be considered ln assessíng fhe
systemrs operation.
(1 ) Time Delays in the Emerqency Care System
(a) The Siqnif icance of Time Delays
The assertion that Time delays are important in emergency medical
care neecls litlle substantiation for clinicians who have observed lheeffects of irreversible shock on the sevenely injurod patient. ln extreme
situations, lhe importance of delays in treafment is obvious. The patientwhose airway is occluded will die in minules if that airway is not cleared,The patient bleeding from a severed major arlery will exsanguinate unless
measures are taken promptly to slop the bleeding and resuscitate him.
ln such cases lime delays are critical and the neod for treaTment :
i mmed i ate.
Furfher evidence of this is provided by the experience in war
zones, discussed in Chapter 2 of lhis thesis, where lhe use of an
efficienï emergency care systern has resulted in an improvement in case
falalify rates associated wîlh reduclion of fhe delays ín instltutingtreatment. (1"4ítchell, 1968. ) lrr civilian practlce, coronary care unitshave been infroduced irr hospilals as a means of providing immediate,
skilled treafment for patients in the acule phase of illness, with con-
sequent improvements in mortal îfy rates. Fol lowing on from this,coronary care ambulances have been introduced as a means of gettingsimilar care to patients before they reach hospital. Undoubfedly, the
rapid provislon of skilled care can be lifç.-saving in certaln situaf lons.
The signif icance of time delays for the deve lopment of morbld-
ity is, however, more difficuli to define. The majorily of emergency
164
care is proviclc.tJ for patients with less than critical degrees of injury,wherc thc urgency is less and the effects of treatment are less obvious.
ln these cases, sÌandards for accepfable dolays in instituti'ng therapy
have never bcen sef and the evalualion of tlre importance of a given time
delay is thus d¡fficult. The rela'tionship h.retween time delay and deter-
ioration in clinical condilion îs complex and unprediclable and thls is
one of the main reasons thaf standards for fime delays in lhe provision
of emergency care have nevcr been c1efined beyond the general, somewhat
nebulous, princîple that the best possible care should be provided in
lhe shorlest possible time.
The feeling anrong many sections of the community lhat high
qualily care is not being provídecl witirin a minimum possible time has
lecJ to the suggestion of several allernafives to the established methods
of provi d i ng emergency care. For examp I e, he I i copters have been
suggeslod as allernafives lo road ambulances and emergency care ambul-
ances aro considereci by many lay and professlonal people to be desirable
¡: I tt¡rnali ves or add ít ions lo ex i st i ng ambu lance serv i ces. A case may be
made for the availability of both facililies, since both off-er advant-
ages over normal services in particular situafions. Bofh, however,
represenf .rxpensive additions to the emergency services and their use
and cost-ef fectiveness must therefore bc-. caref ul ly evaluated in fhe lightof the performance of the existing system in the area under sfudy.
(b) The Observed Time Delavs
ln examining the significance of time delays În the emergency
care syslem, one is obliged to examîne the delays in the separate care
phases. By this means lhe ex.lenl to which the rshortest possiblel
criterion is being met can be determined and the areas which need
modification to improve the operation of lhe system identified.
The response times observe<J in lhis study suggesT that delays
in lhe separate phases of the ambulance call are short. Although ¡t
165
ìilas nol possible to determíne notif ication delays for the study crashes,
it seems fronr interviews conducted aJ--ihe crash scene lhat bystanders
notify urban crashes promptly. l'he median time for an ambulance toarrive at the scene of a road crash after lhe notifying call was
received was observed lo be l2ninutes wíth an average response-iime of10.8 minutcs. (Table 7/6, p.1?7.) The modian treatment and transportlime for fhese calls was 17 minutes, as is shown by the time distríb-ution in Table 7/7 þ.127), Furthermore, the ambulance service time
distrîbution (Table 7/8, p.128) indicates that ambulance vicf ims reach
hospital from crashes in the ¿rea sludied in a mean time of 30 minutes
(wîth a median of 25 ninutes).
After arrivirrg in hospil'al patients wait to see the medical
off icer. The average time u¡aited for this service by road crash victimswas 26 minules; just four minules less than the average lotal elapsed
time during ambulance service. Standards for lhis delay have nof been
prescribed for thc study hospiTals, but since this consultation wifh the
medical officcr ís lhe important event in casualty care, ¡t is apparent
that the service provided does not meet the standard implied in the
administrafive inslruclion (Alfred Hospital, 1969) whích stafes thafpatienls should receiv,,: rprompt examination, appropriate special invest-iga-lions and diagnosis of their conditionr.
The mean total lime spe.,nt in the deparTment by the observed
crash victíms was 190 minutes. (Table 7/8, p.128.) Although crash
victims represenf a small proportion of tlre tofal casualty load, they
form a much larger-proportion of the enrergency patienls freated ln the
departmenf. Thus ¡t is of somo concern thal treatmenl tímes are so
long for this patienl group, and, once aga ín, if is reasonable toconclude that the s-i'atr:d objectivc of tprompt f reatmcnf.....andspeedy dc;spalch to the required clestinalion? (Alfred Hospital, 1969)
is not being met.
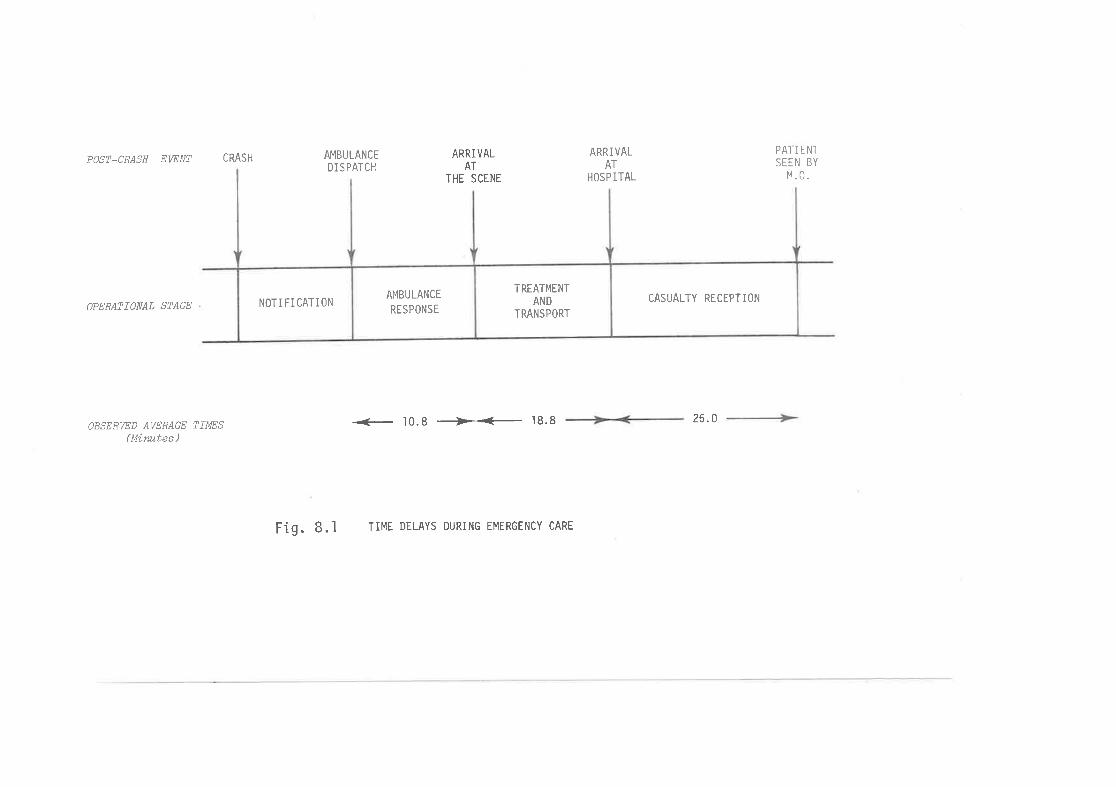
POST-CRASH EWNT CRASH
OPERATIONAL STAGE
OBSERWD AWRAGE TIMES(Mírwtes )
AMBULANCEDI S PATCH
ARRIVALAT
THE SCENE
ARRIVALAT
HOSP ITAL
PAI I ENT
SEEN BY
M.0.
+ 10.8 *+ .t8.8 26.0
Fig. 8.1 TIME DELAYS DURING EMERGENcY cARE
NOTIFICATIONAMBULANCE
RESPONSE
TREAÏMENTAND
TRANSPORT
CASUALTY RECEPTION
166
The r elationship bet,*een 'lhe important ambulance and casualty
deparlment treatmenT delays is shown in Fî9. 8.1. The lenglh of the
delays for patients waiting to sr¡e the doc'lor suggests thal- many of the
time saving advanlages-tc' be gairred by improved amtrulance transporlsystems may be lost because of the delays involved in casualty freat-mont. (The mean waiting fime for severely injured patients in thiscare phase was seventeen minutes. )
ln summary, the observed time distributiorrs suggest thatcJelays in ambulance service in the area studied are usually small.
Delays in casualty treatment are, howe;\,er, almosl invarlably long ancJ
apply to all phases of tile care. Thu:;, in terms of time-saving in the
emergency care system, 'there i:; more room for improvement i n casua lfydepartment organ i zaliorr and c;pcra:f ions than i n lhe ambu I ance serv ice.
(c) Waitinq Times in Hosoital Casually Departments'fhe waii.ing and lreafmenl lime distribulîons observed in the
study werre derived f rom obse;rvations made in three metropolitan hospitals.Ninety-five per ccnt of the palients observed werr¡ trt'aled in fhe AlfredHospital ancl the observerd waifing antl trcatmenl limes are thus largely
characterisfic of a single hospilr:l and its pattern of operations.
Therefore, it is desirable fhe-l waiting and lreatmenl fimes in other
hospilals should be compared with lhose observed to delermine how lhe
observed pattern correlaters lvith waiting limes in otlrer hospitals.
Tho research committee of 1'he Viclorian Seclion of the Ausfral-ian lnstilule of Hospital Adminislrators reported the resulfs of a
survey irr which the walting and treatmonÌ times in eleven VictorianPublic Hospital casualty depi:r-lments were reviewcd. (Brand et al., 1971
(1), (2), (3).) The sarn¡lle of hospitals íncluded fcur teaching hospitals
but did not include lher Alf rrld llospilal. Dala were collecled on alltypes of casualty attenders incl udi ng, pnesumably, road crash victíms.
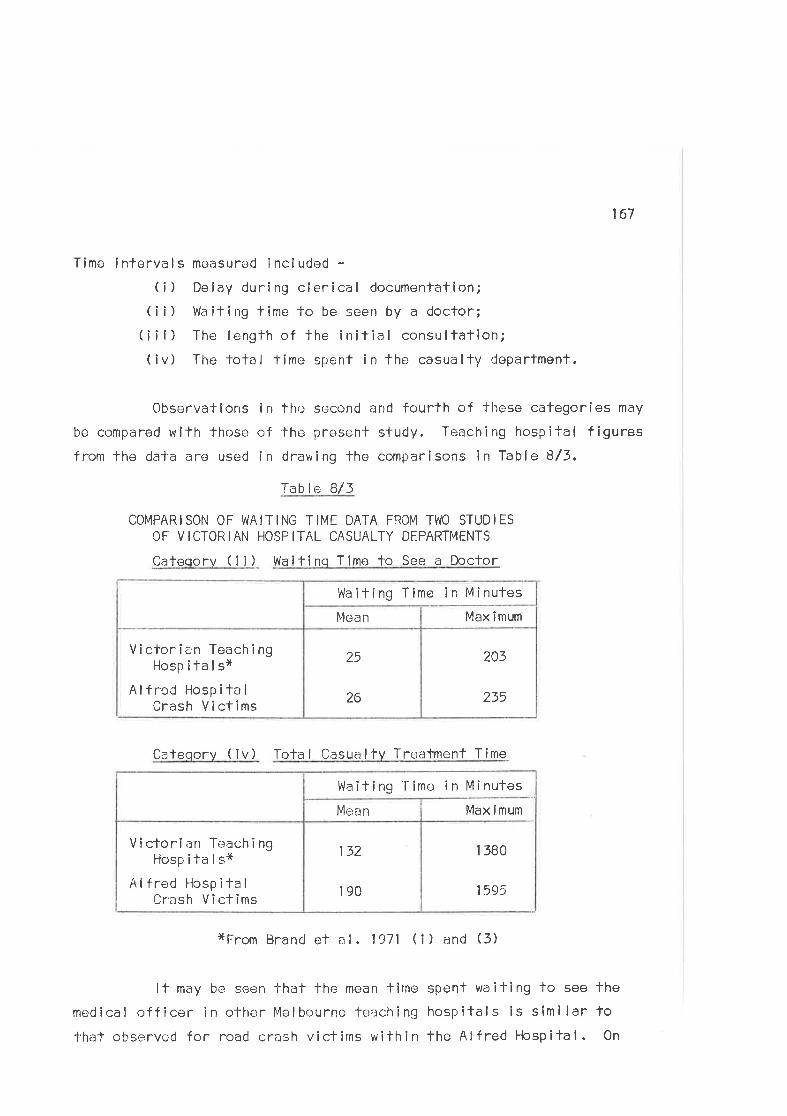
167
Time i nterve I s mcasured i ncl uded -(¡) Delay during clerical documentation;
( i i ) Wa it i ng t ime to be seen by a docfor;(¡il) The lengthofthe initial consultation;(iv) The lotal time spent in the casualty deparfmenl.
Observations ln thr¡ second and fourth of these categories may
be compared with those of the F.¡reseñt study. Teaching hospilal figuresf rom the daJ'a are used in drawing fhe comparísons in Table 8/3,
Table 8/3
COMPARISON OF WAITING TIME DATA FROM T\,vO STUDIESOF VICTOFTIAN HOSPITAL CASUALTY DEPARTMENTS
Cateqorv ( ¡i) Waif inq Time to See a Doctor
ttrlaiting Time ln Minutes
Cafeqory ( iv) Tola I Casua ltv Tre¿¡tment T ime
1 380
1 595
132
190
V ictorian Te;ach ingHosp ita I sx
Al fred Hosp ita I
Crash Victims
Max ímumMeran
Waiting'Iime in Minufes
xFrom Brand et a L 1971 ('l ) and (3)
It may be seen that the mean lime spent waiting to see the
medical of f icer in other Melbourne teraching hospitals is similar fo'l'hat observed for road crash viclims within the Alf red Hospital. 0n
203
235
25
26
Victorian TeachingHospifalsx
Alfrod HospilalCrash Vi ctims
Max îmumMean
168
the averacteo crash victinrs spent longor receiving their casualty treat-monf in the Alfr,:d Hospital 'lh¿¡n thei ovcrall leaching hospltal average.
'[oach i ng irosp ita I pat i errts wcjre categor i zed ¿:ccord i ng to whetherthcy wore urgcnt/non*urgent and s-lrctcher or ambulant. The figures used
in J'ile aL;ove comparisons are based on the over¡.¡ll average assossments
whcre these weri) recorrJod. it is worth noting that'lhe mean casualfytreatment li¡ne in the teachíng hospi-lals studled for the urgenf,/stretchergroup (whir:h would re¡rresent rrìore ne¿-ìt ly the populaiion of road crashvictims) was 227 minutes wilh a maximum waiting timc-: of 1380 minutes.
(d) The Effects of Alfr-:rnatívo Patlerns of Ambulance Serviceon Time Delays
llel icopfe;rs have bc.en suggested as alternaf ive ambulance trans-port vehicles as a resulJ'of fl¡eir usc in war zones. particularly inVietnam. ln the existîng systcm in thc. area under stuciy ít is extremelydoublf u I l'ihcthc:r ambu I ance rcsponse t imes cou I d be improved by the use ofhelicoptor services vrere lhese lo be boTh feasible anrj permitted in thebuilt-up melropolitan area. h/ith response times as shorl as thoseobserved, the time advantages of air lransport would be lergely nega'led
by the relativoly lonq turn-around times whîch accompany civilian heli-copter operations. Hc:l icopters Érreì, hcwevcr, admirab ly suited to ambul-ance service in those situations where travel times make a larger con-trîbution 1'o the ove rall ambulance service lirnc. [ffectively, in thel4elbourne eroð, this means ¡ì range of approximafely 20 fo 100 miles f rcm
the cily centre.
Hel icopters have been uscd in operations on the MorningtonPeninsula in Victoria for fransporting emcrgency patients'fo the majormetropolitan hospitals. Their oLìèratíons have been limi'ied and thussorvice routines are relatively unsophîstic¿rtcd. ln particular thecommunications subsystem and procedures fr¡r palienl pick-up and
transfer neecj development. -l-his is demonstrafed by recent observations
169
of patient reception procedurcs at lhe Alfred Hospifal. The hel icopterlands in a park immedialely opposite the hospilal, and it has been
ol¡serveci thal the average time to unload a pationt and lransfer hlrn tolhe casua lly clepartment is between 4 ar¡d 5 m inu-t'es. (Th is representsan improvemenf on the 6 to 7 minule delays which were noled at the time
the service commenced. ) The normal f lyíng time f rorn Frankston isapproximately 11 minutes and compares favouratlly with the road trip time
of 45 mînutes. The aircrafl is an ef f icient means of 'l-ransporf over
lhese dislancers but its efficiency is tempered by the communications and
de livery faci lilies at each enc1 of the f líghl. Moreover, the delays'that patients may experience wilhin hospilal must also t¡e considered.
A second a I fernat î ve -lo ex i sti ng patterns of ambu I ance servi ce
is the use; of emcrgency ambulânccs. Such a service has recently been
commenced as a combíncd project of the Royal l4elbourne Hospital and theV.C.A.S. with the supporl of the llospitals and Charities Commission ofVictoria. Figures based on en evaluation of the first lhree monthst
operat ion of tlre ve h ic le have no-|, as yet, been re leased " The ambu lance
is based at the Royal Mclbourne Hospifal and is staffed by a medical
registrar from the hospital and a senior ambulance offícer who has
recelved speclal tralning in intensive care.
T!'rc ambulance may bc called out by doctors in the case of such
emergencies as cardiac arresl, asphyxia and drowning, whe;n the equipr¡s¡ffor inlensive resuscitation which the vehicle carries is invaluable. lnother situations, including road crashes, fhe vehicle can be called outby ambulance officers or such persons as police or doctors at the scene.
0verall conlrol of lhe servicc lios with the senior ambulance control leron duly. Such a screening mechanism has been lhoughl necessary because
in the case of road crashes, for example, a relatively small proporlion(approximately 10/') of Ìhose injured recoive severe injuries. Further-more, only a small proportion of those severely in.jured are likely torequire inlensive care at the scene, Therefore, it is necessary to have
170
d f iltering ntechanism to ensure lhe eff icient use of tho service.
ln rc¡aci crash si'tuations, fhe current call out policy means
that lhe pcirsc'n summoning the ambulance ís likely to be the ,Ambulance
Officer already in altendance. The ambulance response times observed in
this sludy suggest lhat, in an ideal system, thore may br: more advantage
in terms of time savîng during extra-hospífal care, in rapidly loading
anC lransporf ing -lhe patienl to an ef f icie nt hosp ital casualty department.
Using lhe avcrage elapsed times observed, it can be seen that thc response
timo for the f îrst ambulance is approximately B minutes. To this must be
added a proporl'ion of th+: treatment and assessment time (say 2 minutes)
in which the i:mbulance off icer determines the nature and severity of the
injuries an'C makes radio conlact fo cal I out fhe emargency ambu lance.
The total elapsed time for Ìhe nclification call for the emergency
ambulance is thus in excess of 1O minutes. The emergency ambulance willtake as long tc.'l-ravel lo the scenü as the ambulance al the scene would
take on the relurn trip. The time saving advanfages of the omergency
vehicle during exf ra-hospifal care are thus marginal. This situationrepresenls lhe pessimislic extreme¡ of emergency ambulance operations
and in practice the vehicler should usual ly bc dispatched wilh some tlme
advantage,
lrr the existing systcm, however, the emergency ambulance
hes ber¡n observed lo make signif icant contribu't'ions nol only to lhe care
the ¡Lalients receive, but also J-o-t'he speed with which fhey receive it.Because a senior member of the hospital medical staff is employod on the
ambulance, the hospital is made aware of a scriously ill patienlfsimminent arrival and preparations are madc for his rercepfion. 0n arrívalat the casually department, the pafient is admitted directly to the
appropriate trealmenf service and thus avoids lhe delays which normal ly
accompôny côsua lty trea-tmen-|. Patients are resuscitated earl ier and
reach the in-palient services ln l¡etter cl inical condltion than isnormal ly observed affer casualty admission. Many of the advantages of
171
this emergency ambulance service are thus derived from the effects thalit has on 'the service and p atienf care wifhin hospital.
ln fhose medical si1-uations, for example, hoart cases, drownings
and industrial accidents, where erarly notificalion and rapid response ofthe vehicle providos definilive medical care al the scene for palientswhcse clinical condition is serious, an emcrgency ambulance is of valueand its adoptlon anc1 use is thus warranted. Af the scene of road crashes,
however, lhe value of fhe service should norrnally be limíted to those
cases where seriously injured victims are trapped in vehicles and requireextricalion, cr wherLì several severely injured patienfs make friage and
resuscitation dif f iculf for a síngle ambulance crew.
Q) The Qua I ify of Emerqoncy þled ica I Care
The second important variable lo be considered in examining
the process of emerqency care is thc quallfy of the care provlded. lnpraclice, this rcquires examination and assessment of 'l-he actual servicesrenCered fo those who entr¡r the syslem. The measuremenf is based on the
assumpfion thaf at any time there is a s;cienfific conscnsus among experlson what conslilutes good or high qual ity emergency care" This consensus
should idoal ly be basi.:C on a br:dy of emplrical data and may thus be
relatecJ to actual practice within tho system under study. The extent towhich performance wilhin the sysfom matches standards els defined isregarded as a me¿rsure of the quality of fhe care provided.
Standards
ln practice" standards and criteria have rarely boen definedfor fhc elements of the medical care process and thus reliable and validcriferia which can be used Tr: interpret valid and useful measures ofqual ity are few. Nevertheless, normative standards for the management
of roed crash injury urere def inecl by the Royal Australasian College ofSurgeons (1970) in a book published as a result of a semînar aÌtended by
Ìhe leading surgeons of the country in 1969. ln recording the consensus
172
of surgical opinion exÞressed at the seminar, the book examines in con-sicjerable detail all aspects of the managemenf ol. crash injury and may
thus be accepted as represenfing the normative standards for pracfice inAuslra I i a.
Sfandar,Cs for ambu lance service used in th is sf udy inc I ude theAmbu I ance Handbook of the V i ctor ian l-iosp ila I s and Char if ies Comm i ss ion(1970) and fhe Manual of Ambulance Transport lJursing published by theSl. John Ambulance Brigaclr-r in South Australia (1963). Both of thesepubl ications describe treatmenl methods and ambulance service practiceswhich may be regarded as standards fo be followed in the performance ofambu I ance serv i ce.
Final ly, the standards for patienl management in the casualtydeparlmen'l of the Alfred Hospital are described in fhc hospitalts hand-
bookrlnstructions to Casualty Residentsr issued to all residenls at thetime they commence work in fhe department. (Alfred Hospital, 1969.)
The sfandards described in the relevant sections of these sourcedocumenls are used in evaluatÍng the qualify of lhe emergency care pro-vided for road crash victims in fhis study.
Thc Melhod of EvaluationEven in the presenco of acceptable slandards against which
qualily can be measured, the peirformance in a given situa'lion is diff lcultto assess objecf irre ly, s ince treafment is s ituation dependenl. The pro-cedures and methods employed necd lo be considered in lhe lighf of pre-vailing circumsfances at the time of trealrnent. Even more importanf thanlhe actual procedure performed is the decisíon pafh followed by theprofesslonals in the process of. providlng lroalment. Since individualclinical sítuations are variable and conrplex, it is often diff icult losÌate that a precise form of care should be performed in a given clinicalsituatic,n. For example, the procedure of sp I ínf ing a f racture in a
173
casualty departmenl may be of secondary imporlance in lhe case of a
soverely injured patient who nceds immediate resuscitafion and emorgency
surgery. Moreover, the doc i s ion ma ki ng procoss i n emergency s ituaT íons
is to a large exlont time depcndent, r:nd the time scale within which
trealmenl is performed mus'f be consiclered in assessing fhe appropriate-ness ¡:nd quality of lhaf performance.
The followlng discìussion of the qualî'ty of the care provided
for crash victims is divided into Two secfîons. l-he first section relatesfo the observations made during Phase One of fhe study, when crash
victims were observed at the sceno of lhe crash ancl during casualtycare. The procedures performod during tneatment were enumerafed
previously and, in lhis chapler, the quality of tho performance isassesseri in ther light of fhe d<;f ined standards for ambulance and casualfyca re.
ln the second section a more delailed analysis of fhe qualityof casualty care focusses on specif ic aspec-l-s of fhe cars process as
it was observed for the victims in Phase Two of the study. The qualifyof thc casualty history and physical examination performed, the adequacy
of the performance c'f certain procedures and lhe overall assessment ofthe qualily of care are examined. Finally, tho results of the postal
qucslionnaire, in which patîents recorded their opinions of the care they
received, are; ¿ìnelysed as an outcome measure of the qualit.v of care
provided for these patients.
ln making The qual ity assessments, fhe observers rated lheperformance of care by comparing the observed perfonrrance with the
defined standards. The categories and cri'leria used in makíng fhe
comparisons are I isted in Appendix 3. lnevitably, subjectîve assess-
ments ancl judgements were involved, but fhe effects of these influenceswere conlrolled as much as possible by inlerprefing each element of care
according fo the specific criteria. These críleria were defined before
the sccorrd phase of fhc sludy uias undertaken,
174
The Qual ity of the Emerqency Care Provided for the Victims
of I 00 Road Crashes i n Me I bourne
ln Phase One of the study, fhe quality of the care provided foreach patient was determined by the two observers at the end of the patlentrsambulance and casualty care. Assessments of quality were based on a consen-
sus of opinion befween the two observers based on their observations of fhecare performed for the víclims.
The assessments were subjective and the care for each patlentwas rated as either satisfacfory or unsatisfaclory. Both observers were
medical pracfitioners who were au fait with the prevalling standards forthe management of road crash and trauma victlms, and who had had prevlous
experience of working both in and with ambulance services and hospifalcasualty departments. The detai led criteria descrlbed for the second
phase were not used in this phase.
ln the majority of cases, procedures were performed salisfactori lyduring ambulance care and the ambulance officers showed satisfactoryjudgement in determining treatment prlorities. One hundred and forty-seven patients were lreated by the ambulance officers, of whom lwo (1.4/")
were judged to lrave received unsatísfacfory care. A further elght patients
from four crashes díd not receive examinafion and treatment when such were
indícatcd. Ambulance offîcers drove up to the scene of two of those
crashes and, wîthout al ighting from the vehicle, enquired whether anyone
was injured. 0n receiving a rcply in the negative, they drove off. One
of the victims involved in these crashes had clínícal slgns of rib frac-tures and a second patient had suffered minor lacerations. The injuriesof all eight of these patîents were relatively minor, and the absence
of examination and treatment would not have affected their subsequenl
management sîgnificantly. The overal I incidence of cases of unsafisfactoryambulance freatment was thus I in 16 rc.4%).
The two cases of unsatisfactory care involved inappropriate
175
care of victíms with severe injuries. The case, mentioned in Chapter 7,
of the unconscious man who was left lying on his t¡ack at the roadside in
the care of bystanders was one example. The second was fhe followingca 5e.
CASE 31010 A 20 year old female car passengcr sustained a
compound f racture of her left wris'|., minor abras ions, lacerations and
concussion in an intersection col I ision. She was found at the scene,
sitting in the passengerrs seat of the vehicle. She had fo be liftedfrom the vehicle lo be placed on fhe ambulance stretcher. The ambulance
officers considered spl inling the fracture before removing her from fhe
car - a procedune which could have been simply performed. ln theirhasle to removo lhe woman, they omitted 1-o splint the fracfure and she
suffereC considerable pain from the fraclure sile during exfrica'lion.An air splint was c-¡ventually applied when she had been placed on the
s-lretcher. Thc trichlorethylene inhaler was offere;d fo her, after she
had been removed from the vehicle,, but its operation was not explained
sal isfactori ly and iJ' was thus îrr{-rf fective.
The "iudgemenf
of unsatisfacfory côre was based on the series
of errors involvcd in this u¡o¡n¿rnrs carre. lt was noleworthy that, whÎlsfmi nor def i ci enci es i n the performance of procedures occurred occas iona I I y,
multiple errors were rare and rarely were the palients exposed to the
risk of exacerbarting or compounding injuries as a result of these
erro 15.
A summary of the obsrèrversr assessmenls of lhe quality of care
provided for each patienf by ambulance officers aÌ lhe scene is shown
în Table B/4 (see p.176),
Approximate-;ly 6Í, of patients received unsatisfactory care atthe scene ¿rnd it may be seen from the Table that-the differences between
the two groups by cJegree of injury are not stalistically signif icant.
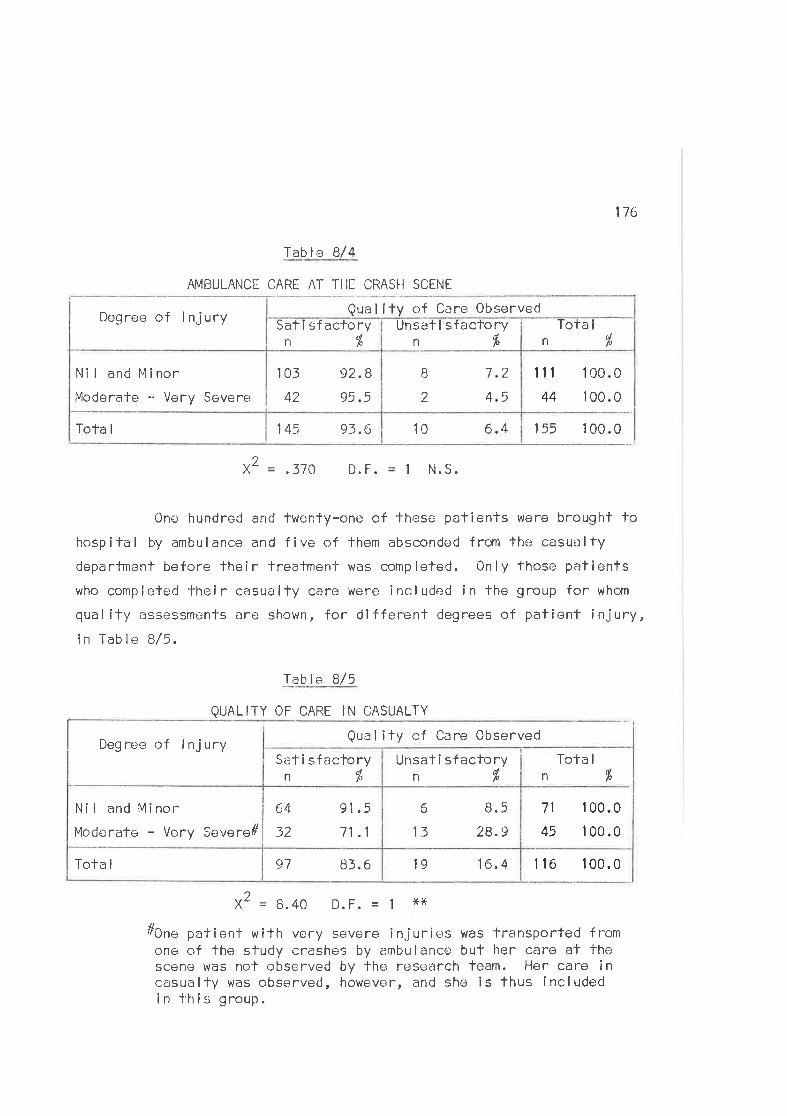
176
Table B/4
AMBULANCE CARE AT THI CRASI.I SCENE
Quall of Care Observed
x2 .37C D. F. 1 N.S.
One hundred and twenty-one of those palienls were brought tohospital by ambuiance and five of Them absconded from fhe casualty
departmenl before lheir freatmenl was completed. 0nly those patienlswho completed their casl¡alty care were included in the group for whom
qual ify assessments are shown, for dlfferent degrees of pafienf injury,ín Table B/5.
Tab le B/5
QUALITY OF CARE IN CASUALTY
Degree of lnjury Qual ity of Care Observed
x2 B. 40 D. F. 1 xt(
#One patienf with very severe injuries was transported fromone of the sludy crashes by ambulance but her care al thescene was nof observed by fhe research feam. Her care incasualty was observerJ, however, and she is thus includedin lhis group.
155 1 00.010 6.4145 93.6Tota I
1r1
44
I 00
00
0
01
I2
7
4
2
5
103
42
92
95
B
5
Nî I and Minor
Moderate .. Very Severer
Tota I
n oípUnsafi sfactory
n%Sati sfactoryn%
Dogree of lnjury
1 'l 6 100.016.4198t.697Tota I
13
6 8.5
28.9
91 ,5
11.1
64
32
Ni I and Mí nor
Moderate - Very Sovere#
Sati sfacloryn%
1 00.0
1 00.0
Tofa I
%n
71
45
Unsafi sfacloryn%
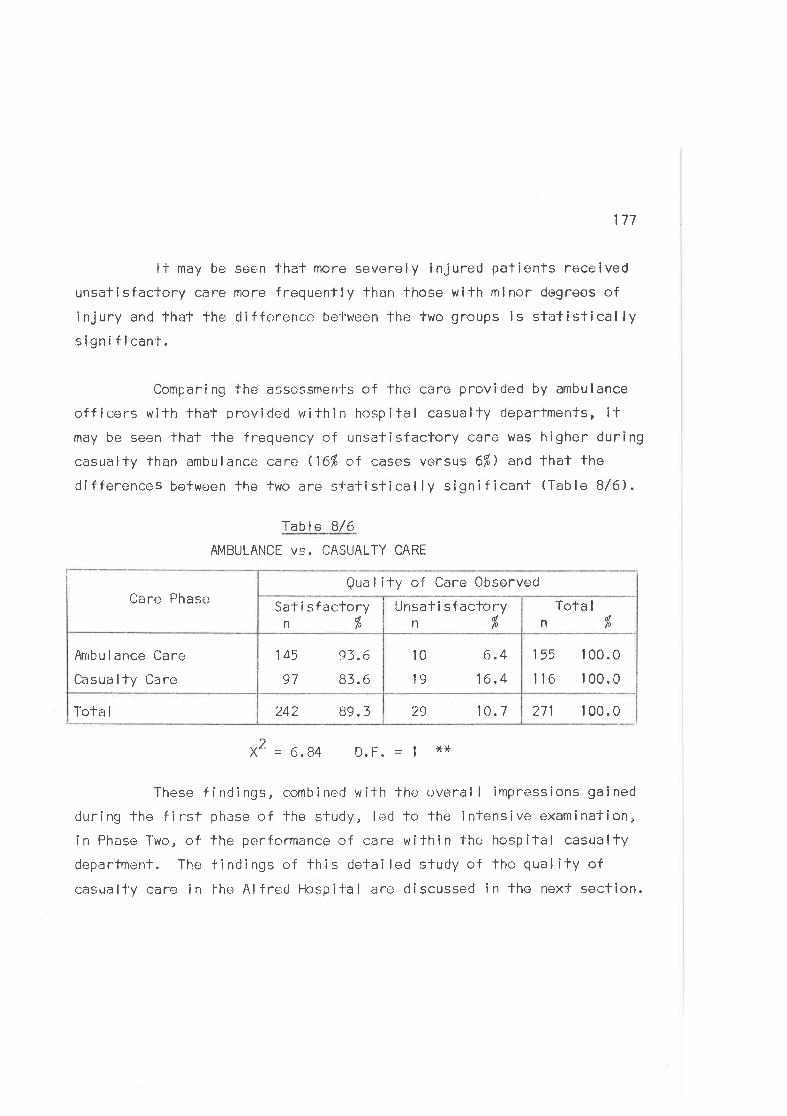
177
It may be seen thal more severely injured patients received
unsatisfactory care more frequently than those with mlnor degrees ofinjury and that the differencc be'l'ween thr; two groups is slatislicallysignif ican't.
Comparing the asses-smerrl-s of f he care provided by ambu lance
officers with that providod vrithin hospital casualty cJepartmenls, itmay be seen lhat lhe frequency of unsatisfactory care was higher during
casuôlTy than ambulance côre (16% of cases versus 611,) an¿ that the
di fferences befween fhe two are slalistical ly significanf (Tabl e B/6).
Tab I e 8/6
AMBULANCE Vs. CASUALTY CARE
271 1 00.029 10.1242 89.3Tofa I
155
116
I 00.0
1 00.0
10
19
6.416.4
145
97
93.(t
83.6
,tr¡bu lance Care
Casua I ly Care
Tota I
n ollo
Unsatisfactoryn%
Sal i sfactoryn/"
Care PhaseQua I i ty of Care Observed
2X = 6.84 D.F. - I **
These findings, combined with the overal I impressions gained
during fhe first phase of fhe study, led to the intensive examination,
in Phase Two, of the performance of care withínthe hospiTal casualty
departmenl. The findings of this detai led study of lhe qual ity ofcasualty care in the Alf red Hospil-al are discussed in the nexf section.
178
The Oual itv of Casualtv Care in Phase Two
The qualily of the care provided for crash viclims admitted tothe Alfred Hospîtal Casualty Departmenl during Phace Two of the study was
assessed by the author as sole observer.
Experience during the first phase had shcwn that crash victitnsreceive emergency care accorciing to a predictable pattern. Each medical
of f icer should elicit a medical history f rom the paf ient before perform-
ing a detai led physical examînation. Many patients require and receiveradi'ological investigation for suspecfed fractures and mosÌ are observed
in casualty for a variable period after lheir examination and inveslig-ation is completed. A proporfion of those severely injured are shocked
and require intravenous fherapy. Those with fracfures need to have theirfracfures spl inied and immobi I ized. Most crash victims who presenf tohospital have sustained bruises, abrasions or lacerations, which requiredressings or suturo. Many are observed in casualty before being dis-charged from the departmenf and either admitfed for in-palient care orreferred for out-patient fol low-up.
ln lhe fol lowing discussion of f he qua I íty of the care províded
for a sample of 328 crash vicflms presenting to the casualty deparlment
of the Alfred Hospital, the elements of the care provided wil I be examined
in the fol lowing categories:-1. Hisfory taking and lhe performance of the physical
exam i nat i on .
2. The casualty treatment performed.(a) lntensive resuscitation.(b) lntravenous fherapy.(c) Fracture management.
(d) Wound care.
3. The overal I assessment of casualty care.
4. Rel iabi I ily of the assessments.
5. Paf ients? attiTudes fo the care they received.
179
(1) THE HTSTORY AND PHYSTCAL ENAMTTIATION
(d The MedieaL Histona
ln mosf cases involving trauma, lhe hisfory of tho presenfing
cornplainl is clear cut and there is thus little need for detailed enquiry
into the patienf ?s previous medical and social history during casualty
frealment. Neverlheless, ft ¡s of some importance to know not only thatpatients have been involved in a road crash, but also fheir type ofinvolvement. Slnce patferns and mc¡chanisms of crash injury are well
documented, the types of injury lhaf differenl pafients are likely tohave sustained may be inferred Îf the crash lype is known. Hence know-
ledge of tho type of involvement can be of considerable assistance in
diagnosis.
It was observed that most crash victims were labelled with the
diagnosis M.C,A. (Motor Car Accidenf) vicfim on admission to lhe depart-
ment. This al l-embracing diagnostic misnomer was used to cover al I types
of victim wifh all degrees of injury ranging f rom minor to very severe.
It was commonly used as an admîssion dîagnosis, particularly by members
of the nursing staff, and the admifting nurse was often observed toreport tM.C.A. in cubiclerto the sister-in-charge after writing M.C.A.
in the casualty admission regisler'. Additional details on the patientts
type of injuries may or may nof be noted and reported at this lime. The
use of this term occasionally masked the pnesence and detection ofpatlents with severe injuries who were awaiting medical attentlon. 0n
one occasion a 68 year old man, who had sustained head injuries, a
fraclure of his left upper arm and fractured ribs with a flall lhoracic
segment, waîted 12 minufes to be soen by a doctor as a rosult of These
factors. 0n a second occasion, a 42 year old pedeslrian who had sustained
a fracfure of his righl femoral shaft lay in a cubicle for 85 minutes
before he was assessed. His provisional diagnosis was I isted in the
casualty register as M.C.A.
The knowledge that a patient was involved in a crash usually
180
leads the examining medical officer to ask two direct quostions, which
frequently complete lhe medical history obtained.(ì) rWere you knocked out ?t or eDo you remember what happened
i n the crash ?r
These questions are deslgned to determine whether the
patient lost consciousness in the crash and the patientrs
response is of some importance, since it determines
whether he is observed in casualty for a minimum of four
hou rs .
(ii) ?frlhere does it hurt ?f designed lo determine the major
sites of lnjury for subsequent examinafion.
Although mosl doctors accepted involvemenf in a crash as
evidence of probable injury, they often failed lo elicil the important
informafion about the type of involvement which can be of considerable
assistance in diagnosis. Moreover, lhe poor communications which existed
between ambulance officers and casualfy staff members, and befween
casually staff members (see Chapler 7) was frequently observed to limifthe amount of informafion avallable to fhe doctor at the fime of his
inillal examination. Thls situation was further compounded by the fact
that ambulance officers rarely compleled the Ambulance Report Forms for
each palient.
The hislory-taking process was observed lor 255 patients. 0n
five occasîons (21Ð nedical officers obtained a complete and detai led
medical history from the patients, all of whom had minor or moderate
injuries. On nineteen occasions fi,4%), an incomplete hisfory was ob-
tained when more detailed informafion could and should have been gathered
from eilher fhe palîent or other sources. Seven of these patienls had
suffered severe or greater injuries and represented lgfi of the severely
injured patienfs for whom lhe history laken was observed. These
observations are summarized in Table B/7.
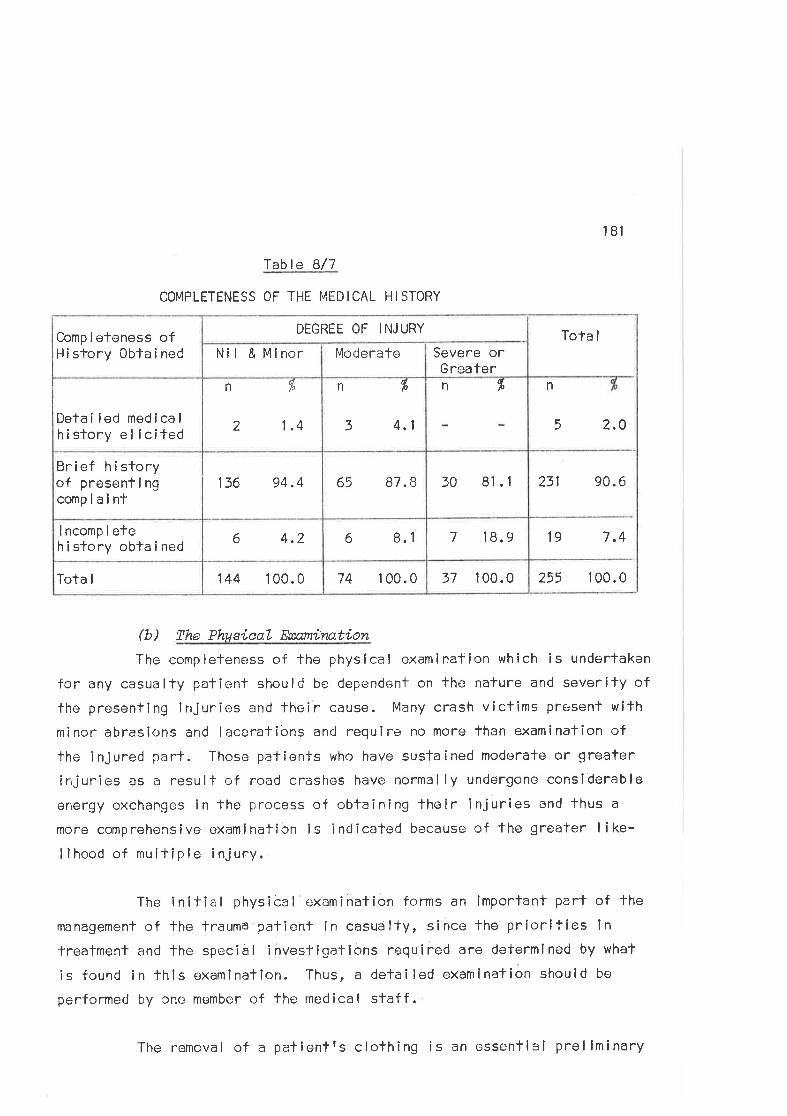
18'l
fable Bl7
COMPLETENESS OF THE I'4EDICAL HISTORY
231 90.6
19 7.4
255 100.037 100.074 1 00.0144 1 00.0Tota I
7 18.96 8.16 4.2I ncomp I etehi story obta i ned
30 81.165 87. B136 94.4Brief hi sforyof presenti ngcomplaint
Tota I
n
5 2.O
n ftn f"
3 4.1
n 7"
2 1.4Detai led medicalhistory el lcited
Severe orGreater
ModerateNil & MlnorComp I eteness ofH i sfory 0bla i ned
DEGREE OF INJURY
ft) The PhusieaL Eæamíiwtion
The completeness of the physical examinalion which is undertaken
for any casualty patient should be dependent on the nature and severity of
the prosenting injuries and their cause. Many crash victims pF€:senf wifh
minor abrasions and lacerations and require no more than examination of
the lnjured part. Those patients who have sustained moderale or greater
injuries as a resulf of road crashes have normel ly undergone considerable
energy exchanges in the process of obtaining lheir lnjuries and lhus a
more comprehensive examlnation is indicatod because of the greater I ike-
lìhood of multîple injury.
The initial physical examihation forms an ímportant part of the
management of the lrauma patienf in casualty, since the priorifies in
treatmenl and the special investigations required are determined by what
is found in thls examlnation. Thus, a detai led examination should be
performed by one member of the medical staff.
The removal of a patientts clothing is an essenfial prel iminary
182
to the performance of a satisfactory physlcal examination. Ë¡ghfy-Two
per cent of the patienls observed were completely undressed before fhey
were examined by the doctor, 14/o were examined through clothing or were
parfly undressed with adequale exposure of the affecfed part. 0nly alof patienfs were examined fhrough clothing in a manner which made
adequate examination d¡ff¡cull. Vlith respect to fhis criterion, the
casualty examina'lion was rated as good.
Patients are usual ly undressed by members of fhe nursing staff,frequently by lrainee nurses. lt was observed that, whi lsf nurses are
careful in removing clothes, inexperience and a reluctance to cut clolhingoccasional ly resulf în considerable discomfort for lhe patienf. Moreover,
the manipulation involved may enhance fhe risk of exacerbaling injuries.One palient wíth a suspected cervical spinal injury was rolled over and
sat up while his jumper, shîrt and underclofhing were removed over his
head rather than cut off. Patients with I imb fractures wer@ occasional ly
subjected to pain from movemenf af tho fracture sife while clolhing was
removed intacl. The decision fo cut clothíng cannot be faken lightly in
view of the resulting cost and inconvenience to the patient, and repres-
enÌs another reason why a frained member of lhe nursing staff should be
present al the fime of the inítial nursing examination and procodures.
ln assessing lhe qual ily of the examinations performed for fhe
study patients, attention was paid fo lhe compleleness and appropriateness
of lhe examinalion in the prevai I ing circumsfances. Thus when a medical
officer examined a patienl thoroughly, paying particular attention to the
injured body regions and establishing a base line for the patienles
overall clinical condition, he rated a favourable score for that examin-
ation. lt was considered lhat all crash victims with moderate or greafer
degrees of injury warranted a physical examinafion whích included examin-
alion of fhe head and neck; testing of pupillary reactions; chest examin-
afion with ausculTation and checking for possible rib fracturss; abdominal
palpaf ion; assessment of the bony pelvîs and limbs; and cardiovascular
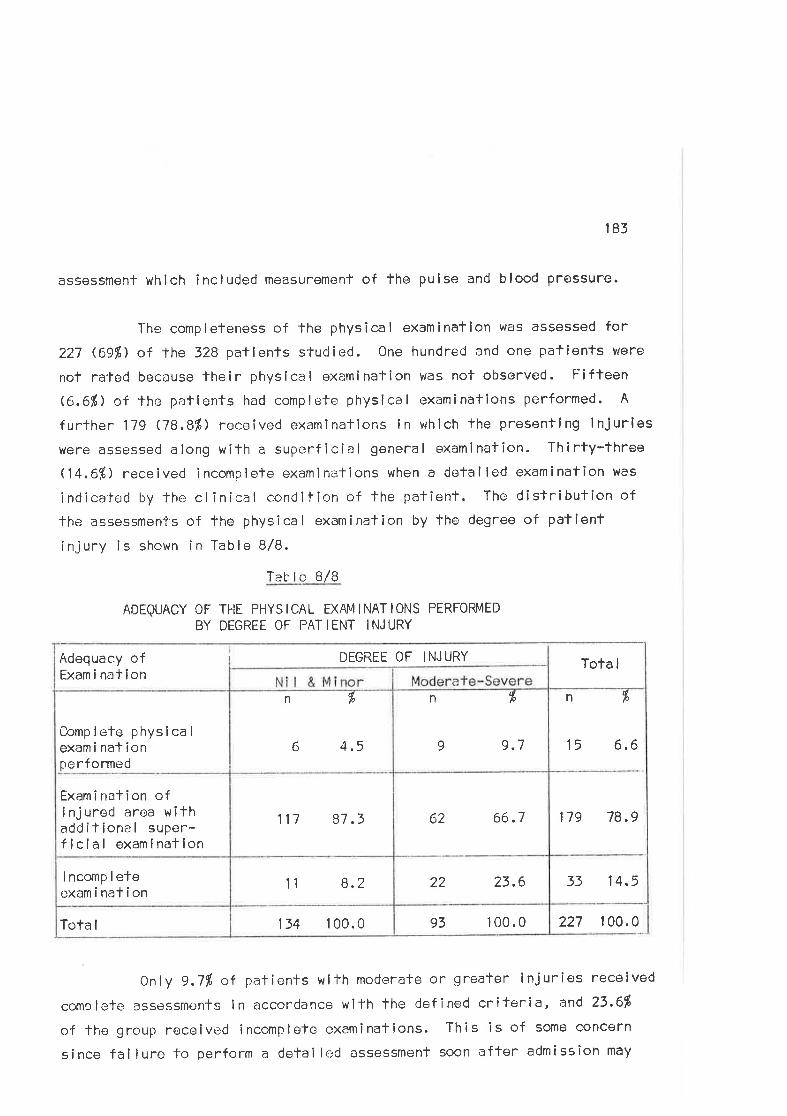
185
assessment which included measurêment of the pulse and blood Pressure.
The compleleness of the physical examination was assessed for
227 (69Ð of lhe 328 patlents studied. One hundred and one patients vlere
not rafed because lheir physical examination was nof observed. Ëifleen
rc.6%) of the pat ients had comp I ete phys i ca I exam i nal ions perf ormed. A
further 179 Jl.81) receíved examÌnations in which fhe presentíng lnjurieswere assessed along with a superficial general examinatic¡n. Thirty-three(14.6%) received incomplefe examinations when a detailod examination was
indicated by lhe clinical condilion of the paf ient. The dislribuf ion of
the assessmen-ls of the physical examination by the degreo of patlent
injury is shown in Table B/8.
Tab I e B/B
ADEQUACY 0F Tl-lE PHYSICAL EXAlvllNATloNS PERFoRMED
BY DEGREE OF PATIENT INJURY
0nly 9.7% o+ patients wilh moderate or greater injurios received
complefe assessmenfs in accordance wiTh the defined criteria, and 23.6fi
of lhe group received incomplefe examinations. This Îs of some concern
since failure to perform a detailed assessment soon after admission may
227 100.093 100.0134 1 00.0Tota I
33 14.522 23.6t1 8.2I ncomp I eteexaminafion
n r,
15 6,6
179 78.962 66.7
n %
6 4.5
117 87.3
Comp lele physica I
exami naf ionpe rformed
Exami nation ofinjured area wifhadditional super-ficial examinatlon
n fr
9 9.7
Tota IAdequacy ofExam i nal ion
DEGREE OF INJURY
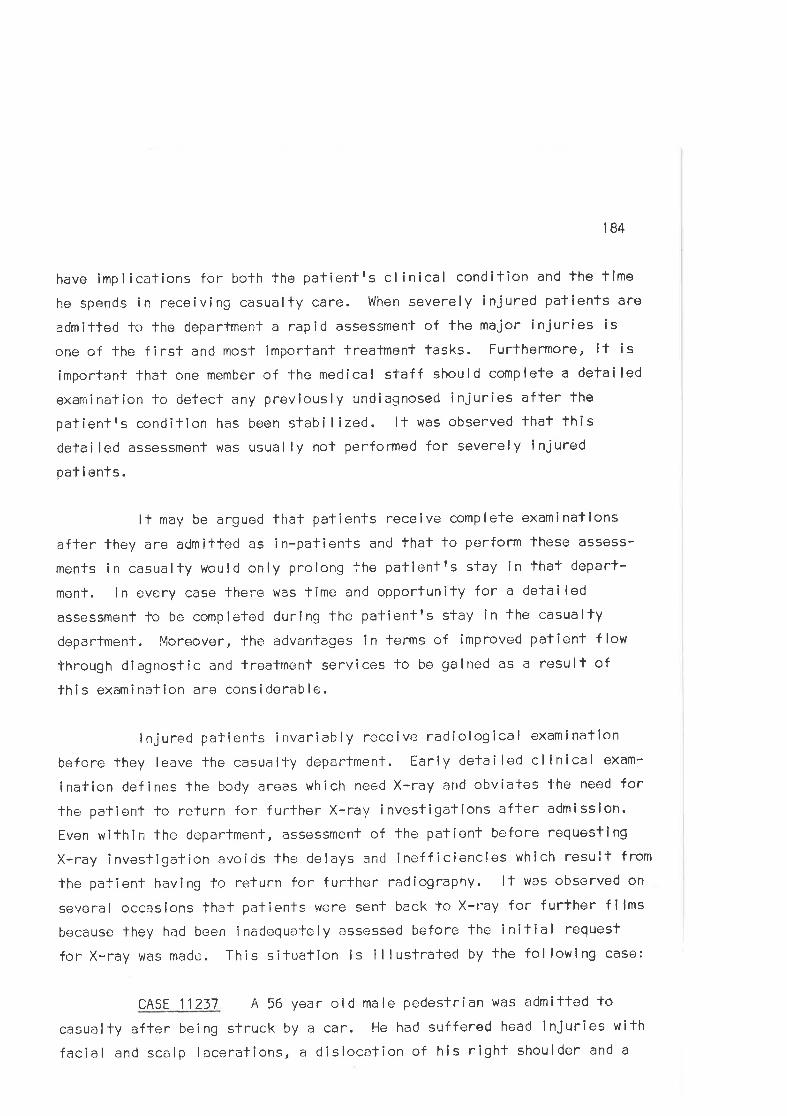
184
have implicalions for both the palientrs clínical condilion and the time
he spends in receiving casualty care. When severely lnjured palients are
admitted lo the deparlment a rapid assessment of lhe major injuries is
one of the f irst and rnosf imporfant trealment tasks. Furthermore, if is
imporïant that one member of the medical staff should complete a detailed
examinaTion fo detect any previously undiagnosed injuries after lhe
palientrs condition has been stabi lized. lt was observed thaf thisdeïai led assessment was usual ly not performed for severely ínjured
paÌ i ents.
It may be argued that pafienÌs receive complete examinations
after they are admitted as in-patients ancl fhat fo porform lhese assess-
ments in casualty would only prolong Ìhe patientfs slay in that depart-
ment. ln every case lhere was time and opportunity for a detailed
assessment lo be completod durlng the patientrs stay in the casualfy
dopartment. Moreover, the advantages in lerms of improved patient flow
through diagnostic and treatment services fo be gained as a result of
lhi s exami nation are considerable.
lnjured palients invariably receive radiological examination
before they leave the casualty department. Ëarly detai led cl ínical exam-
ination defines lhe body aroas which need X-ray and obviales 1-he need for
the patient to return for furfher X-ray investigafions after admissîon.
Even wilhin thr: department, assessment of the patient before requesting
X-ray invesligation avoids lhe delays and inefficiencles which result from
lhe patient having to return for further radiography. lt was observed on
several occasions that patienÌs were sent back to X-r-ay for f urther f ilms
because lhey had been inadequately assessed before the initial request
for X-ray was made . This situation is illustrated by the followlng case:
cASE 1 1 237 A 56 year old male pedestrian was admitted to
casualty after being struck by a car. He had suffered head injuries with
facial and scalp lacerations, a dislocafion of his righf shoulder and a
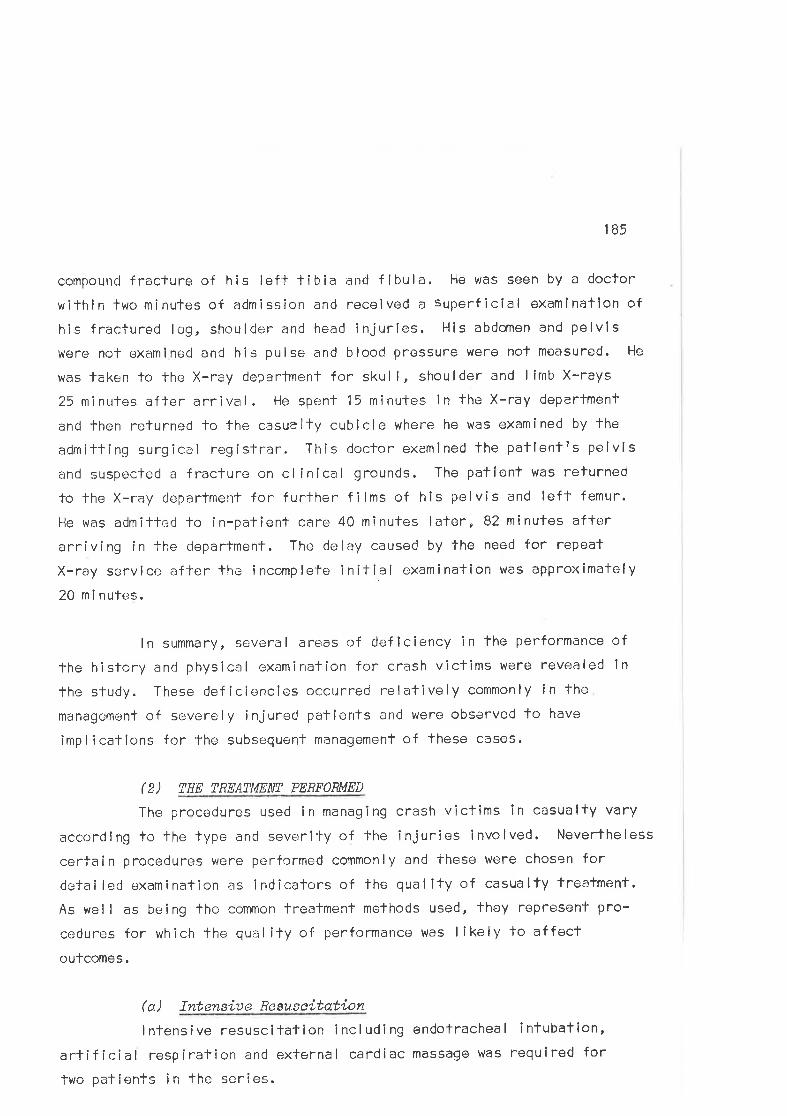
185
compouncJ fracture of his left tibia and f íbula. He was seen by a doctor
within lwo mînules of admission and received a superficial examination of
his fracturedl"g, shoulder and head injuríes. His abdomen and pelvis
were not examined and his pulse¡ and blood pressure were noT measured. He
was laken to the X-ray department for skull, shoulder and limb X-rays
25 minules after arrival. He spenl 15 minutes in the X-ray depertment
and then relurned lo the casualty cubicle where he was examined by the
admitting surgical registrar. This doctor examined the patlenlrs pelvis
and suspected a fracture on cl inical grounds. The palient was returned
to fhe X-ray dcpartment for further films of his pelvis and left femur.
He was admillod lo in-patient care 40 minutes later, 82 nínutes afferarriving in the department. The delay caused by the need for repeat
X-ray service afler lhe incomplete initial examination was aPProximafely
2O ni nutes.
ln summary, several areas of deficiency in the performance of
the history an<1 physical examination for crash vlcfims were revealed ln
the sludy. These def icie;ncies occurred relatively commonly in the
mänagement of severely injured patients and were observed to have
impl icatÌons for the subsequenl management of these cases.
(2) THE TRF:ATMENT PERFORMED
The procedures used in managing crash victíms in casualty vary
according to the lype and severi'ly of the injuries involved. Nevertheless
certain procedures vvere pcrfcrmed cornmonly and these were chosen fordetai led examínation as indicators of the qual ity of casualfy trealment.
As well as beíng lhe common treatment methods used, they represenf pro-
cedures for which 'the qualily of performance was likely to af fect
outcomes.
(Ð lntensiue Resu.seitation
lntensive resuscitation including endotracheal intubation,
artificial respiratîon and external cardiac massage was required for
two palients in thc series.
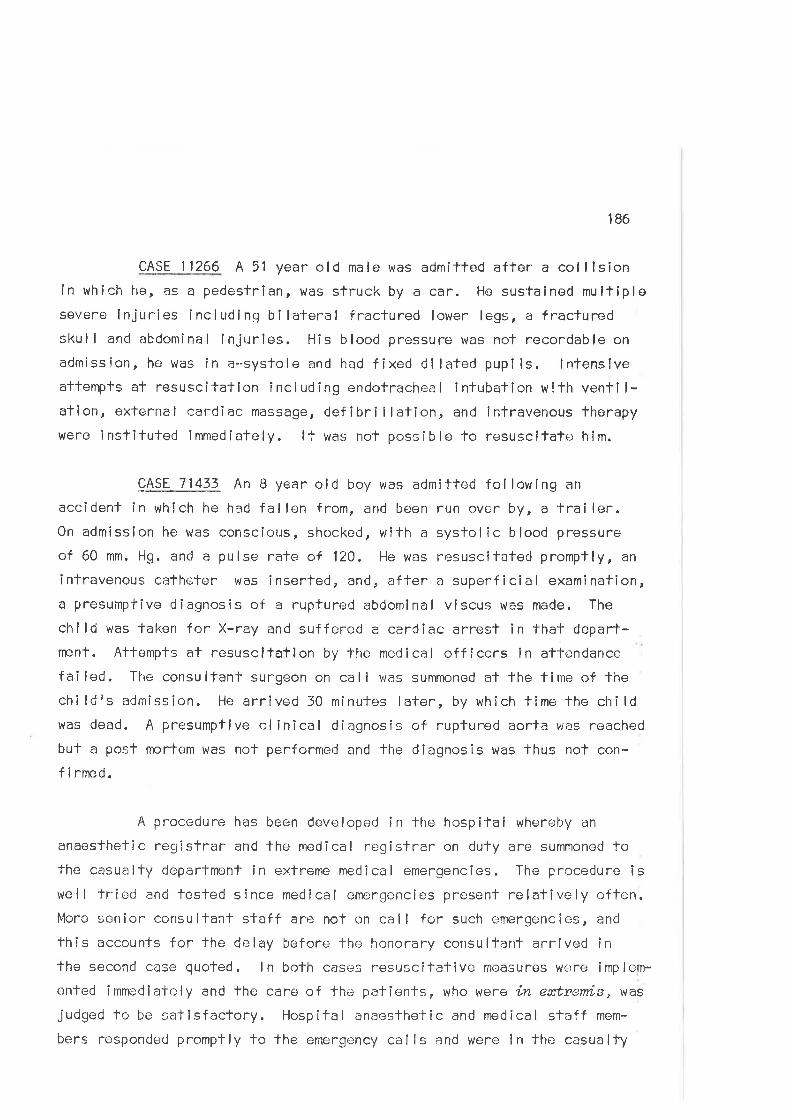
186
CASE 11266 A 51 year old male was admitted after a colllsíonin which he, as a pedesfrîan, vras struck by a car. He sus'tained multiplesevene lnjuries including bi laferal fraclured lower legs, a fracturedskull and abdominal injttrles. His blood pressure was not recordable on
admission, he was in a-systole and had l'ixed dilated pupi ls. lnfenslveattempts at resuscitaffon incl uding endofrachea I i ntubalion w!th venti l-ation, external cardiac massage, defibri I lalion, and intravenous therapywere inslituted fmmediately. lt was not possible fo resuscitatE: hîm.
çASE_Z|_133- An B year old boy was admitted following an
accident în which he had fallen from, and been run over by, a trailer.0n admission he was conscious, shockod, wlth a syslolic blood pressure
of 60 mm. Hg. and a pulse rate of 120. He was resuscitated promptly, an
infravenous catheter was inserfed, and, affer a superficial examination,a presumptîve diagnosis of a rupfured abdomlnal viscus was made. The
child uras laken for X-ray and suffered a carCiac arrest in that depart-npnt. Affempts at resuscltatlon by the medical offîcers in atlendancefailed. -Ihe consulfant surgeon on call v/as summoned al fhe time of thechildrs admission. lie arrived 30 minutes later, by which f ime the childwas dead. A presumptive clinical diagnosîs of ruptured aorta we-'s reached
buf a post mortem was not performed and the diagnosîs was thus not con-
f i rrned.
A procedure has been developed ín the hospifal whereby an
anaeslhetic registrar and the medical regisfrar on duty are summoned tothe casualfy department in extreme medical emergencies. The procedure îswel I lried and tested since medical emcrgencies presenf relatively oftcn.More senior consultant staff are not on call for such emergencies, and
this accounts for fhe delay before the honorary consulfant arrived inthe second case quoted. ln bofh casr:s resuscitative rneasures were imp le¡n-
enfed immediatcly and fhe care of fhe patienfs, who were in eætnenris, was
judged to be satisfacfory. Hospital anaesthetic and medical staff mem-
bers nesponded promptly to the emergency calls and were in thc casualty
187
department assisTing with care within four minules in both cases.
General observation of these, and olher, emergency patients
suggestecj thal when ernergency patients p resented and were recoqnized as
such, they received prompt care.
(b) fntnauenous T?terapu
An establ ished maxim in trauma managemenl slates fhat fsevere
trauma is lhe earl iesl sign of hypovolaemic shockf. (Newhouser, 1955. )
The replacement of circulating f luicl volume is the accepted treatment of
this condition and inlravenous therapy is the procedure of choice for
achieving 1'his goal. Several speakers at lhe symposium of the Royal
Auslralasian College of Surgeons in 1969 reiterated the prîmarr¡ import-
ance of lhe early commencemcnt of intraverrous therapy for maintaining
circulalory physiology in frauma palients. The L¡enef its of the procedure
have been demonstrated in war zones (Howard, \956; Hardaway, 1968), where
the effoctiveness of early intravenous therapy in resuscitation has been
proven. As a resull, many doclors now advocate lhat drips should be used
to resuscifate severely injured pafienfs at the scene of the crash, or
in the ambulance. (Royal Australasian Col lege of Surgeons, 1970. )
lntravenous therapy was instltuted in casualty for fourteen of
lhe palienls admilte;d during Fhase Two of the study. Forty-seven
palienls had sustained severe injuries and il was apparent thal medical
officers were conservativE: in their use of this procedure for injured
victims.
One of the reasons for this conservatism was staled to be lhe
danger of over-hydration of patients wilh head lnjuries. Head injuries
often accompany olher severe injuries in road crashes and thus thiscaution may be justi f iab le. Neverthe less lhe ri sks of over-hydration i n
the acute phase of the management of severe shock are sa i d lo have been
exaggerafed (Simpson, 1g7O) and potential mismanagement of pafients
1BB
(which over-hydration ropresenl's) îs an uns¿¡tisf actory reason for wif h-
holding a useful fherapeufic measure. The study observalions suggested
lhat a more likely reason for this conservatism was that resident medlcal
officers were simply nof aftuned to the llkelihood of severely injuredpatients Ceveloping hypovolaemic shock. lt was noted, in conlrast, thatthe cardiogenic shock v¡as a well recognized problem and pationts who had
suffered myocardial infarc'fions roufinely received intravenous trans-fusions in casualty.
ln most cases, medical officers did noi commence infravenous
tlrerapy until the patienÌs had developed overt clinical signs and symptoms
of shock. The following lvro sludy cases illustrate observed pracf ice.
CASE 1 1456 An 18 year old man was admitfed lo hospital
following a collision between his motor cycle and a car, in which he
suffered head injuries. Thesr: included e massive soft fissue avulsion
involving the left cheek, I ips and nose. His other injuries included
minor abrasions of tho lhorax, arms and legs. His blood pressure on
admission was 140/180 with a pulse rate of 120, Continual and coplous
blceding was observed from arteries in fhe <lepths of the facial wound.
He was seen within two minutr:s of arrival by the in-patienf surgical
registrar and a consultanf surgeon, who inspected the wound and sfated
that he required plastic surgery. The wound was subsequenfly re-dressed
by lhe nursing staff, but was rû-examined on 4 subsequenÌ occasions by
different membeirs of lhe mcdical and nursing staff. Fifty-níne minufes
after admission l're was laken for X-ray and, whílst being X-rayed, he
became clinicalty shocked. His blood pressure dropped to 90/50 mm. H9.
and his pulse ral'e was 1?-0 beafs/minute. Affer fhe attention of the
medical off icer was drawn 1-o his condÎtion a drip was inserted - 94
minutes after the patient had been admÎlted.
CASE 1 1 421 A 42 year old male pedesfrian sustained head
injuries with multiple minor facial lacerations and a fracture of the
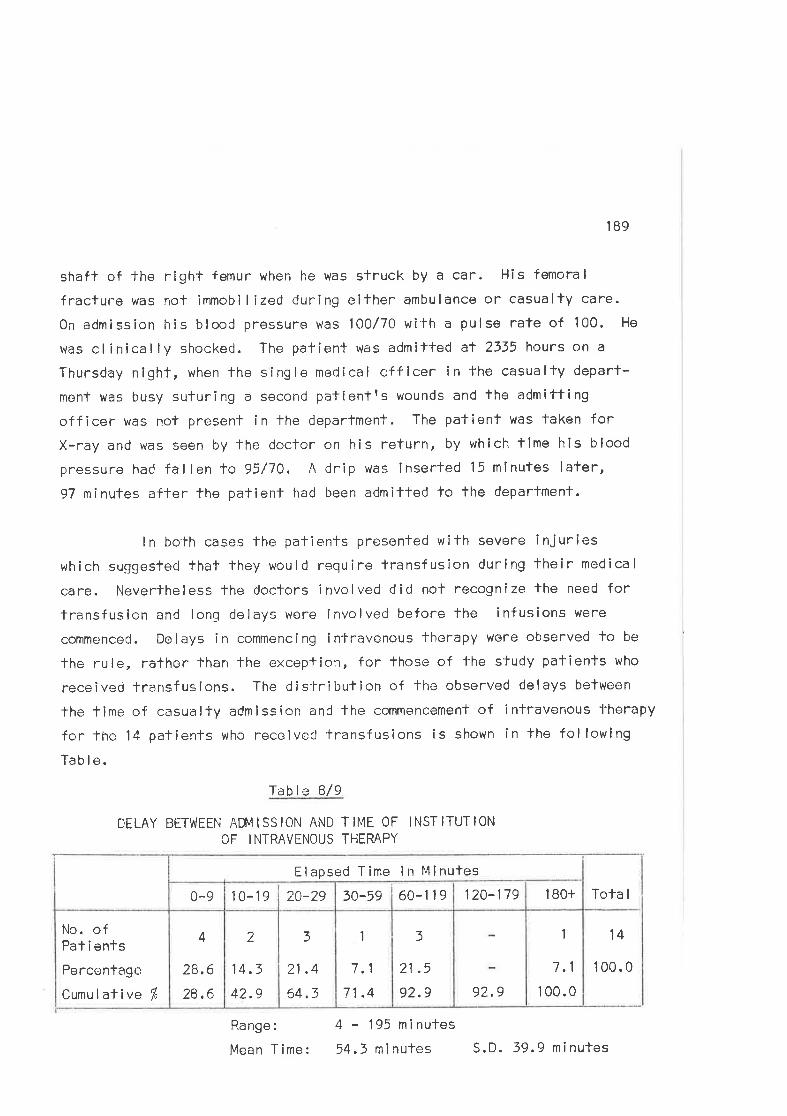
189
shaft of the right femur when he was struck by a car. His femoral
fracture was not immobi I ized during eifher ambulance or casualty care.
0n admission his blood pressure was 100/70 with a pulse rate of 100. He
was clinically shocked. The patient was admilted at 2335 hours on a
Thursday night, when lhe sîngle medical offlcer in the casually deparf-
menl was busy suluring a second palientrs wounds and fhe admítting
officer was nof present in the deparfment. The patienf was Ìaken forX-ray and was seen by the doctor on his return, by which time his blood
pressure had fallen to 95/70. A drip was inserted 15 minutes lafer,97 ninutes after the palient had been a<Jmitted to the department.
ln bolh cases the patients presented with sevene injurieswhich suggestecl thaT they would require transfusion during their medical
care. Neverlheless the doctors involved did nol recognize the need fortransfuslon and long delays were involved before the infusions were
commenced. Delays in commencing intravenous fherapy were observed to be
the rule, rafher than the exception, for those of 'f'he study patîenls who
received lransfusions. The dis-lribution of the observed delays belween
the time of casualty admission and fhe commencement of întravenous therapy
for lhe 14 patienls who receiveC transfusions is shown in the following
Tab I e.
Tab I e B/9
DELAY BETWEEN AM4ISSION AND TIME OF INSTITUTIONOF INTRAVENOUS THERAPY
Tota I
14
100.0
1
7.1
1 00.092.9
3
21 .5
92.9
1
7.1
71 .4
3
21 .4
64.3
2
14.3
42.9
4
28,6
28,6
No. ofPat i ents
Percentage
Cumu I aÌive f'
1 80+120-17960-1 1 930-5920-2910-190-9
Elapsed Time in Minules
Range:
Mean T ime:
4 - 195 mlnutes
54.3 n inutes S. D. 39.9 ni nules
190
These long delays and lhe practice of nol- instituting treatment
until the patÌents were clinically shocked are contrary to the currenflyrecommí-JnderJ slanCards for trauma managemenl, wh ich requ ire the ea:rly
commencement cf intr¿rvenous therapy. (Sando , 1970.)
Although the commencement of transfusîons al the scene of the
crash has bcen advocated by some doctors (ambulances carry lhe necessary
equipmenl fo permil doclors fo perform the procedures), none of the study
patients had received such lreatmenl at the scene. The observers consid-
erecl thaf lransfusion would not havo been necessary at the scene of any
of fhe study crashcs. Morcovcr, conditions for setfing up fransfusíons
at the roadside are far from îdeal. Hence, in the observerst opinion, ¡tis norrnally preferable, in the oxisting system, fhat patlents be taken foa def initive care facility for i-his procedure. ln me-tropolilan areas the
delays in resuscitating patients as a resull of lhis lransport should be
smal l, givcn efficiency in fhe casuelty departmenf. ln practíce they are
long because of dclays incurred v¡ithin fhaf deparlment.
phera I
was
Three palients had had infusions commenced in country or peri-hospitals before they arrived at the study hospital. One of these
cAsE 1 1444. A 60 year old male was fransferred from a country
hospital r¡fler initial resuscifalion in that hospital. A pedestrien, he
had been struck by a car and suffered a fractured sku I I , compound fracfure
of the le"ift femur and minor abrasTons. He had been resuscitaled by a
country geneìraI practitioner who had commenced an íntravenous infusion,
immobilized the femoral fracture wiTh a Thomas splinf, and confirmed his
clinical diagnoses radiologically. The general practitioner rang the
admifting officer of the study hospital to advise him that he was trans-ferring thc p;:fi'.rnt. The admítting off icer did not warn the casualty
slaff of his impending arrival and they wclre thus unprepared when the
pationt arrived at 2155 hours. His blood pressure on arrival was 95/60
191
and he was admitted to the acute emergency cubicle where he was seen by
a doclor within fwo minutes. This tjoclor did not measure fhe patientfsblood pressure in his initial clinical examination, buf he did nofice
that lhe drip'was into Ìhe tissues. ll was then removed and not replaced,
in spite of the fact fhaf lhe palient was still clinically shocked. The
Thomas splint þ/as removed from the fraclured leg and not replaced. A
head injury chart was commenced after 35 minutes and he was admltted toin-patient care, 55 minutes affer arrìving in the casualty department.
This case involved a serîes of deficiencfes in the management
of a severely injured palient. Similar siluations, wherein the combin-
ation of a superf icial clinical examinaf ion, unsatîsfactory trealment
and long time delays resulted in the patient receiving poor qualify care
in the casualty deparlment, wero observed on several occasions during
the study.
Allhough 14 of lhe 47 patienls received Transfusions, the pro-
cedure was indicated for several olher patienfs in vïew of their cllnÎcalcondîtion, bul it was no1- performed. For example,
CASE 1 1237. Tho 56 year old male pedestrian, whose case was
described in lhe prevlous section, sus'ta ined a compound f racf ure of his
left lower limb with a suspected f ractured pelvis. He was clinicallyshocked. The resident medical officer made lhree at1-empts to insert a
drlp into forearm veins before abandoning the procedure. The patlent was
in casualty for B0 minutes before he was admltted to in-patient care and
r¿/as clinically shocked lhroughout this period.
The qualiÌy of the performance of lntravenous therapy for the
14 persons who received the procodure was assessed by lhe observer. The
înfusion was inserted properly with good techníque in 6 cases. ln a
further 6 cases the infusion was sel up with satisfactory technique aftera considerable delay. ln the remaining two cases, long delays and
192
non-recognîtlon of the need for the procedure were coupled wlth poor
technique in ils perfofinance.
ln summary, fhe performance of infravenous fherapy in the
emergency care syslem diverged considerably from the practices expecfed
on the t¡asis of the normativo standards. Considerable delays lninstituting the procedure were common. l{oreover, if was used conservaf-
ively wilh mosf patients not receiving inf usíons untl I they were
cllnically shocked. This praclice is at variance with currentlyrecommended standards.
(e) The Itlanaqernent of Línb Eractures
Thirty-seven patients admitted during lhe second phase of the
sludy had sustained a total of 52 limb fraclures. Thirty-one of these
patienls had had their fractures immobí I ized by ambulance officers bofore
they arrived in the casualty department. Air splinfs were used for 21 offhese patients. As wos menfíoned in an earl îer chapter, ambulance offíc-ors used air splints to immobilize long bone fractures whenevor possîble
and, allhough Thomas splints were available for immobilizlng femoral
shaft fractures, they were rarely used.
It was common Þractice for these ambulance spl ints to be
rcmoved in lhe casually department and replaced by a padded wooden splintor, as oflen happened, not replaced at all. The alr splint was retained
in use Ìhroughout casually care in four cases. Eleven patients had lhe
air splint removed and replaced by a padded wooden splint. Six patients,
whose fractures had been splinted by the ambulance officers, had the
spl ints removed in casualfy and not replaced. Two pafienfs, whose
femoral fractures had been immobi I ìzed wifh modifTed Thomas spl ínts by
country doctors, had the splints removed and not replaced in lhe casualty
department.
Aîr spl ints are a salisfactory and effective method of
193
ímmobilizíng fractures (Gartrell, 1965) and there ís no good reason why
they should be removed and not reapplied in casual-iy departments, partic-ularly since changeover splints were avaílable fo replace The amblulance
spl int. Moreover, thc wooden spl ints which were commonly used fo replace
the air splinfs usually failed lo immobilize the f raclure. (Fig. 8.2,)Sand bags, which were used to support fractures on two occasions, were
equally inef fective. (Fig. B.l. ) lmmobilizat íon of f ractures ls a long
standing and accepfed principle in fhe treatmenl of trauma. Since most
patients spenl a considerable fime waílîng for admission and treatment in
casualty departmenls lhere can be no good reason why this comparatively
simple procedure was not used roulinely in the casualty departments of
teach i ng hosp i ta I s.
Failure fo spl int fracÌures was observed t<¡ resull in consider-
able discomforl for palíents. Pafients suffered pain from movemenls at-lhe fracture site, particularly when members of lhe nursing and medical
staff were observedtomanÌpulate unsplinted limbs in the course of per-
forming other procedures. Moreover, thcre is a risk of exacerbating softtissue in.jury when f ractures are ncf immobilized. The following case f rom
lhe series illustrates a clinical situatíon in which several of these
factors were involved.
CASE 1 1485 A 62 year old oedestrian sustained concussion,
minor abrasions of his lefl'arm and a comminuted fracture of his righttibia and fibula when he was struck by a car. His leg was splinted by
the ambulance officers at fhe scene and he was gîven trichlorelhylenefor pain during ambulance transporl'. 'Ihe splint v¿as removed after he
arrived ín casually. He was seen by a doclor wilhin 10 minutes of
arriving in the deparlment and was subsequently taken for X-nay. 0n
relurning from X-ray 15 minutes lafer, a member of the nursing slafflifted his fraclured leg by lhe foot bccause it was profruding from the
blankets al lhe foot of fhe barouche. Since there were no empty bods
in the hospilal on The nighl, it was decided lo manage the patient from
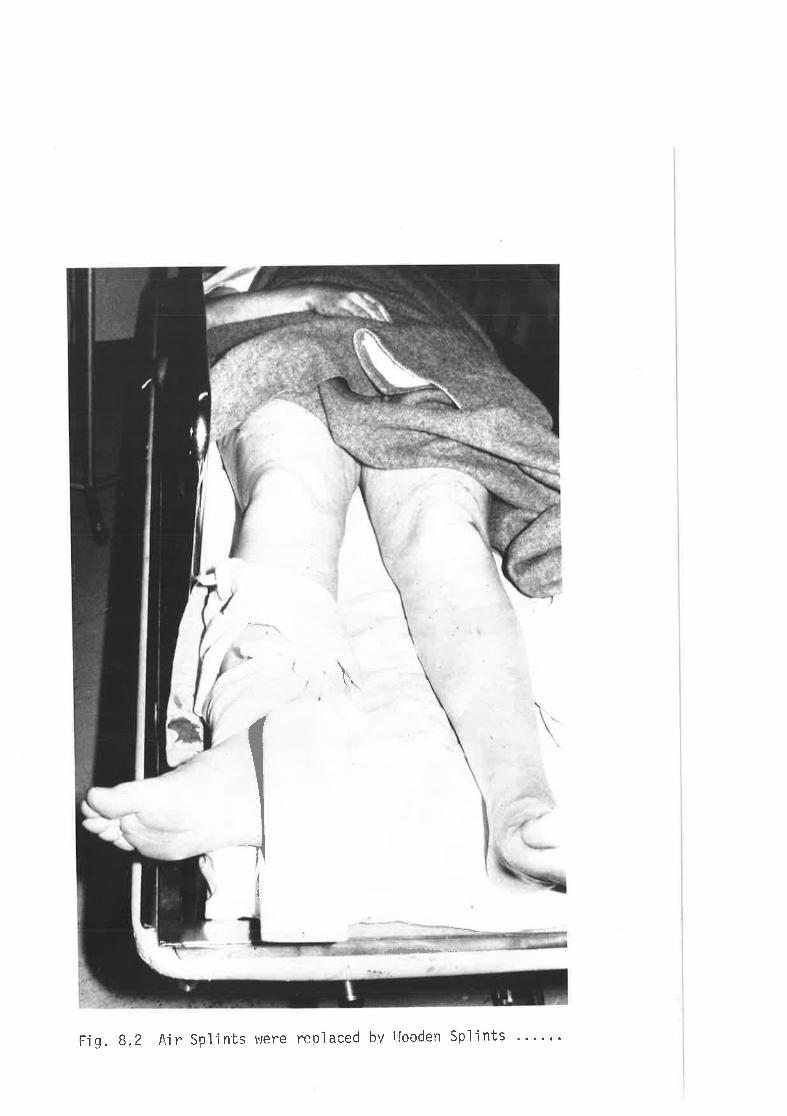
' sluL[dS uapooil ^q
paspldðr orant s1ui[dS rlV Z'B '0t¡
------:r.#l*a
¡
I
t\
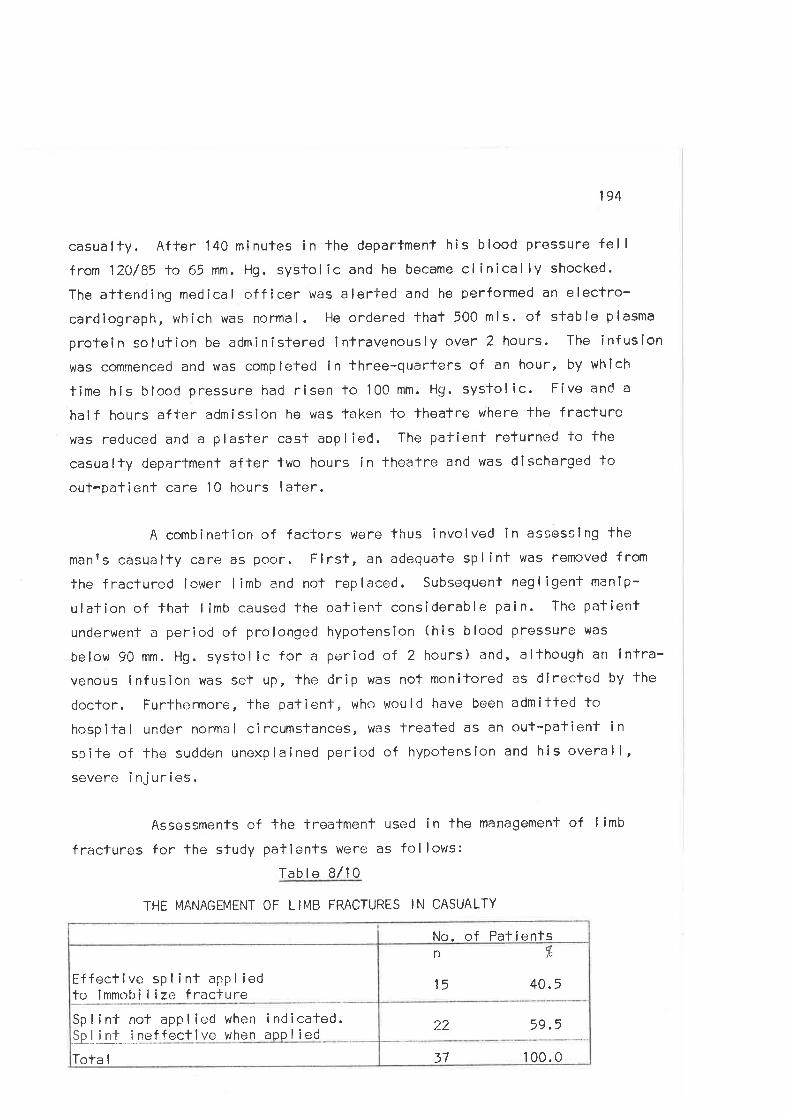
194
casualty. After 140 mínutes in the department his blood pressure fel I
from 120/85 to 65 mm. Hg. systolic and he became clínically shocked.
The attending medical officer was alerted and he performed an electro-cardiograph" which was normal. l-le ordered that 500 mls. of stable plasma
protein solutîon be adminisïered intravenously over 2 hours. The infusion
was commenced and was completed in three-quarters of an hour, by which
time his blood pressure had risen to 100 mm. Hg. sysfolîc. Five and a
half hours after admission he was faken lo Ìheatre where fhe fracture
was reduced and a plaster casf applied. The patient returned to fhe
casually department after two hours in lheatre and vras discharged loout-patient care l0 hours laÌer.
A combination of factors were thus involved in assesslng the
manrs casualty care as poor. Firsl, an adequate splint was removed from
the fractured lower I imb and not replaced. Subsequent negl igent manip-
ulalion of that I imb caused fhe patient considerable pain. The patient
underwenf a period of prolonged hypotension (his blood pressure was
below 90 mm. Hg. systolic for a period of 2 hours) and, although an íntra-venous lnfuslon was set up, the drip was not monitored as dlrected by the
doctor. Furthermore, the patienf, who would have been admiTted to
hospilal under normal circumstances, was treated as an out-patient in
spite of the sudden unexplained period of hypotension and his overall,severe i nj ur i es.
Assessments of the freatment used in the management of limb
fractures for the sfudy patients were as fol lows:
Table B/10
?_2 59.5
37 100.0
Sp I i nt not app I i ed when i nd i cated.Þliú-,1neffect i ve when app I i ed
Tota I
n %
15 40. 5Effecti ve sp I i nt app I iedto immobi I ize fraclure
No. of Patients
THE MANAGEMENT OF LIMB FRACTURES IN CASUALTY
195
The management of limb fractures in fhe casualty departments
vanied considerably from that expected on the basis of the normative
standards for the manâgement of such patients.
ø) þlound Marwgement in CasuaLtg
The commonest ínjuries sustained by victims of road crashes
are bruises, abrasions and lacerations, and most of the study patients
had received such injuries to one or more body areas. These injurieswere usually treated in casually by members of lhe medical and nurslng
staf f , or by rned ica I students.
Abras ions
t4inor abrasions were cleaned and dressed by nursing staffmer,nbers. Mercurochrome paint was commonly used as an antibacterlalagent. One patienf in the series had sustained severe abrasions.
cAsE 1 2033 A 20 year old man received extensive
abrasions of his thorax, abdomen and back when he was ejected from the
car he was driving and dragged along a bifumen road. Extensive bitumen
tattooing had occurred. He was seen in casually by a rosident medical
officer who consulled lhe admitting surgicaf registrar and was advised
that lhe abrasions should be scrubbed in casualty, The patient was given
10 mg. Morphia and an attempf was made to clean the bitumen from the
abrasions wilh Savlon and-lowels. Predicfably, the procedure was halted
by the patíentts puin and proteslations. He had suslained minor lacer-
alions to his head and left elbow which were sutured before he was
discharged from casualty, 11 hours after admission. The bifumen had not
been scrubbed from the wounds when he was discharged.
The fallure to clean these abrasions was contrary to the stand-
ards for the management of such wounds which should have been thoroughly
scrubbed and cleaned, after the patient was adequately anaosthetized.
The patient dicl nol return for further follow-up and thus the extent of
196
any resultant lattoolng could not be determined.
\l/ith this nofable exception, the overall managemenf of minor
abrasions in the department was considered lo be satisfactory.
Lace rat i ons
Lacerations and cpen wounds had offen been dressed by
ambulance officers befora the patienls reached the casualty department.
They were usually cleanod and re-dressed by members of fhe nursing
staff dur ing the verious weitîng periods in casualfy care. Subsequenfly,
they were usually inspected by several medical and nursíng staff members
and students before definitive 'trealment was undertaken.
l4ulfiple wound lnspectlr:n was common. ln the case of fhemolor cyclisl tn¡ho had suf fered massive soft tissue lnjuríes (Case 11456,
see p. 1BB), lhe facial wounds r¡rere inspected on f ive separate occasions
by different slaff members, before the patient was admitfed for in-patienfcarc. Oflen Cressings were nof replaced afler such inspections wilh theresult fhat open wcunds were left exposed beneath hospl-lal bedding.(Fig. 8.4. ) This presumably enhanccd the rîsks of wound contamination and
cross infection.
l-acerations were the second most common type of injurysuslained by palients in lhe study. Facial and head lacerationsaccountc;d for approximately three-quarfers of all lacerations recorded.
The lrealment of f acia I lacerations is based on f timeproven concepts of surgical managemenfr and includes tfhorough cleansÌng,
debridement, moficulous haemostasis, exploration of the depth of the
wound, repair layer by layer with oblileration of the dead space by means
of deep sutures ¿:nd fhe use of appropriate, fine suture material toapproximate the skinr. (Howol l, 1967. ) Similar management principleswere described by lhe members of the Royal Australasian College of
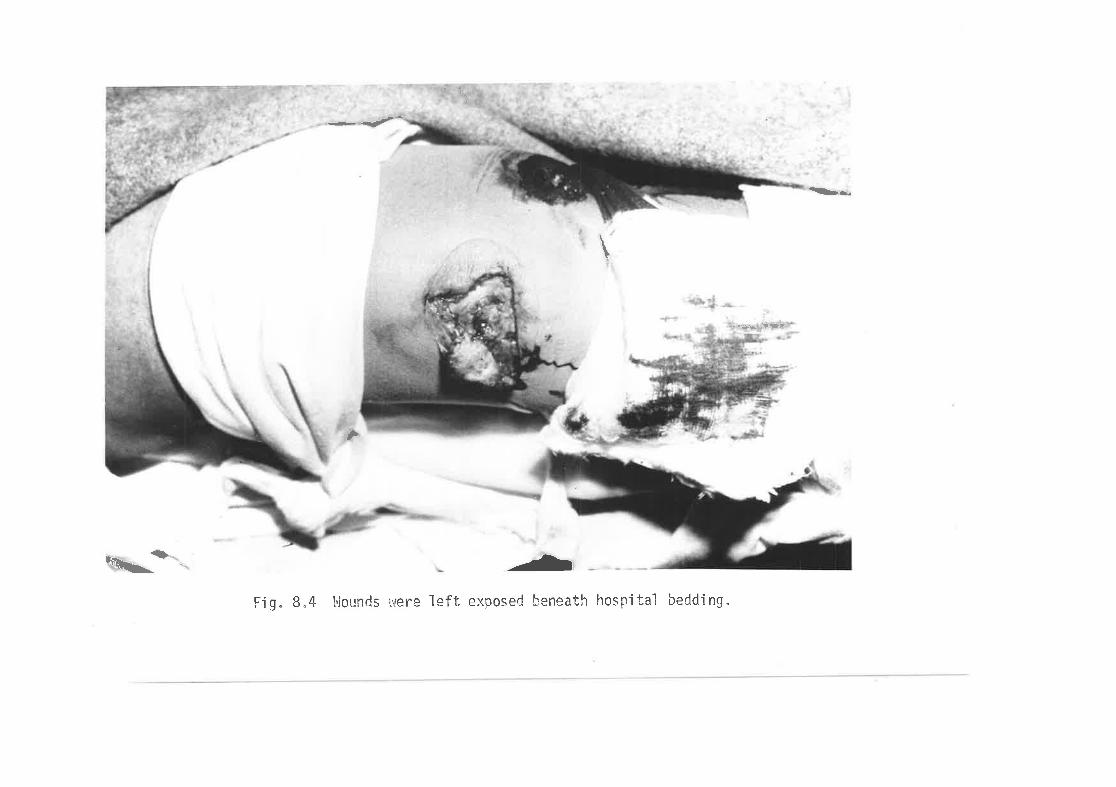
-<--
ì¡ry
\
r..è.s .lÜrr
,
nt'Ðt-----
Fìg" 8.4 þlounds were left exposed benreath hospital bedding.
197
Surgeons in emphasizlng the fact lhat lhe rhighest standards of wound
repair and care should always be applied to facial wounds to achieve themaximum cosmetic and f unctlonal resulf r. (Royal Australasian Col lege ofSurgeons, 1910.')
Since facial lacerations were common and aval lable hospitalbeds fow, mosf lacerations were sutured in casualfy and managed on on
out-patient basîs. Patients wilh major soft tissue injuries, and thosepalients with c¡ther injuries which warrantecl in-patienf care, were usual lyadmitted lo hospital. Nevertheless, many patienfs who required admlssion
for ín-palient surgical care had their soft fissue injuries sutured incasually before they were admitled to the wards.
Casually theatres were avai lable for these procedures but were
rarely used. Most lacerations were sutured in the acute receivlng ordressing cubicles. Since faci I ities for the performance of these proced-
ures were less than ideal in lhe cubicles as compared to fhe theatres,their use represents an unsatlsfactory compromise which resulled in less
tlran idea I standards of asepsis and treatment.
The limlled availability of medical staff for minor procedures
meant that many of these lacerations were sulured by medical students.Students who had never previously inserted sufures were observed toperform the prlmary closure of facial lacerations and were nêitherinslructed nor dlrectly supervlsed by medical staff members at the time
the procedure was performed. ln general, lhe technical competence dis-played in the sulure of lacerafions was commensurate wîth the experience
of the surgeöns and was thus rarely compafible with fhe normative stand-
ards as descrÌbed by the Col lege of Surgeons.
The equipmenl used for minor surgical procedures was good.
lnstrumonts, drugs and dressings were conveniently packed ln s-leri lecontaíners. Surgeons usual ly masked for procedures; gowns were worn
198
occasional ly and g loves rarely.
Wounds þ/ere usually prepared for surgeny by swabblng them with
skin antiseptic. Hair was usually, but nol always, clipped or shaved frqn
the edges of scalp laceralions. lf was observed that halrs had been in-cluded ln many of lhe scalp wounds vrhich were inspected after the sutur-
ing was completed.
Anaesthesia was usually induced try local infiltralion fhrough
the wound edges. Regional nerve blocks were not usecJ in any of the ob-
served cases. A common defecl in surglcal fechnique was that inspeclion
and suture of the wound was commenced before the anaesfhetÌc had had time
lo lake effect.
Thorough inspection and cleansing of the depfhs of lacerations
was nol well performed, and frequently the involvement of deeper struct-ures was nof assessed. This Is i I lustrated by the fol lowing case.
CASE 11224 A 59 year old male was admitfed following a crash
in which his head struck and shaftered fhe windscreen of his car. He was
concussed and had suslained a deep laccraticn of the bridge of lhe nose
involving the medial canthus and left lower eyelid. The nasal bones were
fractured. The casualty resident consulted the senior surgical regisfrarwho inspected the wound superficially but did not probe ifs depths. The
resident was lold to suluro the wound and lhîs was done using skin sufures
only. Subsequently, when the palient was obs€rved as an out-patient,considerable cosmetic deformity of the nose was noled along with evidence
of naso-lacrimal duct damage.
This wound required careful inspectíon for glass fragments,
assessmenl for the involvemenl of deeper strucfures, and meficulous
suture, none of which were performed.
199
A nolable deficiency in the management of wounds was thefailure ol'the surgeons to close wounds in layers. The inexperience ofthose performing'fhe procedures was reflecled in a reluctance to probe
wcunds and define analomica I structures for definifive repair. As a
nesull subculaneous sutures r¡rere not used to cbliterate dead space and
haematoma formation was often observed beneath scalp and facial wounds
as a resull. The following cases involved several of these fypical freat-menl deficiencies.
CASE 11106 A 55 year old male was admitted after sufferinga 41r laceraf ion of thr? right ternpora I region in a crash. The wound in-volved the skin, subcutaneous tissues, lemporal fascia and muscle, ond
fhe rîght superficial lemporal arfery which was bleeding profusely. The
palienl l.las seen briefly, l3 minutes affer admission, by a docfor who
ordered that fhe wound should be re-dressed. No aftempt was made lo clipoff the artery. A second doctor examirred lhe patient 45 ninutes later and
ordered a skull X-ray. At thîs stage the palient had lost a lof of blcod
and his blood prossure had fallen lo 100 mm. Hg. The observer thus
suggesfed Ìh¿:t lhe wound should be repairecl and the arlery clipped. This
was performed, 93 minutes affer the patient was admitted. Suosequently
hair around lhe margins of the scalp wound was trimmed (but not shaved)
and an al1'ernpf vras made to anaesfhetizc The wound by inf iltration of local
anaesthetîc lhrough its marg i ns. The superficial temporal arfery was fiedoff and lhe resident then commenced to close lhe skin without resforîngthe deeper anatomical struclures. After further advice from fhe observer,
the muscle and fascial layers were îdenlified and reconstituted. The
patient became hypotensive during the procedure, which took the residentapproximatelV 4* hours -lo completo. No specific lreatmenf was undertaken
for the hypotension, but he uras observed for 5 hours in the department
before being discharged, 11 hours after casualty admission.
The rcpair of this laceration should have been a relativelystraighfforr,iard surgical procedure. Nevertheless, the inexperíence of
200
lhe casually staff and their complete lack of supervision and directionmeanl that the procedure t+as unnecessarí ly time consuming, poorly per-
formed and resulled in considerable discomfort for fhe patient.
The adequacy of the performance of wound repair for the study
patients was assessed as fol lows.
Table 8/l 1
PERFOFü\4ANCE OF WOUND REPA IR
No. of Patients
Tota I
56 72.7
12 15.6Poor wound closure wlth poorsuture lechnique
Fair wound repalr
n fr
9 11 ,7Sufure performed wifh adequatelocal anaeslhesla, correcfmaterials and good technique
77 100.0
The ulf imate ar'biter of the quality of minor surgical proced-
ures is the cosmetic result. lt is diff iculf to predict what this willbe at lhe fime the procedure is performed. A review of case histories of
these palienls was atlempted in order to delermine the relevant treatment
outcomes. lt was found that details of wound healing were rarely recorded
by lhe out-patlent surgeons and it was lhus impossible to assess the
resu I ts.
Several organizetional factors were observed lo be important
for the management of minor wounds in casualty. During the day when
casualty work loads were heavy, one member of the resldenf medical slaffwas rostered to perform fhe minor procedures required in lreating these
injuries. This staffing arrangement usual ly handled the work load salls-faclori ly. At night, however, a single medical officer was rostered forduty in the deparlment after 2300 hours on most nights of the week and
201
was responsible for al I assessmenf and lreatment procedures performed.
He thus managed both major and rninor emergencies presenting to thedepa rtment.
This sílualion had several impl ications for casualty care. Once
a doclor had commonced a surgical procedure, his availability for assess-
ing other patients was I imitcd and, occasional ly, severely injurodpatients were not seen promptly on admission as a result. Conversely,
the arrîval of new pafíenls was observed to delay lhe performance of minor
procedures, and therefore prolonged lhe casualty waiting and lreatment
times. Whl lst admitting officens and in-patient staff were theoretical lyavailable to support casualty slaff at these times, it was observed thaflhey werc rarely summoned. Residents on duty preferred to work on untilthe work-load had decreased and lhe back-log of palients was cleared.Although long casualty queues developed at all hours of the day because ofdemands orr sfaf f and facililîes, it was only at nighTs that non-availabil-ily of staff was a potenf facfor in producing these queues. The absence
of a formal mechanism urhereby additional slaff were called to casualty tohelp out at fhese times was considered to be one of lhe most important
causes of dolays in casually care. The development of such situationsrepresents a derel iction of responsibi I iTy by admitting officers and more
senior supervisory staff .
l4edical sfudents were rostered for casualty duty and often per-
formed sutures and minor procedures, lhcreby helping lo rel ieve thepressures on the residenf slaff. ln doing so they performed a useful
servíce and gained valuable experience. l.levertheless, it was slgnif icantthal they were unsupervised (as were fhe fîrst year casualty residents)and lhus lacked practical instruction in correct surgical techniques.
Hence lhe technical compelence displayed in lhe performance of procedures
was usual ly poor. Practical experience is the most valuable form oflearning, but it should be backed with aclequate super-vision and instruct-ion. Moreover, the fact lhat junior staff rarely had fhe opportunity to
202
rev¡ew their palients when'they relurned for subsequent treatment,diminished the value of the learning experience. They lacked even theopportunity to learn by their mistakes.
Casualty residents and students cannot be expecled to provldegood qual ity care withoul aCequafe supervision and instruction from
trained slaff members. Furlhermore, since most of the minor surgery lsperformed by these persons, there is I i+tle chance of high quality care
beirrg provided for patients wlthin lhe deparfmenfs. As a result, theerrors in primary repair of sutures which were singled out for partic-ular cornment by members of the Royal Australasian Col lege of Surgeons(1970) were the errors fhat were observed mosf commonly in the managemenf
of the study patients, viz.(i ) Fai lure to remove dlrt and foreign bodíes from
abrasive type of wounds and lacerations.(¡¡) Failure to suture the muscle layers and irregular
skin lacerations back fo their correct positions.(iii) Suluring wounds under lension with large sutures.
( iv) Fa i I ut-e to exp lore ad.equafe ly the depths of f ho
wound and recognize derepe--r structures.
(3) AN OVERALL ASSESSILENT OE THE SUALTTT OF CASUALTY CNNE
It is apparenf from fhe preceding descriptions of parlicularaspects of lhe care provîded for crash victims in casualty, fhat large
discrepancies exisf between lhe normative standards and the care acfual lyperformed. ln an attempl to quantify these differences, and thereby
assess the overall quatlty of the care, lhe correlalîon between fhe care
provided for each patienl and that expected on the basis of the standards
was rated on a fhree point scale.
Those patients whose care was compafible with fhat described by
the normative slandards were assessed as havíng received good caro.Divergence from the normative standard was assessed in fwo categories.
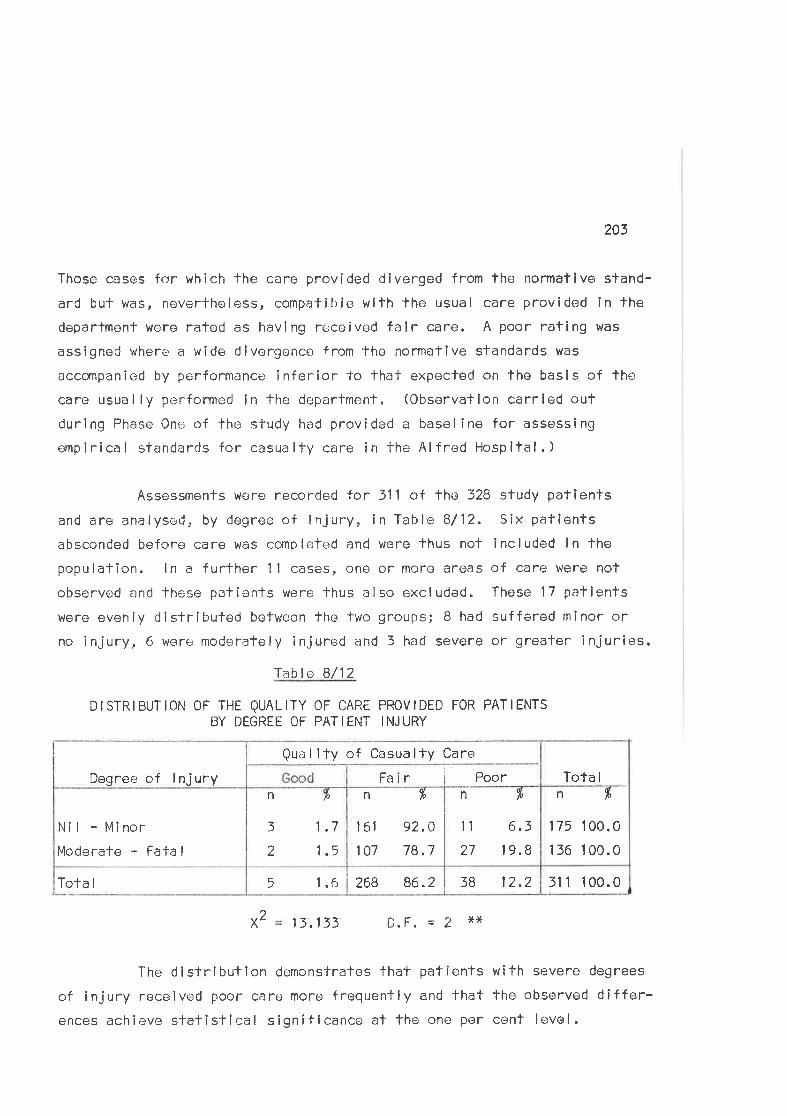
203
Those cases for which the care provided diverged from the normatlve stand-
arC bul was, nevertheless, compatible wilh the usual care provided in the
deparlment were rafed as having received falr care. A poor rafing was
assigned where a wide divergence from the normative standards was
accompanied by performance inferior to that expecled on the basis of the
care usual ly performed in the department. (Obsorvation carrled out
during Phase One of the study had provided a baseline for assessing
ompirical standards for casualty care in the Alfred Hospifal.)
Assessments were recorded Íor 311 of lhe 328 study palients
and are analysed, by degree of injury, in Table B/12. Six patientsabsconded before care was completed and wore thus not included ln the
populalion. ln a further 11 cases, one or more areas of care were not
observed and these patienls were lhus also excludod. These 17 patientswere evenly cjisfrîbuted between the two groups; B had suffered minor or
no injury, 6 were moderalely injured and f had severe or greater injuries.
Tablo 8/12
DtsTRrBUT|ON 0F THE QUALITY 0F CARE PROVIDED FoR PATIENTSBY DEGREE OF PATIENT INJURY
38 12.2268 86.25 1.6
nft1 75 100.0
1 56 1 00.0
nqlù
6.3
1 9.8
11
27
n
151
101
fr
92.0
78.7
n þ
3 1.7
2 1.5
Nil - Minor
Moderate - FaÌa I
Tota I
Qual ity of Casualty Care
Fa ir PoorDegree of lnjury
Tota I
X 13.133 ñE-.lt*Ur I .
The distributlon demonstrates fhat patients with severe degrees
of injury received poor care more frequenfly and that the observed differ-ences achieve statistical significance at the one per cenf level.
311 100.0
2
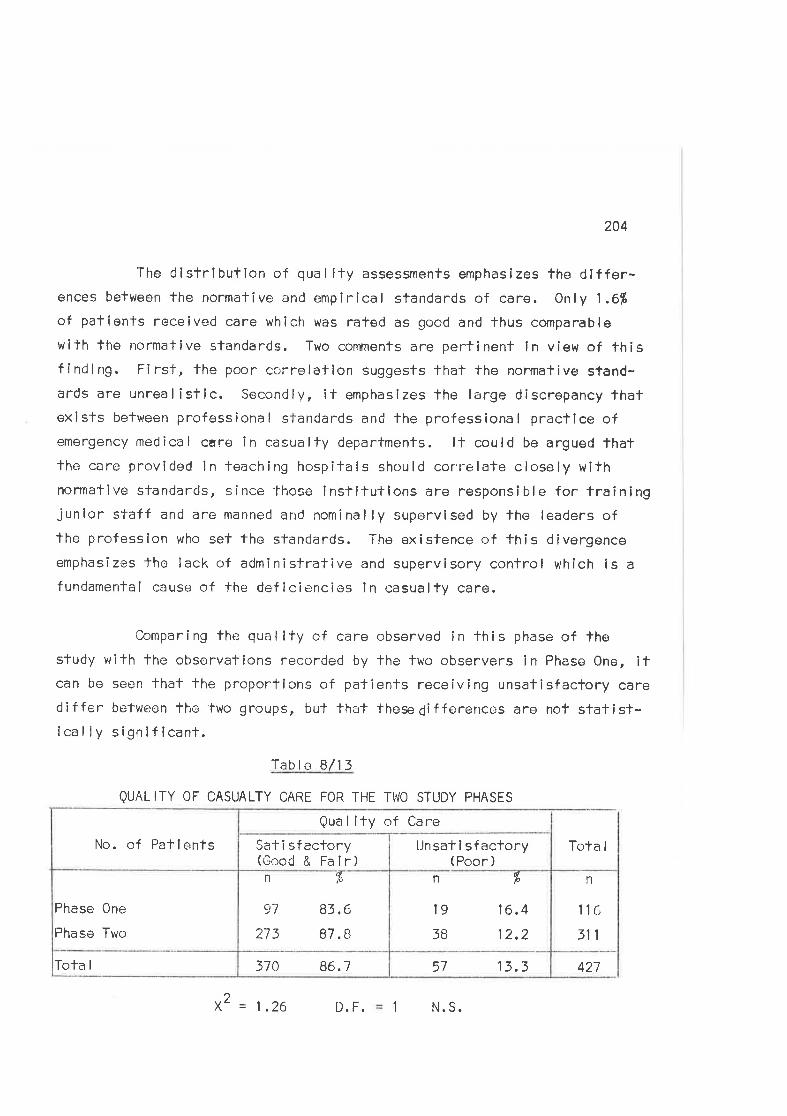
204
The dlstrlbution of qual lty assessments emphasizes the differ-ences befween the normative and empirîcal standards of care. Only 1.6fiof palienls received care which was rated as good and thus comparable
wilh lhe normative standards, Two comments are pertlnent ln view of fhisfinding. First, fhe poor correlafion suggests that the normative stand-ards are unrealistlc. Secondly, ît emphasizes the large discrepancy fhatexists belr¡reen professiona I slandards and the professiona I pracf lce ofemergency medical care in casualty departmenfs. lt could be argued thatlhe care provided in teaching hospitals should correlate closely withnormative sTandards, since those institulions are responsible for trainingjunior staff and are manned and nominally supervised by fhe leaders ofthe professlon who set the slandards. The existence of fhis divergenceemphasizes lhe lack of administrative and supervisory confrol which is a
fundamental cause of the deflciencios in casualty care.
Comparing the quality of care observed în this phase of thestudy with the observations recorded by the lwo observers in Phase One, itcan be seen lhat fhe proportions of patîenfs receiving unsatisfactory carediffer betweon the two groups, but that these6ifferences are nof statist-lcal ly signifícanl.
Table B/i5
QUALITY 0F CASUALTY CARE FoR THE Th'O STUDY PHASES
42757 13.3370 86.7Tota I
n
116
311
n
l938
þ
16.4
12,2
n
97
273
lL\
83.6
87. B
Phaso One
Phase Two
Unsatisfactory(Poor )
Sat i sfactory(Good & Fair)
No. of PafientsQual îty of Care
Tota I
x2= 1.26 D. F. 1 N.S.
205
On the basis of fhese observalions approximatelV 13fi of the
crash victims observed during bolh phases of -lhe sludy received unsatis-factory care ín casualty. lt w¡s shown in the earlier sectlon that approx-
imately 6fi of patienls received unsalisfaclory ambulance care al fhe
scene. Ir,lhile the care provided in casualty is not directly comparable
with thal provided al the sccne, both ôre elements of an imporlant and
continuous medical care process. The fact fhat a larger propcrtíon ofpatients receive unsatisfactory care in casualty is of concern and
supports the contention thal planners of emergency services should
consider care within casualty when planning changes in fhe emergency care
system.
(4) RELTABILTTY OF THE ASSESSMENTS
The assessments of quality made by the two observers during the
firsl phase of the study represented a combined judgement of the care they
had witnessed. ln the seccnd phasc observations were made by a singleobserver. More detailed cri'ierie were used for specifying the standards
and procodures for assessment of the care in an attempt to reduce lhe
varialion whîch must inevifably occur due torwifhin-observerr inconsisf-encies. No specific measures were taken in the study to control such
influences, beyond the general awareness by the observers of the problems
i nvo I ved. Neverthe I ess, the fact that 1 6% of paf i enls were j udged as
having rece îr,,ed unsatisf actory care dur ing the Phase One sf udy as compared
with 12% in lhe second phase suggests that there was consistency between
lhe observations in thc two sfudy phases.
One may argue thaf c¡bservers are likely to be more critical in
assessing the car-e of severely injured patients, who usually require more
treatment procedures moro urgently lhan lhose with minor injuries, and
that this inf luence could affect lhe assessmerrts made. ln vieur of this,three faclors should be consiclered with respect to the present study.
First, the observers were aware of these influences af lhe time of the
sTudy and thus tried to control for fhem. Secondly, more severely
206
injured patients neecl hlgh quality care for their optimum managemenf and
any divergence from such standards is undesirable and thus noteworthy.
Thirdly, similar inf luences would have prevailed and, were they signif ic-ant, should have been revealeC during the observafions of ambulance care.
Observer bias is o factor which is difficult to control in
direct observafion studies and here again, beyond the general awareness
of the problems by the observers, no specific measures were taken tocontrol this aspect of qual ity assessrnent.
The i nf I uence of lhe cl¡server on the process under study i s a
thírd important facfor in direct observation studies. lt was felf, in
both pl-rases of the sludy, lhaf the inf luence of the observer on the
system was small. Thís factor was dîscussed and tested in Chapter 6. lfis worth noting that the observerrs presence is mosl likely to resulf inthe performance of be'lter caro in a relatively shorter time. ln vievr ofseveral of the findings in this study if ls to be hoped that the care
provicjed under these circumslances did not represent the optimal capacity
to perform which would be expected on the basis of this premise.
(5) PAMENTSI ATIITADES TO TT]E CARE THEY RECETVED
A postal queslionnaire was used -lo determine patientst opinions
of their ambulance and casualty trealment in the second phase of the
study. One hunclred and e ighty-three $5.5%) of the pat ients responded
to the questionnaire.
The characterlslics of lhe respondenls and non-respondenfs in
thq qust ionna ire samp le w,.:re compared ln Chapter 6, where f he two groups
were compared for age, sex, degree of injury, and time spent in the
casually deparlment. ln Table B/14, the assessmenfs of lhe qual ity ofcare Drovided for the two populalions, as raTed by the observor al the
time of casualty treatmenl, are compared.
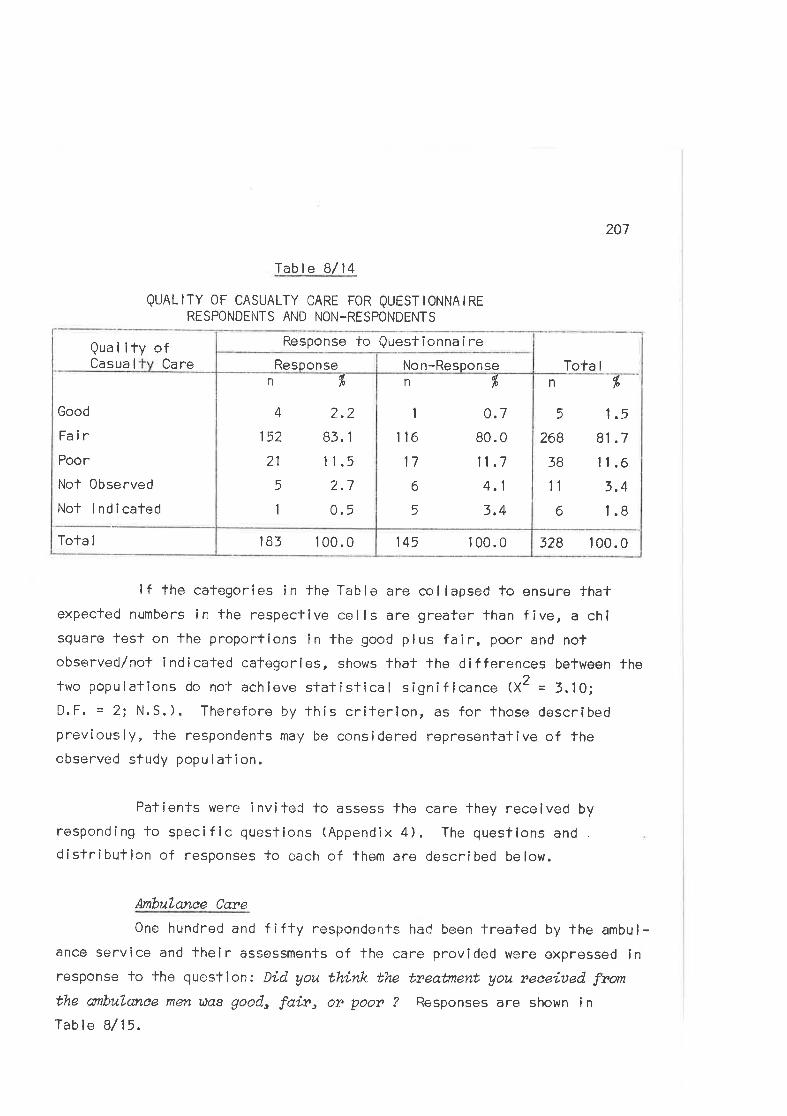
207
Tab I e B/14
QUALITY OF CASUALTY CARE FOR QUESTIONNAIRERESPONDENTS AND NON-RESPONDENTS
Qual lty ofCasua I Ca re
lf the categories in the Table are collapsed to ensure thatexpected numbers in the respective cells are greater than five, a chisquare fest on fhe proportions in the good plus fair, poor and notobserved/not lndicated calogories, shows that the differences between thefwo populallons do not achleve statislical signif icance (XZ = 3.10;D.F. = 2i N.S.). Therefore by this criterlon, as for those describedpreviously, the respondents may be considered representafive of theobserved study population.
Pafíenls were invited lo assess fhe care they received by
responding Ìo specific questions (Appendix 4). The quesfions and
distribution of responsês to each of them are described below.
Atnbulanee Caye
One hundred and f i fty respondenls hacl been treated by the ambu l -ance servíce and fheir assessments of the care provided were expressed inresponse to fhe questlon: Did you think the treaünent you nece.iued fromthe anbulanee men üas good" fair, o? poo? ? Responses are shown i n
Table B/15,
328 100.0145 1 00.0l83 100.0Tofa I
Tota I
n
5
268
3B
11
6
%
1.5
8t .7
11.6
3.4
l.B
Non-Responsen
I
116
17
6
5
dþ
0.7
80.0
11 .7
4.1
3,4
Responsen %
2.283.1
11 .5
l. t
0.5
4
152
21
5
1
Good
Fa irPoor
Not Observed
Not lndicated
Response to Questionnaire
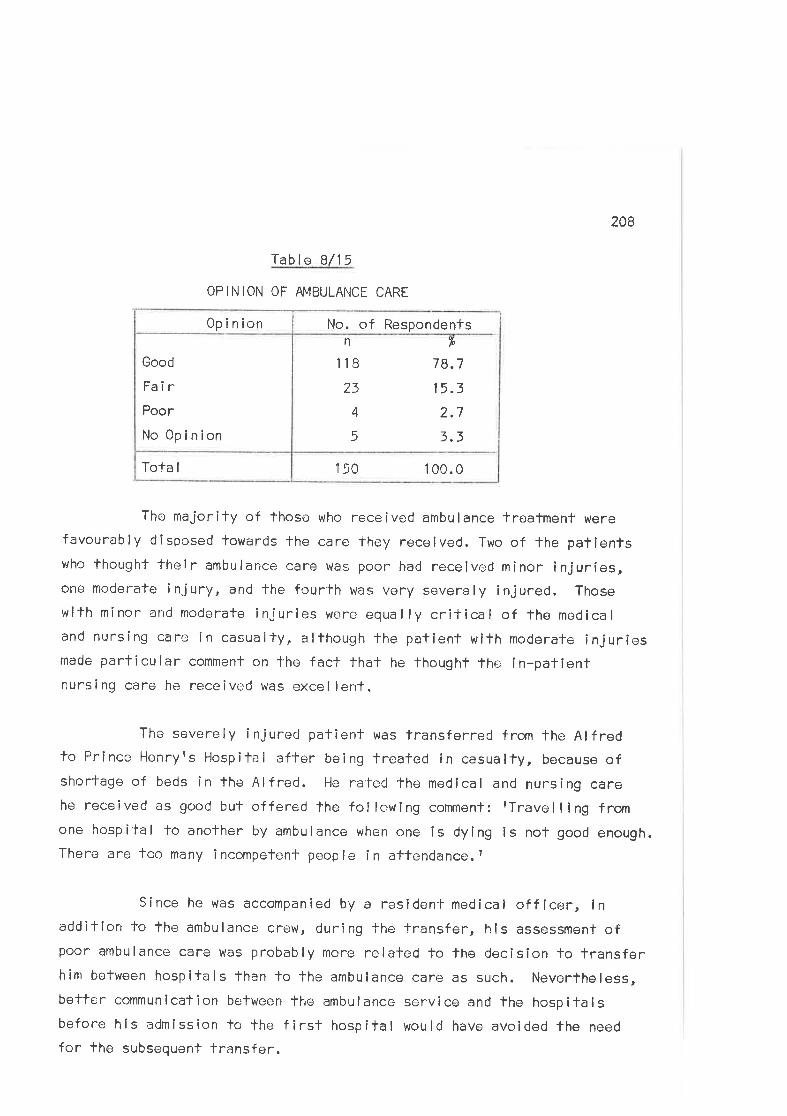
208
Table B/15
OPINION OF AMBULANCE CARE
150 I 00.0ïofa I
n
118
23
4
5
lo
78.7
15.3
2.7
3.3
Good
FairPoor
I'lo 0pinion
No. of Respondents0pinion
The majority of those who received ambulance lreatment were
favourably disposed towards the care they received. Two of the patientswho thought their ambulance care was poor had received minor injuríes,one moderate injury, and the fourfh was very severely injured. Those
with minor and rnoderate injurles were equally crif ical of fhe medicaland nursing care in casualty, although fhe patient with moderate injurîesmade parlîcular comment on the fact thal he thought the ín-pailentnursi ng care he receivc.d was excel lent.
The severely injured patient was transferrecj from the Alfredto Prince Henryrs HospitaI after being treafed in casualty, because ofshortage of beds Ìn the Alfred. He ra'led the medical and nursing carehe received as good but offered the fcllowing comment: rTravelling fromone hospital to another by ambulance when one is dying is nof good enough.There are too many incompetenf people in attendance.t
Since he was accompanied by a resìden-l- medical off icer, inadditlon to the ambulance crew, during the transfer, hls assessment ofpoor ambulance care was probably more relaled to the decision lo transferhim befween hospitals than to lhe ambulance care as such. Neverlheless,bettcr communlcation between the ambulance service and the hospitalsbefore his admission lo the first hospifal would have avoided the need
for the subsequent transfer.
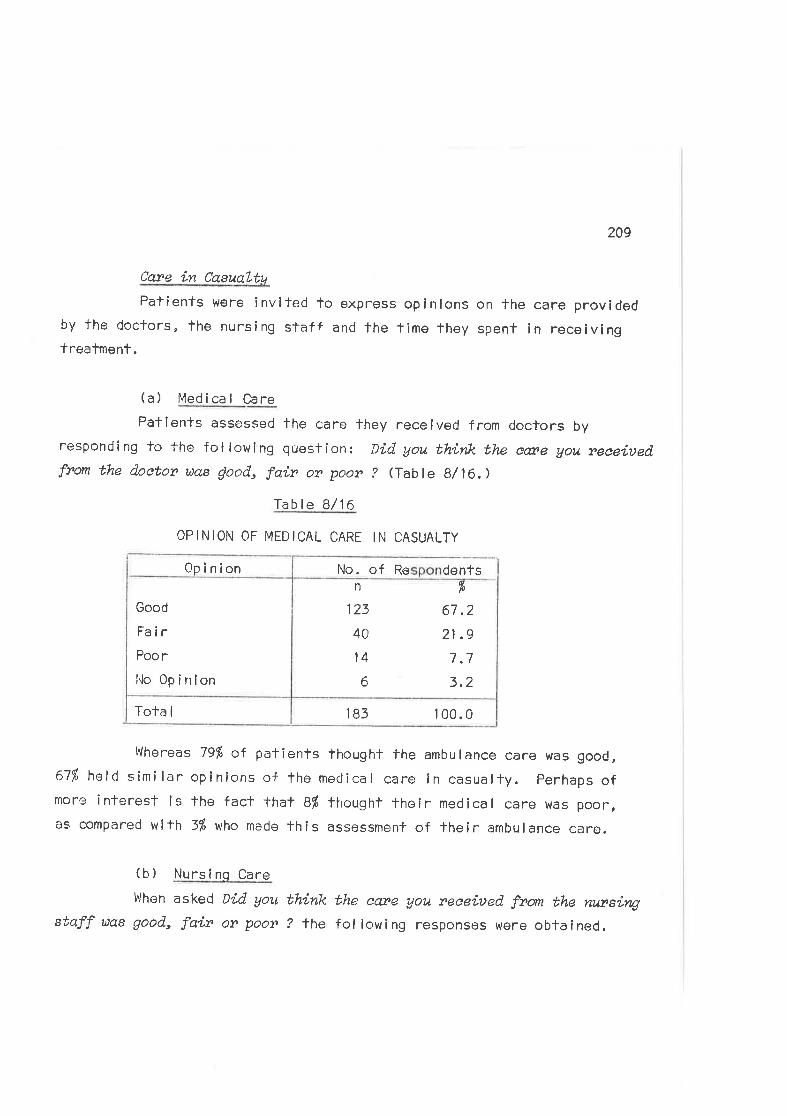
209
Cav'e in. CasuaLtt¿
Patients were invlted to express opinions on the care providedby fhe doctors, lhe nursing staff and fhe time they spent in receivingtrealment.
(a) Medical Care
Patlents assessed the care they received from doctors by
responding to fhe followÌng question: Díd you think the cæe gou reeeitsed,
from the doetor uas jood, fair or poor ? (Tabl e 8/16,)
Table B/16
OPINION OF MEDICAL CARE IN CASUALTY
183 1 00.0Tota I
n
123
40
14
6
fr
67 .2
21 .9
7.7
3.2
Good
Fa irPoor
iio 0pinion
0pinion No. of Re dents
Whereas 79% of patienfs lhought the ambulance care was good,671Á held similar opinions of the meclica I care in casualfy. perhaps ofmore interest is lhe fact lhat BÍ thought their medical care tvas poor,as comPared wi+h 3f" who made this assessment of their ambulance care.
(b) Nursinq Care
l¡Jhen asked Díd you think the eate you neeeiued ftorn the rutnsírqstaff uas good, faín on poon ? the following responses wore obtained.
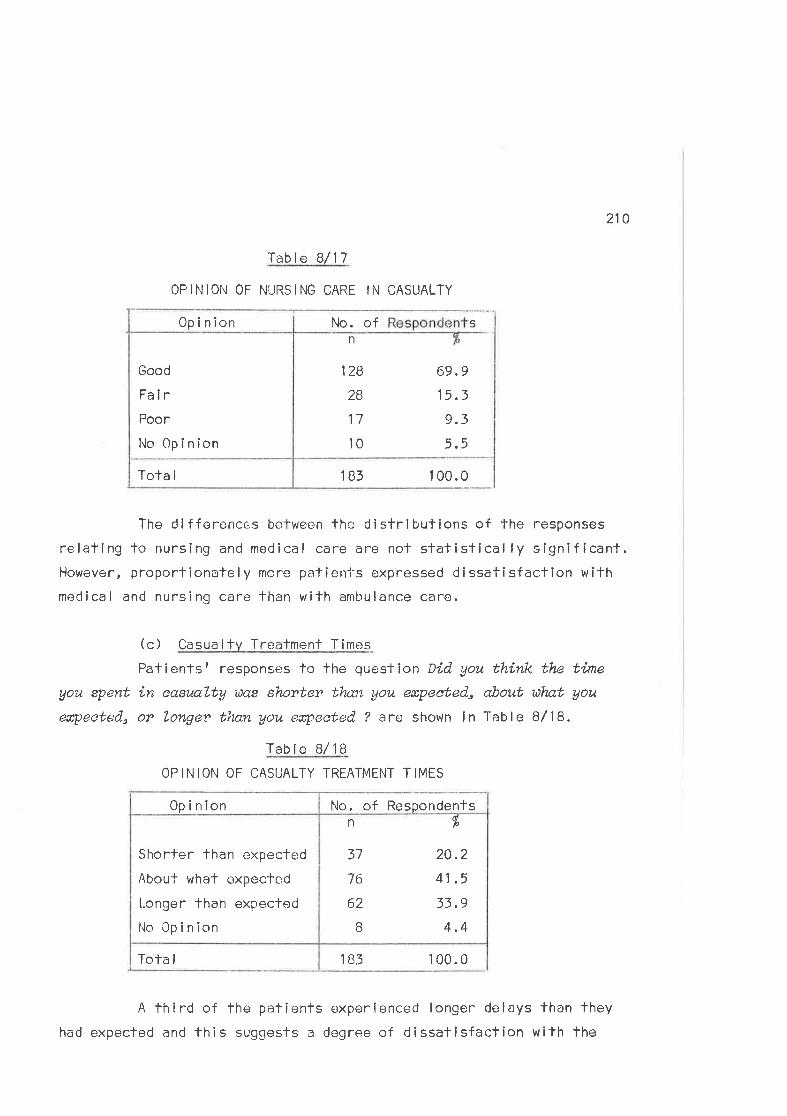
210
Table B/17
0PINlotl 0F NURSING CARE IN CASUALTY
183 1 00.0Tota I
Good
FairPoor
l{o 0p in ion
0pinion SNo. ofn
128
28
17
l0
69.9
15.3
9.3
5.5
The difference,s between the distribufions of the responses
relating to nursing and medical care are not sfatistically signif icant.However, proportionately more patienl-s expressed dissatisfaclion vlithmeclica I and nurs i ng care than w ith amlru lance care.
(c) Casualty Trealment Times
Patienlst response'rs to the question Did you think the time
you spent ín easl/a,Lty uas shorter tlmn gou eæpeeted, about u\nt you
eapeeted" or Longer tlnn you erpeeted ? are shown in Table B/18.
Table B/18
OPINION OF CASUALTY TREATMENT TIMES
183 1 00.0ïota I
n
37
76
62
B
dlo
20.2
41 .5
33.9
4.4
Shorter than expected
Abouf what expected
l-onger than expectod
I'lo 0p in ion
No. of Respondents0pinlon
A lhird of the patienls experíenced longer delays than they
had expected and this suggests a degree of dissalisfaction wilh fhe
211
ïreatment times. Mosf pafîenfs are aware that casualty departmenls are
busy and fhat waiTing times may thus be long. Their expectafions as fowhat represents a reasonable waifing timc are, no doubt, tempered by
their perceptlon of their own illness and its severity. Thus it was notsurprising thaf comparison of fhe patienl'st responses with the actualtimes spent in receiving care did nol shour any significant correlalion.
Elghteen patients added sponTaneous comments to lheir questionn-aires in which they stated that wailing limes were too long. Waifinglimes to see the docfor ernd wailing for X-ray were singled out forparticular comment.
)ueraLl. Opinion of Etnez,qeney Tneatrnent
The majority of patients wcre satisfied wilh the treatment lheyreceived, as was shown by'fhe response to The question: Did you thinkthe otsanaLl treabnent you y,eceiued fon yow injwðes uas good" fai,n orpoon ?
Tablo B/19
CPINION OF OVERALL TREATMËNT
183 1 00.0Tota I
n
129
35
17
2
dtl0
70.5
19.1
9.3
1.1
Good
Fa irPoor
No 0pinion
No. of Respondents0p in ion
One hundred patienls added comments relating to their trealmentto their repl ies. Forty of these were favourable and sîxty unfavourable.Eighteen of the unfavourable group related to time delays, 34 to treat-ment deficiencies and I to other areas of the care performed. Fivepatients commented on lhe anxiety caused to parents or relatives due to
212
poor communications between casualty staff and waiting relallves.
(6 ) suwLry_
The quality of care provided for lhe pallents observed in the
second phase of the study has been reviewed in this section by examining
elements of the process of lhe care provided. A considerable discrepancy
has been demonstrated between the normative standards of care as propounded
by senior members of the profession and the acfual standards of care
practised in the casualty department, with less lhen 2fr of patientsreceiving lreatment compatible with fhese standards. Moreover, approx'-
imately 13ft of patients were assessed as receiving unsatisfactory care
in comparison wilh lhe empirical standards for the managemen't of road
crash victims in fhe Alfred Hospital.
Patienfsfatlitudes lo care, as determined by responses to a
postal questîonnaire, indicated that, whi lst most patienls consldered
tlreir f reatmenl saiisfactory, a large proportion ß4%) felt thatcasualty waiting times were longer lhan they expected. Three per cent
of patients felt that the ambulance care lhey received was Poor, and
10% held similer opïnion.s of casualty care. Ratings of the quality ofcare by two observers in the first phase of the study found similarproportions of unsafisfactory care, wilh 6$ of patients being assessed
as having receìved unsatîsfactory ambulance care and 16É unsatisfactorycasua lty treatment.
(3) An Analvsis of Patterns of Casualtv Service for Road Crash Viclims
Data relating to patient flow patferns through the casualty
deparlmenl have been described in this study and may be usecJ for such
administralive purposes as planning mociif ications of exisling systems
or set-l i ng rea I i sl I c operat i ng standards.
lf modificalions are intended, îf is useful (and of some
213
imporlarnce to management) to be able to preclict tho likely effects ofany projec-led charnges. Onc method of making such predictions involves
the use of simul¿:lion models. Simulalion modelling provides a means
whereby management can lest the effects of changes in an operating
system without changing the existing system. Thus, for example, theeffects on casualty waifing times of changing staff ratîos or treatmentpriorilies can be assessed by si,mulating the exisling system and examin-
ing lhe effects of various altv-rnative operatîng methods on lhe outpuls
of the mode I .
Simulalion models ¿ìre used for the descriptíon of system
operations in those situations where malhernatical analysis is likely tobe e ither too complex or foc costly to be benef icial. Such situationsusually involve many interactîng variables which are dif f icult to describe
în terms of mathematical functions, but which can be successful ly
simulated by fho use of a model which represents the essential featuresof the system. The lechniques have been used for management problems
ranging from the planning of servicing and repair requiremenfs formachinery breakdowns in factories to the determînafion of unloading
schedules for ships in dockyards. ln lhe emergency care field, simulationmethods have been used to solve ambulance location problems (Savas,1969)
and fo analyse service and detection systenrs on freeways. (Kel ler, 1971.)
(ù THþ} TECHNTSAE OF SflVULATED SAIIPLTNG
l4onte Carlo, or simulated sampling, ís an operations research
technique which permifs the introduction ínfo a system of data whîch have
the properlies of a given distribution. A model is developed which
describes the essential features of the system and thîs model is fhen
driven by input data from the observed system. The reactions of the
syslem components and its outpufs fo infroducod changes can be assessed
try analysing thc distribulion of the output variables produced by
running the simulation. The value of a simulation is determined by itsabi I ily lo predicf the bcrhaviour of lhe system under study.
214
Four slages are necessary in simulating a given system and
are i I lustraled below by reference to casually deparlment operations.( i ) The frequency distribufions of patient arrivals
and e lapsed t imes r:ur i irg the var ious f reatment
phases are measurod and converfed into cumulativeprobabi I ity distributions.
(¡i) A simulation model describing the elcments of the
system lo be studied is derived.( i¡ i) Randc.rm sampling f rom the cumulative distributions
determines lhe specif íc arriva l, waitíng and
treatment times for use in simulating the casualtylrealment system.
By using random numbers fo enfer fhe cumulaf-
ive distributíons, specif ic fime values which
are associated with each rando'm number are
gathered in proporÌion to lhe probabi I ify oftheir occurrence as doscribed by the originalf requency d I stri bulion.
(iv) The actual operation of the casually treafment iss imu lated.
Simulation involves selection of a patientarrival from the observed arrival distribution.Adclitional sampling from fhe mcdícal of f icers¿:rvice time distribution, fhe probabillfy ofthe patient requiring X-ray, the time spenl inX-ray distribulion, and fhe observation and
treatmenl time díslributlon drives lhe model and
allows examination of the outputs, of waitinglime fo see The medical offlcer, and total tlmc
spent within the system.
ln fhe fcl lowing seclions, lhe observed patterns of casuallyoperation will be discussed, using a simulalion model to fest the
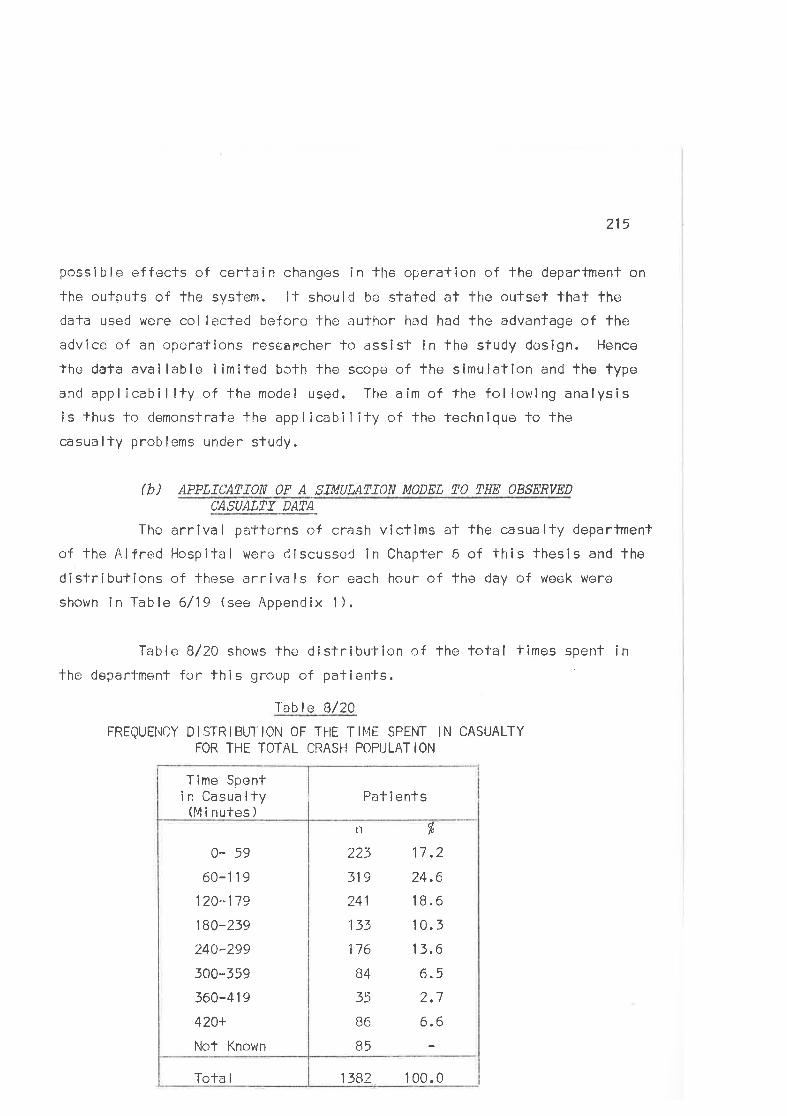
215
possible effecls of certain changes in fhe operation of the department on
the outputs of the system. lt should be stated al the outset lhat thedata used were col lected before lhe author had had the advantage of f'he
advice of an operations reseapcher to assist in the study design. Hence
the data available limited bcth the scope of fhe simulalion and the typeand applicabillty of the model used. The aím of the followlng analysisis thus fo demonsfrate the applicability of the technique to the
casually problems under sludy.
(b) APPLTCATTON OF A STMULATTON MODEL TO THE OBSERVED
CASUALIY DATA
The arrival patterns of crash viclims al fhe casualty department
of the Alfr.ed Hospital were dlscussed in Chapter 6 of this lhesis and fhe
dislributions of these arrivals for each hour of the day of week were
shown in Table 6/19 (see Appendix l).
Table B/20 shows the dislribufion of fhe total times spent inthe department for fhis group of patients
Tab I e B/20
FREQUENCY DISTR|BUTtON 0F THE Tl¡4E SPENT tN CASUALTYFOR THE TOTAL CRASH POPULATION
n
223
319
241
133
176
B4
35
B6
B5
dlo
17 .2
24.6
1 8.6
10.5
13.6
Cr. 5
J1
6.6
1382 100.0Tola I
0- 59
60-1 1 9
120-1 ,19
180-239
240-299
300-359
360-419
420+
Not Known
Pat i enlsT ime Spent
i n Casua lty(M i nutes )
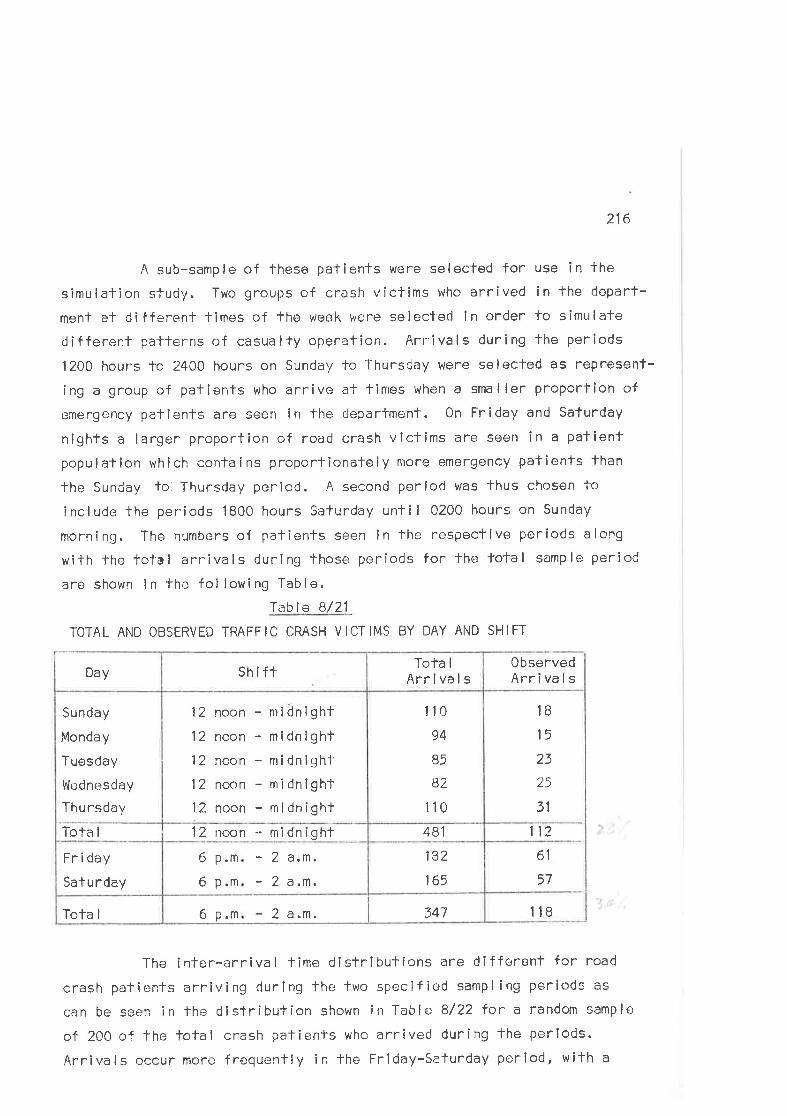
216
A sub-sample of these patients were selected for use in the
simulation study. Two groups of crash víctims who arrived in fhe depart-
ment at different times of tho week were selecteci in order fo simulate
different palterns of casualTy operation. Arrivals during the periods
12OO hours lo 2400 hours on Sunday to Thursday were selected as represent-
ing a group of pafients who arrive ai times when a smaller ProporTion of
emergcncy palients are seen in the deparfment. 0n Friday and Safurday
nighfs a larger proportion of road crash victims are seen in a patient
population which contains proportionalely nrore emergency patients fhan
fhe Sunday lo' ThurscJay poriod. A second period was lhus chosen io
include the periods 1800 hours Saturday until 0200 hours on Sunday
morning. The numbers of patients seen in the respective periods along
with lhe tolal arrivals during those periods for the total samPle period
are shown in the fol lowing Table.
Table B/21
TOTAL AND OBSERVED TRAFFIC CRASH VICTIMS BY DAY AND SHIFT
3476 p.m 2 a.n,Tofa I
bt
57
182
165
5 p.m - 2 a.m.
- 2 a.m.6 p.m
Fn i day
Saturday
11?48112 noon - midnightTofa I
1B
15
23
25
31
110
94
B5
82
110
12 noon - nridnight
12 noon - midnight
12 noon - midniqht12 noon - midnight12 noon - midnight
Sunday
Monday
Tuesday
Wt:dnesday
Thursday
0bservedArrivals
Tola I
ArrivalsshiftDay
1lB
The inter-arrival lime distributions are dlfferent for road
crash palienls arriving during the lwo specified sampl ing periods as
can be seen in the distribution shown in Table 8/22 for a random sample
of 200 cf lhe tofal crash patients who arrived during the periods.
Arrivals occur more frequenlly ín the Friday-Saturday period, with a
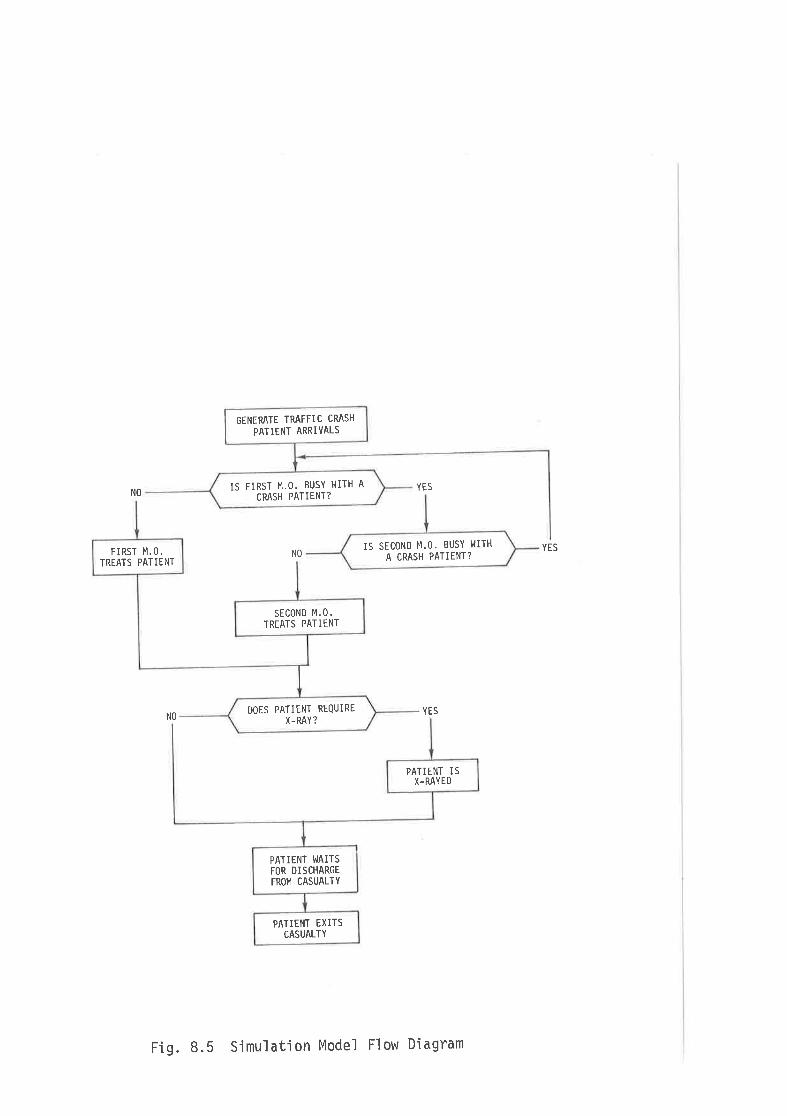
IS FIRST M.O. BUSY I'IITH A
CRASH PATIENT?
GENERATE TRAFFIC CRASH
PATIENT ARRIVALS
IS SECOND M.O. BUSY l.lITH
A CRASH PATIENT?
PATIETIT TXITSCASUALTY
PATIINT WAITSFOR DISCHARGEFROM CASUALTY
PATIENT ISX-RAYED
DOES PATIENT REQUIRE
X-RAY ?
SECOND M,O.TREATS PATIENT
FIRST M.O.TREATS PATIENT
NOYES
YES
YESNO
NO
Fig. 8.5 Simulation Model Flow Diagram
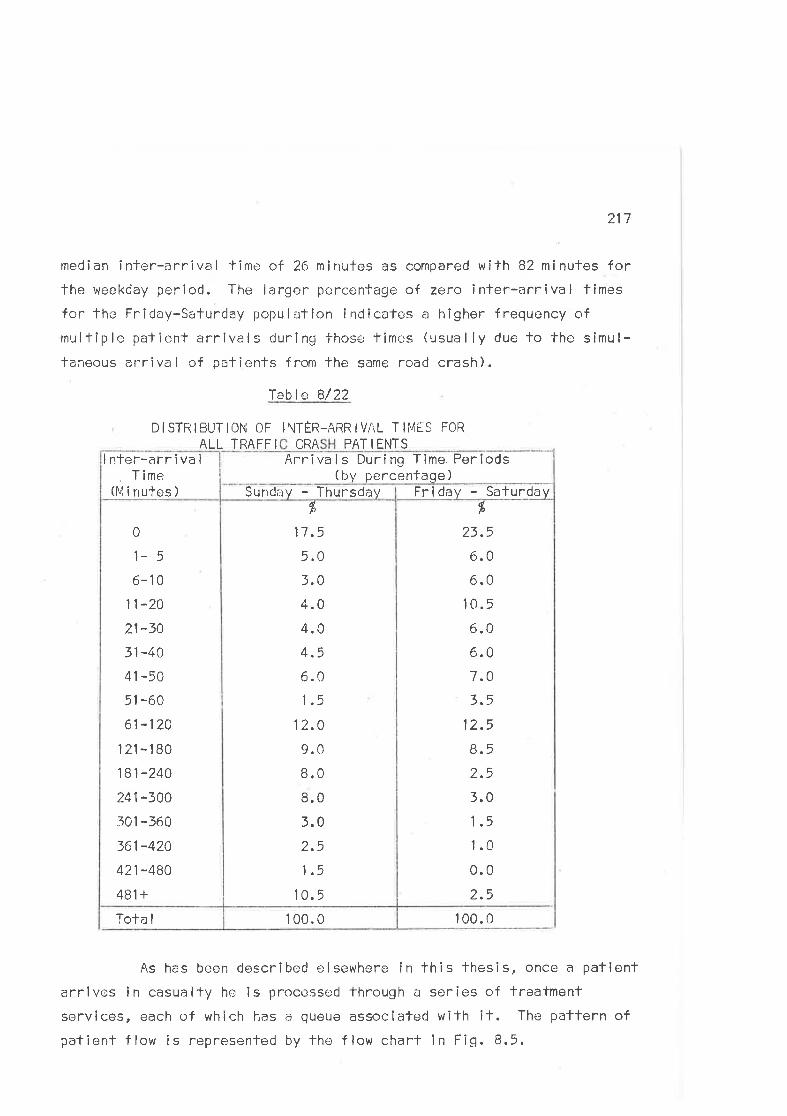
217
med¡an inter-arrival time of 26 minufes as compared with 82 minules forthe weekday perÍod. The larger percentage of zero inter-arríval times
for fhe Friday-Saturday population inclicafes a higher frequency ofmultiple patient arrivals during fhoso timcs (usually due to the simul-taneous arrival of palients from the same road crash).
Iable B/22
DISTRIBUTIOI'{ OF
ALL TRAFF I
I\TËR-ARR I VAL T IiVES FOR
CRA PAT I ENTS
Tola I
As has been described elsewhere in this thesis, once a patlentarrives in casually he is processed through a series of treatment
services, each of which has a queue associafed with it. The pattern ofpatient f low is represented by lhe f low chart in Fig. 8.5.
1 00.0 100.0
fr
23.5
6.0
6.0
1 tl.5
6.06.07.03.5
12.5
8.5ÔEL.)
3,0
1.5
1.0
0.0
2.5
dlD
17,5
5.0
3.0
4.04.04.5
6.0
1.5
12.0
9.0
8.0
8.0
3.0
2.5
1.5
10.5
\J
1- 5
6-10
11-20
21-30
31-40
41-50
51 -60
61-120
121-180
181-240
?_41-300
301 -360
361-420
421-480
481 +
Friday - SaturdaySund¡:y - Thursdav
Arrîva ls During Time Periods( t¡y pe rcenfage )
I nter-arr î va I
, Time(l"li nutos )
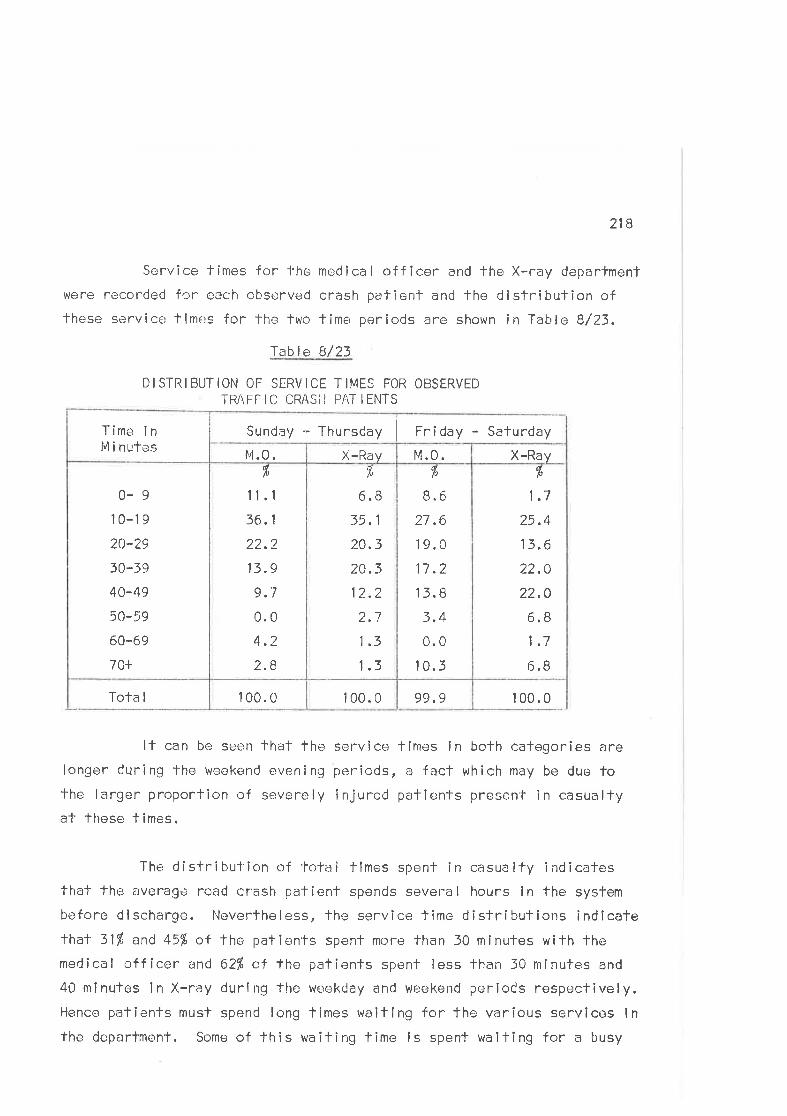
218
Service límes for l'he medical officer and fhe X-ray department
vlere recorded for each observed crash patienf and lhe dlsfribulion oflhese serviccl times for the two time periods are shown in Table B/23.
fable B/23
DISTRIBUTION OF SERVICE TIMES FOR OBSERVEDTRAFFIC CRASiI PAT IENTS
99.9100.0100.0Tota I
f'
1.7
25.4
13.6
22.0
22.0
6.81.7
6.8
ft
8.6
27.6
19.0
11.2
r3.B
3.4
0.0
10.3
,Ã
6.8
35.1
?_0.3
20.3
12.2
2.7
1.3
1.3
r,
'tl.r16. 1
22.2
13.9
9.7
0.0
4.2
2.8
0-910-19
20-?9
30-39
40-49
50-59
60-69
70+
X-RayM.0.X-Rayt4.0.
Time inlnlinutes
Sunday - Thursday Fnîday - Saturday
1 00.0
lf can be seen that the service times in both categories are
longer during the weekend evening pericds, a fact which may be due folhe larger proportion of severely injured pafîents present in casualtya1- these times.
The distribulion of lotal limes spent in casualty indicatesthat the averagc road crash patient spends several hour-c in the system
bcfore dischar ge. Neverfheless, lhe service f íme distributions indlcatethal 311, and 45'1" of the patÌents spenl more than 30 minutes with thomedîcal officer and 621' oÍ the patients spenf less than J0 minutes and
40 mlnutes ln X-ray durlrrg the weekCay and weekend periods respectively.Hence patients must spend long limes r^raitlng for the various services lnthe deparfmenl. Some of this waiting time ls spent walting for a busy
219
serv¡ce - for example, fhe medical officer or the X-ray deparfment'
Another portion of it represenls a part of fhe treatmenl process and
includes time spenf waillng for the results of diagnostic procedures and
llme spenl under observation.
Aims of bhe SírruLatíon,
The reducfion of walling and treatment times in casualty is a
general ly accepted adminisfralive goal. ln the next sectíon two posslble
alfernatives for reducing the total fime a patient spends in casualty
are considered by using a simulation model.
First, fhe effecl- of givlng priority to crash patients over
all ofher pafienls is examined. The hypothesís is thaf signiflcantreductions in total casually service time will result f rom glvÎng
casualty patienls priority in the gueue waÎfing fo see the medical
of f i cer.
Secondly, the effecf of a reduction in lhe amount of time fhe
medical officer spends with each patienf is examined, uslng a medical
officer service time distribution derived from observatlons made in
another Vicforian l-lospital. One would predict that reducing medical
officer service times would increase the oatienf flow and thus save
casua lty treatment time.
The Simúation MadeL
The casualty treatment system can be represented by a Monte
Carlo simulation model Four queueing situalions are evidenf in the
syslem flow diagram (Fig. 8.5). Patients may be subject fo delays
while waif îng for clerical processing on admission to casualfy, waiting
for lhe initial consultafion with a medical off icer, waiting in X-ray,
and waiting for discharge, either after lhe initial medical off icerconsullation or after X-ray. WaitÌng fimes during this latter phase
may include several modical consultations, observation, and treatment
220
procedures (e.9. suture of lacerations). These four queueing services
within casualty can be described mathematical ly by their respective
service lime distributions. The delays at each service are a funcfionof the service timos. Altering the service tlmes has an exfra lmpact
on lhe Total time in fhe system, since it also affects the waifîng tlmes
f or subsequen-l serv icos.
The palient arrlvals used for the simulation are generated
from fhe distribution of infor-arrival times determined for lhe road
crash population prosentlng to the Alfred Hospital casualfy department
during the study periods and shown in Table B/22.
The lnitlal assessment and documentation by lhe admittingnurse was assumed to have a constant service time of 2 minutes and thistime is lhus added to lhe arrival time of each patient in fhe simulationin recognifion of lhe service.
During most of the time periods chosen for lhis study the
casualty department was staffed by two residenf medical officers who
were responsible for fhe reception, assessment and treatmenl of acute
casualty admissions.
Once lhe palienf is admitTed fo the deparfment he is seen by
one of these two medical officers. The flrst medical officer corresponds
to the tfirst onr resident in the hospifal and he is the doctor glven
preference if bolh are idle when a netlt admission occurs.
It is assumed that road crash victims have prlorily over
other casualty patients. Therefore these pallenls have only to waif fora medical officer when bofh doctors are examining road crash patienfs.The observed service times of lhe medical officers for the two differenttime periods are presented in Table B/23,
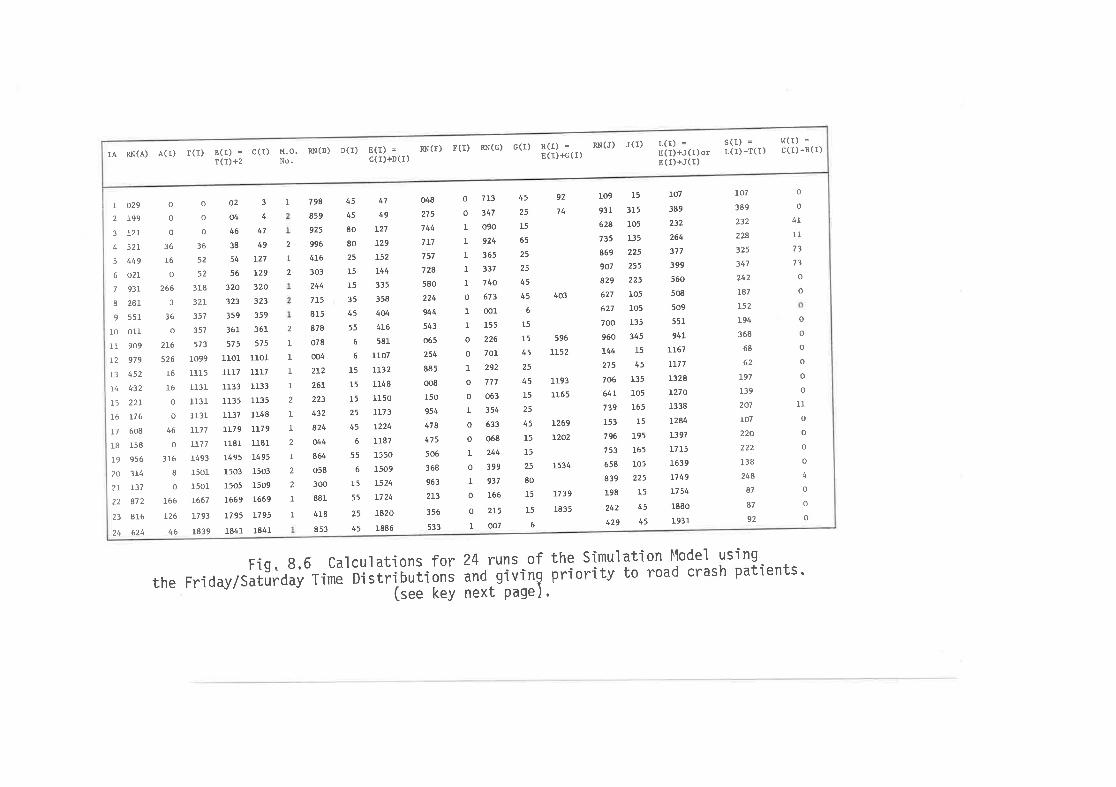
RN(J)RN(r) r(r) Rx(G)IA RN(A) A(l) r(I) B(I) = c(I)
T(r)+2M.O. RN(D)No.
D(I) E(I) =c(r)+D(r)
c(r) s(l) =E(t)€(r)
J(l) L(r) =H(l)+J(I)orE (r) +J(r)
S (I)L(t)
= w(r) =
-r(r) c(r) -B(r)
o
o
o
36
52
52
318
32L
357
357
573
to99
l1t5113r
1131
t r31
LI17
]-77
1493
r50l1501
t667
t793
1839
47
49
L27
L29
L52
t44335
358
4ú4L6
581
1107
LL32
1148
1150
LL73
L224
1187
1550
1509
L524
t724
1820
1886
048
2?5
744
7L7
757
728
580
224
944
543
065
254
885
oo8
150
954
478
475
506
368
963
2L3
356
533
o 713
o 347
I O90
| 924
1 365
I 337
1 740
o 673
I 001
r t55
o 226
o 701
L 292
o 777
o 063
L 354
o 633
o 068
L 244
o 399
L 937
0 166
o 215
1 007
596
LLs2
1193
1165
t269
120.2
r09
931
628
735
869
907
829
627
627
700
960
144
275
706
64r739
153
796
753
658
839
198
242
429
15
3r5
105
135
225
255
225
r05
105
135
345
15
45
135
105
165
15
r95
165
105
225
t5
45
45
r07
389
232
264
317
399
560
508
509
551
94L
LL61
LL71
L32g
I270
1338
1284
t397
L7L5
r639
r749
rt 54
1880
r931
t07
389
232
224
125
347
242
r87
¡52
194
368
68
62
L97
139
207
r07
220,tt
138
244
87
a7
92
o
I2
3
4
5
6
7
8
9
IO
llL2
t3
t4
l5I6
t7
lgl920
2l
23
24
c29
199
t2L
521
449
o2l931
28L
551
oll909
979
452
4'32
22L
116
608
158
956
314
137
872
816
624
o
o
o
36
I6
o
266
3
36
o
216
526
t6t6
0
o
46
o
3r6
Io
166
126
46
798
859
925
996
416
303
244
715
815
878
078
oo4
2L2
26r
223
432
824
ú4864
o58
300
881
4r8
853
45
45
80
80
25
15
L5
35
45
55
6
6
l515
I525
45
6
55
6
15
55
25
45
02304446 47
38 49
54 r27
56 L29
320 320
323 323
359 359
361 361
575 575
1101 lrol1117 1117
1133 1133
r135 1135
1137 1148
1r79 1179
r18r l18l1495 1495
1503 1503
1505 1509
L669 L669
L?95 1795
1841 1841
I 92
74
45
25
15
65
25
25
45
45
6
15
15
45
25
45
15
25
45
15
15
25
80
15
15
6
o
t1l
I173
73
o
2
I2
o
o
o
o
o
o
o
IIo
o
o
o
4
o
o
o
t
1
I1
I2
1
I2
I2
2
II
403
1s34
rt39
1835
Fig, 8.6 Calculations f or 24 runs of the Simulation ttlodel using
rhe Friday/sarurdãv-ri*ã Disrri-buitàñi ãn¿ givtng prioritv ro road crash parients"--J (see keY next-Page) '
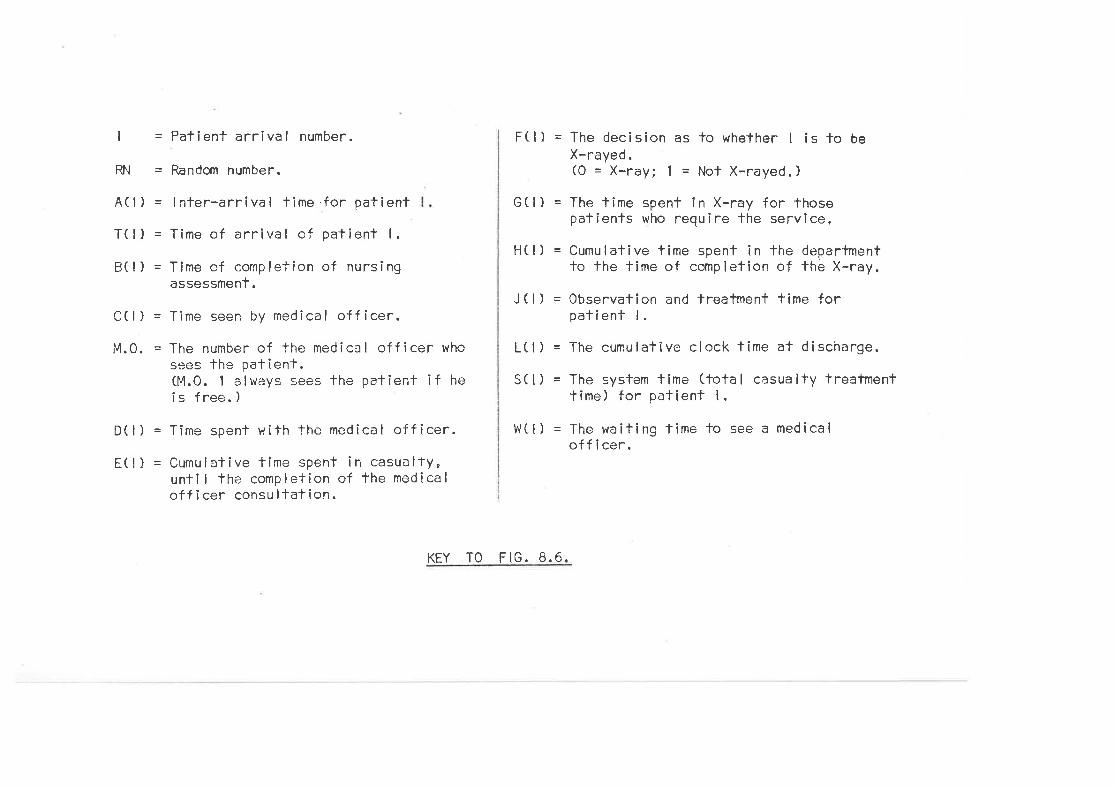
l=
RN=
A(l) =
T(l) =
B(l) =
C(l) =
Patient arr¡val number.
Random number.
I nter-arrival time .for patient
Time of arrîva I of patient I .
Time cf completion of nursingassessmenf.
Time seen by medical officer.
F(l) = The decisîon as to whether I is to beX-rayed.(0 = X-ray; 1 = Nol X-rayed.)
G(l) = The lime spent in X-ray for thosepatients who require lhe servlce.
H(l ) = Cumulative time spent in the deparfmentto the tîme of completion of the X-ray.
J ( l) = Observatîon and treatrnent time forpatienf l.
L(l ) = The cumulative clock time at discharge.
S(l) = The system time (total casualty treatmentt irne ) for pat ient I .
W(-I) = The waiting lime to see a medicaloff i cer.
M.0. = The number of the medical officer whosees the patienf.04.0. 1 always sees the patient if hei s free. )
D(l) = Time spent with the medical offÎcer.
E( l) = Cumulalive time spent in casualty,unti I the completion of the medicalofficer consultation.
KEY TO FIG. 8.6.
7_21
After beíng seen by a medical officer, palienfs are sent toX-ray, discharged, or they wait for some additional service. For thepurposes of the simulation patients either go fo X-ray or they are dis-charged from casualty. Seventy per cent of the sunday to Thursdaypopulalion received X-rays as compared with onlv 50l of lhe Friday-saturday patienfs. Those patients who are discharged from casualtywithout X-rays waif for variable periods before fhey are discharged.The service time of this discharge operation (the observation and treaf-menf time) varies considerably since mosf patients are not dischargedimmediately. For example, many pafienls with head injuries are observedfor at least four hours and fhose who require in-pafienf admissíon waitfor the completion of admission documentation procedures before theyleave the casualty department.
Two separafe simulations of 100 arrivals at the casualfydepartmenl were run using fhe inter-arrival and service time distrlb-utions shown in Tables 6/22 end B/23, a conslanf nurse assessment timeof fwo minules and the dislribution of times to discharge after service.One run represented the Sunday-Thursday time period and lhe other simul-ated the Friday-Saturday situatíon. Twenty-four runs of the Friday-Saturday simulation are shown in trlg.8.6. The resulting simulatedwaÎting times to see the medlcal officer during both time periods arecompared in Table B/24 (see p,22D,
During bolh time periods the wailing f îmes are subslanlf allyreduced by giving priorify fo road crash patients, but even with theprlority policy, 6f, of lhe Friday-saturday crash patlenls wall longerthan 50 minutes for their first medical consultation.
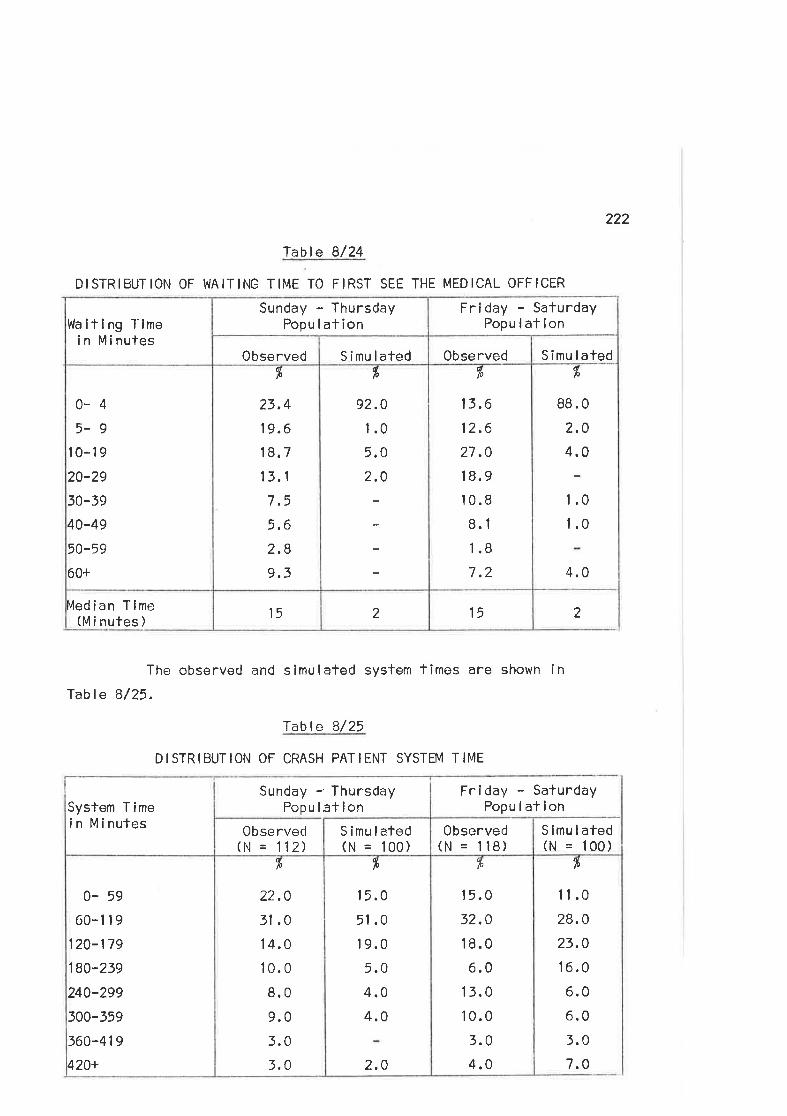
222
fable 8/24
DISTRIBUTION OF I{AI-TING TIME TO FIRST SEE THE MEDICAL OFFICER
The observed and simulated system fimos are shown in
Table B/25.
Table B/25
DISTRIBUTION OF CRASH PATIENT SYSTEM TIME
215215Vedian Tlme
(M i nufes )
dfo
88.0
2.04,0
1.0
1.0
4.0
olo
13.6
12.6
2t.0I8.910.8
8.1
1.8
7.2
fr
92.0
1.0
5.0
2.0
al0
23,4
19.6
18.7
13.1
7.5
5,6
2.89.3
0-45-9
l0-19
20-29
30-39
40-49
50-59
60+
Simulafed0bservedSimulated0bserved
Waiting Tlmei n Mi nutes
Friday - SafurdayPopulation
Sunday - ThursdayPopu lat ion
fr
11.0
28.0
23,0
16.0
6.06.0
3.0
7,0
fr
1 5.0
32,0
18.0
6.0
1 3.0
10.0
3.0
4.0
fr
15.0
51 .0
19.0
5.0
4.04.0
2.0
dlo
22,0
31 .0
1 4.0
10.0
8.0
9.0
5.0
t.0
0- 59
60-1 1 9
120-179
180-239
240-299
300-359
360-419
420+
S imu lated(N = 100)
0bserved(N = ll8)
Sunday -'ïhursdayPopuletion
0bse rved(hl = 1 12)
S imu lated(N = 100)
System Timein Minules
Frlday - SaturdayPopulafion
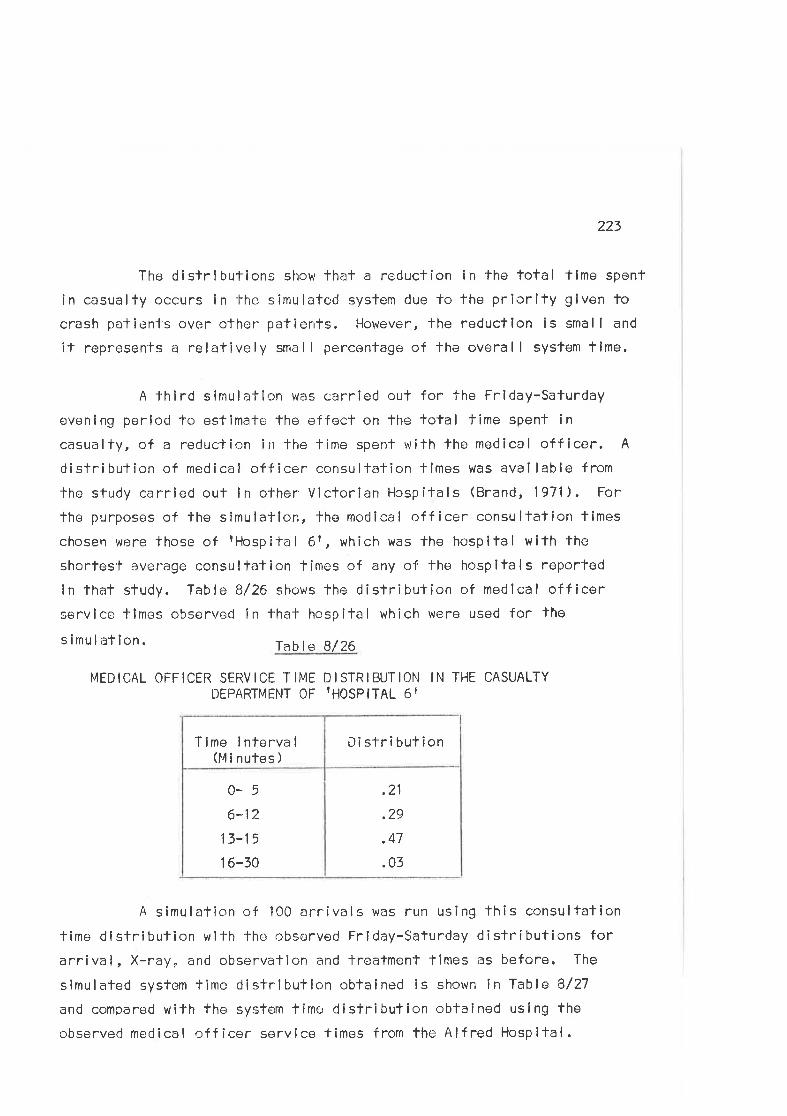
223
The distrlbutions show that a reduclion in the total lime spenf
in casualty occurs in -l-he simulated system due to the priorlfy glven tocrash patients over othor pafients. However, fhe reduction is smal I and
if represents a relatively small percenfage of the overall sysfem time.
A third simulation was carried out for the Frlday-Saturday
evening perlod to estimate the effect on the lotal fime spent incasualty, of a reductic;n in Ìhe time spent wifh the medical off icer. A
distribution of medical officer consultation tlmes was avai lable from
tho study carried ouf in olher Victorian Hospltals (Brand,1971). For
the purposes of the simulation, the medical c.rff icer consultation fimes
chosen were those of rHospifal 6r, which was the hospital with the
shorlesÌ average consulfation times of any of'the hospitals reported
in that sludy. Table 8/26 shows the distribufion of medlcal officerservice tlmes observed in thaf hospital whîch were used for the
s imu lation. Table 8/26
MEDICAL OFFICER SERVICE TIME DISTRIBUTION IN THE CASUALTYDEPARTMEI{T OF 'HOSPITAL 6T
.21
2A
.47
.03
0-56-12
l3-15
1 6-50
DislributionT íme I nterva I
(M i nutes )
A simulation of 100 arrivals was run using this consultalion
fime dlstribution wifh the obsorved Friday-Saturday distributions forarrival, X-ray, and observalion and treatment TÎmes as before. The
slmulated system time dislributlon obtained is shown ín Table B/27
and compared with the system time distribution obtained using the
observed medical oÍl icer service times f rom the Alf red Hospital.
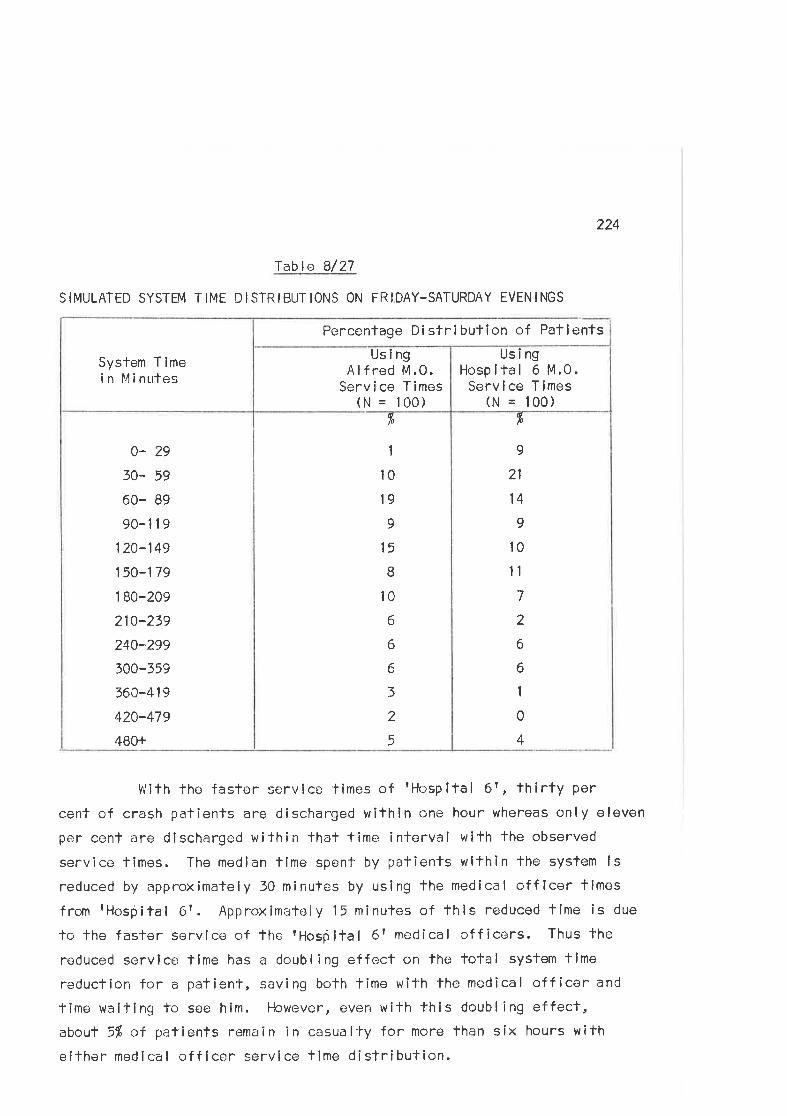
224
fable 8/27
S IMULATED SYSTEM T IME D ISTR IBUT IONS ON FR IDAY-SATURDAY EVEN INGS
fr
o
21
14
I10
1l
7
2
6
6
1
0
4
r,
1
10
19
9
15
B
10
6
6
6
3
2
5
0- 29
30" 59
60- 89
90-119
120-149
150-179
1 B0-209
210-239
240^299
300-559
360-4 1 9
420-479
480+
UsingHospifal 6 M.0.Servíce Times
(N = 100)
UsingA lf red M.0.
Service Times(N = 100)
System Timei n Mi nutes
Percentage Di stri bulion of Patients
VÍith the faster service times of rHospltal 6r, thirty per
cenf of crash patients are discharged within one hour whereas only eleven
per cenl are discharged within that time interval wlth the observed
service times. The median time spent by patients wlthin the system ls
reduced by approximately 30 minutes by using the medical off icer llmes
from fHosþital 6r. Approximately 15 minutes of this reduced time is due
fo the faster service of the rHosþltal 6rme<lical officers. Thus the
reduced service llme has a doubling effect on the total systan time
reducfion for a patient, saving both time with the medical off icor and
time waiting to see him. However, even with this doubling effect,about 5% oÍ patients remain in casualfy for more than síx hours with
elther medical off icer servlce lime distribulion.
225
DiscussionThis simple simulatlon model is used to demonstrate fhe
methodology and potential appl icabi I ity of the technique to casualty
care problems. Because the data col lected related to lhe observed road
crash victims only, the f îndings of the simulatlon cannot be extrapolated
to lhe total casualty case mix. Moreover, the data aval lable from
casualty records does not permit the validity of the model used to be
tested. The only elapsed time which could be calculated for patients,
other than those observed in fhe study, was the total lime spent În the
casually deparfment. Hence the validity of the model cannot be defin-itely fested. Nevertheless, the results reflect reallfy and suggesl thatmore detailed time sludies could be expected to offer pracf ical solutions
to problems in casualty department administration.
þ) CONCLUSTONS
The analysls of lhe time study data permifs the followingconclusions about casually services to be drawn.
( i ) Road crash patients experience considerable delays incasualty.
(i i ) Road crash patients arrive more frequently on Friday and
Saturday nights fhan during the week nights.(i i i ) Medical officers spend more fime treating the average
weekend evening road crash patient than they do in treatingthose that arrive on weekday evenings.
(iv) Road crash palients spend more lime in casualty on weekend
evenings than during the weokday evenings.
ln addition, the use of a simulation model to tesf the effectof changes in sysïem operalions on The casualty medical officer waitlng
times and syslem time has shown lhat(v) Reducing the medical officer servíce time seems fo reduce
the lotal system time for a patient more than slmply
giving priority to road crash patients over otherpatients in the casualty deparlmenf.
226
(vi) Reducing lhe medical off icer service time in lhe AlfredHospífal casually departmenf lo that of rHospital 6t
saves, on the avcrage, 30 minutes in the casualty depart-ment per pafient; 15 ninulos in reduced time with the
medîcal off icer and 15 minutes in the time spent wailingfo see that doctor.
Operations research has been widely used in indusfry for solv-ing queueing problems which are very similar lo those experienced in
hospifal out-patienf and casualty departments. Problerns of delays in fheseparate 'freatment services caused by pressures on space, equipment and
manpower can be solved by applying fhese analyfical methods. The partic-ular value of mathematical modelling of complox svstems lies ín the ease
with which lhe variables used in formulating the model can be manipulaled
and the effects of lhese manipulations on the various system outputs
observed.
The results of the simuIation performed in this study predictthe effecls of two changes in the method of processing road crash
palien-ls lhrough freatment services in fhe hospital casualty department.
The collection of dala from a more comprehensive patienl group would
permit the study and manipulallon of f low characferistics for allpalienfs passing through the emergency deparfment. Such factors as
increasing the number of trealmenl personnel, or altering patterns ofservice, may be examined and lheir effects on waiting times and patientflow predicted. Results of analyses such as these could be used by
hospilal administrators lo improve manpower a llocations and admlnísten
the processing of patienÌs lhrough the treatment system more efficiently.
Larger simulalions involving many variables can be rapidly and
simply processed by computor. The computer pcrmifs the performance oflarge numbers of simulation runs wlth large numbcrs of differenfvariables, since fhe memory capabi I ities of the machine al low lhe
227
storage and progress¡ve bui ld up of the outpuf variables. Using such
facilities, ê slmulation model can become very realistic, ref lectinglhe contingencies which apply in the roal situation. A particularfeature of the operation is the ability to program for the costs ofeach alternative examined and deduce, as an oulput, the cosl-effective-ness of fhe measures.
An lmportant limltation on the use of operations research
techniques at present is lhe lack of suitable dala descrlbing system
operalions. Most hospital recording systems do nol permit the recal I
of informafion useful for such purposes. Slmi larly, the present rocord-ing systems used by other emergency se¡rvicos do nof record useful data
for such analyses. Special studies must lhus be underfaken to obtainfhe necessary data or, alternatlvely, special dala systems or modlfic-ations of existing recordirrg systems need to be introduced. ln eithercase forward planning is required to ensure the applicabllity and uso-
f u I ness of the clata wh i ch i s co I lected.
Operalïons research has much to offer the health care syslem,
particularly in view of the cost-effectiveness calculafions which can
be included in the studies. t4odifications of data systems to perml+
the routine collection of usable informalion would allow the techniques
to be used mcre widely. Applicaf ion of the methodology should aidadministrative decision making and organizational efficiency.
228
Chapter 9
CONCLUS IONS AND RECOMMENDAT IONS
This study of road crashes and crash pafients was undertakento invesfigate the operation of the emergency care system in an area ofMelbourne. The care provîded at fhe scene and during ambulance frans-port has been related to that provided wilhin the hospital casualtydepartnent and fwo imporlant variables, time delays and the qualify ofpatient care, used fo evaluafe the performance of the emergency
serv i ces .
The major tîme delays during êmergerìcy care occurred withinhospital casualty departments. Ambu lance response times were shortand delays during the phases of ambulance service were generally small.ln casualty departments, however, long delays in al I the treatmenlphases were the rule and applied lo patients irrespective of theirdegree of injury.
Simí larly, the assessments of fhe quality of Ìhe care pro-vided for patients within the system showed fhat significanlly more
patients received unsafisfactory care during casualty than duringambulance frealment. Moreover, the care provîdod wíthin casualfydepartments divergod widely from the normative standards as defined by
seníor members of fhe medical profession. Such large discrepancieswere nof apparont between the ambu I ance care and the def i ned standardsfor fhaf process.
These findings substanfiate the assertion that planners ofemergency services should consider care within the casualty deparfment
when planning modif icatîons to existing services. ln the system studied,particular emphasis should be placed on împroving the effíciency and
qual ity of care provided in hospital casualty departments.
229
A systems approach was used in the study to analyse theemergency care of road crash victims in terms of fhe communications,transport, documentation and treatment subsystems which conrprlse theemergency care system. The major conclusions and recornmendafions ''r
arising from the sfudy will be discussed as they relate to each ofthese four major subsystems.
COMMUNICATIONS
(l ) Communicaflons between Emergency Services (see pp .105-112)Poor communications belween fhe ambulance servlce and
casualty departmenfs affocf patient care in the system and result inthe loss of important ínformation relating to the patienlrs careduring the early post-crash phase. These communicafions broakdowns
are unlikely to be resolved by the installation of împroved tele-communicatlon I inks between the services. They are the result offai lures in inter-professional communicafion betwoen the providers ofemergency care and are thus likely fo require more than fechnicalinnovations for lheir correcflon.
Reeonmendatíons(a) Ambulance and casualty staff members should be encouraged
to liaíse more closely, in order to facllitate mutual
understanding and respect for their tasks within theemergency care system. Case review segsions may be ofvalue in achleving this objective.
(b) Ambulance officers should be regarded as para-medicalprofessionals.
(c) A medical practitioner should be appointed to the sfaffof the ambulance communicatlons centre.ln the flrst insfanco this doctor should administer the
230
bed bureau for the cify. He should also be aval lable toprovido medlcal advico for ambulanco officers at thescene of emergencies and be responslble for advislngcasualty slaf f of imminenf patient arrivals. ulf imately,he should conlrol admissions to emergency beds in al I
fhe major city hospitals ancl be responsible for ensuringthe even distrit¡ution of patients between hospltals.Finally, lf telemetry of patlent data becomes feasible,this doctor shoulC rmonitor the equtpment, advlseambulance officers on treafment, and transmif rolevantdafa to tho receiving casualty staff.
Q) Communications wlthin Hospital (see pp,113-115)A lack of communicatíon was observed between members of the
casualty staff, patients, and their relatives. several patients com-plained of the lack of information provlded during emergency care.Hospital slaff occasional ly attempted to keep patients and relatlvesinformed cf their progress. Nevertheless, the lack of a formal mechanismfor aftending to this important are.¡a of care meant that it was oftenoverlooked.
Rqcormnendøtíon
One member of the trained nursing staff in the departmentshould be appcinted to I ialse between doctors, patientsand their relatives.
(3) Communications Eoui pmenf (see pp.49; 102)
Ambulanco communicalions equipment is adequate for exístingoperations but considerable benefits could be expected from theinstal lation of more sophisticated equipment to assisf data recordlngand processing and faci I itate overal I fleet control. computerlzedsysfems are used for this purpose in several overseas counfries.Existing government departments, notably tho Postmasler-General ts and
231
Army Departments, have communícations experience whlch is relevant fothe emergency care siluation. This expe;rtise should be made avaílableto fhe civi I ian emergency services.
Reeomnenåation
The use of more sophisticated communicatíons systems
should be investigated by the emergency scrvices.
TFANSPORT
(l ) Ambulance Vehiclcs ( see Pp.48; l68-171)Existing ambulance vehicles in Melbourne are wel I designed and
equipped for routine ambulance work. one vehicle is equipped as an
emergency care ambulance and is manned by medical and frained ambulance
staff. This servícers role has yet to be complefely defined and itsusefulness af lhe scene of road crashes ís likely to be limíted.Nevertheless, fhe avai labi I lfy of such services for al I emergencíes isa deslrable development in ambulance care. These ambulances should be
hosp ita I based.
Reeormpndations
(a) Subjecl to the findings of the demonstration project,additional emergency ambulances should be based atselecfed major cily hospitals to service the metropol itanarea. Existing demands are unl íkely to warrant lhedeployment of more than three such ambulances.
(b) Given existing ambulance response limes and traff icconditions in Melbourne, there are no indications forthe use of hel icopters as alternative ambulance
vehicles in the Melbourne metropolitan area.
2t2
(2) Ambu lance Loc ron
The deployment of the ambulance fleef wifhin fhe metropol ltanarea is a complex problem. lt is complicated ln the Melbourne area by
the fact that fhe major public hospitals, parlicularly fhose servíng thearea studied, are al I located close lo fhe cify centre. Ambulance
service limes are affected by the relative locafions of the ambulance,the emergency and the hosplÌal. Operations research analysts could. helplo resol're the problems of ambulance locatlon in the metropolitan area.
Reeotmtenåation
Operations research techniques should be used lo analyzeproblems of ambulance deployment in the metropol ifan area.
(3) Ambulance Transport (see pp.120-123)
lf was nof possible fo demonslrafe any significant change inthe condition of paflenfs as a result of their road Transporf. Two
factors which relaled lo paTient safety and comfort during Transportwere the lack of resfraint mechanisms for seated ambulance patients and
fhe lack of changeover stretchers in casualty departmenfs.
Reeor¡tnenÅa.tione
(a) The Jordan I ifting frame should be used for I iftingseverely injured pafients throughouf theír ambulance
and casualfy care.
(b) Ambulance pafients should not be permitted to sif on
the strelchers in the rear cabin of ambulances withoutadequate crash reslraint.
(4) Protecf ion of the Crash Scene (see pp. l lB-l l9)Present arrangemenls for protecting those lnvolved in
emêrgency care af the crash scene are inadequate.
253
Reeontmendatíons
(a) Emergency services should be required to carry and use
warning devices (e.9. f wifches hatsr, safety triangles)to alert oncoming motorists. The towing services should
be requíred to set out these devices, since they are
usual ly the firsf on fhe scene and perform a secondary
role in the early posl-crash phase.
(b) Al I emergency service personnel should be required towear high visibility safety clothing.
DOCUMENTATI0N (see pp,148-154)
ln present operations data are recorded by each of fhe emerg-
ency services to moet their individual neods, and important operatinginformation is difficult to recal l. As a result, comparisons of per-formance within fhe various areas of the system cannoÌ be made. Forexample, the V.C.A.S. hes for some years recorded fhe times of occurrenceof several of the more imporlant events during fhe ambulance call. The
d¡ff¡culty in collating these separate data items has meant that, unfílrecently, no review of ambulance response fimes has been made by theservice. Furthermore, I i+tle information ls avai lable on the types ofambulance cal I attended and the proportlon of the workload thaf each
represents. Equal ly therc is I ittle data by which performancê and work-loads in hospifal casualty departments may be assessed. such basicinformation is essential for assessing existing servlces and rationallyp I ann i ng future needs.
Existing recording systems have deficiencies over and above
those relating lo the recal I of usoful data. Observafions made duringthis study suggest fhat the recording instruments used are unsafis-factory. Ambulance report forms were raroly used, and fhe casualtymedical record offen contalned incomplete or irrelevant dala. lt ls
234
essential that data shoulcl be simple to collect, useful to those
collecling it, and collected in a manner which is compatible with
modern data processing techniques. Presenl recording systems lack
most of lhese fc;afures.
A co-ordinated documentation subsysfem ls required to col lectdata relallng to the services, fhe crashes and the care received by
the patients. Two types of dala need fo be collected on a routine basis:
(i) lnventory Dala
This information relates to the strucfural aspecfs of
care and needs fo be updated regularly lo permif regular
assessmenf of fhe state of the services.
(ii) Response Dafa
This includes information on response times, utl I izationrates and other performance measures which permlf the
assessment of the efficlency and qual ity of the services
prov i ded.
Documentatlon sysfems for emergency medical services have been
Invesllgated and designed in the United Stales (Bordner, ,l968; Stanford
Research lnstitute, 1969) as a means of recording data which are
demonsfrably useful lo the services. Difficulfies have been experienced
in introducing lhese systems. (Norlhrop, 1911; Stanford Research
lnstitule, 1970,) The intrcduction of new data systems is a difficullunderl'aking in a singl<; service, to say nothing of an integrated
system to involve several services. Therefore it is importanT thatthey should replace or complement exisfíng instruments ralher than add
to the already large volume of paper work that confronts those vrorking
in the services.
235
Reeorrunendatíons
(a) A co-orclinated documenfafion subsystem should be
considererJ for use by the emergency services involvedin caring for road crash victims.
(b) Existing recording instruments, notably the ambulance
report form on a casualty and fhe hospital casualtymedlcal record, should be complefed in appropriatedetai I for each patient,
TREATMENT
(l) Firsf Aid at the Cras h Scene (see p,129)Although the ambulance service was the major provider of first
aid af the scene of the sfudy crashes, members of the general publicoffen performed effectivo first aid during fhe early post-crash phase.Mass education campaigns have been suggested as methods of raising thegeneral level of f irsf aid skill in fhe ccrnmunity, wilh the aím ofimproving the emergency care of victims. lt should be noted that, intruly I ífe-saving sifuafions, the ski r rs of the anaesthefist orresuscllatíonist are likely to be required; skills whích are beyond
fhe training of many medical practltioners to say nothing of fírstaiders. l+ is noteworthy that docfors rarely altended the studycrashes. They can contribute to the welfare of those ínvolved and
should thus be encouraged fo atfend and treaf patients at the sceno.The life-saving potenf ial of f irsl aid is diff icult to determine, bufits very existence is sufficient fo encourage rational allempts toachieve ¡t. voluntary first aid schemes should be encouraged, and, ifwider first aid training ís fo be adopted, it should be directed ln thefirst insfance fo selected occupational groups such as faxi and towtruck drivers.
2t6
(2) Ambulance Care
T.he performance of ambulance care for crash victlms was
observed to be satisfactory given the level of fraining and skÍll offhe ambulance officers. Training and equipmenf standards are commensur-
able with those described for similar services overseas. As with allprofessionals, it ís desirable thaf ambulance officers should be as
skÎ lled as possible and ambulance authorlties in Victoria are apparentlytakíng positíve steps fo improve the standards of care within theservice. Def iciencies in care occurrecJ infrequently and on no occasionwas fhe palientrs condition adversely affected by the care (or lack ofit) providecl.
(3) Casua lty Care
Major deficiencies were detected in the performance of carewilhin hospital casualty deparfments. Tlme delays during casualtywere excûssivo, departments were manned by junior staff who lacked
supervision, and poor qual ify care was frequently observed.
Reeornnendations
(a) Senior medical off icers should be appointed to supr,:rvise
casualty operafions lhroughouf the day.
These docfors should take over the supervisory functionsof the existing casualty surgeons (see pp. 138; 160).
(b) Casualty medical sfaff should be rostered so fhat daí lyworking shifts can be reduced to a length which iscompatible with personal ancJ departmenfal eflíciency(see p.160).
(c) Admiffing officers should be present in the casuallydepartment lhroughout their rosfered duty periods(see p.201).
237
(d) A formal mechanlsm is needed to summon back-up doctors
fo casualty when workloads become excessive, parllcularlyduring the late night hours (see p,201),
(e) An exporienced doctor should be presenT in the casualtydeparfment at al I tlmes to consult wilh junior sfaffmembers,
(f) Existíng arrangements for patíenf lriage are total lyinadequate (see pp.134; 179).( ¡ ) A senior nursing sister should assess al I pafients
on admission and report directly to a trlage medica I
off i cer.(i¡) Palionts should be seen by medical officers accord-
ing to priorities determined by their severity ofinjury rafher than their posif ion in the palionfqueue.
(g) An obscrvafion ward, manned by traíned nursing staff,should be avai lable lo provide faci I it¡es for the observ-atlon of pafienls awalting transfer or discharge from
emergency care (see p ,146),
(h) Junior sfaff need instrucfion and supervision in theperformance of:(l ) Resuscítation, notably intravenous therapy.
( i i ) The management of fracfures.(¡ii) Minor surgical procedures (see pp,185-202).
239
SUMMARY
Many of the defíciencies ln the emergency care system,particularly those occurring in casualfy deparfmenls, wi I I requireremedial changes in patterns of organization. ln thls regard,considerable benefit could be expecled from further defai led study ofthe system, using operations research technlques. The casualfydepartment, as lhe weakest I ink in the syslem, warrants partícularattenf i on.
Reeornnendation
A sysfems analysis of the casualty department shouldbe undertaken wifh the objective of developing a
model for eff icient casualty operations.
No
Appendix 1
TABLES
V.C.A.S. EMERGËNCY CALLS DURING THE TOTAL SAIVIPLE
PER I OD
V.C.A.S. EMERGENCY CALLS DURING TIMES ON DUTY
PROPORTION OF SAMPLE CRASHES TO THE ESTIMATEDCRASHES OCCURRING IN THE STUDY AREA DURINGTHE STUDY PERIODS
AGË & SEX DISTRIBUTION OF CRASH VICTIMS
ARRIVALS OF THE OBSERVED CRASH VICTIMS AT THE ALFREDHOSPITAL CASUALTY DEPARTMENT BY EACH HOUR OF T}IEDAY OF THE hIEEK
AGE & SEX DISTRIBUTION OF THE STUDY PATIENTS(PHASE TI'JO)
PATTERNS OF CRASH INJURY
ARRIVALS OF ROAD CRASH VICTIMS AT THE CASUALTYDEPART}4ENT OF THE ALFRED HOSPITAL BY HOUR OF DAYOF WEEK DURING THE TOTAL SAMPLE PERIOD
NUKIBER OF PATIENTS OBSERVED DURING DUTY PERIODS,|YvITH THE TOTAL NUMBER OF ROAD CRASH VICTIMSADMITTED DURING THOSE PËRIODS
OBSERVED PATIENTS, AS A PROPORTION OF THE TOTALROAD CRASH VICTIMS ADi4ITTED TO THE CASUALTYDEPARÏI4ENT DURING THE TOTAL STUDY PERIOD
AGE AND SEX DISTRIBUTION OF ROAD CRASH VICTIMSADMITTED TO THE ALFRED HOSPITAL DURING THE TOTALSAMPLE PER IOD
239
Paqe
240
241
242
243
244
245
246
247
248
249
6/1
6/2
6/4
6/7
6/ 11
6/ 12
6/ 15
6/ 19
6/20
6/21
6/22 250
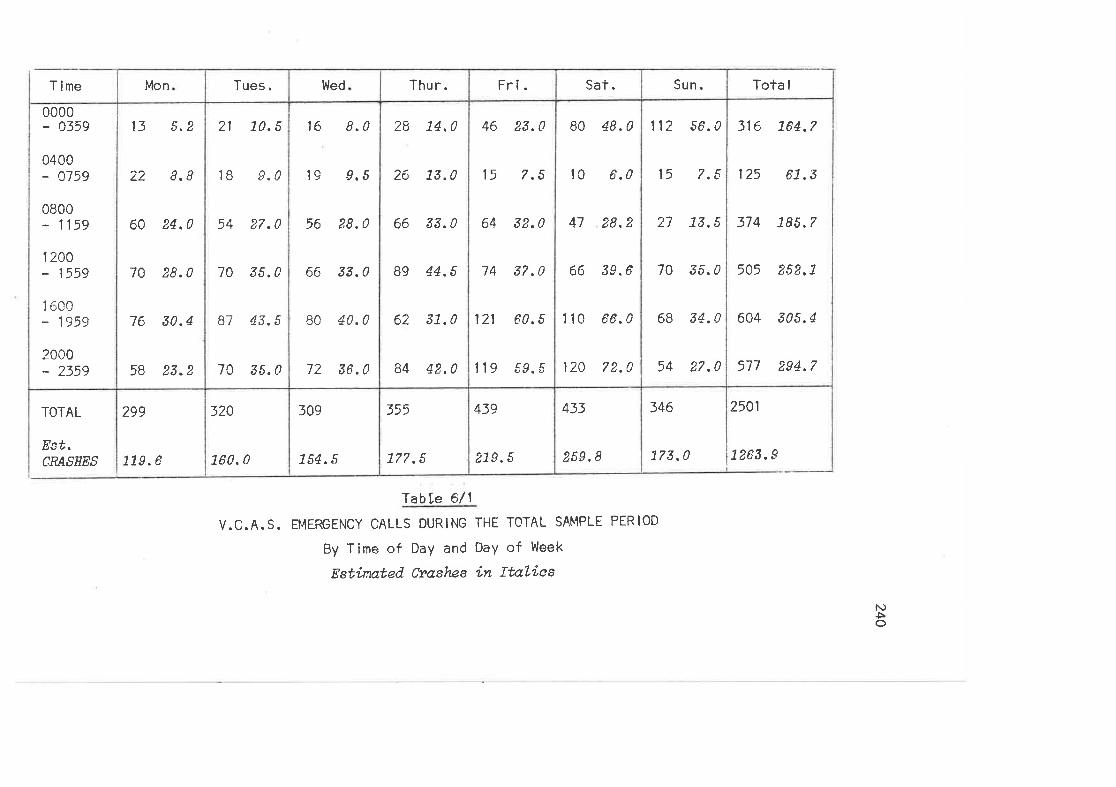
T ime
TOTAL
Est.CRASHES
0000- 0359
0400- 0159
0800- 1159
1200- 1559
1 600- 1959
2000- 2359
299
779.6
13 5.2
22 8.8
60 24.0
70 28.0
76 30.4
58 23.2
Mon
320
L60. 0
21 10.5
1B 9.0
54 27.0
70 35.0
87 43.5
70 3s.0
Tues.
109
754. s
16 8.0
19 9,5
56 28.0
66 33.0
80 40.0
72 36.0
Wed
355
L77 ,5
28 L4,0
26 13.0
66 33.0
89 44.5
62 3L.0
84 42,0
Thur.
439
2L9. 5
46 23.0
15 7.5
64 32.0
74 s?.0
121 60.5
119 59.5
Fri.
433
259.8
B0 48.0
l0 6,0
47 28.2
66 39.6
1 10 66.0
120 72.0
Sat.
346
17s .0
l1?
l5
27
70
6B
54
56.0
7.5
73,5
35.0
34.0
2? .0
Sun .
2501
1263.9
316 764.7
125 67.3
374 78õ.7
505 252.L
604 305.4
577 294,7
Tota I
f abLe 6/ 1
V.C.A. S. EMERGENCY CALLS DURlNG THE TOTAL SAMPLE PERIOD
By Time of DaY and DaY of Week
Estinated Cvashes in ftaLì'es
N)Þo
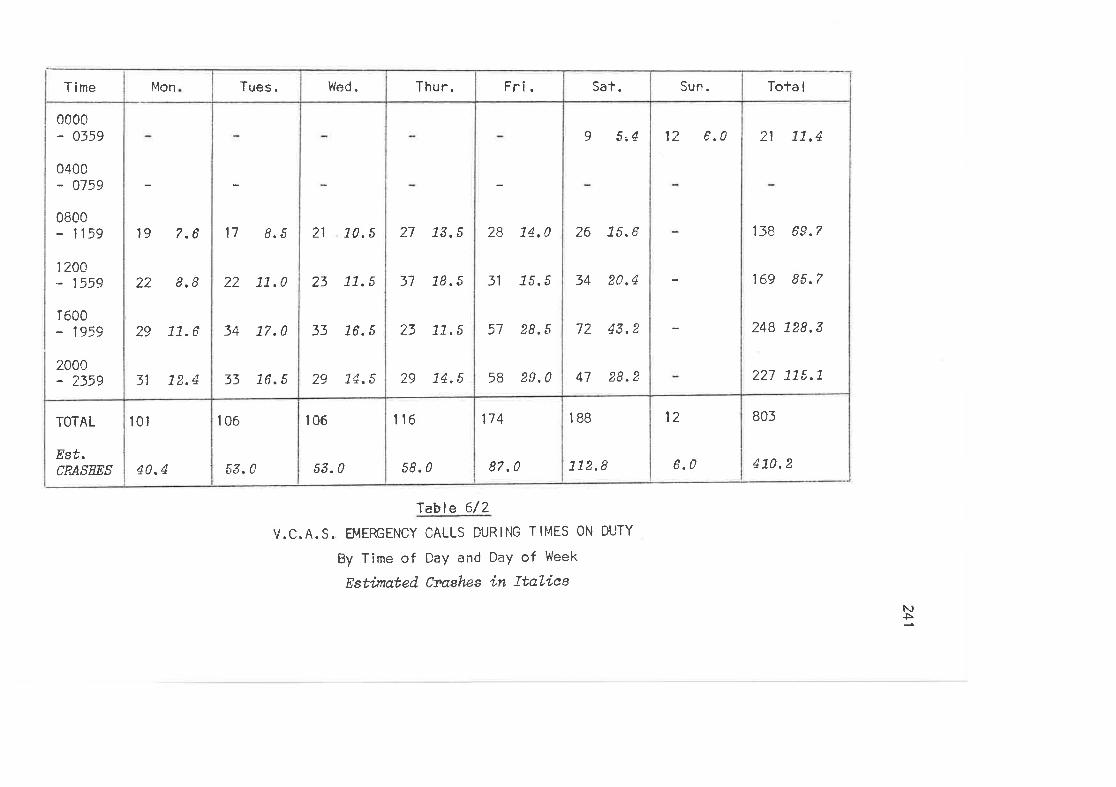
TOTAL
Est.CRASEES
0c00- 0359
0400- 0759
0800- 1159
I 20C- 1559
1600- 1959
2000- 2359
Time
l0l
40.4
19 7.6
22 8.8
29 L7.6
31 72.4
Itilon
106
53. 0
17 8.5
22 7L.0
34 17.0
33 L6.5
Tues.
106
53. 0
21 L0,5
23 L1.5
33 16.5
29 L4.5
Wed.
116
58.0
?7
31
23
29
73. 5
78. 5
77.5
74. 5
Thu r.
174
87 ,0
28 L4,0
31 15.5
57 28.5
58 29.0
Fri.
l88
112.8
9 5,4
26 75.6
34 20,4
72 43,2
47 28.2
Sat.
12
6.0
t2 6.0
Sun.
805
170. 2
21 77,4
I fB 69.7
169 85.7
248 128.3
227 77î,.7
ïota I
'leble 6/2
V.C.A.S. EMERGENCY CALLS DURING TtI"lES ON DUTY
By Time of DaY and DaY of Week
Estínated Ctashes ín ItaLiesNÞ
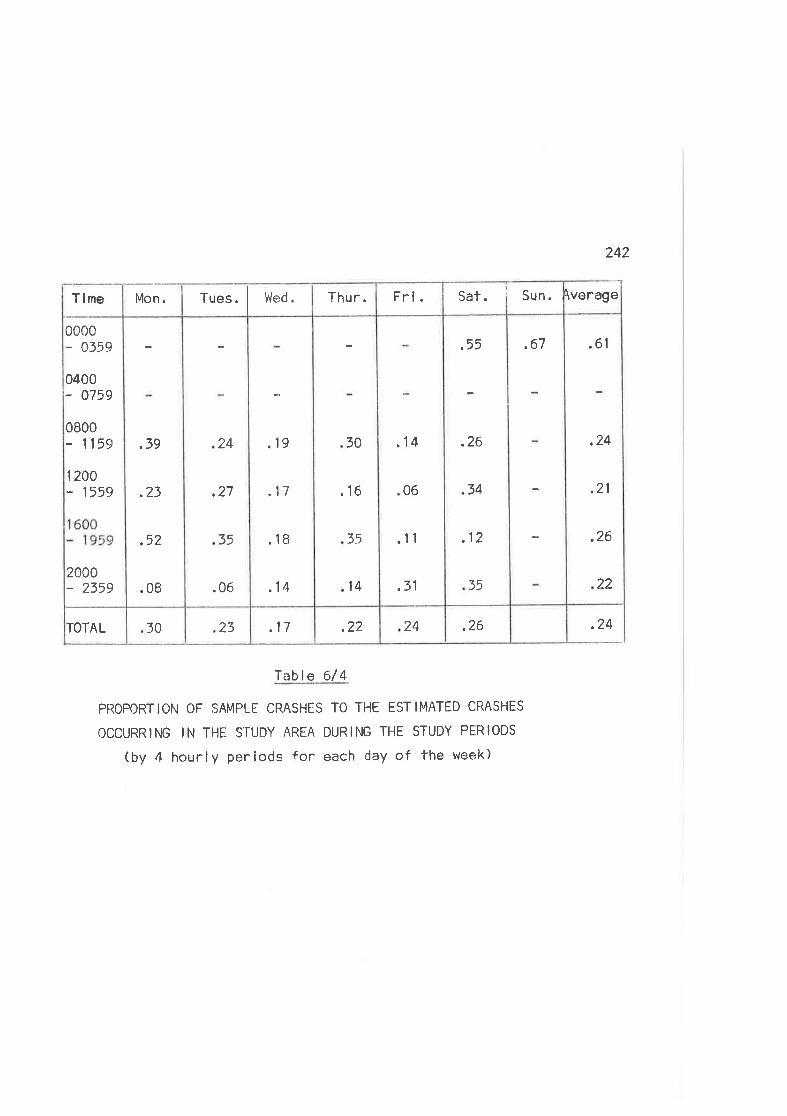
242
.2624.¿¿.172330ÏOTAL
.61
,24
.21
.26
22
,67,55
.26
34
.12
35
.14
06
.11
.31
30
.16
t5
.14
.19
.17
.18
.14
24
,27
35
.0f:
,39
.23
.52
.08
0000- 0559
0400- 0759
0800- 1159
lzaa- 1559
1 600- 1959
2000- 235s
\verageSun.Sat.Fri.Thur.Tues. WedMon.Tlme
.24
f able 6/ 4
PROPORTION OF SAMPLE CRASHES TO THE ESTIMATED CRASHES
OCCURRING IN THË STUDY AREA DURING THE STUDY PERIODS
(by 4 hourly periods for each day of the week)
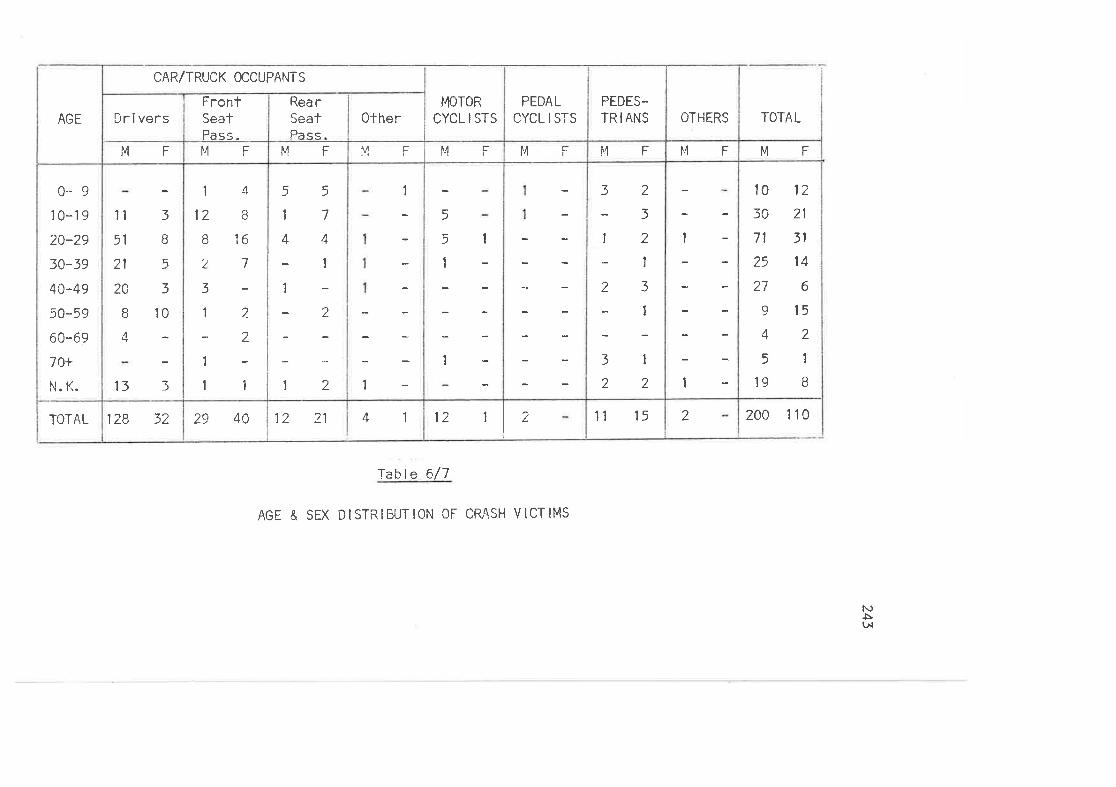
TOTAL
0-9r0-19
20-29
30-39
40-49
50-59
60-69
1O+
N. K.
AGE
128 32
t1
51
21
2A
B
4
3
d
5
3
10
133
MF
Dri vers
CAR/TRUCK OCCUPANTS
29 40
1
t2
B
z
3
I
1
1
(t
16
7
I
aL
1
MF
FrcntSeatPass.
12 21
5
1
4
5
7
4
1
2
2
1
MF
Rea rSeatPass
41
1
1
MF
0ther
12 1 2
5
5
I
I
1
f",1 F
MOTOR
CYCL I STS
f"l F
PEDAL
cYcL I STS
tl 15
32
12-123-t
3122
MF
PEDES-ÏR I ANS
2
,l
1
[.1 F
OTHERS
200 1 10
10
50
71
25
27
9
4
5
19
12
21
3t
14
6
l52
1
MF
TOTAL
Table 6/7
AGE & SEX DISTRIBUTION OF CRASH VICTIMS
f\)è\¡
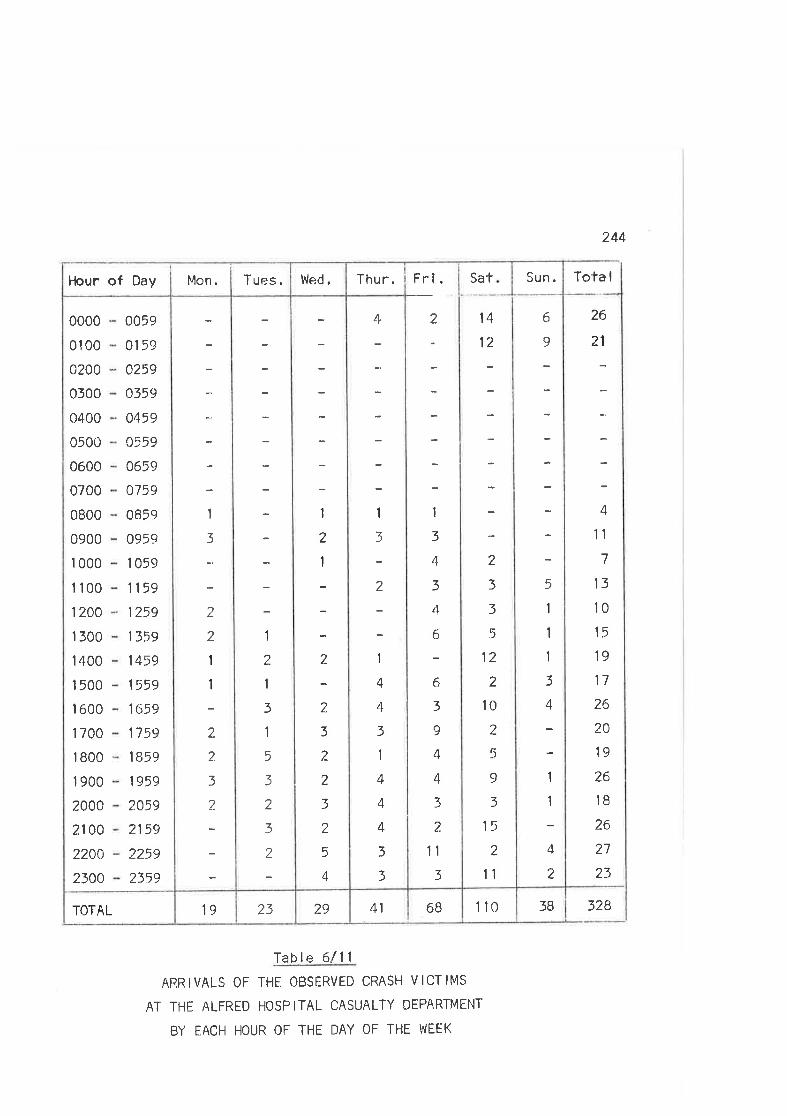
244
3283811041 6B292319TOTAL
26
21
4
11
7
13
10
15
19
17
26
20
19
26
18
26
27
23
6
9
5
1
1
I
3
+̂
1
1
4
2
Sat
\4
12
2
3
3
5
12
2
10
2
5
9
3
15
2
11
Fri.
2
1
3
4
3
tl
6
6
3
9
4
4
3
2
1tz)
4
1
2
1
4
4
3
1
4
4
4
3
3
1
2
1
2
2
3
2
2
3
2
5
ÂT
1
2
1
3
1
5
3
2
3
2
1
3
.,L
2
1
I
2
2
3
2
0000
01 00
0200
0300
0400
0500
0600
0700
0800
0900
1 000
I 100
1200
1 300
1 400
1 500
I 600
I 700
1 800
1 900
2000
21AO
2200
2300
0059
0159
0259
0359
0459
0559
0659
0759
0859
0959
1 059
1159
1?59
1359
1459
1559
1659
1759
1859
1959
2.059
2159
2259
2359
ïota ISun.Thur.Wed.Tues.Mon.Hour of Day
Table 6/11
ARRIVALS OF THE OBSERVED CRASH VICTIMS
AT THE ALFRED HOSPITAL CASUALTY DEPART}4ENT
BY EACH HOUR OF THE DAY OF THE WEEK
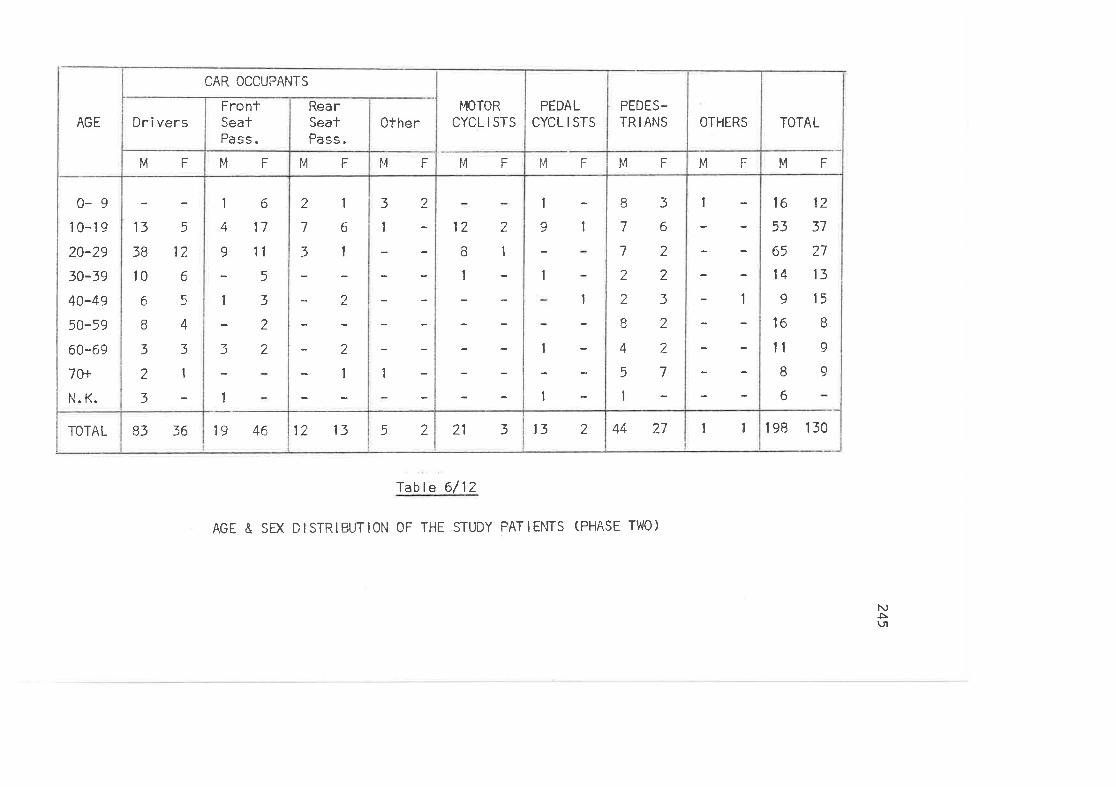
TOTAL
0-910-19
20-29
30-39
40-49
50-59
60-69
70+
I'1. K.
AGE
83 36
13538 12
10 6
Á, çi
B433213-
MF
Dr i vers
CAR OCCUPANTS
19 46
1 6
17
11
5
3
2
2
9
1
3
1
MF
FrontSeatPass.
12 13
2
7
3
1
6
I
)
2
I
MF
RearSealPass.
52
3
I
2
1
MF
Cther
21 3
122B11
t"t F
t40ToRCYCL I STS
132
1
9 I
I
I
1
1
MF
PEDALCYCL I STS
44 27
I7
7
2
2
o(J
4
5
1
3
6
2
2
3
2
2
7
t"1 F
PEDES-TR I ANS
t1
t
1
l''l F
OTHERS
198 130
16
53
65
14
9
16
llI6
12
37
?7
13
15
B
9
9
MF
TOTAL
Íable 6/ 12
AGE & SEX DISTRIBUTION OF THE STUDY PATIENTS (PHASE TWO)
N)5\t
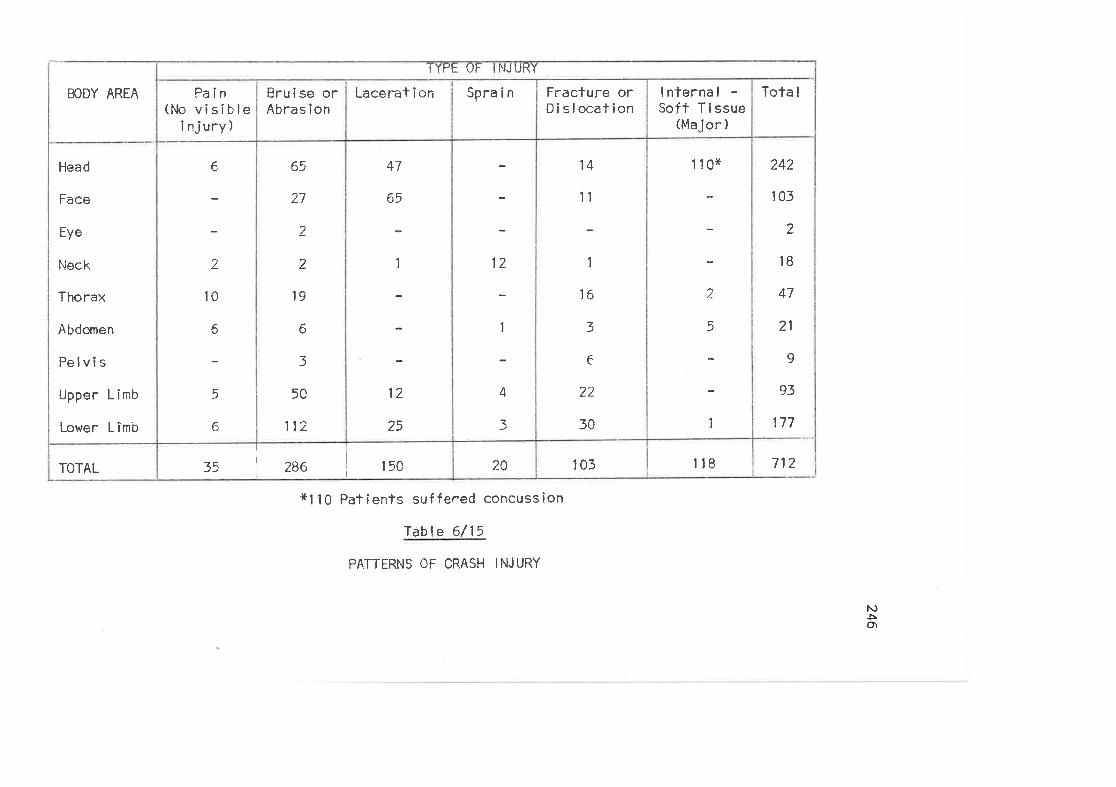
TOTAL
Head
Face
Eye
l,ieck
Thorax
Abdomen
Pelvis
Upper Lirnb
Lower L imb
BODY AREA
35 286 t5c
6
2
10
A
5
^
Fa in(No visible
injury)
TYPE OF INJURY
65
27
2
2
19
6
3
5C
112
Bru i se orAbras ion
47
65
1
12
25
Lacerat i on
20
12
1
4
3
Spra i n
105
14
'll
1
16
3
6
22
30
Fracture orDislocation
r t8
1 10x
.)L
c
I
I nterna I -Soft Tissue
(lvlajor )
712
242
105
2
18
47
21
9
93
177
Tota I
xl 10 Patients suffered concussion
Table 6/ 15
PATTERNS OF CRASH INJURY
1\)ÞOt
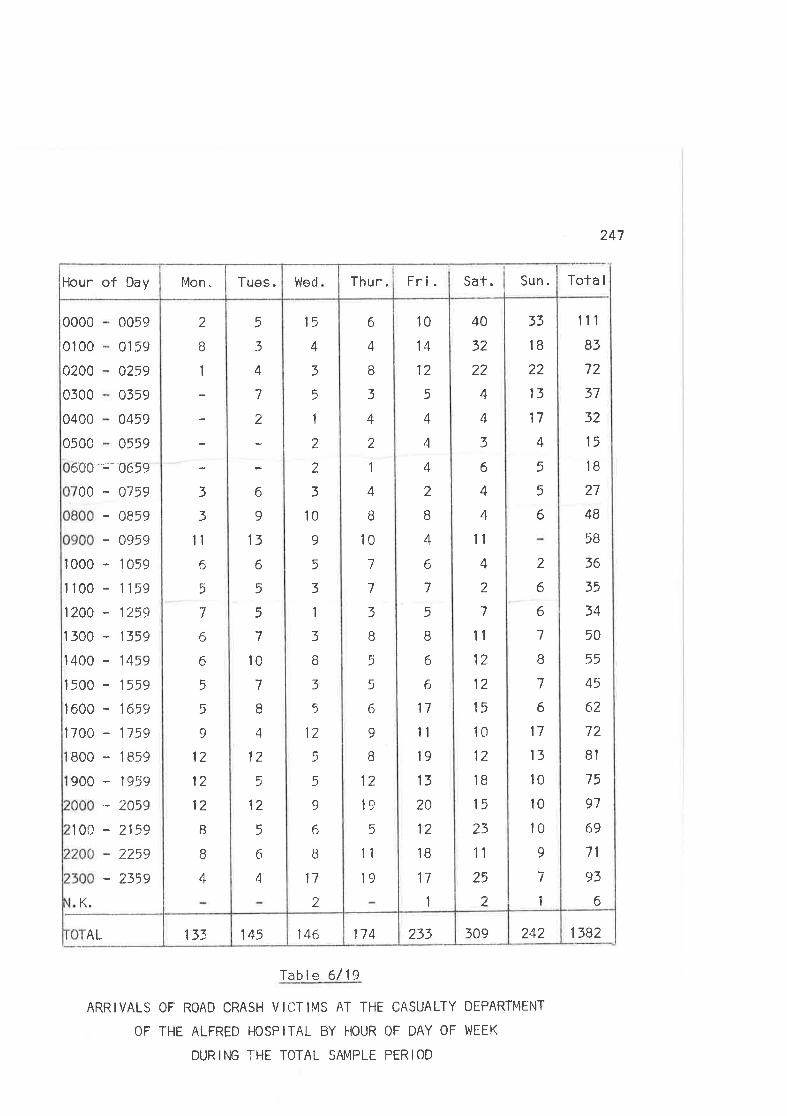
247
Tota I
133AL 146145 109233114 1382242
3
3
tl6
5
1
6
6
È
5
9
12
t2
12
8
B
4
2
ö
I
r 0659
- 0759
- 0859
- 0959
- 1059
- 1159
- 1259
- 1359
- 1459
- 1559
- 1659
- 1759
- 1859
- 195<)
- 2059
- 2159
- 2259
- 2359
K.
100
900
800
00
600'
I 000
1r00
1200
1 500
I 400
1 500
I 600
I 700
0059
8159
o259
0359
0459
0559
0000
01 00
0200
0500
0400
0500
10
14
12
5
4
4
4
2
B
4
6
7
5
B
6
6
17
t1
19
13
2A
12
1B
17
1
6
4
I3
4
2
1
4
B
l07
7
3
o
5
5
6
9
I12
19
5
11
1c)
15
4
3
5
1
2
2
3
10
o
5
3
1
3
ö
3
5
12
5
5
I6
B
17
2
5
3
4
7
:
6
I13
6
5
5
7
10
7
I4
12
5
12
5
6
4
33
IB
22
13
17
4
5
5
6
2
6
6
7
B
7
6
17
13
10
l010
9
7
1
40
32
22
4
4
3
6
4
4
1l
4
2
7
11
12
12
15
1C)
12
18
15
23
1'l
25
2
11r
B3
72
37
32
15
IB
27
4B
5B
36
35
34
50
55
45
6?.
72
B1
75
97
69
71
93
6
Sun.Sat.Fri.Thur.WedTues.Mon.Hour of Day
Table 6/19
ARRIVALS OF ROAD CRASH VICTIMS AT THE CASUALTY DEPARTMENT
OF THE ALFRED HOSPITAL BY FIOUR OF DAY OF WEEK
DURING THE TOTAL SAMPLE PERIOD
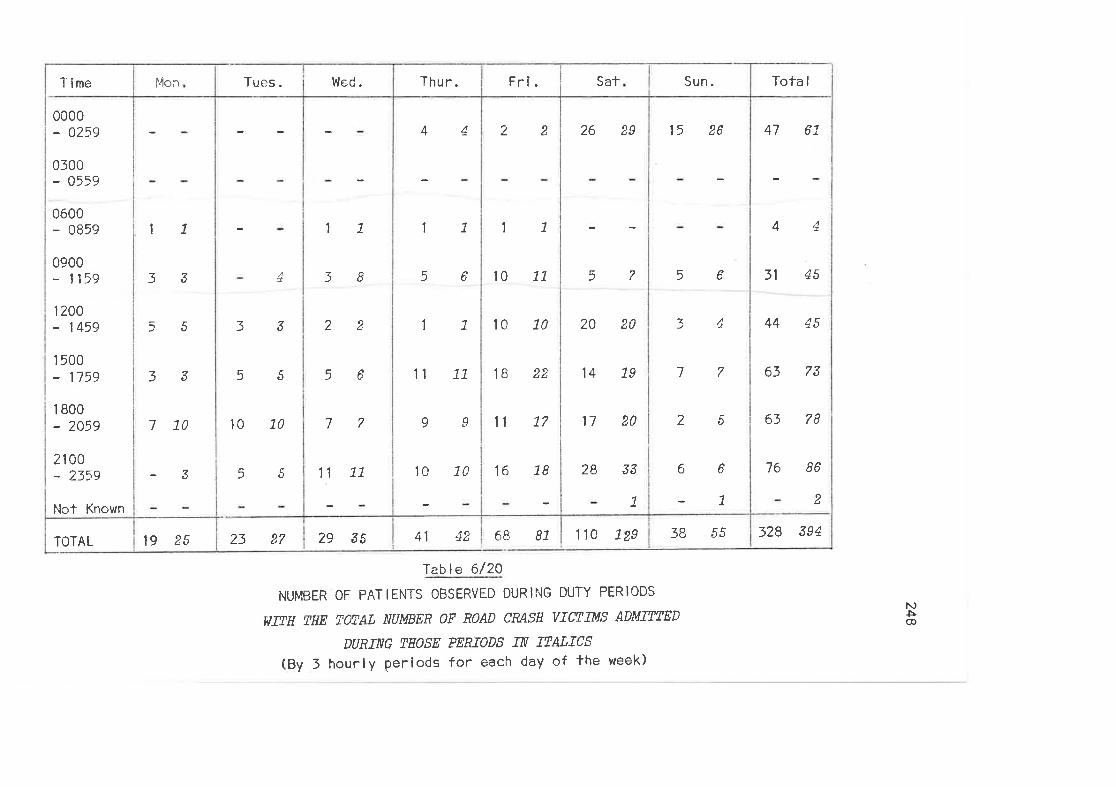
TOTAL
Time
0000- 0259
0300- 0559
0600- 0859
0900- 1159
1200- 1459
1 500- 1759
1 800- 2A59
2100- 2359
Nct Known
19 25
l1
33
5 5
33
770
?
It'lo¡
11
+ 38
zz 22
55 56
to 70 77
55 11 77
23 27 29 35
Tues. Wed.
41 42
44
11
)ô
1L
11 71
oo
10 7C
Thur.
68 81
22
11
10 11
l0 10
18 22
l1 L7
16 L8
Fri.
1 10 129
26 29
57
20 20
14 79
17 20
28 33
7
Sat
JB 55
15 26
56
34
77
25
6 6
7
Sun.
328 394
47 67
44
31 45
44 45
63 73
63 78
76 86
2
Tota I
lable 6/20
NUMBER OF PATIENTS OBSERVED DURII'IG DUTY PERIODS
ïIIH, TIIE ræAL NUMBER oF Rono CRASH vIæLuS AD'\'IIIIED
ÐT]RTNG THOSE PERTADS TX T?ALTCS
(By 3 hourly periods for each day of the week)
NÞ@
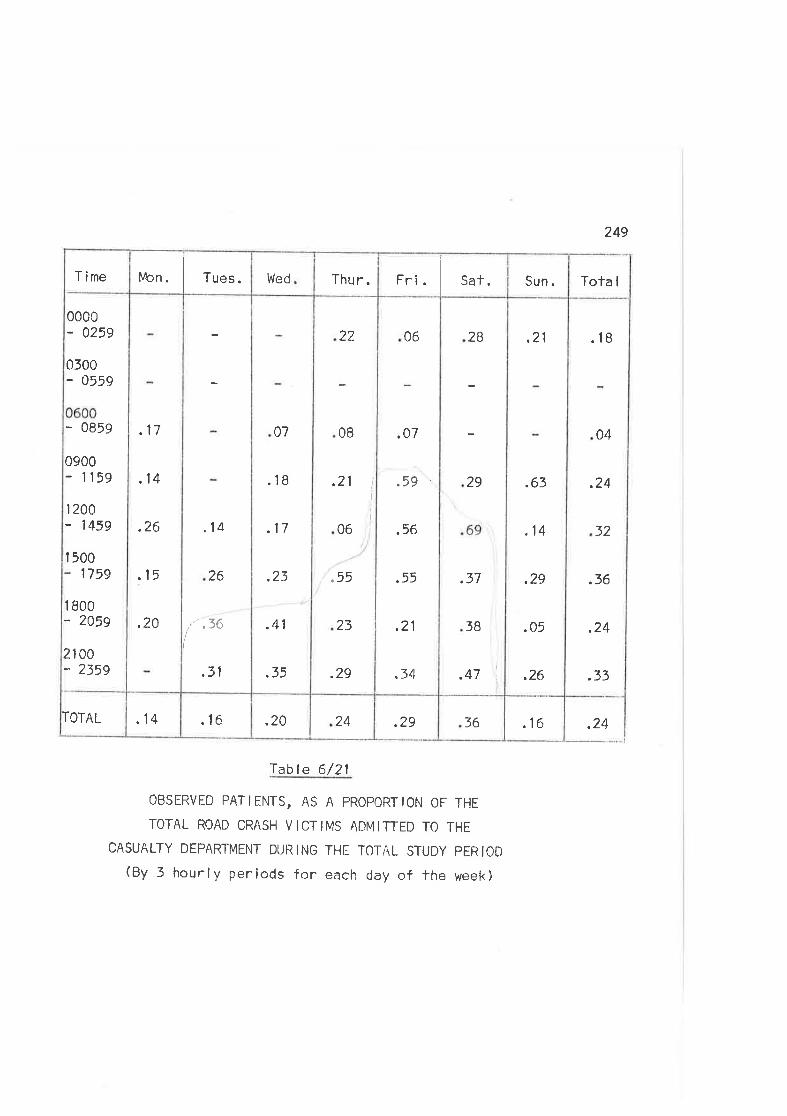
249
.1636.2924.20.16.14TOTAL
.18
04
.24
32
.36
.24
.33
,21
.63
.14
.29
.05
.26
28
29
.37
3B
.47
06
.07
.59
.56
qtr
.21
.34
22
08
.21f
f
06
55
23
.29
07
.18
.17
.23
.41
.35
.14
26
l"tu.31
.17
,14
.26
.15
.20
T ime
0000- 0259
0300- 0559
- 0859
0900- 1159
120Q- 1459
I 5001759
I 800- 2059
2100- 2359
Tola ISun.Fri. Sat.Thu r.Wedi4on . Tues.
.24
Table 6/21
OBSERVED pATtENTS, AS A PROPORTtON OF THE
TOTAL ROAD CRASH VICTIMS ADMITTED TO THE
CASUALTY DEPARTMENT DUIìING THE TOTÂL STUDY PERIOD
(By 3 hourly periods for each day of the week)
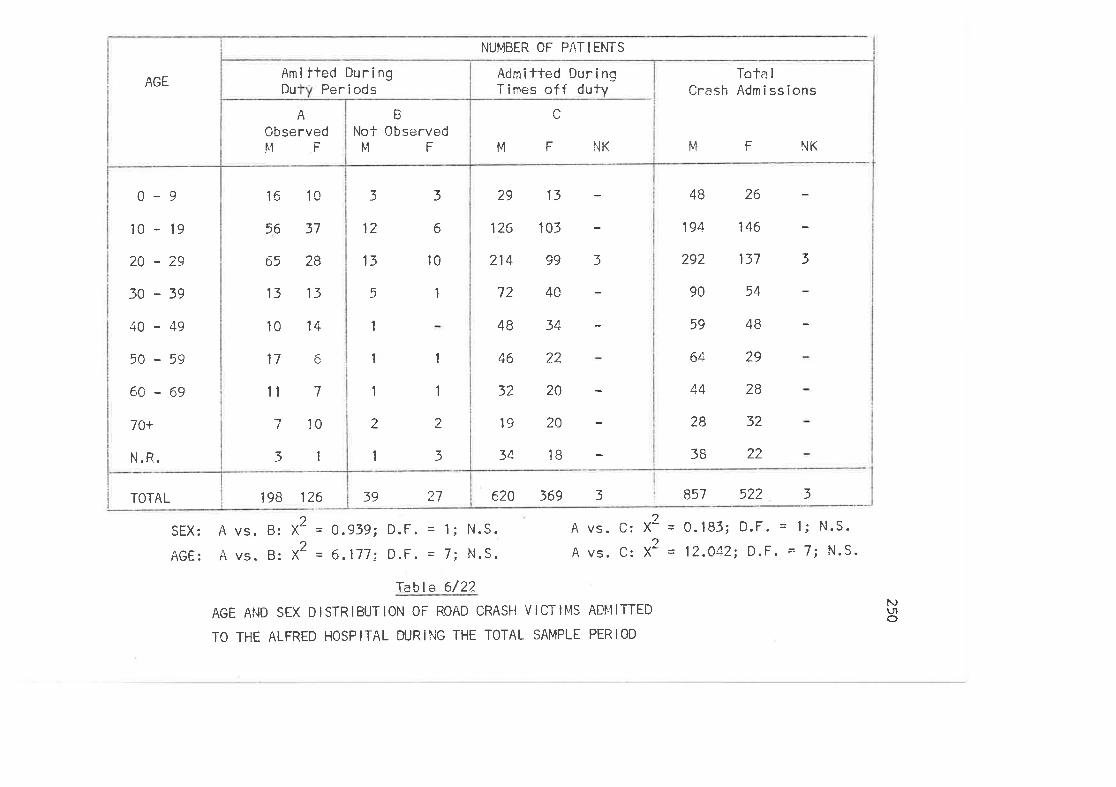
NUMBER OF PATIENTS
TOTAL
0-9
10 - l9
2A-29
30-39
4C-49
50-59
6A-69
7O+
N.R.
AGE
A
0bservedMF
2739
16
56
65
13
10
17
1t
-I
3
14
7 1
I
1
1
2
1
1
6
3
2
31
10
13
28
37
10
5
13
12
3
1
10
B
Not 0bserved¡,1 F
Amitted DuringDu Per i ods
29
126
214
72
48
46
32
l9
34
40
34
22
?0
20
18
13
101
993
NKMF
Admilted DuringTirnes of f duty
4B
194
292
90
59
64
44
28
38
26
146
137
54
48
29
28
3?
22
NKl"l F
620 369 3 857 522 3
3
Tota I
Crash Admissions
198 1?6
SËX;
AGE:
/\ vs. B: X2 = 0.939; D.F. = 1; N.S.
A vs. B: X2 = 6.177; D.F. = 7i N.S.
Table 6/22
AGE AND SEX DISTRIBUTION OF ROAD CRASI] VICTII"IS ADI4ITTED
TO THE ALFRED HOSPITAL DURING THE TOTAL SAMPLE PERIOD
A vs. C:
A vs. C:
2X-
2X'
= 0.18f; D,F. = 1; N.S.
= 12.042; D.F. = 7; N.S.
NL'To
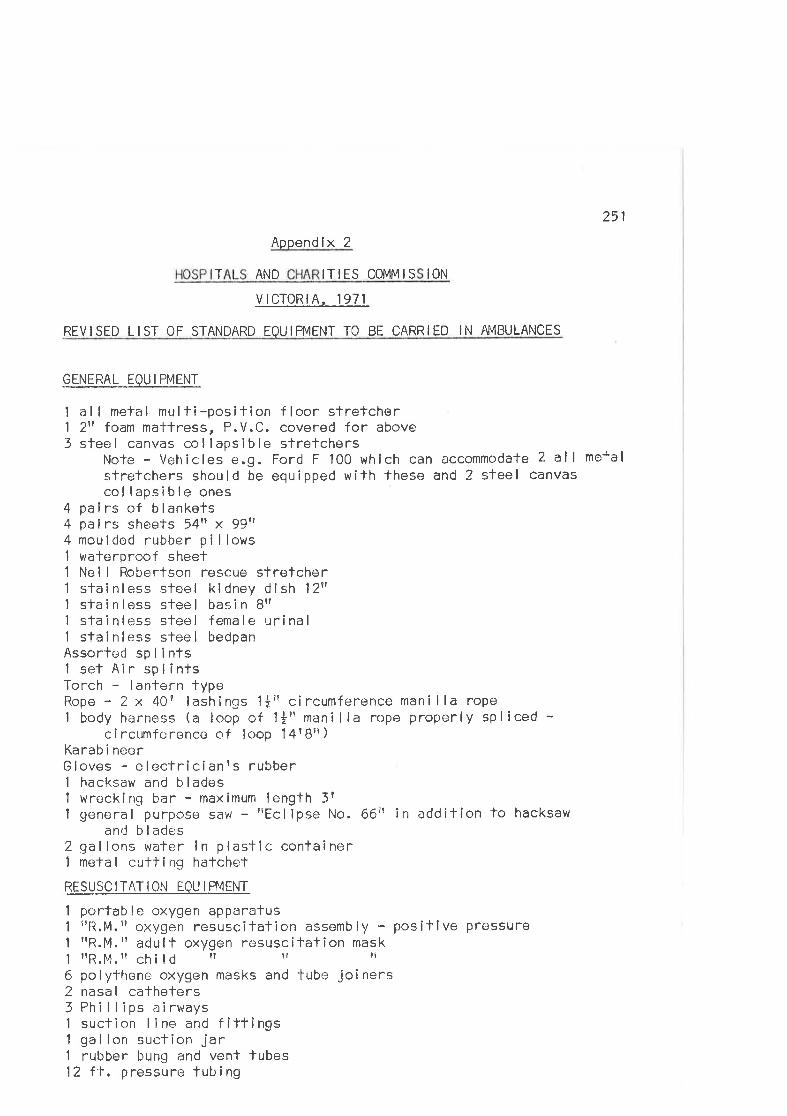
251
Appendlx 2
T AND ITIES COMMIS t0N
vtcToRtA, 1971
REVISËD LIST OF STANDARD EOUIPMENT TO BE CARRIED IN AT4BULANCES
-GENERAL_EQU I PMENT
I al I metal multi-position floor sïretcher1 2rrfoam mattress, P.V.C. covered for above3 steel canvas col lapsible slretchers
Note - Vehicles e.g. Ford F 100 which can accommodate 2 all metalstreTchers should be equipped with these and 2 steel canvascol lapsible ones
4 pa i rs of b I ankets4 palrs sheets 54tt x 99tt4 moulded rubber pi I lows1 walerproof sheef1 Nel I Robertson rêscue stretcher1 stainle;ss sleel kidney dish 12"I sfainloss steel basin Brllstainless sleel female urinal1 stainless steel bedpanAssorled splinfsI set Air splinfsTorch - lanlern typeRope - 2 x 40? lashlngs 'lått circumference mani lla rope1 body harness (a loop of llr? manilla rope properly sPliced -
c i rcumf c rence of loop 1 4 r Br? )
Karab i neerGloves - electricianrs rubbert hacksaw and b I ades1 wrecking bar - maximum length 3?
I general purpose saw - rlEclipse No. 66r' in addition to hacksawand b lacjes
2 gal lons water in plastic conlainr¡r1 metal cutling hatchet
.RESUSC I-TAT ION EO
I porfable oxygen apparatus1 rlR.M.troxygen resuscilation assembly - positlve pressure1 rrR.M. " adu I t oxygen rêsusc itat îon mask1 nR.M.n chiId il ?? Ît
6 polythene oxygen masks and tube joiners2 nasal catheters5 Phillips airways1 suction I ine and fîttings1 gallon suction jar1 rubber bung and vent lubes12 ft, pressure tubing
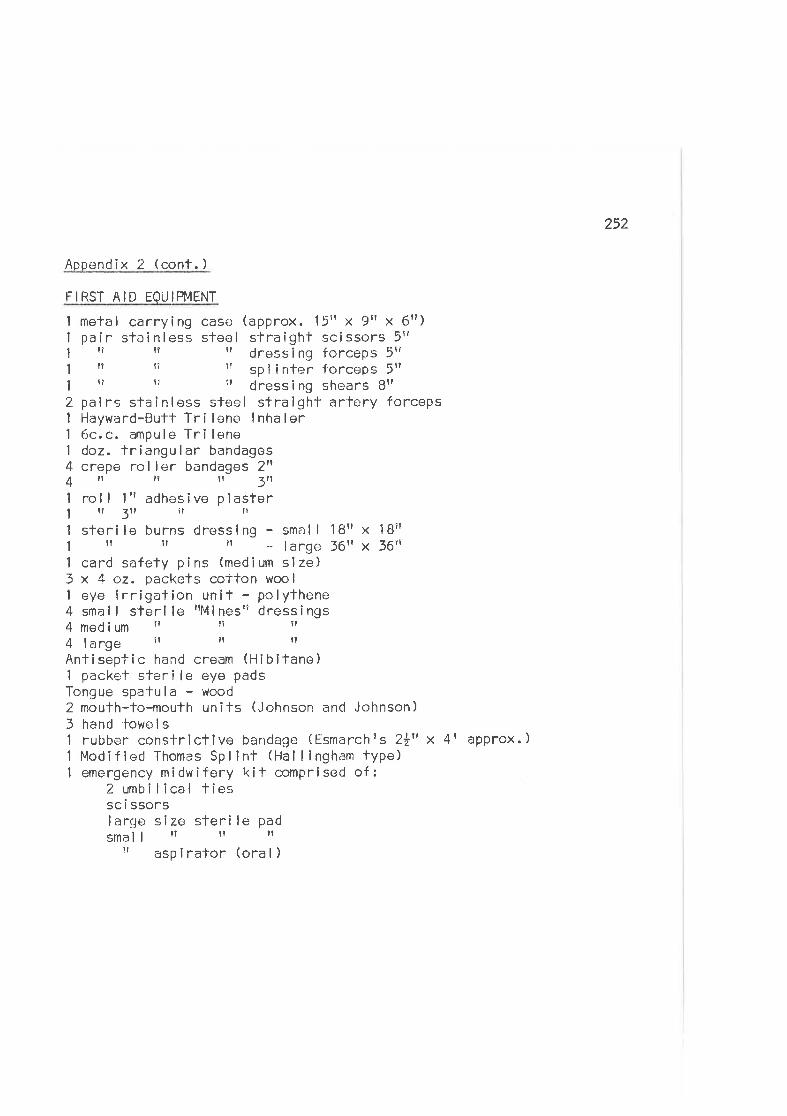
252
Appendix 2 (cont. )
FIRST AID EOUIPNIENT
I metal carrying case (approx. 15t' x 9tr x 6r¡)1 pair stainless steel straighl scissors 5rt1 rr tr rr dressing forceps 5ttI tr tî It sp I inter forceps 5rr
1 er r? 1r dress i ng shears Btr
2 pairs slainless steel straight artcry forceps1 Hayward-Butt Tri lene lnhaler1 6c.c. ampulo Tri lene1 doz. triangular bandages4 crepe roller bandages 2ff4rlil 1r3n1 roll lrradhesive plaster1il3ilifrr1 sterile burns dressing - small lBrr x lBrtI il rr il _lange36tf x36tr1 card safety pins (medium slze)3 x 4 oz. packets cotton woo I
1 eye irrigation unit - po lythene4 sma I I ster i le rrM i nestr dress Ì ngs4 med ium r? re rr
4 I arge lr tr rr
Antiseptic hand cream (Hlbifane)1 packe'f ster i le eye padsTongue spalula - wood2 mouth-to-mouth units (Johnson and Johnson)3 hand lowe I s1 rubber constrictive bandage (Ësmarchis Zttt x 4l1 Modified Thomas Spl int (Hal I ingham type)1 emergency midwifery kit comprised of:
2 unb i lical tiessc i ssorslarge slze sterile padsmall rt rl It
t' asp irafor (ora I )
approx. )
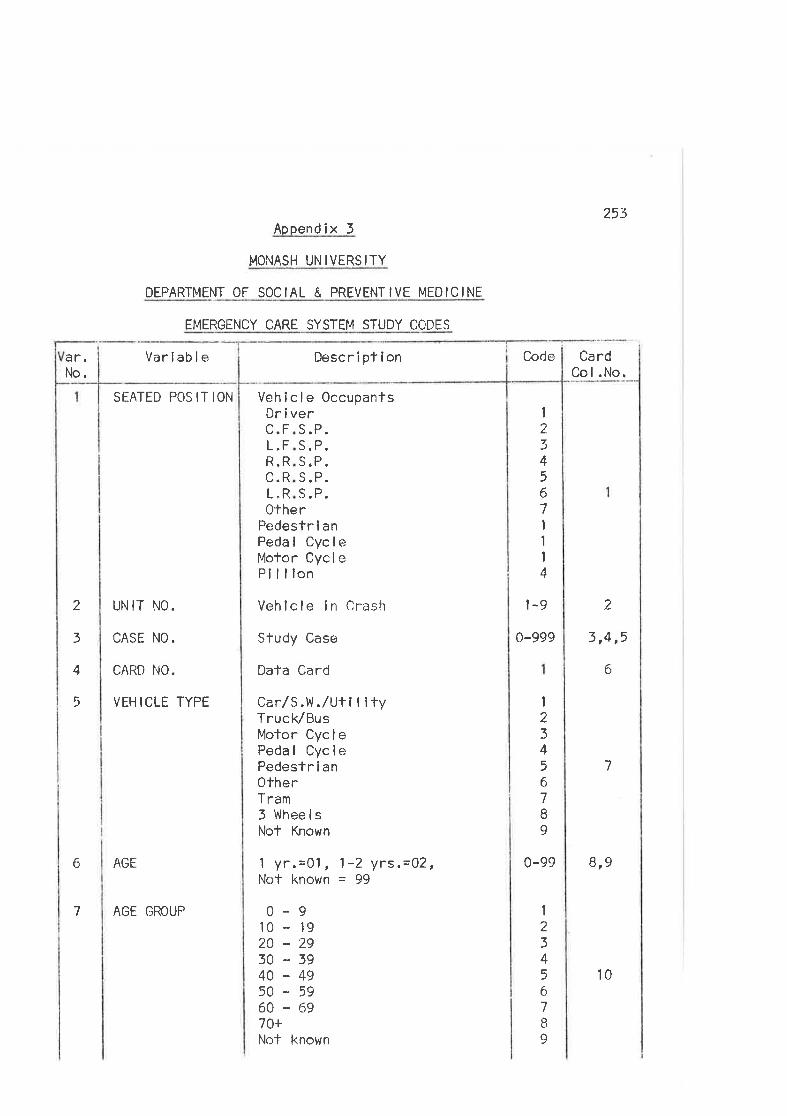
ar.No.
Aopendix 3
MONASH UNIVERSITY
DEPARTMENT OF SOCIAL & PREVENTIVE MEDICINE
EMËRGENCY CARE SYSTEM STUDY CODES
Variable
SEATED POS IT ION Vehicle Occupants
0thePedestr î anPedal CycleMofor Cycl ePillion
253
CardCol.No.
VEDric.FL.FR.RC.RL"R
r 1
2345671
1
I4
s.P.eoS.P.s. P.S.P.r
2
3
4
5
UN IT NO.
CASE NO.
cARt) NO.
VEH ICLE TYPE
AGE
Vehlcle in Crash
Sfudy Caso
Data Card
CarlS.V.l./Uti lltyTruck/BusMotor CyclePedal CyclePedestr i anOtherTram3 WheelsNot Known
1 yr.=01, 1-2 yrs,=02,Not known = 99
0-910 - 1920-2930-3940-495Q '5960-6970+Not known
1-9 2
0-999
6
7
0-99 819
3,4,5
6
7
I234567I9
I234567a
9
CodeDescriplion
AGE GROUP
10
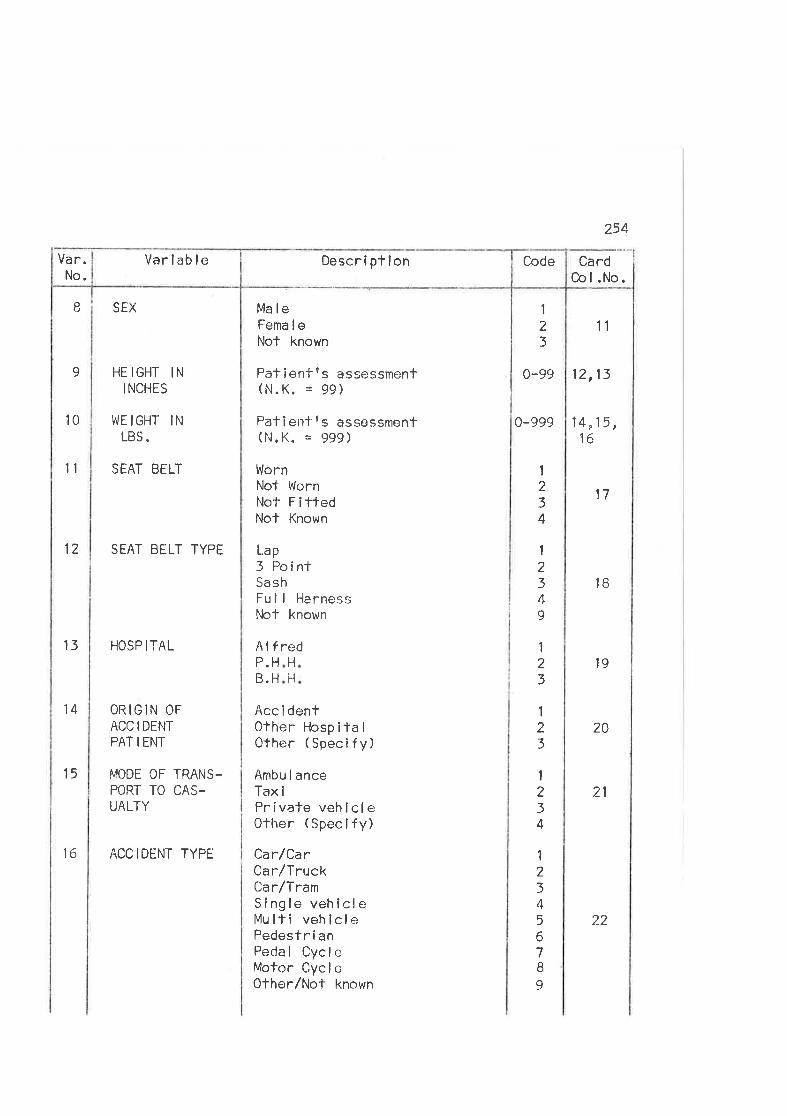
254
I SEX
HE IGHT INI NCHES
10 llJEIGHT INLBS.
11 SEAT BELT
12 SEAT BELÏ TYPE
13 HOSP ITAL
14 ORIGIN OF
ACC I DENT
PAÏ I ENI-
15 MODE OF TRANS,POFJ TO CAS-UALTY
16 ACCIDENT TYPË
Ma loFema I eNot known
Patienfes assessmenf(N.K. = 99)
Pallenfts assessment(N.K. = 999)
WornNot WornNot FittedNot Known
L.ap
3 PointSashFu I I HarnessNlot known
H
Acc i denlOfher Hosp ita I
Other (Specify)
Ambu I anceTax iPrivate vehicleOther (Spec i fy)
Car/CarCarlTruckCa r/TramSingle vehlcleMu lti veh lcl ePedestr i anPecJal CycleMofor CycleOther/Not known
I23
11
14,15,16
17
1B
12,130-99
0-999
9
red
FI
AtfP.HB.H
19
20
21
1
234
I
2349
1
23
1
23
1
234
I234567I9
Card0ol.No.
CodeDescriptlonVariableVa r.No.
22
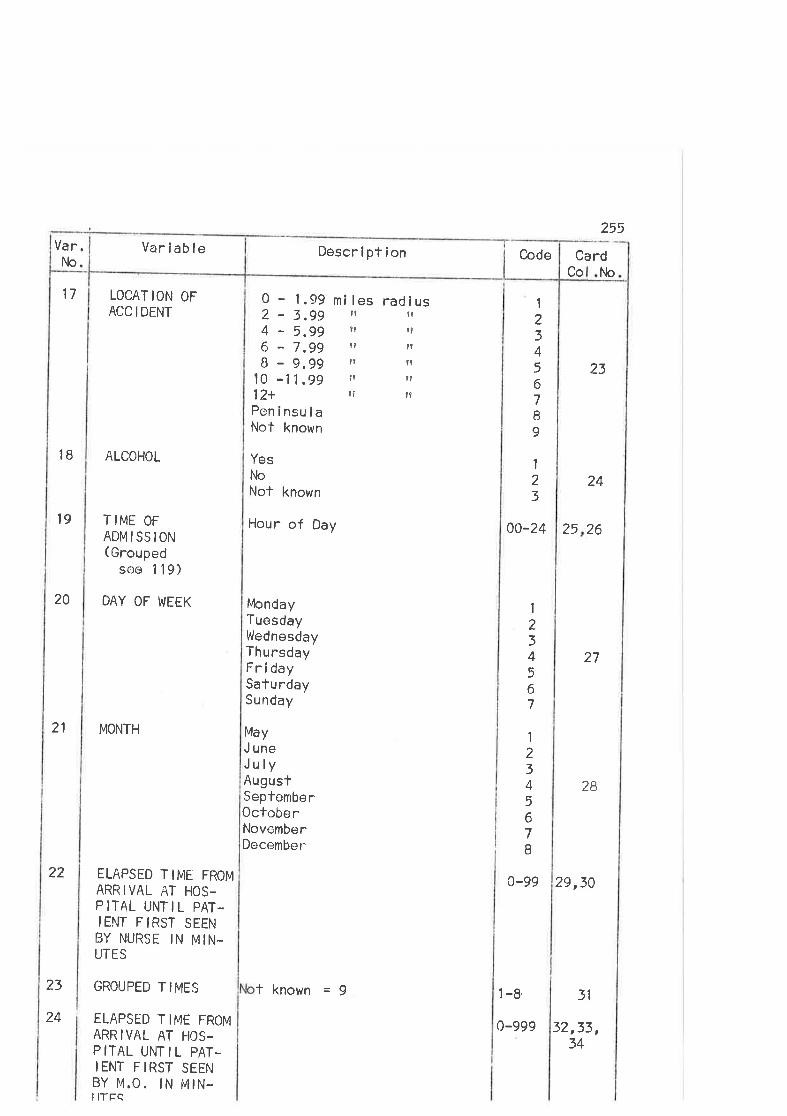
255
17 LOCAT ION OFACC I DENT
IB ALCOHOL
l9 T IME OF
ADMISSION( Grouped
see 1 l9)
20 DAY OF WEEK
21 MONTH
ELAPSED TIME FROMARRIVAL AT HOS.P ITAL UNT IL PAT-IENT FIRST SEENBY NURSF IN MIN.UTES
GROUPED TIMES
ELAPSËD T IME FROMARRIVAL AT HOS.P ITAL UNT IL PAT-IENT FIRST SEENBY M,O. IN MIN-IITtrC
0 - 1.99 mi les radius
Card
23
24
0a-24 25 26
27
28
0-99 29,30
t{oCo
2 - 3.994 - 5,996 - 7.99B - 9.99
l0 -11.9912+PeninsulaNot known
YesNlo
Nof known
Hour of Day
IrtlcndayTuesdayWednesdayThursdayFridaySaturdaySunday
MayJ uneJulyAugusfSeptemberOctoberNovemberDecember
illtItt?
lr
t9
ltn
ilnt?
t1
1
234567I9
I23
1
234567
I23Â
567B
22
23
24
l -8,
0-999
3l
32,33,
CodeDescrlptionVariableVar.Nlo.
f known = j
34
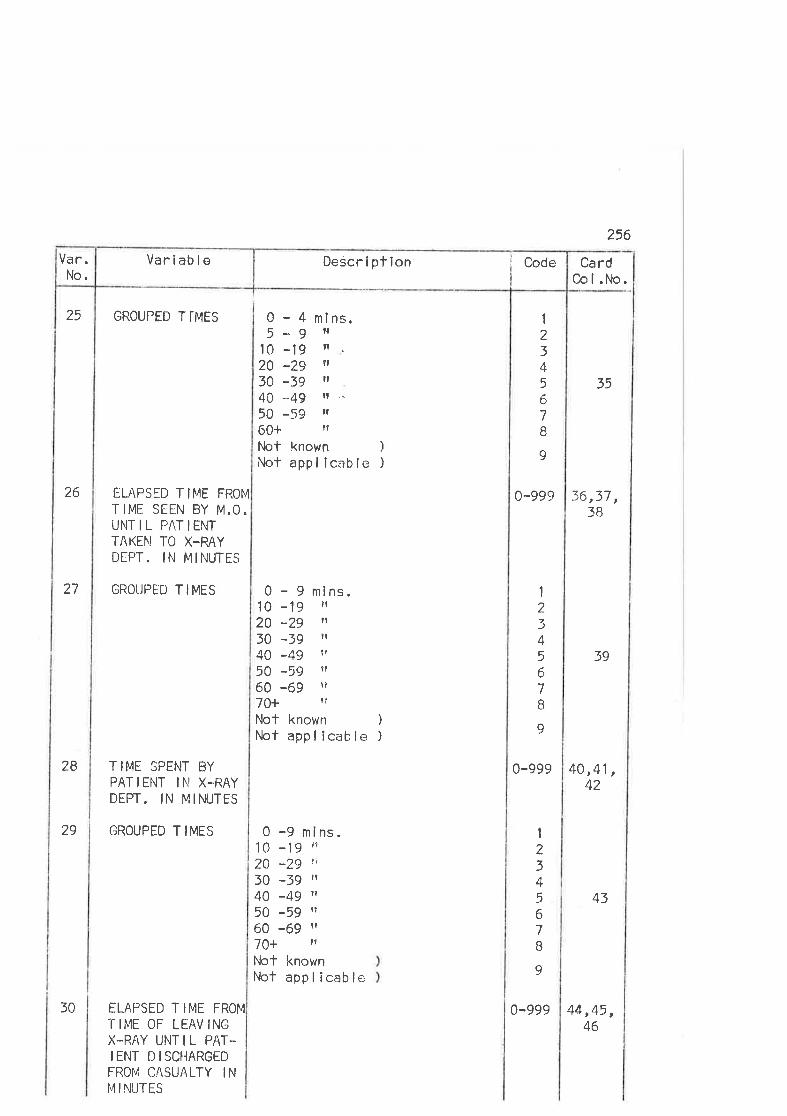
25 GROUPED T I-MES
26 ELAPSED TIME FROI4
TIME SEEN BY M.O.UNIT IL PAT IENTTAKEI\I TO X.RAYDEPT. IN MINUTES
27 GROUPED TIMES
TIME SPENT BYPATIENT IN X-RAYDEPT. IN MINUTES
2B
29 GROUPED T IMES
ELAPSED T IME FROM
Ï IME OF LËAV INGX-RAY UNTIL PAT-IENT DISCHARGEDFROI¡ CASUALTY INM INTJTES
30 0-999 44,45,46
Descr i pf ion iI
CodeVariableVar.No.
0-4m5-9
l0 -1920 -2930 -3940 -4950 -5960+Not known )
Not appl lcable )
0 - 9 mins.l0 -19 'l20 -29 '1
30 -39 il
40 -49 r?
50 *59 11
60 -69 fr
70+ lt
Not known )fùct app I icab le )
i ns.lrtl.Itillt .-
ilr
0-99çr 36
256
Ca rdCol.No,
35
39
1
2345
67B
9
400-999
1
234567B
9
1
234567B
9
,37,3B
,41 ,42
0 -9 mins.l0 -19 "2A -29 \1
30 -fg il
40 -49 t1
50 -59 rr
60 -69 H
70+ I'
Not knownI'irct app I icab le
43
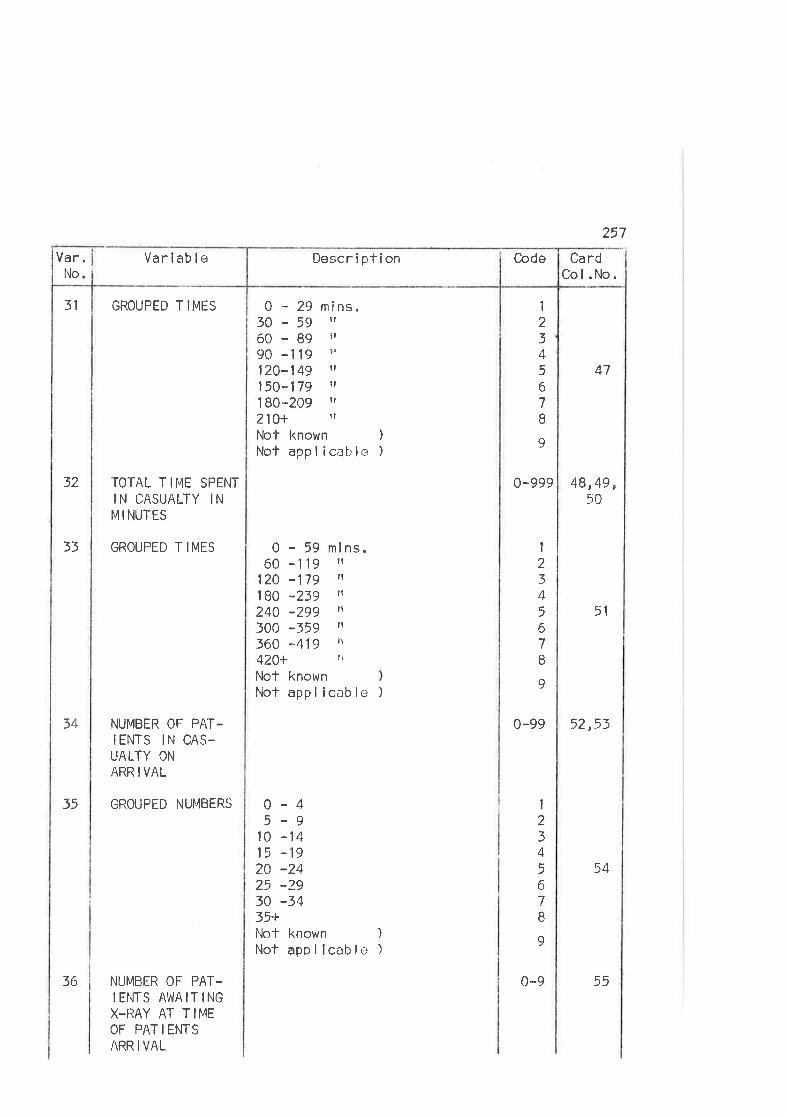
257
0-99932
31 GROUPËD TIMES
TOTAL TIME SPENTIN CASUALTY INM I NUTES
33 GROUPED T IMES
34 NUMBER OF PAT.IENTS IN CAS-UALTY ON
ARR I VAL
35 GROUPED NUÍ'4BERS
NUMBER OF PAT.I ENTS At',lAIÏINGX-IìAY AT T IMEOF PAT I ENTSARR I VAL
0 - 29 mins.30-59 rÍ
60-89 e,
9A -119 îr
120-.149 il
150-179 ?r
1 80-209 il
210+ eî
Nof known )
Not appl icable )
0-5960 -t19
124 .179180 -239240 -299300 -359360 -419420+Not knownNot appl icable )
0-45-9
10 -1415 :1920 -2425 -2930 -3435+llct known )Not appl icable )
1
23+567I9
1
234567II
ml ns.ilIt
It
ft
tr
?l
47
48,49,
51
0-99 52,53
54
50
1
234567B
9
Code CardCol.No.
DescriptionVariableI'lo
Var.
36 0-9 55
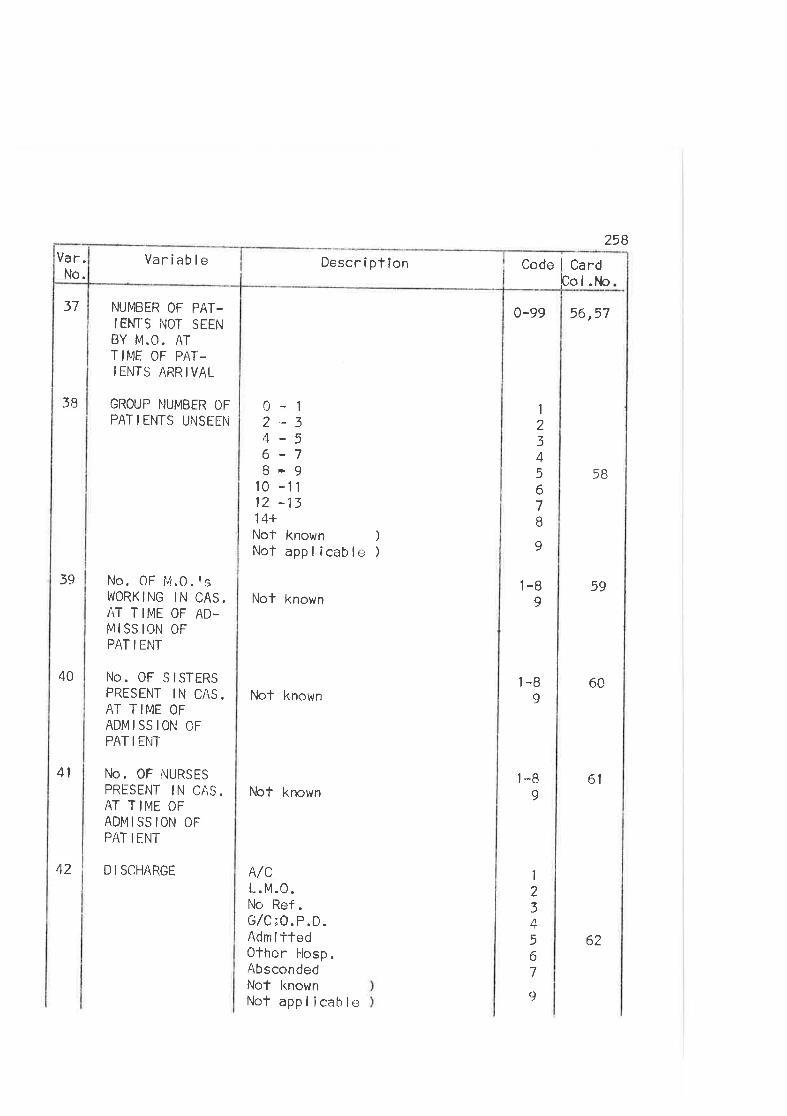
258
37
3B
39
NUMBER OF PAT-IEM'S NOT SEENBY M.O. ATTI¡4E OF PAT-IENTS ARRIVAL
GROUP NUMBER OFPAT I ENTS UNSËEN
No. 0F 14.0 . t sI'/ORK ING IN CAS.AT TIME OF AD-M ISS ION OFPAT I ENT
No. 0F SISTERSPRESENT IN CAS.AT TIME OFADMISSION CFPAT IENT
No. 0F NURSESPRTSENT IN CAS.AT TIME OFADMISSION OFPAT I ENT
42 D I SCHARGE
10 -1112 -1314+Not known )
Not appl icable )
Not known
Not known
l,lct known
A/CL. M.0.No Ref.G/C;O.P.D.Adm i ttedOther l-losp.AbscondedNot knownNot appl icable
0-12-34-56-7B-9
0-99 56,57
58
1-B 599
'l-B 609
l-B 6t9
1
234567B
9
40
41
1
234567
9
Code i Cardþo I .l',*¡
Descr i pt ionVariableVar.No.
62
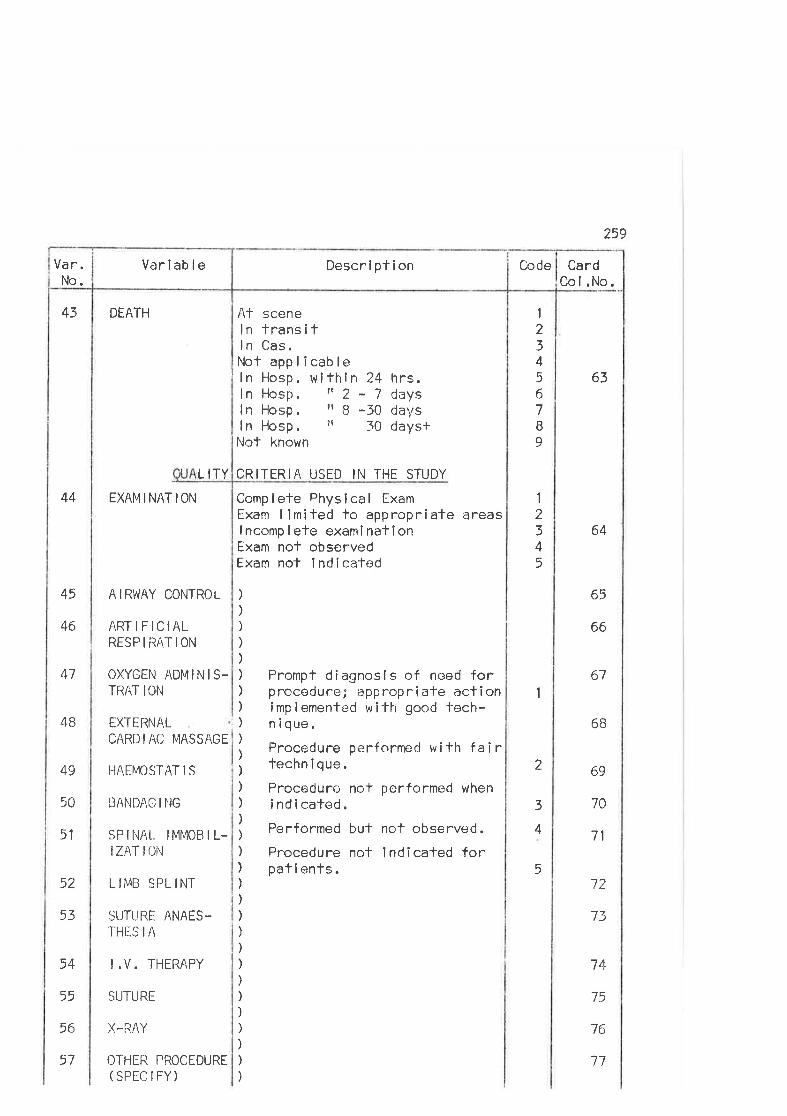
259
43 DEATH
44 EXAMINATION
At sceneln transifI n Cas.Nof applicableln Hosp, wiThin 24 hrs.ln Hosp. 'r 2 - 7 daysln Hosp . rr B -30 daysln Hosp . r' 30 days+Not known
L ITY CRITERIA USED IN THE STUDY
Complefe Physical ExamExarn llmíted lo appropriate areasI ncomp I ete examÍ natîonExam nof observedExam nol I nd Í catod
1
234567B
9
I2345
63
64
65
67
6B
69
70
71
72
73
74
75
76
66
1
45
46
47
4B
AIRWAY CONTROL
ARTIFICIALRESP I iìAT ION
OXYGEN ADMINIS.TRAT ION
EXTERNALCARD I AC I4ASSAGE
I-IAEMOSTAT IS
EANDAO I NG
SP I IiA[. IMMOB I L-IZATION
SUTURE ANAES.THES I A
I.V. THERAPY
SUTURE
X-RAY
OTHER PROCEDURE(SPECIFY)
Prompt diagnosls of need forproceclure; appropri ate actionimp I emented w i -lh good fech-n i que.
Procedure perforrnerJ wilh fairtechn i que.
Procedure not performed wheni nd i caled.
Performed but not observed.
Procedure not indicated forpat i ents .
)
)
)
))
)
))
)
)
)
)
)
))ì
)
))
)
)
)
))
)
)
)
)
)
)
)
49
50
51
2
3
4
552 I- IMB SPL INT
53
54
55
56
57
CardCol.No.
CodeDescrlptionVari ab I eVar.No.
17
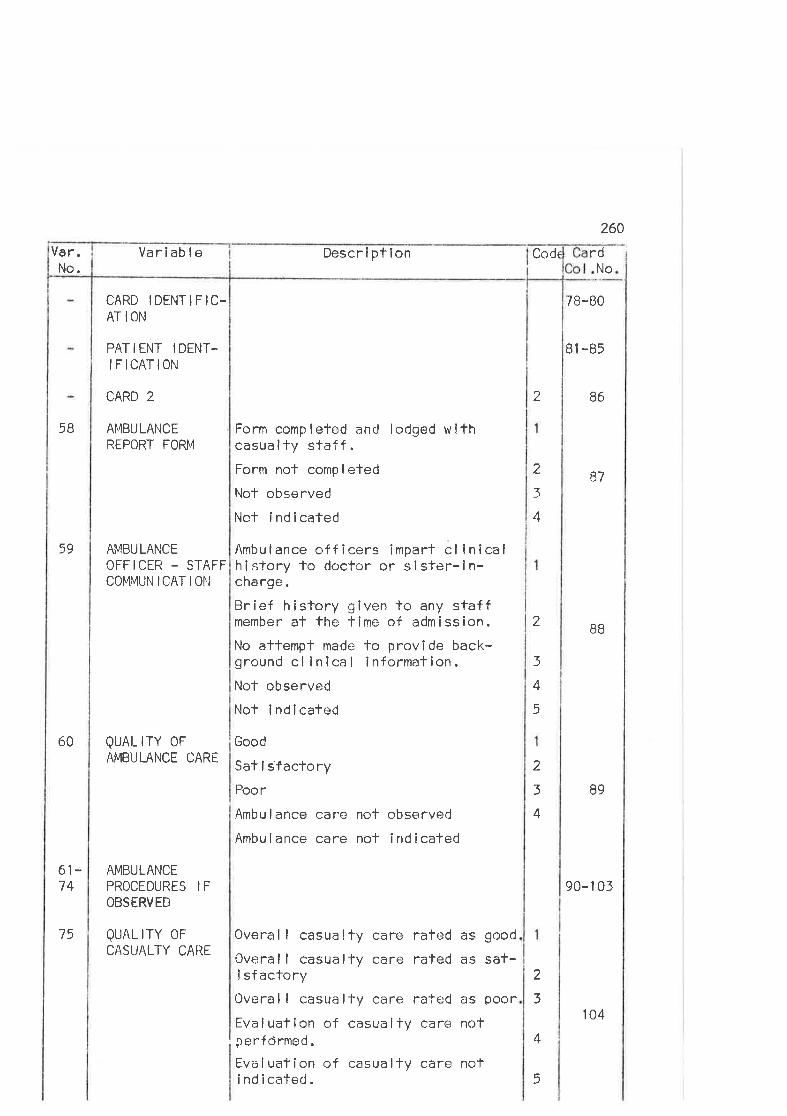
as good
as sa+-
as poor
not
rd
7B-BO
B1 -85
2 86
90-1 03
260
No
5B
CARD IDENTIFIC-ATION
PATIENT IDENT-IFICATION
CARD 2
AMBULANCEREPORÏ FORß4
59 AMBULANCEOFFICER - STAFFCOMI\4U|'ì ICAT I 0¡.J
60 QUAL rïY 0FAMBULANCE CARÉ
Form completed and lodged withcasualty staff.Form not comp I eted
Not observed
Not indicated
Ambulance officers imparl cl inicalhistory to doctor or sister-in-charge.
Brief history given lo any staffmember at the time of admission.
No altempt made to provîde back-ground cl inical infornnation.Not observed
Not lndicated
Good
Sat I sfactoryPoor
Ambu I ance care not observed
Ambulance care not indicated
7_
3
4
87
B8
89
2
3
4
5
2
3
4
61-74
AMBULANCEPROCEDURES I F
OBSERVED
QUAL ITY OF
CASUALTY CAREOveral I casualty care ratedOveral I casualfy care ratedÌ sfactoryOveral I casually cere ratedEva I uation of casua I ty careperfdrmed
"
Evaluation of casualty carei nd i cated .
2
3
4
5
CodeDescriptionVariableVar.No.
75
not
104
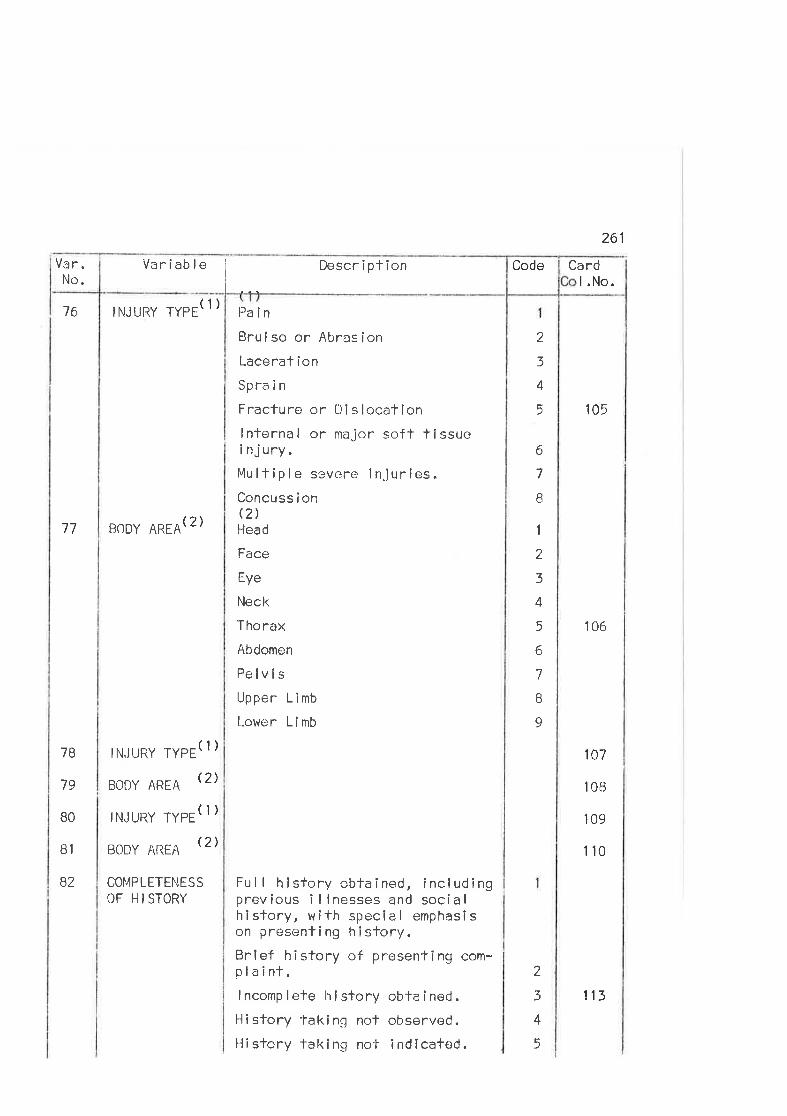
Code
I
DescriplionVariableVar.No.
(1)
261
Cardl.No.
105
106
107
l0B
109
110
76 INJURY TYPE
77 BODY AREA(2)
Pa in
Bruise or Abrasion
Lacerat ion
Spra i n
tracture or Di slocationlnternal or major soff tissuei nj ury.Mulf ipl e sevcre injuries.Concuss ionQ)Head
Face
Eye
Neck
Thorax
Abdomen
PelvisUpper Limb
[-ower Limb
Ful I history obtained, includingprev ious i I I nesses and soci a I
history, wlth special emphasîson presenling hlstory.Bnlef hîstory of presenting com-plaint.Incomp Iete hí stor y obta ined.History takingtr not observr:d.
History laking no-l- indlcated.
2
3
4
5
6
7
I
1
?
3
4
5
6
7
B
9
7B
79
BO
B1
82
(1)
(2)
(1)
(2)
IN.JURY 'TYPE
BODY AREA
INJURY TYPE
BODY AREA
CO¡4PLETENESSOF HI STORY
2
3
4
5
113
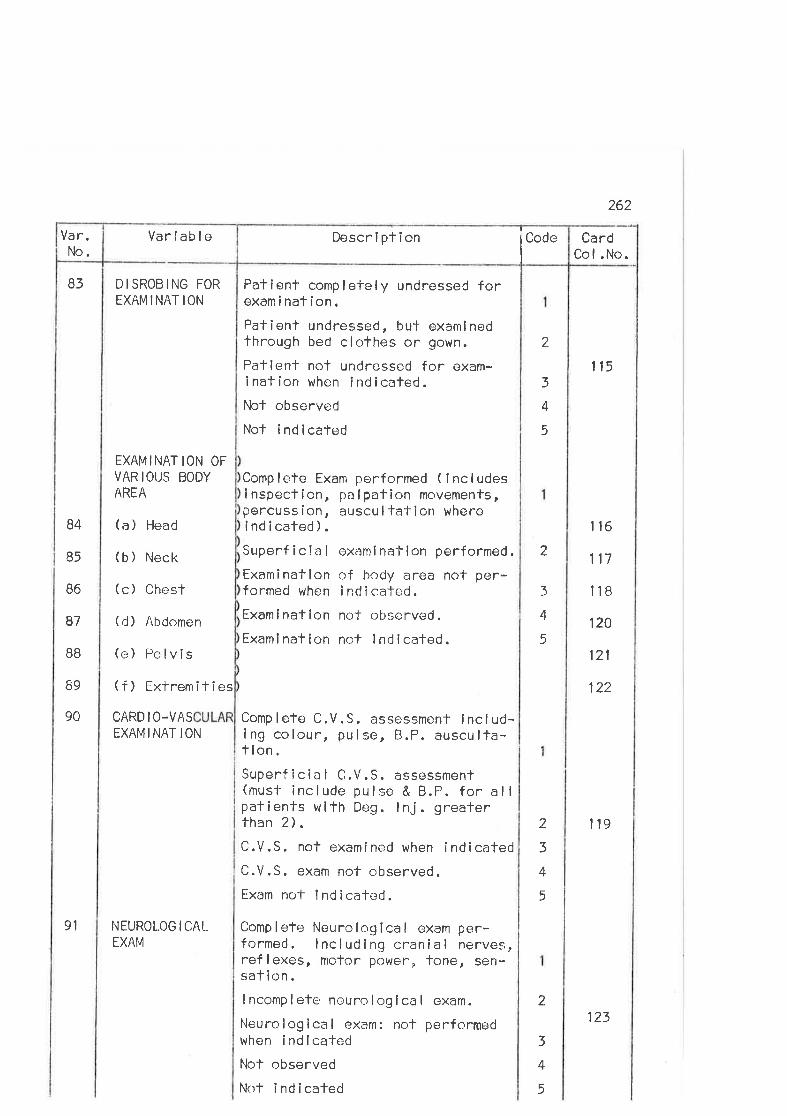
262
83
Variable
D I SROB I NG FOR
EXAMINATION
EXAMINAT ION OFVARIOUS BODYAREA
(a) Head
(b) Neck
(c) Chest
(d) Abdomen
(e) Pelvis
(f) Extremíties
CARD I O-VASEXAMINATION
NEUROLOG I CALEXAM
Patient completely undressed forexam i nat ion.Patient undressed, but examlnedthrough bed clothes or gown.
Patlent not undressed for exam-ination when indicated.Not observed
Not indicated
Comp lete Exam performed ( I ncl udesi nspection, pa I pation movements,percuss ion, auscu I fation whereindicated).Superf icla I ox¡:mlnalion performed.
Examination of body area not per-formed when i ncJ i cafed .
Examination nol observed.
Examinaf ion not lndlcafed.
Comp lefe C.V.S. assessment lnclud-ing colour, pulse, B.P. ausculfa-f lon.Superf icia I C.V.S. assessment(must include pulse & B.P. for allpat ients w ith Deig . I nJ . greaterthan 2).C.V.S. not examined when indicatedC.V.S. exam not observed.Ëxam not 1 nd i cated.
Complete Neurological exam per-formed. lncludlng cnanial nerves,reflexes, motor power¡ tone, sen-sation.I ncomp I ete neuro I og I ca I cxam.
Neurological exam: not performedwhon indlcatedNot observed
Not indicated
?
3
4
5
115
116
117
118
120
121
122
1t9
B4
85
B6
87
BB
B9
9o
2
3
4
5
2
3
4
5
2
3
4
5
CardCol.No.
Descrlption eCodVar.No.
91
123
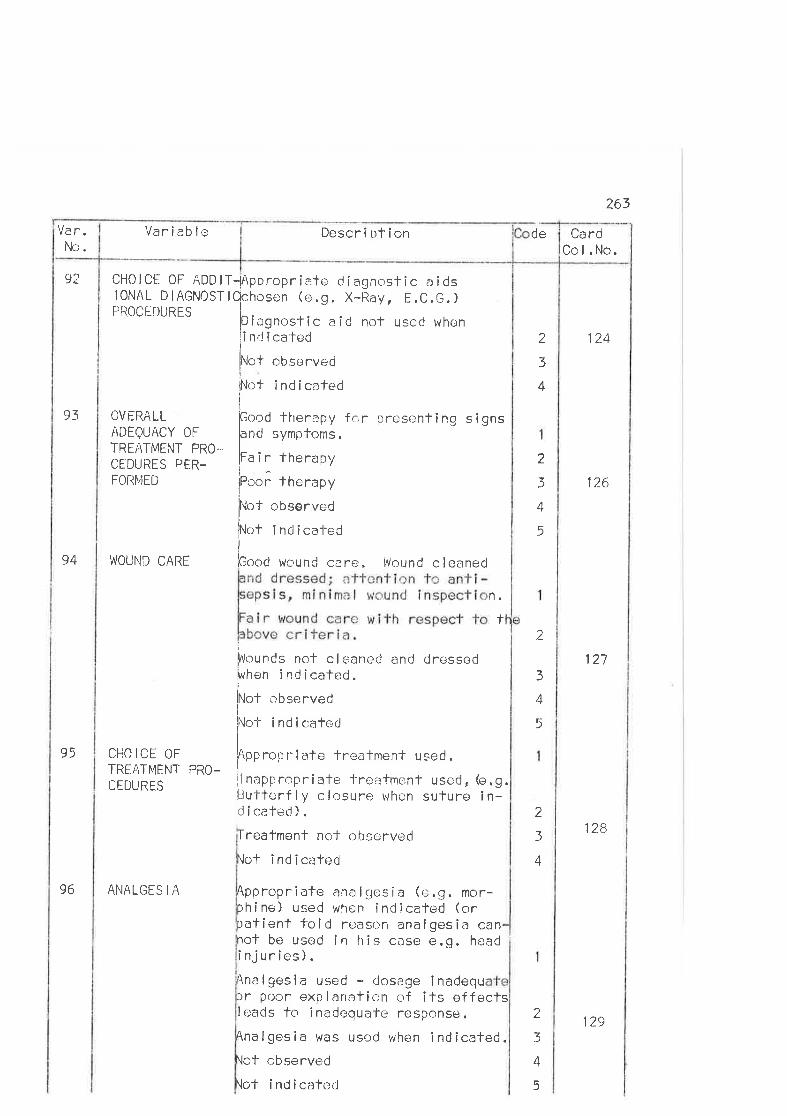
263
Va r.Nc.
Variable de
92 CHOICË OF ADDIIONAL DIAGNOSTPROCEDURES
93 OVERALL/\DEQUACY 0FTREATMENT PRO".
CEDURES PER.FORþIED
94 WOUND CARE
95 CHOICË OFTREATMENI' PRO_CEDURES
96 ANALGES I A
T-lAppropriate cj i agnostic a i dslQchosen (e.9. X-l-ìay, E.C.G.)
I
lDíi:gnostic aid rrof used whenii nrJ ica'tedI
lNlot obsorved
irunt ind icatedi
pood therapy fc;r presenting sigþnd sympfoms.I
lFa ir therapy!^¡Poor therapy
iNol observec
Not i nd ical-edi
bood wound care: . Wol¡nd c leaned
ì
þVouncls nof c I c¡aned and dressedþhen indîcated.
lÌrlot observed
flot i nd icalerjI
lApp.onrîate treatment used "t"
ns
n.
t
1?4
126
127
1?-8
2
3
4
2
3
+
5
2
l4
5
nappropriate -l-reatmenf used, (e.9.u'tterf ly closure when suture in-i cated ) .
irE
ioI
freatment nof observed
'lot ind icated
Appropriate analgesia (e.9. mor-:hine) uEed when indîcated (orratient told reason analgesiô canrot be used in tris case e.g. headinjuries).inalgesia used - dosage inadequ)r poor explanation of its effectsleacls to inade¡quale response .
Ana I ges ia was used when i nd icated.\ot observed
\of indicaÌed
2
3
4
2
3
A
5
CardCcl.No.
Description
129
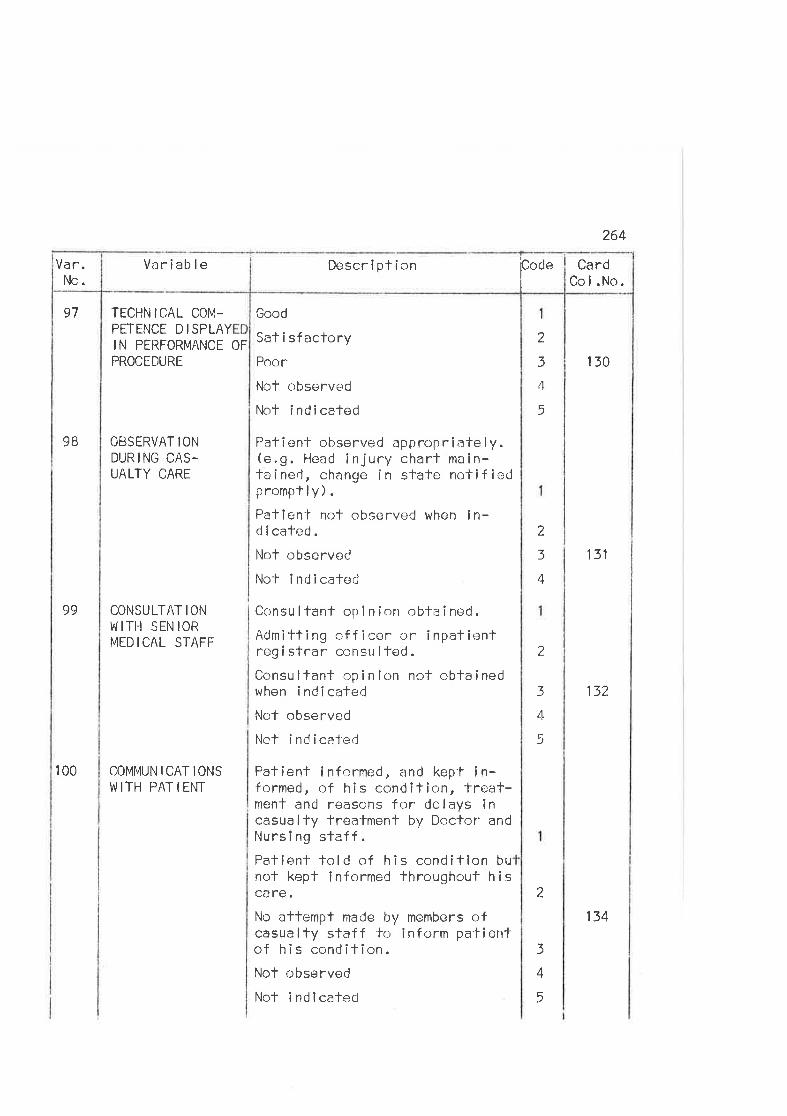
264
97
Variable
TECHNICAL COM-PETENCE DISPLAYIN PERFORMANCE OF
PROCEDURE
OtsSERVAT IOî'J
DURING CAS-UALTY CARE
CONSULTAT IONul ITH s EN toRMED IC/iL STAFF
COMMUNICATIONSW ITH PAT I ENT
Good
Sat i sfactoryPoor
Not observed
No+ indicated
Patien-f observed appropriate ly.(e.9. Head injury charl main-ta i ned, change i n state noti f iedpromptly).Patîent nof observed when in-d i cated .
Not observed
Nof i ndi cated
Consu ltanf opi nion obtained.Admitting officen or inpalientreg i sfrar consu I ted .
Consultant opinion nol obtainedwhen i ndi cafed
Not observed
Not i nd ica'f'ed
Patient informed, and kep'l in-fcnmed, of his conditîon, freat-ment and reasons for delays incasually treafment by Doctor ancJ
Nursi ng staff.Paflent told of his conditlon bunot kept informed througlrout hiscare.No alfempt made by members ofcasualty sfaff to inform patientof his condifion.Not observed
Nof indlcated
2
3
4
5
130
131
132
9B
99
100
2
3
4
2
3
4
5
2
3
4
5
CardCo I .No.
Descrfption['0"
Var.No.
134
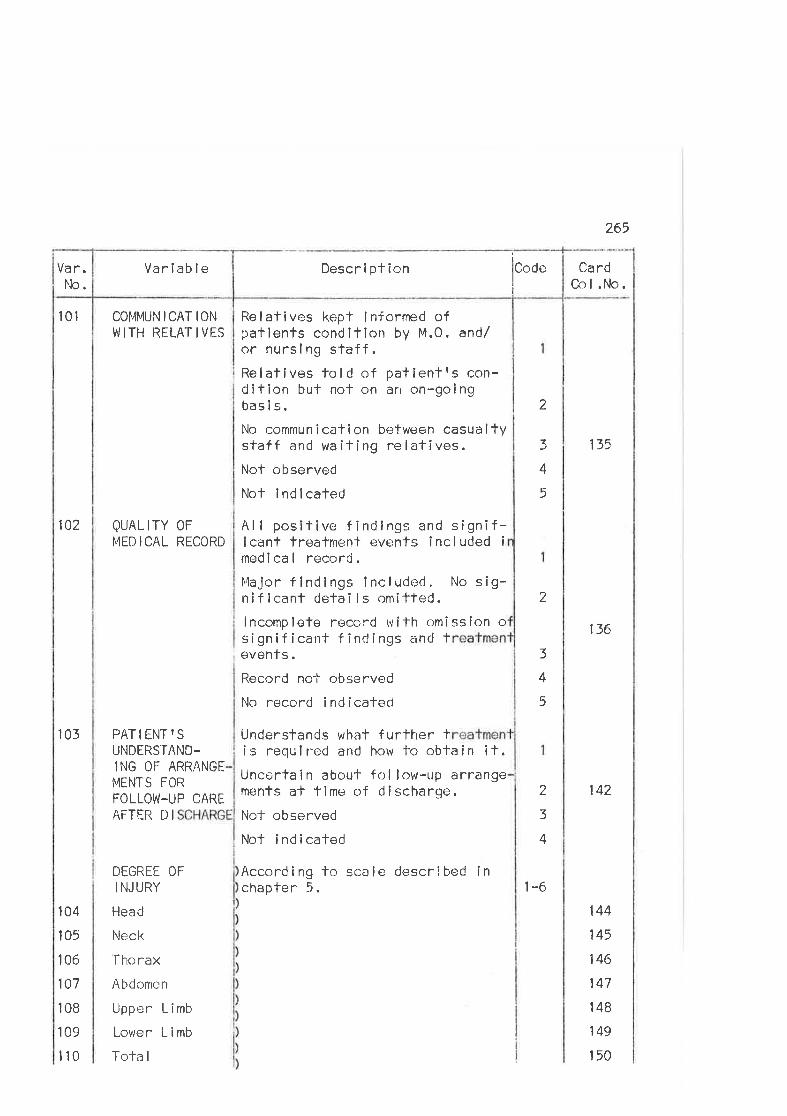
r01
102
103
104
105
106
107
108
109
110
COMMUN I CAT IONW I TH RELAT I VES
QUALITY 0FMEDICAL RECORD
PATIENTISUNDERSTAND-ING OF ARRANGE
MENTS FOR
FOLLOW-UP CARE
AFTER tJ I
DEGREE OF
I NJ LIRY
Head
Neck
ïho rax
Abdomen
Upper Limb
Lower L i mb
Tota I
Relatives kepf informed ofpatienfs condition by M.0. and/or nurslng slaff.Re I at i ves to I d of pat i ent fs con-dition but nof on an on-goingbas I s.
No communication between casualtystaff and waiting relafives.Nof observed
Nof lndlcated
Al I posîtive findings and signif-icant Ìreatment events included i
rned i ca I record .
It4ajor f indlngs included, No sig-niflcant detai ls omitfed.lncomplete record wiTh omission osignificanl findings and tevents.Record nol observed
No record indicatecl
Underslands what further tis required and how to obtain it.Uncertain abouÌ fol low-up arrangements af time of discharge.
Nol- observed
Nof indicated
According to scale described inchapter 5.
2
265
CardCol.No.
135
136
142
144
145
146
147
148
149
150
3
4
5
2
3
4
5
2
3
4
t-6
I
lCodeII
I
Descri ptionVarlableVa r.No.
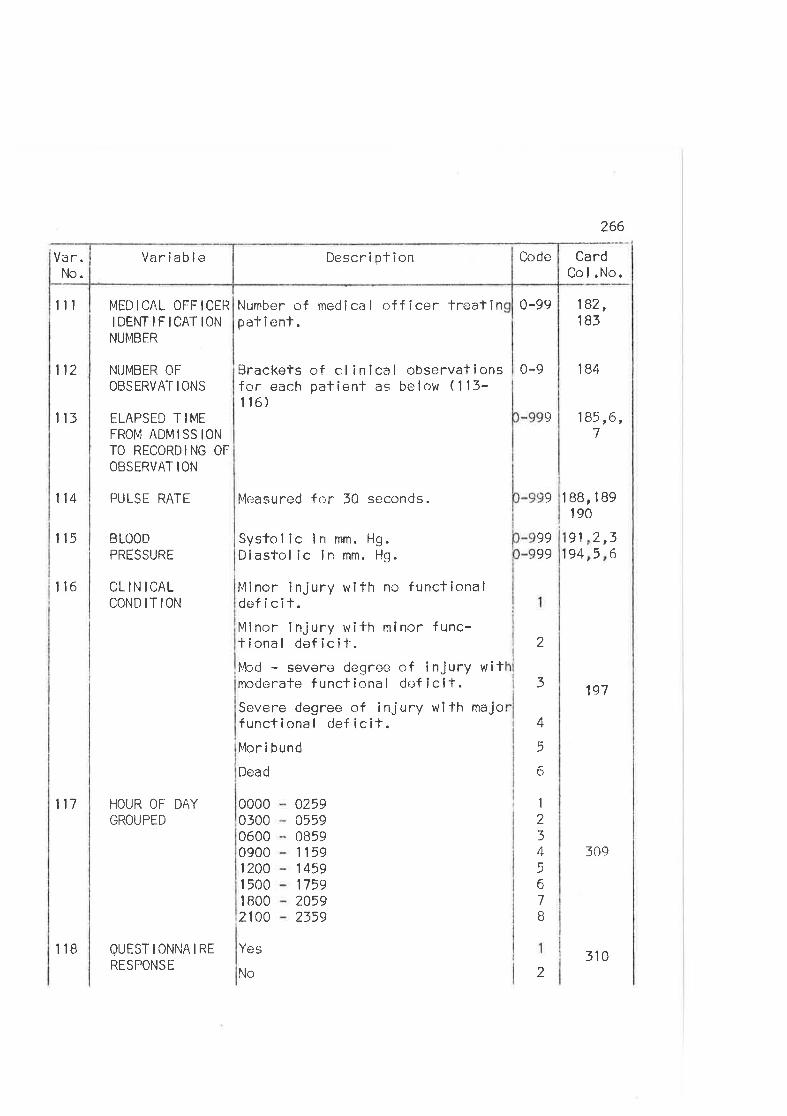
Var.No.
111 MËDICAL OFFICER Number of me.J i ca I of f icer treat in 0-99IDENTIFICATION pat i ent.NUMBER
112 l840-9
266
CardCol.No.
182,183
185 ,6,7
190
197
309
114 PULSE RAÏE
115 BLOODPRESSURE
116 CLINICALCONDITION
117
NUMBER OF
OBSERVAT I ONS
ELAPSED T IMEFROM ADMI SS IONÏO RECORDING OF
OBSERVAT ION
HOUR OF DAYGROUPED
QUESTTONNAtRERESPONSË
113
Brackefs of cl inical observationsf or each pat ient as be I ow ( 1 'l 3-116)
Measured for 30 seconds.
Systol ic in mm. Hg.Diastol ic in mm. Hg.
Minor injury with nc functionaldeficif.Minor injury with mínor func-tional deficît.ft&rd - severe degree of injury witmoderale f unctional dc:f icit.Scvere degree of injury wifh majofuncfional def icit.l,¿lor i bund
Dead
9
9
9999
1BB,l89
36
9194
,.)L
5
00000300060009001 2001 5001 8002100
Yes
No
02590559085911591 459175920592359
2
3
4
5
6
1
234567B
2
Descrlption CodeVaríable
118 310
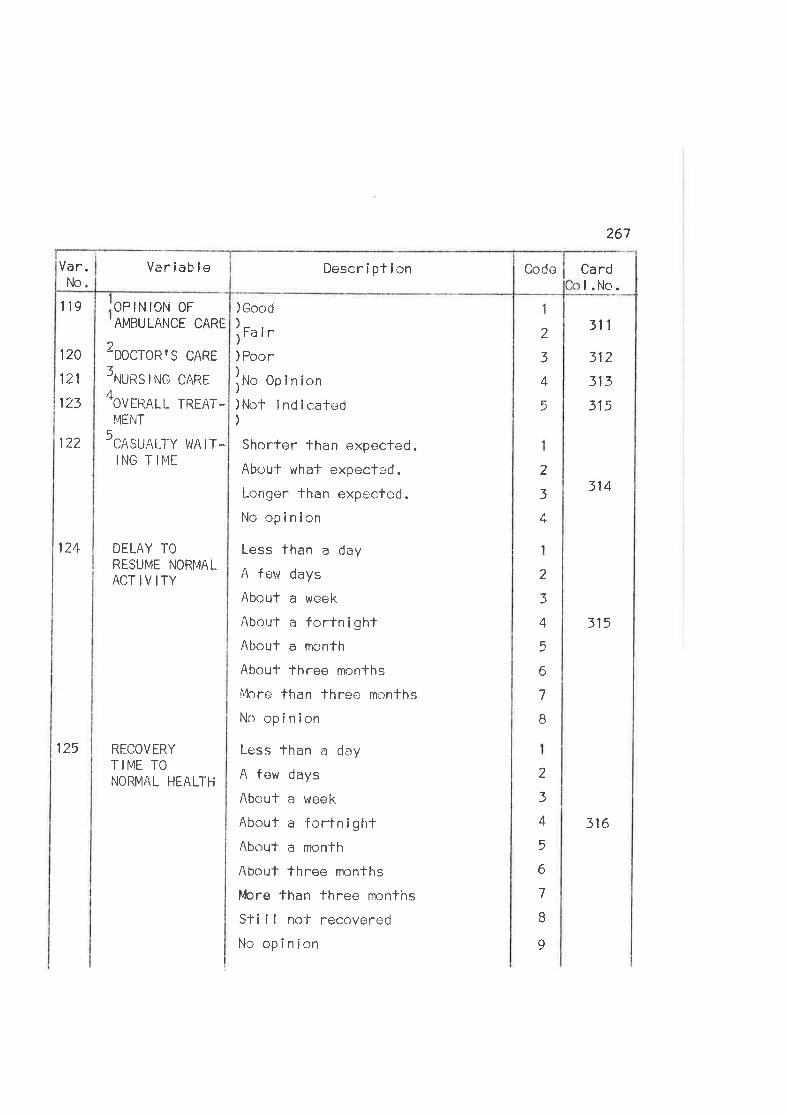
119
120
121
123
122
124
125
OP IN ION OF
AMBULANCE CARE
2ooctoRfs cARE
3ruuns r NG cARE
4ovrnRtl rREAT-
MENT
5cRsuRLty lvA rr-
ING TIME
DELAY TORESUME NORMAL
AOTIVITY
RÊCOVERYTIME TONORMAL HEALTH
Pocr
No 0plnionNot indicated
Shorter than expec-led.
About what expecfsd.
l-ongelthan expecfcd.
No opinion
Less than a cJay
A few days
About a week
About a forlnightAbout a month
About three monlhs
l"{ore than lhree months
No opinion
Loss than a day
A few days
About a week
About a fortnightAboul a rnonth
Abouf three months
i¡lcre than fhree months
Slí ll no'l recovered
No opinion
Good
Fa ir)
)
))
)
)
)
)
267
Cardl.No.
311
312
313
315
314
315
316
2
3
4
5
2
3
4
2
3
4
5
6
7
B
2
3
4
5
6
7
B
9
CodeDescriptionVariableNo
Var.
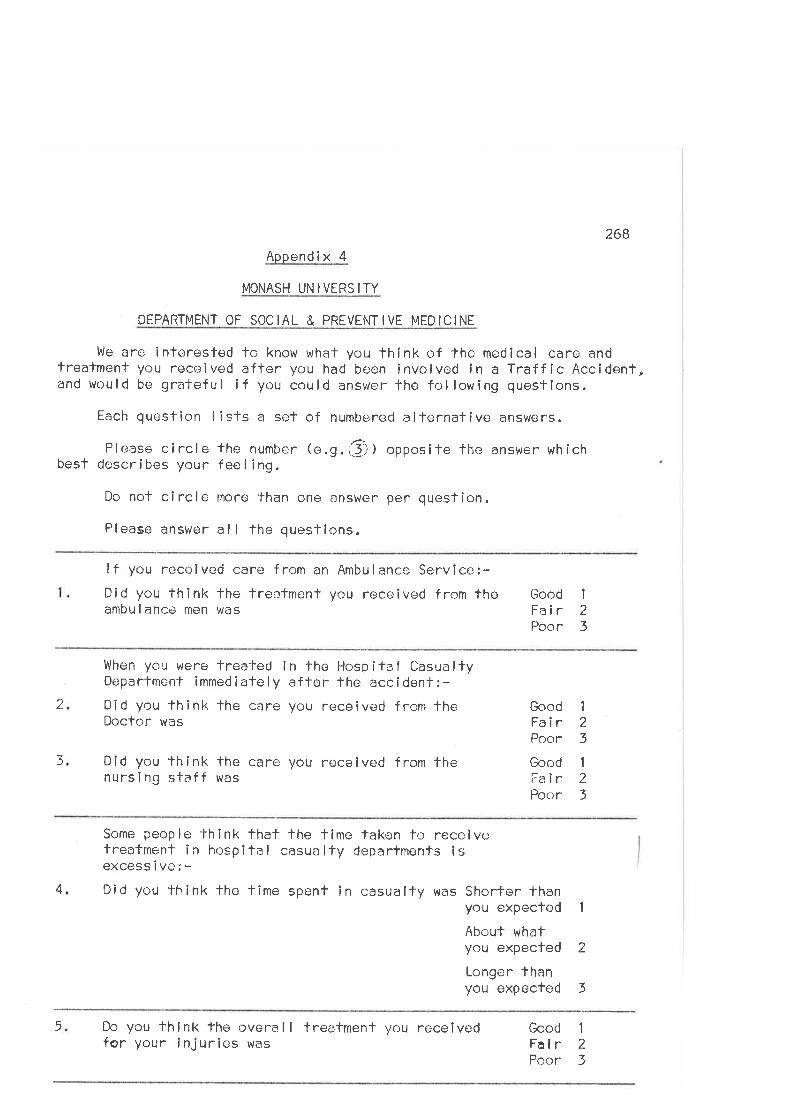
268
Appendix 4
MONASH UN IVERS ITY
DEPARTMENT OF SOCIAL & PREVENTIVE MEDICINE
We are interested to know whal you think of the medical care andtreatment you received after you had been involved in a Traffic Accident,and would be grateful if you could answer the following questions.
Each question I ists a set of numbered alternative answers.
Please circle the number (e.g.{!j I opposite the answer whîchbest descri bes your fee I i ng.
Do nof circle moro than one answer per question.
Please answer al I the questions.
lf you received care from an Ambulance Service:-Did you think the treafment you received from thoambu I ancè men was
Good IFair 2Poor 3
2
)
When you were treated in fhe t{ospifal OasualtyDepartment immediately affer the accident:-Did you fhink'lhe care you received from theDoctor was
Did you think lhe care you rÐceived from thenursing staff was
Good 1
Fair 2Poor 3
Good 1
Falr 2Poor 3
4
Some people fhink that the time taken fo receivefreafment in hospîtal casualty deparfments isexcess i ve: -Did you think thc time spent in casualty was Shorter fhan
you expected 1
About whatyou expected 2
Longer thanyou expected 3
5 Do you fhink fhe r:verall treatrnenl you receivedfor your injuries was
Good 1
Falr 2Poor 3
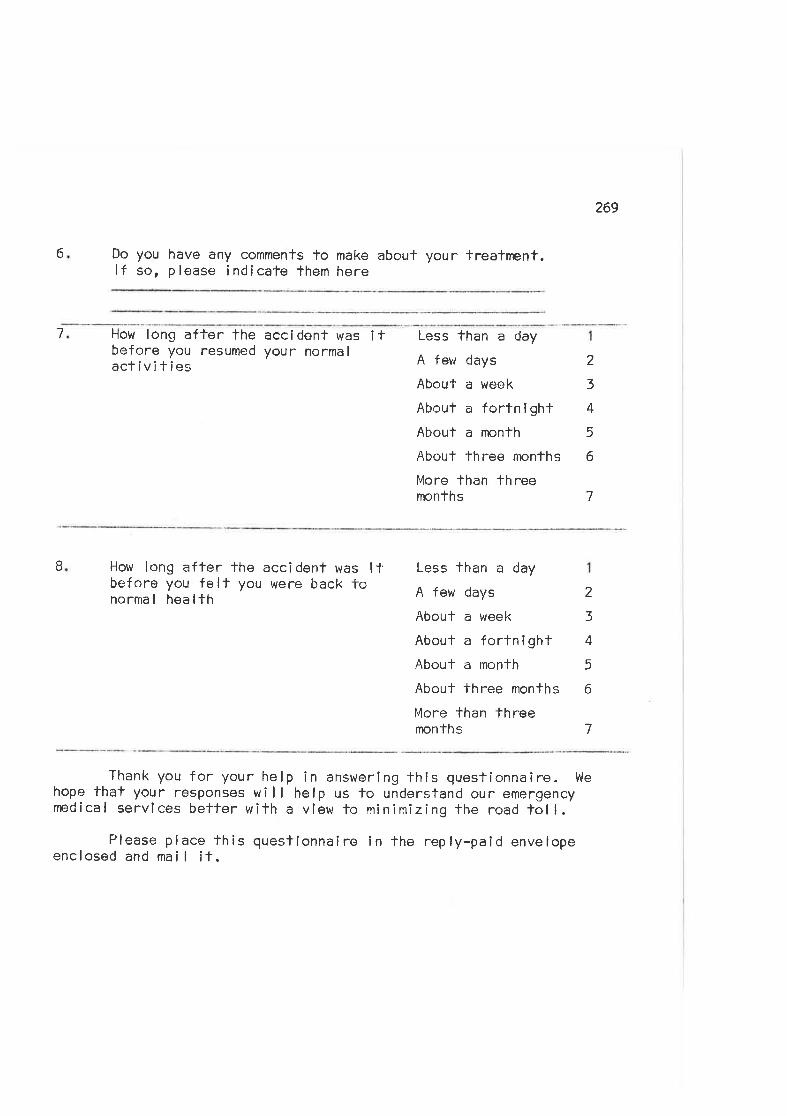
269
6 Do you have any commenfs to make about your treafnent.lf so, please indlcate them here
7 How long after the accidenf was itbefore you resumed your normalacfivities
Less than a day
A feur days
Abou'l- a weok
About a fortnlghtAbouï a month
About three monfhs
More than threemonths
2
3
4
5
6
7
B How long after the accídenf was l.l'before you felt you were back tonormal healfh
Less than a day
A few days
About a week
About a fortnighlAbout a month
About three months
More than threemonths
2
3
4
5
6
7
Thank you for your help in answerlng this questionnaire. Wehope that your responses will help us lo understand our emergencynedical services better with a view to minimizing the road toll.
Please place this queslionnaire in the reply-paid envelopeenclosed and mai I ¡t.
270
BIBLIOGRAPHY
ADAMS, A. l. (1967) rrDeath and lnjury on Country Roads - A Sludy of816 persons involved in Rural Treffic Accidents.'rtvled. J. Aust. 22799
ALFRED HOSPITAL (1969) rrlnstructicns for Casualty Residents.ltA I fred Hospilal, lulel bourne.
ALFRED HOSPITAL (1970) Unpublished Staf istics 1970. Alf red Hospital,Mel bourne.
MERICAN COLLEGE 0F SURGEONS (1963) Committee on Trauma. I'Standards forEmergency Departments.?ì Am. Col l. Surg. Bul letin.
A[\4ERICAN COLLEGE 0F SURGEONS (1954) Commiltee on Trauma. lrA li4odel of aHospilal Emergency Department.'r Chícago.
AVIER ICAN
A,f\4ER I CAN
A¡4ER ICAN
AMER I CAN
AI\4ERlCAl'l
AIVIER ICAN
COLLEGE CF SURGEONS (1967 ) Comm i ltee on Trauma . rrM i n ima I
Equipment for Ambulances.îf Am. Coll. Surg. Bulletin, 52292.
COLLEGE 0F SURGEONS (961) Committee on Trauma. çeStandards forEmergency Ambulance Servicas.rr Am. Coll. Surg. Bullef în, 52:131
HOSPITAL ASSOCIATI0N (1960) rrThe Hospital Emergency Department -en approach for examining emergency service.!t Chicago,
HCSPITAL ASSOCIATI0N (1962) "The Emergency Department in lheHospital: A Guide lo Organization and Managem'lnt.r' A.H.A.,Ch I cago.
MEDICAL ASSOCIATI0N (1966) lrEmergency Department - A Handbookfor Med i ca I Staf f . rt Department of llosp ita I s and Med lca I
Faci I ities, Chlcago, I I I lnois.
MEDICAL ASSOClATl0N, Department of Hospilals and MedicalFac i I it ies ( 1 966 ) rrThe Emergency Departmenr Prob lem. I'
J .A.M.A. I 98 (4) :380.
AIvIERICAN SOCIETY OF ANÂESTHESIOLOGISTS (1968)MedicaI Services." J.A.N'l.A. 204:595.
rf0ommunity Wlde Emergency
ANDERSON, V.W . (1969 ) rrThe Road Accident Af ter-care Scheme Sympos ium.tlJ. Roy. Coll. Gen. Practit. 1B:108.
ANDREWS, R.B. U969) rrOriteria Selectlon in Emergency Nledical SystemsAnalysis." U,C.L.A. Graduate School of Business Administration.
ANON. U963) 'rHlstory of the Victorian Civil Ambulance Service andAmbulance Transport Services of Vicforia.r? White Cross 4(1):4.
ANON.
ANON.
271
(1970) ?rAccidenl and Ëmergency Services.rr Brif . Med. J., 4:58.
(1971) rlAccidenl and Ernergency Services.er Brît. Med. J., 3:385,
ARCHER, F.L. (1970) ieCare Before Casu¿rlfy - Current Shorfcomings.tÌp .35 i n ltThe Manageme nl of Road Traf f ic Casua lt ies. I' Roya I
¡\ustralasian Col legc of Surgeons, Melbourne,
ARIZONA STATE UNIVERSITY (1970) lrAir Medical Evacualion System -(1) /lna lysis of Data Reporting and Use of Accident RecondsQ) Final Reporl and Appendîces.1r N.T.l.S. Accession Nos.PB 1937?4, PB 193725, PB 193864,
AUDETTE, L.G. & KEGGI, K.J. (1910) r¡Portable Television for EmergencyVehicles.tr l4ed. & Biol. lllus., 2Oz1 .
AUSTRALIAN POST 0FFICË (1911) Personal Communication.
BARTLETT, H.C. (1971) ilHelîcop'l'er Ambulances: An Evaluaf ion of theirOpe national and Economîc Feasibility.tr Traf f ic Digest &
Review, 19(7):1-7.
BELOFF, J.S. (1968) rrAdapting the Hospital Emergency Servíce to PatientNeeds. il Hosp i ta I s (J . A. H. A. ) , 42:65
BERRY, H"G. ( 1971 ) rtThe Hartnett Genera I Purpose Ambu lance - aneffective compromîse"r? White Cross: 23.
BERRY, H.G. (1968) I'A Report on thc Trial of a Helícopter as an AirAmbulance.lr Victorian Air Ambulance Service.
BËRRY, l-i.G. & TOYNE, A.[-1. (1970) I'The Recruiting and Training ofAmbu lance 0f f icens i n V ictoria.tr ln rrfi4anagement of RoadTraffic Casualties'1, p.49, Royal Auslralasian Col lege ofSurgeons, Melbourne ('1970).
BERRY, H. G. (1972) rl0rganizafion and Operation cf Rural AmbulanceServices.?t Paper presented to the National Road SafefySymposium of the Commonwealth Deparfment of Shipping andTransport, Canberra.
BöHLER, J . (1963) lrOrgan i zat ion and lvlanagemen-l of Trauma Surgery i nAusfria.rr Bull. Am. Coll. Surg.,48:107.
UO|ILER, J . ( 1970) rrOrgan izationa I and Mater ia I Requ irements for a TraumaService.re J. Trauma, lQ:92.
BONNER, Paul A. (1968) rrThe Applîcation of Computer Simulation Techniquesfo an Emergency Room Service.It Masferts Thesis, YaIe Universíty
272
BOODMAN, D.M. (1967) rrRole of Systems Analysis in Traff ic Safety.f?Society of Automotive Englneers Paper No. 670012, New York.
BoRDNER, K.R., BURKHART, C., HOUJARD, J.M. & LEVY, A.G.D. (1968)!iEmergency Care Systems Demonstratl on Projecf s.te Frank I i nlnslilute Research Labs., Philadelphia Pa. N.T.l.S. AccessionNos. PB 179847-179850.
BOUGHEY, ttJ.N. F. ( 1968) 'lAccldents, Emergencies and Ambulances: A Surveyin Porlsmoufh.lr Bril. Med. J., 1:369,
BOURRET, P., FRANCOU, J., DENANTE, F. and THOMAS, P. (1971 ) 'rEmergencyMedical Treafment, Transporfation and Hospifal Admission forVictims of Road Accidenls.'r lnfernaf íonal Microf llm Journalof Lega I Med íc ine, 6(2.) 22.
BRAND, I.A.G.,(1)(2)(3)
STEELE, S.K. & SlÄ/tNDEN, L.B. (1971)rrPafienfs in Casualty." Hospífal and Health CatrPatience in Casualty." HospitaI and Health CaI'lmpatience in fjasualty." Hospital and Health2(1) :25.
F€,1ê,Ca re
1(11):41 (12):11
BRAND, l.A.G, (911) 1?lmprovement in Casualty l,/ailing Time.rr Naf íonalHospital, 15:27.
LIRAYDROOK, R.l4 . (1970) î?The Commun ica't ions Prob lem and the Po I ice. r' I nriThe Managemenf of Road Traff Ic Casualtles.rr Royal Austral-asian Col lege of Sungeons, Melbourne.
BRECHMANI'ì, h/. (1969) 'TDas Heidelberger l4odell ChirurgischerErstvc:rsorgung am Unf a I lort. tt Langenbeckrs Archives f urCh i rurg i e, 325 2265 ,
BRITISH 0RTHCPAIDIC ASSOCIATI0N U959) I'Memorandum on Accident Services.rlJ. Eìone & Jt. Sur . 4lB.
BR00K, R.iJ. & STEVENSOI'{, R. L. ( 1970) rrEf f ecf iveness of Paf ient Care inan Emergency Room.î1 New Eng. J. Med., 283:904,
BUSH, J . P. (1971 ) ??A Cons I derat ion of Road Traf f ic Acc i dents - the i rProvention, and the Treatment of those lnvolved.tt Annals ofGeneral Practice, 16:46.
CADMUS, R.R. & KETNER, J.H. (1965) î'Organízíng Ambulance Services in lhePub I ic lnterost. r' Norlh Carol ina Hosp ita I Education andResearch Foundation. Chapel H¡ll, N.C.
CALDI¡/ELL, L.A. (1961) I'Ambulance Servîces and Íraf f ic Casualf ies.ltOnlario Medical Review, 28:172.
273
CARTER, J. (1971 ) r?Expenience wilh an ln-Depth Survey of Emergency Room
Trauma in a Large Urban Hospital.rt lnternaf ional Microf ilmJournal of Legal l4edicine, 6(l):10.
cAsHt4AN, B
cAVE, E. F.
CLARK, J . E
(1970 ) 'rRecord i ng Ma jor Trauma. 1r I nj ury , 2:11 ,
(1968) "Trauma: Past and Present.rr J. Trauma, B:104.
. (1971) ltlr4 iss iss ípp i Sfale Un ivers if y Deve lops a Tota I
Emergency Med i ca I Care System. ri Traff i c Safety , 71 :22.
CLUTE, K.F. (1963) 'rThe General Pracli*ioner: A Study of Medical Educationand Practi ce i n Ontar io and I'lova Scot ia. tr Un i vers ity of TorontoPress.
COLL lNS, J . (1966) 'rOrganiza"fion and Funclion of an Accident FlyingSquad. rr Br it. l.4ed. J . , 3:578 ,
COMMONWEALTH 0F AUSTRALIA, BUREAU 0F CENISUS AND STATISTICS (1910) I'Road
Traff ic Accidents lnvolving Casualties, 1969.t1 Bureau ofCensus and Stat i sl ics, F'le I bourne.
COMMONWEALTH 0F AUSTRALIA, tsUREAU 0F CENSUS AND STATISTICS (1971 ) rrRoad
Traff i.c Accidents lnvolvîng Casualties, 197O.tt Bureau ofCensus and Stati stics, Mel bourne.
COMI'{oNWEALTH 0F AUSTRALITi, BUREAU 0F CENSUS AND STATISTICS (1972}Persona I Commun ication.
COI4MONWEÂLTH OF AUSTRALIA, DEPARTMENT 0F THE ARMY (1971 ) PersonalCommun i caT ion.
COOPER, C. ( 1968 ) rrDescr ipt íon and Ana I ys i s of E íghteen Proven EmergencyAmbulance Servîce Sysfems.ii Vols. I & I l. National Assoc-iation of Counties Research Foundation. Washington D.C.N.T.l.S. Accession I'los. PB 179651-179652.
CORCORAN, J. (1961) luAcciclent and Emergency Services in Dublin.rl Journa I
of the lrish Medical Associa-iion, 60:71.
CURRIE, D. J. (1966) rrEarly Manageme;nt of lhe Critically lnjured.rr Can.Med. Ass. J., 95:862.
CURRY, G.J. (1968) rtTransportaf ion of lnjured Persons.rr Cl inical Ortho-paedics, 59:189.
CURRY, G. J. & LYTTLE, S.N. (1957 ) 'rThe Speeding Ambulance.rr Journal ofMichigan State Medical Sociefy, 56:1140.
DRYE, J.C. & HYDE, C.J (1965) rrThe Louisvi I le Plan for Care of 274
the lnjured.'? Postgrad. fied .:43,DE HAVEN, H. (1942) rrMechanÌcal Analysis of Survlval in Falls f rom Heights
of Fifty to One Hundred and Fifly Feet.tl p,539 in Haddon,Suchman & Klein, tiAccident Researchrt, Harper & Row, New York,1964.
DlXON, C.W., EI'4ERY, G.M. & SPEARS, G.F.S. (1970) 1?Casualty DepartmentUtilizetion Survey.l' I'lsw Zealand Medical Journal, 71:272.
DONABEDIAI'1, A. (1967 ) 'rEvaluating fhe Qua I ity of Medica I Care.'1 lnl4ainland D.E. (Ed, ) ??Health Services Researchrt. M¡ lbankMemorial Fund, New York.
DONABEDIAN, A. (1969) "A Guide to Medical Care Administratíon. Vol. I l:Medical Care Appraisal: Qualify and Utilizaf ion.lr AmericanPublic Flealth Association, New York.
DUNLAP AND ASSOCIATES INCORPOR/r,TED (1968) rrEconomics of Highway EmergencyAmbulance Se rvice.ì' Dunlap & Assoc. Inc., Darien, Conn., 1968.C.S.F.T.l. Accession No. PB l7BB37,
DUNLAP AND ASSOCIATES INCORPORATED (1969) l'Basic Training Program forEmergeircy Medical Technician - Ambulance: Concepts and Recommend-aticns.ir Dunlap & Assoc. lnc., D¿-.rion, Conn
DUNLAP AND ASSOC IATES l|.ICORPORATED ( 1969) tlBas ic Tra i n i ng Prog ram f orEmergency Medical Technician - Ambulance: Course Guide andCourse Coordinalor 0rienlation Program.tt Dun lap & Assoc. lnc. ,Darien. Conn.
DURBIN, E.P. (1969) 'rThe U.C.L.A. Emergency Medíca I Care Project.'1Traffic Digest and Review, 1723
EASTON, K.C. ('1969) 'tRoad Íraffic Accidents * The Therapeutic Vacuum,r'Brit. J. Surg., 56:717.
EASTON, K.C. (1970) trTrauma and lhe Genera I Practitioner: Road AccidenÌs.rrFroc. Roy. Soc. l'4ed . , 63:1321 .
EISEMAN, B. (1967 ) 'rCombat Casualty Management in Vietnam.ri J. Trauma,1:53.
FAtRLEY, J. & HEWETT, W.C.Greater Londcn. ??
(1969) 'iSurvey of Casualfy Departmenfs inBrî1. Med. J., 2:375.
Ft SCHER-HOMBERGER, E. ( 1 970)lmage Roche, 38:28.
r10n f he Deve lopmenl of Rescue 0rgan i zat ions. tt
FLAGLE, C.D. (1970) rlThe Role of Simulation in the Health Services.r'Amer. Journal of Publ ic Health, 60:2386,
FITZSIMMONS, J.A. (1971 ) riOomputerized Ambulance Locatiorrpres. et 1 8th I nternat ion¿¡ I Mee-i i ng of the I nst.Sciencos, Washington D.C., March 1971.
275
Log i c. rr Paperof l'4anagement
FREY, C.F., HINDS, R.J., DOW, R."4., & TURCOTTE, J.G. (1970) ilFrom
Ernc.:reoncy Ror-rm to Emergency Department: An Evaluatlon of lheEm.-rgoncy Departmonl. I' The Un i vers iiy of M i ch igan Med I ca I
Centre Journal, 36:6?.
FREY, C. F , HIJELKE, D. F. & G IKAS, P.W. (1969 ) I'Resuscitation andSut-vival in Motor Vehicle Accidents.lr J. Trauma. 9:2-q2.
FREY, 0.F. (1971) ttWhors Responsible for Emergency Medical Services.rrlnternalional lvlicrofi lm Journ(îl cf Legal Medicine, 6(1 ):1 1.
FRIEDHOFF, E. & H0FFI4AN, V. (1959) lrArtzliche Versorgung Schwerverlelzeram Unf;¡llortund auf den Transport.tr i\4unch. Med. Wschr., 101:1430
FRY, J. (1960) "Casualfy Services and their Sefting.?r Oxford lJ.P.
GARTRELL, P. (1965 ) frRece nt /tdvances ín Ambu lance Transporf Nurs lng inSouf h Austra I i a. rr Med. J . Aust. , 2:720 ,
GIBSCN, G., BUGBEE, C. & ANDERSON, 0.W. (1970) rfEmergency Medical Servicesin thr: Chicago Area.l' Centre for Healfh Admlnlstration Sfudies,Universily of Chicago.
G I SSANE, (1969) 'lThe Carc of lhe lnjured: The Development and Purposean Accident Hospifal." Anna ls of the Royal Col lege; of SurgeonsEng I and , 41 :335,
GISSANE, W., BULL, J. & ROBERTS, B. (1970) rtsequelae of Road lnjuries -A Review r¡f one yearrs admissions to an Accidont Hospifal.rrI njury, 1:195.
GOGLER, Ë. (1969) I'Chlrurgie am UnfallorT.'r Langenbeckf s Archiv FurCn i rurg i e , 325:214 .
GORDON, J.E. (1949) rrThe Epidemiology of Accidenls.'r Am.39:504.
J. Pub. Health,
GREGORIEVA, N. (1961) i'Ambulance Service ln the U.S.S.R.'' CanadianFamí ly Physician, 43.
GROUNDS, A.D. (1969) 'rAccident and Emergency Services.rt Australianl'4ed ica I Assoc i at ion Sludy Group on Med ica I P lann i ng .
HADDON, !V. (1963) 'rA Note concerning Accidenf Theory and Research wllhspecial referencc fo Motor Vehicle Accidenfs.rr Ann. N.Y. Acad.Sciences, 1C7:635.
HAACKER, L.P. (1969) 'rTime and ils Effecfs on Casualties in World War lland Vietnam.r' Arch. Surg. , 98:39.
W.
ofof
HADDON,
HADDON,
276
t,/. (1968) rrThe Changing Approach to the Ëpidemiology, Preventionand Ame I iorat ion of Trauma.lr Amer ican Journa I of Pub I ic
!{. (1970) ?iA Lcgical Framework for Categorizing Highway SafelyPhenomena ancj Actîvify." Paper dcl ivered to Tenfh lnternationalSfudy Week in Traffic and Safety Engineering. Rotterdam, Sept.1970.
HALL, M.H. & G¡\RDEN, R.S. (1961) rtRadio Communication and the ËmergencyDepartment.?r ilrit. Med. J .,. 3:17O.
HAMPTON, 0.P. (1960) rrTransporfation of -lhe lnjured.rr tsull. Amer. Coll,Surg. , 45:55.
HAMPTON, 0.P. (1970) rrThe Challenge of the Trauma Froblem To Organizedlulecjicine.rr J. Trauma, 1A:926.
HANDYSIDE, A.J. & MORRlS, D. (1967) rrsimulation of Emergency BedOccupancy.lr Healfh Services Rosearch, 2:287 .
HARLìlSON, R.F.F. (1969) r?Patient Transporfation.r' Med. J. Aust., 2:302,
HARDAWAY, R.þ1. (1968) rlclînical l4anagemenl of Shock.'1 Charles C. Thomas,I I I inois.
HELFER, R.E. (967 ) 'rEstimating the Quality of Care in a PaediatricEmergency Room. r? J . N{ed i ca I Educal ion, 42:244.
HENDERSON, l'4. (1910 ) erThe Prevention of Traf f ic Trauma. r' Bu I I . Posf -Grad.Comrn. in l4ecj., Universily of Sydney" Nov. 1970:144
IJOCKlNG, F. (962) 'rMorbidify în a General Teaching Hospital; Thelncidence of some lr4edical, Surgical and Psychiatric Conditions.reMed. J. AusT., 2:259.
HODGE, P.R. (1962) "Fatal Traffic Accidenls in Adelaíde." Med. J. AusT.,1 :509,
HOSPITALS AND CHARITIES C0Ml'4lSSl0N, VICTORIA (1970) îfAmbulance Handbook.frMe I bourne.
HOWARD, J.M. & DE BAKEY, M.E. (1956) lrThe Cost of Delayed Modical Care.r'14i I îfary lt4ed., 118:343.
HOWELL, J.Å. (1967) rrManaqement of Minor Facial Trauma in the EmergencyRoom.r? The Amcrican Surgeorl ,33:973.
HUELKE, D.F. , GRABB, W.C. , D INGMAN, R. D. & ONËAL, R.M. ( 1968) frThe New
Automobile Windshield and ifs Effectiveness in Reduclng FacíalLaceralions.?r Plastic and Reconsfrucf ive Surg., 41 :554.
HUELKE,
HUGHES,
J ACOBS,
J ACOBS,
277D.F. & HARBER, J.H. (1969) trMaxillo-facíal lnjuries: lheir nature
and mechanísms of production.?r J. Oral Surgery, 27t451
A.D. (1970) î?The Availability of Accidenf and Emergency HealthServi ces to the Me I bourne and Metropo I lfan Genera I Pub I i c.'rUnpublished l'4asferls Thesis, Dept. of Health Administration,Un i vers i ty of New South Wa I es.
4.R., GAVETT, J .fti. & WERS INGER, R. (1971) rrEmergency DeparfmentUti I ízation ln an Urban Community." J.A.M.A., 216:307
A.R. & McLAUGIJLIN, C.P. (1967) "Analysing fhe Role of theHel icopfer in Emergency Medical Care for a Community."Medical Care, 5:343.
K.G. (1971) 'tTraffic lnjuries in Brisbane - General Study.îtlnternalional Microf ilnn Journal of Legal Medlcine, 6(1):2,
K.G., DUGGAN, A.UJ., TWEDDELL, J., popE, L. I . & ZV'|RBULlS, J.E.(1911 ) trTraffic crashes in Brisbane.rt Austral ian Road ResearchBoa rd , Spec i a I Repo rt No. 2 .
JAMIESON, K,G. (1966) 'rThe Tolt ofMed. J. Ausl. o 2:157
the Road - Cllnical Aspects.rl
JAMIESON, K.G. & TAIT, l.A. (1966) lrTraff íc lnjury in Brisbane.fiNational Health and Medical Research Counci l, SpecÌal ReporlSeri es No. 1 3.
J AM I ESOI'I,
J AM 1 ESON,
JENKINS, A.McL., McQUlNLANo,t,,r. 14. & McNAlR, T.J. (1969) 'rResuscitaf ionRoom Survey.rr Scotlish Medical Journal, 14:29.
JONES, R.c. & sHlRES, G.T. (1969) trEmergency Room Triage - PreliminaryLifesaving Methods.ri J. 0ral Surg., 27:461,
JUNGFER, C.C. & LAST, J.M. (1965) rrClinical Performance in AustralianGeneral Practice.rr Medical Care, Z(2):71.
KAFJHAUSER" C.p., GEFMAN, J.D., SWEETMAN, J.L.& HAITH, p.R. ( 1969)rlNebraskars Aír Ambulance Project: ?Operation Sky-Aidt - FlnalReport.rr Nebraska Sfate Patrol, Lincoln N35BOO.
KEGGI, K.J., WEBB, s.B. & BROADBENT, E.J. (19j0) '?A Method for studyinglhe Emergency Care of lhe Trauma Patient: Results of the YaleTrauma Study.!r Connecticut Medicine, 342107,
KELLER, H. (1971) frAnalysís of Service and Delection Syslems on Freeways.?rAccid. Anal. & Prev., 3:149.
KENNEDY, R.H. (1963) lrGuidelines for an Effective Emergency Department.?rllospitals (J.A.H.A. ) 37.
278
KENNEDY, R.H. (1969) I'Convnunity Responsibillty in the Care of EmergencyPafients.rr J. Ora I Surgery, 27 :533.
KEY, J.D. (1968) ieu.S. Army Modical Departmenf and Civi I War Medicine.rlMi I itary Medicine, 113:181.
Kll4BALL, K. F. (1967 ) rrObservaf ions of Emergency Medica I Services andDispatch in Europe During Apri I and May 1967.r1 UniversiTy ofNebraska Co I lege ,of Med ic i ne.
KING, B.G. & SOX, E.D. (196i) rrAn Emergency Medical Servlce System.rlPubl lc Health Reports, 82:995,
KING. B.G. ( 1968) rrEstimating Communify Requirements for the EmergencyCare of Highway Accident Víctims.eI American Journal of PublicHea I th, 58: 1 422.
KOSSUTH, L.C. (1967) frlmmediate Care to Vehicle Accident Victims.trPostgraduate [t{edicine, 41 z4A7 .
KOVACS, G.T. (1971) Personal Communicatlon.
LEHMAN, S.P. & HOLLINGSWORTH, K.H. (1960) rîAmbulance Service in Seattle.'lPubl ic Health Reporls, 75:343,
LE IN IGER, W.J . ( 1968) I'Deve lopment of a Cost-Ef fect iveness System forEval uating Accident Counter-M€asures.lt Vols. 1-6. OperalionsResearch lnc., Silver Spring MÐ. N.T.l.S. Accesslon Nos.1 83440-1 -2-3-4-5 .
LEWIN, M.L. (19ó9) 'rManagement of Facial Lacerafions due fo Vehicle¡\ccidenfs.rt J. Med. Soc. Ner¡¡ Jersey, 66:120.
LINDLEY, D.V. & MILLER, J.C.D. (1962) Cambridge Elementary StatisticalTab les, Cambrldge University Press.
LITTLE, ARTHUR D., lNC. (1966) ltThe State of the Art of Traf f ic Safety.r'r\rthur D. L¡+tle lnc. , New York.
LITTLE, ARTHUR D., lNC. (19ó6) llCost Ef fectíveness and Traf f ic Safefy.t'Frederick A. Praeger, New York.
LONDON, P.S. (1969) rtTreatment of Soff Tissue lnjuries at the Roadslde."tsrlt. Med. J., 4:284.
LONDON, P.S. (1970) 'rAccident Services.er Brit. J. Hospital Surgery, 4246Q,
LOUGHEED, J.C. (1965) rrThe Current Status of Emergency Trealment inAulomobi le Accidents.r! Soulhern Medical Journal, 58:1083.
279
LUKANOV, A. & STOYANOV, R. (1971) rrOrganization and Cllnical Principlesof the Emergency l4edîcal A¡d by the complex Trafflc Traumatismin Bulgaria.rr lnternational Microfilm Journal of LegalMedicine, 6(2);3,
MAINE DEPARTMENT OF HEALTH AND WELFARE (1966) ?tAmbulance and EmergencyDepa rtment Serv ices Ì n fr4a i ne. rt Ma i ne.
MAI{EGOLD, R.F. & slLVER, M.H. (1967) eeAn overview of Emergency MedicalCare Services. r' J .4..M.4. , 200(4) :300-j04.
MAXWELL, T,M. (1971) 'lshock in severe Traff ic lnjury.Ì1 lnternaflonal14icrof ilm Journal of Legal l4edicine, 6(1):10.
MEDICAL COMMISSI0N 0N ACCIDENT PREVENTI0N (1970) rtDesign Criteria for theEmergency Ambulance." Report of an lnternational Seminararranged by fhe Medical Commission on Accidenl Prevenlion, 1969.I njury, 1 :245.
[4lcHoN, J.4., EERNST, J.T. & KOUTSALL, G.A. (1969) rtsafety clothing forHuman Traff ic 0bsfacles.ri Ergonomics, 12:61 .
MILLER, l'4.c. & PAGE, l¡l.R. (1968) t'The Effect on survival of Delay inEmergency Care in Motor Vehicle lnjuries in Louisiana.lrJ. Louisiana State Med. Society, 120:1,
l'4lLLAR, E.l-.M. (1966) e'Ambulance Training and Equipmenf: Report by theU.K. Worklng Party.t' H.M.S.0. London.
M I LLER, P.J . (911) rrThe Management of lvla.jor Accidents.tr lnj ury , z:169.
MlrcHELL, A. (1972) rrThe Hospital south of the Yarra.rt ph.D. Thesis,Melbourne University. Depl. of History, Melbourne.
14ITCHELL, A. (910) I'Highlights in the History of the Alfred Hospital.rtAlf red Hospital : Annua I Report 1969-70, Melbourne.
l'IlTCHELL, H.H. (1968) lrEmergency Medical Care and Traf f ic Fatalilies.?tRand Corporation, SantaMonica, Calif . Rand R.M. - 5637 - D.O.T.
MUL, A. (1953) 'f0rganizacja Doraznej Pomocy Lekarskiej W.M, St. Warszawle.rlTdrow ie Publ iczne, 1:99.
MURCOTT J . (1971) I'Largest Tow Truck in the Counf ry.rt The Age,Mel bourne , 24/7 /71 .
MUSTARD, R.A. ( 1961 ) îlEmergency Treatment of Common Traf f ic Accidents.rlCanadian Medical Association Journal, 84 :1054.
McFARLAND, R.A. & l400RE. R.C. (1962)Ann. Rev. Med., 13:371.
MACKAY, G.M. (1969) rtTraff ic Accidenfs - The tìoadside Requlremenfs oflhe Emergency Ambulance.rl lnternational Seminar on DesignCri'ter i a f or the Emergency Ambu I ance. London.
McKËNi''lY, E.M. (1967) lil-iistory of the lt4oforized Ambulance Transporf.rrMi I ifary l4edicine, 1322819.
NAGEL, E.L. (1968) "Telemetry of Physiologic Data." Southern MedicalJournal, 61l.598.
NAGEL, E .1., HIRSCHMAN, J.C., NUSSENFELD,(1970) 'fTelemetry Medical CommaEmerEency Care Systems.'r J .4.M.
280
îlAccidenfs and Accident Prevention.rt
.¡ RANKIN, D. & LUNDBLAD, E.in Coronary and Other Mobí le214:332,
S.RnC
¡iAl-lUM, A.l'1. (1971) "Emergency Medical Care Systems.r! J.A.M.A. 21721530.
I'IATlONAL HIGHI{AY SAFETY BUREAU (1969) rrProceedings of fhe Highway SafetyProgram Priorifies Seminar held at Fredericksburg, Virglnia,July 18-20th, 1969.rr National Technical lnformation Service,Accessíon No. PB 186270.
NEEL, S ( 1968) t'Armv Aero-medica I Evacuatlon Procedures in Vietnam.rrJ . A.14 . A. , 2O4:309 .
NEWHOUSER, L.R. (1956) rrBlood and Plasma Volume Expanders in lhe Treatmentof l4ass Casualties.'r l.4ilítary Medicine, 1182364.
NORTHROP, H.L. (1971 ) 1?Emergency Care Systems: The Documentafion Sub-System: A Pílof Tesf.tt lnlernational Microf ilm Journal ofLeqal trledicine, 6(1 ) :10.
NUTTON, V (1969 ) I'Medicíne and the Roman Army: A Furf her Reconslderaf ion."l4ed. l{isl. , l3:260.
OGLE RESEARCH (1969) lfA Report for the N.Iì.D.C. on the Feaslb¡líty ofPrcducing an Emergency Ambulance.rr Letchworth, U.K.
OR-IMANN, G.H. (1971) - Chief Execuf ive 0ff ícer,Service. Persona I Communication.
Victorian Civi I Ambulance
OWEN, J .K. (1967) r\Checklists for Analyzing a Communítyrs Emergencyl4cdical Servíces.rt J.A.M.A., 200(4)z 305-308.
OWEN, J K. (1966) ttEmergency Services musfHcspltal, 107:84.
be Reorgan i zed. tr The l4odern
OWENS, J.C. (1965) î'Colorado Study of Emergency Treôfmenf Fací I itîes.'1Bi-Regional Emergency f4edical Services Seminar, University ofNevada, iìeno, Ne:vada, September 1965 .
OI{ENS, J . C. (1966 ) 'rEmergency Med i ca I Serv icesRocky Mountain lr4ed. J., 63:23.
281
i n the Sma I I Communlty. "
PACY, H. (1961) rlRoad Acciclents: The Medical Rescuer.r?1 :806.
Med. J. Aust.,
PETERSON, 0.1., ANDREWS, 1.p., SpAlN, R.S. & GREENBERG, B.G. (1956)ltAn Analytical Study of North Carolina General Practice.riJ . Med. Educ. " 31 (12) :l .
PETERSON,0"L. (1963) leMedical care: lfs social and 0rganlzationalAspects : Eva I uat ion of the Qua I Íty of Med i ca I Care . I' Nerv Eng .J. Med., 269:1238.
PETERSON, 0.1. (1966) r'Evaluation of the Quality of Medical Care.'rCh. 19 in DE GR00T, L.J., ffl\4edical Care.'n Charles C. Thomas,Springfield lil.
PHELAN, lvl.D. (1911) lrNotes concerning the Formation of the Sf . JohnAmbulance Association, Vlctoria Cenlre, and lhe Foundation andGrowth of lhe St. John Ambulance Brigade, Víctoria Disfricl.t'St. John Ambulance Association, Melbourne.
.F. ('1968) 'rThe Management of Multiple lnjury Patients.'rJ . Trauma, B: 9 I
PlzTl , w
PLATT, tl .S. (1969) 'tThe Evolution of 0rthopaedic Surgery in Norlh-WestEngland.rr J. Roy. Coll. Surg. Eclin. , 14 126,
POYNTER, F.N.L. & KEELE, K.D. (1961) '?A Short Hístory of Medicine.trMi I ls & Boon, London.
RACE, D. (1972) 'rThe Developmenl of a Hospital DaTa Base.lr Med. J, Aust.,1 :78.
REl.lt¡/lcK, E.D. & t¡/lLLlAMS, l.M. (1969) r?A short llistory of the Order ofSt. John.'r S'f. John Ambulance Associalion, London.
ROBERTSON, J.S., McLEAN, A.J. & RYAN, G.A, (1966) llTraf f ic Accidents inAdelaide, South Australia.rT Australian Road Research Board,Speci a I Reporf No.1 .
rcBERTSON, J.S. & TONGE, J.l. (1968) 'îDuration of Survival in l'raf f icAcci dent Fata I i ti es. " Med. J . Ausl. , 2:1 .
ROBERTSON, J . S . (1969 ) r?The Patho logy of Road AccidentManagement of Road Traff ic Casualties.li RoyaCo I I ege of Surgeons, Me I bourne.
lnjury.it lntrTheAustralasian
ROBERTSON, J.S. (1971) '?The A.M.A. Road AccidenT Survey.Load in Rural S.A. in the years 1968 and 1970.t|2|121 .
l. The AmbulanceMed. J. Aust.,
ROBlNSON, J.S. & McLEAN, A.C.J. (1970)Aust, , 2:439.
282
lrMobile Coronary Care.t' Med. J.
ROCHESTER ACADEMY 0F MEDICINE (1967 ) r?Proceedings of the Rochesfor Forumon Emergency Hea I th Serv i ces. " New York, 1967 .
ROSS, J.C. rtThe Role of the Hel icopter.rr p.43 i n ?eThe Managemenl of RoadTraffic Casualties.rr Royal Australasian Col lege of Surgeons,Mel bourne, 197O.
ROYAL AUSTRAL-ASIAN C0LLEGE 0F SURGEONS (1970) 'rThe Management of RoadTraffic Casualties." Proceedíngs of the First Seminar conductedby lhe Royal Australasian Col lege of Surgeons, October 1969.McCarron Bi rd, Mel bourne.
RUFFEL-SMlTH, H.P. (1970) riTime to Die from lnjuries Received in RoadTraf f ic Accidents.'r lnj ury , 2:99.
RYAN, G.A. (1965 ) ri I njuríes and I njury Production i n Traff ic Accidentsin Metropolitan Adelaide.rr M.D. Thesis, University of Adelaide,South Austral ia.
RYAN, G.A. & CRANSWICK, P.J. (1971 ) Personal Communication.
RYAN, G.A. & GARRETT, J.W. (1968) t'A Quantitative Scale of lmpact lnjury.l'Cornel I Aer. Lab. A.C. l.R.,C.A.L. Nr¡. VJ-1823-R34., New York.
SAFAR, P., ESPOSIT0, G. & BENSON, D.M. (1971) 'rAmbulance Design andEquipment for lt4obile lntensive Care.rr Arch. Surg., 1022163.
ST. JOHN AMBULANCE BRIGADE (1963)S.¡\. District.
:rl.4anua I of Ambu I ance Transporf I'lurs i ng . rf
SANDO, þ1.W. & CORNlSH, B. (1970) p.63 in "The Management of Road TrafficCasualties.tr Royal Australasian College of Surgeons, Melbourne.
SAVAS, E.S. (1969) '?Simulation and Cost Ef fectiveness Analysis of NewYork Emergency Ambulance Service.r? Management Scíence, 15:136-8.
SCOTT, 8.Y., T0URlN, B. & HOLLENBERG, C.S. (1970) "Operations Research:InpI ications for Safety Syslems l4anagement.r? BehaviouraIResearch in Highway Safety, l:227.
scOTT, J .C. (967) "Report on the Oxford Accident Service afler 25 Years.rlBrit. Med. J., 22632.
SCOTT, J.C. (1970) IrAccident Services in the 1970rs.?' lnjury,2:1.
283
SH00K' L. L. (1966) r?A Study of lowa Ambulance Service.?' Bureau of Pol!ceScience, Universlfy of lowa, lowa City.
sll"4PSON, D. (1970) '?Priorities in Managemenl.t' p.85 inrlThe Managementof fìoad Traf l ic Casua I ties. Ît Roya I Austra las ian Co I legc ofSurqeons, Mel bourne.
slNGER, c. & UNDERWOOD, Ë.4. (1962). ?14 shorf History of Medicine.rrOxford U.P., Oxford.
SKUDDER,
SKUDDER,
STOREY, P.B. & ROTH
Un ion . rt
P.A. & McCARROLL, J.R. (1961 ) r'Hospital Emergency Facilif ies andS<¡rvices, a Survey.?e Bull. Am. Coll. Surg.,46(2):44,
P.A. & WADE, P.A. (1964) trThe Organizaf ion of Emergency l4edica I
Facilitiss and Services.rl J. Trauma,4:358,
sN00K, R. (1969) (1) ltExfrication of rrapped casualties.rr Bril. t4ed. J.4:478.Q) tiRoad Accidenls and the Family Doctor; Resuscitaf lon at RoadAccidents.lr Brît. I4ed. J., 4:348,
SN00K, R. 11971) erRoarj Accident Rescue Technîques.'r Med. & Biol. lllus.,21 :66,
STANFORD RESEARCH INST ITUTE (1967-70 ) 'rl,4ef hods f or Survey i ng H ighwayEmergency N4edical Services.r? Stanford Research lnstitule,Menlo Park, Calif . N.T.l.S. Accession Nos. PB 192735, PB 194390,PB 178231, PB 178232,
, R.BJ.A.M
(1911 ) "Emergency MedicaI Care in the SovíefA. , 217 z5BB.
ST JOHNSTON (slR) THOMAS ERlc (1911) rrA Reporf on the Victoria PolíceForce.rr Victoria Parliament, Parliamenlary Paper D5 of 1970/71.
TONGE, J 1., CZECHOIIIICZ, A.S. & ROBERTSOI{, J.S. (1967 ) rrsurvival afterFatal Tral't ic Accîdents.tr Lancet ll:670.
TONGE, J.1., 0rRElLLY, M.J.J. & DAVISON, A. (1964) rrFatal Traf f icAccidents in Brisbane from 1935 to 1964.tî Med. J. Ausf., Z:Bll.
TORRENS, P.R. & YEDVAB, D.G. (1970) I'Variations among Emergency RoomPopulations: A Comparison of Four Hospilals in New York Cíty."l4edical Care, Vl I I :60.
TURNER, H.S. & ELLINGSON, H.V. (1970) rrllse of the Helicopter as anEmergency Vehicle in the Civi I ian Environment: Results of aSurvey Queslionnaire.?' Aerospace Medicine, 41 :135.
284
UNIVERS ITY OF CALI FORNIA,GRADUATE SCHOOL OF BUSINESS ADMINISTRATION,Division of Research, at Los Angeles (1969). TrE.f'4.S. Project,Quarterly Repcrf, August I - Ocfober 31, 1969.11
UNIVERSITY0FMELBOURNE (1961) ttAlfrecJ llospital Accident Survey, 1960-6l.trDepartmenl of Surgery, [Jniversily of Melbourne, Melbourne.
UNITED STATES GOVERNI\4ENT, DEPARTMENT OF TRANSPORTATION, NATIONAL HIGHWAYSAFETY BUREAU, I^JASH I NGTON, D. C.(1) llHighway Safety Program SÌandards.rr (1968)(2) '?A Summary of 1968-69 Multidisciplinary Accident
I nvestigalions. fr (1969)(3) ;'Highway Safety Program f4anual. Vol.ll - Emergency
Med ica I Serv ices. rr ( I 969 )
G) rrEconom i cs of H ighway Emergency Ambu I ance Serv i ce. rt (1969)( 5 ) çtAmbu
I ance Des ign Cr ifer ia. " (1970)
VAN WAGONER, F.H. (1961) r?Died in Hospital; a Three Year Study of DeathsFollowing Trauma.r? J. Trauma, 1:401 .
VARLEY, C. (1969) trCare Before Casualty. A. The Process.rr lnrrTheManagement of Road Traff ic Casualties.'r Royal AustralaslanCol lege of Surgeons, Melbourne.
VAUGHAN, R.G. (1971) itMolor Vehicle Design Effecls on Pedestrianlnjuries.'? Thesis submitted to fhe Dept. of Engineering,Universlty of New Soulh Wales.
VICTORIAN CIVIL AMBULANCE SERVICE (1970) lfAnnual Roport 1969-70.11V.C.A.S., Melbourne.
VICTORIAI'J ClVl L AMBULANCE SERVICE (1970-71) Unpubl ished Sfatistlcs.
WADE, P.A. (1959) rrThe Responsibility of the Me<Jical Professíon to theViclim of the Automobi le Accidenf.tl Am. J. Surg., 98:526.
WALLER, J.A. (1954) trTraf f ìc Deaf hs: A Preliminary Sfudy of Urban andRural Fatalities in California.r' California l4edicine, 101 2272.
WALLER, J .4. , CURRAN, R. & NOYES, F. (1964) lrMore Rura I lnjurles areFata I . re Ca I i f orn iars Hea lf h, 22:65 ,
WALLER, J.4., GARDNER, R. & LAWRENCE, B.S. (1966) "Uti I ization ofAmbulance Services in a Rural Community.tt American J.P.H. , 56:513
WALLER, J.A. (1967 ) 'lConIrol of Accidents in Rural Areas.rt J.4.M.4.201 :176
WATSON, P. A. ( 1970) 'rAmbu lance AccTdents - is there a Common Denomi nator?ttPanacea , 3262,
WEBB,
WEED,
WEED, L. L
WEST, I
285
M.L. (1969) rtThe Emergency Medical Care Systern in a MetropolitanArea.'i D.P.H. Thesis, School of ltygiene and Public Healfh,Johns Hopki ns University, Ba ltirnore.
L.L. (1970) rrl4edical Records, fr4edícal Education and Palient Care.rtYear Book Medical Publ ishers, Chicago.
,
(1971) "Quality Control and lhe l4edical Record.tf Arch.I nterna I Med ici ne, 127:101 .
KLEtNMAN, G., TAYLOR, E.8., MAJORS, A. & MITCHELL, H.W. (1964)ItSpeeding Ambulance Survey.tt AlD, Sept-Oct. :8.
wElNERI'1AN, E.R. & EDWARDS, H.R. (1964) r'Yale studies in Ambulatory care:l. Changing Patterns in Hospifal Emergency Service.rrHosp i ta I s , 38 255 .
I¡JEINERMAN, E.R., RATNER, R.S., ROBBINS, A. & LAVERHAR, Nî.A. (1966)rrYale Sludîes in Ambulatory Medical Care: V. Deferminants of Use0f Hospital Faci I ities.lr Amer. J.P.H., 56:1037,
l{EINERMAN, E.R., RUTZEN, S.R. & PEARSON, D.A. (1965) ?tYale Studies inAmbulatory Care: ll. Effects of Medical rTriagef in HospitalEmergency Service.?r Pub. Health Rep. B0:589.
V/HlTE, H.A. & O1CONNOR, P.A. (1970) î'Use of an Emergency Room in aCommunily Hospital.rr Pub. Health Report, 85:16f.
ltlILDER, R.J . & JUDE, J .R. ( 1969) îlCarrJiopulmonary Resuscitation byTrained Ambulance Personne> l.rr J.A.M.A., 190:551 .
r¡lORLD HËALTH ORGANIZATI0N (.l968) ltThe Organization of Resuscifaflon andCasualty Se.'rvices - Report of a Seminar held in [-eningrad1967.r? lrl.H.0. Regîonal Office for Europe, 1968, DocumenfNo. EURO 0256.
WORMAN, 1.W., C00K, H.E. & KING, J.1.4. (1962) rrThe Trauma Patient vs.Emergency Care: The Role of the Emergency Hospital.riEmergency Hospital and Trauma Care:340
-9M.D t::::9 4-
<":'
Appendix 5
TREATMENT DELAYS BY TIME OF WEEK
During the second ~hase of the study, proportionately more of
the patients presenting to the casualty department on Friday and
Saturday nights than of those presenting at other times of the week
were included in the sample. This excess of Friday/Saturday patients
resulted partly from the fact that every Friday and Saturday was worked
as a requirement of the sampling frame and partly from the pattern of
arrivals of crash victims at the department during times off duty.
In the following tables the delays experienced by patients at
different times in the week are analyzed in an attempt to determine the
effects of this stratification in the sample on the waiting times in
the separate care phases . The periods 0800 - 1159 hours and 1200 -
1759 hou rs on weekdays (Monday - Friday) and 1800 - 2359 hours from
Sunday -· Thursday are compared with the evening periods from 1800 -
0159 hours on Friday and Saturday nights. Staffing patterns and work-
loads in the casualty depa1~tmentwere broadly similar within each of
these time groups. Thus each group :;;ay be compared v,1ith the othc:~:; ~,1 determi ni ng the effects cf the stratification on the overall time
d12 lays fc,· the w,2ek 0
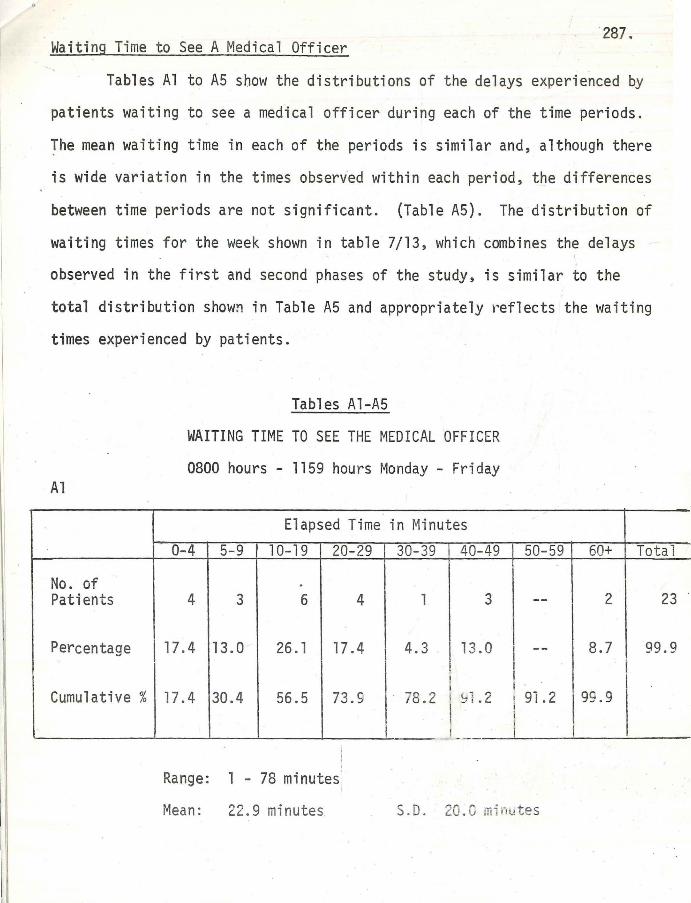
·2a1. Waiting Time to See A Medical Officer
Tables Al to A5 show the distributions of the delays experienced by
patients waiting to see a medical officer during each of the time periods.
The mean waiting time in each of the periods is similar and, although there
is wide variation in the times obser~ed within each period, the differences
between time periods are not significant. (Table A5). The distribution of
waiting times for the week shown in table 7/13, which combines the delays
observed in the first and second phases of the study, is similar to the
total distribution show~ in Table A5 and appropriately reflects the waiting
times experienced by patients.
Al
Tables Al-A5
WAITING TIME TO SEE THE MEDICAL OFFICER
0800 hours - 1159 hours Monday - Friday
Elapsed Time in Minutes
0-4 5-9 10-19 20-29 30-39 .40-49 50-59 60+ Total
No. of Patients
Percentage
Cumulative%
. 4 3 6 4
17.4 13.0 26. 1 17.4
17.4 30.4 56.5 73.S
Range: l - 78 minutes
Mean: 22 . 9 minutes
l 3 -- 2 23
4.3 13.0 I -- 8.7 99.9 I I I I
1a. 2 I ~11. 2 I . I 9i. 2 9S.9
I I ! .J,_
S.D. 20.C minutes
I
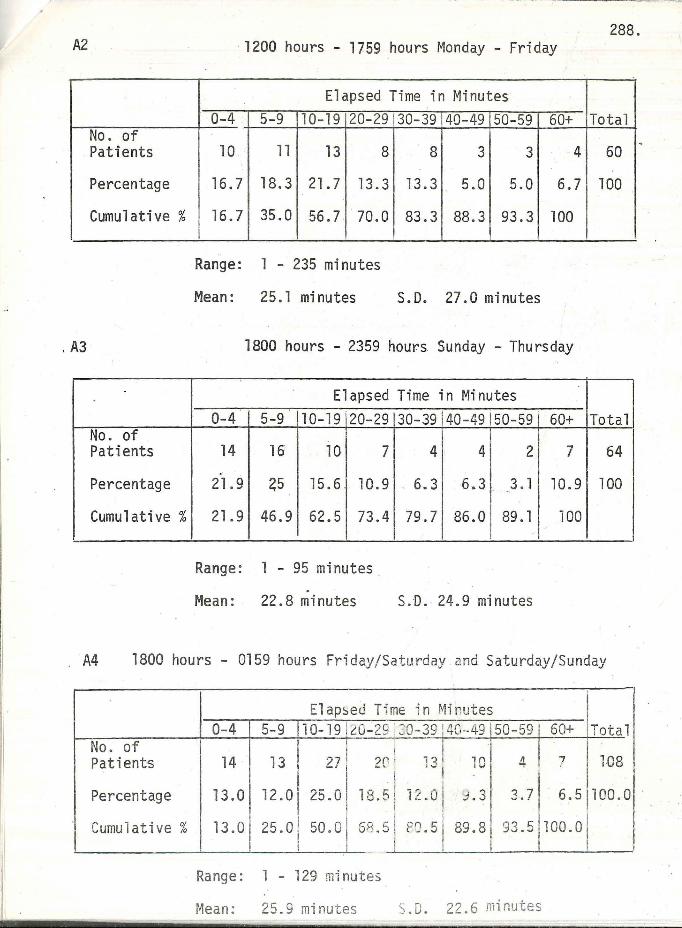
288. A2 1200 hours - 1759 hours Monday - Friday
No. of Patients
Percentage
Cumulative%
Elapsed Time in Minutes 0-4 5-9 10-19 20-29
10 · 11 13 8
16.7 18. 3 21. 7 13.3
16.7 35.0 56.7 70.0
Range: 1 - 235 minutes
Mean: 25.l minutes
30-39 40-49 50-59
8 3 3
13.3 5.0 5.0
83.3 88.3 93.3
S.D. 27.0 minutes
60+
4
6.7
100
. A3 1800 hours - 2359 hours Sunday - Thursday
No. of Patients
Percentage
Cumulative%
Elapsed Time in Minutes 0-4 5-9 10-19 20-29 30-39 40-49 50-59
14 16 10 7
21.9 ~5 15.6 10.9
21.9 46.9 62.5 73.4
Range: l - 95 minutes .
Mean: 22.8 minutes
4 4 2
. 6. 3 6.3 3. l - · .
79.7 86.0 89 . l
S.D . 24.9 minutes
60+
7
10.9
100
Total
60
100
Total
64
100
A4 1800 hours - 0159 hours Friday/Satu rday and Saturday/Sunday
No. of Patients
Percentage
Cumulative%
Elap~eJ Time in Minutes 0-4 5-9 10- 19 ~0-29 ! 30-39 140 --49 50-59 60+ Tota l
I
, -~ I 27 1 i
14 13 2C1 • , (\ 4 7 108 · - · 1
l\,J
I .
13.0 12.0125.0 12.s l 11..o l 9. 3 3.7 6.5 100.0 I I
13.0 25.0 : 50.0 I I
GR.s ! PO.S i 89.8 93.51100.01 . I . I I
Range: 1 - 129 minutes
Mean: 25.9 minutes S.O. 22.6 mir.u tes
l
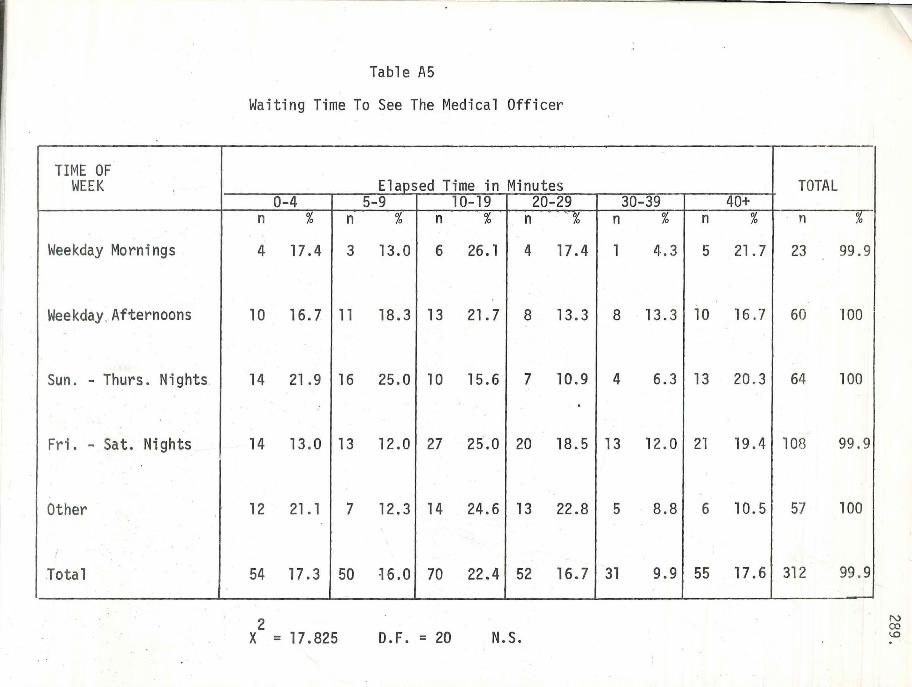
Table A5
Waiting Time To See The Medical Officer
TIME OF WEEK Elaosed Time in Minutes
0-4 5-9 l 0-19 20-29 n % n % n % . n "L ,o
Weekday Mornings 4 17.4 3 13. 0 6 26. l 4 17 .4
Weekday, Afternoons 10 16.7 11 18.3 13 21. 7 8 13.3
Sun. - Thurs. Nights 14 21.9 16 25.0 10 15.6 7 10.9
: .
Fr i. - Sat. Nights 14 13.0 13 12 .0 27 25.0 20 18.5
Other 12 21. l 7 12. 3 14 24.6 13 22.8
I
Tot al 54 17.3 50 ~ 6.0 70 22.4 52 16. 7
2 X = 17.825 D.F. = 20 N.S.
30-39 n % n
l 4.3 5
8 13. 3 10
4 6.3 13
13 12.0 21
5 8.8 6
31 9.9 55
TOTAL 40+
% n
21. 7 23
16. 7 60
20 .3 64
19.4 108
l 0. 5 57
17.6 312
%
99. 9
100
100
99.9
100
99 .9
N (X) I..O
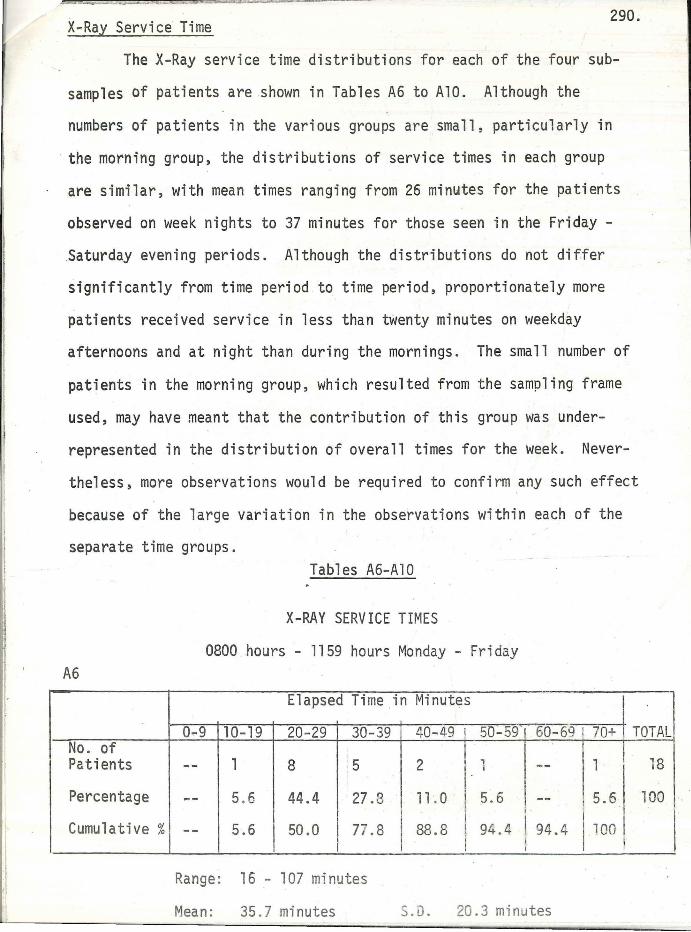
/ .
X-Ray Service Time 290.
The X-Ray service time distributions for each of the four sub-
samples of patients are .shown in Tables A6 to AlO. Although the
numbers of patients in the various groups are small, particularly in
the morning group, the distributions of service times in each group
are similar, with mean times ranging from 26 minutes for the patients
observed on week nights to 37 minutes for those seen in the Friday -
Saturday evening periods. Although the distributions do not differ
significantly from time period to time period, proportionately more
patients received service in less than twenty minutes on weekday
afternoons and at night than during the mornings. The small number of
patients in the morning group, which resulted from the sampling frame
used, may have meant that the contribution of this group was under
represented in the distribution of overall times for the week. Never
theless, more observations would be required to confirm any such effect
because of the large variation in the observations within each of the
separate time groups. Tables A6-Al0
X-RAY SERVICE TIMES
0800 hours - 1159 hours Monday - Friday A6
Elapsed Time in Minutes
0-9 10-19 20 -29 30-39 l ~0-49 i 50-59160-69 I 70+ TOTAL No. of I , Patients -- l 8 :5 2 -- l 18 I
Percentage -- 5.6 44.4 27.3 i1 . 0 5.6 -- 5.6 100 I '
Cumulative% -- 5.6 50.0 77.8 88.8 , 94.4 1 94.4 1,00 I I j
Range: 16 - 107 minutes
Mean : 35 .7 minutes S.0. 20.3 minu tes
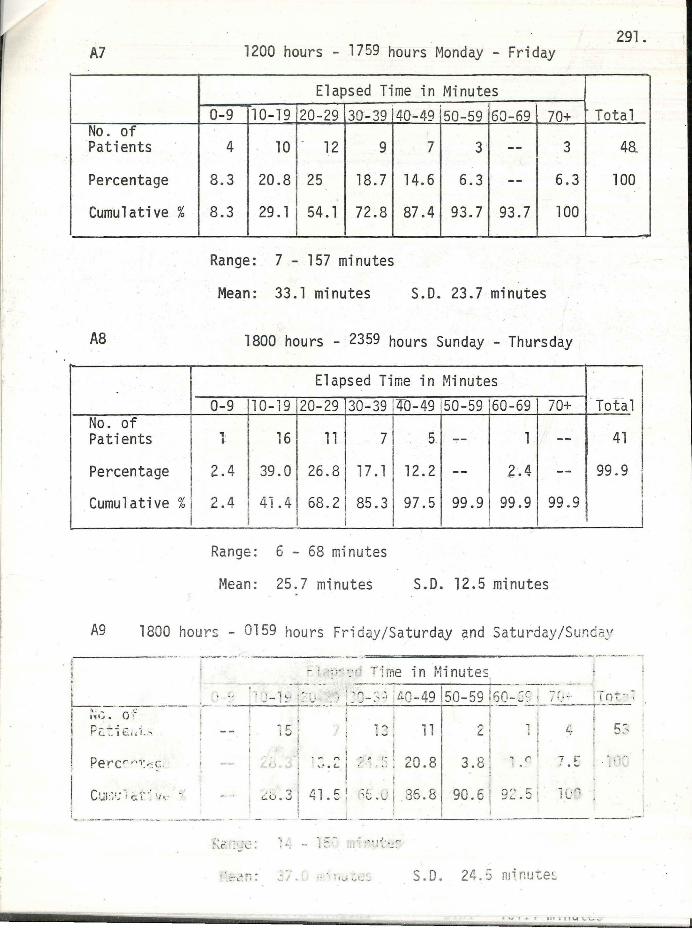
A7
No . of Patients
Percentage
Cumulative%
AB
No. of Patients
Percentage
Cumulative%
1200 hours - 1759 hours Monday - Friday
Elapsed Time in Minutes 0-9 10-19 20-29 30- 39
4 10 - 12 9
8.3 20 .8 25 18. 7
8 .3 29 .1 54. 1 72.8
Range: 7 - 157 minutes
Mean: 33.1 minutes
40--49 50-59 60-69
7 3 --
14. 6 6.3 --87.4 93.7 93.7
S.D. 23.7 minutes
70+
3
6.3
100
1800 hours - 2359 hours Sunday - Thursday
Elapsed Time in Minutes
0-9 10-19 20-29 30-39
1 16 11 7
2.4 39.0 26.8 17. 1
2.4 41.4 68.2 j 85.3 I
Range: 6 - 68 minutes
Mean: 25.7 minutes
40-49 50-59 60-69
5. 1
12.2 -- z·.4
97.5 99.9 99.9
S.D. 12.5 minutes
70+
--
--99.9
. 291.
Total
4a
100
· rota 1
41
99.9
I
A9 1800 hour!: - 0159 hours Fri day /Saturday and Saturday /Sur:d a:' ·----·-·- ---------- =--=,~-------------·· --·-·· ··---· -!
!
' t '---------- ---i :1,~. o -t.:
. p;:: "'.': ~ t.i ; i..,
Percr ,·;:~=c.
Ctn:1;; ~r c. t ·: t, , ..
- · ··;":"·_-,- Tirne in Minutes, - ··· l --- --·-· -· i - , • · • ' , ~ ... .. • t · . ,_ ... r • ·- ~ - •· :: - 1~· '. '): .~:' L.:c_-' _ _ , _, lc,Q-49 jso-59 ?o-~~; 1_ I , _, - ! IQ, • '
f~ C' < .::~:
' ·.::-~ft:
. l
., ,-i ;:;; ;
I t
1 " 11 I
; - " I : , ,: i 20 8 ,,. c.. l . . ., . . . :
,,_. ';• !:.l ,:: I ;1 .. ,•1· Q,~ Q i..U. ~ , •"' ! · 'v.,""' ,,.,v. U
I ,... i 1 ! C. I , I l
3.8 '. ... (' . 9" 6 ' ::i-· ,.. ' u. i :.,.._. ::i !
- _ _j _ __ : - _· --'-- --- -
: ··.· 1 f. - nr-: :" J"'..· ·.::
., \ ~,.;, .:c .. , S.D. 24 .S rninu ~e~
l.,.
7 I-"
1 l;r-,
I~~ , ., i 1 11 i 11""' \ . \..- ...
5:-
}.
_ !
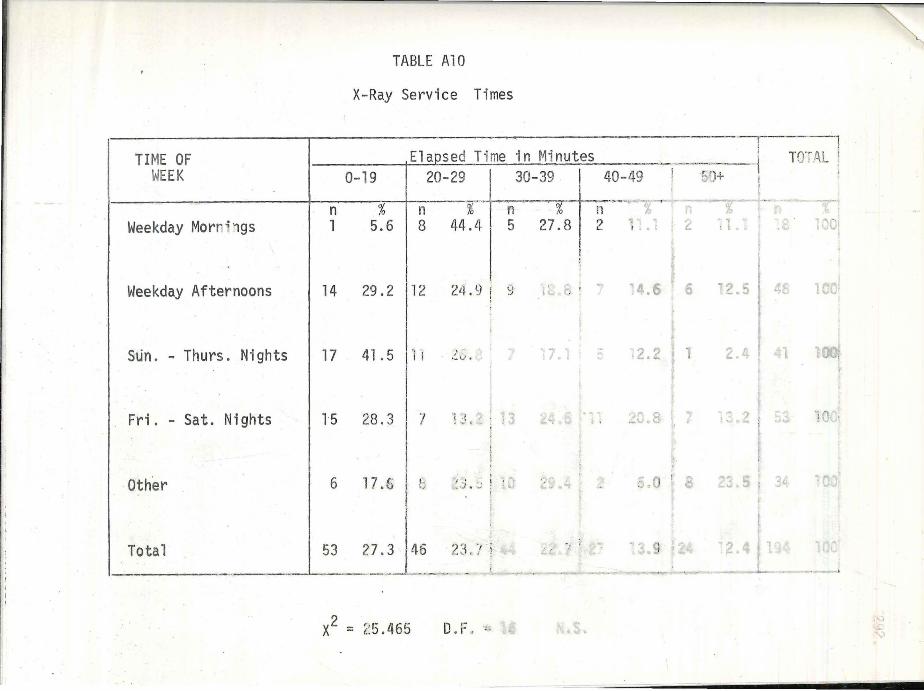
,,,
TIME OF WEEK
Weekday Morr~1gs
Weekday Afternoons
Sun. - Thurs. Nights
Fri. - Sat. Nights
Other
TABLE AlO
X-Ray Service Times
0-19
n % l 5.6
Elapsed Time in Minutes ______ ,. _ _ : 20-29 I 30-39 t 40-49 ! C' )+ I
n %·tn-~% l1_,_, ___ -··;;- -i'"-~?o
8 44.4 ! 5 27.8 2 1:.1
l
14 29. 2 I 12 2il. 9 ! 9 14. 6 ·2 .5 I 4
17 41 . 5 In .:: :, . . 2 •
1·5 "8 ., I I ·, 1 .::'. • ,J , ~ ' 13 • a.
6 17 .s / ·. ,, ~ ~ . :; \.
Total ___ _,___s3_ 2~~J~--~~'!_L_
2 'i- 465 D ,.. X = ~~- .r.
TOT,AL
1
:O• ,
",;' ~,<'l!
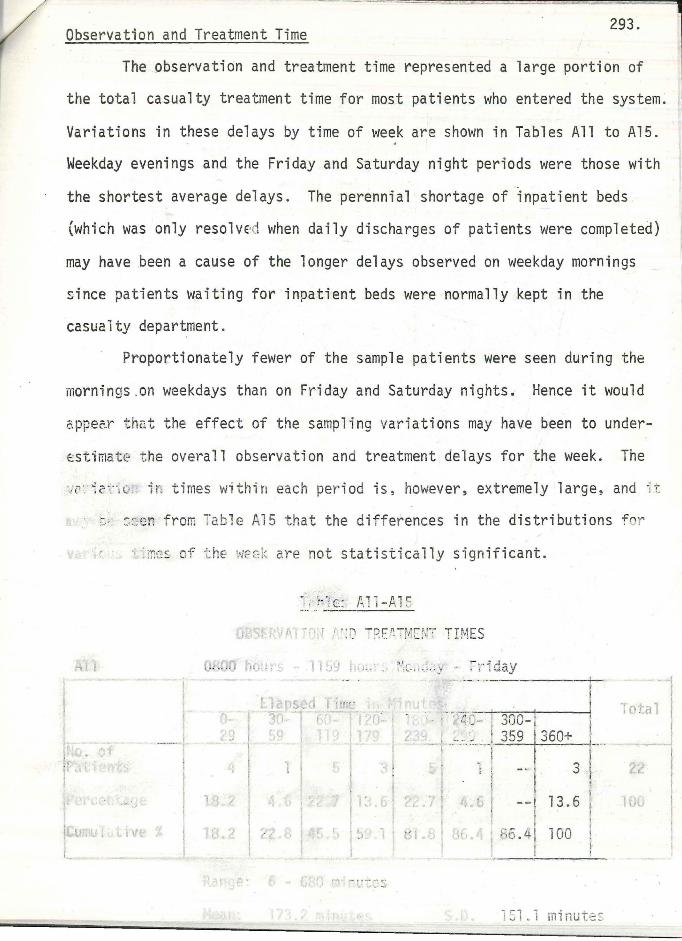
Observation and Treatment Time 293.
The observation and treatment time represented a large portion of
the total casualty treatment time for most patients who entered the system.
Variations in these delays by time of week are shown in Tables All to Al5 . . Weekday evenings and the Friday and Saturday night periods were those with
the shortest average delays. The perennial shortage of inpatient beds
(which was only resolved when daily discharges of patients were completed)
may have been a cause of the longer delays observed on weekday mornings
since patients waiting for inpatient beds were normally kept in the
casualty department.
Proportionately fewer of the sample patients were seen during the
mornings.on weekdays than on Friday and Saturday nights. Hence it would
appe~r th2t the effect of the sampling variations may have been to under
estimate the overall observation and treatment delays for the week. The
·-' c- : ~2r ·, t:: .. "ir! t imes within each period is, however, extremely large, and it
~ ~:en from Ta ble Al5 that the differences in the distributions fe r
~mes of t h~ WF0k are not statistically significant.
·. ; f0 fc: f~11 --tU2
• ·:D -!Jf /\_ 7 f-11[ r~-r TIMES
-, . fie.,-' . ! l !,, .~ ~-':t:-: ;,. 1 --y :- r 1da.y
. ~ ,:.;·;;·r l ,..,,,_..O [ , , .. _ .. ·, -:>u-
I .. a, I
1
'-!··;~ - ..- • .. .. ~- ·- r·
____ J_ ~.-·.:'---! 359 1360+ ! 3 •i
,: .• Gr --1 13.6
i;6 . 4I 100 r
I !
I
1Sl.1 minute:
I
2,~7 I
r ., I
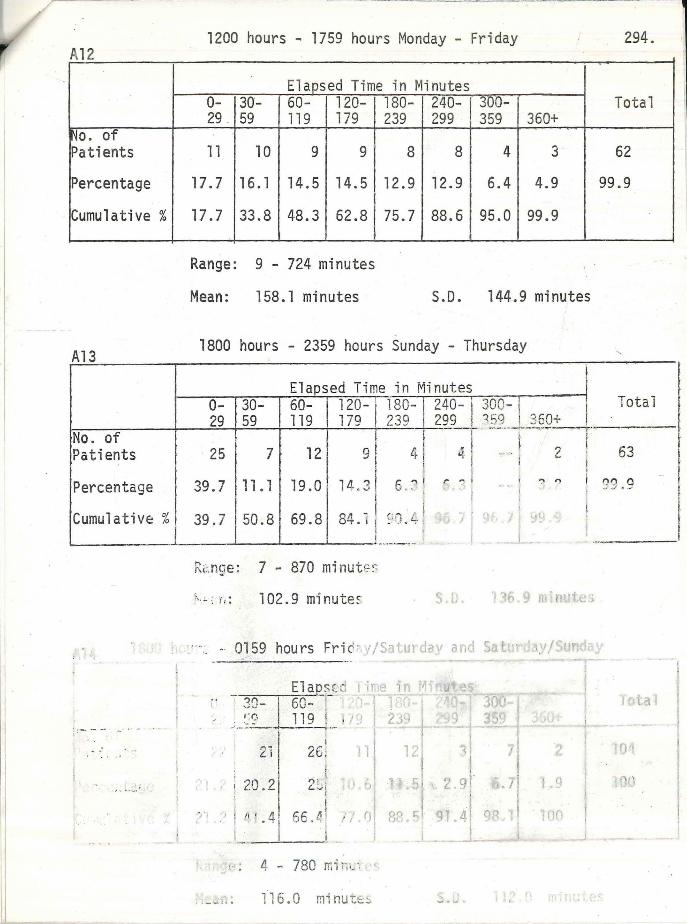
A12
No. of Patients
Percentage
Cumulative%
A13
1200 hours - 1759 hours Monday - Friday
Elapsed Time in Minutes 0- 30- 60- 120- 180- 240- 300-29 _ 59 119 179 239 299 359 360+
11 10 9 9 8 8 4 3
17. 7 16 .1 14.5 14. 5 12.9 12.9 6.4 4.9
17. 7 33.8 48.3 62.8 75.7 88.6 95.0 99.9
Range: 9 - 724 minutes
Mean: 158.1 minutes S.D. 144.9 minutes
1800 hours - 2359 hours Sunday - Thursday
Elaosed Time in Minutes
294.
Total
62
99.9
Total 0- 30- I 60- 120- f 180- 240- 1· 300- 1 . I 29 59 119 179 I 239 2,99 , ?5Y __ ,. ~§9~-~-~~-
No. of I t ~ Patients · 25 7 12 91 41 ~-1 --··~ 2 !
Percentage
Cumulative:%
I , - - --
39. 7 111. 1 I 19 . o I 1.1 .. 31 6 -:' !
39, 7 l 50. 8 I 69. 8 I 84. 1 ! ~·G. ~ I
R~nge : 7 - 870 minutE~
r. ~, t, : 102.9 minute~
0159
-:in ' ,.; \ } -
r:a
I"";, LI
.• 1 20 . 2
:1 ! ,, . . 4
i 26 !
2Ll ' !
66.t: 1 I
_ _,_ __ l
:1 , , ; 4 - 780 Tr. F;i_c ·.
--~ ": 11 6.0 mi nu-css
I ,.. ~ 1 t ':" ')
63
?3. 9
0
,:'\ -.,
I '
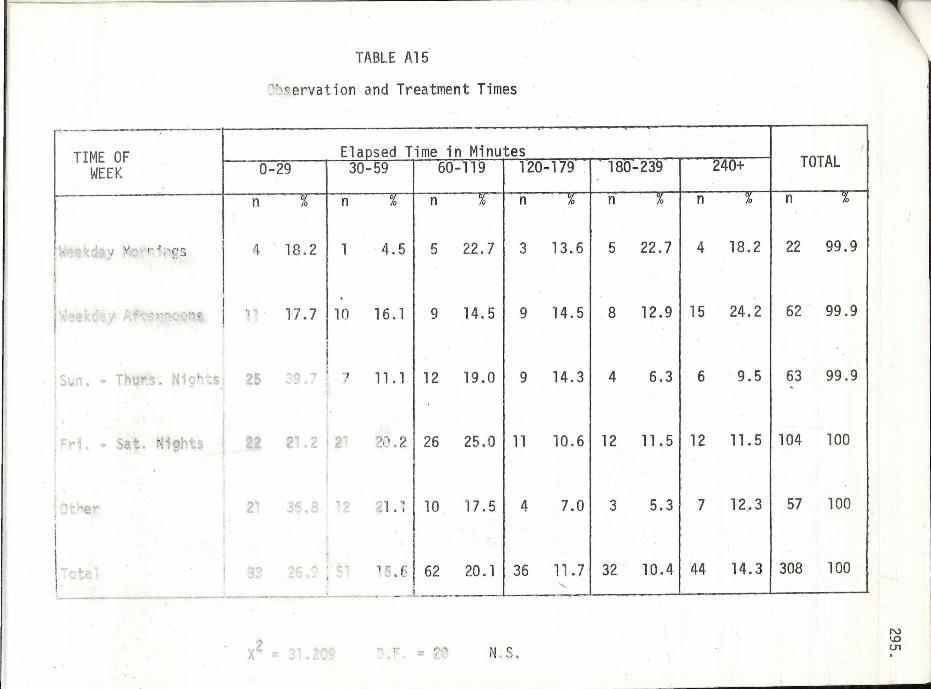
TI ME OF WEEK
:!, .... -:..:.~rs
S~n. - Thurs . Nig~ts
. • Sa~.
e
TABLE Al5
~~~ ervation and Treatment Times
Elapsed Time in Minutes 0-29 30-59 1 60-l19 1 120-119--1·· 1so~23 40+ TOTAL
n iO n "00 n n n n n 'O
,i 18.2 I 1 4. 5 I 5 22. 7 I 3 13. 6 I 5 22. 7 I 4 18. 2 I 22 99. 9
'P l7. 7 110 16 . l I 9 14. 5 I 9 14. 5 I 8 12. 9 I 15 24. 2 I 62 . 99. 9
5 7 ., 11 . 1112 19.0 9 14.3 4 6.3 6 9.5 63 99.9
:: ,: . 2 I 26 25. o I 11 lo. 6 I 12 11 . 5 I 12 11 . 5 I 104 loo
.. , ~1 . -: I 1 o '17. 5 I 4 7 .o I 3 5. 3 I 7 12 .. 3 I 5 7 1 oo
.-, "'!I.I~ 1 :: • 6 I 62 20 . l I 36 11 . 7 I 32 lo. 4 I 44 14. 3 I 308 loo :---~-- --L ----L----"'
X .. NS. N '-0 <.n
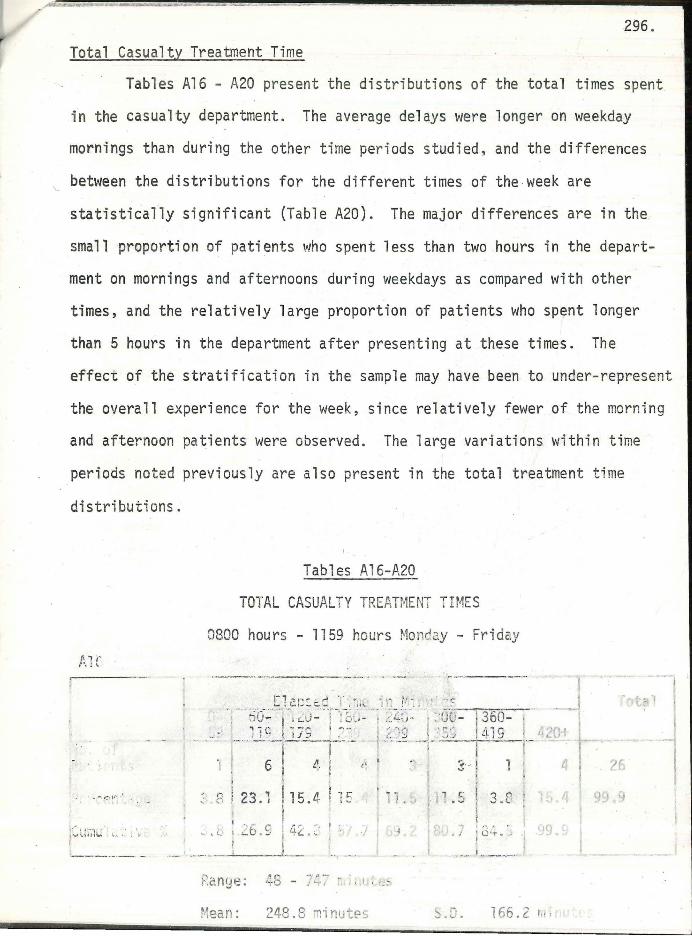
~
296 .
Total Casualty Treatment Time
Tables Al6 - A20 present the distributions of the total times spent
in the casualty department. The average delays were longer on weekday
mornings than during the other time periods studied. and the differences
between the distributions for the different times of the week are
statistically significant (Table A20). The major differences are in the
small proportion of patients who spent less than two hours in the depart
ment on mornings and afternoons during weekdays as compared with other
times, and the relatively large proportion of patients who spent longer
than 5 hours in the department after presenting at these times. The
effect of the stratification in the sample may have been to under-represent
the overall experience for the week, since relatively fewer of the morning
and afternoon patients were observed. The large variations within time
periods noted previously are also present in the total treatment time
distributions.
'
. l ;· -. ~ "
. .-, r.~,r
ii ' '""l" ;...., l',i, I.,, ~ .• ' • ;.
L_ ___ __ ,_ , ·-
Tables Al 6-A20
TOTAL CASUALTY TREATMENT TIMES
0800 hours - 1159 ho urs Mor.c2.y - Fr iday
• • ,._,w,_ _ _ _ . -·
.~-1._c~c: .~¢-~.J~·._~~· '"· __ ~i_'~- _r~·;:. ,_·-:f ·· ? . ~ ri 1jw: 1 ~ LU- \ -: o:_.. - : / li.0 1
~ ; ~-uo- 360-~ 1 ~ ~ j JS I ~-" . l ( :·.g f' . ·,;/; ~i 1 S
i 6 I
I
- i-··· - 1 · ·--· ·-i -i! I . l . , . ";. ') Ip:- ~ ' ;. I .-..• ·t •• ,r· .• . •
' :· ! . f
.~ ' " 3 " I 1 i:: ll 1· ~ r.: (";~ t,.. ·,.~ I .J • • \ ; ..) , ' n. , r-;. I 1 (, .~ I -· L: I.
' ·-. t
I ., - - f .• r -. i • ' b l. I I.J./ . -.. , •'-• -' - r &... 11o·- ' . ' /3~. ·,
·-" . --- · ---''-------'- ~ . - ·' --- ------
~2n~e:
~9
Mean: 248.8 minutes .. ,_ ... LI ,. 166. 2 111;
!
_J ---i
·1 ?6 I
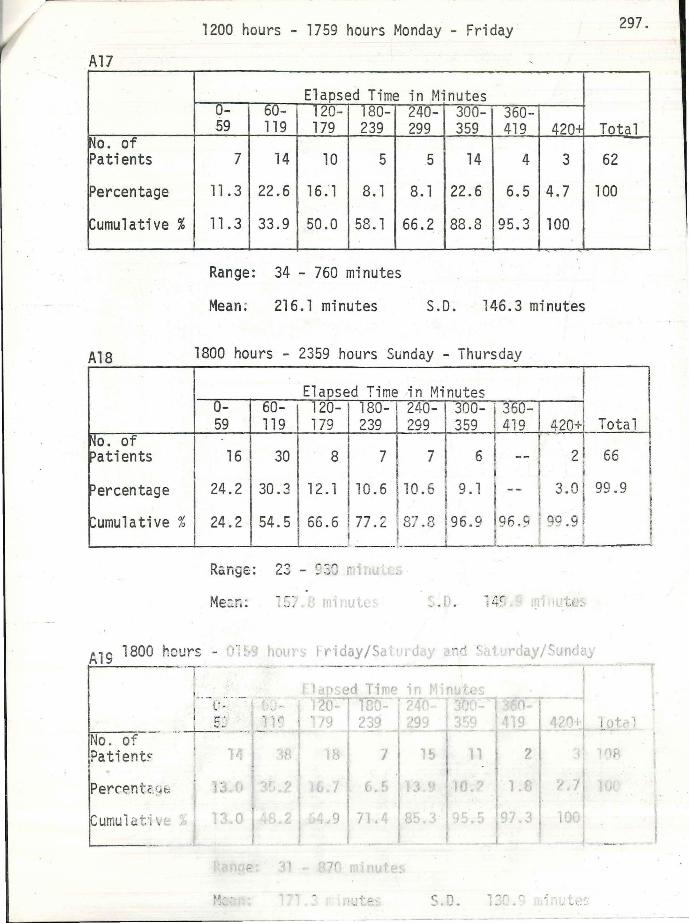
A17
No. of Patients
Percentage
~umulative %
Al8
~o. of :>ati ents
'ercentage
:umulative %
1200 hours - 1759 hours Monday - Friday 297.
Elapsed Time in Minutes 0- 60- 120- 180- 240- 300- 360-59 119 179 239 299 359 419 420+ Total
7 14 10 5 5 14 4 3 62
11. 3 22.6 16. l 8. l 8. l 22.6 6.5 4.7 100
11.3 33.9 50.0 58. l 66.2 88.8 95.3 100
Range: 34 - 760 minutes
Mean; 216.l minutes S.D. 146.3 minutes
1800 hours - 2359 hours Sunday - Thursday
Elapsed Time in Minutes 0- 60- 120- 180- 240- 1 300- 360-59 119 179 239 299 359 419 420+ Total
8 7 7 I 6 -- . 2 66 I 16 30 l .
24.2 30.3 ,2.1 10.6 10.6 i 9., -- 3.o 99.9 I I . .
24.2 54.5 66.6 77.2 87.e !96 .9 196 .s 19si .9 1 I I I , r ______ __ ,_ i I • I ---l
R&nge: 23 - ~21 r1 ,
Me~.r.: ~ s: (-i mrnu ( ·1 ., J, _, . I • t .. I t(_:
A19 1800 hours - J~! t1 rd , ... .... , ·'
1--~·7·-, - ----
1--- .. ·-; l' . I ,- .
No . of Patient~
Perrentr./4b
umukti \.~
' ... .. . ~ -
11,, .... l'h ..
7
;._;tf: ~ ~ ll ... __, . ' . :.....::: :.-
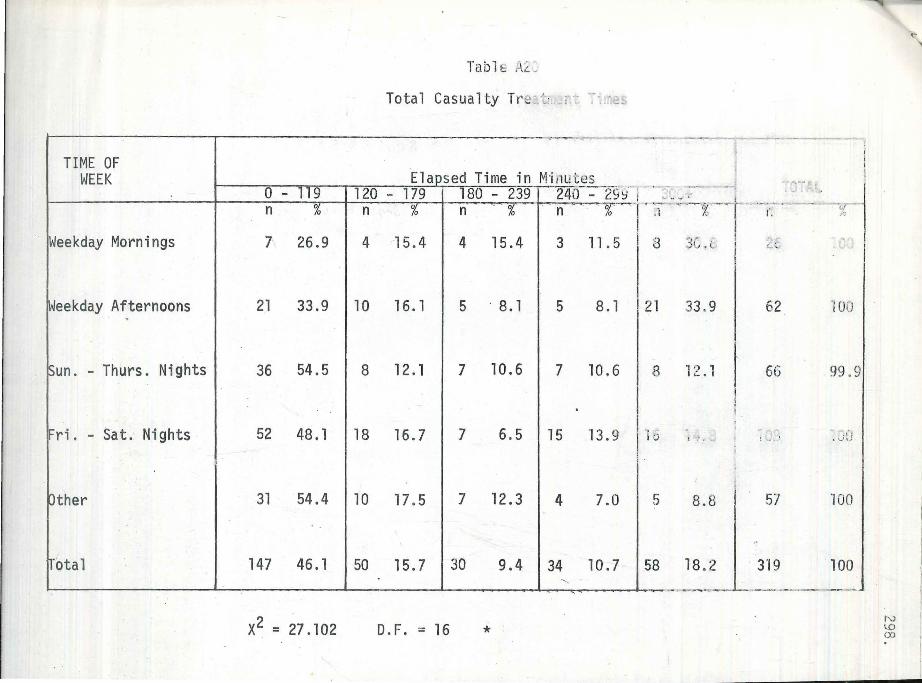
TIME OF WEEK
0 - 119 n 0
0
Weekday Mornings 7 26.9
Weekday Afternoons 21 33.9 .
Sun. - Thurs. Nights 36 54.5
Fri . - Sat. Nights 52 48 . l
Other 31 54.4
fetal 147 46.1
x2 = 21.102
Tabl e i.\L~
Total Casualty i re < :· .. .: :·: :··,'.r:e:,
.........,.._ ·-
Elapsed Time in Midu tes 120 - 179 180 - 239 240 - 29Y- I .
n % n % ' . n %_......, . ~
4 15 . 4 4 15.4 3 11. 5
10 16. l 5 · 8. l 5 8.1 2
8 12. 1 7 10.6 7 10.6
. 18 16. 7 7 6.5 15 13.9 1
10 17.5 7 12.3 4 7.0
50 15. 7 30 9.4 34 10.7 5 "
D. F. = 16 *
·----;:_ ~ :- - -~ ' "' ' ·"t ' 1 --.r ...... ~?, ---- r· , cc ,_, _ __ ,,, _ ,....:. ::.....-- , ·-
.1 % I: . ~o
8 3C , c I l),: :, ·,
l
8
0
5
8
33 .9
, ') , I.:. , I
t -: •
8.8
18 . 2
r .. 1..,-:-
62
66
r L'1r~
5/
319
·1ou
99 .9
,, ' d ,)
'JOO
100
-----~ f-.) lO co
Copyright © 2022 FDOKUMEN