
Modeling treatment motivation in substance-abusing women with children
11
Child Abuse & Neglect 29 (2005) 1313–1323 Modeling treatment motivation in substance-abusing women with children Dina J. Wilke a,∗ , Akihito Kamata b , Scottye J. Cash c a Florida State University, College of Social Work, Tallahassee, FL 32306-2570, USA b Florida State University, College of Education, Tallahassee, FL, USA c Ohio State University, College of Social Work, Columbus, OH, USA Received 14 June 2004; received in revised form 5 April 2005; accepted 7 May 2005 Abstract Objectives: Children are often considered a primary motivator for women seeking substance abuse treatment. This study tested a model predicting treatment motivation in substance-abusing mothers. Methods: This study was a secondary analysis of the Drug Absue Treatment Outcome Study (DATOS). It used structural equation modeling to describe factors influencing motivation for treatment. DATOS is a national study of substance abusers entering treatment. Treatment was provided by a sampling of community-based programs, free-standing hospitals, hospital units, county-funded programs, modified therapeutic communities, and criminal justice programs. The subsample of women with children under the age of 18 for whom custody of children could be determined was selected (n = 1371). The variables comprising each factor were based on self-report, and standardized scales measuring level of drug involvement, psychological functioning, children, and a desire to stop using drugs were used. Results: Drug involvement was positively related to poorer psychological functioning, child custody issues, and the desire to stop using drugs. Child custody issues had a negative influence, while poorer psychological functioning and a desire to stop using drugs positively influenced treatment motivation. Conclusions: The negative influence that children have on treatment motivation may reflect the practical or emotional difficulties of having to leave children behind or in some instances having children placed in foster care. Specifically, losing custody of children, particularly with little expectation they will be reunified, may serve as a detriment to motivation. Popular beliefs hold that children serve as a primary source of a mother’s treatment motivation; ∗ Corresponding author. 0145-2134/$ – see front matter © 2005 Elsevier Ltd. All rights reserved. doi:10.1016/j.chiabu.2005.05.002
Transcript of Modeling treatment motivation in substance-abusing women with children

Child Abuse & Neglect 29 (2005) 1313–1323
Modeling treatment motivation in substance-abusingwomen with children
Dina J. Wilkea,∗, Akihito Kamatab, Scottye J. Cashc
a Florida State University, College of Social Work,Tallahassee, FL 32306-2570, USA
b Florida State University, College of Education,Tallahassee, FL, USA
c Ohio State University, College of Social Work,Columbus, OH, USA
Received 14 June 2004; received in revised form 5 April 2005; accepted 7 May 2005
Abstract
Objectives: Children are often considered a primary motivator for women seeking substance abuse treatment. Thisstudy tested a model predicting treatment motivation in substance-abusing mothers.Methods: This study was a secondary analysis of the Drug Absue Treatment Outcome Study (DATOS). It usedstructural equation modeling to describe factors influencing motivation for treatment. DATOS is a national studyof substance abusers entering treatment. Treatment was provided by a sampling of community-based programs,free-standing hospitals, hospital units, county-funded programs, modified therapeutic communities, and criminaljustice programs. The subsample of women with children under the age of 18 for whom custody of childrencould be determined was selected (n = 1371). The variables comprising each factor were based on self-report, andstandardized scales measuring level of drug involvement, psychological functioning, children, and a desire to stopusing drugs were used.Results: Drug involvement was positively related to poorer psychological functioning, child custody issues, and thedesire to stop using drugs. Child custody issues had a negative influence, while poorer psychological functioningand a desire to stop using drugs positively influenced treatment motivation.Conclusions: The negative influence that children have on treatment motivation may reflect the practical or emotionaldifficulties of having to leave children behind or in some instances having children placed in foster care. Specifically,losing custody of children, particularly with little expectation they will be reunified, may serve as a detrimentto motivation. Popular beliefs hold that children serve as a primary source of a mother’s treatment motivation;
∗ Corresponding author.
0145-2134/$ – see front matter © 2005 Elsevier Ltd. All rights reserved.doi:10.1016/j.chiabu.2005.05.002

1314 D.J. Wilke et al. / Child Abuse & Neglect 29 (2005) 1313–1323
however this study found the opposite was true. Children should not automatically be considered a primary sourceof motivation for participation in treatment.© 2005 Elsevier Ltd. All rights reserved.
Keywords: Motivation; Substance abuse; Women with children
Introduction
Maternal substance abuse is a major factor in referrals to the child welfare system for abuse and neglect.The increase of alcohol and other drug (AOD) use among women, particularly cocaine and more recently,methamphetamine (Bartholet, 1999) has led to research which suggests that between 40 and 80% of allthe families in the child welfare system involve AOD abuse (Young, Gardner, & Dennis, 1998). Druguse contributes to child maltreatment in many ways. Substance abusing parents are likely to use moneyto buy drugs that would otherwise be used for necessities, provide inadequate supervision while they areusing or recovering from episodes of intoxication, or expose children to criminal activity such as drugdealing or prostitution (Dore, Doris, & Wright, 1995; Munkel, 1996).
Child neglect, though difficult to define, is the most common form of child maltreatment. Recent datasuggest that an estimated 896,000 children were victims of maltreatment in 2002 and that 60.5% of thosereferrals were for neglect (US Department of Health & Human Services, 2004). It is estimated that thereported rate of child neglect is 7.2 per 1000 children (US Department of Health and Human Services,2004). The definition of child neglect includes inadequate nutrition, supervision, and provision of medicalcare, and living in an unsafe environment (Sedlack & Broadhurst, 1996). Arguments exist over whetherthere needs to be evidence of actual harm to the child and whether intent to harm should be included inthe definition (US Department of Health & Human Services, 2001).
There are many factors that predict if substance-abusing women will neglect their children, includingboth historical and present day factors. Historical predictors of neglect include sexual abuse as a childand substance abuse in the extended family, while present day factors include severity of drug problems,drug of choice (cocaine or heroin) and difficulties finding child care (Cash & Wilke, 2003). Additionally,parents who neglect their children tend to be socially isolated with few social supports, and comorbiddepression and/or other mental illness is common (Berry, Charlson, & Dawson, 2003; Menahem & Halasz,2000). It may be that in addition to the direct impact parental substance abuse has on child development,there is an indirect effect through the occurrence of ineffective parenting (Dunn et al., 2002).
Case-control studies of substance abusing and non-substance abusing parents in the child welfaresystem found that substance abusing parents more often failed to follow through with court mandates andwere more likely to lose their children than parents without a substance abuse problem (Murphy et al.,1991). Another study matched parents of children born with and without positive cocaine toxin screens(Kelley, 1992). Almost eight times as many parents of babies born positive for cocaine had substantiatedabuse or neglect reports (60%) compared to the control group. Further, about 50% of the drug-exposedchildren had been removed from the home by the end of the first year, compared to no children fromthe control group. Finally, a longitudinal study found that substance abuse of any kind, particularlypolysubstance abuse, most strongly predicted re-referrals to the child welfare system (Wolock & Magura,1996).
D.J. Wilke et al. / Child Abuse & Neglect 29 (2005) 1313–1323 1315
If the assumption is that substance abuse is a major risk factor in the abuse and neglect of children,then it follows that resolving drug or alcohol problems could facilitate improvement in the level of familyfunctioning. A referral for substance abuse treatment is a logical step toward that goal. However, whilesubstance abuse and involvement in the child welfare system often overlap, one study found that almosthalf of families receiving child welfare services were never referred to substance abuse treatment (ChildWelfare League of America, 2001). Further, treatment success depends on many factors including anindividual’s readiness to change (Prochaska, DiClemente, & Norcross, 1992) and the source of motivation(e.g., intrinsic vs. extrinsic).
Children have often been assumed to be a principle source of motivation for mothers to change drug-abusing lifestyles (Tracy, 1994; Wilke, 1994). Indeed, most substance abusing mothers enter treatmentwith an awareness of the impact of substance abuse on their children, or out of fear that their children willbe removed from the home if they do not successfully complete a treatment program (Berry et al., 2003).The purpose of this study was to test a model describing factors that influence motivation for treatment ina sample of drug or alcohol abusing mothers who were in substance abuse treatment. This study adds tothe current knowledge base by testing the assumption that having children will have a positive influenceon a mother’s willingness to seek treatment.
Methods
This study was a secondary data analysis of the Drug Abuse Treatment Outcome Study (DATOS), aNIDA-funded, national, multisite, longitudinal study of men and women in community-based drug andalcohol treatment programs between 1991 and 1993 (Flynn, Craddock, Hubbard, Anderson, & Etheridge,1997). The treatment was provided by a sampling of for-profit, not-for-profit, and public programs includ-ing community-based programs, free-standing hospitals, hospital units, county-funded programs, modi-fied therapeutic communities, and criminal justice programs (Etheridge, Hubbard, Anderson, Craddock,& Flynn, 1997).
A total of 10,010 clients were interviewed as they entered AOD treatment resulting in a comprehensivedatabase of demographic, alcohol and drug, mental and physical health, and social functioning variables.The subsample of women with children under the age of 18 (n = 2,146) was selected for this study.However, an additional 775 participants were excluded due to missing data on a key variable of interest(custody of children at admission), most often because the item was not included on all versions of theinstrument. This resulted in a final sample size of 1,371. IRB approval was not needed as this was asecondary analysis of a publicly available dataset.
Measures
Motivation
A standardized scale was used to measure motivation for treatment (Simpson & Joe, 1993). It is a5-item scale and includes items such as “I came to this program because I really felt that I am ready todeal with myself in treatment,” and “The only thing that will help me now is some kind of treatment.”Responses were measured using a 3-point Likert scale (not at all, agree somewhat, and very much agree),
1316 D.J. Wilke et al. / Child Abuse & Neglect 29 (2005) 1313–1323
and the subscale scores were derived by summing the response categories. The alpha reliability coefficientin this sample was .75.
Drug involvement factor
Items used to measure the drug involvement factor included having cocaine or heroin as a primary drugof choice (both of these measures were dummy coded with “no” being the omitted category). Womenwere also asked if they were in a primary sexual relationship, and if yes, was that individual abusingdrugs or alcohol. This was used as a dichotomous variable with “no” being the omitted category. Finally,a variable was created to assess the degree of substance abuse risk in the mother’s personal network andwas defined using four items. Respondents were asked to indicate the number of people they knew (none,one or a few, and many) who: (1) used drugs for nonmedical purposes; (2) drank alcohol heavily; (3)entered treatment; and (4) quit using drugs. The last two items were reverse scored and the responseswere summed. Higher scores indicated a greater level of AOD risk in the mother’s personal environment.
Psychological functioning factor
Standardized scales were used to assess indicators of psychological functioning. The Rosenberg Self-Esteem Scale (Rosenberg, 1965) is a 10-item scale used to measure levels of self-esteem. In this sample,the Cronbach’s alpha score for self-esteem was .85. The TCU Psychosocial Functioning Scales wereused to measure depression, anxiety, and anger control problems (Knight, Holcom, & Simpson, 1994).Depression was measured using a 14-item scale that included items such as crying easily, feeling blue,feeling no interest in things, and so forth (Cronbach’s alpha = .94). Anxiety was measured using a 10-itemscale that included items such as feeling fearful, tense, keyed up, or restless (Cronbach’s alpha = .93).Finally, anger control was measured using a 6-item scale that included items such as temper outbursts,getting into frequent arguments, and having urges to break or smash things (Cronbach’s alpha = .88). Forall of these scales, responses were summed for an overall scale score, and higher scores indicated greaterlevels of the indicator measured.
Children factor
Several indicators were used to measure the children factor including signs of child neglect, custodyof children at admission, number of children at home, and whether participating in treatment will affectcustody status. Child neglect was a self-report measure whereby participants were asked if in the 12months prior to treatment they had ever: (1) left a child under the age of 6 home alone; (2) had someoneelse feed their child because of not cooking or not having food in the house; (3) had been told by aprofessional (e.g., social worker, nurse) that a child was not receiving the care he/she needed; (4) run outof money because it was spent on going out/“partying”; and (5) not provided required financial supportfor a child. The signs of neglect indicator was measured as the sum of positive responses.
Legal custody was used as a dichotomous variable, and was created by using responses to two differentquestions. Respondents were asked how many children they had given birth to, and then asked each child’scurrent legal custody status. Women who indicated that they did not have legal custody of at least oneof their children, regardless of whether others remained in the home, were coded as “yes” with all otherwomen in the omitted category. Further, women were asked to indicate the total number of children in

D.J. Wilke et al. / Child Abuse & Neglect 29 (2005) 1313–1323 1317
their home for whom they were providing care, and if receiving treatment now would affect the legalcustody of their children. This was measured as a dichotomous variable with “no” being the omittedcategory.
Finally, respondents were asked to indicate up to four reasons why they entered treatment. One of thesereasons, “wanting to get off drugs,” was entered into the model as an observed variable and representeda woman’s desire to stop her AOD use. This item was dummy coded with “not selected” as the omittedcategory.
Data analysis
Structural equation modeling was used to analyze a hypothesized model predicting treatment moti-vation in substance abusing women with children by factors including level of drug involvement,psychological functioning, child welfare, and having a desire to stop using drugs. Structural equationmodeling allows for testing the relationship between latent (not directly observed) constructs and observedindicators that are theoretically related on a specified dependent variable. SEM has advantages over mul-tiple regression in its ability to analyze the relationships between latent constructs, factor loadings, andobserved indicators simultaneously. In addition, there are exogenous variables (independent variables),endogenous variables (intermediary dependent variables) and the main dependent variable, which allowsthe researcher to determine how a construct or observed indicator mediates or moderates the relationshipsin the equation. Further, models have various fit indices. We reported the comparative fit index (CFI) asit is one of the most widely accepted fit indices in the literature. The standard for determining a goodmodel fit is generally considered to be a CFI greater than .90, where values range from 0 to 1 (Bollen,1989; Byrne, 1994).
Results
Demographic data of the final sample indicated that 59% of the respondents were African-American,26% were Caucasian, and 13% were Hispanic. Thirty-five percent of the sample was married or livingas married, while 43% indicated that they had never been married. Fully 73% of the sample reported noweeks of full-time work in the previous 12 months, and 46% did not finish high school. The average ageof the respondents was 31 years old (SD = 5.6 years), and 66% were not currently involved in the criminaljustice system.Table 1provides the means and the standard deviations for the observed variables andthe variables that constitute the latent constructs. Desire to stop using drugs and motivation for treatmentwere measured as observed variables. Finally, each measurement model was first examined separately,and then relationships between constructs were examined in the structural model.
Drug involvement
The first measurement model is for drug involvement, with its five indicators, primary drug—heroin,primary drug—cocaine, high-risk AOD environment, and AOD-abusing partner. Heroin use, cocaine use,and AOD-abusing partner are dichotomously scored, so that the weighted least square (WLS) methodwas used. The model fit values were CFI = .993 and RMSEA = .046, which showed a very good fit withχ2 = 7.744 withdf = 2 (χ2/df = 3.872). When the coefficients were estimated in the final structural model,

1318 D.J. Wilke et al. / Child Abuse & Neglect 29 (2005) 1313–1323
Table 1Descriptive statistics for observed variables and corresponding constructs (n = 1371)
Construct Variable
M SD Range %
Psychological functioningDepression 10.45 10.03 0–40Anxiety 22.00 14.48 0–56Anger 6.73 6.12 0–24Self-esteem 2.81 .50 1–4
Drug involvementPrimary drug—heroin 21.6Primary drug—cocaine 61.7High risk AOD environment 9.34 1.50 5–12Pre-treatment severity 4.91 2.25 0–7AOD abusing partner (% yes) 18.0
ChildrenNo. of children in the home 1.73 1.32 0–6Indicators of neglect 1.10 1.32 0–5Lost custody at admission (% yes) 55.6Treatment affects custody (% yes) 46.4
Desire to get off drugsa (% yes) 75.0Motivation for treatmenta 14.04 1.61 6–15
a This construct was measured as an observed variable.
they were−.400, .367,−.092, and .452 for heroin use, cocaine use, partner use, and high-risk AODenvironment, respectively. The coefficient for high-risk AOD environment is standardized, while thecoefficients for heroin use, cocaine use, and partner use are in a logit scale. These coefficients were allsignificant at theα = .05 level, except for partner use.
Psychological functioning
The second measurement model is for psychological functioning, with four indicators, depression,anxiety, anger control and self-esteem. They are all continuous variables, so maximum-likelihood (ML)method was used to evaluate the model fit. Fit indices showed a good fit of the model; CFI = .997and RMSEA = .047, with reasonably lowχ2 to df ratio (χ2/df = 4.016). In the final structure model, thestandardized coefficients were estimated to be .791, .898, .737 and−.380 for depression, anxiety, anger,and self-esteem, respectively, with anxiety having the largest impact on the psychological functioningfactor with anR2 = .806. These coefficients were all significant atα = .05 level.
Children
The third measurement model is for children with four indicators, number of children in the home,number of neglect indicators, custody status of children at admission to treatment (custody), and ifengaging in treatment will affect custody status (treatment affects custody). Two of the variables are
D.J. Wilke et al. / Child Abuse & Neglect 29 (2005) 1313–1323 1319
dichotomously scored (custody and treatment affects custody), so weighted least square method was usedto evaluate the model. The model fit values were CFI = .999 and RMSEA = .012, with a very smallχ2 todf ratio (χ2/df = 2.306/2 = 1.158), indicating a very good fit. In the final structure model, the coefficientswere estimated to be−.281 for the number of children in the home, .597 for the number of neglectindicators, .356 for custody status of children at admission to treatment, and .243 for treatment affectingcustody status, with greater number of neglect indicators having the largest impact on this factor withanR2 = .356. The coefficients for the number of children at home and number of neglect indicators arestandardized, while coefficients for custody and treatment affecting custody are in a logit scale. Thesecoefficients were all significant at theα = .05 level.
Structural model
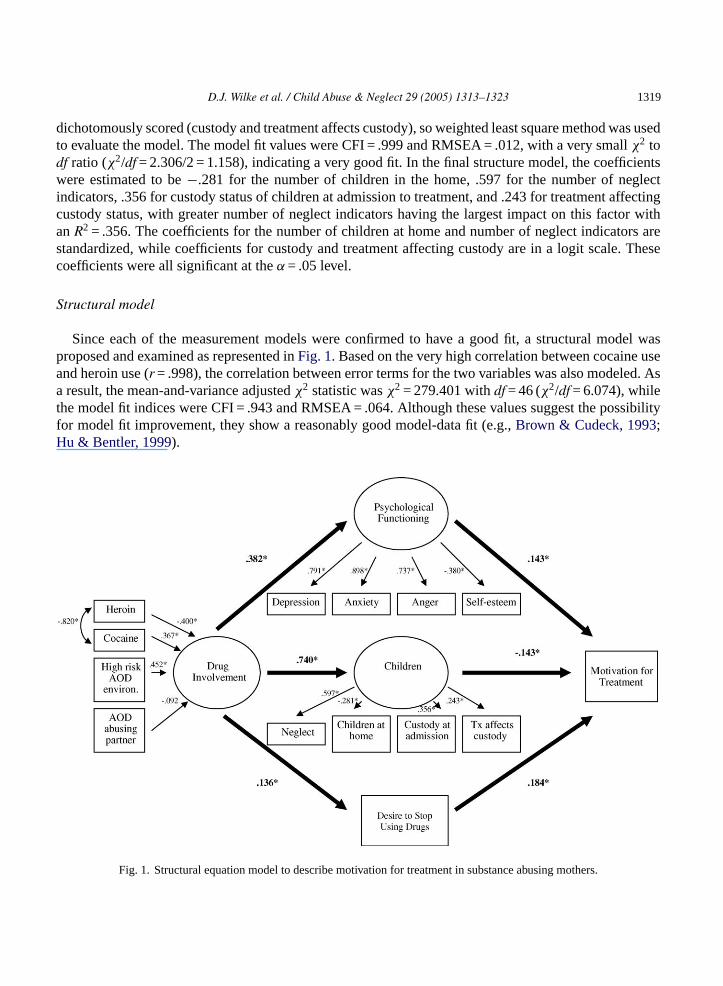
Since each of the measurement models were confirmed to have a good fit, a structural model wasproposed and examined as represented inFig. 1. Based on the very high correlation between cocaine useand heroin use (r = .998), the correlation between error terms for the two variables was also modeled. Asa result, the mean-and-variance adjustedχ2 statistic wasχ2 = 279.401 withdf = 46 (χ2/df = 6.074), whilethe model fit indices were CFI = .943 and RMSEA = .064. Although these values suggest the possibilityfor model fit improvement, they show a reasonably good model-data fit (e.g.,Brown & Cudeck, 1993;Hu & Bentler, 1999).
Fig. 1. Structural equation model to describe motivation for treatment in substance abusing mothers.
1320 D.J. Wilke et al. / Child Abuse & Neglect 29 (2005) 1313–1323
The path between drug involvement and psychological functioning was significant atp ≤ .05 level witha standardized path coefficient of .382 (R2 = .146). This finding suggests that increased drug involvement(specifically the use of heroin and/or cocaine, living in a high-risk AOD environment, and having anAOD-abusing partner) is predictive of an increase in difficulties with psychological functioning (i.e.,increased depression, anxiety, and anger, and lower self-esteem).
The drug involvement factor was also highly predictive of issues associated with children. This rela-tionship was significant atα = .05 level with a standardized path coefficient of .740 (R2 = .548) reflectingthe consequences of drug involvement on the status of children in the lives of substance abusing women.Finally, the drug involvement factor had a positive relationship with the desire to stop using drugs. Thepath coefficient was .136 (R2 = .019) in the scale of logit, which was significant at theα = .05 level. Thisindicates that an increase in the drug involvement factor increases the desire to stop using drugs.
Regarding the final endogenous variable, motivation for treatment was significantly related to thepsychological functioning and children factor, and with the desire to stop using drugs (R2 = .061). Thepsychological functioning factor (.143) and the desire to stop using drugs (.184) were both positivelyassociated with an increase in motivation for treatment. These indicate that women with higher psy-chological functioning factor scores (measured as greater symptoms of anxiety, depression, and angermanagement problems, in addition to a lower level of self-esteem) had higher motivation for treatment,while those with a desire to stop using drugs also had higher motivation for treatment. However, there wasa negative relationship between the children factor and motivation for treatment (−.143), indicating thathigher scores on the children items (number of children in the home, custody loss, indicators of neglect,and participation in treatment affecting custody) reduced overall motivation for participating in treatment.These coefficients, while significant, are small in size. The small sizes coupled with the overallR2 (.061)indicate that other factors not measured in this model also contribute to higher levels of motivation fortreatment. However, they provide an initial glimpse of what influences treatment motivation among drugusing women with children.
Discussion
There are a number of interesting results from the test of this model that warrant attention. The first ofthese is the negative relationship between the children factor and motivation for treatment. This wouldseem to indicate that issues related to children might serve to depress treatment motivation for mothers.On the one hand, this may be considered surprising given the expectation that children are a powerfulsource of motivation for substance abusing mothers. It may be important then to examine the indicatorscomprising the children factor more closely. Higher scores on the children factor are related to havingfewer children in the home, having a greater number of indicators of child neglect, having custodydecisions being influenced by involvement in treatment, and having lost custody of one or more childrenat the time of admission. It may be that losing custody of children, particularly if coupled with littleexpectation that custody will be regained, serves to depress treatment motivation. These results may alsoreflect the neglectful environment of child rearing in that a mother may be apathetic towards treatmentand other aspects of life including parenting.
On the other hand, finding that the children factor had a negative influence on treatment motivationcould be expected given the barriers that children have often presented for women attempting to receivetreatment services. However, the mothers in this study were already in treatment so it can be assumed

D.J. Wilke et al. / Child Abuse & Neglect 29 (2005) 1313–1323 1321
those potential barriers had been resolved. An important implication here could be that issues related tochild custody reduce treatment motivation despite the successful resolution of barriers to treatment.
Finally, the children factor could also be conceptualized as something external to the mother, whereaspsychological functioning and a desire to stop using drugs could be considered internal or intrinsicvariables. To that extent, the positive relationships between psychological functioning (in this study,poorer functioning) and treatment motivation and a desire to stop using drugs and treatment motivationare consistent with other research suggesting that behavior influenced by intrinsic factors is often moresuccessful than behavior influenced by extrinsic factors (DiClemente, Bellino, & Neavins, 1999). Further,there is little difference in the magnitude of the effect on treatment motivation between the psychologicalfunctioning factor and a desire to stop using drugs.
Beyond treatment motivation, when examining the entire model, the strongest predictive relationshipis between the drug involvement factor and the children factor. This indicates that there is clearly aneed to evaluate the children-related consequences of drug use for substance abusing women thoroughly,including the more insidious indications of child neglect, which had the strongest influence on the childrenfactor. Although the indicators comprising the children factor may reduce treatment motivation, they arenonetheless important issues for treatment planning. This planning represents the essential intersectionbetween the substance abuse treatment and child welfare systems.
Children remain a complicated circumstance for substance-abusing women, (and by extension, sub-stance abuse providers), particularly mothers involved in the child welfare system. On the one hand,caring for children can present as a significant barrier to entering treatment, primarily due to the needfor adequate child care and concerns about losing custody of their children if they do enter treatment(Berry et al., 2003). On the other hand, once custody has been lost, there may be little motivation to entertreatment, particularly if the chance to regain custody is small. This idea is supported by other studies,which have found that mothers who had custody of their children had a higher retention rate in treatmentthan the women whose children were in someone else’s care (Strantz & Welch, 1995). None of this,however, speaks to the role that children have in motivating change, which is an important area for futureresearch.
The discussion presented herein should be considered in light of the study’s strengths and limitations.The large, representative sample of women with children in treatment should be considered a strengthboth in terms of the study’s generalizability and its statistical power. However, these data are all self-report and may have been influenced by an under- or over-reporting bias depending on perceived benefitsor consequences. It is also important to note that all of these data are derived from women who havealready entered treatment. In some respects, this indicates that there exists a base level of motivation fortreatment that may not be found in those outside of treatment. We would argue that these results thenwould be conservative estimates. One might expect that the negative relationship reported here betweenthe children factor and treatment motivation would be even stronger in a sample of women with littledesire to participate in a formal program. Finally, the only maltreatment indicator included in this studywas neglect; physical and sexual abuse were not included.
An important implication for substance abuse treatment providers is that children, in or out of the childwelfare system, should not automatically be considered a primary source of motivation for participationin treatment, or even an intrinsic motivator. Indeed, identifying children as a primary source of motivationfor treatment may only reinforce guilt or shame. Instead, it appears that the intrapersonal consequencesof drug use such as symptoms of depression or anxiety, or simply having a desire to quit using drugsare what positively influence treatment motivation, indicating that intervention strategies that address the

1322 D.J. Wilke et al. / Child Abuse & Neglect 29 (2005) 1313–1323
person rather than the role (e.g., mother) may be what is needed to motivate a substance abusing motherinto treatment.
It is important to note that we are not suggesting that children serve as a disincentive to change.DiClemente (1999)points to a conceptual distinction between motivation to change versus motivationfor treatment. One can have a high level of motivation to change with a comparatively low level ofmotivation for participation in a formal treatment program. An important implication for child welfareproviders is to identify what intrinsic factors would motivate a substance-abusing mother to changeher drug using lifestyle, recognizing that formal treatment may not be the only way to accomplish thatgoal. The negative influence that children have on treatment motivation may simply reflect the practicalor emotional difficulties of leaving children behind. In that event, it becomes especially important toprovide substance abuse services for women that include their children, in an effort to see if that improvesmotivation for treatment.
References
Bartholet, E. (1999).Nobody’s children. Boston, MA: Beacon Press.Berry, M., Charlson, R., & Dawson, K. (2003). Promising practices in understanding and treating child neglect.Child & Family
Social Work, 8, 13–24.Bollen, K. A. (1989).Structural equations with latent variables. Indianapolis, IN: John Wiley & Sons.Brown, M. W., & Cudeck, R. (1993). Alternative ways of assessing model fit. In K. A. Bollen & J. S. Long (Eds.),Testing
structural equation models (pp. 132–162). Newbury, CA: Sage.Byrne, B. M. (1994).Structural equation modeling with EQS and EQS/Windows. Thousand Oaks, CA: Sage Publications.Cash, S. J., & Wilke, D. J. (2003). An ecological model of maternal substance abuse and child neglect: Issues, analyses, and
recommendations.American Journal of Orthopsychiatry, 73, 392–404.Child Welfare League of America. (2001). National fact sheet. Washington, DC: Child Welfare League of America.DiClemente, C. C. (1999). Motivation for change: Implications for substance abuse treatment.Psychological Science, 10(3),
209–213.DiClemente, C. C., Bellino, L. E., & Neavins, T. M. (1999). Motivation for change and alcoholism treatment.Alcohol Research
& Health, 23(2), 86–92.Dore, M. M., Doris, J. M., & Wright, P. (1995). Identifying substance abuse in maltreating families: A child welfare challenge.
Child Abuse & Neglect, 19, 531–543.Dunn, R. G., Tarter, R. E., Mezzich, A. C., Vanyukov, M., Kirisci, L., & Kirillova, G. (2002). Origins and consequences of child
neglect in substance abuse families.Clinical Psychology Review, 22, 1063–1090.Etheridge, R. M., Hubbard, R. L., Anderson, J., Craddock, S. G., & Flynn, P. M. (1997). Treatment structure and program
services in the Drug Abuse Treatment Outcome Study (DATOS).Psychology of Addictions, 11, 244–260.Flynn, P. M., Craddock, S. G., Hubbard, R. L., Anderson, J., & Etheridge, R. (1997). Methodological overview and research
design for the Drug Abuse Treatment Outcome Study (DATOS).Psychology of Addictive Behaviors, 11(4), 230–243.Hu, L., & Bentler, P. M. (1999). Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new
alternatives.Structural Equation Modeling, 6, 1–55.Kelley, S. J. (1992). Parenting stress and child maltreatment in drug-exposed children.Child Abuse & Neglect, 16, 317–328.Knight, K., Holcom, M., & Simpson, D. D. (1994).TCU psychosocial functioning and motivation scales: Manual on psychometric
properties. Fort Worth, TX: Texas Christian University, Institute of Behavioral Research.Menahem, S., & Halasz, G. (2000). Parental non-compliance-a pediatric dilemma: A medical and psychodynamic perspective.
Child: Care, Health and Development, 26, 61–72.Munkel, W. I. (1996). Neglect and abandonment. In J. A. Monteleone (Ed.),Recognition of child abuse for the mandated reporter
(pp. 39–54). St. Louis, MO: G.W. Medical Publishing, Inc.Murphy, M. J., Jellinek, M. S., Quinn, D., Smith, G., Poitrast, F. G., & Goshko, M. (1991). Substance abuse and serious child
mistreatment: Prevalence, risk, and outcome in a court sample.Child Abuse & Neglect, 15, 197–211.
D.J. Wilke et al. / Child Abuse & Neglect 29 (2005) 1313–1323 1323
Prochaska, J. O., DiClemente, C. C., & Norcross, J. C. (1992). In search of how people change: Applications to addictivebehaviors.American Psychologist, 47(9), 1102–1114.
Rosenberg, M. (1965).Society and the adolescent self-image. Princeton, NJ: Princeton University Press.Sedlack, A. J., & Broadhurst, D. D. (1996).The third national incidence study of child abuse and neglect (NIS-3). Washington,
DC: US Department of Health and Human Services.Simpson, D. D., & Joe, G. W. (1993). Motivation as a predictor of early dropout from drug abuse treatment.Psychotherapy, 30,
357–368.Strantz, I. H., & Welch, S. P. (1995). Postpartum women in outpatient drug abuse treatment: Correlates of retention/completion.
Journal of Psychoactive Drugs, 27(4), 357–373.Tracy, E. M. (1994). Maternal substance abuse: protecting the child, preserving the family.Social Work, 39, 534–540.US Department of Health & Human Services. (2004). Child maltreatment.http://www.acf.hhs.gov/programs/cb/
publications/cm02/index.htm. Retrieved 23 March 2005.US Department of Health & Human Services. (2001).Acts of omission: An overview of child neglect. Washington DC: Author.Wilke, D. (1994). Women and alcoholism: How a male-as-norm bias affects research, assessment, and treatment.Health &
Social Work, 19, 29–36.Wolock, I., & Magura, S. (1996). Parental substance abuse as a predictor of child maltreatment re-reports.Child Abuse & Neglect,
20, 1183–1193.Young, N. K., Gardner, S. L., & Dennis, K. (1998).Responding to alcohol and other drug problems in child welfare: Weaving
together practice and policy. Washington, DC: CWLA Press.
Resume
French-language abstract not available at time of publication.
Resumen
Spanish-language abstract not available at time of publication.




















