
Substance use in college students with ADHD
15
http://jad.sagepub.com/ Journal of Attention Disorders http://jad.sagepub.com/content/early/2011/01/19/1087054710392536 The online version of this article can be found at: DOI: 10.1177/1087054710392536 published online 2 February 2011 Journal of Attention Disorders Mary Rooney, Andrea Chronis-Tuscano and Yesel Yoon Substance Use in College Students With ADHD Published by: http://www.sagepublications.com can be found at: Journal of Attention Disorders Additional services and information for http://jad.sagepub.com/cgi/alerts Email Alerts: http://jad.sagepub.com/subscriptions Subscriptions: http://www.sagepub.com/journalsReprints.nav Reprints: http://www.sagepub.com/journalsPermissions.nav Permissions: at UCSF KALMANOVITZ LIB & CKM on February 14, 2011 jad.sagepub.com Downloaded from
Transcript of Substance use in college students with ADHD

http://jad.sagepub.com/Journal of Attention Disorders
http://jad.sagepub.com/content/early/2011/01/19/1087054710392536The online version of this article can be found at:
DOI: 10.1177/1087054710392536
published online 2 February 2011Journal of Attention DisordersMary Rooney, Andrea Chronis-Tuscano and Yesel YoonSubstance Use in College Students With ADHD
Published by:
http://www.sagepublications.com
can be found at:Journal of Attention DisordersAdditional services and information for
http://jad.sagepub.com/cgi/alertsEmail Alerts:
http://jad.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
at UCSF KALMANOVITZ LIB & CKM on February 14, 2011jad.sagepub.comDownloaded from

Journal of Attention DisordersXX(X) 1 –14© 2011 SAGE PublicationsReprints and permission:sagepub.com/journalsPermissions.navDOI: 10.1177/1087054710392536http://jad.sagepub.com
ADHD is characterized by developmentally inappropriate inattention and hyperactivity-impulsivity resulting in academic and social impairment (American Psychological Association [APA], 2000). Once conceptualized as a disorder specific to childhood, it is now estimated that ADHD persists into adult-hood in 58% to 70% of cases (Barkley, Fischer, Smallish, & Fletcher, 2002). Individuals with ADHD have been found to engage in higher rates of risky behavior across the life span (Barkley, Fischer, Smallish, & Fletcher, 2004; Flory, Molina, Pelham, Gnagy, & Smith, 2006; Lahey et al., 2004) and begin-ning in adolescence are at elevated risk for problematic sub-stance use (Barkley et al., 2004; Molina, Marshal, Pelham, & Wirth, 2005; Weiss & Hechtman, 1993; Wilens et al., 2008). The college years overlap with the peak developmental period for problematic substance use (Littlefield, Sher, & Wood, 2009) and may represent a time of unique vulnerability for students with ADHD (Brown et al., 2008).
Advances in the use and effectiveness of psychosocial and pharmacological interventions and increased legislative sup-port have made higher education more accessible to students with ADHD (Gallagher, Sysko, & Zhang, 2001). The actual proportion of college students meeting full diagnostic criteria for ADHD is currently unknown. Studies suggest, however, that 2% to 8% of college students self-report symptoms con-sistent with a diagnosis of ADHD (Weyandt & DuPaul, 2008), with the percentage varying as a functional postsecondary institution characteristics and study design. In addition, it is
estimated that individuals with ADHD represent 25% of col-lege students who self-refer to campus disability support ser-vices (DSS; Wolf, 2001). College students with ADHD likely represent a unique subgroup of individuals with the disorder who have thus far achieved a relatively high level of academic functioning. Nonetheless, challenges such as moving away from home, making autonomous decisions, establishing a new peer group, and managing unstructured social and aca-demic environments may be particularly difficult for these students (DuPaul et al., 2001; Weyandt & DuPaul, 2008).
Despite the fact that students with ADHD appear to repre-sent a significant population on college campuses, little is known about how this group adapts to developmental chal-lenges unique to the college experience. Recent theories have attributed the core symptoms of ADHD to deficits in execu-tive functioning (e.g., difficulties with impulse control, plan-ning, goal persistence, inhibition of prepotent responses, and working memory; Barkley, 1997; Nigg, 2001). When consid-ering problematic substance use in this population, it is nota-ble that there is significant overlap between executive functioning deficits independently associated with ADHD
392536 JADXXX10.1177/1087054710392536Rooney et al.Journal of Attention Disorders© 2011 SAGE Publications
Reprints and permission:sagepub.com/journalsPermissions.nav
1University of Maryland, College Park
Corresponding Author:Mary Rooney, Clinical Psychology, University of Maryland, College Park, MD 20742, United States Email: [email protected]
Substance Use in College Students With ADHD
Mary Rooney1, Andrea Chronis-Tuscano1, and Yesel Yoon1
AbstractObjective: The college years represent a developmental transition during which the initiation and escalation of heavy drinking set the stage for lifelong difficulties with alcohol and other drugs. Evidence from studies of adolescents and young adults with ADHD suggests that college students with the disorder may be uniquely vulnerable to alcohol- and drug-related problems. However, no studies have examined substance use in college students with ADHD. Method: Tobacco, alcohol, illicit drug use, and associated impairment were examined in 91 college students with (n = 53) and without (n = 38) ADHD. Results: ADHD was associated with increased frequency of tobacco use, higher rates of dangerous or hazardous patterns of alcohol use, and higher levels of impairment related to marijuana and nonmarijuana illicit drug use, independent of conduct disorder history. Conclusion: These findings suggest that college students with ADHD may be at elevated risk for problematic patterns of substance use.
KeywordsADHD, CD, substance use, alcohol, college students, risky behavior
at UCSF KALMANOVITZ LIB & CKM on February 14, 2011jad.sagepub.comDownloaded from

2 Journal of Attention Disorders XX(X)
(Barkley, 1997) and substance use disorder (Giancola & Tarter, 1999; Grant, Contoreggi, & London, 2000). Impairments that emerge when ADHD persists into adoles-cence (e.g., difficulty adapting to increasing academic demands, interpersonal problems, and higher rates of crimi-nal offending; Smith, Waschbusch, Willoghby, & Evans, 2000) are additional risk factors for problematic substance use. In addition, the decrease in external structure and adult supervision that occurs during adolescence may be particu-larly problematic for individuals with ADHD given their reli-ance on external sources for structure and regulation (Pelham & Fabiano, 2008). The presence or history of comorbid con-duct disorder (CD), found in 7% to 50% of children and ado-lescents with ADHD (Barkley, 1998; Ford, Goodman, & Meltzer, 2003; Lahey, McBurnett, & Loeber, 2000), confers an additional risk for substance-related problems. Adolescents and young adults with ADHD and comorbid CD typically evidence the riskiest patterns of substance use (Barkley et al., 2004; Molina & Pelham, 2003; Molina, Smith, & Pelham, 1999; Wilens et al., 2008). To the best of our knowledge, however, no studies have examined how these risk factors may operate in the context of the college environment.
In contrast to the absence of studies examining substance use in college students with ADHD, numerous studies have identified risky patterns of substance use among adoles-cents and young adults with confirmed ADHD diagnoses. Across studies, adolescents and young adults with ADHD have been found to use tobacco at higher rates and begin using at an earlier age relative to their nondisordered peers (Milberger, Biederman, Faraone, Chen, & Jones, 1997; Molina & Pelham, 2003; Wilens et al., 2008). Although rates of cigarette smoking are consistently highest among adolescents with co-occurring ADHD and CD (hereafter referred to as ADHD + CD), ADHD alone does appear to confer a unique risk (Molina et al., 2005).
Findings from studies of alcohol and illicit drug use in this population are less consistent than those related to tobacco. In earlier research, substance use behavior in adolescents with ADHD was examined as a secondary outcome in sev-eral large-scale longitudinal studies (Barkley, Fischer, Edelbrock, & Smallish, 1990; Biederman et al., 1997; Gittelman, Mannuzza, Shenker, & Bonagura, 1985; Hartsough & Lambert, 1987; Mannuzza & Klein, 1999). Many of these early studies failed to include questions about behaviors prognostic of later use (e.g., age of first use and a history of having used multiple illicit drugs), included only male participants, and rarely considered the role of comorbid CD. When using developmentally sensitive indicators and examining the role of comorbid CD, Molina and Pelham (2003) found higher rates and earlier initiation of both alco-hol and nonmarijuana drug use and substance use disorder among adolescents with ADHD compared with those with-out ADHD. The highest rates were found among those with ADHD + CD. Given that substance use during adolescence
predicts continued substance use during young adulthood (Johnston, O’Malley, Bachman, & Schulenberg, 2009) and that individuals with ADHD begin using alcohol and illicit drugs at an earlier age and with greater frequency than their peers, higher rates of substance use and substance use disor-der (SUD) can be expected among young adults with ADHD.
Longitudinal studies have identified important differ-ences in the alcohol use patterns of young adults with and without ADHD (Weiss & Hechtman, 1993; Wilens, Biederman, & Mick, 1998; Wilens, Biederman, & Spencer, 2002). Although young adults with ADHD do not appear to use alcohol at higher rates than their peers without the dis-order, they are significantly more likely to abuse alcohol or have alcohol use disorder (Smith, Molina, & Pelham, 2002; Weiss & Hechtman, 1993). The absence of a between-group difference in rates of use may be explained by the fact that increased alcohol use is normative during young adulthood (Johnston et al., 2009). In contrast, behavior patterns that constitute alcohol abuse or dependence are outside the norm. Although illicit drug use has been studied to a lesser extent than alcohol use in this population, findings indicate significantly higher levels of illicit drug use among young adults with ADHD compared with those without ADHD (Biederman et al., 2006; Hechtman, 1984; Lambert & Hartsough, 1998; Mannuzza & Klein, 2000; Milberger, Biederman, Faraone, Wilens, & Chu, 1997; Weiss, 1979). In the only study that considered comorbid CD, Barkley et al. (2004) found that young adults with ADHD alone had a significantly higher rate of illicit drug use relative to con-trols. Those with ADHD + CD, however, had the highest rate of use among all groups. Additional studies are needed to further examine the associations between substance use, ADHD, and CD in young adults.
The college years overlap with the peak developmental period for problematic substance use (Littlefield et al., 2009). For college students with ADHD, environmental influences specific to the traditional college experience may uniquely influence patterns of alcohol and illicit drug use (Brown et al., 2008). However, up to this point, substance use in college students with ADHD has largely gone unstud-ied. In contrast, substance use behaviors in the general col-lege student population have been studied extensively. Three large-scale projects—the Monitoring the Future Study (Johnston et al., 2009), the College Alcohol Survey (Wechsler, Lee, Kuo, & Lee, 2000), and the Core Alcohol and Drug Survey (CORE; Core Institute, 2005; Presley, 1994)—found that patterns of alcohol and substance use among college students differ from those of the general young adult population. For example, findings consistently show that college students engage in riskier alcohol con-sumption behaviors than their peers who are not attending college and that those who are members of fraternities or sororities engage in the riskiest patterns of use (Johnston et al., 2009). Results from the Monitoring the Future Study
at UCSF KALMANOVITZ LIB & CKM on February 14, 2011jad.sagepub.comDownloaded from

Rooney et al. 3
show that illicit drug use is also a significant concern on college campuses. One third of all college students report past-year marijuana use and one fifth report past-year non-marijuana illicit drug use. As with alcohol use, patterns of illicit drug use in college students differ from those of young adults not attending college. Although marijuana use is similar between these two groups, current daily mari-juana use is significantly lower among college students. When considering all illicit drugs other than marijuana, col-lege students report significantly lower rates of use in the past year than their noncollege peers. As these studies dem-onstrate, patterns of substance use differ between college students and their same-age, noncollege peers. Findings derived from studies of noncollege young adults may not apply to the college student population.
In summary, a robust literature demonstrates that adoles-cents and young adults with ADHD engage in riskier pat-terns of substance use than their non-ADHD peers. Unique vulnerabilities associated with ADHD may intensify the challenges associated with the transition from adolescence to young adulthood that occurs within the context of the college environment. These vulnerabilities may place col-lege students with ADHD at elevated risk for engagement in risky substance use behaviors. For the reasons described earlier, findings from studies of adolescents and young adults with ADHD may not generalize to college students with ADHD. The absence of studies examining these issues in college students with ADHD therefore represents a sig-nificant gap in the literature.
The current study aimed to evaluate associations between ADHD diagnosis and patterns of substance use in a college student sample. We addressed limitations in the existing lit-erature in three important ways: (a) by utilizing a sample of college students with retrospectively confirmed childhood ADHD diagnoses, (b) by examining the role of CD when studying associations between ADHD and substance use, and (c) by including a large proportion of female partici-pants. On the basis of the existing literature of adolescents and young adults with ADHD, we hypothesized that in our college student sample the presence of Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV; APA, 2000) ADHD would be associated with higher rates of current tobacco, alcohol, and illicit drug use; earlier age of first use across substances; patterns of harm-ful or hazardous use across substances; and greater sub-stance-related impairment.
MethodParticipants
Participants included 91 full-time undergraduate students enrolled in a large, public, Mid-Atlantic university: 53 with ADHD and 38 without ADHD. Participants were recruited
through flyers advertising a study of substance use in stu-dents with and without ADHD and through electronic post-ings for extra credit opportunities available to students in introductory psychology courses. Following a brief tele-phone screen, respondents were invited for a onetime appointment at our ADHD Program within the university’s Department of Psychology. All participants in the ADHD group met DSM-IV criteria for current ADHD, based on guidelines outlined in the seminal article by McGough and Barkley (2004). Within the fields of psychology and psy-chiatry, there is an ongoing debate about how to best apply the DSM-IV ADHD criteria in adults given that the DSM-IV diagnostic criteria were based on field trials conducted with elementary school-age boys (Lahey, Applegate, McBurnett, & Biederman, 1994). As a result, several of the DSM-IV symptoms are reflective of ADHD in children and less rel-evant to adults (e.g., running or climbing on things exces-sively, difficulty playing quietly, etc.). For this reason, McGough and Barkley, in their seminal paper, recommend that a diagnosis be made during adulthood (a) only when there exists clear evidence of childhood DSM-IV ADHD symptoms and impairment based on retrospective report and (b) when participants meet reduced current DSM-IV symptom criteria (i.e., a minimum of four or five current DSM-IV symptoms of inattention or four or five current DSM-IV symptoms of hyperactivity-impulsivity) and present clear evidence of functional impairment.
For inclusion in the present study, participants with ADHD were required to (a) retrospectively meet full DSM-IV diagnostic criteria for ADHD during childhood (i.e., a minimum of six DSM-IV symptoms of inattention or six symptoms of hyperactivity-impulsivity), according to self- or parent-report; (b) have a minimum of four current DSM-IV symptoms of inattention or four current DSM-IV symptoms of hyperactivity-impulsivity according to self- or parent-report and clear evidence of current functional impairment; and (c) have a Conners Adult ADHD Rating Scale (CAARS) ADHD Index T-score above 60 (i.e., one standard deviation above the mean). Although a prior diag-nosis of ADHD was not required for participation in the ADHD group, it should be noted that 66% (n = 35) of par-ticipants in the ADHD group reported that they had received a prior ADHD diagnosis. As noted previously, all partici-pants in the ADHD group were required to retrospectively meet full DSM-IV symptom and impairment criteria for ADHD during childhood based on self- or parent-report.
Participants in the non-ADHD comparison group were required to have the following: (a) no history of an ADHD diagnosis or prescription of ADHD medication according to self-report, (b) fewer than three DSM-IV symptoms of inat-tention and fewer than three DSM-IV symptoms of hyperac-tivity-impulsivity, (c) fewer than three DSM-IV symptoms of CD with no history of the disorder according to self-report, and (4) a CAARS ADHD Index T-score below 40 (i.e., one
at UCSF KALMANOVITZ LIB & CKM on February 14, 2011jad.sagepub.comDownloaded from

4 Journal of Attention Disorders XX(X)
standard deviation below the mean). To enhance generaliz-ability, participants in either group were not excluded on the basis of having a self-reported learning disability (LD) diag-nosis or other psychiatric disorder. In addition, all partici-pants were required to be enrolled as full-time undergraduate students and to be living away from their parents during the academic year. The residency criteria ensured that partici-pants were college students who were no longer living at home and relying on their parents as a principle source of external structure.
Participant demographic and diagnostic characteristics are presented in Table 1.
ProcedureADHD group classification was determined through (a) the administration of a semistructured interview assessing DSM-IV ADHD symptoms during childhood and young adulthood, (b) parent responses to questionnaires about the presence of past and current ADHD symptoms in their child (when available), and (c) responses on the CAARS self-report questionnaire. In accordance with procedures previ-ously used in our research laboratory (Chronis-Tuscano, Raggi, et al., 2008; Chronis-Tuscano et al., 2010; Chronis-Tuscano, Seymour, et al., 2008) and by others (Biederman & Spencer, 2002; Faraone, Biederman, & Milberger, 1995;
Faraone, Biederman, & Monuteaux, 2002), investigators administered the ADHD and CD modules of the Kiddie-Schedule for Affective Disorders and Schizophrenia for School-Age Children (K-SADS; Ambrosini, 2000) to the participants with modifications appropriate for retrospec-tive and current self-report by adults. A clinical psychology doctoral student administered a majority of the diagnostic interviews (n = 80) under the close supervision of a licensed clinical psychologist who directs the Department of Psychology’s ADHD Program. A senior undergraduate research assistant administered 11 interviews under the close supervision of the advanced doctoral student and faculty supervisor. Supervision included having the clinical psy-chology doctoral student present in the interview room with the research assistant to aid with interview administration when necessary. All interviews were audio recorded for supervision purposes and a second interviewer coded 20% of the interviews. Interrater reliability analyses using the kappa statistic were performed to determine consistency among raters for ADHD diagnosis and CD diagnosis. Kappa values were 1.0 for ADHD and 1.0 for CD.
Informant ratings of participant ADHD symptoms are frequently used in ADHD diagnosis (for a review, see Katz, Petscher, & Wells, 2009). Studies have shown that adults with ADHD may report fewer ADHD symptoms and impairment than collateral informants (Mannuzza, Klein,
Table 1. Demographic and Diagnostic Characteristics
Non-ADHD (n = 38) ADHD (n = 53)
Characteristic n (%) n (%)
Age (M, SD) 19.6 0.67 20.13 1.50a
Year in school (M, SD) 14.63 0.67 14.56 0.97Fraternity or sorority member 9 (23.7) 19 (35.8)Sex Male 19 (50.0) 36 (67.9) Female 19 (50.0) 17 (32.1)Race/ethnicity Non-Hispanic White 27 (71.1) 42 (79.2) African American 4 (10.5) 0 (0.0)a
Latino or Hispanic 2 (5.3) 4 (7.5) Asian 5 (3.2) 2 (3.8) Biracial 0 (0.0) 4 (7.5)a
DSM-IV diagnoses ADHD Predominately inattentive 0 (0.0) 16 30.2 Hyperactive-impulsive 0 (0.0) 6 11.3 Combined 0 (0.0) 31 58.5 CD: Childhood onset 0 (0.0) 0 0.0 CD: Adolescent-onset 0 (0.0) 9 17.0 Learning disability 4 (10.5) 9 17.0a
ADHD medication—Current 0 (0.0) 30 56.6
Note: DSM-IV = Diagnostic and Statistical Manual of Mental Disorders (4th edition); CD = conduct disorder.aDifferences between groups at p < .05.
at UCSF KALMANOVITZ LIB & CKM on February 14, 2011jad.sagepub.comDownloaded from

Rooney et al. 5
Klein, Bessler, & Shrout, 2002; Murphy & Schachar, 2000). Therefore, informant reports of childhood and current symptoms were obtained whenever possible from a parent who had frequent contact with the participant both at the time of the interview and during childhood (Belendiuk, Clarke, Chronis, & Raggi, 2006; McGough & Barkley, 2004; Murphy & Schachar, 2000).
Participants were asked to provide consent for the researcher to contact a parent for the purpose of obtaining informant ratings of ADHD symptoms but were explicitly told that they would not be excluded from the study if they did not allow parental contact. Including only the partici-pants who consented to parental contact would have pro-duced a biased sample and may have limited the degree to which participants felt comfortable responding candidly to questions about substance use. A total of 88% of ADHD participants (n = 47) and 56% of non-ADHD participants (n = 22) provided consent for parent participation. Informant report forms, an informant consent form, and a stamped self-addressed return envelope were mailed to the parents of students who provided consent for parental participation. A single reminder call was placed to parents who did not return forms within 3 weeks. Parents were not compensated for completing forms. Informant ratings were received for 73% of ADHD participants (n = 38) and 29% of non-ADHD participants (n = 11). The large discrepancy between groups in the percentage of informant reports received was driven largely by a group difference participant willingness to pro-vide consent for parental contact. Possible reasons for this difference include (a) students with ADHD may be more likely to have a history of parental involvement in mental health treatment or educational intervention, (b) partici-pants in the ADHD group felt more invested in the study because they are directly affected by the diagnosis under examination, or (c) participants in the ADHD group may have been less likely to consider consequences associated with the researcher contacting their parents.
Guidelines for the use of informant ratings in diagnosing ADHD have not yet been established (Katz et al., 2009). Piacentini, Cohen, and Cohen (1992) have recommended combining self- and informant-reports such that any symp-tom endorsed by either source was counted toward the symptom total (i.e., the “or rule”). As with prior studies conducted in our laboratory (Chronis-Tuscano, Raggi, et al., 2008; Chronis-Tuscano et al., 2010; Chronis-Tuscano, Seymour, et al., 2008), we followed Piacentini’s recommen-dation and combined self- and informant-reports using the “or” rule. As informant ratings were not available for all participants, it is possible that differences in symptom count emerged between those whose parents participated and those whose parents did not participate. In a post hoc review of the data, all participants in the ADHD group with infor-mant reports were found to meet symptom criteria for an ADHD diagnosis based on self-report alone. When
informant reports were integrated using the “or rule,” the number of symptoms per participant increased, and for 4 participants, subtype classification changed from inatten-tive type to combined type. ADHD group classification (i.e., ADHD vs. non-ADHD group), however, did not change for any participants.
CD diagnosis was based solely on participant responses to questions from the CD module of the K-SADS (Ambrosini, 2000). This module inquires about CD symp-toms present during childhood and adolescence (i.e., before age 18). Notably, all participants with a history of CD met criteria for the adolescent-onset subtype and primarily endorsed symptoms and impairment related to truancy, breaking curfew, lying, and shoplifting.
The study protocol was approved by the university’s Institutional Review Board. Participants provided written informed consent after procedures were described in detail. Compensation for participation was provided in the form of extra-credit points for introductory psychology classes or a US$12 cash payment.
MeasuresAssessment of ADHD and CD. The CAARS (Conners
et al., 1999) provided a dimensional measurement of par-ticipants’ current ADHD symptoms. The CAARS ADHD Index score was one indicator used to determine placement in the ADHD or comparison group. The CAARS is a reli-able and valid measure that assesses the core features of ADHD as seen in children and adolescents, while adding content unique to adult expression of ADHD (Erhardt, Epstein, Conners, Parker, & Sitarenios, 1999). This mea-sure has excellent psychometric properties and provides essential age- and gender-based normative data to supple-ment the adult ADHD diagnosis based on diagnostic interview.
The ADHD and CD modules of the K-SADS (Ambrosini, 2000; Biederman & Montreaux, 2002), modified for past and current self-report by adults (Biederman & Spencer, 2002; Faraone et al., 1995; Faraone et al., 2002), were administered to participants. The K-SADS has well-established reliability for the diagnosis of ADHD and CD in children (Ambrosini, 2000) and has been used by our labo-ratory and others in studies of adult ADHD (Biederman & Spencer, 2002; Chronis-Tuscano, Raggi, et al., 2008; Chronis-Tuscano et al., 2010; Chronis-Tuscano, Seymour, et al., 2008). To facilitate retrospective recall of symptoms, interviewers asked participants whether symptoms were present during “early elementary school” that was then defined as third grade or earlier. At times, participants pro-vided examples of childhood symptoms and impairment that were present around the age of 9 or 10 because they were unable to recall specific examples from kindergarten through second grade. In so far as we required that all
at UCSF KALMANOVITZ LIB & CKM on February 14, 2011jad.sagepub.comDownloaded from

6 Journal of Attention Disorders XX(X)
participants in the ADHD group endorsed symptoms and impairment present during “early elementary school,” we did not adhere to the DSM-IV age of onset criteria with the strin-gency found in studies of children with ADHD. McGough and Barkley (2004) and others (Faraone et al., 2006) recom-mend an age of symptom onset before the age of 12, and our procedures were consistent with these guidelines.
The Childhood Symptom Scale—Other Report Form and Current Symptoms Scale—(Barkley & Murphy, 2006) were mailed to parents to obtain informant ratings of the participants’ past and current ADHD symptoms. These measures each contain 18 items that map directly onto DSM-IV symptoms of ADHD. Responses range from rarely or never to very often, with the two highest responses (often and very often) considered clinically significant. The mea-sures also inquire about age of symptom onset and related impairment. Internal consistency coefficients were calcu-lated for the Childhood and Current Symptom Scales using data from the current study. Cronbach’s alphas were .76 for the Childhood Symptom Scale and .68 for the Current Symptom Scale.
Substance UseThe alcohol use disorders identification test (AUDIT; Saunders, Aasland, Babor, De La Fuenta, & Grant, 1993) was developed by the World Health Organization as a simple, brief method of screening for excessive drinking and related impairment (Babor, Higgins-Biddle, Saunders, & Monteiro, 2001). This self-report questionnaire provides a continuous score comprising 10 items on three factors: (a) consumption: 3 items assessing quantity and frequency of alcohol consumption, (b) dependence: 3 items assessing alcohol dependence, and (c) hazardous use: 4 items assess-ing problems caused by drinking (Rist, Glockner-Rist, & Demmel, 2009; Saunders et al., 1993). Each question is scored according to a 5-point scale (0-4). Higher total scores on the AUDIT indicate higher levels of risky alcohol use (Babor et al., 2001). Internal consistency for the AUDIT has been shown to be strong. Analyses of the con-sumption factor (Shields, Guttmannova, & Caruso, 2004) and the total score (Kokotailo et al., 2004) have produced Cronbach’s alphas of .81 and .80, respectively, in college samples. Test–retest reliability has been shown to be satis-factory in a general population sample with an intraclass correlation coefficient of .84 (Selin, 2003).
The drug use disorders identification test (DUDIT; Berman, Bergman, Palmstierna, & Schlyter, 2005) is an 11-item self-report instrument intended for use with the AUDIT. Like the AUDIT, each question is scored accord-ing to a 5-point scale (0-4) and provides a continuous score of drug use and related impairment. Studies of young adults have yielded different findings when marijuana use was considered independently of other illicit drug use. Therefore, the DUDIT was modified to obtain separate
scores for marijuana and nonmarijuana illicit drug use. Psychometric properties for this scale are not available in the existing literature. In the current sample, internal consistency coefficients were calculated separately for the DUDIT–marijuana and DUDIT–nonmarijuana measures. Calculations included all items in each measure. Cronbach’s alphas were .77 for the DUDIT–marijuana and .68 for the DUDIT–nonmarijuana.
The CORE (Core Institute, 2005) is a 198-item rating scale with a number of subscales designed to assesses quan-tity and frequency of alcohol and illicit substance use, con-sequences associated with substance use (e.g., “How often have you gotten into an argument or fight due to your drink-ing or drug use?”), and reasons for use of alcohol or drugs (e.g., “Do you believe alcohol facilitates a connection with peers?”) in a college student population. It was selected for its strong psychometric properties (Core Institute, 2005) and its relevance to the study’s research questions. In the current study, we used subscales related to the quantity and frequency of drug use and negative consequences of alco-hol use (Johnston et al., 2009).
ResultsAnalytic Approach
Regression analyses were used to examine the association between ADHD diagnosis and several indices of substance use outcomes, while also examining associations with CD. Preliminary analyses were first conducted to examine the extent to which the demographic variables of age, race/ ethnicity, gender, fraternity/sorority membership, current ADHD medication status, and LD diagnosis were associated with the outcome variables. These control variables were selected on the basis of prior literature, suggesting a rela-tionship, positive or negative, to substance use behaviors in college students and/or young adults (Douglas et al., 1997; Kollins, 2008; Mannuzza et al., 2008; Volkow & Swanson, 2008; Wechsler, Dowdall, Davenport, & Castillo, 1995), or because the difference between ADHD and non-ADHD groups was statistically significant in the current sample. Demographic variables significantly associated with each outcome variable were included on the first step of the regression equation. ADHD and CD diagnoses (dummy coded) were entered on the next step. Finally, although our sample size did not allow for sufficiently powered analyses, exploratory analyses were then conducted to examine the association between the interaction of ADHD and CD (ADHD + CD comorbidity) and the outcome variables.
Preliminary AnalysesAge was frequently associated with the variables of interest, and these associations were always in a positive direction, suggesting greater use with increasing age (see Tables 2-4).
at UCSF KALMANOVITZ LIB & CKM on February 14, 2011jad.sagepub.comDownloaded from

Rooney et al. 7
In addition, fraternity/sorority membership was positively associated with all alcohol-related variables with the exception of age of first use (see Table 3) and with frequency of current nonmarijuana illicit drug use (see Table 4). African American race/ethnicity status was posi-tively associated with having ever used marijuana (see Table 4), and Asian race/ethnicity status was positively associated with frequency of arguments or fights resulting from alcohol use (see Table 3). Finally, male gender was positively associated with the DUDIT–marijuana total score (see Table 4). Surprisingly, neither current ADHD medication use nor self-reported LD was significantly asso-ciated with any of the outcome variables.
TobaccoThe presence of ADHD was uniquely associated (i.e., inde-pendent of CD history) with having first used tobacco at an earlier age. In addition, when compared to their peers with-out ADHD, those with ADHD were 3.6 times more likely to have ever used tobacco (95% CI [1.424, 9.431]). ADHD was also independently associated with a greater frequency of tobacco use during the past 30 days. Associations between ADHD + CD and tobacco use were not significant (see Table 2).
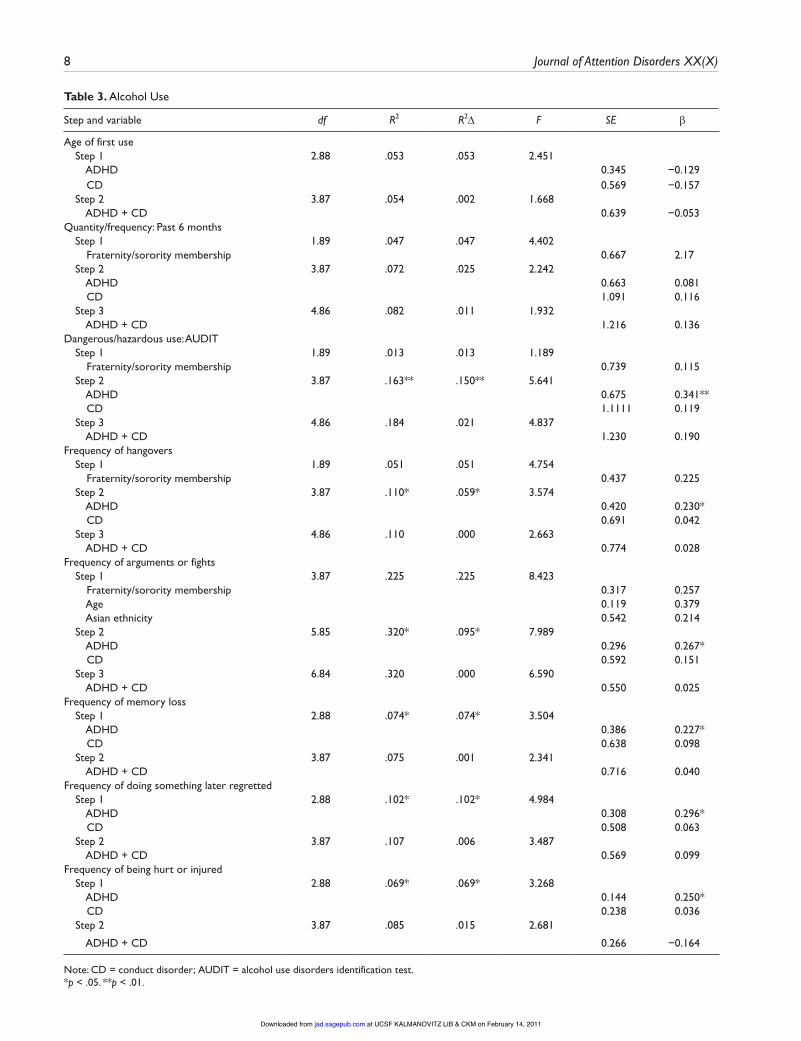
AlcoholADHD, independent of CD, was not associated with an earlier age of alcohol use initiation, with the likelihood of having ever used alcohol, or with the quantity or frequency of alcohol use during the past 6 months. However, ADHD was independently associated with higher total scores on the AUDIT, higher scores on the dangerous or hazardous
use subscale of the AUDIT, and with a greater likelihood of having endorsed an item indicative of dependence or emerging dependence on the AUDIT (odds ratio = 3.70, CI [1.397, 9.821]). Findings are displayed in Table 3.
Among those who had used alcohol in the past year (n = 87), ADHD was associated with a greater frequency of the following consequences of use: having a hangover, getting into an argument or fight, getting nauseated or having vom-ited, experiencing memory loss, doing something he or she later regretted, and being hurt or injured. Associations between ADHD + CD and each measure of alcohol use or consequences of use were not significant (Table 3).
Drug UseWhen compared to their peers without ADHD, those with ADHD were 3.3 times more likely to have ever used mari-juana (95% CI [1.208, 8.553]) and 4.5 times more likely to have ever used nonmarijuana illicit drugs (95% CI [1.353, 15.282]). ADHD was also independently associated with having first used marijuana and nonmarijuana drugs at an earlier age and with higher levels of current substance-related impairment on measures of both marijuana and non-marijuana illicit drug use (Table 4). ADHD was not, however, independently associated with a greater frequency of mari-juana or nonmarijuana illicit drug use during the past 30 days (Table 4).
Results of exploratory analyses showed that ADHD + CD were significantly associated with higher scores on the global measure of impairment related to marijuana use (DUDIT–marijuana). However, no significant associations between ADHD + CD and nonmarijuana illicit drug use (DUDIT–nonmarijuana) were identified. Results are pre-sented in Table 4.
Table 2. Tobacco Use
Step and variable df R2 R2 F SE
Age of first use Step 1 2.88 .077* .77* 3.676 ADHD 0.546 0.273* CD 0.902 0.015 Step 2 3.87 .082 .005 2.605 ADHD + CD 1.010 0.096Frequency of use: Past 30 days Step 1 1.89 .054 .054 5.036 Age 0.163 0.231 Step 2 3.87 .140* .086* 4.731 ADHD 0.409 0.284* CD 0.738 !1.94 Step 3 4.86 .150 .0101 3.801 ADHD + CD 0.767 0.137
Note: CD = conduct disorder.*p < .05.
at UCSF KALMANOVITZ LIB & CKM on February 14, 2011jad.sagepub.comDownloaded from
8 Journal of Attention Disorders XX(X)
Table 3. Alcohol Use
Step and variable df R2 R2 F SE
Age of first use Step 1 2.88 .053 .053 2.451 ADHD 0.345 !0.129 CD 0.569 !0.157 Step 2 3.87 .054 .002 1.668 ADHD + CD 0.639 !0.053Quantity/frequency: Past 6 months Step 1 1.89 .047 .047 4.402 Fraternity/sorority membership 0.667 2.17 Step 2 3.87 .072 .025 2.242 ADHD 0.663 0.081 CD 1.091 0.116 Step 3 4.86 .082 .011 1.932 ADHD + CD 1.216 0.136Dangerous/hazardous use: AUDIT Step 1 1.89 .013 .013 1.189 Fraternity/sorority membership 0.739 0.115 Step 2 3.87 .163** .150** 5.641 ADHD 0.675 0.341** CD 1.1111 0.119 Step 3 4.86 .184 .021 4.837 ADHD + CD 1.230 0.190Frequency of hangovers Step 1 1.89 .051 .051 4.754 Fraternity/sorority membership 0.437 0.225 Step 2 3.87 .110* .059* 3.574 ADHD 0.420 0.230* CD 0.691 0.042 Step 3 4.86 .110 .000 2.663 ADHD + CD 0.774 0.028Frequency of arguments or fights Step 1 3.87 .225 .225 8.423 Fraternity/sorority membership 0.317 0.257 Age 0.119 0.379 Asian ethnicity 0.542 0.214 Step 2 5.85 .320* .095* 7.989 ADHD 0.296 0.267* CD 0.592 0.151 Step 3 6.84 .320 .000 6.590 ADHD + CD 0.550 0.025Frequency of memory loss Step 1 2.88 .074* .074* 3.504 ADHD 0.386 0.227* CD 0.638 0.098 Step 2 3.87 .075 .001 2.341 ADHD + CD 0.716 0.040Frequency of doing something later regretted Step 1 2.88 .102* .102* 4.984 ADHD 0.308 0.296* CD 0.508 0.063 Step 2 3.87 .107 .006 3.487 ADHD + CD 0.569 0.099Frequency of being hurt or injured Step 1 2.88 .069* .069* 3.268 ADHD 0.144 0.250* CD 0.238 0.036 Step 2 3.87 .085 .015 2.681
ADHD + CD 0.266 !0.164
Note: CD = conduct disorder; AUDIT = alcohol use disorders identification test.*p < .05. **p < .01.
at UCSF KALMANOVITZ LIB & CKM on February 14, 2011jad.sagepub.comDownloaded from

Rooney et al. 9
Discussion
The present study is the very first to examine associations between DSM-IV ADHD and substance use in college
students. Although the existing adolescent and young adult ADHD literature provides a useful foundation, findings from these studies may not generalize to the college student popu-lation. Three categories of substances were examined in the
Table 4. Illicit Drug Use
Step and variable df R2 R2 F SE
Age of first use: Marijuana Step 1 1.89 .090 .090 8.805 Age 0.209 .300 Step 2 3.87 .153* .063* 5.255 ADHD 0.531 .226* CD 0.958 .088 Step 3 4.86 .156 .117 3.979 ADHD + CD 1.000 .070Age of first use: Nonmarijuana illicit drugs Step 1 1.88 .073 .073 6.921 Age 0.091 .270 Step 2 3.86 .163* .090* 5.569 ADHD 0.230 .273* CD 0.412 .097 Step 3 4.85 .186 .023 4.857 ADHD + CD 3.819 .205Frequency past 30 days: Marijuana Step 1 2.88 .024 .024 1.077 ADHD 0.344 .111 CD 0.576 .081 Step 2 3.86 .039 .015 1.177 ADHD + CD 0.633 .162Frequency past 30 days: Non-marijuana illicit drugs Step 1 1.89 .014 .014 1.255 Fraternity/
sorority membership
0.337 .118
Step 2 3.87 .048 .034 1.466 ADHD 0.328 .121 CD 0.540 .113 Step 3 4.86 .048 .000 ADHD + CD 1.093 0.605 .021DUDIT-marijuana total score Step 1 1.89 .036 .36 3.355 Male 1.127 .191 Step 2 ADHD 3.89 .124* .088* 4.117 1.145 .250* CD 1.861 .110 Step 3 4.86 .207** .083** 5.628 ADHD + CD 2.002 .384**DUDIT-nonmarijuana total score Step 1 2.88 .075* .075* 3.577 ADHD 0.727 .279* CD 1.201 !.18 Step 2 3.87 .110 .035 3.587 ADHD + CD 1.323 .246
Note: CD = conduct disorder; DUDIT = drug use disorders identification test.*p < .05. **p < .01.
at UCSF KALMANOVITZ LIB & CKM on February 14, 2011jad.sagepub.comDownloaded from

10 Journal of Attention Disorders XX(X)
current study: (a) tobacco, (b) alcohol, and (c) illicit drugs. Consistent with our predictions and with the existing ADHD literature, ADHD was independently associated with a greater likelihood of having ever used tobacco, using tobacco at an earlier age, and higher rates of current tobacco use. It has been hypothesized that individuals with ADHD may be self-medicating with nicotine, a stimulant found to improve mood and performance on tests of attention and processing speed in individuals with and without ADHD (Levin, Conners, Silva, Canu, & March, 2001; Poltavski & Petros, 2006; Rezani, 2001; Trimmel & Wittberger, 2004). Recent studies have tested alternative hypothesis to explain the high rates of tobacco use among this population. Specifically, researchers have found that adult smokers with ADHD expe-rience a greater disruption in cognitive processes when they abstain from smoking relative to smokers without ADHD (Kollins, McClernon, & Epstein, 2009). This same group also found that cognitive functioning may be differentially affected in smokers with ADHD because of an overlap in the neural circuitry implicated in nicotine addiction and ADHD (McClernon et al., 2008).
Consistent with studies of adolescents with ADHD, col-lege students with ADHD did not report consuming alcohol in greater quantities or with greater frequency than their non-ADHD peers (Weiss & Hechtman, 1993; Wilens et al., 1998, 2002). As noted by Smith, Molina, and Pelham (2002), however, this should not be interpreted as evidence that young adults with ADHD are not consuming alcohol at high rates. Rather, high rates of alcohol consumption are normative at this developmental stage, and young adults with ADHD appear to be “keeping up” with their non-ADHD peers. Given this finding, it does not appear to be the amount of alcohol consumed by college students with ADHD that puts them at risk for alcohol-related problems. Rather, this population appears to be more vulnerable in developing alcohol dependence or experiencing other nega-tive consequences (e.g., doing something he or she later regretted, being hurt or injured, and having a hangover) as a result of their alcohol use.
In contrast to previous studies, linking CD to increased rates of alcohol dependence in young adults with ADHD (Barkley et al., 1990; Gittelman et al., 1985), the present study identified an increased risk for alcohol dependence or emerging dependence specific to ADHD, independent of CD history. Differences in alcohol use assessment methods and sample composition may partially explain these inconsisten-cies. In addition, differences in CD subtype (childhood- vs. adolescent-onset) may have influenced these findings. Specifically, individuals with adolescent onset, the subtype endorsed by all participants with CD in the present study, have largely been found to demonstrate less severe dysfunc-tion (see Moffitt, 2003, for a review). However, additional studies are needed to conclusively determine the factors that may contribute to the discrepant CD-related findings.
Consistent with our predictions of marijuana and non-marijuana illicit drug use, ADHD, independent of CD his-tory, was associated with the following: (a) an increased likelihood of having ever used marijuana or nonmarijuana illicit drugs, (b) an earlier age of first use for both illicit drug categories, and (c) higher levels of impairment related to illicit drug use. Despite higher impairment ratings, cur-rent frequency of marijuana and nonmarijuana illicit drug use was not predicted by ADHD alone or by ADHD with a history of CD. Consistent with the existing literature (Barkley et al. 2004) in exploratory analyses, the highest level of marijuana-related impairment was predicted by ADHD with a history of adolescent-onset CD.
Limitations and Future DirectionsA number of limitations should be considered when inter-preting the current findings. This study was conducted at a large, public, Mid-Atlantic university with stringent admis-sions criteria and included only “traditional” college stu-dents (i.e., those attending college full-time immediately or shortly after completing high school). Therefore, results can only be generalized to similar students with ADHD attend-ing universities with similar characteristics. Additional stud-ies that use more diverse samples at multiple universities are needed. In addition, although the current study addresses a gap in the existing literature by including a large proportion of females in the ADHD sample, this gender distribution may not be representative of the actual college student ADHD population. Likewise, the way in which the sample was collected (i.e., reliance on volunteers who responded to flyers or received extra credit for class) may have resulted in a biased sample. For example, participants who volunteered may have had lower rates of CD or substance use.
Our relatively small sample limited our ability to con-duct a number of potentially important analyses. These include examining interactions between ADHD and history of CD as well as studying the moderating effects of factors such as gender, ADHD subtype, and ADHD medication sta-tus. As each of these factors is accompanied by different correlates and comorbidity profiles, they should be exam-ined in future studies with larger samples. In addition, the cross-sectional nature of the study design did not allow for the identification of developmental precursors to the sub-stance use behaviors under examination. The current study also lacked a noncollege student ADHD comparison group. The absence of this comparison group limited our ability to interpret differences between current study findings and those of previous studies examining noncollege young adults with ADHD. Future studies should consider includ-ing noncollege comparison groups.
The present study relied solely on the use of self-report data for information related to substance use. Objective measures of use (e.g., hair follicle testing) could potentially
at UCSF KALMANOVITZ LIB & CKM on February 14, 2011jad.sagepub.comDownloaded from

Rooney et al. 11
provide more accurate indicators of substance use behav-iors (Harrison & Huges, 1997) and should be incorporated into future studies. Collateral informant ratings of past and current ADHD symptoms were available for only a portion of participants. In future studies, researchers should con-sider the benefits of requiring informant reports for all par-ticipants while weighing the impact of this requirement on sample composition. In addition, the method of data collec-tion differed between participants and informants. Future studies should include interviews with informants as well as participants. Likewise, future studies should include a more thorough assessment of learning disabilities. In the present study, LD diagnosis was captured by participant responses to a single self-report question about presence or absence of an LD diagnosis. This is likely to be an inadequate method for accurately capturing students with an LD.
Clinical ImplicationsDespite these limitations, the study findings suggest that college students with ADHD are at risk for problematic alcohol and drug use. Although these findings are prelimi-nary, they are useful for informing current intervention and prevention efforts on college campuses. Therapists working with this population should consider the role of substance use in patient symptom and impairment profiles and incor-porate substance use treatment when necessary. Likewise, parents of students with ADHD and the students themselves should be aware of the elevated risk for problematic sub-stance use. With this knowledge, they may opt to select a college with fewer known environmental risk factors for excessive alcohol use (Wechsler & Nelson, 2008) or choose living environments that reduce the risk of problematic substance use (i.e., substance-free housing, living at home with parents, and avoiding fraternity/sorority housing; Park, Sher, & Krull, 2009). In addition, medical doctors prescribing stimulant medication should be particularly vigilant about assessing current substance use and provide extensive education about the hazards of mixing stimulant medication with alcohol or illicit drugs. Future research is needed to replicate the current findings and examine mech-anisms underlying the association between ADHD and substance-related problems. These studies would provide an empirical foundation for the development of prevention and treatment programs addressing substance use problems in college students with ADHD.
Declaration of Conflicting InterestsThe authors declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
FundingThis research was supported by a grant from the National Institute on Drug Abuse (F31 DA024946-01).
References
Ambrosini, P. (2000). Historical development and present sta-tus of the schedule for affective disorders and schizophrenia for school-age children (K-SADS). Journal Of the American Academy of Child & Adolescent Psychiatry, 39, 49-58.
American Psychological Association. (2000). Diagnostic andstatistical manual of mental disorders (4th ed., text rev.). Washington, DC: Author.
Babor, T., Higgins-Biddle, J., Saunders, J., & Monteiro, M. (2001). AUDIT: The alcohol use disorders identification test. Guide-lines for use in primary care. Geneva, Switzerland: World Health Organization.
Barkley, R. A. (1997). ADHD and the nature of self-control. New York, NY: Guilford.
Barkley, R. A. (1998). Attention deficit hyperactivity disorder: A handbook for diagnosis and treatment (2nd ed.). New York, NY: Guilford.
Barkley, R. A., Fischer, M., Edelbrock, C. S., & Smallish, L. (1990). The adolescent outcome of hyperactive children diag-nosed by research criteria: I. An 8-year prospective follow-up study. Journal Of the American Academy of Child & Adoles-cent Psychiatry, 29, 546-557.
Barkley, R. A., Fischer, M., Smallish, L., & Fletcher, K. E. (2002). The persistence of attention-deficit/hyperactivity disorder into young adulthood as a function of reporting source and definition of disorder. Journal of Abnormal Psychology, 111,279-289.
Barkley, R. A., Fischer, M., Smallish, L., & Fletcher, K. E. (2004). Young adult follow-up of hyperactive children: antisocial activities and drug use. Journal of Child Psychology and Psy-chiatry, 45, 195-211.
Barkley, R. A., & Murphy, K. R. (2006). Current Symptoms Scale Attention Deficit Hyperactivity Disorder: A Clinical Workbook (3rd ed.). New York, NY: Guilford.
Belendiuk, K. A., Clarke, T. L., Chronis, A. M., & Raggi, V. (2006). Assessing the concordance of measures used to diag-nose adult ADHD. Journal of Attention Disorders, 20, 1-12.
Berman, A., Bergman, H., Palmstierna, T., & Schlyter, F. (2005). Evaluation of the drug use disorders identification test (DUDIT) in criminal justice and detoxification settings and in a Swedish population sample. European Addition Resources, 11, 22-31.
Biederman, J., Monuteaux, M. C., Mick, E., Wilens, T. E., Fontanella, J. A., Poetzl, K. M., . . . Faraone, S. V. (2006). Is cigarette smoking a gateway to alcohol and illicit drug use disorders? A study of youths with and without attention deficit hyperactivity disorder. Biological Psychiatry, 59, 258-264.
Biederman, J., & Spencer, T. J. (2002). Methylphenidate in treat-ment of adults with attention-deficit/hyperactivity disorder. Journal of Attention Disorders, 6(Suppl. 1), S101-107.
Biederman, J., Wilens, T. E., Mick, E., Faraone, S. V., Weber, W., Curtis, S., . . . Soriano, J. (1997). Is ADHD a risk factor for psychoactive substance use disorders? Findings from a
at UCSF KALMANOVITZ LIB & CKM on February 14, 2011jad.sagepub.comDownloaded from

12 Journal of Attention Disorders XX(X)
four-year prospective study. Journal Of the American Acad-emy of Child & Adolescent Psychiatry, 36, 21-29.
Brown, S. A., McGue, M., Maggs, J. L., Schulenberg, J. E., Hingson, R. W., Swartzwelder, S., . . . Murphy, S. (2008). A develop-mental perspective on alcohol and youths 16 to 20 years of age. Pediatrics, 121, S290-S310.
Chronis-Tuscano, A. M., Raggi, V., Clarke, T. L., Rooney, M., Diaz, Y., & Pian, J. (2008). Associations between maternal attention-deficit/hyperactivity disorder symptoms and parent-ing. Journal of Abnormal Child Psychology, 36, 1237-1250.
Chronis-Tuscano, A. M., Rooney, M., Seymour, K. E., Lavin-Jones, H., Pian, J., Robb, A. S., et al. (2010). Effects of maternal stimulant medication on observed parenting in mother-child dyads with attention-deficit/hyperactivity disorder. Journal of Clinical Child & Adolescent Psychology, 39, 581-587.
Chronis-Tuscano, A. M., Seymour, K. E., Stein, M. A., Jones, H., Jiles, C. D., Rooney, M., et al. (2008). Methylphenidate for mothers with ADHD: Preliminary effects on ADHD symp-toms and parenting. Journal of the American Academy of Child & Adolescent Psychiatry, 69.
Conners, C. K., Erhardt, D., Epstein, J. N., Parker, J. D. A., Sitarenios, G., & Sparrow, E. (1999). Self-ratings of ADHD symptoms in adults: I. Factor structure and normative data. Journal of Attention Disorders, 3, 141-151.
Core Institute. (2005). Validity and reliability core alcohol and drug survey long form. Retrieved October 19, 2006, from http://www.core.siuc.edu/surveys.html
Douglas, K. A., Collins, J. L., Warren, C., Kann, L., Gold, R., Clayton, S., . . . Kolbe, L. J. (1997). Results from the 1995 National College Health Risk Behavior Survey. Journal of American College Health, 46, 55-66.
DuPaul, G. J., Schaughency, E. A., Weyandt, L. L., Tripp, G., Kiesner, J., Ota, K., . . . Stanish, H. (2001). Self-report of ADHD symptoms in university students: Cross-gender and cross-national prevalence. Journal of Learning Disabilities, 34, 370-379.
Erhardt, D., Epstein, J. N., Conners, C. K., Parker, J. D. A., & Sitarenios, G. (1999). Self-ratings of ADHD symptoms in adults: II. Reliability, validity, and diagnostic sensitivity. Journal of Attention Disorders, 3, 153-158.
Faraone, S. V., Biederman, J., & Milberger, S. (1995). How reli-able are maternal reports of their children’s psychopathology? One-year recall of psychiatric diagnoses of ADHD children. Journal of the American Academy of Child & Adolescent Psy-chiatry, 34, 1001-1008.
Faraone, S. V., Biederman, J., & Monuteaux, M. C. (2002). Fur-ther evidence for the diagnostic continuity between child and adolescent ADHD. Journal of Attention Disorders, 6, 5-13.
Faraone, S., Biederman, J., Spencer, T. J., Mick, E., Murray, K., Carter, P., et al. (2006). Diagnosing adult attention deficit hyperactivity disorder. Are late onset and subthreshold diag-noses valid? The American Journal of Psychiatry, 163, 1720-1729.
Flory, K., Molina, B. S. G., Pelham, W. E., Jr., Gnagy, E., & Smith, B. H. (2006). Childhood ADHD predicts risky sexual behavior in young adulthood. Journal of Clinical Child & Adolescent Psychology, 35, 571-577.
Ford, T., Goodman, R., & Meltzer, H. (2003). The British Child and Adolescent Mental Health Survey 1999: The prevalence of DSM-IV disorders. Journal of the American Academy of Child & Adolescent Psychiatry, 42, 1203-1211.
Gallagher, R., Sysko, H., & Zhang, B. (2001). National survey of counseling center directors. Alexandria, VA: International Association of Counseling Services.
Giancola, P. R., & Tarter, R. E. (1999). Executive cognitive func-tioning and risk for substance abuse. Psychological Science, 10, 203-205.
Gittelman, R., Mannuzza, S., Shenker, R., & Bonagura, N. (1985). Hyperactive boys almost grown up: I. Psychiatric status. Archives of General Psychiatry, 42, 937-947.
Grant, S., Contoreggi, C., & London, E. D. (2000). Drug abusers show impaired performance in a laboratory test of decision making. Neuropsychologia, 38, 1180-1187.
Harrison, L., & Huges, A. (1997). The validity of self-reported drug use: Improving the accuracy of survey estimates. NIDA Research Monograph, p. 167.
Hartsough, C. S., & Lambert, N. M. (1987). Pattern and pro-gression of drug use among hyperactives and controls: A prospective short-term longitudinal study. Journal of Child Psychology and Psychiatry, 28, 543-553.
Hechtman, L. (1984). Hyperactives as young adults: Past and cur-rent substance abuse and antisocial behavior. American Jour-nal of Orthopsychiatry, 54, 415-425.
Johnston, L. D., O’Malley, P. M., Bachman, J. G., & Schulenberg, J. E. (2009). Monitoring the future national survey on drug use, 1975-2008. Volume II: College students and adults ages 19-50 (NIH Publication No. 09-7402). Bethesda, MD: National Institute on Drug Abuse.
Katz, N., Petscher, Y., & Wells, T. (2009). Diagnosing attention-deficit hyperactivity disorder in college students. Journal of Attention Disorders, 13, 227-283.
Kokotailo, P., Egan, J., Gangnon, R., Brown, D., Mundt, M., & Fleming, M. (2004). Validity of the alcohol use disorders identification test in college students. Alcoholism: Clinical & Experimental Research, 28, 914-920.
Kollins, S. H. (2008). ADHD, substance use disorders, and psy-chostimulant treatment: Current literature and treatment guidelines. Journal of Attention Disorders, 12, 115-125.
Kollins, S. H., McClernon, F. J., & Epstein, J. N. (2009). Effects of smoking on abstinence on reaction time variability in smokers with and without ADHD: An ex-Gaussian analysis. Drug and Alcohol Dependence, 100, 169-172.
Lahey, B., Applegate, B., McBurnett, K., & Biederman, J. (1994). DSM-IV field trials for attention deficit hyperactivity disorder in children and adolescents. American Journal of Psychiatry, 151, 1673-1685.
at UCSF KALMANOVITZ LIB & CKM on February 14, 2011jad.sagepub.comDownloaded from

Rooney et al. 13
Lahey, B. B., McBurnett, K., & Loeber, R. (2000). Are attention-def-icit/hyperactivity disorder and oppositional defiant disorder pre-cursors to conduct disorder? In J. Sameroff, M. Lewis, & S. M. Miller (Eds.), Handbook of developmental psychopathology (2nd ed., pp. 431-446). New York, NY: Kluwer Academic/Plenum.
Lahey, B. B., Pelham, W. E., Jr., Loney, J., Kipp, H. L., Ehrhardt, A., Lee, S. S., . . . Massetti, G. (2004). Three-year predictive validity of DSM-IV attention deficit hyperactivity disorder in children diagnosed at 4-6 years of age. American Journal of Psychiatry, 161, 2014-2020.
Lambert, N. M., & Hartsough, C. S. (1998). Prospective study of tobacco smoking and substance dependencies among samples of ADHD and non-ADHD participants. Journal of Learning Disabilities, 31, 533-544.
Levin, E. D., Conners, C. K., Silva, D., Canu, W., & March, J. (2001). Effects of chronic nicotine and methylphenidate in adults with attention-deficit/hyperactivity disorder. Experi-mental and Clinical Psychopharmacology, 9, 83-90.
Littlefield, A. K., Sher, K. J., & Wood, P. K. (2009). “Maturing out” of problematic alcohol involvement related to personality change? Journal of Abnormal Psychology, 118, 360-374.
Mannuzza, S., & Klein, R. G. (1999). Adolescent and adult out-comes in attention-deficit/hyperactivity disorder. In H. Quay & A. E. Hogan (Eds.), Handbook of disruptive behavior disorders (pp. 279-294). New York, NY: Kluwer Academic/Plenum.
Mannuzza, S., & Klein, R. G. (2000). Long-term prognosis in attention-deficit/hyperactivity disorder. Child and Adolescent Psychiatric Clinics of North America, 9, 711-726.
Mannuzza, S., Klein, R. G., Klein, D., Bessler, A., & Shrout, P. (2002). Accuracy of adult recall of childhood attention-deficit/hyperactivity disorder. American Journal of Psychiatry, 159, 1882-1888.
Mannuzza, S., Klein, R. G., Troung, N. L., Moulton, J. L., Roizen, E. R., Howell, K. H., . . . Castellanos, F. X. (2008). Age of methylphenidate treatment initiation in children with ADHD and later substance abuse: Prospective follow-up into adult-hood. American Journal of Psychiatry, 165, 604-609.
McClernon, F. J., Kollins, S. H., Lutz, A. M., Fitzgerald, D. P., Murray, D. W., Redman, C., & Rose, J. E. (2008). Effects of smoking abstinence on adult smokers with and without atten-tion deficit hyperactivity disorder: Results of a preliminary study. Psychopharmacology, 197, 95-105.
McGough, J. J., & Barkley, R. A. (2004). Diagnostic controver-sies in adult attention deficit hyperactivity disorder. American Journal of Psychiatry, 161, 1948-1956.
Milberger, S., Biederman, J., Faraone, S. V., Chen, L., & Jones, J. (1997). ADHD is associated with early initiation of cigarette smoking in children and adolescents. Journal of the American Academy of Child & Adolescent Psychiatry, 36, 37-44.
Milberger, S., Biederman, J., Faraone, S. V., Wilens, T. E., & Chu, M. P. (1997). Associations between ADHD and psychoactive substance use disorders: Findings from a longitudinal study of high-risk siblings of ADHD children. American Journal on Addictions, 6, 318-329.
Moffitt, T. E. (2003). Life-course persistent and adolescence-limited antisocial behavior: A 10-year research review and research agenda. In B. B. Lahey, T. E. Moffitt, & A. Caspi (Eds.), Causes of conduct disorder and juvenile delinquency (pp. 49-75). New York, NY: Guilford.
Molina, B. S. G., Marshal, M. P., Pelham, W. E., Jr., & Wirth, R. J. (2005). Coping skills and parent support mediate the association between childhood attention-deficit/hyperactiv-ity disorder and adolescent cigarette use. Journal of Pediatric Psychology, 30, 345-357.
Molina, B. S. G., & Pelham, W. E., Jr. (2003). Childhood pre-dictors of adolescent substance use in a longitudinal study of children with ADHD. Journal of Abnormal Psychology, 112, 497-507.
Molina, B. S. G., Smith, B. H., & Pelham, W. E., Jr (1999). Inter-active Effects of Attention Deficit Hyperactivity Disorder and conduct Disorder on Early Adolescent Substance Use. Psy-chology of Addictive Behaviors, 13, 348-358.
Murphy, P., & Schachar, R. J. (2000). Use of self-ratings in the assessment of symptoms of attention-deficit/hyperactivity disorder in adults. American Journal of Psychiatry, 157,1156-1159.
Nigg, J. T. (2001). Is ADHD a disinhibitory disorder? Psychologi-cal Bulletin, 127, 571-598.
Park, A., Sher, K., & Krull, J. (2009). Selection and socialization of risky drinking during the college transition: The importance of microenvironments associated with specific living units. Psychology of Addictive Behaviors, 23, 404-414.
Pelham, W. E., Jr., & Fabiano, G. A. (2008). Evidence-based psy-chosocial treatments for attention-deficit/hyperactivity disor-der. Journal of Clinical Child & Adolescent Psychology, 37, 184-214.
Piacentini, J. C., Cohen, P., & Cohen, J. (1992). Combining dis-crepant diagnostic information from multiple sources: Are complex algorithms better than simple ones? Journal of Abnor-mal Child Psychology, 20, 51-63.
Poltavski, D. V., & Petros, T. (2006). Effects of transdermal nico-tine on attention in adult non-smokers with and without atten-tional deficits. Physiology & Behavior, 87, 614-624.
Presley, C. A. (1994). Development of the core alcohol and drug survey: Initial findings and future directions. Journal of Amer-ican College Health, 42, 248-255.
Rezani, A. (2001). Cognitive effects of nicotine. Biological Psy-chiatry, 49, 258-267.
Rist, F., Glockner-Rist, A., & Demmel, R. (2009). The alcohol use disorders identification test revisited: Establishing its struc-ture using nonlinear factor analysis identifying subgroups of respondents using latent class factor analysis. Drug and Alco-hol Dependence, 100, 71-82.
Saunders, J., Aasland, O., Babor, T., De La Fuenta, J., & Grant, M. (1993). Development of the alcohol use disorders identifi-cation test (AUDIT): WHO collaborative project on early detection of persons with harmful alcohol consumption-II. Addiction, 88, 791-804.
at UCSF KALMANOVITZ LIB & CKM on February 14, 2011jad.sagepub.comDownloaded from

14 Journal of Attention Disorders XX(X)
Selin, K. H. (2003). Test-retest reliability of the alcohol use disor-der identification test in a general population sample. Alcohol-ism: Clinical & Experimental Research, 27, 1428-1435.
Shields, A. L., Guttmannova, K., & Caruso, J. C. (2004). An examination of the factor structure of the alcohol use disorders identification test in two high-risk samples. Substance Use & Misuse, 39, 1161-1182.
Smith, B. H., Waschbusch, D. A., Willoughby, M. T., & Evans, S. W. (2000). The efficacy, safety, and practicality of treatments for adolescents with attention-deficit/hyperactivity disorder. Clinical Child and Family Psychology Review, 3, 243-267.
Smith, B. H., Molina, B. S. G., & Pelham, W. E., Jr. (2002). The clin-ically meaningful link between alcohol use and attention deficit hyperactivity disorder. Alcohol Research & Health, 26, 122-129.
Trimmel, M., & Wittberger, S. (2004). Effects of transdermally administered nicotine on aspects of attention, task load, and mood in women and men. Pharmacology Biochemistry and Behavior, 78, 639-645.
Volkow, N. D., & Swanson, J. M. (2008). Does childhood treatment of ADHD with stimulant medication affect substance abuse in adulthood? American Journal of Psychiatry, 165, 553-555.
Wechsler, H., Dowdall, G. W., Davenport, A., & Castillo, S. (1995). Correlates of college student binge drinking. Ameri-can Journal of Public Health, 85, 921-926.
Wechsler, H., Lee, J. E., Kuo, M., & Lee, H. (2000). College binge drinking in the 1990s: A continuing problem: Results of the Harvard School of Public Health 1999 College Alcohol Study. Journal of American College Health, 48, 199-210.
Wechsler, H., & Nelson, T. F. (2008). What we have learned from the Harvard School of Public Health College Alcohol Study: Focusing attention on college student alcohol consumption and the environmental conditions that promote it. Journal of Studies on Alcohol and Drugs, 69, 481-490.
Weiss, G. (1979). Hyperactives as young adults: A controlled pro-spective ten-year follow-up of 75 children. Archives of Gen-eral Psychiatry, 36, 675-681.
Weiss, G., & Hechtman, L. (1993). Hyperactive children grown up: ADHD in children, adolescents, and adults (2nd ed.). New York, NY: Guilford.
Weyandt, L. L., & DuPaul, G. J. (2008). ADHD in college stu-dents: Developmental findings. Developmental Disabilities Research Reviews, 14, 311-319.
Wilens, T. E., Biederman, J., & Mick, E. (1998). Does ADHD affect the course of substance abuse? Findings from a sam-ple of adults with and without ADHD. American Journal on Addictions, 7, 156-163.
Wilens, T. E., Biederman, J., & Spencer, T. J. (2002). Attention deficit/hyperactivity disorder across the lifespan. Annual Review of Medicine, 53, 113-131.
Wilens, T. E., Vitulano, M., Upadhyaya, H., Adamson, J., Sawtelle, R., Utzinger, L., & Biederman, J. (2008). Cigarette smoking associated with attention deficit hyperactivity disor-der. Journal of Pediatrics, 153, 414-419.
Wolf, L. (2001). College students with ADHD and other hidden disabilities: Outcomes and interventions. Annals of the New York Academy of Sciences, 931, 385-395.
Bios
Mary Rooney, MS, is a doctoral candidate in clinical psychology at the University of Maryland, College Park, and a predoctoral intern at the University of California, San Francisco. Her research applies a developmental psychopathology approach to the study of risky behavior in college students with ADHD.
Andrea Chronis-Tuscano is an associate professor of psychol-ogy at the University of Maryland, College Park. Her research focuses broadly on evidence-based treatment for ADHD. Her specific research interest involves the impact of parental psycho-pathology and parenting on the developmental and treatment outcomes of children with ADHD.
Yesel Yoon, BA, is a graduate of the University of Maryland, College Park. As an undergraduate, she worked as a research assistant with the Maryland ADHD Program at the University of Maryland College Park. Currently, she is a doctoral student in clinical psychology at the University of Massachusetts Amherst.
at UCSF KALMANOVITZ LIB & CKM on February 14, 2011jad.sagepub.comDownloaded from




















