
The hytrin community assessment trial study: A one-year study of terazosin versus placebo in the...
10
RAPID COMMUNICATION THE HYTRIN COMMUNITY ASSESSMENT TRIAL STUDY: A ONE-YEAR STUDY OF TERAZOSIN VERSUS PLACEBO IN THE TREATMENT OF MEN WITH SYMPTOMATIC BENIGN PROSTATIC HYPERPLASIA* CLAUS G. ROEHRBORN, JOSEPH E. OESTERLING, STEPHEN AUERBACH, STEPHEN A. KAPLAN, L. KEITH LLOYD, DOUGLAS E MILAM, AND ROBERT J. PADLEY, FOR THE HYCAT INVESTIGATOR GROUP+ ABSTRACT Objectives. To determine the clinical effectiveness and safety of alpha,-blockade therapy versus placebo in the treatment of men with moderate to severe symptoms of prostatism in a community-based population under usual care conditions. Methods. The Hytrin Community Assessment Trial is a prospective, placebo-controlled, randomized, double- blinded, 1-year clinical trial, conducted at 15 academic medical centers (regional sites) and 14 1 private urol- ogy practices (satellite sites). A total of 2084 men at least 55 years old with moderate to severe symptoms of benign prostatic hyperplasia (BPH) as determined by an American Urological Association (AUA) Symptom Score (AUA-SS) of 13 or more points and a bother score (AUA-BS) of 8 or more were enrolled. Randomized patients at regional sites were required to have a peak urinary flow rate less than 15 mlfs with a voided volume of at least 150 mL. Treatment with terazosin was initiated with 1 mg daily for 3 days, followed by 2 mg daily for 25 days. Thereafter, patients were titrated stepwise to 5 or 10 mg if they failed to achieve a 35% or greater improvement in the AUA-SS. Primary outcome measures were AUA-SS, AUA-BS, BPH Impact Index (BII), dis- ease-specific quality of life (QOL) score, and treatment failure as defined as discontinuation due to persistent or worsening symptoms or need for surgical intervention for BPH. Secondary outcome measures were peak urinary flow rate and postvoid residual urine volume. Results. AUA-SS (0 to 35 point scale) improved from a baseline mean of 20.1 points by 37.8% during tera- zosin (n = 976) and by 18.4% during placebo (n = 973) treatment (P <O.OOl). Similarly, statistically su- perior improvements were observed in regard to the AUA-BS, BII, and the QOL score in the terazosin-treated patients. Peak urinary flow rate improved from a baseline of 9.6 mUs (both regional treatment groups) by 2.2 mUs in the terazosin group (n = 137) and by 0.7 mUs in the placebo group (n = 140) (P 10.05). Treat- ment failure occurred in 1 1.2% of terazosin- and 25.4% of placebo-treated patients (f c 0.00 1; Kaplan-Meier adjusted withdrawal rates at 365 days). Withdrawal from study drug treatment due to adverse events occurred in 19.7% of terazosin- and 15.2% of placebo-treated patients (P <O.OOl). Conclusions. Terazosin given once daily in a dose ranging from 2 to 10 mg in community-based urology prac- tices under conditions simulating usual care is effective in reducing the symptoms, perception of bother, and the impairment of QOL due to urinary symptoms in men with moderate to severe symptoms of prostatism. This effect is superior to placebo and maintained over 12 months of follow-up. Clinical research outcome stud- ies in BPH can be conducted in community-based practices, thus simulating as closely as possible “usual care” conditions. UROLCGY@ 47: 159- 168, 1996. *This study was funded by Abbott Laboratories, Abbott Park, Ill. +See appendix for list of investigators. From the Division of Urology, University of Texas Southwestern Medical Center, Dallas, Texas; Department of Urology, University of Michigan, Ann Arbor, Michigan; Columbia-Presbyterian Medical Center, New York, New York; Vanderbilt University, Nashville, Tennessee; Department of Urology, University of Alabama, Birmingham, Alabama; and Abbott Laboratories, Abbott Park, Illinois Reprint requests: Claus G. Roehrbom, M.D., Department of Surgery, Division of Urology, University of Texas Southwestern Medical Center, 5323 Harry Hines Boulevard, Dallas, TX 7.5235-9110 Submitted: September 1, 1995, accepted (with revisions): October 11, 1995 UROLCX?’ 47 (2), 1996 B enign prostatic hyperplasia (BPH) is a preva- lent disease in aging men, characterized by ir- ritative and obstructive symptoms. Although other factors play an important role in health care seek- ing behavior,’ most men receive treatment for BPH because of their symptoms and the bother associ- ated with them.2 Although the pathophysiology of BPH and its symptoms are poorly understood, it has been postulated that both a static and a dy- namic component are responsible for the infra- vesical obstruction and development of symptoms. The dynamic component is mediated by the tone of the smooth muscle in the prostate adenoma, the 159
-
Upload
utsouthwestern -
Category
Documents
-
view
4 -
download
0
Transcript of The hytrin community assessment trial study: A one-year study of terazosin versus placebo in the...
RAPID COMMUNICATION
THE HYTRIN COMMUNITY ASSESSMENT TRIAL STUDY: A ONE-YEAR STUDY OF TERAZOSIN VERSUS PLACEBO IN THE
TREATMENT OF MEN WITH SYMPTOMATIC BENIGN PROSTATIC HYPERPLASIA*
CLAUS G. ROEHRBORN, JOSEPH E. OESTERLING, STEPHEN AUERBACH, STEPHEN A. KAPLAN, L. KEITH LLOYD, DOUGLAS E MILAM, AND ROBERT J. PADLEY, FOR THE HYCAT INVESTIGATOR GROUP+
ABSTRACT Objectives. To determine the clinical effectiveness and safety of alpha,-blockade therapy versus placebo in the treatment of men with moderate to severe symptoms of prostatism in a community-based population under usual care conditions. Methods. The Hytrin Community Assessment Trial is a prospective, placebo-controlled, randomized, double- blinded, 1 -year clinical trial, conducted at 15 academic medical centers (regional sites) and 14 1 private urol- ogy practices (satellite sites). A total of 2084 men at least 55 years old with moderate to severe symptoms of benign prostatic hyperplasia (BPH) as determined by an American Urological Association (AUA) Symptom Score (AUA-SS) of 13 or more points and a bother score (AUA-BS) of 8 or more were enrolled. Randomized patients at regional sites were required to have a peak urinary flow rate less than 15 mlfs with a voided volume of at least 150 mL. Treatment with terazosin was initiated with 1 mg daily for 3 days, followed by 2 mg daily for 25 days. Thereafter, patients were titrated stepwise to 5 or 10 mg if they failed to achieve a 35% or greater improvement in the AUA-SS. Primary outcome measures were AUA-SS, AUA-BS, BPH Impact Index (BII), dis- ease-specific quality of life (QOL) score, and treatment failure as defined as discontinuation due to persistent or worsening symptoms or need for surgical intervention for BPH. Secondary outcome measures were peak urinary flow rate and postvoid residual urine volume. Results. AUA-SS (0 to 35 point scale) improved from a baseline mean of 20.1 points by 37.8% during tera- zosin (n = 976) and by 18.4% during placebo (n = 973) treatment (P <O.OOl). Similarly, statistically su- perior improvements were observed in regard to the AUA-BS, BII, and the QOL score in the terazosin-treated patients. Peak urinary flow rate improved from a baseline of 9.6 mUs (both regional treatment groups) by 2.2 mUs in the terazosin group (n = 137) and by 0.7 mUs in the placebo group (n = 140) (P 10.05). Treat- ment failure occurred in 1 1.2% of terazosin- and 25.4% of placebo-treated patients (f c 0.00 1; Kaplan-Meier adjusted withdrawal rates at 365 days). Withdrawal from study drug treatment due to adverse events occurred in 19.7% of terazosin- and 15.2% of placebo-treated patients (P <O.OOl). Conclusions. Terazosin given once daily in a dose ranging from 2 to 10 mg in community-based urology prac- tices under conditions simulating usual care is effective in reducing the symptoms, perception of bother, and the impairment of QOL due to urinary symptoms in men with moderate to severe symptoms of prostatism. This effect is superior to placebo and maintained over 12 months of follow-up. Clinical research outcome stud- ies in BPH can be conducted in community-based practices, thus simulating as closely as possible “usual care” conditions. UROLCGY@ 47: 159- 168, 1996.
*This study was funded by Abbott Laboratories, Abbott Park, Ill. +See appendix for list of investigators.
From the Division of Urology, University of Texas Southwestern Medical Center, Dallas, Texas; Department of Urology, University of Michigan, Ann Arbor, Michigan; Columbia-Presbyterian Medical Center, New York, New York; Vanderbilt University, Nashville, Tennessee; Department of Urology, University of Alabama, Birmingham, Alabama; and Abbott Laboratories, Abbott Park, Illinois
Reprint requests: Claus G. Roehrbom, M.D., Department of Surgery, Division of Urology, University of Texas Southwestern Medical Center, 5323 Harry Hines Boulevard, Dallas, TX 7.5235-9110
Submitted: September 1, 1995, accepted (with revisions): October 11, 1995
UROLCX?’ 47 (2), 1996
B enign prostatic hyperplasia (BPH) is a preva- lent disease in aging men, characterized by ir-
ritative and obstructive symptoms. Although other factors play an important role in health care seek- ing behavior,’ most men receive treatment for BPH because of their symptoms and the bother associ- ated with them.2 Although the pathophysiology of BPH and its symptoms are poorly understood, it has been postulated that both a static and a dy- namic component are responsible for the infra- vesical obstruction and development of symptoms. The dynamic component is mediated by the tone of the smooth muscle in the prostate adenoma, the
159

prostate capsule, and the bladder neck.3 Smooth muscle tone is regulated by the sympathetic ner- vous system via alpha,-receptors located in these structures.4’5 Alpha-receptor blockade as a thera- peutic concept in the treatment of prostatism was first explored by Caine et al. in 1976.6 With the demonstration of efficacy in randomized placebo- controlled clinical trials7-13 long-acting alpha,- specific antagonists are currently prescribed for this indication.
Long-term compliance with treatment and a low rate of treatment failure with resulting retreat- ments are key to a successful therapy for a chronic disease process, such as BPH characterized by a 40% response rate to placebo therapy.14 Although long-term, open-label extension studies have demonstrated the maintenance of therapeutic ef- ficacy up to 42 months, l5 they often benefit from an enrichment of the study population by re- sponders during the preceding placebo-controlled period and therefore are of limited value in as- sessing the true efficacy and safety of therapy
Clinical research in BPH has mostly been con- ducted in academic centers with a select popula- tion of patients. A concern might be whether such patients and their responses to therapy are truly comparable to those patients who on their own ini- tiative seek consultation with a physician because they are bothered by symptoms of prostatism.
The goal of the present study was to assess in pri- marily community-based patients with moderate to severe symptoms of prostatism the efficacy of the alpha,-adrenergic antagonist, terazosin (Hytrin), compared with placebo over a period of 1 year in regard to improvement in American Urological Association (AUA) Symptom Score (AUA-SS), AUA Bother Score (AUA-BS) , BPH Impact Index (BII) , and a disease-specific quality of life (QOL) score.16-18 Further goals were to assess the feasibility of com- munity-based clinical research in patients with
Month 0 1 2 3 4 6 6 T 6 6 10 11 12
Health Care Utilization Interview
Visit 1 2 3 4 6 6 7 6
low , I I I 1
S.! ., ;( ., .I
..z.me +.. . . . . . . . . . . . . . . . . .., I
Terazosin
Placebo
t ., , I
A , , , /
I I 1 Lead,” Period I
R
BPH, to assess the safety of terazosin over a 12- month treatment period, and to determine the cost- effectiveness of terazosin versus placebo treatment by an overall cost analysis. The results of the eco- nomic analysis are presented elsewhere. l9
MATERIAL AND METHODS
The Hytrin Community Assessment Trial (HYCAT) was conducted at 15 academic regional centers and 141 commu- nity-based, private urology practices. The regional sites were chosen to achieve geographic representation of the various regions of the United States and were located in New York, NY (2); Boston, Mass; Washington, DC; Rochester, Minn; Columbus, Ohio; Philadelphia, Pa; Kansas City, Kan; Mem- phis, Tenn; Durham, NC; Birmingham, Ala; Miami, Fla; Dal- las, Tex; Los Newport Beach, Calif; and Seattle, Wash. The satellite investigators were selected from geographic regions corresponding to the regional academic centers.
To participate in the study, patients had to be at least 55 years of age, score 13 or more points on the 0 to 35 point scale of the AUA-SS and 8 or more points on the 0 to 28 point scale of the AUA-BS on two consecutive occasions (first visit and visit at end of 2 weeks of placebo lead-in pe- riod), and be willing to participate in a randomized, placebo- controlled trial over a 12-month period. The study was ap- proved by an Institutional Review Board. Exclusion criteria were treatment with an alpha-adrenergic antagonist or some form of antiandrogen therapy during the preceding 3 months, treatment with medications that could interfere with normal detrusor or sphincter activity, history of myo- cardial infarction or cerebrovascular accident within 2 months prior to the study, unstable angina, heart failure, significant arrhythmia, history of orthostatic hypotension, hypotension (blood pressure of less than 100/70 mm Hg), history of prostate cancer, pelvic irradiation, urethral stric- ture, prior BPH surgery, current prostate cancer, impaired renal function (serum creatinine more than 2.0 mg/dL), his- tory of urinary tract infections, neurogenic bladder disor- ders, bladder stones, or a cystoscopy within 2 weeks of study entry.
The study design is shown in Figure 1A. All patients un- derwent the following tests at entry into the study: history and physical examination, vital signs, digital rectal examina- tion, AUA-SS, AUA-BS, BII, QOL, urinalysis, and serum cre- atinine. In addition, patients at the regional sites underwent flow rate recording (Dantec Urodyne 1000), measurement of
FIGURE 1. Study schematic (A) and patient disposition (B) of the Hytrin Community Assessment Trial.
160 uROLOf3Ym47 (21, 1996

TABLE I. Demographics and baseline data (mean f SE, range, and number of patients for whom data are available)
Placebo Terazosin Mean f SE Range No. Mean f SE Range No. P Value
Arice WI 65.7 f 0.22 46-85 1031 65.7 k 0.22 50-94 1053 0.78 Weight (lb) 189 f 1 .OO 106-346 1003 187 f 0.99 119-340 1017 0.23 Systolic BP (mm Hg) 134.9 + 0.55 loo-204 984 134.7 * 0.55 100-212 987 0.74 Diastolic BP (mm Hg) 81.2 f 0.31 40-l 20 984 80.7 f 0.31 50-l 10 987 0.24 AUA-SS 20.1 f 0.17 2-35 973 20.1 + 0.17 1 o-35 976 0.94 AUA-BS 15.7 + 0.16 4-28 971 15.9 f 0.16 7-28 972 0.38 BII 5.8 f 0.09 o-13 927 6.0 f 0.09 o-13 934 0.17 QOL 3.8 f 0.04 O-6 937 3.9 + 0.04 O-6 943 0.38 Q,,, (mW * 9.6 f 0.3 2.4- 15.0 140 9.6 + 0.3 3.0- 15.0 137 0.95 Voided volume (ml] * 253 + 10.3 129-598 140 261 f 10.3 1 16-648 137 0.58 Residual urine (mL] * 97.5 If: 8.7 O-384 139 88.7 f 8.7 O-463 137 0.48 PSA (ng/mL) * 2.4 k 0.21 o-12 128 2.8 + 0.22 o-17 118 0.247
KEY: AUA-SS = American Urological Association Symptom Score (tJ to 35 point scale); AUA-BS = AUA Bother Score (0 to 28 point scale); BII = BPH Impact Index (0 to 13 point scale); Q,, = maximum perfusion; gOL = Quality ofLi$e Index (0 to 6 point scale); PSA measured by Abbott IUU monoclonal assay; P valuefor di;fference between placebo and terazosin, two-way ANOVA, exceptfor blood pressure (BP) and PSA, one-way ANOVA. *Done only at regional sites.
postvoid residual urine by transabdominal ultrasound (Blad- derscan, Seattle, Wash), measurement of prostate-specific antigen (PSA) (Abbott IMx monoclonal-polyclonal assay), and measurement of terazosin blood levels.
During each of the seven subsequent visits, minimal pro- cedures were protocol mandated with patients at all sites un- dergoing assessment by AUA-SS, AUA-BS, BII, QOL, vital signs, and questioning about adverse events. Only at regional sites were flow rate recordings and postvoid residual urine measurements performed, and patients also underwent serum PSA testing at baseline and at weeks 8, 26, 39, and 52.
Patients were randomized to terazosin or placebo treatment in blocks of four at each site if they met all entry criteria. Those treated with terazosin received 1 mg daily for 3 days, followed by 2 mg terazosin daily for the next 25 days. There- after the dose was titrated to 5 or 10 mg terazosin daily based on the patient’s therapeutic response defined as a minimum reduction in the AUA-SS by 35% or greater from the baseline AUA-SS at visit 2. Patients who did not meet the 35% im- provement criterion at the highest dose level were allowed to remain in the study at the discretion of the investigator. Down- titration was allowable in case of intolerance for any reason.
A monthly telephone survey to collect health care utiliza- tion data was administered to patients by Mathematics Pol- icy Research (Princeton, NJ).
STATISTICAL METHODS All hypothesis testing followed the a priori analysis plan es-
tablished at the initiation of the protocol and was by treatment assignment (intent-to-treat). The efficacy endpoints were time to treatment failure for all randomized patients, and the symp- tom and uroflow variables for the intent-to-treat dataset, which was comprised of those patients with a baseline and at least one postrandomization visit. Time to treatment failure (dis- continuation of treatment due to an immediate need for surgery or because of persistent or worsening BPH symptoms) was an- alyzed by computing Kaplan-Meier survival estimates, and the survival curves were compared with the log-rank test.
Changes in symptom scores and flow rates were analyzed with a two-way repeated measures analysis of variance with interaction. The factors used in the model were treatment group and region. Missing data from the study visits were han- dled with the carry-forward technique. Adverse event rates were evaluated with Fisher’s exact test comparison between
uRoLoGYa 47 (2), 1996
treatment groups.The study was designed to provide statisti- cal power exceeding 80% for detecting prespecified differences in failure rates with the type I error controlled to be 0.05.
RESULTS Altogether, 2469 patients were screened in both
regional (357) and satellite (2113) sites (Fig. 1B). The 2084, who fulfilled the eligibility criteria at the baseline (second) visit, were randomized to either terazosin (1053) or placebo (1031) treat- ment. In the placebo group, 560 (54%) completed the study versus 657 (62%) in the terazosin group (P ~0.001) (Fig. 1B).
Demographic and baseline data at randomiza- tion of the 2084 patients who participated in the trial categorized by treatment are shown in Table I. Effective randomization was achieved in terms of age, weight, blood pressure, the health out- comes measures, flow rate variables, PSA, and co- morbidities, particularly cardiovascular diseases.
Overall, 93% of the patients were Caucasian, 4% were African American, 2% Hispanic, and 1% of other ethnic origin. The five most com- mon comorbidities noted during the entry ex- amination were arthritis (placebo, 32.1%; tera- zosin, 35.9%; P = 0.071), hypertension (placebo, 31.1%; terazosin 30.7% P = O.SS>, hearing loss (placebo, 28.8%; terazosin, 27%; P = 0.35), visual disturbances (placebo, 27.8%; terazosin, 26.9%; P = 0.62), and impotence (placebo, 24.3%; tera- zosin, 28.2%; P = 0.047).
There were only minor differences between the 295 patients enrolled in the regional sites and the 1789 patients enrolled in the satellite sites. The mean age was 64.4 versus 66.0 (P <O.OOl) years, respectively. The ethnic distribution was almost identical in these two subgroups. The AUA-SS
161

TABLE II. Analyses of changes in health outcomes and biologic measures from baseline to final visit
Group No. Baseline
Mean
Within Group Change From Baseline
Mean [Cl]
Between Treatment Croups Comparison
Mean [Cl] P Value
AUA-SS Placebo 973* 20.1 -3.7 [-4.1, -3.21 -3.9 I-4.5, -3.31 < 0.001 Terazosin 976* 20.1 -7.6 [-8.0, -7. l]
AUA-BS
Placebo 971* 15.7 -3.1 I-3.5, -2.71 Terazosin 972* 15.9 -6.3 [-6.7, -5.91 -3.2 [-3.7, -2.71 < 0.001
BII Placebo 927* 5.8 -1.1 [-1.3,-1.01 -1.2 < 0.00 1 Terazosin 934* 6.0 -2.4 [-2.5, -2.21 [-1.5, -0.91
QOL Placebo 937* 3.8 -0.6 I-0.7, -0.51 Terazosin 943* 3.9 -1.3 [-1.4,-1.21 -0.7 I-0.8, -0.51 < 0.00 1
Peak flow rate
Placebo 140+ 9.6 0.8 [-0.2, 1.71 Terazosin 137+ 9.6 2.2 11.3, 3.11 1.4 [O. 2.71 1, 0.03
Mean flow rate Placebo 140+ 5.1 0.2 [-0.4, 0.71 137+ 0.01 Terazosin 5.1 1.2 [0.6, 1.71 1 .o [0.2, 1.71
KEY: CI = 95% confidence interval. For other abbreviations, see Table I. *intent-to-treat patients with a baseline and at least one additional visit. ‘Regional patients with a baseline and at least one additional visit (295 total patients randomized at regional sites: terazosin equals 147; placebo equals 148).
was 20.1 * 0.31 in the regional sites and 20.2 * 0.13 in the satellite sites (P = 0.73); and the AUA- BS was 15.4 + 0.29 in the regional sites and 15.9 f 0.12 in the satellite sites (P = 0.12).
The improvements in health and biologic out- come measures from baseline to final visit (mean changes and 95% confidence intervals), displayed in Table II, demonstrate the response of BPH pa- tients to alpha,-antagonist therapy The AUA-SS decreased (improved) from a baseline score of 20.1 f 0.17 (placebo and terazosin) by -3.7 + 0.22 (placebo) and by-7.6 f 0.21 (terazosin) (P <O.OOl) at the last visit with a statistically significant im- provement for terazosin-treated patients over placebo-treated patients at all follow-up visits (Table 11). Comparable improvements in the AUA- BS, BII, and QOL were observed for terazosin pa- tients over that of placebo patients (Table II). The time course of the improvements in AUA-SS, AUA- BS, BII, and QOL for the placebo- and terazosin- treated patients is shown in Figure 2A-D.
We present the percentage improvement as mea- sured by the various instruments in two different ways, namely, as a percentage of baseline and as a total percentage of scale range, a method first uti- lized in the Agency for Health Care Policy and Re- search (AHCPR) BPH Guidelines to standardize the comparison of BPH interventions.14 The terazosin- treated patients exhibited a percentage improve- ment, calculated by either method, twofold greater than that of the placebo-treated patients as mea-
sured by all indices (Table III). Improvements in terms of the health outcomes measures were also analyzed between the regional and the satellite pa- tients, and no significant differences were identified for any of the indices.
A categorical display of absolute and percentage improvement in the AUA-SS stratified by baseline scores into six strata from 13 to 35 points is shown in Table IV This stratification shows that a signif- icant improvement in AUA-SS can be demon- strated with terazosin for patients with moderate or severe baseline symptoms, even if their pre- senting symptoms are in the highest stratum (32-35 points). The absolute improvement in AUA-SS was about four points greater for tera- zosin over placebo-treated patients in all six base- line strata groups (Table IV).
A clinically significant improvement in lower urinary tract symptoms was prospectively defined as a 35% or better improvement in the AUA-SS from baseline. At the last visit, 55% of patients re- ceiving terazosin had achieved at least a 35% level of improvement versus 28% of patients receiving placebo (Fig. 3). Patients with less than a 35% im- provement in AUA-SS were allowed to remain in the study at the discretion of the investigator.
Uroflowmetry was only performed on patients randomized at regional sites. Data are available on 137 patients treated with terazosin and 140 pa- tients treated with placebo. The average peak urinary flow rate improved from a baseline of
162 uRoLcGYm 47 (21, 1996
Recommended DosIng Schedule (mg) Recommended DosIng Schedule (mg)
1.2 z-6 5.10 5.10 * c
Recomnwnded Chlng Schedule (m9)
5-10
Placaba (” I971) (man basalins z 15.7)
Terarosln (n s 972) (mom baseline z 15.9)
*
I
Weeks
Terazosin ,” = 943) (mean blrellne = 3.9,
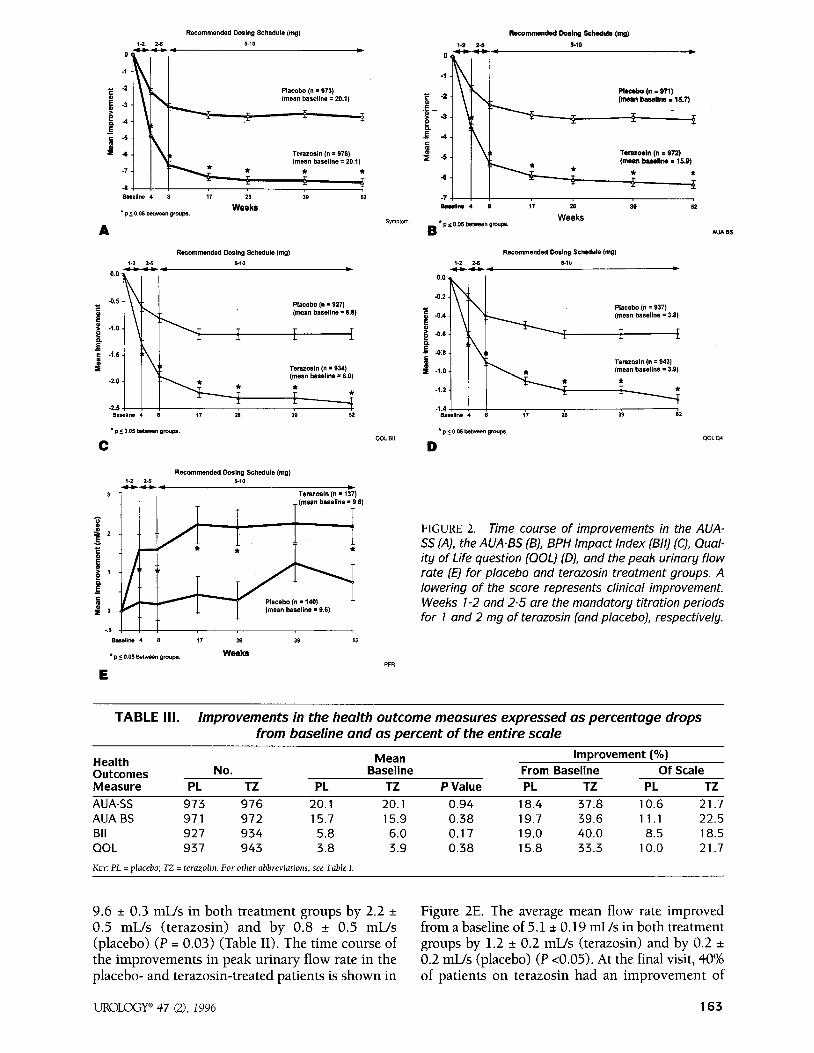
FIGURE 2. Time course of improvements in the AUA- SS (A), the AUA-BS (B), BPH Impact Index (B/l) (C), Qual- ity of Life question [QOL) (D), and the peak urinary flow rate (E) for placebo and terazosin treatment groups. A lowering of the score represents clinical improvement. Weeks l-2 and 2-5 are the mandatory titration periods for 1 and 2 mg of terazosin [and placebo), respectively.
TABLE III. Improvements in the health outcome measures expressed as percentage drops from baseline and as percent of the entire scale
Health Outcomes Measure
AUA-SS AUA-BS Bll QOL
Mean Improvement (%) No. Baseline From Baseline Of Scale
PL TZ PL TZ P Value PL TZ PL TZ 973 976 20.1 20.1 0.94 18.4 37.8 10.6 21.7 971 972 15.7 15.9 0.38 19.7 39.6 11.1 22.5 927 934 5.8 6.0 0.17 19.0 40.0 8.5 18.5 937 943 3.8 3.9 0.38 15.8 33.3 10.0 21.7
KEY: PL = olacebo: TZ = termolin. For other abbreviations. see Table I
9.6 f 0.3 mUs in both treatment groups by 2.2 + Figure 2E. The average mean flow rate improved 0.5 mL/s (terazosin) and by 0.8 f 0.5 mUs from a baseline of 5.1 f 0.19 mUs in both treatment (placebo) (P = 0.03) (Table II). The time course of groups by 1.2 + 0.2 mUs (terazosin) and by 0.2 * the improvements in peak urinary flow rate in the 0.2 mUs (placebo) (P ~0.05). At the final visit, 40% placebo- and terazosin-treated patients is shown in of patients on terazosin had an improvement of
UROLCGY@ 47 (2), 1996 163
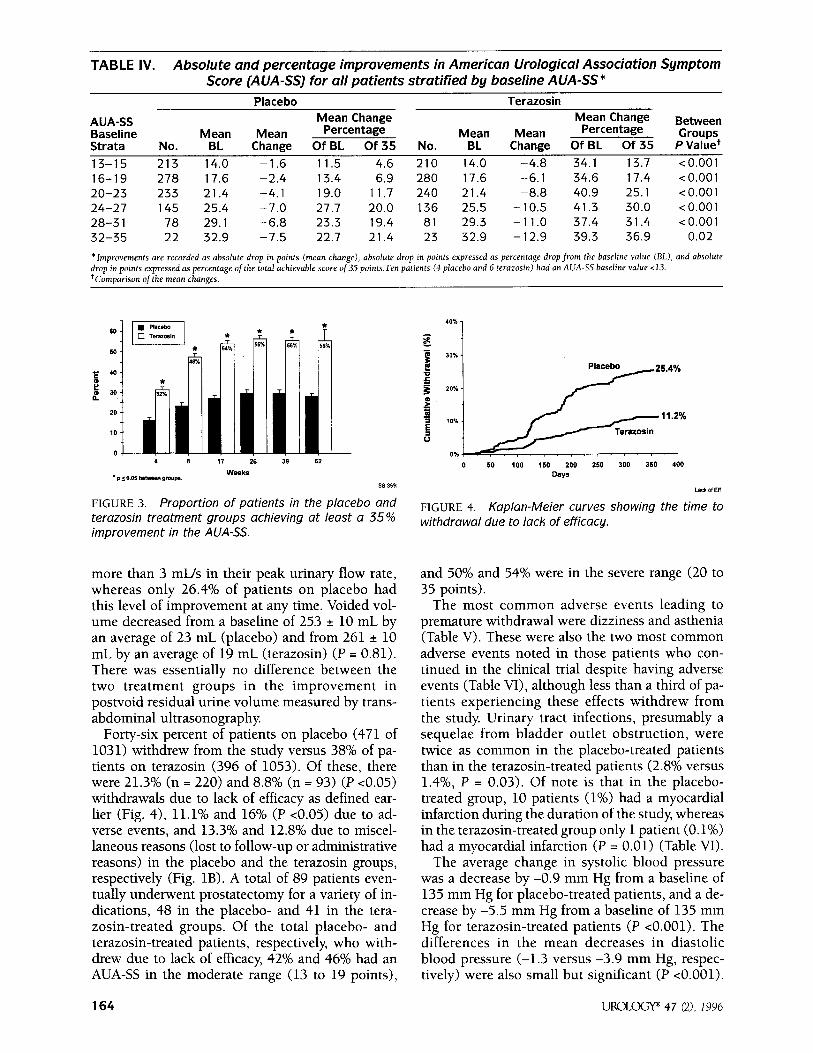
TABLE IV. Absolute and percentage improvements in American Urological Association Symptom Score (AUA-SS) for all patients stratified by baseline AlJA-SS*
Placebo Terazosin
AUA-SS Mean Change Mean Change Percentage Percentage
Between Baseline Mean Mean Mean Mean Groups Strata No. BL Change Of BL Of 35 No. BL Change Of BL Of 35 P Value+ 13-15 213 14.0 -1.6 11.5 4.6 210 14.0 -4.8 34.1 13.7 < 0.001 16-19 278 17.6 -2.4 13.4 6.9 280 17.6 -6.1 34.6 17.4 < 0.001 20-23 233 21.4 -4.1 19.0 11.7 240 21.4 -8.8 40.9 25.1 <O.OOl 24-27 145 25.4 -7.0 27.7 20.0 136 25.5 -10.5 41.3 30.0 <O.OOl 28-31 78 29.1 -6.8 23.3 19.4 81 29.3 -11.0 37.4 31.4 < 0.001 32-35 22 32.9 -7.5 22.7 21.4 23 32.9 -12.9 39.3 36.9 0.02
*Improvements are recorded as absolute drop in points (mean change), absolute drop in points expressed as percentage drop from the baseline value IBL), and absolute drop in points expressed as percentage ofthe total achievable score of35 points.Ten patients (4 placebo and 6 terazosin) had an AUA-SS baseline value ~13. tCommrison of the mean chanaes.
ss 35%
FIGURE 3. Proportion of patients in the placebo and terazosin treatment groups achieving at least a 35% improvement in the AUA-SS.
more than 3 mUs in their peak urinary flow rate, whereas only 26.4% of patients on placebo had this level of improvement at any time. Voided vol- ume decreased from a baseline of 253 f 10 mL by an average of 23 mL (placebo) and from 261 f 10 mL by an average of 19 mL (terazosin) (P = 0.81). There was essentially no difference between the two treatment groups in the improvement in postvoid residual urine volume measured by trans- abdominal ultrasonography.
Forty-six percent of patients on placebo (471 of 1031) withdrew from the study versus 38% of pa- tients on terazosin (396 of 1053). Of these, there were 21.3% (n = 220) and 8.8% (n = 93) (P ~0.05) withdrawals due to lack of efficacy as defined ear- lier (Fig. 4), 11.1% and 16% (P ~0.05) due to ad- verse events, and 13.3% and 12.8% due to miscel- laneous reasons (lost to follow-up or administrative reasons) in the placebo and the terazosin groups, respectively (Fig. 1B). A total of 89 patients even- tually underwent prostatectomy for a variety of in- dications, 48 in the placebo- and 41 in the tera- zosin-treated groups. Of the total placebo- and terazosin-treated patients, respectively, who with- drew due to lack of efficacy, 42% and 46% had an AUA-SS in the moderate range (13 to 19 points),
0 50 100 150 200 250 300 350 400 Days
I.& Of 5”
FIGURE 4. Kaplan-Meier curves showing the time to withdrawal due to lack of efficacy.
and 50% and 54% were in the severe range (20 to 35 points).
The most common adverse events leading to premature withdrawal were dizziness and asthenia (Table V). These were also the two most common adverse events noted in those patients who con- tinued in the clinical trial despite having adverse events (Table VI), although less than a third of pa- tients experiencing these effects withdrew from the study Urinary tract infections, presumably a sequelae from bladder outlet obstruction, were twice as common in the placebo-treated patients than in the terazosin-treated patients (2.8% versus 1.4%, P = 0.03). Of note is that in the placebo- treated group, 10 patients (1%) had a myocardial infarction during the duration of the study, whereas in the terazosin-treated group only 1 patient (0.1%) had a myocardial infarction (P = 0.01) (Table VI).
The average change in systolic blood pressure was a decrease by -0.9 mm Hg from a baseline of 135 mm Hg for placebo-treated patients, and a de- crease by -5.5 mm Hg from a baseline of 135 mm Hg for terazosin-treated patients (P ~0.001). The differences in the mean decreases in diastolic blood pressure (-1.3 versus -3.9 mm Hg, respec- tively) were also small but significant (P ~0.001).
164 UROLOGY@ 47 (2), 1996

TABLE V. Statistically signifkan t treatment emergent adverse events leading to premature withdrawal from Hytrin Community Assessment Trial
Dizziness Asthenia Peripheral edema Tachycardia Weight gain Myocardial infarction
Placebo (n = 1031) No. (%) 16 (1.6) 12 (1.2)
1 (0.1) 0 (0.0) 0 (0.0) 7 (0.7)
Terazosin (n = 1053) No. (%)
34 (3.2) 30 (2.8)
8 (0.8) 6 (0.6) 6 [0.6) 1 (0.1)
P Value 0.01 0.01 0.04 0.03 0.03 0.04
TABLE VI. Statistically significant treatment emergent adverse events
Dizziness Asthenia Peripheral edema Chest pain * Hernia+ Postural dizziness Nausea Dyspnea Abnormal ejaculation Hypotension Malaise Tachycardia Weight gain Epistaxis Urticaria Urinary tract infection Myocardial infarction
*Nonspecific. ‘Includes ventral, inmind, hiatal hernia.
Placebo (n = 1031) Terazosin (n = 1053) No. (%) No. (%) 60 (5.8) 123 (1 1.7) 30 (2.9) 79 (7.5)
9 (0.9) 42 (4.0) 18 (1.7) 41 (3.9) 5 (0.5) 23 (2.2) 5 (0.5) 20 (1.9) 9 (0.9) 22 (2.1) 6 (0.6) 20 (1.9) 2 (0.2) 15 (1.4) 4 (0.4) 14 (1.3) 3 (0.3 13 (1.2) 0 (0.0) 10 (0.9) 1 (0.1) 9 (0.9) 0 (0.0) 7 (0.7) 0 (0.0) 6 (0.6)
29 [2.8) 15 (1.4) 10 (1.0) 1 (0.1)
P Value
10.00 1 10.00 1 10.00 1
0.01 SO.00 1
0.01 0.03 0.01 0.01 0.03 0.02 0.01 0.02 0.02 0.03 0.03 0.01
COMMENTS Medical and surgical interventions in BPH are di-
rected at relieving the symptoms of prostatism and their bothersomeness,20-22 which degrade the pa- tients’ QOL. 1,23 Due to various shortcomings in the assessment of the efficacy of BPH interventions, the vigorous placebo response observed in BPH inter- vention trials,14 and the poorly described conse- quences of failing therapy the AHCPR14 and a World Health Organization sponsored International Con- sultation on BPH24 have independently published guidelines for the assessment of BPH interventions.
In the spirit of these guidelines, HYCAT is the first randomized, double-blind, placebo-controlled study conducted in a largely community-based population to assess prospectively a pharmacologic treatment for the symptoms of BPH and the outcomes that de- termine the interventions clinical effectiveness, as described here, as well as its cost-effectiveness.19
The rather strict entry criterion of an AUA-SS of 13 or more points and an AUA-BS of 8 or more points assured the enrollment of patients with moderate to severe symptoms of BPH, who at the
same time were also at least moderately bothered by their symptoms, the most appropriate candi- dates for the pharmacologic therapy of BPH.14
As a result of this design, the symptom severity of the primarily community-based patient popula- tion was greater at baseline than in other BPH tri- a1s.10,12,25 However, the symptomatic response of the patients to terazosin therapy over 12 months, when expressed as an absolute change or percent improvement of total scale range,14 was equivalent or superior to that of alphai-blocker trials of shorter duration,10,12,26 and superior to that observed with 1 year of Sa-reductase inhibitor treatment.25 The percent change from baseline was 37.8% for the AUA-SS, 39.6% for the AUA-BS, 40% for the BII, and 33.3% for the QOL scores. The drop expressed as percentage drop of the individual scales was 21.7%, 22.5%, 18.5%, and 21.7%, respectively (Table III). In a 12-month Sa-reductase inhibitor trial 25 the symptom score fell by 2.7 points from 10.2 to 7.5 points (26.5% of baseline, or 7.5% drop of the 36 point scale). In a 26-week alphai-blocker trial with alfuzosin, the symptom score fell by 4.0
uRoLoGYa 47 (2), 1996 165

points from 9.5 to 5.5 points (42% of baseline, or 19% of the 21 point scale).12 In a 12-week tera- zosin trial, the score fell by 4.6 points from 10.1 to 5.5 points (45.5%, or 17% of the 27 point scale).‘O
Stratification of patients in this trial by baseline symptom severity (Table IV) demonstrated that treatment with terazosin provides meaningful re- lief of symptoms superior to the placebo effect for patients with moderate and even severe symptoms, the cohort for which surgical treatment is usually recommended. The mean absolute change in AUA- SS for all strata was about four points greater in the terazosin- versus the placebo-treated patients. When considering this margin of benefit of tera- zosin over placebo across all symptom severity strata, it should be noted that the minimal im- provement in symptom score noticeable to pa- tients is about three points on the AUA-SS scale.27
The improvement noted in regard to the peak urinary flow rate (Table II and Fig. 2E) is compa- rable to the effect seen in a 12-month finasteride tria125 and prior trials with alpha-blockers of shorter duration.1°,12 A mean improvement from 12.1 to 13.5 mUs was noted in a 26-week trial with alfuzosin,12 and in a 12-week trial with ter- azosin mean improvements from 9.3 to 10.9 mL/s (5-mg dose) and from 8.8 to 12.2 mIJs (lo-mg dose) were observed. lo However, changes in flow rate measures do not correlate with symptomatic relief,2s and at present, it is unknown which level of improvement in peak urinary flow rate repre- sents a change perceived by the patient as such.
A key factor in the success of a pharmacologic intervention for BPH is its long-term effectiveness as determined by patients’ continued use of the therapy l4 The nearly twofold greater withdrawal rate of placebo-treated patients due to treatment failure at 1 year (Fig. 4) compared with those treated with terazosin is consistent with the ther- apeutic response to the study drug (Fig. ZA-D). Although the studied population was primarily community-based, the 4.4% greater withdrawal rate of terazosin-treated patients due to adverse events compared with placebo at 1 year was less than observed in trials of shorter duration26 and more selective eligibility criteria.
In regard to adverse events, the findings are similar to those previously reported with either alfuzosin,12 doxazosin,13,29 or terazosin.7,10,30 In contrast to these reports, the incidence of several common adverse events (headaches, syncope) was not found to be statistically significantly different from placebo. One hundred fourteen (11.1%) of patients on placebo and 168 (16%) of patients on terazosin withdrew from the trial because of ad- verse events, the most common being dizziness and asthenia. These two adverse events were also the two most common adverse events overall in
the terazosin-treated patients with an incidence of 11.7% and 7.5%, respectively Urinary tract infec- tions are believed to be a sequelae of bladder out- let obstruction, and indeed recurrent infection represents an indication for prostate surgery.14 They occurred twice as commonly in the placebo- treated than in the terazosin-treated patients (2.8% versus 1.4%; P = 0.03). Alpha blockers are postu- lated to convey a cardioprotective effect via sev- eral mechanisms31 In this context, it is an in- triguing finding that in the placebo group 10 patients (1%) had a myocardial infarction versus only 1 (0.1%) (P = 0.01) in the terazosin-treated group. In this l-year study, a total of 89 patients eventually underwent prostatectomy for a variety of indications, 48 in the placebo- and 41 in the terazosin-treated group.19
The present study sets a new direction for clini- cal BPH research. The use of community-based sites for patient enrollment proved to be feasible from a viewpoint of logistics as well as data consistency Patients enrolled at satellite sites (private urology offices) were at baseline similar in all respects to those patients enrolled at the regional (academic centers) sites, and responded to a similar extent in regard to improvements in outcome measures.
REFERENCES 1. Roberts RO, Rhodes T, Panser LA, Girman CJ, Chute
CG, Oesterling JE, Lieber MM, and Jacobsen SJ: Natural his- tory of prostatism: worry and embarrassment from urinary symptoms and health care-seeking behavior. Urology 43: 621-628, 1994.
2. Hohgrewe HL, Mebust WK, Dowd JB, Cockett AT, Pe- ters PC, and Proctor C: Transurethral prostatectomy: prac- tice aspects of the dominant operation in American urology. J Urol 141: 248-253, 1989.
3. Lepor H: Nonoperative management of benign pros- tatic hyperplasia. J Urol 141: 1283-1289, 1989.
4. Lepor H: Alpha adrenergic antagonists for the treat- ment of symptomatic BPH. Int J Clin Pharmacol27: 151-155, 1989.
5. Gup DI, Shapiro E, Baumann M, and Lepor H: Con- tractile properties of human prostate adenomas and the de- velopment of infravesical obstruction. Prostate 15: 105-114, 1989.
6. Caine M, Pfau A, and Perlberg S: The use of alpha- adrenergic blockers in benign prostatic obstruction. Br J Urol 48: 255-263, 1976.
7. Lepor H, Knapp-Maloney G, and Wozniak-Petrofsky J: The safety and efficacy of terazosin for the treatment of be- nign prostatic hyperplasia. Int J Clin Pharmacol27: 392-397, 1989.
8. Lepor H, and Laddu A: Terazosin in the treatment of benign prostatic hyperplasia: the United States experience. Br J Urol 70 (suppl 1): 2-9, 1992.
9. Lepor H, Meretyk S, and Knapp-Maloney G: The safety, efficacy and compliance of terazosin therapy for benign pros- tatic hyperplasia. J Urol 147: 1554-1557, 1992.
10. Lepor H, Auerbach S, Puras-Baez A, Narayan P, Soloway M, Lowe F, Moon T, Leifer G, and Madsen P: A ran- domized, placebo-controlled multicenter study of the effi- cacy and safety of terazosin in the treatment of benign pros- tatic hyperplasia. J Urol 148: 1467-1474, 1992.
166 UROLOGYm 47 (21, 1996
11. Christensen MM, Bendix Holme J, Rasmussen PC, Ja- cobsen F, Nielsen J, Norgaard JP, Olesen S, Noer I, Wolf H, and Husted SE: Doxazosin treatment in patients with pros- tatic obstruction. A double-blind placebo-controlled study. Stand J Urol Nephrol 27: 39-44, 1993.
12. Jardin A, Bensadoun H, Delauche-Cavallier MC, and Attali P: Alfuzosin for treatment of benign prostatic hyper- trophy. The BPH-ALF Group. Lancet 337: 1457-1461,1991.
13. Chapple CR, Carter P, Christmas TJ, Kirby RS, Bryan J, Milroy EJ, and Abrams P: A three month double-blind study of doxazosin as treatment for benign prostatic bladder outlet obstruction. Br J Urol 74: 50-56, 1994.
14. McConnell JD, Barry MJ, and Bruskewitz RC: Benign Prostatic Hyperplasia: Diagnosis and Treatment. Agency for Health Care Policy and Research. Clinical Practice Guideline 8: l-17, 1994.
15. Lepor H: Long-term efficacy and safety of terazosin in patients with benign prostatic hyperplasia. Terazosin Re- search Group. Urology 45: 406-413, 1995.
16. Barry MJ, Fowler FJ, O’Leary MP, Bruskewitz RC, Holtgrewe HL, Mebust WK, and Cockett ATL: The American Urological Association’s symptom index for benign prostatic hyperplasia. J Urol 148: 1549-1557, 1992.
17. O’Leary MP, Barry MJ, and Fowler FJ Jr: Hard mea- sures of subjective outcomes: validating symptom indexes in urology. J Urol 148: 1546-1548, 1992.
18. Barry MJ, Fowler FJ, O’Leary MP, Bruskewitz RC, Holtgrewe HL, and Mebust WK: Measuring disease-specific health status in men with benign prostatic hyperplasia. Med Care 33: AS145-155, 1995.
19. Hillman AL, Schwartz JS, Willian MK, Peskin E, Roehrborn CG, Oesterling JE, Mason MF, Maurath C, Dev- erka PA, and Padley RJ: The cost-effectiveness of terazosin and placebo in the treatment of moderate-to-severe benign prostatic hyperplasia. Urology 47: 169-178, 1996.
20. Fowler FJ Jr, Wennberg JE, Timothy RP, Barry MJ, Mulley AG Jr, and Hanley D: Symptom status and quality of life following prostatectomy. JAMA 259: 3018-3022, 1988.
21. Barry MJ, Mulley AG Jr, Fowler FJ, and Wennberg JW: Watchful waiting vs immediate transurethral resection for symptomatic prostatism. The importance of patients’ pref- erences. JAMA 259: 3010-3017, 1988.
22. Barry MJ: Medical outcomes research and benign pros- tatic hyperplasia. Prostate 3 (suppl): 61-74, 1990.
23. Girman CJ, Epstein RS, Jacobsen SJ. Guess HA, Panser LA, Oesterling JE, and Lieber MM: Natural history of prosta- tism: impact of urinary symptoms on quality of life in 2115 ran- domly selected community men. Urology 44: 825-831, 1994.
24. Cockett ATK, Khoury S, Aso Y, Chatelain C, Denis L, Griffiths K, and Murphy G: The 2nd International Consulta- tion on Benign Prostatic Hyperplasia (BPH). Proceedings, Jersey, Channel Islands, Scientific Communication lnterna- tional Ltd, 1993.
25. Gormley GJ, Stoner E, Bruskewitz RC, lmperato- McGinley J, Walsh PC, McConnell JD, Andriole GL, Geller J, Bracken BR, Tenover JS, et al: The effect of finasteride in men with benign prostatic hyperplasia. The Finasteride Study Group. N Engl J Med 327: 1185-1191, 1992.
26. Brawer MK, Adams G, and Epstein H: Terazosin in the treatment of benign prostatic hyperplasia. Terazosin Benign Prostatic Hyperplasia Study Group. Arch Fam Med 2: 929-935, 1993.
27. Barry MJ, Williford WO, Chang YC, Machi M, Jones KM, Walker-Corkery W, and Lepor H: BPH-specific health status measures in clinical research: how much change in AUA Symptom Index and the BPH Impact Index is percepti- ble to patients? J Urol 154: 1770-1774, 1995.
28. Barry MJ, Cockett AT, Holtgrewe HL, McConnell JD, Sihelnik SA, and Winfield HN: Relationship of symptoms of
prostatism to commonly used physiological and anatomical measures of the severity of benign prostatic hyperplasia. J Ural 150: 351-358, 1993.
29. Christensen MM, Bendix Holme J, Rasmussen PC, Ja- cobsen F, Nielsen J, Norgaard JP, Olesen S, Noer I, Wolf H, and Husted SE: Doxazosin treatment in patients with pros- tatic obstruction. A double-blind placebo-controlled study. Stand J Urol Nephro127: 39-44, 1993.
30. Lepor H, Henry D, and Laddu AR: The efficacy and safety of terazosin for the treatment of symptomatic BPH. Prostate 18: 345-355, 1991.
31. Khoury AF, and Kaplan NM: Alpha-blocker therapy of hypertension. An unfulfilled promise. JAMA 266: 394-398, 1991.
APPENDIX The following investigators randomized patients in the
study at regional sites: Drs. Stephen Auerbach (Newport Beach, CA); Michael Brawer (Seattle, WA); Culley Carson (Durham, NC); Steven Kapian (New York, NY); L. Keith Lloyd (Birmingham, AL); Kevin Loughlin (Boston, MA); Franklin Lowe (New York, NY); John Lynch (Washington, DC); Samuel Manfrey (Philadelphia, PA); Claus Roehrborn and John McConnell (Dallas, TX); Winston Mebust (Kansas City, KS); Douglas Milam (Nashville, TN); Joseph Oesterling (Rochester, MN); Mark Soloway (Miami, FL); William Somers (Columbus, OH).
The following investigators randomized patients in the study at community sites: Drs. Brett B. Abernathy (Wheat Ridge, CO); George Wilburn Adams, Jr. (Birmingham, AL); J. Robert Adams (Memphis, TN); Kenneth W. Aldridge (Tuscaloosa, AL); Vincent A. Andaloro, Jr. (Norwood, MA); Rodney A. Appell (Gretna, LA); John A. Arcadi (Whittier, CA); W. Landon Banfield (Washington, DC); John Bardole (Des Moines, IA); John R. Beahrs (St. Paul, MN); James K. Bennett (Atlanta, GA); Yitzhak Berger (West Orange, NJ); Robert J. Biester (Haddon Heights, NJ); Michael Blum (Win- netka, IL); Robert D. Blute, Jr. (Worcester, MA); Barry H. Bodie (New Orleans, LA); Ted B. Boone (Dallas, TX); Richard J. Boxer (Milwaukee, WI); William Brannan (Covington, LA); William C. M. Brown (Greenwich, CT); Hernan M. Car- rion (Miami, FL); Stacy J. Childs (Alabaster, AL); Douglas 0. Chinn (Arcadia, CA); Arnold C. Cinman (Beverly Hills, CA); William R. Clark (Anchorage, AK); William Cohen (Miami, FL); Jerry L. Coles (Anchorage, AK); Raoul S. Conception (Nashville, TN); Lynn W. Conrad (Memphis, TN); Darrell R. Cornelius (Mount Vernon, WA); John W. Davis (Fullerton, CA); Noel P. Defelippo (Lynn, MA); Michael Dourmashkin (Paramus, NJ); Leonidas W. Dowlen, Jr. (Coral Gables, FL); Eugene Dula (Van Nuys, CA); Sidney W. Ecker (Rockville, MD); Charles W. E&stein (Nashville, TN); Rainer M. E. En- gel (Baltimore, MD); Cesar J. Ercole (St. Paul, MN); Patrick 0. Faricy (Colorado Springs, CO); Nathan H. Fischman (Jef- ferson, LA); Mark D. Flora (Nashville, TN); Lionel S. Foster (San Jose, CA); Emanuel Friedman (Natick, MA); Pat F. Ful- gham (Dallas, TX); Norman R. Galen (New Orleans, LA); John E. Garnett (Chicago, IL); Phillip C. Ginsberg (Philadel- phia, PA); Marc C. Gittelman (North Miami, FL); Robert E. Glesne (Alexandria, MN); L. Michael Goldstein (Dallas, TX); Robert S. Grajewski (Statesville, NC); Gedas M. Grinis (Hutchinson, KS); Adel B. Guirguis (Winchester, VA); Leon C. Hamrick, Jr. (Fairfield, AL); Richard G. Harris (Melrose Park, IL); Richard K. Heppe (Englewood, CO); H. Pat Hez- mall (Arlington, TX); Gerald P. Hoke (New York, NY); Jef- frey S. lsen (Worcester, MA); Albert P. lsenhour, Jr. (Nashville, TN); David K. Johnson (Lansing, Ml); Jeffrey R. Johnson (Springfield, MO); John H. Jurige, Jr. (Louisville, KY); Richard D. Kane (Raleigh, NC); Marshall M. Kaplan (Fort Lauderdale, FL); Lawrence I. Karsh (Denver, CO);
UROLOGY~ 47 (21, 1996 167

Nabet Kasabian (New York, NY); Stuart E. Katz (Falls Church, VA); David G. Kaufman (Brooklyn, NY); Ansar Khan (Fremont, NE); Dieter Kirchheim (Olympia, WA); Hugh Lamensdorf (Fort Worth, TX); John Landsberger (Long Beach, CA); Albert G. LeRoy, Jr. (Rock Hill, SC); Gary Leifer (Kansas City, MO); Charles E. Libby (Great Neck, NJ); Joseph N. Macaluso (Gretna, LA); Luis F. Maggiolo (Coral Gables, FL); Conrad C. Maitland (Highland Park, MI); Terrence R. Malloy (Philadelphia, PA); John Mandler (Abington Hospi- tal, Philadelphia, PA); Hal K. Mardis (Omaha, NE); Sheldon H. F. Marks (Tucson, AZ); Donald L. McKay, Jr. (Dallas, TX); Robert H. McLaren (Neenah, WI); James J. Meyer (Ed- ina, MN); Richard Milsten (Voorhees, NJ); Thomas E. Moody (Bessemer, AL); Joseph B. Murphy (Towson, MD); Alex M. Nading (Birmingham, AL); Steven D. Nash (Kansas City, MO); Carl T. Newman (Denver, CO); Ian Nisonson (Miami, FL); James R. Noble (Shreveport, LA); Frank M. O’Kelly (Westminster, CA); Kimball R. Orton (Tucson, AZ); Richard S. Pelman (Bellevue, WA); Jill M. Peters-Gee (Hartford, CT); W. Henry Purvis (Sanford, NC); Leslie Mark Rainwater (St. Paul, MN); David Reed (Seattle, WA); Gary W. Rheinschild (Anaheim, CA); Stephen C. Rochman (Fayetteville, NC); Timothy M. Roddy (Edmonds, WA); James G. Saalfield (Ir-
ving, TX); Eric J. Sacknoff (Cambridge, MA); Thomas C. Sansone (Bryn Mawr, PA); George Schuster (Joliet, IL); Bipin N. Shah (Columbus, OH); Robert S. Shahon (Phoenix, AZ); Kerry L. Short (Louisville, KY); John D. Siegel (Millburn, NJ); Larry E. Siref (Omaha, NE); Jeffrey A. Snyder (Denver, CO); Gus Spector (Phoenixville, PA); Key H. Stage (Dallas, TX); Peter J. Standard (Fort Collins, CO); Christopher P. Steidle (Fort Wayne, IN); Karl Sturge (Miami, FL); Stephen Jay Sweitzer (Louisville, KY); Paul E. Tocci (Fort Lauderdale, FL); Eugene R. Todd (Dallas, TX); Jeffrey Troxell (Portsmouth, NH); Albert J. Tully, Jr. (Birmingham, AL); John P. Tuttle, Jr. (Lexington, KY); Steven M. Wahle (Cedar Rapids, IA); Michael C. Walter (Fort Worth, TX); Don H. Wasserman (Ranch0 Mirage, CA); Samuel R. Watkins, Jr. (Louisville, KY); Alex J. Weinstein (Santa Barbara, CA); Mark B. Weitzenfeld (North Miami Beach, FL); James C. West, Jr. (Kansas City, MO); Reginald D. Westmacott (Denver, CO); Matthew Wilner (Dallas, TX); Phillip Winslow (Ponca City, OK); Henry A. Wise, II (Columbus, OH); Michael R. Wolff (Burlington, NC); Richard K. Wonderly (Seattle, WA); Abra- ham Woods, III (Sebring, FL); Jay Marshall Young (Laguna Hills, CA); Steven M. Zappala (North Andover, MA); Jeffrey Zipkin (Cincinnati, OH).
168 uRoLoGYa 47 (21, I996




















