
Immunohistochemical Study of a Non-invasive Canine Thymoma: A Case Report
Upload
independentCategory
view
0download
0
www.elsevier.com/locate/humpath
Human Pathology (2014) 45, 437–445
Progress in pathology
The histomorphologic spectrum of spindle cell thymoma☆
Annikka Weissferdt MD, FRCPath⁎, Cesar A. Moran MD
Department of Pathology, MD Anderson Cancer Center, Houston, TX 77030
Received 27 July 2012; revised 25 August 2012; accepted 29 August 2012
o
0h
Keywords:Anterior mediastinum;Thymus;Spindle cell thymoma;Histopathology;Subtypes
Summary Spindle cell thymomas are a subset of thymoma that is characterized by great morphologicvariability. This histologic complexity coupled with the overall rarity of these lesions can easily causediagnostic confusion with other spindle cell neoplasms of the anterior mediastinum. In this review, wesummarize the various morphologic patterns that have been described in the peer-reviewed literature andpresent additional patterns that we have encountered in our practice. Familiarity with the histomorphologicspectrum of spindle cell thymomas is essential to diagnose these tumors correctly and distinguish themfrom other mediastinal spindle cell lesions that require different treatment modalities.© 2014 Elsevier Inc. All rights reserved.
1. Introduction
Thymomas are the most common epithelial tumor of theanterior mediastinum; however, the general incidence ofthese tumors is low [1]. Histologically, these tumors arecomposed of neoplastic thymic epithelial cells and a variablenumber of lymphocytes leading to a myriad of histologicsubtypes depending on the proportion of these elements. Overthe years, several attempts of classifying these tumors havebeen proposed with no universal acceptance of a single one,to date [2–6]. Spindle cell thymomas (World HealthOrganization type A) are a subtype of thymoma that isdifferent from the conventional types of thymoma in severalaspects. Spindle cell thymomas are characterized by fusiformor oval-shaped neoplastic epithelial cells and a lower numberof lymphocytes than those in conventional thymoma.Nevertheless, the lymphocytic component can be more
☆ Conflict of interest statement: The authors declare no conflictf interest.⁎ Corresponding author.E-mail address: [email protected] (A. Weissferdt).
046-8177/$ – see front matter © 2014 Elsevier Inc. All rights reserved.ttp://dx.doi.org/10.1016/j.humpath.2012.08.025
prominent, and what is considered a type AB thymoma inthe current World Health Organization schema is probablybest regarded as a spindle cell thymoma with a more markedlymphoid component. In addition, spindle cell thymomaslack most of the organotypical features seen in conventionalthymomas, namely, a well-developed lobular architecture,prominent fibrous bands, and dilated perivascular spaces.Furthermore, spindle cell thymomas are unique with respectto their histomorphologic variability. These tumors can showa wide morphologic spectrum and can easily cause diagnosticconfusion with other spindle cell neoplasms of the medias-tinum not only on small mediastinoscopic biopsies but alsoon resected tumor material. This review aims to highlight thevarious morphologic patterns displayed by these tumors.Familiarity with these growth patterns is vital to correctlydiagnose these neoplasms as spindle cell thymomas.
2. Clinical features
Spindle cell thymomas account for up to 22% of allthymomas [7]. The age at manifestation ranges from 7 to 83years, with a mean age in the sixth decade [2,8–16]. Males

438 A. Weissferdt, C. A. Moran
and females appear to be affected equally. Similar toconventional thymomas, spindle cell thymomas may beassociated with autoimmune diseases, most commonlymyasthenia gravis. Patients present with chest pain, cough,or dyspnea or may be entirely asymptomatic, and the tumorsare found incidentally on imaging for unrelated problems.
3. Gross features
Grossly, the tumors are encapsulated or invasive massesranging in size from 2.5 to 18 cm [2,8–16]. The cut surfacecan vary from subtype to subtype and show solid or cysticpatterns. The solid elements can be composed of rubberyfirm gray-white or brownish friable tissue with or withoutfocal calcification. Grossly identifiable cystic spaces canrange in size from microscopic to more than 3.5 cm indiameter. Hemorrhage and/or necrosis is not a commonfeature of spindle cell thymomas.
Fig. 1 A, Spindle cell thymoma of diffuse type separated fromsurrounding thymic adipose tissue by a fibrous capsule (hematox-ylin and eosin, ×2). B, Storiform pattern of diffuse spindle cellthymoma. Note the sparse lymphocytic component (hematoxylinand eosin, ×10).
4. Histologic features
4.1. Diffuse spindle cell thymoma
The most commonly encountered pattern of spindle cellthymoma is the diffuse pattern. This pattern is characterizedby spindle or oval-shaped cells with bland nuclei, dispersedchromatin, and inconspicuous nucleoli either arranged insolid sheets without any particular architecture or in astoriform or fascicular pattern [17,18] (Fig. 1A and B). Theremay be mild nuclear pleomorphism, and scattered mitoticfigures may be present. These tumors often have few or nolymphocytes and show neither distinct lobules nor dissectingfibrous bands or prominent perivascular spaces as seen inother types of thymoma [17,18]. In some instances, however,the spindle cells may be accompanied by a more conspicuouslymphocytic component. In practice, those tumors are bestgrouped under spindle cell thymoma because the associationof spindle cell and conventional (lymphocyte-rich) thymo-mas can occur, as recently amply documented [7]. As in alltypes of thymoma, extensive sampling of the tumors isnecessary to detect these mixed-type histologic patterns [7].
4.2. Micronodular thymoma with lympyhoidB-cell hyperplasia
First described by Suster and Moran [8] in 1999, thisthymoma is a peculiar subtype of spindle cell thymomathat consists of multiple small tumor nodules separatedby prominent lymphoid tissue (Fig. 2A). The tumornodules are composed of neoplastic epithelial spindlecells with elongated nuclei and inconspicuous nucleoli. Insome areas, these tumor nodules can coalesce and form
elongated solid structures. Mitotic activity or cytologicatypia are not observed. The stroma separating the tumorislands is composed of a dense proliferation of smalllymphocytes with formation of lymphoid follicles andgerminal centers. Occasional plasma cells may be part ofthis lymphoid component, and scattered small lympho-cytes can also be observed infiltrating the epithelial tumornodules. Although this lymphoid infiltrate was initiallythought to be primarily of B-cell lineage [8], subsequentreports using more modern immunohistochemical anti-bodies have demonstrated a mixed B- and T-cellpopulation [9,10,19,20], including occasional immatureT cells, as commonly seen in the conventional types ofthymoma. Rare clonality studies have shown thelymphoid elements to be of polyclonal nature [10].
4.3. Desmoplastic spindle cell thymoma
Spindle cell thymomas with prominent desmoplasticchanges are characterized by extensive areas of hyalinized
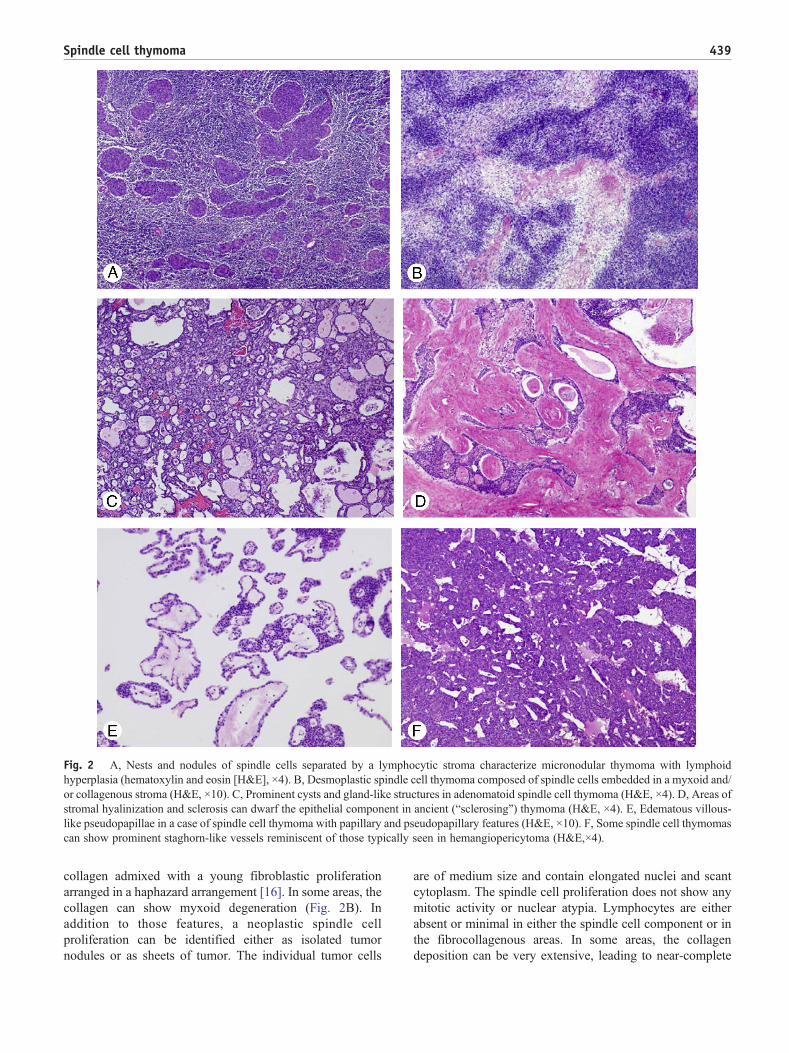
Fig. 2 A, Nests and nodules of spindle cells separated by a lymphocytic stroma characterize micronodular thymoma with lymphoidhyperplasia (hematoxylin and eosin [H&E], ×4). B, Desmoplastic spindle cell thymoma composed of spindle cells embedded in a myxoid and/or collagenous stroma (H&E, ×10). C, Prominent cysts and gland-like structures in adenomatoid spindle cell thymoma (H&E, ×4). D, Areas ofstromal hyalinization and sclerosis can dwarf the epithelial component in ancient (“sclerosing”) thymoma (H&E, ×4). E, Edematous villous-like pseudopapillae in a case of spindle cell thymoma with papillary and pseudopapillary features (H&E, ×10). F, Some spindle cell thymomascan show prominent staghorn-like vessels reminiscent of those typically seen in hemangiopericytoma (H&E,×4).
439Spindle cell thymoma
collagen admixed with a young fibroblastic proliferationarranged in a haphazard arrangement [16]. In some areas, thecollagen can show myxoid degeneration (Fig. 2B). Inaddition to those features, a neoplastic spindle cellproliferation can be identified either as isolated tumornodules or as sheets of tumor. The individual tumor cells
are of medium size and contain elongated nuclei and scantcytoplasm. The spindle cell proliferation does not show anymitotic activity or nuclear atypia. Lymphocytes are eitherabsent or minimal in either the spindle cell component or inthe fibrocollagenous areas. In some areas, the collagendeposition can be very extensive, leading to near-complete
440 A. Weissferdt, C. A. Moran
obliteration of the epithelial tumor elements. Hemorrhage ornecrosis is not a feature of these tumors.
4.4. Adenomatoid spindle cell thymoma
Spindle cell thymoma with an adenomatoid pattern is arecently described subtype of thymoma that is exclusivelyfound in the spindle cell type [14]. The predominant growthpattern in this type is composed of adenomatoid-like andmicrovesicular areas alternating with short spindled epithe-lial cells arranged in diffuse, subtle storiform and hemangio-pericytic growth patterns (Fig. 2C). Although scatteredlymphocytes can be seen associated with the neoplasticproliferation, the presence of thick fibrous bands typical forconventional thymoma is not identified. Cytologically, thecells forming the adenomatoid-like areas are bland, with noevidence of nuclear pleomorphism or necrosis and onlyscattered mitotic figures. Importantly, in some areas ofadenomatoid growth, the spindle cells can have prominentcytoplasmic vacuolation imparting a signet ring cell–likeappearance [14].
4.5. Ancient (sclerosing) thymoma
Extensive areas of hyalinization and sclerosis constitutingmore than 85% of the tumor mass can be seen in all types ofthymoma, including spindle cell thymomas [13]. Initiallydescribed by Kuo [12] in 1994 and interpreted to be aregressive change, Moran and Suster [13] subsequentlyreported a larger number of cases with these changes andattributed them to degenerate or “ancient” changes. Inaddition to extensive hyalinization and sclerosis, furtherchanges include cholesterol cleft granulomas and areas ofcalcification. The residual thymoma component may besmall, once again highlighting the importance of sufficienttumor sampling (Fig. 2D). In cases of spindle cell thymoma,the cells will be fusiform in shape with scanty eosinophiliccytoplasm and an absence of cellular atypia or mitoticactivity [13].
4.6. Spindle cell thymoma with prominent papillaryand pseudopapillary features
Papillary and pseudopapillary growth patterns can beseen in a small subset of spindle cell thymomas andusually do not comprise more than 50% of the tumor mass[15]. Three patterns can be recognized: (a) a solid patternwith papillary projections, (b) an edematous pseudopapil-lary proliferation, and (c) hyalinized pseudopapillarystructures. In the first pattern, fibrovascular cores can beidentified that are generally lined by the same spindledepithelial cells that comprise the rest of the tumor;however, focally, a more columnar epithelial lining canalso be seen. In the second pattern, no definitivefibrovascular cores are identified, but larger villous-like
stromal projections are present with central edematouschanges and areas of calcification and occasional psam-moma body formation (Fig. 2E). The lining cells areflattened and show no evidence of mitotic activity ornuclear atypia. Lastly, the third pattern is characterized byhyalinized pseudopapillary structures lined by blandepithelial cells. In some areas, this pattern is reminiscentof the pseudopapillary hyperplasia associated with vascularstructures. Necrosis and hemorrhage are not usually seen inthis type of spindle cell thymoma.
4.7. Spindle cell thymoma withhemangiopericytoma-like pattern
Another unusual pattern of spindle cell thymoma is thehemangiopericytoma-like pattern. This is primarily charac-terized by a prominent vasculature composed of small and/orlarge branching vascular spaces imparting a staghorn-likepattern (Fig. 2F). The cells separating these vessels are thesame spindle cells seen in any other type of spindle cellthymoma. Hemangiopericytoma-like vessels are generallydistributed in otherwise diffuse spindle cell thymomas ormay be associated with other variants of this tumor.
4.8. Spindle cell thymoma withneuroendocrine-like pattern
Histologic features reminiscent of a neuroendocrinegrowth pattern is not an uncommon finding in spindle cellthymomas. Most commonly, these take the form of rosette-like structures composed of neoplastic spindled epithelialcells that may or may not demonstrate central lumina(Fig. 3A). In addition, the spindle cells may grow inrounded organoid nests, cords, or ribbons. In some cases, acomplex trabecular pattern can be identified. Prominenthyaline or myxoid stromal changes may be associated withsome of these cases. Contrary to true neuroendocrinecarcinomas, the individual cells in these tumors areidentical to those found in diffuse spindle cell thymomas,that is, bland fusiform cells with no evidence of cytologicatypia, mitotic activity, or necrosis. Although neuroendo-crine-like changes may be extensive, in some cases, thesefeatures are only focal and associated with areas of othertypes of spindle cell thymoma.
4.9. Spindle cell thymoma with neural patterns
Cases of otherwise diffuse spindle cell thymoma mayrarely contain areas showing morphologic features remi-niscent of neural lesions. These include meningothelial orschwannoma-like patterns. In the former case, the tumorscontain scattered epithelioid cell nests with a whorledconfiguration reminiscent of those typically seen inmeningothelial type meningiomas (Fig. 3B). The schwan-noma-like pattern is characterized by a bland spindle cell
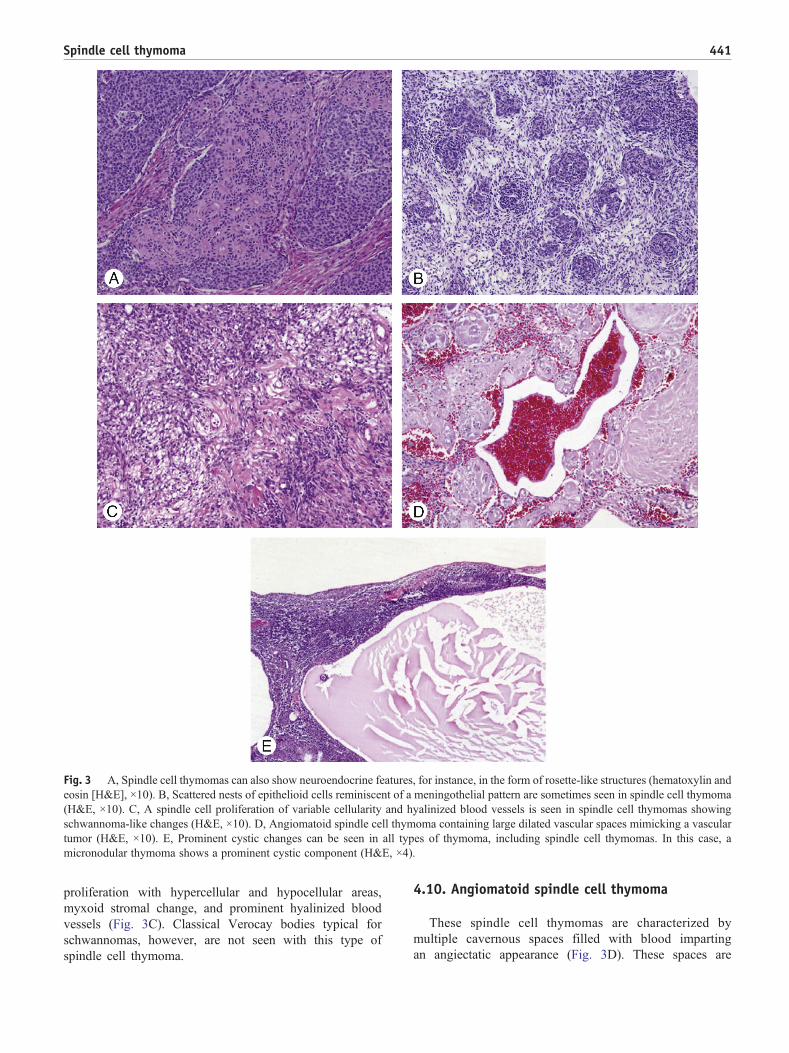
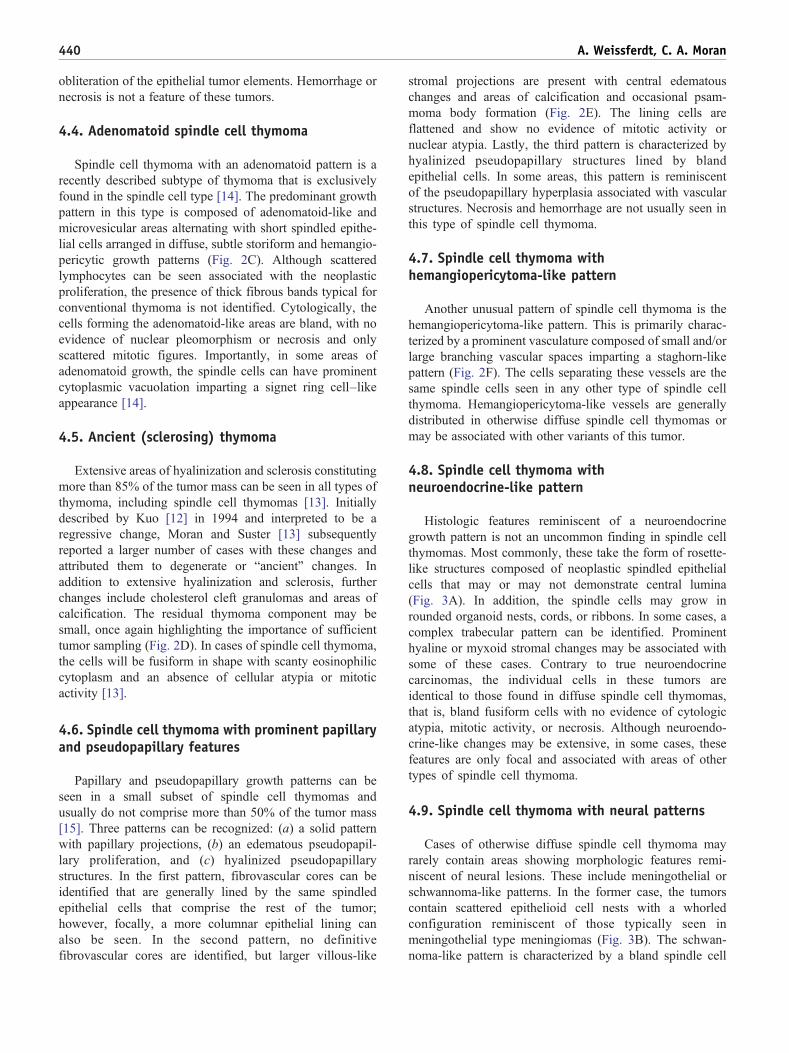
Fig. 3 A, Spindle cell thymomas can also show neuroendocrine features, for instance, in the form of rosette-like structures (hematoxylin andeosin [H&E], ×10). B, Scattered nests of epithelioid cells reminiscent of a meningothelial pattern are sometimes seen in spindle cell thymoma(H&E, ×10). C, A spindle cell proliferation of variable cellularity and hyalinized blood vessels is seen in spindle cell thymomas showingschwannoma-like changes (H&E, ×10). D, Angiomatoid spindle cell thymoma containing large dilated vascular spaces mimicking a vasculartumor (H&E, ×10). E, Prominent cystic changes can be seen in all types of thymoma, including spindle cell thymomas. In this case, amicronodular thymoma shows a prominent cystic component (H&E, ×4).
441Spindle cell thymoma
proliferation with hypercellular and hypocellular areas,myxoid stromal change, and prominent hyalinized bloodvessels (Fig. 3C). Classical Verocay bodies typical forschwannomas, however, are not seen with this type ofspindle cell thymoma.
4.10. Angiomatoid spindle cell thymoma
These spindle cell thymomas are characterized bymultiple cavernous spaces filled with blood impartingan angiectatic appearance (Fig. 3D). These spaces are

Table 1 Summary of subtypes, main histologic features, and differential diagnosis of spindle cell thymomas
Type Main histologic features Main differential diagnosis
Diffuse (conventional) spindlecell thymoma
Storiform or fascicular pattern; spindle or oval-shapedepithelial cells with bland nuclear features; fine nuclearchromatin; small or absent nucleoli; absence of mitoticactivity; variable lymphocytes
Spindle cell neuroendocrine thymiccarcinoma, spindle cell thymic carcinoma,monophasic synovial sarcoma
Micronodular spindle cellthymoma with lymphoidhyperplasia
Multiple tumor nests or nodules composed of spindledepithelial cells; bland nuclear features; prominentlymphocytic stroma with germinal centers
Metastatic carcinoma/sarcoma in lymphnode; micronodular thymic carcinoma withlymphoid hyperplasia
Desmoplastic spindle cellthymoma
Neoplastic bland-appearing spindle cells set in a stromawith prominent hyalinized or fibroblastic-appearingstroma; minimal lymphocytes
Solitary fibrous tumor
Adenomatoid spindle cellthymoma
Short spindled epithelial cells alternating with microcysticareas; scarce lymphocytes; subtle storiform orhemangiopericytoma-like pattern
Metastatic carcinoma, yolk sac tumor
Ancient (sclerosing) thymoma Sclerosis constituting N85% of the tumor with only scantresidual neoplastic spindle cell proliferation; cholesterolcleft granulomas; calcification
Solitary fibrous tumor
Spindle cell thymoma withprominent papillary andpseudopapillary features
Solid areas with papillary pattern, edematouspseudopapillary changes, hyalinized pseudopapillarystructures usually in b50% of the tumor
Papillary thyroid carcinoma, papillary thymiccarcinoma
Spindle cell thymoma withhemangiopericytoma-likepattern
Neoplastic spindled epithelial cells with prominentstaghorn-like vasculature
Solitary fibrous tumor
Spindle cell thymoma withneuroendocrine-like pattern
Organoid nests, cords, ribbons or rosette-like arrangementof neoplastic spindle cells
Spindle cell neuroendocrine thymiccarcinoma
Spindle cell thymoma withneural patterns
Dispersed whorls of epithelioid cell nests (meningothelialpattern) or hypocellular and hypercellular spindle cellproliferation with myxoid stromal change and hyalinizedblood vessels (schwannoma-like pattern)
Meningioma, schwannoma
Angiomatoid spindle cellthymoma
Prominent cavernous blood-filled spaces separatingspindled epithelial cells
Hemangioma, angiosarcoma
Cystic thymoma Confluent large cystic spaces devoid of an epitheliallining; spindled epithelial cells and occasionallymphocytes in cyst wall; inflammation, cholesterolclefts, granulomas, hemorrhage and focal necrosis notuncommon
Multilocular thymic cyst
442 A. Weissferdt, C. A. Moran
surrounded by the spindled neoplastic cells that, in keepingwith the nature of spindle cell thymoma, show nocytologic atypia or mitotic activity. These angiomatoidareas are often seen in association with the diffuse type ofspindle cell thymoma.
4.11. Cystic thymoma
Cystic changes are not restricted to spindle cell thymomasbut can be seen in any type of thymoma [21]. Confluent largecystic spaces characterize these tumors. The fibrous wallsseparating the cystic spaces contain the neoplastic thymicepithelial elements; in spindle cell thymomas, these aretightly packed bland spindle cells with scarce lymphoidelements (Fig. 3E). The walls of the cysts are devoid of anycyst lining but can show severe inflammation, areas ofhemorrhage, hemosiderin deposition, cholesterol cleft gran-ulomas, and focal necrosis [21].
A summary of the subtypes, their main histologicfeatures, and their differential diagnoses is provided inTable 1.
5. Immunohistochemical andmolecular features
Immunohistochemical studies targeting specifically spin-dle cell thymomas are scarce [18]. In a comprehensive studyapplying a wide immunopanel to 30 spindle cell thymomasincluding diffuse, micronodular, adenomatoid, and neuroen-docrine-like subtypes, Weissferdt et al [18] could demon-strate that there is generalized and diffuse positivity of thespindled epithelial cells for pancytokeratin and cytokeratin(CK) 5/6 (Fig. 4A and B). More variable or focalimmunoreactivity can be observed for CK7, synaptophysin,

Fig. 4 A, Strong and diffuse pancytokeratin positivity in a case ofadenomatoid spindle cell thymoma (pancytokeratin, ×4). B, CK5/6decorates the spindled epithelial cells in micronodular thymomawith lymphoid hyperplasia (CK5/6, ×4). C, Diffuse nuclearexpression of Pax8 in a spindle cell thymoma with neuroendo-crine-like features (Pax8, ×4).
Table 2 Summary of immunohistochemical phenotype ofspindle cell thymomas
Marker Immunohistochemical expression
CK +++CK5/6 +++Pax8 +++FoxN1 +++CD205 ++CK7 ++Synaptophysin +SMA +Bcl-2 +Calretinin +/−TTF-1 +/−CK20 −EMA −Chromogranin −CD34 −S100 protein −Desmin −
Abbreviations: SMA, smooth muscle actin; EMA, epithelial membraneantigen; TTF-1, thyroid transcription factor 1.
443Spindle cell thymoma
calretinin, Bcl-2, and smooth muscle actin. Of note,occasional cases can also show weak nuclear staining forthyroid transcription factor 1. More recently, a studyinvestigating Pax8 expression in thymic epithelial neoplasmsshowed that strong and diffuse positive staining with this
antibody was seen in all 30 cases of spindle cell thymoma[22] (Fig. 4C). In addition, 2 novel makers, FoxN1 andCD205, have been shown to be sensitive and specificmarkers for thymic epithelial tumors including spindle cellthymomas [23]. Interestingly, in a study by Pan et al [17],CD20 positivity was observed in the epithelial cells of up to90% of cases of diffuse spindle cell thymoma but not in themicronodular variant. Negative markers for this tumorinclude CD5, CK20, S100 protein, CD34, chromogranin,and desmin [18,24,25]. Stains for epithelial membraneantigen can highlight subtle stromal fibroblastic elementsbut are generally negative in the neoplastic spindle cells [18](Table 2). The scanty lymphoid component of spindle cellthymomas is primarily composed of mature CD3- and CD5-positive T cells and only a small proportion of immatureCD99+/CD1a+ T lymphocytes [2].
To date, there are no studies exclusively investigatingthe molecular changes associated with spindle cell thymo-mas, the rarity and heterogeneity of thymic epithelialneoplasms in general limiting the research on theseneoplasms. Despite this, few attempts at molecularcharacterization of thymomas have yielded several yetinconsistent abnormalities including immunohistochemicaloverexpression and amplification of epidermal growthfactor receptor, overexpression of Kras and p53, and lossof expression of p16 [26].
6. Differential diagnosis
The differential diagnosis of spindle cell thymomas canbe extensive and will largely depend on the morphologic
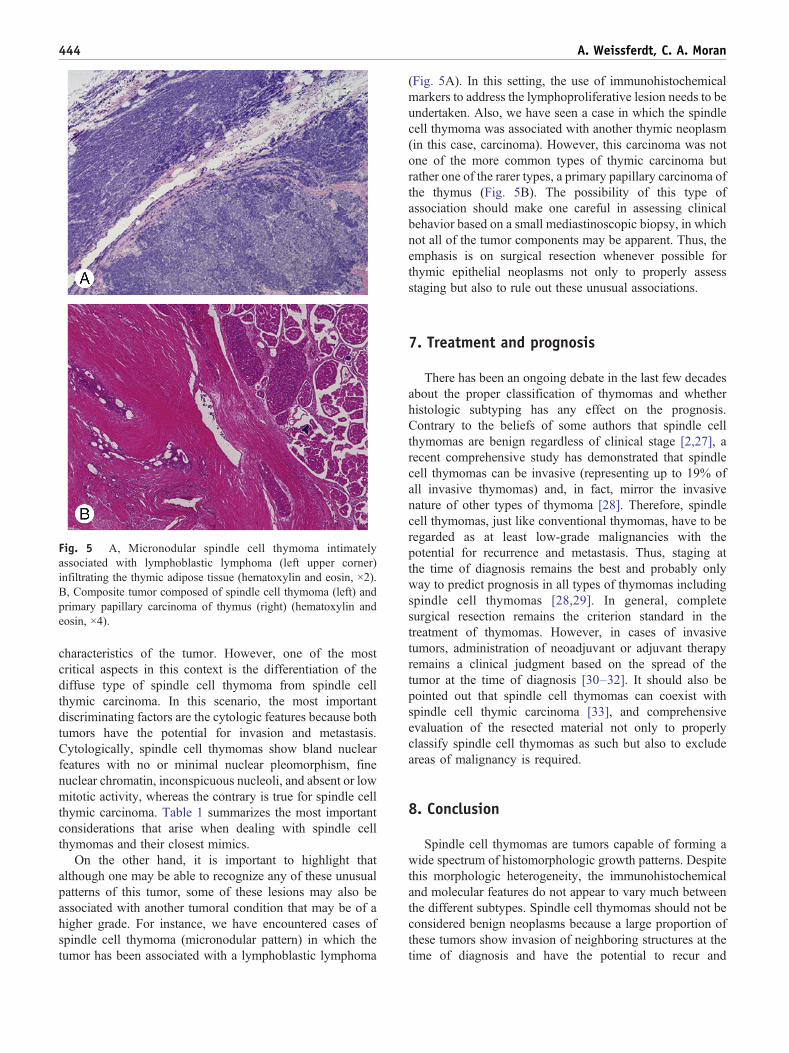
Fig. 5 A, Micronodular spindle cell thymoma intimatelyassociated with lymphoblastic lymphoma (left upper corner)infiltrating the thymic adipose tissue (hematoxylin and eosin, ×2).B, Composite tumor composed of spindle cell thymoma (left) andprimary papillary carcinoma of thymus (right) (hematoxylin andeosin, ×4).
444 A. Weissferdt, C. A. Moran
characteristics of the tumor. However, one of the mostcritical aspects in this context is the differentiation of thediffuse type of spindle cell thymoma from spindle cellthymic carcinoma. In this scenario, the most importantdiscriminating factors are the cytologic features because bothtumors have the potential for invasion and metastasis.Cytologically, spindle cell thymomas show bland nuclearfeatures with no or minimal nuclear pleomorphism, finenuclear chromatin, inconspicuous nucleoli, and absent or lowmitotic activity, whereas the contrary is true for spindle cellthymic carcinoma. Table 1 summarizes the most importantconsiderations that arise when dealing with spindle cellthymomas and their closest mimics.
On the other hand, it is important to highlight thatalthough one may be able to recognize any of these unusualpatterns of this tumor, some of these lesions may also beassociated with another tumoral condition that may be of ahigher grade. For instance, we have encountered cases ofspindle cell thymoma (micronodular pattern) in which thetumor has been associated with a lymphoblastic lymphoma
(Fig. 5A). In this setting, the use of immunohistochemicalmarkers to address the lymphoproliferative lesion needs to beundertaken. Also, we have seen a case in which the spindlecell thymoma was associated with another thymic neoplasm(in this case, carcinoma). However, this carcinoma was notone of the more common types of thymic carcinoma butrather one of the rarer types, a primary papillary carcinoma ofthe thymus (Fig. 5B). The possibility of this type ofassociation should make one careful in assessing clinicalbehavior based on a small mediastinoscopic biopsy, in whichnot all of the tumor components may be apparent. Thus, theemphasis is on surgical resection whenever possible forthymic epithelial neoplasms not only to properly assessstaging but also to rule out these unusual associations.
7. Treatment and prognosis
There has been an ongoing debate in the last few decadesabout the proper classification of thymomas and whetherhistologic subtyping has any effect on the prognosis.Contrary to the beliefs of some authors that spindle cellthymomas are benign regardless of clinical stage [2,27], arecent comprehensive study has demonstrated that spindlecell thymomas can be invasive (representing up to 19% ofall invasive thymomas) and, in fact, mirror the invasivenature of other types of thymoma [28]. Therefore, spindlecell thymomas, just like conventional thymomas, have to beregarded as at least low-grade malignancies with thepotential for recurrence and metastasis. Thus, staging atthe time of diagnosis remains the best and probably onlyway to predict prognosis in all types of thymomas includingspindle cell thymomas [28,29]. In general, completesurgical resection remains the criterion standard in thetreatment of thymomas. However, in cases of invasivetumors, administration of neoadjuvant or adjuvant therapyremains a clinical judgment based on the spread of thetumor at the time of diagnosis [30–32]. It should also bepointed out that spindle cell thymomas can coexist withspindle cell thymic carcinoma [33], and comprehensiveevaluation of the resected material not only to properlyclassify spindle cell thymomas as such but also to excludeareas of malignancy is required.
8. Conclusion
Spindle cell thymomas are tumors capable of forming awide spectrum of histomorphologic growth patterns. Despitethis morphologic heterogeneity, the immunohistochemicaland molecular features do not appear to vary much betweenthe different subtypes. Spindle cell thymomas should not beconsidered benign neoplasms because a large proportion ofthese tumors show invasion of neighboring structures at thetime of diagnosis and have the potential to recur and

445Spindle cell thymoma
metastasize just like the conventional types of thymoma.Treatment usually consists of complete surgical resectionwith or without additional therapy, depending on tumor stageat diagnosis. Familiarity with the histologic features of thedifferent variants of spindle cell thymoma is of utmostimportance for pathologists dealing with mediastinal lesionsbecause these tumors can mimic a range of other processesthat require different treatment modalities. Another impor-tant fact is that any of the patterns described in this reviewmay also be seen in association with other patterns ofthymoma, be it another spindle cell variant or a moreconventional lymphocyte-rich thymoma. In this setting, itbecomes significant to recognize a mixed-pattern thymomaas such and not to misinterpret these lesions as a thymomaassociated with another spindle cell neoplasm.
References
[1] Engels EA, Pfeiffer RM. Malignant thymoma in the United States:demographic patterns in incidence and associations with subsequentmalignancies. Int J Cancer 2003;105:546-51.
[2] Kuo TT, Mukai K, Eimoto T, et al. Type A thymoma. In: Travis WD,Brambilla E, Müller-Hermelink HK, et al, editors. Pathology andgenetics of tumours of the lung, pleura, thymus and heart. Lyon,France: IARC Press; 2004. p. 154-7.
[3] Suster S, Moran CA. Thymoma, atypical thymoma, and thymiccarcinoma. A novel conceptual approach to the classification of thymicepithelial neoplasms. Am J Clin Pathol 1999;111:826-33.
[4] Bernatz PE, Harrison EG, Clagett OT. Thymoma: a clinicopathologicstudy. J Thorac Cardiovasc Surg 1961;42:424-44.
[5] Rosai J, Levine GD. Tumors of the thymus. Armed Forces Institute ofPathology, Second Series, Fascicle 13; 1976. Washington D.C.
[6] Marino M, Muller-Hermelink HK. Thymoma and thymic carcinoma:relation of thymoma epithelial cells to the cortical and medullarydifferentiation of thymus. Virch Arch A Pathol Anat Histopathol 1985;407:119-49.
[7] Moran CA, Weissferdt A, Kalhor N, et al. Thymomas I: aclinicopathologic correlation of 250 cases with emphasis on the WorldHealth Organization schema. Am J Clin Pathol 2012;137:444-50.
[8] Suster S, Moran CA. Micronodular thymoma with lymphoid B-cellhyperplasia: clinicopathologic and immunohistochemical study ofeighteen cases of a distinctive morphologic variant of thymic epithelialneoplasm. Am J Surg Pathol 1999;23:955-62.
[9] Tateyama H, Saito Y, Fujii Y, et al. The spectrum of micronodularthymic epithelial tumours with lymphoid B-cell hyperplasia. Histopa-thology 2001;38:519-27.
[10] Mende S, Moschopulos M, Marx A, et al. Ectopic micronodularthymoma with lymphoid stroma. Virchows Arch 2004;444:397-9.
[11] Lu HS, Gan MF, Zhou T, et al. Sarcomatoid thymic carcinoma arisingin metaplastic thymoma: a case report. Int J Surg Pathol 2011;19:677-80.
[12] Kuo T. Sclerosing thymoma—a possible phenomenon of regression.Histopathology 1994;25:289-91.
[13] Moran CA, Suster S. “Ancient” (sclerosing) thymomas: a clinicopath-ologic study of 10 cases. Am J Clin Pathol 2004;12:867-71.
[14] Weissferdt A, Kalhor N, Suster S, et al. Adenomatoid spindle cellthymomas: a clinicopathological and immunohistochemical study of20 cases. Am J Surg Pathol 2010;34:1544-9.
[15] Kalhor N, Suster S, Moran CA. Spindle cell thymomas (WHO type A)with prominent papillary and pseudopapillary features: a clinicopath-ologic and immunohistochemical study of 10 cases. Am J Surg Pathol2011;35:372-7.
[16] Weissferdt A, Moran CA. Desmoplastic spindle cell thymoma: aclinicopathologic and immunohistochemical study. HUM PATHOL2012, http://dx.doi.org/10.1016/j.humpath.2012.07.011.
[17] Pan CC, Chen WY, Chiang H. Spindle cell and mixed spindle/lym-phocytic thymomas: an integrated clinicopathologic and immunohis-tochemical study of 81 cases. Am J Surg Pathol 2001;25:111-20.
[18] Weissferdt A, Hernandez JC, Kalhor N, et al. Spindle cell thymomas:an immunohistochemical study of 30 cases. Appl ImmunohistochemMol Morphol 2011;19:329-35.
[19] Ströbel P, Marino M, Feuchtenberger M, et al. Micronodularthymoma: an epithelial tumour with abnormal chemokine expressionsetting the stage for lymphoma development. J Pathol 2005;207:72-82.
[20] El MF, Braham E, Ayadi A, Ismail O, Kilani T. Micronodularthymoma with lymphoid stroma: report of two cases and particularassociation with thymic lymphoid hyperplasia in one case. Pathology2006;38:586-8.
[21] Suster S, Rosai J. Cystic thymomas. A clinicopathologic study of tencases. Cancer 1992;69:92-7.
[22] Weissferdt A, Moran CA. Pax8 expression in thymic epithelialneoplasms: an immunohistochemical analysis. Am J Surg Pathol 2011;35:1305-10.
[23] Nonaka D, Henley JD, Chiriboga L, et al. Diagnostic utility of thymicepithelial markers CD205 (DEC205) and Foxn1 in thymic epithelialneoplasms. Am J Surg Pathol 2007;31:1038-44.
[24] Saad RS, Landreneau RJ, Liu Y, et al. Utility of immunohistochem-istry in separating thymic neoplasms from germ cell tumors andmetastatic lung cancer involving the anterior mediastinum. ApplImmunohistochem Mol Morphol 2003;11:107-12.
[25] Pan CC, Chen PC, Chou TY, et al. Expression of calretinin and othermesothelioma-related markers in thymic carcinoma and thymoma.HUM PATHOL 2003;34:1155-62.
[26] Kuhn E, Wistuba II. Molecular pathology of thymic epithelialneoplasms. Hematol Oncol Clin North Am 2008;22:443-55.
[27] Quintanilla-Martinez L, Wilkins Jr EW, Choi N, et al. Thymoma.Histologic subclassification is an independent prognostic factor.Cancer 1994;74:606-17.
[28] Moran CA, Kalhor N, Suster S. Invasive spindle cell thymomas (WHOtype A): a clinicopatholgic correlation of 41 cases. Am J Clin Pathol2010;134:793-8.
[29] Moran CA, Walsh G, Suster S, et al. Thymomas II: a clinicopathologiccorrelation of 250 cases with a proposed staging system with emphasison pathologic assessment. Am J Clin Pathol 2012;137:451-61.
[30] Loehrer Sr PJ, Perez CA, Roth LM, et al. Chemotherapy for advancedthymoma. Preliminary results of an intergroup study. Ann Intern Med1990;113:520-4.
[31] Göldel N, Böning L, Fredrik A, et al. Chemotherapy of invasivethymoma. A retrospective study of 22 cases. Cancer 1989;63:1493-500.
[32] Curran Jr WJ, Kornstein MJ, Brooks JJ, et al. Invasive thymoma: therole of mediastinal irradiation following complete or incompletesurgical resection. J Clin Oncol 1988;6:1722-7.
[33] Suster S, Moran CA. Primary thymic epithelial neoplasms showingcombined features of thymoma and thymic carcinoma. A clinicopath-ologic study of 22 cases. Am J Surg Pathol 1996;20:1469-80.
Copyright © 2022 FDOKUMEN



















