
The Gliding Nail, a Universal Implant in the Treatment of Proximal Femur Fractures
8
Original Article 562 European Journal of Trauma 2006 · No. 6 © Urban & Vogel European Journal of Trauma The Gliding Nail, a Universal Implant in the Treatment of Proximal Femur Fractures Jonas Gehr, Tim Arnold, Florian Hilsenbeck, Wilhelm Friedl 1 Abstract Introduction: Due to the increase in the incidence of osteoporosis with age and the high biochemical load on the proximal femur, the pertrochanteric femur frac- ture is the typical fracture of the elderly. The number of different fracture types and the characteristic fea- tures of this patient population places high demands on any universally applicable implant. The rotational instability of the head–neck fragment in the case of a trochanter minor defect, in particular, is a significant factor in the care of pertrochanteric femur factures. The object of this study was to show that the gliding nail constitutes a universal implant for the care of proximal femur fractures with constantly maintained stability under load. Material and Methods: Between March 1996 and April 2001, 501 patients with per- and subtrochanteric frac- tures and an average age of 76 were included in the study. All osteosyntheses were carried out using the gliding nail which has an I-beam cross-section profile blade. 73.2% were treated operatively for closed iso- lated per- or subtrochanteric femur fractures. Results: All patients were restored to full weight-bear- ing postoperatively. The combined overall early and late complication rate following gliding nail synthesis was only 5.4%. Neither blade cut-out nor head–neck rota- tion was observed following gliding nail osteosynthe- sis. Three-month mortality rose from 2.4% in patients with no complications to 90% in patients with four complications. 92.1% of patients were independently mobile at the time of the follow-up examination. Conclusion: With its low complication rate and the ever-present possibility of full weight bearing, the gliding nail fulfills all the requirements of a modern implant for the treatment of proximal femur fractures. In our opinion, its most advantageous features are the high moment of resistance of the I-beam cross-section profile blade which ensures the possibility of gliding, the minimalized risk of proximal cut-out due to the large surface area with two planes of support in the bone, and its secure rotational stability in terms of both nail and bone. The impaction of the blade, which requires no reaming with its resulting loss of bone sub- stance, is responsible for the excellent bone–implant interface. Eur J Trauma 2006;32:562–9 DOI 10.1007/s00068-006-5117-2 Introduction Proximal femur fractures have a particular socioecono- mic significance due to the constantly ageing population. The pertrochanteric femur fracture is the typical frac- ture of the elderly due to the increase in the incidence of osteoporosis with age and the high biochemical load on the proximal femur. Even when walking slowly, the load while standing on one leg is three times the body weight. This leads to a high risk of implant avulsions, a serious complication in the osteosynthesis of proximal femur fractures. In addition, the many different fracture types place high demands on any universally applicable imp- lant. The rotational instability of the head–neck frag- ment in the case of a trochanter minor defect poses a particular problem. This dorso-medially located defect leads to the rotation of the calcar into dorsal displace- ment. This in turn results in an uncontrolled fracture impaction and a high risk of proximal cut-out. By using 1 Klinikum Aschaffenburg – Unfallchirurgie, Aschaffenburg, Germany Received: September 23, 2005; revision accepted: June 07, 2006
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of The Gliding Nail, a Universal Implant in the Treatment of Proximal Femur Fractures
Original Article
562European Journal of Trauma 2006 · No. 6 © Urban & Vogel
European Journal of Trauma
The Gliding Nail, a Universal Implant in the Treatment of Proximal Femur FracturesJonas Gehr, Tim Arnold, Florian Hilsenbeck, Wilhelm Friedl1
AbstractIntroduction: Due to the increase in the incidence of osteoporosis with age and the high biochemical load on the proximal femur, the pertrochanteric femur frac-ture is the typical fracture of the elderly. The number of different fracture types and the characteristic fea-tures of this patient population places high demands on any universally applicable implant. The rotational instability of the head–neck fragment in the case of a trochanter minor defect, in particular, is a significant factor in the care of pertrochanteric femur factures. The object of this study was to show that the gliding nail constitutes a universal implant for the care of proximal femur fractures with constantly maintained stability under load.Material and Methods: Between March 1996 and April 2001, 501 patients with per- and subtrochanteric frac-tures and an average age of 76 were included in the study. All osteosyntheses were carried out using the gliding nail which has an I-beam cross-section profile blade. 73.2% were treated operatively for closed iso-lated per- or subtrochanteric femur fractures.Results: All patients were restored to full weight-bear-ing postoperatively. The combined overall early and late complication rate following gliding nail synthesis was only 5.4%. Neither blade cut-out nor head–neck rota-tion was observed following gliding nail osteosynthe-sis. Three-month mortality rose from 2.4% in patients with no complications to 90% in patients with four complications. 92.1% of patients were independently mobile at the time of the follow-up examination.Conclusion: With its low complication rate and the ever-present possibility of full weight bearing, the gliding nail fulfills all the requirements of a modern
implant for the treatment of proximal femur fractures. In our opinion, its most advantageous features are the high moment of resistance of the I-beam cross-section profile blade which ensures the possibility of gliding, the minimalized risk of proximal cut-out due to the large surface area with two planes of support in the bone, and its secure rotational stability in terms of both nail and bone. The impaction of the blade, which requires no reaming with its resulting loss of bone sub-stance, is responsible for the excellent bone–implant interface.
Eur J Trau ma 2006;32:562–9
DOI 10.1007/s00068-006-5117-2
IntroductionProximal femur fractures have a particular socioecono-mic significance due to the constantly ageing population. The pertrochanteric femur fracture is the typical frac-ture of the elderly due to the increase in the incidence of osteoporosis with age and the high biochemical load on the proximal femur. Even when walking slowly, the load while standing on one leg is three times the body weight. This leads to a high risk of implant avulsions, a serious complication in the osteosynthesis of proximal femur fractures. In addition, the many different fracture types place high demands on any universally applicable imp-lant. The rotational instability of the head–neck frag-ment in the case of a trochanter minor defect poses a particular problem. This dorso-medially located defect leads to the rotation of the calcar into dorsal displace-ment. This in turn results in an uncontrolled fracture impaction and a high risk of proximal cut-out. By using
1 Klinikum Aschaffenburg – Unfallchirurgie, Aschaffenburg, Germany
Received: September 23, 2005; revision accepted: June 07, 2006
Gehr J, et al. The Gliding Nail
563European Journal of Trauma 2006 · No. 6 © Urban & Vogel
a rotationally stable blade profile, such as that of the gliding nail, it is possible to prevent this rotation. In order to develop an implant which is stable while being loaded, biomechanical principles were analyzed using osteotomy models on plastic and cadaver models [10]. The tests were carried out in a similar manner to physio-logical step-loading tests in the form of alternating load tests (4,000 cycles up to 2,000 N load) and an additional maximum-load test.
In experimental tests it was possible to show a reduction of 50% in the transmigration rate using the double-T profile of the gliding nail blade compared to the single screw of the gamma nail and 75% in compari-son to the PFN double screw. One significant advantage of the gliding nail is that, in contrast to screws, no drill-ing of the head and neck is necessary since the blade is inserted using a guide wire without losing any bone substance thus impacting the bone stock [10].
The objective of this study was to show that the glid-ing nail constitutes a universal implant for the treatment of proximal femur fractures with constantly maintained stability under load.
Materials and MethodsDescription of the Implant
The standard gliding nail has a length of 220 mm, a diameter of 12 mm distal and 19 mm proximal and an angle in the frontal plane of 6°. To adapt to the ana-tomical variability of the neck–shaft angle the gliding nail is available in 125° and 135° versions. The diffe-rent lengths are 220, 340, 400 and 440 mm. For nar-row medullary cavity, there exists a nail with a distal diameter of 11 mm and a proximal diameter of 17 mm and a length of 180 or 220 mm. The intramedullary position of the nail results in a low bending moment.
The oval profile of the distal holes allows dynamic and static locking for secure rotational stability and exact length. The proximal blade with its I-beam cross-section profile is available in lengths from 80 to 125 mm in 5 mm increments. It is 16 mm high and thus ensures a high moment of resistance. The I-beam cross-section profile pro-vides perfect rotational stability of the head–neck fragment and the blade–nail interface. The gliding principle enables fracture compression in line with the femoral neck.
In order to avoid irritations of the tractus iliotibialis the lateral blade end has been angled so that the implant ends in line with the lateral cortex.
Case MaterialBetween March 1996 and April 2001 all patients with per- and subtrochanteric fractures of the proximal femur (n = 501) presented at the University of Heidel-berg Trauma Unit were treated using the gliding nail as a universal implant.
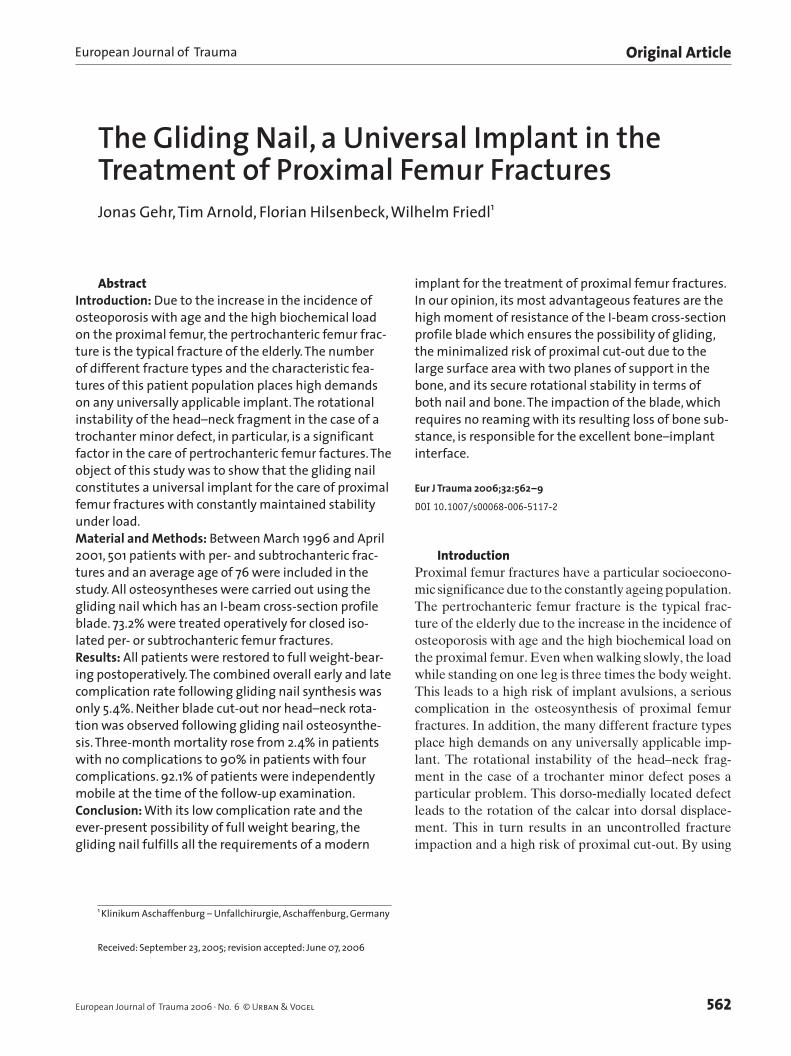
The follow-up consisted of the study of patient doc-umentation, the analysis of patients’ X-rays and clini-cal examinations 3 months and an analysis of mortality 3 months and 1 year after initial treatment. All patients lived locally making it possible for the reviewer to visit them personally or interview the general practitioners treating them. This explains the exceptional follow-up rate. The average age of the patients was 76.2, the young-est being 14 and the oldest 96 years old. Among them 70% were women and 30% were men. The average age of the men was 63.5 and that of the women 79.8 (Figure 1).
In 301 cases the fracture was on the right side, in 198 cases on the left and in 2 cases both left and right sides were fractured. 59.5% of patients were independ-ently mobile without a walking aid, 23.6% with a walk-ing stick or underarm crutches and 10.4% with a rolling walker. 6.5% of the patients were wheel-chair bound or bed-ridden.
Only 18% of our patients had no relevant under-lying disease. 54.5% had relevant cardiac and 19.6% relevant pulmonary diseases. 22.3% of patients were diabetics.
18.4% of patients presented special local risk fac-tors. One percent suffered from a sacral decubitus and 0.2% from a decubitus right above the trochanter major.
Age distribution (n = 501 cases)
19 1122
48
144158
96
0
20
40
60
80
100
120
140
160
180
Age
n P
at.
30-39 40-49 50-59 60-69 70-79 80-89 90-99
Figure 1. Age distribution of the 501 patients with proximal femoral fractures treated with gliding nail osteosynthesis (from 03/96March 1996 to 03/2001March 2001).
Gehr J, et al. The Gliding Nail
564 European Journal of Trauma 2006 · No. 6 © Urban & Vogel
Eleven percent had a preexisting arthrosis coxae. All fractures were closed.
Four groups were distinguished in terms of accident history. Eighty percent of injuries were minor injuries characteristic of old age. 16.8% of our patient popula-tion had suffered high-energy traumas, 2.2% had patho-logical fractures and in 1% of cases gliding nail osteo-synthesis was carried out due to corrective osteotomies.
One hundred and seventy-nine (35.7%) patients were operated on the day of the accident itself, 245 (48.9%) on the following day, 44 (8.8%) after 2 days
and 33 (6.6%) patients after 4 days. The latter figure was because of the necessity of preoperative diagnostics and treatment to achieve operability with preexisting multimorbidity of the patients.
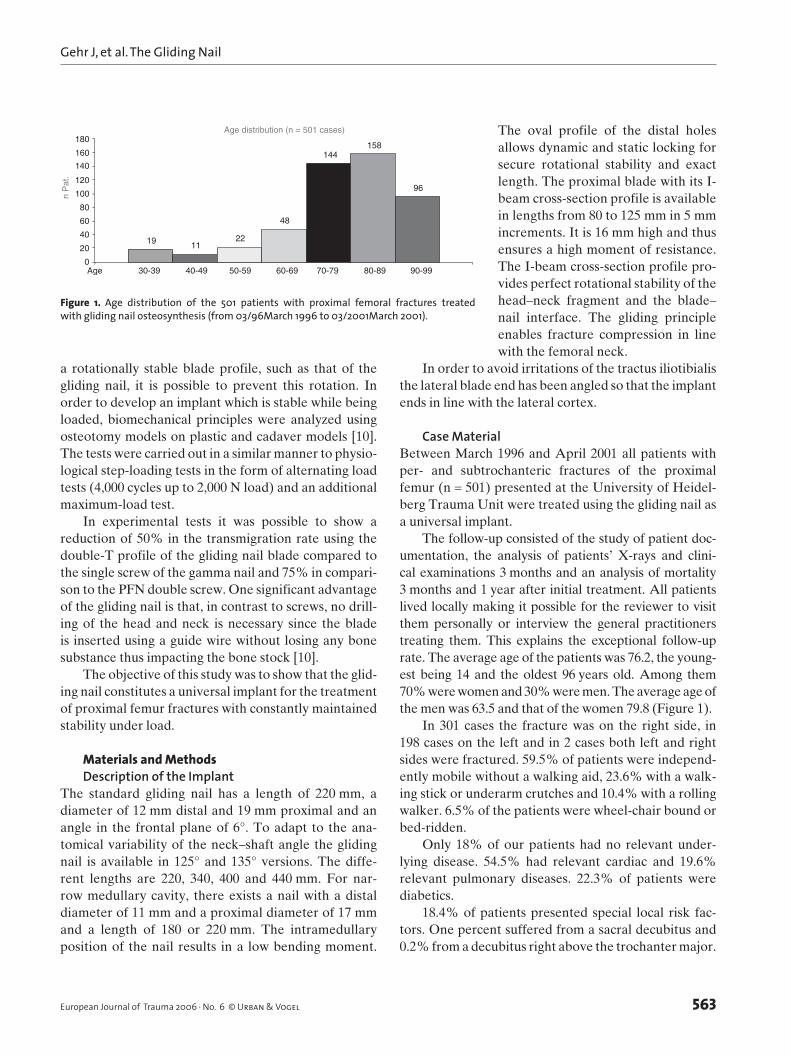
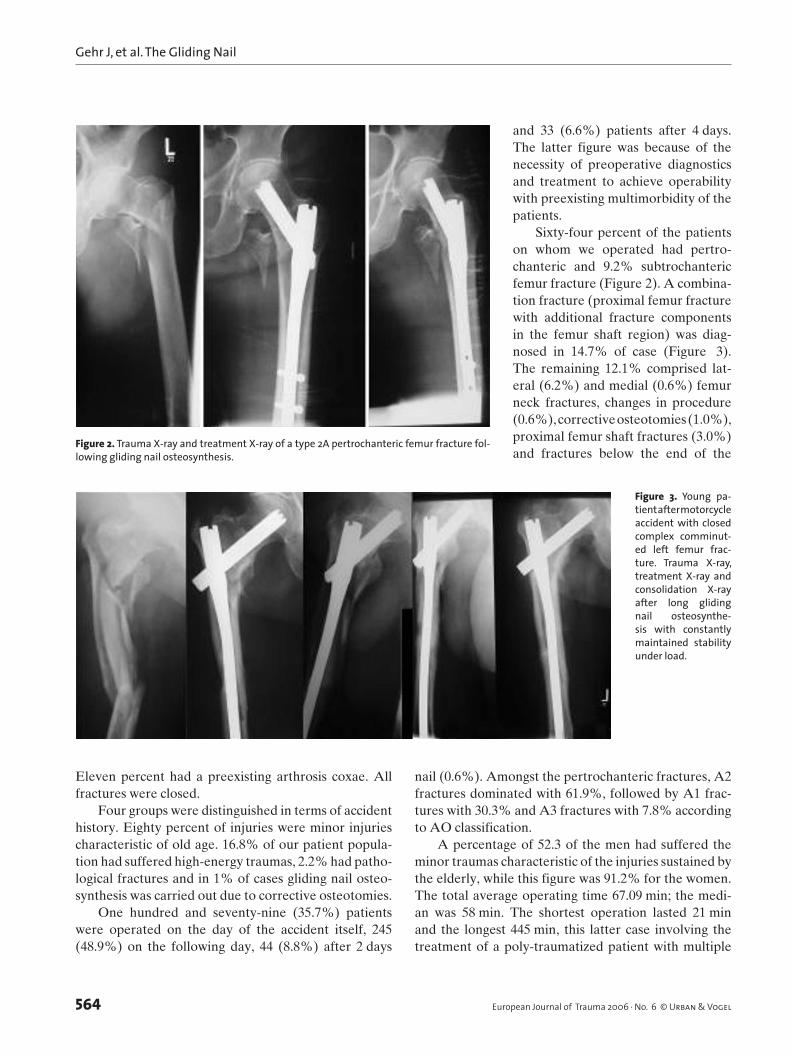
Sixty-four percent of the patients on whom we operated had pertro-chanteric and 9.2% subtrochanteric femur fracture (Figure 2). A combina-tion fracture (proximal femur fracture with additional fracture components in the femur shaft region) was diag-nosed in 14.7% of case (Figure 3). The remaining 12.1% comprised lat-eral (6.2%) and medial (0.6%) femur neck fractures, changes in procedure (0.6%), corrective osteotomies (1.0%), proximal femur shaft fractures (3.0%) and fractures below the end of the
nail (0.6%). Amongst the pertrochanteric fractures, A2 fractures dominated with 61.9%, followed by A1 frac-tures with 30.3% and A3 fractures with 7.8% according to AO classification.
A percentage of 52.3 of the men had suffered the minor traumas characteristic of the injuries sustained by the elderly, while this figure was 91.2% for the women. The total average operating time 67.09 min; the medi-an was 58 min. The shortest operation lasted 21 min and the longest 445 min, this latter case involving the treatment of a poly-traumatized patient with multiple
Figure 2. Trauma X-ray and treatment X-ray of a type 2A pertrochanteric femur fracture fol-lowing gliding nail osteosynthesis.
Figure 3. Young pa-tient after motorcycle accident with closed complex comminut-ed left femur frac-ture. Trauma X-ray, treatment X-ray and consolidation X-ray after long gliding nail osteosynthe-sis with constantly maintained stability under load.

Gehr J, et al. The Gliding Nail
565European Journal of Trauma 2006 · No. 6 © Urban & Vogel
fractures. Isolated proximal femur fractures took a mean operating time of 61 min (21–210 min.). The aver-age hospital stay was 16.3 days.
ResultsAs standard, patients were placed on a traction table and fractures were reduced in closed technique. Forty-six (9.2%) patients required open reduction.
Technical problems were experienced with 35 patients (7%). These included, on a patient-specific basis, three complicated reductions due to knee joint contractions (0.6%), four complicated reductions with arthrosis coxae (0.8%) and two retrograde drillings in cases with extended trochanteric metastasis (0.4%).
Technical problems encountered included a tro-chanteric fracture (0.2%), two poor reductions (0.4%), insertion of only one distal bolt five times (1%), mis-drilling with bracket loosening of the distal bolts five times (1%), without resulting in a misplacement, bro-ken drill three times (0.6%), bending of the blade guide wire three times (0.6%) and the distraction of the fracture gap during insertion of the blade twice (0.4%). In no case, load restriction was required or a reopera-tion carried out. Similarly, no additional fractures or fissures in the shaft region were observed (Table 1). In a total of 185 patients (36.9%) it was possible to carry out a radiological check as part of the follow-up examination. The assessment of postoperative X-rays showed a perfect blade position in the lower and cen-tral third of the femoral head in 94.3% of cases. Even in the 5.7% of cases with unfavorable cranial blade position neither blade cut-out nor head rotation was observed.
The average distance between blade end and fem-oral head was 11.6 mm. The compression of the frac-ture due to postoperative load was observable by the increase in the blade–cortex distance of 2.2 mm, while the blade–head distan pression into the head fragment was only slight. All patients with no other load-limiting injury to the same limb were permitted to return to full weight-bearing (98%).
In 5.4% of cases an operative revision was required due to early (within first 30 days) or late complications. Early complications were limited to hematomas. Over-all we recorded 33 (6.6%) subcutaneous hematomas. It was possible to treat 22 (4.4 %) patients conservatively, while 11 (2.2%) had to be revised due to a hemato-ma, five (1.0%) had positive intraoperative smear findings.
Late complications were medial blade perforation (0.7%), fracture below the nail end (0.7%) and lateral backing out of the blade (1.2%). We had to carry out a recompression due to a dehiscent fracture gap on two occasions; one late infection was treated by opera-tion. Neither fatigue fractures of the implant, such as rotations of the head–neck fragment, nor pseudarthro-sis occurred. No cranial perforations (cut-outs) were observed. Furthermore, three patients suffered a femur shaft fracture distal of the nail end not affecting the locking-bolt bearing, following a fall on the same leg. These patients were treated by using a long gliding nail. Similarly, the 26 (6.1%) patients with tractus iliotibialis irritation did not need intervention. Due to the change in blade design with its angled lateral blade end, this complication no longer occurs.
In the period of the follow-up examination, 28.5% of the patients suffered from one or more general complica-tions, 6.8% suffered from cardiovascular diseases, 8.4% from urinary tract infections and 4% from deep leg vein thrombosis, while 1% developed a manifest stasis ulcer.
In patients without general complications, 3-month mortality rate stood at 2.4%. Where a patient had two complications, 3-month mortality increased to 32% and
Tables 2. Hospital lethality dependent on complications following the osteosynthetic treatment of 501 patients using the gliding nail after proximal femoral fractures.
Number of complications n – patients n – deceased patients0 371 9 ( 2.4%)
1 60 15 (25.0%)
2 53 17 (32.0%)
3 7 3 (42.8%)
4 10 9 (90.0%)
Tables 1. Breakdown of complications following gliding nail osteosyn-thesis in 501 patients with proximal femoral fractures.
Purulent infection 2 (0.4%)
Haematoma, infected haematoma 11 (2.2%)
Fracture distal of the nail 3 (0.6%)
Blade slide 5 (1.0%)
Blade impaction 3 (0.6%)
Secondary distal dynamisation 2 (0.4%)
Implant failure 0
Rotational instability 0
Secondary endoprosthetic treatment 0
Total wound revision rate 2.6%
Total implant revision rate 2.6%
Total re-operation rate 2.6%
Cut out 0.0%

Gehr J, et al. The Gliding Nail
566 European Journal of Trauma 2006 · No. 6 © Urban & Vogel
with four complications it rose to 90% (Table 2). Cardiac complications in particular (15 out of 34 patients dying), pneumonia (10/39) and renal complications (3/10) were associated with high levels of mortality. Age was also a factor influencing mortality. The lethality rate dur-ing the observation period was 6.9% in patients under 80 years, and 22.8% in those over 80 years. In contrast, however, diabetes and osteoporosis, for example, had no influence. Overall, the hospital mortality rate was 3.9%, 3-month mortality was 14.9% and mortality after 1 year was 26.9% (Figures 4, 5).
Fifty-eight percent of patients were able to be transferred to rehabilitation clinics, 36% were dis-charged home, only 4.3% were readmitted to nursing
homes and 1.7% were transferred to other hospital departments.
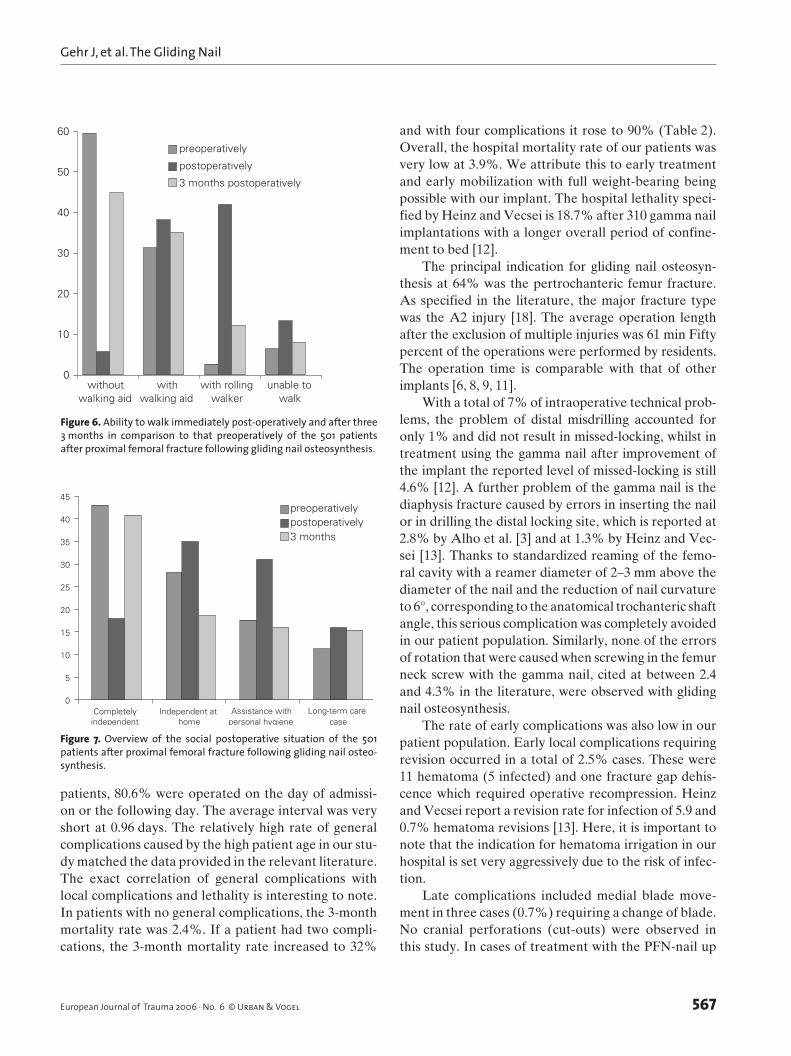
In order to measure the postoperative social situ-ation, ability to walk and independence of care were compared to the preoperative situation. Three months postoperatively 44.8% of the patients were mobile without a walking aid compared to a preoperative fig-ure of 59.5%. 11.3% required underarm crutches, 36% required rolling walkers and 7.9% were unable to walk. Thus 92.1% of patients were independently mobile at the time of the follow-up examination. Preoperatively a total of 6.5% of patients were immobile. This cor-responds to an increase in immobility of only 1.4% (Figure 6).
Four groups were distinguished in terms of social independence. Forty-three percent were fully inde-pendent preoperatively against 40.7% postoperatively. Domes tic independence was possible for 28.2% of patients preoperatively, 18.6% postoperatively. 17.6% of patients required assistance with personal hygiene preoperatively as compared to 25.4% postoperatively. 15.3% of patients were classified as long-term care cases postoperatively, as opposed to 11.2% preoperatively. This indicates a small number of patients with a dete-riorating social situation, which was also reflected in the low rate of readmissions to nursing homes (Figure 7 ).
DiscussionThis study is based on the follow-up examination of 501 consecutive patients who had been treated operatively at the University of Heidelberg Trauma Hospital for a proximal femur fracture using gliding nail osteosyn-thesis in the period from May 1996 to March 2001. All fractures were treated using the gliding nail in order to test its suitability as a universal implant. Eighty per-cent of the patients suffered this injury at an advanced age, a phenomenon also reported by other authors in their patient groups [4, 5, 15, 22]. If one considers the underlying diseases, only 18% of these patients could be considered as healthy, while 54.5% had cardiovas-cular conditions, 22.3% diabetes mellitus and 19.6% a COPD. Overall, this gave a rate of two preexisting relevant underlying diseases per patient. Other authors also highlight the polymorbidity of the predominantly geriatric patient population with similar data [19, 20]. In order to minimize the risk of pneumonia, throm-bosis and stasis ulcer early operative intervention is required. Under Müller [21] almost 91% were tre-ated on the first day, under Heinz [12] 45.8%. Of our
Figure 4. Deceased patients in each age group of the 501 patients after proximal femoral fracture following gliding nail osteosynthesis.
0
10
20
30
40
50
60
<60 <80 >90
Hospital lethality
3 months
1-6 years
0
10
20
30
40
50
60
70
80
90
100
0RF 1RF 2RF 3RF 4RF 5RF 6RF
Hospital lethality
3-month lethality
Figure 5. Lethality and preoperative risk factors (RF) in 501 patients after proximal femoral fracture following gliding nail osteosynthesis.
Gehr J, et al. The Gliding Nail
567European Journal of Trauma 2006 · No. 6 © Urban & Vogel
and with four complications it rose to 90% (Table 2). Overall, the hospital mortality rate of our patients was very low at 3.9%. We attribute this to early treatment and early mobilization with full weight-bearing being possible with our implant. The hospital lethality speci-fied by Heinz and Vecsei is 18.7% after 310 gamma nail implantations with a longer overall period of confine-ment to bed [12].
The principal indication for gliding nail osteosyn-thesis at 64% was the pertrochanteric femur fracture. As specified in the literature, the major fracture type was the A2 injury [18]. The average operation length after the exclusion of multiple injuries was 61 min Fifty percent of the operations were performed by residents. The operation time is comparable with that of other implants [6, 8, 9, 11].
With a total of 7% of intraoperative technical prob-lems, the problem of distal misdrilling accounted for only 1% and did not result in missed-locking, whilst in treatment using the gamma nail after improvement of the implant the reported level of missed-locking is still 4.6% [12]. A further problem of the gamma nail is the diaphysis fracture caused by errors in inserting the nail or in drilling the distal locking site, which is reported at 2.8% by Alho et al. [3] and at 1.3% by Heinz and Vec-sei [13]. Thanks to standardized reaming of the femo-ral cavity with a reamer diameter of 2–3 mm above the diameter of the nail and the reduction of nail curvature to 6°, corresponding to the anatomical trochanteric shaft angle, this serious complication was completely avoided in our patient population. Similarly, none of the errors of rotation that were caused when screwing in the femur neck screw with the gamma nail, cited at between 2.4 and 4.3% in the literature, were observed with gliding nail osteosynthesis.
The rate of early complications was also low in our patient population. Early local complications requiring revision occurred in a total of 2.5% cases. These were 11 hematoma (5 infected) and one fracture gap dehis-cence which required operative recompression. Heinz and Vecsei report a revision rate for infection of 5.9 and 0.7% hematoma revisions [13]. Here, it is important to note that the indication for hematoma irrigation in our hospital is set very aggressively due to the risk of infec-tion.
Late complications included medial blade move-ment in three cases (0.7%) requiring a change of blade. No cranial perforations (cut-outs) were observed in this study. In cases of treatment with the PFN-nail up
patients, 80.6% were operated on the day of admissi-on or the following day. The average interval was very short at 0.96 days. The relatively high rate of general complications caused by the high patient age in our stu-dy matched the data provided in the relevant literature. The exact correlation of general complications with local complications and lethality is interesting to note. In patients with no general complications, the 3-month mortality rate was 2.4%. If a patient had two compli-cations, the 3-month mortality rate increased to 32%
0
10
20
30
40
50
60
withoutwalking aid
withwalking aid
with rollingwalker
unable towalk
preoperatively
postoperatively
3 months postoperatively
Figure 6. Ability to walk immediately post-operatively and after three 3 months in comparison to that preoperatively of the 501 patients after proximal femoral fracture following gliding nail osteosynthesis.
0
5
10
15
20
25
30
35
40
45
Completelyindependent
Independent athome
Assistance withpersonal hygiene
Long-term carecase
preoperativelypostoperatively3 months
Figure 7. Overview of the social postoperative situation of the 501 patients after proximal femoral fracture following gliding nail osteo-synthesis.

Gehr J, et al. The Gliding Nail
568 European Journal of Trauma 2006 · No. 6 © Urban & Vogel
to 8% of cut-outs were reported [1, 14, 23–25]. Five patients (1.2%) experienced lateral blade slide with irritation of the tractus iliotibialis. In these cases the blade was blocked statically using a grub screw with-out further complications. In two patients, dynamiza-tion by removing the distal locking bolt was carried out after 3 months with a still visible fracture gap. Overall, therefore, the revision rate for 501 gliding nails is very low at 5.2%. Higher revision rates after PFN-osteosyn-thesis are reported. These range from 7.1 up to 27.3% [1, 14]. The frequency of femur shaft fractures follow-ing gamma nail treatment is recorded at 2.9–5.6% by various authors [2, 3, 7, 8]. With gliding nail osteosyn-thesis, this serious complication arose in only three cases (0.6%) all after re-trauma. In these cases a long gliding nail was implanted. The occasional breakages of the implant of gamma nails reported in the litera-ture [8, 11, 13] were not observed with the clearly more stable gliding nail in this study.
The average stay in our hospital was 16.3 days for proximal femur fractures. Various authors report peri-ods of confinement to bed of between 22 and 63.8 days [4, 7, 16, 18]. Thanks to close co-operation with acute geriatric services Manner [20] was able to reduce the average hospital stay of men and women to only 7 days. In this respect, there is much to be achieved by opti-mizing co-operation between aftercare services and acute clinics. A study of 330 gamma nail osteosynthe-ses reported a readmission rate into nursing homes of 17.5% [11]. In our study, the rate was very low with a total of 4.3% readmissions to nursing homes, highlight-ing the excellent social rehabilitation after gliding nail osteosynthesis.
To further assess social rehabilitation, ability to walk and independence of care were compared with preoperative status. With 92.1% of patients independ-ently mobile with and without aids, we achieved very good results. The use of walking aids should be regard-ed relatively here, since the indication was extremely generous in terms of fall prevention and patients’ fears of falling. 11.2% of patients were considered long-term care cases preoperatively and 15.3% postoperatively. These figures provide powerful evidence of the good levels of social rehabilitation after gliding nail osteosyn-thesis. Removal of the gliding nail is not recommended, especially in elderly patients. We follow the opinion of other authors to leave this type of device in place even after fracture healing except in cases of deep and chron-ic infection [17].
References 1. AL- Yassari G, Langstaff RJ, Jones JW, et al. The AO/AISF proximal
femoral nail (PFN) for treatment of unstable trochanteric femo-ral fracture. Injury Int J Care Injured 2002;33:395–9.
2. Albareda J, Ladergia A, Palanca D, et al. Complications and tech-nical problems with the gamma nail. Int Orthop 1996;20:47–50.
3. Aune AK, Ekeland A, Odegaard B, et al. Gamma nail vs compres-sion screw for trochenteric femoral fractures. 15 reoperations in a prospective, randomized study of 378 patients. Acta Orthop Scand 1994;65:127–30.
4. Augeneder M, Boszotta H, Ohrenberger G, et al. Zur Letalität nach Endernagelung pertrochanterer Frakturen. Unfallchirurg 1987;90:380–385.
5. Benz K, Jasarevic M, Rüb M. Die Ender-Nagelung – Versuch einer Standortbestimmung. Unfallchirurg 1991;17:156–65.
6. Bridle S, Patel A, Bircher M, et. al. Fixation of interochanteric fractures of the femur. A randomised prospective comparison of the gamma nail and the dynamic hip screw. J Bone Joint Surg (Br) 1991;73:330–4.
7. Bonnaire F, Götschin U, Kuner EH. Früh- und Spätergebnisse nach 200 DHS-Osteosynthesen zur Versorgung pertrochanterer Femurfrakturen Unfallchirurg 1992;95:246–53.
8. Boriani S, De Lure F, Campanacci L, et al. A technical report re-viewing the use of the 11-mm Gamma nail: intraoperative femur fracture incidence. Orthopedics 1996;19:597–600.
9. Eberle C, Guyer P, Keller H, Metzger U. Der Gammanagel, ein ideales Implantat zur Behandlung instabiler Frakturen beim alten Menschen. Helv Chir Acta 1993;59:527–31.
10. Friedl W, Clausen J. Experimental examination for optimized stabilisation of trochanteric femur fractures. Intra- or extramed-ullary implant localisation and influence of femur neck compo-nent profile on cut-out risk. Chirurg 2001;72:1344–52.
11. Friedl W, Colombo Benkmann M, Dockter S, et al. Gammana-gel-Osteosynthese per- und subtrochanterer Femurfrakturen. Chirurg 1994;65:953–63.
12. Heinz T, Wöhry G, Vecsei V. Stellenwert der Gammanagelung bei der Versorgung von hüftgelenknahen Frakturen. Unfallchirurg 1994;97:132–8.
13. Heinz Th, Vecsei V. Komplikationen und Fehler bei der Anwend-ung des Gammanagels. Chirurg 1994;65:943–52.
14. Hohendorff B, Meyer P, Menezes D, et al. Behandlungsergebnisse und Komplikationen nach PFN-Osteosynthese. Unfallchirurg 2005;108:938–53.
15. Huberts U, et al. Hat die 130-Grad-Winkelplatte bei der Stabi-lisierung hüftgelenksnaher Frakturen noch ihre Berechtigung? In: Rahmenzadeh R, Meißner A, Würtenberger C (eds.) Unfall- und Wiederherstellungs-Chirurgie des proximalen Femurs und des Beckengürtels, Einhorn, Reinbek, 1994;169–71.
16. Kaiser W, Gulielmos V, David T. Zum klinischen Verlauf operativ versorgter hüftgelenksnaher Femurfrakturen in der geria-trischen Chirurgie Unfallchirurg 1994;20:30–6.
17. Kukla C, Pichl W, Prokesch R, et al. Femoral neck fracture after removal of the standard gamma interlocking nail: a cadaveric study to determine factors influencing the biomechanical prop-erties of the proximal femur. J Biomech. 2001;34:1519–26.
18. Lucke C, Phillip J, Krause D. Operative Ergebnisse pertrochanterer Frakturen Unfallchirurg 1995;98:272–7.
19. Lustenberger A, Bekie J, Ganz R. Roatationsstabilität tro-chanterer Femurfrakturen fixiert mit der DHS. Unfallchirurg 1995;98:514–7.
20. Manner M, Ruf W. Die dynamische Hüftschraube. Unfallchirurg 1994;91:299–306
Gehr J, et al. The Gliding Nail
569European Journal of Trauma 2006 · No. 6 © Urban & Vogel
21. Müller-Färber J, Wittner B, Reichel R. Spätergebnisse nach Ver-sorgung pertrochanterer Femurfrakturen des alten Menschen mit DHS Unfallchirurg 1988;91:341–50.
22. Muller B, Bonnaire F, Heckel T, et al. Ender-Nagel mit Verriege-lung oder dynamische Hüftschraube bei petrochanteren Frak-turen? Unfallchirurg 1994;20:18–29.
23. Saudan M, Lubbeke A, Sadowski C, et al. Pertrochanteric frac-tures: is there an advantage to an intramedullary nail? J Orthop Trauma 2002;16:386–93.
24. Simmeracher RKJ, Bosch AN, Van der Werken C. The AO/ASIF-proximal femoral nail (PFN): a new device fort he treat-ment of unstable proximal femoral. Injury Int J Care Injured 1999;30:327–32.
25. Werner-Tutschku W, Lajtai G, Schmiedhuber G, et al. Intra and perioperative complications in stabilization of per- and sub-trochanteric femoral fractures by mean of PFN. Unfallchirurg 2002;105:881–5.
Address for CorrespondenceJonas GehrKlinikum Aschaffenburg – UnfallchirurgieAm HasenkopfAschaffenburg 63739Germanye-mail: mailto: [email protected]




















