Idiopathic hypereosinophilic syndrome: a rare cause of erythroderma
Upload
independentCategory
view
1download
0
The Spine Journal - (2013) -
Clinical Study
The effects of backpack load and carrying method on the balanceof adolescent idiopathic scoliosis subjects
Sonia Sahli, PhDa,*, Haithem Rebai, PhDb, Sameh Ghroubi, MDa,c, Abdelmonem Yahia, MDa,c,Mohamed Guermazi, MDa,c, Mohamed Habib Elleuch, MD, PhDa,c
aUnit�e de Recherche sur les Pathologies de l’Appareil Locomoteur 04 UR 07/08, CHU Habib Bourguiba, Universit�e du Sud, 3029 Sfax, TunisiabUnit�e de Recherche Adaptations Cardio-circulatoires, Respiratoires, M�etaboliques et Hormonales �a l’Exercice Musculaire,
Facult�e de M�edecine Ibn El Jazzar, Universit�e du Centre, 4002 Sousse, TunisiacService de M�edecine Physique et R�eadaptation Fonctionnelle, CHU Habib Bourguiba, Universit�e du Sud, 3029 Sfax, Tunisia
Received 18 January 2012; revised 29 October 2012; accepted 1 June 2013
Abstract BACKGROUND CONTEXT: Concerns have
FDA device/drug
Author disclosures
SG: Nothing to discl
close. MHE: Nothing
* Corresponding
R�eadaptation Fonctio
3029 Sfax, Tunisia. T
E-mail address: s
1529-9430/$ - see fro
http://dx.doi.org/10.10
been raised about the effect of backpack carryingon adolescent balance. For adolescent idiopathic scoliosis (AIS) subjects, the effect of backpackcarrying method on their balance has not been determined. Our aim is to examine the effects ofbackpack load and carrying method on AIS subjects’ balance.STUDY DESIGN/SETTING: Paired sample matched for age and sex.PATIENT SAMPLE: Twelve healthy adolescents matched for age and sex with 14 adolescentswith mild AIS participated in this study.OUTCOMEMEASURES: A test battery including clinical examination, radiological assessment,and stabilometric measurements of the postural sways in the upright standing posture wereconducted.METHODS: Center of pressure excursions of our subjects were recorded with a stabilometricplatform during the upright standing posture without a backpack and while carrying a backpacksymmetrically and asymmetrically on each shoulder. For each carrying method, the backpack isloaded at 10% and 15% of body weight (BW).RESULTS: Our results indicated that postural sways increased with increasing backpack load.These postural sways were observed when normal adolescents carried a backpack loaded with15% BW load, whereas, for age- and sex-matched AIS subjects, these postural responses were ob-served for the 10% BW load. The symmetrical backpack carrying induced better balance comparedwith the asymmetrical one. Asymmetrical carrying on the convex side of the scoliotic curve affectsAIS subjects’ balance more than carrying it on the concave side.CONCLUSIONS: Load carriage of 10% BW seems to alter AIS subjects’ balance. Asymmetricalcarrying should be avoided especially on the convex side of the scoliotic curve because it causesbalance impairments that may increase spinal pain. � 2013 Elsevier Inc. All rights reserved.
Keywords: Balance; Adolescent idiopathic scoliosis; Backpack load; Backpack carrying method
Introduction
Idiopathic scoliosis is a lateral and rotational spinal cur-vature in the absence of associated congenital or neurologic
status: Not applicable.
: SS: Nothing to disclose. HR: Nothing to disclose.
ose. AY: Nothing to disclose. MG: Nothing to dis-
to disclose.
author. Service de M�edecine Physique et
nnelle, CHU Habib Bourrguiba, Universit�e du Sud,
el.: (216) 20001928; fax: (216) 74278502.
[email protected] (S. Sahli)
nt matter � 2013 Elsevier Inc. All rights reserved.
16/j.spinee.2013.06.023
abnormalities [1]. The adolescent form accounts for mostcases of this disease [1]. Although there is no establishedcause, idiopathic scoliosis has been associated with severalsensory and motor impairments [2]. These impairmentswould lead to balance control problems [3,4]. Posturalchanges in the body attitude associated with scoliosis couldbe responsible for the balance problems that have beenreported in adolescent idiopathic scoliosis (AIS) [5]. Formany studies, the postural stability control of AIS patientswould exhibit lesser stability than the healthy controls[5–9]. For others, scoliosis has no significant effect[10,11] or induces greater stability [12].

2 S. Sahli et al. / The Spine Journal - (2013) -
The balance of upright standing posture is also influ-enced by external factors such as load carriage that is ofparticular concern in children with AIS [13] as there are in-dications that postural disequilibrium may be a contributoryetiological factor in AIS [6]. Therefore, further impairmentof balance because of schoolbag carrying may play a role inthe development of the scoliotic deformity [13]. Severalstudies on normal adolescents showed an increase in thetrunk forward inclination [3,14,15] and an increase in thehead forward inclination [14,16] because of load carrying.Relatively little experimental data about the effect of back-pack carriage on standing balance have been reported. Gohet al. [17] proposed that backpack carriage would increasestability. However, an increase in the center of pressure(CoP) range of motion in the anteroposterior [13,18] andthe mediolateral [13] directions has been observed with in-creasing load. The same effect of backpack carriage on bal-ance control has been reported for subjects with mild AISincluding an increase in the range of sway with increasingbackpack load [13].
Concerns have been raised about the effects of school-bag load on adolescents, and Sahlstrand et al. [6] recom-mended that the load should be limited between 10% to15% body weight (BW). Based on trunk inclination mea-surements, Hong and Cheung [19] suggested a maximumpermissible backpack load of 15% BW, whereas posturalresponses to increasing load suggested a critical load of ap-proximately 10% BW [20]. However, is the recommendedload limit for normal adolescents equally applicable tothose with musculoskeletal disorders and in particularAIS? To our knowledge, there are no experimental dataother than those reported by Chow et al. [13] suggestingthat lower backpack loads than 10% BW may be appropri-ate for subjects with AIS.
Although both AIS and backpack weight affect standingposture and balance, no studies could be found reportingthe effect of the method in which the load is carried onthe balance of these subjects. For normal adolescents, ithas been found that, compared with the two-strap back-pack, carrying schoolbags on one shoulder significantly al-ters the posture of adolescents [14,21–23] and maycontribute to the development of back pain [23].
The purpose of this study was to determine the effect ofbackpack load and carrying method on the CoP sway dur-ing the upright standing posture in AIS subjects comparedwith normal subjects to help establish the recommendedbackpack load limits and the best method of carriage forthese subjects. In this context, we hypothesized that pos-tural sway induced by backpack carrying would increasewith increasing backpack load, and the recommended loadlimit for normal adolescents would not be applicable to AISsubjects. We further hypothesized that similarly to normaladolescents, asymmetrical backpack carrying would alterpostural stability of AIS subjects more than do symmetricalcarrying.
Methods
Design
The study methodology was based on a controlled re-peated measures design where a group of AIS subjects werecompared with normal subjects matched for age and sex.The dependent variables were CoP sway area and lateraland anteroposterior mean positions. The independent vari-ables consisted of three backpack loads (0%, 10%, and15% BW) and three backpack carrying methods (a symmet-rical carrying method with the two straps on both shouldersand two asymmetrical carrying methods with one strapacross one shoulder).
Patients
A scoliotic group of 14 adolescents with idiopathic sco-liosis (13 females and 1 male) and a control group of 12healthy subjects matched for age, height, and weight partic-ipated in this study. The subjects of the scoliotic group wererecruited from the Orthopaedic and Traumatology Serviceof the University Hospital Habib Bourguiba in Sfax, Tuni-sia. The mean age, height, and weight for this group were14.1761.64 years, 1.6060.09 m, and 51.7568.77 kg, re-spectively. Their inclusion criteria were X-ray evidence ofmild AIS with a lumbar or thoracolumbar curve definedby a Cobb angle between 10� and 28� and no previous con-servative or surgical treatment for the scoliosis. The majorcurve was to the left in 4 subjects and to the right in 10. Ex-clusion criteria were previous orthopedic surgery, central orperipheral neurologic disorders, or other spinal disorders.The control group subjects were recruited from the generalcommunity and friends and family of the researchers. Themean age, height, and weight for the control group were13.261.62 years, 1.5960.08 m, and 45.366.55 kg, respec-tively. Their inclusion criteria were a normal X-ray of thespine (no thoracic, thoracolumbar, or lumbar prominenceO5� screened with a scoliometer in the forward bendingposition [24], no previous spinal disorders, no previous or-thopedic surgery, and no central or peripheral neurologicdisorders). All clinical examinations performed for sub-jects’ screening were done by the same clinician.
All subjects participated voluntarily in this study andgave, with their parents, informed consent before datacollection.
Procedure and data collection
It has been suggested that force-plate CoP data can beused to determine differences in the standing balance be-tween children and adolescents of different ages and thosewith movement and balance abnormalities [25]. Therefore,our subjects were asked to stand barefoot on a static stabi-lometric platform (SATEL, Blagnac, France) that com-prised a steel plate (480�480 mm) supported by three

Fig. 2. Picture of a subject wearing backpack.
3S. Sahli et al. / The Spine Journal - (2013) -
sensors and in level with the surrounding floor (Fig. 1). Theforce sensors used in this platform are SP4 (type ‘‘constantmoment beams,’’ sensibility 260.1 mV/V, maximal weight100 kg, and frequency 40 Hz) manufactured by HBM orSCAIME.
Foot positions were marked appropriately to standardizestance with the heels 5 cm apart and a 30�angle between thelong axes of the feet. They were instructed to maintain a re-laxed upright standing posture as still as possible with armscomfortably placed downward at either side of the bodyand gaze fixed straight ahead at a white cross placed ontothe wall 2 m away at the eye level.
The upright standing posture of each subject was re-corded while carrying a backpack loaded at 0%, 10%,and 15% BW (Fig. 2). The percentage of BW, rather thanabsolute weight, was used to classify the carrying load sothat normalization across subjects could be achieved. Thebackpack used for all tests was a standardized dual strap de-sign comprising a soft backpack with no internal framing orback support, two padded adjustable shoulder straps, nowaist or chest compression straps, no internal compart-ments, and one size only. The carrying methods comparedin this study were a symmetrical carrying method with thetwo straps on both shoulders and two asymmetrical carry-ing methods with one strap across the shoulder. For the con-trol group, the two asymmetrical carrying methods wereacross the right shoulder and across the left shoulder. Forthe clinical relevance, these asymmetrical carrying methodsfor the scoliotic group were across the shoulder on the con-vex side of the scoliotic curve and across the shoulder onthe concave side of the scoliotic curve. Therefore, nine dif-ferent experimental conditions of backpack load and carry-ing method were investigated in this study. There werethree trials in each experimental condition for a total of27 trials for each subject. Following French PosturologyAssociation norms (Normes 85), each trial lasted 51.2 s.A resting period of 30 s was allowed between trials to can-cel fatigue effects. Trials were presented in a random orderto cancel learning or fatigue effects. Data collection was
Fig. 1. The experimental device used (static stabilometric platform
SATEL).
initiated after subjects had adopted the required postureon the platform, stabilized their postural sway, and signaledto the examiner that they were ready to begin. During therecording session, the examiner remained near the subjectfor security without touching him or providing additionalinstructions and took care that the posture was maintainedthroughout the trials. All these measurements were per-formed by the same examiner who is well trained withyears of expertise.
Data analysis
To analyze the postural balance of the two groups, threeCoP parameters were calculated: the CoP sway area andlateral and anteroposterior mean positions. The sway areaparameter is considered as subject postural stability criteria,whereas the mediolateral and anteroposterior mean posi-tions are considered as subject bodily orientation criteria[26]. The best postural balance is for the lower values ofsway area and mediolateral and anteroposterior mean posi-tions of the CoP. The three parameters were averaged forthe three trials per condition and per subject to obtain a rep-resentative measure of the postural balance. All posturaldata were interpreted by the same researcher with at least5-year experience in this field.
Statistical analysis
Statistics were performed with Statistica software(StatSoft, Maisons-Alfort, France), and statisticians were

4 S. Sahli et al. / The Spine Journal - (2013) -
blinded. Shapiro-Wilk test used to assess the normality of thedata revealed that the data were normally distributed.Mauchly sphericity test was performed to examine data sphe-ricity. Results revealed that all chi-square approximationswere associated with p value greater than .05. Therefore,the sphericity assumption has not been violated, and accord-ing to this, analysis of variance (ANOVA) for repeated mea-sures was performed. As the backpack carrying methodfactor for theAIS group differs from that of the control group,data related to each group were first analyzed separately. Foreach group, a two-way repeated measures ANOVA (back-pack carrying method and backpack load) was applied to de-termine the effect of backpack load and/or carrying methodon the dependent variables. The backpack carrying methodfactor has three levels: one symmetrical carrying and twoasymmetrical ones (on the right/left shoulder for the controlgroup and on the convex/concave side of the scoliotic curvefor AIS group). The backpack load factor has three levels:0%, 10%, and 15% BW conditions. The effect of groupwas investigated by applying a three-way repeated measuresANOVA. For each statistically significant effect of main fac-tor and interaction, a post hoc analysis was performed usingthe TukeyHSD test. Effect sizeswere calculated as partial etasquared hp
2 to assess the practical significance of our find-ings. The alpha level of statistical significance was set at pvalue less than .05.
Results
The three-way repeated measures ANOVA revealed sig-nificant main effect of group, on all the stability and bodilyorientation parameters (Table). Post hoc analysis showedthat these parameters were significantly higher in the AISgroup (Figs. 3–5). No significant group�load interaction,
Table
A summary of the results of statistical analyses
Parameters
Sway area A
p, hp2
Group .002, 0.65 .0
Load !.001, 0.74 !Carrying method NS !Group�load NS .0
Load�carrying method NS .0
Group�carrying method .002, 0.48 .0
Group�load�carrying method NS .0
AIS group results
Load !.001, 0.59 !Carrying method .002, 0.41 !Load�carrying method NS !
Control group results
Load !.001, 0.62 .0
Carrying method NS N
Load�carrying method NS N
AIS, adolescent idiopathic scoliosis.
Note: p and, hp2 values are indicated for significant main effects and interactio
NS where not significant.
except on the CoP anteroposterior mean position, was seen(Table). Results of the separate statistical analysis appliedin each group revealed significant effect of load on all the de-pendent parameters. Post hoc analysis showed that the pos-tural stability and bodily orientation parameters increasedsignificantly as the backpack load increased (Figs. 3–5).However, for the control group, this increase was not signif-icant between the 0% and 10% load conditions (Figs. 3–5).The carrying method effect on the postural stability andbodily orientation parameters was found to be significantfor the AIS group but not for the control group (Table).Values of all of these parameters were significantly lowerwhen the backpack was carried symmetrically across thetwo shoulders compared with when it was carried asymmet-rically across one shoulder in the convex side of the scolioticcurve (Figs. 3–5). Significant lower values of all these pa-rameters were also found for the asymmetrical backpack car-riage across one shoulder in the concave side of the scolioticcurve compared with those recorded for the carriage acrossone shoulder in the convex side of the scoliotic curve (Figs.3–5). However, no significant difference was seen betweenpostural stability and bodily orientation values recorded withschoolbag carried symmetrically across the two shouldersand those recorded with backpack carried asymmetricallyacross one shoulder in the concave side of the scoliotic curve(Figs. 3–5). Significant carrying method�load interactionwas found on the bodily orientation parameters but not onthe postural stability parameter (Table). No adverse eventsoccurred during testing.
Discussion
Postural balance results assessed by postural stabilityand bodily orientation parameters indicated that the AIS
nteroposterior mean position Mediolateral mean position
4, 0.61 .04, 0.38
.001, 0.65 .001, 0.63
.001, 0.65 NS
31 .03, 0.31
08, 0.31 NS
01, 0.54 .02, 0.33
1, 0.27 NS—
.001, 0.59 !.001, 0.58
.014, 0.64 !.014, 0.31
.02, 0.35 !.027, 0.22
01, 0.5 .011, 0.39
S NS
S NS
ns among group, load, and carrying method as appropriate and are marked
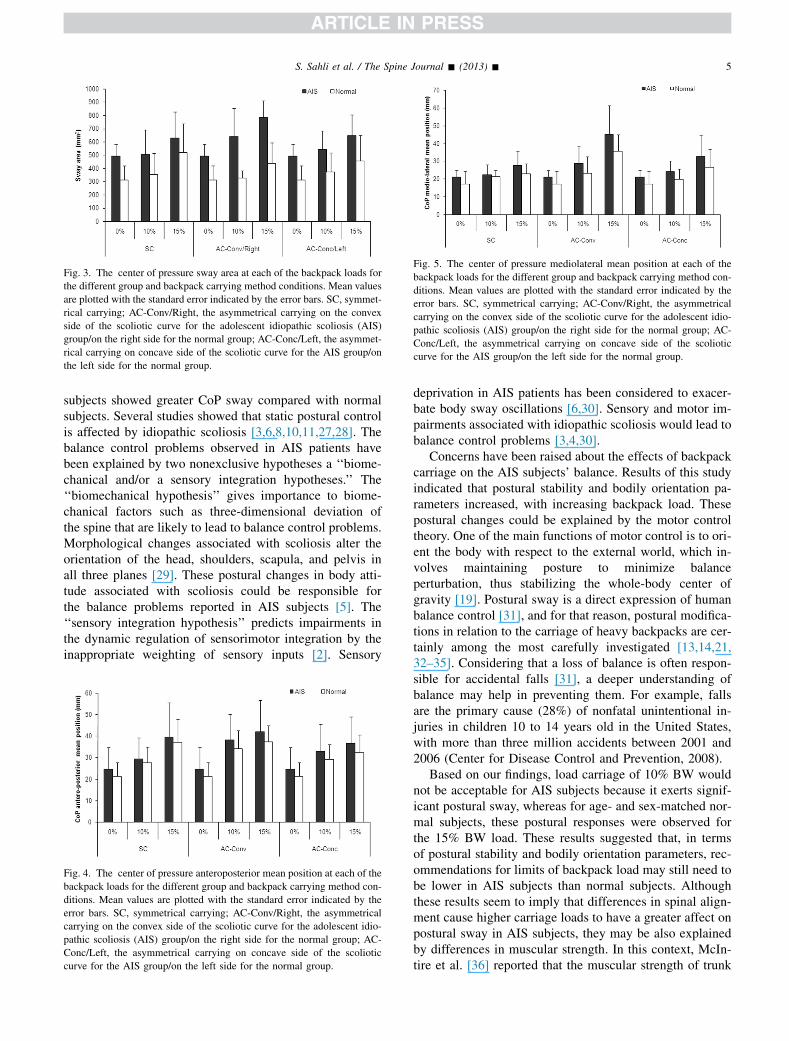
Fig. 3. The center of pressure sway area at each of the backpack loads for
the different group and backpack carrying method conditions. Mean values
are plotted with the standard error indicated by the error bars. SC, symmet-
rical carrying; AC-Conv/Right, the asymmetrical carrying on the convex
side of the scoliotic curve for the adolescent idiopathic scoliosis (AIS)
group/on the right side for the normal group; AC-Conc/Left, the asymmet-
rical carrying on concave side of the scoliotic curve for the AIS group/on
the left side for the normal group.
Fig. 5. The center of pressure mediolateral mean position at each of the
backpack loads for the different group and backpack carrying method con-
ditions. Mean values are plotted with the standard error indicated by the
error bars. SC, symmetrical carrying; AC-Conv/Right, the asymmetrical
carrying on the convex side of the scoliotic curve for the adolescent idio-
pathic scoliosis (AIS) group/on the right side for the normal group; AC-
Conc/Left, the asymmetrical carrying on concave side of the scoliotic
curve for the AIS group/on the left side for the normal group.
5S. Sahli et al. / The Spine Journal - (2013) -
subjects showed greater CoP sway compared with normalsubjects. Several studies showed that static postural controlis affected by idiopathic scoliosis [3,6,8,10,11,27,28]. Thebalance control problems observed in AIS patients havebeen explained by two nonexclusive hypotheses a ‘‘biome-chanical and/or a sensory integration hypotheses.’’ The‘‘biomechanical hypothesis’’ gives importance to biome-chanical factors such as three-dimensional deviation ofthe spine that are likely to lead to balance control problems.Morphological changes associated with scoliosis alter theorientation of the head, shoulders, scapula, and pelvis inall three planes [29]. These postural changes in body atti-tude associated with scoliosis could be responsible forthe balance problems reported in AIS subjects [5]. The‘‘sensory integration hypothesis’’ predicts impairments inthe dynamic regulation of sensorimotor integration by theinappropriate weighting of sensory inputs [2]. Sensory
Fig. 4. The center of pressure anteroposterior mean position at each of the
backpack loads for the different group and backpack carrying method con-
ditions. Mean values are plotted with the standard error indicated by the
error bars. SC, symmetrical carrying; AC-Conv/Right, the asymmetrical
carrying on the convex side of the scoliotic curve for the adolescent idio-
pathic scoliosis (AIS) group/on the right side for the normal group; AC-
Conc/Left, the asymmetrical carrying on concave side of the scoliotic
curve for the AIS group/on the left side for the normal group.
deprivation in AIS patients has been considered to exacer-bate body sway oscillations [6,30]. Sensory and motor im-pairments associated with idiopathic scoliosis would lead tobalance control problems [3,4,30].
Concerns have been raised about the effects of backpackcarriage on the AIS subjects’ balance. Results of this studyindicated that postural stability and bodily orientation pa-rameters increased, with increasing backpack load. Thesepostural changes could be explained by the motor controltheory. One of the main functions of motor control is to ori-ent the body with respect to the external world, which in-volves maintaining posture to minimize balanceperturbation, thus stabilizing the whole-body center ofgravity [19]. Postural sway is a direct expression of humanbalance control [31], and for that reason, postural modifica-tions in relation to the carriage of heavy backpacks are cer-tainly among the most carefully investigated [13,14,21,32–35]. Considering that a loss of balance is often respon-sible for accidental falls [31], a deeper understanding ofbalance may help in preventing them. For example, fallsare the primary cause (28%) of nonfatal unintentional in-juries in children 10 to 14 years old in the United States,with more than three million accidents between 2001 and2006 (Center for Disease Control and Prevention, 2008).
Based on our findings, load carriage of 10% BW wouldnot be acceptable for AIS subjects because it exerts signif-icant postural sway, whereas for age- and sex-matched nor-mal subjects, these postural responses were observed forthe 15% BW load. These results suggested that, in termsof postural stability and bodily orientation parameters, rec-ommendations for limits of backpack load may still need tobe lower in AIS subjects than normal subjects. Althoughthese results seem to imply that differences in spinal align-ment cause higher carriage loads to have a greater affect onpostural sway in AIS subjects, they may be also explainedby differences in muscular strength. In this context, McIn-tire et al. [36] reported that the muscular strength of trunk

6 S. Sahli et al. / The Spine Journal - (2013) -
muscles is weaker in AIS females compared with healthyones. Caution should be taken when recommending loadlimits. The relevance of the parameter(s) used to determineany load limit should be considered carefully as differingchoice of parameters may lead to different recommenda-tions for load limits [37] Hong and Brueggemann [38] rec-ommended a backpack load limit of 10% BW on the basisof significant changes in forward trunk lean and blood pres-sure recovery time of 10-year-old boys walking on a tread-mill. For college-aged students, carrying loads of 10% BWand above should be avoided because these loads inducesignificant changes in electromyography, kinematics, andsubjective scores [32]. Carrying a backpack weighing15% BW changes all the postural angles in preadolescentchildren [33,39]. Investigation of gait parameters indicatinga critical response to increasing load appears to suggest thatthis critical load may be lower for AIS subjects (7.5% BW)than normal controls (10% BW) [37]. No interaction be-tween load carriage and group was found, which means thatbackpack carriage seems to have a similar effect on pos-tural stability of both normal and AIS subjects. This indi-cates that the effects of AIS and backpack load factors onpostural stability appear to be independent and are likelyto be additive as reported in a previous study [13]. It hasbeen demonstrated that postural disequilibrium may bea contributory etiological factor in AIS [6]; therefore, fur-ther balance impairment because of backpack carriagemay play a role in the development of the scoliotic defor-mity [13]. In addition, although excessive backpack loadis unlikely to be the primary cause of falls in children[40], the compromise of balance because of the AIS, com-bined with backpack carrying, may decrease their toleranceof perturbation before fall occurs compared with normalsubjects [13].
Because of concerns raised about the effects of school-bag carriage on adolescent balance, many studies investi-gated the effects of symmetrical and asymmetrical loadcarriage on the balance of normal adolescents. However,these effects are not known in AIS subjects. Our AIS groupresults showed that, in all load conditions, the symmetricalbackpack carriage induced better postural stability andbodily orientation compared with the asymmetrical one.This result was statistically significant when symmetricalbackpack carriage was compared with the asymmetricalbackpack carriage on the convex side. Based on the kine-matics of the upright standing posture [14,22,34] and/orgait patterns [14,22,34,41,42], it has been concluded thatnormal adolescents are more stable when they carry a back-pack bilaterally than unilaterally. Pascoe et al. [14] foundpostural changes only when youths carried book bags onone shoulder and concluded that the daily physical stressassociated with this carrying method significantly altersthe posture and gait of the youth, whereas when they walkwith a backpack, trunk co-contraction increases to continueto provide both static and dynamic stability. Unilateralbackpack carrying causes an asymmetrical external
moment about the spinal column [42] to counteract theasymmetrical external load disturbance. This can beachieved by trunk lateral inclination away from the load[41] and shoulder elevation [42]. Such postural adjustmentsreflect the need to bring toward the central body line a loadthat is positioned too laterally [34] that may alter posturalstability and bodily orientation. It has been shown that,for normal schoolgirls, postural effects of asymmetricalload carrying were the same regardless of which shoulderwas used (right or left) [34]. Our AIS group data showedthat carrying the backpack on the convex side of the curveaffects postural performance more than carrying it on theconcave one. The most probable explanation of these find-ings is the asymmetrical back muscle activity associatedwith the asymmetrical load carrying in AIS subjects. Infact, one-sided carrying technique may be prone to fatiguebecause of increased muscular activity on the side oppositeto the load [23,42]. On the other hand, data from the previ-ous studies demonstrated that back muscles of the convexside of the scoliotic curve produced more EMG than backmuscles of the concave side [43,44]. That is, asymmetricalbackpack carrying on the convex side of the curve imposesa higher load demand on the concave side muscles inducinga probable fatigue because of the weakness of these mus-cles, which could increase the perceived spinal pain, as ithas been found that weak back extensors play a role inthe development of spinal pain [45].
Clinical relevance
The most important clinical implication of this study isprevention. It has been shown that injuries associated withbackpack use by children usually involve falls; therefore,educating them on the importance of backpack carryingis likely to prevent future injury and back pain caused bycarrying a backpack [42]. As the compromise of balancebecause of the combination of backpack carrying and AISmay decrease tolerance of perturbation before fall occurs,the risk of balance loss and associated injury may be greaterin AIS subjects [13]. Although there is no evidence for anyinteraction between AIS and carried load effects on the re-corded postural stability and bodily orientation parameters,examination of our results indicating a critical response toincreasing load appears to suggest that the backpack loadlimit may be lesser for AIS subjects (10% BW) than age-and sex-matched normal controls (15% BW). The findingsof our study highlight the fact that preventing back pain andinjury may be best accomplished through adolescent’s com-pliance not only with suggested load limits but also withrecommended backpack carrying method. In fact, AIS sub-jects should be advised to carry their backpack on twoshoulders rather than on one shoulder because asymmetri-cal backpack carrying alters postural stability and bodilyorientation more than symmetrical backpack carrying does.Nevertheless, most of our adolescent population prefer to

7S. Sahli et al. / The Spine Journal - (2013) -
carry their backpack on one shoulder. In this case, carryingbackpack on the convex side of the scoliotic curve shouldbe avoided because it significantly increases postural sway.As postural sway represents an effective indicator of bal-ance abilities, the alterations observed suggest that thisbackpack carrying method leads to balance impairment.
In addition, because subjects leaned laterally away fromthe side on which the backpack was carried [41] and elevatetheir shoulder [42], a backpack carried on the convex sideof a scoliotic curve may lead to a development of the per-ceived spinal pain.
Limitations
It is important to recall that the present study is limitedto an investigation of the immediate effects of backpackcarriage on stability and bodily orientation in a restedstanding posture, which is not consistent with the habitualuse of backpack [33]. In habitual loading conditions, ado-lescents are frequently walking while carrying a backpack.The duration of the backpack carriage may have a signifi-cant effect on the balance parameters [33] as muscular fa-tigue becomes evident [46]. Therefore, the longer termeffects of load carriage and associated fatigue should be in-vestigated in future studies of AIS subjects’ balance.
Our results suggest that a 10% BW load, fairly commonin this population, seems to alter postural stability andbodily orientation. The effects of this load were studied onlyin relation to those of a 15% BW load; thus, we do not knowwhat findings would emerge considering the question in re-lation to lighter loads. It has been demonstrated that the spi-nal level at which the backpack is carried can affect thepostural changes observed [33,46]. Although we carefullychanged individually the length of the straps, so as to applythe load in the higher buttocks as usually done by the sub-jects of our study, obviously, in real life, the load applied tothe spine can change according to the leverage generated bythe distribution of the load in the backpack and to the straptension [47], which may be a source of some error. Further-more, other features of pack design may affect these results,such as adding sternum straps, frame sheets, or waist belts.Likewise, only mild cases of AIS (Cobb angles of between10� and 28�) were considered in the present study. Yamadaet al. [48] indicated that the degree of balance dysfunctionwas related to curve severity. Therefore, the effects of thesefactors need to be evaluated too.
Conclusions
Significant postural sways were observed when normaladolescents carried a backpack loaded with 15% BW load.This backpack load limit should be lower for age- and sex-matched AIS subjects as load carriage of 10% BW seems toalter their postural stability and bodily orientation. Thecompromise of balance because of the AIS combined with
backpack carrying may decrease their tolerance of pertur-bation before a fall occurs. The symmetrical backpackcarrying induced better postural stability and bodily orien-tation compared with the asymmetrical one. But if AIS sub-jects prefer to carry their backpack asymmetrically,carrying it on the convex side of the scoliotic curve shouldbe avoided because it affects postural stability more thancarrying it on the concave one. Such carrying methodcauses balance impairment and may potentially increasespinal pain. Overall, AIS subjects were recommended tocarry a backpack loaded less than 10% BW and to carryit on both shoulders, particularly avoiding carrying it onthe convex side of their scoliotic curve.
Acknowledgments
We would like to thank all the adolescent participantsand their families. We also thank the head of the orthopae-dic and traumatologic department of the University Hospi-tal Habib Bourguiba in Sfax, Tunisia, for collaboration andhelps in AIS subject recruitment.
References
[1] Greiner KA. Adolescent idiopathic scoliosis: radiologic decision-
making. Am Fam Physician 2002;65:1817–22.
[2] Simoneau M, Mercier P, Blouin J, et al. Altered sensory-weighting
mechanisms is observed in adolescents with idiopathic scoliosis.
BMC Neurosci 2006;7:1–9.
[3] Byl NN, Holland S, Jurek A, Hu SS. Postural imbalance and vibra-
tory sensitivity in patients with idiopathic scoliosis: implications
for treatment. J Orthop Sports Phys Ther 1997;26:60–8.
[4] Gauchard GC, Lascombes P, Kuhnast M, Perrin PP. Influence of dif-
ferent types of progressive idiopathic scoliosis on static and dynamic
postural control. Spine 2001;26:1052–8.
[5] Nault ML, Allard P, Hinse S, et al. Relations between standing stabil-
ity and body posture parameters in adolescent idiopathic scoliosis.
Spine 2002;27:1911–7.
[6] Sahlstrand T, Ortengren R, Nachemson A. Postural equilibrium in ad-
olescent idiopathic scoliosis. Acta Orthop Scand 1978;49:354–65.
[7] Chen TH, Tsuang YH. Body center of pressure in idiopathic scolio-
sis. J Orthop Surg ROC 1994;11:215–21.
[8] Chen PQ, Wang JL, Tsuang YH, et al. The postural stability control
and gait pattern of idiopathic scoliosis adolescents. Clin Biomech
(Bristol, Avon) 1998;13:S52–8.
[9] Silferi V, Rougier P, Labelle H, Allard A. Postural control in idio-
pathic scoliosis: comparison between healthy and scoliotic subjects.
Rev Chir Orthop Reparatrice Appar Mot 2004;90:215–25.
[10] Gregoric M, Pecak F, Trondelj JV, Dimitrijevic MR. Postural control
of scoliosis. A statokinesimetric study in patients due to neuromuscu-
lar disorders and in patients with idiopathic scoliosis. Acta Orthop
Scand 1981;52:59–63.
[11] Driscoll DM, Newton RA, Lamb RL, Nozi J. A study of postural
equilibrium in idiopathic scoliosis. J Pediatr Orthop 1984;6:
677–81.
[12] Adler N, Bleck EE, Ringsky LA, Young W. Balance reactions and
eye-hand coordinations in idiopathic scoliosis. J Orthop Res
1986;4:102–7.
[13] Chow DHK, Kwok MLY, Cheng JCY, et al. The effect of backpack
weight on the standing posture and balance of schoolgirls with ado-
lescent idiopathic scoliosis and normal controls. Gait Posture
2006;24:173–81.

8 S. Sahli et al. / The Spine Journal - (2013) -
[14] Pascoe DD, Pascoe DE, Wang YT, et al. Influence of carrying book
backpacks on gait cycle and posture of youths. Ergonomics 1997;40:
631–41.
[15] Li JX, Hong Y, Robinson PD. The effect of load carriage on move-
ment kinematics and respiratory parameters in children during walk-
ing. Eur J Appl Physiol 2003;29:35–43.
[16] Grimmer KA, Williams MT, Gill TK. The associations between ad-
olescent head-on-neck posture, backpack weight, and anthropometric
features. Spine 1999;24:2262–7.
[17] Goh JH, Thambyah A, Bose K. Effects of varying backpack loads on
peak forces in the lumbosacral spine during walking. Clin Biomech
1998;13:S26–31.
[18] Palumbo N, George B, Johnson A, Cade D. The effects of backpack
load carrying on dynamic balance as measured by limits of stability.
Work 2000;16:123–9.
[19] Hong Y, Cheung CK. Gait and posture responses to backpack load
during level walking in children. Gait Posture 2003;17:28–33.
[20] Chow DH, KwokML, Au-Yang AC, et al. The effect of backpack load
on the gait of normal adolescent girls. Ergonomics 2005;48:642–56.
[21] Cottalorda J, Rahmani A, Diop M, et al. Influence of school bag car-
rying on gait kinetics. J Pediatr Orthop B 2003;12:357–64.
[22] Cottalorda J, Bourelle S, Gautheron V, Kohler R. Backpack and spi-
nal disease: myth or reality? Rev Chir Orthop Reparatrice Appar Mot
2004;90:207–14.
[23] Motmans RR, Tomlow S, Vissers D. Trunk muscle activity in differ-
ent modes of carrying schoolbags. Ergonomics 2006;49:127–38.
[24] Bunnell WP, Delaware W. An objective criterion for scoliosis screen-
ing. J Bone Surg Am 1984;66:1381–7.
[25] Wolff DR, Rose J, Jones VK, et al. Postural balance measurements
for children and adolescents. J Orthop Res 1998;16:271–5.
[26] P�erennou D, Decavel P, Manckoundia P, et al. Evaluation of balance in
neurologic and geriatric disorders. Ann Readapt Med Phys 2005;48:
317–35.
[27] Byl NN, Gray JM. Complex balance reactions in different sensory
conditions: adolescents with and without idiopathic scoliosis. J Or-
thop Res 1993;11:215–27.
[28] Allard P, Chavet P, Barbier F, et al. Effect of body morphology on
standing balance in adolescent idiopathic scoliosis. Am J Phys Med
Rehabil 2004;83:689–97.
[29] Le Blanc R, Labelle H, Forest F, et al. Possible relationship between
idiopathic scoliosis and morphologic somatotypes in adolescent fe-
males. Ann Chir 1995;49:762–7.
[30] Simoneau M, Richer N, Mercier P, et al. Sensory deprivation and bal-
ance control in idiopathic scoliosis adolescent. Exp Brain Res
2006;170:576–82.
[31] Winter A. Human balance and posture control during standing and
walking. Gait Posture 1995;3:193–214.
[32] Devroey C, Jonkers I, de Becker A, et al. Evaluation of the effect of
backpack load and position during standing and walking using
biomechanical, physiological and subjective measures. Ergonomics
2007;50:728–42.
[33] Brackley HM, Stevenson JM, Selinger JC. Effect of backpack load
placement on posture and spinal curvature in prepubescent children.
Work 2009;32:351–60.
[34] Negrini S, Negrini A. Postural effects of symmetrical and
asymmetrical loads on the spines of schoolchildren. Scoliosis
2007;2:8.
[35] Grimmer K, Dansie B, Milanese S, et al. Adolescent standing pos-
tural response to backpack loads: a randomized controlled experi-
mental study. BMC Musculoskelet Disord 2002;17:3–10.
[36] McIntire KL, Asher MA, Burton DC, Liu W. Trunk rotational
strength asymmetry in adolescents with idiopathic scoliosis: an ob-
servational study. Scoliosis 2007;2:9.
[37] Chow DHK, Kwok MLY, Au-Yang ACK, et al. The effect of load car-
riage on the gait of girls with adolescent idiopathic scoliosis and nor-
mal controls. Med Eng Phys 2006;28:430–7.
[38] Hong Y, Brueggemann P-G. Changes in gait patterns in 10-yearold
boys with increasing loads when walking on a treadmill. Gait Posture
2000;11:254–9.
[39] Ramprasad M, Alias J, Raghuveer AK. Effect of backpack weight on
postural angles in preadolescent children. Indian Pediatr 2010;47:
575–80.
[40] Pau M, Pau M. Postural sway modifications induced by backpack car-
riage in primary school children: a case study in Italy. Ergonomics
2010;53:872–81.
[41] Hong Y, Li JX. Influence of load and carrying methods on gait phase
and ground reactions in children’s stair walking. Gait Posture
2005;22:63–8.
[42] Smith B, Ashton KM, Bohl D, et al. Influence of carrying a backpack
on pelvic tilt, rotation, and obliquity in female college students. Gait
Posture 2006;23:263–7.
[43] Avikainen VJ, Rezasoltani A, Kauhanen HA. Asymmetry of paraspi-
nal EMG-time characteristics in idiopathic scoliosis. J Spinal Disord
1999;12:61–7.
[44] Gaudreault N, Arsenault AB, Larivi�ere C, et al. Assessment of the
paraspinal muscles of subjects presenting an idiopathic scoliosis: an
EMG pilot study. BMC Musculoskelet Disord 2005;6:14.
[45] Bo Andersen L, Wedderkopp N, Leboeuf-Yde C. Association be-
tween back pain and physical fitness in adolescents. Spine 2006;31:
1740–4.
[46] Chow DHK, Leung DSS, Holmes AD. The effect of load carriage and
bracing on the balance of schoolgirls with adolescent idiopathic sco-
liosis. Eur Spine J 2007;16:1351–8.
[47] Negrini S, Carabalona R. Backpacks on! Schoolchildren’s percep-
tions of load, associations with back pain and factors determining
the load. Spine 2002;27:187–95.
[48] Yamada K, Yamamoto H, Nakagawa Y, et al. Etiology of idiopathic
scoliosis. Clin Orthop Relat Res 1984;184:50–7.
Copyright © 2022 FDOKUMEN