
The effectiveness of current dentin desensitizing agents used to treat dental hypersensitivity: a...
12
doi: ##.####/j.qi.a##### 1 QUINTESSENCE INTERNATIONAL GENERAL DENTISTRY The effectiveness of current dentin desensitizing agents used to treat dental hypersensitivity: A systematic review Wellington Luiz de Oliveira da Rosa 1 /Rafael Guerra Lund, PhD 2 /Evandro Piva, PhD 2 /Adriana Fernandes da Silva, PhD 2 Objective: Dentin desensitizing agents are used in the treatment of dentin hypersensitivity, which is defined as a painful response in the exposed dentin to stimuli that are thermal, evaporative, tactile, osmotic, or chemical. A systematic review was conducted to analyze the clinical effectiveness of current desensitizer with at least 3-months follow-up. Method and Materials: Eight electronic databases were searched: MedLine (PubMed), Embase, Lilacs, Ibecs, Web of Science, Scopus, Scielo, and The Cochrane Library. Only those clini- cal trials published from 2000 to 2012 were included. Results: A total of 3,029 relevant records were identified. After title and abstract examination, 2,645 articles were excluded. A data extraction form was designed and completed by reviewers from the selected stud- ies for a retrospective comparison. From the 99 studies retrieved for detailed review, only 17 had an evaluation time of at least 3-months follow-up and fulfilled the selection criteria. Conclusion: Cervitec Plus, SE Bond & Protect Liner F, laser, and iontophoresis have shown satisfactory posttreatment results between 3 and 6 months. However, additional clinical trials are warranted to better compare the different types of treatments and their effectiveness in the longer term. (Quintessence Int 201#;##:1–12; doi: ##.####/j.qi.a#####) Key words: dentin desensitizing agents, dental materials, dentin sensitivity, systematic review 1 Undergraduate Student, Faculty of Dentistry, Federal Universi- ty of Pelotas, Pelotas, Brazil. 2 Professor, Department of Restorative Dentistry, Federal Univer- sity of Pelotas, Pelotas, Brazil. Correspondence: Professor Adriana Fernandes da Silva, Restor- ative Dentistry, Department of Restorative Dentistry, College of Dentistry, Federal University of Pelotas, Gonçalves Chaves St. 457/504, Centro, Pelotas - RS – Brazil 96015-560. Email: adrisil- [email protected] Dentin hypersensitivity (DH) is one of the most common painful conditions affecting oral comfort and function. 1,2 It is also one of the least successfully resolved problems of the teeth. 3 DH can be defined as temporary pain or an exaggerated response in exposed dentin to stimuli that are typically thermal, evaporative, tactile, osmotic, or chemical, which cannot be explained as arising from other forms of dental defect or pathology. 1,3-8 Primary treatment strategies should undoubtedly aim to eliminate predis- posing factors, such as abfraction, abra- sion, or erosive components, thereby preventing recurrence. 1,9,10 Under normal conditions, dentin is cov- ered by enamel or cement and does not suffer direct stimulation. 11 However, the exposure of dentinal tubules due to enamel loss by abrasion, erosion, abfraction, or root surface exposure caused by gingival reces- sion, periodontal treatment, or a combina- tion of both may produce strong dentin sen- sitivity. 4,12 Root area exposures with cervical lesions may be multifactorial, resulting from chronic trauma from tooth brushing, tooth flexure due to abnormal occlusal loading forces, parafunctional habits, acute and chronic inflammatory gingivitis, and peri- odontal diseases. 3,9 Although several hypotheses have been presented to characterize DH, the generally accepted basis for its physiological cause is Brännstrom’s hydrodynamic theory. 4,13-16 According to its principles, exposed and open dentinal tubules at the tooth surface permit fluid movement inside the tubules that leads to sensorial activation of the nerve cells in the pulp, thus causing pain. 4,13,17
Transcript of The effectiveness of current dentin desensitizing agents used to treat dental hypersensitivity: a...
doi: ##.####/j.qi.a##### 1
QUINTESSENCE INTERNATIONAL
GENERAL DENTISTRY
The effectiveness of current dentin desensitizing
agents used to treat dental hypersensitivity: A
systematic review
Wellington Luiz de Oliveira da Rosa1/Rafael Guerra Lund, PhD2/Evandro
Piva, PhD2/Adriana Fernandes da Silva, PhD2
Objective: Dentin desensitizing agents are used in the treatment of dentin hypersensitivity,
which is defined as a painful response in the exposed dentin to stimuli that are thermal,
evaporative, tactile, osmotic, or chemical. A systematic review was conducted to analyze
the clinical effectiveness of current desensitizer with at least 3-months follow-up. Method
and Materials: Eight electronic databases were searched: MedLine (PubMed), Embase,
Lilacs, Ibecs, Web of Science, Scopus, Scielo, and The Cochrane Library. Only those clini-
cal trials published from 2000 to 2012 were included. Results: A total of 3,029 relevant
records were identified. After title and abstract examination, 2,645 articles were excluded.
A data extraction form was designed and completed by reviewers from the selected stud-
ies for a retrospective comparison. From the 99 studies retrieved for detailed review, only
17 had an evaluation time of at least 3-months follow-up and fulfilled the selection criteria.
Conclusion: Cervitec Plus, SE Bond & Protect Liner F, laser, and iontophoresis have
shown satisfactory posttreatment results between 3 and 6 months. However, additional
clinical trials are warranted to better compare the different types of treatments and their
effectiveness in the longer term. (Quintessence Int 201#;##:1–12; doi: ##.####/j.qi.a#####)
Key words: dentin desensitizing agents, dental materials, dentin sensitivity,
systematic review
1Undergraduate Student, Faculty of Dentistry, Federal Universi-
ty of Pelotas, Pelotas, Brazil.
2Professor, Department of Restorative Dentistry, Federal Univer-
sity of Pelotas, Pelotas, Brazil.
Correspondence: Professor Adriana Fernandes da Silva, Restor-
ative Dentistry, Department of Restorative Dentistry, College of
Dentistry, Federal University of Pelotas, Gonçalves Chaves St.
457/504, Centro, Pelotas - RS – Brazil 96015-560. Email: adrisil-
Dentin hypersensitivity (DH) is one of the
most common painful conditions affecting
oral comfort and function.1,2 It is also one of
the least successfully resolved problems of
the teeth.3 DH can be defined as temporary
pain or an exaggerated response in
exposed dentin to stimuli that are typically
thermal, evaporative, tactile, osmotic, or
chemical, which cannot be explained as
arising from other forms of dental defect or
pathology.1,3-8 Primary treatment strategies
should undoubtedly aim to eliminate predis-
posing factors, such as abfraction, abra-
sion, or erosive components, thereby
preventing recurrence.1,9,10
Under normal conditions, dentin is cov-
ered by enamel or cement and does not
suffer direct stimulation.11 However, the
exposure of dentinal tubules due to enamel
loss by abrasion, erosion, abfraction, or root
surface exposure caused by gingival reces-
sion, periodontal treatment, or a combina-
tion of both may produce strong dentin sen-
sitivity.4,12 Root area exposures with cervical
lesions may be multifactorial, resulting from
chronic trauma from tooth brushing, tooth
flexure due to abnormal occlusal loading
forces, parafunctional habits, acute and
chronic inflammatory gingivitis, and peri-
odontal diseases.3,9
Although several hypotheses have been
presented to characterize DH, the generally
accepted basis for its physiological cause
is Brännstrom’s hydrodynamic theory.4,13-16
According to its principles, exposed and
open dentinal tubules at the tooth surface
permit fluid movement inside the tubules
that leads to sensorial activation of the
nerve cells in the pulp, thus causing
pain.4,13,17
2 doi: ##.####/j.qi.a#####
QUINTESSENCE INTERNATIONALda Rosa et al
There are many approaches to the treat-
ment and prevention of DH.13 Extensive
research has been conducted regarding its
treatment, although no single treatment is
accepted universally.14 Treatment with a
chemical agent (eg potassium nitrate) that
penetrates into the dentinal tubules and
depolarizes the nerve synapse, thereby
reducing sensitivity by preventing the con-
duction of pain impulses, is a method used
in daily use toothpastes.13 An alternative
approach is to treat the tooth with a chemi-
cal or physical agent that creates a layer
that mechanically occludes the exposed
dentinal tubules, thus reducing sensitivity
by preventing dentinal fluid flow. This
method is used by prophylaxis pastes and
varnishes.13,16
Numerous desensitizing agents also
have been clinically tested over several
decades in an effort to alleviate DH.3,14 Due
to the different methodologies employed,
variability of the subjective responses, and
influence of the placebo effect, results have
been variable and to some extent inconclu-
sive.13,18 For immediate alleviation of mild to
moderate symptoms, occlusion of dentinal
tubules can be noninvasively achieved with
toothpastes containing strontium salts and/
or highly concentrated fluoride lacquers or
varnishes.11,19,20 Another approach is to use
potassium salt formulations that modulate
intradental nerve excitability.21,22 In the case
of pronounced severity, a semi-invasive
treatment can block dentin tubules via the
application of a bonding agent or an adhe-
sive restorative material.23,24 These different
modalities have shown variable results over
time.1,11,21,23-28
Current therapies provide only tempo-
rary effects and require multiple applica-
tions to take effect, which explains the large
number of studies evaluating the reduction
of pain in the short-term as well as the lack
of long-term effects associated with these
materials.28-31 The aim of this study was to
analyze the clinical effectiveness of the
treatments for DH with at least 3-months
follow-up.
METHOD AND MATERIALS
Search strategies
This systematic review was performed
according to the PRISMA (Preferred Report-
ing Items for Systematic Reviews and Meta-
Analyses) Statement.32 The literature search
was carried out by two independent review-
ers (WLOR and AFS) involving publications
between January 2000 and August 2012.
Eight databases – MedLine (Pubmed),
Embase, Lilacs, Ibecs, Web of Science,
Scopus, Scielo, and The Cochrane Library
– were searched using the keywords “den-
tin sensitivity”, “dentine sensitivity”, “dentine
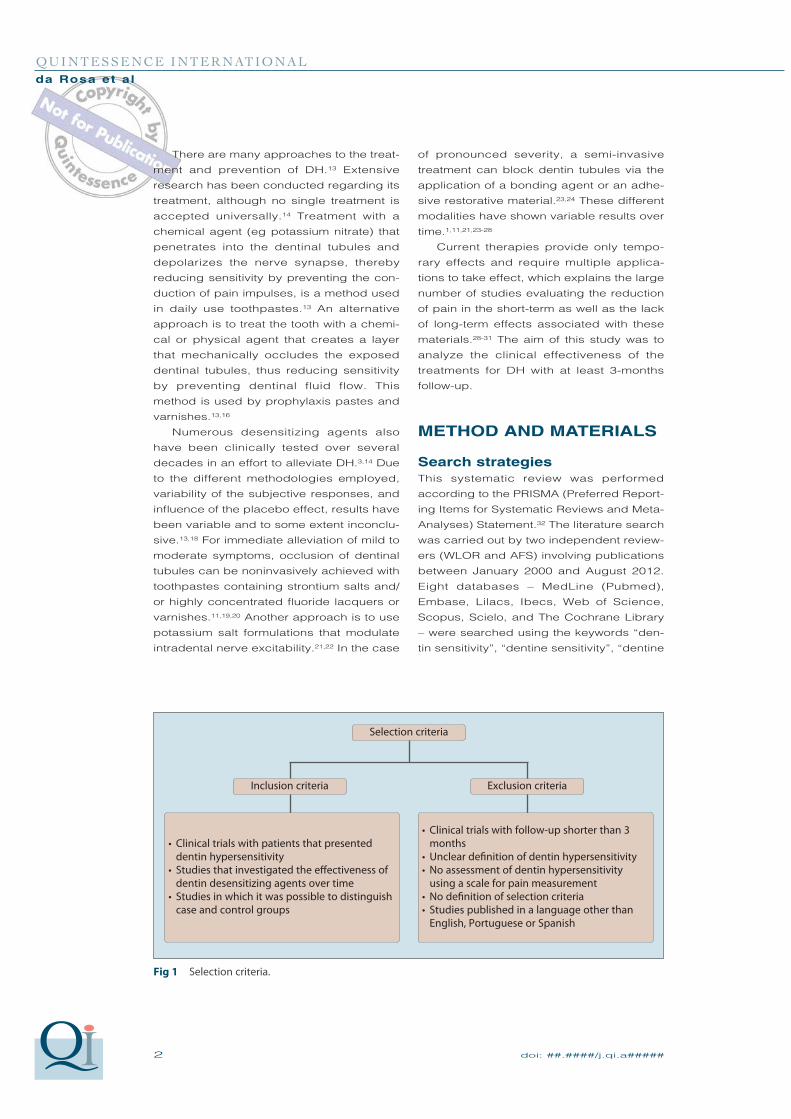
Fig 1 Selection criteria.
Clinical trials with patients that presented dentin hypersensitivityStudies that investigated the effectiveness of dentin desensitizing agents over timeStudies in which it was possible to distinguish case and control groups
Clinical trials with follow-up shorter than 3 monthsUnclear definition of dentin hypersensitivityNo assessment of dentin hypersensitivity using a scale for pain measurementNo definition of selection criteriaStudies published in a language other than English, Portuguese or Spanish
Exclusion criteria
Selection criteria
Inclusion criteria

doi: ##.####/j.qi.a##### 3
QUINTESSENCE INTERNATIONALda Rosa et al
hypersensitivity”, “desensitizing dentin”,
“dental sensitivity”, “hypersensitivity teeth”,
“dentin desensitizing agents”, “teeth desen-
sitizer”, and “dental desensitizer”. Only
those clinical trials that evaluated dentin
desensitizing agents over time were
selected. All identified papers were evalu-
ated and chosen based on the following
inclusion criteria (Fig 1): any in vivo study
with a protocol for dentin hypersensitivity
with at least 3 months of follow-up.
Study selection
According to the PRISMA Statement,32 the
abstracts were independently reviewed by
two reviewers (WLOR and AFS). After the
screening and eligibility criteria were indi-
vidually accomplished, the article was
included if a consensus was reached. If
not, a third author was invited to discuss the
article. The studies were analyzed accord-
ing to the selection criteria (Fig 1). Only
those studies that fulfilled all criteria were
admitted.
The authors of selected manuscripts
were contacted by email when it was nec-
essary to retrieve some missing data or
information. If no answer was received by 2
weeks after the first email message was
sent, then a second email was forwarded. If
no answer was provided by the author 1
month after the first contact, the missing
Table 1 Demographics of the included studies
Study Year Country Study design Patients Teeth Posttreatment time
Aranha et al3 2009 Brazil CCT; split-mouth 39 101 1 wk, 1 mo, 3 mo, 6 mo
Birang et al29 2007 Iran RCT; alternate allo-
cation
9 63 1 mo, 3 mo, 6 mo
Brahmbhatt
et al14
2011 India RCT; split-mouth 25 260 15 d, 1 mo, 3 mo
Ciaramicoli
et al43
2003 Brazil CCT; alternate allo-
cation
20 145 6 mo
Clavijo
et al45
2009 Brazil RCT, alternate allo-
cation
10 28 7 d, 14 d, 1 mo, 2 mo, 3 mo
Drebenstedt
et al51
2012 Germany RCT, parallel groups 120 NS 1 d, 7 d, 1 mo, 3 mo
Duran and
Sengun52
2004 Turkey RCT; split-mouth 52 277 10 d, 3 mo
Ipci et al55 2009 Turkey RCT, parallel groups 50 450 1 wk, 1 mo, 6 mo
Kobler et al46 2008 Germany RCT; split-mouth 132 NS 2 wk, 2mo, 3 mo, 6 mo
Lier et al59 2002 Norway RCT; split-mouth 17 34 1 wk, 1 mo, 4 mo
Polderman
and
Frencken26
2007 Netherlands RCT; split-mouth 14 28 1 mo, 3 mo, 19.2 mo, 25.2 mo
Sethna
et al47
2011 India RCT; split-mouth 250 500 1 mo, 3 mo
Singal et al48 2005 India RCT, alternate allo-
cation
50 425 2 wk, 1 mo, 3 mo
Vieira et al28 2009 Brazil RCT; split-mouth 30 164 3 mo
Yilmaz et al31 2011 Turkey RCT; alternate allo-
cation
42 146 1 wk, 1 mo, 3 mo
Yilmaz et al60 2011 Turkey RCT; split-mouth 48 244 1 wk, 1 mo, 3 mo, 6 mo
Yilmaz et al57 2011 Turkey RCT; split-mouth 51 174 1 wk, 1 mo, 3 mo
CCT, controlled clinical trial; NS, not specified; RCT, randomized clinical trial.
4 doi: ##.####/j.qi.a#####
QUINTESSENCE INTERNATIONALda Rosa et al
information was not included in this review.
When papers from the same group of
authors were identified, with very similar
databases of patients, materials, methods,
and outcomes, the authors were also con-
tacted to clarify whether the pool of patients
was indeed the same.
Data extraction
A data extraction form was designed ad
hoc and filled by reviewers to register data
from the selected studies. Demographic
data (eg number of patients, country) were
recorded for each of the studies (Table 1).
The number of patients and teeth evaluated
were also recorded. For each study, the
type of materials tested (Table 2) and the
main results (Table 3) were recorded, as
described in the study.
Assessment of methodologic
quality
Due to the high degree of heterogeneity in
terms of the different studies, the materials
tested, the number of treatment sessions,
and the variety of follow-up periods used, a
meta-analysis among the selected studies
was considered inappropriate. Decreases
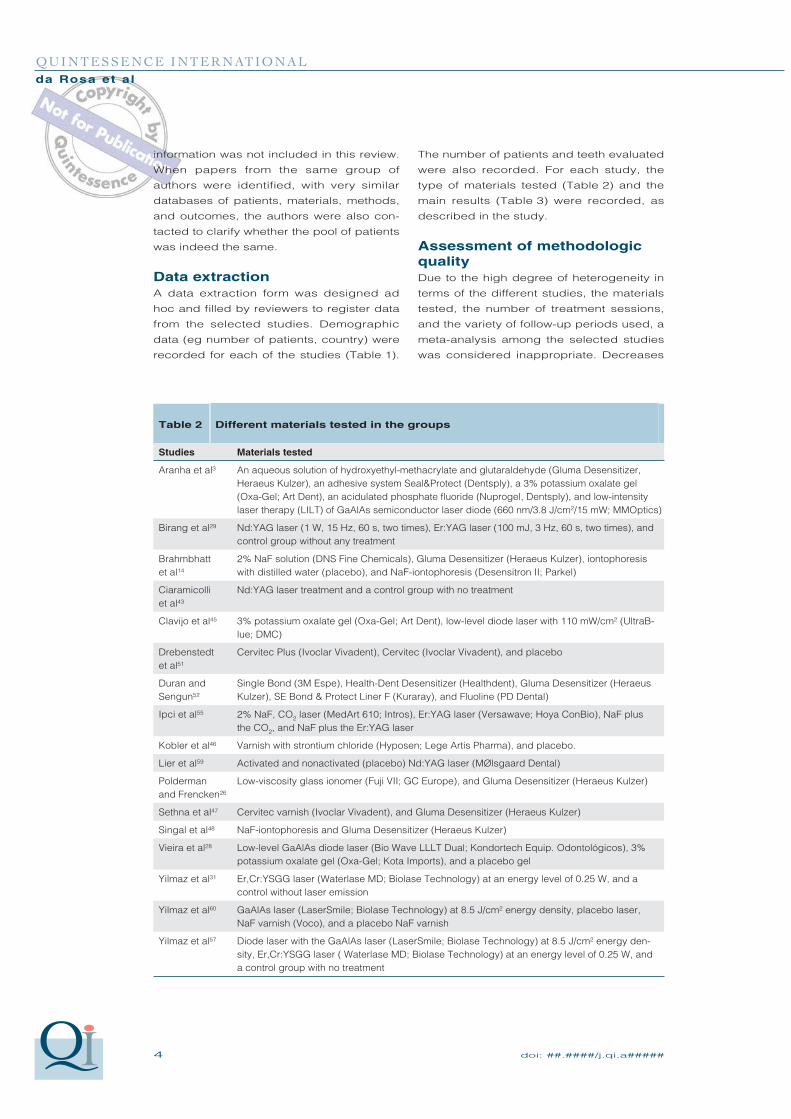
Table 2 Different materials tested in the groups
Studies Materials tested
Aranha et al3 An aqueous solution of hydroxyethyl-methacrylate and glutaraldehyde (Gluma Desensitizer,
Heraeus Kulzer), an adhesive system Seal&Protect (Dentsply), a 3% potassium oxalate gel
(Oxa-Gel; Art Dent), an acidulated phosphate fluoride (Nuprogel, Dentsply), and low-intensity
laser therapy (LILT) of GaAlAs semiconductor laser diode (660 nm/3.8 J/cm²/15 mW; MMOptics)
Birang et al29 Nd:YAG laser (1 W, 15 Hz, 60 s, two times), Er:YAG laser (100 mJ, 3 Hz, 60 s, two times), and
control group without any treatment
Brahmbhatt
et al14
2% NaF solution (DNS Fine Chemicals), Gluma Desensitizer (Heraeus Kulzer), iontophoresis
with distilled water (placebo), and NaF-iontophoresis (Desensitron II; Parkel)
Ciaramicolli
et al43
Nd:YAG laser treatment and a control group with no treatment
Clavijo et al45 3% potassium oxalate gel (Oxa-Gel; Art Dent), low-level diode laser with 110 mW/cm2 (UltraB-
lue; DMC)
Drebenstedt
et al51
Cervitec Plus (Ivoclar Vivadent), Cervitec (Ivoclar Vivadent), and placebo
Duran and
Sengun52
Single Bond (3M Espe), Health-Dent Desensitizer (Healthdent), Gluma Desensitizer (Heraeus
Kulzer), SE Bond & Protect Liner F (Kuraray), and Fluoline (PD Dental)
Ipci et al55 2% NaF, CO2 laser (MedArt 610; Intros), Er:YAG laser (Versawave; Hoya ConBio), NaF plus
the CO2, and NaF plus the Er:YAG laser
Kobler et al46 Varnish with strontium chloride (Hyposen; Lege Artis Pharma), and placebo.
Lier et al59 Activated and nonactivated (placebo) Nd:YAG laser (MØlsgaard Dental)
Polderman
and Frencken26
Low-viscosity glass ionomer (Fuji VII; GC Europe), and Gluma Desensitizer (Heraeus Kulzer)
Sethna et al47 Cervitec varnish (Ivoclar Vivadent), and Gluma Desensitizer (Heraeus Kulzer)
Singal et al48 NaF-iontophoresis and Gluma Desensitizer (Heraeus Kulzer)
Vieira et al28 Low-level GaAlAs diode laser (Bio Wave LLLT Dual; Kondortech Equip. Odontológicos), 3%
potassium oxalate gel (Oxa-Gel; Kota Imports), and a placebo gel
Yilmaz et al31 Er,Cr:YSGG laser (Waterlase MD; Biolase Technology) at an energy level of 0.25 W, and a
control without laser emission
Yilmaz et al60 GaAlAs laser (LaserSmile; Biolase Technology) at 8.5 J/cm2 energy density, placebo laser,
NaF varnish (Voco), and a placebo NaF varnish
Yilmaz et al57 Diode laser with the GaAlAs laser (LaserSmile; Biolase Technology) at 8.5 J/cm2 energy den-
sity, Er,Cr:YSGG laser ( Waterlase MD; Biolase Technology) at an energy level of 0.25 W, and
a control group with no treatment
doi: ##.####/j.qi.a##### 5
QUINTESSENCE INTERNATIONALda Rosa et al
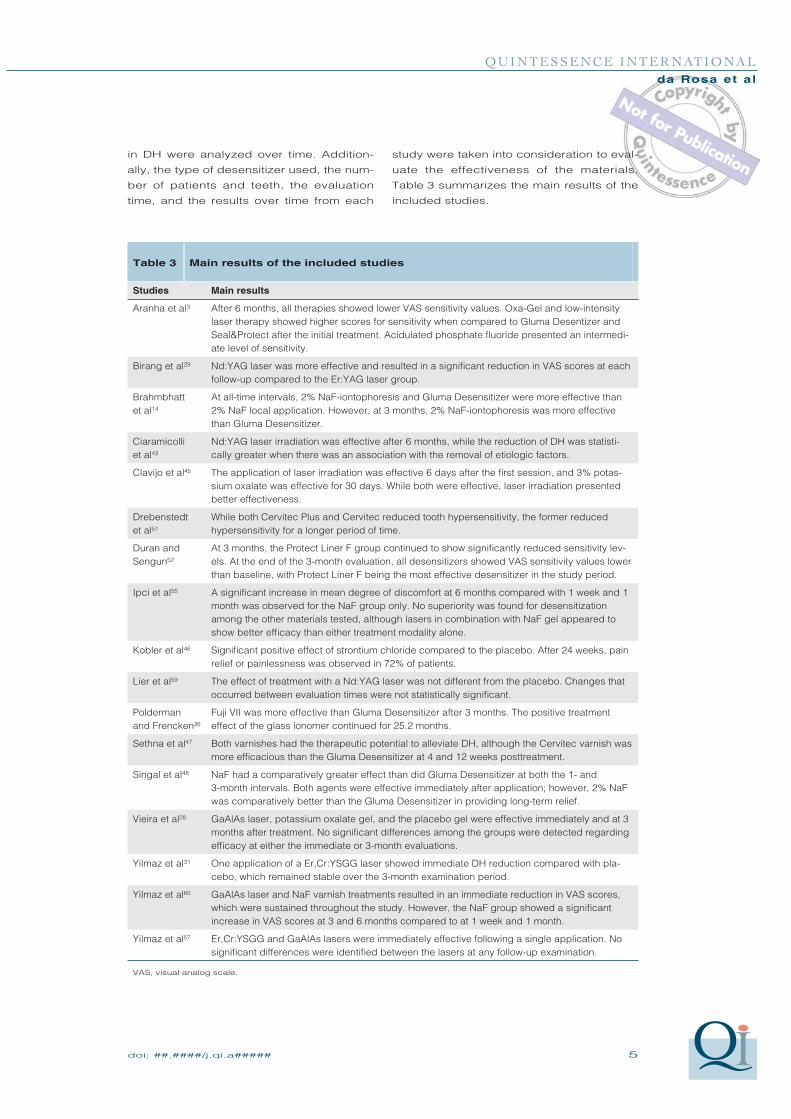
Table 3 Main results of the included studies
Studies Main results
Aranha et al3 After 6 months, all therapies showed lower VAS sensitivity values. Oxa-Gel and low-intensity
laser therapy showed higher scores for sensitivity when compared to Gluma Desentizer and
Seal&Protect after the initial treatment. Acidulated phosphate fluoride presented an intermedi-
ate level of sensitivity.
Birang et al29 Nd:YAG laser was more effective and resulted in a significant reduction in VAS scores at each
follow-up compared to the Er:YAG laser group.
Brahmbhatt
et al14
At all-time intervals, 2% NaF-iontophoresis and Gluma Desensitizer were more effective than
2% NaF local application. However, at 3 months, 2% NaF-iontophoresis was more effective
than Gluma Desensitizer.
Ciaramicolli
et al43
Nd:YAG laser irradiation was effective after 6 months, while the reduction of DH was statisti-
cally greater when there was an association with the removal of etiologic factors.
Clavijo et al45 The application of laser irradiation was effective 6 days after the first session, and 3% potas-
sium oxalate was effective for 30 days. While both were effective, laser irradiation presented
better effectiveness.
Drebenstedt
et al51
While both Cervitec Plus and Cervitec reduced tooth hypersensitivity, the former reduced
hypersensitivity for a longer period of time.
Duran and
Sengun52
At 3 months, the Protect Liner F group continued to show significantly reduced sensitivity lev-
els. At the end of the 3-month evaluation, all desensitizers showed VAS sensitivity values lower
than baseline, with Protect Liner F being the most effective desensitizer in the study period.
Ipci et al55 A significant increase in mean degree of discomfort at 6 months compared with 1 week and 1
month was observed for the NaF group only. No superiority was found for desensitization
among the other materials tested, although lasers in combination with NaF gel appeared to
show better efficacy than either treatment modality alone.
Kobler et al46 Significant positive effect of strontium chloride compared to the placebo. After 24 weeks, pain
relief or painlessness was observed in 72% of patients.
Lier et al59 The effect of treatment with a Nd:YAG laser was not different from the placebo. Changes that
occurred between evaluation times were not statistically significant.
Polderman
and Frencken26
Fuji VII was more effective than Gluma Desensitizer after 3 months. The positive treatment
effect of the glass ionomer continued for 25.2 months.
Sethna et al47 Both varnishes had the therapeutic potential to alleviate DH, although the Cervitec varnish was
more efficacious than the Gluma Desensitizer at 4 and 12 weeks posttreatment.
Singal et al48 NaF had a comparatively greater effect than did Gluma Desensitizer at both the 1- and
3-month intervals. Both agents were effective immediately after application; however, 2% NaF
was comparatively better than the Gluma Desensitizer in providing long-term relief.
Vieira et al28 GaAlAs laser, potassium oxalate gel, and the placebo gel were effective immediately and at 3
months after treatment. No significant differences among the groups were detected regarding
efficacy at either the immediate or 3-month evaluations.
Yilmaz et al31 One application of a Er,Cr:YSGG laser showed immediate DH reduction compared with pla-
cebo, which remained stable over the 3-month examination period.
Yilmaz et al60 GaAlAs laser and NaF varnish treatments resulted in an immediate reduction in VAS scores,
which were sustained throughout the study. However, the NaF group showed a significant
increase in VAS scores at 3 and 6 months compared to at 1 week and 1 month.
Yilmaz et al57 Er,Cr:YSGG and GaAlAs lasers were immediately effective following a single application. No
significant differences were identified between the lasers at any follow-up examination.
VAS, visual analog scale.
in DH were analyzed over time. Addition-
ally, the type of desensitizer used, the num-
ber of patients and teeth, the evaluation
time, and the results over time from each
study were taken into consideration to eval-
uate the effectiveness of the materials.
Table 3 summarizes the main results of the
included studies.
6 doi: ##.####/j.qi.a#####
QUINTESSENCE INTERNATIONALda Rosa et al
RESULTS
Study characteristics
The last electronic search was conducted
on August 2012. A total of 3,029 potentially
relevant records were identified from all
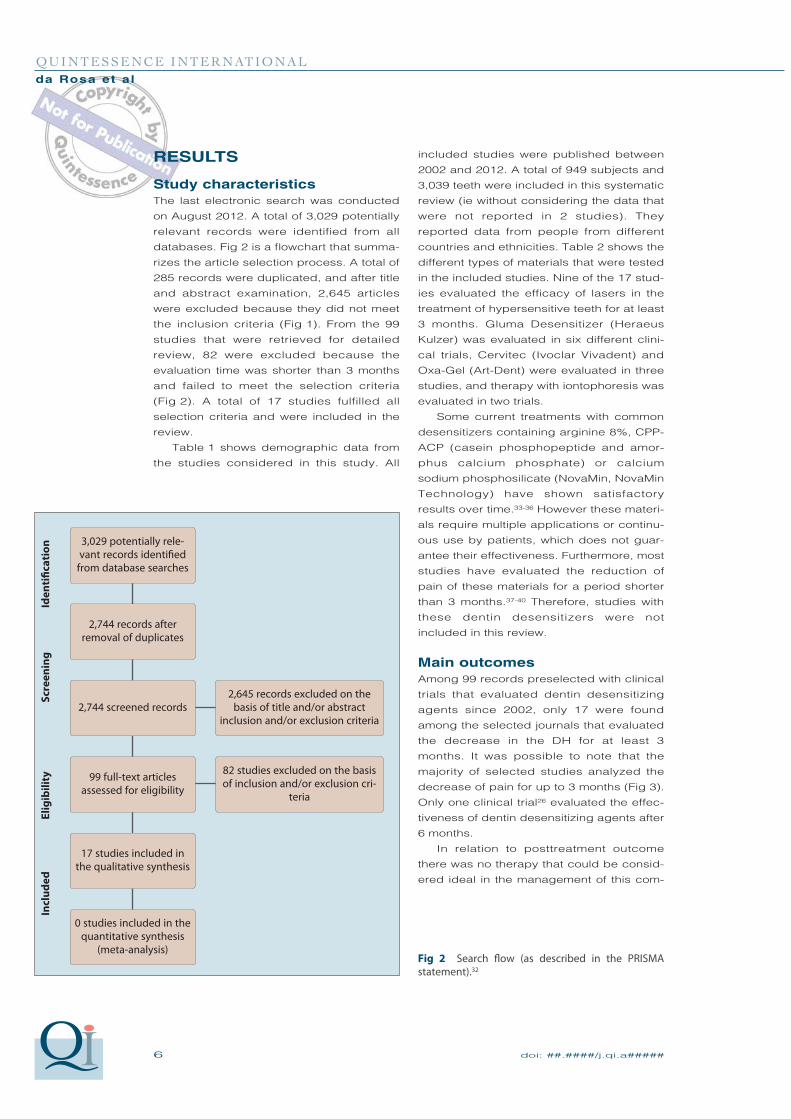
databases. Fig 2 is a flowchart that summa-
rizes the article selection process. A total of
285 records were duplicated, and after title
and abstract examination, 2,645 articles
were excluded because they did not meet
the inclusion criteria (Fig 1). From the 99
studies that were retrieved for detailed
review, 82 were excluded because the
evaluation time was shorter than 3 months
and failed to meet the selection criteria
(Fig 2). A total of 17 studies fulfilled all
selection criteria and were included in the
review.
Table 1 shows demographic data from
the studies considered in this study. All
included studies were published between
2002 and 2012. A total of 949 subjects and
3,039 teeth were included in this systematic
review (ie without considering the data that
were not reported in 2 studies). They
reported data from people from different
countries and ethnicities. Table 2 shows the
different types of materials that were tested
in the included studies. Nine of the 17 stud-
ies evaluated the efficacy of lasers in the
treatment of hypersensitive teeth for at least
3 months. Gluma Desensitizer (Heraeus
Kulzer) was evaluated in six different clini-
cal trials, Cervitec (Ivoclar Vivadent) and
Oxa-Gel (Art-Dent) were evaluated in three
studies, and therapy with iontophoresis was
evaluated in two trials.
Some current treatments with common
desensitizers containing arginine 8%, CPP-
ACP (casein phosphopeptide and amor-
phus calcium phosphate) or calcium
sodium phosphosilicate (NovaMin, NovaMin
Technology) have shown satisfactory
results over time.33-36 However these materi-
als require multiple applications or continu-
ous use by patients, which does not guar-
antee their effectiveness. Furthermore, most
studies have evaluated the reduction of
pain of these materials for a period shorter
than 3 months.37-40 Therefore, studies with
these dentin desensitizers were not
included in this review.
Main outcomes
Among 99 records preselected with clinical
trials that evaluated dentin desensitizing
agents since 2002, only 17 were found
among the selected journals that evaluated
the decrease in the DH for at least 3
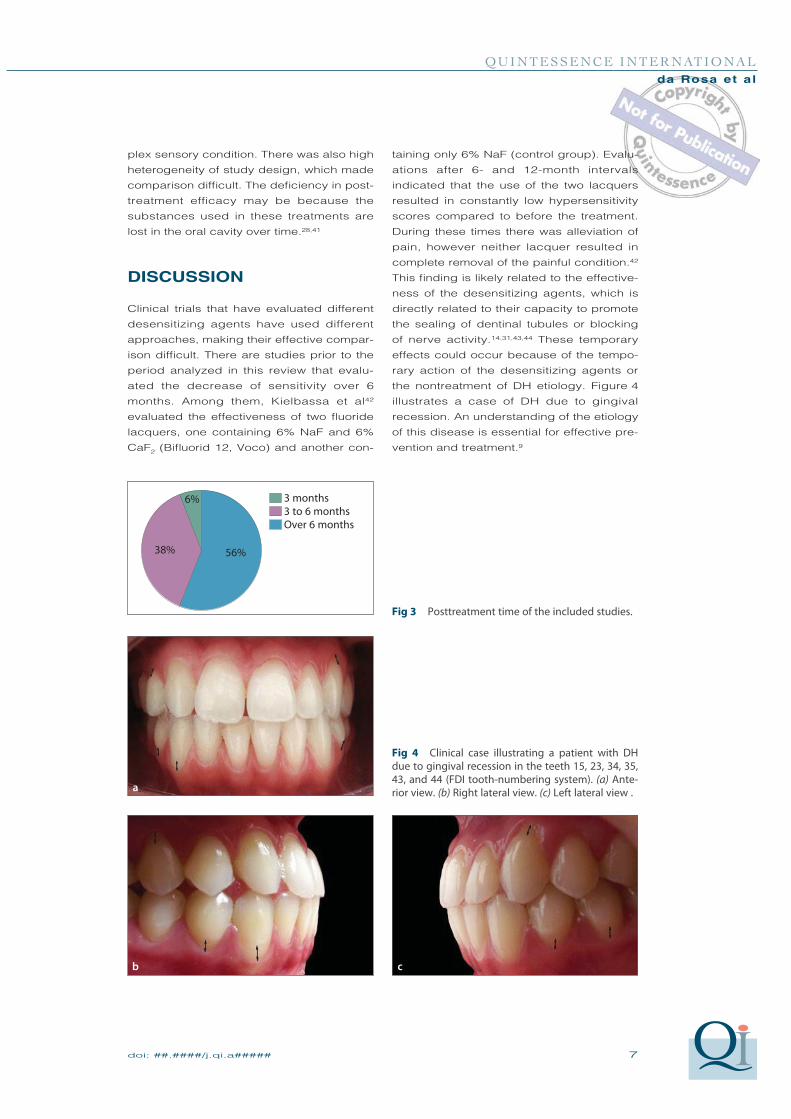
months. It was possible to note that the
majority of selected studies analyzed the
decrease of pain for up to 3 months (Fig 3).
Only one clinical trial26 evaluated the effec-
tiveness of dentin desensitizing agents after
6 months.
In relation to posttreatment outcome
there was no therapy that could be consid-
ered ideal in the management of this com-
Fig 2 Search flow (as described in the PRISMA statement).32
3,029 potentially rele-vant records identified
from database searches
2,744 records after removal of duplicates
2,744 screened records2,645 records excluded on the
basis of title and/or abstract inclusion and/or exclusion criteria
99 full-text articles assessed for eligibility
82 studies excluded on the basis of inclusion and/or exclusion cri-
teria
17 studies included in the qualitative synthesis
0 studies included in the quantitative synthesis
(meta-analysis)
Iden
tific
atio
nSc
reen
ing
Elig
ibili
tyIn
clud
ed
doi: ##.####/j.qi.a##### 7
QUINTESSENCE INTERNATIONALda Rosa et al
plex sensory condition. There was also high
heterogeneity of study design, which made
comparison difficult. The deficiency in post-
treatment efficacy may be because the
substances used in these treatments are
lost in the oral cavity over time.28,41
DISCUSSION
Clinical trials that have evaluated different
desensitizing agents have used different
approaches, making their effective compar-
ison difficult. There are studies prior to the
period analyzed in this review that evalu-
ated the decrease of sensitivity over 6
months. Among them, Kielbassa et al42
evaluated the effectiveness of two fluoride
lacquers, one containing 6% NaF and 6%
CaF2 (Bifluorid 12, Voco) and another con-
taining only 6% NaF (control group). Evalu-
ations after 6- and 12-month intervals
indicated that the use of the two lacquers
resulted in constantly low hypersensitivity
scores compared to before the treatment.
During these times there was alleviation of
pain, however neither lacquer resulted in
complete removal of the painful condition.42
This finding is likely related to the effective-
ness of the desensitizing agents, which is
directly related to their capacity to promote
the sealing of dentinal tubules or blocking
of nerve activity.14,31,43,44 These temporary
effects could occur because of the tempo-
rary action of the desensitizing agents or
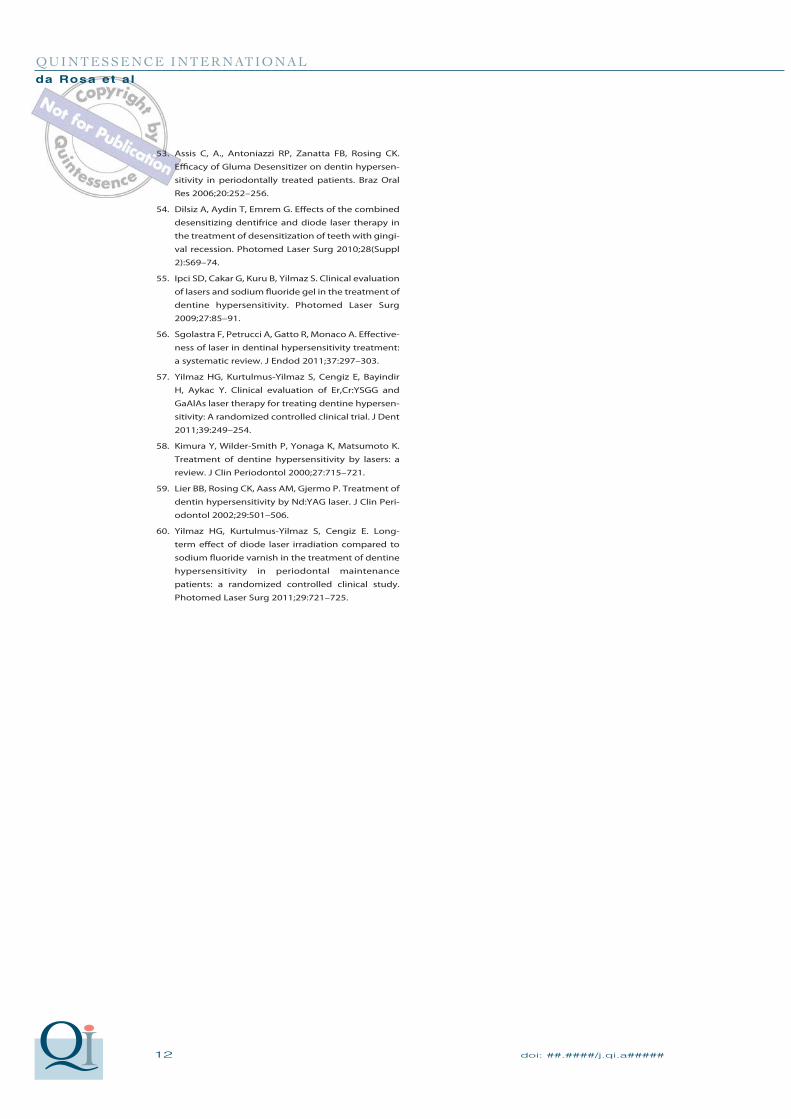
the nontreatment of DH etiology. Figure 4
illustrates a case of DH due to gingival
recession. An understanding of the etiology
of this disease is essential for effective pre-
vention and treatment.9
Fig 3 Posttreatment time of the included studies.
Fig 4 Clinical case illustrating a patient with DH due to gingival recession in the teeth 15, 23, 34, 35, 43, and 44 (FDI tooth-numbering system). (a) Ante-rior view. (b) Right lateral view. (c) Left lateral view .
3 months 3 to 6 months Over 6 months
56%38%
6%
a
b c

8 doi: ##.####/j.qi.a#####
QUINTESSENCE INTERNATIONALda Rosa et al
Some researchers43,45,46 have included
patients submitted to periodontal therapy
procedures in their studies. Although
defined as short and sharp pain arising
from exposed dentin which cannot be
ascribed to any other form of dental defect
or disease,26,47,48 many authors have consid-
ered the possibility of DH arising after peri-
odontal therapy, which is an obvious out-
come and can be described only as
temporary sensitivity. While there is no con-
sensus on the definition of this disease, the
studies included in this review evaluated
patients who also had DH after periodontal
procedures. On the other hand, clinical
studies which evaluated the sensitivity after
dental bleaching were not included in this
review because this sensitivity seems to be
a transient outcome after the bleaching pro-
cedure. Although many patients undergo-
ing bleaching procedures complain of post-
operative sensitivity, there is a lack of
clinical investigations correlating the altera-
tions of the dentin-pulp complex with tooth
sensitivity.49,50 It is hypothesized that direct
activation of the intradental nerve via the
chemosensitive ion channel TRPA1 triggers
the sensitivity mechanism during bleach-
ing.49
Among the conventional treatments for
DH, two types of varnish designed to treat
exposed root surfaces (Cervitec Plus and
Cervitec; Ivoclar Vivadent) were evaluated
for 3 months.51 Both equally reduced hyper-
sensitivity for a certain period of time. How-
ever, the efficacy of Cervitec Plus was still
observed 90 days after application
because of better adhesion of the varnish.
When Cervitec was compared to Gluma
Desensitizer in another study,47 the first was
more efficacious after 1 and 3 months.
Gluma Desensitizer was also compared to
Single Bond (3M Espe), Health-Dent
Desensitizer (Healthdent), SE Bond & Pro-
tect Liner F (Kuraray), and Fluoline (PD
Dental) in another clinical trial52 included in
the present review. At the end of the
3-month evaluation period, all desensitizers
showed lower sensitivity values compared
to baseline. Only SE Bond & Protect Liner F
contain colloidal silica, which has consider-
able treatment potential, especially in terms
of tubule blockage. It may have been this
different substance that made SE Bond &
Protect Liner F the most effective agents in
the study period.52
Only one study26 included in the present
review evaluated the decrease of hypersen-
sitivity over 6 months. In this study the
hypersensitive teeth were treated with low-
viscosity glass ionomer (Fuji VII, GC) and a
resin-based glutaraldehyde-containing
primer (Gluma Desensitizer). Fuji VII was
more effective than Gluma Desensitizer
after 3 months and its effect continued for
about 25 months. This indicated that the
glass ionomer was retained longer and still
covered dentin tubules after many episodes
of plaque removal using a toothbrush.
In relation to current treatments, ionto-
phoresis is another therapy that has gained
some popularity. It is a technique in which
fluoride can be transferred under electrical
pressure deep into the dentinal
tubules.10,14,53,54 It may cause calcium fluo-
ride precipitation when used with sodium
fluoride (NaF), which may decrease fluid
movement in dentin tubules, thereby reduc-
ing DH.14 The clinical trials14,48 that evalu-
ated for 3 months 2% NaF-iontophoresis
observed that iontophoresis was more
effective than other treatments (Table 2).
These studies were consistent with the
hypothesis that electrically driven fluoride
ions react with calcium in the hydroxyapa-
tite to form fluorapatite, which blocks the
dentinal tubules.10,27,48
Due to the absence of effective success
in the routine treatment for DH, laser ther-
apy was first introduced in the mid-1980s
as a potential treatment modality.29,55,56 Nine
of the studies evaluated in the present
review included laser therapy. With its
growing utilization in dentistry, many
improvements have occurred in both the
quality and quantity of available laser
types.55,56 In the absence of established
protocols for DH treatment using low-level
laser therapy, comparisons between stud-
ies become difficult.45 Furthermore, com-
pared with conventional approaches, in-
office laser treatment has several
disadvantages, including high cost, com-
plexity of use, and decreasing effectiveness
over time, all of which limit its clinical util-
ity.14,23
Various laser types are used, including
neodymium or erbium-doped yttrium alumi-

doi: ##.####/j.qi.a##### 9
QUINTESSENCE INTERNATIONALda Rosa et al
num garnet (Nd:YAG or Er:YAG), CO2,
He-Ne, and diode (ie GaAlA) lasers, all of
which can be applied at various energy set-
tings and wavelengths ranging from
632.8 nm (He-Ne) to 10,600 nm (Er:YAG,
CO2).56 Furthermore, Er,Cr:YSGG laser
(wavelength 2,780 nm) has recently been
tested and its use showed a stable effect
for at least 3 months.31,57 It is important to
consider that the clinical effect of low-level
lasers on DH relies not only on an immedi-
ate analgesic effect, but also on changes in
neural transmission networks and delayed
obliteration of dentinal tubules by tertiary
dentin, the latter of which is due to
increased metabolic activity of odonto-
blasts.44,46,58 However, its efficacy and
mechanism of action are controversial
because of the lack of information related to
the irradiation protocol and the subjectivity
of the evaluation of DH.28,56
In another 6-month evaluation3 that com-
pared five different treatment modalities
(Oxa-Gel, Gluma Desensitizer, Seal&Protect
[Dentsply], Nuprogel [Dentsply], and low-
intensity laser therapy [LILT] of GaAlAs), it
was demonstrated that laser did not pro-
vide an immediate reduction of sensitivity.
After 6 months, all desensitizing agents
were capable of reducing DH. Another simi-
lar clinical trial28 showed that after 3 months
GaAlAs and potassium oxalate gel reduced
the degree of sensitivity; however, a pla-
cebo gel also showed similar effectiveness
over time. Further, in a randomized clinical
trial55 CO2 and Er:YAG lasers showed
potential desensitizing effects for 6 months.
In addition, lasers in combination with NaF
gel appeared to show better efficacy than
either treatment modality alone. Although
the decrease in sensitivity has been verified
in these studies, neither treatment resulted
in complete remove of dentin sensitivity.
In a 4-month posttreatment evaluation,59
the effects of activated Nd:YAG laser were
not statistically significant or different from
the placebo group (non-activated laser) in
reducing pain sensation. However, it was
noted in another study43 that after 6 months
there was significant reduction in DH in
patients who received treatment with
Nd:YAG laser and whose etiologic factors
were removed. In another clinical trial29
using the same laser it was demonstrated
that Nd:YAG was more effective than
Er:YAG laser in reducing pain after 6
months. These studies demonstrated the
potential effectiveness of laser therapy for
DH, although more comparative studies
over 6 months must be conducted to con-
firm its effectiveness.
From these studies, it can be under-
stood that although many therapies aim to
treat DH, there is no agent that is able to
effectively obliterate the dentin tubules
because the substances used are lost over
time and require many applications. The
removal of DH etiologic factors is another
important factor that was little reported in all
selected studies and should be taken into
consideration by researchers, since it can
become a bias in the study design if not
observed. Among all studies included in
this review, therapies involving laser and
iontophoresis showed satisfactory results
for 6 and 3 months, respectively, although
they are more expensive than other modali-
ties and they have not been directly com-
pared. Treatments using mechanical barri-
ers such as Cervitec Plus or SE Bond &
Protect Liner F also seem to have efficacy
until 3 months. However, studies with post-
treatment evaluation over 3 months are
required to evaluate the effectiveness of
these treatments for longer periods. Fur-
thermore, the effective treatment for DH
may be achieved when the desensitizing
agent induces the biomineralization of den-
tin tubules and results in a biological
response of the tooth, thereby obliterating
the tubules and directly addressing the
pathology. Research using biological treat-
ments associated with the removal of DH
etiologic factors is required, since current
therapies have led to recurring sensitivity.
CONCLUSION
There is lack of clinical trials that evaluate
different types of dentin desensitizing
agents over 6 months. Some treatments
with Cervitec Plus, SE Bond & Protect Liner
F, laser, and iontophoresis have shown sat-
isfactory posttreatment results between 3
and 6 months. However, additional clinical
trials are warranted to better compare the

10 doi: ##.####/j.qi.a#####
QUINTESSENCE INTERNATIONALda Rosa et al
different types of treatments and their effec-
tiveness in the longer term.
REFERENCES
1. Aparna S, Setty S, Thakur S. Comparative efficacy of
two treatment modalities for dentinal hypersensi-
tivity: a clinical trial. Indian J Dent Res 2010;21:544–
548.
2. Kumar NG, Mehta DS. Short-term assessment of the
Nd:YAG laser with and without sodium fluoride
varnish in the treatment of dentin hypersensitivity:
a clinical and scanning electron microscopy study. J
Periodontol 2005;76:1140–1147.
3. Aranha AC, Pimenta LA, Marchi GM. Clinical evalua-
tion of desensitizing treatments for cervical dentin
hypersensitivity. Braz Oral Res 2009;23:333–339.
4. Assis JS, Rodrigues LK, Fonteles CS, Colares RC,
Souza AM, Santiago SL. Dentin hypersensitivity
after treatment with desensitizing agents: a ran-
domized, double-blind, split-mouth clinical trial.
Braz Dent J 2011;22:157–161.
5. Hoang-Dao BT, Hoang-Tu H, Tran-Thi NN, Koubi G,
Camps J, About I. Clinical efficiency of a natural resin
fluoride varnish (Shellac F) in reducing dentin
hypersensitivity. J Oral Rehabil 2009;36:124–131.
6. Kara C, Orbak R. Comparative evaluation of Nd:YAG
laser and fluoride varnish for the treatment of den-
tinal hypersensitivity. J Endod 2009;35:971–974.
7. Sowinski J, Ayad F, Petrone M, et al. Comparative
investigations of the desensitising efficacy of a new
dentifrice. J Clin Periodontol 2001;28:1032–1036.
8. Zappa U. Self-applied treatments in the manage-
ment of dentine hypersensitivity. Arch Oral Biol
1994;39(Suppl):107S–112S.
9. Addy M, Pearce N. Aetiological, predisposing and
environmental factors in dentine hypersensitivity.
Arch Oral Biol 1994;39(Suppl):33S–38S.
10. Gangarosa LP Sr. Current strategies for dentist-
applied treatment in the management of hypersen-
sitive dentine. Arch Oral Biol 1994;39(Suppl):101S–
106S.
11. Orsini G, Procaccini M, Manzoli L, Giuliodori F,
Lorenzini A, Putignano A. A double-blind random-
ized-controlled trial comparing the desensitizing
efficacy of a new dentifrice containing carbonate/
hydroxyapatite nanocrystals and a sodium fluoride/
potassium nitrate dentifrice. J Clin Periodontol
2010;37:510–517.
12. Kishore A, Mehrotra KK, Saimbi CS. Effectiveness of
desensitizing agents. J Endod 2002;28:34–35.
13. Banerjee A, Hajatdoost-Sani M, Farrell S, Thompson
I. A clinical evaluation and comparison of bioactive
glass and sodium bicarbonate air-polishing pow-
ders. J Dent 2010;38:475–479.
14. Brahmbhatt N, Bhavsar N, Sahayata V, Acharya A,
Kshatriya P. A double blind controlled trial compar-
ing three treatment modalities for dentin hypersen-
sitivity. Med Oral Patol Oral Cir Bucal 2012;17:e483–
490.
15. Brannstrom M, Astrom A. The hydrodynamics of the
dentine; its possible relationship to dentinal pain.
Int Dent J 1972;22:219–227.
16. Corona SA, Nascimento TN, Catirse AB, Lizarelli RF,
Dinelli W, Palma-Dibb RG. Clinical evaluation of low-
level laser therapy and fluoride varnish for treating
cervical dentinal hypersensitivity. J Oral Rehabil
2003;30:1183–1189.
17. Castillo JL, Rivera S, Aparicio T, et al. The short-term
effects of diamine silver fluoride on tooth sensitivi-
ty: a randomized controlled trial. J Dent Res
2011;90:203–208.
18. West NX, Addy M, Jackson RJ, Ridge DB. Dentine
hypersensitivity and the placebo response. A com-
parison of the effect of strontium acetate, potassi-
um nitrate and fluoride toothpastes. J Clin Peri-
odontol 1997;24:209–215.
19. Gillam DG, Newman HN, Davies EH, Bulman JS,
Troullos ES, Curro FA. Clinical evaluation of ferric
oxalate in relieving dentine hypersensitivity. J Oral
Rehabil 2004;31:245–250.
20. Ozen T, Orhan K, Avsever H, Tunca YM, Ulker AE,
Akyol M. Dentin hypersensitivity: a randomized
clinical comparison of three different agents in a
short-term treatment period. Oper Dent
2009;34:392–398.
21. Pradeep AR, Sharma A. Comparison of clinical effi-
cacy of a dentifrice containing calcium sodium
phosphosilicate to a dentifrice containing potassi-
um nitrate and to a placebo on dentinal hypersensi-
tivity: a randomized clinical trial. J Periodontol
2010;81:1167–1173.
22. Wara-aswapati N, Krongnawakul D, Jiraviboon D,
Adulyanon S, Karimbux N, Pitiphat W. The effect of
a new toothpaste containing potassium nitrate and
triclosan on gingival health, plaque formation and
dentine hypersensitivity. J Clin Periodontol
2005;32:53–58.
23. Tengrungsun T, Sangkla W. Comparative study in
desensitizing efficacy using the GaAlAs laser and
dentin bonding agent. J Dent 2008;36:392–395.
24. Yu X, Liang B, Jin X, Fu B, Hannig M. Comparative in
vivo study on the desensitizing efficacy of dentin
desensitizers and one-bottle self-etching adhesives.
Oper Dent 2010;35:279–286.
25. Liu H, Hu D. Efficacy of a commercial dentifrice con-
taining 2% strontium chloride and 5% potassium
nitrate for dentin hypersensitivity: a 3-day clinical
study in adults in China. Clin Ther 2006;34:614–622.
26. Polderman RN, Frencken JE. Comparison between
effectiveness of a low-viscosity glass ionomer and a
resin-based glutaraldehyde containing primer in
treating dentine hypersensitivity: a 25.2-month
evaluation. J Dent 2007;35:144–149.

doi: ##.####/j.qi.a##### 11
QUINTESSENCE INTERNATIONALda Rosa et al
27. Prasad KV, Sohoni R, Tikare S, Yalamalli M, Rajesh G,
Javali SB. Efficacy of two commercially available
dentifrices in reducing dentinal hypersensitivity.
Indian J Dent Res 2010;21:224–230.
28. Vieira AH, Passos VF, de Assis JS, Mendonca JS, San-
tiago SL. Clinical evaluation of a 3% potassium oxa-
late gel and a GaAlAs laser for the treatment of
dentinal hypersensitivity. Photomed Laser Surg
2009;27:807–812.
29. Birang R, Poursamimi J, Gutknecht N, Lampert F, Mir
M. Comparative evaluation of the effects of Nd:YAG
and Er:YAG laser in dentin hypersensitivity treat-
ment. Lasers Med Sci 2007;22:21–24.
30. Goodis HE, White JM, Marshall GW Jr, et al. Effects of
Nd: and Ho:yttrium-aluminium-garnet lasers on
human dentine fluid flow and dental pulp-chamber
temperature in vitro. Arch Oral Biol 1997;42:845–
854.
31. Yilmaz HG, Cengiz E, Kurtulmus-Yilmaz S, Leblebi-
cioglu B. Effectiveness of Er,Cr:YSGG laser on den-
tine hypersensitivity: a controlled clinical trial. J Clin
Periodontol 2011;38:341–346.
32. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred
reporting items for systematic reviews and meta-
analyses: the PRISMA statement. J Clin Epidemiol
2009;62:1006–1012.
33. Fu Y, Li X, Que K, et al. Instant dentin hypersensitiv-
ity relief of a new desensitizing dentifrice contain-
ing 8.0% arginine, a high cleaning calcium carbon-
ate system and 1450 ppm fluoride: a 3-day clinical
study in Chengdu, China. Am J Dent 2011;23(Spec
No A):20A–27A.
34. Kowalczyk A, Botulinski B, Jaworska M, Kierklo A,
Pawinska M, Dabrowska E. Evaluation of the prod-
uct based on Recaldent technology in the treat-
ment of dentin hypersensitivity. Adv Med Sci
2006;51(Suppl 1):40–42.
35. Que K, Fu Y, Lin L, et al. Dentin hypersensitivity
reduction of a new toothpaste containing 8.0%
arginine and 1450 ppm fluoride: an 8-week clinical
study on Chinese adults. Am J Dent 2011;23(Spec
No A):28A–35A.
36. Sharma N, Roy S, Kakar A, Greenspan DC, Scott R. A
clinical study comparing oral formulations contain-
ing 7.5% calcium sodium phosphosilicate (Nova-
Min), 5% potassium nitrate, and 0.4% stannous fluo-
ride for the management of dentin hypersensitivity.
J Clin Dent 2011;21:88–92.
37. Du Min Q, Bian Z, Jiang H, et al. Clinical evaluation of
a dentifrice containing calcium sodium phospho-
silicate (NovaMin) for the treatment of dentin
hypersensitivity. Am J Dent 2008;21:210–214.
38. He T, Chang J, Cheng R, Li X, Sun L, Biesbrock AR.
Clinical evaluation of the fast onset and sustained
sensitivity relief of a 0.454% stannous fluoride den-
tifrice compared to an 8.0% arginine-calcium car-
bonate-sodium monofluorophosphate dentifrice.
Am J Dent 2012;24:336–340.
39. Kakar A, Kakar K, Sreenivasan PK, DeVizio W, Kohli R.
Comparison of the clinical efficacy of a new denti-
frice containing 8.0% arginine, calcium carbonate,
and 1000 ppm fluoride to a commercially available
sensitive toothpaste containing 2% potassium ion
on dentin hypersensitivity: a randomized clinical
trial. J Clin Dent 2012;23:40–47.
40. Salian S, Thakur S, Kulkarni S, LaTorre G. A random-
ized controlled clinical study evaluating the efficacy
of two desensitizing dentifrices. J Clin Dent
2011;21:82–87.
41. Azarpazhooh A, Limeback H, Lawrence HP, Fillery
ED. Evaluating the effect of an ozone delivery sys-
tem on the reversal of dentin hypersensitivity: a
randomized, double-blinded clinical trial. J Endod
2009;35:1–9.
42. Kielbassa AM, Attin T, Hellwig E, Schade-Brittinger
C. In vivo study on the effectiveness of a lacquer
containing CaF2/NaF in treating dentine hypersen-
sitivity. Clin Oral Investig 1997;1:95–99.
43. Ciaramicoli MT, Carvalho RC, Eduardo CP. Treat-
ment of cervical dentin hypersensitivity using neo-
dymium: Yttrium-aluminum-garnet laser. Clinical
evaluation. Lasers Surg Med 2003;33:358–362.
44. Ladalardo TC, Pinheiro A, Campos RA, et al. Laser
therapy in the treatment of dentine hypersensitivi-
ty. Braz Dent J 2004;15:144–150.
45. Clavijo EMA, Clavijo VRG, Bandeca MC, et al. Clinical
efficiency of low-level diode laser in reducing den-
tin hypersensitivity. Laser Physics 2009;19:2041–
2044.
46. Kobler A, Kuss O, Schaller HG, Gernhardt CR. Clinical
effectiveness of a strontium chloride-containing
desensitizing agent over 6 months: A randomized,
double-blind, placebo-controlled study. Quintes-
sence Int 2008;39:321–325.
47. Sethna GD, Prabhuji MLV, Karthikeyan BV. Compari-
son of two different forms of varnishes in the treat-
ment of dentine hypersensitivity: a subject-blind
randomised clinical study. Oral Health Prev Dent
2011;9:143–150.
48. Singal P, Gupta R, Pandit N. 2% sodium fluoride-
iontophoresis compared to a commercially avail-
able desensitizing agent. J Periodontol 2005;76:351–
357.
49. Markowitz K. Pretty painful: why does tooth bleach-
ing hurt? Med Hypotheses 2010;74:835–840.
50. Reis A, Dalanhol AP, Cunha TS, Kossatz S, Loguercio
AD. Assessment of tooth sensitivity using a desensi-
tizer before light-activated bleaching. Oper Dent
2011;36:12–17.
51. Drebenstedt S, Zapf A, Rodig T, Mausberg R, Ziebolz
D. Efficacy of two different CHX-containing desensi-
tizers: a controlled double-blind study. Oper Dent
2012;37:161–171.
52. Duran I, Sengun A. The long-term effectiveness of
five current desensitizing products on cervical den-
tine sensitivity. J Oral Rehabil 2004;31:351–356.
12 doi: ##.####/j.qi.a#####
QUINTESSENCE INTERNATIONALda Rosa et al
53. Assis C, A., Antoniazzi RP, Zanatta FB, Rosing CK.
Efficacy of Gluma Desensitizer on dentin hypersen-
sitivity in periodontally treated patients. Braz Oral
Res 2006;20:252–256.
54. Dilsiz A, Aydin T, Emrem G. Effects of the combined
desensitizing dentifrice and diode laser therapy in
the treatment of desensitization of teeth with gingi-
val recession. Photomed Laser Surg 2010;28(Suppl
2):S69–74.
55. Ipci SD, Cakar G, Kuru B, Yilmaz S. Clinical evaluation
of lasers and sodium fluoride gel in the treatment of
dentine hypersensitivity. Photomed Laser Surg
2009;27:85–91.
56. Sgolastra F, Petrucci A, Gatto R, Monaco A. Effective-
ness of laser in dentinal hypersensitivity treatment:
a systematic review. J Endod 2011;37:297–303.
57. Yilmaz HG, Kurtulmus-Yilmaz S, Cengiz E, Bayindir
H, Aykac Y. Clinical evaluation of Er,Cr:YSGG and
GaAlAs laser therapy for treating dentine hypersen-
sitivity: A randomized controlled clinical trial. J Dent
2011;39:249–254.
58. Kimura Y, Wilder-Smith P, Yonaga K, Matsumoto K.
Treatment of dentine hypersensitivity by lasers: a
review. J Clin Periodontol 2000;27:715–721.
59. Lier BB, Rosing CK, Aass AM, Gjermo P. Treatment of
dentin hypersensitivity by Nd:YAG laser. J Clin Peri-
odontol 2002;29:501–506.
60. Yilmaz HG, Kurtulmus-Yilmaz S, Cengiz E. Long-
term effect of diode laser irradiation compared to
sodium fluoride varnish in the treatment of dentine
hypersensitivity in periodontal maintenance
patients: a randomized controlled clinical study.
Photomed Laser Surg 2011;29:721–725.




















