
Biological evaluation of the apical dentin chip plug
7
0099-2399/85/1101-0018/$02.00/0 JOURNALOF ENDODONTICS Copyright 1985 by The American Association of Endodontists Printed in U.S.A. VOL. 11, NO. 1,JANUARY 1988 Biological Evaluation of the Apical Dentin Chip Plug Evaluacion Biologica del Tapon de Virutas en la Zona Apical Kamran Safavi, DMD,MEd, Preben Hc~rsted, DDS, Elizeu A. Pascon, DDS, MSD, and Kaare Langeland, DDS, PhD Autologous dentin chips were packed in the apical part of root canals of baboon teeth. Root canals were then filled with Hydron using a pressure sy- ringe technique. Histological periapical response was evaluated up to 114 wk. Complete apical clo- sure did not occur and material particles were ob- served in periapical tissues. All root canal sealers studied until now are known to be toxic (1,2). Extrusion of root filling materials into the periapical tissue causes an inflammation, including for- eign body reaction, and contributes to poor prognosis and failures in root canal treatment (3). Apical dentin chip plugs are suggested to prevent overfilling during root canal obturation (4, 5) and, at least in noninfected root canals, appear to be compatible to periapical tis- sues (6-11). A technique for pulpectomy and the simultaneous creation of an autologous dentin plug is described by Baume et al. (12). The purpose of the present study was to examine periapical tissue reaction to a dentin chip plug and to investigate if such a plug can act as a biocompatible barrier between periapical tissue and root canal filling material. Se sabe que todos los selladores o cementos de obturacion estudiados hasta ahora son toxicos. La extrusi6n de materiales de obturacion de conductos en el tejido periapical causa inflamaci6n incluyendo reacci6n a los cuerpos extra~os y contribuye a un peor pronostico y fracasos en los tratamientos de conductos. El tap6n de virutas dentinarias en la zona apical se sugiere para impedir la sobreobturacion del conducto, y al menos, en conductos no infecta- dos, parece ser compatible con los tejidos periapi- cales. Una tecnica para la pulpectomia y la creaci6n simultanea de un tapon dentinario autologico es descripta por Baume (1971). El proposito de este estudio fue examinar la re- 18 accion del tejido periapical al tapon de virutas de dentina, e investigar si ese tapon puede actuar como una barrera biocompatible entre el tejido per- iapical y el material de obturacion del conducto. MATERIALS AND MEq'HODS Four 14-kg baboons were used for this study. The baboons were anesthetized with an intramuscular in- jection of an initial dose of 5 ml of solution combining 2 ml of 100 mg of ketamine HCI/ml (Ketaset; Bristol Laboratories), 1.5 ml of 10 mg of acepromacine/ml, and 1.5 ml of 0.4 mg of atropine/ml. Additional one-half doses were injected when required. A full-mouth series of radiographs were taken of each baboon and 24 teeth, with complete root formation, were selected for the study. Teeth were scaled and individually isolated with a rubber dam. The crowns of the teeth were scrubbed with a 30% hydrogen peroxide solution using a cotton applicator and then dried by air syringe. With the use of a fresh cotton applicator, a 5% solution of tincture of iodine was applied over the crown, the clamp, and the surrounding rubber dam. The access cavity was prepared with a sterile, round high-speed bur and no water spray. The coronal pulp tissue was removed with sterile spoon excavators and/or low- speed round burs, and the canal orifices were located with an endodontic explorer. A 1% sodium hypochlorite solution and suction was used for irrigation. The method described by Baume et al. (12) was used to establish the dentin chip plug. By using the periapical radiograph and the root canal diameter, the tentative working length was estimated and a flat-ended reamer slightly larger than the root canal diameter was selected and inserted into the canal 2 to 5 mm short of the radiographic apex. If the tip of the reamer did not come into contact with the canal walls at this level, the reamer was removed and a larger size was inserted into the root canal until it bound to the dentin walls 2 to 5 mm short of the radiographic apex. A working length radi- ograph was taken at this time (Fig. 1). If the tip of the reamer was more than 5 mm short of the radiographic
-
Upload
independent -
Category
Documents
-
view
13 -
download
0
Transcript of Biological evaluation of the apical dentin chip plug

0099-2399/85/1101-0018/$02.00/0 JOURNAL OF ENDODONTICS Copyright �9 1985 by The American Association of Endodontists
Printed in U.S.A. VOL. 11, NO. 1,JANUARY 1988
Biological Evaluation of the Apical Dentin Chip Plug
Evaluacion Biologica del Tapon de Virutas en la Zona Apical
Kamran Safavi, DMD, MEd, Preben Hc~rsted, DDS, Elizeu A. Pascon, DDS, MSD, and Kaare Langeland, DDS, PhD
Autologous dentin chips were packed in the apical part of root canals of baboon teeth. Root canals were then filled with Hydron using a pressure sy- ringe technique. Histological periapical response was evaluated up to 114 wk. Complete apical clo- sure did not occur and material particles were ob- served in periapical tissues.
All root canal sealers studied until now are known to be toxic (1,2). Extrusion of root filling materials into the periapical tissue causes an inflammation, including for- eign body reaction, and contributes to poor prognosis and failures in root canal treatment (3). Apical dentin chip plugs are suggested to prevent overfilling during root canal obturation (4, 5) and, at least in noninfected root canals, appear to be compatible to periapical tis- sues (6-11).
A technique for pulpectomy and the simultaneous creation of an autologous dentin plug is described by Baume et al. (12).
The purpose of the present study was to examine periapical tissue reaction to a dentin chip plug and to investigate if such a plug can act as a biocompatible barrier between periapical tissue and root canal filling material.
Se sabe que todos los selladores o cementos de obturacion estudiados hasta ahora son toxicos. La extrusi6n de materiales de obturacion de conductos en el tejido periapical causa inflamaci6n incluyendo reacci6n a los cuerpos extra~os y contribuye a un peor pronostico y fracasos en los tratamientos de conductos. El tap6n de virutas dentinarias en la zona apical se sugiere para impedir la sobreobturacion del conducto, y al menos, en conductos no infecta- dos, parece ser compatible con los tejidos periapi- cales. Una tecnica para la pulpectomia y la creaci6n simultanea de un tapon dentinario autologico es descripta por Baume (1971).
El proposito de este estudio fue examinar la re- 18
accion del tejido periapical al tapon de virutas de dentina, e investigar si ese tapon puede actuar como una barrera biocompatible entre el tejido per- iapical y el material de obturacion del conducto.
MATERIALS AND MEq'HODS
Four 14-kg baboons were used for this study. The baboons were anesthetized with an intramuscular in- jection of an initial dose of 5 ml of solution combining 2 ml of 100 mg of ketamine HCI/ml (Ketaset; Bristol Laboratories), 1.5 ml of 10 mg of acepromacine/ml, and 1.5 ml of 0.4 mg of atropine/ml. Additional one-half doses were injected when required. A full-mouth series of radiographs were taken of each baboon and 24 teeth, with complete root formation, were selected for the study. Teeth were scaled and individually isolated with a rubber dam. The crowns of the teeth were scrubbed with a 30% hydrogen peroxide solution using a cotton applicator and then dried by air syringe. With the use of a fresh cotton applicator, a 5% solution of tincture of iodine was applied over the crown, the clamp, and the surrounding rubber dam. The access cavity was prepared with a sterile, round high-speed bur and no water spray. The coronal pulp tissue was removed with sterile spoon excavators and/or low- speed round burs, and the canal orifices were located with an endodontic explorer. A 1% sodium hypochlorite solution and suction was used for irrigation. The method described by Baume et al. (12) was used to establish the dentin chip plug. By using the periapical radiograph and the root canal diameter, the tentative working length was estimated and a flat-ended reamer slightly larger than the root canal diameter was selected and inserted into the canal 2 to 5 mm short of the radiographic apex. If the tip of the reamer did not come into contact with the canal walls at this level, the reamer was removed and a larger size was inserted into the root canal until it bound to the dentin walls 2 to 5 mm short of the radiographic apex. A working length radi- ograph was taken at this time (Fig. 1). If the tip of the reamer was more than 5 mm short of the radiographic
Vol. 11, No. 1, January 1985
b : m . , , ~z, ~il
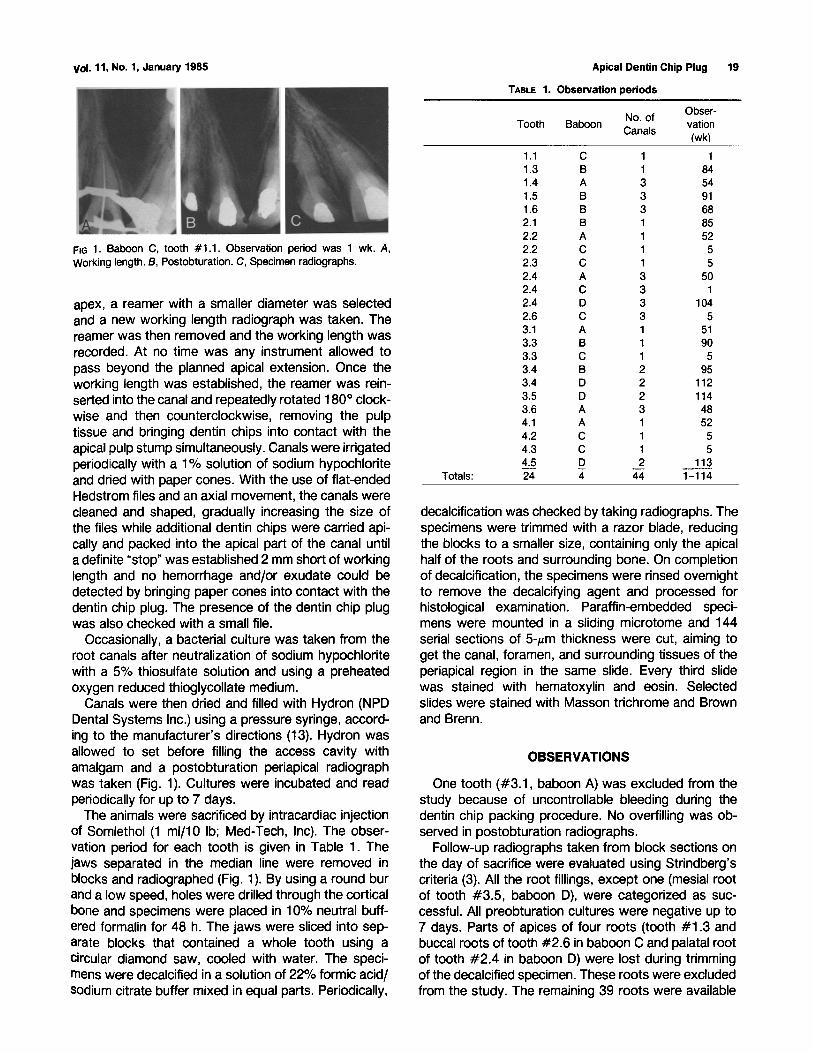
FiG 1. Baboon C, tooth #1.1. Observation period was 1 wk. A, Working length. B, Postobturation. C, Specimen radi~:jraphs.
apex, a reamer with a smaller diameter was selected and a new working length radiograph was taken. The reamer was then removed and the working length was recorded. At no time was any instrument allowed to pass beyond the planned apical extension. Once the working length was established, the reamer was rein- serted into the canal and repeatedly rotated 180 ~ clock- wise and then counterclockwise, removing the pulp tissue and bringing dentin chips into contact with the apical pulp stump simultaneously. Canals were irrigated periodically with a 1% solution of sodium hypochlorite and dried with paper cones. With the use of flat-ended Hedstrom files and an axial movement, the canals were cleaned and shaped, gradually increasing the size of the files while additional dentin chips were carried api- cally and packed into the apical part of the canal until a definite "stop" was established 2 mm short of working length and no hemorrhage and/or exudate could be detected by bringing paper cones into contact with the dentin chip plug. The presence of the dentin chip plug was also checked with a small file.
Occasionally, a bacterial culture was taken from the root canals after neutralization of sodium hypochlorite with a 5% thiosulfate solution and using a preheated oxygen reduced thioglycollate medium.
Canals were then dried and filled with Hydron (NPD Dental Systems Inc.) using a pressure syringe, accord- ing to the manufacturer's directions (13). Hydron was allowed to set before filling the access cavity with amalgam and a postobturation periapical radiograph was taken (Fig. 1). Cultures were incubated and read periodically for up to 7 days.
The animals were sacrificed by intracardiac injection of Somlethol (1 ml/10 Ib; Med-Tech, Inc). The obser- vation period for each tooth is given in Table 1. The jaws separated in the median line were removed in blocks and radiographed (Fig. 1). By using a round bur and a low speed, holes were drilled through the cortical bone and specimens were placed in 10% neutral buff- ered formalin for 48 h. The jaws were sliced into sep- arate blocks that contained a whole tooth using a circular diamond saw, cooled with water. The speci- mens were decalcified in a solution of 22% formic acid/ sodium citrate buffer mixed in equal parts. Periodically,
Apical Dentin Chip Plug 19
TABLE 1. Observation periods
Obser- No. of
Tooth Baboon vation Canals
(wk)
TOtals:
1.1 C 1 1 1.3 B 1 84 1.4 A 3 54 1.5 B 3 91 1.6 B 3 68 2.1 B 1 85 2.2 A 1 52 2.2 C 1 5 2.3 C 1 5 2.4 A 3 50 2.4 C 3 1 2.4 D 3 104 2.6 C 3 5 3.1 A 1 51 3.3 B 1 90 3.3 C 1 5 3.4 B 2 95 3.4 D 2 112 3.5 D 2 114 3.6 A 3 48 4.1 A 1 52 4.2 C 1 5 4.3 C 1 5 4.5 D 2 113 24 4 44 1-114
decalcification was checked by taking radiographs. The specimens were trimmed with a razor blade, reducing the blocks to a smaller size, containing only the apical half of the roots and surrounding bone. On completion of decalcification, the specimens were rinsed overnight to remove the decalcifying agent and processed for histological examination. Paraffin-embedded speci- mens were mounted in a sliding microtome and 144 serial sections of 5-#m thickness were cut, aiming to get the canal, foramen, and surrounding tissues of the periapical region in the same slide. Every third slide was stained with hematoxylin and eosin. Selected slides were stained with Masson trichrome and Brown and Brenn.
OBSERVATIONS
One tooth (#3.1, baboon A) was excluded from the study because of uncontrollable bleeding during the dentin chip packing procedure. No overfilling was ob- served in postobturation radiographs.
Follow-up radiographs taken from block sections on the day of sacrifice were evaluated using Strindberg's criteria (3). All the root fillings, except one (mesial root of tooth #3.5, baboon D), were categorized as suc- cessful. All preobturation cultures were negative up to 7 days. Parts of apices of four roots (tooth #1.3 and buccal roots of tooth #2.6 in baboon C and palatal root of tooth #2.4 in baboon D) were lost during trimming of the decalcified specimen. These roots were excluded from the study. The remaining 39 roots were available
20 Safavi et al. Journal of Endodontics
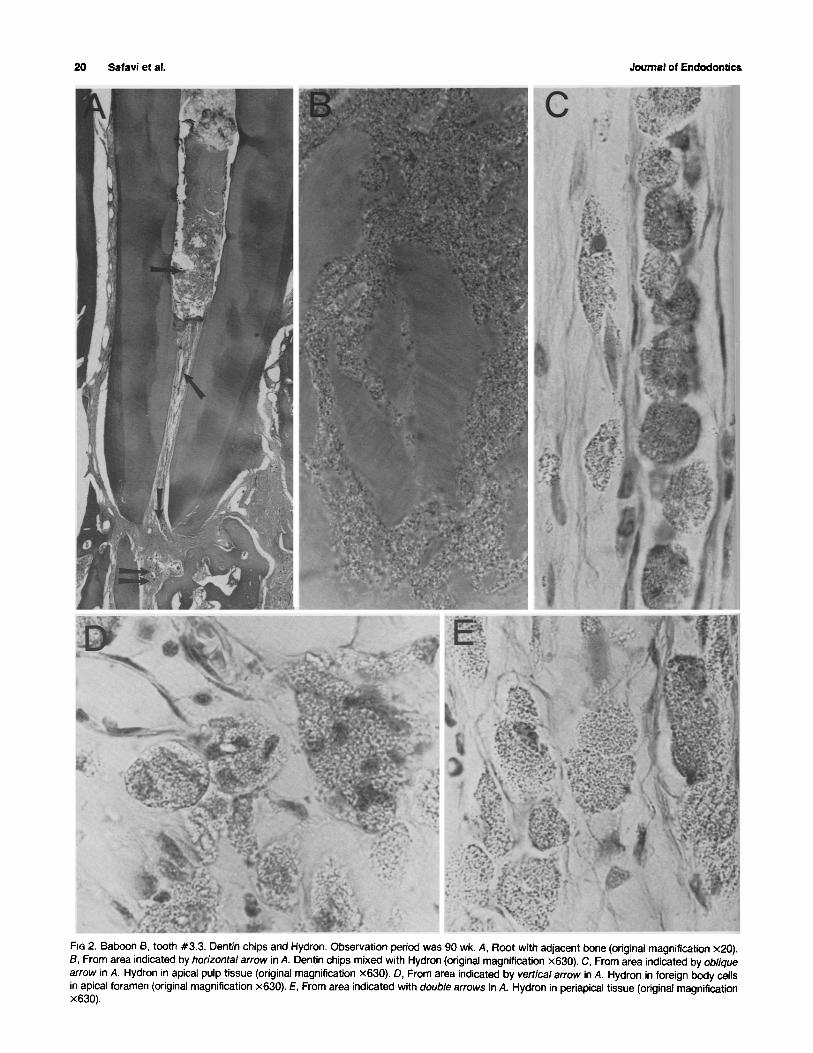
FIG 2. Baboon 8, tooth #3.3, Dentin chips and Hydron. Observation period was 90 wk. A, Root with adjacent bone (original magnification x20). B, From area indicated by horizontal arrow in A. Dentin chips mixed with Hydron (original magnification x630). C, From area indicated by oblique arrow in A. Hydron in apical pulp tissue (original magnification x630). D, From area indicated by vertical arrow in A. Hydron in foreign body cells in apical foramen (original magnification x630). E, From area indicated with double arrows in A. Hydron in periapical tissue (original magnification x630).
Vol. 11, No. 1, January 1985
for light microscope observation. Six roots, in which sections did not contain apical root canal including the foramen with direct connection into the periodontal ligament, were also eliminated from the study. Thus, 33 roots in which root filling material, dentin chip plug, apical foramen, and surrounding periapical tissue were all present in serial sections were evaluated in this study (Fig. 2).
The filling material was observed short of the dentin chip plug in some sections and mixed with dentin chips in others (Fig. 2).
The length of the dentin chip plug varied in different root canals and different sections of the same root canal. The distance between the material/dentin chip "interface" and the apical foramen ranged from 0.8 to 6.9 mm. Hydron particles were observed in the apical
Apical Dentin Chip Plug 21
pulp tissue of 12 canals extending to periapical ligament in some sections (Fig. 2).
Extruded particles were observed among dentin chips in macrophages, foreign body cells, in vessels in the remaining apical pulp tissue, in the periapical tissue, and in the periodontal ligament apical to the apex (Fig. 2).
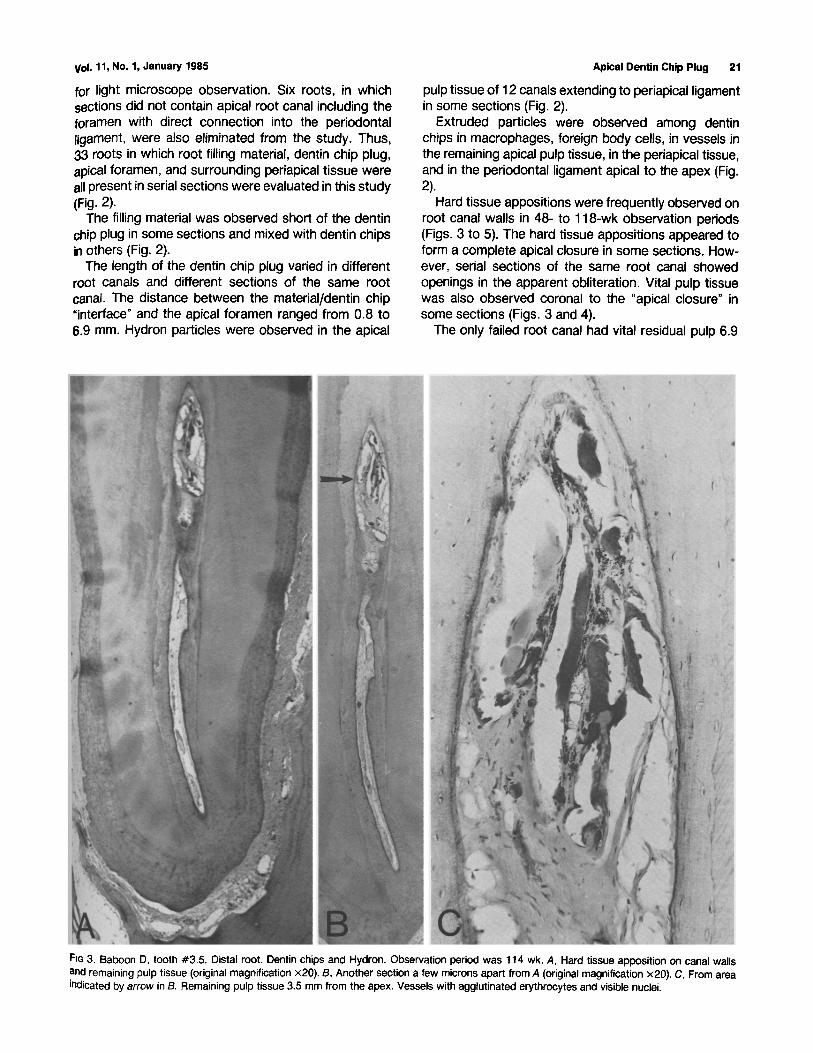
Hard tissue appositions were frequently observed on root canal walls in 48- to 118-wk observation periods (Figs. 3 to 5). The hard tissue appositions appeared to form a complete apical closure in some sections. How- ever, serial sections of the same root canal showed openings in the apparent obliteration. Vital pulp tissue was also observed coronal to the "apical closure" in some sections (Figs. 3 and 4).
The only failed root canal had vital residual pulp 6.9
FiG 3. Baboon D, tooth #3.5. Distal root. Dentin chips and Hydron. Observation period was 114 wk. A, Hard tissue apposition on canal walls and remaining pulp tissue (original magnification x20). B, Another section a few microns apart from A (original magnification x20). C, From area indicated by ar row in B. Remaining pulp tissue 3.5 mm from the apex. Vessels with agglutinated erythrocytes and visible nuclei.

22 Safavi et ai, Journal of Endodontics
FIG 4. Baboon B, tooth #1.5. Palatal root. Dentin chips and Hydron. Observation period was 91 wk. A, Dentin chip plug indicated with horizontal arrow (original magnification x28). B, Another section, a few microns apart from A. Apparent apical closure indicated with horizonta/arrow (original magnification x28). C, From area indicated with vertical arrow in A. Erythrocytes 2 mm coronal to the =apical closure" (original magnification x1250). D, From area indicated with vertical arrow in B. Soft tissue 2 mm coronal to the apex. The apparent closure is a section of the root canal wall.
Vol. 11, No. 1, January 1985
a
Apical Dentin Chip Plug 23
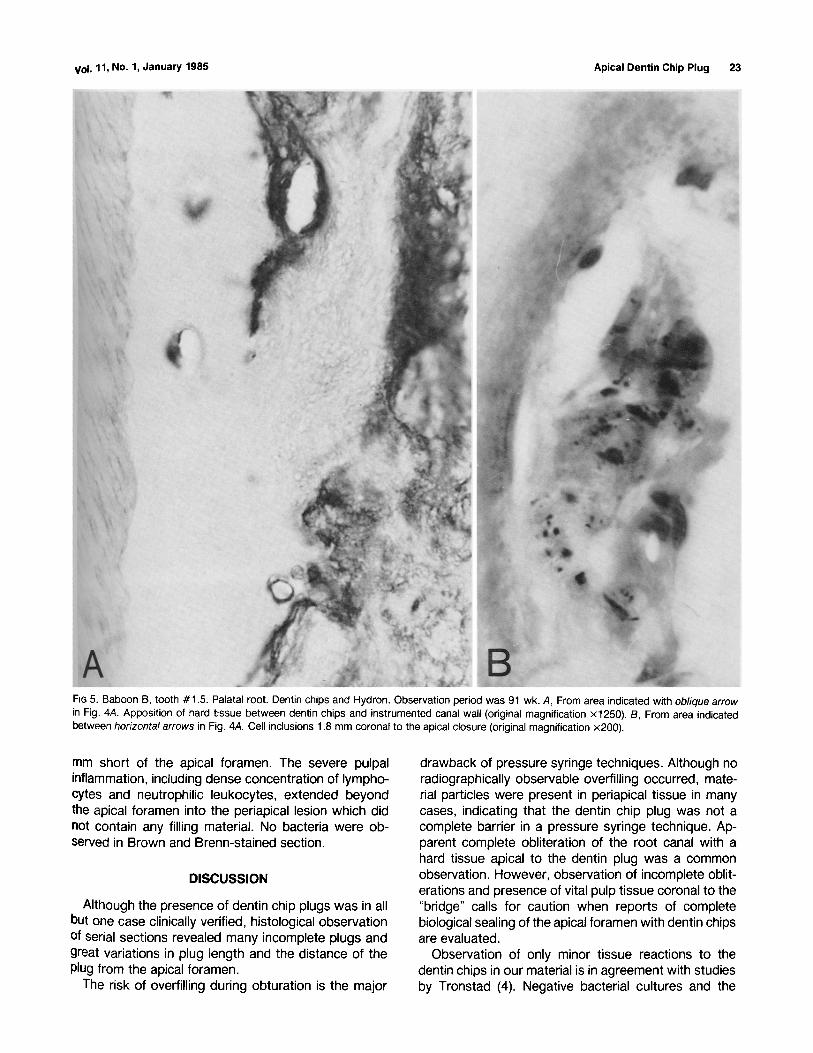
FIG 5. Baboon B, tooth #1.5. Palatal root. Dentin chips and Hydron. Observation period was 91 wk. A, From area indicated with oblique arrow in Fig. 4A. Apposition of hard tissue between dentin chips and instrumented canal wall (original magnification x1250). B, From area indicated between horizontal arrows in Fig. 4A. Cell inclusions 1.8 mm coronal to the apical closure (original magnification •
mm short of the apical foramen. The severe pulpal inflammation, including dense concentration of lympho- cytes and neutrophilic leukocytes, extended beyond the apical foramen into the periapical lesion which did not contain any filling material. No bacteria were ob- served in Brown and Brenn-stained section.
DISCUSSION
Although the presence of dentin chip plugs was in all but one case clinically verified, histological observation of serial sections revealed many incomplete plugs and great variations in plug length and the distance of the plug from the apical foramen.
The risk of overfilling during obturation is the major
drawback of pressure syringe techniques. Although no radiographically observable overfilling occurred, mate- rial particles were present in periapical tissue in many cases, indicating that the dentin chip plug was not a complete barrier in a pressure syringe technique. Ap- parent complete obliteration of the root canal with a hard tissue apical to the dentin plug was a common observation. However, observation of incomplete oblit- erations and presence of vital pulp tissue coronal to the "bridge" calls for caution when reports of complete biological sealing of the apical foramen with dentin chips are evaluated.
Observation of only minor tissue reactions to the dentin chips in our material is in agreement with studies by Tronstad (4). Negative bacterial cultures and the

24 Safavi et al.
absence of bacteria in Brown and Brenn-stained sec- tions indicate that in our materials the dentin chips were not contaminated. In the case of necrotic pulps, dentin chips may contain bacteria (14, 15) and cause an unfavorable periapical tissue response (16).
CONCLUSIONS 1. Complete dentin chip barrier to root filling materials
could not be achieved with the method used. 2. Hard tissue formation was common but no total
apical closure occurred, 3. Tissue response to dentin chips was generally
favorable.
This study was supported by United States Public Health Service Grant 5 RO1 DE04096-05.
Dr. Safavi is assistant professor and director of the Graduate Endodontic Program, Department of Endodontics, School of Dental Medicine, University of Connecticut Health Center, Farmington, CT. Dr. Horsted is associate professor, Department of Dental Pathology and Operative Dentistry, Arhus Tandlaege- h~jskole, The Royal Dental College, Vennelyst Boulevard, DK-8000 Arhus C., Denmark. Dr. Pascon is assistant professor, Department of Endodontics, School of Dental Medicine, University of Connecticut Health Center. Dr. Lange- land is professor and chairman, Department of Endedontics, and chief, Endo- dontic Service, John Dempsey Hospital, University of Connecticut Health Cen- ter.
References
1. Sp&ngberg L. Biological effects of root canal filling materials. Experimen- tal investigation of toxicity of root canal filling materials in vitro and in vivo.
Journal of Endodontic8
Odont Revy 1969;20(supp116). 2. Langeland K. Root canal sealants and pastes. Dent Clin North Ann
1974;18:309-27. 3. Strindberg LZ. The dependence of the results of pulp therapy on certain
factors. Acta Odontol Scand 1956;14(supp121):1-175. 4. Tronstad L. Tissue reactions following apical plugging of the root canal
with dentin chips in monkey teeth subjected to pulpectomy. Oral Surg 1978;45:297-304.
5. EIDeeb ME, Thur-Quyen NT, Jensen JR. The dentinal plug: its effect on confining substances to the canal and-on the apical seal. J Endodon 1984;9:355-9.
6. Petersson K, Hasselgren G, Petersson A, Tr~nsted L. Clinical experience with the use of dentin chips in pulpectomies. Int End J 1982;15:161-7.
7. Safavi K, Pascon E, Langeland K. Dentin chip plug and root canal obturation [Abstract 254]. General Session, International Association for Dental Research. J Dent Res 1982;61:207.
8. Kuttler Y. A precision and biologic root canal filling technique. J Am Dent Assoc 1958;56:38-50.
9. Nyborg H, Hailing A. Amputation instruments for partial pulp extirpation. II. A comparison between the efficiency of the antheos root canal reamer and the HedstrSm file with cut tip. Odontol Tidskr 1963;71:277-283.
10. Holland GR. Periapical response to apical plugs of dentin chip and calcium hydroxide in ferret canines. J Endodon 1984;10:71-4.
11. Holland R, Nery M J, Souza V, Bernabe PFE, Mello W, Otoboni Filho JA. The effect of the filling material in the tissue reactions following apical plugging of the root canal with dentin chips. A histologic study in monkeys' teeth. Oral Surg 1983;55:398-401.
12. Baume L J, Holz J, Risk LB. Radicular pulpotomy for category III pulps. Part II. Instrumentation and technique. J Prosthet Dent 1971 ;25:525-31.
13. Langeland K, OIsson B, Pascon E. Biological evaluation of Hydron. J Endodon 1981 ;7:196-204.
14. Shovelton DS. The presence and distribution of microorganisms within non-vital teeth. Br Dent J 1964;117:101-7.
15. Lin L, Langeland K. Light and electron microscopic study of teeth with carious pulp exposures. Oral Surg 1981 ;57:297-319.
16. Holland R, De Souza V, Nery M J, de Mello W, Bernabe PFE, Otoboni Filho JA. Tissue reactions following apical plugging of the root canal with infected dentin chips. A histologic study in dogs' teeth. Oral Surg 1980;49: 366-9.




















