Do Dentin Bond Strength Tests Serve a Useful Purpose?
11
Do Dentin Bond Strength Tests Serve a Useful Purpose? Somsri SudsangiamVRichard van Noort'' Purpose: The publication of dentin bond strength data is prolific in the dental literature and will remain so as more and more new dentin bonding agents are marketed. It is the purpose of this presentation to as- sess the usefuiness of this information. Methods: The limitations of dentir bond strength tests are examined in the contert of current knowledge about the methods used. Results: The evidence provided shows that dentin bond strength measurement techniques provide data that \s not sbie to act as a consistent predictor of clinical performance. Fundamental fiaws in the most popular methods adopted have been identified and alternative approaches need to be explored. Unfortu- nately, we do not as yet have in place methodologies that siiow us to establish a reliabie link between iab- oratory bond strength data and clinical performance. Conclusion: For the present, oiinicslly based evidence remains the only reliabie means for the selection of dentin bonding agents. J Adhesive Dent 1999:1:57-67 SuOmitteû for putilicatlon: 13.08.98: accepted for publication: 28.09.98. A S a consequence of a growing demand for mate- rials that bond well to dentin, new and improved versions of bonding systems are constantly being marketed, making it difficult for dental practitioners to choose the most appropriate materials for clini- cal use. Since long-term clinical trials are costly and time consuming, and manufacturers are not obliged to carry out such studies prior to launching a new product, laboratory bond strength test data are usu- ally used to demonstrate the quality of a dentm adhesive relative to its competitors. Many manufac- turers promote their products on the basis of mean values of shear bond strength measurements, im- plying that high bond strength values are indicative of good clinical performance. But has it been shown that such measurements provide useful and reli- ^ Postgraduate student. Department of Restorative Dentistry, Uni- versity of Sheffield, United Kingdom. " Professor, Department of Restorative Dentistry, University of Sheffield, United Kingdom. Reprint requests: Prof R. van Noort, Department of Restorative Den- tistry, University of Sheffield, Claremont Crescent, Sheffield SIO 2TA, United Kingdom. E-mail: r.vannoortmheffieid.ac.uk. able information relevant to clinical adhesive be- havior? This paper reviews the validity of commonly used methods of measuring dentin bond strengths and their relevance to clinical performance. BOND STRENGTH TESTS In a tensile bond strength test using extracted human or bovine teeth stored In a suitable medium, a flat bonding site is prepared on a dentin surface by wet grinding with silicone carbide paper. The pre- pared bonding site is usually treated according to manufacturers' instructions for the adhesive sys- tem being evaluated. A cylindrical-shaped restora- tive material is then bonded to the treated dentin surface. After short- or long-term specimen storage, possibly combined with cyclic fatigue or thermal stress aging, the bonded specimen is placed in a universal testing machine and subjected to tensile force perpendicular to the tooth surface. The test arrangement is shown in Eig 1. A major difficulty with this type of test is maintaining the alignment during both bonding and testing to avoid stress con- centrations due to incorrect interfacial geometry. Vol 1, No L 57
-
Upload
khangminh22 -
Category
Documents
-
view
4 -
download
0
Transcript of Do Dentin Bond Strength Tests Serve a Useful Purpose?

Do Dentin Bond Strength Tests Serve aUseful Purpose?
Somsri SudsangiamVRichard van Noort''
Purpose: The publication of dentin bond strength data is prolific in the dental literature and will remain soas more and more new dentin bonding agents are marketed. It is the purpose of this presentation to as-sess the usefuiness of this information.
Methods: The limitations of dentir bond strength tests are examined in the contert of current knowledgeabout the methods used.
Results: The evidence provided shows that dentin bond strength measurement techniques provide datathat \s not sbie to act as a consistent predictor of clinical performance. Fundamental fiaws in the mostpopular methods adopted have been identified and alternative approaches need to be explored. Unfortu-nately, we do not as yet have in place methodologies that siiow us to establish a reliabie link between iab-oratory bond strength data and clinical performance.
Conclusion: For the present, oiinicslly based evidence remains the only reliabie means for the selection ofdentin bonding agents.
J Adhesive Dent 1999:1:57-67 SuOmitteû for putilicatlon: 13.08.98: accepted for publication: 28.09.98.
AS a consequence of a growing demand for mate-rials that bond well to dentin, new and improved
versions of bonding systems are constantly beingmarketed, making it difficult for dental practitionersto choose the most appropriate materials for clini-cal use. Since long-term clinical trials are costly andtime consuming, and manufacturers are not obligedto carry out such studies prior to launching a newproduct, laboratory bond strength test data are usu-ally used to demonstrate the quality of a dentmadhesive relative to its competitors. Many manufac-turers promote their products on the basis of meanvalues of shear bond strength measurements, im-plying that high bond strength values are indicativeof good clinical performance. But has it been shownthat such measurements provide useful and reli-
^ Postgraduate student. Department of Restorative Dentistry, Uni-versity of Sheffield, United Kingdom.
" Professor, Department of Restorative Dentistry, University ofSheffield, United Kingdom.
Reprint requests: Prof R. van Noort, Department of Restorative Den-tistry, University of Sheffield, Claremont Crescent, Sheffield SIO 2TA,United Kingdom. E-mail: r.vannoortmheffieid.ac.uk.
able information relevant to clinical adhesive be-havior? This paper reviews the validity of commonlyused methods of measuring dentin bond strengthsand their relevance to clinical performance.
BOND STRENGTH TESTS
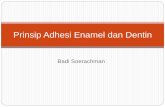
In a tensile bond strength test using extractedhuman or bovine teeth stored In a suitable medium,a flat bonding site is prepared on a dentin surfaceby wet grinding with silicone carbide paper. The pre-pared bonding site is usually treated according tomanufacturers' instructions for the adhesive sys-tem being evaluated. A cylindrical-shaped restora-tive material is then bonded to the treated dentinsurface. After short- or long-term specimen storage,possibly combined with cyclic fatigue or thermalstress aging, the bonded specimen is placed in auniversal testing machine and subjected to tensileforce perpendicular to the tooth surface. The testarrangement is shown in Eig 1. A major difficultywith this type of test is maintaining the alignmentduring both bonding and testing to avoid stress con-centrations due to incorrect interfacial geometry.
Vol 1, No L 57

Sudsangiam/van Noort
LOAD
ADHESIVE
O
DENTIN
(a)
I fTensile stress [Compressive stress
Fig 1 Cross SGCtioh of a tensile bond test speoirnen (a) and non-uniform stress formation due to misalignment |b).
LOAD
ADHERENDA
ADHEREND B
Fig 2 View of shear bond test arrangement.
Such problems as alignment are iargely over-come in the shear bond strength test. Specimenpreparation is essentially the same as for the ten-sile test, but in the shear bond strength test thebond is broken by a force applied paraiiei to the
tooth surfaoe (Fig 2). The advantage ofthis methodis that specimens and loading arrangements areeasy to produce, which makes it by far the mostpopular measurement system used. However, thistest may easily transform to a bend or cleavagetype of test where tensile and not shear stressesdominate (Fig 3).
It has been shown repeatediy that dentin bondstrength data suffer from considerabie scatter andlack of consistency when results from different lab-oratories are compared."^s Therefore, the compar-ison of the reported bond strength values must betreated with caution. Alternatively, ranking of bondstrength values has been claimed to be moremeaningfui than the absolute values obtained.^While it may be the case in some studies that theshear and tensile bond strength tests produce thesame ranking of the products,i^ aithough withsomewhat higher values in shear than in tension,other studies^^ do not show this, as illustrated inFig 4.
An enormous number of variables can influencethe bond strength test. Broad categories of vari-abies influencing the test resuits have been sum-marized by Pashiey et al.̂ s Factors relating to theselection, storage, and preparation ofthe substratefor bond strength tests to tooth structure have aisobeen thoroughly reviewed by Rueggeberg.̂ ^ poten-
58 The Journal of Adhesive Dentistry

Sudsangiam/van Noort
DISTRIBUTED LOAD
SUBSTRATE
ADHE
Ben
- • /ADHEREND
SIVE
ding
INTERRACIAL LOAD
SUBSTRATE ADHEREND
ADHESIVE
Cleavage
Fig 3 Bending and cleavage arising in the shear bond strength test.
^Tensile• Shear
^ Tensile• Shear
Fig 4 Comparison of bond strength vaiues from tensile and stiear bond strength testing. Left: From Kitasai^o et al,is Right: From
iVlay et ai,^3
59

Sudsangiam/van Moort
TB5 (MPal
^Scotchbond 2Ö Gluma
TBS (MPa)
with flash
without flash
Adhesive application meltiod
Fig 5 Comparison of bond strength vaiues with smaii modifications to the methods. Left; From Oiio et ai.2' Right: From van Noortet al.^e
tially of much greater influence and significance isthat different methods or smaii modifications of thesame method can give two- to four-fold differencesin bond strength values for one and the same prod-uct. This has been shov^n to be the case by Oilo eta\^^ and van Noort et al,''^ as illustrated in Fig 5.
The lack of consistency in the use of dentin bondstrength measurement techniques has novjreached the stage that editoriais requesting devel-opment of a standardized bonding test are beingwritten.39 A group of experts working for the Inter-national Organization for Standardization (ISO) havedeveloped guidelines [CD TR 11405, Dental Materi-als "Guidance on testing of adhesion to tooth struc-ture"] Viiith the intention to standardize the bondtesting procedures as much as possible.^^ Both ten-sile and shear tests are described in the ISO docu-ment. However, this standard has not been givenmuch recognition and has been harshiy criticized.^^Inherent in the process of standardization is the be-lief that the results derived from the bond strengthtest wili have some vaiidity and meaning as long asbond strength can be measured consistently. Thisis highly questionable, as discussed beiow, be-cause no amount of standardization will overcomeinconsistency problems if a test is fundamentaliyflawed.
Aithough a strict standardization scheme maysoive part of the inconsistency of the test resuits,there are more fundamental concerns with regardto the mechanics of the test method. Severai re-searchers have shown that a non-uniform stressdistribution is generated aiong the bonded inter-face in both the tensile and shear bond strengthtests.'•"Ë'''^ The occurrence of prominent stress con-centrations is in conflict with the underlying as-sumption o f the nominal bond strength, which isdefined as the average stress value of the crosssection. Van Noort et al^^.J? used finite elementstress analysis (FEA) to demonstrate that the maxi-mum stresses generated in tensiie and shear bondstrength measurements are at the edge ofthe inter-face and far exceed the nominal bond strength.This was confirmed in a more detailed 3-D FFAanalysis by DeHoff et al.? Fracture is probably initi-ated from some point around the circumference ofthe bonded interface where there is a flaw of a criti-cal size, coincident with the high localized tensilestress, and then propagates aiong the interface. Inthese anaiyses,^•''S''̂ ? the interfacial stress distribu-tion in both tests was found to be highly dependenton the geometry of the test arrangement, the na-ture of the load application, the presence or ab-sence of adhesive f iash, and the physical
60 The Journal of Adhesive Dentistry

Table 1 Strength of dentin
Source
Mineralized dentinBowen et a 1,61962Smith et ai,3äl97SSano et al,331994Watahabeetal,i3i996
Demineralized dentinSano et a 1,331994
Cohesive strength (MPa)
51.7±10,3103,0 ± 135,0
93,8±11,17S,4±13,3
29,6±5,9
Resin-infiltrated demineraiizerl rlpntmSano et a 1,351995 121,6±20-3 (AB]
111,5±14,5 (MP)117,6±12,2 (SB ]102,6+3,7 (CL)57,6±16.4 (PB)
AB = All Bond 2, MP ̂ ScotcliBond MultipjrDOse, SB = SuperBonfl C&PB = Clearfil Phoiobnnd.
Type of hoiid strength test
TensiieShear (micropunch)
TensiieShear
Tensiie
Tensiie
3, CL = Clearfil Liner Bond 2,
properties of the materials involved. The sensitivitylo the loading geometry is particularly acute inshear type tests. Shearing force can be applied witha wide variety of configurations, including loops,points, and knife edges. Clearly differing configura-tions of ioad application will lead to differing stressdistributions. Moreover, in the shear test the trueshear stresses at the interface were invariabiy over-shadowed by high tensile stresses.
Versluis et ai,"^ using a failure accumuiation sim-ulation program to determine iocaiized failure inter-activeiy with a f in i te e lement solver, was inagreement with van Noort et al, ' '^"^ They confirmedthat dentin pull-out in the shear bond strengthtest was, in part, due to the mechanics of the testset-up, such as crosshead speed, load applicationoffsets, and adhesive layer thickness. They aisonoted that failure in dentin did not mean that theadhesive strength exceeded the cohesive strengthof the dent in , as concluded by many re-sea rc hers, ̂ ^'^^ but is a consequence of the experi-mental design.
The mode of failure is another important aspectof bond strength tests, although not reported on asoften as it shouid. A detailed inspection of the frac-tured surfaces can indicate the failure mode of abonded assembly. The failure mode can be adhe-
sive [located in the adhesive interface), cohesive (afracture in one ofthe materials on either side oftheinterface), or a mixture of the two. As reported byseverai investigators, a high percentage of fracturesin dentin are observed at bond strengths over 15 to20 MPa when using current adhesive systems,^^'^^However, the ultimate tensile strengtii of humandentin has been consistently reported to be in arange of 50 to 138 MPa (Table i).6,33,35,38,49 jhe ex-planation for this discrepancy, with identin fracturesoccurring at seemingly iower stresses in the shearbond strength test, is simple. Due to uneven stressdistributions deveioped during the test, the calcu-lated nominai stresses are far beiow the actualstress experienced at the adhesive interface. Thisexplanation can also be applied when cohesive fail-ure occurs within the restorative materials. For ex-ampie, the bond strength of glass-ionomer cements,typically 1 to 5 MPa'̂ and with largely cohesive fail-ures within the cement, are lower than those re-ported for resin-modified giass-ionomer cementsand resin composites,^•^•*'° However, their low bondstrength vaiue is primariiy due to the iack of tensilestrength of the materials themselves" rather thanany inability to bond to the dentin. The higher bondstrength of resin-modified glass-ionomer cementscompared with conventionai glass-ionomer ce-
Vol 1, No 1, 1999 61

Sudsangiam/uan Noort
mehts can be attributed to the improved oohesivestrength of the resin-modified cements.is There-fore, It Is questionable what is being measured inthese tests; it certainly is not the adhesive strengthofthe cements.
Thus, variations in test results can be easily in-troduced by the design of the experimental set-up.This means that relying solely on bond strengthdata is not a reliable method of material selection.Furthermore, the conventional bond strength testsmay no longer be able to measure the adhesiveproperties of the dentin adhesive. The popularity ofthese tests, especially the shear type, can be ex-plained by their relative simplicity. However, this isnot a good reason for their continued use.
The non-uniformity of the stress distribution gen-erated during the conventional tensile and shearbond strength tests will create areas of high localstress, and fracture will be initiated from flaws atthe interface or in the substrate in these areas ofhigh local stress. The local stress at which failureoccurs cannot easily be calculated and is not repre-sented by the average stress quoted in most arti-cles. A new approach for the evaluation of biologicinterfaces is clearly needed to provide a better in-terpretation of the dentin adhesive properties.There are a number of ways this could be dealtwith. One possibility is to design a test configura-tion that is more akin to the clinical situation—whatone might consider a usage test. An example ofsuch an approach is the push-out test used byKrämer et al^o and Frankenburger et al^o providinga measure of the retention of an inlay in dentin.However, there is no doubt that the interfacialstresses in such an experimental design will againbe highly non-uniform and potentially influenced bythe stiffness characteristics of the materials, thedesign of the plunger, and the exact geometry anddimensions of the test arrangement. Thus, as a testfor in-house comparison, it will serve a useful pur-pose but will be difficult to duplicate elsewhere.Also, the data obtained should not be expressed interms of the extrusion stress, ie, MPa, but shouldbe reported simply as the extrusion force. The ratio-nale for this recommendation is that the interfacialstresses are highly complex and non-uniform, mak-ing the average value of stress calculated of littlevalue as a measurement ofthe actual stresses ex-perienced at the adhesive interfaoe. This will haveno effect on the relative ranking of the data as longas the dimensions are standardized. It will alsoavoid any tendency on the part of others to carry
out what would be an invalid comparison with theequally incorrect stresses calculated from shearbond strength experiments.
An alternative approach is to design an experi-meht in which the interfacial stresses will be as uni-form as possible to achieve, so that the true in-terfaoial stresses can be readily calculated. Sano etal^" developed a bond test that sought to eliminatethe non-uniform stress distribution at the adhesiveinterface by reverting to the more traditional dumb-bell-shaped specimen design. The so-called "mi-crotensile" method involves bonding adhesiveresins to the entire flat occlusal surface of thetooth, which is then covered with a resin composite.After curing and storage, the specimen is verticallysectioned into multiple serial sections. The trimmedsection is then attached to microgrips and sub-jected to a tensile force (Eig 6). By this method, theauthors found that bond strengths to dentin wereinversely related to the bonding surface areas. Thelarger surface areas showed lower tensile bondstrengths, whereas the smaller surface areas wereassociated with higher tensile bond strengths. At abonded surface area below 2.0 mm^, the bondstrength values showed minimum scatter, and all ofthe failures were adhesive in nature even thoughthe bond strengths increased to 50 to 60 MPa. Thisphenomenon is due to a reduction of the numberand size of flaws, which is a consequence ofthe re-duction in specimen size. It follows the same pat-tern observed many years ago by Griffith whehchanging from low-strength glass sheets to highstrength glass fibers.^3 These results provide addi-tional evidence that the cohesive strength of dentinis much higher than the values measured in shearbond testing when dentin fails cohesively. Thehigher bond strength values obtained with the mi-crotensile method are also consistent with the finiteelement analysis prediction of van Noort et al,''^which suggested that the actual tensile stresses ex-perienced under the loading point in the shear testcan be as much as a factor of three higher than thenominal bond strength values. Schreiner et al^scompared the microtensile bond strength test withthe shear bond strength test, and found that signifi-cantly more failures In dentln and composite wereseen in the shear test. Thus, the results obtainedfrom the microtensile testing method may better re-flect the actual interfaoial bond strengths to dentin.
Another experimental approach for evaluation ofthe adhesion of dentin-bonded interfaces is thefracture toughness test.^i The fracture toughness
62 The Journai of Adhesive Dentistry

PMMA ^^T^t\
CompositeDentin
CompositeDentin
H
Fig 6 Bonding procedure ahd specimen preparation for the miorotensiie bond strength test. A,B: Preparation of tooth for bonding.C: Composite crown bonded to dentin, D: Preparation of bonded specimen for sectioning. E: Serial seotioning of specimen. F: Indi-vidual slab shown in profile and full view. G: Slab trimmed at bonded interface. H: Trimmed slab in special grips. (Adapted fromSaho et al.s")
Vol 1, No. 63

Sudsangiam/van Noort
value (Kic) reflects the ability of a materiai to resistcrack initiation and unstable propagation, Tam andPilliar'^i compared a fracture toughness test ofdentin-resin interfaces with a tensiie bond strengthtest. Although the relative rankings of the groupedmeans for the dentin bonding agents were thesame for both tests, light microscopy examinationrevealed a greater number of total or partial cohe-sive fractures after the tensile bond strength test-ing compared with fracture toughness testing. Theyconcluded that the fracture toughness test provideda vaiid method of characterizing the fracture resis-tance of the denttn-resin interface both quanti-tatively, with respect to the Kic results, and qua-litativeiy, with respect to the fracture surfaces.
Both the microtensile test and the fracture me-chanics approach show promise in improving ourunderstanding of the properties of the adhesive in-terface. Despite this, the acceptance of these ap-proaches by the wider research community willprobabiy be poor because they are much more diffi-cuit to do.
CLINICAL VALUE OF BOND STRENGTH TESTS
As discussed above, bond strength vaiues dependon the method used, and thus it is advisable not todirectly compare the reported values. The purposeof breaking apart a bonded assembly is to try to es-tablish how strong the bond is and where there areweaknesses in the system. Identification of theseweaknesses and their eiiminetion ieads to improve-ments, in engineering appiications it is often reia-tiveiy straightforward to design bond strengthexperiments that are exactly the same as the bond-ed assembly to be used in service, eg, lap joints orbutt joints. However, given the complexity of adhe-sively retained restorations in dentistry, this is notpossible. The most popular methods to evaiuatebond strengths to enamei and dentin cleariy bearno relationship to the ciinicai situation. This in itselfshould not present a problem, as long as the infor-mation obtained in the laboratory has value in as-sessing the merits of the bonding system beingevaiuated, which is a matter of interpretation anduse of the data. Ideally the data gathered can sub-sequently be used to determine the potential per-formance of the adhesive in service. This is how anengineer wiil use fundamental properties (eg, elas-tic modulus, yield strength, and fracture toughness)of a material such as high tensile steel to deter-
mine if it wiii perform its intended function as partof a structurai unit, be it a bridge, boat, or car. At nostage is the materiai judged for its suitabiiity for aparticular purpose solely on the data gathered iniaboratory experiments on the material. In dentistrythis seems to be what we are trying to do. It shouldtherefore come as no surprise that this naive ap-proach does not work,
if bond strength data are to be of enduring value,a number of things will need to happen. First, thedata obtained must be transferabie from one situa-tion to another. The microtensiie test data appearpromising in this respect, and the fracture tough-ness approach may aiso be the way to gain greaterinsight to what is actuaiiy happening at the adhe-sive interface. Second, the means by which thistransfer is to be achieved needs to be explored. Theengineer has the advantage in that the process ofdesigning a suspension bridge, for example, iendsitself to an analytical soiution of the stresses andstrains the bridge components wili be required tosupport. Thus it is possible to teli from its funda-mental properties, obtained from laboratory experi-ments, if a material has adequate strength andstiffness for its intended purpose. When the struc-ture to be built does not lend itself to a simple ana-lytical solution, the engineer calls upon othertechniques, such as photoelasticity or finite ele-ment modeling of the structure. In engineeringthese are tried and trusted procedures; however, indentistry the use of such techniques is new andmuch needs to be learned before they can be usedwith any degree of confidence. We can takecourage from the fact that the worid of industrialadhesives is not much ahead of dentistry and theyare also still working to understand what is happen-ing atthe adhesive interface.^^
While this situation remains, clinical evidencewill continue to be the only conclusive measure ofadhesive performance, despite its own inherentproblems. The clinical evaluation of dentin adhe-sive materials is based primarily on the retention ofthe restorations. Few studies have attempted to cor-relate laboratory bond strength measurements di-rectiy with the clinical performance of the ad-hesives used. This may be partiy because of theiarge number of dentin adhesive materials on themarket, and partly because of the changes in prod-uct chemistry that occur periodicaily, Platt et al^^conducted both a shear bond strength test and ciin-icai evaiuation of four dentin adhesive materials.They concluded that the popuiar laboratory test
64 The Journai of Adhesive Dentistry

Fig 7 Comparison of 3-year clinical re-tention rate of two different adhesiverestorative materiais, reported by Po-well et al,30 and their bond strengthvalues published by severai laborato-
Rétention rats 1%)
inn —
90
BO
/O
40
30
20
ID
S7
Bond ali-angth (MPa|
•4 Ketac-Fil ^ * - Scotchbond Z/Sl lux-^
12
s
6
• Retention rats
g Bond slrangth
1
may not be a good means of predicting ciinicai per-formance ofthe materiais.
Given the differences in clinioal results withmany systems, such as Scotchbond Muitipurposeand Prisma Universai Bond 3 dentin bonding sys-tems, '̂3.*3,45 ¡I; ¡5 apparent that various factors mayalter the apparent clinioai efficacy of adhesives.Some of these factors could be tooth preparation,operator, patient, material, and intraoral location.""
Figure 7 illustrates the results of a recently pub-lished study on the 3-year clinicai retention rate oftwo different adhesive restorative materials.3° Alsoincluded are the bond strength values of each ma-terial as reported from several laboratories.^-ii'^i"^Glass-ionomer cements consistently produce excel-ient retention rates, yet their bond strengths are ai-ways very low; dentin bonding agents producemuch higher bond strengths but have poorer reten-tion rates. The impression this creates is that thelaboratory bond strength values of dentin adhesivesystems have little correlation with clinical retentionrates. Neither the bond strength values nor theirranking appear able to predict the longevity ofdentin-bonded restorations. As already noted, oneconspicuous exampie of this is giass-ionomer ce-ment {eg, Ketac-Fil), which has been shown to havea favorable clinical retention rate up to 10 years^^but very low bond strength values."*" Neo et al^snoted that Imperva Bond had high loss rate (35%)in their clinioal trial despite its high shear bondstrength.^3
CONCLUSION
Adhesion tests, while not perfect, have enabied thedevelopment of improved bonding systems andtechniques. The shear bond strength test has beenof vaiue in differentiating between materials thathave littie or no adhesion to dentin and those thatshow good promise as a dentin adhesive. However,it must be recognized that bond strength values de-pend on the method used, should be carefully inter-preted, and that comparison of the results fromdifferent laboratories is not possible. In terms ofnew information it can provide, the shear bondstrength test has reached the end ofthe road. Newtesting methods need to be developed to provideresearchers with the tools needed to make furtheradvances in adhesion to dentin.
Research is based on experimentation and iogicsuch that the empirical method stresses the factsand at the same time chaiienges the theoreticaliyminded to make deductions from them. Most publi-cations on bond strength tests provide what areperceived as facts-that is, bond strength data. Atfirst sight this appears to be adequate, but the du-bious validity of these data makes the job of thetheoretical thinker, who seeks an expianation of thefacts, difficult if not impossible. Thus we need firstto establish the truth behind the facts if we are everto make sense of the data being generated.
The abiiity of the bonded interface between toothand restoration to resist fracture is complex andcannot be simply correlated with laboratory bondstrength values. We need to learn to make the linkbetween laboratory-generated data on dental mate-
Vnl 1 No L 1999 65

udsangiam/van hJoort
rials and their ciinical appiication. We have dentalmaterials scientists and we have dental clinicians;perhaps we need more dental engineers. Until suchtime that we know how to produce the missing link,dentin bond strength data may be of some use inthe laboratory duringthe development of new adhe-sives but cannot and should not be used as ameans of predicting clinicai performance, whetherdirectly or by inference.
For the present, therefore, the oniy reliablesource of information for the seiection of dentin ad-hesives remains comparison of clinicai perfor-mance of different products over a significantperiod of time.
REFERENCES
1, Abdalia Al, Garcia-Godoy F, Bond strengths ot resin-mod if iedgiass ionomers and poiyacid-modified resin composites todentin. Am J Dent 1997:10:291-294,
2, Aihadainy HA, Abdaiia Ai, 2-year clinical evaluation of dentinbonding systems. Am J Dent 1996:9:77-79,
3, Barnes DM, BianK LW, Gingeii JC, Gilner PR A ciinicai evalua-tion of a resih-nioOified glass ionomer restorative materiai, JAm Dent Assoc 1995:126:1245-1253,
4, Berry EA, Powers JM. Bond strength of glass ionomers tocoronal snd radicular dentin, Oper Dent 1994:19:122-126,
5, Bordin-Aykroyd S, Sefton J, Davies EH, In vitro bond strengthsof three current dentin adhesives to primary and permanentteeth, Oent Mater 1992:8:74-78,
6, Bowen RL, Rodriguez MS, Tensile strength and modulus ofelasticity of tooth structure and several restorative materials,J Am Dent Assoc 1962:64:378-387,
7, DeHoff PH, Anusavice KJ, Wang Z. Three-dimensional finite element analysis of the shear bond test. Dent Mater 1995;11:126-131,
S, Federation Dentaire Internationaie, FDI technicai report No,35, Dentin bonding. Int Dent J 1990,1:127-128,
9. Fowier CS, Svuartz ML, Moore BK, Rhodes BF, Influence of se-iected variables on adhesion testing. Dent Mater 1992:8:265-269,
10, Frankenburger R, Sindel J, Krämer N, Petscheit A, Dentinhaf-tung von Keramikinlays in simulierten Kavitäten, Dtsch Zahn-artzi 2 1998:53:507-512,
11, Fritz UB, Finger WJ, Uno S, Resin-modified giass ionomer ce-ments: Bonding to enamei and dentin. Dent Iviater 1996:12:161-166,
12, Garcia-Godoy F, Neuman E, Dentastic bond strength todentin. Am J Dent 1996:9:130-132.
13, Gordon JE. The New Science of Strong Materials, ed 2, Mid-diesex: Penguin Books Ltd, 1976:Chapter 5,
14, Holten JR, Nystrom GP, Oiin PS, Pheips RA, Phiiiips JJ, Doug-las WH, Bond strength of six dentinal adhesives, J Dent1994:22:92-96,
15, internationai Organization for Standardization, ISO/TR11405, Dentai materials: Guidance on testing of adhesion totooth structure. Geneva, Switzeriand: WHO,
16, Jiang KR, Penn LS, improved anaiysis and expérimentai eval-uation of the singie filament puii-out test. Composites SciTechnol 1992:45:89-103,
17, Kerby RE, Knobioch L, Strength charaoteristics of glass-ionomer cements, Oper Dent 1992:17:170-174,
18, Kerby RE, Knoblooh L, Thakur A. Strength properties of visi-ble-light-cured resin-modified glass-ionomer cements, OperDent 1997:22:79-83,
19, Kitasako V, Burrow MF, Nikaido T, Harada N, inokoshi S, Ya-mada T, Takatsu T Shear and tensiie bond testing for resincement evaiuation. Dent Mater 1995:11:298-304,
20, Krämer N, Popp J, Sindei J, Frankenburger R, Einfluß der Vor-öehandiung von Kompositinlays auf die Verbundfestigkeit,Dtsch Zahnartzi Z 1996:51:598-601,
21, Mason PN, Ferrari M, Cagidraco MC, Davidson CL, Shearbond strength of four dentinal adhesives applied in vivo andm vitro, J Dent 1996:24:217-222,
22, Matis BA, Cochran M, Carison T. Longevity of glass-ionomerrestorative materiais: Resuit of a 10-year evaluation.Quintessence int 1996:27:373-382,
23, May KN Jr, Swift EJ Jr, Bayne SC, Bond strengths of a newdentin adhesive system. Am J Deht 1997:10:195-198,
24, Mechoisky JJ Jr Fracture mechanics principies. Dent Mater1995:11:111-112,
25, Neo J, Chew CL, Yap A, Clinical evaluation of tooth-ccloredmateriais in cervioai lesions. Am J Dent 1996:9:15-18,
26, 0ilo G, Austrheim EK. In vitro quaiity testing of dentm adhe-sives. Acta Odontoi Scand 1993:51:263-269,
27 0iio G, CIsson S, Tensiie bond strength of dentin adhesives: Acomparison of materials and methods. Dent Mater1990:6:138-144,
28, Pashley DH, Sano H, Ciucchi B, Yoshiyama M, Carvaiho RM,Adhesion testing of dentin bonding agents: A review. DentMater 1995:11:117-125,
29, Piatt JA, Winkier MM, Matis BA, Moore BK, Correlation ofdentin adhesive laboratory and clinicai performance at 3years [abstract 1044], J Dent Res 1998:77:236,
30, Powell LV, Johnson GH, Gordon GE, Factors associated withclinical success of cervical abrasion/erosion restorations,Oper Dent 1995:20:7-13,
31, Retief DH, Mandras RS, Russell CM, Shear bond strength re-quired to prevent microieakage ofthe den tin/restora tion in-terface. Am J Dent 1994:7:44-46,
32, Rueggeberg FA, Substrate for adhesion testing to tooth struc-ture. Review of the literature: A report of the ASC MC156Task Group on test methods for the adhesion of restorativemateriais. Dent Mater 1991:7:2-10,
33, Sano H, Ciucchi B, Matthews WG, Pashley DH, Tensile proper-ties of mineralized and demineraiized human and bovinedentin, J Dent Res 1994:73:1205-1211,
34, Sano H, Shono T, Sonoda H, Takatsu T, Ciucchi B, Carvalho R,Pashiey D, Reiatiohship between surface area for adhesionand tensiie bond strength: Evaiuation of a micro-tensiie bondtest. Dent Mater 1994:10:236-240,
35, Sano H, Takatsu T, Ciucchi B, Russeii CM, Pashley DH, Tensiieproperties of resm-infiitrated demineraiized human dentin, JDent Res 1995:74:1093-1102,
66 The Journal of Adhesive Dentistry

Sudsangiam/van Noort
Í6. Schreiner R, Chappell R. Eick J. Microtensiie testing of üentinadhesives (abstract 2133]. J Dent Res 1997:76:280.
37. Sheriff M. Dentai materiais 1991 literature review: Adhesionand mechanisms. J Dent 1993:31:10-11.
33. Smith DC, Cocper WEG. The determination of shear strength,A method using a micropunch apparatus. Br Dent J 1971:130:333-337.
39. Staniey HR. Guest editorial: An urgent piea for a stanOardiseObonding (adhesion) test. J Dent Res 1993,72:1362-1363.
40. Swift EF Jr, Pawius MA, Vargas MA. Shear bend strengths ofresir-modified glass-ionomer restorative matenals. Oper Dent1995:20:138-143.
41. Tam LE, Pilliar RM, Fracture toughness of dentm/res in-com-posite adhesive Interfaces. J Dent Res 1993:72:953-959.
42. Triólo PT Jr. Swift EJ Jr, Barkmeier WW Shear bond strengthsof composite to dentin using sis dental adhesive systems.Oper Dent 1995:20:46-50.
43. Tyas MJ. Ciinicai performance of two dentin adhesives: 2-yeairesults. Aust Dent J 1996:41:324-327.
44. Tyas MJ. Clinicai testing-Has it proved the efficacy of adhe-sives? int Dent J 1993:43:343-347.
45. Van Dijken JWV. Clinical effectiveness of nine aühesives inclass V cervical lesions [abstract 1369]. J Dent Res 1997:76:185.
46. Van Ncort R, Cardew GE, Howard iC, Noroozi S. The effect oflocai interfacial geometry en the measurement of the tensileOond strength to dentin. J Dent Res 1991:70:889-893.
47. Van Noort R, Noroozi S. Howard IC, Cardew G. A critique ofbond strength measurements. J Dent 1989:17:61-67.
48. Versiuis A. Tantbirojn D, Douglas WH. Why do shear bondtests pull out dentin? J Dent Res 1997,76:1298-1307.
49. Watanabe LG, Marshali GW. Marshall SJ. Dentin shearstrength: Effects of tubule orientation and mtratooth location.Dent Mater 1995:12:109-115.
Vol 1, No 1,
InflammationA Review of the Process
Fifth Edition
H c n i j O.Trowbi-idge. DDS. PhD. anJ
Robert C. Emling, MS. EdD
This new edition of a popular textbook includes
a clinical-connections section and new illustra-
tions. With backgrounds ill pathologj' and educa-
tion, the authors create a refreshing "self-study"
approach that explains this complicated field using
direct language and useful metaphors. Self-tests are
.strategically placed for quick review. Ideal as
preparation for the board examinations, or as a
refi esher for busy practitioners seeking to update
their knowledge in this rapidly changing area.
Contents
200 pp (soltcover): 96¡lljslratinns {15 color):ISBN 0-86715-310-5;US$42
I Acute Inflammatory ProcessVascular Response to ln|uryChemical Mediators of the Vascular
ResponseThe Blood LeukocytesSysleniio Manitestations of infiammation
II ImmunityThe Immune SystemHypersensilivity ReactionsChronic Inflammatory Processes
III Repair of Host TissuesHealing
IV Application of Basic PrinciplesClinical Connections
FOR FAST SERVICE
CallToll Free 1-800-621-0387
or Fax 1-630-682-3288
boelu Quintessence Publishing Co, Inc