
The Effect of Chronic Low Back Pain on Trunk Muscle Activations in Target Reaching Movements With...
8
SPINE Volume 32, Number 26, pp E801–E808 ©2007, Lippincott Williams & Wilkins, Inc. The Effect of Chronic Low Back Pain on Trunk Muscle Activations in Target Reaching Movements With Various Loads James S. Thomas, PhD, PT,* Christopher R. France, PhD,† DaoHang Sha, PhD,* Nicole Vander Wiele, DPT,* Stacey Moenter, DPT,* and Kevin Swank, BS* Study Design. A cross-sectional study of the timing of trunk muscle activations between 19 participants with chronic low back pain (LBP) compared with 19 matched controls. Objective. To determine the effects of target height and load on trunk muscle coordination in whole body reaching tasks, and whether participants with chronic LBP display a shift in trunk muscle coordination performing these tasks. Summary of Background Data. Changes in the precise timing of trunk muscle activation may cause an initial episode of back pain, or contribute to the development of recurrent or chronic symptoms. However, most para- digms used to examine timing of trunk muscle activation did not necessitate large displacements of the trunk. Methods. Participants with and without chronic LBP performed a series of bilateral reaching tasks to 3 target heights with 3 different loads held in the reaching hands. During reaching, joint motions were recorded with an optoelectric system and surface electromyographic sig- nals were collected bilaterally from 5 trunk muscles: rec- tus abdominis, external oblique, internal oblique, iliocos- talis lumborum, and the multifidis, and bilaterally from the deltoid muscle. The onset latencies of the antagonist trunk muscles relative to the deltoid muscle were ana- lyzed to determine the effects of group, target height and load. Results. Onset of trunk extensor muscles was signifi- cantly delayed in participants with chronic LBP compared with control subjects. Further, the onset latency of the antagonist trunk muscles increased with target distance, but decreased with target load. Conclusion. These findings suggest that a well docu- mented control strategy generalizes beyond single joint movements and that individuals with chronic LBP display a shift in this strategy. Key words: low back pain, muscle activation, coordi- nation, reaching. Spine 2007;32:E801–E808 Changes in the precise timing of trunk muscle activation may cause an initial episode of back pain, 1–3 or contrib- ute to the development of recurrent or chronic symp- toms. 2 Consistent with this notion, numerous studies have demonstrated differences in the timing of trunk muscle recruitment between healthy controls and indi- viduals with low back pain (LBP). 2,4 –7 However, these paradigms did not necessitate large displacements of the trunk, and often the implicit goal was to maintain a neu- tral trunk position. Because the risk of low back injury is often associated with large trunk displacements, 8,9 it is important to determine the timing of agonist and antag- onist trunk muscles using tasks that necessitate signifi- cant trunk motion. Timing and coordination of agonist and antagonist muscle activity has been studied extensively in single joint movements. 10 –16 Gottlieb et al proposed the term “speed-insensitive” strategy for a control strategy in which movement speed is not explicitly controlled for, but varies due to task constraints of distance and inertial load. 13 In the speed-insensitive strategy, the rising phase of agonist activity and the early latency of the antagonist burst are invariant to distance or load. In contrast, the latency of the later phase of the antagonist burst in- creases with distance and load. 13 Empirical support for speed-insensitive strategy has been provided for single joint movements of the elbow, wrist, and ankle suggest- ing that a common set of control rules is used at different joints. 17 However, it is not known whether the speed- insensitive strategy generalizes to more complex move- ments involving multiple joints such as whole body reaching movements, and whether pain influences this control strategy. Whole body target reaching movements generally in- volve shoulder flexion and lumbar spine flexion to reach targets placed at various heights. 18 –20 Starting from an upright posture, shoulder flexion will create a reactive moment on the torso that will result in lumbar flexion if not counteracted by lumbar paraspinal muscle activity. 21 Additionally, it has been shown that simple trunk flexion movements made at a comfortable pace do not require active abdominal muscle activity but simply a reduction in tonic activity of the lumbar paraspinal muscles. 22 Thus, in these complex reaching tasks, the shoulder flex- From the *School of Physical Therapy, Ohio University, Athens, OH; and †Department of Psychology, Ohio University, Athens, OH. Acknowledgment date: January 26, 2007. First revision date: May 1, 2007. Second revision date: July 16, 2007. Acceptance date: September 4, 2007. This work was supported by National Institutes of Health Grant RO1- HD045512. The manuscript submitted does not contain information about medical device(s)/drug(s). Federal funds were received in support of this work. No benefits in any form have been or will be received from a commercial party related directly or indirectly to the subject of this manuscript. The authors of the manuscript have no financial or other relationships that might lead to a conflict of interest, and the study was conducted in accordance with the current American Psychological Association guidelines for human research and was approved by the Ohio Univer- sity Institutional Review Board. Address correspondence and reprint requests to James S. Thomas, PhD, PT, Ohio University School of Physical Therapy, W277 Grover Center, Athens, OH 45701; E-mail: [email protected] E801
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of The Effect of Chronic Low Back Pain on Trunk Muscle Activations in Target Reaching Movements With...

SPINE Volume 32, Number 26, pp E801–E808©2007, Lippincott Williams & Wilkins, Inc.
The Effect of Chronic Low Back Pain on Trunk MuscleActivations in Target Reaching Movements WithVarious Loads
James S. Thomas, PhD, PT,* Christopher R. France, PhD,† DaoHang Sha, PhD,*Nicole Vander Wiele, DPT,* Stacey Moenter, DPT,* and Kevin Swank, BS*
Study Design. A cross-sectional study of the timing oftrunk muscle activations between 19 participants withchronic low back pain (LBP) compared with 19 matchedcontrols.
Objective. To determine the effects of target heightand load on trunk muscle coordination in whole bodyreaching tasks, and whether participants with chronic LBPdisplay a shift in trunk muscle coordination performingthese tasks.
Summary of Background Data. Changes in the precisetiming of trunk muscle activation may cause an initialepisode of back pain, or contribute to the development ofrecurrent or chronic symptoms. However, most para-digms used to examine timing of trunk muscle activationdid not necessitate large displacements of the trunk.
Methods. Participants with and without chronic LBPperformed a series of bilateral reaching tasks to 3 targetheights with 3 different loads held in the reaching hands.During reaching, joint motions were recorded with anoptoelectric system and surface electromyographic sig-nals were collected bilaterally from 5 trunk muscles: rec-tus abdominis, external oblique, internal oblique, iliocos-talis lumborum, and the multifidis, and bilaterally fromthe deltoid muscle. The onset latencies of the antagonisttrunk muscles relative to the deltoid muscle were ana-lyzed to determine the effects of group, target height andload.
Results. Onset of trunk extensor muscles was signifi-cantly delayed in participants with chronic LBP comparedwith control subjects. Further, the onset latency of theantagonist trunk muscles increased with target distance,but decreased with target load.
Conclusion. These findings suggest that a well docu-mented control strategy generalizes beyond single jointmovements and that individuals with chronic LBP displaya shift in this strategy.
Key words: low back pain, muscle activation, coordi-nation, reaching. Spine 2007;32:E801–E808
Changes in the precise timing of trunk muscle activationmay cause an initial episode of back pain,1–3 or contrib-ute to the development of recurrent or chronic symp-toms.2 Consistent with this notion, numerous studieshave demonstrated differences in the timing of trunkmuscle recruitment between healthy controls and indi-viduals with low back pain (LBP).2,4–7 However, theseparadigms did not necessitate large displacements of thetrunk, and often the implicit goal was to maintain a neu-tral trunk position. Because the risk of low back injury isoften associated with large trunk displacements,8,9 it isimportant to determine the timing of agonist and antag-onist trunk muscles using tasks that necessitate signifi-cant trunk motion.
Timing and coordination of agonist and antagonistmuscle activity has been studied extensively in singlejoint movements.10–16 Gottlieb et al proposed the term“speed-insensitive” strategy for a control strategy inwhich movement speed is not explicitly controlled for,but varies due to task constraints of distance and inertialload.13 In the speed-insensitive strategy, the rising phaseof agonist activity and the early latency of the antagonistburst are invariant to distance or load. In contrast, thelatency of the later phase of the antagonist burst in-creases with distance and load.13 Empirical support forspeed-insensitive strategy has been provided for singlejoint movements of the elbow, wrist, and ankle suggest-ing that a common set of control rules is used at differentjoints.17 However, it is not known whether the speed-insensitive strategy generalizes to more complex move-ments involving multiple joints such as whole bodyreaching movements, and whether pain influences thiscontrol strategy.
Whole body target reaching movements generally in-volve shoulder flexion and lumbar spine flexion to reachtargets placed at various heights.18–20 Starting from anupright posture, shoulder flexion will create a reactivemoment on the torso that will result in lumbar flexion ifnot counteracted by lumbar paraspinal muscle activity.21
Additionally, it has been shown that simple trunk flexionmovements made at a comfortable pace do not requireactive abdominal muscle activity but simply a reductionin tonic activity of the lumbar paraspinal muscles.22
Thus, in these complex reaching tasks, the shoulder flex-
From the *School of Physical Therapy, Ohio University, Athens, OH;and †Department of Psychology, Ohio University, Athens, OH.Acknowledgment date: January 26, 2007. First revision date: May 1,2007. Second revision date: July 16, 2007. Acceptance date: September4, 2007.This work was supported by National Institutes of Health Grant RO1-HD045512.The manuscript submitted does not contain information about medicaldevice(s)/drug(s).Federal funds were received in support of this work. No benefits in anyform have been or will be received from a commercial party relateddirectly or indirectly to the subject of this manuscript.The authors of the manuscript have no financial or other relationshipsthat might lead to a conflict of interest, and the study was conducted inaccordance with the current American Psychological Associationguidelines for human research and was approved by the Ohio Univer-sity Institutional Review Board.Address correspondence and reprint requests to James S. Thomas,PhD, PT, Ohio University School of Physical Therapy, W277 GroverCenter, Athens, OH 45701; E-mail: [email protected]
E801
ors act as the agonist muscles that initiate lumbar flexionand the lumbar paraspinals work as antagonists to breaklumbar motion. The abdominal muscles, particularly theinternal obliques, purportedly act to ensure spinal stabil-ity during the reaching task.4
The present study examined activation timing oftrunk muscles in participants with LBP and matchedcontrols while they performed full body reaching move-ments to different target heights with various loads in thereaching hands. We hypothesized that for all targetheights and loads trunk muscle onset latencies would belonger in participants with LBP. Further, we hypothe-sized that trunk muscle onset latencies would increase astarget height was lowered and decrease as load increased.
Methods
Our final sample included a total of 38 participants. Specifi-cally, we recruited 11 women and 8 men with a history ofchronic LBP and an equivalent number of controls matched on
sex, age, height, and weight (Table 1). Based on a conservativeestimate of effect size of d � 1.0, this sample size would yieldpower �0.90 with � � 0.05. Compared with healthy controls,participants with back pain reported greater pain (P � 0.001)and disability (P � 0.001) on the McGill Pain Question-naire,23,24 and the Roland Morris Disability Question-naire,25–27 respectively.
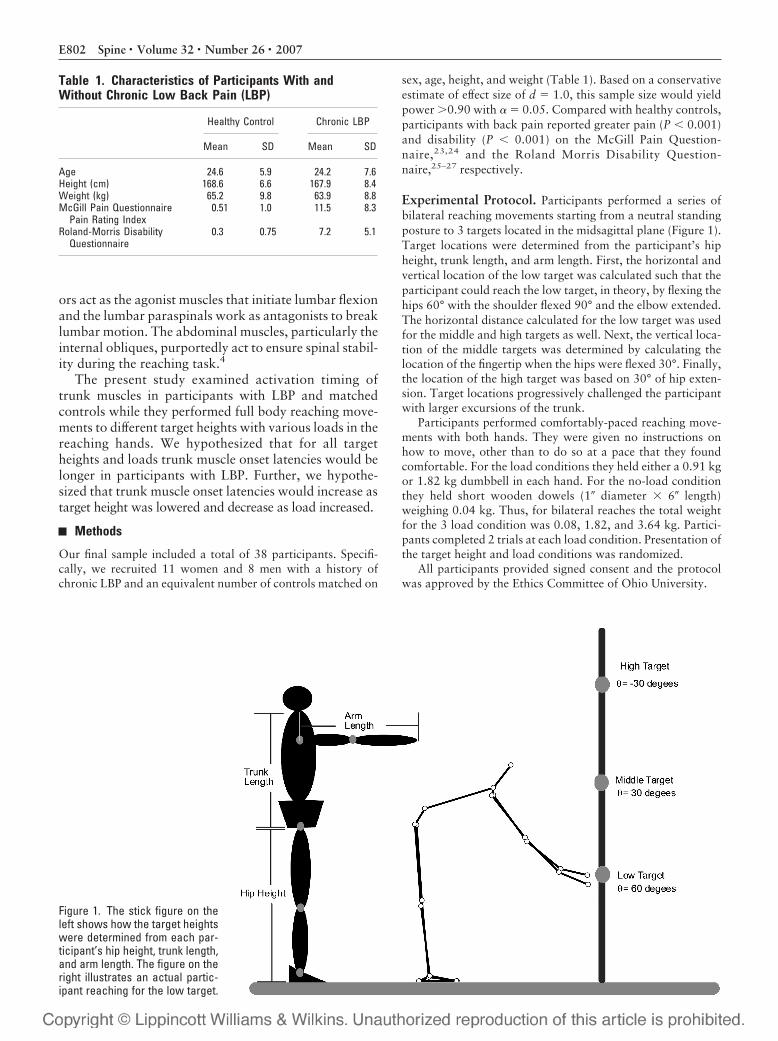
Experimental Protocol. Participants performed a series ofbilateral reaching movements starting from a neutral standingposture to 3 targets located in the midsagittal plane (Figure 1).Target locations were determined from the participant’s hipheight, trunk length, and arm length. First, the horizontal andvertical location of the low target was calculated such that theparticipant could reach the low target, in theory, by flexing thehips 60° with the shoulder flexed 90° and the elbow extended.The horizontal distance calculated for the low target was usedfor the middle and high targets as well. Next, the vertical loca-tion of the middle targets was determined by calculating thelocation of the fingertip when the hips were flexed 30°. Finally,the location of the high target was based on 30° of hip exten-sion. Target locations progressively challenged the participantwith larger excursions of the trunk.
Participants performed comfortably-paced reaching move-ments with both hands. They were given no instructions onhow to move, other than to do so at a pace that they foundcomfortable. For the load conditions they held either a 0.91 kgor 1.82 kg dumbbell in each hand. For the no-load conditionthey held short wooden dowels (1� diameter � 6� length)weighing 0.04 kg. Thus, for bilateral reaches the total weightfor the 3 load condition was 0.08, 1.82, and 3.64 kg. Partici-pants completed 2 trials at each load condition. Presentation ofthe target height and load conditions was randomized.
All participants provided signed consent and the protocolwas approved by the Ethics Committee of Ohio University.
Table 1. Characteristics of Participants With andWithout Chronic Low Back Pain (LBP)
Healthy Control Chronic LBP
Mean SD Mean SD
Age 24.6 5.9 24.2 7.6Height (cm) 168.6 6.6 167.9 8.4Weight (kg) 65.2 9.8 63.9 8.8McGill Pain Questionnaire
Pain Rating Index0.51 1.0 11.5 8.3
Roland-Morris DisabilityQuestionnaire
0.3 0.75 7.2 5.1
Figure 1. The stick figure on theleft shows how the target heightswere determined from each par-ticipant’s hip height, trunk length,and arm length. The figure on theright illustrates an actual partic-ipant reaching for the low target.
E802 Spine • Volume 32 • Number 26 • 2007

Data Collection. As part of a larger experiment, motions ofthe trunk and limb segments were recorded using a 7 cameraVicon MX-13 system, which has a spatial resolution of 0.10mm. The plug-in-gait marker placement for the infrared reflec-tive markers was used with slight modification. Four markerswere used on the posterior pelvis and virtual anterior superioriliac spine (ASIS) markers were determined from the orienta-tion of the markers on the posterior pelvis. Motion data weresampled for 5 seconds at 100 Hz. An Euler angles sequence(flexion, abduction, and rotation) was used to extract the timeseries 3-dimensional joint angles using BodyBuilder software.
Surface EMG electrodes were placed bilaterally over themuscle belly of the anterior deltoid in a vertical direction cen-tered below the lateral end of the clavicle28 and on the follow-ing trunk muscles using double sided tape collars29: (1) RectusAbdominis 1 cm above the umbilicus and 2 cm lateral to themidline, (2) External Oblique just below the rib cage along aline connecting the most inferior portion of the costal marginand the contralateral pubic tubercle, (3) Internal Oblique 1 cmmedial to the ASIS and just beneath a line joining both ASIS, (4)Iliocostalis Lumborum at the L2 level aligned parallel to theline between the posterior superior iliac spine and the lateralborder of the muscle at the 12th rib, and (5) Multifidus at theL5 level aligned parallel to the line between the posterior supe-rior iliac spine and the L1–L2 interspinous space. EMG signalswere collected using a 16 channel Delsys Bagnoli system (band-width of 20–450 Hz). The raw EMG data were amplified,sampled at 1000 Hz, filtered with a 60 Hz notch filter, and thenrectified. Finally, the rectified EMG data were filtered using afourth zero-lag Butterworth filter with a cut-off frequency of100 Hz. To ensure proper electrode placement and signal qual-ity, participants performed a series of maximal isometric exer-tions designed to activate each muscle group (e.g., the signalsfor the internal and external obliques were tested using maxi-mum effort left and right rotations).
Data Processing. Movement onset (t0) was defined as thepoint where finger-tip velocity exceeded 2.5% of peak velocityand movement offset (t1) was defined as the point where fin-gertip velocity dropped below 2.5% peak velocity. Movementtime was simply t0 to t1. Movement onset and offset weredetermined using custom algorithms written in Matlab.
The onset of muscle activity was determined automaticallyusing custom algorithms developed in Matlab. Each muscleonset determined by the algorithm was visually inspected toensure that appropriate onsets and not spurious events (e.g.,EMG artifacts) were chosen. To determine onset of EMG ac-tivity, first the baseline and standard deviation were calculatedfrom 100 data points beginning 200 milliseconds before t0.The algorithm initially determined onset by searching thesmoothed EMG signal from the point 100 milliseconds beforet0 until the point at which the EMG signal was greater than orequal to threshold criteria (baseline � 4 SD). Once onset wasdetermined for each muscle the latencies of the trunk musclerelative to the deltoid were determined.
Statistics Analysis. Movement time, joint excursions, peakangular velocities, and trunk muscle onset latencies were ana-lyzed using separate 3-way mixed-model analysis of variancesin which target height (high, middle, low) and load (0.08, 1.82,3.64 kg) were within subject variables and group (healthy,chronic LBP) was the between subjects variable.
Results
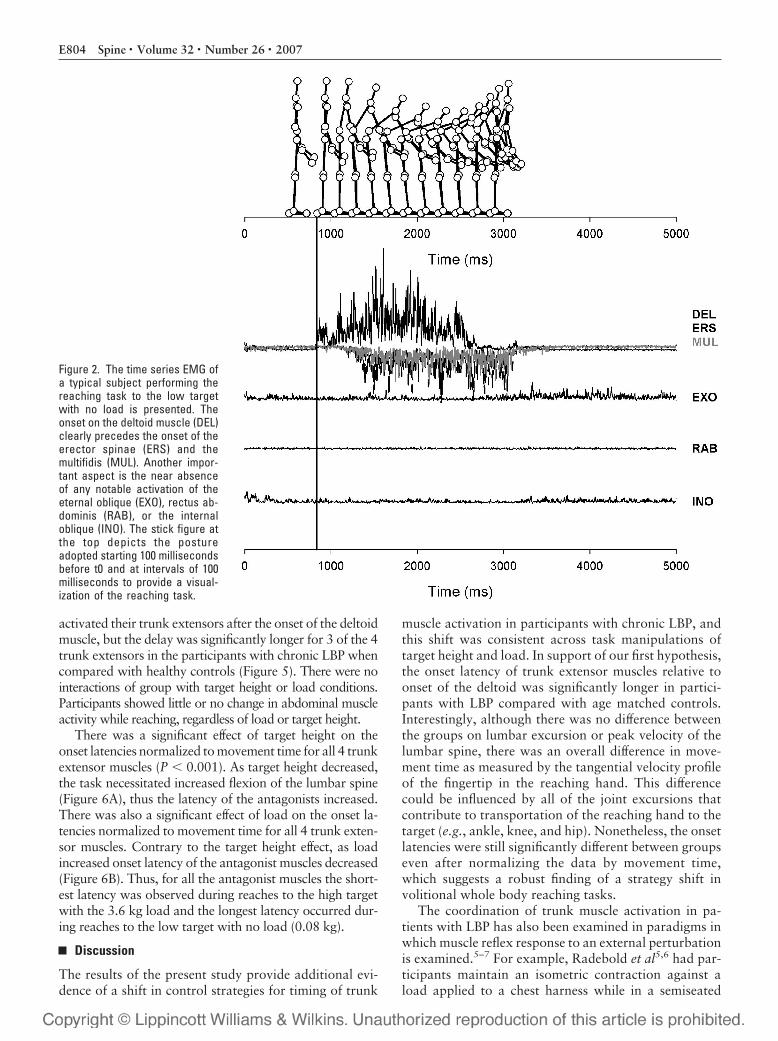
Figure 2 illustrates the time series EMG of a typical healthyparticipant performing a reaching movement to the lowtarget with no load. There are 2 important aspects to thisfigure. One is the obvious latencies of the erector spinaeand multifidis muscles relative to the deltoid muscles.The second is the lack of an abdominal muscle responseduring this task. Unexpectedly, we were unable to detecta discernable onset of abdominal muscle EMG for mostmovement trials of both groups. Below we focus on theactivation patterns of the trunk extensors.
Movement TimeOn average, across all target heights and load conditions,participants with chronic LBP reached the targets in1421 milliseconds whereas healthy participants reachedthe targets in 1203 milliseconds (P � 0.01). As illustratedin Figure 3, there was a significant interaction of load bytarget height on movement time (P � 0.005). Movementtime increased for each load condition only for reaches tothe low target. In contrast, for reaches to the high andmiddle targets, there was no difference in movement timebetween the no load and 1.8 kg load conditions. Becauseof significant effects of group, target height, and load onmovement time, all onset latencies were normalized tomovement time before performing the repeated measuresanalyses.
Joint KinematicsThere was no effect of group on the excursions of thelumbar spine or shoulder for these reaching tasks. Inter-estingly, although there were significant differences inmovement time derived from tangential velocity of thefingertip, there was no effect of group on peak angularvelocity of the lumbar spine or shoulder.
As illustrated in Figure 4A, lumbar spine excursions in-creased (P � 0.001) and peak angular velocity increased(P � 0.001) as target height decreased. In contrast, as illus-trated in Figure 4B, shoulder excursions were greatest forthe high target and least for the middle target (P � 0.001).Although there was a significant effect of target height onshoulder peak angular velocity (P � 0.001) pairwise com-parisons revealed no difference between the middle and lowtargets. The greatest peak velocity was observed for reachesto the high target and the least for reaches to the middle andlow targets. Although there was no effect of load on lumbarspine excursions, shoulder excursions increased as load in-creased (P � 0.001). There was also an interaction of targetheight and load on peak angular velocity for lumbar spine(P � 0.01) and shoulder (P � 0.05). For both the lumbarspine and shoulder, pairwise comparisons revealed thatload influenced peak velocity only for reaches to the lowtarget. As load increased, peak angular velocity decreased.
Onset LatenciesA main effect of group was observed for onset latenciesnormalized to movement time for the right erector spinaeand right and left multifidis (all P � 0.05). On average,across all target heights and load conditions, both groups
E803Muscle Latencies in LBP • Thomas et al
activated their trunk extensors after the onset of the deltoidmuscle, but the delay was significantly longer for 3 of the 4trunk extensors in the participants with chronic LBP whencompared with healthy controls (Figure 5). There were nointeractions of group with target height or load conditions.Participants showed little or no change in abdominal muscleactivity while reaching, regardless of load or target height.
There was a significant effect of target height on theonset latencies normalized to movement time for all 4 trunkextensor muscles (P � 0.001). As target height decreased,the task necessitated increased flexion of the lumbar spine(Figure 6A), thus the latency of the antagonists increased.There was also a significant effect of load on the onset la-tencies normalized to movement time for all 4 trunk exten-sor muscles. Contrary to the target height effect, as loadincreased onset latency of the antagonist muscles decreased(Figure 6B). Thus, for all the antagonist muscles the short-est latency was observed during reaches to the high targetwith the 3.6 kg load and the longest latency occurred dur-ing reaches to the low target with no load (0.08 kg).
Discussion
The results of the present study provide additional evi-dence of a shift in control strategies for timing of trunk
muscle activation in participants with chronic LBP, andthis shift was consistent across task manipulations oftarget height and load. In support of our first hypothesis,the onset latency of trunk extensor muscles relative toonset of the deltoid was significantly longer in partici-pants with LBP compared with age matched controls.Interestingly, although there was no difference betweenthe groups on lumbar excursion or peak velocity of thelumbar spine, there was an overall difference in move-ment time as measured by the tangential velocity profileof the fingertip in the reaching hand. This differencecould be influenced by all of the joint excursions thatcontribute to transportation of the reaching hand to thetarget (e.g., ankle, knee, and hip). Nonetheless, the onsetlatencies were still significantly different between groupseven after normalizing the data by movement time,which suggests a robust finding of a strategy shift involitional whole body reaching tasks.
The coordination of trunk muscle activation in pa-tients with LBP has also been examined in paradigms inwhich muscle reflex response to an external perturbationis examined.5–7 For example, Radebold et al5,6 had par-ticipants maintain an isometric contraction against aload applied to a chest harness while in a semiseated
Figure 2. The time series EMG ofa typical subject performing thereaching task to the low targetwith no load is presented. Theonset on the deltoid muscle (DEL)clearly precedes the onset of theerector spinae (ERS) and themultifidis (MUL). Another impor-tant aspect is the near absenceof any notable activation of theeternal oblique (EXO), rectus ab-dominis (RAB), or the internaloblique (INO). The stick figure atthe top depicts the postureadopted starting 100 millisecondsbefore t0 and at intervals of 100milliseconds to provide a visual-ization of the reaching task.
E804 Spine • Volume 32 • Number 26 • 2007

position. They then examined the timing of the onset andoffset of trunk agonist and antagonist muscles when theload was released. Results indicated that participantswith LBP had longer reaction times for switching mus-cles on and off. Similarly, patients with LBP have alsobeen reported to have delayed response of the trunk mus-cles to externally applied perturbations while stand-ing.7,30 The delay in responses to the perturbation couldbe the result of an impairment of the feedback loops thatcontrol the initial response to the perturbation in indi-viduals who have suffered soft tissue injury. Alterna-
tively, the delayed response could be a precipitating fac-tor in the development of LBP. An important caveat isthat there is some disagreement whether surface EMG issufficiently sensitive when recording from the multifidus,or whether intramuscular electrodes are required toavoid cross talk from the longissimus.31,32 Ideally, theseresults will need to be replicated in future studies usingintramuscular electrodes.
Hodges and Richardson4 found no group differencesfor erector spinae latency in arm raising tasks, regardlessof arm movement speed, suggesting that LBP did not
Figure 3. The interaction of tar-get height and load on movementtime calculated from tangentialvelocity profiles of the finger-tipis plotted. This plot shows thatalthough there is an increase inmovement time as the load in-crease from the no load to the3.64 kg load, this increase isgreatest for the low target andleast for the middle target.
Figure 4. A and B, The mean joint excursions collapsed across load conditions for each target height is plotted against peak angularvelocity for (A) lumbar spine, which displays a monotonic increase as target height decreases, and (B) right shoulder, which displays thegreatest excursion and peak velocity for the high target and least for the middle target.
E805Muscle Latencies in LBP • Thomas et al

alter feedforward control of the trunk extensors. Differ-ences between Hodges and Richardson4 and the presentstudy could be driven by the implicit goals of rapid armraising versus target reaching tasks. In the former, thegoal is to maintain the trunk in an upright posture whilemoving the upper limb. In the later, the trunk must flexto complete the task. Thus, early activation of the trunkextensors is logical when the task requires one to resist
flexion moments, but is unnecessary when the task ne-cessitates movement with gravity.10
Although our findings indicate clear differences in on-set latencies of the trunk extensor muscles, a surprisingfinding was the near absence of any clear abdominalmuscle activity, particularly because it has been sug-gested that coactivation of the trunk muscles is a strategyused by patients with LBP to enhance spinal stability.33
Figure 5. The onset latencies ofthe right, erector spinae (R ERS),right multifidis (R MULT), lefterector spinae (L ERS), and leftmultifidis (L MULT) averagedacross target height and load areplotted for the chronic low backpain group and the matched con-trols. Although the analyses wereoriginally conducted on the timenormalized latencies, follow-upanalyses on non-normalized laten-cies displayed the same signifi-cant findings and are thereforepresented for easier interpretation.*Indicate significance P � 0.05.
Figure 6. A and B, The onset latencies of the right, erector spinae (R ERS) and multifidis (R MULT) averaged across all subjects are plottedfor (A) Target height (collapsed across load) and (B) load (collapsed across target height). Although the analyses were originallyconducted on the time normalized latencies, follow-up analyses on non-normalized latencies displayed the same significant findings andare therefore presented for easier interpretation.
E806 Spine • Volume 32 • Number 26 • 2007

In this reaching task neither healthy participants northose with chronic LBP displayed any systematic activa-tion of the abdominals either to initiate lumbar flexiontowards the target or to increase trunk stiffness and po-tentially increase spinal stability (Figure 2).
Consistent with previous studies of the speed-insensitivecontrol strategy, the tasks manipulations resulted in an in-crease in peak lumbar velocity as the target height was low-ered (Figure 4A). Further the latency of the trunk exten-sors increased with increased target distance which is acommon finding from the single joint literature.13,17
However, the load manipulation resulted in a reductionof peak lumbar velocity only for reaches to the low targetlocation. Nonetheless, onset latency of the trunk exten-sors decreased as load increased which is the oppositeof what has been reported for the speed-insensitivestrategy.13,17 The fact that there was no clear effect ofload on peak joint velocity, combined with the fact thattrunk motion was performed with gravity, could accountfor the differences between the present study and single-joint studies. Though the speed-insensitive strategywould predict an increase in antagonist latency with in-creased load, in the present reaching tasks the load in thereaching hand creates a significant increase in flexionmoment on the lumbar spine that must be countered byan earlier onset of antagonist muscles to provide a suffi-cient braking force. Finally, since timing was comparedto the deltoid muscle, which was not a true agonist to thetrunk extensors, it is not unexpected that differences be-tween the speed-insensitive control strategy defined forsingle joint movements and whole body reaching wouldemerge.
Conclusion
The present study demonstrated that, in whole bodyreaching tasks, onset of trunk extensor muscles is de-layed in individuals with chronic LBP when comparedwith healthy matched controls. These findings provide apartial extension of the speed-insensitive control strategyto whole body reaching tasks.
Key Points
● The onset timing of 8 trunk muscles were as-sessed in 19 individuals with chronic LBP and 19matched healthy controls performing whole bodyreaches to different target heights and various loadsin the reaching hands.● The onset latency of trunk extensor muscles rel-ative to onset of the deltoid was significantly longerin participants with LBP compared with agematched controls.● Neither healthy participants nor those withchronic LBP displayed any systematic activation ofthe abdominals either to initiate lumbar flexion to-ward the target or to increase trunk stiffness andpotentially increase spinal stability.
● These findings indicate a shift in control strategyfor individuals with chronic LBP and provide a par-tial extension of the speed-insensitive control strat-egy to whole body reaching tasks.
AcknowledgmentsThe authors thank Candace Kochman and Sara Claggfor their assistance in data collection.
References
1. Cholewicki J, McGill SM. Mechanical stability of the in vivo lumbar spine:implications for injury and chronic low back pain. Clin Biomech (Bristol,Avon) 1996;11:1–15.
2. Hodges PW, Richardson CA. Inefficient muscular stabilization of the lumbarspine associated with low back pain. A motor control evaluation of trans-versus abdominis. Spine 1996;21:2640–50.
3. McGill SM, Grenier S, Kavcic N, et al. Coordination of muscle activity toassure stability of the lumbar spine. J Electromyogr Kinesiol 2003;13:353–9.
4. Hodges PW, Richardson CA. Altered trunk muscle recruitment in peoplewith low back pain with upper limb movement at different speeds. Arch PhysMed Rehabil 1999;80:1005–12.
5. Radebold A, Cholewicki J, Panjabi MM, et al. Muscle response pattern tosudden trunk loading in healthy individuals and in patients with chronic lowback pain. Spine 2000;25:947–54.
6. Radebold A, Cholewicki J, Polzhofer GK, et al. Impaired postural control ofthe lumbar spine is associated with delayed muscle response times in patientswith chronic idiopathic low back pain. Spine 2001;26:724–30.
7. Wilder DG, Aleksiev AR, Magnusson ML, et al. Muscular response to suddenload. A tool to evaluate fatigue and rehabilitation. Spine 1996;21:2628–39.
8. Marras WS, Lavender SA, Leurgans SE, et al. The role of dynamic three-dimensional trunk motion in occupationally-related low back disorders. Theeffects of workplace factors, trunk position, and trunk motion characteristicson risk of injury. Spine 1993;18:617–28.
9. Punnett L, Fine LJ, Keyserling WM, et al. Back disorders and nonneutraltrunk postures of automobile assembly workers. Scand J Work EnvironHealth 1991;17:337–46.
10. Virji-Babul N, Cooke JD, Brown SH. Effects of gravitational forces on singlejoint arm movements in humans. Exp Brain Res 1994;99:338–46.
11. Khan MA, Garry MI, Franks IM. The effect of target size and inertial load onthe control of rapid aiming movements. A test of speed-sensitive and speed-insensitive strategies. Exp Brain Res 1999;124:151–8.
12. Hoffman DS, Strick PL. Step-tracking movements of the wrist. IV. Muscleactivity associated with movements in different directions. J Neurophysiol1999;81:319–33.
13. Gottlieb GL, Corcos DM, Agarwal GC. Organizing principles for single-joint movements. I. A speed-insensitive strategy. J Neurophysiol 1989;62:342–57.
14. Corcos DM, Gottlieb GL, Jaric S, et al. Organizing principles underlyingmotor skill acquisition. In: Winters JM, Woo SL-Y, eds. Mulitiple MuscleSystems: Biomechanics and Movement Organization. New York: Springer-Verlag; 1990:251–67.
15. Karst GM, Hasan Z. Antagonist muscle activity during human forearmmovements under varying kinematic and loading conditions. Exp Brain Res1987;67:391–401.
16. Gielen CC, van den Oosten K, Pull ter Gunne F. Relation between EMGactivation patterns and kinematic properties of aimed arm movements. J MotBehav 1985;17:421–42.
17. Pfann KD, Hoffman DS, Gottlieb GL, et al. Common principles underlyingthe control of rapid, single degree-of- freedom movements at different joints.Exp Brain Res 1998;118:35–51.
18. Thomas JS, Corcos DM, Hasan Z. The influence of gender on spine, hip,knee, and ankle motions during a reaching task. J Mot Behav 1998;30:98 –103.
19. Thomas JS, Corcos DM, Hasan Z. Effect of movement speed on limb seg-ment motions for reaching from a standing position. Exp Brain Res 2003;148:377–87.
20. Thomas JS, Corcos DM, Hasan Z. Kinematic and kinetic constraints on arm,trunk, and leg segments in target-reaching movements. J Neurophysiol 2005;93:352–64.
21. Eng JJ, Winter DA, MacKinnon CD, et al. Interaction of the reactive mo-
E807Muscle Latencies in LBP • Thomas et al
ments and centre of mass displacement for postural control during voluntaryarm movements. Neurosci Res Commun 1992;11:73–80.
22. Oddsson L, Thorstensson A. Fast voluntary trunk flexion movements instanding: motor patterns. Acta Physiol Scand Suppl 1987;129:93–106.
23. Melzack R. The McGill pain questionnaire: major properties and scoringmethods. Pain 1975;1:277–99.
24. Melzack R, Katz J. The McGill Pain Questionnaire: appraisal and currentstatus. In: Turk DC, Melzack R, eds. Handbook of Pain Assessment. NewYork: Guilford Press; 2001.
25. Kori KS, Miller RP, Todd DD. Kinesiophobia: a new view of chronic behav-ior. Pain Manag 1990;3:35–43.
26. Roland M, Morris R. A study of the natural history of back pain. I. Devel-opment of a reliable and sensitive measure of disability in low-back pain.Spine 1983;8:141–4.
27. Stratford PW, Binkley JM, Riddle DL. Development and initial validation ofthe back pain functional scale. Spine 2000;25:2095–102.
28. Basmajian JV, Blumenstein R. Electrode placement in electromyographic
biofeedback. In: Basmajian JV, ed. Biofeedback: Principles and Practice forClinicians. 3rd ed. Baltimore: Williams & Wilkins; 1989:369–82.
29. Ng JK, Parnianpour M, Richardson CA, et al. Functional roles of abdominaland back muscles during isometric axial rotation of the trunk. J Orthop Res2001;19:463–71.
30. Magnusson ML, Aleksiev A, Wilder DG, et al. European Spine Society—theAcroMed Prize for Spinal Research 1995. Unexpected load and asymmetricposture as etiologic factors in low back pain. Eur Spine J 1996;5:23–35.
31. Arokoski JP, Kankaanpaa M, Valta T, et al. Back and hip extensor musclefunction during therapeutic exercises. Arch Phys Med Rehabil 1999;80:842–50.
32. Stokes IA, Henry SM, Single RM. Surface EMG electrodes do not accuratelyrecord from lumbar multifidus muscles. Clin Biomech (Bristol, Avon) 2003;18:9–13.
33. Van Dieen JH, Cholewicki J, Radebold A. Trunk muscle recruitment pat-terns in patients with low back pain enhance the stability of the lumbar spine.Spine 2003;28:834–41.
E808 Spine • Volume 32 • Number 26 • 2007




















