Molecular mechanisms of neuroprotection by two natural antioxidant polyphenols
Upload
independentCategory
view
2download
0
Original article 427
The combination of vitamin C and grape-seed polyphenolsincreases blood pressure: a randomized, double-blind,placebo-controlled trialNatalie C. Ward, Jonathan M. Hodgson, Kevin D. Croft, Valerie Burke,Lawrence J. Beilin and Ian B. Puddey
Background There is growing evidence that oxidative
stress contributes to the pathogenesis of hypertension and
endothelial dysfunction. Thus, dietary antioxidants may
beneficially influence blood pressure (BP) and endothelial
function by reducing oxidative stress.
Objective To determine if vitamin C and polyphenols, alone
or in combination, can lower BP, improve endothelial
function and reduce oxidative stress in hypertensive
individuals.
Design A total of 69 treated hypertensive individuals with a
mean 24-h ambulatory systolic blood pressure
>— 125 mmHg participated in a randomized, double-blind,
placebo-controlled, factorial trial. Following a 3-week
washout, participants received 500 mg/day vitamin C,
1000 mg/day grape-seed polyphenols, both vitamin C and
polyphenols, or neither for 6 weeks. At baseline and post-
intervention, 24-h ambulatory BP, ultrasound-assessed
endothelium-dependent and -independent vasodilation of
the brachial artery, and markers of oxidative damage,
(plasma and urinary F2-isoprostanes, oxidized
low-density lipoproteins and plasma tocopherols), were
measured.
Results A significant interaction between grape-seed and
vitamin C treatments for effects on BP was observed.
Vitamin C alone reduced systolic BP versus placebo
(S1.8 W 0.8 mmHg, P U 0.03), while polyphenols did not
(S1.3 W 0.8 mmHg, P U 0.12). However, treatment with the
combination of vitamin C and polyphenols increased
0263-6352 � 2005 Lippincott Williams & Wilkins
systolic BP (4.8 W 0.9 mmHg versus placebo;
6.6 W 0.8 mmHg versus vitamin C; 6.1 W 0.9 mmHg versus
polyphenols mmHg, each P < 0.0001) and diastolic BP
(2.7 W 0.6 mmHg, P < 0.0001 versus placebo;
1.5 W 0.6 mmHg, P U 0.016 versus vitamin C;
3.2 W 0.7 mmHg, P < 0.0001 versus polyphenols).
Endothelium-dependent and -independent vasodilation,
and markers of oxidative damage were not significantly
altered.
Conclusion Although the mechanism remains to be
elucidated, these results suggest caution for hypertensive
subjects taking supplements containing combinations of
vitamin C and polyphenols. J Hypertens 23:427–434 Q 2005
Lippincott Williams & Wilkins.
Journal of Hypertension 2005, 23:427–434
Keywords: blood pressure, endothelial function, oxidative stress,polyphenols, vitamin C
School of Medicine and Pharmacology, University of Western Australia and WestAustralian Institute for Medical Research (WAIMR), Perth, Australia.
Sponsorship: This study was funded by the National Health and MedicalResearch Council (NHMRC) of Australia (Project Grant 139067). All tablets wereprovided by Taractechnologies (Australia).
Correspondence and requests for reprints to Natalie Ward, School of Medicine &Pharmacology (RPH), Box X2213 GPO Perth, WA 6847, Australia.Tel: +61 8 92240381; fax: +61 8 9224 0246;e-mail: [email protected]
Received 8 June 2004 Revised 2 September 2004Accepted 15 September 2004
IntroductionHypertension has been postulated to be a state of
increased oxidative stress [1]. This may be related to
increased production of free radicals in the arterial wall, a
reduction in nitric oxide bioavailability [1] and endothe-
lial dysfunction [2]. If oxidative stress plays a role in
hypertension and endothelial dysfunction, then dietary
antioxidants could be expected to beneficially influence
both blood pressure (BP) and endothelial function. Avail-
able evidence suggests water-soluble antioxidants may
play an important role and vitamin C and polyphenolic
compounds represent two major dietary water-soluble
antioxidants.
Cross-sectional population studies indicate a consistent
association of higher vitamin C intake or status with lower
BP [3] Controlled intervention trials have been incon-
clusive, with some suggesting that vitamin C supplemen-
tation may lower BP [4,5], while others have shown no
effect [6,7]. Studies examining the effect of polyphenolic
compounds on BP have provided conflicting results [8,9].
However, a recent report has shown a reduction in clinic

428 Journal of Hypertension 2005, Vol 23 No 2
BP following treatment with dark chocolate versus
polyphenol-free white chocolate, which may be due to
the cocoa polyphenols [10].
The effect of vitamin C on endothelial dysfunction also
remains unclear. A number of studies have demonstrated
vitamin C’s ability to improve vasodilation [11,12] in
hypertensive subjects, but not controls [13]. However,
Duffy et al. [14] observed no improvement in vasodilation
in hypertensive subjects, despite a reduction in BP [14].
Improvement in vasodilation by polyphenolic com-
pounds has been observed in subjects with coronary
artery disease [15], hyperlipidemia [16] and healthy sub-
jects [17]. However, studies have not been carried out in
hypertensive subjects.
The ability of vitamin C and polyphenols to reduce
markers of oxidative stress is also inconclusive. Vitamin
C has been shown to reduce urinary isoprostanes in non-
smokers [18], yet have no effect on urinary isoprostanes in
hypertensive subjects [4]. Polyphenols from tea [19], red
wine [20] and purple grape juice [21], have been shown to
reduce ex vivo LDL oxidation. However, effects of poly-
phenols on isoprostanes are variable [19,22,23].
Arachidonic acid can be metabolized by cytochrome
P450 enzymes to form 20-hydroxyeicosatetraenoic acid
(20-HETE), which has been postulated to play a role in
BP regulation and vascular tone [24,25]. Several in vitrostudies have shown inhibitory effects of various polyphe-
nols and phenolic acids on cytochrome P450 isoforms
[26,27]. The effect of vitamin C either alone or in combi-
nation with polyphenols on the activity of the cytochrome
P450 enzyme has not been previously investigated.
To date no studies have examined possible additive or
synergistic effects of vitamin C and polyphenols on BP,
endothelial dysfunction and markers of oxidative
damage. The aims of this study were to determine if
vitamin C and grape-seed polyphenols, alone and in
combination, lower ambulatory BP and improve endothe-
lial dysfunction in hypertensive subjects. We also sought
to determine if any changes in BP were related to changes
in oxidative stress, inflammation or 20-HETE.
Materials and MethodsSubjectsBetween February 2002 and May 2003, 74 men and
women (mean age 62 � 7 years) with a previous physician
diagnosis of hypertension were recruited from the Perth
general population to the School of Medicine and Phar-
macology at the University of Western Australia. All
individuals were taking one or more antihypertensive
drugs for � 3 months, had a mean 24-h ambulatory sys-
tolic BP of � 125 mmHg and at least one additional
cardiovascular disease (CVD) risk factor. Risk factors
included previous coronary or cerebrovascular event
> 6 months, hyperlipidaemia (total cholesterol > 6
mmol/l), use of lipid-lowering therapy, or smoking
> 5 cigarettes/day. All volunteers ceased any vitamin,
fish oil or antioxidant supplements for at least 3 weeks
prior to study entry. All usual medication was taken as
prescribed on the morning of each visit and maintained
for the duration of the trial. Exclusion criteria included:
previous coronary or cerebrovascular event � 6 months,
heart failure or unstable disease, premenopausal, use of
nitrate medication, use of oral contraceptive, body mass
index > 35 kg/m2, diabetes mellitus, fasting gluco-
se � 7 mmol/l, or elevated serum creatinine (men >110 mmol/l or women > 100 mmol/l). Individuals were
asked to limit tea and coffee intake to 3 cups/day, and
cease all red wine and commercial fruit juice for the
duration of the study. All individuals provided a written
informed consent. The study was approved by the Royal
Perth Hospital Human Ethics Committee and was car-
ried out in accordance with the Declaration of Helsinki
(1989) of the World Medical Association.
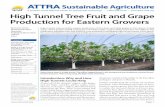
DesignFollowing a 3-week washout period, subjects were allo-
cated to a study treatment via block randomization using
computer-generated random numbers, devised by the
statistician. Volunteers were assigned to receive either
(1) 500 mg/day vitamin C and matched grape-seed poly-
phenol placebo, (2) 1000 mg/day grape-seed polyphenols
and matched vitamin C placebo, (3) 500 mg/day vitamin
C and 1000 mg/day grape-seed polyphenols, or (4)
matched placebo tablets for both grape-seed polyphenols
and vitamin C, for 6 weeks in a double-blind fashion
(Fig. 1). Tablets were taken twice daily at meal times as
250 mg and 500 mg of vitamin C and polyphenols,
respectively. Vitamin C doses chosen for the present
study as well as the treatment duration were in keeping
with previous studies [4,5]. Average daily intake of poly-
phenols was estimated to be approximately 1000 mg/day,
and the present dose was chosen to double polyphenol
intake. All tablets were identical in appearance, size and
colour and were prepared by Taractechnologies (Austra-
lia). All study personnel and participants were blinded to
treatment assignment for the duration of the study. The
chief investigator held the code for the tablets in a sealed
envelope, which was not broken until the end of the trial.
At the end of the washout and intervention periods, all
subjects completed a 24-h ambulatory BP monitoring,
provided a 24-h urine collection, underwent fasting bra-
chial artery ultrasound to assess endothelium-dependent
and -independent vasodilation and provided a fasting
blood sample.
Methods24-h ambulatory blood pressure
Twenty-four hour BP monitoring was performed using
an ambulatory BP monitoring device (Spacelabs 90207;

Antioxidant supplementation and blood pressure Ward et al. 429
Fig. 1
weeks-6
C nimatiV yad/gm 005
obecalp +
91 = n
yad/gm 0001
obecalp + slonehpyloP
81 = n
C nimatiV yad/gm 005
yad/gm 0001 +
slonehpylop
81 = n
obecalp + obecalP
91 = n
Randomizationweeks-3
letepmoc ton diD
0 = n
ton diD
2 = n
ton diD
2 = n
ton diD
1 = n
for Analysed forAnalysed
stniopdne
91 = n
stniopdne
61 = n
stniopdne
61 = n
stniopdne
81 = n
forAnalysed forAnalysed forAnalysed
letepmoc letepmoc letepmoc
Treated hypertensive patients
24-h systolic BP ≥ 125 mmHg +
≥ 1 CVD risk factors
Study design. BP, blood pressure; CVD, cardiovascular disease.
Australia), set to take oscillometric readings at 20-min
intervals while awake and 30-min intervals while asleep.
The monitor was fitted to the non-dominant arm 2.5 cm
above the antecubital fossa by a trained researcher. While
sitting and with the arm resting at heart level, BP was
calibrated with the monitor connected to a mercury
sphygmomanometer and at least three readings, recorded
by the monitor, were within � 7 mmHg of the readings
observed on the sphygmomanometer. Patients were
instructed to continue their normal routine and maintain
a diary while awake. A valid 24-h recording was accepted
as a minimum of 80% successful readings with all cali-
bration and error readings excluded from analysis. Read-
ings were aggregated for each hour, and mean BP
determined for the 24-h period and for awake and asleep
times based on the patient’s diary.
Brachial artery ultrasonography
Brachial artery ultrasonography was carried out as pre-
viously described [28]. Briefly, patients were studied fol-
lowing a 12-h fast and resting supine in a quiet,
temperature-controlled room (21–258C). Endothelium-
dependent vasodilation was assessed as response to
forearm ischaemic flow-mediated dilation (FMD) and
independent dilation as response to glyceryl trinitrate
(GTN)-mediated dilation. An experienced observer blind-
ed to the patient’s treatment status performed the analysis.
Responses were calculated as the percentage change in
brachial artery diameter from baseline at maximum peak
time. Reproducibility studies have previously demon-
strated an intrasubject coefficient of variation of 14.7
and 17.6% for FMD and GTN response, respectively [28].
Biochemical parameters
Oxidative stress was assessed via measurement of plasma
and 24-h urinary F2-isoprostanes by gas chromatography
mass spectrometry (GC/MS) [29]. Oxidized low-density
lipoproteins (oxLDL) were analysed using an enzyme-
linked immunosorbent assay (ELISA) kit (Mercodia,
Sweden) [30] and plasma a- and g-tocopherol concentra-
tions were analysed by high-performance liquid chroma-
tography (HPLC) with electrochemical detection using
Tocol as an internal standard [31]. Twenty-four hour
urinary 20-hydroxyeicosatetraenoic acid (20-HETE) was
analysed by GC/MS [32]. The Core Clinical Laboratory at
Royal Perth Hospital analysed high-sensitivity C-reactive
protein (HS-CRP) with particle-enhanced immunone-
phelometry using BN Systems (Dade-Behring, Germany)
and full blood picture was analysed using a Cell-Dyn 4000
analyser.
Compliance
Compliance was assessed via tablet count and analysis of
plasma vitamin C and urinary polyphenol metabolites.

430 Journal of Hypertension 2005, Vol 23 No 2
Table 1 Baseline patient characteristics
Vitamin C Polyphenols Vitamin C þ polyphenols Placebo
n 19 16 16 18Age (years) 59.5 � 5.9 61.3 � 6.3 62.3 � 7.1 63.6 � 8.2Gender (M/F) 12/7 12/4 10/6 14/4BMI (kg/m2) 28.7 � 3.6 27.7 � 3.4 28.6 � 2.6 29.3 � 4.3Smokers n (%) 1 (5) 2 (13) 1 (6) 0 (0)Mean 24-h SBP (mmHg) 133.6 � 9.8 133.6 � 11.6 138.8 � 11.0 134.1 � 8.2Mean 24-h DBP (mmHg) 80.8 � 7.9 79.8 � 9.8 79.6 � 11.0 78.2 � 7.1Plasma vitamin C (mmol/l) 40.8 � 14.6 41.8 � 17.2 35.2 � 17.4 40.1 � 12.3Urinary 3-HPP (mg/24-h)
�712 (346, 1467) 382 (219, 666) 518 (296, 906) 913 (517, 1613)
Mean result � SD or. �Geometric mean (95% confidence intervals). 3-HPP, 3-hydroxyphenylpropionic acid No significant differences. SBP, systolic blood pressure; DBP,diastolic blood pressure; BMI, body mass index; M, male; F, female.
Table 2 Differences in the use of each antihypertensive drug classand statin therapy between the treatment groups
Vitamin C PolyphenolsVitamin C þpolyphenols Placebo x2 P-value
ACE inhibitors 10 10 9 13 0.642At II receptor
blockers5 2 4 3 0.707
b-blockers 9 8 5 6 0.589Calcium
channel entryblockers
8 5 6 4 0.612
Diuretics 8 6 6 5 0.834Statins 14 12 12 16 0.653
ACE, angiotensin-converting enzyme; At II, angiotensin II.
Plasma vitamin C was measured by HPLC with electro-
chemical detection, using a modified version of a previous
method [33]. Twenty-four hour urinary excretion of 3-
hydroxyphenylpropionic acid (3-HPP), a phenolic acid
metabolite of proanthocyanadins [34], were analysed
using GC/MS [35].
Statistical analysis
Sample size was calculated using BP as the primary
endpoint; 16 subjects in each group provided us with
> 80% power to observe a 5 mmHg change in BP. Ambu-
latory BP was analysed using mixed models (PROC
Mixed) with the Statistical Analysis Systems (SAS Insti-
tute, Cary, North Carolina, USA). All other analysis was
carried out using the Statistical Package for the Social
Sciences (SPSS Version 11.5, Chicago, Illinois, USA).
Non-normally distributed data were log-transformed.
Results are presented as mean result � SEM or geometric
mean (95% confidence intervals) as appropriate. Univari-
ate and multivariate analysis was carried out with Bonfer-
roni post-hoc comparisons to assess the effect of treatment
on BP, endothelial function and markers of oxidative
damage, inflammation and 20-HETE production.
ResultsA total of 69 subjects completed the study. One subject
was excluded due to a myocardial infarction during the
study period; one ceased antihypertensive treatment; two
experienced gastrointestinal side-effects from the poly-
phenol tablets and one was unrelated to the study. The
primary analysis was according to the protocol and
involved all individuals who successfully completed
the study. Treatment groups were well matched at base-
line (Table 1), and there were no significant differences
between groups for age, body mass index, BP, urinary
phenolic acid excretion or plasma levels of vitamin C.
Number and type of antihypertensive medication did not
differ between the groups (Table 2).
Mean compliance assessed by tablet count, was reported
as 96%. Plasma vitamin C concentrations increased by
approximately 50% in those receiving vitamin C
(40.8 � 3.4 to 62.9 � 3.1 mmol/l, P < 0.001) and the com-
bination (35.2 � 4.4 to 62.9 � 2.9 mmol/l, P < 0.001).
Urinary excretion of the polyphenol metabolite increased
significantly following supplementation with the poly-
phenols (3-HPP, 382 (219, 666) to 1111 (628, 1966) mg/
24 h, P < 0.001). A similar increase was observed follow-
ing supplementation with the combination (3-HPP, 518
(296, 906) to 1033 (630, 1695) mg/24 h, P < 0.001).
There was a significant interaction between the vitamin
C and polyphenol treatments that affected BP. That is,
the effects of vitamin C and polyphenols were different
when provided in combination. Therefore results could
not be analysed for main effects and were analysed by
group, following adjustment for baseline levels. Treat-
ment with vitamin C alone significantly reduced systolic
BP versus placebo (�1.8 � 0.8 mmHg, P ¼ 0.02), while
treatment with polyphenols alone did not (�1.3 �0.8 mmHg, P ¼ 0.12). However, treatment with the com-
bination of vitamin C and polyphenols resulted in a
significant increase in mean 24-h systolic BP versus
treatment with placebo (4.8 � 0.9 mmHg, P < 0.0001),
vitamin C (6.6 � 0.8 mmHg, P < 0.0001) or polyphenols
(6.1 � 0.9 mmHg, P < 0.0001) (Fig. 2a). Treatment
with the combination also resulted in a significant
increase in diastolic BP versus placebo (2.7 � 0.6 mmHg,
P < 0.0001), vitamin C (1.5 � 0.6 mmHg, P ¼ 0.02) and
polyphenols (3.2 � 0.7 mmHg, P < 0.0001) (Fig. 2b).
Mean 24-h heart rate (HR) was significantly increased
following treatment with vitamin C compared with treat-
ment with placebo (1.6 � 0.6 beats/min, P ¼ 0.007) or
polyphenols (3.7 � 0.6 beats/min, P < 0.0001). Treat-
ment with the combination significantly increased HR

Antioxidant supplementation and blood pressure Ward et al. 431
Fig. 2
4−3−2−1−01234567
Mea
n s
ysto
lic B
P (
mm
Hg
)
a)(
*
‡†*
Poly + CV Poly + CV
Poly + CV
PolyPoly
Poly
CV 2−
1−
0
1
2
3
4
Mea
n d
iast
olic
BP
(m
mH
g)
b)(‡†*
CV
CV
3−
2−
1−
0
1
2
3B
eats
/min
c)( ‡* ‡
Mean 24-h ambulatory (a) systolic blood pressure (BP), (b) diastolic BP and (c) heart rate. Mixed model Statistical Analysis Systems (SAS) analysisfollowing adjustment for baseline, �versus placebo, yversus vitamin C and zversus polyphenols, P < 0.001. VC, vitamin C; Poly, polyphenols.
compared with polyphenols alone (3.2 � 0.6 beats/min,
P < 0.0001) (Fig. 2c). These changes were unaltered
after adjustment for age and gender. Mean systolic and
diastolic BP for awake and asleep periods were signifi-
cantly increased following treatment with the vitamin C
and polyphenol combination compared with placebo,
vitamin C alone and polyphenols alone (data not pre-
sented). Addition of dosage time to the model did not
alter the observed increases following treatment with the
combination and this variable was not statistically sig-
nificant (data not presented).
FMD and GTN responses were not significantly altered
by treatment with vitamin C alone, polyphenols alone or
the combination (Fig. 3). Plasma and urinary F2-isopros-
tanes, oxidized LDL or a- and g-tocopherol were not
significantly affected by any of the treatments (Table 3).
Markers of inflammation including HS-CRP, leukocytes
Fig. 3
2− Poly + CVPolyCV
1− 5.1−
0− 5.0.0 51.1 52
Mea
n c
han
ge
FM
D (%
)
(a)
Mean percentage change in (a) flow-mediated dilation (FMD) and (b) glyceryfollowing adjustment for age and gender with Bonferroni post-hoc compari
and monocytes were not altered by any of the study
treatments. However, neutrophils were significantly ele-
vated following treatment with the combination of vita-
min C and polyphenols (Table 3). Urinary 20-HETE
excretion (pmol/24 h) was not significantly different
between the groups and was not affected by any of the
study treatments (Table 3). Adjustment for age, gender,
smoking or alcohol intake did not alter the interpretation
of the findings.
DiscussionGiven the evidence linking hypertension with oxidative
stress, it is reasonable to speculate that antioxidants
would beneficially influence oxidative stress, BP and
endothelial function. However, the present study indi-
cates that a combination of vitamin C and grape-seed
polyphenols results in a clinically significant increase in
BP. In contrast, treatment with vitamin C alone resulted
(b)
CV4−3−2−1−0123456
Mea
n c
han
ge
GT
N (%
)
Poly + CVPoly
l trinitrate (GTN) response versus the placebo group. Univariate analysissons. VC, vitamin C; Poly, polyphenols.

432 Journal of Hypertension 2005, Vol 23 No 2
Table 3 Treatment effects on biomarkers of oxidative stress, plasma tocopherols, inflammation and urinary excretion of 20-HETE
Vitamin C Polyphenols Vitamin C þ polyphenols Placebo
Urinary 24-h F2-isoprostanes (pmol/24-h)§ �648 � 435 �1111 � 1355 �834 � 293 �348 � 260Plasma F2-isoprostanes (pmol/l)§ �232 � 93 �14 � 78 �80 � 87 �23 � 87Oxidized LDL (mg/ml)§ �0.01 � 0.43 �0.10 � 0.62 0.04 � 0.33 �0.12 � 0.57a-tocopherol �1.14 � 1.15 �0.58 � 1.04 0.38 � 1.00 0.50 � 0.50g-tocopherol 0.01 � 0.15 �0.11 � 0.12 0.01 � 0.12 0.13 � 0.06Leucocytes ( 109/l) �0.26 � 0.20 �0.01 � 0.18 0.33 � 0.25 �0.04 � 0.13Neutrophils ( 109/l) �0.26 � 0.13 �0.09 � 0.13 0.40 � 0.21�,y �0.08 � 0.09Monocytes ( 109/l) �0.05 � 0.04 0.02 � 0.02 0.04 � 0.02 0.01 � 0.03HS-CRP (mg/l)§ �4.88 � 4.89 �0.31 � 0.40 1.16 � 1.31 �0.24 � 0.4420-HETE (pmol/24-h)§ �18.7 � 138.3 7.5 � 75.1 �156.1 � 246.9 �68.1 � 160.4
Mean difference � SEM versus baseline. Between treatment group univariate analysis with Bonferroni post-hoc comparisons. �versus placebo. yversus vitamin C andzversus polyphenols, P < 0.05. §Data was log-transformed for analysis. HS-CRP, high-sensitivity C-reactive protein; 20-HETE, 20-hydroxyeicosatetraenoic acid; LDL, low-density lipoprotein.
in a small, but significant reduction in systolic BP. To our
knowledge this is the first study to demonstrate a pressor
effect of this combination supplement on BP. Although
this result is unexpected, it is in agreement with a recent
review that there is widespread misconception that the
use of antioxidants will always be beneficial. In fact,
depending on the circumstances, such compounds, which
are better described as redox agents, may be pro-oxidant
rather than antioxidant [36].
However, in our study, there was no effect of the combina-
tion supplement on any of the measured markers of
oxidative stress. This suggests that the increase in BP
may not have been a result of increased oxidative stress,
at least as measured by markers of lipid peroxidation
(urinary and plasma F2-isoprostanes), oxidized LDL or
plasma tocopherols. The effects of supplementation with
combination vitamin C and polyphenols on oxidative
stress have not been previously investigated. An in vitrostudy has shown a synergistic effect of phenolic acids and
ascorbate in preventing oxidation of LDL [37]. The
potential mechanism was thought to be the ability of
vitamin C to recycle the highly reactive phenoxyl radicals.
Alternatively, flavonoids have been shown to inhibit
uptake of ascorbate in cultured cells [38]. However, in
the present study, we have seen no apparent effects of
polyphenols on the bioavailability of ascorbate, with simi-
lar increases in plasma vitamin C with and without poly-
phenol treatment. Furthermore, there appears to be no
effect of vitamin C on the bioavailability of polyphenols.
An alternative mechanism investigated was a possible
effect of treatment on the production of 20-HETE.
20-HETE is a vasoactive cytochrome P450 metabolite
of arachidonic acid that has been implicated in the
pathogenesis of hypertension [24,25,39]. It is thought
to cause constriction via inhibition of potassium channels
[40], and contribute to the vascular actions of endothelin-1
and angiotensin [41,42]. Data on the regulation of
20-HETE in humans are limited. Studies have suggested
that polyphenolic compounds may be able to inhibit
various isoforms of cytochrome P450, which may alter
drug metabolism [26,27]. The present study however,
revealed that polyphenol treatment, either alone or in
combination with vitamin C, had no effect on 20-HETE
production. The possibility that the combination of vita-
min C and grape-seed polyphenols may be interfering
with the metabolism of antihypertensive drugs has not
been ruled out.
There is evidence to suggest that chronic or low-grade
inflammation is a risk factor for hypertension [43]. Alter-
natively, increased BP may itself be a stimulus for
inflammation, resulting from increased hydrostatic pres-
sure and strain, which in turn affects endothelial cell
function [43,44]. Inflammation may also contribute to
vascular problems associated with hypertension, via the
release of vasoconstrictors, reduction of nitric oxide and
promotion of platelet aggregation [43,45]. The increase in
circulating neutrophils following supplementation with
the combination is consistent with this explanation.
However, HS-CRP, total leucocyte count and monocytes
were not significantly altered, so although some of our
results provide support for an inflammatory mechanism,
the overall evidence is weak.
The non-significant reduction in FMD response follow-
ing treatment with the vitamin C, polyphenol combina-
tion suggests the increase in BP may be associated with a
small decrease in endothelium-dependent vasodilation.
The lack of significance for the change in FMD response
may be related to power. The study was originally pow-
ered for a main effects analysis. However, because of the
significant interaction for blood pressure, all analysis was
by group. This gave us 80% power to see a 3.8% change
in FMD response. We saw a < 1% change in FMD
response.
We also observed a small, but significant reduction in
systolic BP following treatment with vitamin C alone,
while the reduction seen with the polyphenols alone was
not significant. This is in contrast to the result observed
with the combination. Some previous studies have shown
a reduction in BP with vitamin C [4,5], while in others,

Antioxidant supplementation and blood pressure Ward et al. 433
vitamin C has had no effect [6,7]. Duffy et al. [4] provided
500 mg/day vitamin C, for 4 weeks, and observed
13 mmHg reduction in clinic systolic BP, but not diastolic
BP. Fotherby et al. [5] also examined 500 mg/day of
vitamin C for 3 months and observed a 3 mmHg reduc-
tion in ambulatory day systolic BP, but not diastolic or
clinic BP. There have been no other studies examining
the effects of grape-seed polyphenols on BP, but studies
examining other polyphenols [8,9] remain inconclusive.
In our study, although treatment with vitamin C alone
was able to reduce systolic BP, there was no correspond-
ing reduction in oxidative stress biomarkers or improve-
ment in endothelial function. This is in agreement with a
previous study that showed reductions in BP following
treatment with vitamin C, but no change in urinary
isoprostanes [4].
There is increasing evidence suggesting oxidative stress
is involved in the pathogenesis of hypertension. This has
resulted in the concept that dietary supplementation with
antioxidants may be able to reduce blood pressure by
reducing oxidative stress. However, the present study
provides evidence that combined supplementation with
vitamin C and grape-seed polyphenols actually increases
blood pressure in treated hypertensive individuals. While
the mechanism behind this increase in BP following
supplementation with the vitamin C and grape-seed
polyphenol combination remains to be elucidated, the
results indicate that the effect is unlikely to be due to
increased oxidative stress or 20-HETE production, but
still allow the possibility that it may be related to inflam-
mation or endothelial dysfunction. Although this result
was unexpected, it suggests that careful evaluation in
controlled clinical trials is required before the use of this
combination by treated hypertensive individuals can be
supported.
AcknowledgementsN.C.W. gratefully acknowledges the assistance of a
University of Western Australia Postgraduate Award.
The authors thank Michael Clarke, Jennifer Rivera
and Lisa Rich for expert technical assistance and the
volunteers who took part in the study.
References1 Kumar KV, Das UN. Are free radicals involved in the pathobiology of human
essential hypertension? Free Radic Res Commun 1993; 19:59–66.
2 Panza JA, Quyyumi AA, Brush JE Jr, Epstein SE. Abnormal endothelium-dependent vascular relaxation in patients with essential hypertension.N Engl J Med 1990; 323:22–27.
3 Ness AR, Chee D, Elliott P. Vitamin C and blood pressure – an overview.J Hum Hypertens 1997; 11:343–350.
4 Duffy SJ, Gokce N, Holbrook M, Huang A, Frei B, Keaney JF Jr, et al.Treatment of hypertension with ascorbic acid. Lancet 1999; 354:2048–2049.
5 Fotherby MD, Williams JC, Forster LA, Craner P, Ferns GA. Effect ofvitamin C on ambulatory blood pressure and plasma lipids in olderpersons. J Hypertens 2000; 18:411–415.
6 Ghosh SK, Ekpo EB, Shah IU, Girling AJ, Jenkins C, Sinclair AJ. A double-blind, placebo-controlled parallel trial of vitamin C treatment in elderlypatients with hypertension. Gerontology 1994; 40:268–272.
7 Kim MK, Sasaki S, Sasazuki S, Okubo S, Hayashi M, Tsugane S. Lack oflong-term effect of vitamin C supplementation on blood pressure.Hypertension 2002; 40:797–803.
8 Hodgson JM, Puddey IB, Beilin LJ, Mori TA, Burke V, Croft KD, et al.Effects of isoflavonoids on blood pressure in subjects with high-normalambulatory blood pressure levels: a randomized controlled trial. Am JHypertens 1999; 12:47–53.
9 Hosseini S, Lee J, Sepulveda RT, Rohdewald P, Watson RR. Arandomised, double-blind, placebo-controlled, prospective, 16 weekcross-over study to determine the role of Pycnogenol in modifying bloodpressure in mildly hypertensive patients. Nutr Res 2001; 21:1251–1260.
10 Taubert D, Berkels R, Roesen R, Klaus W. Chocolate and blood pressurein elderly individuals with isolated systolic hypertension. JAMA 2003;290:1029–1030.
11 Taddei S, Virdis A, Ghiadoni L, Magagna A, Salvetti A. Vitamin C improvesendothelium-dependent vasodilation by restoring nitric oxide activity inessential hypertension. Circulation 1998; 97:2222–2229.
12 Sherman DL, Keaney JF Jr, Biegelsen ES, Duffy SJ, Coffman JD, Vita JA.Pharmacological concentrations of ascorbic acid are required for thebeneficial effect on endothelial vasomotor function in hypertension.Hypertension 2000; 35:936–941.
13 Singh N, Graves J, Taylor PD, MacAllister RJ, Singer DR. Effects of a‘healthy’ diet and of acute and long-term vitamin C on vascular function inhealthy older subjects. Cardiovasc Res 2002; 56:118–125.
14 Duffy SJ, Gokce N, Holbrook M, Hunter LM, Biegelsen ES, Huang A, et al.Effect of ascorbic acid treatment on conduit vessel endothelial dysfunctionin patients with hypertension. Am J Physiol 2001; 280:H528–H534.
15 Stein JH, Keevil JG, Wiebe DA, Aeschlimann S, Folts JD. Purple grapejuice improves endothelial function and reduces the susceptibility of LDLcholesterol to oxidation in patients with coronary artery disease.Circulation 1999; 100:1050–1055.
16 Hodgson JM, Puddey IB, Burke V, Watts GF, Beilin LJ. Regular ingestionof black tea improves brachial artery vasodilator function. Clin Sci 2002;102:195–201.
17 Cuevas AM, Guasch V, Castillo O, Irribarra E, Mizon C, San Martin A, et al.A high-fat diet induces and red wine counteracts endothelial dysfunction inhuman volunteers. Lipids 2000; 35:143–148.
18 Huang HY, Appel LJ, Croft KD, Miller ER III, Mori TA, Puddey IB. Effects ofvitamin C and vitamin E on in vivo lipid peroxidation: results of arandomized controlled trial. Am J Clin Nutr 2002; 76:549–555.
19 Hodgson JM, Puddey IB, Croft KD, Burek V, Mori TA, Caccetta RA, et al.Acute effects of ingestion of black and green tea on lipoprotein oxidation.Am J Clin Nutr 2000; 71:1103–1107.
20 Abu-Amsha R, Croft KD, Puddey IB, Proudfoot JM, Beilin LJ. Phenoliccontent of various beverages determines the extent of inhibition of humanserum and low-density lipoprotein oxidation in vitro: identification andmechanism of action of some cinnamic acid derivatives from red wine. ClinSci 1996; 91:449–458.
21 O’Byrne DJ, Devaraj S, Grundy SM, Jialal I. Comparison of the antioxidanteffects of Concord grape juice flavonoids a-tocopherol on markers ofoxidative stress in healthy adults. Am J Clin Nutr 2002; 76:1367–1374.
22 Abu-Amsha CR, Burke V, Mori TA, Beilin LJ, Puddey IB, Croft KD. Redwine polyphenols, in the absence of alcohol, reduce lipid peroxidativestress in smoking subjects. Free Radic Biol Med 2001; 30:636–642.
23 Hodgson JM, Croft KD, Mori TA, Burke V, Beilin LJ, Puddey IB. Regularingestion of tea does not inhibit in vivo lipid peroxidation in humans. J Nutr2002; 132:55–58.
24 McGiff JC, Quilley J. 20-hydroxyeicosatetraenoic acid andepoxyeicosatrienoic acids and blood pressure. Curr Opin NephrolHypertens 2001; 10:231–237.
25 Roman RJ. P-450 metabolites of arachidonic acid in the control ofcardiovascular function. Physiol Rev 2002; 82:131–185.
26 Ow YY, Stupans I. Gallic acid and gallic acid derivatives: effects on drugmetabolizing enzymes. Curr Drug Metab 2003; 4:241–248.
27 Piver B, Berthou F, Dreano Y, Lucas D. Differential inhibition of humancytochrome P450 enzymes by epsilon-viniferin, the dimer of resveratrol:comparison with resveratrol and polyphenols from alcoholized beverages.Life Sci 2003; 73:1199–1213.
28 Woodman RJ, Playford DA, Watts GF, Cheetham C, Reed C, Taylor RR,et al. Improved analysis of brachial artery ultrasound using a novel edge-detection software system. J Appl Physiol 2001; 91:929–937.
29 Mori TA, Croft KD, Puddey IB, Beilin LJ. An improved method for themeasurement of urinary and plasma F2- isoprostanes using gaschromatography-mass spectrometry. Anal Biochem 1999; 268:117–125.
30 Holvoet P, Vanhaecke J, Janssens S, Van de WF, Collen D. Oxidized LDLand malondialdehyde-modified LDL in patients with acute coronarysyndromes and stable coronary artery disease. Circulation 1998;98:1487–1494.

434 Journal of Hypertension 2005, Vol 23 No 2
31 Su Q, Rowley KG, O’Dea K. Stability of individual carotenoids, retinol andtocopherols in human plasma during exposure to light and after extraction.J Chromatogr 1999; 729:191–198.
32 Rivera J, Ward N, Hodgson J, Puddey IB, Falck JR, Croft KD. Measurementof 20-hydroxyeicosatetraenoic acid in human urine by gaschromatography-mass spectrometry. Clin Chem 2004; 50:224–226.
33 McCulloch RK, Vandongen R. Measurement of ascorbic acid in plateletsand its relationship to polymorphonuclear leukocyte levels. Clin Chim Acta1992; 213:15–22.
34 Deprez S, Brezillon C, Rabot S, Philippe C, Mila I, Lapierre C, et al.Polymeric proanthocyanidins are catabolized by human colonic microflorainto low-molecular-weight phenolic acids. J Nutr 2000; 130:2733–2738.
35 Hodgson JM, Morton LW, Puddey IB, Beilin LJ, Croft KD. Gallic acidmetabolites are markers of black tea intake in humans. J Agric Food Chem2000; 48:2276–2280.
36 Azzi A, Davies KJ, Kelly F. Free radical biology - terminology and criticalthinking. FEBS Lett 2004; 558:3–6.
37 Vieira O, Laranjinha J, Madeira V, Almeida L. Cholesteryl esterhydroperoxide formation in myoglobin-catalyzed low density lipoproteinoxidation: concerted antioxidant activity of caffeic and p-coumaric acidswith ascorbate. Biochem Pharm 1998; 55:333–340.
38 Park JB, Levine M. Intracellular accumulation of ascorbic acid is inhibitedby flavonoids via blocking of dehydroascorbic acid and ascorbic aciduptakes in HL-60, U937 and Jurkat cells. J Nutr 2000; 130:1297–1302.
39 Imig JD, Zou AP, Stec DE, Harder DR, Falck JR, Roman RJ. Formation andactions of 20-hydroxyeicosatetraenoic acid in rat renal arterioles. Am JPhysiol 1996; 270:R217–R227.
40 Roman RJ. Does 20-HETE mediate the cGMP independent actions ofNO? High Blood Press Res Newsl 1999; Fall:20–22.
41 Croft KD, McGiff JC, Sanchez-Mendoza A, Carroll MA. Angiotensin IIreleases 20-HETE from rat renal microvessels. Am J Physiol 2000;279:F544–F551.
42 Hercule HC, Oyekan AO. Cytochrome P450 omega/omega-1hydroxylase-derived eicosanoids contribute to endothelin(A) andendothelin(B) receptor-mediated vasoconstriction to endothelin-1 in therat preglomerular arteriole. J Pharm Exp Ther 2000; 292:1153–1160.
43 Nakanishi N, Sato M, Shirai K, Suzuki K, Tatara K. White blood cell countas a risk factor for hypertension; a study of Japanese male office workers.J Hypertens 2002; 20:851–857.
44 Chae CU, Lee RT, Rifai N, Ridker PM. Blood pressure and inflammation inapparently healthy men. Hypertens 2001; 38:399–403.
45 Brown DW, Giles WH, Croft JB. White blood cell count: an independentpredictor of coronary heart disease mortality among a national cohort.J Clin Epidemiol 2001; 54:316–322.
Copyright © 2022 FDOKUMEN