
Bilirubin From Heme Oxygenase1 Attenuates Vascular Endothelial Activation and Dysfunction
Upload
khangminh22Category
view
0download
0
Seediscussions,stats,andauthorprofilesforthispublicationat:https://www.researchgate.net/publication/5603653
TheClinicalImplicationsofEndothelialDysfunction
ArticleinJournaloftheAmericanCollegeofCardiology·November2003
ImpactFactor:16.5·DOI:10.1016/S0735-1097(03)00994-X·Source:PubMed
CITATIONS
828
READS
74
4authors,including:
MichaelEWidlansky
MedicalCollegeofWisconsin
51PUBLICATIONS2,845CITATIONS
SEEPROFILE
JosephAVita
BostonUniversity
251PUBLICATIONS26,629CITATIONS
SEEPROFILE
Allin-textreferencesunderlinedinbluearelinkedtopublicationsonResearchGate,
lettingyouaccessandreadthemimmediately.
Availablefrom:MichaelEWidlansky
Retrievedon:16May2016

STATE-OF-THE-ART PAPER
The Clinical Implications of Endothelial DysfunctionMichael E. Widlansky, MD, Noyan Gokce, MD, FACC, John F. Keaney, JR, MD, FACC,Joseph A. Vita, MD, FACCBoston, Massachusetts
Defining new approaches for the prevention and treatment of atherosclerosis is an importantpriority. Recently, measurement of endothelial function in patients has emerged as a usefultool for atherosclerosis research. Risk factors are associated with impaired endothelialfunction, and clinical syndromes relate, in part, to a loss of endothelial control of vascularhomeostasis. Recent studies have shown that the severity of endothelial dysfunction relates tocardiovascular risk. A growing number of interventions known to reduce cardiovascular riskhave been shown to improve endothelial function. This work suggests that studies ofendothelial function could be used in the care of patients and as a surrogate marker for theevaluation of new therapeutic strategies. This article will review this growing literature in aneffort to evaluate the current clinical utility of endothelial dysfunction. (J Am Coll Cardiol2003;42:1149–60) © 2003 by the American College of Cardiology Foundation
Measurement of endothelial function in patients has re-cently emerged as a useful tool for atherosclerosis research.In the setting of cardiovascular disease (CVD) risk factors,the endothelium loses its normal regulatory functions.Clinical syndromes such as stable and unstable angina, acutemyocardial infarction, claudication, and stroke relate, inpart, to a loss of endothelial control of vascular tone,thrombosis, and the composition of the vascular wall.Recent studies have shown that the severity of endothelialdysfunction relates to the risk for an initial or recurrentcardiovascular event. Finally, a growing number of interven-tions known to reduce cardiovascular risk also improveendothelial function. This work has prompted speculationthat endothelial function serves as a “barometer” for cardio-vascular health that can be used for patient care andevaluation of new therapeutic strategies (1). This article willreview this growing literature in an effort to evaluate thecurrent clinical utility of assessing endothelial dysfunction.Normal functions of the endothelium. The endotheliumacts to maintain vascular homeostasis through multiplecomplex interactions with cells in the vessel wall and lumen(reviewed by Gokce et al. [2]). Table 1 lists many of themajor factors regulated and elaborated by vascular endothe-lium. Specifically, the endothelium regulates vascular toneby balancing production of vasodilators, including nitricoxide (NO), and vasoconstrictors. Furthermore, the endo-
thelium controls blood fluidity and coagulation through theproduction of factors that regulate platelet activity, theclotting cascade, and the fibrinolytic system. Finally, theendothelium has the capacity to produce cytokines andadhesion molecules that regulate and direct the inflamma-tory process (3).Pathophysiology of endothelial dysfunction. Under ho-meostatic conditions, the endothelium maintains normalvascular tone and blood fluidity, and there is little to noexpression of pro-inflammatory factors. However, bothtraditional and novel CVD risk factors initiate a chronicinflammatory process that is accompanied by a loss ofvasodilator and anti-thrombotic factors and an increase invasoconstrictor and pro-thrombotic products. As outlinedin Figure 1, risk factors as diverse as smoking, aging,hypercholesterolemia, hypertension, hyperglycemia, and afamily history of premature atherosclerotic disease are allassociated with an attenuation/loss of endothelium-dependent vasodilation in both adults and children (2,4,5).More recently recognized risk factors such as obesity (6),elevated C-reactive protein (7), and chronic systemic infec-tion (8) also are associated with endothelial dysfunction.
Abnormal vasoreactivity is not the only imbalance presentin high-risk individuals. Endothelial cells may adopt apro-thrombotic phenotype, portending an elevated risk ofcardiovascular events in high-risk individuals (9,10). Fur-thermore, when exposed to certain pathogenic pro-inflammatory stimuli, the endothelium expresses leukocytechemotactic factors, adhesion molecules, and inflammatorycytokines (11). The precise extent and order in which thenormal control mechanisms are affected have yet to be fullyelucidated.
The term “endothelial dysfunction” refers to this broadalteration in endothelial phenotype that may contribute tothe development and clinical expression of atherosclerosis(12). While the precise mechanisms remain to be eluci-
From the Evans Department of Medicine and Whitaker Cardiovascular Institute,Boston University School of Medicine, Boston, Massachusetts. Dr. Widlansky issupported by NIH Training Grant (T32 HL 07224). Dr. Gokce is supported by aMentored Patient-Oriented Research Career Transition Award from the NationalInstitutes of Health (K23 HL04425). Dr. Keaney is an Established Investigator of theAmerican Heart Association and is supported by the NIH (DK55656; HL60886;HL67206). Dr. Vita is supported by a Specialized Center of Research in IschemicHeart Disease grant from the National Institutes of Health (HL55993), the GeneralClinical Research Center, Boston Medical Center (M01RR00533), and by NIHgrants PO1HL60886 and HL52936.
Manuscript received February 18, 2003; revised manuscript received April 27,2003, accepted June 5, 2003.
Journal of the American College of Cardiology Vol. 42, No. 7, 2003© 2003 by the American College of Cardiology Foundation ISSN 0735-1097/03/$30.00Published by Elsevier Inc. doi:10.1016/S0735-1097(03)00994-X

dated, endothelial dysfunction appears to participate in a“positive feedback loop” in which inflammatory factorspromote monocyte and T-cell adhesion, foam cell forma-tion, extracellular matrix digestion, and vascular smoothmuscle migration and proliferation leading to atheroscle-rotic plaque formation (3,13). Endothelial dysfunction alsois relevant to the later stages of the disease, and appears toplay a role in acute coronary syndromes (14). Given thispossible causal pathway from endothelial dysfunction toatherosclerosis (Fig. 1), numerous methods have been em-ployed to measure endothelial dysfunction in humans.Methods of evaluating endothelial dysfunction in humans.While atherosclerosis is associated with a broad alteration inendothelial phenotype, the assessment of endothelium-dependent vasodilation has emerged as an accessible indi-cator of endothelial health. In particular, stimuli that in-crease production of endothelium-derived NO have provenuseful in assessing endothelium-dependent vasodilation inhumans. Such stimuli include increased shear stress fromincreased blood flow, and receptor-dependent agonists, suchas acetylcholine, bradykinin, or substance P. Basal NOrelease can be assessed using specific inhibitors of NO
synthase, such as NG-monomethyl-L-arginine. Investiga-tors have employed several methods in the evaluation ofendothelial function, each with its own advantages anddisadvantages (Table 2).
The earliest studies of endothelial control of vasomotionused quantitative coronary angiography to examine thevasomotor responses of the epicardial coronary artery duringinfusion of acetylcholine (15) or increased blood flow (16).In healthy individuals, the endothelium responds to thesestimuli by releasing vasodilator factors, particularly NO.Early studies demonstrated that patients with angiographi-cally proven coronary artery disease (CAD) display impairedflow-mediated dilation (FMD) and a vasoconstrictor re-sponse to acetylcholine rather than the normal vasodilatorresponse, likely reflecting loss of NO and unopposed con-strictor effects of acetylcholine on vascular smooth muscle(15). More recent studies suggest that acetylcholine-mediated coronary constriction may also result, in part, fromenhanced endothelial release of the potent vasoconstrictorendothelin (17).
Invasive studies in the arm involve infusion of endothelium-dependent agonists into the brachial artery and measuringthe vasodilator responses of forearm resistance vessels usingvenous occlusion plethysmography (18). Like studies in thecoronary circulation, this approach allows investigators toexamine dose-response relations and use specific agonistsand antagonists in a more accessible vascular bed. However,the technique requires an arterial catheter and, thus, haslimited applicability for large-scale studies or future devel-opment as a clinical tool.
Measures of arterial stiffness, including pulse wave veloc-ity and arterial distensibility, are also being investigated asnon-invasive means of measuring vascular health (19).Several studies have demonstrated that such measures pre-dict cardiovascular events (20,21). While dynamic factors,such as release of endothelium-derived NO, play a role,arterial stiffness is also highly dependent on fixed structuralfeatures of the vascular wall including the degree of fibrosisand calcification (19). Elucidation of the precise relationshipbetween endothelial function and vascular stiffness awaitsfurther study.
Finally, there has been considerable interest in non-invasive examination of endothelium-dependent FMD ofthe conduit brachial artery using vascular ultrasound (22).This response has been shown to depend in large part onNO synthesis (23,24), but also reflects release of otherendothelium-derived vasodilators. Like measures of vascularstiffness, this technique can safely be applied to large andvaried groups of patients and can be used to make repeatedmeasurements over time. As in the coronary circulation,endothelial function in the brachial circulation is impairedin the setting of traditional and novel risk factors andresponds to interventions known to reduce CVD risk (1).Importantly, studies suggest that endothelial function de-tected non-invasively in the brachial artery correlates withfunction in conduit coronary arteries (25). Despite the many
Abbreviations and AcronymsBP � blood pressureCAD � coronary artery diseaseCVD � cardiovascular diseaseFMD � flow-mediated dilationHRT � hormone replacement therapyICAM � intercellular adhesion moleculeNO � nitric oxideVCAM-1 � vascular cell adhesion molecule-1
Table 1. Normal Functions of the Vascular Endothelium and aPartial List of Factors Elaborated and Regulated by theEndothelium to Maintain Vascular Homeostasis
Maintenance of vascular toneNitric oxideProstaglandins (prostacyclin [PGI2], thromboxane A2 [TxA2])Endothelial hyperpolarizing factorEndothelin-1Angiotensin IIC-type natriuretic peptide
Balancing blood fluidity and thrombosisNitric oxideTissue plasminogen activatorHeparinsThrombomodulinProstaglandinsPlasminogen activator inhibitor-1 (PAI-1)Tissue factorVon Willibrand’s factor
Control of the vascular inflammatory processMonocyte chemotactic factor-1 (MCP-1)Adhesion molecule expression (VCAM-1, ICAM-1, selectins)Interleukins 1, 6, and 18Tumor necrosis factor
ICAM-1 � intercellular adhesion molecule-1; VCAM-1 � vascular cell adhesionmolecule-1.
1150 Widlansky et al. JACC Vol. 42, No. 7, 2003Endothelial Dysfunction October 1, 2003:1149–60

parallel findings, one modest-sized study suggested that,within individual subjects, brachial artery FMD does notcorrelate with resistance vessel (microvascular) function asmeasured by infusion studies (26). Indeed, it is likely thatthere is differential regulation of vascular tone in conduitand resistance vessels, and that the different measures ofvascular function may have relevance to different aspects ofCVD.Studies evaluating the prognostic value of endothelialdysfunction. Although case-control studies indicate anassociation between endothelial dysfunction and acute cor-onary syndromes (14), more convincing evidence for apathogenic role is provided by studies demonstrating thatendothelial dysfunction identifies patients at increased riskfor future events. To date, 10 published studies haveexamined this issue (Table 3).
Three studies evaluated the prognostic value of endothe-lial dysfunction in the coronary circulation in patients withCAD (27–29). In each study, endothelial dysfunction pre-dicted the occurrence of CVD events, such as cardiac death,myocardial infarction, unstable angina, ischemic stroke, andrevascularization procedures, after controlling for knownrisk factors. The studies are limited because there was noprospective plan to obtain long-term follow-up at the timeof enrollment and because the methods for studying endo-thelial function may have evolved over time. Nevertheless,these three studies involved a sizable number of patients andhad consistent results. The study by Halcox et al. (29) isparticularly convincing because of the larger sample size and
because the combined end point did not involve revascular-ization procedures, which, unlike spontaneous cardiovascu-lar events, are more likely to be influenced by non-biologicalfactors. In these studies, it is interesting that future eventswere poorly predicted by the angiographic severity ofdisease.
Two additional studies involved patients with CAD, butexamined endothelial dysfunction in the brachial rather thancoronary circulation. Heitzer et al. (30) observed that theforearm blood flow responses to intra-arterial acetylcholinewas an independent predictor of cardiovascular events,further suggesting that the forearm circulation is a reason-able surrogate for the coronary circulation. These investiga-tors also examined the degree to which a concomitantascorbic acid infusion improved endothelial function. Pa-tients with the largest improvement in endothelial functionduring ascorbic acid infusion had the highest risk, suggest-ing that increased oxidative stress may be a contributingmechanism for endothelial dysfunction and events. Neun-teufl et al. (31) examined brachial artery FMD usingultrasound. Although limited by a relatively small samplesize, retrospective design, and a heterogeneous mix of stableand unstable patients, this study also suggested that endo-thelial dysfunction in the brachial artery has prognosticvalue.
Gokce et al. (32) prospectively examined patients withatherosclerotic peripheral arterial disease awaiting non-emergent vascular surgery. Such patients are known to havea high incidence of recognized and undiagnosed CAD, and
Figure 1. The role of endothelial dysfunction in the pathogenesis of cardiovascular disease events. Cardiovascular disease risk factors adversely affect adiverse range of endothelial homeostatic functions and contribute mechanistically to the development, progression, and clinical expression of atherosclerosis.The response of the endothelium to the cumulative effects of risk factors may, in part, relate to intrinsic and environmental factors such as geneticpolymorphisms, dietary factors, exercise, and other factors. Thus, endothelial function may serve as a barometer for cardiovascular risk.
1151JACC Vol. 42, No. 7, 2003 Widlansky et al.October 1, 2003:1149–60 Endothelial Dysfunction

they have high short-term post-operative risk. Endothelialfunction was determined by brachial ultrasound beforesurgery, and patients were followed for 30 days after surgery.The study demonstrated that impaired FMD was a strongindependent predictor of post-operative events. The post-operative state is associated with pain, fluid shifts, increasedsympathetic nervous system activity, and inflammation, and,in this setting, endothelial dysfunction might increase therisk for plaque rupture or a mismatch between myocardialoxygen demand and supply. On longer term follow-up(mean of 1.2 years), impaired brachial artery FMD re-mained an independent predictor of events, even after thepatients had recovered from the immediate stress of surgery(33). Notably, the study demonstrated that this non-
invasive method for studying endothelial function had highsensitivity and negative predictive value, suggesting that itmight have utility as a screening test to identify low-riskpatients who might undergo surgery without further evalu-ation.
In addition to studies that examined patients with estab-lished atherosclerosis, several studies have examined theprognostic value of endothelial function in patients with riskfactors, but no known atherosclerosis. Two of these studieswere done in the brachial artery (34,35). Perticone et al. (34)examined the forearm blood flow responses to acetylcholinein untreated male and female patients with hypertension,and observed that endothelial dysfunction identified pa-tients at risk. Modena et al. (35) examined brachial arteryFMD in post-menopausal women with newly diagnosedhypertension. Patients had increased risk over the next fiveyears when endothelial dysfunction was not reversed by sixmonths of antihypertensive therapy. Although treatmentwas not standardized, the type of antihypertensive therapyor the degree of blood pressure (BP) lowering did notexplain the difference in prognosis. Importantly, these twostudies raise the possibility that endothelial function couldbe used as a screening test for the primary prevention ofCVD and as a guide to therapy.
Studies in patients with angiographically normal coronaryarteries provide further evidence that endothelial dysfunc-tion precedes and portends the development of athero-sclerosis. Halcox et al. (29) found both epicardial andmicrovascular endothelial dysfunction predicted future car-diovascular events independently of the angiographic pres-ence of CAD at the time of enrollment. Recently, Schindleret al. (36) reported that a coronary vasoconstrictor responseto the cold pressor test, which reflects, in part, endothelialdysfunction, independently predicts future cardiovascularevents in patients with normal coronary angiograms andelevated C-reactive protein levels.
Overall, the 10 studies examining the prognostic value ofendothelial vasomotor function involved 1,920 patients withatherosclerosis or hypertension and 333 patients withevents. These studies strongly and consistently demonstratethat endothelial dysfunction identifies patients who haveincreased risk for CVD events in the short and long term.Importantly, endothelial vasomotor dysfunction appears tobe a systemic process that can be identified in vascular bedsremote from the coronary and cerebral circulations whereevents occur.
In addition, vasomotor dysfunction, circulating bloodmarkers of endothelial dysfunction, also have prognosticvalue. In patients without known CVD, elevated levels ofsoluble intercellular adhesion molecule (ICAM) (37), andtissue plasminogen activator (9), are independent predictorsof future cardiovascular events. In patients with knowncoronary disease, soluble ICAM (38), von Willebrand factor(39), tissue plasminogen activator (39), plasminogen activa-tor inhibitor (40), and endothelin (41) all have prognosticvalue. As mentioned previously, markers of systemic inflam-
Table 2. Advantages and Disadvantages of Methods to QuantifyEndothelial Function in Humans
1. Intracoronary agonist infusion with quantitative coronary angiographyAdvantages
Direct quantification of endothelial function in the vascular bedof interest
Allows for mapping dose-response relationships of endothelialagonists and antagonists
Allows for examination of basal endothelial function (with NOSantagonist infusion)
DisadvantagesInvasiveExpensiveCarries risks inherent with coronary artery catheterization
(stroke, MI, infection, vascular injury)2. Brachial artery catheterization with venous occlusive plethysmography
AdvantagesMore accessible circulation than coronary arteriesAllows for mapping dose-response relationships of endothelial
agonists and antagonistsAllows for examination of basal endothelial function (with NOS
antagonist infusion)Disadvantages
InvasiveRisk of median nerve injury, infection, vascular injury
3. Vascular tonometry and measurements of vascular stiffnessAdvantages
NoninvasiveSafer and faster than either invasive methodLower operator dependence than brachial artery ultrasoundMay reflect basal endothelial function
DisadvantagesImportantly influenced by structural aspects of the vasculature
beyond the endothelium4. Brachial artery ultrasound with FMD
AdvantagesNoninvasiveSafer and faster than either invasive methodReactivity correlates to endothelial dysfunction in coronary
circulationFlow is a physiological stimulus for vasodilation unlike
agonists such as acetylcholineDisadvantages
Poor resolution relative to arterial sizeVariability in measurementsHighly operator-dependent
FMD � flow-mediated dilation; MI � myocardial infarction; NOS � nitric oxidesynthase.
1152 Widlansky et al. JACC Vol. 42, No. 7, 2003Endothelial Dysfunction October 1, 2003:1149–60

Table 3. Studies Evaluating the Predictive Value of Endothelial Dysfunction
Lead AuthorDesign/
Mean Follow-Up Patient PopulationVascular
BedMarker of Endothelial
Function End Points Examined Findings
Al Suwaidi (27) Retrospective/28 months 157 patients with mild CAD Coronary Acetylcholine response Cardiac death, MI, CHF,CABG, or PCI
6 patients with event. Acetylcholineresponse independent predictor ofevents.
Schachinger (28) Retrospective/7.7 years 147 patients with CAD Coronary Acetylcholine, cold pressortest, FMD, NTG
MI, UA, ischemic stroke, CABG,PTCA, peripheral bypass
28 patients with event. Vasomotorfunction independent predictor ofevents.
Neunteufl (31) Retrospective/5 years 73 patients with CAD Brachial FMD Death, MI, PTCA, or CABG 27 patients with event. FMD�10% predictive of events. Effectlost when controlling for extent ofCAD.
Heitzer (30) Prospective/4.5 years 281 patients with CAD Brachial Forearm blood flow responseto acetylcholine
CVD death, stroke, MI, CABG,PTCA, peripheral bypass
91 patients with event. Acetylcholineresponse independent predictor ofevents.
Perticone (34) Prospective/32 months 225 patients withhypertension
Brachial Forearm blood flow responseto acetylcholine
CVD death, MI, stroke, TIA,UA, CABG, PTCA, PVD
29 subjects with event. Acetylcholineresponse predictive of events.
Gokce (32) Prospective/30 days 187 patients undergoingvascular, surgery
Brachial FMD CVD death, MI, UA, stroke 45 patients with event. FMDindependent predictor of events.
Modena (35) Prospective/67 months 400 hypertensive post-menopausal women
Brachial FMD Hospitalization for CVD event(not otherwise specified)
47 patients with event. Failure toimprove FMD with 6 months ofantihypertensive therapyindependent predictor of events.
Halcox (29) Retrospective/46 months 308 patients referred forcardiac catheterization
Coronary Acetylcholine response CVD death, MI, ischemic stroke,UA
35 subjects with event. Acetylcholineresponse independent predictor ofevents.
Schindler (36) Prospective/45 months 130 patients with normalcoronary angiograms
Coronary Cold presser test CVD death, UA, MI, PTCA,CABG, stroke, peripheralbypass
26 patients with event. Cold pressortest response independentpredictor of events.
Gokce (33) Prospective/1.2 years 199 patients undergoingvascular surgery
Brachial FMD CVD, death, MI, UA, stroke 35 patients with events. FMDindependent predictor of long-term events.
CABG � coronary artery bypass graft surgery; CAD � coronary artery disease; CHF � congestive heart failure; CVD � cardiovascular disease; FMD � flow-mediated dilation; MI � myocardial infarction; NTG � nitroglycerin-mediateddilation; PCI � percutaneous coronary intervention (e.g., angioplasty or stent); PTCA � percutaneous transluminal coronary angioplasty; PVD � peripheral vascular disease; TIA � transient ischemic attack; UA � unstable angina.
1153JACC
Vol.42,No.7,2003W
idlanskyet
al.October1,2003:1149–60
EndothelialDysfunction

mation, including increased levels of C-reactive protein (7),are also associated with endothelial dysfunction in humansubjects (8,42,43). Overall, these studies illustrate thatidentifying endothelial phenotype using systemic markershas prognostic value. It remains unknown which individualmarker or combination of markers will prove most useful.Interventions to reverse endothelial dysfunction. An im-portant corollary to the hypothesis that endothelial dysfunc-tion contributes to the pathogenesis of CVD is the idea thatreversing endothelial dysfunction will reduce risk. Althoughthis corollary has not been tested directly, numerous studieshave evaluated lifestyle and pharmacologic interventions toimprove endothelial function, and many of these sameinterventions are known to limit cardiovascular risk. Theeffects of some of these treatments on endothelial functionand CVD risk are summarized in Table 4.Lifestyle modification. Exercise is an important lifestylefactor that reduces cardiovascular risk (44), and exercise hasbeen repeatedly shown to improve endothelial vasomotorfunction in healthy subjects (45,46) and in disease statesincluding hypertension (47), congestive heart failure (48),and CAD (49). These effects appear to be mediated in largepart by increased NO bioavailability (50) and may begreatest in vascular beds exposed to repetitive increases inblood flow during exercise (51), which includes the coronarycirculation for all types of exercise.
In contrast, a sedentary lifestyle is linked to obesity and isassociated with endothelial dysfunction, increased oxidativestress, and elevated systemic markers of inflammation. In
obese women, a yearlong program of low fat diet andexercise reduced plasma levels of tumor necrosis factor-alpha, interleukin-6, soluble ICAM-1, and soluble vascularcell adhesion molecule-1 (VCAM-1) (52). In that study,weight loss improved “endothelial function” as reflected bythe degree of BP reduction after infusion of L-arginine. Nopublished study has examined the effects of weight loss onendothelium-dependent vasodilation. Minimizing othertraditional risk factors for CVD also improves endothelialfunction. For example, BP reduction (35), drug therapy toincrease insulin sensitivity in diabetics (53), and smokingcessation (54) have been associated with improved endothe-lial function.Dietary modifications. Diets low in fat and high in fruitsand vegetables have been recommended by the AmericanHeart Association to decrease cardiovascular risk (55). Aportion of the benefit could result from increased intake offlavonoids, which may improve endothelial function. Forexample, endothelial dysfunction is reversed after intake offlavonoid-containing beverages including tea (56) grapejuice (57), and de-alcoholized red wine (58).
Conversely, poor dietary habits may worsen endothelialfunction. Several studies suggest that a high-fat meal willinduce acute impairment of FMD (59), although a portionof this effect may relate to other non-endothelium-dependent systemic effects on the vasculature (60). The typeof fat consumed may also be important (61), as a diet highin n-3 fatty acids (i.e., fish oil) may improve endothelium-dependent vasodilation (62).Antioxidant therapy. Oxidative stress is a central cause ofendothelial dysfunction in atherosclerosis (63), and therehas been great interest in the effects of antioxidant therapy.Regarding lipid-soluble antioxidants, probucol combinedwith lovastatin improved coronary endothelial function inpatients with CAD (64). However, the data for vitamin Eare quite mixed (reviewed by Duffy et al. [65]). Vitamin Ehas been shown to improve endothelial function in patientswith multiple risk factors, particularly cigarette smoking(66). However, a number of other studies have failed toshow a benefit (67–70). These latter results may be consis-tent with the recently published Heart Outcomes Preven-tion Evaluation (HOPE) study (71), which failed to dem-onstrate any effect of vitamin E on CVD events in alarge-scale randomized trial.
Regarding water-soluble antioxidants, vitamin C admin-istration consistently improves endothelium-dependent va-sodilation in patients with CVD (65). Some epidemiologicstudies suggest that individuals with low plasma concentra-tions (72) or low dietary intake (73) of ascorbic acid haveincreased cardiovascular risk. However, no randomizedclinical trial has addressed the benefits of ascorbic acidtreatment in a patient population with evidence of inade-quate ascorbic acid intake or unsaturated tissue stores.
Studies of combinations of antioxidants, typically vitaminC, vitamin E, and beta-carotene, have provided disappoint-ing results. Two studies failed to demonstrate a beneficial
Table 4. Effect of Interventions on Endothelial Function andCVD
Intervention
Effect onEndothelial
FunctionEffect on
CVD Events
Lipid-lowering therapy � �Smoking cessation � �Exercise � �ACE inhibitors � �Angiotensin receptor blockers � �N-3 fatty acids � �Glycemic control in diabetes mellitus � �Hormone replacement therapy � �Vitamin E � �Combination antioxidants � �L-arginine � ?Dietary flavonoids � ?Vitamin C � ?Folate � ?Tetrahydrobiopterin � ?Specific metal ion chelation therapy � ?Protein kinase C inhibition � ?Cyclooxygenase-2 inhibition � ?Thromboxane A2 inhibition � ?Troglitazone treatment in diabetes � ?Xanthine oxidase inhibition � ?Tumor necrosis factor inhibition � ?
� � weight of evidence indicates an improvement; � � weight of evidence indicatesno effect or worsening; ? � there are insufficient data at the present time.
ACE � angiotensin converting enzyme; CVD � cardiovascular disease.
1154 Widlansky et al. JACC Vol. 42, No. 7, 2003Endothelial Dysfunction October 1, 2003:1149–60

effect of this combination on endothelium-dependent vaso-dilation (74,75). The recent Heart Protection Study exam-ined such a combination in 20,536 individuals with CAD,diabetes, or peripheral vascular disease and demonstrated nobenefit on cardiovascular events (76).
Despite the strong evidence that oxidative stress contrib-utes to atherogenesis (77) and endothelial dysfunction (63),there are a number of possible reasons why antioxidanttreatment has failed to show a benefit. For example, thestudied antioxidants may have insufficient activity againstthe, as yet, undefined oxidants most relevant to CVD andendothelial dysfunction. The background antioxidant statusof participants may have obscured any beneficial effect.Finally, it is possible that an antioxidant strategy designed toact on the sources of oxidant stress may be more effectivethan treatment with agents that act on selected “down-stream” consequences, as has been suggested by Munzel andKeaney (78).Lipid-lowering therapy. There is strong and consistentevidence that reduction of plasma low-density lipoproteinimproves endothelial function. This benefit has been ob-served when low-density lipoprotein is lowered by non-pharmacologic means such as diet in animals (79), and withbile acid resins and plasma apheresis in humans (80,81).Treatment with HMG CoA reductase inhibitors (statins)has been consistently shown to reduce cardiovascular risk(82) and reverse endothelial dysfunction (64,80,83–86).Although two studies have failed to demonstrate a benefiton coronary endothelial function, these studies involvedshort-term treatment of patients with relatively low baselinecholesterol levels and had methodological problems includ-ing limited statistical power and improved endothelialfunction in the placebo group (87,88). While statins havebeen shown to induce regression of atherosclerotic plaques,the available data strongly suggest that that the interrelatedeffects of statins on the endothelium, inflammation, andplaque composition are more important than lesion regres-sion in regard to the observed reduction in cardiovascularrisk (12).
While reduction of serum cholesterol is likely the majormechanism by which statins improve endothelial function,in vitro studies suggest that pleiotropic effects of statins mayalso be relevant. In addition to reducing cholesterol levels,HMG CoA reductase inhibition reduces cellular concentra-tions of important and biologically active intermediates thatinfluence endothelial phenotype. By this mechanism, statinshave been shown to directly enhance expression, phosphor-ylation state, and activity of the endothelial isoform of NOsynthase (89,90). Moreover, C-reactive protein reduces NOsynthase expression (91), suggesting that statins may spe-cifically protect against the adverse effects of inflammationon the vasculature. It remains uncertain whether the pleio-tropic effects of statins are relevant at the concentrations ofstatins achievable in patients.
Angiotensin-converting enzyme inhibition and angio-tensin-II receptor blockade. Large-scale outcome trials(92) have clearly demonstrated that angiotensin-convertingenzyme (ACE) inhibitors reduce CVD events in patientswith CAD and diabetes, independent of BP reduction.Similarly, ACE inhibitors also improve endothelial function(93–96). Angiotensin converting enzyme inhibitors mayaffect endothelium-derived NO by several mechanisms. Forexample, angiotensin-II increases nicotinamide adeninedinucleotide phosphate (reduced) oxidase activity (97) lead-ing to increased production of reactive oxygen species and“inactivation” of NO. Furthermore, ACE inhibitors inhibitthe breakdown of bradykinin, a substance that stimulatesNO production. Indeed, investigators have proposed thatthe balance between angiotensin II and NO is one of themajor determinants of endothelial and vascular phenotype(98). The importance of angiotensin-II is further supportedby the observation that angiotensin receptor blockers alsoappear to improve endothelial function and reduce endo-thelial markers of inflammation and oxidative stress(99,100).Hormone replacement therapy. There has been extensivestudy of hormone replacement therapy (HRT) and endo-thelial function (101). Studies in post-menopausal womenhave repeatedly shown that estrogen replacement improvesendothelium-dependent dilation and reduces systemic plas-minogen activator inhibitor-1 levels (102). Combinationtherapy with a progesterone preparation blunts the benefitsof estrogen in some, but not all studies (103,104). The issueof whether estrogen treatment has a beneficial effect onendothelial function in patients with established CVD hasbeen less well studied, but a large cross-sectional studysuggests that the beneficial effects are less than thoseobserved in younger women without CVD (105). Despitethe apparent beneficial effects on endothelial function,outcome studies have failed to show a beneficial effect ofHRT (combination of estrogen and progesterone) for pri-mary (106) or secondary (107) prevention of CVD events.Indeed, reduction in cardiovascular risk is no longer anaccepted indication for HRT.
The explanations for the apparently disparate resultsremain uncertain. However, estrogen and progesterone havecomplex cellular effects, and it is possible that adverseeffects, including pro-thrombotic effects, outweigh the ben-efits of improved endothelial function. Furthermore, it isunclear whether benefits of estrogen might have beenconfounded by concurrent progesterone therapy. Neverthe-less, these results suggest that not every therapy thatimproves endothelial function translates directly into areduction in cardiovascular risk.Newer interventions. Finally, a number of newer therapieshave been shown to improve endothelial function in humansubjects, and a partial list is provided in Table 4. Forexample, L-arginine, which is the precursor for NO syn-thesis, has been administered in high doses to humansubjects and has been shown in some studies to improve
1155JACC Vol. 42, No. 7, 2003 Widlansky et al.October 1, 2003:1149–60 Endothelial Dysfunction

endothelium-dependent dilation (108,109). Other examplesinclude tetrahydrobiopterin, an essential co-factor for endo-thelial NO synthase (110), protein kinase C inhibition(111), iron chelation (112), and cyclooxygenase-2 inhibition(113). It is likely that many additional therapies will emergeas the pathophysiologic mechanisms of endothelial dysfunc-tion in specific disease states are elucidated.Clinical utility of studying endothelial function. In sum-mary, the reviewed studies suggest that: 1) the endotheliumplays a central role in vascular homeostasis and the patho-genesis of CVD; 2) endothelial vasomotor function canreadily be measured in the coronary and peripheral circula-tions and that systemic markers of endothelial phenotypecan be measured in blood; 3) endothelial vasomotor dysfunc-tion detected in the coronary or peripheral circulation hasprognostic value; and 4) many, but not all, interventions thatreverse endothelial dysfunction also reduce cardiovascular risk.The question at hand is how these results can be used from apublic health and/or clinical perspective (Table 5).
The available evidence suggests that endothelial functionreflects the integrated effects of risk factors on the vascula-ture and that the development of endothelial dysfunction isan early event in the atherogenic process. There are strongand consistent relationships between mechanistically diverserisk factors and endothelial dysfunction. Furthermore, en-dothelial dysfunction identifies individuals at risk, before thedevelopment of clinically apparent CVD. These observa-tions suggest that study of endothelial dysfunction hasutility for the identification of novel risk factors for CVD.The finding that a potential risk factor is associated withendothelial dysfunction in carefully controlled cross-sectional studies would strongly suggest that this factor isassociated with the development of CVD. Further evidencewould be provided by studies showing the reversal ofendothelial dysfunction by a specific intervention also re-duces the cardiovascular risk associated with the risk factor.Often such studies are performed in the context of support-ive epidemiologic outcome studies and mechanistic basicstudies suggesting a causal relationship between the riskfactor and atherosclerosis. Recent examples of the utility ofendothelial function in regard to novel risk factors includeobesity (6) and certain systemic infections (8).
Another current role for study of endothelial dysfunctionis evaluation of interventions to reduce CVD risk. There isgreat interest in identifying “surrogate markers” of risk thatcan be used as an end point to evaluate a potentialintervention before undertaking a longer term and consid-erably more expensive study that involves CVD events asthe end point. Given the prognostic value of endothelialdysfunction and the strong correlation between improvedendothelial dysfunction and reduced cardiovascular risk(Table 4), it is reasonable to consider endothelial dysfunc-tion for this purpose. The possibility of using endothelialfunction to screen patients for evidence of high cardiovas-cular risk is further supported by high sensitivity andnegative predictive values (�90%, respectively) (32). Again,studies evaluating the utility of endothelial function as ascreening test must be evaluated in the context of otheravailable epidemiologic, clinical, and experimental data. Asis the case for HRT, potential confounding effects of theintervention must be considered.
A number of other modalities have been consideredpotential surrogate end points for CVD, including carotid-intimal thickness measured by ultrasound and coronarycalcification assessed by computed tomography or magneticresonance imaging scan. These modalities largely provide ameasure of the presence and extent of fixed atherosclerosis.Studies of endothelial function may prove advantageousbecause they provide insight into vascular function, whichappears to be more relevant to the pathogenesis of plaquerupture and the ensuing thrombosis that underlies cardio-vascular events. Measurement of serum markers of inflam-mation (e.g., C-reactive protein) is another promising ap-proach to this issue, but may not reflect the susceptibility ofthe vasculature to the adverse effects of systemic inflamma-tion. It is possible that the state of the endothelium mayreflect the degree to which the vasculature has been alteredby inflammatory stimuli, and, thus, may provide additionalprognostic information. Also unknown is the potential roleof more specific serum markers of endothelial dysfunctionsuch as plasminogen activator inhibitor-1, endothelin, andadhesion molecules (ICAM-1, VCAM-1). Direct compar-ative studies of the relative utility of available surrogates arelacking at the present time.
The available studies linking endothelial dysfunction tocardiovascular events (Table 3) raise the intriguing possibil-ity that the technique could have utility for the managementof individual patients. In regard to brachial artery FMD,studies of patients with hypertension and established coro-nary disease suggest that endothelial dysfunction identifiesindividuals who might benefit from more intensive treat-ment (31,35). Similarly, the prospective studies by Gokce etal. (32,33) might suggest that patients with peripheralarterial disease with preserved endothelial function are atlow risk for perioperative and long-term events and mightbe managed differently than patients with poor function.The study by Modena et al. (35) raises the further possibilitythat persistent endothelial dysfunction during antihyperten-
Table 5. Clinical Utility of Endothelial Dysfunction
Current usesIdentification of novel risk factors for CVDInvestigation of mechanisms of atherosclerosis and vascular
dysfunctionSurrogate marker of cardiovascular risk for intervention studies
involving groups of patientsPotential future uses
Screening individuals for future cardiovascular riskEvaluating CVD patients for lifestyle, pharmacologic, and/or
mechanical interventionPreoperative evaluationMonitoring response to primary and secondary prevention therapies/
strategies
CVD � cardiovascular disease.
1156 Widlansky et al. JACC Vol. 42, No. 7, 2003Endothelial Dysfunction October 1, 2003:1149–60

sive therapy identifies high-risk individuals and that endo-thelial function might be used to monitor the effectivenessof risk reduction therapy. Thus, evaluation of endothelialfunction could be advantageous in prevention of bothprimary and secondary events. A paradigm shift from thecurrent reactive, symptom-based, screening system lookingfor active disease to a non-invasive, relatively inexpensive,screening system based on vascular function would also be ofbenefit to both the general health of the population and thealready overburdened and costly medical system.
Although highly appealing, there are insufficient data tosupport these possible applications for individual patients atthe present time. Reproducible evaluation of endothelialfunction is limited to facilities with extensive experience inthese techniques. The applicability of testing endothelialfunction on a population-wide basis is further diminished bythe lack of large prospective trials evaluating its efficacy as ascreening tool in the general population and by the lack oftrials demonstrating that improving endothelial functiondecreases cardiovascular risk. Further studies are needed toconfirm the available results and to carefully evaluate thesensitivity and specificity of the techniques relative to or incombination with other available measures of risk forindividual patients. The recently initiated Multi-EthnicStudy of Atherosclerosis (MESA) will clarify some of theseissues by simultaneously examining the predictive value ofseveral measures of endothelial function and other subclin-ical markers of atherosclerosis (114). However, furtherstudies are needed to demonstrate that clinical use ofendothelial function can be used to guide risk reductiontherapy.Future directions. The available methods for studyingendothelial function are currently useful for evaluating riskfactors, mechanisms of CVD, and potential interventions ingroups of patients. However, as outlined in Table 2, thereare important limitations associated with each of thesetechniques. Development of improved or novel methodol-ogy to assess endothelial vasomotor function would beextremely useful. One approach would be to develop ameans to obtain higher-resolution imaging of arterial diam-eter. Ideally, such imaging would be performed in thecoronary circulation, although the available data indicatethat peripheral arteries are reasonable surrogates. The mostcurrent non-invasive methodology requires off-line analysis,and another potential advance would be the development ofcontinuous on-line measurement and reporting of vasomo-tor responses. At the present time, study of nitric-oxide-dependent responses requires imaging of blood vessels,measurement of changes in blood flow, or pulse waveanalysis. Development of simpler indirect methods to assessendothelium-dependent responses may hold some promisefor the future. For example, there is recent interest in asimple pulse amplitude tonometry method to measureFMD of small vessels in the finger (115–117). There alsomay be utility in further study of other manifestations of thepathologic endothelial phenotype, including pro-
thrombotic, vasoconstrictor, and pro-inflammatory factorsthat can be measured in blood. Most important for thefuture use of endothelial function in the care of patients isthe need for a standardized approach that is supported bylarge-scale outcome studies.
Reprint requests and correspondence: Dr. Joseph A. Vita,Section of Cardiology, Boston Medical Center, 88 East NewtonStreet, Boston, Massachusetts 02118. E-mail: [email protected].
REFERENCES
1. Vita JA, Keaney JF Jr. Endothelial function: a barometer forcardiovascular risk? Circulation 2002;106:640–2.
2. Gokce N, Vita JA. Clinical manifestations of endothelial dysfunction.In: Loscalzo J, Schafer AI, editors. Thrombosis and Hemorrhage.Philadelphia, PA: Lippincott Williams & Wilkins, 2002:685–706.
3. Libby P, Ridker PM, Maseri A. Inflammation and atherosclerosis.Circulation 2002;105:1135–43.
4. Sorensen KE, Celermajer DS, Georgakopoulos D, Hatcher G,Betteridge DJ, Deanfield JE. Impairment of endothelium-dependentdilation is an early event in children with familial hypercholesterol-emia and is related to the lipoprotein (a) level. J Clin Invest1994;93:50–5.
5. Celermajer DS, Sorensen KE, Gooch VM, et al. Non-invasivedetection of endothelial dysfunction in children and adults at risk ofatherosclerosis. Lancet 1992;340:1111–5.
6. Steinberg HO, Chaker H, Leaming R, Johnson A, Brechtel G,Baron AD. Obesity/insulin resistance is associated with endothelialdysfunction: implications for the syndrome of insulin resistance.J Clin Invest 1996;97:2601–10.
7. Fichtlscherer S, Rosenberger G, Walter DH, Breuer S, Dimmeler S,Zeiher AM. Elevated C-reactive protein levels and impaired endo-thelial vasoreactivity in patients with coronary artery disease. Circu-lation 2000;102:1000–6.
8. Prasad A, Zhu J, Halcox JP, Waclawiw MA, Epstein SE, QuyyumiAA. Predisposition to atherosclerosis by infections: role of endothe-lial dysfunction. Circulation 2002;106:184–90.
9. Thogersen AM, Jansson J, Boman K, Nilsson TK, Weinehall L.High plasminogen activator inhibitor and tissue plasminogen activa-tor levels in plasma precede a first acute myocardial infarction in bothmen and women: evidence for the fibrinolytic system as an indepen-dent primary risk factor. Circulation 1998;98:2241–7.
10. Cushman M, Lemaitre RN, Kuller LH, et al. Fibrinolytic activationmarkers predict myocardial infarction in the elderly: the Cardiovas-cular Health study. Arterioscler Thromb Vasc Biol 1999;19:493–8.
11. Ruiz-Ortega M, Lorenzo O, Ruperez M, et al. Role of the renin-angiotensin system in vascular diseases: expanding the field. Hyper-tension 2001;38:1382–7.
12. Levine GN, Keaney JF Jr., Vita JA. Cholesterol reduction incardiovascular disease: clinical benefits and possible mechanisms.N Engl J Med 1995;332:512–21.
13. Ross R. Atherosclerosis—an inflammatory disease. N Engl J Med1999;340:115–26.
14. Okumura K, Yasue H, Matsuyama K, et al. Effect of acetylcholine onthe highly stenotic coronary artery: difference between the constrictorresponse of the infarct-related coronary artery and that of thenoninfarct-related artery. J Am Coll Cardiol 1992;19:752–8.
15. Ludmer PL, Selwyn AP, Shook TL, et al. Paradoxical vasoconstric-tion induced by acetylcholine in atherosclerotic coronary arteries.N Engl J Med 1986;315:1046–51.
16. Cox DA, Vita JA, Treasure CB, et al. Atherosclerosis impairsflow-mediated dilation of coronary arteries in humans. Circulation1989;80:458–65.
17. Lerman A, Holmes DR, Bell MR, Garratt KN, Nishimura RA,Burnett JC. Endothelin in coronary endothelial dysfunction and earlyatherosclerosis in humans. Circulation 1995;92:2426–31.
18. Creager MA, Cooke JP, Mendelsohn ME, et al. Impaired vasodila-tion of forearm resistance vessels in hypercholesterolemic humans.J Clin Invest 1990;86:228–34.
1157JACC Vol. 42, No. 7, 2003 Widlansky et al.October 1, 2003:1149–60 Endothelial Dysfunction
19. Oliver JJ, Webb DJ. Noninvasive assessment of arterial stiffness andrisk of atherosclerotic events. Arterioscler Thromb Vasc Biol 2003;23:554–66.
20. Laurent S, Boutouyrie P, Asmar R, et al. Aortic stiffness is anindependent predictor of all-cause and cardiovascular mortality inhypertensive patients. Hypertension 2001;37:1236–41.
21. Grey E, Bratteli C, Glasser SP, et al. Reduced small artery but notlarge artery elasticity is an independent risk marker for cardiovascularevents. Am J Hypertens 2003;16:265–9.
22. Corretti MC, Anderson TJ, Benjamin EJ, et al. Guidelines for theultrasound assessment of endothelial-dependent flow-mediated vaso-dilation of the brachial artery: a report of the International BrachialArtery Reactivity Task Force. J Am Coll Cardiol 2002;39:257–65.
23. Joannides R, Haefeli WE, Linder L, et al. Nitric oxide is responsiblefor flow-dependent dilatation of human peripheral conduit arteries invivo. Circulation 1995;91:1314–9.
24. Lieberman EH, Gerhard MD, Uehata A, et al. Flow-inducedvasodilation of the human brachial artery is impaired in patients �40years of age with coronary artery disease. Am J Cardiol 1996;78:1210–4.
25. Anderson TJ, Uehata A, Gerhard MD, et al. Close relation ofendothelial function in the human coronary and peripheral circula-tions. J Am Coll Cardiol 1995;26:1235–41.
26. Eskurza I, Seals DR, DeSouza CA, Tanaka H. Pharmacological vs.flow-mediated assessments of peripheral vascular endothelial vasodi-latory function in humans. Am J Cardiol 2001;88:1067–9.
27. Suwaidi JA, Hamasaki S, Higano ST, Nishimura RA, Holmes DR,Lerman A. Long-term follow-up of patients with mild coronaryartery disease and endothelial dysfunction. Circulation 2000;101:948–54.
28. Schachinger V, Britten MB, Zeiher AM. Prognostic impact ofcoronary vasodilator dysfunction on adverse long-term outcome ofcoronary heart disease. Circulation 2000;101:1899–906.
29. Halcox JP, Schenke WH, Zalos G, et al. Prognostic value of coronaryvascular endothelial dysfunction. Circulation 2002;106:653–8.
30. Heitzer T, Schlinzig T, Krohn K, Meinertz T, Munzel T. Endothe-lial dysfunction, oxidative stress, and risk of cardiovascular events inpatients with coronary artery disease. Circulation 2001;104:2673–8.
31. Neunteufl T, Heher S, Katzenschlager R, et al. Late prognostic valueof flow-mediated dilation in the brachial artery of patients with chestpain. Am J Cardiol 2000;86:207–10.
32. Gokce N, Keaney JF Jr., Menzoian JO, et al. Risk stratification forpostoperative cardiovascular events via noninvasive assessment ofendothelial function. Circulation 2002;105:1567–72.
33. Gokce N, Keaney JF Jr., Hunter LM, et al. Predictive value ofnon-invasively-determined endothelial dysfunction for long-termcardiovascular events in patients with peripheral vascular disease.J Am Coll Cardiol 2003;41:1769–75.
34. Perticone F, Ceravolo R, Pujia A, et al. Prognostic significance ofendothelial dysfunction in hypertensive patients. Circulation 2001;104:191–6.
35. Modena MG, Bonetti L, Coppi F, Bursi F, Rossi R. Prognostic roleof reversible endothelial dysfunction in hypertensive postmenopausalwomen. J Am Coll Cardiol 2002;40:505–10.
36. Schindler TH, Hornig B, Buser PT, et al. Prognostic value ofabnormal vasoreactivity of epicardial coronary arteries to sympatheticstimulation in patients with normal coronary angiograms. Arterio-scler Thromb Vasc Biol 2003;23:495–501.
37. Ridker PM, Hennekens CH, Roitman-Johnson B, Allen J. Plasmaconcentration of soluble intercellular adhesion molecule 1 and risks offuture myocardial infarction in apparently healthy men. Lancet1998;351:88–92.
38. Haim M, Tanne D, Boyko V, et al. Soluble intercellular adhesionmolecule-1 and long-term risk of acute coronary events in patientswith chronic coronary heart disease: data from the BezafibrateInfarction Prevention (BIP) study. J Am Coll Cardiol 2002;39:1133–8.
39. Thompson SG, Kienast J, Pyke SD, Haverkate F, van de Loo JCW.Hemostatic factors and the risk of myocardial infarction or suddendeath in patients with angina pectoris. N Engl J Med 1995;332:635–41.
40. Hamsten A, de Faire U, Walldius G, et al. Plasminogen activatorinhibitor in plasma: risk factor for recurrent myocardial infarction.Lancet 1987;2:3–9.
41. Omland T, Lie RT, Aakvaag A, Aarsland T, Dickstein K. Plasmaendothelin determination as a prognostic indicator of 1-year mortal-ity after acute myocardial infarction. Circulation 1994;89:1573–9.
42. Hingorani AD, Cross J, Kharbanda RK, et al. Acute systemicinflammation impairs endothelium-dependent dilatation in humans.Circulation 2000;102:994–9.
43. Vita JA, Loscalzo J. Shouldering the risk factor burden: infection,atherosclerosis, and the vascular endothelium. Circulation 2002;106:164–6.
44. Smith SC Jr., Blair SN, Bonow RO, et al. AHA/ACC guidelines forpreventing heart attack and death in patients with atheroscleroticcardiovascular disease: 2001 update. A statement for healthcareprofessionals from the American Heart Association and the Ameri-can College of Cardiology. J Am Coll Cardiol 2001;38:1581–3.
45. Clarkson P, Montgomery HE, Mullen MJ, et al. Exercise trainingenhances endothelial function in young men. J Am Coll Cardiol1999;33:1379–85.
46. DeSouza CA, Shapiro LF, Clevenger CM, et al. Regular aerobicexercise prevents and restores age-related declines in endothelium-dependent vasodilation in healthy men. Circulation 2000;102:1351–7.
47. Higashi Y, Sasaki S, Kurisu S, et al. Regular aerobic exerciseaugments endothelium-dependent vascular relaxation in normoten-sive as well as hypertensive subjects: role of endothelium-derivednitric oxide. Circulation 1999;100:1194–202.
48. Hambrecht R, Fiehn E, Weigl C, Gielen S, Hamann C. Regularphysical exercise corrects endothelial dysfunction and improves exer-cise capacity in patients with chronic heart failure. Circulation1998;98:2709–15.
49. Hambrecht R, Wolf A, Gielen S, et al. Effect of physical exercise oncoronary endothelial function in coronary artery disease. N EnglJ Med 2000;342:454–60.
50. Gielen S, Schuler G, Hambrecht R. Exercise training in coronaryartery disease and coronary vasomotion. Circulation 2001;103:E1–6.
51. Gokce N, Vita JA, Bader DS, et al. Effect of exercise on upper andlower extremity endothelial function in patients with coronary arterydisease. Am J Cardiol 2002;90:124–7.
52. Ziccardi P, Nappo F, Giugliano G, et al. Reduction of inflammatorycytokine concentrations and improvement of endothelial functions inobese women after weight loss over one year. Circulation 2002;105:804–9.
53. Mather KJ, Verma S, Anderson TJ. Improved endothelial functionwith metformin in type 2 diabetes mellitus. J Am Coll Cardiol2001;37:1344–50.
54. Celermajer DS, Sorensen KE, Georgakopoulos D, et al. Cigarettesmoking is associated with dose-related and potentially reversibleimpairment of endothelium-dependent dilation in healthy youngadults. Circulation 1993;88:2149–55.
55. Krauss RM, Eckel RH, Howard B, et al. AHA dietary guidelines:revision 2000: a statement for healthcare professionals from theNutrition Committee of the American Heart Association. Circula-tion 2000;102:2284–99.
56. Duffy SJ, Keaney JF Jr., Holbrook M, et al. Short- and long-termblack tea consumption reverses endothelial dysfunction in patientswith coronary artery disease. Circulation 2001;104:151–6.
57. Stein JH, Keevil JG, Wiebe DA, Aeschlimann S, Folts JD. Purplegrape juice improves endothelial function and reduces the suscepti-bility of LDL cholesterol to oxidation in patients with coronary arterydisease. Circulation 1999;100:1050–5.
58. Agewall S, Wright S, Doughty RN, Whalley GA, Duxbury M,Sharpe N. Does a glass of red wine improve endothelial function? EurHeart J 2000;21:74–8.
59. Vogel RA, Corretti MC, Plotnick GD. Effect of a single high-fatmeal on endothelial function in healthy subjects. Am J Cardiol1997;79:350–4.
60. Gokce N, Duffy SJ, Hunter LM, Keaney JF Jr., Vita JA. Acutehypertriglyceridemia is associated with peripheral vasodilation andincreased basal flow in healthy young adults. Am J Cardiol 2001;88:153–9.
61. Vogel RA, Corretti MC, Plotnick GD. The postprandial effect ofcomponents of the Mediterranean diet on endothelial function. J AmColl Cardiol 2000;36:1455–60.
62. Goodfellow J, Bellamy MF, Ramsey MW, Jones CJ, Lewis MJ.Dietary supplementation with marine omega-3 fatty acids improve
1158 Widlansky et al. JACC Vol. 42, No. 7, 2003Endothelial Dysfunction October 1, 2003:1149–60
systemic large artery endothelial function in subjects with hypercho-lesterolemia. J Am Coll Cardiol 2000;35:265–70.
63. Keaney JF Jr. Atherosclerosis, oxidative stress, and endothelialfunction. In: Keaney JF Jr., editor. Oxidative Stress and VascularDisease. Boston, MA: Kluwer Academic Publishers, 2000:155–81.
64. Anderson TJ, Meredith IT, Yeung AC, Frei B, Selwyn A, Ganz P.The effect of cholesterol lowering and antioxidant therapy onendothelium-dependent coronary vasomotion. N Engl J Med 1995;332:488–93.
65. Duffy SJ, Vita JA, Keaney JF Jr. Antioxidants and endothelialfunction. Heart Failure 1999;15:135–52.
66. Heitzer T, Yla HS, Wild E, Luoma J, Drexler H. Effect of vitaminE on endothelial vasodilator function in patients with hypercholes-terolemia, chronic smoking or both. J Am Coll Cardiol 1999;33:499–505.
67. Gazis A, White DJ, Page SR, Cockcroft JR. Effect of oral vitamin E(alpha-tocopherol) supplementation on vascular endothelial functionin type 2 diabetes mellitus. Diabetes Med 1999;16:304–11.
68. Title LM, Cummings PM, Giddens K, Genest JJ Jr., Nassar BA.Effect of folic acid and antioxidant vitamins on endothelial dysfunc-tion in patients with coronary artery disease. J Am Coll Cardiol2000;36:758–65.
69. Elliott TG, Barth JD, Mancini GBJ. Effects of vitamin E onendothelial function in men after myocardial infarction. Am J Cardiol1995;76:1188–90.
70. Chowienczyk PJ, Kneale BJ, Brett SE, Paganga G, Jenkins BS, RitterJM. Lack of effect of vitamin E on L-arginine responsive endothelialdysfunction in patients with mild hypercholesterolemia and coronaryartery disease. Clin Sci 1998;94:129–34.
71. Yusuf S, Dagenais G, Pogue J, Bosch J, Sleight P. Vitamin Esupplementation and cardiovascular events in high-risk patients: theHeart Outcomes Prevention Evaluation study investigators. N EnglJ Med 2000;342:154–60.
72. Khaw KT, Bingham S, Welch A, et al. Relation between plasmaascorbic acid and mortality in men and women in EPIC-Norfolkprospective study: a prospective population study. European Prospec-tive Investigation into Cancer and Nutrition. Lancet 2001;357:657–63.
73. Enstrom JE, Kanim LE, Klein MA. Vitamin C intake and mortalityamong a sample of the United States population. Epidemiology1992;3:194–202.
74. Gilligan DM, Sack MN, Guetta V, et al. Effect of antioxidantvitamins on low density lipoprotein oxidation and impairedendothelium-dependent vasodilation in patients with hypercholester-olemia. J Am Coll Cardiol 1994;24:1611–7.
75. McKechnie R, Rubenfire M, Mosca L. Antioxidant nutrient supple-mentation and brachial reactivity in patients with coronary arterydisease. J Lab Clin Med 2002;139:133–9.
76. MRC/BHF Heart Protection Study Group. MRC/BHF HeartProtection study of antioxidant vitamin supplementation in 20,536high-risk individuals: a randomised placebo-controlled trial. Lancet2002;360:23–33.
77. Diaz MN, Frei B, Vita JA, Keaney JF Jr. Antioxidants and athero-sclerotic heart disease. N Engl J Med 1997;337:408–17.
78. Munzel T, Keaney JF Jr. Are ACE-inhibitors a “magic bullet” againstoxidative stress? Circulation 2001;104:1571–4.
79. Harrison DG, Armstrong ML, Frieman PC, Heistad DD. Restora-tion of endothelium-dependent relaxation by dietary treatment ofatherosclerosis. J Clin Invest 1987;80:1808–11.
80. Leung WH, Lau CP, Wong CK. Beneficial effect of cholesterol-lowering therapy on coronary endothelium-dependent relaxation inhypercholesterolemic patients. Lancet 1993;341:1496–500.
81. Tamai O, Matsuoka H, Itabe H, Wada Y, Kohno K, Iamaizumi T.Single LDL apheresis improves endothelium-dependent vasodilationin hypercholesterolemic humans. Circulation 1997;95:76–82.
82. Libby P. Current concepts of the pathogenesis of the acute coronarysyndromes. Circulation 2001;104:365–72.
83. Egashira K, Hirooka Y, Kai H, et al. Reduction in serum cholesterolwith pravastatin improves endothelium-dependent coronary vasomo-tion in patients with hypercholesterolemia. Circulation 1994;89:2519–24.
84. Treasure CB, Klein JL, Weintraub WS, et al. Beneficial effects ofcholesterol-lowering therapy on the coronary endothelium in patientswith coronary artery disease. N Engl J Med 1995;332:481–7.
85. Masumoto A, Hirooka Y, Hironaga K, et al. Effect of pravastatin onendothelial function in patients with coronary artery disease(cholesterol-independent effect of pravastatin). Am J Cardiol 2001;88:1291–4.
86. Perticone F, Ceravolo R, Maio R, et al. Effects of atorvastatin andvitamin C on endothelial function of hypercholesterolemic patients.Atherosclerosis 2000;152:511–8.
87. Vita JA, Yeung AC, Winniford M, et al. Effect of cholesterol-lowering therapy on coronary endothelial vasomotor function inpatients with coronary artery disease. Circulation 2000;102:846–51.
88. The ENCORE Investigators. Effect of nifedipine and cerivastatin oncoronary endothelial function in patients with coronary artery disease:the ENCORE I study (Evaluation of Nifedipine and Cerivastatin OnRecovery of coronary Endothelial function). Circulation 2003;107:422–8.
89. Laufs U, La Fata V, Plutzky J, Liao JK. Upregulation of endothelialnitric oxide synthase by HMG CoA reductase inhibitors. Circulation1998;97:1129–35.
90. Kureishi Y, Luo Z, Shiojima I, et al. The HMG-CoA reductaseinhibitor simvastatin activates the protein kinase Akt and promotesangiogenesis in normocholesterolemic animals. Nat Med 2000;6:1004–10.
91. Verma S, Wang CH, Li SH, et al. A self-fulfilling prophecy:C-reactive protein attenuates nitric oxide production and inhibitsangiogenesis. Circulation 2002;106:913–9.
92. Yusuf S, Sleight P, Pogue J, Bosch J, Davies R, Dagenais G. Effectsof an angiotensin-converting-enzyme inhibitor, ramipril, on cardio-vascular events in high-risk patients: the Heart Outcomes PreventionEvaluation study investigators. N Engl J Med 2000;342:145–53.
93. Mancini GB, Henry GC, Macaya C, et al. Angiotensin-convertingenzyme inhibition with quinapril improves endothelial vasomotordysfunction in patients with coronary artery disease: the TREND(Trial on Reversing ENdothelial Dysfunction) study. Circulation1996;94:258–65.
94. Prasad A, Husain S, Quyyumi AA. Abnormal flow-mediated epicar-dial vasomotion in human coronary arteries is improved byangiotensin-converting enzyme inhibition: a potential role of brady-kinin. J Am Coll Cardiol 1999;33:796–804.
95. Prasad A, Tupas-Habib T, Schenke WH, et al. Acute and chronicangiotensin-1 receptor antagonism reverses endothelial dysfunctionin atherosclerosis. Circulation 2000;101:2349–54.
96. Higashi Y, Sasaki S, Nakagawa K, et al. A comparison ofangiotensin-converting enzyme inhibitors, calcium antagonists, beta-blockers and diuretic agents on reactive hyperemia in patients withessential hypertension: a multicenter study. J Am Coll Cardiol2000;35:284–91.
97. Griendling KK, Minieri CA, Ollerenshaw JD, Alexander RW.Angiotensin II stimulates NADH and NADPH oxidase activity incultured vascular smooth muscle cells. Circ Res 1994;74:1141–8.
98. Gibbons GH. Cardioprotective mechanisms of ACE inhibition: theangiotensin II-nitric oxide balance. Drugs 1997;54 Suppl 5:1–11.
99. Wassmann S, Hilgers S, Laufs U, Bohm M, Nickenig G. Angioten-sin II type 1 receptor antagonism improves hypercholesterolemia-associated endothelial dysfunction. Arterioscler Thromb Vasc Biol2002;22:1208–12.
100. Hornig B, Landmesser U, Kohler C, et al. Comparative effect ofACE inhibition and angiotensin II type 1 receptor antagonism onbioavailability of nitric oxide in patients with coronary artery disease:role of superoxide dismutase. Circulation 2001;103:799–805.
101. Vita JA, Keaney JF Jr. Hormone replacement therapy and endothelialfunction: the exception that proves the rule? Arterioscler ThrombVasc Biol 2001;21:1867–9.
102. Brown NJ, Abbas A, Byrne D, Schoenhard JA, Vaughan DE.Comparative effects of estrogen and angiotensin-converting enzymeinhibition on plasminogen activator inhibitor-1 in healthy postmeno-pausal women. Circulation 2002;105:304–9.
103. Gerhard M, Walsh MW, Tawakol A, Haley EA, Creager SJ.Estradiol therapy combined with progesterone and endothelium-dependent vasodilation in postmenopausal women. Circulation 1998;98:1158–63.
104. Sorensen KE, Dorup I, Hermann AP, Mosekilde L. Combinedhormone replacement therapy does not protect women against theage-related decline in endothelium-dependent vasomotor function.Circulation 1998;97:1234–8.
1159JACC Vol. 42, No. 7, 2003 Widlansky et al.October 1, 2003:1149–60 Endothelial Dysfunction

105. Herrington DM, Espeland MA, Crouse JR III, et al. Estrogenreplacement and brachial artery flow-mediated vasodilation in olderwomen. Arterioscler Thromb Vasc Biol 2001;21:1955–61.
106. Women’s Health Initiative Study Group. Risks and benefits ofestrogen plus progestin in healthy postmenopausal women: principalresults from the Women’s Health Initiative randomized controlledtrial. JAMA 2002;288:321–33.
107. Hulley S, Grady D, Bush T, et al. Randomized trial of estrogen plusprogestin for secondary prevention of coronary heart disease inpostmenopausal women: Heart and Estrogen/progestin ReplacementStudy (HERS) research group. JAMA 1998;280:605–13.
108. Adams MR, McCredie R, Jessup W, Robinson J, Sullivan D,Celermajer DS. Oral L-arginine improves endothelium-dependentdilatation and reduces monocyte adhesion to endothelial cells inyoung men with coronary artery disease. Atherosclerosis 1997;129:261–9.
109. Lerman A, Burnett JCJ, Higano ST, McKinley LJ, Holmes DRJ.Long-term L-arginine supplementation improves small-vessel coro-nary endothelial function in humans. Circulation 1998;97:2123–8.
110. Heitzer T, Krohn K, Albers S, Meinertz T. Tetrahydrobiopterinimproves endothelium-dependent vasodilation by increasing nitricoxide activity in patients with type II diabetes mellitus. Diabetologia2000;43:1435–8.
111. Beckman JA, Goldfine AB, Gordon MB, Garrett LA, Creager MA.Inhibition of protein kinase C-beta prevents impaired endothelium-dependent vasodilation caused by hyperglycemia in humans. Circ Res2002;90:107–11.
112. Duffy SJ, Biegelsen ES, Holbrook M, et al. Iron chelation improvesendothelial function in patients with coronary artery disease. Circu-lation 2001;103:2799–804.
113. Chenevard R, Hurlimann D, Bechir M, et al. Selective COX-2inhibition improves endothelial function in coronary artery disease.Circulation 2003;107:405–9.
114. Bild DE, Bluemke DA, Burke GL, et al. Multi-ethnic study ofatherosclerosis: objectives and design. Am J Epidemiol 2002;156:871–81.
115. Kuvin JT, Patel AR, Sliney KA, et al. Assessment of peripheralvascular endothelial function with finger arterial pulse wave ampli-tude. Am Heart J 2003;146:168–74.
116. Gerhard-Herman M, Hurley S, Mitra D, Creager MA, Ganz P.Assessment of endothelial function (nitric oxide) at the tip of a finger(abstr). Circulation 2002;106:II170.
117. Bonetti PO, Pumper GM, Higano ST, Holmes DR, Lerman A.Reactive hyperemia peripheral arterial tonometry, a novel non-invasive index of peripheral vascular function, is attenuated inpatients with coronary endothelial dysfunction (abstr). Circulation2002;106:II579.
1160 Widlansky et al. JACC Vol. 42, No. 7, 2003Endothelial Dysfunction October 1, 2003:1149–60

CLINICAL RESEARCH Clinical Trials
Seven-Year Outcome in the RITA-2 Trial:Coronary Angioplasty Versus Medical TherapyRobert A. Henderson, FRCP, FESC,* Stuart J. Pocock, PHD,† Tim C. Clayton, MSC,†Rosemary Knight, RGN,† Keith A. A. Fox, FRCP, FESC,‡ Desmond G. Julian, FRCP, FESC,§Douglas A. Chamberlain, FRCP, FESC,� for the Second Randomized Intervention Treatment of Angina(RITA-2) Trial ParticipantsNottingham, London, Edinburgh, and Cardiff, United Kingdom
OBJECTIVES This study was designed to compare the long-term consequences of percutaneous translu-minal coronary angioplasty (PTCA) and continued medical treatment.
BACKGROUND The long-term effects of percutaneous coronary intervention need evaluating, especially incomparison with an alternative policy of continued medical treatment.
METHODS The Second Randomized Intervention Treatment of Angina (RITA-2) is a randomized trialof PTCA versus conservative (medical) care in 1,018 patients considered suitable for eithertreatment option. Information on clinical events, interventions, and symptoms is available fora median seven years follow-up.
RESULTS Death or myocardial infarction (MI) occurred in 73 (14.5%) PTCA patients and 63 (12.3%)medical patients (difference �2.2%, 95% confidence interval �2.0% to �6.4%, p � 0.21).There were 43 deaths in both groups, of which 41% were cardiac-related. Among patientsassigned PTCA 12.7% subsequently had coronary artery bypass grafts, and 14.5% requiredadditional non-randomized PTCA. Most of these re-interventions occurred within a year ofrandomization, and after two years the re-intervention rate was 2.3% per annum. In themedical group, 35.4% required myocardial revascularization: 15.0% in the first year and anannual rate of 3.6% after two years. An initial policy of PTCA was associated with improvedanginal symptoms and exercise times. These treatment differences narrowed over time, mainlybecause of coronary interventions in medical patients with severe symptoms.
CONCLUSIONS In RITA-2 an initial strategy of PTCA did not influence the risk of death or MI, but itimproved angina and exercise tolerance. Patients considered suitable for PTCA or medicaltherapy can be safely managed with continued medical therapy, but percutaneous interventionis appropriate if symptoms are not controlled. (J Am Coll Cardiol 2003;42:1161–70)© 2003 by the American College of Cardiology Foundation
The optimal management of patients with angina pectorisremains controversial, but options include anti-anginalmedication, percutaneous coronary intervention (PCI), orcoronary artery bypass surgery. Several randomized clinicaltrials have compared percutaneous and surgical methods of
See page 1171
myocardial revascularization, and some have reported long-term results (1–3). Overall, these trials suggest that percu-taneous intervention is slightly less effective at relievingangina than is coronary artery bypass surgery, but there is no
evidence that either revascularization strategy provides aprognostic advantage in the majority of patients.
For some patients with angina, revascularization is notconsidered essential for symptom relief or for prognosticreasons. Several small trials have compared percutaneousintervention with alternative medical treatment strategies insuch patients, but most have reported only limitedfollow-up data (4–8). A meta-analysis of data available in1998 concluded that percutaneous transluminal coronaryangioplasty (PTCA) provides superior relief of angina at thecost of more coronary artery bypass surgery, but it could notreliably estimate the effects of the two treatment strategieson the risk of death or myocardial infarction (MI) (9).
The second Randomized Intervention Treatment of An-gina (RITA-2) trial was designed to compare PTCA withcontinued medical treatment in patients in whom eitherstrategy was considered a clinically acceptable treatmentoption. The primary trial end point was the five-year rate ofdeath or non-fatal MI. The trial recruited 1,018 patients,and interim results have been published (10,11). In thisarticle we report extended follow-up of the RITA-2 patientsto a median seven years.
From the *Nottingham City Hospital, Nottingham, United Kingdom; †LondonSchool of Hygiene and Tropical Medicine, London, United Kingdom; ‡RoyalInfirmary, Edinburgh, United Kingdom; §London, United Kingdom; and �Pre-hospital Emergency Research Unit and Wales Heart Institute, University of WalesCollege of Medicine, Cardiff, United Kingdom. The trial was supported by grantsfrom the British Heart Foundation and Medical Research Council. Additionalsupport was provided by Advanced Cardiovascular Systems Inc (U.S.), InterventionLtd (U.K.), Cordis Ltd, Schneider (U.K.) and Nycomed Ltd.
Manuscript received September 13, 2002; revised manuscript received March 31,2003, accepted April 3, 2003.
Journal of the American College of Cardiology Vol. 42, No. 7, 2003© 2003 by the American College of Cardiology Foundation ISSN 0735-1097/03/$30.00Published by Elsevier Inc. doi:10.1016/S0735-1097(03)00951-3
METHODS
Trial design. The design of RITA-2 has been reportedpreviously (10). Patients were recruited at 20 centers in theU.K. and Ireland, and the ethics committee of each partic-ipating center approved the trial protocol. In brief, patientswith arteriographically proven coronary artery disease(CAD) were considered for the trial if the supervisingcardiologist thought that continued medical therapy andPTCA were both acceptable treatment options. Patientshad to be over 18 years of age, but there was no upper agelimit. Patients were not required to have current symptoms,but patients with multi-vessel disease, occluded coronaryarteries, or impaired left ventricular (LV) function werepotentially eligible for the trial. Patients with previousmyocardial revascularization, significant left main stem dis-ease, recent (within seven days) acute coronary syndrome,hemodynamically significant valve disease, or life-threatening non-cardiac disease likely to have a majorinfluence on survival were excluded. Patients in whomrevascularization was considered necessary for symptomrelief or for prognostic reasons were also ineligible.
Before randomization, a participating interventional car-diologist reviewed the coronary arteriogram of a potentiallyeligible patient and identified at least one significant coro-nary stenosis in a major epicardial vessel that could betreated by coronary angioplasty. Patients who satisfied theeligibility criteria and consented to participate were subse-quently randomized to initial treatment strategies of PTCAor continued medical management. Patients were stratifiedby center and by extent of disease (single or multi-vesseldisease).
The trial protocol required that patients assigned toPTCA underwent dilation of the target stenosis (or steno-ses) within three months of randomization. Stents and othercoronary interventional techniques were used only if theinitial balloon angioplasty result was unsatisfactory. Thechoice of medication after a randomized PTCA was notmandated, although clinicians were encouraged to discon-tinue anti-anginal drugs if a patient no longer had symp-toms of angina. Patients in the PTCA group underwentadditional coronary arteriography and revascularization pro-cedures if considered appropriate by the supervising clini-cian, with the objective of detecting and treating restenosis.
Patients randomized to an initial strategy of medicalmanagement were prescribed appropriate anti-anginal med-
ication for symptom relief. Coronary arteriography wasrepeated only for compelling clinical reasons, and myocar-dial revascularization procedures were reserved for patientswhose symptoms were not controlled by optimal anti-anginal medication (usually a beta-adrenoceptor blocker,with a calcium antagonist, and/or with long-acting nitratein maximally tolerated doses).Data collection. Patients were assessed at three months,six months, and yearly intervals after randomization. Re-search assistants at each participating center recorded trialdata on specially prepared forms.
The pre-defined primary trial end point was the five-yearrate of death and definite MI. An independent eventvalidation committee, unaware of treatment assignment,reviewed all available information on deaths and MIs. Thecause of death was classified as cardiac, other cardiovascular,or non-cardiovascular. Definite MI was diagnosed whennew pathological Q-waves appeared on a follow-up electro-cardiogram, or when a convincing clinical history wasassociated with electrocardiographic changes consistentwith non–Q-wave infarction and cardiac enzyme activityabove twice the upper limit of normal on at least tworelevant serum samples.
As previously reported, angina was assessed with theCanadian Cardiovascular Society classification and breath-lessness and physical activity were assessed by ordinal scales(10,12). Symptom-limited exercise tolerance tests werecarried out using the Bruce protocol at three and six monthsand one and three years after randomization. Left ventric-ular function was assessed from LV angiograms using a wallmotion score.Statistical analysis. A total of 1,018 patients were random-ized at 20 participating centers. All data were analyzed byintention to treat, using standard methods. The percentagesof patients with the primary end point of death or MI at fiveyears in each treatment group were compared using Kaplan-Meier estimates. Times to death and death/MI are pre-sented using Kaplan-Meier curves. The percentages ofpatients reporting other outcomes from follow-up inter-views were compared using chi-squared tests. Analysis ofco-variance was used to compare exercise time at threemonths and three years. Prognostic factors were determinedby forward stepwise regression modeling: for the outcome ofcardiac death or non-fatal MI, Cox regression was used, andfor angina grade 2� at five years, logistic regression wasused.
RESULTS
The 1,018 patients were randomized to coronary angio-plasty (n � 504) or continued medical treatment (n � 514)from July 1992 to May 1996. Follow-up to September 30,2001, is included in this report, the median follow-upperiod being seven years. Eighteen patients (1.8%) havebeen lost to follow-up. The five-year follow-up rate is99.1%.
Abbreviations and AcronymsCABG � coronary artery bypass graftCAD � coronary artery diseaseLV � left ventricularMI � myocardial infarctionPCI � percutaneous coronary interventionPTCA � percutaneous transluminal coronary angioplastyRITA � Randomized Intervention Treatment of
Angina
1162 Henderson et al. JACC Vol. 42, No. 7, 2003Seven-Year Outcome in RITA-2 October 1, 2003:1161–70

Baseline data and randomized PTCA. Detailed informa-tion on baseline comparability and the randomized PTCAhas been published earlier (10). In brief, 60% of patients hadsingle-vessel disease, 53% had angina grade 2 or worse, 18%were female, and the median age was 58 years. At random-ization 53% were receiving two or more anti-anginal drugs,13% were taking lipid-lowering medication, 47% had had aprevious MI, and 9% were treated for diabetes. The PTCAand medical treatment groups were similar with regard to allthese baseline features.
The intended randomized PTCA was performed on 471(93%) patients in the PTCA group, the median time fromrandomization to PTCA being five weeks. Angioplasty wasattempted in a mean 1.4 vessel segments per patient (means1.2, 1.6, and 1.9 segments for those with significant diseasein 1, 2, and 3 epicardial vessels, respectively), of which 93%were successfully dilated. The randomized PTCA wascomplicated by emergency coronary artery bypass graft(CABG) in seven patients, non-fatal MI in seven patients(of whom 4 developed new electrocardiographic Q-waves),and one procedure-related death. Patient recruitment beganbefore the widespread use of coronary stents, which wereimplanted during 44 (9%) randomized PTCAs. Of these,32 occurred in the 160 patients randomized to PTCAduring 1995 and 1996, the last 17 months of patientrecruitment.Death and MI. To date, 43 patients have died in bothtreatment groups (Table 1). The survival plot (Fig. 1A)reveals comparable mortality between groups over eightyears of follow-up. At five years follow-up, the mortalityrate was 4.6% and 4.7% in the PTCA and medical groups,respectively (difference �0.1%, 95% confidence interval[CI] �2.7% to �2.5%).
Almost half the deaths were from non-cardiovascularcauses. Although there were fewer cardiac deaths in thePTCA group—13 PTCA versus 22 medical—this differ-ence is not statistically significant. Three of the sevencardiovascular deaths in the PTCA group were due tostroke.
To date, 32 and 23 patients in the PTCA and medicalgroups respectively have had a definite non-fatal MI (Table1), five of whom (2 PTCA, 3 medical) have subsequentlydied. Thus, death or definite MI has occurred in 73 PTCAand 63 medical patients. The time-to-event plot (Fig. 1B)reveals an excess risk of this combined end point in thePTCA group in the first two months after randomization,which can be attributed to the eight procedure-relatedevents mentioned earlier. Thereafter, the plots run parallelwith a steady rate of end points up to eight years offollow-up. If the eight events related to the randomizedPTCA are discounted, the subsequent rates of death ordefinite MI in the PTCA and medical groups are 2.0 and1.8 per 100 patient-years of follow-up, respectively (differ-ence �0.2, 95% CI from �0.5 to �0.8).
The pre-defined primary end point of death or definite
Table 1. Deaths, MIs, and New Interventions During a MedianSeven Year Follow-Up
OutcomePTCA
(n � 504)Medical
(n � 514)
DeathsCardiac 13 22Other cardiovascular 7 2Non-cardiovascular 23 19
All causes 43 43Definite non-fatal MI
Related to randomized PTCA 7 –Related to other intervention 4 3Other 21 20
Total 32 23Death or definite MI (primary end point) 73 63Cardiac death or definite MI 44 42Patients with non-randomized
interventions (total number ofprocedures in brackets)
CABG 64 (65) 63 (63)Non-randomized PTCA 86 (106) 139 (174)CABG and/or non-randomized PTCA 137 (171) 182 (237)Coronary arteriography 191 (278) 182 (244)
CABG � coronary artery bypass graft; MI � myocardial infarction; PTCA �percutaneous transluminal coronary angioplasty.
Figure 1. Cumulative risk of (A) death and (B) death or definite non-fatalmyocardial infarction (MI). Bars show 95% confidence interval. Numbersshow patients at risk of death or non-fatal MI. PTCA � percutaneoustransluminal coronary angioplasty.
1163JACC Vol. 42, No. 7, 2003 Henderson et al.October 1, 2003:1161–70 Seven-Year Outcome in RITA-2
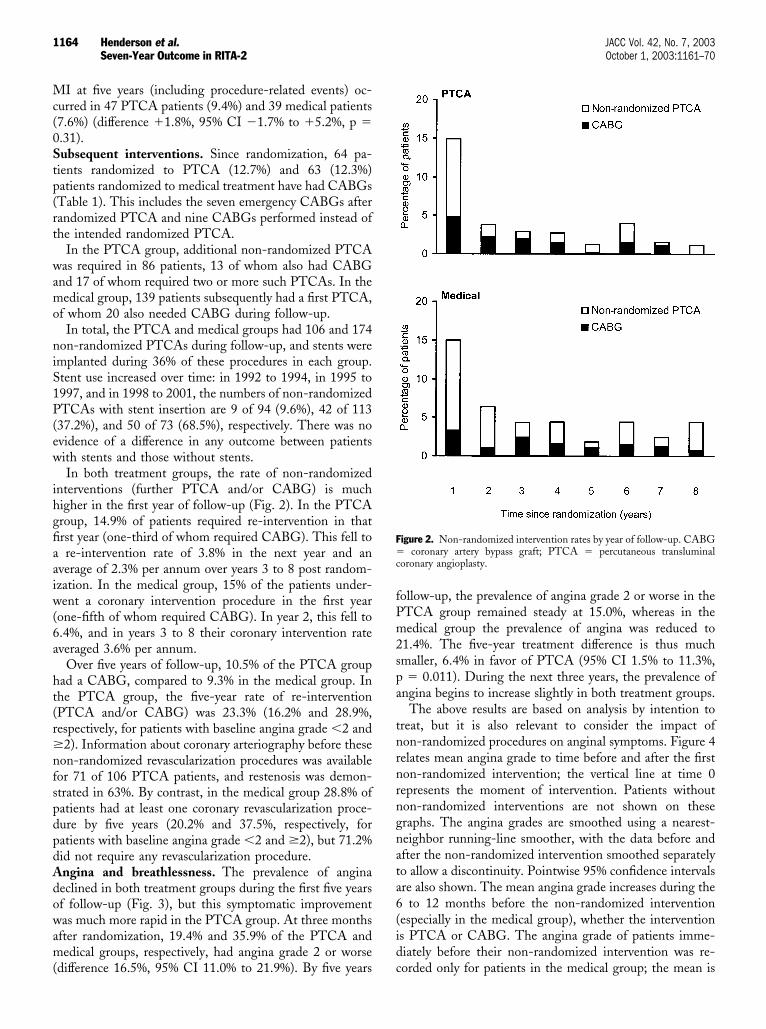
MI at five years (including procedure-related events) oc-curred in 47 PTCA patients (9.4%) and 39 medical patients(7.6%) (difference �1.8%, 95% CI �1.7% to �5.2%, p �0.31).Subsequent interventions. Since randomization, 64 pa-tients randomized to PTCA (12.7%) and 63 (12.3%)patients randomized to medical treatment have had CABGs(Table 1). This includes the seven emergency CABGs afterrandomized PTCA and nine CABGs performed instead ofthe intended randomized PTCA.
In the PTCA group, additional non-randomized PTCAwas required in 86 patients, 13 of whom also had CABGand 17 of whom required two or more such PTCAs. In themedical group, 139 patients subsequently had a first PTCA,of whom 20 also needed CABG during follow-up.
In total, the PTCA and medical groups had 106 and 174non-randomized PTCAs during follow-up, and stents wereimplanted during 36% of these procedures in each group.Stent use increased over time: in 1992 to 1994, in 1995 to1997, and in 1998 to 2001, the numbers of non-randomizedPTCAs with stent insertion are 9 of 94 (9.6%), 42 of 113(37.2%), and 50 of 73 (68.5%), respectively. There was noevidence of a difference in any outcome between patientswith stents and those without stents.
In both treatment groups, the rate of non-randomizedinterventions (further PTCA and/or CABG) is muchhigher in the first year of follow-up (Fig. 2). In the PTCAgroup, 14.9% of patients required re-intervention in thatfirst year (one-third of whom required CABG). This fell toa re-intervention rate of 3.8% in the next year and anaverage of 2.3% per annum over years 3 to 8 post random-ization. In the medical group, 15% of the patients under-went a coronary intervention procedure in the first year(one-fifth of whom required CABG). In year 2, this fell to6.4%, and in years 3 to 8 their coronary intervention rateaveraged 3.6% per annum.
Over five years of follow-up, 10.5% of the PTCA grouphad a CABG, compared to 9.3% in the medical group. Inthe PTCA group, the five-year rate of re-intervention(PTCA and/or CABG) was 23.3% (16.2% and 28.9%,respectively, for patients with baseline angina grade �2 and�2). Information about coronary arteriography before thesenon-randomized revascularization procedures was availablefor 71 of 106 PTCA patients, and restenosis was demon-strated in 63%. By contrast, in the medical group 28.8% ofpatients had at least one coronary revascularization proce-dure by five years (20.2% and 37.5%, respectively, forpatients with baseline angina grade �2 and �2), but 71.2%did not require any revascularization procedure.Angina and breathlessness. The prevalence of anginadeclined in both treatment groups during the first five yearsof follow-up (Fig. 3), but this symptomatic improvementwas much more rapid in the PTCA group. At three monthsafter randomization, 19.4% and 35.9% of the PTCA andmedical groups, respectively, had angina grade 2 or worse(difference 16.5%, 95% CI 11.0% to 21.9%). By five years
follow-up, the prevalence of angina grade 2 or worse in thePTCA group remained steady at 15.0%, whereas in themedical group the prevalence of angina was reduced to21.4%. The five-year treatment difference is thus muchsmaller, 6.4% in favor of PTCA (95% CI 1.5% to 11.3%,p � 0.011). During the next three years, the prevalence ofangina begins to increase slightly in both treatment groups.
The above results are based on analysis by intention totreat, but it is also relevant to consider the impact ofnon-randomized procedures on anginal symptoms. Figure 4relates mean angina grade to time before and after the firstnon-randomized intervention; the vertical line at time 0represents the moment of intervention. Patients withoutnon-randomized interventions are not shown on thesegraphs. The angina grades are smoothed using a nearest-neighbor running-line smoother, with the data before andafter the non-randomized intervention smoothed separatelyto allow a discontinuity. Pointwise 95% confidence intervalsare also shown. The mean angina grade increases during the6 to 12 months before the non-randomized intervention(especially in the medical group), whether the interventionis PTCA or CABG. The angina grade of patients imme-diately before their non-randomized intervention was re-corded only for patients in the medical group; the mean is
Figure 2. Non-randomized intervention rates by year of follow-up. CABG� coronary artery bypass graft; PTCA � percutaneous transluminalcoronary angioplasty.
1164 Henderson et al. JACC Vol. 42, No. 7, 2003Seven-Year Outcome in RITA-2 October 1, 2003:1161–70

marked with a triangle (Fig. 4) and is consistent with theprior trend. After the non-randomized intervention, anginagrade improves rapidly, especially where a CABG was done(Figs. 4B and 4D).
Patients in the PTCA group had less use of anti-anginaldrugs up to eight years follow-up compared with themedical group. For instance, at five years 70% and 83% ofthe PTCA and medical groups, respectively, were receivingat least one anti-anginal drug, 23% and 34% were receivingtwo drugs, and 8% and 11% were receiving triple-drugtherapy. Anti-anginal treatment included a beta-blocker in42% of the PTCA group and 53% of the medical group. Inthe PTCA group, 92% were taking aspirin, compared with91% of the medical group. The use of HMG CoA reductaseinhibitors increased over time, and at five years 51% of thePTCA group and 47% of the medical group were prescribedlipid-lowering medication. Angiotensin-converting enzymeinhibitors were prescribed for 20% of the PTCA group and17% of the medical group.
The highly significant treatment difference in prevalenceof breathlessness in early follow-up had largely disappearedafter a few years: 42% versus 57% breathless at three months(p � 0.001) in the PTCA and medical groups, respectively,compared to 46% versus 50% at three years (p � 0.30).
Similarly the mean difference in Bruce exercise treadmilltime at three months, �37 s in favor of PTCA based on 864patients (95% CI 21 to 52 s), had reduced to �25 s meanbenefit based on 749 patients (95% CI 6 to 44 s) by threeyears follow-up.Prognostic factors. In determining which patient baselinefactors are linked to subsequent prognosis we consideredtwo outcomes:
1) The combined incidence of cardiac death and definitenon-fatal MI, excluding the eight such events related to
randomized PTCA, since they are likely to have a differentetiology. Thus 78 patients experienced this outcome.
2) The presence of angina grade 2 or worse five years afterrandomization: this affected 173 of 948 patients seen atfive years.
For each outcome the following baseline factors wereconsidered: angina grade, unstable angina in the past threemonths, number of anti-anginal drugs, breathlessness grade,exercise treadmill time, age, gender, previous MI, treatmentfor diabetes mellitus (with diet, drugs, or insulin), treatmentfor hypertension, blood pressure, serum cholesterol, weight,height, body mass index, smoking history, electrocardio-graphic abnormality, LV function score, number of diseasedvessels, and �50% stenosis in the proximal left anteriordescending or other proximal vessel. By using forwardstepwise regression modeling procedures the predictivemodels shown in Table 2 were derived.
For cardiac death and non-fatal MI, angina grade atrandomization was the strongest predictor. Patients withboth proximal left anterior descending and at least one otherdiseased proximal vessel (i.e., �50% stenosis) had an esti-mated three-fold increase in risk, but there were only 71patients in this category. There was no treatment differencein risk after adjusting for these two factors.
For prevalence of angina grade 2� after five years, thebaseline exercise time and breathlessness at baseline werestrongly predictive. Patients with more severe angina atbaseline also had an increased risk; but angina grade wasstrongly associated with breathlessness and exercise time,and after taking these variables into account, baseline anginagrade was less independently predictive of outcome. Afteradjusting for these three factors, there remained a 33% oddsreduction in angina at five years for PTCA versus medicaltreatment (p � 0.031).
Figure 3. Prevalence of angina over time at baseline (base), three, and six months, and yearly intervals after randomization. P � coronary angioplasty group;M � medical group.
1165JACC Vol. 42, No. 7, 2003 Henderson et al.October 1, 2003:1161–70 Seven-Year Outcome in RITA-2

There was a trend for the 90 patients with diabetesmellitus to be at greater risk of death or MI (hazard ratio1.17, 95% CI 0.56 to 2.43) or angina grade 2� duringfollow-up (odds ratio 1.43, 95% CI 0.80 to 2.58), but therewas no evidence of an interaction between diabetes andtreatment for these two outcomes. Other subgroup analyseswere explored for each of the baseline variables listed above,but for neither outcome were there any statistically signifi-
cant interactions between treatment group and baselinefactors.
DISCUSSION
The RITA-2 trial provides the only currently availablerandomized evidence comparing the long-term conse-quences of PCI and medical treatment in patients with
Figure 4. Mean angina grades before and after non-randomized intervention. Panels A and B show data for the percutaneous transluminal coronaryangioplasty (PTCA) group. Panels C and D show data for the medical group. Lines are smoothed averages and 95% confidence intervals. The circles showindividual data points. Continued on next page.
1166 Henderson et al. JACC Vol. 42, No. 7, 2003Seven-Year Outcome in RITA-2 October 1, 2003:1161–70

angina. Over a median seven years follow-up, we havedemonstrated that initial policies of PTCA and medicaltherapy in patients considered suitable for either treatmentare comparable with regard to risk of death and non-fatalMI, but an initial policy of PTCA was associated with alower prevalence of angina and improved exercise tolerance.
The patients in our trial were selected from a large groupof patients undergoing coronary arteriography and rangedfrom patients with no angina and single-vessel disease tothose with severe symptoms and advanced coronary disease
(10). Nevertheless our patients were at low cardiovascularrisk, with a mortality of �1% per annum in both groups.The trial results therefore cannot be generalized to allpatients undergoing PCI but are relevant to a substantialgroup of patients for whom optimal treatment has beenuncertain and for whom percutaneous intervention or con-tinued medical therapy both seem appropriate.
Other trials of coronary angioplasty versus medical ther-apy (4–8) provide important additional information but aretoo small to reliably estimate the effects of the two treatment
Figure 4 Continued. For the medical group (C and D), the triangle indicates angina grade immediately before non-randomized intervention. CABG �coronary artery bypass graft.
1167JACC Vol. 42, No. 7, 2003 Henderson et al.October 1, 2003:1161–70 Seven-Year Outcome in RITA-2
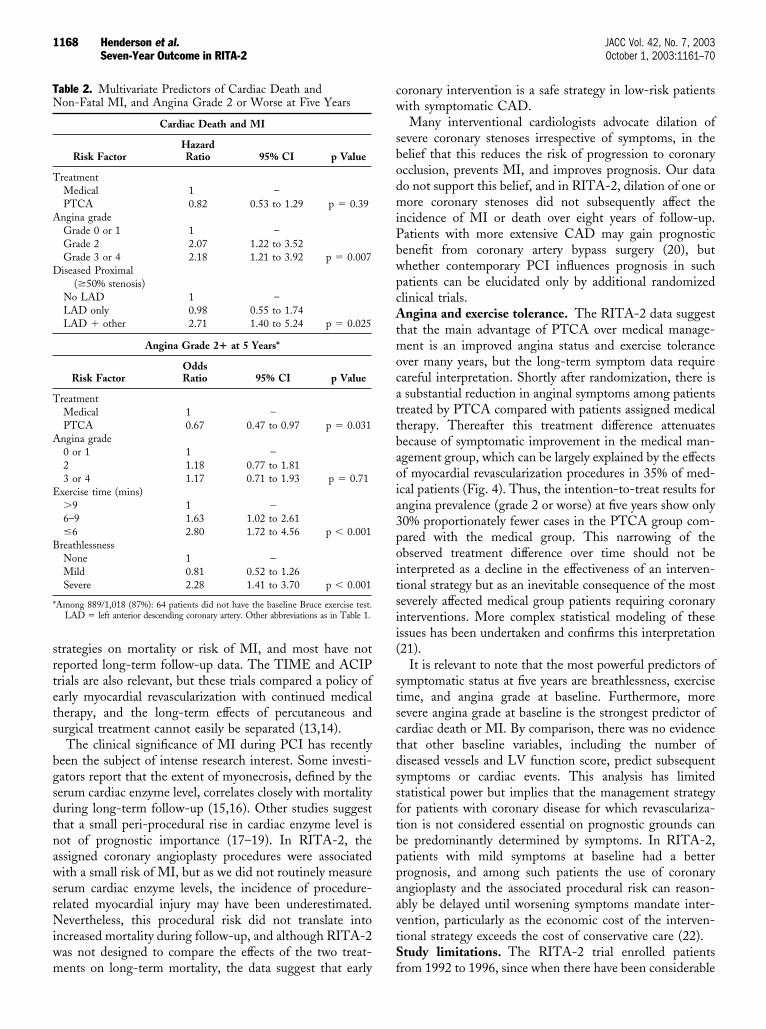
strategies on mortality or risk of MI, and most have notreported long-term follow-up data. The TIME and ACIPtrials are also relevant, but these trials compared a policy ofearly myocardial revascularization with continued medicaltherapy, and the long-term effects of percutaneous andsurgical treatment cannot easily be separated (13,14).
The clinical significance of MI during PCI has recentlybeen the subject of intense research interest. Some investi-gators report that the extent of myonecrosis, defined by theserum cardiac enzyme level, correlates closely with mortalityduring long-term follow-up (15,16). Other studies suggestthat a small peri-procedural rise in cardiac enzyme level isnot of prognostic importance (17–19). In RITA-2, theassigned coronary angioplasty procedures were associatedwith a small risk of MI, but as we did not routinely measureserum cardiac enzyme levels, the incidence of procedure-related myocardial injury may have been underestimated.Nevertheless, this procedural risk did not translate intoincreased mortality during follow-up, and although RITA-2was not designed to compare the effects of the two treat-ments on long-term mortality, the data suggest that early
coronary intervention is a safe strategy in low-risk patientswith symptomatic CAD.
Many interventional cardiologists advocate dilation ofsevere coronary stenoses irrespective of symptoms, in thebelief that this reduces the risk of progression to coronaryocclusion, prevents MI, and improves prognosis. Our datado not support this belief, and in RITA-2, dilation of one ormore coronary stenoses did not subsequently affect theincidence of MI or death over eight years of follow-up.Patients with more extensive CAD may gain prognosticbenefit from coronary artery bypass surgery (20), butwhether contemporary PCI influences prognosis in suchpatients can be elucidated only by additional randomizedclinical trials.Angina and exercise tolerance. The RITA-2 data suggestthat the main advantage of PTCA over medical manage-ment is an improved angina status and exercise toleranceover many years, but the long-term symptom data requirecareful interpretation. Shortly after randomization, there isa substantial reduction in anginal symptoms among patientstreated by PTCA compared with patients assigned medicaltherapy. Thereafter this treatment difference attenuatesbecause of symptomatic improvement in the medical man-agement group, which can be largely explained by the effectsof myocardial revascularization procedures in 35% of med-ical patients (Fig. 4). Thus, the intention-to-treat results forangina prevalence (grade 2 or worse) at five years show only30% proportionately fewer cases in the PTCA group com-pared with the medical group. This narrowing of theobserved treatment difference over time should not beinterpreted as a decline in the effectiveness of an interven-tional strategy but as an inevitable consequence of the mostseverely affected medical group patients requiring coronaryinterventions. More complex statistical modeling of theseissues has been undertaken and confirms this interpretation(21).
It is relevant to note that the most powerful predictors ofsymptomatic status at five years are breathlessness, exercisetime, and angina grade at baseline. Furthermore, moresevere angina grade at baseline is the strongest predictor ofcardiac death or MI. By comparison, there was no evidencethat other baseline variables, including the number ofdiseased vessels and LV function score, predict subsequentsymptoms or cardiac events. This analysis has limitedstatistical power but implies that the management strategyfor patients with coronary disease for which revasculariza-tion is not considered essential on prognostic grounds canbe predominantly determined by symptoms. In RITA-2,patients with mild symptoms at baseline had a betterprognosis, and among such patients the use of coronaryangioplasty and the associated procedural risk can reason-ably be delayed until worsening symptoms mandate inter-vention, particularly as the economic cost of the interven-tional strategy exceeds the cost of conservative care (22).Study limitations. The RITA-2 trial enrolled patientsfrom 1992 to 1996, since when there have been considerable
Table 2. Multivariate Predictors of Cardiac Death andNon-Fatal MI, and Angina Grade 2 or Worse at Five Years
Cardiac Death and MI
Risk FactorHazardRatio 95% CI p Value
TreatmentMedical 1 –PTCA 0.82 0.53 to 1.29 p � 0.39
Angina gradeGrade 0 or 1 1 –Grade 2 2.07 1.22 to 3.52Grade 3 or 4 2.18 1.21 to 3.92 p � 0.007
Diseased Proximal(�50% stenosis)
No LAD 1 –LAD only 0.98 0.55 to 1.74LAD � other 2.71 1.40 to 5.24 p � 0.025
Angina Grade 2� at 5 Years*
Risk FactorOddsRatio 95% CI p Value
TreatmentMedical 1 –PTCA 0.67 0.47 to 0.97 p � 0.031
Angina grade0 or 1 1 –2 1.18 0.77 to 1.813 or 4 1.17 0.71 to 1.93 p � 0.71
Exercise time (mins)�9 1 –6–9 1.63 1.02 to 2.61�6 2.80 1.72 to 4.56 p � 0.001
BreathlessnessNone 1 –Mild 0.81 0.52 to 1.26Severe 2.28 1.41 to 3.70 p � 0.001
*Among 889/1,018 (87%): 64 patients did not have the baseline Bruce exercise test.LAD � left anterior descending coronary artery. Other abbreviations as in Table 1.
1168 Henderson et al. JACC Vol. 42, No. 7, 2003Seven-Year Outcome in RITA-2 October 1, 2003:1161–70

advances in both medical and interventional treatment. Theuse of coronary stents has increased markedly, and develop-ments in stent design and deployment techniques, togetherwith adjunctive use of clopidogrel and glycoprotein IIb/IIIareceptor antagonists, have all contributed to improvementsin outcome after PCI (23,24). Randomized trials of multi-vessel stenting versus CABG, such as ARTS (25),ERACI-2 (26), and SOS (27) provide valuable information,but their follow-up period is still relatively short. Theintroduction of drug-coated stents has been heralded as amajor advance, but there are no data concerning thelong-term effects of this new technology (28). Otherchanges in practice include increasing use of hydroxymethylglutaryl coenzyme A (HMG-CoA) reductase inhibitors(29,30), angiotensin-converting enzyme inhibitors (31), andthienopyridines (32) in patients with CAD.
The long-term prognostic and symptomatic implicationsof all these developments for patients considered eligible forPCI remain largely unexplored to date. The Clinical Out-come Utilizing Revascularization and Aggressive DrugEvaluation (COURAGE) trial is testing the hypothesis inmore than 3,000 patients that optimal catheter-based cor-onary revascularization combined with intensive medicaltherapy is superior to intensive medical therapy alone (33).Further data will be available from the BARI-2D trial, acomparison of medical therapy and revascularization inpatients with type 2 diabetes mellitus. These trials will beimportant contributions; but recruitment in both trials isongoing, and hence, long-term results will not be known forseveral years. Meantime RITA-2 provides the best currentlyavailable insight into outcome many years after initialpolicies of percutaneous intervention or conservative man-agement in patients with angina.Conclusions. In conclusion, we have demonstrated thatPTCA reduces anginal symptoms and improves exercisetolerance in the long-term for patients who are consideredsuitable for treatment by percutaneous intervention or bycontinued medical therapy. However, among such patientsPTCA does not appear to influence the disease naturalhistory favorably with regard to risk of death and non-fatalMI. Treatment choice can therefore be determined princi-pally by symptom status. Patients with mild to moderateangina can be safely managed with continued medicaltherapy, but percutaneous intervention is appropriate ifsymptoms are not controlled by medication. Other trialevidence is needed to update these long-term findingsregarding percutaneous interventional treatment, in thelight of increased use of coronary stents and recent devel-opments in medical treatments.
AcknowledgmentsWe thank the 1,018 patients who consented to participatein the trial. We greatly value the work of past RITA-2 trialcoordinators (Bronwen Youard [1992 to 1996] and ClaireMarley [1996 to 1998]) and RITA-2 trialists. We alsothank Ian White for calculating the data analysis for Figure
4. The randomization service was provided by the RoyalFree Hospital coronary care unit.
We particularly acknowledge the work and contributionof Rosemary Carey, who died on June 6, 2003.
Reprint requests and correspondence: Dr. Robert A. Hender-son, Department of Cardiology, Nottingham City Hospital,Hucknall Road, Nottingham NG5 1PB, United Kingdom. E-mail: [email protected].
REFERENCES
1. Henderson RA, Pocock SJ, Sharp SJ, et al. Long-term results ofRITA-1 trial: clinical and cost comparisons of coronary angioplastyand coronary-artery bypass grafting. Lancet 1998;352:1419–25.
2. BARI Investigators. Seven-year outcome in the Bypass AngioplastyRevascularization Investigation (BARI) by treatment and diabeticstatus. J Am Coll Cardiol 2000;35:1122–9.
3. King SB, Kosinski AS, Guyton RA, Lembo NJ, Weintraub WS.Eight-year mortality in the Emory Angioplasty versus Surgery Trial(EAST). J Am Coll Cardiol 2000;35:1116–21.
4. Folland ED, Hartigan PM, Parisi AF. Percutaneous transluminalcoronary angioplasty versus medical therapy for stable angina pectoris:outcomes for patients with double-vessel versus single-vessel coronaryartery disease in a Veterans Affairs Cooperative randomized trial. J AmColl Cardiol 1997;29:1505–11.
5. Hartigan PM, Giacomini JC, Folland ED, Parisi AF. Two- tothree-year follow-up of patients with single-vessel coronary arterydisease randomized to coronary angioplasty or medical therapy (resultsof a VA cooperative study). Am J Cardiol 1998;82:1445–50.
6. Hueb WA, Soares PR, Almeida DO, et al. Five-year follow-up of theMedicine, Angioplasty, or Surgery Study (MASS): a prospective,randomized trial of medical therapy, balloon angioplasty, or bypasssurgery for single proximal left anterior descending coronary arterystenosis. Circulation 1999;100 Suppl:II107–13.
7. Pitt B, Waters D, Brown WV, et al. Aggressive lipid-lowering therapycompared with angioplasty in stable coronary artery disease. N EnglJ Med 1999;341:70–6.
8. Dakik HA, Kleiman NS, Farmer JA, et al. Intensive medical therapyversus coronary angioplasty for suppression of myocardial ischemia insurvivors of acute myocardial infarction: a prospective, randomizedpilot study. Circulation 1998;98:2017–23.
9. Bucher HC, Hengstler P, Schindler C, Guyatt GH. Percutaneoustransluminal coronary angioplasty versus medical treatment for non-acute coronary heart disease: meta-analysis of randomised controlledtrials. BMJ 2000;321:73–7.
10. RITA-2 Trial Participants. Coronary angioplasty versus medicaltherapy for angina: the second Randomised Intervention Treatment ofAngina (RITA-2) trial. Lancet 1997;350:461–8.
11. Pocock SJ, Henderson RA, Clayton T, Lyman GH, Chamberlain DA.Quality of life after coronary angioplasty or continued medical treat-ment for angina: three-year follow-up in the RITA-2 trial. J Am CollCardiol 2000;35:907–14.
12. Campeau L. Grading of angina pectoris (letter). Circulation 1976;54:522–3.
13. TIME Investigators. Trial of invasive versus medical therapy in elderlypatients with chronic symptomatic coronary-artery disease (TIME): arandomised trial. Lancet 2001;358:951–7.
14. Davies RF, Goldberg AD, Forman S, et al. Asymptomatic cardiacischaemia pilot (ACIP) study two-year follow-up. Outcomes ofpatients randomized to initial strategies of medical therapy versusrevascularization. Circulation 1997;95:2037–43.
15. Califf RM, Abdelmeguid AE, Kuntz RE, et al. Myonecrosis afterrevascularization procedures. J Am Coll Cardiol 1998;31:241–51.
16. Abdelmeguid AE, Topol EJ, Whitlow PL, Sapp SK, Ellis SG.Significance of mild transient release of creatine kinase-MB fractionafter percutaneous coronary interventions. Circulation 1996;94:1528–36.
1169JACC Vol. 42, No. 7, 2003 Henderson et al.October 1, 2003:1161–70 Seven-Year Outcome in RITA-2

17. Stone GW, Mehran R, Dangas G, Lansky AJ, Kornowski R, LeonMB. Differential impact on survival of electrocardiographic Q-waveversus enzymatic myocardial infarction after percutaneous interven-tion: a device-specific analysis of 7147 patients. Circulation 2001;104:642–7.
18. Saucedo JF, Mehran R, Dangas G, et al. Long-term clinical eventsfollowing creatine kinase myocardial band isoenzyme elevation aftersuccessful coronary stenting. J Am Coll Cardiol 2000;35:1134–41.
19. Kini A, Marmur JD, Kini S, et al. Creatine kinase-MB elevation aftercoronary intervention correlates with diffuse atherosclerosis, and low-to-medium level elevation has a benign clinical course: implications forearly discharge after coronary intervention. J Am Coll Cardiol 1999;34:663–71.
20. Yusuf S, Zucker D, Peduzzi P, et al. Effect of coronary artery bypassgraft surgery on survival: overview of 10-year results from randomisedtrials by the Coronary Artery Bypass Graft Surgery Trialists Collab-oration. Lancet 1994;344:563–70.
21. White IR, Carpenter J, Pocock SJ, Henderson RA. Adjusting treat-ment comparisons to account for non-randomised interventions: anexample from an angina trial. Stat Med 2003;22:781–93.
22. Sculpher MJ, Smith DH, Clayton T, et al. Coronary angioplastyversus medical therapy for angina. Health service costs based on thesecond Randomised Intervention Treatment of Angina (RITA-2)trial. Eur Heart J 2002;23:1291–1300.
23. Bhatt DL, Bertrand ME, Berger PB, et al. Meta-analysis of random-ized and registry comparisons of ticlopidine with clopidogrel afterstenting. J Am Coll Cardiol 2002;39:9–14.
24. Topol EJ, Mark DB, Lincoff AM, et al. Outcomes at 1 year andeconomic implications of platelet glycoprotein IIb/IIIa blockade inpatients undergoing coronary stenting: results from a multicentrerandomised trial. Lancet 1999;354:2019–24.
25. Serruys PW, Unger F, Sousa JE, et al. Comparison of coronary-arterybypass surgery and stenting for the treatment of multivessel disease.N Engl J Med 2001;344:1117–24.
26. Rodriguez A, Bernardi V, Navia J, et al. Coronary angioplasty withstenting versus coronary bypass surgery in patients with multiple-vesseldisease (ERACI II): 30-day and one-year follow-up results. J Am CollCardiol 2001;37:51–8.
27. The SOS Investigators. Coronary artery bypass surgery versus percu-taneous coronary intervention with stent implantation in patients withmultivessel coronary artery disease (the Stent or Surgery trial). Lancet2002;360:965–70.
28. Morice MC, Serruys PW, Sousa JE, et al. A randomized comparisonof a sirolimus-eluting stent with a standard stent for coronary revas-cularization. N Engl J Med 2002;346:1773–80.
29. Scandinavian Simvastatin Survival Study Group. Randomised trial ofcholesterol lowering in 4444 patients with coronary heart disease: theScandinavian simvastatin survival study (4S). Lancet 1994;344:1383–9.
30. LIPID Study Group. Prevention of cardiovascular events and deathwith pravastatin in patients with coronary heart disease and a broadrange of initial cholesterol levels. N Engl J Med 1998;339:1349–57.
31. Yusuf S, Sleight P, Pogue J, Bosch J, Davies R, Dugenais G. TheHOPE Investigators. Effects of an angiotensin converting enzymeinhibitor, ramipril, on cardiovascular events in high-risk patients.N Engl J Med 2000;342:145–53.
32. CURE Investigators. Effects of clopidogrel in addition to aspirin inpatients with acute coronary syndromes without ST-segment eleva-tion. N Engl J Med 2001;345:494–502.
33. Boden W, O’Rourke R. Clinical outcome utilizing revascularizationand aggressive drug evaluation. The COURAGE trial. Available at:http://www.cardiosource.com/trials/. Accessed September 6, 2002.
APPENDIX
For a complete list of participants in the RITA-2 trial,please see the October 1, 2003, issue of JACC at www.cardiosource.com/jacc.html.
1170 Henderson et al. JACC Vol. 42, No. 7, 2003Seven-Year Outcome in RITA-2 October 1, 2003:1161–70

EDITORIAL COMMENT
Dilate or Defer?View of a Skeptic*Spencer B. King III, MD, MACCAtlanta, Georgia
Coronary angioplasty was developed by Andreas Gruentzigas a less invasive method to alleviate ischemia and thedebilitating angina it causes. The introduction of balloondilation and the subsequent improvements, especially stent-ing, is a resounding success story in medicine. Bypasssurgery has been safely avoided as demonstrated in manyrandomized trials. Although subsets of patients with exten-sive disease, especially those with diabetes, have fared betterwith surgery, angioplasty and stenting have far surpassedsurgery as the most frequently performed revascularizationprocedures.
See page 1161
Many patients with coronary artery disease do not havedebilitating symptoms, and the data to support revascular-ization in these have undergone less scrutiny. The absenceof severe symptoms does not assure a good prognosis, andthe extent of coronary artery disease, the magnitude ofischemia, and left ventricular function define patients whohave an improved prognosis with surgery and probably (byinference) percutaneous intervention. There are, however,many patients without refractory symptoms who lack theprognostic indicators mandating revascularization. Many ofthese are undergoing percutaneous interventions all over theworld and, yet, evidence for the true value of that approachhas been sparse.
The Randomized Treatment of Angina (RITA)-2 trialwas designed to compare the strategy of performing percu-taneous transluminal coronary angioplasty (PTCA) or med-ical therapy alone on patients who were judged eligible foreither approach. The primary end point was death ormyocardial infarction (MI) at five years. In this issue of theJournal, Henderson et al. (1) report the results: the primaryend point, death or MI, was not different, and death alonewas not different (43 in each group). The need for subse-quent bypass surgery was not different. Repeat percutaneousintervention was more in the patients who did not receive itin the first place, but that difference was not great, 17% ofthe medical group and 27% in the PTCA group at five years.Subsequent revascularization (percutaneous coronary inter-vention [PCI] or coronary artery bypass grafting [CABG])was used in 23.3% of the PTCA and 28.8% of the surgery
patients. As reported by Henderson et al. (1), angina wasimproved, especially during the first year; however, thatdifference narrowed over time due to the performance ofPCI in symptomatic patients in the medical group. Whywas the outcome so disappointing for PTCA? Many willdismiss this study as dated. “It is so 90s.” This may be true.Let this skeptic examine the evidence.
The skeptic: “This is a low-risk group.” The overallmortality at five years of 4.6% in the PTCA group and 4.7%in the medical group would not argue for an abundance ofhigh-risk features. Sixty percent of the patients had single-vessel disease at baseline. The National Heart, Lung, andBlood Institute Dynamic registry of PCI in high volumecenters was composed of one-vessel disease (40.6%), two-vessel disease (32.3%), and three-vessel (26.8%), and asingle lesion was treated in 68.2% of these cases (2). So, arethe lesions treated in this study markedly different fromthose in elective patients, without the exclusions listed inthis trial, who are undergoing PCI today? I suspect not.
The skeptic: “This is old technology, results would bemuch better today.” Stenting was used in this trial only tobail out complications of PTCA. Emergency surgery wasused in 1.5% (7 of 471), which is not an unusually highnumber even in the stent era. In the NHLBI Dynamicregistry, it has been 1.1% (2).
The skeptic: “Surely stenting has a better outcome thanplain old balloon angioplasty.” The findings of a recentmeta-analysis of 29 trials of routine stenting versus balloonangioplasty and stenting only for complications or residualstenosis may be surprising. Death, death or MI, andsubsequent coronary bypass surgery were not different (3).Repeat PCI was more common in the balloon angioplastywith provisional stenting group, but the absolute differencewas only 5 patients per 100 treated. Stenting was used morecommonly in the control group in these trials, but thealmost identical death, MI, and CABG rates by treatmentgroup are reminiscent of the present study. Routine stentingmay have changed the primary outcome of this trial, but theevidence to assume that is lacking.
The skeptic: “English patients will put up with anything.”American colleagues may feel that the subjects of this trialwill keep the proverbial “stiff upper lip” and que passively forstaggering doses of anti-anginal medications to combat theirangina. (English colleagues in turn may feel that Americanshave the “princess and the pea” syndrome and will be dilatedat the slightest twinge or any hint of ischemia). Medicalsystems are different, but the consumption of antianginalswas not dramatically different between these treatmentgroups. At all time points there was more angina in themedical group, and this may have been reduced by moreaggressive interventions. However, the absence of moreinterventions in the medical group did not seem to adverselyaffect the primary end point of death or MI.
The skeptic: “It is true that the use of beta-blockers,angiotensin-converting enzyme inhibitors, lipid-lowering
*Editorials published in the Journal of the American College of Cardiology reflect theviews of the authors and do not necessarily represent the views of JACC or theAmerican College of Cardiology.
From the Fuqua Heart Center, Atlanta, Georgia.
Journal of the American College of Cardiology Vol. 42, No. 7, 2003© 2003 by the American College of Cardiology Foundation ISSN 0735-1097/03/$30.00Published by Elsevier Inc. doi:10.1016/S0735-1097(03)00952-5

agents, and thianopyridines seem very low by currentstandards.” These agents exert their beneficial effect primar-ily over the extended follow-up and would be expected tobenefit the medical group as well as the PTCA group. Onlyglycoprotein IIb/IIIa agents have been shown to reduceperiprocedural MI significantly. Routine biomarkers werenot obtained in this study, but the occurrence of periproce-dural MI, although small, did not translate into an increasein late events.
The skeptic: “Let’s get back to the angina. At the end ofthe follow-up, grade II or more angina was present in 21.4%of the medical patients but only 15.0% of the PTCA group.(�6.4%; 95% confidence interval, 1.5 to 11.3; p � 0.011).That is about a 30% reduction in angina.” Of course, forpatients with a less stiff upper lip, an intervention could bedone.
The skeptic: “At least they could exercise more.” Yes, 25 smore at 3 years!
This skeptic is beginning to run out of ammunition.Maybe the Clinical Outcome Utilizing Revascularizationand Aggressive drug Evaluation (COURAGE) trial and theBypass Angioplasty Revascularization Investigation-2 Dia-betes (BARI 2D) will come to my rescue at least in somesubsets, like diabetes (only 9% of the patients in this trialhad treated diabetes).
What can we learn from this trial that can be applied tothe next patient we see? As the authors point out, if there isno evident prognostic marker that the patient is at increasedrisk, then use revascularization to solve refractory symptoms.This will vary among patients. Some will have a strongdesire to avoid angina so as to engage in vigorous activities.
Others will be intolerant of beta-blockers. We must, how-ever, be honest with ourselves as well as our patients. Ifprognosis is not an issue, that should be clearly stated.Physicians have been accused of having the “oculostenoticreflex.” Patients who are told that they have a “blockage”often have an “auditorystenotic reflex.” “If it is blocked, Iwant it fixed.” If there is no evidence to support improve-ment in prognosis, the patient needs to hear and understandthat. Then, if the symptoms warrant an intervention, thepatient can help make the decision.
In the coming era of drug-eluting stents, the cost to themedical system will increase. Physicians must evaluate thisadvance for its contribution to preventing the hard endpoints of death and MI. Industry and payors must providea balance in pricing and reimbursement for all patients whorequire revascularization. Cost containment can be achievedby avoiding intervention in those who do not. RITA-2supports what we all should know and practice.
Reprint requests and correspondence: Dr. Spencer B. King III,Fuqua Heart Center, Ste. 2075, 95 Collier Road NW, Atlanta,Georgia 30309. E-mail: [email protected].
REFERENCES
1. Henderson RA, Pocock SJ, Clayton TC, et al. Seven-year outcome inthe RITA-2 trial: coronary angioplasty versus medical therapy. J AmColl Cardiol 2003;42:1161–70.
2. The NHLBI Dynamic Registry Investigators Meeting. Chicago, IL:March, 2003.
3. Brophy JM, Belisle P, Joseph L. The evidence for coronary stents—ahierarchical Bayesian meta-analysis. Ann Intern Med 2003. In Press.
1172 King III JACC Vol. 42, No. 7, 2003Editorial Comment October 1, 2003:1171–2

Acute Myocardial Infarction
The Incidence, Predictors, andOutcomes of Early Reinfarction AfterPrimary Angioplasty for Acute Myocardial InfarctionSteven J. Kernis, MD,* Kishore J. Harjai, MD, FACC,* Gregg W. Stone, MD, FACC,†Lorelei L. Grines, PHD,* Judith A. Boura, MS,* Michael W. Yerkey, MD,* William O’Neill, MD, FACC,*Cindy L. Grines, MD, FACC*Royal Oak, Michigan; and New York, New York
OBJECTIVES We sought to identify the incidence, predictors, and clinical consequences of one-monthreinfarction (RE-MI) in patients undergoing primary percutaneous coronary intervention(PCI) for acute myocardial infarction (AMI).
BACKGROUND One-month reinfarction after AMI significantly increases long-term mortality; however, littleis known about the incidence and predictors of RE-MI in patients undergoing primaryangioplasty.
METHODS We analyzed data from 3,646 patients who underwent primary PCI in the PrimaryAngioplasty in Acute Myocardial Infarction (PAMI) studies. We studied the incidence,correlates, and clinical outcomes of 30-day RE-MI.
RESULTS Reinfarction within one month of index hospitalization occurred in 77 (2.1%) of patients. Inmultivariate analysis, admission Killip class �1 (odds ratio [OR] 2.02, 95% confidenceinterval [CI] 1.09 to 3.76), left ventricular ejection fraction �50% (OR 2.49, 95% CI 1.30 to4.74), final coronary stenosis �30% (OR 2.57, 95% CI 1.28 to 5.15), and presence ofcoronary dissection (OR 2.40, 95% CI 1.36 to 4.24) and thrombus (OR 2.36, 95% CI 1.23to 4.53) on the final angiogram were independent correlates of RE-MI. One-monthreinfarction was independently associated with death (OR 7.14, 95% CI 3.28 to 15.5) andischemic target vessel revascularization (I-TVR) (OR 15.0, 95% CI 8.68 to 26.0) at sixmonths.
CONCLUSIONS We conclude that, although early RE-MI is uncommon in patients treated by primary PCI,it is a significant independent predictor of death and I-TVR at six months. Admission Killipclass �1 and left ventricular systolic dysfunction were associated with higher incidence ofRE-MI. Our results suggest that optimal revascularization during primary PCI may decreaseRE-MI rates. (J Am Coll Cardiol 2003;42:1173–7) © 2003 by the American College ofCardiology Foundation
Reinfarction (RE-MI) after acute myocardial infarction(AMI) leads to increased morbidity and mortality (1–4).Before the advent of revascularization therapy using throm-bolytics or primary angioplasty, nearly one-quarter of allQ-wave myocardial infarction patients suffered RE-MIwithin 10 years (5). With increased use of aspirin andbeta-blockers, thrombolytic therapy led to a reduction inone-year RE-MI rates by about 2% per year between 1987and 1994 (4–10). Donges et al. (3) studied AMI patientsenrolled in a large registry and found that 4.7% of patientshad in-hospital RE-MI and that the incidence of RE-MIwas lower in patients treated with percutaneous coronaryintervention (PCI) compared with thrombolytics.
Little is known about RE-MI occurring early after AMIin the era of primary angioplasty. Because primary angio-plasty is associated with better Thrombolysis In MyocardialInfarction (TIMI) flow in the infarct-related artery, the
incidence of RE-MI is expected to be lower than that notedhistorically in thrombolytic studies. More recently, Keeley etal. (11) performed a pooled analysis of 23 randomized trialsof PCI versus thrombolytics and found a significant de-crease in RE-MI with PCI. We performed this analysis tostudy the incidence, clinical, and angiographic predictors,and clinical consequences of one-month RE-MI in patientsundergoing primary angioplasty.
METHODS
Study population. We analyzed data available in 3,646patients treated by primary PCI in seven Primary Angio-plasty in Acute Myocardial Infarction (PAMI) studies,including PAMI-1 (12), PAMI-2 (13), Stent PAMI (14),Local PAMI (15), Stent Pilot (10), PAMI No Surgery onSite, and Air PAMI (16) (Table 1).PAMI study protocol. All patients enrolled presentedwithin 12 h of onset of chest pain and electrocardiographicchanges (ST elevation in two contiguous leads or left bundlebranch block). The trials excluded patients presenting withcardiogenic shock, high bleeding risk, and those who did
From the *Cardiology Division, William Beaumont Hospital, Royal Oak, Mich-igan; and †Cardiology Division, Lenox Hill Hospital, New York, New York.
Manuscript received March 5, 2003; revised manuscript received May 14, 2003,accepted May 21, 2003.
Journal of the American College of Cardiology Vol. 42, No. 7, 2003© 2003 by the American College of Cardiology Foundation ISSN 0735-1097/03/$30.00Published by Elsevier Inc. doi:10.1016/S0735-1097(03)00920-3
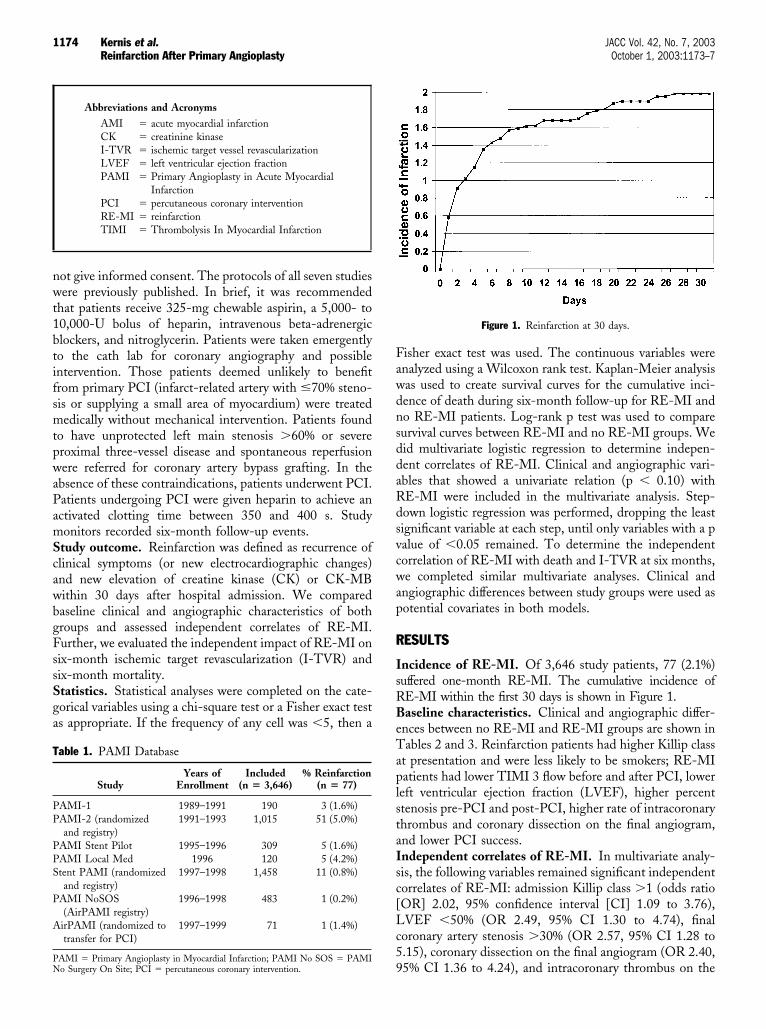
not give informed consent. The protocols of all seven studieswere previously published. In brief, it was recommendedthat patients receive 325-mg chewable aspirin, a 5,000- to10,000-U bolus of heparin, intravenous beta-adrenergicblockers, and nitroglycerin. Patients were taken emergentlyto the cath lab for coronary angiography and possibleintervention. Those patients deemed unlikely to benefitfrom primary PCI (infarct-related artery with �70% steno-sis or supplying a small area of myocardium) were treatedmedically without mechanical intervention. Patients foundto have unprotected left main stenosis �60% or severeproximal three-vessel disease and spontaneous reperfusionwere referred for coronary artery bypass grafting. In theabsence of these contraindications, patients underwent PCI.Patients undergoing PCI were given heparin to achieve anactivated clotting time between 350 and 400 s. Studymonitors recorded six-month follow-up events.Study outcome. Reinfarction was defined as recurrence ofclinical symptoms (or new electrocardiographic changes)and new elevation of creatine kinase (CK) or CK-MBwithin 30 days after hospital admission. We comparedbaseline clinical and angiographic characteristics of bothgroups and assessed independent correlates of RE-MI.Further, we evaluated the independent impact of RE-MI onsix-month ischemic target revascularization (I-TVR) andsix-month mortality.Statistics. Statistical analyses were completed on the cate-gorical variables using a chi-square test or a Fisher exact testas appropriate. If the frequency of any cell was �5, then a
Fisher exact test was used. The continuous variables wereanalyzed using a Wilcoxon rank test. Kaplan-Meier analysiswas used to create survival curves for the cumulative inci-dence of death during six-month follow-up for RE-MI andno RE-MI patients. Log-rank p test was used to comparesurvival curves between RE-MI and no RE-MI groups. Wedid multivariate logistic regression to determine indepen-dent correlates of RE-MI. Clinical and angiographic vari-ables that showed a univariate relation (p � 0.10) withRE-MI were included in the multivariate analysis. Step-down logistic regression was performed, dropping the leastsignificant variable at each step, until only variables with a pvalue of �0.05 remained. To determine the independentcorrelation of RE-MI with death and I-TVR at six months,we completed similar multivariate analyses. Clinical andangiographic differences between study groups were used aspotential covariates in both models.
RESULTS
Incidence of RE-MI. Of 3,646 study patients, 77 (2.1%)suffered one-month RE-MI. The cumulative incidence ofRE-MI within the first 30 days is shown in Figure 1.Baseline characteristics. Clinical and angiographic differ-ences between no RE-MI and RE-MI groups are shown inTables 2 and 3. Reinfarction patients had higher Killip classat presentation and were less likely to be smokers; RE-MIpatients had lower TIMI 3 flow before and after PCI, lowerleft ventricular ejection fraction (LVEF), higher percentstenosis pre-PCI and post-PCI, higher rate of intracoronarythrombus and coronary dissection on the final angiogram,and lower PCI success.Independent correlates of RE-MI. In multivariate analy-sis, the following variables remained significant independentcorrelates of RE-MI: admission Killip class �1 (odds ratio[OR] 2.02, 95% confidence interval [CI] 1.09 to 3.76),LVEF �50% (OR 2.49, 95% CI 1.30 to 4.74), finalcoronary artery stenosis �30% (OR 2.57, 95% CI 1.28 to5.15), coronary dissection on the final angiogram (OR 2.40,95% CI 1.36 to 4.24), and intracoronary thrombus on the
Abbreviations and AcronymsAMI � acute myocardial infarctionCK � creatinine kinaseI-TVR � ischemic target vessel revascularizationLVEF � left ventricular ejection fractionPAMI � Primary Angioplasty in Acute Myocardial
InfarctionPCI � percutaneous coronary interventionRE-MI � reinfarctionTIMI � Thrombolysis In Myocardial Infarction
Table 1. PAMI Database
StudyYears of
EnrollmentIncluded
(n � 3,646)% Reinfarction
(n � 77)
PAMI-1 1989–1991 190 3 (1.6%)PAMI-2 (randomized
and registry)1991–1993 1,015 51 (5.0%)
PAMI Stent Pilot 1995–1996 309 5 (1.6%)PAMI Local Med 1996 120 5 (4.2%)Stent PAMI (randomized
and registry)1997–1998 1,458 11 (0.8%)
PAMI NoSOS(AirPAMI registry)
1996–1998 483 1 (0.2%)
AirPAMI (randomized totransfer for PCI)
1997–1999 71 1 (1.4%)
PAMI � Primary Angioplasty in Myocardial Infarction; PAMI No SOS � PAMINo Surgery On Site; PCI � percutaneous coronary intervention.
Figure 1. Reinfarction at 30 days.
1174 Kernis et al. JACC Vol. 42, No. 7, 2003Reinfarction After Primary Angioplasty October 1, 2003:1173–7

final angiogram (OR 2.36, 95% CI 1.23 to 4.53) (Fig. 2).The percent of patients suffering RE-MI increases signifi-cantly with an increasing number of independent riskfactors. Patients with zero risk factors had a one-monthRE-MI rate of 0.6% compared with a 22% incidence inthose with four risk factors.The relation of RE-MI with six-month clinical outcomes.Of the patients who had RE-MI, 16% died at six monthscompared with 3% of those without RE-MI (p � 0.0001).Similarly, I-TVR during six-month follow-up was per-formed in 54% of RE-MI patients and 9.1% of patientswithout RE-MI (p � 0.0001) (Fig. 3). Cumulative survivalof patients with RE-MI was significantly worse than pa-tients without RE-MI (p � 0.0001) (Fig. 4). Step-down,multivariate, logistic regression analysis revealed thatRE-MI was a significant independent predictor of bothsix-month I-TVR (OR 15.0, 95% CI 8.68 to 26.0) anddeath (OR 7.14, 95% CI 3.28 to 15.5).
DISCUSSION
Early reinfarction after an AMI treated with primary PCI isrelatively uncommon. In our analysis, 2.1% of patientssuffered one-month RE-MI. This incidence is lower thanthat reported in the several large, randomized AMI throm-bolytic trials in the last 20 years, with in-hospital RE-MIrates ranging from 2.5% to 4.3% (1,8,17), and one-monthRE-MI rate of 3.4% (18). Our incidence is also lower than
that seen in previous studies that included patients revascu-larized by primary angioplasty. In Global Utilization ofStreptokinase and Tissue Plasminogen Activator in Oc-
Table 2. Baseline Clinical Characteristics of Patients With andWithout RE-MI
VariablesNo RE-MI(n � 3,569)
RE-MI(n � 77) p Value
Age (mean � SD) 60.9 � 12 62.6 � 12 0.24Women 959 (27%) 24 (31%) 0.40Heart rate* 88 � 21 89 � 20 0.49SBP* 111 � 26 112 � 24 0.84Diabetes mellitus 592 (17%) 12 (16%) 0.81Ever smoker 2,221 (65%) 37 (51%) 0.019Prior myocardial
infarction519 (15%) 11 (14%) 0.93
Prior angioplasty 353 (10%) 6 (8%) 0.53Prior congestive heart
failure87 (2.5%) 1 (1.4%) 1.00
Prior CABG 145 (4.5%) 5 (7.5%) 0.23Peripheral vascular
disease214 (6.2%) 6 (8%) 0.47
Hypertension 1,629 (46%) 37 (49%) 0.62Hyperlipidemia 1,036/2,599 (40%) 29/66 (44%) 0.50Stroke or TIA 185 (5.2%) 4 (5.3%) 1.00Chronic obstructive lung
disease105/2,089 (5%) 0/18 (0%) 1.00
Killip class on admission (n � 3,526) Killip � 11 3,064 (89%) 55 (74%) 0.00032 387 (11%) 19 (25%)3 67 (1.9%) 2 (2.6%)4 8 (0.2%) 0 (0%)
*Highest heart rate and lowest systolic blood pressure (SBP) recorded from presen-tation to emergency room until arrival in the cath lab is shown here.
CABG � coronary artery bypass grafting; RE-MI � reinfarction; TIA �transient-ischemic attack.
Table 3. Angiographic Characteristics
No RE-MI(n � 3,569)
RE-MI(n � 77)
pValue
Pre-PCI variablesEjection fraction �50% 61% 83% 0.0002TIMI flow in culprit artery 0.039
0 62% 75%1 11% 3%2 16% 12%3 11% 10%
Diameter stenosis in culpritartery %
97 � 7 98 � 7 0.035
PCI variablesInfarct related artery location
RCA 42% 43% 0.95LAD 41% 48% 0.24LCX 14% 8% 0.12Other* 6% 4%
Stent 35% 17% 0.0016Abciximab 10% 1% 0.017
Post-PCI variablesTIMI flow in culprit artery 0.053
0 1% 4%1 1% 0%2 5% 9%3 94% 87% 0.049
Diameter stenosis in culpritartery %
15 � 17 28 � 24 � 0.0001
Thrombus† 10% 23% 0.0002Dissection‡ 15% 31% 0.0005
PCI success§ 92% 81% 0.001
*Left main, saphenous vein graft, internal mammary artery, or unidentified; †In StentPrimary Angioplasty in Acute Myocardial Infarction (PAMI) thrombus was definedas post-PCI intraluminal filling defect or lucency surrounded by contrast material inmultiple projections, persistence of contrast material within the lumen, or visibleembolization of intraluminal material downstream. In PAMI-2 and PAMI No-SOS,thrombus was defined as a filling defect at least half the vessel diameter, or if the vesselremained occluded after PCI; ‡Dissection classified as post-PCI type 1 (grade A orB dissection), type 2 (grade C dissection), or type 3 (grade D1, D2, E, F) post-PCIcoronary dissection; §PCI success was defined as TIMI 3 flow with final diameterstenosis �50%.
LAD � left anterior descending artery; LCX � left circumflex artery; PCI �percutaneous coronary intervention; RCA � right coronary artery; RE-MI �reinfarction; TIMI � Thrombolysis In Myocardial Infarction.
Figure 2. Multivariate correlates of reinfarction (Re-MI).
1175JACC Vol. 42, No. 7, 2003 Kernis et al.October 1, 2003:1173–7 Reinfarction After Primary Angioplasty

cluded Arteries (GUSTO) IIb, 30 day RE-MI occurred in4.5% of patients (19). A meta-analysis of 23 randomizedtrials conducted by Keeley et al. (11) reported that RE-MIoccurred in 3% of patients undergoing primary angioplasty.Although our trial did not address a direct comparison ofPCI versus thrombolysis, prior literature has shown thatRE-MI occurs less frequently with primary PCI than it doeswith thrombolytics (19). We found that most cases ofRE-MI occurred within four days of hospital admission.
Our study identified several independent determinants ofRE-MI (Fig. 1). Admission Killip class �1, LVEF �50%,final coronary stenosis �30%, post-PCI coronary dissec-tion, and post-PCI intracoronary thrombus were significantpredictors of one-month RE-MI. Unlike previous trials(1,3–5,8,9,20), admission Killip class �1 was the onlyclinical characteristic that identified patients at higher riskof RE-MI. Rather, angiographic variables were the pre-dominant predictors of one-month RE-MI. This is proba-bly because previous studies had less detailed angiographicdata. The availability of such data in PAMI studies likelyoverwhelms the predictive ability of clinical variables. Thus,the occurrence of reinfarction is a function of poor angio-graphic outcomes, and is less dependent upon clinicalfactors identified in prior studies, such as age, gender, or ahistory of diabetes.
Finally, we found RE-MI to be strongly associated withincreased mortality and revascularization at six months.Those suffering one-month RE-MI had more than seven-fold increased adjusted mortality at six months. Moreover,the risk of I-TVR in RE-MI patients was 15-fold higher inadjusted incidence. These findings are in accord with severaltrials that all show strong associations between RE-MI anddeath (1). This increased mortality underscores the need foridentification of high-risk patients, as well as effectiveprimary revascularization by PCI (4).Implications. Angiographic predictors are stronger riskfactors for RE-MI than clinical factors; RE-MI may bepreventable by optimal coronary revascularization and treat-ment of dissection and thrombus.Summary. Reinfarction in the era of primary PCI for AMIis rare, and less common then that reported previously. Wefound one clinical characteristic and several angiographicvariables that are associated with higher RE-MI risk;RE-MI, although infrequent, imparts a significantly higherrisk of future revascularization and death. Reinfarction maybe preventable, by optimal coronary revascularization andaggressive treatment of post-PCI dissection and thrombus.Study limitations. This study may suffer from bias relatedto its retrospective analysis design. Our results cannot beextrapolated to cardiogenic shock patients, as the PAMIstudies excluded these patients. Furthermore, our resultsmay be less representative of contemporary practice, due tolower rates of glycoprotein IIb/IIIa and thienopyridinemedications, and lower stent use. The majority of RE-MIcases occurred in PAMI II where balloon angioplastywithout stenting was the dominant treatment modality.
AcknowledgmentsThe authors thank the people and institutions that partici-pated in the PAMI trials.
Reprint requests and correspondence: Dr. Cindy L. Grines,Division of Cardiovascular Medicine, William Beaumont Hospi-tal, 3601 West 13 Mile Road, Royal Oak, Michigan 48073-6769.E-mail: [email protected].
REFERENCES
1. Hudson MP, Granger CB, Topol EJ, et al. Early reinfarction afterfibrinolysis: experience from the global utilization of streptokinase andtissue plasminogen activator (alteplase) for occluded coronary arteries(GUSTO I) and global use of strategies to open occluded coronaryarteries (GUSTO III) trials. Circulation 2001;104:1229–35.
2. Marmor A, Sobel BE, Roberts R. Factors presaging early recurrentmyocardial infarction (“extension”). Am J Cardiol 1981;48:603–10.
3. Donges K, Schiele R, Gitt A, et al. Incidence, determinants, andclinical course of reinfarction in-hospital after index acute myocardialinfarction (results from the pooled data of the maximal individualtherapy in acute myocardial infarction [MITRA], and the myocardialinfarction registry [MIR]). Am J Cardiol 2001;87:1039–44.
4. Kornowski R, Goldbourt U, Zion M, et al. Predictors and long-termprognostic significance of recurrent infarction in the year after a firstmyocardial infarction: SPRINT study group. Am J Cardiol 1993;72:883–8.
5. Berger CJ, Murabito JM, Evans JC, Anderson KM, Levy D. Prognosisafter first myocardial infarction: comparison of Q-wave and non–Q-
Figure 3. Six-month clinical outcomes. ReMI � reinfarction; TVR �target vessel revascularization.
Figure 4. Mortality at six-months. ReMI � reinfarction.
1176 Kernis et al. JACC Vol. 42, No. 7, 2003Reinfarction After Primary Angioplasty October 1, 2003:1173–7

wave myocardial infarction in the Framingham Heart study. JAMA1992;268:1545–51.
6. Rosamond WD, Chambless LE, Folsom AR, et al. Trends in theincidence of myocardial infarction and in mortality due to coronaryheart disease, 1987 to 1994. N Engl J Med 1998;339:861–7.
7. Gilpin E, Ricou F, Dittrich H, Nicod P, Henning H, Ross J, Jr.Factors associated with recurrent myocardial infarction within one yearafter acute myocardial infarction. Am Heart J 1991;121:457–65.
8. Volpi A, de Vita C, Franzosi MG, et al. Predictors of nonfatalreinfarction in survivors of myocardial infarction after thrombolysis: resultsof the Gruppo Italiano per lo Studio della Sopravvivenza nell’InfartoMiocardico (GISSI-2) data base. J Am Coll Cardiol 1994;24:608–15.
9. Dwyer EM, Jr., McMaster P, Greenberg H. Nonfatal cardiac eventsand recurrent infarction in the year after acute myocardial infarction.J Am Coll Cardiol 1984;4:695–702.
10. Stone GW, Brodie BR, Griffin JJ, et al. Prospective, multicenter studyof the safety and feasibility of primary stenting in acute myocardialinfarction: in-hospital and 30-day results of the PAMI stent pilot trial:Primary Angioplasty in Myocardial Infarction Stent Pilot trial inves-tigators. J Am Coll Cardiol 1998;31:23–30.
11. Keeley EC, Boura JA, Grines CL. Primary angioplasty versus intra-venous thrombolytic therapy for acute myocardial infarction: a quan-titative review of 23 randomised trials. Lancet 2003;361:13–20.
12. Grines CL, Browne KF, Marco J, et al. A comparison of immediateangioplasty with thrombolytic therapy for acute myocardial infarction:the Primary Angioplasty in Myocardial Infarction study group. N EnglJ Med 1993;328:673–9.
13. Stone GW, Marsalese D, Brodie BR, et al. A prospective, randomizedevaluation of prophylactic intraaortic balloon counterpulsation in highrisk patients with acute myocardial infarction treated with primaryangioplasty: Second Primary Angioplasty in Myocardial Infarction(PAMI-II) trial investigators. J Am Coll Cardiol 1997;29:1459–67.
14. Grines CL, Cox DA, Stone GW, et al. Coronary angioplasty with orwithout stent implantation for acute myocardial infarction: StentPrimary Angioplasty in Myocardial Infarction study group. N EnglJ Med 1999;341:1949–56.
15. Esente P, Kaplan AV, Ford JK, et al. Local intramural heparin deliveryduring primary angioplasty for acute myocardial infarction: results ofthe Local PAMI pilot study. Catheter Cardiovasc Intervent 1999;47:237–42.
16. Grines CL, Westerhausen DR, Jr., Grines LL, et al. A randomizedtrial of transfer for primary angioplasty versus on-site thrombolysis inpatients with high-risk myocardial infarction: the Air Primary Angio-plasty in Myocardial Infarction study. J Am Coll Cardiol 2003. InPress.
17. Gruppo Italiano per lo Studio della Sopravvivenza nell’Infarto Mio-cardico. GISSI-2: a factorial randomised trial of alteplase versusstreptokinase and heparin versus no heparin among 12,490 patientswith acute myocardial infarction. Lancet 1990;336:65–71.
18. ISIS-3 (Third International Study of Infarct Survival) CollaborativeGroup. ISIS-3: a randomised comparison of streptokinase vs tissueplasminogen activator vs anistreplase and of aspirin plus heparin vsaspirin alone among 41,299 cases of suspected acute myocardialinfarction. Lancet 1992;339:753–70.
19. The Global Use of Strategies to Open Occluded Coronary Arteries inAcute Coronary Syndromes (GUSTO IIb) Angioplasty SubstudyInvestigators. A clinical trial comparing primary coronary angioplastywith tissue plasminogen activator for acute myocardial infarction.N Engl J Med 1997;336:1621–8.
20. Birnbaum Y, Herz I, Sclarovsky S, et al. Admission clinical andelectrocardiographic characteristics predicting an increased risk forearly reinfarction after thrombolytic therapy. Am Heart J 1998;135:805–12.
1177JACC Vol. 42, No. 7, 2003 Kernis et al.October 1, 2003:1173–7 Reinfarction After Primary Angioplasty
Percutaneous Intervention and Anticoagulation
Outcome of Urgent and Elective PercutaneousCoronary Interventions After PharmacologicReperfusion With Tenecteplase Combined WithUnfractionated Heparin, Enoxaparin, or AbciximabChristophe L. Dubois, MD,* Ann Belmans, MSC,*† Christopher B. Granger, MD, FACC,‡Paul W. Armstrong, MD, FACC,§ Lars Wallentin, MD, FACC,� Paolo M. Fioretti, MD, FACC,¶Jose L. Lopez-Sendon, MD, FACC,# Freek W. Verheugt, MD, FACC,** Jurgen Meyer, MD, FACC,††Frans Van de Werf, MD, FACC,* on behalf of the ASSENT-3 InvestigatorsLeuven, Belgium; Durham, North Carolina; Edmonton, Canada; Uppsala, Sweden; Udine, Italy; Madrid, Spain;Nijmegen, The Netherlands; and Mainz, Germany
OBJECTIVES The aim of this study was to evaluate percutaneous coronary intervention (PCI) in theAssessment of the Safety and Efficacy of New Thrombolytic Regimens (ASSENT-3) trial.
BACKGROUND In the ASSENT-3 trial, co-therapy with abciximab (ABC) or enoxaparin (ENOX) reducedischemic complications after ST-elevation acute myocardial infarction treated with tenect-eplase when compared with unfractionated heparin (UFH). The effect of these newco-therapies on the results of PCI is unknown.
METHODS Clinical outcomes in patients who received co-therapy with ABC, ENOX, or UFH andsubsequently underwent an elective (n � 1,064) or urgent (n � 716) PCI in the ASSENT-3trial were compared.
RESULTS No significant differences in clinical end points were observed in patients who underwent anelective PCI. A non-significant trend toward fewer in-hospital myocardial re-infarctions wasseen with ABC and ENOX when compared with UFH (0.5% vs. 0.6% vs. 1.5%, respectively).The incidence of bleeding complications was similar in the three treatment arms. Significantlyfewer ABC- and ENOX-treated patients needed urgent PCI compared with UFH (9.1% vs.11.9% vs. 14.3%; p � 0.0001), but outcomes in these patients were in general less favorable(30-day mortality: 8.2% vs. 5.4% vs. 4.5%; 1-year mortality: 11.0% vs. 8.5% vs. 5.6%;in-hospital re-infarction: 3.9% vs. 2.5% vs. 2.7%; major bleeding complications: 8.8% vs. 7.0%vs. 3.4%). In pairwise comparisons with UFH, the higher one-year mortality and majorbleeding rates after ABC were statistically significant (p � 0.045 and p � 0.012, respectively).
CONCLUSIONS Clinical outcomes after elective PCI were similar with the three antithrombotic co-therapiesstudied in ASSENT-3. Although fewer patients needed urgent PCI with ABC and ENOX,clinical outcomes were less favorable in this selected population, especially withABC. (J Am Coll Cardiol 2003;42:1178–85) © 2003 by the American College ofCardiology Foundation
Reperfusion therapy has been one of the major advances inthe treatment of acute myocardial infarction (AMI) since
See page 1186
the introduction of the coronary care unit. The combinedadministration of a fibrinolytic agent, unfractionated hepa-rin (UFH), and aspirin became the standard of care in the
late 1980s (1,2). Although significant improvements infibrinolytic therapy were made, substantial challenges re-main (3–5). Optimal reperfusion of the infarct-relatedepicardial coronary artery is achieved in only 50% to 60% ofthe patients 60 to 90 min after initiation of treatment(6–10). Other concerns are reperfusion at the tissue level,recurrent ischemia or re-infarction, and bleeding complica-tions (11,12). Newer co-therapies, including low-molecular-weight heparin and platelet glycoprotein IIb/IIIainhibitors were tested in recent trials in conjunction withfibrinolytics (13–15). Although no mortality benefit wasseen, these newer treatment regimens led to a consistentreduction in ischemic complications, including re-infarctionand refractory ischemia. This benefit was partly counterbal-anced by an increased rate of non-intracranial bleedingcomplications.
A substantial proportion of patients with ST-elevationAMI who receive thrombolytic therapy subsequently un-
From the *Department of Cardiology, University Hospitals Leuven, Leuven,Belgium; †Department of Public Health, Biostatistical Centre, Catholic UniversityLeuven, Leuven, Belgium; ‡Duke Clinical Research Institute, Durham, NorthCarolina; §Department of Cardiology, University of Alberta, Edmonton, Canada;�Department of Cardiology, University of Uppsala, Uppsala, Sweden; ¶Departmentof Cardiology, Istituto di Cardiologia, Udine, Italy; #Department of Cardiology,Hospital Gregorio Maranon, Madrid, Spain; **Department of Cardiology, UniversityMedical Center Nijmegen, Nijmegen, The Netherlands; ††Department of Cardiol-ogy, Johannes Gutenberg-University, Mainz, Germany.
Manuscript received January 10, 2003; revised manuscript received March 6, 2003,accepted March 12, 2003.
Journal of the American College of Cardiology Vol. 42, No. 7, 2003© 2003 by the American College of Cardiology Foundation ISSN 0735-1097/03/$30.00Published by Elsevier Inc. doi:10.1016/S0735-1097(03)00917-3

dergo a percutaneous coronary intervention (PCI). Unfrac-tionated heparin has been the anticoagulant of choiceduring PCI. As in acute coronary syndromes, newer anti-coagulants (low-molecular-weight heparin or direct anti-thrombins) and antiplatelet agents (platelet glycoproteinIIb/IIIa inhibitors) emerged and have been proven to be safeand perhaps even superior in elective and urgent PCI(16–24). However, the effect of these newer treatmentregimens on the outcome of PCI performed after lytictherapy is largely unknown.
We analyzed clinical outcomes in patients who under-went PCI after lytic therapy in the Assessment of the Safetyand Efficacy of New Thrombolytic Regimens (ASSENT-3)trial. In this trial, 6,095 patients with ST-elevation AMI of�6 h were randomly assigned to one of three regimens:half-dose tenecteplase (TNK-tPA) with weight-adjustedlow-dose UFH and a 12-h infusion of abciximab (ABC),full-dose TNK-tPA and enoxaparin (ENOX) for a maxi-mum of seven days, or full-dose TNK-tPA with weight-adjusted UFH for 48 h. The main results of this trial havebeen published (15).
METHODS
Data management. Using the ASSENT-3 database, weselected all patients who underwent urgent or elective PCIduring the initial hospitalization and evaluated them sepa-rately. Elective PCI referred to a planned procedure and wasperformed in 1,064 patients (17.5% of the total ASSENT-3study population). A total of 716 patients (11.7%) under-went an urgent PCI, defined as an ischemia-driven revas-cularization before hospital discharge. Patients who under-went both an urgent and an elective PCI (n � 15) wereincluded in the analysis of urgent PCI. Outcomes of earlyPCI (urgent or non-urgent), performed on the same day orthe day after thrombolytic treatment, were also assessedseparately. This group comprised 667 patients (11.0%).These patients are of special interest because the treatmenteffects of ABC and UFH have been thought to be mostpronounced during the first 24 to 48 h. Furthermore, mostefficacy end points of interest (death, re-infarction, refrac-tory ischemia) occur early and could be influenced by earlyintervention (25).
Analyzed data included the allocated trial medication,
time of randomization, death at 30 days, one-year mortality,in-hospital myocardial re-infarction, in-hospital refractoryischemia, in-hospital major and minor bleeds, puncture-site-related bleeds as well as day of PCI, re-infarction, orrefractory ischemia. In the case of urgent PCI, reason forurgency was also assessed (per protocol defined as myocar-dial re-infarction, myocardial ischemia, or “others”). Datawere checked for completeness and for internal consistencywith source documents.Definitions of efficacy and safety end points. We ana-lyzed the composite end point of 30-day mortality, in-hospital re-infarction, or in-hospital refractory ischemia(efficacy end point) as well as the individual components ofthe efficacy end point. Because one-year follow-up wasrecently completed, one-year mortality data were also in-cluded in our analysis. The incidence of in-hospital intra-cranial hemorrhage (ICH), major non-cerebral bleeds, andmajor and minor bleeds at the arterial puncture site (safetyend points) was also assessed. The same definitions forre-infarction, refractory ischemia, and major versus minorbleeding, as described in the main report of ASSENT-3,were also used in our analysis (15).Data analysis. Baseline characteristics were tabulated foreach treatment group. For binary and categorical variables,differences between treatment groups were assessed usingthe chi-square test. For continuous variables, an overall Ftest was performed.
The end point data were analyzed using a proportionalhazards regression. To allow for the timing of the outcome(before or after PCI) to be taken into account, PCI wasincluded as a time-dependent covariate (coded as 0 beforethe performance of PCI, coded as 1 afterwards). In addition,an interaction term between this time-dependent covariateand treatment was also included in the model to allow fordifferent treatment effects before and after the performanceof a PCI. Furthermore, propensity scores (probability ofreceiving treatment based on baseline characteristics) werecalculated for all patients and included in the model (26). Byincluding propensity scores in the model, it is hoped thatany imbalances in risk factors between the treatment groupsafter the performance of a PCI will be reduced or removed.For each of the three subgroups that were analyzed, apropensity score analysis was performed, in which theprobability of receiving one of the three treatments wasmodeled on the basis of patients’ baseline characteristics,using a logistic regression. The models used to determinethe propensity scores included patients’ baseline character-istics and their second-order interactions: gender, age,weight, infarct location, previous myocardial infarction,systolic and diastolic blood pressure, Killip class at entry,time from symptom onset to treatment initiation, heart rate,diabetes, previous coronary artery bypass surgery, previousPCI, country (U.S./Europe/other), and randomization date.Visual inspection of exploratory plots revealed that notransformation of the continuous variables was necessary forinclusion into the propensity model. For the urgent and
Abbreviations and AcronymsABC � abciximabAMI � acute myocardial infarctionASSENT � ASsessment of the Safety and Efficacy of
New Thrombolytic RegimensENOX � enoxaparinICH � intracranial hemorrhagePCI � percutaneous coronary interventionTNK-tPA � tenecteplaseUFH � unfractionated heparin
1179JACC Vol. 42, No. 7, 2003 Dubois et al.October 1, 2003:1178–85 Outcome of PCI in ASSENT-3

early PCI groups, the concordance obtained with thepropensity model was good with C-statistics of 0.82 (UFHvs. ENOX) and 0.83 (UFH vs. ABC) for the group ofpatients with urgent PCI and C-statistics of 0.82 (UFH vs.ENOX) and 0.85 (UFH vs. ABC) for the patients whounderwent an early PCI. For the subgroup of patients whounderwent an elective PCI, the C-statistics were 0.74 (UFHvs. ENOX) and 0.73 (UFH vs. ABC). Then, based on theobtained propensity scores, all patients were divided intoquintiles. For all subgroups studied, patient numbers andbaseline characteristics were tabulated by treatment groupwithin each of the obtained quintiles. The results indicatedthat baseline characteristics were balanced within quintileand that none of the covariates that were included in thepropensity model induced an inappropriate separation of thetreatments.
Based on the proportional hazards regression, pair wisetreatment comparisons between ENOX and UFH andbetween ABC and UFH were calculated, together withtheir corresponding 95% confidence interval. A chi-squaretest was performed to assess the statistical significance of thepairwise comparisons.
RESULTS
The distribution of patients who underwent an early,elective, or urgent PCI in the three treatment arms is shownin Table 1. Fewer patients in the ABC arm than in theUFH arm underwent an urgent or early PCI. There was asimilar trend for urgent PCI with ENOX.
The baseline characteristics of the patients who under-went an elective PCI were similar in the three treatmentarms (Table 2). Median time to revascularization was fivedays in each group. The composite end point of 30-daymortality, in-hospital myocardial re-infarction, or in-hospital refractory ischemia, its individual components,one-year mortality and non-intracranial bleeding complica-tions in patients who underwent elective PCI are shown inFigure 1.
There was one ICH in the UFH arm (0.30%) and one inthe ENOX arm (0.29%). No ICH was seen in the ABCarm. No significant differences were observed between thedifferent treatment regimens. A trend towards fewer in-hospital myocardial re-infarctions was seen in the ABC andENOX arms compared with the UFH arm, but statistical
significance was not reached. Low 30-day and one-yearmortality rates were observed after elective PCI, the lowestin the ENOX arm. The incidences of in-hospital majornon-cerebral bleeds and arterial puncture-related majorbleeds were also similar in the three treatment arms. Theproportion of patients who received additional UFH duringPCI was similar in the three groups (77% for ABC, 79% forENOX, and 75% for UFH). Pair wise treatment compari-sons with hazard ratios and corresponding 95% confidenceintervals for outcome after elective PCI are also shown inFigure 1. Overall, there was a slightly more favorablecomposite efficacy outcome with ENOX treatment, whereassafety outcome was slightly better with ABC.
There was a significantly lower need for urgent PCI inpatients given ABC or ENOX when compared with UFH(Table 1). Fewer early PCI were performed in the ABC arm(Table 1). Of the urgent PCI performed, 75% were earlyPCI. The baseline characteristics in patients who neededurgent PCI or who underwent an early PCI are given inTables 3 and 4. Except for age in the urgent PCI analysisand for time from onset of symptoms to TNK-tPA in theearly PCI analysis, baseline characteristics were similar.Efficacy end points are summarized in Figures 2 and 3.There was a trend towards reduced efficacy in the ABC arm,with even a significantly higher one-year mortality whencompared with UFH.
The safety end points in the urgent and early PCI patientpopulation as well as the pairwise comparisons are shown inFigures 2 and 3. One ICH was seen in each group (0.55%for ABC, 0.41% for ENOX, and 0.34% for UFH) in urgentPCI. Significantly more major, non-cerebral bleeding com-plications were seen in the ABC group compared with the
Table 1. Distribution of Patients in the Different Subgroups
ABC(n � 2,009)
ENOX(n � 2,037)
UFH(n � 2,035) p Value*
Elective PCI 384 (19.1%) 348 (17.1%) 332 (16.3%) 0.0539Urgent PCI 182 (9.1%) 242 (11.9%) 292 (14.3%) � 0.0001PCI on day 1
or 2174 (8.7%) 232 (11.4%) 261 (12.8%) � 0.0001
*p value: chi-square test for overall difference between treatment groups.ABC � abciximab; ENOX � enoxaparin; PCI � percutancous coronary inter-
vention; UFH � unfractionated heparin.
Table 2. Baseline Characteristics in Patients With Elective PCI
VariableABC
(n � 384)ENOX
(n � 348)UFH
(n � 332)p
Value*
Age (yrs) 59 � 11† 59 � 12 60 � 12 0.60Male gender (%) 73 77 75 0.59Weight (kg) 82 � 18 80 � 16 80 � 16 0.09Hypertension (%) 42 38 40 0.62Diabetes mellitus (%) 14 15 15 0.82Previous myocardial
infarction (%)14 13 13 0.86
Previous PCI (%) 9 9 9 0.95Previous CABG (%) 5 3 3 0.22Anterior infarction (%) 34 34 36 0.76Killip class I (%) 90 93 93 0.30Systolic blood pressure
(mm Hg)134 � 22 133 � 21 134 � 21 0.94
Heart rate (beats/min) 74 � 16 74 � 16 74 � 16 0.99Hours from symptom
onset to TNK-tPA3.0 � 1.5 2.8 � 1.5 2.9 � 1.4 0.20
*p value: chi-square test for binary and categorical variables, overall F-test forcontinuous variables. †Continuous variables are mean � SD. Propensity scores: ABCvs. UFH: 0.39 � 0.19 for the ABC group, 0.54 � 0.17 for the UFH group; ENOXvs. UFH: 0.40 � 0.19 for the ENOX group, 0.58 � 0.19 for the UFH group.
ABC � abciximab; CABG � coronary artery bypass grafting; ENOX �enoxaparin; PCI � percutaneous coronary intervention; TNK-tPA � tenecteplase;UFH � unfractionated heparin.
1180 Dubois et al. JACC Vol. 42, No. 7, 2003Outcome of PCI in ASSENT-3 October 1, 2003:1178–85
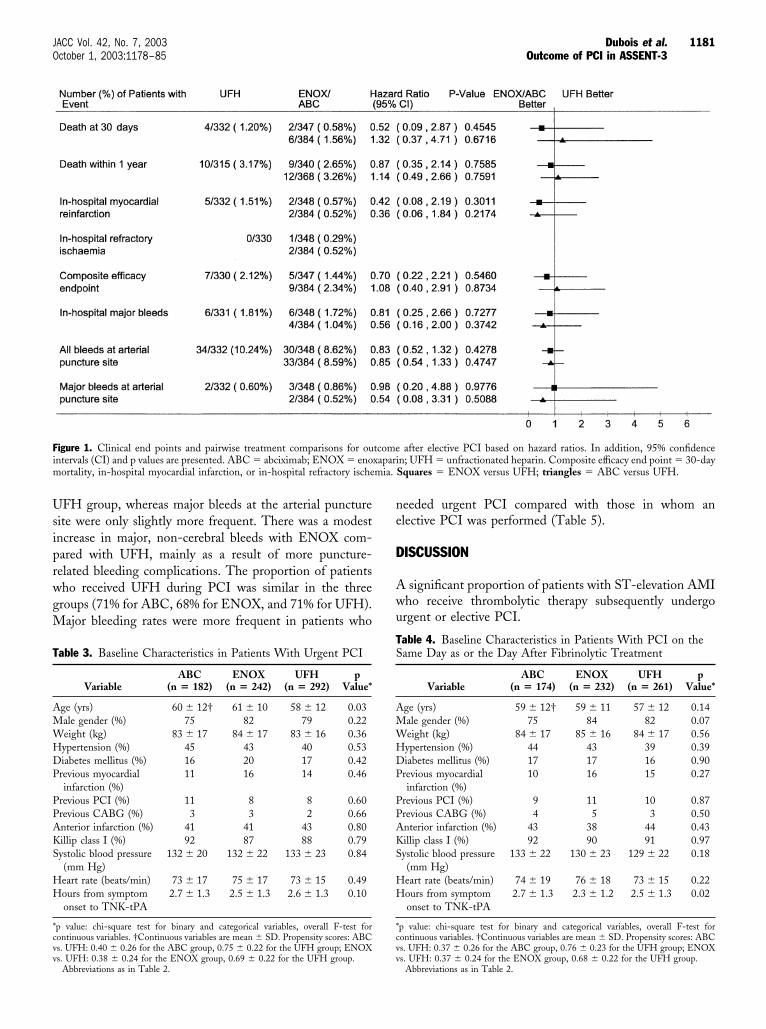
UFH group, whereas major bleeds at the arterial puncturesite were only slightly more frequent. There was a modestincrease in major, non-cerebral bleeds with ENOX com-pared with UFH, mainly as a result of more puncture-related bleeding complications. The proportion of patientswho received UFH during PCI was similar in the threegroups (71% for ABC, 68% for ENOX, and 71% for UFH).Major bleeding rates were more frequent in patients who
needed urgent PCI compared with those in whom anelective PCI was performed (Table 5).
DISCUSSION
A significant proportion of patients with ST-elevation AMIwho receive thrombolytic therapy subsequently undergourgent or elective PCI.
Figure 1. Clinical end points and pairwise treatment comparisons for outcome after elective PCI based on hazard ratios. In addition, 95% confidenceintervals (CI) and p values are presented. ABC � abciximab; ENOX � enoxaparin; UFH � unfractionated heparin. Composite efficacy end point � 30-daymortality, in-hospital myocardial infarction, or in-hospital refractory ischemia. Squares � ENOX versus UFH; triangles � ABC versus UFH.
Table 3. Baseline Characteristics in Patients With Urgent PCI
VariableABC
(n � 182)ENOX
(n � 242)UFH
(n � 292)p
Value*
Age (yrs) 60 � 12† 61 � 10 58 � 12 0.03Male gender (%) 75 82 79 0.22Weight (kg) 83 � 17 84 � 17 83 � 16 0.36Hypertension (%) 45 43 40 0.53Diabetes mellitus (%) 16 20 17 0.42Previous myocardial
infarction (%)11 16 14 0.46
Previous PCI (%) 11 8 8 0.60Previous CABG (%) 3 3 2 0.66Anterior infarction (%) 41 41 43 0.80Killip class I (%) 92 87 88 0.79Systolic blood pressure
(mm Hg)132 � 20 132 � 22 133 � 23 0.84
Heart rate (beats/min) 73 � 17 75 � 17 73 � 15 0.49Hours from symptom
onset to TNK-tPA2.7 � 1.3 2.5 � 1.3 2.6 � 1.3 0.10
*p value: chi-square test for binary and categorical variables, overall F-test forcontinuous variables. †Continuous variables are mean � SD. Propensity scores: ABCvs. UFH: 0.40 � 0.26 for the ABC group, 0.75 � 0.22 for the UFH group; ENOXvs. UFH: 0.38 � 0.24 for the ENOX group, 0.69 � 0.22 for the UFH group.
Abbreviations as in Table 2.
Table 4. Baseline Characteristics in Patients With PCI on theSame Day as or the Day After Fibrinolytic Treatment
VariableABC
(n � 174)ENOX
(n � 232)UFH
(n � 261)p
Value*
Age (yrs) 59 � 12† 59 � 11 57 � 12 0.14Male gender (%) 75 84 82 0.07Weight (kg) 84 � 17 85 � 16 84 � 17 0.56Hypertension (%) 44 43 39 0.39Diabetes mellitus (%) 17 17 16 0.90Previous myocardial
infarction (%)10 16 15 0.27
Previous PCI (%) 9 11 10 0.87Previous CABG (%) 4 5 3 0.50Anterior infarction (%) 43 38 44 0.43Killip class I (%) 92 90 91 0.97Systolic blood pressure
(mm Hg)133 � 22 130 � 23 129 � 22 0.18
Heart rate (beats/min) 74 � 19 76 � 18 73 � 15 0.22Hours from symptom
onset to TNK-tPA2.7 � 1.3 2.3 � 1.2 2.5 � 1.3 0.02
*p value: chi-square test for binary and categorical variables, overall F-test forcontinuous variables. †Continuous variables are mean � SD. Propensity scores: ABCvs. UFH: 0.37 � 0.26 for the ABC group, 0.76 � 0.23 for the UFH group; ENOXvs. UFH: 0.37 � 0.24 for the ENOX group, 0.68 � 0.22 for the UFH group.
Abbreviations as in Table 2.
1181JACC Vol. 42, No. 7, 2003 Dubois et al.October 1, 2003:1178–85 Outcome of PCI in ASSENT-3

The aim of our study was to evaluate clinical outcomes inpatients who underwent PCI during initial hospitalizationin the ASSENT-3 trial. In light of the pharmacologic
properties attributable to ENOX, ease of administrationand proven safety and efficacy in non–ST-elevation acutecoronary syndromes and PCI, evaluation of the possible
Figure 2. Clinical end points and pairwise treatment comparisons for outcome after urgent PCI based on hazard ratios. In addition, 95% confidenceintervals (CI) and p values are presented. ABC � abciximab; ENOX � enoxaparin; UFH � unfractionated heparin. Composite efficacy end point � 30-daymortality, in-hospital myocardial infarction, or in-hospital refractory ischemia. Squares � ENOX versus UFH; triangles � ABC versus UFH.
Figure 3. Clinical end points and pairwise treatment comparisons for outcome after early PCI based on hazard ratios. In addition, 95% confidence intervals(CI) and p values are presented. ABC � abciximab; ENOX � enoxaparin; UFH � unfractionated heparin. Composite efficacy end point � 30-daymortality, in-hospital myocardial infarction, or in-hospital refractory ischemia. Squares � ENOX versus UFH; triangles � ABC versus UFH.
1182 Dubois et al. JACC Vol. 42, No. 7, 2003Outcome of PCI in ASSENT-3 October 1, 2003:1178–85

benefit or harm of ENOX in PCI early after thrombolysis ofan ST-elevation AMI is important (16–18,27,28). Al-though there is clear evidence that ABC reduces thromboticcardiac complications in patients undergoing PCI, it is notknown whether ABC is beneficial after PCI in patients withST-elevation AMI previously treated with reduced dosethrombolytics (19–22).
No significant difference in the primary composite effi-cacy end point or its components between the three treat-ment regimens was seen in the population who underwentelective PCI in ASSENT-3. Nevertheless, a trend towardsfewer in-hospital myocardial re-infarctions was seen in theENOX and ABC arms. Median time to elective revascu-larization was rather long (five days after randomization).Because per protocol ENOX was to be administered untilrevascularization or discharge with a maximum of sevendays and because prolonged low-level platelet receptorblockade may still be present up to 10 days after thecessation of an ABC infusion, the antithrombotic effects ofABC and ENOX may have been responsible for thesefavorable outcomes, supporting the results of trials inelective PCI (16,17,19,20,22).
In patients who underwent an urgent PCI during theinitial hospital stay in the ASSENT-3 trial, the overall lowevent rates after the procedure make the interpretation ofdifferences in post-procedural outcome very hazardous. Ouranalysis shows a somewhat higher incidence of the efficacyend points after PCI in the ABC arm. More specifically,there was a significantly higher one-year mortality and alsoa slight excess in re-infarction. These worse outcomes aredifficult to understand because one would have expectedbenefit in this regard from ABC (19,21,24). Althoughbaseline characteristics were similar in the three post-randomization subgroups, differences in risk-profile (selec-tion of a higher-risk population) could have played a roledespite our attempts to adjust for these imbalances.
An alternative explanation could be the observed differ-ences as to the urgency of PCI. In ASSENT-3, total PCIrates were similar in the three treatment arms with asignificantly lower need for urgent intervention in the ABCarm and to a lesser extent in the ENOX arm and a
borderline significant excess of elective PCI in the ABCarm. Patient characteristics (and hence probably lesioncharacteristics and extent of disease) were similar in thethree treatment groups in ASSENT-3 (15). Because differ-ences in urgency for revascularization are likely to be a directtreatment effect, patients with similar lesion complexitycould potentially have been shifted from urgent to electivePCI or even medical therapy, as a consequence of theplaque-stabilizing characteristics of ABC. This could haveresulted in a concentration of very complex “ABC-resistant”lesions in a smaller group of patients undergoing urgentrevascularization and a selection of “ABC-stabilized” butcomplex lesions in the group of patients undergoing anelective intervention. Percutaneous coronary intervention inthese patients with complex lesions might have a worseprognosis, and this could explain in part the higher mortal-ity rates. On the other hand, some “ABC-stabilized” pa-tients who were treated medically could have benefited froma PCI, preventing late re-infarction and death.
Safety of the new antithrombotic co-therapies was not anissue after elective PCI. The rates of in-hospital non-cerebral major bleeds as well as puncture-related bleeds werelow and similar in the three treatment arms. These resultsare in accordance with other recent trials (16,17,20,22). Thetime to elective PCI in ASSENT-3 was long (�5 days),which may partly explain the low rates of major bleedings atthe puncture site.
An excess of major bleeds was observed in patients whoneeded urgent PCI compared with those who underwent anelective PCI (Table 5). This excess was small in the UFHgroup but larger in the ABC and ENOX groups. Whencompared with UFH, the incidence of major, non-cerebralbleeds in patients undergoing urgent PCI was significantlyhigher with ABC, whereas there was a modest increase inpatients treated with ENOX. Overall, puncture-relatedbleeds (major and minor) were similar in the three arms.Nevertheless, the incidence of major puncture-relatedbleeds was higher in the ENOX arm. It is unlikely that thisdifference could be attributed to additional administrationof UFH during the procedure, because the proportion of
Table 5. Bleeding Episodes After Urgent PCI Compared With Elective PCI and No PCI inASSENT-3 Population
End PointsUrgent PCIASSENT-3
Elective PCIASSENT-3
No PCIASSENT-3
In-hospital major bleeds (excluding ICH)UFH 10/292 (3.4%) 6/332 (1.8%) 24/1411 (1.7%)ENOX 17/242 (7.0%) 6/348 (1.7%) 38/1446 (2.6%)ABC 16/182 (8.8%) 4/384 (1.0%) 57/1443 (4.0%)
Puncture-related bleedsUFH 56/292 (19.2%) 34/332 (10.2%)ENOX 55/242 (22.7%) 30/348 (8.6%)ABC 34/182 (18.7%) 33/384 (8.6%)
ABC � abciximab; ASSENT-3 � Assessment of the Safety and Efficacy of New Thrombolytic Regimens; ENOX �enoxaparin; ICH � intracranial hemorrhage; PCI � percutaneous coronary intervention; UFH � unfractionated heparin.
1183JACC Vol. 42, No. 7, 2003 Dubois et al.October 1, 2003:1178–85 Outcome of PCI in ASSENT-3

patients who received additional UFH during PCI wassimilar in the three groups.
Bleeding sites differed among the three treatment arms:one-fourth of the major bleeds occurred at the arterialpuncture site in the ABC arm, in contrast with one-half andalmost two-thirds in the UFH and ENOX arms, respec-tively (Fig. 2). These observations are in line with those ofthe Global Use of Strategies To open Occluded coronaryarteries (GUSTO V) trial (14). No single bleeding site couldexplain the relatively higher proportion of non-puncture-related major bleeding episodes in the ABC arm. New trialsof facilitated PCI will evaluate the safety of differentpre-PCI pharmacologic reperfusion regimens.
Our study has several limitations. Because this was a posthoc analysis, caution is needed when interpreting differencesbetween treatment groups, because the performance of PCIcould have been influenced by the study treatments. Inaddition, interactions between study treatment and PCI canfurther obscure the study treatment effect. We tried toaddress some of these issues by analyzing data using aproportional hazards regression that included the interac-tion between occurrence of PCI and treatment, in whichPCI was included as a time-dependent covariate, and bycalculating propensity scores in order to avoid or to reduceimbalances between treatment groups after the performanceof a PCI. It should be kept in mind that even when takingthe above measures, it is impossible to ascertain the trueeffect of the study treatment in the group of patients whounderwent a PCI. No adjustments for multiplicity weremade, and false positive results can therefore not be ex-cluded. On the other hand, event rates were low, and truedifferences might have been missed because of the smallsample size.
CONCLUSIONS
Clinical outcomes in patients with an ST-elevation AMIundergoing an elective PCI after treatment with TNK-tPAwere similar in the three treatment arms studied inASSENT-3, and no excess of bleeding complications wasobserved.
Although fewer patients needed urgent PCI after co-therapy with ABC and ENOX, clinical outcomes were lessfavorable in this selected population, especially with ABC.
Reprint requests and correspondence: Prof. Frans Van de Werf,Department of Cardiology, University Hospital GasthuisbergLeuven, Herestraat 49, B 3000 Leuven, Belgium. E-mail:[email protected].
REFERENCES
1. Gruppo Italiano per lo Studio della Streptochinasi nell’Infarcto Mio-cardio (GISSI). Effectiveness of intravenous thrombolytic treatment inacute myocardial infarction. Lancet 1986;1:397–401.
2. ISIS-2 (Second International Study of Infarct Survival) Collaborativegroup. Randomized trial of intravenous streptokinase, oral aspirin,
both, or neither among 17187 cases of suspected acute myocardialinfarction: ISIS-2. Lancet 1988;2:349–60.
3. The GUSTO Investigators. An international randomized trial com-paring four thrombolytic strategies for acute myocardial infarction.N Engl J Med 1993;329:673–82.
4. The GUSTO-III Investigators. An international, multicenter, ran-domized comparison of reteplase with alteplase for acute myocardialinfarction. N Engl J Med 1997;337:1118–23.
5. The ASSENT-2 Investigators. Single-bolus tenecteplase comparedwith front-loaded alteplase in acute myocardial infarction: theASSENT-2 double-blind randomized trial. Lancet 1999;354:716–22.
6. The GUSTO Angiographic Investigators. The effects of tissue plas-minogen activator, streptokinase, or both on coronary artery patency,ventricular function and survival after acute myocardial infarction.N Engl J Med 1993;329:1615–22.
7. Smalling RW, Bode C, Kalbfleisch J, et al., for the RAPID Investi-gators. More rapid, complete and stable coronary thrombolysis withbolus administration of reteplase compared with alteplase infusion inacute myocardial infarction. Circulation 1995;91:2725–32.
8. Bode C, Smalling RW, Berg G, et al. Randomized comparison ofcoronary thrombolysis achieved with double bolus reteplase andfront-loaded alteplase in patients with acute myocardial infarction.Circulation 1996;94:891–98.
9. Cannon CP, Gibson CM, McCabe CH, et al. TNK-tissue plasmin-ogen activator compared with front-loaded alteplase in acute myocar-dial infarction: results of the TIMI 10B trial. Circulation 1998;98:2805–14.
10. den Heijer P, Vermeer F, Ambrosioni E, et al. Evaluation ofweight-adjusted single-bolus plasminogen activator in patients withmyocardial infarction: a double-blind, randomized angiographic trialof lanoteplase versus alteplase. Circulation 1998;98:2117–25.
11. White H, Van de Werf F. Thrombolysis for acute myocardialinfarction. Circulation 1998;97:1632–46.
12. Armstrong PW, Collen D. Fibrinolysis for acute myocardial infarc-tion: current status and new horizons for pharmacological reperfusion,part I. Circulation 2001;103:2862–6.
13. Ross AM, Molhoek P, Lundergan C, et al. Randomized comparisonof enoxaparin, a low-molecular-weight heparin, with unfractionatedheparin adjunctive to recombinant tissue plasminogen activator throm-bolysis and aspirin. Second Trial of Heparin and Aspirin ReperfusionTherapy (HART II). Circulation 2001;104:648–52.
14. The GUSTO-V Investigators. Reperfusion therapy for acute myocar-dial infarction with fibrinolytic therapy or combination reduced fi-brinolytic therapy and platelet glycoprotein IIb/IIIa inhibition: theGUSTO V randomized trial. Lancet 2001;357:1905–14.
15. The ASSENT-3 Investigators. Efficacy and safety of tenecteplase incombination with enoxaparin, abciximab, or unfractionated heparin:the ASSENT-3 randomized trial in acute myocardial infarction.Lancet 2001;358:605–13.
16. Rabah MM, Premmereur J, Graham M, et al. Usefulness of intrave-nous enoxaparin for percutaneous coronary intervention in stableangina pectoris. Am J Cardiol 1999;84:1391–5.
17. Kereiakes DJ, Grines C, Fry E, et al., for the NICE 1 and NICE 4Investigators. National Investigators Collaborating on Enoxaparin.Enoxaparin and abciximab adjunctive pharmacotherapy during percu-taneous coronary intervention. J Invasive Cardiol 2001;13:272–8.
18. Collet JP, Montalescot G, Lison L, et al. Percutaneous coronaryintervention after subcutaneous enoxaparin pretreatment in patientswith unstable angina pectoris. Circulation 2001;103:658–63.
19. The EPIC Investigators. Use of a monoclonal antibody directedagainst the platelet glycoprotein IIb/IIIa receptor in high-risk coronaryangioplasty. N Engl J Med 1994;330:956–61.
20. The EPILOG Investigators. Platelet glycoprotein IIb/IIIa receptorblockade and low-dose heparin during percutaneous coronary revas-cularization. N Engl J Med 1997;336:1689–96.
21. The CAPTURE Investigators. Randomised placebo-controlled trialof abciximab before and during coronary intervention in refractoryunstable angina: the CAPTURE study. Lancet 1997;349:1429–35.
22. The EPISTENT Investigators. Randomised placebo-controlled andballoon-angioplasty-controlled trial to assess safety of coronary stent-ing with use of platelet glycoprotein-IIb/IIIa blockade. Lancet 1998;352:87–92.
23. Stone GW, Grines CL, Cox DA, et al., for the CADILLACInvestigators. Comparison of angioplasty with stenting, with or
1184 Dubois et al. JACC Vol. 42, No. 7, 2003Outcome of PCI in ASSENT-3 October 1, 2003:1178–85

without abciximab, in acute myocardial infarction. N Engl J Med2002;346:957–66.
24. Montalescot G, Barragan P, Wittenberg O, et al., for the ADMIRALInvestigators. Platelet glycoprotein IIb/IIIa inhibition with coronarystenting for acute myocardial infarction. N Engl J Med 2001;344:1895–903.
25. Hudson MP, Granger CB, Topol EJ, et al. Early reinfarction afterfibrinolysis: experience from the global utilization of streptokinase andtissue plasminogen activator (alteplase) for occluded coronary arteries(GUSTO I) and global use of strategies to open occluded coronaryarteries (GUSTO III) trials. Circulation 2001;104:1229–35.
26. Rosenbaum PR, Rubin DB. The central role of the propensity score inobservational studies for causal effects. Biometrika 1983;70:41–55.
27. Antman EM, McCabe CH, Gurfinkel EP, et al. Enoxaparin preventsdeath and cardiac ischemic events in unstable angina/non–Q-wavemyocardial infarction: results of the thrombolysis in myocardial infarc-tion (TIMI) 11B trial. Circulation 1999;100:1593–601.
28. Cohen M, Demers C, Gurfinkel EP, et al, for the Efficacy and Safetyof Subcutaneous Enoxaparin in Non–Q-Wave Coronary Events StudyGroup. A comparison of low-molecular-weight heparin with unfrac-tionated heparin for unstable coronary artery disease. N Engl J Med1997;337:447–52.
1185JACC Vol. 42, No. 7, 2003 Dubois et al.October 1, 2003:1178–85 Outcome of PCI in ASSENT-3

Triple Antiplatelet Therapy During PercutaneousCoronary Intervention Is Associated WithImproved Outcomes Including One-Year SurvivalResults From the Do Tirofiban and ReoProGive Similar Efficacy Outcome Trial (TARGET)Albert W. Chan, MD,* David J. Moliterno, MD,† Peter B. Berger, MD,‡ Gregg W. Stone, MD,§Peter M. DiBattiste, MD,� Steven L. Yakubov, MD,¶ Shelly K. Sapp, MS,# Kathy Wolski, MPH,#Deepak L. Bhatt, MD,† Eric J. Topol, MD,† for the TARGET Investigators**New Orleans, Louisiana; Cleveland and Columbus, Ohio; Rochester, Minnesota; New York, New York; and WestPoint, Pennsylvania
OBJECTIVES We sought to examine if clopidogrel treatment initiated before coronary stenting improvedclinical outcomes among patients receiving aspirin and a glycoprotein (GP) IIb/IIIa inhibitor.
BACKGROUND Antiplatelet therapy plays a pivotal role in contemporary percutaneous coronary interventions(PCI).
METHODS Outcomes among 4,809 patients randomized to tirofiban or abciximab during PCI with stentplacement were compared according to whether they received 300 mg of clopidogrel beforePCI (93.1%) versus immediately after the procedure.
RESULTS The 30-day primary composite end point (death, myocardial infarction [MI], or urgent targetvessel revascularization [TVR]) was lower among clopidogrel-pretreated patients (6.6% vs.10.4%, p � 0.009), mainly because of reduction of MI (6.0% vs. 9.5%, p � 0.012). Thebenefit of clopidogrel pretreatment was sustained at six months (death, MI, any TVR: 14.6%vs. 19.8%, HR � 0.71, p � 0.010), and this was due mainly to lowering of death and MI(7.8% vs. 13.0%, p � 0.001). At one year, clopidogrel pretreatment was associated with alower mortality rate (1.7% vs. 3.6%, p � 0.011). Because clopidogrel pretreatment was notrandomized, multivariable and propensity analyses were performed. After adjusting forbaseline heterogeneity, clopidogrel pretreatment was an independent predictor for death orMI at 30 days (HR � 0.63, p � 0.012) and at six months (HR � 0.61, p � 0.003), andsurvival at one year (HR � 0.53, p � 0.044). No excess in 30-day bleeding events was notedwith clopidogrel pretreatment.
CONCLUSIONS Among patients undergoing coronary stent placement with aspirin and a GP IIb/IIIainhibitor, clopidogrel pretreatment is associated with a reduction of death and MI irrespectiveof the type of GP IIb/IIIa inhibitor used. (J Am Coll Cardiol 2003;42:1188–95) © 2003by the American College of Cardiology Foundation
Antiplatelet therapy plays a pivotal role in percutaneouscoronary interventions (PCI). The use of aspirin duringcoronary balloon angioplasty reduces the incidence of acute
See page 1196
thrombotic complications (1–3). When added to aspirin,intravenous glycoprotein (GP) IIb/IIIa receptors furtherimprove clinical outcome during elective, urgent, and emer-gency PCI (4–10). The administration of ticlopidine aftercoronary stenting also improves clinical outcome (11–18).
In a subanalysis of the Evaluation of Platelet IIb/IIIaInhibitor for Stenting (EPISTENT) trial (19), ticlopidinegiven before PCI was associated with a reduction of subse-quent major adverse cardiac events during the first year.However, this benefit was evident only among patientsrandomly assigned to placebo and not among those patientsreceiving the GP IIb/IIIa inhibitor abciximab.
Clopidogrel is a selective, irreversible adenosine diphos-phate (ADP) receptor antagonist (20). It has a more rapidplatelet anti-aggregatory effect than ticlopidine, andachieves near maximal platelet inhibition within 2 to 6 husing a 300 mg oral loading dose (21–23). Given after PCI,the combination of aspirin and clopidogrel appears to havea superior safety profile as compared with aspirin plusticlopidine (24–28). In a recent substudy from the Clopi-dogrel in Unstable Angina to Prevent Recurrent Events trial(PCI-CURE) (29), clopidogrel treatment before PCI (withor without stent placement) was associated with improvedoutcome, though less than one-fourth of the patientsreceived IIb/IIIa inhibitors. Because GP IIb/IIIa antago-nists provide potent inhibition of platelet aggregation and
From the *Department of Cardiology, Ochsner Clinic Foundation, New Orleans,Louisiana; †Department of Cardiovascular Medicine, The Cleveland Clinic Foun-dation, Cleveland, Ohio; ‡Division of Cardiology, Mayo Clinic Foundation, Roch-ester, Minnesota; §Lenox Hill Heart and Vascular Institute, New York, New York;�Merck, West Point, Pennsylvania; ¶Riverside Methodist Hospital, Columbus, Ohio;and #Department of Biostatistics and Epidemiology, The Cleveland Clinic Founda-tion, Cleveland, Ohio. The TARGET study was supported by Merck, Inc., WestPoint, Pennsylvania. Dr. DiBattiste is an employee of Merck. **For the full list ofTARGET investigators, please refer to N Engl J Med 2001;344:1888–94.
Manuscript received December 12, 2002; revised manuscript received April 22,2003, accepted May 9, 2003.
Journal of the American College of Cardiology Vol. 42, No. 7, 2003© 2003 by the American College of Cardiology Foundation ISSN 0735-1097/03/$30.00Published by Elsevier Inc. doi:10.1016/S0735-1097(03)00944-6

have become a standard pharmacologic adjunct in contem-porary PCI, whether clopidogrel pretreatment providesimportant additional benefits among patients receiving IIb/IIIa inhibitors remains uncertain. Therefore, we examinedthe impact of clopidogrel pretreatment among patients inthe Do Tirofiban and ReoPro Give Similar Efficacy Out-come Trial (TARGET) (30).
METHODS
Study protocol. The design and methods of TARGEThave been previously detailed (30,31). In brief, 4,809 pa-tients undergoing elective or urgent PCI-stent of nativecoronary vessels or bypass grafts were enrolled betweenDecember 1999 and August 2000 in 149 hospitals in NorthAmerica, Australia, and Europe. Patients were randomizedin a double-blind, double-dummy fashion to receive a bolusand infusion of either abciximab or tirofiban. All patientsreceived 250 to 500 mg of aspirin within 24 h before theprocedure and 75 to 325 mg/day following the procedure. Aloading dose of 300 mg of clopidogrel at least 2 to 6 h beforethe procedure was recommended. Alternatively, the samedose of clopidogrel could be given just before the PCIprocedure if it were performed immediately following diag-nostic angiography. The timing of clopidogrel administra-tion was at the interventional cardiologists’ discretion.Patients who received clopidogrel before either abciximab ortirofiban was given were categorized into the clopidogrelpretreatment group. Otherwise, a 300-mg loading dose ofclopidogrel was to be given as early as possible after theprocedure. Clopidogrel was continued for 30 days after PCIat a dose of 75 mg daily. At the time of procedure, heparinwas administered to achieve an activated clotting time �250s. Interventional procedures were performed as per institu-tional standard.Study end points. The primary end point of TARGETwas the composite of death, nonfatal myocardial infarction(MI), or urgent TVR within 30 days of the index procedure.Prespecified secondary end points included the composite of
death, nonfatal MI, or any TVR at six months and mortalityat one year. Treatment assignment remained blinded to oneyear. The definition of MI during index hospitalization andto six months was described previously (30). Target vesselrevascularization was defined as any repeat revascularizationof the vessel treated during the index procedure. For thesafety analysis, the end points of major and minor bleedingwere defined using the Thrombolysis In Myocardial Infarc-tion (TIMI) criteria (32). End points were reported byinvestigators, and were reviewed and adjudicated by anindependent Clinical Events Committee.Statistical analysis. All patients were categorized accord-ing to whether they received pretreatment with clopidogrelor not. The time of first clopidogrel administration wasrecorded, and subanalysis was performed separating patientsinto pretreatment intervals: no pretreatment; treatment 0 to2 h, 2 to 6 h, or �6 h before PCI (time zero defined as whenIIb/IIIa inhibitor bolus was given). The demographic,procedural, and safety data are reported as percentages fordiscrete variables, and as means � 1 SD for continuousvariables. Comparisons of the baseline characteristics be-tween clopidogrel pretreatment and no pretreatment weremade by means of chi-square statistics for categoricalvariables and Mann-Whitney-Wilcoxon tests for continu-ous variables. Fisher’s exact test was used to compareinfrequent events such as major and minor bleeding.Kaplan-Meier methods were used to estimate end points at30 days, 6 months, and 1 year, and log-rank tests were usedto compare the clopidogrel pretreatment and no pretreat-ment groups.
Because the timing of clopidogrel administration relativeto the PCI procedure was not randomized, a propensityanalysis was performed (33) to adjust for potential biasinherent in treating patients with clopidogrel before ratherthan following PCI. Based on the individual demographicand preprocedural clinical characteristics, a propensity scorewas developed for each patient using a multivariable logisticregression model in order to estimate the probability ofclopidogrel pretreatment. Covariates that were tested in themodel included demographic characteristics (age, gender,race, body mass index), cardiovascular risk factors (cigarettesmoking, hypertension, diabetes, hypercholesterolemia, andfamily history of coronary artery disease), cardiovascular andmajor noncardiac comorbidities (prior history of coronarybypass, PCI, MI, heart failure, stroke, peripheral arterialdisease, gastrointestinal disorders, and bleeding diathesis),acuity of presentation (recent Q-wave MI, non–Q-waveMI, unstable angina, and stable angina), and concomitantmedication use (aspirin, angiotensin-converting enzymeinhibitors, beta-blockers, calcium-receptor antagonist,lipid-lowering agent, nitrates, anti-inflammatory agents,anti-ulcerants, insulin, and hypoglycemic agents). To exam-ine the impact of clopidogrel pretreatment on outcome, thepropensity score was entered into the Cox proportionalhazards model as a continuous variable along with potentialcovariates that might affect outcome. These variables in-
Abbreviations and AcronymsACS � acute coronary syndromeADP � adenosine diphosphateCREDO � Clopidogrel for Reduction of Events
During ObservationEPISTENT � Evaluation of Platelet IIb/IIIa Inhibitor
for StentingGOLD � Assessing Ultegra-AU StudyGP � glycoproteinMI � myocardial infarctionPCI � percutaneous coronary interventionPCI-CURE � PCI substudy of the Clopidogrel in
Unstable Angina to Prevent RecurrentEvents Trial
TIMI � Thrombolysis In Myocardial InfarctionTVR � target vessel revascularization
1189JACC Vol. 42, No. 7, 2003 Chan et al.October 1, 2003:1188–95 Clopidogrel Pretreatment in TARGET

cluded those entered into the propensity score model, andthe procedural variables (assigned study drug, prior heparinuse, number of diseased vessels, target vessel(s), lesionlength, multivessel PCI, pre-TIMI flow, U.S. vs. non-U.S.enrollment). A p value of �0.05 was considered statisticallysignificant in all analyses.
RESULTS
Of the 4,809 patients enrolled, 4,477 (93.1%) were givenclopidogrel before PCI. Baseline clinical characteristics ofthe two groups are shown in Table 1. Of note, the twogroups were similar regarding cardiovascular risk profile, theprevalence of comorbidities, and indication for coronaryrevascularization. Compared with patients who did notreceive clopidogrel before PCI, clopidogrel-pretreated pa-tients were more likely to receive aspirin, beta-blockers,calcium-channel blockers, and lipid-lowering therapy beforetheir procedures. Among the patients who received pre-treatment, 2,535 patients (56.6%) received the loading dosewithin 2 h before procedures, 1,216 patients (27.2%) within2 to 6 h, and 726 patients (16.2%) for �6 h before the indexprocedure. The mean duration from clopidogrel adminis-tration to initiation of PCI was 2.1 h.30-day outcomes. The primary composite end point ofdeath, MI, or urgent TVR at 30 days occurred in 10.4% ofpatients without pretreatment and in 6.6% of patients withclopidogrel pretreatment (p � 0.009, Table 2). The benefitof clopidogrel pretreatment was predominantly due to areduction in MI (9.5% vs. 6%, p � 0.012). There was nosignificant difference in the triple end point event ratesbetween patients who received pretreatment for 0 to 2 h andthose who were pretreated for 2 to 6 h (6.5% vs. 7.7%,respectively; p � 0.198). Compared with patients who didnot receive clopidogrel until after PCI, those who werepretreated 0 to 6 h before the procedure had a 34% lowercomposite event rate (6.9% vs. 10.4%, p � 0.021). Further-more, as compared with those who were pretreated for �6h, patients who were clopidogrel-loaded for �6 h beforePCI had a 29% lowering in 30-day events (6.9% vs. 4.9%, p� 0.045); this difference was due mainly to fewer MI events(6.3% vs. 4.2%, p � 0.028).
Figure 1 illustrates the rates of primary end point accord-ing to clopidogrel pretreatment and IIb/IIIa drug assign-ment. When given to patients randomized to tirofibantherapy, clopidogrel pretreatment relatively reduced the30-day event rate by 43%, from 12.8% to 7.3% (p � 0.017).Likewise, patients who were pretreated with clopidogrel andreceived abciximab had a 30% relative reduction in thecomposite event rate (from 8.4% to 5.9%, p � 0.168)compared with abciximab without clopidogrel pretreatment.Whereas the overall TARGET study showed a 26% relativerisk reduction in primary end point with abciximab ascompared with tirofiban, the superiority of abciximab wasattenuated among patients who received clopidogrel pre-treatment (Table 3).
Table 1. Baseline Clinical and Target Lesion Characteristics ofPatients Who Were Pretreated and Those Who Were NotPretreated With Clopidogrel
ClopidogrelPretreatment(n � 4,477)
NoClopidogrel
Pretreatment(n � 332) p
Age, yrs 62.3 � 10.9 62.5 � 11.3 0.954Female, % 26.4 28.3 0.441Weight, kg 86.0 � 17.6 87.6 � 18.5 0.121Caucasian, % 91.4 88.0 0.034Risk factors, %
Cigarette smoking 21.8 24.2 0.306Diabetes mellitus 23.3 22.0 0.579Hypertension 64.5 68.9 0.110Hypercholesterolemia 75.1 72.0 0.214Family history of coronary
artery disease54.7 53.1 0.577
Medical history, %Coronary bypass grafting 17.2 13.3 0.064Prior PCI 29.7 27.5 0.404Heart failure 9.7 11.5 0.292Myocardial infarction 39.6 36.6 0.267Prior stroke 2.7 2.4 0.722Peripheral arterial disease 9.6 11.5 0.265Gastrointestinal disorders 23.9 24.8 0.719Bleeding disorders 0.8 1.2 0.330
Medications, %Aspirin (within 24 h) 97.3 93.6 � 0.001ACE inhibitors 36.9 32.5 0.113Beta-blockers 66.0 57.8 0.003Calcium-channel antagonists 31.7 24.4 0.006Lipid-lowering agents 60.7 48.8 � 0.001Nitrates 59.5 58.7 0.789Thombolytics during index
admission5.3 4.2 0.395
Anti-inflammatory agents 15.1 16.9 0.393Anti-ulcerants 32.5 29.8 0.310Insulin 8.2 8.1 0.944Oral hypoglycemic agents 16.6 15.4 0.573
Randomized to abciximab, % 49.8 54.2 0.123Indication for PCI, % 0.541
Q-wave MI 5.5 5.4Non–Q-wave MI 10.3 9.3Unstable angina 46.9 51.5Stable angina and others 37.3 33.8
Lesion locationLeft anterior descending artery 42.6 42.3 0.920Circumflex artery 28.1 29.3 0.643Right coronary artery 37.3 38.1 0.776Left main coronary artery 1.3 1.8 0.454Bypass graft 6.1 5.4 0.625
Severity of stenosis before PCI 87.6 � 9.7% 88.4 � 9.8% 0.117Lesion length, % 0.912
�10 mm 24.9 25.210–20 mm 59.2 58.2�20 mm 15.9 16.7
Left ventricular ejection fraction 0.244�50% 72.6 73.130%–50% 25.0 22.9�30% 2.5 4.0
ACE � angiotensin-converting enzyme; MI � myocardial infarction; PCI �percutaneous coronary intervention.
1190 Chan et al. JACC Vol. 42, No. 7, 2003Clopidogrel Pretreatment in TARGET October 1, 2003:1188–95
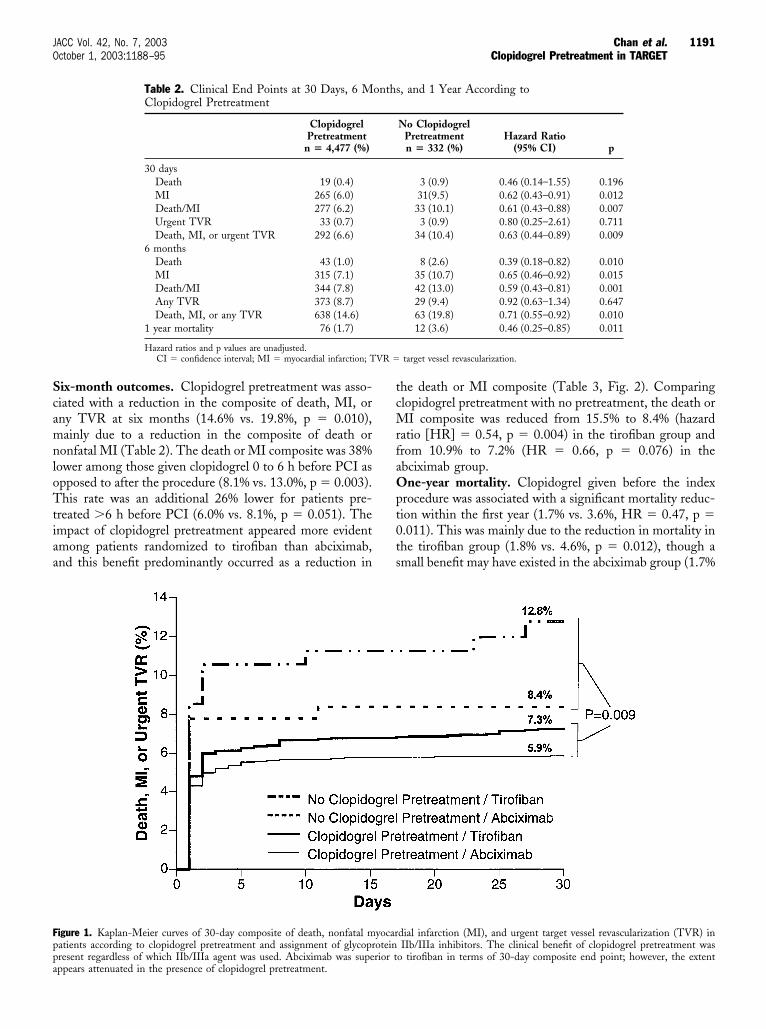
Six-month outcomes. Clopidogrel pretreatment was asso-ciated with a reduction in the composite of death, MI, orany TVR at six months (14.6% vs. 19.8%, p � 0.010),mainly due to a reduction in the composite of death ornonfatal MI (Table 2). The death or MI composite was 38%lower among those given clopidogrel 0 to 6 h before PCI asopposed to after the procedure (8.1% vs. 13.0%, p � 0.003).This rate was an additional 26% lower for patients pre-treated �6 h before PCI (6.0% vs. 8.1%, p � 0.051). Theimpact of clopidogrel pretreatment appeared more evidentamong patients randomized to tirofiban than abciximab,and this benefit predominantly occurred as a reduction in
the death or MI composite (Table 3, Fig. 2). Comparingclopidogrel pretreatment with no pretreatment, the death orMI composite was reduced from 15.5% to 8.4% (hazardratio [HR] � 0.54, p � 0.004) in the tirofiban group andfrom 10.9% to 7.2% (HR � 0.66, p � 0.076) in theabciximab group.One-year mortality. Clopidogrel given before the indexprocedure was associated with a significant mortality reduc-tion within the first year (1.7% vs. 3.6%, HR � 0.47, p �0.011). This was mainly due to the reduction in mortality inthe tirofiban group (1.8% vs. 4.6%, p � 0.012), though asmall benefit may have existed in the abciximab group (1.7%
Table 2. Clinical End Points at 30 Days, 6 Months, and 1 Year According toClopidogrel Pretreatment
ClopidogrelPretreatment
n � 4,477 (%)
No ClopidogrelPretreatmentn � 332 (%)
Hazard Ratio(95% CI) p
30 daysDeath 19 (0.4) 3 (0.9) 0.46 (0.14–1.55) 0.196MI 265 (6.0) 31(9.5) 0.62 (0.43–0.91) 0.012Death/MI 277 (6.2) 33 (10.1) 0.61 (0.43–0.88) 0.007Urgent TVR 33 (0.7) 3 (0.9) 0.80 (0.25–2.61) 0.711Death, MI, or urgent TVR 292 (6.6) 34 (10.4) 0.63 (0.44–0.89) 0.009
6 monthsDeath 43 (1.0) 8 (2.6) 0.39 (0.18–0.82) 0.010MI 315 (7.1) 35 (10.7) 0.65 (0.46–0.92) 0.015Death/MI 344 (7.8) 42 (13.0) 0.59 (0.43–0.81) 0.001Any TVR 373 (8.7) 29 (9.4) 0.92 (0.63–1.34) 0.647Death, MI, or any TVR 638 (14.6) 63 (19.8) 0.71 (0.55–0.92) 0.010
1 year mortality 76 (1.7) 12 (3.6) 0.46 (0.25–0.85) 0.011
Hazard ratios and p values are unadjusted.CI � confidence interval; MI � myocardial infarction; TVR � target vessel revascularization.
Figure 1. Kaplan-Meier curves of 30-day composite of death, nonfatal myocardial infarction (MI), and urgent target vessel revascularization (TVR) inpatients according to clopidogrel pretreatment and assignment of glycoprotein IIb/IIIa inhibitors. The clinical benefit of clopidogrel pretreatment waspresent regardless of which IIb/IIIa agent was used. Abciximab was superior to tirofiban in terms of 30-day composite end point; however, the extentappears attenuated in the presence of clopidogrel pretreatment.
1191JACC Vol. 42, No. 7, 2003 Chan et al.October 1, 2003:1188–95 Clopidogrel Pretreatment in TARGET

vs. 2.8%, p � 0.257). For patients who did not receiveclopidogrel pretreatment, abciximab administration was as-sociated with a numerically lower but statistically similarmortality rate at one year compared with tirofiban (2.8% vs.4.6%, p � 0.390).Multivariable analysis. Within the propensity score anal-ysis, variables that independently predicted the use ofclopidogrel before PCI were (in descending order) prescrip-tion of lipid-lowering agents, concomitant aspirin use andhistory of angina. The following variables were also includedin the logistic model using intersections statistics to developthe final propensity score: BMI �30, race, hypertension,and use of prior medications such as angiotensin-convertingenzyme inhibitors, beta-blockers, and calcium channel
blockers. The goodness-of-fit for the propensity score asassessed by the c-statistic was 0.64. Using Cox proportionalhazards modeling to adjust for potential variables and thepropensity of prescribing clopidogrel before the procedure,clopidogrel pretreatment remained an independent predic-tor for a lower composite of death or MI at 30 days and sixmonths. Other independent correlates for death or MI at 30days and 6 months are provided in Table 4.
Not surprisingly, the strongest predictors for outcomeincluded advanced age, acuity of disease (acute coronarysyndrome [ACS]), and extent of atheroma (lesion lengthand number of vessels revascularized). Adding statisticalinteractions to several proportional hazard models, clopi-dogrel continued to provide independent predictive value.
Table 3. Influence of Clopidogrel Pretreatment on Relative Efficacy of Tirofiban Versus Abciximab on Various End Points
Clopidogrel Pretreatment (n � 4,477)
p
No Clopidogrel Pretreatment (n � 332)
pAbciximab
n � 2,231 (%)Tirofiban
n � 2,246 (%)Hazard Ratio*
(95% CI)Abciximab
n � 180 (%)Tirofiban
n � 152 (%)Hazard Ratio*
(95% CI)
30 daysDeath 8 (0.4) 11 (0.5) 0.73 (0.29–1.81) 0.497 2 (1.2) 1 (0.7) 1.72 (0.16–20.00) 0.655MI 118 (5.3) 147 (6.6) 0.81 (0.63–1.03) 0.080 13 (7.2) 18 (12.1) 0.61 (0.30–1.23) 0.167Death/MI 124 (5.6) 153 (6.9) 0.81 (0.64–1.03) 0.087 14 (7.8) 19 (12.8) 0.62 (0.31–1.23) 0.170Urgent TVR 15 (0.7) 18 (0.8) 0.83 (0.42–1.67) 0.609 1 (0.6) 2 (1.4) 0.42 (0.04–4.76) 0.470Death, MI, or urgent TVR 130 (5.9) 162 (7.3) 0.81 (0.64–1.01) 0.065 15 (8.4) 19 (12.8) 0.67 (0.33–1.32) 0.234
6 monthsDeath 21 (1.0) 22 (1.0) 0.96 (0.53–1.75) 0.891 4 (2.4) 4 (2.9) 0.91 (0.23–3.57) 0.883MI 143 (6.5) 172 (7.8) 0.83 (0.67–1.04) 0.108 16 (9.1) 19 (12.6) 0.71 (0.37–1.39) 0.324Death/MI 159 (7.2) 185 (8.4) 0.86 (0.69–1.06) 0.167 19 (10.9) 23 (15.5) 0.70 (0.38–1.30) 0.856Any TVR 193 (9.0) 180 (8.3) 1.08 (0.88–1.32) 0.470 15 (9.3) 14 (9.5) 0.96 (0.46–2.00) 0.909Death, MI, or any TVR 314 (14.4) 324 (14.7) 0.97 (0.83–1.34) 0.688 31 (18.3) 32 (21.6) 0.83 (0.51–1.35) 0.459
1-year mortality 37 (1.7) 39 (1.8) 0.95 (0.61–1.49) 0.840 5 (2.8) 7 (4.6) 0.61 (0.19–1.92) 0.390
*Refers to the unadjusted hazard ratios for abciximab vs. tirofiban.Abbreviations as in Table 2.
Figure 2. Kaplan-Meier curves of composite of death and nonfatal myocardial infarction (MI) to six months, based on the use of clopidogrel pretreatmentand assignment of glycoprotein IIb/IIIa inhibitors.
1192 Chan et al. JACC Vol. 42, No. 7, 2003Clopidogrel Pretreatment in TARGET October 1, 2003:1188–95

Interestingly, in one analysis, the use of antidepressantscontributed to the overall model (chi-squared � 6), andwhen adding the interaction term preprocedural clopidogrel� antidepressant use, the separate contribution of clopi-dogrel pretreatment was decreased whereas the contributionof antidepressants was increased. At one-year follow-up,clopidogrel pretreatment remained an independent predic-tor for survival (HR � 0.53; 95% CI, 0.29 to 0.98; p �0.044) after adjusting for the study drug treatment, age,gender, body mass index, presentation acuity, cardiac andvascular comorbidities, cardiovascular risk factors, bleedingdisorders, and medication use.Bleeding. The incidence of major and minor bleeding, andfrequency of transfusion according to clopidogrel pretreat-ment, are listed in Table 5. The frequency of these compli-cations was low, and there was no significant increase inbleeding events among patients treated with clopidogrelbefore undergoing PCI with adjunctive GP IIb/IIIainhibitors.
DISCUSSIONAmong PCI patients undergoing stent placement withadjunctive aspirin and a GP IIb/IIIa inhibitor, clopidogreladministered as an oral loading dose before the procedurewas associated with superior clinical outcome, which wasevident within 24 to 48 h after the procedure and wassustained at 6 months. Although the outcome with �6 h ofpretreatment was more favorable than that of 0 to 6 h ofpretreatment, clopidogrel loading within 6 h before theprocedure was also associated with significantly better out-come as compared with no pretreatment. Clopidogrel pre-treatment was predominantly associated with a reduction inischemic events (MI), though its benefit appears to extendto mortality reduction at one year. These associationsremained markedly significant following adjustment forbaseline clinical and procedural characteristics, as well as thepropensity for receiving preprocedural clopidogrel. Theobservations remained significant even when broadening thecomposite six-month outcome to include target vessel re-vascularization.
The efficacy of thienopyridine pretreatment before PCIhas been reported (19,29,34). In the EPISTENT trial (19),pretreatment with a thienopyridine (ticlopidine) was asso-ciated with a reduction of major adverse cardiac events,though the benefit was not seen among patients randomizedto IIb/IIIa inhibition. In the PCI-CURE study (29), theduration of clopidogrel pretreatment was markedly longerthan in the current study (days versus hours), but cardiacenzymes were not routinely measured postprocedure. Thepresence of an interaction between clopidogrel pretreatmentand IIb/IIIa inhibitor use could not be readily assessedbecause IIb/IIIa inhibitors were administered to a minorityof PCI-CURE patients. The results of the Clopidogrel forReduction of Events During Observation (CREDO) trialshowed that clopidogrel pretreatment before PCI reduced a28-day composite of death, MI, or urgent revascularization18.5% (from 8.3% to 6.8%, p � 0.23), though the benefitdid not reach statistical significance perhaps owing tosample size (35). However, similar to the PCI-CURE trial,less than one-fourth of the CREDO patients receivedplanned GP IIb/IIIa inhibitor treatment, and a similarlysmall percentage of patients were treated with IIb/IIIatherapy as part of a bailout strategy. Consistent with theearly report from CREDO, we observed the lowest adverseevent rate among those with �6 h of clopidogrel pretreat-ment. Given the large sample size in TARGET, it isimpressive that treatment with clopidogrel prior to coronarystenting was associated with incremental benefit in thepresence of both aspirin and a IIb/IIIa inhibitor. Thisbenefit seems extraordinary and likely reflects the impor-tance of inflammation and platelets in PCI associated withvascular injury (36).
The mechanism of benefit with clopidogrel pretreatmentdeserves particular attention. When combined with aspirintherapy, clopidogrel provides synergistic antiplatelet effects
Table 4. Independent Predictors for Death or MI AfterCoronary Stenting
CharacteristicsHazard
Ratio95% Confidence
Interval p
30 daysClopidogrel pretreatment 0.63 0.43–0.90 0.012RCA intervention 0.75 0.59–0.95 0.017Abciximab vs. tirofiban 0.80 0.64–1.00 0.048Propensity score 0.99 0.72–1.38 0.979Age � 65 years 1.53 1.22–1.91 � 0.001Multivessel PCI 1.60 1.22–2.10 0.001Maximal lesion length* 1.86 1.55–2.24 � 0.001
6 monthsClopidogrel pretreatment 0.61 0.44–0.84 0.003RCA intervention 0.78 0.63–0.97 0.022Propensity score 0.99 0.75–1.35 0.977Age � 65 years 1.31 1.07–1.61 0.008Acute coronary syndrome 1.39 1.10–1.75 0.005Heart failure 1.51 1.14–2.00 0.005Multivessel PCI 1.51 1.18–1.93 0.001Maximal lesion length* 1.68 1.43–1.98 � 0.001
*Classified as �10 mm vs. 10–20 mm vs. �20 mm.MI � myocardial infarction; PCI � percutaneous coronary intervention; RCA �
right coronary artery.
Table 5. Incidence of Bleeding and Transfusion DuringIndex Hospitalization
ClopidogrelPretreatment
(n � 4,477)
No ClopidogrelPretreatment
(n � 332) p
Major or minor bleeding, % 4.3 3.9 0.718Major bleeding, % 0.8 0.9 0.754Minor bleeding, % 3.6 3.3 0.821Transfusion, %
Packed red blood cells 1.3 0.9 0.800Platelet 0.4 0.9 0.191Plasma 0.2 0.3 0.475
1193JACC Vol. 42, No. 7, 2003 Chan et al.October 1, 2003:1188–95 Clopidogrel Pretreatment in TARGET

via concurrent inhibition of ADP and thromboxane A2pathways (37,38). Based on the results from the AssessingUltegra-AU (GOLD) study (39), optimal PCI outcomeregarding death or MI was observed with �95% inhibitionof platelet aggregation at 10 min after initiation of therapy.Interestingly, using ADP-induced platelet aggregation test-ing, the tirofiban regimen used in TARGET produced�70% platelet inhibition during the first 60 min of proce-dure, in contrast to abciximab, which consistently achieved�90% inhibition during this time (40,41). As such, clopi-dogrel pretreatment may lower the risk of myocardialnecrosis during the window of vulnerability following thetirofiban bolus and before the drug infusion can achieveadequate plasma levels (40,42,43). Even among abciximab-receiving patients with PCI, the current analysis suggeststhat clopidogrel pretreatment provides benefit.
Additionally, it is possible that a benefit of clopidogrelpretreatment is separately related to a reduction in plateletactivation and inflammation. Elevated C-reactive protein(CRP) level has been linked to the risk of cardiovasculardeath and MI after PCI (44,45). This association wasblunted in the presence of clopidogrel pretreatment (46),implying that patients with elevated baseline CRP mayderive particular benefit from clopidogrel pretreatment.Indeed, formation of platelet-leukocyte aggregates was re-duced by clopidogrel through lowering CD62 expression inan in vitro model (47), suggestive of a link between plateletactivation and inflammation. Although patients with ACSare more likely to have an associated heightened inflamma-tory state, both ACS and non-ACS patients received similarbenefit from clopidogrel pretreatment in the TARGET trial(48).Study limitations. Clopidogrel pretreatment in this studywas not randomized. Despite the use of contemporarystatistical methods to adjust for imbalances between thepretreatment and no pretreatment groups, unmeasured con-founders might have influenced the decision regarding thetiming of clopidogrel administration (selection bias), andthe intermediate goodness-of-fit of the propensity model(C-statistic 0.64) may reflect this. Alternatively, the model’sfit may only be modest because the covariates were alreadyfairly balanced between the groups. It is worth noting thatthe major determinants of early and intermediate outcomeafter PCI, such as age, left ventricular function, indicationfor procedure, and diabetic status were similar between thetwo study groups. As noted in Table 4, the propensity scoreitself was not independently predictive of outcome. Thissuggests that decisions regarding pretreatment with clopi-dogrel were not systematically biased according to baselineprognostic profiles. Finally, the duration of clopidogreltherapy before the index procedure was variable amongpatients. The quick onset of effect for the 300-mg bolusdosing reduces the effect of dose duration, although patientstreated more than 6 h in advance had the best outcome.However, by including all patients who received clopidogrelregardless of how soon before beginning PCI, our observa-
tions should only underestimate the effect of clopidogrelpretreatment.Conclusions. Our analysis suggests that in addition toplatelet inhibition provided by aspirin and GP IIb/IIIainhibitors, administration of clopidogrel before coronarystenting further reduces ischemic complications during bothelective and urgent PCI procedures. Even a relatively briefperiod of clopidogrel pretreatment, such as a loading doseseveral hours before PCI, is associated with improvedoutcomes. Pretreatment for �6 h was associated with evengreater antithrombotic protection and was found to be safe.This triple therapy antiplatelet regimen should be consid-ered for all PCI-stent patients.
Reprint requests and correspondence: Dr. David J. Moliterno,Department of Cardiovascular Medicine, The Cleveland ClinicFoundation, 9500 Euclid Avenue, Desk F25, Cleveland, Ohio44195. E-mail: [email protected].
REFERENCES
1. Barnathan ES, Schwartz JS, Taylor L, et al. Aspirin and dipyridamolein the prevention of acute coronary thrombosis complicating coronaryangioplasty. Circulation 1987;76:125–34.
2. Schwartz L, Bourassa MG, Lesperance J, et al. Aspirin and dipyrid-amole in the prevention of restenosis after percutaneous transluminalcoronary angioplasty. N Engl J Med 1988;318:1714–9.
3. Savage MP, Goldberg S, Bove AA, et al. Effect of thromboxane A2blockade on clinical outcome and restenosis after successful coronaryangioplasty. Multi-Hospital Eastern Atlantic Restenosis Trial (M-HEART II). Circulation 1995;92:3194–200.
4. Topol EJ, Califf RM, Weisman HF, et al. Randomised trial ofcoronary intervention with antibody against platelet IIb/IIIa integrinfor reduction of clinical restenosis: results at six months. The EPICInvestigators. Lancet 1994;343:881–6.
5. The CAPTURE Investigators. Randomised placebo-controlled trialof abciximab before and during coronary intervention in refractoryunstable angina: the CAPTURE Study. Lancet 1997;349:1429–35.
6. The IMPACT-II Investigators. Randomised placebo-controlled trialof effect of eptifibatide on complications of percutaneous coronaryintervention: IMPACT-II. Integrilin to Minimise Platelet Aggrega-tion and Coronary Thrombosis-II. Lancet 1997;349:1422–8.
7. The EPILOG Investigators. Platelet glycoprotein IIb/IIIa receptorblockade and low-dose heparin during percutaneous coronary revas-cularization. N Engl J Med 1997;336:1689–96.
8. The RESTORE Investigators. Effects of platelet glycoprotein IIb/IIIablockade with tirofiban on adverse cardiac events in patients withunstable angina or acute myocardial infarction undergoing coronaryangioplasty. Randomized Efficacy Study of Tirofiban for Outcomesand REstenosis. Circulation 1997;96:1445–53.
9. Lincoff AM, Califf RM, Moliterno DJ, et al. Complementary clinicalbenefits of coronary-artery stenting and blockade of platelet glycopro-tein IIb/IIIa receptors. Evaluation of Platelet IIb/IIIa Inhibition inStenting Investigators. N Engl J Med 1999;341:319–27.
10. The ESPRIT Investigators. Novel dosing regimen of eptifibatide inplanned coronary stent implantation (ESPRIT): a randomised,placebo-controlled trial. Lancet 2000;356:2037–44.
11. Schomig A, Neumann FJ, Kastrati A, et al. A randomized comparisonof antiplatelet and anticoagulant therapy after the placement ofcoronary-artery stents. N Engl J Med 1996;334:1084–9.
12. Urban P, Macaya C, Rupprecht HJ, et al. Randomized evaluation ofanticoagulation versus antiplatelet therapy after coronary stent implan-tation in high-risk patients: the Multicenter Aspirin and TiclopidineTrial after Intracoronary Stenting (MATTIS). Circulation 1998;98:2126–32.
13. Rupprecht HJ, Darius H, Borkowski U, et al. Comparison of anti-platelet effects of aspirin, ticlopidine, or their combination after stentimplantation. Circulation 1998;97:1046–52.
1194 Chan et al. JACC Vol. 42, No. 7, 2003Clopidogrel Pretreatment in TARGET October 1, 2003:1188–95

14. Leon MB, Baim DS, Popma JJ, et al. A clinical trial comparing threeantithrombotic-drug regimens after coronary-artery stenting. StentAnticoagulation Restenosis Study Investigators. N Engl J Med 1998;339:1665–71.
15. Schuhlen H, Kastrati A, Pache J, Dirschinger J, Schomig A. Sustainedbenefit over four years from an initial combined antiplatelet regimenafter coronary stent placement in the ISAR trial. IntracoronaryStenting and Antithrombotic Regimen. Am J Cardiol 2001;87:397–400.
16. Cutlip DE, Baim DS, Ho KK, et al. Stent thrombosis in the modernera: a pooled analysis of multicenter coronary stent clinical trials.Circulation 2001;103:1967–71.
17. Schuhlen H, Kastrati A, Pache J, Dirschinger J, Schomig A. Incidenceof thrombotic occlusion and major adverse cardiac events between twoand four weeks after coronary stent placement: analysis of 5,678patients with a four-week ticlopidine regimen. J Am Coll Cardiol2001;37:2066–73.
18. Berger PB, Mahaffey KW, Meier SJ, et al. Safety and efficacy of only2 weeks of ticlopidine therapy in patients at increased risk of coronarystent thrombosis: results from the Antiplatelet Therapy alone versusLovenox plus Antiplatelet therapy in patients at increased risk of StentThrombosis (ATLAST) trial. Am Heart J 2002;143:841–6.
19. Steinhubl S, Ellis S, Wolski K, Lincoff A, Topol E, for theEPISTENT Investigators. Ticlopidine pretreatment before coronarystenting is associated with sustained decrease in adverse cardiac events.Data from the Evaluation of Platelet IIb/IIIa Inhibitor for Stenting(EPISTENT) Trial. Circulation 2001;103:1403–9.
20. Geiger J, Brich J, Honig-Liedl P, et al. Specific impairment of humanplatelet P2Y(AC) ADP receptor-mediated signaling by the antiplate-let drug clopidogrel. Arterioscler Thromb Vasc Biol 1999;19:2007–11.
21. Thebault JJ, Kieffer G, Cariou R. Single-dose pharmacodynamics ofclopidogrel. Semin Thromb Hemost 1999;25:3–8.
22. Savcic M, Hauert J, Bachmann F, Wyld PJ, Geudelin B, Cariou R.Clopidogrel loading dose regimens: kinetic profile of pharmacody-namic response in healthy subjects. Semin Thromb Hemost 1999;25:15–9.
23. Cadroy Y, Bossavy JP, Thalamas C, Sagnard L, Sakariassen K, BoneuB. Early potent antithrombotic effect with combined aspirin and aloading dose of clopidogrel on experimental arterial thrombogenesis inhumans. Circulation 2000;101:2823–8.
24. Moussa I, Oetgen M, Roubin G, et al. Effectiveness of clopidogrel andaspirin versus ticlopidine and aspirin in preventing stent thrombosisafter coronary stent implantation. Circulation 1999;99:2364–6.
25. Berger PB, Bell MR, Rihal CS, et al. Clopidogrel versus ticlopidineafter intracoronary stent placement. J Am Coll Cardiol 1999;34:1891–4.
26. Bertrand ME, Rupprecht HJ, Urban P, Gershlick AH, InvestigatorsFT. Double-blind study of the safety of clopidogrel with and withouta loading dose in combination with aspirin compared with ticlopidinein combination with aspirin after coronary stenting: the clopidogrelaspirin stent international cooperative study (CLASSICS). Circulation2000;102:624–9.
27. Taniuchi M, Kurz HI, Lasala JM. Randomized comparison ofticlopidine and clopidogrel after intracoronary stent implantation in abroad patient population. Circulation 2001;104:539–43.
28. Bhatt DL, Bertrand ME, Berger PB, et al. Meta-analysis of random-ized and registry comparisons of ticlopidine with clopidogrel afterstenting. J Am Coll Cardiol 2002;39:9–14.
29. Mehta SR, Yusuf S, Peters RJ, et al. Effects of pretreatment withclopidogrel and aspirin followed by long- term therapy in patientsundergoing percutaneous coronary intervention: the PCI-CUREstudy. Lancet 2001;358:527–33.
30. Topol EJ, Moliterno DJ, Herrmann HC, et al. Comparison of twoplatelet glycoprotein IIb/IIIa inhibitors, tirofiban and abciximab, forthe prevention of ischemic events with percutaneous coronary revas-cularization. N Engl J Med 2001;344:1888–94.
31. Moliterno DJ, Topol EJ. A direct comparison of tirofiban andabciximab during percutaneous coronary revascularization and stent
placement: rationale and design of the TARGET study. Am Heart J2000;140:722–6.
32. Rao AK, Pratt C, Berke A, et al. Thrombolysis In MyocardialInfarction (TIMI) Trial—phase I: hemorrhagic manifestations andchanges in plasma fibrinogen and the fibrinolytic system in patientstreated with recombinant tissue plasminogen activator and streptoki-nase. J Am Coll Cardiol 1988;11:1–11.
33. D’Agostino RB. Propensity score methods for bias reduction in thecomparison of a treatment to a non-randomized control group. StatMed 1998;17:2265–81.
34. Assali AR, Salloum J, Sdringola S, et al. Effects of clopidogrelpretreatment before percutaneous coronary intervention in patientstreated with glycoprotein IIb/IIIa inhibitors (abciximab or tirofiban).Am J Cardiol 2001;88:884–6, A6.
35. Steinhubl SR, Berger PB, Mann JT 3rd, et al. Early and sustained dualoral antiplatelet therapy following percutaneous coronary intervention:a randomized controlled trial. JAMA 2002;288:2411–20.
36. Quinn MJ, Plow EF, Topol EJ. Platelet glycoprotein IIb/IIIa inhib-itors: recognition of a two-edged sword? Circulation 2002;106:379–85.
37. Harker LA, Marzec UM, Kelly AB, et al. Clopidogrel inhibition ofstent, graft, and vascular thrombogenesis with antithrombotic en-hancement by aspirin in nonhuman primates. Circulation 1998;98:2461–9.
38. Herbert JM, Dol F, Bernat A, Falotico R, Lale A, Savi P. Theantiaggregating and antithrombotic activity of clopidogrel is potenti-ated by aspirin in several experimental models in the rabbit. ThrombHaemost 1998;80:512–8.
39. Steinhubl SR, Talley JD, Braden GA, et al. Point-of-care measuredplatelet inhibition correlates with a reduced risk of an adverse cardiacevent after percutaneous coronary intervention: results of the GOLD(AU-Assessing Ultegra) multicenter study. Circulation 2001;103:2572–8.
40. Kabbani SS, Aggarwal A, Terrien EF, DiBattiste PM, Sobel BE,Schneider DJ. Suboptimal early inhibition of platelets by treatmentwith tirofiban and implications for coronary interventions. Am JCardiol 2002;89:647–50.
41. Lakkis NM, George S, Thomas E, Ali M, Guyer K, Carville D. Useof ICHOR-platelet works to assess platelet function in patients treatedwith GP IIb/IIIa inhibitors. Catheter Cardiovasc Interv 2001;53:346–51.
42. Simon D, Liu G, Ganz P, et al. A comparative study of lighttransmission aggregometry and automated bedside platelet functionassays in patients undergoing percutaneous coronary intervention andreceiving abciximab, eptifibatide, or tirofiban. Catheter CardiovascInterv 2001;52:433–4.
43. Swieirkosz TA, Kapoor S, Tardiff DC, et al. Does greater plateletinhibition explain abciximab’s superiority in the TARGET trial? Arandomized comparison. Circulation 2001;104:II–385.
44. Chew DP, Bhatt DL, Robbins MA, et al. Incremental prognosticvalue of elevated baseline C-reactive protein among established mark-ers of risk in percutaneous coronary intervention. Circulation 2001;104:992–7.
45. Walter DH, Fichtlscherer S, Sellwig M, Auch-Schwelk W, Schach-inger V, Zeiher AM. Preprocedural C-reactive protein levels andcardiovascular events after coronary stent implantation. J Am CollCardiol 2001;37:839–46.
46. Chew DP, Bhatt DL, Robbins MA, et al. Effect of clopidogrel addedto aspirin before percutaneous coronary intervention on the riskassociated with C-reactive protein. Am J Cardiol 2001;88:672–4.
47. Klinkhardt U, Graff J, Harder S. Clopidogrel, but not abciximab,reduces platelet leukocyte conjugates and P-selectin expression in ahuman ex vivo in vitro model. Clin Pharmacol Ther 2002;71:176–85.
48. Stone GW, Moliterno DJ, Bertrand M, et al. Impact of clinicalsyndrome acuity on the differential response to 2 glycoprotein IIb/IIIainhibitors in patients undergoing coronary stenting: the TARGETtrial. Circulation 2002;105:2347–54.
1195JACC Vol. 42, No. 7, 2003 Chan et al.October 1, 2003:1188–95 Clopidogrel Pretreatment in TARGET

EDITORIAL COMMENT
Platelet Inhibition Strategies inPercutaneous CoronaryInterventionCompetition or Coopetition?*James E. Tcheng, MD, FACC,Mark E. Campbell, MDDurham, North Carolina
Over the past two and a half decades, a remarkable series oftools, technologies, and techniques have been created,developed, and refined for the performance of percutaneouscoronary intervention (PCI). A constant over time, how-ever, has been the therapeutic framework of enlargement ofthe luminal dimensions of diseased coronary vessels as thehallmark of PCI. Within this construct, an obligatorydisruption of the integrity of the vascular endothelium andother vessel components is produced. An inherent andinevitable consequence of PCI is, thus, the creation of alocal environment conducive to thrombosis.
See page 1188
In parallel with developments in the technology of PCIhas been the detailed elucidation of platelet physiology,coupled with a deeper understanding of the role of theplatelet in the thrombosis cascade (1,2). The complexities ofthe platelet can be distilled into several overlapping func-tions: adhesion, activation, secretion, and aggregation. Inthe setting of PCI, numerous clinical trials have establishedthe independent efficacies of agents that target the platelet,namely aspirin, the thienopyridines, and platelet glycopro-tein (GP) IIb/IIIa receptor blockers (3–8). Classified bytheir respective targets, aspirin inhibits platelet activation viathe irreversible acetylation of cyclooxygenase and conse-quent suppression of the synthesis of thromboxane A2, apotent platelet stimulant. The thienopyridines (ticlopidineand clopidogrel) also irreversibly inhibit platelet activation,albeit via a different pathway, blockade of the P2T typeadenosine diphosphate (ADP) receptor (9). Adenosinediphosphate modulates the change of the GP IIb/IIIareceptor from an inactive, inert state to a ligand receptiveconformation. The platelet GP IIb/IIIa receptor antagonistsinhibit platelet aggregation via blockade of the RGD-specific binding site for fibrinogen and other adhesionmolecules to the IIb/IIIa integrin on platelets (10). Sinceactivation is a prerequisite to secretion and aggregation,
both aspirin and the thienopyridines (partially) inhibit thesefunctions; conversely, GP IIb/IIIa blockade indirectly re-duces platelet secretion by reducing platelet mass whilehaving little direct effect on platelet activation.
Rather than clarifying the landscape, clinical trials ofantiplatelet therapies have led to a bewildering array ofuncertainties regarding the appropriate selection, timing,and duration of the various treatment options. Althoughthere is universal acceptance of aspirin as a mainstay oftreatment, less certain are the answers about clopidogrel andthe GP IIb/IIIa antagonists. With respect to clopidogreltherapy as an adjunct to contemporary PCI, the key remain-ing questions include the following. First, what is theoptimal timing of the initiation of thienopyridine therapyrelative to the start of a PCI procedure—along with thecorollary question, is ad hoc treatment (i.e., on the cathe-terization table during a “cath possible” case) as good asseveral hours (or days) of pretreatment? Second, what isactually being accomplished with clopidogrel pretreat-ment—again with a corollary question, is post-treatment(after PCI) effective in preventing subacute stent thrombo-sis? Third, can a thienopyridine be used as a substitute for aGP IIb/IIIa integrin antagonist (and vice versa), or are theseagents complementary and best used concurrently? Fourth,what is the appropriate loading dose of clopidogrel, partic-ularly in the ad hoc situation? And fifth, how long shouldclopidogrel be administered after the procedure?
In this issue of the Journal, Chan et al. (11) haveaddressed the first three of these key questions. A series ofpost hoc analyses of the 4,809-patient TARGET (DoTirofiban and ReoPro Give Similar Efficacy OutcomesTrial) study of tirofiban versus abciximab in stent PCI (12)were conducted, incorporating statistical approaches to ad-just and account for differences among groups. The keyfindings have a high degree of relevance to the practice ofcontemporary stent PCI.
With respect to the first question (timing of clopidogrelrelative to intervention), outcomes of patients were im-proved with the administration of a 300-mg loading dose ofclopidogrel when given at any time before the PCI proce-dure (including just before the procedure) relative to thesubgroup that had clopidogrel started after PCI. In thisreport, the majority (57%) of patients who were pretreatedreceived drug within 2 h of PCI, with only 16% ofpretreated patients having received clopidogrel �6 h beforePCI. The benefit of �6 h of pretreatment was marginalrelative to treatment for �6 h, suggesting a slight, butperhaps still meaningful, additional advantage to a longerperiod of pretreatment before PCI.
The crucial point of the analysis is that benefit is greatestwhen clopidogrel is started before PCI. This is consistentwith both the pathophysiology of PCI (wherein a relativelyinert blood vessel is abruptly converted into a prothromboticmilieu) and the rapid bioavailability of the active metaboliteof clopidogrel, generally within minutes of drug adminis-
*Editorials published in the Journal of the American College of Cardiology reflect theviews of the authors and do not necessarily represent the views of JACC or theAmerican College of Cardiology.
From the Duke University Medical Center, Durham, North Carolina.
Journal of the American College of Cardiology Vol. 42, No. 7, 2003© 2003 by the American College of Cardiology Foundation ISSN 0735-1097/03/$30.00Published by Elsevier Inc. doi:10.1016/S0735-1097(03)00945-8

tration (13–15). Delaying treatment until after PCI hasbeen completed (i.e., after activation of the thrombosiscascade) would seem somewhat imprudent, particularlybecause administration even in an ad hoc fashion is notespecially difficult. Coupled with the known liabilities ofclopidogrel treatment vis a vis the excessive rates of bleedingin the patient undergoing coronary artery bypass surgery,(16,17), this would argue for pretreatment of patients postedfor elective PCI who have already undergone diagnosticcatheterization, and for the ad hoc treatment of “cathpossible” patients who may (or may not) subsequentlyundergo PCI.
These data are thus both congruous and expand upon theresults of the recent PCI-CURE (Clopidogrel in UnstableAngina to Prevent Recurrent Events) and CREDO (Clo-pidogrel for the Reduction of Events During Observation)trials (6,16). In these studies, patients undergoing PCI wererandomized to treatment with clopidogrel for either severaldays (PCI-CURE) or 3 to 24 h (CREDO) before PCI andwere found to have 30% (p � 0.03) and 18.5% (p � 0.23)relative risk reductions in the composite of death, myocar-dial infarction (MI), or urgent target vessel revascularization(TVR) to 28 days, respectively, compared with those startedon clopidogrel after PCI. The unique contribution of thecurrent work is the efficacy observed in the large group ofpatients treated within 0 to 2 h before PCI, a groupheretofore left unstudied in randomized clinical trials. Thiscompelling observation speaks to the absence of a specifictrial addressing the question of ad hoc treatment; a random-ized clinical trial comparing �6 h of treatment versus ad hoctreatment (perhaps with 300 mg vs. 600 mg dosing sched-ules) would seem to be in order to verify these post hocfindings.
A mild damper on the pro forma conclusions to the firstquestion relates to the second question (characterization ofthe benefits of clopidogrel treatment). In the mid 1990s, thewholesale substitution of thienopyridine therapy for warfa-rin anticoagulation after stent PCI was driven largely byreductions in bleeding and subacute stent thrombosis (18–21). However, most of the efficacy of pretreatment withclopidogrel in the current study was in reducing death orMI. There were no reported differences in rates of urgentTVR between the pretreatment and post-treatment groups,suggesting that subacute stent thrombosis is an infrequentevent that can be suppressed by administration of clopi-dogrel as long as it is started around the time (either beforeor immediately following) of PCI. If the goal is thus tosimply prevent subacute stent thrombosis, the timing ofclopidogrel administration would appear to be less relevantprovided a 300-mg loading dose is administered shortlyafter PCI. However, this would be obviating the potentialbenefits of reducing death or MI simply as a matter ofconvenience and would overall seem ill advised.
Finally, the third question (the relative contributions ofclopidogrel and platelet GP IIb/IIIa blockade to reducingischemic complications) can be inferentially approached by
examining the current study in the context of the existingliterature. Pretreatment with clopidogrel provided addi-tional efficacy to patients already receiving a GP IIb/IIIainhibitor in the TARGET trial. The converse was ad-dressed in two other studies, the Evaluation of IIb/IIIaPlatelet Inhibition for Stenting (EPISTENT) and theESPRIT (Enhanced Suppression of the Platelet IIb/IIIaReceptor with Integrilin Therapy) trials. In these trials,improvements in outcomes were seen with adjunctive treat-ment with abciximab or eptifibatide compared with placebo,even in the presence of ticlopidine (EPISTENT) or clopi-dogrel (ESPRIT) (22,23). In particular, in the 2,064-patient ESPRIT stent PCI study, an additional 35% (p �0.003) relative risk reduction in the composite end point ofdeath, MI, and urgent TVR at 30 days was observed witheptifibatide treatment with concurrent thienopyridine ad-ministration. These observations should thus help put torest the ongoing debate about whether to consider thien-opyridine and platelet GP IIb/IIIa blockade as therapeuticcompetitors or synergistic collaborators in favor of strategiesthat use these agents in a concomitant fashion. This is inaccordance with our current understanding of the physiol-ogy of platelets and the pharmacology of the antiplateletagents. Platelet activation, inhibited by thienopyridine ther-apy, is not affected by platelet GP IIb/IIIa blockade, andplatelet aggregation, suppressed by blockade of the plateletGP IIb/IIIa integrin, is only modestly inhibited by thien-opyridine therapy. Even with platelet GP IIb/IIIa blockade,secretion of vasoactive humors and proinflammatory cyto-kines can occur; conversely, even with inhibition of theADP receptor with thienopyridine therapy, platelet aggre-gation can occur. The body of evidence thus argues for acomplementary, rather than competitive role for antiplatelettherapies. To borrow a term coined by the founder of theNovell Corporation, Ray Noorda, this would be an exampleof “coopetition,” both at the pharmacologic and drugindustry levels. Although this is admittedly an inferentialdeduction that demands formal testing in randomizedclinical trials, available data would suggest that outcomes arebest optimized by combining aspirin, thienopyridine, andGP IIb/IIIa antagonist therapies in patients undergoingstent PCI.
Answers to queries four (optimizing the loading dose)and five (duration of treatment) are not addressed in thisreport, but need to be mentioned to complete the list ofpertinent questions relevant to the positioning of clopi-dogrel as an adjunct to PCI. Provocative data suggest thatfurther optimization of the loading dose may be possible(24), whereas the PCI-CURE and CREDO trials suggestthat continued therapy to one year is of particular benefit inpatients following PCI, a benefit even greater than thatimparted to patients managed with medical therapy alone(5,6).
In conclusion, there is a compelling and consistentliterature that argues for the use of triple antiplatelet therapyincluding aspirin, clopidogrel, and platelet GP IIb/IIIa
1197JACC Vol. 42, No. 7, 2003 Tcheng and CampbellOctober 1, 2003:1196–8 Editorial Comment

inhibitors in the setting of stent PCI. This broad approachto inhibiting the platelet at several different loci is effectivein improving the prothrombotic environment created dur-ing PCI while diminishing the inflammatory responseassociated with platelet activation. Triple therapy remainssafe and is associated with a lower incidence of subacutestent thrombosis, periprocedural MI, TVR, and death.Based on the current report along with a compilation ofprevious work, prudent specific recommendations concern-ing clopidogrel include the following:
1) Clopidogrel should be started as early as possible (�6 h)before PCI when the anatomy has been defined and thepatient is scheduled for elective PCI.
2) Clopidogrel should be started in an ad hoc fashionbefore PCI (but after diagnostic catheterization) in “cathpossible” patients.
3) Both GP IIb/IIIa antagonists and clopidogrel should beused together and started before PCI, particularly inhigher risk patients; neither is a complete substitute forthe other.
4) Still more information is needed about the optimumloading dose of clopidogrel preprocedure; a minimum of300 mg is recommended, with up to 600 mg appearingreasonable.
5) Clopidogrel treatment should be continued for up to oneyear after PCI.
The platelet remains a “black box” that is incompletelyunderstood; unfortunately, there remain patients with the-oretically adequate antiplatelet therapy who develop throm-bosis. Although we have learned much in the recent yearsabout how to improve our management of patients in theperiprocedural timeframe, more investigation with appro-priately designed and sized trials will be required to defin-itively answer the remaining questions and further refinetreatment algorithms.
Reprint requests and correspondence: Dr. James E. Tcheng,7021 Duke North Pavilion, 2400 Pratt Street, Durham, NorthCarolina 27705. E-mail: [email protected].
REFERENCES
1. Schafer AI. Antiplatelet therapy. Am J Med 1996;101:199–209.2. Stein B, Fuster V, Israel DH, et al. Platelet inhibitor agents in
cardiovascular disease: an update. J Am Coll Cardiol 1989;14:813–36.3. Collaborative overview of randomised trials of antiplatelet therapy—I:
prevention of death, myocardial infarction, and stroke by prolongedantiplatelet therapy in various categories of patients. AntiplateletTrialists’ Collaboration. BMJ 1994;308:81–106.
4. Leon MB, Baim DS, Popma JJ, et al. A clinical trial comparing threeantithrombotic-drug regimens after coronary-artery stenting. StentAnticoagulation Restenosis Study Investigators. N Engl J Med 1998;339:1665–71.
5. Mehta SR, Yusuf S, Peters RJ, et al. Effects of pretreatment withclopidogrel and aspirin followed by long-term therapy in patientsundergoing percutaneous coronary intervention: the PCI-CUREstudy. Lancet 2001;358:527–33.
6. Steinhubl SR, Berger PB, Mann JT III, et al. Early and sustained dualoral antiplatelet therapy following percutaneous coronary intervention:a randomized controlled trial. JAMA 2002;288:2411–20.
7. Madan M, Berkowitz SD, Tcheng JE. Glycoprotein IIb/IIIa integrinblockade. Circulation 1998;98:2629–35.
8. Kong DF, Califf RM, Miller DP, et al. Clinical outcomes oftherapeutic agents that block the platelet glycoprotein IIb/IIIa integrinin ischemic heart disease. Circulation 1998;98:2829–35.
9. Geiger J, Brich J, Honig-Liedl P, et al. Specific impairment of humanplatelet P2YAC ADP receptor-mediated signaling by the antiplateletdrug clopidogrel. Arterioscler Thromb Vasc Biol 1999;19:2007–11.
10. Scarborough RM, Kleiman NS, Phillips DR. Platelet glycoproteinIIb/IIIa antagonists. What are the relevant issues concerning theirpharmacology and clinical use? Circulation 1999;100:437–44.
11. Chan AW, Moliterno DJ, Berger PB, et al. Triple antiplatelet therapyduring percutaneous coronary intervention is associated with improvedoutcomes including one-year survival: results from the Do Tirofibanand ReoPro Give Similar Efficacy Outcome Trial (TARGET). J AmColl Cardiol 2003;42:1188–95.
12. Topol EJ, Moliterno DJ, Herrmann HC, et al. Comparison of twoplatelet glycoprotein IIb/IIIa inhibitors, tirofiban and abciximab, forthe prevention of ischemic events with percutaneous coronary revas-cularization. N Engl J Med 2001;344:1888–94.
13. Thebault JJ, Kieffer G, Cariou R. Single-dose pharmacodynamics ofclopidogrel. Semin Thromb Hemost 1999;25 Suppl 2:3–8.
14. Savcic M, Hauert J, Bachmann F, Wyld PJ, Geudelin B, Cariou R.Clopidogrel loading dose regimens: kinetic profile of pharmacody-namic response in healthy subjects. Semin Thromb Hemost 1999;25Suppl 2:15–9.
15. Cadroy Y, Bossavy JP, Thalamas C, Sagnard L, Sakariassen K, BoneuB. Early potent antithrombotic effect with combined aspirin and aloading dose of clopidogrel on experimental arterial thrombogenesis inhumans. Circulation 2000;101:2823–8.
16. Mehta SR, Yusuf S, Clopidogrel in Unstable angina to preventRecurrent Events (CURE) Study Investigators. The Clopidogrel inUnstable angina to prevent Recurrent Events (CURE) trial pro-gramme; rationale, design and baseline characteristics including ameta-analysis of the effects of thienopyridines in vascular disease. EurHeart J 2000;21:2033–41.
17. Hongo RH, Ley J, Dick SE, Yee RR. The effect of clopidogrel incombination with aspirin when given before coronary artery bypassgrafting. J Am Coll Cardiol 2002;40:231–7.
18. Schomig A, Neumann FJ, Kastrati A, et al. A randomized comparisonof antiplatelet and anticoagulant therapy after the placement ofcoronary-artery stents. N Engl J Med 1996;334:1084–9.
19. Urban P, Macaya C, Rupprecht HJ, et al. Randomized evaluation ofanticoagulation versus antiplatelet therapy after coronary stent implan-tation in high risk patients: the multicenter aspirin and ticlopidine trialafter intracoronary stenting (MATTIS). Circulation 1998;98:2126–32.
20. Rupprecht HJ, Darius H, Borkowski U, et al. Comparison of anti-platelet effects of aspirin, ticlopidine, or their combination after stentinplantation. Circulation 1998;97:1046–52.
21. Leon MB, Baim DS, Popma JJ, et al. A clinical trial comparing threeantithrombotic-drug regimens after coronary-artery stenting. StentAnticoagulation Restenosis Study Investigators. N Engl J Med 1998;339:1665–71.
22. Steinhubl S, Ellis S, Wolski K, Lincoff AM, Topol EJ, for theEPISTENT Investigators. Ticlopidine pretreatment before coronarystenting is associated with sustained decrease in adverse cardiac events:data from the Evaluation of Platelet IIb/IIIa Inhibitor for Stenting(EPISTENT) Trial. Circulation 2001;103:1403–9.
23. The ESPRIT Investigators. Novel dosing regimen of eptifibatide inplanned coronary stent implantation (ESPRIT): a randomised,placebo-controlled trial. Lancet 2000;356:2037–44.
24. Gurbel PA, Cummings CC, Bell CR, Alford AB, Meister AF,Serebruany VL. Onset and extent of platelet inhibition by clopidogrelloading in patients undergoing elective coronary stenting: the PlavixReduction Of New Thrombus Occurrence (PRONTO) trial. AmHeart J 2003;145:239–47.
1198 Tcheng and Campbell JACC Vol. 42, No. 7, 2003Editorial Comment October 1, 2003:1196–8
Age and Cardiovascular Disease
Prediction of Risk for First Age-RelatedCardiovascular Events in an Elderly Population:The Incremental Value of EchocardiographyTeresa S. M. Tsang, MD, FACC,* Marion E. Barnes, MSC,* Bernard J. Gersh, MB, CHB, DPHIL, FACC,*Yasuhiko Takemoto, MD,* A. Gabriela Rosales, MS,† Kent R. Bailey, PHD,†James B. Seward, MD, FACC*Rochester, Minnesota
OBJECTIVES We sought to determine if echocardiography enhances prediction of first age-relatedcardiovascular events.
BACKGROUND Whether echocardiographic assessment improves risk stratification for first cardiovascularevents is not well known.
METHODS This retrospective cohort study included randomly selected residents of Olmsted County,Minnesota, age �65 years, who had �1 transthoracic echocardiograms at the Mayo Clinicbetween 1990 and 1998, in sinus rhythm, without valvular or congenital heart disease, andfollowed through medical records for first myocardial infarction (MI), coronary revascular-ization, atrial fibrillation (AF), congestive heart failure (CHF), transient ischemic attack(TIA), stroke, or cardiovascular death. Patients were excluded if they had any of these eventsbefore the baseline echocardiogram.
RESULTS Of 1,160 patients (age 75 � 7 years; 746 women) followed for a mean of 3.8 � 2.7 years, 333(29%) first events occurred (70 AF, 67 coronary revascularization procedures, 65 CHF, 48MI, 38 stroke, 25 TIA, and 20 cardiovascular deaths). In a multivariate model, age (p �0.001), male gender (p � 0.001), diabetes mellitus (p � 0.005), systemic hypertension (p �0.001), left atrial volume/body surface area �32 ml/m2 (p � 0.003), left ventricular (LV)mass/height �120 g/m (p � 0.014), LV systolic dysfunction (p � 0.001), and LV diastolicdysfunction (p � 0.029) were independent predictors. A risk-scoring algorithm wasdeveloped and validated for the prediction of first events. The five-year event-free survival was90%, 74%, and 50% for low-, medium-, and high-risk groups, respectively.
CONCLUSIONS Echocardiography enhanced prediction of first cardiovascular events in this referral-basedelderly cohort. Its role in risk stratification for primary prevention of these events in thecommunity warrants further investigations. (J Am Coll Cardiol 2003;42:1199–205)© 2003 by the American College of Cardiology Foundation
Congestive heart failure (CHF) and atrial fibrillation (AF)have reached epidemic proportions in the U.S. (1,2). Cor-onary heart disease remains the number one cause of deathin the country, while stroke is the leading cause of disabilityfor both men and women (3). The magnitude of these
See page 1206
age-related conditions is expected to increase because of theburgeoning older population. Significant progress has beenmade in the evaluation and treatment of certain clinical riskfactors for primary and secondary prevention of cardiovas-cular diseases. The value of echocardiographic assessment ofsubclinical abnormalities for stratification of risk for age-related cardiovascular outcomes is not well known.
Our aim in this study was to determine, within an elderlycohort, which subclinical abnormalities detected by nonin-vasive echocardiography are predictive of first age-relatedcardiovascular events including CHF, AF, myocardial in-farction (MI), coronary revascularization, stroke, transientischemic attack (TIA), and cardiovascular death. We hy-pothesized that certain abnormalities, which may not beclinically overt, portend greater risk for future cardiovascularevents, independent of and incremental to conventionalclinical cardiovascular risk factors.
METHODS
Study design and population. A retrospective cohort de-sign was used. After obtaining approval from the MayoFoundation Institutional Review Board, a list of potentialsubjects was identified from a computerized search of theechocardiography database. Search criteria were residence inOlmsted County, Minnesota, and record of �1 transtho-racic echocardiograms performed at Mayo Clinic or Olm-sted Medical Center or their affiliated hospitals betweenJanuary 1, 1990, and December 31, 1998. Olmsted County
From the *Division of Cardiovascular Diseases and Internal Medicine, and the†Section of Biostatistics, Mayo Clinic, Rochester, Minnesota. Grant support pro-vided by the American Heart Association and the American Society of Echocardi-ography.
Manuscript received January 18, 2003; revised manuscript received May 6, 2003,accepted May 12, 2003.
Journal of the American College of Cardiology Vol. 42, No. 7, 2003© 2003 by the American College of Cardiology Foundation ISSN 0735-1097/03/$30.00Published by Elsevier Inc. doi:10.1016/S0735-1097(03)00943-4

is relatively isolated geographically, with healthcare pro-vided by a few well-defined health providers, the largest ofwhich is Mayo Clinic, which provides all echocardiographicservices. In a prior study, it was demonstrated that 96% ofOlmsted County residents age 65 to 74 years had �1encounters with the Mayo medical system within a three-year period (4).
The population from which the study sample was drawnincluded all Olmsted County residents of age �65 years,who were referred for a transthoracic echocardiogram be-tween 1990 and 1998 and had provided permission to usetheir records for research purposes. The earliest examinationwithin the study period was designated as the baseline study.The list of patients was cross-referenced with the comput-erized Mayo Clinic registration file, medical index (contain-ing diagnostic codes), surgical database, and electrocardio-graphic database. These administrative databases allowedscreening of patients with conditions that were exclusioncriteria. A total of 3,520 patients remained eligible aftercross-referencing the administrative databases, and a ran-dom sample of 2,240 (64%) was drawn by SAS randomnumber selection program. Retrospective comprehensivereview of the Mayo Clinic medical records of these 2,240patients was undertaken. During this review, a further 1,080patients were excluded, 942 of these owing to baselinepresence of more than mild valvular disease by echocardio-graphic criteria, and 138 because of presence of exclusioncriteria not detected by the administrative databases. Theremaining 1,160 patients constituted the study population.Clinical and echocardiographic data. The medical recordsof each of the 1,160 eligible patients were comprehensivelyreviewed for the clinical data. The indication for echocar-diography was directly retrieved from a specific field fromthe Echocardiography Laboratory database called “indica-tion or referral diagnosis,” which had to be entered at thetime of booking for echocardiography study. The definitionsof coronary artery disease, peripheral artery disease, carotidartery disease, smoking status, hyperlipidemia, systemichypertension, diabetes mellitus, and family history of coro-nary artery disease were as per standard clinical diagnoses,and had previously been described in detail (5).
Criteria defining the outcomes of interest were specifieda priori. The patients with any of these outcomes on orbefore the date of baseline echocardiogram were excluded
from the study. The type and date of detection of eachoutcome were abstracted. Congestive heart failure wasdefined according to Framingham criteria, requiring thepresence of two major, or one major and two minorFramingham criteria (6). A history of MI was consideredpresent if �2 of the three diagnostic criteria were fulfilled:compatible clinical presentation, diagnostic cardiac enzymelevels, and electrocardiographic changes consistent with MI.Coronary revascularization referred to coronary artery by-pass grafting or percutaneous coronary intervention. Atrialfibrillation was defined as the presence of clinically docu-mented and electrocardiographically confirmed irregularrhythm with disorganized atrial activity and without discreteP-waves. Stroke in this study included development of anytype of stroke, as defined by clinical documentation of thediagnosis with confirmatory findings on imaging studies. ATIA was defined by the clinical documentation of thediagnosis, in the absence of other conditions that could beresponsible for the neurological symptoms.
Left atrial (LA) volume was measured offline using thebiplane area-length method (7) and was indexed to bodysurface area (indexed LA volume). The cardiologists mea-suring LA volume were blinded to patients’ clinical data andoutcome status. All other echocardiographic data wereretrieved electronically from the computerized echocardio-graphic database.
The transmitral Doppler flow profile is integral to theassessment of diastolic function (8). Abnormal relaxation isthe mildest form of diastolic dysfunction. In our study, thepresence of mitral E/A �0.75 or deceleration time �240 mswas considered evidence of abnormal relaxation. In patientswith pseudonormal LV filling, or moderate diastolic dys-function, transmitral flow characteristics are similar to thoseobserved in normal diastolic function, although the leftatrium is typically enlarged from elevated LV filling pres-sures. In this study, both pseudonormal and normal LVfilling were defined by the presence of mitral E/A of 0.75 to1.5 and deceleration time of 151 to 240 ms, but distin-guished by whether LA volume was �28 ml/m2 (pseudo-normal) or �28 ml/m2 (normal) (9). The severe form ofdiastolic dysfunction is characterized by the presence ofrestrictive diastolic filling with markedly elevated fillingpressures (8). In this study, the presence of mitral E/A �1.5or deceleration time �150 ms was considered evidence ofrestrictive diastolic filling. Unlike other transmitral flowparameters, isovolumic relaxation time was not routinelymeasured during the study period and was therefore notused for analyses.Outcome ascertainment. The outcomes of interest for thisstudy were first documented MI, coronary revascularization,CHF, AF, stroke, TIA, and cardiovascular death. Theascertainment of any of these outcomes was accomplishedthrough comprehensive review of the medical records andcross-referencing the multiple administrative databasesavailable (medical, surgical, electrocardiography, and echo-cardiography) to detect any inconsistencies. The same
Abbreviations and AcronymsAF � atrial fibrillationCHF � congestive heart failureCI � confidence intervalHR � hazard ratioLA � left atrialLV � left ventricleMI � myocardial infarctionSD � standard deviationTIA � transient ischemic attack
1200 Tsang et al. JACC Vol. 42, No. 7, 2003Age-Related Cardiovascular Events October 1, 2003:1199–205

definitions and criteria for adjudication of events were usedfor all patients throughout the study period.Statistical methods. Differences in baseline characteristicsbetween patients who did and did not develop outcomeevents of interest after baseline echocardiography wereassessed using chi-square analyses for categorical variables(Table 1). For continuous variables, two-sample t tests wereused for variables that had a normal distribution, andWilcoxon rank-sum tests for those with a non-normaldistribution. Descriptive statistics for both groups weretabulated as means and standard deviations (SD) or fre-quency percentages.
To evaluate the incremental prognostic value of echocar-diographic variables, the global log likelihood ratio chi-square statistics for models developed using: 1) clinical riskfactors alone; 2) echocardiographic variables alone; and 3)combined clinical and echocardiographic variables weredetermined by Cox proportional hazards regression. In allcases, statistical significance was defined as two-tailed p �0.05.Development of model and risk-scoring algorithm.Using Cox proportional hazards analyses, age- and gender-adjusted models, as well as models with multiple adjust-ments, were developed to estimate the associations betweenclinical and echocardiographic variables, and time to firstcardiovascular event. From these models, hazard ratios(HR), 95% confidence intervals (CI), and the associated pvalues were generated. Ordinal versions of each of theechocardiographic variables of the multivariate model, withtwo to four levels, were created, and represented by thresh-old indicator variables. When a certain echocardiographicmeasurement was missing in a patient, an additional level
(missing) for that variable was assigned. With the exceptionof age, the clinical variables were dichotomous.
Next, a backward stepwise Cox regression procedure wasused, starting with the four clinical variables and 14 echo-cardiographic indicator variables. In addition to requiringthat each variable remain significant at p � 0.05 level, it wasalso mandated that the degree of risk change unidirection-ally with each step-up in level for all echocardiographicvariables. The missing category for each echocardiographicvariable was simply combined with whichever of the corre-sponding ordinal levels it most closely resembled in relativerisk.
Finally, a risk score was developed by assigning smallinteger values to each category (clinical or echocardiograph-ic), which were approximately proportional to the model-based log hazard differences between the categories. The log(hazard) associated with a 10-year age increase was similarlyconverted to an integer value. It was anticipated that theresulting score would account appropriately for the missingvalues, and therefore would be generalizable to other situ-ations with different patterns of missingness. Cumulativeevent-free survival, stratified by three risk groups (low-,medium-, and high-risk scores), was estimated by Kaplan-Meier analysis.Validation of model and score. The multivariate modelfor prediction and risk scoring algorithm were displayed inTables 2 and 3. We investigated the robustness of the modelusing two approaches. First, a bootstrap (10) resamplingstudy (n � 500) was done relative to the backward stepwiseprocedure to determine the likelihood that all of the clinicaland echocardiographic variables in our final models wouldappear also in the final model of these bootstrap samples. It
Table 1. Baseline Clinical, Electrocardiographic, and Echocardiographic Characteristics of StudyPopulation Stratified by Event Status
Characteristic (Number With Data)Had Events
(333)No Events
(827) p
Age, mean � SD, yr (1,160) 77 � 7 74 � 6 � 0.001*Men, % (1,160) 38 35 0.269Pulse rate, mean � SD, beats/min (1,117) 67 � 19 64 � 18 0.044Systolic blood pressure, mean � SD, mm Hg (948) 146 � 23 142 � 23 0.011Pulse pressure, mean � SD, mm Hg (948) 67 � 19 64 � 18 0.044History of hypertension, % (1,160) 63 48 � 0.001History of vascular disease, % (960) 26 13 � 0.001History of diabetes mellitus, % (1,160) 11 7 0.026LVH on ECG, % (1,160) 6 3 0.043M-mode LA dimension, mean � SD, mm (1,014) 41 � 7 40 � 6 0.001*LA volume, mean � SD, ml (1,018) 64 � 22 56 � 21 � 0.001*Indexed LA volume, mean � SD, ml/m2 (1,018) 36 � 12 31 � 12 � 0.001LV diastolic septal wall thickness, mean � SD, mm (765) 12 � 3 11 � 2 � 0.001*LV diastolic posterior wall thickness, mean � SD, mm (792) 11 � 2 10 � 2 � 0.001*LV mass/height, mean � SD, g/m (733) 131 � 44 109 � 26 � 0.001*LV ejection fraction, mean � SD, % (866) 61 � 11 63 � 9 0.018*
*Rank-sum test was used. Other variables that did not differ significantly between the two groups: weight, height, body surfacearea, body mass index, diastolic blood pressure, hyperlipidemia, smoking (current or past), family history of coronary arterydisease, chronic obstructive pulmonary disease, LV end-systolic and end-diastolic dimensions, pulmonary venous systolic anddiastolic forward flow velocities, pulmonary venous atrial reversal velocity, mitral peak E and peak A velocities, mitral earlydeceleration time, and tricuspid regurgitation velocity.
ECG � electrocardiography; LA � left atrial; LV � left ventricular; LVH � left ventricular hypertrophy.
1201JACC Vol. 42, No. 7, 2003 Tsang et al.October 1, 2003:1199–205 Age-Related Cardiovascular Events

was not required that the same set of threshold variables foreach echocardiographic variable be selected, but merely thatthe variable was represented by at least one of the thresholdvariables.
The second method of validation was to apply the modelto a separate population of a prospective study (referredfrom here on as the prospective validation cohort). In thisprospective cohort, all 410 patients were referred to theechocardiography laboratory subsequent to 1998, and wererecruited and followed prospectively. A total of 62 outcomeevents occurred during a two-year follow-up in this pro-spective cohort. This prospective study had no residencyrequirement and included many non-Olmsted County res-idents. The final model (ordinal variable version) wasre-estimated on this prospective validation cohort, and themodel chi-square statistics (normalized to the number ofevents) compared. In addition, risk scores were calculatedfor the 410 patients in the prospective validation cohort, andused to stratify the patients in the same way as in studycohort. The corresponding Kaplan-Meier event-free sur-vival curves were generated and compared with those of the
study cohort. The empiric risk estimates at year 1 and year2 were compared between the study population and theprospective validation cohort (Table 4).
RESULTS
Baseline characteristics of the study population. A totalof 1,160 residents (746 women; 414 men) of OlmstedCounty, Minnesota, mean age 75 � 7 years (range 65 to100 years) fulfilled all study criteria and constituted thestudy population. The principal indications for echocardio-graphic assessment were dyspnea (32%), chest discomfort(20%), palpitations, lightheadedness, presyncope or syncope(18%), cardiac function assessment (20%), murmurs (8%),and other reasons (2%). Further review of the records of thegroup of patients with a referral indication of “cardiacfunction assessment” showed that 38% had dyspnea as apredominant symptom, 32% had chest discomfort, 20% hadfatigue, and 10% had various combinations of these symp-toms. Over a mean follow-up period of 3.8 � 2.7 years, 333(29%) patients had a total of 536 events of interest. A totalof 307 patients died during the follow-up period. Firstevents (n � 333) included 70 AF, 67 coronary revascular-ization procedures, 65 CHF, 48 MI, 38 stroke, 25 TIA, and20 cardiovascular deaths. A number of baseline character-istics differed between the patients who had �1 outcomeevent versus those who did not have an event duringfollow-up (Table 1). The majority of the patients (1,113patients; 96%) had normal LV systolic function with ejec-tion fraction �50%. Left ventricular diastolic function wasclassified as normal in 150 patients, mildly abnormal (ab-
Table 2. Multivariate Model for Prediction of First Age-Related Events
VariablesParameterEstimate HR (95% CI) p
Age, yrs 0.06 1.06 (1.04–1.08) � 0.001Male gender 0.41 1.50 (1.19–1.88) � 0.001Diabetes mellitus 0.50 1.64 (1.16–2.32) 0.005Systemic hypertension 0.50 1.64 (1.30–2.06) � 0.001Indexed LA volume � 32 ml/m2 0.35 1.42 (1.13–1.78) 0.003LV mass/height � 120 g/m 0.45 1.57 (1.10–2.26) 0.014LV ejection fraction � 50% 0.80 2.22 (1.44–3.42) � 0.001Presence of any diastolic dysfunction 0.49 1.64 (1.10–2.55) 0.029
*p � 0.05 for the following variables: systolic blood pressure, diastolic blood pressure, pulse pressure, pulse rate, hyperlipidemia,carotid artery disease, smoking (current or past), chronic obstructive pulmonary disease.
CI � confidence interval; HR � hazard ratio; LA � left atrial; LV � left ventricular.
Table 3. Risk-Scoring Algorithm for the Prediction of FirstAge-Related Cardiovascular Events
VariableRisk
Score
ClinicalAge 65–69.9 yrs 0Age 70–74.9 yrs �1Age 75–79.9 yrs �2Age 80–84.9 yrs �3Age �85 yrs �4Male gender �1Diabetes mellitus �1Systemic hypertension �1
EchocardiographicLV ejection fraction � 50% or missing 0LV ejection fraction � 50% �2Normal diastolic function 0Any diastolic dysfunction or missing �1Indexed LA volume � 32 ml/m2 or missing 0Indexed LA volume � 32 ml/m2 �1LV mass/height �120 g/m or missing 0LV mass/height �120 g/m �1
LA � left atrial; LV � left ventricular.
Table 4. Kaplan-Meier Event Rates for the Study Populationand Prospective Validation Cohort
RiskGroups
StudyPopulation
ValidationCohort
At year 1Low 3 2Medium 8 7High 17 13
At year 2Low 5 2Medium 12 10High 25 23
1202 Tsang et al. JACC Vol. 42, No. 7, 2003Age-Related Cardiovascular Events October 1, 2003:1199–205

normal relaxation) in 473 patients, moderately abnormal(pseudonormal) in 192 patients, and severely abnormal(restrictive) in 32 patients.Prediction of first age-related cardiovascular events. AGE
AND GENDER-ADJUSTED MODELS FOR PREDICTION OF
FIRST EVENTS. When adjusted for both age and gender, thesignificant clinical and echocardiographic predictors in-cluded age (per year) (HR 1.06; 95% CI 1.05 to 1.08; p �0.001); male gender (HR 1.20; 95% CI 0.96 to 1.50; p �0.105); body mass index (per 5 kg/m2) (HR 1.02; 95% CI1.01 to 1.05; p � 0.037); systemic hypertension (HR 1.75;95% CI 1.40 to 2.19; p � 0.001); coronary artery disease(HR 1.85; 95% CI, 1.08 to 3.17; p � 0.025); diabetesmellitus (HR 1.84; 95% CI 1.31 to 2.60; p � 0.001), andthe following echocardiographic variables: indexed LA vol-ume (per 10 ml/m2) (HR 1.29; 95% CI 1.19 to 1.40; p �0.001); LV end-systolic dimension (per 5 mm) (HR 1.23;95% CI 1.10 to 1.36; p � 0.001); LV ejection fraction (per10%) (HR 0.77; 95% CI 0.68 to 0.86; p � 0.001); LVmass/height (per 10 g/m) (HR 1.01; 95% CI 1.01 to 1.02;p � 0.001); and presence of diastolic dysfunction (HR 1.36;95% CI 1.16 to 1.60; p � 0.001).
MULTIVARIATE MODEL FOR PREDICTION OF FIRST
EVENTS. A multivariate model was developed for the pre-diction of first events. This contained four clinical and fourechocardiographic variables, all statistically independent ofeach other: age, gender, diabetes mellitus, systemic hyper-tension, LV systolic function, LV diastolic function, LVmass, and LA volume (Table 2). The global log likelihoodratio chi-square statistics for the models containing: 1) thefour clinical risk factors only; 2) the four echocardiographicvariables only; and 3) combined four clinical and fourechocardiographic variables were 99, 54, and 143 (vs. 99 or54, p � 0.001), respectively. We also tested for anyindependent predictive value of symptoms (chest pain,dyspnea, lightheadedness, palpitations, presyncope, synco-pe), and found that presenting symptoms that led toechocardiography referral were not independently predictiveof first events in univariate or multivariate model. Also,adding symptoms to the multivariate model with the eightindependent clinical and echocardiographic variables (Table2) did not diminish the predictive value of any of theparameters in the model.
RISK-SCORING ALGORITHM FOR PREDICTION OF FIRST
EVENTS. A risk score was generated for each patient basedon the multivariate model of four clinical and four echocar-diographic variables, using the method outlined in theMethods section. The minimum score was 0 and themaximum score was 12 (Table 3). The Kaplan-Meierfive-year event-free survival stratified by low (�2), medium(3 to 4), and high (�5) risk scores were 90%, 74%, and 50%(Fig. 1).
The risk score was validated both within the studypopulation, as well as in a prospective validation cohort of410 patients (see Methods). Within the study population
from which 500 random samples were drawn by thebootstrapping technique, only 2% did not include at leastseven of the eight predictor variables of the multivariatemodel. This means that the multivariate model was highlystable when subjected to random sampling within the studypopulation. Notably, indexed LA volume was the onlyechocardiographic variable that appeared in 100% of thesamples in this random sampling. The risk score in thisstudy population was associated with a HR of 1.44 (95% CI1.35 to 1.53; p � 0.001), so that every increment of onepoint was associated with a hazard increase of 44%.
We also validated the model and risk score with acompletely separate population of 410 patients, who werereferred to the echocardiography laboratory and followedprospectively in a different study. Over a two-year follow-up, a total of 62 outcome events developed. In this prospec-tive population, the model fitting was highly acceptable(global model chi-square of 38 for 62 events, versus globalmodel chi-square of 143 for 333 events in the studypopulation). The risk score calculated for the prospectivevalidation cohort was associated with a HR of 1.40 (95% CI1.25 to 1.58; p � 0.001). Thus, the hazard associated withthe risk score in the study population (HR 1.44) and thatwith the validation cohort (HR 1.40) compared closely.Further, the Kaplan-Meier event-free survival curves for theprospective validation cohort and the study populationcompared closely, when stratified by the low-, medium-,and high-risk scores, as did the estimated cumulative eventrates at one and two years (Fig. 2, Table 4).
DISCUSSION
Prediction of age-related cardiovascular events in theelderly: beyond clinical risk factor assessment. This studyprovides evidence that assessment of certain subclinicalparameters by noninvasive echocardiography improves riskstratification for the development of first age-related car-diovascular events in the elderly. The events considered in
Figure 1. Kaplan-Meier estimates of cumulative event-free survival for thestudy population.
1203JACC Vol. 42, No. 7, 2003 Tsang et al.October 1, 2003:1199–205 Age-Related Cardiovascular Events

this study are common age-related conditions. Nearly one-third of the entire cohort who were free from any events ofinterest at baseline developed at least one event during amean follow-up time of only 3.8 years.
Advancing age, male gender, systemic hypertension, anddiabetes mellitus are well-established cardiovascular riskfactors, and were independent predictors of first events inthis study, even after echocardiographic parameters wereadded to the model. From the risk modification standpoint,chronologic age and male gender are immutable. In con-trast, systemic hypertension is highly treatable, yet hasremained grossly undertreated in the community (11,12).Diabetes mellitus is a potent cardiovascular risk factor, andis now considered equivalent to established coronary heartdisease in terms of its status as a risk factor (13). Earlydiagnosis and control of this metabolic disease has majorimplications on cardiovascular outcomes. Although thereare abundant data on the impact of detection and treatmentof these clinical risk factors on cardiovascular outcomes,there is a paucity of data with regard to assessment andtreatment of echocardiographic risk markers.
The echocardiographic predictors of first events identifiedin this study can be readily obtained with any echocardiog-raphy system, including the more advanced hand-helddevices. Based on the multivariate model in this study(Table 2), simple identification of whether an elderlyindividual has: 1) abnormal systolic function (LV ejectionfraction �50%); 2) evidence of any diastolic dysfunction; 3)LA volume/body surface area �32 ml/m2 (�2 SD from thenormal mean value); and 4) LV mass/height of �120 g/mcontributes to the prediction of first events. Although LVsystolic function (14,15), diastolic function (5,16), and mass(17) have been shown to be important prognostic indicatorsfor various cardiovascular outcomes, few studies have dem-onstrated LA volume to be independent of all these echo-
cardiographic risk markers, and of clinical risk factors, forthe prediction of the first cardiovascular events in theelderly. Notably, LA volume was the only echocardio-graphic predictor that was represented in the model for eachof the 500 samples randomly drawn from the study popu-lation in the risk score validation procedure, attesting to itsrobustness as a predictor for first events.
Symptoms that led to echocardiographic referral, such aschest pain, dyspnea, palpitations, lightheadedness, presyn-cope, or syncope, were not independently predictive of firstevents. This could be related to the relatively nonspecificnature of these symptoms, which are often subjective andnot readily quantifiable. In contrast, echocardiography pro-vides a more objective, quantifiable, and reproducible as-sessment.Risk-scoring algorithm for prediction of first events inthe elderly. A risk-scoring algorithm was developed in thisstudy, based on the multivariate model for the prediction offirst events, which was validated both within the studypopulation and in a separate cohort containing 410 patientsfollowed prospectively for two years. The Framinghaminvestigators have been instrumental in the development ofalgorithms for risk stratification and event prediction. TheFramingham data used to generate equations for estimatingrisk of manifest cardiovascular disease were derived from amiddle-aged population of white men and women (18), andnot from an elderly population as in this study. TheFramingham investigators had also described a generalstroke risk profile (19,20), as had the investigators of IsraeliIschemic Heart Disease project (21) and the CardiovascularHealth Study (22). Subclinical risk factors, such as thosemeasured by echocardiography in our study, have not beenincluded in these risk-scoring algorithms. Further, mostrisk-scoring methods to date were developed to predict aspecific condition. Therefore, different risk prediction ruleshave to be applied to estimate the risks for differentoutcomes of interest. The clinical application of multiplemetrics for quantifying the risks for different events can beintimidating. In the case of primary prevention of a firstcardiovascular event, it is desirable to having a simpleunifying algorithm that enables point-of-care risk stratifi-cation for common age-related conditions that share similarrisk factors, such as AF, stroke, MI, CHF, revascularization,and cardiovascular death.
The feasibility of utilizing echocardiography to screen theelderly population for subclinical predictors and applying asimple scoring algorithm for risk stratification requiresprospective investigation. The impact of detection andtreatment of these abnormalities on cardiovascular outcomesand the cost-effectiveness of such a program will need to bedetermined. With the availability of highly sophisticatedhand-held echocardiographic devices that now allow mea-surement of these subclinical parameters readily in an officesetting, the future possibility of applying noninvasive echo-cardiographic technology effectively at the point of care for
Figure 2. Comparison of Kaplan-Meier estimates of cumulative event-freesurvival between the study population and the prospective validationcohort, stratified by risk groups.
1204 Tsang et al. JACC Vol. 42, No. 7, 2003Age-Related Cardiovascular Events October 1, 2003:1199–205

risk stratification in primary prevention is appealing andwarrants further investigation.Study limitations. This is a retrospective referral-basedcohort study, and subject to biases inherent to the design.The majority of this elderly cohort was of Caucasian descent,and the generalizability of the findings to other racial/ethnicgroups and to non-referral-based populations could not bedetermined. Outcome ascertainment, based on chart review,might have underestimated the number of events. However,given the relative geographic isolation of Olmsted County, andthe near exclusive utilization of Mayo Clinic as the healthprovider by the residents of this county (4), it is relativelyunlikely that the underestimation would be significant.
Because of the era in which the echocardiograms wereperformed, pulmonary venous flow velocities and tissueDoppler mitral annular velocities were not available in asignificant number of the patients. The categorization ofdiastolic function status was based on simple mitral inflowcharacteristics and LA volume, and therefore, misclassifica-tion of diastolic function status was possible.
The echocardiographic variables in the multivariatemodel for the prediction of first events were purposely definedcategorically to preserve simplicity. It is possible that the abilityto predict first age-related cardiovascular events may be furtherenhanced if the echocardiographic variables were evaluated ascontinuous variables. Such a model, however, would be morecumbersome to use clinically.
In this study, we also did not develop a unique predictionmodel specific for each outcome event. Our intent was todevelop a unifying prediction metric, or risk-scoringmethod, for estimating the overall risk for first cardiovas-cular events of interest that share similar risk factors. Thisrisk stratification approach does sacrifice event-specific pre-diction, but is eminently more practical and feasible. Al-though the risk-scoring algorithm was validated within thestudy population, and also in a separate referral-basedpopulation prospectively followed for outcome events, fur-ther validation procedures using community-based non-referral-based populations would be important.Conclusions. The noninvasive echocardiographic identifi-cation of subclinical risk markers, such as LV systolic ordiastolic dysfunction, enlarged left atrium, and increased LVmass, enhanced risk stratification for the development offirst age-related cardiovascular events in our referral-basedelderly cohort, incremental to clinical risk profiling alone.Prospective studies to confirm these findings in otherpopulations, including community free-living individuals,and to determine the cost-effectiveness of primary preven-tion programs that incorporate echocardiographic evalua-tion in risk stratification for first events in the elderly mayhave important public health implications.
Reprint requests and correspondence: Dr. Teresa S. M. Tsang,Mayo Clinic, 200 First Street SW, Rochester, Minnesota 55905.E-mail: [email protected].
REFERENCES
1. Scheinman MM. Atrial fibrillation and congestive heart failure: theintersection of two common diseases. Circulation 1998;98:941–2.
2. Braunwald E. Shattuck lecture: cardiovascular medicine at the turn ofthe millennium: triumphs, concerns and opportunities. N Engl J Med1997;337:1360–9.
3. 2003 Heart and Stroke Statistical Update. Dallas, TX: AmericanHeart Association, 2002.
4. Melton LJ. History of the Rochester Epidemiology Project. MayoClin Proc 1996;71:266–74.
5. Tsang TSM, Gersh BJ, Tajik AJ, et al. Left ventricular diastolicdysfunction: an important predictor of the first diagnosed nonvalvularatrial fibrillation in 840 elderly men and women. J Am Coll Cardiol2002;40:1636–44.
6. McKee P, Castelli W, McNamara P, Kannel W. The natural historyof congestive heart failure: the Framingham Study. N Engl J Med1971;285:1441–6.
7. Ren J-F, Kotler MN, DePace NL, et al. Two-dimensional echocar-diographic determination of left atrial emptying volume: a noninvasiveindex in quantifying the degree of nonrheumatic mitral regurgitation.J Am Coll Cardiol 1983;2:729–36.
8. Nishimura RA, Tajik AJ. Evaluation of diastolic filling of left ventriclein health and disease: Doppler echocardiography is the clinician’sRosetta Stone. J Am Coll Cardiol 1997;30:8–18.
9. Tsang T, Barnes M, Gersh B, Bailey K, Seward J. Left atrial volumeas a morphophysiologic expression of diastolic dysfunction and relationto cardiovascular risk burden. Am J Cardiol 2002;90:1284–9.
10. Efron B. The jackknife, the bootstrap and other resampling plans.Regional Conference Series in Applied Mathematics, 38. SIAM,Philadelphia, PA: 1982.
11. Meissner I, Whisnant JP, Sheps SG, et al. Detection and control ofhigh blood pressure in the community: do we need a wake-up call?Hypertension 1999;34:466–71.
12. He J, Muntner P, Chen J, Roccella E, Streiffer R, Whelton P. Factorsassociated with hypertension control in the general population of theUnited States. Arch Intern Med 2002;162:1051–8.
13. Expert Panel on Detection, Evaluation, and Treatment of HighBlood Cholesterol in Adults. Executive Summary of the ThirdReport of the National Cholesterol Education Program (NCEP)Expert Panel on Detection, Evaluation, and Treatment of High BloodCholesterol in Adults (Adult Treatment Panel III). JAMA 2001;285:2486–97.
14. The SOLVED Investigators. Effect of enalapril on survival in patientswith reduced left ventricular ejection fraction and congestive heartfailure. N Engl J Med 1991;325:293–302.
15. Pfeffer MA, Braunwald E, Moye LA, et al. Effect of captopril onmortality and morbidity in patients with left ventricular dysfunctionafter myocardial infarction. Results of the survival and ventricularenlargement trial. The SAVE Investigators. N Engl J Med 1992;327:669–77.
16. Redfield MM, Jacobsen SJ, Burnett JC, Mahoney DW, Bailey KR,Rodeheffer RJ. Burden of systolic and diastolic ventricular dysfunctionin the community. JAMA 2003;289:194–202.
17. Levy D, Garrison RJ, Savage DD, Kannel WB, Castelli WP. Prog-nostic implications of echocardiographically determined left ventricu-lar mass in the Framingham Heart Study. N Engl J Med 1990;322:1561–6.
18. Wilson PWF, D’Agostino RB, Levy D, Belanger AM, Silbershatz H,Kannel WB. Prediction of coronary heart disease using risk factorcategories. Circulation 1998;97:1837–47.
19. Wolf PA, D’Agostino RB, Belanger AJ, Kannel WB. Probability ofstroke: a risk profile from the Framingham Study. Stroke 1991;22:312–8.
20. D’Agostino RB, Wolf PA, Belanger AJ, Kannel WB. Stroke riskprofile: adjustment for antihypertensive medication. The FraminghamStudy. Stroke 1994;25:40–3.
21. Tanne D, Yaari S, Goldbourt U. Risk profile and prediction oflong-term ischemic stroke mortality. Circulation 1998;98:1365–71.
22. Lumley T, Kronmal R, Cushman M, Manolio T, Goldstein S. Astroke prediction score in the elderly: validation and web-basedapplication. J Clin Epidemiol 2002;55:129–36.
1205JACC Vol. 42, No. 7, 2003 Tsang et al.October 1, 2003:1199–205 Age-Related Cardiovascular Events

EDITORIAL COMMENT
The Left AtriumA Biomarker of ChronicDiastolic Dysfunction andCardiovascular Disease Risk*Pamela S. Douglas, MD, FACCMadison, Wisconsin
Since Framingham Heart Study investigators first con-firmed the existence and importance of cardiac risk factorsin 1961 (1), clinicians and scientists have been seeking torefine our ability to predict cardiovascular disease risk.These efforts stem from an appreciation that atherosclerosisbegins at a very young age but is clinically silent for manyyears and also that during this latent period it is possible todelay or prevent the onset of its devastating and systemicclinical manifestations. Thus, efforts have focused on iden-tifying risk factors, not for their own sake, but so that theymay be modified and, through this modification, reduce theburden of disease. This trio—risk stratification, risk modi-fication, and altered outcomes—is one of the foundations ofcardiovascular medicine and defines a preventive paradigmof medical care that is increasingly receiving attention fromcaregivers across many specialties, patients, and the public.
See page 1199
At the present time, the state of the art in cardiovascularrisk assessment and modification is the National Choles-terol Education Program Adult Treatment Panel III, aNational Institutes of Health–convened, consensus panel–endorsed risk assessment tool based largely on age andcounting major risk factors to estimate 10-year coronaryheart disease (CHD) risk based on Framingham data. It iseasy to perform and scientifically well validated for themiddle-aged, Caucasian population from which it wasderived. However, it is not perfect, particularly in predictingrisk in other populations and in individuals. There are alsoother reasons why we should seek to improve our ability toestimate risk. In the Framingham risk score, the significanceof advancing age overwhelms most risk factors, making itdifficult to identify low-risk elderly individuals, even amongthose without risk factors. The Framingham risk score alsofails to adjust for the severity of risk factors, their treatment,other genetic factors, lifestyle, and interactions between riskfactors. Finally, because CHD is so common, many affectedindividuals actually fall within the normal range of variables
such as cholesterol, making it even harder to predictindividual risk.
In this issue of the Journal, Tsang et al. (2) propose thattransthoracic echocardiography adds significantly to ourcurrent ability to assess risk. Drawing on a moderately sized(for epidemiologic studies) community-based population ofelderly patients undergoing clinically indicated echocardio-grams, the authors compare a variety of clinical and echo-cardiographic variables to the development of virtually anyform of cardiovascular disease. Of the clinical variables, age,gender, diabetes, and high blood pressure predict outcomes,whereas smoking, cholesterol levels, or a family history ofCHD does not. Although some of these findings areexpected, the lack of significance of some known risk factorsis of concern. Other limitations relate to the cohort studied,particularly their homogeneity and that they were clinicallyreferred rather than being a community sample.
Of the echocardiographic variables examined, reducedejection fraction, left ventricular (LV) hypertrophy, anddiastolic dysfunction score were associated with pooreroutcomes, as has been noted by others. However, left atrial(LA) volume (but not dimension) was also associated withpoorer outcomes. Because LA diameter would be expectedto track with LA volume, it is unclear why there should bethis disconnect. Nevertheless, the finding that LA size isrelated to prognosis is new and of interest. Perhaps itsnovelty is related to the fact that few evaluations of cardiacrisk in otherwise healthy individuals have considered de-tailed echocardiographic findings as predictive variables.Exceptions include the Framingham study, which pro-nounced LV hypertrophy a risk factor 13 years ago (3) and,along with the present authors, has noted a poorer outcomein those with asymptomatic systolic and/or diastolic dys-function (4). The Tsang et al. (2) data suggest that echo-cardiography in general, and evaluation of LA size inparticular, should be included among tests and variablesoffering insight into cardiovascular risk.
There is substantial biologic plausibility to the prognosticsignificance of LA volume. The left atrium (LA) is mostcommonly thought of as a transporting chamber, receivingblood from the pulmonary veins and conveying it to the leftventricle (LV) through both passive and active diastolicfilling. However, the LA also functions as a volume sensorof the heart, releasing natriuretic peptides in response tostretch and other neurohormones and generating a reflextachycardia in response to increased venous return (Bain-bridge reflex). The LA also reflects LV filling pressure andis capable of remodeling (enlarging) in response to itselevation. It is in this final role, as an ongoing biomarker ortransducer of sustained elevations in LV filling pressures,that LA size captures our attention.
A great deal of research has been conducted on nonin-vasive assessments of diastolic function. Investigators andclinicians alike have struggled with the load dependence ofeasy-to-obtain measures, such as rapid filling rates and
*Editorials published in the Journal of the American College of Cardiology reflect theviews of the authors and do not necessarily represent the views of JACC or theAmerican College of Cardiology.
From the Cardiovascular Medicine Section, Department of Medicine, University ofWisconsin, Madison, Wisconsin.
Journal of the American College of Cardiology Vol. 42, No. 7, 2003© 2003 by the American College of Cardiology Foundation ISSN 0735-1097/03/$30.00Published by Elsevier Inc. doi:10.1016/S0735-1097(03)00956-2

mitral E and A velocities, and with the technical difficultiesof obtaining pulmonary vein flows and assessing the angle ofthe color M-mode LV inflow. At best, these techniquespresent only a snapshot view of diastolic function—thepattern would be altered if loading conditions changed.Clinicians need a measure of diastolic dysfunction that iseasy to obtain, adequately reflects underlying abnormalities,and has similar prognostic significance. The Tsang et al. (2)data suggest that this elusive measure is LA volume.
Left atrial size is certainly easy to assess. With the adventof hand-carried ultrasound, it can be a bedside or point ofcare measure, possibly routinely obtainable as part of acomprehensive physical examination. Even more important,the Tsang et al. (2) data suggest that the hypothesis that LAsize represents the integration of LV diastolic performanceover time is clinically valid. Left atrial volume therebyprovides a long-term view of whether or not the patient hasthe “disease” of diastolic dysfunction, regardless of whateverloading conditions are present at the time of the examina-tion. Drawing a parallel to two of the most commonly useddiagnostic tests in diabetes is nearly irresistible. Just asserum glucose is used to assess transient diabetic control,LV filling pressure is used to assess transient loadingconditions. In turn, the diastolic function corollary ofmeasurement of hemoglobin A1C (a long-term biomarker ofaverage metabolic state) is LA size (a long-term biomarkerof average LV diastolic pressure, and hence, when increased,of diastolic dysfunction). The message is simple: in theabsence of other contributing pathology such as mitral valvedisease, if the LA is large, the patient has had a sustainedelevation in LV filling pressure, and hence has chronicdiastolic dysfunction.
The Tsang et al. (2) report is of interest in other ways aswell. Epidemiologic studies rarely include such large num-bers of the elderly (average age 75 years), despite theirgrowing demographic importance. More interestingly, fewepidemiologic studies have considered and combined such abroad range of cardiovascular outcomes—heart failure,atrial fibrillation, myocardial infarction, surgical or percuta-neous revascularization, stroke or transient ischemic at-tack—in addition to death. This novel combined end pointallowed the authors to develop a single, unifying predictionmodel, rather than separate models for each type of event.This is arguably more clinically relevant than determiningrisk for any single one of its component events. Interest-ingly, in contrast to epidemiologic studies, randomizedclinical trials routinely utilize a combined end point(MACE, or major adverse cardiovascular events), similar tothe present study’s. The Tsang et al. (2) approach is worthkeeping in mind for future studies.
Many studies evaluating cardiovascular risk place an
emphasis on the presence of clinical disease—diabetes,hypertension, hyperlipidemia—and minimize subclinical ormechanistic markers that may be more predictive. In thissense, the prognostic value of high sensitivity C-reactiveprotein is an important example, as it detects the inflam-matory component of the disease process as it is occurring,and not simply its end point. Other “non-traditional” teststhat detect the actual burden of subclinical disease are also ofvalue. The best studied of these, carotid intima medialthickness, has been proven in multiple cohorts to prospec-tively predict both heart attack and stroke (5). A $68 millionNIH-funded trial, the Multi-Ethnic Study of Atheroscle-rosis (MESA), involving six centers and 6,500 participantsage 45 to 84 years, is examining the relative value of suchtests, including cardiac magnetic resonance imaging, carotidintima medial thickness, ankle-brachial index, coronarycalcium scores, and inflammatory and genetic markers.Echocardiography is not included in the trial, which couldhave made it an excellent validation of the Tsang et al. (2)data in a much larger population. Future studies will beneeded to determine the relative value of LA size in relationto other noninvasive tests.
Tsang et al. (2) have taken the relationship between LAsize and diastolic dysfunction and analyzed its clinicalrelevance. The association needs to be studied prospectively,and the applicability of these data to clinical care remains tobe defined. Nevertheless, their findings suggest that echo-cardiographically determined LA size may become an im-portant clinical risk stratifier in pre-clinical cardiovasculardisease.
Reprint requests and correspondence: Dr. Pamela S. Douglas,Cardiovascular Medicine, University of Wisconsin MedicalSchool, H6/352 Clinical Science Center, 600 HighlandAvenue, Madison, Wisconsin 53792-3248. E-mail: [email protected].
REFERENCES
1. Kannel WB, Dawber TR, Kagan A, Revotskie N, Stokes JI. Factors ofrisk in the development of coronary heart disease—six year follow-upexperience: the Framingham Study. Ann Intern Med 1961;55:33–50.
2. Tsang TSM, Barnes ME, Gersh BJ, et al. Prediction of risk for firstage-related cardiovascular events in an elderly population: the incre-mental value of echocardiography. J Am Coll Cardiol 2003;42:1199–205.
3. Levy D, Garrison RJ, Savage DD, Kannel WB, Castelli WP. Prognos-tic implications of echocardiographically determined left ventricularmass in the Framingham Heart Study. N Engl J Med 1990;322:1561–6.
4. Redfield MM, Jacobsen SJ, Burnett JC, Mahoney DW, Bailey KR,Rodeheffer RJ. Burden of systolic and diastolic ventricular dysfunctionin the community. JAMA 2003;289:194–202.
5. Lakatta EG, Levy D. Arterial and cardiac aging: major shareholders incardiovascular disease enterprises: Part I: aging arteries: a “set up” forvascular disease. Circulation 2003;107:139–46.
1207JACC Vol. 42, No. 7, 2003 DouglasOctober 1, 2003:1206–7 Editorial Comment

Age Does Not Limit Quality of LifeImprovement in Cardiac Valve SurgeryArtyom Sedrakyan, MD,* Viola Vaccarino, MD, PHD,† A. David Paltiel, PHD,*John A. Elefteriades, MD, FACC,‡ Jennifer A. Mattera, MPH,§ Sarah A. Roumanis, RN,§Zhenqiu Lin, PHD,§ Harlan M. Krumholz, MD, FACC*§�
New Haven, Connecticut; and Atlanta, Georgia
OBJECTIVES We sought to determine the association of age with the change in quality of life (QOL) aftervalve surgery.
BACKGROUND Improvement in QOL is one of the principal goals of valve surgery. These procedures arebeing done with increasing frequency for older patients.
METHODS We prospectively studied 148 patients with aortic valve procedures and 72 patients withmitral valve procedures. Patients’ QOL was measured at baseline and at 18 months using theMedical Outcomes Trust Short Form 36-Item (SF-36) Health Survey (response rate 90%).The association of age with change in QOL was measured by multiple regression analysis andbased on two meta-scores of the SF-36: the Mental Component Summary (MCS) and thePhysical Component Summary (PCS).
RESULTS Overall improvement in most domains of the SF-36, including the MCS and the PCS scores,was substantial. Improvement in the MCS score was not influenced by age in either aortic(0.09 score point improvement per 10-year age increments; p � 0.9) or mitral (0.90 scorepoint improvement per 10-year age increments; p � 0.3) patients. Similarly, improvement inthe PCS score did not vary by age in aortic patients (�1.00 score points per 10-year ageincrements; p � 0.2) and only slightly varied by age in mitral patients (�1.90 score points per10-year age increments, p � 0.02). In the latter, despite statistical significance, the associationwas not substantial or clinically important.
CONCLUSIONS Among patients referred for cardiac valve surgery, age does not appear to limit the QOLbenefits of surgery. (J Am Coll Cardiol 2003;42:1208–14) © 2003 by the American Collegeof Cardiology Foundation
More than 79,000 cardiac valve replacement procedures areperformed annually in the U.S. (1,2), with more than 16%performed for patients who are older than 75 years of age(3,4). Given the rapidly growing older population (5) andthe increasing prevalence of symptomatic valve disease withadvancing age (6,7), the number of elderly patients referredfor cardiac valve surgery is likely to grow.
See page 1215
Several recent studies have reported “acceptable” opera-tive risk (in-hospital mortality 11% to 14%) and late survival(five-year survival �70%) for elderly patients undergoingcardiac surgery (8–10). However, because the long-termconsequences of cardiac valve surgery extend beyond meresurvival and morbidity, physicians are often hesitant torecommend surgery based on mortality data alone (11). In
addition, cardiac valve surgery in elderly patients is stillassociated with higher resource utilization and morbiditythan in younger patients (9,10,12).
There is a growing interest in the use of health status toevaluate clinical strategies. Improvement in quality of life(QOL) is considered to be one of the principal goals of valvesurgery (13). Patients deciding among treatment optionsmay value information about the change in QOL that theycan expect after valve surgery. It is particularly important toevaluate QOL in elderly patients, who have a higherprevalence of comorbidity, stress of surgery, and rate ofcomplications—all factors that may hinder improvement inQOL. Moreover, whether age modifies the expected QOLbenefit is not known. Previous studies addressing QOL inpatients undergoing cardiac valve surgery and the impor-tance of age as a predictor of QOL were limited by theabsence of younger controls, cross-sectional design, smallsample size, retrospective design, and use of substandardQOL instruments (11,14–16).
The relative lack of information on change in QOL aftermajor valve surgery impedes informed decision-making byphysicians and patients. Accordingly, we sought to investi-gate whether older patients derived less health status andQOL benefit after valve surgery than did younger patients.To achieve this objective, we prospectively studied whetherage is associated with change in QOL at 18 months afteraortic or mitral valve surgery.
From the *Division of Health Policy and Administration, Department of Epide-miology and Public Health, Yale University School of Medicine, New Haven,Connecticut; the †Department of Medicine, Division of Cardiology, Emory Univer-sity School of Medicine, and Rollins School of Public Health, Atlanta, Georgia; the‡Section of Cardiothoracic Surgery, Yale University School of Medicine, New Haven,Connecticut; the §Center for Outcomes Research and Evaluation, Yale-New HavenHospital, New Haven, Connecticut; and the �Section of Cardiovascular Medicine,Department of Medicine, Yale University School of Medicine, New Haven, Con-necticut. Dr. Sedrakyan was supported with a Fulbright scholarship (1999–2000) andfellowships at Yale University and Bayer Corporation (2000–2001).
Manuscript received December 31, 2002; revised manuscript received March 12,2003, accepted April 10, 2003.
Journal of the American College of Cardiology Vol. 42, No. 7, 2003© 2003 by the American College of Cardiology Foundation ISSN 0735-1097/03/$30.00Published by Elsevier Inc. doi:10.1016/S0735-1097(03)00949-5

METHODS
Study sample. We performed a longitudinal prospectivecohort study of consecutive patients undergoing isolatedvalve or simultaneous valve-coronary artery bypass graft(CABG) procedures at Yale-New Haven Hospital fromMarch 31, 1998, to March 30, 1999. Detailed clinical andnon-clinical information was abstracted from medicalrecords. During the first week after surgery, patients com-pleted baseline questionnaires focusing on their functioningin the month before surgery. Patients were contacted at 18months after surgery for outcome status assessment. Therewas a six-week time window allowed for follow-up ques-tionnaire completion.Measurement of QOL. Quality of life was measured atbaseline and at follow-up using the Medical OutcomesTrust Short Form 36-Item Health Survey (SF-36), a surveywith demonstrated high reliability and validity (17–20). TheSF-36 consists of 36 questions, grouped into the followingeight multi-item domains, which measure functioning indifferent aspects of daily life:
1) Physical functioning: limitations in lifting, climbing,bending, kneeling, walking, or running;
2) Role physical: degree of physical health to performactivities typical for the specific age and social responsi-bility, such as a job, community activities, and volunteerwork;
3) Bodily pain: intensity and duration of bodily pain andlimitations in activities due to pain;
4) General health: beliefs and evaluations of overall health;5) Vitality: feelings of energy, pep, fatigue, and tiredness;6) Social functioning: ability to develop, maintain, and
nurture mature social relationships (including family,friends, and spouse);
7) Role emotional: personal feelings about job performance,work, or other activities;
8) Mental health: emotional, cognitive, and intellectualstatus.
The Mental Component Summary (MCS) and the Phys-ical Component Summary (PCS) are two meta-scores of theSF-36. They combine eight multi-item domains and rep-resent overall physical functioning and mental functioning(17). These summary scales are used in this study as theprimary health-related QOL outcome variables for the
multivariable analyses. Validated U.S. population norms fordifferent age groups were used to gauge the significance ofthe improvement in QOL after surgery (21).Study variables. Society of Thoracic Surgery forms anddefinitions were used for clinical data collection (22).Socio-demographic variables included age, gender, andbody mass index (cut-offs: �22, 22 to 30, �30 kg/m2).Comorbidities included renal disease, peripheral vasculardisease (PVD), chronic obstructive pulmonary disease, dia-betes, and hypertension. Heart disease–related variableswere history of heart failure, New York Heart Association(NYHA) functional class, ejection fraction (mainly ab-stracted from ventriculography reports), cardiomegaly,chronic atrial fibrillation, previous myocardial infarction,aortic stenosis, mitral stenosis, angina type (stable or unsta-ble), previous CABG, and previous valve procedure.Procedure-related variables were implant type (tissue, me-chanical, or repair), simultaneous coronary bypass, andurgency of operation.Statistical analysis. First, we calculated descriptive statis-tics for the study variables. Next, after stratification of ageinto three groups (�64, 65 to 74, �75 years), we deter-mined the improvement in QOL after valve surgery bycomparing QOL at baseline and at 18 months after surgeryand comparing these values with U.S. population norms.Mean values and 95% confidence intervals were used todemonstrate the difference. Patient scores were consideredsimilar to the U.S. norms if the scores were within one-fourth of one standard deviation (SD) of the mean. This wasa conservative standard, as published guidelines to interpretthese scores suggest that even differences of one-half of oneSD are small (23). In addition, one-fourth of one SD (i.e.,5 to 10 points) represents the difference that is consideredclinically relevant for SF-36 domains (24). For MCS andPCS meta-scores, a clinically relevant difference is likely tobe 4 to 7 points (one-half of one SD) (25), which is, again,larger than our conservative estimate of one-fourth of oneSD. Given our set effect size, we had over 80% power todetermine statistical significance of the change in QOLwith 95% confidence (alpha level of 0.05). Finally, wemeasured the impact of age (continuous variable) on changein QOL by multiple regression analysis of the change in twometa-scores of the SF-36: the MCS and the PCS. Weconstructed four multiple regression models (2 for aorticand 2 for mitral subgroups). Aortic and mitral patients wereanalyzed separately to determine if the association of agewith change in QOL is different after aortic or mitralsurgery. Baseline score (MCS or PCS, depending onwhether change in MCS or PCS was predicted) was themost significant predictor of change in score from thebaseline and was included in all models. Because thevariance inflation factor did not exceed 2.5 and the tolerancewas �0.4, there was little or no evidence of colinearityamong predictors in determining the change in QOL. Wealso adjusted for disease severity characteristics (cardiomeg-aly, NYHA class), procedure type (isolated valve vs. valve
Abbreviations and AcronymsCABG � coronary artery bypass graft surgeryMCS � Mental Component SummaryNYHA � New York Heart AssociationPCS � Physical Component SummaryPVD � peripheral vascular diseaseQOL � quality of lifeSD � standard deviationSF-36 � Medical Outcomes Trust Short Form 36-Item
Health Survey
1209JACC Vol. 42, No. 7, 2003 Sedrakyan et al.October 1, 2003:1208–14 Age and Quality of Life in Cardiac Valve Surgery

plus CABG), and valve implant type (tissue vs. mechanical).In addition, we adjusted for gender and comorbid condi-tions (hypertension, body mass index, PVD) that mayinfluence the change in QOL.
The generalized estimating equations method was used todetermine age-related differences in QOL changes by test-ing the interaction between age and time and adjusting formeasurement correlation. The latter was confirmatory tomultiple regression, and only results of the multiple regres-sion are reported here. We used the Statistical AnalysisSystem (SAS Institute, release 8.02, Cary, North Carolina)for data management and analysis.
RESULTS
Cohort characteristics. Of the 285 consecutive patientswho underwent cardiac valve procedures, 220 (77.2%) par-ticipated in the study. Reasons for non-participation in-cluded death (n � 13), neurological problems (n � 10), dataentry problems (n � 10), inability to administer the QOLquestionnaire before discharge (n � 10), refusal (n � 9),language barriers (n � 4), and other reasons (n � 9). Therewas no difference between the baseline participants andnon-participants with regard to age and gender. For othercharacteristics, cerebrovascular accidents, PVD, and urgentsurgeries were more frequent in non-participants (Table 1).
Of 220 baseline participants, 14 patients (6.4%) diedwithin 18 months, leaving 206 patients available for follow-up. All but one of the deceased patients were �65 years ofage, and half were �75 years of age. There were sevenpatients (3%) who did not reply within the six-weekresponse period, four (2%) who refused to complete thequestionnaire, and nine (4%) who were lost to follow-up.Thus, of the baseline participants, follow-up QOL mea-surements at 18 months were obtained in 186 (90%) cases.
At baseline, there were 148 (67%) patients who had aorticvalve surgery and 72 (33%) patients who had mitral valvesurgery. Simultaneous valve and CABG procedures wereperformed in 38% of patients, and the proportion of patients�75 years of age was 34%. Elderly patients (age �75 years)were more likely than younger patients (age groups �65 and65 to 75 years) to have hypertension and higher NYHAclass, and they more often had valve-CABG procedures(data not presented). They were similar to younger patientsin terms of mean ejection fraction, diabetes, and chronicobstructive pulmonary disease.Improvement of QOL after surgery and comparison withnormative values. There were 126 aortic and 60 mitralpatients who reported both their baseline and follow-upQOL. Improvement in QOL after surgery was similar inboth aortic and mitral patients after stratification into threeage groups (scores were within one-fourth of one SDcompared with normative values). Thus, after age stratifi-cation into three categories and comparisons with popula-tion norms, the groups were combined.
All age groups showed improvement in most QOLdomains at 18 months. In the younger age group (�64years), there were statistically significant improvements inall domains except those of general health and role emo-tional (Fig. 1, Table 2). In the latter scales, pre-operativenorms were comparable with population norms, thus lim-iting the possibility of recording higher absolute improve-ments.
Among older patients (age groups 65 to 74 and �75years), overall absolute improvements in QOL were notedin the domains of physical functioning, role physical,vitality, and mental health, as well as in the MCS and thePCS meta-scores (Figs. 2 and 3, Table 2). As found inyounger patients, there was little or no absolute improve-ment reported on the general health, role emotional, bodilypain, and social functioning scales, where pre-operativescores were comparable with population norms. In all agegroups, mean values for the QOL domains at 18 monthsafter surgery were comparable and sometimes higher thanpopulation norms.Effect of age on the improvement in QOL in regressionanalysis. The multivariable models had good predictivepower in both aortic (R-square: 0.34 for change in MCSand 0.48 for change in PCS) and mitral (R-square: 0.48 forchange in MCS and 0.61 for change in PCS) samples. Inthe multiple regression analysis of overall mental function-ing as measured by MCS, age was not a significant predictorof change in score (Table 3). Similarly, after controlling forclinically relevant factors, the association of age with thechange in overall physical functioning as measured by PCSwas small and not statistically significant in the aortic sample(see statistical analysis) (Table 3). In contrast, age had astatistically significant association with PCS for patients un-dergoing mitral valve surgery. However, it was modest inmagnitude, with a 10-year increment in age resulting in a scorereduction of 1.90 (less than one-fourth of one SD).
Table 1. Comparison of Responders With Non-Responders*
VariablesParticipants
(n � 220)Non-Participants
(n � 65) p
Age, mean (SD) 66.5 � 14.4 65.1 � 15.1 0.52LVEF, mean (SD) 50.8 � 13.2 50.0 � 15.8 0.74Male gender (%) 54.5 64.6 0.15NYHA (III–IV) class† (%) 56.4 63.1 0.53History of MI (%) 23.6 28.1 0.46Urgent surgery (%) 33.0 50.0 0.013PVD (%) 13.6 26.1 0.017CVA (%) 5.0 16.9 0.002Diabetes (%) 15.9 23.1 0.18Hypertension (%) 58.9 55.4 0.61Cardiomegaly (%) 41.8 44.6 0.68COPD (%) 20.2 29.1 0.15Angina (%) 41.7 33.8 0.26Aortic stenosis (%) 54.1 43.1 0.12
*Groups were also not different with regard to arrhythmia, mitral stenosis cases,pulmonary artery pressure, family history of coronary disease, body mass index, andreoperation. †NYHA class I–II was the reference category.
COPD � chronic obstructive pulmonary disease; CVA � cerebrovascular acci-dent; LVEF � left ventricular ejection fraction; MI � myocardial infarction; NYHA� New York Heart Association; PVD � peripheral vascular disease; SD � standarddeviation.
1210 Sedrakyan et al. JACC Vol. 42, No. 7, 2003Age and Quality of Life in Cardiac Valve Surgery October 1, 2003:1208–14

DISCUSSION
We found that patients reported improvement in theirQOL after valve surgery in all age groups and across almostall QOL domains. The improvements from the baselineafter 18 months were larger than one-half of one SD inmost scales of the SF-36, as well as for overall mentalfunctioning and physical functioning (MCS and PCS meta-scores), supporting the clinical importance of the changes.In addition, we found that 18 months after surgery, QOLmean scores were comparable to U.S. population normativescores in all age groups of patients undergoing either aortic
or mitral surgery. This is notable, given that the nationalnorms used for comparison with our study population werederived from a general population of “healthy” people notreporting any symptomatic illness (21,26).
After adjusting for clinically relevant variables, we foundthat age alone was not strongly predictive of QOL improve-ment after surgery. We did not find an association betweenage and change in global mental health functioning (MCSmeta-score) for aortic or mitral patients (Table 3). Themagnitude of improvement in mental health was similar inelderly and younger patients. Similar conclusions can bedrawn with regard to physical functioning (PCS meta-
Figure 1. Quality of life (QOL) values with 95% confidence intervals in the �64-year age group (combined mitral and aortic patients). Open boxes �pre-operative QOL scores; open circles � 18-month follow-up QOL scores; closed triangles � U.S. population QOL norms for the �64-year age group.BP � bodily pain; GH � general health; MCS � mental component summary; MH � mental health; PCS � physical component summary; PF � physicalfunctioning; RE � role emotional; RP � role physical; SF � social functioning; VT � vitality.
Table 2. Preoperative, Postoperative, and Normative Mean QOL Values* in Different Age Groups
QOLScales
QOL Values in the<64-Year Age Group
QOL Values in the65–74-Year Age Group
QOL Values in the>75-Year Age Group
Preoperative Postoperative Norms Preoperative Postoperative Norms Preoperative Postoperative Norms
PF 61 � 31 81 � 20 76 49 � 30 72 � 28 69 40 � 25 58 � 26 53RP 43 � 44 80 � 30 74 33 � 41 63 � 41 65 17 � 29 42 � 42 45BP 66 � 32 84 � 21 68 71 � 28 80 � 24 68 64 � 32 75 � 27 61GH 59 � 11 59 � 9 65 57 � 14 59 � 8 63 55 � 12 58 � 8 57VT 44 � 25 63 � 23 60 42 � 19 61 � 22 60 38 � 22 50 � 21 50SF 71 � 29 84 � 22 81 74 � 25 83 � 23 81 71 � 25 75 � 26 74RE 64 � 45 79 � 36 80 62 � 44 74 � 41 81 59 � 46 56 � 43 63MH 59 � 11 75 � 19 75 59 � 13 78 � 18 81 58 � 11 76 � 16 74MCS 45 � 9 50 � 10 51 46 � 9 51 � 11 53 46 � 9 49 � 11 50PCS 41 � 10 49 � 6 46 39 � 10 45 � 10 43 34 � 8 41 � 9 38
*QOL values presented as means � SD.BP � bodily pain; GH � general health; MCS � mental component summary; MH � mental health; PCS � physical component summary; PF � physical functioning;
QOL � quality of life; RE � role emotional; RP � role physical; SF � social functioning; VT � vitality.
1211JACC Vol. 42, No. 7, 2003 Sedrakyan et al.October 1, 2003:1208–14 Age and Quality of Life in Cardiac Valve Surgery

score). In the aortic sample, the parameter estimate for agewas small (�1.00; less than one-fourth of one SD for a10-year increment) and not statistically significant (p �0.22) in predicting the improvement in overall physicalfunctioning (Table 3). In the mitral sample, the parameterestimate for age was slightly larger (�0.19) and statisticallysignificant (p � 0.02). However, interpretation of thisestimate suggests that two otherwise identical patientswhose ages differ by 10 years can expect a PCS differentialof 1.9 points (less than one-fourth of one SD). This isclearly a small difference, as the SD for the PCS score is 10and differences up to one-half of one SD are consideredsmall in health-related QOL evaluations (23). Furthermore,the overall results of our study suggest that older age doesnot limit the QOL benefits of cardiac valve surgery.
Although other studies have compared QOL before andafter valve surgery to population norms, they were limited bysamples that excluded older or younger patients, as well asby other aspects of study design. A study of 100 participantsby Phillips et al. (26) considered only younger patients andobtained 67% follow-up. Later prospective studies (14,27)that evaluated QOL after valve surgery had only six monthsof follow-up, and one of these studies, based on only 32patients, had no younger controls (14). Another cross-sectional study included 147 elderly patients; however,pre-operative QOL data were not available, and the studywas limited to aortic valve procedures (11). Additionalstudies did not separate valve patients from isolated coro-nary bypass patients (16,27). All previous studies reported
considerable improvement in QOL among elderly patients,and the consistency of the results in a variety of studydesigns supports the validity of the findings in the currentstudy.
The advantages of our study are its prospective design,relatively large sample size, accurate control over possibleconfounding, and use of a validated and widely acceptedinstrument for QOL assessment. In addition, this study isthe first to evaluate long-term outcomes (18 months), aswell as the first to evaluate the impact of age on improve-ment in QOL in aortic and mitral patients using a regres-sion approach. Comparison of QOL scores before and aftersurgery with population norms provided another estimate ofthe effect of cardiac surgery on QOL improvement inelderly and younger patients.Study limitations. First, this study was conducted at asingle center, perhaps limiting its generalizability. However,we compared our sample with the Society of ThoracicSurgeons summary data from 1991 to 1995 (28) and foundthe patients to be similar. Second, because we were unableto interview patients before surgery, baseline QOL datawere obtained during the first week after surgery. However,patients were asked to report their QOL in the monthbefore surgery. Third, we attempted to enroll every patientbut were not able to do so. In addition, we comparedparticipants with non-participants and found that the twogroups were not different with regard to major risk factors.Fourth, we did not test for cognitive decline that canpotentially be associated with QOL. Finally, our findings
Figure 2. Quality of life (QOL) values with 95% confidence intervals in the 65- to 74-year age group (combined mitral and aortic patients). Open boxes� pre-operative QOL scores; open circles � 18-month follow-up QOL scores; closed triangles � U.S. population norms for the 65- to 74-year age group.BP � bodily pain; GH � general health; MCS � mental component summary; MH � mental health; PCS � physical component summary; PF � physicalfunctioning; RE � role emotional; RP � role physical; SF � social functioning; VT � vitality.
1212 Sedrakyan et al. JACC Vol. 42, No. 7, 2003Age and Quality of Life in Cardiac Valve Surgery October 1, 2003:1208–14
are relevant to patients being referred for valve surgery, andtheir relevance to patients with mitral or aortic disease whodid not undergo surgery is unknown. It is possible thatconcerns about recovery lead some physicians not to recom-mend surgery to some older patients who might have adifferent recovery experience. Nevertheless, we believe thatthese limitations had a minor impact on our finding that agedoes not limit QOL benefits that can be attained aftersurgery.Conclusions. Patients reported improved QOL at 18months after aortic and mitral surgery that was comparableto population norms for their age. Among patients currentlyreferred for cardiac valve surgery, age does not appear toindependently influence or limit the improvement in QOL.Elderly patients should be educated about the expectedhealth status benefits associated with valve surgery. Further-more, these findings should help surgeons and elderly
patients to make informed decisions regarding the suitabil-ity of the valve surgery.
AcknowledgmentsThe authors acknowledge the staff of the Center forOutcomes Research and Evaluation at Yale-New HavenHospital for their kind assistance during the importantstages of the research.
Reprint requests and correspondence: Dr. Harlan M. Krum-holz, Yale University School of Medicine, 333 Cedar Street, P. O.Box 208025, New Haven, Connecticut 06520-8025. E-mail:[email protected].
REFERENCES
1. American Heart Association. 1999 Heart and Stroke Statistical Up-date. Dallas, TX: American Heart Association.
2. CDC/NCHS and the American Heart Association. National Healthand Nutrition Examination Survey III (NHANES III), 1988–1994.
3. Jamieson WR, Thompson DM, Munro AL. Cardiac valve replace-ment in elderly patients. CMAJ 1980;123:628–32.
4. Jaeger AA, Hlatky MA, Paul SM, Gortner SR. Functional capacityafter cardiac surgery in elderly patients. J Am Coll Cardiol 1994;24:104–8.
5. Greengross S, Murphy E, Quam L, Rochon P, Smith R. Aging: asubject that must be at the top of world agendas. BMJ 1997;315:1029–30.
6. Singh JP, Evans JC, Levy D, et al. Prevalence and clinical determi-nants of mitral, tricuspid and aortic regurgitation (the FraminghamHeart Study). Am J Cardiol 1999;83:897–902.
7. Hinchman DA, Otto CM. Valvular disease in the elderly. CardiolClin 1999;17:137–58.
Figure 3. Quality of life (QOL) values with 95% confidence intervals in the �75-year age group (combined mitral and aortic patients). Open boxes �pre-operative QOL scores; open circles � 18-month follow-up QOL scores; closed triangles � U.S. population norms for the �75-year age group. BP� bodily pain; GH � general health; MCS � mental component summary; MH � mental health; PCS � physical component summary; PF � physicalfunctioning; RE � role emotional; RP � role physical; SF � social functioning; VT � vitality.
Table 3. Multivariable Analysis of the Effect of Age on Changein MCS and PCS Scores
Subgroupsof ValvePatients
Age Effect(1-Year Increments)for Change in MCS p
Age Effect(1-Year Increments)for Change in PCS p
Aortic* 0.09 0.29 �0.10 0.22Mitral† 0.009 0.94 �0.19 0.02
*Multiple regression including all variables in aortic sample (n � 126) (see statisticalanalysis section for the list of variables in the final models). †Multiple regressionincluding all variables in mitral sample (n � 60) (forward selection procedure wasconsidered because of the small sample size, but it did not affect parameter estimate).
MCS � mental component summary; PCS � physical component summary.
1213JACC Vol. 42, No. 7, 2003 Sedrakyan et al.October 1, 2003:1208–14 Age and Quality of Life in Cardiac Valve Surgery

8. Khan JH, McElhinney DB, Hall TS, Merrick SH. Cardiac valvesurgery in octogenarians: improving quality of life and functionalstatus. Arch Surg 1998;133:887–93.
9. Kirsch M, Guesnier L, LeBesnerais P, et al. Cardiac operations inoctogenarians: perioperative risk factors for death and impaired auton-omy. Ann Thorac Surg 1998;66:60–7.
10. Gehlot A, Mullany CJ, Ilstrup D, et al. Aortic valve replacement inpatients aged eighty years and older: early and long-term results.J Thorac Cardiovasc Surg 1996;111:1026–36.
11. Sundt TM, Bailey MS, Moon MR, et al. Quality of life after aorticvalve replacement at the age of �80 years. Circulation 2000;102 Suppl3:III70–4.
12. Dalrymple-Hay MJ, Alzetani A, Aboel-Nazar S, Haw M, Livesey S,Monro J. Cardiac surgery in the elderly. Eur J Cardiothorac Surg1999;15:61–6.
13. Bonow RO, Carabello B, de Leon AC Jr., et al. ACC/AHA guidelinesfor the management of patients with valvular heart disease: a report ofthe American College of Cardiology/American Heart AssociationTask Force on Practice Guidelines (Committee on Management ofPatients with Valvular Heart Disease). J Am Coll Cardiol 1998;32:1486–588.
14. Olsson M, Janfjall H, Orth-Gomer K, Unden A, Rosenqvist M.Quality of life in octogenarians after valve replacement due to aorticstenosis. A prospective comparison with younger patients. Eur Heart J1996;17:583–9.
15. Fruitman DS, MacDougall CE, Ross DB. Cardiac surgery in octoge-narians: can elderly patients benefit? Quality of life after cardiacsurgery. Ann Thorac Surg 1999;68:2129–35.
16. Heijmeriks JA, Pourrier S, Dassen P, Prenger K, Wellens HJ.Comparison of quality of life after coronary and/or valvular cardiacsurgery in patients �75 years of age with younger patients. Am JCardiol 1999;83:1129–32.
17. Beaton DE, Hogg-Johnson S, Bombardier C. Evaluating changes inhealth status: reliability and responsiveness of five generic health statusmeasures in workers with musculoskeletal disorders. J Clin Epidemiol1997;50:79–93.
18. Jenkinson C, Lawrence K, McWhinnie D, Gordon J. Sensitivity tochange of health status measures in a randomized controlled trial:comparison of the COOP charts and the SF-36. Qual Life Res1995;4:47–52.
19. The Bypass Angioplasty Revascularization Investigation (BARI) In-vestigators. Comparison of coronary bypass surgery and angioplasty inpatients with multivessel disease. N Engl J Med 1996;335:217–25.
20. Rumsfeld JS, Whinney SM, McCarthy M Jr, et al. Health-relatedquality of life as a predictor of mortality following coronary arterybypass graft surgery. JAMA 1999;281:1298–303.
21. Ware JE Jr., Kosinski M, Keller SD. SF-36 Physical and MentalHealth Summary Scales: A User’s Manual. Boston, MA: The HealthInstitute, New England Medical Center, 1994.
22. Clark RE. Definitions of terms of the Society of Thoracic SurgeonsNational Cardiac Surgery Database. Ann Thorac Surg 1994;58:271–3.
23. Revicki DA, Osoba D, Fairclough D, et al. Recommendations ofhealth-related quality of life research to support labeling and promo-tional claims in the United States. Qual Life Res 2000;9:887–900.
24. Ware JE Jr., Kosinski M, Bayliss MS, McHorney CA, Rogers WH,Raczek A. Comparison of methods for the scoring and statisticalanalysis of SF-36 health profile and summary measures: summary ofresults from the Medical Outcomes Study. Med Care 1995;33 Suppl4:AS264–79.
25. Ware JE Jr., Bayliss MS, Rogers WH, Kosinski M, Tarlov AM.Differences in 4-year health outcomes for elderly and poor, chronicallyill patients treated in HMO and fee-for-service systems. Results fromthe Medical Outcomes Study. JAMA 1996;276:1039–47.
26. Phillips RC, Lansky DJ. Outcomes management in heart valvereplacement surgery: early experience. J Heart Valve Dis 1992;1:42–50.
27. Chocron S, Etievent JP, Viel JF, et al. Prospective study of quality oflife before and after open heart operations. Ann Thorac Surg 1996;61:153–7.
28. Jamieson WR, Edwards FH, Schwartz M, Bero JW, Clark RE,Grover FL. Risk stratification for cardiac valve replacement. NationalCardiac Surgery Database. Database Committee of the Society ofThoracic Surgeons. Ann Thorac Surg 1999;67:943–51.
1214 Sedrakyan et al. JACC Vol. 42, No. 7, 2003Age and Quality of Life in Cardiac Valve Surgery October 1, 2003:1208–14

EDITORIAL COMMENT
Valve Surgery in the ElderlyA Question of Quality (of Life)?*John S. Rumsfeld, MD, PHD, FACCDenver, Colorado
Over the next two decades, the aging of the population willforce a major shift in clinical care in the U.S. By 2010, over40 million Americans will be age 65 years and older, 18million Americans will be over the age of 75 years, and theburden of cardiac disease among older persons will continueto rise (1,2). Clinicians caring for patients with cardiovas-cular disease will need to make tough decisions about theuse of therapies and interventions in older persons. This willbe a tremendous challenge for multiple reasons. First, olderage is an independent risk factor for higher mortality andmorbidity in cardiac populations (3). Second, elderly pa-tients have a heavy burden of comorbid diseases, whichcomplicates management and further increase the risk ofadverse outcomes (4,5). Third, the evidence base for most
See page 1208
cardiovascular therapies stems from clinical trials that haveexcluded elderly patients (particularly those �75 years ofage), leaving clinicians with relatively little direct evidenceto guide treatment (3,6). And finally, few studies havefocused on patient-centered outcomes, including health-related quality of life (HRQL). Ultimately, for clinicians tomake the best decisions about cardiovascular therapies, aclear understanding of the impact of these therapies on theHRQL of patients is essential. This is particularly true forelderly patients because many older persons express apreference for quality of life over quantity of life, andsurvival benefits may not be the primary therapeutic goal(7).
Cardiac valve surgery is an excellent example whereHRQL considerations are critical, but where evidence islacking. Valve surgery is increasingly performed on olderpatients, including those over 75 years (6,8). At the sametime, advanced age is a risk factor for operative mortalitywith valve surgery (6,8,9). While data is limited, studies ofvalve surgery in octogenarians have reported short-term(e.g., 30-day) mortality rates of approximately 8% to 20%,with lower mortality for isolated aortic valve surgery andhigher mortality for mitral valve, multiple valve, and valve-coronary artery bypass graft (CABG) operations (6,8,10–
12). Very limited data on valve surgery on nonagenarianssuggests operative mortality in excess of 15% (13). Clearly,the elevated operative mortality risk in older persons under-going valve surgery must be balanced against the potentialbenefits of the operation.
A principal goal of cardiac valve surgery is improvementin HRQL through reduction of symptoms and betterphysical function. Although valve surgery will be under-taken in select elderly patients for potential survival benefit(e.g., isolated severe aortic stenosis in a patient withoutsignificant comorbidities), the primary goal of the operationfor most elderly persons should be improvement in HRQL.Unfortunately, the potential HRQL benefits of the opera-tion may be offset in older patients by neurocognitivedeficits after surgery, increased short- and long-term com-plications, and incomplete recovery resulting in significantresidual functional limitations (6). Coupled with the tech-nical challenges of valve surgery in older persons, includingthe potential for extensive calcification of the aortic valve,annulus, and aortic root, and the prevalence of ischemicmitral regurgitation, it cannot be assumed that surgery tocorrect valvular pathology will improve HRQL. Withoutevidence supporting HRQL benefits of valve surgery in theelderly, clinicians are faced with the decision of recom-mending an intervention for which the risks may outweighthe potential gains.
In this issue of the Journal, Sedrakyan et al. (14) evaluatedwhether older age attenuates the HRQL benefits of cardiacvalve surgery in a cohort of 220 patients undergoing aorticor mitral valve operations. They measured HRQL at base-line and 18 months after the operation using the Short-Form 36 (SF-36) health status survey. The SF-36 does notcontain disease-specific questions (i.e., there are no ques-tions directly relating to symptoms or functional limitationsfrom valve disease), but is a widely validated measure ofoverall physical and mental health status (15). The authorsfound clinically significant mean improvements in overallphysical and mental health status for patients in the �65-,65- to 74-, and �75-year-old age groups. The averageimprovements in SF-36 scores were similar across the agespectrum and for both aortic and mitral valve operations.Remarkably, postoperative SF-36 scores were restored topopulation norms for all age groups. Therefore, the authorsconcluded that age does not appear to limit the HRQLbenefits of valve surgery.
Several limitations of the Seredkyan et al. (14) studyshould be noted. First, the study was performed at a singletertiary care center, which may limit generalizability. Sec-ond, over one-third of the patients had combined valve-CABG procedures, so the relative HRQL improvement dueto repair of the valve lesion versus coronary revascularizationcannot be determined. Finally, the baseline HRQL assess-ment was administered after surgery, raising some concernof bias. It is possible that patients who have survived acardiac operation would overstate their preoperative HRQL
*Editorials published in the Journal of the American College of Cardiology reflect theviews of the authors and do not necessarily represent the views of JACC or theAmerican College of Cardiology.
From the Veterans Affairs Medical Center/University of Colorado Health SciencesCenter, Denver, Colorado. Dr. Rumsfeld is supported by a VA Health ServicesResearch Career Development Award.
Journal of the American College of Cardiology Vol. 42, No. 7, 2003© 2003 by the American College of Cardiology Foundation ISSN 0735-1097/03/$30.00Published by Elsevier Inc. doi:10.1016/S0735-1097(03)00950-1

deficits, leading to an overestimation of the improvement inHRQL after the operation. Furthermore, this study designleads to the exclusion of patients with early deaths and thosethat were too ill or cognitively impaired after the operationto participate. This may result in a study cohort largelycomposed of patients who benefited from the procedure.
Nonetheless, the results of this study are consistent withprevious studies that have examined HRQL after valvesurgery in the elderly (10–12,16–18). Furthermore, thecurrent study avoids many of the limitations of previousstudies, such as very small sample sizes, short follow-up,failure to use validated HRQL measures, and/or failure toassess HRQL longitudinally. The study by Seredkyn et al.(14), therefore, moves us toward a better understanding ofthe impact of valve surgery on HRQL.
The primary implication of the study by Sedrakyan et al.(14) is that older patients undergoing cardiac valve surgerycan have significant improvements in HRQL, on par withimprovements seen in younger patients. It is essential torecognize, however, that the average HRQL improvementsreported in this study will not be realized in all patientsundergoing the operation. More importantly, the study doesnot tell us which elderly patients should be chosen for theoperation. The decision to recommend valve surgery for agiven older patient will need to be individualized based onthe specific valvular pathology and severity, the actual age ofthe patient (because the term “elderly” remains a broadconcept), associated comorbid diseases, and patient prefer-ences regarding the potential risks and benefits of theoperation. It will be essential to supplement this decision-making with an understanding of which patients are mostlikely to derive an HRQL benefit from the operation.
Therefore, the study by Sedrakyan et al. (14) should beviewed as an important first step toward a greater under-standing of how to choose cardiac therapies to optimizepatient-centered outcomes. To achieve this goal, expandedresearch efforts are needed to measure the impact of cardiactherapies on the HRQL of older cardiovascular patients.Studies are also needed to identify the determinants ofHRQL in cardiac populations and to evaluate interventionsto improve patient-centered outcomes. Ideally, new clinicaltrials will be undertaken, such as the recently publishedTrial of Invasive versus Medical therapy in Elderly patients(TIME) (19). In many instances, however, new clinicaltrials are not likely to be forthcoming, and we must rely oncareful observational studies like the one by Seredkyn et al.(14). Registries are a potentially rich source of data forobservational studies, and there are several well-establishedregistries for cardiac surgery (20). However, a key deficiencyof existing cardiovascular registries is the lack of data onpatient-centered outcomes. The time has come for HRQLmeasures to be incorporated in all cardiovascular clinicaltrials, observational studies, and cardiovascular registries.
Although further research is critical, we can gain someinsight from the existing literature on how HRQL measuresmay be helpful in clinical decision-making. It has been
shown in multiple cardiac populations that HRQL inde-pendently predicts subsequent mortality (21–23). This hasnot yet been evaluated for valve surgery, but we cananticipate that patients with diminished preoperativeHRQL will be at higher risk for operative mortality. On theother hand, it is likely that only those patients withsignificant HRQL deficits will derive HRQL benefits withthe operation (24). This paradox is directly analogous topatients with reduced left ventricular ejection fraction, whoare at increased risk for CABG surgery, but can derive agreater survival benefit (25). Thus, clinicians should stronglyconsider formal measurement of HRQL before cardiacvalve surgery to aid in risk stratification.
In conclusion, cardiovascular clinicians will increasinglybe faced with the challenges of decision-making in elderlypatients. The issues prominent in the growing field of“geriatric cardiology” are moving into mainstream cardiol-ogy. An understanding of the impact of therapies on theHRQL of older cardiac patients, and an understanding ofhow HRQL data can be used in the clinical management ofelderly patients, will be critical. Only through dedicatedresearch and clinical practice efforts will we be ready to makedecisions in elderly patients that will optimize patient-centered outcomes, and, ultimately, provide the highestquality of care.
Reprint requests and correspondence: Dr. John S. Rumsfeld,Cardiology (111B), Denver VA Medical Center, 1055 ClermontStreet, Denver, Colorado 80220. E-mail: [email protected].
REFERENCES
1. American Heart Association. 2003 Heart and Stroke Statistical Up-date. Available at: http://www.americanheart.org. Accessed on April1, 2003.
2. U.S. Census Bureau. Population Projections. Available at: http://www.census.gov/population/www/projections/popproj.html. Accessedon April 1, 2003.
3. Cheitlin MD, Gerstenblith G, Hazzard WR, et al. Database Confer-ence January 27–30, 2000, Washington, DC. Do existing databasesanswer clinical questions about geriatric cardiovascular disease andstroke? Am J Geriatr Cardiol 2001;10:207–23.
4. Lee PY, Alexander KP, Hammill BG, Pasquali SK, Peterson ED.Representation of elderly persons and women in published randomizedtrials of acute coronary syndromes. JAMA 2001;286:708–13.
5. Wolff JL. Prevalence, expenditures, and complications of multiplechronic conditions in the elderly. Arch Intern Med 2002;162:2269–76.
6. Aziz S, Grover FL. Cardiovascular surgery in the elderly. Cardiol Clin1999;17:213–31.
7. Tsevat J, Dawson NV, Wu AW, et al. Health values of hospitalizedpatients 80 years or older: Hospitalized Elderly Longitudinal Project.JAMA 1998;279:371–5.
8. Hinchman DA, Otto CM. Valvular disease in the elderly. CardiolClin 1999;17:137–58.
9. Edwards FH, Peterson ED, Coombs LP, et al. Predition of operativemortality after valve replacement surgery. J Am Coll Cardiol 2001;37:885–92.
10. Sundt TM, Bailey MS, Moon MR, et al. Quality of life after aorticvalve replacement at the age of �80 years. Circulation 2000;102 SupplIII:70–4.
1216 Rumsfeld JACC Vol. 42, No. 7, 2003Editorial Comment October 1, 2003:1215–7

11. Khan JH, McElhinney DB, Hall TS, Merrick SH. Cardiac valvesurgery in octogenarians: improving quality of life and functionalstatus. Arch Surg 1998;133:887–93.
12. Shapira OM, Kelleher RM, Zelingher J, et al. Prognosis and quality oflife after valve surgery in patients older than 75 years. Chest 1997;112:885–94.
13. Edwards MB, Taylor KM. Outcomes in nonagenarians after heartvalve replacement operation. Ann Thorac Surg 2003;75:830–4.
14. Sedrakyan A, Vaccarino V, Paltiel AD, et al. Age does not limitquality of life improvement in cardiac valve surgery. J Am Coll Cardiol2003;42:1208–14.
15. Ware J, Kosinski M. SF-36 Physical and Mental Health SummaryScales: A Manual for Users of Version 1. 2nd edition. Lincoln, RI:QualityMetric Inc., 2001.
16. Chocron S, Rude N, Dussaucy A, et al. Quality of life after open-heartsurgery in patients over 75 years old. Age Ageing 1996;25:8–11.
17. Heijmeriks JA, Pourrier S, Dassen P, Prenger K, Wellens HJ.Comparison of quality of life after coronary and/or valvular cardiacsurgery in patients �75 years of age with younger patients. Am JCardiol 1999;83:1129–32.
18. Olsson M, Janfjall H, Orth-Gomer K, Unden A, Rosenqvist M.Quality of life in octogenarians after valve replacement due to aorticstenosis: a prospective comparison with younger patients. Eur Heart J1996;17:583–9.
19. Pfisterer M, Buser P, Osswald S, et al. Outcome of elderly patients
with chronic symptomatic coronary artery disease with an invasive vs.optimized medical treatment strategy: one-year results of the random-ized TIME trial. JAMA 2003;289:1117–23.
20. Jones RH, Hannan EL, Hammermeister KE, et al. Identification ofpreoperative variables needed for risk adjustment of short-term mor-tality after coronary artery bypass graft surgery. The Working GroupPanel on the Cooperative CABG Database Project. J Am Coll Cardiol1996;28:1478–87.
21. Spertus JA, Jones P, McDonell M, et al. Health status predictslong-term outcome in outpatients with coronary disease. Circulation2002;106:43–9.
22. Rumsfeld JS, MaWhinney S, McCarthy M, et al. Health-relatedquality of life as a predictor of mortality following coronary arterybypass graft surgery. JAMA 1999;281:1298–303.
23. Konstam V, Salem D, Pouleur H, et al. Baseline quality of life as apredictor of mortality and hospitalization in 5,025 patients withcongestive heart failure. SOLVD Investigations. Studies Of LeftVentricular Dysfunction Investigators. Am J Cardiol 1996;78:890–5.
24. Rumsfeld JS, Magid DJ, O’Brien M, et al. Changes in health-relatedquality of life following coronary artery bypass graft surgery. AnnThorac Surg 2001;72:2026–32.
25. Eagle KA, Guyton RA, Davidoff R, et al. ACC/AHA guidelines forcoronary artery bypass graft surgery: a report of the American Collegeof Cardiology/American Heart Association Task Force on PracticeGuidelines. J Am Coll Cardiol 1999;34:1262–346.
1217JACC Vol. 42, No. 7, 2003 RumsfeldOctober 1, 2003:1215–7 Editorial Comment
Heart Failure
Is Nutritional Intake Adequatein Chronic Heart Failure Patients?Roberto Aquilani, MD,* Cristina Opasich, MD,† Manuela Verri, PHD,‡ Federica Boschi, PHD,‡Oreste Febo, MD,§ Evasio Pasini, MD,� Ornella Pastoris, PHD‡Pavia, Montescano, and Brescia, Italy
OBJECTIVES The goal of this study was to investigate the nutrition adequacy and energy availability forphysical activity in free-living, clinically stable patients with chronic heart failure (CHF).
BACKGROUND Little information exists regarding the nutrition adequacy and alimentary habits of patientswith clinically stable CHF. We hypothesized that CHF patients have an inadequate intakeof calories and protein, leading to a negative calorie and nitrogen balance, an expression ofincreased tissue breakdown.
METHODS In 57 non-obese patients with CHF (52 males and 5 females; 52 � 3 years; body mass index�25 kg/m2) and in 49 healthy subjects (39 males and 10 females) matched for age, body massindex, and sedentary life style we evaluated total energy expenditure (TEE), calorie intake(kcalI), and nitrogen intake (NI) from a seven-day food diary, total nitrogen excretion (TNE),and energy availability (EA � kcalI � resting energy expenditure). A zero calorie balance(CB) occurred when kcalI � TEE; a nitrogen balance (NB) in equilibrium was set at NB (�NI � TNE) 0 � 1 g/day.
RESULTS In patients and controls kcalI and NI were similar. However, in CHF patients the kcalI was�TEE with a consequent negative CB (�186 � 305 kcal/day vs. � 104.2 � 273 kcal/dayof controls; p � 0.01). Nitrogen balance resulted negative in CHF (�1.7 � 3.2 g/24 h vs. �2.2 � 3.6 g/24 h in controls; p � 0.01). Energy availability in CHF patients was 41% lowerthan in controls (p � 0.05).
CONCLUSIONS Non-obese, free-living patients with clinically stable CHF have an inadequate intake ofcalories and protein and reduced energy availability for physical activity. (J Am Coll Cardiol2003;42:1218–23) © 2003 by the American College of Cardiology Foundation
Nutritional intake is adequate to body needs when itprovides energy substrates for current body energy needsand restores catabolized endogenous proteins, thus increas-ing the low glycogen content in muscles. These prioritiesmay be particularly relevant in patients with chronic heartfailure (CHF) who can be hypermetabolic (1,2), hypercata-bolic (3), and have low glycogen content (4).
See page 1224
In clinical practice a useful method to assess nutritionaladequacy is to calculate the calorie-nitrogen balance (CNB),that is the difference over a day, between calorie-nitrogenintake and total calorie expenditure-nitrogen excretion.Previous studies dealing with nutrition in CHF did notcalculate CNB (5).
We hypothesized that the calorie and protein intakes of
non-obese patients with CHF, although clinically stable andliving freely at home, might be inadequate to meet bodyrequirements, thus causing negative CNB, as in clinicalpractice, non-obese ambulatory CHF patients are not rou-tinely provided a personalized nutritional prescription oradvice despite their possible catabolic factors.
We, therefore, assessed nutritional adequacy and calcu-lated energy availability for daily life physical activities innon-obese, clinically stable patients with CHF, living athome.
METHODS
Population. Fifty-seven non-obese patients (body massindex �25 kg/m2) with CHF, admitted to the Heart FailureUnit of Montescano for assessment or reassessment ofindications for cardiac transplantation, were enrolled for thestudy three days before their discharge from the unit.Patients with diabetes mellitus, liver, and renal insufficiencywere excluded from the study.
Table 1 summarizes the demographic, clinical, func-tional, neurohormonal, and treatment characteristics of thepatients recorded while they were clinically stable (noevidence of fluid retention—peripheral or pulmonary ede-ma; jugular venous pressure not raised; no changes inmedication for at least seven days).
No patient had clinical signs of intestinal malabsorption
From the *Servizio di Fisiopatologia Metabolico-Nutrizionale e NutrizioneClinica, Fondazione S. Maugeri, IRCCS, Istituto Scientifico di Montescano,Montescano-Pavia, Italy; †Divisione di Cardiologia, Fondazione S. Maugeri,IRCCS, Istituto Scientifico di Pavia, Pavia, Italy; ‡Dipartimento di Scienze Fisio-Farmacologiche, Sezione di Farmacologia, Universita degli Studi di Pavia, Pavia,Italy; §Divisione di Cardiologia-Unita Scompenso, Fondazione S. Maugeri, IRCCS,Istituto Scientifico di Montescano, Montescano-Pavia, Italy; and �Centro di RicercaCardiovascolare, Fondazione S. Maugeri, IRCCS, Istituto Scientifico di Gussago,Brescia, Italy.
Manuscript received December 18, 2002; revised manuscript received March 25,2003, accepted April 17, 2003.
Journal of the American College of Cardiology Vol. 42, No. 7, 2003© 2003 by the American College of Cardiology Foundation ISSN 0735-1097/03/$30.00Published by Elsevier Inc. doi:10.1016/S0735-1097(03)00946-X

such as steatorrhea, diarrhea. Twenty patients (35%) haddigestive disturbances such as early satiety, abdominal dis-comfort and fullness after meals.
The patients were adequately informed about the aimsand methods of the study and gave written consent for their
participation. The study was approved by our institution’sethical scientific committee.Materials. CHF NUTRITIONAL-HORMONAL EVALUATIONS.
Triceps skinfold thickness and midarm muscle circumfer-ence were measured in all patients in order to calculate armmuscle area (AMA) (6). Body weight (BW) was recordedand compared with the usual BW in the last six to 12months before hospital admission.
A non-intentional loss of �10% of BW in the precedingyear or �7.5% in the last six months was considered as amarker of energy depletion (7). Severe muscle proteinmalnutrition and, hence, loss of lean body mass was diag-nosed when the AMA was below the 5th percentile (6). Theco-presence of BW loss and a reduced AMA was diagnosticof combined calorie and protein malnutrition.
Resting energy expenditure (REE) was measured byindirect calorimetry (8) and expressed in kcal/day, kcal/kgBW, and kcal/m2 body surface.
A normal REE value lies between 90% to 110% of thevalue predicted by the Harris-Benedict equation (HB) (9).
At 8 AM peripheral venous blood samples were drawn forassays of cortisol (nmol/l) and insulin (�UI/ml) levels(commercial kits Cord-CT Radioimmunoassay Kit CISFrance, Coat A Count Insuline, D.P.C., Los Angeles,California).
The patients were extensively informed on how to keep aseven-day food diary at home and asked to collect three-day24-h urine samples for determination of urea nitrogenexcretion (UNE) (in g/24 h) (10). After receiving thepatients’ food diaries and UNE results, we used computer-ized nutritional analysis to calculate the macronutrient(carbohydrates [CHO], proteins, lipids) and calorie intakes(kcalI).
Total energy expenditure (TEE) (kcal/day) was estimatedas REE � 1.3 where 1.3 is a correction factor for physicalactivity (1). Energy availability (EA) (kcal/day) for dailyphysical activity was calculated as kcalI � REE.
CRITERIA FOR NUTRITION ADEQUACY TO BODY NEEDS.
1) Adequate calorie intake: a neutral or positive caloriebalance (CB), where CB (�kcal/day) � kcalI � TEE.
2) Adequate protein intake: a neutral or positive nitrogenbalance (NB), where NB (g/24 h) � daily nitrogenintake (NI) � total nitrogen loss (TNL). NI � nitrogenintake with food (� protein intake: 6.25); TNL � totalnitrogen loss (g/24 h) � UNE (g/24 h) � 2g (11).
If NB � 0 � 1 g/24 h, body anabolic and catabolicprocesses were in equilibrium; a negative NB (��1 g/24 h)denoted an excess of endogenous protein consumption(catabolic process) while a positive NB (��1 g/24 h)indicated a predominance of anabolic processes.
CONTROL GROUP ENROLLMENT. A control group of 49healthy subjects (39 males and 10 females) was selected tomeet the following criteria: 1) comparable age (44 � 16years; p � NS); 2) a very sedentary lifestyle (12); 3) no
Abbreviations and AcronymsAMA � arm muscle areaBW � body weightCB � calorie balanceCHF � chronic heart failureCHO � carbohydratesCNB � calorie-nitrogen balanceEA � energy availabilityHB � Harris-Benedict equationkcalI � daily calorie intakeNB � nitrogen balanceNI � daily nitrogen intakeREE � resting energy expenditureTEE � total energy expenditureTNL � total nitrogen lossUNE � urine nitrogen excretion
Table 1. Patients’ Demographic, Clinical, Functional,Neurohormonal, and Treatment Characteristics
Number (n): 57 ptsAge (yrs): 52 � 3Men/women: 52/5Etiology
Coronary artery disease 31 pts (� 54.3%)Idiopathic cardiomyopathy 20 pts (� 35%)Valvular heart disease 6 pts (� 10.5%)
Duration of disease (months)�18 23 pts�18 34 pts
NYHA classI 5 pts (� 8.7%)II 28 pts (� 49%)III 21 pts (� 37%)IV 3 pts (� 5.3%)
Left ventricular ejection fraction 20.3 � 5.6%Peak VO2 (ml O2/kg/min)
�14 (11.8 � 2.5) 26 pts�14 (18.5 � 4.7) 31 pts
Anaerobic threshold (ml O2/kg/min)peak VO2 � 14 10 � 2.1peak VO2 � 14 14.8 � 3.7
Respiratory exchange ratiobaseline 0.84 � 0.1peak VO2 1.1 � 0.1
Neurovegetative status evaluationnorepinephrine (pg � ml�1) 330.0 � 19
(reference values from our laboratory: 278 � 75)Medication
ACE inhibition 45 pts (79%)Digoxin 16 pts (28%)Diuretics 54 pts (95%)Warfarin 17 pts (29.8%)Calcium antagonists 8 pts (14%)Oral nitrates 14 pts (24.6%)
ACE � angiotensin-converting enzyme; NYHA � New York Heart Association;pts � patients.
1219JACC Vol. 42, No. 7, 2003 Aquilani et al.October 1, 2003:1218–23 Nutrition in Chronic Heart Failure

symptoms or signs of heart disease or diabetes; 4) weightstability (� 1 kg) during the three months before theirenrollment; 5) comparable body mass index. To achieve thislast match we selected people with a body mass indexranging from 17 kg/m2 (underweight individuals) to 25kg/m2 (normal weight individuals). The underweight sub-jects were people who deliberately, and without advice froma nutritionist, had chosen to reduce their food intake in thelast year.
The control group underwent the same experimentalprotocol as CHF patients.Statistical analysis. Results are presented as the meanvalue � SD. Comparisons between groups were performedwith t tests. Differences were considered statistically signif-icant at p � 0.05.
Furthermore, simple linear regression analysis was used toshow possible correlations between plasma cortisol levels,plasma insulin levels, cortisol/insulin ratio, and anthropo-metric parameters and resting energy expenditure.
RESULTS
Patients’ nutritional status and resting energy expendi-ture. The study showed that 31/57 patients (54.4%) weremalnourished: nine had combined protein-calorie malnutri-tion (15.8% population), 22 (38.5%) had protein malnutri-tion with a normal BW (90% to 110% desirable BW) (Table2).
Patients and controls were designated as follows: allpatients with CHF (All-CHF) (n � 57); normally nour-ished CHF patients (Normo-CHF) (n � 26); malnourishedCHF (Maln-CHF) patients (n � 31); all healthy controls(All-C) (n � 49); normal weight controls (Normo-C) (n �33); underweight controls (Under-C) (n � 16).
Compared with controls, CHF patients had similar
REEs/kg (hence, TEEs) but different REEs/m2. They lostmetabolic adaptation to body tissue wasting (13), as theirREEs percent predicted HB was higher than that in controls.Nutritional intake, calorie and nitrogen balance, energyavailability. Negative CB and NB occurred in 70.1% and59.6% of CHF patients, respectively, despite them havingsimilar calorie (kcalI/kg) and nitrogen (NI/kg) intakes ascontrols (Table 3). A combined negative CNB was found in40.3% of the patients.
Patients with CHF had a lower energy availability (EA)for physical tasks of daily life than did controls (�41%:292.5 kcal/day).
From diaries, patients with CHF ingested less lipids thancontrols but similar amounts of CHO. The contributions ofCHOs and lipids to ingested calories (% kcal) were higherand lower, respectively, in CHF patients than in controls(p � 0.01). As regards alimentary habits, CHF concen-trated 82 � 8% ingested calories over a day in the two mainmeals (lunch and dinner).
Thirty-five percent of CHF patients confirmed, in theirdiaries, the persistence of digestive disturbances.Plasma cortisol and insulin concentrations, cortisol/insulin ratio. Plasma cortisol levels, higher in CHF pa-tients than in controls, although within the normal range ofvalues, were positively correlated with REE/kg (r � 0.38,p � 0.02) (Table 4).
Plasma insulin concentrations, similar between patientsand controls, were correlated with BW (r � 0.6, p � 0.01),triceps skinfold thickness (r � 0.45, p � 0.01), AMA (r �0.48, p � 0.01), but not with REE (p � NS).
Thus, the calculated cortisol/insulin ratio was higher inCHF patients than in controls, although this was onlysignificant for All-CHF versus All-C (p � 0.01). The ratiowas negatively correlated with BW (r � �0.52, p � 0.01)and AMA (r � �0.46, p � 0.02).
Table 2. Anthropometric Measures, Resting Energy Expenditure for Basal Homeostasis, and Calculated Total Daily-EnergyExpenditure in Patients and Controls of the Study
All-CHF(n � 57)
All-C(n � 49)
Normo-CHF(n � 26)
Normo-C(n � 33)
Maln-CHF(n � 31)
Under-C(n � 16)
BMI kg/m2 22.4 � 3 23 � 6.2 25 � 1.5 25.1 � 1.8† 21.5 � 2.9¶ 18 � 1.7‡BW
kg 64.9 � 9.9 62.5 � 18.2 74.2 � 7.6 77.9 � 15.9 60.2 � 9.2¶ 49.7 � 5.3% Usual 96 � 9 98 � 3 101 � 5 102 � 4 90 � 7 85.4 � 8.8
AMA cm2 47 � 9.8 (46)* — 55.7 � 4.9 — 41.8 � 9¶ —REE
kcal/day 1,499 � 228 1,309 � 315# 1,609 � 256 1,494 � 312 1,461 � 192 1,156 � 242§kcal/kg 22.9 � 2.4 21.4 � 3.4 21.9 � 2.4 19.3 � 2.8 23.9 � 2.3 23 � 2.9kcal/m2 870 � 98.7 777 � 113** 856.7 � 92 812 � 103 872 � 94 749 � 123§% Predicted 103.2 � 11 92 � 13** 102.8 � 8.8 94.8 � 8.5 105 � 12 92 � 13§
TEE � REE � 1.3kcal/day 1,949 � 296 1,702 � 409# 2,092 � 333 1,942 � 406 1,898 � 250 1,503 � 315§kcal/kg 29.8 � 3.1 27.8 � 4.4 28.5 � 3.1 25.1 � 3.6 31.1 � 3 30 � 3.8
Data are given as mean � SD. *In brackets: value under the fifth percentile of normal values. Statistical analysis: t test. Statistical significance was set at p � 0.05. Normo-CHFvs. Normo-C: †p � 0.05; Maln-CHF vs. Under-C: ‡p � 0.05; §p � 0.01; Normo-CHF vs. Maln-CHF: ¶p � 0.01; All CHF vs All-C: #p � 0.05; **p � 0.01. All-CHF �all patients with CHF; All-C � all healthy controls; Normo-CHF � normally nourished CHF patients; Normo-C � normal weight controls; Maln-CHF � malnourished CHFpatients; Under-C � underweight controls.
AMA � arm muscle area; BMI � body mass index; BW � body weight; CHF � chronic heart failure; REE � resting energy expenditure; TEE � total energy expenditure.
1220 Aquilani et al. JACC Vol. 42, No. 7, 2003Nutrition in Chronic Heart Failure October 1, 2003:1218–23
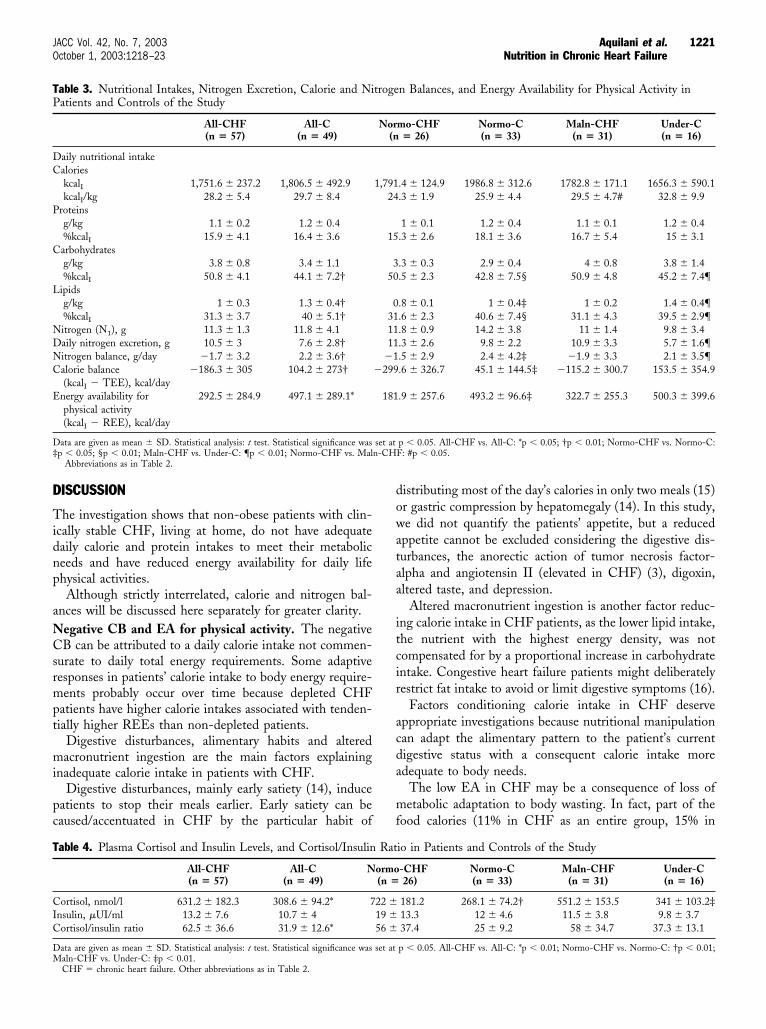
DISCUSSION
The investigation shows that non-obese patients with clin-ically stable CHF, living at home, do not have adequatedaily calorie and protein intakes to meet their metabolicneeds and have reduced energy availability for daily lifephysical activities.
Although strictly interrelated, calorie and nitrogen bal-ances will be discussed here separately for greater clarity.Negative CB and EA for physical activity. The negativeCB can be attributed to a daily calorie intake not commen-surate to daily total energy requirements. Some adaptiveresponses in patients’ calorie intake to body energy require-ments probably occur over time because depleted CHFpatients have higher calorie intakes associated with tenden-tially higher REEs than non-depleted patients.
Digestive disturbances, alimentary habits and alteredmacronutrient ingestion are the main factors explaininginadequate calorie intake in patients with CHF.
Digestive disturbances, mainly early satiety (14), inducepatients to stop their meals earlier. Early satiety can becaused/accentuated in CHF by the particular habit of
distributing most of the day’s calories in only two meals (15)or gastric compression by hepatomegaly (14). In this study,we did not quantify the patients’ appetite, but a reducedappetite cannot be excluded considering the digestive dis-turbances, the anorectic action of tumor necrosis factor-alpha and angiotensin II (elevated in CHF) (3), digoxin,altered taste, and depression.
Altered macronutrient ingestion is another factor reduc-ing calorie intake in CHF patients, as the lower lipid intake,the nutrient with the highest energy density, was notcompensated for by a proportional increase in carbohydrateintake. Congestive heart failure patients might deliberatelyrestrict fat intake to avoid or limit digestive symptoms (16).
Factors conditioning calorie intake in CHF deserveappropriate investigations because nutritional manipulationcan adapt the alimentary pattern to the patient’s currentdigestive status with a consequent calorie intake moreadequate to body needs.
The low EA in CHF may be a consequence of loss ofmetabolic adaptation to body wasting. In fact, part of thefood calories (11% in CHF as an entire group, 15% in
Table 3. Nutritional Intakes, Nitrogen Excretion, Calorie and Nitrogen Balances, and Energy Availability for Physical Activity inPatients and Controls of the Study
All-CHF(n � 57)
All-C(n � 49)
Normo-CHF(n � 26)
Normo-C(n � 33)
Maln-CHF(n � 31)
Under-C(n � 16)
Daily nutritional intakeCalories
kcalI 1,751.6 � 237.2 1,806.5 � 492.9 1,791.4 � 124.9 1986.8 � 312.6 1782.8 � 171.1 1656.3 � 590.1kcalI/kg 28.2 � 5.4 29.7 � 8.4 24.3 � 1.9 25.9 � 4.4 29.5 � 4.7# 32.8 � 9.9
Proteinsg/kg 1.1 � 0.2 1.2 � 0.4 1 � 0.1 1.2 � 0.4 1.1 � 0.1 1.2 � 0.4%kcalI 15.9 � 4.1 16.4 � 3.6 15.3 � 2.6 18.1 � 3.6 16.7 � 5.4 15 � 3.1
Carbohydratesg/kg 3.8 � 0.8 3.4 � 1.1 3.3 � 0.3 2.9 � 0.4 4 � 0.8 3.8 � 1.4%kcalI 50.8 � 4.1 44.1 � 7.2† 50.5 � 2.3 42.8 � 7.5§ 50.9 � 4.8 45.2 � 7.4¶
Lipidsg/kg 1 � 0.3 1.3 � 0.4† 0.8 � 0.1 1 � 0.4‡ 1 � 0.2 1.4 � 0.4¶%kcalI 31.3 � 3.7 40 � 5.1† 31.6 � 2.3 40.6 � 7.4§ 31.1 � 4.3 39.5 � 2.9¶
Nitrogen (N1), g 11.3 � 1.3 11.8 � 4.1 11.8 � 0.9 14.2 � 3.8 11 � 1.4 9.8 � 3.4Daily nitrogen excretion, g 10.5 � 3 7.6 � 2.8† 11.3 � 2.6 9.8 � 2.2 10.9 � 3.3 5.7 � 1.6¶Nitrogen balance, g/day �1.7 � 3.2 2.2 � 3.6† �1.5 � 2.9 2.4 � 4.2‡ �1.9 � 3.3 2.1 � 3.5¶Calorie balance
(kcalI � TEE), kcal/day�186.3 � 305 104.2 � 273† �299.6 � 326.7 45.1 � 144.5‡ �115.2 � 300.7 153.5 � 354.9
Energy availability forphysical activity(kcalI � REE), kcal/day
292.5 � 284.9 497.1 � 289.1* 181.9 � 257.6 493.2 � 96.6‡ 322.7 � 255.3 500.3 � 399.6
Data are given as mean � SD. Statistical analysis: t test. Statistical significance was set at p � 0.05. All-CHF vs. All-C: *p � 0.05; †p � 0.01; Normo-CHF vs. Normo-C:‡p � 0.05; §p � 0.01; Maln-CHF vs. Under-C: ¶p � 0.01; Normo-CHF vs. Maln-CHF: #p � 0.05.
Abbreviations as in Table 2.
Table 4. Plasma Cortisol and Insulin Levels, and Cortisol/Insulin Ratio in Patients and Controls of the Study
All-CHF(n � 57)
All-C(n � 49)
Normo-CHF(n � 26)
Normo-C(n � 33)
Maln-CHF(n � 31)
Under-C(n � 16)
Cortisol, nmol/l 631.2 � 182.3 308.6 � 94.2* 722 � 181.2 268.1 � 74.2† 551.2 � 153.5 341 � 103.2‡Insulin, �UI/ml 13.2 � 7.6 10.7 � 4 19 � 13.3 12 � 4.6 11.5 � 3.8 9.8 � 3.7Cortisol/insulin ratio 62.5 � 36.6 31.9 � 12.6* 56 � 37.4 25 � 9.2 58 � 34.7 37.3 � 13.1
Data are given as mean � SD. Statistical analysis: t test. Statistical significance was set at p � 0.05. All-CHF vs. All-C: *p � 0.01; Normo-CHF vs. Normo-C: †p � 0.01;Maln-CHF vs. Under-C: ‡p � 0.01.
CHF � chronic heart failure. Other abbreviations as in Table 2.
1221JACC Vol. 42, No. 7, 2003 Aquilani et al.October 1, 2003:1218–23 Nutrition in Chronic Heart Failure

depleted CHF, 8% in non-depleted ones) are not availablefor physical activity but serve to meet the not-reducedamount of REE as normally expected as an adaptiveresponse to BW and lean body mass wasting (13).
The loss of adaptation is probably caused by increasedwork of visceral organs and tissues, as indirectly suggestedby REE/m2 (2) and accentuated, in turn, by the increasedcortisol levels as this hormone is correlated to REE. Ofinterest, simple elevations of cortisol seem sufficient toelevate the energy consumption for basal homeostasis.Negative nitrogen balance. The finding of a negativenitrogen balance, indicating a hypercatabolic status, accordswith results from Minotti’s investigation documenting anegative protein balance across leg tissues in patients withcardiac cachexia (17).
Our investigation offers clear evidence that spontaneousnutrition of clinically stable CHF patients may not com-pensate for the various catabolic factors that can be presentand that a normal protein intake (1.1 g/kg/day) is notsynonymous with an adequate protein intake.
Inadequate calorie intake or hormonal derangements areprobably responsible for the negative nitrogen balance. Anegative nitrogen balance can be caused or exacerbated byinadequate calorie intake because even a partial restriction ofnormal calorie intake increases nitrogen excretion (18).
The hormonal derangements observed in this studyconfirm previous findings (7) and may play a role ininducing protein catabolism, given the catabolic action ofcortisol and the negative correlation of the cortisol/insulinratio with skeletal muscle protein stores and BW.
The normal insulin concentrations confirm that, overtime, the patients’ calorie intake was not in excess, thusexplaining the discrepancy with results of previous investi-gations (7,19) and suggesting a lack of body anabolicresponse to the catabolic action of cortisol.
The coexistence of severe muscle protein malnutritionwith normal BW was found in previous investigations (7)and may be explained by non-proportional rates of loss andapposition of adipose and muscular tissues during catabolicperiods (hemodynamic instabilization) and anabolic periods(after resolution of acute decompensation).Significance of an inadequate calorie protein intake inCHF. In clinically stable CHF patients, an inadequatecalorie protein intake should be considered an additivecatabolic insult contributing to 1) progressive deteriorationof important cellular substrate concentrations such as mus-cle glycogen and amino acids (4), 2) exacerbation of musclecell energy crisis (4), and 3) muscle protein breakdown.
In this way, increased wasting of lean mass occurs, whichis critical for activities of daily life, and, hence, the subject’squality of life and survival (20).
In summary, inadequate calorie-protein intake in clini-cally stable, non-obese CHF patients assumes a greatermetabolic relevance than would be suspected from its degree.Clinical implications. The present study has some impli-cations for clinical practice.
Daily intakes of 29.5 kcal/kg � 1.1 g protein/kg byfree-living, clinically stable, depleted CHF patients and 24.3kcal/kg � 1 g protein/kg by normally nourished ones maynot be sufficient to ensure a neutral calorie nitrogen balanceand tissue conservation.
Clinically stable, depleted CHF patients should have adaily intake of at least 31.8 kcal/kg � 1.37 g protein/kg andnormally nourished ones a daily intake of at least 28.1kcal/kg � 1.12 g protein/kg in order to preserve their actualbody composition or limit the effects of hypercatabolism.This study indirectly suggests that great caution should bepaid in prescribing a hypocaloric diet in overweight/obeseCHF patients, as 24.3 kcal/kg, a calorie allowance higherthan usually advised for dieting, is associated with increasedbody protein breakdown; this could be particularly impor-tant for patients with anabolic/catabolic hormone imbal-ance. The risk is that overweight CHF patients will losemore muscle than fat.
The study also highlights the need to calculate calorienitrogen balance and not only macronutrient intakes in allpatients with CHF in order to determine the patients’metabolic status.
Calculation of energy availability may be clinically usefulas they can allow physician to prescribe or advise physicalactivity more commensurate to the patient’s current meta-bolic possibility.Study limitations. This investigation was not planned toprovide any information about possible causality betweeninsufficient nutrition and the patient’s metabolic, tissuedeterioration over time. This is a major limitation of thestudy. Proof of causality, if any, would require an appropri-ate longitudinal study.
Diary records of seven days may be too short a period todiagnose the presence of lasting inadequate alimentaryhabits in patients with CHF. We suggest that, in clinicallystable, non-obese CHF, three periods of seven-days diaryrecords (and calorie nitrogen balance calculations) over threemonths would be more representative of the patient’s realalimentary habits.
In this study we deliberately avoided the term cachexia todefine patients with involuntary reduction of total BW overthe last six (7) or 12 months. Although useful in clinicalsettings, from a nutritional standpoint, cachexia shouldconnote individuals with loss of �10% lean body mass, atwhich point impaired immune function can generally bedocumented (21).
Thus, in our study, the term cachexia would probablyhave been more pertinent for the non-obese patients withsevere muscle protein malnutrition (54.4% population).
Reprint requests and correspondence: Dr. Pastoris Ornella,Sezione di Farmacologia e Biotecnologie Farmacologiche, Facoltadi Scienze MM.FF.NN., Universita degli Studi di Pavia-PiazzaBotta 11, 27100 Pavia, Italia. E-mail: [email protected].
1222 Aquilani et al. JACC Vol. 42, No. 7, 2003Nutrition in Chronic Heart Failure October 1, 2003:1218–23

REFERENCES
1. Toth MJ, Gottlieb SS, Fisher ML, Poehlman ET. Daily energyrequirements in heart failure patients. Metabolism 1997;46:1294–8.
2. Opasich C, Pasini E, Aquilani R, et al. Skeletal mass function at lowwork level as a model for daily activities in patients with chronic heartfailure. Eur Heart J 1997;18:1626–31.
3. Berry C, Clarck AL. Catabolism in chronic heart failure. Eur Heart J2000;21:521–32.
4. Opasich C, Aquilani R, Dossena M, et al. Biochemical analysis ofmuscle biopsy in overnight fasting patients with severe chronic heartfailure. Eur Heart J 1996;17:1686–93.
5. Mancini DM, Walter G, Reichek N, et al. Contribution of skeletalmuscle atrophy to exercise intolerance and altered muscle metabolismin heart failure. Circulation 1992;85:1364–73.
6. Frisancho AR. New forms of upper limb fat and muscle areas forassessment of nutritional status. Am J Clin Nutr 1981;34:2540–5.
7. Anker SD, Chva TP, Ponikowski PP, et al. Hormonal changes andcatabolic/anabolic imbalance in chronic heart failure and their impor-tance for cardiac cachexia. Circulation 1997;96:526–34.
8. Frayn KN. Calculation of substrate oxidation rates in vivo fromgaseous exchange. J Appl Physiol 1983;55:626–34.
9. Harris JS, Benedict FG. A Biometric Study of Basal Metabolism inMan (Carnegie Institution of Washington publication #279). Wash-ington, DC: Carnegie Institute, 1919.
10. Aquilani R, Dossena M, Foppa P, et al. Low protein diet improvesmuscle energy metabolism in chronic renal failure. Nutr Clin Prac1997;12:6.
11. Bistrian BR, Blackburn GL, Sherman M. Therapeutic index of
nutritional depletion in hospitalised patients. Surg Gynecol Obstet1975;141:512–6.
12. Nielsen DH, Amundsen LR. Exercise physiology: an overview withemphasis on aerobic capacity and energy cost. In: Amadsen LR, editor.Cardiac Rehabilitation. New York, NY: Churchill Livingstone, 1981:11–28.
13. Golden MHN, Jackson AA. Chronic severe undernutrition. In: OlsonRE, editor. Present Knowledge in Nutrition. 5th edition. Washington,DC: The Nutrition Foundation, 1984:57.
14. Carr JG, Stevenson LW, Walden JA, Heber D. Prevalence andhemodynamic correlates of malnutrition in severe congestive heartfailure secondary to ischemic or idiopathic dilated cardiomyopathy.Am J Cardiol 1989;63:709–13.
15. Moore JG, Christian PE, Brown JA, et al. Influence of meal weightand caloric content on gastric emptying of meals in man. Dig Dis Sci1984;29:513–9.
16. Hunt JN, Stubbs DE. The volume and energy content of meals asdeterminants of gastric emptying. J Physiol 1975;245:209–25.
17. Minotti J, Simonini A, Samarel AM. Skeletal muscle protein synthesisin congestive heart failure. Circulation 1993;88:1414.
18. Keys A, Brozek J, Henschel A. The Biology of Human Starvation.Minneapolis, MN: University of Minnesota Press, 1950;1:383.
19. Swan JW, Walton C, Godsland IF, Clark AL, Coats AJS, Oliver MF.Insulin resistance in chronic heart failure. Eur Heart J 1994;15:1528 –32.
20. Walesby RK, Goode AW, Spinks TJ, Herring A, Ranicar AS, BentallHH. Nutritional status of patients requiring cardiac surgery. J ThoracCardiovasc Surg 1979;77:570–6.
21. Freeman LM, Roubenoff R. The nutrition implications of cardiaccachexia. Nutr Rev 1994;52:340–7.
1223JACC Vol. 42, No. 7, 2003 Aquilani et al.October 1, 2003:1218–23 Nutrition in Chronic Heart Failure

EDITORIAL COMMENT
Dietary Research in Heart FailureBeyond the Salt Shaker*Marc A. Silver, MD, FACCOak Lawn, Illinois
Anyone caring for patients with heart failure (HF) is awareof the importance of dietary instruction for these patients.Because of the patients’ salt-avid state, these instructionsgenerally follow the admonition for a reduction of sodiumintake. In a related fashion, particularly for patients withevidence of volume overload and diuretic therapy require-ments, fluid restriction is the next most common instruction.Finally, often related to an atherogenic substrate, dietaryrestriction of saturated fats is commonly the third admonition.In general, aside from the dietary restrictions related to apatient’s evidence of edema or the diagnosis of coronary arterydisease or hyperlipidemia, little attention has been paid todietary assessment, evaluation, instruction, or research for thevast majority of HF patients. This is, indeed, unfortunatebecause there are suggestions that as many as 50% of patientshospitalized with HF are malnourished (1).
See page 1218
Heart failure textbooks and guidelines add little addi-tional information or suggestion of the magnitude of theneed for information regarding nutritional assessment ofpatients with HF (2–4). A single text contains one page outof 929 focusing only on cachexia (2). And among thepaucity of data exists the widest spectrum of opinion. Arecent Framingham analysis related increased body massindex (BMI) with worsened survival (5). Conversely, otherstudies have suggested that survival may in fact be betterwith higher BMIs or, in fact, with obesity (6,7).
Were a student or resident to ask me about informationon the general nutritional status of patients with HF, myresponse would suggest that weight loss in advanced diseasedue to malabsorption and wastage of nutrients coupled witha decrease in appetite seen in the volume overloaded patientis common. I would also mumble something about the needto attain ideal body weight. But the response would lackcritical data, conviction, or, more importantly, suggestionsaimed at proper nutritional replacement and support.
Therefore, I welcome the paper by Aquilani et al. (8) inthis issue of the Journal. In the background information forthis study the authors rightfully explain, “little informationexists regarding the nutritional adequacy and alimentary
habits of patients with clinically stable chronic HF.” Theauthors looked beyond simple morphometrics and per-formed a prospective analysis of nutritional balance. Theauthors studied carefully 57 non-obese, community-livingpatients mostly with mild to moderate HF. The populationis not perfect for broader extrapolation; the patients werebriefly hospitalized for transplant evaluation, and, despitetheir moderate functional class, many had exceedingly lowpeak oxygen uptake. Nonetheless, the only neurohormonemeasured was plasma norepinephrine and these levels wereonly modestly elevated. Importantly, the authors excludedpatients taking beta-blockers, concerned that metabolic ratemight be affected. The population therefore might best bedescribed as having Stage C (4) disease on suboptimaltherapy—akin to many general HF populations! Age-,BMI-, and activity-matched subjects served as a suitablecontrol group.
More important, however, is the author’s study of thecalorie-nutrition balance (CNB), which reflects a dailyhomeostasis between calorie-nitrogen intake over excretionand its relationship to total energy expenditure. The meth-ods seem adequate, although one might debate how restingenergy expenditure (REE) is measured or calorie/nitrogenintake (based on seven-day food diaries) assessed; again notan important point to belabor.
The authors demonstrate a remarkable proportion ofpatients having a negative calorie balance (70.1%), negativenitrogen balance (59.6%), or negative combined CNB(40.3%). This occurred despite similar calorie and nitrogenintake, not only in HF patients but also in controls; onlyunderweight controls took in fewer calories. The next impor-tant finding is that total energy expenditure was the same inHF patients and controls. Doing the math, one then readilyunderstands the authors’ conclusions—these patients simply donot have enough energy available for physical expenditure onactivity, let alone stresses related to periods of decompensation,infection, or enhanced physical training.
The authors’ work, however, (and that of the HF com-munity) remains undone. No new information is offered asto how or why the nutritional balance is so poor in thesepatients. Presumed is a progressive change in dietary habitscoupled with chronic malabsorption of macro and micro-nutrients. Much could be learned by studying CNB inpatients earlier along the HF path (Stages A and B).Whether cytokine activity, drug effects on taste, or evensubclinical depression alters intake is not well known. Also,we do not know what forces may be at play to keep theenergy expenditure of the “sedentary” HF patient so high.We also do not know what role the negative balance plays inthe symptoms of the HF syndrome nor on its progression.And finally, we do not know the impact of prescribedweight loss or exercise training on these patients.
What we do now know is that our patients are likelystarving before us, and we may be inadvertently making itworse. Unfortunately, calculating CNB is not a simple
*Editorials published in the Journal of the American College of Cardiology reflect theviews of the authors and do not necessarily represent the views of JACC or theAmerican College of Cardiology.
From the Department of Medicine, Heart Failure Institute, Advocate ChristMedical Center, Oak Lawn, Illinois.
Journal of the American College of Cardiology Vol. 42, No. 7, 2003© 2003 by the American College of Cardiology Foundation ISSN 0735-1097/03/$30.00Published by Elsevier Inc. doi:10.1016/S0735-1097(03)00957-4

bedside procedure. Also, nutrition in HF patients is notlikely to either share the exciting spotlight of new drug ordevice development in HF or have similar access to fundingresources. Yet, many questions remain—questions that mayplay an important role in limiting our HF epidemic. Weshould applaud the authors on this novel approach. I alsoencourage young investigators, and all of us, to begin tothink “beyond the salt shaker.”
Reprint requests and correspondence: Dr. Marc A. Silver,Department of Medicine, Director, Heart Failure Institute,Advocate Christ Medical Center, Suite 428 South, 4440 West95th Street, Oak Lawn, Illinois 60453-2600. E-mail: [email protected].
REFERENCES
1. Freeman LM, Roubenoff R. The nutritional implications of cardiaccachexia. Nutr Rev 1994;52:340–7.
2. Poole-Wilson PA, Colucci WS, Massie BM, et al. Heart Failure. NewYork, NY: Churchill Livingstone, 1997.
3. Hosenpud JD, Greenberg BH. Congestive Heart Failure. Pathophysi-ology, Diagnosis, and Comprehensive Approach to Management. 2nded. Philadelphia, PA: Lippincott, Williams and Wilkins, 2000.
4. Hunt SA, Baker DW, Chin MH, et al. ACC/AHA guidelines for theevaluation and management of chronic heart failure in the adult: areport of the American College of Cardiology/American Heart Asso-ciation Task Force on Practice Guidelines (Committee to Revise the1995 Guidelines for the Evaluation and Management of Heart Failure).2001. American College of Cardiology Web site. Available at: http://www.acc.org/clinical/guidelines/failure/hf_index.htm.
5. Kenchaiah S, Evans JC, Levy D, et al. Obesity and the risk of heartfailure. N Engl J Med 2002;347:305–13.
6. Horwich TB, Fonarow GC, Hamilton MA, et al. The relationshipbetween obesity and mortality in patients with heart failure. J Am CollCardiol 2001;38:789–95.
7. Davos CH, Doehner W, Rauchhaus M, et al. Body mass and survivalin patients with chronic heart failure without cachexia: the importanceof obesity. J Card Fail 2003;1:29–35.
8. Aquilani R, Opasich C, Verri M, et al. Is nutritional intake adequatein chronic heart failure patients? J Am Coll Cardiol 2003;42:1218 –23.
1225JACC Vol. 42, No. 7, 2003 SilverOctober 1, 2003:1224–5 Editorial Comment

Noncardiac Comorbidity IncreasesPreventable Hospitalizations and Mortality AmongMedicare Beneficiaries With Chronic Heart FailureJoel B. Braunstein, MD,*† Gerard F. Anderson, PHD,*‡ Gary Gerstenblith, MD,† Wendy Weller, PHD,‡Marlene Niefeld, MPP,‡ Robert Herbert,‡ Albert W. Wu, MD, MPH*‡Baltimore, Maryland
OBJECTIVES We studied the impact of noncardiac comorbidity on potentially preventable hospitalizationsand mortality in elderly patients with chronic heart failure (CHF).
BACKGROUND Chronic HF disproportionately affects older individuals, who typically have extensivecomorbidity. However, little is known about how noncardiac comorbidity complicates care inthese patients.
METHODS This was a cross-sectional study of 122,630 individuals age �65 years with CHF identifiedthrough a 5% random sample of all U.S. Medicare beneficiaries. We assessed the relationshipof the 20 most common noncardiac comorbidities to one-year potentially preventablehospitalizations and total mortality. Preventable hospitalizations were determined by admis-sions for ambulatory care sensitive conditions using predefined criteria.
RESULTS Sixty-five percent of the sample had at least one hospitalization, of which 50% werepotentially preventable. Exacerbations of CHF accounted for 55% of potentially preventablehospitalizations. Nearly 40% of patients with CHF had �5 noncardiac comorbidities, andthis group accounted for 81% of the total inpatient hospital days experienced by all CHFpatients. The risk of hospitalization and potentially preventable hospitalization stronglyincreased with the number of chronic conditions (both p � 0.0001). After controlling fordemographic factors and other diagnoses, comorbidities that were associated consistently withnotably higher risks for CHF-preventable and all-cause preventable hospitalizations, andmortality, included chronic obstructive pulmonary disease/bronchiectasis, renal failure,diabetes, depression, and other lower respiratory diseases (all p � 0.01).
CONCLUSIONS Noncardiac comorbidities are highly prevalent in older patients with CHF and stronglyassociate with adverse clinical outcomes. Cardiologists and other providers routinely caringfor older patients with CHF may improve outcomes in this high-risk population by betterrecognizing non-CHF conditions, which may complicate traditional CHF managementstrategies. (J Am Coll Cardiol 2003;42:1226–33) © 2003 by the American College ofCardiology Foundation
Despite advances in the care of individuals with chronicheart failure (CHF), uncertainty remains about how best tomanage CHF in elderly patients with complex comorbidi-ties (1). Although a few reports have examined the impactof chronic disease comorbidity in elderly patients with CHF(2–8), most of these have been limited by their use of index
See page 1234
scores rather than specific conditions to describe comorbid-ity (7,8), or use of local, non-U.S. representative (6,8) ornon-U.S. samples (2,4,5). Brown and Cleland (2) studied aScottish cohort of 25,000 individuals with a hospital diag-nosis of CHF, and evaluated the relationship of comorbidi-ties to death and hospitalization. They concluded thatnon-CHF conditions that may be overlooked during rou-
tine CHF management frequently precipitate, complicate,or contribute to admissions. Redelmeier and colleagues (9)demonstrated that when one serious condition is the centralfocus of care, care for other chronic disorders is compro-mised.
In this study, we examined whether noncardiac chronicdiseases influence potentially preventable hospitalizationsand mortality in Medicare beneficiaries with CHF. Wefocused on individuals age �65 years because they accountfor approximately 80% (10) of the one million reportedCHF-related hospitalizations (11) and 88% (12) of the287,000 annually reported CHF deaths (11). We definedpotentially preventable hospitalizations by admissions forambulatory care sensitive conditions (ACSCs). Widelyviewed as an indicator of adequate primary care, ACSCsreflect conditions for which timely and effective primary carecan reduce the risks of hospitalization by preventing condi-tion onset, controlling an acute episodic illness, or managinga chronic condition (13–15). We hypothesized that forMedicare beneficiaries with CHF, the probability of pre-ventable hospitalization due to any ACSC, and morespecifically to CHF-related ACSC, would increase withgreater numbers of noncardiac comorbidities. We also
From the *Robert Wood Johnson Clinical Scholars Program and †Division ofCardiology, Department of Medicine, Johns Hopkins Medical Institutions; ‡Depart-ment of Health Policy and Management, Johns Hopkins Bloomberg School of PublicHealth, Baltimore, Maryland. This research has been sponsored by Partnerships forSolutions, Robert Wood Johnson Foundation, Princeton, New Jersey.
Manuscript received December 26, 2002; revised manuscript received February 26,2003, accepted April 3, 2003.
Journal of the American College of Cardiology Vol. 42, No. 7, 2003© 2003 by the American College of Cardiology Foundation ISSN 0735-1097/03/$30.00Published by Elsevier Inc. doi:10.1016/S0735-1097(03)00947-1

hypothesized that comorbidities typically responsive to reg-ular outpatient management (such as diabetes mellitus[DM] or chronic renal failure) would be associated withhigher probabilities of preventable hospitalization and mor-tality. The presence of such relationships would suggest theneed for physicians caring for CHF to better recognizenon-CHF conditions that complicate management of olderindividuals.
METHODS
Study design and sample population. This was a cross-sectional analysis of U.S. Medicare beneficiaries age �65years. We obtained data from a 5% nationally representativerandom sample of Medicare beneficiaries with both Part A(hospitalization services costs) and Part B (mainly physicianand outpatient services costs) fee-for-service coverage in1999. This file, managed by the Centers for Medicare andMedicaid Services (formerly the Health Care FinancingAdministration), is commonly used for research purposes.The enrollment file contains demographic information; theclaims files contain fee-for-service expenditures, health careutilization (that is hospital and physician visits, services usedand procedures performed), and primary and secondaryinpatient and outpatient diagnosis billing data at the indi-vidual beneficiary level for all Medicare covered services. Wecombined the enrollment and claims files to develop indi-vidual records for each beneficiary included in our sample.We supplemented these data with county of residence datafrom the 1999 Area Resource File (Health Resources andServices Administration).
We used the Clinical Classification System (CCS) (16),developed by the Agency for Health Research and Quality,to identify individuals with CHF and chronic comorbidi-ties. The CCS system clusters diagnoses and proceduresassigned by providers based on International Classificationof Diagnoses-9th revision (ICD-9) codes into clinicallyhomogenous categories. To be classified with CHF, bene-ficiaries required at least two claims with CCS code 108(ICD-9 codes 398.91, 428, 428.0, 428.1, and 428.9) fornon-hypertensive CHF, with at least one claim originatingfrom Medicare Part B outpatient visit data. We used thecriteria of two claims rather than one to increase thespecificity of diagnoses and to eliminate “rule out” encoun-ters. We defined a chronic form of heart failure using CCScode 108, rather than one that also included ICD-9 code402.11, which is heart failure with hypertension, because we
felt this latter diagnosis better represented an acute cardio-vascular diagnosis (one that might be coded during ahospitalization) than a chronic disease state. IncludingICD-9 code 402.11 into our CHF definition expanded thesample by �0.1% and insignificantly influenced results.Therefore, we used only CCS code 108 to define oursample.
Initially, 148,384 beneficiaries qualified as having CHF.We excluded beneficiaries if they were age �65 years (n �11,276), had incomplete enrollment (n � 7,826) or countydata (n � 80), had any non-death-related termination ofcoverage during 1999 (n � 2,751), were non-U.S. residents(n � 1,356), had zero-dollar claims associated with quali-fying CCS codes (n � 61), or were enrolled in managed careduring any part of 1999 (n � 2,404), because these latterpatients frequently have incomplete utilization data. Ourfinal sample consisted of 122,630 individuals.
We used similar exclusions to create the analysis file forall Medicare beneficiaries. Beginning with 2,055,561 ben-eficiaries, we excluded those �65 years (n � 363,564),without parts A and B coverage for all 12 months (n �105,017), with HMO coverage (331,591), or of non-U.S.residence (n � 16,493). Remaining were 1,285,895 Medi-care beneficiaries, of which 122,630 (9.5%) met CHFsample definition.Dependent variables. Main outcomes in this analysis werepotentially preventable hospitalizations, designated as eitherACSC hospitalization due to CHF (CHF-ACSC) or anyACSC hospitalization (ACSC), and all-cause mortalityoccurring at any time in 1999. We also examined totalhospitalizations to determine the percentage potentiallypreventable. On the basis of a previously published method(17), we defined ACSCs using ICD-9 codes listed as eithera primary or secondary billing diagnosis from inpatienthospitalization administrative claims. Examples of ACSCsbeyond CHF exacerbation include bronchopneumonia, de-hydration, gastroenteritis, and diabetes with hyperosmolar,nonketotic coma. Mortality was coded present when abeneficiary had a 1999 date of death specified administratively.Measures of noncardiac comorbidity. We characterizedMedicare beneficiaries by their number and types of non-cardiac comorbidities. Noncardiac comorbidities were iden-tified using CCS coding and included all conditions exceptthe following cardiac comorbidities: coronary atherosclero-sis, cardiac dysrhythmias, valvular disorders, pericarditis,endocarditis and myocarditis cardiomyopathy, and conduc-tion disorders.
We combined a few CCS codes (such as Type 1 and 2DM) to simplify chronic disease classification and groupclinically similar conditions (available upon request). Weidentified the 20 most common noncardiac comorbiditiesamong CHF beneficiaries and treated these conditions asindependent variables associated with preventable hospital-ization and mortality.
Abbreviations and AcronymsACSC � ambulatory care sensitive conditionsCCS � Clinical Classification SystemCHF � chronic heart failureCOPD � chronic obstructive pulmonary diseaseDM � diabetes mellitusICD-9 � International Classification of Diagnoses-
9th revision
1227JACC Vol. 42, No. 7, 2003 Braunstein et al.October 1, 2003:1226–33 Comorbidity in the Elderly With Heart Failure

Other independent variables. Our regression models forpreventable hospitalization and mortality included otherexplanatory variables: gender, age, race, and primary pro-vider type defined by the provider type that most filedoutpatient claims during 1999 (categorized as cardiologist;generalist [general practice, family practice, internal medi-cine, obstetrics/gynecology, geriatric medicine, preventivemedicine], or noncardiac specialist). We included the Deyo-Charlson comorbidity score (18), which is a general comor-bidity index used for case-mix adjustment, and the fivecardiac comorbidities defined here in preliminary analyses.Because these variables did not significantly alter parameterestimates of individual noncardiac comorbidities, however,we excluded them from final models. Because availability ofhospitals and specialist care for chronic conditions caninfluence clinical outcomes, we accounted for patients’ localaccess to hospital services, physicians, and cardiovascularphysicians at the resident county level. We also evaluatedthe impact of living in a Health Professional Shortage Area;we excluded it from final models, however, because it didnot influence results.Data analysis. We used descriptive statistics to examinedemographic characteristics and noncardiac comorbidity.The probability of experiencing hospitalization or hospi-talization due to CHF-ACSC or any ACSC was calcu-lated for the entire population and by burden of noncar-diac comorbidity. A test of linear trend tested thehypothesis that hospitalizations were associated withgreater comorbidity.
We calculated period prevalences for the 20 most fre-quent noncardiac comorbidities. We used multivariablelog-linear Poisson regression to assess the impact of eachnoncardiac comorbidity on probability of a beneficiaryexperiencing outcomes: CHF-ACSC or any ACSC hospi-talization, and mortality, while adjusting for potential con-founders. The Poisson regression allows for an unbiasedestimate of risk conferred by an exploratory variable on anoutcome that occurs frequently, as was the case for the threeoutcomes we measured. Dummy-coded variables in the finalregression models included: age (65 to 69, 70 to 74, 75 to79, 80 to 84, 85�), gender, race (white or nonwhite),primary provider type (cardiologist, generalist, or noncar-diac specialist), and each of the 20 most prevalent noncar-diac conditions. We performed age- and gender-stratifiedmodels in preliminary analyses, but refrained from reportingthem because interactions between these variables andcomorbidities did not materially influence findings. Datafrom the regression models are reported as maximumlikelihood risk ratios (RR) with 95% confidence limits,where risk of outcome in the presence of exploratoryvariable is compared to risk of outcome in the absence ofexploratory variable. We used Stata v7.0 (Stata Corporation,College Station, Texas) and SAS v8.0 (SAS, Cary, NorthCarolina) for all analyses.
RESULTS
Patient characteristics. Most CHF beneficiaries werewomen (60%) and white (88%). Mean age was 79.6 years.Although these data are consistent with demographics ofthe entire Medicare population, beneficiaries with CHFwere, on average, 4.4 years older than the overall Medicarepopulation (19). Generalist physicians were the most fre-quent source of care for 64,183 (52%) patients, noncardi-ologist specialists for 38%, and cardiologists for 10% ofpatients. The most common forms of cardiac comorbiditywere atherosclerotic heart disease, cardiac dysrhythmias, andvalvular disorders (Table 1).
Noncardiac comorbidities were highly prevalent (Tables 1and 2). Thirty-nine percent of patients had �5 noncardiacconditions, and only 4% had CHF alone. The most com-
Table 1. Characteristics of Patients Age �65 Years With CHF
Characteristics
Total Samplen � 122,630
(%)
GenderMen 48,690 (40)Women 73,940 (60)
RaceWhite 108,093 (88)Black 10,673 (9)Other 3,864 (3)
Age, yrs (%)65–69 13,821 (11)70–74 21,562 (18)75–79 25,958 (21)80–84 26,330 (21)85� 34,959 (29)
Primary provider type in 1999Cardiologist 12,479 (10)Generalist 64,183 (52)Noncardiac specialist 45,968 (38)
Associated cardiac conditionsCoronary atherosclerosis and other related
heart disease62,087 (51)
Cardiac dysrhythmias 50,826 (41)Valvular disorders 26,941 (22)Peri-, endo-, and myocarditis, cardiomyopathy 14,180 (12)Conduction disorders 12,693 (10)
Total # of noncardiac comorbidities0 5,122 (4)1 12,360 (10)2 18,204 (15)3 19,961 (16)4 18,599 (15)5 15,029 (12)6 11,283 (9)7 7,860 (6)8 5,418 (4)9 3,383 (3)10� 5,411 (4)
Any inpatient stay, % (SE) 65 (0.1)Inpatient stay for any ACSC, % (SE) 32 (0.1)Inpatient stay for CHF ACSC, % (SE) 17 (0.1)Mortality in 1999 22,481 (18)
ACSC � ambulatory care sensitive conditions; CHF � chronic heart failure; SE �standard error.
1228 Braunstein et al. JACC Vol. 42, No. 7, 2003Comorbidity in the Elderly With Heart Failure October 1, 2003:1226–33

mon noncardiac conditions were: essential hypertension(55%), DM (31%), and chronic obstructive pulmonarydisease (COPD)/bronchiectasis (26%) (Table 2). Seventy-five percent of patients with CHF had at least one of thesethree conditions, and 93% had at least one of the 20conditions specified in Table 2.
Approximately 65% of CHF beneficiaries had at least onehospitalization during 1999. Mean CHF-ACSC andACSC hospitalization rates were 17% and 32%, respectively(Table 1). The most common ACSCs besides CHF (55%)were pneumonia (21%), COPD exacerbation (13%), anddehydration (5%). Death occurred in 22,481 patients (18%).Noncardiac chronic disease burden and hospitalizationrates. Figure 1 depicts the relationship between number ofnoncardiac comorbidities and probability of hospitalization.Beneficiaries with CHF and no other comorbidities had amean probability of hospitalization of 35% (SE 1%). Theprobability increased to 72% for five comorbidities and 94%for �10 comorbidities (p � 0.0001). Although patientswith �5 comorbidities comprised only 39% of the popula-tion, they accounted for 81% of total hospital days.
Among beneficiaries with CHF and no comorbidities,the probability of CHF-ACSC was 10%. This probabilityincreased to 19% in the presence of five comorbidities and
29% in the presence of �10 comorbidities. For any ACSChospitalization, the probability was 17% in patients withCHF alone, 35% in the presence of five comorbidities, and52% in the presence of �10 comorbidities (p � 0.001 forboth CHF-ACSC and any ACSC hospitalization).
To determine whether high probabilities of ACSC hos-pitalizations were unique to CHF beneficiaries and notelderly patients in general, we compared risks of hospital-ization and ACSC hospitalization in CHF beneficiaries torisks in non-CHF beneficiaries from the overall Medicarepopulation, while controlling for number of comorbidities.Relative to non-CHF beneficiaries, CHF beneficiaries hada 1.27-fold (�10 comorbidities) to 8.75-fold (no comor-bidities) higher risk of overall hospitalization and a 3.25-fold (�10 comorbidities) to 21-fold (no comorbidities)higher risk of any ACSC hospitalization. Non-CHF ben-eficiaries also had close to zero percent risk for experiencingCHF-ACSC hospitalization (data not shown).Specific noncardiac comorbidity on CHF-ACSC and anyACSC admissions, and total mortality. Tables 3, 4, and 5present results of the unadjusted and adjusted Poissonregressions to determine how each of the 20 most prevalentconditions influenced the risk of a CHF beneficiary expe-riencing CHF-ACSC, any ACSC, and death, respectively.Complicated or secondary hypertension conveyed the great-est adjusted RR of CHF-ACSC admission (RR 1.51, 95%CI � 1.45 to 1.56), followed by chronic renal failure (RR1.43, 95% CI � 1.36 to 1.50) and COPD/bronchiectasis(RR 1.40, 95% CI � 1.36 to 1.44) (Table 3).
Pulmonary conditions, including COPD/bronchiectasis,lower respiratory disease/failure/or insufficiency, and asthmawere associated with the highest unadjusted RR of anyACSC hospitalization in CHF beneficiaries (Table 4).After adjustment, pulmonary conditions remained stronglyassociated with ACSC hospitalization, as did essential andcomplicated hypertension, late-stage cerebrovascular dis-ease, chronic renal failure, Alzheimer’s disease/dementia,DM, and depression/affective disorders.
Chronic lower respiratory disease/failure/insufficiencywas associated with the greatest adjusted risk for deathamong our study population (RR 2.34, 95% CI � 2.27 to2.41) (Table 5). Renal failure conferred the next highestadjusted RR (1.65, 95% CI � 1.58 to 1.73). Interestingly,some conditions (such as essential hypertension and hyper-lipidemia) appeared “protective” for mortality, with riskratios significantly below 1.00.
Although not the focus of our study, the influences ofsome demographic variables we used in our multivariablemodels on patient outcomes were of some clinical interest.Age, although an important determinant of mortality (RR2.04, 95% CI � 1.93 to 2.15 for those 85� relative to those65 to 69), had only weak positive associations with CHF-ACSC and ACSC hospitalizations. Gender and race min-imally influenced outcomes.
Table 2. Twenty Most Common Noncardiac Chronic DiseaseConditions for Patients Age �65 Years With CHF (n �122,630)
Chronic Disease Defined by CCS Code% Prevalence
(n)
Essential hypertension 55 (67,211)Diabetes mellitus 31 (38,175)COPD and bronchiectasis 26 (32,275)Ocular disorders (retinopathy, macular disease,
cataract, glaucoma)24 (29,548)
Hypercholesterolemia 21 (25,219)Peripheral and visceral atherosclerosis 16 (20,027)Osteoarthritis 16 (19,929)Chronic respiratory failure/insufficiency/ arrest
or other lower respiratory disease excludingCOPD/bronchiectasis
14 (17,610)
Thyroid disorders 14 (16,751)Hypertension with complications and
secondary hypertension11 (13,732)
Alzheimer’s disease/dementia 9 (10,839)Depression/affective disorders 8 (9,371)Chronic renal failure 7 (8,652)Prostatic hyperplasia 7 (8,077)Intravertebral injury, spondylosis, or other
chronic back disorders7 (8,469)
Asthma 5 (6,717)Osteoporosis 5 (6,688)Renal insufficiency (acute and unspecified
renal failure)4 (5,259)
Anxiety, somatoform disorders, andpersonality disorders
3 (3,978)
Cerebrovascular disease, late effects 3 (3,750)
CCS � Clinical Classification System; CHF � chronic heart failure; COPD �chronic obstructive pulmonary disease.
1229JACC Vol. 42, No. 7, 2003 Braunstein et al.October 1, 2003:1226–33 Comorbidity in the Elderly With Heart Failure

DISCUSSION
Whereas burden of chronic illness complicates the manage-ment of all seniors (19), the adverse impact of chronicdisease comorbidity on the care of elderly individuals withCHF appears especially profound. In our sample, patientswith �5 comorbidities comprised approximately 40% ofMedicare beneficiaries with CHF but accounted for 81% oftotal inpatient hospital days. Approximately 65% of patientshad at least one hospitalization. Half of these hospitaliza-
tions were regarded as potentially preventable, of which 55%were CHF-related. Individuals with CHF, at any level ofchronic disease comorbidity, had markedly higher risks forexperiencing at least one preventable hospitalization relativeto individuals without CHF.
Although our study is the first to report trends for ACSChospitalizations in aged CHF patients, several reports haveidentified inadequacies in primary care for older individualswith multiple chronic illnesses (9,20). Wolff et al. (19)demonstrated in a nonselective group of Medicare benefi-ciaries, that chronic disease burden is strongly associatedwith one’s risk of experiencing both ACSC admissions andpreventable complications incurred during hospitalization.Recognizing that access to care powerfully predicts ACSChospitalizations (14), multiple comorbidities may impedeappropriate access to primary care that could forestall acuteevents requiring hospitalization (19). The fact that multiplecomorbidities predispose individuals to medical undertreat-ment supports this hypothesis (9).
Our observations of potentially preventable hospitaliza-tions among patients with CHF are consistent with previ-ously published data, mainly from smaller samples(3,7,10,21,22). Vinson et al. (21) determined that among161 patients age �70 years with index CHF hospitaliza-tions, approximately 50% of readmissions by 90 days wereeither possibly or probably preventable. Michalsen et al. (22)studied 179 elderly patients hospitalized with decompen-sated preexisting CHF and identified 54.2% of admissionsas preventable.
A number of reasons may explain why older CHF
Figure 1. Impact of noncardiac comorbidity burden on the annual prob-ability of a Medicare beneficiary with chronic heart failure (n � 122,630)experiencing a hospitalization due to any cause, a preventable hospitaliza-tion or a preventable hospitalization due to chronic heart failure (CHF).Data are represented as mean probabilities. p � 0.0001 for linear trend forall outcomes. ACSC � ambulatory care sensitive conditions.
Table 3. Association of Noncardiac Comorbidity With Ambulatory Care Sensitive CHFHospitalization Among Medicare Beneficiaries With CHF
Condition
Risk Ratio (95% CI) (n � 122,630)
Unadjusted Adjusted*
Chronic renal failure 1.91 (1.83–1.99) 1.43 (1.36–1.50)Acute and unspecified renal failure 1.83 (1.74–1.93) 1.18 (1.11–1.25)Hypertension—with complications or secondary 1.82 (1.76–1.88) 1.51 (1.45–1.56)Lower respiratory disease, failure or insufficiency 1.57 (1.52–1.63) 1.34 (1.30–1.39)COPD/bronchiectasis 1.49 (1.45–1.53) 1.40 (1.36–1.44)Diabetes mellitus 1.41 (1.37–1.44) 1.33 (1.29–1.37)Essential hypertension 1.31 (1.28–1.35) 1.23 (1.20–1.27)Asthma 1.31 (1.23–1.39) 1.05 (1.00–1.11)Anxiety, somatoform disorders, and personality disorders 1.22 (1.14–1.31) 1.15 (1.07–1.23)Peripheral or visceral atherosclerosis 1.19 (1.15–1.23) 1.08 (1.04–1.11)Depression/affective disorders 1.16 (1.10–1.21) 1.11 (1.05–1.16)Thyroid disorders 1.05 (1.01–1.09) 1.04 (1.00–1.08)Chronic back disorders† 1.01 (0.96–1.06) 1.00 (0.95–1.06)Osteoarthritis 1.01 (0.97–1.05) 1.01 (0.97–1.05)Cerebrovascular disease, late effects 0.98 (0.91–1.07) 0.91 (0.84–0.98)Ocular disorders 0.98 (0.95–1.01) 0.96 (0.93–0.99)Prostatic hyperplasia 0.93 (0.88–0.99) 0.92 (0.86–0.97)Osteoporosis 0.91 (0.86–0.97) 0.93 (0.87–0.99)Hypercholesterolemia 0.90 (0.87–0.93) 0.84 (0.81–0.87)Alzheimer’s disease/dementia 0.82 (0.78–0.86) 0.81 (0.77–0.85)
*Adjusted for patient race (white or nonwhite), age (65–69, 70–74, 75–79, 80–84, 85�) and gender, primary caring providertype (cardiologist, generalist, non-cardiac specialist), patient’s county of residence per capita hospital beds, total physicians andcardiovascular specialists; †Includes intravertebral injury, spondylosis, or other chronic back disorders.
CHF � chronic heart failure; CI � confidence interval; COPD � chronic obstructive pulmonary disease.
1230 Braunstein et al. JACC Vol. 42, No. 7, 2003Comorbidity in the Elderly With Heart Failure October 1, 2003:1226–33

patients with greater comorbidity may experience moreadverse events that lead to preventable hospitalizations.These include underutilization of effective CHF therapies inthe presence of other conditions because of safety concerns(for example, use of beta-blockers in asthma or angiotensin-converting enzyme inhibitors in renal insufficiency), patient
nonadherence to or inability to recall complex dietary ormedication regimens, inadequate postdischarge care, failedsocial support, and failure to promptly seek medical atten-tion during symptom recurrence (21–25). Psychologicalstress from chronically poor health may also predispose tobad outcomes. Emotional stress can induce left ventricular
Table 4. Association of Noncardiac Comorbidity With Any Ambulatory Care SensitiveCondition Hospitalization Among Medicare Beneficiaries With CHF
Condition
Risk Ratio (95% CI)(n � 122,630)
Unadjusted Adjusted*
COPD/bronchiectasis 1.92 (1.88–1.96) 1.46 (1.42–1.51)Lower respiratory disease, failure or insufficiency 1.82 (1.77–1.86) 1.70 (1.65–1.76)Asthma 1.54 (1.48–1.60) 1.13 (1.07–1.19)Acute and unspecified renal failure 1.51 (1.45–1.57) 1.09 (1.02–1.16)Chronic renal failure 1.51 (1.46–1.56) 1.22 (1.16–1.28)Hypertension—with complications or secondary 1.44 (1.40–1.48) 1.29 (1.24–1.34)Anxiety, somatoform disorders and personality disorders 1.35 (1.29–1.42) 1.11 (1.04–1.19)Depression/affective disorders 1.30 (1.26–1.35) 1.17 (1.12–1.23)Cerebrovascular disease, late effects 1.22 (1.16–1.29) 1.39 (1.30–1.48)Diabetes mellitus 1.21 (1.18–1.23) 1.17 (1.14–1.21)Peripheral or visceral atherosclerosis 1.20 (1.17–1.23) 1.13 (1.09–1.16)Essential hypertension 1.18 (1.16–1.21) 1.50 (1.45–1.54)Alzheimer’s disease/dementia 1.18 (1.14–1.22) 1.24 (1.19–1.30)Osteoporosis 1.10 (1.05–1.15) 1.02 (0.96–1.08)Thyroid disorders 1.05 (1.02–1.08) 0.99 (0.95–1.03)Osteoarthritis 1.03 (1.00–1.05) 0.98 (0.94–1.01)Chronic back disorders† 1.01 (0.97–1.05) 1.01 (0.96–1.07)Ocular disorders 0.95 (0.92–0.97) 0.96 (0.93–0.99)Prostatic hyperplasia 0.94 (0.90–0.98) 0.93 (0.88–0.99)Hypercholesterolemia 0.80 (0.78–0.82) 1.09 (1.06–1.13)
*Adjusted for same variables as in Table 3. †Includes intravertebral injury, spondylosis or other chronic back disorders.Abbreviations as in Table 2.
Table 5. Association of Noncardiac Comorbidity With Death Among Medicare BeneficiariesWith CHF
Condition
Risk Ratio (95% CI)(n � 122,630)
Unadjusted Adjusted*
Lower respiratory disease, failure or insufficiency 2.56 (2.48–2.63) 2.34 (2.27–2.41)Acute and unspecified renal failure 2.06 (1.96–2.16) 1.46 (1.38–1.54)Chronic renal failure 1.92 (1.84–1.99) 1.65 (1.58–1.73)Alzheimer’s disease/dementia 1.64 (1.58–1.70) 1.24 (1.20–1.29)Cerebrovascular disease, late effects 1.41 (1.32–1.51) 1.23 (1.15–1.31)COPD/bronchiectasis 1.31 (1.27–1.34) 1.12 (1.09–1.16)Depression/affective disorders 1.12 (1.07–1.18) 1.07 (1.02–1.13)Peripheral or visceral atherosclerosis 1.03 (0.99–1.07) 0.95 (0.92–0.99)Hypertension—with complications or secondary 0.97 (0.93–1.02) 0.94 (0.90–0.98)Diabetes mellitus 0.94 (0.91–0.97) 1.11 (1.07–1.14)Anxiety, somatoform disorders and personality disorders 0.89 (0.82–0.96) 0.89 (0.83–0.97)Asthma 0.78 (0.73–0.83) 0.81 (0.75–0.86)Osteoporosis 0.78 (0.73–0.83) 0.84 (0.79–0.90)Thyroid disorder 0.73 (0.70–0.76) 0.81 (0.78–0.85)Essential hypertension 0.61 (0.59–0.63) 0.70 (0.68–0.72)Chronic back disorders† 0.60 (0.56–0.64) 0.78 (0.73–0.83)Prostatic hyperplasia 0.59 (0.55–0.63) 0.63 (0.58–0.67)Osteoarthritis 0.56 (0.54–0.59) 0.65 (0.62–0.68)Ocular disorders 0.40 (0.39–0.42) 0.46 (0.44–0.48)Hypercholesterolemia 0.33 (0.31–0.35) 0.47 (0.44–0.49)
*Adjusted for same variables as in Table 3; †Includes intravertebral injury, spondylosis, or other chronic back disorders.Abbreviations as in Table 2.
1231JACC Vol. 42, No. 7, 2003 Braunstein et al.October 1, 2003:1226–33 Comorbidity in the Elderly With Heart Failure

dysfunction in patients with idiopathic cardiomyopathy(26), and in one study preceded CHF hospitalization in49% of patients (27). Elderly patients with multiple comor-bidities and polypharmacy are also susceptible to poor coordi-nation of care (19) and at increased risk for experiencingadverse drug reactions from drug-drug interactions (28). Fi-nally, it may be that greater chronic disease burden results indiminished physiologic reserve and hence more acute events.
In this study, we found that renal disease, hypertension,COPD/bronchiectasis, anxiety/somatoform/and personalitydisorders, and DM associate with the highest risks of ACSChospitalizations. The association of these comorbidities withpotentially preventable hospitalizations is clinically relevantbecause these conditions are all typically responsive to effectiveoutpatient management, and possibly, to care coordinationwith non-cardiologists. Although it remains unproven thatimproving outpatient access and care integration necessarilyimproves outcomes among older CHF patients with thesecomorbidities, these strategies clearly target two importantindicators of healthcare quality (14).
Some of our results might seem unexpected withoutfurther discussion. Alzheimer’s disease/dementia conferreda lower preventable CHF hospitalization risk, but higheroverall preventable hospitalization and mortality risk. Sloanand Taylor (29) also observed Medicare patients withAlzheimer’s disease to have high rates of mortality andhospitalization for conditions like pneumonia and hip frac-ture, but low rates of hospitalization for CHF; it may bethat caregivers or chronic care institutions have high thresh-olds for hospitalizing near-terminal patients with dementiafor CHF exacerbations. Hypertension also associated withunexpected outcomes, conferring a higher preventable hos-pitalization risk but lower overall mortality risk. Althoughuncontrolled hypertension can frequently precipitate CHFhospitalizations (21,22), uncomplicated hypertension maybe “protective” in the CHF setting (30,31). This may relateto differences in prognosis between CHF due to diastolicdysfunction with blood pressures in the “hypertensive” rangeand CHF due to systolic dysfunction with blood pressuresin the low-output failure range (30). Finally, hypercholes-terolemia appeared protective in the setting of CHF byconferring a 53% lower mortality risk than those withouthypercholesterolemia. Several other studies have correlatedhigh lipoprotein levels with improved survival rates amongindividuals with CHF (32,33). One proposed mechanism isthe capacity for lipoproteins to bind lipopolysaccharide, andcurtail proinflammatory cytokine production and cytokine-induced catabolism (34). An additional explanation is acoding artifact. Healthier patients may more likely havehypercholesterolemia coded on an administrative billingform than do patients with serious conditions requiringfrequent medical attention (35).Study limitations. This study has several noteworthy lim-itations. First, we used administrative claims data to drawinferences about care outcomes. This precluded assessmentsof heart failure etiology, ejection fraction, disease severity,
medication usage and several sociodemographic factors.Thus, we cannot ignore the potential impact of unmeasuredconfounders on our results. Because we were unable todistinguish diastolic from systolic dysfunction, we are alsounable to conclude whether the impact of chronic diseasecomorbidity on outcomes is the same for these two forms ofCHF. The lack of significant age and gender interactionswith the comorbidities we studied on outcomes providessome suggestion that these differences are unlikely substan-tial, given that the predominant forms of CHF for elderlyfemales and younger males are diastolic and systolic dys-function, respectively.
A second limitation is that we used ICD-9 codes todefine chronic conditions. Whereas ICD-9 codings forchronic conditions can have variable sensitivity, the speci-ficity of this method to identify a condition is typicallyexceptional, with levels exceeding 96% (36). In addition tocoding practices varying by providers and institutions, sev-eral studies, including those that evaluated coding in pa-tients with heart failure, suggest that severe, acute compli-cations take coding precedence over chronic conditions,particularly during hospitalizations (31,35). The reason forunderreporting chronic diseases may also relate to influencesof reimbursement incentives on ICD-9 coding. Althoughclaims-based selection and misclassification bias likely bi-ased the prevalence rates of our chronic conditions down-ward, we do not believe such biases invalidate the majorimplications of our analysis.
Because we focused on patients age �65 years andexcluded beneficiaries enrolled in managed care, our resultsmay not be generalizable to the entire Medicare CHFpopulation. Also, because we used two CHF-coded claimsrather than one to increase the specificity of our definedsample, we may have favorably or adversely selected apopulation by excluding incident CHF cases with just oneclaim. We performed a sensitivity analysis to estimate theimpact of this potential selection bias. As this resulted inlittle change to probabilities of outcomes, selection bias onthese grounds appears minimal. A final study limitation isthat we did not account for time-dependent variables in ourmultivariable regression models. Beneficiaries who devel-oped incident CHF beyond year onset or who died beforeyear-end would have had shortened periods of risk exposureto the outcomes we measured compared to those with CHFfor the entire 1999 study period.Conclusions. Noncardiac comorbidity clearly complicatesCHF care and is prevalent in one form or another for over95% of elderly individuals with CHF. These data suggestthat the health system’s current “cardiologic” approach formanaging elderly patients with CHF needs strong consid-eration of change. Parmley (37) recently recognized thisneed and outlined the growing importance for cardiologiststo better recognize the frailty of the primary population theyincreasingly treat. Optimal approaches to managing elderlypatients with CHF also need clearer definition. The strin-gent entry criteria of most randomized-controlled CHF
1232 Braunstein et al. JACC Vol. 42, No. 7, 2003Comorbidity in the Elderly With Heart Failure October 1, 2003:1226–33

treatment trials typically exclude elderly patients and thosewith one or more significant comorbidities (38,39). Under-representation of these individuals makes it difficult togeneralize findings to patients with CHF more likely to beencountered in routine clinical practice.
In conclusion, this study highlights how noncardiaccomorbidities negatively influence individuals with CHF.Responses from cardiologists might include increased vigi-lance to conditions that complicate care, reorganized prac-tices to reduce access barriers and improved communica-tions with other providers when quality of comprehensivecare seems suboptimal. Medicare responses might includemultidisciplinary disease management teams, explicit pay-ment for care coordination and new case-mix-adjustedreimbursement strategies that reward cardiologists for rec-ognizing and referring, when necessary, patients with inap-propriately treated noncardiac conditions. Given the steadyrise in CHF incidence and prevalence in an aging popula-tion, optimizing outcomes for this high-risk population is apublic health imperative.
Reprint requests and correspondence: Dr. Joel B. Braunstein,Johns Hopkins Medical Institutions, 600 North Wolfe Street,Carnegie #568, Baltimore, Maryland 21287. E-mail: [email protected].
REFERENCES1. Rich MW. Heart failure in the 21st century: a cardiogeriatric syn-
drome. J Gerontol A Biol Sci Med Sci 2001;56:M88–96.2. Brown AM, Cleland JG. Influence of concomitant disease on patterns
of hospitalization in patients with heart failure discharged fromScottish hospitals in 1995. Eur Heart J 1998;19:1063–9.
3. Gambassi G, Forman DE, Lapane KL, et al. Management of heartfailure among very old persons living in long-term care: has the voiceof trials spread? The SAGE Study Group. Am Heart J 2000;139:85–93.
4. Khand AU, Gemmell I, Rankin AC, Cleland JG. Clinical eventsleading to the progression of heart failure: insights from a nationaldatabase of hospital discharges. Eur Heart J 2001;22:153–64.
5. Cleland JG, Gemmell I, Khand AU, Boddy A. Is the prognosis ofheart failure improving? Eur J Heart Fail 1999;1:229–41.
6. Philbin EF, DiSalvo TG. Prediction of hospital readmission for heartfailure: development of a simple risk score based on administrativedata. J Am Coll Cardiol 1999;33:1560–6.
7. Krumholz HM, Parent EM, Tu N, et al. Readmission after hospital-ization for congestive heart failure among Medicare beneficiaries. ArchIntern Med 1997;157:99–104.
8. Chin MH, Goldman L. Factors contributing to the hospitalization ofpatients with congestive heart failure. Am J Public Health 1997;87:643–8.
9. Redelmeier DA, Tan SH, Booth GL. The treatment of unrelateddisorders in patients with chronic medical diseases. N Engl J Med1998;338:1516–20.
10. Haldeman GA, Croft JB, Giles WH, Rashidee A. Hospitalization ofpatients with heart failure: National Hospital Discharge Survey, 1985to 1995. Am Heart J 1999;137:352–60.
11. American Heart Association. 2002 Heart and Stroke Statistical Up-date. Dallas, TX: American Heart Association, 2001.
12. Graves EJ. Detailed diagnoses and procedures, national hospitaldischarge survey, 1990. Vital Health Stat 13 1992;113:1–225.
13. Billings J, Zeitel L, Lukomnik J, Carey TS, Blank AE, Newman L.Impact of socioeconomic status on hospital use in New York City.Health Aff (Millwood) 1993;12:162–73.
14. Bindman AB, Grumbach K, Osmond D, et al. Preventable hospital-izations and access to health care. JAMA 1995;274:305–11.
15. Blustein J, Hanson K, Shea S. Preventable hospitalizations andsocioeconomic status. Health Aff (Millwood) 1998;17:177–89.
16. Clinical Classifications Software (ICD-9-CM) Summary and Down-load. Rockville, MD: Agency for Health Care Policy and Research,1999.
17. Culler SD, Parchman ML, Przybylski M. Factors related to potentiallypreventable hospitalizations among the elderly. Med Care 1998;36:804–17.
18. Deyo RA, Cherkin DC, Ciol MA. Adapting a clinical comorbidityindex for use with ICD-9-CM administrative databases. J ClinEpidemiol 1992;45:613–9.
19. Wolff JL, Starfield B, Anderson G. Prevalence, expenditures, andcomplications of multiple chronic conditions in the elderly. ArchIntern Med 2002;162:2269–76.
20. Asch SM, Sloss EM, Hogan C, Brook RH, Kravitz RL. Measuringunderuse of necessary care among elderly Medicare beneficiaries usinginpatient and outpatient claims. JAMA 2000;284:2325–33.
21. Vinson JM, Rich MW, Sperry JC, Shah AS, McNamara T. Earlyreadmission of elderly patients with congestive heart failure. J AmGeriatr Soc 1990;38:1290–5.
22. Michalsen A, Konig G, Thimme W. Preventable causative factorsleading to hospital admission with decompensated heart failure. Heart1998;80:437–41.
23. Ghali JK, Kadakia S, Cooper R, Ferlinz J. Precipitating factors leadingto decompensation of heart failure. Traits among urban blacks. ArchIntern Med 1988;148:2013–6.
24. Opasich C, Febo O, Riccardi PG, et al. Concomitant factors ofdecompensation in chronic heart failure. Am J Cardiol 1996;78:354–7.
25. Kravitz RL, Hays RD, Sherbourne CD, et al. Recall of recommen-dations and adherence to advice among patients with chronic medicalconditions. Arch Intern Med 1993;153:1869–78.
26. Giannuzzi P, Shabetai R, Imparato A, et al. Effects of mental exercisein patients with dilated cardiomyopathy and congestive heart failure.An echocardiographic Doppler study. Circulation 1991;83:II155–65.
27. Perlman LV, Ferguson S, Bergum K, Isenberg EL, Hammarsten JF.Precipitation of congestive heart failure: social and emotional factors.Ann Intern Med 1971;75:1–7.
28. Ebbesen J, Buajordet I, Erikssen J, et al. Drug-related deaths in adepartment of internal medicine. Arch Intern Med 2001;161:2317–23.
29. Sloan FA, Taylor DH Jr. Effect of Alzheimer disease on the cost oftreating other diseases. Alzheimer Dis Assoc Disord 2002;16:137–43.
30. Croft JB, Giles WH, Pollard RA, Keenan NL, Casper ML, Anda RF.Heart failure survival among older adults in the United States: a poorprognosis for an emerging epidemic in the Medicare population. ArchIntern Med 1999;159:505–10.
31. Jencks SF, Williams DK, Kay TL. Assessing hospital-associateddeaths from discharge data. The role of length of stay and comorbidi-ties. JAMA 1988;260:2240–6.
32. Horwich TB, Fonarow GC, Hamilton MA, MacLellan WR, WooMA, Tillisch JH. The relationship between obesity and mortality inpatients with heart failure. J Am Coll Cardiol 2001;38:789–95.
33. Vredvoc DL, Woo MA, Doering LV, Brecht ML, Hamilton MA,Fonarow GC. Skin test anergy in advanced heart failure secondary toeither ischemic or idiopathic dilated cardiomyopathy. Am J Cardiol1998;82:323–8.
34. Rauchhaus M, Coats AJ, Anker SD. The endotoxin-lipoproteinhypothesis. Lancet 2000;356:930–3.
35. Iezzoni LI, Foley SM, Daley J, Hughes J, Fisher ES, Heeren T.Comorbidities, complications, and coding bias. Does the number ofdiagnosis codes matter in predicting in-hospital mortality? JAMA1992;267:2197–203.
36. Quan H, Parsons GA, Ghali WA. Validity of information oncomorbidity derived from ICD-9-CCM administrative data. MedCare 2002;40:675–85.
37. Parmley WW. Do we practice geriatric cardiology? J Am Coll Cardiol1997;29:217–8.
38. Cleland JG. ACE inhibitors for “diastolic” heart failure? Reasons notto jump to premature conclusions about the efficacy of ACE inhibitorsamong older patients with heart failure. Eur J Heart Fail 2001;3:637–9.
39. Heiat A, Gross CP, Krumholz HM. Representation of the elderly,women, and minorities in heart failure clinical trials. Arch Intern Med2002;162:1682–8.
1233JACC Vol. 42, No. 7, 2003 Braunstein et al.October 1, 2003:1226–33 Comorbidity in the Elderly With Heart Failure

EDITORIAL COMMENT
Delivering theCumulative Benefits ofTriple Therapy to ImproveOutcomes in Heart FailureToo Many Cooks Will Spoil the Broth*John G. F. Cleland, MD, FACC,Andrew L. Clark, MDKingston-Upon-Hull, United Kingdom
One of the great scourges of the Victorian era was tuber-culosis. A huge research effort led to dramatic advances in abroad range of medical sciences, from epidemiology tothoracic surgery. Even before treatment was very effective,sanitoria were established near most large communities,staffed by doctors, nurses, therapists, and surgeons capableof delivering a wide range of therapy. Initially, nonpharma-cological and pharmacological treatments, including digi-talis (1), were ineffective. The first breakthrough in the1940s, streptomycin, led to optimism, but hopes weredashed as the disease evolved and became resistant totherapy. Subsequently, the development of dual and thentriple therapy overcame the problem of resistance, allowingthe disease to be contained, although not eliminated.
See page 1226
The analogy between tuberculosis and heart failure (HF)in Western society is striking, but our response to theseepidemics are disparate. Heart failure, just like tuberculosis,progressed and evolved despite the introduction of singletherapies. Triple-therapy for HF secondary to left ventric-ular systolic dysfunction has arrived (2), as has the need forcareful monitoring to avoid toxic side effects and for patientsto adhere to relatively complex treatment regimens. Awell-proven series of interventions, each with a relativelymodest benefit (Fig. 1), may reduce two-year mortalitycumulatively by 50% to 60% (Fig. 2) (2). However, heartfailure appears a more complex and recalcitrant conditionthan tuberculosis. Most patients with HF require chronicdiuretic therapy and some would consider routine use ofantithrombotic agents, statins, and digoxin, although evi-dence of a worthwhile benefit for any of these for mostpatients is lacking (3–6). There is evidence that implantabledefibrillators, cardiac resynchronization devices, and possi-bly left ventricular assist systems have an important role forthe management of a substantial minority of patients
(2,7,8). Unfortunately, although a lot of money is spenttreating patients with HF in a haphazard fashion, littleeffort has been spent, so far, on organizing infrastructure fortheir care.
A city with a population of one million should provideservices to manage at least 10,000 patients with HF, provideabout 140 hospital beds for its management, and expectabout 2,000 to 3,000 new cases each year and about 5,000admissions (9,10). How then should care for patients withHF be organized? Disseminating information to all physi-cians and expecting them all to implement guidelines for themanagement of HF is not effective (11–13) because of therelative complexity of diagnosis and management and be-cause there are many competing guidelines for other cardi-ological and noncardiological conditions. Most hospital-based physicians have already become specialists in somedisease area and most will feel it inappropriate that theyshould take the lead in organizing services for patients withHF (12,13). Primary care physicians could provide thecommon investigations required and manage triple therapy,but by seeking out a large enough number of patients toacquire the necessary skills and experience, they wouldinevitably become specialists. Subspecialization means thatmany cardiologists do not have the skills, experience, orinclination to organize and implement a high standard ofcare for patients with HF (14).
Braunstein et al. (15), in this issue of the Journal,examined the Medicare records of over 100,000 patients age�65 years with HF and examined the effect of noncardiaccomorbidities on outcome over one year. Fifty percent ofpatients were age �80 years, 60% were women, only 51%were reported to have coronary disease, and only 10% wereprimarily looked after by a cardiologist, consistent withpreviously known data (16–18). It is likely that mostpatients had preserved left ventricular systolic function (18).Sixty-five percent of the patients had one or more hospital-izations during one-year follow-up, a remarkable statistic initself and higher than epidemiological studies (10,17) orclinical trials have suggested, perhaps reflecting the age ofthe patients (10). Forty percent of patients had �5 noncar-diac comorbidities, and these patients accounted for �80%of admissions. The most common comorbidities were hy-pertension (55%), diabetes mellitus (31%), chronic lungdisease (26%), ocular disease (24%), and hypercholesterol-emia (21%). Only 50% of admissions were thought to bepreventable, of which slightly more than half were for HF.Many comorbidities were associated with a modest increasein the risk of preventable admissions and mortality but,intriguingly, some were associated with a substantially lowerrisk, most notably hypercholesterolemia and hypertension.
Excessive attention to comorbidity may impair the treat-ment of HF (16,19). Braunstein et al. (15) suggest that toomuch focus on the management of HF may lead to neglectof comorbid conditions and that this could be detrimental topatient care. However, it is far from clear that advice
*Editorials published in the Journal of the American College of Cardiology reflect theviews of the authors and do not necessarily represent the views of JACC or theAmerican College of Cardiology.
From the University of Hull, Kingston-Upon-Hull, United Kingdom.
Journal of the American College of Cardiology Vol. 42, No. 7, 2003© 2003 by the American College of Cardiology Foundation ISSN 0735-1097/03/$30.00Published by Elsevier Inc. doi:10.1016/S0735-1097(03)00948-3

proffered by those who are not HF specialists is safe oreffective for patients with HF. There is no specific role forrenal physicians in the management of patients with HFuntil dialysis is required. There is no evidence that bettercontrol of glycemia improves the outcome of diabeticpatients with HF. There is no evidence of improvedoutcome with specialist care for most patients with chroniclung disease; only now is the safety and efficacy of steroidsand bronchodilator therapy being tested (20). Likewise,there is no evidence that mood disorders in patients withHF respond to conventional therapy, that pharmacological
treatment for depression is safe, or that specialist advice ismore effective than a sympathetic “ear” from a nurse ordoctor (21,22). What is important is to ensure that theabove comorbidities are not used as false excuses forwithholding effective triple therapy given in adequate doses.
Cardiologists also fail to practice evidence-based medi-cine, are often to blame for unnecessary investigation andunwarranted polytherapy (23), and have generally failed torecognize that the relationships between traditional riskmarkers for cardiovascular disease, such as hypertension,hypercholesterolemia, obesity, and cardiovascular morbidity
Figure 1. Effects of therapy on two-year mortality in landmark trials of heart failure of varying symptomatic severity. �B � beta-blocker; AA � aldosteroneantagonist; ACEi � angiotensin-converting enzyme inhibitor; NYHA � New York Heart Association; Prev. � Prevention; Treat. � Treatment. CIBIS-II� Cardiac Insufficiency Bisoprolol Study-part II; CONSENSUS � Cooperative North Scandinavian Enalapril Survival Study; COPERNICUS �Carvedilol Prospective Randomised Cumulative Survival trial; EPHESUS � Eplerenone’s Neurohormonal Efficacy and Survival Study; MERIT �Metoprolol CR/XL Randomized Intervention Trial in Heart Failure; RALES � Randomized Aldactone Evaluation Study; SOLVD � Studies Of LeftVentricular Dysfunction.
Figure 2. The cumulative effects of triple therapy with angiotensin-converting enzyme inhibitors, beta-blockers, and aldosterone antagonists over two yearsshowing the potential number of lives saved over two years. These studies also showed a reduction in hospitalization and an improvement in patients’symptoms amongst survivors.
1235JACC Vol. 42, No. 7, 2003 Cleland and ClarkOctober 1, 2003:1234–7 Editorial Comment

fail to operate in a conventional manner once patientsdevelop HF (24). Hypertension is consistently associatedwith a better prognosis in patients with HF and provides anadditional substrate for the actions of triple therapy (25).The lack of evidence for and potential futility or dangers ofaspirin therapy in patients with HF are widely known, yetcardiologists refuse to give up old habits (3,4). Hypercho-lesterolemia is also associated with a better outcome eitherbecause it is a marker of an intrinsically better prognosis orbecause it provides cardiovascular protection in this setting(5,6,26). If the former is true, lipid-lowering therapy couldstill be an important adjunctive treatment for many patientswith HF and coronary disease. If the latter is true thenlipid-lowering therapy is not only adding to wasteful poly-therapy but may also have an adverse effect on patientoutcome (5). The large post-infarction trials effectivelyexcluded HF, as evidenced by the low annual mortality inthese studies (about 2% per annum) (2,27). Three largestudies of statins in patients at increased risk of developingHF, one in older patients and two in patients with hyper-tension, showed no effect of statins on mortality or chronicdisability, further suggesting that such treatment may befutile for patients with HF (2). Two large placebo-controlled trials examining the effects of statins in over10,000 patients with HF and coronary disease are nowunderway and will provide evidence for the safety andefficacy of statins (2).
Misuse of pharmacotherapy is not the only or, indeed,most expensive problem. Many cardiologists recommendedangiography as part of the investigation of HF (28). How-ever, there is no evidence that revascularization, even forhibernating or ischemic myocardium, improves patient out-come; therefore, investigation of coronary disease shouldusually be confined to patients with angina intractable tomedical management (29). Two large randomized-controlled outcome studies are underway investigating thesafety and efficacy of revascularization for patients with HF(29). Their results should be awaited before jumping toexpensive investigations and potentially deleterious or futileinterventions. For now, there is more evidence in favor ofinterventions such as enhanced external counterpulsationthan for angioplasty or coronary bypass grafting in patientswith HF and coronary disease (30,31). There is growingevidence that a range of implantable devices may be usefulfor the management of HF, although the issue of patientselection to ensure cost-effectiveness is unresolved (32).Although electrophysiologists may be the most appropriatespecialists to implant devices, it may be more appropriate forHF physicians to select patients and provide continuingmedical management.
The growing complexity of selecting and monitoringtreatment for HF due to left ventricular systolic dysfunctionmeans that it is difficult to disseminate best medical practiceto all health professionals who might encounter such pa-tients. A network of family physicians supported by HFspecialists (possibly recruited from amongst cardiologists,
geriatricians, primary care physicians, or nurses) who couldevaluate new patients, reevaluate them regularly, and man-age them when they require admission to hospital may bethe most, and possibly only, effective option. The support ofphysicians with expertise in the care and rehabilitation offrail elderly patients will be essential. Depending on thelevel of nonspecialist support, a specialist could support acase-load of 200 to 500 patients. Assuming a prevalence ofHF due to left ventricular systolic dysfunction of 1%, anycommunity of �20,000 people might require the support ofat least one HF specialist, 20 to 50 such specialists would berequired per million population, translating to between10,000 to 20,000 specialists in the U.S. or about 1,500 to3,000 in the UK. The complexity and arguments in favor ofspecialist management of left ventricular systolic dysfunc-tion contrast starkly with the lack of such arguments for“diastolic” HF, which is equally common but for which aspecialist role is distinctly unproved, so far (33).
Braunstein et al. (15) have highlighted the high preva-lence and prognostic associations of noncardiac comorbidi-ties in patients with HF. The study does not provideinformation on how these comorbidities should be man-aged. According to current evidence, it seems more appro-priate for HF specialists to be educated in the key aspects ofthe management of common comorbid medical conditions,resorting to specialist advice where evidence of real benefitexists, rather than to try to educate all physicians about howto manage HF well. The current disorganized state of affairsin which no group has been allowed to properly championthe needs of victims of HF, the most common malignantdisease in Europe and North America (34), should not beallowed to persist. Patients need coordinated services, withclear management plans that serve their needs and offersociety value-for-money. Too many “cooks” will ensure thateffective policy and management decisions are not made.
Reprint requests and correspondence: Dr. John G. F. Cleland,Castle Hill Hospital, University of Hull, Castle Hill Road,Kingston-Upon-Hull, Cottingham HU16 5JQ, United Kingdom.E-mail: [email protected].
REFERENCES
1. Lee MR. William Withering (1741–1799): a Birmingham lunatic.Proc R Coll Physicians Edinb 2001;31:77–83.
2. Cleland JGF, Coletta AP, Nikitin N, Louis A, Clark A. Update ofclinical trials from the American College of Cardiology 2003. EPHE-SUS, SPORTIF-III, ASCOT, COMPANION, UK-PACE, andT-wave alternans. Eur J Heart Fail 2003;5:391–8.
3. Cleland JGF. For debate: preventing atherosclerotic events withaspirin. BMJ 2002;324:103–5.
4. Cleland JGF. Is aspirin “the weakest link” in cardiovascular prophy-laxis? The surprising lack of evidence supporting the use of aspirin forcardiovascular disease. Prog Cardiovasc Dis 2002;44:275–92.
5. Louis A, Cleland JGF, Crabbe S, et al. Clinical trials update:CAPRICORN, COPERNICUS, MIRACLE, STAF, RITZ-2,RECOVER and RENAISSANCE and cachexia and cholesterol inheart failure. Highlights of the scientific sessions of the AmericanCollege of Cardiology, 2001. Eur J Heart Fail 2001;3:381–7.
6. Krum H, McMurray JJ. Statins and chronic heart failure: do we needa large-scale outcome trial? J Am Coll Cardiol 2002;39:1567–73.
1236 Cleland and Clark JACC Vol. 42, No. 7, 2003Editorial Comment October 1, 2003:1234–7

7. Cleland JGF, Ghosh J, Khan NK, Ghio S, Tavazzi L, Kaye G.Multi-chamber pacing: a perfect solution for cardiac mechanicaldyssynchrony? Eur Heart J 2003;24:384–90.
8. Cleland JGF, Thackray S, Goodge L, Kaye GC, Cooklin M. Outcomestudies with device therapy in patients with heart failure. J CardiovascElectrophysiol 2002;13:S73–91.
9. Cleland JGF, Khand A, Clark AC. The heart failure epidemic: exactlyhow big is it? Eur Heart J 2001;22:623–6.
10. Cleland JGF, Gemmel I, Khand A, Boddy A. Is the prognosis of heartfailure improving? Eur J Heart Fail 1999;1:229–41.
11. Weinberger M, Oddone EZ, Henderson WG. Does increased accessto primary care reduce hospital readmissions? N Engl J Med 1996;334:1441–7.
12. Indridason OS, Coffman CJ, Oddone EZ. Is specialty care associatedwith improved survival of patients with congestive heart failure? AmHeart J 2003;145:209–13.
13. Reis SE, Holubkov R, Edmundowicz D, et al. Treatment of patientsadmitted to the hospital with congestive heart failure: specialty-relateddisparities in practice patterns and outcomes. J Am Coll Cardiol1997;30:733–8.
14. Sakakibara M, Kongoji K, Samejima H, et al. Specialty-relateddisparities of readmission in patients with chronic heart failure: theimportance of hospital-clinic cooperation. Intern Med 1999;38:705–9.
15. Braunstein JB, Anderson GF, Gerstenblith G, et al. Noncardiaccomorbidity increases preventable hospitalizations and mortalityamong Medicare beneficiaries with chronic heart failure. J Am CollCardiol 2003;42:1226–33.
16. Brown A, Cleland JGF. Influence of concomitant disease on patternsof hospitalisation in patients with heart failure discharged fromScottish hospitals in 1995. Eur Heart J 1998;19:1063–9.
17. Cleland JGF, Cohen-Solal A, Cosin-Aguilar J, et al. Management ofheart failure in primary care (the IMPROVEMENT of Heart FailureProgramme): an international survey. Lancet 2002;360:1631–9.
18. Cleland JGF, Swedberg K, Follath F, et al. The EuroHeart FailureSurvey Programme: survey on the quality of care among patients withheart failure in Europe. Part 1: patient characteristics and diagnosis.Eur Heart J 2003;24:422–63.
19. Komajda M, Follath F, Swedberg K, et al. The EuroHeart FailureSurvey Programme. A survey on the quality of care among patientswith heart failure in Europe. Part 2: treatment. Eur Heart J 2003;24:464–74.
20. Jones PW, Willits LR, Burge PS, Claverley PM, Inhaled Steroids inObstructive Lung Disease in Europe Study Investigators. Disease
severity and the effect of fluticasone propionate on chronic obstructivepulmonary disease excacerbations. Eur Respir J 2003;21:68–73.
21. Cleland JGF, Wang M. Depression and heart failure—not yet a targetfor therapy? Eur Heart J 1999;20:1529–30.
22. Miller AB. Heart failure and depression. Eur J Heart Fail 2002;4:402.23. Cleland JGF, Baksh A, Louis A. Polypharmacy (or polytherapy) in the
treatment of heart failure. Heart Fail Monit 2000;1:8–13.24. Davos CH, Doehner W, Rauchhaus M, et al. Body mass and survival
in patients with chronic heart failure without cachexia: the importanceof obesity. J Card Fail 2003;9:29–35.
25. Cowburn PJ, Cleland JGF, Coats AJS, Komajda M. Risk stratificationin chronic heart failure. Eur Heart J 1998;19:696–710.
26. Clark AL, Loebe M, Potapov EV, et al. Ventricular assist device insevere heart failure. Effects on cytokines, complement and bodyweight. Eur Heart J 2001;22:2275–83.
27. Louis A, Manousos R, Coletta A, Clark AL, Cleland JGF. Clinicaltrials update: The Heart Protection Study, IONA, CARISA,ENRICHD, ACUTE, ALIVE, MADIT II and REMATCH. EurJ Heart Fail 2002;4:111–6.
28. Hunt SA, Baker DW, Chin MH, et al. ACC/AHA guidelines for theevaluation and management of chronic heart failure in the adult:executive summary a report of the American College of Cardiology/American Heart Association task force on practice guidelines. Circu-lation 2001;104:2996–3007.
29. Cleland JGF, Freemantle N, Ball SG, et al. The Heart FailureRevascularisation Trial (HEART): rationale, design and methodology.Eur J Heart Fail 2003;5:295–303.
30. Lawson WE, Kennard ED, Holubkov R, et al. Benefit and safety ofenhanced external counterpulsation in treating coronary artery diseasepatients with a history of congestive heart failure. Cardiology 2001;96:78–84.
31. Soran O, Fleishman B, DeMarco T, et al. Enhanced external coun-terpulsation in patients with heart failure: a multicenter feasibilitystudy. Congest Heart Fail 2002;8:201–3.
32. Owens DK, Sanders GD, Heidenreich PA, McDonald KM, HlatkyMA. Effect of risk stratification on cost-effectiveness of the implant-able cardioverter defibrillator. Am Heart J 2002;144:440–8.
33. Banerjee P, Banerjee T, Khand A, Clark AL, Cleland JGF. Diastolicheart failure—neglected or misdiagnosed? J Am Coll Cardiol 2002;39:138–41.
34. Stewart S, MacIntyre K, Hole DJ, Capewell S, McMurray JJ. More‘malignant’ than cancer? Five-year survival following a first admissionwith heart failure. Eur J Heart Fail 2001;3:315–22.
1237JACC Vol. 42, No. 7, 2003 Cleland and ClarkOctober 1, 2003:1234–7 Editorial Comment

Hormone Replacement TherapyIs Associated With Improved Survivalin Women With Advanced Heart FailureJoAnn Lindenfeld, MD,* Jalal K. Ghali, MD,† Heidi J. Krause-Steinrauf, MS,‡ Steven Khan, MD,§Kirkwood Adams, JR, MD,� Steven Goldman, MD,¶ Mary Ann Peberdy, MD,# Clyde Yancy, MD,**Surai Thaneemit-Chen, MS,†† Rhonda L. Larsen, RN,‡‡ James Young, MD,§§ Brian Lowes, MD,*Yves D. Rosenberg, MD,‡ for the BEST InvestigatorsDenver, Colorado; Shreveport, Louisiana; Bethesda, Maryland; Los Angeles and Palo Alto, California;Chapel Hill and Durham, North Carolina; Tucson, Arizona; Richmond, Virginia; Dallas, Texas; andCleveland, Ohio
OBJECTIVES We sought to determine whether hormone replacement therapy (HRT) is associated with animproved prognosis in women with advanced heart failure (HF) and systolic dysfunction.
BACKGROUND There are about two million postmenopausal women in the U.S. with HF. However, limiteddata are available to assess the effects of HRT on survival in this large group of patients.
METHODS A retrospective analysis of women age 50 years and over entered into the Beta-BlockerEvaluation of Survival Trial (BEST) was conducted using Cox regression analysis comparingsurvival in HRT users and non-users after correcting for baseline variables known to predictsurvival in women with HF and systolic dysfunction.
RESULTS In 493 women age 50 years and older, HRT was associated with a significant reduction inmortality—21% mortality in HRT users and 34% in non-users (p � 0.025). Multivariateanalysis demonstrated a hazard ratio for mortality of 0.6 (95% confidence interval � 0.36 to0.97) (p � 0.039) for HRT users. The benefits of HRT were noted only in women with anonischemic etiology of HF (n � 237).
CONCLUSIONS Hormone replacement therapy is associated with a marked improvement in survival inpostmenopausal women with advanced HF. A prospective, randomized trial of HRT shouldbe performed in this large group of patients. (J Am Coll Cardiol 2003;42:1238–45) © 2003by the American College of Cardiology Foundation
Heart failure (HF) is a common cause of morbidity andmortality in both men and women. It is estimated that fourto five million people in the U.S. have HF and that one-halfof these are women (1,2). Data from the Framingham HeartStudy and the National Health and Nutrition Examination
See page 1246
and Survey-I suggest that at least 70% of women with HFare over age 50 years—the average age of menopause in theU.S. (3,4). Thus, there are at least two million menopausalwomen in the U.S. with HF. Mortality is high in womenwith HF, with estimates of 50% to 90% mortality over 10
years (3,4). Despite the frequency and severity of advancedHF in postmenopausal women, there is only one studyinvestigating the effect of hormone replacement therapy(HRT) in these women. This retrospective study combinedtrials comparing vesnarinone with placebo in patients withadvanced HF (5). After accounting for known predictors ofmortality, estrogen use was associated with a 32% decreasein HF mortality. We sought to confirm whether HRT isassociated with an improved prognosis in women withadvanced HF and systolic dysfunction using data collectedin the Beta-Blocker Evaluation of Survival Trial (BEST).
METHODS
The BEST study. The BEST trial was a multicenter,prospective, randomized trial comparing a nonselectivebeta-blocker, bucindolol, with placebo in patients with NewYork Heart Association (NYHA) functional class III or IVHF and an ejection fraction of �35%. The design of thistrial and the study results have been published (6,7).Exclusion criteria included a reversible cause of HF andinfarction within the previous six months (6). Other exclu-sion criteria included a coronary revascularization procedurewithin 60 days, patients who were candidates to be listed forheart transplantation, unstable angina defined as uncor-rected thyroid disease, obstructive or hypertrophic cardio-myopathy, amyloidosis, active myocarditis, malfunctioning
From the *University of Colorado Health Sciences Center and Center for Women’sHealth Research, Denver, Colorado; †Cardiac Centers of Louisiana, Shreveport,Louisiana; ‡National Heart, Lung, and Blood Institute, Bethesda, Maryland;§Cedars-Sinai Medical Center, Los Angeles, California; �University of NorthCarolina, Chapel Hill, North Carolina; ¶Tucson SAVAHCS, Tucson, Arizona;#Virginia Commonwealth University, Medical College of Virginia, Richmond,Virginia; **University of Texas Southwestern, Dallas, Texas; ††VA Palo Alto HealthCare System Cooperative Studies Program, Palo Alto, California; ‡‡Duke ClinicalResearch Institute, Durham, North Carolina; and the §§Cleveland Clinic Founda-tion, Cleveland, Ohio. The BEST trial was sponsored by the Division of Epidemi-ology and Clinical Applications of the National Heart, Lung, and Blood Institute andthe Department of Veterans Affairs Cooperative Studies Program through aninteragency agreement. Additional support was provided by Incara PharmaceuticalsCorporation, which also supplied bucindolol and placebo.
Manuscript received February 5, 2003; revised manuscript received April 9, 2003,accepted April 18, 2003.
Journal of the American College of Cardiology Vol. 42, No. 7, 2003© 2003 by the American College of Cardiology Foundation ISSN 0735-1097/03/$30.00Published by Elsevier Inc. doi:10.1016/S0735-1097(03)00938-0

prosthetic heart valve, or myocardial use of �6 nitroglycerintablets per week, heart rate �50 beats/min, life expectancyof �3 years, or a serum creatinine level �3 mg/dl. Patientswith decompensated HF, pulmonary edema, or systolicblood pressure �80 mm Hg were also excluded. Patientswere excluded if they required a drug in one of fourcategories: 1) beta-adrenergic blocking agents within 30days of baseline evaluation; 2) calcium channel blockingagents, theophylline, tricyclic antidepressants, monoamineoxidase inhibitors, or beta-adrenergic agonists within oneweek of baseline evaluation; 3) flecainide, encainide,propafenone, or disopyramide within two weeks of random-ization; or 4) amiodarone within eight weeks of baselineevaluation.
Randomization at each clinical site was stratified byetiology of HF (ischemic or nonischemic), left ventricularejection fraction (LVEF) (�0.20 vs. �0.20), gender, andrace. Follow-up visits occurred at 3, 6, and 12 months afterrandomization and at 6-month intervals thereafter. Theprimary end point was all-cause mortality. Secondary endpoints included cardiovascular mortality, all-cause and con-gestive heart failure (CHF)-specific hospitalization, thecombination of death and cardiac transplantation, LVEF at3 and 12 months, myocardial infarction, quality of life, anda change in the need for cotherapy.
We conducted a retrospective analysis to examine theeffect of HRT in postmenopausal women on survival and toevaluate whether the effect varied according to etiology ofHF. We also examined HRT-by-treatment effect(bucindolol-placebo) interactions for mortality.Definition of postmenopausal and HRT. Women in thistrial were considered to be postmenopausal if they were �50years of age. Women were classified as using HRT if theywere taking estrogen, progestin, or a combination of both atthe baseline evaluation.Assessment of compliance and health status. Compli-ance to follow-up was estimated by percent attendance atthe three-month follow-up visit. Health status was esti-mated by the prevalence of current smoking and body massindex (BMI) at the baseline evaluation. Coronary arterydisease (CAD) was defined as the presence of significantdisease by angiography or evidence of a previous myocardialinfarction.
Statistical analysis. Means and standard deviations ormedians are reported for continuous data. Proportions arereported for categorical data. The p values reported for thecomparisons of the HRT and non-HRT subgroups arefrom the t test, except when the data were non-normal andthe Wilcoxon rank sum test for continuous variables wasused. For categorical variables the chi-square test was used,except in cases when the expected cell counts were �5 andthe Fisher’s exact test was used. Two-sided tests of signif-icance were performed using an alpha of 0.05. Cox propor-tional hazards regression was used to examine the effect ofHRT on survival, adjusting for prespecified variables and toestimate risk (hazard) ratios and corresponding confidenceintervals (CIs). A backward elimination process was used toderive the multivariate model, which examined the follow-ing predictors: LVEF, NYHA functional classification,etiology of HF (ischemia � CAD, no ischemia � noCAD), race, age, diabetes, cardiothoracic ratio (CTR),HRT, and treatment group assignment (bucindolol orplacebo). Cox regression models were also used to examineHRT-by-CAD and HRT-by-treatment interactions. Themodel-based Kaplan-Meier curves were corrected for po-tential confounders, including CTR, NYHA functionalclassification, etiology (CAD vs. non-CAD), LVEF, andtreatment group.
RESULTS
Patient characteristics. A total of 2,708 patients wererandomized in the BEST study, including 593 women. Ofthe 593 women, 435 (73%) were �50 years of age and wereconsidered to be postmenopausal. Subjects were consideredto be using HRT if they were taking oral or transdermalestrogen alone, a progestin, or a combination of estrogenand progestin. Of the 435 women age 50 years or older, 122(23%) were using HRT. No woman age 50 years or abovewas using oral contraceptives. Of the 102 HRT users, 72were using estrogen alone, 3 were using a progestin alone,and 27 were using a combination of the two hormones. Thebaseline characteristics of the HRT users and non-HRTusers are shown in Table 1. Hormone replacement therapyusers were younger and more often non-black comparedwith the HRT non-users. Hormone replacement therapyusers had a lower BMI compared with the non-HRTsubgroup, primarily because of a height difference. Hor-mone replacement therapy users were less likely to have ahistory of hypertension and diabetes than the non-users.Systolic and diastolic blood pressure, heart rate, LVEF andright ventricular ejection fraction, and the prevalence ofatrial fibrillation were not different between the two sub-groups. Medications at baseline were similar, with theexception of fewer vasodilators being taken by HRT userscompared with non-users (p � 0.047). Hormone replace-ment therapy users had slightly lower creatinine, serumsodium, and alanine aminotransferase levels than theirnon-HRT counterparts. Median plasma norepinephrine
Abbreviations and AcronymsBMI � body mass indexCAD � coronary artery diseaseCHF � congestive heart failureCI � confidence intervalCTR � cardiothoracic ratioHF � heart failureHR � hazard ratioHRT � hormone replacement therapyLVEF � left ventricular ejection fractionMAPK � mitogen-activated protein kinaseNYHA � New York Heart Association
1239JACC Vol. 42, No. 7, 2003 Lindenfeld et al.October 1, 2003:1238–45 HRT and Heart Failure

Table 1. Baseline Clinical Characteristics by HRT User Status*
Characteristics
HRT User (n � 102) HRT Non-User (n � 333)
OverallP Value
Placebo(n � 49)
Bucindolol(n � 53) Overall
Placebo(n � 165)
Bucindolol(n � 168) Overall
DemographicAge (yrs) 61.8 � 7.5 61.2 � 7.3 61.5 � 7.4 63.8 � 8.6 65.1 � 9.0 64.5 � 8.8 0.004
Range 50–78 50–77 50–78 50–86 50–93 50–93Weight (lbs) 150.3 � 34.0 152.4 � 27.1 151.4 � 30.5 155.5 � 37.7 156.5 � 35.5 156.0 � 36.5 0.204Height (in) 64.0 � 2.5 64.2 � 2.5 64.1 � 2.5 63.4 � 2.6 63.1 � 2.8 63.3 � 2.7 0.007Body mass index (kg/m2) 25.9 � 6.2 26.1 � 5.1 26.0 � 5.6 27.1 � 6.0 27.6 � 6.2 27.4 � 6.1 0.048Median duration of CHF (months) 48.0 46.0 47.5 36.0 40.5 39.0 0.178*
Range 1–240 1–288 1–288 1–199 1–456 1–456 –Current smoker 5 (10%) 7 (13%) 12 (12%) 12 (7%) 19 (11%) 31 (9%) 0.467Ever smoked 30 (61%) 32 (60%) 62 (61%) 83 (51%) 87 (53%) 170 (52%) 0.120
RaceWhite non-Hispanic 41 (84%) 47 (89%) 88 (86%) 106 (64%) 105 (63%) 211 (63%) 0.000Black non-Hispanic 7 (14%) 5 (9%) 12 (12%) 46 (28%) 52 (31%) 98 (29%)Hispanic or Latino 1 (2%) 1 (2%) 2 (2%) 10 (6%) 10 (6%) 20 (6%)Other 0 (0%) 0 (0%) 0 (0%) 3 (2%) 1 (1%) 4 (1%)
NYHA functional classIII 44 (90%) 50 (94%) 94 (92%) 149 (90%) 154 (92%) 303 (91%) 0.715IV 5 (10%) 3 (6%) 8 (8%) 16 (10%) 14 (8%) 30 (9%)
Heart failure etiologyIschemic 17 (35%) 23 (43%) 40 (39%) 74 (45%) 84 (50%) 158 (47%) 0.144Nonischemic 32 (65%) 30 (57%) 62 (61%) 91 (55%) 84 (50%) 175 (53%)
History of related illnessHypertension 24 (49%) 26 (49%) 50 (49%) 99 (60%) 107 (64%) 206 (62%) 0.021Hyperlipidemia 25 (51%) 26 (49%) 51 (50%) 81 (49%) 74 (44%) 155 (47%) 0.541Diabetes mellitus 12 (24%) 18 (34%) 30 (29%) 72 (44%) 73 (43%) 145 (44%) 0.011
Hemodynamics/ventricular functionHeart rate (beats/min) 82.0 � 11.0 81.4 � 10.3 81.7 � 10.6 83.4 � 13.5 82.0 � 11.4 82.7 � 12.5 0.404Blood pressure (mm Hg)
Systolic 117.4 � 17.1 119.8 � 17.5 118.7 � 17.3 119.0 � 19.0 117.9 � 18.7 118.5 � 18.8 0.771Diastolic 70 � 12 71 � 10 71 � 11 70 � 11 69 � 11 69 � 11 0.290
LVEF (%) 24.9 � 6.0 24.1 � 7.2 24.5 � 6.6 24.5 � 7.0 24.6 � 7.5 24.6 � 7.3 0.917RVEF (%) 40.8 � 14.4 39.4 � 12.7 40.1 � 13.5 37.9 � 14.3 36.1 � 14.2 37.0 � 14.2 0.081Atrial fibrillation 2 (4%) 3 (6%) 5 (5%) 8 (5%) 12 (7%) 20 (6%) 0.675
Routine medicationsACE inhibitor 43 (88%) 45 (85%) 88 (86%) 147 (89%) 153 (91%) 300 (90%) 0.277Angiotensin receptor blocker 6 (12%) 7 (13%) 13 (13%) 18 (11%) 9 (5%) 27 (8%) 0.156Digitalis 46 (94%) 50 (94%) 96 (94%) 152 (92%) 152 (90%) 304 (91%) 0.359Diuretic 44 (90%) 50 (94%) 94 (92%) 156 (95%) 165 (98%) 321 (96%) 0.101Aldactone (spironolactone) 4 (8%) 2 (4%) 6 (6%) 9 (5%) 4 (2%) 13 (4%) 0.101Vasodilator 17 (35%) 23 (43%) 40 (39%) 90 (55%) 78 (46%) 168 (50%) 0.047Hydralazine/isosorbide 13 (27%) 18 (34%) 31 (30%) 57 (35%) 63 (38%) 120 (36%) 0.295Antiarrhythmic 2 (4%) 0 (0%) 2 (2%) 1 (1%) 1 (1%) 2 (1%) 0.235Anticoagulant 18 (37%) 26 (49%) 44 (43%) 63 (38%) 65 (39%) 128 (38%) 0.396Aspirin 21 (43%) 22 (42%) 43 (42%) 70 (42%) 61 (36%) 131 (39%) 0.611Statin lipid-lowering agents 9 (18%) 13 (25%) 22 (22%) 41 (25%) 32 (19%) 73 (22%) 0.940
Laboratory valuesCreatinine (mg/dl) 1.0 � 0.3 1.0 � 0.4 1.0 � 0.3 1.1 � 0.4 1.1 � 0.4 1.1 � 0.4 0.007*Serum sodium (mg/dl) 138.6 � 2.7 137.8 � 2.8 138.2 � 2.7 139.5 � 3.4 139.3 � 3.0 139.4 � 3.2 0.001Serum potassium (mg/dl) 4.3 � 0.5 4.3 � 0.5 4.3 � 0.5 4.3 � 0.5 4.3 � 0.5 4.3 � 0.5 0.607Serum ALT (mg/dl) 19.3 � 9.2 19.1 � 8.5 19.2 � 8.8 25.7 � 16.3 25.4 � 18.7 25.5 � 17.5 0.0001*Median plasma norepinephrine (pg/ml) 392.0 423.0 420.0 460.0 423.0 441.0 0.413*
ECG/X-rayQRS duration, (ms) 137.1 � 32.3 137.5 � 34.4 137.4 � 33.2 131.4 � 36.2 129.8 � 34.7 130.6 � 35.4 0.087QT duration–corrected (ms) 450.6 � 45.7 458.7 � 53.0 454.8 � 49.6 451.9 � 45.8 446.0 � 47.6 448.9 � 46.7 0.273LBBB 22 (45%) 24 (45%) 46 (45%) 60 (36%) 63 (38%) 123 (37%) 0.139Cardio/thoracic ratio 58.6 � 6.6 56.6 � 7.6 57.6 � 7.2 60.4 � 8.0 60.2 � 7.2 60.3 � 7.6 0.002
*Mean � SD unless otherwise indicated. p Value based on Wilcoxon rank sum test.ACE � angiotensin converting enzyme; ALT � alanine aminotransferase; CHF � congestive heart failure; ECG � electrocardiogram; HRT � hormone replacement
therapy; LBBB � left bundle blanch block; LVEF � left ventricular ejection fraction; NYHA � New York Heart Association; RVEF � right ventricular ejection fraction.
1240 Lindenfeld et al. JACC Vol. 42, No. 7, 2003HRT and Heart Failure October 1, 2003:1238–45

values were not different between the two subgroups. Therewere no differences in the QRS or corrected QT durationsor the incidence of left bundle branch block. Hormonereplacement therapy users had a smaller CTR comparedwith non-HRT users (p � 0.002).
Figure 1 depicts the model-based survival curves adjustedfor potential confounders for HRT users and non-users.There were 134 deaths in the 435 women age 50 and overwith a mean follow-up of 2 years. Twenty-one deaths (21%)occurred in the 102 HRT users and 113 deaths (34%) in the333 non-HRT users. There was a significant difference insurvival favoring HRT users (Wald chi-square p value forHRT � 0.04). Table 2 presents the results from themultivariate analysis using prespecified risk factors known topredict mortality in patients with HF and adjusting fortreatment group assignment (bucindolol or placebo). Sig-nificant factors predicting higher mortality included NYHAfunctional class IV vs. III and an ischemic etiology of HF.A higher LVEF and HRT use were associated with a lowermortality. After adjusting for the effect of HRT, treatmentgroup assignment and etiology of CHF, we found nosignificant effect of HRT-by-treatment interaction (p �0.85) or HRT-by-etiology of CHF (CAD vs. no CAD)interaction (p � 0.09) on mortality.
Survival curves adjusted for potential confounders com-paring HRT users with non-HRT users by etiology ofdisease are presented in Figure 2. Of the 198 women with
ischemic etiology, there was no difference in survival be-tween HRT users and non-users (HR � 0.74, 95% CI �0.41 to 1.33, Wald chi-square p value � 0.31). However,there was a significant survival benefit for HRT users in the237 nonischemic postmenopausal women (HR � 0.35, 95%CI � 0.14 to 0.87, Wald chi-square p value � 0.02).
We compared the survival between unopposed estrogenHRT users (n � 72) to those users on a combination ofestrogen plus progestin (n � 27). A total of 21 deathsoccurred, 15 (21%) in unopposed estrogen users and 6(22%) in those using combination estrogen and progestin.
Figure 1. Model-based survival curves for survival by hormone replacement therapy (HRT) use in postmenopausal women. Difference between HRTsubgroups is significant. (Wald chi-square p value for HRT � 0.04) Adjustment was made for etiology of disease (coronary artery disease vs. non-coronaryartery disease), cardiothoracic ratio, New York Heart Association functional classification, left ventricular ejection fraction, and treatment group. CI �confidence interval; HR � hazard ratio.
Table 2. Multivariate Predictors of Mortality IncludingTreatment Group Assignment
CovariateRelative
Risk 95% CI p Value
NYHA (IV vs. III) 2.610 1.659–4.107 0.0001CAD (ischemic vs. nonischemic) 2.492 1.737–3.573 0.0001LVEF (per 1 EF unit increase) 0.961 0.935–0.988 0.0042HRT (taking vs. not taking) 0.595 0.364–0.973 0.0387Cardio/thoracic ratio 1.026 1.000–1.053 0.0502Treatment (bucindolol vs. placebo) 0.710 0.502–1.005 0.0534
n � 426, total deaths � 131. Estimates from Cox proportional hazards regressionmodel. Model derived using a backwards elimination process considering thefollowing covariates: left ventricular ejection fraction (LVEF), New York HeartAssociation (NYHA) classification, etiology of heart failure (ischemia � coronaryartery disease [CAD] or no ischemia � no CAD), race, age, diabetes, cardiothoracicratio, hormone replacement therapy (HRT), and treatment group assignment(bucindolol or placebo).
CI � confidence interval; EF � ejection fraction.
1241JACC Vol. 42, No. 7, 2003 Lindenfeld et al.October 1, 2003:1238–45 HRT and Heart Failure

There was no difference in survival between combinationHRT and unopposed estrogen subgroups (HR � 1.09, 95%CI � 0.42 to 2.82, p � 0.86).
The results of the multivariate analysis including BMIand current smoking status as measures of health status andusing attendance at the three-month visit as a measure ofcompliance are presented in Table 3. The frequency ofcurrent smoking status and the BMIs for HRT users andnon-users are shown in Table 1. Attendance at the three-month clinic visit was 93% among both HRT users andnon-users. Forcing measures of health status and compli-
ance into the multivariate analysis resulted in an estimatedrelative risk for mortality for HRT of 0.54 (95% CI � 0.33to 0.91) and p value of 0.019.
DISCUSSION
Our study suggests that the use of HRT in women withadvanced HF and systolic dysfunction is associated with asignificant survival benefit. Hormone replacement therapyusers had a number of baseline features that are known topredict a better prognosis. These included a younger age, ahigher percentage of non-black subjects, less hypertensionand diabetes, and a higher frequency of nonischemic etiol-ogy. When these factors are accounted for in a multivariateanalysis, HRT remains a significant predictor of mortalitywith a relative risk of 0.60 (p � 0.039).
Only one previous study has addressed the issue of HRTin women with HF. Using data combined from three trialsof patients with advanced HF comparing vesnarinone withplacebo, the relative risk of HRT for survival was 0.68 (5).The baseline characteristics in that study were similar to ourstudy with HRT users being younger, less often black, andmore frequently having a nonischemic etiology. In bothstudies, 21% to 22% of women age 50 years and older wereusing HRT. In both studies, multivariate analysis did notalter the apparent association of HRT with survival. Ourstudy had a mean follow-up of two years, compared with amean follow-up of �1 year in the study of Reis et al. (5).Thus, our findings confirm the study of Reis et al. (5) and
Figure 2. Model-based survival curves by hormone replacement therapy (HRT) use within etiology of disease. Differences are significant for women witha non-coronary artery disease (CAD) etiology but not for those with a CAD etiology. Adjustment was made for cardiothoracic ratio, New York HeartAssociation functional classification, left ventricular ejection fraction, and treatment group. CI � confidence interval; HR � hazard ratio.
Table 3. Multivariate Predictors of Mortality IncludingMeasures of Compliance and Health Status
CovariateRelative
Risk 95% CI P Value
NYHA functional class (IV vs. III) 2.766 1.738–4.402 0.0001CAD (ischemic vs. nonischemic) 2.171 1.494–3.155 0.0001Compliance (yes vs. no) 0.235 0.142–0.389 0.0001LVEF (per 1 EF unit increase) 0.952 0.925–0.980 0.0007Current smoker (yes vs. no) 0.464 0.224–0.959 0.0381BMI (per kg/m2) 0.970 0.939–1.003 0.0742Cardio/thoracic ratio 1.020 0.994–1.047 0.1379HRT (taking vs. not taking) 0.544 0.327–0.906 0.0193Treatment (bucindolol vs. placebo) 0.697 0.489–0.994 0.0462
*Table 2 model with BMI � smoker � compliance with treatment. N � 425, totaldeaths � 130. estimates from Cox proportional hazards regression model. Compli-ance at three-month visit defined as a patient attending her three month visit andhaving a physical exam completed.
BMI � body mass index; CAD � coronary artery disease; CI � confidenceinterval; HRT � hormone replacement therapy; LVEF � left ventricular ejectionfraction; NYHA � New York Heart Association.
1242 Lindenfeld et al. JACC Vol. 42, No. 7, 2003HRT and Heart Failure October 1, 2003:1238–45

also suggest that the association of HRT with improvedmortality in women with advanced HF is present even withprolonged follow-up.
Hormone replacement therapy was associated with amarked improvement in survival in women with a nonisch-emic etiology of HF (HR � 0.35, 95% CI � 0.14 to 0.87,p � 0.02) but no improvement in women with an ischemicetiology (HR � 0.74, 95% CI � 0.41 to 1.33, p � 0.31)(Fig. 2). This effect of etiology differs from the study of Reiset al. (5), in which etiology of HF did not impact the benefitof HRT. However, in that study the benefits of HRT werenot statistically significant in either ischemic or nonischemicetiologies when the groups were considered separately. Atest of interaction of benefit of HRT by etiology had a pvalue of 0.09. Although not statistically significant, this pvalue certainly does not exclude the possibility of an inter-action between etiology of CHF and HRT. Indeed, a largerstudy will be necessary to be certain if etiology of HF isimportant for the benefits of HRT.
We found no difference in the benefits of combinationestrogen and progestin versus unopposed estrogen. Reis etal. (5) reported a trend for estrogen alone to be associatedwith improved mortality. The small numbers of patients inboth studies do not allow firm conclusions.Potential mechanisms of benefit of HRT. Hormonereplacement therapy may improve survival in postmeno-pausal women with advanced HF through effects on endo-thelial function, neurohormonal activation, myocardial re-modeling, CAD, or any combination of these.Postmenopausal women have impaired endothelial functionas measured by flow-mediated vasodilation (8,9). ChronicHRT with estrogen alone or with the combination of17�-estradiol and norethisterone acetate improvesendothelial-dependent vasodilation in postmenopausalwomen (9–11). Improved endothelial function may result inlower systemic vascular resistance and improved cardiacoutput in women with advanced HF, although no studies ofHRT have been conducted in postmenopausal women withHF.
Neurohormonal activation is associated with a poorerprognosis in patients with HF (12,13). Increasing levels ofnorepinephrine, renin, angiotensin II, and endothelin haveall been correlated with poorer survival in patients with HF(12–14). Hormone replacement therapy, particularly estro-gen, is associated with reduced activation of a number ofneurohormonal systems. Estrogen is known to suppressmuscle sympathetic nerve activity, both at rest and afterexercise in postmenopausal women (15). It is not known ifcardiac sympathetic activity is also suppressed by estrogen,but muscle sympathetic nerve activity is known to reflectcardiac sympathetic activity (16). Estrogen supplementationto perimenopausal women for eight weeks decreased systolicand diastolic blood pressure and total body norepinephrinespillover in response to mental stress (17). Estrogen andprogesterone decrease angiotensin-converting enzyme levelswhile increasing bradykinin levels in hypertensive post-
menopausal women (18,19). Estrogen is known to decreaseendothelin levels in healthy postmenopausal women (9,11).Thus, there is evidence that HRT might reduce activationof a number of neurohormonal systems that are known to beassociated with increased mortality in HF. There are nodata addressing the effects of HRT on neurohormonalactivation in women with HF. However, if HRT providessimilar benefits in women with advanced HF as in healthypostmenopausal women, an effect of HRT on mortality inHF might be expected.
There are substantial gender differences in myocardialremodeling due, at least in part, to the influence of sexhormones. In the general population there is a progressiveage-related increase in myocardial mass in healthy womenthat is not seen in their male counterparts (20). Thesefindings were confirmed in a healthy, nonobese, normoten-sive subset of the Framingham Heart Study (21). Thesestudies demonstrate the increase in myocardial mass occursprimarily in postmenopausal women. Indeed, premeno-pausal women with essential hypertension have thinnerposterior left ventricular walls, smaller left ventricular mass,and better cardiac function than age-matched men (22). Inone study, women using HRT for more than 10 years hada significant reduction in septal and posterior left ventricularwall thickness when compared with controls (23). Elderly(postmenopausal) women with systolic hypertension oraortic stenosis have more concentric remodeling and betterpreserved left ventricular systolic function than their malecounterparts both at rest and with exercise (24–28). Thesedata suggest that female sex hormones, estrogen and pro-gesterone, influence myocardial hypertrophy and myocardialremodeling by suppressing cardiac hypertrophy and preserv-ing myocardial function. Studies in animals subjected to aleft ventricular pressure load also demonstrate a substantialeffect of female sex hormones on myocardial remodeling.Female rats subjected to pressure loads demonstrate lesshypertrophy than male rats (29). Furthermore, female micesubjected to pressure overloads have less progression to HFthan do the males (29–31). Female rats demonstrate geneexpression changes in beta-myosin and sarcoplasmic retic-ulum calcium adenosine triphosphatase expression consis-tent with less hypertrophy and preserved systolic function(32). It is known that estrogen receptors are present in themyocardium (33). Recently two studies have contributedinformation linking 17�-estradiol with cardiac hypertrophy.van Eickels et al. (34) have shown that 17�-estradiolreduces left ventricular hypertrophy in ovariectomized micesubjected to aortic constriction. Estrogen therapy was asso-ciated with reduced levels of p38 mitogen-activated proteinkinase (MAPK). The MAPK proteins are important in theactivation and maintenance of cardiac hypertrophy andp38MAPK may be important in the progression to HF(35). In another study, Xin et al. (36) have demonstratedthat male FKBP 12.6 knockout mice develop left ventricularhypertrophy, whereas the female knockouts do not. FKBP12.6 is an intracellular binding protein that modulates the
1243JACC Vol. 42, No. 7, 2003 Lindenfeld et al.October 1, 2003:1238–45 HRT and Heart Failure

action of the cardiac ryanodine receptor complex, whichregulates sarcoplasmic reticulum calcium release. Blockingestradiol receptors in the female mice resulted in hypertro-phy similar to that seen in the male mice. Thus, estrogenmay have effects on more than one pathway influencingcardiac hypertrophy.
Myocyte apoptosis may also be important in myocardialremodeling. Olivetti et al. (37), in an autopsy study, dem-onstrated that myoctye number and volume are betterpreserved in women than in men. This intriguing study issupported by recent findings that estrogen may be importantin the activation of the antiapoptotic protein AKT in theheart (38). Thus HRT, and particularly estrogen, positivelyeffect myocardial hypertrophy and remodeling, and thismechanism seems the most plausible explanation for theimproved survival with HRT in women with advanced HF.
Recent studies differ about whether HRT alters thenatural history of CAD in women. Data from the Heart andEstrogen/progestin Replacement Study (HERS) and Heartand Estrogen/progestin Replacement Study follow-up dem-onstrated no increase in the rate of primary coronary heartdisease events or secondary cardiovascular events with com-bination estrogen and progesterone therapy in postmeno-pausal women with known coronary heart disease (39,40).However the Women’s Health Initiative (WHI) found aHR of 1.29 for coronary heart disease with combined HRTin healthy postmenopausal women (41). Our study did notdemonstrate any benefit of HRT on survival in women withan ischemic etiology for HF. The absence of benefit in thissubgroup may represent the sum of the positive benefit seenin women with a nonischemic etiology and a negative effecton CAD, such as was noted in WHI. Both the WHI andHERS studies have demonstrated a �2-fold risk in throm-boembolic disease in women on combination HRT (39–41). However, the baseline risk of thromboembolic diseasewas about two-fold higher in the women with coronarydisease enrolled in HERS than in the healthy postmeno-pausal women enrolled in WHI. In the Studies Of LeftVentricular Dysfunction (SOLVD) trials, women with HFhad an increasing rate of thromboembolic events withdecreasing ejection fraction that was not seen in the men(42). Most of the subjects in SOLVD had underlyingcoronary disease, and it is not known if the excess inthromboembolic events in the women in SOLVD wasrelated to etiology of CHF. Our results could be explainedif there were an excess risk of thromboembolic events inwomen with an ischemic etiology of disease compared withthose with a nonischemic etiology. Although the test forinteraction between the effect of HRT and etiology ofdisease was not statistically significant (p � 0.09), thenumber of women in these subgroups was small, and,accordingly, the power to detect an interaction effect waslow.
Our results may also reflect a difference in the healthstatus or compliance of HRT users compared with non-users. It is known that women who take HRT have
healthier lifestyles than do non-HRT users and that thismay be an explanation of the reported benefits of HRT inretrospective studies (43). Furthermore, compliance biasmay have influenced our study (44,45). However, when weattempted to correct for the “healthy subject” bias and forcompliance bias as measured by compliance to treatmentvisits, the benefit of HRT was the same or even larger.Although these adjustments are rudimentary, they do notsuggest a “healthy subject” or compliance bias in our studyparticipants.
We have demonstrated a significant benefit of HRT useon survival in postmenopausal women with advanced HF. Itwill be important to determine if this benefit is confirmed ina prospective, randomized trial of HRT in postmenopausalwomen with HF because there are more than two millionpostmenopausal women in the U.S. with HF, and thisnumber will continue to increase as our population ages(46).Study limitations. This was a retrospective study andmenopausal status was not collected prospectively. Hor-mone replacement therapy use was only documented atrandomization and not during follow-up. This study couldnot completely address the possibility that either preventionbias or compliance bias or other factors not controlled forcould have influenced these results, as has been suggested instudies of HRT and CAD (43–45). Although there was nostatistically significant interaction between the effect ofHRT and etiology of disease, there was low power to detectan interaction effect because of the small number of womenin these subgroups.Conclusions. We have demonstrated an association ofHRT with improved survival in postmenopausal womenwith advanced HF and systolic dysfunction over a follow-upof two years. The 40% reduction in mortality is nearlyidentical to the 38% reduction noted in a previous study.Our finding that this benefit is noted in women with anonischemic etiology of HF requires confirmation. Withmore than two million postmenopausal women with HF inthe U.S., a prospective, randomized trial evaluating thebenefits of HRT in this population, particularly those witha nonischemic etiology of HF, would be important.
Reprint requests and correspondence: Dr. JoAnn Lindenfeld,University of Colorado Health Sciences Center, 4200 East NinthAvenue, B-130, Denver, Colorado 80262. E-mail: [email protected].
REFERENCES
1. American Heart Association. 2000 Heart and Stroke Statistical Up-date. Available at: http://www.americanheart.org/statistics/index.html. Accessed July 2000.
2. Lindenfeld J, Krause-Steinrauf H, Salerno J. Where are all the womenwith heart failure? J Am Coll Cardiol 1997;30:1417–9.
3. Ho KKL, Pinsky JL, Kannel WB, Levy D. The epidemiology of heartfailure: the Framingham study. J Am Coll Cardiol 1993;22:6A–13A.
4. Schocken DD, Arrieta MI, Leaverton PE, Rosse A. Prevalence andmortality rate of congestive heart failure in the United States. J AmColl Cardiol 1992;20:301–6.
1244 Lindenfeld et al. JACC Vol. 42, No. 7, 2003HRT and Heart Failure October 1, 2003:1238–45

5. Reis SE, Holubkov R, Young JB, White BG, Cohn JN, Feldman AM.Estrogen is associated with improved survival in aging women withcongestive heart failure: an analysis of the vesnarinone studies. J AmColl Cardiol 2000;36:529–33.
6. The BEST Steering Committee. Design of the beta-blocker evalua-tion of survival trial (BEST). Am J Cardiol 1995;75:1220–3.
7. The Beta-Blocker Evaluation of Survival Trial Investigators. A trial ofbeta-blocker bucindolol in patients with advanced chronic heartfailure. N Engl J Med 2001;344:1659–67.
8. Gilligan DM, Badar DM, Panza JA, et al. Acute vascular effects ofestrogen in post-menopausal women. Circulation 1994;90:786–91.
9. Ylikarkala O, Orpana A, Puolakka J, et al. Postmenopausal hormonalreplacement decreases plasma levels of endothelin-I. J Clin EndocrinolMetab 1995;80:3384–7.
10. Lieberman EH, Gerhard MD, Uehata A, et al. Estrogen improvesendothelial dependent flow-mediated vasodilation in post-menopausalwomen. Ann Intern Med 1994;121:936–41.
11. Siatta A, Altavilla D, Cucinotta D, et al. Randomized, double-blind,placebo-controlled study on effects of raloxifene and hormone replace-ment therapy on plasma NO concentrations, endothelin-1 levels, andendothelium-dependent vasodilation in postmenopausal women. Ar-terioscler Thromb Vasc Biol 2001;21:1512–9.
12. Cohn JN, Levine TB, Olivari MT, et al. Plasma norepinephrine as aguide to prognosis in patients with chronic congestive heart failure.N Engl J Med 1984;311:819–23.
13. Francis GS, Cohn JN, Johnson G, Rector TS, Goldman S, Simon A.Plasma norepinephrine, plasma renin activity, and congestive heartfailure. Relations to survival and the effects of therapy in V-HeFT II.The V-HeFT VA Cooperative Studies Group. Circulation 1993;87Suppl 6:VI40–8.
14. Pousset F, Isnard R, Lechat P, et al. Prognostic value of plasmaendothelin-1 in patients with chronic heart failure. Eur Heart J1997;18:254–8.
15. Weitz G, Elam M, Born J, et al. Postmenopausal estrogen adminis-tration suppresses muscle sympathetic nerve activity. J Clin EndocrinolMetab 2001;86:344–8.
16. Esler M, Kaye D, Lambert G, Esler D, Jennings G. Adrenergicnervous system in heart failure. Am J Cardiol 1997;80:7L–14L.
17. Komesaroff PA, Esler MD, Sudhir K. Estrogen supplementationattenuates glucocorticoid and catecholamine responses to mental stressin perimenopausal women. J Clin Endocrinol Metab 1999;84:606–10.
18. Nogawa N, Ichikawa S, Kanda T, et al. Hormone replacement therapyin postmenopausal women with essential hypertension increases cir-culating plasma levels of bradykinin. Am J Hypertens 1999;12:1044–7.
19. Nogawa N, Sumino H, Ichikawa S, et al. Effect of long-term hormonereplacement therapy on angiotensin-converting enzyme activity andbradykinin in postmenopausal women with essential hypertension andnormotensive postmenopausal women. Menopause 2001;8:210–5.
20. Marcus R, Krause L, Weder AB, et al. Sex-specific determinants ofincreased left ventricular mass in the Tecumseh Blood Pressure Study.Circulation 1995;92:3249–54.
21. Dannenberg AL, Levy D, Garrison RJ. Impact of age on echocardio-graphic left ventricular mass in a healthy population. (The Framing-ham Study). Am J Cardiol 1989;64:1066–8.
22. Garavaglia GE, Messerli FH, Schmieder RE, et al. Sex differences incardiac adaptation to essential hypertension. Eur Heart J 1989;10:1110–4.
23. Lim WK, Wren B, Jepson N, et al. Effect of hormone replacementtherapy on left ventricular hypertrophy. Am J Cardiol 1999;83:1132–4.
24. Krumholz HM, Larson M, Levy D. Sex differences in cardiacadaptation to isolated systolic hypertension. Am J Cardiol 1993;72:310–3.
25. Carroll JD, Carroll EP, Feldman T, et al. Sex-associated differences inleft ventricular function in aortic stenosis of the elderly. Circulation1992;86:1099–107.
26. Douglas PS, Otto CM, Mickel MC, Labovitz A, Reid CL, Davis KB.Gender differences in left ventricular geometry and function in patientsundergoing balloon dilatation of the aortic valve for isolated aorticstenosis. Br Heart J 1995;73:548–54.
27. Leggett ME, Kuusisto J, Healy NL, et al. Gender differences in leftventricular function at rest and with exercise in asymptomatic aorticstenosis. Am Heart J 1996;131:94–100.
28. Aurigemma GP, Silver KH, McLaughlin M, et al. Left ventricularsystolic function in older patients with aortic stenosis: importance ofchamber geometry and gender. Am J Cardiol 1994;74:794–8.
29. Douglas PS, Katz SE, Weinberg EO, et al. Hypertrophic remodeling:gender differences in the early response to left ventricular pressureoverload. J Am Coll Cardiol 1998;32:1118–25.
30. Pfeffer JM, Pfeffer MA, Fletcher P, Braunwald E. Alterations ofcardiac performance in rats with established spontaneous hypertension.Am J Cardiol 1979;44:994–8.
31. Tamura T, Said S, Gerdes AM. Gender-related differences in myocyteremodeling in progression to heart failure. Hypertension 1999;33:676–80.
32. Weinberg EO, Thienelt CD, Katz SE, et al. Gender differences inmolecular remodeling in pressure overload hypertrophy. J Am CollCardiol 1999;34:264–73.
33. Grohe C, Kahlert S, Lobbert K, et al. Cardiac myocytes and fibroblastscontain functional estrogen receptors. FEBS Lett 1997;416:107–12.
34. Van Eickels M, Grohe C, Cleutjens JP, et al. 17beta-estradiolattenuates the development of pressure-overload hypertrophy. Circu-lation 2001;104:1419–23.
35. Haq S, Shoudroun G, Lim H, et al. Differential activation of signaltransduction pathways in human hearts with hypertrophy versusadvanced heart failure. Circulation 2001;103:670–7.
36. Xin H-B, Senbonmatsu T, Cheng D-S, et al. Oestrogen protectsFKBP 12.6 null mice from cardiac hypertrophy. Nature 2002;416:334–8.
37. Olivetti G, Giogano G, Corradi D, et al. Gender differences andaging: effects on the human heart. J Am Coll Cardiol 1995;26:1068–79.
38. Camper-Kirby D, Welch S, Walker A, et al. Myocardial Akt activa-tion and gender: increased nuclear activity in females versus males.Circ Res 2001;88:1020–7.
39. Hulley S, Grady D, Bush T, et al. Randomized trial of estrogen plusprogestin for secondary prevention of coronary heart disease inpostmenopausal women. Heart and Estrogen/progestin ReplacementStudy (HERS) Research Group. JAMA 1998;280:605–13.
40. Grady D, Herrington D, Bittner V, et al. Cardiovascular diseaseoutcomes during 6.8 years of hormone therapy: Heart and estrogen/progestin replacement study follow-up (HERS II). JAMA 2002;288:49–57.
41. Writing Group for the Women’s Health Initiative Investigators. Risksand benefits of estrogen plus progestin in healthy postmenopausalwomen: principal results from the Women’s Health Initiative random-ized controlled trial. JAMA 2002;288:321–33.
42. Dries DL, Rosenberg YD, Waclawiw MA, Domanski MJ. Ejectionfraction and risk of thromboembolic events in patients with systolicdysfunction and sinus rhythm: evidence for gender differences in theStudies of Left Ventricular Dysfunction Trials. J Am Coll Cardiol1997;29:1074–80.
43. Barrett-Connor E. Postmenopausal estrogen and prevention bias. AnnIntern Med 1991;115:455–6.
44. Petitti DB. Coronary heart disease and estrogen replacement therapy.Can compliance bias explain the results of observational studies? AnnEpidemiol 1994;4:115–8.
45. Gallagher EJ, Viscoli CM, Horwitz RI. The relationship of treatmentadherence to the risk of death after myocardial infarction in women.JAMA 1993;270:742–4.
46. Lenfant C. Fixing the failing heart. Circulation 1997;95:771–2.
1245JACC Vol. 42, No. 7, 2003 Lindenfeld et al.October 1, 2003:1238–45 HRT and Heart Failure

EDITORIAL COMMENT
New Hope for HormoneReplacement and the Heart?*Diana B. Petitti, MD, MPHPasadena, California
In this issue of the Journal, Lindenfeld et al. (1) report ananalysis examining the association between postmenopausalhormone replacement therapy (HRT) and survival inwomen with moderate to severe heart failure (HF). Thedata in the analysis are derived from the Beta-BlockerEvaluation of Survival Trial (BEST), which was a random-ized trial that compared the effect on survival of a nonse-lective beta-blocker, bucindolol, with that of placebo in menand women with moderate to severe HF (2). In the 435women who were 50 or more years of age, the adjustedprobability of survival 42 months after study entry was 58%in non-users of HRT and 78% in users. These results areconsistent with those of Reis et al. (3), who examined theassociation of postmenopausal HRT with survival in womenwith advanced HF based on pooled data from three trialscomparing vesnarinone with placebo. In the Reis et al. (3)analysis, 12 months after entry, survival was 73% in 897women who were non-users of HRT and 85% in 237 usersof HRT.
See page 1238
Until five years ago, postmenopausal HRT appeared tohold great promise in the primary and secondary preventionof coronary heart disease. Widespread use of postmeno-pausal hormones for “heart health” was based on data fromobservational studies that showed lower incidence andmortality from coronary disease in users of HRT who werefree of coronary disease and better survival in hormone userswith established coronary disease (4).
The 1998 publication of the results of the Heart andEstrogen/progestin Replacement study (HERS) (5)—a ran-domized, placebo-controlled trial of the effect of combinedestrogen/progestin HRT on coronary events in women withestablished coronary disease—followed closely by the pub-lication of the results of the Estrogen Replacement Athero-sclerosis (ERA) trial (6)—a randomized, placebo-controlledtrial of the effect of combined estrogen/progestin therapyand estrogen alone on progression of atherosclerosis—dampened enthusiasm for hormones in prevention of coro-nary disease. Lack of enthusiasm turned to downrightpessimism with the 2003 publication of further results fromHERS (7) and, more importantly, results of the combined
estrogen/progestin arm of the randomized trial componentof the Women’s Health Initiative (WHI) (8). This arm ofWHI, which involved more than 16,000 women, wasdesigned to test the effect of hormone replacement in theprimary prevention of coronary heart disease. It unexpect-edly found a significantly increased risk of coronary heartdisease in women assigned to combined estrogen/progestinHRT.
In spite of this gloomy picture, hope persists that estrogenalone—where WHI results are not yet available—or estro-gen/progestin combinations that were not used in WHI, orhormones initiated at ages earlier than in WHI might havea beneficial effect on some aspect of cardiovascular health(9). The data suggesting that postmenopausal hormonetherapy might affect survival in women with HF are sure tofuel this hope.
How should this analysis of HF be interpreted in thecontext of recent findings from randomized trials of HRT?Both Lindenfeld et al. (1) and Reis et al. (3) call for arandomized trial of HRT in women with HF. Is this thebest next step?
The use of data from randomized trials to exploreassociations with end points of factors that were not thesubject of the randomization capitalizes on the collection ofdata on prognostic factors in HF based on standardizedprotocols. Other positive features of well-conducted ran-domized trials, such as systematic monitoring of the qualityof data collection and careful verification of end points, carryover to these analyses. Notwithstanding these strengths inthe data from randomized trials, the comparison of hor-mone users with non-users is vulnerable to uncontrolled,and even controllable, confounding.
At entry to BEST, users of HRT differed from non-usersin many ways. They were younger, taller, less obese, andmore likely to be white, non-Hispanic. Their HF was morelikely to be nonischemic in origin, and they were less likelyto have history of hypertension and diabetes. Serum creat-inine, sodium, and ALT, all independent predictors ofmortality in patients with HF, were all significantly lower inhormone users than in non-users. Statistical adjustment wasused to try to take these differences into account in drawingconclusions about the effect of hormones on survival.
It has been suggested that “compliance bias” mightexplain the lower risk of coronary disease found in obser-vational studies of hormones and coronary disease (10).Preventive behaviors differ between hormone users andnon-users (11), leading to the hypothesis that “preventionbias” might explain the findings of observational studies.Lindenfeld et al. (1) attempt to eliminate compliance biasand prevention bias by including measures of health statusand compliance with treatment with study medication inBEST in a multivariate analysis.
It is doubtful that a measure of health status captures fullyall of the many possible differences in preventive behavior,health habits, and lifestyle between hormone users and
*Editorials published in the Journal of the American College of Cardiology reflect theviews of the authors and do not necessarily represent the views of JACC or theAmerican College of Cardiology.
From Kaiser Permanente Southern California, Pasadena, California.
Journal of the American College of Cardiology Vol. 42, No. 7, 2003© 2003 by the American College of Cardiology Foundation ISSN 0735-1097/03/$30.00Published by Elsevier Inc. doi:10.1016/C0735-1097(03)00939-2

non-users. Multivariate analysis does not adjust for what ispoorly measured. With so many measured differences be-tween the hormone users and non-users in BEST, there arealso likely to be unmeasured differences. Multivariate anal-ysis does not account for what is not measured. Bias due tocompliance arises not from a specific behavior but from apanoply of differences that are captured by the decision to becompliant. It is no surprise that adjustment for compliancedid not alter the relationship between hormone use andsurvival. Multivariate analysis does not adjust for what isunmeasurable. The discrepancy between observational stud-ies and randomized trials of hormone replacement forcoronary disease should teach us to be not just skeptical, butextremely skeptical, of the ability of statistical adjustment toyield valid conclusions about drug efficacy.
Lindenfeld et al. (1) provide an exhaustive review of thepossible mechanisms by which exogenous estrogen or pro-gestin might have a true biologic effect in decreasingmortality in women with HF. Absence of a mechanisticexplanation for the observed association would raise seriousquestions about whether the observation is real. However,mechanistic arguments must be viewed cautiously in light ofthe randomized trials. The hormone regimens used in therandomized trials examining coronary heart disease andmeasures of coronary atherosclerosis have extensive data toestablish a mechanism for a benefit in preventing coronarydisease and delaying progression of atherosclerosis, includ-ing favorable effects on total cholesterol, low-density li-poprotein cholesterol, high-density lipoprotein cholesterol,fibrinogen, and fasting insulin and glucose (12,13).
Data from both HERS and WHI show that combinedestrogen/progestin HRT at least doubles the risk of venousthromboembolism (8,14), and several observational studiesshow that estrogen alone also increases the risk of venousthromboembolic disease (15–17). In the WHI, the risk ofischemic stroke was also increased in users of combinedestrogen/progestin therapy (8). Given the high risk ofvenous thromboembolism and stroke in women with HF,concerns are sure to be raised about the ethics of a trial ofeither combined estrogen/progestin therapy or estrogenalone. Recruitment of women with HF to a trial is likely tobe challenging, even if deemed ethical.
Taken together, the results of the analysis of BEST andthe three vesnarinone trials do not provide much data uponwhich to select a regimen of hormone replacement for arandomized trial. Lindenfeld et al. (1) found no difference insurvival in users of combined estrogen/progestin therapycompared with estrogen alone. The analysis of data from thevesnarinone trials found a nonsignificant trend toward lessbenefit of combined estrogen/progestin therapy comparedwith estrogen alone. The statistical power of the comparisonof estrogen/progestin with estrogen alone was low in bothanalyses, and the data are compatible with large differencesin the effect of combined therapy compared with estrogenalone.
Lindenfeld et al. (1) make much of the fact that the
magnitude of the association between HRT and improvedsurvival was greater in women whose HF was nonischemicin origin (hazard ratio 0.35) than in women whose HF wasischemic (hazard ratio 0.74). The confidence intervals (CIs)for these estimates of HRT overlap (95% CI 0.14 to 0.87 fornonischemic HF; 95% CI 0.41 to 1.33 for ischemic HF),and the claim for a difference between any effect of HRT onsurvival in ischemic and nonischemic HF is very tentative.Importantly, the Reis et al. (3) analysis of data from thevesnarinone trials did not find any difference in the associ-ation of HRT with survival between ischemic and nonisch-emic HF.
The immediate practical importance of having moreclarity on this point is for the design of a randomized trialthat would address the question of a possible effect of HRTon survival in women with HF. A study that includes HF ofboth ischemic and nonischemic etiology would need to belarger than a study of one or the other type of HF and, thus,would be more expensive. Given the results of HERS,recruitment of women with HF with an ischemic etiology toa trial of hormone replacement would perhaps be moredifficult than recruitment of women with HF without anischemic etiology.
A number of relatively recent randomized trials of HF[e.g., OVERTURE (18), ATLAS (19), CIBIS II (20),IMPRESS (21)] included reasonably large numbers ofwomen. Analysis of data from other HF trials with infor-mation on HRT would be the most important next step toguide a decision about whether to conduct a randomizedtrial of hormone replacement in women with HF. Informa-tion from such analyses would permit design of the safestpossible trial that would enroll women with the types of HFthat are most likely to benefit from hormone use.
The HF data are a minor reprieve for hormones and theheart. Knowledge of the past suggests extreme caution, andclinical practice should not be changed based on thesefindings. The path from hormone replacement to cardio-vascular health is littered with plausible mechanisms, ele-gant models, consistent data, and anguished analysts.
Reprint requests and correspondence: Dr. Diana B. Petitti,Director of Research, Kaiser Permanente Southern California, 393East Walnut, Pasadena, California 91188. E-mail: [email protected].
REFERENCES
1. Lindenfeld J, Ghali JK, Krause-Steinrauf HJ, et al. Hormone replace-ment therapy is associated with improved survival in women withadvanced heart failure. J Am Coll Cardiol 2003;42:1238–45.
2. The Beta-Blocker Evaluation of Survival Trial Investigators. A trial ofthe beta-blocker bucindolol in patients with advanced chronic heartfailure. N Engl J Med 2001;344:1659–67.
3. Reis SE, Holubkov R, Young JB, White EG, Cohn JN, Feldman AM.Estrogen is associated with improved survival in aging women withcongestive heart failure: analysis of the vesnarinone studies. J Am CollCardiol 2000;36:529–33.
1247JACC Vol. 42, No. 7, 2003 PetittiOctober 1, 2003:1246–8 Editorial Comment

4. Stampfer MJ, Colditz GA. Estrogen replacement therapy and coro-nary heart disease: a quantitative assessment of the epidemiologicevidence. Prev Med 1991;20:47–63.
5. Hulley S, Grady D, Bush T, et al. Randomized trial of estrogen plusprogestin for secondary prevention of coronary heart disease inpostmenopausal women. Heart and Estrogen/progestin ReplacementStudy (HERS) Research Group. JAMA 1998;280:605–13.
6. Herrington DM, Reboussin DM, Brosnihan KB, et al. Effects ofestrogen replacement on the progression of coronary artery atheroscle-rosis. N Engl J Med 2000;343:522–9.
7. Grady D, Herrington D, Bittner V, et al. Cardiovascular diseaseoutcomes during 6.8 years of hormone therapy. Heart and Estrogen/progestin Replacement Study follow-up (HERS II). JAMA 2002;288:49–57.
8. Rossouw JE, Anderson GL, Prentice RL, et al. Risks and benefits ofestrogen plus progestin in healthy postmenopausal women: principalresults From the Women’s Health Initiative randomized controlledtrial. JAMA 2002;288:321–33.
9. Grodstein F, Clarkson TB, Manson JE. Understanding the divergentdata on postmenopausal hormone therapy. N Engl J Med 2003;348:645–50.
10. Petitti DB. Coronary heart disease and estrogen replacement therapy.Can compliance bias explain the results of observational studies? AnnEpidemiol 1994;4:115–8.
11. Barrett-Connor E. Postmenopausal estrogen and prevention bias. AnnIntern Med 1991;115:455–6.
12. Espeland MA, Hogan PE, Fineberg SE, et al. Effect of postmeno-pausal hormone therapy on glucose and insulin concentrations. PEPIInvestigators. Postmenopausal Estrogen/Progestin Interventions. Di-abetes Care 1998;21:1589–95.
13. The Writing Group for the PEPI Trial. Effects of estrogen orestrogen/progestin regimens on heart disease risk factors in postmeno-pausal women. The Postmenopausal Estrogen/Progestin Interventions(PEPI) trial. JAMA 1995;273:199–208.
14. Grady D, Wenger NK, Herrington D, et al. Postmenopausal hormonetherapy increases risk for venous thromboembolic disease. The Heartand Estrogen/progestin Replacement Study. Ann Intern Med 2000;132:689–96.
15. Daly E, Vessey MP, Hawkins MM, Carson JL, Gough P, Marsh S.Risk of venous thromboembolism in users of hormone replacementtherapy. Lancet 1996;348:977–80.
16. Jick H, Derby LE, Myers MW, Vasilakis C, Newton KM. Risk ofhospital admission for idiopathic venous thromboembolism amongusers of postmenopausal oestrogens. Lancet 1996;348:981–3.
17. Perez GS, Garcia Rodriguez LA, Castellsague J, Duque OA. Hor-mone replacement therapy and risk of venous thromboembolism:population based case-control study. BMJ 1997;314:796–800.
18. Packer M, Califf RM, Konstam MA, et al. Comparison of omapatrilatand enalapril in patients with chronic heart failure: the OmapatrilatVersus Enalapril Randomized Trial of Utility in Reducing Events(OVERTURE). Circulation 2002;106:920–6.
19. Packer M, Poole-Wilson PA, Armstrong PW, et al. Comparativeeffects of low and high doses of the angiotensin-converting enzymeinhibitor, lisinopril, on morbidity and mortality in chronic heartfailure. ATLAS Study Group. Circulation 1999;100:2312–8.
20. The Cardiac Insufficiency Bisoprolol Study II (CIBIS-II): a random-ised trial. Lancet 1999;353:9–13.
21. Rouleau JL, Pfeffer MA, Stewart DJ, et al. Comparison of vasopep-tidase inhibitor, omapatrilat, and lisinopril on exercise tolerance andmorbidity in patients with heart failure: IMPRESS randomised trial.Lancet 2000;356:615–20.
1248 Petitti JACC Vol. 42, No. 7, 2003Editorial Comment October 1, 2003:1246–8

Left Atrial Appendage Obliteration in Atrial Fibrillation
Thoracoscopic Extracardiac Obliterationof the Left Atrial Appendage forStroke Risk Reduction in Atrial FibrillationJoseph L. Blackshear, MD,* W. Dudley Johnson, MD,† John A. Odell, MD,* Vickie S. Baker, RN,*Mary Howard, RN,† Lesly Pearce, MS,‡ Christopher Stone, MD,† Douglas L. Packer, MD,§Hartzell V. Schaff, MD§Jacksonville, Florida; Milwaukee, Wisconsin; Minot, North Dakota; and Rochester, Minnesota
OBJECTIVES We evaluated left atrial appendage obliteration in high-risk patients with atrial fibrillation(AF).
BACKGROUND Left atrial appendage thrombosis and embolization is the principal mechanism of stroke inAF. Anticoagulation is underutilized and often contraindicated.
METHODS Thoracoscopic Left Appendage, Total Obliteration, No cardiac Invasion (LAPTONI) wasundertaken with a loop snare in eight patients and a stapler in seven patients, median age 71years, with clinical risk factors for stroke and with an absolute contraindication to or failureof prior thrombosis prevention with warfarin. Eleven patients had a history of priorthromboembolism. One patient took sustained warfarin during follow-up.
RESULTS The LAPTONI procedure was completed in 14 of 15 patients, and 1 patient required urgentconversion to open thoracotomy because of bleeding. Patients have been followed up for 8 to60 months, mean 42 � 14 months. One fatal stroke occurred 55 months after surgery, andone non-disabling stroke three months after surgery. Two other deaths occurred, one aftercoronary bypass surgery and the other from hepatic failure. The subgroup of 11 patients withprior thromboembolism had an annualized rate of stroke of 5.2% per year (95% confidenceinterval [CI] 1.3 to 21) after LAPTONI, which compares to a rate of 13% per year (95% CI9.0 to 19) for similar aspirin-treated patients from the Stroke Prevention in Atrial Fibrillationtrials (p � 0.15).
CONCLUSIONS The LAPTONI procedure appears technically feasible without immediate disabling neuro-logic morbidity or mortality, and it demonstrates low post-operative event rates and astatistical trend toward thromboembolic risk reduction in high-risk AF patients. (J Am CollCardiol 2003;42:1249–52) © 2003 by the American College of Cardiology Foundation
The stroke rate in patients with atrial fibrillation (AF) olderthan 75 years of age is 8.1% per year with one clinical risk factorand is 12% per year at any age in clinical trial populations witha history of prior thromboembolism (1,2). Three-year strokerates in elderly nursing home patients not anticoagulated are inexcess of 50% (3). Fear of hemorrhagic complications preventsutilization of anticoagulation in these high-risk patients.
See page 1259
Most thrombi in non-rheumatic AF originate in the leftatrial (LA) appendage (4), suggesting the origin of throm-boembolism (5). Left atrial appendage obliteration is com-monly performed in a variety of cardiac surgical operations,but its feasibility and value as a stand-alone stroke preven-tative strategy is undefined. A catheter-based LA appendageoccluder device has recently been developed and tested in
animals, and a first group of humans has undergone deviceimplantation (6). However, there are no data to support thehypothesis that appendage obliteration reduces stroke. Wepresent data on isolated surgical obliteration of the LAappendage in 15 patients with a mean follow-up in excess ofthree years. Data on seven of these patients were previouslypublished shortly after surgery (7).
METHODS
Patient population. Patients at two medical centers withchronic or intermittent AF were identified from routineclinical practice with at least one risk factor for stroke (priorthromboembolism, hypertension, age �75 years, left ven-tricular dysfunction, or diabetes mellitus) and either anabsolute contraindication to warfarin or documentation ofprior LA appendage thrombosis despite adequate oral an-ticoagulation. The protocol was approved by the institu-tional review boards of both institutions.Thoracoscopic closure of the LA appendage. Informedconsent was obtained before surgery. Each patient wasanesthetized and intubated with a double lumen endotra-cheal tube. Transesophageal echocardiography (TEE) con-
From the *Mayo Clinic Jacksonville, Jacksonville, Florida; †W. Dudley JohnsonHeart Care Center, Milwaukee, Wisconsin; ‡Biostatistical Consultant, Minot, NorthDakota; §Mayo Clinic, Rochester, Minnesota. Supported by grants from EthiconEndosurgery and the Mayo Foundation for Medical Research.
Manuscript received December 5, 2002; revised manuscript received January 30,2003, accepted February 20, 2003.
Journal of the American College of Cardiology Vol. 42, No. 7, 2003© 2003 by the American College of Cardiology Foundation ISSN 0735-1097/03/$30.00Published by Elsevier Inc. doi:10.1016/S0735-1097(03)00953-7

firmed the absence of LA appendage thrombus at the timeof surgery. Patients were positioned, prepared, and drapedas for a left or left-lateral thorocotomy. Three to fivethoracoscopic incisions were made to introduce the video-assisted thoracoscopic instruments. Using a double-lumenendotracheal tube, the volume of the left lung was reduced.Up to 4 cm pressure CO2 insufflation in the left pleuralspace was used specifically to reduce or eliminate thepotential for air embolus in the event of an inadvertent tear.The pericardium was opened with scissors at a site parallelto the phrenic nerve. The atrial appendage tip was graspedusing a non-traumatic clamp, and an endoloop snare wasfixed as a tie to the appendiceal tip. A second endoloop wasintroduced over the first tie and manipulated with theassistance of instruments to the appendiceal base, where itwas cinched to occlude the appendage. Alternatively, a rowof staples was placed. Occlusion was documented by TEEas the abrupt appearance of dense, stationary, high-contrastechoes (Fig. 1). At the conclusion of the procedure, thepericardium was left open, the CO2 was evacuated, and tubethoracoscopy suction was employed.Follow-up. Patients were regularly contacted after theprocedure and questioned regarding neurologic symptoms.Contact was by telephone interview at six-month intervals.Medical records from hospitalizations were reviewed. The
protocols did not include late imaging for verification ofpersistent occlusion of the LA appendage.Statistical methods. Patient exposure for stroke was com-puted as the number of days from LAPTONI to date of firststroke, with exposure censored on the date of death or lastday of follow-up if no stroke occurred. Similarly, patientexposure for death was computed as the number of daysfrom LAPTONI to the date of death, with censorship onthe last day of follow-up. Overall event rates were calculatedby dividing the number of events by the total patientobservation, with 95% confidence intervals calculated usinga Poisson distribution. Survival curves were computed usingthe Kaplan-Meier method and compared to reference pop-ulations. All statistical tests were two-sided, and statisticalsignificance was accepted at the 0.05 level.
RESULTS
Patients’ characteristics are listed in Table 1. Ages variedfrom 24 to 81 years, mean � SD 67 � 15 years, median 71years. Eleven patients had a history of prior thromboembo-lism, 12 had a history of hypertension, and 11 had bleedingdiatheses including five with prior intracranial hemorrhageand one with prior meningioma surgery. Hospital length ofstay varied with from two to 20 days. Post-operativecomplications included bleeding from a torn accessory atrialappendage, necessitating urgent thoracotomy in one patient.One patient with hypertrophic nonobstructive cardiomyop-athy experienced refractory pump failure and a prolongedintensive care unit stay after the procedure. One patient hadatelactasis, one had prolonged air leak, one underwentinvestigation and treatment of genitourinary bleeding, andone had chronic pleuritic pain. There were no peri-operativeneurologic events.
Median follow-up duration was 42 months. During thistime, two strokes—one non-disabling and one fatal—
Abbreviations and AcronymsAF � atrial fibrillationAFI � Atrial Fibrillation InvestigatorsEAFT � European Atrial Fibrillation TrialLA � left atrialLAPTONI � Left Appendage Total Obliteration,
No cardiac InvasionSPAF � Stroke Prevention in Atrial FibrillationTEE � transesophageal echocardiography
Figure 1. Intraoperative transesophageal echocardiographic images of the left atrial appendage before (left) and after (right) LAPTONI.
1250 Blackshear et al. JACC Vol. 42, No. 7, 2003Thoracoscopic Atrial Appendage Obliteration October 1, 2003:1249–52

occurred. One patient with a history of multiple priorstrokes had a small stroke during hospitalization for pneu-monia. He made a complete recovery and remains well 40months after surgery. One patient, age 79 at surgery, withprior stroke, congestive heart failure, severe left ventriculardysfunction, and multiple subdural hematomas, suffered afatal stroke and intracranial hemorrhage 55 months aftersurgery. One patient died after coronary bypass surgery,performed 34 months after LAPTONI. One patient withchronic hepatitis C, variceal and small intestinal blood loss,and prior systemic embolism died from hepatic failure.Overall rate of stroke was 4.0% per patient-year, 95%confidence interval (CI) 1.0 to 16. Rate of fatal stroke was2.0% per patient-year, 95% CI 0.3 to 13. Rate of death orstroke was 6.0% per patient-year, 95% CI 2.0 to 19. Amongthe 11 patients with a history of prior thromboembolism,stroke rate was 5.2% per year, 95% CI 1.3 to 21, whichcompares to 13% per year, 95% CI 9.0 to 19 in aspirin-treatedpatients with prior thromboembolism in the Stroke Preventionin Atrial Fibrillation (SPAF) studies (p � 0.15, not significant)(8). In four patients without a history of prior stroke, the strokerate was 0% per year after LAPTONI, compared to a rate of2.6% per year, 95% CI 1.9 to 3.6% per year rate of stroke inSPAF (not statistically significant). Figure 2 presents cumula-tive freedom from thromboembolism with comparison to ratesin prior studies of similar patients (1,2).
DISCUSSION
The recent publication of a catheter-based LA appendageoccluder device and its use in 30 patients (6) and the absenceof data supporting the safety and efficacy of such a procedureprovided us the impetus to present our results. Our two-center experience utilized surgical appendage obliterationwith either a loop snare or a stapler, with placement of theocclusion device at the appendiceal base. Pre-clinical expe-
rience with both techniques documented a smooth LAarchitecture with complete obliteration (9). The site ofclosure is similar to that documented with the transvascularoccluder (6)—but without the foreign body in immediatecontact with the circulation. Although underpowered forstatistical significance, the observed event rate in our seriesof patients with a history of prior thormboembolism isconsistent with the benefits proposed for appendage oblit-eration. This observation would appear to support thefurther development and testing of strategies to reducestroke risk in this highest risk segment of the AF population
Table 1. Patient Characteristics and Outcomes
Age/Gender Prior TE Htn ICHGI/GU
Bleed/Ulcer LOSMonths Free of
Thomboembolism
Months Free ofDeath or DisablingThomboembolism
81/M* yes no no yes 10 d 46 4679/F yes no yes no 5 d 60 6063/M yes yes yes no 3 d 60 6079/M yes yes no no 3 d 58 5856/F yes no no yes 10 d 54 5479/M† yes yes yes yes 2 d 55 5570/F no yes yes no 6 d 29 2976/M yes yes yes no 3 d 8 863/M yes yes no no 7 d 41 4178/M‡ yes yes no§ no 20 d 3 4071/M no yes no yes 3 d 38 3850/M yes yes no no 4 d 38 3824/F yes yes no no 5 d 37 3774/M� no yes no yes 12 d 34 3469/M no yes no yes 7 d 34 34
*Died of hepatic failure, †Fatal stroke 55 months after surgery, ‡Nondisabling stroke 3 months after surgery with full recovery, alive and well 40 months after surgery, §Priorsurgery for meningioma, �Died after coronary bypass surgery done 34 months after first surgery.
Htn � hypertension; ICH � intracranial hemorrhage; GI/GU � gastrointestinal/genitourinary; LOS � length of stay; TE � thromboembolism.
Figure 2. Cumulative proportion of 15 patients with atrial fibrillation (AF)after surgical left atrial appendage obliteration (LAPTONI) withoutthromboembolism (straight line). The reference lines are based onthromboembolism rates for non-anticoagulated AF patients aged 65 to 75years in the Atrial Fibrillation Investigators’ (AFI) meta-analysis with atleast one risk factor (upper dashed line) (1) and for non-anticoagulated AFpatients of any age with a history of prior thromboembolism in AFI andthe European Atrial Fibrillation Trial (EAFT) (bottom dashed line) (1,2).
1251JACC Vol. 42, No. 7, 2003 Blackshear et al.October 1, 2003:1249–52 Thoracoscopic Atrial Appendage Obliteration

(1,2) in whom the preferred therapy, anticoagulation, iscontraindicated or has previously been insufficient to pre-vent embolism. Clearly the magnitude of risk varies but maybe very high. In a study of secondary stroke prevention inAF, non-anticoagulated patients had a 17% per year rate ofstroke or death (2). Age, itself a significant AF stroke riskfactor, was lower in the anticoagulation clinical trials thanthe AF population median of 75 years, suggesting thatclinical trial data underestimate the true risk for this group.Consistent with this, Aronow et al. (3) described 312persons with AF with an average age of 84 years whoresided in a chronic care facility. Rates of stroke over threeyears in those not anticoagulated were 56% in those with noprior history of thromboembolism and 81% in those withprior history of thromboembolism (3).
Definitive proof that appendage obliteration by anytechnique reduces the risk of thromboembolism can beobtained only through a randomized clinical trial. However,data from Cox et al. (10) support the hypothesis thatappendage ligation, a part of the maze procedure, may beeffective in preventing stroke. More than 40% of patientswho undergo the maze operation have transient post-operative AF, yet only those with mitral valve replacement,mechanical aortic valve replacement, or Benthall procedureare routinely anticoagulated. Despite this high rate ofpost-operative AF, the rate of post-operative stroke in themaze procedure population was 0.7% (10). Rates of peri-operative stroke for coronary bypass associated AF withoutmaze vary from 2% to 7% (11), and post-operative AF wasa highly significant independent predictor of stroke in thestudy of Stamou et al. (12). In addition, despite somereduction in atrial function in a portion of the post-mazepopulation, during follow-up of between three months and11.5 years, the stroke rate has been 0.4% (10). Patientsundergoing maze surgery were relatively young and probablyhad a lower intrinsic risk of thromboembolism.Study limitations. The obvious limitation of this study isthe small numbers of study patients, yielding very wide CIsfor event rates and preventing a definitive statement regard-ing efficacy. While they suggest a trend toward benefit, theevent rates after LAPTONI fall within the confidence limitsreported in clinical trials with aspirin or no therapy. Second,the absence of a simultaneous randomized control groupprevents a truly accurate assessment of risk reduction.Despite the absence of mortality or neurologic morbidityfrom LAPTONI in the short term, we did experiencesignificant, although not unexpected, non-stroke morbidityin our small series, suggesting that refinements in theprocedure or more careful patient selection may be required.Cardiac failure in our patient with hypertrophic cardiomy-opathy, and the prior report from Cox et al. that two of 10peri-operative deaths in patients undergoing the mazeprocedure occurred in patients with hypertrophic cardiomy-opathy (10), suggest that these patients should be excludedfrom the initial application of this procedure.
Conclusions. Surgery to prevent stroke is widely accepted,as in the case of carotid endarterectomy. Our initial humanexperience with LAPTONI in AF documents that it istechnically feasible to perform this procedure without car-diac invasion, in a relatively elderly population at substantialrisk for AF-related stroke, without producing any disablingneurologic morbidity in the short term. Our study differsfrom the endovascular approach thus far described (6), inthat our patients had higher estimated risk, that no cardiacinvasion or intracardiac foreign body was placed, and thatno immediate post-procedure antithrombotic therapy wasutilized. A statistical trend toward benefit in our patientswith prior thromboembolism was demonstrated with anaverage follow-up of 42 months. These data provide supportfor the further development of this or other techniques forappendage obliteration, in hopes of providing an effectiveprophylaxis for patients with the highest risk and absolutecontraindications to, or proven inefficacy of, anticoagulation.
Reprint requests and correspondence: Dr. Joseph L. Blackshear,Mayo Clinic Jacksonville, 4500 San Pablo Road, Jacksonville,Florida 32224. E-mail: [email protected].
REFERENCES
1. Atrial Fibrillation Investigators. Risk factors for stroke and efficacy ofantithrombotic therapy in atrial fibrillation. Analysis of pooled datafrom five randomized controlled trials. Arch Intern Med 1994;154:1449–57.
2. EAFT (European Atrial Fibrillation Trial) Study Group. Secondaryprevention in non-rheumatic atrial fibrillation after transient ischaemicattack or minor stroke. Lancet 1993;342:1255–62.
3. Aronow WS, Ahn C, Kronzon I, et al. Incidence of new thrombo-embolic stroke in persons 62 years and older with chronic atrialfibrillation treated with warfarin versus aspirin. J Am Geriatr Soc1999;47:366–8.
4. Blackshear JL, Odell JA. Appendage obliteration to reduce stroke incardiac surgical patients with atrial fibrillation. Ann Thorac Surg1996;61:755–9.
5. Hart RG, Halperin JL. Atrial fibrillation and stroke. Revisiting thedilemmas. Stroke 1994;25:1337–41.
6. Sievert H, Lesh MD, Trepels T, et al. Percutaneous left atrialappendage transcatheter occlusion to prevent stroke in high-riskpatients with atrial fibrillation: early clinical experience. Circulation2002;105:1887–9.
7. Johnson WD, Ganjoo AK, Stone CD, et al. The left atrial appendage:our most lethal human attachment! Surgical implications. Eur J Car-diothorac Surg 2000;17:718–22.
8. Hart RG, Pearce LA, McBride R, et al. Factors associated withischemic stroke during aspirin therapy in atrial fibrillation: analysis of2012 participants in the SPAF I-III clinical trials. The StrokePrevention in Atrial Fibrillation (SPAF) Investigators. Stroke 1999;30:1223–9.
9. Odell JA, Blackshear JL, Davies E, et al. Thoracoscopic obliteration ofthe left atrial appendage: potential for stroke reduction? Ann ThoracSurg 1996;61:565–9.
10. Cox JL, Ad N, Palazzo T. Impact of the maze procedure on the strokerate in patients with atrial fibrillation. J Thorac Cardiovasc Surg1999;118:833–40.
11. Blackshear JL. Prevention of thromboembolism in patients with newonset or recently discovered atrial fibrillation. Cardiac ElectrophysiolRev 1997;1:32–9.
12. Stamou SC, Hill PC, Dangas G, et al. Stroke after coronary arterybypass: incidence, predictors, and clinical outcome. Stroke 2001;32:1508–13.
1252 Blackshear et al. JACC Vol. 42, No. 7, 2003Thoracoscopic Atrial Appendage Obliteration October 1, 2003:1249–52

Role of Left Atrial AppendageObliteration in Stroke Reductionin Patients With Mitral Valve ProsthesisA Transesophageal Echocardiographic StudyMiguel Angel Garcıa-Fernandez, MD, PHD, Esther Perez-David, MD, Juan Quiles, MD,Juan Peralta, MD, Ismael Garcıa-Rojas, MD, Javier Bermejo, MD, Mar Moreno, MD, Jacobo Silva, MDMadrid, Spain
OBJECTIVES The aim of our study was to assess whether left atrial appendage (LAA) ligation in patientsundergoing mitral valve replacement is associated with the risk of future embolisms.
BACKGROUND Previous studies show that the LAA plays an important role in the development ofintracardiac thrombus. According to this decisive role, LAA surgical closure in patientsundergoing cardiac surgery may be an attractive choice for reducing stroke.
METHODS We retrospectively studied 205 patients with previous mitral valve replacement and referredfor echocardiography study. Patients were excluded if other causes of systemic embolism werefound. The main outcome measure was the occurrence of an embolic event.
RESULTS Ligation of LAA was performed in 58 patients. However, an incomplete ligation was verifiedin six patients. During a median time from valve replacement to echocardiography study of69.4 months (1 to 329), 27 patients had an embolism. Multivariate analysis identified theabsence of LAA ligation (odds ratio [OR] 6.7 [95% confidence interval {CI} 1.5 to 31.0]; p �0.02) and the presence of left atrial thrombus as the only independent predictors of occurrenceof an embolic event. Moreover, when the identification of an incomplete LAA ligation wasconsidered together with the absence of LAA ligation, risk of embolism increased up to11.9 � (OR 11.9 [95% CI 1.5 to 93.6]; p � 0.02).
CONCLUSIONS Our study shows that LAA ligation during surgery of mitral valve replacement, performed ina high-risk population, is consistent with a reduction of the risk of late embolism and supportsthis technique if a mitral valve replacement is indicated. (J Am Coll Cardiol 2003;42:1253–8) © 2003 by the American College of Cardiology Foundation
The left atrial appendage (LAA) plays a fundamental role inthe formation of atrial thrombus in patients with atrialfibrillation (AF). In patients with nonrheumatic AF, LAAis the origin of at least 90% of all left atrial (LA) clots (1–3),and the resulting systemic emboli cause approximately 25%of all strokes (4,5). Moreover, in patients in sinus rhythm inwhom an LA thrombus was diagnosed with standardechocardiography, LAA location was involved in 95% of thecases (6).
See page 1259
Transesophageal echocardiography (TEE) is the gold-standard diagnostic method for the detection of thrombusin the LAA. The size of the LAA, the reduction of LAAflow velocities (7–11), and the detection of spontaneousecho contrast in either the LA or the LAA have beensuggested as markers of increased embolism risk (12–16).
According to the decisive role of LAA in thrombusformation, LAA surgical ligation in patients undergoingcardiac surgery may be an attractive choice for reducingstroke risk (17,18). In addition, LAA closure can be nowachieved through different approaches such as thoracoscopic
LAA ligation (19) and, more recently, percutaneous LAAocclusion (20,21).
However, to our knowledge, no prior study in a large andhomogeneous population has analyzed the role of LAAligation in the prevention of strokes or systemic embolicphenomena after a surgical intervention. As a result, inter-mittent and unsystematic LAA ligation is performed bysurgeons worldwide. We hypothesized that LAA ligationwould be associated with lower stroke risk and designed aretrospective study of patients undergoing mitral valvereplacement. The aim of our study was to assess whetherLAA ligation is associated with the risk of future embolism.
METHODSStudy population. A total of 242 patients with prior mitralvalve replacement, referred to our echocardiography labora-tory from February 1996 to October 2001, were included forthe study. Patients were referred for echocardiography bytheir physician and were both studied with transthoracicand TEE. The indications for referral were 82 patients forquantification of mitral valve regurgitation, 48 patients thatwere investigated for suspected mitral valve endocarditis, 42patients for investigation of an embolic source, 30 patientsfor evaluation of right or left ventricular function, 25patients for further evaluation of a detected increase inmitral prosthesis diastolic gradient, and 15 patients werestudied for miscellaneous indications.
From the Seccion de Cardiologıa No Invasiva, Servicio de Cardiologıa, HospitalGeneral Universitario Gregorio Maranon, Madrid, Spain. Presented, in part, at the75th Scientific Session of the American Heart Association, Chicago, November 2002.
Manuscript received February 7, 2003; revised manuscript received April 22, 2003,accepted May 9, 2003.
Journal of the American College of Cardiology Vol. 42, No. 7, 2003© 2003 by the American College of Cardiology Foundation ISSN 0735-1097/03/$30.00Published by Elsevier Inc. doi:10.1016/S0735-1095(03)00954-9

Patients were excluded if other potential causes of sys-temic embolism were found in the echocardiographic study:thrombotic occlusion of the prosthetic valve (n � 11),confirmed endocarditis (n � 9), aortic dissection (n � 1),and if an extracardiac source were found to be the origin ofthe embolism (n � 16).
The final study group consisted of 205 patients (130women) with a mean age of 62.4 years. The reason for themitral valve replacement was rheumatic valve disease in 170patients, mitral valve endocarditis in 10 patients, severeischemic regurgitation in 6 patients, and mitral valve pro-lapse in 19 patients. All patients with mechanical prosthesesunderwent anticoagulation treatment with acenocumarin,and those with biological valves were either anticoagulatedor received antiplatelet therapy.Study flow. Retrospective analysis of the patients aftermitral valve replacement was supported by a review ofpatient records. Main outcome measure was the occurrenceof an embolic event, considering only those appearing after48 h of the surgery. An embolic event was defined by thepresence of clinical signs and the verification with at leastone of the following diagnostic tools: computed tomography(neurological events) or angiography and/or surgery (pe-ripheral artery events).
The clinical diagnosis of an embolic transient ischemicattack, or stroke, was made by a neurologist. Those patientswith deficits in the posterior cerebral circulation territory orwith lacunar strokes were excluded.Echocardiography. Conventional transthoracic echocardi-ography was performed with either a Sonos 5500 (PhilipsTechnologies, Andover, Massachusetts) or an Acuson Se-
quoia 256 (Siemens Technologies, Mountain View, Cali-fornia) using a phased array transducer. Transesophagealechocardiography was performed using an omniplane probein 182 patients and with a biplane TEE probe in theremaining patients.
Cardiac structures and the aorta were visualized frommultiple esophageal and transgastric views. Prosthetic mitralvalve area was estimated using the pressure half-timemethod (22). Mitral regurgitation jet was visualized usingcolor Doppler flow and graded to determine the severity ofmitral regurgitation by a previously validated method (23).Maximal LAA areas were measured by tracing a line fromthe top of the upper pulmonary vein limbus along the entireendocardial LAA border (8).
The LA and LAA were closely inspected for the presenceof thrombi and spontaneous echo contrast. The severity ofLAA spontaneous echo contrast (LASEC) was graded from0 to 4 following the classification of Fatkin et al. (24).Surgical ligation of the LAA was clearly identified by thelack of any anatomical structure between the mitral valvebase and the upper left pulmonary artery (25) (Fig. 1A and1B). Incomplete ligation was diagnosed by color Dopplerflow, demonstrating a jet traversing the separation betweenLAA and the LA body (25) (Fig. 2).Statistical analysis. Data are expressed as mean � SD.Proportions were compared with the chi-square test. If anyof the cells from a 2 � 2 table had an expected count below5, then a Fisher exact test was applied. Quantitative vari-ables were normally distributed and compared with aStudent t test. The independent contribution of the poten-tial factors involved in embolism was analyzed with alogistic regression. In the multiple regression analysis, thedependent variable was the occurrence of an embolic event,and the independent variables were those that showed, onunivariate analysis, a significant correlation with the occur-rence of an embolic event as well as variables that showed atrend (p � 0.25) and those with well-known clinicalrelevance. Differences were considered to be statisticallysignificant if the null hypothesis could be rejected with
Abbreviations and AcronymsAF � atrial fibrillationLA � left atrial/atriumLAA � left atrial appendageLASEC � left atrial appendage spontaneous echo
contrastTEE � transesophageal echocardiography
Figure 1. (A) Transesophageal echocardiogram in a patient with Saint Jude medical prosthesis in mitral position and without ligation of the left atrialappendage (LAA) (arrows). (B) Postoperative transesophageal echocardiographic study showing the absence of the LAA with complete obliteration of thecavity (arrows). LA � left atrium; P � prosthesis.
1254 Garcıa-Fernandez et al. JACC Vol. 42, No. 7, 2003Left Atrial Appendage Ligation Reduces Stroke Risk October 1, 2003:1253–8
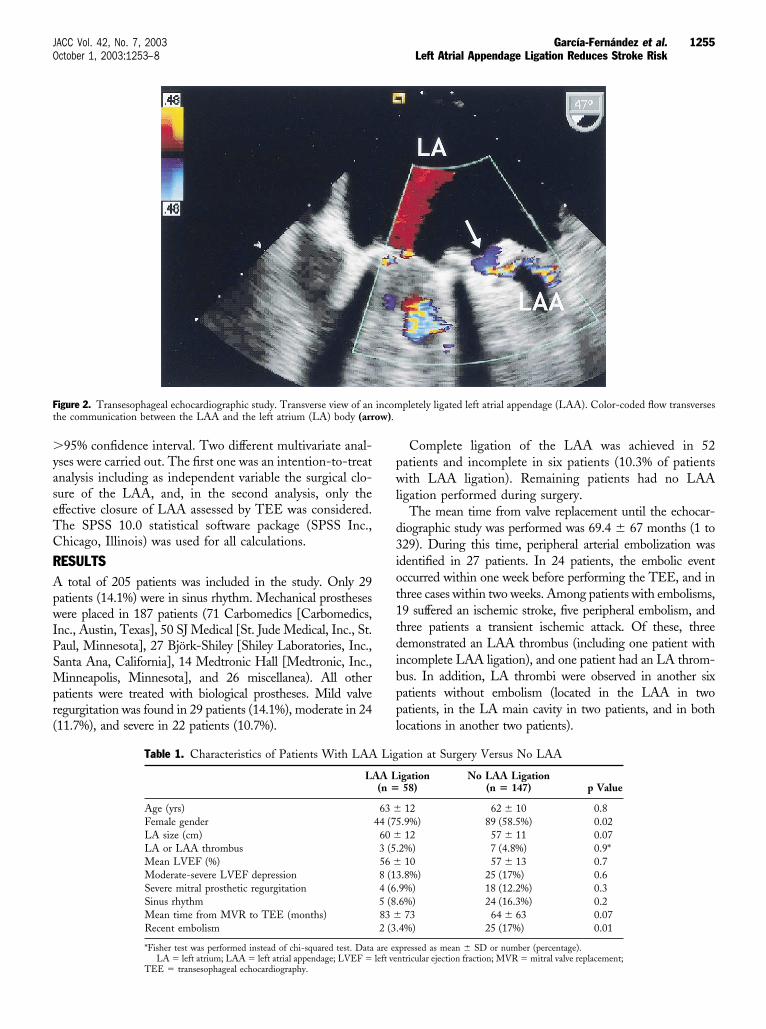
�95% confidence interval. Two different multivariate anal-yses were carried out. The first one was an intention-to-treatanalysis including as independent variable the surgical clo-sure of the LAA, and, in the second analysis, only theeffective closure of LAA assessed by TEE was considered.The SPSS 10.0 statistical software package (SPSS Inc.,Chicago, Illinois) was used for all calculations.
RESULTSA total of 205 patients was included in the study. Only 29patients (14.1%) were in sinus rhythm. Mechanical prostheseswere placed in 187 patients (71 Carbomedics [Carbomedics,Inc., Austin, Texas], 50 SJ Medical [St. Jude Medical, Inc., St.Paul, Minnesota], 27 Bjork-Shiley [Shiley Laboratories, Inc.,Santa Ana, California], 14 Medtronic Hall [Medtronic, Inc.,Minneapolis, Minnesota], and 26 miscellanea). All otherpatients were treated with biological prostheses. Mild valveregurgitation was found in 29 patients (14.1%), moderate in 24(11.7%), and severe in 22 patients (10.7%).
Complete ligation of the LAA was achieved in 52patients and incomplete in six patients (10.3% of patientswith LAA ligation). Remaining patients had no LAAligation performed during surgery.
The mean time from valve replacement until the echocar-diographic study was performed was 69.4 � 67 months (1 to329). During this time, peripheral arterial embolization wasidentified in 27 patients. In 24 patients, the embolic eventoccurred within one week before performing the TEE, and inthree cases within two weeks. Among patients with embolisms,19 suffered an ischemic stroke, five peripheral embolism, andthree patients a transient ischemic attack. Of these, threedemonstrated an LAA thrombus (including one patient withincomplete LAA ligation), and one patient had an LA throm-bus. In addition, LA thrombi were observed in another sixpatients without embolism (located in the LAA in twopatients, in the LA main cavity in two patients, and in bothlocations in another two patients).
Figure 2. Transesophageal echocardiographic study. Transverse view of an incompletely ligated left atrial appendage (LAA). Color-coded flow transversesthe communication between the LAA and the left atrium (LA) body (arrow).
Table 1. Characteristics of Patients With LAA Ligation at Surgery Versus No LAA
LAA Ligation(n � 58)
No LAA Ligation(n � 147) p Value
Age (yrs) 63 � 12 62 � 10 0.8Female gender 44 (75.9%) 89 (58.5%) 0.02LA size (cm) 60 � 12 57 � 11 0.07LA or LAA thrombus 3 (5.2%) 7 (4.8%) 0.9*Mean LVEF (%) 56 � 10 57 � 13 0.7Moderate-severe LVEF depression 8 (13.8%) 25 (17%) 0.6Severe mitral prosthetic regurgitation 4 (6.9%) 18 (12.2%) 0.3Sinus rhythm 5 (8.6%) 24 (16.3%) 0.2Mean time from MVR to TEE (months) 83 � 73 64 � 63 0.07Recent embolism 2 (3.4%) 25 (17%) 0.01
*Fisher test was performed instead of chi-squared test. Data are expressed as mean � SD or number (percentage).LA � left atrium; LAA � left atrial appendage; LVEF � left ventricular ejection fraction; MVR � mitral valve replacement;
TEE � transesophageal echocardiography.
1255JACC Vol. 42, No. 7, 2003 Garcıa-Fernandez et al.October 1, 2003:1253–8 Left Atrial Appendage Ligation Reduces Stroke Risk
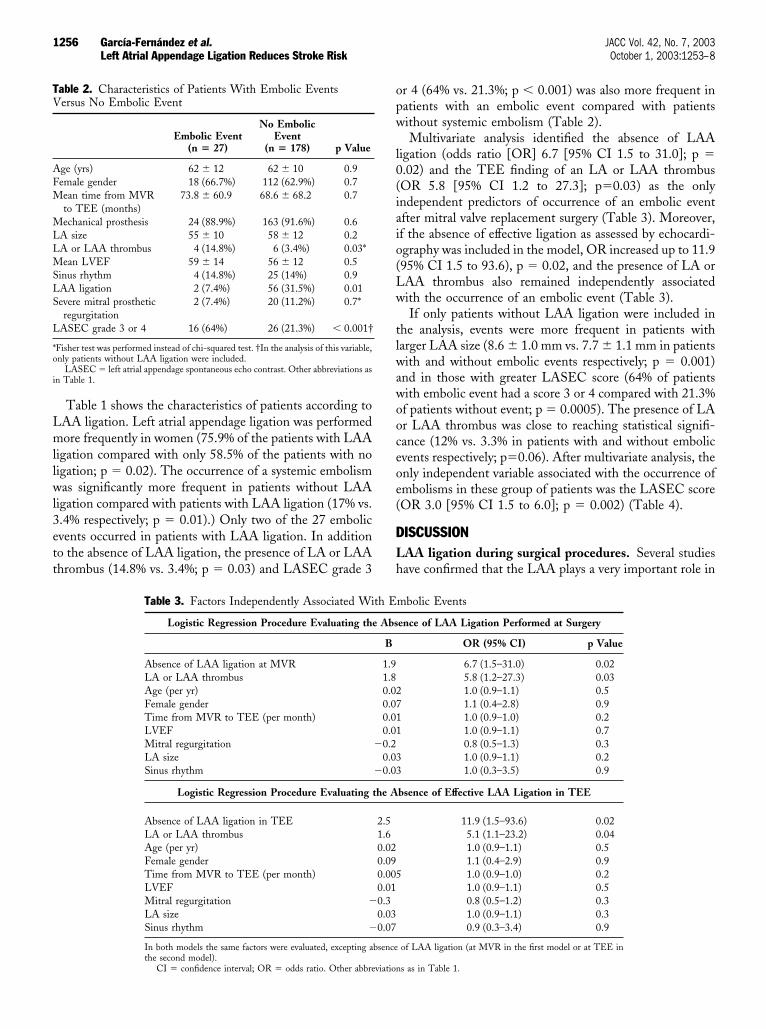
Table 1 shows the characteristics of patients according toLAA ligation. Left atrial appendage ligation was performedmore frequently in women (75.9% of the patients with LAAligation compared with only 58.5% of the patients with noligation; p � 0.02). The occurrence of a systemic embolismwas significantly more frequent in patients without LAAligation compared with patients with LAA ligation (17% vs.3.4% respectively; p � 0.01).) Only two of the 27 embolicevents occurred in patients with LAA ligation. In additionto the absence of LAA ligation, the presence of LA or LAAthrombus (14.8% vs. 3.4%; p � 0.03) and LASEC grade 3
or 4 (64% vs. 21.3%; p � 0.001) was also more frequent inpatients with an embolic event compared with patientswithout systemic embolism (Table 2).
Multivariate analysis identified the absence of LAAligation (odds ratio [OR] 6.7 [95% CI 1.5 to 31.0]; p �0.02) and the TEE finding of an LA or LAA thrombus(OR 5.8 [95% CI 1.2 to 27.3]; p�0.03) as the onlyindependent predictors of occurrence of an embolic eventafter mitral valve replacement surgery (Table 3). Moreover,if the absence of effective ligation as assessed by echocardi-ography was included in the model, OR increased up to 11.9(95% CI 1.5 to 93.6), p � 0.02, and the presence of LA orLAA thrombus also remained independently associatedwith the occurrence of an embolic event (Table 3).
If only patients without LAA ligation were included inthe analysis, events were more frequent in patients withlarger LAA size (8.6 � 1.0 mm vs. 7.7 � 1.1 mm in patientswith and without embolic events respectively; p � 0.001)and in those with greater LASEC score (64% of patientswith embolic event had a score 3 or 4 compared with 21.3%of patients without event; p � 0.0005). The presence of LAor LAA thrombus was close to reaching statistical signifi-cance (12% vs. 3.3% in patients with and without embolicevents respectively; p�0.06). After multivariate analysis, theonly independent variable associated with the occurrence ofembolisms in these group of patients was the LASEC score(OR 3.0 [95% CI 1.5 to 6.0]; p � 0.002) (Table 4).
DISCUSSIONLAA ligation during surgical procedures. Several studieshave confirmed that the LAA plays a very important role in
Table 2. Characteristics of Patients With Embolic EventsVersus No Embolic Event
Embolic Event(n � 27)
No EmbolicEvent
(n � 178) p Value
Age (yrs) 62 � 12 62 � 10 0.9Female gender 18 (66.7%) 112 (62.9%) 0.7Mean time from MVR
to TEE (months)73.8 � 60.9 68.6 � 68.2 0.7
Mechanical prosthesis 24 (88.9%) 163 (91.6%) 0.6LA size 55 � 10 58 � 12 0.2LA or LAA thrombus 4 (14.8%) 6 (3.4%) 0.03*Mean LVEF 59 � 14 56 � 12 0.5Sinus rhythm 4 (14.8%) 25 (14%) 0.9LAA ligation 2 (7.4%) 56 (31.5%) 0.01Severe mitral prosthetic
regurgitation2 (7.4%) 20 (11.2%) 0.7*
LASEC grade 3 or 4 16 (64%) 26 (21.3%) � 0.001†
*Fisher test was performed instead of chi-squared test. †In the analysis of this variable,only patients without LAA ligation were included.
LASEC � left atrial appendage spontaneous echo contrast. Other abbreviations asin Table 1.
Table 3. Factors Independently Associated With Embolic Events
Logistic Regression Procedure Evaluating the Absence of LAA Ligation Performed at Surgery
B OR (95% CI) p Value
Absence of LAA ligation at MVR 1.9 6.7 (1.5–31.0) 0.02LA or LAA thrombus 1.8 5.8 (1.2–27.3) 0.03Age (per yr) 0.02 1.0 (0.9–1.1) 0.5Female gender 0.07 1.1 (0.4–2.8) 0.9Time from MVR to TEE (per month) 0.01 1.0 (0.9–1.0) 0.2LVEF 0.01 1.0 (0.9–1.1) 0.7Mitral regurgitation �0.2 0.8 (0.5–1.3) 0.3LA size 0.03 1.0 (0.9–1.1) 0.2Sinus rhythm �0.03 1.0 (0.3–3.5) 0.9
Logistic Regression Procedure Evaluating the Absence of Effective LAA Ligation in TEE
Absence of LAA ligation in TEE 2.5 11.9 (1.5–93.6) 0.02LA or LAA thrombus 1.6 5.1 (1.1–23.2) 0.04Age (per yr) 0.02 1.0 (0.9–1.1) 0.5Female gender 0.09 1.1 (0.4–2.9) 0.9Time from MVR to TEE (per month) 0.005 1.0 (0.9–1.0) 0.2LVEF 0.01 1.0 (0.9–1.1) 0.5Mitral regurgitation �0.3 0.8 (0.5–1.2) 0.3LA size 0.03 1.0 (0.9–1.1) 0.3Sinus rhythm �0.07 0.9 (0.3–3.4) 0.9
In both models the same factors were evaluated, excepting absence of LAA ligation (at MVR in the first model or at TEE inthe second model).
CI � confidence interval; OR � odds ratio. Other abbreviations as in Table 1.
1256 Garcıa-Fernandez et al. JACC Vol. 42, No. 7, 2003Left Atrial Appendage Ligation Reduces Stroke Risk October 1, 2003:1253–8

the development of thromboembolic strokes. In patientswith rheumatic and nonrheumatic AF, at least 60% and90% of LA thrombi, respectively, are located in the LAA(1–3). Therefore, it is likely that ligation of the LAA wouldgreatly reduce the risk of stroke.
Since the early rheumatic mitral stenosis surgical proce-dures (17,18), LAA ligation has been performed attemptingto reduce the risk of embolization. Ligation of the LAAduring mitral valve replacement surgery is still controversial.Some authors propose that prophylactic appendage removalshould be performed whenever the chest is open as amethod of preventing future strokes (26). Surprisingly, thebenefit of carrying out such a commonly performed proce-dure is poorly documented in scientific literature, and its usehas been sporadic and governed by intuition alone (3). Theutilization of this technique depends on the methodologyand insight of the different surgical teams despite that it isa recommended procedure in the ACC guidelines (27).
Orszulak et al. (28) evaluated the risk of stroke in elderlypatients during the early postoperative period after a mitralvalve replacement with a Carpentier-Edwards biologicalprosthesis and found a strong correlation between latestroke in patients having the LAA ligated when patientsunderwent mitral valve replacement and coronary bypassgrafts. However, in the group of patients with isolatedmitral valve replacement and in the overall group, the onlyindependent variable associated with a greater risk of latestroke was an advanced heart class.
Juratli et al. (29) analyzed the use of LAA ligation duringmitral valve surgery (50% underwent mitral valve repair and23% received a mechanical prosthesis) as an alternative toanticoagulant treatment with warfarin. Left atrial append-age ligation did not provide an adequate protection fromthromboembolic events in the absence of effective antico-agulation treatment with warfarin. Our study population,unlike the patient population studied by Juratli et al. (29) andOrszulak et al. (28), had received acenocumarin treatment in82% of cases, and in all the cases when a patient received amechanical prosthesis. In addition, the majority of subjects
were diagnosed with chronic rheumatic mitral valve disease,and a greater enlargement of the LA was observed.LAA incomplete ligation. A special group of patients arethose with incomplete surgical ligation of the LAA. Katz etal. (25) recently reported that 36% of patients had incom-plete ligation of the LAA after a mitral valve surgery, and22% of them suffered an embolic event. In our study thefrequency of incomplete ligation of the LAA was only10.3%, of which only one case suffered an embolic event.There is no doubt about the influence of the surgicaltechnique on these findings. In the series of Katz et al. (25),a running suture was performed, whereas our surgeonscarried out a double suture (a purse string suture as well asa running suture). This double suture probably provides amore stable LAA ligation. The high incidence of incom-plete ligation of the LAA should be noted, and furtherinvestigation is required to establish if this can result in anincreased incidence of postoperative embolic events.Selection of patients for LAA ligation. The physiologicalrole of the LAA is minimal, and consequently, its removalhas been advocated over the years to reduce stroke risk. Atthis point, an interesting application of TEE may be toidentify patients for LAA ligation; TEE can define ahigh-risk population if a low or absent LAA flow velocityprofile or the presence of LASEC is identified (8). It couldbe argued that ligation of the LAA is unnecessary in thosehigh-risk patients because they will receive anticoagulationtherapy for decades. However, it is well known that, despiteclear guidelines, warfarin is either not used or used improp-erly on a large scale (30–32). In addition, warfarin levels areaffected by a large number of dietary and drug factors (3).Thus, it is clear that variations in the therapeutic effective-ness of long-term treatments are almost the norm, and it isin these changes where the appearance of embolic events cantake place. Thus, it would appear sensible to eliminate thefundamental origin of the embolic events.
Our study shows for the first time that LAA ligationduring surgery of mitral valve replacement, performed in ahigh-risk population, is consistent with a reduction of therisk of late embolism (6.7-fold reduction in embolic risk).Moreover, if a complete ligation is achieved and confirmedwith TEE, a further reduction in embolism risk is observed(11.9-fold reduction in embolic risk). In addition, the TEEidentification of LAA or LA thrombus, higher LA size, orhigher degrees of LASEC is associated with a higher risk oflate embolisms. These findings represent a strong negativeassociation between an embolic event and ligation of theLAA during surgical intervention, thus providing clearevidence for the benefit of ligation of the LAA duringsurgical procedure as a method of preventing a postoperativeembolic event. Because we studied mainly patients withrheumatic valvular disease, our results may be applicableonly to this population. However, an ongoing randomizedtrial of LAA occlusion during routine coronary artery bypassgraft surgery (Left Atrial Appendage Occlusion Study[LAAOS] study) (33) will be able to provide definitive
Table 4. Factors Independently Associated With EmbolicEvents Evaluated Only in Patients Without LAA LigationPerformed at Surgery (n � 147)
B OR (95% CI) p Value
LASEC* 1.09 3.0 (1.5–6.0) 0.002Age (per yr) 0.01 1.0 (0.9–1.17) 0.7Female gender 0.37 1.5 (0.5–4.4) 0.5Mechanical mitral
prosthesis0.004 1.0 (0.9–1.2) 0.9
Mitral regurgitation 0.37 1.4 (0.7–3.0) 0.3LAA size 0.29 1.3 (0.8–2.2) 0.3LA size �0.03 1.0 (0.9–1.1) 0.2Sinus rhythm 0.18 1.2 (0.2–6.9) 0.8LA or LAA thrombus 1.13 3.1 (0.6–17.6) 0.2
*OR related to each grade of increase of severity. Logistic regression procedureincluding the following variables: age, gender, mechanical mitral prosthesis, LA size,LAA size, sinus rhythm, LA thrombus, mitral prosthetic regurgitation.
Abbreviations as in Tables 1, 2, and 3.
1257JACC Vol. 42, No. 7, 2003 Garcıa-Fernandez et al.October 1, 2003:1253–8 Left Atrial Appendage Ligation Reduces Stroke Risk

evidence about LAA ligation in patients without rheumaticvalvular disease.Study limitations. The study population consisted of pa-tients referred to the echocardiography laboratory for mitralvalve prosthesis evaluation using TEE. This pretest referralbias can result in an amplification of the beneficial effect ofLAA ligation if fewer patients who had mitral valve replace-ment and LAA ligation would be referred for echocardio-graphic study. Another limitation is the lack of informationabout anticoagulation levels in these patients. Although allpatients with a mechanical prosthesis were anticoagulated, itcould be possible that lower international normalized ratiolevels influenced the development of an embolic event.Despite its evident clinical relevance, there is no reason to thinkthat patients with LA appendectomy have a different chronicanticoagulation profile than patients without it. Thus, thedegree of chronic anticoagulation should not be a confoundingfactor in this setting.
Our study supports the surgical LAA ligation togetherwith the mitral valve replacement. It provides new informa-tion about potential impact of LAA ligation until new dataof a randomized study with blinded event verification areavailable (33).
Reprint requests and correspondence: Dr. Miguel AngelGarcıa-Fernandez, Laboratorio de Ecocardiografıa, Servicio deCardiologıa, Hospital General Universitario Gregorio Maranon,Doctor Esquerdo 46, 28007, Madrid, Spain. E-mail: [email protected].
REFERENCES1. Al Saady NM, Obel OA, Camm AJ. Left atrial appendage: structure,
function, and role in thromboembolism. Heart 1999;82:547–54.2. Ischemic stroke associated with atrial fibrillation: the demographic and
clinical characteristics and 30-day mortality in a hospital strokeregistry: the European Community Stroke Project, Florence unit. AnnItal Med Int 1996;11:20–6.
3. Blackshear JL, Odell JA. Appendage obliteration to reduce stroke incardiac surgical patients with atrial fibrillation. Ann Thorac Surg1996;61:755–9.
4. Vemmos KN, Bots ML, Tsibouris PK, et al. Stroke incidence and casefatality in southern Greece: the Arcadia Stroke registry. Stroke1999;30:363–70.
5. Petersen P, Godtfredsen J. Risk factors for stroke in chronic atrialfibrillation. Eur Heart J 1988;9:291–4.
6. Agmon Y, Khandheria BK, Gentile F, Seward JB. Clinical andechocardiographic characteristics of patients with left atrial thrombusand sinus rhythm: experience in 20,643 consecutive transesophagealechocardiographic examinations. Circulation 2002;105:27–31.
7. Pollick C, Taylor D. Assessment of left atrial appendage function bytransesophageal echocardiography: implications for the developmentof thrombus. Circulation 1991;84:223–31.
8. Garcia-Fernandez MA, Torrecilla EG, San Roman D, et al. Left atrialappendage Doppler flow patterns: implications on thrombus forma-tion. Am Heart J 1992;124:955–61.
9. Mugge A, Kuhn H, Nikutta P, Grote J, Lopez JA, Daniel WG.Assessment of left atrial appendage function by biplane transesopha-geal echocardiography in patients with nonrheumatic atrial fibrillation:identification of a subgroup of patients at increased embolic risk. J AmColl Cardiol 1994;23:599–607.
10. Kamp O, Verhorst PM, Welling RC, Visser CA. Importance of leftatrial appendage flow as a predictor of thromboembolic events inpatients with atrial fibrillation. Eur Heart J 1999;20:979–85.
11. Kato H, Nakanishi M, Maekawa N, Ohnishi T, Yamamoto M.Evaluation of left atrial appendage stasis in patients with atrial
fibrillation using transesophageal echocardiography with an intrave-nous albumin-contrast agent. Am J Cardiol 1996;78:365–9.
12. Daniel WG, Nellessen U, Schroder E, et al. Left atrial spontaneousecho contrast in mitral valve disease: an indicator for an increasedthromboembolic risk. J Am Coll Cardiol 1988;11:1204–11.
13. Black IW, Hopkins AP, Lee LC, Walsh WF. Left atrial spontaneousecho contrast: a clinical and echocardiographic analysis. J Am CollCardiol 1991;18:398–404.
14. Tsai LM, Chen JH, Fang CJ, Lin LJ, Kwan CM. Clinical implicationsof left atrial spontaneous echo contrast in nonrheumatic atrial fibril-lation. Am J Cardiol 1992;70:327–31.
15. Gonzalez-Torrecilla E, Garcia-Fernandez MA, Perez-David E, Ber-mejo J, Moreno M, Delcan JL. Predictors of left atrial spontaneousecho contrast and thrombi in patients with mitral stenosis and atrialfibrillation. Am J Cardiol 2000;86:529–34.
16. Hwang JJ, Kuan P, Chen JJ, et al. Significance of left atrial sponta-neous echo contrast in rheumatic mitral valve disease as a predictor ofsystemic arterial embolization: a transesophageal echocardiographicstudy. Am Heart J 1994;127:880–5.
17. Bailey C, Olsen A, Keown K, et al. Commisurotomy for mitralstenosis technique for prevention cerebral complications. JAMA 1952;149:1085–91.
18. Madden J. Resection of the left auricular appendix. JAMA 1948;140:769–72.
19. Odell JA, Blackshear JL, Davies E, et al. Thoracoscopic obliteration ofthe left atrial appendage: potential for stroke reduction? Ann ThoracSurg 1996;61:565–9.
20. Nakai T, Lesh MD, Gerstenfeld EP, Virmani R, Jones R, Lee RJ.Percutaneous left atrial appendage occlusion (PLAATO) for prevent-ing cardioembolism: first experience in canine model. Circulation2002;105:2217–22.
21. Sievert H, Lesh MD, Trepels T, et al. Percutaneous left atrialappendage transcatheter occlusion to prevent stroke in high-riskpatients with atrial fibrillation: early clinical experience. Circulation2002;105:1887–9.
22. Hatle L, Angelsen BA, Tromsdal A. Non-invasive assessment ofaortic stenosis by Doppler ultrasound. Br Heart J 1980;43:284–92.
23. Cooper JW, Nanda NC, Philpot EF, Fan P. Evaluation of valvularregurgitation by color Doppler. J Am Soc Echocardiogr 1989;2:56–66.
24. Fatkin D, Kelly RP, Feneley MP. Relations between left atrial append-age blood flow velocity, spontaneous echocardiographic contrast andthromboembolic risk in vivo. J Am Coll Cardiol 1994;23:961–9.
25. Katz ES, Tsiamtsiouris T, Applebaum RM, Schwartzbard A, TunickPA, Kronzon I. Surgical left atrial appendage ligation is frequentlyincomplete: a transesophageal echocardiographic study. J Am CollCardiol 2000;36:468–71.
26. Johnson WD, Ganjoo AK, Stone CD, Srivyas RC, Howard M. Theleft atrial appendage: our most lethal human attachment! Surgicalimplications. Eur J Cardiothorac Surg 2000;17:718–22.
27. Bonow RO, Carabello B, de Leon AC, et al. ACC/AHA Guidelinesfor the Management of Patients With Valvular Heart Disease:Executive Summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines(Committee on Management of Patients with Valvular Heart Dis-ease). J Heart Valve Dis 1998;7:672–707.
28. Orszulak TA, Schaff HV, Pluth JR, et al. The risk of stroke in the earlypostoperative period following mitral valve replacement. Eur J Car-diothorac Surg 1995;9:615–9.
29. Juratli N, Wilkoff B, Tchou P, et al. Left atrial appendage ligationduring mitral valve surgery may increase the risk of late thromboem-bolic event (abstr). J Am Coll Cardiol 2002;39:85A.
30. Munschauer FE, Priore RL, Hens M, Castilone A. Thromboembo-lism prophylaxis in chronic atrial fibrillation: practice patterns incommunity and tertiary-care hospitals. Stroke 1997;28:72–6.
31. Schlicht JR, Davis RC, Naqi K, Cooper W, Rao BV. Physicianpractices regarding anticoagulation and cardioversion of atrial fibrilla-tion. Arch Intern Med 1996;156:290–4.
32. Stafford RS, Singer DE. National patterns of warfarin use in atrialfibrillation. Arch Intern Med 1996;156:2537–41.
33. Crystal E, Lamy A, Connolly SJ, et al. Left Atrial AppendageOcclusion Study (LAAOS): a randomized clinical trial of left atrialappendage occlusion during routine coronary artery bypass graftsurgery for long-term stroke prevention. Am Heart J 2003;145:174–8.
1258 Garcıa-Fernandez et al. JACC Vol. 42, No. 7, 2003Left Atrial Appendage Ligation Reduces Stroke Risk October 1, 2003:1253–8

EDITORIAL COMMENT
Obliteration of the LeftAtrial Appendage forPrevention of Thromboembolism*Jonathan L. Halperin, MD, FACC,†Mardi Gomberg-Maitland, MD, MSC‡New York, New York; and Chicago, Illinois
Shaped like a wizard’s hat but long considered functionallyinsignificant, the conical, trabeculated left atrial appendage(LAA) arises from the embryonic left atrium during thethird week of gestation and extends superiorly from theanterolateral surface of the left atrium (1). This accessorychamber extends over an area of 3 to 6 cm2, is morecompliant than the atrium, and is actively contractile innormal hearts—filling and emptying in response to bothventricular and atrial dynamics (2,3). Receptors in the LAAinfluence heart rate, and granules secrete atrial natriureticpeptide, contributing to regulation of intravascular pressureand volume in response to stretch (3–7).
See pages 1249 and 1253
The LAA is seldom imaged clearly by precordial echo-cardiography, but, through transesophageal echocardiogra-phy (TEE), the LAA has been recognized as a prime nidusof thrombus formation in patients with atrial fibrillation(AF) and, indeed, the leading source of cardiogenic stroke(8–10). When fibrillating, the LAA undulates at a rate�350 cycles/min, and outflow velocity is considerably re-duced. With long-standing AF, the ejection velocity fromthe LAA often decreases to negligible levels, and theappendage dilates at least as quickly as the rest of the atriumin patients with chronic mitral valve disease, sometimesreaching an area of 12 cm2. Communication with the atrialcavity increases proportionally, hypothetically facilitatingthe first stage of embolism by allowing a thrombotic mass tocross the orifice more easily.
In a meta-analysis of 23 studies in which the LAA wasexamined by TEE, autopsy, or direct intra-operative inspec-tion, intracardiac thrombus was identified in 17% of patientswith non-valvular AF and in 13% of cases in which AF wasassociated with valvular heart disease. These thrombi werelocated in the LAA in 91% of the patients with non-valvularAF, compared with 57% of those with valvular disease (11).
In patients with mitral stenosis, stasis is generalized in boththe atrium and the LAA, while, in cases of mitral regurgi-tation, the LAA may be more prone to this phenomenonthan the body of the left atrium (12).
In patients with AF, several risk factors that predictthromboembolism in clinical studies correlate with reducedflow velocity in the LAA, accounting in part for their linksto cardiogenic embolism (13,14). There are also strongcorrelations between reduced LAA flow velocity, thrombusformation, hypertension, and atheromatous disease of theaorta (15,16). Hypertension may be a key factor linkingvascular lesions with the pathogenesis of thrombus in theappendage, and the consistent association of hypertensionwith stroke in AF patients may be attributed to atrial stasisor to associated disease of the vasculature supplying thebrain. This may help explain why recent trials have notfound control of the dysrhythmia and maintenance of sinusrhythm more effective than rate control and anticoagulationfor prevention of adverse clinical outcomes in patients withAF (17,18).
At present, protection against ischemic stroke due tocardiogenic embolism in high-risk patients involves oralanticoagulation at a dose adjusted to maintain internationalnormalized ratio between 2 and 3. Though highly effective,warfarin use is associated with a considerable risk of bleed-ing, including intracranial hemorrhage, which occurs at arate of 0.5%/year. When the risk of bleeding or otherimpediment to anticoagulation outweighs the risk of isch-emic stroke, removing or otherwise isolating the LAArepresents a theoretically attractive alternative strategy forprevention of embolic events.
The LAA is relatively easy to exclude from communica-tion with the left atrium at the time of cardiac surgery byligation, plication, or amputation. The procedure, firstapplied in the 1930s to patients with rheumatic mitralstenosis (19), is now performed routinely in many centersand recommended in practice guidelines to reduce strokerisk in patients with valvular heart disease undergoingcardiac operation (20). The appendage is also routinelyisolated during the Maze operation for treatment of refrac-tory AF (21). With any of these techniques, there is a riskof incomplete exclusion, which has been reported on early(33%) and later (40%) postoperative TEE examinations(22).
Two articles in this issue of the Journal address elimina-tion of the LAA for prevention of ischemic (presumablyembolic) clinical events. Garcia-Fernandez et al. (23) reportthe outcome of LAA obliteration in patients with prostheticmitral valves. Although the majority of the patients in theirstudy had a cardiac rhythm other than sinus (presumablyAF or flutter in most), the intensity of anticoagulation wasnot described, and the performance of LAA obliteration atthe time of cardiac operation was not randomized. Eventhough prosthetic heart valves were potential sources ofembolism in all cases, the LAA isolation procedure was
*Editorials published in the Journal of the American College of Cardiology reflect theviews of the authors and do not necessarily represent the views of JACC or theAmerican College of Cardiology.
From the †Mount Sinai Medical Center, The Zena and Michael A. WienerCardiovascular Institute, New York, New York; and ‡Rush Heart Institute, Chicago,Illinois.
Journal of the American College of Cardiology Vol. 42, No. 7, 2003© 2003 by the American College of Cardiology Foundation ISSN 0735-1097/03/$30.00Published by Elsevier Inc. doi:10.1016/S0735-1097(03)00958-6

associated with a reduced rate of ischemic events. Furtherstudy will be needed to establish whether incomplete liga-tion (2.9% in this report) compromises this protective effect.
The feasibility of less invasive approaches to isolating orremoving the LAA has raised interest in applying thisstrategy to selected patients with AF who do not otherwiserequire cardiac surgery. Techniques for thoracoscopic liga-tion (24) and initial experience with catheter deployment ofan implantable device to seal the mouth of the LAA havebeen described (25,26). As testimony to the limited functionof the LAA in patients with chronic AF, its thoracoscopicremoval from 437 patients appeared safe and unencumberedby clinical sequelae (24). Proof that one or another of thesetechniques is both effective and safe would provide avaluable alternative for patients unable to sustain systemicanticoagulant therapy. No such validation, however, hasbeen produced to date. The logistical difficulties of mount-ing a proper randomized trial are compounded by consid-erable comorbidity in the subset of patients with AF whohave risk factors for thromboembolism and contraindica-tions to long-term anticoagulation.
In another article in this issue of the Journal, Blackshearet al. (27) describe their experience in 15 high-risk patientswith AF and compare longitudinal outcomes of LAAexclusion with those of participants in the control groups ofrandomized trials of antithrombotic therapy for AF toderive the first estimates of the efficacy of this strategy as analternative to anticoagulation. The patients had AF and oneor more additional risk factors for stroke; anticoagulanttherapy was either contraindicated or not sufficiently effec-tive to eradicate LA thrombus demonstrated by TEE. Afterobliteration of the appendage by either surgical staples orsnare under general anesthesia, there was a trend suggestingreduction in thromboembolism compared with historicalcohorts over a median follow-up of 42 months, but statis-tical power to demonstrate proof of the concept was lackingin this small number of patients.
It is important to point out that the patients to whom theappendage exclusion procedure was applied differed fromthose in the earlier trials, who were deemed eligible foranticoagulation. Other advances in medical treatment mayhave also contributed to the apparent favorable outcome.The efficacy of the technique is presumably related to thecompleteness and permanence of elimination of blood flowinto and out of the LAA. This was demonstrated by TEEat the time of intervention, but the durability of the effectwas not confirmed by subsequent examinations.
Despite these limitations, this work is important as a testof how the concept that the pathogenesis of ischemic eventsin patients with AF is related to embolism of thrombusfrom the LAA can be exploited to clinical advantage. Onereason for uncertainty is that many patients with AF harborother forms of cardiovascular pathology, including hyper-tension and atherosclerosis. Patients with this commoncardiac rhythm disturbance come cloaked in cardiovascularcomorbidity that contributes to stroke risk and responds to
antithrombotic therapy. Whether mechanical measures tointercede in this presumed mechanism will prove compara-bly effective and safer for some patients remains to beestablished as a therapeutic principle. We might swipe orseal the wizard’s hat, yet the rabbit could still appear.
Reprint requests and correspondence: Dr. Jonathan L. Hal-perin, Mount Sinai Medical Center, The Zena and Michael A.Wiener Cardiovascular Institute, Box 1030, 1 Gustave L. Levy Place,New York, New York 10029-0310. E-mail: [email protected].
REFERENCES
1. Sadler T. Cardiovascular system. In: Langman J, editor. Langman’sMedical Embryology. 6th edition. Baltimore, MD: Williams andWilkins, 1990:179–227.
2. Akosah KO, Funai JT, Porter TR, Jesse RL, Mohanty PK. Left atrialappendage contractile function in atrial fibrillation: influence of heartrate and cardioversion to sinus rhythm. Chest 1995;107:690–6.
3. Tabata T, Oki T, Yamada H, et al. Role of left atrial appendage in leftatrial reservoir function as evaluated by left atrial appendage clampingduring cardiac surgery. Am J Cardiol 1998;81:327–32.
4. Kappagoda CT, Linden RJ, Saunders DA. The effect on heart rate ofdistending the atrial appendages in the dog. J Physiol 1972;225:705–19.
5. Kappagoda CT, Linden RJ, Snow HM. The effect of distending theatrial appendages on urine flow in the dog. J Physiol 1972;227:233–42.
6. Davis CA 3rd, Rembert JC, Greenfield JC Jr. Compliance of leftatrium with and without left atrium appendage. Am J Physiol1990;259:H1006–8.
7. Chapeau C, Gutkowska J, Schiller PW, et al. Localization of immu-noreactive synthetic atrial natriuretic factor (ANF) in the heart ofvarious animal species. J Histochem Cytochem 1985;33:541–50.
8. Grimm RA, Stewart WJ, Maloney JD, et al. Impact of electricalcardioversion for atrial fibrillation on left atrial appendage function andspontaneous echo contrast: characterization by simultaneous trans-esophageal echocardiography. J Am Coll Cardiol 1993;22:1359–66.
9. Halperin JL, Hart RG. Atrial fibrillation and stroke: new ideas,persisting dilemmas. Stroke 1988;19:937–41.
10. Lindsay BD. Obliteration of the left atrial appendage: a concept worthtesting. Ann Thorac Surg 1996;61:515.
11. Blackshear JL, Odell JA. Appendage obliteration to reduce stroke incardiac surgical patients with atrial fibrillation. Ann Thorac Surg1996;61:755–9.
12. Blackshear JL, Pearce LA, Asinger RW, et al. Mitral regurgitationassociated with reduced thromboembolic events in high-risk patientswith nonrheumatic atrial fibrillation: Stroke Prevention in AtrialFibrillation Investigators. Am J Cardiol 1993;72:840–3.
13. Hwang JJ, Ko FN, Li YH, et al. Clinical implications and factorsrelated to left atrial spontaneous echo contrast in chronic nonvalvularatrial fibrillation. Cardiology 1994;85:69–75.
14. Mitusch R, Lange V, Stierle U, Maurer B, Sheikhzadeh A. Trans-esophageal echocardiographic determinants of embolism in nonrheu-matic atrial fibrillation. Int J Cardiac Imaging 1995;11:27–34.
15. Goldman ME, Pearce LA, Hart RG, et al. Pathophysiologic correlatesof thromboembolism in nonvalvular atrial fibrillation. I. Reduced flowvelocity in the left atrial appendage (The Stroke Prevention in AtrialFibrillation [SPAF-III] study). J Am Soc Echocardiogr 1999;12:1080–7.
16. Asinger RW, Koehler J, Pearce LA, et al. Pathophysiologic correlatesof thromboembolism in nonvalvular atrial fibrillation. II. Densespontaneous echocardiographic contrast (The Stroke Prevention inAtrial Fibrillation [SPAF-III] study). J Am Soc Echocardiogr 1999;12:1088–96.
17. Wyse DG, Waldo AL, DiMarco JP, et al. A comparison of rate
1260 Halperin and Gomberg-Maitland JACC Vol. 42, No. 7, 2003Editorial Comment October 1, 2003:1259–61

control and rhythm control in patients with atrial fibrillation. N EnglJ Med 2002;347:1825–33.
18. Van Gelder IC, Hagens VE, Bosker HA, et al. A comparison of ratecontrol and rhythm control in patients with recurrent persistent atrialfibrillation. N Engl J Med 2002;347:1834–40.
19. Madden J. Resection of the left auricular appendix. JAMA 1948;140:769–72.
20. Bonow RO, Carabello B, de Leon AC Jr., et al. Guidelines for themanagement of patients with valvular heart disease: executive sum-mary. A report of the American College of Cardiology/AmericanHeart Association Task Force on Practice Guidelines (Committee onManagement of Patients with Valvular Heart Disease). Circulation1998;98:1949–84.
21. Cox JL. The surgical treatment of atrial fibrillation. IV. Surgicaltechnique. J Thorac Cardiovasc Surg 1991;101:584–92.
22. Katz ES, Tsiamtsiouris T, Applebaum RM, Schwartzbard A, TunickPA, Kronzon I. Surgical left atrial appendage ligation is frequentlyincomplete: a transesophageal echocardiographic study. J Am CollCardiol 2000;36:468–71.
23. Garcıa-Fernandez MA, Perez-David E, Quiles J, et al. Role of leftatrial appendage obliteration in stroke reduction in patients with mitralvalve prosthesis: a transesophageal echocardiographic study. J Am CollCardiol 2003;42:1253–8.
24. Johnson WD, Ganjoo AK, Stone CD, Srivyas RC, Howard M. Theleft atrial appendage: our most lethal human attachment! Surgicalimplications. Eur J Cardiothorac Surg 2000;17:718–22.
25. Sievert H, Lesh MD, Trepels T, et al. Percutaneous left atrialappendage transcatheter occlusion to prevent stroke in high-riskpatients with atrial fibrillation: early clinical experience. Circulation2002;105:1887–9.
26. Nakai T, Lesh MD, Gerstenfeld EP, Virmani R, Jones R, Lee RJ.Percutaneous left atrial appendage occlusion (PLAATO) for prevent-ing cardioembolism: first experience in canine model. Circulation2002;105:2217–22.
27. Blackshear JL, Johnson WD, Odell JA, et al. Thoracoscopic extracar-diac obliteration of the left atrial appendage for stroke risk reduction inatrial fibrillation. J Am Coll Cardiol 2003;42:1249–52.
1261JACC Vol. 42, No. 7, 2003 Halperin and Gomberg-MaitlandOctober 1, 2003:1259–61 Editorial Comment

Mechanisms and Treatment of Atrial Fibrillation
Competing Autonomic Mechanisms Precedethe Onset of Postoperative Atrial FibrillationDavid Amar, MD,* Hao Zhang, MD,* Saul Miodownik, MEE,† Alan H. Kadish, MD‡New York, New York; and Chicago, Illinois
OBJECTIVES This study was designed to evaluate autonomic changes preceding atrial fibrillation/flutter(AF) after thoracotomy.
BACKGROUND Autonomic fluctuations before the onset of postoperative AF have been reported but withconflicting results.
METHODS In 48 patients with postoperative AF, 2-h Holter recordings before the onset of AF werecompared with corresponding data from 48 age- and gender-matched surgical controlswithout AF. Five-minute segments of heart rate variability (HRV) were studied using linearregression methods.
RESULTS There was a near-significant trend for the RR interval among patients with AF to be lowerthan controls (p � 0.06), whereas the standard deviation of RRs (p � 0.0001), root meansquare of successive RR differences (p � 0.0001), proportion of RRs �50 ms different (p �0.0001), low-frequency power (p � 0.0003) and its log (p � 0.0001), and high-frequency-power (p � 0.0001) and its log (p � 0.0001) were all significantly greater in patients with AF,respectively. In comparison to controls, AF patients had a significant decrease in RR interval(p � 0.02) and significant increments in all time- and frequency-domain analyses studied.
CONCLUSIONS In the period before the onset of postoperative AF, there are significant increases in HRVduring a time when heart rate also increases. These novel findings are consistent withparasympathetic resurgence competing with increasing sympathetic activity as the triggeringmechanism for postoperative AF. (J Am Coll Cardiol 2003;42:1262–8) © 2003 by theAmerican College of Cardiology Foundation
Postoperative atrial arrhythmias, including specifically atrialfibrillation/flutter (AF), are seen in 6.1% of elderly patientsundergoing non-cardiothoracic surgery and in 10% to 65%of patients after cardiothoracic operations (1–4). The clin-ical symptoms, time of AF onset, and natural course of thearrhythmia are similar whether a patient has had cardiac,thoracic, or other surgery (1–5). As in AF unrelated to
See page 1269
surgery, age �60 years is consistently the only independentpreoperative risk factor most strongly associated with post-operative AF (1–6). It is well known that aging causesdegenerative and inflammatory changes in atrial myocar-dium that lead to alterations in electrical properties of theatria (7,8). The utility of signal-averaged P-wave duration topredict postoperative AF remains controversial (9–12). Weand others have observed that a greater preoperative heartrate (HR) was an independent predictor of AF aftercardiothoracic surgery, suggesting that lower preoperative
vagal tone further stratifies those susceptible to AF amongthe elderly (4,6,13).
The mechanisms of postoperative AF, however, have notbeen well defined. Increased atrial ectopy can trigger post-operative AF (14). Although autonomic imbalance has alsobeen implicated as a possible trigger of postoperative AF,there is some controversy as to whether this is primarilyvagal or sympathetic in nature (15,16). Having a betterunderstanding of the mechanisms of postoperative AF couldlead to more targeted preventative or therapeutic interven-tions. To gain insight into autonomic influences precedingpostoperative AF, we compared time and frequency domainparameters of heart rate variability (HRV) of patients whodeveloped this arrhythmia with those of matched postoper-ative controls without AF.
METHODS
The data used in this study were obtained from an ongoingprospective database of 412 patients in sinus rhythm whohad major thoracic surgery beginning in October 1990 toSeptember 1999 at Memorial Sloan-Kettering Cancer Cen-ter and had Holter recordings postoperatively. With Insti-tutional Review Board approval and written informed con-sent, patients participated in consecutive trials focused onthe study of postoperative AF (2,17,18). All patients sched-uled for thoracic surgery who met inclusion criteria wereapproached to enroll in the studies subject to the availabilityof research staff. Excluded from this study were 216 patients
From the *Departments of Anesthesiology and Critical Care Medicine and†Biomedical Engineering, Memorial Sloan-Kettering Cancer Center and WeillMedical College of Cornell University, New York, New York, and ‡Division ofCardiology, Northwestern University School of Medicine, Chicago, Illinois. Pre-sented in part at the 52nd Annual Scientific Session of the American College ofCardiology, March 2003, Chicago, Illinois.
Manuscript received September 24, 2002; revised manuscript received March 25,2003, accepted April 3, 2003.
Journal of the American College of Cardiology Vol. 42, No. 7, 2003© 2003 by the American College of Cardiology Foundation ISSN 0735-1097/03/$30.00Published by Elsevier Inc. doi:10.1016/S0735-1097(03)00955-0

receiving drugs such as prophylactic intravenous diltiazemor class I and III antiarrhythmic drugs that may reduce thefrequency of AF episodes. Preoperative beta-blockers werecontinued postoperatively to avoid withdrawal. Patientswho were taking calcium channel blockers for hypertensionor coronary artery disease resumed taking these medicationson the first postoperative day. The primary end point of thisstudy was the new onset of sustained (�30 s) AF defined byan irregularly irregular cardiac rhythm other than sinuswithin 96 h after surgery and detected by Holter recordings.We examined the first episode in every patient because atthat time no prior antiarrhythmic medications were giventhat might interfere with our results of subsequent episodes.Of the remaining 196 patients, 48 patients who developedpostoperative AF and met the inclusion criteria were com-pared with 48 age- and gender-matched controls whounderwent the same operation but did not develop AF. Theoperations were performed using standard thoracotomyapproaches. Postoperative pain relief was provided to allpatients by continuous administration of either an epiduralopioid (usually fentanyl) (n � 49) or an intravenous opioid(usually morphine) patient-controlled analgesia (n � 47).Patient-controlled analgesia pumps were used in all patientswith the goal of achieving a visual analog pain score of 3 orless.Ambulatory electrocardiography and HRV analysis.Dual-lead electrocardiographic recordings (leads CM2 andCM1 or CM5) were made on Marquette 8500 Holterrecorders. Recordings were made continuously beginningupon arrival in the post-anesthesia care unit for 72 to 96 h.The Holter tapes were digitized on a Marquette series 8000scanner. The signal was sampled at 128 Hz. The decisionsmade automatically by the computer were reviewed andcorrected by an experienced technician and then by acardiologist. When calculating the HRV parameters onlynormal-to-normal (NN) intervals were used. Thus, bothectopic coupling intervals and post-ectopic pauses wereexcluded. For frequency-domain analysis, each interval thatwas to be excluded because of ectopic beats or artifact wasreplaced by holding the previous coupling interval levelthroughout the time interval to the next valid couplinginterval. The HRV analysis was done during the 2 hpreceding AF onset and in a corresponding time window in
controls. The HRV indices measured were: mean RRinterval (ms) and its standard deviation (SD; ms); root meansquare of difference of successive RRs (rMSSD; ms); pro-portion of adjacent RRs �50 ms different (pNN50; %); low(LF; 0.04 to 0.15 Hz) and high frequency (HF; 0.15 to0.40 Hz) power (ms2) (19). Fast Fourier transformation wasused to compute the power within the defined frequencylimits for each 5-min interval. The LF/HF ratio has beenproposed by some to be an index of sympathovagal balance(20).
Continuous data are presented as mean value � SD.Patient and operative characteristics between patients withand without AF were compared using the Student t test fornormally distributed variables; the Mann-Whitney U testwas used for comparisons of supraventricular and ventricularectopy. Categorical variables were compared using theFisher exact test. Time and frequency domain parameters inthe two hours period preceding AF were assessed usingmixed effects linear regression models in which the non-independence of data from the same patient is taken intoaccount. The difference in the slope coefficient over timebetween patients with and without AF for HRV variableswas assessed for statistical significance. Each HRV variablewas of interest and tested a priori. Analysis of LF and HFis presented with and without log transformation. Toprovide additional information on HRV between thegroups, a secondary analysis of data selected from four timepoints before AF onset was done using paired t tests withBonferroni correction for multiple comparisons. All statis-tical tests were two-tailed, and p � 0.05 was regarded asstatistically significant.
RESULTS
Characteristics and surgical data of patients who did (n �48) or did not (n � 48) develop AF are presented in Table1. The mean sinus rate 5 min before AF onset was 93 � 16versus 86 � 15 beats/min in controls, p � 0.04. The meannumber of atrial premature beats during the 2 h precedingAF was significantly greater among patients with AF thancontrols, 392 � 561 versus 28 � 58, p � 0.0001, as was thenumber of supraventricular runs (3 or more beats), 1.8 � 3.8versus 0.02 � 0.14, p � 0.0001, and premature ventricularbeats 30 � 67 versus 7 � 23, p � 0.0001, respectively.ST-segment changes (up- or downsloping) occurred in 6/48patients with AF compared to 10/48 patients without AF,p � 0.41. When patients who had evidence of pericarditiswere excluded, regional ST-segment changes were presentin 5/48 patients with AF compared to 6/48 patients withoutAF, p � 0.99. None of the patients studied developed amyocardial infarction postoperatively.Time-domain HRV parameters. There was a near-significant trend for the RR-interval among AF patients tobe lower than controls (p � 0.06, Fig. 1A), whereas SD(p � 0.0001, Fig. 1B), rMSSD (p � 0.0001, Fig. 1C), andpNN50 (p � 0.0001, Fig. 1D) were all significantly greater
Abbreviations and AcronymsAF � atrial fibrillation/flutterCABG � coronary artery bypass graftingHF � high-frequency powerHR � heart rateHRV � heart rate variabilityLF � low-frequency powerpNN50 � proportion of adjacent RRs �50 ms differentRMSSD � root mean square of difference of successive
RRsSD � standard deviation
1263JACC Vol. 42, No. 7, 2003 Amar et al.October 1, 2003:1262–8 Mechanisms of Postoperative AF

in patients with AF, respectively (Table 2). When allpatients were considered together, there were no significantchanges in time-domain parameters of HRV over the 2 hstudy window (Table 2). However, in comparison to con-trols patients with AF had significant changes in HRVparameters over time: RR decreased while SD, rMSSD, andpNN50 all increased (Figs. 1A to 1D, Table 2). To provideadditional information on HRV between the groups, asecondary analysis of data selected from four time pointsbefore AF onset was done (Table 3). For example, incomparison to controls time-domain parameters of HRVstudied were significantly different 5 min before AF onset:mean RR interval was 657 � 112 versus 717 � 134 ms, p �0.05; SD was 73 � 42 versus 40 � 33 ms, p � 0.005;rMSSD was 108 � 70 versus 46 � 56 ms, p � 0.005; andpNN50 was 12.8 � 11.9 versus 2.7 � 6.9%, p � 0.005,respectively (Table 3).Frequency-domain HRV parameters. Patients with AFhad significantly greater values in LF (p � 0.0003, Fig. 2A),Ln LF (p � 0.0001, not shown), HF (p � 0.0001, Fig. 2B),Ln HF (p � 0.0001, not shown), but lower LF/HF ratio(p � 0.006, Fig. 2C) than controls (Table 2). When allpatients were considered together, there were no significantchanges in frequency-domain parameters of HRV over the2 h study window (Table 2). However, in comparison to
controls, patients with AF had significant increments in LF,Ln LF, HF, and Ln HF, but not in LF/HF ratio (Figs. 2Ato 2C, Table 2). Table 3 shows HRV data selected fromfour time points before AF onset. In comparison to controls,all frequency-domain parameters of HRV studied weresignificantly different 5 min before AF onset: LF was2,529 � 3,799 versus 705 � 1,452 ms2, p � 0.02; Ln LFwas 6.9 � 1.5 versus 5.5 � 1.4 (ms2), p � 0.005; HF was7,325 � 7,049 versus 2,282 � 8,433 ms2, p � 0.01; and LnHF was 8.1 � 1.6 versus 5.7 � 1.8 (ms2), p � 0.005; andLF/HF ratio was 0.5 � 0.7 versus 2.0 � 2.8, p � 0.004,respectively (Table 3).
DISCUSSION
The main findings of this study are that patients whodevelop postoperative AF have a significant elevation of HRthat is accompanied by a consistent and significant rise intime- and frequency-domain parameters of HRV during the2 h preceding the onset of AF in comparison to age- andgender-matched controls undergoing major noncardiac tho-racic surgery. These data suggest that vagal activation in thesetting of sympathetic predominance contribute strongly topostoperative AF.
Dissecting sympathetic and parasympathetic influenceson the sinus node using HRV measures has been extensivelyutilized despite some well-defined limitations (20,21). Timedomain indices represent respiratory modulation of vagalactivity. Frequency domain indices are more complex tointerpret, but in general the HF component has beenthought to reflect primarily vagal activity whereas LFreflects both sympathetic and vagal activity (20). Theimpressive elevations in time-domain indices of HRV weobserved simultaneously with an increasing HR suggestvagal resurgence in a background of increasing sympatheticactivity immediately before AF onset. These findings are incontrast to classic examples as described by Coumel ofadrenergically or vagally mediated AF characterized by anincreasing or decreasing HR before arrhythmia onset, re-spectively (22). The independence of neural modulation ofRR cycle length from HRV has been described in nonsur-gical patients and may be interpreted differently in postop-erative patients in whom changing respiratory patterns andvarying systemic opioid concentrations occur (23).
Although experimental models have shown that increasedvagal tone alone may produce AF, vagally mediated AF isuncommon, and it may be the heightened backgroundsympathetic tone that helps promote AF with increasedvagal activity. It is conceivable that vagal rebound promotesectopy by shortening refractoriness in a heterogeneousmatter and that the increased background sympatheticactivity may then promote AF (24). The LF/HF ratio mayrepresent sympathovagal balance, but the utility of thisindex has been challenged (20,21). Recent work in volun-teers studied under conditions of autonomic blockade orstimulation showed that HR but not LF/HF ratio is a
Table 1. Patient Characteristics
AF(n � 48)
Controls(n � 48) p
PreoperativeAge, yrs 70 � 8 70 � 8 0.99Weight, kg 76 � 16 72 � 14 0.27Male (%) 32 (67) 32 (67) 0.99Heart rate, beats/min 73 � 13 74 � 14 0.88Smoking (%) 35 (73) 35 (73) 0.99Hypertension (%) 20 (42) 15 (31) 0.29Coronary artery disease (%) 7 (15) 4 (8) 0.52Diabetes mellitus (%) 4 (8) 6 (13) 0.74Chemotherapy (%) 7 (15) 11 (23) 0.30Medication
ACE-inhibitors (%) 5 (10) 6 (13) 0.68Beta-blockers (%) 6 (13) 6 (13) 0.99Ca-channel blockers (%) 7 (15) 6 (13) 0.77
Pulmonary functionFEV1, % predicted 80 � 29 84 � 23 0.53FVC, % predicted 90 � 27 97 � 22 0.17DCO, % predicted 78 � 20 79 � 17 0.77
IntraoperativeLobectomy (%) 32 (67) 39 (81) 0.16Pneumonectomy (%) 9 (19) 7 (15)Extrapleural pneumonectomy 7 (15) 2 (4)Estimated blood loss, l 0.5 � 0.6 0.4 � 0.4 0.20Fluid replacement, l 2.8 � 3.2 2.6 � 2.1 0.62
PostoperativeEpidural analgesia (%) 25 (52) 24 (50) 0.84Pericarditis (%) 5 (10) 5 (10) 0.99Pneumonia or acute
respiratory failure (%)4 (8) 3 (6) 0.99
ACE � angiotensin-converting enzyme; AF � atrial fibrillation/flutter; DCO �diffusion capacity of carbon monoxide; FEV1 � forced expiratory volume; FVC �forced vital capacity.
1264 Amar et al. JACC Vol. 42, No. 7, 2003Mechanisms of Postoperative AF October 1, 2003:1262–8

reliable and practical index of sympathovagal balance (21).Nevertheless, in the current study the LF/HF ratio wassignificantly lower among patients with AF in comparisonto controls, which is consistent with vagal resurgence butshowed no significant change over time in either group sinceboth components increased in parallel. The mechanismresponsible for AF in our patients is not entirely clear but
may represent a combination of the effects of alteredsympathovagal balance, intraoperative trauma to autonomicfibers, and inflammatory changes that occur in response tomajor pulmonary resection (25). Observations made inpatients with focal ectopy originating from the pulmonaryveins have suggested a primary increase in adrenergic drivefollowed by marked modulation toward vagal predominancebefore the onset of paroxysmal AF unrelated to surgery (26).Whether ectopic atrial activity from the pulmonary veinscontributes to the genesis of postoperative AF remainsunknown.
In the present study, patients with AF had more frequentatrial and ventricular ectopy than controls. Atrial fibrillationis often initiated by an atrial premature contraction (8,14).Once initiated, AF can cause further alterations in atrialelectrical and structural properties (remodeling), whichpromote the maintenance of the arrhythmia and facilitate itsre-initiation should it terminate (8). The use of temporarybi-atrial overdrive pacing was shown to be effective toprevent AF after coronary artery bypass grafting (CABG)(27,28). The proposed mechanism for this beneficial effectwas that overdrive pacing primarily decreased the incidence
Figure 1. Continuous 5-min data of time-domain parameters of heart rate variability (HRV) during the 2 h preceding the onset of atrial fibrillation/flutter(AF) (filled circles) or in the corresponding study window in controls (unfilled circles). A � RR interval; B � SD; C � rMSSD; D � pNN50. See textfor abbreviations. P values in the figures represent the group by time interaction results.
Table 2. p Values Representing Heart Rate Variability Differences
Time(5 Min Intervals)
Group(AF vs. Controls)
Interaction(Time and Group)
RR, ms 0.53 0.06 0.02SD, ms 0.59 � 0.0001 0.01rMSSD, ms 0.94 � 0.0001 0.03pNN50, % 0.40 � 0.001 0.03LF, ms2 0.94 0.0003 0.05Ln LF, ms2 0.42 � 0.0001 0.0008HF, ms2 0.74 � 0.0001 0.009Ln HF, ms2 0.87 � 0.0001 0.007LF/HF ratio 0.57 0.006 0.24
AF � atrial fibrillation/flutter; HF � high frequency (0.15–0.40 Hz); LF � lowfrequency (0.04–0.15 Hz); rMSSD � root mean square of difference of successiveRRs; pNN50 � proportion of adjacent RRs � 50 ms different; SD � standarddeviation of RRs.
1265JACC Vol. 42, No. 7, 2003 Amar et al.October 1, 2003:1262–8 Mechanisms of Postoperative AF

of atrial ectopy after surgery by reducing rate-dependentelectrophysiologic changes and helped reduce atrial disper-sion of refractoriness (27–29). The observation that prophy-lactic atrial pacing prevents AF after CABG does notexclude the possibility that the autonomic changes weobserved may promote AF. For example, fixed rate atrialpacing may suppress ectopy in making refractoriness morehomogenous, thus decreasing the susceptibility of atrialmyocardium to autonomic changes. Furthermore, vagalrebound may explain why the efficacy of beta-adrenergicblockers to reduce the incidence of postoperative AF iscontroversial (3,4).
Little work has been done using HRV to understandautonomic mechanisms before postoperative AF (15,16,30).
Whereas Jideus et al. (30) found that patients who devel-oped postoperative AF did not differ from controls in HRVmeasures after CABG, Dimmer et al. (15) showed thatpatients with AF had a modest increase in HR, SD, and
Table 3. HRV Preceding the Onset of AF
AF Controls p value
RR, ms120 min 672 � 109 708 � 130 0.5560 min 685 � 109 709 � 130 0.9930 min 670 � 119 705 � 130 0.565 min 657 � 112 717 � 134 0.05
SD, ms120 min 60 � 37 35 � 28 0.00460 min 50 � 37 33 � 37 0.1230 min 62 � 43 32 � 31 � 0.0055 min 73 � 42 40 � 33 � 0.005
rMSSD, ms120 min 87 � 63 40 � 48 � 0.00560 min 69 � 61 38 � 58 0.0830 min 89 � 70 36 � 53 � 0.0055 min 108 � 70 46 � 56 � 0.005
pNN50%120 min 9.1 � 9.8 2.3 � 5.5 � 0.00560 min 7.3 � 10.1 2.2 � 5.6 0.00430 min 9.3 � 10.4 2.5 � 6.7 � 0.0055 min 12.8 � 11.9 2.7 � 6.6 � 0.005
LF, ms2
120 min 2,217 � 2,543 657 � 812 � 0.00560 min 1,060 � 1,389 743 � 2,136 0.9930 min 2,647 � 3,802 523 � 919 0.0045 min 2,529 � 3,799 705 � 1,452 0.02
Ln LF, ms2
120 min 7.1 � 1.2 5.8 � 1.3 � 0.00560 min 6.1 � 1.5 5.5 � 1.5 0.2630 min 6.7 � 1.9 5.2 � 1.5 � 0.0055 min 6.9 � 1.5 5.5 � 1.4 � 0.005
HF, ms2
120 min 7,522 � 9,640 1,625 � 2,806 � 0.00560 min 3,412 � 4,601 1,400 � 2,624 0.0330 min 8,995 � 14,665 2,430 � 10,682 0.095 min 7,325 � 7,049 2,282 � 8,433 0.01
Ln HF, ms2
120 min 8.1 � 1.5 6.2 � 1.6 � 0.00560 min 6.8 � 2.0 5.6 � 1.9 0.0330 min 7.6 � 2.2 5.5 � 1.8 � 0.0055 min 8.1 � 1.6 5.7 � 1.8 � 0.005
LF/HF ratio120 min 0.6 � 0.7 1.3 � 1.7 0.0460 min 1.0 � 1.2 2.2 � 3.1 0.0930 min 1.0 � 2.0 3.0 � 7.5 0.365 min 0.5 � 0.7 2.0 � 2.8 0.004
Abbreviations as in Table 2.
Figure 2. Continuous 5-min data of frequency-domain parameters ofHRV during the 2 h preceding the onset of AF (filled circles) or in thecorresponding study window in controls (unfilled circles). A � LF; B �HF; C � LF/HF ratio. See text for abbreviations. P values in the figuresrepresent the group by time interaction results.
1266 Amar et al. JACC Vol. 42, No. 7, 2003Mechanisms of Postoperative AF October 1, 2003:1262–8

LF/HF ratio before AF onset. The latter results wereinterpreted to suggest that vagal withdrawal and increase insympathetic tone were the primary triggers of postoperativeAF (15). Hogue et al. (16) used linear and nonlinearmeasures of HRV in 18 patients who developed AF aftercardiac surgery and found that patients with AF had agreater HR and lower approximate entropy 1 h before AFonset in comparison to controls. These investigators alsofound that among the patients with AF there were 19 AFepisodes that were preceded by low HRV and 5 AF episodesby high HRV (16). They suggested that their preliminaryfindings may represent two different autonomic patternsunderlying AF after CABG: one of heightened vagal toneand one of adrenergic predominance. Our results in a muchlarger group of noncardiac thoracic surgical patients supportone autonomic mechanism for the trigger of postoperativeAF. However, our data differ from Hogue et al. (16) in thatthe two patient populations studied differ in severity ofcardiac disease, lower use of beta-blockers, and in surgerythat does not involve cardiopulmonary bypass.
There have been conflicting reports on the meaning ofHRV changes before paroxysmal AF unrelated to surgery(31–33). The most recent study showed that the increases inHRV were preceded by a decreasing RR interval (33).These data in nonsurgical patients are comparable to ours,where RR decreased and frequency domain parameters ofHRV increased before AF onset. In addition, time domainparameters of HRV also increased in our patients, providingconsistent data to suggest that vagal rebound or resurgencewas occurring in addition to an elevation in sympathetictone before the trigger of postoperative AF.Study limitations. Our patient population consists of pro-spectively collected data in an ongoing database of consec-utive trials, but not necessarily of all consecutive patientswho had surgery at our institution during the study period.Nevertheless, this population of patients represents one ofthe more comprehensive and large prospective databases ofpatients undergoing major noncardiac thoracic surgery fo-cused on the problem of postoperative AF with Holter data.Our results may not apply to patients with illnesses thatmight affect autonomic state and regulation. We chose tostudy 5-min HRV over a 2-h period preceding AF insteadof 24-h periods, as this represented a critical time whereshort-term autonomic changes influencing the trigger ofthis arrhythmia were likely to occur (15,16). Heart ratevariability is only an indirect measure of autonomic influ-ences on the sinus node, and therefore interpretation con-cerning the exact mechanism of postoperative AF should bemade with caution (23). Linear methods of HRV analysis(Fast Fourier) may be influenced by several importantconditions, including age, posture, respiratory rate, circadianrhythms, disease states, and medications. Posture and respi-ratory rate could not be controlled, and we uniformly treatedour patients with opioids postoperatively according to astandard protocol. Patients with AF had significantly moresupraventricular and ventricular ectopy than controls, and
this could have artifactually increased HRV in the AFgroup. On the contrary, because ectopic and post-ectopicintervals were excluded from the time domain analysis andconstant RR intervals were substituted for these intervals inthe frequency domain analysis, increased ectopy wouldactually tend to decrease HRV in the AF group because theintervals were otherwise assumed to be constant.Conclusions and clinical implications. In comparison tomatched controls, patients who developed AF after majornoncardiac thoracic surgery demonstrated significantchanges in HRV that are consistent with vagal resurgencecompeting in a background of increasing sympathetic activ-ity as the primary autonomic mechanism responsible for thetrigger of postoperative AF. To the best of our knowledge,these novel results represent the largest study using HRV tounderstand autonomic influences preceding postoperativeAF, and suggest that interventions that modulate both thesympathetic and parasympathetic nervous systems may bebeneficial in suppressing postoperative AF.
Reprint requests and correspondence: Dr. David Amar, Profes-sor of Anesthesiology, Memorial Sloan-Kettering Cancer Center,1275 York Avenue, M-304, New York, New York 10021. E-mail:[email protected].
REFERENCES
1. Polanczyk CA, Goldman L, Marcantonio ER, Orav EJ, Lee TH.Supraventricular arrhythmia in patients having noncardiac surgery:clinical correlates and effect on length of stay. Ann Intern Med1998;129:279–85.
2. Amar D, Roistacher N, Burt M, Reinsel RA, Ginsberg RJ, WilsonRS. Clinical and echocardiographic correlates of symptomatic tachy-dysrhythmias after non-cardiac thoracic surgery. Chest 1995;108:349–54.
3. Maisel WH, Rawn JD, Stevenson WG. Atrial fibrillation after cardiacsurgery. Ann Intern Med 2001;135:1061–73.
4. Mathew JP, Parks R, Savino JS, et al., for the Multicenter Study ofPerioperative Ischemia Research Group. Atrial fibrillation followingcoronary artery bypass graft surgery: predictors, outcomes, and re-source utilization. JAMA 1996;276:300–6.
5. Cox JL. A perspective of postoperative atrial fibrillation in cardiacoperations. Ann Thorac Surg 1993;56:405–9.
6. Amar D, Zhang H, Leung DHY, Roistacher N, Kadish AH. Olderage is the strongest predictor of postoperative atrial fibrillation.Anesthesiology 2002;96:352–6.
7. Spach MS, Dolber PC. Relating extracellular potentials and theirderivatives to anisotropic propagation at a microscopic level in humancardiac muscle. Evidence for electrical uncoupling of side-to-side fiberconnections with increasing age. Circ Res 1986;58:356–71.
8. Allessie MA, Boyden PA, Camm AJ, et al. Pathophysiology andprevention of atrial fibrillation. Circulation 2001;103:769–77.
9. Steinberg JS, Zelenkofske S, Wong SC, Gelernt M, Sciacca R,Menchavez E. Value of the P-wave signal-averaged ECG for predict-ing atrial fibrillation after cardiac surgery. Circulation 1993;88:2618–22.
10. Frost L, Lund B, Pilegaard H, Christiansen EH. Re-evaluation ofP-wave duration and morphology as predictors of atrial fibrillation andflutter after coronary artery bypass surgery. Eur Heart J 1996;17:1065–71.
11. Zaman AG, Archbold RA, Helft G, Paul EA, Curzen NP, Mills PG.Atrial fibrillation after coronary artery bypass surgery. A model forpreoperative risk stratification. Circulation 2000;101:1403–8.
12. Amar D, Roistacher N, Zhang H, Baum MS, Ginsburg I, SteinbergJS. Signal averaged P-wave duration does not predict atrial fibrillationafter thoracic surgery. Anesthesiology 1999;91:16–23.
1267JACC Vol. 42, No. 7, 2003 Amar et al.October 1, 2003:1262–8 Mechanisms of Postoperative AF

13. Giri S, White CM, Dunn AB, et al. Oral amiodarone for preventionof atrial fibrillation after open heart surgery, the atrial fibrillationsuppression trial (AFIST): a randomized placebo-controlled trial.Lancet 2001;357:830–6.
14. Frost L, Christiansen EH, Molgaard H, Jacobsen C-J, Allermand H,Thomsen PEB. Premature atrial beat eliciting atrial fibrillation aftercoronary artery bypass grafting. J Electrocardiol 1995;28:297–305.
15. Dimmer C, Tavernier R, Gjorgov N, Nooten GV, Clement DL,Jordaens L. Variations of autonomic tone preceding onset of atrialfibrillation after coronary artery bypass grafting. Am J Cardiol 1998;82:22–5.
16. Hogue CW, Domitrovich PP, Stein PK, et al. RR interval dynamicsbefore atrial fibrillation in patients after coronary artery bypass graftsurgery. Circulation 1998;98:429–34.
17. Amar D, Roistacher N, Burt ME, et al. Effects of diltiazem versusdigoxin on dysrhythmias and cardiac function after pneumonectomy.Ann Thorac Surg 1997;63:1374–82.
18. Amar D, Roistacher N, Rusch VW, et al. Effects of diltiazemprophylaxis on the incidence and clinical outcome of atrial arrhythmiasafter thoracic surgery. J Thorac Cardiovasc Surg 2000;120:790–8.
19. Myers GA, Martin GJ, Magid NM, et al. Power spectral analysis ofheart rate variability in sudden cardiac death: comparison to othermethods. IEEE Trans Biomed Eng 1986;33:1149–56.
20. Task Force of European Society of Cardiology and the NorthAmerican Society for Pacing and Electrophysiology. Heart rate vari-ability: standards of measurement, physiological interpretation, andclinical use. Circulation 1996;93:1043–65.
21. Goldberger JJ. Sympathovagal balance: how should we measure it?Am J Physiol 1999;276:H1273–80.
22. Coumel P. Paroxysmal atrial fibrillation: a disorder of autonomic tone?Eur Heart J 1994;15 Suppl A:9–16.
23. Zaza A, Lombardi F. Autonomic indexes based on the analysis ofheart rate variability: a view from the sinus node. Cardiovasc Res2001;50:434–42.
24. Chen Y, Chen S, Tai C, et al. Role of atrial electrophysiology andautonomic nervous system in patients with supraventricular tachycar-dia and paroxysmal atrial fibrillation. J Am Coll Cardiol 1998;32:732–8.
25. Amar D. Perioperative atrial tachyarrhythmias. Anesthesiology 2002;97:1618–23.
26. Zimmermann M, Kalusche D. Fluctuation in autonomic tone is amajor determinant of sustained atrial arrhythmias in patients with focalectopy originating from the pulmonary veins. J Cardiovasc Electro-physiol 2001;12:285–91.
27. Blommaert D, Gonzalez M, Mucumbitsi J, et al. Effective preventionof atrial fibrillation by continuous atrial overdrive pacing after coronaryartery bypass surgery. J Am Coll Cardiol 2000;35:1411–5.
28. Levy T, Fotopoulos G, Walker S, et al. Randomized controlled studyinvestigating the effect of biatrial pacing in prevention of atrialfibrillation after coronary artery bypass grafting. Circulation 2000;102:1382–7.
29. Daubert JC, Mabo P. Atrial pacing for the prevention of postoperativeatrial fibrillation: how and where to pace? J Am Coll Cardiol2000;35:1423–7.
30. Jideus L, Ericson M, Stridsberg M, Nilsson L, Blomstrom P,Blomstrom-Lundqvist C. Diminished circadian variation in heart ratevariability before surgery in patients developing postoperative atrialfibrillation. Scand Cardiovasc J 2001;35:238–44.
31. Lombardi F, Colombo A, Basilico B, et al. Heart rate variability andearly recurrence of atrial fibrillation after electrical cardioversion. J AmColl Cardiol 2001;37:157–62.
32. Herweg B, Dalal P, Nagy B, Schweitzer P. Power spectral analysis ofheart period variability of preceding sinus rhythm before initiation ofparoxysmal atrial fibrillation. Am J Cardiol 1998;82:869–74.
33. Bettoni M, Zimmermann M. Autonomic tone variations beforethe onset of paroxysmal atrial fibrillation. Circulation 2002;105:2753–9.
1268 Amar et al. JACC Vol. 42, No. 7, 2003Mechanisms of Postoperative AF October 1, 2003:1262–8

EDITORIAL COMMENT
Autonomic Modulation Precedingthe Onset of Atrial Fibrillation*William H. Maisel, MD, MPHBoston, Massachusetts
Autonomic influences on the heart have been recognized formany centuries. It was not until 1921, however, that aGerman physiologist named Otto Loewi stimulated a frog’svagus nerve, collected the released substance, and applied itto a second, different frog heart to demonstrate its effects.For his discovery of this “vagusstuff” (subsequently shown tobe acetylcholine), Loewi (1) shared the 1936 Nobel Prize inPhysiology or Medicine. We now know that acetylcholinereleased by the vagus nerve is the predominant parasympa-thetic influence on the heart while epinephrine and norepi-nephrine mediate the principal cardiac sympathetic effects (2).
See page 1262
The measurement of autonomic tone in humans nonin-vasively presented new challenges. Subtle beat-to-beat vari-ations in heart rate are influenced by autonomic tone, givingrise to the measure of heart rate variability (HRV). Thatchanges in the RR-interval (heart rate) precede and predictclinically relevant events was first appreciated in the mid-1960s when beat-to-beat variations in heart rate were shownto portend fetal distress (2). Later, it was appreciated thatreduced HRV was an independent predictor of ventriculararrhythmias, sudden cardiac death, and total mortality aftermyocardial infarction and predicted increased mortality inother patient populations such as those with heart failure ordiabetes (2–4).
Experimental studies utilizing vagus nerve stimulation,vagotomy, and muscarinic receptor blockade have demon-strated that efferent vagal activity contributes significantly tothe high-frequency (HF) component of HRV (2). Whileinterpretation of the low-frequency (LF) component ofHRV is more controversial, most agree that at least someportion reflects sympathetic modulation of the autonomicnervous system (2). The LF/HF ratio is viewed by many,therefore, to represent sympathovagal “balance” (2). Impor-tantly, HRV measures changes in the relative degree ofautonomic modulation of heart rate, not the absolute levelof sympathetic or parasympathetic tone.
In this issue of the Journal, Amar et al. (5) report theresults of their investigation into the autonomic fluctuationspreceding the development of postoperative atrial fibrilla-
tion (AF) in patients undergoing major thoracic surgery.They utilized HRV measures as an indicator of autonomictone. Compared with control patients, those who developedAF had an increase in LF and HF power and a decrease inLF/HF ratio in the period preceding AF onset. Thesefindings are consistent with activation of both the sympa-thetic and parasympathetic systems with a shift towardsparasympathetic predominance. These findings add to thegrowing body of literature suggesting that autonomic influ-ences play an important role in the initiation of AF.
A number of other studies have also demonstrated thatfluctuations in autonomic tone, as measured by HRV,precede the onset of AF (6–10). Yet while these investiga-tions consistently demonstrate that dynamic changes inautonomic tone occur prior to AF, the frequency, character,and degree of change varies considerably from study tostudy. For example, among patients with structurally normalhearts, some have observed an increase in vagal predomi-nance in the minutes preceding AF onset, while others havenoted a marked shift towards sympathetic predominance(10,11). Other patients with paroxysmal AF or AF triggeredby pulmonary vein foci may experience a rise in sympathetictone followed by a marked shift towards vagal predomi-nance in the minutes preceding AF onset (6,7), findingsmore consistent with those of Amar et al. In contrast,patients undergoing cardiac surgery experience a relativedecrease in vagal tone and an increase in sympathetic tonebefore developing AF (9). To explain these various obser-vations, some have suggested that vagally mediated AFoccurs most often in patients with normal hearts and occurspredominantly at night when vagal tone is relatively high,while adrenergically induced AF occurs more frequently inpatients with organic heart disease and occurs more fre-quently during the day (11). However, not all studiessupport this simplified interpretation of the data. Indeed,there are many exceptions to this “rule.”
A number of important electrophysiologic changes occurin atrial myocardium in response to an increase in vagusnerve activity. Acetylcholine, acting via its effect on musca-rinic receptors, reduces the slope of spontaneous depolar-ization of the sinoatrial node pacemaker cells and results ina slowing of the heart rate. Acetylcholine also shortens theatrial refractory period and increases the heterogeneity ofatrial refractoriness, effects that predispose to reentry(12,13). It appears that the relative sympathovagal balance isas important, or more important, than the absolute sympa-thetic or parasympathetic tone. Indeed, experimental re-gional cardiac denervation (e.g., withdrawal of sympathetictone from a specific atrial site) can result in a relativeincrease in vagal tone without a change in the absolute vagaltone. This can result in regional shortening of the atrialrefractory period, heterogeneity of atrial repolarization, andpredisposition to induction of AF (14–16). This importantinterplay between sympathetic and parasympathetic tone isfurther underscored by the observation that AF induction in
*Editorials published in the Journal of the American College of Cardiology reflect theviews of the authors and do not necessarily represent the views of JACC or theAmerican College of Cardiology.
From the Cardiovascular Division, Department of Medicine, Brigham and Wom-en’s Hospital, Boston, Massachusetts.
Journal of the American College of Cardiology Vol. 42, No. 7, 2003© 2003 by the American College of Cardiology Foundation ISSN 0735-1097/03/$30.00Published by Elsevier Inc. doi:10.1016/S0735-1097(03)00959-8

dogs occurs much more readily with infusion of isoproter-enol and acetylcholine than with either isoproterenol oracetylcholine alone (17).
That increased vagal tone can predispose to the develop-ment of AF has been recognized since the initial descriptionby Coumel et al. (18). Perhaps most exciting are the newtherapeutic avenues that have been opened by our increasedunderstanding of the autonomic influences that predisposeto AF. Parasympathetic ganglia have been localized todiscrete epicardial fat pads. Radiofrequency ablation ofspecific fat pads causes regional alterations of cardiac para-sympathetic tone and, as a result, affects atrial refractoryperiods, atrioventricular nodal conduction properties, andheterogeneity of atrial conduction (15,19,20). In dogs,catheter ablation of parasympathetic nervous input to theatrium can abolish vagally mediated AF (21).
Loewi’s (1) initial description of “vagusstuff” opened thedoor to important advances in our understanding of cardiacautonomic regulation. Similarly, improved understanding ofthe autonomic influences that predispose to AF will becritical to the development of novel therapies. While thereis much that remains to be learned, specific pharmacologic,catheter, or device-based therapies that alter or regulateautonomic tone may someday prove to be useful weapons inthe battle against AF.
Reprint requests and correspondence: Dr. William H. Maisel,Cardiovascular Division, Brigham and Women’s Hospital, 75Francis Street, Boston, Massachusetts 02115. E-mail: [email protected].
REFERENCES
1. Loewi O. The Nobel Prize in Physiology or Medicine: Nobel Lecture.December 12, 1936. Available at: www.nobel.se/medicine/laureates/1936. Accessed on March 24, 2003.
2. Task Force of the European Society of Cardiology and the NorthAmerican Society of Pacing and Electrophysiology. Heart rate vari-ability: standards of measurement, physiological interpretation, andclinical use. Circulation 1996;93:1043–65.
3. Lombardi F. Chaos theory, heart rate variability, and arrhythmicmortality. Circulation 2000;101:8–13.
4. Stein PK, Bosner MS, Kleiger RE, Conger BM. Heart rate variability:a measure of cardiac autonomic tone. Am Heart J 1994;127:1376–81.
5. Amar D, Zhang H, Miodownik S, Kadish AH. Competing autonomicmechanisms precede the onset of postoperative atrial fibrillation. J AmColl Cardiol 2003;42:1262–8.
6. Bettoni M, Zimmermann M. Autonomic tone variations before theonset of paroxysmal atrial fibrillation. Circulation 2002;105:2753–9.
7. Zimmerman M, Kalusche D. Fluctuation in autonomic tone is amarker determinant of sustained atrial arrhythmias in patients withfocal ectopy originating from the pulmonary veins. J CardiovascElectrophysiol 2001;12:285–91.
8. Wen ZC, Chen S-A, Tai C-T, Huang J-L, Chang M-S. Role ofautonomic tone in facilitating spontaneous onset of typical atrialflutter. J Am Coll Cardiol 1998;31:602–7.
9. Dimmer C, Tavernier R, Gjorgov N, Van Nooten G, Clement DL,Jordaens L. Variations of autonomic tone preceding onset of atrialfibrillation after coronary artery bypass grafting. Am J Cardiol 1998;82:22–5.
10. Fioranelli M, Piccoli M, Mileto GM, et al. Analysis of heart ratevariability five minutes before the onset of paroxysmal atrial fibrilla-tion. Pacing Clin Electrophysiol 1999;22:743–9.
11. Herweg B, Dalal P, Nagy B, Schweitzer P. Power spectral analysis ofheart period variability of preceding sinus rhythm before initiation ofparoxysmal atrial fibrillation. Am J Cardiol 1998;82:869–74.
12. Wang J, Liu L, Feng J, Nattel S. Regional and functional factorsdetermining induction and maintenance of atrial fibrillation in dogs.Am J Physiol 1996;271:H148–58.
13. Ninomyia I. Direct evidence of nonuniform distribution of vagaleffects on dog atria. Circ Res 1966;19:576–83.
14. Olgin JE, Sih HJ, Hanish S, et al. Heterogeneous atrial denervationcreates substrate for sustained atrial fibrillation. Circulation 1998;98:2608–14.
15. Hirose M, Leatmanoratn Z, Laurita KR, Carlson MD. Partial vagaldenervation increases vulnerability to vagally induced atrial fibrillation.J Cardiovasc Electrophsyiol 2002;13:1272–9.
16. Chen YJ, Chen S-A, Tai C-T, et al. Role of atrial electrophysiologyand autonomic nervous system in patients with supraventriculartachycardia and paroxysmal atrial fibrillation. J Am Coll Cardiol1998;32:732–8.
17. Sharifov OF, Federov VV, Beloshapko GG, Iushmanova AV, Roz-enshtraukh LV. Isoproterenol potentiates atrial fibrillation induced byacetylcholine. Ross Fiziol Zh Im I M Sechenova 2001;87:1296–308.
18. Coumel P, Attuel P, Lavallee J, Flammang D, Leclercq JF, Slama R.Syndrome d’arythmie auriculaire d’origine vagale [The atrial arrhyth-mia syndrome of vagal origin]. Arch Mal Coeur 1978;71:645–56.
19. Chiou C-W, Eble JN, Zipes DP. Efferent vagal innervation of thecanine atria and sinus and atrioventricular nodes: the third fat pad.Circulation 1997;95:2573–84.
20. Quan KJ, Lee JH, Van Hare GF, Biblo LA, Mackall JA, Carlson MD.Identification and characterization of atrioventricular parasympatheticinnervation in humans. J Cardiovasc Electrophysiol 2002;13:735–9.
21. Schauerte P, Scherlag BJ, Pitha J, et al. Catheter ablation of cardiacautonomic nerves for prevention of atrial fibrillation. Circulation2000;102:2774–80.
1270 Maisel JACC Vol. 42, No. 7, 2003Editorial Comment October 1, 2003:1269–70

Catheter-Induced Linear Lesions in theLeft Atrium in Patients With Atrial FibrillationAn Electroanatomic StudySabine Ernst, MD, Feifan Ouyang, MD, Felix Lober, Matthias Antz, MD, Karl-Heinz Kuck, MDHamburg, Germany
OBJECTIVES In this study using radiofrequency current and the electroanatomic mapping system CARTO,four line designs were tested in 84 patients suffering from drug-refractory atrial fibrillation(AFib).
BACKGROUND Prevention of AFib by trigger elimination within the pulmonary veins (PVs) has been recentlyreported, but the success may be lesser in patients with chronic AFib or large atria requiringlinear lesion deployment.
METHODS Type A encircled the ostia of all four PVs with a connection to the mitral annulus (MA). Intype B, three lines connected anatomic barriers. Type C encircled both septal and lateral PVswith connections between PVs and to the MA. Type D encircled PVs only. In the initial 12patients (type D/1), line validation was performed without, and in 23 patients (type D/2)with, an additional catheter inside the encircled PVs.
RESULTS The ability to achieve completeness of all intended lines was 5% in type A, 21% in type B,29% in C, 66% in type D/1, and 61% in type D/2. This resulted in stable sinus rhythm in 19%(4/21 patients) in type A, 32% (6/19 patients) in type B, 50% (7/14 patients) in type C, 58%(7/12 patients) in type D/1, and 65% (15/23 patients) in type D/2, respectively, over a meanfollow-up of 620 � 376 days. Besides thromboembolic events (one stroke and one transientischemic attack), total occlusion of a PV was a major complication in one patient, and acutetamponade in two patients.
CONCLUSIONS Complete lesions in the left atrium were difficult to achieve using conventional radiofrequencycurrent technology, but were associated with sinus rhythm in 74% of patients duringlong-term follow-up, whereas incomplete lesions led mostly to recurrences of AFib orgap-related atrial tachycardia. (J Am Coll Cardiol 2003;42:1271–82) © 2003 by theAmerican College of Cardiology Foundation
Catheter ablation of atrial fibrillation (AFib) has beenattempted by either elimination of the initiating trigger orby modifying the substrate for maintenance of the arrhyth-mia. Prevention of AFib by trigger elimination within thepulmonary veins (PVs) can be successful in up to 71% ofpatients (1–3). The success rate may be lower in patientswith chronic AFib or large atria mostly due to extra-PV
See page 1283
triggers that cannot be ablated during electrophysiologicalstudy. Therefore, substrate modification may be mandatoryeither as primary or as additional treatment after successfulisolation of the PVs. We have recently shown that multiplelinear lesions may be successfully deployed within the rightatrium (RA), but do not prevent AFib episodes in the vastmajority of patients (4).
Compartmentalization of the left atrium (LA) by surgi-cally deployed linear lesions has prevented AFib episodes(5,6). Application of linear lesions within the LA bycatheter techniques has been reported with variable success
(7,8). In those reports, completeness of lines was notvalidated in detail. Thus, it was unclear whether AFibrecurrences were due to incomplete lines or an inadequateline design. Furthermore, incomplete linear lesions predis-pose to gap-related tachycardia (AT) (9).
This paper presents four different line designs within theLA aiming at modification of the myocardial substrate forAFib and/or isolation of PVs in humans.
METHODS
Patient population. Between June 1997 and August 2000,a total of 84 patients (66 male; mean age, 58.3 � 8.7 years)underwent primary catheter ablation for AFib in the LA.All patients suffered from either intermittent or chronicsymptomatic (n � 15) AFib for a mean duration of 10 � 8years and were refractory to a median number of fourantiarrhythmic agents (including amiodarone in 64 pa-tients). A total of 46 patients had undergone previousablation procedures that failed to change their arrhythmia:34 patients an RA linear lesion ablation for AFib, threepatients a PV isolation attempt using ultrasound energy,nine patients a bidirectional isthmus blockade for atrialflutter. All patients suffered from symptomatic AFib pre-senting with symptoms such as palpitations, dizziness, orpresyncope despite antiarrhythmic treatment. The ethicalcommittee in Freiburg, Germany, had approved the study
From the II. Med. Abteilung, Allgemeines Krankenhaus St. Georg, Hamburg,Germany. Drs. Ernst, Ouyang, Antz, and Kuck are trainers of the EuropeanTeaching Course of the CARTO system (Biosense Webster, Europe).
Manuscript received January 6, 2003; revised manuscript received April 9, 2003,accepted April 17, 2003.
Journal of the American College of Cardiology Vol. 42, No. 7, 2003© 2003 by the American College of Cardiology Foundation ISSN 0735-1097/03/$30.00Published by Elsevier Inc. doi:10.1016/S0735-1097(03)00940-9

protocol, and all patients gave their written consent. Afterexclusion of intracardiac thrombi by transesophageal echo-cardiography, patients were studied in a fasting state undercontinuous sedation.Electrophysiologic study. Two standard catheters werepositioned: a His bundle recording catheter (Parahis, Bio-sense Webster, Waterloo, Belgium) advanced via femoralvein access, as well as a multipolar catheter (A 20, BiosenseWebster) advanced in the distal coronary sinus (CS) via theleft subclavian vein. Subsequently, trans-septal access usinga modified Brockenbrough technique was performed andeither a single standard 8F sheath (SL1, DAIG, St. JudeMedical, Minnetonka, Minnesota) or a custom-made 11Fdouble sheath system (Cordis Roden, Roden, the Nether-lands) was advanced. Using this double-sheath technique(in nine patients of group A and B), the inner preformedsheath guides the catheter tip so that it is in parallel and nottangential orientation to the atrial wall and can be gentlydragged along the intended line (10). In type D/2 ablationprocedures, a double trans-septal puncture with two 8Fsheaths was performed. After trans-septal puncture, acti-vated clotting time was adjusted to 250 to 300 s by repeatintravenous.Heparin bolus throughout the procedure. In addition, acontinuous infusion with heparinized saline was connectedto the trans-septal sheaths (flow rate 15 ml/h) to avoidthrombus formation or air embolism.Three-dimensional mapping. The electroanatomic map-ping system (CARTO) was used to reconstruct the LA,which has been previously described in detail (11). In brief,a 4-mm tip mapping and ablation catheter (NAVI-Star,Biosense Webster) was advanced to the LA via the trans-septal sheath. Mapping was performed during stable pacingconditions from the CS or from the RA septum. In case ofAFib, sinus rhythm (SR) was restored by external cardio-version. If DC shock failed, intravenous flecainide (up to 1.5mg/kg body weight, n � 12 patients) was administered andcardioversion repeated. After completion of the mapping, allendocardial potentials were manually annotated.Ablation design. Type A consisted of two lines: a circularlesion, which incorporated all PV ostia and a connectionfrom the encircling line (close to the inferior lateral PV) tothe mitral annulus (MA) (Fig. 1A). This concept copies the
“core” line of the surgical Maze procedure and interrupts bythe lateral connection to the MA the potential macroreentryaround the annulus.
Type B consisted of three lines: the first connecting thesuperior septal to the superior lateral PV (roof line), thesecond connecting the middle of the roof line to the anteriorMA, and the third connecting the roof line towards theposterior MA leaving an intentional gap of 2 to 3 cm toallow activation of the LA appendage (Fig. 1B). This designinvestigates a pure substrate modification attempt withoutany trigger elimination by PV isolation.
Type C consisted of two encircling lines around the septalsuperior and inferior PV ostia as well as the lateral superiorand inferior PV ostia, respectively. In addition, linearconnections along the posterior wall between the twoencircling lines and towards the lateral MA were deployed(Fig. 1C). This design combines both the PV isolation withthe substrate modification attempt to interrupt potentialreentry circuits between the PV segments and around theMA.
Type D, as type C without the connections between thePV encircling lines (Fig. 1D). After the experience ofincomplete lesion deployment in type C, the connectionswere omitted to avoid iatronegic gap-related tachycardia.Ablation. The linear lesions were applied by moving theablation catheter along the previously designed lines intemperature-controlled mode (maximum temperature 55°C,maximum duration of 180 s, maximum 50 W).
End point for radiofrequency current (RFC) delivery waseither the total elimination of the local potential or amaximum of 180 s. In case of an impedance drop by �10 �,RFC energy was immediately stopped to prevent carbon-ization at the catheter tip.Line validation. Validation was performed by conven-tional mapping criteria followed by a repeat three-dimensional reconstruction while pacing either from CS orRA septum.
In type A, complete lines lead to an isolation of theencircled area, as previously described (10). The electroana-tomic activation map showed a sudden change from early tolate activation along the ablation line and/or no potentials atall within the isolated area. Conduction gaps were identifiedby sites with single potentials and by local early activation(Fig. 2A).
In type B, completion of the anterior line was character-ized by an abrupt change of the activation sequence re-corded from the multipolar catheter placed distally in theCS while pacing from the RA septum (Fig. 2B). Further-more, double potentials could be found along the lines whenpacing from sites opposite to the ablation line: from RAseptum for the anterior and posterior line and from the CSfor the LA roof line. Accordingly, the electroanatomic mapshowed a sudden change of the local activation times.
In type C, isolation of the PV segments was defined by adecrease of local voltage amplitude of �70% within theisolated areas using the amplitude voltage feature of the
Abbreviations and AcronymsAFib � atrial fibrillationAT � atrial tachycardiaCS � coronary sinusLA � left atrium/atrialLAA � left atrial appendageMA � mitral annulusPV � pulmonary veinRA � right atrium/atrialRFC � radiofrequency currentSR � sinus rhythm
1272 Ernst et al. JACC Vol. 42, No. 7, 2003Catheter-Induced Linear Lesions in the Left Atrium October 1, 2003:1271–82

CARTO system and a cut-off limit of 0.1 mV (12).Completion of the connecting lesions in type C wasdetermined by pacing maneuvers from the proximal anddistal CS while recording double potentials along theablation lines (Fig. 2C).
In type D, two different approaches were used: in the
initial 12 patients (type D/1), successful encircling of the PVsegments was defined as in type C (Fig 2D). In theremaining 23 patients (type D/2), an additional catheter(ParaHis, Biosense Webster, Diamond Bar, California) wasplaced inside the respective PV before lesion deployment todemonstrate a PV spike potential on one or more bipolar
Figure 1. Intended line designs: anterior posterior projections of a mesh graph of the electroanatomic mapping system CARTO of an LA with thepulmonary veins (PV) and the trans-septal sheath depicted as colored tubes. Ablation lines are depicted by multiple red dots. (A) A long encircling linearound all four PV ostia (roof line) and a connection to the lateral mitral annulus (MA). (B) Roof line between the right and left superior PV ostium. Theanterior line connects the middle of the roof line to the superior MA; the posterior line aims at the inferior MA with an intentional gap of approximately3 cm. (C) Two encircling lines around the ostia of the superior and inferior PVs on both the septal and lateral sides. Additional connections between thePV segments (posterior line), the lateral PV segment, and the MA. (D) Encircling lines around the PVs on both sides without additional connection lines.
1273JACC Vol. 42, No. 7, 2003 Ernst et al.October 1, 2003:1271–82 Catheter-Induced Linear Lesions in the Left Atrium

Figure 2. Line validation (A) pulmonary artery (PA) projection of an activation map of the electroanatomic mapping system in the patient with a single persisting gap in the lateral aspect of the posteriorline as depicted by the gradual change of colors at the site of the conduction gap. Complete lesions demonstrate double potential while constantly pacing from the coronary sinus (CS). Continued on next page.
1274Ernstetal.
JACCVol.42,No.7,2003
Catheter-InducedLinear
Lesionsin
theLeftAtrium
October1,2003:1271–82

Figure 2 Continued. (B) Comparison of the pre- and post-ablation activation map in a left anterior oblique projection for type B. The right-hand paneldemonstrates the activation sequence along a multipolar catheter advanced in the distal CS while constantly pacing from the RA septal site. Please notethe prolongation of the activation time after complete anterior line deployment in the distal CS electrodes. Continued on next page.
1275JACC Vol. 42, No. 7, 2003 Ernst et al.October 1, 2003:1271–82 Catheter-Induced Linear Lesions in the Left Atrium

electrograms. Validation of the completeness of the encir-cling PV isolation line was demonstrated by loss or disso-ciation of the PV spikes (Fig. 2E).Definitions. Lines were classified as being either complete,having a single or multiple conduction gaps.
Upon completion of the post-ablation maps, a manualcontrast injection in the ostia of all PVs was performed aftertype C and D line deployment to exclude acute PV stenosis.Follow-up. All patients were initially followed on theirprevious antiarrhythmic medication that was continued
throughout the ablation procedure. Anticoagulation wasadvised with warfarin (international normalized ratio 2 to3), or with aspirin (300 mg per day) if the patient refused totake warfarin. One day after the procedure, a 12-leadelectrocardiogram (ECG), transthoracic echocardiography,and a 24-h Holter recording were performed. These wererepeated after one, three, and six months by the referringphysicians or by the ablation center (where all data wascollected and reviewed). In case of stable SR after threemonths, antiarrhythmic medication was discontinued. Pa-
Figure 2 Continued. (C) Post-ablation activation map after pulmonary vein (PV) isolation during pacing from the CS catheter shown in a PA projection.Double potentials are marked with blue dots. Continued on next page.
1276 Ernst et al. JACC Vol. 42, No. 7, 2003Catheter-Induced Linear Lesions in the Left Atrium October 1, 2003:1271–82

Figure 2 Continued. (D) Comparison of voltage in the pre- and post-ablation maps in a posterior-anterior projection of the LA. The voltage is depicted according to the color spectrum shown in the rightupper corner, ranging from low (�0.1 mV, red) to high-voltage (�1.5 mV, purple). Continued on next page.
1277JACC
Vol.42,No.7,2003Ernst
etal.
October1,2003:1271–82Catheter-Induced
LinearLesions
inthe
LeftAtrium

tients were advised to obtain a 12-lead ECG in case ofrecurrent palpitations. After completion of the six-monthfollow-up, patients were contacted and interviewed viatelephone at regular intervals. Patients were offered a re-attempt at catheter ablation if AFib persisted.Study end points. The primary end point was the completedeployment of the intended ablation lines.
Secondary end points were either recurrences of symp-tomatic or documented AFib, stable SR, and new-onset ATs.Statistical analysis. Continuous variables are expressed asmean � 1 SD.
RESULTS
Procedural data. The 84 patients underwent a total of 107procedures. The average procedure time was 8.4 � 1.7 hfrom sheath insertion to sheath extraction. A mean durationof 33.3 � 30.5 min of fluoroscopy was used, ranging fromup to 145 min (Patient 8) in the first 10 procedures to as lowas 7.1 min with increasing experience of the investigators. A
mean number of 43.2 � 15.3 radiofrequency applicationswere deployed (Table 1).Validation of line completeness and results of follow-up.In type A, a mean number of 49.2 � 15.7 RFC applicationswere delivered over a mean total line length of 202 � 32mm (185 � 28 mm for the PV isolation segment) (Table 2,Fig. 3). Complete lines were achieved in a single patient(during the second ablation session). This resulted in thecreation of a silent area in the posterior part of the LA (10).In a second patient, a single gap persisted despite multipleradiofrequency applications at the inferior lateral part of theLA (Fig. 2A). In the remaining patients, multiple conduc-tion gaps persisted in the roof (12 patients) and septal (10patients) lines.
During a mean follow-up of 974 � 408 days, the patientwith complete lines remained in SR without antiarrhythmicmedication. The patient with the single gap was in SR withfrequent atrial extrasystoles on antiarrhythmic medication.Of the 18 patients with incomplete lines, only two were in
Figure 2 Continued. (E) Left-hand panel depicts the multipolar catheter in the right upper PV (RUPV) during contrast injection through the secondtrans-septal sheath. The right panel demonstrates the loss of the PV spike potential (arrow) during radiofrequency current application. Surface lead II, aswell as a bipolar electrogram from the 4-mm ablation catheter (Mp), four bipolar electrograms of the PV catheter (from distal to proximal), and from theproximal CS are shown. MA � mitral annulus.
Table 1. Overview of Patient Demographics and Procedural Data for Each Line Design
Type A Type B Type C Type D/1 Type D/2 Total
# of patients treated 21 20 (19 ablated) 14 12 23 84# of procedures 27 20 16 14 30 107Mean age (yrs) 60 � 6 56 � 10 62.1 � 6.4 54.2 � 9.6 62.1 � 6.4 58.3 � 8.7Gender (M/F) 19/2 15/4 10/4 7/5 20/3 66/18AFib duration 11.3 � 9 8.2 � 5.9 11.7 � 10 9.8 � 6.4 8.7 � 7.5 9.9 � 8.2# of chronic AFib 3 4 4 0 5 15# of intermittent AFib 18 16 10 12 18 69Mean number of episodes/months 12 � 8 16 � 11 16 � 11 17 � 14 16 � 11 –Mean duration of episodes (h) 21 � 23 20 � 19 21 � 20 20 � 16 26 � 23 –Procedure duration (h) 8.7 � 1.6 8.8 � 2 9.4 � 0.8 7.3 � 1.5 7.7 � 1.8 8.4 � 1.7Fluoroscopy (min) 63 � 44.1 29 � 11.8 19.3 � 8.4 15.7 � 6.2 23.2 � 9.9 33.3 � 30.5# of RFC application 49.2 � 15.7 46.7 � 15.7 46.4 � 14.7 33.9 � 9.0 34.1 � 16.1 43.2 � 15.3Total length of ablation line (mm) 202 � 32 177 � 23 309 � 96 188 � 36 215 � 39 –Length of PV isolation line(s) (mm) 185 � 28 – septal: 109 � 28 septal: 101 � 16 septal: 114 � 16 –
lateral: 120 � 40 lateral: 96 � 20 lateral: 110 � 24
Numbers are given as mean � SD.AFib � Atrial fibrillation; PV � pulmonary vein; RFC � radiofrequency current.
1278 Ernst et al. JACC Vol. 42, No. 7, 2003Catheter-Induced Linear Lesions in the Left Atrium October 1, 2003:1271–82

SR, but 14 patients experienced recurrences of AFib (onepatient underwent a second ablation attempt with designC). Two patients (with multiple gaps) presented withincessant atrial macroreentrant tachycardia around the MAand underwent subsequent successful ablation.
In type B (Fig. 3B), a mean number of 46.7 � 15.7 RFCapplications were given over a mean total line length of 177� 23 mm. All three lines could be successfully deployed infour patients (in all these patients the custom-made doublesheaths were used). Despite multiple RFC applications,conduction gaps persisted in 15/19 patients, at the roof linein 11 patients and the anterior line in eight patients. Duringfollow-up (827 � 330 days), complete lines resulted in SRwith occasional atrial extrasystoles in three patients, whereasthe remaining patient changed from chronic to intermittentAFib on antiarrhythmic medication. Only one patient withincomplete lesions remained in SR; all other patients hadrecurrences of AFib on their medication. Two patientssuffered from incessant LA macroreentrant tachycardia dueto persisting gaps in either the roof or anterior line andunderwent subsequent successful ablation.
In type C (Fig. 3C), a mean number of 46.4 � 14.7 RFCapplications were delivered over a mean line length of 308 �96 mm (109 � 28 mm and 120 � 40 mm for the septal andlateral PV isolation segment, respectively). Complete encir-cling of the septal PV ostia was achieved in all 14 patients.The lateral encircling line was incomplete in nine patients,with conduction gaps located close to the base of the leftatrial appendage (LAA). The connections between the PVsegments towards the mitral annulus were incomplete inseven patients. Overall, lines were complete in only fourpatients, whereas, in the remaining 10 patients, multipleconduction gaps persisted despite repeat RFC applications.During a follow-up of 511 � 142 days, three of the fourpatients with complete lines remained in SR without anti-arrhythmic medication. Of the remaining patients, only twowere in SR, whereas six patients had recurrences of AFib.Two patients with incomplete connections towards the MA
had incessant AT and underwent subsequent catheter abla-tion.
In type D/1 (Fig. 3D), a mean number of 33.7 � 9.0RFC applications were delivered over a mean total linelength of 188 � 36 mm (101 � 16 mm and 96 � 20 mmfor the septal and lateral PV isolation segment, respectively).Complete encircling was achieved around the septal PVs inall patients, around the lateral PVs in 7/12 patients. Aftertwo repeat procedures, this segment was completed in onemore patient. During a follow-up of 400 � 126 days, fourof the eight patients with complete linear lesions were instable SR without antiarrhythmic medication, whereas fourpatients had persistent AFib episodes despite continuedantiarrhythmic medication. Three of the four patients withan incomplete lateral PV segment remained in SR.
In type D/2 (Fig. 3E), a mean number of 34.1 � 16.1RFC applications were given over a mean total line lengthof 215 � 39 mm (114 � 16 mm and 110 � 24 mm for theseptal and lateral PV segment, respectively). Complete PVencircling was achieved in all but one patient for the septalsegment, but remained incomplete in 10/23 patients for thelateral segment after the initial ablation procedure. In repeatprocedures this linear lesion was completed in four addi-tional patients. During a mean follow-up of 324 � 140days, 12/14 patients with complete lines remained in stableSR, whereas only 3/9 patients with incomplete lines re-mained arrhythmia-free.Complications. In two patients (type A and B) trans-septal puncture resulted in acute tamponade, requiringimmediate pericardiocentesis. One patient (type A) under-went the same procedure four weeks later; the other shiftedto type C six months later. Although no impedance rise hadbeen evident during the ablation session, one patient (typeA) suffered a stroke, leading to vision disturbances within48 h after the procedure, and one patient (type D/2) suffereda transient ischemic attack (without morphologic changes insequential computed tomography scans). The symptomsresolved gradually during follow-up. In one patient of group
Table 2. Follow-Up of Treated Patients With Regard to the Respective Ablation Type: Patients Are Categorized With Respect toResults of Line Validation After the Final Ablation Session
Type A Type B Type C Type D/1 Type D/2
# of patients treated 21 20 (19 ablated) 14 12 23# of procedures 27 20 16 14 30Mean follow-up duration 974 � 408 827 � 330 511 � 142 400 � 126 324 � 140Complete lines (n) with
rhythm outcome1/20 4/19 4/14 8/12 14/23
1 pt SR 3 pts SR � AES 3 pts SR 4 pts SR 12 pts SR1 pt i.AFib 1 pt AFib 4 pts AFib 2 pts AFib
Incomplete lines (n) withrhythm outcome
19/20 15/19 10/14 4/12 9/23
3 pts SR (single gap:SR � AES)
1 pt SR 2 pts SR 3 pts SR 3 pts SR
14 pts AFib 12 pts AFib 6 pts AFib 1 pt AFib 6 pts AFib2 pts AT 2 pts AT 2 pts AT
AA-TX � antiarrhythmic medication; AES � atrial extrasystoles; AFib � atrial fibrillation; AT � atrial tachycardia; i.AFib � intermittent atrial fibrillation; pt � patient; SR� sinus rhythm.
1279JACC Vol. 42, No. 7, 2003 Ernst et al.October 1, 2003:1271–82 Catheter-Induced Linear Lesions in the Left Atrium
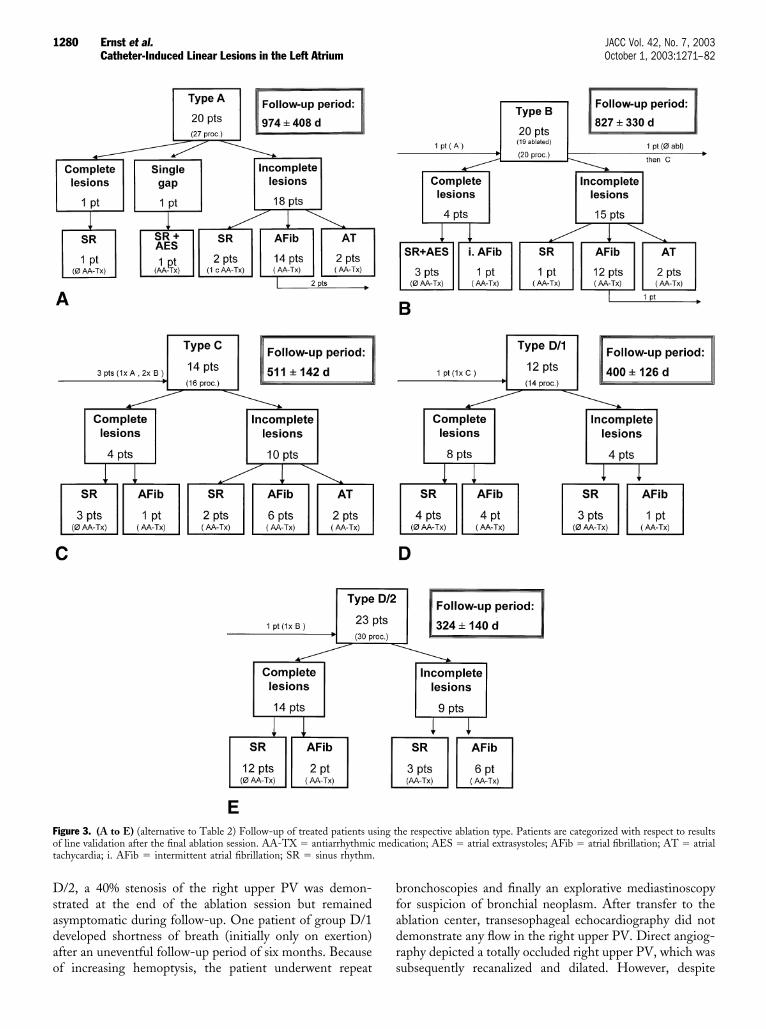
D/2, a 40% stenosis of the right upper PV was demon-strated at the end of the ablation session but remainedasymptomatic during follow-up. One patient of group D/1developed shortness of breath (initially only on exertion)after an uneventful follow-up period of six months. Becauseof increasing hemoptysis, the patient underwent repeat
bronchoscopies and finally an explorative mediastinoscopyfor suspicion of bronchial neoplasm. After transfer to theablation center, transesophageal echocardiography did notdemonstrate any flow in the right upper PV. Direct angiog-raphy depicted a totally occluded right upper PV, which wassubsequently recanalized and dilated. However, despite
Figure 3. (A to E) (alternative to Table 2) Follow-up of treated patients using the respective ablation type. Patients are categorized with respect to resultsof line validation after the final ablation session. AA-TX � antiarrhythmic medication; AES � atrial extrasystoles; AFib � atrial fibrillation; AT � atrialtachycardia; i. AFib � intermittent atrial fibrillation; SR � sinus rhythm.
1280 Ernst et al. JACC Vol. 42, No. 7, 2003Catheter-Induced Linear Lesions in the Left Atrium October 1, 2003:1271–82

antiplatelet and anticoagulation therapy, re-stenosis oc-curred, necessitating repeat balloon dilation and, finally,stent implantation.
DISCUSSION
We have recently shown that linear lesions within the RAcan be successfully deployed and validated using the elec-troanatomic mapping system (4).
In contrast with previously reported data (8,13), RAlinear lesions did not prevent AFib recurrences, even whenthese lesions were complete. Therefore, this study focusedon the efficacy of linear lesions within the LA. As in the RAstudy, the electroanatomic mapping system was used forlesion deployment. Special care was taken on line validationby conventional electrophysiologic criteria and the use of theelectroanatomic mapping system, which might explain thedifference in procedure time and RFC delivery in otherstudies (8,12).
The first line design (type A) was intended to compart-mentalize a large part of the LA including all four PVs, and,thereby, copy the “core” line of the maze operation. Thislong single ablation line could only be completed in one of18 patients, who stayed in SR. All other patients were leftwith incomplete lines. All except two had recurrences ofAFib or AT. The second line design (type B) was aimingsolely at the interruption of possible macro–re-entriesaround anatomic barriers such as PV ostia or the MA.However, the only line that could be completed in 15/19patients (79%) was the anterior line. In contrast, the roofline turned out to be very difficult, which was mostly due tocatheter instability. Catheter stability was enhanced by theuse of the double sheath technique allowing a parallel ratherthan tangential catheter tip orientation at the roof line. Asbefore, complete lines were associated with freedom fromAFib recurrences. In type C, encircling of PV segments mayalso eliminate triggers from within the PVs. Each ablationsegment had a shorter lesion length (approximately 11 cm)and, thereby, was easier to achieve. Inability to encircle thelateral PVs can be explained by the anatomic location of theintended line between the ostium of the lateral PVs and thebase of the LAA (14). The connections were intended toprevent possible macro–re-entry around the newly pre-formed barriers and the MA. These connections wereextremely difficult to achieve and remained incomplete in alarge proportion of patients (50%), causing iatrogenic gap-related tachycardia during follow-up.
Therefore, in type D, the additional connections betweenthe PVs were omitted. During follow-up in type D/1, thevalidation criterion of the reduced signal amplitude (�70%reduction as compared with the pre-ablation map and acut-off value of 0.1 mV) proved not to be discriminativebecause only 4/8 patients with complete PV lesions re-mained in SR, whereas 3/4 patients with incomplete lesionswere also in SR. In type D/2, loss of the PV spike potentialas the ablation end point demonstrated an improved dis-
criminative power: 12/14 patients with complete linearlesions stayed in SR, compared with only 3/9 patients withincomplete lesions. In contrast, when the end point was onlyamplitude reduction, no correlation was found betweencompleteness of lines and maintenance of SR. These find-ings are not in agreement with previously published data(12). Although there might be a small difference in theablation design (separate isolation of each PV as comparedwith an encircling line around both upper and lower PVs),RFC delivery is extremely short (15 to 30 s) and might noteven result in a transmural lesion or have an effect onepicardially located autonomic nervous endings.
The high incidence of incomplete ablation lines using asolid 4-mm tip electrode demands further technologicalimprovement. The use of custom-made sheaths improvedthe catheter-tissue contact, especially at the roof line. Othertechniques, such as irrigated tip catheters, were not availableat the time of study, but may improve lesion deploymentsignificantly and lower the risk of thromboembolic compli-cations, which was 2.4% in this study.
Although the ablation lines were designed to be at theatrial side, PV occlusion occurred in one patient. Even usingthe enhanced mapping and navigation tools of the electro-anatomic mapping system, assessment of the complex three-dimensional anatomy of the PV-LA junction is difficult,and intrapulmonary ablation cannot be ruled out becausedistinctive markers for the PV ostia are missing. Even moredisturbing, PV occlusion developed slowly. The symptomssuch as hemoptysis and shortness of breath were, in ourpatient, not related to the ablation procedure by the initiallyinvolved physicians and led to numerous procedures beforethe diagnosis of PV occlusion was made.Study limitations. The evidence of complete linear lesionsat the end of the ablation session may only be a transientphenomenon, and re-conduction may occur during follow-up, which may account for recurrences, although completelines were acutely demonstrated. On the other hand, RFC-induced lesions may mature after the ablation session,accounting for the effective treatment of patients defined as“incomplete.” Finally, the growing experience of the inves-tigators in deploying linear lesions in the LA using sequen-tial RFC applications have to be taken into account whenjudging the effectiveness of the line designs.Conclusions. Complete lesions in the LA were difficult toachieve using conventional RFC technology, but wereassociated with SR in 74% of patients during long-termfollow-up, whereas incomplete lesions led mostly to recur-rences of AFib or gap-related AT. Further technologicalimprovement (catheter design, ablation energy, specificallydesigned trans-septal sheaths) is necessary to improve linecompleteness and to facilitate line deployment.
Reprint requests and correspondence: Dr. Karl-Heinz Kuck,AK St. Georg, 2. Med. Abteilung (Kardiologie), Lohmuhlenstr. 5,20099 Hamburg Germany. E-mail: [email protected].
1281JACC Vol. 42, No. 7, 2003 Ernst et al.October 1, 2003:1271–82 Catheter-Induced Linear Lesions in the Left Atrium

REFERENCES
1. Oral H, Knight BP, Tada H, et al. Pulmonary vein isolation forparoxysmal and persistent atrial fibrillation. Circulation 2002;105:1077–81.
2. Shah DC, Haıssaguerre M, Jais P, et al. Curative catheter ablation ofparoxysmal atrial fibrillation in 200 patients: strategy for presentationsranging from sustained atrial fibrillation to no arrhythmias. PacingClin Electrophysiol 2001;24:1541–58.
3. Chen SA, Hsieh MH, Tai CT, et al. Initiation of atrial fibrillation byectopic beats originating from the PVs: electrophysiological character-istics, pharmacological responses, and effects of radiofrequency abla-tion. Circulation 1999;100:1879–86.
4. Ernst S, Schluter M, Ouyang F, et al. Modification of the substrate formaintenance of idiopathic human atrial fibrillation. Circulation 1999;100:2085–92.
5. Cox JL, Boineau JP, Schuessler RB, et al. Five-year experience withthe maze procedure for atrial fibrillation. Ann Thorac Surg 1993;56:814–23.
6. Kottkamp H, Hindricks G, Hammel D, et al. Intraoperative radio-frequency ablation of chronic atrial fibrillation: a left atrial curativeapproach by elimination of anatomic “anchor” reentrant circuits.J Cardiovasc Electrophysiol 1999;10:772–80.
7. Haıssaguerre M, Jais P, Shah D, et al. Right and left atrial radiofre-
quency catheter therapy of paroxysmal atrial fibrillation. J CardiovascElectrophysiol 1996;12:1132–44.
8. Pappone C, Oreto G, Lamberti F, et al. Catheter ablation ofparoxysmal atrial fibrillation using a 3D mapping system. Circulation1999;100:1203–8.
9. Duru F, Hindricks G, Kottkamp H. Atypical left atrial flutter afterintraoperative radiofrequency ablation of chronic atrial fibrillation:successful ablation using three-dimensional electroanatomic mapping.J Cardiovasc Electrophysiol 2001;12:602–5.
10. Ernst S, Ouyang F, Schneider B, Kuck KH. Prevention of atrialfibrillation by complete compartmentalization of the LA using acatheter technique. J Cardiovasc Electropysiol 2000;11:686–90.
11. Shpun S, Gepstein L, Hayam G, Ben-Haim SA. Guidance ofradiofrequency endocardial ablation with real-time three-dimensionalmagnetic navigation system. Circulation 1997;96:2016–21.
12. Pappone C, Oreto G, Rosanio S, et al. Atrial electroanatomicremodeling after circumferential radiofrequency pulmonary vein abla-tion: efficacy of an anatomic approach in a large cohort of patients withatrial fibrillation. Circulation 2001;104:2539–44.
13. Gaita F, Riccardi R, Calo L, et al. Atrial mapping and radiofrequencycatheter ablation in patients with idiopathic atrial fibrillation: electrophys-iological findings and ablation results. Circulation 1998;97:2136–45.
14. Ho SY, Sanchez-Quintana D, Cabrera JA, Anderson RH. Anatomyof the LA: implications for radiofrequency ablation of atrial fibrilla-tion. J Cardiovasc Electrophysiol 1999;10:1525–33.
1282 Ernst et al. JACC Vol. 42, No. 7, 2003Catheter-Induced Linear Lesions in the Left Atrium October 1, 2003:1271–82

EDITORIAL COMMENT
Linear Ablationfor Atrial FibrillationHave We Come Full Circle?*David J. Wilber, MD, FACCMaywood, Illinois
The evolution of effective and broadly applicable strategiesfor percutaneous ablation of atrial fibrillation (AF) hasfollowed a complex course over the past decade. In 1994,Swartz et al. (1) reported successful percutaneous ablation ofAF with multiple long linear lesions. Conceived as areplication of the surgical MAZE, the procedure deployedspecifically tailored long sheaths to facilitate fluoroscopicallyguided sequential radiofrequency application along a prede-termined set of ablation lines in both atria. Subsequentlong-term follow-up in 40 patients with chronic AF dem-onstrated the remarkable efficacy of this procedure (90% insinus rhythm), but with prolonged procedure times (10 to15 h), and a 22% incidence of major complications (includ-ing stroke, significant pericardial effusion/tamponade, andpulmonary vein [PV] occlusion) (2).
See page 1271
Other groups subsequently tested a variety of linearstrategies employing the sequential application technique inattempts to simplify the procedure and reduce risks, pre-dominantly in patients with paroxysmal AF (3–8). Severallessons emerged from that experience. Right atrial lesionsalone or in combination with left linear lesions appeared tocontribute little to overall procedural efficacy and werelargely abandoned. During follow-up, elimination of AFwithout antiarrhythmic drugs occurred in 40% to 50% ofpatients with left linear lesions; an additional 20% hadcomplete suppression of AF after adjunctive antiarrhythmicdrug therapy. These results fell short of the 80% to 90%success rates reported for surgically based simplified MAZEprocedures (9,10), as well as the original Swartz procedure.Continuous transmural lesions were technically difficult toproduce, and gaps in the ablation line resulted not only inrecurrent AF, but also promoted a new form a proarrhyth-mia, left atrial (LA) macroreentry, often requiring addi-tional intervention. Subsequent experimental data con-firmed that gaps from 2 to 5 mm were capable of permittingconduction and could facilitate LA macroreentry (11,12).Use of irrigated catheters did not completely eliminate the
problem of incomplete lines (7). Finally, the risk of majorcomplications associated with these procedures remainedsubstantial (12).
With the recognition of venous triggers for AF initiationand maintenance by Haıssaguerre et al. (13), enthusiasm forlong linear lesion strategies waned. Initial approaches tar-geted spontaneous focal triggers within one or more “ar-rhythmogenic” PVs (13,14). However, the unreliable prov-ocation of focal firing in the laboratory, frequent recurrencesnecessitating repeated interventions, and a modest risk ofPV stenosis led to procedural modifications whereby focalsegmental ablation was performed at the LA-PV junction,with the aim of electrical disconnection of the vein from theLA (15). The use of circular recording catheters that couldmonitor electrograms around the circumference of the veinfacilitated this approach (16). Elimination of high frequencypotentials indicative of local activation from within the veinduring atrial pacing (entrance block) and the inability ofpaced or spontaneous depolarizations within the vein toactivate the LA (exit block) became easily recognized andwell-defined acute end points. Extension of the segmentalostial isolation procedure to all four PVs resulted in suc-cessful elimination of paroxysmal AF in 70% to 80% of suchpatients during short-term follow-up, with a low risk ofsymptomatic PV stenosis and other major complications(17–19). The reported success of this procedure for persis-tent and chronic AF has been variable, but appears lower(19,20).
Subsequently, Pappone et al. (21,22) developed a PVisolation procedure based on encircling point-by-point ra-diofrequency lesions placed in atrial tissue outside theLA-PV junction and utilizing electroanatomical mapping.The end point of the procedure was the recording of onlydelayed low voltage (�0.10 mV) far-field electrograms fromwithin the isolated area. Elimination of AF duringfollow-up was reported in 85% of 179 patients with parox-ysmal AF and 68% of 72 patients with chronic AF.Successful outcome correlated poorly with the designatedprocedural end points and was best predicted by a largerpercentage of total LA surface area incorporated within thecircular lesions.
It is with this perspective that the manuscript of Ernst etal. (23), published in this issue of the Journal, is bestunderstood. These investigators examined the outcome oflinear radiofrequency ablation with a standard 4 mm elec-trode guided by electroanatomical imaging in 84 patientswith predominantly paroxysmal AF. Four different strate-gies for lesion deployment were evaluated, with systematicuse of electrophysiologic criteria to assess completeness ofconduction block across the ablation line. For the initial twostrategies, 1) a circular line around all four PVs with aseparate line connecting the circle to the posterior mitralannulus, and 2) three separate nonencircling LA lines,complete lines were rarely accomplished and consequentlyelimination of AF during follow-up was uncommon. In
*Editorials published in the Journal of the American College of Cardiology reflect theviews of the authors and do not necessarily represent the views of JACC or theAmerican College of Cardiology.
From the Cardiovascular Institute, Loyola University Medical Center, Maywood,Illinois.
Journal of the American College of Cardiology Vol. 42, No. 7, 2003© 2003 by the American College of Cardiology Foundation ISSN 0735-1097/03/$30.00Published by Elsevier Inc. doi:10.1016/S0735-1097(03)00942-2

addition to recurrence of AF, gaps in the nonencircling linespromoted the occurrence of LA macroreentry (11% ofpatients).
The final two strategies: 1) separate encircling linesaround the septal and lateral PVs, with an additional linearconnection between these circles and the posterior mitralannulus, and 2) separate encirclement of the septal andlateral PVs alone, without additional lines, mimic moreclosely the method of Pappone et al. (21,22). These proce-dures resulted in elimination of AF in nearly two-thirds ofpatients during follow-up. Low voltage within the isolatedarea was a poor predictor of outcome. However, eliminationof high frequency potentials within the isolated veins wasfound to be relatively specific for a favorable outcome.Inclusion of an additional long linear lesion between the PVencircling lesions and the mitral annulus failed to improveoutcome and facilitated the occurrence of LA macroreentry.Two patients had PV stenosis or occlusion, raising concernsthat the ostium may not have been appropriately visualizedbefore ablation.
How should the findings of Ernst et al. (5) influence ourconceptual approach to the ablation of AF? First, it is clearthat isolation of the PVs remains the cornerstone forsuccessful percutaneous ablation of AF. Second, this studyconfirms the previously described technical difficulties andpotential proarrhythmia associated with long linear lesionsin the LA. Third, encircling linear lesions placed in atrialtissue outside the PVs are a viable alternative to segmentalostial isolation at the putative LA-PV junction.
Is the inclusion of LA tissue adjacent to the ostiumdesirable during PV isolation? There are several reasons thatthis may be so. The anatomy of the venoatrial junction iscomplex, with both longitudinally and spirally orientedfibers from the adjacent LA entering and investing themedia of the proximal PV (24–27). This region and theadjacent proximal PVs are also the site of greatest electro-gram fractionation, conduction slowing, and repolarizationheterogeneity, all potential substrates for reentry (28,29).Left atrial tissue adjacent to the PV is the predominantsource of discrete high frequency periodic activity duringAF (30). Spontaneously discharging foci are frequentlyfound in atrial tissue near the LA-PV junction in bothexperimental preparations (29) and in clinical experience(19). It may be overly simplistic to envision the LA-PVjunction as a discrete anatomic ring. Rather, at least func-tionally, it may be more useful to consider the junction as abroader band incorporating both proximal venous andadjacent LA tissue. Given the importance of this region, itis perhaps surprising that there has been little rigorousattention to the accurate assessment of the location of theLA-PV junction during clinical procedures. Contrastvenography (16,17,19), intracardiac echo (31,32), and tissueimpedance (21,22) have each been used to identify the PVostium, but few attempts have been made to correlate thesetechniques with each other, or with histologic and electro-physiologic findings.
One attractive aspect of circular linear lesions placeddeliberately several millimeters outside the putative LA-PVjunction is that the impact of inaccuracies in locating thisstructure and leaving behind a remnant of arrhythmogenictissue, may be minimized. In the experience of Pappone etal. (21,22), high frequency potentials were identified at 35%of LA sites thought to be adjacent to, but not within, thePV. Both Pappone et al. (22) and Ernst et al. (23) foundthat gaps in the peri-PV circular lesions, as demonstrated byactivation or voltage mapping, did not predict proceduralfailure. The experience of Ernst and coworkers indicatesthat the elimination of high frequency potentials within theisolated area may be a better end point. Circular lesionsplaced outside the os (when properly identified) may alsofurther reduce the risk of PV stenosis. Finally, targetingatrial tissue outside the LA-PV junction may permit the safeuse of higher power applications that could reduce theincidence of delayed recovery of activation within the PVs,an important cause of recurrent AF after apparently suc-cessful segmental ostial isolation procedures (17,19).
Strategies for the percutaneous ablation of AF continueto evolve. It is likely that for some patients, such as thosewith more extensive structural abnormalities, PV isolationalone will be insufficient. However, until we are able toreliably produce durable complete isolation of the PVs andthe LA-PV junction, it will be difficult to judge who maybenefit from additional long linear lesions, with theirattendant risk and extended procedural times, elsewhere inthe atria.
Reprint requests and correspondence: Dr. David J. Wilber,Cardiovascular Institute, Loyola University Medical Center,2160 South First Avenue, Maywood, Illinois 60153. E-mail:[email protected].
REFERENCES
1. Swartz JF, Perrersels G, Silvers J, et al. A catheter based curativeapproach to atrial fibrillation in humans (abstr). Circulation 1994;90Suppl:I35.
2. Cannom DS. Atrial fibrillation: nonpharmacologic approaches. Am JCardiol 2000;85:25D–35D.
3. Haissaguerre M, Jais P, Shah DC, et al. Right and left atrialradiofrequency catheter therapy of paroxysmal atrial fibrillation. J Car-diovasc Electrophysiol 1996;12:1132–44.
4. Nademanee K, Kosar E, Mehra A, et al. Catheter-based MAZEprocedure for atrial fibrillation (abstr). Circulation 1998;98 Suppl:I283.
5. Ernst S, Shluter M, Ouyang F, et al. Modification of the substrate formaintenance of idiopathic human atrial fibrillation: efficacy of radio-frequency ablation using nonfluoroscopic catheter guidance. Circula-tion 1999;100:2085–92.
6. Pappone C, Oreto G, Lamberti F, et al. Catheter ablation ofparoxysmal atrial fibrillation using a 3D mapping system. Circulation1999;100:1203–8.
7. Jais P, Shah DC, Haissaguerre M, et al. Efficacy and safety of septaland left atrial linear ablation for atrial fibrillation. Am J Cardiol1999;84:139R–46R.
8. Garg A, Finneran W, Mollerus M, et al. Right atrial compartmental-ization using radiofrequency catheter ablation for management ofpatients with refractory atrial fibrillation. J Cardiovasc Electrophysiol1999;10:763–71.
1284 Wilber JACC Vol. 42, No. 7, 2003Editorial Comment October 1, 2003:1283–5
9. Cox JL, Schuessler RB, Lappas DG, Boineau JP. An 8 1/2 year clinicalexperience with surgery for atrial fibrillation. Ann Surg 1996;224:267–75.
10. Kosakai Y, Kawaguchi AT, Isobe F, et al. Modified Maze procedurefor patients with atrial fibrillation undergoing simultaneous open heartsurgery. Circulation 1995;92 Suppl 9:II359–64.
11. Mitchell MA, McRury ID, Everett TH, Li H, Mangrum JM, HainesDE. Morphological and physiological characteristics of discontinuouslinear atrial ablations during atrial pacing and atrial fibrillation.J Cardiovasc Electrophysiol 1999;10:378–86.
12. Packer DL. Linear ablation for atrial fibrillation: the pendulum swingsback. In: Zipes DP, Haissaguerre M, eds. Catheter Ablation ofArrhythmias. Armonk, NY: Futura, 2002:107–29.
13. Haissaguerre M, Jaıs P, Shah DC, et al. Spontaneous initiation ofatrial fibrillation by ectopic beats originating in the pulmonary veins.N Engl J Med 1998;339:659–66.
14. Chen SA, Hsieh MH, Tai CT, et al. Initiation of atrial fibrillation byectopic beats originating from the pulmonary veins: electrophysiolog-ical characteristics, pharmacological responses, and effects of radiofre-quency ablation. Circulation 1999;100:1879–86.
15. Haissaguerre M, Jais P, Shah DC, et al. Electrophysiological end pointfor catheter ablation of atrial fibrillation initiated from multiplepulmonary venous foci. Circulation 2000;101:1409–17.
16. Haissaguerre M, Shah DC, Jais P, et al. Electrophysiological break-throughs from the left atrium to the pulmonary veins. Circulation2000;102:2463–5.
17. Macle L, Jais P, Weerasooriya R, et al. Irrigated-tip catheter ablationof pulmonary veins for treatment of atrial fibrillation. J CardiovascElectrophysiol 2002;13:1067–73.
18. Oral H, Knight BP, Tada H, et al. Pulmonary vein isolation forparoxysmal and persistent atrial fibrillation. Circulation 2002;105:1077–81.
19. Marrouche NF, Dresing T, Cole C, et al. Circular mapping andablation of the pulmonary vein for treatment of atrial fibrillation:impact of different catheter technologies. J Am Coll Cardiol 2002;40:464–74.
20. Haissaguerre M, Jais P, Shah DC, et al. Catheter ablation of chronicatrial fibrillation targeting the reinitiating triggers. J Cardiovasc Elec-trophysiol 2000;11:2–10.
21. Pappone C, Rosanio S, Oreto G, et al. Circumferential radiofrequencyablation of pulmonary vein ostia: a new anatomic approach for curingatrial fibrillation. Circulation 2000;102:2619–28.
22. Pappone C, Oreto G, Rosanio S, et al. Atrial electroanatomicremodeling after circumferential radiofrequency pulmonary vein abla-tion: efficacy of an anatomic approach in a large cohort of patients withatrial fibrillation. Circulation 2001;104:2539–44.
23. Ernst S, Ouyang F, Lober F, Antz M, Kuck K–H. Catheter-inducedlinear lesions in the left atrium in patients with atrial fibrillation: anelectroanatomic study. J Am Coll Cardiol 2003;42:1271–82.
24. Ho SY, Sanchez-Quintana D, Cabrera JA, Anderson RH. Anatomyof the left atrium: implications for radiofrequency ablation of atrialfibrillation. J Cardiovasc Electrophysiol 1999;10:1525–33.
25. Ho SY, Cabrera JA, Tran VH, Farre J, Anderson RH, Sanchez-Quintana D. Architecture of the pulmonary veins: relevance toradiofrequency ablation. Heart 2001;86:265–70.
26. Saito T, Waki K, Becker AE. Left atrial myocardial extension ontopulmonary veins in humans: anatomic observations relevant for atrialarrhythmias. J Cardiovasc Electrophysiol 2000;11:888–94.
27. Moubarak JB, Rozwadowski JV, Strzalka CT, et al. Pulmonaryveins–left atrial junction: anatomic and histological study. Pacing ClinElectrophysiol 2000;23:1836–8.
28. Hocini M, Ho SY, Kawara T, et al. Electrical conduction in caninepulmonary veins: electrophysiological and anatomic correlation. Cir-culation 2002;105:2442–8.
29. Arora R, Verheule S, Scott L, et al. Arrhythmogenic substrate of thepulmonary veins assessed by high-resolution optical mapping. Circu-lation 2003;107:1816–21.
30. Mandapati R, Skanes A, Chen J, Berenfeld O, Jalife J. Stablemicroreentrant sources as a mechanism of atrial fibrillation in theisolated sheep heart. Circulation 2000;101:194–9.
31. Martin RE, Ellenbogen KA, Lau YR, et al. Phased-array intra-cardiac echocardiography during pulmonary vein isolation and linearablation for atrial fibrillation. J Cardiovasc Electrophysiol 2002;13:873–9.
32. Swarup V, Azegami K, Arruda MS, Burke MC, Lin AC, Wilber DJ.Four vessel pulmonary vein isolation guided by intracardiac echocar-diography without contrast venography in patients with drug refractoryparoxysmal atrial fibrillation (abstr). J Am Coll Cardiol 2002;39Suppl:114A.
1285JACC Vol. 42, No. 7, 2003 WilberOctober 1, 2003:1283–5 Editorial Comment

Cardiac Imaging
Is There a Referral Bias AgainstCatheterization of Patients WithReduced Left Ventricular Ejection Fraction?Influence of Ejection Fraction and Inducible Ischemia onPost–Single-Photon Emission Computed TomographyManagement of Patients Without a History of Coronary Artery DiseaseRory Hachamovitch, MD, MSC, FACC,* Sean W. Hayes, MD,†‡ John D. Friedman, MD, FACC,†‡Ishac Cohen, PHD,†‡ Xingping Kang, MD,†‡ Guido Germano, PHD, FACC,†‡Daniel S. Berman, MD, FACC†‡Los Angeles, California
OBJECTIVES The objective of this work was to define the relationship between left ventricular perfusion/function measures and referral rates to catheterization and revascularization early after stressgated myocardial perfusion single-photon emission computed tomography (MPS).
BACKGROUND Although revascularization yields the greatest survival benefit in patients with low ejectionfraction (EF) and extensive coronary artery disease, referral patterns to catheterization andrevascularization after noninvasive testing are not well defined.
METHODS We identified 3,369 patients without previous myocardial infarction or revascularization whounderwent exercise or adenosine stress MPS and who were followed-up (97% complete) foroccurrence of early (�60 days) post–single-photon emission computed tomography (SPECT)revascularization. Multivariable logistic regression modeling was used to determine theassociation of various patient characteristics and test results with performance of catheter-ization and revascularization as separate end points.
RESULTS In the first 60 days after stress MPS, 445 catheterizations (13.2%) and 254 revascularizations(7.5%) occurred, including 140 coronary artery bypass graft surgeries (4.1%) and 114percutaneous coronary interventions (3.4%). Both post-stress gated EF and percent of themyocardium ischemic by stress MPS were independent predictors of revascularization.Logistic regression revealed that the likelihood of catheterization increased with bothincreasing ischemia and decreasing EF (c-index � 0.94, chi-square � 590). Predicted referralrates to catheterization increased with decreasing EF except in patients with severe ischemia(�15% of myocardium), where rates decreased with decreasing EF. Similar modeling ofrevascularization (c-index � 0.94, chi-square � 329) revealed that the likelihood ofrevascularization increased with increasing ischemia but, in general, decreased with decreasingEF.
CONCLUSIONS Although post-SPECT referral to both catheterization and revascularization is driven byischemia, EF has the opposite effect on these two outcomes. Further studies evaluating theappropriateness of these referral patterns are warranted. (J Am Coll Cardiol 2003;42:1286–94) © 2003 by the American College of Cardiology Foundation
Numerous studies have evaluated the absolute and relativevalues of various markers for risk identification in patientswith known or suspected coronary artery disease (CAD).The presence of extensive anatomic CAD, stress, or rest leftventricular (LV) dysfunction; exercise-induced electrocar-diogram (ECG) changes; and the extent and severity of
stress perfusion defects on myocardial perfusion single-photon emission computed tomography (MPS) all havebeen associated with an increased risk of cardiovascularmortality (1–10). Both randomized, clinical trials and large,observational data series have demonstrated that this risk,and its reduction by revascularization, increases with theextent of angiographic disease (1–3,11). The presence of LVdysfunction further identifies patients with an enhancedsurvival benefit as a result of revascularization (1), particu-larly in the presence of exercise-induced ECG changes(1,2). Using gated MPS, the combination of LV perfusionand function measures yield added prognostic informationcompared with either measure separately (6,7,12).
Previous studies have examined resource use early afterMPS and the relationship between patient risk and physi-
From the *Cardiovascular Division, Department of Medicine, Keck School ofMedicine, University of Southern California, Los Angeles, California; †Departmentsof Imaging (Division of Nuclear Medicine) and Medicine (Division of Cardiology),Cedars-Sinai Medical Center, Los Angeles, California; and the ‡Department ofMedicine, UCLA School of Medicine, Los Angeles, California. This work wassupported in part by grants from Bristol-Myers Squibb Medical Imaging andFujisawa Healthcare, Inc. Gottlieb Friesinger, MD, acted as the guest editor for thismanuscript.
Manuscript received December 23, 2002; revised manuscript received June 2, 2003,accepted June 13, 2003.
Journal of the American College of Cardiology Vol. 42, No. 7, 2003© 2003 by the American College of Cardiology Foundation ISSN 0735-1097/03/$30.00Published by Elsevier Inc. doi:10.1016/S0735-1097(03)00991-4

cian action (13–17) and showed that referrals to catheter-ization and revascularization tracked closely with patientrisk. However, observed and risk-adjusted referral rates torevascularization early after the use of stress MPS have notbeen examined in the context of both LV function andperfusion data. Our goal was to define the relationshipbetween MPS-measured LV perfusion and function andsubsequent resource use, as defined by early post-MPSreferral to catheterization and revascularization.
METHODS
Study population. We identified 5,370 consecutive uniquepatients who underwent exercise or adenosine stress gatedMPS between July 1992 and November 1998. Patients withprevious myocardial infarction, revascularization, or knowncardiomyopathy were excluded, leaving 3,481 patients (65%of initial cohort). Of these patients, 112 (3.4%) were lost tofollow-up; hence, a final study population of 3,369 patientswas used.Imaging and stress protocol. Patients were injected intra-venously at rest with thallium-201 (3.0 to 4.5 mCi) withdose variation based on patient weight. Rest thallium-201single-photon emission computed tomography (SPECT)was initiated 10 min after injection of the radionuclide (14).
EXERCISE STRESS MPS PROTOCOL. Immediately after im-aging, patients performed symptom-limited exercise tread-mill testing using standard protocols. Exercise end pointsincluded physical exhaustion, severe angina, ventriculartachycardia, significant supraventricular arrhythmias, or sig-nificant exertional hypotension. At near-maximal exercise, a25- to 40-mCi dose of technetium-99m sestamibi wasinjected and exercise continued for 1 min after injection(18).
ADENOSINE STRESS MPS PROTOCOL. Patients were in-structed not to consume caffeine products for 24 h beforestress MPS. After rest thallium-201 SPECT was com-pleted, pharmacologic stress was performed using adenosineinfusion (140 �g/kg/min for 5 to 6 min). Technetium-99msestamibi (25 to 40 mCi) was injected at the end of thesecond or third minute of infusion (14). For patients whounderwent exercise as an adjunct to adenosine infusion,low-level exercise treadmill testing was performed at 0% to10% grade at 1 to 1.7 mph.
During both types of stress, 12-lead ECG recording wasperformed at each minute of stress with continuous moni-toring of leads aVF, V1, and V5. Blood pressure wasrecorded at rest, at the end of each stress stage, and at peakstress. Maximal ST-segment change at 80 ms after the Jpoint was assessed as horizontal, upsloping, or downsloping.Post-stress gated SPECT acquisition protocol. Eight-frame post-stress gated SPECT was initiated 15 to 30 minafter exercise or 15 to 60 min after adenosine stress. Circularor elliptical acquisitions were performed using a two-detector, three-detector, or single-detector camera, obtain-ing 60 to 64 projections over 180 projections for 35 s(thallium-201) or 25 s (technetium-99m sestamibi) perprojection (18). The eight projection sets were summed togenerate an “ungated” set for assessment of perfusion.Projection images were reconstructed into transaxial imagesusing filtered backprojection. No attenuation or scattercorrection was used. After automatic reorientation (19),gated short-axis tomograms were processed automatically tomeasure ejection fraction (EF) (20). The post-stress gatedEF was used in all analyses.Image interpretation. A semiquantitative visual interpre-tation was performed using 20 segments for each rest andstress image (18). Each segment was scored by consensus oftwo experienced observers by using a five-point scoringsystem (0 � normal, 1 � equivocal, 2 � moderate, 3 �severe reduction of radioisotope uptake, and 4 � absence ofdetectable tracer uptake in a segment) as describedpreviously.Scintigraphic perfusion indices. Summed stress and restscores were obtained by adding the scores of the 20segments of the stress and rest images, respectively (21).The difference between the summed stress and rest scoreswas defined as the summed difference score, representingthe amount of ischemia. These indices, incorporating theextent and severity of perfusion defects, were converted topercent of the myocardium manifesting stress, ischemic, orfixed defects by dividing the summed scores by 80, which isthe maximum potential score (4 � 20), and multiplying by100 (11).Patient follow-up. Individuals who were blinded to thepatients’ test results performed follow-up by scripted tele-phone interview. The end point of the current study wasreferral to catheterization or revascularization early (�60days) after stress MPS. This time point was selected becauseit has been shown to be a temporal threshold distinguishingreferrals to revascularization made on the basis of the scanresults (�60 days) as opposed to worsening of the patients’clinical status prompting intervention (�60 days) (22).Statistical analysis. Baseline characteristics of patientswere described in terms of mean � 1 SD for continuousvariables and frequencies for categorical variables. Theformer was compared using analysis of variance and thelatter using a chi-square test for comparisons of discretevariables. A value of p � 0.05 was considered statisticallysignificant.
Abbreviations and AcronymsCABG � coronary artery bypass graft surgeryCAD � coronary artery diseaseECG � electrocardiogram/electrocardiographicEF � ejection fractionLV � left ventricle/left ventricularMPS � myocardial perfusion single-photon emission
computed tomographyPCI � percutaneous coronary interventionSPECT � single-photon emission computed tomography
1287JACC Vol. 42, No. 7, 2003 Hachamovitch et al.October 1, 2003:1286–94 Predictors of Post-SPECT Resource Use

MULTIVARIABLE MODELING. A logistic regression modelwas used to perform covariate adjustment to determine theassociation of patient characteristics and test results withperformance of: 1) catheterization, and 2) revascularizationas separate end points. Additional models were developedfor coronary artery bypass graft surgery (CABG) andpercutaneous coronary intervention (PCI) as separate endpoints. Candidate variables for modeling are listed onTable 1.
Based on univariate analysis and clinical judgment, allfactors known to influence these referral decisions wereconsidered for entry into a logistic regression model withinthe constraints of overfitting (23,24). The threshold forentry of variables into all models was p � 0.10. Based onthese models, risk-adjusted survival curves were determined.Care was given to examination of the assumptions oflinearity and additivity (23,24). S plus 2000 (Mathsoft Inc.,Cambridge, Massachusetts) using supplemental librarieswas used for all analyses.
RESULTS
Patient characteristics. The baseline characteristics of pa-tients in this study are shown in Table 1. Of the patients,approximately two-thirds underwent exercise stress, approx-imately one-half were male, and most had a history ofhypertension, hypercholesterolemia, abnormal rest ECG, oranginal symptoms at the time of presentation. Small num-bers of patients had a previous catheterization, were usingdigoxin, had diabetes mellitus, were smokers, or had a
family history of premature CAD. The mean age was 65 �13 years, and the mean stress defect size was within theupper limits of normal and was predominantly reversiblerather than fixed. The mean EF (62 � 13%) was well withinthe normal range.
The distribution of EF was skewed toward higher values(�35%: 4%; 35% to 50%: 13%; �50%: 83%). The distri-bution of ischemia was also skewed toward having noischemia; 66% of patients were not ischemic and 15%, 7%,7%, and 5% were 1% to 5%, 6% to 10%, 11% to 20%, and�20% myocardium ischemic, respectively.
Figure 1. Univariate relationship between the likelihood (Lk) of catheter-ization referral and percent of the myocardium ischemic (solid line) with95% confidence intervals (dotted lines). Increase in likelihood, p � 0.001.
Table 1. Patient Characteristics and Univariate Predictors of Catheterizationand Revascularization
Referral toCatheterization
Referral toRevascularization
Chi-Squared Odds Ratio Chi-Squared Odds Ratio
N 3,369 (100%)Exercise stress 2,146 (64%) 26.0* 0.59 4.0* 0.77Male 1,742 (52%) 33.2* 1.83 29.8* 2.13History catheterization 352 (10%) 9.0* 1.55 8.1* 1.67Digoxin use 135 (4%) 1.2 1.30 0.1 0.91Hypertension 1,630 (48%) 9.9* 1.38 17.2* 1.75Diabetes mellitus 446 (13%) 34.3* 2.95 26.5* 2.22Hypercholesterolemia 1,439 (43%) 0.1 0.97 0.3 1.09Smoking 371 (11%) 2.7 1.28 0.7 1.18Family history CAD 753 (22%) 6.4* 0.72 1.5 0.82Anginal symptoms 1,575 (47%) 9.8* 1.37 25.6* 1.96Abnormal rest ECG 1,837 (55%) 56.0* 2.28 23.4* 1.97Age (yrs) 65 � 13 45.2* 1.67 28.6* 1.03% myocardium total 4.1 � 8.6% 549.3* 1.18 439.3* 1.15% myocardium ischemic 3.4 � 7.2% 556.8* 1.23 442.8* 1.18% myocardium fixed 0.7 � 3.5% 77.4* 1.12 51.9* 1.09Post-stress ejection fraction 62 � 13 257.4* 0.94 152.4* 0.95Year of stress myocardial perfusion
SPECT study1994: 1501995: 4001996: 8761997: 12031998: 740
13.5* 0.81 3.7* 0.81
*p � 0.05.CAD � coronary artery disease; ECG � electrocardiogram; SPECT � single-photon emission computed tomography.
1288 Hachamovitch et al. JACC Vol. 42, No. 7, 2003Predictors of Post-SPECT Resource Use October 1, 2003:1286–94
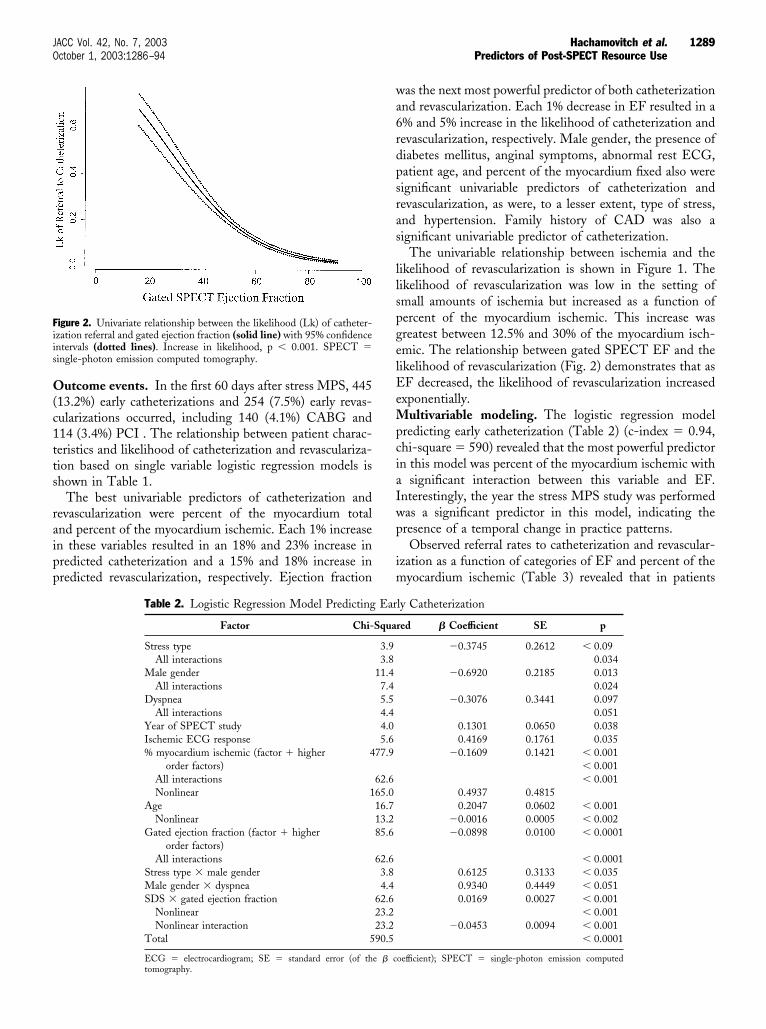
Outcome events. In the first 60 days after stress MPS, 445(13.2%) early catheterizations and 254 (7.5%) early revas-cularizations occurred, including 140 (4.1%) CABG and114 (3.4%) PCI . The relationship between patient charac-teristics and likelihood of catheterization and revasculariza-tion based on single variable logistic regression models isshown in Table 1.
The best univariable predictors of catheterization andrevascularization were percent of the myocardium totaland percent of the myocardium ischemic. Each 1% increasein these variables resulted in an 18% and 23% increase inpredicted catheterization and a 15% and 18% increase inpredicted revascularization, respectively. Ejection fraction
was the next most powerful predictor of both catheterizationand revascularization. Each 1% decrease in EF resulted in a6% and 5% increase in the likelihood of catheterization andrevascularization, respectively. Male gender, the presence ofdiabetes mellitus, anginal symptoms, abnormal rest ECG,patient age, and percent of the myocardium fixed also weresignificant univariable predictors of catheterization andrevascularization, as were, to a lesser extent, type of stress,and hypertension. Family history of CAD was also asignificant univariable predictor of catheterization.
The univariable relationship between ischemia and thelikelihood of revascularization is shown in Figure 1. Thelikelihood of revascularization was low in the setting ofsmall amounts of ischemia but increased as a function ofpercent of the myocardium ischemic. This increase wasgreatest between 12.5% and 30% of the myocardium isch-emic. The relationship between gated SPECT EF and thelikelihood of revascularization (Fig. 2) demonstrates that asEF decreased, the likelihood of revascularization increasedexponentially.Multivariable modeling. The logistic regression modelpredicting early catheterization (Table 2) (c-index � 0.94,chi-square � 590) revealed that the most powerful predictorin this model was percent of the myocardium ischemic witha significant interaction between this variable and EF.Interestingly, the year the stress MPS study was performedwas a significant predictor in this model, indicating thepresence of a temporal change in practice patterns.
Observed referral rates to catheterization and revascular-ization as a function of categories of EF and percent of themyocardium ischemic (Table 3) revealed that in patients
Figure 2. Univariate relationship between the likelihood (Lk) of catheter-ization referral and gated ejection fraction (solid line) with 95% confidenceintervals (dotted lines). Increase in likelihood, p � 0.001. SPECT �single-photon emission computed tomography.
Table 2. Logistic Regression Model Predicting Early Catheterization
Factor Chi-Squared � Coefficient SE p
Stress type 3.9 �0.3745 0.2612 � 0.09All interactions 3.8 0.034
Male gender 11.4 �0.6920 0.2185 0.013All interactions 7.4 0.024
Dyspnea 5.5 �0.3076 0.3441 0.097All interactions 4.4 0.051
Year of SPECT study 4.0 0.1301 0.0650 0.038Ischemic ECG response 5.6 0.4169 0.1761 0.035% myocardium ischemic (factor � higher
order factors)477.9 �0.1609 0.1421 � 0.001
� 0.001All interactions 62.6 � 0.001Nonlinear 165.0 0.4937 0.4815
Age 16.7 0.2047 0.0602 � 0.001Nonlinear 13.2 �0.0016 0.0005 � 0.002
Gated ejection fraction (factor � higherorder factors)
85.6 �0.0898 0.0100 � 0.0001
All interactions 62.6 � 0.0001Stress type � male gender 3.8 0.6125 0.3133 � 0.035Male gender � dyspnea 4.4 0.9340 0.4449 � 0.051SDS � gated ejection fraction 62.6 0.0169 0.0027 � 0.001
Nonlinear 23.2 � 0.001Nonlinear interaction 23.2 �0.0453 0.0094 � 0.001
Total 590.5 � 0.0001
ECG � electrocardiogram; SE � standard error (of the � coefficient); SPECT � single-photon emission computedtomography.
1289JACC Vol. 42, No. 7, 2003 Hachamovitch et al.October 1, 2003:1286–94 Predictors of Post-SPECT Resource Use

with �10% myocardium ischemic, referral rates to cathe-terization decreased with increasing EF. However, forpatients with 10% to 20% and �20% myocardium ischemic,no differences in referral rates to catheterization were notedas a function of EF.
The relationship defined by the percent of the myocar-dium ischemic/EF interaction (Fig. 3) reveals a markedincrease in the likelihood of referral to catheterization withincreasing amounts of ischemia, with the maximal slope ofthis increase occurring between 5% to 15% of the myocar-dium ischemic in patients with normal EF. In patients with�10% of the myocardium ischemic, the likelihood of thisreferral decreased as a function of decreasing EF. However,patients with low EF (�45%) and small amounts of percentof the myocardium ischemic (�10%) had an increasinglikelihood of referral to catheterization with decreasingischemia and decreasing EF. Further, this model also
revealed that the year the index SPECT study was per-formed influenced the likelihood of referral to catheteriza-tion, with progressive increases each year from 1994 to1998.
The logistic regression model predicting revascularization(Table 4) (c-index � 0.94, chi-square � 329) revealedpercent of the myocardium ischemic as the most powerfulpredictor with a significant interaction between this variableand EF. The contribution of percent of the myocardiumfixed was significant but smaller. The relationship definedby the percent of the myocardium ischemic/ EF interaction(Fig. 4) indicates that in patients with normal EF, a markedincrease in the likelihood of revascularization occurred withincreasing amounts of ischemia. The slope of this increasewas maximal between 5% to 15% of the myocardiumischemic and plateaued beyond that point. Importantly, forvalues of EF below 50%, a linear relationship was present.This relationship was further investigated by examiningCABG and PCI as separate end points. The logisticregression model predicting CABG (c-index � 0.94, chi-square � 204) included anginal symptoms, ST-segmentchanges with stress, gated EF, percent of the myocardiumfixed, and percent of the myocardium ischemic. The latterwas again the most powerful predictor (�80% of overallchi-square), interacted powerfully with gated EF, and wasmodeled non-linearly. The relationship defined by thepercent of the myocardium ischemic/EF interaction for thismodel is shown in Figure 5. In contrast to the likelihood ofreferral to revascularization (Fig. 4), this relationship dem-onstrates an increase in the likelihood of referral to CABGas a function of increasing percent of the myocardiumischemic with a small increase in likelihood as a function ofdecreasing EF. The logistic regression model predictingPCI (c-index � 0.90, chi-square � 223) included hyper-tension, anginal symptoms, gated EF, and percent of themyocardium ischemic, with the latter interacting with gatedEF and being the most powerful individual predictor in themodel (�80% overall chi-square). The relationship definedby the percent of the myocardium ischemic/EF interactionis shown in Figure 6. There was a low likelihood of referralto PCI in the setting of an EF �35% irrespective of theamount of ischemia present. In the setting of an EF 35% to50%, the likelihood of revascularization was low when theamount of ischemia was small to moderate but rose whenthe amount of ischemia was large (�15% of the myocar-dium ischemic). When EF was �50%, the likelihood ofreferral to PCI increased steeply for patients with percent ofthe myocardium ischemic 15% to 30% and reached a plateauin patients with percent of the myocardium ischemic �30%.Multivariable modeling in patients with ischemia andreduced EFs. We performed a subgroup analysis in asubgroup of 273 patients with EF �50% and �5% of themyocardium ischemic. These patients had 154 early cath-eterizations on follow-up. The logistic model most predic-tive of referral to catheterization included stress type, patientgender, the year the SPECT study was performed, percent
Figure 3. Relationship between gated ejection fraction and percent of themyocardium ischemia with respect to prediction of likelihood (Lk) ofcatheterization referral based on logistic regression model. Results areshown for percent of the myocardium ischemia values of 0%, 5%, 7.5%,10%, 12.5%, 15%, 20%, and 30%. SPECT � single-photon emissioncomputed tomography.
Table 3. Observed Referral Rates to Catheterization as aFunction of EF and %Myocardium Ischemic
%MyocardiumIschemic
ObservedReferral Rate toCatheterization
n (%)
% of PatientsReferred to EarlyRevascularization
After EarlyCatheterization
�10% EF � 35% 39% (70) 30%�10% EF � 35%,
�50%11% (289) 36%
�10% EF � 50% 4% (2,560) 42%10–20% EF � 35% 65% (48) 64%10–20% EF � 35%,
�50%61% (71) 58%
10–20% EF � 50% 63% (175) 61%�20% EF � 35% 61% (26) 75%�20% EF � 35%,
�50%65% (65) 81%
�20% EF � 50% 77% (64) 73%
EF � ejection fraction.
1290 Hachamovitch et al. JACC Vol. 42, No. 7, 2003Predictors of Post-SPECT Resource Use October 1, 2003:1286–94
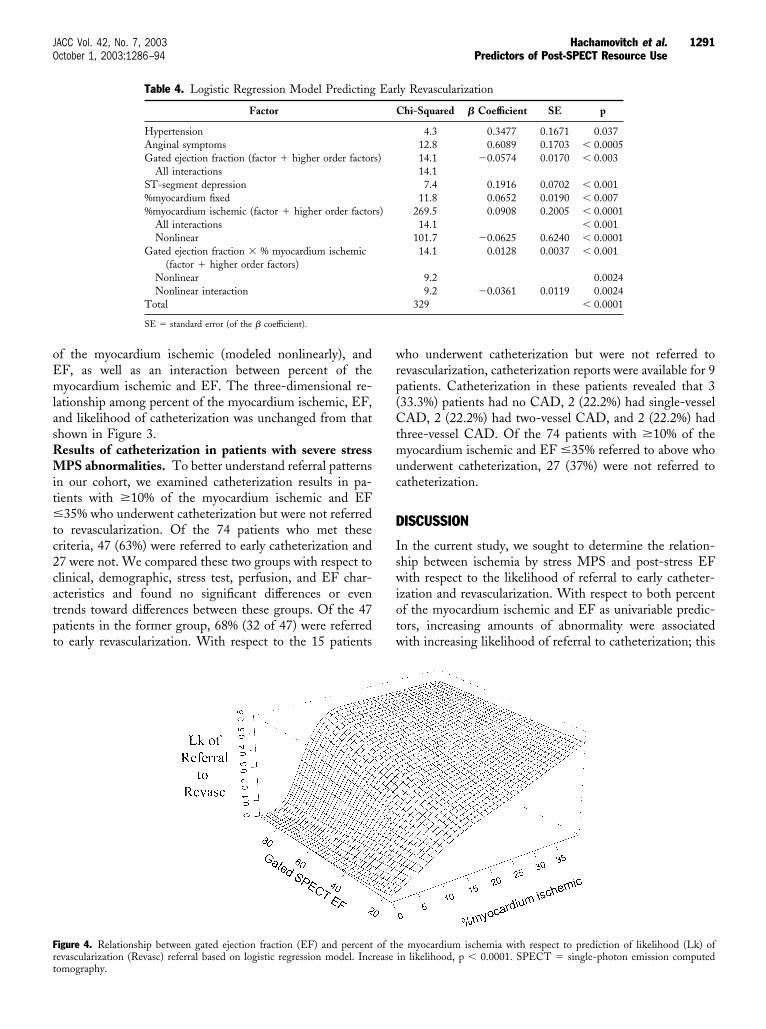
of the myocardium ischemic (modeled nonlinearly), andEF, as well as an interaction between percent of themyocardium ischemic and EF. The three-dimensional re-lationship among percent of the myocardium ischemic, EF,and likelihood of catheterization was unchanged from thatshown in Figure 3.Results of catheterization in patients with severe stressMPS abnormalities. To better understand referral patternsin our cohort, we examined catheterization results in pa-tients with �10% of the myocardium ischemic and EF�35% who underwent catheterization but were not referredto revascularization. Of the 74 patients who met thesecriteria, 47 (63%) were referred to early catheterization and27 were not. We compared these two groups with respect toclinical, demographic, stress test, perfusion, and EF char-acteristics and found no significant differences or eventrends toward differences between these groups. Of the 47patients in the former group, 68% (32 of 47) were referredto early revascularization. With respect to the 15 patients
who underwent catheterization but were not referred torevascularization, catheterization reports were available for 9patients. Catheterization in these patients revealed that 3(33.3%) patients had no CAD, 2 (22.2%) had single-vesselCAD, 2 (22.2%) had two-vessel CAD, and 2 (22.2%) hadthree-vessel CAD. Of the 74 patients with �10% of themyocardium ischemic and EF �35% referred to above whounderwent catheterization, 27 (37%) were not referred tocatheterization.
DISCUSSION
In the current study, we sought to determine the relation-ship between ischemia by stress MPS and post-stress EFwith respect to the likelihood of referral to early catheter-ization and revascularization. With respect to both percentof the myocardium ischemic and EF as univariable predic-tors, increasing amounts of abnormality were associatedwith increasing likelihood of referral to catheterization; this
Figure 4. Relationship between gated ejection fraction (EF) and percent of the myocardium ischemia with respect to prediction of likelihood (Lk) ofrevascularization (Revasc) referral based on logistic regression model. Increase in likelihood, p � 0.0001. SPECT � single-photon emission computedtomography.
Table 4. Logistic Regression Model Predicting Early Revascularization
Factor Chi-Squared � Coefficient SE p
Hypertension 4.3 0.3477 0.1671 0.037Anginal symptoms 12.8 0.6089 0.1703 � 0.0005Gated ejection fraction (factor � higher order factors) 14.1 �0.0574 0.0170 � 0.003
All interactions 14.1ST-segment depression 7.4 0.1916 0.0702 � 0.001%myocardium fixed 11.8 0.0652 0.0190 � 0.007%myocardium ischemic (factor � higher order factors) 269.5 0.0908 0.2005 � 0.0001
All interactions 14.1 � 0.001Nonlinear 101.7 �0.0625 0.6240 � 0.0001
Gated ejection fraction � % myocardium ischemic(factor � higher order factors)
14.1 0.0128 0.0037 � 0.001
Nonlinear 9.2 0.0024Nonlinear interaction 9.2 �0.0361 0.0119 0.0024
Total 329 � 0.0001
SE � standard error (of the � coefficient).
1291JACC Vol. 42, No. 7, 2003 Hachamovitch et al.October 1, 2003:1286–94 Predictors of Post-SPECT Resource Use

relationship was steeper in the setting of moderate andsevere rather than mild abnormalities. Logistic regressionmodeling of referral to both catheterization and revascular-ization yielded robust models (c-indices both 0.94). Bothmodels indicated that the majority of referrals to eitherprocedure could be explained by percent of the myocardiumischemia with an interaction present between percent of themyocardium ischemic and EF for both end points. Referralrates to catheterization increased with decreasing values ofEF in the setting of no (�5% of the myocardium ischemic)or mild to moderate amounts of ischemia (5% to 15% of themyocardium ischemic), but this pattern was reversed inpatients with severe ischemia (�15% of the myocardiumischemic) wherein predicted referral rates to catheterizationdecreased with decreasing EF. Referral rates to revascular-ization increased markedly with increasing amounts ofischemia, plateauing beyond 15% of the myocardium isch-
emia, and demonstrated a mild decrease in referral rateswith decreasing EF that was quantitatively not as significantas that found in the referral to catheterization model.Although referral to revascularization seemed to be inproportion to the anticipated risk in these patients, cathe-terization was the rate-limiting step in the evaluation ofthese patients and was significantly influenced by an EF-related referral bias.Comparison of the current study to previous studies:post-stress MPS resource use. A number of previousstudies have demonstrated the preeminent role of MPS-demonstrated ischemia and post-SPECT referral rates tocatheterization and revascularization (14–17). Our groupshowed that in patients without previous CAD, this is thecase in all (low, intermediate, and high) clinical risk subsets(14). The current study supports these previous findings andextends them by demonstrating the positive effect of post-stress EF on catheterization referral in the setting of little orno ischemia but its negative effect on this referral in thesetting of extensive ischemia. Ejection fraction tended toadversely affect referral to revascularization, but this wasquantitatively less significant than the effect on catheteriza-tion referral. With respect to referral to CABG, percent ofthe myocardium ischemic but not EF influenced referralrates. Because the former and not the latter defined poten-tially salvageable myocardium, this referral pattern is prob-ably appropriate and reflects an attempt to intervene inproportion to potential benefit. Of concern, however, is thatPCI referral patterns suggest that a referral bias is presentsuch that patients with compromised LV function may beselectively under-referred to PCI.Previous studies: risk as a function of CAD extent andLVEF. Previous studies have shown that the combinationof LV perfusion and function measures yield increasedprognostic information compared with either of these twomeasures separately (6,7,12). We have previously shownthat with respect to annualized cardiac death risk in medi-cally treated patients, both patients with EF �50% and alarge amount of ischemia, as well as patients with EF 30%to 50% and mild or moderate ischemia, were at intermediaterisk (2% to 3%). Also, patients with mild or moderateischemia and EF �50% were at low risk (�1%) (25).Further, patients with EF �30% were at high risk (�4%)irrespective of ischemia amount. In light of these findings,the current study indicates that post-SPECT referral tocatheterization in patients with low EF is disproportionatelylow relative to their risk. Recent studies have extended thesefindings and shown that the survival benefit associated withrevascularization increases as a function of percent of themyocardium ischemic (11), even in the setting of a reducedEF (12).Is there a referral bias against catheterization of patientswith low EF and significant inducible ischemia? Toclassify a pattern of clinical care as “bias,” a pattern ofreferral contrary to accepted, recommended, or optimalpractice must be shown. Numerous studies have shown that
Figure 5. Relationship between gated ejection fraction (EF) and percent ofthe myocardium ischemia with respect to prediction of likelihood (Lk) ofcoronary artery bypass graft surgery (CABG) referral based on a logisticregression model. Increase in likelihood, p � 0.0001.
Figure 6. Relationship between gated ejection fraction (EF) and percent ofthe myocardium ischemia with respect to prediction of likelihood (Lk) ofpercutaneous coronary intervention (PCI) referral based on logistic regres-sion model. Increase in likelihood, p � 0.0001.
1292 Hachamovitch et al. JACC Vol. 42, No. 7, 2003Predictors of Post-SPECT Resource Use October 1, 2003:1286–94

risk—and survival benefit with revascularization—increasesin the setting of low EF (1,3,12). As discussed in thepreceding text, low gated SPECT EF is associated withgreater risk and a potential survival benefit if ischemia ispresent (7,12). Hence, the failure of referral rates to cathe-terization to increase in proportion to patient risk wouldappear to potentially be less than optimal practice and maythus be considered a referral bias.Impact of referral bias on assessment of prognosticvalue. With respect to diagnostic testing, the preferentialreferral of patients with positive test responses to a goldstandard results in a post-test referral bias when the sensi-tivity and specificity of this test are subsequently examined(26). Similar referral biases can occur with respect toprognostic testing. Observational studies assessing the prog-nostic value of noninvasive testing censor patients undergo-ing early post-testing revascularization because of the rela-tionship between this revascularization and the test results(22,26). We have previously hypothesized that with increas-ing physician acceptance of stress MPS and the strongdependence of post-MPS revascularization referral on theseresults, a post-test referral bias may develop that results inan underestimation of the test’s prognostic value as a resultof the revascularization (and censoring) of the highest riskpatients (9,26,27).
The current study suggests that this source of post-testreferral bias may adversely affect the observed prognosticvalue of stress-induced ischemia but not EF. In this study,the likelihood of referral to revascularization was positivelyaffected by ischemia but only minimally affected by the EF,especially in patients with severe ischemia, thus adverselyaffecting the observed relationship between risk and isch-emia, but less so the relationship between risk and EF. Theprevious results of Sharir et al. (7), that post-stress gatedSPECT EF yields greater prognostic value than perfusiondata, may have been due, in part, to this referral bias. In thefuture, these types of studies may benefit from an analyticapproach that incorporates (and adjusts for) this referralbias.Study limitations. STATISTICAL AND CLINICAL. The prob-lems associated with the use of multivariable techniquesapplied to observational data to adjust for differences inbaseline characteristics are well described (23,24,26). None-theless, this remains an observational study with all the flawsinherent in its design. The impact of various biases, missingcovariates, and the limits of single-site data from a centerwhose referral and testing patterns may be unique all limitthe reliability and generalizability of the current results. Inaddition, as single-center data, the interpretive and/or referralpatterns reported may not be generalizable. Finally, althoughthis study is well-powered overall, certain conclusions of thisstudy are based on a relatively small number of patients.
TECHNICAL. Scintigraphic studies in the current work wereinterpreted by experienced observers using a standardized,semiquantitative approach to visual interpretation that we
have developed and have documented to be highly repro-ducible (28,29). These form the basis for existent quantita-tive analysis programs that have been shown to correlatestrongly with those of quantitative analysis (28,29). All EFdata reported in the current study were obtained as apost-stress measurement in which the acquisition was ini-tiated as early as 15 min (exercise stress) and as late as 60min or more (adenosine stress) post-stress. Importantly,although the type of stress performed was a potential sourceof variation, it was not a significant predictor of revascular-ization in the logistic model for any of the end points weexamined.Conclusions. Although post-SPECT referral to catheter-ization and revascularization is primarily driven by theextent and severity of ischemia on gated stress MPS, referralrates are less affected by EF in patients with ischemia.Hence, a post-SPECT referral bias is present with respectto referral to catheterization, resulting in a relative under-catheterization of patients with low EF and significantischemia. Further studies evaluating the appropriateness ofthese referral patterns would be warranted.
Reprint requests and correspondence: Dr. Daniel S. Berman,Cedars-Sinai Medical Center, Room A042, 8700 BeverlyBoulevard, Los Angeles, California 90048. E-mail: [email protected].
REFERENCES
1. Yusuf S, Zucker D, Peduzzi P, et al. Effect of coronary artery bypassgraft surgery on survival: overview of 10-year results from randomisedtrials by the Coronary Artery Bypass Graft Surgery Trialists Collab-oration. Lancet 1994;344:563–70.
2. Weiner DA, Ryan TJ, McCabe CH, et al. The role of exercise testingin identifying patients with improved survival after coronary arterybypass surgery. J Am Coll Cardiol 1986;8:741–8.
3. Califf RM, Harrell FE Jr., Lee KL, et al. The evolution of medical andsurgical therapy for coronary artery disease: a 15-year perspective.JAMA 1989;261:2077–86.
4. Ladenheim ML, Pollock BH, Rozanski A, et al. Extent and severityof myocardial hypoperfusion as predictors of prognosis in patientswith suspected coronary artery disease. J Am Coll Cardiol 1986;7:464 –71.
5. Harris PJ, Harrell FE Jr., Lee KL, et al. Survival in medically treatedcoronary artery disease. Circulation 1979;60:1259–69.
6. Marie PY, Danchin N, Durand JF, et al. Long-term prediction ofmajor ischemic events by exercise thallium-201 single-photon emis-sion computed tomography. Incremental prognostic value comparedwith clinical, exercise testing, catheterization and radionuclide angio-graphic data. J Am Coll Cardiol 1995;26:879–86.
7. Sharir T, Germano G, Kavanagh PB, et al. Incremental prognosticvalue of post-stress left ventricular ejection fraction and volume bygated myocardial perfusion single photon emission computed tomog-raphy. Circulation 1999;100:1035–42.
8. Hachamovitch R, Hayes S, Friedman JD, et al. Determinants of riskand its temporal variation in patients with normal stress myocardialperfusion scans: what is the warranty period of a normal scan? J AmColl Cardiol 2003;41:1329–40.
9. Hachamovitch R, Hayes S, Friedman JD, Cohen I, Berman DS. Stressmyocardial perfusion SPECT is clinically effective and cost-effective inrisk-stratification of patients with a high likelihood of CAD but noknown CAD. J Am Coll Cardiol 2003. In Press.
10. Abidov A, Bax JJ, Hayes SW, et al. Transient ischemic dilation of theleft ventricle is a significant predictor of future cardiac events in
1293JACC Vol. 42, No. 7, 2003 Hachamovitch et al.October 1, 2003:1286–94 Predictors of Post-SPECT Resource Use

patients with otherwise normal myocardial perfusion SPECT. J AmColl Cardiol 2003. In Press.
11. Hachamovitch R, Hayes SW, Friedman JD, Cohen I, Berman DS.Identification of a threshold of inducible ischemia associated with ashort-term survival benefit with revascularization compared to medicaltherapy in patients with no prior CAD undergoing stress myocardialperfusion SPECT. Circulation 2003;107:2900–7.
12. Hachamovitch R, Hayes S, Cohen I, Germano G, Berman DS.Inducible ischemia is superior to EF for identification of short-termsurvival benefit with revascularization vs. medical therapy (abstr).Circulation 2002;106 Suppl:II523.
13. Hachamovitch R, Berman DS, Kiat H, et al. Gender-related differ-ences in clinical management after exercise nuclear testing. J Am CollCardiol 1995;26:1457–64.
14. Hachamovitch R, Berman DS, Kiat H, et al. Exercise myocardialperfusion SPECT in patients without known coronary artery disease:incremental prognostic value and use in risk stratification. Circulation1996;93:905–14.
15. Bateman TM, O’Keefe JH Jr., Dong VM, et al. Coronary angio-graphic rates after stress single-photon emission computed tomo-graphic scintigraphy. J Nucl Cardiol 1995;2:217–23.
16. Travin MI, Duca MD, Kline GM, et al. Relation of gender tophysician use of test results and to the prognostic value of stresstechnetium 99m sestamibi myocardial single-photon emission com-puted tomography scintigraphy. Am Heart J 1997;134:73–82.
17. Berman DS, Kang X, Hayes SW, et al. Adenosine myocardialperfusion SPECT in women compared to men: incremental prognos-tic value, effect on patient management and impact on diabetesmellitus. J Am Coll Cardiol 2003;41:1125–33.
18. Berman DS, Kiat H, Friedman JD, et al. Separate acquisition restthallium-201/stress technetium-99m sestamibi dual-isotope myocar-dial perfusion single-photon emission computed tomography: a clini-cal validation study. J Am Coll Cardiol 1993;22:1455–64.
19. Germano G, Kavanagh PB, Chen J, et al. Operator-less processing ofmyocardial perfusion SPECT studies. J Nucl Med 1995;36:2127–32.
20. Germano G, Kiat H, Kavanagh PB, et al. Automatic quantification ofejection fraction from gated myocardial perfusion SPECT. J NuclMed 1995;36:2138–47.
21. Berman DS, Hachamovitch R, Kiat H, et al. Incremental value ofprognostic testing in patients with known or suspected ischemic heartdisease: a basis for optimal utilization of exercise technetium-99msestamibi myocardial perfusion single-photon emission computedtomography. J Am Coll Cardiol 1995;26:639–47.
22. Staniloff HM, Forrester JS, Berman DS, et al. Prediction of death,myocardial infarction, and worsening chest pain using thallium scin-tigraphy and exercise electrocardiography. J Nucl Med 1986;27:1842–8.
23. Greenland S. Modeling and variable selection in epidemiologic anal-ysis. Am J Public Health 1989;79:340–9.
24. Harrell FE Jr., Lee KL, Mark DB. Multivariable prognostic models:issues in developing models, evaluating assumptions and adequacy, andmeasuring and reducing errors. Stat Med 1996;15:361–87.
25. Sharir T, Germano G, Kang X, et al. Prediction of myocardialinfarction versus cardiac death by gated myocardial perfusion SPECT:risk stratification by the amount of stress-induced ischemia and thepoststress ejection fraction. J Nucl Med 2001;42:831–7.
26. Hachamovitch R, Shaw L, Berman DS. Methodological considerationsin the assessment of noninvasive testing using outcomes research: pitfallsand limitations. Prog Cardiovasc Dis 2000;43:215–30.
27. Berman DS, Germano G, Shaw LJ. Nuclear cardiology. In: FusterVAR, King S, O’Rourke RA, Wellens HJJ, editors. Hurst’s TheHeart. New York, NY: McGraw-Hill Companies, 2000:525–65.
28. Berman DS, Kang X, Van Train KF, et al. Comparative prognosticvalue of automatic quantitative analysis versus semiquantitative visualanalysis of exercise myocardial perfusion single-photon emission com-puted tomography. J Am Coll Cardiol 1998;32:1987–95.
29. Van Train KF, Garcia EV, Maddahi J, et al. Multicenter trialvalidation for quantitative analysis of same-day rest-stress technetium-99m-sestamibi myocardial tomograms. J Nucl Med 1994;35:609–18.
1294 Hachamovitch et al. JACC Vol. 42, No. 7, 2003Predictors of Post-SPECT Resource Use October 1, 2003:1286–94

Clinical Safety of Magnetic ResonanceImaging Early After Coronary Artery Stent PlacementThomas C. Gerber, MD, FACC,* Panayotis Fasseas, MD,† Ryan J. Lennon, MS,‡Venkata U. Valeti, MD,† Christopher P. Wood, MD,§ Jerome F. Breen, MD,§Peter B. Berger, MD, FACC†Jacksonville, Florida; and Rochester, Minnesota
OBJECTIVES Our aim was to examine the rate of adverse cardiac events in patients undergoing magneticresonance imaging (MRI) �8 weeks after coronary stent placement.
BACKGROUND The risk of coronary stent thrombosis from dislodgement due to MRI early after stentplacement is not well defined. Manufacturers recommend postponing MRI studies until eightweeks after coronary stent placement.
METHODS We analyzed the Mayo Clinic Rochester Percutaneous Coronary Intervention Database andexamined records of 111 patients who underwent MRI �8 weeks after coronary stentplacement treated with aspirin and a thienopyridine. Occurrence of death, myocardialinfarction (MI), and repeat revascularization within 30 days of MRI were recorded.
RESULTS Magnetic resonance imaging (1.5 tesla) was performed within a median of 18 days (range, 0to 54 days) after coronary stent placement. Four noncardiac deaths occurred, and threepatients had repeat revascularization procedures. Stent thrombosis did not occur (95%confidence interval, 0% to 3.3%).
CONCLUSIONS Magnetic resonance imaging �8 weeks after coronary stent placement appears to be safe, andthe risk of cardiac death or MI due to stent thrombosis is low. Postponing MRI does notappear to be necessary. (J Am Coll Cardiol 2003;42:1295–8) © 2003 by the AmericanCollege of Cardiology Foundation
Magnetic resonance imaging (MRI) is considered unsafe inthe presence of many metallic cardiovascular devices becauseit may cause dislodgement of the device by ferromagneticforce, device heating, flow of electrical currents, or malfunc-tion of a device’s electrical system (1–3). Every year approx-imately 457,000 metallic coronary artery stents (CASs) areplaced (4). In patients with CASs, MRI is believed to besafe once endothelialization (5) has occurred, because en-dothelialization presumably opposes possible dislodgement(3). Therefore, manufacturers of CASs (6,7) and profes-sional associations of cardiologists (8) recommend postpon-ing elective MRI examinations for four to eight weeks afterstent placement.
However, the need for urgent or emergent MRI can arisewithin this period. Opinions differ about whether it is safeto perform MRI �8 weeks after CAS placement (9,10), andphysicians may choose to avoid MRI because of safetyconcerns. Dislodgement could theoretically increase theexposure of metallic coronary stent material to platelets,which may trigger stent thrombosis, resulting in cardiacdeath, myocardial infarction (MI), or emergent revascular-ization. In vitro and animal studies (11–14) have shown thatferromagneticity and stent migration are absent or minimalwith MRI of currently available stents. However, very fewclinical data are available on the outcome of patients whoundergo MRI early after CAS placement (15,16).
In addition to their clinical importance, data on the safetyof MRI early after CAS placement are also needed fordesigning clinical studies that use MRI (e.g., to compare theefficacy of different treatment modes for acute MI or toassess the status of CASs) (16–18). Therefore, we retro-spectively examined the rates of adverse cardiac eventsoccurring within 30 days after MRI performed �8 weeksafter placement of a CAS.
METHODS
Patients. We analyzed the Mayo Clinic Rochester Percu-taneous Coronary Intervention Database, which containsdemographic, clinical, angiographic, and procedural data.Immediate and in-hospital events are recorded, and allpatients are contacted for follow-up at six and 12 monthsand yearly thereafter. For the present analysis, we identifiedall patients who had CAS placement between July 1, 1994,and November 30, 2001. After CAS placement, all patientshad received a thienopyridine for no longer than four weeksin addition to aspirin. By cross-referencing the archivesystem of the Mayo Clinic Department of Radiology, weidentified all patients who had undergone an MRI exami-nation �8 weeks after CAS placement. If more than oneCAS placement preceded MRI, the time interval to MRIwas counted from the latest CAS placement.
The study was approved by the Mayo Foundation Insti-tutional Review Board. Patients who denied access to theirmedical record for research purposes (n � 4) were excluded.Outcomes. We queried the database for the occurrence ofdeath from any cause, MI, or repeat revascularizationprocedures within 30 days after the MRI examination. If
From the *Division of Cardiovascular Diseases and Department of Radiology,Mayo Clinic, Jacksonville, Florida; and †Division of Cardiovascular Diseases andInternal Medicine, ‡Division of Biostatistics, and §Department of Radiology, MayoClinic, Rochester, Minnesota.
Manuscript received February 6, 2003; revised manuscript received May 21, 2003,accepted May 30, 2003.
Journal of the American College of Cardiology Vol. 42, No. 7, 2003© 2003 by the American College of Cardiology Foundation ISSN 0735-1097/03/$30.00Published by Elsevier Inc. doi:10.1016/S0735-1097(03)00993-8

more than one MRI was performed �8 weeks after CASplacement, the follow-up period was extended to 30 daysfrom the latest MRI. An investigator reviewed medicalrecords to establish the nature of clinical events recorded inthe database. For patients who died, clinical data andautopsy reports were reviewed, and death was classified ascardiac or noncardiac. For repeat percutaneous coronaryinterventions, catheterization reports and films werereviewed.
An MI was diagnosed if any two of the following threecriteria were met: 1) “typical” chest pain that lasted �20min; 2) an elevation of creatine kinase or of its MBisoenzyme �2 times the upper limit of normal; or 3) newQ-waves or ST-T segment changes suggestive of MI on anelectrocardiogram.
Stent thrombosis was considered to have occurred if atleast one of the following was present: 1) confirmation onautopsy or by coronary angiography; 2) MI in the territoryof the treated vessel without definite exclusion of stentthrombosis; 3) sudden death without a clear noncardiaccause.Statistical analysis. Data are presented as mean � SD,median, or percentages. Exact binomial confidence intervalswere calculated.
RESULTS
Of 112 patients who underwent CAS placement followedby MRI within eight weeks and were eligible for the study,one was lost to follow-up. The remaining 111 (mean age, 67� 12 years) had a median of two stents placed (range, oneto six). Comorbid conditions and angiographic and proce-dural characteristics are shown in Table 1.
All MRI examinations were performed on one of twotypes of 1.5-tesla MRI units (Signa, General ElectricMedical Systems, Waukesha, Wisconsin, or Gyroscan,Philips Medical Systems, Best, The Netherlands). Duringthe eight weeks after CAS placement, 128 MRI examina-tions were performed. The following body parts wereimaged: head or neck, 50 (39%); spine, 27 (21%); abdomenor pelvis, 18 (14%); extremities, 13 (10%); chest, 11 (9%);and combined examination of several body parts, 9 (7%).Fifteen patients had �1 MRIs (13 patients had 2; 2 patientshad 3).
The mean time interval from CAS placement to MRIwas 21 � 17 days (median, 18; range, 0 to 54 days).Magnetic resonance imaging was performed within twodays after CAS placement in 15 patients (14%) and within14 days in 52 patients (47%).
Stent thrombosis as defined by the study criteria did not
occur. The 95% exact confidence interval for no events in111 patients is 0% to 3.3%. Seven clinical events occurred insix (5%) of the 111 patients during the 30 days after MRI(Table 2), including four noncardiac deaths and three repeatrevascularization procedures (all percutaneous coronary in-terventions).
DISCUSSION
This study shows that the risk of cardiac death, MI, or needfor repeat revascularization due to stent thrombosis associ-ated with MRI performed �8 weeks after CAS placementis very low. The results are consistent with the 30-daycardiac event rates (0.5% to 1.9%) after CAS placementwith contemporary antiplatelet therapy in patients notundergoing MRI (19).MRI after coronary stent placement. In a series of 13patients who underwent MRI 3 � 1 days after CASplacement for MI, no early adverse cardiac events occurredin the postinfarct period (16). In other small observationalstudies with longer intervals from elective CAS placementto MRI, stent thrombosis was also rare (15,17).
Our study includes the largest series to date of patientswho underwent MRI before CASs could be fully endothe-lialized (5). For all MRIs, the heart was at or near theisocenter of the magnet, and therefore, the CAS wereexposed to the scanners’ full magnetic field strength andspatial gradient. Our patients underwent MRI early afterCAS placement, contrary to conventional clinical practice,
Abbreviations and AcronymsCAS(s) � coronary artery stent(s)MI � myocardial infarctionMRI � magnetic resonance imaging
Table 1. Baseline Clinical and Procedural Characteristics of theStudy Population at Time of Coronary Artery Stent Placement(n � 111)
Characteristics Value*
Men 81 (73)Prior MI 60 (54)Prior PTCA 30 (27)Prior CABG 20 (18)Prior CVA/TIA 25 (23)Diabetes 38 (34)Current/former smoker 75 (68)Moderate/severe renal disease† 12 (11)Cancer 3 (3)Acute coronary syndrome 59 (53)CHF on presentation 14 (13)Preprocedural shock 3 (3)No. of coronary arteries with significant stenoses
2 41 (37)3 43 (39)
Type B2 or C lesion (20) 89 (80)Thrombus in any lesion 30 (27)Summed length of stents used, mm 22 � 15�3 Stents placed 16 (14)Average stent size, mm 3.3 � 0.6Stent diameter �3 mm 17 (15)
*Categorical variables are expressed as number (percentage) and continuous variablesas mean � SD; †Creatinine �265 �mol/l, current dialysis, or history of kidneytransplant.
CABG � coronary artery bypass graft; CHF � congestive heart failure; CVA �cerebrovascular accident; MI � myocardial infarction; PTCA � percutaneoustransluminal coronary angioplasty; TIA � transient ischemic attack.
1296 Gerber et al. JACC Vol. 42, No. 7, 2003Safety of MRI After Coronary Artery Stenting October 1, 2003:1295–8

because of severe comorbidity (Table 1). Accordingly, alldeaths during the follow-up period resulted from with-drawal of respiratory support or from stroke (Table 2).
The prevalence in our study group of factors known to beassociated with increased risk of stent thrombosis (19,20)(Table 1) suggests that our patients were at least at inter-mediate risk of adverse cardiac events. Therefore, theabsence of CAS thrombosis in our study cannot be attrib-uted to selection bias toward patients with low proceduralrisk. The three repeat percutaneous coronary interventionswere performed remote from the original treatment sites (n� 2) or for in-stent restenosis (n � 1), which was easilydistinguished from stent thrombosis by its far less acutecourse (21).Study limitations. Without complete 30-day angiographicfollow-up, we cannot exclude the possibility that the pres-ence of subclinical stent thrombosis was not detected insome patients with concurrent, critical illness. However,subclinical stent thrombosis is believed to be a very rareoccurrence, and the close observation of this patient groupwarranted by their comorbid conditions may actually haveresulted in higher than normal sensitivity for detectingcardiac events.
Despite the large number of patients in this series, theconfidence intervals remain wide, and a stent thrombosisrate as high as 3.3% cannot be excluded with certainty. Inaddition, the MRI field strength in our study was limited to1.5 T. Thus, it may not be appropriate to extrapolate fromour data to newer, higher field strength MRI scanners.
Nevertheless, our data suggest that MRI with fieldstrengths up to 1.5 T can be performed safely �8 weeksafter CAS placement. Current clinical practice and recom-mendations by manufacturers of CASs to postpone MRI
studies until after eight weeks from CAS placement do notseem necessary.
Reprint requests and correspondence: Dr. Thomas C. Gerber,Division of Cardiovascular Diseases, Mayo Clinic, 4500 San PabloRoad, Jacksonville, Florida 32224. E-mail: [email protected].
REFERENCES
1. Bhachu DS, Kanal E. Implantable pulse generators (pacemakers) andelectrodes: safety in the magnetic resonance imaging scanner environ-ment. J Magn Reson Imaging 2000;12:201–4.
2. Pinski SL, Trohman RG. Interference with cardiac pacing. CardiolClin 2000;18:219–39.
3. Shellock FG. Pocket Guide to MR Procedures and Metallic Objects:Update 2001. Philadelphia, PA: Lippincott Williams & Wilkins,2001:51–3.
4. 2002 Heart and Stroke Statistical Update. Dallas, TX: AmericanHeart Association, 2001:31–2.
5. Roubin GS, Robinson KA, King SB, III, et al. Early and late resultsof intracoronary arterial stenting after coronary angioplasty in dogs.Circulation 1987;76:891–7.
6. Medtronic AVE. Coronary artery disease: after treatment. Availableat: http://www.medtronicave.com/noflash/patients/coronaryartery_posttreatment.shtml. Accessed April 23, 2003.
7. Guidant Corporation. Instructions for use: coronary stent system.Available at: http://www.Guidant.com/condition/cad/ifu.shtml. Ac-cessed April 23, 2003.
8. American Heart Association. Stent procedure. Available at: http://www.americanheart.org/presenter.jhtml?identifier�4721. AccessedApril 23, 2003.
9. Jost C, Kumar VV. Are current cardiovascular stents MRI safe?J Invasive Cardiol 1998;10:477–9.
10. Kotsakis A, Tan KH, Jackson G. Is MRI a safe procedure in patientswith coronary stents in situ? Int J Clin Pract 1997;51:349.
11. Scott NA, Pettigrew RI. Absence of movement of coronary stents afterplacement in a magnetic resonance imaging field. Am J Cardiol1994;73:900–1.
Table 2. Clinical Events During 30-Day Follow-up in Six of 111 Patients Who Underwent MRI Within Eight Weeks of CoronaryStent Placement
Patient GenderAge,yrs
Vessel/LesionType (20)
Comorbid Conditionsat Time of Stent
Placement
StentPlacement
to MRI,days
Body PartImaged
MRI toClinical
Event, days Event
1 M 45 RCA/B1 ACS, prior MI, 3-VD 2 Extremity 1 PCI in different vessel (LAD)2 M 81 LM/C, LAD/C ACS, shock, CHF,
prior MI, 3-VD,DM, CRF
14 Head 7 Death (withdrawal ofrespiratory support)
3 F 67 LAD/B2 CHF, prior PCI, 2-VD, DM, CRF
15 Head 6 Death (withdrawal ofrespiratory support)
4 F 77 LAD/B2, LCx/B2, RCA/B2
ACS, prior MI, 3-VD,prior CVA
2 Head 4 Death (recurrent stroke)
5 M 68 LAD/C ACS, prior MI, priorPCI, prior CABG,2-VD
40 Extremity 9 Repeat PCI of LAD (in-stentrestenosis)
6 F 62 RCA/C ACS 7 Head 8 Repeat PCI of RCA (remotefrom original treatmentsite)
24 Head/spine 25 Death (withdrawal ofrespiratory support)
ACS � acute coronary syndrome; CABG � coronary artery bypass graft; CHF � congestive heart failure; CRF � chronic renal failure; CVA � cerebrovascular accident; DM� diabetes mellitus; F � female; LAD � left anterior descending coronary artery; LCx � left circumflex coronary artery; LM � left main coronary artery; M � male; MI �myocardial infarction; MRI � magnetic resonance imaging; PCI � percutaneous coronary intervention; RCA � right coronary artery; 2-VD � two-vessel disease; 3-VD �three-vessel disease.
1297JACC Vol. 42, No. 7, 2003 Gerber et al.October 1, 2003:1295–8 Safety of MRI After Coronary Artery Stenting

12. Strohm O, Kivelitz D, Gross W, et al. Safety of implantable coronarystents during 1H-magnetic resonance imaging at 1.0 and 1.5 T.J Cardiovasc Magn Reson 1999;1:239–45.
13. Hug J, Nagel E, Bornstedt A, Schnackenburg B, Oswald H, Fleck E.Coronary arterial stents: safety and artifacts during MR imaging.Radiology 2000;216:781–7.
14. Matsumoto AH, Teitelbaum GP, Barth KH, Carvlin MJ, Savin MA,Strecker EP. Tantalum vascular stents: in vivo evaluation with MRimaging. Radiology 1989;170:753–5.
15. Schroeder AP, Houlind K, Pedersen EM, Thuesen L, Nielsen TT,Egeblad H. Magnetic resonance imaging seems safe in patients withintracoronary stents. J Cardiovasc Magn Reson 2000;2:43–9.
16. Kramer CM, Rogers WJ, Jr., Pakstis DL. Absence of adverseoutcomes after magnetic resonance imaging early after stent placementfor acute myocardial infarction: a preliminary study. J CardiovascMagn Reson 2000;2:257–61.
17. De Cobelli F, Cappio S, Vanzulli A, Del Maschio A. MRI assessmentof coronary stents. Rays 1999;24:140–8.
18. Mohiaddin RH, Roberts RH, Underwood R, Rothman M. Localiza-tion of a misplaced coronary artery stent by magnetic resonanceimaging. Clin Cardiol 1995;18:175–7.
19. Orford JL, Lennon R, Melby S, et al. Frequency and correlates ofcoronary stent thrombosis in the modern era: analysis of a single centerregistry. J Am Coll Cardiol 2002;40:1567–72.
20. Ellis SG, Vandormael MG, Cowley MJ, et al. Coronary morphologicand clinical determinants of procedural outcome with angioplasty formultivessel coronary disease: implications for patient selection. Mul-tivessel Angioplasty Prognosis study group. Circulation 1990;82:1193–202.
21. Lowe HC, Oesterle SN, Khachigian LM. Coronary in-stent resteno-sis: current status and future strategies. J Am Coll Cardiol 2002;39:183–93.
1298 Gerber et al. JACC Vol. 42, No. 7, 2003Safety of MRI After Coronary Artery Stenting October 1, 2003:1295–8

BASIC SCIENCE STUDY
Effect of Tumor Necrosis Factor-Alphaon Endothelial and Inducible Nitric OxideSynthase Messenger Ribonucleic AcidExpression and Nitric Oxide Synthesisin Ischemic and Nonischemic Isolated Rat HeartYosef Paz, MD,* Inna Frolkis, MD, PHD,* Dimitri Pevni, MD,* Itzhak Shapira, MD,* Yael Yuhas, PHD,‡Adrian Iaina, MD,† Yoram Wollman, PHD,† Tamara Chernichovski, MSC,† Nahum Nesher, MD,*Chaim Locker, MD,* Rephael Mohr, MD,* Gideon Uretzky, MD*Tel-Aviv and Petah-Tikva, Israel
OBJECTIVES The present study aimed to investigate the influence of endogenous tumor necrosisfactor-alpha (TNF-�) that was synthesized during ischemia and exogenous TNF-� onendothelial and inducible nitric oxide synthase (eNOS and iNOS) messenger ribonucleic acid(mRNA) expression and nitric oxide (NO) production in the isolated rat heart.
BACKGROUND Tumor necrosis factor-� is recognized as being a proinflammatory cytokine with a significantcardiodepressant effect. One of the proposed mechanisms for TNF-�-induced cardiaccontractile dysfunction is increased NO production via iNOS mRNA upregulation, but therole of NO in TNF-�-induced myocardial dysfunction is highly controversial.
METHODS Isolated rat hearts studied by a modified Langendorff model were randomly divided intosubgroups to investigate the effect of 1-h global cardioplegic ischemia or the effect of 1-hperfusion with exogenous TNF-� on the expression of eNOS mRNA and iNOS mRNA andon NO production.
RESULTS After 1 h of ischemia, there were significant increases in TNF levels in the effluent (fromhearts), and eNOS mRNA expression had declined (from 0.91 � 0.08 to 0.68 � 0.19, p �0.001); but there were no changes in iNOS mRNA expression, and NO was below detectablelevels. Perfusion of isolated hearts with TNF-� had a cardiodepressant effect and decreasedeNOS mRNA expression to 0.67 � 0.04 (p � 0.002). Inducible nitric oxide synthase mRNAwas unchanged, and NO was below detectable levels.
CONCLUSIONS We believe this is the first study to directly show that TNF-� does not increase NO synthesisand release but does downregulate eNOS mRNA in the ischemic and nonischemic isolatedrat heart. (J Am Coll Cardiol 2003;42:1299–305) © 2003 by the American College ofCardiology Foundation
Tumor necrosis factor-alpha (TNF-�) is a trimeric 17-kDapolypeptide produced by monocytes and macrophages,which are known to be proinflammatory cytokines (1,2). Itsclassic trilogy action on the body is the induction ofnecrosis, shock, and cachexia. Tumor necrosis factor-alphahas a potent negative inotropic effect (3,4), and the hemo-dynamic influence of TNF-� is characterized by decreasedmyocardial contraction and reduced ejection fraction, hypo-tension, decreased systemic vascular resistance, and biven-tricular dilatation (5,6). Recent studies have demonstratedthat TNF-� is produced during ischemia-reperfusion injuryand activates nuclear factor kappa-�, which initiates the
cytokine cascade and facilitates the expression of chemo-kines and adhesion molecules (7,8). Experiments with micelacking TNF-� have demonstrated an improvement inmyocardial ischemia-reperfusion injury (9).
Myocardial cells themselves can produce TNF-� in theisolated perfused heart under endotoxin treatment (10). Ourgroup previously reported that TNF-� is released from theisolated heart undergoing ischemia and that this cytokineproduction is directly correlated with the degree of myocar-dial dysfunction (11,12). Moreover, the administration ofmonoclonal antibodies to TNF-� eliminates this cytokinein effluent and attenuates the postischemic myocardialinjury (13).
One of the mechanisms suggested for TNF-� cardiaccontractile dysfunction is increased nitric oxide (NO) pro-duction by the myocardium, which causes depression ofcardiac function. In the heart, NO is synthesized fromL-arginine by two types of nitric oxide synthases (NOS):endothelial (eNOS) and inducible (iNOS). A constitutive
From the *Department of Thoracic and Cardiovascular Surgery and †Departmentof Nephrology, Tel-Aviv Medical Center, Sackler Faculty of Medicine, Tel-AvivUniversity, Tel-Aviv, Israel; and the ‡Felsenstein Medical Research Center, Petah-Tikva, Israel. This study was supported by the Research Fund of the Department ofThoracic and Cardiovascular Surgery, Sourasky Tel-Aviv Medical Center, Israel.
Manuscript received February 3, 2003; revised manuscript received May 19, 2003,accepted June 4, 2003.
Journal of the American College of Cardiology Vol. 42, No. 7, 2003© 2003 by the American College of Cardiology Foundation ISSN 0735-1097/03/$30.00Published by Elsevier Inc. doi:10.1016/S0735-1097(03)00992-6

isoform of NOS, eNOS, which is calcium/calmodulinregulated and was originally described in endothelial cells,causes continuous NO production and plays an importantrole in vascular tone regulation (14). The second type ofNOS described in cardiac myocytes is calcium-independentiNOS, which can be activated by cytokines, leading to NOoverproduction and causing a negative inotropic effect,probably by activation of the enzyme guanylate cyclase(15,16). Some studies have found that cardiac myocytesexpress both eNOS and iNOS (16)
Finkel et al. (17) demonstrated that NOS inhibitionprevents the myocardial-depressant effect of TNF-� andconcluded that the negative inotropic effect is mediated byNO. Wang and Zweier (18) observed increased NO andperoxinitrite release from the isolated rat heart after 30 minof global ischemia. Pretreatment with the NOS inhibitorsresulted in a fourfold increase in postischemic functionalrecovery. The role of NO in TNF-�-induced myocardialdysfunction, however, is highly controversial. Avontuur etal. (19) showed that inhibition of NO synthesis causesmyocardial ischemia in endotoxemic rats. Yocoyama et al.(4) reported that increased levels of NO did not mediateTNF-�-induced myocardial contractile abnormalities. Inanother study, TNF-� showed no significant effect on NOproduction in cultured cardiac myocytes (20). Lastly, NOSinhibitors did not prevent a decrease of either intracellularcalcium or the amplitude of cell shortening caused byTNF-� in isolated ventricular myocytes (21). Most of theseabove-cited studies incorporated evidence provided indi-rectly by NOS inhibitors.
The present study investigated whether endogenous(paracrine) TNF-� that was synthesized during globalcardioplegic ischemia and exogenous TNF-� given in per-fusion solution have a direct influence on eNOS and iNOSmessenger ribonucleic acid (mRNA) expression and NOrelease in the isolated rat heart.
METHODS
Male Wistar rats were anesthetized by intraperitoneal in-jection of pentobarbital sodium (30 mg/kg). Their heartswere rapidly excised, immersed in cold saline (4°C),mounted on the stainless-steel cannula of a modified Lan-gendorff apparatus, and perfused with Krebs-Henseleit
(KH) solution exactly as detailed in four of our previouslyreported studies (11–13).
Left ventricular (LV) hemodynamic parameters (peaksystolic developed pressure) and coronary flow (CF) werecontinuously measured at 10-min intervals, and the firstderivative of the rise in LV pressure (dP/dtmax) and time-pressure integral were calculated.Ethics. All animals received humane care as described in“Principles of Laboratory Animal Care” formulated by theNational Society for Medical Research and the “Guide forthe Care and Use of Laboratory Animals” prepared by theNational Academy of Sciences and published by the Na-tional Institutes of Health (NIH Publication No. 80-23,revised 1985).Experimental protocol. The rats were randomly dividedinto two subgroups to assess the effect of 1-h globalcardioplegic ischemia on TNF-� and NO synthesis andproduction. Control measurements were recorded after a15-min period of stabilization (baseline). All hearts wereperfused thereafter for a 30-min period. Left ventricularhemodynamic parameters were measured at 10-min inter-vals. Effluent for TNF-� and NO levels was withdrawn atthe end of the 30-min period (n � 8). Warm cardioplegiawas then administered for 2 min (37°C, perfusion pressure73 mm Hg, KCl � 16 mEq/l in KH solution) followed bya 60-min period of global ischemia at 31°C to the arrestedhearts (group A, n � 8).
Group B was similar to group A, but these rats receivedpolyclonal rabbit anti-rat TNF-� antibodies (anti-TNF-�Ab, n � 8). Concentration of anti-TNF-� Ab was selectedaccording to specific activity: approximately 1 �g of theseantibodies completely neutralized 25 pg of rat TNF-�. Wefound that the TNF-� level in effluent was 805 � 230pg/ml after a 60-min period of global ischemia. We used 1.5�g/ml of anti-TNF-� antibodies (total dose 45 �g) for totalneutralization of TNF-� in the heart tissue, after whichTNF-� was not found in the effluent from the coronarysinus of ischemic hearts.
The first milliliter of reperfusion effluent was withdrawnat the end of ischemia to determine TNF-� and NO levelsin both groups. Additional hearts were assayed at baseline(n � 7) and immediately at the end of ischemia (n � 7 foreach group) to determine LV TNF-�, eNOS, and iNOSmRNA expression.
Two additional subgroups (groups C and D) formed byother rats were used to investigate the direct effect ofexogenous TNF-� on nonischemic perfused hearts. Controlmeasurements were recorded after a 15-min period ofstabilization. Thereafter, the hearts were perfused for a60-min period with KH solution to which either saline(group C, n � 10, “controls”) or 16 ng/ml (pathophysio-logical relevant concentration) TNF-� (group D, n � 7)were added to KH solution using an infusion pump (0.5ml/min). The dose of TNF-� was selected according theresults of group A’s postischemic TNF-� level measure-ments. Hemodynamic measurements were recorded every
Abbreviations and AcronymsCF � coronary floweNOS � endothelial nitric oxide synthaseiNOS � inducible nitric oxide synthaseKH � Krebs-HenseleitLV � left ventricularmRNA � messenger ribonucleic acidNO � nitric oxideNOS � nitric oxide synthasePCR � polymerase chain reactionTNF-� � tumor necrosis factor-alpha
1300 Paz et al. JACC Vol. 42, No. 7, 2003Effect of TNF-� on eNOS and iNOS mRNA Expression October 1, 2003:1299–305

10 min, and effluent was withdrawn to determine TNF-�and NO levels. Five hearts in each group were removed forLV iNOS and eNOS mRNA assays immediately at the endof the 60-min perfusion period.TNF-� determination. Tumor necrosis factor-� levelswere detected in the effluent from the coronary sinus of theisolated rat hearts. Tumor necrosis factor-� activity wasmeasured using the commercially available enzyme-linkedimmunoassay kit Cytoscreen TM rat kit TNF-�, Immuno-assay kit (Biosource, Camarillo, California). The limit ofdetection was 4 pg/ml.NO measurement. Effluent nitrite (NO2)- and nitrate(NO3)-stable metabolites of NO representing NO produc-tion were detected in the heart perfusate samples andcardiac myocyte culture supernatant as described previously(22). The limit of detection was 2 �mol/l.Myocardial tissue TNF-�, eNOS, and iNOS mRNAdetermination. Immediately after stabilization (baseline)or after 1 h of global cardioplegic ischemia, the LVmyocardium was excised and placed in cold Hank’s balancedsolution. Total RNA was extracted from myocardial sam-ples using the guanidinium thiocyanate method (23). Ribo-nucleic acid pellets were maintained at �20°C with 75%ethanol until assay. Dried sediments were dissolved in sterileRNAse free water and quantitated spectrophotometricallyat � � 260 nm.
Reverse-transcription polymerase chain reaction (PCR)amplification and quantitative analysis were prepared aspreviously described (12). The primer sequences, annealingtemperature, number of cycles, and PCR product size arelisted in Table 1.
All TNF-�, eNOS, and iNOS band intensities werenormalized by respective for glyceraldehyde-phospate dehy-drogenase values. Each PCR reaction was performed at leasttwice, and four to five hearts were used for each experimen-tal group.Drugs. Polyclonal rabbit anti-rat TNF-� Ab was pur-chased from R&D Systems (Minneapolis, Minnesota).Specific activity was as follows: approximately 1 �g of theseantibodies completely neutralized 25 pg of rat TNF-�.
Recombinant human TNF-� was purchased from Repro-gen Ltd. (Rehovot, Israel).Statistics. The results are presented as mean � SD. Allhemodynamic measurements were subjected to two-wayanalysis of variance with repeated measures. This designincludes one between-subject factor (the experimentalgroup) and one within-subject factor (the time of measure-ment). Whenever a significant time trend was demon-strated, we used contrast analysis to compare each measure-ment to its successive one (SIMPLE; SPSS Inc., Chicago,Illinois). Only one contrast was used to eliminate theproblem of multiple comparisons. Student t tests were usedto assess significant differences between relative opticaldensities of the mRNA bands in groups and betweengroups. Significance was established at p � 0.05. Allstatistical analyses were performed by the Statistical Depart-ment at our Medical Center.
RESULTS
The baseline values (groups A and B) for different LVhemodynamic parameters are given in Table 2. No signifi-cant differences were found between the experimentalgroups. A two-way analysis of variance (comparing groupmeans and group-time interaction) was conducted to revealpossible differences in LV hemodynamic parameters for theexperimental groups before cardioplegic ischemia (baselinevalues, 10, 20, and 30 min perfusion); none of the p valuesattained statistical significance.
Table 1. Specification of the Primer Sets Used to Analyze Messenger Ribonucleic Acid Expression
Size Primer SetNumber of
CyclesAnnealing Temperature
(°C)PCR Product
(bp)
TNF-�Sense CACGCTCTTCTGTCTACTGA 30 57 546Antisense GGACTCCGTGATGTCTAAGT
eNOSSense CCGGAATTCGAATACCAGCCTGATCCATGGAA 45 65 614Antisense GCCGGATCCTCCAGGAGGGTGTCCACCGCATG
iNOSSense GTGTTCCACCAGGAGATGTTG 35 60 576Antisense CTCCTGCCCACTGAGTTCGTC
GAPDHSense AATGCATCCTGCACCACCAA 30 60 515Antisense GTAGCCATATTCATTGTCAT
eNOS � endothelial nitric oxide synthase; GAPDH � glyceraldehyde-phosphate dehydrogenase; iNOS � inducible nitric oxide synthase; PCR � polymerase chain reaction;TNF-� � tumor necrosis factor–alpha.
Table 2. Baseline Measurements
Group A Group B
Peak systolic pressure 121 � 4 123 � 5 (mm Hg)dP/dtmax (mm Hg/s) 4015 � 381 4176 � 174Time-pressure integral 8.3 � 0.5 8.5 � 0.7 (mm Hg � s)Coronary flow (ml/min) 17.6 � 0.7 18.6 � 1.2
Data presented as mean values � SE. All variables were identical for all groups ofhearts (p � nonsignificant).
dP/dt max � first derivative of the rise of left ventricular pressure.
1301JACC Vol. 42, No. 7, 2003 Paz et al.October 1, 2003:1299–305 Effect of TNF-� on eNOS and iNOS mRNA Expression

Effect of global cardioplegic ischemia on TNF-�, eNOS,and iNOS mRNA expression. The baseline TNF-�mRNA expression that had been detected in LV specimensafter a period of stabilization and that did not change aftera 90-min period of nonischemic perfusion served as anadditional control (n � 7) to the postischemic TNF-�,iNOS, and eNOS mRNA measurements. Intensities of thebands at baseline and at the end of perfusion were 0.55 �0.2 and 0.53 � 0.1, respectively (p � NS, Fig. 1A). Onehour of global cardioplegic ischemia led to a 1.6-foldincrease of TNF-� mRNA expression, which was signifi-cantly higher than the levels detected in nonischemic,normally perfused hearts (p � 0.003, Fig. 1A).
Baseline eNOS and iNOS mRNA expression was de-tected in LV samples after a period of stabilization and didnot change after a 90-min period of nonischemic perfusion(Fig. 1B and 1C). No upregulation of iNOS mRNAexpression was registered in postischemic LV myocardialtissue compared with baseline values or after a 90-minperiod of nonischemic perfusion. There was, however, asignificant downregulation of eNOS mRNA expression (p� 0.01, Fig. 1C) after 1 h of global cardioplegic ischemia.Effect of global cardioplegic ischemia on TNF-� andNO release. Tumor necrosis factor-� was not detected inthe myocardial effluent after 15 min of stabilization, beforeischemia (after 30 min of perfusion), or after 90 min ofnormal nonischemic perfusion. Significant amounts ofTNF-� were detected in the effluent after 1 h of globalcardioplegic ischemia upon the first minute of reperfusion(805 � 230 pg/ml). The NO2 and NO3 values in theeffluent from isolated perfused hearts in all groups werebelow detectable levels.Effect of TNF-� depletion on myocardial TNF-�,eNOS, and iNOS mRNA expression and release. Anti-TNF-� Ab was added to the cardioplegic solution toneutralize TNF-� in the ischemic heart. In hearts treatedwith anti-TNF-� Ab, TNF-� mRNA expression was atbasal levels after 1 h of global ischemia (Fig. 1A), which wassignificantly lower than the levels detected in untreatedischemic hearts.
There was an increase of eNOS mRNA in the ischemicheart pretreated with anti-TNF-� Ab compared with un-treated ischemic hearts (1.07 � 0.1 and 0.67 � 0.2,respectively, p � 0.01). There were no significant differ-ences in iNOS mRNA band intensities between anti-TNF-� Ab-treated and control hearts (Fig. 1B and 1C).Tumor necrosis factor-� protein production and NO2 andNO3 in the effluent from the ischemic hearts treated withanti-TNF-� Ab were below detectable levels.Effect of exogenous TNF-� on LV hemodynamic per-formances. No significant differences in baseline values forLV hemodynamic parameters were found between groupsC and D (Fig. 2). Hearts treated with TNF-� demonstrateda significant deterioration in all hemodynamic measure-ments after only 10 min of perfusion (Fig. 2) and, after 60min of TNF-� treatment, peak-systolic pressure fell to 45.1
Figure 1. Effects of global cardioplegic ischemia on myocardial tumornecrosis factor-� (TNF-�) (A), endothelial nitric oxide synthase (eNOS)(B), and inducible nitric oxide synthase (iNOS) (C) mRNA expression:relative optical densities of polymerase chain reaction signals. Data werenormalized to the glyceraldehyde 3-phosphate dehydrogenase (GAPDH)polymerase chain reaction signal. Shown are samples of left ventricularmyocardium withdrawn at the end of stabilization [1], after ischemia [2],after ischemia with anti-TNF-� antibodies in the cardioplegia [3], andafter 90 min of normal nonischemic perfusion [4].
1302 Paz et al. JACC Vol. 42, No. 7, 2003Effect of TNF-� on eNOS and iNOS mRNA Expression October 1, 2003:1299–305

� 3.7%; dP/dtmax to 51.8 � 5.5%, time-pressure integral to73.5 � 4.8%, and CF to 54.7 � 2.8% (p � 0.001 for allmeasurements compared with baseline). The decrease of LVfunction parameters in TNF-�-treated hearts was signifi-cant compared wit untreated hearts (Fig. 2, p � 0.0001 forall measurements).Effect of exogenous TNF-� on eNOS and iNOS mRNAexpression. Endothelial nitric oxide synthase mRNA ex-pression in LV specimens after a period of stabilization didnot change after a 60-min period of nonischemic perfusion,but 60 min of TNF-� treatment led to significant down-regulation of eNOS mRNA expression (Fig. 3A; p � 0.01).There were no significant differences in iNOS mRNA bandintensities between TNF-�-treated and control hearts(Fig. 3B).
DISCUSSION
In the present study, we have demonstrated that endoge-nous (i.e., released during ischemia) and exogenous TNF-�cause depression of LV function associated with undetect-
able NO levels in the effluent from the heart, unchangediNOS mRNA expression, and eNOS mRNA downregula-tion.The role of TNF-� in cardiac dysfunction. Tumor ne-crosis factor-� is an essential mediator of the profoundcardiovascular changes observed during the shocked stateassociated with bacterial sepsis and its experimental coun-terpart, endotoxic shock (24,25). Recent investigations haveconfirmed that the TNF-� levels were increased in patientswith congestive heart failure and demonstrated a directrelationship between circulating levels of TNF-� and clin-ical features of the disease (26). Tumor necrosis factor-�also plays an important role in reperfusion injury aftermyocardial revascularization (27). Tumor necrosis factor-�is synthesized and released from the isolated heart under-going ischemia (11,12). The results of current experimentssupport this previous observation. Immunohistochemicalstudies localized TNF-� in ischemic hearts to cardiacmyocytes and endothelial cells (13). The myocardium hasbeen shown to be a major source of TNF-� in patientsundergoing cardiopulmonary bypass (in vivo acute global
Figure 2. Effect of exogenous tumor necrosis factor-� on hemodynamic performance of isolated rat hearts during 1 h of perfusion: control group (opencircles) and hearts treated with tumor necrosis factor-� (black circles), p � 0.0001 (analysis of variance) for all measurements vs. control.
1303JACC Vol. 42, No. 7, 2003 Paz et al.October 1, 2003:1299–305 Effect of TNF-� on eNOS and iNOS mRNA Expression

ischemia) (28). A blood-free model was intentionally usedin this study to exclude the possibility of involvement ofsystemic blood factors in endogenous TNF-� and NOformation and in exogenous TNF-� action on the heart. Amodel of cardioplegic ischemia was chosen because of theextensive use of cardioplegic solutions in cardiopulmonarybypass.
The cardiac depressant effect of TNF-� on an isolatedmyocardium was previously shown with relatively highconcentrations of this cytokine (17,29). In the present study,perfusion with TNF-� in a low, pathophysiologically rele-vant concentration led to a significant decrease of LVpeak-systolic pressure, dP/dtmax, and time-pressure integral.Mechanisms of TNF-� action. The exact mechanismsresponsible for TNF-�-induced cardiac damage are contro-versial (30). Several mechanisms have been suggested tocause TNF-�-induced myocardial dysfunction. Tumor ne-crosis factor-� decreases the intracellular free calcium andleads to dysfunctional excitation-contraction coupling, caus-ing systolic/diastolic dysfunction (4,21). Several in vitro andin vivo studies have shown involvement of sphingosine in
TNF-�-mediated cardiac depression (29,31). Tumor necro-sis factor-� induces apoptosis (programmed cell death) invarious cell types, including cardiac myocytes (2,31). Otherpossible mechanisms are direct cytotoxicity and oxidantstress (30).Current hypothesis. Some previous studies using NOsynthesis inhibitors confirm that NO is responsible forTNF-�-induced negative inotropism (17,18). It is proposedthat TNF-� stimulates iNOS which, in turn, controls theconversion of L-arginine to NO. Excessive production ofNO by cardiomyocytes causes contractile dysfunction anddepression of cardiac function.
Recent investigations, however, have shown that theNOS inhibitors do not ameliorate the decreased contractil-ity of isolated perfused hearts observed with TNF-� (29).Tumor necrosis factor-� had no significant effect on NOand cGMP production in cultured cardiac myocytes (20). Ina model of isolated cardiac myocytes, NOS inhibitors do notattenuate the negative inotropic effect of TNF-�, andincubation with TNF-� did not increase NO and cGMPproduction (4). NOS inhibitors did not prevent a decreasein either intracellular calcium or the amplitude of cellshortening caused by TNF in isolated ventricular myocytes(21). In addition, it has been shown that the massivecardiospecific overexpression of iNOS in transgenic mice isnot associated with deleterious effects on cardiac hemody-namics and energetics (32). The participation of eNOSmRNA expression in cardiodepressant action of TNF-� hasnot been investigated in depth.New insights. The present study clearly has demonstratedthat endogenous (paracrine) TNF-� synthesized during 1 hof global cardioplegic ischemia or exogenous TNF-� addedfor 1 h to perfusion solution does not increase iNOS mRNAexpression and NO release in the isolated rat heart. In thepresent study, we have demonstrated that the endogenousand exogenous TNF-� caused a decrease in eNOS mRNAexpression. Moreover, depletion of TNF-� with anti-TNF-� Ab resulted in an increase in eNOS mRNA in theischemic heart compared with untreated ischemic hearts,recovering eNOS mRNA expression to baseline levels.
We have shown that CF significantly decreased after 1 hof perfusion with a TNF-�-containing solution. Previousexperiments demonstrated that TNF-� caused coronaryconstriction in the rat heart, which might accentuate directnegative inotropic action of TNF-� (29). In the currentstudy, we found that eNOS mRNA downregulation inhearts undergoing ischemia or TNF-� perfusion may leadto a decrease in endothelial NO production, coronaryvasoconstriction, and a decrease of CF. This might be oneof the possible mechanisms of TNF-�-induced cardiode-pressant action. It is theoretically possible that a moreprolonged (3 to 6 h) TNF-� influence could lead to achange in iNOS mRNA expression, but this duration wouldbe considered excessive in a model such as ours.Study limitations. Our study had several limitations. First,it was performed in vitro. Second, nonblood perfusion
Figure 3. Effect of exogenous tumor necrosis factor-� on myocardialendothelial nitric oxide synthase (eNOS) (A) and inducible nitric oxidesynthase (iNOS) (B) messenger ribonucleic acid expression: relative opticaldensities of polymerase chain reaction signals. Data were normalized toglyceraldehyde 3-phosphate dehydrogenase (GAPDH) polymerase chainreaction signal. Samples of left ventricular myocardium withdrawn at theend of stabilization [1], after 1-h perfusion with normal Krebs-Henseleitsolution [2], and after 1 h of perfusion with tumor necrosis factor-� [3].
1304 Paz et al. JACC Vol. 42, No. 7, 2003Effect of TNF-� on eNOS and iNOS mRNA Expression October 1, 2003:1299–305

excluded an influence of blood immunological and proin-flammatory factors and also excluded the influence of severaltypes of blood cells that are an important source of TNF-�and NO. Caution must be exercised when drawing directclinical conclusions from the use of anti-TNF-� Ab in aclinical setting because our study was performed on anisolated rat heart model.Conclusions. This study demonstrated that endogenous(i.e., released during ischemia) and exogenous TNF-� donot influence iNOS mRNA expression and that they do notenhance NO release. This study did reveal eNOS mRNAdownregulation in the isolated rat heart. Depletion ofendogenous TNF-� caused by anti-TNF-� Ab led to thedecrease of TNF-� mRNA expression, the elimination ofTNF-� protein from effluent solution, and an increase ineNOS mRNA expression to baseline levels in ischemichearts. These findings suggest that eNOS downregulationoccurs as a result of endogenous TNF-� synthesis. Wehypothesize that the TNF-�-related eNOS mRNA down-regulation that is associated with CF decreases and that LVdysfunction may be one of the mechanisms of TNF-�-mediated myocardial depression.
AcknowledgmentsThe authors thank Esther L. Shabtai, MSc, for statisticalassistance and Esther Eshkol, MA, for editorial assistance.
Reprint requests and correspondence: Dr. Inna Frolkis, Depart-ment of Thoracic and Cardiovascular Surgery, Tel Aviv SouraskyMedical Center, 6 Weizmann Street, Tel Aviv 64239, Israel.E-mail: [email protected].
REFERENCES
1. Aggarwal B, Natarjan K. Tumor necrosis factor: development duringthe decade. Eur Cytokine Netw 1996;7:93–124.
2. Meldrum DR. Tumor necrosis factor in the heart. Am J Physiol1998;274:R577–95.
3. Pagani FD, Baker LS, His C, Knox M, Fink MP, Visner MS. Leftventricular systolic and diastolic dysfunction after infusion of tumornecrosis factor-alpha in conscious dogs. J Clin Invest 1992;90:389–98.
4. Yokoyama T, Vaca L, Rossen RD, Durante W, Hazarika P, MannDL. Cellular basis for the negative inotropic effect of tumor necrosisfactor-alpha. J Clin Invest 1993;92:2303–12.
5. Parker MM, McCarty KE, Ognibene FP, Parrillo JE. Right ventric-ular dysfunction and dilatation, similar to left ventricular changes,characterize the cardiac depression of septic shock in humans. Chest1990;97:126–31.
6. Ellrodt AG, Riedinger MS, Kimchi A, et al. Left ventricular perfor-mance in septic shock: reversible segmental and global abnormalities.Am Heart J 1985;110:402–9.
7. Frangogiannis NG, Lindsey ML, Michael LH, et al. Resident cardiacmast cells degranulate and release preformed TNF-alpha, initiating thecytokine cascade in experimental canine myocardial ischemia/reperfusion. Circulation 1998;98:699–710.
8. Kupatt C, Habazettl H, Goedecke A, et al. Tumor necrosis factor-alpha contributes to ischemia- and reperfusion-induced endothelialactivation in isolated hearts. Circ Res 1999;84:392–400.
9. Maekawa N, Wada H, Kanda T, et al. Improved myocardial ischemia/reperfusion injury in mice lacking tumor necrosis factor-�. J Am CollCardiol 2002;39:1229–35.
10. Kapadia S, Lee J, Torre AG, Birdsall HH, Ma TS, Mann DL. Tumornecrosis factor-alpha gene and protein expression in adult felinemyocardium after endotoxin administration. J Clin Invest 1995;96:1042–52.
11. Gurevitch J, Frolkis I, Yuhas Y, et al. Tumor necrosis factor-alpha isreleased from the isolated heart undergoing ischemia and reperfusion.J Am Coll Cardiol 1996;28:247–52.
12. Frolkis I, Gurevitch J, Yuhas Y, et al. Interaction between paracrinetumor necrosis factor-alpha and paracrine angiotensin II duringmyocardial ischemia. J Am Coll Cardiol 2001;385:729–33.
13. Gurevitch J, Frolkis I, Yuhas Y, et al. Anti-tumor necrosis factor-alphaimproves myocardial recovery after ischemia and reperfusion. J AmColl Cardiol 1997;30:1554–61.
14. Buockley BS, Mirza Z, Whorton AR. Regulation of Ca2� dependentnitric oxide synthase in bovine aortic endothelial cells. Am J Physiol1995;269:C757–65.
15. Joe IK, Schussheim AE, Longrois D, et al. Regulation of cardiacmyocytes contractile function by inducible nitric oxide synthase(iNOS): mechanisms of contractile depression by nitric oxide. J MolCell Cardiol 1998;30:303–15.
16. Balligand JL, Kobzik L, Han X, et al. Nitric oxide-dependentparasympathetic signaling is due to activation of constitutive endothe-lial (type III) nitric oxide synthase in cardiac myocytes. J Biol Chem1995;270:14582–6.
17. Finkel MS, Oddis CV, Jacob TD, Watkins SC, Hattler BG, SimmonsRL. Negative inotropic effect of cytokines on the heart mediated bynitric oxide. Science 1992;257:387–9.
18. Wang P, Zweier JL. Measurement of nitric oxide and peroxinitritegeneration in the postischemic heart: evidence of peroxinitrite-mediated reperfusion injury. J Biol Chem 1996;271:29223–30.
19. Avontuur JAM, Bruining HA, Ince S. Inhibition of nitric oxidesynthesis causes myocardial ischemia in endotoxemic rats. Circ Res1995;76:418–25.
20. Shindo T, Ikeda U, Ohkawa F, Kawahara Y, Yokoyama M, ShimadaK. Nitric oxide synthesis in cardiac myocytes and fibroblasts byinflammatory cytokines. Cardiovasc Res 1995;29:813–9.
21. Sugishita K, Kinugawa K, Shimizu T, et al. Cellular basis for the acuteinhibitory effect of IL-6 and TNF-alpha on excitation-contractioncoupling. J Mol Cell Cardiol 1999;31:1457–67.
22. Pevni D, Frolkis I, Iaina A, et al. Protamine cardiotoxicity and nitricoxide. Eur J Cardiothorac Surg 2001;20:147–52.
23. Sambrook J, Fritsch EF, Maniatis T. Molecular cloning: extraction ofRNA with guanidinium thiocyanate followed by centrifugation inserum chloride solution. In: Nolan SH, editor. Laboratory Manual.Book 1, Cold Spring Harbor Laboratory Series. New York, NY: ColdSpring Harbor, 1989:719–32.
24. Tracay KJ, Beutler B, Lowry SF, et al. Shock and tissue injury inducedby recombinant human cachectin. Science 1986;234:470–4.
25. Mathison JS, Wolfson E, Ulevitch RJ. Participation of tumor necrosisfactor in the mediation of gram negative bacterial lipopolysaccharide-induced injury in rabbits. J Clin Invest 1988;81:1925–37.
26. Packer M. Is tumor necrosis factor an important neurohormonalmechanism in chronic heart failure? Circulation 1995;92:1382–97.
27. Wei M, Kuukasjarvi P, Laurikka E, et al. Inflammatory cytokines andsoluble receptors after coronary artery bypass grafting. Cytokines2001;15:223–8.
28. Meldrum DR, Meng X, Dinarello CA, et al. Human myocardial tissueTNF-alpha expression following acute global ischemia in vivo. J MolCell Cardiol 1998;30:1683–9.
29. Edmuds NJ, Lal H, Woodward B. Effect of tumor necrosis factor-�on left ventricular function in the rat isolated perfused heart: possiblemechanisms for a decline in cardiac function. Br J Pharmacol 1999;126:189–96.
30. Retter AS, Frishman WH. The role of tumor necrosis factor in cardiacdisease. Heart Disease 2001;3:319–25.
31. Hakan O, Dorn GW, Mann DL. Sphingosine mediates the immedi-ate negative inotropic effect of tumor necrosis factor-� in the adultcardiac myocyte. J Biol Chem 1997;272:4836–42.
32. Heger J, Godecke A, Flogel U, et al. Cardiac-specific overexpression ofinducible nitric oxide synthase does not result in severe cardiacdysfunction. Circ Res 2002;90:93–9.
1305JACC Vol. 42, No. 7, 2003 Paz et al.October 1, 2003:1299–305 Effect of TNF-� on eNOS and iNOS mRNA Expression

EXPEDITED REVIEW
Androgens Up-Regulate Atherosclerosis-RelatedGenes in Macrophages From Males But Not FemalesMolecular Insights Into Gender Differences in AtherosclerosisMartin K. C. Ng, MBBS, FRACP,*† Carmel M. Quinn, DPHIL,‡Jane A. McCrohon, MBBS, PHD, FRACP,† Shirley Nakhla, BSC,† Wendy Jessup, PHD,‡David J. Handelsman, MBBS, PHD, FRACP,§ David S. Celermajer, MBBS, PHD, FRACP,*†�Alison K. Death, PHD�
Sydney, Australia
OBJECTIVES This study investigated the effects of androgens on gene expression in male- and female-donor macrophages.
BACKGROUND Men have more severe coronary disease than women. Androgen exposure increases foam cellformation in male but not female macrophages, and male macrophages express �4-fold moreandrogen receptor messenger ribonucleic acid than female macrophages. Therefore, androgenexposure may have gender-specific and potentially pro-atherogenic effects in macrophages.
METHODS Utilizing complementary deoxyribonucleic acid arrays, we studied the effects of a pureandrogen (dihydrotestosterone, 40 nmol/l) on human monocyte-derived macrophages fromhealthy male and female donors (n � 4 hybridizations; 2 men, 2 women). Differentialexpression of atherosclerosis-related genes was confirmed by real-time reverse transcription-polymerase chain reaction (RT-PCR) in five male and five female donors. Functionalcorroboration of foam cell formation-related findings was undertaken by experiments using125I-acetylated low-density lipoprotein (AcLDL).
RESULTS In male macrophages, androgen treatment produced differential up-regulation of 27 genesconcentrated in five functional classes: 1) lipoprotein processing; 2) cell-surface adhesion; 3)extracellular signaling; 4) coagulation and fibrinolysis; and 5) transport protein genes. Bycontrast, none of 588 genes were up-regulated in female macrophages. By RT-PCR, weconfirmed the gender-specific up-regulation of six of these atherosclerosis-related genes: acylcoenzyme A:cholesterol acyl transferase I, lysosomal acid lipase (LAL), caveolin-2, CD40,vascular endothelial growth factor-165 receptor, and tissue factor pathway inhibitor. Func-tionally, androgen-treated male macrophages showed increased rates of lysosomal AcLDLdegradation, by 45% to 75% after 15 to 20 h of 125I-AcLDL incubation (p � 0.001),consistent with increased LAL activity.
CONCLUSIONS Androgens increase expression of atherosclerosis-related genes in male but not femalemacrophages, with functional consequences. These findings may contribute to the malepredisposition to atherosclerosis. (J Am Coll Cardiol 2003;42:1306–13) © 2003 by theAmerican College of Cardiology Foundation
Men have earlier and more severe atherosclerosis thanwomen, independent of environmental risk factor exposure(1). Indeed, the incidence of coronary deaths in men age 35to 64 years exceeds that in age-matched women by up to500% (2). To date, the causes of this gender differenceremain unclear. Such observations have produced consider-able interest in the potential role of sex hormones inatherogenesis. The apparent atheroprotective effect of es-trogen has been studied extensively, and, contrary to expec-
tations, the first prospective randomized controlled trials totest this hypothesis have shown adverse effects (3,4). Therole of androgens is now also being scrutinized.
Macrophages play a key role in both the early (via foamcell formation) and late (via inflammatory and other medi-ators) stages of atherosclerosis (5). Formation of the mac-rophage foam cell is due to the uptake of modified lipopro-teins by monocyte-derived macrophages (MDMs) in thearterial wall (6). A growing body of evidence shows that sexsteroid hormones regulate processes integral to humanmacrophage foam cell formation (7). Furthermore, sexsteroids may act in a gender-specific manner, with greatereffects of estrogens and/or androgens in male or female cells(7). This gender-related regulation might have importantimplications for understanding the basis of (and developingtreatments for) the gender gap in atherosclerosis.
We recently demonstrated that androgen exposure in-creases foam cell formation in male- but not female-donor
From the *Department of Cardiology, Royal Prince Alfred Hospital; †HeartResearch Institute; ‡Centre for Vascular Research, University of New South Wales;§ANZAC Research Institute; and the �Department of Medicine, University ofSydney, Sydney, Australia. Drs. Ng, Quinn, Jessup, and Death are supported by theNational Health and Medical Research Council, and Dr. Celermajer is supported bythe Medical Foundation, University of Sydney.
Manuscript received May 11, 2003; revised manuscript received July 16, 2003,accepted July 22, 2003.
Journal of the American College of Cardiology Vol. 42, No. 7, 2003© 2003 by the American College of Cardiology Foundation ISSN 0735-1097/03/$30.00Published by Elsevier Inc. doi:10.1016/S0735-1097(03)01091-X

human MDMs, via an androgen receptor (AR)-mediatedpathway (8). Furthermore, male-donor MDMs express atleast four-fold more AR messenger ribonucleic acid (RNA)than MDMs from female donors (8). As the AR mediatesthe genomic effects of androgen action, androgens may havegender-specific and potentially pro-atherogenic effects onmacrophage gene expression. Utilizing complementary de-oxyribonucleic acid (cDNA) array analysis, we have system-atically investigated the effects of androgen exposure ongene expression in male- and female-donor human MDMsin order to identify: 1) atherosclerosis-related genes poten-tially regulated by androgen exposure; and 2) cellular mech-anisms involved in the androgen regulation of macrophagefoam cell formation.
METHODS
Isolation, culture, and hormone treatment of humanmonocytes. Monocytes were isolated from whole blood ofyoung healthy adult male and premenopausal female donors(inclusion criteria: Caucasian, �35 years of age, withoutpre-existing cardiovascular disease or cardiovascular risks,and no hormone therapy) by counterflow centrifugationelutriation (9) and cultured in phenol red-free RPMI (LifeTechnologies, Carlsbad, California) containing 10% post-menopausal human serum (17�-estradiol �75 pmol/l, pro-gesterone �0.8 nmol/l, and testosterone �2 nmol/l), pen-icillin G (50 U/ml), and streptomycin (50 �g/ml). Over anine-day maturation period, the following treatments wereadded with each media change from days 3 to 9: 1)dihydrotestosterone (DHT) at 40 nmol/l, or 2) vehiclecontrol (0.1% ethanol). Monocyte purity was �95% andviability �95% (trypan blue) in all experiments.RNA isolation and cDNA array experiments. To identifyatherosclerosis-related genes potentially regulated by andro-gen exposure, cDNA arrays were used (ATLAS HumanCardiovascular Array containing 588 genes and 9 house-keeping genes, Clontech Laboratories, Palo Alto, Califor-nia). Total RNA was isolated from both control- andandrogen-treated macrophages at maturation (day 9). Fourseparate array analyses of gene expression in control- versusandrogen-treated MDMs from four consecutive donors
(two men and two women) were undertaken. Probe synthe-sis, array hybridization, and phosphorimager analysis wereperformed using a modification of published methods (10).Briefly, cDNA probes both control- and androgen-treatedMDMs, synthesized by reverse transcription of 5 �g totalRNA in the presence of �32P-dATP, were hybridized for16 h onto separate but identical array membranes, and thesignal intensities were measured by phosphorimager analysis(Fujix Bas 1500 Phosphorimager, Fuji, Tokyo, Japan).Pairwise comparative gene expression between controls andandrogen-treated MDMs from each donor was undertakenafter signal intensities were converted to a ratio adjusted forbackground and housekeeping gene (60S rRNA) expres-sion. Data for each gene were used only when the signals forthat gene from both membranes were at least 50% abovebackground. Hence, our experiments preferentially detectedup-regulation rather than down-regulation.
The cDNA array reproducibility was evaluated by under-taking two consecutive array hybridizations using the sametwo samples of control- and androgen-treated RNA. Thesedata demonstrated that 97% of differential expression valuesin each experiment were within two-fold of each other.
DIFFERENTIAL EXPRESSION CRITERIA. Individual genesthat exhibited at least two-fold up-regulation in theandrogen-treated cells relative to control in both mem-branes for each gender were defined as being differentiallyexpressed.
SELECTION OF HOUSEKEEPER GENE. A non-linear powerregression analysis of cDNA array signal intensities fromboth control- and androgen-treated arrays of each subjectwas used to identify the housekeeper gene. On all regressionplots, 60S rRNA did not exhibit differential expression withandrogen treatment and was selected as the housekeepergene.Relative real time reverse transcription-polymerase chainreaction (RT-PCR). Confirmation of array findings in sixatherosclerosis-related genes was undertaken in MDMsfrom five male and five female donors by relative real-timeRT-PCR with SYBR Green I (Molecular Probes, Eugene,Oregon) monitoring using a modification of publishedmethods (11). The MDMs for these experiments werecultured using the same protocols and treated in the samehormonal conditions as for the cDNA array studies. Thegenes assayed included: acyl coenzyme A:cholesterol acyl-transferase I (ACAT); lysosomal acid lipase (LAL); caveo-lin-2; CD40; vascular endothelial growth factor (VEGF)-165 receptor; and tissue factor pathway inhibitor (TFPI).Reverse transcription of each RNA sample was performedin duplicate according to standard protocols. Relative real-time PCR reactions were performed in duplicate for eachcDNA sample for each gene of interest (Applied BiosystemsIncorporated [ABI] Model 7700 Sequence Detector, PEBiosystems, Foster City, California) and analyzed usingABI Prism Sequence Detector Software version 1.6.3 (PE
Abbreviations and AcronymsACAT � acyl coenzyme A:cholesterol acyl transferase IAcLDL � acetylated low-density lipoproteinAR � androgen receptorcDNA � complementary deoxyribonucleic acidDHT � dihydrotestosteroneLAL � lysosomal acid lipaseMDM � monocyte-derived macrophageRNA � ribonucleic acidRT-PCR � reverse transcription-polymerase chain
reactionTFPI � tissue factor pathway inhibitorVEGF � vascular endothelial growth factor
1307JACC Vol. 42, No. 7, 2003 Ng et al.October 1, 2003:1306–13 Gender Differences in Macrophage Gene Regulation

Biosystems). The housekeeping gene, 60S rRNA, was alsomeasured for normalization of real-time PCR results.
The primer sequences were: ACAT forward 5� AGT-TGACAGCAGAGGCAGAG 3�, reverse 5� GGATA-AAGAGAATGAGGAGGG 3�; LAL forward 5�GCAACAGCAGAGGAAATAC 3� , reverse 5�GAGAATGACCCACATAATACAC 3�; caveolin-2forward 5� TGCAGACAATATGGAAGAG 3�, reverse5� GAAATGAACAGAACAGTGG 3�; CD40 forward5� GCACCTCAGAAACAGACAC 3�, reverse 5�GGACCACAGACAACATCAG 3�; VEGF-165 recep-tor forward 5� CTCATCACCATCATAGCC 3�, reverse5� CAACTTCACACCATCCAC 3�; TFPI forward 5�GTGAATAACTCCCTGACTCC 3�, reverse 5� TT-TCACTCTCTGCTTCTTTC 3�; and 60S rRNA for-ward 5� GGAGAAGAGGAAAGAGAAAG 3�, reverse5� CAACGCATGAGGAATTAAC 3�.Functional studies on lipoprotein metabolism. Lipopro-tein uptake and lysosomal degradation studies were con-ducted in both control- and androgen-treated (DHT 400nmol/l) male-donor MDMs after incubation with 125I-acetylated low-density lipoprotein (AcLDL). Cell-surface–bound AcLDL was determined after a 4-h incubation at4°C with 125I-AcLDL with and without a 30-fold excess ofunlabeled AcLDL. Specific binding was calculated by sub-tracting the results in the presence of unlabeled AcLDLfrom that in its absence (12). Binding parameters wereanalyzed using the LIGAND computer program (BIO-SOFT, Cambridge, United Kingdom). Lysosomal degrada-tion of AcLDL was determined as trichloroacetic acid-soluble, non-iodide 125I in the post-incubation medium (12)following incubation at 37°C with 20 �g/ml 125I-AcLDL(with or without a 30-fold excess of unlabeled Ac LDL) for6, 16, and 20 h. Retroendocytosis studies were conducted tousing a modification of published methods (13). Briefly,MDMs were incubated with 20 �g/ml 125I-AcLDL at37°C for up to 120 min. Following incubation, cells werecooled to 4°C and washed five times with phosphatebuffered saline containing 2 mg/ml bovine serum albumin,once with an acid wash (0.2 mol/l acetic acid, 0.5 mol/lsodium chloride, pH 2.4), followed by three times withphosphate buffered saline. Retroendocytosis of AcLDL wasdetermined by measuring release of trichloroacetic acid-precipitable 125I-material during a 1-h chase period at 37°C(13).Statistical analysis. All results are expressed as mean �SEM. Statistical comparisons were performed using pairedor unpaired t tests, as appropriate. In the RT-PCR exper-iments, a repeated measures design was adopted in that bothcontrol- and DHT-treated macrophages are derived fromthe same subject. For these experiments, gene expression incontrol- versus DHT-treated cells in each gender werecompared one gene at a time using a paired t test. Wheremultiple comparisons were performed—for example, whencomparing gene expression by real-time RT-PCR, p valueswere adjusted according to Hochberg’s modification of the
Bonferroni procedure (14). Statistical analysis was per-formed using GraphPad Prism version 3.0a (GraphPadSoftware, San Diego, California), and regression plots weregenerated using Kaleidagraph 3.0 (Synergy Software, Read-ing, Pennsylvania).
RESULTS
Effects of androgen exposure on male and female donormacrophage gene expression: cDNA array findings. IncDNA array analyses of MDMs from two consecutivesubjects for each gender, androgen exposure in male-donorMDMs up-regulated the expression of 27 genes. The genesencoded for proteins that were categorizable into fivefunctional clusters: 1) lipoprotein and other metabolicpathways; 2) adhesion, inflammation, and cell-surface anti-gens; 3) coagulation and fibrinolysis; 4) extracellularsignaling/receptor-associated proteins; and 5) transport pro-teins (Table 1, Figs. 1A and 1B). By contrast, in female-donor MDMs, no gene met our criteria of being up-regulated at least two-fold in two consecutive individuals bycDNA array analysis.Real time relative RT-PCR. The androgen-dependent,gender-specific up-regulation of six atherosclerosis-relatedgenes was confirmed by real time RT-PCR, by comparingthe expression of each gene in androgen- versus control-treated MDMs from five consecutive male and five consec-utive female donors. Gene expression for each subject wasquantified four times—twice on each of two separate cDNAsyntheses). In male-donor MDMs, androgen exposure up-regulated the expression of ACAT by 5-fold, LAL by3.8-fold, caveolin-2 by 3.4-fold, CD40 by 5.5-fold, VEGF-165 receptor-1 by 3.7-fold, and TFPI by 4.8-fold, respec-tively (p � 0.005 vs. control for all genes). By comparison,androgen exposure had no significant effect on the expres-sion of the same genes in female donor MDMs whencompared with control (p � 0.1 vs. control for all genes)(Fig. 1C).Functional studies: the effect of androgen exposure andmacrophage lipoprotein metabolism. Because DHT in-creases cholesteryl ester accumulation in male-donorMDMs (8), we used the cDNA array findings to identifycellular mechanisms for androgen action. Functional anal-ysis of cDNA array findings indicated that androgen effectson foam-cell-formation–related processes involved up-regulation of genes involved in lysosomal degradation(LAL) and post-lysosomal processing (ACAT and hor-mone sensitive lipase). In contrast, the expression of genesinvolved in pre-lysosomal processes, such as modified low-density lipoprotein binding and uptake (macrophage scav-enger receptor types A1 and A2), were unaffected byandrogen exposure. Therefore, in vitro experiments wereundertaken to evaluate the effects of androgen exposure onthe uptake and lysosomal processing of modified low-density lipoprotein by male-donor MDMs and to corrobo-rate the functional implications of our array findings.
1308 Ng et al. JACC Vol. 42, No. 7, 2003Gender Differences in Macrophage Gene Regulation October 1, 2003:1306–13

LYSOSOMAL DEGRADATION OF MODIFIED LOW-DENSITY
LIPOPROTEIN. To evaluate the functional significance ofincreased LAL expression, we studied the effects of andro-gen exposure on lysosomal lipoprotein degradation in male-donor macrophages by incubation of macrophages withradiolabelled AcLDL. Androgen-treated male donor mac-rophages showed increased rates of lysosomal degradation ofAcLDL at 37°C compared with controls (Fig. 2A). Thisdifference was highly significant by 20 h of incubation withradiolabelled AcLDL (p � 0.001).
SCAVENGER RECEPTOR BINDING AND RETROENDOCYTOSIS
STUDIES. No difference existed between control- andDHT-treated male MDMs in specific or non-specificcell-surface binding of AcLDL with increasing concentra-tions of radiolabelled ligand (Fig. 2B). This was confirmedby computational analysis of binding parameters (LIGANDprogram, BIOSOFT), which showed no difference in bind-ing affinity (Kd 1.77 � 10�8 mol/l and Kd 1.91 � 108 mol/lin controls and DHT-treated cells, respectively; p � 0.9) orreceptor site concentrations (1.23 � 10�10 mol/l and 1.35� 10�10 mol/l in controls and DHT-treated cells, respec-tively; p � 0.3) between androgen and control treatments.In addition, there was no difference in retroendocytosis ofundegraded AcLDL between control- and DHT-treatedcells during pulse-chase experiments where the only source
of labeled lipoprotein was from an intracellular site ofpreviously endocytosed I125-AcLDL (100 � 5 % and 103 �4% for control- and DHT-treated cells, respectively; p �0.1).
In the absence of androgen effects on scavenger receptorbinding and retroendocytosis, the effect of DHT on lyso-somal lipoprotein degradation is consistent with a primaryeffect on increasing the activity of LAL. Overall, thesefunctional data are consistent with the gene expressionfindings noted above.
DISCUSSION
Male gender is a strong risk factor for atherosclerosis,independent of environmental risk factor exposure (1).Therefore, gender differences in sex hormones and geneticsmay contribute to the male predisposition to atherosclerosis.To date, few studies have investigated gender-dependentdifferences in the regulation of atherosclerosis-related genes.Using cDNA array analysis, we report that androgensregulate the macrophage expression of a large number ofatherosclerosis-related genes in a strikingly gender-dependent manner. In male-donor human MDMs, andro-gen exposure up-regulated the expression of 27 genes witha range of atherosclerosis-related functions, including li-poprotein metabolism, adhesion, inflammation, coagula-
Table 1. Genes Up-Regulated by Androgen Exposure in Male- and Female-Donor Human Macrophages*
Gender Gene Functional Class Accession No. Gene Name
Male Lipoprotein and other metabolic pathways L21934 Acyl coenzyme A:cholesterol acyltransferaseU40002 Hormone-sensitive lipaseM74775 Lysosomal acid lipaseAF035752 Caveolin-2X17025 Isopentenyl diphosphate delta isomeraseM34788 Adrenodoxin/ferredoxin 1L19501 Cystathionine beta-synthaseM58342 Iduronate 2-sulfataseM36693 Superoxide dismutase 2
Adhesion, inflammation, and cell surface antigens X60592 CD40AF047826 Cadherin 19, type 2U41070 Leukotriene B4 receptorX05908 Annexin IU34802 Gap junction protein alpha-8U49240 Symplekin
Coagulation and fibrinolysis D00017 Annexin IIJ03225 Tissue factor pathway inhibitorD29992 Tissue factor pathway inhibitor 2V00595 Prothrombin precursor
Extracellular signaling/receptor-associated genes L25615 Arginine vasopressin receptor 1AX15357 Atrial natriuretic peptide receptor AL13436 Atrial natriuretic peptide receptor BAF016050 Vascular endothelial cell growth factor 165 receptorAF016098 Vascular endothelial cell growth factor 165 receptor 2
Transport proteins Y10255 Fatty acid binding protein 3M94856 Fatty acid binding protein 5M20747 Insulin-responsive glucose transporter type 4
Female Nil Nil Nil
*Differential up-regulation was defined as an at least two-fold up-regulation in androgen-treated cells versus control in both arrays for each gender.
1309JACC Vol. 42, No. 7, 2003 Ng et al.October 1, 2003:1306–13 Gender Differences in Macrophage Gene Regulation

Figure 1. Effects of androgen exposure on macrophage gene expression. (A, B) Gene expression profiles in control- and androgen-treated malemacrophages, respectively. There is enhanced expression of a large number of atherosclerosis-related genes (see Table 1). For example, the boxed areascontaining lysosomal acid lipase (LAL) and acyl coA:cholesterol acyl transferase (ACAT) are enlarged and shown on the right. (C) Differential geneexpression examined by reverse transcription-polymerase chain reaction (RT-PCR) shows the androgen-dependent gender-specific up-regulation of sixatherosclerosis-associated genes: 1) ACAT; 2) LAL; 3) caveolin-2; 4) CD40; 5) tissue factor pathway inhibitor; and 6) vascular endothelial growth factor(VEGF)-165 receptor. In all genes studied by RT-PCR, androgen exposure produced up-regulation in gene expression in male-donor but not female-donormacrophages (p � 0.005 vs. control for all genes in male-donor cells as compared with p � 0.1 vs. control for all genes in female-donor cells). Open bars� controls; striped bars � 40 nmol/l dihydrotestosterone.
1310 Ng et al. JACC Vol. 42, No. 7, 2003Gender Differences in Macrophage Gene Regulation October 1, 2003:1306–13

tion, and angiogenesis (Table 1). By contrast, no genes wereaffected in female-donor MDMs. These array findings wereconfirmed by real-time RT-PCR findings, as well as by thedemonstration of functional effects of androgen exposure onmacrophage lipoprotein metabolism.
We previously reported that androgen exposure increaseshuman macrophage foam cell formation in male-donor but
not in female-donor MDMs (8). The present study extendsthese findings by demonstrating that androgens exert com-plex and gender-specific effects on the expression of lipopro-tein metabolism genes in male-donor MDMs. This involvesthe up-regulation of genes involved in: 1) lysosomal lipopro-tein processing (LAL), and 2) post-lysosomal processesincluding intracytoplasmic cholesterol esterification (ACAT)and cholesteryl ester hydrolysis (hormone-sensitive lipase). Bycontrast, the expression of genes involved in modified low-density lipoprotein binding and uptake (scavenger receptorsclass A1 and A2) were unaffected by androgen exposure. Asandrogens exert both genomic and non-genomic effects andas changes in gene expression do not always reflect func-tional changes, we undertook a series of lipoprotein metab-olism studies to examine androgen regulation of modifiedlow-density lipoprotein cell surface binding, retroendocyto-sis, and lysosomal degradation of lipoproteins. Our geneexpression findings are corroborated by in vitro functionalstudies demonstrating that androgen exposure increases therate of lysosomal hydrolysis of lipoproteins in male-donorMDMs, in the absence of androgen effects on scavengerreceptor binding, or retroendocytosis. These findings are inkeeping with an androgen-dependent up-regulation of LALactivity in male-donor MDMs. The LAL plays a major rolein the delivery of atherogenic lipoproteins to the cell, byhydrolyzing the cholesteryl ester moiety from lipoproteinsdelivered to the lysosome via endocytosis or phagocytosisinto free cholesterol, thereby making free cholesterol avail-able for intracytoplasmic re-esterification by ACAT (15).Increase in LAL activity has thus been implicated inpromoting macrophage foam cell formation (15,16). Ourcurrent findings also support a previous observation ofpositive correlation between serum testosterone levels dur-ing development and hormone-sensitive lipase protein levelsand enzymatic activity in the guinea pig testis (17). In maleMDMs, therefore, androgen exposure exerts widespreadeffects on the expression of genes involved in lipoproteinmetabolism, with a net functional effect of increasing theaccumulation of cholesteryl esters.
The adherence of monocytes to vascular endothelium andtheir subsequent transmigration into the vessel wall are keyearly events in atherogenesis (5). We have previously re-ported that androgen treatment of endothelial cells increaseshuman monocyte adhesion to endothelium in male-donorcells via up-regulation of endothelial cell expression ofvascular cell adhesion molecule-1 (18). The present studyextends these observations from endothelial cells to mono-cytes. In the current study, we found that androgen exposurein macrophages produced a gender-specific up-regulation ofgenes implicated in promoting the adherence of monocytesto vascular endothelium (including CD40, leukotriene B4receptor, and cadherin 19). CD40 ligation in human mac-rophages has been shown to trigger the expression ofadhesion molecules including lymphocyte function-associated antigen-1 and intercellular adhesion molecule-1(19). Leukotriene B4, a potent chemoattractant and pro-
Figure 2. Effects of androgen exposure on macrophage lipoprotein metab-olism. (A) Androgen exposure increased the rate of lysosomal degradationof acetylated low-density lipoprotein (AcLDL) by male-donor monocyte-derived macrophages—a finding consistent with increased lysosomal acidlipase activity (p � 0.001 for dihydrotestosterone [DHT]-treated vs.control cells, at 20 h). (B) Androgen exposure had no effect on cell surfacebinding of 125I-AcLDL (p � 0.1 for androgen vs. control macrophages).
1311JACC Vol. 42, No. 7, 2003 Ng et al.October 1, 2003:1306–13 Gender Differences in Macrophage Gene Regulation

inflammatory mediator, has also been implicated in mono-cyte recruitment, activation, and adhesion. Leukotriene B4receptor antagonism has been shown to reduce monocyteinfiltration and lipid accumulation in apoE-deficient mice(20).
A number of the array findings from this study are alsoconsistent with available observational data. In clinicalstudies evaluating the effect of androgens on coagulation,exogenous testosterone has been reported to increase plasmalevels of prothrombin fragment F1.2 in healthy men (21),but not in women with severe premenstrual syndrome (22),which is consistent with a gender-dependent effect. Inanimal models, androgen exposure up-regulates argininevasopressin receptor 1A messenger RNA in the male Syrianhamster brain (23) and increases fatty acid binding proteincontent in rat heart and skeletal muscle (24). Increasingevidence shows the role of androgens in the control ofangiogenesis. Dihydrotestosterone up-regulates the expres-sion of VEGF messenger RNA and VEGF biologicalactivity in an adult rat prostate (25), and testosteroneincreases VEGF expression via an AR-dependent manner,in an immortalized cell line S115 (26).
We and others have previously shown that male humanmacrophages express higher levels of AR message thanfemale-donor cells (8,27). Moreover, in rat aortic smoothmuscle cells, AR protein levels are higher in male than infemale animals (28). Therefore, the marked gender speci-ficity of androgen effects on macrophage gene expression ismost likely related to gender differences in MDM ARcontent. Hence, gender differences in AR content may be akey mediator of gender differences in vascular biology. Thishypothesis is supported by a recent study using maletesticular feminized rats, which express a non-functionalAR. In rats, the contractile response of the thoracic aorta tovasopressin is three-fold higher in females than in males(29). Stallone et al. (29) found that this gender difference invascular reactivity in rat aortas was abolished in AR-deficient male testicular feminized rats, where responses tovasopressin were similar to normal female rather than maleanimals.
Regarding limitations, we used arrays with 588 cDNAswith a high concentration of genes with established rele-vance to atherosclerosis and vascular biology. A larger,genome-wide screen might identify more androgen-regulated genes within macrophages.
Dihydrotestosterone, a potent physiologic androgen spe-cific for AR, was used at a concentration of 40 nmol/l on thebasis of previous foam cell and cell adhesion experiments(8,18). As DHT is not aromatizable to estrogenic metabo-lites, unlike testosterone (30), its use avoids the potentiallyconfounding effects of estrogens, as they have also beenshown to influence both gene expression and macrophagelipid loading (31). Whereas DHT at 40 nmol/l is higherthan normal circulating levels (being ten-fold above thenormal serum concentration for male adults), this concen-tration is physiologically relevant in our experiments as: 1)
testosterone, the major circulating androgen (usual serumconcentrations 20 to 32 nmol/l in men), is absent from ourculture milieu; and 2) plasma levels of DHT do not reflecttissue formation (32), particularly in tissues possessing5�-reductase activity, such as macrophages (33,34). The5�-reductase enzyme converts testosterone to DHT, ac-counting for 75% of tissue DHT, which is the finalandrogenic messenger in many target tissues. This enzymeis also present in the other major cell types in the athero-sclerotic lesion: the endothelial cell (35) and the vascularsmooth muscle cell (36). Therefore, in the absence oftestosterone, the use of 40 nmol/l DHT for in vitrotreatment of MDMs is likely to be physiologically relevantbecause DHT concentrations in tissues possessing 5�-reductase activity can approach concentrations in the orderof 100 nmol/l (34,37). Moreover, the functional effects ofgender-dependent, AR-mediated up-regulation of genes areevident at DHT concentrations as low as 4 nmol/l (8). Inour previous dose-ranging studies, DHT produced a dose-dependent, AR-dependent increase in male-donor MDMcholesteryl ester accumulation which was demonstrablebetween 4 to 400 nmol/l (inclusive), but had no effect oncholesteryl ester accumulation in female-donor MDMseven at concentrations as high as 400 nmol/l (8).
In summary, using differential gene-expression techniques,we report for the first time that androgens regulate themacrophage expression of a large number of atherosclerosis-related genes in a highly gender-dependent manner. An-drogen exposure up-regulated the expression of 27 genes,many with known atherosclerosis-related functions, inmale-donor MDMs but had no significant effect on geneexpression in female-donor MDMs. These findings providenovel insights into the effects of androgens on gene expres-sion in the macrophage and suggest that androgens may beinvolved in the complex and gender-dependent regulationof a range of atherosclerosis-related processes includingfoam cell formation, adhesion, inflammation, coagulation,and angiogenesis. These gene expression findings are cor-roborated by functional data confirming the androgen-dependent up-regulation of lysosomal degradation of mod-ified lipoproteins in male-donor MDMs—a process integralto the delivery of atherogenic lipoproteins to the macro-phage. These effects may contribute to the male predispo-sition to atherosclerosis.
Reprint address and correspondence: Dr. David S. Celermajer,Department of Cardiology, Royal Prince Alfred Hospital, Camper-down, Sydney NSW 2050, Australia. E-mail: [email protected].
REFERENCES
1. Wingard DL, Suarez L, Barrett-Connor E. The sex differential inmortality from all causes and ischaemic heart disease. Am J Epidemiol1983;117:165–72.
2. Tunstall-Pedoe H, Kuulasmaa K, Amouyel P, Arveiler D, RajakangasAM, Pajak A. Myocardial infarction and coronary deaths in the WorldHealth Organization MONICA Project. Registration procedures,
1312 Ng et al. JACC Vol. 42, No. 7, 2003Gender Differences in Macrophage Gene Regulation October 1, 2003:1306–13
event rates, and case-fatality rates in 38 populations from 21 countriesin four continents. Circulation 1994;90:583–612.
3. Hulley S, Grady D, Bush T, et al. Randomized trial of estrogen plusprogestin for secondary prevention of coronary heart disease inpostmenopausal women. Heart and Estrogen/progestin ReplacementStudy (HERS) Research Group. JAMA 1998;280:605–13.
4. Writing Group for the Women’s Health Initiative Investigators. Risksand benefits of estrogen plus progestin in healthy postmenopausalwomen. JAMA 2002;288:321–33.
5. Ross R. The pathogenesis of atherosclerosis: a perspective for the1990’s. Nature 1993;362:801–9.
6. Tabas I. The stimulation of the cholesterol esterification pathway byatherogenic lipoproteins in macrophages. Curr Opin Lipidol 1995;6:260–8.
7. Ng MKC, Jessup W, Celermajer DS. Sex-related differences in theregulation of macrophage cholesterol metabolism. Curr Opin Lipidol2001;12:505–10.
8. McCrohon JA, Death AK, Nakhla S, et al. Androgen receptorexpression is greater in macrophages from male than from femaledonors. A sex difference with implications for atherogenesis. Circula-tion 2000;101:224–6.
9. Garner B, Dean RT, Jessup W. Human macrophage-mediated oxi-dation of low-density lipoprotein is delayed and independent ofsuperoxide production. Biochem J 1994:421–8.
10. Huang P, Feng L, Oldham EA, Keating MJ, Plunkett W. Superoxidedismutase as a target for the selective killing of cancer cells. Nature2000;407:390–5.
11. Morrison TB, Weiss JJ, Wittwer CT. Quantification of low-copytranscripts by continuous SYBR Green I monitoring during amplifi-cation. Biotechniques 1998;24:954–62.
12. Goldstein JL, Basu SK, Brown MS. Receptor-mediated endocytosis oflow-density lipoprotein in cultured cells. Methods Enzymol 1983;98:241–60.
13. Greenspan G, St. Clair RW. Retroendocytosis of low-density lipopro-tein. Effect of lysosomal inhibitors on the release of undegraded125I-low density lipoprotein of altered composition from skin fibro-blasts in culture. J Biol Chem 1984;259:1703–13.
14. Hochberg Y. A sharper Bonferroni procedure for multiple tests ofsignificance. Biometrika 1988;75:800–2.
15. Kritharides L, Jessup W. Macrophage lipid metabolism and athero-sclerosis. In: Dean RT, Kelly DT, editors. Atherosclerosis. New York,NY: Oxford University Press, 2000;176–206.
16. Stary HC, Chandler B, Glagov S, et al. A definition of initial, fattystreak, and intermediate lesions of atherosclerosis. ArteriosclerThromb 1994;14:840–56.
17. Kabbaj O, Holm C, Vitale C, Pelletier R-M. Expression, activity, andsubcellular localization of testicular hormone-sensitive lipase duringpostnatal development in the guinea pig. Biol Reprod 2001;65:601–12.
18. McCrohon JA, Jessup W, Handelsman DJ, Celermajer DS. Androgenexposure increases human monocyte adhesion to vascular endotheliumand endothelial cell expression of vascular cell adhesion molecule-1.Circulation 1999;99:2317–22.
19. Schonbeck U, Libby P. CD40 signaling and plaque instability. CircRes 2001;89:1092–103.
20. Aiello RJ, Bourassa P-A, Lindsay S, Weng W, Freeman A, ShowellHJ. Leukotriene B4 receptor antagonism reduces monocytic foam cellsin mice. Arterioscler Thromb Vasc Biol 2002;22:443–9.
21. Anderson RA, Ludlam CA, Wu FCW. Haemostatic effects ofsupraphysiological levels of testosterone in normal men. ThrombHaemost 1995;74:693–7.
22. Buckler HM, McElhone K, Durrington PN, Mackness MI, LudlamCA, Wu FC. The effects of low-dose testosterone treatment on lipidmetabolism, clotting factors and ultrasonographic ovarian morphologyin women. Clin Endocrinol (Oxf) 1998;49:159–60.
23. Young LJ, Wang Z, Cooper TT, Albers HE. Vasopressin (V1a)receptor binding, mRNA expression and transcriptional regulation byandrogen in the Syrian hamster brain. J Neuroendocrinol 2000;12:1179–85.
24. van Breda E, Keizer HA, Vork MM, et al. Modulation of fatty-acid–binding protein content of rat heart and skeletal muscle by endurancetraining and testosterone treatment. Pflugers Arch 1992;421:274–9.
25. Sordello S, Bertrand N, Plouet J. Vascular endothelial growth factor isup-regulated in vitro and in vivo by androgens. Biochem Biophys ResCommun 1998;251:287–90.
26. Ruohola JK, Valve EM, Karkkainen MJ, Joukov V, Alitalo K,Harkonen PL. Vascular endothelial growth factors are differentiallyregulated by steroid hormones and antiestrogens in breast cancer cells.Mol Cell Endocrinol 1999;149:29–40.
27. Cutolo M, Accardo S, Villaggio B, et al. Androgen and estrogenreceptors are present in primary cultures of human synovial macro-phages. J Clin Endocrinol Metab 1996;81:820–7.
28. Higashiura K, Mathur RS, Halushka PV. Gender-related differencesin androgen regulation of thromboxane A2 receptors in rat smoothmuscle cells. J Cardiovasc Pharmacol 1997;29:311–5.
29. Stallone JN, Salisbury RL, Fulton CT. Androgen-receptor defectabolishes sex differences in nitric oxide and reactivity to vasopressin inthe rat aorta. J Appl Physiol 2001;91:2602–10.
30. Simpson ER, Zhao Y, Agarwal VR, et al. Aromatase expression inhealth and disease. Recent Prog Horm Res 1997;52:185–213.
31. McCrohon JA, Nakhla S, Jessup W, Stanley KK, Celermajer DS.Estrogen and progesterone reduce lipid accumulation in humanmonocyte-derived macrophages: a sex-specific effect. Circulation 1999;100:2319–25.
32. Toscano V, Horton R. Circulating dihydrotestosterone may not reflectperipheral formation. J Clin Invest 1987;79:1653–8.
33. Milewich L, Kaimal V, Toews GB. Androstenedione metabolism inhuman alveolar macrophages. J Clin Endocrinol Metab 1983;56:920–4.
34. Araneo BA, Dowell T, Diegel M, Daynes RA. Dihydrotestosteroneexerts a depressive influence on the production of interleukin-4 (IL-4),IL-5 and �-interferon, but not IL-2 by activated murine T cells. Blood1991;78:688–99.
35. Milewich L, Kaimal V, Johnson AR. Steroid 5 alpha-reductase activityin endothelial cells from human umbilical cord vessels. J SteroidBiochem 1987;26:561–7.
36. Fujimoto R, Morimoto I, Morita E, Sugimoto H, Ito Y, Eto S.Androgen receptors, 5 alpha-reductase activity and androgen-dependent proliferation of vascular smooth muscle cells. J SteroidBiochem Mol Biol 1994;50:169–74.
37. Siiteri PK, Wilson JD. Dihydrotestosterone in prostatic hypertrophy.I. The formation and content of dihydrotestosterone in the hypertro-phic prostate of man. J Clin Invest 1970;49:1737–45.
1313JACC Vol. 42, No. 7, 2003 Ng et al.October 1, 2003:1306–13 Gender Differences in Macrophage Gene Regulation

EDITOR’S PAGE
What Constitutes a Great Review?Anthony N. DeMaria, MD, MACCEditor-in-Chief, Journal of the American College of Cardiology
The last Editor’s Page dealt with the topic of a report cardfor journals. Just as journals are subject to grading, so are thecritiques of manuscripts prepared by reviewers. In fact, theEditors grade each review for quality based on a number ofcharacteristics we have found to be of value. However, thesecharacteristics have not been well disseminated. During ourrecent Editorial Board retreat, a number of Editorial Boardmembers indicated that they had never received counselingon how best to review an original research manuscript. Theconsensus was that it would be useful for the Editors todefine what we regard as the attributes of an outstandingreview. We discussed this topic at one of our weeklymeetings, and the following summarizes our thoughts onthe matter.
As I have previously indicated, when a manuscript cri-tique is done well, it requires time, effort, and often a certainamount of background research. The rewards for suchefforts are meager and generally consist of an insight intothe latest developments in the area of research and theopportunity to influence the material being read by thecardiovascular community. Generally, the function of re-viewing manuscripts is regarded as a contribution to theacademic pool and as reciprocation for having someone elseundertake to review one’s own articles. Nevertheless, reviewscan vary from excellent to cursory, and their value is notlimited to the crucial role they play in determining accep-tance or rejection. Perhaps even more importantly, they canmarkedly improve an article for final publication. Therefore,it is hoped that reviewers will attempt to be as proficient inthis task as they are in authoring articles.
Many critiques begin with a brief summary of themanuscript being reviewed. This may at first seem redun-dant, since the Editors have clearly read the manuscriptthemselves. However, the summary provides us with avaluable insight into the reviewer’s perspective of how thestudy was conducted and the findings reported in the paper.Perhaps not surprisingly, individual reviewers will oftencome away from the same manuscript with very differentimpressions of the nature of the study. Even just a descrip-tion of the hypothesis tested, methods applied, and resultsfound often conveys an indication of the impression thearticle had on the referee. Therefore, although it is notabsolutely necessary, a brief overview of the manuscript isvery useful to the Editors in determining its priority forpublication.
The heart and soul of a manuscript review is, of course, an
evaluation of how well it serves the scientific process. Wasthere a rationale for the objectives of the study, and was thehypothesis to be tested important? Were the methods usedappropriate and accurate, and was the resulting data appro-priately measured and analyzed? Were the conclusionsdrawn justified, and the findings significant? In short, wasthe article original, accurate, and relevant? It is surprisinghow often this basic information is never commented on ina critique. Very often the reviewer will merely begin byraising specific issues related to some aspect of the paper.The Editors are left to wonder whether the omission ofcomments regarding the basic structure of the work impliesthat it was well done or that it was never evaluated. We askfor specific grades for each of these categories, of course, butas will be discussed below, we often get grades withoutjustification.
The best reviews place the manuscript in proper perspec-tive. Such critiques indicate the state of knowledge in thefield being studied and how the manuscript contributes theknowledge in the area. It is, of course, the responsibility ofthe authors to provide the appropriate background for theirwork. On occasion, however, the true significance of orig-inal research is missed by the author and first identified onlyby the reviewer. The Editors, who are often not expert in anarea, certainly appreciate the orientation that a review canprovide for a manuscript.
One of the most consistent characteristics of an excellentreview is the inclusion of references and citations from theliterature to support statements made by the referee. This is,of course, most important in assessing the originality ofmanuscripts. Very often a reviewer will comment that thereis “little new information” contained in a research article.However, the authors of the manuscript typically disagree,having stated in their introduction that few or no data exist.Moreover, the natural bias of the Editors is to assume thatif the information contained is new to them, it is likely toseem original to the majority of readers. The citation ofprevious work reporting the same or similar data as in thesubmission under consideration is therefore of inestimablevalue in determining the priority for publication. In thesame vein, literature citations are of great value in substan-tiating the criticisms leveled by reviewers against manu-scripts. The claim in a review that methods are inappropri-ate or that variables capable of influencing data are ignoredis most effective when supported by appropriate citations.The Editors are often adjudicating differing opinions re-
Journal of the American College of Cardiology Vol. 42, No. 7, 2003© 2003 by the American College of Cardiology Foundation ISSN 0735-1097/03/$30.00Published by Elsevier Inc. doi:10.1016/S0735-1097(03)01181-1

garding the same manuscript by individual reviewers, andthe opinions supported by data are always the ones assignedthe greatest significance.
It never ceases to surprise us how often reviewers neglectto provide any comments in the space provided for “Com-ments to the Editors.” Often the referees merely repeat theircomments to the authors. The “Comments to the Editors”should provide a summary assessment of the manuscript andjustifications for the accept/reject recommendation and thepriority scores assigned. Most critiques include both positiveand negative statements in the “Comments to the Authors”section. In addition, individuals differ considerably in as-signing priority scores, just as some teachers and professorsare “easy graders” and others are “hard graders.” Therefore,it is of enormous value for the reviewers to put into prosetheir overall assessment of the article and the reasonssupporting this assessment in their “Comments to theEditors.” While the ultimate decision to reject or accept anarticle must rest with the Editors, a review that provides anopinion for or against acceptance, with supporting reasons,is always regarded with appreciation.
It goes without saying that the best reviews will conveythe same message to the authors and to the Editors. Thenumber of manuscript evaluations we have received thatconvey one opinion of the work to the authors and adifferent one to the Editors was quite unexpected. Suchcritiques are neither helpful to the authors in improvingtheir manuscripts nor helpful to the Editors in explainingour editorial decision. The Editors dread such reviews andimmediately prepare for letters of appeal from the authors.
I have heard it said that editors of medical journals areeither “abortionists” or “midwives.” I think this statementvery well summarizes the charge to the reviewers. Firstly,the reviewer is asked to represent the journal in selectingonly those manuscripts that are of the highest quality forpublication. The referee must protect the journal fromaccepting flawed manuscripts that contain errors in methodsand analysis or inaccurate conclusions. In addition, giventhe low acceptance rate of most journals, the reviewer isasked to help the journal prioritize the merit of individualsubmissions within the limited number of pages available.In this role, the reviewer is clearly sitting as a judge andemphasizing the identification of significant flaws in the
paper. However, the reviewer is also asked to seize theopportunity to act as consultant to the authors and improvetheir papers. The Editors have seen numerous instances inwhich manuscripts have been enormously upgraded by thepeer-review process, and virtually all manuscripts are im-proved afterwards. In this “midwife” role, an excellentreview is one that is objective and constructive, one thatavoids antagonism and points out areas in which the articlecan be improved.
A last issue worthy of discussion relates to reviewsjudging that manuscripts are not well suited for publicationin JACC. Clearly, there is some subject matter that will be oflittle interest to most of our readers. However, reviewsindicating that original research submissions are “not for ouraudience” are assuming a knowledge of what the bulk ofJACC readers will find of value. Although the Editors nearlyalways agree with those reviews that assess manuscripts asnot suitable for JACC, the best reviews include a justificationfor this opinion and provide evidence that the manuscriptwill not be of interest either to the reviewers or the generalreadership.
Just like parenthood, the reviewing of manuscripts is oneof those things in life for which there is very little formaltraining. Although the task itself seems quite straightfor-ward, critiques differ significantly in their quality. Given theimportance of the undertaking to both the authors and thescientific community in general, manuscript review is aresponsibility that should not be undertaken lightly. Fromthe standpoint of the Editors and the Journal, the peer-review process is fundamental to our existence. When thecharacteristics previously described are present in a review, italways gets commented upon when the paper is discussed inour weekly meetings. The real evidence of the value of aquality review lies in the fact that the Editors are all familiarwith the names of those individuals whose critiques areconsistently excellent.
Address correspondence to: Anthony N. DeMaria, MD,MACC, Editor-in-Chief, Journal of the American College of Car-diology, 3655 Nobel Drive, Suite 400, San Diego, California92122.
1315JACC Vol. 42, No. 7, 2003 DeMariaOctober 1, 2003:1314–5 Editor’s Page
ACC NEWS
Rethink Retirement:Plan a Second Career in CardiologyCarl J. Pepine, MD, MACCPresident, American College of Cardiology
A physician shortage in cardiology has prompted the Amer-ican College of Cardiology (ACC) to establish a task forceto study and recommend workforce solutions. Recent re-ports from the federal government, the media, and physicianrecruiters suggest that fellows entering the field of cardiol-ogy cannot keep pace with the replacement of veterancardiovascular (CV) physicians who are retiring. But onefactor, perhaps most within our power to influence orchange, is the relatively new phenomenon of early retire-ment from cardiology practice. This exit from the professionis draining and adversely affecting our CV workforce,already under stress.
For a moment, consider the opportunities that exist incardiology after retirement:
● Continuing intellectual stimulation;● Sharing your wealth of knowledge through teaching;● Participation in an office-based practice, perhaps in a
different subspecialty area (e.g., moving from interven-tional to general cardiology);
● Nonprofit/volunteer work (domestic, international, leg-islative, cause-oriented);
● Research; and● Part-time hours in a practice situation that may be
different from the high-volume demand of your currentpractice.
Many CV specialists, as they reach retirement, want toexit the field due to frustration with managed care, issuesrelated to Medicare reimbursement and compliance, and therising cost of malpractice insurance. But largely, theseconcerns evaporate in a second career, where opportunitiesshift from an emphasis on career- and practice-building toone of enjoying the practice of CV medicine. Medicalschools present the opportunity to teach young people andvery likely also offer the opportunity to obtain malpracticeinsurance at lower rates. In addition to teaching, largemedical school groups present a smorgasbord of professionalofferings, including the opportunity to practice in an officesetting—often without night or weekend call.
Aside from assuming some of the currently overwhelmingburden of patient care, returning cardiologists can signifi-cantly contribute to the health care environment as potentknowledge resources, especially where fellows-in-trainingare concerned. They bring a plethora of knowledge and
experience to the teaching environment, along with arefreshing disregard for appointment schedules, constraintson time spent with patients, or practice-related frustrations.
Returning (recent) retirees also can make meaningfulcontributions to cardiology-oriented organizations such asthe ACC and the American Heart Association (AHA) inareas such as advocacy, education, and content develop-ment. I would submit that everything done at the ACC byactively practicing Fellows could be done just as well—orbetter—by retired cardiologists (or those nearing retire-ment) using their perspective of years of experience andhaving the advantage of more time to volunteer. They couldattend political action committee meetings and visit legis-lators on Capitol Hill. Who could better speak our piece?Or who could cast a more realistic light on what they’ve seenin our profession?
Returning (recent) retirees also could effectively partici-pate in fund-raising committees for the ACC or other CVdisease-related nonprofit organizations. Committee partic-ipation becomes more rewarding and fulfilling when youhave time to thoughtfully and strategically contribute on aregular basis.
In the past, many cardiologists often worked into their70s, garnering seniority, honors, heightened peer and com-munity respect, and often, privilege. However, currentanecdotal evidence shows that by the time cardiologists turn50, they are looking toward retirement. A survey of physi-cians 50 years old and older undertaken in the year 2000 bya physician recruiting firm (Merritt, Hawkins & Associates)revealed that close to 80% of physicians 50 years old or olderwere planning to change their practice patterns in the nextone to three years. Of these, 38% planned to retire, and ofthose who were planning to retire, the decision was signif-icantly linked to managed care (48%), noted as their greatestsource of professional frustration. Conversely, the greatestsource of professional satisfaction was identified as thepatient-physician relationship (300 physicians participatedin this survey in approximately the same proportion thatexists in the physician population as a whole: 35% primarycare physicians and 65% medical specialists).
My own experience recruiting a cardiologist from retire-ment has been entirely a productive, happy one. Three yearsago, I hired a 25-year veteran of CV medicine, coaxing himout of retirement. He had business interests to keep him
Journal of the American College of Cardiology Vol. 42, No. 7, 2003© 2003 by the American College of Cardiology Foundation ISSN 0735-1097/03/$30.00Published by Elsevier Inc. doi:10.1016/S7035-1097(03)01092-1

busy; nonetheless, he was bored—but still attending cardi-ology conferences and going to medical grand rounds in his“spare time.”
As a returning retiree, my colleague works an unusuallyflexible schedule based on short hours—2 to 5 h perday—rotating weeks on and off. He oversees the consultservice at one of the teaching hospitals associated with theUniversity of Florida. If I could hire five more like him, Iwould tomorrow.
Recently, the back-from-retirement cardiologist (nowspecializing in nuclear cardiology, a switch from his pre-retirement specialty in invasive and general cardiology)presided over our fellows’ graduation and realized he hadhelped select them, contributed to their training, and nowwas watching them move into the profession as independentphysicians. Proud and pleased, he had completed a veryrewarding, meaningful, and satisfying professional experi-ence with them.
For his part, my “new hire” says he’s having a ball andloves what he’s doing. Instead of shouldering the responsi-bilities of the multi-specialty group he founded nearly threedecades ago, he’s teaching fellows how to give a propercardiac examination, evaluating patients for nearly an hourat a time on grand rounds, taking his time with each caseand each fellow, concentrating on the quality of care, andnot looking at his watch or his numbers.
Obviously, my colleague’s daily practice is no longerabout earning money. According to him, it’s about “leavinga legacy, teaching how to think, how to talk to people, howto do a physical examination—a lost art.” He is drawingfrom his retirement fund, drawing small salaries from theuniversity and the hospital, and enjoying the heck out ofcardiology again, with very little distracting him from purepatient care.
Opportunities in practice, in education, and in the vol-unteer sector hold potential for very fulfilling professionalexperiences, at a much slower pace, void of frustration.Retired cardiologists in the field can make a huge differenceas teachers, role models, and backup physicians—whorequire virtually no training—in easing the pace for ex-tremely overworked colleagues in their peak years.
Part of the problem in bringing back retirees and utilizingtheir expertise is that there is no formal venue where suchopportunities are exchanged. With interest from our mem-bership, however, the ACC could add a category to theACC Practice Opportunity Line (an online job search toolfor CV specialists) for retired cardiologists who would liketo find alternative careers in cardiology. In markets likeFlorida, veteran cardiologists could be hired seasonally.(Merritt, Hawkins & Associates report that up to 1,000cardiologists work on a temporary basis every year, thatthere are 2.4 opportunities for every physician in cardiologylooking for a new challenge, and that only 41% of temporarycardiology openings are ever filled.) Additionally, physicianrecruiters are seeing more and more health care facilitiessetting up local networks of retired and semi-retired physi-cians as a means to prepare for temporary or urgent staffingneeds.
Personally, I believe that many physicians look forward toretirement at some time in the future—but with therealization that they still want to make contributions to theprofession and that they don’t want to cut off their partic-ipation completely.
For many of us, cardiology is not only a career but alifetime endeavor. Let’s recast retirement as an opportunityto change what we’re doing, or how we’re doing it—but notstop altogether. Our professional long-term career invest-ments in ourselves are too valuable not to recycle.
Note: Retired cardiologists or those near retirement whoare interested in participating in an ACC “job board” shouldindicate their interest by phoning or e-mailing MoiraDavenport, associate director of the ACC Member Rela-tions and Chapter Affairs Department: telephone 800-253-4636, ext. 672, or e-mail: [email protected].
Send correspondence to: Carl J. Pepine, MD, MACC, Professorand Chief, Division of Cardiovascular Medicine, University ofFlorida College of Medicine, Box 100277, 1600 Archer Road,Gainsville, Florida 32610-0277. E-mail: [email protected].
1317JACC Vol. 42, No. 7, 2003 PepineOctober 1, 2003:1316–7 President’s Page

ACC/AHA/ASNC Guidelines for the Clinical Use of CardiacRadionuclide Imaging—Executive Summary
A Report of the American College of Cardiology/American HeartAssociation Task Force on Practice Guidelines
(ACC/AHA/ASNC Committee to Revise the 1995 Guidelinesfor the Clinical Use of Cardiac Radionuclide Imaging)
Committee Members
Francis J. Klocke, MD, MACC, FAHA, Chair;Michael G. Baird, MD, FACC, FAHA; Beverly H. Lorell, MD, FACC, FAHA;
Timothy M. Bateman, MD, FACC, FAHA; Joseph V. Messer, MD, MACC, FAHA;Daniel S. Berman, MD, FACC, FAHA; Patrick T. O’Gara, MD, FACC;
Blase A. Carabello, MD, FACC, FAHA; Richard O. Russell, Jr, MD, FACC;Manuel D. Cerqueira, MD, FACC, FAHA; Martin G. St. John Sutton, MBBS, FACC;
Anthony N. DeMaria, MD, MACC, FAHA; James E. Udelson, MD, FACC;J. Ward Kennedy, MD, MACC, FAHA; Mario S. Verani, MD, FACC*;
Kim Allan Williams, MD, FACC, FAHA
Task Force Members
Elliott M. Antman, MD, FACC, FAHA, Chair; Sidney C. Smith, Jr, MD, FACC, FAHA, Vice-Chair;Joseph S. Alpert, MD, FACC; Gabriel Gregoratos, MD, FACC, FAHA;
Jeffrey L. Anderson, MD, FACC; Loren F. Hiratzka, MD, FACC, FAHA;David P. Faxon, MD, FACC, FAHA; Sharon Ann Hunt, MD, FACC, FAHA;
Valentin Fuster, MD, PhD, FACC, FAHA; Alice K. Jacobs, MD, FACC, FAHA;Raymond J. Gibbons, MD, FACC, FAHA†‡; Richard O. Russell, MD, FACC†
Table of Contents
I. Introduction.............................................................. 1319II. Acute Syndromes..................................................... 1320
A. Myocardial Perfusion Imaging in the Assessmentof Patients Presenting With Chest Pain to theEmergency Department ..................................... 1320
B. Detection of AMI When Conventional MeasuresAre Nondiagnostic ............................................. 1320
C. Radionuclide Testing in Risk Assessment: Prognosisand Assessment of Therapy After STEMI ........... 1320
D. Radionuclide Testing in Risk Assessment: Prognosisand Assessment of Therapy After NSTEMI or UA. 1320
III. Chronic Syndromes ................................................. 1321
The ACC/AHA Task Force on Practice Guidelines makes every effort to avoid any actual or potential conflicts of interest that might arise as a resultof an outside relationship or personal interest of a member of the writing panel. Specifically, all members of the writing panel are asked to providedisclosure statements of all such relationships that might be perceived as real or potential conflicts of interest. These statements are reviewed by the parenttask force, reported orally to all members of the writing panel at the first meeting, and updated as changes occur.
This document was approved by the American College of Cardiology Foundation Board of Trustees in July, 2003, the American Heart AssociationScience Advisory and Coordinating Committee in July, 2003, and the American Society of Nuclear Cardiology Board of Directors in July, 2003.
When citing this document, the American College of Cardiology Foundation, the American Heart Association, and the American Society of NuclearCardiology request that the following citation format be used: Klocke FJ, Baird MG, Bateman TM, Berman DS, Carabello BA, Cerqueira MD, DeMariaAN, Kennedy JW, Lorell BH, Messer JV, O’Gara PT, Russell RO Jr, St. John Sutton MG, Udelson JE, Verani MS, Williams KA. ACC/AHA/ASNCguidelines for the clinical use of cardiac radionuclide imaging—executive summary: a report of the American College of Cardiology/American HeartAssociation Task Force on Practice Guidelines (ACC/AHA/ASNC Committee to Revise the 1995 Guidelines for the Clinical Use of RadionuclideImaging). J Am Coll Cardiol 2003;42:1318–33.
*Deceased.†Former Task Force Member.‡Former Task Force Chair.(J Am Coll Cardiol 2003;42:1318–33)©2003 by the American College of Cardiology Foundation and the American Heart Association, Inc.
DOI: 10.1016/S0735-1097(03)01090-8
ACC/AHA Guideline

A. Detection (Diagnosis) of CAD.......................... 13211. Sensitivity and Specificity.......................... 13212. Effect of Referral Bias ............................... 13213. Quantitative Analysis ................................. 13224. ECG-Gated SPECT .................................... 13225. Attenuation Correction ............................... 13226. Positron Emission Tomography ................. 1322
B. Management of Patients With Known orSuspected Chronic CAD: Assessment of DiseaseSeverity, Risk Stratification, Prognosis ............ 13221. Nongated Myocardial Perfusion Imaging.. 13222. Gated SPECT.............................................. 13223. Radionuclide Angiography......................... 13224. Cost Effectiveness ...................................... 13225. Frequency of Testing.................................. 13226. Evaluation of the Effects of Medical Therapy.. 1322
C. Specific Patient Populations.............................. 13221. African Americans...................................... 13222. Women........................................................ 13223. Normal Resting ECG, Able to Exercise.... 13234. Intermediate-Risk Duke Treadmill Score .. 13235. Normal Resting ECG, Unable to Exercise. 13236. LBBB/Pacemakers...................................... 13237. Left Ventricular Hypertrophy..................... 13238. Patients With Nonspecific ST-T-Wave
Changes....................................................... 13239. Elderly......................................................... 1323
10. Asymptomatic Patients ............................... 132311. Obese Patients............................................. 132312. Diabetes....................................................... 132313. After Coronary Calcium Screening ........... 132414. Before and After Revascularization........... 132415. Radionuclide Imaging Before Noncardiac
Surgery........................................................ 1324D. Recommendations.............................................. 1324
IV. Heart Failure ............................................................ 1326A. Introduction........................................................ 1326B. Assessment of LV Function.............................. 1327
1. Assessment of LV Systolic Dysfunction ... 13272. Assessment of LV Diastolic Dysfunction . 1327
C. Assessment of CAD .......................................... 13271. Importance of Detecting CAD in Heart
Failure Patients ........................................... 13272. Myocardial Perfusion Imaging to Detect CAD
in Heart Failure Patients............................. 1327D. Assessment of Myocardial Viability................. 1327
1. Goals of Assessing Myocardial Viability.. 13272. General Principles of Assessing Myocardial
Viability by Radionuclide Techniques....... 13283. Techniques and Protocols for Assessing
Myocardial Viability................................... 13284. Image Interpretation for Myocardial
Viability: Quantitative Versus VisualAnalysis of Tracer Activities ..................... 1328
5. Comparison of Techniques......................... 1328E. Etiologies of Heart Failure................................ 1329
1. Dilated Cardiomyopathy............................. 13292. Dilated Cardiomyopathy Due to
Doxorubicin/Anthracycline Cardiotoxicity. 1329
3. Dilated Cardiomyopathy Due toMyocarditis ................................................. 1329
4. Posttransplantation Rejection and AllograftVasculopathy............................................... 1329
5. Chagas Myocarditis and/or Cardiomyopathy... 13306. Sarcoid Heart Disease ................................ 13307. Cardiac Amyloidosis .................................. 13308. RV Dysplasia.............................................. 13309. Hypertrophic Cardiomyopathy ................... 1330
10. Hypertensive Heart Disease ....................... 133011. Valvular Heart Disease............................... 133012. Adults With Congenital Heart Disease...... 1331
References ....................................................................... 1331
I. IntroductionThe American College of Cardiology (ACC)/American HeartAssociation (AHA) Task Force on Practice Guidelines regularlyreviews existing guidelines to determine when an update or fullrevision is needed. Guidelines for the Clinical Use of CardiacRadionuclide Imaging were originally published in 1986 andupdated in 1995. Important new developments have continued tooccur since 1995, particularly in the areas of acute and chronicischemic syndromes and heart failure. The Task Force thereforebelieved the topic should be revisited de novo and invited theAmerican Society for Nuclear Cardiology (ASNC) to cosponsor theundertaking, which represents a joint effort of the 3 organizations.
The full-text guideline is available on the Internet (www.acc.org,www.americanheart.org, and www.asnc.org). It discusses the use-fulness of nuclear cardiological techniques in 3 broad areas: acuteischemic syndromes, chronic syndromes, and heart failure. Utility isconsidered for diagnosis, severity of disease/risk assessment/prog-nosis, and assessment of therapy. An appendix provides descrip-tions of individual techniques. This Executive Summary includesrecommended indications for the use of specific techniques andsummary evaluations of topics addressed in the full-text document.Additional supporting evidence and a complete reference list arepresented in the full-text document.
The current guideline overlaps with several previouslypublished ACC/AHA guidelines for patient treatment thatpotentially involve cardiac radionuclide imaging. These in-clude published guidelines for chronic stable angina (SA;2002), unstable angina and non–ST-elevation myocardialinfarction (UA/NSTEMI; 2002), heart failure (2001), periop-erative cardiovascular evaluation for noncardiac surgery(2002), exercise testing (2002), valvular heart disease (1998),and acute myocardial infarction (AMI; 1999). The presentreport is not intended to include information previouslycovered in these guidelines or to provide a comprehensivetreatment of the topics addressed in these guidelines.
The ACC/AHA classifications I, II, and III are used tosummarize indications as follows:
Class I: Conditions for which there is evidence and/orgeneral agreement that a given procedure ortreatment is useful and effective
Class II: Conditions for which there is conflicting evi-dence and/or a divergence of opinion about theusefulness/efficacy of a procedure or treatment
1319JACC Vol. 42, No. 7, 2003 Klocke et al.October 1, 2003:1318–33 ACC/AHA Guidelines for Cardiac Radionuclide Imaging

IIa: Weight of evidence/opinion is in favor ofusefulness/efficacy
IIb: Usefulness/efficacy is less well established byevidence/opinion
Class III: Conditions for which there is evidence and/orgeneral agreement that the procedure/treat-ment is not useful/effective and in some casesmay be harmful
Levels of evidence for individual class assignments aredesignated as follows:
A: Data derived from multiple randomized clinical trialsB: Data derived from a single randomized trial or from
nonrandomized studiesC: Consensus opinion of experts
These guidelines will be reviewed annually by the TaskForce and will be considered current unless the Task Forcerevises or withdraws them from distribution.
II. Acute SyndromesA. Myocardial Perfusion Imaging in theAssessment of Patients Presenting With Chest Painto the Emergency DepartmentOptimal decision-making in patients seen in the emergencydepartment with chest pain requires triage into risk categorieson the basis of the probability of AMI, UA, or both and thesubsequent risk and potential interventional options. Withinsuch an algorithm, radionuclide imaging provides clinicallyuseful information for diagnosis and management. The UAguidelines use 4 risk levels for chest pain: noncardiac, chronicSA, possible acute coronary syndrome (ACS), and definiteACS (http://www.acc.org/clinical/guidelines/unstable/unstable.pdf) (1). Radionuclide imaging is most appropriatein patients with possible ACS. After initial triage on the basisof symptoms, ECG, and history, rest single-photon emissionCT (SPECT) imaging appears to be useful for identifyingpatients at high risk (those with perfusion defects), whoshould be admitted, and patients with low risk (those withnormal scans), who in general may be discharged home witha low risk for subsequent ischemic events. Randomized
clinical trials (2,3) now support several observational studies(see Table 1 in the full-text guideline) indicating a highnegative predictive value for excluding ACS. Table 1 listsrecommendations for emergency department imaging forsuspected ACS.
B. Detection of AMI When Conventional MeasuresAre NondiagnosticRest myocardial perfusion imaging with 99mTc tracers has ahigh sensitivity for diagnosing AMI. Because there is mini-mal redistribution of the radiopharmaceutical over time,imaging can be delayed for a few hours after the injection andstill provide accurate information about myocardial perfusionat the time of injection, which reflects the area of myocardi-um at risk. Perfusion defects, however, do not distinguishamong acute ischemia, acute infarction, or previousinfarction.
C. Radionuclide Testing in Risk Assessment:Prognosis and Assessment of TherapyAfter STEMIAs discussed in the ACC/AHA Guidelines for the Manage-ment of Patients with Acute Myocardial Infarction: 1999Update (4) (http://www.acc.org/clinical/guidelines/nov96/1999/index.htm), the prognosis of STEMI is primarily afunction of ejection fraction (EF), infarct size, and residualmyocardium at risk. Thus, acute or late measurement of EF,infarct size, and myocardium at risk provides importantprognostic management information. Radionuclide tech-niques are also useful for assessing the presence and extent ofstress-induced myocardial ischemia—information that is use-ful for immediate and long-term patient management (5–9).Table 2 lists recommendations for radionuclide testing indiagnosis, risk assessment, prognosis, and assessment oftherapy after acute STEMI.
D. Radionuclide Testing in Risk Assessment:Prognosis and Assessment of Therapy AfterNSTEMI or UAThe ACC/AHA 2002 Guideline Update for the Managementof Patients with UA/NSTEMI (1) recommends an earlyinvasive strategy in patients with any of several high-risk
TABLE 1. Recommendations for Emergency Department Imaging for Suspected ACS
Indication Test ClassLevel ofEvidence
1. Assessment of myocardial risk in possible ACS patients withnondiagnostic ECG and initial serum markers and enzymes, if available.
Rest MPI I A
2. Diagnosis of CAD in possible ACS patients with chest pain withnondiagnostic ECG and negative serum markers and enzymes or normalresting scan.
Same day rest/stressperfusion imaging
I B
3. Routine imaging of patients with myocardial ischemia/necrosis alreadydocumented clinically, by ECG and/or serum markers or enzymes
Rest MPI III C
See Figure 6 of ACC/AHA 2002 Guideline Update for the Management of Patients With Unstable Angina and Non–ST-SegmentElevation Myocardial Infarction at http://www.acc.org/clinical/guidelines/unstable/incorporated/figure6.htm and Figure 1 of ACC/AHAGuidelines for the Management of Patients with Acute Myocardial Infarction at www.acc.org/clinical/guidelines/nov96/1999/jac1716f01.htm.
ACS indicates acute coronary syndromes; CAD, coronary artery disease; ECG, electrocardiogram; MPI, myocardial perfusionimaging.
1320 Klocke et al. JACC Vol. 42, No. 7, 2003ACC/AHA Guidelines for Cardiac Radionuclide Imaging October 1, 2003:1318–33

indicators and no serious comorbidities. High-risk findings onnoninvasive stress testing (eg, myocardial perfusion imaging)are one such indication. In the absence of high-risk findings,the guidelines endorse either an early conservative or earlyinvasive strategy in patients without contraindications forrevascularization. Myocardial perfusion imaging is particu-larly useful in the predischarge risk stratification of patientswith UA. The presence and extent of reversible perfusiondefects on stress testing after the patient is stabilized arehighly predictive of future events (10–14). Table 3 listsrecommendations for radionuclide testing for risk assess-ment/prognosis in patients with NSTEMI or UA.
III. Chronic SyndromesA. Detection (Diagnosis) of Coronary Artery DiseaseA thorough discussion of the concepts of likelihood ofcoronary artery disease (CAD) is provided in the ACC/AHA2002 Guideline Update for the Management of Patients WithChronic Stable Angina (15) (http://www.acc.org/clinical/guidelines/stable/stable_clean.pdf), accompanied by a simpli-fied table for estimating pretest probability ranges. Myocar-dial perfusion imaging is most useful in patients with an
intermediate likelihood of angiographically significant CADon the basis of age, sex, symptoms, risk factors, and theresults of stress testing (for patients who have undergoneprior stress testing).
1. Sensitivity and SpecificityTables 5 and 6 in the full-text guideline summarize studiesreporting sensitivities and specificities of exercise and vaso-dilator stress perfusion SPECT for the detection of angio-graphically significant (more than 50% stenosis) CAD. Sen-sitivities (generally uncorrected for referral bias) average 87%and 89%, respectively; specificities (also uncorrected) average73% and 75%.
2. Effect of Referral BiasIn estimating the true sensitivity and specificity of noninva-sive testing, referral or work-up bias needs to be taken intoaccount. Table 7 in the full-text guideline summarizes studiesin which effects of referral bias have been estimated. Becauseof the profound impact of referral bias on specificity, theconcept of the normalcy rate has been developed. The termnormalcy rate is used to describe the frequency of normal testresults in patients with a low likelihood of CAD, to differen-tiate it from specificity.
TABLE 2. Recommendations for Use of Radionuclide Testing in Diagnosis, Risk Assessment, Prognosis, andAssessment of Therapy After Acute STEMI
Patient Subgroup(s) Indication Test ClassLevel ofEvidence
All 1. Rest LV function Rest RNA or ECG-gated SPECT I B
Thrombolytic therapy withoutcatheterization
2. Detection of inducible ischemia andmyocardium at risk
Stress MPI with ECG-gated SPECTwhenever possible
I B
Acute STEMI 3. Assessment of infarct size andresidual viable myocardium
MPI at rest or with stress using gatedSPECT
I B
4. Assessment of RV function withsuspected RV infarction
Equilibrium or FPRNA IIa B
ECG indicates electrocardiography; FPRNA, first-pass radionuclide angiography; LV, left ventricular; MPI, myocardial perfusion imaging; RNA,radionuclide angiography; RV, right ventricular; SPECT, single-photon emission computed tomography; STEMI, ST-segment elevation myocardialinfarction.
TABLE 3. Recommendations for Use of Radionuclide Testing for Risk Assessment/Prognosis in Patients With NSTEMIand UA
Indication Test ClassLevel ofEvidence
1. Identification of inducible ischemia in the distribution of the “culpritlesion” or in remote areas in patients at intermediate or low risk formajor adverse cardiac events.
Stress MPI with ECG gatingwhenever possible
I B
2. Identification of the severity/extent of inducible ischemia in patientswhose angina is satisfactorily stabilized with medical therapy or inwhom diagnosis is uncertain.
Stress MPI with ECG gatingwhenever possible
I A
3. Identification of hemodynamic significance of coronary stenosis aftercoronary arteriography.
Stress MPI I B
4. Measurement of baseline LV function. RNA or gated SPECT I B
5. Identification of the severity/extent of disease in patients with ongoingsuspected ischemia symptoms when ECG changes are not diagnostic.
Rest MPI IIa B
ECG indicates electrocardiography; LV, left ventricular; MPI, myocardial perfusion imaging; RNA, radionuclide angiography; SPECT, single-photonemission computed tomography.
1321JACC Vol. 42, No. 7, 2003 Klocke et al.October 1, 2003:1318–33 ACC/AHA Guidelines for Cardiac Radionuclide Imaging

3. Quantitative AnalysisQuantitative analysis of myocardial perfusion SPECT hasbeen developed using a variety of approaches and, in general,has similar sensitivities and specificities compared with thoseof expert visual analysis.
4. ECG-Gated SPECTThe current state of the art is ECG-gated myocardial perfu-sion SPECT (gated SPECT). The ability to observe myocar-dial contraction in segments with apparent fixed perfusiondefects permits the nuclear test reader to discern attenuationartifacts from true perfusion abnormalities. The ability ofgated SPECT to provide measurement of left ventricular (LV)EF (LVEF), segmental wall motion, and absolute LV vol-umes also adds to the prognostic information that can bederived from a SPECT study.
5. Attenuation CorrectionThe field of attenuation correction continues to evolve rap-idly, with some available systems having undergone moredetailed and successful clinical validation than others. On thebasis of current information and the rate of technologyimprovement, the Society of Nuclear Medicine and theAmerican Society of Nuclear Cardiology have concluded thatattenuation correction has become a method for which theweight of evidence/opinion is in favor of its usefulness (16).
6. Positron Emission TomographyStudies involving several hundred patients (see Table 10 inthe full-text guideline) indicate that perfusion imaging withpositron emission tomography (PET) using dipyridamole andeither 82Rb or 13N ammonia is also a sensitive and specificclinical means to diagnose CAD.
B. Management of Patients With Known orSuspected Chronic CAD: Assessment of DiseaseSeverity, Risk Stratification, PrognosisNuclear tests are best applied for risk stratification in patientswith a clinically intermediate risk of a subsequent cardiacevent, analogous to the optimal diagnostic application ofnuclear testing to patients with an intermediate likelihood ofhaving CAD. Many of the major determinants of prognosis inCAD can be assessed by measurements of stress-inducedperfusion and function. Studies including large patient sam-ples have now demonstrated that factors estimating the extentof LV dysfunction (LVEF, the extent of infarcted myocardi-um, transient ischemic dilation of the LV, and increased lunguptake) are excellent predictors of cardiac mortality. Incontrast, markers of provocative ischemia (exertional symp-toms, electrocardiographic changes, the extent of reversibleperfusion defects, and stress-induced ventricular dyssynergy)are better predictors of the subsequent development of acuteischemic syndromes (17).
1. Nongated Myocardial Perfusion ImagingNot withstanding the now well-demonstrated advantages ofgated imaging, nongated perfusion scintigraphy has played amajor role in risk stratification of CAD patients. The full-textguideline summarizes studies of stress myocardial perfusionimaging in definite or suspected CAD (see Table 12 in thefull-text guideline). Normal stress perfusion SPECT results
are consistently predictive of a less than 1% annual risk ofcardiac death or myocardial infarction.
2. Gated SPECTThe information contained in the combined assessment ofperfusion and function with gated myocardial perfusionSPECT is likely to enhance its prognostic and diagnosticcontent. The most common current approach combines post-stress and/or rest LV function by gated SPECT with rest/stress perfusion measurements.
3. Radionuclide AngiographyRest LVEF is universally recognized as one of the mostimportant determinants of long-term prognosis in patientswith chronic stable CAD. Radionuclide angiography (RNA)can also be helpful in evaluating dyspnea by establishing thestate of right ventricular (RV) and LV performance. LVfunction during exercise reflects disease severity and pro-vides prognostic information.
4. Cost EffectivenessAs indicated in the ACC/AHA 2002 Guideline Update for theManagement of Patients With Chronic Stable Angina (15),cardiac imaging can serve as a gatekeeper to cardiac cathe-terization to minimize the rate of normal catheterizations andto enrich the angiographic population with a greater propor-tion of patients with significant, yet treatable, disease.
5. Frequency of TestingConsiderations for follow-up testing are also summarized inthe ACC/AHA 2002 Guideline Update for the Managementof Patients With Chronic Stable Angina (15). If patientsdevelop new signs or symptoms suggesting a worsenedclinical state, repeat testing at the time of worsening would beappropriate. In the absence of a change in clinical state, theestimated patient risk after initial testing (high, intermediate,or low, as defined earlier) should play an important role inindividual recommendations (18).
6. Evaluation of the Effects of Medical TherapyAlthough the available evidence suggests that the efficacy oftherapy can be assessed with repeat SPECT procedures whilethe patient is under the effects of the medical treatment,information about the effects of medical therapy on outcomesis limited.
C. Specific Patient Populations
1. African AmericansThe role of noninvasive imaging has been studied infre-quently in African Americans or other minorities. Normal restand stress SPECT perfusion studies have been associatedwith higher rates of AMI and/or cardiac death in AfricanAmericans than in other populations (19,20), but includedhigher than usual cardiac risk patients and did not account forthe incidence of LV hypertrophy (LVH) (21).
2. WomenAs discussed in the ACC/AHA 2002 Guideline Update forExercise Testing (22) (http://www.acc.org/clinical/guide-lines/exercise/exercise_clean.pdf), the use of radionuclidetesting in women is influenced importantly by the later
1322 Klocke et al. JACC Vol. 42, No. 7, 2003ACC/AHA Guidelines for Cardiac Radionuclide Imaging October 1, 2003:1318–33

presentation of CAD in women than in men and by sex-related limitations in exercise stress testing. These issues haveprovoked interest in the potential additive benefit of stressperfusion imaging in women, particularly those with at leastan intermediate likelihood of coronary disease (23–26).
3. Normal Resting ECG, Able to ExercisePatients with a normal resting ECG constitute a large andimportant subgroup. Most patients who present with multiplerisk factors with or without cardiac symptoms have a normalresting ECG. Such patients are likely to have normal LVfunction and an excellent prognosis. For these reasons, astepwise strategy is generally recommended in which anexercise ECG, and not a stress imaging procedure, is per-formed as the initial test in patients with an intermediatepretest likelihood of CAD who are not taking digoxin, have anormal resting ECG, and are able to exercise. A stressimaging technique should be used for patients with wide-spread rest ST depression (more than 1 mm), complete leftbundle-branch block (LBBB), ventricular-paced rhythm, pre-excitation, or LVH with repolarization changes (15).
4. Intermediate-Risk Duke Treadmill ScoreThe Duke treadmill score combines various forms of infor-mation from stress testing and provides a simple way tocalculate risk (27). Annual mortality rates according to riskgroups are presented in the ACC/AHA 2002 Chronic StableAngina Guideline Update (15). The score has been reportedto work well for both inpatients and outpatients and equallywell for men and women. Only a small number of elderlypatients, however, have been studied. Several studies havedemonstrated value of myocardial perfusion scintigraphy infurther risk assessment of patients with an intermediate scoreassociated with an intermediate risk of cardiac death (28–30).
5. Normal Resting ECG, Unable to ExerciseIn patients with an intermediate to high likelihood of CADwho have a normal resting ECG but are unable to exercise,pharmacologic myocardial perfusion SPECT with adenosineor dipyridamole has been shown to be highly effective indiagnosis and risk stratification.
6. LBBB/PacemakersPharmacologic stress perfusion imaging is preferable toexercise perfusion imaging for purposes of both diagnosisand risk stratification (31,32). Several studies have observedan increased prevalence of myocardial perfusion defectsduring exercise imaging, in the absence of angiographiccoronary disease, in patients with LBBB. Given that ECGtesting is nondiagnostic in patients with ventricular pacing ina manner similar to that observed with LBBB, it is likely thatthe considerations with regard to the use of radionuclidetechniques for diagnostic and risk stratification purposes inpatients with ventricular pacemakers are the same as thoseapplied to patients with LBBB.
7. Left Ventricular HypertrophyIn patients with LVH, with or without resting ST-segmentabnormality, ST depression during exercise is frequentlypresent in the absence of significant CAD. In these patients,stress nuclear techniques have similar diagnostic sensitivity
and specificity to those observed in patients without LVH.The diagnostic value of myocardial perfusion SPECT is notgenerally degraded by the presence of hypertension withoutevidence of LVH (33), although an increased frequency offalse-positive studies has been reported in athletes (34).Similarly, although the number of reports is small, theprognostic value of myocardial perfusion SPECT in patientswith LVH appears to be equal to that observed in patientswithout LVH (35).
8. Patients With Nonspecific ST-T-Wave ChangesPatients with nonspecific ST-T-wave changes, such as mightoccur with digoxin, Wolff-Parkinson-White syndrome(WPW), or other conditions, are considered to have nondi-agnostic stress ECG responses with regard to ST-segmentdepression. Although there are limited data on the diagnosticand prognostic information for myocardial perfusion SPECTin these patients, those with intermediate to high likelihood ofcoronary disease can perhaps be effectively assessed fordetection and risk stratification with myocardial perfusionSPECT.
9. ElderlyPrognostic value of perfusion scintigraphy in elderly patientshas been reported (36).
10. Asymptomatic PatientsThe relatively low prevalence of CAD and risk of futureevents will affect the performance of any diagnostic test in amanner predictable by Bayesian principles (ie, positive pre-dictive value will usually be low). It is not clear that detectingasymptomatic preclinical CAD will lead to therapeutic inter-vention that will reduce risk beyond that indicated by riskfactor profiling and currently recommended strategies toreduce risk (37).
Persons whose occupations may affect public safety (eg,airline pilots, truckers, bus drivers) or who are professional orhigh-profile athletes commonly undergo periodic exercisetesting for statutory reasons (22). In some asymptomaticpatients, testing may be appropriate when there is a high-riskclinical situation (eg, diabetes or multiple risk factors) (22).Patients with a more than 20% 10-year risk of developingcoronary heart disease are considered to be at high risk incurrent National Cholesterol Education Program guidelines(37).
11. Obese PatientsVery obese patients constitute a special problem becausemost imaging tables used for SPECT have weight-bearinglimits (often 300 lb [135 kg]) that preclude imaging veryheavy subjects. These subjects can still be imaged by planarscintigraphy.
12. DiabetesThe increasing recognition of diabetes mellitus as a majorrisk factor for cardiovascular disease (38) has heightenedinterest in myocardial perfusion imaging for CAD diagnosisand risk stratification. Available studies are based on retro-spective analyses of patients referred to the nuclear cardiol-ogy laboratory (24,39,40). Prospective information in asymp-tomatic diabetic patients drawn from the general diabetic
1323JACC Vol. 42, No. 7, 2003 Klocke et al.October 1, 2003:1318–33 ACC/AHA Guidelines for Cardiac Radionuclide Imaging

population is awaited (41). Currently available studies indi-cate that (1) 99mTc-sestamibi myocardial perfusion SPECT hascomparable sensitivity, specificity, and normalcy rates for thediagnosis of CAD in diabetic and nondiabetic patients; (2)risk-adjusted event-free survival in patients with mildly andmoderately to severely abnormal scans is worse in patientswith diabetes than in those without diabetes; (3) the presenceand extent of myocardial perfusion SPECT abnormality is anindependent predictor of cardiac death alone, or of cardiacdeath and MI, in patients with or without diabetes; and (4)diabetic women have the worst outcome for any given extentof reversible myocardial defect.
13. After Coronary Calcium ScreeningAlthough some patients can benefit from nuclear stresstesting after electron-beam CT, it would clearly not becost-effective for all patients with atherosclerosis accordingto electron-beam CT to go on to the more expensive nuclearcardiology testing. In general, when the electron-beam CTscore is higher than the 75th percentile for age and sex, stressnuclear testing may sometimes be appropriate for purposes ofrisk stratification.
14. Before and After Revascularization
a. Radionuclide Imaging Before Revascularization Interven-tions
When there is uncertainty with regard to the appropriatechoice of therapy after coronary angiography, stress nucleartesting can risk stratify 25% to 75% lesions usefully (42).
b. Radionuclide Imaging After Percutaneous Coronary Inter-vention
The ACC/AHA 2002 Guideline Update for Exercise Test-ing (22) summarizes the available information on exercisetesting after percutaneous coronary intervention (PCI). Symp-tom status is an unreliable index of development of resteno-sis, with 25% of asymptomatic patients documented ashaving ischemia on exercise testing. Myocardial perfusionimaging can be helpful in appropriately selected patients. Themajor indication for perfusion imaging in patients aftersuccessful PCI is to evaluate symptoms suggesting newdisease.
c. Radionuclide Imaging After Coronary Artery Bypass GraftSurgery
Myocardial perfusion scintigraphy can be useful in deter-mining the location, extent, and severity of ischemia. Prog-nostic value has been demonstrated both early (43) and late(44,45) after coronary artery bypass graft (CABG) surgery.
15. Radionuclide Imaging Before Noncardiac SurgeryThe ACC/AHA Guideline Update for Perioperative CardiacEvaluation for Noncardiac Surgery (46) (http://www.acc.org/clinical/guidelines/perio/update/pdf/perio_update.pdf) hasemphasized the importance of clinical, demographic, andsurgical indicators of risk. In general, noninvasive preopera-tive testing is best directed at patients considered to be atintermediate clinical risk (diabetes, stable CAD, compensatedheart failure) who are scheduled to undergo intermediate- orhigh-risk surgery. A thorough evaluation of appropriatelyselected patients will also afford an assessment of cardiacprognosis over the long term. Exercise stress is preferred in
patients capable of achieving adequate workloads; radionu-clide techniques should be reserved for patients whosebaseline ECGs render exercise interpretation invalid or whorequire pharmacologic stress because of the inability toexercise.
a. Myocardial Perfusion ImagingThe full-text guideline summarizes studies of perfusion
imaging in the preoperative assessment of cardiac risk forvascular and nonvascular surgery (see Table 14 in thefull-text guideline). For patients with radionuclide evidenceof ischemia, the positive predictive value of such testing isuniformly low, in the range of 4% to 20%. The negativepredictive value of a normal scan, however, is very high (96%to 100%). Patients with reversible defects are at greater riskfor perioperative ischemia than are those with fixed defects;the latter defects may, in turn, be a marker for longer-termrisk. The positive predictive value of perfusion imaging canbe improved when testing is applied selectively to patientswith a higher pretest likelihood of CAD and when the resultsare integrated into a clinical risk assessment. If a noninvasiveassessment of ischemic jeopardy before noncardiac surgery isnecessary, the choice between radionuclide stress perfusionimaging and dobutamine stress echocardiography should bemade on the basis of institutional expertise and patient-specific attributes.
b. Radionuclide VentriculographyExercise radionuclide ventriculography is rarely performed
to assess ischemic jeopardy before noncardiac surgery. Theevaluation of resting LV function, however, is an importantcomponent of the preoperative assessment of patients withsymptoms and/or signs of heart failure. LV systolic functionis now routinely assessed with gated SPECT techniques at thetime of myocardial perfusion imaging. Not unexpectedly, therisk of perioperative complications is highest among patientswith a resting LVEF more than 0.35. Reduced LV systolicfunction is a predictor of perioperative heart failure but bearsno consistent correlation with the risk of perioperativeischemia.
D. Recommendations
I. Cardiac Stress Myocardial Perfusion SPECT in Pa-tients Able to Exercise: Recommendations for Diag-nosis of Patients With an Intermediate Likelihood ofCAD and/or Risk Stratification of Patients With anIntermediate or High Likelihood of CAD Who AreAble to Exercise (to at least 85% of Maximal Pre-dicted Heart Rate)
Class I1. Exercise myocardial perfusion SPECT
to identify the extent, severity, and loca-tion of ischemia in patients who do nothave LBBB or an electronically-pacedventricular rhythm but do have a base-line ECG abnormality that interfereswith the interpretation of exercise-induced ST-segment changes (ventricu-lar pre-excitation, LVH, digoxin ther-
1324 Klocke et al. JACC Vol. 42, No. 7, 2003ACC/AHA Guidelines for Cardiac Radionuclide Imaging October 1, 2003:1318–33

apy, or more than 1-mm ST depression).(Level of Evidence: B)
2. Adenosine or dipyridamole myocardialperfusion SPECT in patients with LBBBor electronically-paced ventricularrhythm. (Level of Evidence: B)
3. Exercise myocardial perfusion SPECTto assess the functional significance ofintermediate (25% to 75%) coronarylesions. (Level of Evidence: B)
4. Exercise myocardial perfusion SPECT inpatients with intermediate Duke treadmillscore. (Level of Evidence: B)
5. Repeat exercise myocardial perfusionimaging after initial perfusion imagingin patients whose symptoms havechanged to redefine the risk for cardiacevent. (Level of Evidence: C)
Class IIa1. Exercise myocardial perfusion SPECT at 3
to 5 years after revascularization (either PCIor CABG) in selected high-risk asymptom-atic patients. (Level of Evidence: B)
2. Exercise myocardial perfusion SPECTas the initial test in patients who areconsidered to be at high risk (patientswith diabetes or patients otherwise de-fined as having a more than 20% 10-year risk of a coronary heart diseaseevent). (Level of Evidence: B)
Class IIb1. Repeat exercise myocardial perfusion
SPECT 1 to 3 years after initial perfu-sion imaging in patients with known or ahigh likelihood of CAD and stable symp-toms and a predicted annual mortalityof more than 1% to redefine the risk ofa cardiac event. (Level of Evidence: C)
2. Repeat exercise myocardial perfusionSPECT on cardiac active medicationsafter initial abnormal perfusion imagingto assess the efficacy of medical therapy.(Level of Evidence: C)
3. Exercise myocardial perfusion SPECT insymptomatic or asymptomatic patientswho have severe coronary calcification(CT coronary calcium score more than the75th percentile for age and sex) in thepresence on the resting ECG of pre-excitation [Wolff-Parkinson-White syn-drome] or more than 1 mm ST-segmentdepression. (Level of Evidence: B)
4. Exercise myocardial perfusion SPECT inasymptomatic patients who have a high-risk occupation. (Level of Evidence: B)
II. Cardiac Stress Myocardial Perfusion SPECT in Pa-tients Unable to Exercise: Recommendations for Di-agnosis of Patients With an Intermediate Likelihood
of CAD and/or Risk Stratification of Patients With anIntermediate or High Likelihood of CAD Who AreUnable to Exercise.
Class I1. Adenosine or dipyridamole myocardial
perfusion SPECT to identify the extent,severity, and location of ischemia. (Levelof Evidence: B)
2. Adenosine or dipyridamole myocardialperfusion SPECT to assess the func-tional significance of intermediate (25%to 75%) coronary lesions. (Level of Evi-dence: B)
3. Adenosine or dipyridamole myocardialperfusion SPECT after initial perfusionimaging in patients whose symptomshave changed to redefine the risk forcardiac event. (Level of Evidence: C)
Class IIa1. Adenosine or dipyridamole myocardial
perfusion SPECT at 3 to 5 years afterrevascularization (either PCI or CABG)in selected high-risk asymptomatic pa-tients. (Level of Evidence: B)
2. Adenosine or dipyridamole myocardialperfusion SPECT as the initial test inpatients who are considered to be at highrisk (patients with diabetes or patientsotherwise defined as having a more than20% 10-year risk of a coronary heartdisease event). (Level of Evidence: B)
3. Dobutamine myocardial perfusionSPECT in patients who have a contrain-dication to adenosine or dipyridamole.(Level of Evidence: C)
Class IIb1. Repeat adenosine or dipyridamole myo-
cardial perfusion imaging 1 to 3 yearsafter initial perfusion imaging in pa-tients with known or a high likelihood ofCAD and stable symptoms, and a pre-dicted annual mortality of more than1%, to redefine the risk of a cardiacevent. (Level of Evidence: C)
2. Repeat adenosine or dipyridamole myo-cardial perfusion SPECT on cardiac ac-tive medications after initial abnormalperfusion imaging to assess the efficacyof medical therapy. (Level of Evidence: C)
3. Adenosine or dipyridamole myocardialperfusion SPECT in symptomatic orasymptomatic patients who have severecoronary calcification (CT CoronaryCalcium Score more than the 75th per-centile for age and sex) in the presenceon the resting ECG of LBBB or anelectronically-paced ventricular rhythm.(Level of Evidence: B)
1325JACC Vol. 42, No. 7, 2003 Klocke et al.October 1, 2003:1318–33 ACC/AHA Guidelines for Cardiac Radionuclide Imaging

4. Adenosine or dipyridamole myocardialperfusion SPECT in asymptomatic pa-tients who have a high-risk occupation.(Level of Evidence: C)
III. Cardiac Stress Myocardial Perfusion PET: Recom-mendations for Diagnosis of Patients With an Inter-mediate Likelihood of CAD and/or Risk Stratificationof Patients With an Intermediate or High Likelihoodof CAD
Class I1. Adenosine or dipyridamole myocardial
perfusion PET in patients in whom anappropriately indicated myocardial per-fusion SPECT study has been found to beequivocal for diagnostic or risk stratifica-tion purposes. (Level of Evidence: B)
Class IIa1. Adenosine or dipyridamole myocardial
perfusion PET to identify the extent,severity, and location of ischemia as theinitial diagnostic test in patients who areunable to exercise. (Level of Evidence: B)
2. Adenosine or dipyridamole myocardialperfusion PET to identify the extent, se-verity, and location of ischemia as theinitial diagnostic test in patients who areable to exercise but have LBBB or anelectronically-paced rhythm. (Level of Ev-idence: B)
IV. Cardiac Stress Perfusion Imaging Before NoncardiacSurgery: Recommendations
Class I1. Initial diagnosis of CAD in patients with
intermediate pretest probability of diseaseand abnormal baseline ECG1 or inabilityto exercise. (Level of Evidence: B)
2. Prognostic assessment of patients under-going initial evaluation for suspected orproven CAD with abnormal baselineECG1 or inability to exercise. (Level ofEvidence: B)
3. Evaluation of patients following achange in clinical status (eg, ACS) withabnormal baseline ECG1 or inability toexercise. (Level of Evidence: B)
4. Initial diagnosis of CAD in patients withLBBB and intermediate pretest proba-bility of disease, when used in conjunc-tion with vasodilator stress. (Level ofEvidence: B)
5. Prognostic assessment of patients withLBBB undergoing initial evaluation forsuspected or proven CAD, when used in
conjunction with vasodilator stress.(Level of Evidence: B)
6. Assessment of patients with intermedi-ate or minor clinical risk predictors2 andpoor functional capacity (less than 4METS) who require high-risk noncar-diac surgery3, when used in conjunctionwith pharmacologic stress. (Level of Ev-idence: C)
7. Assessment of patients with intermedi-ate clinical risk predictors2, abnormalbaseline ECGs1, and moderate or excel-lent functional capacity (more than 4METS) who require high-risk noncar-diac surgery. (Level of Evidence: C)
Class IIb1. Routine assessment of active, asymptom-
atic patients who have remained stablefor up to 5 years after CABG surgery.(Level of Evidence: C)
2. Routine evaluation of active asymptom-atic patients who have remained stablefor up to 2 years after previous abnor-mal coronary angiography or noninva-sive assessment of myocardial perfusion.(Level of Evidence: C)
3. Diagnosis of restenosis and regional is-chemia in active asymptomatic patientswithin weeks to months after PCI. (Levelof Evidence: C)
4. Initial diagnosis or prognostic assess-ment of CAD in patients with rightbundle-branch block or less than 1-mmST depression on resting ECG. (Level ofEvidence: C)
Class III1. Routine screening of asymptomatic men
or women with low pretest likelihood ofCAD. (Level of Evidence: C)
2. Evaluation of patients with severe co-morbidities that limit life expectancy orcandidacy for myocardial revasculariza-tion. (Level of Evidence: C)
3. Initial diagnosis or prognostic assess-ment of CAD in patients who requireemergency noncardiac surgery. (Level ofEvidence: C)
IV. Heart FailureA. IntroductionThe clinical syndrome of heart failure in adults is commonlyassociated with the etiologies of ischemic and nonischemic
1Baseline ECG abnormalities that interfere with interpretation ofexercise-induced ST-segment changes include LBBB, ventricular pre-excitation, ventricular pacing, LVH with repolarization changes, morethan 1-mm ST depression, and digoxin therapy.
2As defined in the ACC/AHA Guideline Update for Perioperative Cardio-vascular Evaluation for Noncardiac Surgery (46), intermediate clinical riskpredictors include mild angina, prior MI, compensated or prior heart failure,diabetes, and renal insufficiency. Minor clinical risk predictors includeadvanced age, abnormal ECG, rhythm other than sinus, low functionalcapacity, history of cerebrovascular accident, and uncontrolled hypertension.3High-risk surgery is defined by emergent operations (particularly in theelderly), aortic and other major vascular surgery, peripheral vascular surgery,and other prolonged operations in which major fluid shifts are anticipated (ie,reported cardiac risk often more than 5%).
1326 Klocke et al. JACC Vol. 42, No. 7, 2003ACC/AHA Guidelines for Cardiac Radionuclide Imaging October 1, 2003:1318–33

dilated cardiomyopathy, hypertrophic cardiomyopathy, hy-pertensive heart disease, and valvular heart disease. Commonprinciples of assessment that influence prognosis and therapyinclude the assessment of (1) LV function and remodeling,(2) the contribution of myocardial ischemia due to CAD, and(3) myocardial viability.
B. Assessment of LV Function
1. Assessment of LV Systolic DysfunctionThe clinician’s choice of noninvasive imaging modality todetect and quantify LV systolic dysfunction in the individualpatient with heart failure depends on several variables,including cost, ease of access at point-of-care, need forprecise computed quantitative measurement, and local exper-tise. RNA can be used to compute quantitative estimates ofLV, as well as RV, EF, and absolute volumes. A strength ofRNA is that the quantitative computation of EF and chambervolumes does not depend on mathematical assumptions ofventricular geometry. Thus, radionuclide quantitative compu-tations of LV chamber volume and EF are obtainable in�100% of patients. The long biological half-life of 99mTc-labeled blood pool agents in gated equilibrium studies alsopermits serial acquisition of data at rest and during exercise.
2. Assessment of LV Diastolic DysfunctionThe objective determination of the presence and severity ofdiastolic dysfunction is increasingly important in patientswith the clinical syndrome of heart failure. The rate of changeof counts in diastole can be analyzed to calculate indices ofdiastolic filling, including the peak LV filling rate, time topeak filling, and atrial contribution to filling. In contemporarypractice, Doppler blood flow velocity indices of transmitralflow are more commonly used to assess LV diastolic fillingparameters. Large population-based criteria, adjusted for ageand sex, for normal versus abnormal diastolic function usingRNA have not yet been established.
C. Assessment of CAD
1. Importance of Detecting CAD in Heart Failure PatientsDetermining whether LV dysfunction is caused predomi-nantly by the consequences of CAD or by one of the many
other etiologies included in the term “nonischemic” cardio-myopathy is a critical early step in the management of heartfailure patients. Decisions about the need for cardiac cathe-terization and coronary angiography will be informed by theinitial clinical and noninvasive assessment of these patients.A significant subgroup of patients with heart failure andunderlying CAD has a potentially reversible degree of LVdysfunction with revascularization.
2. Myocardial Perfusion Imaging to Detect CAD in HeartFailure PatientsThe sensitivity and negative predictive value of myocardialperfusion imaging in detecting CAD in patients with heartfailure and LV dysfunction have been excellent in publishedstudies. However, it is not clear how these studies, some ofwhich involved relatively small numbers of patients and oldertechniques, may generalize to current patients and contempo-rary imaging techniques. The specificity of perfusion imagingto rule out coronary disease is modest, on the average 40% to50%. The frequent false-positive studies are due to perfusionabnormalities in a significant number of patients with “nonis-chemic” cardiomyopathy, ie, those patients without epicardialcoronary disease. Table 4 lists recommendations for radionu-clide imaging in patients with heart failure.
D. Assessment of Myocardial Viability
1. Goals of Assessing Myocardial ViabilityIn patients with chronic coronary disease and LV dysfunc-tion, an important subpopulation exists in which revascular-ization may significantly improve regional or global LVfunction, as well as symptoms and potentially natural history.The underlying pathophysiology involves reversible myocar-dial dysfunction (hibernation or stunning). Meta-analysis of asubstantial body of literature indicates that those with evi-dence of preserved myocardial viability who underwentrevascularization had a substantial reduction in the risk ofdeath during long-term follow-up (47). If nonviability waspredominant, the risk of death was intermediate and notaffected by revascularization. These conclusions, however,are limited by lack of randomization and the fact thatobservational cohorts analyses are subject to selection biases.
TABLE 4. Recommendations for the Use of Radionuclide Imaging in Patients With Heart Failure:Fundamental Assessment
Indication Test ClassLevel ofEvidence
1. Initial assessment of LV and RV function at rest* Rest RNA I A
2. Assessment of myocardial viability for consideration ofrevascularization in patients with CAD and LV systolic dysfunctionwho do not have angina
MPI (see Table 5), PET I B
3. Assessment of the copresence of CAD in patients without angina MPI IIa B
4. Routine serial assessment of LV and RV function at rest Rest RNA IIb B
5. Initial or serial assessment of ventricular function with exercise Exercise RNA IIb B
*National consensus treatment guidelines are directed by quantitative assessment of LVEF and identification of LVEF less than orequal to 40%.
CAD indicates coronary artery disease; LV, left ventricular; MPI, myocardial perfusion imaging; PET, positron emission tomography;RNA, radionuclide angiography.
1327JACC Vol. 42, No. 7, 2003 Klocke et al.October 1, 2003:1318–33 ACC/AHA Guidelines for Cardiac Radionuclide Imaging

2. General Principles of Assessing Myocardial Viability byRadionuclide TechniquesPreservation of myocardial viability exists as a spectrum in aterritory with regional ventricular dysfunction, from thepossibility of no preserved viability (ie, complete transmuralinfarction) to completely preserved viability (ie, transmuralhibernation or stunning with the potential for full recovery offunction). Most studies evaluating the radionuclide tech-niques for assessing viability have focused on analysis ofresting tracer uptake (as with 201Tl, sestamibi, or tetrofosmin)or evidence of preserved metabolic activity at rest (by18F-2-fluorodeoxyglucose [FDG] or 11C-acetate).
3. Techniques and Protocols for Assessing MyocardialViability
a. 201Tl Stress RedistributionThe uptake of 201Tl is an energy-dependent process requir-
ing intact cell membrane integrity, and the presence of 201Tlimplies preserved myocyte cellular viability. The redistribu-tion properties of 201Tl have been used as an important markerof myocardial viability in stress imaging followed by a 3- to4-hour redistribution image. The presence of a reversibleperfusion defect and/or preserved 201Tl uptake on the 3- to4-hour redistribution images is an important sign of regionalviability.
b. 201Tl ReinjectionThe 2 most widely studied protocols for assessing viability
in the presence of an inconclusive result on initial stress/redistribution imaging involve 201Tl reinjection and late redis-tribution imaging. The presence of a severe 201Tl defect afterreinjection identifies areas with a very low probability ofimprovement in function.
c. Late Redistribution ImagingAlthough improvement in uptake on late redistribution
images (24 to 48 hours after the initial stress 201Tl injection)has good positive predictive value for identifying regionswith potential improvement in function, the negative predic-tive value is suboptimal in some patients.
d. 201Tl Rest RedistributionThe identification of a “reversible resting defect” (in 3- to
4-hour versus 15- to 20-minute images) generally reflectspreserved viability. The finding appears to be an insensitivethough specific sign of potential improvement in regionalfunction.
e. 99mTc-Sestamibi and TetrofosminAlthough the 99mTc-based tracers sestamibi and tetrofosmin
do not share the redistribution properties of 201Tl, theirperformance characteristics for predicting improvement inregional function after revascularization appear to be similarto those seen with 201Tl.
f. PET ImagingPositron tracers of blood flow and metabolism have been
extensively studied for evaluation of myocardial viability.The most commonly used PET protocol involves evaluationof myocardial glucose metabolism with 18F-FDG in conjunc-tion with PET or SPECT examination of MBF with 13N-ammonia or 99mTc-sestamibi, respectively. This approachappears to have slightly better overall accuracy for predictingrecovery of regional function after revascularization than dosingle-photon techniques (48). The magnitude of improve-ment in heart failure symptoms after revascularization inpatients with LV dysfunction correlates with the preoperativeextent of 18F-FDG “mismatch” pattern (49).
Table 5 lists recommendations for the use of radionuclidetechniques to assess myocardial viability.
4. Image Interpretation for Myocardial Viability:Quantitative Versus Visual Analysis of Tracer ActivitiesWhether quantitative analysis of tracer uptake in radionuclidetechniques is required for assessing viability is not estab-lished. Visual analyses need to be at least semiquantitative,accounting for defect severity.
5. Comparison of TechniquesAll radionuclide techniques (and dobutamine echocardiography)perform in a relatively similar manner with regard to positiveand negative predictive values for predicting improvements inregional function (48). A meta-analysis of outcome studies
TABLE 5. Recommendations for the Use of Radionuclide Techniques to Assess Myocardial Viability
Indication Test Class Level of Evidence
1. Predicting improvement in regional andglobal LV function after revascularization
Stress/redistribution/reinjection 201TlRest-redistribution imaging
Perfusion plus PET FDG imagingResting sestamibi imaging
Gated SPECT sestamibi imagingLate 201Tl redistribution imaging
(after stress)Dobutamine RNAPostexercise RNA
Postnitroglycerin RNA
IIII
IIaIIb
IIbIIbIIb
BBBBBB
CCC
2. Predicting improvement in heart failuresymptoms after revascularization.
Perfusion plus PET FDG imaging IIa B
3. Predicting improvement in natural historyafter revascularization
201Tl imaging (rest-redistribution andstress/redistribution/reinjection)
Perfusion plus PET FDG imaging
I
I
B
B
FDG indicates flurodeoxyglucose; PET, positron emission tomography; RNA, radionuclide angiography; SPECT, single-photonemission computed tomography; 201Tl, thallium-201.
1328 Klocke et al. JACC Vol. 42, No. 7, 2003ACC/AHA Guidelines for Cardiac Radionuclide Imaging October 1, 2003:1318–33

related to myocardial viability has demonstrated no differenceamong techniques commonly used to assess viability (PETversus single-photon radionuclide versus dobutamine echocar-diography) with regard to reduction of mortality or unfavorablecardiac events after revascularization (47).
E. Etiologies of Heart Failure
1. Dilated CardiomyopathyTable 6 lists recommendations for the use of radionuclideimaging to diagnose specific causes of dilatedcardiomyopathy.
2. Dilated Cardiomyopathy Due to Doxorubicin/Anthracycline CardiotoxicityRNA is an ideal noninvasive tool to provide longitudinalquantitative assessment of LV function in patients receivingdoxorubicin and other anthracyclines such as epirubicin. EFshould be measured in all patients before receiving doxoru-bicin; those with pre-existing heart disease and/or LV dys-function are at greater risk of congestive heart failure.Continued use of doxorubicin after LV dysfunction hasdeveloped causes progressive chamber dilatation and deteri-oration in systolic function. Therapy with trastuzumab, amonoclonal antibody directed against the HER2 receptor,
may increase the risk of developing heart failure duringstandard-dose doxorubicin therapy (50). Radionuclide evalu-ation of EF is also important in monitoring the cardioprotec-tive effects of agents such as dexrazoxane when doxorubicinis used in high dosages for solid malignant tumors (51).
3. Dilated Cardiomyopathy Due to MyocarditisRadioisotope imaging has been reported to identify myocar-ditis of diverse etiologies with gallium (which detects inflam-mation), antimyosin antibody (which detects myocardialnecrosis and is myosin specific), and metaiodobenzylguani-dine (MIBG; which assesses adrenergic neuronal function).The usefulness of radionuclide imaging to detect myocarditisin heart failure patients is not well established, however, anddata describing use of this approach are based on nonrandom-ized studies.
4. Posttransplantation Rejection and AllograftVasculopathy111In antimyosin antibody imaging has been described as atechnique to detect rejection after cardiac transplantation insmall observational studies. Because of many false-positiveresults, endomyocardial biopsy continues to be the techniqueof choice for serial monitoring and detection of acute rejec-tion. Radionuclide evaluation of allograft vasculopathy, the
TABLE 7. Recommendations for the Use of Radionuclide Imaging to EvaluateHypertrophic Heart Disease
Indication Test ClassLevel ofEvidence
1. Diagnosis of CAD in hypertrophiccardiomyopathy
Rest and exerciseperfusion imaging
IIb B
2. Diagnosis and serial monitoring ofhypertensive hypertrophic heart disease
Rest RNA IIb B
3. Diagnosis and serial monitoring ofhypertrophic cardiomyopathy, with andwithout outflow obstruction
Rest RNA III B
CAD indicates coronary artery disease; RNA, radionuclide angiography.
TABLE 6. Recommendations for the Use of Radionuclide Imaging to Diagnose Specific Causes ofDilated Cardiomyopathy
Indication Test ClassLevel ofEvidence
1. Baseline and serial monitoring of LV functionduring therapy with cardiotoxic drugs (eg,doxorubicin)
Rest RNA I A
2. RV dysplasia Rest RNA IIa B
3. Assessment of posttransplant obstructive CAD Exercise perfusion imaging IIb B
4. Diagnosis and serial monitoring of Chagasdisease
Exercise perfusion imaging IIb B
5. Diagnosis of amyloid heart disease 99mTc-pyrophosphate imaging IIb B
6. Diagnosis and serial monitoring of sarcoidheart disease
Rest perfusion imagingRest 67Ga imaging
IIbIIb
BB
7. Detection of myocarditis Rest 67Ga imaging111In antimyosin antibody imaging
IIbIIb
BC
67Ga indicates gallium-67; 99mTc-pyrophosphate, Tc-99m-pyrophosphate; 111In, indium-111; CAD, coronary artery disease; LV, leftventricular; RNA, radionuclide angiography; RV, right ventricular.
1329JACC Vol. 42, No. 7, 2003 Klocke et al.October 1, 2003:1318–33 ACC/AHA Guidelines for Cardiac Radionuclide Imaging

major limitation for long-term survival in transplant recipi-ents, is limited by variable sensitivity and specificity. ASPECT study with no reversible perfusion defects may beuseful in excluding coronary lesions appropriate for revascu-larization (52).
5. Chagas Myocarditis and/or CardiomyopathyChagas myocarditis and/or cardiomyopathy has several dis-tinctive features in comparison with dilated cardiomyopathydue to presumed viral myocarditis. Observational studiesusing RNA and perfusion imaging have reported that chronicChagas cardiomyopathy is frequently associated with LVregional wall motion abnormalities and perfusion defects inthe absence of epicardial CAD, and RV dyssynergy iscommon in asymptomatic patients with no other clinical signsof heart failure (53). In correlative investigations, there hasbeen a topographic association between regional defects insympathetic denervation detected by 123I-MIBG imaging andperfusion defects detected by 201Tl imaging (54).
6. Sarcoid Heart DiseaseMyocardial SPECT with 99mTc-sestamibi has been used todetect myocardial involvement in patients with sarcoidosis.Perfusion defects are more common in the RV than the in LVand correlate with atrioventricular block, heart failure, andventricular tachycardia of RV origin (55). These defects arefrequently reversible, which makes it unlikely that theyrepresent deposition of granulomata or fibrosis. 67Ga wasformerly used in sarcoidosis as a marker of the activity andextent of the disease and for predicting the efficacy ofcorticosteroids, but it has been largely superseded by serialchest CT and pulmonary function tests.
7. Cardiac AmyloidosisRadionuclide angiography enables assessment of diastolicand systolic function, including peak filling rates and LVfilling volumes during rapid filling and atrial contraction,respectively (56). 131I-MIBG imaging has indicated a highincidence of sympathetically denervated but viable myocar-dium (57). Although 99mTc-pyrophosphate imaging has beenreported to have diagnostic utility, echocardiography appearsto be more useful because it enables complete characteriza-tion of the altered LV and RV myocardium, as well asvalvular and pericardial involvement.
8. RV DysplasiaThe RV in arrhythmogenic RV dysplasia is characterized bymarked dilatation and depressed EF, which can be readilyidentified with RV RNA (58).
9. Hypertrophic CardiomyopathyRadionuclide angiographic studies are not usually indicatedin the diagnosis of hypertrophic cardiomyopathy. Chest painis a frequent symptom, raising the possibility of coexistentCAD. However, fixed and reversible exercise-induced myo-cardial perfusion defects suggesting scar or ischemia occur inthe absence of significant epicardial coronary artery stenoses.Reversible perfusion defects may reflect ischemia related todiminished coronary flow reserve or decreased sympathoneu-ral function in hypertrophied areas. Table 7 lists recommen-dations for the use of radionuclide imaging to evaluatehypertrophic heart disease.
10. Hypertensive Heart DiseaseRNA allows recognition of abnormal diastolic and systolicfunction in hypertensive subjects, even when resting systolicglobal function and regional function are normal. A signifi-cant proportion of such patients have hypertensive hypertro-phic heart disease.
Hypertension is common in patients presenting with chestpain for stress testing in whom CAD is suspected. The role ofstress perfusion imaging in patients with and without LVHhas been covered in the section on Chronic Syndromes.
11. Valvular Heart Disease
a. Diagnosis and Risk StratificationIn daily practice, 2D Doppler echocardiography studies
have become the modality of choice for diagnosing valvularheart disease. The potential usefulness of RNA in assessingvalvular heart disease stems from the ability of RNA toquantify LV and RV function. In addition, myocardial per-fusion imaging has been used to examine for the presence offlow-limiting coronary disease, especially in aortic stenosis.
b. Aortic StenosisBecause of the lack of specificity and sensitivity of angina
for the concomitant presence of coronary disease in aortic
TABLE 8. Recommendations for the Use of Radionuclide Imaging in Valvular Heart Disease
Indication Test ClassLevel ofEvidence
1. Initial and serial assessment of LV and RV function Rest RNA I B
2. Initial and serial assessment of LV function Exercise RNA IIb B
3. Assessment of the copresence of coronary disease MPI IIb B
LV indicates left ventricular; RNA, radionuclide imaging angiography; RV, right ventricular; MPI, myocardial perfusion imaging.
TABLE 9. Recommendations for the Use of RadionuclideImaging in Adults With Congenital Heart Disease
Indication Test ClassLevel ofEvidence
1. Initial and serial assessment ofLV and RV function
Rest RNA I B
2. Shunt detection and quantification FPRNA IIa B
FPRNA indicates first-pass radionuclide angiography; LV, left ventricular; RV,right ventricular; RNA, radionuclide angiography.
1330 Klocke et al. JACC Vol. 42, No. 7, 2003ACC/AHA Guidelines for Cardiac Radionuclide Imaging October 1, 2003:1318–33

stenosis, there has been much interest in the use of myocar-dial perfusion imaging in preoperative evaluation. The sen-sitivity and specificity of stress perfusion are relatively goodbut probably not adequate for patients about to undergo valvesurgery. Thus, in practice, perfusion imaging has not sup-planted coronary angiography in the preoperative work-up ofpatients with aortic stenosis.
c. Aortic RegurgitationThe most promising use of RNA in valvular heart disease
initially appeared to be in the evaluation of patients withaortic regurgitation, in whom a failure of EF to rise duringexercise seemed to mark the onset of LV dysfunction andpredict a poorer prognosis or indicate that the asymptom-atic patient would soon become symptomatic (59). Subse-quent studies indicated that exercise angiography does notusually add additional prognostic information to the mea-surement of resting LVEF and end-systolic dimension inpredicting the response to aortic valve replacement (60).Enhanced prognostic ability of exercise RNA has beenreported when the calculation of systolic wall stress isadded (61).
d. Mitral RegurgitationPerhaps the most compelling current use of RNA in
valvular heart disease is in the preoperative evaluation ofpatients with mitral regurgitation. The echocardiogramdoes not evaluate RV function well, whereas RV functionassessment is a strength of RNA. As with aortic regurgi-tation, resting EF is a useful guide to valve repair orreplacement. Again, however, Doppler echocardiographycan make this assessment and add other anatomic andprognostic information. RNA is useful postoperatively ingauging changes in LV and RV performance. Table 8 listsrecommendations for the use of radionuclide imaging invalvular heart disease.
12. Adults With Congenital Heart DiseaseAs in other forms of heart disease, RNA can be usedeffectively to assess RV and LV systolic performance. Inaddition, left-to-right shunting causes persistently high levelsof activity in the lung or RV during FPRNA because of earlyrecirculation. The resultant time-activity curve can be used tocalculate pulmonary to systemic flow ratios. The earlyappearance of tracer in the left chambers of the heart can beused to detect right-to-left shunts. 99mTc RNA appears to beuseful in evaluating abnormal lung flow after the Fontan andGlenn procedures (62).
In general, however, radionuclide studies are now utilizedinfrequently in assessing congenital heart disease and areunlikely to be accurate if performed only occasionally. Table9 lists recommendations for the use of radionuclide imagingin adults with congenital heart disease.
References1. Braunwald E, Antman E, Beasley J. ACC/AHA 2002 guideline update
for the management of patients with unstable angina and non–ST-segment elevation myocardial infarction: a report of the AmericanCollege of Cardiology/American Heart Association Task Force onPractice Guidelines (Committee to Update Guidelines on the Man-agement of Patients with Unstable Angina). 2002; American Collegeof Cardiology Web site. Available at: http://www.acc.org/clinical/guidelines/unstable/incorporated/UA_incorporated.pdf. AccessedJune 12, 2003.
2. Stowers SA, Eisenstein EL, Th Wackers FJ, et al. An economic analysisof an aggressive diagnostic strategy with single photon emissioncomputed tomography myocardial perfusion imaging and early exercisestress testing in emergency department patients who present with chestpain but nondiagnostic electrocardiograms: results from a randomizedtrial. Ann Emerg Med 2000;35:17–25.
3. Udelson JE, Beshansky JR, Ballin DS, et al. Myocardial perfusionimaging for evaluation and triage of patients with suspected acutecardiac ischemia: a randomized controlled trial. JAMA 2002;288:2693–700.
4. Ryan TJ, Antman EL, Brooks NH, et al. ACC/AHA guidelines for themanagement of patients with acute myocardial infarction: 1999 update: areport of the American College of Cardiology/American Heart Asso-ciation Task Force on Practice Guidelines (Committee on Management ofAcute Myocardial Infarction). 1999; American College of CardiologyWeb site. Available at: http://www.acc.org/clinical/guidelines/nov96/1999/amipdf99.pdf. Accessed July 30, 2002.
5. Basu S, Senior R, Dore C, et al. Value of thallium-201 imaging indetecting adverse cardiac events after myocardial infarction andthrombolysis: a follow up of 100 consecutive patients. BMJ 1996;313:844–8.
6. Brown KA, Heller GV, Landin RS, et al. Early dipyridamole (99m)Tc-sestamibi single photon emission computed tomographic imaging 2 to 4days after acute myocardial infarction predicts in-hospital and postdis-charge cardiac events: comparison with submaximal exercise imaging.Circulation 1999;100:2060–6.
7. Dakik HA, Mahmarian JJ, Kimball KT, et al. Prognostic value of exercise201Tl tomography in patients treated with thrombolytic therapy duringacute myocardial infarction. Circulation 1996;94:2735–42.
8. Shaw LJ, Eagle KA, Gersh BJ, et al. Meta-analysis of intravenousdipyridamole-thallium-201 imaging (1985 to 1994) and dobutamineechocardiography (1991 to 1994) for risk stratification before vascularsurgery. J Am Coll Cardiol 1996;27:787–98.
9. Verani MS. Risk stratifying patients who survive an acute myocardialinfarction. J Nucl Cardiol 1998;5:96–108.
10. Bodenheimer MM, Wackers FJ, Schwartz RG, et al. Prognostic signif-icance of a fixed thallium defect one to six months after onset of acutemyocardial infarction or unstable angina. Multicenter Myocardial Ische-mia Research Group. Am J Cardiol 1994;74:1196–200.
11. Kroll D, Farah W, McKendall GR, et al. Prognostic value of stress-gatedTc-99m sestamibi SPECT after acute myocardial infarction. Am J Cardiol2001;87:381–6.
12. Miller DD, Stratmann HG, Shaw L, et al. Dipyridamole technetium 99msestamibi myocardial tomography as an independent predictor of cardiacevent-free survival after acute ischemic events. J Nucl Cardiol 1994;1:72–82.
13. Brown KA. Prognostic value of thallium-201 myocardial perfusionimaging in patients with unstable angina who respond to medicaltreatment. J Am Coll Cardiol 1991;17:1053–7.
14. Stratmann HG, Younis LT, Wittry MD, et al. Exercise technetium-99mmyocardial tomography for the risk stratification of men with medicallytreated unstable angina pectoris. Am J Cardiol 1995;76:236–40.
15. Gibbons RJ, Chatterjee K, Daley J, et al. ACC/AHA 2002 guidelineupdate for the management of patients with chronic stable angina: a reportof the American College of Cardiology/American Heart Association TaskForce on Practice Guidelines (Committee to Update the 1999 ChronicStable Angina Guidelines). 2002; American College of Cardiology Website. Available at: http://www.acc.org/clinical/guidelines/stable/stable_clean.pdf. Accessed August 20, 2002.
16. Hendel RC, Corbett JR, Cullom SJ, et al. The value and practice ofattenuation correction for myocardial perfusion SPECT imaging: a jointposition statement from the American Society of Nuclear Cardiology andthe Society of Nuclear Medicine. J Nucl Cardiol 2002;9:135–43.
17. Sharir T, Germano G, Kang X, et al. Prediction of myocardial infarctionversus cardiac death by gated myocardial perfusion SPECT: risk strati-fication by the amount of stress- induced ischemia and the poststressejection fraction. J Nucl Med 2001;42:831–7.
18. Hachamovitch R, Hayes S, Friedman JD, et al. Determinants of risk andits temporal variation in patients with normal stress myocardial perfusionscans: what is the warranty period of a normal scan? J Am Coll Cardiol2003;41:1329–40.
19. Akinboboye OO, Idris O, Onwuanyi A, et al. Incidence of major cardio-vascular events in black patients with normal myocardial stress perfusionstudies. J Nucl Cardiol 2001;8:541–7.
20. Alkeylani A, Miller DD, Shaw LJ, et al. Influence of race on the pre-diction of cardiac events with stress technetium-99m sestamibi tomo-
1331JACC Vol. 42, No. 7, 2003 Klocke et al.October 1, 2003:1318–33 ACC/AHA Guidelines for Cardiac Radionuclide Imaging

graphic imaging in patients with stable angina pectoris. Am J Cardiol1998;81:293–7.
21. Liao Y, Cooper RS, McGee D, et al. The relative effects of left ventricularhypertrophy, coronary artery disease, and ventricular dysfunction onsurvival among black adults. JAMA 1995;273:1592–7.
22. Gibbons RJ, Balady GJ, Bricker JT, et al. ACC/AHA 2002 guidelineupdate for exercise testing: a report of the American College of Cardiol-ogy/American Heart Association Task Force on Practice Guidelines(Committee on Exercise Testing). 2003; American College of CardiologyWeb site. Available at: http://www.acc.org/clinical/guidelines/exercise/exercise_clean.pdf. Accessed February 26, 2003.
23. Amanullah AM, Kiat H, Friedman JD, et al. Adenosine technetium-99msestamibi myocardial perfusion SPECT in women: diagnostic efficacy indetection of coronary artery disease. J Am Coll Cardiol 1996;27:803–9.
24. Berman DS, Kang X, Hayes SW, et al. Adenosine myocardial per-fusion single-photon emission computed tomography in womencompared with men: impact of diabetes mellitus on incremental prog-nostic value and effect on patient management. J Am Coll Cardiol2003;41:1125–33.
25. Iskandrian AE, Heo J, Nallamothu N. Detection of coronary arterydisease in women with use of stress single-photon emission computedtomography myocardial perfusion imaging. J Nucl Cardiol 1997;4:329–35.
26. Taillefer R, DePuey EG, Udelson JE, et al. Comparative diagnosticaccuracy of Tl-201 and Tc-99m sestamibi SPECT imaging (perfusion andECG-gated SPECT) in detecting coronary artery disease in women. J AmColl Cardiol 1997;29:69–77.
27. Mark DB, Shaw L, Harrell FE Jr., et al. Prognostic value of a treadmillexercise score in outpatients with suspected coronary artery disease.N Engl J Med 1991;325:849–53.
28. Gibbons RJ, Hodge DO, Berman DS, et al. Long-term outcome ofpatients with intermediate-risk exercise electrocardiograms who do nothave myocardial perfusion defects on radionuclide imaging. Circulation1999;100:2140–5.
29. Hachamovitch R, Berman DS, Kiat H, et al. Exercise myocardial per-fusion SPECT in patients without known coronary artery disease: incre-mental prognostic value and use in risk stratification. Circulation 1996;93:905–14.
30. Shaw LJ, Hachamovitch R, Peterson ED, et al. Using an outcomes-basedapproach to identify candidates for risk stratification after exercisetreadmill testing. J Gen Intern Med 1999;14:1–9.
31. Gil VM, Almeida M, Ventosa A, et al. Prognosis in patients with leftbundle branch block and normal dipyridamole thallium-201 scintigraphy.J Nucl Cardiol 1998;5:414–7.
32. Wagdy HM, Hodge D, Christian TF, et al. Prognostic value of vasodilatormyocardial perfusion imaging in patients with left bundle-branch block.Circulation 1998;97:1563–70.
33. Elhendy A, van Domburg RT, Sozzi FB, et al. Impact of hypertension onthe accuracy of exercise stress myocardial perfusion imaging for thediagnosis of coronary artery disease. Heart 2001;85:655–61.
34. Bartram P, Toft J, Hanel B, et al. False-positive defects in technetium-99m sestamibi myocardial single-photon emission tomography in healthyathletes with left ventricular hypertrophy. Eur J Nucl Med 1998;25:1308–12.
35. Amanullah AM, Berman DS, Kang X, et al. Enhanced prognostic strat-ification of patients with left ventricular hypertrophy with the use ofsingle-photon emission computed tomography. Am Heart J 2000;140:456–62.
36. Hilton TC, Shaw LJ, Chaitman BR, et al. Prognostic significance ofexercise thallium-201 testing in patients aged greater than or equal to 70years with known or suspected coronary artery disease. Am J Cardiol1992;69:45–50.
37. Grundy SM, Pasternak R, Greenland P, et al. Assessment of cardio-vascular risk by use of multiple-risk-factor assessment equations: astatement for healthcare professionals from the American Heart Asso-ciation and the American College of Cardiology. Circulation 1999;100:1481–92.
38. Diabetes mellitus: a major risk factor for cardiovascular disease. A jointeditorial statement by the American Diabetes Association; The NationalHeart, Lung, and Blood Institute; The Juvenile Diabetes FoundationInternational; The National Institute of Diabetes and Digestive andKidney Diseases; and The American Heart Association. Circulation 1999;100:1132–3.
39. Giri S, Shaw LJ, Murthy DR, et al. Impact of diabetes on the riskstratification using stress single-photon emission computed tomography
myocardial perfusion imaging in patients with symptoms suggestive ofcoronary artery disease. Circulation 2002;105:32–40.
40. Kang X, Berman DS, Lewin HC, et al. Incremental prognostic value ofmyocardial perfusion single photon emission computed tomography inpatients with diabetes mellitus. Am Heart J 1999;138:1025–32.
41. Wackers FJ, Zaret BL. Detection of myocardial ischemia in patients withdiabetes mellitus. Circulation 2002;105:5–7.
42. Miller DD, Donohue TJ, Younis LT, et al. Correlation of pharmacological99mTc-sestamibi myocardial perfusion imaging with poststenotic coro-nary flow reserve in patients with angiographically intermediate coronaryartery stenoses. Circulation 1994;89:2150–60.
43. Miller TD, Christian TF, Hodge DO, et al. Prognostic value of exercisethallium-201 imaging performed within 2 years of coronary artery bypassgraft surgery. J Am Coll Cardiol 1998;31:848–54.
44. Lauer MS, Lytle B, Pashkow F, et al. Prediction of death and myocardialinfarction by screening with exercise-thallium testing after coronary-artery-bypass grafting. Lancet 1998;351:615–22.
45. Zellweger MJ, Lewin HC, Lai S, et al. When to stress patients aftercoronary artery bypass surgery? Risk stratification in patients earlyand late post-CABG using stress myocardial perfusion SPECT: impli-cations of appropriate clinical strategies. J Am Coll Cardiol 2001;37:144 –52.
46. Eagle KA, Berger PB, Calkins H, et al. ACC/AHA guideline update forperioperative cardiovascular evaluation for noncardiac surgery: a reportof the American College of Cardiology/American Heart Association TaskForce on Practice Guidelines (Committee to Update the 1996 Guidelineson Perioperative Cardiovascular Evaluation for Noncardiac Surgery).2002; American College of Cardiology Web site. Available at: http://www.acc.org/clinical/guidelines/perio/clean/pdf/perio_pdf.pdf. AccessedJune 11, 2002.
47. Allman KC, Shaw LJ, Hachamovitch R, et al. Myocardial viability testingand impact of revascularization on prognosis in patients with coronaryartery disease and left ventricular dysfunction: a meta-analysis. J Am CollCardiol 2002;39:1151–8.
48. Bax JJ, Wijns W, Cornel JH, et al. Accuracy of currently availabletechniques for prediction of functional recovery after revascularization inpatients with left ventricular dysfunction due to chronic coronary arterydisease: comparison of pooled data. J Am Coll Cardiol 1997;30:1451–60.
49. Di Carli MF, Davidson M, Little R, et al. Value of metabolic imagingwith positron emission tomography for evaluating prognosis in patientswith coronary artery disease and left ventricular dysfunction. Am JCardiol 1994;73:527–33.
50. Feldman AM, Lorell BH, Reis SE. Trastuzumab in the treatment ofmetastatic breast cancer: anticancer therapy versus cardiotoxicity. Circu-lation 2000;102:272–4.
51. Lopez M, Vici P, Di Lauro K, et al. Randomized prospective clinicaltrial of high-dose epirubicin and dexrazoxane in patients withadvanced breast cancer and soft tissue sarcomas. J Clin Oncol 1998;16:86 –92.
52. Carlsen J, Toft JC, Mortensen SA, et al. Myocardial perfusion scin-tigraphy as a screening method for significant coronary artery stenosisin cardiac transplant recipients. J Heart Lung Transplant 2000;19:873– 8.
53. Marin-Neto JA, Bromberg-Marin G, Pazin-Filho A, et al. Cardiacautonomic impairment and early myocardial damage involving the rightventricle are independent phenomena in Chagas’ disease. Int J Cardiol1998;65:261–9.
54. Simoes MV, Pintya AO, Bromberg-Marin G, et al. Relation of regionalsympathetic denervation and myocardial perfusion disturbance to wallmotion impairment in Chagas’ cardiomyopathy. Am J Cardiol 2000;86:975–81.
55. Eguchi M, Tsuchihashi K, Hotta D, et al. Technetium-99m sestamibi/tetrofosmin myocardial perfusion scanning in cardiac and noncardiacsarcoidosis. Cardiology 2000;94:193–9.
56. Hongo M, Fujii T, Hirayama J, et al. Radionuclide angiographicassessment of left ventricular diastolic filling in amyloid heart disease: astudy of patients with familial amyloid polyneuropathy. J Am CollCardiol 1989;13:48–53.
57. Tanaka M, Hongo M, Kinoshita O, et al. Iodine-123 metaiodobenzylgua-nidine scintigraphic assessment of myocardial sympathetic innervation inpatients with familial amyloid polyneuropathy. J Am Coll Cardiol 1997;29:168–74.
58. Le Guludec D, Gauthier H, Porcher R, et al. Prognostic value of radio-nuclide angiography in patients with right ventricular arrhythmias. Cir-culation 2001;103:1972–6.
1332 Klocke et al. JACC Vol. 42, No. 7, 2003ACC/AHA Guidelines for Cardiac Radionuclide Imaging October 1, 2003:1318–33

59. Borer JS, Bacharach SL, Green MV, et al. Exercise-induced left ventric-ular dysfunction in symptomatic and asymptomatic patients with aorticregurgitation: assessment by radionuclide cineangiography. Am J Cardiol1978;42:351–7.
60. Bonow RO, Lakatos E, Maron BJ, et al. Serial long-term assessment of thenatural history of asymptomatic patients with chronic aortic regurgitation andnormal left ventricular systolic function. Circulation 1991;84:1625–35.
61. Borer JS, Hochreiter C, Herrold EM, et al. Prediction of indications forvalve replacement among asymptomatic or minimally symptomatic
patients with chronic aortic regurgitation and normal left ventricularperformance. Circulation 1998;97:525–34.
62. Pruckmayer M, Zacherl S, Salzer-Muhar U, et al. Scintigraphic assessment ofpulmonary and whole-body blood flow patterns after surgical intervention incongenital heart disease. J Nucl Med 1999;40:1477–83.
KEY WORDS: ACC/AHA Guidelines � imaging � radioisotopes � testing
1333JACC Vol. 42, No. 7, 2003 Klocke et al.October 1, 2003:1318–33 ACC/AHA Guidelines for Cardiac Radionuclide Imaging

LETTERS TO THE EDITOR
Is the Tolerability of Long-TermThiazolidinedione Therapy Overstated?The study by Tang et al. (1) concluded that their retrospectivechart review demonstrated the tolerability of long-term thiazo-lidinedione (TZD) therapy in a diabetic population with estab-lished chronic heart failure (HF). Although we applaud theirefforts to study this important topic, we believe the data presentedare not so clear, and that their conclusions that a large majority ofchronic HF patients tolerate these agents are overstated.
First, we believe the definition of TZD-related fluid retention,as a 10-pound weight gain from baseline, in addition to signs orsymptoms of volume overload, is far too exclusive of important levelsof fluid retention. By using this cut-off, we can be sure that thosepatients had severe fluid retention. However, we do not know thenumber of other patients who had important levels of weight gain oredema and who were missed by the investigators’ likely insensitivecriteria. Heart failure guidelines recommend action when weightincreases by 2 to 4 pounds depending on how quickly it occurs.
Second, we disagree that the reported incidence of fluid reten-tion of 17.1% is an overestimate due to selection bias. In fact, it isprobably an underestimate. Obtaining data from a chart review canonly lead to under-reporting the true incidence of fluid retentionand adverse events. Furthermore, the majority of patients hadstable New York Heart Association functional class I or II heartfailure where TZD therapy is not contraindicated. (The incidenceof edema [with or without weight gain] in TZD randomizedcontrolled trials ranged between 2% and 15% [2,3].)
Third, the intolerability of these agents in this population isfurther illustrated by the fact that 31% discontinued TZD therapywithin one year of initiation (most due to fluid retention), whereasthe rate of discontinuation was far �0.1% in randomized con-trolled trials (2,3). Also of concern is that 26% of patients who metthe criteria for fluid retention were hospitalized. Finally, we areconcerned that both the data and the discussion regarding theincidence of fluid retention and characteristics of the non-TZDcontrol group were very limited. This data would likely providemore insight into the true tolerability of these medications in thispopulation.
In summary, we agree that further studies are needed toexamine the relationship between TZD-related fluid retention andpatient cardiac status. We believe this study and its conclusionsshould be interpreted very carefully, as the true risks of adverseeffects related to volume expansion are likely understated.
Robb M. Malone, PharmD, CDE, CPPUniversity of North Carolina School of MedicineDivision of General Internal Medicine5039 Old Clinic BuildingCB #7110Chapel Hill, NC 27599-7110E-mail: [email protected]
Darren A. DeWalt, MD, MPHMike P. Pignone, MD, MPHTimothy J. Ives, PharmD, MPH
doi:10.1016/S0735-1097(03)00995-1
REFERENCES
1. Tang WHW, Francis GS, Hoogwerf BJ, Young JB. Fluid retentionafter initiation of thiazolidinedione therapy in diabetic patients withestablished chronic heart failure. J Am Coll Cardiol 2003;41:1394–8.
2. GlaxoSmithKline Pharmaceuticals. Avandia (rosiglitazone) packageinsert. Research Triangle Park, NC: 2001.
3. Takeda Pharmaceuticals America. Actos (pioglitazone) package insert.Lincolnshire, IL: 2002.
REPLY
We appreciate the comments by Dr. Malone and his colleaguesregarding our recent report on the characteristics of fluid retentionafter initiation of thiazolidinedione (TZD) therapy in diabeticpatients with established chronic heart failure (HF). In our report,we fully acknowledged that fluid retention does occur with TZDuse in patients with established HF, and until we have moreexperience with this drug class “there is little doubt thatTZDs. . .should be avoided in highly symptomatic patients withHF who are already having difficulty maintaining a balancedvolume status” (1). Although we recognize that the definition offluid retention is arbitrary, there is currently no gold standard for“important levels of fluid retention.” We chose the 10-pound limitto account for the long-term, nonedematous weight gain associ-ated with TZD use that has been previously reported in theliterature (2). It is noteworthy that 68% of patients received 12months of TZD therapy without demonstrating significant fluidretention. Also, 20% of patients in our cohort had TZD discon-tinued owing to reasons other than edema. Until we have moreobjective measures to quantify the degree of fluid retention (such assequential plasma volume analyses or surrogate markers like plasmaB-type natriuretic peptide levels), observations of this nature canonly rely on “insensitive” clinical criteria.
The selection bias in this retrospective observational studyoriginated from the referral nature of the specialized HF clinic,where a large number of patients are seen specifically because offluid retention following TZD initiation. Meanwhile, the non-TZD user “control” group in our study was used in a nestedcase-controlled manner to illustrate the discrepancy in clinicalpresentation between TZD-related fluid retention and what wecommonly consider to be HF exacerbation independent of TZDuse. As stated in our discussion, the incomplete nature of retro-spective data collection precludes any statistical comparisons be-tween groups (including drug tolerability) so as to avoid falseinferences. Although we agree that any association between TZD-related fluid retention and patient’s cardiac status should beinterpreted with caution, we argue against the proscription of thisdrug class in patients with HF simply by equating fluid retentionwith HF exacerbation. What is more alarming to us is the paucityof published reports in this area (limited to sporadic case reports)over the past few years despite widespread recognition of themetabolic syndrome and the potential benefits of this class of drugsin such patients. The true incidence of TZD-related fluid reten-tion and TZD tolerability in patients with HF can only bedetermined by well-designed prospective studies specifically ad-dressing patients with HF.
Journal of the American College of Cardiology Vol. 42, No. 7, 2003© 2003 by the American College of Cardiology Foundation ISSN 0735-1097/03/$30.00Published by Elsevier Inc.

W.H. Wilson Tang, MDDepartment of Cardiovascular MedicineCleveland Clinic Foundation9500 Euclid AvenueDesk F25Cleveland, OH 44195E-mail: [email protected]
Gary S. Francis, MD, FACCByron J. Hoogwerf, MDJames B. Young, MD, FACC
doi:10.1016/S0735-1097(03)00996-3
REFERENCES
1. Tang WHW, Francis GS, Hoogwerf BJ, Young JB. Fluid retentionafter initiation of thiazolidinedione therapy in diabetic patients withestablished chronic heart failure. J Am Coll Cardiol 2003;41:1394–8.
2. Larsen TM, Toubro S, Astrup A. PPARgamma agonists in thetreatment of type II diabetes: is increased fatness commensurate withlong-term efficacy? Int J Obes Relat Metab Disord 2003;27:147–61.
Is Diastolic Heart FailureSynonymous With Heart FailureWith Preserved Ejection Fraction?In his excellent Editorial Comment, Dr. Zile states that “heartfailure with a preserved ejection fraction” and “diastolic heartfailure” are synonymous (1). Respectfully, I must disagree. Not allpatients with diastolic heart failure have left ventricular hypertro-phy. Therefore, the general applicability of the study cited sup-porting the equivalency of the two terms might be limited becauseall patients in that study had echocardiographic evidence for leftventricular hypertrophy, and diastolic dysfunction is generallyaccepted to precede hypertrophy. In our early experience aboutone-third of patients with heart failure with a preserved ejectionfraction had explanations for the signs and symptoms of failureother than diastolic dysfunction, predominately right heart failuredue to pulmonary disease and regurgitant valvular heart disease (2).The nonspecific nature of the symptoms of heart failure andiatrogenic volume overload were also noted. It is unclear to whatextent stricter diagnostic criteria for heart failure would affect thesefindings, and I believe that our initial criteria would still lead mostclinicians to the diagnosis of heart failure. Furthermore, a patientwith heart failure due to chronic, severe mitral regurgitation withan ejection fraction of 40% or even 50% has predominately systolic,not diastolic, heart failure. Therefore, I believe it is best toconclude that patients with “diastolic heart failure” form a sub-group of patients with “heart failure with a preserved ejectionfraction.”
Until a uniformly accepted and therapeutically meaningfulmeasure of diastolic dysfunction is defined, diastolic heart failure isin many ways a diagnosis of exclusion. The value of initially usingthe term “heart failure with preserved, or normal, ejection fraction”underscores the need to define left ventricular function in virtuallyall patients with heart failure (3) as well as the need to carefullyeliminate other cardiac and noncardiac possibilities from thepatient’s signs and symptoms. After eliminating other possibilities,I agree that the term “diastolic heart failure” seems most appro-priate, and I hope, as Dr. Zile does, that accepting the term
promotes the investigative efforts that are long overdue for thesepatients.
Kenneth M. Kessler, MDUniversity of Miami School of MedicineDivision of Cardiology26 William Howard DriveGlen Mills, PA 19342E-mail: [email protected]
doi:10.1016/S0735-1097(03)00997-5
REFERENCES
1. Zile MR. Heart failure with preserved ejection fraction: is this diastolicheart failure? J Am Coll Cardiol 2003;41:1519–22.
2. Echeverria HH, Bilsker MS, Myerburg RJ, Kessler KM. Congestiveheart failure: echocardiographic insights. Am J Med 1983;75:750–5.
3. Hunt SA, Baker DW, Chin MH, et al. ACC/AHA guidelines for theevaluation and management of chronic heart failure in the adult:executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Com-mittee to Revise the 1995 Guidelines for the Evaluation and Manage-ment of Heart Failure). J Am Coll Cardiol 2001;38:2101–13.
REPLY
One of the first, if not the first, study to use the term “diastolicheart failure” was by Dr. Kessler in 1988 (1). His report was trulyinnovative and showed remarkable insight into a difficult clinicalproblem. I enthusiastically agree with Dr. Kessler’s point of viewand I am grateful to receive his support. In his letter to the editorof the JACC, he raises three important issues: 1) some patients withdiastolic heart failure do not have left ventricular (LV) hypertro-phy; 2) the diagnosis of diastolic heart failure should excludepatients with noncardiac (such as pulmonary disease) and othercardiac (such as mitral stenosis, regurgitant valve disease) causes ofheart failure; and 3) left ventricular (LV) function must bemeasured in every patient with heart failure.
In the study that Dr. Kessler refers to in his letter (2), only aboutone-third of the patients had LV hypertrophy defined as LV mass�125 g/m2. However, all patients had concentric hypertrophicremodeling characterized by a decreased LV end diastolicvolume/mass ratio or LV end diastolic dimension/wall thicknessratio or an increased relative wall thickness. I believe that amajority of patients with diastolic heart failure in fact haveeither concentric remodeling or some other evidence of myo-cardial or cardiac structural alterations such as an enlarged leftatrium. With or without concentric remodeling, if a patienttruly has objective signs and symptoms of heart failure andnoncardiac and other cardiac causes have been ruled out, thenheart failure with a normal ejection fraction (EF) is caused bydiastolic dysfunction and the appellation “diastolic heart failure”should be applied.
Dr. Kessler correctly points out that in patients with primaryright heart failure (caused by chronic lung disease, pulmonicstenosis, tricuspid regurgitation) or mitral stenosis or left-sidedregurgitant valvular disease, this can result in heart failure with anormal EF. I am grateful that Dr. Kessler emphasized this pointbecause our previous publications (2,3) did not make it explicitlyclear that we had in fact excluded patients with noncardiac andother cardiac causes of heart failure in this study patient cohort.
1335JACC Vol. 42, No. 7, 2003 Letters to the EditorOctober 1, 2003:1334–7

It is critical that LV function, both systolic and diastolic, bemeasured in every patient with heart failure. The advent of tissueDoppler (and other echo-Doppler techniques) has made it easierand more practical to identify abnormalities in diastolic function.Nonetheless, precise and comprehensive assessment of diastolicfunction requires the use of invasive catheterization techniques.However, if noncardiac and other cardiac causes of heart failure areexcluded, the remaining patients with heart failure and a normalEF all have abnormalities of diastolic function making measure-ment of diastolic function confirmatory rather than a mandatorycomponent of diagnostic criteria.
Finally, I join Dr. Kessler in his enthusiastic use of the term“diastolic heart failure” and renew my editorial plea: “Stop thediscrimination against the term diastolic heart failure.”
Michael R. Zile, MDCardiology/MedicineMedical University of South Carolina135 Rutledge AvenueSuite 816P.O. Box 250592Charleston, SC 29425E-mail: [email protected]
doi:10.1016/S0735-1097(03)00998-7
REFERENCES
1. Kessler KM. Heart failure with normal systolic function. Arch InternMed 1988;148:2109–11.
2. Zile MR, Gaasch WH, Carroll JD, et al. Heart failure with a normalejection fraction. Is measurement of diastolic function necessary to makethe diagnosis of diastolic heart failure? Circulation 2001;104:779–82.
3. Zile MR. Heart failure with preserved ejection fraction: is this diastolicheart failure? J Am Coll Cardiol 2003;41:1519–22.
Determination of the NaturalHistory of Aspirin Resistance AmongStable Patients With Cardiovascular DiseaseWe read with interest the recent study by Gum et al. (1) regardingaspirin resistance. Their results, in particular the focus on long-term follow-up, offer important information in the confusing butclinically important area of aspirin resistance. They were able toshow that, by using standard light-transmittance aggregometry ina population of patients already on aspirin therapy, the response totwo different platelet agonists could predict long-term outcome.However, in these investigators’ original study of baseline aspirinresponsiveness in this identical patient population, a point-of-caretest, the platelet function analyzer (PFA)-100, was also used todetermine aspirin responsiveness along with light transmittanceaggregometry (2). In the first study, minimal correlation betweenthe two methods was found. It is unclear to us, though, whylong-term outcomes based on baseline aspirin responsiveness asdetermined by the PFA-100 were not also included in their presentreport. Clearly the routine determination of aspirin responsivenesswill depend upon the ability to measure it with a point-of-caredevice. Therefore, whether or not the PFA-100 results correlatedwith long-term clinical outcomes would have important implica-tions regarding its utility in that role. The importance of thisquestion is highlighted in the editorial following the Gum et al. (3)
study as well as in a recent review of the topic, as both suggest thatthe PFA-100 may be well suited for the routine determination ofaspirin resistance (3,4). However, this would likely not be the caseif PFA-100 results were found to not have any clinical relevance interms of future thrombotic events.
Steven R. SteinhublUniversity of North CarolinaDivision of CardiologyCB #7075Chapel Hill, NC 27599E-mail: [email protected]
Jay S. Varinasi, MDLee Goldberg, MD
doi:10.1016/S0735-1097(03)00999-9
REFERENCES
1. Gum PA, Kottke-Marchant K, Welsh PA, White J, Topol EJ. Aprospective, blinded determination of the natural history of aspirinresistance among stable patients with cardiovascular disease. J Am CollCardiol 2003;41:961–5.
2. Gum PA, Kottke-Marchant K, Poggio ED, et al. Profile and prevalenceof aspirin resistance in patients with cardiovascular disease. Am JCardiol 2001;88:230–5.
3. Eikelboom JW, Hankey G. Aspirin resistance: a new independentpredictor of vascular events. J Am Coll Cardiol 2003;41:966–8.
4. McKee SA, Sane DC, Deliargyris EN. Aspirin resistance in cardiovas-cular disease: a review of prevalence, mechanisms, and clinical signifi-cance. Thromb Haemost 2002;88:711–5.
REPLY
We appreciate and share the interest of Dr. Varinasi and colleaguesin aspirin resistance and its clinical relevance. Previously, wedocumented the profile and prevalence of aspirin resistance instable patients with cardiovascular disease (1). In this initial study,we used both optical platelet aggregation, which we consider to bethe gold standard for the determination of platelet reactivity in thepresence of aspirin, and a rapid, whole-blood assay, the plateletfunction analyzer (PFA)-100, to determine the prevalence ofaspirin resistance. The kappa statistic between these two methodswas 0.1 (95% confidence interval 0.045 to 0.246), indicating a poorcorrelation between optical platelet aggregation and the PFA-100in detection of aspirin resistance.
In our more recently published work (2), we reported anincreased risk of death, myocardial infarction (MI), or strokeassociated with aspirin resistance as determined by optical plateletaggregation. In analysis, long-term outcomes (death/MI/stroke)were not related to aspirin resistance status as determined by thePFA-100 (12.9% aspirin sensitive vs. 15.1% aspirin resistant, p �0.4). These findings seem to indicate that the PFA-100 is not asspecific a test as compared to optical platelet aggregation fordetermining clinically relevant aspirin resistance. In fact, thissupposition may be supported by the poor kappa statistic betweenthe two tests. However, prior to categorically drawing this conclu-sion, one must acknowledge the real possibility of a type II error.Although there may be no statistical association between thePFA-100 and clinical outcomes in our investigation, a real asso-ciation may have been missed by the small sample size of our study.
1336 Letters to the Editor JACC Vol. 42, No. 7, 2003October 1, 2003:1334–7

As reported, our study did demonstrate aspirin resistance asmeasured by optical platelet aggregation to be independentlypredictive of poor long-term outcomes, but further work is neededin this area. Larger studies evaluating more widely availablepoint-of-care tests are needed to define a test that has both ease ofuse and clinical relevance.
Eric J. Topol, MDThe Cleveland Clinic FoundationDepartment of Cardiovascular Medicine9500 Euclid Avenue, F-25Cleveland, OH 44195E-mail: [email protected]
Patricia Gum, MDKandice Kottke-Marchant, MD
doi:10.1016/S0735-1097(03)01000-3
REFERENCES
1. Gum PA, Kottke-Marchant K, Poggio ED, et al. Profile and prevalenceof aspirin resistance in patients with cardiovascular disease. Am JCardiol 2001;88:230–5.
2. Gum PA, Kottke-Marchant K, Welsh PA, White J, Topol EJ. Aprospective, blinded determination of the natural history of aspirinresistance among stable patients with cardiovascular disease. J Am CollCardiol 2003;41:961–5.
1337JACC Vol. 42, No. 7, 2003 Letters to the EditorOctober 1, 2003:1334–7
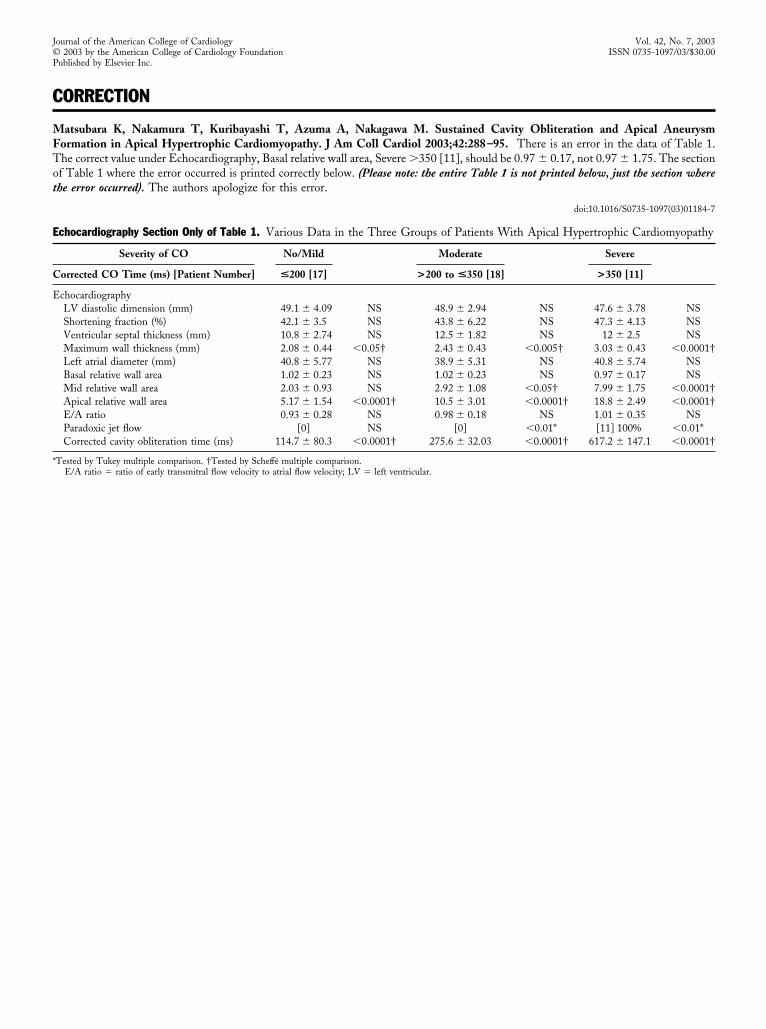
CORRECTION
Matsubara K, Nakamura T, Kuribayashi T, Azuma A, Nakagawa M. Sustained Cavity Obliteration and Apical AneurysmFormation in Apical Hypertrophic Cardiomyopathy. J Am Coll Cardiol 2003;42:288 –95. There is an error in the data of Table 1.The correct value under Echocardiography, Basal relative wall area, Severe �350 [11], should be 0.97 � 0.17, not 0.97 � 1.75. The sectionof Table 1 where the error occurred is printed correctly below. (Please note: the entire Table 1 is not printed below, just the section wherethe error occurred). The authors apologize for this error.
doi:10.1016/S0735-1097(03)01184-7
Echocardiography Section Only of Table 1. Various Data in the Three Groups of Patients With Apical Hypertrophic Cardiomyopathy
Severity of CO No/Mild Moderate Severe
Corrected CO Time (ms) [Patient Number] <200 [17] >200 to <350 [18] >350 [11]
EchocardiographyLV diastolic dimension (mm) 49.1 � 4.09 NS 48.9 � 2.94 NS 47.6 � 3.78 NSShortening fraction (%) 42.1 � 3.5 NS 43.8 � 6.22 NS 47.3 � 4.13 NSVentricular septal thickness (mm) 10.8 � 2.74 NS 12.5 � 1.82 NS 12 � 2.5 NSMaximum wall thickness (mm) 2.08 � 0.44 �0.05† 2.43 � 0.43 �0.005† 3.03 � 0.43 �0.0001†Left atrial diameter (mm) 40.8 � 5.77 NS 38.9 � 5.31 NS 40.8 � 5.74 NSBasal relative wall area 1.02 � 0.23 NS 1.02 � 0.23 NS 0.97 � 0.17 NSMid relative wall area 2.03 � 0.93 NS 2.92 � 1.08 �0.05† 7.99 � 1.75 �0.0001†Apical relative wall area 5.17 � 1.54 �0.0001† 10.5 � 3.01 �0.0001† 18.8 � 2.49 �0.0001†E/A ratio 0.93 � 0.28 NS 0.98 � 0.18 NS 1.01 � 0.35 NSParadoxic jet flow [0] NS [0] �0.01* [11] 100% �0.01*Corrected cavity obliteration time (ms) 114.7 � 80.3 �0.0001† 275.6 � 32.03 �0.0001† 617.2 � 147.1 �0.0001†
*Tested by Tukey multiple comparison. †Tested by Scheffe multiple comparison.E/A ratio � ratio of early transmitral flow velocity to atrial flow velocity; LV � left ventricular.
Journal of the American College of Cardiology Vol. 42, No. 7, 2003© 2003 by the American College of Cardiology Foundation ISSN 0735-1097/03/$30.00Published by Elsevier Inc.
Copyright © 2022 FDOKUMEN




















