
Reliability and diagnostic accuracy of clinical special tests for myelopathy in patients seen for...
11
RESEARCH ARTICLE Reliability and Diagnostic Accuracy of Clinical Tests of Vestibular Function for Children Jennifer B. Christy, PT, PhD; JoAnne Payne, MA, CCC-A; Andres Azuero, PhD, MBA; Craig Formby, PhD Department of Physical Therapy, School of Health Professions (Dr Christy), and Department of Community Health, Outcomes and Systems, School of Nursing (Dr Azuero), The University of Alabama at Birmingham, Birmingham, Alabama; Department of Communicative Disorders (Ms Payne and Dr Formby), College of Arts and Sciences, The University of Alabama, Tuscaloosa, Alabama. Purpose: To determine reliability, diagnostic values, and minimal detectable change scores, 90% confidence (MDC 90 ) of pediatric clinical tests of vestibular function. Methods: Twenty children with severe to profound bilateral sensorineural hearing loss and 23 children with typical development, aged 6 to 12 years, participated. The Head Thrust Test, Emory Clinical Vestibular Chair Test, Bucket Test, Dynamic Visual Acuity, Modified Clinical Test of Sensory Interaction on Balance, and Sensory Organization Test were completed twice for reliability. Reference standard diagnostic tests were rotary chair and vestibular evoked myogenic potential. Reliability, sensitivity, specificity, predictive values, likelihood ratios, and MDC 90 scores were calculated. Results: Reliability ranged from an intraclass correlation coefficient of 0.73 to 0.95. Sensitivity, specificity, and predictive values, using cutoff scores for each test representing the largest area under the curve, ranged from 63% to 100%. The MDC 90 for Dynamic Visual Acuity and Modified Clinical Test of Sensory Interaction on Balance were 8 optotypes and 16.75 seconds, respectively. Conclusions: Clinical tests can be used accurately to identify children with vestibular hypofunction. (Pediatr Phys Ther 2014;26:180–190) Key words: child, diagnostic tests/standards, postural balance, reproducibility of results, ROC curves, sensitivity and specificity, sensorineural hearing loss, vestibular function tests INTRODUCTION The reported incidence of vestibular-related deficits in children has grown. 1,2 Impairments identified in this group are poor gaze stability with head movement, as well as delayed development of postural control and motor skills. 3-6 These impairments persist and progress through- out childhood, adversely affecting high-level gross mo- tor function, reading ability, and school performance. 7-11 0898-5669/110/2602-0180 Pediatric Physical Therapy Copyright C 2014 Wolters Kluwer Health | Lippincott Williams & Wilkins and Section on Pediatrics of the American Physical Therapy Association Correspondence: Jennifer B. Christy, PT, PhD, Department of Physical Therapy, The University of Alabama at Birmingham, 1720 2nd Ave S, SHPB 360X, Birmingham, AL 35294 ([email protected]). Grant Support: This study was funded by a research grant from the Section on Pediatrics, awarded to Dr Christy. The authors declare no conflicts of interest. DOI: 10.1097/PEP.0000000000000039 Although studies demonstrate the effectiveness of vestibu- lar exercise in children with hypofunction, 3,12,13 vestibular function is rarely tested because simple inexpensive clini- cal tests of vestibular function have not been developed for children. Because of the known adverse effect of vestibu- lar impairment on motor function, postural control, and stability of gaze, there is a pressing need for valid, reliable, and simple tests to assess children’s peripheral vestibular system integrity. The development of valid and reliable testing tools for pediatric assessment is warranted because of increas- ing reports of vestibular dysfunction in children, including benign positional vertigo, 14 vestibular neuronitis, 15,16 oti- tis media, 17 and drug-induced vestibulopathy. 18 Variabil- ity of reported incidence of vestibular hypofunction (VH) (30%-100%) in children with sensorineural hearing loss (SNHL) exists because of differences in study populations and vestibular testing. 19-23 Cushing et al 20,21 measured vestibular function by using reference standard tests of caloric, rotary chair and vestibular evoked myogenic potential (VEMP). 24 Caloric testing detects unilateral vestibular hypofunction (UVH) of Copyright © 2014 Wolters Kluwer Health | Lippincott Williams & Wilkins and the Section on Pediatrics of the American Physical Therapy Association. Unauthorized reproduction of this article is prohibited. 180 Christy et al Pediatric Physical Therapy
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Reliability and diagnostic accuracy of clinical special tests for myelopathy in patients seen for...

R E S E A R C H A R T I C L E
Reliability and Diagnostic Accuracyof Clinical Tests of VestibularFunction for ChildrenJennifer B. Christy, PT, PhD; JoAnne Payne, MA, CCC-A; Andres Azuero, PhD, MBA; Craig Formby, PhD
Department of Physical Therapy, School of Health Professions (Dr Christy), and Department of Community Health,Outcomes and Systems, School of Nursing (Dr Azuero), The University of Alabama at Birmingham, Birmingham,Alabama; Department of Communicative Disorders (Ms Payne and Dr Formby), College of Arts and Sciences, TheUniversity of Alabama, Tuscaloosa, Alabama.
Purpose: To determine reliability, diagnostic values, and minimal detectable change scores, 90% confidence(MDC90) of pediatric clinical tests of vestibular function. Methods: Twenty children with severe to profoundbilateral sensorineural hearing loss and 23 children with typical development, aged 6 to 12 years, participated.The Head Thrust Test, Emory Clinical Vestibular Chair Test, Bucket Test, Dynamic Visual Acuity, Modified ClinicalTest of Sensory Interaction on Balance, and Sensory Organization Test were completed twice for reliability.Reference standard diagnostic tests were rotary chair and vestibular evoked myogenic potential. Reliability,sensitivity, specificity, predictive values, likelihood ratios, and MDC90 scores were calculated. Results: Reliabilityranged from an intraclass correlation coefficient of 0.73 to 0.95. Sensitivity, specificity, and predictive values,using cutoff scores for each test representing the largest area under the curve, ranged from 63% to 100%. TheMDC90 for Dynamic Visual Acuity and Modified Clinical Test of Sensory Interaction on Balance were 8 optotypesand 16.75 seconds, respectively. Conclusions: Clinical tests can be used accurately to identify children withvestibular hypofunction. (Pediatr Phys Ther 2014;26:180–190) Key words: child, diagnostic tests/standards,postural balance, reproducibility of results, ROC curves, sensitivity and specificity, sensorineural hearing loss,vestibular function tests
INTRODUCTION
The reported incidence of vestibular-related deficitsin children has grown.1,2 Impairments identified in thisgroup are poor gaze stability with head movement, aswell as delayed development of postural control and motorskills.3-6 These impairments persist and progress through-out childhood, adversely affecting high-level gross mo-tor function, reading ability, and school performance.7-11
0898-5669/110/2602-0180Pediatric Physical TherapyCopyright C© 2014 Wolters Kluwer Health | Lippincott Williams &Wilkins and Section on Pediatrics of the American Physical TherapyAssociation
Correspondence: Jennifer B. Christy, PT, PhD, Department of PhysicalTherapy, The University of Alabama at Birmingham, 1720 2nd Ave S,SHPB 360X, Birmingham, AL 35294 ([email protected]).
Grant Support: This study was funded by a research grant from theSection on Pediatrics, awarded to Dr Christy.
The authors declare no conflicts of interest.
DOI: 10.1097/PEP.0000000000000039
Although studies demonstrate the effectiveness of vestibu-lar exercise in children with hypofunction,3,12,13 vestibularfunction is rarely tested because simple inexpensive clini-cal tests of vestibular function have not been developed forchildren. Because of the known adverse effect of vestibu-lar impairment on motor function, postural control, andstability of gaze, there is a pressing need for valid, reliable,and simple tests to assess children’s peripheral vestibularsystem integrity.
The development of valid and reliable testing toolsfor pediatric assessment is warranted because of increas-ing reports of vestibular dysfunction in children, includingbenign positional vertigo,14 vestibular neuronitis,15,16 oti-tis media,17 and drug-induced vestibulopathy.18 Variabil-ity of reported incidence of vestibular hypofunction (VH)(30%-100%) in children with sensorineural hearing loss(SNHL) exists because of differences in study populationsand vestibular testing.19-23
Cushing et al20,21 measured vestibular function byusing reference standard tests of caloric, rotary chair andvestibular evoked myogenic potential (VEMP).24 Calorictesting detects unilateral vestibular hypofunction (UVH) of
Copyright © 2014 Wolters Kluwer Health | Lippincott Williams & Wilkins and the Section on Pediatrics of the American Physical TherapyAssociation. Unauthorized reproduction of this article is prohibited.
180 Christy et al Pediatric Physical Therapy

the horizontal canal. Caloric testing is a potentially fright-ening experience for children since cold and warm watermust be placed in the ear, which elicits vertigo.25 The rotarychair test also evaluates horizontal canal function. It usesnatural rotational stimulation to detect bilateral vestibu-lar hypofunction (BVH) and is tolerated by most children.Vestibular evoked myogenic potential tests the saccule,which contributes to the vestibulospinal system and pos-tural control.24 Pediatric normative data are available forthe rotary chair and VEMP tests.26–28 Cushing et al20 foundthat 9 of 9 children with profound deafness following bac-terial meningitis had VH. Their balance scores, measuredusing the balance subscale of the Bruininks-Oseretsky Testof Motor Proficiency, were less than that of peers who werenot hearing impaired and children with SNHL but normalvestibular function. In a separate study, Cushing et al21
tested 153 children with congenital and acquired SNHL ofvarying etiologies and found that 50% had measurable VH;37% of these children had severe VH or areflexia.
Clinical tests of the vestibulo-ocular reflex or hori-zontal canal function include the Head Thrust Test (HTT;response to head turns right/left), the Dynamic Visual Acu-ity test (DVA; acuity difference with head still and movingat 2 Hz), and the Emory Clinical Vestibular Chair Test(ECVCT; time of nystagmus following rotations in thedark). A clinical test of utricular function is the BucketTest of subjective visual vertical (SVV): ability to perceivea line as vertical in the absence of visual cues. Althoughreliability and validity of these tests have been reported foradults,29-32 the only test with reported reliability, sensitiv-ity, and specificity for children is the DVA test.33,34 TheDVA test had good inter- and intratester reliability (intr-aclass correlation coefficient [ICC] = 0.94 and 0.84, re-spectively) and 100% sensitivity/specificity for identifyingchildren with confirmed BVH.33 The HTT had good sen-sitivity/specificity for adults with unilateral and bilateralcaloric weakness.29,30 The ECVCT had moderate to goodtest-retest, intrarater, and interrater reliability for adults(r > 0.70). Sensitivity was 78%, specificity was 92% foridentifying 5 adult subjects with VH.35 The Bucket Test isa low-technical version of the laser SVV that tests utricu-lar function. Zwergal et al31 reported that healthy adultswere able to perceive true vertical within 0.9 ± 0.7◦. Sub-jects with vestibular deficits perceived vertical within 8.9± 5.4◦. Inter- and intratester reliability of the Bucket Testwere r = 0.90 and r = 0.92, respectively.
Postural control involves input from the vestibular, vi-sual, and somatosensory systems. Studies have shown thatchildren with VH also have poor postural control.3,22 Aclinical test of postural control is the Sensory OrganizationTest (SOT). The SOT is not a direct measure of vestibu-lospinal function but determines how vestibular informa-tion is used to control posture.36 The ICC demonstratingreliability of the SOT was greater than 0.75 for childrenwith and without VH.37,38 However, many clinics do nothave access to the equipment required to complete theSOT. The Clinical Test of Sensory Interaction on Balance(CTSIB)39 was designed as a low-technical SOT and has
been used in studies of postural control in adults40,41 andchildren.42,43 The original test had 6 conditions to mimicSOT. A dome was used for sway-referenced visual condi-tions and thick foam for sway-referenced somatosensoryconditions. The pediatric version (P-CTSIB) also includedtandem and single-legged stance conditions.42,43 TheCTSIB was modified, dome conditions were removed, andthe test was validated for adults at risk for falls.41,44 Goodtest-retest and interrater reliability (r ≥ 0.75), and moder-ate correlations with SOT, were reported for adults.41,45,46
Reliability and validity of the Modified Clinical Test ofSensory Interaction on Balance (MCTSIB), without extraconditions used in the P-CTSIB, have not been establishedfor children.
The purpose of this preliminary study was to deter-mine reliability, sensitivity, specificity, predictive values,likelihood ratios, and cutoff scores for clinical tests ofvestibular function. The clinical tests (ie, HTT, BucketTest, DVA, MCTSIB, and ECVCT) were compared withreference standard tests (ie, VEMP and rotary chair) in asmall cohort of children with severe to profound SNHL.
METHODS
A convenience sample was recruited from the Birm-ingham, Alabama, community. To be included, subjectshad to be between 6 and 12 years of age and diagnosedwith severe to profound SNHL as determined by audio-metric testing. Subjects were excluded if they showed ev-idence of neurological, central visual, or musculoskeletalabnormalities, fear of darkness, motion sensitivity, or ahistory of neck trauma. Inclusion and exclusion criteriawere determined via phone interview with a parent be-fore the first testing session and via neuromuscular screen.Twenty children with severe to profound SNHL (mean age= 8.9 ± 1.8 years) and 23 children with typical develop-ment (mean age = 9.5 ± 2.9 years) participated (Table 1).The Institutional Review Boards at The University of Al-abama at Birmingham and The University of Alabama,Tuscaloosa, approved this study. Parents and children pro-vided informed consent.
Clinical Tests
After obtaining informed consent, subjects completed3 testing sessions. The first session began with a neuromus-cular screen composed of oculomotor tests (ie, smoothpursuit, saccades, vergence, ocular range of motion); cere-bellar tests (ie, rapid alternating movements, heel to shin);manual muscle testing and range of motion. Children withabnormal results were excluded.
The same examiner, with 20 years of pediatric physi-cal therapy experience and advanced training in vestibularrehabilitation, completed clinical tests (J.B.C.). Publishedmethods29 were used for HTT. Facing the subject at eyelevel, the examiner flexed the neck 30◦ to maximally stimu-late the horizontal canal. This was done using an imaginaryline between the lateral canthus of the eye and the external
Copyright © 2014 Wolters Kluwer Health | Lippincott Williams & Wilkins and the Section on Pediatrics of the American Physical TherapyAssociation. Unauthorized reproduction of this article is prohibited.
Pediatric Physical Therapy Clinical Tests of Vestibular Function for Children 181

TABLE 1Subject Characteristics
SNHL TD(n = 20) (n = 23)
Age in years, mean (SD) 8.9 (1.8) 9.5 (2.9)Gender, n
Male 14 10Female 6 13
Ethnicity, nWhite 16 22African American 1 1Hispanic 1 0Other 2 0
Hearing level, nBilateral profound 7Bilateral severe/profound 8Bilateral moderate/severe 5
Etiology of hearing loss, nConexin 26 4Enlarged vestibular aqueduct
syndrome2
Pendred syndrome 1Goldenhar syndrome 1Heredity 5Unknown 7
Cochlear implants, nBilateral 10Unilateral right 3None 7
Abbreviations: SNHL, sensorineural hearing loss; TD, typical develop-ment.
acoustic meatus. The subject attempted to keep the eyes onthe examiner’s nose, which was decorated with a sticker.The subject’s head was unpredictably and quickly turnedto the right and left from center at an amplitude of 5◦ to 10◦.The examiner watched for a corrective saccade followingeach HTT, and then the head was returned to center. Thismaneuver was randomly repeated 3 times in each direc-tion. The HTT was positive if at least 2 corrective saccadeswere observed to the right and/or the left.
Modified methods were used for the modified ECVCT(m-ECVCT).35 The subject sat in a rotating office chairwith the head centered and slightly flexed and eyes closed.The chair was rotated right for 30 seconds at 0.5 Hz, us-ing a metronome. This timing differed from the originaltest,35 which rotated adult subjects for 60 seconds. Duringdevelopment of the protocol before data collection began,it was determined that younger children became restlessand tried to open their eyes after 30 seconds. Therefore,after 30 seconds of rotation, the chair was stopped and thetimer started. The subject did not open the eyes until in-frared camera goggles were placed over the eyes, blockingfixation. The goggles were not placed on the eyes duringrotation to avoid damage to the goggle cables. Nystagmuswas observed on the monitor and timed until it subsided.The subject rested for 2 minutes or double the durationof nystagmus to dampen the effect of the first rotation.35
The test was then repeated to the left. All subjects receivedrightward and then leftward rotations. We used 2 examin-ers. One examiner rotated the chair and held the goggles
on the subject’s face. The other examiner timed durationof nystagmus. The examiners were trained by the primaryinvestigator (J.B.C.) and practiced before testing. To deter-mine interrater reliability, nystagmus was videorecordedso that raters could later watch and time the nystagmus.To determine whether or not goggles were necessary, thetest was repeated without goggles. After rotating with eyesclosed, the subject looked at a white sheet and nystagmuswas timed. Nystagmus was again videotaped so that in-terrater reliability could be determined later. Four trainedexaminers scored the videos, and scored the same videos1 week later. For intra- and interrater reliability of the m-ECVCT, fixation removed, 2 examiners scored the videos.
For the Bucket Test, a straight line was drawn intothe bottom of an opaque bucket (23.5-cm diameter and24-cm long). An angle finder was placed on the bottom ofthe bucket in the same plane as the line.31 Each subjectpracticed with the bucket held away from the face (ie,available visual cues) until the examiner was certain thatthe subject understood the task. Subjects also confirmedthat the only object they could see when the bucket washeld over the face was the line. After training, the subjectwas seated with eyes closed. The mouth of the bucket wasplaced around the subject’s face and the examiner turnedthe bucket to set the line off vertical. The subject thenopened the eyes. As the examiner slowly turned the bucket,the subject said “now” when the line reached vertical. Theangle of degrees and direction off 0◦ was recorded for 10trials of clockwise and counterclockwise rotations. Themean degrees off 0◦ and mode of direction tilted (ie, left,right, or straight) were calculated.
For the DVA test, the subject sat 10′ away from theLea Symbols (ie, house, circle, heart, and square) chart. Thechart had a total of 15 lines of 5 optotypes, ranging fromSnellen acuity levels of 20/200 to 20/8. The subject beganat an acuity level where all symbols on a line could be cor-rectly identified, and continued to identify progressivelysmaller symbols until no symbol could be identified.33 Thenumber of optotypes unable to be identified was static vi-sual acuity. For the DVA, the neck was flexed 30◦ by usingthe same anatomical landmarks as for the HTT, the headwas moved at 2 Hz (120◦ per second) to a metronome inthe yaw plane, and the number of unidentified optotypeswas recorded. The DVA was completed twice, averaged,and scored as the difference in optotypes missed betweenthe DVA and static visual acuity tests.
For the SOT, the subject wore a safety harness andstood on the SMART EquiTest platform (NeuroCom, adivision of Natus, Clackamas, Oregon). The subject stoodstill during 6 conditions: (1) stable platform, (2) stableplatform eyes closed, (3) sway-referenced visual surround,(4) sway-referenced platform, (5) sway-referenced plat-form eyes closed, and (6) sway-referenced visual surroundand platform. A blindfold was used for eyes closed condi-tions. Each condition lasted 20 seconds, and 3 trials werecompleted. On the basis of reports that children withhypofunction have low visual, vestibular, and somatosen-sory effectiveness ratios,3,47 these ratios were calculated as
Copyright © 2014 Wolters Kluwer Health | Lippincott Williams & Wilkins and the Section on Pediatrics of the American Physical TherapyAssociation. Unauthorized reproduction of this article is prohibited.
182 Christy et al Pediatric Physical Therapy

follows: somatosensory = 3/1; visual = 4/1; and vestibular= 5/1.48
For the MCTSIB, the subject stood barefoot with armsacross the chest and feet together for 30 seconds during 4conditions: (1) floor eyes opened; (2) floor eyes closed; (3)Neurocom foam eyes opened; and (4) Neurocom foam eyesclosed. A blindfold was used for eyes closed conditions. Oneyes opened conditions, subjects faced a white sheet. Threetrials of each condition were completed only if the subjectwas unable to complete the entire 30 seconds on the first orsecond trial. If the child completed 30 seconds on the firsttrial, a score of 30 seconds was given for that condition.The mean of the 3 trials was calculated for each conditionand then added for a total score (maximum = 120 seconds,30 seconds for each of the 4 conditions).
The HTT, Bucket Test, DVA, MCTSIB, and m-ECVCTwere completed a second time, 4 hours to 7 days later,for test-retest reliability. Some children were unable tobe tested on 2 separate days, whereas others preferred toreturn on a different day. Given the nature of the tests,we felt that 4 hours was sufficient time to negate effectsof the first testing session, and 7 days was short enoughto negate effects of maturation. Reference standard testswere completed within 1 month after the clinical testsby an audiologist with 24 years of experience, blinded toclinical test results. Reference standard test results werenot expected to change in 1 month.
Reference Standard Tests
The cervical VEMP (cVEMP) assessed the function ofthe saccule and inferior vestibular nerve following proto-cols previously reported.49,50 Before testing, subjects wereexamined with otoscopy and tympanometry to ensure theears were free of obstruction. Subjects sat in a semireclinedposition during the test. Following electrode placement,subjects turned the head to activate the sternocleidomas-toid. Electromyography with video feedback assured thatbaseline sternocleidomastoid muscle activity was between35 and 50 μV. Tone burst stimuli (ie, 500 Hz with 2-0-2rise-plateau-fall) were presented at 97 dB normal hearinglevel (nHL) or 105 dB nHL at a rate of 5 per second with rar-efaction polarity. One subject had complete atresia of bothear canals, requiring protocol modification. For this sub-ject, stimuli were presented via B71-10 bone conductionvibrator placed on the mastoid bone.51 Recordings wereamplified with a gain of 5000×, for a bandpass settingof 2 to 250 Hz, and time window of 30 millisecond. Theinitial positive and negative peaks were marked, and theP1-N1 amplitude asymmetry ratio was calculated. Subjectresponses were compared with normative data.27,52 Re-sponses greater than 2 SDs from the normative mean wereconsidered positive.
Oculomotor tests, laser SVV, and sinusoidal harmonicacceleration (SHA) were completed as was step rotationtesting using a Neuro Kinetics, Inc (Pittsburgh, Pennsyl-vania) Rotary Chair with VEST 6.10 software. Videonys-tagmography measured eye movements through infrared
cameras on I-Portal 100-Hz binocular video oculographygoggles. Subjects were seated in a chair with a computer-controlled motor within a closed booth in complete dark-ness. If necessary, small children sat in the lap of an adult.Calibration of eye movement was performed before test-ing. An adult investigator sat in the darkened room andused a radio for communication with the audiologist, whovisually monitored the test via infrared cameras. Alertingtasks were used.12,27,28
Oculomotor tests (ie, smooth pursuit, saccades, andoptokinetic nystagmus) were completed to rule out centralvisual problems. The gain and accuracy of eye movementswere compared with pediatric normative data (Neuro Ki-netics, Inc). The SVV paradigm was based on previouslyreported methods.53 The subject practiced the techniquein room light until he or she understood. In completedarkness, the subject set the off-vertical laser line to per-ceived vertical, using buttons that rotated the line clock-wise or counterclockwise in 0.1◦ increments. The subjectsaid “now” when he or she perceived that the line wasvertical. The test was repeated 5 times to each side andresponses were averaged.
Rotary chair tests included the SHA and step rota-tions to measure horizontal canal function. The subject’shead was pitched forward 30◦ and gently immobilized.For the SHA test, 5 frequencies were examined (ie, 0.01,0.04, 0.08, 0.16, and 0.64 Hz) at 60◦ per second over 3to 9 cycles. Data included phase, gain, and asymmetry ofthe vestibulo-ocular reflex response. Step rotation testingincluded a series of complete chair rotations to both theright and left (ie, 100◦ per second for 60 seconds). Pre- andpostrotary time constants (ie, the amount of time requiredfor nystagmus to decrease to 37% of its original strength)were measured. Results were compared with normativedata and scored as follows: (1) negative, within 1.5 SDs ofthe comparative sample mean; (2) bilateral loss (positive),reduced gain values outside the comparative range; and (3)unilateral loss (also positive), abnormal phase and asym-metry values in the presence of normal gain values.12,27,28
If either the rotary chair (ie, SHA, step rotation) or cVEMPtests were positive, the vestibular result was classified as a“positive” diagnosis. Subjective visual vertical was not usedfor classification due to lack of pediatric normative data.
Data Analysis
Descriptive statistics were computed for participantcharacteristics and clinical tests scores. For each clinicaltest, a receiver operating characteristic curve determinedoptimal cutoff scores for classification of VH as diagnosedby reference standard tests. The area under the ROCcurve (AUC) was tabulated for comparison of accuracyamong clinical tests. The closer an AUC to the maximumvalue of 1, the more accurate the test. After cutoff scoreswere determined, cross-tabulations between hypofunctionstatus and clinical test results were conducted to estimatethe frequencies of true positive (TP), false positive (FP),true negative (TN), and false negative (FN) classifications.
Copyright © 2014 Wolters Kluwer Health | Lippincott Williams & Wilkins and the Section on Pediatrics of the American Physical TherapyAssociation. Unauthorized reproduction of this article is prohibited.
Pediatric Physical Therapy Clinical Tests of Vestibular Function for Children 183
Measures of sensitivity (TP/(TP+FN)), specificity(TN/(TN+FP)), positive predictive value (TP/(TP+FP)),negative predictive value (TN/(TN+FN)), positive like-lihood ratio (sensitivity/(1 − specificity)) and negativelikelihood ratio ((1 − sensitivity)/specificity), and 95%confidence intervals (CIs) were computed. The Delta logitmethod54 and the method by Simel et al55 were used toestimate proportion and likelihood ratio CIs, respectively.Repeated assessments estimated test-retest reliability andinterrater reliability with the ICC;56 95% CIs for thesemeasures were computed with the Fisher z transforma-tion. Pearson correlations were used to examine linearassociations. To determine the minimal detectable change(90% confidence) (MDC90), the following formula was
applied:57 MDC90 = 1.65 × pooled SD ×√
(2[1 − ICC]).Analyses were conducted using SAS version 9.3 (SASInstitute, Cary, North Carolina).
RESULTS
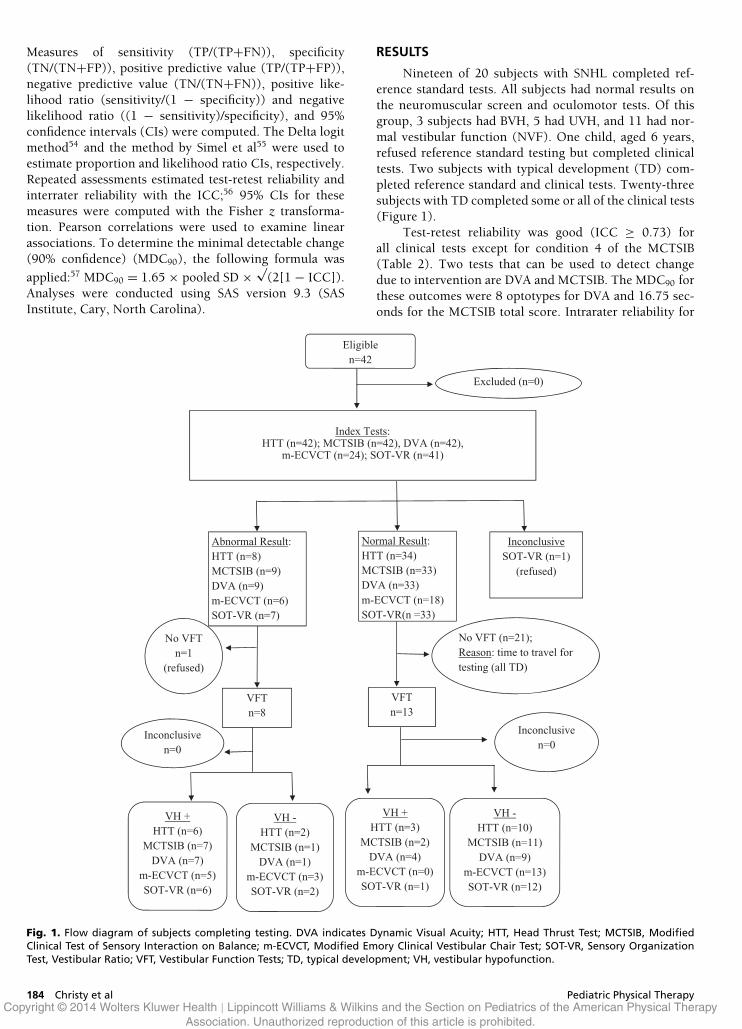
Nineteen of 20 subjects with SNHL completed ref-erence standard tests. All subjects had normal results onthe neuromuscular screen and oculomotor tests. Of thisgroup, 3 subjects had BVH, 5 had UVH, and 11 had nor-mal vestibular function (NVF). One child, aged 6 years,refused reference standard testing but completed clinicaltests. Two subjects with typical development (TD) com-pleted reference standard and clinical tests. Twenty-threesubjects with TD completed some or all of the clinical tests(Figure 1).
Test-retest reliability was good (ICC ≥ 0.73) forall clinical tests except for condition 4 of the MCTSIB(Table 2). Two tests that can be used to detect changedue to intervention are DVA and MCTSIB. The MDC90 forthese outcomes were 8 optotypes for DVA and 16.75 sec-onds for the MCTSIB total score. Intrarater reliability for
Eligible n=42
Excluded (n=0)
Index Tests: HTT (n=42); MCTSIB (n=42), DVA (n=42),
m-ECVCT (n=24); SOT-VR (n=41)
Abnormal Result: HTT (n=8) MCTSIB (n=9) DVA (n=9) m-ECVCT (n=6) SOT-VR (n=7)
Normal Result: HTT (n=34) MCTSIB (n=33) DVA (n=33) m-ECVCT (n=18) SOT-VR(n =33)
Inconclusive SOT-VR (n=1)
(refused)
No VFT n=1
(refused)
No VFT (n=21); Reason: time to travel for testing (all TD)
VFT n=8
VFT n=13
Inconclusive n=0
Inconclusive n=0
VH + HTT (n=6)
MCTSIB (n=7) DVA (n=7)
m-ECVCT (n=5) SOT-VR (n=6)
VH - HTT (n=2)
MCTSIB (n=1) DVA (n=1)
m-ECVCT (n=3) SOT-VR (n=2)
VH + HTT (n=3)
MCTSIB (n=2) DVA (n=4)
m-ECVCT (n=0) SOT-VR (n=1)
VH - HTT (n=10)
MCTSIB (n=11) DVA (n=9)
m-ECVCT (n=13) SOT-VR (n=12)
Fig. 1. Flow diagram of subjects completing testing. DVA indicates Dynamic Visual Acuity; HTT, Head Thrust Test; MCTSIB, ModifiedClinical Test of Sensory Interaction on Balance; m-ECVCT, Modified Emory Clinical Vestibular Chair Test; SOT-VR, Sensory OrganizationTest, Vestibular Ratio; VFT, Vestibular Function Tests; TD, typical development; VH, vestibular hypofunction.
Copyright © 2014 Wolters Kluwer Health | Lippincott Williams & Wilkins and the Section on Pediatrics of the American Physical TherapyAssociation. Unauthorized reproduction of this article is prohibited.
184 Christy et al Pediatric Physical Therapy

TABLE 2Test-Retest Reliability
Name of Test n (TD) n (SNHL) ICC (95% CI)
HTT, +/− 17 20 0.73 (0.53-0.85)DVA score, # optotypes 15 20 0.81 (0.66-0.90)m-ECVCT room light, total seconds
left + right4 18 0.88 (0.75-0.95)
m-ECVCT fixation removed, totalseconds left + right
5 15 0.95 (0.88-0.98)
MCTSIB total score, s 18 20 0.74 (0.55-0.86)MCTSIB condition 4, s 18 20 0.56 (0.15-0.77)Bucket Test, mean degrees off
center15 20 0.74 (0.49-0.87)
Bucket Test Direction, most oftentilted: right, left, straight
15 20 κ : 0.24 (0.00-0.49)
Abbreviations: CI, confidence interval; DVA, Dynamic Visual Acuity; HTT, Head Thrust Test; ICC, intraclass correlation coefficient; κ , kappa; MCTSIB,modified clinical test of sensory interaction for balance; m-ECVCT, modified Emory Clinical Vestibular Chair Test; SNHL, sensorineural hearing loss;TD, typical development.
the m-ECVCT in room light was good for the 4 raters. TheICC ranged from 0.76 (95% CI, 0.51-0.89) to 0.97 (95%CI, 0.92-0.99). However, interrater reliability was poor forthe 4 raters on the m-ECVCT room light. The ICC rangedfrom 0.37 (95% CI, 0.10-0.62) for left rotations to 0.40(95% CI, 0.13-0.65) for right rotations. Intra- and inter-rater reliability was high for 2 raters on m-ECVCT withfixation removed; ICC = 0.86 (95% CI, 0.67-0.93) for left+ right rotations.
Moderate to good correlations were found betweenthe m-ECVCT fixation removed, the m-ECVCT room light,and the rotary chair time constant. The m-ECVCT roomlight total score correlated with the m-ECVCT fixation re-moved total score (r = 0.59 [95% CI, 0.22-0.80]). Them-ECVCT fixation removed after spinning right/left cor-related moderately with the rotary chair time constant afterspinning right/left—right: r = 0.66 (95% CI, 0.31-0.84);left: r = 0.81 (95% CI, 0.55-0.92). A fair correlation wasfound between SOT composite scores and the MCTSIB to-tal scores (r = 0.37; P = .02). However, a moderate to goodcorrelation was found between the MCTSIB total scoresand SOT vestibular ratios (r = 0.58; P < .001). The cor-relation between the Bucket Test mean degrees off centerand laser SVV mean scores was not statistically significant(r = −0.34; P = .13).
Means and SDs for all clinical tests are provided inTable 3. The optimal cutoff scores to predict hypofunctionfor clinical tests, on the basis of the AUC, are summarizedin Table 4. Positive and negative likelihood ratios with CIsare provided in Table 5. Except for the Bucket Test, allclinical tests had an AUC ranging from 0.64 to 0.89. TheBucket Test had an AUC of 0.55, indicating slightly betterthan chance prediction of hypofunction. The highestoverall values were obtained with the HTT (sensitivity= 75%; specificity = 91%), the MCTSIB total score(sensitivity = 88%; specificity = 85%), the m-ECVCTfixation removed (sensitivity = 63%; specificity = 100%),the SOT vestibular ratio (sensitivity = 75%; specificity= 92%), and the DVA (sensitivity = 88%; specificity =
69%). Likelihood ratio CIs were wide because of the lowprevalence of hypofunction in the sample.
All 5 subjects with UVH had a laser SVV result greaterthan 2◦, tilted to the lesioned side in all but 1 subject. Onesubject with BVH had an abnormal laser SVV. Forty-fivepercent of subjects with normal rotary chair and cVEMPresults had abnormal laser SVV results. Both subjects withTD who completed testing had laser SVV results less than2◦. Laser SVV results agreed with the Bucket Test resultsin only 38% of cases.
DISCUSSION
This is the first study to determine reliability and di-agnostic accuracy for pediatric clinical tests of vestibularfunction. The HTT had good test-retest reliability and cor-rectly predicted vestibular function scores with 88% agree-ment. Schubert et al29 tested subjects with UVH/BVH andcompared the HTT with caloric tests. Sensitivities for sub-jects with UVH and BVH were 71% and 84%, respectively.Specificity was 82%. In the current study, we combinedsubjects with UVH (n = 5) and BVH (n = 3) because oflow prevalence. Even so, the HTT was reliable (ICC =0.73), sensitive (75%), and specific (91%). The HTT wassimple and required no special equipment. However, clin-icians should practice correct technique.
Similar to adult performance,41 the MCTSIB totalscore was reliable. The sensitivity, specificity, and pre-dictive values were 78% or greater for a cutoff score of110 total seconds. However, if only doing condition 4of the MCTSIB, test-retest reliability decreased (ICC =0.56). Therefore, we recommend that all conditions of theMCTSIB be completed. If using the MCTSIB as an outcometool to measure improvement, then the MDC90 score of16.76 seconds should be used. The moderate to good cor-relation between the SOT vestibular ratio and the MCTSIBscore indicated that the latter provided information aboutvestibular input to postural control. This differed from thefindings of Gagnon et al,58 who reported that the Pediatric
Copyright © 2014 Wolters Kluwer Health | Lippincott Williams & Wilkins and the Section on Pediatrics of the American Physical TherapyAssociation. Unauthorized reproduction of this article is prohibited.
Pediatric Physical Therapy Clinical Tests of Vestibular Function for Children 185

TABLE 3Means and SDs
Clinical Test TD SNHL NVF SNHL BVH SNHL UVH
HTT R n = 23 n = 11 n = 3 n = 5# positive results 0 2 1 4HTT L n = 23 n = 11 n = 3 n = 5# positive results 0 3 1 2DVA score n = 23 n = 11 n = 3 n = 5Mean optotypes (SD) 11.6 (8.7) 8.3 (3.4) 19.3 (13.5) 15 (5.6)m-ECVCT room light n = 6 n = 10 n = 3 n = 5Mean total seconds (SD) 19.3 (7.6) 17.9 (9.3) 2.7 (2.5) 15.3 (10.8)m-ECVCT fixation removed n = 5 n = 11 n = 3 n = 5Mean total seconds (SD) 52.1 (7.5) 48.3 (9.5) 9.7 (16.9) 41.9 (17.7)Bucket Test n = 21 n = 11 n = 3 n = 5Mean degrees off center (SD) 1.8 (0.44) 1.7 (0.47) 1.7 (0.58) 1.6 (0.54)Laser SVV score n = 2 n = 11 n = 3 n = 5Mean degrees off center (SD) 0.49 (0.62) 2.15 (1.5) 2.7 (2.2) 5.0 (2.7)MCTSIB total score n = 23 n = 11 n = 3 n = 5Mean seconds (SD) 118.6 (4.3) 116.0 (6.3) 84.4 (23.3) 98.4 (20.4)SOT visual ratio n = 22 n = 11 n = 3 n = 5Mean ratio (SD) 0.76 (0.18) 0.59 (0.18) 0.64 (0.29) 0.69 (0.15)SOT vestibular ratio n = 22 n = 11 n = 3 n = 5Mean ratio (SD) 0.57 (0.17) 0.43 (0.17) 0.00 0.22 (0.16)SOT somatosensory ratio n = 22 n = 11 n = 3 n = 5Mean ratio (SD) 0.96 (0.05) 0.95 (0.67) 0.95 (0.05) 0.99 (0.05)
Abbreviations: BVH, bilateral vestibular hypofunction; DVA, Dynamic Visual Acuity; HTT, Head Thrust Test; L, left; m-ECVCT, modified Emory ClinicalVestibular Chair Test; MCTSIB, modified clinical test of sensory interaction for balance; NVF, normal vestibular function; R, right; SNHL, sensorineuralhearing loss; SOT, sensory organization test; SVV, subjective visual vertical; TD, typical development; UVH, unilateral vestibular hypofunction.
CTSIB and SOT did not correlate and concluded that the2 tests measured sensory organization differently. In thecurrent study, we did not do tandem or single-leggedstance conditions. We also used the vestibular ratio ratherthan the SOT stability scores. The clinical DVA test wasreliable and predicted vestibular function test results witha 76% success rate, using a cutoff score of 10 optotypes(ie, 2 lines). This differed from a previous study that re-ported a 100% success rate for predicting hypofunction.33
Unlike original study methods, we continued testing untilthe subject missed all optotypes on a line and then countedthe total number of missed optotypes, pushing subjects totheir limit of the DVA. The original test33 ended when sub-jects missed 3 optotypes on a line. The DVA test can be
used to determine whether or not gaze stability exercisesare working.59 A change in the DVA score of greater than 8optotypes (or approximately 1.6 lines) can be considereda change that is greater than error.
The m-ECVCT with fixation removed was reliableand predicted vestibular function with 86% accuracy, us-ing a cutoff of 29.2 seconds (ie, following 30-second left+ right rotations). It correlated moderately with the ro-tary chair time constant. The m-ECVCT in room light hadgood test-retest and poor interrater reliability. The cutoffscore of 15.3 seconds yielded only 65% correct prediction.The 4 raters who participated in the interrater reliabilitystudy commented that it was difficult to determine whennystagmus stopped in room light. Some children fixated
TABLE 4Diagnostic Values and Cutoff Scoresa
Optimal Sensitivity Specificity PPV NPVClinical Test AUC Cutoff Score % Agree (95% CI) (95% CI) (95% CI) (95% CI)
HTT (pos or neg) NA NA 88 0.75 (0.25-0.89) 0.77 (0.32-0.86) 0.67 (0.25-0.84) 0.83 (0.31-0.90)MCTSIB condition 4 only 0.89 20 s 90 0.88 (0.22-0.95) 0.92 (0.28-0.96) 0.88 (0.22-0.95) 0.92 (0.28-0.96)SOT vestibular ratio 0.88 0.20 (ratio) 86 0.75 (0.25-0.88) 0.92 (0.28-0.96) 0.86 (0.21-0.95) 0.86 (0.33-0.91)MCTSIB total 0.88 110 s 86 0.88 (0.22-0.95) 0.85 (0.32-0.90) 0.78 (0.26-0.89) 0.92 (0.27-0.96)DVA score 0.85 10 optotypes 76 0.88 (0.22-0.95) 0.69 (0.30-0.82) 0.64 (0.27-0.81) 0.90 (0.25-0.95)m-ECVCT, room light 0.74 15.3 s (total) 65 0.75 (0.25-0.89) 0.58 (0.27-0.78) 0.55 (0.25-0.78) 0.78 (0.26-0.89)m-ECVCT, fixation removed 0.74 29.2 s (total) 86 0.63 (0.23-0.84) 1.00 (NA) 1.00 (NA) 0.81 (0.35-0.87)SOT visual ratio 0.67 0.76 (ratio) 76 0.63 (0.23-0.84) 0.85 (0.32-0.90) 0.71 (0.22-0.88) 0.79 (0.33-0.86)SOT somatosensory ratio 0.64 0.98 (ratio) 67 0.50 (0.20-0.80) 0.77 (0.32-0.86) 0.57 (0.20-0.84) 0.71 (0.32-0.81)
Abbreviations: AUC, area under the curve; CI, confidence interval; cVEMP, cervical vestibular evoked myogenic potential; DVA, Dynamic Visual Acuity;HTT, Head Thrust Test; MCTSIB, Modified Clinical Test of Sensory Interaction on Balance; m-ECVCT, modified Emory Clinical Vestibular Chair Test;NA, not applicable; neg, negative; NPV, negative predictive value; pos, positive; PPV, positive predictive value; SOT, Sensory Organization Test.aPositive cases tested positive on the cVEMP or rotary chair test or both.
Copyright © 2014 Wolters Kluwer Health | Lippincott Williams & Wilkins and the Section on Pediatrics of the American Physical TherapyAssociation. Unauthorized reproduction of this article is prohibited.
186 Christy et al Pediatric Physical Therapy

TABLE 5Likelihood Ratios
Clinical Test LR+ (95% CI) LR− (95% CI)
HTT (pos or neg) 3.25 (1.11-9.48) 0.33 (0.09-1.12)MCTSIB condition 4 only 11.38 (1.70-76.14) 0.13 (0.02-0.85)SOT vestibular ratio 9.75 (1.42-66.85) 0.27 (0.08-0.91)MCTSIB total 5.87 (1.54-20.90) 0.14 (0.02-0.94)DVA score 2.84 (1.20-6.70) 0.18 (0.03-1.17)m-ECVCT, room light 1.80 (0.83-3.93) 0.43 (0.12-1.56)m-ECVCT, fixation removed NA 0.38 (0.15-0.92)SOT visual ratio 4.06 (1.02-16.20) 0.44 (0.18-1.12)SOT somatosensory ratio 2.17 (0.65-7.27) 0.65 (0.31-1.38)
Abbreviations: CI, confidence interval; DVA, Dynamic Visual Acuity; HTT, Head Thrust Test; LR+, positive likelihood ratio; LR−, negative likelihoodratio; MCTSIB, Modified Clinical Test of Sensory Interaction on Balance; m-ECVCT, modified Emory Clinical Vestibular Chair Test; NA, not applicable;SOT, Sensory Organization Test.
and stopped nystagmus immediately. Therefore, this testshould be done with fixation removed.
The Bucket Test had good test-retest reliability ofmean degrees off vertical, poor reliability for direction,and did not correlate with the laser SVV results. A cut-off score could not be determined because the AUC wasonly slightly better than chance. These results differed fromthose obtained by Zwergal et al,31 who found good reliabil-ity, sensitivity, and specificity of the Bucket Test. In adults,SVV in the acute stage following UVH tilts toward the sideof the lesion. Studies differ as to when or if SVV ever fullycompensates.60 We do not know how SVV compensatesin children with VH because adult paradigms of utriculartesting have not been tested in children.61,62 To our knowl-edge, this is the first study to report SVV results in childrenwith VH. Given the results of the laser SVV in this study,it is tempting to hypothesize that the children with UVHhad static uncompensated deficits, whereas the 5 subjectswith normal vestibular function tests but abnormal perfor-mance for laser SVV had a utricular deficit. Except for 1,subjects with BVH did not have asymmetric SVV, whichwas expected. Utricular function should be tested in largernumbers of children with and without VH using the ocularVEMP, a laboratory test of utricular function.63
Cochlear implantation is increasingly being offeredfor individuals with severe to profound SNHL.64 Thesurgery involves an array of electrodes inserted into thecochlea to send electrical signals to the auditory nerve.65
Histological studies revealed saccular damage in some chil-dren who received cochlear implantation, ostensibly dueto trauma during electrode insertion into the cochlea,which lies in close proximity to the saccule.66,67 In thesecases, persisting vertigo occurred when the device wasactivated.66 In contrast, some subjects demonstrated bet-ter balance with the cochlear implant turned on thanoff.19,68,69 Importantly, children undergoing cochlear im-plant surgery should be screened for vestibular deficits.
The timing of vestibular injury is important. Thevestibulo-ocular reflex develops rapidly during the first2 years of life.70 The use of vestibular input for posturalcontrol does not become adult-like until after the age of 15years.71 Therefore, an adult who developed typically andacquired VH will differ from a child who did not develop
with a functioning vestibular system. The current studyincluded subjects with chronic VH. It is possible that testresults might differ in subjects with acute lesions.
Clinical Implications
To apply the results of this study in a clinicalcontext, we will consider the subject who refused ref-erence standard tests. This was a 6-year-old girl withSNHL, of unknown origin. She had bilateral cochlearimplant surgery at the age of 4 years. She walked in-dependently at 15 months of age and had a normalneurological and oculomotor screen. She presented withpositive HTT bilaterally and a static visual acuity andDVA score difference of 34 (>10 optotypes cutoff). HerMCTSIB total score was 95.57 seconds (<110 cutoff). Allconditions on the MCTSIB were normal except for thefoam eyes closed condition (5.57 seconds). She refused theSOT. The m-ECVCT score was 23.3 seconds (<cutoff of29.2 seconds). According to clinical tests, this child likelyhas BVH affecting gaze stability and balance. This childcould potentially benefit from vestibular exercises.3,59
LIMITATIONS
First, only 8 of 19 children with SNHL had confirmedVH. This contributed to the wide 95% CIs for diagnosticvalues and likelihood ratios. The low number of subjectsmay have also contributed to the low diagnostic capacitiesof the Bucket Test and condition 4 of the MCTSIB. Moresubjects with confirmed pathology are needed to add tothis preliminary data. Second, the reliability of laser SVVin children has not been established. We do not knowhow development or the presence of a vestibular deficitaffects SVV in children. Third, this study can only begeneralized to children aged 6 to 12 years with severe toprofound SNHL and without other neurologic problems.This battery of tests should be completed on other groupsof children with VH.
CONCLUSION
The best tests to determine whether a child with anotherwise normal neurological system has VH include (1)
Copyright © 2014 Wolters Kluwer Health | Lippincott Williams & Wilkins and the Section on Pediatrics of the American Physical TherapyAssociation. Unauthorized reproduction of this article is prohibited.
Pediatric Physical Therapy Clinical Tests of Vestibular Function for Children 187

the HTT, (2) the m-ECVCT fixation removed, (3) the DVA,(4) the MCTSIB, and (5) SOT vestibular ratio. The MDC90
scores should be considered if using the DVA and MCTSIBas outcome tools to detect improvement due to interven-tion. Tests of utricular function require further study inpediatric populations.
REFERENCES
1. Rine RM. Growing evidence for balance and vestibular problems inchildren. Audiol Med. 2009;99999:1.
2. O’Reilly RC, Morlet T, Nicholas BD, et al. Prevalence of vestibular andbalance disorders in children. Otol Neurotol. 2010;31(9):1441-1444.
3. Rine RM, Braswell J, Fisher D, Joyce K, Kalar K, Shaffer M. Improve-ment of motor development and postural control following inter-vention in children with sensorineural hearing loss and vestibularimpairment. Int J Pediatr Otorhinolaryngol. 2004;68(9):1141-1148.
4. Rine RM, Spielholz NI, Buchman C. Postural control in childrenwith sensorineural hearing loss and vestibular hypofunction: deficitsin sensory system effectiveness and vestibulospinal function. In: Duy-sens j, Smits-Engelsman BCM, Kingma H, eds. Control of Posture andGait. Amsterdam, the Netherlands: Springer-Verlag; 2001:40-45.
5. Inoue A, Iwasaki S, Ushio M, et al. Effect of vestibular dysfunction onthe development of gross motor function in children with profoundhearing loss. Audiol Neurootol. 2013;18(3):143-151.
6. Shall MS. The importance of saccular function to motor developmentin children with hearing impairments. Int J Otolaryngol. 2009;2009:1-5.
7. Braswell J, Rine RM. Evidence that vestibular hypofunction af-fects reading acuity in children. Int J Pediatr Otorhinolaryngol.2006;70:1957-1965.
8. Kaga K. Vestibular compensation in infants and children with con-genital and acquired vestibular loss in both ears. Otorhinolaryngology.1999;49:215-224.
9. Rine RM, Cornwall G, Gan K, et al. Evidence of progressive delay ofmotor development in children with sensorineural hearing loss andconcurrent vestibular dysfunction. Percept Mot Skills. 2000;90:1101-1112.
10. Hlavacka F, Mergner T, Krizkova M. Control of the body ver-tical by vestibular and proprioceptive inputs. Brain Res Bull.1999;40(5/6):431-435.
11. Franco ES, Panboca I. Vestibular function in children underperform-ing in school. Braz J Otorhinolaryngol. 2008;74(6):815-825.
12. Casselbrant ML, Mandel EM, Sparto PJ, et al. Longitudinal postur-ography and rotational testing in children three to nine years of age:normative data. Otolaryngol Head Neck Surg. 2010;142(5):708-714.
13. Rine RM, Wiener-Vacher S. Evaluation and treatment of vestibulardysfunction in children. NeuroRehabilitation. 2013;32(3):507-518.
14. Saka N, Imai T, Seo T, et al. Analysis of benign paroxysmalpositional nystagmus in children. Int J Pediatr Otorhinolaryngol.2013;77(2):233-236.
15. Monobe H, Murofushi T. Vestibular neuritis in a child with otitis me-dia with effusion; clinical application of vestibular evoked myogenicpotential by bond-conducted sound. Int J Pediatr Otorhinolaryngol.2004;68:1455-1458.
16. Zannolli R, Zazzi M, Muraca MC, Macucci F, Buoni S, Nuti D. Achild with vestibular neuritis. Is adenovirus implicated? Brain Dev.2006;28(6):410-412.
17. Casselbrant ML, Villardo RJ, Mandel EM. Balance and otitis mediawith effusion. Int J Audiol. 2008;47(9):584-589.
18. Contopoulos-Ioannidis DG, Giotis ND, Baliatsa DV, Ioannidis JP.Extended-interval aminoglycoside administration for children: ameta-analysis. Pediatrics. 2004;114(1):e111-e118.
19. Buchman CA, Joy J, Hodges A, Telischi FF, Balkany TJ. Vestibulareffects of cochlear implantation. Laryngoscope. 2004;114:1-22.
20. Cushing SL, Papsin BC, Rutka JA, James AL, Blaser SL, GordonKA. Vestibular end-organ and balance deficits after meningitis and
cochlear implantation in children correlate poorly with functionaloutcome. Otol Neurotol. 2009;30(4):488-495.
21. Cushing SL, Gordon KA, Rutka JA, James AL, Papsin BC. Vestibularend-organ dysfunction in children with sensorineural hearing lossand cochlear implants: an expanded cohort and etiologic assessment.Otol Neurotol. 2013;34(3):422-428.
22. Suarez H, Angeli S, Suarez A, Rosales B, Carrera X, Alonso R. Balancesensory organization in children with profound hearing loss andcochlear implants. Int J Pediatr Otorhinolaryngol. 2007;71(4):629-637.
23. Tribukait A, Brantberg K, Bergenius J. Function of semicircularcanals, utricles and saccules in deaf children. Acta Otolaryngol.2004;124:41-48.
24. Sheykholesami K, Kaga K, Megerian CA, Arnold JE. Vestibular-evoked myogenic potentials in infancy and early childhood. Laryn-goscope. 2005;115:1440-1444.
25. Wuyts FL, Furman J, Vanspauwen R, Van de HP. Vestibular functiontesting. Curr Opin Neurol. 2007;20(1):19-24.
26. Eviatar L, Eviatar A. The normal nystagmic response of infants tocaloric and perrotatory stimulation. Laryngoscope. 1979;89:1036-1045.
27. Valente M. Maturational effects of the vestibular system: a studyof rotary chair, computerized dynamic posturography, and vestibu-lar evoked myogenic potentials with children. J Am Acad Audiol.2007;18(6):461-481.
28. Staller SJ, Goin DW, Hildebrandt M. Pediatric vestibular evalu-ation with harmonic acceleration. Otolaryngol Head Neck Surg.1986;95(4):471-476.
29. Schubert MC, Tusa RJ, Grine LE, Herdman SJ. Optimizing the sensi-tivity of the Head Thrust Test for identifying vestibular hypofunction.Phys Ther. 2004;84(2):151-158.
30. Halmagyi GM, Curthoys LS, Cremer PD, et al. The human horizon-tal vestibulo-ocular reflex in response to high acceleration stimula-tion before and after unilateral vestibular neurectomy. Exp Brain Res.1990;81:479-490.
31. Zwergal A, Rettinger N, Frenzel C, Dieterich M, Brandt T, Strupp M.A bucket of static vestibular function. Neurology. 2009;72(19):1689-1692.
32. Hall CD, Hoover J, Jacobs M, et al. A new measurement tool forvestibular hypofunction: validity of the Emory Clinical VestibularChair Test. J Neurol Phys Ther. 2009;33(4):232.
33. Rine RM, Braswell J. A clinical test of Dynamic Visual Acuity forchildren. Int J Pediatr Otorhinolaryngol. 2003;69(11):1195-1201.
34. Rine RM, Roberts D, Corbin BA, et al. A new portable tool to screenvestibular and visual function: National Institutes of Health ToolboxInitiative. J Rehabil Res Dev. 2012;49(2):209-220.
35. Hall CD, Abbott KN, Lane EC, et al. Measurement of vestibularhypofunction: validity of the Emory Clinical Vestibular Chair Test(ECVCT). J Neurol Phys Ther. 2007;31(4):210-211.
36. Evans MK, Krebs DE. Posturography does not test vestibulospinalfunction. Otolaryngol Head Neck Surg. 1999;120(2):164-173.
37. Gabriel LS, Mu K. Computerized platform posturography for chil-dren: test-retest reliability of the sensory test of the VSR System. PhysOccup Ther Pediatr. 2002;22(3/4):101-117.
38. Rine RM, Rubish K, Feeney C. Measurement of sensory system ef-fectiveness and maturational changes in postural control in youngchildren. Pediatr Phys Ther. 1998;10:16-22.
39. Shumway-Cook A, Horak FB. Assessing the influence of sensory in-teraction on balance. Phys Ther. 1986;66:1548-1550.
40. Horak FB. Clinical measurement of postural control in adults. PhysTher. 1987;67(12):1881-1885.
41. Cohen H, Blatchly CA, Gombash LL. A study of the clinical test ofsensory interaction and balance. Phys Ther. 1993;73(6):346-351.
42. Crowe TK, Deitz JC, Richardson PK, Atwater SW. Interrater reliabilityof the pediatric clinical test of sensory interaction for balance. PhysOccup Ther Pediatr. 1990;10(4):1-27.
43. Westcott SL, Lowes L, Richardson PK. Evaluation of postural sta-bility in children: current theories and assessment tools. Phys Ther.1997;77(6):629-645.
Copyright © 2014 Wolters Kluwer Health | Lippincott Williams & Wilkins and the Section on Pediatrics of the American Physical TherapyAssociation. Unauthorized reproduction of this article is prohibited.
188 Christy et al Pediatric Physical Therapy

44. Wrisley DM, Whitney SL. The effect of foot position on the modifiedclinical test of sensory interaction and balance. Arch Phys Med Rehabil.2004;85(2):335-338.
45. Weber PC, Cass SP. Clinical assessment of postural stability. Am JOtol. 1993;14(6):566-569.
46. El-Kashlan HK, Shepard NT, Asher AM, Smith-Wheelock M, TelianS. Evaluation of clinical measures of equilibrium. Laryngoscope.1998;108(March):311-319.
47. Enbom H, Magnusson M, Pyyko I. Postural compensation in childrenwith congenital or early acquired bilateral vestibular loss. Ann OtolRhinol Laryngol. 1991;100:472-478.
48. Charpiot A, Tringali S, Iionescu E, Vital-Durand F, Ferber-Viart C.Vestibulo-ocular reflex and balance maturation in healthy childrenaged from six to twelve years. Audiol Neurootol. 2010;15(4):203-210.
49. Akin FW, Murnane OD, Panus PC, Caruthers SK, WilkinsonAE, Proffitt TM. The influence of voluntary tonic EMG levelon the vestibular-evoked myogenic potential. J Rehabil Res Dev.2004;41(3B):473-480.
50. Halmagyi GM, Curthoys IS. Clinical testing of otolith function. AnnN Y Acad Sci. 1999;871:195-204.
51. McNerney KM, Burkard RF. The vestibular evoked myogenic po-tential (VEMP): air- versus bone-conducted stimuli. Ear Hear.2011;32(6):e6-e15.
52. Zhou G, Kenna MA, Stevens K, Licamelli G. Assessment of saccularfunction in children with sensorineural hearing loss. Arch OtolaryngolHead Neck Surg. 2009;135(1):40-44.
53. Bohmer A, Mast F. Assessing otolith function by the subjective visualvertical. Ann N Y Acad Sci. 1999;871:221-231.
54. Agresti A. Categorical Data Analysis. 2nd ed. Hoboken, NJ: Wiley;2002.
55. Simel DL, Samsa GP, Matchar DB. Likelihood ratios with confidence:sample size estimation for diagnostic test studies. J Clin Epidemiol.1991;44(8):763-770.
56. Rousson V, Gasser T, Seifert B. Assessing intrarater, interraterand test-retest reliability of continuous measurements. Stat Med.2002;21(22):3431-3446.
57. Haley SM, Fragala-Pinkham MA. Interpreting change scores of testsand measures used in physical therapy. Phys Ther. 2006;86(5):735-743.
58. Gagnon I, Swaine B, Forget R. Exploring the comparability of theSensory Organization Test and the Pediatric Clinical Test of Sen-sory Interaction for Balance in children. Phys Occup Ther Pediatr.2006;26(1/2):23-41.
59. Braswell J, Rine RM. Preliminary evidence of improved gaze stabilityfollowing exercise in two children with vestibular hypofunction. IntJ Pediatr Otorhinolaryngol. 2006;70:1967-1973.
60. Hafstrom A, Fransson PA, Karlberg M, Magnusson M. Subjectivevisual tilt and lateral instability after vestibular deafferentation. ActaOtolaryngol. 2006;126(11):1176-1181.
61. Clarke AH, Schonfeld U, Helling K. Unilateral examinationof utricle and saccule function. J Vestib Res. 2003;13(4-6):215-225.
62. Bohmer A. The subjective visual vertical as a clinical parameter foracute and chronic vestibular (otolith) disorders. Acta Otolaryngol.1999;119:126-127.
63. Iwasaki S, Smulders YE, Burgess AM, et al. Ocular vestibular evokedmyogenic potentials in response to bone-conducted vibration of themidline forehead at Fz. A new indicator of unilateral otolithic loss.Audiol Neurootol. 2008;13(6):396-404.
64. Rubin LG, Papsin B. Cochlear implants in children: surgical siteinfections and prevention and treatment of acute otitis media andmeningitis. Pediatrics. 2010;126(2):381-391.
65. James AL, Papsin BC. Cochlear implant surgery at 12months of age or younger. Laryngoscope. 2004;114(12):2191-2195.
66. Basta D, Todt I, Goepel F, Ernst A. Loss of saccular function aftercochlear implantation: the diagnostic impact of intracochlear electri-cally elicited vestibular evoked myogenic potentials. Audiol Neurootol.2008;13(3):187-192.
67. Tien HC, Linthicum FH Jr. Histopathologic changes in thevestibule after cochlear implantation. Otolaryngol Head Neck Surg.2002;127(4):260-264.
68. Ribari O, Kustel M, Szirmai A, Repassy G. Cochlear implantationinfluences contralateral hearing and vestibular responsiveness. ActaOtolaryngol. 1999;119(2):225-228.
69. Bonucci AS, Costa Filho OA, Mariotto LD, Amantini RC, AlvarengaKF. Vestibular function in cochlear implant users. Braz J Otorhino-laryngol. 2008;74(2):273-278.
70. Fife TD, Tusa RJ, Furman JM, et al. Assessment: vestibular testingtechniques in adults and children: report of the Therapeutics andTechnology Assessment Subcommittee of the American Academy ofNeurology. Neurology. 2000;55:1431-1441.
71. Ferber-Viart C, Onescu E, Orlet T, Roehlich P, Ubreuil C. Balance inhealthy individuals assessed with Equitest: maturation and normativedata for children and young adults. Int J Pediatr Otorhinolaryngol.2007;71(7):1041-1046.
C L I N I C A L B O T T O M L I N E
Commentary on “Reliability and Diagnostic Accuracy of Clinical Tests of Vestibular Function for Children”
“How could I apply this information?”Clinicians can use the positive and negative likelihood ratios (LR+, LR−) provided in Table 5 to determine
the likelihood that a specific child diagnosed with severe to profound sensorineural hearing loss (SNHL) hasvestibular hypofunction (VH). We use the example of the 6-year-old child with SNHL in this study who did notundergo reference standard Vestibular Function Testing (VFT) yet had positive results on 4 clinical tests: (1) HeadThrust Test, (2) Dynamic Visual Acuity Test, (3) Modified Clinical Test of Sensory Interaction on Balance totalscore, and (4) Modified Emory Clinical Vestibular Chair Test with fixation removed. Her pretest probability forVH was 42%, on the basis of the fact that 8 of 19 children with SNHL in this study had VH as diagnosed by VFT.Using a nomogram1 and the LR+ from each clinical test (range, 2.84-5.87), her posttest probability of having VHas diagnosed by VFT would be approximately 65% to 82% (Figure 1). If each clinical test had been negative (LR−range, 0.14-0.38), her posttest probability of having VH as diagnosed by VFT would be approximately 8% to 20%(Figure 2). In this case, the use of a nomogram and the LR of each clinical test provided critical quantitativeinformation that increased certainty that the child had VH to make appropriate referrals for reference standardVFT and determine the most appropriate intervention plan.
Copyright © 2014 Wolters Kluwer Health | Lippincott Williams & Wilkins and the Section on Pediatrics of the American Physical TherapyAssociation. Unauthorized reproduction of this article is prohibited.
Pediatric Physical Therapy Clinical Tests of Vestibular Function for Children 189

“What should I be mindful about when applying this information?”Clinicians must be mindful that only 8 participants had VH as diagnosed by reference standard VFT and
that the psychometric properties of the 5 clinical tests of vestibular function can only be generalized to 6- to12-year-old children with severe to profound SNHL from chronic lesions. Furthermore, 13 of 20 participants withSNHL used cochlear implants, yet no mention was made as to whether these children had a higher incidence ofVH or whether their implants were on or off during the clinical tests of vestibular function.
Fig. 1. Using a nomogram to find the posttest probabil-ity of VH based on positive test results. Pretest probabil-ity = 42%. MCTSIB total +LR = 5.87, posttest probabil-ity = 82%. HTT +LR = 3.25, posttest probability = 70%.DVA +LR = 2.84, posttest probability = 65%. A positiveresult on each of these 3 clinical tests changes the prob-ability of the child having VH from 42% (pretest) to 65%to 82% (posttest), depending on the test. DVA indicatesDynamic Visual Acuity; HTT, Head Thrust Test; LR, like-lihood ratio; MCTSIB, Modified Clinical Test of SensoryInteraction on Balance.
REFERENCE
1. Fagan T. Nomogram for Bayes’s theorem. N Engl J Med. 1975;293:257.
Fig. 2. Using a nomogram to find the posttest probabil-ity based on negative test results. Pretest probability =42%. m-ECVCT-fixation removed − LR = 0.38, posttestprobability = 20%. HTT − LR = 0.33, posttest proba-bility = 18%. DVA − LR = 0.18, posttest probability =10%. MCTSIB total − LR = 0.14, posttest probability =8%. A negative result on each of these 4 clinical testschanges the probability of the child having VH from42% (pretest) to 8% to 20% (posttest), depending onthe test. DVA indicates Dynamic Visual Acuity; HTT, HeadThrust Test; LR, likelihood ratio; MCTSIB, Modified Clin-ical Test of Sensory Interaction on Balance; m-ECVCT,Modified Emory Clinical Vestibular Chair Test.
Barabara Sargent, PT, PhD, PCSUniversity of Southern California
Los Angeles, California
Jennifer Pate, PT, DPTLos Angeles Children’s Hospital
Los Angeles, California
The authors declare no conflicts of interest.
DOI: 10.1097/PEP.0000000000000040
Copyright © 2014 Wolters Kluwer Health | Lippincott Williams & Wilkins and the Section on Pediatrics of the American Physical TherapyAssociation. Unauthorized reproduction of this article is prohibited.
190 Christy et al Pediatric Physical Therapy




















