Terapi SLE Peralmuni2011
23
Treatment of SLE Dr.B.P.Putra Suryana, SpPD-KR Rheumatology, Internal Medicine Brawijaya University-Dr.Saiful Anwar General Hospital Malang Indonesian Rheumatism Association Workshop SLE Peralmuni Cabang Malang 29 Oktober 2011
-
Upload
independent -
Category
Documents
-
view
4 -
download
0
Transcript of Terapi SLE Peralmuni2011

Treatment of SLE
Dr.B.P.Putra Suryana, SpPD-KRRheumatology, Internal Medicine
Brawijaya University-Dr.Saiful Anwar General HospitalMalang
Indonesian Rheumatism Association
Workshop SLEPeralmuni Cabang Malang
29 Oktober 2011

Problem in treatment• Very wide clinical spectrum and disease activities of SLE.
• Individual response to treatment.
• Delayed initiation of disease-modifying treatment.
• Inadequate patient education.

10-Year survival rate of SLE in Asia
Source Country Period Survival Rates
(10 years) %PH Feng Singapor
e1970-80 60
F Wang Malaysia 1974-90 71DM Chang Taiwan 1983-96 75A N Changdra-sekaran
South India
1994 82
SL Chen China 1980-98 84H Hashimoto
Japan 1970-79 86Shun-le Chen. International Congress on SLE. Shanghai 2007.

Clinical Manifestation
N=32Percentage
Kejang 3 9.3Vasculitis 7 22.5Arthritis 20 64.5Proteinuria 5 16.1Skin rash 23 71.8Alopecia 13 41.9Mucosal Ulcer 14 43.7Pleuritis 4 12.5Trombositopeni 2 6.2Leukopenia 2 6.2Raynaud’s 2 6.2Anemia 23 71.8Hemolytic anemia 5 16.1
Clinical manifestation of SLE in Malang
Fatoni A, Kusworini Handono, Suryana BPP. Brawijaya University, Malang. 2007

Non-pharmacologic• Education : disease manifestation, treatment, prognosis, complication.
• Skin protection from UV-light• Rehabilitation• Nutrition

Treatment and Disease Severity
• Mild to moderate lupus :– Paracetamol, NSAIDs– Corticosteroids– DMARDs : chloroquine, MTX• Severe lupus :
- NSAIDs- Corticosteroids (high dose – mega dose)- DMARDs and immunosuppresive : azatioprine, cyclophosphamide, MMF, cyclosporine
- Biologic agent : rituximab

Malar rash
Malar rash in SLE with positive ANASlide from Rheumatology Clinic Dr.Saiful Anwar Hospital, Malang, Indonesia
MTX 7.5 mg / weekFolic acid 1x1 tabPrednison 5 mg (1-0-0)Calcium 500 mg / dayMeloxicam 15 mg prn
Monitoring :CBC (Hb, WBC)LFT (SGOT, SGPT)

Discoid rash in cutaneous lupus

Arthritis and other musculoskeletal

Vasculitis
Erythematous and raised skin lesions represent vasculitis in
42 year-old with SLE Slide from Rheumatology Clinic Dr.Saiful Anwar Hospital, Malang, Indonesia
Azatioprine 50 mg 2x1Methyl-prednisolone 3x8 mg (tap off)Calcium 500 mg / day

Livedo reticularis

Raynaud’s phenomenon

SLE with Polymyositis Dermatomyositis
Male 18-year-old with generalized muscle weakness and typical skin rash (heliotrope) and papules on hands
Slide from Rheumatology Clinic Dr.Saiful Anwar Hospital, Malang, Indonesia

SLE PM-DM : Gottron’s papules
Slide from Rheumatology Clinic Dr.Saiful Anwar Hospital, Malang, Indonesia
Cyclophosphamide pulse 750 mg / monthMethyl-prednisolone 3x16 mgCalcium 1000 mg/day
Monitoring :CBC (Hb, WBC)LFT (SGOT, SGPT)UrinalysisRenal function

Digital vasculitis and necrosis
Digital vasculitis and necrosis in 32 year-old female with SLE
Slide from Rheumatology Clinic Dr.Saiful Anwar Hospital, Malang, Indonesia
Azatioprine 50 mg 2x1Methyl-prednisolone 3x16 mg (tap off)Aspirin 80 mg/dayCalcium 1000 mg / day
Monitoring :CBC (Hb, WBC)LFT (SGOT, SGPT)UrinalysisRenal function
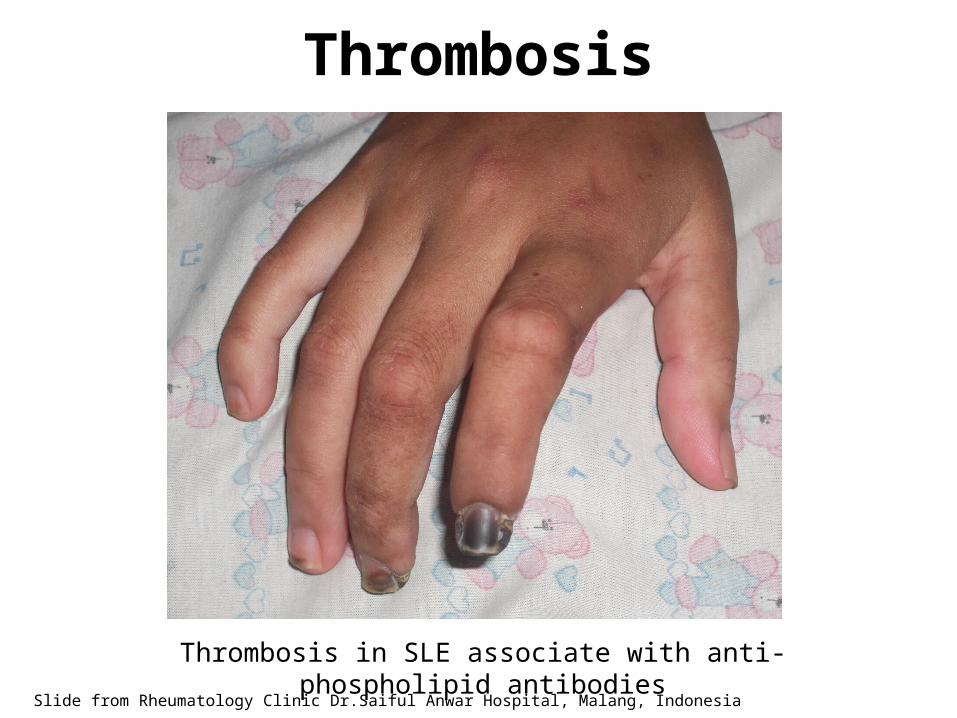
Thrombosis
Slide from Rheumatology Clinic Dr.Saiful Anwar Hospital, Malang, Indonesia
Thrombosis in SLE associate with anti-phospholipid antibodies

SLE with panniculitis, lipo-atrophy
Slide from Rheumatology Clinic Dr.Saiful Anwar Hospital, Malang, Indonesia
MTX 7.5 mg/week, Folic acid 1x1 tab

Pericardial Effusion in SLE
Slide from Rheumatology Clinic Dr.Saiful Anwar Hospital, Malang, Indonesia
Referred to CardiologistCyclophosphamide pulse 750 mg / monthMethylprednisolone 3x16 mg (Tap offf)

Osteoporosis and Fracture
Slide from Rheumatology Clinic Dr.Saiful Anwar Hospital, Malang, Indonesia
MTX 7.5 mg / weekChloroquine 250 mg / dayMethyl-prednisolone 8 mg/dayFolic acid 1x1 tabBisphosphonate infusCalcium 1000 mg/day

Is reducing Anti-dsDNA levels would reduce disease activity?
• Immunosuppresive and steroid reduced mean anti-dsDNA level and fewer flares of disease (Bootsma et al, Lancet 1995).
• Anti-CD20 in refractory SLE showed impressive clinical responses associated with falls in levels of anti-dsDNA
(Cambridge et al, Arthritis Rheum 2006).Isenberg et al. Rheumatology 2007

Future : Immunotherapy in SLE
Karim et al. Rheumatology 2009;48.
Referring and Consultation
• Diagnosis confirmation• Initiation of DMARDs or immunosuppresant
• Poor response to treatment• Severe or life-threatening condition
• Co-morbidity : osteoporosis, cardiovascular disease, drug side effects etc

SUMMARY• SLE is a systemic auto-immune disease with wide clinical spectrum, variable course and prognosis.
• Patient education, exercise, rehabilitation, and nutrition should be advised for all patients.
• Pharmacotherapy include paracetamol, NSAIDs, corticosteroids, DMARDs, and immunosupressant. Also treat concomitant diseases.
Terima kasih, semoga bermanfaat.