
Targeted Radionuclide Therapy - An Overview
29
Send Orders for Reprints to [email protected] Current Radiopharmaceuticals, 2013, 6, 000-000 1 1874-4710/13 $58.00+.00 © 2013 Bentham Science Publishers Targeted Radionuclide Therapy - An Overview Ashutosh Dash 1 , F. F. (Russ) Knapp Jr 2 . and M.R.A. Pillai 1 * 1 Radiopharmaceuticals Division, Bhabha Atomic Research Centre, Mumbai 400 085, India; 2 Emeritus, Medical Radioi- sotopes Program, Isotope Development Group, MS 6229, Bldg, 4501, Oak Ridge National Laboratory (ORNL), PO Box 2008, 1 Bethel Valley Road, Oak Ridge, TN, 37831, USA Abstract: Radionuclide therapy (RNT) based on the concept of delivering cytotoxic levels of radiation to disease sites is one of the rap- idly growing fields of nuclear medicine. Unlike conventional external beam therapy, RNT targets diseases at the cellular level rather than on a gross anatomical level. This concept is a blend of a tracer moiety that mediates a site specific accumulation followed by induction of cytotoxicity with the short-range biological effectiveness of particulate radiations. Knowledge of the biochemical reactions taking place at cellular levels has stimulated the development of sophisticated molecular carriers, catalyzing a shift towards using more specific target- ing radiolabelled agents. There is also improved understanding of factors of importance for choice of appropriate radionuclides based on availability, the types of emissions, linear energy transfer (LET), and physical half-life. This article discusses the applications of radionu- clide therapy for treatment of cancer as well as other diseases. The primary objective of this review is to provide an overview on the role of radionuclide therapy in the treatment of different diseases such as polycythaemia, thyroid malignancies, metastatic bone pain, radiation synovectomy, hepatocellular carcinoma (HCC), neuroendocrine tumors (NETs), non-Hodgkin’s lymphoma (NHL) and others. In addi- tion, recent developments on the systematic approach in designing treatment regimens as well as recent progress, challenges and future perspectives are discussed. An examination of the progress of radionuclide therapy indicates that although a rapid stride has been made for treating hematological tumors, the development for treating solid tumors has, so far, been limited. However, the emergence of novel tumor-specific targeting agents coupled with successful characterization of new target structures would be expected to pave the way for future treatment for such tumors. Keywords: Antibodies, Auger electron, cytotoxic, hepatocellular carcinoma (HCC), nanoparticles, non-Hodgkin’s lymphoma (NHL), neuroendocrine tumors (NET), osteogenesis, peptides, phagocytosis, radioisotopes, radionuclides, radiosynovectomy, somatostatin (SST) receptor. INTRODUCTION Therapeutic radiopharmaceuticals are radiolabeled molecules consisting of a target-specific moiety, such as antibody or antibody fragments, peptides or low molecular weight ligands, linked to an appropriate radionuclide de- signed to deliver therapeutic doses of ionizing radiation to specific disease sites. In recent years, there has been a great acceleration in the development of therapeutic radiopharma- ceuticals using a wide variety of therapeutic radionuclides for treatment of cancers. Cancer is one of the main health problems with high mortality and morbidity globally [1]. In spite of the unprece- dented advances in research and treatment, cancer is cur- rently ranked among the second leading cause of death worldwide, being only surpassed by cardiovascular diseases [2]. The past few decades have witnessed considerable pro- gress towards the use of ionizing radiation as a therapeutic armamentarium with the intent of cure as well as an effective modality of palliative treatment to relieve patients from can- cer symptoms. Approximately half of all cancer patients re- ceive radiation in some form including external beam and brachytherapy, either alone or in combination with other treatment modalities such as surgery or chemotherapy [3]. *Address correspondence to this author at the Radiopharmaceuticals Divi- sion, Bhabha Atomic Research Centre, Mumbai 400 085, India; Tel: 91-22- 25593676; Fax: +91-22-25505151; E-mail: [email protected] Currently, radiation therapy is primarily based on three mo- dalities. The most widely used procedure involves the use of external beams of rays from radioactive sources (e.g. 60 Co), Electrons, x-rays, high-energy Bremsstrahlung x-rays, and hadrons (e.g. neutrons, protons and heavy ions) from accel- erators, which has seen significant expansion over the past two decades [4]. The second modality involves the introduc- tion of certain radionuclides in the form of sealed radiation sources at the disease site by mechanical precise placement which is known as brachytherapy which lies in the realm of radiation oncology [5]. The third modality uses a biochemi- cal pathway to target the radionuclide to the site of cancer and is called radionuclide therapy (RNT), endoradiotherapy, ‘in vivo targeted radiotherapy’ or ‘targeted radionuclide ther- apy’. RNT uses radiolabeled molecules referred to as ‘thera- peutic radiopharmaceuticals’, and is a unique treatment mo- dality lying between chemotherapy and external beam radio- therapy. The goal of RNT is to kill tumor cells selectively by delivering high radiation doses to a specific target while minimizing damage to normal cells. The importance of radionuclide therapy has generated an enormous number of excellent review articles describing many innovative and exciting developments [6-17]. The goal of this article is to provide an update of the current advances in radionuclide therapy to serve as a resource for scientists and clinicians involved in this area of fascinating research and therapy strategies. This overview is not a comprehensive review but is rather focussed on the principles of radionu- clide therapy and surveys major treatment options by dis-
Transcript of Targeted Radionuclide Therapy - An Overview

Send Orders for Reprints to [email protected]
Current Radiopharmaceuticals, 2013, 6, 000-000 1
1874-4710/13 $58.00+.00 © 2013 Bentham Science Publishers
Targeted Radionuclide Therapy - An Overview
Ashutosh Dash1, F. F. (Russ) Knapp Jr
2. and M.R.A. Pillai
1*
1Radiopharmaceuticals Division, Bhabha Atomic Research Centre, Mumbai 400 085, India;
2Emeritus,
Medical Radioi-
sotopes Program, Isotope Development Group, MS 6229, Bldg, 4501, Oak Ridge National Laboratory (ORNL), PO Box
2008, 1 Bethel Valley Road, Oak Ridge, TN, 37831, USA
Abstract: Radionuclide therapy (RNT) based on the concept of delivering cytotoxic levels of radiation to disease sites is one of the rap-
idly growing fields of nuclear medicine. Unlike conventional external beam therapy, RNT targets diseases at the cellular level rather than
on a gross anatomical level. This concept is a blend of a tracer moiety that mediates a site specific accumulation followed by induction of
cytotoxicity with the short-range biological effectiveness of particulate radiations. Knowledge of the biochemical reactions taking place
at cellular levels has stimulated the development of sophisticated molecular carriers, catalyzing a shift towards using more specific target-
ing radiolabelled agents. There is also improved understanding of factors of importance for choice of appropriate radionuclides based on
availability, the types of emissions, linear energy transfer (LET), and physical half-life. This article discusses the applications of radionu-
clide therapy for treatment of cancer as well as other diseases. The primary objective of this review is to provide an overview on the role
of radionuclide therapy in the treatment of different diseases such as polycythaemia, thyroid malignancies, metastatic bone pain, radiation
synovectomy, hepatocellular carcinoma (HCC), neuroendocrine tumors (NETs), non-Hodgkin’s lymphoma (NHL) and others. In addi-
tion, recent developments on the systematic approach in designing treatment regimens as well as recent progress, challenges and future
perspectives are discussed. An examination of the progress of radionuclide therapy indicates that although a rapid stride has been made
for treating hematological tumors, the development for treating solid tumors has, so far, been limited. However, the emergence of novel
tumor-specific targeting agents coupled with successful characterization of new target structures would be expected to pave the way for
future treatment for such tumors.
Keywords: Antibodies, Auger electron, cytotoxic, hepatocellular carcinoma (HCC), nanoparticles, non-Hodgkin’s lymphoma (NHL), neuroendocrine tumors (NET), osteogenesis, peptides, phagocytosis, radioisotopes, radionuclides, radiosynovectomy, somatostatin (SST) receptor.
INTRODUCTION
Therapeutic radiopharmaceuticals are radiolabeled
molecules consisting of a target-specific moiety, such as
antibody or antibody fragments, peptides or low molecular
weight ligands, linked to an appropriate radionuclide de-
signed to deliver therapeutic doses of ionizing radiation to
specific disease sites. In recent years, there has been a great
acceleration in the development of therapeutic radiopharma-
ceuticals using a wide variety of therapeutic radionuclides for treatment of cancers.
Cancer is one of the main health problems with high
mortality and morbidity globally [1]. In spite of the unprece-
dented advances in research and treatment, cancer is cur-
rently ranked among the second leading cause of death
worldwide, being only surpassed by cardiovascular diseases
[2]. The past few decades have witnessed considerable pro-
gress towards the use of ionizing radiation as a therapeutic
armamentarium with the intent of cure as well as an effective
modality of palliative treatment to relieve patients from can-
cer symptoms. Approximately half of all cancer patients re-
ceive radiation in some form including external beam and
brachytherapy, either alone or in combination with other
treatment modalities such as surgery or chemotherapy [3].
*Address correspondence to this author at the Radiopharmaceuticals Divi-sion, Bhabha Atomic Research Centre, Mumbai 400 085, India; Tel: 91-22-25593676; Fax: +91-22-25505151; E-mail: [email protected]
Currently, radiation therapy is primarily based on three mo-dalities. The most widely used procedure involves the use of external beams of rays from radioactive sources (e.g.
60Co),
Electrons, x-rays, high-energy Bremsstrahlung x-rays, and hadrons (e.g. neutrons, protons and heavy ions) from accel-erators, which has seen significant expansion over the past two decades [4]. The second modality involves the introduc-tion of certain radionuclides in the form of sealed radiation sources at the disease site by mechanical precise placement which is known as brachytherapy which lies in the realm of radiation oncology [5]. The third modality uses a biochemi-cal pathway to target the radionuclide to the site of cancer and is called radionuclide therapy (RNT), endoradiotherapy, ‘in vivo targeted radiotherapy’ or ‘targeted radionuclide ther-apy’. RNT uses radiolabeled molecules referred to as ‘thera-peutic radiopharmaceuticals’, and is a unique treatment mo-dality lying between chemotherapy and external beam radio-therapy. The goal of RNT is to kill tumor cells selectively by delivering high radiation doses to a specific target while minimizing damage to normal cells.
The importance of radionuclide therapy has generated an enormous number of excellent review articles describing many innovative and exciting developments [6-17]. The goal of this article is to provide an update of the current advances in radionuclide therapy to serve as a resource for scientists and clinicians involved in this area of fascinating research and therapy strategies. This overview is not a comprehensive review but is rather focussed on the principles of radionu-clide therapy and surveys major treatment options by dis-

2 Current Radiopharmaceuticals, 2013, Vol. 6, No. 3 Dash et al.
ease, discusses recent developments and current status, and outlines key challenges and opportunities for further devel-opment. Given the expansive of this multidisciplinary field, topics mainly of academic interest are not included and the authors apologize for possible oversights of important con-tributions.
THERAPEUTIC RADIOPHARMACEUTICALS
While RNT using radionuclides has been established
even longer than diagnostic imaging, the importance for their
use in treating neoplasia other than thyroid cancer has been
realized only in the last decade [18-19]. In RNT, a radio-
pharmaceutical can consists of a simple ion (e.g. 131
I-), a
complex (e.g. 188
Re-HEDP) or a carrier molecule labelled
with a particulate emitting radionuclide (e.g. 90
Y-DOTA-
TATE). These agents have a desired biodstribution used to
target the radiation specifically to the disease sites. A major
goal is retention at the target site long enough to deliver a
prolonged radiation dose sparing surrounding normal tissues.
The path length of the emitted radiation should be short
enough to allow effective therapy following uptake of the
radiopharmaceutical in the targeted sub-population of cells.
A number of different mechanisms are used for targeting the radiopharmaceutical to cancer cells. These include taking advantage of cellular metabolic processes such as sodium
iodide symporter (NIS) for accumulation of 131
I in thyroid cancer cells [20], the use of specific cell surface receptors for accumulating radiolabelled peptides [21] and cell surface antigens to target monoclonal antibodies. Different extracel-lular metabolic mechanisms are used to achieve selective uptake of bone seeking radiopharmaceuticals in the targeted tissues [22].
The most important direct and indirect targeting of radia-tion is the nuclear DNA. Direct action is the dominant proc-ess in the interaction of high LET particles with biological materials. The indirect effect involves, the radiation interac-tion with other molecules within the cell to produce numer-ous radiolytic reactive products such as free radicals (OH
•,
H•), O2 and H2O2. These reactive products break chemical
bonds and produce chemical changes that can result in DNA damage. Double strand DNA breaks are much more difficult to repair and are primarily responsible for cell death. The localized delivery of controlled doses of ionizing radiation initiates genomic instability that in turn induces cell death in tumor cells. Apoptosis, mitotic catastrophe, necrosis, senes-cence and autophagy are forms of cell death induced by ra-diation.
Table 1 summarizes the characteristic of therapeutic ra-dionuclides based on their radioactive decay [23]. The depo-sition of energy by ionizing radiation ( , and Auger-electrons) in cells lead to ionizations within the cells. The type of damage created within DNA depends upon the nature
Table 1. Characteristics of therapeutic radionuclides based on radioactive decay characteristics.
Characteristic Beta Decay Alpha Decay Low Energy
Electron Decay
Emission Negative charged electron Helium nucleus Auger and Coster Kronig (CK) elec-
trons
Energy 0.05 – 2.5 MeV 2-10 MeV 10 eV-10 keV
Range 0.2 – 15 mm 50-100 μm Nanometers
Path track Tortuous Straight Contorted
Ionizations Less dense Dense
Relatively dense but
only in immediate
vicinity
Linear Energy
Transfer 0.2 keV/μm 80 – 300 keV/μm 4 – 26 keV/μm
Mechanism
Cross fire effect, half life
and radioactivity
dependent, oxygen
dependent
Traversed path
length in the cell
nuclei, oxygen
independent
Breaks in DNA
Strands
("Bystander" effect)
Relative Biological
Effectiveness Low High Low
Requisite Close to target/cell
surface
Binding to cancer
cell
Incorporation into
nucleus
Cross fire effect Yes No No
Clinical application Some of the application are FDA
approved
223RaCl2 is FDA approved
(For treatment of patients with
Castration-resistant cancer who have
bone metastases)
Experimental

Targeted Radionuclide Therapy Current Radiopharmaceuticals, 2013, Vol. 6, No. 3 3
of the ionizing radiation and its energy. Schematic illustra-tion of ionization densities produced along tracks of particu-late radiation of different type is illustrated in Fig. 1.
RADIONUCLIDE CHOICE CRITERIA
In light of the explicit role of therapeutic radionuclides to
deliver a cytotoxic radiation dose sufficient to overcome the
cell response in terms of repair and proliferation, a therapeu-
tic radiopharmaceutical must meet several specifications.
The inherent determinant for the success of radionuclide
therapy therefore resides in the selection of appropriate radi-
onuclides which is based on a number of considerations de-scribed below.
• Particle emitting radionuclides ( particle, - particle or
Auger electron emitters) are suitable for therapy as they
tend to be effective at delivering localized cytotoxic ion-izing radiation [24-26].
• The choice of emission type depends on the size of the
tumor to be treated, intratumor distribution (i.e., degree
of heterogeneity of radionuclide deposition), pharma-
cokinetics, and other factors [27]. The range of - parti-
cles is in millimeters and is effective for large tumors.
The range of particles is 50-100 m so they will also
be effective for small tumors as well as micrometasta-
ses. Radionuclides that emit Auger and Coster-Kronig
(C-K) electrons are usually effective only when tagged
with carrier molecules which can cross the cell mem-
brane and reach the nucleus to cause damage to the
DNA (e.g. 111
In-Octreotide) when internalized into
the cytoplasm can help to achieve effective therapy be-cause of “bystander” effect.
• The physical half-life of the radionuclide should be matched well with the in vivo pharmacokinetics of the radiolabeled targeting molecule. The half-life must be long enough for target uptake as well as tumor irradia-tion during period of biolocalization of the radiolabeled compound in target tissue. The half-lives of most radi-onuclides used for radionuclide therapy are usually rela-tively short. Strontium-89, has 50 day half life and is widely used as
89SrCl2 for bone pain palliation and is the
longest lived radionuclide currently used in therapy RNT.
• Energy of particulate emission: The linear energy trans-fer (LET) of particles is ~ 80 keV/ m while for
- par-
ticles it is 0.2 keV/ m. Consequently, alpha particles can cause irreparable damage to DNA and 2-3 tracks of the radiation will be enough to induce cell death as compared to10
3-10
4 tracks required in the case of
particles. The energy of - particles has more implica-
tions on the success of radionuclide therapy. Depending on the energy,
- emitting radionuclides have been used
for treating different diseases. In the case of targeted therapy of other cancers, metastasis will prefer to have low energy whereas high energy
- particles are pre-
ferred for solid tumors. Bone marrow toxicity can be a major challenge while using hard
- emitters and the
amount of radionuclide which can be injected will be limited by the dose burden to the bone marrow and kid-ney.
• The specific activity of the radionuclide can be an im-
portant criterion for selecting a radionuclide for therapy.
High specific activity radionuclides are mandatory for
preparation of radiopharmaceuticals in receptor-targeted therapy and radioimmunotherapy.
• The radionuclide used for RNT should be available with
high purity (radionuclidic, radiochemical, and elemental
purity) and usually free from trace metal contamination.
Trace metal contaminants are a concern while using me-
tallic radionuclides in particular, as they interfere with radiolabelling of the chelates.
• While the particulate emission property of the radionu-
clide determines the therapeutic potential, a -emission
component is advantageous for low-dose imaging stud-
ies for dosimetry estimates and for monitoring response
to therapy. Ideally, gamma-radiation should be of low
abundance to minimize the contribution to non-target
organs and low energy (100-200 keV) to provide effec-
tive gamma camera imaging. This is becoming a more
important attribute in the emerging personalized medi-cine.
• The radionuclide should have chemistry amenable to its
attachment with a broad class of carrier molecules and
binding must exhibit high in vivo stability when attached to the radiopharmaceutical.
• Large scale production of radionuclides with high spe-
cific activity and purity for use in therapeutic application
should be carried out in a cost effective manner. Radi-
onuclides which exhibit attractive characteristics but
which lack a cost effective production route will find difficulty for wide scale utility.
Fig. (1). Schematic illustration of ionization densities produced
along tracks of particulate radiation. Alpha particles produce a high
density, beta particles create a low density and Auger cascades,
clusters of high ionization density.

4 Current Radiopharmaceuticals, 2013, Vol. 6, No. 3 Dash et al.
There is a steadily expanding list of therapeutic of radi-onuclides with different emission characteristics, which are currently being used or can potentially be used for clinical therapy. Production of therapeutic radionuclides is not only the first step in the preparation of therapeutic radiopharma-ceuticals but also the cornerstone for the success of radionu-clide therapy. Their production is carried out by the nuclear reactions either in a reactor or in particle accelerators such as cyclotron. (Fig. 2) depicts the issues associated with the se-lection and production of radionuclides for therapy. A de-tailed discussion on production of radionuclides [28-34] is beyond the scope of this article and thus not pursued further.
- Particle Emitting Radionuclides
Beta particles are negatively charged electrons emitted
from the nucleus of decaying radioactive atoms (one electron
per nuclear transformation) and have a continuous energy
spectrum ranging from zero up to the maximum - energy.
The average energy of a - particle is about one-third of its
maximum energy. Kinetic energy is lost as - particle trav-
erses through matter. The recoil energy of - radiation
is negligible. Beta particle emitters, due to low LET, produce
sparsely ionizing tracks with lower killing efficacy compared
to particle and Auger electron emitters. Beta particles used
for therapy generally have energies ranging from 0.05 to 2.5
MeV and an average LET in the order of 0.2 keV/μm of path
length. Beta particles have the longest range in tissues fol-
lowed by alpha particles and Auger electrons. The long
range of these emitted electrons leads to the production of a
‘cross fire’ effect [35] which is important and negates the
need to target every cell within the tumor as long as all the
target cells are within the range of the decay path. This so-
called crossfire effect will compensate to some degree for
heterogeneous tumor uptake [15]. Tumor response to beta
particle radiation depends on several parameters [36] which include:
• The position of the decaying atom in the targeted cell.
• Distance of the decaying atom from the cell nucleus and
• The radius of the cell nucleus
The energy of the - particles should match target site,
and as example higher energy - particles are inappropriate
for smaller metastasis as the target site will receive a reduced radiation dose per emission, due to the unwanted deposition of a larger fraction of the particle energy in normal tissue outside the target volume. In contrast, when the tumor size is large in comparison to the range of
- particle, most of the
energy is deposited within the tumor. In this context, - par-
ticle emitting radionuclides used for radiosynovectomy is a good example. The low-energy beta emitters such as
169Er
are effective in treating smaller joints (finger), the medium range beta emitters such as
175Yb,
177Lu,
186Re, etc. are useful
for medium joints (wrist, elbow, shoulder, ankle and hip joints) and high energy beta emitters
32P,
90Y,
188Re are use-
ful for knee joints. Beta particle emitting radionuclides offer a wide range of choice in terms of availability, costs, particle energy (thereby range) and chemical properties. Depending upon their energy,
- emitting radionuclides can be classified
into the following three groups.
• Low-energy emitters: Radionuclides having Eavg = 0.08–0.18 MeV and mean range of 0.4–0.9 mm are best suited for treatment of small target sites (d ~ 1–2 mm) [37]. Iodine-131 and
177Lu
are the most common radi-
onuclides in this group that has been clinically used and another good candidate in this group is
105Rh.
• Medium-energy emitters : Radionuclides having Eavg = 0.23–0.36 MeV and mean range of 1.2–1.8 mm in-clude
153Sm,
186Re ,
143Pr and
77As in this group.
• High-energy emitters: The radionuclides with Eavg = 0.5–1.0 MeV and mean range 2.2–5.0 mm are most ef-fective in treating large treatment sites (> 1 cm) [38] and 32
P, 89
Sr, 90
Y and 188
Re are commonly used radionu-clides belonging to this group.
Alpha Particle Emitting Radionuclides
Alpha particles are helium nuclei and are ~8,000 times larger than
- particles (electrons). Among charged particle
radiations particles are the least penetrating and have a very short soft tissue range. Radionuclides that emit alpha particles are highly energetic and release enormous amounts of energy over a very short soft tissue distance, typically in the range of 50-100 m. They have high LET with a mean energy deposition of 80-300 keV/ m of path length. Conse-quently, use of alpha therapy allows the specific targeting and in turn a more specific tumor cell killing ability without damage to the surrounding normal tissues. The high cytotox-icity of alpha particles in combination with the selective fea-tures of targeting vectors for membrane bound receptors of-fer the possibility for the elimination of minimal residual or micrometastases by selectively killing readily accessible isolated and pre-angiogenic clusters of cancer cells. Unlike Auger electrons, alpha particles do not require internaliza-tion, and has the capability to kill tumor cells with non-heterogeneous antigen expression in the neighborhood. Other advantages of -particles include their independence from cell cycle position as well as oxygen level [39]. This
Fig. (2). Steps involved in the production of radionuclides for
therapeutic radiopharmaceuticals preparation.

Targeted Radionuclide Therapy Current Radiopharmaceuticals, 2013, Vol. 6, No. 3 5
feature makes them proficient for eliciting tumoricidal ef-fects on both the oxic and hypoxic cell populations. Al-though the radiobiological properties of alpha-particles have been recognized since the early 20
th Century [35-39], their
use in targeted therapy has accelerated relatively recently [40]. The selection of an particle emitting radionuclide for treatment of micrometastatic lesions is primarily based on the deposition of a large amount of energy and thereby pro-vide a high dose rate. As the tumor size decreases, the poten-tial advantage of -particles over
- emitters should increase.
Auger-electrons Emitting Radionuclides
Auger electrons are emitted by radionuclides that decay by electron capture (EC) or internal conversion (IC) and as a consequence create a vacancy in an inner atomic shell. The filling of this vacancy by electrons dropping from higher shells leads to a cascade of atomic electron transitions with the emission of characteristic x-ray photons or Auger, Cos-ter-Kronig, or super Coster-Kronig monoenergetic electrons. These electrons are distinguished by the shells involved with the transition and are often collectively referred to as Auger electrons. On an average, 5-30 electrons with energies rang-ing from a few eV to keV, are emitted from an EC decay or an IC process [41]. This form of decay leaves the resultan-tant atoms transiently with a high positive charge, resulting in subsequent charge-transfer processes and leads to the deposition of highly localized energy around the decay site [42]. Auger-electron-emitting radionuclides have the follow-ing properties:
• As the radioactive atom undergoes electron capture (EC)
or internal conversion (IC) decay, multiple electrons are
emitted per decaying atom;
• These electrons traverse a very short distance (only
few nm diameters);
• the LET of the electrons is 20-fold higher than that ob-
served along the tracks of energetic (>50 keV) beta par-
ticles.
• These electrons dissipate their energy around the decay
site, and molecules in the immediate vicinity of the de-
caying atoms and results deposition of 106 to 10
9
cGy/decay in an extremely small volume (in a few cubic
nanometers)
The evaluation and potential use of Auger emitters for
therapy has been essentially focused on cancer therapy. The
possibility of incorporating an Auger emitter in close prox-
imity to the cancer cell DNA has immense therapeutic poten-
tial. The double stranded DNA helix presents a diameter of 2
nm. In a typical Auger radiation decay, the highest energy
deposition occurs in spheres of 1-2 nm [43]. This means that
the local energy deposition of an Auger emitter is sufficient
to disrupt both DNA strands over distances of several nu-
cleotides [44,45]. Besides the direct effect, indirect effects
caused by radical species that arise principally from the ra-
diolysis of water can cause further DNA damage. In addi-
tion, the molecule containing the excited atom is also sub-
jected to damage caused by charge neutralization. As a con-
sequence, biomolecules incorporating Auger electron emit-
ting radionuclides offer the opportunity to deliver a high
radiation dose to the tumor cells with high radiotoxicity
while minimizing toxicity to normal tissue [46]. Further-
more, many Auger-electron emitters also emit -radiation,
this property makes Auger emitting radionuclides attractive
option as ‘theranostic’ agents for molecular imaging as well
a targeted therapy of cancer.
CARRIER MOLECULES USED IN RADIONUCLIDE THERAPY
The carrier molecule for an ideal therapeutic radiophar-maceutical preparation should meet certain requirements such as:
• Non toxic as determined with a high LD50 (lethal dose at
50% survival) value.
• Resistance to radiological degradation.
• Availability with required purity or easy to prepare or
synthesize without much chemical manipulation.
• Amenable to site specific chemical modifications for
radiolabeling.
• Non-immunogenic.
• High binding affinity and specificity towards target
site/cells.
• Exhibit in vivo stability to preclude the degradation of
the radiolabeled biomolecules after cellular internaliza-
tion and/ or binding.
• The radiolabeled species should be minimally affected
by changes in pH, temperature and other denaturing
agents or environmental conditions.
Some typical examples of radionuclide carriers used in the preparation of therapeutic radiopharmaceuticals include:
Liposomes
Liposomes have been studied to serve as carriers of radi-
onuclides for vascularised tumors [47]. Liposomes are single
bilayer capsules with distinct interior compartments in which
therapeutic agents can be sequestered from the exterior envi-
ronment. The polar parts of the individual lipids face the
vascular water compartment, while the hydrophobic parts of
the lipid provide a barrier in which hydrophilic or charged
molecules are poorly soluble. Hydrophobic molecules can be
dissolved within the bilayer [48]. Phospholipid bilayer mem-
branes have a thickness of about 4 nm and liposomes may
entrap thousands of water soluble molecules in their internal
aqueous compartment [49]. Liver and spleen are common
accumulation sites for liposomes.
Dextran
Dextran is a branched polysaccharide made of many glu-
cose molecules joined into chains of varying lengths. Dex-
tran seems suitable as a carrier of radionuclides for passive
accumulation at the sites of vascularized tumors aimed for
therapy and has also been extensively studied [50]. Similar
to liposomes, the size of dextran is of a few nm; and liver
and spleen are common accumulation sites.

6 Current Radiopharmaceuticals, 2013, Vol. 6, No. 3 Dash et al.
Bisphosphonates
Bisphosphonates are biologically stable analogs of natu-
rally occurring pyrophosphates. They inhibit osteoclast-
mediated bone resorption by binding to bone mineral and
interfere with osteoclast activation. They also promote repair
by stimulating osteoblast differentiation and bone formation.
As a result, these agents are successfully used to deliver -
particle emitting radiometals [e.g. 153
Sm, 186/188
Re, 166
Ho, 177
Lu] for bone-pain palliation. These radiolabelled bisphos-
phonates bind to hydroxyapatite at sites of active bone for-
mation (osteogenesis) [51-54].
Peptides
The over-expression of many peptide receptors on human tumor cells compare to normal tissues makes these receptor attractive molecular targets for radiotherapy. The most commonly used peptide based therapy is the use of soma-tostatin (SST) analogs for the treatment of neuroendocrine tumors (NETs) [55-57].
Peptidomimetics
Peptidomimetics are small protein-like chains which arise either from modification of an existing peptide, or by designing similar systems that mimic peptides, such as pep-toids and -peptides [58]. The altered chemical structure is tailored to improve the molecular properties such as, stability or biological activity to develop improved target from exist-ing peptides [59-60].
Antibodies
The exquisite specificity afforded by monoclonal anti-
bodies and their fragments has long been recognized for their
ability to serve as carriers in the development of therapeutic
radiopharmaceuticals [61]. Most tumors over-express some
tumor antigens and once these antigens are identified, mono-
clonal antibodies (MoAb) can be prepared against them by
following the hybridoma technique [62]. Monoclonal anti-
bodies are prepared fusing B lymphocytes cells obtained
from antigen immunized mice with myeloma cells. Through
repeated cloning and selection, the hybridoma cells which
are responsible for making the specific antibodies are iso-
lated and propagated in culture medium for the preparation
of specific monoclonal antibodies. Monoclonal antibodies of
the immunoglublin G (IgG) type are macro molecules with
molecular weight of about 150,000 Da. These macromole-
cules have slower in vivo kinetics compared to peptides. The
monoclonal antibodies are of mice origin and hence will
create human anti mouse antibody (HAMA) response on
repeated injections. Most monoclonal antibodies which are
now used in therapy thus are mainly humanized to avoid the
HAMA response [63]. If adequate antibody localization at
the site of disease is achieved, a therapeutic dose of the same
antibody could be administered after labeling with a radi-
onuclide capable of inducing curative effects. In most cases,
antibody radiolabeling is accomplished either by iodination
of tyrosine residue for radiolabeling with 131
I or by conjuga-
tion of chelating moieties for conjugation of radiometals to the antibody molecules [64-66].
Affibody
Affibody molecules are engineered proteins developed to
bind peptides or proteins and are therefore categorized as
antibody mimetics. They are typically of about 6000 Da hav-
ing helices with no disulphide bridges. Being smaller in
molecular weight they have faster in vivo uptake and exhibit
renal clearance. The antigen binding sites are engineered by
having randomization of 13 amino acids located in the two
helices. Affibodies modified with chelators and labeled with
radiometals offer the potential to develop therapeutic radio-
pharmaceuticals [67].
RADIOLABELING
The ultimate aim of any radiolabeling strategy is to achieve a high specific activity radiolabeled formulation in which the radioisotope is attached to maximum number of molecules. High specific activity labeling is generally achieved by the following two general approaches:
• Direct labeling method,
• Indirect labeling approach using a bifunctional chelate (BFC).
Several requirements need to be fulfilled for effective la-beling of a target molecule and in general the labelling chemistry should be fast, regiospecific, reproducible and provide a stable, labeled product in high radiochemical yield.
Characteristics of the Radiolabeled Species
With the exception of those radionuclides which are
aministered directly as ionic species (e.g 131
I, 89
Sr, 223
Ra etc),
the radionuclide must be incorporated into bioactive mole-
cules rapidly, efficiently, and in such a way that the radiola-
belled product retains biological activity.
• The procedure adapted should exhibit high radiolabeling efficiency and provide high specific activity of the ra-
diolabeled preparation.
• The radiolabeling procedure should be simple, rapid,
reproducible and adaptable for kit formulation proce-
dure. A cold kit contains the ligand to which radiometal
is to be complexed, a buffer agent to adjust the pH to
suit the labelling conditions, stabilizing agents and ex-cipients. The kits are prepared in a freeze-dried form and
have a long shelf life, ranging from several months to
years
• Near qunatitiave radiolabelling is desirable to avoid the
necessities of post radiolabeling purification of the ra-
diolabelled product. In most cases, this is difficult and a
suitable purification step is thus essential and often re-quires microcolumn or HPLC purification.
• Biological activity of radiolabeled molecule should be
preserved during and after radiolabeling.
• An important parameter to consider is the in vitro and in
vivo stability of the radiolabelled species. Any decom-position or leaching of the radionuclide from the carrier
molecule should be within acceptably defined limits.

Targeted Radionuclide Therapy Current Radiopharmaceuticals, 2013, Vol. 6, No. 3 7
Pre-clinical validation is a prerequisite before translation of radiolabeled products into clinical trials and consists of the following steps:
• Development of animal models.
• Translational development from animal models into clinical models to population level.
• Validation of clinical models for the purpose of progno-sis, diagnosis, staging of disease, and selection and monitoring of therapy.
The practice of studying the distribution of radiation re-sulting from the systemic or locoregional administration of a therapeutic radiopharmaceutical in patients is termed ‘do-simetry’ which requires not only a thorough understanding of its biodistribution and pharmacokinetics but also a meth-odology for translating total number of radionuclide disinte-gration in a particular anatomical volume to the absorbed dose to the volume [68]. Dosimetry in targeted therapy is evolving from a standard anatomical model-based calcula-tion that provides mean absorbed dose over a target organ volume to a calculation that provides the spatial distribution of absorbed dose over the individual patient target and organ geometry and that also incorporates radiobiological model-ing as a step towards assessing the biological consequences of the dose distribution.
Issues relating to the above requirements are outside the scope of this paper and thus not discussed further, but have been discussed in detail in recent reviews [69-76].
RADIONUCLIDE THERAPY FOR DIFFERENT DIS-EASES
This section provides a brief overview of the radionu-clide therapy methods currently used for treatment of various types of diseases.
Polycythaemia
Polycythemia vera is a clonal disorder of the hema-topoietic stem cell compartment characterized by an increase in red cell volume. The primary form, polycythemia rubra vera, presents as a clonal neoplastic disorder, and in secon-dary forms due to appropriate or inappropriate increases in levels of erythropoietin. Phosphorous-32 as
32P-
orthophosphate (32
PO43-
) has been used for the treatment of elderly patients with polycythemia vera and essential throm-bocytopenia with remarkable myelosuppressive efficacy [77,78]. Treatment regimens for polycythaemia are usually based on an intravenous injection of 74-111 MBq of
32P per
square meter body surface area but should not exceed 185 MBq (5 mCi) for each injection [79]. Any relapse or failure to respond within 12 weeks may require retreatment with dosages up to 260 MBq (7 mCi). The therapeutic aim is to suppress rather than eradicats hyperproliferative cells [80]. The therapeutic dose is usually well tolerated and complete remission is obtained in up to 98% of cases [81]. Based on evidence of effectiveness and side effects of
32P, this form of
therapy is well suited for elderly patients (>65 years), par-ticularly those with poor venous access or unable to attend regularly for medical care [82,83]. It is not recommended for the young and middle-aged populations owing to an in-
creased incidence of hematological and non-hematological malignancies that lead to the risk of leukaemia and myelo-dysplastic syndromes after therapy [80,84]. This mode of therapy is now rarely practiced as drug based alternatives are available.
Thyroid Cancer
Use of iodine-131 for the treatment of thyroid cancer pa-tients is a key example of the early and most successful clinical use of radionuclide therapy [85]. Thyroid carcinoma is the most common malignant tumor of the endocrine glands. Ninety percent of malignant thyroid nodes are well-differentiated thyroid carcinomas (DTC), including papillary and follicular carcinomas [86]. Iodine-131 therapy is used increasingly as a first-line therapy for adult in many clinical situations.
Based on its concentration by thyroid cancer cells, ra-dioiodine therapy in patients with papillary and follicular thyroid carcinoma has frequently been divided into ablation of thyroid remnants and treatment of metastases. For abla-tion therapy,
131I as sodium iodide is administered to elimi-
nate postoperative remaining normal thyroid tissues and de-stroy occult microscopic carcinoma. It is prescribed in a dose of 1.85-3.7 GBq (50-100 mCi) 4 to 6 weeks after total or near-total thyroidectomy [87]. For pre-ablation diagnos-tic scintigraphy tracer dosages of
131I is recommended in
order to avoid thyroid tissue stunning [88].
For treatment of metastases, 131
I is often administered ei-ther in liquid form or as capsules, following thyroid stimulat-ing hormone (TSH) stimulation obtained after thyroid hor-mone withdrawal, in a dosage of upto 7.4 GBq (200 mCi). It is rapidly absorbed from the gastrointestinal mucosa. Within the thyroid gland, iodine is taken up by differentiated follicu-lar thyroid cells through an enzymatic pathway which con-verts inorganic iodide to protein bound iodine. The efficacy of the therapy not only depends on the concentration of
131I
in the tumor but also on the time period it takes to accumu-late in the thyroid gland. The biological half life of
131I in
tumor tissue is about 10 days whereas in normal thyroid it is more than 60 days [89]. Lower dosage is recommended (80-120 mCi) if diffuse lung metastases are present in order to prevent lung fibrosis (pneumocities) [90]. In order to reduce the risk of bone marrow supression,
131I retention in the body
should not be greater than 4.44 GBq (120 mCi) at 48 hours and the delivery of less than 2 Gy to the blood [91]. While the use of
131I for thyroid cancer treatment constitutes the
most successful form of radionuclide therapy, the high inci-dence of early or late hypothyroidism makes it obligatory to monitor patients adequately after treatment [92]. There is large and growing body of literature demonstrating the effec-tiveness of
131I in the management of well differentiated thy-
roid cancers. Today, 131
I therapy is the most effective therapy in the treatment of differentiated thyroid carcinomas (up to 95%). It is expected that
131I therapy will remain as one of
the main forms of treatment for thyroid cancers in the fore-seeable future.
Neuroendocrine Tumors (NETs) using 131
I-mIBG
Metaiodobenzylguanidine (mIBG) is a catecholamine analogue similar to noradrenalin, uptake of
131I-mIBG radio-

8 Current Radiopharmaceuticals, 2013, Vol. 6, No. 3 Dash et al.
pharmaceutical occurs in the medullary adrenal catechola-mine storage vesicles.
131I-mIBG is useful to image as well
as treat sympatomatic medulla neoplasms, such as neuroblas-toma and pheochromocytoma. Neuroblastoma is the most common intra-abdominal malignancy of infancy and the most common extracranial solid tumor of childhood. It arises from the sympathetic nervous system primary sites in adre-nal glands and in paraspinal locations from neck to pelvis [93]. Since mIBG structurally resembles norepinephrine, it enters neuroendocrine cells by an active uptake mechanism and is stored in the neurosecretory granules [94]. Phaeo-chromocytomas and paragangliomas are tumors originating from chromaffin tissue, phaeochromocytoma arising from the adrenal medulla and paragangliomas are from extra-adrenal sites along the sympathetic or parasympathetic chain [95]. mIBG is selectively concentrated by these tumors as well as occasional carcinoid tumors and medullary carci-noma of the thyroid, entering the cells via the vanillylman-delic acid (VMA) transporters VMAT1 and VMAT2 [96]. Avid uptake of
131I-mIBG in pheochromocytoma and neuro-
blastoma permits its use as a therapeutic agent for NETs [97]. Although a variety of therapeutic regimens have been described in the literature, activities ranging from 3.7 to 11.1 GBq per administration are widely accepted. The cumulative administered doses varies from case to case basis [98]. Sev-eral treatments may be required at intervals of 3–6 months to obtain therapeutic success [99].
131I-mIBG is probably one of
the treatments of choice for patients with advanced NET disease, since the invasiveness and toxicity of this therapy compare favorably with that of chemotherapy, external beam radiotherapy and immunotherapy.
Bone Pain Palliation Therapy
Bone metastasis is a common complication in cancer pa-tients and often present with severe bone pain. Bone metas-tases may occur in almost all tumors at different frequencies, however, prostate, lung, and breast cancer most commonly results in skelatal metastasis. More than 50% of patients with advanced breast or prostate cancer develop bone metastases at one stage or the other. If undiagnosed or inadequately treated, metastasis will often lead to spinal cord compres-sion, hypercalcemia, and pathological fracture of involved bones. The general tendency is to significantly affect the quality of life.
Radiopharmaceutical treatment of metastatic bone pain has emerged as an effective modality that provides palliation of pain to multiple areas of the skeleton simultaneously without the significant soft-tissue toxicity [100-101]. It is one of the treatment modalities that have been around for 70 years [102]. Radiopharmaceuticals used for the palliation of painful bone metastases should possess the following crite-ria:
• Selective uptake and prolonged retention of the radio-pharmaceutical at metastatic sites in contrast to normal bone i.e. high tumor-to-normal bone ratio;
• Fast clearance from normal bone and soft tissues[103];
• Biodistribution patterns predictable based on bone scin-tigraphy;
• In vivo stability of the radiopharmaceutical must be en-sured to provide therapeutic outcome.
Radionuclide bone therapy can be used for:
• The treatment of primary bone tumors such as osteosar-coma, where the bone-seeking radiopharmaceutical be-haves like a tumor-seeking agent.
• Targeting the tumor-produced osteoid of not only the primary tumor and its skeletal metastases, but also the extra-osseous metastases.
• Therapy using bone-seeking radiopharmaceuticals for the palliation of painful skeletal metastases.
While the use of radiopharmaceuticals in tumor therapy involves their incorporation into or fixated to the tumor cell; bone therapy targets the reactive osteoblastic reaction in the normal bone directly adjacent to the metastasis, which is generally the cause of pain.
Common Radionuclides Used for Bone Pain Palliation
A summary of the common beta emitting radionuclides used for bone pain palliation treatment and their characteris-tics is shown in Table 2. The radionculides used and pro-posed for bone pain palliation have wide ranging nuclear characteristics such as half life, decay energy, availability, imageable photons, etc. One important advantage is that there is no need to have high specific activity radionuclides for preparing bone pain palliating agents. Several radionu-clides are approved and reimbursed for rourine clinical use are promising candidates for expanded clinical evaluation. A brief description of some of the commonly used radionu-clides is given below.
Phosphorus-32
32P in the form of sodium orthophosphate was the first
systemic radionuclide to be used for the treatment of bone metastases. Phosphorus is one of the major components of bone and is taken up by the calcium hydroxy apatite struc-ture. However,
32P also has strong incorporation into phos-
phorus containing intracellular constituents such as RNA and DNA. The standard dose for therapy is 148 MBq (4 mCi). Phosphorus-32 is no longer in common use since the 1980s because of induced bone marrow toxicity [104].
Strontium-89
89Sr behaves biologically like calcium and is taken up in
areas of osteoblastic bone metastases and the unbound 89
Sr activity is eliminated from the body through both the urinary and gastrointestinal systems [105]. The standard prescribed dose for
89Sr as SrCl2 (Metastron
®) is 148 MBq (4 mCi) for
all patients. The US Food and Drug Administration (FDA) has approved the use of
89Sr for therapy [106]. Due to the
long half life of 89
Sr, it is generally recommended for use in patients with moderate pain and a reasonable life expectancy.
Samarium-153
A major impediment using 32
P and 89
Sr is the relatively long range of the energetic
- particles in soft tissues and
bone resulting in significant irradiation of the marrow com-partment which can lead to usual transient depression of bone marrow function. Bone marrow toxicity limits the dose which can be administered to patients. As a result, signifi-cant research has been focussed on the prospects of using other radionuclides with more favorable radiation proper-

Targeted Radionuclide Therapy Current Radiopharmaceuticals, 2013, Vol. 6, No. 3 9
ties with distinct mechanisms of action. Among these, 153
Sm-EDTMP merits attention but because of the absence of in-herent bone-seeking properties,
153Sm is chelated to ethylene
diamine tetramethylene phosphonate (EDTMP), which tar-gets the bone matrix as a polyphosphonate [107].
153Sm-
EDTMP concentrates in the skeleton, in proportion to os-teoblastic activity. Several studies have shown the effective-ness of
153Sm-EDTMP in palliating pain from bone metasta-
ses [108-111]. The standard prescribed activity of 153
Sm for patients with bone metastases is 37 MBq (1 mCi)/kg to a maximum of 5.55 GBq (150 mCi) per patient.
153Sm-EDTMP
(Quadramet®
) is the most widely used agent in the United States for the treatment of bone pain palliation.
Investigational Radionuclides for Bone Pain Palliation
Rhenium-186 and 188
Re are the two radionuclides which
form stable bisphosphonate complexes with hydroxyeth-
ylidene diphosphonate (HEDP) and are also used for bone
pain palliation. Among the two radionuclides, 186
Re will
cause minimal myelosuppression due to its lower - energy
[112,113] and hence will be useful in patients with poor
bone marrow reserve [114]. The maximum tolerated dose of 186
Re-HEDP is reported to be 2.4 GBq (65 mCi) [115]. Evi-
dently this agent is no longer available on physician pre-
scription in Europe. Similar to 186
Re, targeting with 188
Re is
achieved by chelation with HEDP. The short physical half-
life resulted in high dose rates and relatively high doses [up
to 2.59 GBq (70 mCi)] can be administered to patients lead-
ing to rapid symptom response. The higher beta energy of 188
Re can also result in transitory bone marrow involvement [116,117].
Fractionated therapy has been shown to prolong
response duration and progression-free survival in a small
series of patients [116].
Tin-117m is an Auger electron emitting radionuclide and
has been under investigation for a long time for the treatment
of bone metastases. It differs from other radionuclides as
regards to its mode of radioactive decay and bone deposition.
While this radiometal is a natural bone-seeker, its highest
specificity for bone necessitates the element to be in its
quatravalent state (4+). In order to circumvent this drawback,
it is chelated with diethylenetriaminepentaacetic acid
(DTPA) that stabilizes Sn in this preferred 4+ state, protect-
ing it from competing redox reactions in vivo [118]. The
decay of 117m
Sn to 117
Sn by an internal conversion process is
accompanied by the ejection of conversion electrons that
have 1.7-5.5 times lower energy than the other - emitting
radionuclides discussed above. The low energy and short
range of the emitted conversion electrons are reported to
provide an optimal therapeutic window [119,120]. It has
been reported that pain relief with 117m
Sn in patients with
metastatic prostate cancer has been effective, with a low risk
of myelosuppression [121,122]. Techno-economic feasibility
of large-scale production of 117m
Sn emerges as the major
roadblock for the wide scale use of this reagent.
More recently, attention has been focused on the use of the -emitting radionuclide
223Ra. Radium has a natural af-
finity for metabolically active bone due its chemical similar-ity with calcium. Owing to the limited range and high linear energy transfer of the alpha particle, use of
223Ra allows a
highly localized density of ionizing radiation to nearby tu-mor cells, causing significant amount of irreparable double-stranded DNA damage rendering cellular repair mechanisms ineffective [123], with minimal exposure to the nearby bone marrow, resulting in a high therapeutic index [124]. Use of 223
Ra is recommended for patients with skeletal metastases having therapy-resistant disease. It is commonly adminis-
Table 2. Key examples of beta emitting radionuclides for bone pain palliation
Radionuclide Half Life
(days)
E max.
(Mev)
Maximum
Range (mm)
Gamma
Emission
(keV )
Imaging Chemical Form Usual Adminis-
tered Activity
32P 14.3 1.71 8.7 none Brems Phosphate
444 MBq
[fractionated]
89Sr 50.5 1.46 8.0 none Brems Chloride 148 MBq
186Re 3.77 1.07 5.0 137 Gamma HEDP 1.3 GBq
188Re 0.7 2.12 3.0 none Gamma HEDP 1.3–4.4 GBq
153Sm 1.95 0.805 3.0 103 Gamma EDTMP 37 MBq/kg
117mSn 13.6 <0.001
0.13 and 0.16
(conversion
electron)
0.159 Gamma DTPA 2–10 MBq/kg
223Ra 11.4
5.78 ( )
average <0.01 0.154 Gamma Chloride 50–200 kBq/kg
177Lu 6.7 0.497 1.8 208 Gamma
EDTMP
DOTMP
Not
established
170Tm
128 0.968 3.1 84 Gamma EDTMP Not established
DTPA=diethylenetriamine pentaacetic acid; EDTMP=ethylenediamine tetramethylene phosphonic acid; HEDP=1-hydroxy ethylidene-1,1-diphosphonic acid; DOTMP (Tetra-azacyclo-dodecano1,4,7,10 Tetra-amino methylene phosphonate)

10 Current Radiopharmaceuticals, 2013, Vol. 6, No. 3 Dash et al.
tered as 223
RaCl2. It is predominantly excreted via the gastro-intestinal tract, with less than 10% renal clearance [125]. On May 15,2013, the US FDA approved
223RaCl2 for the treat-
ment of patients with Castration-resistant prostate cancer who have bone metastates.
Potential Radionuclides for Bone Pain Palliation
Lutetium-177 is an attractive radionuclide for develop-ing bone pain palliation agents (Table 2). The lower energy
- particles are expected to minimize any possible damage to
the bone marrow. The 6.7 day half life is logistically favor-able for shipment of
177Lu radiopharmaceuticals. There is
abundant international capability for the large scale produc-tion of relatively high specific activity
177Lu suitable for
preparation of bone pain palliation radiopharmaceuticals. Preclinical studies and initial clinical trials of
177Lu-EDTMP
have shown encouraging results [126-129]. Results of clini-cal trials reveal that
177Lu-EDTMP is an effective option for
palliation of metastatic bone pain in patients with prostate or breast cancer. A dose of 1295 MBq (35 mCi) is sufficient for bone pain palliation therapy, and doses as high as 2590 MBq (70 mCi) are well tolerated.
There are also other radioisotopes which decay with emission of low energy particles which are good candidates for bone pain palliation. Ytterbium-175 is another low en-ergy
- emitter which has also been suggested for bone pain
palliation. The low - energy of
175Yb (480 keV) will induce
minimum radiation dose to bone marrow and hence will al-low higher levels of radioactivity to potentially obtain even a therapeutic efficacy similar to that demonstrated for
153Sm
and 188
Re. Similar to 153
Sm, it can also be chelated to poly-amino-poly phosphonate ligands [130]. In addition, thulium-170 in combination with EDTMP is considered as an alterna-tive to
89SrCl2 in palliative therapy of bone metastases. The
use of 170
Tm would exhibit low myelosupression since emis-sion of lower energy
– particles [E (max) = 968 keV] than
those emitted by 89Sr, and the -photons emitted can be used
for scintigraphy to detect the accumulated activity and bioki-netics at the target sites [131]. The long half life of 128.6 days could be advantageous and as a mixed radionuclide therapy using
170Tm together with
153Sm,
177Lu or
175Yb could
provide both early and sustained long term pain relief to pa-tients in early stage of disease.
Radiosynovectomy
As a non-cancer application of therapeutic radiopharma-ceuticals, the use of therapeutic radioisotopes for treatment of arthritis is widespread. Rheumatoid arthritis (RA) is one of the most common autoimmune inflammatory diseases caused from destruction of diarthrodial or synovial tissues which causes severe pain, disability, and immobility in these individuals [132,133]. Radiosynovectomy or radiosyno-viorthesis is defined as the restoration of inflamed and dam-aged synovial membrane of the joints after intra articular injection of radionuclide based preparations. In this proce-dure, a beta-emitting radionuclide in colloidal or particulate form is injected into the articular cavity in which they are phagocytized by the outermost cellular layer of the synovial membrane and deliver radiation dose to the synovium with-out excessive irradiation of surrounding tissue.
Principle of the Therapy
The presence of the radiolabelled particulates or radionu-clide loaded colloid particles in the joint cavity are recog-nized as foreign bodies by the outermost cellular layer of the synovial membrane and as a result are phagocytosed by these cells. This selective irradiation of the synovial mem-brane leads to a fibrotic and sclerosed synovial membrane. The result is apoptosis and ablation of the inflamed synovial membrane [134, 135]. This is followed by progressive fibro-sis of the synovial stroma, the vessels and infrequently, mild diffuse damage to the joint bones [136]. There is also a re-duction in the filtration and reabsorption of the synovial fluid. After a few months, the synovial membrane is fibrosed without signs of mononuclear infiltration. In this way, fur-ther destruction of the joint cavity by immunological reac-tions is prevented and a long term remission is achieved [137]. This process results in alleviation of the pain, improve mobility and preserve joint function which all contribute to significant improvement in quality of life.
Advantage of Radiosynovectomy
• Minimally invasive intervention.
• Radiosynovectomy is generally performed as an outpa-tient procedure.
• Provides an attractive treatment option for inoperable patients.
• Intensity and duration of rehabilitation is minimal.
• Effective radiation dose for the treatment is low.
• Multiple joints may be treated simultaneously or at short intervals.
• Multiple radioactive dose administration to achieve maximum response.
Selection of Radionuclides
Radionuclides that can be used for radiosynovectomy should have the following properties:
• Since beta radiation can penetrate only a few hundred
cell diameters, microparticles labeled with beta emitting radionuclides are effective in treating the disease by ra-
diation in confined spaces without endangering nearby normal tissue [138].
• The energy of beta radiation should be sufficient to af-
fect only the synovial membrane without affecting the cartilage, adjacent bone underneath.
• The radionuclide particles should be sufficiently small enough to be phagocytosed in the joint, but not too small to leave the joint space through lymphatic drainage be-
fore being phagocytosed. The ideal size is between 2 – 5 M [139].
• The particles should ideally be biodegradable to prevent formation of granulation tissue at the local site. Any bio-
logically induced degradation of the agent should ideally release the radionuclide in a chemical form that would
be rapidly excreted from the body.
Many beta emitters in different particulate chemical forms have been used as radiosynovectomy agents

Targeted Radionuclide Therapy Current Radiopharmaceuticals, 2013, Vol. 6, No. 3 11
[140,141]. The selection of radionuclides for radiosynovec-tomy of specific joint is critical since the synovial thickness (e.g., finger, wrist, knee, etc.) varies substantially. Selection of the radioparticle and thus degree of soft tissue penetration is therefore primarily based on the size of the joint to be treated. For smaller joints lower energy is preferable and the short range beta emitters such as
169Er are effective in treat-
ing smaller joints (finger). The medium range beta emitters such as
175Yb,
177Lu,
186Re etc. are useful for medium joints
(wrist, elbow, shoulder, ankle and hip joints) and high en-ergy beta emitters
32P,
90Y,
188Re with tissue penetration of 3
to 11 mm are useful for knee joints. Effective dose to be de-livered to the joints is determined by the size of the joint, synovial thickness, synovial structures (smooth, villous-fine/rough edematous), condition of the joint fluid (watery or gelatinous) and inflammatory activity of synovium. How-ever, the usual dose is a few MBq (millicuries). Table 3
summarizes the nuclear characteristics of radionuclides commonly used in radiosynovectomy.
With over 35 years record in clinical practice, radio-synovectomy of the joints has been found to be an effective alternative procedure for treating early stages of chronic synovitis in rheumatoid arthritis patients [142-145]. As for the future prospects of the technique, many promising radi-onuclides such as
177Lu,
153Sm with favorable decay charac-
teristics and cost-effective production routes are expected to be used in this modality of treatment [146,147].
Treatment of Hepatocellular Carcinoma (HCC) and Hepatic Malignancies
Hepatocellular carcinoma (HCC) is a malignant tumor of the liver hepatocyte which may present either as primary
liver cancer or as secondary liver tumors. HCC represents the sixth most common malignancy worldwide and the third most common cause of cancer-related mortality causes with almost half a million deaths annually [148-150]. Normal hepatocytes have a lower tolerance to the effects of radiation than neoplastic tissue. The required cytotoxic radiation dose for HCC is estimated to be 70 Gy which is far greater than the liver tolerance dose of 35 Gy [151]. Radioembolization is one of the intriguing therapies for the treatment of liver ma-lignancies for administering radiotherapy internally to pro-vide the cytotoxic radiation dose. The technique of trans-arterial radio-embolization exploits HCC preferential blood supply from the hepatic artery [152] to deliver the radioac-tive particles which end up in hepatic end-arterioles, allow-ing localized delivery of therapeutic doses, while sparing the surrounding liver parenchyma.
Thus, it is essentially a flow-
directed mode of treatment that is dependent of neoangio-genesis.
Advantages
• The tumor destroying effect of the radiation does not
depend upon the cellular characteristics of HCC as it is
not necessary for the radionuclide to be taken up by the
tumor cells for effectiveness.
• Since the hepatic artery is usually not embolised, it can
be safely used in patients with compromised liver func-
tion or portal vein thrombosis.
• Use of gamma emitting radionuclides, such as 131
I and 188
Re makes external dosimetry possible which can help
in individualising the treatment procedure and thus in
avoiding/reducing side effects/toxicity and achieving
Table 3. Decay characteristics of key radionuclides used in radiosynovectomy
Radionuclide Half Life
[days]
Max. -
energy [MeV]
Tissue Penetration
Depth [mm]
-energy
[keV] Particle Size Dose Remarks
165Dy 0.1 1.29 5.7 95 3-10nm 9.99 GBq
(270 mCi)
Large joints
166Ho 1.2 1.85 / 1.77 8.5 81 5-10 m 370 MBq
(10 mCi)
Large joints
198Au 2.7 0.96 3.6 411 20-70 m 259 MBq
(7 mCi)
Large joints
90Y 2.7 2.28 11.0 - 100 m 148 MBq
(4 mCi)
Large joints
186Re 3.7 1.07 / 0.93 3.6 137 5-10 m 92.5 MBq
(2.5 mCi)
Medium size
joints
32P 14 1.71 7.9 - 0.6-4 m 74 MBq
(2 mCi)
Large
joint
169 Er 9,4 0.34 / 0.35 1.0 - 2-5 m 37 MBq
(1 mCi)
Small
joints

12 Current Radiopharmaceuticals, 2013, Vol. 6, No. 3 Dash et al.
better tumor response by administering the tumoricidal
dose.
• Prophylactic irradiation of apparently normal liver pa-renchyma can reduce the risk of recurrence (adju-vant/neoadjuvant role).
Selection of Radionuclide
Radionuclides that can be used for the treatment of HCC should meet the following criteria:
• High energy - radiation with low mean free path is de-
sirable for the effective delivery of a cytotoxic radiation dose to the tumor and at the same time limit the radia-tion exposure to the vicinity of the tumor while main-taining healthy hepatic parenchymal exposure to toler-able levels.
• The physical half-life of the radionuclide used should be relatively short.
• The chemical characteristic of the radionuclide prepara-tion should be amenable for incorporation into a wide range of embolic particles.
• Detectable percentage of emission for imaging and dosimetry.
Selection of Carrier
The carrier for intra-arterial therapy should possess the following properties [153].
• Mechanically robust enough to withstand the capillary force during passage through the capillary network.
• Good stability to circumvent elution of the radioactivity by macrophage removal or radiolysis.
• Near uniform size.
• Density of the particles should be optimum to prevent settling or streaming.
• Chemical characteristics should permit simple and effi-cient radiolabeling.
• Non toxic, biocompatible and preferably biodegradable.
In this modality, 131
I or 188
Re labeled lipiodol, 90
Y or 166
Ho labeled microspheres/particles are some of the radio-pharmaceuticals that have been extensively studied. Physical characteristic of these radionuclides are shown in Table 4.
A large number of studies using 131
I-lipiodol have been reported for the treatment of unresectable HCC [154-162]. Lipiodol is a mixture of iodinated fatty acid ethyl esters of poppy seed oil which contains 38% of iodine by weight and
has traditionally been used as a contrast medium for the de-tection of HCC. Lipiodol remains in these tumors for a longer period compared to normal liver or in other tissues. In order to preclude the toxicity of
131I, it is essential to block
the thyroid gland before and after the treatment. The proce-dure involves a selective hepatic artery injection of 2 to 3 mL of
131I-lipiodol with an activity of 0.9 to 2.4 GBq
[163,164]. The response of HCC and therapeutic outcome is very much dependent on the size of the tumor as well as the activity level delivered for treatment. The required activity for therapy is calculated for a given tumor mass according to its size. There is also a role for
131I-lipiodol as an effective
therapy option in patients with portal vein thrombosis [165,166]. One of the main limiting factors for
131I-lipiodol
is the requirement of long period of patient isolation owing to the long half life of
131I. Availability of
131I-lipiodol, pre-
dictability of the radiolabeling yield, stability and cost are major issues. No significant tumor reduction is usually seen after single treatment of liver metastases. In order to achieve optimum response, multiple sessions may be required. Some authors have expressed their concern about inducement of hypothyroidism in treated patients, however, can be taken care by hormone supplement therapy, if it occurs [167].
Other beta-emitting radioisotopes have been evaluated for this application and a number of embolic platforms of 188
Re such as glass microspheres [168], human serum albu-min microspheres [169], poly (L-lactide) (PLA) micro-spheres [170], and lipiodol have been studied for their possi-ble use in the treatment of inoperable HCC [171]. Among these agents,
188Re-4-hexadecyl-1,2,9,9-tetramethyl-4,7-
diaza-1,10-decanethiol (HDD) labeled iodized lipiodol has received maximum attention [172-178]. Rhenium-188 has advantages over
131I due to lower energy emission (155
KeV vs 365 KeV), greater - penetration, shorter half life
(16.9 h vs 8 d), higher dose value as well as availability from a generator. The quantity of
188Re-HDD-lipiodol adminis-
tered is based on the radiation absorbed dose to critical or-gans, which is calculated after administration of test dose of the radioconjugate, transarterially [175]. An International Atomic Energy Agency (IAEA) sponsored multicentre study using intra-arterial
188Re lipiodol for the treatment of inoper-
able HCC showed safety and efficacy of this radioconjugate [175]. The limited availability as well as the current high cost of
188W/
188Re generator aren impediments towards its
wide scale applicability. The requirement of greater patient dose due to its shorter half-life is also an impediment. How-ever, one could use reactor produced
188Re prepared by irra-
diating 187
Re enriched targets and the specific activity of the product obtained will also be sufficient for making radio-pharmaceuticals for the treatment of hepatocarcinoma.
Table 4. Characteristics of radionuclides used for treatment of HCC
Radionuclide Emission Half Life
[days]
Mean Soft Tissue Penetration Depth
[mm] Imaging Possibilities
131I , 8.04 0.4 Yes
90Y 2.7 3.0 No
188Re , 0.709 4.0 Yes
166Ho , 1.2 1.23 Yes

Targeted Radionuclide Therapy Current Radiopharmaceuticals, 2013, Vol. 6, No. 3 13
Holmium-166 is used in a complex with poly (L-lactide) (PLA) [179, 180] and chitosan as the embolic platform. Chi-tosan is a unique substance derived from chitin a marine source and has the ability to dissolve in water under acidic conditions but forms a gel in basic environments. The use of holmium/chitosan complex is found to be effective in treat-ing small HCCs (< 3 cm in size) [181]. Their effectiveness in large size HCCs are under evaluation [182 -184].
Therapy with 90
Y-microspheres is emerging as a main-stream treatment modality due to the availability of approved products. Currently, there are two commercially available microsphere devices in which
90Y is incorporated; one with
microspheres made of glass (TheraSphere®
; MDS Nordion, Ottawa, ON, Canada) and the other with microspheres made of resin (SIR-Spheres
®; Sirtex Medical, Sydney, Australia).
TheraSphere®
consisting of 90
Y embedded into glass micro-spheres of ~25 m diameter size is approved by the Food and Drug Administration for treatment of unresectable HCC. SIR-Spheres
® consist of biocompatible resin-based micro-
spheres containing 90
Y was granted approval for metastatic colorectal cancer in 2002.
Peptide Receptor Radionuclide Therapy (PRRT)
In the last two decades, there has been an explosive growth in the development of radiolabeled peptides for both diagnostic and therapeutic applications [185-187]. Peptides are molecules consisting two or more amino acids linked together with peptide bonds. As the number of aminoacids in the peptide keeps increasing beyond 50 they are designated as proteins. Typically, peptides have molecular weights <5000 Da and do not possess well-defined three-dimensional (tertiary) structure characteristics of proteins. Peptides regu-late many physiological processes, acting at some sites as endocrine or paracrine signals and at others as neurotrans-mitters or growth factors [188]. In general terms, regulatory peptides represent a group of different families of molecules
known to act at extremely low concentrations on multiple targets in the human body. Regulatory peptides include neu-ropeptides, gut peptides and neuroendocrine peptides [189]. These peptides are known to bind with receptors present on the cell surface. The receptors are protein molecules found on plasma membrane, cytoplasm or even in the cell nucleus. Several types of molecules other than peptides also can bind to receptors and these include hormones, neurotransmitters, drugs and toxins. There are several receptor types found within a typical cell and each of these type is linked to a spe-cific biochemical pathway. Each of this receptor recognizes and binds only a certain type of ligand shape ensuring very high specificity. The ligand receptor binding generates chemical signals to direct the cell to perform an action such as for division or cell death, or to allow certain molecules to enter or exit the cell. The ligand-receptor interactions are thus very convenient tools to be explored for the develop-ment of both diagnostic and therapeutic radiopharmaceuti-cals. The receptors are often over-expressed in cancer cells or during cell proliferation and targeting these receptors us-ing suitable ligands such as peptides is the basis of diagnosis as well as therapy. Peptides can be used as transport vehicles to guide the radionuclides to tissues which express a particu-lar receptor [190]. Peptides have low molecular weight and hence diffuse to the target tissues relatively fast. The main reason to prefer regulatory peptide receptors in therapy is due to their presence on the plasma membrane. After binding with the radioligand, the complex is internalized thereby allowing retention of radioactivity within cells. The labeled peptides usually clear rapidly from the blood and non-target tissues, resulting in high tumor-to-background ratios. In ad-dition, peptides are non-immunogenic and hence can be in-jected repeatedly. Table 5 summarizes the expression of some of the important regulatory peptide receptors found in human tumors [185, 191,192].
Radiolabelled peptides have several advantages over
other biologically active molecules in therapy [193].
Table 5. Regulatory peptide receptors overexpressed in human tumors
Peptide Receptor Known Subtypes Tumour Type
Somatostatin SSTR 1-5 Neuroendocrine tumors, nonHodkgin lymphoma, melanoma, breast
cancer.
Bombesin/GRP BB1-4 (BB2=GRP) SCLC, colon, breast, glioblastoma, prostate.
Gastrin/CCK CCK1,2 MTC, SCLC, pancreatic, astrocytoma, stromal ovarian cancer.
Substance P NK1 glioblastoma, astrocytoma, MTC, breast cancer, intra- and peritumoral
blood vessels.
Neurotensin (NT) NT1-3 Exocrine pancreatic tumors, small cell lung cancer, neuroblastoma, colo-
nic cancer.
-MSH -MSH Melanoma.
VIP/PACAP VPAC1,2 SCLC, colon, gastric, pancreatic.
Substance P NK1 glioblastoma, astrocytoma, MTC, breast cancer, intra- and peritumoral
blood vessels.
Oxytocin Oxytocin glial tumors, neuroblastoma, breast and endometrial cancers.
Calcitonin Calcitonin Bone, MTC.
Endothelin ET A,B Breast, ovary, lung cancer.
SSTR= Somatostatin receptor, CCK = Cholecystokinin, NK1 = Neurokinin 1, MSH = melanocyte stimulating hormone, VPAC= Vasoactive intestinal polypeptide, MTC= medullary thyroid carcinoma, SCLC= small cell lung cancer, MTC= Medullarry thyroid carcinoma

14 Current Radiopharmaceuticals, 2013, Vol. 6, No. 3 Dash et al.
• Peptides have very high affinity to specifically bind with
the target receptors.
• The small size and low molecular weight of peptides, compared to proteins and antibodies, facilitate rapid ac-cess to target tissue.
• Peptides usually display favorable pharmacokinetics characterized by high concentration in the target tissues and rapid clearance from the blood and non-target tis-sues.
• Elimination processes can be tailored to accommodate the desired routes of excretion or metabolism.
• Not immunogenic.
• Easy to synthesize either using an automated peptide synthesizer or by manual synthesis.
• Possibility to radiolabel with a variety of radionuclides using both conventional and novel chelating moieties.
• Amenable to extensive chemical/molecular modifica-tions to optimize affinity for a particular receptor and to display a more specific biodistribution pattern.
• Ability to tolerate the harsh conditions such as pH, high temperature etc. during radiolabelling.
Limitation
• The short blood half-lives represent a major road block for successful in vivo application owing to their suscep-tibility to degradation before reaching the intended tar-get. In order to circumvent such enzymatic destruction, most peptides need to be modified synthetically [185].
• Owing to their ability to induce pharmacologic effects at relatively low concentrations, high specific activity for-mulations are desirable that necessitates the use of radi-onuclides that are obtained in no carrier added form or at very high specific activity.
• The cellular receptor concentrations are limited and hence only small quantities of labeled peptides can be injected in order to avoid saturation of binding sites.
• The potential loss of binding affinity to the receptor and in vivo metabolism upon coupling with a chelator to hold the radionuclide can be circumvented to an extent by site-directed radiolabeling that can be achieved by in-serting a spacer group between the binding sequence and the chelating moiety [185]. One appealing approach is the cyclization of the peptide around a metal core which
not only makes the peptide analogs resistant to chemical and proteolytic degradation in vivo, and at times in-creases the affinity for its target [194,195].
• High uptake and retention by the kidneys, which is a concern, particularly for radionuclide therapy because of the potential nephrotoxicity [196-198].
Neuroendocrine Tumors
Neuroendocrine tumors (NETs) constitute a distinct het-
erogeneous group of neoplasia, characterized by their endo-
crine metabolism and histological pattern. NETs originate
from gastroenteropancreatic tract (GEP NETs) which secrete
biogenic amines and polypeptide hormones. Though rela-
tively rare and slow-growing neoplasms, they collectively
represent a major clinical problem. It has been well estab-
lished that the expression of peptide receptors on NET cells
is significantly higher as compared to normal tissues and
cells [199-200]. Somatostatin receptors (SSTR) are ex-
pressed on the cell surface and upon binding to the peptide,
the receptor-peptide complex is partly internalized [201].
The peptide, somatostatin (SST) and its analogues not only
inhibit the growth of normal but also malignant cells and
hence used in therapy of neuroendocrine tumors [202-203].
The vast majority of human tumors with neuroendocrine
origin over-express one or the other of the five distinct SSTR
subtype receptors (SSTR1 5) [204,205]. Somatostatin has a
very short half life of 2 min and hence several analogues of
somatostin have been synthetically produced and radiola-
belled with different radionuclides for the development of
diagnostic and therapeutic radiopharmaceuticals. The thera-
peutic radionuclides, 90
Y and 177Lu have been used in most of
these clinical studies. A number of radiolabeled SST peptide
analogs are currently in use to treat patients with SST recep-
tor-expressing tumors in neuroendocrine tumor (NETs). The
nuclear decay characteristics characteristics of 111
In, 90
Y and 177
Lu used in PRRT are shown in Table 6.
PRRT Studies with [111
In-DTPA0]octreotide
Researchers in the mid- to late-1990s used [111
In-DTPA] octreotide for PRRT as a natural extension of diagnostic im-aging to therapy. While the use of high activities of [
111In-
DTPA] octreotide in patients with metastasised neuroendo-crine tumors were encouraging with regard to symptom re-lief, tumor size regression was unsatisfactory [206,207]. The major roadblocks in the use of
111In-coupled peptides are
their small particle range, short tissue penetration (~10 μm) and radiotoxicity [208,209]. Additionally,
111In is also a -
Table 6. Characteristics of Radionuclides often used for Peptides Labeling
Radionuclide Half-life Emissions Mean Energy (keV) Maximum Tissue Penetration
Range of Particle Source BFC
rays 171 and 245 Indium-111 67.2 h
Auger electrons 3.6 and 19
10 m Cyclotron DTPA, DOTA
Yttrium-90 64.1 h particles 934 12 mm Generator DOTA
particles 149 Lutetium-177 160.8 h
rays 208 2 mm Reactor DOTA

Targeted Radionuclide Therapy Current Radiopharmaceuticals, 2013, Vol. 6, No. 3 15
emitter and not optimal for internal radiotherapy. The 111
In radionuclide was replaced by more effective therapeutic ra-dionuclides, such as
90Y and
177Lu with sufficient
- energy
to cause cell damage without radiation penetration of sur-rounding tissue [210].
[90
Y-DOTA0,Tyr
3]octreotide (
90Y-DOTA-TOC) and [
90Y-
DOTA0,Tyr
3]octreotate (DOTA-TATE)
In an attempt to develop a more effective somatostatin analog for peptide receptor radionuclide therapy, [DOTA,-Tyr
3] octreotide (DOTA-TOC) was synthesized and used for
radiolabelling with 90
Y. DOTA-TOC had higher affinity for somatostatin receptor subtype-2 and provided a stable bind-ing to the radionuclide,
90Y. In clinical trials conducted in
different institutions with 90
Y-DOTA-TOC [211,212], treat-ment outcome was effective for complete or partial remis-sions (10–34%) in patients with neuroendocrine tumors (NETs). These ranges were higher than those obtained with 111
In-DTPA-octreotide. In further studies, [DOTA,Tyr3] octreotate (DOTA-TATE) was developed by replacing the C-terminal threoninol in DOTATOC with threonine. This small change of molecular structure was shown to have higher affinity for the SSTR2 compared with DOTA-TOC in vitro [213,214]. Table 7 gives the affinity profiles of differ-ent somatostatin analogues and their BFCA conjugates.
Somatostatin Receptor Radiotherapy with [177
Lu-DOTA
0,Tyr
3]octreotate (DOTA-TATE)
The use of lutetium-177 is relatively new for targeted therapy and this therapeutic radionuclide has emerged as important due to its more favorable radionuclidic characteris-tics. In addition it is relatively easily produced in high spe-cific activity and high activity [215-217]. Targeted radionu-clide therapy with
177Lu-DOTA-TATE [218-221] shows an
overall response of 30-38% and a significantly high median overall survival of 48 months has been reported. It was ob-served that the quality of life improved significantly after treatment with
177Lu-DOTA-TATE.
Animal experiments have demonstrated that 90
Y-labelled somatostatin analogues may be more effective in larger tu-mors, whereas
177Lu-labelled somatostatin analogues may be
more effective in smaller tumors, but their combination may be even more effective [222]. In this context the studies car-ried out by Kunikowska et al. [223] using a cocktail of 50%
90Y-DOTATATE + 50%
177Lu-DOTATATE in 25 patients
and comparison with another group of 25 patients treated by 90
Y-DOTATATE alone is important. These investigators found striking differences in overall survival and progressive disease in favour of the combination
90Y+
177Lu compared
with each single-agent treatment. While the tandem therapy was reported to be more effective, there were no significant differences with respect to tumor response and progression free survival.
Radioimmunotherapy (RIT)
Radioimmunotherapy (RIT) uses monoclonal antibodies
as the vector for transport of the radioactivity to cancer cells
[224]. The radiolabeled antibodies are directed against vari-
ous antigens overexpressed on tumor cells or blood vessels
formed during angiogenesis [225-227]. These radioimmuno-
conjugates exploit the exquisite targeting specificity of the
humoral immune system to deliver lethal doses of cytotoxic
radiation by the decaying radionuclides to the tumor [228].
Although considered as one of the classic techniques, RIT
has significantly progressed in the past decade due to several
factors which include the large scale availability of MAbs,
humanization of MAbs, development of new chelate mole-
cules and novel targeting techniques [229]. This modality is
primarily used for the treatment for hematopoietic malignan-
cies where targeting is rapid such as non-Hodgkin’s lym-
phoma, which require only low doses of radiation (~15 Gy)
[230-234].
Advantages of RIT
• There are abundant and well characterized cell surface
antigens overexpressed on the cells in the case of several
major cancers. The ability to target specific antigens ex-
pressed on the surfaces of human cancer cells provide
the prospect of using radiolabeled antibodies to guide
the radionuclides to the tumor.
• RIT provides a comprehensive route to the identification
of tumor cells which generally overexpress antigens.
• Lymphomas are very sensitive to radiation in a dose-
dependent fashion, thus making them ideal targets for
RIT.
Table 7. Affinity Profiles of Somatostatin Analogs for Different human Somatostatin Receptor Subtypes (SSTR1-5)
IC50 (S.E.M) Peptide
SSTR1 SSTR2 SSTR3 SSTR4 SSTR5
Somatostatin 5.2 (0.3) 2.7 (0.3) 7.7 (0.9) 5.6 (0.4) 4.0(0.30)
Octreotide >10,000 2.0 (0.7) 187 (55) >1000 22 (6)
DTPA-Octreotide >10,000 12 (2) 376 (84) >1000 299 (50)
DOTA-[Tyr3]Octreotide >10,000 14 (2.6) 880 (324) >1000 393 (84)
DOTA-[Tyr3]Octreotate >10,000 1.5 (0.4) >1000 453(176) 547(160)
DOTA-lanreotide >10,000 26(3.4) 771(229) >10000 73 (12)
SSTR= Somatostatin receptor

16 Current Radiopharmaceuticals, 2013, Vol. 6, No. 3 Dash et al.
• The level of radiation that reaches the target can be ac-
curately determined using predose imaging techniques
and therefore offer the possibility to administer higher
radiation doses to the tumor site.
• The amount of radiation to non-target organs is predict-
able from imaging studies.
• Therapeutic effectiveness of RIT depends mainly on its
radionuclide payload, rather than antibody-dependent
cellular cytotoxicity and complement-dependent cyto-
toxicity [235,236]. Unlike unconjugated antibodies, ra-
dioimmunoconjugates can be effective when the host
immune system is not fully functional, can destroy anti-
gen-negative cells within tumors, and can overcome
poor penetration of the antibody into tumors. This strat-
egy thus offers the scope of treating patients who failed
treatment with non-radiolabelled monoclonal antibodies.
• An added advantage of radioimmunotherapy is the rele-
vant “crossfire effect”. Since the radiation emitted from
the radionuclides carried by the radioimmunoconjugate
may be deposited in an area covering several cell diame-
ters, poorly perfused or non-antigen expressing cells
within the tumor mass also could suffer the cytotoxic
radiation effect.
Selection of Target Antigen
Choice of the target antigen plays a key role in determin-ing the success of RIT.
• The antigen should be confined to the malignant cells for effective targeting and prevent a subpopulation of antigen-negative cells from proliferating.
• A favorable antigen expression profile is desirable for successful tumor targeting.
• To ensure specificity, the antigen must be over ex-pressed in target cells and have minimum presence in healthy cells.
• Effective antibody mediated cytotoxicity is achieved if the target antigen is not internalized or shed following antibody binding.
• In order to achieve effective therapy, a high density of antibody binding to the cell surface is essential. Anti-gens that shed from the cell surface and circulate in the peripheral blood at high concentration are not useful tar-gets.
• The chosen antigen should not mutate in a way that al-lows cancer cells to avoid destruction by the immune system.
Based on the above criteria, a wide variety of antigens on
cell surface have been considered as targets for a variety of
tumors which fulfill such criteria to differing degrees [237-
239].
Selection of Antibody
The success of RIT largely depends on the selection of
the MAbs which must possess the following key features.
• The MAbs should have the ability to recognize target
antigens with high affinity and specificity.
• In order to be therapeutically useful, the antibody should
have the ability to activate host effector functions such
as complement dependent cytotoxicity (CDC) and anti-
body-dependent cell cytotoxicity (ADCC).
• They should induce apoptosis or inhibit survival signals in the targeted neoplastic cells.
Monoclonal antibodies which are already approved for immunotherapy are ideal candidates for making radioimmu-notherpaeutic conjugates.
Selection of a Radionuclide for RIT
Selection of a radionuclide for RIT primarily resides on the type of particle, energy of particulate emission, the physical half-life and ability to be incorporated into the anti-body either directly or through BFC agents. The choice of the radionuclide is also influenced by the clinical disease, such as tumor size, physiological behavior and tumor radio-sensitivity.
Radionuclides with beta radiation (-) are advantageous
for RIT owing to cost effective availability and the ‘cross-fire’ effect where surrounding cells not receiving sufficient antibody binding, are also destroyed by radiation from adja-cent targeted cells. A low abudance of low energy gamma radiation emission is helpful for imaging and dosimetry. On the basis of in vitro cytotoxicity findings, in vivo studies and upon theoretical dosimetry calculations, it is well established that -emitting radionuclides and Auger electron emitting radionuclides have the ability to treat even single tumor cells in the circulation, micrometastases and in certain cases, minimal residual disease [240-248]. It has been suggested that shorter range radionuclides are effective for the treat-ment of cancers, such as neoplastic meningitis and ovarian cancer [249]. Characteristics of radionuclides with potential for use in radioimmunotherapy are depicted in Table 8.
Treatment of Non-Hodgkin’s B-cell lymphoma
Lymphomas are malignancies of the lymphoid tissue which are broadly classified into Hodgkin’s lymphoma (HD) and non-Hodgkin’s lymphomas (NHL). Non-Hodgkin’s lymphomas are a heterogeneous group of lymphoreticular malignancies with a wide range of aggressiveness. The ma-jority of NHL are B-cell lymphomas, with the follicular and diffused large B-cell lymphomas constituting up to 50 per-cent of NHL [250].
NHL provides an ideal candidate for RIT owing to its ac-cessibility to the therapeutic antibodies as well as sensitivity to apoptosis, complement dependent cytotoxicity (CDC) and antibody-dependent cellular cytotoxicity (ADCC) mediated killing of cancer cells. The CD20 antigen is one of the many epitopes expressed on the mature B cells, making it a suit-able target antigen for therapeutic radioactive monoclonal antibodies. CD20 is not present on stem cells and its expres-sion does not vary at different stages of the cell cycle. Moreover, it does not internalize or shed from the cell sur-face in response to antibody binding. By linking anti-CD20 monoclonal antibodies to an appropriate therapeutic radionu-clide, disseminated disease sites can effectively be targeted [245]. Although several radionuclides have been considered for RIT, most attention has been focused on the use of io-
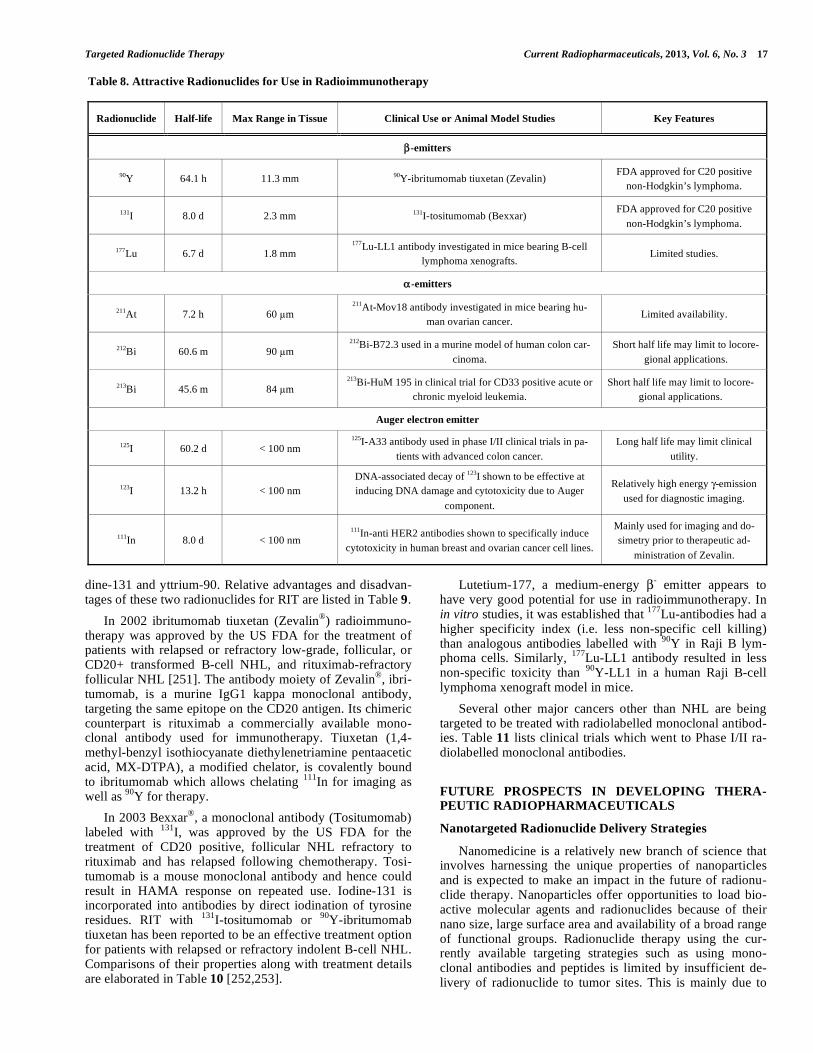
Targeted Radionuclide Therapy Current Radiopharmaceuticals, 2013, Vol. 6, No. 3 17
dine-131 and yttrium-90. Relative advantages and disadvan-tages of these two radionuclides for RIT are listed in Table 9.
In 2002 ibritumomab tiuxetan (Zevalin®
) radioimmuno-therapy was approved by the US FDA for the treatment of patients with relapsed or refractory low-grade, follicular, or CD20+ transformed B-cell NHL, and rituximab-refractory follicular NHL [251]. The antibody moiety of Zevalin
®, ibri-
tumomab, is a murine IgG1 kappa monoclonal antibody, targeting the same epitope on the CD20 antigen. Its chimeric counterpart is rituximab a commercially available mono-clonal antibody used for immunotherapy. Tiuxetan (1,4-methyl-benzyl isothiocyanate diethylenetriamine pentaacetic acid, MX-DTPA), a modified chelator, is covalently bound to ibritumomab which allows chelating
111In for imaging as
well as 90
Y for therapy.
In 2003 Bexxar®
, a monoclonal antibody (Tositumomab) labeled with
131I, was approved by the US FDA for the
treatment of CD20 positive, follicular NHL refractory to rituximab and has relapsed following chemotherapy. Tosi-tumomab is a mouse monoclonal antibody and hence could result in HAMA response on repeated use. Iodine-131 is incorporated into antibodies by direct iodination of tyrosine residues. RIT with
131I-tositumomab or
90Y-ibritumomab
tiuxetan has been reported to be an effective treatment option for patients with relapsed or refractory indolent B-cell NHL. Comparisons of their properties along with treatment details are elaborated in Table 10 [252,253].
Lutetium-177, a medium-energy - emitter appears to
have very good potential for use in radioimmunotherapy. In in vitro studies, it was established that
177Lu-antibodies had a
higher specificity index (i.e. less non-specific cell killing) than analogous antibodies labelled with
90Y in Raji B lym-
phoma cells. Similarly, 177
Lu-LL1 antibody resulted in less non-specific toxicity than
90Y-LL1 in a human Raji B-cell
lymphoma xenograft model in mice.
Several other major cancers other than NHL are being targeted to be treated with radiolabelled monoclonal antibod-ies. Table 11 lists clinical trials which went to Phase I/II ra-diolabelled monoclonal antibodies.
FUTURE PROSPECTS IN DEVELOPING THERA-PEUTIC RADIOPHARMACEUTICALS
Nanotargeted Radionuclide Delivery Strategies
Nanomedicine is a relatively new branch of science that involves harnessing the unique properties of nanoparticles and is expected to make an impact in the future of radionu-clide therapy. Nanoparticles offer opportunities to load bio-active molecular agents and radionuclides because of their nano size, large surface area and availability of a broad range of functional groups. Radionuclide therapy using the cur-rently available targeting strategies such as using mono-clonal antibodies and peptides is limited by insufficient de-livery of radionuclide to tumor sites. This is mainly due to
Table 8. Attractive Radionuclides for Use in Radioimmunotherapy
Radionuclide Half-life Max Range in Tissue Clinical Use or Animal Model Studies Key Features
-emitters
90Y 64.1 h 11.3 mm 90Y-ibritumomab tiuxetan (Zevalin) FDA approved for C20 positive
non-Hodgkin’s lymphoma.
131I 8.0 d 2.3 mm 131I-tositumomab (Bexxar) FDA approved for C20 positive
non-Hodgkin’s lymphoma.
177Lu 6.7 d 1.8 mm 177Lu-LL1 antibody investigated in mice bearing B-cell
lymphoma xenografts. Limited studies.
-emitters
211At 7.2 h 60 m 211At-Mov18 antibody investigated in mice bearing hu-
man ovarian cancer. Limited availability.
212Bi 60.6 m 90 m 212Bi-B72.3 used in a murine model of human colon car-
cinoma.
Short half life may limit to locore-
gional applications.
213Bi 45.6 m 84 m 213Bi-HuM 195 in clinical trial for CD33 positive acute or
chronic myeloid leukemia.
Short half life may limit to locore-
gional applications.
Auger electron emitter
125I 60.2 d < 100 nm 125I-A33 antibody used in phase I/II clinical trials in pa-
tients with advanced colon cancer.
Long half life may limit clinical
utility.
123I 13.2 h < 100 nm
DNA-associated decay of 123I shown to be effective at
inducing DNA damage and cytotoxicity due to Auger
component.
Relatively high energy -emission
used for diagnostic imaging.
111In 8.0 d < 100 nm 111In-anti HER2 antibodies shown to specifically induce
cytotoxicity in human breast and ovarian cancer cell lines.
Mainly used for imaging and do-
simetry prior to therapeutic ad-
ministration of Zevalin.

18 Current Radiopharmaceuticals, 2013, Vol. 6, No. 3 Dash et al.
relatively low and heterogeneous expression of receptor on tumor cells, rapid elimination of the agents from the targets and dose-limiting toxicities to normal tissues. Even though there is no technical impediment to administer large quantity of the agent as one of the possible solutions, there are con-cerns about undesirable toxicity. Ensuring maximum thera-peutic index with minimum toxicity represents an important initiative to deliver the radionuclides to the target at higher concentration and at optimal time. In this context, use of biocompatible nanoparticles with appropriate polymer coat-ings offers interesting platforms for carrying therapeutic agents to the tumor. Major advantages of using nanoparticles to deliver therapeutic agents are:
• Nanoparticles have prolonged blood retention time, ranging from 30 minutes to more than 24 hours. Their retention time depends on the morphology and size of the particle, coating materials, and composition of nanoparticle conjugates.
• Nanoparticle carriers enhance the accumulation of therapeutic agents at the target site.
• Capability to use radionuclide of lower specific activity owing to large surface areas.
• Internalization of receptor targeted nanoparticles leads to a high payload of radionuclide in the target cells, re-sulting in effective killing of tumor cells with a rela-tively low level of receptor-expression.
• The unique chemical and physical properties of nanoparticles, such as magnetization and photosensitiz-ing, provide additional capabilities and functions for im-proving delivery of the radionuclides (for example the external application of a magnetic field) and monitoring the therapeutic response.
Major challenges in developing nanoparticles for carry-ing and delivering therapeutic radionuclides for radionuclide therapy include:
• Synthesis of nanocarriers with characteristics which are able to decrease uptake of delivered therapeutic agents in cells of the reticuloendothelial system (RES) and pro-long blood circulation.
• Production of multifunctional nanoparticles with im-proved in vivo targeting capabilities, and interaction with biological carrier at the molecular level.
• Development of reliable procedures to assess the in vitro and in vivo stability of these new materials.
With the controlled formulation of nanoparticles and
careful radiolabeling strategies, nanoparticle platforms may
offer the appropriate pharmacokinetics to enable optimal
delivery of radionuclides for therapy.
Selective Targeting Strategies for Nano Particles
Two mechanisms, passive and active strategies, could be used to target nanoparticles to tumors.
Passive Targeting
Most nanoparticles are expected to accumulate in tumors
due to the pathophysiologic characteristics of tumor blood
vessels. The rich, chaotic, and highly permeable tumor vas-
culature together with the lack of a well-defined lymphatic
system of tumors offer an enhanced permeability and reten-
tion (EPR) effect for the passive targeting and selective ac-
cumulation of nanoparticles in the tumor interstitium [254-
259]. In passive targeting, nanoparticles and payloads could
reach the tumor and subsequently remain in the tumor due to
its lack of lymphatic drainage.
However, passive targeting approaches suffer from the
limitations that would be expected to obstruct the path to-
ward wide scale utility. Owing to the large variation on the
degree of tumor vascularization and porosity of tumor ves-
sels in different tumor type and status, such a targeting strat-
Table 9. Advantages and Disadvantages of Iodine-131 and Yttrium-90 for RIT
Radionuclide Advantages Disadvantages
Iodine-131
• Relatively inexpensive and readily available.
• The gamma component makes it amenable
to imaging using conventional gamma
cameras.
• The long path length of the gamma component can result in increased exposure to
hospital staff during treatment administration and follow-up.
• Retention of radionuclide in the tumor is lower due to dehalogenation and release
of the 131I from the targeted antibody.
• Iodine-131 that detaches from the antibody is typically taken up into the thyroid
gland, and such accumulation could potentially lead to hypothyroidism as a late
effect of treatment.
• Large variability among patients in radionuclide excretion, thus requiring dosime-
try for customized patient dosing.
Yttrium-90
• The beta emission from 90Y has a longer
path length than that of 131I, which is advan-
tageous in tumors with heterogeneous anti-
body distribution as it permits radiation to a
larger area.
• Since 90Y has no gamma component, shield-
ing of hospital personnel or using high pa-
tient doses are easily managed and do not
require hospital stay after administration
• Direct attachment to the antibody is not feasible; therefore, a bifunctional chelat-
ing agent is first attached to the antibody.
• The lack of a gamma component requires bremsstrahlung imaging or the use of a
surrogate isotope if an imaging component is desired. Typically, 111In is used since
binding to the targeting antibody conjugate is similar to that of yttrium-90.
• If freed from the chelated mAb, it accumulates in bone, thereby increasing radia-
tion to the marrow.
• Require on site availability of a 90Sr/90Y generator. Relatively expensive and not
available widely.

Targeted Radionuclide Therapy Current Radiopharmaceuticals, 2013, Vol. 6, No. 3 19
egy is not feasible in all tumors [260]. Internalization of
nanoparticles is also hampered by the reduced number of
specific interactions of cancer cells.
Active Targeting
In order to circumvent the above limitations, active tar-geting has also been pursued in which nanoparticles are en-gineered to attach targeting moieties at their surfaces. Such a strategy seemed attractive as the nanoparticles containing target specific biomarker molecules such as antibodies, pep-tides, and small molecules provide an opportunity to bind the radionuclide and at the same time offer the scope of targeting the related receptors that are over expressed in tumor cells [261-263]. Although such strategies have not yet made any clinical impact on human health, clinical translation of the concept is considered not far away [264].
Types of Targeting Moieties for Nanoparticles
Some examples of targeting moieties used in nanoparticle platforms for the delivery of therapeutic radionuclides are as follows.
• Proteins (mainly antibodies and their fragments): Con-jugates composed of nanoparticles and antibodies were
found to maintain the properties of both the antibody and the nanoparticles.
• Peptides: Peptides are attractive targeting molecules due
to their small size, low immunogenicity, and ease of
manufacture [265].
• Nucleic acids (aptamers): Aptamers are small nucleic
acid ligands (15–40 bases) that bind to targets with high
specificity due to the ability of the molecules to fold into
unique conformations with three-dimensional structures
[266]. The high affinity and specificity of aptamers
make them ideal targeting agents.
• Small molecules or others (vitamins or carbohydrates):
Small molecules with infinitely diverse structures and
properties have great potential as a class of targeting moieties.
Conjugation of Functional Moieties to Nano Particles
Conjugation of targeting moieties and a radionuclide to
nanoparticle surfaces could be performed through a wide
range of chemical strategies. To be effective, this coupling
must be fast and stable, including in physiological medium
in vitro and in vivo, and it must be carried in such a manner
Table 10. Comparison of Zevalin(TM)
and Bexxar(TM)
Properties Zevalin Bexxar
Isotope used 90Y 131I
Type of radiation and
Max beta energy (mean) 2.29 MeV (0.9 MeV) 0.6 MeV (0.19 MeV)
Path length 0. 8 mm 5. 3 mm
Isotope half life 64 hours 8 days
Source of radionuclide 90Sr/90Y gererator Reactor production
Availability of radionuclide Limited Widely
Antibody Murine IgG-1 kappa antibody to CD20+ Murine IgG2a lambda antibody to CD20+
Ease of Labeling More complex Ease
Pre-infusion antibody chimeric (rituximab) murine (tositumomab)
Pre-infusion dose 250 mg of rituximab 450 mg of tositumomab
Tracer imaging 185 MBq(5 mCi) of 111In 185 MBq (5 mCi) of 131I
Clearance Urinary Urinary, (faster)
Purpose of diagnostic scan using tracer 1- 2 scans to visually assess distribution. 3 scans to determine clearance and determine
therapeutic dose
Therapeutic dose 18.4 MBq(0.4 mCi)/kg ([maximum of 1.18
GBq(32 mCi)] Dose to deliver 75 cGy to total body dose
Critical organ Spleen, testes Thyroid
Dose determination Fixed based on weight and platelets [18.4-11.1
MBq (0.4 or 0.3 mCi0/kg)]
Clearance rate/dosimetry based to deliver 75cGy
or 65cGy total body dose.
Pre-therapy preparation Antihistamines/NSAID Additional thyroid blocking
Hematological toxicity Predominant toxicity Predominant toxicity, less severe than Zevalin
Other unique toxicities Dehalogenation in liver, and effect on marrow Hypothyroidism
Radiation precautions Universal for 1 week Additional precautions for gamma radiation
Therapy setting Outpatient Majority outpatient

20 Current Radiopharmaceuticals, 2013, Vol. 6, No. 3 Dash et al.
Table 11. Examples of Key Radioimmunoconjugates Currently in Clinical Trials for Therapeutic Applications Under active Devel-
opment
Monoclonal
Antibody
Brand
Name Radionuclide Highest Phase Description Type of Cancer Organization
ch-TNT-1/B Cotara 131I
Phase II
131I-labeled chimeric monoclonal
antibody chTNT-1/B for tumor
necrosis therapy.
Anaplastic astrocytoma,
biliary
cancer, colorectal cancer,
liver cancer, pancreas cancer,
glioblastoma multiforme,
glioma, sarcoma.
Peregrine Pharmaceuticals
Tustin, CA 92780.
BC8 131I
Phase II
131I-labeled murine anti-CD45
monoclonal IgG1 antibody.
Acute myeloid leukemia.
Fred Hutchinson Cancer
Research Center; Seattle, WA
98109
National Cancer Institute;
University of Washington.
J591 111In, 177Lu
Phase II
111In/177Lu labeled
humanized monoclonal
antibody to prostate
specific membrane
antigen/extracellular
domain (PSMAext).
Prostate cancer.
BZL Biologics; Cornell
University, New York; Memorial
Sloan-Kettering Cancer
Center, New York; Millennium
Pharmaceuticals Cambridge, MA
02139.
Metuximab Licartin 131I
Phase II
131I-labeled murine monoclonal
antibody HAb18 F(ab0)2
fragment against the
HCC-associated antigen
HAb18G/CD147.
Liver cancer.
Eastern Hepatobiliary
Surgery Hospital Shanghai;
Fourth Military
Medical University,
Xi'an,Shaanxi, PRC.
cG250 177Lu
Phase II
Chimeric monoclonal
antibody G250 conjugated
to DOTA and radiolabeled
with 177Lu
Kidney cancer.
(renal cell carcinoma)
Ludwig Institute for Cancer Re-
search, Melbourne ;
Radboud Universiteit
Nijmege, The Netherlands.
3F8 131I
Phase II
131I-labeled anti-GD2
ganglioside murine IgG3
monoclonal antibody
Cancer, medulloblastoma,
neuroblastoma
Memorial Sloan-Kettering
Cancer Center, New York ;
National
Cancer Institute, New York.
L19 Radre-
tumab 131I
Phase II
131I-labeled SIP composed
of L19 that binds to the ED-B domain
of human
fibronectin.
Non–small cell lung cancer,
solid tumors,
hematologic/blood
cancer.
Philogen, Zurich.
F16 Tena-
Rad 131I
Phase II
131I-labeled human monoclonal
antibody against the A1 domain of
tenascin-C.
Hematological cancer,
solid tumors. Philogen, Zurich.
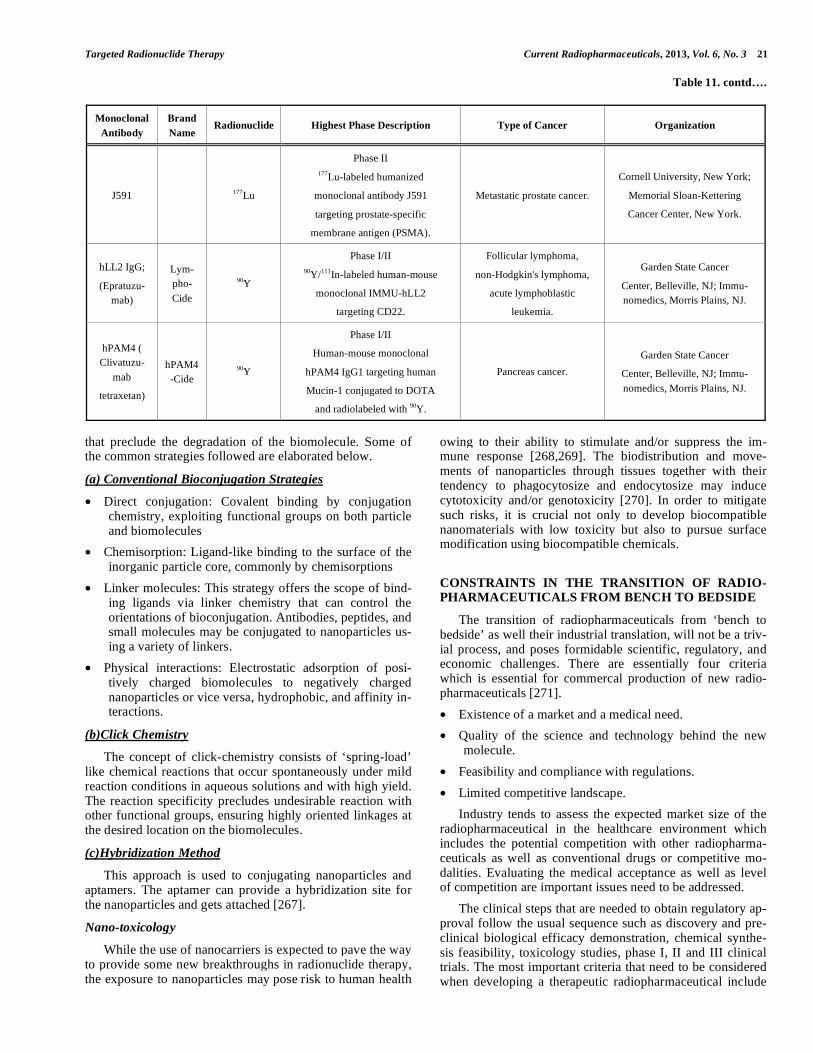
Targeted Radionuclide Therapy Current Radiopharmaceuticals, 2013, Vol. 6, No. 3 21
Table 11. contd….
Monoclonal
Antibody
Brand
Name Radionuclide Highest Phase Description Type of Cancer Organization
J591 177Lu
Phase II
177Lu-labeled humanized
monoclonal antibody J591
targeting prostate-specific
membrane antigen (PSMA).
Metastatic prostate cancer.
Cornell University, New York;
Memorial Sloan-Kettering
Cancer Center, New York.
hLL2 IgG;
(Epratuzu-
mab)
Lym-
pho-
Cide
90Y
Phase I/II
90Y/111In-labeled human-mouse
monoclonal IMMU-hLL2
targeting CD22.
Follicular lymphoma,
non-Hodgkin's lymphoma,
acute lymphoblastic
leukemia.
Garden State Cancer
Center, Belleville, NJ; Immu-
nomedics, Morris Plains, NJ.
hPAM4 (
Clivatuzu-
mab
tetraxetan)
hPAM4
-Cide
90Y
Phase I/II
Human-mouse monoclonal
hPAM4 IgG1 targeting human
Mucin-1 conjugated to DOTA
and radiolabeled with 90Y.
Pancreas cancer.
Garden State Cancer
Center, Belleville, NJ; Immu-
nomedics, Morris Plains, NJ.
that preclude the degradation of the biomolecule. Some of the common strategies followed are elaborated below.
(a) Conventional Bioconjugation Strategies
• Direct conjugation: Covalent binding by conjugation chemistry, exploiting functional groups on both particle and biomolecules
• Chemisorption: Ligand-like binding to the surface of the inorganic particle core, commonly by chemisorptions
• Linker molecules: This strategy offers the scope of bind-ing ligands via linker chemistry that can control the orientations of bioconjugation. Antibodies, peptides, and small molecules may be conjugated to nanoparticles us-ing a variety of linkers.
• Physical interactions: Electrostatic adsorption of posi-tively charged biomolecules to negatively charged nanoparticles or vice versa, hydrophobic, and affinity in-teractions.
(b)Click Chemistry
The concept of click-chemistry consists of ‘spring-load’ like chemical reactions that occur spontaneously under mild reaction conditions in aqueous solutions and with high yield. The reaction specificity precludes undesirable reaction with other functional groups, ensuring highly oriented linkages at the desired location on the biomolecules.
(c)Hybridization Method
This approach is used to conjugating nanoparticles and aptamers. The aptamer can provide a hybridization site for the nanoparticles and gets attached [267].
Nano-toxicology
While the use of nanocarriers is expected to pave the way to provide some new breakthroughs in radionuclide therapy, the exposure to nanoparticles may pose risk to human health
owing to their ability to stimulate and/or suppress the im-mune response [268,269]. The biodistribution and move-ments of nanoparticles through tissues together with their tendency to phagocytosize and endocytosize may induce cytotoxicity and/or genotoxicity [270]. In order to mitigate such risks, it is crucial not only to develop biocompatible nanomaterials with low toxicity but also to pursue surface modification using biocompatible chemicals.
CONSTRAINTS IN THE TRANSITION OF RADIO-PHARMACEUTICALS FROM BENCH TO BEDSIDE
The transition of radiopharmaceuticals from ‘bench to bedside’ as well their industrial translation, will not be a triv-ial process, and poses formidable scientific, regulatory, and economic challenges. There are essentially four criteria which is essential for commercal production of new radio-pharmaceuticals [271].
• Existence of a market and a medical need.
• Quality of the science and technology behind the new molecule.
• Feasibility and compliance with regulations.
• Limited competitive landscape.
Industry tends to assess the expected market size of the radiopharmaceutical in the healthcare environment which includes the potential competition with other radiopharma-ceuticals as well as conventional drugs or competitive mo-dalities. Evaluating the medical acceptance as well as level of competition are important issues need to be addressed.
The clinical steps that are needed to obtain regulatory ap-proval follow the usual sequence such as discovery and pre-clinical biological efficacy demonstration, chemical synthe-sis feasibility, toxicology studies, phase I, II and III clinical trials. The most important criteria that need to be considered when developing a therapeutic radiopharmaceutical include

22 Current Radiopharmaceuticals, 2013, Vol. 6, No. 3 Dash et al.
selection of appropriate ligands and radionuclide, standardi-zation of radiolabeling procedure, evaluation of chemical stability, suitable mechanism of action, monitoring of bio-logical binding through in vitro and in vivo models, ensuring minimal accumulation in sensitive tissues such as the liver or kidney and no accumulation in non-targeted tissues, asse-ment of metabolic and biological stability and evaluation of potential side effects and toxicity.
Positive preclinical results then pave the way for clinical trials which follow the principal I, II and III clinical trial phases.
• Phase I trial to demonstrate absence of toxicity in human.
• Phase II to demonstrate efficacy and to choose the most adequate dose.
• Phase III confirms efficacy and absence of side-effects at the selected dose.
All of these trials are required to be performed under Good Clinical Practice (GCP) conditions, while the Phase III trial needs to be performed with the radiopharmaceuticals produced under GMP conditions. All these trials must be performed in specialized healthcare departments that have expertise and adequate equipment.
In order to adhere to regulatory requirements and safety regulations, some simple rules needs to be followed. They are:
• The radiopharmaceutical must above all show efficacy for the claimed indication, as well as safety for the pa-tient.
• All results provided in the NDA (New Drug Application) dossier must be reproducible and have been generated under Good Laboratory Practices (GLP), GCP and GMP conditions.
• A GMP manufacturing process must also be in place at the time of dossier filing.
Appropiate radiologic safety measures need to be in place for the patient, hospital staff handling the radiophar-maceutical and technicians involved in the manufacturing of radiopharmaceutical and logistics process.
SUMMARY AND CONCLUSION
Advances in molecular and cellular biology are opening
up the possibility of identifying several targeting vectors
which are suitable for radionuclide therapy. New monoclonal
antibodies, peptides and other biomolecules are being devel-
oped to which radionuclides can be attached for developing
therapeutic radiopharmaceuticals. The availability of thera-
peutic radionuclides having desirable nuclear characetristics
at high specific activity together with chemical methods to
attach them stably to the targeting vectors have also im-
proved tremendously in the recent past. With the appropriate
combination of an optimally engineered targeting vector and
a suitable radionuclide, the benefit of radionuclide therapy is expected to increase substantially in the future.
Advances made in targeted alpha-particle therapy so far are encouraging. However, the major current impediment for widespread implementation of alpha-particle therapy is the
limited suppy of alpha emitting radionuclides. The most promising benefit of alpha radionuclide therapy thus far ap-pears to be for palliation in patients with skeletal metastasis using
223RaCl2 (alpharadin
®). Radionuclide therapy using
Auger-electron–emitting radionuclides will require very in-novative delivery capability wherein the radionuclide targets the cell nucleus. Despite impressive progress in the nuclear localization sequences to transport radiolabeled peptides or proteins from cytoplasmatic compartments to the nucleus, the challenge to develop useful products remains.
Small peptides are important biological agents, success-fully used as transport vehicles to guide the radionuclides to the tissues expressing a particular receptor. After many years of intense research activities, radiolabeled regulatory pep-tides are beginning to be used clinically for cancer therapy and
90Y/
177Lu labeled somatostin analogs have already found
a nich area for the treatment of neuroendocrine tumors. With the identification of several new peptide-receptor combina-tions, peptide radionuclide therapy could effectively come to be useful for the treatment of several major cancers.
Radioimmunotherapy had early start but has not devel-oped to the extent expected for wide scale applications. Cur-rently, this technology is accepted as an efficacious therapy for patients suffering from NHL. Both
131I-tositumomab
(Bexaar®
) and 90Y-ibritumomab tiuxetan (Zevalin
®) are ap-
proved for the treatment of NHL and demonstrated favorable clinical results. Several clinical trials are also underway with several other radiolabelled monoclonal antibodies. The ad-vances in engineering antibody fragments will permit greater control of tumor targeting, clearance and pharmacokinetics.
Although only few selected radionuclides are currently used in the existing treatment modalities, there are a number of radionuclides that appear promising and thus warrant con-tinued investigation. Technical and logistical challenges as-sociated with the reliable availability of radionuclides are obstacles that continue to challenge the wider use of targeted therapy. The most preferred radionuclides at present are the
- emitters for targeted therapy. Iodine-131,
177Lu and
90Y
are the three - emitting radionuclides that offer wider avail-
ability with desired specific activity and suitable to be used in a variety of targeted radionuclide therapies [18]. Each country needs to assess the available options and infrastruc-ture to undertake regular production of therapeutic radionu-clides for research as well as for routine clinical use to meet their needs. Countries that acquire therapeutic radionuclide production capability will be best placed to meet their own needs as well as for export. Ensuring sustainable production and supply of radionuclides of required quantities and qual-ity represents a bold initiative to avail the proven benefit of radionuclide therapy in the coming years [19,33,34].
Despite spectacular progresses achieved thus far, there is still a need to find better tumor targeting with novel agents, different radionuclides, more accessible targets, and innova-tive pretargeting strategies for a wide range of therapeutic applications. Nanotargeted radionuclide delivery strategies have seen dramatic progress and is expanding rapidly, though still in infancy could contribute significantly in the future.
A major challenge is to cross the regulatory barrier while translating from pre-clinical animal studies to human clinical

Targeted Radionuclide Therapy Current Radiopharmaceuticals, 2013, Vol. 6, No. 3 23
trials. Therapeutic radiopharmaceuticals are not lucrative areas which attract investments from large drug manufactur-ers as the sales are far lower than conventional drugs. The scientific efforts are now mostly confined to small research groups in publicly funded laboratiories or in universities whose interests are mainly academic and hence lack the re-sources for translating good scientific outcome to clinical products [271]. Adequate resources and multidisciplinary commitments together with a sensible strategy are essential to translate preclinical research into clinical settings. Interna-tional bodies such as the International Atomic Energy Agency (IAEA), the World Health Organization (WHO), and the Nuclear Energy Agency (NEA) could contribute to the development and clinical translation of new therapeutic ra-diopharmaceuticals by pooling resources of different stake holders.
ACKNOWLEDGEMENTS
Research at the Bhabha Atomic Research Centre is part of the ongoing activities of the Department of Atomic En-ergy, India and is fully supported by government funding. Research at the Oak Ridge National Laboratory is supported by the US Department of Energy under contract DE-AC05-00OR22725 with UT-Battelle, LLC.
CONFLICT OF INTEREST
The authors have declared that no conflicting financial interest.
DISCLAIMER
This manuscript has been authored by UT-Battelle, LLC, under contract DE-AC05-00OR22725 with the U.S. Depart-ment of Energy. The United States Government retains and the publisher, by accepting the article for publication, ac-knowledges that the United States Government retains a non-exclusive, paid-up, irrevocable, world-wide license to pub-lish or reproduce the published form of this manuscript, or allow others to do so, for United States Government pur-poses.
REFERENCES
[1] Ferlay, J.; Shin, H.R.; Bray, F.; Forman, D.; Mathers, C.; Parkin,
D.M. Estimates of worldwide burden of cancer in 2008: GLOBO-CAN 2008. Int. J. Cancer. 2010, 127, 2893-2917.
[2] World Health Organization Fact Sheet no. 297 – Cancer, 2009. Available at: https://www.who.int.mediacenter/factsheets/fs297/en.
[3] Baskar, R.; Lee, K.A.; Yeo, R.; Yeoh, K.W. Cancer and Radiation Therapy: Current Advances and Future Directions. Int. J. Med.
Sci. 2012, 9, 193-199. [4] Carlsson, J. ; Forssell-Aronsson, E. ; Hietala, S.O. ; Stigbrand, T.;
Tennvall, J. Tumor therapy with radionuclides: assessment of pro-gress and problems. Radiother. Oncol. 2003, 66, 107-117.
[5] Carlsson, J.; Forssell-Aronsson, E.; Glimelius, B.; Mattsson, S. Therapy with radiopharmaceuticals. Acta. Oncol. 2002, 41, 623-
628. [6] Ercan, M.T.; Caglar, M. Therapeutic radiopharmaceuticals. Cur.
Pharm. Design. 2000, 6, 1085-1121. [7] Srivastava, S.C. Therapeutic radionuclides: Making the right
choice, in Mather SJ (ed): Current Directions in Radiopharmaceuti-cal Research and Development, Dordrecht, The Netherlands, Klu-
wer Academic Publishers, 1996, 63-79.
[8] Williams, L.E.;DeNardo, G.L.;Meredith, R.F.Targeted radionuclide
therapy. Med Phys. 2008, 35, 3062-3068 [9] Srivastava, S.C.; Dadachova, E. Recent advances in radionuclide
therapy, http://www.seminarsinnuclearmedicine.com/article/S0001-2998%2801%2980012-X/abstract - article-footnote-1Sem. Nucl.
Med. 2001, 31, 330-341. [10] Cuaron, J.J.; Hirsch, J.A.; Medich, D.C.; Rosenstein, B.S.; Martel,
C.B.; Hirsch, A.E. A proposed methodology to select radioisotopes for use in radionuclide therapy. AJNR. Am. J. Neuroradiol. 2009,
30, 1824-1829. [11] Tolmachev, V.; Carlsson, J.; Lundqvist, H. A limiting factor for the
progress of radionuclide-based cancer diagnostics and therapy-availability of suitable radionuclides. Acta. Oncol. 2004, 43, 264-
275. [12] Unak, P. Targeted Tumor Radiotherapy. Braz. Arch. Biol. Tech.
2002, 45, 97-110, [13] Stanciu, A.E. Radionuclide in targeted therapy of cancer. Rev.
Roum. Chim. 2012, 57, 5-13. [14] Das, T.; Pillai, M.R.A. Options to meet the future global demand of
radionuclides for radionuclide therapy. Nucl. Med. Biol. 2013, 40, 23–32.
[15 ] Sofou, S. Radionuclide carriers for targeting of cancer. Int J Nanomedicine. 2008, 3, 181–199.
[16] Kassis, A.I. Therapeutic Radionuclides: Biophysical and Radiobi-ologic Principles. Semin. Nucl. Med. 2008, 38, 358–366.
[17] Howell, R.W.; Rao, D. V. ; Sastry, K. S. Macroscopic dosimetry for radioimmunotherapy: nonuniform activity distributions in solid
tumors Med. Phys. 1989, 16, 66–74. [18] Volkert, W.A.; Hoffman, T.J. Therapeutic radiopharmaceuticals.
Chem. Rev. 1999, 99, 2269-2292. [19] Volkert, W.A.; Goeckler, W.F.; Ehrhardt, G.J.; Ehrhardt, G.J.;
Ketring, A.R. Therapeutic radionuclides: Production and decay property considerations. J. Nucl. Med. 1991, 32, 174-185.
[20] Spitzweg, C.;Morris, J.C. Sodium iodide symporter (NIS) and thyroid. Hormones (Athens). 2002, 1, 22-34
[21] Wheldon, T.E. Targeting radiation to tumors. Int. J. Radiat. Biol. 1994, 65, 109-116.
[22] O'Donoghue, J.A.; Bardibs, M.; Wheldon, T.E.; Relationships between tumor size and curability for uniformly targeted therapy
with beta-emitting radionuclides. J. Nucl. Med. 1995, 36, 1902-1909.
[23] Kassis, A.I.; Adelstein, S.J. Radiobiologic principles in radionu-clide therapy. J Nucl Med 2005, 46(Suppl 1), 4S-12S.
[24] Hall, E.J. Radiobiology for the radiologist. Philadelphia, Lippin-cott, 1994, 153–164.
[25] Barendsen, G.W.; Beusker, T.L.J. Effects of different ionizing radiations on human cells in tissue culture. 1. Irradiation techniques
and dosimetry. Radiat. Res. 1960, 13, 832–840. [26] Barendsen, G.W.; Beusker, T.L.J.; Vergroesen, A.J.; Budke, L.
Effect of different ionizing radiations on human cells in tissue cul-ture. 2. Biological experiments, Radiat. Res. 1960, 13, 841–849.
[27] Barendsen, G.W. ; Vergroesen, A.J. Irradiation of human cells in tissue culture with alpha-rays, beta-rays and X-rays, Int. J. Radiat.
Biol. Relat. Stud. Phys. Chem.Med. 1960, 2, 441. [28] Ruth, T. J.; Pate, B. D.; Robertson, and Porter, J. K. Radionuclide
production for biosciences. Nucl. Med. Biol. 198916, 323-336. [29] Ehrhardt, G. J.; Ketring, A. R.; and Ayers, L. M. Reactor-produced
radionuclides at the University of Missouri Research Reactior. Appl. Radiat. Isot. 1998, 49, 295-297.
[30] Karenlin, Y. A.; Toporov, Y. G. RIAR reactor produced radionu-clides. Appl. Radiat. Isot. 1998, 49, 299-304.
[31] Knapp, F. F., Jr., (Russ); Mirzadeh, S.; Beets, A. L.; O’Doherty, M.; Blower, P. J.; Verdera, E. S.; Gaudiano, J. S.; Kropp, J., Gi-
hlke;J., Palmedo, H.; Biersack, H.-J. Reactor-produced radioiso-topes from ORNL for bone pain palliation. Appl. Radiat. Isot.
1998, 49, 309-315. [32] Mausner, L. F.; Kolsky, K. L.; Joshi, V.; Srivastava, S. C. Radi-
onuclide development at BNL for nuclear medicine therapy. Appl. Radiat. Isot. 1998, 49, 285–294.
[33] Qaim, S. M. The present and future of medical radionuclide pro-duction, Radiochim. Acta. 2012 , 100, 635–651.
[34] Neves, M.; Kling, A. ; Oliveira, A. Radionuclides used for therapy and suggestion for new candidates, Journal of Radioanalytical and
Nuclear Chemistry, 2005 , 266, 377–384. [35] Barendsen, G.W. Dose-survival curves of human cells in tissue
culture irradiated with alpha-, beta-, 20-kV X- and 200-kV X-

24 Current Radiopharmaceuticals, 2013, Vol. 6, No. 3 Dash et al.
radiation. Nature 1962, 193, 1153-1156.
[36] Barendsen, G.W.; Walter, H.M.D.; Bewley, D.K. ; Fowler, J.F. Effects of different ionizing radiations on human cells in tissue cul-
ture. 3. Experiments with cyclotron accelerated alpha-particles and deuterons. Radiat. Res. 1963, 18, 106–119.
[37] Barendsen, G.W.; Walter, H.M.D. Effects of different ionizing radiations on human cells in tissue culture. 4. Modification of ra-
diation damage. Radiat. Res. 1964, 21, 314–329. [38] Barendsen, G.W.; Modification of radiation damage by fractiona-
tion of dose anoxia+chemical protectors in relation to LET. Ann. N.Y. Acad. Sci. 1964, 114, 96–114.
[39] Barendsen, G.W. Impairment of the proliferative capacity of hu-man cells in culture by alpha-particles with differing linear-energy
transfer. Int. J. Radiat. Biol. Relat. Stud. Phys. Chem. Med. 1964, 8, 453–466.
[40] Allen, B.J. Future prospects for targeted alpha therapy. Curr Ra-diopharm. 2011, 4, 336-342.
[41] Kassis, A.I.; Adelstein, S.J. Radiobiologic principles in radionu-clide therapy. J. Nucl. Med. 2005, 46, 4S–12S.
[42] Kassis A. I.; Fayad F.;Kinsey B. M.; Sastry K. S. R.; Taube R. A.; Adelstein S. J. Radiotoxicity of 125I in mammalian cells. Radiat.
Res. 1987, 111, 305–318. [43] Humm, J. L.; Howell, R. W.; Rao, D. V. Dosimetry of Auger-
Electron-Emitting Radionuclides, Report No. 3 of AAPM Nuclear Medicine, Task Group No. 6. Med. Phy. 1994, 21, 1901-1915.
[44] Howell, R. W.; Narra, V. R.; Sastry, K. S.; Rao, D. V. Auger Elec-tron Dosimetry, Report No. 37 of AAPM Nuclear Medicine, Task
Group No. 2. Med. Phy., 1992, 19, 1352-1383. [45] Thisgaard, H. Accelerator Based Production of Auger- Electron
Emitting Isotopes for Radionuclide Therapy, Denmark, Risø-PhD-42(EN), 2008, 2-6.
[46] Kassis, A.I.; Adelstein, S.J. Radiobiologic principles in radionu-clide therapy. J. Nucl. Med. 2005, 46, 4S-12S.
[47] Henriksen, G.; Schoultz, B.W.; Michaelsen, T.E.; Bruland, O.S.; Larsen, L.H. Sterically stabilized liposomes as a carrier for alpha-
emitting radium and actinium radionuclides Nucl. Med. Biol. 2004, 31, 441-449.
[48] Sofou, S.; Kappel, B.J.; Jaggi, J.S.; McDevitt, M.R.; Scheinberg, D.A.; Sgouros, G. Enhanced retention of the alpha-particle-
emitting daughters of Actinium-225 by liposome carriers. Biocon-jug. Chem., 2007, 18, 2061-2067.
[49] Lasic, D.D.;Liposomes from Physics to Applications.Elsevier, Amsterdam, 1993, 43-62.
[50] Du, J.; Marquez, M.; Hiltunen, J.; Marquez, M.; Nilsson S.;Holmberg, A.R. Radiolabeling of dextran with rhenium-188.
Appl. Radiat. Isot., 2000, 53, 443-448. [51] Brenner, W.; Kampen, W.U.; Brümmer, C.; von Forstner, C.;
Zuhayra. M.;Czech, N.;Muhle, C.; Henze, E. Bone uptake studies in rabbits before and after high-dose treatment with 153Sm-EDTMP
or 186Re-HEDP. J. Nucl. Med. 2003, 44, 247-251. [52] Maini, C.L.;Bergomi, S.;Romano, L.; Sciuto, R.153Sm-EDTMP for
bone pain palliation in skeletal metastases. Eur. J. Nucl. Med. Mol. Imaging. 2004, 31, S171-S178.
[53] Lam, M.G.; de Klerk, J.M.; van Rijk, P.P.;186Re-HEDP for metas-tatic bone pain in breast cancer patients. Eur. J. Nucl. Med. Mol.
Imaging. 2004, 31, S162-S170. [54] Lam, M.G.; de Klerk, J.M.; van Rijk, P.P.; Zonnenberg, B.A. Bone
seeking radiopharmaceuticals for palliation of pain in cancer pa-tients with osseous metastases. Anticancer. Agents. Med. Chem.
2007, 7, 381-97. [55] Eriksson, B. New drugs in neuroendocrine tumors: rising of new
therapeutic philosophies? Curr.Opin. Oncol. 2010, 22, 381-386. [56] Okarvi, S.M. Peptide based radiopharmaceuticals and cytotoxic
conjugates: potential tools against cancer. Cancer. Treat. Rev. 2008, 34, 13-26.
[57] Reubi, J.C.;Mäcke, H.R.;Krenning, E.P. Candidates for peptide receptor radiotherapy today and in the future. J. Nucl. Med. 2005,
46, 67S-75S. [58] Milton, R.C.;. Milton, S.C; Kent, S.B. Total chemical synthesis of
a D-enzyme: the enantiomers of HIV-1 protease show demonstra-tion of reciprocal chiral substrate specificity. Science. 1992, 256,
1445-1448. [59] Welch, B.D.; Van Demark, A.P.; Heroux, A.; Hill, C.P.; Kay, M.S.
Potent D-peptide inhibitors of HIV-1 entry.Proc. Natl. Acad. Sci. 2007, 104, 16828-16833.
[60] Walensky, L.D.; Kung, A.L.; Escher, I. Activation of apoptosis in
vivo bv a hydrocarbon-stapled BH3 helix, Science. 2004, 305, 1466-1470.
[61] Xia, H.C.; Hu, W.G.; Yang, X.X.; Li. F.; Zhang, Z.C. Preparation and primary application of monoclonal antibodies against a novel
ribosome-inactivating protein Moschatin from pumpkin seeds. Acta. Biochim. Biophys. Sin (Shanghai). 2004, 36, 105-110.
[62] Breedveld, F. C. Therapeutic monoclonal antibodies. Lancet. 2000, 355, 735-740.
[63] Steiner, M.;Neri, D.Antibody-radionuclideconjugates for cancer therapy: historical considerations and new trends. Clin Cancer
Res. 2011, 17, 6406 -6416. [64] Teicher, B.A.;Chari, R.V. Antibody conjugate therapeutics: chal-
lenges and potential. Clin Cancer Res. 2011, 17, 6389-6397. [65] Wong, J.Y. Basic immunology of antibody targeted radiotherapy.
Int. J. Radiat. Oncol. Biol. Phys. 2006, 66, S8-S14. [66] Goldmacher, V.S.; Kovtun, Y.V. Antibody-drug conjugates: using
monoclonal antibodies for delivery of cytotoxic payloads to can-cer cells. Ther. Deliv. 2011, 2, 397-416.
[67] Susan Hoppmann, S. ; Miao, Z.;Shuanglong Liu, S.; Liu, H.; Ren, G.; Bao, A.; Cheng.Z. Radiolabeled Affibody Albumin Bioconju-
gates for HER2-Positive Cancer Targeting. Bioconjugate. Chem. 2011, 22, 413-421.
[68] Eberlein, U.; Bröer, J.H.; Vandevoorde, C.; Santos, P.; Bardiès, M.; Bacher, K.; Nosske, D.; Lassmann, M. Biokinetics and dosi-
metry of commonly used radiopharmaceuticals in diagnostic nu-clearmedicine – a review. Eur. J. Nucl. Med. Mol. Imaging. 2011,
38, 2269-2281. [69] Lassmann, M.; Chiesa, C.; Flux, G.; Bardiès, M., EANM Dosime-
try Committee guidance document: good practice of clinical dosi-metry reporting. Eur. J. Nucl. Med. Mol. Imaging. 2011, 38, 192-
200. [70] Bacher, K.; Thierens, H.M. Accurate dosimetry: an essential step
towards good clinical practice in nuclear medicine. Nucl. Med. Commun. 2005 , 26, 581-586.
[71] Strigari, L.; Benassi, M.; Chiesa, C.;Cremonesi, M.; Bodei, L.; D'Andrea, M. Dosimetry in nuclear medicine therapy: radiobio-
logy application and results.Q. J. Nucl. Med. Mol. Imaging. 2011, 55, 205-221.
[72] Sgouros, G.; Frey, E.; Wahl, R.; He, B.; Prideaux, A.; Hobbs, R.Three-dimensional imaging-based radiobiological dosimetry.
Semin. Nucl. Med. 2008 , 38, 321-334. [73] Hobbs, R.F.;Baechler, S.;Fu, D.X.;Esaias, C.; Pomper, M.G.;
Ambinder, R.F.; Sgouros, G. A model of cellular dosimetry for macroscopic tumors in radiopharmaceutical therapy. Med.
Phys. 2011, 38, 2892-2903. [74] Flux, G.;Bardies, M.; Chiesa, C.; Monsieurs, M.; Savolainen, S.;
Strand, S.E.; Lassmann, M.Clinical radionuclide therapy dosime-try: the quest for the "Holy Gray".Eur. J. Nucl. Med. Mol. Ima-
ging. 2007, 34, 1699-1700. [75] Brans, B.; Bodei, L.; Giammarile, F.; Linden, O.;Luster, M.; Oyen,
W.J.; Tennvall, J. Clinical radionuclide therapy dosimetry: the quest for the "Holy Gray". Eur. J. Nucl. Med. Mol. Imaging. 2007,
34, 772-86. [76] Bardiès, M.; Buvat, I.Dosimetry in nuclear medicine therapy:
what are the specifics in image quantification for dosimetry? Q. J. Nucl. Med. Mo.l Imaging. 2011, 55, 5-20.
[77] Meuret, G.; Hoffmann, G.; Gmelin, R. 32
P-therapy in polycythe-mia vera. Klin. Wochenschr. 1975, 53(11):519-521.
[78] Meuret, G. Present status of 32
P-therapy in management of polycythemia vera. Klin. Wochenschr. 1975, 53, 555-558.
[79] Tennvall, J.; Boudewijn, B. EANM procedure guideline for 32P phosphate treatment of myeloproliferative diseases. Eur. J. Nucl.
Med. 2007, 34, 1324-1327. [80] Petrini, B.; Blomgren, H.; Wasserman, J.; Svedmyr, E.; Stedingk,
L.V.; Schnell, P.O. Effect of 32
P treatment for polycythaemia vera on blood lymphocyte subpopulations and their functions. Eur. J.
Haematol. 1987, 39, 221-227. [81] Najean, Y.; Rain, J-D. The very long-term evolution of polycy-
themia vera: an analysis of 318 patients initially treated by phlebo-tomy of
32P between 1969 and 1981. Semin.Hematol. 1997, 34, 6-
16. [82] Tennvall, J.; Brans, B. EANM procedure guideline for
32P phos-
phate treatment of myeloproliferative diseases. Eur. J. Nucl. Med. Mol. Imaging. 2007, 34, 1324–1327.

Targeted Radionuclide Therapy Current Radiopharmaceuticals, 2013, Vol. 6, No. 3 25
[83] Pearson, T.C.; Barbui, T. The management of polycythemia vera.
Hematology 1997, 2, 55-64. [84] Berk, P.D.; Goldberg, J.D.; Donovan, P.B.; Fruchtman, S.M.; Ber-
lin, N.I.; Wasserman, L.R. Therapeutic recommendations in polycythemia vera based on Polycythemia Vera Study Group
protocols. Semin. Hematol. 1986, 23, 132-143. [85] Beierwaltes, W.H. The history of the use of radioactive iodine.
Semin. Nucl. Med. 1979, 3, 151-155. [86] Goldsmith, S.J. Thyroid carcinoma. In: Khalikhali I, Maublant JC,
Goldsmith SJ, editors. Nuclear oncology: Diagnosis & Therapy. Philadelphia: Lippincott Williams & Wilkins, 2001. 197-219.
[87] Beierwaltes, W.H.; Nishitama, R.H.;Thompson, N.W.; Copp, J.E.; Cuba, A. Survival Time "Cure" in Papillary and Follicular Thyroid
Carcinoma with Distant Metastases: Statistics Following University of Michigan Therapy. J. Nucl. Med. 1982, 23, 561-568.
[88] Klain, M.; Ricard, M.; Leboulleux, S.; Baudin, E, ; Schlumberger, M. Radioiodine therapy for papillary and follicular thyroid carci-
noma. Eur. J. Nucl. Med. 2002. 29, S479-S485. [89] Movious, E.G.; Robbins, J.; Pierce, L.R, ; Reynolds, J.C.; Keenan,
A.M.; Phyillaier, M.A. In: Medeiros, N.G.; Gaitan, E. [eds], Fron-tiers in thyroidology, New York, Plenum Press, 1986, 2, 1269-
1272. [90] Meier, D.A.; Brill, D.R.; Becker, D.V.; Clarke, S.E.M.; Silberstein,
E.B.; Royal, H.D.; Balon, H.R. Procedure guidelines for therapy of thyroid disease with
131Iodine. J. Nucl. Med. 2002, 43, 856-861.
[91] Leeper, R.D.; Shimaoka, K. Endocrinol. Metab. Clin. North Am. 1980, 9, 383-405
[92] Lun, Y.; Wu, X.; Xia, Q.; Han, Y.; Zhang, X.; Liu, Z.; Wang, F.; Duan, Z.; Xin, S.; Zhang, J. Hashimoto's thyroiditis as a risk factor
of papillary thyroid cancer may improve cancer prognosis. Oto-laryngol .Head Neck Surg.. 2013 , 148, 396-402.
[93] Miller, R.W.; Young, J.L. Jr, Novakovic, B. Childhood cancer. Cancer 1994, 75, 395–405.
[94] Gasnier, B.; Roisin, M.P.; Scherman, D.; Coornaert, S.; Desplan-ches, G.; Henry, J.P. Uptake of meta-iodobenzylguanidine by bo-
vine chromaffin granule membranes. Mol. Pharmacol. 1986, 29, 275 280.
[95] Chrisoulidou, A.; Kaltsas, G.; Ilias, I.; Grossman, A.B. The diag-nosis and management of malignant phaeochromocytoma and pa-
raganglioma. Endocr. Relat. Cancer. 2007, 14, 569–585. [96 ] Ahlman, H. Malignant pheochromocytoma: state of the field with
future projections. Ann. N. Y. Acad. Sci. 2006, 1073, 449-464. [97] Hoefnagel, C.A.; de Hraker, J.; Valdes Olmos, R.A.; Voute P.A.
131I-MIBG as first-line treatment in high risk neuroblastoma pati-
ents. Nucl Med Comm 1994, 15, 712-717
[98] Kaltsas. G.A.; Papadogias, D.; Makras, P.; Grossman, A.B. Tre-atment of advanced neuroendocrine tumors with radiolabelled
somatostatin analogues. Endocr. Relat. Cancer. 2005, 12, 683–699.
[99] Kolby, L.; Bernhardt, P.; Johanson, V.; Wangberg, B.; Muth, A.; Jansson, S.; Forssell-Aronsson, E.; Nilsson, O.; Ahlman, H. Can
quantification of VMAT and SSTR expression be helpful for plan-ning radionuclide therapy of malignant pheochromocytomas?
Ann. N. Y. Acad. Sci. 2006, 1073, 491–497. [100] Cuccurullo, V.; Cascini, G.L.; Tamburrini, O.; Rotondo, A.; Mansi,
L. Bone metastases radiopharmaceuticals: an overview. Curr. Ra-diopharm. 2013, 6, 41-47.
[101] Paes, F.M.; Serafini, A.N. Systemic metabolic radiopharmaceutical therapy in the treatment of metastatic bone pain. Semin. Nucl. Med.
2010, 40, 89-104. [102] Pecher, C. Biological Investigations with Radioactive Calcium and
trontium: Preliminary Report on the Use of Radioactive Strontium in the Treatment of Metastatic Bone Cancer. Univ. Calif. Publ.
Pharmacol. 1942, 2, 117–149.
[103] Cuccurullo, V.; Cascini, G.; Rossi, A.; Tamburrini, O.; Rotondo,
A.; Mansi, L. Pathophysiological premises to radiotracers for bone metastases. Q. J. Nucl. Med. Mol. Imaging. 2011, 55, 353-73
[104] Silberstein, E.B. Advances in our understanding of the treatment of painful bone metastases. J. Nucl. Med. 2000, 41, 655.657.
[105] Blake, G.M.; Zivanovic, M.A.; Blaquiere, R.M.; Fine. D.R.; McEwan, A.J.; Ackery, D.M.;.Strontium-89 therapy: meas-
urement of absorbed dose to skeletal metastases. J. Nucl. Med. 1988; 29, 549-557.
[106] Collins, C.; Eary, J.F.; Donaldson, G.; Vernon, C.;Bush, N.E.; Petersdorf, S, .; Livingston, R.B.; Gordon, E.E.; Chapman,
C.R.; Appelbaum, F.R. Samarium-153-EDTMP in bone metastases
of hormone refractory prostate carcinoma: a phase I/II trial. J. Nucl.
Med. 1993, 34, 1839-1844.
[107] Dolezal, J. Systemic radionuclide therapy with samarium-153-
EDTMP for painful bone metastases. Nucl. Med. Rev. Cent. East.
Eur. 2000, 3, 161-163.
[108] Dolezal, J.; Vizda, J.; Odrazka, K. Prospective evaluation of samar-
ium- 153-EDTMP radionuclide treatment for bone metastases in
patients with hormone-refractory prostate cancer. Urol. Int. 2007,
78, 50-57.
[109] Tian, J.H.; Zhang, J.M; Hou, Q.T; Oyang, Q.H;Wang, J.M; Luan,
Z.S; Chuan, L; He, Y.J.Multicentre trial on the effi cacy and toxic-
ity of single-dose samarium-153-ethylene diamine tetramethylene
phosphonate as a palliative treatment for painful skeletal metastases
in China. Eur. J. Nucl. Med. 1999;26 :2-7.
[110] Etchebehere, E.C.; Pereira Neto, C.A.; Lima, M.C. ; Santos Ade,
O.; Ramos, C.D.; Silva, C.M.; Camargo, E.E. Treatment of bone
pain secondary to metastases using samarium-153-EDTMP. Sao.
Paulo. Med. J. 2004, 122, 208-212.
[111] Sapienza, M.T.; Ono, C.R.; Guimarães, M.I.; Watanabe, T.; Costa,
P.A.; Buchpiguel, C.A. Retrospective evaluation of bone pain pal-
liation after samarium-153-EDTMP therapy. Rev. Hosp. Clin. Fac.
Med. Sao. Paulo. 2004, 59, 321-328.
[112] Palmedo, H.; Guhlke, S.; Bender, H.; Sartor, J.; Schoeneich,
G.; Risse, J.; Grünwald, F.; Knapp, F.F. Jr.; Biersack, H.J. Dose es-
calation study with 188Re-HEDP in prostate cancer patients with os-
seous metastases. Eur. J. Nucl. Med. 2000, 27, 123-130.
[113] Sciuto, R.; Festa, A.; Pasqualoni, R.; Semprebene, A; Rea,
S.; Bergomi, S.; Maini, C.L. Metastatic bone pain palliation with
89-Sr and 186-Re-HEDP in breast cancer patients. Breast. Cancer.
Res. Treat. 2001, 66, 101-109.
[114] De Klerk, J.M.; Zonnenberg, B.A.; Blijham, G.H.; Van Het Schip,
A.D.; Hoekstra, A.; Han, S.H.; Quirijnen, J.M.; Van Dijk, A.; Van
Rijk, P.P.Treatment of metastatic bone pain using the bone seeking
radiopharmaceutical Re-186-HEDP. Anticancer. Res. 1997, 17,
1773-1777.
[115] de Klerk, J.M.; van het Schip, A.D.; Zonnenberg, B.A.; van Dijk,
A.; Quirijnen J.M.; Blijham, G.H.; van Rijk, P.P.Phase 1 study of
rhenium-186-HEDP in patients with bone metastases originating
from breast cancer. J. Nucl. Med. 1996, 37, 244-249.
[116] Palmedo, H.; Guhlke, S.; Bender, H.; Sartor, J.; Schoeneich,
G.; Risse, J.; Grünwald, F.; Knapp, F.F. Jr.; Biersack, H.J. Dose es-
calation study with rhenium-188 hydroxyethylidene diphosphonate
in prostate cancer patients with osseous metastases. Eur. J. Nucl.
Med. 2000, 27, 123-130.
[117] Palmedo H, Manka-Waluch A, Albers P, Schmidt-Wolf,
I.G.; Reinhardt, M.; Ezziddin, S.; Joe, A.; Roedel, R.; Fimmers,
R.; Knapp, F.F.Jr.; Guhlke, S.; Biersack, H.J. Repeated bone tar-
geted therapy for hormone refractory prostate carcinoma: random-
ized phase II trials with the new high-energy radiopharmaceutical
rhenium-188 hydroxythylidine-diphosphonate. J. Clin. Oncol.
2003, 21, 2869-2875.
[118] Krishnamurthy, G.T.; Swailem, F.M.; Srivastava, S.C.; Atkins,
H.L.; Simpson, L.J.; Walsh, T.K.; Ahmann, F.R.; Meinken,
G.E.; Shah, J.H. Tin-117m(4+) DTPA: pharmacokinetics and imag-
ing characteristics in patients with metastatic bone pain. J. Nucl.
Med. 1997, 38, 230-237.
[119] Bishayee, A.; Rao, D.V.; Srivastava, S.C.; Bouchet, L.G.; Bolch,
W.E.; Howell, R. W. ; Marrow-sparing effects of 117mSn(4+) dieth-
ylenetriaminepentaacetic acid for radionuclide therapy of bone
cancer. J. Nucl. Med. 2000, 41, 2043-2050.
[120] Bouchet, L.G.; Bolch, W.E.; Goddu, S.M.; Howell, R.W.; Rao,
D.V.; Considerations in the selection of radiopharmaceuticals for
palliation of bone pain from metastatic osseous lesions. J. Nucl.
Med. 2000, 41, 682-687.
[121] Srivastava, S.C.; Atkins, H.L.; Krishnamurthy, G.T.; Zanzi,
I.;Silberstein, E.B.; Meinken, G.;Mausner. L.F.; Swailem, F.;
D'Alessandro, T.; Cabahug, C.J.; Lau, Y.;Park, T.;Madajewicz, S.
Treatment of metastatic bone pain with tin-117m stannic diethyle-
netriaminepentaacetic acid: a phase I/II clinical study. Clin. Can-
cer. Res. 1998, 4, 61-68.
[122] Atkins, H.L, ; Mausner, L.F.; Srivastava, S.C.; Meinken,
G.E.; Cabahug, C.J.; D'Alessandro, T.Tin-117m(4+)-DTPA for pal-

26 Current Radiopharmaceuticals, 2013, Vol. 6, No. 3 Dash et al.
liation of pain from osseous metastases: a pilot study. J. Nucl. Med.
1995, 36, 725-729.
[123] Ritter, M.A.; Cleaver, J.E.; Tobias, C.A. High-LET radiations
induce a large proportion of non-rejoining DNA-breaks. Nature. 1977, 266, 653–655.
[124] Cheetham, P.J.; Petrylak, D.P. Alpha particles as radiopharmaceu-ticals in the treatment of bone metastases: mechanism of action of
radium-223 chloride (Alpharadin) and radiation protection. Oncology. 2012, 26, 330-337.
[125] Henriksen, G.; Fisher, D.R.; Roeske, J.C.; Bruland, O.S.; Larsen, R.H. Targeting of osseous sites with alpha-emitting 223Ra: com-
parison with the -emitter 89Sr in mice. J. Nucl. Med. 2003, 44, 252–259.
[126] Solá, G.A.R.; Argüelles, M.G.; Bottazzini, D.L.; Furnari, J.C.; Parada, I.G.; Rojo, A.; Ruiz, H.V. Lutetium-177-EDTMP for bone
pain palliation. Preparation, biodistribution and pre-clinical studies. Radiochimica Acta. 2000, 88, 157-161.
[127] Chakraborty, S.; Das, T.; Banerjee, S.; Balogh, L.; Chaudhari, P.R.; Sarma, H.D.; Polyák, A.; Máthé, D.; Venkatesh, M.; Janoki,
G.; Pillai, M.R. A. 177Lu-EDTMP: a viable bone pain palliative in skeletal metastasis. Cancer. Biother. Radiopharm. 2008, 23, 202-
213. [128] Máthé, D.; Balogh, L.; Polyák, A, Király, R.; Márián, T.; Pawlak,
D.; Zaknun, J.J.; Pillai, M.R.A.; Jánoki, G.A. Multispecies animal investigation on biodistribution, pharmacokinetics and toxicity of 177Lu-EDTMP, a potential bone pain palliation agent. Nucl. Med. Biol. 2010, 37, 215-226.
[129] Liu, C.; Brasic, J.R.; Liu, X.; Li, H.; Xiang, X.; Luo, Z.; Wang, Y.; Kuai, D.; Zhang, G.; Zaknun, J.J. Timing and optimized acqui-
sition parameters for the whole-body imaging of 177Lu-EDTMP to-ward performing bone palliation treatment. Nucl. Med. Commun.
2012, 33, 90-96. [130] Mathew, B.; Chakraborty, S.; Das, T.; Sarma, H.D. Banerjee, S.;
Samuel, G.; Venkatesh, M.; Pillai , M.R.A.175Yb labeled poly-aminophosphonates as potential agents for bone pain palliation.
Appl. Radiat. Isot. 2004, 60, 635-642
[131] Das, T.; Chakraborty, S.; Sarma, H.D.; Tandon, P.; Banerjee, S.;
Venkatesh, M.; Pillai , M.R.A.170Tm-EDTMP: a potential cost-effective alternative to 89SrCl2 for bone pain palliation. Nucl. Med.
Biol. 2009, 36, 561-568.. [132] Schneider, P.; Farahati, J.; Reiners, C. Radiosynovectomy in rheu-
matology, orthopedics, and hemophilia. J. Nucl. Med. 2005, 46, 48S-54S.
[133] Modder, G. Radiosynoviorthesis-involvement of nuclear medicine in rheumatology and orthopaedics. Warlich Druck und Verlagsges.
MbH: Meckenheim, Germany, 1995. [134] Yates, D.B. Arthroscopy of the knee after the injection of 90Y. Ann.
Rheum. Dis. 1973, 32 , 48-50. [135] Wang SJ.; Lin WY.; Chen MN.; Chen JT.;Ho WL.;Hsieh
BT.; Huang H.; Shen LH.; Ting G.; Knapp F.F. Jr. Histologic study of effects of radiation synovectomy with Rhenium-188 micro-
sphere. Nucl. Med. Biol. 2001, 28, 727-732. [136] Mohr, W, ; Mohing, W.; Hersener, J. Morphological changes in the
articular capsule tissue after preliminary synoviorthesis. Z. Rheu-matol. 1977, 36, 316-331.
[137] Menkes, C.J. Gelenkverodung mittels radioaktiver Isotpe bei rheu-matoider Arthritis. Therapiewoche. 1979, 29, 498-501.
[138] Shortkroff, S.; Sledge, C.B. Radiation synovectomy. In: Principles of Nuclear Medicine 2nd edition. Edited by: Wagner HN Jr, Szabo
Z, Buchanan JW. Philadelphia: WB Saunders Co.1995, 1021-1028. [139] Noble, J.; Jones, A.G.; Davies, M.A.; Sledge, C.B. ; Kramer, R.I.;
Livni, E. Leakage of radioactive practice system from synovial joint studied with a gamma camera; its application to radiation
synovectomy. J. Bone. Joint. Surg. 1983, 65, 381-389. [140] Murray, T.; Erskine Hilditch, T. Therapeutic applications of radio-
pharmaceuticals. In: Textbook of Radiopharmacy. Theory and Practice 3rd edition. Edited by: Sampson CB. Cambridge: Gordon
and Breach Science Publishers. 1999:380. [141] Clunie, G.; Ell, P.J. A survey of radiation synovectomy in Europe,
1991–1993. Eur. J. Nucl. Med. 1995, 22, 970-976. [142] Lee, E.B.; Shin, K.C.; Lee, Y.J.; Lee, Y.J.; Cheon, G.J.; Jeong,
J.M.; Son, M.W.; Song, Y. W.188Re-tin colloid as a new therapeutic agent for rheumatoid arthritis. Nucl. Med. Commun. 2003, 24, 689-
696.
[143] Harbert, J.C. Radionuclide Therapy in Joint Diseases. In: Harbert,
J.C. ed. Nuclear Medicine Diagnosis and Therapy. New York; Thieme Medical Publishers. Inc. 1996, 1093–1110.
[144] Siegel, M. Siegel, H.J.; Luck, J.V. Radiosynovectomy’s Clinical Applications and Cost Effectiveness: A Review. Semin. Nucl. Med.
1997, 27, 364–371. [145] Clunie, G.; Fischer, M. EANM procedure guidelines for radio-
synovectomy. Eur. J. Nucl. Med. Mol. Imaging. 2003, 30, BP12-BP16.
[146] Schneider, P.; Farahati, J.; Reiners, C. Radiosynovectomy in rheu-matology, orthopedics, and hemophilia. J. Nucl. Med. 2005, 46,
48S-54S. [147] Kat, S.; Kutz, R.; Elbracht, T.; Weseloh, G.; Kuwert, T. Radio-
synovectomy in pigmented villonodular synovitis. Nuklearmedizin. 2000, 39, 209-213.
[148] Parkin, D.M.; Bray, F.; Ferlay, J.; Pisani, P. Global cancer statis-tics, 2002. CA. Cancer. J. Clin. 2005, 55, 74-108.
[149] Bosch, F.X.; Ribes, J.; Diaz, M.; Cleries, R. Primary Liver cancer: worldwide incidence and trends. Gastroenterology. 2004, 127, S5-
S16. [150] El-Serag, H.B.; Davila, J.A.; Petersen, N.J.; McGlynn, K.A.The
continuing increase in the incidence of hepatocellular carcinoma in the UnitedStates: an update. Ann. Intern. Med. 2003, 139, 817-823.
[151] Kennedy, A.; Nag, S.; Salem, R.; Murthy, R.; McEwan, A.J.; Nutting, C.; Benson, A.; Espat, J.; Bilbao, J. I.; Sharma, R. A.;
Thomas, J. P.;Coldwell, D. Recommendations for radioemboliza-tion of hepatic malignancies using yttrium-90 microsphere
brachytherapy: a consensus panel report from the radioemboliza-tion brachytherapy oncology consortium. Int. J. Radiat. Oncol.
Biol. Phys. 2007, 68, 13-23. [152] Ackerman, N.B.; Lien, W.M.; Kondi, E.S., Silverman, N.A.The
blood supply of experimental liver metastases. I: The distribution of hepatic artery and portal vein blood to “small” and “large” tu-
mors. Surgery. 1970, 66, 1067-1072. [153] Harbert, J.C.; In Nuclear Medicine: Diagnosis and Therapy; Har-
bert JC, Eckelman WC and Neumann RD. Thieme Medical Pub-lishers, Inc., New York, 1996, 1141-1155.
[154] Leung, W.T.; Lau, W.Y.; Ho. S.; Chan, M.; Leung, N.; Lin, J.; Ho, K.C. Metreweli C, Johnson PJ, Li AK.Selective internal radiation
therapy with intra-arterial iodine-131-Lipiodol in inoperable hepa-tocellular carcinoma. J. Nucl. Med. 1994, 35, 1313-1318
[155] Raoul, J.L.; Guyader, D.; Bretagne, J.F.; Duvauferrier, R.; Bourguet, P.; Bekhechi, D.; Deugnier, Y.M.; Gosselin, M. Ran-
domized controlled trial for hepatocellular carcinoma with portal vein thrombosis: intra-arterial iodine-131-iodized oil versus medi-
cal support. J. Nucl. Med. 1994, 35, 1782-1787. [156] Bhattacharya, S.; Novell, J.R.; Dusheiko, G.M.; Hilson, A.J.; Dick,
R.; Hobbs, K.E. Epirubicin-Lipiodol chemotherapy versus 131iodine-Lipiodol radiotherapy in the treatment of unresectable
hepatocellular carcinoma. Cancer. 1995, 76, 2202-2210. [157] Risse, J.H.; Grunwald, F.; Kersjes, W.; Strunk, H.; Caselmann,
W.H.; Palmedo, H.; Bender, H.; Biersack, H.J.Intraarterial HCC therapy with I-131-Lipiodol. Cancer. Biother. Radiopharm. 2000,
15, 65-70. [158] Boucher, E.; Corbinais, S.; Rolland, Y.; Bourguet. P.; Guyader,
D.; Boudjema, K.; Meunier, B.; Raoul, J.L.Adjuvant Intra-arterial Injection of Iodine-131-Labeled Lipiodol after Resection of Hepa-
tocellular Carcinoma, Hepatology. 2003, 38, 1237–1241. [159] Risse, J.H.; Rabe, C.; Pauleit, D.; Reichmann, K.; Menzel,
C.; Grünwald, F.; Strunk, H.; Biersack, H.J.; Palmedo, H. Therapy of hepatocellular carcinoma with iodine-131-lipiodol. Results in a
large German cohort. Nuklearmedizin. 2006, 45, 185-192. [160] Boucher, E.; Garin, E.; Guylligomarc'h, A.; Olivie, D.; Boudjema,
K.; Raoul, J.L. Intra-arterial injection of iodine-131-labeled lipio-dol for treatment of hepatocellular carcinoma. Radiothe.r Oncol.
2007, 82, 76-82. [161] Kanhere, H.A.; Leopardi, L.N.; Fischer, L.; Kitchener, M.I.; Mad-
dern, G.J. Treatment of unresectable hepatocellular carcinoma with radiolabelled lipiodol. ANZ. J. Surg. 2008, 78, 371-376.
[162] Chua, T.C.; Chu, F.; Butler, S.P.; Quinn, R.J.; Glenn, D.; Liauw, W.; Morris, D.L.Intra-arterial iodine-131-lipiodol for unresectable
hepatocellular carcinoma. Cancer. 2010, 116, 4069-4077 [163] Becker, S.; Laffont, S.; Vitry, F.; Rolland, Y.; Lecloirec, J.;
Boucher, E.; Raoul, J.L.;Herry, J.Y.; Bourguet, P.; Garin, E.Dosimetric evaluation and therapeutic response to internal radia-

Targeted Radionuclide Therapy Current Radiopharmaceuticals, 2013, Vol. 6, No. 3 27
tion therapy of hepatocarcinomas using iodine-131-labelled lipio-
dol. Nucl. Med. Commun. 2008, 29, 815-825. [164] Bretagne, J.F.; Raoul, J.L.; Bourguet, P.; Duvauferrier, R.;
Deugnier, Y.; Faroux, R.; Ramée, A.; Herry, J.Y.; Gastard J. He-patic artery injection of I-131-labelled lipiodol - Part 2. Radiology.
1998, 168, 547-550 [165] Raoul, J.L.; Boucher, E.; Roland, V.; Garin, E. 131-iodine Lipiodol
therapy in hepatocellular carcinoma. Q. J. Nucl. Med. Mol. Imag-ing. 2009, 53, 348-355.
[166] Raoul, J.L.; Guyader, D.; Bretagne, J.F.; Duvauferrier, R.; Bourguet, P.; Bekhechi, D.; Deugnier Y.M.; Gosselin,
M.Randomized controlled trial for hepatocellular carcinoma with portal vein thrombosis: intra-arterial iodine-131-iodized oil versus
medical support. J. Nucl. Med. 1994, 35, 1782-1787. [167] Toubeau, M.; Touzery, C.; Berriolo-Riedinger, A.; Cochet,
A.; Brunotte, F.; Bedenne, L.; Cercueil, J.P.; Krause, D.131I thyroid uptake in patients treated with 131I-Lipiodol for hepatocellular car-
cinoma. Eur. J. Nucl. Med. 2001, 28, 669-670. [168] Chang M.C.;Lin, W.Y. The Effect of Intratumoral Injection of
188Re-Microspheres on the Hematologic, Hepatic and Renal Func-tions in the Treatment of VX2 Hepatic Tumor: An Animal Study.
Ann. Nucl. Med. Sci. 2007, 20, 187-192. [169] Wunderlich, G.; Drews, A.; Kotzerke, J. A kit for labeling of
[188Re] human serum albumin microspheres for therapeutic use in nuclear medicine. Appl. Radiat. Isot. 2005 , 62, 915-918.
[170] Hafeli, U.O. Roberts, W.K.; Pauer, G.J.; Kraeft, S.K.; Macklis, R.M.Stability of biodegradable radioactive rhenium (Re-186 and
Re-188) microspheres after neutron-activation. Appl. Radiat. Isot. 2001, 54, 869-79
[171] Andreana, L.; Isgrò, G.; Marelli, L.; Davies, N.; Yu, D.; Navalkissoor, S.;Burroughs, A.K. Treatment of hepatocellular car-
cinoma (HCC) by intra-arterial infusion of radio-emitter com-pounds: trans-arterial radio-embolisation of HCC. Cancer. Treat.
Rev. 2012, 38:641-649. [172] Kumar, A.; Srivastava, D.N.; Chau, T.T.; Long, H.D.;Bal,
C.;Chandra, P.;Chien le T.; Hoa, N.V.;Thulkar, S.;Sharma, S.;Tam le, H.;Xuan, T.Q.;Canh, N.X.;Pant, G.S.;Bandopadhyaya, G.P. In-
operable hepatocellular carcinoma: transarterial 188Re HDD-labeled iodized oil for treatment--prospective multicenter clinical trial.
Radiology. 2007, 243, 509-519. [173] Sundram, F.;Chau, T.C.;Onkhuudai, P.;Bernal, P.;Padhy, A.K.
Preliminary results of transarterial rhenium-188 HDD lipiodol in the treatment of inoperable primary hepatocellular carcinoma. Eur.
J. Nucl. Med. Mol. Imaging. 2004, 31, 250-257. [174] Bernal, P.;Raoul, J.L.;Stare, J.;Sereegotov, E.; Sundram, F.X.;
Kumar, A.; Jeong, J.M.; Pusuwan, P.; Divgi, C.; Zanzonico, P.; Vidmar, G.; Buscombe, J.; Chau, T.T.; Saw, M.M.; Chen, S.;
Ogbac, R.; Dondi, M.; Padhy, A.K. International Atomic Energy Agency-sponsored multination study of intra-arterial rhenium-188-
labeled lipiodol in the treatment of inoperable hepatocellular carci-noma: results with special emphasis on prognostic value of do-
simetric study. Semin. Nucl. Med. 2008, 38, S40-S45. [175] Bernal, P, Raoul, J.L, .;Vidmar, G.;Sereegotov, E.;Sundram,
F.X.;Kumar, A.;Jeong, J.M.;Pusuwan, P.;Divgi, C.;Zanzonico, P.;Stare, J.; Buscombe, J.;Minh, C.T.;Saw, M.M.;Chen, S.;Ogbac,
R.;Padhy, A.K.Intra-arterial rhenium-188 lipiodol in the treatment of inoperable hepatocellular carcinoma: results of an IAEA-
sponsored multination study. Int. J. Radiat. Oncol. Biol. Phys. 2007, 69, 1448-1455.
[176] Lambert, B.;Bacher, K.;Defreyne, L. Rhenium-188 based radio-pharmaceuticals for treatment of liver tumors. Q. J. Nucl. Med.
Mol. Imaging. 2009, 53, 305-310. [177] Liepe, K.; Brogsitter, C.; Leonhard, J.; Wunderlich, G.; Hliscs, R.;
Pinkert, J.; Folprecht, G.; Kotzerke, J. Feasibility of high activity rhenium-188-microsphere in hepatic radioembolization. Jpn. J.
Clin. Oncol. 2007, 37, 942-950. [178] Lambert, B.;Bacher, K.; De Keukeleire, K.;Smeets, P.;Colle,
I.;Jeong, J.M.;Thierens, H.;Troisi, R.;De Vos, F.;Van de Wiele, C.188Re-HDD/lipiodol for treatment of hepatocellular carcinoma: a
feasibility study in patients with advanced cirrhosis. J. Nucl. Med. 2005, 46, 1326-1332.
[179] Vente, M.A.; de Wit, T.C.; van den Bosch, M.A.; Bult, W.; Seevinck, P.R. Holmium-166 poly(L: -lactic acid) microsphere ra-
dioembolisation of the liver:technical aspects studied in a large animal model. Eur. Radiol. 2009, 20, 862-869.
[180] Smits, ML, Nijsen, JF, van den Bosch, MA, Lam, MG, Vente, MA,
Huijbregts, J.E.; van het Schip, A.D.; Elschot, M.; Bult, W.; de Jong, H.W.;Meulenhoff, P.C.; Zonnenberg, B.A. Holmium-166 ra-
dioembolization for the treatment of patients with liver metastases: design of the phase I HEPAR trial. J. Exp. Clin. Cancer. Res. 2010,
29, 70. [181] Kim, J.K.; Han, K.H.; Lee, J.T.; Paik, Y.H.; Ahn, S.H.; Lee,
J.D.; Lee, K.S.; Chon, C.Y.; Moon, Y.M. Long-term clinical out-come of phase IIb clinical trial of percutaneous injection with hol-
mium-166/chitosan complex (Milican) for the treatment of small hepatocellular carcinoma. Clin Cancer Res. 2006, 12, 543–548.
[182] Sohn, J.H.; Choi, H.J.; Lee, J.T.; Lee, J.D.; Kim, J.H.; Kim, J.H.;Moon, Y.M.; Park, K.; Park, K.B.; Kim, E.; Yoo, N.C. Phase
II study of transarterial holmium-166-chitosan complex treatment in patients with a single, large hepatocellular carcinoma. Oncology.
2009, 76, 1-9. [183] Lee, I.J.; Seong, J.; Koom, W.S.; Kim, Y.B.; Jeon, B.C.; Kim, J.H.;
Han, K.J. Selection of the Optimal Radiotherapy Technique for Lo-cally Advanced Hepatocellular Carcinoma, Jpn. J. Clin. Oncol.
2011, 41, 882-889. [184] Lee, I.J.; Seong, J.The Optimal Selection of Radiotherapy Treat-
ment for Hepatocellular Carcinoma, Gut. Liver. 2012, 6, 139-48[185] Okarvi, S.M. Peptide-based radiopharmaceuticals: fu-
ture tools for diagnostic imaging of cancers and other diseases. Med. Res. Rev. 2004, 24, 357-397.
[186] Heppeler, A.; Froidevaux, S.; Eberle, A.N.; Maecke, H.R. Receptor targeting for tumor localisation and therapy with radiopeptides.
Curr. Med. Chem. 2000, 7, 971-994. [187] Van Den Bossche, B.; Van de Wiele, C. Receptor imaging in on-
cology by means of nuclear medicine: current status. J. Clin. On-col. 2004, 22, 3593–3607.
[188] Santos, S.; Torcato, I.; Castanho M.A.Biomedical applications of dipeptides and tripeptides. Biopolymers. 2012;98.288-393.
[189] Reubi, J.C. Peptide receptors as molecular targets for cancer diag-nosis and therapy. Endocr Rev. 2003, 24, 389-427.
[190] Gotthardt, M.; Dijkgraaf, I., Boerman, O.C.; Oyen, W.J.G. Nu-clear medicine imaging and therapy of neuroendocrine tumors
Cancer Imaging.2006, 6, S178–S184. [191] Reubi, J.C.; Macke, H.R.; Krenning, E.P. Candidates for peptide
receptor radiotherapy today and in the future. J. Nucl. Med. 2005, 46, 67S–75S.
[192] Rufini, V.; Calcagni, M.L.; Baum, R.P. Imaging of neuroendocrine tumors. Semin. Nucl. Med. 2006, 36, 228-247.
[193] Fani, M.;. Maecke, H. R.; Okarvi , S. M. Radiolabeled Peptides: Valuable Tools for the Detection and Treatment of Cancer, Ther-
anostics, 2012, 2, 481-501. [194] Chen, J.Q.; Giblin, M.F.; Wang, N.; Jurisson, S.S.; Quinn, T.P. In
vivo evaluation of 99mTc/188Re-labeled linear alpha-melanocyte stimulating hormone analogs for specific melanoma targeting.
Nucl. Med. Biol. 1999, 26, 687–693. [195] Miao, Y.; Benwell, K.; Quinn, T.P. 99mTc- and 111In-labeled amela-
nocyte-stimulating hormone peptides as imaging probes for pri-mary and pulmonary metastatic melanoma detection. J. Nucl. Med.
2007, 48, 73–80. [196] Valkema, R, Pauwels, SA, Kvols, LK, Kwekkeboom, DJ, Jamar, F,
de Jong, M, Barone, R.; Walrand, S.; Kooij, P.P.; Bakker, W.H.; Lasher, J.; Krenning, E.P. Long-term follow-up of renal
function after peptide receptor radiation therapy with 90Y-DOTA0, Tyr3-octreotide and 177Lu-DOTA0, Tyr3-octreotate. J. Nucl. Med.
2005, 46, 83S-91S. [197] Imhof, A.; Brunner, P.; Marincek, N.; Briel, M.; Schindler,
C.; Rasch, H.; Mäcke, H.R.; Rochlitz, C.; Müller-Brand, J.; Walter, M. A. Response, survival, and long-term toxicity after therapy with
the radio-labeled somatostatin analogue [90Y-DOTA]-TOC in me-tastasized neu-roendocrine cancers. J. Clin. Oncol. 2011, 29, 2416-
2423. [198] Teunissen, J.J.; Kwekkeboom, D.J.; de Jong, M.; Esser, J.P.;
Valkema, R.; Kren-ning, E.P. Endocrine tumors of the gastrointes-tinal tract. Peptide receptor radionuclide therapy. Best. Pract. Res.
Clin. Gastroenterol. 2005, 19, 595-616. [199] Barbieri F, Bajetto A, Pattarozzi A, Gatti M, Würth R, Thellung S,
Corsaro A, Villa V, Nizzari M, Florio T.Peptide Receptor Target-ing in Cancer: The Somatostatin Paradigm Int J Pept. 2013 (In
press) [200] Ginj M, Zhang H, Waser B, Cescato R, Wild D, Wang X, Erchegyi
J, Rivier J, Mäcke HR, Reubi JC.Radiolabeled somatostatin recep-

28 Current Radiopharmaceuticals, 2013, Vol. 6, No. 3 Dash et al.
tor antagonists are preferable to agonists for in vivo peptide recep-
tor targeting of tumors. Proc Natl Acad Sci USA. 2006, 103, 16436-16441.
[201] Prinster, S.C.; Hague, C.; Hall, R.A. Heterodimerization of g pro-tein-coupled receptors: specificity and functional significance.
Pharmacol Rev. 2005, 57, 289-98 [202] Oberg, K. Carcinoid tumors: molecular genetics, tumor biology,
and update of diagnosis and treatment. Curr. Opin. Oncol. 2002, 14, 38–45.
[203] Oberg, K. Future aspects of somatostatin-receptor mediated ther-apy. Neuroendocrinol. 2004, 80 (Suppl 1), 57–61.
[204] Cescato, R.; Schulz, S.; Waser, B.; Eltschinger, V.; Rivier, J.E.; Wester, H.J.; Culler, M.; Ginj, M.; Liu, Q.; Schonbrunn,
A.; Reubi, J.C.Internalization of sst2, sst3, and sst5 receptors: ef-fects of somatostatin agonists and antagonists. J. Nucl. Med. 2006,
47, 502 511. [205] Reubi, J.C.; Scha¨r, J.C.; Waser, B.; Wenger S.; Heppeler,
A.; Schmitt, J.S.; Mäcke, H.R.. Affinity profiles for human soma-tostatin receptor subtypes SST1-SST5 of somatostatin radiotracers
selected for scintigraphic and radiotherapeutic use. Eur. J. Nucl. Med. 2000, 27, 273-282.
[206] Valkema, R.; de Jong, M.; Bakker, W.H.; Breeman, W.A.; Kooij, P.P.; Lugtenburg, P.J.; De Jong, F.H.; Christiansen, A.; Kam,
B.L.; De Herder, W.W.;Stridsberg, M.; Lindemans, J.; Ensing, G.; Krenning, E.P. Phase I study of peptide receptor radionuclide
therapy with [111In-DTPA0]Octreotide: The Rotterdam experience. Semin. Nucl. Med. 2002, 32, 110-122.
[207] Anthony, L.B.; Woltering, E.A.; Espanan, G.D.; Cronin, M.D.; Maloney, T.J.; McCarthy, K.E. Indium-111-pentetreotide prolongs
survival in gastroenteropancreatic malignancies. Semin. Nucl. Med. 2002, 32, 123-132.
[208] Kaltsas, G.A.; Papadogias, D.; Makras, P.; Grossman, A.B. Treat-ment of ad-vanced neuroendocrine tumors with radiolabelled soma-
tostatin ana-logues. Endocr. Relat. Cancer. 2005, 12, 683-699. [209] Kwekkeboom, D.J.; Teunissen, J.J.; Bakker, W.H.; Kooij, P.P.; de
Herder, W.W.; Feelders, R.A.; van Eijck, C.H.;Esser, J.P.; Kam, B.L.; Krenning, E.P. Radiolabeled somatostatin analog [177Lu-
DOTA0, Tyr3]octreotate in patients with endocrine gastroentero-pancreatic tumors. J. Clin. Oncol. 2005, 23, 2754-2762.
[210] Otte, A.; Mueller-Brand, J.; Dellas, S.; Nitzsche, E.U.; Herrmann, R.; Maecke, H.R. Yttrium-90-labelled somatostatin-analogue for
cancer treatment. Lancet. 1998, 351:417-418. [211] Imhof, A.; Brunner, P.; Marincek, N.; Briel, M.; Schindler,
C.; Rasch, H.; Mäcke, H.R.; Rochlitz, C. Müller-Brand, J.; Walter, M.A.Response, survival, and long-term toxicity after therapy with
the radio-labeled somatostatin analogue [90Y-DOTA]-TOC in me-tastasized neu-roendocrine cancers. J. Clin. Oncol. 2011, 29, 2416-
2423. [212] Waldherr, C.; Pless, M.; Maecke, HR.; Schumacher, T.; Crazzo-
lara, A.; Nitzsche, E.U.; Haldemann, A.; Mueller-Brand, J.Tumor response and clinical benefit in neuroendocrine tumors after 7.4
GBq 90Y-DOTATOC. J. Nucl. Med. 2002, 43, 610-616. [213] Bodei, L.; Cremonesi, M.; Grana, C.; Rocca, P.; Bartolomei, M.;
Chinol M.; Paganelli, G. Receptor radionuclide therapy with 90Y-[DOTA]0-Tyr3-octreotide (90Y-DOTATOC) in neuroendocrine
tumors. Eur. J. Nucl. Med. Mol. Imaging. 2004, 31, 1038-1046. [214] Valkema, R.; Pauwels, S.; Kvols, L.K.; Barone, R.; Jamar, F.;
Bakker, W.H.; Kwekkeboom, D.J.; Bouterfa, H.; Krenning, E.P.Survival and response after peptide receptor radionuclide ther-
apy with [90Y-DOTA0, Tyr3]octreotide in patients with advanced gastroentero-pancreatic neuroendocrine tumors. Semin. Nucl. Med.
2006; 36:147-56. [215] Dvorakova, Z.; Henkelmann, R.; Lin, X.; Türler, A.;Gerstenberg,
H. Production of 177Lu at the new research reactor FRM-II: Irradia-tion yield of 176Lu(n, gamma)177Lu., Appl. Radia.t Isot. 2008, 66,
147-151. [216] Pillai, M.R.A; Chakraborty, S.; Das, T.; Venkatesh , M.; Rama-
moorthy, N. Production logistics of 177Lu for radionuclide therapy. Appl. Radiat. Isot. 2003, 59, 109-118
[217] Chakravarty, R.; Das, T.; Dash, A.; Venkatesh, M. An electro-amalgamation approach to isolate no-carrier-added 177Lu from neu-
tron irradiated Yb for biomedical applications. Nucl. Med. Biol. 2010, 37, 811-820.
[218] Kwekkeboom, D.J.; de Herder, W.W.; Kam, B.L, van Eijck, C.H.; van Essen, M.; Kooij, P.P.; Feelders, R.A.; van Aken,
M.O.; Krenning, E.P.Treatment with the radiolabeled somatostatin
analog [177Lu-DOTA0, Tyr3]octreotate: toxicity, efficacy, and sur-
vival. J. Clin. Oncol. 2008, 26, 2124-2130. [219] Kwekkeboom, D.J.; Teunissen, J.J.; Bakker, W.H.; Kooij, P.P.; de
Herder, W.W.; Feelders, R.A.; van Eijck, C.H.; Esser, J.P.; Kam, B.L.; Krenning, E.P. Radiolabeled somatostatin analog [177Lu-
DOTA0, Tyr3]octreotate in patients with endocrine gastroentero-pancreatic tumors. J. Clin. Oncol. 2005, 23, 2754-2762.
[220] van Essen, M.; Krenning, E.P.; Bakker, W.H.; de Herder, W.W.; van Aken, M.O.; Kwekkeboom, D.J. Peptide receptor radionuclide
therapy with 177Lu-octreotate in patients with foregut carcinoid tu-mors of bronchial, gastric and thymic origin. Eur. J. Nucl. Med.
Mol. Imaging. 2007, 34, 1219-1227. [221] van Essen, M.; Krenning, E.P.; De Jong, M.; Valkema, R.; Kwek-
keboom, D.J. Peptide receptor radionuclide therapy with radiola-belled somatostatin analogues in patients with somatostatin recep-
tor positive tumors. Acta. Oncol. 2007, 46, 723-734. [222] Jong, M.; Valkema, R.; Jamar, F.; Kvols, L.K.; Kwekkeboom, D.J.;
Breeman, W.A.; Bakker, W.H.; Smith, C.; Pauwels, S.; Krenning, E.P. Somatostatin receptor-targeted radionuclide therapy of tumors:
preclinical and clinical findings. Semin. Nucl. Med. 2002, 32, 133-140.
[223] Kunikowska, J.; Krolicki, L.; Hubalewska-Dydejczyk, A.; Mikola-jczak, R.; Sowa-Staszczak, A.; Pawlak, D. Clinical results of radi-
onuclide therapy of neuroendocrine tumors with (90)Y-DOTATATE and tandem (90)Y/(177)Lu-DOTATATE: which is a
better therapy option? Eur. J. Nucl. Med. Mol. Imaging. 2011, 38, 1788–1797.
[224] Chatal, J.F.; Mahé, M. Therapeutic use of radiolabelled antibodies. In Murray IPC, Ell PJ, eds. Nuclear Medicine in clinical diagnosis
and treatment. Edinburgh : Churchill Livingstone 1998, 1101-1114. [225] Carmeliet, P. Angiogenesis in health and disease. Nat. Med. 2003,
9, 653-660. [226] Folkman, J. Angiogenesis in cancer, vascular, rheumatoid and other
disease. “Angiogenesis in cancer, vascular, rheumatoid and other disease”. Nat. Med. 1995, 1, 27-31.
[227] Ahlskog, J.; Paganelli, G.; Neri, D. Vascular tumor targeting. Q. J. Nucl. Med. Mol. Imaging. 2006, 50, 296-309.
[228] Kitson, S.L.; Cuccurullo, V.; Moody, T.S.; Mansi, L. Radionuclide antibody-conjugates, a targeted therapy towards cancer. Curr. Ra-
diopharm. 2013, 6, 57-71 [229] Sharkey, R.M.; Brenner, A.; Burton, J.; Hajjar, G.; Toder, S.P.;
Alavi, A.; Matthies, A.; Tsai, D.E.; Schuster, S.J.; Stadtmauer, E.A.; Czuczman, M.S.; Lamonica, D.; Kraeber-Bodere, F.; Mahe,
B.; Chatal, J.F.; Rogatko, A.; Mardirrosian, G.; Goldenberg, D.M. Radioimmunotherapy of non-Hodgkin's lymphoma with 90Y-
DOTA humanized anti-CD22 IgG (90Y-Epratuzumab): do tumor targeting and dosimetry predict therapeutic response? J. Nucl. Med.
2003, 44, 2000-2018. [230] Postema, E. J.; Boerman, O. C.; Oyen, W. J.; Raemaekers, J. M.;
Corstens, F. H. Radioimmunotherapy of B-cell non-Hodgkin’s lymphoma. Eur. J. Nucl. Med. 2001, 28, 1725-1735. .
[231] Witzig, T. E. Radioimmunotherapy for patients with relapsed B-cell non- Hodgkin lymphoma. Cancer. Chemother. Pharmacol.
2001, 48, 91S-95S. [232] White, C.A.; Berlfein, J. R.; Grillo-Lopez, A. J. Antibody-targeted
immunotherapy for treatment of non-Hodgkin’s lymphoma. Curr. Pharm. Biotechnol. 2000, 1, 303–312.
[233] Goldenberg, D. M. The role of radiolabeled antibodies in the treat-ment of non-Hodgkin’s lymphoma: the coming of age of radioim-
munotherapy. Crit. Rev. Oncol. Hematol. 2001, 39, 195–201. [234] Wiseman, G. A.; White, C. A.; Sparks, R. B.; Erwin, W. D.; Pod-
oloff, D. A.; Lamonica, D.; Bartlett, N. L.; Anthony Parker, J.; Dunn, W. L.; Spies, S. M.; Belanger, R.; Witzig, T. E.; ; Leigh, B.
R. Biodistribution and dosimetry results from a phase III prospec-tively randomized controlled trial of Zevalin radioimmunotherapy
for low-grade, follicular, or transformed B-cell non-Hodgkin’s lymphoma. Crit. Rev. Oncol. Hematol. 2001, 39, 181-194.
[235] Kaminski, M.S.; Zasadny, K.R.; Francis, I.R.; Milik, A.W.; Ross, C.W.; Moon, S.D.; Crawford, S.M.; Burgess, J.M.; Petry, N.A.;
Butchko, G.M.; Glenn, S.D.; Wahl, R.L. Radioimmunotherapy of B-cell lymphoma with [131I]anti-B1 (anti-CD20) antibody. N. Engl.
J. Med. 1993, 329, 459-465. [236] Trikha, M.; Yan, L.; Nakada, M.T. Monoclonal antibodies as
therapeutics in oncology. Curr. Opin. Biotechnol. 2002, 13, 609-614.

Targeted Radionuclide Therapy Current Radiopharmaceuticals, 2013, Vol. 6, No. 3 29
[237] Caron, P.C.; Schwartz, M.A.; Co, M.S.; Queen, C.; Finn, R.D.;
Graham, M.C.; Divgi, C.R.; Larson, S.M.; Scheinberg, D.A. (Mur-ine and humanized constructs of monoclonal antibody M195 (anti-
CD33) for the therapy of acute myelogenous leukemia. Cancer. 1994, 73, 1049–1056.
[238] Goldenberg, D.M.; Gaffar, S.A.; Bennett, S.J.; Beach, J.L. Experi-mental radioimmunotherapy of a xenografted human colonic tumor
(GW-39) producing carcinoembryonic antigen. Cancer. Res. 1981, 41, 4354–4360.
[239] Schlom, J.; Colcher, D.; Siler, K.; Thor. A.; Bryant, G.; Johnston, W.W.; Szpak, C.A.; Sugarbaker, P.; Carrasquillo, J. A. ; Reynolds,
J.C.; Keenan, A. M.; Larson, S. M. Tumor targeting with mono-clonal antibody B72.3: experimental and clinical results. Cancer.
Treat. Res. 1990, 51, 313–335. [240] Humm, J.L. Problems and advances in the dosimetry of radionu-
clide targeted therapy. In: Systemic radiotherapy with monoclonal antibodies, options and problems, Bihl S ML, Bihl H, Wannen-
macher M (eds.) Springer-Verlag, Berlin, Heidelberg, Germany, 1996, 37-66.
[241] Kozak, R.W.; Atcher, R.W.; Gansow, O.A.; Friedman, A.M.; Hines, J.J.; Waldmann, T.A.. Bismuth-212-labeled anti-TAC
monoclonal antibody: alpha-particle-emitting radionuclides as mo-dalities for radioiimunotherapy. Proc. Natl. Acad. Sci. 1986, 83,
474-478. [242] Humm, J.L. A microdosimetric model of astatine-211 labeled anti-
bodies for radioimmunotherapy. Int. J. Radiat. Oncol. Biol. Phys. 1987, 13, 1767-1773.
[243] Zalutsky, M.R.; Schuster, J.M.; Garg, P.K.; Archer, G.E. Jr., De-whirst, M.W.; Bigner, D.D. Two approaches for enhancing radio-
immunotherapy: a emitters and hyperthermia. In: Systemic radio-therapy with monoclonal antibodies, options and problems, Bihl
SML, Bihl H, Wannenmacher M (eds). Springer-Verlag, Berlin, Heidelberg, Germany. 1996, 101-122.
[244] Behr TM, Sgouros G, Vougiokas V., Memtsoudis, S.; Gratz, S.; Schmidberger, H.; Blumenthal, R.D.; Goldenberg, D.M.; Becker,
W. Therapeutic efficacy and doselimiting toxicity of Auger-electron versus beta emitters in radioimmunotherapy with internal-
izing antibodies: evaluation of 125I-versus 131Ilabeled CO17-1A in a human colorectal cancer model. Int. J. Cancer. 1998, 76, 738-
748. [245] Griffiths, G.L.; Govindan, S.V.; Sgouros, G.; Ong, G.L.;
Goldenberg, D. M.; Mattes, M. J. Cytotoxicity with auger electron- emitting radionuclides delivered by antibodies. Int. J. Cancer.
1999, 81, 985-992. [246] Barendswaard, E.C.; Humm, J.L.; O’Donoghue, J.A.; Sgouros, G.;
Finn, R.D.; Scott, A.M.; Larson, S.M.; Welt, S.Therapeutic effi-cacy of 125I- and 131I-labeled monoclonal antibody A33 in a human
colon cancer xenograft. J. Nucl. Med. 2001, 42, 1251-1256. [247] Heyerdahl, H.; Abbas, N; Sponheim, K.; Mollatt, C.; Bruland, Ø.;
Dahle, J. Targeted alpha therapy with 227Th-trastuzumab of intrape-ritoneal ovarian cancer in nude mice. Curr. Radiopharm. 2013, 6,
106-116. [248] Abbas N, Heyerdahl H, Bruland ØS, Brevik EM, Dahle J. Compar-
ing high LET 227Th- and low LET 177Lu-trastuzumab in mice with HER-2 positive SKBR-3 xenografts. Curr. Radiopharm. 2013, 6,
78-86. [249] Goldsmith, S.J. Radioimmunotherapy of lymphoma: Bexxar and
Zevalin. Semin. Nucl. Med. 2010, 40, 122–135. [250] Azinovic, I.; DeNardo, G.L.; Lamborn, K.R.; Mirick, G.;
Goldstein, D.; Bradt, B.M.; DeNardo, S.J. Survival benefit associ-ated with human anti-mouse antibody (HAMA) in patients with B-
Cell malignancies. Cancer. Immunol. Immunother. 2006, 55, 1451-1458.
[251] Schroff, R.W.; Foon, K.A.; Beatty, S.M.; Oldham, R.K.; Morgan,
A.C. Jr. Human antimurine immunoglobulin responses in patients receiving MoAb therapy. Cancer. Res. 1985, 45, 879-885.
[252] Goldenberg, D.M.; Sharkey, R.M. Advances in cancer therapy with radiolabeled monoclonal antibodies. Q.J. Nucl. Med. Mol. Imaging.
2006, 50, 248-264. [253] Michel, R.B.; Andrews, P.M.; Rosario, A.V.; Goldenberg,
D.M.; Mattes, M.J.177Lu-antibody conjugates for single-cell kill of B-lymphoma cells in vitro and for therapy of micrometastases in
vivo. Nucl. Med. Biol. 2005, 32, 269-278. [254] Jones, A.; Harris, A.L. New developments in angiogenesis: a
major mechanism for tumor growth and target for therapy. Can-cer. J. Sci. Am. 1998, 4, 209-217.
[255] Hobbs, S.K.; Monsky, W.L.; Yuan, F.; Roberts, W.G.; Griffith, L.; Tor-chilin, V.P.; Jain, R.K. Regulation of transport pathways in
tumor vessels: role of tumor type and microenvironment. Proc. Natl. Acad. Sci. USA. 1998, 95, 4607-4612.
[256] Shubik, P. Vascularization of tumors: a review. J. Cancer. Res. Clin. Oncol. 1982, 103, 211-226.
[257] Yaun, F.; Dellian, M.; Fukumura, D.; Leunig, M.; Berk, D.A.; Torchilin, V.P.; Jain, R.K. Vascular permeability in a human tu-
mor xenograft: molecular size dependence and cutoff size. Can-cer. Res. 1995, 55, 3752-56.
[258] Allen, T.M.; Cullis, P.R. Drug delivery systems: entering the ma-instream. Science. 2004, 303, 1818-1822.
[259] Byrne, J.D.; Betancourt, T.; Brannon-Peppas, L. Active targeting schemes for nanoparticle systems in cancer therapeutics. Adv.
Drug. Deliv. Rev. 2008, 60, 1615-1626. [260] Bae, Y.H; Drug targeting and tumor heterogeneity. J. Control
Release. 2009, 133, 2-3. [261] Kukowska-Latallo, J.F.; Candido, K.A.; Cao, Z.; Nigavekar,
S.S; Majoros, I.J; Thomas, T.P; Balogh, L.P; Khan, M.K; Baker, J.R. Jr. Nanoparticle targeting of anticancer drug improves thera-
peutic response in animal model of human epithelial cancer. Can-cer. Res. 2005, 65, 5317-5324.
[262] Weissleder, R.; Kelly, K.; Sun, E.Y.; Shtatland, T.; Josephson, L. Cell-specific targeting of nanoparticles by multivalent attachment
of small molecules. Nat. Biotechnol. 2005 , 23, 1418-1423. [263] Liu, Z.; Cai, W.; He, L.; Nakayama, N.; Chen, K.;Sun, X.; Chen,
X.; Dai, H. In vivo biodistribution and highly efficient tumour tar-geting of carbon nanotubes in mice. Nat. Nanotechnol. 2007, 2,
47–52. [264] Shi, J.; Xiao, Z.; Kamaly, N.; Farokhzad, O.C. Self-Assembled
Tar-geted Nanoparticles: Evolution of Technologies and Bench to Bedside Translation. Acc. Chem. Res. 2011, 44, 1123-34.
[265] Wang, A.Z.; Gu, F.; Zhang, L.; Chan, J.M.; Radovic-Moreno, A.; Shaikh, M.R.; Farokhzad, O.C. Biofunctionalized targeted nano-
particles for thera-peutic applications. Expert. Opin. Biol. Ther. 2008, 8, 1063-1070.
[266] Wilson, D.S.; Szostak, J.W. In vitro selection of functional nucleic acids. Ann. Rev. Biochem. 1999, 68, 611-647.
[267] Javier, D.J.; Nitin, N.; Levy, M.; Ellington, A.; Richards-Kortum, R. Aptamer-targeted gold nanoparticles as molecular-specific
contrast agents for reflectance imaging. Bioconjug. Chem. 2008, 19, 1309-1312.
[268] Garnett, M. C.; Kallinteri, P. Nanomedicines and nanotoxicology: some physiological principles, Occup. Med. 2006, 56, 307-311.
[269] Nel, A.; Xia, T.; Mädler, L.; Li, N. Toxic potential of materials at the nanolevel. Science. 2006, 311, 622-627.
[270] Vega-Villa, K. R.; Takemoto, J. K.; Yáñez, J. A.; Remsberg, C. M.; Forrest, M. L.; Davies, N. M. Clinical toxicities of nanocarrier
systems. Adv. Drug. Deliv. Rev. 2008, 60, 929-938. [271] Zimmermann, R.G. Why are investors not interested in my radio-
tracer? The industrial and regulatory constraints in the develop-ment of radiopharmaceuticals. Nucl. Med. Biol. 2013, 40, 155-66.





![Intrinsically radiolabelled [(59)Fe]-SPIONs for dual MRI/radionuclide detection](https://static.fdokumen.com/doc/165x107/6335c40d379741109e00c5c6/intrinsically-radiolabelled-59fe-spions-for-dual-mriradionuclide-detection.jpg)














