
Radionuclide regurgitant index: Value and limitations
7
Radionuclide Regurgitant Index: Value and Limitations WILFRED LAM, MD, FACC DAN PAVEL, MD ERNEST BYROM, PhD AMJAD SHEIKH, MD DAVID BEST, MD KENNETH ROSEN, MD, FACC Chicago, Illinois From the Section of Cardiology, Department of Medicine, and the Section of Nuclear Medicine, Department of Radiology, Abraham Lincoln School of Medicine, Unlversity of Illinois College of Medicine, Chicago, Ilnnois. This study was supported in part by Institutional Training Grant HL 07387 from the National Heart, Lung, and Blood Institute, National Institutes of Health, Bethesda, Maryland. Manuscript received June 16, 1980; revised manuscript received September 23, 1980, accepted September 26, 1980. Address for reprints: Wilfred Lam, MD, Uni- versity of Illinois Hospiil, Cardiology Section, P.O. Box 6998, Chicago, Illinois 60680. The radionuclide regurgitant index, defined as left ventricular/right ven- tricular stroke counts obtained from gated equilibrium studies, has been reported to predict the presence and severity of left-sided valve regur- gitation. This study evaluated the radionuclide regurgitant index in 100 patients in whom left-sided valve regurgitation was angiographically graded (0 to 4+) with regard to most severe mitral or aortic regurgitation. Regurgitation was graded 0 in 44 of the 100 patients, l+ in 22, 2-I in 8, 3-F in 8 and 4+ in 20. The radionuclide regurgitant index was 0.9 to 1.5 in 51 patients, 1.8 to 2.4 in 23 and 2.5 to 12.0 in 28. The mean radionuclide regurgitant index was 1.34 in the group with no regurgitation and 1.80 in those with l+, 2.01 in those with 2-i-, 2.80 in those with 3-F and 3.85 in those with 4-F regur- gitation. There was a significant difference (p <0.05) in the radionuclide regurgitant index between patients with no regurgitation and each group with regurgitation and between groups with regurgitation separated by two or more grades of angiographic regurgitation. Twelve patients had a discordant radionuclide regurgitant index; their index either predicted clinically significant or severe regurgitation when they had no or trivial regurgitation, or predicted no or trivial regurgitation when they had clinically significant regurgitation. Eight of 10 patients with a left ventricular ejection fraction of less than 0.30 had a discordant index (p <O.OOOS). All three patients with mitral valve prolapse associated with frequent ventricular extrasystoles had a discordant index (p <O.OOOS). Recently, gated radionuclide equilibrium studies have been utilized as a noninvasive technique for measuring the severity of valve regurgitation. Rigo et a1.l reported a radionuclide index of left-sided valve regurgitation derived from gated cardiac blood pool studies. This index was defined as the ratio of left to right ventricular stroke counts, calculated from the difference in counts in each ventricle between end-diastole and end- systole. On the basis of studies iti 40 patients (31 with cardiac catheter- ization), they suggested that this index was useful in assessing the presence and severity of aortic or mitral regurgitation, or both. In this study, we measured the radionuclide regurgitant index in 100 patients undergoing both cardiac catheterization and electrocardi- ographically synchronized radionuclide cardiac studies in an attempt to assess further the utility of this new noninvasive measure of left-sided valve regurgitation. In addition, we attempted to define subgroups of patients whose radionuclide regurgitant index appeared to predict spuriously the presence or absence of significant regurgitation. Methods Patient selection: The study group consisted of 100 consecutive patients undergoing clinically indicated diagnostic cardiac catheterization and radio- nuclide cardiac equilibrium studies. The catheterization and radionuclide studies were performed within a period of 2 weeks in all patients and within 3 days in 66 patients. There was no change in the clinical or hemodynamic status of any patient between the two studies. Patients were excluded from consideration and 292 February 1981 The American Journal of CARDIOLOGY Volume 47
-
Upload
neuroscience -
Category
Documents
-
view
1 -
download
0
Transcript of Radionuclide regurgitant index: Value and limitations

Radionuclide Regurgitant Index: Value and Limitations
WILFRED LAM, MD, FACC DAN PAVEL, MD ERNEST BYROM, PhD AMJAD SHEIKH, MD DAVID BEST, MD KENNETH ROSEN, MD, FACC
Chicago, Illinois
From the Section of Cardiology, Department of Medicine, and the Section of Nuclear Medicine, Department of Radiology, Abraham Lincoln School of Medicine, Unlversity of Illinois College of Medicine, Chicago, Ilnnois. This study was supported in part by Institutional Training Grant HL 07387 from the National Heart, Lung, and Blood Institute, National Institutes of Health, Bethesda, Maryland. Manuscript received June 16, 1980; revised manuscript received September 23, 1980, accepted September 26, 1980.
Address for reprints: Wilfred Lam, MD, Uni- versity of Illinois Hospiil, Cardiology Section, P.O. Box 6998, Chicago, Illinois 60680.
The radionuclide regurgitant index, defined as left ventricular/right ven- tricular stroke counts obtained from gated equilibrium studies, has been reported to predict the presence and severity of left-sided valve regur- gitation. This study evaluated the radionuclide regurgitant index in 100 patients in whom left-sided valve regurgitation was angiographically graded (0 to 4+) with regard to most severe mitral or aortic regurgitation. Regurgitation was graded 0 in 44 of the 100 patients, l+ in 22, 2-I in 8, 3-F in 8 and 4+ in 20.
The radionuclide regurgitant index was 0.9 to 1.5 in 51 patients, 1.8 to 2.4 in 23 and 2.5 to 12.0 in 28. The mean radionuclide regurgitant index was 1.34 in the group with no regurgitation and 1.80 in those with l+, 2.01 in those with 2-i-, 2.80 in those with 3-F and 3.85 in those with 4-F regur- gitation. There was a significant difference (p <0.05) in the radionuclide regurgitant index between patients with no regurgitation and each group with regurgitation and between groups with regurgitation separated by two or more grades of angiographic regurgitation.
Twelve patients had a discordant radionuclide regurgitant index; their index either predicted clinically significant or severe regurgitation when they had no or trivial regurgitation, or predicted no or trivial regurgitation when they had clinically significant regurgitation. Eight of 10 patients with a left ventricular ejection fraction of less than 0.30 had a discordant index (p <O.OOOS). All three patients with mitral valve prolapse associated with frequent ventricular extrasystoles had a discordant index (p <O.OOOS).
Recently, gated radionuclide equilibrium studies have been utilized as a noninvasive technique for measuring the severity of valve regurgitation. Rigo et a1.l reported a radionuclide index of left-sided valve regurgitation derived from gated cardiac blood pool studies. This index was defined as the ratio of left to right ventricular stroke counts, calculated from the difference in counts in each ventricle between end-diastole and end- systole. On the basis of studies iti 40 patients (31 with cardiac catheter- ization), they suggested that this index was useful in assessing the presence and severity of aortic or mitral regurgitation, or both.
In this study, we measured the radionuclide regurgitant index in 100 patients undergoing both cardiac catheterization and electrocardi- ographically synchronized radionuclide cardiac studies in an attempt to assess further the utility of this new noninvasive measure of left-sided valve regurgitation. In addition, we attempted to define subgroups of patients whose radionuclide regurgitant index appeared to predict spuriously the presence or absence of significant regurgitation.
Methods
Patient selection: The study group consisted of 100 consecutive patients undergoing clinically indicated diagnostic cardiac catheterization and radio- nuclide cardiac equilibrium studies. The catheterization and radionuclide studies were performed within a period of 2 weeks in all patients and within 3 days in 66 patients. There was no change in the clinical or hemodynamic status of any patient between the two studies. Patients were excluded from consideration and
292 February 1981 The American Journal of CARDIOLOGY Volume 47

RADIONUCLIDE REGURGITANT INDEX-LAM ET AL.
were not included in this analysis if they had an intracardiac shunt or clinically evident tricuspid regurgitation.
Angiographic studies: The angiographic methods in- cluded biplane left cineventriculography (30’ right anterior oblique and 60” left anterior oblique projections) in all pa- tients, and ascending aortography (45” left anterior oblique projection) for aortic regurgitation when clinically indicated. The severity of mitral and aortic regurgitation was angio- graphically graded (only during conducted beats) by con- sensus of two of us on a 0 to 4+ scale modified from Sellers et al.” The grading scale was as follows: 0 = no regurgitation visualized; 1+ = slight opacification of the proximal chamber clearing completely in one cycle; 2+ = moderate opacification of the proximal chamber not completely clearing in one cycle but without progressive opacification; 3+ = progressive opacification of the proximal chamber over three or more cycles; 4+ = total opacification of the proximal chamber within one or two cycles.
For purposes of this study, patients with combined aortic and mitral regurgitation were categorized according to the most severe lesion. This categorization, rather than algebraic addition of graded aortic and mitral regurgitation, was utilized because the angiographic grading is not necessarily a linear function for which addition would be appropriate. For ex- ample, the severity of regurgitation in a patient with 2+ aortic and 2+ mitral regurgitation is not necessarily the same a~ that in a patient with a 4+ mitral regurgitation, and is of less clinical importance.
Radionuclide studies: The radionuclide cardiac studies were performed with 15 to 25 mCi of technetium-99m in vivo labeled red blood cells.” A large field of view Anger camera with a low energy all-purpose collimator was positioned in the left anterior oblique projection, chosen for best visualization of the ventricular septum, with a 10’ to 15’ caudal tilt. The electrocardiographically synchronized cardiac equilibrium study was acquired onto a dedicated mini-computer SIMIS- III (Informatek State, Inc., Norcross, Georgia), in 16 frames of 64 by 64 matrix resolution. Acquisition was continued until there were 500,000 counts/frame. Frame duration ranged from 30 to 60 ms depending on the patient’s heart rate. The left ventricular ejection fraction was calculated in a standard manner previously described.4
For calculation of the regurgitant index, the end-diastolic frame. was considered the first frame after the R wave. The end-systolic frame was taken from the nadir of the left ven- tricular time-activity curve derived during the calculation of ejection fraction. A region of interest for each ventricle in end-diastole (drawn by consensus of three of us) was utilized to calculate the regurgitant index. These regions of interest were drawn on simultaneously displayed end-diastolic and end-systolic frames, and on subtraction images (obtained from subtracting the end-systolic from the end-diastolic frame and vice versa) using a double cursor technique.5 For the right ventricle, the subtraction images were particularly useful for delineating the right ventricular region of interest. In this way, the best delineation of the boundary between the right atrium and right ventricle was possible (Fig. 1). The left ventricular region of interest was actually obtained during the ejection fraction processing so that the determination of the regurgi- tant index added only a small amount to the overall processing time. The regurgitant index was calculated by the following formula:
Regurgitant index = LV stroke counts
RV stroke counts ’ where LV stroke counts = (counts in end-diastolic frame from left ventricular end-diastolic region of interest) minus (counts
b
FIGURE 1. Delineation of right and left ventricular regions of interest for calculation of the radionuclide regurgitant index is performed on simultaneously displayed end-diastolic (a), end-systolic (b) and sub- traction images [end-diastole minus end-systole (c) and end-systole minus enddiastole (d)].
in end-systolic frame from left ventricular end-diastolic region of interest), and right ventricular stroke counts = (counts in end-diastolic frame from right ventricular end-diastolic region of interest) minus (counts in end-systolic frame from right ventricular end-diastolic region of interest).
Thus, no background was subtracted in this calculation and the same end-diastolic and end-systolic frames were used for both ventricles. Also, only the end-diastolic regions of interest were utilized for counts from the ventricles in end-systole as well as end-diastole.
Statistical analysis: The calculation of the radionuclide regurgitant index and angiographic grading were performed independently. The radionuclide regurgitant index was compared with angiographically graded regurgitation using a logarithmic transformation and one way analysis of variance. The chi-square test with the Yates correction was utilized t,o compare patient subgroups.
Results
Patient characteristics: Of the 100 patients studied, 57 were male and 43 female; their ages ranged from I4 to 73 years (mean f standard deviation 44.6 f 16.3 years). Table I lists the cardiac diagnosis in these 100 patients. Ninety-four patients had sinus rhythm, in- cluding 16 patients who had frequent (6 or more/min) ventricular extrasystoles. Six paCents had chronic atria1 fibrillation.
February 1981 The American Journal of CARDIOLOGY Volume 47 293
RADIONUCLIDE REGURGITANT INDEX-LAM ET AL.
TABLE I
Cardiac Diagnoses of Study Group _
Diagnosis
No structural heart disease Coronary artery disease Rheumatic heart disease Primary myocardial disease Mitral valve prolapse Bacterial endocarditis Other valvular heart disease Other nonvalvular heart disease Total
Patients (n)
14
9: 16 11
z 2
100
15
r
Regurgitant Index vs. Angiagraphic Regurgitation
The left ventricular ejection fraction obtained from the radionuclide study ranged from 0.15 to 0.82 (mean 0.55 f 0.16). Left ventricular ejection fraction was greater than 0.50 in 68 patients, between 0.30 and 0.50 in 22 patients and less than 0.30 in 10 patients.
Angiographic regurgitation: Angiography dem- onstrated no left-sided regurgitation in 44 patients, mitral regurgitation in.29, aortic regurgitation in 14 and both mitral and aortic regurgitation in 13 patients.
Among the 56 patients with regurgitation, the regurgitation was graded l+ in 22,2+ in 8,3+ in 6 and 4+ in 20. The 56 patients included 4 patients with fre- quent ventricular extrasystoles (3 with l+, 1 with 2+ regurgitation) and 3 patients with atria1 fibrillation (1 with l+, 1 with 2+ and 1 with 4+ regurgitation).
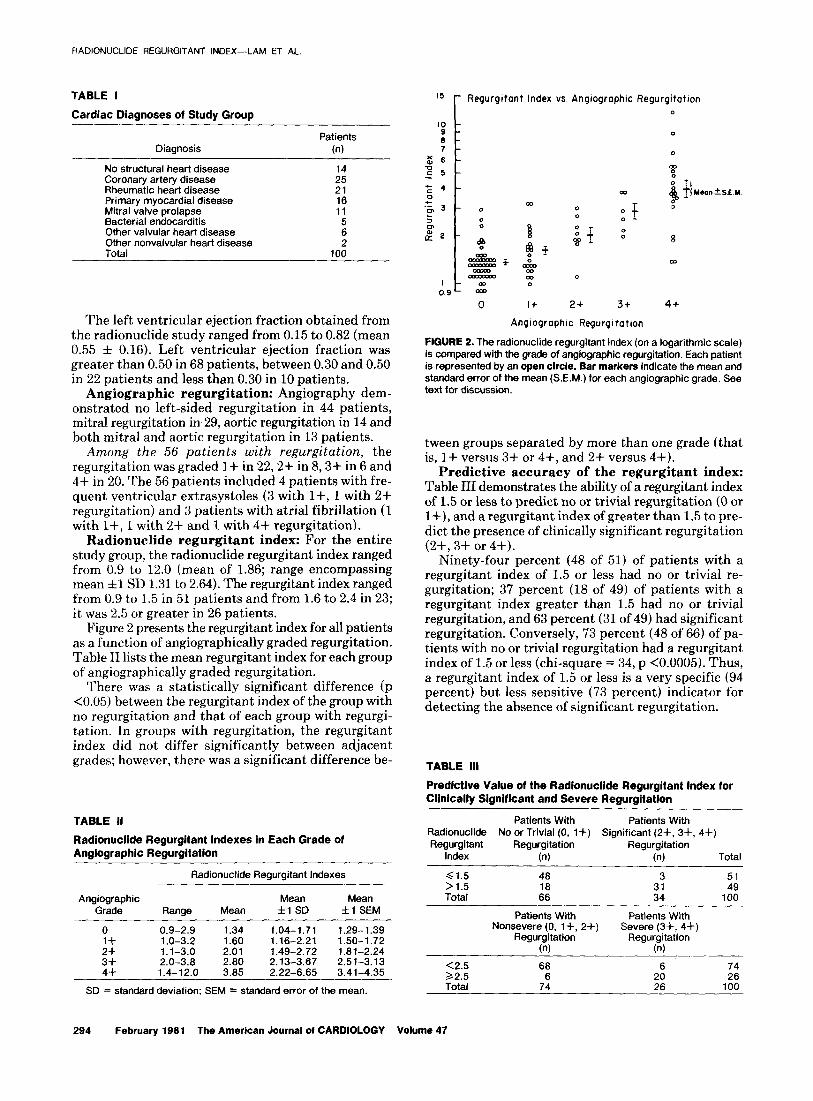
Radionuclide regurgitant index: For the entire study group, the radionuclide regurgitant index ranged from 0.9 to 12.0 (mean of 1.86; range encompassing mean fl SD 1.31 to 2.64). The regurgitant index ranged from 0.9 to 1.5 in 51 patients and from 1.6 to 2.4 in 23; it was 2.5 or greater in 26 patients.
Figure 2 presents the regurgitant index for all patients as a function of angiographically graded regurgitation. Table II lists the mean regurgitant index for each group of angiographically graded regurgitation.
There was a statistically significant difference (p <0.05) between the regurgitant index of the group with no regurgitation and that of each group with regurgi- tation. In groups with regurgitation, the regurgitant index did not differ significantly between adjacent grades; however, there was a significant difference be-
FIGURE 2. The radionuclide regurgitant index (on a logarithmic scale) is compared with the grade of angiographic regurgitation. Each patient is represented by an open circle. Bar markers indicate the mean and standard error of the mean (S.E.M.) for each angiographic grade. See text for discussion.
tween groups separated by more than one grade (that is, l+ versus 3+ or 4+, and 2+ versus 4+).
Predictive accuracy of the regurgitant index: Table III demonstrates the ability of a regurgitant index of 1.5 or less to predict no or trivial regurgitation (0 or l+), and a regurgitant index of greater than 1.5 to pre- dict the presence of clinically significant regurgitation (2+, 3+ or 4+).
Ninety-four percent (48 of 51) of patients with a regurgitant index of 1.5 or less had no or trivial re- gurgitation; 37 percent (18 of 49) of patients with a regurgitant index greater than 1.5 had no or trivial regurgitation, and 63 percent (31 of 49) had significant regurgitation. Conversely, 73 percent (48 of 66) of pa- tients with no or trivial regurgitation had a regurgitant index of 1.5 or less (chi-square = 34, p <0.0005). Thus, a regurgitant index of 1.5 or less is a very specific (94 percent) but less sensitive (73 percent) indicator for detecting the absence of significant regurgitation.
TABLE Ill
Predictive Value of the Radionuclide Regurgitant Index for Clinically Significant and Severe Regurgitation
TABLE II
Radionuclide Regurgitant Indexes in Each Grade of Angiographlc Regurgitation
Radionuclide Regurgitant Indexes
Patients With Patients With Radionuclide No or Trivial (0, l+) Significant (2-l-, 3+, 4+) Regurgitant Regurgitation Regurgitation
Index (n) (n) Total
Angiographic Mean Mean Grade Range Mean fl SD fl SEM
0 0.9-2.9 1.34 1.04-1.71 1.29- 1.39 1+ 1 .O-3.2 1.60 1.16-2.21 1.50-1.72
3:: 1.1-3.0 2.01 1.49-2.72 1.81-2.24 2.0-3.8 2.80 2.13-3.67 2.51-3.13
4+ 1.4-12.0 3.85 2.22-6.65 3.41-4.35
SD = standard deviation: SEM = standard error of the mean.
61.5 48 3 >1.5 :: Total :: 3”: 100
Patients With Patients With Nonsevere (0, l-k, 2+) Severe (3+, 4+)
Regurgitation Regurgitation (n) (n)
<2.5 68 32.5 6
2: 74 26
Total 74 26 100
294 February 1981 The American Journal of CARDIOLOGY Volume 47
0
0
: T y$pf
a
2+ 3t 4+
Angiographic Regurgitation

RADIONUCLIDE REGURGITANT INDEX-LAM ET AL.
Table III demonstrates the ability of a regurgitant index of 2.5 or greater to predict the presence of clini- cally severe regurgitation (3+ or 4+) and a regurgitant index of less than 2.5 to predict the absence of severe regurgitation (0, l+ or 2+).
Seventy-seven percent (20 of 26) of patients with a regurgitant index of 2.5 or greater had severe regurgi- tation; 92 percent (68 of 74) of patients with a regurgi- tant index of less than 2.5 did not have severe regurgi- tation. Conversely, 77 percent (20 of 26) of patients with severe regurgitation had a regurgitant index of 2.5 or greater (chi-square = 45, p <0.0005). Thus, a regurgi- tant index of 2.5 or greater was a relatively sensitive (77 percent) and specific (77 percent) indicator of severe regurgitation.
Clinical characteristics of patients with a dis- cordant regurgitant index: The regurgitant index was arbitrarily defined as discordant if it was greater than 1.5 in patients with no regurgitation or greater than 2.5 in patients with 1+ regurgitation (Fig. 3). In patients with 2+, 3+ and 4+ regurgitation, the regurgitant index was also arbitrarily defined as discordant if it was 1.5 or less.
Twelve patients had a discordant regurgitant index. Nine of these had false positive discordance (that is, a regurgitant index predicting significant or severe regurgitation in patients with no or trivial regurgita- tion). Three of these nine patients had both mitral valve prolapse and frequent ventricular extrasystoles, five had a left ventricular ejection fraction of less than 0.30, and one had coronary artery disease with an ejection fraction of 0.47.
Three patients had false negative discordance (that is, a regurgitant index predicting no or trivial regurgi- tation in patients with significant regurgitation). All three had a left ventricular ejection fraction of less than 0.30.
Table IV presents the incidence of discordance in specific patient groups. There was a significant associ- ation of discordance with a left ventricular ejection fraction of less than 0.30 and with mitral valve prolapse associated with frequent ventricular extrasystoles. Patients with frequent ventricular extrasystoles alone (without an ejection fraction of less than 0.30 or mitral valve prolapse), atria1 fibrillation or mitral valve pro- lapse without frequent ventricular extrasystoles did not have a discordant regurgitant index.
TABLE IV
Incidence of Discordant Radionuclide Regurgitant Indexes
Patlents with DIscardant RR1 0
0
0.9L -
0 I+ 2+ 3t 4t
Angiographtc Regurgitation
FIGURE 3. The radionuclide regurgitant index (RRI) is compared with the grade of angiographic regurgitation as in Figure 2. Patients with a regurgitant index considered discordant (see text for discussion) are represented by crosses. The remaining patients, whose regurgitant index was not discordant, are represented by open circles.
Discussion
Gated cardiac blood pool studies have previously been validated for the noninvasive evaluation of right and left ventricular function.s-l0 These studies have been demonstrated to be useful for measuring ventric- ular ejection fraction and assessing regional wall motion abnormalities. Recently, Rigo et al.’ proposed the ratio of left to right ventricular stroke counts (defined as the difference between end-diastolic and end-systolic counts for each ventricle) as a measurement of the presence and severity of left-sided valve regurgitation. In their patients with significant mitral or aortic regurgitation, or both, the ratio of left to right ventric- ular stroke counts was significantly greater than unity. In their patients without regurgitation, this ratio ranged from 0.9 to 1.4 (mean 1.15). Baxter et al.lr provided quantitative verification of this hypothesis utilizing a dog model with experimentally induced acute aortic regurgitation. Bough et a1.12 recently reported reason- able correlation of this stroke count ratio with quanti- tative catheterization methods.
Rigo et al.’ demonstrated that this ratio of left to right ventricular stroke counts, or regurgitant index, was
Patients in Total
Series (n)
Patients With Index Discordant
n % P
Value*
Entire study group 100 12 Ejection fraction <0.30 10
: A’0 <0.0005
Mitral prolapse without PVCs 8 0 NS PVCs without mitral prolapse 13 2+ Mitral prolapse with PVCs
“6 3 lb”,
Atrial fibrillation 0 0
l Probability (p) value of chi-square test comparing presence of discordance and presence or absence of clinical characteristic listed. + Two patients with PVCs without mitral prolapse with a discordant regurgitant index had an ejection fraction of less than 0.30. NS = not significant; PVCs = frequent ventricular contractions.
February 1981 The American Journal of CARDIOLOGY Volume 47 295

?A3’OV_‘C!_‘?’ QFG’JRG”ANT INDEX-LAN ET AL.
reprduc ible when calculated by different observers. Because we also have found little interobserver vari- abil!it:y in calculation of the radionuclide regurgitant index” we did not formally repeat this study. Rigo et al. showed a significant correlation between the regurgitant index and the severity of left-sided valve regurgitation in 40 patients (of whom 31 underwent catheterization and 20 manifested regurgitation of varying degrees of severity). There was no overlap in the regurgitant in- dexes calculated in patients with no regurgitation and in those with moderate or severe regurgitation. The patients studied had good overall left ventricular function, only four having a reduced left ventricular ejection fraction (less than 0.50).
Methodologic considerations: In this study, we attempted to assess the usefulness of the radionuclide regurgitant index in a variety of cardiac disorders, rhythms and ranges of cardiac function. Our radionu- elide method was based on the principle outlined by Rigo et al.’ utilizing a single end-diastolic region of in- terest for each ventricle without background subtrac- tion. Our technique differed from that of Rigo et al. because we used (1) in vivo labeled red blood cells rather than labeled albumins; (2) a caudal tilt in the left an- terior oblique position; (3) subtraction images (in- cluding end-diastole minus end-systole and end-systole minus end-diastole)5t8,g; and (4) the continuous elec- trocardiographically synchronized equilibrium mode of acquisition for all studies.4 The use of the caudal tilt allowed improved separation of the atria from the ventricles, especially in the right side of the heart. Subtraction images, especially the “stroke volume image” (obtained from the subtraction of end-systole from end-diastole), aided in the delineation of the right and left ventricular regions of interest. The radionuclide methods we utilized are virtually identical to the methods used in the recent report of Bough et a1.12 However, Bough et al. utilized a 30” caudal slant hole collimator of intermediate sensitivity as opposed to a caudal tilt.
We applied the continuous electrocardiographically synchronized mode of acquisition and display to all patients studied. Rigo et a1.l applied this mode of dis- play in only 19 of 40 patients. For simplicity, we utilized only the nadir of the left ventricular time-activity curve in identifying the end-systolic frame for both ventricles. Although there is a potential for error because right and left ventricular end-systole may not coincide, Rigo et al. found no systematic difference between using the same end-systolic frame for both ventricles as opposed to using separate time-activity curves to identify each ventricular end-systole.
In our method, the cardiac cycle was divided into 16 frames. Theoretically, increasing the number of frames would appear to increase the accuracy of the regurgitant index because the peak and nadir of time-activity curves would be sharper. However, to obtain the same number of overall counts/frame, a longer acquisition time would be necessary because the time interval of each frame would be shorter. Otherwise, for the same acquisition time, increasing the number of frames would result in
a lower number of counts/frame and more statistical variation.
Correlation of radionuclide and angiographic regurgitation: In our series, the radionuclide re- gurgitant index generally correlated with the presence and severity of angiographic left-sided valve regurgi- tation. There was a significant difference between the regurgitant index of patients without angiographic regurgitation and that of patients with 1+ or greater regurgitation. There was no significant difference be- tween the indexes of patients with adjacent angio- graphic grades of regurgitation, a finding that may re- flect the small number of patients with angiographically graded 2+ and 3+ regurgitation. Comparison of the regurgitant indexes of patients separated by more than one grade of regurgitation (that is, 1+ versus 3+, 2+ versus 4+) showed a significant difference.
A regurgitant index of 1.5 or less generally indicated no or trivial regurgitation. This separation was more specific (94 percent) than it was sensitive (73 percent). A regurgitant index of 2.5 or greater was a relatively sensitive (77 percent) and specific (77 percent) predictor of severe regurgitation. Patients with a regurgitant index between 1.5 and 2.4 had a wide range of angio- graphic regurgitation. Generally, they had 0, l+ or 2+ regurgitation rather than 3+ or 4+ regurgitation, but this trend did not appear to be of statistical signifi- cance.
Causes of discrepancies between angiographic grading and regurgitant index: Unlike the patients studied by Rigo et al.,l our patients demonstrated some overlap in the range of regurgitant indexes in all angi- ographic grades of regurgitation. The study by Bough et a1.12 illustrated some discrepancies between the an- giographic grading and the radionuclide assessment of the severity of valve regurgitation; however, there was no explanation of these discrepancies. In attempting to identify the characteristics of patients whose regurgi- tant index appeared to be obviously discordant, we ex- amined a group of arbitrarily classified patients on the basis of regurgitant indexes shown to separate no and trivial from significant regurgitation, and severe from nonsevere regurgitation. Patients with a greatly reduced left ventricular ejection fraction (less than 0.30) had a significantly greater incidence of discordance than did patients with an ejection fraction of 0.30 or greater. We can only postulate why the regurgitant index appears to predict inaccurately the presence or severity of regurgitation in patients with a greatly decreased left ventricular ejection fraction. Such patients generally have elevated pulmonary arterial pressures or right ventricular failure and may have clinically silent tri- cuspid regurgitation. These conditions would tend to reduce the radionuclide regurgitant index in patients with significant left-sided regurgitation. Conversely, the severity of regurgitation may be overestimated angio- graphically in these patients because of a relatively slow washout of contrast medium with a greatly reduced forward output. These explanations would not account for the discrepancies noted in patients with a low ejec-
tion fraction, no angiographic regurgitation and a high
296 February 1961 The American Journal of CARDIOLOGY Volume 47

regurgitant index. The precision with which the stroke counts can be measured may be reduced in patients with low right and left ventricular ejection fractions and markedly dilated ventricular chambers. This factor may account for these discrepancies.
Limitations of method and sources of error: The inability of the radionuclide regurgitant index to detect the presence of severity of regurgitation in patients with a very low ejection fraction limits its usefulness in as- sessing the significance of a mitral regurgitant murmur in these patients. Thus, the regurgitant index would not be able to discriminate adequately between a patient with a cardiomyopathy with mild mitral regurgitation (secondary to distortion of the supporting structures of the mitral valve) and a patient with severe long-standing mitral regurgitation with resultant depressed left ven- tricular dysfunction (secondary to the volume overload) if the ejection fraction was less than 0.30.
All three patients with mitral valve prolapse associ- ated with frequent ventricular extrasystoles had a high regurgitant index in the absence of angiographic mitral regurgitation during conducted beats. There were eight patients with mitral valve prolapse alone and 11 pa- tients with frequent ventricular extrasystoles alone (without either prolapse or a greatly reduced ventricular ejection fraction). None of these patients had a discor- dant regurgitant index. Possibly, the patients with both mitral valve prolapse and frequent ventricular extra- systoles had mitral regurgitation with extrasystoles during the radionuclide study that was not noted during angiography (when only conducted beats were ana- lyzed). The presence of atria1 fibrillation did not in- validate the regurgitant index.
This radionuclide method is also theoretically limited in clinical conditions with volume overload of the right ventricle such as tricuspid regurgitation or atria1 septal defect. Also, the method does not allow discrimination of aortic from mitral regurgitation.
Previous angiographic studies have demonstrated nearly equal right and left ventricular stroke volumes in the absence of shunts and valve regurgitation.13 It was not immediately clear why the regurgitant index was greater than 1.0 in some patients with no regurgitation. It is more difficult to separate the right atrium from the right ventricle than it is to separate the left atrium from the left ventricle in the radionuclide study. Because the right atria1 time-activity curve peaks during right ven- tricular systole, inclusion of a portion of the right atrium in the right ventricular region of interest would result in a dampening of the right ventricular time-activity curve. This reduction in the right ventricular stroke counts would systematically increase the ratio of left to right ventricular stroke counts.
RADIONUCLIDE aEGC;“G’- AS’ ‘N?=,“--‘_A% ‘- ,t’..
There may be other geometric far tars : f:at ma\. result in different absorption characteristics ()I’ each vt:ntric- ular blood pool. Reported data”.. I suggesl that better separation of the atria from the Lrntricles witt-: a 30” slant hole collimat,or results in regurgitant indexeh closer to unity and with less variability 11 .i)O i 0.08) in pa- tients with no regurgitation. We were able to obt.ain only a loo to 15O caudal angulation, a factor that might ex- plain our higher values. Our mean value for regurgitant index (1.34) was also higher than that (1.15) reported by Rigo et al. for patients with nl:, regurgitation. Our method utilized a 10” to 15” caudal tilt, whereas Rigo et al. did not utilize any caudal tilt. Thus, the caudal tilt would not appear to explain the difference in this in- stance. Our inclusion of patients with a wider range of cardiac function (including patients with a discordant index and a low ejection fraction) than that of patients in the study by Rigo and co-workers may explain the difference.
Limitations of angiographically graded re- gurgitation: Unfortunately there is no ideal “gold standard” for the quantitation of valve regurgitation. Angiographicalfv graded regurgitation is the method most widely utlhzed clinically. This visual grading of angiographic regurgitation is affected by the size of the ventricular and atria1 chambers. Regurgitant fractions can be calculated by comparing the angiographic left ventricular stroke volume with the forward stroke vol- ume calculated from the cardiac output and heart rate. The presence of any arrhythmia during angiography invalidates this calculation because only a few beats are available for analysis. The angiographically calculated regurgitant fraction also is subject to the limitations of calculating the stroke volumes with angiography and with cardiac output determinations. This limitation is a particular problem in patients with a very low cardiac output and stroke volume and large ventricular vol- umes. Limiting analysis to patients in whom a mea- surement of an angiographic regurgitant fraction was possible or whose regurgitant index corresponded to the angiographic grading would preselect patients and thus might lead to false conclusions of the accuracy of the radionuclide regurgitant index.
Implications: The radionuclide regurgitant index is useful for assessing the presence and severity of left- sided valve regurgitation. The presence of a markedly reduced left ventricular ejection fraction may result in both false positive and false negative discordant regurgitant indexes. Mitral valve prolapse associated with frequent ventricular extrasystoles may result in a false positive discordant regurgitant index. Recognizing these potential sources of error should make the ra- dionuclide regurgitant index more useful.
References
1. Rigo P, Alderson PO, Robertson RM, Becker LC, Wagner HN. 1964; 14:437-47. Measurement of aortic and mitral regurgitation by gated cardiac 3. blood pool scans. Circulation 1979;60:306-12.
Pave1 DG, Zlmmer AM, Patterson VN. In vivo labeling of red blood
2. Sellers RD, Levy MJ, Amplalz K, Llllehei CW. Left retrograde cells with 99Tc: a new approach to blood pool visualization. J Nucl Med 1977;18:305-8.
cardioangiography in acquired cardiac disease. Am J Cardiol 4. Pave1 DG, Byrom E, Ayres B, Pietras RJ, Bianco JA, Kanakis C.
February 1981 The American Journal of CARDIOLOGY Volume 47 297

Multifaceted evaluation of lefi vantricular function by the first transit technique using Anger type cameras and an optimized protocol: correlation with biplane roentgen angiography. In: Sorenson JA, ed. Nuclear Cardiology: Selected Computer Aspects. Atlanta: Society of Nuclear Medicine, 1978: 129-38.
5. Byrom E, Pave1 DG. Improved computer definition of regions of interest by using a double-cursor method. J Nucl Med 1978;19: 959-60.
rate from gated images. J Nucl Med 1978; 19:880-3. 10. Maddahi J, Berman DS, Matsuoka DT, et al. A new technique for
assessing right ventricular ejection fraction using rapid multiple- gated equilibrium cardiac blood pool scintigraphy. Circulation 1979;60:581-9.
11. Baxter RH, Becker LC, Alderson PO, et al. Quantification of aortic valvular regurgitation in dogs by nuclear imaging. Circulation 1980;61:404-10.
6. Burow RD, Strauss HW, Singleton T, et al. Analysis of left ven- tricular function from multiple gated acquisition cardiac blood pool imaging. Circulation 1977;56: 1024-8.
7. Seeker-Walker RH, Resnick L, Kunz H, Parker JA, Hill RL, Potchen RJ. Measurement of left ventricular ejection fraction. J Nucl Med 1973;14:798-802.
12. Bough EW, Gandsman EJ, North DL, Shulman RS. Gated radio- nuclide angiographic evaluation of valve regurgitation. Am J Cardiol 1980;46:423-8.
13. Carlsson E, Keene RJ, Lee P, George RJ. Angiographic stroke volume correlation of the two cardiac ventricles in man. Invest Radio1 1971;6:44-51.
8. Maddox DE, Holman BL, Wynne J, et al. Ejection fraction: a 14. Gandsman E, Bough E, North D, Shulman R. The ventricular stroke non-invasive index of regional left ventricular wall motion. Am J volume ratio: requirements for accurate quantitation (abstr). Cir- Cardiol 1978;41:1230-8. culation 1979;6O:Suppl li:ll-62.
9. Green MV, Brady WR, Douglas MA, et al. Ejection fraction by count
298 February 1981 The American Journal of CARDIOLOGY Volume 47




















